The Project Gutenberg EBook of A Treatise on Fractures, Luxations, and other Affections of the Bones, by Pierre-Joseph Desault This eBook is for the use of anyone anywhere in the United States and most other parts of the world at no cost and with almost no restrictions whatsoever. You may copy it, give it away or re-use it under the terms of the Project Gutenberg License included with this eBook or online at www.gutenberg.org. If you are not located in the United States, you'll have to check the laws of the country where you are located before using this ebook. Title: A Treatise on Fractures, Luxations, and other Affections of the Bones Author: Pierre-Joseph Desault Editor: Xavier Bichat Translator: Charles Caldwell Release Date: January 3, 2019 [EBook #58602] Language: English Character set encoding: UTF-8 *** START OF THIS PROJECT GUTENBERG EBOOK A TREATISE ON FRACTURES *** Produced by Thiers Halliwell, Sonya Schermann and the Online Distributed Proofreading Team at http://www.pgdp.net (This file was produced from images generously made available by The Internet Archive)
The text of this e-book has been preserved as in the original, including inconsistent capitalisation and hyphenation. Archaic and inconsistent spellings have also been preserved except where obviously misspelled in the original. A list of corrections and inconsistencies is appended at the end of the book.
A black underline indicates a hyperlink to a page, illustration or footnote (hyperlinks are also highlighted when the mouse pointer hovers over them). A grey dashed underline indicates the presence of a concealed comment which is revealed when the mouse pointer hovers over the underlined text. Page numbers are shown in the right margin. Footnotes have been renumbered sequentially and are located at the end.
The book contains several lllustrations, but details cannot be seen clearly with small-screen e-readers. A standard browser is recommended.
The cover image of the book was created by the transcriber and is placed in the public domain.
District of Pennsylvania, to wit:
BE IT REMEMBERED, That on the twentieth day of February, in the twenty-ninth year of the independence of the United States of America, A. D. 1805, Charles Caldwell, M. D. of the said district, hath deposited in this Office, the Title of a Book, the Right whereof he claims as proprietor, in the words following to wit:
“A Treatise on Fractures, Luxations, and other Affections of the Bones, by P. J. Desault, surgeon in chief to the Hotel-Dieu of Paris, wherein his Opinions and Practice, in such cases, are stated and exemplified. Edited by Xav. Bichat; with Plates. Translated from the French, by Charles Caldwell, M. D. With Notes, and an Appendix containing several late improvements in surgery.”
In conformity to the act of the Congress of the United States, intituled, “An act for the encouragement of learning, by securing the copies of maps, charts, and books, to the authors and proprietors of such copies during the times therein mentioned:” And also to the act, entitled, “An act supplementary to an act, entitled, “An act for the encouragement of learning, by securing the copies of maps, charts, and books, to the authors and proprietors of such copies during the times therein mentioned,” and extending the benefits thereof to the arts of designing, engraving and etching historical and other prints.”
D. CALDWELL,
Clerk of the District of Pennsylvania.
| MEMOIR I. | PAGE |
| On the Fracture of the Condyls of the lower Jaw, | |
| MEMOIR II. | |
| On the Fracture of the Clavicle, | |
| Explanation of the first Plate, | |
| MEMOIR III. | |
| On the Luxation of the Clavicle, | |
| Luxation of the Sternal extremity, | |
| of the Humeral extremity, | |
| MEMOIR IV. | |
| On Fractures of the Acromion, and of the lower angle of the Scapula, | |
| Fracture of the Acromion, | |
| of the lower angle of the Scapula, | |
| MEMOIR V. | |
| On the Fractures of the upper end or neck of the Humerus, | |
| MEMOIR VI. | |
| On the Fracture of the lower extremity of the Humerus, with a separation of the Condyls, | |
| MEMOIR VII. | |
| On the Luxation of the Humerus, | |
| MEMOIR VIII. | |
| On the Fracture of the bones of the Fore-arm, | |
| Fracture of the Radius, | |
| of the Ulna, | |
| of the Olecranon, | |
| MEMOIR IX. | |
| On the Luxation of the Fore-arm, | |
| MEMOIR X. | |
| On the Luxations of the Radius over the Ulna, | |
| Luxation of the lower extremity of the Radius, | |
| MEMOIR XI. | |
| On the Fractures of the Thigh, | |
| Fractures of the body of the Os Femoris, | |
| of the upper end of the Os Femoris, | |
| of the great Trochanter, | |
| of the neck of the Os Femoris, | |
| of the lower extremity of the Os Femoris, | |
| Explanation of the second Plate, | |
| Thoughts on Luxations of the Os Femoris upward and forward, | |
| MEMOIR XII. | |
| On spontaneous Luxations of the Os Femoris, | 299 |
| MEMOIR XIII. | |
| On the Fracture of the Rotula, | |
| MEMOIR XIV. | |
| On the formation of foreign bodies in the joint of the knee, | |
| Observations and Reflections on forms of Apparatus1 for fractures of the leg, | |
| MEMOIR XV. | |
| On the Division of the Tendo Achillis, | |
| MEMOIR XVI. | |
| On the Fracture of the Os Calcis, | |
| MEMOIR XVII. | |
| On complicated Luxations of the Foot, | |
| APPENDIX. | |
| ARTICLE I. | |
| Dr. Physick’s new and successful method of treating an old and obstinate fracture of the os humeri, | |
| ARTICLE II. | |
| An account of Dr. Physick’s improvement of Desault’s apparatus for making permanent extension in oblique fractures of the os femoris, | |
| ARTICLE III. | |
| Explanation of the third Plate, | |
BY THE TRANSLATOR.
The business of a translator, though very limited as to its range, may be extensive and important in its consequences, and, though humble in its end, is oftentimes extremely difficult in its nature. Prohibited from adding any thing to, or in any measure transgressing the bounds of, the meaning of his original, he is obligated to interpret that meaning with faithfulness and accuracy. In this latter point consists the difficulty of his task. If several different readers oftentimes attach as many different meanings to parts and sentences of works written in their own language, how much more likely will this be to occur with respect to such as are written in a foreign language? For readers to differ in the former case is common, in the latter unavoidable.
The translator of the following work is far from affirming, that he has in no instance deviated from the meaning of his original. To hazard an assertion like this, would be assuming to himself more than is consistent with modesty or, perhaps, with truth. He trusts, however, that such deviations are very rare, that if they do occur they are but slight in themselves, and never connected with facts or principles of practical importance. He can, at least, very confidently declare, that they have never been the offspring of carelessness or design.
Should any one open this volume in quest of the flowers of fancy, or the embellishments of style, he will close it again without being gratified. Ambitious only of communicating new and useful matter, and too intent on things to be in any measure choice of his words, the celebrated original was regardless, perhaps to a fault, of the ornaments of diction. Rich in the resources of a capacious and exalted intellect, he poured forth his knowledge like precious ore from the mine, leaving to others of inferior capacities the humbler task of refining and polishing it.
With such an example before him, the translator thought it best to follow in some measure the footsteps of his illustrious guide, without venturing to chalk out a new and different track for himself. As his principal object, throughout the work, has been to make himself clearly understood, and that in as few words as practicable, he has never hesitated, when they came in competition, to sacrifice elegance to precision and ornament to perspicuity. He has even in some instances been guilty of intentional tautology, for the purpose of rendering his meaning the more clear and definite. For this he flatters himself he need offer no apology to those, who prefer utility to pleasure and sense to sound. And, as to readers of an opposite cast of mind, should any such choose to sit in judgment on him, he neither deprecates their censure nor courts their approbation.
A circumstantial analysis of the following memoirs would constitute a paper too extensive to be introduced here in the form of a preface, and a mere outline or general character of them would be altogether useless. The translation is now before the public, and every reader must judge of its merit for himself. On this point the translator will only observe, that the attention which he has been necessarily led to bestow on the work, has been to him the best school of surgery he ever attended, as far as relates to affections of the bones. Should other practitioners throughout the United States derive equal benefit from perusing his translation, he will rejoice in a consciousness of having, at least in one instance, been of service to his country.
Such are the extent and importance of Desault’s improvements in some branches of practical surgery, as to constitute a new epoch in the history of the profession. His different forms of apparatus for fractures and luxations are certainly more rational in their construction, and more efficacious in their action, than those of any other writer. But their excellence does not arise from these circumstances alone. Their cheapness and simplicity, taken in conjunction with the ease and quickness with which they may be every where made and applied, greatly enhance their value, particularly to practitioners in the country. If they be not already at hand, they can be easily prepared by the surgeon or his assistants, without any material loss of time. The sufferings of the patient, therefore, whatever may be the form of fracture or luxation under which he labours, need never be prolonged, by any delay in obtaining the necessary apparatus. It is thus that the means and processes of every art become simple and easy, in proportion as the art itself approaches perfection: and thus that the truly great artist is known, not by the multiplicity and the complex nature of his forms of apparatus, but by the numerous ends which he accomplishes by means the most simple and easy of construction.
Several French practitioners, in projecting improvements on the forms of apparatus of Desault, have evidently rendered them more complex, more expensive, and therefore more difficult to be constructed or procured, without adding in the smallest degree to the efficacy of their action. This is particularly the case with respect to Boyer, in his attempt to substitute a new apparatus for a fractured clavicle, in place of that invented by Desault. The latter can be constructed in a very few minutes by the surgeon or one of his assistants, without any expense, whereas the former must be made by a workman employed for the purpose, and is necessarily attended with both cost and delay. Nor is it always practicable, particularly in the country, to procure a workman capable of making this apparatus. But this is not all. On Desault’s plan, the same apparatus for a fractured clavicle will fit, and may be applied to, persons of different sizes and figures; whereas, on the plan of Boyer, each patient must have an apparatus constructed particularly for himself. No practitioner, therefore, can hesitate a moment in deciding to which of these two forms of apparatus the preference is due.
Similar remarks may be made respecting Boyer’s apparatus for making permanent extension in oblique fractures of the os femoris. It is much more complex and difficult to be constructed than that of Desault. Nor does it possess a single advantage over it as improved by Drs. Physick and Hutchinson. In a word, the forms of apparatus of Boyer may answer well enough in hospitals and in cities, where the expence of such articles is not much regarded, and where workmen to make them can be readily procured. But, as the practitioner in the country is generally obliged to be himself the constructor of the forms of apparatus which he uses, and as he is not at all times prepared to meet heavy expenses, it is to those recommended and employed by Desault that he must necessarily have recourse.
With these remarks the translator submits to the good sense and candour of his countrymen the following sheets, as the offspring of some of his hours of leisure throughout the winter. He hopes that the appendix subjoined by himself will not be regarded as either an useless or an unpleasing addition. Every native of the United States, whose bosom glows as it ought, with that noblest of passions, the amor patriæ, will witness with pride and exultation the improvements that are daily making in the arts and sciences, by the industry and enterprize of his enlightened countrymen. Such a mind will enjoy in anticipation the glory of his country, at that period, when she will be able to reflect back, with increased splendour, the light which she has so long been borrowing from the countries of Europe.
The translator does not plead the want of time as an apology for any imperfections or errors which his translation may exhibit. Yet he believes it to be true, that had he had more time to bestow on it, he could probably have rendered it more worthy of public patronage.
ON
FRACTURES, DISLOCATIONS, &c.
§ I.
1. The lower jaw, a kind of moveable hammer, destined, to use the words of a certain physiologist, to triturate the aliments against the almost immoveable anvil of the upper jaw, is more exposed to the action of external bodies, and consequently to fractures, than most of the other bones of the face. But all parts of it are not alike subject to such accidents. Common in its body, but less frequent in its branches or sides, fractures sometimes occur in the two processes in which its branches terminate. One of these processes, concealed by the zygoma, embosomed in the temporal muscle, and covered by the masseter, is less liable to fractures than the other, which serves as the centre of the motions performed by the bone, and is protected externally only by the parotid gland.
§ II.
2. A fracture of the condyle may sometimes arise from a counter-stroke, as when, in consequence of some external force being applied from before backwards, and from below upwards against the chin, this process is driven against the projecting rim of the glenoid cavity; at other times it may be the effect of an immediate or direct stroke, as when a body in motion strikes with force against the region of the joint, and does violence to that portion of the bone.
3. But in whatever manner the fracture may be produced, it generally occurs in the slender part of the bone which supports the condyle, below the insertion of the pterygoideus externus. It is characterized by a pain more or less acute, necessarily accompanying the motions of the jaw; by a difficulty more or less considerable, in the performance of these motions; by a crepitation, oftentimes distinct, when, in consequence of the angle of the jaw being pushed forward, or the jaw itself alternately depressed and elevated, the separated surfaces rub against each other; by an inequality of surface sometimes perceptible directly over the fractured condyle; by the ease with which, on being pushed forward, it may be forced into the depression beneath the zygoma; and by its remaining stationary, during the movements of the lower jaw, from which it is separated. These signs, though generally characteristic, are subject to an uncertainty proportioned to the swelling that occurs in the part.
4. In this accident a displacement is almost always produced by muscular action. The pterygoideus externus, being attached to the condyle, draws it forward and upward, towards the external wing of the pterygoid apophysis, its fixed point of insertion. On the other hand, the body of the bone is left behind, being held by the masseter and external pterygoid muscles, the course of which is opposed to a displacement in the same direction; so that there always exists a separation, more or less perceptible, between the two fragments of bone.
5. Hence, if proper means be not used to restore the contact between the broken ends of the bone, the following consequences will be likely to occur: 1st. Their reunion will be tedious, because in every bone this process is, in point of rapidity, inversely proportioned to the separation of the divided surfaces: 2dly, This reunion may even entirely fail to take place, if the bone be subject to the slightest movements, as I have witnessed in a particular case, where the condyle, not being reunited to the other part, exfoliated, and was in part discharged through the external integuments: 3dly, Under such circumstances, the callus produced in the process of healing, being situated near to the joint, and rendered irregular and deformed by the separation of the parts, is apt to impede muscular action, and do a permanent injury to the functions of the jaw.
§ III.
6. As the whole apparatus in this case consists in a passive resistance to the active powers employed in producing a displacement, it follows from what has been said (4), that the bandage intended to prevent this displacement, and by that means to guard against the accidents specified above (5), ought, either effectually to bring back to its natural situation, the condyle which is drawn forward, or pull in this last direction (that is, forward) the body of the bone which is still retained in its usual position, in order that it may thus be brought into contact with the condyle.
The first of these measures is impracticable, in consequence of the situation of the condyles, which are too deeply enveloped by the surrounding parts, and offer a hold too small to be acted on. The second, therefore, remains to be adopted, and is the more easily executed, in as much as the angle of the jaw, from its projecting and being but slightly covered by the integuments, may without difficulty be directed from behind forward by a proper force.
7. The fingers of the surgeon temporarily supply this force, at the time of reduction; but it is necessary that it should be permanently kept up by means of the apparatus. This end is attained, in the following manner:
Place behind the angle of the jaw, which must be first pushed forward, thick compresses, to fill up the hollow under the ear, and form an eminence higher than the surface of the surrounding parts; pass over these compresses, in an oblique manner, the bandage commonly used in lateral fractures of the bone, the application of which must in this case commence on the sound side.
These compresses, being more projecting than the surrounding surface, will necessarily sustain a greater pressure, because the compression made by a bandage is in proportion to the projection of the part on which it is applied. Hence, being firmly supported, they will retain the body of the bone in a line with the displaced condyle (4).
8. In addition to this mode of applying the bandage, it is necessary that the fractured bone should be kept in a state of perfect rest. The internal pterygoid and masseter muscles, tending by their contractile efforts to draw the angle of the jaw backwards, sometimes overcome the resistance of the apparatus, and, by producing a second displacement, give rise to the accidents formerly mentioned (5).
Let the lower jaw be now brought into perfect contact with the upper one, and not separated from it during the first few days after the injury, except so far as may be necessary for the admission of nourishing broths. Should a tooth have been lost, the space which it occupied will furnish, without disturbing the bone, an opening for the conveyance of nourishment to the patient. Let talking, laughing, and every thing that might produce a separation between the body of the bone and the condyle, be carefully avoided. The further treatment of the accident should be such as is generally applicable to all fractures of bones, and need not be at present particularly detailed.
The following cases, reported by citizen Giraud, second surgeon to the Hotel-Dieu, will confirm the advantages of this mode of treatment.
Case I. Margaret Bessonet, aged thirty-four, was admitted into the hospital on the 10th of May, 1791. On the preceding day she had received a violent fall on her chin: a severe pain, and a preternatural mobility in the left side of the jaw, had been the immediate consequences of the accident: from these symptoms, taken in conjunction with those formerly mentioned (3), Desault discovered that a fracture of the condyle existed, which he reduced and supported in the usual manner (7).
After being somewhat uneasy during the first few days, the patient became reconciled to the action of the bandage, which, by inattention, had been two or three times disturbed and put out of order, but which, by being carefully reapplied, and aided by the necessary precautions (8), restored to the bone its natural form and solidity, by the thirtieth day, and on the thirty-sixth the patient was discharged perfectly cured. The only inconvenience she experienced, was a slight difficulty in the motions of the jaw, an effect naturally resulting from the long continued inactivity of the muscles, but which was soon removed by means of exercise.
Case II. Claudius Laurat, aged twenty-seven, fell as he was carrying a heavy burden. In his fall his chin struck with violence against a beam that lay in his way. In an instant he experienced a sharp pain in his right temple, and found it almost impossible to move his jaw. Two hours afterwards a considerable swelling appeared in the part, extending from the angle of the jaw above the ear. The patient was admitted into the Hotel-Dieu, where the circumstances of the fall and the symptoms that followed, gave satisfactory evidence of a fracture of the condyle. It was reduced and supported as in the preceding case. On the day following, the swelling was removed, doubtless by means of the compression which had been made on it; the other symptoms (3), hitherto scarcely perceptible, became more obvious; the bandage was reapplied, and the disease terminated, in about twenty-nine days, in the same manner with that of case 1.
§ I.
1. Man enjoys an advantage which nature has bestowed on but few of the quadrupeds, namely, a power of moving his upper extremities in every direction. The clavicle being a kind of arch placed between the breast and shoulder, forms a centre, moveable indeed but solid, for these motions, a part of which can no longer be performed, when this arch, in consequence of being broken, ceases to afford them a point of support. Hence it follows, that the fracture of this bone may be said to reduce the individual who sustains it, when considered in relation to its functions, to a level with that numerous division of animals that are destitute of clavicles.
2. Few diseases of the kind are more frequently met with than this. The natural curve of the clavicle, its situation immediately under the skin, the want of a support to its middle part, the great proportion of spongy substance which enters into its composition, the projection of the shoulder exposing it to the action of external bodies; all these circumstances concur in rendering the accident frequent, particularly among that class of men subject, from their occupations, to violent exertions of the upper extremities.
Here then, more than in the generality of fractures, we should feel an interest in the advancement of the art of surgery; and yet, having hitherto employed in it but feeble means, our efforts have been attended with imperfect success. Hippocrates has observed, that some degree of deformity almost always accompanies the reunion of a fractured clavicle; all writers since his time have made the same remark; experience has confirmed the truth of it, and as much time has been spent in hypothetical speculations to explain the accident, as in serious inquiries how to prevent it. At length Desault proved that a feeble and unskilful mode of treatment was the sole cause of a want of success, and that, by being more correct and judicious, art might be as successful here, as in other fractures. In order to give a correct view of his practice in this disease, I will examine the causes, varieties, and signs of a fracture of the clavicle; the accidents of which it is susceptible; the mode and the causes of the displacement of the broken ends of the bone; the indications that arise out of those causes, and the manner of answering these indications as well during, as after, the reduction.
§ II.
3. The action of external bodies is almost the only known cause of this fracture, whether these bodies strike the shoulder with violence, or the shoulder be forcibly driven against them. But this action is not in every case the same; its application is most frequently mediate or indirect, but is sometimes immediate or direct.
In the first case there is a true counter-stroke, the ordinary effect, either of a severe blow on the point of the shoulder, which is the most common occurrence; or, as happens less frequently, of a fall on the arm when it is extended for the purpose of guarding the body from the force of the accident. Under these circumstances, being pressed between the sternum, which makes resistance, and the body which acts on its extremity, the clavicle is bent in that direction which is most natural to it; but, not being sufficiently flexible, it gives way generally in the place where its curvature is the greatest. Thus the ribs are broken, when the sternum, by being violently driven backward, forces them to bend in the centre beyond their natural flexibility.
In the second case, the fracture occurs at the spot where the stroke is given. Here the momentum or quantity of force applied on the bone, surpassing the solidity which the bone possesses, its continuity is necessarily destroyed.
4. But in whatever way the fracture is produced, it is either oblique or transverse, single or double, in the middle or towards the extremities of the bone, simple or compound.
An oblique fracture is most frequently the effect of a counter-stroke; a transverse fracture is the more common result of the immediate action of external bodies; a counter-stroke seldom produces any thing but a simple fracture; while compound fractures are generally owing to a direct stroke. The one produces a solution of continuity in the middle of the bone, or thereabout; because in that part the curvature is most considerable. The other is almost always the cause of this solution, when it occurs at the extremities. To the latter alone, is a double division to be attributed. The reason of these differences is already so plain, that it would be a waste of time to dwell on an explanation of them.
§ III.
5. The several phenomena that attend a fracture of the clavicle, taken together, leave in general but little doubt as to its existence, particularly when the fracture is oblique. As is the case in most other instances of the kind, so here, an acute pain is felt at the instant of the stroke; sometimes a cracking of the bone is distinctly heard by the person injured; on every occasion, it becomes suddenly impracticable to perform circular or rotatory motions with the arm; motions from before backwards can still be executed, but are difficult and painful, and, as I have already observed (1), the individual injured is reduced to the class of animals destitute of clavicles.
Oftentimes the shoulder of the injured side, being more or less depressed, loses its level with the other. It is also evidently drawn forward and inward. The distance between the acromion and sternum, on the affected side, is found on comparison, to be evidently less than on the opposite side. In almost every case, that portion of the fractured bone, which adheres to the sternum, forms a visible protuberance above and on the inside of the shoulder.
6. In the mean time the pain continues. The painful drawing or dragging occasioned by the weight of the arm forces the patient, for the purpose of relieving it, to bend his body towards the side affected, and incline his head in the same direction. This forms a peculiar attitude, which of itself was frequently sufficient to disclose to Desault the nature of the disease. We have oftentimes witnessed him establishing the truth of this diagnostic, by merely looking at patients entering the amphitheatre, who had been brought thither for the reduction of such fractures.
By this position, the pains are generally relieved, because the arm finds some degree of support; but should the patient wish to change his position, or perform any particular motions, the pains return almost as acutely as at first.
7. If to these signs, which are almost all of them founded in reason, we add those that are still more palpable to the senses, such as the mobility of the two broken ends of the bone; the crepitation produced by their friction against each other; the depression felt at the point of fracture, by passing the fingers over the upper surface of the bone; and the facility of restoring to it its natural form and direction, by moving the shoulder upwards, outwards, and backwards; it will be difficult to be mistaken respecting the nature of this fracture. This is perhaps more particularly the case, when the fracture is oblique, as this kind offers the most striking diagnosis, and cannot be involved in uncertainty, unless when a considerable swelling occurs in the parts around the fracture. But, even then, as the circumspection of the practitioner will necessarily direct his attention to this circumstance, the obscurity of the signs will have no unfavourable influence on the cure.
8. When the fracture is transverse, there is sometimes more difficulty attending the diagnosis. The corresponding inequalities of the divided surfaces may mutually penetrate each other and interlock, and thus prevent a displacement. Does any uncertainty on this score exist? Placing your fingers on the two extremities of the bone, order an assistant to move the arm in every direction, and the motions will be communicated to the clavicle; but, if a fracture exist, they will be most perceptible in the fragment adjoining the shoulder, and will separate it from that attached to the sternum. This method will seldom deceive us, is easily employed, and subjects the patient to but a momentary pain.
§ IV.
9. We do not generally find fractures of the clavicle accompanied by such accidents as the anatomical relations of the parts might lead us to apprehend. The external force being all expended in fracturing the bone, extends but feebly to the brachial plexus, which would be much injured by the shock, were the bone to yield, without breaking, to the action of external bodies striking against it. Hence, without doubt, would arise serious affections, as may be fairly inferred from the analogy of blows on the head and vertebral column, and as is indeed confirmed by certain cases reported by Desault.
Case I. Two bricklayers were brought to the Hotel-Dieu, who had met with similar accidents. A piece of timber, thrown from a building, in which they were engaged, had struck them, the one on the external part of the left clavicle, the other about the middle of the right. A considerable wound pointed out in each the place on which the blow had been received. But the former, having escaped a fracture, experienced nothing but an acute pain, while the second had the bone broken in two places.
The customary apparatus was applied to the latter, and the treatment which we shall presently describe, being pursued, the result was that complete success which never failed to crown the attentions of Desault. In the other patient a considerable swelling made its appearance the day after the accident. On the third day a numbness and partial loss of the power of motion occurred in the arm of the affected side. Soon afterwards an insensibility came on, and by the seventh day, the paralysis of the arm was complete. It was not till after a tedious treatment, an account of which would be foreign from my present subject, that the limb recovered in part its original strength.
From whatever cause the fracture of the clavicle in this latter patient was prevented, it is evident, that the whole of the force employed to produce the fracture in the other, acted here on the brachial plexus, and gave rise, by means of concussion, to the accidents which followed.
10. The axillary artery, though running near to the clavicle, in common with the brachial nerves, experiences, notwithstanding, less frequently than they do, injurious effects from the fracture of this bone. I know not of any instance where a puncture from the broken ends of the clavicle has produced in this artery a false aneurism. To conclude, like all other fractures, that of which we are now treating, may be connected with wounds, splinters, &c. But in general, as Hippocrates remarks, the fracture of the clavicle assumes in common cases a mild aspect.
§ V.
11. Most of the symptoms formerly mentioned (5 and 6) as accompanying a fracture of the clavicle, are evidently the result of a displacement of its broken ends. Yet this phenomenon, taken notice of by all authors, and considered by them as a necessary effect of the disease, does not occur in every case (8). There are instances, in cases of transverse fractures, where the extremity attached to the shoulder, has retained its natural position. Three examples of this kind occurred in the Hotel-Dieu in the course of the year 1787.
12. Instances have also been known, in which the sternal fragment, when fractured obliquely upwards, has supported the end of the humeral in such a manner as to prevent any derangement. Desault was accustomed to relate several cases, where similar occurrences took place; but, in general, this state of things is rare, in comparison with that in which the fragments lose their natural level.
Almost always, then, there is more or less of a perceptible overlapping (chevauchement) produced, either, by the elevation (a circumstance which is very rare) of the external fragment over the internal; or, (as commonly occurs) by the depression of the former beneath the latter.
13. Of the first of these modes of displacement (a mode but rarely mentioned by authors) a few examples are to be found among the observations of Desault, one of which he has recorded in his journal. Hippocrates speaks of the phenomenon as a thing that was familiar to him.
14. The second kind of displacement, that which we constantly find in practice, and which the laws of muscular action render almost inevitable, takes place in such a manner that the shoulder appears to obey the impulse of two powers, one of which draws it downwards, and along with it the external fragment of the clavicle, which is displaced by this power in the direction of its transverse diameter, or thickness. The other power approximates the shoulder to the breast, and draws it forward, carrying along with it the same fragment, which is by this means displaced in a longitudinal direction.
That we may the better understand them and their effects, let us, in our minds, separate these two powers, although they are perfectly simultaneous in their action. A knowledge of them will lead us to a knowledge of the resistances which ought to be opposed to them. But let us first remark, that the humeral fragment, being drawn downward and inward, takes sometimes such a direction, that its internal extremity passes backward under the sternal fragment, its external end continuing to point forward: this disposition can be understood from its natural direction.
15. The first of these powers, namely, that which depresses the point of the shoulder, appears to have escaped the notice of the ancient physicians of Greece, who attributed the apparent depression of this part, to the elevation of the sternal fragment, and, accordingly, endeavoured by making compression on the latter, to restore it to a level with the other. Hippocrates, more judicious than those who had preceded him, demonstrated that their doctrine, false in its principles, was still more dangerous in its consequences, and that the sternal fragment being immoveable, lost its relative position with respect to the humeral, only because the latter was depressed by the weight of the arm. This doctrine of the father of physic is satisfactorily proved, by a comparison of the sound shoulder with the diseased one, and has since been admitted by all practitioners. Indeed, the mere recollection that one of the uses of the clavicle is to support the shoulder at that level necessary for the performance of its functions, is alone sufficient to convince us, that, in case of its ceasing to fulfil that office, the shoulder must obey the laws of its own gravity, increased by that of the hand and arm.
16. The illustrious Petit, and with him Duverney, in acknowledging this cause of displacement, have added to it as another the action of the deltoid muscle on the external end of the bone; in this action, the end of the clavicle is the moveable point, while the humerus affords the fixed point. But how can we admit this cause, when the humeral fragment, in passing under the sternal, moves in a backward direction? So far is the deltoid muscle from drawing the bone downward, that here the bone rather draws the muscle in part backward, and yet, in such a case, the displacement is as perceptible as in any other. Besides, when the sternal fragment, broken obliquely upwards, supports the humeral and prevents a displacement, why does not the deltoid produce this displacement?
It is then in the weight of the arm and shoulder alone, that we must look for the passive power, which depresses them, and which produces a displacement in the direction of the transverse diameter or thickness of the clavicle.
17. A second power, highly active, co-operates with this. I allude to the permanent contraction of the muscles, that extend from the breast to the clavicle and shoulder: from this cause arises the displacement in the longitudinal direction of the bone.
The pectoralis major, the pectoralis minor, the subclavius, the serratus major, and the trapezius, unite their efforts in producing this displacement. These muscles are, in certain respects, antagonists to each other, but they all unite in drawing the shoulder forward and inward. None of them appears to act with more effect than the pectoralis major. To this, in particular, is to be attributed the displacement in a forward direction.
Except in the instances stated above, the action of the muscles is not immediate. They act only secondarily on the external fragment, which, being stedfastly attached to the scapula and humerus, is obedient to the motions impressed by the muscles on these two bones; motions which, in a sound state, the clavicle has a power of controlling.
18. To the weight of the lower extremity (15 and 16), and the spontaneous action of the muscles (17) must be added, as another cause of displacement, the motions which are communicated to the arm by external bodies, and which, being imparted ultimately to the clavicle, derange the fragments, by separating them, approximating them, or making them overlap each other, according to the direction in which they act.
19. When a fracture occurs at the extremity next the shoulder, no displacement of the fragments in general takes place. This circumstance is attributed to the action of the trapezius, which draws each fragment upwards with equal force. However this may be, it is doubtless to such cases that we must refer the complete cures, obtained without any retentive apparatus, by Gasparetti, Brown, and other writers. Hence also, without doubt, arise the difficulties experienced by certain practitioners, such as Duverney, with respect to the diagnosis of this disease. These fractures may be mistaken for fractures of the acromion, being situated so immediately in its vicinity.
§ VI.
20. On looking into the causes of that displacement (15...18), so common in fractures of the clavicle, it appears that in almost every case, the external extremity of the humeral fragment is drawn, by a double power, downward, inward, and forward. Hence it follows, 1st. That the resistance opposed to this power, by the means used for the purpose of reduction, and the retentive apparatus subsequently employed, ought to be directed upward, backward, and outward, these directions being the reverse of those in which the powers of displacement act: 2dly. That, in as much as these powers, viz. the weight of the parts and the action of the muscles, are in constant operation, and, besides, as the motions of the arm are continually disturbing the fragments of the bone, the apparatus ought to be equally constant in its action, and should keep up, without any remission, the effect produced, at first, by the means of reduction. This principle is applicable to every case, and ought to be the standard of comparison, for determining the advantages or disadvantages of different bandages, and processes for the reduction of fractures of the clavicle.
21. But we are not to suppose, that these processes have heretofore manifested an exact application of this rule. Hippocrates directed to press the arm close to the ribs, and at the same time to push it upwards, in such a manner, as to make the shoulder appear as sharp and pointed as possible. Hence his precept, to lay the patient down on his back, the back being supported by some projecting body, and then to press the shoulders backward; hence again, when the humeral fragment is drawn inward, his advice to press the elbow close to the breast. This twofold expedient was attended with great difficulties, even under the direction of the father of medicine. Celsus only copied Hippocrates, adding nothing whatever to his mode of practice. Paul of Egina, more judicious in this case, conceived, that for the purpose of forcing the shoulder outward, and rendering it, agreeably to the idea of Hippocrates, very projecting and sharp, it would be advisable to place the fulcrum or point of support, not in the middle of the back, but under the arm-pit. A woollen ball was employed by him for this purpose, a practice which would, at once, have carried the art near to perfection, if, after being employed to reduce the fragments, this process had been continued for the purpose of retaining them in apposition.
22. No new method distinguished the surgery of the Arabians. It is necessary to come down to the time of Guy of Chauliac, before we meet with the method which is almost universally adopted at present, and which consists in placing between the shoulders, the knee of an assistant, whose hands are to be employed in drawing them forcibly backwards. But it is evident that this is only doing, while the patient is in an erect position, what Hippocrates did, after having laid him with his back on a projecting body. Here, then, the art seems to have degenerated, after the time of Paul of Egina: and, indeed, on comparing this process with the general principles already established (20), it will be immediately perceived, that the powers of replacement do not here act in an opposite direction to those of displacement.
Hence the difficulties of reduction, the time spent in the operation, and the sufferings by which it was sure to be accompanied. The fragments were brought together, it is true; but it was only by varying the movements, and changing their direction, that the point of contact was ultimately found.
23. Desault conceived, in the year 1768, that to reduce, in the most effectual manner, a fracture of the clavicle, it was necessary not only to push the shoulder backward and upward, as was commonly done, but, above all, to force it outward, and that the power destined to draw it in this latter direction, ought to act horizontally, according to the course of the clavicle, in the same way, as, in an oblique fracture of the thigh or leg, the extension for replacing the fragments is made in the direction of the bone.
24. As the union of the humerus to the clavicle, by means of the scapula, communicates to the one the movements of the other, it is easy, by placing the ball used by Paul of Egina, under the arm-pit, to convert the arm into a lever of the first kind.2
The lower extremity of the arm being then pressed towards the body, the upper end is separated from it, and becomes, with regard to the clavicle, what the efforts of an assistant who makes the extension, in a fracture of the leg, are to the foot of the patient.
The mode of reduction being established, it was necessary, in the next place, to invent a bandage, calculated to retain the broken ends of the bone in contact. Desault thought it practicable to unite these two points of treatment, in the same process, that is to say, to reduce, and at the same time to retain the fracture. Here the art is indebted to him for an improvement, which, I will venture to say, carries it near to perfection. To judge of this, it will be necessary only to take a hasty survey of the different kinds of apparatus proposed by different writers.
§ VII.
25. Here all authors seem to have been directed by the same principle. This is to keep the shoulder of the affected side, 1st, drawn forcibly backwards, 2dly, approximated towards the shoulder of the sound side. Such was the practice of the Greek physicians, whom we have seen in common with Hippocrates, Celsus, and Paul of Egina, employing a kind of bandage, varied in its form, according to the displacement it was intended to remedy.
Above all others, we find an application of this principle, in the figure of 8 bandage, a particular form, which was employed in practice by Albulasis, an Arabian, and afterwards by his countrymen, as well as by Lanfranc, Guy of Chauliac, and their contemporaries. The use of this bandage was continued by Pare and his successors, and has been lately modified by several authors, such as Heister, Petit, Brunninghausen, &c.
26. But under whatever form it shows itself, its action is always the same, and always insufficient. On comparing its effect with the general principle, on which every apparatus for the clavicle should be constructed (20), we perceive, that it by no means answers the threefold indication, of retaining the shoulder backward, outward, and upward.
27. In relation to carrying the shoulder backward it loses half of its effect, because, its force being decomposed (so to speak) by the obliquity of its direction, is divided into two channels. One of these runs parallel to the shoulder and acts to no purpose, while the other, being perpendicular to it, is alone effective; hence it must act with a force equal to 10, in order to produce an effect equal to 5.
28. The indication, to draw the humeral fragment outward, far from being fulfilled, is here diametrically counteracted. The scapula, being approximated to that of the opposite side, draws the humeral fragment towards the trunk, making it underlap the internal one, and, in this respect, the figure of 8 bandage acts posteriorly in precisely the same manner, during the treatment, that the contractions of the muscles did anteriorly before the reduction.
29. Should the shoulder be supported, at such an elevation, as might have a constant tendency to destroy the influence of its own gravity? this is evidently prevented by the very oblique direction of the turns of the bandage. Suspending the arm in a sling, is the only way, in which that end can be attained. But does this mode always possess sufficient firmness and stability? The arm, not being here sufficiently fixed, may be constantly in motion, which, by deranging its situation, must communicate very troublesome and injurious movements to the fragments of the clavicle. One of the principal faults of all bandages consists, in not preventing these movements, by restraining the movements of the arm.
To the other disadvantages of this mode, need I add that of its making, by the turns of the bandage, an undue compression on the projecting edges of the arm-pit, and producing thereon troublesome and painful excoriations?
30. From the want of a mutual correspondence and fitness between the indications already enumerated (20), and the manner in which the figure of 8 bandage acts, it is evident that the former can never be satisfactorily fulfilled by the latter. Hence we may judge, what improvement the art has received from the iron cross of Heister, the compress of Petit, drawn transversely over the oblique turns of the bandage, the waistcoat which Brasdor fastened round the thorax of his patients, and the leathern apparatus, lately proposed by a German practitioner. These means, though diversified in their form, are similar in their effect, and, being nothing but modifications of the figure of 8 bandage, possess, like it, the radical fault of not offering a resistance directly opposed to the two-fold power, arising from the muscular action and the gravitation of the shoulder.
