The Project Gutenberg EBook of Obstetrics for Nurses, by Charles B. Reed
This eBook is for the use of anyone anywhere in the United States and most
other parts of the world at no cost and with almost no restrictions
whatsoever. You may copy it, give it away or re-use it under the terms of
the Project Gutenberg License included with this eBook or online at
www.gutenberg.org. If you are not located in the United States, you'll have
to check the laws of the country where you are located before using this ebook.
Title: Obstetrics for Nurses
Author: Charles B. Reed
Release Date: February 21, 2020 [EBook #61476]
Language: English
Character set encoding: UTF-8
*** START OF THIS PROJECT GUTENBERG EBOOK OBSTETRICS FOR NURSES ***
Produced by Richard Tonsing, Mark C. Orton, and the Online
Distributed Proofreading Team at http://www.pgdp.net
Transcriber’s Note:
The cover image was created by the transcriber and is placed in the public domain.
OBSTETRICS
FOR NURSES
BY
CHARLES B. REED, M.D.,
Obstetrician to Wesley Memorial Hospital, Chicago.
ONE HUNDRED THIRTY ILLUSTRATIONS
ST. LOUIS
C. V. MOSBY COMPANY
1917
Copyright, 1917, by C. V. Mosby Company
Press of
C. V. Mosby Company
St. Louis
TO HIS LOYAL FRIEND
EUGENE S. GILMORE
THIS BOOK IS AFFECTIONATELY DEDICATED BY THE AUTHOR
7
PREFACE
It might seem that an apology was necessary for
presenting a new textbook on obstetrics for nurses
when so many are to be had for the asking. But when
a teacher is rarely or never satisfied with his own
work it is too much to expect that he will ever fully
endorse the product of another. It may be therefore
largely a personal matter that none of the existent
books seem to exhibit the fullness of information, the
conciseness of expression, and the emphasis due to certain
subjects that the present writer would hope to
find.
The necessities apparently demand such an arrangement
of our obstetrical doctrine that the book may
serve for class instruction and at the same time be
complete enough for post-graduate reference.
To secure this much discrimination is necessary. The
confusion attendant upon overabundance must be
avoided as well as the discouragement that is not infrequently
produced by a large book or a periphrastic
style.
Hitherto there has been a tendency to teach the
nurse too little rather than too much but conditions
have changed. Vocational instruction is not only more
methodical and far reaching but it is developmental.
The present day nurse expects not merely to assist
the physician and earn a stipulated reward, but she
is constantly alert to attain her own maturity as a professional
woman.
To be a capable and intelligent assistant it is not
sufficient to have a clear comprehension of her particular
8duties, but she must have a defined and critical conception
of what the doctor is aiming to accomplish.
This is especially true in obstetrics where the nurse
has the additional responsibility of giving support and
counsel to her patient in the various emergencies that
arise. Moreover, to attain her intellectual maturity the
nurse must strive unremittingly to understand the
complicated processes that take place under her observation.
She must cooperate with her doctor whose associate
she is and secure the confidence of her patient who relies
upon her for guidance in the perils she is facing.
For childbirth is a peril. It is no longer the normal
process it once was. Civilization has changed the shape
of the pelvic bones, altered the muscles of parturition
and weakened the nerve centers that control the event.
The birth of a child is equal in severity and seriousness
to many of the major operations. It is not an
affair to be entered upon lightly nor managed without
the utmost foresight and care.
The dangers that are recognized and prepared for
in this book by what may seem to some to be an extravagant
technic, are very real dangers, extremely
subtle, and against them at times every precaution and
every defense proves unavailing.
Nevertheless, skill, thoughtfulness, and above all,
cleanliness, will avert the worst, as well as unhappily
the most common of these disasters. If our nurses
could be convinced of this, the difficulties and apprehensions
of childbirth would be greatly diminished.
The nurse should see to it that her patient is surrounded
by all the precautions and safeguards against
infection that she would demand for a member of her
own family. This means of course that her work will
9be far more exacting and onerous but also it will save
many nights of anxiety and not infrequently a life.
This book represents the obstetric ideas and technic
which the writer has endeavored for years to impress
upon his students and nurses with such emendations
and changes as experience and scientific progress have
suggested. It is a selective essence distilled from the
recurrent harvests that workers in this field have
brought forth during centuries of consecrated effort.
To all these forerunners the writer acknowledges a
deep personal indebtedness.
In the preparation of the book thanks are due particularly
to Charlotte Gregory, Head Nurse of the
Wesley Maternity, whose rare ability as teacher, technician
and executive and whose untiring vigilance has
been a leading factor in securing and maintaining the
high state of efficiency in this department. She has
kindly contributed Chapters XXIII and XXIV, together
with valuable suggestions and criticisms in other
portions of the text.
The author also takes pleasure in acknowledging his
obligations to Florence Olmstead, Head Nurse of the
Dispensary of the Northwestern University Medical
School, whose long experience in feeding babies gives
to her words an unquestioned authority. Chapter XXII
is almost entirely her work.
To the various publishers who have courteously allowed
the reproduction of valuable illustrations from
the books of other writers thanks are also extended,
and to his own publishers especially for their cordial
and sympathetic cooperation the author wishes to express
his warmest gratitude.
11
CONTENTS
| CHAPTER I |
|
PAGE |
| |
| Anatomy |
17 |
| |
| CHAPTER II |
| |
| Physiology |
33 |
| |
| CHAPTER III |
| |
| Normal Pregnancy |
51 |
| |
| CHAPTER IV |
| |
| Hygiene of Normal Pregnancy |
66 |
| |
| CHAPTER V |
| |
| Abnormal Pregnancy |
74 |
| |
| CHAPTER VI |
| |
| Abnormal Pregnancy (Continued) |
89 |
| |
| CHAPTER VII |
| |
| Preparations for Labor and the Normal Course of Labor |
98 |
| |
| CHAPTER VIII |
| |
| The Mechanism of Normal Labor |
120 |
| |
| CHAPTER IX |
| |
| The Care of the Patient During Normal Labor |
129 |
| |
| CHAPTER X |
| |
| The Normal Puerperium |
151 |
| |
| CHAPTER XI |
| |
| Unusual Presentations and Positions |
165 |
| |
| CHAPTER XII |
| |
| Operations |
179 |
| |
| 12CHAPTER XIII |
| |
| Minor Operations |
200 |
| |
| CHAPTER XIV |
| |
| Complications in Labor |
214 |
| |
| CHAPTER XV |
| |
| Complications in Labor (Continued) |
228 |
| |
| CHAPTER XVI |
| |
| The Abnormal Puerperium |
242 |
| |
| CHAPTER XVII |
| |
| Infection |
255 |
| |
| CHAPTER XVIII |
| |
| The Care of the Child |
265 |
| |
| CHAPTER XIX |
| |
| The Care of the Child (Continued) |
278 |
| |
| CHAPTER XX |
| |
| The Care of the Child (Continued) |
287 |
| |
| CHAPTER XXI |
| |
| The Care of the Child (Continued) |
298 |
| |
| CHAPTER XXII |
| |
| Infant Feeding |
310 |
| |
| CHAPTER XXIII |
| |
| Cleanliness and Sterilization |
323 |
| |
| CHAPTER XXIV |
| |
| Diets and Formulæ |
330 |
| |
| CHAPTER XXV |
| |
| Solutions and Therapeutic Index |
340 |
13
ILLUSTRATIONS
| FIG. |
|
PAGE |
| |
| 1. |
The normal female pelvis |
18 |
| |
| 2. |
The planes of the brim, the cavity, and the outlet |
19 |
| |
| 3. |
Visceral relations |
20 |
| |
| 4. |
Uterus and appendages |
22 |
| |
| 5. |
Normal position of pelvic organs |
24 |
| |
| 6. |
The external genitals |
25 |
| |
| 7A. |
Varieties of hymen |
27 |
| |
| 7B. |
Varieties of hymen |
28 |
| |
| 8A. |
The excreting ducts of the mammary gland |
29 |
| |
| 8B. |
Lobules and duct of the mammary gland |
29 |
| |
| 9. |
Nipple, areola, and the glands of Montgomery |
30 |
| |
| 10. |
Supernumerary milk glands in the axillæ |
31 |
| |
| 11. |
The three ages of the breast |
31 |
| |
| 12. |
Development of the ovary |
34 |
| |
| 13. |
Graafian follicles |
35 |
| |
| 14. |
Human spermatozoa |
36 |
| |
| 15. |
The chorionic villi about the third week of pregnancy |
38 |
| |
| 16. |
Diagram illustrating relations of structures of the human uterus at the end of the seventh week of pregnancy |
39 |
| |
| 17. |
Maternal surface of the placenta and membranes |
40 |
| |
| 18. |
Fœtal surface of human placenta |
41 |
| |
| 19. |
The egg at term with uterus removed |
42 |
| |
| 20. |
Normal attitude of fœtus |
43 |
| |
| 21. |
Fœtal skulls showing sutures |
44 |
| |
| 22A. and B. |
Child’s head at term, showing diameters |
45 |
| |
| 23. |
The fœtal circulation |
49 |
| |
| 24. |
Gravid uterus at the end of the eighth week |
52 |
| |
| 25. |
Striæ gravidarum |
54 |
| |
| 26. |
Bimanual examination |
60 |
| |
| 27. |
Abdominal enlargement at different months of pregnancy |
63 |
| |
| 28. |
Height of the uterus at various months of pregnancy |
64 |
| |
| 29. |
Twins |
83 |
| |
| 30. |
Diagram representing the sites for the various forms of tubal pregnancy |
90 |
| |
| 31. |
Abdominal binder with crosspiece to hold vulvar pads |
100 |
| |
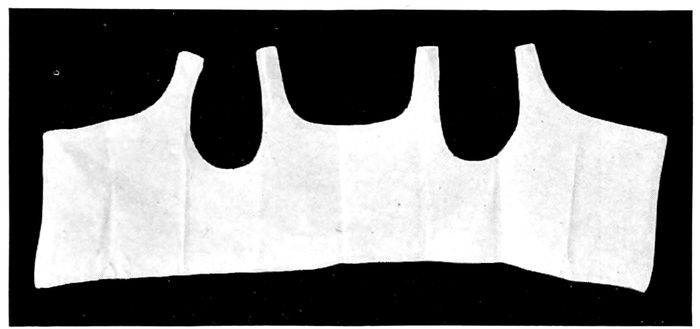
| 1432. |
T-binder, used in all cases after the fifth day post partum |
100 |
| |
| 33. |
Breast binder |
101 |
| |
| 34. |
Baby’s dress with winged sleeves |
102 |
| |
| 35. |
The bag of waters begins to act on the cervix |
111 |
| |
| 36. |
The effect of the pains. The cervix before labor begins |
112 |
| |
| 37. |
The effect of the pains. The cervix begins to be “effaced” |
112 |
| |
| 38. |
The effect of the pains. The cervix is effaced, and the dilatation of the os begins |
113 |
| |
| 39. |
The effect of the pains. The cervix is effaced and the os continues to dilate |
113 |
| |
| 40. |
The cervix is effaced and the os dilated |
115 |
| |
| 41. |
Child in second stage of labor |
116 |
| |
| 42. |
The head passing over the perineum |
117 |
| |
| 43. |
Normal expulsion of the placenta according to Schultze |
118 |
| |
| 44. |
The child in left-occipito-anterior position |
122 |
| |
| 45. |
The child in right-occipito-anterior position |
123 |
| |
| 46. |
The descent of the head in right-occipito-anterior position |
124 |
| |
| 47. |
Internal anterior rotation and extension of the head in a left-occipito-anterior position |
124 |
| |
| 48. |
Extension |
125 |
| |
| 49. |
Extension completed. Expulsion |
125 |
| |
| 50. |
A cephalhæmatoma |
127 |
| |
| 51. |
Points of greatest intensity of fœtal heart tones |
130 |
| |
| 52. |
Handling forceps, kept sterile in a jar of alcohol |
132 |
| |
| 53. |
Palpation. What is in the pelvis? |
134 |
| |
| 54. |
Palpation. What is in the fundus? |
135 |
| |
| 55. |
Palpation. Where is the back? Where are the small parts? |
136 |
| |
| 56. |
Patient draped for internal examination |
137 |
| |
| 57. |
Delivery in side position |
141 |
| |
| 58. |
Sheet twisted into a sling |
147 |
| |
| 59. |
Repair of perineum |
148 |
| |
| 60. |
The progress of involution |
152 |
| |
| 61. |
The breech. Left-sacro-anterior position |
166 |
| |
| 62. |
The breech. Left-sacro-posterior position |
167 |
| |
| 63. |
Extraction of the breech |
170 |
| |
| 64. |
Breech delivery. Extraction of the trunk |
171 |
| |
| 65. |
Breech delivery. Delivering the shoulder |
172 |
| |
| 66. |
The delivery of the after-coming head by the Smellie-Veit maneuver |
172 |
| |
| 67. |
Shoulder presentation |
173 |
| |
| 1568. |
Face presentation |
175 |
| |
| 69. |
Descent of the chin in face presentation |
176 |
| |
| 70. |
Delivery in face presentation |
177 |
| |
| 71. |
Exaggerated lithotomy position |
181 |
| |
| 72. |
Dorsal position when assistants are available |
182 |
| |
| 73. |
Instruments for artificial delivery of the head |
183 |
| |
| 74. |
Forceps operation. Introduction of the left blade |
186 |
| |
| 75. |
Forceps operation. The introduction of the right blade |
187 |
| |
| 76. |
Forceps operation. Locking the handles |
187 |
| |
| 77. |
Forceps operation. The way the blades should grasp the fœtal head |
188 |
| |
| 78. |
Forceps operation. Traction on the handles |
189 |
| |
| 79. |
Forceps operation. The delivery of the head |
189 |
| |
| 80. |
Version. Seizing a foot |
190 |
| |
| 81. |
Version. The child rotates as pressure is made upon the head and traction upon the foot |
191 |
| |
| 82. |
Version is complete when the knee appears at the vulva |
192 |
| |
| 83. |
The Walcher position |
194 |
| |
| 84. |
The Wiegand compression of the child’s head to force it into the pelvis |
195 |
| |
| 85. |
The Naegele perforator |
196 |
| |
| 86. |
Apparatus for getting a sterile specimen of urine from an infant |
201 |
| |
| 87. |
Tampon of the uterus |
203 |
| |
| 88. |
Tampon of vagina |
204 |
| |
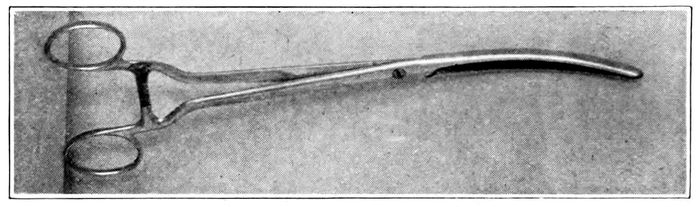
| 89. |
Pean forceps |
208 |
| |
| 90. |
Hand bulb syringe; and Vorhees bags; bag rolled and grasped by Pean forceps ready for introduction |
209 |
| |
| 91. |
Vorhees bag in place |
210 |
| |
| 92. |
Episiotomy |
212 |
| |
| 93. |
Various forms of pelvic deformity |
215 |
| |
| 94. |
The pelvimeter |
216 |
| |
| 95. |
The various diameters of the inlet |
216 |
| |
| 96. |
Measuring the distance between the anterior superior spines of the pelvis |
217 |
| |
| 97. |
Measuring the external conjugate |
218 |
| |
| 98. |
Measuring the diagonal conjugate with the finger |
219 |
| |
| 99. |
Various forms of placenta prævia |
229 |
| |
| 100. |
The knee-elbow posture |
236 |
| |
| 101. |
The knee-chest posture |
236 |
| |
| 16102. |
The exaggerated lithotomy position obtained with a sheet sling |
237 |
| |
| 103. |
The improvised Trendelenburg position |
237 |
| |
| 104. |
The dorsal position with stirrups |
238 |
| |
| 105. |
Dorsal position across the bed |
239 |
| |
| 106. |
Flexed dorsal position with feet on the table |
240 |
| |
| 107. |
The Sims position |
241 |
| |
| 108. |
Examples of imperfect nipples |
245 |
| |
| 109. |
A standard nipple shield |
246 |
| |
| 110. |
A standard breast pump |
251 |
| |
| 111. |
Germs most frequently found in cases of puerperal fever |
256 |
| |
| 112. |
Rubber bath tub |
266 |
| |
| 113. |
The Pettit cord clamp |
268 |
| |
| 114. |
Standard breast pump; Standard nursing bottle; the breast tray; the Wansbrough lead nipple shield; the Brophy nipple for harelip and cleft palate |
271 |
| |
| 115. |
Proper position of mother while nursing child |
274 |
| |
| 116. |
Proper method of taking rectal temperature |
276 |
| |
| 117. |
Method of passing the tracheal catheter |
279 |
| |
| 118. |
Byrd’s method of artificial respiration. Extension and inspiration |
280 |
| |
| 119. |
Byrd’s method of artificial respiration. Beginning flexion and expiration |
280 |
| |
| 120. |
Byrd’s method of artificial respiration. Flexion and compression |
281 |
| |
| 121. |
Method of giving gavage |
284 |
| |
| 122. |
Apparatus for gavage or lavage |
286 |
| |
| 123. |
Cleft palate nipple |
288 |
| |
| 124. |
The device for feeding the child with cleft palate |
288 |
| |
| 125. |
Device for assisting the cleft palate child to nurse |
289 |
| |
| 126. |
Method of strapping an umbilical hernia |
290 |
| |
| 127. |
Proper position for introduction of a suppository |
299 |
| |
| 128. |
Hydrocephalus |
307 |
| |
| 129. |
Anencephalus |
308 |
| |
| 130. |
Elements of human milk |
312 |
17
CHAPTER I
ANATOMY
The study of obstetrics is an investigation of the
passage, the passenger, and the driving powers of labor,
as well as of the various complications and anomalies
that may attend the process of reproduction.
The passage is composed of a bony canal, called the
pelvis, and the soft tissues which line and almost close
its outlet.
The pelvis is made up of four bones; the sacrum, the
coccyx, and two other large structures of irregular
shape, called the hip, or innominate bones. Joined by
cartilage and held in place by ligaments, they form a
cavity or basin which, in the male is deep, narrow,
small and funnel-shaped, while in the female, slighter
bones, expanded openings and wider arches make a
broad, shallow channel, through which the child is born.
The bony pelvis is divided for description into two
parts, the upper or false pelvis, and the lower or true
pelvis. The upper pelvis is formed by the wings of
the innominate bones and has but two functions of importance
to child-bearing. It acts as a guide to direct
the child into the true passage, and when measured by
the pelvimeter, it gives information as to the shape
and size of the inlet to the true pelvis. The true pelvis
is of most concern to the obstetrician, because anomalies
in its size or shape may impede the progress of labor or
18render it impossible. The pelvis is divided conveniently
into three parts: the brim, the outlet, and the cavity.
The brim, inlet, or upper pelvic strait, is the boundary
line between the false and true pelvis. It is traced from
the upper border of the symphysis along the iliopectineal
line on both sides to the promontory of the sacrum.
The shape and size of this opening varies much in different
races and individuals, both normally and through
disease; and when pathologically altered, both shape
and size may exercise a marked influence on the course
of labor. In American women, the outline of the brim
is roughly heart-shaped, like an ovoid with an indentation
where the promontory of the sacrum impinges upon
the opening.
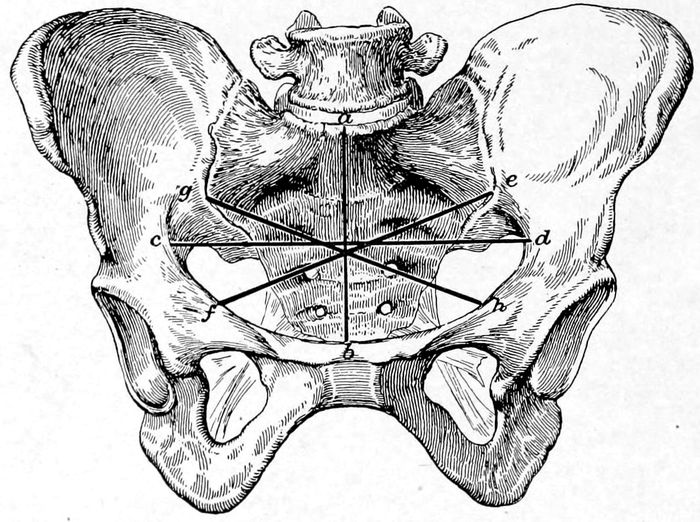
Fig. 1.—The normal female pelvis. (Eden.) The lines ab and cd divide the pelvis into the right and left anterior and the right and left posterior quadrants. ab indicates the anteroposterior diameter of the brim, cd shows the transverse diameter while gh and ef represent, respectively, the right and left oblique diameters.
19The brim or inlet has four important diameters to be
remembered; important because the hard, round head
of the child must pass through them by accommodating
its diameters as favorably as possible to those of this
opening. These diameters are named respectively the
anteroposterior or conjugate diameter, the transverse,
and the right and left oblique diameters. The two
oblique diameters attain their greatest importance when
the pelvis is irregularly distorted, but the others are
essential in every case where labor impends. It is to
secure an estimate of these latter diameters that the
bony prominences are measured. This upper opening
lies not horizontally, but in oblique relation to the body
in standing position, and the weight of the abdominal
viscera rests largely upon the bones and in consequence
does not crowd into the inlet unless forced in by corsets
or faulty habits.
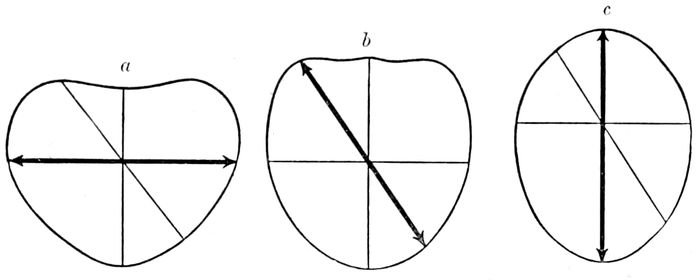
Fig. 2.—The planes of (a) the brim, (b) the cavity and (c) the outlet. (Eden.)
Passing through the brim, a cavity is found below it,
midway between the inlet and outlet, which is nearly
round in shape. This is the “excavation,” or the true
pelvis. Then comes the outlet, bounded in front by the
pubic arch and soft parts, and behind by the coccyx
pushed back as far as it can go. It is ovoid in shape,
but the long axis of this ovoid lies at right angles with
the axis of the ovoid inlet.
20We find, therefore, a succession of three geometric
figures or planes through which the head must pass by
means of a spiral motion called rotation. These figures
are inclined to one another so markedly in front that
a line drawn through the center of each will curve
forward at both ends, one end passing out near the umbilicus,
the other through the vulva. This is known as
the axis of the pelvis or the curve of Carus.
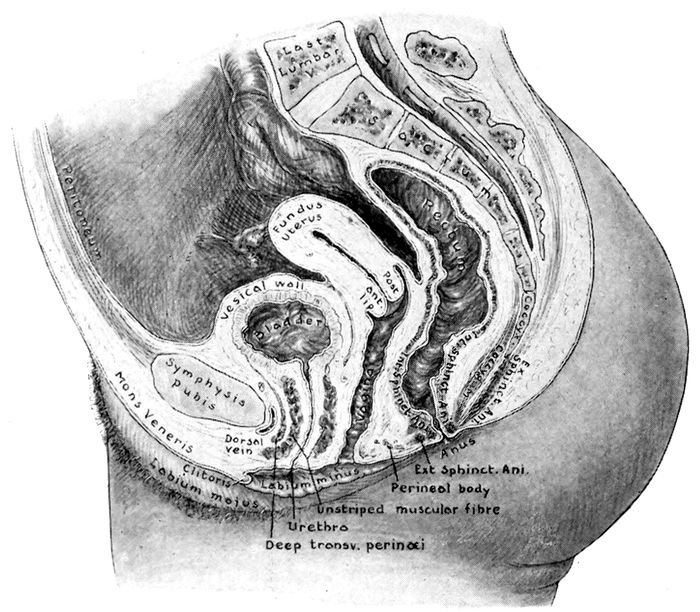
Fig. 3.—Visceral relations. (Redrawn from Gray.)
THE SOFT PARTS
Inside the pelvis are the organs of generation with
their accessory structures and supporting tissues.
21Of first importance are the ovaries, tubes and uterus,
together with the vagina. These special structures are
the true genital organs. They are bounded in front by
the bladder, behind by the rectum, above by the abdominal
viscera, and surrounded everywhere by muscular,
mucous and fatty tissues, which support them and
aid their function.
The Vagina.—The vagina is a hollow organ, about
four inches long, attached to the cervix above and the
vulva below. It is an elastic sheath bounded in front
by the bladder and behind by the rectum. Under normal
conditions, this tube easily admits one or two fingers,
but during labor it dilates enormously to allow the
head to pass. The vagina is lined with a thick mucous
membrane, ridged and roughened by folds, which are
called rugæ. Thus a continuous channel connects the
ovary with the outside and through it pass, at appropriate
times, the ovule, the menstrual blood, the uterine
secretions, the child, the placenta, and the lochia.
The Uterus.—The uterus (womb) is a pear-shaped
organ, flattened from before backward, and composed of
unstriped or involuntary muscle cells and connective
tissue. Normally the virgin uterus measures from two
and one-half to three inches in length, and weighs about
two ounces. It is suspended in the middle of the pelvis
by strong ligaments, so that the fundus inclines gently
forward against the bladder. When the bladder fills,
the uterus is pushed backward. Most of the organ is
internal, but a small part of the lower pole is grasped
by the vagina, in which the lower end with its invaluable
aperture, the os, dips and swings. The part above
the vagina is called the body or fundus, and is covered
with the serous membrane (peritoneum) that lines the
abdominal cavity. Below the fundus is the cervix or
neck, which lies partly above and partly within the
22vagina. The cavity of the uterus is usually closed by
the apposition of the walls. The inner surface is covered
with a peculiar kind of membrane called the endometrium,
which is highly vascular. The uterine cavity
opens into the vagina through the os, which is small
and round in the nulliparous woman, and slit-shaped or
gaping in the woman who has borne a child.
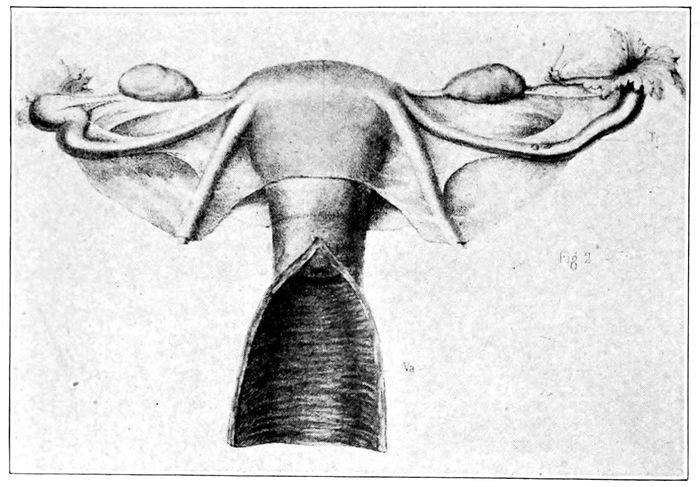
Fig. 4.—Uterus and appendages. On either side of the uterus will be seen the ovary, the fimbriated extremity of the tube, the tube, and the round ligament. The vagina lies open below. (Lenoir and Tarnier.)
Fallopian Tubes.—On either side of the upper end of
the uterus are the orifices of the Fallopian tubes, through
which the egg, escaping from the ovary, finds access to
the uterine cavity. These tubes extend outward from
the uterus about four inches, and terminate in a bell-shaped
opening with long, ragged fingers which hang
loosely down toward the ovary. The tubes are lined by
epithelial cells having hair-like projections, (ciliæ)
which wave automatically toward the uterus. Thus impelled
23by a gentle current, the egg moves definitely
along the tube toward the uterus and against this current
the spermatozoa force their way to meet and fertilize
the egg.
The Ovaries.—On either side of the pelvis, close to
the fringed end of the Fallopian tube and attached to
it, lies a small, hard, almond-shaped organ, called the
ovary. This is the intrinsic sexual gland of the female.
It contains the small cells which are to ripen and become
eggs. Each ovary is said to contain about thirty-six
thousand eggs, or ovules.
The Bladder.—The bladder lies between the pubic
bone and the uterus. It is a reservoir for urine, filled
by means of two little tubes called ureters, that run
down from the kidneys. It drains through the urethra
which opens just below the pubic bone in front of, and
just above, the vaginal opening. The bladder should be
emptied frequently during labor.
The Anus.—The large bowel (colon) terminates in an
opening near the middle of the genital crease. This
opening is called the anus. It is closed by a contracting
muscle, the sphincter, which acts like a puckering
string. Just inside of the opening is a group of large
veins which may become enlarged, inflamed, and bleed
during pregnancy. They are then called hæmorrhoids.
The Rectum.—Upward from the anus and to the left
of the uterus extends the rectum. This is the end of the
intestinal canal and is supplied with an abundance of
nerves. When the head presses upon it, it gives the
sensation of a bowel movement, and warns the observer
of the low position of the head. The anus pouts as the
head comes down and the anterior walls become visible.
In severe cases of labor, the sphincter is sometimes
torn. The bowels should be emptied by an enema
as early as possible in the first stage of labor.
24The Peritoneum.—The peritoneum is a thin, glistening,
serous membrane, which lines the abdominal cavity
and drops down from above over the uprising tops of
the bladder and uterus. Folding together at the sides
and extending to the walls of the pelvis, it encloses the
tubes and round ligaments in deep, flat masses, called
the broad ligaments. This is the structure that becomes
so perilously inflamed (peritonitis) when infected by
germs that find entrance through the genital passage.
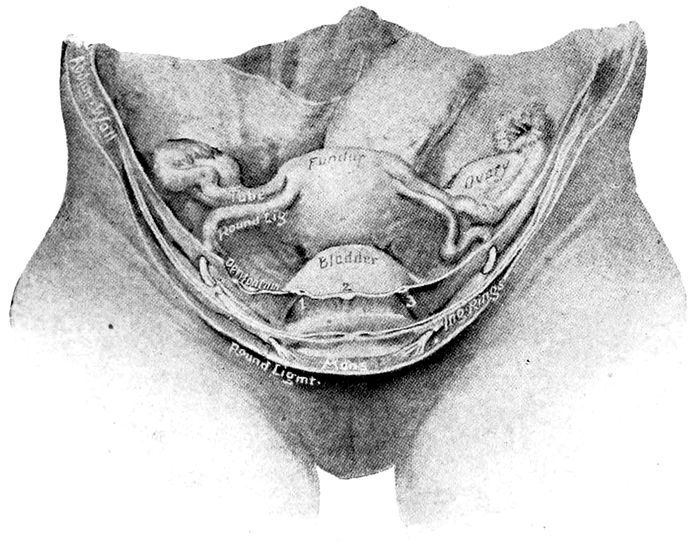
Fig. 5.—Normal position of pelvic organs, seen from above and in front. They are enveloped in peritoneum. (Bougery and Jacob, in American Text Book.)
THE EXTERNAL GENITALS
The external genitals form the vulva. Under this
name are included the mons veneris, the labia majora,
the labia minora, the clitoris, the vestibule, the hymen
and the glands of Bartholin.
25The entire groove from the mons veneris to a point
well up on the sacrum forms a deep fold or crevice,
which is known as the genital crease. That part of the
genital crease lying between the anus and vulva is technically
known as the perineum (q.v.)
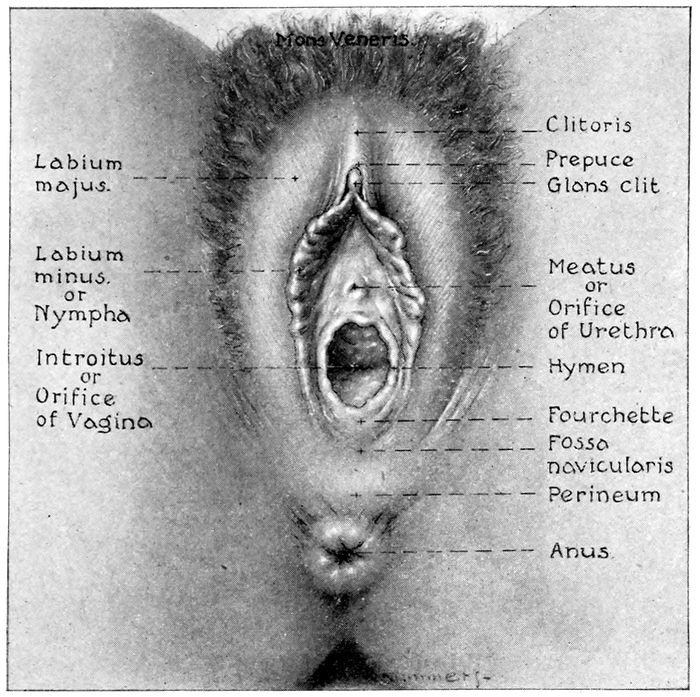
Fig. 6.—The external genitals. (Redrawn from Gray.)
The Mons Veneris.—The mons veneris is a gently
rounded pad of fat lying just above the junction of the
pubic bones (the symphysis). The overlying integument
is filled with sebaceous glands and covered with
hair at puberty.
The Labia Majora.—The labia majora are the large
26lips of the vulva. They are loose, double folds of skin
extending downward from the mons veneris to the anterior
boundary of the perineum and covered externally
with hair. Normally they lie in apposition and
conceal the vaginal opening. They correspond to the
male scrotum.
The Labia Minora.—The labia minora, or nymphæ,
are two small folds of skin and mucous membrane, that
extend from the clitoris obliquely downward and outward
for an inch and a half on each side of the entrance
to the vagina. On the upper side, where they meet and
invest the clitoris, the fold is called the prepuce, but
on the under side they constitute the frænum.
The labia minora are sometimes enormously enlarged
in the black races and are then called the Hottentot
apron.
The Clitoris.—The clitoris is an erectile structure analogous
to the erectile tissue of the penis. The free
extremity is a small, rounded, extremely sensitive tubercle,
called the glans of the clitoris. About the clitoris
there forms a whitish substance called smegma. This
is a good culture medium for germs and must be carefully
sponged away when the vulva is prepared for delivery.
The Vestibule.—The vestibule is bounded by the clitoris
above, the labia minora on the sides, and the
vaginal orifice below. It contains the opening of the
urethra, which is called the meatus urinarius.
The Hymen.—The hymen is a thin fold of membrane
which closes the vaginal opening to a greater or lesser
extent in virgins. It varies much in shape and consistency.
It is sometimes absent, or it may persist after
copulation, hence its presence or absence can not be
considered a test of virginity. When torn, the edges
27shrink up and form little irregularities called carunculæ
myrtiformes.
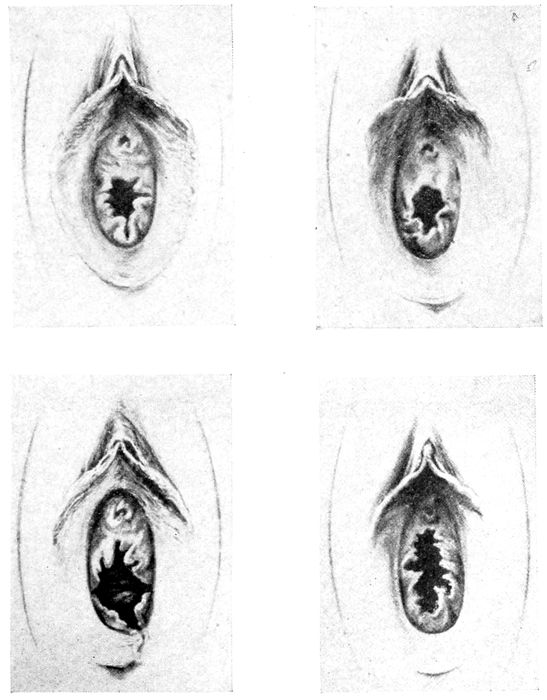
Fig. 7 A.—Varieties of hymen. (American Text Book.)
Bartholin Glands.—Bartholin glands are located on
each side of the commencement of the vagina. Each
gland discharges by a small duct just external to the
hymen. They are often the seat of a chronic gonorrhœal
28inflammation and must be watched carefully, lest infection
extend to the mother after labor, or to the eyes of
the child in passing.
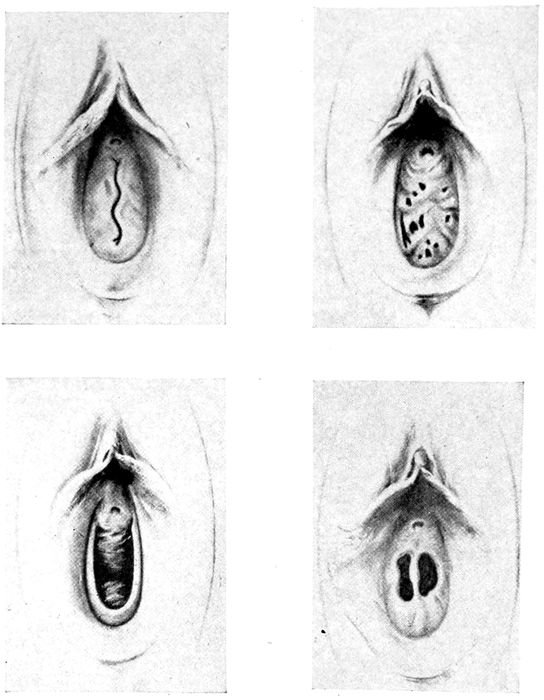
Fig. 7 B.—Varieties of hymen. (American Text Book.)
The Perineum.—The perineum is a body of muscle,
fascia, connective tissue, and skin, situated between
the vagina and the rectum. The vagina bends forward
29and the rectum backward, so a triangular area is left
between them which is filled by the perineal body. It
is about two inches long from before backward, and becomes
progressively thinner the deeper it extends.
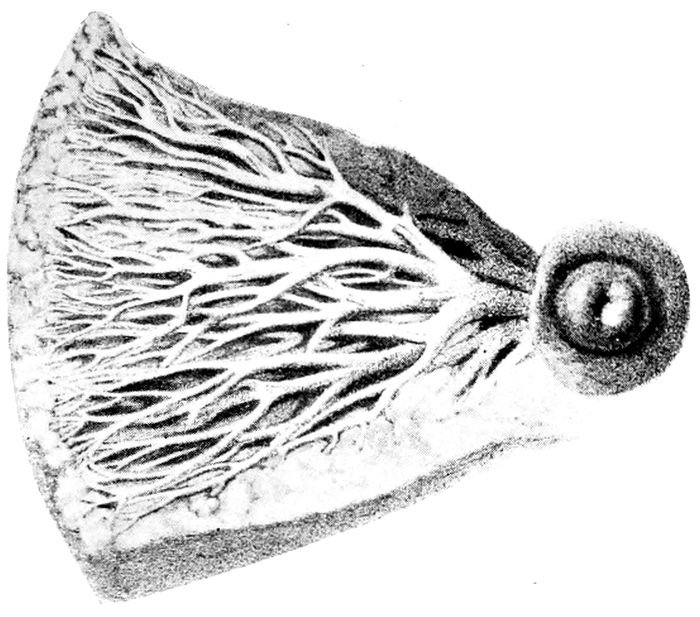
Fig. 8 A.—The excreting ducts of the mammary gland. (Lenoir and Tarnier.)
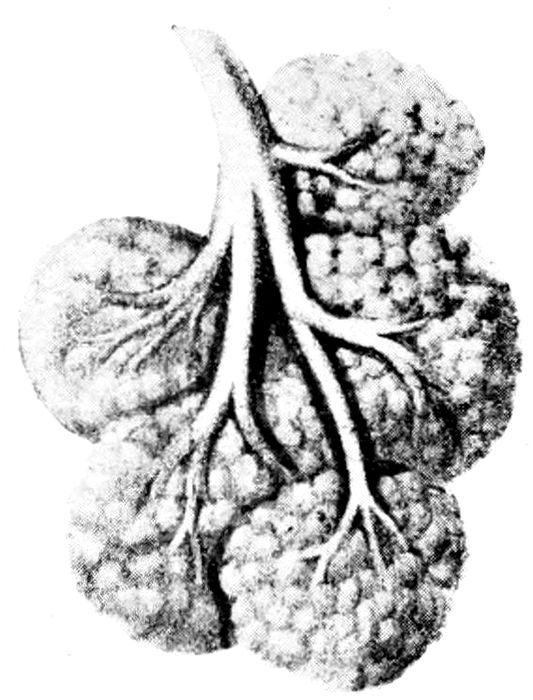
Fig. 8 B.—Lobules and duct of the mammary gland. (Lenoir and Tarnier.)
The perineal body is flattened out and compressed
30by the passage of the head and in many cases torn.
(Thirty per cent of primiparas and ten to fifteen per
cent of multiparas.) It should be repaired immediately.
The Mammary Glands.—The mammary glands are
secondary but highly important parts of the genital system.
They are formed by a dipping down of skin glands
and they perform the special function of secreting milk.
The breast is made up of fifteen or twenty lobes, each
of which, like a bunch of grapes, clusters about and
discharges into a single tube which, in turn, leads to
the nipple. The area between the lobes is filled with
fat and connective tissue.
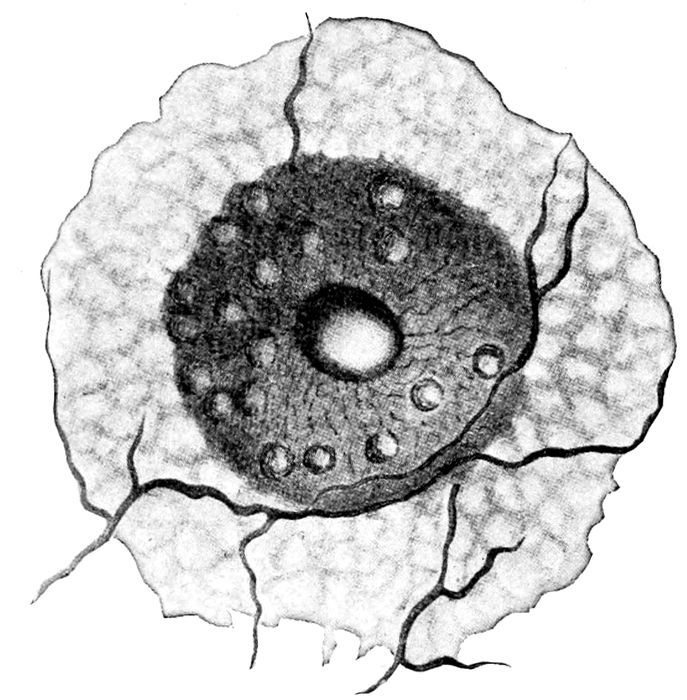
Fig. 9.—Nipple, areola, and the glands of Montgomery. (Eden.)
The nipple is pink or darkly pigmented. It is composed
of erectile tissue and under stimulation, it rises
from the surface of the gland so that it is easily taken
into the mouth.
31
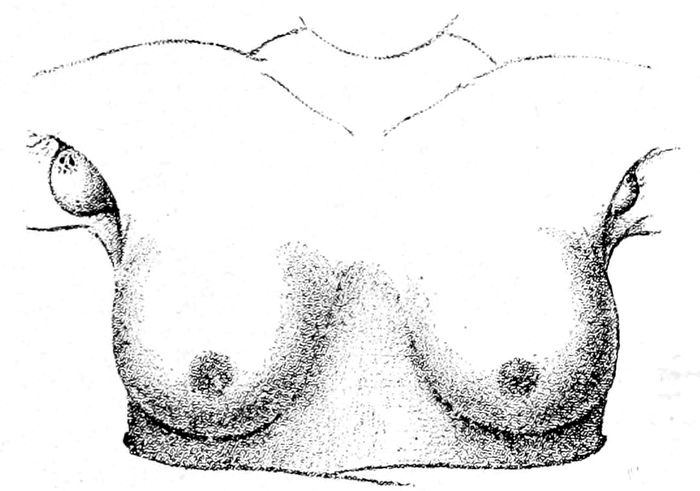
Fig. 10.—Supernumerary milk glands in the axillæ. They may be found also below the breasts. (Witkowski.)
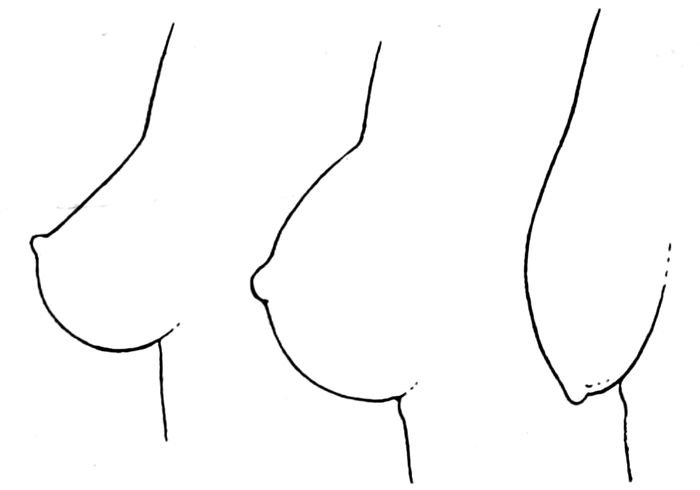
Fig. 11.—The three ages of the breast—virginity, maturity, and senescence. (Witkowski.)
Surrounding the nipple is a darkly pigmented area
from one inch to four inches in diameter that is called
the areola. It contains hard, shot-like nodules, the
glands, or tubercles, of Montgomery. These often secrete
milk and sometimes become infected. It occasionally happens
that more than two breasts may be found on the
human female, and not infrequently pieces of mammary
32tissue may be discovered in the axilla or on the chest or
back.
The mammary gland is undeveloped at birth, but, nevertheless
it may fill with milk (witches’ milk). At puberty,
after marriage, and during pregnancy, the gland
reaches maturity. It is only after delivery, however,
that the functional climax is attained.
33
CHAPTER II
PHYSIOLOGY
Ovulation.—Ovulation is the process whereby the eggs
are discharged from the Graafian follicle which matures
and protects them in the ovary. The egg is a true cell
with one, and sometimes more than one, nucleus.
The ripening of the eggs, as well as their discharge,
is attended with much general disturbance and great
physical changes. This phenomenon begins from the
twelfth to the fifteenth year, depending on race, climate,
occupation and temperament, and marks the transition
of the individual from childhood into maturity.
This period is called puberty. At this time the breasts
enlarge, the hips round out, the vagina, uterus and external
genitals increase in size. Hair appears upon the
vulva, the emotions become more evident, and modesty develops
through a consciousness of sexual difference and
attraction.
Simultaneously a new function appears—
Menstruation.—Menstruation may be defined as a
process wherein a bloody fluid is discharged from the
uterus at regularly recurring periods between puberty
and the menopause, except during pregnancy and lactation.
It is a hæmorrhage which in some way is
closely associated with ovulation, but it is not known
positively which is the precedent of the other,
or whether one causes the other.
Menstruation is not essential to pregnancy, for pregnancy
may occur when the flow is normally absent, as before
puberty, after the menopause, or during lactation.
34Nevertheless, regularity of menstruation is the rule in fertile
women and clinicians agree that while conception may
occur at any part of the menstrual cycle, it is most likely
to happen just before or just after the menstrual flow.
The best authorities at present support the theory
that ovulation usually occurs soon after the close of
the menstrual period. This is confirmed by the similarity
of the physical changes that take place in the endometrium
during menstruation and after conception.
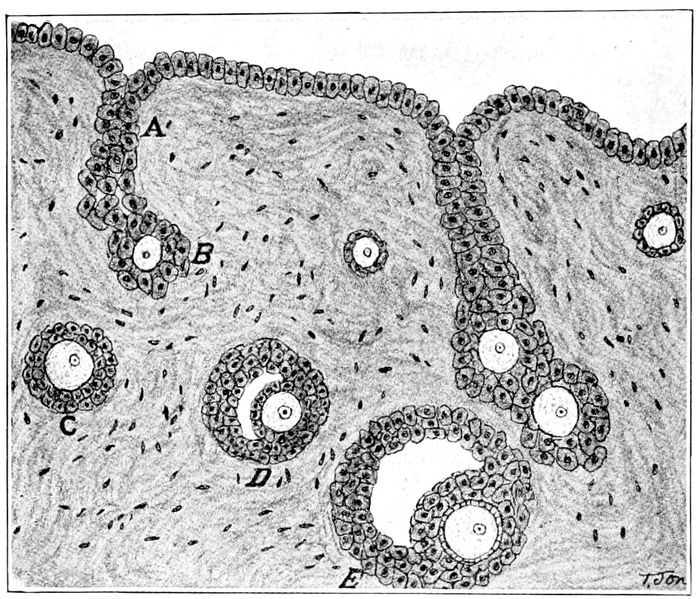
Fig. 12.—Development of the ovary (after Wiedersheim). A, an ingrowth of the germinal epithelium, forming a cell-cord, which breaks up into primitive Graafian follicles; B, a primitive Graafian follicle, with its contained primitive ovum; C, D, E, later stages in the development of the Graafian follicle. (Crossen.)
As the period of the flow approaches, the lining membrane
of the uterus becomes hyperæmic and swollen
35with blood, serum, and glandular secretions. The blood
vessels are engorged, the glands become longer and
more tortuous, little hæmorrhages appear, and the superficial
epithelium is thrown off. A large amount of
mucus is produced by the increased activity of the
glands, and all is discharged into the vagina as a
bloody, incoagulable flow with an odor of marigolds.
The process continues usually from three to seven days,
when the discharge ceases and the endometrium slowly
resumes its uncongested state.
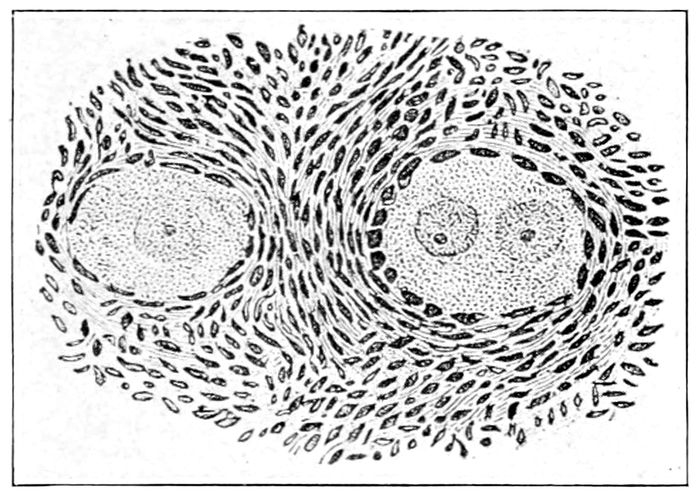
Fig. 13.—Graafian follicles. One contains two ovules which, if fertilized, will produce twins. If all three ovules are fertilized, triplets will result. (Bumm.)
Meanwhile, the psychic and bodily conditions have
not remained unaffected. The nervous system is disturbed,
the disposition is irritable and capricious and the
head may ache. The woman takes cold easily. She is
indisposed to exertion from a sense of languor and
malaise. Pain may develop in the back, or cramps in
the pelvis, so severe as to keep the woman in bed. Frequently
the approach of the period is signalized by skin
changes, such as a marked odor or an eruption of acne
pustules.
36The flow usually returns every twenty-eight days, but
it may vary within normal limits from twenty-one to
thirty days. The flow continues at such intervals regularly
from puberty to the menopause (change of life),
which occurs between the ages of forty-five and fifty.
Conception, or Fertilization.—This is the process
wherein the male element (spermatozoon) meets and
unites with the female egg. From what is known from
investigations of lower animals, this meeting usually
takes place in the Fallopian tube.
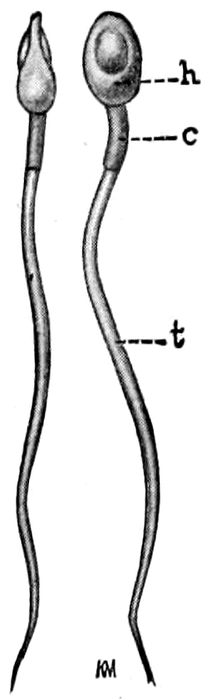
Fig. 14.—Human spermatozoa. h, head; c, intermediate portion; t, tail. (Williams.)
The egg expelled from the ovary is carried into the
open end of the tube by peritoneal currents and passed
on toward the uterus by the waving action of the hair-like
outgrowths of the cells (ciliæ) that line the tube, aided,
possibly, by the tubal muscle.
The spermatozoon makes its way upward from the
vagina by means of its tail. This activity, like the tail
of a fish, or snake, or as a boat is sculled, drives the cell
37forward through the thin layer of fluid that covers the
mucous membranes.
The arrow-shaped spermatozoon travels at a rate that
completes the passage to the ovary in twenty-four hours,
but spermatozoa may lie in wait for the egg a considerable
time, as is shown by the fact that they have
been found alive in Fallopian tubes removed three and
a half weeks after copulation. As soon as the male and
female elements approach each other, they exercise a
powerful magnetic attraction, which draws them together,
and as soon as they touch, the two cells unite
and the spermatozoon almost immediately disappears.
Only one spermatozoon is required for the fertilization
of an egg, and hence enormous numbers must perish
without achieving their destiny.
The fertilized egg has become the ovum, and originally
1/125 of an inch in diameter, it now begins to grow,
and filled with a new energy, it passes down the tube
and enters the uterus. Here it comes into contact with
the soft mucosa and digs a hole for itself—a nest, very
much as a warm bullet might sink into ice or snow—and
is soon completely surrounded by a proliferating tissue
called the decidua. The woman is now pregnant. The
menstrual flow does not appear, and local and systematic
changes are inaugurated.
The egg enlarges rapidly. Little glove-finger-like projections
(the villi) appear on its surface and dip
down into the maternal tissues. Through these villi
the egg gets nourishment until about the twelfth week,
when the placenta forms. Externally the ovum resembles
a chestnut burr. As the egg grows, the villi on
the surface find it more and more difficult to secure
nutriment, and except at one place, all gradually shrink
and disappear. At this significant point, they increase
38greatly in size, number, and complexity to form the
thick, cake-like placenta.
The egg or ovum is simply a growing cyst, filled with
a fluid, normally sterile, in which the developing embryo
lives and swims. This fluid is the liquor amnii and
it is retained by a cystic wall made up of two layers—the
chorion, which represents the original cell membrane,
and the amnion, which develops out of the fœtus. At
maturity, the ovum will contain from one to two pints
of liquor amnii.
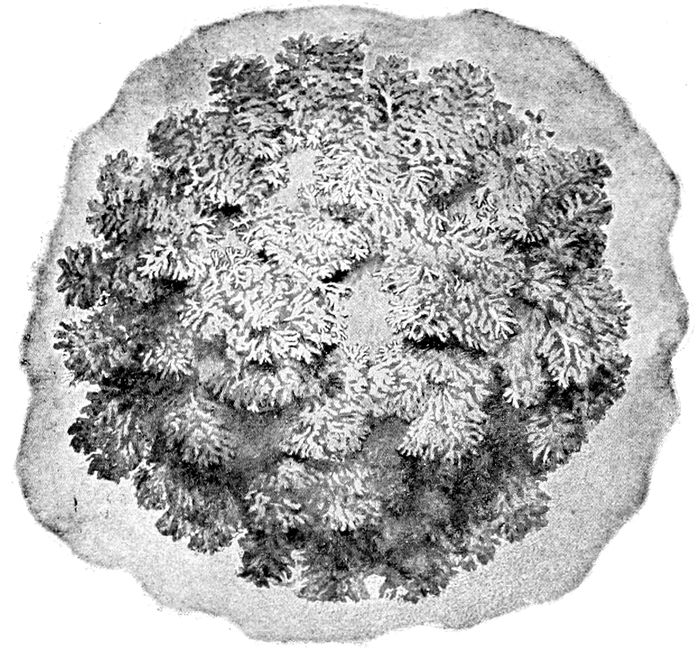
Fig. 15.—The chorionic villi about the third week of pregnancy. (Edgar.)
The Liquor Amnii.—The liquor amnii is of vast importance
to the child. It allows free movement for the
growing limbs and body, protects the child from sudden
changes of temperature, prevents injury both from
39without and within, saves the child from birthmarks
and deformities by keeping it from contact with the
surrounding walls, and in labor lubricates the passages
for the advancing part. In a measure, too, it probably
serves as a food. In labor it forms a pouch called the
bag of waters, which aids in dilating the os.
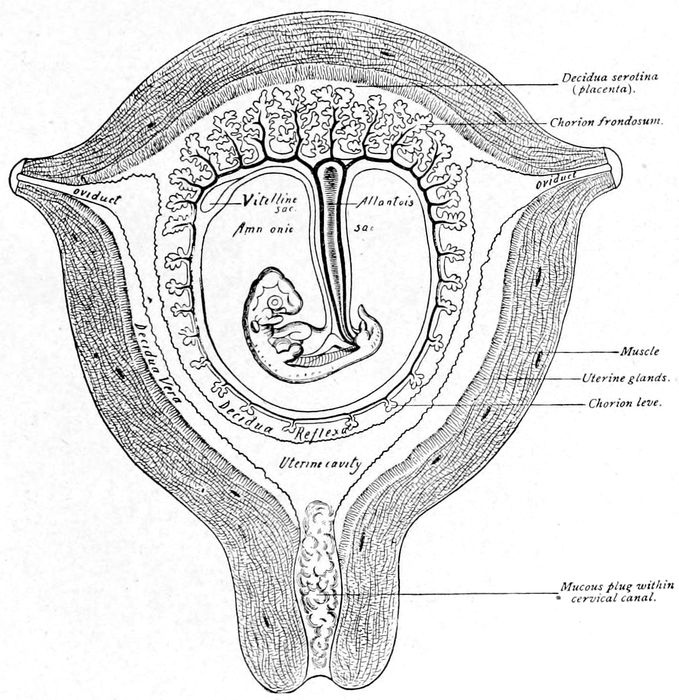
Fig. 16.—Diagram illustrating relations of structures of the human uterus at the end of the seventh week of pregnancy. (American Text Book.)
Gradually, as nutrition becomes more abundant at the
site of the growing placenta, a stalk-like structure
thrusts out from the fœtal abdomen and forms an attachment
40with the formative placenta. This is called
the ventral stalk and as soon as the communication
with the placenta is established, it is combined with
other parallel structures and becomes vascularized, to
form the umbilical cord.
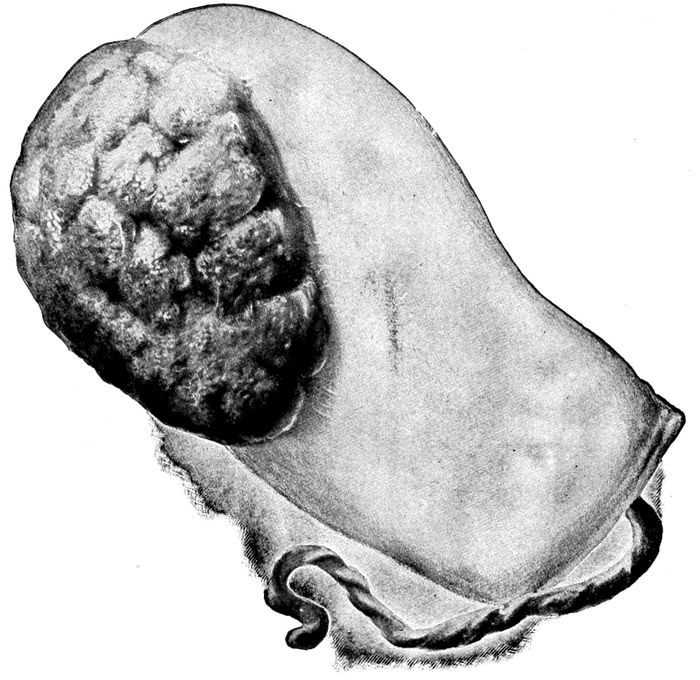
Fig. 17.—Maternal surface of the placenta and membranes. The cord protrudes from the cavity which held the fœtus. (Edgar.)
The Umbilical Cord.—The umbilical cord at maturity
measures from five to fifty inches in length and from
one-half to one inch in thickness. The cord is composed
of a gelatinous connective tissue, called Wharton’s
jelly, in the midst of which lie the twisted vessels (two
41arteries and a vein) that supply the embryo with air
and food and carry off the waste.
The Placenta.—The placenta or “after-birth” is an
oval or circular somewhat flattened disc, six to ten inches
in diameter, and three-quarters to one and one-half inches
thick. It weighs about a pound and a half. It is the organ
of respiration and nutrition for the fœtus.
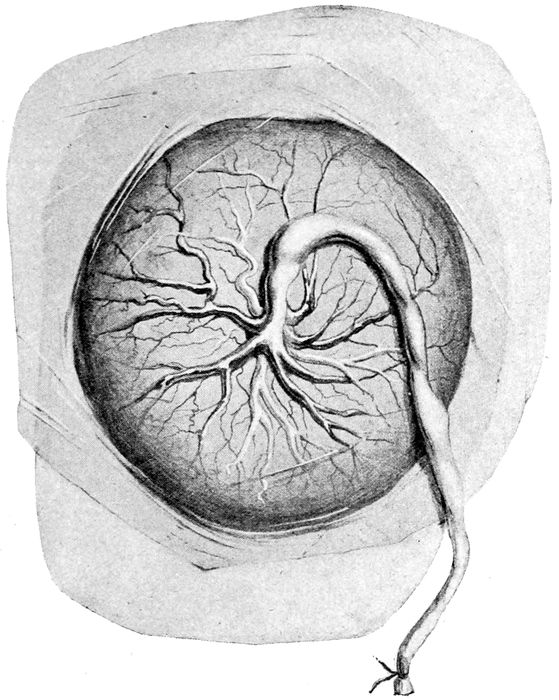
Fig. 18.—Fœtal surface of human placenta. (Eden.)
42
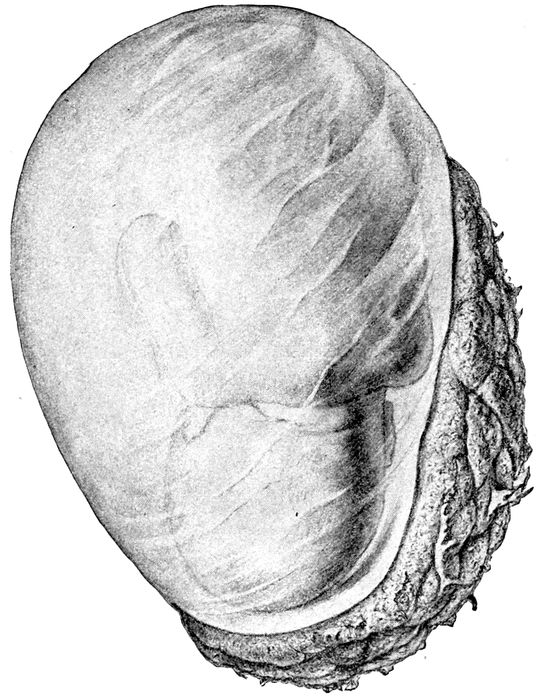
Fig. 19.—The egg at term with uterus removed and child showing through the membranes. (Edgar.)
It is formed about the third month outside the membranes
covering the child and is more or less loosely attached
to the uterine wall. The umbilical cord is attached
to its fœtal surface, inside the ovum. Like a flat
sponge it takes oxygen, blood, and the nourishing fluids
from the blood vessels in the uterine wall, carries them to
the child by means of the umbilical vein, and carries back
43the carbonized blood and waste products by the umbilical
arteries to the placenta, and there returns them to
the maternal blood for disposal. The blood of the veins
is bright red, and of the arteries, dark and turbid.
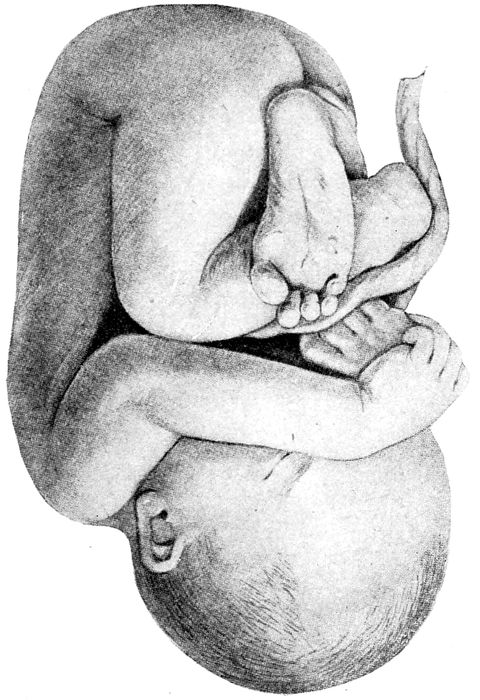
Fig. 20.—Normal attitude of fœtus (complete flexion). (Barbour.)
There is no direct communication between the maternal
tissues and the placenta, hence all the changes
occur by osmosis, and by the activity of the cells which
form the walls of the villi.
44The liver of the child is large and active. The stomach
and intestines functionate mildly. The kidneys
act, and urine is discharged into the liquor amnii,
which the child occasionally swallows.
During development, the movements of the child become
more and more pronounced. Arms, legs, and entire
body participate in turn. Periods of rest are also
observed. Gradually the child assumes a definite attitude
in the uterus. It becomes more and more folded
and flexed to accommodate its size to the limitations of
space. The head bends on the chest, the arms are
folded, the thighs flex against the abdomen, the legs
on the thighs, and even the back ultimately becomes
convex. It attains a complete flexion, the normal attitude
of the child. As maturity approaches, the head
becomes more and more palpable and seeks its usual location
in the lower pole of the uterus, resting on the
pelvic brim.
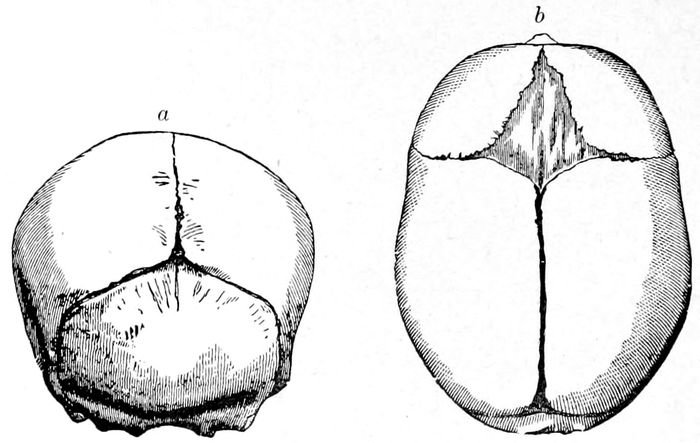
Fig. 21.—Fœtal skulls showing sutures. Note the differences between the anterior and posterior fontanelles. (Eden.)
45
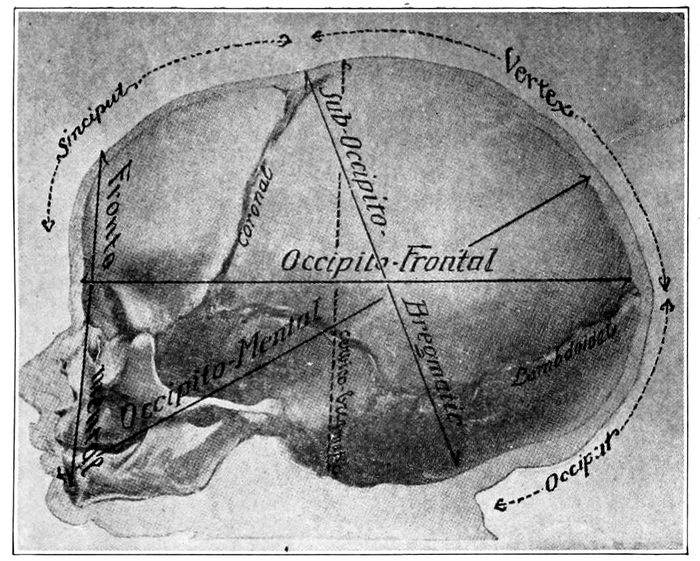
Fig. 22 A.—Child’s head at term (from side), showing diameter. (American Text Book.)
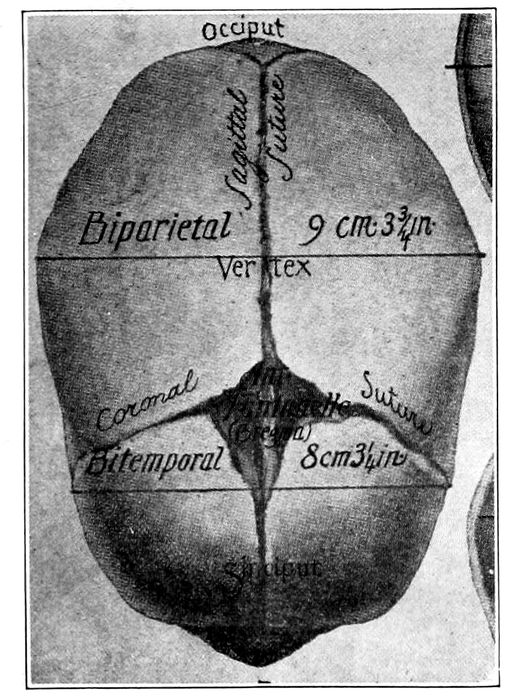
Fig. 22 B.—The child’s head at term (from above), showing diameters and fontanelles. (American Text Book.)
46The fœtal skull at maturity (at term) is still incompletely ossified. The bones are thin and pliable and
separated at their edges by intervals of unossified membrane
which form the sutures and fontanelles. Thus
the skull is compressible to a slight degree and capable
of much change in shape. It can be measurably moulded
by the uterine contractions to suit the pelvis.
In front, the two coronary sutures meet the frontal
and sagittal sutures to produce a kite-shaped figure,
called the large or anterior fontanelle, or the bregma.
Behind, the lambdoidal suture meets the sagittal suture
to form the small or posterior fontanelle.
The large fontanelle is made up of four bones and
four angles; the small, of three bones and three angles,
and are usually easy to differentiate. Furthermore,
the difference between these fontanelles is of great importance
in labor, since by it the observer is enabled to
determine the position of the head. In America, the
shape of the head is that of an ovoid with the long
diameter anteroposterior (Dolico-cephalic). Thus it
happens that when the head is completely flexed, the
smallest diameters are presented for delivery.
The important diameters of the head, with their measurements
and names, are as follows:
Nape of neck to center of bregma, 9.5 cm.—Suboccipito-bregmatic
diameter. Occipital protuberance to root
of nose, 11.25 cm.—Occipito-frontal diameter. Between
the eminences of parietal bones, 9.25 cm.—Biparietal
diameter. Between anterior ends of coronal sutures, 8
cm.—Bitemporal diameter.
The smallest circumference is that of the suboccipito-bregmatic
plane, which comes into relation with
the brim of the pelvis when the flexion of the head is
complete. It measures 27.5 centimeters.
The fœtus grows at a definite rate throughout gestation
47and so regularly that the increase is rarely simulated
by any other condition.
To find the probable length of the fœtus at any given
time, square the month of the pregnancy (up to five)
and the result is the fœtal length in centimeters. After
the fifth month, multiply the number of the month by
five. Thus:
7th month ×5=35 cm., the approximate length of the fœtus
at the lunar month.—(Hasse’s rule.)
The Mature Fœtus.—Although subject to considerable
variation, the fœtus at term will weigh about seven and
one-fourth pounds, and measure 50 cm. in length. The
weight is far more uncertain than the length, and therefore
not so reliable as a sign of maturity.
To obtain an estimate of the weight of the child at any
given month of the pregnancy, the number of lunar
months minus 2, is squared and divided by 2, and the
result is the average weight of the child at that time in
hundreds of grams. Thus:
8th month −2=6. 6×6=36. 36÷2=18, or in hundreds of grams,
1800, the weight of the child.—(Tuttle’s rule.)
Differences between the mature and immature
fœtus:
| Mature |
Immature |
| |
| 1. |
Skin smooth, plump, pink covered with vernix caseosa. |
1. |
Skin lax, wrinkled, dull red in color; little vernix caseosa. |
| |
| 2. |
Generous amount of subcutaneous fat. |
2. |
Subcutaneous fat scanty. |
| |
| 3. |
Hair abundant and from 1 to 2 inches long. |
3. |
Hair on scalp short. |
| |
| 4. |
Lanugo mostly absent. |
4. |
Lanugo present all over body. |
| |
| 5. |
Nails project from finger tips. |
5. |
Short nails on fingers and toes. |
| |
| 486. |
Skull bones in contact except at fontanelles. |
6. |
Skull sutures open. |
| |
| 7. |
Length 50 cm. born. |
7. |
Moves and cries feebly when |
| |
| 8. |
Weight five to eight pounds. |
8. |
Weight less than five pounds. |
| |
| 9. |
Cartilage in ear well developed. |
|
|
| |
| 10. |
Navel in middle of body. |
|
|
| |
| 11. |
Testes have descended in the male, and the labia majora in the female usually cover the labia minora. |
|
|
| |
| 12. |
Moves and cries vigorously when born. |
|
|
The Fœtal Circulation.—The placenta is an organ
of nutrition as well as respiration, and through the
umbilical vessels the food materials are brought to the
fœtus and the waste products removed.
Surrounded by the jelly of Wharton that fills out the
cord, and running in and out between the two arteries,
the umbilical vein passes into the fœtal abdomen and divides
into two branches, one, the larger, short-circuits directly
into the inferior vena cava. This branch is called the
ductus venosus. The other joins the portal vein and
passes through the liver, after which it also enters the
vena cava.
Thus the heart is fed with a mixed blood, part coming
fresh from the placenta and part coming up from
the lower half of the fœtus. This blood is poured into
the right auricle, where it becomes mixed again with
the blood coming down from the upper pole of the fœtus
through the superior vena cava.
49
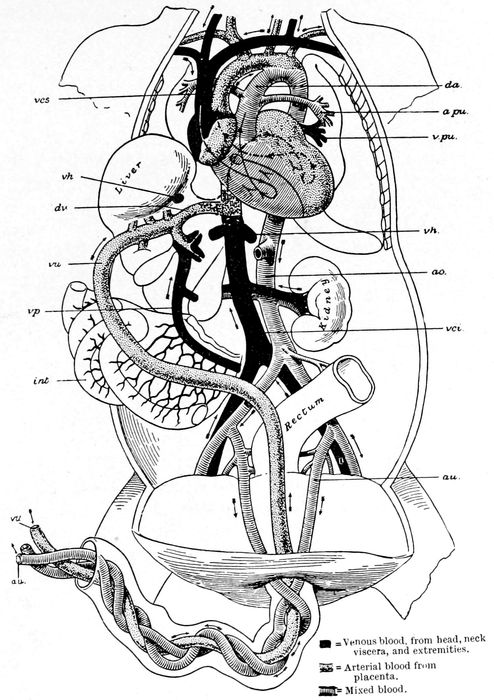
Fig. 23.—The fœtal circulation. (Edgar.)
50Now a small part goes down into the right ventricle
and is forced into the pulmonary arteries to supply
the lungs. But the lungs are not functionating, hence
the greater part is again short-circuited through the ductus
arteriosus into the arch of the aorta, where it meets
with the great volume of blood which passed over into the
left auricle through the hole in the septum between the
right and left auricles, called the foramen ovale, thence
down into the left ventricle and out through the aorta to
supply the rest of the fœtal body.
With the exception of the ductus venosus and the
ductus arteriosus and the foramen ovale, the circulation
is the same as in the adult.
The blood in the descending aorta again divides and
part goes on to supply the lower extremities while the
greater part leaves the internal iliac arteries by means
of the hypogastric vessels and returns through the umbilical
arteries to the placenta for oxygenation.
As soon as the child is born, the fœtal structures are
altered. The child breathes, the pulmonary circulation
is established and the ductus arteriosus is closed. The
placental circulation is abolished, and the ductus venosus
and the hypogastric arteries are converted into solid
fibrous cords. Owing to the immediate change of pressure
in the auricles, the foramen ovale closes and the
circulation assumes the adult type.
51
CHAPTER III
NORMAL PREGNANCY
The entire body participates in the changes brought
about by pregnancy. The hips and breasts become
fuller, the back broadens, and the woman puts on fat.
She becomes mature in appearance, but, of course, the
phenomena connected with alterations in the breasts
and genitals are most important, and late in pregnancy,
most conspicuous.
The uterus exhibits the most marked alteration.
From an organ that weighs two ounces, it becomes the
largest in the body, and increases in size from two and
one-half or three inches to fifteen inches. The typical
pear-shape becomes spheroidal near the end of the third
month, becomes pyriform again at the fifth month, and
continues thus until term.
Up to the fourth month the walls become thicker,
heavier and more muscular, but as pregnancy advances,
more and more tissue is demanded, until at the end, a
muscle wall of only moderate thickness protects the
ovum. Meanwhile the muscular functions of contractibility
and irritability are greatly increased.
At the fourth month the womb, which has occupied a
position of anteversion against the bladder, rises out
of the pelvis. It is now an abdominal organ and as it
gets heavier and heavier, it rests a certain amount of
its bulk on the brim of the pelvis. About the sixth
month, the uppermost part of the uterus (fundus) is at
the level of the umbilicus. At the eighth month, the
fundus is found a little more than midway between the
52umbilicus and the ensiform cartilage. About two weeks
before term, it reaches its highest point, the ensiform
cartilage, and then sometimes sinks a little lower in
the abdomen.
The ovum, or egg, does not completely fill the uterine
cavity at first, but grows from its side like a fungus until
the third month. Then the uterine cavity is entirely occupied
and thereafter the egg and the uterus develop
at an equal rate. As the uterus rises in the abdomen,
it rotates to one side, usually the right, forward on its
vertical axis.
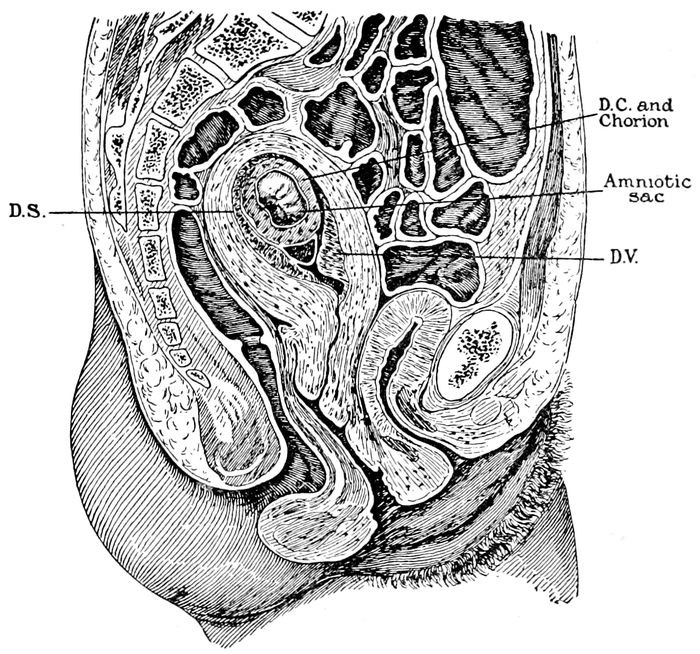
Fig. 24.—Gravid uterus at the end of the eighth week. (Braune.)
The blood vessels and lymphatics also increase in size,
number, and tortuosity. Many of the veins become
53sinuses as large as the little finger. This increased
amount of fluid both within and without the uterus has
a marked effect upon its consistency. The walls of the
uterus, vagina, and cervix become softened, infiltrated
and more distensible. There is also an increase in size
and in number of the muscle cells.
During pregnancy the uterine muscle exhibits a definite
functional activity. Intermittent contractions occur,
feeble at first, but growing markedly stronger as
pregnancy advances. These are the contractions of
Braxton Hicks. They are irregular and painless, but
can be felt by the examining hand. At term they merge
into, and are lost in, the regular, painful contractions
of labor.
The breasts can not be said to be fully developed until
lactation has occurred, nevertheless, the glands show
pronounced changes as a result of marriage and pregnancy.
The size of the gland, as well as the size and appearance
of the nipple and areola, varies greatly in different
women; but under the stimulation of pregnancy the
whole gland enlarges, including the connective tissue
stroma.
About the fourth month a pale yellow secretion can
be squeezed from the nipple. This is called colostrum.
The pigmentation extends over a wider area and deepens
in color, while the increased vascularity is shown
by the appearance of the blue veins under the thin tender
skin. Light pinkish lines sometimes radiate from
the nipple. These are striæ and are more evident in
blondes.
The milk comes into the breasts about the third day
after labor, and normally continues to flow for six, to
ten or twelve months.
54Why the pregnancy and labor induce such marked
mammary activity is not known, but the fact is patent.
The skin reacts both mechanically and biologically to
the stimulus of pregnancy.
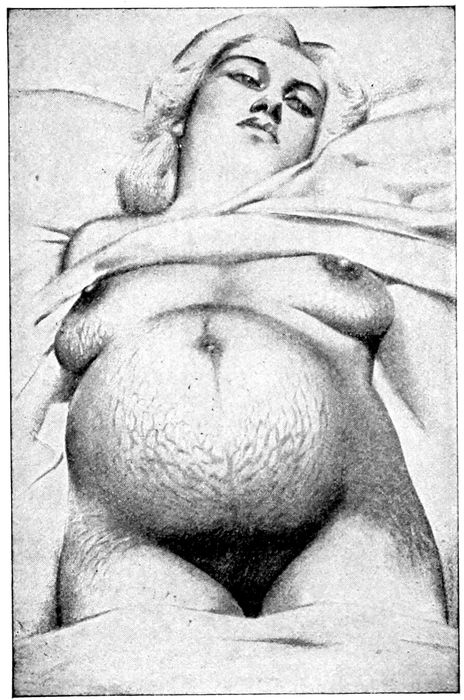
Fig. 25.—Striæ Gravidarum. (Edgar.)
Striæ Gravidarum.—Striæ gravidarum appear on the
abdomen similar to those observed on the breasts and
are due to the same cause—mechanical stretching.
When fresh, they are pinkish in color and variable in
length and breadth, but attain the greatest size below
55the umbilicus. Occasionally they extend to the thighs
and buttocks.
After labor, they become pale, silvery, and scar-like
and are called linea albicantes. They are sometimes
found in other conditions than pregnancy, such as tumors
or ascites.
Increased Pigmentation.—Pigmentation is not limited
to the breasts. On the abdomen, a dark line will appear
between the umbilicus and the pubes. This is the linea
nigra, and it becomes most conspicuous in the latter
half of pregnancy. In the groins, the axillæ, and over
the genitals, the deposit is common, and sometimes
patches appear on the face, either discrete or in coalescence,
to form a continuous discoloration, called chloasma;
or when extensive, the “mask of pregnancy.” The
pigmentation is absorbed, or at least greatly diminished,
after labor. The sebaceous and sweat glands are
more active.
The hair may fall out and the teeth decay. “With
every child a tooth,” is the cry of tradition. These
changes are due to imperfect nutrition, or to the presence
of toxins in the circulation.
Eruptions of an erythematous, eczematous, papular
or pustular type are not uncommon; and itching, either
local or general, may make life miserable.
The blood undergoes certain modifications that are
fairly constant. The total amount is increased, but the
quality is poorer, especially by an increase in water and
white cells and a diminution of red cells. The amount
of calcium is slightly increased and the fibrin is diminished
up to the sixth month, when it rises to normal
again at term.
The heart is slightly hypertrophied on the right side
and blood pressure somewhat raised. A marked increase
in blood pressure is suggestive of eclampsia.
56The thyroid gland enlarges frequently, both as a consequence
of menstrual irritation and of pregnancy.
Goiters may show an increase of development, which
remains after labor.
The urine is diminished in amount, but increased in
frequency of evacuation. The bladder is more irritable
during the first and last months, and micturition may
be painful and unsatisfactory. The kidneys must be
watched carefully during gestation.
The nervous system is disordered in most women, but
especially in those of neurotic tendencies.
Irritability, insomnia, neuralgia of face or teeth, or
perversion of appetite in the so-called “longings” are
the more common manifestations.
Cramps occur in the muscles of the legs, owing to
varicose veins or pressure upon the lumbar and sacral
plexus of nerves.
The lungs are crowded by the growing uterus and the
respiration interfered with.
The liver is enlarged, but functionally it is less competent,
and constipation is common.
It is probable that most of the changes enumerated
above are due to the circulation through the body of
some definite product of fœtal activity, which is more or
less toxic in character. The more pronounced effects of
this toxin will be studied under the abnormal conditions
of pregnancy.
Generally, if the pregnancy is normal, the whole body
responds to the stimulating influence. After the nausea
and vomiting of the early months subside, the
woman feels energetic and ambitious. She is eager to
do something at all times and feels fatigue but slightly.
Music, literature or housework engages her attention
and is zealously and joyfully practiced. The world
57seems bright and the thought of her labor does not
bring solicitude, but pleasant anticipations. The body
fills out in all directions and the woman takes on the
appearance of maturity.
DIAGNOSIS OF PREGNANCY
The presence of pregnancy is naturally determined
by the recognition of those changes in the maternal
system which the growing ovum produces.
During the second half of the period the fœtus can
be made out distinctly by palpation, or by its movements,
and the heart tones observed by auscultation.
During the first half this is impossible and the diagnosis
must be made from subjective symptoms elicited
from the patient and upon physical signs observed by
the physician.
It is of extreme practical importance to be able to
recognize a pregnancy at all periods. The subjective
symptoms of the first half are—amenorrhœa, morning
sickness, irritability of the bladder, discomfort and
swelling of the breasts, enlargement of the abdomen
and quickening; but the appearance of any or all of
these phenomena is not to be regarded as conclusive,
but merely as a presumption that pregnancy exists.
Either through ignorance, intent to deceive, or from
pathological conditions, any or all of these symptoms
may be present, but not until the tenth week are the
changes in the uterus sufficiently definite to confirm a
diagnosis unless the circumstances are especially favorable.
Amenorrhœa.—Cessation of the menses is practically
invariable in pregnancy. One or two periods may occur
after conception, but care must be used to exclude other
causes of hæmorrhage. Sudden cessation of the periods
58in a healthy woman of regular habits who is not
near the menopause, is strongly suggestive of pregnancy.
Why a developing ovum causes an immediate
arrest of menstruation is not understood.
Amenorrhœa may occur in consequence of chlorosis,
heart disease, hysteria, tuberculosis, fright, grief, and
some forms of insanity; a change from a low to a high
altitude, or an ocean voyage not infrequently causes the
flow to remain absent for one or more months. In
addition to its value as a presumptive symptom, the
amenorrhœa affords a common and convenient method
of estimating the date of confinement. The method is
fallacious but practical, and will be discussed later.
Morning Sickness.—This symptom is not invariable.
It is most frequent in primiparas, but not so likely to
occur in subsequent pregnancies. It usually appears
about the second month, shortly after the first period
missed. It varies in intensity. Some women have a
little nausea on arising and no further trouble during
the day, others are nauseated and vomit either on rising
or after the first meal, and yet others after each
meal; but the general health is not ordinarily affected
and the tongue remains clean. Some cases are of extreme
severity (hyperemesis) and will be discussed
elsewhere.
The morning sickness is probably toxic in origin. It
must be remembered that chronic alcoholism is accompanied
by morning sickness, but with it the tongue is
furred.
Irritability of bladder is shown by a frequency of
urination. It is caused by the congestion and stretching
of the tissues that lie between the uterus and
bladder and hold them in relation to one another. After
the third month an accommodation is established and
the symptom does not reappear until late in pregnancy,
59when the pressure of the heavy uterus tends to keep
the bladder empty. If especially annoying, this irritability
may be much relieved by putting the patient in
the knee-chest position night and morning.
Enlargement of the breasts is common in primiparas,
but this, with changes in the areola, may occur at menstrual
periods in nervous women. Tingling, pricking
and shooting sensations may also be noted.
Enlargement of the abdomen is only noticeable toward
the latter part of the first half, when the uterus
rises out of the abdomen.
Quickening means “coming to life,” and refers to the
first movements of the fœtus that are felt by the mother.
It is described as similar to the flutter of a bird in the
closed hand. It is sometimes accompanied by nausea
and faintness. Quickening usually occurs about the
seventeenth week of pregnancy, and continues to the
end. Gas in the intestines will sometimes simulate
quickening.
The movements are important in the second half as
indicating that the child is alive.
Physical Signs.—During the first weeks no conclusive
changes occur that can be detected by examination,
and unless conditions are especially favorable, the earliest
time for the definite diagnosis of pregnancy is the
eighth week. Previous to this it is presumptive only.
At the eighth week, the breasts may show enlargement
and tenderness, with some secretion. In the multipara,
this sign has no significance. Secretion is present
sometimes in the breast of nonpregnant women with
uterine disease (fibroids).
Examination of the abdomen at this time is of little
value, but changes in the uterus can be detected by
careful bimanual examination. It is needless to say
60that all internal examinations should be made with the
utmost care and gentleness.
Softening of the lips of the os (Goodell’s sign) may
be found, but it must not be confused with erosions of
the os. The os of a nonpregnant woman feels like the
tip of the nose, and that of the pregnant woman like the
lips.
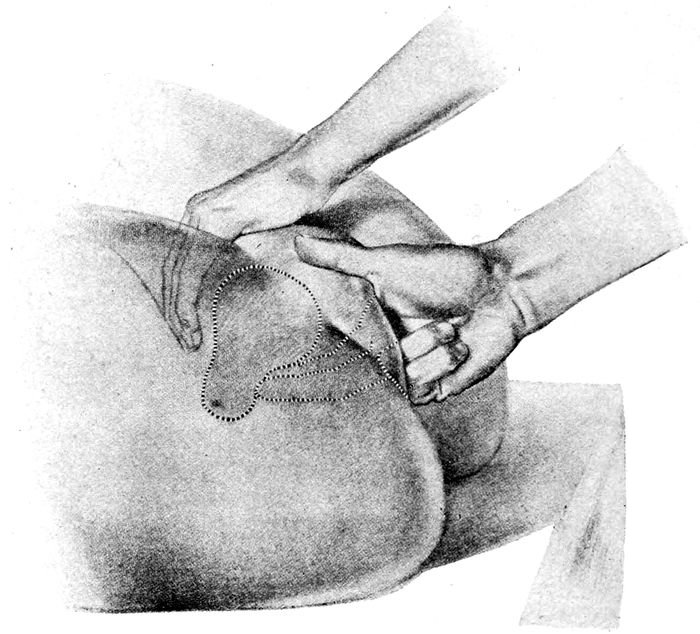
Fig. 26.—Bimanual examination. (Edgar.)
The increased size and globular shape must also be
considered as confirmatory.
Hegar’s Sign.—The upper part of the uterus is soft
and distended by the ovum, the lower part is soft and
not filled out by the ovum. Between the two is an
61isthmus that is compressible between the fingers of one
hand in the vagina, and of the other upon the abdomen.
When found, this sign is of great value.
At the eighth week, pregnancy can be regarded as
highly probable by the conjunction of the following
symptoms and signs: Amenorrhœa, morning sickness,
irritability of bladder, slight breast changes in primiparas,
lips of os externum softened, uterine body enlarged,
softened, and nearly globular in shape, and
Hegar’s sign.
Abderhalden’s test is a serum reaction based on the
well established principle that the introduction into the
blood of an organic foreign substance leads to the formation
of a ferment to destroy it. Abderhalden’s plan
was to discover whether the blood of a pregnant woman
contained a ferment capable of destroying placental
protein. It is a very complicated test, and subject to
many inaccuracies and numerous sources of error. At
the same time, the main features of this reaction have
been confirmed, and when it is worked out, it will be
of immense value not alone in early uterine pregnancies,
but in extrauterine pregnancy. This view very properly
demands that pregnancy be regarded as a parasitic
disease. It is practicable as early as the sixth week to
make a diagnosis, and it only fails in possibly ten per
cent of the cases. The negative test is equally definite
as eliminating pregnancy.
Sixteenth Week.—Morning sickness and urinary
symptoms have disappeared but amenorrhœa remains.
Enlargement of the breasts is noticeable, as well as the
increased pigmentation. The uterus begins to rise above
the symphysis as an elastic, somewhat ill-defined, boggy
mass. The cervix is softer. The characteristic dull
lavender coloration of the vulvar mucous membrane is
62now evident. It is due to the congestion and is called
Jacquemins’ sign.
Two New Signs.—Irregular, painless contractions of
the uterus (Braxton Hicks’ sign), and ballottement.
The contractions of Braxton Hicks now become more
easily palpable.
Ballottement consists in the detection in the uterus
of a movable solid body surrounded by fluid. In a
standing position, the fœtus rests in the lower part of
the uterus, just above the cervix. The woman stands
with one foot on a low stool, and two fingers of one
hand are pushed into the vagina until they touch the
cervix, the other hand is placed on the fundus. A
smart upward blow by the internal hand is transmitted
to the fœtus, and it can be felt to leave the cervix,
strike lightly the tissues underneath the external hand,
and return to the cervix. It is simulated by so few
things, and so rarely, that in practice it must be regarded
as a positive sign.
During the second half, the subjective symptoms are
of minor importance since unmistakable evidence is
furnished by the physical signs. The symptoms of this
period are mostly discomforts. Increased intraabdominal
pressure brings on edema of the feet, cramps in the
legs, varicose veins of the legs and vulva, dyspnœa, and
palpitations.
Twenty-sixth Week.—About the twenty-sixth week,
or, at the end of the sixth calendar month, the hypertrophy
of the breasts, the presence of secretion, and the
marked pigmentation are unmistakable. The abdominal
protrusion is now clearly visible, and the fundus will
be found at the level of the upper border of the umbilicus.
Spontaneous fœtal movements appear and may be felt
by the palpating hand.
63Auscultation reveals the uterine souffle and the fœtal
heart sounds. The heart sounds and the fœtal movements,
when obtained by the observer, are positive signs.
Uterine souffle is a soft, blowing murmur, synchronous
with the mother’s pulse. It is best heard at the
lower parts of the lateral borders of the uterus. It is
due to the passage of blood through the greatly dilated
uterine arteries. It may be heard also in cases of fibroid
tumors of the uterus.
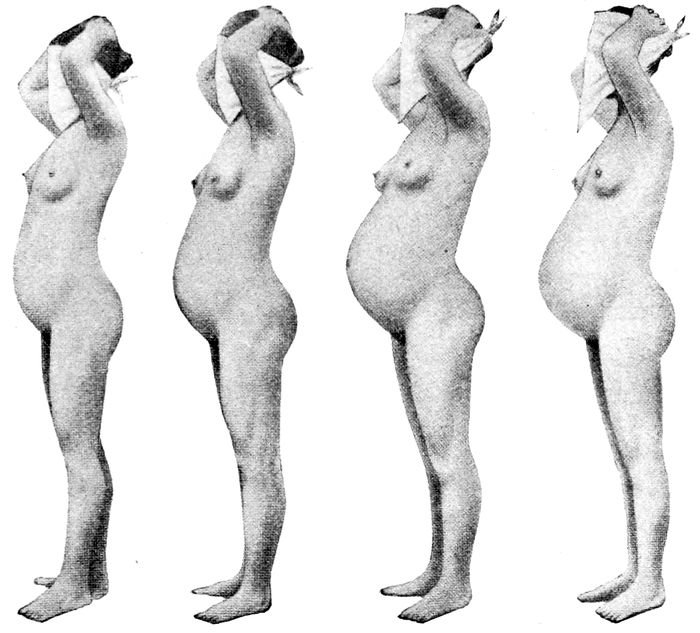
Fig. 27.—Abdominal enlargement at third, sixth, ninth, and tenth months of pregnancy. (Williams.)
64
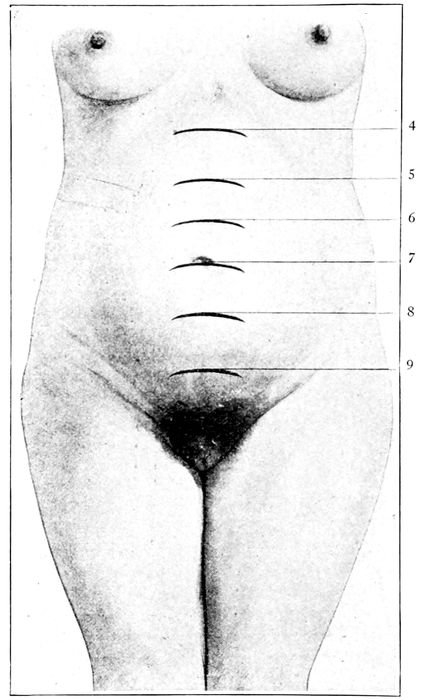
Fig. 28.—Height of the uterus at various months of pregnancy. (Bumm.)
The fœtal heart sounds are the most anxiously sought
for of all the signs of pregnancy. They are conclusive.
They not only determine the diagnosis, but afford valuable information during labor, and nurse and student
should lose no opportunity of becoming familiar with
them. The heart tones can be heard as early as the
twenty-sixth week, but they become more and more distinct
as pregnancy advances. They vary from 140 to
160 beats to the minute at the twenty-sixth week, and at
65term, from 120 to 140. When they rise above 160 or sink
below 120, some danger threatens the child. The fœtal
heart tones have no significance as an indication of sex.
Funic souffle is the sound made by the passage of
blood through the umbilical cord when a loop accidentally
lies under the tip of the stethoscope. It is synchronous
with the fœtal heart tones, but of no great
practical importance when the heart tones can be obtained.
Determination of the period to which pregnancy has
advanced is sometimes important. This can be approximated
by a calculation of the time that has elapsed since
the last period, or from the date on which quickening
has occurred. Measurement of the height of the fundus
and comparison with such scales as Spiegelberg’s, may
be carried out, but it is not often required.
A method of estimation in gross, that is approximately
correct, in many cases depends on the observation
of the steady growth of the womb.
Thus, the uterus rises out of the pelvis at the fourth
month, and may be found well above the symphysis
pubis. At the fifth month the fundus is midway between
the symphysis and the umbilicus. At the sixth month it
reaches the umbilical level. At the eighth month it is
a little more than midway between the umbilicus and
the ensiform cartilage, which it attains in another month,
the ninth. Then it usually sinks a little, especially in
primiparas during the last two or three weeks. This is
called lightening.
66
CHAPTER IV
HYGIENE OF NORMAL PREGNANCY
The time of confinement can never be accurately determined,
because the onset of labor is purely an
accident, dependent on many factors. Furthermore,
conception does not take place necessarily at the time
of intercourse, and we have no means of knowing
whether conception occurred just after the last period
present or just before the first period missed. So there
is always a possible error of three weeks.
Pregnancy in the human family normally lasts from
275 to 280 days, and the approximate date of confinement
can be obtained by the following convenient rules:
1. Take the first day of the last menstruation, count
back three months and add seven days.
2. Or, assuming that quickening occurs at the seventeenth
week, count ahead twenty-two weeks from the
day on which quickening was observed.
3. Or, count two weeks from the day of lightening.
4. Or, with a pelvimeter, get the length of the fœtus
by Ahlfeld’s rule (measure from symphysis to breech of
child, subtract two cm. for thickness of abdominal wall
and multiply by two. The result is the length of the child
in centimeters) and compare with fifty centimeters,
which is the average length of a mature child. After the
seventh month, the child in utero grows at the rate of
about 1 cm. a week (0.9 cm.).
5. Or, by the tape, according to Spiegelberg’s standard
of growth, as previously mentioned.
The hygienic rules to be observed during pregnancy
67are founded on three basic principles: (1) To watch
attentively the different organs and see that they functionate
normally; (2) To eliminate all those conditions
that favor the premature expulsion of the egg; and (3)
To provide, so far as possible, for the normal gestation
and the physiological delivery of the child. These factors
will be taken up in detail.
The Diet.—The appetite is usually somewhat increased,
but it is unnecessary to indulge the stomach on
the ground that the mother “must eat for two.” Longings,
however, should be gratified so far as the demand
is not for unwholesome things. Food should be simple
and plainly cooked. Meat is permitted in moderation
unless some organic change exists to contraindicate it.
Rich pastries and gravies should be avoided, but cereals,
fruits and vegetables should be used in abundance. It
may be better to eat four times a day instead of three.
Fluids should be taken freely, from one to two quarts
daily. Milk is especially valuable, and alkaline, natural
and charged waters, such as Vichy and seltzer, are useful.
Wine, beer and other alcohols should not be taken, or
if the patient is habituated to their use, the amount
should be restricted on account of danger to the pregnancy
and danger to the child.
In contracted pelves it is sometimes desired to furnish
a special diet, with the idea of controlling the size
of the child (see Prochownick’s Diet, p. 332) but this
is an emergency. Certain books on maternity, designed
for popular reading, advocate diets that are supposed,
by depriving the child of lime salts, to keep its bones
soft and make the labor easy. If it succeeds, the child
will be injuriously affected. If it does not succeed, the
claim is false.
Exercise.—Exercise should be taken, but it should not
be violent, nor attended by risk. Golf, swimming, tennis,
68dancing, horseback or bicycle riding and fast driving
in automobiles should be forbidden, lest abortion
follow. General exhaustion must be avoided and all
conditions that even approximate traumatism. Walking
and slow driving are best, and housework is excellent
up to a mild degree of fatigue. Travel should be
restricted. If exercise is not feasible, massage will
furnish the required stimulation to the circulation.
The menstrual epochs are peculiarly favorable to abortive
influences.
The Bowels.—Most women have a tendency to constipation
during pregnancy. Many times this can be corrected
by increasing the “roughening” in the food;
more vegetables and fruits, bran bread and muffins,
whole wheat bread, spinach, beans, carrots, turnips,
peas and especially potatoes, baked and eaten, skin and
all. Prunes, figs, and dates are valuable aids. Agar
may be eaten three or four times daily. Russian oil
(liquid petrolatum), taken in tablespoon doses three
times daily, is an adjuvant, and finally, some form of
cascara or aperient pill may be taken, if necessary.
Violent cathartics should not be used at all, and
enemas as little as possible; only when quick results
are necessary.
Heartburn.—Heartburn is a frequent complication,
especially in the later months. It is due to an inordinate
secretion of acid in the stomach. Soda mint tablets,
bicarbonate of soda, and magnesia, in cake or as
milk of magnesia, will relieve. The magnesia is also a
laxative.
The kidneys require particular care during pregnancy,
and in every case the urine should be examined
monthly, up to the fifth month, and every two weeks
thereafter, until the last six weeks, when a weekly test
should be made.
69The amount passed in twenty-four hours should be
measured. Three pints is an average quantity. Albumin,
sugar, and casts must be looked for and reported.
Albumin may or may not be a serious symptom.
Casts are significant of nephritis and indicate
danger. Sugar may be lactose and be derived from the
milk secreted in the breast. Edema of feet, hands and
eyelids must always be investigated, with the possibility
in mind, of heart and kidney lesions. Blindness,
dizzy spells, headaches and spots before the eyes are
always alarming symptoms until their innocence is
established.
Through constant watchfulness of the urine, many
cases of eclampsia may be averted.
Bathing is more important in pregnancy than at other
times. The more the skin secretes, the less the burden
on the kidneys. The skin must be kept warm, clean, and
active. Then again, during pregnancy the skin is often
unusually sensitive and only the mildest soaps and blandest
applications can be used. The water must be neither
hot nor cold, but just a comfortable temperature. Cold
bathing, whether shower, plunge, or sitz, must be denied.
Sea bathing is also unwise. The warm tub bath of plain
water or with bran answers all conditions until the expected
labor is near, then the warm shower or sponge
bath should be substituted, lest germs from the bath
water enter the vagina.
If the kidneys need aid, a hot pack may be used; but
in all cases, frequent rubbing of the skin with a coarse
towel should follow the bath.
The dress must be warm, loose, simple and suspended
from the shoulders. To prevent chilling, wool or silk,
or a mixture of both, should be worn next to the skin,—light
in summer and heavy in winter.
The patient must be sensibly clad in broad, loose, low-heeled
70shoes. There should be no constriction about
chest or abdomen. Circular garters must not be worn.
If a corset is insisted upon, it must support the abdomen
from below and lift it up. No corset is admissible
that pushes down on the abdomen. This is especially
true if the woman has borne one or more children and
has a pendulous abdomen. The breasts may get heavy
and require the rest and ease supplied by a properly
fitting bust supporter.
Fainting is an annoying symptom in some women.
It may come when quickening is first perceived, or from
the excitement of crowds, or from hysteria. It usually
passes quickly. The pallor is not deep, the pulse is not
affected, and consciousness is not lost. It does not affect
the ovum. Heart trouble should be excluded, and
the daily habits of dress, diet, and bowels investigated.
Smelling salts will usually suffice for the attack.
The abdominal walls may be strengthened by appropriate
exercise before and after gestation, so that the
muscles will preserve their tone. After delivery nursing
the child will help greatly in the preservation of the
waist line and figure, by aiding involution.
About the seventh month in primiparas, the abdomen
gets very tense and in places the skin is stretched
until it gives way and forms striæ. This tightness can
be relieved to a considerable degree by inunctions of
cocoanut oil or albolene.
Pain in the abdomen at this time may be due to mechanical
distention, to strain on the muscles, to stretching
of operative adhesions, to gas, constipation, or appendicitis.
The physician should be informed of it. In
every case, constipation, swelling of feet, hands or eyelids,
blurring of vision, ringing in the ears, vomiting,
persistent backache, or the passage of blood, no matter
how slight, should be reported to the doctor.
71The Breasts.—There should be no pressure on the
glands and they should be warmly covered. The nipples
must be kept clean and soft by soap and water, and
about a month before the labor is expected, the nipple
should be anointed with albolene or cocoanut oil and
rubbed and pulled for a few minutes every night. This
removes the crusts and dried secretions that collect on
the nipple and prepare it for the macerating action of
the baby’s mouth. No alcohol or strongly astringent
washes should be used. Injuries must be avoided. If
the nipples become tender they may be protected from
external irritation by the lead nipple shield or by a
wooden shield with a hollow center, such as Williams
recommends.
Leucorrhœa.—This is one of the commonest discomforts
of pregnancy, and the sense of uncleanliness, if
the discharge is excessive, as well as the resulting irritation,
may demand attention. It must be kept in mind,
however, that the normal vaginal discharge of a healthy
pregnant woman is strongly germicidal and should not
be douched away without definite indications.
Vaginal douches of warm boric acid solution will do
for cleanliness, but the douche bag must not be higher
than the waist. Stronger and more antiseptic solutions
are potassium permanganate 1:5000, or chinosol 1:1000.
A suppository may be used, consisting of extract belladonna,
gr. ss; tannic acid, gr. v, and boroglyceride
dr. ss.
Sexual intercourse is distasteful to most pregnant
women, but sometimes the inclination is intensified.
Coitus often causes much pelvic discomfort and may
be an influential factor in producing abortion. It should
be forbidden during the early months, at all menstrual
epochs, and for at least two weeks before labor. The
72uterus may be infected by germs beneath the foreskin
and hæmorrhage may follow the act if the placenta is
low. In healthy persons, at the instance of the female,
intercourse in moderation is permissible.
The mental condition should be placid without either
excitement or fatigue. Anxiety should be dissipated by
cheerful company and surroundings. Judicious amusement
is desirable and a congenial occupation, but neighbors
who tell frightful tales of disaster in labor, or
nurses who relate the details of their critical cases, are
equally to be avoided.
Many women of neurotic temperament dread the labor
desperately. They are sure that death impends and
they dwell with tragic interest on the stories of complicated
cases related by thoughtless or malicious neighbors.
The nurse can do much to allay these apprehensions by
cheerfulness, optimism, and gentleness. Her buoyant
temperament will drive away the patient’s fears just as
effectively as the assurances of the physician.
Great allowances must be made for attacks of irritability,
for the changes going on in the woman’s pelvis
keep her in a capricious and whimsical condition. A
good book to read at this time is, the “Prospective
Mother,” by Slemons.
The subject of maternal impressions is the cause of
much anxiety during pregnancy. It is safe to assure
the mother that it is nearly impossible to mark her
child by emotional stress. There is no demonstrable
nervous communication between mother and child, and
most of the deformities that occur and are attributable
to shock, etc., can be explained by our knowledge of
intrauterine changes. Furthermore, the same deformities
occur in lower animals, to which it is difficult to ascribe
such high nervous organization.
Many of the birthmarks, supposedly due to shock,
73occur too late in the pregnancy to affect the child, even
if it were possible, for the child is completely formed before
the fourteenth week.
The Determination of Sex.—It is not possible to know
in advance of delivery whether the child will be a male
or a female. It is equally impossible to determine or
even to influence the sex of the coming child. Many
theories have been advanced, and much talent has been
wasted in trying to solve this problem.
Reasoning by analogy from the facts obtained from
lower animals, the sex of the child is unalterably decided
the moment conception occurs. The responsibility
for the decisions seems to lie with the male cell.
All we really know is that the sexes appear in the ratio
of 100 girls to 106 boys.
74
CHAPTER V
ABNORMAL PREGNANCY
After the diagnosis of pregnancy has been satisfactorily
established, no further internal examinations are
necessary in the absence of special indications, until
about the thirtieth week.
At this time a series of complete physical examinations
may be required to determine the presentation
and position of the child, the presence and rate of fœtal
heart tones, the diameters of the head, the length and
approximate maturity of the child, as well as the condition
of the bony and soft passages of the mother.
It is thus that an appreciation of the obstetrical problem
is secured and a course laid out for its successful
solution.
Pregnancy is not a disease, but a normal function;
but the woman is exposed, nevertheless, to many grave
risks that are peculiar to her condition and to many
complications accidental or otherwise which are more
serious on account of her pregnancy.
The Toxæmias.—The growing ovum brings about
changes in the maternal metabolism that are manifested
by characteristic symptoms which in other better
known conditions are recognized as due to toxæmia.
Therefore, while there is no positive proof as yet that
these symptoms, arising during pregnancy, are toxæmic
in origin, the evidence goes to show that they are; and,
therefore, should be classified as toxic.
Postmortem findings in eclampsia and pernicious
75vomiting such as extensive thromboses, cell necrosis,
and interstitial hæmorrhages are very suggestive.
Clinical findings in regard to the excretion of nitrogen
(urea, ammonia, uric acid, etc.), the occurrence of
acidosis, elevation of blood pressure, fever, diminished
excretion, coma and convulsions, all point to toxæmia.
It is the minor disturbances, however, that the nurse
will come in contact with most. They are nearly all
toxæmic in origin, and a brief description of them must
be given, together with suggestions for their management.
Salivation or Ptyalism.—In the majority of cases, saliva
is not especially noticeable; but at times the secretion
shows an enormous increase, and may even demand
abortion. Patients will have saliva running constantly
from the mouth. The amount may reach a pint or a
quart a day, and the skin of the lower lip becomes
greatly inflamed.
The only satisfactory treatment is a rigorous milk
diet on the theory that the disturbance is an intoxication.
In extreme cases abortion may be indicated.
Gingivitis.—The gums may become inflamed, spongy
and hæmorrhagic during pregnancy, usually in patients
of low vitality. If a generous diet and astringent mouth
washes do not relieve the condition, the milk diet
should be considered.
Toothache and Dental Decay.—The patient may be
given hypophosphites, and the teeth should be put in
good condition by a dentist.
Constipation has already been referred to. Strong
cathartics should be avoided lest abortion follow.
Condylomata of pregnancy occur most frequently
around the labia, perineum, and anus. They are wart-like
growths that develop slowly or quickly and may
76remain discrete or cover the entire area with masses as
small as beans or as large as cauliflowers, which in appearance
they much resemble. The etiology is obscure,
but they are generally associated with irritating vaginal
discharges, such as an old gonorrhœa.
Treatment consists in stopping the discharge or neutralizing
it, and in keeping the growths dry with a salicylic
acid dusting powder. (See Therapeutic Index.)
Pruritus is often distressing. The itching may be
limited to the genitals or appear on other parts of the
body. It may be due to the irritation of local discharges
or to a condition of the nervous system, arising from
toxæmia. Astringent douches and protective ointments
will relieve some cases.
Bromides and milk diet, bran or alkaline baths give
good results, and local applications of sedative lotions
and ointments containing menthol, carbolic acid or cocaine
(cautiously) will aid. The woman in some instances
becomes almost frantic, and tears at the vulva
with her nails until it bleeds.
The iodine treatment of Hensler is simple and often
effective. If no skin changes are visible and but little
leucorrhœa, the vulva is thoroughly prepared as for a
vaginal operation, dried and painted with a 10 per cent
solution of tincture of iodine. Generally one application
suffices, but when the leucorrhœa is bad, it may be
necessary to repeat the treatment on the third and fifth
day thereafter. Between treatments, the vulvar surfaces
and even the vaginal walls (by insufflation) are
kept dry with zinc oxide powder. If all measures fail
and exhaustion is imminent, emptying the uterus may
be advisable.
Herpes is an inflammatory, superficial eruption, characterized
by red patches, blisters, or pustules. It is
77accompanied by burning, itching, and nervous depression.
The origin is probably toxic and the termination
may be fatal. Milk diet, soothing lotions, and, if necessary,
abortion, constitute the means of treatment.
Areas of pigmentation (the chloasmata) are not amenable
to treatment. They usually disappear after labor.
Albuminuria of Pregnancy.—Albuminuria is so common
as to be almost physiological when the amount
of albumin is small. When the amount of albumin in
the urine is large, it may be due to pre-existing disease,
which is first discovered when the urinalysis is made
during pregnancy. (Chronic nephritis?).
If it makes its debut during gestation and continues
as a mere trace without casts, it is spoken of as the albuminuria
of pregnancy, but the patient must be watched
with great care, since the albuminuria may be a premonitory
sign of eclampsia.
Albuminuria and eclampsia must be considered together,
because, while the two conditions may exist
separately, they are most frequently associated, and it
is believed that they have a common causation. It is
true that most cases of albuminuria terminate favorably,
yet the higher the albumin content, the greater the
danger of eclampsia.
Albumin appears in the urine in from three to five
per cent of all pregnancies. It is more common in the
latter half of gestation and the attacks differ greatly
in severity.
Symptoms.—In the early stages the urine shows an
abundant, pale fluid of low specific gravity.
The seriousness of the case is generally indicated by
the amount of albumin, although this is not a reliable
guide as to the danger of eclampsia. Casts and red
and white blood corpuscles are occasionally found. The
78output of urea usually remains normal, but diminution
usually occurs in connection with eclampsia. Anæmia
and anasarca are common, but it is a hopeful clinical
sign that the cases of extensive edema rarely develop
eclampsia.
In albuminuria of pregnancy there is a large fœtal
mortality which, to a degree, is independent of eclampsia.
The infant dies in utero or is born feeble, or prematurely.
Eclampsia is the sudden appearance of convulsions
in the course of pregnancy. It may precede, follow, or
accompany albuminuria. It occurs rarely in the absence
of albuminuria in a woman who was apparently
in good health. The two phenomena are best explained
as a consequence of toxæmia due to poisons at present
unidentified.
Treatment of the albuminuria is treatment for impending
eclampsia. Regular examination of the urine
is indispensable. The presence of albumin suggests
toxæmia. The daily output of urine and the output of
urea must be compared, for a fall in urea is a premonitory
sign of eclampsia. The bowels and the skin should
be stimulated, respectively, by saline cathartics, hot
baths and packs. The digestive organs must be spared
as much work as possible, especially the liver. Water
is given in abundance, and milk is the staple diet. Koumiss,
butter milk and ice cream may be allowed. As the
patient improves, vegetables are allowed. The food
should be salt-free; and alcohol, as well as rich, indigestible
things should be forbidden. In the milder cases
boiled fish and a little chicken may be permitted.
The course of the disease and the condition of the
patient is determined by frequent examinations of the
urine, while in all serious cases an examination of the
79fundus of the eye must be made to detect a possible
albuminuric retinitis.
The treatment of eclampsia will be considered under
the complications of labor, where the attack usually
begins.
Pyelitis of pregnancy is an acute, and rarely, a chronic
infection of the pelvis of the kidney, due to the Bacillus
coli. It usually appears after the fourth month
(fifth to eighth) and attacks by preference the right
side. Extension to the kidney substance, ureters, and
bladder is occasionally observed.
Symptoms.—Sudden, acute abdominal pain, at first
diffuse, but after a few hours, becoming localized in the
right side, and on this account is often confused with
appendicitis, especially as vomiting is not infrequent.
A chill may mark the onset and the temperature rise to
103° F. or 104° F. The bowels are constipated, the
tongue coated, and there is tenderness over the kidney.
The urine is scanty, turbid, slightly albuminous
and contains pus and epithelium in the urinary canal.
A culture reveals the bacillus which has obtained access
to the kidney, either by extension of the ureter from the
bladder, by direct invasion of the tissues from the adjacent
colon, or through the circulation.
Treatment.—The diet should be fluid and mostly milk,
the bowels should be moved freely and frequently. The
urine is alkalinized with sodium citrate, since the Bacillus
coli lives only in an acid medium. As the symptoms
subside, urotropin may be administered. If the
patient does not improve within two weeks, abortion
must be seriously considered. Nephrotomy is not to be
thought of unless abortion has failed.
Hyperemesis Gravidarum.—The nausea and vomiting
of pregnancy is so usual as to be regarded as normal.
80It usually ceases from the fourth to the fifth month
spontaneously; has no ill effect upon the ovum, and
may respond readily to treatment.
Hyperemesis comes on at the same period and exhibits
all stages of violence, from the mild form above
described, to cases that end fatally.
Three classes of this serious disorder may be distinguished
as associated (Eden), neurotic, and toxæmic
vomiting.
Associated vomiting is the vomiting that comes with
gastric ulcer or cancer, chronic gastritis, cirrhosis of
the liver, and cerebral disease. These conditions must
be excluded in diagnosis.
Neurotic vomiting—severe and persistent nausea and
retching—is common in pregnant women of the nervous
type. It does not lead to loss of flesh ordinarily; the
urine is somewhat diminished in quantity from the
lack of fluids, but the amount of nitrogen excreted remains
normal. This is important.
Toxæmic vomiting includes a small but very important
class of cases, for all are severe and intractable and
some end in death.
Clinical Features.—The normal nausea and vomiting
may seem unusually severe. It persists and gets worse.
Then vomiting occurs when no food is taken and nothing
is held on the stomach. The vomit is stained with bile
or blood. The tongue remains clean, and the general
condition is good.
Next, weight is lost and the pulse quickens. A persistent
pulse of over 100 is serious. The tongue becomes
coated, sordes develops, sleeplessness and muscular
twitching appear, and the patient complains of epigastric
pain. Abortion may now occur and the condition
clear up.
81In its final stage, the urine becomes scanty and albuminous,
icterus may appear and the temperature rise to
100° F. or more, though sometimes it is subnormal. The
pulse may go to 120. Delirium and coma supervene,
and emptying the uterus is of no value. Fifty per cent
of these bad cases die.
The especially prominent points to be noted are the
urine, which shows acetone, albumin and blood, either
one or all, as well as an increased amount of ammonia.
A persistently rapid pulse, marked loss of flesh, coated
tongue, jaundice and delirium are regularly present.
Treatment.—Organic disease must be excluded and a
diagnosis of pregnancy strongly evident.
For the neurotic type, the patient must be segregated
from her friends, and a competent, cheerful nurse put
in charge. A cool, darkened room is best. If the patient
can be transferred to a hospital, the results are
more satisfactory. Here the isolation from external
interests and irritations can be made complete. The patient
does not talk, even the nurse comes with food, attends
to the obvious necessities, and departs in silence.
Once a day a sedative bath is given (see Baths, p. 325)
and medication in kind and frequency as the conditions
demand.
In any case, the patient should be put to bed and fed
carefully every two or three hours on milk, peptonized
food or barley water. If this is not retained, albumin
water may be given for twenty-four hours at regular
intervals, or rectal alimentation may be tried after stopping
all foods by mouth. Iced champagne, seltzer or
Vichy, either alone or with milk, may be tried. A dry
diet is sometimes effective, rusk, toast, toasted shredded
wheat biscuit, crackers, etc., taken early in the morning,
as one eats cheese. No exercise is permitted except
82such muscular and nervous excitation as may be
derived from massage or the sedative bath.
Drugs are sometimes of great value—the bromides, in
full doses, or 1 m. doses of tincture of iodine, well diluted,
every hour; or bismuth with hydrocyanic acid; or cocaine
or oxalate of cerium. Occasionally good results are
reported from a capsule of pepsin, 2 gr. and ¼ gr.
silver nitrate given just before meals; and adrenalin in
10 drop doses may be considered. Extract of corpus
lutea has been tried by Hirst with favorable results.
Sinapisms to the epigastrium and ice bags to the spine
have been found useful, and washing out the stomach
is efficient at times. In washing out the stomach, be sure
the stomach tube is iced before it is introduced.
When the case gets worse in spite of treatment and
acidosis supervenes, bicarbonate of soda may be given
in sixty grain doses every four hours, by rectum, if
necessary, until the urine gives an alkaline reaction.
Glucose as a readily assimilable carbohydrate may
be given in doses up to 10 oz. of a 6 per cent solution
(Eden) or sugar infusions by rectum, 1000 c.c. in twenty-four
hours by drop method.
The obstetric treatment is the emptying of the uterus.
To be effective the abortion must be done before the
condition of the patient is desperate. It is most favorable
before the febrile stage. If the vomiting persists
in spite of treatment and is accompanied by emaciation,
a pulse of over 100, albumin in the urine, with an increase
of the ammonia output, the pregnancy should be
terminated at once. If the patient can not go to a
hospital, the nurse should prepare the room as described
for operations.
After emptying the uterus, the vomiting usually
ceases but much labor is thrown upon the nurse in supplying
83nourishment and caring for an exhausted and
whimsical patient.
The back must be inspected daily for decubitus (bed
sores) and her position changed frequently. A daily
rub with alcohol and water (50 per cent) followed by an
oil inunction will be valuable. The teeth and gums
should be cleaned with gauze, wrapped around the
finger and dipped in solution of boric acid. No brush
should be used.
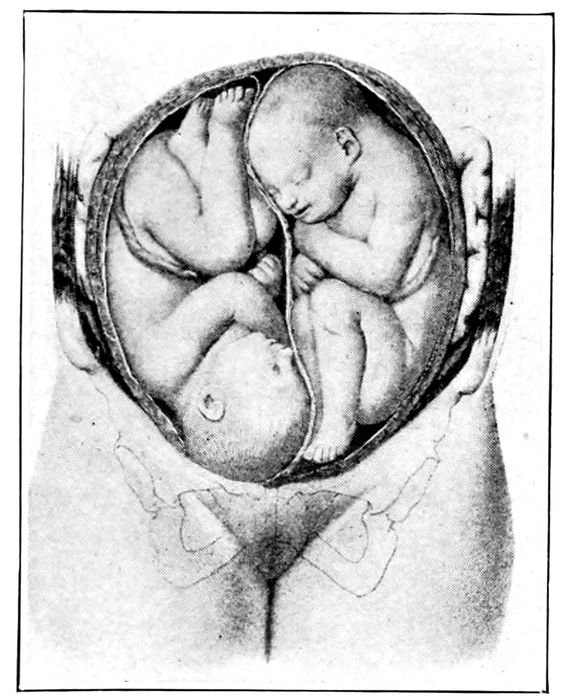
Fig. 29.—Twins. (Lenoir and Tarnier.)
Multiple Pregnancy.—Twins occur about once in
ninety labors, triplets, once in seven thousand.
Heredity and multiparity seem to be the only recognized
predisposing factors. The more pregnancies a
woman has, the more liable she is to have twins.
Twins may occur through a division of the primitive
cell through the fertilization of two ova from the same
84or different ovaries, or by fertilization of a single ovum
having two nuclei. (See Fig. 13). The former are
called binovular twins, and may or may not be of
the same sex. The latter are called uniovular twins and
are always of the same sex. Twins are usually somewhat
smaller than a single child, and frequently associated
with hydramnios. Binovular twins have separate
placentæ and uniovular twins have one placenta, with
separate cords.
Twin pregnancies usually go into labor earlier than
the single child, possibly on account of the over-distention
of the uterus.
The diagnosis is occasionally difficult and at other
times easy. Two sets of heart tones must be distinguished
and differentiated by their variation in frequency,
heard at the same time by different observers.
The presence of twins may be strongly suspected also
when the external measurements of child and uterus
greatly exceed the average. In such cases a systematic
and persistent search must be made for the two fœtal
heart tones.
The delivery is generally uncomplicated, unless the
chins become locked.
Displacements of the Uterus.—In most cases displacements
of the uterus are a consequence of conception in
organs that are previously retroflected or retroverted.
They rarely produce symptoms until the end of the third
month, when the attention is directed to the bladder.
There may be absolute retention or a constant dribbling
from a full bladder (ischuria paradoxa), possibly
associated with pain. If recognized early, an attempt
should be made to replace the uterus by posture (knee
chest) and when replaced, to hold it by pessary or tampon.
The prone position in bed will aid.
85After retention has occurred, the patient should be
put to bed and the bladder catheterized regularly every
eight or ten hours for three or four days. As a rule, the
organ will rise spontaneously into the abdomen. If it
does not, it is probably incarcerated under the promontory,
and the physician must try to replace the uterus
by manipulation or by continuous pressure, but in bad
cases, he will empty the uterus before the condition of
the patient becomes too serious.
In multiparas with weak abdominal walls, or women
with spinal curvature or contracted pelves, the uterus
may fall forward and, passing between the recti muscles,
continue to drop until the fundus lies lower than
the symphysis pubis.
Management, until labor occurs, may be made more effective
by using a strong, well-fitting abdominal bandage.
Malformation of the uterus may possess an obstetric
interest at times. The double uterus (uterus didelphys)
and the uterus with a rudimentary horn (uterus
bicornis) are examples. These are congenital conditions,
due to imperfect development, and pregnancy may
take place in one or both sides. If in one side only, the
other half will also exhibit the softening and other
changes as in normal cases. Binovular twins may be the
result of a pregnancy in each side.
Pressure Symptoms.—Edema of legs and sometimes
of the vulva occurs during the last trimester. It is due
to increased intraabdominal pressure and to direct interference
with the return circulation by the pressure
of the heavy uterus on the iliac veins at the brim of the
pelvis. The urine should be examined for albumin and
the patient put in the horizontal position if the edema
is troublesome.
Varicose veins of legs and vulva may cause much distress.
86The limbs should be bound with flannel spirals
or with rubber bandages in the recumbent position, or
elastic stockings may be obtained. Operation during
pregnancy is not to be considered. The vulva can only
be relieved by a double bandage, which is sewed at the
point where it crosses the vulva, and buckled or tied
to a waistband above the hips, both before and behind.
This brings support to the vulva. If the veins rupture,
the part should be elevated and compressed with an aseptic
pad.
Hæmorrhoids may either appear or grow worse late
in pregnancy. If they protrude, they should be replaced.
Ointments and iced applications may be used and the
bowels kept loose.
Cramps may occur in the muscles of the legs, due
sometimes to the varicose veins and sometimes to pressure
on the lumbosacral plexus.
Moles.—Mole is the name given to an ovum which is
destroyed by disease of its coverings during the early
months of gestation. Two kinds are known, the blood
mole (carneous mole, fleshy mole, or hæmatoma mole)
and the hydatidiform mole (vesicular mole).
The blood mole results from progressive or recurrent
slight hæmorrhages during the first three months
of pregnancy, but hæmorrhages insufficient in quantity
to produce an abortion. The blood forms a clot, which
may be retained for several months and become solidified.
Hydatidiform mole is a disease of the young chorionic
villi, characterized by the growth of an immense
number of irregular clusters and chains of grape-like
cysts from the very minute to bodies four-fifths of an
inch in diameter. The causation is unknown.
Both forms occur in the first half of the pregnancy
87and are characterized by undue enlargement of the
uterus and hæmorrhagic discharge.
Diseases of the Membranes.—Hydramnios, or polyhydramnios,
is the name applied to the condition where an
excess of liquor amnii is formed. The amount normally
present varies, but anything in excess of four pints
could be called hydramnios. Six gallons have been reported.
Since the source of the liquor amnii is not
positively known, the etiology of hydramnios must be
equally obscure.
It is occasionally associated with morbid conditions of
the mother, such as hepatic or cardiac dropsy, but more
frequently with developmental anomalies of the fœtus.
Since the mother is usually healthy and the fœtus frequently
deformed, the theory is advanced that the disease
is fœtal in origin. It frequently occurs with twin
pregnancies, and in the first months it is most plausible
that the liquor amnii is in some way derived from the
fœtus.
The disease is more common in multiparas. It is
generally slow in onset, but it may be acute, and an
immense amount of fluid may be formed in a few weeks.
The symptoms are those due to pressure from the extremely
large uterus.
The treatment, if interference with heart or lungs
becomes pronounced, is puncture of the membranes.
The child need not be considered for it is usually dead
or deformed.
Oligohydramnios is the condition where the liquor
amnii is deficient in amount. It gives no maternal
symptoms, but it is the cause of many birthmarks and
fœtal deformities (club-foot, spinal curvature, wry-neck,
ankylosis of joints).
Amniotic adhesions are usually associated with oligohydranmios
88and cause deformities by amputation of
limbs, strangulation of cord, and production of six
fingers.
The placenta may show anomalies of size and shape.
Thus, there may be two lobes, or three. There may be
the main placenta and a small out-lying mass connected
by membrane and vessels with the larger segment.
The cord may be inserted in the middle or at
the edge and yellowish-white masses called infarcts may
be found in its substance.
Unusual size and weight of the placenta are suggestive
of syphilis.
Abnormal conditions of the fœtus may arise from primary
or transmitted disease or from errors of development.
The developmental errors may be monsters, hydrocephalus
spina bifida, etc., which may not influence
the pregnancy. The most commonly transmitted disease
is syphilis, which may produce abortion, premature
labor, or a child born with syphilitic skin changes
on palms and soles, as well as internally.
89
CHAPTER VI
ABNORMAL PREGNANCY (Cont’d)
Extrauterine Pregnancy.—This is a pregnancy which
occurs outside the uterus, and while the event usually
happens in the tube, cases have been reported where
the egg developed in the ovary or abdomen.
The ovum, owing to some delay in passage to the
uterus, is fertilized either in the ovary or in the tube,
and by reason of a chronic inflammation of the tube
or pelvis, or of overgrowth does not succeed in reaching
the uterus at all.
As the ovum develops, the tube expands, but it does
not possess the power of growing into a large organ
like the uterus, hence a sudden jar, a strain, or a blow
may cause it to rupture and discharge the egg into the
abdomen (ruptured tubal pregnancy) or force it out
through the end of the tube (tubal abortion).
This phenomenon may be accompanied by a severe or
even fatal hæmorrhage; or the prostration may pass off
in a few days or weeks, and leave the patient well.
In the early stages the ovum is absorbed, but after the
pregnancy becomes more advanced, it may remain as a
tumor, or require an operation for its removal.
Infection may occur and the mass ulcerate its way
into neighboring organs (rectum, vagina, or bladder)
and discharge itself in a long, suppurative process.
Most cases of ectopic (extrauterine)gestation present
definite and even dangerous symptoms between the second
and fourth month. The symptoms are those of pregnancy,
together with irregular hæmorrhages from the uterus,
90which may result in the expulsion of pieces of tissue or
of membrane. Besides this, there is a vomiting and
acute irregular pain on one side, associated with a sense
of fullness. Such symptoms should be brought to the
attention of the physician, who will learn the true condition
of the pelvis by internal examination, conducted
as gently as possible so as not to produce rupture.
If rupture occurs, it will be ushered in by a sharp
lancinating pain on one side, followed by faintness,
nausea, vomiting, prostration, rapid pulse, sighing
respiration, and collapse. The temperature is subnormal
and death may occur in a few hours, unless an
operation is done.
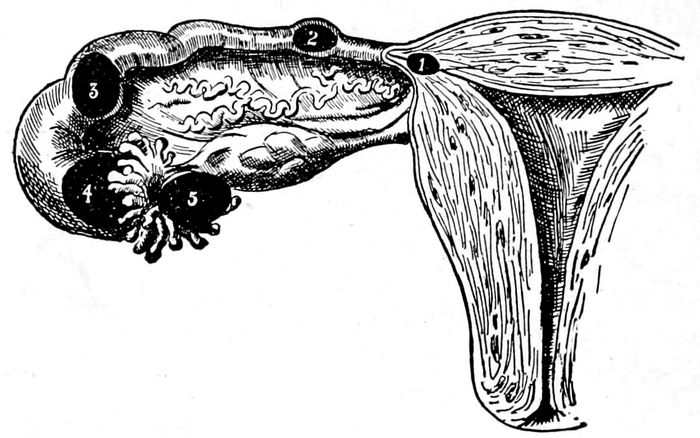
Fig. 30.—Diagram representing the sites for the various forms of tubal pregnancy. 1, interstitial pregnancy; 2, isthmial pregnancy; 3, ampullar pregnancy; 4, infundibular pregnancy; 5, tubo-ovarian pregnancy. (Gilliam.)
In cases of tubal abortion (where the ovum escapes
through the end of the tube) the symptoms are very
similar, but the patient soon rallies and gradual recovery
takes place.
If the diagnosis is made before rupture or abortion
the treatment is laparotomy. If rupture occurs, the
91laparotomy must be done immediately to check the
hæmorrhage, which threatens the life of the patient. In
tubal abortion, if the diagnosis is certain, some delay
may be permitted under extreme watchfulness of the
nurse and physician. In such case, the nurse will
keep the patient absolutely quiet and forbid exertion of
any kind.
If operation is necessary, the utmost gentleness must
be used in preparing the abdomen. The tincture of
iodine application to the site of the incision is sufficient
preparation, and, of course, an abundance of sterile
gauze, cotton, and towels should be supplied, as in every
case where laparotomy is done.
If the rupture occurs while the nurse is present, the
doctor should be notified at once, and if not at home,
another doctor should be summoned. Meanwhile, the
nurse prepares the room, solutions and utensils for an
abdominal operation. Immediate incision to check the
hæmorrhage and remove the mass offers the greatest
safety.
The after-care is the same as for any laparotomy,
with the additional duty of making up the lost blood
as soon as possible by nourishing foods, normal saline
solution by rectum, and, if necessary, by hypodermoclysis.
Acute fevers are a serious complication of pregnancy
on account of the danger of abortion or premature
labor, which may come on either from the associated
high temperature or from the transmission of the disease
to the ovum.
The following diseases are known to affect the fœtus
in utero: cholera, yellow fever, small pox, scarlet fever,
typhoid, measles, erysipelas, meningitis and syphilis.
92
CHRONIC INFECTIONS
Tuberculosis does not affect fertility or the course
of the pregnancy, but the progress of the disease is
hastened, and the maternal death accelerated.
The question of artificial abortion in the early months
must be seriously considered, and if the case goes on
to term, the child must not be nursed or cared for by
the mother.
Syphilis is the most frequent systemic cause of the
interruption of pregnancy. It is a blood disease, due to
an organism, called spirochæta pallida, and it appears
in three distinct stages. The first is the primary stage,
wherein a hard, nodular ulcer appears on some part of
the body, as the vulva, lips, gums, tonsils, or hand. It
is not always venereal in origin. The second stage begins
six or eight weeks after the sore, and is marked by
a general eruption of red spots, chronic sore throat, falling
hair, and rheumatic pains in the joints. The third
stage is the name given to the later conditions of the
disease which affect the bones, blood vessels, and nervous
system.
Infection of the ovum may usually be traced to the
father, who may transmit syphilis at any stage of the
disease. In the third stage, the child alone will be infected;
the mother escapes.
The mother may or may not transmit the disease,
depending on the period of pregnancy wherein her infection
occurs. If she gets the disease at, before, or
just about, the time of conception, she will abort three
times out of four, and the ovum will show definite
lesions. If infected later, abortion occurs less frequently;
and if the disease is contracted late in pregnancy,
the child may be born apparently free from infection.
93Symptoms.—A child with congenital syphilis will show
the eruption of coppery spots, blisters on palms and soles,
deep cracks on the feet, snuffles, cracks and ulcers around
the mouth and rectum, and the weakly, marasmic condition
of the body.
The diagnosis in suspected cases can be rendered more
certain by the Wassermann reaction. This is a laboratory
test of the blood which should always be made before
a wet nurse is allowed to nurse a child, or before
a suspected child is nursed by a clean woman. In all
cases of transfusion of blood, it is imperative.
Treatment.—Antisyphilitic treatment of an infected
mother or child by salvarsan, mercury, and potassium
iodide must be carried out vigorously in all cases.
The syphilitic patient must be prevented from spreading
the infection by having dishes and utensils of her
own, which are kept sterile. Discharges are collected
and burned, and the nurse in charge of these cases must
carefully cover her hands with rubber gloves, and see
that all cracks and fissures are properly protected from
contact with sources of infection.
Gonorrhœa is an acute or chronic disease of the mucous
membranes due to a germ called the gonococcus.
Beginning with a sharp inflammatory disturbance of
the urethra or vagina, it may pass slowly up through
the genital passage and produce chronic and permanent
disabilities, such as sterility, pus tubes, and pelvic peritonitis.
The symptoms are painful urination, painful inflammation
of the vagina, with a purulent discharge. During
pregnancy all these symptoms are intensified, and
warty growths (condylomata) may appear on the vulva.
If infection occurs after pregnancy has begun, the
course of the gestation is rarely affected, as the uterus
is closed to germ invasion. During delivery, however,
94there is a serious danger of infection of mouth or eyes
of the child if they come in contact with the discharge.
Prophylaxis.—The eyes at birth must be immediately
instilled with a drop or two of 1 per cent solution of silver
nitrate in water. This is not neutralized by normal saline.
Great care must be used that the discharge does not come
in contact with the eyes of the mother or attendants, lest
infection follow.
Treatment.—Scrupulous cleanliness must be observed.
Douches of potassium permanganate, 1:5000, or painting
the vagina with iodine or solution of silver nitrate, or
suppositories of argyrol or protargol furnish the best
means of treatment before labor.
Neither syphilis nor gonorrhea is necessarily caused
by venereal infection. They may be spread by barbers,
dentists, physicians, and nurses,—by anyone who is unclean;
and may be acquired innocently everywhere.
These diseases should not be discussed by the nurse or
physician except with the patient. Certainly nothing
from the sick room should be repeated elsewhere.
The valves of the heart are not uncommonly found to
be diseased in pregnancy, the mitral being the most
often affected, either as an insufficiency or as a stenosis
(a narrowing of the mitral opening). Mitral stenosis
is the most serious of all heart complications of pregnancy,
and where this is present, a woman should be
advised to avoid conception.
In other mitral lesions, many pregnancies may be
successfully passed, if compensation is maintained; but
every one brings further damage to the already weakened
heart, and reduces its reserve of force. If the heart
breaks down early in pregnancy, and does not respond
to medication, abortion should be induced. In the second
half of pregnancy, the mother should be given the
prior chance, but the child should be saved, if possible.
95Renal diseases, such as nephritis, may not only induce
abortion by destroying the fœtus, but the kidney lesion
may be greatly aggravated by the pregnancy. The most
careful observation of the patient’s condition, the regular
examination of the urine, and the scientific management
of the diet is necessary to relieve the work on the
kidneys and keep the patient in a moderate degree of
health.
It is the duty of the nurse to protect her patient
against fatigue and chill, and to see that the proper diet
is followed; but other symptoms, such as headache and
disturbance of vision and developing edema, must be
noted and reported to the physician at once.
Diseases of Liver.—Acute yellow atrophy is a rare
condition, which, for reasons unknown, is promoted by
pregnancy.
The symptoms are intense headache and pain in the
abdomen, possibly accompanied by vomiting and purging,
which are soon followed by coma. There is generally
a certain amount of jaundice. The urine is diminished
in amount and contains albumin, casts, and sometimes
blood. There is no known treatment, and the end is
death.
Diabetes is seldom found associated with pregnancy.
Its presence is unfavorable to conception and to gestation.
Mother and child are both less secure. Abortion or
premature labor is the rule.
The hæmorrhages of pregnancy in the first half generally
mean abortion, and in the last half, either placenta
prævia or premature detachment of the normally implanted
placenta (see p. 228).
Abortion is the expulsion of the ovum before the
fœtus is viable, that is, before it is capable of maintaining
life after birth. This means the twenty-eighth week,
or the seventh month. Subsequent to the seventh month,
96the interruption is called premature labor. Abortion is
a miniature labor, consisting of a stage of dilatation, a
stage of expulsion, and a stage of involution.
The interruption of the pregnancy may occur spontaneously
or be induced. In spontaneous cases the
causes may be sought in diseases of the ovum, or in the
mother, in injuries to the uterus or its contents, and
such systemic affections as syphilis, Bright’s disease,
alcoholism, lead poisoning, etc.
Abortions happen about once in every five or six pregnancies,
and more frequently at the third month than
at any other time.
The symptoms are hæmorrhage and pain. The dangers
are hæmorrhage and infection.
Infection is most common and most serious in abortions
that are brought about mechanically.
Hæmorrhage, in some degree, is an invariable symptom,
which has its origin in the separation of the ovum
from the uterine wall. Hæmorrhage from the uterus is
serious at whatever stage of pregnancy it appears.
The duty of the nurse is to put the patient in a cool,
dark room, on her back, elevate the foot of the bed, put
ice bags on the lower abdomen, and summon the attending
physician, with the hope that an abortion can
be averted. Bromides and opium are the drugs most
to be relied upon. Opium may be given in suppository,
1 grain night and morning.
If the hæmorrhage is alarmingly profuse and the
nurse is skillful and clean, under exceptional circumstances
she may pack the vagina with sterile cotton
while waiting for the doctor. Then the room should be
set for operation.
Dead Ovum.—The ovum may be discharged in pieces
or in a single complete mass.
The egg may die at any period of the pregnancy, and
97be discharged in a few hours, or it may not be expelled
for weeks, if at all. Fœtal death in the uterus may
have its cause on the paternal side in a father too old or
too young, or affected with such diseases as diabetes,
nephritis, tuberculosis, syphilis, or chronic lead poisoning;
on the maternal side, the same diseases, plus cancer,
anæmia, insufficient food, and inflammation of the
uterus; on the part of the embryo, syphilis or any transmitted
or primary disease of the ovum.
The results of retention of the dead ovum vary with
the case. Infection of the ovum is rare, except where
the membranes have ruptured and an open channel exists.
No harm follows the death of the fœtus, except
in the presence of infections, all other changes are benign.
The embryo in the first and second months may
be absorbed, but at later periods, it becomes macerated
petrified, or otherwise altered.
Among the signs of fœtal death are prolonged cessation
of fœtal movements after being definitely observed,
chilliness, languor and malaise of the mother, sense of
weight in abdomen, and possibly a bad taste in the
mouth. Furthermore, the uterus does not correspond to
the period of pregnancy, and may have become smaller.
Retrogressive changes take place in the breasts.
The diagnosis is only certain when the heart tones
are persistently absent, or the macerated head of the
fœtus is felt through the partly dilated os as a flabby
bag of bones.
Treatment in noninfective cases is expectant. Spontaneous
expulsion will occur sooner or later and there is
no necessitous indication for interference. Local signs
of putrefaction, however, make the immediate emptying
of the uterus necessary.
98
CHAPTER VII
PREPARATIONS FOR LABOR AND THE NORMAL COURSE OF LABOR
The Nurse.—Scientific obstetric nursing is a specialty
that enlists the interest of exceptional women only.
It demands a high sense of duty, a strong physique,
broad training, unusual judgment, and rare tact. The
nurse must be professionally aseptic and personally
clean. She should keep herself free from odors, and
bathe at least three times a week. The presence of pus
anywhere on her body disqualifies her at once, and she
should report off duty.
The compensation should always be somewhat higher
than for other work, because there are two patients to
be cared for.
An obstetric nurse should specialize in her work, and
not take infectious cases. Unhappily the haphazard
character of the onset of labor presents a difficulty.
The patient frequently can not afford to have the nurse
for a long time in advance of labor, and the nurse whose
income is limited by the number of her cases can not
afford to be idle. Hence, it is better for two nurses to
work in alternation with one another, so that one is always
available in an emergency.
Both doctor and nurse should visit the lying-in room
before labor begins, and plan its rearrangement. At
least a week before the expected confinement, the chamber
selected should be thoroughly cleaned and the woodwork
wiped off. Curtains, draperies and bric-a-brac and
all useless furniture should be removed. Carpets must
99be taken up, or at time of confinement, well protected.
Rugs can be easily managed. A chair, a bed, and the
various tables for instruments and solutions are all that
are required.
The nurse usually is called to the case first, and upon
her falls the responsibility of the diagnosis and the
burden of the preparation. As soon as she arrives and
satisfies herself that the patient is really in labor, she
puts the final touches to the room. In her own mind
she goes over all possible emergencies and prepares to
meet them.
The following supplies should be in the house for
the labor:
3 hand basins, 10 inches in diameter.
3 hand brushes.
1 two-quart douche bag.
15 yards nonsterile gauze.
2 lb. each of cotton batting and absorbent cotton for making bed pads.
2 pieces of rubber sheeting 1 by 2 yards.
5–yd. jar of borated gauze.
4 oz. lysol (or ziratol).
100 c.c. of Squibb’s chloroform.
2 oz. green soap.
2 oz. solid albolene.
8 oz. alcohol.
½ oz. ergotol.
½ oz. bismuth subnitrate and ½ oz. boric acid powder mixed.
1 nail file.
Nurse’s outfit consists of the following: Nail file, surgical
scissors, catheter (silver is best), hypodermic syringe
with tablets of morphine, strychnine, and digitalis; two
fever thermometers, one for mouth and one for rectum;
a pair of tissue forceps and a razor.
Some time before the labor, the nurse should call on
the patient and establish a working acquaintance. It
adds greatly to her authority and to the patient’s confidence in her. Her advice will be sought on a multitude
of subjects, partly real and partly to try her out.
100
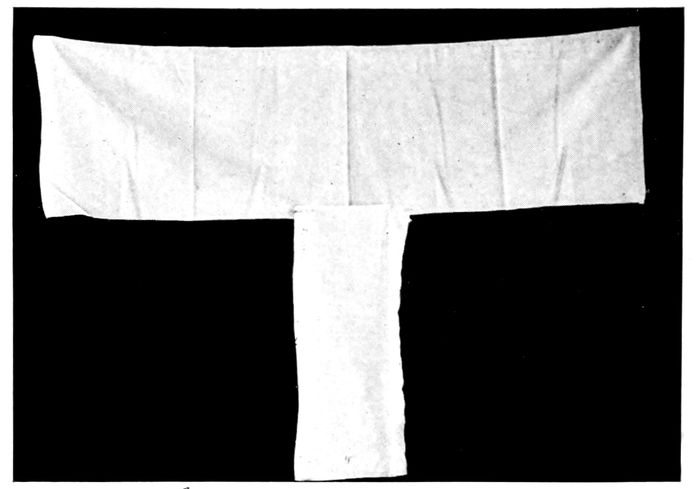
Fig. 31.—Abdominal binder with crosspiece to hold vulvar pads.