As to what remains, it will be sufficient to show the insufficiency of the process of reduction (22), by means of the knee placed between the shoulders, in order to demonstrate the existence of a like insufficiency in all those forms of apparatus, which, as Brasdor remarks, have for their object a continuance, during the treatment, of the effect produced by that process.
31. On the other hand, those indications will be fulfilled with exactness, by such a form of apparatus as will render permanent the action of the means of reduction which were employed by Paul of Egina, by certain Arabian physicians, and by Pare; which have been renewed by Desault, and tend to draw the shoulder upward, backward, and outward (23 and 24).
Pecceti appears, in the last century, to have had a faint view of the proper indication on this subject, when, under the article of fractures, he advises the ball to be suffered to remain under the arm during the treatment of the injury. But the figure of 8 bandage, united to this expedient, counterbalances its effect, rendering it of no avail, and Pecceti was therefore no more successful than others, in obtaining a cure of the fracture, unaccompanied by deformity.
32. An overlapping more or less perceptible never failed to accompany the consolidation or knitting of the bone, and here, as in many other cases, practitioners laboured to explain what they knew not how to prevent. The impracticability of surrounding the part, as in other fractures, with a circular bandage, appeared to Heister, Petit, and Duverney, to be the cause of this deformity. They supposed that to be a superabundant callus, which was nothing but a displacement of the fragments. These visionary hypotheses ceased to exist, as soon as this displacement was prevented by a proper apparatus.
Desault sought for this form of apparatus, as well as for his other bandages, in the multiplied application of means already known, without inventing new ones. Bandages and compresses, easy to be procured, and already rendered familiar to surgeons by daily use, served him for the construction of his apparatus, for which several machines had been already proposed.
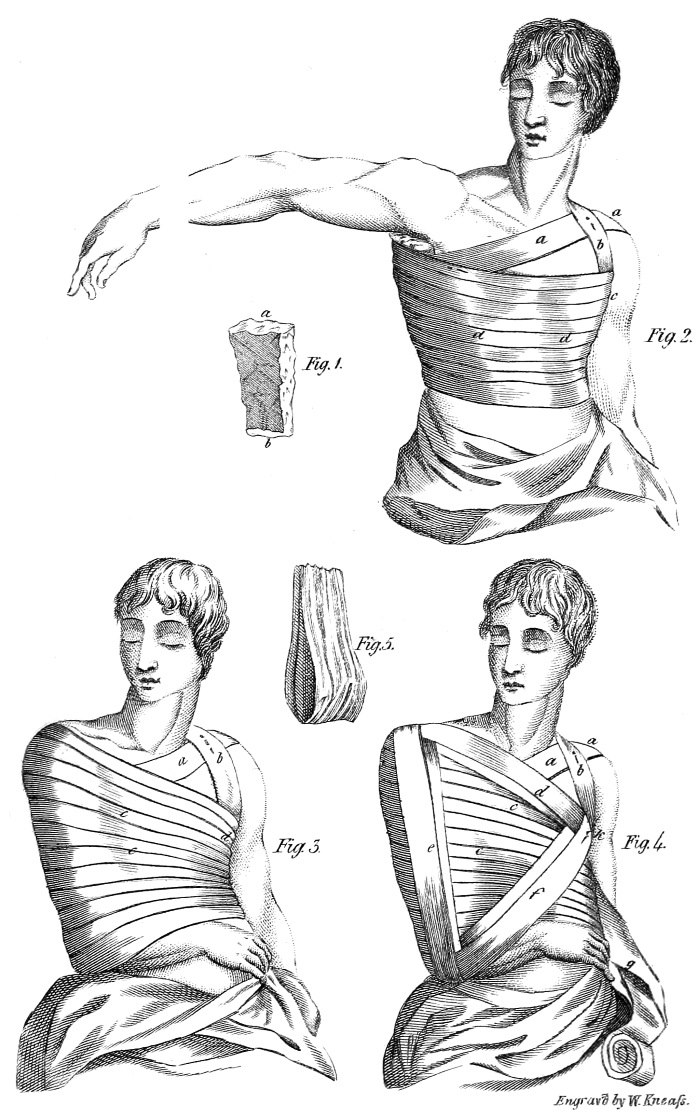
33. The pieces of which this apparatus is composed, are,
1st. Three rollers, three inches broad; the two first, six, and the other eight, ells long, each one rolled up separately.
2dly. A bolster or pad (a, b, Fig. 1), made in the form of a wedge, out of pieces of old linen. Its length should be equal to that of the humerus, its breadth four or five inches, and its thickness at the base (a), about three inches.
3dly. Two or three long compresses.
4thly. A small sling for the arm, (Fig. 5).
5thly. A piece of linen large enough to cover the whole bandage.
Every thing being properly arranged, the following is the mode of applying the apparatus, which of itself reduces the fracture.
34. The patient being placed in a standing position, or, if his case render that impracticable, on a seat without a back, an assistant elevates the arm of the affected side, and supports it at nearly a right angle with the body (Fig. 2), while the surgeon places under the arm-pit the head of the bolster, which descends along the side of the thorax, and which another assistant, situated at the patient’s sound side, holds by the two upper corners.
35. The surgeon now takes one of the first rollers, applies the end of it on the middle of the bolster, fixes it there by two circular turns round the body, and passes a turn obliquely (a a) along the fore part of the thorax, ascending to the sound shoulder: the roller then descends behind, passes under the arm, and returning in front of the thorax, makes a circular turn and a half, horizontally. Having reached the hind part of the thorax, it reascends obliquely by the cast (b), as it had done before, and passes over, before, and under, the sound shoulder; having thus crossed the turn (a a), the roller again passes across the hind part of the thorax, and finishes by circular turns, which completely cover the bolster. A pin is now to be fixed in the place of crossing of the roller on the sound shoulder, to prevent the turn (a) from slipping downward.
The application of this first roller is intended for no other purpose, than firmly to fix the bolster which is held up by the two oblique turns before and behind, and secured against the body, by the subsequent circular turns.
36. The bolster being fixed, the surgeon applying one hand to its external surface, pushes it upwards, and, with the other, taking hold of the elbow, after having half-bent the fore arm, lowers the arm, till it is laid along the bolster. He then presses its lower extremity forcibly against the side of the thorax, pushing it upwards at the same time, and directing its upper extremity a little backwards.
The application of the bandage constitutes a part of the process of reduction. The humerus, now converted into a lever of the first kind, is drawn at its upper end from the shoulder, in proportion as its lower end, is approximated to the thorax. The scapulary fragment being drawn along with it, and directed at the same time upward and backward, comes into contact with the sternal fragment, and in an instant the deformity of the part disappears.
37. The arm being thus situated, is given in charge to an assistant, who retains it in the same position in which he received it from the surgeon, by pressing on it with one hand, and with the other supporting the fore arm half bent, and placed horizontally across the breast.
The second roller is next to be applied. The end of this is carried under the arm-pit of the sound side. It is then brought across the breast, over the superior part of the diseased arm, and extends across the thorax behind till it passes under the arm-pit. Two circular turns cover the first. The roller must then ascend to the lower part of the shoulder, by oblique turns (c. c. Fig. 3), each of which must be overlapped by the succeeding one, to the extent of about the third part of its breadth. It is necessary that these turns be applied in such a way, as to bind but very gently above, and to increase in tightness, as they descend nearer to the lower extremity of the humerus.
The use of this second roller is, to supply the place of the hand of the assistant, in pressing the arm against the side of the thorax; its effect evidently is to draw the upper extremity of the arm outwards, and, as it is already directed backwards, to retain it in that position. The compression of the circular turns on the arm, being thus gradually augmented, becomes, on the one hand, more efficacious, because it acts on a greater surface, and on the other, less troublesome, because, being more divided, it is less felt at the lower extremity of the arm, where it bears with most force.
38. A third indication remains still to be fulfilled, namely, to retain the shoulder in its elevated position, and, by that means, to assist in the extension of the fragments, which already has some effect in preventing a depression.
To fulfil this indication, an assistant sustains the elbow in its elevated position, with one hand, and, with the other, supports the patient’s hand before his breast, while the surgeon fills with lint the hollow spaces around the clavicle. He then applies on the clavicle, at the place where it is fractured, the two long compresses, wet with vegeto-mineral water, or some other cooling liquid. Taking now the last roller, he fixes the end of it under the sound shoulder; from thence he brings it obliquely across the breast, over the long compresses, and carries it down behind the shoulder along the posterior part of the arm, till it passes under the elbow. From this point, he again carries it obliquely upwards across the breast to the arm-pit, then across the back, over the compresses, and brings it down again before the shoulder, along the front of the humerus till it again reaches the elbow. From thence the roller again ascends obliquely behind the thorax, passing under the arm-pit, where the first cast of the roller is covered, and from whence it again starts, to run the same course we have just described. This constitutes a second round, which covers in part the first, and forms a kind of double triangle (e, f, d), situated before the breast, and over the circular turns of the other rollers (c. c. Fig. 4). The remaining part of the roller, brought from behind forward, is employed in circular turns over the arm, and round the thorax, for the purpose of preventing the displacement of the first part. To make it the more secure, it is fastened with pins at its different places of crossing.
The sling (Fig. 4) is next passed under the hand, and fastened above to the ascending turns (d), and not to the circular (c c), which the weight of the hand would be likely to draw downward.
39. It is only necessary to examine the course of this third roller, to see, that, united to the sling, it is well calculated to support the external fragment, which the weight of the shoulder has a tendency to depress, on a level with the internal one. It supplies the place of the assistant, who raises the elbow and supports the hand of the patient, in like manner as the second roller performs the office of the assistant, who presses the lower part of the humerus against the side of the thorax.
On the other hand, the circular turns, by which the application of the third roller is finished, being directed from before backward, push in the same direction the arm and shoulder, which have been already carried that way, by the process of reduction, and thus retain them in their proper places.
Hence may be inferred the truth of the proposition, which we have been endeavouring to demonstrate; namely, that the bandage of Desault, constructed according to the general principle formerly established (20), for fractures of the body of the clavicle, is calculated to retain the external extremity of the humeral fragment upward, outward, and backward.
40. The casts of the rollers, thus surrounding the thorax, however well they may be secured, are yet liable to be displaced, particularly when the patient is in bed. This inconvenience may be avoided, by surrounding the whole with a piece of linen, leaving nothing uncovered, but the sound arm, which is at liberty to perform its usual motions.
The arm of the diseased side, being thus fixed in such a manner, as to constitute a whole or entire body with the thorax, follows its movements, without producing any displacement. It is thus, that by the apparatus for a continued extension of the thigh, the fragments of the os femoris, forming an immoveable whole with the pelvis, cannot change their situation, even in following the motions of the trunk.
Hence arises, in fractures of the clavicle, this advantage, that the patient is not obliged to keep his bed, but is able even to attend to his business, during the progress of the cure.
41. I will not dwell on the numerous objections urged by different authors against the bandage which has just been described. What answer, indeed, can be given to those writers, who fancy that they behold the patient in the greatest danger of immediate suffocation; who dread an approaching mortification of the arm of the diseased side; who allege, contrary to the rules of the art, that there is no impression made immediately on the clavicle, but on a neighbouring bone; who, &c. &c.? Twenty times in a year, has experience answered those objections, in the Hotel-Dieu; and there is not a pupil of Desault, who has not, as well in this, as in many other cases, seen that objections, plausible, indeed, when considered in the closet, or at a distance from a sick room, dwindle to nothing at the bed-side of the patient.
42. In those cases (which, as Hippocrates remarks, very rarely occur) where the external fragment projects over the internal one (12), the bandage must be somewhat varied, although the two principal indications, of drawing the shoulder backward and outward, must still, as in other cases, be fulfilled. The only additional circumstance, therefore, necessary to be attended to here, is, not to elevate the shoulder, by pushing it upwards. This may be easily avoided, 1st, by omitting to raise the elbow, when applying the bandage; 2dly, by drawing the third roller a little tighter than usual.3
The fragments, being reduced to the same level, and brought into apposition, by this two-fold attention, will unite as in ordinary cases.
If the fracture exist at the end of the clavicle next to the humerus, the difficulty of their being displaced renders the application of the bandage less necessary. Prudence, however, demands that it be not altogether neglected.
§ VIII.
The regimen to be pursued during the reunion of the clavicle, varies according to circumstances. It is impracticable to lay down general rules, applicable to all affections of this kind. Here, however, much more than in other cases, if the division of the bone be simple, and no unfortunate accident occur, it is always unnecessary to restrain the patient from his usual course of life, beyond the second or third day. But, though internal means are for the most part omitted in the treatment, the apparatus is a subject on which too much attention cannot be bestowed. With whatever degree of exactness it may be at first applied, it will soon become loose, and oppose a diminished resistance to the weight of the shoulder, and the action of the muscles. Hence, unless it be frequently examined, the fragments will be displaced. The following case furnishes a detail of the treatment subsequent to the reduction, to which, in ordinary cases, Desault had recourse.
Case III. Mary Adel, aged thirty, as she was crossing a path covered with ice, in the severe winter of 1788, fell on the point of her left shoulder, and fractured the clavicle about the middle. Being brought to the Hotel-Dieu a few hours after the accident, she was dressed in the manner just described, and, as the fracture was simple, it was judged sufficient to make a slight diminution in the quantity of her aliment, during the two or three first days. The dressing was moistened every morning, with vegeto-mineral water, at the place corresponding to the fracture.
On the fourth day the piece of linen that surrounded the bandage was removed, for the purpose of examining the state of the parts. Every thing was found in its proper situation, and the covering was replaced till the seventh day, when the rollers appeared to be somewhat relaxed. The apparatus was taken off, and reapplied as at first, the compresses being carefully moistened with vegeto-mineral water, at the part lying over the fracture. After the third day the patient was permitted to return to her usual regimen. The third roller being a little deranged on the tenth day, it was taken off, and reapplied as at first, together with the sling. The fragments were examined and found in perfect contact. The patient was up during the whole day, walked about the house, and experienced no other inconvenience than that of not being able to use the left arm.
On the thirteenth day, the bandage was again reapplied, and allowed to remain till the sixteenth, when the patient having disturbed it, it was once more changed. At this period, the fragments, already firmly united, exhibited scarcely a vestige of the division they had sustained.
The reunion was complete by the twentieth day, when all the pieces of apparatus were dispensed with, except the bolster and the second roller, which were also removed two days afterwards, as they were found to be no longer necessary.
The continued inactivity of the limb, during the treatment, had occasioned a stiffness in the shoulder. This was gradually done away by making the patient move her arm in all directions, twice a day, each time, for the space of an hour.
On the twenty-ninth day she left the hospital, carrying with her nothing to remind her of the injury she had sustained. She was free from that uneasiness which is the consequence of a tedious and ill-managed treatment, during which the exercise of the limb has been neglected.
§ IX.
44. We are in possession of but few observations particularly relative to the different complications, that may accompany fractures of the clavicle. The treatment, in such cases, varied according to circumstances, must be accommodated to the indications common to all fractures of this kind.
When splinters, displaced in different directions, whether adhering to the bone or not, irritate the soft parts, and, having passed through the integuments, appear without, most practitioners advise to remove them and cut off such parts as project beyond the fractured end of the bone, previously to reduction. This direction is founded on the severe pains which, in such cases, accompany the common treatment of the injury, and which the figure of 8 bandage always augments, by drawing the shoulder inward, and consequently pressing the soft parts against the projecting parts of the fragment, or the points of the splinters. But if the splinters, adhering as yet to each other and to the bone, by means of the periosteum, have not assumed the nature of foreign bodies, (that is, if they be not actually dead) it is always proper to replace them. It is here only that we meet with an occasion for that part of the process, of reduction denominated conformation,4 which is never requisite in other cases.
A fragment which has penetrated the soft parts, but has not been long exposed to the air, disappears, and is replaced by extension, provided it be properly directed. Being retained afterwards in a state of constant extension, it can neither be displaced, nor cause pain by irritating the parts, which is the inevitable result of the figure of 8 bandage.
In cases of this kind, it is useful to protect the shoulder with a small splint, which may support the turns of the bandage, and prevent their pressure on the splinters, or the broken ends, which they might otherwise disturb. These precautions are alike indispensable when the fracture is double.
Case IV. Francis Ricord, twenty-five years of age, was received in the month of July, 1790, into the Hotel-Dieu of Paris. On the preceding day, a piece of timber having fallen from a considerable height on his right shoulder, had broken the clavicle of that side into several pieces. Severe pains, which occurred at the moment of the accident, had continued throughout the night, and were still sensibly felt. The slightest motion of the part augmented them to such a degree, as to extort from the patient piercing cries.
The point of the shoulder being very much depressed, was also drawn perceptibly forward and inward; and a large echymosis, without any external wound, occupied its whole extent.
Desault being satisfied that the several fragments were all connected together, and that none of them was separated from the periosteum, placed, as in ordinary cases, the bolster under the arm, completed the reduction, and applied a splint along the course of the clavicle, after having, with his hands, brought the fractured pieces into contact. Confident, then, that the form of the part was perfectly restored, he applied the bandage, which was moistened with vegeto-mineral water, twice or thrice a day.
At the moment of reduction the pains ceased, and were felt no more till the fifth day, when the bandage being a little relaxed, admitted of a slight displacement of the fragments. This displacement was removed, and the pains along with it, by the reapplication of the apparatus.
During the six first days a very strict diet was enjoined. This, however, was dispensed with by degrees, till, on the thirteenth day, the patient returned to his usual regimen. On the seventeenth day, there remained nothing of the echymosis, but a yellow tinge, the customary consequence, of such an accident. The precautions inculcated in the preceding case, were employed also in this, and the patient was discharged perfectly cured, on the forty-second day from the time of his admission. Nor had he experienced, during his treatment, those severe and long continued pains, which, under a different management, so frequently accompany this kind of fracture.
Fig. 1. A bolster made in the form of a wedge, intended to be placed between the arm and the side of the thorax.
a. Its base, which should fit the hollow of the arm-pit.
b. Its summit reversed, against which the elbow is to be applied.
Fig. 2. The first roller applied for the purpose of fixing the bolster against the side of the thorax.
a a. Oblique casts before, passing over the opposite shoulder, in order to hold it up.
b. Oblique casts from behind, crossing the first ones on the shoulder.
d d. Circular casts round the trunk, covering the bolster, which they fix laterally.
Fig. 3. The second roller, applied to fix the arm against the bolster.
a & b. Portions of the oblique casts of the first roller, left uncovered by this one.
c c. Turns of the second roller, covering those of the first, loose above, and tighter below, for the purpose of drawing the superior extremity of the humerus outwards.
d. Their passage over the side opposite to the bolster.
Fig. 4. The third roller intended to keep the point of the shoulder raised.
a a & b. Oblique casts of the first roller, remaining uncovered.
c c. Turns of the second, seen through the opening of those of the third.
d. Oblique casts of the third, ascending from the arm-pit over the shoulder of the diseased side, to descend again behind, along the arm, and pass under the elbow.
f k. A continuation of the preceding casts, reascending under the sound arm-pit, and from thence behind the thorax, over the diseased shoulder.
e. A continuation of the same casts, descending on the fore side of the arm, passing under the elbow, and ascending again under the arm-pit of the sound side.
g. The remainder of the roller, intended to be employed in circular turns, in order to secure the casts e, and prevent them from slipping outward.
Fig. 5. A sling which should be fastened to the oblique cast d (Fig. 4), to support the hand.
§ I.
1. The clavicle, which forms a moveable abutment for the shoulder, and receives and sets bounds to most of the movements of that part, and of the arm, exhibits at its extremities, two articulations, essentially different from each other in their form, dispositions, and uses. These differences give rise to differences equally essential with regard to the dislocations to which they are subject.
2. On the sternal extremity, a small surface, convex from above downwards, and concave from before backwards, is fitted, by means of an intervening cartilage, to a much smaller surface of the sternum, concave and convex in opposite directions.
One capsule, two ligaments, viz. the interclavicular and costo-clavicular ligaments,5 and the anterior portion of the sterno-cleido-mastoideus muscle, strengthen the connexion of these two surfaces, and tend, on one hand, to prevent their luxation, while, on the other, this luxation is favoured and facilitated by the following circumstances: 1st, the disproportion between the dimensions of the two articulating surfaces; 2dly, the mobility of the joint; and 3dly, by this joint’s constituting a kind of centre for the motions of the arm.
3. On the humeral side, an elliptical surface, slightly convex, and inclined downwards, is immediately joined to a corresponding surface of the acromion, elliptical also, a little concave and directed upwards. Hence two kinds of inclined plains, which would be very liable to dislocations, by sliding easily over each other, were they not firmly secured by a capsule, by accessory fibres, by the intersection of those of the deltoid and trapezius muscles, and, above all, by two ligaments, the rhomboid and the conoid.6
Having laid down these preliminary considerations, let us proceed to examine, in particular, each kind of luxation to which the clavicle is subject.
§ II.
4. The sternal articulation of the clavicle experiences different changes, according to the different movements of this bone. If these movements be in a backward direction, the articulating surface is turned forward, straining the anterior part of the capsule, the corresponding ligament, and the extremity of the sterno-cleido-mastoideus muscle. If, on the other hand, they be in a forward direction, the posterior ligament, and the adjacent portion of the capsule are overstretched. In motions directed upwards, the costo-clavicular ligament, and the external and inferior part of the capsule, and in those directed downwards, the inter-clavicular ligament, and the internal portion of the capsule, experience a similar degree of tension.
5. Hence it follows, 1st. That the natural movements of the shoulder may be regarded as predisposing causes of luxation, because at the part where tension is excessive, the ligaments are disposed to give way, and suffer the sternal extremity to escape: 2dly. That the efficient causes will be, all external forces acting on the clavicle in such a way as to increase its motions beyond their natural degree, and beyond the resistance which the ligaments are capable of making. Thus a fall on the point of the shoulder, forcing it suddenly backward and inward, produces a luxation forward. But, in general, as the strength of the articular ligaments is superior to the resistance of the clavicle itself, a fracture takes place more frequently than a luxation, in the proportion of nearly six to one.
Though falls on the point of the shoulder are oftentimes productive of luxation of the clavicle, they are not the exclusive causes of that accident. Desault has seen the sternal extremity forced from its cavity by the knee being pushed violently against the middle of the back, while the shoulders were drawn at the same time backwards.
Case I. A porter dislocated his clavicle in the following manner. He was carrying a very heavy burden, suspended from his shoulders by cords that passed under each arm-pit. Being desirous of resting himself by the way, he placed on a block the burden he carried, which slipping backward, drew his shoulders in the same direction, and at the instant of his attempting to retain it and prevent it from falling, produced a luxation of the clavicle.
7. It follows from what has been said respecting the different states of the articulation, during its various motions (4), that the clavicle is not equally liable to be luxated in every direction. Inclining naturally backward, but a very slight degree of motion in that direction is necessary, to effect a luxation forward. To produce a luxation backward or inward, it is necessary, on the other hand, that the humeral extremity of the bone should make a sweep at least three times the extent of that required in the preceding case. Besides, motions in this direction are accompanied with pain, particularly if they be made by force. Luxation downward is prevented, on the one hand, by the cartilage of the first rib, which presents to the bone an insurmountable barrier. On the other hand, to produce this kind of luxation, it would be necessary for the external extremity of the clavicle to be forced upwards, an occurrence very seldom occasioned by falls. Luxation upward, or over the superior edge of the sternum, must be the effect of a stroke, which, by depressing the point of the shoulder, and forcing it at the same time forward, presses the sternal extremity against the internal and superior part of the capsule, which, being thus lacerated, suffers a luxation to take place. But such a derangement of the articulating surfaces is very rarely produced by falls. Whence it follows, that of the different kinds of luxation of the clavicle, that in a downward direction is altogether impracticable. Those backward and upward, though possible, occur but rarely in practice; while that in a forward direction, on the contrary, is not an unfrequent accident. This tends to confirm the observations of practitioners, and particularly of Desault, whose immense collection on the subject furnishes examples of the last kind of luxation only.
8. In these luxations, there is for the most part, a rupture of the capsular ligament, and an escape of the bone through the opening. But sometimes the ligament is only preternaturally distended, and then the luxation is incomplete.
§ III.
9. But whatever may be the causes or kind of the luxation, its diagnosis is always easy. If it be forward, the direction of the stroke which the shoulder has received, furnishes, at first, some ground of suspicion. The accident is certainly known by the appearance of a hard and unnatural protuberance in front of the sternum, and behind the extremity of the sterno-cleido-mastoideus muscle, by the existence of a sensible depression or hollow at the joint, and by the situation of the shoulder, which is pushed further backward, and is less projecting and more approximated to the trunk, than in its natural state. Add to these, a difficulty in performing motions in a forward direction, which, when somewhat forced, reduce, in proportion as they are accomplished, the size of the protuberance formed by the displaced end. The head is always inclined towards the side where the luxation exists; an attitude which relieves the painful drawing or tension produced in the sterno-mastoideus muscle, by the humeral extremity pushing it forward.
10. A protuberance over the superior edge of the sternum, a difficulty in raising the shoulder, the pain which results from attempting such a motion, the diminution of the protuberance which it occasions, the absence of the sternal extremity from its natural cavity, the approximation of the shoulder to the thorax, and its depression and diminished projection, compared to its usual state, afford evidence of a luxation upwards.
11. A luxation inward or backward, would be characterized by a projection of the shoulder exteriorly, by a difficulty in performing motions in a backward direction, by the alarming effects, which, as Petit remarks, the compression of the trachea would doubtless produce, and by a depression or hollow at the joint, more perceptible here than in the two preceding cases.
12. These appearances will be more or less striking, accordingly as the membranes, lacerated or only distended, offer a greater or less resistance.
§ IV.
13. To reduce a luxation, is, in general, to make the bone re-enter its cavity, by retracing, or returning along, the same route which it followed in escaping from it. Now, in a forward luxation, the displacement is from behind forward, in an upward one from below upward, in an inward or backward one from before backward, but, in each of the three, it is more particularly from without inward. In the first case, therefore it is backward, in the second, forward, in the third downward, but, in each of the three, more particularly outward, that the powers for producing extension must be directed.
14. Hence the method generally employed by most practitioners, recommended by almost every author who has written on the subject, adopted by Petit, Duverney, Heister, &c. and which consists in placing the knee between the shoulders of the patient, as a point of resistance, by the aid of which the shoulders may be drawn backward, fulfils only half of the indication of cure; because at the time that the humeral extremity is drawn backward, it is not directed sufficiently outward.
Hence a difficulty of replacing the bone sometimes occurs, a difficulty always removed, when, pursuant to the method employed by Desault in fractures of the clavicle (see Desault’s method), the arm is made to serve as a lever of the first kind, to carry backward and outward, the head of the bone, which is displaced in the opposite directions, when the luxation is forward. This method possesses the advantage, not only of giving the powers of extension a proper direction, but also of increasing them to a degree even beyond what is necessary for effecting a reduction, by removing them further from the resisting force. Hence it is unnecessary to adopt any particular measures for restoring and preserving the form of the part, as the extension is alone sufficient for that purpose.
These principles, evidently applicable in effecting a reduction, are still more strikingly so in the means destined for retaining it. Let us apply what I have just said, to a case of dislocation in a forward direction. It will be easy to transfer it afterwards to the other kinds of luxation.
§ V.
15. Few luxations are so speedily reduced, but few are more easily displaced again, than that of the clavicle. This disposition is the reverse of that of most other luxations, which are reduced indeed with difficulty, but seldom afterwards suffer a displacement. The cause of this we find, 1st, in the extreme mobility of the clavicle, to which all the motions of the arm are communicated; 2dly, in this further consideration, that most of the muscles, which have their insertion towards the shoulder, tend to draw this bone inward, when the ligaments, in consequence of being either broken or distended, as happens in this accident, do not offer a sufficient resistance.
16. From this two-fold cause of displacement, arises a two-fold indication in the arrangement and application of the apparatus. These are, 1st, to render the clavicle immoveable, by restraining every kind of motion in the shoulder and arm; 2dly, to retain the extremity of the clavicle outward, a direction opposed to that in which it has a tendency to be displaced. But if to those indications we compare the forms of apparatus hitherto used, we will readily perceive that they are insufficient to fulfil them.
17. The figure of 8 bandage, so generally in use, and all the various modifications, under which it has been revived, without being improved, fix the clavicle in the very direction most favourable to a displacement, and even do it in the very manner in which that accident is sometimes brought about; as maybe seen in the history of the case of the porter (6). This bandage does not, under any of its modifications, prevent the motions of the shoulder, because it does not restrain those of the arm, which remains free and unencumbered. Far from constituting an antagonist power to, it even co-operates with, that which has produced the displacement. (For further light on this subject, see what has been already said on the fracture of the clavicle, pages 22 and 25.)
Bell, in condemning the figure of 8 bandage, not so much because of its action being insufficient, as because of its obstructing respiration, proposes, as a substitute for it, a kind of machine analogous to the iron cross of Heister, which, being fixed by straps passing under the arm-pit, and round the neck and body, is intended to retain the parts firm and immoveable. But the motions of the arm not being restrained, nor the action of the muscles of the shoulder opposed by an antagonizing power, places this piece of apparatus in the same class with those, which, from not being devised and constructed on a proper view and conception of the causes of displacement, have no affinity to rational practice.
18. The apparatus for a continued extension, invented by Desault, for fractures of the clavicle, fulfil here all those indications in which the others fail.
By this, 1st. The aim, being firmly fixed against the side, by means of the roller (c c Fig. 3), can communicate no motion either to the shoulder, or the clavicle. 2dly. The shoulder itself, being forcibly drawn outward, with the upper extremity of the humerus, by the action of the kind of lever into which this bone is converted, and to which the bolster (a b Fig. 1) serves as a fulcrum, cannot, by its movements, derange the luxated bone. 3dly. The sternal extremity, being drawn both by the muscles which tend to displace it inwardly, and by the bandage which acts on it in an opposite direction, remains fixed between those two antagonizing forces, which thus destroy each other. Hence the apparatus of Desault, when accurately applied, offers to both of these powers of displacement, a resistance perfectly calculated to combat them.
20. We must, however, admit that this apparatus partakes of one inconvenience, common indeed to all bandages, but which is perhaps more particularly applicable to this in consequence of the numerous casts of the rollers that form it, namely, the great facility with which it becomes relaxed. Hence one cause of displacement, which the most exact and scrupulous attention cannot at all times prevent.
Case. Desault had, for a long time, the care of a patient, whose luxation, having been neglected for four days, was reduced on the fifth, by a surgeon, who, for the purpose of retaining it, employed a bandage of a particular kind. An hour afterwards, a motion of the shoulder backward, displaced the luxated extremity: a new reduction was the consequence; on the day following, another displacement, and so on in succession, for ten days, at the expiration of which, Desault being consulted, applied to the part the bandage formerly described.
On being examined the next day, the apparatus was found in a favourable state. On the day following, a slight displacement rendered necessary a new application of the bandage, which, this time, continued longer than before. But, about the expiration of the third day, the projection of the bone was again considerable. Finally, the patient recovered, with a very perceptible protuberance in front of the sternum, and a difficulty of motion, great at first, but less afterwards, and which exercise succeeded ultimately in removing.
21. The application of the apparatus differs from that intended for a fracture of the clavicle, only in this, that it is of service to place on the luxated extremity, graduated compresses,7 calculated to make pressure backward and outward, and which are to be secured by the turns of the roller (b Fig. 4).
A second precaution, not less essential, is, to push the humeral extremity of the clavicle, a little forward, and fix it in that direction, in order that the sternal being directed backward, may be removed from the place8 through which it has a tendency to escape.
22. Desault almost always obtained complete success by this process, and by the most accurate attention to prevent the relaxation of the bandage. In the mean time, a stiffness, more or less considerable, always remains in the joint for a long time after the reduction, and it is not unfrequently a month or two before the part recovers its usual facility of motion.
The following cases, collected by Brochier, confirm the doctrine for which I have been contending.
Case II. A man luxated the clavicle by falling on the point of his shoulder, and forcing it backward. He was immediately brought to the Hotel-Dieu, where Desault demonstrated to his pupils, that the head of the bone, carried in front of the sternum, was removed nearly an inch from its natural cavity, the ligaments of which were no doubt lacerated.
Here, as in the fracture of the clavicle, the application of the bandage answered the purpose of reduction, and removed the protuberance formed by the extremity of the bone.
The patient, being strong and vigorous, and having received besides a violent contusion, was bled twice, and confined to a low diet. On the following day, no derangement; on the fourth day, a slight displacement of the bone, the rollers a little relaxed, bandage applied anew. Eighth day, no sensible displacement. Eleventh day, some swelling around the joint; compresses, wet with vegeto-mineral water, ordered to be frequently renewed. Twentieth day, the swelling almost gone, and no disposition to a displacement; the apparatus was removed; motions at first difficult, and contracted. Twenty-ninth day, more free and easy. Thirty-fourth day, returned to their natural state.
Case III. Mary Rivert luxated her clavicle, on the seventh day of January 1789. Being brought some time afterwards, to the Hotel-Dieu, she was treated in the same manner as the foregoing patient, and with the same result, except that a very slight protuberance remained at the extremity of the bone, and the confined state of the motions continued a little longer. Desault related, in his lectures, other instances of cures being performed without the least remaining deformity.
After all, even supposing the method just proposed, to possess no other advantage, than that of diminishing the protuberance of the bone, which, under other modes of treatment, is almost inevitable, and by that means preventing the motions of the part from being confined, it would still, without doubt, be a great step towards the perfection of the art.
23. Should a luxation backwards occur, the same process of reduction should be adopted, with this difference, that the extension ought to be made forward and outward; and the same apparatus should be applied for retaining the parts, except that the humeral extremity ought to be directed a little backward, in order that the sternal extremity, being carried forward, may be removed from the place of laceration in the capsule.
In like manner, should the bone be luxated upwards, it would be necessary to draw the arm outwards, and elevate slightly the point of the shoulder, for the purpose of depressing the sternal extremity.
§ V.
24. Luxations of the humeral extremity of the clavicle, take place, according to Petit, in two ways, 1st, under, and 2dly, over the acromion. If we attend to the disposition of the articulating surfaces, the superior of which rests obliquely on the inferior; if we examine, in particular, the relative position of the corocoid apophysis with respect to the clavicle, it will be difficult to conceive how the first kind of luxation can occur, without being accompanied by a fracture. Yet some facts added by Desault to the doctrine of Petit, on this point, seem to demonstrate the possibility of the clavicle sliding under the acromion. As to luxations forward and backward, the mobility of the shoulder, the facility with which it yields to motions impressed on it in these two directions, and the want of a resisting power, make the two bones that compose it, move together, still preserving their relative position.
The luxation upward, then, is that which ought chiefly to occupy the attention of the practitioner. Yet even this is less frequent than the luxation of the sternal extremity, on account of the very great strength of the retaining ligaments, which, when this luxation occurs, must be, if not lacerated, at least very much distended.
§ VI.
25. A fall on the point of the shoulder is the most frequent cause of this luxation. The two articulating surfaces, representing an inclined plain, slide along each other, in such a manner, that that which belongs to the acromion is pushed inward, while that of the clavicle is directed outward. The capsule being stretched, gives way, and then the displacement is manifested by a preternatural protuberance over the acromion; by a stiffness in the motion of the shoulder; by the direction of this part, which is evidently drawn inward and downward; by the inclination of the head of the patient to the side affected; by a bending of the body; and by severe pains in the luxated part. These characters are essentially distinct, and ought to have prevented the error of Galen, who mistook a case of this kind for a luxation of the os humeri downward. Hippocrates and Ambrose Pare have foreseen the possibility of this mistake and even warned young practitioners to be on their guard against it. But, as citizen Sabattier judiciously observes, the position of the head of the humerus, under the arm, in a luxation of that bone, will remove all uncertainty respecting the nature of the injury.
§ VII.
26. The reduction, in this case, is generally attended with but little difficulty. The acromion being drawn outward, by the upper end of the os humeri, which, by means of a fulcrum placed under the armpit, is made to act as a lever of the first kind, is restored, without much trouble, to its natural contact with the corresponding surface of the clavicle. But, it soon becomes deranged again, unless it be retained in its place by a proper apparatus. Now, on what principle ought this apparatus to be constructed? To prevent the displacement, which generally occurs from without inwards, it ought evidently to act from within outwards. Whence it follows, that the rollers in the figure of 8 bandage, recommended in this case by all writers, instead of preventing, actually favour the displacement (17), because they act in the same direction with, and therefore assist, the powers that produce it.
27. Here, in like manner as in the preceding case, the bandage of Desault fulfils with precision the indications of cure, because, by it, the point of the shoulder is, particularly, drawn outward; and if, in certain cases, a slight projection of the humeral extremity still remains, it is to be attributed to the inefficacy of the means of execution, and not to the principles on which they are founded.
§ I.
1. There is no part of the scapula more liable to fractures than the acromion. Being but slightly covered by the soft parts, this insulated kind of appendix has not, in all positions of the humerus, a solid point of support. A strong muscular force oftentimes acts on it with great energy. Being large in front, it presents in that direction a considerable surface to receive the action of external bodies. Whence it follows, that if it is not oftentimes broken, this is to be attributed, not so much to its natural disposition, as to the position which it generally assumes in falls.
2. The fracture, which is almost always transverse, is sometimes at the summit, and sometimes at the base of this apophysis, and is usually produced by a violent shock from a body falling on the shoulder, by a blow received on that part, &c.
3. But in whatever place it occurs, it greatly resembles a fracture of the humeral extremity of the clavicle, of which the acromion appears like a continuation. There is accordingly a strong analogy between the phenomena, the consequences, and the modes of treating these two kinds of fractures.
4. This accident is characterized, 1st, By a severe pain experienced by the patient, at the place of the fracture. This pain is increased by the elevation of the arm, which, generally hangs motionless down along the side. 2dly, If the humerus be removed from the trunk, the hand being at the same time placed on the acromion, the extremity of this apophysis is felt sinking downward, creating thereby an evident depression in the part. 3dly, Generally, the two fragments lose, of their own accord, their relative position; and unless the precaution about to be mentioned be used, their displacement becomes manifest, being produced by the weight of the arm, and the contractions of the deltoid muscle. 4thly, The head is inclined to the affected side.
§ II.
5. Two different processes have been long in use for the reduction of fractures of the acromion. One consists in elevating the arm almost to a right angle with the body, in order, as Heister remarks, to throw the deltoid muscle into a state of relaxation, and then to be able, with the fingers, to place the fragments in their natural situation. In the other mode, the humerus is suffered to retain the position it has assumed, that is, to hang down the side; the surgeon then taking hold of the elbow, pushes it vertically from below upwards, in such a manner, that the head of the bone, pressing against the acromion, elevates and replaces it.
6. Petit seems to have adopted indiscriminately these two methods, one of which, however, is greatly superior to the other. Indeed, it is evident, that if the humerus be removed from the trunk, its head will necessarily sink down in the glenoid cavity. Being thus separated from the fractured apophysis, it leaves beneath it a hollow or vacancy, into which the fragment will be pushed, should it be in any measure, compressed by the casts of the roller, during the application of the bandage.
7. On the other hand, if the arm still fixed against the side, be pushed upwards, it will afford to the acromion a solid point of support, which, during the application of the apparatus, will prevent its displacement downwards. This consideration is unquestionably of moment, during the process of reduction; but ought more particularly, to command the attention of the practitioner, in the choice of means destined to maintain the reduction.
§ III.
8. As the displacement is most likely to occur downwards, particularly in motions of the arm, it is necessary that a continued resistance be opposed to this tendency. But this resistance should be made by the head of the humerus, which, if properly directed, will represent, during the treatment, a kind of splint, which art ought to render fixt and immoveable lest, being contiguous to the divided surfaces, it might derange, by its motions, the work of nature in effecting their reunion. Hence it follows, that the precise and immediate intention of the whole apparatus destined to support fractures of the acromion apophysis, is, 1st, to keep the head of the humerus constantly elevated or pushed upwards: 2dly, carefully to prevent all motions of the arm and shoulder.
9. If the means, heretofore employed in this fracture, be examined, it will be perceived that they by no means fulfil this twofold indication.
A compress placed immediately over the fracture; a roller passed round this to secure it; a ball or bolster9 put into the hand; the fore-arm supported in a sling; such is the apparatus recommended by Petit. In addition to this, Duverney judiciously advises to keep the sling elevated, for the purpose of keeping the head of the humerus applied under the fractured pieces. He employed also the spica-bandage which has been equally recommended by Heister.
10. But, in the employment of these means, the arm, not being confined against the trunk, can move with ease, and derange the fragments, and, therefore, the second indication is not fulfilled. Will even the first be fulfilled? By no means. The sling, being soon deranged, by the movements of the arm, which are oftentimes involuntary, suffers it to sink down again, and then the fragments, being no longer supported, are displaced. Hence the difficulties attending the treatment, difficulties which have not escaped the notice of authors, and which Heister thus expresses: “Nemo ita curari solet, ut brachium postea, liberi sursum attollere queat,” an observation, which the celebrated Cheselden made before him, in describing the scapula.
11. These inconveniences will be avoided, by fixing the arm, as recommended by Desault, firmly against the trunk, by converting, so to speak, the arm and the trunk into one single and solid piece, in such a manner, that the humerus having no other motions but those in common to it and the thorax, may not be able to communicate any others to the fragments, which are supported by its head. This advantage can be easily obtained, by means of the bandage, already described, for fractures of the clavicle, modified agreeably to the circumstances of the case, in which it is to act.
12. A bolster or pad of an equal thickness in all its parts, is placed under the arm. The arm is then to be pressed down on this, in like manner as in the bandage for the clavicle. The fractured apophysis is now to be covered by two compresses; one extending from the clavicle to the spinous processes of the vertebræ, while the other, lying over this, and running in a contrary direction, crosses it at the place of the fracture. The whole is then to be secured by a roller, which, starting from the arm-pit of the sound side, pursues nearly the same course with that destined, in fractures of the clavicle, to retain the shoulder upwards. (See what has been said on this subject, when treating of the structure of the bandage.)
13. By this mean, the two-fold indication of keeping the humerus immoveable, and directed upwards (8), is evidently fulfilled, as I have already proven at full length, when treating of fractures of the clavicle; and a reunion, without deformity, may be looked for, of which we have an instance in the following case, recorded by Derrecagaix.
Case I. Nicholas Gay, aged twenty-nine, was struck, in passing under a decayed building, by a stone, which, having become loosened, fell on the point of his shoulder. In an instant he experienced severe pain, and a difficulty of moving his arm, particularly upwards. Soon afterwards there occurred a swelling of the shoulder, and a large echymosis at the place where the blow was received. The pain, not so acute during a state of rest, was increased by the motions of the arm, and even by leaning the head towards the opposite side, which latter circumstance was, no doubt, owing to the contraction of the trapezius muscle.
A surgeon being called, judged it sufficient to make use of discutient applications, to which the swelling and the echymosis appeared to yield in the course of a few days. On a more accurate examination, a fracture was discovered, supposed to be in the external part of the clavicle, and for which the patient was sent to the Hotel-Dieu.
The fracture was discovered to be in the middle of the acromion, which it divided transversely. The bandage already mentioned (12) was applied, and, from the first day, the patient was left to his usual regimen. Fifth day, a renewal of the apparatus which had become relaxed: seventh day, a fresh displacement, in consequence of an unguarded motion: a fresh application of the bandage, which continued in its place till the sixteenth day, when it was replaced anew: thirty-second day, reunion complete; a stiffness in the motions of the part, which exercise removed by degrees, and of which the patient felt no remains after the forty-eighth day.
§ IV.
14. Next to the acromion, the lower angle of the scapula is that portion of the bone most liable to be fractured. The usual causes of it are, falls on the side, or blows received on the part. It is characterized by a displacement which is always perceptible. On the one hand, the fleshy portion of the serratus-major, which is attached to the inferior fragment, draws it directly forward, while it is drawn upward by the teres-major, and some of the fibres of the latissimus dorsi. On the other hand, the body of the bone itself remains behind, being held by the rhomboid muscles. Hence arises a separation, which renders it difficult to mistake the fracture. Should any doubts still remain, let the shoulder be drawn backwards and the scapula along with it: let the fingers be, at the same time, placed on the lower angle, to ascertain whether or not it follows the motions of the bone; if it does, there is no division: but if, on the contrary, it remains stationary, the existence of the fracture is evident.
§ V.
15. Here, as in all other fractures, the means of reduction must be founded on the causes of displacement. To effect the replacement, therefore, it is necessary, either to push backward and downward, the angle which is displaced in a contrary direction, in order that it may be brought into contact with the body of the bone, or else to draw the body of the bone forward and upward, that it may meet the displaced angle. It is thus, that in a fracture of the condyle, the body of the jaw, is drawn into contact with the fragment.
16. But the first mode of reduction is difficult, and the means of maintaining it impracticable. It is necessary, therefore to have recourse to the second, which is the more easily executed, as the scapula follows the movements of the arm, and as, by drawing this limb forward, and the elbow of it outward, that bone is removed from the spinous processes of the vertebræ, and directed in such a manner, as to be brought into contact with its inferior fragment. This situation possesses another advantage, as it throws into a state of relaxation the muscles which tend to displace the lower fragment.
Hence it follows, 1st, That here, in like manner as in fractures of the clavicle, it is not on the fractured bone, that the force must act, but on the humerus. 2dly, That the humerus ought to be, during the whole treatment, immoveably fixed, because its motions, being communicated to the scapula, must soon derange the contact necessary to a reunion.
18. On these principles were founded the apparatus of Desault, and his process of reduction, which consisted, 1st, in drawing the arm forward, and separating the elbow a little from the thorax; 2dly, in fixing the fore-arm at an angle sufficiently acute, to direct the hand to the point of the opposite shoulder; and 3dly, to bring afterwards into proper apposition and form, the fragments already approximated to each other by the first movements.
19. To retain this reduction, the arm and fore-arm must be permanently fixed in the above position. This object is attained in the following manner, 1st, A bolster in form of a wedge, being placed between the arm and the side, its apex situated in the arm-pit, affords the double advantage of keeping the elbow at a distance from the thorax, and of rendering the position of the arm less fatiguing by serving as a point of support to it. 2dly, Compresses wet with some discutient liquid, are applied on the part corresponding to the fracture. 3dly, The whole is now to be secured by a roller, seven or eight yards long. The first turns of this roller, must secure the hand of the affected side on the sound shoulder to which it had been applied, during the reduction, and running afterwards from before backwards, pass over the place of the fracture, for the purpose of retaining the compresses on it. The wedge-formed bolster is to be secured on the thorax, by circular turns around it. Then, passing under the sound arm-pit, after having made these circular turns, the roller must be brought behind again, conducted obliquely over the shoulder of the diseased side, along the anterior part of the arm, under the elbow, and behind the thorax, where it is carried obliquely, in order to pass again under the sound arm-pit. From this place it ascends again anteriorly over the affected shoulder, redescends along the posterior part of the arm, repasses under the elbow, returns under the arm-pit, and terminates finally in circular turns round the trunk, and arm together. Hence it may be observed, that, in the first turns of the roller, this bandage greatly resembles the third roller applied in the fracture of the clavicle, to retain the point of the shoulder upward and backward (Fig. 4. plate I.)
20. By this, 1st, The movements of the arm being entirely impeded, they cannot have any influence on those of the shoulder; hence, in this respect, the fragments are suffered to remain in contact. 2dly, The serratus-major and teres-major muscles, being kept in a state of habitual relaxation, can no longer draw the inferior fragment forward, which cannot, therefore, be separated from the body of the bone. 3dly, Nor can the body of the bone, being permanently held in this situation, be removed from the fragment; whence, in both respects, a displacement will be effectually prevented. This threefold advantage is not possessed by any of the different kinds of apparatus hitherto proposed, such as the sling and cross-bandage, employed by Petit, which have the fault of suffering the arm to move backward, of allowing the scapula to be easily separated from its insulated angle, of retarding by that means the cure, and even of preventing it entirely, while, by the process just described, it is usually completed by the thirtieth day.
1. The language of the surgeon differs, in this case, from that of the anatomist, and by the expression, “fracture of the neck of the humerus,” is here meant not that of the slight circular depression, which separates the head from the tuberosities of the bone, but rather that of the contracted or diminished portion of the bone, which commences at the tuberosities above, and being continued down the body of the bone, receives at its lower end the insertion of the tendons of the pectoralis major, the latissimus dorsi, and the teres major. Many practitioners consider this neck or contracted portion as extending even to the insertion of the deltoid muscle.
2. Several facts, the truth of which it is difficult to call in question, attest the possibility of a fracture of the neck of the bone, so called in anatomical language. I have myself seen, in the humerus of a young man, aged seventeen years, the head of the bone exactly separated from its body, by a division which had but slightly affected the upper extremity of the tuberosities. But the examples of this nature which occur in the annals of surgery are too few, to enable us to lay down any general principles for the treatment of such fractures.
§ II.
3. The operation of external bodies, active, when they are thrown against the shoulder, passive, when the shoulder, or the arm, is forcibly driven against them, is always the cause of a fracture of the neck of the humerus. From the mechanism of the part, the division is sometimes direct, and sometimes the effect of a counter-stroke.
The first of these arises very generally from a fall on the point of the shoulder, and as in such a case, the commotion or shock must be very great, to extend with sufficient force through the thick mass which forms the deltoid muscle, that muscle sometimes suffers both contusion and an echymosis. Blood may even escape from a rupture of some of the arteries or veins of the joint, and form, as Desault has observed, a collection or tumour which it would be imprudent to open.
The other is the effect of a fall on the elbow, separated, at the time, some distance from the trunk, or on the hand, which, by a natural instinct, is thrown out, together with the arm and fore-arm, in order to break the violence of the fall.
4. The varieties of this kind of fracture originate, 1st, from the spot which it occupies, being either the middle or the lower part, rarely the upper part, of the neck of the humerus: 2dly, from the state of the surrounding soft parts, which sometimes remain quite natural, and at other times become distended and tumefied. This circumstance always involves the diagnosis in more or less uncertainty; 3dly, from the direction of the fracture, which is sometimes transverse, but usually oblique, particularly when produced in the second mode, that is, by a counter-stroke (3); 4thly, from the relative situation of the fragments, which may remain in contact, an occurrence however but very rare, or may separate from one another in a direction inwardly or upward; and, 5thly, from different complications, with which it may be attended.
§ III.
The whole of the signs of a fracture of the neck of the humerus, taken together, characterize its existence in a manner sufficiently evident. But it is not always an easy matter to take a view of them all at once, and in such a case, there are more difficulties attending the diagnosis here, than in any other fracture of the humerus.
An acute pain is felt at the instant of the fall; and sometimes a crack or report is plainly heard. There is always a sudden inability to move the limb, which, being left to itself, hangs motionless. But if any external force act on it, it yields to it without resistance, and may be moved by it with great ease in every direction.
These motions are accompanied with severe pain, and, if carried too far, may give rise to very troublesome affections, as has been observed in patients, where the fracture was mistaken for a luxation.
Beneath the acromion, is discovered a depression, always situated lower down, than that which accompanies the fracture of that apophysis. If one hand be placed on the head of the bone, while the other is employed in moving the lower fragment in different directions, or, while an assistant, engaged in making the necessary extension, communicates to this fragment a rotatory motion, 1st, the head will be perceived to remain motionless; 2dly, the friction of the two divided ends will produce a crepitation more or less perceptible. This twofold sign is always decisive as to the existence of a fracture; but the swelling of the joint may occasionally prevent the practitioner from availing himself of it.
The fragments remain sometimes in contact, without experiencing any displacement, in which case, most of the signs not manifesting themselves, the diagnosis is rendered more difficult. But most frequently a displacement occurs, and then it is the inferior fragment that is deranged, and not the superior one which is so short that it can be but little effected by the action of the muscles.
7. The displacement is in general but slightly perceptible in the longitudinal direction of the bone, unless when, in a very oblique fracture, the fragments present points which irritate the muscles, excite them to contraction, and augment their force; or, when a blow of great violence, continuing to act after the bone is broken, causes the fragments to overlap each other. Thus has the body of the bone been forcibly drawn upwards, or driven in the same direction, till having passed through the deltoid muscle, and the external integuments, it has even risen considerably above the level of its head.
But in general, as Petit observes, the weight of the limb hanging down the side, opposes to the action of the muscles a sufficient degree of resistance; and it is in the direction of the cross-diameter or thickness of the bone, that the displacement most frequently occurs. It is to be observed, that the lower fragment is driven either inward or outward, rarely in any other direction. In the first case, which is by far the most common, the elbow is somewhat removed from the body, and cannot be brought near to it without pain; in the second, which is more rarely met with, it is moved in an opposite direction.
In the one, the contractions of the deltoid muscle and the natural curve of the humerus, in the other, the united action of the pectoralis major, the latissimus dorsi, and the teres-major, appear to have an essential influence on the displacement.
In each case, the displacement is facilitated by the mobility of the lower fragment, and of the shoulder, when an apparatus from being improperly constructed, fails to prevent the movements of the whole extremity.
8. The signs which have just been detailed, do not always furnish such luminous evidence, particularly to an inexperienced practitioner, as to prevent the occurrence of very serious mistakes. Of this Desault related many examples in his lectures.
Case. J. M*** Est*** falling on his elbow, fractured the neck of the humerus. A surgeon was immediately called, who, finding a depression beneath the acromion, a protuberance in the hollow of the arm-pit, and the humerus directed outwards, pronounced, without further examination, that there existed a luxation in a downward direction. Wishing to reduce it immediately, he employed, to no purpose, the common processes. Acute pains were the consequence. The opening in the capsule being too narrow was irritated, and the member subjected to great violence of motion. At length the pains became insupportable; the operators gave over their fruitless efforts, and Desault was called.
He discovered the mistake from the immobility of the head; from the depression beneath the acromion being lower down than in a luxation; and from the existence of a crepitation. A reduction was effected without loss of time; the apparatus was applied, but in the evening a considerable swelling occurred around the arm-pit; soon afterwards inflammation was superadded; a vast collection of matter succeeded, and, notwithstanding the utmost attention, it was five months before the patient was restored to health.
9. To this example, I could add others, where the most serious accidents have resulted from a similar mistake. It must be acknowledged, however, that, if, in a fracture, the displacement be inward and a little forward, the greater part of the signs herein detailed (5) apply equally to a fracture and a luxation: but then, as we have just seen in the preceding case, the immobility of the head, the place of the depression beneath the acromion, and the crepitation, will remove any doubts that may be excited in the mind of the surgeon, by the protuberance in the arm-pit, the direction of the arm, &c. &c.
§ IV.
10. A fracture of the neck of the humerus assumes, in general, a character not very troublesome; and if, as Heister says, “a fracture near the head is worse, and more difficult to be cured,” this is less owing to the nature and seat of the disease, than to the difficulty of keeping the fragments in contact.
Seldom have the reunion of the bone, and the removal of all the disagreeable effects accompanying the accident, required a longer time than is necessary for the cure of other fractures. The numerous examples, which occurred in the Hotel-Dieu, during Desault’s direction of the surgical department, confirm the truth of this assertion, notwithstanding some doubts that may have been raised respecting it, by prejudices formerly entertained, on the subject of fractures in the vicinity of joints.
From twenty-six to thirty days are sufficient for the reunion: this was the term commonly required in the Hotel-Dieu.
11. If judiciously managed, art readily removes all the accidents attendant on this fracture; but, if otherwise, the consequences are apt to prove troublesome. It is here, much more particularly than in other places, that all deformity of the part ought to be prevented; because, the neck of the humerus being near to the centre of the motions of the arm, will very essentially impede those motions if it be not properly reunited. A deformed callus has been known to produce, in the hollow of the arm-pit, a protuberance, which has, in part, prevented abduction, and appeared to keep up an habitual swelling in the limb.
It is, then, from the perfection of the apparatus, and not from the vicinity of the injury to a joint, that the prognosis is to be formed, both as to the consequences, and as to the duration of the fracture. Keep the fragments in exact and regular contact, and there will be no obstacle to that success which seldom forsook Desault.
§ V.
12. The reduction in this case is usually attended with but little difficulty, and the great multiplicity of means hitherto used for that purpose, demonstrate only the barrenness of the art.
Most of the machines destined to reduce the luxation of the humerus, have been applied to this fracture. Thus the ladder,11* the door,† and the club,‡ placed under the arm-pit, served at once the purposes of counter-extension, and conformation, while the powers for producing extension were applied to the elbow, and more rarely to the wrist. Thus Hippocrates recommended a wooden cross, the effect and mode of action of which are nearly the same. These means, in general, besides being insufficient, are liable to a further objection, in consequence of their acting on the edges of the pectoralis major, latissimus dorsi, and teres major, which being thus forced upwards, draw the fragment to which they adhere in the same direction, and thereby constitute an obstacle to the reduction. (See what will be advanced on the subject of luxations of the humerus.)
13. To machines succeeded the use of straps, weights suspended to the limb, &c. These processes were entirely useless, in as much as they were intended only to increase the natural powers of the operator, which are already more than sufficient of themselves. They will, therefore, in a short time, exist only in the history of surgery.
Petit proposed to reduce this fracture, by first raising the arm to a right angle with the body, and then directing one assistant to make the requisite extension, by taking hold of the elbow with his hands, while another grasped the point of the shoulder, for the purpose of counter-extension. This method was attended with the threefold inconvenience, of subjecting the patient to great fatigue and pain, of weakening the extending powers, by bringing them too near to the point required to be moved, and of irritating the muscles that draw the lower fragment upwards, and thus exciting them to contract. Hence the difficulties sometimes attendant on reduction, which is always simple in itself, when, after the trunk is properly fixed, gentle extensions are made by taking hold of the fore-arm in a half-bent state. The following is the mode of reduction practised by Desault.
14. The patient is seated either on a chair or on the side of a bed. The arm is slightly separated from the body, and carried a little forward.
One assistant is directed to fix and secure the trunk in a proper manner. This he does by pulling at the arm of the sound side, taking hold of it near to the hand, and extending it in a direction perpendicular to the axis of the body. This mode of counter-extension is preferable to that commonly employed, which consists in applying the hands to the upper part of the patient’s shoulder. Indeed, on the one hand, the power being farther removed from the resisting force, need not be so great. And, on the other, the body being entirely unencumbered, renders it easy for the surgeon to apply the roller without discontinuing, or in any way disturbing, the extension.
Another assistant makes extension on the fore-arm, which serves him as a lever, where, one hand being placed behind or on the back of the wrist, forms the point of support, (or fulcrum), while the other applied to the anterior and middle part of the fore arm, on which it makes pressure from above downward, represents the power; the fragments to be brought into contact constitute the resistance.
The relaxation of the muscles produced by this semi-flexion of the fore-arm, and the slight separation of the arm from the trunk, greatly favour this mode of extension; a mode recommended by the ancients, adhered to by the English, and which possesses the advantage of leaving uncovered all that portion of the limb on which the apparatus is to be applied, and by that means of allowing the hands of the assistant to keep the same position during the whole time of the application.
A small degree of force, judiciously directed according as the displacement is inward or outward, is sufficient to effect the reduction, which even takes place of its own accord, under this process. If the surgeon lays his hands on the place of fracture, it is rather to examine the state of the fragments, than to assist in bringing them into apposition.
§ VI.
16. All kinds of apparatus for fractures, being nothing but resistances opposed by art, to the powers which produce displacement, it follows, that they should all act in directions precisely opposed to the directions of those powers. But, we have seen (7), that, in the present case, these powers are, 1st, the action of external bodies, favoured by the extreme mobility of the arm and shoulder; 2dly, the action of the latissimus dorsi, the pectoralis major, and the teres major, which carry the inferior fragment inward, or, what is more common, of the deltoid muscle, which draws it outward; 3dly, the contractions of the muscles of the arm, which have a slight tendency to draw the same fragment upwards.
17. Therefore, 1st, to render the arm and shoulder immoveable; 2dly, to carry the upper end of the lower fragment outward or inward, according to the direction in which it is displaced; and, 3dly, to draw this fragment downward, are the three indications that ought to be fulfilled by every bandage intended for a fracture of the neck of the humerus. The last merits less attention than the other two, because, as already observed, the weight of the limb alone is nearly sufficient to answer it.
18. Let us inquire, whether or not the kinds of apparatus, hitherto employed, have been adequate to the fulfilment of these indications.
The ancients, in obedience to the precept of Hippocrates, fixed the arm against the breast, and confined it there by a bandage recommended by Celsus, and constantly employed by Paul of Egina. “Præstat antem, says he, brachium, ad thoracem moderate deligare, ut ne, si id commoveatur, figuram avertat.” Pare still preserved this process, which the moderns have now entirely abandoned, and which, taken alone, could properly fulfil only the first indication. The second indication was less happily fulfilled, by a kind of bandage added to the first, by Celsus, Paul of Egina, and the Arabians, the necessary effect of which was, to force the lower fragment outwards. It is surprising that Heister and Lamotte should have confined themselves to the use of this for the retention of the fragments.
What shall we say of the eighteen-tailed bandage exclusively adopted by Petit and Duverney? The arm, not being fixed by it, was liable to be moved, and the fragments to be displaced by the least shock. There was nothing to prevent the lower fragment from obeying the powers tending to carry it either inward or outward. Indeed the bandage was of no avail whatever in giving support to a fracture, as was observed by Louis, in his “Dissertation on Petit’s Diseases of the Bones.”
Suppose the arm, as some have advised, to be supported only by a sling. Not one of the indications just established (17) could by such means be fulfilled.
Perhaps the bolster of tow proposed by Moscatti, would have surpassed all these means, in the advantages it offered, had it not, by leaving the arm moveable below, and the shoulder above, still favoured a displacement.
Le Dran has also advised the use of a bolster composed of that of Moscatti, and bole Armenian. It fixed the arm more firmly against the trunk and in this respect, certainly approached nearer to the attainment of the object in view.
19. It is obvious, from this comparison between the indications of cure (17), and the means hitherto employed for the fulfilment of them (18), that nothing satisfactory had yet been done, and that a proper apparatus was still a desideratum. The success experienced by Desault, in the use of that which we are about to describe, has perhaps proven, that this desideratum exists no longer.
20. The pieces which compose it, are, 1st, Two rollers, the one from five to six, and the other from eight to ten yards long, each one about three inches wide: 2dly, Three strong splints, of different lengths, each about two inches broad: 3dly, A small bolster made of linen, from three to four inches thick, at one end, tapering like a wedge to the other, and of a sufficient length to reach from the arm-pit to the elbow; 4thly, A sling for the purpose of supporting the fore-arm; 5thly, A piece of linen to surround the whole apparatus.
Every thing being properly arranged, the reduction, effected in the manner already stated (14), and the assistants still continuing the extension:
1st, The surgeon takes the first roller, wet with vegeto-mineral water, fixes one end of it by two circular turns on the upper part of the fore-arm, and carries it up along the arm by oblique turns, moderately tight, and overlapping each other about two-thirds of their breadth. Having reached the upper part of the limb, he makes some reversed turns to prevent the wrinkles that would be caused by the unevenness that occurs in this place. He then passes two casts of the roller under the opposite arm-pit, and bringing the ball to the top of the shoulder again, gives it into the hand of an assistant.
2dly, The first splint is then placed before, and reaches from the fold of the arm, to a level with the acromion. The second on the outside, reaching from the external condyle to the same level. The third behind, reaching from the olecranon to the fold of the arm-pit. The bolster placed between the arm and the thorax is a substitute for a fourth splint, which is by that rendered unnecessary. An assistant now secures them, by grasping them with his hand towards the curvature of the elbow, so as not to hinder the application of the remaining part of the bandage.
3dly, The surgeon takes hold of the roller again, descends by oblique and reversed turns along the splints, which he fixes by binding them moderately tight, and terminates the bandage at the upper part of the fore-arm, where he had commenced.
4. The assistants still continuing the extension, the surgeon places the bolster between the arm and the trunk, taking care that the thick end be uppermost, if the displacement be in an inward direction, but lowermost, if it be in an outward one, as is most commonly the case (7). The bolster is to be fastened at top by two pins to a cast of the roller.
5. The arm is now pressed towards the trunk, and fixed against the bolster, by means of the second roller. This roller is applied like that which, in fractures of the clavicle, fastens down the arm to the bolster, by the oblique turns c. c. (Fig. 3. plate I.), with this difference, that in the present case, the turns ought to be very tight below, and looser above, if the displacement be in an inward direction. But, on the other hand, if it be outwardly, they must be loose below, and tight above.
6. The fore-arm is now to be suspended in a sling, and the whole apparatus afterwards surrounded by a piece of linen, which, by protecting the casts of the roller from friction, prevents them from being disturbed.
21. If we now compare the action of this apparatus with the indications of cure formerly laid down (17), it will be easy to perceive, that, by it, they are extremely well fulfilled. Indeed, the arm, being firmly fixed against the trunk, cannot move, otherwise than by motions common to it and the trunk, and nothing can derange the lower fragment, which is equally immoveable. Nor can the shoulder communicate any motion to the superior fragment. The bolster being differently disposed, according to the direction in which the lower fragment is displaced, will serve to move it in an opposite direction.
Should this fragment be forced inwards, the thick head of the bolster will separate it to a distance from the thorax. It will be maintained in this state of separation, by the casts of the roller, which, being very tight below, will act on it as on a lever of the first kind, of which the bolster, forms the fulcrum, while the resistance to be overcome is the action of the latissimus dorsi, the pectoralis major and the teres major. The casts of the roller, by pressing the elbow to the body, will draw the fractured end of the bone in a contrary direction; and, in this respect, the bandage may be considered as an artificial muscle, forming a perfect antagonist to the natural ones.
22. If the displacement be in an external direction, as most commonly occurs (7), a contrary effect must be produced, as well by the pressure made by the bandage, on the upper extremity of the displaced fragment, as by the situation of the elbow which is directed outwards by means of the thick end of the bolster being placed lowermost. The external splint will also prevent the displacement outwards, as well by opposing to the bone a mechanical resistance, as in compressing the deltoid muscle, which is the principal cause of the displacement. The derangement of the lower fragment forward and backward, will be prevented by the two splints before and behind.
The displacement longitudinally, already checked by the weight of the limb, will be still further prevented, by the compression made on the muscles of the arm, which are the instruments of displacement, by the splints and the bandage.
23. To the advantage of keeping the fragments exactly in place, this apparatus unites that of not confining the patient, who is not obliged to keep his bed, and to whom a lying position is even, in general, more troublesome and injurious than an erect one. This observation applies to the treatment of fractures of the clavicle, of the scapula, and even of the fore-arm, when no accident has rendered them complicated.
Desault has cured several patients, but more particularly two, who, being obliged to travel daily, did not, except on the day of the accident, deviate in any measure from their usual mode of life.
An inexperienced surgeon sometimes applies the rollers too tight, in which case, a swelling of the fore-arm is the consequence. This is remedied by relaxing the bandage; but if, notwithstanding this, the swelling still continues, it will be necessary to extend the bandage from the hand to the shoulder.
§ VII.
24. The pain ceases as soon as the apparatus is applied, because the fragments, now brought into perfect contact, cease to irritate the surrounding parts. Nor does it return during the treatment, as they are firmly retained, and not suffered again to separate.
It is rare that any serious accident follows this fracture, and, among the numerous examples met with by Desault, he has scarcely ever had one such to encounter: yet he generally paid but little attention to those internal means which are usually combined with external ones. In most cases, the patients pursued the regimen to which they had been accustomed.
In cases, where a considerable swelling attacked the upper part of the joint, a circumstance which occasionally occurs in practice, one or two bleedings, a diet more or less strict, and the use of diluent drinks, constituted the internal treatment. Of this the following case, related by Brochier, furnishes a detail.
Case II. Maria Catharine Bardelle, aged forty-five, of a high complexion, fell, as she was carrying a heavy load, on the elbow of the right side, the arm being extended a little from the body. The neck of the humerus was fractured, and all the usual signs combined in pointing out the nature of the accident.
A surgeon was immediately called, who mistaking it for a luxation, made useless attempts to reduce it, tormented the patient for half an hour, and then left her to be sent to the Hotel-Dieu.
Desault discovered it at first sight to be a fracture, and foreseeing the consequences of the improper steps that had been taken, ordered blood-letting, and a low diet, after having effected the reduction, and applied the apparatus already described (20).
In the evening, a considerable swelling appeared around the articulation; the pains continued; a diluting drink composed of dog-grass and oxymel was prescribed. Second day, the swelling is gaining ground; pains increased; blood drawn again; diet and drink continued; apparatus is frequently wet with vegeto-mineral water, particularly at the upper part. Third day, a little better; pains diminished, swelling checked; weak soup is allowed. Fourth day, a diminution of the swelling; pains almost gone. Sixth day, the swelling has almost disappeared; light food; bandage, having become loosened, is reapplied.
Tenth day, tongue foul; nausea; want of appetite; symptoms of a bilious diathesis. Bitter drink is prescribed; the day following, a grain of tartar emetic is given in solution.
Thirteenth day, the patient is in her ordinary state; the apparatus is renewed. Twenty-fourth day, the reunion is evidently advancing. Thirty-second day, the consolidation is complete.
The patient now began to perform gentle motions with the limb, which she gradually increased, till about the fortieth day, when she was perfectly well, and free in all her motions.
25. I will here repeat an observation, already made, on the subject of the bandage for the clavicle, of which this is nothing else than a modification. In a short time the bolster sinking downward, the bandage becoming relaxed, and the splints less tight, do not effectually oppose a displacement, unless the bandage be daily examined, and reapplied, when it seems to act too feebly. There are many surgeons, who have not been fortunate in retaining the fragments with exactness, because, trusting too far to the action of the bandage, they have for a long time neglected to examine it; this remark is applicable to every apparatus composed of rollers.
26. Here, much more than in other cases, it is all-important that the limb be accustomed to motion, after the process of consolidation. Situated near to the joint, the fracture always leaves some stiffness in it, which time no doubt wears away, but which will sooner disappear under the above treatment.
§ VIII.
27. Complicated fractures of the neck of the humerus are to be classed with all other accidents of a similar nature, and it would be difficult here to lay down such general rules as would be applicable to every case. The practitioner must be always governed by circumstances. The necessity of the case sometimes urges him to the adoption of daring measures, which, in developing the resources of the art, do honour to the talents of him who exercises it. Of this the following case is a proof.
Case III. Pierre Lena, aged fifteen, as he was at work on a scaffold, forty feet from the ground, fell from that height on the corner of a stone. He experienced instantly such severe pains, that he was unable to rise. He was carried to the house of a surgeon, who, believing that he had suffered a luxation, made fruitless attempts to reduce it, produced in the part an enormous swelling, augmented his pains, and all to no purpose.
The patient was carried to the Hospital of Charity, where Desault at the time was surgeon in chief. A fracture of the neck of the humerus was discovered, through the tumefaction and echymosis, which had overspread the whole shoulder. A suitable bandage was applied.
A few days afterwards, a manifest fluctuation, an evidence of an effusion of blood, disclosed the necessity of making an opening. This was accordingly done, and the fingers being introduced into the part, several large splinters were discovered, and a sharp-pointed bone, the end of the lower fragment, pricking the deltoid muscle, and occasioning, no doubt, the pains which had hitherto continued without intermission.
The indication was evident. To give vent to all the splinters, and cut off the point of the bone, or to amputate the limb, was the only alternative that was left. Most of the practitioners that were consulted were in favour of the last measure. But Desault ventured to repose a hope in the first, the successful issue of which would be the certain preservation of the limb. He performed the operation as follows.
A large incision made in the posterior, and one still larger in the anterior part of the arm, enabled him to remove with ease all the splinters. Then taking hold of the pointed extremity of the inferior fragment, he drew it through the anterior opening, and cut it off with a saw and a pair of cutting forceps. He then replaced it with his fingers, and fixing the head of the bone in its proper position, applied an apparatus somewhat similar to that intended for the retention of fractures.
A suppuration taking place, the patient was dressed every day. Several abscesses were formed during the course of the treatment; each time the pus was discharged by means of an incision.
At the end of four months, the bone was perceived to be in a state of necrosis. The dressings were regularly continued; but the patient, becoming tired of his residence in the hospital, left it, being able to move without difficulty, and having, in the upper part of his arm, a deep fistula, from whence there was a constant escape of ichorous matter, and through which several splinters were discharged, in the space of six months which he passed at his own house.
About the expiration of this period he returned to the Hospital of Charity. Desault had, in the mean time, left this institution to take charge of the Hotel-Dieu. Amputation was proposed to the patient as his only resource. He refused to comply, and went to Desault, who, examining the state of the parts, found an irregular callus formed, which he removed, together with a portion of the soft parts corresponding to the fracture. At the end of two months and a half, the patient was discharged perfectly cured, except a weakness in the limb, which disqualified him for hard labour.
28. This case may throw considerable light on the difficult question relative to amputations at the joint. But this is not the place to state the ideas of Desault on that point of practice.
I will only observe, that in many cases of gun-shot wounds, a similar treatment would probably save life, without exposing the wounded to the dangers of an operation, in which so considerable a portion of the system cannot be removed with impunity, and would secure to them a limb, for the preservation of which they ought not to shrink from the pains and hazards of a tedious treatment. To sacrifice a part for the preservation of the whole, is the last resource of the art. It is necessary, before resolving on this, to exhaust those previous ones that might restore the whole of our organs to life and their proper functions.
1. Fractures of the humerus, accompanied with a separation of the condyls, appear to have escaped the notice of most authors who have written on diseases of the bones. The ancients have transmitted nothing to us on this point. Petit, Duverney, and Bell, among the moderns, have made no mention of it. Heister adverts to this fracture of the bone, only to express an unfavourable prognostic respecting it, without determining the mode in which it is to be remedied. Yet it is by no means rare to meet with examples of it in practice. Desault, in particular, has had frequent occasions to observe it.
§ I.
2. These fractures, like those of the condyls of the os femoris, are rarely the effect of a counter-stroke. They are almost always produced by the immediate action of external bodies; such, for instance, as a fall on the joint of the arm; the wheel of a carriage passing over this part, &c. &c.
3. Whatever may be their cause, they generally occur in such a manner, that a longitudinal division separates the condyls from each other, and, extending upwards to a greater or less distance, is terminated by another transverse or oblique division, which passes through the whole thickness of the body of the bone, so that there are three fragments, and two fractures.
4. Sometimes the division is simple; in which case, being directed outwards or inwards, it crosses the lower end of the humerus, obliquely from above downwards, and terminating at the joint, separates but one of the condyls from the body of the bone, leaving the other adhering to it.