Fig. 32.—T-binder, used in all cases after the fifth day post partum.
101Sterilizing may be done in a hospital, or, if this is not
feasible, the nurse should go to the house two or three
weeks before the expected labor and sterilize in an
Arnold or Rochester sterilizer the following articles:
½ doz. sheets.
3 doz. towels.
2 pillow slips.
3 abdominal binders of unbleached cotton, 16 in. wide and 36 in. long, folded and hemmed.
4 T bandages.
3 breast binders.
2 jacket parts of pajama suits.
3 pairs of long white stockings.
3 packages of vulvar dressings (see Preparation of Supplies, p.
326).
2 obstetric pads 1 by 36 by 36 inches.
1 pillow slip full of cotton pledgets for sponges.
1 jar applicators (cotton twisted about toothpicks).
1 jar of gauze pledgets for perineorrhaphy and cord dressings.
Everything must be neatly wrapped and labeled.
102
Fig. 34.—Baby’s dress with winged sleeves.
Infant’s Outfit.—
12 plain slips 27 inches long of dimity or nainsook (with winged sleeves).
3 long sleeve shirts, silk and wool (size No. 2).
6 pinning blankets, made of outing flannel, if it is a winter baby.
3 bands, 6 by 18 inches, clip or notch edges, do not hem.
3 petticoats, flannel bottoms and muslin waists, without sleeves and with small button on shoulders.
3 outing flannel wrappers.
6 plain, soft muslin dresses.
3 (Arnold) knitted night gowns, light weight.
4 doz. light weight cotton diapers, 20 x 40 inches. Bird’s-eye linen is the best. Wash and dry these in the air before using.
4 soft towels (linen preferred).
2 quilted pads.
4 soft wash cloths.
4 wool wrapping blankets.
1 pair scales that weigh ounces and fractions thereof.
4 oz. of olive oil or benzoated lard.
4 oz. of alcohol (95 per cent).
¼ lb. boric acid crystals.
103½ lb. absorbent cotton.
1 cake of castile soap.
2 oz. solid albolene.
½ oz. subnitrate of bismuth powder and ½ oz. of powdered boric acid mixed.
1 bed pan.
2 basins, holding 2 quarts each.
1 papier mache, rubber, or enamel ware bathtub.
Anæsthetics.—Excessive pain is destructive and disintegrating
to the vital forces. Many a woman who has
passed through a particularly severe labor remembers
her experience with a horror that forever precludes its
repetition.
This is the day of relative painlessness in labor, and all
the world is striving to make childbirth easier and less
lethal. No woman, unless she herself requests it, should
be permitted to go through the agony of labor without
an anæsthetic, judiciously selected and carefully administered.
Pain-deadening agents are numerous and inexpensive,
and it is only a matter of experience and judgment to
choose a method that will reduce the suffering of childbirth
to a minimum. The second and first stages of
labor, in the order named, demand the most in the way
of relief.
A prolonged first stage with nagging, violent and apparently
useless pains may devitalize the patient more
than short, but acute pains of the second stage. In the
first stage, under proper selection of cases and experienced
supervision, “Twilight Sleep” will be successful
in seventy to eighty per cent of the cases.
By success, is meant that the patient is relatively free
from pain. When the drugs do not relieve pain, the
case is a failure (fifteen per cent), although in no case,
when properly given, is the mother or child endangered.
Morphine solution ⅙ gr. and scopolamine hydrobromid
1041/200 gr. to 1/150 gr. is the customary dosage for the
first injection. Another injection of 1/200 gr. is given
in a half or three-quarters of an hour. The room is
darkened, talking is forbidden, and the family exiled.
The patient gets red in the face and very thirsty, the
pulse is rapid but full. She answers questions very
slowly and drowsily, awakes for her contraction but
goes right off to sleep again. In this condition she is
kept through bi-hourly repetitions of the scopolamine
until the delivery. It is this half waking and half sleeping
condition that suggested the name of “Twilight
Sleep.”
Morphine and scopolamine will relieve the pains of
the first stage without greatly protracting the labor.
The same drugs may and probably will prolong the
duration of the second stage. The first dose should be
given as soon as the patient is well started in labor.
“Twilight Sleep” is at present a hospital procedure,
and the technic so exacting as to weary the attendants
greatly. It can not be employed until the woman has
definitely gone into labor and is at least three hours
away from delivery. It is not serviceable where the
pains are weak and shallow; and it must be used with
wise circumspection, if at all, in the presence of complications.
For the second stage, there is a choice of three drugs:
gas, chloroform, and ether. Like twilight sleep each is
open to some objection, but each may be of the greatest
assistance if used under appropriate indications and conditions.
Gas has one advantage, in that it in no way interferes
with the pain activities; and Lynch and Davis have shown
that with a proper admixture of oxygen, it may be
given with comparative safety for the two or three hours
105which may mark a normal second stage. To administer
it a competent machine for mixing the gas is necessary.
It should not be given to patients who have bad hearts,
high blood pressure, or toxæmia. Neither is it a satisfactory
anæsthetic when the head delivers, for the mother
being less relaxed and more rigid, the legs and muscle
action are harder to control and unnecessary perineal
lacerations are liable to occur. The patient is instructed
to take several deep breaths just as the uterine contraction
comes on and the gas bags supply about 75 per cent
nitrous oxide and 25 per cent oxygen. As the pain passes
off the oxygen is increased and the nitrous oxide diminished
until the mind is again clear.
To save the perineum and better to control the patient,
when the head is about to pass the vulva, it is wiser to
abandon the gas for chloroform or ether.
Obstetrical operations, such as forceps and version,
require ether or chloroform, and not gas. The dangers
vary with the anæsthetic chosen, as well as the amount
and the method of administration. Ether affects the
respiration, chloroform attacks the heart. Ether must
not be given near an open flame. Chloroform is not
explosive but is decomposed by fire into an irritating
gas. Chloroform must be diluted with 90 per cent of
air, hence the mask must be open, or the napkin held
free from the face, so that plenty of air can enter. Ether
and chloroform, when given “a la reine;” i. e., a few
drops on the mask at the beginning of each pain and
increased up to the acme, is relatively free from danger.
They have the additional advantage that the sleep may
be instantly deepened if operation is required. Chloroform,
it is now believed, predisposes mildly to post
partum hæmorrhage. Davis has shown that neither
ether, gas, nor chloroform affects the child injuriously if
106the administration is intermittent and not too greatly
prolonged.
To summarize: Morphine and scopolamine combined
is a first stage analgesic, which has too much value to be
neglected.
Gas, if an apparatus is to be had, may work well for
the greater part of the second stage, while for operations,
or for the period of expulsion, during which the
head passes the perineum, chloroform and ether give
bests results. Moreover, chloroform “a la reine” may
be given safely and efficiently by a competent nurse
and in many instances must be given by the nurse, if at
all.
When the perineum bulges, or the head becomes visible
at the vulva, the nurse should anoint the lips, cheeks
and tip of the nose with cold cream or olive oil, to avoid
burning the skin, and lay two or three thicknesses of
handkerchief or gauze over the nose (an inhaler is best).
An abundance of room must be left underneath and at
the sides of the mask for air to enter.
At the beginning of the pain a few drops of chloroform
are poured on the cloth and the patient instructed
to breathe vigorously. The cloth is removed as soon
as the pain ceases and when the next contraction comes
on, the process is repeated. As the head passes the
perineum, the chloroform should be pushed to complete
anæsthesia, both to save suffering and to give the doctor
full control of the perineum. When the nurse gives the
anæsthetic, she should watch the doctor for his signal to
increase the vapor or remove the mask.
Summary.—Cover the eyes with a wet towel and anoint
the face with cream or oil before using chloroform. Remove
false teeth, if present.
Obstetric degree—a few drops on mask at beginning
of each pain.
107Surgical degree—complete anæsthesia.
Watch pulse and respiration.
A nurse should never leave a patient who has had an
anæsthetic until she is conscious. Vomiting is especially
dangerous.
Normal Labor.—Labor is the process by which a
fœtus of viable age is expelled from the uterus.
By normal labor is meant a case where the fœtus presents
by the vertex and terminates naturally without
artificial aid, or complications. It varies greatly in severity,
duration and danger to mother and child. A first
labor is more prolonged and difficult than later confinements.
A woman in her first delivery is called a primipara,
in subsequent cases, a multipara.
The date at which labor comes on is difficult to determine
accurately. The average duration of pregnancy is
from 275 to 280 days, forty weeks, or ten lunar months,
but conception does not occur necessarily at the time of
coitus, nor is it possible to know with any certainty
when it does occur.
Labor may occur two weeks earlier than calculated,
with benefit to the mother, and no harm to the child;
but if the woman goes over time, the child becomes much
larger and the labor harder and more dangerous to
both.
Causes of Labor.—Why labor should occur at all is not
known. Many theories have been advanced, none of
which is entirely satisfactory. Some of the best known
are the growing irritability of the uterus accompanied
by an increase in the frequency and strength of the intermittent
uterine contractions or increasing distention
of the uterus. Thus it is believed that when the uterus is
distended up to a certain point, it will try to relieve
itself like the bladder, or a baby’s stomach. It may be
108that any one of the following factors, or all of them
acting together, are influential.
Dilatation of the cervix by the presenting part.
Increasing distention of the lower half of the uterus
with pressure on neighboring nerve structures.
The circulation of fœtal products of metabolism
(toxins) acting on the nerve centers.
The menstrual periodicity.
Heredity and habit.
Physical and emotional causes.
The onset of labor probably is not purely accidental,
and yet it is so inconstant in appearance and so indifferently
early or late, that it has every appearance of being
an affair of chance. The time when labor will come on
is highly speculative in general, but the phenomenon is
preceded by certain definite symptoms:
The lightening.
False pains.
Show.
Rupture of membranes.
The pains.
Lightening.—About two weeks before labor, especially
in a primipara, the uterus and the head sometimes descend
into the pelvis. The body of the child falls forward and
the abdomen protrudes, the stomach is flatter, the patient
breathes easier and feels, as she says, “lighter.”
But walking is more difficult, the bladder is stimulated
to frequent evacuations and the rectum is compressed.
This occurrence is a premonitory sign of labor, and
also favorable inasmuch as it demonstrates that this
particular head is not too large to pass this particular
pelvis.
False pains may appear, especially in multiparas, from
two to four weeks before labor. In some of these cases
109the pains may be due to gas or indigestion and respond
to hot applications and enemas, or there may be definite
uterine contractions, as shown by the hardness of that
organ during a pain, but the phenomena are irregular
and therefore not typical of labor pains.
Usually they pass off in a few hours, but if the patient
is nervous, the doctor or nurse may be called needlessly.
The patient, therefore, should be instructed to have the
pains timed by the watch for half an hour or an hour.
If they are regular during this period, the physician
should be notified. Upon his arrival, an internal examination
will reveal the true character of the disturbance
by the condition of the cervix and os.
The show is a discharge of thick, white mucus, slightly
stained with blood. This is the mucus plug which occludes
the cervix during pregnancy and when the os begins to dilate,
the mass is released and passes out. Labor usually
comes on vigorously within twelve hours.
The membranes may rupture before labor begins and
much fluid escape. The advantage of the dilating bag
of water and lubricating qualities of the liquor amnii
are thus lost. Such a labor is called a “dry birth” and
is frequently slow, exhausting, and extremely painful.
The pains are the subjective manifestations of the
powers of labor. The forces concerned are uterine and
abdominal muscles, principally assisted by those of the
back, legs, and arms. Their constricting action on the
nerve fibers in the walls of the uterus is the cause of
the pains in the first stage. The onset may be violent
and go on to a quick delivery, but generally the inception
is more insidious.
The irregular, painless contractions, (of Braxton Hicks)
that were mentioned on an earlier page, gradually at term
change their character and become regular and painful.
110At first they may be slight and vague, lasting only half
a minute and separated by intervals of ten or fifteen
minutes and scarcely attract the patient’s attention.
They are felt chiefly in the abdomen.
More or less rapidly they increase in frequency, severity
and duration. They last from a minute to a minute
and a half and come every three minutes. The whole
uterus hardens and its outline is clearly defined during
the contraction; it relaxes and becomes soft in the interval.
The woman is now in labor. The pains become
grinding and the patient feels that she is not accomplishing
anything, yet under the influence of these contractions
the cervix is effaced and the os is dilated.
The Course of Labor.—Labor is divided for convenience
into three stages as follows:
The first stage, from the beginning of pains until the
complete dilatation of the os.
The second stage, from the complete dilatation of the
os to the delivery of the child.
The third stage, from the delivery of the child to the
expulsion of the placenta.
The first stage is the stage of dilatation.
Usually at term, the cervix is columnar and unshortened,
the canal intact, and closed at both ends, as shown
in Fig. 36.
In multiparas the outer opening will usually admit
the tip of the finger.
As labor proceeds, the cervix is effaced, the os slowly
dilates, and the bag of waters forms.
The Bag of Waters.—When the cervix is effaced and
only the os remains, the lower end of the egg with its
fluid restrained by the membranes, bulges forward into
the canal. The fœtal head, or breech presses into the
pelvis, and the fluid in the membranes, compressed between
111the presenting part above and the cervix below,
is called the bag of waters.
When the contraction comes on the longitudinal muscular
fibers of the uterus are drawn upward and the bag of
waters becomes tense and pushes farther and farther
down into the opening; and by its even and universal
pressure, mechanically and slowly increases the size of
the opening which the muscular traction is pulling apart.
At the same time, the fluid around the child prevents, for
a time, direct and injurious compression on the body.
When no definite cervical projection can be felt, and
when the teat-like protrusion of the cervix has disappeared,
the cervix is said to be effaced.
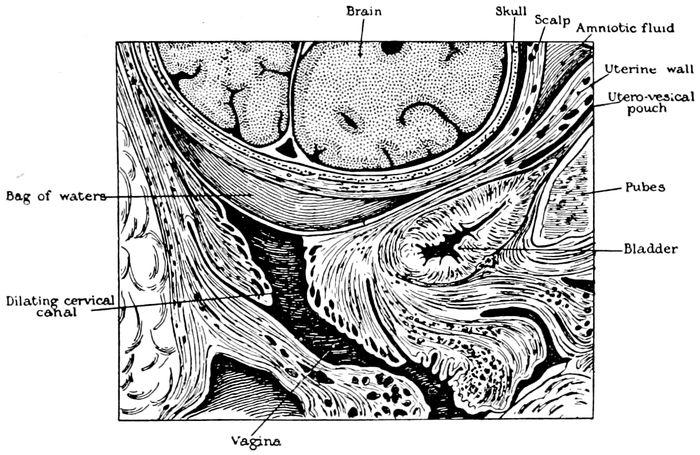
Fig. 35.—The bag of waters begins to act on the cervix. (Eden.)
The os now begins to stretch and widen, the bag of
waters becomes more and more evident, vomiting occurs,
and at last, when the os has expanded to a diameter of
four inches (ten centimeters), the membrane can withstand
the pressure no longer. It ruptures, a certain
amount of fluid escapes, the presenting part comes down
against the opening, and like a valve, prevents the outflow
of the waters from above.
112
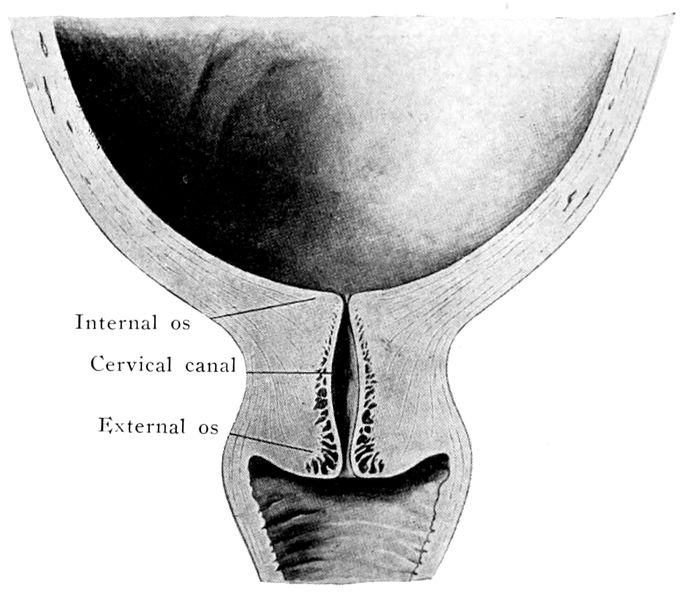
Fig. 36.—The effect of the pains. The cervix before labor begins. (Bumm.)
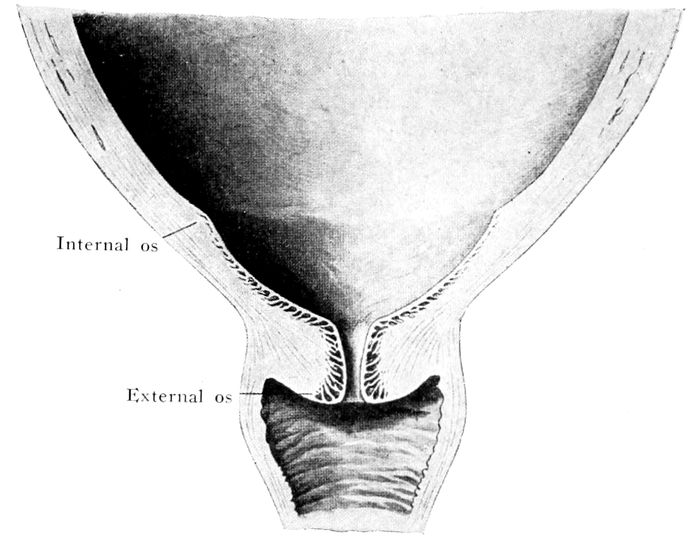
Fig. 37.—The effect of the pains. The cervix begins to be “effaced.” (Bumm.)
113
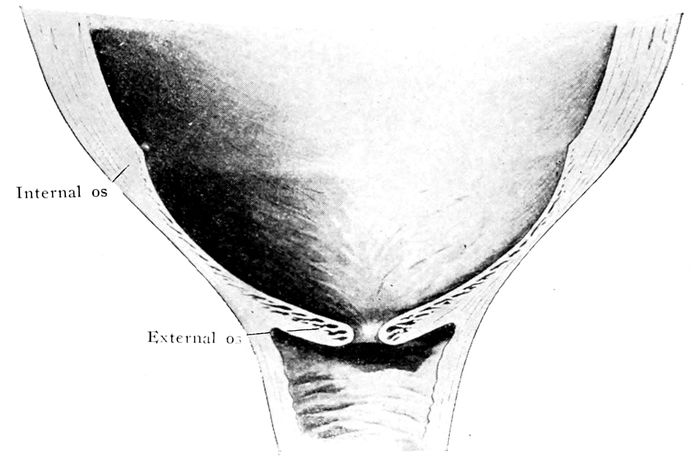
Fig. 38.—The effect of the pains. The cervix is effaced, and the dilatation of the os begins. (Bumm.)
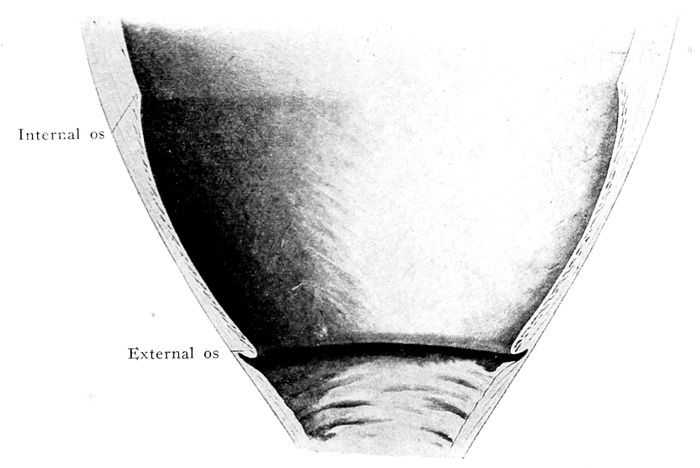
Fig. 39.—The effect of the pains. The cervix is effaced, and the os continues to dilate. (Bumm.)
114Sometimes the labor may be preceded by some hours
(two or three), or days (two or three), even weeks
(two or three), by the rupture of the membrane, and
sometimes when the structure is thick and tough, the
rupture may be delayed until well into the second stage,
or even until the child is born. In the latter case, the
head comes out, covered with membrane. In the old
days, this was called being “born with a caul.” It was
supposed to be a lucky omen, but it was lucky only that
the babe escaped suffocation. The membrane should be
torn open quickly.
The duration of this stage is variable. It is much
longer in primiparas than multiparas. It averages sixteen
hours in the former, and eight hours in the latter.
Vomiting during this stage is quite common, but the
pulse and temperature remain normal. The first stage of
labor is usually under the entire control of the nurse. It
is her responsibility.
With complete dilatation of the os, the second stage, or
stage of expulsion, begins, whether the membranes rupture
or not. The presenting part, usually the head,
passes from the cervix into the vagina. The vagina in
turn gradually dilates from above downward until
uterus, cervix and vagina form a single, wide channel of
the same diameter. The child is driven forward by the
uterine contractions, strongly reinforced by the abdominal
muscles, which the patient uses vigorously. The
onset of each pain is accompanied by a deep inspiration,
followed by straining or bearing down with the abdominal
muscles as in a highly exaggerated bowel movement.
The patient holds her breath, braces her feet,
fastens her hands on bed or attendant, and uses all the
trunk muscles in the effort. The face becomes congested,
115the pulse quickened, she perspires some, and
groans deeply during the contraction. The pain is extreme
and is due partly to the stretching of the vagina
and vulva and partly to the distention of deeper sensitive
structures.
When the head reaches the pelvic floor, the first
change observed in the external genitals is the stretching
(bulging) of the perineal body. Next, the anus becomes
turgid, dilates slightly, the anterior wall becomes
visible, and the hairy scalp of the child appears at the
vulva. The actual expulsion of the head in a primipara is
accomplished by a series of prolonged and severe contractions,
accompanied by violent straining.
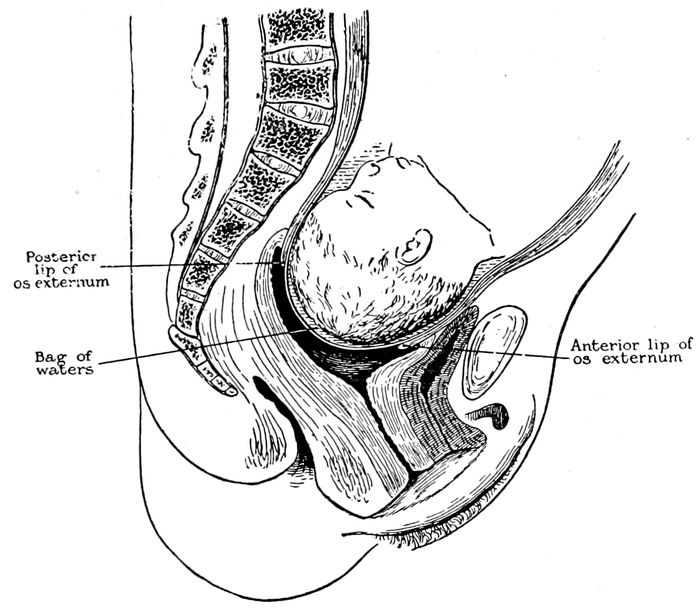
Fig. 40.—The cervix is effaced, and the os dilated. The second stage begins. (Eden.)
116
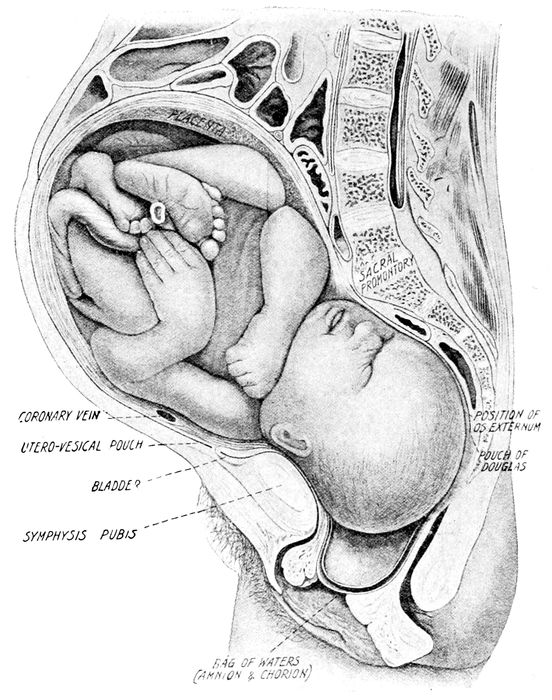
Fig. 41.—Child in second stage of labor with bag of waters unruptured and presenting at the vulva. (Braune, from Barbour.)
A short pause ensues, followed in two or three minutes
by a return of the pains, which expel first the
shoulders and then the trunk. As the body escapes it
is followed by a rush of blood-stained liquor amnii.
This is the fluid that has been pent up in the uterus by
117the obstructing body of the child. The second stage
lasts about two hours in a primipara and from fifteen
minutes to one hour in a multipara.
The third stage is the delivery of the after-birth. The
after-birth sometimes called the secundines, consists of
placenta, umbilical cord, and membranes.
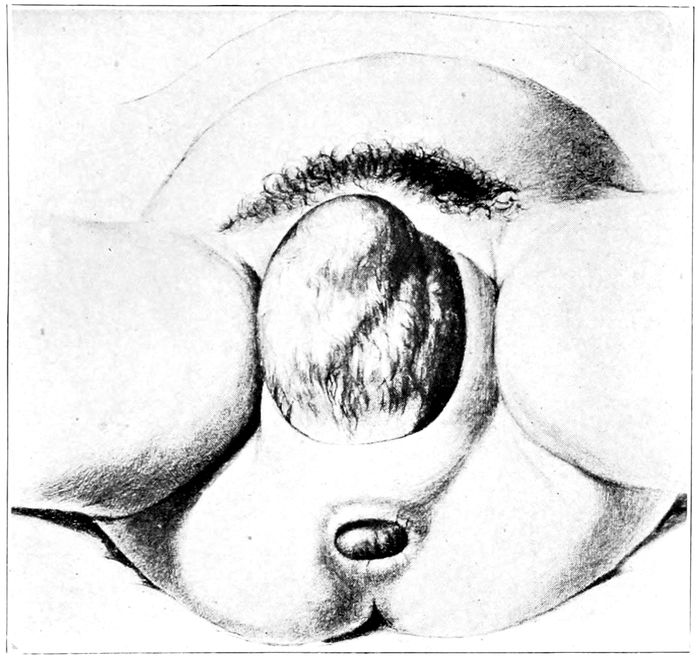
Fig. 42.—The head passing over the perineum. (Bumm.)
After the expulsion of the fœtus, the uterus undergoes
a sudden diminution in size. It is about as large as the
child’s head, and the fundus lies near the level of the
umbilicus. The contractions still persist feebly, but they
are practically painless, and the patient is greatly relieved,
possibly sleeping.
118In from ten to thirty minutes, the uterus becomes
smaller, harder, more globular in shape and more movable.
The patient brings the voluntary muscles of the
abdomen strongly into action again. The nurse presents
a sterile basin and the physician sustains and slowly
twists the membranes free from their final attachment
and out of the uterus. When the placenta passes the
vulva, a moderate sized blood clot follows it.
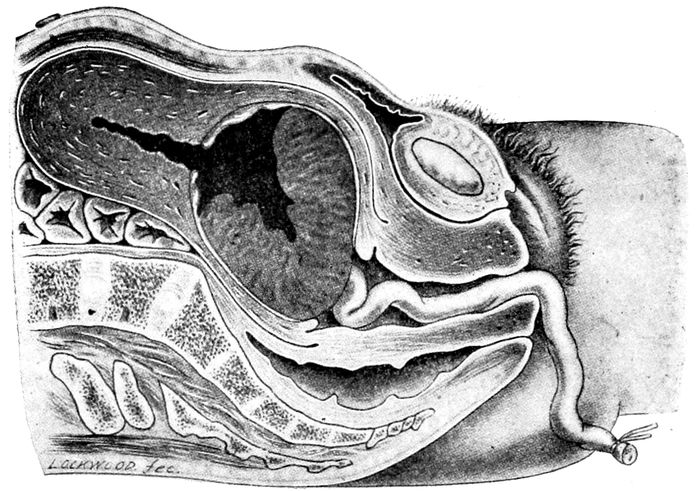
Fig. 43.—Normal expulsion of the placenta like an inverted umbrella according to Schultze. (Williams.)
The uterus is now much smaller, and hard and firm
in consistency, but for some hours the contractions are
intermittent, and while this continues, there is risk of
hæmorrhage.
General Effects.—The mother’s pulse is quickened during
the contraction. The fœtal heart beats more slowly
and feebly during a contraction, but quickly recovers in
the interval.
119The amount of blood lost during labor averages from
ten to sixteen ounces. The temperature may be elevated
one or two degrees in a woman of moderate physique,
while one with a fragile body may present the signs and
symptoms of surgical shock. The chill, pallor, cold
limbs and body, rapid and feeble pulse with subnormal
temperature, suggest to the nurse at once the proper
treatment. Heat, to all parts of the body, warm covers
and hot milk or coffee. If hæmorrhage is present and the
uterus relaxed, the nurse should immediately inject pituitrin
(15 ♏︎) into the deltoid muscle and notify her attending
physician.
120
CHAPTER VIII
THE MECHANISM OF NORMAL LABOR
The powers of labor are primarily the uterine contractions
strongly aided by the muscles of the abdomen
and diaphragm. Some assistance is given by the fixation
of the legs and arms and sometimes by gravity,
when a sitting or standing position is maintained.
The resistances are the bony pelvis and its relatively
soft coverings of muscle and fascia.
The problem is to get the awkwardly shaped passenger
through the curiously shaped passage.
In the first, and a part of the second stage, the uterine
contractions do not act directly upon the body of
the child, for the latter is surrounded by a wall of liquor
amnii.
Pressure is transmitted by a fluid medium in all directions,
hence, the weak part of the wall, which is the
cervix, must give way. While the membranes remain intact,
or when sufficient fluid is retained, no amount of
pressure can injure the fœtus. When the membranes
rupture, the force of the pains is exerted directly upon
the child to drive it forward, and prolonged pressure
may produce injurious effects through compression of
fœtus, placenta, or cord.
The progress of labor is registered usually by watching
the advance of the fœtal head.
The relation of the head to the pelvic brim is of
great importance, as it travels much faster and easier
in certain positions than in others. The term “presentation”
121is used to designate that part of the child which
enters or tends to enter the pelvic inlet.
The presentation is named from the part of the child
which comes into apposition with the brim. Thus, one
speaks of a vertex presentation, or a breech presentation,
or a shoulder presentation. The presentation is determined
externally by palpation.
The vertex presents in 96 per cent of all labors. With
the vertex presenting, the head may occupy any one of
four positions. The term “position” is used to explain
the relation which the most distinctive feature of the
presenting part bears to the quadrants of the pelvic inlet.
Thus, the most distinctive feature or landmark of
the vertex is the occiput, which is the point of direction,
and so again, the position is the relation of the point of
direction to the brim of the pelvis. The point of direction
is the part that takes precedence in the process of delivery.
Thus, in all cases where the occiput is in advance,
the occiput is the point of direction and the position is
called occipital. Where the chin is in advance, it is mental
(mentum is Latin for chin.) In breech cases, the
sacrum is the point of direction.
The pelvis is divided by the transverse and anteroposterior
diameters into four quadrants named respectively
the left anterior, the right anterior, and the right and
left posterior. (See Fig. 1.) Thus, in a vertex presentation
the back of the child may be (and in 53 per cent is)
to the front and to the left.
The occiput is the point of direction, and lies in relation
to the left anterior quadrant of the pelvis, and is
spoken of as a left-occipito-anterior position. Similarly
a right-occipito-anterior position is named, and right- and
left-occipito-posterior positions. These occur respectively
in about 21 per cent, 14 per cent and 11 per cent
of the cases. (Eden.)
122In passing the pelvis, the fœtus not only follows the
curved line of the pelvic axis, but it describes a certain
series of movements which alter its relations to the
pelvis.
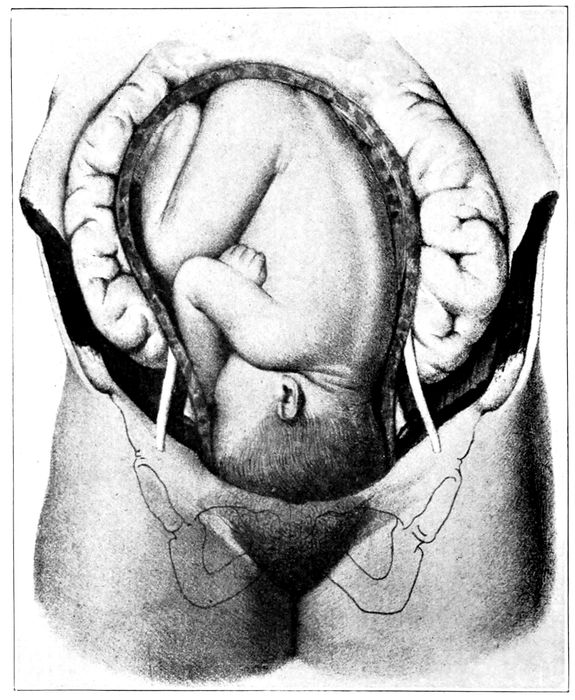
Fig. 44.—The child in left-occipito-anterior position. (Lenoir and Tarnier.)
There are five of these movements: flexion, descent,
internal anterior rotation, extension, and external restitution.
123Flexion.—Flexion is usually present before labor begins.
That is, the head is bent down until the chin
touches the breast. This may be modified by various
conditions, but so far as it becomes extended, the mechanism
is disturbed and the labor complicated, since
large and less favorable diameters are brought to delivery.
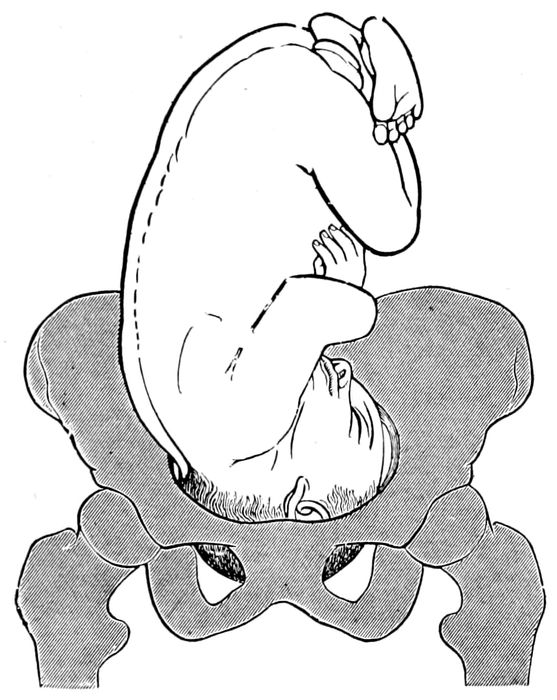
Fig. 45.—The child in right-occipito-anterior position. Shows the flexion of the head intensified at the beginning of labor. (Eden.)
Flexion is increased by pressure against the pelvic
brim as labor begins.
Descent.—As the driving force of the contractions
becomes effective, the head passes the inlet and descends
to the pelvic floor. When the large diameters of the
head (biparietal) have passed the inlet, the head is said
to be engaged.
124
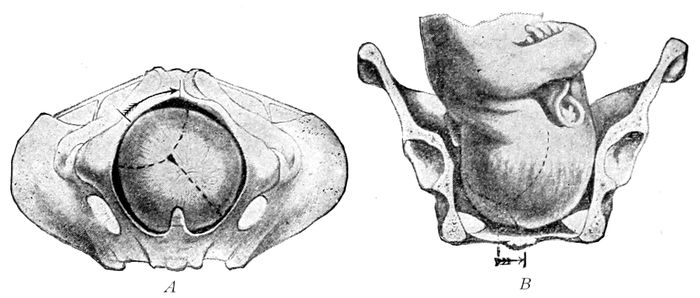
Fig. 46 A.—The descent of the head in right-occipito-anterior position. Seen from below. (Edgar.) Fig. 46 B.—Side view.

Fig. 47.—Internal anterior rotation and extension of the head in a left-occipito-anterior position. (American Text Book.)
Internal Rotation.—The head most frequently enters
the brim with the occiput to the left and anterior
(obliquely) because it finds more room and an easier
passage; but upon passing this strait and entering the
roomy, true pelvis, the head must rotate so that the long
diameter of the head will conform to the long diameter
125of the pelvic outlet, which lies in a direction
just opposite to the long diameter of the inlet or brim;
hence, the occiput turns forward under the pubic arch.
This movement is due largely to the sloping pelvic floor
and the necessity of accommodation between the head
and pelvis as the child is driven forward.
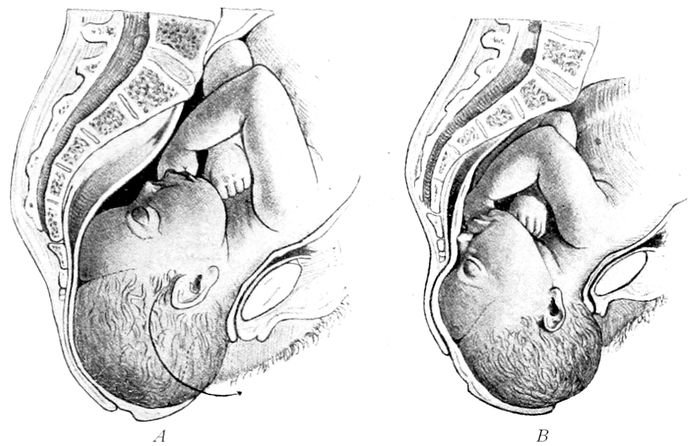
Fig. 48.—Extension. A, the chin leaves the chest; B, extension in progress. (Eden.)
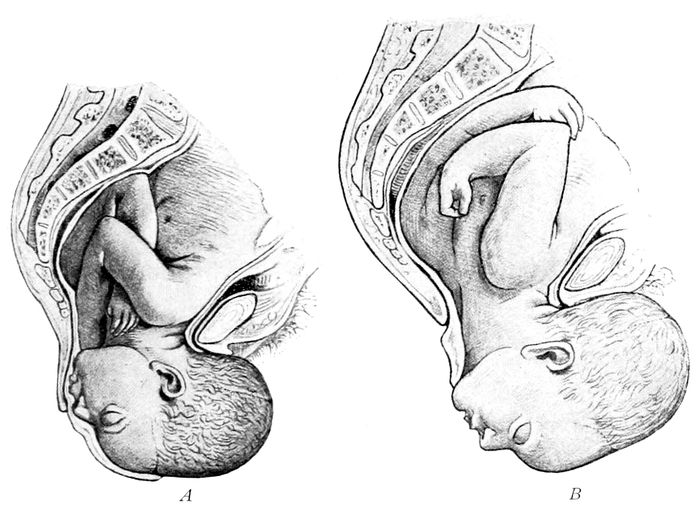
Fig. 49.—A, extension completed; B, expulsion. (Eden.)
126Rotation is much retarded or entirely stopped when
the head is extended instead of flexed or when it enters
the inlet with the occiput posterior instead of anterior.
Extension.—After internal, anterior rotation, the head
emerges at the vulva, the occiput coming out first, then
in succession the vertex, forehead and face and chin.
As the chin rolls out over the perineum, it moves away
from the chest wall—it becomes extended.
External Restitution.—While the head is passing
through the outlet, the shoulders are entering the pelvic
inlet, and so soon as the head is released from the
restraint of the vagina, it naturally falls into its normal
relation to the fœtal back; hence in the position now discussed,
it turns toward the left.
Therefore, we may summarize the mechanism in a
normal left-occipito-anterior position of the head by
saying: The head is flexed and forced into the pelvis.
It descends to the pelvic floor. The occiput rotates to
the front of the pelvis and impinges against the symphysis.
Extension ensues in consequence of the necessity
for an accommodation between the pelvis and the
advancing head, and during this extension, the head delivers
over the perineum. External restitution follows.
The Effect of Labor on the Fœtal Head.—As the head
passes through the canal, it is moulded by contact with
the resistances. The degree of moulding is proportionate
to the pressure required to drive it through. Thus,
in a large head, or a relatively small pelvis, the moulding
may be extreme, and changes in the scalp are common.
127Caput Succedaneum.—Since all parts of the scalp are
in contact with a resistant wall, except in the center of
the birth canal, an effusion of serum takes place here,
which is due to the obstruction of the venous circulation.
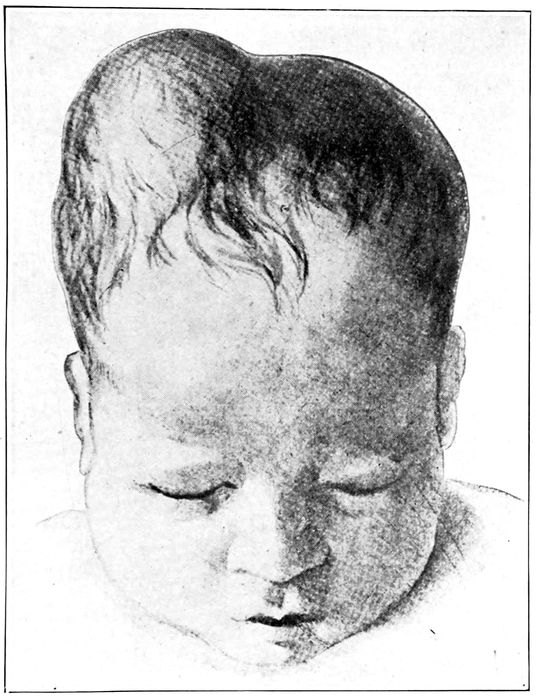
Fig. 50.—A cephalhæmatomata. Do not confuse with caput succedaneum. (Bumm.)
Swelling occurs in the subcutaneous cellular tissue,
and a tumor forms—the caput succedaneum—which
spontaneously disappears in twenty-four or forty-eight
128hours. It is useful in confirming the diagnosis of the
position.
Cephalhæmatoma.—Following labor a tumor is sometimes
found upon the head, which is often confused with
a caput succedaneum.
This tumor is caused by an effusion of blood beneath
the periosteum or the covering of the bone—usually a
parietal bone. It is sometimes single and sometimes
double, and it varies in size from a filbert to a peach.
The swelling never extends across a suture. The effusion
takes place gradually, and may not appear for a
day or so after birth. The cause is unknown, for it occurs
after normal and easy, as well as after difficult,
deliveries, and after breech, as well as vertex, cases.
At first it fluctuates, then becomes hard, and in a
few weeks or months is gradually absorbed. If symptoms
of cerebral pressure develop, it must be remembered
that hæmatoma may occur inside as well as outside
the cranium.
No treatment is necessary. Puncture is inadvisable.
In extremely rare instances the tumor may suppurate
and require incision.
129
CHAPTER IX
THE CARE OF THE PATIENT DURING NORMAL LABOR
Every case of labor must be conducted with the most
scrupulous attention to surgical cleanliness on the part
of the patient, doctor and nurse. Puerperal infection
in most cases is due to the introduction of disease-producing
microbes into the wounded genital canal. To be
sure, the successful enforcement of surgical cleanliness
is attained only in good hospitals, but it can be approximated
in a private house if the patient insists upon delivery
at home.
A nurse or doctor who is clean of person, is most
apt to have an “aseptic conscience.” The possession
of such a conscience may entail financial sacrifices, but
it has many compensations. Neither the nurse nor the
doctor is doing justice to the patient, nor to the profession,
who indiscriminately takes pus cases, contagious
diseases, and confinements. The public will soon learn
that such a nurse and such a doctor are unsafe attendants.
How may the nurse know that the patient is in labor?
This is the final assumption that must be confirmed or
refuted when the nurse is called to her case. It is
ascertained partly by the history and partly by the
conditions found.
Thus, the patient may report the passage of a piece
of blood-stained mucus, and the nurse will observe
that the contractions of the uterus are regular, rhythmical
130and painful. She will observe that when the patient
complains of pain, the uterus gets hard. She will
also observe the definite regularity of the contractions
by timing them.
Under such conditions, the doctor should be called
at once if the symptoms develop between 7 A. M. and
11 P. M. If the pains begin in the night, say from 11
P. M. to 7 A. M., the doctor need not be called unless he
has requested it, or, unless in the judgment of the nurse
or the anxiety of the patient, it is desirable for him to
see her.
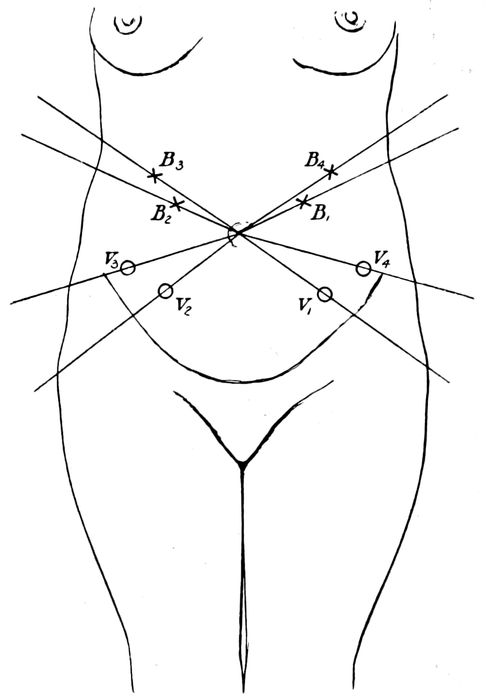
Fig. 51.—Points of greatest intensity of fœtal heart tones. V, vertex presentations; B, breech presentations. (Eden.)
131When the doctor is notified he will want to know, and
the well trained nurse will be able to inform him, when
the pains began, their strength, duration and frequency.
He will want to know whether or not the membranes
have ruptured. Many doctors also require, and a well
trained nurse who specializes in obstetrics should be
able to say by external examination, whether the head
seems high or low, as well as the position and frequency
of the fœtal heart tones.
In the hospital the following rules for summoning
the resident physician may be found useful:
1. For multipara, when pains are regular and five minutes apart.
2. For primipara, when pains are regular and two minutes
apart, or when head is visible if pains are less frequent.
3. If a precipitate is imminent, delivery must be delayed
until arrival of attending man by—
(a) Turning patient on side with legs straight;
(b) Instructing patient to breathe deeply or to cry out
with mouth wide open; then
(c) Place sterile towel over vulva, and at time of pain
prevent expulsion by compressing the head by
means of locking the hands over a towel on the vulva.
It is possible thus to delay delivery two hours, or
until the doctor arrives. Do not permit a precipitate.
After the nurse has completed her preliminary observation,
she starts her history, notes the character
of the pains, the pulse, temperature and respiration. All
unusual phenomena should be recorded; and after the
visit of her attending man, his examination, if any, and
the conditions found, are put down. Then she prepares
the patient and sets up the room for the delivery.
Preparation.—As soon as the patient is known to be
in labor, the bowels are thoroughly cleansed with a soapsuds
enema. A toilet jar should be used and not the
132water closet. The bladder must be emptied at the time
of preparation and at frequent intervals throughout the
labor. As soon as the bowels and bladder are emptied,
the patient is given a bath and thoroughly soaped. The
shower is preferred lest the water, contaminated by
bacteria from the skin and external genitals, should enter
and pollute the vagina.
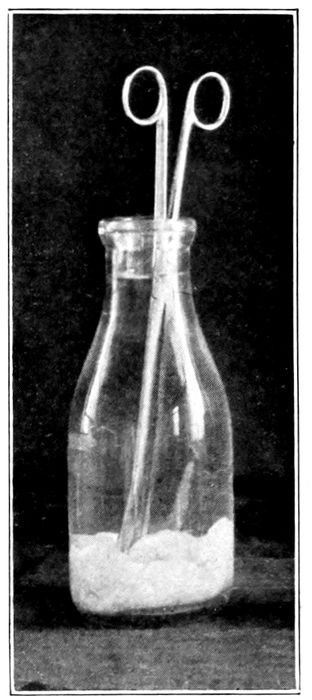
Fig. 52.—Handling forceps, kept sterile in a jar of alcohol.
The hair should be braided in two braids. The vulva
and perineum are shaved. No patient will object to this
when its importance as a feature of protection against
blood poisoning is explained to her.
Scrub thighs, hips, and abdomen as far as the navel
with soap and warm water, then sterile water, followed
133by a 2 per cent solution of lysol. Care must be taken
to remove the smegma and dried secretions from the folds
of the vulva. Put on a fresh pad, a clean gown, and
long stockings. A loose wrapper over all permits the
patient to move about. (See Chapter XXIII.)
Guests are forbidden, and the immediate family is
kept at a distance—if possible.
An air of buoyancy, composure, and competence
should prevail in the sick room, and the patient should
be cheered and encouraged in every possible way.
During the first stage, the patient may be up and
about, as this diverts the mind. She may assist in the
arrangement of the room which should always be the
best room in the house. It should be well warmed and
close to the bathroom. All unnecessary furniture and
hangings should be removed, as previously described.
After the room has been put in order, the bed is made.
Making the Bed.—Put mattress pad over mattress and
cover with rubber sheet or oil cloth, and spread a sheet
over all. Then a smaller rubber sheet is put on, extending
from under the pillows to a couple of feet from
the foot. A plain muslin sheet goes over the rubber,
then the delivery pad.
When the bed is ready, a small table or stand should
be placed near the head, on which is put the anæsthetic,
the mask and the oil or cold cream. The patient may be
lightly covered with a sheet or a sheet and blanket.
During the first stage, light and easily digested food
and drinks may be served, either cold or hot, as the patient
prefers.
When the doctor arrives he may want to examine the
patient either externally or internally, or both. So a
sheet is thrown across the lower part of the body and
the night-dress pulled up as far as the breasts.
134For the external examination the doctor washes his
hands in warm water and green soap and scrubs with
the nail brush for five minutes. This period should be
prolonged to fifteen minutes, if, by any mischance, the
hands have been in contact with pus or infectious material.
It is extremely difficult to get them even approximately
clean after such an experience.

Fig. 53.—Palpation. What is in the pelvis? (Eden.)
He now palpates the abdomen, notes the location of
the head and back, finds and counts the heart tones,
measures the pelvis and child, estimates the descent of
the head and the character of the pains.
135
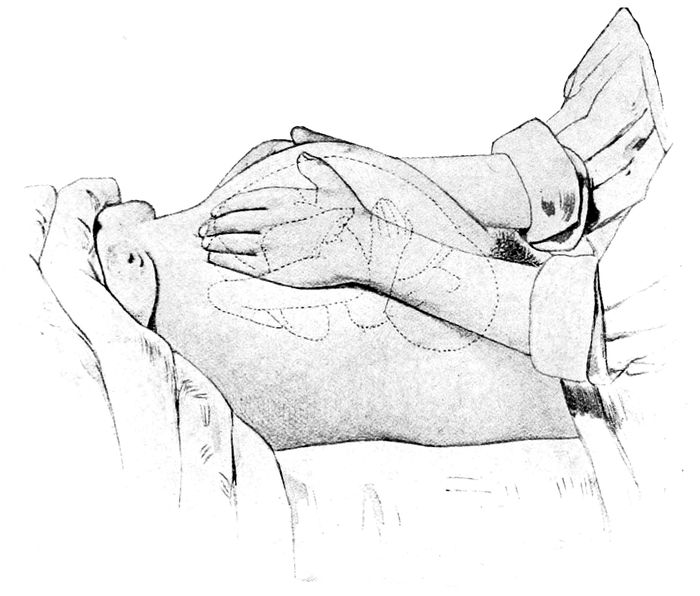
Fig. 54.—Palpation. What is in the fundus? (Eden.)
If he thinks an internal examination is necessary, he
will now return to the bathroom, pare and clean his
nails, scrub hands and arms to elbows for ten minutes
in running water with green soap and a sterile brush,
soak the hands in lysol solution 0.5 per cent for five minutes.
Bichloride of mercury solutions have no place in
obstetrics. They ruin instruments and hands, and are
valueless for asepsis since the mercury unites with the
albumin of the mucoid discharges and forms an albuminate
of mercury, which is inert. The bichloride
solutions also are nonlubricating, harsh and astringent,
as well as poisonous, as soon as the mucoid protection
has been removed. When the doctor takes his hands from
the lysol solution, they should be wiped on a sterile towel.
A sterile gown is put on, if possible. If it is not available,
he should be careful not to touch anything that
may destroy or contaminate his preparation. The hands
136are powdered and sterile rubber gloves pulled on (one
will do.).
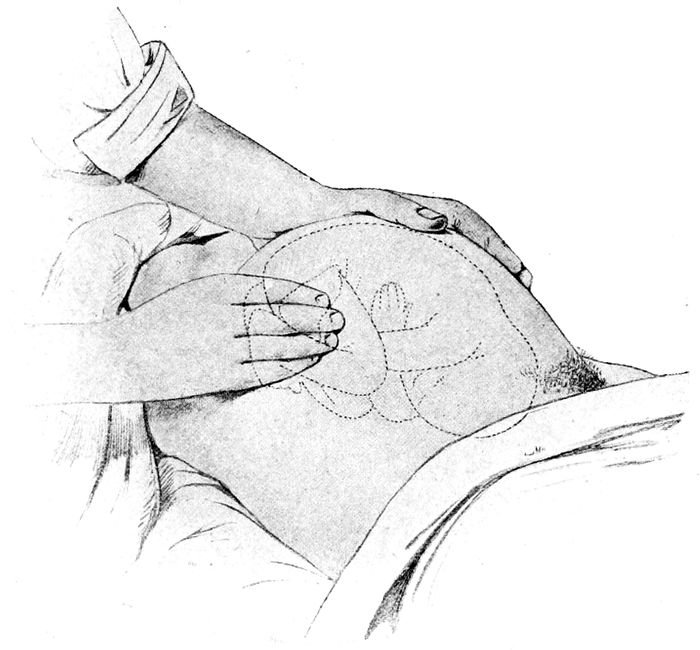
Fig. 55.—Palpation. Where is the back? Where are the small parts? (Eden.)
The nurse, meanwhile, has wrapped the legs of the
patient in the ends of a sterile sheet, the bulk of which
covers the abdomen. The knees are spread apart. The
vulva cleansed with pledgets of cotton soaked in lysol
solution. One or two pledgets are used on either side
of the vulva and the same number for cleansing the introitus.
The fingers are now introduced.
The internal examination may be conveniently postponed
until the waters break, or it may be omitted altogether
137if the heart tones of the child remain good, the
labor progressive, and the head continually advances
into the pelvis, as determined by the external examination.
The great advantage of an internal examination
at this time is the diagnosis of the degree of dilatation
and the assurance that the cord has not been washed
down into the vagina by the rush of fluid.
If the first stage is prolonged, the nurse should try to
get the patient to rest, and she should herself snatch a
few moments of repose if possible.
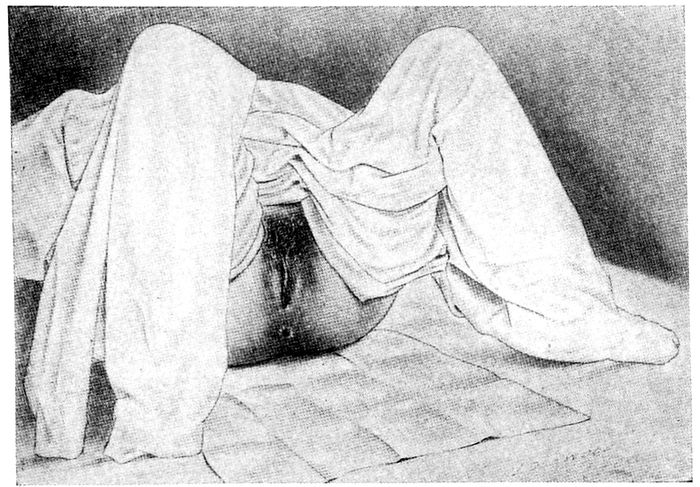
Fig. 56.—Patient draped for internal examination. (Williams.)
The condition of the os and the character of the pains
may make the doctor feel safe in leaving the house,
but his whereabouts and telephone number should be
ascertained and the exact time of his return.
Second Stage.—During this stage, the patient should
go to bed and the doctor should remain nearby. The
138nurse may observe the vulva at intervals and note bulging,
if present, or she may press a finger against the soft
parts outside the labia and see if the hard resistant head
has come into the outlet.
The pains are severe and all accessory muscles are
called into action. Partial anæsthesia should be maintained
in most cases, which should merge into complete
narcosis as the head passes the vulva. The nurse may
have to administer this.
When this stage begins, or is well under way, the
patient should be prepared. A sterile pad should be
placed under her, then a sterile bed pan. The nurse
having prepared her hands and arms as previously directed
for the doctor, scrubs abdomen, legs, and vulva
with green soap and warm water, followed by lysol solution
0.5 per cent and a rinsing with sterile water.
The cleansing of the patient should take about ten minutes.
Cover with a sterile towel and put on the sterile
linen.
If in the hospital, the drums have been packed for
sterilization so that when they are opened each article
will appear in the order of its need:
No. 1. (Beginning at the bottom.) A receiving blanket, which has a ticket, marked with the weight of the blanket, attached to it.
1 abdominal binder with pad holder attached.
1 pillow slip folded half way back.
1 gown for patient.
2 surgeon’s gowns.
3 sheets.
1 pair surgical stockings folded half way.
1 surgeon’s gown for nurse.
No. 2 contains cotton pledgets.
No. 3 contains strips of gauze and combination pads.
Application of Sterile Linen—Normal Case.—Sterile
linen is to be applied as follows, by a clean nurse;
- 1.139
- Lay sheet across foot of bed and half way up.
- 2.
- Put surgical stocking on one foot and draw sheet up for foot to rest upon.
- 3.
- Second foot as above.
- 4.
- Lay sterile sheet across bed under patient, letting ends hang.
- 5.
- Lay sterile sheet over abdomen of patient.
In many hospitals the sterile stockings and protective
sheet are all made in one piece, which greatly simplifies
the application of the linen.
As soon as the second stage begins, the packet containing
the perineorrhaphy and cord set, carefully sterilized,
is brought out and placed in convenient reach of
the doctor.
This set contains—
8 in. forceps.
2 scissors curved on the flat.
1 dissecting forceps.
1 duck bill speculum.
1 needle holder.
1 metal catheter.
8 gauze sponges.
1 medicine dropper.
1 cord clamp, or
2 cord tapes.
2 case numbers, attached.
12 needles, 4 round, 4 half-curved cervix needles, and 4 skin needles.
This is the stage of expulsion and the patient may
want to pull or push on something to aid the straining
effort. Unless the nurse needs time to set up the room
or to get the doctor, this tendency may be encouraged.
A sterile sheet may be attached to the foot of the bed
and the ends (corners) given into the patient’s hands
as a knot or loop to pull on, or she may push upward
against the head of the bed. Under no circumstances
must she be permitted to touch or contaminate the clean
140linen in her movements, either consciously or unconsciously.
The hands should be restrained, if necessary,
to avoid this.
The face may be sponged and a cold towel laid across
the eyes. Rubbing of the back and legs will bring great
comfort, and cramps of the limbs may be removed by
straightening the legs and rubbing the muscles underneath.
Everything is now ready for the delivery. If
the husband insists upon being in the room, he should
take off his coat and vest and wear a gown, or if the
labor is in the home, drop a clean night robe over his
clothes.
The prepared room will show at close hand-reach, the
basins of solutions, the pledgets of cotton, tape or clamp
for cord, scissors, nitrate of silver solution (1 per cent)
for the eyes, with dropper, the sterile douche can in
readiness for hæmorrhage and a large reserve of supplies.
Whatever anæsthetic has been chosen for the
second stage, is now administered. Throughout this
stage, the heart tones of the child must be watched, as
well as those of the mother, for intra-partum death
may occur at any moment.
A second examination may be desirable now to confirm
the diagnosis and to secure an estimate of the
advance. As a rule, the examinations should be as few
as possible on account of the danger of infection.
This is the period of greatest responsibility for the
doctor whose duty it is to watch and, if necessary, to
restrain the advance of the head in order to protect
the perineum from rupture.
This may be done at times most successfully, or in the
case of too few assistants, most desirably, by delivery
on the side. To secure this, as the head becomes more
and more visible, the woman is turned upon her left
141side; a pillow rolled tightly and pinned in a sterile
covering is placed between the knees, and a sheet flung
across the body.
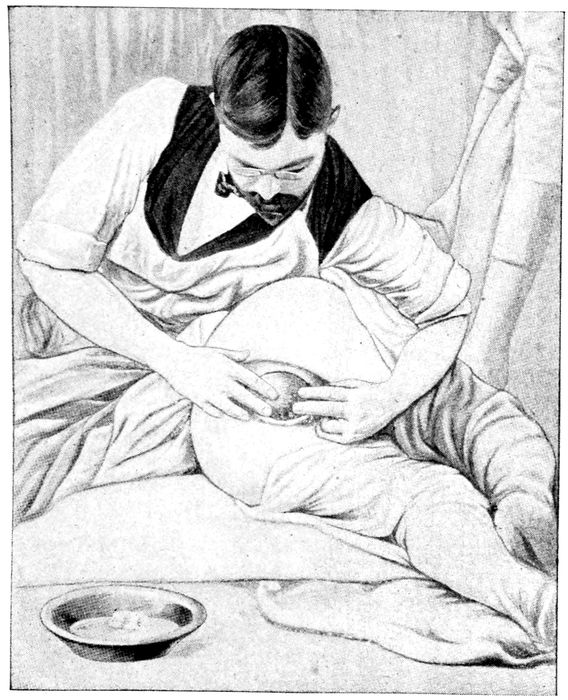
Fig. 57.—Delivery in side position. The hands should be gloved and the upper leg raised on a hard cushion or pillow. (American Text Book.)
The hips must be brought to the edge of the bed
while the chest and head are pulled over to the other
edge of the bed, leaving the legs just enough space to
142double up along the side of the bed parallel with its
long axis.
The doctor may now sit on the edge of the bed, or
on a high stool at the back of the patient and facing
the buttocks. This is a most convenient and easily managed
position.
As the head is born, the fæcal matter, blood and discharges
must be sponged away, and the field kept clean,
with the whole perineum visible. Always sponge from
vagina toward rectum and throw away the sponge.
Should the hand touch nonsterile things or septic material,
like fæces, the glove must be changed. The
hands must be kept surgically clean.
It is a part of the nurse’s duty tactfully to warn the
doctor when such a thing occurs, as it may happen accidentally
while his attention is concentrated elsewhere,
and a conscientious man will be grateful for the information.
As the head passes the perineum the anæsthesia
should be deepened.
As soon as the head is born and the first respiration
established (see Asphyxia, p. 278), the cord is cut and
clamped. There is rarely any necessity for haste in this
maneuver. The eyes are treated, and if in a hospital, a
numbered tape is tied about the wrist and a tape with a
corresponding number about the mother’s wrist.
The baby is now placed in the receiving blanket on
its right side, with artificial warmth at its back and
feet. The head must be lower than the body so any retained
mucus can drain out of nose and mouth. Meanwhile,
the doctor (or nurse) keeps a hand on the fundus
of the uterus to watch its contraction, see that it does
not balloon up, and massage it occasionally if necessary
while he awaits the onset of the third stage.
Third Stage.—The patient is turned upon her back as
143soon as the child is delivered. The pulse and face must
be watched for signs of hæmorrhage. While waiting for
the placenta, the perineum is examined to note the degree
of laceration, if any. To do this, the vulva must be
spread apart with clean fingers so as to bring the posterior
wall into view, and the discharge is sponged away
with cotton pledgets taken from the lysol solution and
squeezed dry.
The patient may now have the saturated dressings removed
and clean, dry ones substituted. The new pads
catch the oozing blood and give an estimate of its
amount.
At this time, if desirable, the perineum can be repaired.
The woman is partly unconscious, the tissues
numbed, and the needle hurts much less than it will
later. Nevertheless, anæsthesia may be required.
In a period varying from a few minutes to an hour,
the hand on the uterus will note a hardening, the mass
will become smaller, more globular, and rise slightly in
the abdomen. A gush of blood appears at the vulva
and usually the placenta follows. If it does not, or if
hæmorrhage or the condition of the mother requires it
earlier, the uterus may be compressed (see Credé expression)
and the placenta constrained to deliver.
The nurse holds a sterile basin for its reception. As
the mass drops into the pan, the membranes drag after
and it should be gently twisted, or the loose portions
drawn upon until the end slips out. The placenta is set
aside for examination, and ergot or pituitrin may be
given to enforce the uterine contraction. The process
of expulsion is generally assisted by a strong voluntary
contraction of the abdominal muscles.
After a short rest, the blood is washed off the genitals,
clean linen and clean pads applied, and the abdominal
144binder or girdle is put on to hold the pads. Warm
blankets are thrown over the patient and within an
hour, a glass of hot milk is administered.
The legs should be kept together, and in case of hæmorrhage,
the feet crossed.
The placenta is now inspected and not only its completeness
or incompleteness noted, but anomalies of every
kind should be looked for.
IMMEDIATELY AFTER LABOR
Perineorrhaphy must be done if required.
A lacerated cervix is not to be repaired at this time,
except in case of hæmorrhage, for the tissues are greatly
swollen, and if sutures are put in tight enough to allow
for sufficient shrinkage, they will cut through; while if
not tight, they will be useless in twenty-four hours.
Care of Mother.—
- 1.
- Cleanse genitals with lysol solution 0.5 per cent from above downward.
- 2.
- Put on sterile pad, with pad holder and binder.
- 3.
- Wash face and hands.
- 4.
- Take temperature, pulse, and respiration.
- 5.
- Glass of hot milk.
- 6.
- Keep on back four hours. Watch uterus for hæmorrhage and keep firm by occasional massage.
- 7.
- Put tape with case number on arm.
Care of Child.—
- 1.
- Clamp for the cord.
- 2.
- Place on right side with head lower than breech.
- 3.
- Keep warm and watch for cord hæmorrhage.
- 4.
- Treat eyes with silver nitrate solution 1 per cent, or argyrol solution, 15 per cent. Do
not neutralize the 1 per cent silver nitrate solution.
- 5.
- Put tape with case number corresponding to mother’s on arm.
145To preserve the perineum from rupture is an important
duty, and in a definite percentage of cases, unsuccessful.
Nevertheless, it is a duty, which, in the absence
of the doctor, may fall upon the nurse. How shall she
meet it?
The greatest danger to the perineum comes from a
too rapid advance of the head; hence, the nurse retards
the delivery by putting the woman on her side where
she can not bear down so successfully, and instructs her
to cry out with her pains. She may also delay the labor
by holding the head back with a clean pad until the
vulva stretches to its fullest capacity.
The rules which the doctor follows in protecting the
perineum as the head advances, may be thus summarized.
- 1.
- Deliver the patient on her side.
- 2.
- Maintain flexion of head.
- 3.
- Delay extension of the head.
- 4.
- Give chloroform to retard delivery and to prevent precipitate delivery.
- 5.
- Deliver between pains, if possible, by Ritgen’s maneuver (modified).
- 6.
- Do episiotomy, if necessary.
Perineorrhaphy.—Lacerations of the perineum occur
in about 30 per cent of all primiparas and in from 10 to
15 per cent of multiparas. They occur when the child
is large or too rapidly delivered, and when the orifice
is small or the tissues inelastic.
For convenience, the lacerations of the perineum are
divided for description into three degrees.
The first degree involves only the fourchette and a
small portion of the mucosa. It is rarely more than one-half
an inch in depth and requires no attention except
cleanliness by the nurse.
The second degree may tear a variable distance into
146the perineal body, sometimes so deeply as to expose the
sphincter ani. It is usually on one side, but may appear
on both sides, and be accompanied by prolongations
into the vagina.
The third degree passes through the sphincter and
sometimes well up the rectal wall. This is also called
a complete tear.
The lacerations of the perineum which require sutures
should be attended to at once unless the patient’s condition
is critical. In such cases the repair may wait
from twelve to twenty-four hours.
For this operation the nurse will assemble and boil
for fifteen minutes:
2 pairs of scissors.
2 tissue forceps, one with teeth and one without.
1 bull-dog forceps.
3 artery forceps.
6 needles, 3 full and 3 half-curved.
1 dressing forceps.
1 needle holder.
Suture material of catgut and silkworm gut should
be ready in sterile containers. The catgut should be
the twenty-day chromicized, No. 3 and 4. Even then the
strands are quickly absorbed when the lochial secretions
flow over them.
Silkworm gut is better, but hard to remove from the
vagina; hence it is customary to use catgut inside the
vagina and silkworm gut for the sutures outside.
The nurse renews the supplies of gauze and cotton
sponges. Hot solutions are prepared, and the patient
brought into a position on table or across the bed so
that the best light may be had. The legs may be held by
the husband or nurse, or both. If help is inadequate, a
sheet sling can be utilized. This is made by twisting
147the sheet from corner to corner and passing it rope-like
over the shoulders, and back of the neck. Then each
end is tied above the patient’s knee on either side as the
legs are flexed in an exaggerated lithotomy position.
The sutures are now introduced and tied loosely from
below upward and from within outward. If tied too
tightly, they will cut through. The success of the operation
depends on two things: the care with which the
levator ani, if torn, is found and restored; and the
scrupulous cleanliness obtained by the nurse in her
after-care. If the stitches become sore, a few drops of
sterile glycerine should be applied with an applicator.
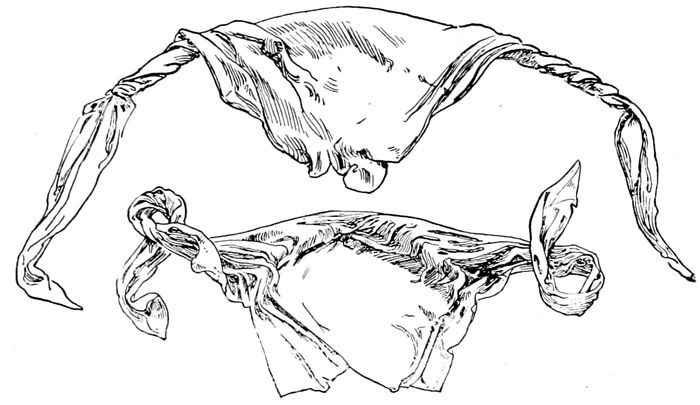
Fig. 58.—Sheet twisted into a sling. The patient lies on the unrolled portion. The rolled cords bearing against the shoulders are tied to the legs below the knees. See Fig. 102. (American Text Book.)
If catgut is used inside the vagina, the counting of
the stitches is gratuitous, since they absorb without removal.
If silkworm gut is used, the number of sutures
must be recorded, lest one be overlooked in removal.
Binding the legs together after repair is not required,
but the sutures must be given aseptic care after each
148bowel movement, each urination, and when the pads are
changed, if they have become contaminated. The sutures
are removed on the tenth day.
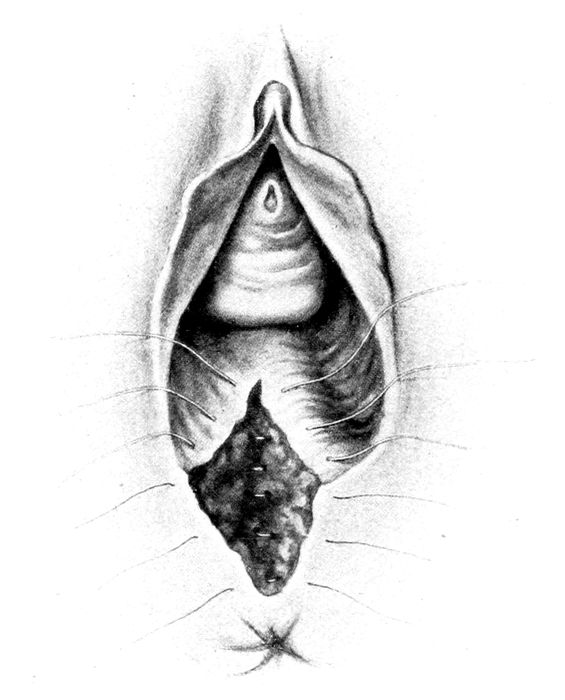
Fig. 59.—Repair of perineum. Sutures in place. (Hammerschlag.)
After complete tears, the bowels are kept constipated
for two or three days, and then moved with a high enema
of sweet oil, followed by castor oil by mouth. After the
bowel movement, the nurse should wash out the rectum
with normal saline solution. The nurse must look carefully
at the stitches every time the pad is changed and
note if the swelling is increasing or diminishing, if
149there is irritation or tenderness, or if they are cutting
out through the tissues.
The external sutures are usually left long and tied together
in a knot, to prevent the ends from sticking into
the patient. If she complains of this, the ends may be
wrapped in sterile gauze. During the progress of the
case the nurse must watch for and report any sign of
fluid passing from bowel through the vagina.
The perineorrhaphy being completed, the woman is
permitted to rest though the nurse will make frequent
examinations of pulse and respiration. She will note
the look of the face and the hardness of the uterus.
The pad should be watched and the amount of blood
discharged, duly estimated. If the flow does not diminish
or if the uterus should balloon up, the doctor
should be notified and the nurse meanwhile should give a
dram of ergot (fluid extract) by mouth or an ampoule
of aseptic ergot hypodermically.
The doctor should remain within call of the patient
for at least an hour after delivery.
In the hospital the following rules may be used as
a concise guide for the conduct of the third stage:
Conduct of Third Stage.
Keep patient on back and keep a hand on fundus. Note
amount of blood lost, its character, its flow, and whether
steady or in gushes. The placenta should detach itself
normally in thirty minutes. After thirty minutes, expulsion
may be assisted by—
(1) Early expression.
(a) Massage, rub and knead the uterus, until it
hardens under the hand.
(b) Seize contracted uterus by fundus with full hand,
fingers behind and thumb in front.
(c) Push slowly but firmly toward the pelvic outlet.
150(2) Credé expression.
Same maneuver as above, except that the fundus is
compressed between thumb and fingers while the
downward movement is progressing.
Conditions for Credé expression:
(a) Uterus must be contracted.
(b) Uterus must be in median line.
(c) Bladder must be empty.
If not successful, wait ten minutes and then repeat maneuver.
Never make traction on the cord. Never use ergot
until uterus is empty.
If placenta does not come away within an hour, manual
removal must be considered. In case of hæmorrhage, it
must be removed at once.
Carefully inspect placenta and be sure it is complete. (See
Post Partum Hæmorrhage, p. 232.)
When the patient is put to bed, the bloody sheets and
towels are put to soak in cold water, and after several
rinsings, may be sent to the laundry. Drapings stained
with fæcal matter must be cleansed separately.
151
CHAPTER X
THE NORMAL PUERPERIUM
The puerperium is the name given to the period succeeding
the birth of the child as far as the time of the
complete restoration of the genitals. It may last from
six to ten weeks, or even longer if complicated.
When the labor is completed, the most urgent desire
of the patient is for rest. She is thoroughly exhausted
in nerves and body. A post partum chill may appear,—a
slight shiver that may last a quarter of an hour. Since
the pulse and temperature remain unaffected, this phenomenon
may be regarded merely as a sign of prostration
or nervous revulsion.
In the course of the first three days, the temperature
may rise to 100° F. in a case entirely normal. It has no
pathological significance unless persistent or increasing.
The temperature should be taken night and morning,
and in complicated cases every four hours. All temperatures
over 100° F., after the initial rise and descent
just described, must be regarded as septic.
The pulse does not rise with the temperature of the
first three days, but remains firm or even falls a little.
When the pulse rises and the temperature sinks, it means
hæmorrhage.
The urine is usually increased for the first few days
and then returns to the normal for that patient. The
labor affects the patient like a surgical operation.
The digestion is disturbed. The appetite is gone, and
152the stomach must be treated gently until its tone is
restored. The body in repose is less urgent in its demands
for food. Liquids in abundance form the staple
diet for the first two days. For the next three days,
semisolids may be added, and after the milk is well established,
a general diet is desirable; but so long as the
mother nurses her child, the liquids must preponderate
in most cases.
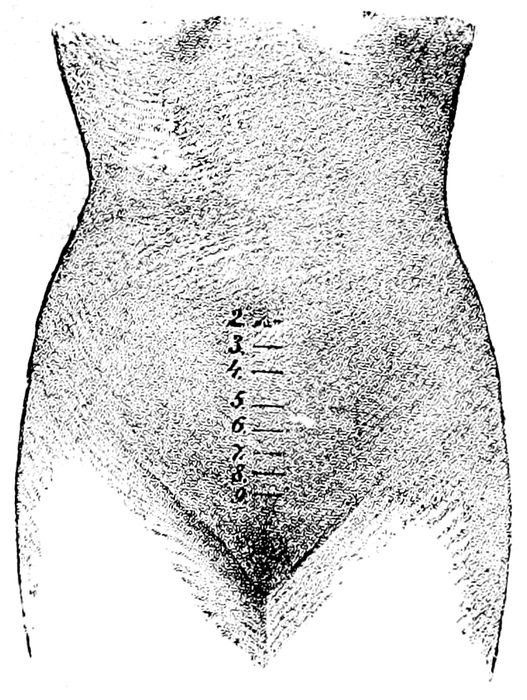
Fig. 60.—The progress of involution on the various days of the puerperium. (von Winchkel, from Knapp.)
Meanwhile, certain changes are taking place in the
pelvis that are highly important.
Involution is the process undergone by the uterus in
returning to its normal nonpregnant state. This shrinkage
can be followed abdominally and is registered by the
nurse in the number of finger-breadths or centimeters
above the symphysis pubis.
153Edgar gives the rate of shrinkage as follows:
| After delivery, |
5.92 in. long, or |
15.8 cm. |
| 2nd day, |
4.63 in. long, or |
11.30 cm. |
| 3rd day, |
4.37 in. long, or |
11.10 cm. |
| 6th day, |
3.42 in. long, or |
8.48 cm. |
| 8th day, |
2.55 in. long, or |
6.40 cm. |
| 10th day, |
2.22 in. long, or |
5.60 cm. |
The rate of involution not only varies greatly with
different women, but varies much after the different
labors of the same woman.
Ordinarily at the end of the first week the fundus
should lie midway between the navel and the pubes,
and should shrink rapidly thereafter.
The necessity for watching the rate of involution is
imperative for a number of reasons. If involution is
slow, or stops, it may indicate fatigue of the muscle
from multiparity or over-distention (twins, hydramnios,
etc.) or it may follow a post partum hæmorrhage. Subinvolution
may also indicate infection, the retention of
clots, or pieces of placenta. It happens also when the
woman gets up too soon or does not nurse her child and
thereby delays the restoration of her waistline, as well
as diminishes her resistance to disease.
The binder is objectionable to some doctors on the
ground that it favors retroversion of the uterus during
involution.
This would be a plausible theory when the uterus
is high, if it were not that the vertebræ of the patient
and the pelvic brim keeps the uterus from being pushed
out of its place and after the uterus descends into the
pelvis the gentle pressure of the binder evenly distributed
over the abdomen can not affect it appreciably.
Furthermore, the uterus in involution shows a persistent
tendency toward anteflexion and anteversion.
The binder is merely a girdle put on just tight enough
154to hold in place the bandage that supports the perineal
pads and to allow the patient more easily to grow accustomed
to the sudden change in intraabdominal pressure
which the delivery of the child creates. However,
if the doctor objects to a binder, it may be left off with
safety.
The Lochia.—When the placenta is delivered, the
uterus normally closes down and all gross hæmorrhages
cease; but for the next two weeks or possibly longer, a
vaginal discharge continues. For the first few days it is
hæmorrhagic in character and it is called lochia rubra,
and consists mostly of fluid blood with occasional small
clots. By the fourth day, usually it has become brown
and thinner. It is now called lochia serosa. By the
tenth day, it is yellowish-white, and is called lochia alba.
The lochia is the wastage from the shrinking uterus,
and is made up of red blood corpuscles, epithelial cells,
leucocytes, and pieces of broken-down deciduæ. The
entire lining of the uterus is loosened, discharged and
a new one formed during the puerperium. The lochia is
regularly infected by bacteria in the vagina. If involution
is slow, the lochial discharge may be prolonged.
The After-Pains.—The puerperium is not infrequently
accompanied by painful contractions of the uterus called
after-pains. These are more common in multiparas and
serve a useful purpose in maintaining a definite contraction
of the uterus.
If the pains are at all severe, they are a suggestive
symptom of the retention of blood clots, a fragment of
placenta, or of membrane. This, of course, will occur
either in a primipara or multipara. In all cases the
after-pains must be differentiated from gas and from
the pains of pelvic inflammation.
Gas pains can be relieved by hot spiced drinks, asafœtida
and the high rectal tube.
155Subinvolution is treated by the administration of fluid
extract of ergot, in twenty to twenty-five drop doses,
three or four times daily. This will bring about the discharge
of the irritating fragment or clot, and the nurse
can aid the process by gently massaging the uterus
several times daily or by giving a hot vaginal douche.
Codeine may be used for after-pains if absolutely necessary.
Diet in Normal Cases.—There is no restriction on the
kind of food the patient may take, so long as she can
digest it cleanly and without gas. Acids or alkalies,
cold or hot, rich or otherwise, fruits, meats or vegetables,
all go to the formation of good milk if properly
digested. The old idea that acids should not be eaten
is fallacious. There is more acid in the stomach normally,
than could be added in a meal made up entirely
of citrus fruits. At the same time, the heavy foods
should be avoided on account of the serious demand on
the liver and kidneys in the absence of exercise.
On the other hand, if the breasts are engorged, the
fluids must be reduced to a minimum, and a relatively
dry diet enforced.
The patient loses about one-ninth of her previous body
weight in the course of labor and the puerperium.
The breasts are made ready for lactation twelve hours
after delivery by cleansing with sterile green soap and
warm water and bathing in 50 per cent alcohol. Next,
the nipple is attended to, and the infant is put to the
breast.
The nipple is prepared by cleansing it with an applicator
soaked in fresh boric acid solution, and after
nursing, the same process is repeated. This is routine,
whether the mother is in bed or walking about. In the
latter case, the mother must be taught to care for her
own breasts.
156The child is put to the breast every three hours and
given six feedings a day. This leaves a six hour interval
at night, which is very necessary for the mother’s rest
and for the child. If the babe is feeble, seven or eight
feedings in the twenty-four hours may be required for
the first two weeks.
At first the breast only secretes a thick, yellowish secretion
called colostrum, of which the child gets from
a drachm to an ounce. It is a mild laxative.
The irritation of the nipple by the child’s mouth is
begun as early as possible in order to stimulate the
breasts to secrete milk and the uterus to contract, and
thus aid involution and the preservation of the maternal
figure.
The milk usually “comes in” on the third day and is
accompanied by a sense of distention and moderate
pains in the breasts. The glands may be hot, hard and
swollen, but normally there is no rise of temperature
with the inflow of the milk, except with nervous women
who stand pain badly. There is no such thing as milk
fever. If fever appears at this time, an infection must
be suspected.
The engorgement of the glands may become so great
that the nipples are drawn in and nothing is left for the
child to grasp. If the engorgement becomes too painful,
fluids are removed from the diet list, and saline cathartics
administered, while ice packs are applied to both
breasts. Heat should never be used except for the purpose
of hastening suppuration.
This engorgement, or so-called “caking” of the breasts
is not due to the milk, but to the infiltration of the connective
tissue around the glands with serum and blood
which stimulate the glands to secrete. The distention
usually disappears in twenty-four or forty-eight hours,
especially if the child is sturdy. Massage of the breasts
157only increases their activity and tends to make the
trouble worse.
The weight of the glands may be considerable and
require the application of a light supporting breast binder.
Pillows under them will also give relief at
times.
In putting the child to breast, the mother should lie
on the side with the arm raised and the child is dropped
into the hollow thus created, facing the mother (see Fig.
113). In this position the nipple will most easily and conveniently
slip into the child’s mouth. The child should
nurse fifteen or twenty minutes and then be removed. The
toilet of the nipple is made by cleansing with boric solution
as previously described, and then placing not gauze
but a piece of aseptic cotton cloth over it, after which the
binder is readjusted. (See Breast Covers, p. 326.)
The menstrual flow ceases during lactation as a rule,
but not invariably. The flow returns in from four to six
weeks after delivery, if the child is not nursing, and
about the same time after lactation ceases. There is a
popular idea that conception can not occur during lactation,
and many women injuriously prolong lactation
in the hope of avoiding another child. The theory is
fallacious and conception during lactation is not uncommon.
The Bowels.—A lying-in woman is regularly constipated.
Lack of exercise, a nutritious diet, but one with
a minimum of wastage, together with relaxed abdominal
walls, contribute to a condition that is primarily due to
changes in intraabdominal pressure, which follow the
delivery. For weeks the intestines have been under
pressure and irritation by the growing uterus, and
when this is suddenly removed the intestines become
sluggish.
On the morning of the second day the patient should
158receive an ounce of castor oil. This dose, suspended in
black coffee, beer, orange juice, or sherry wine can be
taken by nearly everyone. In from four to six hours a
normal saline, or soapsuds enema is given. The enema
may be repeated daily, or if this is objectionable to the
patient, the castor oil or Russian oil, may be given as a
routine. Saline cathartics should not be used unless
there is an oversupply of milk.
There is sometimes a good deal of gas following labor,
which can be removed by the 1–2–3 enema (see Enema, p.
335). In giving enemas, the nurse must use great care
to avoid touching or infecting an injured perineum.
Many women secrete less gas and are agreeably influenced
mentally by a five grain pill of asafœtida taken
thrice daily.
Urination.—One of the commonest difficulties after
labor concerns micturition.
Owing to the swollen and bruised condition of the
urethra and the nerves supplying the neck of the bladder,
the usual stimuli do not act and the woman, conscious
of a painful distention, is unable to pass water.
The helplessness is increased by her position in bed.
The nurse must make every effort to have the bladder
emptied naturally. The process is aided by letting the
water run from the faucet into the toilet basin, by using
hot applications to bladder or vulva, by allowing warm,
sterile water to run down over the vulva and perineum,
by an enema, by putting smelling salts to the nose, by
using slight pressure over the bladder, or by having
the patient sit up on the bedpan.
If these measures fail and moral suasion is fruitless,
the bladder must be catheterized at the end of twelve
hours. The two dangers of catheterization are injury to
mucous membrane, and infection. Many cases of cystitis
159have resulted from an unclean catheter or the improper
use of a sterile instrument.
To catheterize a patient, she is first given aseptic care
during which particular attention is paid to the meatus.
This should be cleansed with an applicator dipped in a
solution of boric acid. Next, the nurse prepares her
hands by scrubbing ten minutes in hot running water
with sterile nail brush and green soap. The catheter
either of soft rubber or glass, is boiled for fifteen minutes
and passed, not by touch, but by sight, and the
flow is received in a clean basin and the amount recorded.
As soon as the urine ceases to flow freely, the
tip of the index finger is placed tightly over the end
of the catheter and the instrument is gently withdrawn.
The finger is placed over the end of the catheter not only
to avoid the dripping of urine as it is removed, but especially
to prevent the disagreeable sensations produced
by the inrush of air.
Usually one catheterization is sufficient, and every
time the bladder fills, the nurse must take the time
and trouble to make the patient urinate spontaneously,
if possible, for some women form a catheter habit, from
which it is difficult to break them. After natural urination
and after catheterization, the aseptic care should
be repeated.
The Genitals.—The vulvar pads should be changed as
often as they are soiled. Four a day is an average number,
and six or eight in the first three days is not unusual.
Every time the pad is changed, the nurse should
give aseptic care, and extra attention whenever the
bowels and bladder are emptied.
The dried secretions should be washed off with sterile
sponges, wiping always toward the rectum and throwing
away the sponge. Smegma collects in the folds of
the labia and about the clitoris. This should be carefully
160sponged away. If it becomes dry and hard, oil or
albolene will soften it and facilitate its removal. Plenty
of soap and warm water should be used, then with a
pitcher or douche point, the whole area is irrigated
with a solution of lysol 1 per cent. Especial care is
given to the stitches if any are present. No traction
must be made on the ends of the sutures, and if unusual
soreness is complained of, the doctor should inspect
them at his next visit.
The nurse should be careful not to get lochia on her
hands as the discharge contains germs which she may
carry to herself, to the baby, or to the patient’s breasts
or eyes.
Painful swelling of the vulva, or edema of the rectal
protrusion may be relieved by hot boric dressings or by
ice bags to the anus.
The vaginal douche is rarely employed at present except
under specific indications.
If the involution is slow, it is safer to use ergot by
mouth, rather than the hot vaginal douche, as sometimes
recommended. The douche is a frequent source of infection,
as well as a useless procedure. Nevertheless, a
dainty woman gets much comfort mentally, as well as
physically, if she is kept clean and free from odors;
hence if the lochial discharge becomes offensive on the
fifth day or sixth day, as sometimes happens, a single
hot vaginal douche may be permitted. A 1:5000 solution
of potassium permanganate, or a teaspoonful of formaldehyde
to a quart of water, or a chinosol solution
1:1000 may be used.
Rest.—Since the patient will be in bed from eight
days to two weeks in normal cases, she must be made as
happy and comfortable as possible, and nothing contributes
so much to her satisfaction as a cheerful, competent
nurse. Her mind is at ease about herself and her
161child, and the companionship of the nurse can be made
one of the pleasantest recollections of her illness.
Any patient who is at all reasonable can be managed
by a tactful nurse without the consciousness of being
opposed or directed. Gossip, hospital stories, criticism
of other cases, other nurses, or of doctors should be
avoided. The patient is deeply interested in her own
case, and the private troubles of the nurse do not concern
her nor enlist her attention for more than a few
polite but unpleasant moments.
The nerves of the patient are highly sensitized, and
therefore she should sleep as much as possible at night,
and take an additional nap in the afternoon. Only the
members of the family should be allowed to see the patient
the first week, and they but for a short time. It
takes the strength of the patient unnecessarily to see
guests even though they be close friends. Importunate
visitors may be pacified frequently by a view of the baby.
The patient must be spared all household responsibilities,
and if necessary, the nurse must take charge. Tact
must be used to avoid being dictatorial, either to family
or servants. If anything unusual arises, the nurse must
show no surprise, annoyance, or bewilderment. Everything
is attended to quietly, firmly, and without friction.
Getting Up.—It is a tradition that the woman is lazy
who does not get out of bed by the ninth day.
There are three factors to be considered, the progressive
involution of the uterus, the strength of the patient,
and the presence of stitches. Involution may be complete
on the fifth day, but the prostration from the
labor may make the woman indifferent to arising. She
may be strong enough to rise on the third day, but the
uterus is large and heavy, and the erect position will put
an unnecessary strain on the supports which may retard
162involution and cause displacement or disease later.
Also, it is not desirable for a woman to sit up until her
perineum is well on the road to restoration.
In general, the woman should not get up until the
uterus has gone down into the pelvis and is nonpalpable.
If this is the case on the fifth day and she feels strong,
she may get up. If she is not strong, time will be saved
by staying in bed until her vigor returns, whether it is
ten days or twenty.
Getting up may be followed by a return of the bloody
discharge. This may come from subinvolution, from a
relaxed and flabby uterus, from a cervical tear, or from
change in posture.
If there has been a retroversion before pregnancy, lying
prone with an occasional knee chest position for a
few moments will aid. Massage and passive exercises
while in bed will aid the patient to recover and to maintain
her strength. Even after she is up and about, she
should lie down frequently during the day and always
when nursing the babe, until she feels quite normal
again.
For the hospital the following standing orders may
be followed:
Standing Orders—Puerperium
Breasts:
1. Prepare for lactation 12 hours after delivery.
(a) Clean breasts and nipples with soapy water and
green soap.
(b) Sponge with sterile water.
(c) Sponge with boric solution.
(d) Sterile compresses over nipples and adjust binder.
2. Babe to breast immediately after breast preparation.
3. Every morning apply fresh compresses over nipples and
oftener, if necessary.
4. Cleanse nipples with boric solution (use applicator) before
and after each nursing.
163To dry up milk:
Restrict fluids; give saline cathartics; apply ice bags to
breasts, as needed; for pain give codeine solution ¼ to
½ gr. hypodermically, if necessary.
Do not massage, do not bind, do not pump. Let breasts alone.
When breast is inflamed:
Apply ice bags constantly until pain subsides and temperature
goes down. Watch for signs of suppuration.
Genitals:
1. S.S. enema each morning, followed by aseptic care.
Cleanse from above downward—1 per cent solution of
lysol and cotton pledgets.
1 pledget for each side.
1 pledget for center.
1 pledget for rectum (last).
External douche of sterile water.
Dry sterile pad.
2. Aseptic care following all bowel movements and urination.
Routine:
1. Record pulse and temperature twice a day, unless otherwise
ordered.
2. Bladder must be emptied in twelve hours. If all persuasive
means fail (may sit up in bed), catheterize.
3. Make daily records of conditions of uterus (firmness and
height), breasts and nipples.
4. No vaginal douche unless ordered.
5. Diet: liquid two days; semisolid two days; then general.
6. Watch for hæmorrhage.
7. Keep uterus firm by occasional massage.
8. All cases to have castor oil, 1 ounce within thirty-six
hours after delivery (before noon).
9. Woman may get up as soon as uterus can not be felt
above pubes, if there is no contraindication.
The history sheet should be kept accurately and
should show every incident in the course of the lying-in
period.
The condition of the bowels, bladder, and lochia, the
temperature, pulse and respiration and the height of
the fundus above the symphysis from day to day must
be set down in finger-breadths or centimeters.
For the hospital, the following system will be found
useful in establishing a routine.
First Stage.
1. When pains began.
2. Frequency and duration of pains.
3. Character vaginal discharge.
4. Time membranes ruptured.
(a) Artificial.
(b) Spontaneous.
Second Stage.
1. Time second stage began and ended.
2. Anæsthetic.
3. Mode of delivery.
4. Who delivered.
5. Sex of child.
(a) Living.
(b) Dead.
6. Perineum.
(a) Condition.
(b) Repair.
Third Stage.
1. Method.
(a) Spontaneous.
(b) Early expression.
(c) Credé expression.
(d) Manual removal.
2. Placenta delivery.
(a) Time.
(b) Size.
(c) Complete or incomplete.
(d) Length of cord.
3. Note.
(a) Hæmorrhage.
(b) Quantity.
(c) Color.
(d) Clots.
General condition—was case number put on mother and child?
Other treatments.
Medications.
Condition of uterus.
Temperature, pulse and respiration before leaving delivery
room.
Signed ..........................
(Nurse’s Name.)
165
CHAPTER XI
UNUSUAL PRESENTATIONS AND POSITIONS
Breech Presentation.—The pelvic pole enters the inlet
first, once in thirty cases and more commonly in primiparas
than otherwise.
Etiology.—Anything that interferes with or deranges
the laws of normal gestation will predispose to, or produce
this anomaly.
Thus, if the head is too large, as in hydrocephalous, or
if the fœtus is too movable, as in hydramnios, or if an
obstacle, like placenta previa, contracted pelvis or tumors
prevent the proper approach of the head to the
inlet, the mechanism will be disturbed and a breech or
possibly a shoulder presentation will result.
Abnormal flaccidity of the uterine or abdominal walls,
prematurity or twins also contribute definitely to its occurrence.
The attitude of the child generally retains its normal
aspect of complete flexion. This pose, however, is not
maintained invariably for on occasion the buttocks and
genitals may rest upon the inlet while one or both feet
may be extended on the thighs and lie beside the neck,
or the thighs may be extended while the knees remain
flexed, and what is known as a knee presentation, or if
the foot comes down, a footling presentation results.
Positions.—The sacrum is the most prominent bony
landmark of the breech, hence the positions are named
from the relation this bone bears to the four quadrants
of the inlet.
166
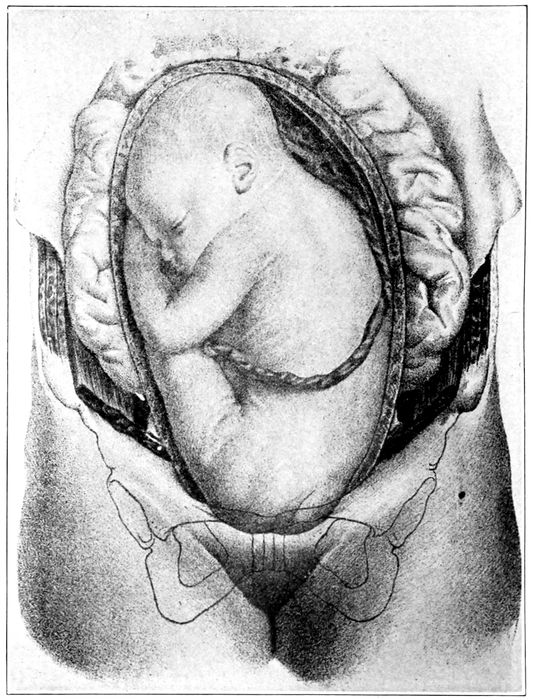
Fig. 61.—The breech. Left-sacro-anterior position. (Lenoir and Tarnier.)
We have therefore in their order of frequency the
following designations: Left-sacro-anterior, where the
sacrum lies to the left of the median line of the mother’s
body and in front; right-sacro-anterior, where the sacrum
lies to the right and in front; right-sacro-posterior,
where the bone lies near the mother’s vertebral column,
and on the right side; and the left-sacro-posterior position,
167where the bone occupies a corresponding place on
the left side.
Diagnosis.—The recognition of this presentation is
most easily secured by external abdominal palpation in
pregnancy, which may be reinforced during labor by
the internal examination.
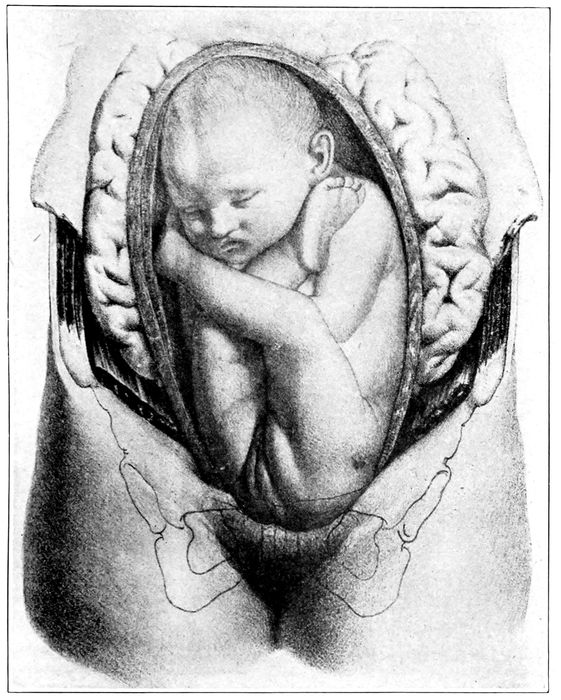
Fig. 62.—The breech. Left-sacro-posterior position. (Lenoir and Tarnier.)
168Externally the palpating fingers at the pelvic brim
will note the absence of the hard, round head, and feel
a mass, softer, quite irregular in shape, and less defined
than customary. Movements also may be appreciated
that would be too far down in the uterus if the head
was presenting.
Next the hard, spherical tumor of the head can be
outlined somewhere in the fundus, and the heart tones,
instead of being below the umbilicus will be on the
same level or even higher.
Vaginally the cervix is not filled out, the presenting
part does not come down, but after labor has begun the
distinctive features of the breech gradually become
more evident, as they are driven into the pelvis.
One or both feet, or the buttocks, may be recognized.
The examining finger may possibly enter the anus and
be stained with meconium or pinched by the sphincter,
which differentiates this orifice from the mouth.
One after another the characteristic landmarks appear
until the diagnosis can not be doubtful. As soon
as the sacrum is found or the legs definitely placed, the
position can be named.
Mechanism.—The hips always enter the inlet in one of
the oblique diameters and the back is turned to the
same part of the uterine wall as in the corresponding
vertex positions.
The acts described in the mechanism for vertex deliveries
show a somewhat different order. Descent is first,
then comes internal anterior rotation, which brings the
anterior hip under the symphysis and its delivery is
quickly followed by the posterior hip, which rolls out
over the perineum.
The body advances, as a rule, with the back toward
the front of the mother. The shoulders with arms folded
169move under the pubic arch and then the head delivers
in a state of flexion. The head, of course, has no caput
and it is not moulded.
This mechanism may be greatly impeded or complicated
at any stage of the movement. The advance may
be retarded to a pathological degree, the belly may be
large and as it passes along the canal one or both arms
may be stripped up alongside the head or even into the
back of the neck. The head may be arrested at the inlet
by the arms, by its degree of deflexion, or by pelvic contraction.
The rotation may not take place, or it may be abnormal,
and the belly of the child look forward toward the
mother’s. Any of these variations adds further to the
difficulty of the labor and to the danger of the partners
in the event.
Artificial aid may be required which brings with it
the possibility of sepsis.
The fœtal mortality which averages five per cent is
due mostly to asphyxiation. Interference with the supply
of oxygen begins as soon as the cord passes the
vulva and the child must be delivered in eight minutes
from that time, or perish. Partial detachment of the
placenta may also cut off the oxygen to a fatal degree,
and the child may be unable to breathe when born on
account of mucus sucked into the trachea by premature
efforts at respiration.
Minor accidents also occur, such as fractures, dislocations,
and paralysis from injury to the nerve trunks.
Management.—In the interest of the child, this presentation
is occasionally converted into a vertex by external
version during the last weeks of pregnancy or
in labor before the membranes have ruptured. It is
difficult, however, to maintain the vertex over the inlet.
170The woman must be kept quiet in a horizontal posture
and long roller splints applied to the side of the child
in utero and bound on.
In primiparas, this is nearly impossible, and it is
wiser, in the absence of some great necessity to warn
the parents of the conditions and dangers and let them
share in the responsibility.
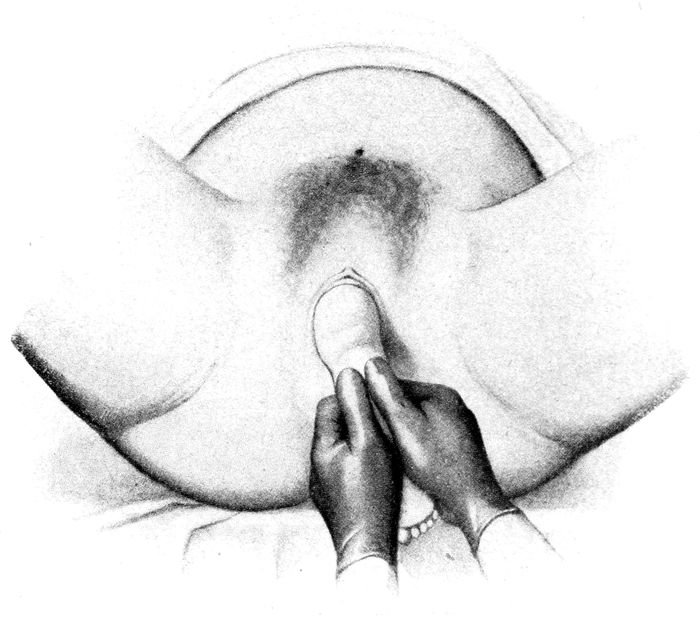
Fig. 63.—Extraction of the breech. Traction on one leg. (Hammerschlag.)
When the labor begins, the bag of waters must be
kept from rupture as long as possible and when it finally
breaks, an internal examination should be made to see
if the cord has come down. If this happens it may be
necessary to expedite the delivery by external assistance.
171

Fig. 64.—Breech delivery. Extraction of the trunk by pulling on the hips. (Hammerschlag.)
The doctor brings down a foot, if it is not already
down, or pulls on the breech until the feet drop out.
Compression of the cord must be always in mind. It is
always compressed after the umbilicus has passed the
navel. The shoulders are delivered by seizing the feet
with the operating hand and swinging the body out of
the way. This brings the posterior shoulder, which
should be first, into the hollow of the pelvis. Extraction
is then completed by what is called the Smellie-Veit
maneuver. The child is put astride one arm, the first
finger of which is hooked into the child’s mouth to maintain
flexion. The fingers of the other hand then grasp
the shoulders of the child astride the back of the neck
and traction is made downward in the axis of the inlet
until the head slips into the excavation.
172
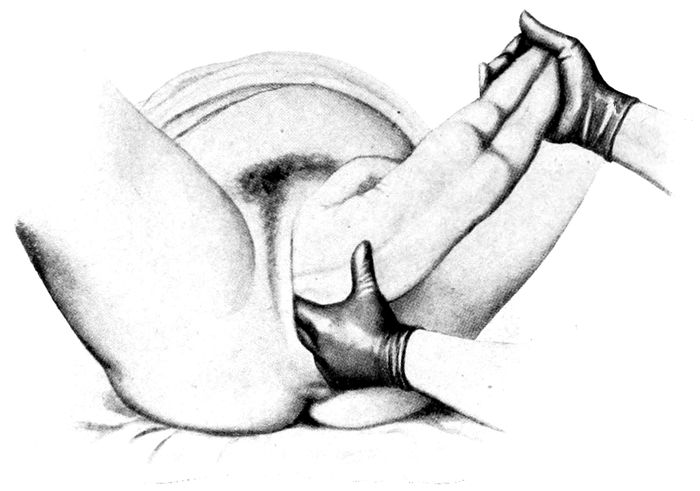
Fig. 65.—Breech delivery. Delivering the shoulder. The body is swung strongly upward and outward to bring posterior shoulder into the pelvis. (Hammerschlag.)
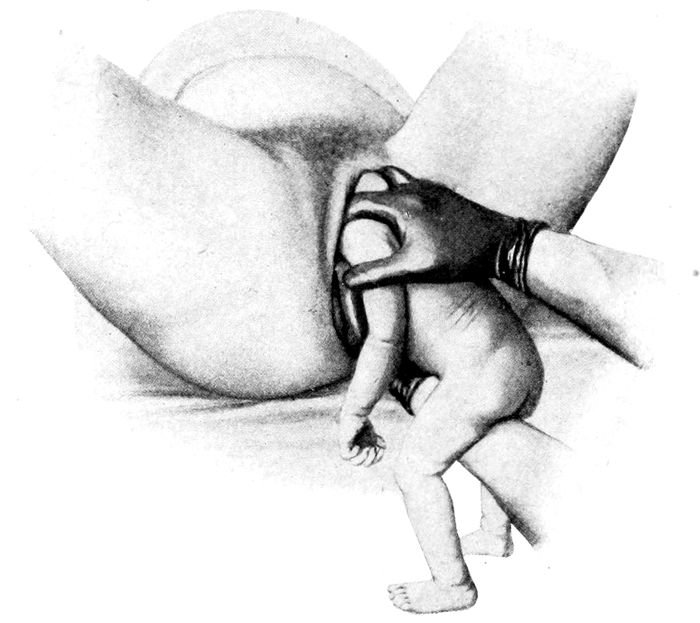
Fig. 66.—The delivery of the after-coming head by the Smellie-Veit maneuver. (Hammerschlag.)
173If the head is delayed at the inlet, it may be necessary
to put the woman in the Walcher position (q. v.)
and for the nurse to use the Wiegand compression
(q. v.). The feet must not be fastened in stirrups for
breech cases.
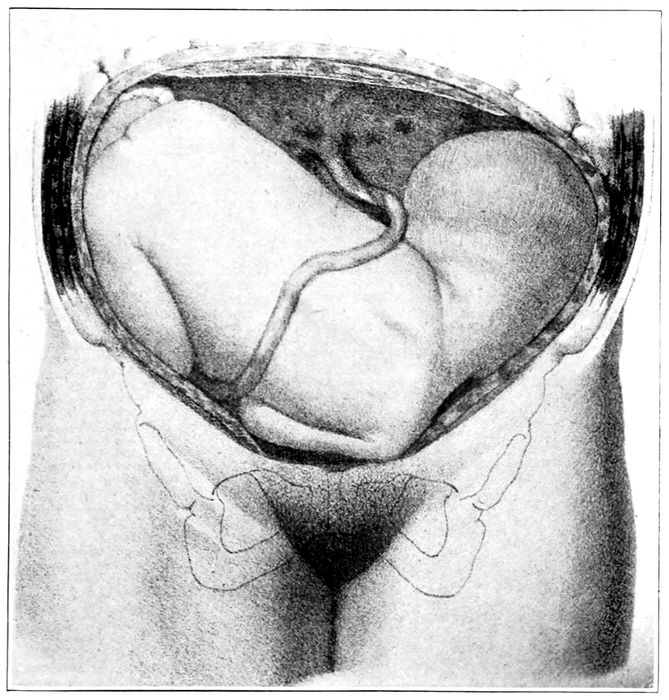
Fig. 67.—Shoulder presentation. Left-scapulo-anterior position. (Lenoir and Tarnier.)
Forceps are not recommended for application to the
breech as they do not fit and are liable to slip off and
injure both child and mother. The fingers are best.
174Forceps are not recommended for the after-coming
head unless the child is dead. If the child lives, the
Smellie-Veit is more-successful; and if the child dies,
the cranioclast, if possible, will save the mother much
suffering and avoid some injury to the tissues.
Transverse or Shoulder Presentations.—These are
cases in which the long axis of the child lies directly
across or obliquely across the long axis of the uterus.
The shoulder (scapula) is the bony landmark, and
the part which most frequently impends over the inlet.
This presentation probably occurs once in two hundred
labors.
It is due to the same conditions that were given for
breech cases; namely, weak abdominal or uterine muscles,
pelvic contraction, placenta previa, hydramnios,
and twins.
It is easily recognized in pregnancy, and must not be
neglected, for it is impossible of delivery without first
changing it into a longitudinal presentation. If this
correction is not done, rupture of the uterus is liable
to occur, with the consequent death of both mother and
child.
The treatment is invariably version.
Face and Brow Presentations.—The face presents
once in about three hundred labors. In this case, the
head is completely extended so that the occiput rests
against the back of the neck. The trunk and spine are
straightened out while the legs and arms remain in the
normal attitude of flexion.
The causes of these anomalies must be sought in those
conditions which bring about the deflexion of the chin.
The most common are pelvic contraction, large child,
175placenta previa, hydramnios, goiter, anencephalus and
multiparity.
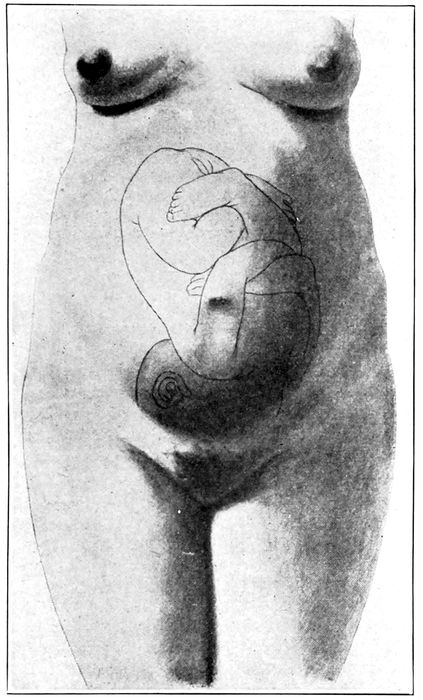
Fig. 68.—Face presentation. (Bumm.)
Face positions take their names from the location of
the chin (mentum—Latin). Thus the most frequent
face position is the right-mento-posterior.
The diagnosis is not easy and may not be conclusive
176until the bony prominences of the face, such as the nose
and orbital ridges can be distinguished by vaginal examination.
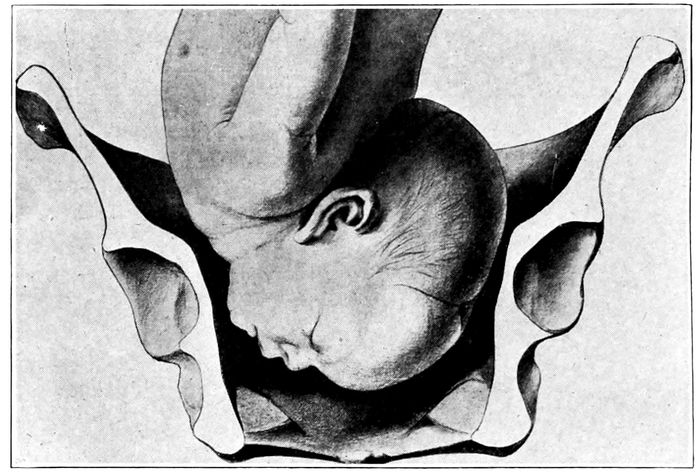
Fig. 69.—Descent of the chin in face presentation. (Bumm.)
The delivery is protracted from three to five hours beyond
the average by this complication, and the mortality
is higher both for mother and child. The face is
badly swollen and disfigured, but the normal condition
of the tissues will be restored by the end of a week.
Most face cases terminate spontaneously, but operative
interference is not infrequent on account of danger to
mother or child.
Version or manual correction of the presentation may
be done before engagement.
Forceps is the operation of choice after the head is
fixed in the pelvis, but it may be necessary to precede
the delivery by a preparatory pubiotomy, or in case of
failure, to do a craniotomy on the dead child.
177If the chin does not rotate forward under the symphysis,
the labor is impossible without pubiotomy or
the destruction of the child. In general, the case should
be left to nature unless some definite indication to interfere
develops.
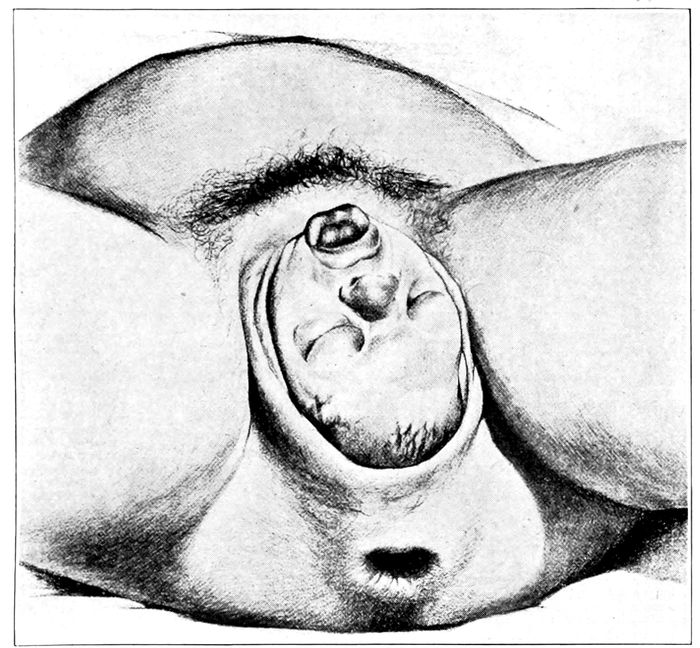
Fig. 70.—Delivery in face presentation. (Bumm.)
The brow presents much more rarely than the face,
possibly once in a thousand labors. It is due to the same
conditions as bring about the presentation of the face.
The mortality for both mother and child is higher than
in face cases. The whole labor is harder and longer,
besides being more dangerous to life and to tissues.
This presentation, if recognized before the head is
178fixed, should be converted into a breech by version, but
after the head comes down, it may be possible by hand
or forceps to deliver either as a face or as an occipito-posterior,
but otherwise the cranioclast must be considered.
Occipito-posterior position is the name given to vertex
cases wherein the occiput lies in one or the other of
the two posterior quadrants of the pelvic inlet.
These labors are necessarily prolonged, both in the
first and second stages, because the mechanism of delivery
is deranged by the larger diameters brought into
relation with the bony canal and by the ineffectiveness
of the contractions.
The pains in the second stage may become violent
and extremely painful, but the labor does not advance
appreciably. After a little experience, mere observation
of the course of the labor will cause the suspicion
to arise in the mind of a competent nurse that the occiput
is posterior. The diagnosis will be cleared up by
the doctor’s internal examination, which shows the
large fontanelle anterior and the sagittal suture running
backward.
The head is partially deflexed and it may not be possible
at first to find the small fontanelle.
The position terminates by delivery uncorrected, by
spontaneous rotation into an anterior position, or is corrected
by the doctor.
Correction should not be attempted until it is apparent
that the anomaly will not right itself, which it will
do in four cases out of five.
179
CHAPTER XII
OPERATIONS
Complications during labor may arise from abnormal
positions of the head, such as face or brow; from abnormal
presentations of the child, such as breech, transverse
or shoulder; from twin labors; or from prolapse
of a part like the foot, arm or cord.
The mother may be responsible for some of these
abnormalities through having a contracted pelvis, a
rigid os, or a rigid pelvic floor.
The uterus, too, may functionate abnormally by acting
too vigorously, as in precipitate labor, or too slowly,
as in uterine inertia. The membranes may rupture
prematurely and produce a dry birth.
There may be hæmorrhages before labor (ante partum
hæmorrhage) during labor (intra partum), and after
labor (post partum hæmorrhage), or the labor may be
preceded, accompanied, or followed by that extreme
example of toxæmia known as eclampsia.
Face and brow presentations are rare and come to the
attention of the nurse only when an operation is required
for their relief. Further conditions may arise,
such as danger to mother or child, which demand an acceleration
of the labor.
If the head is engaged, forceps is the operation most
commonly undertaken, and if not engaged, the problem
may be solved either by an early version and extraction
or by forceps later. The dangers to the mother are
not usually difficult to diagnose if the case has been
followed carefully.
180Signs of danger to child must be looked for constantly.
Such are:
(a) Alteration of the heart tones.
(b) Retardation of pulse in cord between pains.
(c) Escape of meconium is not significant unless occurring
in the pain-free interval, when it may signify
hypercarbonization of blood and a threat of asphyxiation.
The preliminaries for the performance of these operations
may now be described, and the indications and
conditions briefly tabulated.
The preparation should be standardized so that the
same set-up of the room will do for all of the major
obstetrical operations, except Cæsarean section.
The kitchen table is generally regarded as a satisfactory
operating table. Its length is sufficient for delivery
when the legs are doubled up. The table should be
covered with a blanket or comfort on which it laid a
clean sheet. A rubber blanket or piece of oil cloth is
put on, so folded above the place for the patient’s hips,
and so pinned at the sides, that all drainage will flow
off into a bucket or jar at the foot.
In front of the table is placed a straight-backed
chair with flat seat. To the right of the operator, as he
faces the table, stands a bench, or two chairs, side by
side; or, if possible, another table. This is covered with
a clean sheet for the reception of the instruments. To
the operator’s left, another table similarly prepared
carries the solutions, sponges, etc. Every operation for
delivery should have tape and cord scissors within easy
reach, as well as facilities for the resuscitation of the
child.
The light should come from behind the operator and
fall full upon the field of operation. The room should
be warm.
181The patient is laid upon the table and her knees elevated
in the exaggerated lithotomy position. If there
are assistants enough, one can stand on either side
and hold a knee, if not, a sheet sling can be made
and slung round the patient’s shoulders and tied to the
knees as previously described.
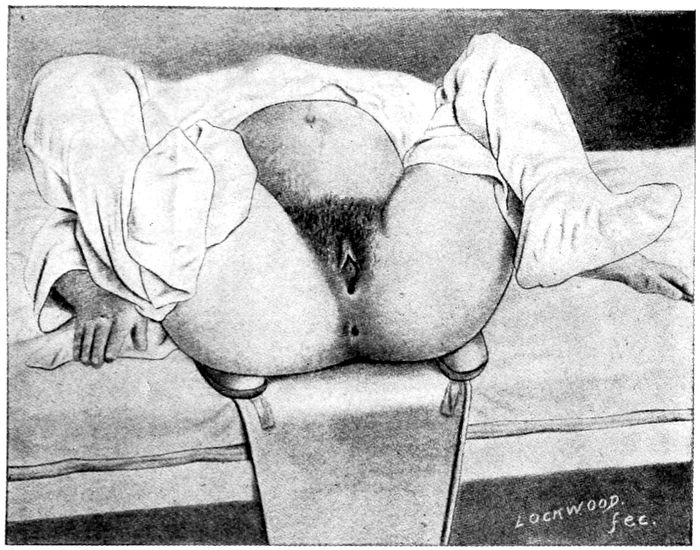
Fig. 71.—Exaggerated lithotomy position. The legs are held by a sheet sling. The vulva should be shaved. (Williams.)
An anæsthetic will be required. If a doctor can not
be had, this duty will fall to the nurse.
A sterile douche bag hangs near the table. A bath
tub of hot water must be provided and a tracheal catheter
must be ready for the removal of mucus from the
child’s windpipe. An abundance of hot and cold sterile
water must not be overlooked. In the hospital the following
182synopsis for the placing of the linen may be
found useful:
Sterile Linen for Operative Case.—
Bring patient to foot of bed.
Put in the stirrups. (For breech deliveries do not use stirrups.)
Same order as for normal case except that feet are put
in stirrups instead of on bed.
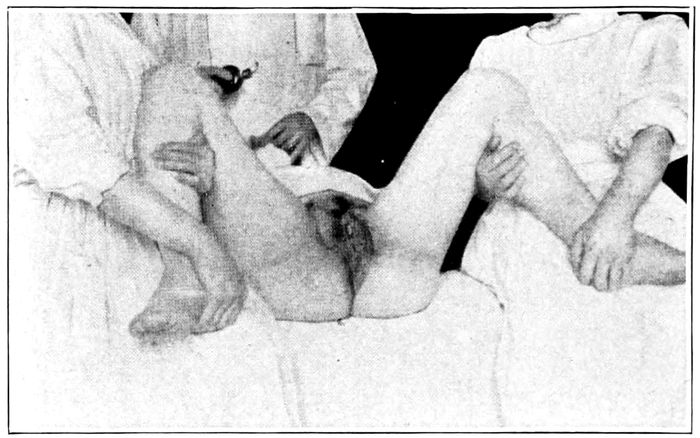
Fig. 72.—Dorsal position when assistants are available. (Hammerschlag.)
Sterile sheet under patient extends now from basin under
bed to buttocks.
Combination pad over field of operation.
Sterile sheet over abdomen.
The genitals of the patient are now cleansed with all
care and attention described for labor. If this has
been done within an hour, she need only be sponged
off thoroughly with lysol solution (1 per cent). The
feet and legs are covered with stockings, the body
kept warm, and protected by sheets and blankets, if
necessary.
183Every operative delivery is preceded by catheterization.
All instruments are boiled for thirty minutes and
brought to the table in the same container in which
they are sterilized. The hot water has been poured off
and a cool, weak solution of lysol (0.5 per cent) added.
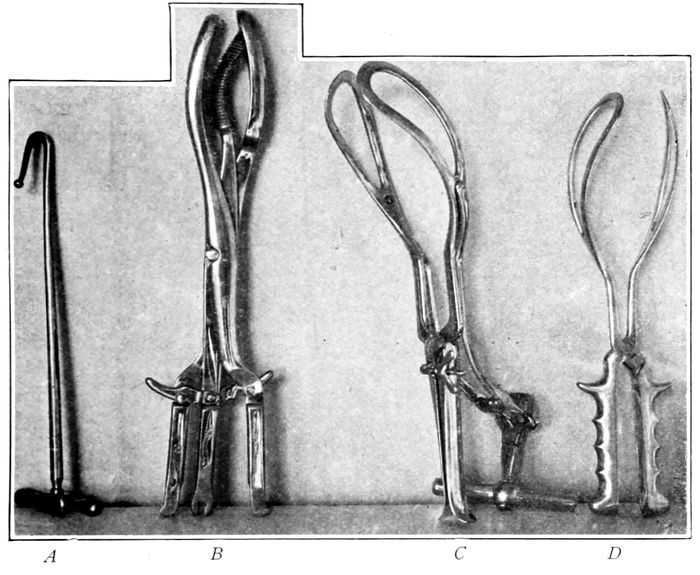
Fig. 73.—Instruments for artificial delivery of the head. A, Braun’s blunt hook; B, Cranioclast (Auvard); C, Axis traction forceps (Webster); D, Low forceps (Simpson).
Forceps.—Before using forceps it should be determined
that the woman can not deliver the child unaided,
or can not be permitted to do so without too
great expenditure of physical and nervous energy. The
exact conditions must be recognized as to the location
and position of the head, the condition of the fœtal
heart tones and the size of the pelvis. When the head
is high up, the axis traction instrument is employed
184and patient put in Walcher’s position for the traction.
Axis traction forceps are extremely dangerous to
mother and child, and should be avoided wherever possible.
The following instruments are required:
The obstetric forceps.
2 eight-inch forceps.
6 artery forceps.
1 vulsellum forceps.
1 tissue forceps.
1 needle forceps and 6 needles.
2 vaginal retractors.
1 pair dressing forceps.
1 douche point.
1 silver catheter.
Suture material—both catgut and silkworm gut.
Besides these instruments, the nurse will also have
solution basins as described for normal labor. For
operations outside of hospitals, the nurse need not be
clean, as her duties will consist for the most part
in changing solutions, refilling basins, handing towels,
etc., all of which can be done with sterile forceps.
The following summary may be serviceable for advanced
study or reference:
Preparation.—
Thorough asepsis, both subjective and objective.
Patient should be pulled down to the foot of the labor bed
with feet in the stirrups, or put upon the kitchen table
or across the bed with the legs held in the lithotomy position.
(For breech cases, legs should not be fastened.)
Bladder and rectum must be empty.
Anæsthetic is necessary.
The position of the head must be accurately known.
Facilities for the treatment of asphyxia neonatorum must
be at hand.
Conditions.—
Cervix effaced and os dilated, except when maternal or fœtal
life is threatened.
185Bag of waters must be ruptured.
The head must be engaged.
The child should be living.
Indications.—
Insufficiency of the powers of labor.
Deep transverse arrest of the head.
Complications in labor, such as:
Eclampsia.
Fever.
Acute or chronic disease.
Hernia—especially if incarcerated.
Placenta previa.
Prolapse of the cord.
Face and brow presentations.
Contracted pelvis.
Occipito-posterior positions.
Dangers From Forceps.—
Injuries to Child.—Overcompression, especially with axis traction
forceps or in contracted pelvis.
Crushing of soft parts, or such lesions as abrasions, pressure
marks, hæmatomata, swelling of face and eyelids.
Bone injuries: Spoon-shaped depression where the head has
been dragged through a narrow inlet; fissures in the
parietal or frontal bones; fractures. When axis traction
forceps are applied antero-posteriorly, the occipital bone
may be sprung inwards until it cuts the medulla.
Compression of the cord, especially if it is around the neck.
Hæmorrhage from the middle meningeal artery.
Injury to eye.
Erb’s paralysis.
Laceration of ears when the forceps are removed.
Facial paralysis from pressure of the blade.
Injury to Mothers.—
Infection.
Improper application of the blades outside the cervix uteri.
Soft parts torn by too rapid extraction. When os is not
dilated, it is first pulled down and then torn. The tear
may extend into the vaginal vault. Fistulæ may be
produced.
Prolapse of the uterus from prolonged traction.
Vaginal tears from the blades or from malplaced head.
Slipping of blades. Traction must be not against the symphysis,
but down.
186The forceps commonly used in this country (Simpson
or Elliott) are so made that the left blade must be
introduced first on account of the lock.
The mortality for the child in forceps cases is about
six per cent.

Fig. 74.—Forceps operation. The left blade, in the left hand, is introduced first into the left side of the mother so that the curve of the blade fits the child’s head (inside the cervix). (Hammerschlag.)
The axis traction instrument is used but seldom by good
obstetricians, since the danger to mother and child in
this operation is very serious and it should be reserved
for emergencies of exceptional character. Pubiotomy may
precede the operation with advantage in many cases.
Asphyxia of the child and maternal hæmorrhage must be
prepared for.
187
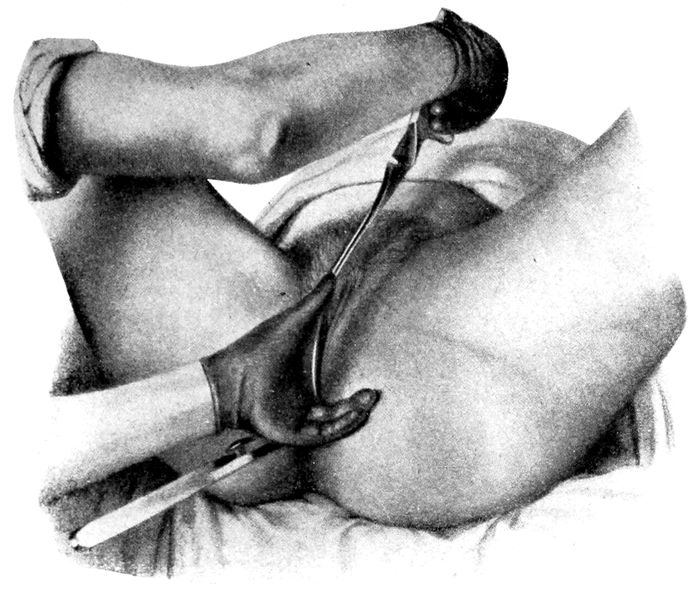
Fig. 75.—Forceps operation. The introduction of the right blade. (Hammerschlag.)
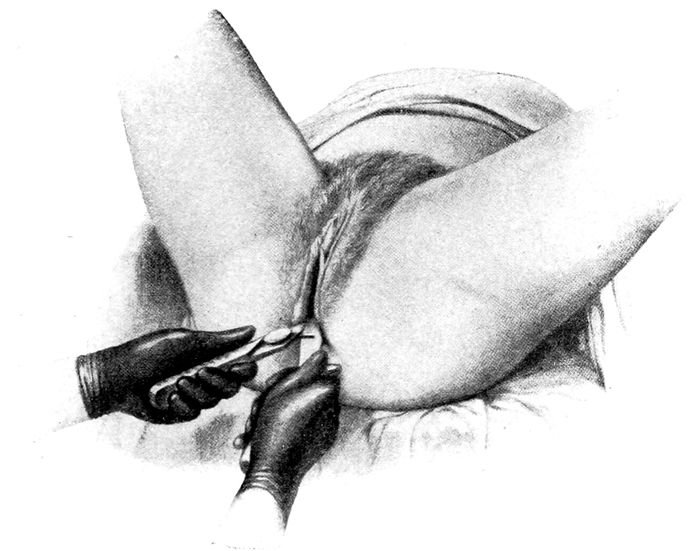
Fig. 76.—Forceps operation. Locking the handles. (Hammerschlag.)
188
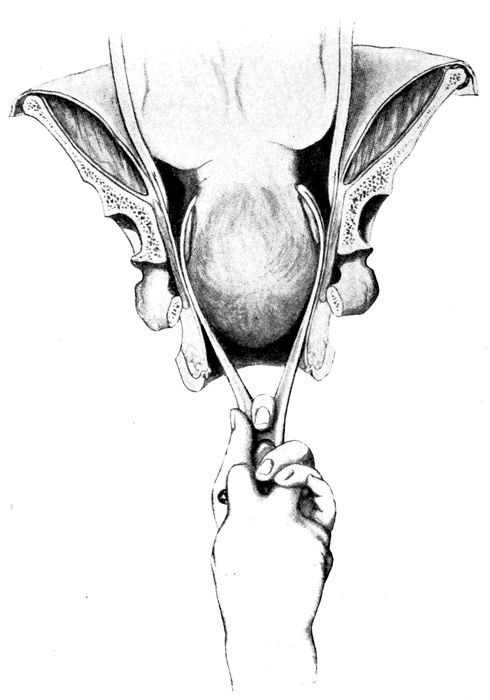
Fig. 77.—Forceps operation. The way the blades should grasp the fœtal head. (Hammerschlag.)
189

Fig. 78.—Forceps operation. Traction on the handles. (Hammerschlag.)
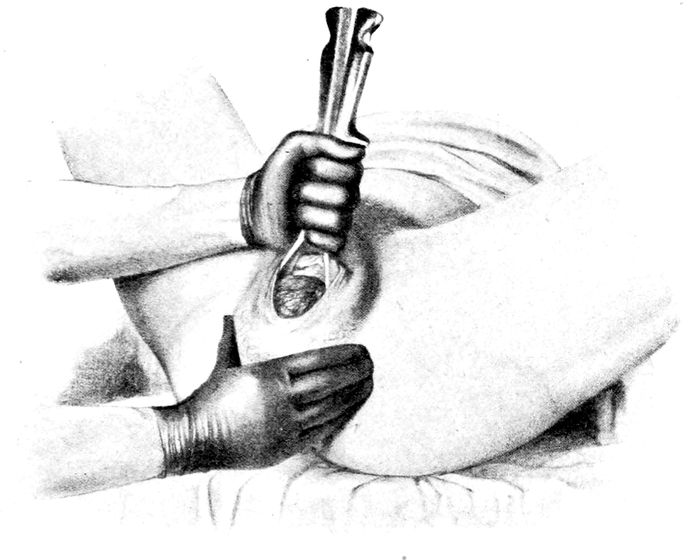
Fig. 79.—Forceps operation. The delivery of the head. (Hammerschlag.)
190
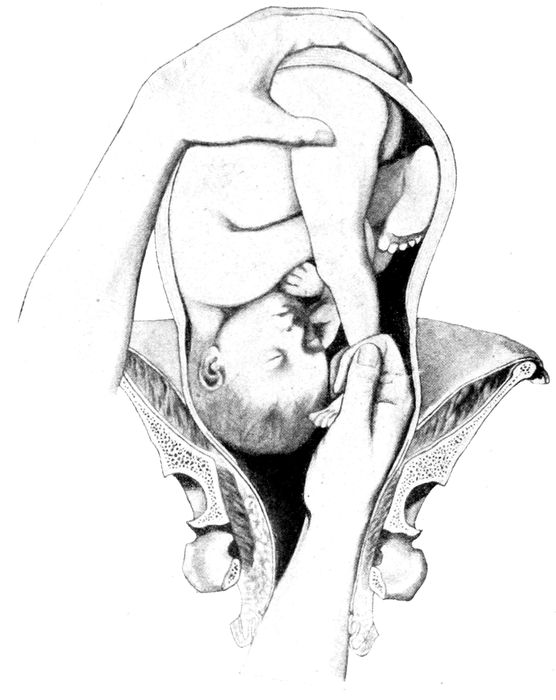
Fig. 80.—Version. Seizing a foot. (Hammerschlag.)
Version (Turning).—Version is a maneuver for altering
the presentation of the child while it is still in the
uterus. A vertex may be converted into a breech, a
breech into a vertex or a transverse into either a vertex
or a breech.
191
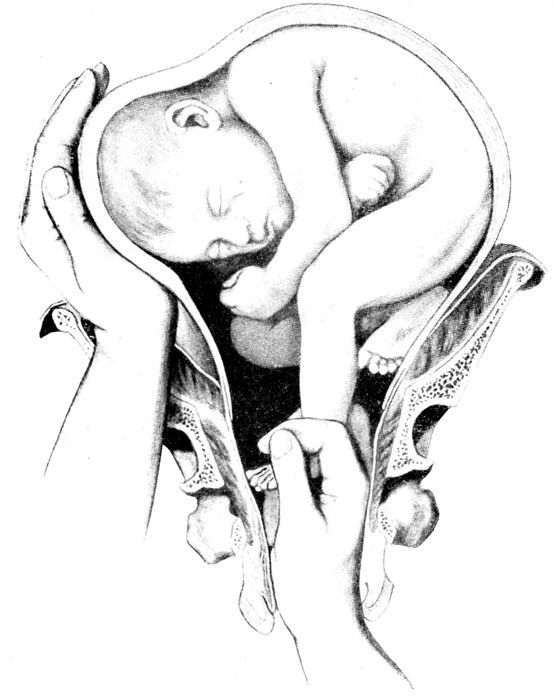
Fig. 81.—Version. The child rotates as pressure is made upon the head and traction upon the foot. (Hammerschlag.)
Version usually means that a transverse or a vertex
presentation is changed into a breech and is followed by
the extraction of the child. The operation is serious
and not to be undertaken without definite indications.
There is always the risk of sepsis and rupture of the
uterus as well as a high probability of a dead child.
192Perineorrhaphy is, if anything, more frequent after this
operation than after forceps.

Fig. 82.—Version is complete when the knee appears at the vulva. (Hammerschlag.)
Preparations.—The room and patient are arranged as
for forceps, except that the stirrups can not be put in.
The legs must be held by assistants, for the delivery of
the after-coming head may be complicated and require
the Walcher position, which can not be quickly obtained
if the legs are fast. Only eight minutes are allowed for
the delivery of the child after the navel passes the
vulva, if it is expected to live.
193The bladder and rectum must be empty.
Asepsis must be rigid and both subjective and objective.
The dorsal position on a table is imperative.
The diagnosis must be accurate and the anæsthesia carried
to the surgical degree.
Facilities for treating asphyxia neonatorum must be provided.
The following summary of the indications and conditions
may be convenient for reference.
Indications.—Contracted pelvis. (Consider pubiotomy.)
Abnormal position of the head. (Face position with chin
posterior.)
Prolapse of cord or an extremity with a presentation of the
head.
Placenta previa.
Transverse position after the seventh month.
Any condition requiring rapid delivery.
Conditions.—Cervix effaced and os dilated.
Uterus not in tetanus nor contracted down over the child.
The fœtus must be movable.
The head should not be engaged.
The Walcher position is produced by bringing the patient
down to the end of the table so that the sacrum rests
upon the edge. The thighs and legs are allowed to hang
down of their own weight and the patient is restrained
from falling off by traction upwards on the axillæ.
In the Walcher position the diameter of the pelvic
inlet is increased from ⅓ to ½ inch (1 cm.) and thereby
the delivery of heads that otherwise could not pass
becomes possible.
In addition to the Walcher position other measures
may be required to help the head through. Thus, traction
from below may be carried to the limit of safety
and in spite of the Walcher position the head may not
pass the inlet.
194Then pressure from above is added. This maneuver
will have to be executed in many cases by the nurse.
The fingers palpate the head above the pubes. Then
one or both fists are placed upon the abdomen over the
head and force is exerted to crowd the head down into
the pelvis. This is known as the Wiegand compression.
For the operations destructive to the child, craniotomy
or decapitation, the same arrangements are made.
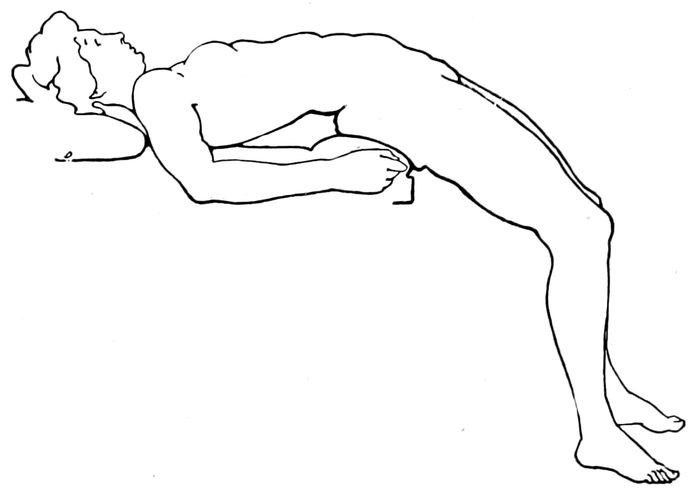
Fig. 83.—The Walcher position. (American Text Book.)
Cranioclasis is the crushing of the fœtal skull so that
in its reduced condition the child can be delivered and
the mother’s life spared. In addition to the solutions,
the only instruments required are the Auvard cranioclast,
a Naegele perforator, and a douche bag with
glass, or any tip that can be sterilized.
In many of these cases, both mother and child could
be saved if seen early enough to have a Cæsarean operation.
Decapitation is done to save the maternal life in cases
of transverse or shoulder presentation. The preparations
195are the same as already described for forceps and
version and the only instrument needed is a Braun blunt
hook. (Fig. 73.)

Fig. 84.—The Wiegand compression of the child’s head to force it into the pelvis. (Hammerschlag.)
Cæsarean section is the delivery of the child through
an opening in the abdomen.
It is made necessary by contraction of the pelvic
196bones, or by the presence of a fleshy or bony mass which
diminishes the size of the inlet. It may be required on
account of the closure of the vagina or cervix by scars
or on account of urgent conditions of the mother, such
as eclampsia, heart disease, and sometimes placenta
previa.
The technic is simple, but good judgment must be
used in knowing when to do it. Many operators find
it so easy that they prefer it to the harder but safer
obstetrical operations.

Fig. 85.—The Naegele perforator. (Hammerschlag.)
The time of election is when the woman is at term
but not in labor. This, of course, can be determined by
the history, but more certainly by careful measurements
of the child.
When it becomes necessary to operate on a woman
who has been in labor a long time and especially if she
has been examined frequently, the mortality is disproportionately
high.
It is a hospital operation, but may be done in the
house. If not an emergency, the bowels are emptied by
a laxative and enema the day before. Regular preparations
for laparotomy are made, plus the equipment
necessary for tieing the cord and resuscitating the
child. A table must be found large enough to hold the
patient in the horizontal position at full length. Solutions
of lysol 1 per cent and sterile water are placed on
197each side of the table. The instrument table carries
towels and suture material as well.
On a stand behind the operator is placed the hot bath
and tracheal catheter. This center is presided over by
someone skilled in the treatment of respiratory difficulties
in the new born. Altogether, five assistants are
required for the operation: an anæsthetizer, a clean
nurse, and a nonsterile nurse to manage supplies, an
operating assistant and one to take charge of the child.
Rubber gloves must be worn by the clean assistants.
2 scalpels.
2 scissors.
8 eight-inch forceps.
10 six-inch artery forceps.
4 sponge carriers.
4 tenaculum forceps.
2 rat-toothed tissue forceps.
4 full curved round needles for uterine wall.
4 smaller needles for the fascia.
2 Hagedorn needles for the skin.
2 needle holders.
1 dressing forceps.
Plenty of suture material, both catgut (No. 3 and 4) and silkworm gut for the abdominal wall.
1 doz. laparotomy sponges with metal rings sewed in or
a long tape attached.
6 large laparotomy pads.
1 large pillow slip full of sterile cotton.
Sponges.
1 laparotomy sheet.
1 dozen towels.
1 pair of leggins.
Gowns and head dressings (gauze will do) for the operator and assistants; rubber gloves, basins and accessories. All are sterilized.
If the woman has been examined, the vagina should
be sponged out with tincture of iodine. The abdomen is
198shaved, scrubbed with green soap, nail brush, and hot
water for five minutes. It is then rinsed with ether and
painted with iodine.
The presentation of the child, the presence and location
of the heart tones must be determined before operation.
The patient is anæsthetized with ether, chloroform or
gas.
The incisions are made; the child delivered to the
proper assistant; the placenta and membranes removed;
the sponges counted; and the uterus and abdominal wall
sutured.
After-care.—The nurse watches the patient for sighing
respiration, rapid pulse, pallor, and other symptoms
of hæmorrhage, either external or internal. Artificial
heat is supplied. Hæmorrhage from vagina should be
looked for. It is normal. Salt solution by hypodermoclysis
may be required. Hot water by mouth in small sips or tap
water by rectum (drop method) will relieve the thirst.
Morphine may be given if pain is extreme. An enema
may be given on the second day or calomel may be
started in the morning of the second day. Distention
from gas, with or without nausea and vomiting, hiccough
and rise of temperature are all signs of danger.
No milk should ever be given on account of the gas it
causes.
The child is put to breast as usual after twelve hours.
The stitches are to be taken out on the tenth or
twelfth day.
Symphyseotomy is a separation of the pelvis at the
pubic joint and is done with a scalpel or a specially devised
knife.
Pubiotomy is the division of the pelvis, three or four
centimeters to the right or left of the pubic joint. The
division passes through the pubic bone and is usually
199done with a serrated wire called the Gigli saw. It is
introduced subcutaneously by a special instrument
called a pubiotomy needle. Both symphyseotomy and
pubiotomy are preparatory to delivery. Pubiotomy is
the more desirable and successful operation. The ends
of the severed bones separate from one and a half to two
inches, and the child delivers easily through the enclosed
opening. The after-care is usually simple.
1 scalpel.
2 Gigli saws.
1 pubiotomy needle.
6 artery forceps.
3 eight-inch forceps.
1 needle holder.
2 retractors.
Suture material and sponges as usual.
The hips are strapped in circumference with zinc adhesive
plaster to support the bones.
The danger of infection of the wound from the lochia
is always present. The main difficulty is in moving the
patient, who is more than usually helpless. The bony
ring of the pelvis is broken and she can not raise her
leg. The repair is cartilaginous at first, but solidifies
in a few months so that locomotion is not impaired. Especial
pains must be taken to avoid bed sores.
200
CHAPTER XIII
MINOR OPERATIONS
Aseptic Care.—Place patient on a clean bed pan. It
need not be sterile. Drape with a sheet and arrange it
so the fold may be easily raised by nurse’s elbow. Have
sterile basin with cotton pledgets to be filled with solution
of lysol 1 per cent. Lysol must be put in basin
first and the water added. Take to bedside. Nurse
scrubs her hands ten minutes with a sterile brush, hot
water, and green soap. Use no towel, no gloves. Keep
hands wet and clean. Cleanse vulva with wet pledgets
from above downward. Apply sterile pad.
Sterile Specimen.—To get a sterile specimen of urine
without catheter, give aseptic care, tampon vagina with
large pledget of sterile cotton. Have patient urinate in
a sterile basin. Remove tampon.
Sterile Specimen from Child.—Take a glass test tube
and thrust its round end through a hole in a square
piece of adhesive plaster. Push it down until the plaster
is caught and stopped by the enlarged rim at the
mouth of the tube, with adhesive side of plaster on same
side as opening of tube. Fasten the tube over the male
penis or female vulva by applying the plaster to the surrounding
skin. Leave until full.
Aseptic Douche.—Boil douche point and basin.
Leave point in sterile basin. Fill douche can with
sterile water, temperature 104° to 110° F. Put clean
bedpan under patient who is draped with a sheet.
Have at hand a sterile basin containing solution of
201lysol 0.5 per cent, or boric acid 5 per cent in which cotton
pledgets are immersed. Scrub the hands as for aseptic
care. Cleanse the vulva with cotton pledgets, washing
always toward the anus, and use each pledget but
once. Adjust the douche point and introduce it just
inside the labia. The douche can should be only a trifle
higher than the pelvis. When can is empty, apply a sterile
pad.
Fig. 86.—Apparatus for getting a sterile specimen of urine from an infant.
202If the douche is to be used as a deodorant after the fifth
day of the puerperium, either of the following solutions
may be employed: Potassium permanganate, 1:5000;
formaldehyde 1 dram to quart, or chinosol 1:1000.
The vaginal douche may be used in cases of gonorrhœal
infection in pregnancy during the last weeks, in
the hope of avoiding infection of the child’s eyes.
It is given like the aseptic douche (q. v.) with potassium
permanganate 1:5000, or chinosol 1:1000. It should
be hot (112° to 120° F.), and be begun not long before
term, so that in case labor comes on, the danger to the
child will be minimized. The reservoir must not be too
high, nor the douche point inserted much beyond the
labia. The woman should be on her back and the
douche point should be rubber or glass.
Removal of Sutures.—On, or about, the tenth day the
removal of sutures is required.
The nurse will sterilize by boiling, 1 pair of long-handled,
sharp-pointed scissors, 1 pair of tissue forceps,
and if the sutures extend far into the vagina, a vaginal
retractor.