5. In the first case (3), there is more deformity at the broken extremity of the humerus; and the mobility is also greater. If the fingers, placed before or behind, press on the limb in the direction of the longitudinal fracture, the two condyls will be separated from each other, the one yielding in an outward, and the other in an inward direction, leaving a fissure or opening between them. The part at the same time expands in breadth. Thus, the two condyls of the os femoris, are seen to separate from each other when in a similar fracture, pressure is made on the rotula. The fore-arm is almost constantly in a state of pronation. When we take hold of one of the condyls in each hand, and endeavour to make them move in opposite directions, they can be brought alternately forward or backward: and, if their surfaces touch, a manifest crepitation is heard.
6. In the second case (4), the condyls cannot be so easily separated from each other; but it is always practicable by taking hold of that one which is divided from the body of the bone, and moving it from before backward, to produce a crepitation, which is a sufficient proof that a fracture exists. In a case where the external condyl was alone separated, Desault found the limb in a constant state of supination, a position to be attributed, without doubt, to the muscles attached to this condyl.
7. An acute pain, the almost inevitable effect of the flexion or extension of the fore-arm, the habitual semi-flexion of the limb, a tumefaction of it sometimes supervening, and a swelling more or less considerable, around the joint, are symptoms which accompany both modes of division (3 and 4). The fracture may further be rendered complicated by means of wounds, splinters, &c. when the blow has been very severe, or when a pointed fragment has made its way through the surrounding soft parts, &c.
§ II.
8. The preceding assemblage of signs, leaves in general but little doubt on the subject of the diagnosis; but is the establishment of a solid prognosis attended with the same facility?
If authors be consulted, they will be all found to agree, in considering the communication of fractures with a joint as a complication of a very serious nature. A swelling of the adjacent parts, their inflammation, a continuance of the pains after the reduction, extensive abscesses, a gangrene even of the soft parts, and a caries of the bones; such, according to these authors, are the almost inevitable consequences of these kinds of fractures, of which an anchylosis is the most favourable termination that can be expected. Petit, Heister, and Duverney, do not describe the evils that accompany these accidents. Pare, in speaking of them, says, “In such cases, the violence done to the tendons generally gives rise to great inflammation.”
9. From whence can arise these exaggerated fears? Can it be, as is pretended, the mere communication of the fracture with a joint, that is productive of such serious affections? What relation, then, can reason discover between the cause and the effect? Does not experience answer in other cases, in a manner that admits of no reply, when it furnishes us with the analogy of fractures of the rotula, the olecranon, &c.?
Modern researches have entirely abolished the ancient theory of an effusion of callus into the joint, and with it one of the principal causes assigned by writers for the accidents and evils which they so much dreaded.
The admission of air into an articular cavity, would be, without doubt, in such cases, a consideration of more weight; but this does not occur except in fractures accompanied with wounds, and yet all those in the vicinity of joints, whether compound of not, are regarded as extremely dangerous. Besides, observation has oftentimes proven to Desault, that even the contact of air is not so dangerous as it has been commonly supposed, and many instances occurred to him in his practice, where, notwithstanding such a complication, a perfect cure was obtained.
10. It is, then, to the want of a skilful mode of treatment, and to the irritation experienced in the parts, in consequence of an ill-constructed apparatus being applied to them, that the accidents formerly mentioned (8) ought to be attributed. Such accidents never occurred to Desault, in any of the numerous cases that fell under his care. It is thus that in the fracture of the neck of the os femoris, the insufficiency of the means, is oftentimes productive of unfavourable results.
§ III.
11. The displacement here is, in general, inconsiderable, because, being drawn in contrary directions, by the muscles of the arm and fore-arm, the condyls separated from the bone remain stationary between these two forces. A fall, a percussion, or some other external cause, can alone produce a displacement, by communicating some degree of motion to the fragments. Now, from what was formerly said (5 & 6), the condyls may, under such an impulse, move either forward or backward, or else may separate from each other, leaving between them an intermediate void. Hence the apparatus ought to oppose to them a resistance in these four directions, namely, inward, outward, forward, and backward; a resistance which it will be easy to make, by means of four splints, placed in these directions, and properly retained by a roller. The two lateral splints, are particularly necessary, when the condyls are both separated from the body of the bone, and divided from each other (3). If one of them be still attached to the humerus (4), a splint on that side becomes less useful.
12. It is needless for the apparatus to extend as high up as in a fracture of the arm. What effect, in sustaining the fragments, would casts of a roller have, when applied to the body of the bone, above the place of division? Their only advantage would consist in compressing the brachial and triceps muscles, and in that way preventing their action.
On the other hand, the roller must be continued along the fore-arm, in order that the elbow joint may correspond, according to the judicious precept of Paul of Egina, to the middle of the bandage, which is in general more compact and solid, in the middle than in any other part, and also, that a slight compression may be thus made on the muscles attached to the condyls.
13. The pieces which compose the apparatus, are 1st, A roller five or six yards long, and three inches broad, made of soft linen or muslin, and rolled up in a ball. 2dly, Four splints (11), two of them flexible in the middle, in order that they may bend to fit the fold of the arm, and the elbow, and the other two very strong and inflexible, intended to be applied at the two sides.
14. Every thing being arranged, the reduction is effected in the following manner. One assistant is directed to make extension at the upper part of the arm, which he grasps with both his hands; another makes extension on the fore-arm half-bent, which he uses as a lever of the second kind,12 where one of his hands, being placed under the wrist, forms a fulcrum, while the other applied towards the fold of the arm, represents the power. The surgeon, in the mean time brings the condyls together, adjusts their level and apposition, both between themselves, and with the body of the bone, and then proceeds to the application of the apparatus, the limb being still kept in a half-bent position, as was long since recommended in such cases by Paul of Egina. “Si in vicinia cubiti brachium fractum est, etiam ipse cubitus deligandus, angulari figura servata.”
15. The roller (13), wet with vegeto-mineral water, which facilitates its application, and prevents the swelling of the part, is fastened by one of its ends, about two-thirds down the fore-arm, and continued upwards by oblique and reverse casts, to the joint. The surgeon then passes a cast of the roller from the anterior and superior part of the fore-arm, to the posterior and inferior part of the arm (humerus), redescends by an oblique cast from the other side, over the fore-arm, and returning along the first track, makes a number of casts in the form of the figure of 8, round the joint, which he next covers by circular casts, applied so close to each other, as to leave no opening between them; he then proceeds upwards by oblique casts, as at the first, to the middle part of the arm (humerus), when the roller is given into the hand of an assistant.
The first of the splints (13) is now placed anteriorly on the fore-arm and arm, and, if it does not bend, in such a manner, as to accommodate itself to the fold of the arm, the vacant space beneath it is filled up with compresses, laid on top of each other, so as to make its compression uniform throughout. The second, being applied on the posterior side part of the arm, moulds itself to the projection of the elbow, while the other two occupy the sides. These are secured below by an assistant, while the surgeon resuming the roller, which he had just given out of his hand, fixes them firmly by circular casts descending along the arm and fore-arm.
The limb is then laid on a pillow, so disposed that the hand may be raised higher than the elbow, in order to prevent the subsequent swelling, which is oftentimes produced by the fracture, as has been already mentioned (7).
16. The effect of this bandage is simple, and has a particular relation to those directions and causes, in and by which, displacements might occur. The two lateral splints prevent the separation of the condyls from each other; the anterior and posterior ones prevent them from moving backward or forward; the muscles are compressed; the motion of the joint is prevented; and, in common, no great length of time is necessary for the reunion of the bone.
As soon as this is accomplished, it is of importance to move the limb in every direction, to prevent that stiffness, which is so commonly the consequence of fractures situated in the neighbourhood of joints. The following case, drawn up by Le-geulle, will furnish the reader with a detailed account of the treatment pursued, in such accidents, by Desault.
Case I. Joseph Kisler, an ostler, aged forty-one, fell from a height of thirty feet, on the left side, his arm being undermost, and fractured the lower end of the humerus. A surgeon gave him immediate assistance, and, at the expiration of two days, he was carried to the Hotel-Dieu.
From the signs formerly mentioned (5 and 7), Desault discovered a fracture, consisting in a separation of the condyls from each other, by a longitudinal division, and from the body of the bone, by a transverse one. The usual apparatus (16) was applied, and, from a state of extreme anguish, which he had till now suffered, the patient experienced immediate relief.
In the mean time, a considerable swelling around the joint, pointed out the necessity of blood-letting, a low diet, and other antiphlogistic remedies. These were immediately had recourse to, and the limb was placed in the proper position (16).
Notwithstanding these precautions, the tumefaction and redness were increased on the following day. The bandage was applied anew, and wet from time to time with vegeto-mineral water.
On the following days, pain less severe, the bandage kept constantly wet with the same fluid.
Eighth day, the swelling almost gone; the apparatus, being loosened, was again reapplied.
Fifteenth day, the fragments, being examined, were found in regular contact, and already united by a substance of considerable firmness; the strictness of regimen gradually relaxed; solid food taken in small quantity.
Nothing new till the twenty-second day, when the splints were laid aside, having become useless, in consequence of the rapid progress of reunion: from this time till the completion of the cure, nothing was used but the simple roller.
On the twenty-fourth day, gentle flexion and extension of the arm and fore-arm were for a short time performed; these movements were attended with acute pain, notwithstanding which, the fortitude of the patient enabled him to persevere in them.
Thirtieth day, no pain accompanies the movements of the arm: the range of these movements visibly increased; the roller laid aside; from this time the range of motion increases rapidly.
On the thirty-seventh day, the patient was discharged perfectly cured, and free from every vestige of his disease, except a trifling stiffness, which was doubtless soon removed by the motions of the joint.
17. When wounds, splinters, or severe contusions, render these kinds of fractures more complicated, an inflammation occurring on the articular surfaces, may cause them to unite together, and by that means give rise to an anchylosis. But this accident, inevitable in such a case, according to writers, does not always occur, provided nature be assisted, by a judicious mode of treatment, in her attempt to reunite the broken bone. Desault has established this truth, in many instances. Here, as in other joints, he has oftentimes obtained a complete cure, without the loss of motion, although the part had sustained the greatest violence. Incisions, easily made, the extraction of splinters, a frequent renewal of dressings, a most vigilant care to prevent all jarring of the limb, and consequently all derangement of the contact of the fragments, an assemblage or combination of those minute attentions, which art cannot teach, which genius suggests, and which characterize the true surgeon; a precaution (not to be dispensed with) to make the limb perform motions, gentle at first, but gradually increased afterwards, when the adhesion of the parts has acquired sufficient solidity to admit of it; such are, in general, the steps and circumstances constituting the bases of that treatment, requisite in these complicated fractures, which, like all others, appear, in each case, to assume a new aspect, and to present different indications.
Case II. A person, carrying a heavy burden, fell with his elbow on a sharp corner of a bar of iron. The external condyl was broken, being separated from the body of the bone, by an oblique division running into the joint. Anteriorly, a large contusion; posteriorly, a transverse wound; on the outside, the end of the condyl projecting through the soft parts, which it had lacerated: such were the complications of a fracture, for which the patient was admitted into the Hotel-Dieu, on the seventh day of January, 1794.
On examining the state of the parts, Desault discovered, in the transverse wound, two splinters which when extracted, gave vent to an effusion of blood. He reduced, instead of cutting it off, as authors have advised, the end of the separated condyl, applied a bandage of strips,13 and, to prevent accidents, ordered a strict diet, copious blood-letting, and diluting drinks.
Compresses wet with vegeto-mineral water, kept the apparatus constantly moist.
On the day following, the dressing was renewed superficially; severe pains in the part; abated towards evening; almost gone next day; low diet continued.
Fourth day, pains returned; an incipient swelling around the joint; more blood drawn.
Sixth day, considerably better; all the apparatus renewed; suppuration beginning to appear.
Tenth day, a small abscess on the external condyl opened, and a splinter extracted posteriorly.
Fifteenth day, the parts assume a flattering aspect; suppuration favourable; fragments in contact; from this time the dressings are less frequent.
Twentieth day, a bilious diathesis; edges of the wounds livid; loss of appetite; nausea; vomiting; an emetic is administered.
Thirtieth day, unfavourable appearances gone; reunion commencing; wounds visibly healing. Fortieth day, all external injuries healed, except the one situated anteriorly; callus already very firm; gentle motions performed with the limb, which is still surrounded by the apparatus.
Forty-seventh day, the apparatus become useless; motions gradually increased; articulation already tolerably free. Fifty-seventh day, bilious diathesis returned; low diet and evacuants. Sixty-fifth day, the patient discharged from the hospital; consolidation perfect; wounds entirely healed; motions of extension still difficult to be performed in their full extent, but are recovered in a great measure, and will doubtless, in a short time, be completely re-established, provided the same mode of treatment be continued.
§ I.
1. Nature, who, according to the wants of different species of animals, has varied the number of their articulations, knows also how to vary their structure, according to the uses of the different parts of their bodies. With great mobility, she has sometimes connected great solidity and strength, as is the case in the vertebral column; in other instances, parts very solid and compact, are capable of performing but feeble motions, as the carpus, the tarsus, &c. And, lastly, other parts, again, capable of great motion, possess so little solidity and firmness as to be easily deranged by the action of external bodies. Such, in man, is the articulation of the humerus with the scapula, of the sternum with the clavicle, &c.
2. Hence there exist three classes of articulations, very different from each other. To the last, as enumerated above, belongs, in a particular manner, the history of luxations, and, in this, as the solidity varies, the frequency of dislocations is equally various; no luxation occurs more frequently than that of the humerus; indeed, in a comparative catalogue of accidents of this kind, it alone has, during certain years, occurred oftener, in the Hotel-Dieu, than that of all the other bones, taken collectively.
3. Every thing seems to favour the escape of this bone from its natural cavity. 1st, On the part of the articulating surfaces, a cavity somewhat oval and very shallow, aided by a slight cartilaginous ring, receives a half-spherical head, twice its own diameter from above downwards, and three times as large from before backwards. 2dly, On the part of the ligaments, this articulation is strengthened by only a simple capsule. This capsule is thin and weak on its lower side, a direction in which there is nothing to prevent a luxation, while it is thicker on its upper side, where the acromion and coracoid apophyses, and a strong ligament, present an obstacle almost insurmountable. 3dly, As far as respects the muscles and the motions of the joint, strong and numerous bundles of fibres surrounding the articulating surfaces, communicate to them motions easily performed in every direction, and which, by pushing the head of the humerus against the different parts of the capsule, distend it, predispose it to laceration, and indeed even rupture it, when the quantum of their force is superior to its resistance. 4thly, As far as relates to external bodies, what bone is more exposed to their action than this, particularly among that class of persons, engaged, for a livelihood, in hard labour?
4. Subject to the influence of these different predisposing causes, the humerus would be constantly liable to luxations, did not the scapula, moveable like itself, furnish it, by accompanying its motions, with a point of support, differently disposed, according to the different position of its superior extremity; so that, to this two-fold mobility of the articulating surfaces, is to be attributed, in a great measure, the stability of their connexion.
§ II.
5. The upper articulation of the humerus, though predisposed, in general, to luxations, is not equally so in every direction. There is a point at which luxation cannot take place. There are others, where, though possible, this accident has never been observed. It is necessary, therefore, before examining the mechanism of this luxation, to mention with precision, the directions in which it may occur. On this point, writers have differed in a very singular manner. Sometimes, to express the same thing, they have used a different language; and, at other times, have, by the same words, expressed things widely different. Always agreeing as to certain modes of dislocation, they have been divided as to others; while, in the midst of those contrarieties, the surgeon being embarrassed, is at a loss on what ground to found his practice.
6. The ancients, knowing but little of the natural relation of the parts surrounding the joint, were ignorant of the accidental ones, which these several parts assume, in the case now under our consideration. Hence, without doubt, arises the confusion, of their opinions on the subject.
Many admitted of four kinds of luxations; a great number acknowledged only three; some subscribed to but two; while others believed in the possibility of none but one.
7. The first divided differently the directions in which the bone might be luxated. Some contended for luxations upward, downward, forward, and backward; and such was the opinion of the first Greek physicians, predecessors to the father of medicine, who has transmitted the opinion to us accompanied with a demonstration of its fallacy. Others have divided them into those that take place downward, upward, outward, and forward. This division is adopted by Galen, who yet produces only an example of a forward luxation, and does not give us to understand what he means by a luxation upward and inward.
8. The second distinguished the modes of this luxation, sometimes into downward, forward, and backward; as was the case with Oribazes; at other times, into downward, outward, and inward, according to the opinion of Paul of Egina, who, no doubt, adopted exactly the preceding division, expressing it only in different words; sometimes into downward, forward, and upward; such was the sentiment of Albucasis, who, notwithstanding, considered a luxation upward, as a very difficult, and very rare occurrence.
9. The third were of opinion, that, in undergoing a displacement, the head of the humerus could be carried only downward, under the arm-pit, which is the most common direction, or forward, a course which it takes more rarely. Celsus is almost the only writer who has contended for this division. “Humerus, says he, modo in alam excidit, modo in partem priorem.”
10. Lastly, The fourth believe, with Hippocrates, in none but a displacement downwards, the only one which that physician has met with in his practice. “At vero humerus, inferiorem in partem excidit; aliam in partem excidere non audivi.”
11. The moderns, in borrowing from the ancients their divisions of luxations, did not, like them, determine a priori and in a vague manner, the precise spot and direction of displacement; but ascertained these points by subsequent observation, with more precision, in proportion as a knowledge of anatomy shed light on them. They also paid particular attention to the essential difference between primitive and consecutive luxations.
12. Petit admitted of four kinds of luxations, 1st, downward, on the edge of the scapula: this is a very rare occurrence: 2dly, outward, under the spine of that bone, a kind very difficult to be primitively produced. 3dly, inwards, under the hollow of the armpit. 4thly, forward, between the corocoid apophysis and the clavicle. With this illustrious practitioner, Heister acknowledged four kinds of displacements; but, here again, was a new variety, both in expression, and in meaning. The one says, downward, under the arm-pit, the other forward, under the pectoralis major; the one, backward, under the scapula, the other outward, under its spine. According to Duverney, luxations are never primitively in any other direction than downward; the others being only the subsequent effect of muscular action.
13. In the midst of these very complicated modes of treating a very simple subject, it is necessary, first, in order to acquire definite ideas, to divide luxations of the humerus into primitive, which are the immediate effect of external violence, and consecutive, which succeed the primitive, through the influence of causes which I am about to consider.
Let us suppose four lines to inscribe, in form of a parallelogram, the oval surface of the glenoid cavity, one representing the superior edge, another the inferior, a third the internal, and the fourth the external.
14. It is evident that the head of the humerus cannot be displaced towards the superior edge. In that direction, must be encountered, the acromion and corocoid apophyses, the strong ligament passing between them, the tendons of the triceps and supra-spinatus muscles, and the fleshy mass of the deltoid; all which, taken together, constitute an insurmountable obstacle to the escape of the head of the bone upwards. Besides, what power could carry it upwards? In order that this kind of luxation might take place, it would be necessary, that the head of the bone should be carried outwards at the same time, as well as upwards, a circumstance which is impossible, because the trunk prevents the lower extremity (the elbow) from being directed sufficiently inward to produce such an effect.
15. On the contrary, in other directions, but very little resistance is to be met with. Towards the inferior edge of the cavity, the long portion of the triceps; the tendon of the subscapularis, towards the internal edge; and towards the external edge, the tendons of the infra-spinatus, and teres minor, yield with ease to a force directed against them, and permit the occurrence of primitive luxations, downward, inward, and outward. Downward, between the tendon of the long portion of the triceps, and that of the subscapularis; inward, between the subscapulary muscle and fossa;14 and outward, between the fossa infra-spinatus and the muscle of the same name. These modes of displacement are not alike frequent, as will be mentioned presently.
16. Having escaped from its cavity, and being primitively placed in one of these three situations, the head of the humerus oftentimes changes its position. Then, to a primitive luxation downward or inward, succeeds a consecutive or secondary one; but never to a luxation in an outward direction, if such ever occur, because the spine of the scapula forms an obstacle to it.
A secondary luxation inward, may succeed a primitive one downward; there is nothing to oppose the head of the humerus in the course it takes, to enter between the subscapulary muscle and fossa. If, on the other hand, it be disposed to pass to the external side, the tendon of the triceps opposes it; and, notwithstanding what Petit has advanced, there is no secondary luxation in that direction.
17. It sometimes happens, that, having escaped either from the internal part, or from the inferior part of the capsule, the head passes behind the clavicle, and forms there a secondary luxation upwards, as has been observed by Ambrose Pare, and by Gallien, and of which an example or specimen was preserved in the cabinet of Desault. But, here, the secondary displacement must take place in a slow manner, and when it has taken place, art can seldom remove it, on account of the strong adhesions formed by the bony surfaces. Thus, in the example mentioned, there was a new cavity formed behind the clavicle, and the humerus adhered to the surrounding parts by a kind of new ligaments.
18. It appears from what has been said, that the humerus is subject to four different kinds of displacement. 1st, Downward: 2dly, outward, in both of which directions the luxation is always primitive; 3dly, inwards, where it is sometimes primitive, and sometimes consecutive; 4thly, upwards, where it can never be otherwise than consecutive.
The second and fourth are very rare occurrences, and bear so small a proportion to the others, that the latter alone ought to command the attention of the practitioner.
§ III.
19. The causes and the mechanism of luxations of the humerus, vary according as the displacement is primitive or consecutive.
The action of external bodies, directed against the arm, but more particularly falls, where this part strikes forcibly against a resisting body, give rise in general to primitive luxations, and, according as it is differently situated at the time of the fall, the humerus determines, by its position, the different kinds.
20. If it be separated from the trunk, without being carried either before or behind it, if the elbow be elevated, and the fall be on the side, the weight of the body, being almost entirely supported by this bone, pushes its upper extremity downward, distends the inferior part of the capsule, lacerates it, and produces a luxation downward, in which it may even be favoured by the action of the pectoralis major, the latissimus dorsi, and the teres major, as has been judiciously observed by Fabre. In such a case, these muscles, involuntarily contracting to support the trunk, act like the power or force in a lever of the second kind, the resistance to which is formed by the head of the bone, which they draw downward, while the lower extremity of the humerus, resting on the ground, constitutes the fulcrum. Some authors even regard, as an immediate cause of luxation, the powerful contraction of the deltoid muscle, which depresses the head of the bone, and forces it through the lower side of the capsule, a mode of displacement, the existence of which observation incontestibly establishes. The case of a scrivener, so often cited, is well known, who in lifting a book of records luxated his humerus in a downward direction.
21. The mechanism of a primitive luxation inwards, differs a little from the preceding. The elbow, being at once separated from the trunk, and carried backward, the person falls: the weight of the body rests on the humerus; the capsule is lacerated in its fore-part; and a displacement in the same direction supervenes.
22. In a luxation outwards, the elbow is carried forward, towards the opposite shoulder; the capsule being stretched outwardly, gives way in that part, provided the humerus be acted on by a sufficient power. But what can this power be? In a fall, the arm being pushed against the trunk, and stopped by it, cannot carry its motion to a sufficient extent to produce a laceration of the capsule. Hence a luxation outwards must be extremely rare. Indeed no instance of it is to be found in books of surgery. Desault, in particular, never witnessed it. Besides, when in a fall, the arm, separated from the body, is carried backward or forward, the weight of the body acts obliquely on it, and it is but partially subjected to the action of the latissimus dorsi, the pectoralis major, and the teres major. So that no kind of luxation ought from these considerations, to be very frequent, except that in a downward direction, where the influence of both causes is direct. Yet luxation inwards is common enough, and in many instances Desault has observed this primitive mode of displacement, though many modern authors doubt the fact, believing, with Hippocrates, that, primitively, all luxations are downwards.
23. It may so happen that in a primitive luxation, the capsule is only greatly stretched, in which case, the articulating surfaces are but partially displaced; but this membrane more frequently suffers a rupture, through which the head of the bone escapes. To this phenomenon writers, in general, have paid too little attention, notwithstanding the opening of dead bodies has oftentimes demonstrated its existence to practitioners, particularly to Desault, who has given two examples of it modelled in wax; one, of a luxation inward, and the other downward, both found in subjects that died in the Hotel-Dieu. Bell relates some analogous facts, and another English surgeon has also had occasion to meet with them.
24. Oftentimes, in compound fractures, one of the fragments passes through the integuments. In the dislocation of the humerus something similar to this occurs. The capsule is sufficiently lacerated to allow the head to escape; but the opening, being then too narrow, forms around the neck of the bone a noose or kind of collar, which prevents it from re-entering the place which it originally occupied. Thus, in the fractures of which I have just spoken, the aperture in the skin does not, at times, admit of the reduction of the fragment, without a previous dilatation.
In this case, an attempt is made to reduce the luxation: the capsule is pressed in folds against the glenoid cavity, and, interposing itself between it and the head of the humerus, renders fruitless the efforts of the surgeon who would replace the bone. Desault was the first who observed this practical fact, two instances of which are recorded in his journal, and which has frequently since occurred in the Hotel-Dieu. In such a case, the head is in general extremely moveable, because, being entirely without the capsule, there is nothing to impede its motion.
25. When, to a primitive luxation a consecutive one succeeds, several causes may concur in its production. If a second fall happen, the arm, being separated from the body, the head of the humerus having nothing to retain and secure it, obeys, with great facility, the power tending to displace it in that direction, and suffers a fresh removal from the bed which it accidentally occupies.
Case I. A man fell in descending a ladder, and luxated his humerus in a downward direction. Desault being immediately called, discovered the nature of the disease, but deferred the reduction till evening. In the interval, the patient went to get into a chaise: his foot slipped, and he fell a second time. The pains became more severe than at the time of the first accident; and Desault, on his return, instead of finding, as in the morning, the head of the humerus under the hollow of the arm-pit, discovered it to be behind the pectoralis major.
26. Muscular action is one permanent cause of a new displacement. Suppose the humerus luxated downward, the pectoralis major, and the deltoid muscles draw its superior extremity upward and inward, which, offering to their action but a feeble resistance, changes its position and that in a two-fold direction.
27. The different motions of the arm may also, according to their direction, produce the same effect. Thus we have often witnessed a luxation inwards succeeding to a luxation downwards, in consequence of unskilful attempts to reduce it.
§ IV.
28. The diagnosis of luxations of the humerus, presents in general, but few difficulties.
Whatever may be the mode or seat of the displacement, there always exists, as Hippocrates has observed, a manifest depression under the acromion, which exhibits a prominence more perceptible than in its natural state. The motions of the part are almost all accompanied with pain; the greater part of them are impracticable; all of them very much confined. The arm cannot move, without a synchronous motion of the shoulder, because, the articulation being no longer able to exercise its functions, these two parts constitute, so to speak, but one body.
29. Besides these signs, which characterize generally every species of luxation of the humerus, each species is marked by certain others peculiar to itself. If the displacement be downward, the arm is a little longer than in its natural state; it can be moved gently outwards; but an acute pain is the inevitable consequence of moving it forward or backward. The elbow is more or less removed from the axis of the body, by the action of the deltoid, the long portion of the biceps, and the supra-spinatus muscles, which, being unnaturally stretched, contract themselves and tend to carry the bone outward. The pains which result from this position, force the patient, in order to relieve them, to lean towards the affected side, to keep the fore-arm half-bent, the elbow resting on the hip, so that the arm, finding a place of support, may be freed from the painful movements, and from the disagreeable sensation produced by its own weight. From this attitude alone, was Desault in the habit of discovering luxations in a downward direction, and was rarely mistaken in his diagnosis. It is thus, that, in a fracture of the clavicle, the inclined position of the patient is oftentimes, at first sight, characteristic of the nature of his complaint. Beneath the hollow of the arm-pit there always exists a protuberance more or less perceptible, formed by the head of the humerus.
30. To the general signs of luxations of the humerus (28), that in an inward direction adds the following: the elbow, being separated from the trunk of the body, is carried a little backward; the humerus seems to direct itself towards the middle of the clavicle; motions backward are not very painful, while those in a forward direction are extremely so; under the pectoralis major a manifest protuberance exists; the arm is but little longer than in a natural state; the attitude is the same as in the preceding case.
31. Should a luxation in an outward direction occur, it would be particularly characterized by a hard tumour under the spine of the scapula, by the direction of the elbow forward, by its separation from the trunk, and by a little increase in the length of the arm.
A protuberance behind the clavicle, an obvious shortening of the arm, together with its direction, would plainly disclose a luxation upwards.
32. The signs discriminative of the nature of luxations of the humerus, are not always accompanied by the same degree of certainty as those that announce merely its existence. Thus, nothing is more difficult than to determine when a luxation inward is primitive, and when it is consecutive, the same phenomena being common to both. Nothing but an exact history of the disease, stating the order in which the phenomena have succeeded each other, can throw light on this point, which is the more interesting and important, as, according to the one or the other state of things, the processes of reduction ought to vary. In the first case, the head re-enters its natural cavity by a short route; whereas, in the second, it arrives there by a much longer one.
If, as Petit pretended, there exist luxations backward, sometimes primitive, and sometimes consecutive, the same remark may be applied to them with equal propriety.
33. Certain signs, common to luxations of the humerus, fractures of its neck, and dislocations of the scapulary extremity of the clavicle, might here create some uncertainty, if in the one, the absence of a tumour under the arm-pit, and of a depression under the acromion, did not prevent a mistake, which Hippocrates declared to be easily committed, into which, according to Galen, the masters of the art of wrestling fell, and which Pare cautions us to avoid; and if, in the other, the appearances proper to a fracture, did not prevent a mistake which would be serious in its consequences, and which sometimes results from the direction of the humerus, and the kind of protuberance formed in the arm-pit, by the end of the inferior fragment. (See Fracture of the neck of the humerus).
§ V.
34. Luxations of the humerus are but rarely followed by any serious accidents. Sometimes a swelling more or less considerable appears, immediately after the fall, in and around the arm-pit. This is the effect of an increased irritability of the part, and is seldom of long duration. Desault’s remedy for it was the application of compresses wet with vegeto-mineral water, or of cataplasms moistened with the same liquid.
35. Several authors, particularly Bell, speak (as if it were a familiar accident) of an œdematous swelling of the whole upper extremity, caused, in inward luxations, by a compression of the axillary glands. This phenomenon has not often occurred in the Hotel-Dieu, except in luxations of long standing: and when it has been met with in certain cases, very happy effects have been produced, by the action, continued for several days, of a roller applied with considerable tightness after the reduction, and reaching from the fingers to the arm-pit.
Case II. Maria ***, falling from some height, her elbow being separated from her body and directed backwards, luxated her shoulder inwardly. Several days elapsed before she received any surgical aid. She was afterwards admitted into the Hotel-Dieu, where the displacement was discovered through a very considerable swelling, which occupied the parts around the articulation of the humerus. The reduction was accomplished, and the swelling left to itself, which, far however from disappearing, with the cause that produced it, seemed to gain ground. A roller was then applied, and on the day following the tumefaction was reduced to half its former size. The same means are continued. The compression is gradually increased, and by the ninth day, the limb restored to its natural form, performs, as before, all its functions.
36. There is another accident, on which authors have dwelt a little, which was known to Avicenna, and which oftentimes fell under the notice of Desault. I allude to a paralysis of the upper extremity, the effect of compression made by the head of the bone, in inward luxations, on the nerves of the brachial plexus. This accident sometimes resists every expedient of art, as appears from the following case, collected by myself, in the Hotel-Dieu.
Case III. Maria Dougour, fell on her right side, and experienced immediately all the signs of a downward luxation. A surgeon was called, who moved the bone violently in every direction; he made no extension; he kept the patient in torture for an hour; and at the expiration of that time pronounced the luxation irreducible, because the head of the bone, instead of returning into its natural cavity, had moved inwardly. Indeed, in the midst of his unskilful efforts, a consecutive luxation inwards had succeeded to a primitive one downwards.
On the same evening, an evident insensibility occurred in the part. A swelling, joined to a sense of coldness, accompanied it. On the fourth day, the paralysis was complete.
On the tenth day the patient was brought to the Hotel-Dieu, where the processes of art which we shall presently describe, replaced the bone, without removing the effects of its luxation.
To remedy this, irritating means were employed, simple at first, but multiplied and combined afterwards, and pushed so far as to occasion redness accompanied by small blisters. These were continued for three weeks; blistering plasters were applied; all in vain; the paralysis continued, and as long as a year afterwards the patient was still affected with it.
37. This accident is, in general, extremely obstinate, when, as in the preceding case, the nerves have experienced a long continued pressure. Under such circumstances, the most powerful means are often ineffectual. Moxa has been oftentimes used by Desault, which he applied over the clavicle, at the very origin of the brachial plexus. The success, with which he at first applied this remedy, did not always accompany his use of it, so that notwithstanding several cures performed by it, yet, to the majority of patients to whom it was applied, it was wholly useless.
39. But, if the head of the humerus make on the nerves but a momentary pressure, and the reduction be accomplished shortly after the paralytic symptoms occur, oftentimes then the insensibility disappears of itself, and the cure may be always greatly assisted by the application of powerful stimulants; such, for instance, as volatile liniment, composed of oil of almonds and ammonia, which Desault frequently employed, and of which he increased the strength, so as to render it rubefacient.
Case IV. Joanna Saq luxated her arm, by falling on her right side, in the month of July, 1788. In the evening of the same day, all the precursory symptoms of paralysis made their appearance. The affection was complete on the day following.
The patient was brought to the Hotel-Dieu, where the reduction, being accomplished, afforded no relief. On the third day, the paralysis still continuing, the volatile liniment was directed, in the proportion at first of two drachms of ammonia to an ounce of the oil of almonds. This produced no effect. Being increased in strength on the fifth day, it still appeared to be useless. On the eighth it was made of such a degree of strength, as to occasion slight pustules over the whole of the diseased extremity. On this, motion began to return, feeble at first, but increasing by degrees, till by the sixteenth day, it was as free and perfect as in a natural state. During all the time, the liniment was applied twice a day over the arm and fore-arm, which were at the same time subjected to strong friction during the space of half an hour.
39. The pains which accompany luxations of the humerus, claim in general some attention from the practitioner. These have sometimes arisen to such a height, as to produce real disorder in the animal economy, particularly in luxations inwardly, where, resulting, no doubt, from the compression of the axillary nerves, they render immediate reduction more necessary, and are generally removed by it.
§ VII.
40. We may throw into two classes the numerous means, under all their variety of modifications, proposed for the reduction of luxations of the humerus. The one consists in forcing, by some mechanical power, the head of the bone into the cavity from which it had escaped, whether extension has been previously employed or not. The other is confined to disengaging it from the situation, into which it has been accidentally driven, leaving to the action of the muscles the care of its replacement.
In the first of these, art does every thing; in the second, it only gives the proper direction to the powers of nature. These latter give but one course or direction to the action of powers externally applied: in the former, the head of the bone always moves in the diagonal of two powers opposed to each other at an angle more or less acute.
41. A history of the means destined to act in the first mode, would be too tedious to be introduced in this place, would throw no light on the processes about to be proposed, and are detailed at full length in many authors, to which the reader is referred. It will be sufficient to observe, that they all act somewhat in the following manner. Some body, placed under the arm-pit, serves as a fulcrum, on which the arm is made to move like a lever of the first kind, the resistance to which is constituted by the displaced head of the humerus, while the power is applied either at the lower part of this bone, or at the wrist. The extremity of the humerus being directed upwards and inwards, moves its head in the opposite directions, towards the glenoid cavity, where it replaces it with more or less facility.
In this manner acted that machine so celebrated among the ancients and moderns, under the name of “Ambi Hippocratis,” whether it was employed in the precise form described by that prince of physicians, or with the additions and corrections, infinitely varied, which it has received from Paul of Egina, Ambrose Pare, Duverney, Freke, &c. By this, a double motion is communicated to the head of the humerus, which is, at the same time, directed, 1st, in the course above mentioned; and, 2dly, in such a manner, as to disengage it from the unnatural situation which it occupies.
42. Extension by the arm produces, in common, the second effect, and this is made in different modes. Sometimes the weight of the body on one side, and pulling by the luxated limb on the other, serve to produce it; and such was the mode of action of the ladder, the door, and the club, described in the treatise on fractures by Hippocrates, and revived in many modern works. At other times, the body was immoveably fixed, and a powerful extension made by the arm. This was the mode in which the machines of Oribasus operated, and also one of the methods formerly consecrated in the public places where the athletæ held their combats.
43. On some occasions, no extension is perceptibly made, but at the same time in which the extremity of the humerus is forced outwards by a body placed under the arm-pit, the surgeon pushes it upwards into the glenoid cavity: and such were the other modes of reduction practised by the masters in the athletic art. Hence it appears, that the first class of the numerous means, employed for the reduction of luxations, may be divided into those which consist in impulsion, those where mere extension is practised, and those where recourse is not had to either. My object here is not to examine into the inconveniences attending each of these means: a sufficient number of authors have already done this; particularly Petit and Bell. I shall only point out the disadvantages, which, being common to all, ought to induce them all to be excluded from a rational mode of practice.
44. The escape of the head of the bone through the ruptured and lacerated capsule, constitutes essentially the displacement under consideration. But, it is never possible to ascertain with precision the place of this rupture: how, then, can the head of the humerus be directed towards it by an artificial force?
45. However well prepared for the purpose the body may be, which is placed under the arm-pit, to serve as a fulcrum, always a chafing more or less troublesome, and oftentimes distensions and serious lacerations are the consequences of its application, when the body is suspended on it, as in the mode by the door, the club, &c. where Petit has seen a fracture of the neck of the humerus occur, and even a laceration, followed by an aneurism of the axillary artery.
46. Every one has not at his command the different means above mentioned (41 and 42), whence the difficulty of procuring them, or of constructing them, and the loss of time, precious in relation to the reduction, which is almost always easily accomplished in proportion to the expedition used; these charges apply, among many other means, to that machine so complicated, and so well known, under the name of the mitten15 of Petit.