A basin of lysol solution (1 per cent) with cotton
sponges, a sterile towel to lay the instruments on, a
dish to receive the soiled dressings, sutures and discarded
sponges, completes the arrangement.
The patient is now draped with sheets as for examination.
The doctor prepares his hands as for operation.
The nurse holds the limbs of the patient in lithotomy
position and the operation is begun.
Uterine Tampon.—Packing the uterus is mostly employed
for hæmorrhage after labor. The patient, therefore,
203has been prepared and only fresh sponging with
lysol solution is required.
The instruments are, 1 vaginal retractor, 1 pair of
dressing forceps, 1 vulsellum forceps and a jar of gauze,
four to six inches wide and ten or twelve feet long. Always
use a single continuous strip. A very large quantity
is necessary to fill the uterine cavity. Any sterile
gauze may be used, but weak iodoform is satisfactory.
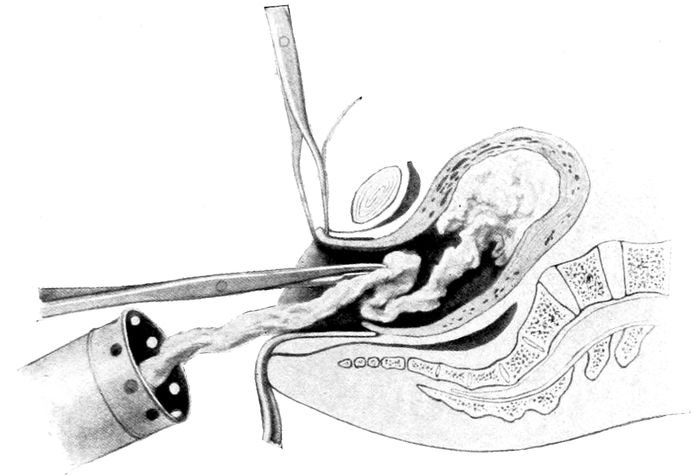
Fig. 87.—Tampon of the uterus. (Hammerschlag.)
The vagina is held open with retractors, the cervix
seized with a tenaculum and pulled down, the end of
the gauze strip is then carried into the uterus as far as
the fundus, the dressing forceps withdrawn and a new
length carried in until the cavity is packed tightly from
the fundus clear to the os.
Care must be taken that the strip of gauze is not contaminated
by vaginal contact during the introduction.
A pad and binder are now applied. If no instruments
are at hand, or there is not time to sterilize, then the
204nurse can grasp the fundus through the abdominal wall
with her hand and push the cervix down to the vulva
where the gauze can be pushed in by the doctor’s fingers,
if necessary.
The tampon acts as a hæmostatic through its direct
mechanical pressure, and dynamically by stimulating
the uterus to contract. It should be removed in from
twelve to twenty-four hours.
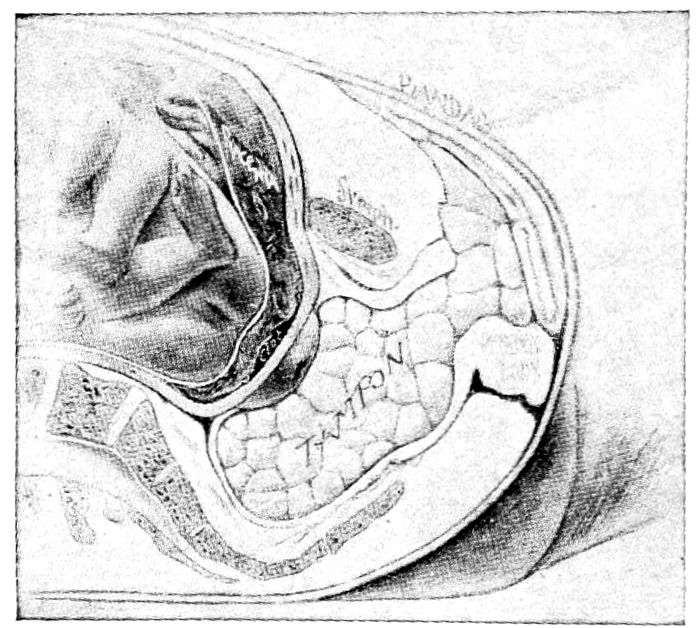
Fig. 88.—Tampon of vagina. (American Text Book.)
To tampon the vagina the woman lies on her back
across the bed, with her feet on the knees of the doctor,
who sits facing her. A sterile retractor holds back the
posterior wall of the vagina.
With a pair of dressing forceps the doctor seizes the
pledgets of cotton or gauze out of the lysol solution
and carries them one by one as far as they will go, in
various directions around the cervix. One is pushed
forwards toward the bladder, the next back toward the
rectum, the next in the middle, and so on until no more
can be introduced. A pad and binder are applied
tightly.
205The uterine douche is sometimes employed for hæmorrhage.
The field of operation and the doctor’s hands are
prepared as usual. The nurse cools the boiled douche
water down to 120° F. and if ordered, adds 2 drams of
sterile salt to each quart.
The instruments are a vaginal retractor, a long uterine
douche point, and one vulsellum forceps.
The cervix is seized and brought down, the long
douche point connected with the tube from the reservoir
is carried to the fundus and the water started. Care
must be used that the return flow is free and unobstructed.
This method is most satisfactory in uterine hæmorrhage
after the uterus has been entirely emptied. It
stimulates a prolonged and profound uterine contraction.
Intravenous Injections.—The vein in the front of the
elbow is usually chosen. (Median basilic or median
cephalic.) A rubber bandage or tourniquet is wound
tightly about the middle of the upper arm to make the
veins stand out prominently. The surface of the skin
should be sterilized for operation by scrubbing with
green soap and hot water and rinsing with 50 per cent
alcohol, followed by 1:2000 solution of bichloride, or
by the application of tincture of iodine.
The hypodermic needle is then introduced after expulsion
of all the contained air and the piston is drawn
up until the blood enters. This assures the operator
that the needle has entered the vein. The bandage is
now loosened and the solution of the drug is introduced
very slowly.
Intravenous infusion or transfusion is given in the
same way. The fluid (normal saline?) must be running
from the needle as it is introduced.
206Hypodermoclysis is the introduction of normal saline
solution, under the skin, or under the breasts. The solution
may be transfused also into a vein.
By this operation, the quantity of fluid in the vessels
is greatly increased and a circulatory stimulant is
provided. Normal saline also promotes diuresis and
aids in the removal of wastage.
The principal dangers arise from too great rapidity or
too large a quantity of the flow.
The skin should be sterilized at the point of attack
by a coating of tincture of iodine.
The instruments required are, a bath thermometer, a
douche can (fountain syringe) with long tubes and an
aspirating needle. A hypodermic needle will do, but
the reservoir must be well elevated since the caliber is
so small. Ordinarily the reservoir need be held only two
or three feet above the point of discharge. The water
should be flowing through the needle when it enters the
tissues. If the fluid is to be introduced under the skin,
the best place is in the loose region between the hips
and the ribs in front. If under the mammary gland, the
needle must go below and under the gland from the outside
edge, not into the gland. If into a vein, such additional
instruments will be needed as a rat-toothed tissue
forceps, a pair of sharp-pointed scissors, a knife and
some fine catgut. From four to sixteen ounces of fluid
may be used at a temperature varying from 105° to
110° F.
The openings where the needles entered are closed by
cotton and collodion.
Curettage of uterus is done for abortion or puerperal
sepsis when foreign fragments are left in the uterus.
The room is prepared as for delivery.
207The instruments are:
1 vaginal retractor.
1 vulsellum forceps.
1 long uterine douche point.
2 dull curettes.
2 sharp curettes of different sizes, together with gauze for packing the uterus.
Rubber gloves should be worn both by nurse and
physician as much for personal protection as for the
patient’s safety. In many cases of incomplete abortion
or of puerperal sepsis the endometrium is more satisfactorily
curetted with the gloved fingers.
Abortion may be indicated in many of the early complications
of pregnancy, such as hyperemesis, nephritis,
uncompensated heart lesions, tuberculosis, insanity,
hydramnios, incarcerated retroversions of the uterus
and the presence of hæmorrhage. These cases require
the operation to be undertaken and finished by the doctor,
but other conditions develop wherein, without volition
on the part of the patient or doctor, the abortion
begins. Some may be saved, but at times the attempt is
futile.
If the emptying of the uterus seems inevitable, the
function of the physician is to see that the process is
finished as quickly and cleanly as possible.
This may be done in the early stages by packing the
cervix and vagina with iodoform gauze and administering
ergot in twenty-five drop doses thrice daily.
In case of dangerous hæmorrhage from spontaneous
abortion, the vagina can be tamponed with cotton pledgets
or gauze by a clean nurse while awaiting the arrival
of the doctor.
When the uterus has partially emptied itself and the
retained fragments prevent the complete contraction
and allow of serious bleeding, or if the fragments are
208septic, then their removal is required. This is done by
the finger or curette.
The preparation of rooms, patient and doctor are the
same whether the operation is for therapeutic or incomplete
abortion. These have been described.
The instruments are:
1 pair dressing forceps.
2 vaginal retractors.
artery forceps.
2 curettes of different sizes.
2 vulsellum forceps.
1 long uterine douche point.
1 pair Goodell dilators.
1 douche can.
The induction of labor at or near term is done for
pelvic contraction, maternal disease, for danger threatening
mother or child, or to avoid the birth of a post-mature
child. A variety of methods may be employed,
but the Vorhees bag is best.
Technic.—Assemble, and sterilize by boiling twenty
minutes, a Vorhees bag No. 3 or 4, Simon speculum or
vaginal retractor, 1 pair long Pean forceps, 2 pairs
vulsellum forceps, 1 dressing forceps, 2 pairs compression
forceps, 1 Goodell dilator, 1 tenaculum forceps,
Davidson hand bulb syringe with glass tubes and rubber
connections for the bag.
Patient, prepared as for delivery, is placed upon the
209table in exaggerated lithotomy position. Stirrups will
serve.
The vagina is retracted, a smear made from cervix,
and the mucous membrane wiped clean with pledgets
of gauze on forceps.
Anæsthesia is only occasionally necessary even in primiparas.
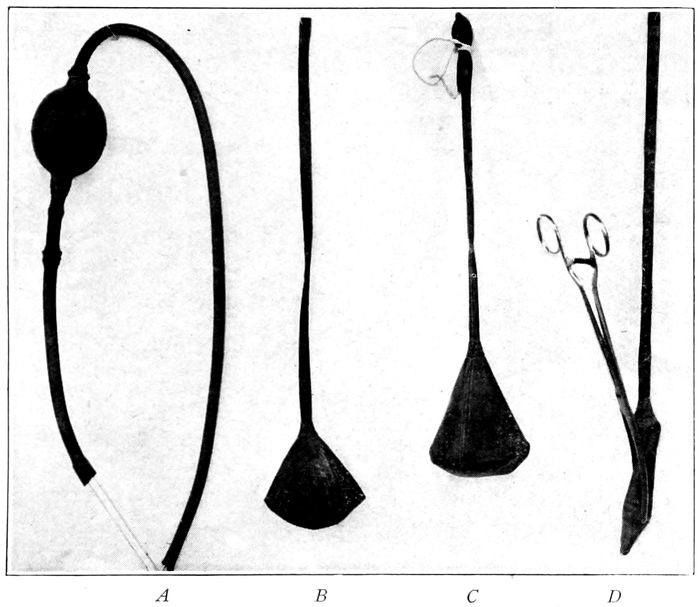
Fig. 90.—A, Hand bulb syringe; B and C, Vorhees bags; D, Bag rolled and grasped by Pean forceps ready for introduction.
Before using, the apparatus must be tested by forcibly
filling the bag with sterile solution.
One lip and sometimes both are seized by vulsellum
forceps and brought down. Usually, even in primiparas,
the os is sufficiently patulous to admit the bag—if not,
dilate.
210
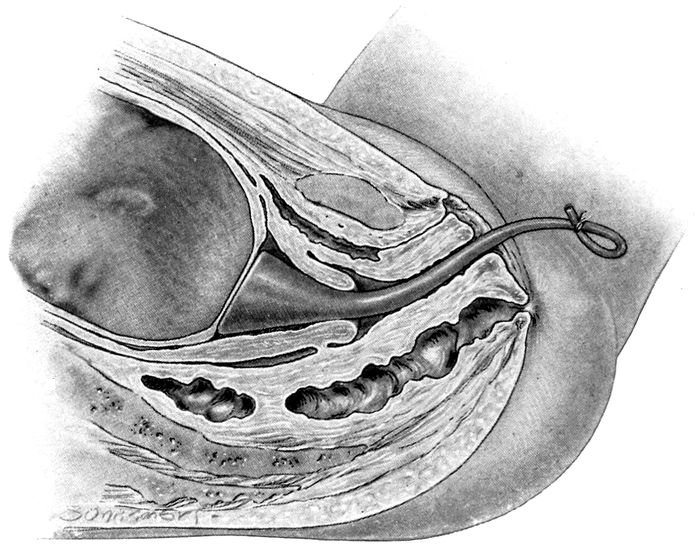
Fig. 91.—Vorhees bag in place.
The bag, emptied of residual air and fluid, is rolled up
into a compact mass like a cigarette, seized with Pean
forceps so that the tips extend just to the end of the
bag. Turn the concavity of forceps toward patient’s left
leg and introduce. As the bag enters turn the mass to
the left—a quarter turn—so that when operation is
completed the forceps curve faces upward. Release the
lock on forceps. Connect the tube of the bag with syringe
tube and force the solution slowly into bag.
Pean forceps may be removed as bag fills. Remove vulsellum.
Tie tube of bag with tape when bag is full—disconnect
syringe. Put sterile pad on either side of
tube.
If pains do not start within an hour, or if compression
is desired as in placenta prævia or a more rapid
211dilatation, then a weight of one or two pounds is attached
by a tape to the protruding tube and passed over
the foot of the bed.
Digital dilatation of cervix may be indicated in cases
of rigid os or where prolonged labor or some danger to
mother or child requires the hastening of the delivery.
No instruments are needed, but a complete anæsthetic
is necessary.
Thorough asepsis must be observed. The patient’s
genitals and the doctor’s hands are prepared as described
for labor, and rubber gloves are imperative.
The gloved hands and the vagina and vulva are well
rinsed with lysol solution 1 per cent. The operation
must be done carefully, patiently and gently, lest the
cervix be lacerated.
The hand is introduced into the vagina, and first the
thumb and index finger are introduced into the os
and separated as widely as possible, then the second
finger and so on, until the dilatation is complete. (Hirst’s
method.)
Another method is the introduction of the tips of both
index fingers, back to back. Force exerted will dilate
the canal so second fingers may also be inserted. Then
patiently and gently the rigid ring of the os is overcome.
(Edgar’s method.)
Episiotomy.—This is a clean incision of the vulva,
which is done to avoid an apparently inevitable and
ragged tear of the perineum.
The instruments required are either a blunt tipped
knife or a pair of blunt scissors.
The operation may be done on one or both sides depending
on the amount of room required. The incision
begins at a point just above the lower third of the
vulvar outlet when distended by the head, and passes
212obliquely downward and outward. This severs unimportant
tissues only, instead of allowing the valuable
perineal body to suffer. It makes a clean wound that
heals readily, instead of a ragged tear through bruised
tissue. The cut is high enough to be free from the
constant bath in infectious lochia, which troubles the
healing of the usual perineal laceration.
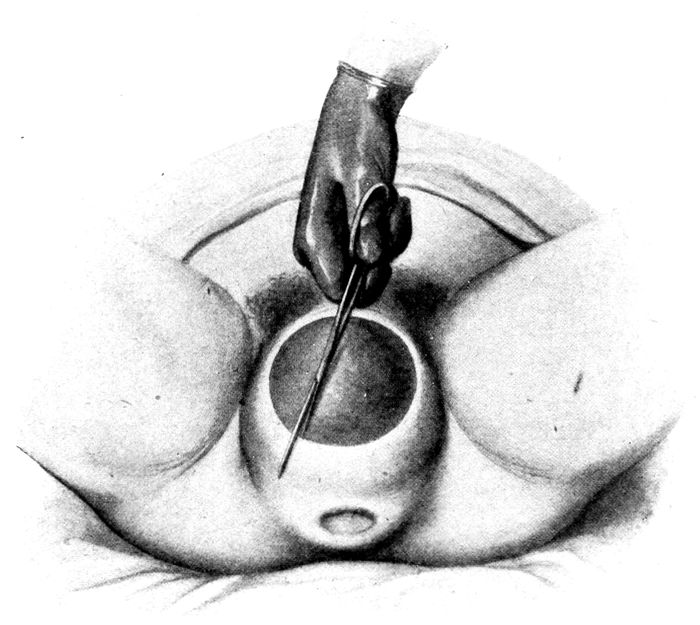
Fig. 92.—Episiotomy. (Hammerschlag.)
Rectal Infusion (Drop Method).—A douche bag containing
normal saline solution is hung near the bed and
kept warm with an electric pad, a hot flatiron, or by a
hot water bag on either side. The tube ends in a catheter
which is inserted into the rectum. The tube is
clamped so that only a drop of solution can escape each
second.
213Wet packs are both sedative and antipyretic and may
be employed for a local or a general effect.
For bronchitis the pack may be applied to the chest
only as follows: The child (or adult) is stripped in a
warm room (75° F.) and the chest swathed front and
back with a thick towel wrung out of hot water (temperature
105° to 110° F.) Over this a woolen shirt may
be drawn or a blanket wrapped, and the patient put to
bed. After six or eight hours, the dressing is removed
in a warm room, a hot bath administered, and the body
well rubbed with alcohol, and dried. The treatment
may be repeated if necessary. Do not burn the patient
by applications too hot.
The general pack is most serviceable in reducing temperature
and producing a diaphoresis to relieve the kidney
and cleanse the system, as in eclampsia. For this
purpose the entire body, naked, is rolled in a sheet
wrung out of hot water and then put between heavy
blankets in bed. The pulse should be taken frequently
and the temperature recorded at intervals. A cool application
to the head is very soothing.
The patient sweats profusely and hot drinks may be
given to promote a more abundant diaphoresis. Usually
the patient drops off to sleep as the fever subsides.
Twenty to forty minutes is the average duration of such
a treatment.
When the pack is removed, the patient is wrapped at
once, without drying, in warm blankets, and left for an
hour or so.
214
CHAPTER XIV
COMPLICATIONS IN LABOR
Pelvic contraction is not infrequently the cause of
difficult or prolonged labor. The deformity is most commonly
due to rickets in childhood.
There are many forms of pelvic contraction, but in
this country only two are at all common; the generally
contracted, and the flat pelvis.
The generally contracted pelvis is, in the main, a well
shaped pelvis, only its measurements are smaller than
normal.
The flat pelvis is marked by a shortening of the anteroposterior
diameter of the inlet. It looks as if it
had been pressed together from before backward while
in a soft condition.
These and other deformities will be recognized in advance
of labor by the routine application of the pelvimeter.
The value of this instrument is so great, that no competent
man does obstetrical work at the present time
without using the pelvimeter as a routine.
The average diameters in normal pelves may be tabulated
as follows:
Interspinous—between the anterior superior iliac
spines—25 cm.
Intercristal—between the iliac crests—28 cm.
External conjugate—taken from the upper border of
the symphysis to the depression below the last lumbar
vertebra—20.5 cm. Take 9.5 cm. from this to get the
true conjugate.
215
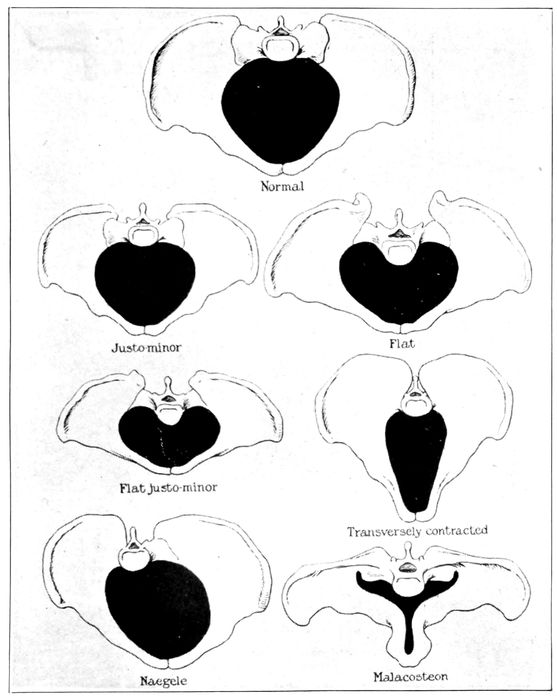
Fig. 93.—Various forms of pelvic deformity compared with the normal inlet. (Bumm.)
The circumference of the hips just below the iliac
crests and above the trochanters—90 cm. It is taken
with a tape line. These are the usual external measurements.
The internal measurements are made with the fingers.
216
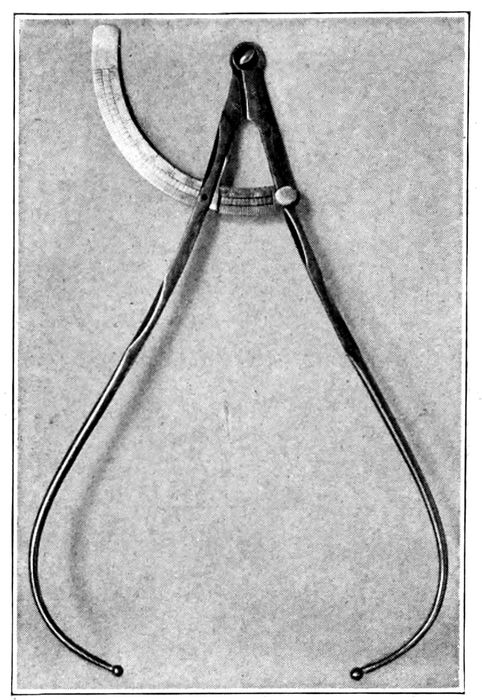
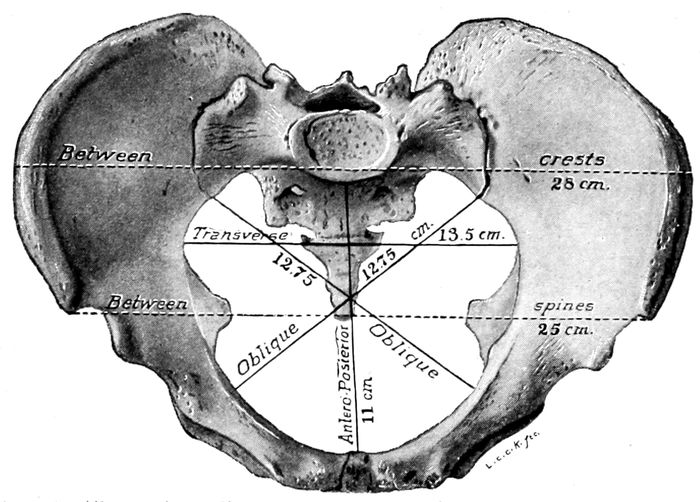
Fig. 95.—The various diameters of the inlet with the lengths given in cubic centimeters. (Williams.)
217
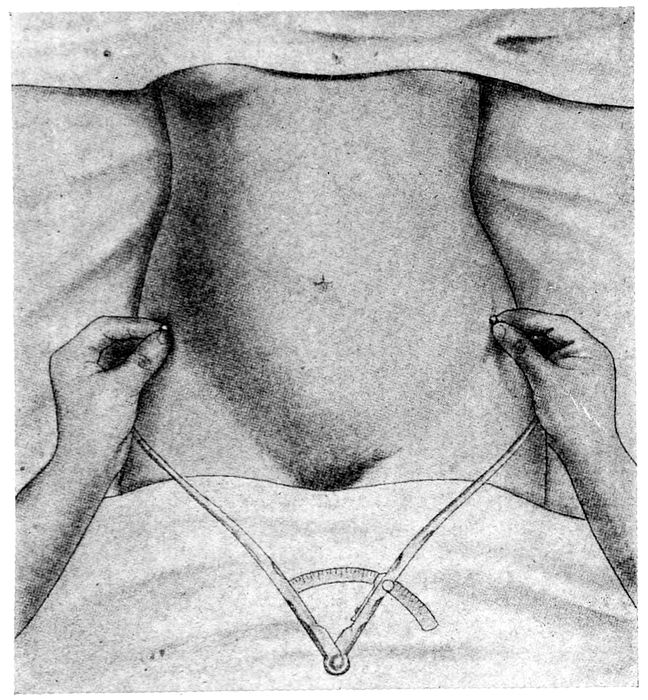
Fig. 96.—Measuring the distance between the anterior superior spines of the pelvis. (Williams.)
The diagonal conjugate is the distance from the lower
border of the symphysis to the promontory of the sacrum.
It should measure 12.5 cm. The first and second
fingers are passed into the vagina and pushed up until
the tip of the second finger touches the promontory of
the sacrum. The finger of the other hand marks the
depth of the examining fingers just below the symphysis.
The distance is measured when the finger is withdrawn,
and 1.5 cm. is subtracted. The result is the true
218conjugate. These measurements carefully made and
the deduction judicially estimated, give one a fairly approximate
idea of size and shape of the pelvic inlet.
The aim of nearly all the pelvic measurements is to get
not only the size and shape of the inlet, but so far as
possible, a working estimate of the anteroposterior diameter
of the brim, which is the most important of all the
diameters. In normal cases this should be 11 cm.
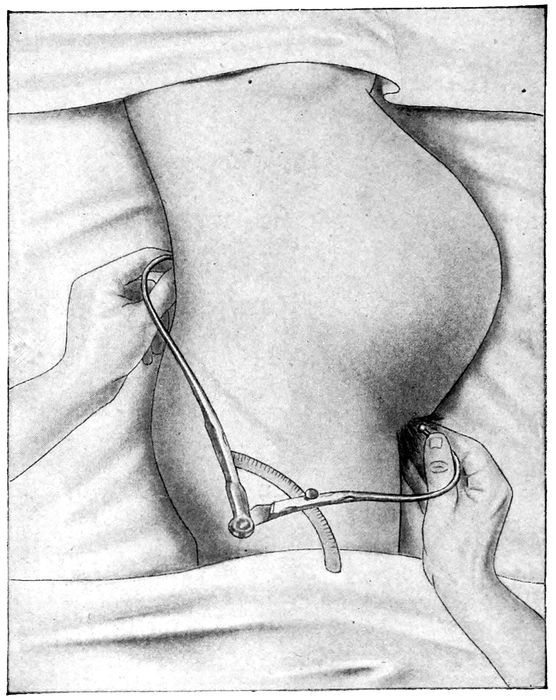
Fig. 97.—Measuring the external conjugate. (Williams.)
219Thus, taking 9.5 cm. from the external conjugate
(20.5 cm.) gives 11 cm.
Subtracting 1.5 cm. from the diagonal conjugate as
obtained with the fingers as above described, (12.5 cm.)
gives 11 cm. The subtraction is made to compensate
for the thickness of the pubic bone and its inclination
outwards.
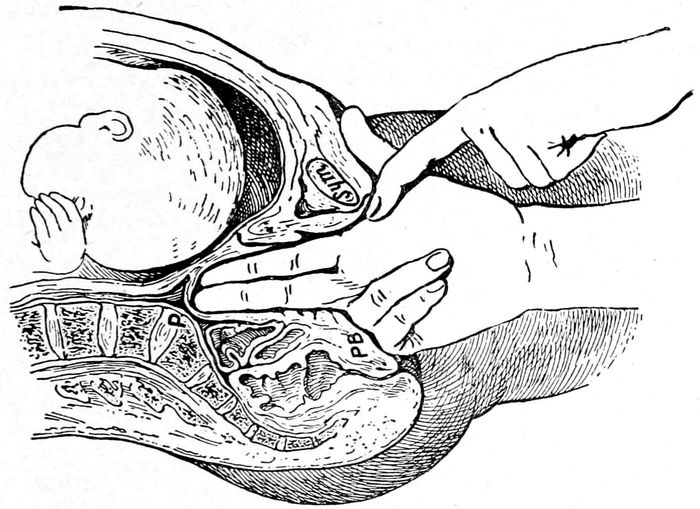
Fig. 98.—Measuring the diagonal conjugate with the finger. (Eden.)
A circumference of 90 cm. corresponds to an inlet of
11 cm. in its anteroposterior diameter, and every variation
of 5 cm. in this circumference makes a difference of
1 cm. (either larger or smaller) in the anteroposterior
diameter.
Thus, 95 cm. in circumference=12 cm. in the diameter;
and 85 cm. in circumference=10 cm.
Complications increase in proportion to the degree
of contraction in the pelvis.
The most frequent difficulties superinduced by the
220small pelvis are prolapse of the cord, malpresentation
and malpositions of the head, prolonged labor, and a
large increase in the number of assisted deliveries.
All the possibilities and probabilities in a given case
will be carefully worked out before labor by the conscientious
obstetrician, and Cæsarean section, induction
of premature labor, pubiotomy, forceps, or version and
extraction, will be done with a sure foreknowledge.
Prolapse of the cord complicates labor once in about
two hundred cases. It is most likely to occur when the
presenting part does not enter or does not entirely fill
the opening, as in transverse or shoulder presentations,
or vertex presentations with small inlets.
The mother is not endangered by this mishap, but the
babe is lost in from 35 to 60 per cent of the cases.
The diagnosis is easily made when a loop of cord protrudes
from cervix or vulva, and the pulsation will differentiate
it from everything else.
If the cord does not pulsate, the family should be informed
that the child is dead and the case may be allowed
to terminate normally.
If it still pulsates, the woman should be placed in
the knee-chest position for ten or fifteen minutes, then
upon the side, opposite to that on which the cord has
prolapsed, and back again as soon as possible to the
knee-chest position. A chair may be used to produce a
Trendelenburg position by placing it so that the edge of
seat and top of back rest on the bed. Then the patient
puts her legs over the lower rungs and lies with her
back against the chair back and her head on the bed.
If the cervix is effaced and the os partly dilated, reposition
may be attempted either with the finger or a male
catheter.
221The operation will, of course, succeed most easily if
done in the knee-chest position, with gravity to aid.
If the cord can be pushed back, a Vorhees bag may
be inserted to keep it from coming down again. This
holds back the cord, dilates the canal and stimulates
the pains.
When the bag comes out, version and extraction can
and should be done at once.
In general, the following summary may be useful:
Causes.—
Contracted pelves.
Breech and transverse presentations.
Malposition of head, or face and forehead presentation.
Hydramnios.
Accident.
Low insertion of placenta.
Diagnosis.—
Before rupture of membranes careful examination will show
pulsating cord in advance of head.
After rupture the cord may be felt in vagina.
Dangers.—
To mother:—None but those due to causative condition.
To child:—Compression of the cord and asphyxiation.
Contraction of exposed vessels of cord.
Patient may lie on cord.
Twenty-five per cent die as a rule under best conditions.
Fifty per cent when left to nature.
Treatment of Cephalic Presentation.—
Extraction of child or reposition of cord, depending upon
the degree of dilatation.
If cervix is small, replace and fill cervix with Vorhees bag.
When cervix admits hand, either replace or do version and
extraction.
With head engaged, reposition or version is not possible.
Child living:—Rapid delivery with forceps.
Child dead:—Craniotomy or leave to nature.
Prolapse of one or both hands may take place. If the head
is engaged, no interference should be attempted. If not,
replacement or version may be done.
222The soft parts may also complicate the labor process.
No time need be spent here on the rarer forms of obstruction
due to uterine or ovarian tumors.
Rigidity of the cervix, or os is not uncommon.
This may be due to a dense, almost cartilaginous consistence
of that tissue, to premature rupture of the bag
of waters, to weak, inefficient contractions in the first
stage, or to a steel-spring-like contraction of the muscular
fibers of the os.
In all cases the first stage of labor is greatly prolonged,
but so long as the membranes are intact, the
child is in no danger.
Two kinds of cases are met with, those in which the
pains are violent, and those in which they are weak
and shallow. In the first class, as soon as the condition
is recognized, a dose of morphine sulphate, ⅙ gr. and
scopolamine hydrobromide 1/150 gr. should be given, hypodermically.
The rigid ring relaxes under the influence
of the narcotic, and labor proceeds rapidly and almost
painlessly. Chloroform may be substituted if the morphine
and scopolamine are not at hand. If the cervix
is effaced and only the rigid ring of the os prevents the
completion of the labor, or if the above methods fail,
then the patient may be anæsthetized and the rigidity
overcome by the fingers. This is an emergency that
should not be attempted until all else has failed and
some danger arises that makes it necessary to hasten the
delivery. (See Minor Operations, p. 211).
Where the constriction is due to unusual density of
the cervix or to cicatricial tissue, it is sometimes necessary
to make incisions under aseptic precautions so
that the rigid ring may expand.
Weak and inefficient contractions can sometimes be
223stimulated satisfactorily by the introduction of a Vorhees
bag.
Rigidity of the pelvic floor may be due to inadequate
elasticity of the tissues as in old primiparas or in young
women who have ridden horseback for many years in
the cross-saddle position.
The head may come down to the pelvic floor but will
not advance further. If the tissues of the vulva do not,
or can not yield sufficiently after appropriate time has
been allowed, episiotomy may be done. (See Minor
Operations, p. 211.)
The uterus itself may functionate abnormally.
Precipitate labor is an over rapid advance of the child
wherein the stages of labor are merged into one another
and the child expelled in two or three pains.
It may be due to unusual capacity of the pelvis, or
to strong contractions which the patient is not aware
of, or both. These cases predispose to post partum
hæmorrhage and to serious lacerations of cervix and
perineum.
The child is usually delivered in an undesirable place,
such as a toilet basin or a street car, and perishes from
the fall, from cold, from umbilical hæmorrhage, or lack
of facilities for revival.
The nurse who is watching a case is responsible for
the prevention of a precipitate. If the event impends,
the woman must be placed upon her side with legs
straight, and she should be instructed to cry out with
every pain. Chloroform may be given and the head
forcibly held back.
Uterine Inertia.—A sluggish state of the uterus may
characterize the labor and the contractions will be slow,
shallow and inefficient. The intervals may be prolonged,
although the patient complains bitterly of pain.
224The condition is seen most frequently in multiparas and
is due to defective innervation of the uterus or to imperfect
reflexes, and in primiparas also it may be due to
the newness of the function that is suddenly called into
play, or to contracted pelvis. Many times the trouble
results from overfatigue and want of sleep. If this is
the case, the remedy may be found in the administration
of morphine sulphate ⅙ gr. and scopolamine
1/150 gr. The pains are diminished or abrogated while
the contractions continue. The scopolamine may be repeated
if necessary. Under proper indications and conditions
this treatment is harmless, both to mother and
child, but requires supervision on the part of the nurse
or physician.
If the patient is not overly fatigued, the introduction
of a Vorhees bag, as described under the head of
Induction of Labor (p. 208) will dynamically increase
the strength and frequency of the contractions, mechanically
aid the effacement of the cervix and the dilatation
of the os, and shorten the first stage anywhere from
six to twelve hours.
As soon as the os is dilated, pituitrin may be given
under due precautions, as hereafter indicated. Pituitrin
has but little influence on the nonfunctionating
organ, but acts well on a uterus which is definitely contracting.
It should not be given during the first stage,
since when the uterus contracts, there must be an adequate
opening for the advance of the child. Five to
seven minims is the usual dose, injected into the deltoid
muscle. The injection may be repeated in an hour, if
required, since the effects, which begin about five minutes
after the injections, will pass off in fifty-five
minutes.
By the use of pituitin many operative procedures are
225altered or avoided. A high forceps case may be converted
into a case for the low instruments, and the latter
in many instances avoided altogether.
The use of pituitin may be briefly summarized as follows:
(Use no alcohol to cleanse syringe or skin before injection.)
Indications.—
1. Inertia uteri or weak, shallow pains in second stage.
2. Multiparity.
3. Post partum hæmorrhage.
4. To avoid use of forceps or to reduce a high forceps case to
a low one.
5. Cæsarean section.
If the patient is a multipara, sterile linen should be on and
attendants ready for the delivery before an injection is
given.
Conditions.—
1. Cervix effaced.
2. Os admits three fingers. (Better if membranes have ruptured.)
3. Head should be engaged.
4. No mechanical obstacle to delivery such as tumors or
markedly contracted pelvis, etc.
Dangers of Long Labors.—
Compression of cord.
{Vesicovaginal fistulæ.
Necrosis of maternal tissues. {
{Rectovaginal fistulæ.
Infection—peritonitis.
Necrosis of skin over skull.
Necrosis of cranium.
Fracture of skull.
Death of child.
Maternal exhaustion and prolonged convalescence.
Premature rupture of the membranes not infrequently
occurs from over-distention, when twins or hydramnios
is present, or at any stage of the pregnancy when
the membranes are weak. The liquor amnii flows off,
226not all at once, but after the first gush by intermittent
discharges, depending on the painless uterine contractions
and the accuracy with which the head fits the
pelvis. Labor usually comes on in from twelve to forty-eight
hours, but it may be postponed for a month.
The labor is sometimes more painful and prolonged
on account of the absence of the fluid wedge and the
generous lubrication of the channel which is supplied by
the liquor amnii.
The danger of infection of the amniotic cavity with consequent
death of the child is always to be apprehended
after the escape of the liquor amnii. Also the fœtal
parts may prolapse and complicate the labor; or if the
cord comes down, the child may be imperiled by its compression.
If near term, the rupture of the membranes is not of
great importance though the case must be watched attentively.
Daily observation must be made of the fœtal heart
tones, the amount of liquor amnii flowing away, and
the presence or absence of infection. If labor does
not determine in a few days or if the heart tones rise
above 160 or go below 120, labor must be inaugurated.
(See Induction of Labor, p. 208.)
Rupture of the uterus is the most serious accident that
occurs in labor. It happens about once in three thousand
confinements. The tear is usually in the lower
part of the uterus and follows a prolonged period of
labor, where the child is in a transverse presentation,
and, therefore, impossible to deliver, or the pelvis is
too small or the child too large. It may also follow ill-advised
or unskillful efforts to change the presentation
by the introduction of the hand into the uterus. Occasionally
rupture is produced by external violence, such
as blows or kicks upon the abdomen.
227It is imperative to be able to recognize the symptoms
when rupture impends or actually occurs.
Signs of Threatened Rupture of Uterus.—
- 1.
- High position of the contracting ring—especially its obliquity. The contracting ring is a
ridge-like formation that may be found running across the anterior and lower portion of
the uterus.
- 2.
- High position of fundus.
- 3.
- Tension of round ligaments.
- 4.
- Rotation of uterus about its long axis.
- 5.
- Tenderness to pressure of lower uterine segment.
- 6.
- Contractions persistent with no pain-free interval.
Signs of Actual Rupture of Uterus.—
- 1.
- Hæmorrhage is one of the earliest and most significant signs, and may be either external
or internal.
- 2.
- Cessation of uterine contractions either abruptly or gradually.
- 3.
- Extreme pain felt by patient.
- 4.
- Recession of presenting part.
The patient gives a sharp cry and has the feeling that
something has given way. Signs of shock rapidly supervene.
A predisposition to rupture may be present from
the scars of a Cæsarean section, uterine tumors, and degeneration
of the muscle.
The treatment depends upon the degree of the injury,
and if investigation shows that the uterus has opened
into the abdominal cavity, immediate laparotomy is
done. In other cases, the morcellation and removal of
the child by the natural passage may permit the use
of a uterine pack and avert the necessity for an abdominal
operation. The child is usually dead and need
not be considered.
228
CHAPTER XV
COMPLICATIONS IN LABOR (Cont’d)
Vomiting in labor frequently occurs near the end of
the first stage. It is due to the sympathetic excitement
of the nerves of the stomach as the last fibers of the
os uteri give way. It requires no treatment.
Hyperemesis in labor is very rare, but when it does
occur, the delivery should be expedited.
Hæmorrhages may occur either before, during, or
after labor. Hæmorrhage is always serious.
Hæmorrhage before labor arises either from a premature
detachment of a normally implanted placenta
or from placenta prævia. The first is sometimes called
“accidental hæmorrhage” to distinguish it from the
latter, or “unavoidable hæmorrhage.”
Accidental hæmorrhage may be the result of an injury
or a blow, but in many cases, there is no such history.
The hæmorrhage is most frequent in the later
months of pregnancy, and may be without any apparent
cause. The hæmorrhage may be entirely inside the
uterus (concealed hæmorrhage) or it may appear externally.
The hæmorrhage, when concealed, takes place back
of the placenta or between the membranes and the
uterine wall. If the hæmorrhage is concealed, it is
usually followed by an attempt to expel the child. If
the hæmorrhage is pronounced, systems of shock appear.
The diagnosis is made by the symptoms which are
summarized in differentiating this condition from
placenta prævia (p. 231).
229From this affection, nearly all the children and half
the mothers die.
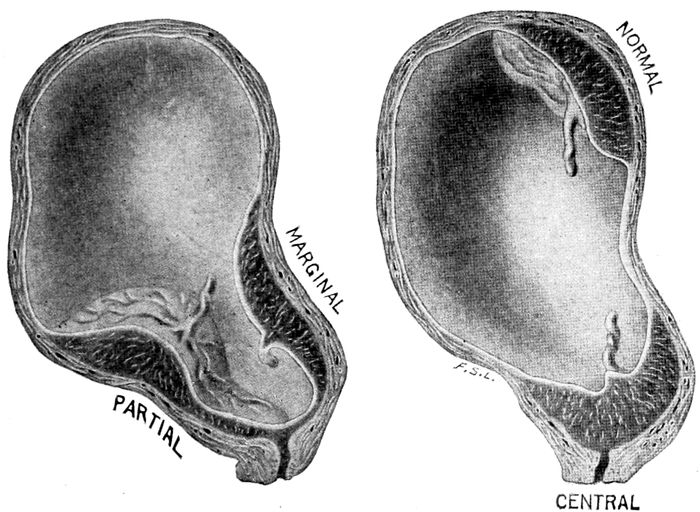
Fig. 99.—Various forms of placenta prævia compared with normal attachment of the placenta. (American Text Book—Williams.)
When the hæmorrhage is external and slight, the
treatment may possibly be expectant for twelve hours,
if carefully watched, but usually the symptoms become
so serious that immediate emptying of the uterus is
required either by the Vorhees bag, digital dilatation,
version and extraction, or Cæsarean section, the method
chosen being dependent upon the amount of the hæmorrhage,
the vigor of the mother and the condition of the
cervix, os, pelvis, and child.
Placenta prævia is the name given to a placenta that
is attached low down in the uterus so that its margin
or a large part of its mass overlies the os. This happens
through the action of the egg which embeds itself
230too far down on the endometrium—too close to the
cervix.
Three different kinds are known and named from
their manner of encroaching on the os, as marginal,
partial, or central implantation of the placenta.
The hæmorrhage is from a loosening of the placental
attachment owing to the stretching and growth of the
uterus.
There is only one symptom of placenta prævia—sudden,
painless, causeless hæmorrhage. The bleeding
seldom appears before the twenty-eighth week, and no
suspicion of a placenta prævia may arise before the appearance
of hæmorrhage, which, as a rule, is soon repeated.
Labor frequently comes on prematurely and malpresentations
naturally result from the inability of the presenting
part to fit itself into the pelvis.
There is no bag of waters, hence the first stage is
longer and bloodier and fraught with much danger.
Interference is regularly indicated to save the life
of the mother, while the child also has a high mortality.
Puerperal infection is not uncommon.
Placenta prævia is always an emergency. If the patient
can be kept under observation in a good hospital,
one may temporize, but under other conditions the
uterus must be emptied at once, even if only a single
hæmorrhage has developed. The indications are, (a)
to control the bleeding, and (b) to empty the uterus.
The life of the child must be disregarded and the mother
alone considered.
If the contractions have not begun, they should be
stimulated by the introduction of a Vorhees bag, which,
at the same time, dilates the canal and mechanically
shuts off the bleeding vessels by compression. In introducing
231the bag, the membranes may be ruptured so
the bag will pass into the uterine cavity. When the
implantation is central, the finger must tear a hole
through the placenta, and through this opening pass
the bag inside the uterus.
If the os is partially dilated, version may be done,
and a foot brought down. The leg may then be pulled
upon until it compresses the bleeding area and the
traction maintained with a slowly developing pressure
sufficient to check the hæmorrhage, until dilatation is
advanced enough for delivery. Occasionally good results
are obtained by tightly packing the cervix and vagina
with gauze or cotton. (See Vaginal Tampon, p. 204.)
Cæsarean section may be done in the interests of the
child, as well as the mother.
The fœtal mortality in placenta prævia is said to be
60 per cent and the maternal 10 per cent.
| Differential diagnosis between |
|---|
| |
| Accidental hæmorrhage and |
Placenta prævia |
| |
| Usually occurs in later months. |
Any time after the twenty-eighth week. |
| |
| May be concealed or open. |
Always open and external. |
| |
| Soon followed by labor pains. |
Labor need not occur. |
| |
| Uterus becomes larger if bleeding is concealed. |
Uterus remains same size. |
| |
| Uterus hard and woodeny. |
Uterus, normal consistency. |
| |
| In severe cases, signs of shock whether hæmorrhage is external or internal. |
In severe cases, signs of shock follow the invariable external hæmorrhage. |
| |
| No placenta can be felt. |
Placenta can be felt through the os. |
| |
| Hæmorrhage continues. |
Hæmorrhage intermittent. |
| |
| No history of previous attack. |
Possibly history of previous attack. |
| |
| No contractions after labor begins in serious cases. |
Contractions as usual. |
| |
| No bogginess of cervix. |
Cervix boggy. |
232Hæmorrhages may occur during labor from retention
of the major part of the placenta while a portion is
detached. This may be due to pre-existent disease, such
as endometritis, or from uterine inertia.
Normally the placenta will separate and be discharged
within an hour after labor and in the absence of hæmorrhage
it may go even longer than this with safety. The
occurrence of severe hæmorrhage, however, requires the
immediate cleaning out of the uterus by inserting the
hand and peeling the placenta from its attachments.
Post partum hæmorrhage includes all hæmorrhages
that occur after the delivery of the placenta.
The “flooding” as it is called by the laity, is most
apt to come on either immediately or within an hour
or so after labor. If it comes on after the first twenty-four
hours, it is called secondary hæmorrhage. Such
predisposing causes as over-distention from twins may
be present, but the hæmorrhage may follow a perfectly
easy and apparently normal labor so suddenly and so
profusely that the woman may die in half an hour.
There are four causes for post partum hæmorrhage:
namely, (a) uterine exhaustion (atonia uteri); (b)
mechanical obstacles to retraction, such as clots or retention
of pieces of placenta or membrane; (c) and
lacerations of some part of genital passage, such as the
vulva, vagina, cervix, or lower uterine segment; and
(d) the systemic condition known as hæmophilia.
“Bleeders” (hæmophilias) are women whose blood
lacks coagulability, owing to the absence of fibrin-producing
elements.
Post partum hæmorrhage is usually an external
hæmorrhage, but the woman may bleed to death into
her own uterus.
Besides the external signs, the patient may show the
233symptoms of acute anæmia, such as the rapid pulse,
hurried, shallow respiration, pallor, cold sweat, yawning,
dizziness, etc.
Nearly all these cases can be saved by prompt recognition
and efficient treatment.
The first step is to grasp the uterus. If the hæmorrhage
is due to a tear low down, the uterus may be hard,
but generally it is relaxed and requires vigorous massage
with both hands before it shows any signs of contraction.
In the absence of the doctor, the nurse must
know how to undertake this maneuver. The uterus,
after labor and especially when relaxed, is sometimes
difficult to identify and the nurse can only make deep
massage in the pelvis until the organ responds and its
hard globular mass can be appreciated. As soon as the
uterus contracts, clots and contained blood are expelled,
and in many cases its bleeding ceases at once. (See
Conduct of Third Stage, p. 149.)
It may be necessary to keep the uterus contracted by
manual massage in this way for several hours. As
soon as possible, the nurse, or someone whom she
directs, prepares a hypodermic of pituitrin—10 to 15 ♏︎.
An injection of ergot may follow because its effect is
more lasting than pituitrin. Next, a hot douche is made
ready and the materials for packing the uterus are assembled.
When the doctor arrives, he sterilizes his hands, puts
on gloves and introduces two fingers or the whole hand
into the uterus to remove clots or any retained fragments
of placenta.
The hot intrauterine douche may follow, and if the
contraction is not firm and the hæmorrhage checked, the
uterus must be packed with gauze. If hæmorrhage
comes from cervix, it should be grasped with long forceps,
234pulled down, and sutured. If from perineum,
pack first, and afterward sutures may be introduced.
If the patient is exsanguinated, the foot of the bed is
raised, coffee given by mouth, camphorated oil hypodermically,
and normal saline transfused under the
breasts.
Pituitrin may be continued in larger doses. 1 c.c.
will raise the blood pressure very definitely. Adrenalin
also may be employed for this purpose.
The following summary may be found convenient:
Etiology, Functional.—
Atony of the uterus, especially after rapid artificial or natural
emptying of the organ.
More common after uterus has previously been greatly distended.
Premature version and extraction.
Hydramnios and twins.
Imperfect development of uterine musculature.
Precipitate labors.
Haste or improper management of third stage.
Etiology, Mechanical.—
Retention of placenta—partial, total or solitary cotyledons.
Inversion of the uterus.
Placenta succenturiata.
Inflammation of decidua serotina.
Conduct of third stage, i.e., wait until placenta separates.
Etiology, Systemic, Hæmophilia.—
Kind of hæmorrhage.
Hæmorrhage before expulsion of placenta due to laceration of
the soft parts, or
Partial release of placenta and failure of uterus to contract,
or
Placenta may be attached to periphery or to one side.
Attempts to expel placenta without waiting for uterine contraction
are sometimes productive of hæmorrhage.
Hæmorrhage after expulsion of placenta.
Hæmorrhage in interval between pains—comes from placental
site.
235Hæmorrhage in stream not checked by uterine contraction
is due to laceration of the canal.
Hæmorrhage in abnormal quantities at beginning of pains.
Pure atony—comes early.
Hæmophilia again.
Diagnosis.—
Palpation of uterus through abdomen.
Placental site excluded from contraction (paralysis).
View of vulva.
Injuries. Flow continuous, fluid and bright red, shows arterial
origin, probably from cervix. Examine.
Atony—bleeding at intervals, clotted and dark.
Hæmorrhage from a tear begins at once.
Uterus contracted and hæmorrhage continues. Look for
tear.
If hæmorrhage does not begin within ten or fifteen minutes
after labor it is not from a tear.
Always have hæmophilia in mind.
Management.—
Third stage must be conducted properly.
Before expulsion of placenta—early expression.
Credé or manual removal—then secure contraction by massage.
Pituitrin, Ergot, or both.
After Third Stage.—
Restore an inverted uterus. Repair lacerations. See that
cavity is clear and clean.
Massage, intrauterine hot water douche, hand in uterus and
hand outside and rub, ergot.
Pituitrin hypodermically. Pack uterus with sterile gauze
or weak iodoform gauze. Strict asepsis for all intrauterine
maneuvers.
Treat anæmia with transfusion, elevation of foot of bed, coffee,
external heat, hot rectal enemas, stimulation, bandaging of
legs.
Strychnine sulphate, adrenalin, or camphorated oil may be required
in usual dosage.
Hypodermoclysis. (See Minor Operations, p. 206.)
After the bleeding stops, the food must be most nutritious—milk,
eggnog, rich soups, chicken and mutton
broths, oyster stew, and beef steak as soon as she can
236take it. A diet of fluids and stimulating foods that
raise the blood pressure will most quickly relieve the
symptoms.
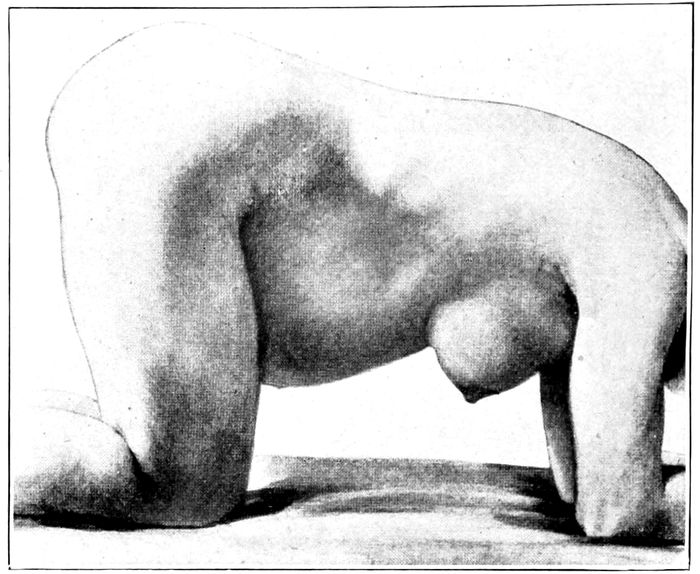
Fig. 100.—The knee-elbow posture. (Bumm.)
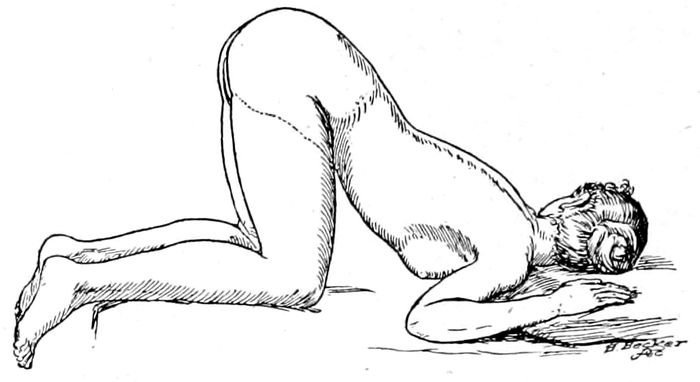
Fig. 101.—The knee-chest posture.
Eclampsia occurs in the last three months of pregnancy
as a rule, and most frequently just before or
during labor.
237In about one sixth of the cases only, the attack may
follow labor. The attack is characterized by violent
convulsions, which come on with little or no warning
unless the urine has been carefully watched.
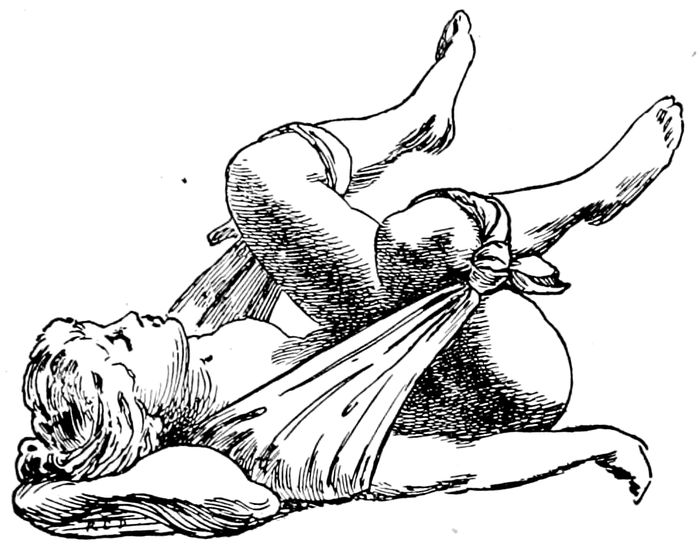
Fig. 102.—The exaggerated lithotomy position obtained with a sheet sling. (American Text Book.)
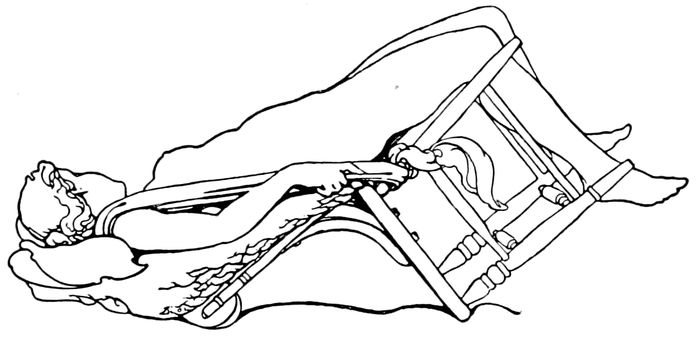
Fig. 103.—The improvised Trendelenburg position. (American Text Book.)
The prodromal symptoms have already been described
under albuminuria in pregnancy (p. 77). The
marked features may be repeated for emphasis: persistent
headaches, disorders of vision, spots before the
eyes, blindness, edema of cheeks, eyelids, feet and hands,
238pain at the pit of the stomach, dizziness, nausea and
vomiting and ringing in the ears. Suddenly the convulsion
occurs, the facial muscles twitch, then the limbs
and body are shaken by violent muscular spasms. The
body becomes rigid, the tongue protrudes and the face
is livid and cyanotic. The spasm usually lasts from one
to five minutes and is succeeded by coma that lasts an
hour or more. In some instances there is no return to
consciousness before the next attack, which comes on
every hour or half hour, though occasionally only one
seizure is noted.
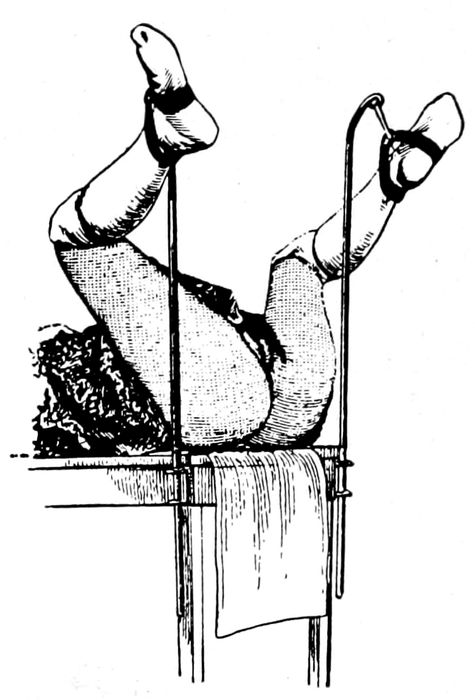
Fig. 104.—The dorsal position with stirrups. (Dorland’s Dictionary.)
The blood pressure is greatly increased and the urine
is diminished, the temperature rises to 101° or 102° F.
When death ensues, it is most frequently due to edema
of the lungs or cerebral hæmorrhage.
The greater the number of convulsions, the more serious
239the outlook as to life, and it is said that after
twenty seizures fifty per cent of the mothers die. Under
the best treatment approximately fifty per cent of
the babies die.
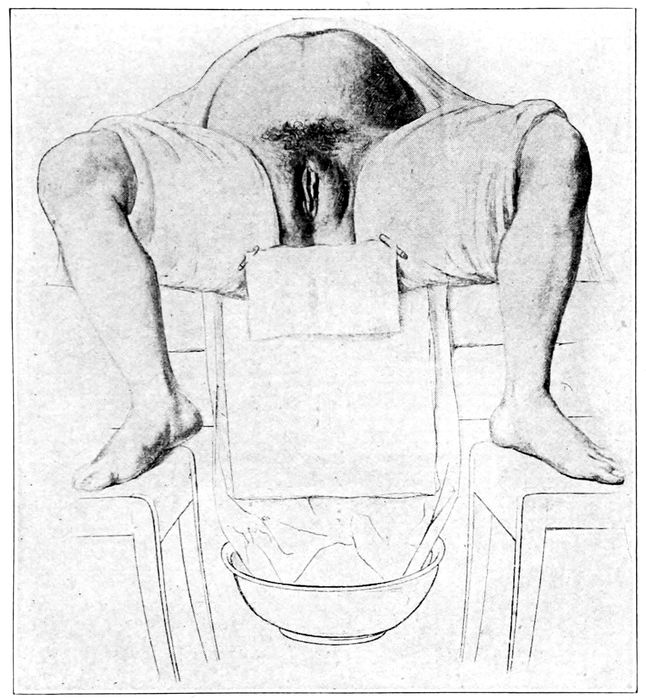
Fig. 105.—Dorsal position across the bed. (Bumm.)
There is no routine treatment for eclampsia.
The principles of management for the attack are (1)
to empty the uterus, on the theory that the disease is
a toxæmia of gestational origin, (2) to eliminate the
poison, and (3) to control the convulsions.
240The albumin in the urine and other eclamptic symptoms
demand urgent attention in prophylaxis.
For the pre-eclamptic period (see Albuminuria of
Pregnancy, p. 77) a rigid milk diet is indicated. The
bowels, kidneys, skin and blood vessels must all be
brought into service.
In the full blooded patient, venesection may be done
and after drawing off ten or twelve ounces of blood,
an equal amount of normal saline may be poured into
the same vein.
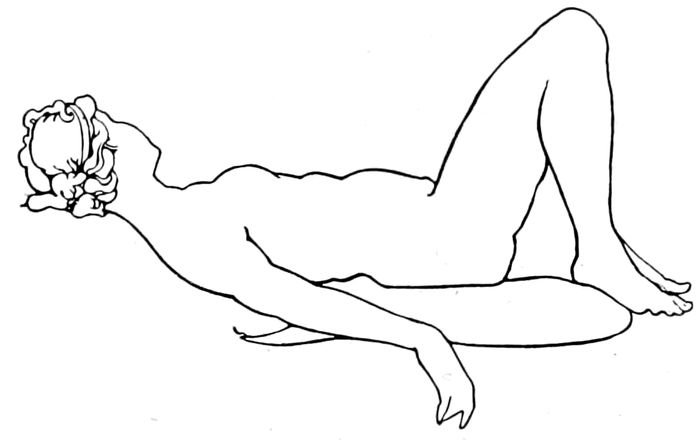
Fig. 106.—Flexed dorsal position with feet on the table. (American Text Book.)
Subcutaneous transfusion or the submammary introduction
of saline solution may be done. The skin is
stimulated by hot wet packs and the bowels by saline
cathartics and frequent irrigation of the colon.
During the attack, the patient must be kept from
injuring herself. A spoon wrapped in gauze or a small,
long roller bandage should be slipped between the teeth
to keep the tongue from injury. The clothing must
be loosened or removed. No food, but only water is
given by mouth, until the patient is conscious.
The convulsions are controlled by morphine, chloral,
or both.
241Morphine sulphate, ¼ gr. is given hypodermically,
followed in an hour by 30 gr. of chloral by mouth. Two
hours later the morphine is repeated and six hours after
the first dose of chloral, it is repeated. In this method
(Stroganoff’s), four doses of chloral and six of morphine
are given in twenty-four hours. That is all.
When the stomach will not retain the chloral it may
be given by rectum in milk. If a general anæsthetic
is used, it should not be chloroform, but ether.
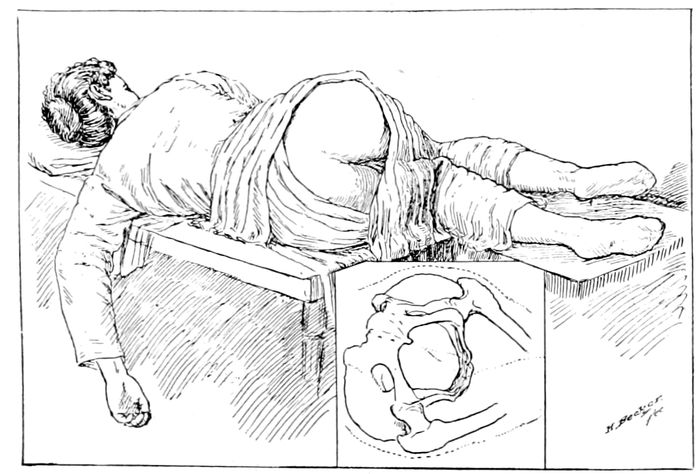
Fig. 107.—The Sims position. (Kelly.)
The labor, if begun, should be expedited by forceps,
or version and extraction. Bleeding during delivery
should be looked upon as desirable. If more rapid
measures of delivery seem demanded and obstacles exist,
such as pelvic contraction, imperfect dilatation, or
the prospect of a prolonged first stage, Cæsarean section
or forcible delivery (accouchment forcé) may be
attempted.
If the labor has not begun, when the convulsion occurs
and a quick delivery by the normal passage does
not seem feasible, then the Cæsarean operation may be
the best treatment.
242
CHAPTER XVI
THE ABNORMAL PUERPERIUM
The practice of obstetrics has many features that are
very gratifying to the nurse and physician.
Instead of a surgical operation, which has come unexpectedly
and undesired; a disaster in which some part
of the body is removed or altered by means of a procedure
associated with extreme pain, mental tribulation
and large expense, a much-wished for addition is
brought to the family, with pain, to be sure, but a
pain that is soon forgotten in the general joy. This is
the normal condition that causes the nurse and the doctor
to rejoice that such a delightful specialty has been
chosen.
Then comes a case in which the labor may be complicated
by some dreadful anomaly, or the puerperium
burdened or disordered by some unwelcome invasion
that tortures the souls of the family and may cost the
life of the mother, or child, or both.
At such a time the nurse and the doctor feel the full
weight of their responsibility, and after a series of
anxious days and sleepless nights, they wonder why
they did not choose gardening or a clerical position for
their life work.
The disorders of the puerperium are many and various,
but naturally the breasts and the pelvic organs are
most frequently affected.
The breasts of the human female are not reservoirs
of milk like the cow’s, but a pair of highly sensitive
organs that functionate and produce only as the demand
243is made. It follows that when the milk comes in,
the breasts become engorged and all the neighboring
structures are involved in the new process. However,
it is not milk that is overfilling the breasts, but serum,
lymph and venous blood, which congest the tissues
surrounding the glands and produce a hard painful
mass.
The breasts become heavy, hot, and painful; supernumerary
glands in the axillæ enlarge, but there is
no fever. There is but little more reason for a fever
when the mammary gland begins to functionate than
when the lungs fill for the first time except in the case
of nervous patients who bear discomfort badly.
If fever appears simultaneously with the milk, the
cause must be sought in some atrium of infection, possibly
in the breasts, but usually elsewhere. There is
no such thing as “milk fever.” The enlarged glands,
the tense mottled skin on which blue veins run visibly
here and there, the nipple, flattened and drawn into
the swelling, so that the child can not grasp it with the
mouth, all produce a sense of disorder that ought to
be associated with fever—but is not. This is the
“caked breast” of the laity, and if let alone, the hyperæmia
subsides and the function remains. The temperature
in possibly two cases out of five may rise to
100° F. for twenty-four hours, but it promptly subsides.
These temperatures generally occur in neurotic
women.
If the breasts are irritated by binders, breast pumps,
or massage,—like the blacksmith’s arm, with exercise—the
trouble, if not increased, is at least much slower
in disappearing.
It is reported that the young virgins of some African
244tribes nurse the babies in the family, the breasts being
stimulated to produce milk largely by massage.
If the condition of the breasts becomes too painful,
the liquids by mouth are reduced to the last degree,
saline cathartics are given until frequent watery stools
result, one or more ice bags are applied to each breast
and codeine sulphate may be given at night. The child
nurses every four hours only. Williams was the first to
show that no tight binder is necessary, but only a supporting
bandage. The tight binder is a cruel and useless barbarism
that has been abandoned by progressive physicians.
No massage is allowed; no pumps; no irritation
whatever, and in twenty-four hours the trouble has disappeared.
Hot dressings to the breast are equally archaic.
They should never be applied to any breast unless
it is desired to hasten suppuration.
If the child dies, or for any reason can not nurse
(inverted nipple, cleft palate, harelip) and it becomes
necessary to dry up the milk, the treatment for “caked
breast” is continued. After twenty-four hours the
breasts are comfortable and rarely give trouble again.
Cracks, Fissures and Abrasions of the Nipple.—The
care of the nipples should be inaugurated about six
weeks before labor, as elsewhere described:
The nipple must be inspected and its possibilities
determined, early in pregnancy, if possible, for many
varieties of badly shaped and ill-developed nipples exist
which may make nursing difficult or impossible.
Imperfect nipples especially are predisposed to fissure
and crack, and will require extreme care on the part of
the nurse. She should inspect them before and after
each nursing and sedulously use cleanliness and asepsis
in her management. In normal and tranquil as well
as in neurotic women, the nipple may become so sore
245as absolutely to preclude nursing, and this entails
much additional work on the nurse and mother, as
well as considerable peril for the child. The condition
usually begins as a fissure or crack, and is accompanied
by much pain. It is serious, furthermore, in another
aspect since all breaks in the surface of the nipple are
avenues of infection that may result in mastitis. The
child may produce fissures or abrasions by rubbing the
nipple with his mouth, by pulling too hard, or by the
habit of holding it in his mouth and macerating it
with his gums when he has finished nursing.
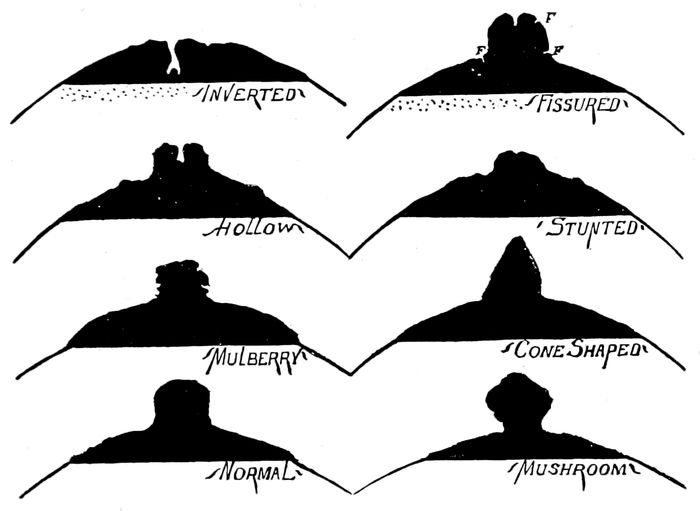
Fig. 108.—Examples of imperfect nipples. (American Text Book.)
The child must not be left at the breast after he has
nursed, but the nipple should be gently removed from
the child’s mouth by passing one finger in beside the
nipple. Fissures and abrasions usually occur within
ten days if at all. Abrasions or erosions are due to
246the wearing away of the epithelial covering of the
nipple in patches more or less extensive.
Thin-skinned blonde women suffer more than those
with dark, dense oily skins.
A fissure is a distinct separation of tissue that goes
deeply into the underlying substance.
A crack is a long abrasion which may deepen into a
fissure.
Both fissure and crack may affect the top, the side
of the apex, or the base of the nipple. They may be
either longitudinal or circular. The entire nipple must
be kept under observation and the instant a raw surface
is detected, treatment must begin.
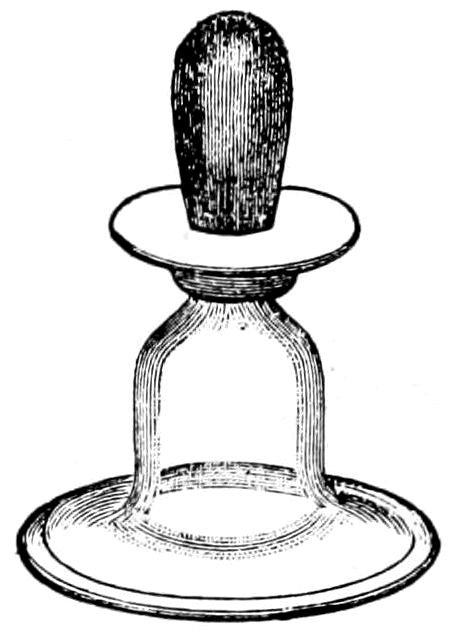
Fig. 109.—A standard nipple shield. (American Text Book.)
Compound tincture of benzoin, liberally applied, is
a favorite and successful remedy. Our routine is to apply
a paste made of equal parts of castor oil and subnitrate
of bismuth. This is put on after the child nurses,
and must be removed carefully before the next nursing.
Sometimes the child’s stools become black and constipated
and the trouble may be traced to imperfect removal
of the bismuth preparation.
247Whatever medication is used, the nipple must be
protected from injurious friction by the clothing. This
is best done by the hat-shaped lead nipple shield, which
is placed over the nipple and held in place by a light
binder. The shield should be boiled before use.
To protect the nipple during nursing, a glass shield
may be used for a day or so, but not long enough for
the babe to get accustomed to it, else he will form a
habit hard to break. This shield must be taken apart
after use, washed and kept in saturated solution of
boric acid until the next nursing.
If all these measures fail, the fissure must be touched
with a nitrate of silver stick once, or have a 2 per cent
solution of nitrate of silver applied night and morning.
It may be necessary to take the child from the breast
for a day or so, in which case he nurses the other
breast and the side with the bad nipple is pumped.
The care of the nipple is highly important since the
apprehension and the actual pain of each nursing may
prevent sleep, destroy the appetite, and diminish the
milk. If begun early, most fissures will heal in twenty-four
to forty-eight hours.
Mastitis.—From three to five per cent of lying-in
women have mastitis in the European clinics, but the
records in America show a much smaller number.
The disease occurs most frequently in blondes and
in primiparas. It is most apt to appear during the
first two weeks, when the congestion accompanying the
new mammary function produces a stasis that favors the
growth of germs, which may enter through the abrasion
or fissures of the nipple produced by zealous activity of
the child’s gums. But it may also occur when the child’s
first teeth come and the nipple is again exposed to injury.
248At times it is impossible to find a plausible
excuse for its occurrence.
Mastitis is usually described in three forms: The
(a) parenchymatous or glandular type, which affects
the substance of the gland or the enveloping connective
tissue; in (b) subcutaneous mastitis the connective tissue
beneath the skin is attacked; and in (c) the sub-glandular
variety, the infection finds a lodging between
the gland and the chest wall.
Mastitis is always due to the presence of microorganisms
which in many cases gain access to the gland
through fissures or abrasions by means of the lymphatics.
In other instances the germs may be in the
blood and a local stasis may encourage the infection.
Still again, they seem to enter through the normal
nipple openings.
Symptoms.—The parenchymatous inflammation begins
with a chill, and the temperature promptly rises to 102°
to 105° F. The pulse is high. The patient complains of
headache and thirst. Examination reveals hard, tender
nodules in some part of the gland. The skin may or
may not be reddened.
If the trouble has begun in the connective tissue,
the skin will be diffusely reddened, the nodule ill-defined,
the temperature will rise gradually and the
chill may be absent.
Treatment.—The breast is put at rest. No tight
binder is applied, no breast pump, no massage. No heat
is allowable.
Ice bags surround the gland night and day. The
liquids by mouth are restricted and saline cathartics
given. Codeine may be administered for pain. Usually
the symptoms subside without suppuration in from
one to two days.
249Should the inflammation persist for more than two
or three days, in most cases the tissue will break down
and form a mammary abscess. When it is evident that
suppuration has begun, heat may be applied to the
gland and the process accelerated. The abscess may
be superficial or deep and will be diagnosed by a bogginess
in a circumscribed area or by fluctuation. The
abscess must be opened as soon as possible.
The nurse sterilizes a bistoury and a pair of long
artery forceps. Lysol solution and cotton sponges are
made and sterile gauze for packing. The hands are
surgically prepared and rubber gloves worn. If an
anæsthetic is required, gas may be used, or chloroform.
The incision is made radially from the nipple so as to
minimize the injury to the milk ducts. A gauze drain
may be required for a few days.
In the after-care, the nurse must be scrupulously
clean and not convey contagion from the breast to the
woman’s genitals, to the child’s eyes, navel or vagina,
nor to her own person.
Excess of milk is rare, but may be observed for a
short time after the glands fill. It seldom requires
treatment, but saline cathartics, restriction of fluids,
and putting the child on a four-hour schedule will
reduce it. Pads may be worn if it runs away freely.
Scarcity of milk is only too common. There may be
enough at first and the quantity gradually diminish, or
it may be deficient from the very beginning.
The faulty secretion may be due to the age of the
mother, to disease (anæmia), to bad nutrition, or to
overwork. It may follow a premature child. Compression
of the breasts by corsets or tight dresses may
prevent development. The amount of gland tissue is
very important. Many women have large, fat breasts,
250but a small glandular development. Mental conditions,
such as fright, worry, and anxiety, will diminish the
flow of milk or stop it altogether.
Symptoms.—The child is fretful, goes to sleep after
nursing but soon wakes up, or may nurse awhile, and
then finding it useless, will cry and refuse the nipple.
He loses weight and when weighed before and after
feeding, the scales scarcely vary. No secretion or very
little can be squeezed from the breasts. The child
may be given a bottle after which he goes to sleep.
Treatment.—When the gland tissue is defective, no
treatment can succeed.
The appetite must be improved by bitter tonics and
the mind relieved of its anxieties, if possible. Change
of scenery may help. The fluids must be increased,
milk, cocoa, chocolate and gruel must be pushed, and
such vegetables added as corn and beets. Oyster
stews, clams, lobsters, and crabs will help. The diet
must be full and nutritious with especial stress on those
foods that raise the blood pressure. Malt drinks or
champagne may avail in some cases. Exercise in moderation
is desirable.
Artificial stimulation of the breast sometimes succeeds.
Massage will irritate the glands, increase the
congestion, and promote functional activity; or a Bier
vacuum apparatus may be put over the gland several
times a day and the air pumped out. The breast should
be kept distended for fifteen to twenty minutes. There
is difficulty in this country in getting glass bells of
sufficient size.
Galactorrhœa is the name applied to an abundant secretion
of milk poor in quality toward the end of a
long lactation or after the child is weaned. The symptoms
251are an almost constant flow of milk with resultant
anæmia.
Treatment.—Elix. of iron, quinine and strychnine with
compression of the gland. A dry diet and the avoidance
of all irritation of the breasts will aid.
To “dry up the milk,” follow the treatment for
“caked breast.”
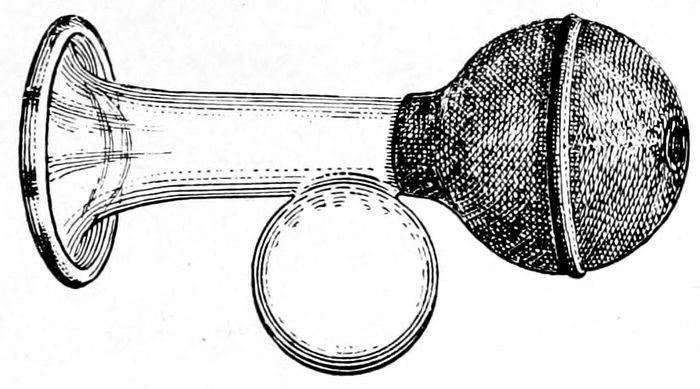
Fig. 110.—A standard breast pump. (American Text Book.)
Quality of the milk may be such that the child will
not take it or, if taken, it fails to nourish. In some
cases this is due to overlong, or to irregular, periods
between feedings; for when the nursing interval is too
short, the milk becomes too rich, when too long, it
becomes thinner and less nutritious.
Fright, anxiety or anger may change the character
of the milk so that colic, vomiting, and diarrhœa and
indigestion are produced in the child. A wet nurse becomes
homesick and the milk dries up. It may become
extremely indigestible, as shown in cases where a wet
nurse quarrels with her husband and her foster child
develops green stools. If the mother’s milk does not
agree, the child may be put on feedings for twenty-four
or forty-eight hours, while the milk, pumped from
the breast, is sent to a laboratory for analysis. If a
252return to the breast is unsatisfactory, artificial feedings
or a wet nurse must be supplied.
Removal of the child from the breast may be required
for a variety of reasons. Thus, the mother’s addiction
to alcohol or opium is good ground for taking
away the child. Arsenic, bromides and iodides of potassium,
saline cathartics, salicylates, alcohol, opium and belladonna
must be given to the mother with great caution
during lactation, for they pass over into the milk.
Acute diseases, such as erysipelas, pneumonia, diphtheria,
typhoid, malaria, pronounced puerperal sepsis
or persistently high fever from any cause, usually dries
up the milk; while cardiac lesions, unless well compensated,
chronic anæmia and tuberculosis, obviously demand
the removal of the child for the sake of both.
Sometimes a new conception, especially when the milk
becomes poor in the last half of gestation, compels
the mother to wean her babe.
A syphilitic woman may nurse her own child, provided
her condition is good and the child also is syphilitic.
Theoretically, the return of menstruation in no way
affects the nursing child, unless the blood is lost to
the point of anæmia. Yet cases do occur in which the
child has indigestion, colic and bad stools, as well as
loses weight, when the mother is menstruating.
The quality of the milk is sometimes altered, but
only for a day or so, and the child should continue at
the breast unless some definite indication for removal
arises.
Weaning ordinarily is completed by the ninth month,
but the child should never be carried beyond the twelfth
month on account of changes in the character of the
milk.
253When a child is weaned, the substitution of an artificial
food may be made gradually,—a bottle a day,
two bottles a day, etc., until, in a couple of weeks,
the breasts are at rest.
The excessive prolongation of lactation is shown
upon the mother by impairment of the health. The
patient is pale, weak, anæmic, fretful, and thin. Headaches,
dizziness, loss of appetite, and constant fatigue
will be complained of.
The treatment is to remove the child at once and
put the mother on stimulating drugs and foods. A
change of air and scenery, if possible, will be highly
beneficial.
The wet nurse is always a tribulation, which must be
endured until the child can be put on artificial food.
She should have a Wassermann test before entering
upon her duties. Syphilis, tuberculosis, and gonorrhœa
must be guarded against. She must be kept like the
family cow, in a placid frame of mind, fed on nutritious
food that is not too rich, and exercised enough
to keep the blood circulating.
Light housework and duties that take her out of
doors part of the time are advisable. Her moral character
can only be assured through those who have
known her. If she brings her own child with her, she
will need watching to provide for an equable distribution
of the milk. The first few days is never a criterion
of a wet nurse’s effectiveness. Change of food and
surroundings may interfere with her usefulness.
Gas may complicate the puerperium after Cæsarean
section, and even after normal labor. A rectal tube of
soft rubber may be passed as high as possible into the
bowel and left for some time, or enemas of S. S., turpentine,
254asafœtida, or milk and molasses may be given.
By mouth calomel or mag. cit. is valuable.
Headache in the puerperium should be watched carefully,
and the cause discovered. Pain in the head may
be a habit with the patient, or it may be a symptom
of some complication either present or developing, such
as toxæmia, eclampsia, or acute yellow atrophy of the
liver. In general, it is due to milder conditions like
exhaustion, too many visitors, excitement, nerves, or
insomnia.
After-pains.—Sometimes patients are greatly annoyed
by after-pains. The pain may be due to a clot retained
in the uterus or possibly a stimulation of the uterus when
the child goes to breast. Gentle massage of uterus, or
ergot, quinine, or codeine may be required to bring
about the expulsion of the clot or to control the pain.
A reasonable degree of after-pain is of favorable significance.
(See p. 154.)
255
CHAPTER XVII
INFECTION
Puerperal fever is a wound infection.
The conditions of the pelvic organs during labor and
post partum, are well adapted to receive and develop
microorganisms, for the healthy antimicrobic power of
the vaginal secretion is absent or diminished.
A long and exhausting labor, possibly accompanied
by hæmorrhage, or terminated by an operation, has
diminished the immunity and broken the resistance of
the tissues to a dangerous degree.
The mucous membrane of vulva and vagina are torn
and bruised, the vitality lowered, and the surface covered
with bloody lochia, which is an excellent nutritive
medium for microbic development. The uterus is
a vast, open wound, filled with fibrin, blood clot, and
decomposing tissue, while the whole pelvis is maintained
at exactly the proper temperature for germ
propagation.
Through these wounds, toxins are carried into the
circulation, and germs, nourished upon the abundant
and favorable culture media, pass through the uterine
walls or by way of the lymph channels first into the
adjacent tissues and thence to all parts of the body.
Certain definite organisms reach the disintegrating
tissues and produce a putrefaction. They do not, however,
once their work is done, pass into the body. But
in producing putrefaction, they also produce injurious
poisons, called toxins, which do enter the body and
cause an absorptive fever known as sapræmia.
256
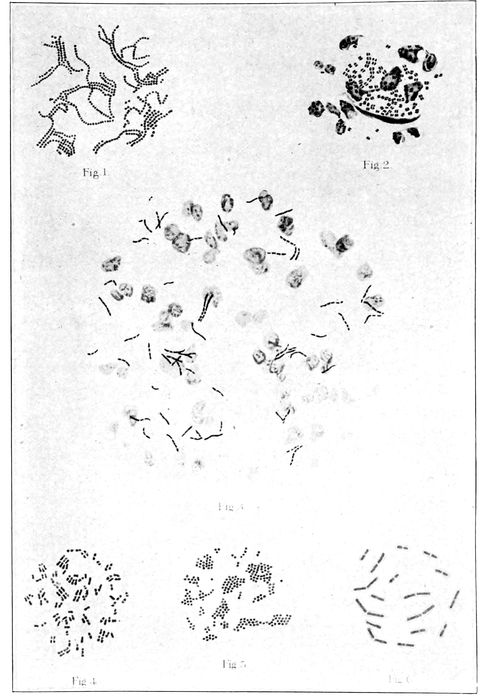
Fig. 111.—Germs most frequently found in cases of puerperal fever. (Kelly’s Gynecology.) 1, streptococci (in chains); 2, gonococci; 3, tubercle bacilli (not a source of puerperal infection); 4, bacillus coli communis; 5, staphylococcus pyogenes aureus; 6, bacillus aerogenes capsulatus.
257Other organisms are the pus microbes, which begin
their growth in any favorable location and continue
to spread and flourish onward and inward by blood
vessel, tissue or lymphatic, until overpowered by the
resistances of the body, or until by general sepsis, they
have killed the patient. These are the streptococcus,
staphylococcus, bacillus coli and bacillus pyocyaneus.
These are the germs that the nurse or the doctor may
bring to the patient on hands, clothing, or hair. These
are the organisms against which our scrupulous asepsis
and antisepsis is directed. It is against them and their
activities that the doctor and nurse prepare by the
long and painful scrubbing of the hands and elbows,
the rubber gloves, by the shaving and scrubbing of the
patient, and by all the paraphernalia and equipment that
go to furnish the modern lying-in-chamber or delivery
room. It is on account of these germs that the conscientious
doctor or nurse lies awake nights and painfully
reviews his technic when his patient has a temperature,
and it is on their account that he shudders at the
callous disregard of human life that is shown by those
who do not observe the known laws of asepsis.
It is true that many women escape when the attendant
is unclean, but this is due to a splendid immunity,
and in no way absolves the man or woman who neglects
his asepsis and has patient after patient running temperatures,
some of whom are bound to die or be crippled
for life. It is for this reason that a surgeon should
do surgery and not general practice; it is for this reason
that an obstetrician should limit himself to the
care of women in childbirth and not endanger them by
taking cases of scarlet fever, erysipelas, and unclean
surgery.
In country practice, all kinds of work must be done
258since there are not enough men to specialize, but it is
inexcusable in the city where a man can always be
clean and keep clean, if he is willing to forego the income
derived from attendance upon septic and infectious
cases. Any article not surgically clean may
contaminate the patient by contact; but ulcers, suppurating
wounds, abscesses, and hands improperly or
insufficiently cleaned are the deadliest causes of post
partum temperature.
Infections are said to be either self-produced or
brought to the patient from without.
The only organism that is demonstrably self-infectious
is the gonococcus, which may be present in the
vagina before labor and may infect the puerperal woman;
but it is wiser, safer, and more nearly accords with
the facts, to regard all infections as alien borne, as
brought to the patient and introduced by the unclean
hands or instruments of her medical attendants.
Prevention.—A conscientious and capable nurse or
doctor will not go from an infected case to a confinement.
Both will keep their bodies clean, the teeth
filled, and pyorrhœas scraped and treated. The occurrence
of pus anywhere on the body is sufficient reason
for the doctor to give up his confinements for a time,
and the nurse to report off duty.
No raw, and but few mucous surfaces should be
touched by the fingers of the attendants, where a sterile
instrument can be used.
The nurse should never make vaginal examinations
unless an emergency exists, and then only when her
instruction has been thorough and her experience great.
Every examination is a possible source of danger, no
matter how carefully the hands and patient are prepared.
The nurse is not to change the pads without
259washing her hands, and she must wash her hands always
after changing the pads, before dressing the
navel of the child.
The navel or eyes of the child may be infected easily
by the hands of nurse, doctor, or patient. The breasts
of the mother may be infected by the hands of nurse,
doctor or patient. The vulva and vagina of the puerperal
woman is highly susceptible to infection from the
hands of nurse, doctor or patient.
Rule.—All temperatures arising in the puerperium are
due to infection, unless satisfactorily explained by finding
the source. The possibility of a slightly elevated
temperature from insignificant causes may be kept in
mind, but such temperatures are transient and yield
quickly to appropriate treatment or to none at all.
Puerperal infection is most apt to appear during the
first week of the lying-in period, and it generally develops
about the third or fourth day post partum. If
the symptoms come on later than this, there is always
a hope that the infection has taken its origin in something
else than the labor.
Symptoms.—In mild cases, a rapid pulse, headache,
and a temperature of 101° or 102° F. may be the only
symptoms. Severe cases begin with a chill, followed by
a marked rise of temperature. The temperature is always
irregular and generally remittent.
The pulse rises to 120 or 130 beats a minute, headache
and prostration appear, occasionally associated with
vomiting.
The flow of lochia may be either increased or diminished
and either offensive or free from odor. Foul-smelling
lochia is a sign of putrefaction but not necessarily
of sepsis.
At the same time there is some tenderness in the
260lower part of the abdomen, usually most marked at
the sides of the uterus. The uterus is larger than it
should be, and not hard, but doughy and sensitive to
touch.
The involution is arrested, except in cases of pure
septicæmia. This is an important reason for the daily
observation and recording of the regular descent of the
organ.
The disease runs a variable and more or less prolonged
course and the prognosis is always doubtful until
the event. Signs of grave import are: repeated
chills, insomnia, pulse above 120, persistent vomiting
and meteorism, with dry, brown tongue.
Treatment.—Mild cases without chill when the uterus
is large and the lochia sometimes offensive, are usually
sapræmic. Free catharsis, ergot in full doses, and a
half-sitting position to aid drainage will cause the
symptoms to subside in two or three days.
In the severe type, the treatment is mostly a case for
careful nursing. The more energetically the doctor
acts, the more liable he is to do harm. The patient
needs all her strength to fight the disease, and should
not be required to fight the consequences of injudicious
interference.
There is still some discussion about the advisability
of assuring oneself that the uterus contains no remnants
of the labor. Some feel that this should be determined
by curetting the uterus with finger or instrument and
following the operation with an intrauterine douche.
If this is the view of the attending man, the nurse must
aid, for the responsibility is his and not hers.
On the other hand, the weight of authority at present
seems inclined to the view that any remnant of the
labor will drain out naturally or be expelled by ergotdriven
261contractions without the necessity of opening
up new raw surfaces by interference and thus spreading
the infection.
The main idea is to promote drainage in every way
possible. No curette, no douche, no uterine packing.
Nevertheless, the vulva may be cleansed and the vagina
carefully retracted and by appropriate means a culture
obtained from the uterus. If this shows streptococci, all
local treatment is to be abandoned at once.
In general, the food must be fluid, and as nutritious
as possible. This means milk, beef and mutton broths,
oyster stew, etc. The nourishment must be pushed artfully
and ingeniously. Alcohol is not indicated. The
bowels are kept open.
Normal saline, drop method, by rectum, will promote
diuresis, skin action, and supply the body with the
much needed fluid. Subinvolution is controlled by ergot
in full doses. The room must be light and as many
windows opened as the weather will permit. Frequent
change of posture, from side to side, from dorsal to
prone and especially to the half-sitting position, will
give the patient comfort and prevent decubitus (bed
sores). The daily bath with an alcohol rub, keeps the
skin in good condition and eases the mind.
The child should be taken from the breast, because
the milk is poor in quality and quantity and it may
be infectious. Besides, the mother needs all her
strength. Nature usually solves the problem by drying
up the milk.
All pads soiled by the patient should be collected
in paper bags or rolled in newspapers and burned.
Sheets, towels, and pillow slips must be boiled in the
house and not sent to the laundry. They should be
soaked for half a day in a 2 per cent solution of lysol
262before being washed, and exposed to the hot sun for
a day or so afterward, if possible. No comforts should
be used on the bed, and the blankets must be left suspended
in the room when it is fumigated at the conclusion
of the case. All dishes and utensils can be
boiled. Plenty of air and sunshine are essential for
the cure of the patient and to prevent the spread of
the disease.
The nurse must use every precaution to avoid carrying
the infection to herself or others. Rubber gloves
should be worn while changing the dressing. It is better
to have the child cared for by another nurse. The
nurse must get her rest and some exercise out of doors
every day. It rejuvenates her and reacts to inspire the
patient.
When she leaves the case the nurse should boil her
linen and wash her hair with soapsuds and hot water,
and bathe frequently.
Milk Leg.—This is an infection characterized by
swelling of one, or rarely, both, limbs, from the foot
to the groin. The leg is white from the edema, and
as the condition is associated with fever and since
the milk diminishes or disappears about the same time,
it was thought in former days that the milk went to
the leg.
The cause of the swelling is a phlebitis of the external
iliac or femoral vein which becomes thrombosed
or so filled with clots that the return circulation is
impeded.
Symptoms.—The attack is signalized by a rise of temperature
to 102° to 104° F. There is headache, pain in
the affected limb, and general prostration. It is a true
sepsis.
The disease appears usually in the latter part of the
263second week of puerperium, when the patient has begun
to congratulate herself that all danger is over.
In many cases the doctor has yielded to importunity
and let the patient get up before involution was sufficiently
advanced and the patient will report that she
got up too early.
The limb must be immobilized and kept warm. The
immobility should be maintained for at least ten days
after the fever has subsided and the pain gone.
The convalescence may be protracted over weeks and
months.
Bed sores may complicate a long convalescence. Bathing
with alcohol or alcohol and alum, and the frequent
change of the patient’s position will usually prevent
them. Rubber rings and sheeting should not be used if
it can be avoided. Ointments containing zinc are of
great value in the cure of this affection.
Phlebitis, in minor degree or in localized sections,
may occur in the veins of the leg and the site of the
invasion will be outlined as red lines or as irregular
nodules. Some fever may attend the condition. Rest
of the affected member, with ice bags for the pain, constitute
the treatment. Bed sores must be guarded
against.
Sudden death in the puerperium is a shocking disaster.
Rapid death may follow the complications of
labor accompanied by hæmorrhage, such as placenta
prævia, rupture of the uterus, etc.; but death may be
sudden, without warning, from pulmonary embolism,
acute myocarditis, fatty degeneration of the heart, or
the entrance of air into the uterine veins. This may
happen several days after labor in a woman who is
passing through a convalescence apparently normal in
every respect. Such an event is probably due to a
thrombus which may form in any of the veins of the
264body, but more frequently in those of the pelvis and
legs. In the latter it may be recognized by hard lumps
that form somewhere along the course of the veins in
consequence of a phlebitis. There is always the menace
that some fragment of this mass, which is merely
a hard clot of blood, may become detached and float
off in the circulation to other parts of the body, such
as heart, lungs, or brain (embolism), and by interference
with those structures, produce paralysis or instant
death. When a thrombus is diagnosed, the affected
part must be kept as quiet as possible. No
massage is permissible. Tincture of iodine or 20 per
cent ichthyol may be applied. The woman should remain
quiet for at least ten days after the apparent
disappearance of the symptoms.
265
CHAPTER XVIII
THE CARE OF THE CHILD
Hitherto the mother and the complications and
changes peculiar to her condition have been selectively
considered, to the neglect of the child; but the labor
being over, and the nurse having assured herself that
the uterus is hard, that there is no hæmorrhage, and
that the mother is resting, now turns to the child lying
in its blanket. A hot water bag, carefully tested,
should lie at its feet wrapped in toweling or napkins.
The eyes have already received the Credé treatment,
1 per cent solution of silver nitrate or possibly a 15
per cent solution of argyrol for prevention of ophthalmia,
and a thorough cleansing comes next.
In a warm room, away from drafts, the nurse takes
the child in her lap, or on a table, with a blanket underneath.
She first anoints the child all over, either with
benzoated lard, liquid albolene, sterile vaseline, or olive
oil. This softens the vernix caseosa that covers the
child and aids its removal.
The skin is wiped carefully with cotton or a soft
cloth, paying particular attention to the folds of the
groin, the arm pits, and the genitals. The nostrils are
gently wiped out with applicators dipped in oil.
The child must be covered as much as possible during
the operation and the work finished quickly. The
whole period should not exceed twenty minutes.
During the cleansing process the nurse should look
closely for anomalies or anatomical imperfections, like an
imperforate anus or urethra, supernumerary digits, etc.
266The Bath.—Daily, until the cord comes off, the baby
is sponged with oiled pledgets, followed by a spray
bath, or a sponging with lukewarm water and castile
soap. The child must not be put into a full bath tub
on account of danger of infecting the umbilicus. The
bath water in a tub or basin quickly becomes filled
with bacteria from the surface of the child’s body and
may be conveyed quite easily to a raw wound.
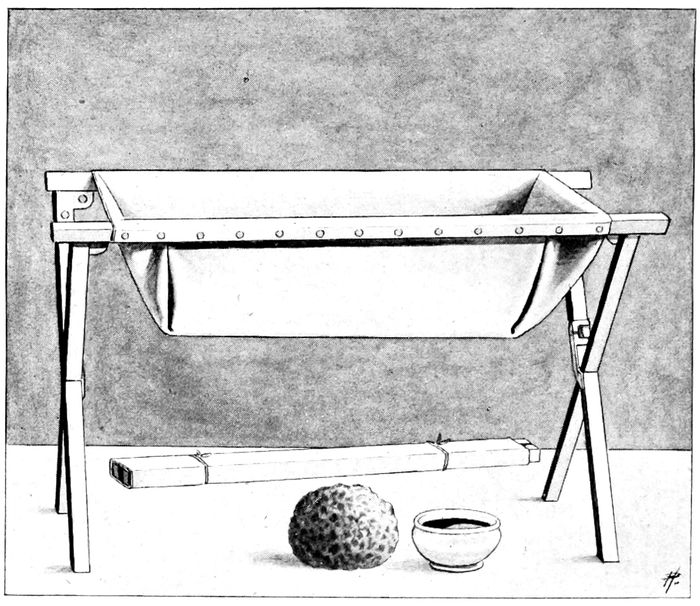
Fig. 112.—Rubber bath tub.
All discharges must be wiped away, and the buttocks
cleansed with oil. If the skin becomes irritated by
urine or otherwise, the child should be well covered
with talcum powder, especially in the folds of the groin
267and in the genital crease. All infants are benefited by
a little mild massage after the bath.
If other babies are handled, a child with infected
eyes, or skin eruptions, must be quarantined and cared
for separately by a special nurse. The color of the skin
should be pink, changing under manipulation to red.
If there is mucus in the mouth, it may be wiped out
with an applicator, if in the throat, the child may be
held up by the feet and the head drawn back for a few
minutes so that gravity will aid the discharge of the
obstruction.
After cleansing the skin, the nurse sterilizes her
hands and dresses the cord. The gauze which was
temporarily wrapped around the stump is removed, the
cord and adjacent skin washed with alcohol and dried.
The stump is powdered above and at the sides with a
mixture of equal parts of boric acid and subnitrate of
bismuth, and then wrapped in gauze. The band is put
on, the temperature taken, and the baby dressed. Some
physicians prefer to have the cord dressed in 95 per
cent alcohol, which is frequently renewed. The normal
separation of the cord takes place through a kind of
dry gangrene, which should be favored by dry rather
than wet dressings. The 95 per cent alcohol does not
remain at 95 per cent after it is exposed to air, hence
it does not absorb moisture from the cord as absolute
alcohol would. However, the attending man is responsible,
and his orders must be followed.
The Umbilicus.—The cord may be severed as soon
as the child has cried lustily or the cessation of pulsation
may be awaited, in either case the child secures
a little more blood, which gives him a better start in
life.
Two tapes are tied about the cord, one close to the
268skin margin of the child and the cord is cut between
them. A kind of mummification or dry gangrene normally
develops and the stump falls off, as a rule, about
the fifth day, leaving a moist, granulating area, which
forms the umbilicus.
A metal clamp may be used in place of a tape to compress
the cord. The advantage of the clamp is that
on account of its greater width and rigidity it does
not cut through the cord when applied. Furthermore,
it can be made and kept more nearly aseptic. It does
not soak up the juices from the cord and form a culture
medium for germs. It can be removed on second day.
The cord usually comes off a day or so sooner than when
the tape is used.
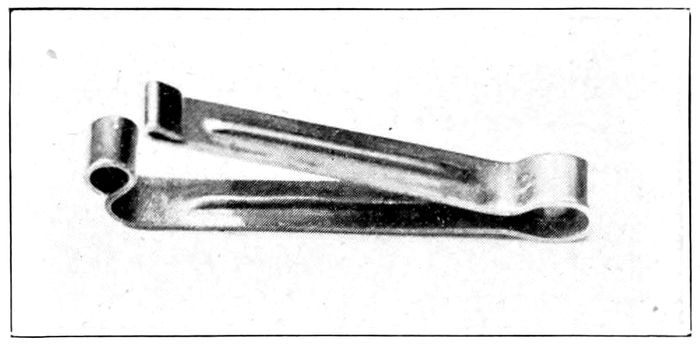
Fig. 113.—The Pettit cord clamp.
The care of the cord is extremely important, as many
infections can be transmitted through it to the child.
At each dressing the cord is inspected, and whether it
is dry or moist, offensive or inodorous, should be noted.
These facts, with the falling off of the cord, are put
down on the history sheet as they are observed. The
binder, after each removal, is not pinned, but sewed
on. The sewing should begin below and go up in order
to have the tightness low down.
Eyes.—After the first instillation of silver nitrate solution,
269a reaction appears with redness, swelling, and
discharge, which passes off without treatment in two
or three days. During the bath, care must be used not
to get anything into the eyes nor anything from the
eyes or nose upon the navel.
At each dressing the nurse should irrigate the edges
of the lids gently with boric acid solution. If the eyes
become red, swollen, and have a purulent discharge
after the second day, the case is possibly ophthalmia
and they must be watched with extreme vigilance. A
smear should be taken for the microscope and preparations
made for energetic treatment.
The following summary may be of service in memorizing
the routine of nursery procedure.
- 1.
- Keep temperature of nursery 68° to 72° F.
- 2.
- During bath, keep temperature of nursery 75° to 80° F.
- 3.
- Temperature of bath water 98° to 99° F.
- 4.
- Never use a diaper that has not been laundered.
- 5.
- Tie case number on child’s arm before leaving delivery room.
- 6.
- Watch cord for hæmorrhage.
- 7.
- Record temperature, stools and urine.
- 8.
- Give water freely between feedings.
- 9.
- Put to breast twelve hours after birth, and every three hours thereafter until the child
begins to gain, then one and possibly (?) two night feedings may be omitted.
- 10.
- Change binder daily.
- 11.
- Oil bath first, then shower bath on subsequent days.
- 12.
- Dress cord with alcohol 95 per cent, dry and apply bismuth subnitrate and boric acid
powder (equal parts) into crevices beneath clamp or tape and under edges of the crust.
Change dressing daily. Cord should fall off fifth day. Report failure to do so.
- 13.
- Clamp may be removed on second day.
270Routine for the Child.—
- 1.
- Temperature.
- 2.
- Undress.
- 3.
- Weight.
- 4.
- Shower bath.
- 5.
- Dress cord—record condition.
- 6.
- Binder daily until discharged.
- 7.
- Diaper and dress.
- 8.
- Sponge eyes with boric solution.
- 9.
- Cleanse nostrils with albolene.
- 10.
- Brush hair.
- 11.
- Drink of warm water.
- 12.
- Observe case number daily.
Clothing.—(See Infant’s Outfit, p. 101.) The clothing
must be light, loose, warm, and not irritating to
the skin. The outside garment should have wing sleeves
which permit free motion of the hands, but do not permit
them to reach the eyes.
The band of plain outing flannel should always be
worn for the first few weeks.
Birds-eye linen makes the best diapers on account of
its superior absorbent qualities.
The feet must be kept warm by stockings, and artificial
heat, if necessary. On hot days much of the
clothing may be removed and the shirt, band and diaper
may be all that are needed.
The care of the shirts and bands is part of the daily
duty of the nurse. They must be washed daily, either
by the nurse herself or under her supervision, as they
are easily injured. After washing, in soft water, if
possible, and with wool soap, they must be dried on a
stretcher. Diapers must be put directly into cold water.
Fæces may be brushed off with a whisk broom, and the
napkin rinsed, boiled and again rinsed. No diaper
should be used a second time until this has been done.
No bluing may be used on the diapers and the soap
271must be mild, otherwise chafing and intertrigo will
follow.
The infant’s toilet basket must contain:
4 soft bath towels.
1 pound of absorbent cotton.
1 dozen wash cloths of soft material.
1 small hair brush.
1 pair nail scissors.
Talcum powder.
Bath thermometer.
Hot water bottle.
Albolene.
Castile soap.
8 oz. boric acid solution.
8 oz. benzoated lard.
Paper bags for waste.
Pitchers and basins.
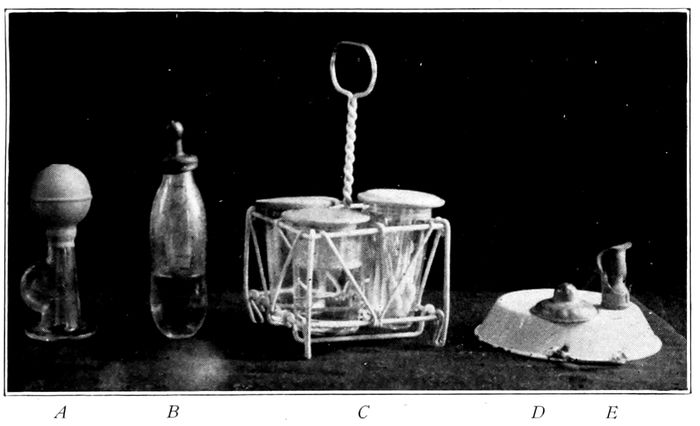
Fig. 114.—A, standard breast pump; B, standard nursing bottle; C, the breast tray; D, the Wansbrough lead nipple shield; E, the Brophy nipple for harelip and cleft palate.
Weight.—The weighing of the child should precede,
for convenience, the first cleaning of the skin and the
daily bath. The child is either put on the scale naked
or weighed in a blanket, and the weight of the blanket,
272ascertained before or after, is subtracted. The daily
weight record is just as important as the temperature.
A scale that registers ounces and fractions thereof
must be used, and the child should be guarded from
falling during the performance. Usually the child loses
from eight ounces to a pound the first week, but it
should gain back to its birth weight, by the end of the
second week. If the child does not gain, it may be due
to lack of milk from the breast, and the weight may
be taken before and after feeding to verify or refute
the suspicion.
The mouth should be inspected each morning, but
not cleansed with the boric acid solution unless definitely
indicated. Spots or any unusual appearance
should be reported.
The Genitals.—The vulva of the female infant usually
requires but little care besides cleanliness. There
is sometimes a whitish discharge which disappears spontaneously
in a few days. It is a drainage of vernix,
smegma and epithelium from the vagina and labia.
With a male, the prepuce must be inspected when
the child is about a week old. If it is long and the
orifice small, circumcision may be suggested. Under
any circumstances, the foreskin must be retracted, the
adhesions broken up, and the smegma removed. This
must be repeated daily until the adhesions do not recur.
The maneuver should be done the first few times
by the physician, for fear of a paraphimosis.
Sleep in the newborn is normally quite deep and almost
continuous, probably twenty-two hours a day, for
the first week. The rather fast respiration of the child,
even when sleeping, is no cause for alarm. A healthy
infant breathes about twenty-five times a minute. The
child should not be rocked, carried about, exhibited, or
273handled more than necessary. It should not sleep with
the mother, lest it become too hot or too cold, be overwhelmed
by bedding, or overlaid by the mother.
Bowels.—The first stools are black and tar-like,—this
is meconium. It disappears by the end of the first
week. The presence or absence and the character of
an evacuation, as well as the number in twenty-four
hours, must be daily recorded. For a breast-fed child,
there should be three or four a day, for the first ten
days and the number should gradually diminish until
a routine of two a day is obtained.
The diaper of bird’s-eye linen should be large and
thick; two may be used if required. They should be
carefully washed after soiling. Bluing must not be
used, because where this substance comes in contact
with the skin, irritation follows.
Weaning should be brought about by the gradual
substitution of other foods, somewhere between the
sixth and twelfth months.
Urination should be copious. The child is always
wet, and frequent changes are necessary to keep the
skin from getting raw and sore.
Both bowels and bladder should be emptied within
the first twenty-four hours. Failure to do so should be
reported, as an imperforate anus or urethra may exist.
Frequently a piece of ice whittled out like a lead
pencil and passed into the rectum will stimulate urination.
Catheterization is practically never necessary. The
child may go three days without injury, but the condition
of the bladder above the pubes must be attentively
watched and its degree of fullness appreciated
by percussion.
Nursing.—The child should be put to the breast
274twelve hours after birth and every three hours thereafter—no
more and no less without definite reasons.
If the child is strong and vigorous, only one feeding
may be given at night, and even this may be omitted in
some cases where the child gets an abundance of food.
Six or seven feedings a day are enough. The child
should stay at the breast from fifteen to twenty minutes,
depending on its activity and the rapidity of the
milk flow, and then be removed. It must not be permitted
to sleep at the breast.
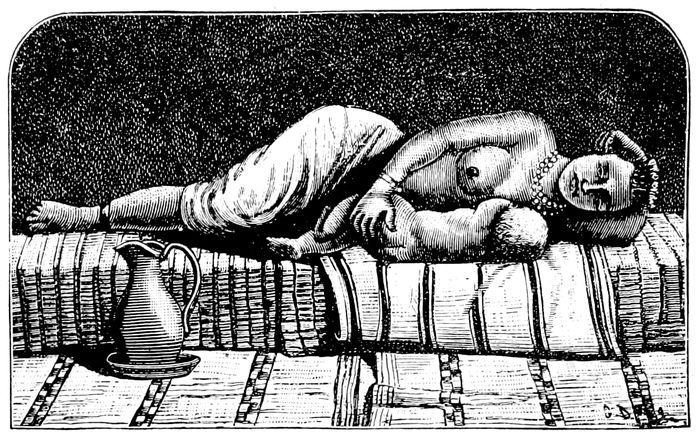
Fig. 115.—Proper position of mother while nursing child. (Witkowski.)
Care must be used that the child gets the nipple over
the tongue and not under it. Many infants have to be
taught to nurse. This may be due to a lack of strong
animal instinct in many cases. There may be an abundance
of milk and a good nipple, but the child will not
learn to nurse without a vast expenditure of time, patience,
and energy on the part of the nurse. Squeezing
a little milk into the mouth or filling a nipple shield
275with milk will sometimes aid in educating the infant,
or even starting the supply with a pump, as many
nurses do, is advantageous. Certain drugs, like castor
oil and turpentine, taken by the mother, may affect the
taste of the milk, and be reason enough for the refusal
of the child to take hold. Other drugs like mercury,
arsenic, potassium iodide, and alcohol may go over in the
milk to the nursing child.
If the child is weak or premature, the milk must be
pumped from the breast and fed to it until strength
comes. The difficulty about this is the bad habit acquired,
but there is no way to avoid it.
A child should get at each feeding half an ounce of
milk to each pound of weight. The capacity of the
stomach at various months is given by Hirst as, first
week, ½ oz.; second week, 2½ oz.; third and fourth
week, 3 oz.; third month, 5 oz.; fifth month, 9 oz.; ninth
month, 12½ oz. Holt says that the capacity at birth
should be one ounce, and increase at the rate of an
ounce a month up to the sixth month.
As hunger stimulates the gastric and salivary glands,
so the sight of the child arouses some emotional center
in the mother, which starts the milk, and the mouth
of the child provides an additional stimulus of great
power. About fourteen ounces is secreted by the seventh
day, and after the second month the daily average
rises to three or four pints. Milk secretion is favored by
drugs and foods that raise the blood pressure and diminished
by substances that lower the blood pressure.
There may be too little milk in the breasts, and if so,
the child will lose weight daily; also the child will
waken before nursing time, fret, refuse water, but
greedily seize the nipple if it is presented. It will continue
to nurse long after its time is up and cling and
276cry when removed. The breast itself may seem flabby
and loose, and no milk, or very little, can be pressed
from the nipple.
Normally, the breasts feel full and tense, both to patient
and nurse, just before feeding time. The real
test, however, is in taking the weight of the child before
and after feeding. Where the milk is insufficient,
the scales will not vary, and after a few repetitions the
nurse can be certain. An infant should be handled as
little as possible after feeding lest the milk be vomited.
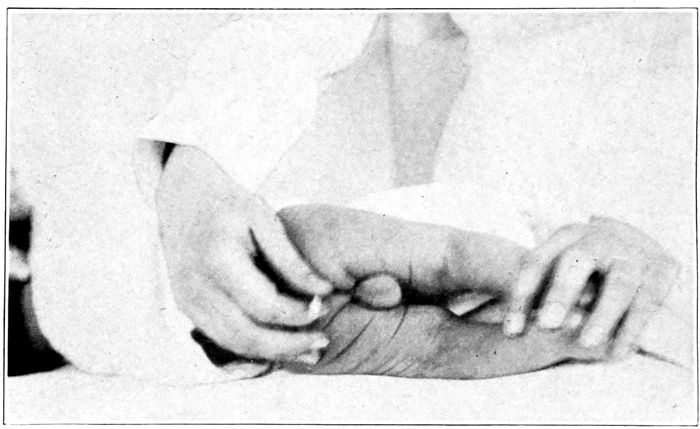
Fig. 116.—Proper method of taking rectal temperature.
Temperature of the newborn child varies from 98° to
99° F. It should be taken morning and evening, or
oftener, if complications are suspected.
The temperature often goes up on the third or fourth
day, and may stay up for several days. This phenomenon
is called by some a starvation or inanition fever.
The temperature may go to 106° F. and the rise is generally
associated with a hot dry skin, dry lips, weak
277pulse, restlessness, and great prostration. The fontanelle
may be sunken and the cry sinks to a fretful,
feeble whine.
It is important that the fever should be recognized and
treated, since the condition may terminate fatally. The
etiology is obscure. The fever should not be confounded
with pyogenic infections, for these rarely begin before the
fifth or sixth day.
The treatment is simple. Give water regularly every
two hours by mouth, and rectal flushings of normal saline
twice daily. The symptoms rapidly subside if the
child is properly nourished. Hence the breasts should be
inspected and the child weighed before and after feeding.
Usually the milk is poor and scanty. If the temperature
does not soon fall the child should be put to another
breast or artificial feedings should be instituted.
278
CHAPTER XIX
THE CARE OF THE CHILD (Cont’d)
Heart.—The heart tones while in the uterus may vary
between 138 and 150 per minute, but when higher than
160 or lower than 120, danger is near. After delivery,
the heart runs from 130 to 140, and during the first
year gradually drops to 115, approximately.
Asphyxia neonatorum is a condition, wherein, for
some reason, the child fails to breathe after delivery.
Out of every one hundred babies born, about six will
die at birth or within the first ten days, and a large
proportion of them from asphyxia in some form.
Asphyxia is found in two degrees: asphyxia livida
(blue) and asphyxia pallida (white).
In the first, the child is deeply cyanosed. This may
be due to patency of the foramen ovale, and yet it is
a question whether this cyanosis is not really a normal
process. The child does not undertake its first respiration
because it needs oxygen, but because an excess of
carbon dioxide (CO2) in the blood acts as a stimulant
to the respiratory center, which is thus set to work,
with the result that oxygen is taken in. The blue
asphyxias, therefore, may be only the first step in the
physiological process of respiration. In these cases,
the pulse is strong and full, and the muscular tone is
preserved, as well as the sensibility of the skin.
In the second degree, the condition is quite different.
The face is pale though the lips may be blue. The
heart is irregular and many times can not be felt.
The cord is soft and flaccid, with its vessels nearly
279empty. The reflexes are abolished, the skin and extremities
cold. A few convulsive efforts at breathing
may occur, but they soon cease.
Treatment is directed first, to opening up the respiratory
passage. The child is held up by the feet so the
mucus, blood, and fluids may escape from the mouth.
Compression of the chest wall will aid. The tracheal
catheter is passed into the trachea and the mucus
sucked out. Next, the skin reflexes are stimulated by
slapping the back, or buttocks, and by blowing upon
the face.
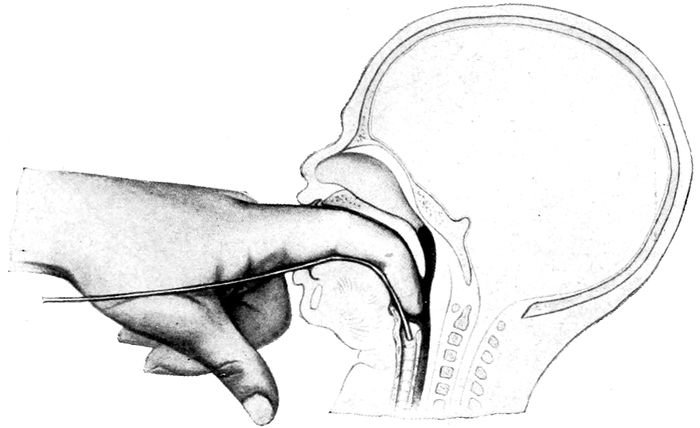
Fig. 117.—Method of passing the tracheal catheter. (Hammerschlag.)
The child at this time may be dipped in a tub of
very warm water, (112° F.) and the chest and face
sprinkled with cold water. Meanwhile, Laborde’s
method of traction on the tongue may be tried. The
tongue is seized with tongue forceps (handkerchief,
napkin, or piece of gauze will do) and rhythmically
drawn out and released about ten times per minute.
Further, the Byrd method of artificial respiration
must be employed.
280
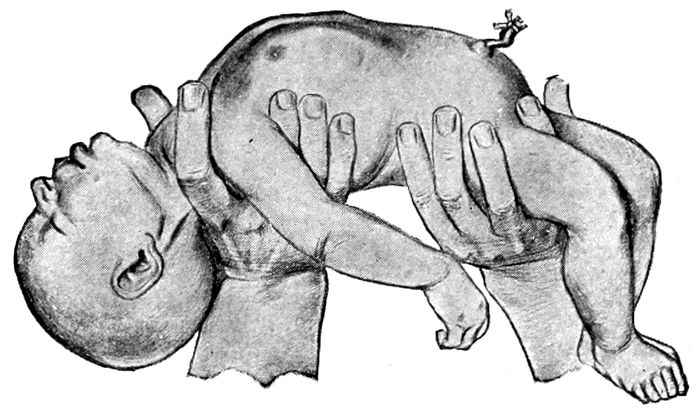
Fig. 118.—Byrd’s method of artificial respiration. Extension and inspiration. (Edgar.)

Fig. 119.—Byrd’s method of artificial respiration. Beginning flexion and expiration. (Edgar.)
The back of the child is held in the right hand, so
that the thumb and forefinger grasp the neck loosely,
the other hand holds the buttocks from behind and
the body is slowly but firmly flexed between them until
the thorax is compressed, then the grip is relaxed and
281the body widely extended to allow the air to rush into
the lungs. This maneuver should be repeated about
twelve times per minute. When the heart ceases to beat,
the child is dead and respiration can not be established.
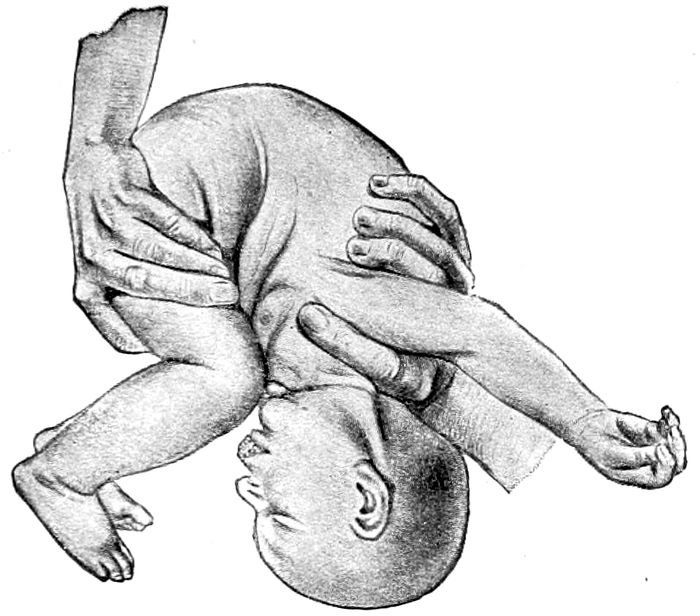
Fig. 120.—Byrd’s method of artificial respiration. Flexion and compression. Note position of child which aids the escape of fluids from the mouth and nose. (Edgar.)
The same treatment is employed for the apnœic child
born in Cæsarean section and the oligopnœic child born
under “Twilight Sleep.” The method called “Schultze
Swinging” is not to be recommended generally, on account
of the chilling which is so necessarily associated
with the exposure. The nurse should learn to practice
all these methods of resuscitation.
After the child breathes it must be watched carefully
for at least forty-eight hours, lest the symptoms recur,
and the child die.
Asphyxia Neonatorum—
(a) Livida—body congested—blue.
(b) Pallida—body limp and pale.
Remember possibility of patent foramen ovale.
282Etiology.—
Too long compression of cord.
Diminished irritability of medulla.
Compression of brain during extraction.
Shock during version.
Aspiration of mucus.
Treatment.—
Hold child by heels with head pulled back to straighten
the trachea, and wipe out mouth and pharynx gently with
cotton wound about the finger.
Stimulate skin reflexes by slapping and blowing.
Tracheal catheter, artificial respiration (Byrd) 8 to 10
times per minute.
Hot and cold bath alternately—rub the skin and knead
the muscles.
Laborde’s method of traction on tongue 10 to 12 times
per minute.
Continue efforts so long as heart beats.
Convulsions occur not infrequently during the first
few weeks. They may develop as a result of injuries to
the head during labor, or as a symptom of toxæmia.
They may arise from constipation, from intestinal indigestion
with curds, from fever or from hæmophila.
Meningitis and other infections are associated with this
symptom, and occasionally atelectasis. They may also
be the manifestation of a spasmophilic diathesis. The
attack may begin with such premonitory phenomena as
restlessness, muscular twitching, and staring of the
eyes, but more frequently the onset is without warning.
The facial muscles are contracted, the neck thrown
back, the hands clenched and the extremities spasmodically
cramped and tightened. There may be frothing
of the mouth and consciousness is lost. Respiration is
feeble, shallow and irregular. The face is discolored
and strange rattling noises come from the larynx. The
bowels and bladder may move involuntarily. The attack
lasts from a few minutes to half an hour.
283Convulsions are not serious in all cases.
The responsibility for the management of this complication
usually falls upon the nurse. She calls the
doctor, to be sure, but the attacks in many cases have
ceased and the child may either be dead or out of danger
of a recurrence before his arrival.
The hot bath is a universal remedy and quite as efficient
as anything. The temperature should be taken
and the bowels washed out.
If the fontanelles are tense when the doctor arrives,
a spinal puncture may relieve the tension. A specimen
of the blood is drawn through a needle and sent to the
laboratory for examination.
The cause must be found, if possible, and removed.
A change of food may be all that is required. Cod-liver
oil may be added to the diet in dram doses, three times
a day, and milk curds, suspended in arrow-root water.
For the acute condition, chloral hydrate is best. It is
given by rectum, one or two grains in an ounce of water,
and may be repeated in four hours.
Atelectasis is the name given to a failure of the lungs
wholly to expand during the efforts at respiration. The
child may live for weeks with this affection, but usually
it expires within a few days.
In this condition, the child has a constant tendency
to get blue, the color deepens, and death may occur
in spite of every aid. The treatment may be permanently
efficacious in some cases, but in most, the revival
is only temporary. Again, the child may live, but in
a weakly, declining state for days, until death comes.
Aside from the physical signs of dullness elicited by
percussion over the lungs, the most conspicuous symptoms
are the cyanosis and the intermittent but persistent
whining cry.
284
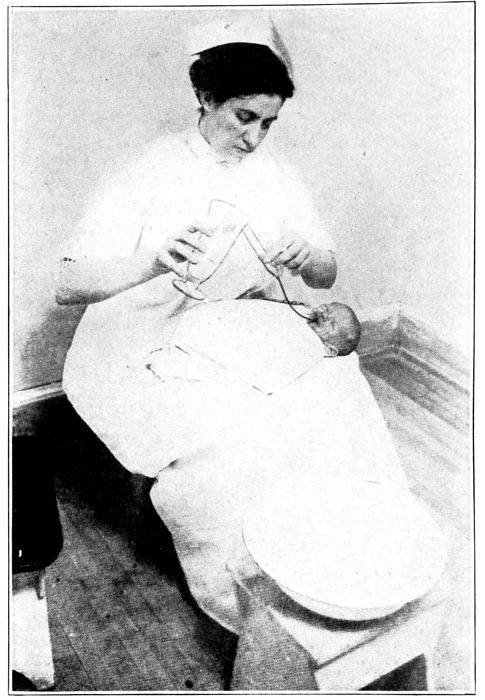
Fig. 121.—Method of giving gavage. (Grulee.)
Treatment is by daily or hourly spanking, and by alternating
hot and cold baths, by sprinkling with cold
water or by massage to stimulate the skin reflexes. The
treatment may have to be repeated every twenty or
thirty minutes, and the earlier it is instituted, the more
persistently carried out, the more chance of success.
Exercise is just as important to the infant as to the
285adult. The kicking of the legs, moving of the arms and
lusty cry are all means of stimulating the circulation,
the muscular development, and the expansion of the
lungs. The position should be changed occasionally in
the crib from back to side and from side to back. Also
the child’s legs and back should be rubbed and massaged
until the skin is red every time the bath is given.
Flushings.—The child is laid across the lap, or on a
table. A rubber sheet is so arranged that the discharge
will drain away.
A soft rubber catheter, No. 18–20 French scale, is
attached to a small funnel. The apparatus is boiled and
filled with normal saline, or sterile water, at a temperature
of 85° F. to 95° F. Half a pint to a pint may be
required.
The catheter is oiled and passed into the rectum just
beyond the sphincter. It must not go farther. The
funnel is then raised and the fluid flows into the bowel.
This flushing must not be confused with the administration
of an enema for constipation, for which, however,
it is often an excellent substitute.
Gavage is forced feeding by means of a tube. A soft
rubber catheter or tube, about No. 7, French scale, is
lubricated with albolene, vaseline or sweet oil. The upper
end is connected with a small tube or glass funnel
holding two or three ounces.
The child is laid upon its back in the arms of mother
or nurse, the baby’s arms are held and the head steadied.
In case of diphtheria or scarlet fever, the tube may
be passed through the nose and down the pharynx and
into the œsophagus five or six inches, or even into the
stomach. It is more convenient and easier when possible
to pass it through the mouth directly into the stomach.
286The food is then poured into the funnel, which, by elevation,
empties itself into the stomach. If regurgitated,
more food must be given. When withdrawn, the tube
should be pinched to prevent leakage into the trachea.
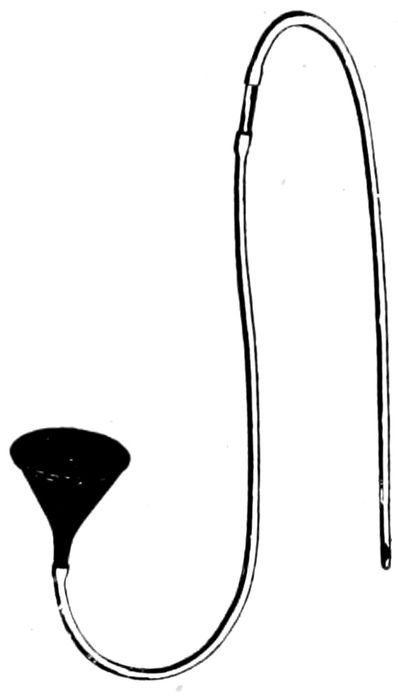
Fig. 122.—Apparatus for gavage or lavage. (Tuley.)
The great danger in these cases is the ease of overfeeding.
Lavage or washing of the stomach may be performed
in the same way with the above apparatus, when necessary.
As soon as the stomach is filled, the tube is lowered
and the fluid siphoned out.
287
CHAPTER XX
THE CARE OF THE CHILD (Cont’d)
Tongue-tie is not met with so frequently as in the old
days. If the child can suck and nurses energetically,
this complication can be excluded. It may, however,
occur. In such a case, the frænum is unusually broad
and seems to extend clear to the tip of the tongue,
which apparently is bound down to the gum and to the
floor of the mouth.
The thin membrane may be snipped with the scissors
close to the tongue and then torn back with the finger.
Harelip and cleft palate interfere with nursing and
require continual attention to keep mucus out of the
throat. Brophy has a rubber flap placed over the nipple
of the bottle in such a way as to occlude the split tissue
and thus enables the child to get nourishment.
These babies must be fed systematically by gavage, if
necessary, until the deformity can be repaired.
Hernia at the navel is a common complication of infancy.
It is not due to crying, to improper tying of the
cord, nor to neglect by the nurse, as frequently charged.
It is a congenital fault, wherein the cord opening does
not close, and in time, crying and straining will drive the
intestines out of the aperture like a pouch. The defect
is revealed by the bulging outward of the navel when
the child cries. Ordinarily the breach will close of its
own accord.
288
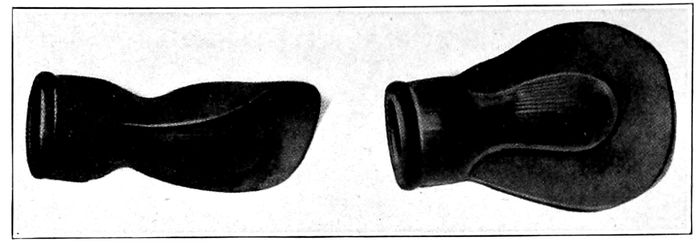
Fig. 123.—Cleft palate nipple. (Brophy.)
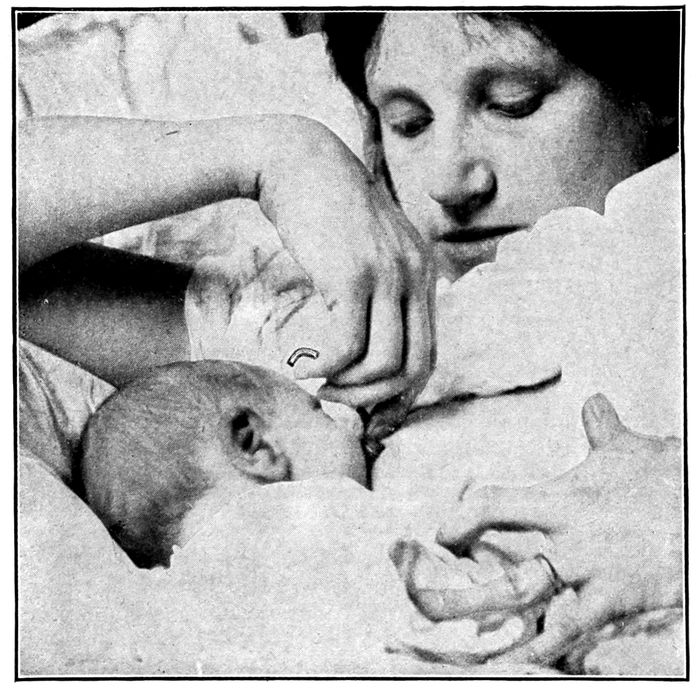
Fig. 124.—The device for feeding the child with cleft palate at the breast. (Brophy.)
289Treatment consists in folding up the skin of the
abdomen so that the groove will be over the umbilicus
and include it. Then adhesive tape is put on to hold it.
The surfaces of skin thus coming in contact should be
dusted with rice powder or stearate of zinc. Another
method of treatment is to place a wooden button form,
round side down, on cotton, over the opening, and bind
it on with a zinc adhesive plaster. The dressing should
be changed at least once a week.
Inguinal hernia usually heals spontaneously also, but
a truss may be required.
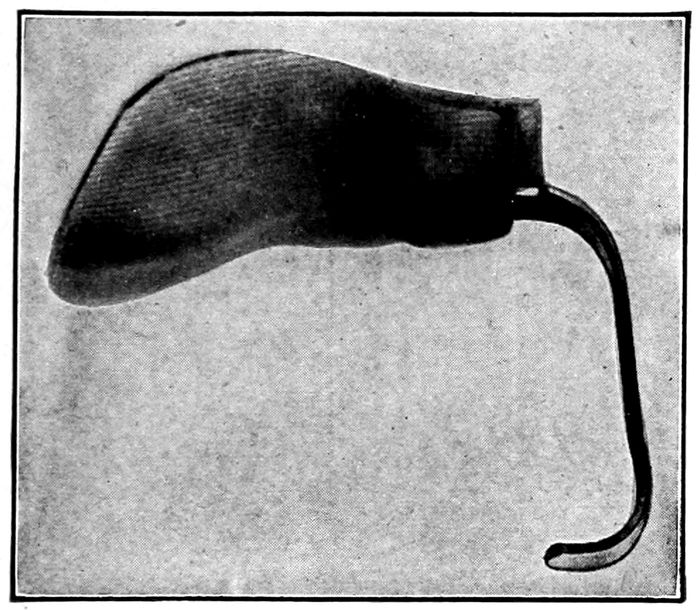
Fig. 125.—Device for assisting the cleft palate child to nurse. (Brophy.)
Hæmorrhage of the newborn is either accidental or
spontaneous. Accidental hæmorrhage may arise from
an imperfectly tied cord, or it may be an effusion,
through compression or rupture, into any of the internal
organs, such as the brain, lungs, or abdominal viscera.
These latter conditions rarely give rise to symptoms,
and are seldom recognized during life. There is no
treatment.
The intracranial hæmorrhages are open to diagnosis
290through the presence of pressure symptoms, but these,
too, are impervious to treatment unless a vessel can be
tied, like the middle meningeal artery.
Spontaneous hæmorrhages may develop during the
first few days of life from sepsis, syphilis, Buhl’s disease,
hæmophilia, and true melæna neonatorum. The
fragile condition of the blood vessels, the great changes
in the blood and circulation after birth, as well as constitutional
dyscrasias, are etiological factors of importance.
All the causes are not as yet known.
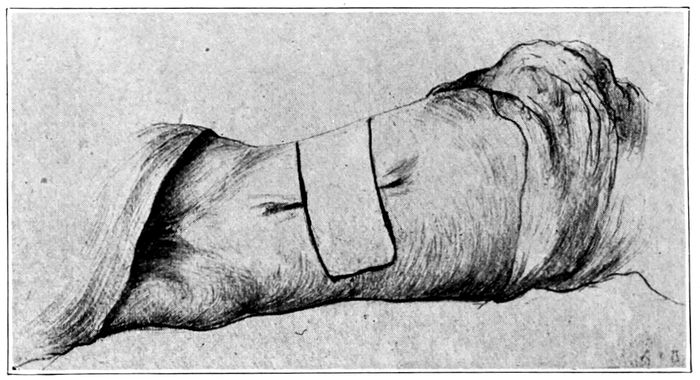
Fig. 126.—Method of strapping an umbilical hernia.
The blood may come from the umbilicus, the mucous
membranes of the eyes, nose, mouth, stomach and intestines.
It may be effused into the tissues beneath the
skin, or into any organ of the body. Marked nosebleed
is generally syphilitic in origin.
As a rule hæmorrhages in the newborn are most common
in males, and strongly hereditary.
The tendency to bleed lasts only a few weeks, and if
recovery takes place, it is permanent. In some cases,
however, where hæmorrhage has developed in the brain,
291clots may form in important centers, and the child be
permanently paralyzed in speech, sight, hearing, or intelligence.
Symptoms of hæmorrhage begin during the first week
and almost never after the twelfth day. The appearance
of blood is the earliest and the most definite sign. The
bleeding may come first from the umbilicus, or from the
stomach, or from the intestines (melæna neonatorum).
The amount lost is small, but the oozing is continuous.
The temperature may be high or subnormal, and may
or may not be due to the hæmorrhage. The skin is pale,
the pulse feeble, prostration marked, and weight is lost
rapidly. Convulsions are not infrequent.
The diagnosis of the condition is simple. It is only
necessary to be certain that the blood is really effused,
and not a temporary or accidental event such as the
regurgitation of swallowed blood. Black tarry stools
will show blood if placed in water.
The prognosis is not good. About two-thirds of these
babies die.
The treatment is to stop the hæmorrhage by ligature,
suture, or compression if possible and to alter the character
of the blood by adding to its fibrin content. This is
brought about, if at all, by the administration of
coagulose, coagulen ciba, or by transfusion from an
adult—preferably the father.
Paralysis of the face (Bell’s paralysis) may follow the
use of forceps. The prognosis is favorable. Paralysis
of the nerve in the neck (musculospiral) is sometimes
known as Erb’s paralysis. It happens in consequence
of difficult breech deliveries or of vertex labors when
much force is required to extract the shoulders.
The deltoid, biceps, and other muscles are affected so
that the arm can not be raised. The failure to raise one
292arm will be the symptom that will attract the attention
of the nurse. Some cases recover in a month or so,
either spontaneously or by the aid of electricity. If not,
the injured nerve must be cut down upon and its continuity
restored.
Ophthalmia neonatorum is an infection of the eyes of
the newborn by the gonococcus. The infection occurs
as the child passes through the vagina or vulva, or when
an unclean finger is put into the eye.
The reaction is violent. The discharge at first is thin,
then thick, pus. If untreated, the eyesight may be lost
by ulceration. In the asylums twenty-five per cent of
the inmates are blind from this infection; and as late
as 1896, seven per cent of the blindness in the state of
New York could be traced to this avoidable disease.
The preventive treatment consists in the frequent
douching of the vagina before labor with potassium
permanganate solution 1:5000, or chinosol 1:1000.
After labor, a drop or so, of 1 per cent solution of nitrate
of silver is dropped into each eye and not neutralized.
After the infection has occurred, iced compresses are
applied to the eye, night and day, and a solution of
argyrol 15 to 20 per cent instilled into the outer corner,
twice a day. In female infants with ophthalmia, the vagina
must be watched for discharge which does not fail
to appear in most cases. Argyrol (20 per cent) should
be injected with a medicine dropper and left to drain out
spontaneously. All dressings used about the child should
be destroyed, and the nurse should use the most scrupulous
cleanliness and care of her own person.
Separation of the cord may be delayed in puny babies
and in cases where the cord is large and thick.
Some of these cases are doubtless due to a patency or
fistulous condition of the urachus. Usually the separation
293may be hastened by touching the constrictured part
with silver nitrate. Or, if the cord does not separate before
the second week, it may be desirable to cut off the
hanging fragment and touch the base with silver nitrate
or dust with alum powder.
Granulations may protrude like a mulberry from the
stump of the navel (“proud flesh”). These are touched
with nitrate of silver stick.
Menstruation may appear occasionally from the vulva
of the newborn. It is really a hæmorrhage, a menstrual
flow, which is associated with uterine activity, but
rarely significant. There is no treatment. It disappears
spontaneously.
The breasts of the newborn may fill with milk and
become indurated and tender. Nothing should be done
to them. Let them alone and the swelling will subside
in a few days and the milk (“witches’ milk”) disappear.
Icterus may develop from the third to the sixth day.
The child becomes yellow and stays yellow for a week,
when the color gradually leaves. It is thought to be due
to the liberation of some embryonic residue in the fœtus,
but nothing is known certainly. For the simple form
no treatment is required. Recovery is prompt and uneventful.
However, jaundice is associated with other
conditions that prove fatal, hence every icterus should
be watched carefully until it disappears.
Child’s Nails.—The nails are frequently rough and
ragged at ends and sides. They should be smoothly
trimmed lest they become infected at the junction with
the skin and give rise to paronychia. If infection does
occur, the skin and flesh may be pushed back with a
sterile applicator, and the point touched with peroxide
294of hydrogen. A syphilitic history may be traced in some
of the babies.
Thrush is a form of contagious soreness, characterized
by white flakes or patches on the mucous membrane of
mouth or anus which look like milk, but can not be
wiped off.
It is due to a vegetable fungus and occurs most frequently
among anæmic or poorly nourished babies or
those suffering from harelip. It is associated with symptoms
of indigestion.
It may always be prevented by keeping the mouth
and nipples clean, as directed on another page, and by
keeping the bottles and rubber nipples in a solution of
boric acid when not in use. When the disease appears,
the mouth must be swabbed three or four times a day
with an applicator soaked in saturated solution of boric
acid. This is curative.
Aphthæ or stomatitis is the name given to whitish
vesicles, followed by superficial ulcers that occur upon
the inside of mouth and lips of the infant. It is rare in
the newborn child. Boric acid solution is cleansing, and
stick alum, frequently applied, will effect a cure.
Wheals, urticaria or “stomach spots” appear as generally
distributed small spots about the size of a split
pea, with a white center and a red periphery. They appear
about the third day and last twenty-four hours.
They may be mistaken for insect bites and they may,
or may not, be accompanied by temperature, which is
probably only a coincidence.
The wheals disappear spontaneously without treatment.
Bednar’s disease is characterized by the appearance
of two ulcers on the hard palate, one on either side and
just above the spot where the last tooth will erupt. It
295is most liable to occur in sickly infants and supposedly
arises from the abrading of the mucous membrane by a
rubber nipple or through the rough cleansing of the
mouth. It is very resistant to treatment. The child
must be put in good condition by attention to the
nourishment and the spots touched with tincture of iodine
on an applicator.
The exudative diathesis is indicated superficially by a
definitely bounded red patch on either cheek, which is
not relieved, or only temporarily, by the common ointments
and powders. The mother says the “face is chapped,”
or that the baby has a “milk eczema.” Otherwise
the skin is pale.
These children are frequently fat, but the tissue is
flabby. The urine is sometimes ammoniacal. There is
no marked disturbance of temperature. Fretfulness
and constipation are the principal symptoms.
The condition is due to too much fat in the food. A
skimmed-milk diet is best for a time. The fat can be
added gradually until the limit of tolerance is found.
If chalky masses appear in the stools, the fat must
be reduced again. Occasionally the child must be taken
off the milk entirely, and a soup or gruel diet substituted.
For local application, the following formula is sometimes
beneficial: (Grulee.)
| ℞ |
Naphthalene |
|
℥i |
| |
Starch |
|
ʒiv |
| |
Zinc stearate |
|
ʒiv |
| |
M. |
|
|
| Sig. Apply frequently. |
The “cradle cap” is a frequent sign of the exudative
diathesis in its milder stages.
The term is applied to a yellowish-gray patch over the
296large fontanelle. The mother calls it “dirt,” which she
finds hard to remove and it always recurs. The mass
is composed of dry scales, which gradually change into
an eczema. Vaseline or sweet oil left on over night
makes the removal of the scales quite easy the next day.
If a raw surface is left, zinc ointment should be applied.
The diet must be changed as previously described.
Erythema, especially of the diaper region, is sometimes
a manifestation of congenital syphilis. It is usually
limited to the inner side of the thighs, the perineum,
scrotum or vulva, and buttocks. It must be associated
with other and more characteristic signs, however, such
as snuffles, cachexia, etc., before it becomes diagnostic
of syphilis. Most erythemas of this area are due to irritation
from moist or soiled diapers, but other factors
may be important. Bluing in the diaper, gastrointestinal
troubles, and circulatory disturbances are contributing
causes. The local treatment is the same as for
intertrigo. If the child is syphilitic, systemic measures
must be instituted.
Intertrigo, or chafing, is a form of eczema due to
moisture, bluing in the diapers or uncleanliness. The
child should be cleaned with oil instead of water, and
well powdered with stearate of zinc or zinc ointment may
be used. Talcum powder which contains boric acid is
contraindicated.
Pemphigus neonatorum is an eruption of blisters or
blebs which seem to follow infection from the maternal
passages or to be communicated by other babies who
have the disease.
From three to fourteen days after birth, the blebs
develop on the abdomen, neck or thighs, and show a
tendency to spread to other parts of the body. The
vesicles vary in size from one-fourth of an inch to two
297inches in diameter, and contain a serous, purulent, or
bloody fluid. Other signs of general sepsis may appear.
In diagnosis care must be used to exclude syphilis,
which also exhibits blebs, but usually on the soles of the
feet or the palms of the hands. Besides, a nonsyphilitic
child is generally better nourished. The prognosis is
unfavorable if the child is weakly, if the blebs spread
rapidly over a large area, or if the infection attacks the
umbilicus.
Treatment.—A rigid quarantine must be enforced.
In the hospital no new cases can be admitted. The
alimentation must be increased, the blisters evacuated,
and the surfaces cleaned and covered with a 25 per cent
ointment of ichthyol, or an ointment of ammoniated
mercury 2 per cent.
Strophulus, red gum, or miliaria rubra are names applied
to an inflammation of the sweat glands when their
secretion is retained. It is a “sweat rash” characterized
by an eruption of scattered red papules or small
vesicles which commonly appear on the cheeks or neck
of young infants, or where skin surfaces come in contact.
It is due to excessive clothing or heat. It is really a
prickly heat. The treatment consists in the removal of
the cause, and a generous use of stearate of zinc powder
or rice powder.
298
CHAPTER XXI
THE CARE OF THE CHILD (Cont’d)
Constipation in the newborn may come from many
causes. The amount of food may be so inadequate that
no residue is left, and the bowels move only once in
forty-eight hours. Over-stimulation of the bowel by
castor oil or colonic flushings in the early weeks of life
to correct colic may diminish its sensitiveness and produce
atonic constipation. In the artificially fed infant
too much fat in the food is a very common cause of the
trouble.
Treatment.—Correct the amount of fat in the milk.
If the child is breast-fed, the mother’s diet should be
non-nitrogenous and vegetables should preponderate.
Drugs should not be given until all else has been tried.
Gluten suppositories will furnish a mild irritation to
the rectum. Orange juice and prune juice may be
given, or Mellin’s food or oatmeal water added to the
milk. Milk of magnesia ½ to 1 teaspoonful, or Husband’s
magnesia, in same dosage, may be given daily.
Senna is also efficacious.
Diarrhœa is generally significant of an error in diet
which is usually a plain indigestion, though there may
be too much sugar in the food.
The stools are more frequent and always softer than
usual, possibly fluid.
Diarrhœa means increased intestinal action due to irritation
from something. It may be due to indigestion,
to the presence of hard curds, to acidosis, or it may accompany
almost any disease of infancy as a symptom
299merely. The odor is due to gases formed in the canal
by bacterial action. There is but little odor in fermentation,
but much in putrefaction. Mucus appears either
as balls or strings. The balls come from the small intestine,
strings from colon. Blood indicates ulceration
at some point in the bowel, or an erosion just above the
sphincter.