47. Supposing the luxation to be consecutive, how can mechanical means make the head of the bone retrace the route it has pursued in becoming displaced? For example, if to a displacement downwards has succeeded a displacement inwards, it will be necessary for the head to return downwards before it can re-enter its cavity. But, can the direction of the movements be thus varied? This whole apparatus of artificial means, for ever contradictory, oftentimes acts in an inverse direction to that of the muscular action, which is the essential and chief agent in the process of reduction.
Should the luxation take place upwards, the insufficiency of these means must be evident.
48. Perhaps, however, they may be employed with some advantage, when a primitive luxation downwards is quite recent, and the head of the bone is near to its cavity. In such a case the lower edge of the scapula presents to it an inclined plane, along which it can easily glide, when pushed by some external force. It is doubtless to this disposition of the bone to replace itself, that we must attribute the successes, greatly exaggerated, but in part real, on which the inventor of every machine endeavours to found the superior merit of his mode of operating.
But, in this case, it is useless to accumulate artificial forces, where natural ones are sufficient, and where the operator may, with his hands, effect the reduction the more easily, as he can with more accuracy vary the direction of his movements.
49. Thus Desault oftentimes employed a process which was attended with great success, and which, like some of the preceding, ought to be referred to impulsion. The patient being seated on a chair of a moderate height, he took hold of the hand of the affected side, placed it between his knees, and carried it downward and backward, for the purpose of making extension, and disengaging the head of the bone; while an assistant held the trunk with a view to counter-extension, which was sometimes effected to a sufficient degree, by the weight of the body and the efforts of the patient. At the same time the hands of the surgeon, applied to the arm, in such a manner that the fingers of each were in contact with the hollow of the arm-pit, and the thumbs with the external part of the arm, drew upwards and a little outwards the head of the humerus, which in common returned with ease into its natural cavity.
50. Petit mentions this process, not such as it is here described, but complicated with the use of a napkin passed under the arm-pit of the patient, and round the neck of the surgeon, who, by raising his head, drew the displaced extremity upwards. This additional mean, always unnecessary, and not judiciously constructed, is generally ineffectual, because, with it, the operator cannot at pleasure vary his movements. The hands alone are always sufficient, and a vast number of examples attest the efficacy of this method, when employed after the manner of Desault.
Case VI. Nicholas Juan fell on his side, his arm being separated from his body, as he was crossing, in January 1790, the place Notre-Dame, opposite to the Hotel-Dieu. An acute pain was immediately experienced; a protuberance appeared suddenly under the arm-pit; and under the acromion a depression equally sudden. He was lifted up, and carried straight to the Hospital, where Desault was just beginning a clinical lecture. The luxation being manifested by these appearances, was immediately reduced by the foregoing means. A few days rest were enjoined on the patient, but, on the same evening, he proceeded on his way, blaming himself, for having lost half of his day’s journey.
51. In analogous cases of very recent luxations downwards, Desault twice or three times effected the reduction by means still more simple, as the following case, reported by Heraut, testifies.
Case VII. Maria Louisa Favert fell, as she was descending a ladder, and having luxated her arm, was carried at her request, immediately after the accident, to the Hotel-Dieu. Desault perceiving the nature of the disease, placed, under the hollow of the arm-pit, his left hand, to serve as a fulcrum while with his right, applied on the inferior and external part of the arm, he approximated the humerus to the trunk, pushing it at the same time upwards. By this double movement, directed upwards and outwards, the head of the humerus re-entered its cavity without the least resistance. The arm was suspended in a sling for two days, and on the fourth the patient returned to her usual labour.
52. There exists some analogy between this method and one of those mentioned, by Hippocrates, to have been practised in ancient times, in the public games, where the exertions of body exposed those engaged to frequent luxations.
It is not only in luxations downwards, that the first of the simple processes which I have mentioned (49), may be applied. Primitive luxations inwardly, yield sometimes to its use, and the Journal of Surgery furnishes two instances of success in similar cases; one in a female sixty-three years of age, and the other in one of fifty-one, of a strong constitution, and in whom the reduction was effected without resistance.
53. But, in general, these means are ineffectual and it becomes necessary to have recourse to extension, which, when employed alone, forms the second class of means intended for reducing luxations of the humerus. Many writers have adopted this exclusively, though some practitioners, indulging their imagination in the vast field of invention, deserted the common track, and had recourse to various kinds of machinery. Celsus depended on extension alone, in common cases of luxation downward and forward. Albucasis employed no other means, Douey, Douglass, and Heister, among the moderns, reject unconditionally the use of machines, as always useless, and often dangerous. Finally, Dupoui and Fabre, examined and analysed with great exactness the process of extension, and pointed out, in every case, the means of rendering it advantageous, by managing in the best manner the extending forces, and in the luxation of the humerus, in particular, to prevent the inconvenience of straps placed under the arm-pit of the patient, demonstrated the inutility of the movement commonly called conformation. In these respects, surgery stands indebted to them for real advancement, and their doctrine, at this day, very generally known and received, was principally reduced to practice by Desault, who made it the basis of his method of reduction in all fractures and luxations.
54. To proceed to the reduction of a luxation of the humerus, it is necessary to have such a number of assistants as to be able, according to the resistance of the parts, to increase the force intended to overcome it. But two are commonly sufficient. They should furnish themselves with a linen ball, thick enough to project beyond the level of the pectoralis major and the latissimus dorsi, when placed in the axilla, and two straps, one formed of flannel doubled several times, four inches broad, and eight or nine feet long, the other of a napkin regularly folded. This latter is not often absolutely necessary.
Every thing being properly arranged, the patient is seated on a chair of a moderate height, or else laid on a table firmly fixed and covered with a simple mattress, in order that the trunk, by being in a horizontal position, may not prevent the motions communicated to the arm from being directed downwards.
55. Desault continued, for a long time, to place the patient in the first of these positions, which, though employed by practitioners generally, is by no means the most favourable. By adopting it indeed the arm may be very well drawn in a transverse direction; but if, as oftentimes happens, it becomes necessary to direct extension upwards or downwards, the assistant, then, being obliged to elevate himself, or to stoop, cannot, in either of these attitudes, exert his strength to advantage, but is confined and embarrassed, and cannot with ease vary, at the pleasure of the surgeon, the direction in which the arm is drawn.
As far as relates to the patient, that situation in which the body is only in part supported, is much more fatiguing than one where the whole of it reposes equally on a horizontal plain. Perhaps, in relation to the surgeon, it would be more advantageous, in enabling him to accomplish the process of conformation16; but, as will be presently observed, this process is always useless. These considerations induced Desault, in the last years of his practice, to renounce the first position, and have recourse only to the second.
56. The patient being properly situated, under the arm-pit of the affected side is placed the linen ball, on which the middle of the first strap is then applied. The two ends of this strap being now brought obliquely upwards, before and behind the thorax, so as to meet on the top of the sound shoulder, and being held by an assistant, serve to fix the body, and to make counter-extension, nor does the action of the strap bear on the edges of the pectoralis major and latissimus dorsi, in consequence of the ball which projects beyond their edges. Were it not for this, these muscles, being pulled upwards, would draw in the same direction the humerus, to which they are attached, and would thus destroy the effect of the extension, which is made in the following manner.
57. Two assistants take hold of the fore-arm above the wrist, or else a folded napkin is fixed on that part, having its two ends twisted around each other. These ends, thus folded together, are given to one or two assistants, who begin to pull in the direction of the humerus. To this first movement, intended to disengage the head of the bone from the bed which it occupies, another succeeds, which must vary according to the kind of luxation. If the luxation be downwards, the surgeon gradually approximates the arm to the trunk, at the same time that he pushes it gently upwards. By this process, the head of the bone, being drawn from the trunk, and brought towards the glenoid cavity, usually re-enters it with but little resistance.
If the luxation be inwards, the extremity of the humerus, after extension according to the direction of the bone, should be carried upward and forward, in order that its head may be directed backwards. Steps the very reverse of these must be pursued, if a luxation in an outward direction is to be reduced.
58. In general, when, by the first extension, the head of the bone is disengaged, the motion communicated to it by the subsequent ones, ought to be in a direction precisely opposite to that which it pursued in escaping from its cavity. But what are the variations of this direction? Extensive experience alone can clearly determine this point. Without experience the practitioner works in darkness. The minutiæ or particulars of the process of reduction, being different in different cases and according to different circumstances, can be neither foreseen, nor taught by precept.
59. If the head of the bone experience any difficulty in re-entering its cavity, it is necessary, when the extensions have been made, to communicate to the bone different movements, varied according to the different directions of displacement, and regulated by the principle just established. Oftentimes this method effects what extensions alone cannot; and the head of the bone, carried by these movements towards its cavity, enters it while they are performing.
60. If the luxation be consecutive, then the first extension made in the direction of the displaced bone, is intended to bring its head into the place where it was primitively lodged, in order that it may be afterwards acted on as if it were a case of primitive luxation. It is oftentimes only at the moment of reduction, that it is practicable to ascertain to which kind of luxation the accident belongs. Indeed, as in most cases, the reduction takes place of itself when the extensions are well executed, if the head be consecutively drawn inward, it is seen to descend along the internal part of the scapula, till it arrives near to the inferior part of that bone, and then to reascend towards the rupture in the capsule through which it passes into its natural situation.
61. I have said that when the extension is properly made, the reduction takes place almost spontaneously. Indeed whatever may be the kind of primitive luxation, it is evident, that the muscles surrounding the articulation must be stretched on one side, while they are relaxed on the other; whence there will necessarily arise a change both in their contractions, and in the direction of these contractions, and such is the nature of this change, that, in case the muscles act, instead of bringing the head towards the rupture in the capsule, they will draw it in another direction, and by that means produce a consecutive luxation.
62. But, if the extensions render the muscles straight, and restore to them their primitive direction, then, obeying their natural irritability, which is still further increased, by means of the extension, they will draw the head to the rupture in the capsule, and force it to re-enter it, with much more certainty than this can be done by the efforts of the surgeon, who is always ignorant of the precise situation of this rupture. On the other hand, if the extension be not judiciously made how can it restore to the muscles their natural direction? In such a case, the head of the bone will be drawn towards some other part of the capsule than that where the rupture exists, and hence, the difficulties that so frequently occur, in reducing luxations of the humerus.
63. From these circumstances it follows; 1st, that the whole art in the treatment of luxations, consists in giving to the extending powers a proper direction; 2dly, that, in general, the process of conformation is unnecessary and useless; 3dly, that to reduce a luxation is not to replace the head of the bone in its cavity, by force, but to restore the muscles to such a state, as to enable them to replace it. Here, therefore, as in every other case, art is only the minister and handmaid of nature.
There are instances, however, where the muscles cannot act properly in consequence of the long standing or age of the luxation, and in consequence of adhesions, more or less strong, having taken place between the surrounding parts. In such cases it is necessary to employ proper measures to force the head of the bone into its cavity, as it cannot be carried thither by the muscles.
64. Reason concurs with experience, which is on all subjects the best authority, in establishing the truth of this doctrine, respecting the reduction of luxations of the humerus. In this operation, Desault employed, in general, nothing but extensions, varied according to circumstances, until the muscles thrown into a favourable state, were themselves enabled to accomplish the reduction. The most immediate success constantly crowned his practice on this point. This success was, no doubt, owing to his judiciously remaining inactive himself, and suffering the muscles to do the work, after the necessary extensions had been made.
65. When the reduction is accomplished, if the arm, in consequence of being very moveable, appears likely to be displaced again, it is necessary, for a few days, to fix it in such a manner as to prevent all motion; an object which may be effectually attained by Desault’s bandage for fractures of the clavicle.
All writers recommend, for this purpose, the use of the Spica bandage.17 But what service can this render? It does not restrain the motions of the humerus, which, hanging down the side, may move forward, backward, &c. and produce a new displacement; an accident that may be always prevented by the bandage proposed.
§ VIII.
66. I will close this memoir by an examination into some circumstances, which may either prevent reduction or render it difficult, and into certain accidents that sometimes accompany it.
I have said that, on some occasions, the rupture of the capsule, being too narrow to admit the head of the humerus to repass it, and return to its cavity, constitutes one of the principal obstacles to a reduction (24). To enlarge this passage, by further lacerating its edges, is evidently the indication that here presents itself. This is fulfilled by communicating to the bone great motion, either by circumduction, or rotation on its own axis, forcing it suddenly in different directions, particularly in that direction in which the luxation has been produced. Its superior extremity must be, at the same time, pushed forcibly against the ruptured capsule, which, by being thus pressed between two resisting bodies, will suffer a more extensive rupture. Reduction, oftentimes impracticable previously to these violent and varied motions, takes place of itself as soon as they have been properly made. Of this the practice of Desault furnishes many examples.
Case VIII. In the Journal of Surgery are recorded two cases, one by Anthaume, the other by Faucheron, which establish this doctrine.
John Seligni, a robust man, forty-four years of age, fell on the point of his shoulder, on the 19th of July 1791; the pain, which was increased by moving his arm, and the swelling which supervened almost immediately, induced him to enter the Hotel-Dieu. The efforts of assistants were at first insufficient, and it was not till after a uniform extension continued for several minutes, that the head of the humerus was drawn by the muscles against the glenoid cavity. The bone appeared to enter the cavity, although the persons present did not hear the collision or clashing of the articulating surfaces, which is almost always perceived in cases of recent luxation: but immediately the humerus was again displaced, without its being practicable to retain it. On the occurrence of this phenomenon, Desault conceived that the head of the bone had pushed before it the capsular ligament, through which it could not pass, in consequence of the narrowness of the opening which had been made at the time of the luxation. He proceeded to move the arm forcibly in every direction, in order to enlarge the opening, and immediately felt a kind of laceration, which satisfied him that his views were accomplished. He then re-commenced extension, which it was again necessary to continue, as at first, for some time, in order to overcome the resistance of the muscles. The reduction was attended with no further difficulty. The humerus continued still to have a great tendency to be displaced, and it was necessary to employ, for several days, a bandage similar to that for a fractured clavicle.
Case IX. Maria Laurencier, aged sixty, fell on her right elbow, and luxated the humerus of the same side. Eight hours afterwards she came to the Hotel-Dieu, on the eighth of March, 1789. The reduction was attempted in the usual manner; but, although the extensions were properly directed, and the head of the humerus brought against the glenoid cavity, it was still displaced again as soon as the limb was let go, a circumstance which created a suspicion, that the opening of the capsule was too narrow to allow the head of the bone to pass. The assistants ceased making extension, and Desault, taking hold of the lower extremity of the arm, impressed on it great motion, particularly in the direction of the luxation, for the purpose of enlarging the laceration of the capsule. The extensions were now renewed, and the reduction succeeded with great ease.
67. A second obstacle, more difficult to be surmounted in the process of reduction, is that arising from the long continuance of the luxation. The head of the bone, having continued for a long time in the bed into which it has been accidentally thrown, forms adhesions to it; the surrounding cellular membrane becomes thickened, and makes, so to speak, a new capsule for the head, which opposes its replacement, and, when the reduction cannot be accomplished, supplies in some measure the office of the old joint, by the movements which it allows to take place.
Most writers, and Bell in particular, advise, in such a case, never to attempt a reduction, which, being of no avail as to the luxation, might prove dangerous to the patient, in consequence of the violence it would do to the parts. This doctrine was for a time, the doctrine of Desault: but experience, in his latter years, led him to a bolder practice.
68. The complete success which he experienced in luxations of fifteen or twenty day’s standing, encouraged him to make the attempt, at the end of thirty and thirty-five days, and we have, three or four times, during the two last years of his life, seen him successful in replacing, after the expiration of two and a half, and even three months, the head of the bone which had escaped, both through the inferior, and the internal side of the capsule.
However powerful, and however long continued the extensions were, none of those terrible accidents occurred, with which we are threatened by authors. Twice only did a phenomenon occur, which it was difficult to foresee, and of which I will presently speak.
69. In cases of this kind, it is necessary, previously to making extension, to move the bone very forcibly in every direction, in order first to break the adhesions, to tear the condensed cellular membrane, which serves as an accidental capsule, and to produce, so to speak, a second luxation, with a view to make way for a perfect reduction of the first. The straps being then applied, as in ordinary cases, serve the purpose of extension, for the accomplishment of which the number of assistants must be increased.
70. Oftentimes the first efforts are fruitless, and the luxated head remains stationary, amidst the most violent efforts. Let the extensions then be discontinued: renew the forcible motions of the limb: carry the humerus upwards, downwards, forward, and backward: force the resistances to give way; make the arm describe a large arch of a circle round the place which it occupies; let the rotatory motions on its own axis be impressed on it anew; and then recommence the extensions, and let them be made in every direction. By these, the head, already disengaged by means of preceding violent motions, will be brought to a level with the glenoid cavity, and ultimately replaced.
It may not be improper to confirm by experience the truth of these precepts, which might to some appear rash, in consequence of the changes that seem likely to occur in the glenoid cavity, during the absence of the head of the humerus. I will relate, among others, a case reported by Giraud, second surgeon to the Hotel-Dieu.
Case X. Maria Gauthier, thirty-four years of age, entered the Hotel-Dieu, on the twentieth of June, 1790, to be cured of a luxation of three months standing, produced originally by a fall on the arm, which was separated, at the time, from the body and carried backward. Different surgeons had, at different times, attempted the reduction, but always without effect, and when every hope of a cure appeared to have expired, Desault, imboldened by reiterated success, tried whether or not he would be equally fortunate in this case.
The patient being placed in a horizontal position, as already directed (55), great motions were first impressed on the limb: extensions were then commenced, first in the direction of the luxation, and afterwards forward and backward. Vain efforts; the head remains immoveable; new motions are again made in every direction, and afterwards, the extensions are renewed: the same want of success. The patient being fatigued, the reduction was deferred till the day following, when the same trials were, after a short time, attended with complete success. The head being at first disengaged, and afterwards drawn slowly along the track through which it had passed in becoming displaced, at length re-entered the capsule. The arm, being supported by the usual apparatus, soon became œdematous, and, notwithstanding the remedies common in such cases, the swelling continued for two months. The motions performed by the limb in the mean time, restored to it, by degrees, its usual suppleness; and, on the sixty-eighth day after her entrance, the patient was discharged cured.
To this case, I might subjoin many others, and, in particular, that of John Putot, also reported by Giraud, and in which the means just described (69 and 70), succeeded in the reduction of a luxation at the expiration of the fourth month. But too great an accumulation of facts distract the attention, and add nothing to conviction, especially when they are already so plain as those just related.
71. But further, in cases of this kind, where a very old luxation presents great obstacles to reduction, although the attempts made to reduce it, do not actually force the head of the bone into the capsule, still they may not prove entirely useless. By bringing the head nearer to the glenoid cavity, or placing it even on that cavity, and making it form new adhesions there, after having destroyed its old ones, the motions of the limb will be facilitated. For, in cases, where the luxation is not fairly reduced, these motions will be always less impeded, in proportion as the head of the bone occupies a place less remote from its natural situation.
72. A third obstacle, common to the reduction, of every kind of luxation, is the muscular force, increased by the irritation of the displaced bone, beyond its natural degree. So great, at times, is this force, that the head of the bone cannot be moved, even by the strongest efforts. What means should then be employed? 1st, Those which diminish general irritability, such as blood-letting, bathing, a relaxing regimen, &c. 2dly, Those which act locally, in diminishing the irritability of the muscles of the shoulder. For example: the application of emollient cataplasms or fomentations to the part; or, what is still better, a powerful extension, continued for some time. In consequence of such extension, the muscles of the part become fatigued, whence their contractions are succeeded by a state of atony, of which advantage may be taken to replace the bone. Frequently this extension ought to be continued for a very long time; and we have known Desault not to complete the reduction in less than half a day, or even a whole day, the limb being suffered to remain all that time in the apparatus for fractures of the clavicle, which draws the shoulder and muscles outwards. Thus, in fractures of the thigh, where muscular contraction prevents the contact of the fragments, permanent extension previously employed, assists in producing this contact.
§ IX.
73. It is rare that any serious accident follows the reduction of a luxation of the humerus. A swelling, more or less extensive, sometimes shows itself around the joint, particularly when extension has been forcible and long continued; but this, being, in general, easily removed, by means of discutients, does not demand particular attention.
74. Another accident which rarely occurs in practice, respecting which but little is to be found in surgical writings, and with which Desault occasionally met, is, a considerable emphysema, suddenly appearing at the time of reduction. In the midst of those powerful extensions, rendered necessary by the ancient state of the luxation, a tumour suddenly appears under the pectoralis major. By a rapid increase it extends itself towards the hollow of the arm-pit, the whole of which it soon occupies. It then propagates itself in a backward direction, and, in the space of a few minutes, its bulk is sometimes equal to that of the head of an infant. A practitioner, if unacquainted with the nature of this accident, might take it for an aneurism, produced by a sudden rupture of the axillary artery, in consequence of the violence done to that vessel by the extensions of the limb. But, if attention be paid to the resistance of the tumour, to its want of pulsation, to the place of its first appearance, (which is usually under the pectoralis major, and not under the hollow of the arm-pit, to which it only propagates itself afterwards, as Desault has observed in similar cases that fell under his notice), to the action of the pulse still continuing, unless the patient should faint from debility, as happened to the subject of the following case, which we had occasion to witness at the amphitheatre, sometime previous to the death of Desault, and to the colour of the skin which suffers no change; if these circumstances be attended to, it will be difficult not to distinguish one of these accidents from the other. In that now under consideration, discutients applied to the tumour, such, for example, as vegeto-mineral water, and a gentle and regular compression made by the bandage intended to support the arm after reduction, are the most efficacious means that art can employ.
Case XI. Simon Cerisiat, sixty years of age, presented himself on the nineteenth of December, 1794, as the subject of a public consultation, which, every day preceded the clinical lecture of Desault, to receive advice for a luxation inwards, which he had suffered a month and a half before, and for the reduction of which no attempt had been yet made.
Convinced, by the example of luxations more ancient, of the practicability of reducing this, Desault undertook it immediately in the presence of his pupils.
The patient being laid on a table, firmly fixed and covered with a mattress, great motions were impressed on the luxated limb upward, forward, and outward, with a view to destroy the adhesions contracted with the surrounding parts. Extensions were then made in the manner already mentioned (66 and 67).
Nothing was gained by the first attempt, the head remaining immoveable, in the midst of the efforts to displace it. Further motions were made in every direction, to break if possible, the attachments which held it; and these were followed by further extensions.
While these were making in a forcible manner, the head was perceived to approach by degrees towards the glenoid cavity, near to the edge of which it reached in two minutes, and was at length replaced, by a sudden movement of the limb from behind forward.
Scarcely was the reduction accomplished, when a tumour rose suddenly under the pectoralis major, propagated itself towards the arm-pit, and occupied immediately its whole extent.
All the assistants, astonished at the phenomenon, knew not to what circumstance to attribute it. Desault himself, a little embarrassed, thought first of an aneurism suddenly produced by the violence of the extension. The pulse of the patient, being scarcely perceptible in the side affected, and a syncope which supervened, appeared at first to favour this suspicion: but immediately the absence of a fluctuation, of a pulsation, and of a change in the colour of the skin, the return of the pulse, the circumscription of the tumour, its resistance, and the sound caused by striking on it, produced a belief that it was owing, not to an effusion of blood, but to a disengagement of air that had been confined in the now lacerated cells of the cellular membrane.
Over the whole of the swelling were applied compresses wet with vegeto-mineral water, while a regular compression was made on it by means of a bandage, which, at the same time, kept the arm fixed against the trunk.
In the night there occurred severe pains around the articulation and the tumour, accompanied with high fever, both which symptoms disappeared on the following day. Third day, a diminution of the emphysematous swelling; and an entire cessation of fever and pain. Eighth day, tumour reduced to half its original size; the arm made to perform gentle motions, and disengaged from the apparatus; discutients continued. Thirteenth day, tumour entirely gone. In the place which it had occupied a large echymosis appeared, produced no doubt, by a rupture of the small vessels at the time of reduction, but which, till now, had not been perceptible externally, in consequence of the emphysematous swelling of the parts, and which was treated by the same means as the emphysema. Seventeenth day, a yellow tinge, mixed with the colour of the echymosis, an evidence of its resolution, which was complete by the twenty-seventh day.
During all this time, the patient had accustomed his limb to constant motion; a facility in the movement of it had thereby returned; and he was perfectly well when he left the Hotel-Dieu, on the thirtieth day from the time of his admission, and the sixty-fifth from the occurrence of the accident.
§ I.
1. The fore-arm, composed of two bones, neither of them very strong, and covered below by a small quantity of soft parts, is exposed still more than the humerus, to the action of external bodies, and is articulated at the upper end in such a manner, as not to yield, like it, in every direction to the impulses which it receives. From these considerations, it is one of those parts where fractures most frequently occur, and, in a comparative view of affections of this kind in the Hotel-Dieu, it has oftentimes held the first place.
2. It would be useless to mention here the disposition of the bones which compose the fore-arm, their irregularly prismatical form, their thickness unequally distributed, their direction obviously different, and their motions differently combined. It is sufficient to observe, that, for the perfection of one part of these motions, a space, wide in the middle, and narrow at the ends, must separate the two bones, that, without this space the radius, impeded in its movements on the cubitus, would compress the muscles, restrain their action, and would be unable to perform the motions of pronation and supination; whence the fore-arm, being confined, as it were, to mere flexion and extension, would not, in its uses, correspond to our wants.
These things being premised, we will observe, that fractures of the fore-arm may have their seat, 1st, in both bones at the same time; 2dly, they may occupy but one of them: hence three kinds of fractures more or less different in their phenomena, their consequences, and their treatment.
§ II.
3. Fractures of both bones of the fore-arm, may occur either at the ends, or in the middle of the limb. Frequent in the middle, and somewhat common below, they seldom occur in its upper part, where the fleshy portions of numerous muscles, combined with a considerable thickness of the ulna, resist the motions which tend to produce them. The two bones, though most commonly broken on the same line, are, however, sometimes broken on different ones. The fracture is almost always single: at times, however, it is double, and Desault, in particular, was once called to a patient, over whose fore-arm the wheels of a carriage had passed, and had broken it both in the middle and at the lower end, so that it evidently exhibited six fragments distinct from each other. The two middle ones, though completely insulated, united again to the others with but very little deformity. Like all other similar affections, these may be rendered compound by wounds, splinters, &c. circumstances which, as they fall within the general class of such injuries, will not be treated of at present.
14. They occur, in general, in two ways, being the result, sometimes of the action of external bodies, immediately applied, and at other times of the same action, operating by way of a counter-stroke. The occasional percussion of a body on the fore-arm, furnishes an example of the first mode of fracture. This is much more frequent, in general, than the other, which usually arises from a fall on the wrist; but, in such a case, as it is the large lower end of the radius that forms the principal point of articulation with the hand, that bone alone sustains almost all the force of the stroke, and is very generally the exclusive seat of the fracture.
§ III.
It is in general difficult to be mistaken with respect to the signs which characterize fractures of the fore-arm. A mobility of the limb where it was before inflexible; a crepitation almost always easily perceived; a depression, sometimes evident, at the place of division; a protuberance sometimes formed under the skin by the fragments; pain produced by the motion of the part; a crack sometimes heard by the patient, at the moment of the accident; an inability to perform the motions of pronation and supination; the almost constant semi-flexion of the fore-arm; such, together with the phenomena common to all fractures, are those which essentially characterize this, and which must generally remove all doubts which the swelling of the limb may temporarily create respecting its existence.
6. There is a circumstance, however, where a fracture near to the joint of the wrist, may give rise to appearances similar to a luxation of that part. In both cases, indeed, a convexity behind, and a depression before, or the reverse, are perceived, and are the effect of a displacement of the fragments. But the styloid apophysis being carefully examined, will always determine, according as it is found above or below the deformity, from which of the two causes the deformity arises. Besides, a greater mobility in one than in the other affection, and a crepitation, will guard the practitioner from an error, into which I saw a surgeon fall in the presence of Desault, whom he called on to consult, in the case of a child six years old, which laboured under a supposed luxation.
§ IV.
7. Most of the phenomena which accompany fractures of the fore-arm (5), are evidently the result of a displacement of the fragments; a displacement, not, in general, very perceptible in the longitudinal direction of the bones, because the muscular action, tending to produce it in that direction, is not very powerful. When it does occur in this way, it is most frequently the immediate effect of the stroke that produced the fracture.
8. But it is different with respect to a displacement in the cross direction of the bone. Here the cause of the separation of the broken ends, may be the same with the cause of their fracture, as happens in the passage of a carriage wheel over the limb, or in the falling of some body against it; and then, 1st, the fragments are separated from before backward, or contrarywise, and hence, a protuberance on the one side of the limb, and a depression on the other; 2dly, or else they are pressed against each other laterally from without inwards. From this latter cause arises that inequality which the limb exhibits at the place of the fracture; the slight depression which it manifests on its sides; and the protrusion or bulging out of its anterior and posterior surfaces, by means of the mass of muscles which are pushed in these directions, by the approximation of the fragments to each other.
9. A proper reduction removes the first kind of displacement, namely, that which occurs in the cross direction of the bone backward or forward (8); and unless an external force be applied anew, it does not again return. On the contrary, how exact soever the reduction may be, in the second kind, namely, that which takes place laterally from without inwards, the fragments are soon found to have approached each other again. Above, the pronator teres presses the superior fragment of the radius against that of the ulna; below, the two fractured extremities are pressed against each other, by the contractions of the pronator quadratus. From this double cause arises, unless something prevent it, the contact of the four fractured ends, which have been sometimes found united together by a common callus, as is proven by several cases sent to Desault, and by the cases of different patients admitted into the Hotel-Dieu, after having undergone an improper treatment. In such cases, the movements of pronation and supination being entirely destroyed, are but imperfectly supplied, as Duverney remarks, by those of a rotation of the arm.
But if the four broken ends should not even be joined together by a common callus, still the space between the bones being evidently diminished, impedes muscular action and the motions of the limb depending thereon.
§ V.
10. It follows from what has been said on the displacement of the fragments (8), and on the causes which have a constant tendency to re-produce this displacement (9), that the extending forces, intended to remove it, should be, in general, less powerful than in most other fractures, because their principal object is, to restore to the limb its natural length, which is here but very little affected.
11. Previously to the application of these, it is necessary, according to the precept of Hippocrates, to place the fore-arm in a middle state between pronation and supination, flexion and extension. This position is highly favourable to the relaxation of the muscles, and is that, above all others, as the father of medicine observes, which those who have sustained a fracture naturally assume, and which alone they can, for a long time, retain, without experiencing any inconvenience.
12. The fore-arm being thus placed, an assistant makes extension, by taking hold of the four fingers; a mode to be adopted in preference to that of Petit, who directs us to make extension at the wrist; for the real momentum or force of a power is in the inverse ratio of its distance from the place of resistance. At the same time, another assistant makes counter-extension on the humerus, which he grasps with both his hands, in such a manner, that his thumbs correspond to the back part of it, while his fingers cross each other anteriorly.
13. It further follows, from what was said (8 and 9), that the process of conformation, so often useless and even injurious, in other fractures of bones, is necessary here, to restore to the fragments that exact contact which they have lost, in a transverse direction. If the displacement be forward, the surgeon pushes both fragments backward, while the assistants maintain the extension. If the bones project backwards, they must be pushed in the contrary direction. As to a lateral displacement (8) in which the broken ends approach each other, it is not altogether useless, as Petit observes, to endeavour to remove it, by forcing the muscles into the space between the bones. This is done by making a moderate pressure on the anterior and posterior surfaces of the fore-arm, in order that the bones, being thus removed from each other, may come in contact with their broken ends. If this be done, when the apparatus is first applied, the reduction is attended with but little difficulty, and the ends of the fragments are easily retained in apposition.
§ VI.
14. Our forms of apparatus are nothing but means of continuing, for a long time, that state of things, which extension and the process of conformation temporarily produce at the time of reduction. This principle, though generally acknowledged, was particularly neglected in such fractures, as that now under consideration, till the time of Petit, who made it the basis of his practice. Before him, there was a common inconvenience attached to every kind of bandage. The two bones being pressed against each other, by circular rollers applied externally, were thus drawn in that very direction, in which the action of the pronator muscles already tended to displace them; because, the form of the fore-arm being irregular, made these rollers act more powerfully on its lateral parts, where it is very convex, than either behind or before, where it is very flat. It is well known that bandages will make the greatest pressure on the most projecting parts of the limbs round which they are applied; so that, if the fore-arm be bound or pressed on behind and before with a force equal to one, it will sustain laterally, that is, on its sides or edges, a pressure equal to two. Hence results, not only a tendency in the radius to approach the ulna, but also, a want of resistance in the muscles situated on the posterior and anterior sides of the fore-arm. For these muscles being, from their flatness, less compressed than the bones, give way, and do not, by forcing themselves between them, oppose the approach of the bones to each other.
15. Such was the disadvantage of the apparatus of Hippocrates, consisting of one roller applied immediately on the skin, of a many-tailed bandage intended to retain this, and of four splints, applied on the seventh day, and secured by another roller. Such was also the inconvenience of several bandages, proposed after the time of Hippocrates, by different authors, who modified his without improving it, and who, in attempting to alter it, even added to its imperfections. Thus, the compresses with which the limb was first covered, previously to the application of the rollers, served only, by becoming wrinkled, to render the compression unequal, fatiguing, and even painful to the patient. In like manner the pasteboard, which many authors, particularly Duverney, have substituted for splints, and which a majority of practitioners employ, even at the present day, soon becoming softened by moisture, bends without resistance, becomes incapable of preventing a displacement, and has at least the inconvenience of being useless.18
16. Is it to be wondered at then that a perfect cure of fractures of the fore-arm has been regarded as a thing of so much difficulty, and that most authors should have advised practitioners, as a thing of prudence, to warn the patient of its being impracticable to cure him, without the loss of the motions of pronation and supination? Thus, in like manner, it was formerly declared, that a constant deformity was the necessary consequence of fractures of the clavicle.
17. Petit first conceived, that he discovered, in the very means destined to prevent the displacement, the cause of its being continued, and that, in order to be effective, the bandage ought to do constantly what the hands of the surgeon do at the time of reduction (13); that is, it ought to oppose to the unremitting action of the pronators, a resistance equally unremitting, by pressing the muscles into the interstice between the bones. But, after having discovered the end to be attained, he accomplished it only in an imperfect manner. For by first applying a roller immediately round the fore-arm, he reproduced, in part, the very inconveniences and disadvantages he wished to prevent, by placing anteriorly and posteriorly two long and thick graduated compresses, intended to keep the bones asunder, by forcing the muscles between them.
18. Duverney, more judicious, proposed to place the graduated compresses of Petit on two circular compresses, previously applied round the fore-arm. But what availed these circular compresses? If they be drawn tight, will they not produce that approximation of the bones which the surgeon wishes to avoid? And if they be not tight, they will, in consequence of their loose and pliable state, form troublesome and inconvenient wrinkles, without being productive of any good to counterbalance this inconvenience.
19. It was from these different considerations, that Desault modified, as I am about to mention, the apparatus for fractures of the fore-arm. To a great degree of simplicity, this apparatus unites, when thus improved, great ease to the patient, and its advantages are proven by the freedom in the different movements of the arm always experienced by the numerous patients, whom he was called to attend. The pieces of the apparatus are, 1st, Two graduated compresses, one of them of such a length as to extend from the elbow to the wrist, and the other from the wrist to the fold of the arm on the inside. They are to be formed each of a single piece of linen, folded seven or eight times on itself, in such a manner, that the lower fold may be an inch wide, while the others, laid on top of each other, gradually diminish in width to the last. The thickness of these compresses ought to be less in very fat persons, where the anterior and posterior surfaces of the arm are more convex. 2dly, A roller about four yards and a half long, and four inches wide. 3dly, Four thin but stiff wooden splints, long enough to reach, one, from the fold of the arm to the wrist, the second, from the interval or hollow space between the olecranon and the condyl to the same part, the third from the internal condyl of the humerus to the styloid process of the ulna, and the fourth from the eternal condyl to the styloid apophysis of the radius. The breadth of the two first ought to be double that of the other two, as the latter occupy a space of but half the width of that occupied by the former.
20. Every thing being arranged, the reduction is to be executed as already directed (11–13); and while the extensions are still continued, the surgeon wets with vegeto-mineral water, or some other discutient liquid, the graduated compresses, and places them on the anterior and posterior part of the fore-arm, (which must be firmly supported in a state between that of pronation and supination, 11), in such a manner, that their broadest part or base may be in immediate contact with the limb. He then secures them with a roller wet with the same liquid, the casts of which, being first fixed at the place of the fracture, descend obliquely to the wrist, and are secured at the hand by being passed between the thumb and the fore-finger. Running across the back of the hand, the roller then reascends, either by oblique or reverse turns, according to the inequalities of the fore-arm, till it reaches the elbow. Here the surgeon relinquishes the roller, giving it into the hand of an assistant, and places the four splints on the parts already mentioned (19), while the hands of a second assistant secures them, by grasping them all at their lower end, next to the wrist. The surgeon then resumes the roller, and, in order to fix the splints immoveably, descends with it along the fore-arm by circular casts, till he reaches the hand, where he finishes.
There is, in the application of this bandage, an essential precaution to be observed; which is, that as each turn of the roller passes over the graduated compresses, the surgeon ought to press on these compresses with the thumb and fore-finger of his left hand, in order that the muscles, by being forced into the interstice between the radius and ulna may prevent their approximation, which would produce an inequality in the compression made by the apparatus.