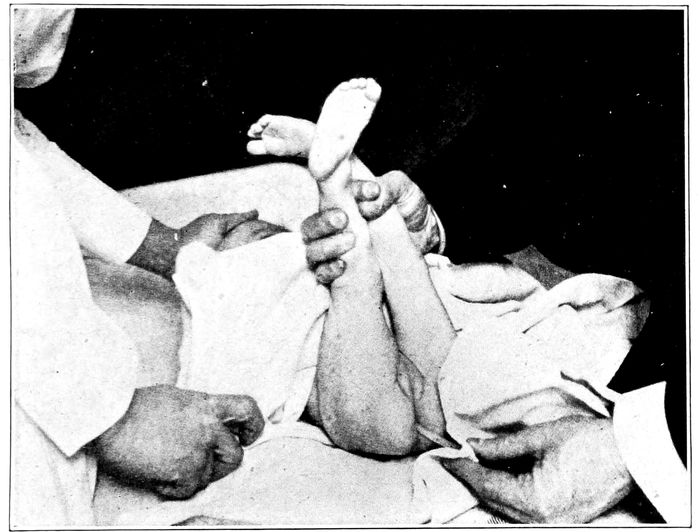
Fig. 127.—Proper position for introduction of a suppository. (Grulee.)
Fatty curds may be either white, granular, sand-like
masses, or small, soft, and yellow. The protein curd is
large and smooth, or white and bean-like. Both occur
only when the artificially fed infant is given raw milk
(Brenneman). If the milk is boiled for two minutes
these masses will not form.
The cause must be determined. The frequent stools,
however, are exhausting, and may have to be checked
with opiates or mechanical astringents.
300When due to indigestion, all food by mouth may be
stopped for two or three days and only barley water
administered.
In a breast-fed child, diarrhœa is sometimes checked
by diluting the milk with a little barley water, given
just before nursing. With these infants, not much
change in the sugar content can be made by alterations
of the maternal diet, but where artificial food is used,
the amount of sugar is easily reduced to a satisfactory
degree.
Colic is a cramp-like pain of the bowels. Previous
to the attack the child is restless, expels some gas, and
has the “colic smile,” which leads the mother to believe
the child is quite well. When the attack comes on, the
thighs are flexed on the abdomen, and the legs on the
thighs. The child has a sharp cry, that is nearly continuous,
but in some way related to the nursing period,
for the attack comes on a few minutes, and sometimes
an hour, after taking the breast. The belly is rigid, the
arms wave aimlessly. Diarrhœa may be present, and
the movements are accompanied by much flatus. Distention
is nearly always present. When the belly is
tapped it gives a drum-like note and the child belches
gas, sometimes accompanied by milk, which seems to
relieve.
Treatment.—Colonic flushings to relieve the bowel
of irritating curds. The child may be laid face down
with a bag of hot water under the belly. Mixture of
asafœtida gtts. xx to xl, or whiskey and hot water
should be given for the attack, followed later by a full
dose of castor oil. The diet should be rigorously investigated.
Vomiting may or may not be serious. The child may
nurse too rapidly or too much, and the over-distended
301stomach simply empties itself. Many infants “spit up”
their excess of milk, and thus relieve themselves. This
is a simple regurgitation, usually of unchanged milk,
though it may be acid from admixture with the gastric
juice.
Vomiting, in a breast-fed child, may come during an
attack of colic when the eructations of gas appear. It
may be a symptom of gastrointestinal intoxication, of
too much fat in the food, too short intervals between
feedings, or too much sugar in the food.
Projectional vomiting awakens suspicion of a pyloric
stenosis or meningitis, and must be reported to the
physician at once.
Vomiting which occurs within twenty minutes after
feedings is not serious ordinarily, even though gas and
large curds are expelled, but all vomiting later than
this, is significant of a pathology.
Treatment.—Regulation of the hours of feeding is
most important, and next, the character of the food.
If the child vomits an hour or so after nursing, it may
be that the milk is too rich (fat). Try a longer interval,
or give an ounce or so of cereal water before putting
the child to the breast.
Prematurity exposes the child to three distinct dangers,
which arise, respectively, from atmosphere, food,
and infection. Very few children born before the
seventh month survive. A child born at the eighth
month, or with a weight of three pounds, or more, can
be saved almost always. The premature child up to
the time of birth, has been protected very carefully
against temperature variations by the liquor amnii, and
when suddenly precipitated into a new environment,
which its vitality barely tolerates, the consequences are
serious.
302These infants have a poor heat production, and the
natural warmth of the body must be preserved. This
is best done by incubators, which supply air and moisture
in stable and appropriate amounts. Chilling of the
child for even a few moments may be fatal. A room
may be fitted up to produce the necessary conditions
of light, air, heat and moisture. The child, wrapped
in sheets of cotton, except the face, is then covered
with a blanket, and surrounded by a temperature varying
from 88° to 95° F., which is gradually lowered to
80° F. as the child gains strength. An occasional whiff
of oxygen, as prescribed for an atelectatic child, is
sometimes advantageous.
Bathing.—Premature infants must not be bathed, but
the skin should be cleansed with cotton and warm
sweet oil or albolene. All unnecessary handling is to be
avoided.
Food.—Breast milk is the secret of success with these
cases. Since most of the infants are too weak to take
the nipple, the breasts must be pumped, and the child
fed with spoon or pipette.
The interval between the feedings depends a little on
the amount taken, but it should not be less than one
and one-half hours, nor more than two hours. As the
child gains, the interval may be lengthened to three
hours. Lack of sufficient nourishment is shown by
cyanosis and loss of weight, and overfeeding, by vomiting
and diarrhœa.
The child must be fed by hand until strong enough
to nurse the breast. In certain cases of prematurity, as
well as in diseases like pneumonia, scarlet fever, and
diphtheria, the child must be fed by gavage. Nutritive
inunctions of benzoated lard or cod-liver oil are also
valuable, not only for the passive exercise supplied, but
303for the absorption of a certain amount of the unguent.
Marasmus means wasting, but the term is applied to
infants that steadily lose weight. The bodies of infants
are so largely composed of fluid, that loss of weight
occurs quite easily and rapidly. Loss of weight may
be sudden or gradual. It comes on rapidly after acute
diarrhœa, either with or without vomiting, or it may
follow persistent vomiting without diarrhœa.
Malnutrition from defective feeding is the most common
cause of wasting in infants. This may be from lack
of sufficient food or lack of proper ingredients, as well
as irregularity of intervals, and disease. Rickets, congenital
stenosis of the pylorus, congenital syphilis, and
tuberculosis are all possible factors in the etiology.
In any case, no treatment can be instituted until these
conditions have been confirmed or excluded.
Pyloric stenosis (the account follows Grulee) may be
a thickening of the muscular coat of the outlet of the
stomach (pylorus) or a spasmodic contraction. The
condition is most frequent in males and in the first
born.
Symptoms usually begin before the second week.
There is constipation with small ribbon-like stools, and
the urine is scanty. The most marked sign, however,
when it is present, is the excessive, uncontrollable vomiting,
which ordinarily occurs fifteen to thirty minutes
after eating, but may be delayed for several hours. The
vomiting may be of the common type, but more frequently
it is projectile in character, like that seen in
meningitis. The contents of the stomach are violently
expelled, sometimes several feet. Physical examination
may reveal the stomach bulging under the arch of the
ribs and peristaltic waves moving back and forth across
304its surface. The pylorus itself may sometimes be felt
as a lump or tumor.
Prognosis.—About fifty per cent die.
Treatment.—Dietetic and surgical. Grulee recommends
small amounts of food, poor in fat, be given at
short intervals. If this fails, operation is required.
Pneumonia in the newborn most frequently results
from the aspiration of mucus out of the maternal passages
as the child is born. This may happen when the
cord is compressed, or at any time when a partial asphyxiation
impels the child to try to breathe.
It may also come on when a feeble child has been
chilled by a prolonged first bath.
The disease develops about twenty-four hours after
birth in a child apparently well. The temperature rises,
respiration becomes rapid, and cough develops. The
child is fretful, restless, refuses the nipple, and gasps for
breath. It may become cyanotic. The prognosis in newborn
infants is very serious.
Treatment is stimulation. A mustard bath will benefit
where the respiration is rapid and the child blue.
Tincture of digitalis may be administered in drop doses
every three or four hours. Carbonate of ammonia,
¼ gr., in mucilage of acacia, half a dram, may be given
for cough.
Child must be fed on mother’s milk pumped from
breast.
Snuffles may be due to improper clothing, to drafts
of air, or to syphilis. If due to cold, camphorated oil
may be rubbed on the nose and the passages kept clean
with an applicator soaked in albolene. If this fails, a
small pellicle of anæsthone may be placed in each nostril,
and the child laid upon its back until the ointment melts
and runs back into the pharynx.
305Furuncles (boils) may be numerous. They come from
irritation of the skin by atmosphere, soap, water, and
clothing, whereby infection enters. This is especially
liable to occur in the hair.
Keep the boils washed with boric acid solution and
open them as soon as the focus, or head, appears.
Phimosis is such a close adjustment of the prepuce
to the glans penis that it can not be retracted. In
some cases there may be obstruction to the outflow of
urine, but generally a tiny portion of the glans can be
seen. The prepuce may or may not be redundant.
This condition makes cleanliness impossible and balanitis
may result.
On account of the straining required to urinate, prolapsus
ani, hernia, and hydrocele of the cord sometimes
develop. Symptoms may arise from preputial adhesions,
as well as phimosis. Frequent or difficult micturition,
nocturnal incontinence, priapism, pruritus, and
masturbation may develop out of the irritation, as well
as nervous manifestations, such as insomnia and night
terrors.
The condition should be recognized and corrected in
infancy. If the adhesions are dense, an incision can be
made down the dorsum of the prepuce, the tissue forcibly
separated from the glans, and the flaps cut off.
Stitches may be required. In other cases circumcision
may be necessary.
Paraphimosis.—When a prepuce with a small orifice
is forcibly retracted over the glans, it occasionally happens
that it cannot be pulled forward again. If allowed
to remain this way, the parts will swell, and the
penis become strangulated as if with a ligature.
The danger arises from the stoppage of the circulation,
which may be followed by ulceration and gangrene.
306Reduction must be brought about by manipulation,
if possible, but where this fails, the constricting band
must be cut through and sedative applications used.
Balanitis is inflammation of the prepuce from the decomposition
of smegma, which collects under a tight
foreskin. The condition is quickly relieved by cleanliness
and a few applications of vaseline or zinc oxide
ointment. Circumcision should not be done until the
inflammation has subsided.
Circumcision, either as a physical necessity or as a
religious rite, is frequently performed.
The nurse prepares a table with sterile linen, a basin
with antiseptic solution and sponges, sterile towel, and
sterile vaseline, with a roll of gauze bandage an inch
wide.
The object of the operation is to remove the prepuce
and leave the glans exposed.
The instruments needed are a pair of sharp scissors,
a pair of dissecting forceps, two pairs of artery forceps,
small, full curved needles, and fine catgut.
The nurse gives the child some gauze to suck, which
has been soaked in brandy and sugar-water, brandy
one dram to an ounce of water. Then taking her place
at the child’s head, she flexes the thighs back upon the
abdomen, and widely separates them. The field of operation
is thoroughly washed with soap and warm water,
the prepuce is then retracted and the smegma
wiped away. Then the body and limbs should be covered
with clean linen, except the penis, or a sterile
towel may be used with a hole in it through which the
penis is drawn. The redundant tissue is removed and
fine catgut sutures put in.
The operation being completed, the wound is covered
307with sterile vaseline and wrapped with a sterile gauze
bandage, leaving the end of the glans exposed.
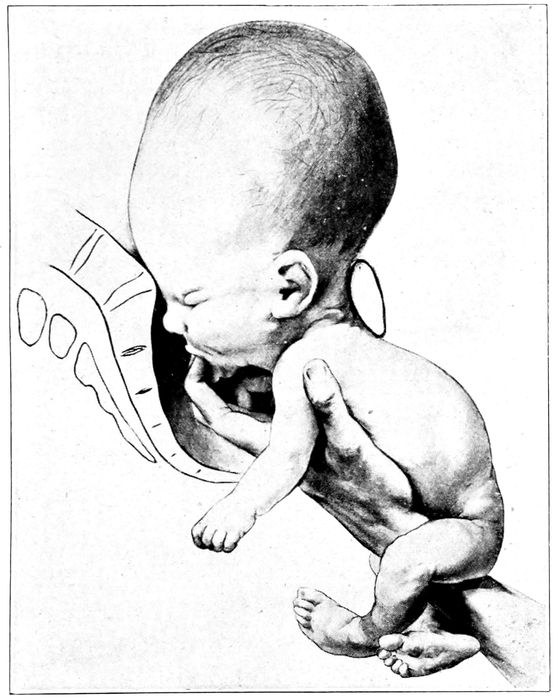
Fig. 128.—Hydrocephalus. (Bumm.)
The gauze and vaseline are changed whenever saturated
with urine. Healing ought to be complete by
the seventh day. The nurse should examine the dressing
at frequent intervals during the first twenty-four
hours, since serious hæmorrhages may occur from vessels
that have not been included in the sutures.
308Priapism is a condition of functional fullness and
firmness of the penis that is more than ordinarily constant.
Its importance lies in the fact that it may be a
symptom of spinal irritation, balanitis, worms, or
phimosis.
Spina bifida is the most common congenital deformity.
It is characterized by a fluid tumor, which protrudes
from an opening in the vertebral column. It
may appear anywhere along the spine, but is found
most frequently in the lumbar or cervical region. The
deformity is supposedly due to an arrest of development.
It is nearly always fatal inside of two weeks,
though cases have been known to reach mature years.
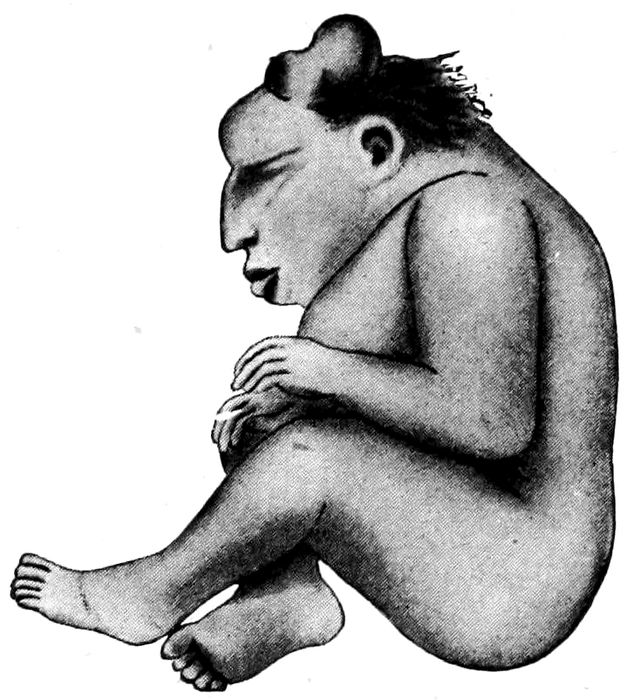
Fig. 129.—Anencephalus. (Williams.)
There is no treatment except protection from injury.
Hydrocephalus is sometimes, but not necessarily, associated
with spina bifida.
The ventricles of the head are filled with cerebrospinal
fluid, and the fontanelles are widely separated.
The cause of the anomaly is unknown.
309This condition may render labor difficult or impossible
until the diagnosis is made and the skull perforated.
Rupture of the uterus may result from the futile
efforts to expel the child. If born alive, the child
nearly always dies, or if it grows up, the intelligence
is imperfect in most cases.
Anencephalus is a monster, having a body, but only
a part of a head. The eyes protrude, the tongue may
hang from the mouth, and the brain is under-developed.
Sudden death of infants that are apparently healthy
comes with a shock to the physician as well as the parents,
and in some instances, no plausible reason can
be assigned for it. Apoplexy, pneumonia and stoppage
of the trachea by milk curds may explain some cases.
Suffocation by lying on the face in wet bedding, or
overlying by the mother will account for others. Internal
hæmorrhage into lungs, pleura, stomach, or brain
is also known to be causative.
310
CHAPTER XXII
INFANT FEEDING
A well fed infant is a happy little animal, who sleeps
approximately twenty-two hours a day, and gains from
four to six ounces a week. If properly fed at the
breast, this condition is easily obtained; but if artificial
food is necessary, the resources and skill of the attendants
may be tried to the utmost before the welcome
result is brought about.
The feeding of infants may be considered under three
heads, (1) the breast; (2) breast and bottle combined
(mixed feeding); and (3) artificial, which is really modified
cow’s milk.
Breast feeding has been taken up elsewhere, but the
same care should be taken in feeding from the bottle
as in feeding from the breast, so far as concerns the
intervals between the feedings and the duration of the
same. Since it takes from one to two hours longer for
cow’s milk to digest than it does for mother’s milk the
longer interval of three or four hours between feedings
is better for the artificially fed child. With such an
interval there will be less vomiting, less colic, less tendency
to overfeed, and a better natured baby.
One feeding should be omitted at night, and if possible,
two.
Length of time for taking the bottle depends somewhat
on the child, but it should not exceed fifteen minutes,
as a rule.
Supplemental Feeding.—A mother who has too little
311milk may have it supplemented by a modified mixture
in one of two ways.
First, the quantity furnished by the breast must be
determined by weighing the infant before and after
feeding, and then the total amount for twenty-four
hours can be deduced. With this information, it is not
difficult for the doctor to know how much cow’s milk
to prescribe. The supplemental feeding may be given
by alternating the bottle and the breast, or by giving
the breast and following it immediately with the bottle.
In the meantime, the mother must be put on tonics
with an abundance of fluids, and a generous diet that
will raise the blood pressure, in the hope that the milk
will increase sufficiently to enable her to feed the child
entirely from the breast.
When it becomes necessary to substitute some other
food for the breast milk, it means that the milk of some
other mammal must be modified for the purpose. The
most convenient and abundant source of supply is the
cow.
While in many respects cow’s milk is similar to mother’s
milk, it is in reality quite a different product.
Mother’s milk is taken, undiluted, directly from the
breast, while cow’s milk is given from a bottle, hours
after milking, and not only must it be diluted, but certain
ingredients must be added to aid its digestibility.
When taken into the stomach in its natural state,
mother’s milk is a liquid, while under the same conditions,
cow’s milk forms a semisolid gelatinous mass.
It is essential that the milk should be as fresh, clean,
and free from bacteria as possible, and this can be approximated
only in certified milk. This milk is required
by law to have its constituents definitely standardized.
Thus, there must be 4 per cent of fat, 4 per cent
of protein, and 4 per cent of sugar, and it must be so free
312from bacteria that not more than 10,000 per cubic centimeter
can be found. The cattle also are tuberculin
tested. The following comparison is from Holt:
| Mother’s Milk |
Cow’s Milk |
| |
| Sp. Gr. |
av. 1.031 |
av. 1.031. |
| Fat |
4. % |
Fat |
4. % |
| Protein |
1.50% |
Protein |
3.50% |
| Sugars |
7. % |
Sugars |
4.50% |
| Salts |
.2 % |
Salts |
.75% |
| Water |
87.3 % |
Water |
87.3 % |
| Reaction |
Alkaline |
Reaction |
Acid |
| Bacteria |
Very few |
Bacteria |
Many |
| |
| Both range from 1.026 to 1.06. |
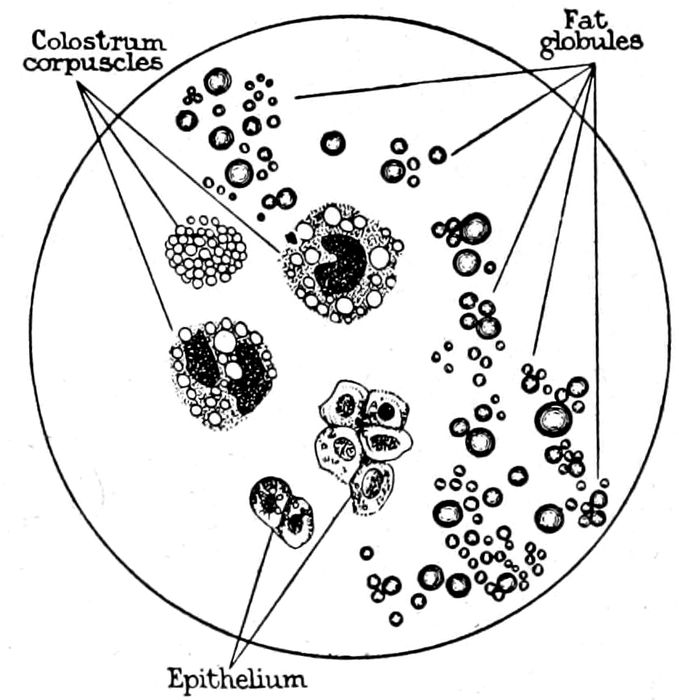
Fig. 130.—Elements of human milk. (Eden.)
The fats are substantially the same, but the fat of
cow’s milk is less easily digested than the fat of mother’s
milk.
The protein of mother’s milk is virtually half lactalbumin
and half casein, which is only slightly coagulated
into soft flocculent curds by the action of rennin
and acids, while the casein of cow’s milk is nearly three
313times greater in amount than the lactalbumin and is
coagulated into coarse, tough curds.
The sugars in both cases are lactose in solution, but
mother’s milk contains a much higher percentage.
Cow’s milk contains three times the quantity of salts
found in human milk, but the water is the same in both.
So, while the two milks seem in comparison to be
much alike, in reality they are quite different; hence it
is necessary to modify cow’s milk in such a way as to
make it not like mother’s milk chemically, but to make
it act like mother’s milk.
It is extremely difficult to bring up an infant on artificial
food, and inasmuch as half the infants that die
during the first year, perish from intestinal disorders,
it is imperative that every resource should be exhausted
before the breast feedings are abandoned. It is fallacious
to believe that anyone can feed a baby, or that
feeding consists merely in trying one food after another
until one is found to agree. Only a competent
physician should prescribe the food, and he should
study his problem and make his modifications just as
he would alter his medicines for a particular disease.
However, it is necessary for the nurse to know how
to carry out the doctor’s orders intelligently and how
to report to him the conditions present.
In prescribing for the child, the doctor usually has
some definite outline in his mind, such as
| Age and weight. |
Example: 3 months old; weight 10 pounds; 7 feedings; 1 every 3 hours. |
Interval, three hours.
Amount in each bottle, four ounces.
Formula:
Milk, 12 oz.
Diluent, 16 oz. (Cereal water or plain water.)
Sugar, ½ oz.
Flour ball, if any, ½ oz.
Boil if ordered.
314The infant should not take more than two ounces of
milk to a pound of weight in each twenty-four hours.
Proprietaries.—Baby foods are not to be recommended
nor condemned. They are placed on the market
as substitutes for mother’s milk with definite instructions
as to preparation. They are also very expensive.
They are not to be condemned, because many
of them are invaluable when used in connection with
cow’s milk. Sometimes a child will not tolerate anything
but malted or condensed milk, or Nestle’s food,
for example. The malt sugars, such as Horlick’s and
Mellin’s, are easily assimilated, fattening, and laxative.
All foods in the modification of milk should be of the
best. The standard sugars are Merck’s milk sugar,
Mead’s Dextri Maltose, Nährzucker, cane sugar, and
Mellin’s and Horlick’s foods. Robinson’s barley flour
or Johnson’s are the best known. Imperial granum is
a partially dextrinized flour and corresponds to the
home-made “flour ball.”
FOOD PREPARATION
Buttermilk Made from a Culture.—Bring two quarts
of milk to a boil, cool to the temperature required for
inoculation (80° to 100° F., depending on the culture
employed). Introduce the culture, and allow it to stand
at the temperature of the room until a solid clabber
forms. Place on ice, whip with an egg beater or break
up with a churn before using. If a fat-free buttermilk
is desired, use skimmed instead of whole milk.
There are many kinds of buttermilk cultures on the
market, but Hansen’s is considered one of the best, because
it is not too acid, besides which, it has a good
flavor, and the culture can be utilized over and over
for a week or ten days.
315In preparing a subsequent portion, it is only necessary
to use two or three ounces of the first buttermilk,
which may be reserved for the purpose. This amount
is introduced into the freshly boiled milk, instead of
the original powder, and the preparation is continued
exactly as described for the mother culture.
In every case the mixture must be placed on ice as
soon as the clabber forms, as it becomes too sour otherwise.
Eiweiss Milk.—Heat one quart of whole milk to
145° F. and coagulate with pepsin, rennin, or chymogen,
which is 10 per cent rennin. Let it stand until
clabbered, which takes about ten minutes. Pour into
a gauze bag and let it stand until all the whey is
drained off. To the dry curd, add ½ ounce of flour
ball, and one pint of skimmed buttermilk, the whole
to be rubbed through a very fine wire mesh sieve (as
fine as a tea-strainer, at least), three separate times;
or, it may be ground twice through a special mill to
break up the curd as minutely as possible. Add a pint
of water and measure. There should be a quart and
three or four ounces over. Place upon a slow fire and
bring to a boil while stirring constantly. Boil two minutes,
then cool, strain, measure, and add water to make
up for evaporation. Shake well before measuring, as
the curd is heavy and settles to the bottom.
Peptonized Milk.—(See p. 338.)
Whey.—To a pint of fresh, warm cow’s milk, add
rennin as pepsin, or chymogen, and stir until mixed.
Let it stand until coagulation is complete. Then the
curd should be broken up with a fork, and the whey
drained off through coarse muslin. This removes the
coagulable proteins from the milk. A ten per cent
cream can be had at home by allowing a quart of milk
316to stand for six hours and then using the upper one-fourth.
Whey-Cream Mixture.—Make whey as described and
mix with cream, in the proportion of whey 1½ ounces
to cream, 1 dram for each feeding.
Barley Water. No. 1.—Use one ounce of barley
pearls to a quart of water. Wash thoroughly, put on
a slow fire and boil for six hours. Add water to make
up for evaporation, and add a pinch of salt. Strain
and cool rapidly.
Barley Water. No. 2.—Use one heaping teaspoonful
of Robinson’s patent barley flour to each pint of cold
water. Boil twenty minutes and add water to make
up for evaporation. Add a little salt, strain and cool
rapidly.
Other cereal waters, like rice and oatmeal, are made
like barley water No. 1, and in the same proportion.
Flour Ball.—Take four cups of ordinary wheat flour
and wrap it in a piece of muslin, and tie it tightly.
Drop the mass into boiling water and boil six hours.
Then take it out, cool it and remove the outer peeling
with a sharp knife. Break into small pieces, the size
of an English walnut, and dry thoroughly in a slow
oven. Pulverize in a mill or meat-grinder, sift and
keep in a dry place.
Milk may be sterilized, pasteurized, or boiled.
Sterilization kills both germs and spores, but it is
not nearly so necessary as it is to have the right proportion
of sugar and fats. Place in an autoclave and
keep at a temperature of 160° F. for an hour.
Pasteurization is desirable when a good, clean milk
is not attainable. It kills the germs, but not the spores.
The process must be carefully attended to, or the milk
will sour more easily. Heat a quart of milk to 160° F.
for twenty minutes. Cool rapidly to 40° F.
317Boiling milk for two minutes kills all bacteria, and
renders the casein more easy of digestion and prevents
the formation of curds.
PUTTING FOODS TOGETHER
Whole milk contains 4 per cent fat, and must be
thoroughly shaken before it is measured, for otherwise
one child will get all the fat and another all the
skimmed milk.
Fat-free, or skimmed milk, contains about 0.1 per
cent fat. The cream has been removed by a siphon or
centrifuge. If unable to get a fat-free milk from a
dairy, the cream can be removed from a quart of whole
milk quite easily with a siphon.
Sugars and flours should be weighed when used, for
they vary greatly in volume.
In using flour ball or imperial granum, the flour must
be mixed with water or cereal water, to make a smooth
paste and brought to a boil. If the milk is to be boiled
also, add the milk to the paste and boil all together.
Cool and strain.
All baby feedings should be strained, as tiny lumps
of food will clog the rubber nipple and the nurse may
think the baby is not taking its feedings well. The following
is a typical formula:
| Whole milk |
15 oz. |
} |
5×6×4 |
| Barley water |
15 oz. |
| Sugar |
½ oz. |
| Flour ball |
½ oz. |
| Boil two minutes. |
|
Weigh the sugar and flour ball and make a paste
with the barley water. Shake the whole milk, measure
out 15 oz. in the graduate, and add the barley water
mixture. Boil two minutes. Cool in running water,
318strain bottle and put on ice. The figures at the side
mean that five feedings of six ounces each are to be
given at four-hour intervals.
It is necessary to cool all feedings as soon as modified,
and keep them on ice for preservation until used.
The only accurate way is to make up the whole quantity
for twenty-four hours, put into separate bottles
the exact amount of each feeding and give at the time
ordered, after the bottle has been properly warmed.
In warming the food, care must be used to get it neither
too hot nor too cold; 100° F., or when it feels
warm to the back of the hand, is about right. The
child should be held in the arms while taking the bottle.
A buttermilk feeding must not be heated to more
than 100° F. because it curdles and can not be used.
The rubber nipples should be washed thoroughly
after use, boiled once a day, and kept in boric acid
solution.
The necessary articles for home modification of milk
can be obtained anywhere. One set of utensils should
be kept for this purpose exclusively and boiled each
time before the food is prepared. A list is convenient:
A 16 ounce glass graduate.
One tablespoon and one teaspoon may be used for measuring
purposes, if unable to get a satisfactory scale.
1 2–quart aluminum cooking dish.
1 long-handled aluminum spoon.
1 fine wire mesh strainer, thirty holes to the inch.
1 dozen bottles, 5 ounce size if the child is small, and 10
ounce if the child takes large feedings.
The bottles should have wide mouths, straight sides,
and round bottoms, which clean easily. Paper caps or
corks that fit tightly should be used instead of cotton
stoppers. Close rubber caps are best, for, as the milk
cools, a vacuum is created, the rubber is drawn in and
319the milk remains air-tight until opened. If infants are
kept on a milk diet alone for too long at a time, they
do not thrive so well, hence as early as six months,
other things may be given. At this stage, the most desirable
additions to the food would be cereal, farina or
cream of wheat, orange juice, vegetable broth, toast
crumbs, etc. The administration of orange juice should
be started when the child is only a few weeks old.
The quantity of all these foods may be increased as
the child gets older, and by the end of a year the diet
is broadened still further. Beside a quart of whole
milk, it may have thickened soups, vegetables, such as
cauliflower, spinach, carrots, creamed celery and a little
baked potato. Fruits, orange juice, grape fruit
juice, prune sauce, apple sauce and scraped apple may
be given, but no bread. In place of bread, use toast,
Huntley and Palmer wafers and biscuits, and soda or
oatmeal crackers. Sweet desserts should be avoided,
but flavored junket or simple custard is unobjectionable.
No meats are permitted until the child is eighteen
months old, except, perhaps, a little crisp bacon, or a
bone to suck.
None of these supplemental foods should be given between
meals, but always at the feeding hour. The
above list supplies a dietary so varied that no child
will tire of it.
In reporting the condition of the infant to the physician,
the following form may be used to advantage. It
is a clear cut, concise summary of what he wishes to
know.
Infant’s Daily Report
- 1.
- Food: Does baby take it all? Is he satisfied?
- 2.
- Bowel movements: How many in last 24 hours? What is the color? Are they hard,
soft, or watery? Any odor? 320Any curds? Any slime? Any blood? Any colic? Much gas?
- 3.
- Does baby vomit? When? How much?
- 4.
- Does baby sleep well? Is he good natured?
- 5.
- Any fever? What is the weight?
Significant Symptoms and Conditions.—In an artificially
fed baby, the normal condition of the bowels is
constipation. The stools are formed, alkaline in reaction,
rather hard, and usually only one a day.
The stools should have a characteristic color, according
to the food taken. Thus:
Sugar or starch will color the movement a dark brown,
like vaseline.
Too much fat gives a pale yellow stool, almost white,
like putty.
Eiweiss feedings show as a pale yellow, somewhat like
the fatty stools, but constipated.
Barley water gives a brown liquid stool.
Starvation stools are thin, slimy, dark brown or green.
The consistency of the movements is also important.
Too much sugar or starch means diarrhœa, with thin,
green, acid stools, and much gas and regurgitation, or,
sometimes foamy, mucous discharges.
Diarrhœa may also be due to indigestion. Mucus in
the stools usually signifies intestinal irritation.
Constipation may exceed the normal limits of the artificially
fed child when the food contains too much fat.
Bad odors of the stools result from putrefaction.
Colic means imperfect digestion with gas. There is
less colic when the intervals between the feedings are
lengthened.
Curds are of two kinds. The soft friable ones due to
fat, and the hard bean-like masses of protein. Curds
occur with feedings of raw milk only, and though associated
with symptoms of indigestion, they signify
321overfeeding. If the sugar content of the food is low,
the child will gain very slowly.
Vomiting is an important phenomenon. It may be
due to overfeeding, to excess of sugar or fat in the
food, or to pyloric stenosis. Excess of fat is shown by
vomiting and regurgitation of small quantities of food
one or two hours after feeding. It may be associated
with constipation.
If vomiting occurs immediately after feeding, it is
probably due to the taking of an excessive amount, or
to the too rapid ingestion of the regular bottle. If the
vomiting takes place later than twenty minutes after
feeding, it is probably pathological. It may be the result
of indigestion, meningitis, or of pyloric stenosis
(q. v.).
For the first weeks of life, mother’s milk should be
obtained at all hazards, if possible, but if this is not to
be had, the artificial feedings may be started.
A desirable milk modification for the first weeks of
life should begin with a low food value. For example,
a child one week old weighing seven pounds, should
start on a formula like this:
| Whole milk |
7 oz. |
| Water |
7 oz. |
| Cane sugar |
½ oz. |
| Boil two minutes. |
|
This will make seven feedings of 2 oz. each, and one
is given every three hours with one feeding omitted at
night.
Cane sugar is less liable to produce colic than sugar
of milk.
Lime water, or sodium citrate may be added, if the
child vomits, or if other indications arise. Both are
alkalies.
322The strength of the mixture, as well as the quantity,
must be increased as the child gets older and it is seen
that the formula will agree.
The percentage of protein is kept down by dilution,
with plain or cereal water, while fats (as cream) and
sugars are added to make up the strength lost by the
dilution.
323
CHAPTER XXIII
CLEANLINESS AND STERILIZATION
The nurse is called to a case on account of her special
qualifications, but also she should lead her patient
in all things, even in gentility. It is her part to anticipate
the wants of the patient, and regard it as a reproach
if the patient has to remind her that it is time
for food, medicine, bath, or for child to come to the
breast. Regularity, promptness, and thoughtfulness
must be supreme. Be on hand when the doctor calls
and stay until he goes. Be as cheerful as Mark Tapley,
however dreary the prospect, and do not make noises
either by the swish of overstarched skirts, the squeak
of shoes, or the moving of equipment. Above all things,
the nurse must keep her patient’s room, her patient,
and her own person rigorously clean. She should not
allow her hands to touch infectious material without
protection by rubber gloves. This is as necessary for
her own safety as for the patient and family. Her
hands should be manicured frequently, her hair shampooed
at short intervals, and her teeth kept in order.
If the hands get hard, take a teaspoonful of sodium carbonate
and one of chloride of lime, mix in the palm of
the hand with enough water to make a cream, and rub
well into palms and about the nails. Rinse in clean
water. (Weir.)
The nurse’s dress should be neat, always mended, and
carefully adjusted. The nurse who is slovenly in appearance
will be slovenly in her mind and slovenly in her
324work. She should not wear her uniform on the street.
It is bad taste, unprofessional, and unsanitary.
She should bathe at least three times a week. There
is always some odor of perspiration about the body,
and especially around the axillary spaces which are
filled with hair. Nothing is more offensive and nauseating
than being leaned over and waited on by a person
who has a strong body smell.
The prodigal use of warm water and soap will aid,
but there are large sebaceous glands in the armpits and
their decomposing excretions are retained by the hair
so lastingly that more radical measures are necessary.
The axillæ should be shaved at least once a month, and
then the soap and water becomes more efficacious.
After thorough cleansing, the armpits should be
dredged with Babcock’s Motiya powder, and the annoying
and offensive odor will disappear.
If the patient is a refined and dainty woman, who
may happen to be afflicted with the same misfortune,
she will be deeply grateful to the nurse who tells her
how to get rid of it.
That some doctors, unfortunately, have strong odors
about the person—the mixed effluvia of tobacco, alcohol,
bad teeth, and uncleanliness—is no excuse for the
nurse. The doctor should know better, but at all
events, his offense rarely needs to be suffered more than
a few minutes at a time, while the nurse is in constant
attendance.
The trained nurse should be polite to, but not familiar
with servants, as she is looked upon as the highest type
of the professionally educated gentlewoman, and she
must be constantly alert that her reputation in this
respect is not diminished.
325
BATHS
Hot Baths.—Temperature from 98° F. to 120° F.
Water should be tepid at first and the hot water
gradually added until the required degree is obtained.
| Warm bath |
92° F. to 98° F. |
| Tepid |
85° F. to 92° F. |
| Cold |
33° F. to 65° F. |
Sedative Bath.—The patient is stripped and stands
for an hour in the hydrotherapy room, while a hot
spray is played up and down the spine. The temperature
of the water is 104° F. to begin with, and gradually
increased to the point of toleration.
An alkaline bath is prepared by adding an ounce of
sodium carbonate to each gallon of water.
Bran Bath.—Add two ounces of bran to each gallon
of water. Mix the bran in a small amount of boiling
water and add to the bath water.
Mustard Bath.—To three gallons of water at a temperature
of 105° F. add a tablespoonful of mustard.
Leave the child in the water for five minutes, all the
while rubbing and stroking the limbs and back. Then
wrap naked in a warm blanket and leave for half an
hour.
STERILE DRESSINGS—ANTISEPTIC SOLUTIONS—STERILIZATION OF INSTRUMENTS
The preparation of sterile dressings, antiseptic solutions
and the sterilization of instruments, is particularly
the work of the nurse, whether in the hospital or in a
private home. The following directions are therefore
desirable:
326As soon as the nurse is sure her patient is in labor,
she boils a milk bottle, fills it two-thirds full of 95 per
cent alcohol, puts a pledget of sterile cotton in the bottom
and then boils a pair of dressing forceps, which are
placed, handle up, in the alcohol. (See Fig. 52, page
132.) With this forceps, she handles all clean dressings,
instruments, and rubber goods that may be contaminated
by touch.
Dressings and Supplies.—The necessary dressings and
supplies may be prepared one or two weeks before labor
according to the following instructions:
Five Yard Packing.—Draw threads at either end of
five yard lengths of gauze to its full width. Fold the
cut edge across until it lies one-third the distance from
the opposite side. Next, fold the double edge over, and
bring it to the outside edge of the first fold. Keep it
perfectly straight. When folded full length, roll from
the end and wrap in strong muslin wrappers. Sterilize
in the autoclave or Arnold sterilizer.
Pads for the Vulva.—Unroll a whole bale of common
cotton and cover it with a ½ inch thickness of absorbent
cotton. Cut in lengths of 12 in. by 4 in. wide. Cover
with gauze cut 12 by 14 inches, and fold the ends of
gauze over absorbent cotton. Roll from the end, wrap
in paper, seal, and sterilize.
Pledgets.—Tear two yard strips, lengthwise of the
roll of absorbent cotton, pull from these, three inch
pieces, roll them in the hands until round, place in
clean bags, and sterilize.
Breast Covers.—Squares of old, soft muslin 4 by 4
inches, with all strings removed, make the best dressings
for the nipple. Do not use gauze, because the papillæ
of the nipple may get caught in the mesh and when it
is taken off, the tender nipple is irritated or abraded.
327Breast Binders.—These are made of single material,
because they would be too warm otherwise. They are
sleeveless and jacket-shaped and measure 16 inches
from shoulder to waist, 40 inches long, and 10 inches for
the arm scallop. A binder of this size, if properly adjusted,
will fit a patient of any size. Three will be
sufficient for the case.
Abdominal Binders.—The abdominal and breast binders
are worn during the bed period only. The abdominal
binder is made of unbleached muslin, double material,
14 by 40 inches, and hemmed. In the center of
the back, on the lower edge, a curved space, six inches
wide, is cut out to prevent the binder from getting
soiled. To this curved edge, the pad holder is attached
by two safety pins, one on either side. The abdominal
binder is adjusted by pinning firmly above the fundus,
and loosely below.
Pad holders are made of unbleached muslin, and measure
6 by 16 inches.
Cord Dressings.—Cut squares of surgical lint 4 by 4
inches, and cut through to the center on one side.
Gauze may be used, but it is not ideal.
Nursery Cotton.—Tear absorbent cotton into narrow
lengths and pull out small one inch pieces. Roll them,
place in a clean bag and sterilize.
Applicators.—Use absorbent cotton and toothpicks.
Tear off small pieces of cotton, moisten the toothpick
point with water, place in the middle of the cotton, and
roll firmly.
Gauze Sponges.—Cut gauze into squares 6 by 6 inches,
and fold from each side to the center. This brings all
the ragged edges inside. Fold into squares, place in
jars, and sterilize.
Sterilization of Instruments.—Place scalpels in carbolic
328acid 95 per cent for ten minutes. Lift with sterile
forceps, and put in a basin of 95 per cent alcohol for
ten minutes. In the absence of carbolic acid and alcohol,
the scalpels may be dropped in a 2 per cent solution of
lysol for twenty minutes. Cleanse with hot sterile
water. (Do not boil scalpels; it dulls the sharp edges.)
All other instruments may be placed in a sterilizer
(dishpan or wash boiler) with enough water to completely
cover them; boil twenty minutes. Cool in sterile
pan, which may be set in cold water. Do not use soda
on the instruments during sterilization, as it makes a
thick, gummy precipitate on the metal.
The sterile handling forceps must be immersed at all
times for two-thirds their length in 95 per cent alcohol.
Brushes.—After using, all brushes should be thoroughly
washed, boiled, and dried, wrapped in waxed
papers, and sterilized in the autoclave. In the absence
of the autoclave, boil thirty minutes.
Basins, pitchers, and douche pans are sterilized by
wrapping in strong muslin bags and put to boil for
forty-five minutes in the basin boiler or wash boiler.
They will not remain sterile longer than one week, even
when kept in a clean place and well wrapped. Bedpans
should be washed in a strong solution of soap and water,
rinsed every morning and boiled for thirty minutes.
Sterilization of Rubber Goods.—
Tracheal Catheters.—Drop in a solution of bichloride
1:5000 and leave for twenty minutes. Lift with sterile
forceps into a basin of warm sterile water and leave for
ten minutes, or until used.
Vorhees Bags.—Boil twenty minutes. The bags and
catheters may be given a longer life by keeping them
in a 25 per cent solution of glycerine and water when
not in use. Kerosene vapor is also preservative.
329Rubber Catheter.—Boil twenty minutes.
Hot Water Bags, Ice Caps, Rubber Bed Rings.—Soak
in 10 per cent lysol solution for two hours, wash with
warm water, and dry thoroughly. The inside of the
ice caps can be dusted with powder.
Never leave rubber gloves in a damp place or lying
in a solution. It stretches them and weakens the rubber.
To sterilize, they must be washed in a strong solution
of soap and water, dried, and paired. Then they
are wrapped in a heavy cloth covering and put in the
autoclave for twenty minutes.
Wet Process for Rubber Gloves.—Wrap in gauze or
cloth and boil for thirty minutes. Lift with sterile forceps
and place in lysol solution 1 per cent until used.
They are easily drawn on by filling them with the solution
as the hand goes in.
The autoclave is not always available, but an Arnold
or Rochester sterilizer is readily portable, and takes the
place of the hospital machine.
Fumigation of rooms is sometimes necessary. Remove
all curtains, bed linen, and other washable fabrics
from the room. Open the drawers of dressers, doors of
closets, and loosen up and separate everything left so
the air can get to it. Close the windows and seal the
crevices with cotton and make the room as air-tight as
possible. Place a large pan containing six ounces of
potassium permanganate crystals in the center of the
room. Pour over this twelve ounces of formalin, close
and seal the outside doors of the room and leave for
twelve hours. If the case has been a very septic one,
it is always a good plan to wash the walls of the room
before using again. The insides of the drawers and the
bed should be thoroughly washed with water and green
soap. A formaldehyde lamp is also quite satisfactory if
obtainable.
330
CHAPTER XXIV
DIETS AND FORMULÆ
The nurse should serve everything in the most cleanly
and appetizing way if it is only a cup of tea; and all
waste, soiled dishes, napkins, and excreta must be removed
as delicately as possible.
Diet for Pregnancy.—Fresh fish, boiled, broiled or
baked; and shell-fish raw or cooked,—any way but
fried.
Meat, once or twice a day, except when contraindicated
by condition of the kidneys. Veal is best
omitted.
All farinaceous foods and vegetables may be eaten
freely.
Desserts should be plain, but tempting.
No alcohol is taken without direct permission from
the doctor, and coffee and tea should be limited.
Diet for Puerperium.—First two days, milk, buttermilk,
soup, gruel, cocoa, toast and tea, chicken, oyster
and clam broth.
In the next two days, under ordinary conditions, the
diet is increased and made somewhat heavier.
Semisolids are added like milk-toast, eggs, poached
or boiled soft, oysters, clams and boiled fish.
After the milk comes in, the woman is put on a
general diet as fast as she can digest it.
Farinaceous diet—melons and oranges.—
Breakfast.—Cereal, coffee with milk and sugar, if desired,
bread and butter, corn bread, rolls, toast, muffins,
hominy, cereal with cream.
331Lunch.—Vegetable soups, bread, butter, potatoes,
beans, rice, macaroni and cereal, peas, buttermilk, pudding,
such as rice, tapioca, bread cornstarch, jellies,
fruit juices, pumpkin, squash, turnips, tomatoes, etc.
Dinner.—Bread, butter, milk-toast, hominy, rice,
celery, fruit salads, lettuce, apples, pears, prunes, stewed
fruits or fresh melons, etc.
The following diets are routine at many hospitals:
General Diet.—Full tray of food in season as furnished
by the hospital. Three meals daily.
Light Diet.—Foods from the following list may be
selected, and served three or five times daily, as desired:
Soups of all kinds. When leguminous foods are employed,
their outer coverings must be removed by rubbing
them through a sieve or colander.
Vegetables of all kinds, except green vegetables (provided
they have been reduced to a pasty consistency).
Those with excess of fiber or cellulose, such as turnips,
celery, asparagus, and cabbage, should be chopped after
thorough boiling, then mashed, while those having tunics
should be sieved or colandered.
Grain foods of all kinds thoroughly cooked, excepting
corn preparations containing much cover, as hulled
corn.
Prepared foods such as tapioca, macaroni, and vermicelli,
require prolonged cooking.
Meats, scraped beef.
Eggs, soft boiled, raw or soft poached.
Bread of all kinds, stale, home-made.
Puddings, ices.
Beverages, all kinds unless otherwise ordered.
Forced Diet.—This includes the general diet with the
addition of one quart of whole milk and four eggs. The
332milk may be given plain or as an eggnog at seven, ten,
three, and eight o’clock. The eggs may be given raw
or cooked soft in any form.
Milk Diet.—Twelve ounces of whole milk (375 c.c.)
may be given every two hours; i. e., at six, eight, ten,
twelve, two, four, five, and eight o’clock, or the patient
may sip it at her pleasure.
The milk may be given raw, boiled, diluted with plain
water, lime water, Vichy, seltzer, or Apollinaris to taste.
The daily amount should include three quarts of whole
milk. Koumiss, buttermilk and milk soups are sometimes
allowed. Note the exact amount taken, and give reasons
for failure. Watch the stools for undigested milk.
Liquid Diet.—Whole milk, buttermilk, koumiss, beef
tea, or beef, chicken, mutton, oyster, or clam broth, in
eight ounce portions, or two ounces of beef juice, every
two hours. Lemonade, orangeade, ice cream, or fruit
ices, at intervals and amounts as desired.
Ulcer Diet.—Whole milk and cream, equal parts,
three ounces every two hours. Sodium bicarbonate,
thirty grains, in a small amount of water, to be given
before and thirty minutes after feeding. Albumin
water, soft boiled eggs, scraped beef, custard, and cream
soups to be added later by direction of the physician. No
seasoning except salt is allowed.
Prochownik Diet.—This diet is advised where some
necessity exists for preventing a large child. It is administered
in the last six weeks of pregnancy only.
Breakfast.—Small cup of coffee, two slices of toast
(1 ounce).
Lunch.—Small piece of meat, fish or an egg, a little
sauce. A vegetable prepared with fat, lettuce, a small
piece of cheese.
Dinner.—Same as lunch with three slices of bread and
butter, and a little milk.
333A pint of water daily is allowed; taken in sips it lasts
longer.
Soup, water, beer (all fluids) and sugar, pastry, and
potatoes are forbidden.
Skimmed Milk Diet (Karell).—Skimmed milk, to
which a pinch of salt is added, 3 to 6 ounces, three
or four times daily, increasing the amount gradually,
taken slowly to allow thorough mixture with saliva,
warmed in winter, room temperature in summer.
Acute Nephritis Diet.—Whole milk, 1000 c.c.; cream,
250 c.c.; water, 150 c.c.; stewed fruit, well sweetened, 50
c.c.
Bread, well buttered, may be toasted, 150 gm. (equal
to three slices).
Green salad of lettuce, celery, apple, pear or grape
fruit, and served either with olive oil, or with a mayonnaise
dressing made from olive oil, egg and lemon juice,
with salt (but no pepper or condiments) may be given
in two small portions daily.
Cooked cereals (cream of wheat, etc.) with cream and
sugar, one portion equal to about two ounces, once daily.
The above represents a daily fluid intake of about
1500 c.c. The diet is to be given in “three meals,” at
eight, one, and six o’clock, with fluid nourishment at
eleven, three, and nine o’clock.
RECTAL FEEDING
Nutrient enemas should be given every six hours, unless
otherwise ordered. It is necessary to cleanse the
lower bowel with a saline or soapsuds enema at least
once a day. The cleansing enema should be given one
hour before the nutrient enema is to be given. The
proper quantity for the nutrient enema is four to six
334ounces for an adult, and one to three ounces for a child.
Nutrient enemas should be given slowly at very low
pressure, the level of the fluid in the can being not over
eight to ten inches above the level of the rectum. If the
injected material is thick, a piston syringe may be required.
The patient should be placed upon the left side
with the hips well elevated and should be kept in that
position for fifteen to twenty minutes after the enema
has been given. The tube should be oiled and not be
inserted more than three or four inches. The temperature
of the enema should be about 98 degrees. If there
is a strong tendency to evacuate the enema, pressure
should be made against the rectum with a pad.
The following nutrient enemas may be ordered by
name.
Glucose Enema.—Glucose (dextrose, grape sugar) 1
ounce, normal salt solution 5 ounces.
The glucose should first be dissolved in hot water.
The amount of glucose may be increased, upon order, if
no irritation is produced.
Pancreatinized Milk Enema.—Add 1 tube of peptonizing
powder, or 1 to 2 drams of “Pancreatic solution”
to 1 pint of skimmed milk. Stir well and place in a
warm water bath for one-half hour. Add 1 dram of salt.
Milk and Egg Enema.—Thoroughly beat the whites
of 2 eggs, add ⅓ dram of salt, and 6 ounces of skimmed
milk. Add one tube of peptonizing powder, or 1
to 2 drams of “pancreatic solution,” stir well, and
place in a warm water bath for one-half hour.
Milk, Egg, and Beef Juice Enema.—Mix the beaten
whites of 2 eggs, 2 ounces of fresh beef juice, 6 ounces
of skimmed milk, and ⅓ dram of salt. Add 1 tube
of peptonizing powder, or 1 to 2 drams of “pancreatic
solution,” stir well, place in a warm water bath for
one-half hour.
335Milk and Glucose Enema.—Add 1 tube of peptonizing
powder to 6 ounces of skimmed milk, stir well, place in
a warm water bath for one-half hour. Add 3 drams of
glucose and ⅓ dram of salt.
ELIMINATIVE ENEMAS
Impaction Enema.—
Castor oil or olive oil, 1 ounce.
Soapsuds (100° F.), 1 quart.
Mix as thoroughly as possible, add one
dram of spirits of turpentine beaten up
with the yoke of one raw egg.
S. S. and G. Enema.—
Soapsuds, 1 quart.
Glycerine, 1 ounce.
Asafœtida Enema.—
Milk of asafœtida, 8 ounces.
Water, 8 ounces.
1–2–3 Enema.—
Magnesium sulphate, 1 ounce.
Glycerine, 2 ounces.
Water, 3 ounces.
Milk and Molasses Enema.—
Milk, ordinary cooking molasses in equal parts, possibly
8 ounces of each. Heat, but do not boil.
Turpentine Enema.—
Soapsuds, 1 pint.
Turpentine, 1 dram.
It acts quickly and effectively.
All enemas should be given through a colon tube.
The patient should be on the left side and the temperature
of the injection should be about 100° F.
336
DIET LIST
Albumin Water.—Take white of 1 egg, stir until
separated. Add a little lemon juice and 1 pint of water.
Ice and serve. Sugar or salt may be used.
Barley Water.—Wash 2 ounces of barley with cold
water. Boil for 5 minutes in fresh water. Strain.
Then cover with 2 quarts of water and cook slowly down
to 1 quart. Flavor with thinly cut lemon rind and
sugar. Do not strain unless patient requests.
Beef Juice.—Cut into cubes 1½ inches each, 1 pound
round steak. Place in a clean, ungreased pan, and fry
one and one-half minutes on each side. Pour into hot
meat press and apply pressure. In absence of a press,
a potato ricer may be used. Season with salt and pepper.
May be served iced or heated by putting in double
boiler and stirred all the time. Do not allow to curdle.
Beef Tea.—Put 1 pound of finely chopped round steak
into a quart glass jar, fill with cold water. Place jar in
kettle of warm water. Leave over slow fire for four
hours. Strain, season with salt and pepper.
Champagne Whey.—Boil 8 ounces milk for fifteen
minutes. Strain through cheesecloth. Add 1½ ounces
champagne.
Chicken Broth.—Skin and chop in small pieces one
small or one-half large fowl. Boil bones and all with
one blade of mace, a sprig of parsley, and 1 tablespoonful
of rice, 1 crust of bread and 1 quart of water,
for one hour. Skim from time to time. Strain through
coarse colander and season to taste.
Cinnamon Water.—One-half ounce stick cinnamon, 2
cups boiling water.
Break sticks in small pieces. Add water, boil twenty
minutes. Strain and serve hot or cold.
337Clam Broth.—Wash thoroughly 6 large clams in shell.
Put in kettle with 1 cup of cold water, bring slowly to
boil, and keep temperature for one minute. Pour off
broth and serve hot. Add salt and pepper.
Eggnog.—Beat an egg, white and yolk separately.
Add to the yolk 1 dram of vanilla extract, a pinch of
salt and 4 oz. fresh milk, and 1 dram of sugar. Add ½
dram of sugar to white of egg, stir a portion into the
glass and heap remainder upon top of glass.
Egg Cordial.—One egg white, 1 teaspoon sugar, 1
tablespoon brandy, 2 grains salt, 2 tablespoons cream.
Beat white until stiff. Add cream, continue beating,
add other ingredients, and serve cold.
Egg Lemonade.—Beat 1 egg and 1 teaspoonful of sugar
until very light, add ¼ cake of yeast dissolved in
one-fourth cup of water, two tablespoonfuls of sugar,
pour into bottles with patent stopper, fill bottles only
two-thirds full, cork tightly. Shake well. Allow to
stand on ice twenty-four hours.
Flaxseed Tea.—One ounce of whole flaxseed, 1 ounce
powdered sugar, ½ ounce licorice root, 1 ounce lemon
juice. Pour over these materials 1 quart of boiling
water and allow to stand four hours. Strain off liquor.
Gum Arabic Water.—Dissolve 1 ounce of gum arabic
in 1 pint boiling water. Add ½ ounce sugar, a wineglassful
of sherry, and juice of one lemon. Serve with
ice.
Junket.—Take ½ pint of fresh milk in a saucepan.
Add 1 teaspoonful of essence of pepsin, stir just enough
to mix. Pour into custard cups. Let stand until
firmly curded. Serve plain or with grated nutmeg.
Sherry may be added.
Koumiss.—Heat four cups of milk, then cool; when
lukewarm, add ¼ cake of yeast dissolved in one-fourth
338cup of water, two tablespoonfuls of sugar, pour into
bottles with patent stopper, fill bottles only two-thirds
full, cork tightly. Shake well, allow to stand on ice
twenty-four hours.
Milk Shake.—White of 1 egg, 1 ounce sugar, 1 ounce
chipped ice, 1 ounce cream. Shake in milk shaker two
minutes. Add milk to fill glass. Flavor with vanilla
and lemon.
Mutton Broth.—Boil slowly 1½ pounds of lean loin
mutton, including the bone. Add a little salt and ½
onion. Pour broth into a basin. Skim off fat when cool.
Warm as used.
Oatmeal Gruel.—One teacup oatmeal flakes, cover with
1 quart cold water. Place on slow fire and soak three
hours. Strain, add 4 teaspoonfuls of sugar and 1 teaspoonful
of salt.
Oatmeal Water.—Cover 1 teacupful oatmeal with 1
quart cold water. Let it stand two hours. Stir often.
Strain. Serve with salt, sugar and ice.
Peptonized Milk. Warm Process.—Dissolve the contents
of Fairchild’s peptonizing tube in 4 tablespoonfuls
cold water. Add to 1 pint of milk. Put in glass jar, and
place jar in vessel of warm water. Heat slowly to 115°
F. Stir slowly and allow it to remain thirty minutes.
Place on ice at once to check further digestion.
Peptonized Milk. Cold Process.—In a clean quart
bottle, put one peptonizing powder (Fairchild). Add 1
teacupful of cold water. Shake. Add 1 pint fresh cold
milk. Shake well. Place on ice. Do not heat before
using.
Rice Water.—Pick over and wash 2 tablespoonfuls of
rice. Put in a saucepan with 1 quart of boiling water;
simmer two hours. When rice is dissolved, strain. Add
339teaspoonful salt. Serve warm or cold. Sherry may be
added.
Rum Punch.—Two teaspoonfuls powdered sugar, 1
egg well beaten, warm milk, 1 large wineglassful; 4
ounces Jamaica rum. Flavor with nutmeg.
Scraped Beef.—Place on breadboard a round steak.
Scrape with table-knife but do not take any shreds of
muscle. Salt and pepper. Spread on thin slices of bread.
Place in toaster until seared.
Toast Water.—Three slices of stale bread well browned,
but do not burn. Put in a pitcher, pour over them 1
quart boiling water. Cover closely, and allow to stand
until very cold. Strain. Wine and sugar may be added,
to stimulate.
Wine Whey.—Put 1 quart new milk in a saucepan and
place over fire. Stir until nearly boiling. Add 2 ounces
of sherry wine. Boil slowly for fifteen minutes. Skim off
curds as they arise. Add 1 tablespoonful sherry. Skim
again, then strain through gauze.
340
CHAPTER XXV
SOLUTIONS AND THERAPEUTIC INDEX
Acid, Boric. 5 dr. in a pint of water makes a 4% solution, or
1:25.
Acid, Carbolic. 15 ♏︎ in a quart of water makes a 0.1% solution,
or 1:1000. 5 dr. to the quart makes a 2% solution;
and 1¼ oz. to the quart, a 5% solution.
Chinosol. 15 gr. to the quart of water makes a solution of 1:1000.
Formalin. 1 dr. to the quart of water makes a solution of about
1:500.
Mercury Bichloride. 15 gr. to the quart of water makes a 0.1%
solution, or 1:1000. 1½ gr. to the quart makes a 0.01% solution,
or 1:10,000.
Normal Salt Solution. 2 dr. of salt to the quart of water, or
0.9%.
Physiological Salt Solution. Take normal salt solution as given
above and to every 3½ oz. add 15 gr. of carbonate of soda.
Potassium Permanganate. 2½ dr. to the quart makes a 1%
solution. 3 gr. to the quart makes a 1:5000 solution.
Silver Nitrate. 4½ gr. to the ounce of water or 1 gr. to 1–7/10
dr. makes a 1% solution.
Ziratol. 2½ teaspoonfuls to a quart of water makes a 1%
solution.
For general reference the following valuable table is appended:
341
| PERCENTAGE SOLUTION TABLE |
|---|
| |
| By Alfred I. Cohn, Phar. D., in Merck’s Report |
|---|
| |
| Quantity of solution to be made |
GRAINS OF SALT OR DRUG REQUIRED TO MAKE SOLUTIONS OF PERCENTAGE STRENGTH INDICATED |
| 0.5% |
1% |
2% |
3% |
4% |
5% |
6% |
8% |
10% |
15% |
20% |
25% |
50% |
1:500 |
1:1000 |
1:2000 |
1:3000 |
1:4000 |
1:5000 |
| ½ fl. oz |
1.15 |
2.3 |
4.6 |
6.9 |
9.3 |
11.7 |
14.1 |
19. |
24. |
36.8 |
50.2 |
65. |
151.2 |
0.46 |
0.228 |
0.12 |
0.075 |
0.06 |
0.05 |
| 1 fl. oz |
2.3 |
4.6 |
9.2 |
13.9 |
18.6 |
23.4 |
28.2 |
37.9 |
47.9 |
73.5 |
100.3 |
130. |
302.5 |
0.91 |
0.456 |
0.23 |
0.15 |
0.12 |
0.09 |
| 2 fl. oz |
4.6 |
9.2 |
18.4 |
27.8 |
37.2 |
46.8 |
56.4 |
75.8 |
95.8 |
147. |
200.6 |
260. |
605. |
1.8 |
0.91 |
0.46 |
0.3 |
0.23 |
0.18 |
| 3 fl. oz |
6.9 |
13.8 |
27.6 |
41.7 |
55.8 |
70.2 |
84.6 |
113.7 |
143.7 |
220.5 |
301. |
390. |
907.5 |
2.7 |
1.37 |
0.68 |
0.46 |
0.34 |
0.27 |
| 4 fl. oz |
9.2 |
18.4 |
36.8 |
55.6 |
74.4 |
93.6 |
112.8 |
151.6 |
191.6 |
294. |
401.2 |
520. |
1210. |
3.64 |
1.82 |
0.91 |
0.61 |
0.46 |
0.36 |
| 5 fl. oz |
11.5 |
23. |
46. |
69.5 |
93. |
117. |
141. |
189.5 |
239.5 |
367.5 |
501.5 |
650. |
1512.5 |
4.55 |
2.28 |
1.14 |
0.76 |
0.57 |
0.46 |
The table shows the quantity of drug required to yield a given volume of solution of the percentage strength desired.
Thus, to make one fluid ounce of a 5 per cent solution it is merely necessary to dissolve 23.4 grains of the salt in sufficient
water to make one fluid ounce.
342
THERAPEUTIC INDEX
Young’s Rule for Dosage: The age of the child is divided
by the age of the child plus 12, and the result is the
appropriate dose for the child. The doses given below
are for the adult unless otherwise specified.
Absorbent. A medicine or dressing that promotes absorption,
such as potassium iodide, Tr. iodine, glycerine, or hot
vaginal douches.
Adrenalin. The blood-raising principle of the suprarenal
glands. It is hæmostatic and astringent. Acts somewhat
like digitalis on the heart.
Uses.—Vomiting of pregnancy, increased glandular activity,
hæmorrhage, inflammation of mucous membranes.
Dose.—Internally, 5–10 m. of the 1:1000 solution. Externally,
the solution of 1:1000 or 1:10,000 may be applied.
Albolene. An oily white substance obtained from petroleum. It
is used on the nipples and skin of the mother and to remove
the vernix caseosa from the skin of the child.
Aloin, Strychnia, and Belladonna. A laxative pill which usually
contains aloin ⅙ gr., strychnia sulph. 1/60 gr., and Belladonna
1/12 gr.
Ammonia Carbonate. Antispasmodic, stimulant, and expectorant.
Uses.—Stimulant to heart. Stimulating expectorant in pneumonia
and bronchitis.
Dose.—5–20 grains in mucilage or syrup.
Anæsthone. A mixture of adrenalin chloride (0.1%) and chlorotone
(5%) in an ointment base of wool fat and petrolatum.
Astringent, antiseptic, anesthetic and germicide. Useful application
to swollen mucous membranes or in coryza.
Argyrol (Silver Vitellin). Antiseptic and germicide.
Uses.—Like Silver Nitrate, but less irritating to the tissues.
3–5% solution in water is an injection for gonorrhœa.
15% solution dropped in the eyes of the newborn may prevent
ophthalmia. 25% solution may be used twice a day
as a remedy for existing ophthalmia, but the strength should
be reduced after three or four days. 10–15% solution is
used as an injection in cystitis. An ounce or more of the
solution may be left in the bladder until the next evacuation.
Asafœtida. A fetid gum resin. Carminative, antispasmodic,
mild stimulant, and expectorant.
Uses.—Gas pains of adults and infants. Hysteria and indigestion.
Dose.—5–10 gr. t.i.d. For infantile colic, an emulsion called
the mistura of asafœtida may be used in 2–4 dram doses.
For adults 1–2 tablespoonfuls.
343Belladonna. Nervine, mydriatic, sedative, narcotic, antispasmodic
and anodyne. Makes the throat dry and dilates the
pupils.
Uses.—Night sweats, nervous cough, pain, incontinence of
urine and to restrain glandular activity.
Dose.—Fl. ext. 1–3 ♏︎; dry ext. ½–1 gr. Tincture 8–20 ♏︎.
Solid ext. ½¼ gr. All for adults. For infants, proportionately
less. See Rule for Dosage.
Benzoin. Antiseptic and externally a styptic and protective for
sores.
Uses.—Sore nipples and urticaria. Lard is also benzoinated
for use in removing vernix caseosa. Compound Tr. of
benzoin contains, benzoin, purified aloes, storax, balsam of
Peru, and alcohol.
Benzoinal. Albolene mixed with benzoin.
Bismuth Subnitrate. A white heavy powder. Antiseptic and
astringent.
Uses.—Subacute gastritis, pyrosis, diarrhœa and vomiting of
pregnancy. Particularly desirable in infancy because it is
free from arsenic, lead and silver.
Dose.—5–60 gr. in the adult.
Boric Acid (Boracic Acid). A white crystalline powder. Antiseptic.
Uses.—As a dressing and lotion for eyes, navel, mouth, nipples,
and all mucous surfaces. In solution to preserve the
sterility of rubber nipples until they are needed.
Dose.—Internally, 5–15 gr. Solutions are usually about 4%
or 5%. A saturated solution in water is about 6%. In hot
water 25%.
Boroglyceride. An antiseptic paste of boric acid and glycerine.
When an excess of glycerine is present the preparation is
called boroglycerol.
Uses.—An oxydizer in endometritis. It is applied to the
cervix on cotton tampons.
Calcium (Lime). Stomach sedative, soothes the irritated or
burned skin, corrects hyperacidity, increases the clotting
power of the blood (?).
Lime water is a saturated solution of calcium hydrate and
is used for nausea, to break up the curds of milk, and to
increase its digestibility. It is mildly constipating.
Calomel. See Mercury.
Camphor. A solid volatile oil. Nerve sedative. Anaphrodisiac.
Antispasmodic. Stimulant.
Uses.—The monobromated camphor is given internally for
hysteria, neuralgia, and as a hypnotic.
Dose.—1–10 gr.
Camphorated Oil. A solution of camphor in cottonseed oil. Rubefacient
and stimulant.
Uses.—Internally in collapse. Externally as an application
to the child for colds of chest and nose.
344Dose.—5–20 ♏︎ hypodermically in collapse. The injection
should be made deep into the muscle.
Carbolic Acid (Phenol). Derived from coal tar. Antiseptic,
deodorant and local anæsthetic.
Uses.—Vomiting of pregnancy, pruritus, eczema, sterilization
of instruments. Usual solution is 2½% to 5%. For
sterilization of knives, scissors and other sharp instruments
the 95% is used. In pruritus, the following wash will aid:
carbolic acid, 12 dr., glycerine 2 dr., alcohol, 4 ʒ water q.s.
1 pt. Apply.
Cascara Sagrada. Stimulant laxative, and cathartic. Useful in
pregnancy, but after labor there is evidence that it may
go over in the milk to the child.
Dose.—Fl. ext. 10–20 ♏︎. The Hinkle pill contains cascara.
Castor Oil. Oil expressed from the seeds of the castor plant.
A cathartic. Acts in four or five hours.
Dose.—For adults, ½ oz. to 1 oz. For infants 10 to 60 drops
given with a dropper—not with a spoon.
Castor oil cocktail.—Rinse out the glass with lemon juice
or whiskey. Pour in teaspoonful of lemon juice and a
teaspoonful of whiskey, add castor oil in amount required,
cover with whiskey and give.
A paste is made from the mixture of castor oil and bismuth
subnitrate in equal parts, which is an excellent preparation
for sore nipples.
Cerium Oxalate (and Cerium Valerianate). Sedative and nerve
tonic. The oxalate is a white crystalline powder, odorless
and tasteless.
Uses.—Vomiting of pregnancy, seasickness.
Dose.—2–10 gr. several times daily.
Charcoal. Administered in tablet form or as a powder between
two slices of buttered bread.
Uses.—Acid stomach. Vomiting of pregnancy.
Chinosol. Nonpoisonous, nonirritating and odorless. Antiseptic
deodorant, styptic and analgesic. Dissolves instead of coagulates
secretions.
Uses.—Antiseptic solutions for hands and sponges, deodorizing
wash for vagina post partum, intrauterine douche, wash
for gonorrhœa and cystitis.
Dose.—For douche or hand solution 1:1000 or 1:5000. For
dusting powder, 1 part to 10 or 20 of starch, talcum, boric
acid, or bismuth subnitrate.
Chinosol will corrode unplated steel. It may be mixed with
salt, but not with soap.
Choral Hydrate. White crystal masses. Pungent in odor and
taste. Hypnotic, antispasmodic, antiseptic and analgesic.
Uses.—Insomnia, eclampsia, convulsions, and to restrain secretion
of milk.
Dose.—By mouth, 10–30 gr. By rectum, not to exceed 60 gr.
In infants 1–2 gr. by rectum in an ounce of water.
345Chymogen. A preparation of rennin (10%) made by Armour &
Company.
Coagulen Ciba. A physiological nontoxic styptic, prepared from
the natural coagulants of the blood. A 10% solution in
water will hasten the beginning and end of coagulation.
May be applied to bleeding surfaces directly, or given under
the skin, into the muscle, or into a vein. 3½% to 5% solution
in distilled water, should be sterilized by boiling 2–3
minutes. Do not filter. Inject.
Cocaine Hydrochlorate. Anæsthetic, sedative, anodyne, anti-pruritic.
Uses.—Vomiting of pregnancy, with caution.
Dose.—Internally ½–1½ gr. Externally a 4%–10% solution
in water.
Codeine. Alkaloid of opium. Less narcotic than morphine.
Uses.—After-pains and pain of over-distended breasts.
Dose.-¼–1½ gr. by mouth. ¼–¾ gr. hypodermically.
Compound Licorice Powder. See Senna.
Condylomata.
Use—
| ℞ |
Acid. Salicyl. |
gr. |
x |
| |
Acid Boric. |
gr. |
xxx |
| |
Calomel. |
ʒ |
i |
| |
M. |
|
|
| |
Sig.: Apply twice daily. |
|
|
Digitalis. Cardiac tonic. Diuretic. Stimulant.
Uses.—Weak heart. Syncope. Collapse.
Dose.—For adult: of the tincture, 5–15 ♏︎, fl. ext. 1–3 ♏︎,
ext. gr. 1/6½.
Digipuratum. A preparation of digitalis from which the inactive
substances have been removed. It is used in the same
conditions as digitalis.
Dose.—The tablets contain 1½ gr. and one is given four
times daily until ten are taken. Then stop. Hypodermically.
Each viol contains 1 c.c. of fluid and equals 1½ gr.
of digipuratum. Each dose contains enough of the active
principle of digitalis to kill a 30 gm. frog.
Ergot (Fungus of Rye). Contracts unstriped muscle fiber.
Uses.—To check hæmorrhage after labor. To promote involution.
Must not be given in labor until the uterus is
empty.
Dose.—By mouth 15–60 ♏︎ of the fl. ext. Hypodermically,
10–20 ♏︎.
Ergotole, Ergotine. Concentrated solutions of ergot, 2½ times
as strong as the fluid extract. They are sterilized and
preserved in glass ampoules.
Uses.—See Ergot.
Dose.—30–60 ♏︎.
Green Soap. A soap made of linseed or other oil, potash, alcohol
and water.
346“The adoption by the U. S. Pharmacopoeia of the term Sapo
Viridis (green soap) is unfortunate, since soft soap even
if made from green hempseed oil will become brown-yellow
unless artificially colored.”—U. S. Dispensatory.
Hæmophilia. A condition of the blood wherein its clotting
power is diminished or absent.
Coagulen, horse serum, or diphtheria antitoxin may be
given hypodermically. Direct transfusion of blood from
another is best.
Hyoscine, Morphine, and Cactin. (H. S. & C. Tablets). A proprietary
combination of drugs. The action is said to be
similar to that of morphine and scopolamine.
Iodine, Tincture.
Uses.—To sterilize the skin before operation. In vomiting
of pregnancy it is sometimes effective. Drop doses may
be given well diluted. Externally it is applied to ulcers,
as in Bednar’s disease, and sometimes as a dressing for
the cord. In pruritus vulvæ it is a valuable application.
Iron. Tonic emmenagogue.
Uses.—To increase the number of red blood corpuscles. To
raise blood pressure and to increase the secretion of milk.
Dose.—3–5 gr. Blaud’s pill contains the carbonate in a form
that is easily assimilated.
Laxatives. Laxatives are unirritating and excite moderate
peristalsis. Sulphur, magnesia, cassia, manna, cascara
sagrada, the Hinkle pill, and the A, B, & S pill are usually
mild in action.
Lysol. Disinfectant and antiseptic for hands and instruments.
It is a brown syrupy fluid made from coal tar oil, which is
distilled and mixed with fat, soap, etc. It has a creosote
odor and contains 50% cresol. Readily soluble in water.
Prepared in ½–4% solutions.
Magnesia, Calcined. Antacid and cathartic. Comes in white
cakes.
Uses.—Acid stomach, vomiting of pregnancy, “heartburn,”
and constipation.
Dose.—30–120 gr.
Magnesia, Milk of. A mixture of magnesia and water. Has the
same properties as the above.
Dose.—For adults, 2–3 teaspoonfuls. For infants, ¼–2 teaspoonfuls.
Magnesia Sulphate (Epsom Salts.). Saline cathartic.
Uses.—The profuse watery stools produced by magnesia are
valuable aids to elimination when the kidneys are overworked
or defective. In congestion of the breasts and
threatened eclampsia, or in any case where it is desirable
to drain off waste or dehydrate the system.
Dose.—1 teaspoonful daily in hot water before breakfast.
½–1 oz. as a single dose or 1 oz. by rectum, as in the 1–2–3
enema.
347Menthol (Mint Camphor, Japanese Peppermint). Analgesic, antiseptic,
anæsthetic, and vascular stimulant.
Uses.—In pruritus vulvæ, vomiting of pregnancy, and hæmorrhoids.
Dose.—By mouth 3–5 gr. In tampons, one part to five of
oil. In ointments one part to sixteen. To the vulva for
pruritus, use the spirits in 5% solution.
Mercury (Hydrargyrum). Cathartic, alterative, antisyphilitic,
antiseptic and disinfectant. Readily absorbed by the unprotected
mucous surface and relatively inert when the
membrane is covered by a discharge. Solutions of the bichloride
when used as a lotion unite with the albumin of
a mucous discharge and form an albuminate of mercury,
which is inactive. Bichloride solutions have small place in
obstetrics. They are hard on the hands and destructive to
instruments. Other agents like lysol, ziratol and chinosol
have satisfactory germicidal properties and in addition are
nonpoisonous, lubricative and cleansing.
Mercury should only be given to the infant in the form of
calomel (the mild chloride). The dose is 1
12-⅛ gr., repeated
if necessary.
Morphine. Alkaloid of opium.
Antispasmodic, hypnotic, analgesic and narcotic.
Uses.—To relieve pain, produce sleep, check diarrhœa, and
to control the pain, as well as the contractions of abortion.
To relax a rigid os.
Dose.—In “Twilight Sleep” and rigid os the first dose is
Morph. sul. 1/6¼ gr. and scopolamine Hydrobromid 1/200–1/150.
The scopolamine to be repeated if required, in one-half
or three-quarters of an hour. The usual dose of morphine
hypodermically is 1
12½ gr.
Nitroglycerine (Glonoin). Vasomotor dilator, arterial stimulant.
Uses.—For the prostration following hæmorrhage.
Dose.-½00–1/50 gr. hypodermically.
Novocaine. Local anæsthetic, similar to cocaine, but less toxic.
For local anæsthesia in solutions of 0.25% to 2% usually in
association with adrenalin (5–10 drops of the 1:1000 solution
to each 10 c.c. of novocaine solution).
Nux Vomica. The plant from which strychnia is derived. Tonic,
stomachic, and stimulant to muscle, nerve, and heart.
Uses.—Bitter tonic and stimulant. Vomiting of pregnancy
and agalactia.
Dose.—Ten drops of the tincture in water before meals.
Opium. The concrete juice of the poppy. Relieves pain. Constipates.
Uses.—Hæmorrhoids in adults, colic and diarrhœa in infants.
Dose.—One grain in suppository night and morning for adult.
For infant, as paragoric only. Two to five drops only, not
repeated. Children bear opium badly.
348Pepsin. A ferment in the gastric juice that digests proteins. In
commerce it is obtained from the pig.
Uses.—Imperfect digestion.
Dose.—For adult, 10–15 grs. For infant, 2 gr.
Phenolphthalein. A nonofficial coal tar derivative. Mild laxative.
Dose.—2–3 gr. Phenolax and chocolax are preparations of
the drug.
Pituitary Extract (Pituitrin). A substance derived from the
infundibular portion or the posterior lobe of the hypophysis
cerebri. Nontoxic, stimulant to unstriped muscle.
Uses.—Uterine inertia, post partum hæmorrhage, Cæsarean
section and tympany. Will not produce abortion nor premature
labor. May be tried in acute anæmia to raise the
blood pressure.
Dose.—5–15 ♏︎. Repeated if necessary.
Potassium (or Sodium) Bromide. White granular powder. Soluble,
1 to 5 in water. Sedative, hypnotic, antiepileptic.
Uses.—Neurasthenia, convulsions, nymphomania, vomiting of
pregnancy.
Dose.—20–60 gr. In enema with chloral. Pot. bromide 40
gr. and chloral 20 gr. in several ounces of water or milk.
Potassium Iodide. Alterative emmenagogue. Uric acid solvent.
Uses.—Syphilis rheumatism, swellings, slow inflammations,
excessive secretion of milk.
Dose.—2–10 gr. increased as required.
Potassium Permanganate. Dark purple opaque prisms. Soluble
in water 1 to 16. Disinfectant, deodorant, antiseptic,
astringent.
Uses.—As an injection in leucorrhœa and gonorrhœa, 1:5000
solution.
Purgatives. Simple purgatives produce free discharges from
the bowels with some griping. Senna, aloes, rheubarb, castor
oil, and calomel are examples. Saline purgatives are followed
by profuse watery evacuations. Magnesia sulphate,
and citrate, potassium and sodium tartrate, and sodium
phosphate belong to this class.
Drastic purgatives bring about a violent action of the bowels
with much griping and tenesmus. Such are jalap, colocynth,
elaterium, and croton oil. Hydrogogue purgatives combine
the results of the salines and drastics. They have much
griping with profuse watery stools. The hydrogogues are
elaterium, gamboge, croton oil, and potassium bitartrate.
Quinine Sulphate. (Derived from Cinchona bark.) Antipyretic,
tonic, antiperiodic, antiseptic, emmenagogue and ecbolic.
Uses.—Valuable stimulant in a slow first stage. It is combined
with castor oil to bring on labor at term. Castor oil 1
oz. and quinine sulphate 10 gr. is given as the first dose, followed
in an hour by another 10 gr. of quinine, and an hour
later by another.
Dose.—2–20 gr.
349Regulin. A mixture of agar-agar in dry form with extract of
cascara sagrada.
Uses.—A laxative in chronic constipation.
Dose.—Teaspoonful to tablespoonful in stewed fruit or
mashed potatoes, once daily.
Russian Oil (Liquid Petrolatum). Laxative in pregnancy and
puerperium. Acts mechanically and as a lubricant. Not
unpleasant to take.
Dose.-½ oz. at bedtime, and, if necessary, before each meal.
May be given to breast-fed babies in doses of gtts. xv three
times daily.
Senna. Laxative and purgative. Acts especially on the large
intestine. Sometimes passes over in the milk to the child.
Dose.—Fl. ext. 1–4 teaspoonfuls. In compound licorice powder
the dose is 30–80 gr. (about 10 gr. of senna to the dose).
Silver Nitrate. Caustic, antiseptic, stimulant, irritant and antigonorrhœic.
Table salt neutralizes it.
Uses.—2% solution in water for pruritus vulvæ. 1% solution
dropped into the eyes of the newborn to prevent ophthalmia
neonatorum. Do not neutralize the 1% solution. ¼
gr. silver nitrate with 2 gr. of pepsin in capsule for pernicious
vomiting of pregnancy.
Sodium Bicarbonate (Baking powder). Antacid, antirheumatic.
Uses.—Gout, dyspepsia, acid stomach, acidosis, vomiting of
pregnancy. Soothes the skin when burned.
Sodium Chloride. (Salt.)
For normal saline use 10 gr. to 3½ oz. of water. For physiological
salt solution, add 15 gr. of Sod. Carb. to every 3½
oz. of normal saline as made above.
Sodium Citrate. A white odorless, granular powder with cooling
salty taste.
Uses.—Diuretic, antipyretic and refrigerant. Retards the
coagulation of albumin in milk and aids the digestibility
of proteins. May be indicated in gout and cystitis.
Dose.—Internally, 15 to 60 gr. In the modification of cow’s
milk about two grains should be used for each ounce of the
mixture.
Spirits of Nitre, Sweet (Spirit Nitrous Ether). 4% solution of
nitrous ether in alcohol. Diaphoretic, diuretic, antipyretic,
stimulant, antispasmodic.
Uses.—Fever, dropsy, vomiting of pregnancy, colic, anuria.
Dose.—For adult, 20–60 gtts. For infants small doses often
repeated.
Stramonium (Jimson Weed). Hypnotic, narcotic, antispasmodic.
Uses.—For hæmorrhoids take Ung. Stramonii and Ung. Galli
in equal amounts and apply.
350Urotropin. A white powder soluble in water. Urinary antiseptic,
diuretic.
Uses.—Cystitis, typhoid bacilli in urine, gout. It makes the
urine irritatingly acid when given long. It does not act
in alkaline media.
Dose.—7½–10 gr. well diluted.
Valerian. Anodyne, stimulant, antispasmodic and nervine.
Uses.—Hysteria, hypochondriasis, headache.
Dose.—30–60 ♏︎ of the fl. ext. by mouth, or by rectum 2 oz.
of the following mixture may be used P.R.N. for hysteria:
Pot. Brom. 1 oz.
Ext. Valerian fl. dr. vi.
Normal saline q.s. oz xii.
Veratrum Viride (Hellebore). Sedative, emetic, diaphoretic,
diuretic. Retards the heart’s action without weakening it.
Uses.—Eclampsia.
Dose.—1 to 4 ♏︎ of the fl. ext. is given hourly until the
pulse comes down to 80.
Veronal. Safe, reliable hypnotic.
Uses.—Insomnia from hysteria, neurasthenia, and mental
disturbance.
Dose.—5 to 15 gr. dissolved in hot tea, milk, or water. May
repeat.
Zinc. Tonic, astringent, antispasmodic.
Uses.—Stearate of zinc is a valuable dressing in excoriations
of buttocks and external genitals.
Zinc Ointment. It is indicated for bedsores (decubitus) eczema,
herpes, and intertrigo. Zinc ointment contains one part of
zine oxide to four parts of benzoinated lard.
Ziratol. A mixture of phenols in soap, water, and glycerine.
Antiseptic, deodorant and germicide. Relatively odorless,
easily soluble and does not injure hands, instruments, or
rubber. It is said to be only ⅐ as toxic as carbolic acid.
Used in solutions of 0.5% up to 5%.
351
GLOSSARY
[Adapted from Dorland and Standard Dictionaries]
Ab-nor´mal. Not normal; contrary
to the usual structure
or condition.
A-bor´tion. 1. The expulsion of
the fœtus before it is viable.
2. Premature stoppage of a
morbid or a natural process.
Ab-ra´sion. 1. A rubbing or
scraping off. 2. A spot rubbed
bare of skin or mucous
membrane.
Ab´scess. A localized collection
of pus in a cavity formed
by the disintegration of tissues.
Ac-couch´e-ment. Delivery in
childbed; confinement.
Ac´e-tone. 1. A colorless liquid
found in pyro-acetic acid and
in naphtha. 2. Any member
of the series to which the normal
or typical acetone belongs.
A´ci-do´´sis. Acid intoxication
of the system from the elaboration
or too much acid
by faulty metabolism or the
imperfect disposition of normal
amounts of acid.
A-ci´nus, pl. acini. One (acini,
more than one) of the smallest
lobules of a compound
gland.
Al´bo-lene. An oily white substance
derived from petroleum.
Al´bu-mi-nu´´ri-a. The presence
of albumin in the urine.
Al´ka-line. Having the reaction
of an alkali.
352A´men-or-rhœ´´a. Absence or
abnormal stoppage of the
menses.
Am-mo´ni-a. A colorless alkaline
gas, NH3, of penetrating
odor, and soluble in water,
forming ammonia-water. Ammoniacal
urine contains ammonia,
which is one form of
nitrogen excretion.
An-æ´mi-a. A condition in
which the blood is deficient in
quantity or in quality.
An´æs-the´´si-a. Loss of feeling
or sensation, especially
loss of tactile sensibility,
though the term is used for
loss of any of the other senses.
An´æs-thet´´ic. 1. Without the
sense of touch or of pain. 2.
A drug that produces anæsthesia.
An´al-ge´´si-a. Absence of sensibility
to pain.
An-aph´ro-dis´´i-ac. A drug that
allays sexual desire.
An´a-sar´´ca. An accumulation
of serum in the cellular tissues
of the body.
An´en-ceph´´al-ous. Having no
brain.
An´ky-lo´´sis. Abnormal rigidity
or stiffness of a joint.
An´o-dyne. A medicine that relieves
pain.
An´te par´tum. Latin for “before delivery.”
An-te´ri-or. Situated in front
of, or in the forward part of.
353An´ti-pe´ri-od´´ic. A drug that
tends to prevent recurrent attacks
of disease.
An´ti-sep´´tic. 1. Preventing decay
or putrefaction. 2. A
substance destructive to poisonous
germs.
A-pe´ri-ent. Mildly cathartic.
Ap-nœ´a. The absence of respiration—especially
that form
which occurs in a child delivered
by the Cæsarean operation.
A-re´o-la. The darkish ring
around the nipple.
As-ci´tes. Dropsy (an accumulation
of fluid) in the abdomen.
A-sep´sis. Absence of septic
matter, or freedom from infection.
As-phyx´i-a. Suffocation.
As-trin´gent. 1. Causing contraction
and arresting discharges.
2. An agent that
arrests discharges.
At´e-lec-ta´´sis. Imperfect expansion
of the lungs at birth;
partial collapse of the lung.
At´on-y. Lack of normal tone
or strength.
A´tri-um. (L., a hall.) The
point of entrance of a bacterial
disease.
At´ti-tude. A posture or position
of the body. The relation
which the various parts
of the child’s body bears to
its own long axis. The attitude
of the fœtus normally is
complete flexion.
Aus´cul-ta´´tion. The act of listening
for sounds within the
body.
Bac-te´ri-a. The vegetable microorganisms
(Schizomycetes)
especially the short-rod forms.
Bal´an-i´´tis. Inflammation of
the glans penis. It is usually
associated with phimosis.
354Bal-lotte´ment. The diagnosis
of pregnancy by pushing up
the uterus by a finger inserted
into the vagina so as
to cause the embryo to rise
and fall again like a heavy
body in water.
Bar´tho-lin glands. The vulvo-vaginal
glands.
Bleb. A skin vesicle filled with
fluid. A blister.
Breg´ma. The point on the surface
of the skull at the junction
of the coronal and sagittal
sutures.
Cæ-sa´re-an sec´tion. (Named
from Julius Cæsar, who is
said to have been thus born).
Delivery of the fœtus by an
incision through the abdominal
and uterine walls.
Ca´put. Any head, or head-like
structure.
Ca´put suc´ce-da´´ne-um. A
swelling formed on the presenting
part of the fœtus
during labor. It is due to
the effusion of fluid into the
subcutaneous tissues of the
scalp and its retention there.
Car-min´a-tive. Drugs that
stimulate the circulation, the
mental faculties, and intestinal
peristalsis. Asafœtida,
camphor, capsicum, cardamon,
chloroform, ether, ginger,
horseradish, mustard, and the
oils of anise, cloves, spearmint,
nutmeg and valerian
are carminatives.
Car´ne-ous. Fleshy.
Cath´e-ter, tra´che-al. A long
slender tube designed for introduction
into the babe’s
trachea as a means of sucking
out mucus.
Cath´´e-ter-ize´. To introduce a
tube and draw off fluid, as
urine or mucus.
355Caul. 1. The great omentum.
2. A piece of amnion which
sometimes envelopes a child’s
head at birth.
Cell. 1. Any one of the minute
protoplasmic masses which
make up organized tissue.
Ceph-al´ic. 1. Pertaining to the
head. 2. A medicine for the
head.
Ceph´al-hæ-ma-to´´ma. 1. A tumor
or swelling filled with
blood beneath the pericranium.
Cer´vix. The neck or any neck-like
part.
Chlo-as´ma. The yellowish brown
spots or patches that appear
on the skin of pregnant women.
Cic´a-tri´´cial. Pertaining to,
or of the nature of, a cicatrix.
Ci-ca´trix. A scar; the mark
left by a sore or wound.
Cil´i-a. 1. The eyelashes. 2.
Minute lash-like processes
that characterize certain cells.
Cli´mac-ter´´ic. A particular
epoch of the ordinary term of
life at which the body is believed
to undergo a radical
change—especially applied to
the menopause.
Cli-ni´cians. Men who teach
and explain diseases by showing
actual cases.
Clit´o-ris. The sensitive organ
of the female, homologous
with the penis in the male.
Coc´cyx. The small bone situated
at the end of the sacrum.
The very last portion of the
spine.
Col-lapse´. A state of extreme
prostration and depression
with failure of circulation.
Col´les’ mem´brane. A layer of
tough sensitive fascia back
of the perineum and on either
side of the vagina.
356Co-los´trum. The first fluid secreted
by the mammary
glands after functional activity
begins. It contains
casein and more albumen than
milk, as well as numerous
fatty globules.
Col´peu-ryn´´ter. A dilatable
bag, used to distend the
vagina.
Co´ma. Profound stupor occurring
in the course of a disease
or after severe injury.
Co´ma-tose. Pertaining to, or
affected with, coma.
Com´pli-ca´´tion. A disease or
diseases concurrent with another
disease.
Con-cep´tion. The fecundation
of the ovum.
Con´dyl-o´´ma. A wart-like excrescence
near the anus or
vulva. It may be as large as
a cauliflower.
Con-gen´i-tal. Born with a person;
existing at or before,
birth.
Con´ju-gate. The anteroposterior
diameter of the pelvic
inlet.
Cor´o-nal. Pertaining to the
crown of the head, as the
coronal suture.
Cra´dle cap. The dirty looking
patch of epithelial scales and
sebaceous material that develops
over the anterior fontanelle
of babies who have
the exudative diathesis.
Cra´ni-ot´´o-my. The cutting in
pieces of the fœtal head to
facilitate delivery.
Cre-dé Expression. The maneuver
in which the uterus is
grasped in the hollow of the
hand and squeezed and
pressed down upon to aid in
the expulsion of the placenta.
357Cre-dé Treatment. The instillation
of a 1% solution of
nitrate of silver into the eyes
of the newborn to prevent
ophthalmia.
Curd. The coagulum of milk,
consisting mainly of casein.
Cy´an-o´´sis. Blueness of the
skin, often due to cardiac
malformation causing insufficient
oxygenation of the
blood.
Cys-ti´tis. Inflammation of the
bladder.
De-cid´u-a. The membranous
structure produced in the
uterus during gestation and
thrown off after parturition.
D. reflexa, the part of decidua
which is reflected upon and
surrounds the ovum. D. serotina,
the late decidua; the
part of the decidua vera
which becomes the maternal
portion of the placenta. D.
Vera, the true decidua; the
portion of the decidua which
lines the uterus.
De-cu´bi-tus. 1. An act of lying
down. 2. A bed-sore.
De-hy´drate. To remove the
water.
Di´a-be´´tes. A disease marked
by an habitual discharge of
an excessive quantity of urine
and the presence of sugar
therein.
Di´´aph-o-re´sis. Perspiration,
and especially profuse perspiration.
Di´´aph-o-ret´ic. 1. Stimulating
the secretion of sweat. 2. A
medicine that increases the
perspiration.
Di-ath´e-sis. Natural or congenital
predisposition to a
special disease.
Dif´fer-en´´tial. Pertaining to a
difference, or differences.
358Dis-crete´. Separate lesions
which do not blend or
coalesce.
Di´u-re´´sis. Increased secretion
of urine.
Dor´sum. The back or any part
corresponding to the back as
the dorsum of the penis or
foot.
Duc´tus ve-no´sus. A fœtal
blood vessel connecting the
umbilical vein with the post-cava.
Dys-cra´si-a. A depraved state
of the system, and especially
of the blood, due to constitutional
disease.
Dysp-nϫa. Difficult or labored
breathing.
Dys-to´ci-a. Painful or slow
delivery or birth.
Ec-bol´ic. An agent that accelerates
labor.
E-clamp´si-a. A sudden attack
of convulsions, especially one
of a peripheral origin.
Ec-top´ic. Out of the normal
place.
E-de´ma. Swelling due to effusion
of watery liquid into
the connective tissue.
Em´bo-lism. The plugging of
an artery or vein by a clot
or obstruction which has been
brought to its place by the
blood-current.
Em´bry-o. The fœtus in its
earlier stages of development,
especially before the end of
the third month.
Em-men´a-gogue. A drug that
aids or stimulates menstruation.
E-mul´sion. An oily or resinous
substance divided and held
in suspension through the
agency of an adhesive, mucilaginous,
or other substance.
En´do-me´´tri-um. The mucous
membrane that lines the cavity
of the uterus.
359En-gage´ment. The head is said
to be engaged when the largest
diameters have passed the
inlet.
En´si-form. Shaped like a
sword.
Ep´i-si-ot´´o-my. Surgical incision
of the vulvar orifice laterally
for obstetric purposes.
E-ro´sion. An eating or gnawing
away.
Er´y-the´´ma. A morbid redness
of the skin due to congestion
of the capillaries, of many
varieties.
E´ti-ol´´o-gy. The study or
theory of the causation of any
disease.
Ex-co´´ri-a´tion. Any superficial
loss of substance such as that
produced on the skin by
scratching.
Ex´os-mo´´sis (Ex-os-mose). Diffusion
or osmosis from within
outward.
Ex-san´guin-a´´tion. An exhaustion
of the blood from a part
or the whole of the body.
Ex-trac´tion. The process or act
of pulling or drawing out,
particularly the removal of a
child by pulling either with
hands or forceps.
Ex´tra-u´´ter-ine. Situated or
occurring outside of the
uterus.
Ex´´u-da´tive di-ath´e-sis. A congenital
predisposition to eczema
in various parts of the
body, as well as to infections
of the respiratory tract.
Fæ´ces (or fe´ces). The excrement
or undigested residue
of the food discharged from
the bowels.
Fen´es-tra-ted. (L., fenestrum,
a window.) Pierced with one
or more openings, like windows.
360Fer´ment. Any substance that
causes fermentation in other
substances with which it
comes in contact.
Fi´brin. A substance which,
becoming solid in shed blood,
plasma and lymph, causes
the coagulation of these fluids.
Fil´let. 1. A loop-shaped structure.
2. A loop, as of cord or
tape, for making traction.
Fis´sure. A cleft or groove,
normal or other.
Fis´tu-la. A deep, sinuous ulcer,
often leading to an internal
hollow organ.
Flu´id ex´tract. A concentrated
solution of the active principle
of a drug in such
strength that 1 c.c. of the
product equals 1 gr. of the
crude drug. The fluid is a
mixture of alcohol, water and
glycerine in varying proportions.
One may be omitted.
Fœ´tus (or fe´tus). The unborn
offspring of any animal that
brings forth living progeny;
the child in the womb after
the third month.
Fon´ta-nelle´´. Any one of the
unossified spots on the cranium
of a young infant. It is
so named because it rises and
falls like a fountain.
Fo-ra´men. A hole or perforation,
especially a hole in a
bone.
Four-chette´. The fold of mucous
membrane at the posterior
junction of the labia majora.
Fræ´num (or fre´num). A fold
of the integument or of the
mucous membrane that checks,
curbs, or limits the movements
of an organ in part—as
the frænum of the tongue.
Func´tion. The normal or
proper action of an organ or
set of organs.
361Func´tion-al. Of or pertaining
to a function.
Fun´dus. The base or part of
a hollow organ remotest from
its mouth.
Ga-lac´tor-rhœ´´a. Excessive secretion
of milk.
Ga-vage´. Feeding by the stomach
tube; also the therapeutic
use of a very full diet.
Gen´it-als. The reproductive organs.
Ger´´mi-cide´. An agent that destroys
germs.
Ges-ta´tion. Pregnancy.
Glans cli-tor´i-dis. The distal
or outside end of the clitoris.
Glans pe´nis. The head, or
terminal end, of the penis.
Gon-or-rhϫa. A contagious
catarrhal inflammation of the
genital mucous membrane.
Graaf´i-an fol´li-cle. Any one
of the small spherical ovarian
bodies, each of which contains
an ovum.
Hæm´o-phil´´i-a. A condition of
the system wherein bleeding
occurs readily, and the blood
clots slowly or not at all.
Hæm´or-rhage. A copious escape
of blood from the vessels;
bleeding. Accidental h.,
hæmorrhage during pregnancy,
due to premature detachment
of the placenta. Post partum
h., that which occurs soon after
labor, or childbirth.
Unavoidable h., that which results
from the detachment of
a placenta prævia.
Hæm´or-rhoid. A pile, or vascular
tumor of the rectal mucous
membrane.
Hy-dat´id. An encysted vesicle
containing an encysted fluid.
From the Greek “Hydatis,”
meaning a drop of water.
362Hy-dat´i-form. Resembling a
hydatid in form.
Hy-dram´ni-os. Dropsy of the
amnion.
Hy´dro-ceph´´a-lous. A fluid effusion
within the cranium.
This disease is marked by
enlargement of the head, with
prominence of the forehead,
atrophy of the brain, mental
weakness, and convulsions.
Hy´giene. The science of health
and of its preservation.
Hy´men. The membranous fold
which partially or wholly occludes
the external orifice of
the vagina, at least during
virginity.
Hy´per-em´´e-sis. Excessive vomiting.
H. gra-vi-da´rum, excessive
vomiting of pregnancy.
Hy´per-æ´´mi-a. Excess of blood
in any part of the body.
Hy-per´tro-phy. The morbid enlargement
or overgrowth of a
part.
Hyp-not´ic. A drug that induces
sleep.
Hy´po-der-moc´´ly-sis. The introduction,
into the subcutaneous
tissues, of fluid in
large quantity.
Hy´po-gas´´tric. Of or pertaining
to the lower anterior region
of the abdomen in the
middle line of the body. The
hypogastric arteries arise
from the internal iliac in addition
to the branches given
off from those vessels in the
adult.
Hy´po-phos´´phite. Any salt of
hypophosphorous acid.
Ic´ter-us. Jaundice.
Id´i-o-syn´´cra-sy. An effect abnormal
to the one usually
produced. An effect peculiar
to the individual.
363Im-mu´ni-ty. The condition of
being immune or exempt from
disease, especially the condition
arising from inoculation,
or from a peculiar resistance
of the organism.
Im´preg-na´´tion. 1. The act of
fecundation or of rendering
pregnant. 2. The process or
act of saturation, a saturated
condition.
In´farct. A mass of substance
extravasated either into the
substance of an organ or into
a vessel due to the obstruction
to the circulation.
In´´fan-tile´ pel´vis. A pelvis
which has not responded to
the developmental stimulation
of the sexual glands at
puberty, and therefore remains
in its infantile shape.
A masculine pelvis.
In´´fan-tile´ u´ter-us. An undeveloped
uterus.
In-fec´tion. The communication
of disease from one person
to another, whether by
effluvia or by contact, mediate
or immediate; also the implantation
of disease from
without.
In´fil-tra´´tion. To cause a liquid
or gas to penetrate or enter
by pores or interstices.
In´flam-ma´´tion. A morbid condition
characterized by pain,
heat, redness and swelling.
In-nom´in-ate. Not having a
name, as the innominate bone.
In-som´ni-a. Inability to sleep;
abnormal wakefulness.
In´ter-sti´tial. Pertaining to, or
situated in, the interstices or
interspaces of a tissue.
In´ter-tri´´go. A chafe, or
chafed patch of the skin; also
the erythema or eczema that
may result from a chafe of
the skin.
364In-tro´i-tus. The entrance to
any cavity or space.
In-ver´sion. A turning inward,
inside out, upside down, or
other reversal of the normal
relation of a part.
In´vo-lu´´tion. 1. A rolling or
turning inward. 2. The return
of the uterus to its normal
size after parturition. 3.
A retrograde change, the reverse
of evolution.
Is-chu´ri-a par-a-dox´a. A condition
in which the bladder is
over-distended with urine, although
the patient continues
to urinate, generally in dribbles.
Jaun´dice. Yellowness of the
skin, eyes, and secretions, due
to the presence of bile pigments
in the blood.
La´bi-a. Lip-shaped organs.
The external folds of the
vulva, labia majora, and the
internal folds of the vulva,
labia minora.
Lac´e-ra´´tion. 1. The act of
tearing. 2. A wound made
by tearing.
Lac-ta´tion. 1. The secretion of
milk. 2. The period of the
secretion of milk. 3. Suckling.
Lan-u´go. The fine hair on the
body of the fetus.
Lav-age´. The irrigation or
washing out of an organ, such
as the stomach or bowel.
Le´sion. Any hurt, wound or
local degeneration.
Leu´cor-rhœ´´a. A whitish, viscid
discharge from the vagina
and uterine cavity.
Light´en-ing. The sense of
lightness and easier breathing
that follows the descent
of the head into the pelvis
during the last three weeks
of pregnancy. It is most
likely to occur in primiparas.
365Lo´chi-a. The vaginal discharge
that takes place during the
first week or two after childbirth.
Lymph. A transparent slightly
yellow liquid of alkaline reaction
which fills the lymphatic
vessels.
Mal-aise´. An uneasiness or indisposition,
discomfort or distress.
Mal´po-si´´tion. Abnormal or
anomalous position.
Mam´ma. The mammary gland;
the breast.
Mam´ma-ry. Pertaining to the
Mamma.
Ma-ras´mus. Progressive wasting
and emaciation, especially
such a wasting in young
children when there is no
obvious or ascertainable
cause.
Mas-sage´. The systematic,
therapeutic friction, stroking
and kneading of the body.
Mas-ti´tis. Inflammation of the
breast.
Me-a´tus. A passage or opening,
as the meatus urinarius.
Me-læ´na ne-o-na-to´rum. The
passage of dark pitchy stools
containing blood pigments
and blood that has been extravasated
into the alimentary
canal of the newborn
babe.
Mem´brane. A thin layer of
tissue which covers a surface
or divides a space or organ.
Men´o-pause. The period when
menstruation normally ceases;
the change of life.
Mis-car´riage. Abortion; premature
expulsion of the
fœtus; birth of the fœtus before
the twenty-eighth week.
366Milk leg (Phlegmasia Alba Dolens).
A condition developing
in one, and rarely, in both,
legs, after delivery. It is due
to occlusion of the veins of
the pelvis and leg by thrombosis
or to septic inflammation
of the pelvic connective
tissue.
Mole. 1. A fleshy mass or tumor
formed in the uterus by
the degeneration or abortive
development of an ovum. 2.
A nevus; also a brownish spot
on the skin.
Mons ven´er-is. A rounded
prominence at the symphysis
pubis of a woman.
Mor-bid´i-ty. The condition of
being diseased or morbid.
Mor´cel-la´´tion. Division and
piecemeal removal.
Mu´cus. The viscid watery secretion
of the mucous glands.
Mul-tip´ar-a. A woman who
has borne more than one
child.
Mum´mi-fi-ca´´tion. Dry gangrene;
also the drying up and
shrivelling of the fœtus.
Myd´ri-at´´ic. A drug that dilates
the pupil.
Nau´se-a. Tendency to vomit;
sickness at the stomach.
Ne-cro´sis. Death of a tissue,
especially of a bone.
Ne-phri´tis. Inflammation of
the kidney.
Neu-rot´ic. 1. Pertaining to or
affected with a neurosis. 2.
Pertaining to the nerves.
Neu´tra-lize. To render neutral
or ineffective.
Ni´tro-gen. A colorless gaseous
element found free in air.
Nod´u-lar. 1. Like a nodule or
node. 2. Marked with nodules.
367Nu´cle-us. 1. a spheroid body
within a cell, forming the essential
and vital part. 2. A
mass of gray matter in the
central nervous system. 3.
In chemistry, the central element
in the molecule of a
compound.
Nu´tri-ent. Nourishing; affording
nutriment.
Nym´phæ. The labia minora.
Ob-stet´rics. The art of managing
childbirth cases; that
branch of surgery which deals
with the management of pregnancy
and labor.
Ob-ste-tri´cian. One who practices
obstetrics.
Oc´ci-put. The back part of the
head.
Ol´i-go-hy-dram´´ni-os. Scantiness
of the liquor amnii.
Ol´i-gop-nœ´´a. A delay following
the birth of a child before
the first respiration is
established.
Oph-thal´mi-a. Severe inflammation
of the eye or of the
conjunctiva.
Or´gan. Any part of the body
having a special function.
Os. (L., a mouth.) The orifice
in the uterus or vagina.
Os-mo´sis. The passage of a
fluid through a membrane.
O´va. Latin plural of ovum,
egg.
O´vu-la´´tion. The formation and
discharge of an unimpregnated
ovum from the ovary.
O´vule. 1. The ovum within
the Graafian vesicle. 2. Any
small egg-like structure.
O´vum. 1. An egg. 2. The
female reproductive cell
which, after fertilization, develops
into a new member of
the same species.
Ox´y-di´´zer. Anything that
combines with oxygen.
368Pal-pa´tion. The act of feeling
with the hand; the application
of the fingers with light
pressure to the surface of the
body for the purpose of determining
the consistence of
the parts beneath in physical
diagnosis.
Par-al´y-sis, Erb’s. 1. Same as
birth-palsy. 2. Partial paralysis
of the brachial plexus affecting
various muscles of the
arm and chest-walls. It is
revealed by an inability to
lift the arm toward the head.
Par-al´y-sis facial (Bell’s).
Paralysis of the face, due to
lesion of the facial nerve or
of its nucleus.
Par´a-me-tri´´tis. Inflammation
of the parametrium, or cellular
tissue about the uterus.
Par´a-phi-mo´´sis. Retraction of
a narrow or inflamed foreskin
which can not be replaced.
Pa-ren´chy-ma. The essential
or functional elements of an
organ as distinguished from
its stroma or framework.
Pa-ri´e-tal. Of, or pertaining
to, the walls of a cavity.
Par´o-nych´´i-a. Infection and
suppuration about the junction
of nails and skin.
Par´ox-ysm. A sudden recurrence
or sudden intensification
of symptoms.
Path-o-log´ic. Pertaining to
pathology.
Pa-thol´o-gy. That branch of
medicine which treats of the
essential nature of disease,
especially of the structural
and functional changes caused
by disease.
Pel-vim´e-ter. An instrument
for measuring the various diameters
of the pelvis.
369Pel-vim´e-try. The act of determining
the dimensions of the
pelvis by means of a pelvimeter.
Per´i-ne-or´´rha-phy. Suturation
of the perineum, performed
for the repair of a laceration.
Per´i-ne´´um. The space or area
between the anus and the
genital opening.
Pe-riph´e-ry. The outward part
or surface.
Per´i-to-ne´´um. The serous
membrane which lines the abdominal
walls.
Per´i-to-ni´´tis. Inflammation of
the peritoneum.
Per´i-stal´´sis. A worm-like
movement by which the alimentary
canal propels its
contents.
Per-ni´cious. Tending to a fatal
issue.
Phe-nom´e-non. Any remarkable
appearance; any sign or
objective symptom.
Phys´i-o-log´´ic. Pertaining to
physiology.
Phys´i-ol´´o-gy. The science
which treats of the functions
of the living organism and
its parts.
Phi-mo´sis. Tightness of the
foreskin such that it can not
be drawn back over the glans.
Phle-bi´tis. Inflammation of a
vein.
Pig´men-ta´´tion. The deposition
of coloring matter.
Pla-cen´ta præ´vi-a. A placenta
which intervenes between the
intrauterine cavity and the
inner orifice of the cervical
canal.
Pla-cen´ta suc´cen-tur´i-a´´ta. An
accessory or subsidiary placenta.
Pled´get. A small compress or
tuft as of wool or lint.
370Pleth´o-ra. A condition marked
by vascular turgescence, excess
of blood and fullness of
pulse.
Po-dal´ic. Pertaining to, or accomplished
by means of, the
feet.
Pol´y-hy-dram´´ni-os. Excess in
the amount of the liquor
amnii in pregnancy.
Po-si´tion. 1. The attitude or
posture of a patient. 2. The
relation of the presenting part
of the fœtus to the quadrants
of the maternal pelvis.
Pos-te´ri-or. Situated behind
or toward the rear.
Post par´tum. After delivery.
Pre´ma-ture. 1. Occurring before
the proper time. 2. An
infant born before its proper
term, but viable.
Pre´ma-tu´´ri-ty. The condition
of a child that has been delivered
before term, and before
maturity or ripening has
taken place.
Pre-mon´i-tory. Serving as a
warning.
Pre´puce. The fold of skin
covering the glans penis; the
foreskin.
Pres´en-ta´´tion. 1. The appearance
in labor of some particular
part of the fœtal body at
the os uteri. 2. That part of
the fœtal body which first
shows itself at the os in labor.
Pri-mip´a-ra. A woman who
has given birth, or who is giving
birth, to her first child.
Prod´ro-mal. Premonitory. Indicating
the approach of an
event, phenomenon, or disease.
Prog-no´sis. A forecast as to
the probable result of an attack
of disease; the prospect
as to recovery from a disease
afforded by the nature and
symptoms of the case.
371Pro-jec´tion-al vom´i-ting. Sudden
violent emesis.
Pro-lapse´. The falling down,
or sinking, of a part or viscus.
Pro-lep´sis. The anticipation
and nullification of complications
before they arise.
Prom´´on-to´ry. A projecting
eminence or process.
Pro´phy-lax´´is. The prevention
of disease.
Pro´te-in. Any one of a group
of nitrogenized, noncrystallizable
compounds similar to
each other, widely distributed
in the animal and vegetable
kingdoms, and forming
the characteristic constituents
of the tissues and fluids
of the animal body. They are
formed by plants, the animal
organism receiving them
as food and transforming and
assimilating them. They all
contain carbon, hydrogen,
nitrogen, oxygen and sulphur.
Some of the most important
are albumin, casein, legumin,
fibrin, myosin and glutin.
Psy´chic. Pertaining to the
mind.
Pu´bes. That part of the lower
central hypogastric region
which, in the adult, is covered
with hair. The pubic
region.
Pu´bic. Pertaining to the
pubes, or os pubis.
Pu´ber-ty. The age at which
the reproductive organs become
functionally operative.
Pu´bi-ot´´o-my. (He-bos´te-ot´´omy.)
The operation of cutting
through the pubic bone, lateral
to the median line.
Pu-er´pe-ral. Pertaining to
childbirth.
372Pu´er-pe´´ri-um. The period or
state of confinement. The
puerperium is the time succeeding
labor which is necessary
for the restoration of
the genitals to their condition
previous to pregnancy,
or as near it as possible. It
varies from 6 weeks to several
months.
Pu´ru-lent. Consisting of or
containing pus.
Py-æ´mia. Blood-poison of microbic
origin.
Py´e-li´´tis. Inflammation of the
pelvis or the kidney.
Py´or-rhœ´´a. A discharge of
pus, especially from infection
around the roots of the teeth.
Py-ro´sis. Heartburn. Acidity
of the stomach. Eructations
of acid.
Re´flex-es. Reflected actions or
movements. Impulses received
and transmitted by the
nervous system without conscious
volition. Involuntary
responses to irritation. Automatic
movements.
Re-frig´e-rant. Relieving fever
and thirst. A cooling remedy.
Acidulous drinks and evaporating
lotions are refrigerant.
Re-gur´gi-ta´´tion. 1. The casting
up of undigested food. 2.
A backward flowing of the
blood through the left auriculo-ventricular
opening, on
account of imperfect closure
of the mitral valve.
Re´lax-a´´tion. 1. A lessening of
tension. 2. A mitigation of
pain.
Re´nal. Pertaining to the kidney.
Res´ti-tu´´tion. 1. An act or
process of restoration. 2.
The rotation of the presenting
part of the fœtus outside
of the vagina.
373Re´tro-gres´´sive. Going or
moving backward. Passing
from a better to a worse condition.
Re´tro-ver´´sion. The tipping of
an entire organ backward.
Rick´ets. (Ra-chi´tis.) A constitutional
disease of childhood
in which the bones become soft
and flexible from retarded ossification,
due to deficiency of
the earthy salts.
Ro-ta´tion. The process of turning
around an axis.
Rough´en-ing. Any rough,
coarse food that gives bulk to
the intestinal contents without
much nutrition.
Ru´be-fa´´ci-ent. An agent that
reddens the skin.
Ru´gæ. Wrinkles or folds.
Rup´ture. 1. Forcible tearing
or breaking of a part. 2.
Hernia.
Sa´crum. The triangular bone
situated at the end of the
spine. It is formed of five
vertebræ, amalgamated and
wedged in between the two
innominate bones.
Sag´it-tal. Shaped like, or resembling,
an arrow.
Sal´i-va´´tion. An excessive discharge
of saliva.
Sal´pin-gi´´tis. Inflammation of
an oviduct or of the eustachian
tube.
Sal´´var-san´. A compound invented
by Ehrlich for the
treatment of diseases caused
by the Spirillæ, such as
syphilis and recurrent fever.
It is popularly called 606.
Sa-præ´mi-a. Poisoning of the
blood by the absorption of
toxins from localized infections
as from the uterus.
Scap´u-la. The shoulder blade.
Scro´tum. The pouch which
contains the testicles and
their accessory organs.
374Se-ba´ceous. 1. Pertaining to
sebum or suet. 2. Secreting a
greasy lubricating substance.
Se-cre´tion. 1. The process or
function of separating various
substances from the blood.
2. Any secreted substance.
Sec´un-dines. All that remains
in the uterus after the birth
of the child is called secundines—placenta,
membrane
and cord.
Se´men. 1. A seed or seed-like
fruit. 2. The thick whitish
liquid fecundating secretion
produced in coition.
Shock. Sudden vital depression,
due to an injury or emotion
which makes a sinister
impression upon the nervous
system.
Show. The appearance of blood
that foreruns a labor or menstruation.
Sin´a-pism. A plaster or paste
of ground mustard-seed; a
mustard plaster.
Sin´ci-put. The portion of the
head lying in front of the anterior
or large fontanelle.
Si´nus. 1. A recess, cavity or
hollow space. 2. A dilated
channel for venous blood,
found chiefly within the cranium
and uterus during gestation.
3. An air-cavity, in one
of the cranial bones, especially
one communicating with
the nose, such are the ethmoidal
frontal maxillary and
sphenoidal sinuses. 4. A suppurating
channel or fistula.
Smeg´ma. A thick, cheesy, ill-smelling
secretion found under
the prepuce and around
the labia minora.
So-lu´tion. 1. The process of
dissolving. 2. A liquid containing
dissolved matter.
375Sor´des. The dark brown matter
which collects on the lips
and teeth in low fevers.
Spas´mo-phil´´ic di-ath´e-sis. Is
a condition characterized by
an increased elective irritability
and a tendency to spasm,
like contractions of one or
more groups of muscles.
(Grulee).
Spe-cif´ic. 1. Pertaining to a
species. 2. Produced by a
single kind of microorganism.
3. A remedy specially indicated
for any particular disease.
Sper´ma-to-zo´´on. The motile
generative element of the semen
which serves to impregnate
the ovum.
Spi´na bif´i-da. Congenital
cleft of the vertebral column
with meningeal protrusion.
Spi´ro-chæ´´te. A genus or form
of flexile spirobacteria.
Sta´sis. A stoppage of the flow
of fluid in any organ or any
part of the body.
Ste-no´sis. Narrowing or stricture
of a duct or canal.
Ster´ile. Nonfertile.
Ster´il-i-za´´tion. The act or
process of rendering sterile.
Still-birth. The birth of a dead
fœtus.
Stim´u-lant. 1. Producing stimulation.
2. An agent or remedy
that produces stimulation.
Strep´to-coc´´cus. A genus or
form of bacterial organism,
which grows in consecutive
links, like a chain.
Stri´a, pl. striæ. Streaks or
lines.
Stro´ma. The tissue which
forms the ground substance,
framework, or matrix of an
organ.
Styp´tic. Astringent, an agent
for arresting hæmorrhage.
376Sub´in-vo-lu´´tion. Incomplete
involution; failure of a part
to return to its normal size
and condition after enlargement
from functional activity.
Sup-pos´i-to-ry. An easily fusible
medicated mass to be introduced
into the vagina, rectum,
or urethra.
Su´ture. 1. Surgical stitch or
seam. 2. The line of junction
of adjacent cranial or
facial bones.
Sym´phys-e-ot´´o-my. The division
of the fibrocartilage of
the symphysis pubis in order
to facilitate delivery by increasing
the anteroposterior
diameter of the pelvis.
Sym´phy-sis. The line of junction
and fusion between bones
originally distinct. The symphysis
pubis.
Syn´chro-nous. Occurring at the
same time.
Syph´i-lis. A contagious venereal
disease leading to many
structural and cutaneous lesions,
due to a microorganism
called the spirochæta pallida.
Tam´pon. A plug made of cotton,
sponge, or oakum.
Te-nac´u-lum. A hook-like instrument
for seizing and holding
tissues.
Te-nes´mus. Straining, especially
ineffectual and painful
straining.
Throm´bus. A plug or clot in
a vessel remaining at the
point of its formation.
Tinc´ture. The solution of medicinal
substances in fluids
other than water or glycerine.
There is usually about
one part of the drug to eight
of alcohol.
Tis´sue. An aggregation of
cells, fibers and various cell-products
forming a structural
element.
377Tox-æ´mi-a. Blood poisoning.
Tox´in. Any poisonous albumin
produced by bacterial action.
Trau´ma. A blow, wound, or
other violent injury.
Trau´ma-tism. A condition of
the system due to injury.
Tu´mor. 1. Swelling; morbid
enlargement. 2. A neoplasm.
A mass of new tissue which
persists and grows independently
of its surrounding structures,
and which has no physiologic
use.
Tym´pa-ni´´tis. Distention of
the abdomen from gas.
Um-bil´i-cal. Pertaining to the
umbilicus.
Um-bi-li´cus. The navel.
U´ra-chus. A cord that extends
from the apex of the bladder
to the navel. It represents
the remains of the canal
in the fœtus which joins the
bladder with the allantois.
U-re´a. A white crystallizable
substance from the urine,
blood and lymph.
U-re´ter. The fibro-muscular
tube which conveys the urine
from the kidney to the bladder.
U-ræ´mi-a. The presence of
urinary constituents in the
blood and the toxic condition
produced thereby.
U-re´thra. A membranous canal
conveying urine from the
bladder to the surface and in
the male conveying the seminal
ejaculations.
U´rin-al´´y-sis. The chemical
analysis of urine.
U´ter-us. The hollow muscular
organ which provides lodgement
for the fœtus from conception
to birth. The womb.
378U´ter-us bi-cor´nis. A womb
wherein the two sides have
been incompletely joined during
development, and two
horns, or protrusions, appear
on the fundus.
U´ter-us di-del´phys. A womb
in which there has been separate
development and incomplete
fusion of the two sides.
U´ter-us du´plex. A double
uterus.
U´ter-us sep´tate. A uterus that
is divided by a partition or
septum.
Var´i-cose veins. Of the nature
of, or pertaining to, a varix.
The permanent dilatation of
a vein.
Ven´e-sec´´tion. The opening of
a vein for the purpose of letting
blood.
Ven´tral stalk. An embryonic
process which is the rudimental
precursor of the umbilical
cord. It is known as the ventral
stalk because somewhat
later in the course of development
it becomes attached to
the ventral (abdominal) surface
of the embryo.
Ver´nix cas´e-o´´sa. A fatty substance
that covers the skin of
the fœtus.
Ver´sion. The act of turning,
especially the manual turning
of the fœtus in delivery.
External v., that which is performed
by outside manipulation.
Internal v., version performed
by the hand introduced
into the uterus. Braxton
Hicks’ Version, a version
done with the whole hand in
the vagina and two fingers
entering the uterus through
the partially dilated os.
Ves´i-cal. Pertaining to the
bladder.
379Vi´a-bil´´i-ty. Able to live after
birth.
Vil´li. 1. The finger-like projections
that develop on the outside
of the egg and connect it
vascularly and otherwise with
the uterus; a vascular chorionic
tuft. 2. A minute club-shaped
projection from the
mucous membrane of the
intestine.
380Vul-sel´lum. A forceps with
teeth on the ends of the jaws.
Walch´er’s position. The patient
on the back with the
hips at the edge of the table
and the legs hanging down.
Whar´ton’s jelly. The soft
pulpy connective tissue that
constitutes the largest part of
the umbilical cord.
Womb. Same as uterus.
382
INDEX
A
- Abderhalden test for pregnancy, 61
- Abdomen:
- care of, 70
- changes in pregnancy, 59
- weakness of, 85
- Abortion, 95
- Accessory articles of diet, 319
- Accidental hæmorrhage, 228
- After-birth, 41, 117
- After-pains, 154, 254
- Albuminuria, 77 (see Eclampsia)
- Amenorrhœa, 57
- during lactation, 158
- in the nonpregnant, 58
- Amnion, 38
- Anæsthetics, 103, 138, 142
- Anencephalus, 309
- Anus, 23
- Aphthæ, 294
- Areola, 31
- Asepsis in delivery, 142
- Aseptic care, 200
- Asphyxia neonatorum, 278
- methods of resuscitation, 279
- Atelectasis, 283
- Attitude of child, 165
B
- Baby:
- anencephalus, 309
- aphthæ, 294
- asphyxia, 142, 278
- balanitis, 306
- bath, 266
- bowels, 273
- breasts, 293
- care after delivery, 144
- care at birth, 142
- circumcision, 306
- cleansing, 265
- clothing, 270
- colic, 299
- constipation, 298
- convulsions, 282
- cradle cap, 295
- diarrhœa, 298
- exercise, 284
- eyes, 268
- furuncles, 305
- flushings, 285
- gavage, 285
- genitals, 272
- hæmorrhage, 289
- harelip and cleft palate, 287
- heart, 278
- hernia, 287
- hydrocephalus, 308
- icterus, 293
- lavage, 286
- marasmus, 303
- menstruation, 293
- mouth, 272
- nails, 289
- nursing periods, 273, 156
- paraphimosis, 305
- phimosis, 305
- pneumonia, 304
- prematurity, 301
- priapism, 308
- respiration, first, 142
- routine for, 270
- significant symptoms and
- conditions, 320
- sleep, 272
- snuffles, 304
- spina bifida, 308
- temperature, 276
- thrush, 294
- tongue-tie, 287
- toilet basket, 271
- 383umbilicus, 267
- urticaria, 294
- vomiting, 300
- weight, 271
- Bag of waters, 39, 110
- Balanitis, 306
- Ballottement, 62
- Barley water, 316
- Baths, 69, 325
- Bed, making, 133
- Bed-linen, care of, 150
- Bed sores, 263
- Bednar’s disease, 294
- Bichloride solution, 135
- Birthmarks and deformities, 72, 87
- Binder, 153
- Bladder, 23
- after delivery, 159
- in pregnancy, 56, 58
- Bleeders, 232, 290
- Blood, in pregnancy, 55
- Bowels, in pregnancy, 68
- Breast milk, quantity, 275
- Breasts, 30
- caked, 156, 243
- care of, 71
- changes due to marriage and pregnancy, 53, 59
- inflow of milk, 53
- massage, 156
- nursing periods, 156
- of puberty, 33
- preparation for lactation, 155
- removal of child, 252, 261
- sensations in pregnancy, 59
- supernumerary, 31
- Breech presentation, 168
- Brow presentation, 177, 179
- Buttermilk, 314
C
- Cæsarean section, 195
- Caput succedaneum, 127
- Case record, nurse’s, 131
- Catheterization,
- after delivery, 159
- before operations, 183
- Caul, 114
- Cephalhæmatoma, 128
- Cervix, effacement, 110
- Child (see Baby)
- Chill in puerperium, 151
- Chloasma, 55
- Chloroform in labor, 103
- Chorion, 38
- Circumcision, 306
- Clamp for cord, 268
- Clitoris, 26
- Coitus, 71
- Colic, 300
- Colostrum, 53
- Conception, 36
- Condylomata, 75
- Confinement, estimating date, 58, 66
- Constipation, 68, 298
- Contraction of pelvis, 214
- Contractions of Braxton Hicks, 53, 62, 109
- Convulsions, of child, 282
- Cord, umbilical, 40
- attachment to placenta, 42
- cutting, 142
- granulations of, 293
- prolapse of, 220, 137
- separation, 292
- Cow’s milk vs. breast milk, 311
- Cradle cap, 295
- Cramps, 56, 86
- Cranioclasis, 194
- Curettage of uterus, 206
- Curve of Carus, 20
D
- Decapitation, 194
- Delivery, asepsis during, 142
- care of mother after, 144
- on side, 140
- Diabetes and pregnancy, 95
- Diapers, 270, 273
- 384Diarrhœa of child, 298
- Diet in puerperium, 152, 155
- Diets, 336
- Doctor, 130
- Douche, vaginal, 202
- Dress in pregnancy, 69
- Drugs affecting the milk, 275
- Dry birth, 225
- Ductus arteriosus, 49
E
- Eclampsia, 78
- blood pressure in, 55
- symptoms and management, 237
- wet packs in, 231
- Ectopic pregnancy, 89
- Edema, 69
- Enemas, eliminative, 355
- Episiotomy, 211
- Ergot, 143
- after delivery, 150
- in abortion, 207
- in post partum hæmorrhage, 233
- Eruptions on the skin, 55
- Erythema, 296
- Ether in labor, 103
- Examination of patient, 134, 140
- Excavation of pelvis, 19
- Extrauterine pregnancy, 89
- Exudative diathesis, 295
- Eye symptoms in pregnancy, 69
F
- Face presentation, 174, 179
- Fallopian tubes, 22
- Fainting, 70
- Fevers and pregnancy, 91
- Flour ball, 316
- Flushings, 285
- Fœtus, attitude, 44
- circulation, 48
- diameters of head, 46
- fontanelles, 46
- heart tones, 63, 180
- movements, 44, 62
- rate of growth, 46
- rule for estimating length, 47
- rule for estimating weight, 47
- signs of danger to, 180
- signs of death, 97
- signs of maturity, 47
- Food mixings, 317
- preparation for infants, 314
- Foramen ovale, 50
- Forceps, application, 186
- conditions for, 185
- dangers of, 185
- in breech cases, 173
- in face presentations, 176
- indications for, 185
- preparations for, 183
- Fumigation, 329
- Furuncles, 305
G
- Galactorrhœa, 250
- Gas analgesia, 104
- Gas pains, 154, 158, 253
- Gavage, 285
- Genital crease, 25
- Genitalia, care after delivery, 142, 148
- preparation for delivery, 131
- preparation for operation, 182
- Getting up, 161
- Gingivitis, 75
- Glands, Bartholin, 27
- mammary, 30
- Montgomery, 31
- thyroid, 56
- Glossary, 351
- Glycosuria, 69
- Gonorrhœa and pregnancy, 93
- Goodell’s sign, 60
- Gossip, 161
- 385Graafian follicle, 33
- Gums in pregnancy, 75
H
- Hæmorrhage, accidental, 228
- in abortion, 207
- in labor, 144, 119, 143
- in the newborn, 289
- in pregnancy, 95
- post partum, 232, 234
- unavoidable, 228
- uterine douche for, 205
- Hæmorrhoids, 86
- Hair, 55, 132
- Hands, care of, 160, 323
- Harelip and cleft palate, 287
- Head, descent, 123
- expulsion of, 115
- effect of labor on, 126
- extension, 126
- external restitution, 126
- flexion, 123
- internal rotation, 124
- Headache, 237, 254
- Heart changes in pregnancy, 55
- Heart tones, fœtal, where
- heard, 130
- significance, 137
- when membranes rupture prematurely, 226
- Hegar’s sign, 60
- Hernia, 287
- Herpes in pregnancy, 76
- Hospital drums, packing, 138
- Hottentot apron, 26
- Hydramnios, 87
- and malpresentations, 175
- and twins, 84
- Hydrocephalus, 308
- Hymen, 26
- Hypodermoclysis, 206
- Hyperemesis gravidarum, 79
I
- Icterus, 293
- Induction of labor, 208
- Infant feeding, 310
- Infection, 226, 255
- Injections, eliminative, 335
- intravenous, 205
- nutrient, 334
- Insomnia, 56
- Intertrigo, 296
- Involution, 152, 160, 161
J
- Jacquemins’ sign, 62
- Jaundice, of child, 293
K
- Kidneys of child, 44
L
- Labia majora, 25
- Labor, care during, 140
- Lactation and menstruation, 157
- Lavage, 286
- Leucorrhœa, 71
- Lightening, 65, 108
- Linea albicantes, 55
- Liquor amnii, 38
- Liver, of child, 44
- of mother in pregnancy, 56, 95
- Lochia, 154
- Longings, 56
- Lungs in pregnancy, 56
M
- Malæna neonatorum, 290
- Marasmus, 303
- 386Mask of pregnancy, 55
- Mastitis, 247
- Maternal impressions, 72
- Membranes, 110
- premature rupture, 225
- relation of rupture to labor, 114
- rupture of, 109, 114
- Menstruation, definition of, 33
- during lactation, 157
- in infant, 298
- physiology of, 34
- relation to conception and pregnancy, 33
- systemic effects, 35
- Milk fever, 243
- Milk, elements of human, 312
- excess of, 249
- fat-free, 317
- inflow, 156
- peptonizing, 338
- pasteurizing, 316
- quality, 251
- scarcity, 249
- sterilization, 316
- to dry up, 163
- whole milk, 317
- Milk leg, 262
- Mind in pregnancy, 72
- Moles, 80
- Monsters, 88, 308
- Mons veneris, 25
- Morning sickness, 58
- Multiple pregnancy, 83
N
- Nausea, 58
- Nervous system, 56
- Neuralgia, 56
- Nipple, 30
- care of, 71
- cracks and fissures, 244
- imperfect, 245
- preparation for lactation, 155
- rubber, 318
- Normal labor, 107
- amount of blood lost, 119
- causes of, 107
- course of, 110
- date of onset, 107
- duration of first stage, 114
- duration of second stage, 114
- general effects, 118
- mechanism, 120
- subjective phenomena, 115
- Nurse, 98
- and cleanliness, 129, 323
- and history sheet, 131
- in obstetrics, 98
- in puerperal fever, 262
- outfit, 99
- qualifications, 323
- sterilizing, 101
- Nursery rules, 269
- Nursing periods, 156
- Nursing the child, 293
O
- Odors of person, 324
- Oligohydramnios, 87
- Operations, preparations for, 180
- Ophthalmia neonatorum, 93, 142, 192
- Os, digital dilatation, 211
- physiology of dilatation, 111
- rigidity of, 222
- Ovaries, 23
- Ovulation, 33
- Ovum, 33
- death of, 96
- fertilization, 36
- implantation, 37
- mode of progress, 23
- relation to uterine cavity, 52
P
- Packs, wet, 213
- Pains, after, 154
- Palpation, 134
- 387Paralysis, facial, 291
- Paraphimosis, 305
- Patient, care of, after delivery, 144
- during second stage, 137
- examination of, 74, 133
- in first stage, 133
- loss of weight post partum, 155
- preparation of, 131, 138
- rest, 160
- visitors, 133, 161
- Pelvic floor rigidity, 223
- Pelvis, 17
- brim, 18
- contracted, 214
- diameters, 214
- false, 17
- measurements, 214
- quadrants of, 121
- shape, 18
- true, 17
- upper strait, 18
- Pemphigus neonatorum, 296
- Perineorrhaphy, 144
- Perineum, 28, 25
- Peritoneum, 24
- Peritonitis, (see Infection)
- Phimosis, 305
- Phlebitis, 263
- Physical signs of pregnancy, 59
- Pigmentation, 55, 77
- Pituitrin, 143, 224
- Placenta prævia, 29
- Placenta, 41
- anomalies, 88
- early expression, 149
- infarcts, 88
- conditions for Crede expression, 150
- manual removal, 150
- Pneumonia in child, 304
- Point of direction, 121
- Position, occipito-posterior, 178
- Pregnancy, Abderhalden’s test for, 61
- age of, 65
- albuminuria in, 77
- at fourth month, 61
- bowels in, 68
- cathartics in, 68
- condylomata, 75
- constipation in, 75
- cramps, 86
- diabetes in, 95
- diagnosis, 57
- duration of, 66, 107
- extra uterine, 89
- fevers and, 91
- general effects, 56
- gingivitis, 75
- gonorrhœa, 93
- hæmorrhages, 95
- hæmorrhoids in, 86
- heart disease and, 94
- heartburn, 68
- herpes, 76
- hydramnios in, 87
- hygiene of, 66
- hyperemesis in, 79
- kidneys in, 68
- local effects, 51
- maternal changes, 51
- mental conditions in, 72
- pressure symptoms, 85
- probable signs, 61
- pruritus, 76
- pyelitis, 79
- salivation, 75
- signs at 26th week, 62
- syphilis, 92
- toothache, 75
- toxæmias, 74
- tuberculosis, 92
- varicose veins, 85
- vomiting in, 79
- Prematurity, 301
- Presentation, definition, 120
- frequency of vertex, 121
- 388of breech, 165
- of face and brow, 174
- transverse, 174
- Pressure symptoms, 85
- Priapism, 308
- Proprietary foods, 314
- Pruritus in pregnancy, 76
- Ptyalism, 75
- Puberty, 33
- Pubiotomy, 198
- Puerperal fever, 255
- disposal of excreta, 261
- etiology, 255
- nurse and, 262
- prevention, 258
- symptoms, 259
- treatment, 260
- Puerperium, 151
- diet in, 152
- laxatives, 158
- standing orders for, 162
- Pulse in puerperium, 151
- Pyelitis, 79
- Pyloric stenosis, 303
Q
- Quickening, 59
R
- Rectal feeding, 333
- Rectal infusions, 212
- Rectum, 23
- Red gum, 297
- Renal disease, 95
- Rest, 160
- Room, setting up, 130, 180
- Rubber gloves, 136
- Rubber nipples, 318
S
- Salivation, 75
- Second stage of labor, 114
- Sex, determination of, 65, 72
- Sexual relations, 71
- Sheet sling, 146, 181
- Show, 109, 129
- Skin, changes, 54
- care of, 69
- eruptions, 55
- pigmentation, 55, 77
- striæ gravidarum, 54
- Snuffles, 304
- Solutions, 340
- Souffle, funic, 65
- Spermatozoa, 36
- Spina bifida, 308
- Standing orders for nurse, 164
- Starvation fever, 276
- Sterile linen, application, 138, 182
- Sterilization, 101, 323
- dressings, 325
- instruments, 327
- rubber goods, 328
- Stitches, care of, 160
- Stomach capacity of child, 275
- Subinvolution, 155, 260, 261
- Subjective signs of pregnancy, 57, 59
- Sudden death of infant, 309
- Sugar in urine, 69
- Sugars and flours, 317
- Supplemental feedings, 310
- Supplies for house, 99
- for sterilization, 101
- preparation of, 326
- Symphyseotomy, 198
- Syphilis and fœtus, 88
- and pregnancy, 92
- of placenta, 88
T
- Tampon of uterus, 202
- Temperature in puerperium, 151
- Third stage of labor, 117, 142, 143
- Thrombus, 263
- Thrush, 294
- 389Thyroid gland, 56
- Toilet basket, 271
- Tongue-tie, 287
- Toothache, 75
- Toxæmia, 74
- Transfusion, 205
- Tubercles of Montgomery, 31
- Tuberculosis and pregnancy, 92
- Twilight sleep, 103
- Twins, 83
U
- Umbilicus, 267
- Unavoidable hæmorrhage, 228
- Urination, after delivery, 158
- Urine, 56
- in pregnancy, 77
- in puerperium, 151
- sterile specimen, 200
- sterile specimen from child, 200
- Urticaria, 294
- Utensils for milk modification, 318
- Uterus, anatomy, 21
- changes in pregnancy, 51, 59
- curettage, 206
- displacements, 84
- height at various months of pregnancy, 64
- inertia, 223
- malformations, 85
- rupture, 226
- Uterine souffle, 63
V
- Vagina, anatomy, 21
- attachments, 21
- distensibility, 21
- Vaginal tampon, 204
- Varicose veins, 85
- Ventral stalk, 40
- Version, 190, 192, 193
- Vestibule, 26
- Vessels of cord, 48
- Villi, 37
- Visitors, 133, 161
- Vomiting, 300, 321
- in pregnancy, 79
- in labor, 228
- uncontrollable, 79
- Vorhees bag, 224, 230
- Vulva, anatomy, 24
W
- Walcher position, 173, 193
- Weaning, 252, 273
- Wet nurse, 253
- Wharton’s jelly, 40
- Whey, 315
- Wiegand compression, 173, 194
- Witch’s milk, 32
- Silently corrected typographical errors and variations in spelling.
- Anachronistic, non-standard, and uncertain spellings retained as printed.
End of Project Gutenberg's Obstetrics for Nurses, by Charles B. Reed
*** END OF THIS PROJECT GUTENBERG EBOOK OBSTETRICS FOR NURSES ***
***** This file should be named 61476-h.htm or 61476-h.zip *****
This and all associated files of various formats will be found in:
http://www.gutenberg.org/6/1/4/7/61476/
Produced by Richard Tonsing, Mark C. Orton, and the Online
Distributed Proofreading Team at http://www.pgdp.net
Updated editions will replace the previous one--the old editions will
be renamed.
Creating the works from print editions not protected by U.S. copyright
law means that no one owns a United States copyright in these works,
so the Foundation (and you!) can copy and distribute it in the United
States without permission and without paying copyright
royalties. Special rules, set forth in the General Terms of Use part
of this license, apply to copying and distributing Project
Gutenberg-tm electronic works to protect the PROJECT GUTENBERG-tm
concept and trademark. Project Gutenberg is a registered trademark,
and may not be used if you charge for the eBooks, unless you receive
specific permission. If you do not charge anything for copies of this
eBook, complying with the rules is very easy. You may use this eBook
for nearly any purpose such as creation of derivative works, reports,
performances and research. They may be modified and printed and given
away--you may do practically ANYTHING in the United States with eBooks
not protected by U.S. copyright law. Redistribution is subject to the
trademark license, especially commercial redistribution.
START: FULL LICENSE
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full
Project Gutenberg-tm License available with this file or online at
www.gutenberg.org/license.
Section 1. General Terms of Use and Redistributing Project
Gutenberg-tm electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or
destroy all copies of Project Gutenberg-tm electronic works in your
possession. If you paid a fee for obtaining a copy of or access to a
Project Gutenberg-tm electronic work and you do not agree to be bound
by the terms of this agreement, you may obtain a refund from the
person or entity to whom you paid the fee as set forth in paragraph
1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this
agreement and help preserve free future access to Project Gutenberg-tm
electronic works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the
Foundation" or PGLAF), owns a compilation copyright in the collection
of Project Gutenberg-tm electronic works. Nearly all the individual
works in the collection are in the public domain in the United
States. If an individual work is unprotected by copyright law in the
United States and you are located in the United States, we do not
claim a right to prevent you from copying, distributing, performing,
displaying or creating derivative works based on the work as long as
all references to Project Gutenberg are removed. Of course, we hope
that you will support the Project Gutenberg-tm mission of promoting
free access to electronic works by freely sharing Project Gutenberg-tm
works in compliance with the terms of this agreement for keeping the
Project Gutenberg-tm name associated with the work. You can easily
comply with the terms of this agreement by keeping this work in the
same format with its attached full Project Gutenberg-tm License when
you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are
in a constant state of change. If you are outside the United States,
check the laws of your country in addition to the terms of this
agreement before downloading, copying, displaying, performing,
distributing or creating derivative works based on this work or any
other Project Gutenberg-tm work. The Foundation makes no
representations concerning the copyright status of any work in any
country outside the United States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other
immediate access to, the full Project Gutenberg-tm License must appear
prominently whenever any copy of a Project Gutenberg-tm work (any work
on which the phrase "Project Gutenberg" appears, or with which the
phrase "Project Gutenberg" is associated) is accessed, displayed,
performed, viewed, copied or distributed:
This eBook is for the use of anyone anywhere in the United States and
most other parts of the world at no cost and with almost no
restrictions whatsoever. You may copy it, give it away or re-use it
under the terms of the Project Gutenberg License included with this
eBook or online at www.gutenberg.org. If you are not located in the
United States, you'll have to check the laws of the country where you
are located before using this ebook.
1.E.2. If an individual Project Gutenberg-tm electronic work is
derived from texts not protected by U.S. copyright law (does not
contain a notice indicating that it is posted with permission of the
copyright holder), the work can be copied and distributed to anyone in
the United States without paying any fees or charges. If you are
redistributing or providing access to a work with the phrase "Project
Gutenberg" associated with or appearing on the work, you must comply
either with the requirements of paragraphs 1.E.1 through 1.E.7 or
obtain permission for the use of the work and the Project Gutenberg-tm
trademark as set forth in paragraphs 1.E.8 or 1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any
additional terms imposed by the copyright holder. Additional terms
will be linked to the Project Gutenberg-tm License for all works
posted with the permission of the copyright holder found at the
beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including
any word processing or hypertext form. However, if you provide access
to or distribute copies of a Project Gutenberg-tm work in a format
other than "Plain Vanilla ASCII" or other format used in the official
version posted on the official Project Gutenberg-tm web site
(www.gutenberg.org), you must, at no additional cost, fee or expense
to the user, provide a copy, a means of exporting a copy, or a means
of obtaining a copy upon request, of the work in its original "Plain
Vanilla ASCII" or other form. Any alternate format must include the
full Project Gutenberg-tm License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works
provided that
* You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is owed
to the owner of the Project Gutenberg-tm trademark, but he has
agreed to donate royalties under this paragraph to the Project
Gutenberg Literary Archive Foundation. Royalty payments must be paid
within 60 days following each date on which you prepare (or are
legally required to prepare) your periodic tax returns. Royalty
payments should be clearly marked as such and sent to the Project
Gutenberg Literary Archive Foundation at the address specified in
Section 4, "Information about donations to the Project Gutenberg
Literary Archive Foundation."
* You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or destroy all
copies of the works possessed in a physical medium and discontinue
all use of and all access to other copies of Project Gutenberg-tm
works.
* You provide, in accordance with paragraph 1.F.3, a full refund of
any money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days of
receipt of the work.
* You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project
Gutenberg-tm electronic work or group of works on different terms than
are set forth in this agreement, you must obtain permission in writing
from both the Project Gutenberg Literary Archive Foundation and The
Project Gutenberg Trademark LLC, the owner of the Project Gutenberg-tm
trademark. Contact the Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
works not protected by U.S. copyright law in creating the Project
Gutenberg-tm collection. Despite these efforts, Project Gutenberg-tm
electronic works, and the medium on which they may be stored, may
contain "Defects," such as, but not limited to, incomplete, inaccurate
or corrupt data, transcription errors, a copyright or other
intellectual property infringement, a defective or damaged disk or
other medium, a computer virus, or computer codes that damage or
cannot be read by your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH 1.F.3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium
with your written explanation. The person or entity that provided you
with the defective work may elect to provide a replacement copy in
lieu of a refund. If you received the work electronically, the person
or entity providing it to you may choose to give you a second
opportunity to receive the work electronically in lieu of a refund. If
the second copy is also defective, you may demand a refund in writing
without further opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS', WITH NO
OTHER WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT
LIMITED TO WARRANTIES OF MERCHANTABILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of
damages. If any disclaimer or limitation set forth in this agreement
violates the law of the state applicable to this agreement, the
agreement shall be interpreted to make the maximum disclaimer or
limitation permitted by the applicable state law. The invalidity or
unenforceability of any provision of this agreement shall not void the
remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in
accordance with this agreement, and any volunteers associated with the
production, promotion and distribution of Project Gutenberg-tm
electronic works, harmless from all liability, costs and expenses,
including legal fees, that arise directly or indirectly from any of
the following which you do or cause to occur: (a) distribution of this
or any Project Gutenberg-tm work, (b) alteration, modification, or
additions or deletions to any Project Gutenberg-tm work, and (c) any
Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of
computers including obsolete, old, middle-aged and new computers. It
exists because of the efforts of hundreds of volunteers and donations
from people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need are critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future
generations. To learn more about the Project Gutenberg Literary
Archive Foundation and how your efforts and donations can help, see
Sections 3 and 4 and the Foundation information page at
www.gutenberg.org
Section 3. Information about the Project Gutenberg Literary Archive Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Contributions to the Project Gutenberg Literary
Archive Foundation are tax deductible to the full extent permitted by
U.S. federal laws and your state's laws.
The Foundation's principal office is in Fairbanks, Alaska, with the
mailing address: PO Box 750175, Fairbanks, AK 99775, but its
volunteers and employees are scattered throughout numerous
locations. Its business office is located at 809 North 1500 West, Salt
Lake City, UT 84116, (801) 596-1887. Email contact links and up to
date contact information can be found at the Foundation's web site and
official page at www.gutenberg.org/contact
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
[email protected]
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To SEND
DONATIONS or determine the status of compliance for any particular
state visit www.gutenberg.org/donate
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including checks, online payments and credit card donations. To
donate, please visit: www.gutenberg.org/donate
Section 5. General Information About Project Gutenberg-tm electronic works.
Professor Michael S. Hart was the originator of the Project
Gutenberg-tm concept of a library of electronic works that could be
freely shared with anyone. For forty years, he produced and
distributed Project Gutenberg-tm eBooks with only a loose network of
volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as not protected by copyright in
the U.S. unless a copyright notice is included. Thus, we do not
necessarily keep eBooks in compliance with any particular paper
edition.
Most people start at our Web site which has the main PG search
facility: www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.