21. After the application of the apparatus, if the patient be obliged to keep his bed, the fore-arm is to be extended on a pillow, taking care to keep it always half-bent, and guarded by hoops from the weight of the bed-clothes. But if the fracture be not a compound one, and if the fall has done no injury to the system in general, it is unnecessary to confine the patient to a position wearisome, and oftentimes insupportable to many persons. Then the limb is to be suspended in a sling, which is always sufficient to support it, without having recourse to the kind of hollow case recommended by Bell, which is seldom at hand, and the use of which must be extremely inconvenient.
22. The subsequent treatment to be adopted in such fractures is simple and easy: to wet the apparatus daily, for a few days, with vegeto-mineral water, to obviate, by proper means, the accidents that may occur; to renew the application of the roller at the end of eight days, or perhaps later, according to the degree of its relaxation; to repeat this application two or three times during the course of the treatment; to allow, at first, but light diet, which may be afterwards more solid, and given in larger quantity, and to admit finally of a return to the patient’s usual mode of living: such was, in cases of fracture, the practice of Desault, which was always attended with happy effects.
23. Sometimes a considerable swelling occurs, after the application of the bandage, on the back and face of the hand; small blisters appear between the fingers; the patient experiences sharp pains along the fore-arm; and other small blisters rise on its surface. It is then necessary to remove the apparatus, to open the blisters by pricking the cuticle, and dress the part with cerate spread on linen rags; replace the apparatus, making it less tight than before, taking care to renew it every day, till the excoriation be entirely gone. This accident, of no great consequence in itself, has frequently occurred to Desault, although the rollers were applied at first with but a moderate degree of tightness.
24. The consolidation being completed generally in twenty-four or twenty-five days, leaves, at this time, a little stiffness in the joints, in consequence of their having remained so long without motion: the movements of pronation and supination are performed but imperfectly. Their return is facilitated and hastened by frequent exercise of the limb, as well at its junction with the os humeri, as in its own proper joints; and, in general, by the fifteenth or twentieth day from the removal of the apparatus, things are in the same state in which they stood before the fracture.
§ VII.
25. The radius, which is the moveable and almost the only support or abutment of the hand, receives, in falls on that part, a much greater share of the shock than the ulna, which is joined to the hand by only a small surface. Hence, without doubt, arises the greater frequency of the fractures of the radius; fractures which, when produced by falls on the hand, are evidently the result of a counter-stroke. Oftentimes also this bone is broken by the immediate action of external bodies, because it is defended below with but a thin covering of muscles.
In whatever way the fracture may be produced, it occurs in the middle or at the extremities of the bone; very rare near its articulation with the os humeri, it is more common in its middle; but more frequent still at its lower end. The difference arises probably from this circumstance, that, in falls on the wrist or hand, the shock is weakened and lost in proportion as it is propagated upwards.
26. In such fractures, displacement is almost constantly observable in the thickness or cross direction of the bone and fore-arm, and is produced by the action of the pronator muscles, which, by forcing the fragments of the radius towards the ulna, tend to diminish the interval between the bones. The ulna remaining unbroken, always prevents any displacement in a longitudinal direction. The first kind of displacement is the more perceptible, in proportion as the fracture is nearer to the middle part of the radius, where the bones are at the greatest distance from each other. This displacement is seldom outwards, because the interosseous ligament prevents that: yet experience furnishes some exceptions to this rule.
Case I. Desault was called, in the month of July, 1781, to visit a mason, who, sleeping at the foot of a wall, with his fore-arm stretched out, received on the anterior part of it, a round stone, of the size of a bowl, which, falling from a scaffold, fractured the radius in its middle, and produced a large contusion, accompanied by an enormous swelling, to which the usual discutient remedies were applied. On the fifth day the swelling had in part disappeared; but then there was discovered a very evident protuberance of the inferior fragment, which, by pointing outwards, separated itself from the superior one, which remained nearly in its place. The interval between the bones was evidently increased below.
The fracture was reduced by pressing the lower fragment inwards, and, instead of employing graduated compresses the whole length of the limb, they reached only to its middle, along the part corresponding to the superior fragment. The roller was drawn a little tighter below than above, in order to keep the inferior part of the radius near to the ulna.
By being treated afterwards in the usual mode, the fracture was cured. But, in consequence of being over-stretched by the separation of the bones, the ligaments of the wrist became the seat of a tedious lymphatic swelling, which left behind it some degree of stiffness.
27. Examples of this kind occur too rarely to affect the general law relative to the direction of the displacement of a fractured radius, a displacement which, if not properly treated, makes the fragments unite in such a manner as to form an angle pointing inwardly towards the ulna, as is evinced by a perceptible depression under the cuticle. In such a case, from this contraction or narrowing of the interval between the bones, arise the inconveniencies already mentioned (9).
§ VIII.
28. The diagnosis of fractures of the radius is in general easy, when they occur at the lower end, or in the middle (25). In these two cases, a depression more or less perceptible, on the external side of the fore-arm; an inability to perform pronation or supination, by the action of the muscles alone; and a severe pain, necessarily resulting from moving the bone in this two-fold direction. Such are the particular signs or appearances which first disclose the existence and the place of the fracture. The reality of the accident is afterwards more fully confirmed by the signs common to all fractures, namely, the flexibility of the bone, the crepitation perceived by moving it in different directions, &c.
29. Desault cautioned his pupils not to confound this last sign or symptom with a kind of noise, sometimes heard in the sheaths of the tendons of the extensor longus, extensor brevis, and abductor longus; a noise resulting from a filtration of synovial fluid into the sheaths, or produced by some other cause. But, besides this crepitus in the sheaths being a very rare occurrence, it is always easy to distinguish it from a crepitation of the bone, by this circumstance, that the first is heard on merely pressing the parts, but the latter only by making the bony surfaces rub against each other. Besides, by an experienced ear there is no danger of any mistake being committed.
30. If the fracture exist at the upper end, the thick muscular covering which there surrounds the radius, renders the diagnosis more difficult. Petit has, however, thrown some light on the subject, by judiciously advising to place one hand on the upper extremity of the radius, and with the other to make the fore-arm rotate on this bone. The solution of continuity or fracture will be rendered evident, if, in the midst of these motions, the head remain stationary. But if, on the other hand, it rotate, it has sustained no injury. These two circumstances can be easily explained; but, it is not so easy for the practitioner to avail himself of them in every case. This precept may also be applied in cases where a considerable swelling, occupying the whole fore-arm, conceals from the touch of the surgeon the fragments of the bone, even when broken in the middle.
§ IX.
31. The reduction of a fracture of the radius is effected in nearly the manner already described for that of the two bones of the fore-arm (10–13), except that, here, the extension must be less, because there exists no displacement in a longitudinal direction (26).
To remove that which exists in a cross direction, an assistant whose business it is to make extension, places the hand in a state of adduction, for the purpose of removing the inferior fragment outwards. This precept cannot be applied to much advantage, if the division exist towards the upper end, on account of the interosseous ligament.
At the same time the surgeon endeavours to bring the ends of the bone into perfect contact, by pushing them in a direction opposite to that of their displacement; and when he has attained this end, he begins the application of a bandage or apparatus the same as that already described (19 and 20), with this difference, that as the ulna is here sound, and performs, in relation to the fractured radius, the office of a natural splint, it is unnecessary to place an artificial one between the internal condyl of the humerus, and the styloid apophysis of the ulna.
32. The consolidation or cure is here always more speedy than in the preceding cases, where nature, with the same amount of means and resources, has twice the quantum of labour to perform, and where she supplies her deficiency of power, by the greater length of the time which she employs. In general the bone is united by the twentieth or twenty-fourth day.
33. When the fracture exists at the superior part of the radius, it is essential, after the removal of the apparatus, to make the limb very frequently perform all its natural motions. In such a case, indeed, the parts sometimes swell, become stiff, and an anchylosis of the fore-arm may be the consequence, as Ambrose Pare observes, in his book on fractures, where he says he has seen many accidents of this kind. Galen has remarked the same thing before him. The following case reported by Jeo. Dol**, confirms the truth of it.
Case II. Jane Rene was received into the Hotel-Dieu, in consequence of a fracture of the upper extremity of the radius, produced by a fall on that part, for which she was subjected to the treatment already described (31). The apparatus being removed at the expiration of twenty-five days, the consolidation was perceived to be complete. The motions of pronation and supination were impracticable; those of flexion and extension very much impeded. The patient was now ordered to have the fore-arm moved daily, in these several directions, for the space of an hour, and this space was even increased morning and evening, notwithstanding the pains which, at first, accompanied the exercise. On the eighth day pronation and supination could already be performed in a small degree; they became more and more free, in proportion as the exercise of the limb was longer continued; finally, on the twenty-second day from the removal of the apparatus, the patient was conducted, according to custom, to the amphitheatre, where all the pupils witnessed the perfect freedom of the motions.
Case III. A few days after this, a man, who had left the Hotel-Dieu about eight months before, while under treatment for a similar fracture, returned, to be the subject of a public consultation in consequence of a different disease.
Desault, on interrogating him, learnt from him that the treatment for the fracture had been continued at his own house (31), but that, when the apparatus was removed, no motion had been impressed on the limb, and that the surgeon had even kept it in a sling. The fore-arm was then examined; it was half bent, constantly in a state of pronation, and could not, by any force, be brought into a state of supination. The motions of flexion and extension, were so limited as to be scarcely sufficient for the common wants of the patient, who, under proper treatment, might have been cured like the preceding one, as Desault remarked to his pupils at the time.
34. The patient who was the subject of this second case, was sent to the mineral springs, but derived no benefit from the use of the waters. If this were a proper occasion, I could mention many instances where this remedy, so highly spoken of by many physicians of the present time, has had no effect, except to deprive the patient of more efficacious means, by making him lose that time, during which exercise frequently repeated, would have effected a cure, but which, coming too late, could be of no avail.
§ X.
35. The ulna, less frequently broken, in general, than the radius, scarcely ever suffers alone from falls on the wrist or hand. Most commonly its fracture is direct, and occurs, in particular, in cases where a person in falling, extends the fore-arm for the purpose of supporting himself, and strikes its internal part against some resisting body.
The division, though it does take place occasionally in all parts of the bone, occurs most frequently near to the lower end, where its slender size, compared to that of its upper end, its more projecting situation, and its thinner covering of soft parts, act as predisposing causes.
36. In whatever part it may exist, the touch must readily detect it, when the fingers are drawn along the internal surface of the ulna, which lies almost immediately under the skin. If moved in contrary directions, the fragments will also, by their mobility and crepitation, disclose the nature of the injury. A depression more or less perceptible is observed on the internal part of the fore-arm, produced by a displacement of the fragments, which are carried towards the radius, more particularly of the inferior fragment, as Petit has well observed, the superior one remaining almost immoveable.
§ XI.
37. The reduction does not differ from that of the radius (31), except in this, that the assistant who makes the extension, must place the hand in the opposite state, namely, that of abduction, in order that the fragments may be brought into contact, while the surgeon assists in this process, by pushing the broken ends of the bone in a direction opposite to that of their displacement.
As in the foregoing case, three splints are sufficient for the apparatus, where the radius, being unbroken, performs the office of a fourth.
The exercise of the limb, after the consolidation of the bone, is in general less necessary here, than in fractures of the radius (34), because the ulna, being an immoveable point of support for the motions of rotation, concurs in them only in a passive manner.
§ XII.
38. The ulna is surmounted, at its upper end, by a considerable appendix, curved before, where it corresponds to the articulation of the fore-arm, and is covered with cartilage; convex behind, where there is nothing to separate it from the external integuments, and is attached at its upper end to the strong tendon of the triceps muscle, which appears to be incorporated with it. This appendix resembles greatly, in its structure, form, and uses, the rotula, from which it would differ in nothing, if the inferior ligament of the latter were ossified, so as to form a bony continuity between it and the tibia. It is exposed to fractures, perfectly similar to those of the rotula, but which differs so essentially from the other fractures of the ulna, as to call for a separate examination.
39. The ancients appear to have had but little knowledge of fractures of the olecranon, respecting which they have transmitted nothing to us, unless with Dalechamps, we find cause to recognize a reference to this affection in the following passage of Paul of Egina: Cubitus frangitur . . . circa partem ad cubiti gilbum.
Most of the moderns have spoken of it only in a vague manner; no one has described with accuracy the signs which characterize it; and few have given satisfactory ideas on its treatment. Petit has not spoken of it separately, and Duverney, who concludes with it his article respecting fractures of the fore-arm, has but imperfectly described for it a bandage which is in itself equally imperfect. Bell does not give us, on this point, an exposition of either his opinions or his practice.
Yet this fracture is by no means so rare as to justify the silence of authors, and its treatment merits a degree of attention beyond that which is requisite in most other fractures.
§ XIII.
40. The olecranon suffers fractures at its base and at its summit, but more frequently in the first, than in the second situation. The division, though very generally transverse, is sometimes oblique. Desault met with an instance of an oblique fracture of the olecranon in a man, who had sustained a violent blow on his fore-arm from a club.
41. The causes which produce it are, either muscular action, a circumstance that very rarely occurs, or the direct action of external bodies, which is by far the most common case. The reverse of this is true with regard to fractures of the rotula, which are almost always produced by the contraction of the muscles attached to that bone.
42. The olecranon has been at times separated from the ulna, by the act of throwing a stone with great force. In such cases, the fracture has been produced by the immediate action of the triceps muscle. This is the first mode of division.
The second occurs when a violent blow is received on the elbow, or, more particularly, from falls on that part: for example, if, when descending a flight of stairs, our heel slip and we fall backwards, the arm is suddenly thrown behind to save the body. In such a case, the olecranon striking forcibly against one of the steps, and being pressed between it and the weight of the body, is broken. In this way was the disease produced in a majority of the patients attended by Desault for fractures of the olecranon.
§ XIV.
43. We meet here with the same appearances and state of things, which constantly occur in fractures of the rotula. The triceps extensor, finding no longer in the continuity or sound state of the ulna, a resistance to its contractions, draws upwards the short fragment to which it adheres, produces between it and the lower one an interval more or less perceptible, and gives rise to the greater part of the other characteristic signs of the affection: these are, 1st, An interval or space between the fragments, corresponding to the posterior part of the articulation. This interval may be increased at pleasure, by increasing the flexion of the fore-arm, or by making the patient contract the triceps muscle, and may be again diminished, by bringing the arm into a state of extension: 2dly, An inability in the patient to extend the fore-arm spontaneously, which is the necessary result of the separation of the triceps from the ulna: 3dly, A constant semiflexion or half-bent state of the fore-arm, produced by the contractions of the biceps and brachialis internus muscles, to which no antagonists are now opposed: 4thly, An elevation, more or less perceptible, of the olecranon above the condyls, which, on the contrary, rise above it, when, in a natural state of the parts, the fore-arm is half-bent: 5thly, A facility of moving the upper fragment in every direction, without communicating any motion to the ulna; 6thly, A peculiar sensation experienced by the patient, to whom it seems, when he makes an effort to extend the fore-arm, as if some body or substance were detached or broken off from his elbow, and carried upwards. The patient may realize the justness of this sign, by comparing it with what he feels on attempting to extend the opposite fore-arm, placed in the same position.
44. If to these signs be added the circumstances which accompany the accident, the severe pain that is always felt, the crack which is sometimes heard by the patient, and the possibility of producing a perceptible crepitation, by rubbing the fragments in contrary directions, after having first brought them together, it will be difficult to be mistaken respecting the existence of the fracture, which indeed the swelling of the part alone can conceal from the practitioner, if, as sometimes happens, it be considerable. But then, being soon dispersed, either spontaneously, or by the action of discutients, it leaves the accident unmasked, accompanied by the signs just enumerated.
45. To the swelling is oftentimes added, an echymosis more or less considerable, when the accident has been produced by a fall on the elbow. But by this, no change is effected in the essential characters, which are always sufficient to distinguish a fracture from a luxation backwards, with which it has been sometimes confounded, as appears from many examples recorded in different works.
§ XV.
46. I will not dwell on the question, so much agitated of late, namely, whether or not the olecranon be susceptible of consolidation or reunion. Already has it been hundreds of times answered by experience. What could theory add to the conviction already impressed on us from that quarter? It was by exhibiting to the crowd of pupils who attended his clinical lectures, fractures of this kind perfectly reunited, that Desault refuted the weak arguments, of the periosteum not being able, in consequence of not covering the anterior surface of the olecranon, to produce a union between its fragments, of the synovia mixing with the matter of callus, diluting it, weakening it, preventing it from becoming sufficiently hard for the purpose of reunion, &c. We will only observe, that these ideas are borrowed from a theory which modern experiments have proven to be unfounded, and which, were it true, would be applied in the present case quite unphilosophically, since it would deny to certain parts of man the power or property of restoration or being healed, a property common to all the component parts of beings endowed with life, and which even constitutes one of their essential and discriminative characters.
47. Is the consolidation of the olecranon effected in the same mode as in other bones? The observations of many practitioners, Camper in particular, seem to prove that a ligamento-cartilaginous substance is always the medium of the union of fragments. Desault once found this substance in a corpse, but it was in a case where the fracture had been improperly treated, and where, of course, no inference could be drawn with regard to ordinary cases.
48. But of what import to us are the means which nature employs? The indication is still the same. The fragments must be always kept in contact, that the reunion may be immediate, and that, as David observes, in his memoir on motion and rest in surgical diseases, the apophysis may not, by becoming too long in consequence of the space occupied by the callus, impede the extension of the forearm on the os humeri.
§ XVI.
49. There are no fractures, the treatment of which demands more attention, or is surrounded with more difficulties, than that of the olecranon. Here art cannot, as in the thigh, and the clavicle, oppose to the ever active power of the natural muscles, a constant resistance produced by the action of a kind of artificial muscle, consisting in permanent extension. The superior fragment, being too small to give any purchase to extending forces, can be only pushed downwards, and kept in that position with a greater or less degree of stability and firmness, while the ulna, so to speak, is drawn to meet it. Whence it follows, that extension here is of little use, and that it is chiefly by position or attitude, aided by a judicious conformation, that the reduction is effected.
50. The position has varied in the hands of different practitioners. Some have proposed that, in which the fore-arm is half-bent, so as to form a right angle with the os humeri. The example mentioned by David, is not the only one where recourse has been had to this. But, by rejecting the general principle respecting the reunion of parts, which requires them to be kept in perfect contact, this mode is exposed to a double inconvenience. The reunion is extremely slow in being accomplished, and, when ultimately obtained, is accompanied by the loss of one part of the movements of the limb, in consequence of the length of the callus. This callus must necessarily fill up the whole space that intervened between the fragments during the treatment, and being thus added to the natural extent of the olecranon, lengthens this appendix to such a degree, that, in extending the fore-arm, its summit or upper end comes too soon into contact with the cavity in the os humeri destined to receive it.
51. This practice appears to have been chiefly owing to an opinion then in existence, that an anchylosis being the necessary consequence of the fracture, it was proper to place the arm in that position in which it would be most likely to be still of some service.
52. We must not, however, by throwing the fore-arm into the greatest possible degree of extension, allow it to be drawn into the opposite extreme. From this error the same inconveniencies would result. In such a case, should the fragments touch each other, and press too hard at their posterior edges, they must inevitably leave an intervening vacuity or space between their anterior edges. Hence a greater thickness of callus on the one side than on the other, and consequently an impediment more or less troublesome in the motions of the joint. If the inferior fragment do not touch the superior one, it sinks into the olecranon cavity, leaves the other behind it, and hence another source of irregularity in the consolidation.
53. Between these two extremes (50 and 51), it remains to choose a middle course, and that position will be best, in which the fore-arm shall be, so to speak, in a state between semi-flexion and extension. By this the fragments, being brought into perfect contact, will experience no obstacle to a reunion, which will be therefore both speedy and uniform.
54. But it would be useless to place the limb in a proper position, if no means were made use of to retain it there. Being immediately submitted to the action and influence of a multitude of causes, it will lose its position, and the work of nature being interrupted, the consolidation will be retarded.
Hence appears, both the necessity of placing a solid body, as Desault did, before the whole of the limb, to prevent its flexion, and the insufficiency of the apparatus proposed by Duverney and others, who directed to lay a thick compress on the fracture, to surround the elbow then by a circular one, to secure the whole by a kind of figure of 8 bandage, similar to that used in blood-letting, and, finally, to place the limb on a pillow, without further precaution.
55. Position alone evidently acts only on the lower fragment, which it directs towards the upper one. But it is also necessary to draw the upper fragment towards the lower one, and fix it there, and this is certainly the most difficult point; because, the triceps muscle having a constant tendency to contract, opposes its action to the approximation of the fragments, and indeed prevents it, if, as in the means usually proposed and adopted, the pieces of the bandage glide easily over each other.
56. These considerations determined Desault to search for some means which, being more efficacious than those already in use, might better fulfil the indications of the fracture. He accordingly invented the apparatus which we are about to describe; some ideas of this apparatus are indeed borrowed from other bandages. The success which attended the use of it at the Hotel-Dieu, will, without doubt, introduce it generally into rational practice, where the insufficiency of the old forms of apparatus is acknowledged.
1st, The fore-arm being placed in the position already directed (53), two assistants retain it in that situation, while the surgeon applies on its lower part the end of a roller five or six yards long, and about four inches wide, wet with some discutient liquid, making with it, at first, one or two circular turns to fasten it. Then ascending from below upwards, he covers the whole of the fore-arm with oblique and reverse turns moderately tight.
2dly, Having arrived at the joint, he stops, and makes an assistant draw the skin of the elbow upwards, lest, being loosened and wrinkled by means of the extension, it might get between the fragments, and create an impediment to their reunion. Then, taking hold of the olecranon, he draws it down towards the ulna, and passes behind it, as a substitute for his fingers which have hitherto kept it firmly fixed, a cast of the roller, which he brings from the anterior part of the fore-arm above the elbow. Descending again with the roller along the external side of the arm, and returning across the anterior part, he pursues again the same course, so as to make the casts of the roller lie on each other, and surround the elbow like a kind of figure of 8.
3dly, The surgeon proceeds now by oblique turns, to the upper part of the arm, where he fixes the roller, by a circular turn, and gives it into the hand of an assistant. He next applies along the arm and fore-arm, a splint very strong, but a little bent at the place which corresponds to the joint, in order to prevent too great an extension of the limb: then, resuming the roller, he employs it, in a descending direction, to secure the splint.
4thly, The apparatus being applied, the limb is placed on a pillow, so as to be equally supported throughout its length, and is protected by hoops from the weight of the bed-clothes.
57. To the bandage which we have just described, Desault added formerly a strip of linen, to be placed all along the posterior part of the arm, secured first at its upper end by circular casts, which began above; this strip was secured afterwards by oblique casts, as far as to the place where it met the olecranon, separated from the ulna. Here, the surgeon quitting the roller, took hold of the bit of linen, and drew it downwards, and along with it the circular casts of the roller, together with the muscles on which these casts were applied, and also the fragment which the muscles drew upwards. An assistant then secured it here, while the surgeon, after having made some casts in form of the figure of 8, descended to the inferior part of the fore-arm, where the end of the strip was made fast by tight circular turns. (See fracture of the rotula.)
58. The intention of this additional piece of apparatus, was to draw down the superior fragment, to prevent the circular casts of the roller from separating by their relaxation, and, by that means, to retain the fragments in apposition. But, on the one hand, may not the superior fragment be drawn by the hand, as well as by a roller employed for the purpose? And, on the other, if the circular casts of the roller be liable to become relaxed, why not the strip of linen also? These considerations induced Desault to lay it aside, and use the bandage in the form just described.
59. The advantages it offers are far from being equivocal. 1st, The limb is kept in a state of invariable extension by the anterior splint, and, on this account, there can be no displacement on the part of the inferior fragment. 2dly, The bandage, which accurately envelopes the whole limb, restrains the action of the muscles by compressing them, and prevents in part the contractions of the triceps; while the casts in the form of the figure of 8, applied with skill and precision, hold down the superior fragment, and render it difficult for it to be displaced. 3dly, Without the application of a roller over the whole limb, a swelling, more or less considerable, would probably be the effect of the constriction at the elbow, which must necessarily be somewhat tight, because, as the turns of the roller, in form of the figure of 8, act on the olecranon obliquely, if they be too loose, they will slip and not perform the office of retention.
60. Like all kinds of apparatus composed of rollers, this ought to be frequently examined, lest, by becoming relaxed, it should not make sufficient resistance to the triceps, which is always disposed to draw itself upwards. There can be no period fixed on for the reapplication of the apparatus; the moment it begins to become slack, it ought to be renewed: three or four times during the course of the treatment are generally sufficient. Should a considerable swelling give reason to suspect that the constriction is too great, it will be necessary to remove the bandage in order to apply it anew.
61. The period necessary for the reunion of fractures of the olecranon varies, according as the bandage is more or less exactly kept in its place. Among ten cases of this kind, collected in the Hotel-Dieu, four united in twenty-four days, three in twenty-eight, and three in thirty-two. Hence, taking the mean term, all other circumstances being alike, the process of cure requires about twenty-six days.
62. When this is completed, it is necessary to impress on the limb motions of flexion and extension, gradually increased every day. This is, as David properly observes, the most certain method of avoiding a stiffness, and even an anchylosis, too often the consequence of this fracture.
63. But that illustrious practitioner, in recommending this salutary remedy, has erred with regard to the mode in which it operates. To consume, by degrees, a superabundant callus in the interior of the articulation, and thus reduce it to a level with the articulating surfaces, is not, as he conceives, the effect which these motions produce. This opinion, founded on the ancient doctrine of an osseous juice, is refuted by the dissection of many bodies of patients that died during the treatment, and in which Desault discovered no trace, either of an effusion of osseous juice, during the reunion, or of its superabundance after this reunion had been completed.
The exercise communicated to the limb, appears to act principally by removing the congestion of the tendons and membranes surrounding the joint, which, being at first irritated by the fracture, are thrown into a state of engorgement; and further by dissipating a kind of numbness which affects the muscles after they have remained too long in a state of rest.
64. But whatever may be its mode of action, it ought to be gradually increased, according to the state of the parts, and continued for at least twenty days, a period sufficiently long to restore to the limb, in general, its natural motions.
65. It is seldom that after this methodical treatment, the patient is exposed to an anchylosis, a thing inevitable in such cases, according to most authors, A celebrated surgeon, believing the long continued extension of the fore-arm to be the cause of this accident, has advised here to abandon every kind of bandage, and to commit the cure entirely to nature. But this doctrine, contrary to the general principles of the reunion of divided parts, has not in its favour the result of experience, which proves that, under such neglect, the stiffness in the parts near to the joint is always as great as in other cases, that the reunion is more tedious and more deformed, and that sometimes it cannot be accomplished at all. The analogy of the inconveniences and disadvantages attributed to the method of Foubert, in fractures of the neck of the os femoris, constitutes another argument against this method, which is now almost entirely abandoned.
66. To the cases already published, proving the success of that which we have proposed, let us add one more, reported by Maublanc.
Case IV. Silvan de la Noue, aged thirty, fell on his elbow, having his fore-arm bent, while the shoulder of the same side supported a heavy load. Acute pains at the instant of the fall; a sudden inability to extend the fore-arm; a considerable swelling appears almost immediately, around the joint; and a superficial echymosis at the hind part.
During the night the pains were augmented, the swelling increased, and, on the day following, February 9th, 1791, the patient was received into the Hotel-Dieu.
From the presence of the signs formerly mentioned (43), Desault recognized the fracture, and applied the apparatus (56), notwithstanding the swelling and echymosis, persuaded that the compression made by this apparatus on the tumefied parts, was the most effectual mode to remove the enlargement.
Next day, pains almost gone; swelling diminished; on the fifth day, the bandage become loose, by the almost entire disappearance of the swelling; a new application of it; the joint wet frequently with vegeto-mineral water.
Seventh day, usual regimen allowed; ninth day, a slightly bilious disposition; evacuants somewhat active administered, to remove it.
Thirteenth day, a third application of the apparatus; echymosis entirely gone.
Thirtieth day, the consolidation complete; the apparatus laid aside; from this time motions gradually impressed on the limb.
Fifty-eighth day, the patient discharged, free in all his motions, except a little stiffness, which exercise will soon remove. Since that time, it has been understood that the limb had completely recovered its natural functions.
§ I.
1. The solidity and security of joints are increased in proportion as the extent of their motions is diminished. This inverse proportion of these two properties to each other, is in a particular manner remarkable in the upper extremities, where the connexion of the humerus with the scapula, of the fore-arm with the humerus, and of the bones of the wrist among themselves, appear, in regular gradation, to acquire the one as they lose the other: hence, their predisposition to luxations is extremely different. We will examine those to which the fore-arm is subject.
2. An angular ginglymus unites to the humerus the bones of the fore-arm, which are again connected with each other by a double lateral ginglymus. Eminences and depressions, reciprocally receiving and received, constitute the first kind of articulation, where, proceeding from without inwardly, we find, 1st, the small head of the humerus, entering or rather joining the upper articular cavity of the radius, which moves on it: 2dly, the external groove of the humerus, receiving the rim of the same cavity of the radius: 3dly, a projection which, rising from the external edge of the coronoide19 cavity, extends to the corresponding edge of that of the olecranon, and is received into the external depression of the sigmoid cavity:20 4thly, the large groove of the humerus, receiving the middle eminence of this same cavity: 5thly, a considerable projection, obliquely applied to the internal depression which receives it.
3. These numerous connexions secure the solidity of the joint, which is still farther strengthened before by the coronoid apophysis, together with the fleshy and tendinous extremities of the biceps, and brachialis muscles, and by the olecranon behind; at the inferior part, by the anconeus; on the sides by two ligaments which descend from the two tuberosities, and strong muscular fasciæ running from the same parts. The whole articulation is also surrounded by a thick capsule, strengthened by numerous accessory fibres. With such powers of resistance, how can this joint suffer a luxation? Yet next to that of the os humeri, it is perhaps most frequently subject to this accident.
§ II.
4. Writers have admitted in general four kinds of displacement; backward, forward, outward, and inward. But all these are not alike frequent, as is proved by experience, and demonstrated by the relative situation of the parts.
5. In a backward direction the olecranon and the radius may pass up behind the humerus, as the coronoid apophysis offers but little resistance in consequence of its slight curvature. On the other hand, the kind of hook formed by the olecranon, prevents it and the radius from passing before the lower articulating extremity of the humerus, and therefore, without a fracture of the olecranon, a luxation in that direction is impracticable: at the sides, the two lateral ligaments, but more particularly the reciprocal joining or interlocking of the uneven articulating surfaces, present almost insurmountable obstacles to luxations laterally. Whence it follows, that luxation backward is much more frequent than the others; compared to lateral luxations, it is, at least, in the proportion of ten to one: with luxations forward, no comparison can be made; neither Petit nor Desault having ever met with such.
6. An external force produces the whole of these luxations, but according to each, this force must vary. In a fall sideways, suppose the hand be applied to the ground, with the arm extended, to save the body. It is evident that the resistance of the ground will tend to make the bones of the fore-arm pass upwards over the humerus, while the weight of the body pushing that bone downward and forward, will make it glide over the coronoid apophysis. Thus, the capsule, being distended before by the humerus, and behind by the bones of the fore-arm, will give way in one or the other place, or in both, as Desault observed in a man, who fell on his side, as he was carrying a heavy load: the weight of the body increased by the load, had such an effect, that the bones overlapped each other nearly two inches.
7. It appears from this, that a state of extension is the position most favourable to a displacement backwards; a doctrine by no means conformable to that of most practitioners, who consider a state of flexion as necessary to the accident. But, then, in what direction should the fall take place, in order that the olecranon may pass upwards? Applied as it is against the side of the cavity that receives it when the arm is extended, would not this apophysis prevent such passage? Whatever may be the mode of displacement, the olecranon, in passing upward and backward, may incline a little to the one or the other side.
8. I have already said, that without a fracture of the olecranon, no luxation forward can occur (5). But what cause can act with sufficient power on the parts to produce both accidents at the same time? It would be necessary that a fall which had produced a fracture should be succeeded by another fall; but in such a case, the fore-arm would be half-bent, and it is in a state of extension alone (7) that the luxation can take place.
9. Lateral luxations, that is, luxations at the sides have been divided into complete, when the two articular ranges of the arm and fore-arm, have lost their connexion entirely, and incomplete, when only one bone or one part of a bone has been separated from its natural connexion with the humerus. But what cause can act with sufficient force to produce the first kind of luxation, namely, that which is complete? In such an accident so great would be the extent of the wreck and ruin of the part, that without doubt amputation would be the only resource.
10. The second kind of lateral displacement is the result of a stroke which forces violently the extremity of the fore-arm outward or inward. A footman, says Petit, in falling from a carriage, had his arm entangled between the spokes of the wheel, and suffered in consequence a luxation outwards. Another produced one inwardly, by being thrown from his horse, and falling with his arm under him, on rough ground. Strokes of this kind may, as that author remarks, vary in a singular manner. But, in general, in all of them, the fore-arm must represent a lever of the first kind, where the power acts on the end next the hand; the resistance being in the joint, and the fulcrum in the middle.
§ III.
11. To form an idea of the signs or appearances of a luxation backwards, let us examine, for a moment, the natural situation of the olecranon, and the condyls of the humerus. As these eminences are easily felt under the skin, a knowledge and recollection of their situation will serve as a standard of comparison, to judge of the changes they experience in a luxation. When the fore-arm is extended, the olecranon is on a level with the internal condyl, and a little above the external one. In a state of flexion, it descends below this level, and is then farther below the internal than the external condyl. In either situation, it is nearer to the first than to the second, the radius separating it from the latter.
12. But, when a luxation has taken place, this apophysis, still remaining on a level with the two condyls, even although the fore-arm be half-bent, is oftentimes separated from the internal one, and driven towards the other: a preternatural protuberance announces this change of position of the olecranon. The coronoid apophysis, whose posterior surface glides in the large groove of the humerus, corresponds to this groove now only with its anterior surface: sometimes the olecranon cavity21 receives its extremity. The radius passes backward over the small head of the humerus. At the fold of the arm, a transverse protuberance, more perceptible on the internal side, announces the presence of the displaced articular extremity of the os humeri. Over this extremity are reflected the biceps and the brachialis muscles in a state of violent distension. These muscles, greatly irritated by such distension, continue in a state of habitual contraction, in consequence of which, they keep the fore-arm half-bent. Nor can the anconeus muscle, which is necessarily relaxed, act so as to prevent this semiflection. Severe pains would be the consequence of attempts to extend the fore-arm; the limb is in a state of pronation; yet I find among the cases collected by Desault, several examples where supination existed; this state is explained by the relaxed condition of the pronator muscles. At the level of or opposite to the coronoid cavity is a depression or hollow manifesting the absence of the apophysis of that name.
13. Should chance give rise to a luxation forward, an anterior projection of the two bones of the forearm, and above all, of the coronoid eminence, a depression corresponding to the olecranon cavity, the extremity of the humerus carried backward and downward, the rigid extension of the fore-arm, a protuberance behind formed by the fractured olecranon (5), and severe pains, necessarily resulting from attempts to bend the limb, &c. would constitute the principal characteristic signs of the displacement.
14. In lateral luxations, a protuberance at the internal or external side of the articulation, always shows of what kind it is. If the displacement be to the internal side, the olecranon is then situated behind the small tuberosity: the middle protuberance of the os humeri bears on the radius, which is sometimes placed even behind the internal articular eminence of that bone, which then rests on the external depression of the great sigmoid cavity. Hence, as Petit judiciously observes, arises the direction of the fore-arm outward, the above eminence presenting a manifest obliquity in that direction. In this luxation, the ulna has been known to lose entirely its connexion with the humerus, and the radius to be brought into contact with the internal condyl of that bone. This is what some authors call a complete luxation. Others reserve that name for cases where, the two articular ranges have lost their correspondence or apposition entirely.
15. In a luxation outwards, the olecranon corresponds to the external condyl; the middle projection of the humerus, to the internal depression of the great sigmoid cavity; the small head of this bone, to the external depression; the radius projects outwards; and the humerus makes a protuberance inwardly.
16. After all, these changes of situation vary remarkably, and it belongs to theory rather than practice, to trace their history, with precision. In general, luxations outwardly happen more frequently than those inwardly, a circumstance which is fully explained by the structure of the joint. In both, the lateral ligaments are almost always lacerated.
A swelling more or less considerable accompanies all the different kinds of luxation, and is sometimes carried so far as to involve the diagnosis in great uncertainty, particularly when the displacement is not very great. This phenomenon (the swelling), seems, in general, to correspond, in a direct ratio, to the force with which the articulation resists. Indeed the violence, and consequently the irritation, are always in proportion to the resistance of the parts.
§ IV.
17. The means of reduction vary according to the different kinds of displacement. They are all, however, founded on nearly the same principles, and it will be easy to form proper ideas of them, when we shall have given an account of the means necessary to be employed in luxations backward, of which the others are only modifications.
Here genius seems to have been as prodigal of resources, as nature has been of obstacles. Indeed, to accomplish the reduction, we sometimes see the surgeon placing his elbow in the fold of the affected arm, interlocking his fingers with those of the same limb, and, then, bending with his whole force, both his own fore-arm, and that of the patient, to effect at the same time extension, counter-extension, and reduction or conformation: at another time we see him fixing the fold of the injured arm against some resisting body, such as a bed-post; and while an assistant, then, pushes the displaced olecranon against this body, he himself, pressing on the shoulder with one hand, and grasping the fore-arm with the other, bends it forcibly, in order, by that means, to produce a replacement: again, a body of some size, being placed in the fold of the arm, serves as a fulcrum, on which the fore-arm, being suddenly flexed, moves and acts like a lever of the first kind, of which the power, being applied at the extremity next the hand, draws it backward and upward, and by that means pushes in a contrary direction its luxated end, where the resistance is made. On some occasions, the fore-arm of the diseased side, bent at a right angle, is placed on a horizontal table, and, while the lower extremity of the humerus is thus resting on the table, the surgeon pushes it backward with one hand, and with the other, taking hold of the extremity of the fore-arm, draws it in a contrary direction.
18. The ancients employed the three first modes. Pare has had engravings of them made: Scultel has also given figures of them as practised by Hippocrates. The Arabians knew of no other modes, nor did their descendants, who were only compilers from them. The practitioners of our own day still continue their use. But, in general, they are chargeable with the numerous inconveniences and faults of producing intense pain, of not being completely under the direction of the surgeon, of bringing the point of luxation too near to the place on which counter-extension is made, and of bruising and doing violence to the parts: nor do they disengage, by means of previous extension, the luxated ends of the bones, to facilitate their replacement in their natural situations.
This last charge is not applicable to the last of the processes proposed by Petit. But, here, the extending forces are most commonly insufficient; the surgeon, having both his hands engaged, is not able to act on the joint to assist in the replacement: and the counter-extension made is too near to the point of luxation.
19. In common cases, Desault employed a method as simple and more efficacious, which few writers have recommended, and none have described with accuracy.
The patient is, indifferently, either seated or standing. The fore-arm being half-bent, an assistant takes hold of the extremity next the hand, to make extension; another, to make counter-extension, takes hold of the humerus a little below its middle, with both hands, the fingers crossing before, and the thumbs behind. The extension is made gradually, and when it begins to move the olecranon, and draw it from the place it accidentally occupies, the surgeon, to aid in the reduction, grasps the lower end of the humerus with both hands, crosses his fingers in the fold of the arm, applies his thumbs to the olecranon, and drawing the first backward, pushes at the same time the latter forward; thus, he favours, on the one hand extension, and on the other counter-extension, and in that way finishes the reduction.
20. This method is most commonly practised with success, in recent luxations, where we have oftentimes seen the reduction effected at the Hotel-Dieu, by the simple process of pushing, as just mentioned, the olecranon forward, the humerus being held backward, without any previous extension, while the fore-arm was merely supported by the assistants.
21. But the luxation being oftentimes of long standing, presents very great difficulties. What means must then be employed? It is an established principle, that the force with which a power acts, is in direct proportion to its distance from the point of resistance. Augment this distance, and the extending forces, being doubled and even trebled, will more easily dislodge the luxated extremity. But this indication is fulfilled, by two long straps, formed each of a towel folded several times, one of which is fixed above the wrist, and the other round the humerus a little below its middle. Extension is then made at their extremities, and is almost always sufficient, when aided by skilful efforts of the surgeon (19), to accomplish the reduction. The application of a strap round the humerus is never necessary, unless when the resistance is very great; because, in counter-extension, it is requisite only to withstand or bear against the efforts of extension, but not to act in a contrary direction.
22. But in cases of this kind, the strap, placed, as we have directed, round the lower part of the humerus, has sometimes the disadvantage of compressing too much the brachialis and the biceps muscles, and thus preventing them from acting; this inconvenience is particularly felt in old luxations, where great force is employed; for, the more active then the contraction of these muscles is, the more it will aid the surgeon in his efforts to draw the bones into their natural situation, when once disengaged by extension, from that which they had accidentally occupied. If, in such a case, we impede the contraction of these muscles, how can they fulfil this office?
23. It was this which, in certain cases, induced Desault to place his counter-extension under the armpit, by means of a strap passing, as in the luxation of the humerus, over a ball previously fixed in this hollow, and crossing, not on the top of the opposite shoulder, but behind that of the diseased side. By this contrivance the humerus was drawn or rather held back, by a force acting perfectly in the line of its direction. But is not this force situated too near to the centre of motion? The strap for making extension, fastened at the wrist, answers very well, as has been already mentioned (21).
24. Should the luxation be forward, the extension must be directed according to the state and position in which the fore-arm is found, which is always extended. The hands of assistants alone (19), or straps (21), may then serve to make the extension, which the surgeon must aid, by grasping, in a direction the reverse of that in the preceding case, the lower extremity of the humerus, that is, by crossing his fingers behind, and placing his thumbs on the coronoid apophysis, to push it downward and backward.
25. The strap for counter-extension, would in such a case, always afford the greatest advantage, by being placed exactly as in luxations of the humerus, that is, by running to, and crossing on, the opposite shoulder; the direction or course of the fore-arm, which is necessarily in a state of extension, sufficiently explains this; finally, the reduction of the luxation must be succeeded by the reduction of the olecranon (5), and by the application of a proper apparatus to retain the whole.
26. The reduction of lateral luxations, differs but little from that of luxations backwards. The displaced extremities must be first dislodged by previous extension (19). The surgeon, then, taking hold of the lower part of the arm, places his fingers before, and with his thumbs, crossed on the olecranon, pushes that apophysis forward and inward, if the displacement be outwardly, but forward and outward if it be inwardly. Does the case prove very difficult, recourse must be had to the other means (21 and 23). The hands of the surgeon must still, according to the direction of the displacement, assist the extension made by the straps.
§ V.
27. Luxations of the fore-arm have, oftentimes, a great disposition to occur anew, after having been reduced, whether they be recent, or of long standing. Extension readily dislodges the olecranon and the radius, and replaces them perfectly in their natural situation; but if any thing interrupt them, the displacement is sometimes immediately renewed: suppose the parts even remaining in contact, the slightest motion may derange this contact, and give rise to a necessity for a new reduction, more difficult, oftentimes, than the first. Hence it is always prudent to employ a retentive apparatus for some time.
28. But, on what principle and for what purpose ought it to be applied? The motions communicated to the fore-arm by external bodies, but, more particularly, the action of the muscles inserted in the bones that have been reduced, are here the causes of their displacement. Hence, 1st, to render the limb immoveable; 2dly, to push the articular ends of the bones in a direction opposite to that in which they are drawn by the muscles, and have a tendency to be displaced: such is the twofold indication of the bandage; an indication not fulfilled by the kind of bandage and the sling which Petit proposed, and which leave the arm free to move, and the muscles free to act.
29. Desault employed the following apparatus: 1st, The arm and fore-arm are first covered by oblique turns of a roller, intended both to protect them from the impression of splints, and to diminish the power and action of the muscles, by the pressure made on them: 2dly, Behind the olecranon is to be placed a thick compress, designed to retain it downwards, and which must be secured by a strong splint, situated behind, and curved at the elbow, to accommodate it to the flexion of the fore-arm: 3dly, On the sides are placed two other splints, chiefly necessary in lateral luxations: 4thly, The whole is to be secured by the remaining part of the roller, by which the arm and fore-arm are already covered.
In this bandage, the immobility of the arm is secured by the splints, while the olecranon is pushed by the compress, in a direction the reverse of that of its displacement. But these circumstances constitute the double indication that was to be fulfilled (28).
30. The period at which these means may be dispensed with, is undetermined. It belongs to the surgeon to examine and ascertain, when the natural connexions of the joint are sufficiently confirmed. Then motions, at first gentle, are to be impressed on the limb; being afterwards gradually increased, they remove by degrees that stiffness, which usually follows a dislocation, particularly an old one. But if it has existed too long, to give the limb motion, is then the only resource: the new attachments or adhesions, contracted by the articulating surfaces in their displaced state, render reduction impracticable. We must then confine ourselves merely to increasing the extent of the motions, which the displaced fore-arm is yet capable of performing.
31. There is, in general, all other things being favourable, a hope of accomplishing the reduction, till the end of the second month after the accident. Desault succeeded in it, at even a later period. What trouble or hardship is it, at last, to try extension? Should no other end be gained, but merely to bring the bones nearer to their natural cavities or situations, even without actually replacing them, this will aid their movements, the extent of which is inversely proportioned to their distance from these cavities.
1st, Most authors who have written on the luxations of the fore-arm, have omitted considering separately those confined to the radius alone. Some detached observations may be found here and there, on the luxations of the upper extremity of this bone, which Duverney alone has treated at some length. Those of its lower extremity, though more frequent, and more easily produced, appear to have almost entirely escaped the attention of the French practitioners, who have transmitted nothing to us on that point, owing, no doubt, to their having had no knowledge of it from experience. But since, at the present day, a sufficient number of facts are collected on the subject, some account of these displacements cannot be a matter of indifference to the art, and it may be traced with as much precision as the accounts of other similar accidents.
§ I.
2. The radius, the moveable agent in pronation and supination, rolls on the ulna its fixed basis or abutment, by means of two small articulating surfaces, the one at its upper end, slightly convex, broad within, and narrow without, corresponding to the small sigmoid cavity, in which it is lodged; and the other at its lower end, concave, semicircular, and fitted to the convex edge of the ulna, which it receives. Hence two kinds of articulation different from each other, with respect to their motions, the connexion of their surfaces, and the ligaments which strengthen them. Let us specify these differences; they will serve to shed light on those that exist between the displacements of the two extremities of the radius.
3. At its upper end, the radius, in performing pronation and supination, moves only on its own axis; at its lower end, it rolls round the axis of the ulna: therefore, being farther removed from their centre, its motions must have both a greater range and greater force, in the latter case than in the former. The head of the radius, turning on itself within the annular ligament, cannot distend it in any direction or part. The cellular membrane attached to this ligament is alone slightly stretched, but being loose and elastic, it yields without resistance. At its lower end, on the contrary, the radius, turning from without inwards during pronation, keeps the capsule posteriorly in a state of tension, and draws it against the immoveable head of the ulna, which tends to pass through it, if the motion be forcible. The same phenomenon occurs in a contrary direction, during supination; the radius is directed backward, and the ulna inward. Being in this case distended before, and relaxed behind, the capsule is disposed to laceration anteriorly.
4. In addition to this disposition, the ligaments of the two articulations are disproportioned in their strength. Thin and weak at the lower articulation, thick and firm at the upper one, they are in this respect strikingly different. The head of the radius, resting against the small but firmly fixed head of the humerus, finds there, in most of its movements, an obstacle to displacement. On the contrary, its lower end, drawing along with it in its movements, the bones of the carpus which are connected with it, derives from them no solid support.
§ II.
5. It follows from what has been said (3 and 4), 1st, that the lower articulation of the radius is not only exposed to the action of more causes of displacement, but possesses fewer means of resisting those causes, and that, from the threefold consideration of its motions, the ligaments which connect its articulating surfaces, and their relation to each other, it must be frequently subject to luxations: 2dly, that for reasons the very reverse of these, its upper articulation must be very seldom subject to luxation.
6. Indeed, what cause is there to produce luxation in this latter joint. Is it from a forcible exertion of pronation or supination that this accident can occur? Surely not: for, on the one hand, as the lower articulation offers less resistance than the upper one, it is evident that, in either state of motion, it being the weakest, will be displaced first, and the motion being thus checked, can no longer operate to the displacement of the other. On the other hand, however forcible the motion may be, there will be in the upper articulation, nothing but a rotation of the bone on its own axis (3). How, then, without being carried forward, backward, &c. can the head be displaced? Indeed, it would be necessary that all the fastenings or bonds of attachment muscular and ligamentous, should be first broken. But these are too strong, and the motion is too weak. Can the displacement be produced by a blow impressed on the radius from below upwards? By no means: because the head of the humerus making, in this case, a solid resistance will not permit it to escape from the capsule (4). Can it arise from a violent extension or flexion of the fore-arm? No. This effort being altogether confined to the ulna, affects the radius in but a very faint degree.
7. It appears from hence, that the accidental luxation of the upper end of the radius, suddenly produced by external causes, must, if it ever occur, be extremely rare. But it is not so with respect to luxations which take place slowly in this joint, particularly in children, where, in consequence of repeated efforts, the ligaments become relaxed. But this kind of displacement, being almost always complicated with a swelling of the joint, and sometimes not to be reduced by the expedients of art, cannot be comprised in my present plan.
9. But experience would seem to have at times exposed the fallacy of these considerations and reasonings, founded merely on the structure of the parts. Duverney relates some instances of luxations of the head of the radius, produced suddenly by external causes. Two other practitioners are also of opinion that they have witnessed similar displacements. But did they examine the subject with all that attention which it required? A similar case was reported to the Academy of Surgery, by one of its associates; but doubts were entertained with regard to its reality: and, ultimately, there were so few facts in its favour, and such strong presumptions against it, that Desault was induced to deny the luxation altogether, till its reality should, by new proofs, be more certainly established.
After all, if it should occur, the same signs which announce the luxation, when the ligaments, in consequence of being gradually relaxed or in some way distended, permit the head of the radius to be insensibly displaced, would then appear as the sudden effect of external violence.
§ III.
9. The causes which produce the displacement of the lower end of the radius, are the same with those that give rise to other similar affections. 1st, The convulsive action of the pronator and supinator muscles, is doubtless a rare cause of the accident, since Desault never met with an instance of it. 2dly, The action of external bodies, which, by forcibly and suddenly producing the motions of pronation, rupture the posterior portion of the capsule, or, by those of supination, lacerate its anterior portion.
10. Hence two kinds of displacement, the one forward, the other backward. The first is somewhat frequent; the second is much less so. The latter was never seen by Desault but once, and that was in the corpse of a man who had had both his arms luxated, but respecting the circumstances of which he could receive no information. The other kind occurred frequently in his practice, of which five examples have been already published. The difference no doubt arises from this circumstance, that the greater part of our powerful motions are performed only in the direction of pronation. This appears to be proven by the following circumstances.
11. If, in several dead bodies, we lay bare the bones of the fore-arm, still united by their ligaments, and push the extremity of the radius forcibly backwards, that is, in the direction of supination, a laceration will as readily occur in the anterior part of the capsule, as it will in its posterior part, when, by forcibly pushing the same extremity forward, the motion of pronation is performed. Hence the difference does not arise from the structure, but from the direction of the motions impressed on the limb.
§ IV.
12. The signs which characterize a luxation of the radius forward, are, 1st, The constant pronation of the limb: 2dly, An inability in it to assume the state of supination, and even severe pains arising from attempting it: 3dly, A protuberance larger than common, formed behind, by the small head of the ulna passing through the capsule: 4thly, The end of the radius being situated more anteriorly than natural: 5thly, The constant adduction, and almost constant extension of the wrist: 6thly, The semiflexion of the fore-arm, and very often of the fingers: this position is generally assumed by the fore-arm, in affections of the bones that form it, and, in the present case, cannot be changed without considerable pain: 7thly, A swelling more or less extensive, which sometimes appears around the articulation, at the moment of the accident, and which never fails to occur afterwards, unless the reduction be immediately effected. This occurrence may conceal the state of the articulation, and make the accident be considered, at first sight, as a sprain, as Desault witnessed in certain cases, where the disease had been mistaken by the surgeons who were first called to the persons injured. It is easy to conceive of the sad consequences of this mistake, which, by preventing any effort at reduction, gives the articular surfaces time to form adhesions, and thus oftentimes renders the mischief irreparable.
13. If to these signs be added, the severe pains experienced by the patient, the circumstances of the fall, in which the fore-arm is violently drawn into a state of pronation, we will have a view of every thing that can here aid the practitioner in his diagnosis.
14. Most of the foregoing signs, taken in the opposite sense, would characterize a luxation of the radius backward, should it occur: such, for example, as a forced supination of the limb, an inability as to pronation, the pains that would result from this movement if performed by force, the tumour formed anteriorly by the extremity of the ulna, the posterior situation of the large head of the radius, and the abduction of the wrist.
15. The dead body, in which Desault observed this kind of displacement (9), being dissected with care, exhibited in the articular parts, the following diseased state. The tendons of the flexor muscles, pushed outwards, adhered to one another and to the skin; a substance of a cellular texture filled up the sigmoid cavity of the radius, and occupied the place of the cartilage which naturally invests it: the inter-articular ligament, which passes between the ulna and the os pyramidalis, scarcely touched the head of the ulna, having followed the radius backwards; and the head of the ulna, situated before the sigmoid cavity of the radius, rested on one of the ossa sesamoidea, to which it was attached by a capsular ligament.
§ V.
16. Extension so important in the reduction of other luxations, renders scarcely any service in this: impulsion alone answers the purpose. If the displacement be forward, it is reduced in the following manner: The patient sits or stands indifferently; the latter position, however, has sometimes this advantage over the former, that by placing the part to be operated on more on a level with the hands of the surgeon, it gives him both more readiness and more force in his motions: one assistant supporting the elbow, separates the arm a little from the body; while another taking hold of the hand and fingers, gives them also an equable support.
17. The surgeon grasps the extremity of the fore-arm, with both hands, one placed on its internal, and the other on its external side, so that his two thumbs may meet before, between the ulna and the radius, and the fingers behind. He then exerts himself to separate the two bones from each other, by pushing the radius backward and outward, and retaining the ulna in its place; in the mean time the assistant who supports the hand, endeavours to move it in the direction of supination, and consequently to draw the radius, with which it is connected, into the same state. Being thus pushed in a direction opposite to that of its displacement, by two forces, the one exerted directly on it, and the other acting indirectly, the radius is forced outwards, and the ulna, returning through the opening in the capsule, is replaced in the sigmoid cavity.
18. Should a luxation of the radius backwards ever occur, the same process executed in an inverse direction, would serve the purposes of reduction. The surgeon with his fingers would have to press the extremity of the radius forward and inward, while a forcible pronatory movement impressed by the assistant on the hand intrusted to him, would favour the effort and finish the reduction.
19. The disappearance of the signs (12...14) of the luxation bespeak its reduction. In general the pain is entirely removed; sometimes a perceptible sound, or report, caused by the passage of the bone through the opening in the capsule, announces the replacement.
20. When the luxation is of long standing, it is always attended with more or less difficulty, occasioned by the adhesions of the surrounding soft parts to the articulating surfaces, by the thickening of the capsule, which diminishes the size of its opening, by the rigidity contracted by the whole part, &c. It is, in such cases, useful to employ emollient applications for some time previously to attempting the reduction, in order to produce such a relaxation, and diminution of the congestion, as may favour the efforts of the surgeon.
21. The first patient whom Desault visited at the Hotel-Dieu in quality of surgeon in chief, had a luxation forward, of more than two months standing, in which the use of these means facilitated the reduction: but they are sometimes insufficient, and then the radius remains immoveable, and the forearm performs its motions but partially.
22. It would seem as if nature, always industrious to provide, amid the disorders of our organs, some resources for the exercise of their functions, has been desirous of preventing here, the inconvenience attendant on a failure of reduction, by rendering luxations backward much more difficult than those forward. Indeed if the fore-arm be kept constantly in a state of supination, it will be much less useful, than if it were always in a state of pronation, the situation in which most of the motions necessary to our existence are performed.
§ VI.
23. When the reduction is finished, the articulating surfaces have sometimes a great tendency to be displaced, by the different movements of the fore-arm, a tendency of which we may easily form an idea, if we observe, that in a state of pronation, the head of the ulna presses against the back part of the strained capsule, and consequently against its opening, when the luxation has been forward: a contrary state of things occurs in a luxation backward. Whence it is always prudent to avoid, for some time, the motions of pronation and supination, according to the direction of the displacement.
24. Should the tendency to displacement be very great, it will be necessary to adopt the simple method pointed out in a case already published by Desault.
Case I. The case was a luxation forward, which was easily reduced. But the easier the reduction, the more difficult was it to retain the replaced parts. This was at length accomplished, by fixing the fore-arm in a state of supination, and applying one thick compress behind the ulna, while the radius was pushed backward by another compress, placed on its anterior part, both secured by a common roller. This apparatus was continued for the space of a month, after which the reduced bones remained in their natural situation. The patient began, at first, to perform gentle motions of the wrist, avoiding those of pronation, on which he afterwards ventured by degrees, and with great caution.
25. These gentle motions frequently repeated, when a displacement is no longer to be apprehended, remove that unavoidable rigidity which, for some time, occupies the parts around the joint. It is advisable, for some time, to apply on the hand and extremity of the fore-arm, compresses wet with some discutient liquor, to prevent the swelling resulting perhaps from the inactivity and sprain of the parts. This was the practice of Desault.
I will close this memoir by two cases, extracted from the Journal of Surgery, in order to confirm, by experience, what has been already settled in theory.
Case I. Desault was called to visit a child five years old, supposed to be labouring under a fracture of the arm. He learnt from the parents of the child, that, as it was lying in a very low bed, a young man who was playing with it, had taken hold of its fore-arm, and drawn it towards him, twisting it forcibly at the same time in the direction of pronation; that the effort had been accompanied by a report, and the child had immediately experienced an acute pain throughout the whole limb, but more particularly along the posterior part of the fore-arm.
When Desault saw the patient, no swelling had as yet supervened; the arm was removed from the body, and carried a little forward, while the fore-arm, half-bent, was kept in a state between pronation and supination. There existed, at its lower and back part, a preternatural tumour, formed by the head of the ulna carried behind the sigmoid cavity of the radius. The hand was a little extended, and in a state of adduction. The patient carefully preserved that position, and, as soon as it was changed, or the part affected touched, manifested signs of the most acute pain.
From these appearances, Desault discovered immediately a luxation of the radius forward, which was reduced in the manner already mentioned (16 and 17). By this process, the bones, being a little separated from each other, were replaced with facility. The suffering of the patient was immediately at an end; the limb resumed its natural state, and performed its functions as freely as before; lest some congestion might be the consequence, the injured parts were covered by compresses wet with camphorated spirits; these were secured by a bandage moderately tight, and no accident whatever supervened.
Case II. On the 29th of January, 1789, Madeleine Fuser, a washer-woman, thirty-four years of age, had the lower extremity of the radius luxated forward.
Just as she had finished wringing a sheet, another washer-woman, who was assisting her to wring it, giving it a forcible jerk, did violence to her left arm, which was at the time in a state of strong pronation.
The woman experienced immediately a severe pain, accompanied by a sensation as if something had been torn. The sheet dropt from her hand, and she fell on the ground. Believing that she had received only a sprain, she neglected to apply for aid, and did not enter the Hotel-Dieu till the sixth day after the accident.
There was then a little swelling at the lower part of the fore-arm and at the wrist: the latter was extended and in a state of adduction; the fingers were bent. This woman suffered but little, when her hand was supported and kept still; but the pains became severe, when she attempted to move it. It was plainly perceived that the radius was placed before the ulna, and that the bones overlapped each other.
Process of reduction the same as in the preceding case. It was accompanied by a kind of report, and its completion was clearly announced by the restoration of the natural shape of the limb, and by the freedom of its motions. Compresses wet with vegeto-mineral water were applied to the wrist.
This patient remained fifteen days in the hospital, at the end of which, she performed with ease the motions of the wrist and hand.
§ I.
1. The os femoris, being in man, a moveable support for the weight of the whole body, appears to be better secured than the other bones, from accidents that might affect its continuity. The numerous masses of muscle that immediately surround it; the thick and compact layers or fasciæ that form its more exterior covering; and an articulation loose, and ready to yield, in every direction, to the motions impressed on it, all seem, on the one hand, calculated for its preservation.
2. But, on the other hand, being visibly curved in its middle, bent at its upper end almost at a right angle, longer in proportion in man than in quadrupeds, placed, in most falls, between the ground which resists, and the weight of the body which presses on it; it would seem, from these latter circumstances, to be less calculated to resist external force. And, if to these considerations be added those of the causes which have an immediate action on it, it will be easy to perceive, that, in a comparative scale of the bones most exposed to fractures, it holds, next to the bones of the leg, one of the highest grades. The proportion which its fractures bear to those of the leg, is, according to the observations of Desault, as one to three; but to that of most other bones it is equal if not superior.
3. The os femoris, being in its body irregularly cylindrical and curved behind, becomes larger towards its lower end, where it terminates in two articulating masses, which rest immediately on two corresponding surfaces of the os tibiæ; changing its direction above, it inclines towards the acetabulum, and inserts into that cavity a round head, supported by a neck which is entirely enclosed in the capsule of the joint.
4. From this different conformation of its different parts, arises such a variety in the fractures which occur in it, that they cannot be treated of under the same head. Hence the division into fractures of the body and of the extremities, which is borrowed from anatomists, and will be followed in the present memoir, where we will consider in order,
1st, The fractures of its body,
2dly, Those of its upper extremity,
3dly, Those of its lower extremity.
§ II.
5. The os femoris may be fractured indifferently at any point between its condyls and its neck. But the part where this accident most frequently occurs, is about the centre of the curve of the bone, where most of the motions and shocks impressed on it by external violence expend their force.
6. Whatever may be the seat of the fracture, its direction is sometimes transverse, but most frequently oblique, a variety which does not affect the real nature of the disease, but which possesses, as to its consequences, a very important influence. As in other affections of the kind, so here, the bone is sometimes affected alone, and, at other times, to a fracture simple or complicated by means of splinters, is added an injury done to the surrounding soft parts. Hence result compound fractures, differently varied, according to the nature of the parts affected, and to the extent and other circumstances of these affections. But, as Petit observes, this bone is less frequently shattered or crushed into several pieces, than those that are more superficially situated.
7. Extraneous causes are known to render falls more frequent in man than in other animals, and to multiply in him the fractures of the lower extremities, by multiplying the action of external bodies on these extremities. This action may be exerted on the os femoris in two modes. Sometimes only passive, it merely offers a resistance to the power which puts the bone in motion; thus, in a fall, the os femoris, being pressed between the ground which resists, and the weight of the body that bears on it, bends beyond the extent of its flexibility or pliancy, and finally gives way. At other times the influence of external bodies is actively and directly exerted in this accident: thus a stone, or a piece of timber, falling on the thigh, fractures the bone, in consequence of communicating to it a degree of motion greater than its power of resistance.
8. In common, the first mode of division is by a true counter-stroke, similar to that which fractures the clavicle, the ribs, &c. In the second mode, the fracture is always direct. The middle part of the bone is generally broken in a counter-stroke: wherever the direct stroke is received, that is the place of the fracture which it produces; the division, most frequently oblique in the first case, is sometimes perpendicular or transverse in the second. From a counter-stroke result most commonly simple fractures, while compound ones are usually owing to a direct stroke.
§ III.
9. In whatever manner a fracture of the os femoris may have occurred (7), its existence is characterized by the following signs: severe local pain at the instant of the accident; a sudden inability to move the limb; a preternatural mobility occurring in some particular part; a crepitation sometimes distinct, when the two fragments are rubbed against each other; and a deformity, which may be considered under the threefold relation, of length, thickness, and direction.22 These signs, being common to most fractures, exhibit but few circumstances peculiar to those of the os femoris, except that of the deformity. Respecting this circumstance, in particular, it is essentially necessary to possess accurate ideas, because, having an incessant tendency to recur, especially in oblique fractures, it must constitute a primary object of attention during the treatment.
10. It may be laid down as a general principle, that all fractures of the os femoris are accompanied with some deformity; the exceptions to this rule are too few to be worthy of notice. If this deformity be considered in relation to length, it will be found that, in oblique fractures, the limb is always shorter than that of the opposite side, a circumstance which plainly points out an overlapping of the fragments. But, on examining the place of fracture, it is easy to discover, that this overlapping arises from the inferior fragment mounting upwards on the superior one, which itself remains immoveable. Now, what power, but the contraction of the surrounding muscles, can communicate to the inferior fragment a motion from below upwards? Attached, on the one hand, to the pelvis, and on the other to this fragment, to the rotula, the tibiæ, and the fibula, these muscles have on the former their fixed, and on the latter their moveable points, and, drawing the leg, the knee, and the inferior portion of the thigh upward, they produce the displacement and shortening either mediately or immediately. In this displacement, the adductores, the semi-tendinosus, the semi-membranosus, the rectus anterior, the rectus internus, &c. are the principal agents.
11. The following case communicated to Desault by a surgeon, who had been formerly his pupil, proves how great the influence of this cause is; a cause which is indeed generally acknowledged, but not sufficiently attended to by practitioners, with a reference to permanent extension. It is this that induces me to relate the case.
Case I. A carpenter falling under the ruins of his scaffold, was immediately taken up and carried home, where a surgeon discovered an oblique fracture of the os femoris, but without any displacement. The thigh, which appeared even a little longer than the other, was fixed in an apparatus too slack to prevent muscular action. Next day, the length of the thigh was the same, but the whole extremity was in a paralytic state, accompanied by an entire inability to discharge urine.
The moxa was proposed. The patient being placed in the position directed by Pott, for fractures of the os femoris, the fire was applied; some movements were the consequence; the application being repeated on the sixth day, the muscles instantly recovered their power of action, and then the shortening of the limb became evident, and still returning immediately after being removed by extension, rendered it necessary to have recourse to an apparatus calculated for permanent extension.
12. In this case, the muscular influence is evident. Indeed the shock having produced a temporary suspension of the excitability of the part, the fragments remained in place and in proper contact with each other: but the moxa having awakened the excitability again in the muscles of the thigh, they resumed their action and caused, as usual, the inferior fragment to mount on the superior.
13. Hence it follows, 1st, that it is principally to the action of the muscles that we must attribute the displacement, in the longitudinal direction of the bone; 2dly, that, as that action, being the effect of an inherent power, is constantly exerted, the limb must have a constant tendency to this displacement, particularly in oblique fractures, where the two extremities of the bone represent two inclined plains, which readily glide along each other.
14. To this must be still added another cause, which operates injuriously in the course of the treatment. However solid the bed may be on which the patient lies, the nates or buttocks, being the most projecting part of the body, soon form a depression in it; hence arises an inclination or descent of the plain or surface on which the body lies. The body therefore sliding downwards, pushes before it the superior fragment, and makes it overlap the inferior one. In consequence of this, the muscles, being irritated by the points of the bones, increase the force of their contractions, and, as we have already observed (10), draw the inferior fragment upwards. This double movement of the two ends of the bone in contrary directions, produces only a single effect, namely, the overlapping of these ends, but carries this overlapping to a higher degree.
15. Transverse fractures are less exposed to displacement, in the longitudinal direction of the bone, because the fragments when in contact, support each other. In such a case, the inferior fragment, drawn by the muscles, finds a point of resistance against the superior one, while the latter, when pressed downward by the weight of the body, pushes the former before it, and thus both preserve their relative position.
16. A deformity of the fractured os femoris, in the direction of its cross-diameter or thickness (9), always accompanies that in its longitudinal direction, and sometimes exists alone. This takes place when, in a transverse fracture the two ends of the bone, losing their contact, are carried, the one outward, and the other inward, or when the one remains in its place, while the other is separated from it. In such a case, the superior fragment is not, as in the preceding one, immoveable by means of muscular action; because the action of the pectineus, the psoas, the illiacus, and the first adductores, derange its natural direction, and contribute to its displacement.
17. The deformity of the limb, in relation to its direction, in other words, the crookedness of the limb (9) is either the result of the stroke which fractured it, or, what is more common, of the ill directed efforts of those who lift and carry the patient, and, by an improper position, bend the two fragments, so as to make them form an angle with each other. Desault was once called to a patient, whom he found seated on a bed, in such a manner, that the upper part of the thigh was in a horizontal position, and the lower, hanging with the leg in almost a perpendicular one. Doubtless the triceps femoralis, equally attached to both fragments, bends them by its contraction, and produces a change in the direction of the limb.
18. Whatever may be the kind of the deformity, whether in a longitudinal or lateral direction, the inferior fragment may either preserve the natural position in which it is placed, or experience a rotatory motion on its axis outwards, which is a common occurrence, or inwards, a circumstance which is more rare. This rotation always renders the displacement more serious, and ought to have an influence, as I shall presently observe, on the means of reduction.
§ IV.
19. Fractures of the os femoris, though seldom very distressing, in common cases, from any accidents that immediately accompany them, are sometimes rendered so, by inconveniences which are the consequences of them, when they are oblique. Celsus declared, that a shortening of the limb, more or less considerable, was always the result of such fractures. Most authors have copied and repeated this assertion, and, even at the present day, the opinion is advocated by a great number of practitioners. It must be acknowledged, that, if we compare the natural powers that are engaged in producing displacement (10...15), with the artificial resistance made by most of our forms of apparatus, we will perceive that there is between the two forces so great a disproportion in point of strength, that the former can never yield to the latter. But, is it in the nature of all forms of apparatus to be unable to overcome the force of the displacing powers? Cannot an equilibrium be established, so as to retain the fragments in contact? The remainder of the present memoir will throw some light on this problem, which will become less difficult of solution, if we call to mind, that the action of muscles, though very powerful at first, diminishes afterwards by degrees, in consequence of their being kept in a state of permanent extension; that even a weaker power may, by acting constantly, accomplish ultimately, what could not have been effected at once, by another power much stronger, if only momentarily applied; and that compression made by circular bandages, tends also to diminish the force and prevent the action of muscles.
Desault has cured, at the Hotel-Dieu, a vast number of fractures of the os femoris, without the least remaining deformity, and there are but few of his pupils who have not witnessed his success, some instances of which will be cited in this memoir.
20. It is, above all, from the well combined use of these two means, the extension and compression of the muscles, that that success was derived. The advantage of extension, in diminishing muscular force, is evident, particularly in the reduction of certain luxations, those of the humerus, for example, where we are frequently unable to succeed, till after having extended the muscles for a longer or shorter time.
Fractures of the rotula and of the olecranon, prove equally the utility of compression in effecting the same purpose; for, when the muscles are not compressed by a bandage, they draw the fragment upwards with a double and even treble force.
21. Accidents relating to complications of the fracture, such as splinters, wounds, &c. are to be classed with compound fractures in general, and cannot be treated of in this place.
§ V.
22. Two great indications enter into the treatment of fractures in general, and of that of the os femoris in particular; namely, to bring the fragments into proper contact, and to maintain them so. Let us examine each of these in all their details.
Hippocrates, and every practitioner since his time, have replaced the fragments by what they call extension, counter-extension, and coaptation.23 This threefold method, though sanctioned by long usage, and rendered almost venerable by age, is by no means necessary at all times in practice, as will presently be observed. Previously to having recourse to it, it is necessary to place the patient in a suitable position. But this position varies: most of the moderns adopt, after the example of the ancients, a horizontal position: so that the thigh may be extended on the body, and the leg on the thigh. This is the common practice at present in France.
23. Pott imagined, on the contrary, that if the lower extremity were kept in a half-bent position, the muscles, being more relaxed, would offer less resistance to the efforts of the extension: he, therefore, proposed to bend the leg on the thigh, and the thigh on the pelvis, and to lay the patient on his side, a position, which, when first employed in reduction, was to be continued throughout the treatment, during which it would render the causes of displacement less active (10...15). Bell adopted this method, which indeed appears to be generally in use in England.
24. But the difficulty of making extension and counter-extension, with the limb thus situated, the necessity of making them on the fractured bone itself, and not on a part distant from the fracture, such as the lower part of the leg; the impossibility of comparing the diseased thigh with the sound one, to judge of the regularity of the conformation; the uneasiness occasioned by this position, if long continued, though it may at first appear the most natural; the troublesome and painful pressure of the body on the great trochanter of the affected side; the derangements to which the fragments are exposed when the patient goes to stool; the difficulty of fixing the leg with sufficient steadiness, to prevent it from affecting the os femoris by its motions; the evident impracticability of this method, when both thighs are broken; and, finally, experience, which, in France, has been by no means favourable to the position recommended by Pott: such were the considerations, which determined Desault to have recourse to it no more, after having tried it on two patients, in one of whom the limb was considerably shortened, notwithstanding the most scrupulous attentions.
25. Besides, all that is gained by the relaxation of some muscles, is lost, by the tension of several others. The knee cannot be bent without the triceps flexor being brought into action; an inconvenience the more serious, as this muscle acts immediately on both fragments. The rectus anterior, though relaxed by the flexion of the thigh, will be thrown into a state of tension by the flexion of the leg. The muscles attached posteriorly to the upper fragment, and even to the superior part of the lower one, will also in certain positions of the limb be rendered tense.
26. Hence it follows, that there can be no just comparison instituted as to the position proper for the limb, between fractures of the upper and those of the lower extremities; that, in the latter, the method pursued by the English surgeons presents an aggregate or general amount of inconveniences so great as to overbalance that of its advantages; and, that the position directed by Hippocrates and the other Greek physicians (22) ought to be adopted.
27. Having determined on the position, the operator proceeds to extension and counter-extension, which are to be made first in the direction of the limb as deformed or altered by the fracture, but must be changed afterwards according to the natural direction of the thigh. I need not here repeat the directions for this double operation: common to all fractures, they contain nothing particular, in relation to that of the thigh. But, on what part should extension be made? Petit, Heister, Duverney, and all their predecessors, recommend to apply the means or powers for making extension above the knee; a precept which is still to be found in the surgical department of the Encyclopedia. A strap surrounding the lower part of the thigh, aided by another placed at the ancle, serves, in this respect, to draw the inferior fragment downward.
28. Dupouy was the first to remark, that this practice rendered it necessary to employ great force, and that it would be better to make extension only on the foot. To this consideration Fabre added that of the inconvenience of the pressure made on the muscles, a pressure which, by irritating them and making them contract, multiplies the obstacles to the reduction.
Desault adopted their doctrine, from nearly the same views of the subject, introduced it into the Hotel-Dieu, and the success which attended it, in his practice, contributed not a little to bring it into general use.
29. For the purpose of making extension, he used the foot as a lever of the first kind. The two hands of an assistant, grasping it in such a manner, as to make the fingers cross on the back of it, while the thumbs, also crossing each other, corresponded to the sole, represented the power; the articulation represented the centre of motion, or fulcrum, and the leg together with the lower fragment, the resistance. The requisite motion was then communicated to the foot, and in that way was the extension effected. This mode is more advantageous than that usually employed, where the hands are applied to the lower extremity of the leg; for the force of the extending power is generally in the inverse ratio of its distance from the resistance intended to be overcome.
30. What I have said of extension (28), applies also to counter-extension. The strap, which was formerly placed for this purpose in the groin of the affected side, by compressing the adductores, and the rectus internus, produced in them a contraction, which, by drawing the lower fragment towards the pelvis, opposed obstacles to the reduction, which are seldom experienced, when, like Desault, the surgeon contents himself with having the trunk held by assistants, either exclusively at the hips, or both at the hips and under the arm-pits. The resistance being always easily overcome in this affection, renders it unnecessary to have recourse to more powerful means.
31. Hippocrates advises, in fractures of the os femoris, to aid extension by coaptation, performed with the hand. All practitioners, since his time, have added this third manœuvre or process to the two first, namely, extension and counter-extension. But, what effect can the hands produce, in most cases, on the bone through the thick covering of the soft parts? Are we able to communicate to it through such a mass whatever lateral movement we please? Being quite lost in the intervening soft parts, will our efforts reach the bone, in the direction which we give them? The muscles bring the fragments into contact, much better than we can, as soon as extension has removed their overlapping. Indeed, if well executed extension makes the lower fragment return along the same track which it pursued in becoming displaced, it will then be inevitably brought into contact with the upper one by the contraction of the muscles. Besides, in most oblique fractures, is it not evident, that the lower fragment must be made to slide from above downward, on the inclined plain presented by the upper one, and on which it has slided from below upward, in becoming displaced? Is it while extension is making that coaptation ought to be performed? Certainly not: because, if the extension be well directed, an attempt at coaptation will derange it; and if it be not well directed, its course ought to be changed. Is it after extension is finished that recourse ought to be had to coaptation? By no means: because if there be then any remains of deformity, it must be owing to extension having been improperly directed. The remedy, therefore, is, to renew the extension, and direct it properly.
32. Hence, it follows, in general, that coaptation is here a feeble assistant towards reduction; that if it renders any service, it is only in cases of displacement laterally, or in the direction of the cross-diameter of the bone; and that it is by giving the proper direction to extension, by managing it according to the disposition of the muscles, and by knowing when to augment and when to slacken it, that the fragments are brought into regular contact.
33. If the inferior fragment has experienced a rotatory motion on its own axis outwards or inwards (18), the assistant ought, in making extension, to turn the limb very gradually in the opposite direction.
34. Extension was formerly attended with difficulties, which are rarely met with at the present day. Oftentimes, if we give credit to authors, it was altogether useless to endeavour, in the first instance, to reduce the fracture, and restore the limb to its natural length, as the contraction of the muscles rendered the operation absolutely impracticable. Hence, applications of a soothing and sedative nature were employed, previously to an attempt at reduction. The following circumstances have been assigned as the cause of these difficulties. The upper strap, irritating and drawing upwards the adductores and the rectus internus, drew the lower fragment in the same direction, while the semi-tendinosus, semi-membranosus, biceps, &c. being drawn downwards by the lower strap applied over them, drew the pelvis also downwards, and, consequently, the superior fragment connected with it. From this double action arose a double motion directly opposed to that which ought to be produced by extension.
35. There are still cases, where the muscles, in consequence of being irritated by projections or points of bone, by the efforts of the assistants, and by a morbid state of the nerves, increase their contraction to such a pitch that no practicable force can bring the fragments into apposition. What means are then to be employed? All those, in general, that diminish irritability, varied according to circumstances, such as diet, venesection, &c. In such cases, Desault obtained the most happy effects, by placing the limb in a state of continued extension; fatigued by the permanent tension in which they are thus kept, the muscles relax by degrees; their force diminishes; at length they yield, and the reduction is accomplished.
§ VI.
36. The mere reduction of a fracture of the os femoris, is but one step towards the cure. In this, more than in the fracture of any other bone, causes which act incessantly (13) tend to subvert the momentary work of art; it is here, then, in particular, that means ought to be devised for maintaining this work. But, the first of these means is a suitable position of the limb. I have already mentioned the inconveniences that result, both as to the reduction and subsequent treatment, from that proposed by Pott (24...26). The patient must, then, be laid horizontally on a plain exactly even, and not capable of being affected or rendered uneven by the weight of the body. Instead of feather beds generally used in other cases at the Hotel-Dieu, Desault, in cases of fractures, substituted firm and hard mattresses, which, not sinking in the least, by the pressure of the body, give no cause to apprehend those continual displacements, to which a soft bed exposes the patient. These mattresses supersede the advice of certain authors who direct a plank to be placed under the patient.
37. The second means, not less efficacious than the first, consist in the forms of apparatus, in which the limb is placed, and which, being differently modified according to the fancies of their different authors, present us with an assemblage of various splints, compresses, &c. To appreciate, with accuracy and correctness, the advantage and disadvantage of these, let us first unfold the curative indications which they ought to fulfil; we will then compare their mode of action with these indications, from whence will result, as necessary inferences, the object of our research.
38. The intention of every form of apparatus being, to prevent the displacement of the fragments, the causes of this displacement ought to be the basis or foundation of its mechanism and construction. But these causes in the present case are, 1st, the muscular action drawing the inferior fragment upwards (10); 2dly, the weight of the body pushing the superior fragment downwards (14); whence every form of apparatus intended to keep the os femoris in place when fractured obliquely, ought, 1st, to draw the lower fragment downward and retain it there; 2dly, to draw and retain upwards the superior fragment, and the trunk which bears on its upper end. This principle is applicable generally, and subject only to a few exceptions which I shall notice when treating of transverse fractures, where the displacement is lateral, or in the direction of the cross-diameter of the bone, or where no displacement at all exists. 3dly, The apparatus must also be so constructed as to prevent the rotatory motions of the lower fragment (18), and secure the immobility of the limb, lest by means of some motion being communicated to it, the fragments might be deranged.
§ VII.
39. If to these indications we compare the mode of action of the different pieces that unite in composing our common forms of apparatus which do not make permanent extension, such as common bandages, splints, compresses, bolsters, &c. we will perceive that they are but ill calculated to fulfil them: and first of bandages. Whether the common roller, or the eighteen-tailed bandage be employed, their mode of operation is the same: their only action is, to add a second exterior and artificial covering to the natural cutaneous and aponeurotic covering of the thigh; to press against the fragments the muscles which form for them a kind of natural case intended to keep them in apposition; and to augment, by this pressure, the lateral resistance of the soft parts. By this contrivance, lateral displacements will, in part, be well guarded against, and, in this respect, these bandages are useful in transverse fractures. But what is there in them to prevent the two inclined plains of an oblique fracture from sliding on each other? What provision is there in them to secure the limb from the effects of motions and shocks which may be accidentally impressed on it from without? Will the pelvis be kept steady by them? or will muscular action be sufficiently checked and kept under by them? The force of the muscles will indeed be slightly diminished by means of compression; and to make this compression is the principal use of these bandages in oblique fractures. But will mere compression be sufficient to prevent a displacement in the longitudinal direction of the bone, particularly if the rollers be slack, as certain practitioners recommend, on the ground of the fallacious theory of Duhamel, who conceived, that a constriction too tight, would injure the action of the periosteum, which, according to him, is the sole agent in the formation of callus? So much, then, for bandages, whose only use is to prevent, by compression, the swelling of the limb, and to diminish, in some degree, the contraction of the muscles, which they press against the fractured bone.
40. These remarks apply equally well to the use of compresses; which make but a very feeble resistance against a powerful cause, and cannot be considered as any obstacle whatever to displacement. What can be said of those surgeons who, from servile attachment to a particular form of apparatus, do not consider a fracture as reduced, unless a certain quantity of compress secured by a given quantity of roller, be applied on the limb. Servile imitators in an art which calls for genius in its votaries, they are only capable of following, without reflection or judgment, the steps of their predecessors.
41. Bandages will do nearly as much harm as good in fractures of the os femoris, if, as was practised by the ancients, they be formed by a single roller surrounding the limb: in such a case, the limb being necessarily raised up at each time of their reapplication, will be exposed to continual displacements. Hence the ingenious idea of applying to simple fractures of the lower extremities the eighteen-tailed bandage, invented for compound fractures, and by means of which the thigh may be suffered to remain at rest. But to this bandage belongs also an inconvenience. The pieces which compose it, being stitched together, cannot be separated, and if one of them be soiled they must all be changed. Hence the superiority of the bandage of slips, known in former times, and engraved by Scultel, but long since forgotten, till Desault revived the use of it, and adopted it exclusively, both in simple and in compound fractures.
42. Splints of different kinds, which form the second division of the pieces of apparatus, used for fractures of the os femoris, have the advantage of fixing the limb in a solid and firm manner, and securing it from any displacement that might result from jolts, or muscular contraction, arising from the inattention of patients: these prevent, more effectually than bandages, any displacement laterally, and, on this account, their use is sufficient, even without extension, in transverse fractures: they also prevent, particularly if they be made of wood, the rotatory motion of the thigh either outwards or inwards (18). But if the division be oblique, will they prevent the gliding of the fragments over one another, and the consequent shortening of the limb? They can evidently produce this effect in no other way, than by the forcible pressure made by the pieces of apparatus, particularly by the straps or bandages that secure the splints, and then, to make effectual resistance, it would be necessary to apply them with such a degree of tightness as would endanger the life of the limb. Will splints prevent the trunk from sinking downwards, and pushing the superior fragment before it? Will they prevent the muscles from acting on the lower fragment? Can they, in a word, fulfil all the indications formerly pointed out (28)? Certainly they cannot. Splints, then, are calculated only to prevent displacement in the lateral or cross direction of the bone, and to secure, better than bandages, the immobility of the limb. Whence it follows, that they ought not, in this case, to be confined to the thigh alone, but should extend to the leg, whose movements, if communicated to the os femoris, may derange the contact of the ends of the bone. The neglect of this precaution, contributed formerly not a little to displacement and deformity.
43. In former times a kind of splints was in use, which were made by securing bundles of straw round sticks proportioned in length to the length of the limb to which they were to be applied. But as these, from being of a round or cylindrical form, touched the limb with but a narrow surface, they did not retain the fracture with sufficient firmness. They were, therefore, very properly exchanged for flat and strong wooden splints, (such as Desault used) which retain the fracture much better, in consequence of presenting to the limb a broad surface, and thereby rendering it in some measure immoveable.
44. The bolsters for filling up interstices, being less intended to prevent displacement, (in which respect they are, notwithstanding useful) than to guard the limb from the immediate pressure of the splints, usually consist of several folds of old linen; this is the form adopted at the Hotel-Dieu; but to these Desault preferred small pallets or bags filled with chaff, which, fashioned according to the form and disposition of the limb, may, at the pleasure of the surgeon, be made thicker or thinner, to suit the inequalities of the surface, in consequence of the ease with which the chaff may be moved from one part of the bag to another.
45. From the foregoing examination of the action of bandages and splints, it appears, that the common apparatus, formed by their union, but not calculated to effect a permanent extension, may perhaps answer in cases of transverse fractures, which indeed but rarely occur, but are always insufficient when the division is oblique, because they cannot fulfil the double indication of drawing the inferior fragment down, and retaining the superior one up (38).
§ VIII.
46. By what means then can this indication be effectually fulfilled? By that which will perpetuate, throughout the whole treatment, the action of those means by which reduction was effected; by that which, to the ever active power of the muscles, will oppose a resistance constant in its action; by that which, forming on the exterior of the thigh a kind of artificial muscle, may become an antagonist to the natural muscles of the part, and neutralize their efforts, by acting in a contrary direction, and which, by pushing up the pelvis and retaining it there, may prevent it from being pushed downward by the weight of the trunk (14). But what other mean than that of permanent extension, unites these advantages? Whatever form of apparatus may be employed to obtain it, it is permanent extension alone that can prevent the displacement, because it alone is founded on principles calculated to meet and obviate the causes by which displacement is produced.
47. The ancients, though less informed than we are respecting the nature of these causes, knew better how to appreciate their effects. All their forms of apparatus made a permanent extension, a measure which has been abandoned by most of the moderns, and regarded, even at present, in France, by a great number of practitioners, as always dangerous, and seldom useful. Let us set in opposition to the vain fears which it inspires, a few thoughts, and much experience.
48. It is from the very object which is proposed to be attained, that the first difficulties arise. What must we think of a limb in a state of preternatural tension, where all the parts being overstretched must experience an uneasiness not to be supported? I answer, that it is not a preternatural elongation that extension produces; on the contrary, being intended to prevent a preternatural shortening, it has for its object to restore the parts to their ordinary state, and to give to the muscles their habitual degree of tension, by opposing such contractions in them as are not habitual: under this point of view, it performs, in relation to the muscles, those very functions which are discharged by the bone itself, when sound and unbroken, as is fully experienced by all patients, when the apparatus is applied. Its use not only does not increase pain, but is alone calculated to diminish it, because, by bringing the fragments into apposition, it prevents the soft parts from being irritated by the points of the bones.
49. Is the swelling of the limb to be dreaded, as some pretend? But whence can this swelling arise? From the over-stretching of the parts? I have already proved that they are not over-stretched. From the pressure of the straps? Perhaps this cause might produce a swelling, if, as formerly, it were applied above the knee; but, by placing it, as Desault did, near to the ancle, by surrounding, with a thick compress, the lower part of the leg, where the straps pass, and by securing the foot with a tight bandage under the straps, if their action be dreaded, this fear must be done away; and, besides, experience, which is the only true test of the dangers of a process, by no means justifies the apprehension. The venæ saphenæ and the absorbents that accompany them, are free from the compression, which bears principally on the tendo Achillis, and the malleoli.
50. What shall we say in reply to the censure thrown on the process of permanent extension, in the memoirs of the academy, where it is charged with having been oftentimes productive of ulceration and even gangrene, in consequence of the pressure of the upper strap? What method can escape censure, if it be unskilfully pursued? What process will not be injurious, if mutilated and ill managed by ignorance or a want of discretion? To represent the thing properly, let us suppose the worst: a circular bandage, in consequence of being drawn too tight, produces mortification in the subjacent parts; must circular bandages be on this account entirely rejected? An unskilful hand, in an operation for cancer, opens the axillary artery; must we therefore cease to search under the arm-pit for schirrous glands?
51. Permanent extension is, say some, insufficient to overcome muscular action; it is opposing to a power equal to 1000, a resistance equal to only 100. But this force of the muscles, which is oftentimes so great at the time of reduction, diminishes gradually, by the pressure of the bandages, by the immobility of the limb, and, above all, by long continued extension; for a continued effort equal to 10, will soon perform what could not be effected by a temporary exertion of a force equal to 100. Let us pass over the more minute objections made against permanent extension, and search among the different modes of performing it, that to which practitioners ought to give a preference.
52. We may throw into two classes the general modes proposed by different authors for effecting permanent extension. Under the one are included those modes requiring simple means, such as straps, splints, &c. while the other embraces such as, from being complex, necessarily call for the use of different machines.
53. In the first class are comprehended:
1st, The method employed in the first instance by the Arabians, adopted afterwards by their successors in medicine, and proposed, at a still later period, by Petit, Heister, and Duverney, and which consists in fixing, at the head and foot of the bed, during the whole treatment, straps intended for the purpose of extension.
2dly, The mode of extension, adopted by many practitioners, which consisted in suspending to a strap fixed at the knee, and reflected over some suitable body, a weight proportioned to the power of the cause which it was intended to combat.
3dly, The ingenious idea of Bruninghausen, who, confining by a kind of stirrup, the diseased leg against the sound one, made the latter serve as a splint to retain the fractured limb on its proper line, and thus preserve its natural length.
4thly, Under this class also must we arrange the means employed by Desault, and which we will presently describe.
54. The second class of means invented for the purpose of making permanent extension, in fractures of the thigh, comprehends:
1st, The Glossocome, the bed of Hippocrates,24 and other machines, used by the ancients, to effect a reduction, in fractures of the os femoris, and, at the same time, to maintain the reduction, by being left on the limb.
2dly, Numerous machines, invented for the purpose of suspending a weight intended to make extension. These have been differently varied and modified, more by the imagination than the judgment. Engravings of some of them are to be found in Scultet, Fabricius of Hilden, Pare, &c.
3dly, The machine of Bellocq, proposed to the Academy of Surgery, a description of which is contained in their memoirs, and which possesses an advantage not found in the others, namely, that of taking its point of extension at the lower part of the leg.
4thly, The machine of Nook, surgeon at Norwich, improved by Aitkin, an engraving of which is given by Bell.
5thly, A new Glossocome, published in the works of Manne, and a great number of other machines, the ephemeral offspring of the genius of their authors, the utility of which experience has seldom confirmed, and which were even dead-born in the opinion of practitioners. I barely mention these, because a circumstantial description of them would lead me from my subject.
55. We may discover at a single glance the comparative merits of these two classes of apparatus. Extension produced by simple means, such as straps, splints, &c. (50), may at all times, and under all circumstances, be had recourse to; because the means necessary for making it may always and every where be found. Are we desirous, on the other hand, of having recourse to machines (54)? These are seldom at hand, and oftentimes not to be obtained: the expense attending the purchase of them, prevents most surgeons from procuring them. They no doubt possess the advantage of multiplying forces, and rendering them more powerful: but, I have already said (51), that a gentle resistance, if long continued, is sufficient to overcome at length the contraction of the muscles, though at first extremely active and energetic.
56. In the first point of view, the first class of means is doubtless preferable to the second. But they both partake generally of the inconvenience of placing the point of extension above the knee. I have already mentioned the effects which this produces with respect to muscular action, at the time of the reduction (28). To the injurious effects there stated may be added the swelling of the limb, arising from the compression made by the straps, the disadvantage of the mobility of the leg, which is not fixed, and the motions of which, being communicated to the thigh, may separate the fragments after they have been brought into apposition. Further, the straps may readily slip down over the knee, and thus leave the fragments subject to the mischievous influence of muscular contraction.
57. To these general disadvantages, add those peculiar to each form of apparatus, which are too tedious to be detailed at present, and you will perceive, that the little success hitherto obtained from continued extension, is owing, not to the nature of the measure itself, but to the manner of employing it, and that, in the present case, as in cases of fractured clavicles, another step towards perfection remained to be made.
58. Desault, in the first instance, attempted only to improve the ancient process, which consisted in fixing the straps for extension to the foot and head of the bed. He remedied the inconvenience of fixing the straps at the knee, by doing, throughout the whole treatment, what Fabre and Dupouy did only at the time of reduction (29); that is, he placed the seat of extension at the foot. The hold for counter-extension was also changed. This he made by a bandage for the body, fastened round the breast, and drawn only moderately tight, lest it might impede the patient’s respiration. The rest of the apparatus was nearly as I shall presently describe.
59. This was, for a long time, the only apparatus which Desault used. He introduced it into the Hotel-Dieu, after having employed it at the hospital of Charity, with great success. In the mean time, the utmost care and attention were here indispensable: every day it was necessary to examine the rollers several times, as they readily became relaxed. The pelvis, not being well secured, could communicate motion to the fracture: it was difficult to raise the patients to the close-stool. Besides, the slightest disease of the chest, rendered the pressure of the body-bandage insupportable. It was this very inconvenience which, having, in a certain case, rendered the preceding apparatus inadmissible, suggested to Desault the following one.
60. This consists, to speak in general terms, in taking the points of extension, above, on the tuberosity of the os ischium of the diseased side, and below, on the malleoli; in securing the straps or rollers, destined for making extension, on the two ends of a strong splint, placed along the outside of the limb; and in converting, so to speak, the pelvis, the thigh, the leg, and the foot into one entire and solid piece.
The pieces which compose it are, 1st, A common junk-cloth25 (FFF plate II.), accommodated to the size of the limb and the splints: 2dly, a bandage for the body (BB) and one passing under the thigh (H) to secure the first on the side opposite to the fracture: 3dly, three stiff splints, an inch and a half wide, the external one of which (AA) being very strong, must be long enough to extend from the spine of the ileum, to the distance of four inches below the sole of the foot. This splint is hollowed out or notched at its lower end, and has a mortise in it a little higher up. The upper splint (CC) occupies the space included between the fold of the groin and the upper part of the knee: and the internal one, which reaches from the upper and internal fold of the thigh, to the sole of the foot: 4thly, three bolsters, an external, an internal, and an upper one (d d d d) consisting of small bags of chaff: 5thly, a bandage of strips (E) accommodated as to number to the circumstances of the case, separate from one another, each three inches broad, and long enough to go twice round the limb, arranged from below upwards, and overlapping each other, about one third of their breadth: 6thly, one long and two circular compresses, intended to be applied immediately on the limb next to the skin: 7thly, two strong rollers (g g and L) intended for extension and counter-extension, at least an ell and a half long: 8thly, one long and thick compress, and a sufficient number of bits of tape.
61. Every thing being ready, previously to putting the patient to bed, the pieces of apparatus are to be arranged on that part of the bed corresponding to the fractured thigh, in the order in which they are to be successively applied. If the patient has been already laid in the place where he is to remain, the limb must be raised with great caution, and, during the extension, each piece gently slipped under it, or the whole must be passed under at once, being first rolled round the several splints, in such a manner, that the apparatus requires only to be opened.
62. Extension is now made in the mode already pointed out (29 and 30), and then the application of the apparatus is begun, for which the surgeon must be situated on the external side of the fractured thigh, while an aid, placed on the other side, gives him assistance.
1st, On the thigh, next to the skin, are first applied the long and circular compresses, accurately spread out so as to have no wrinkles in them, and previously wet with vegeto-mineral water. Around it are then applied, in succession and from below upwards, each strip of the bandage (EE) moderately tight.
2dly, The lower end of the leg is now covered with a thick compress, intended to prevent the impression of the roller (L), which is fixed in such a manner, that its middle is first laid on the tendo Achillis, a little above the heel, while its two ends, crossing each other on the upper part of the foot, are carried on each side to its sole, where crossing again, they are then laid down till the close of the application of the apparatus.
3dly, Along the thigh are placed laterally two bolsters, which, from their thickness being easily increased or diminished in consequence of the moveable nature of the chaff, mould themselves to the inequalities of the limb.
4thly, Around the two lateral splints, the surgeon and his assistant roll, each on his respective side, the two edges of the junk-cloth, so that both splints, by being accurately applied on the bolsters, may make a uniform compression on the whole part.
5thly, The third bolster (d d d d) is then applied on the anterior part of the limb, and over it the splint (CC).
6. The bits of tape passed under the apparatus to the number of four for the thigh, and three for the leg, are tied in succession on the external splint, lest the knots, should they correspond to the thigh, might, by their contact, prove troublesome. That one next to the fracture is tied first, and they are all drawn as tight as the patient can bear them without uneasiness.
7. The body-bandage is now fixed on the pelvis, in such a manner, as to secure laterally the external splint, and is itself retained by the sub-femoral bandage (H), that is, the bandage passing under the thigh.
8. A thick compress placed beneath the tuberosity of the ischium, serves as a cushion or bolster to protect the part from the pressure of the roller (g g) which, being passed first under the apparatus, and drawn afterwards obliquely from within outwards, and from above downwards, takes its points of bearing or action, in one part, on the tuberosity of the ischium, and in the other, on the upper end of the external splint, and is tied in the fold or hollow of the groin.
9. The two ends of the bandage (L) previously made to cross each other on the sole of the foot, are passed the one through the mortise, and the other through the hollow or notch in the lower end of the same splint, and then, being drawn forcibly, are tied in a firm knot, so as to act as a substitute for the hands of the assistant, who now lets go the patient’s foot.
10. If the roller (g g) become relaxed, it is tightened again, and the patient being laid in a suitable position, the limb is protected from the pressure of the bed clothes, by a kind of basket placed over it.
11. A roller (K k) laid first on the sole of the foot, and then brought across over its upper side, and fastened laterally to each splint, serves to secure that part from turning outward or inward, and thus prevents the rotation of the limb.
63. If the mode of operation of this bandage be compared with the general indications formerly established (38) for all oblique fractures of the os femoris, it will be easy to perceive that, conformably to those indications, it tends, 1st, to draw the inferior fragment downward; 2dly, to retain the superior one up; 3dly, and to prevent the rotation of the lower fragment, and secure the immobility of the limb.
64. It is evident that the bandage or roller (g g) so unites the pelvis to the external splint (AA), that the latter cannot be pushed upwards, without drawing the former in the same direction, as well as the superior fragment which adheres to it. But if, after this roller is fixed, the lower one (L) be tightened, the first effect produced is, to push the external splint forcibly upwards; the second, to draw the leg, and with it the inferior fragment downwards; so that, by fixing the roller (L) in the notch and mortise of the splint with the necessary degree of tightness, extension and counter-extension are made permanent. By this means the muscles, being kept on a stretch, lose by degrees their power of contraction, which is still further diminished, by the immoveable state in which they are kept, and by the compression made on them by the bandage of strips. So that, on the one hand, the inferior fragment will have no tendency to rise upwards, and even if it had, it will meet with a sufficient resistance to prevent it; while, on the other hand, the superior fragment will not be pushed downwards by the pelvis.
65. To this advantage is added that of a state of perfect immobility. The pelvis, the leg, the thigh, and the foot being firmly fixed on the external splint, constitute one entire whole, all the parts of which must retain, with respect to each other, the same relative position. Should even a stroke be accidentally given to this assemblage of parts now converted into a solid whole, each portion of it will move at the same time, there will be no partial motion, and the relative position of the parts will not be changed. Hence the advantage of being able to raise the patient without apprehension; a most desirable circumstance indeed, in a position so painful and so long continued (26). The external splint, being extended beyond the sole of the foot, prevents the lower fragment from obeying a tendency, which it sometimes has, to displace itself by a rotation on its axis. Should this tendency be towards the internal side, an occurrence much more rare, the lengthening of the internal splint will effectually prevent it.
66. These considerations induced Desault to renounce his ancient mode of making permanent extension, and employ this exclusively, in the latter years of his practice. Like all other kinds of apparatus, formed principally of rollers, this is very subject to become relaxed; and requires, therefore, great attention on the part of the surgeon. It ought to be examined attentively every day, particularly the two extending bandages (L and g g). As soon as they become relaxed, they must be immediately tightened again: without this precaution, the effect of the apparatus will be lost. Be vigilant also, with respect to the compress placed between the roller (g g) and the tuberosity of the ischium. Should this slip, the roller being frequently tightened, and pressing immediately on the skin, may produce excoriations and ulcers difficult to be healed, particularly in females. The roller itself may slip, and then, having no longer a solid point of support and action on the tuberosity of the ischium, it makes extension in but an imperfect manner.
67. One of the charges brought against this apparatus is, the facility with which the upper roller becomes displaced, a facility that imposes a degree of care and attention, of which few surgeons are capable, and which, when bestowed even by Desault himself, did not always prevent the shortening of the limb.
68. Further, the extension made on the fold of the thigh, partakes, a little, of the inconvenience that accompanied the ancient mode of reduction, namely, that of compressing and irritating the muscles of the upper and internal part of the thigh (30). This inconvenience would be still more sensible, if, for want of extending to a sufficient distance up the pelvis, the upper splint should allow the roller to cross the muscles at an angle somewhat acute, as it would then enclose and press on the greater part of them.
69. If some unfavourable cases, resulting without doubt from these inconveniences, did occur in the practice of Desault, a multitude of successful ones still attest the advantages of this method; and there is not a pupil who attended any time at the Hotel-Dieu, without witnessing them. I will relate but one case, collected by Chorin, to furnish a detail of the treatment subsequent to reduction, referring the reader for further information to the Journal of Surgery.
Case II. Theresa Little-John, aged 45 years, fell, drawn by the weight of her own body, through a window in a balcony, from which she was leaning. She was instantly taken up, carried to her own house, and from thence to the Hotel-Dieu, which she entered on the 28th of October, 1790. From the signs mentioned (9), a fracture was discovered towards the lower part of the thigh; its oblique disposition required an apparatus to make permanent extension. This was applied in the usual manner, and, in an instant, the patient, who had experienced, since her fall, severe pain, became calm, and was completely relieved.
In the night, pains returned; agitation; some spasmodic motions; an anodyne draught administered in the morning. In the course of the day, these troublesome symptoms disappear; a slight swelling at the ancle. Third day, no pain; swelling gone; aliment increased. Sixth day, patient permitted to return to her usual regimen; extending rollers relaxed; lower one tightened: eleventh day, apparatus renewed; fragments in perfect contact: thirteenth day, limb moved incautiously; a slight shortening; apparatus reapplied; extending bandages drawn tight: sixteenth day, a disposition slightly bilious; evacuants administered with success: twenty-fourth day, a third application of the bandage: thirtieth day, progress in consolidation already very evident; the limb straight: fortieth day, extending rollers laid aside: fifty-second day, consolidation complete without the least deformity.
70. The muscular force, in children, being weak, and the weight of the body inconsiderable, have, in general, much less influence in producing a displacement in them than they do in adults. When, therefore, fractures occur in subjects under six or seven years old, the resistance, on the part of the apparatus, need not be so great. In general the lateral pressure which it makes, and the bearing of its different pieces against the limb, are sufficient to prevent the return of deformity, when this has been perfectly removed by reduction.
71. In such cases Desault covered the thigh with a circular bandage, made of a roller seven ells long, and three inches broad. Beginning with this below, near to the condyls, he carried it upwards, by oblique and reversed turns, to the pelvis, round which he threw a cast; then, giving the ball into the hand of an assistant, he applied four splints, one before, another behind, and one on each side: directing these to be held at their lower part near to the knee, he resumed the roller, and secured them firmly by a second series of circular and reversed turns, descending to the lower extremity of the thigh. The limb was then placed in a proper position, and, in general, of whatever kind the fracture was, whether oblique or transverse, this simple bandage, without the aid of permanent extension, was sufficient to retain it.
72. It would be difficult to determine the period necessary for the consolidation of fractures of the os femoris. Numerous circumstances concur to influence this work of nature, which is, in general, extended beyond the term of forty days, vulgarly assigned to it by the people at large. Besides, a stiffness of the limb, the inevitable effect of its long state of rest, still adds to the length of the patient’s confinement, by retarding the necessary motions, the return of which, as in other similar cases, can be accelerated only by exercise.
73. Complicated fractures of the os femoris, being included in the general class of solutions of continuity of that description, cannot be at present particularly considered. We will only remark, that here, in like manner, as in fractures of the clavicle, permanent extension constitutes the most effectual method of preventing the pains, oftentimes insupportable, occasioned by splinters or points of bone irritating the soft parts, from being pressed against them by muscular action in its tendency to shorten the limb.
§ IX.
74. I will close this article by a few remarks on the advantages of permanent extension in old fractures. Nature reunites fractures differently, according to the relation of the divided surfaces to each other. Are those surfaces in perfect contact? If so, they are chiefly instrumental in the formation of callus, which then probably acts in a manner similar to the reunion of wounds. On the other hand, does an overlapping of the fragments separate the divided surfaces from each other; the reunion takes place then principally on the sides, by a kind of enlargement of the bones, produced no doubt by the periosteum. Such is the mode of consolidation, which, on opening dead bodies, is found in most oblique fractures of the os femoris, succeeded by a shortening of the limb.
75. Hence it follows, that this shortening, which would readily yield to extension, at the time of the fracture, becomes obstinate in its resistance, in proportion to the age of the accident. In such a case, indeed, the substances destined to reunite the overlapping fragments, acquiring daily more and more solidity, oppose to the reduction obstacles constantly increasing. Hence, most practitioners regard this reduction as beyond the resources of art, after the expiration of the twelfth or fifteenth day. Nor is this opinion entertained without some foundation, for at a later period, almost all efforts at reduction, however powerful, have proved unavailing. But that which cannot be performed by a very powerful effort, acting momentarily, is, notwithstanding, oftentimes easily attainable by a much weaker one, provided it be long continued. The following cases are in proof of this.
Case III. Ann Gallot, of Melun, aged sixty-nine, having fractured her right thigh, by falling down the steps of a cellar, remained twenty-two days without assistance, and without even knowing the nature of the accident, when, on consulting a surgeon, she was sent to the hospital at Versailles. From the long standing of the disease, a reduction being despaired of, and no one being willing even to undertake it, the patient was sent to the Hotel-Dieu, on the 27th of February, 1791.
A shortening of four inches distinguished the diseased thigh from the sound one. The overlapping was sensible to the touch: in the mean time, a slight mobility at the place of fracture, inspired a hope of being able, if not to restore to the limb its natural form, at least to diminish the contraction. Several efforts were made at first, but without success, as Desault foresaw. The apparatus for permanent extension was applied: on the day following, the extending rollers being a little relaxed, were again tightened. Fourth day, a sensible increase in the length of the limb; apparatus renewed. Ninth day, the left thigh but an inch longer than the other: eleventh day, equality in length almost re-established. After this, the apparatus was kept constantly applied and renewed from time to time.
Fortieth day, consolidation already perceptible: forty-sixth day, symptoms of a putrid fever have made their appearance: fiftieth day, symptoms worse; fifty-second, something better: fifty-fifth, worse again: fifty-seventh, dead. On opening the body, an oblique fracture was found, its surfaces very nearly in apposition, and already united by a very solid callus.
Case IV. Joseph Maugrin, a saddler, broke his thigh in the month of July, 1793. A surgeon being called to him, placed his limb in an old form of apparatus, which did not prevent a shortening, to the extent of an inch and a half, from showing itself on the following day: hence a new reduction, and a new application of the apparatus: but soon afterwards, another shortening; the same means to remove it; the same failure of means. Weary of such trials, the surgeon abandoned the limb to its fate, contenting himself with merely keeping it in the apparatus.
On the twenty-ninth day, Desault being called in consultation, and finding the thigh shorter by three inches than that on the opposite side, proposed permanent extension, persuaded that this expedient alone would soon be sufficient to re-establish the contact of the fragments. The proposal was acceded to. On the day following, the effects were already perceptible; the thigh was lengthened by almost an inch. By the sixth day, it was equal in length to the other: during this period, the extending rollers were tightened twice a day.
At the end of two months the consolidation was complete, and the patient walked perfectly well, except that there was a little shortening of the limb, trifling though indeed, compared to what would have been the consequence, had the original treatment been continued.
76. The lengthening of the limb, in these cases, was evidently owing to the continued action of the apparatus, which effected, in a length of time, what the momentary efforts of the surgeon could not accomplish. This it did, by destroying or gradually lengthening the medium of union, which already connected the overlapping fragments, by that means bringing their separated surfaces or ends into contact, and almost restoring to the bone its primitive form.
Art cannot always, with certainty, command such success, and perhaps, even at a less advanced period, a more rapid progress of reunion might leave but little ground for hope. But, could only an inch in length be gained by permanent extension, would it not be proper to have recourse to it, particularly as no inconvenience can result from the trial? To prevent deformity altogether, is the first object of art; but when that cannot be attained, to lessen it is the second.
The history of fractures of the upper end of the os femoris, includes, 1st, Those of the great trochanter: 2dly, Those of the neck. These fractures, sometimes existing together, and at other times separately, are very different with regard to the frequency of their occurrence: the one taking place very rarely, has but slightly engaged the attention of practitioners, who have multiplied their researches with regard to the other, particularly in late years.
§ X.
77. Fractures of the great trochanter are the effect either of falls on that protuberance, or of the action of bodies striking against it. Oblique or transverse, situated sometimes at its summit, and sometimes at its base, these fractures may be either simple or complicated. They are rendered complicated sometimes by splinters and a swelling, as happens when a ball produces the division, and at other times by a fracture of the neck of the bone, an example of which we find in the Journal of Surgery, in the case of a man seventy years of age, who had been long subject to the itch.
78. Whatever the varieties may be, the fracture will be characterized, 1st, By a facility of moving the great trochanter in every direction, while the pelvis and the thigh remain without motion: 2dly, By a crepitation, arising from the friction of the divided surfaces against each other: 3dly, By there being no shortening of the limb, when the fracture exists alone: 4thly, By the fragments being brought together in abduction, and separated in adduction: 5thly, By the position of the great trochanter being higher and more anterior than natural. The presence of these signs is the more readily perceived, because, being superficially situated, this protuberance can be easily felt, and yields to the motions impressed on it.
§ XI.
79. The reduction is effected, by pushing the separated fragment in the direction opposite to that of its displacement, by bringing it to its natural level, and, in certain cases, by moving the thigh a little outwards; it is retained by means of some compresses placed by its sides, and secured by a roller directed obliquely from the sound hip towards that part of the thigh corresponding to the fracture, and representing a true spica bandage.
80. A fracture produced by a gun-shot wound, always renders large incisions necessary, for the purpose of extracting foreign bodies, and relaxing the aponeurosis of the fascia lata, which suffers too great a degree of tension in this place, and might, if not dilated, produce a very troublesome stricture. A fracture complicated by splinters, but without an external wound, and produced by a body striking against the part, seldom requires any particular apparatus, because, adhering as yet to the periosteum, the separated portions of the os femoris may unite again, either among themselves, or with the fragments.
§ XII.
81. The neck of the os femoris, being surrounded by a large mass of soft parts, and protected by the great trochanter, which forms its external boundary, is almost completely secured from the immediate action of external bodies, and consequently from direct fractures. Whenever it sustains a fracture, it is always by a true counter-stroke, resulting from a fall, sometimes on the great trochanter, and at other times on the sole of the foot or the knee. But fractures produced in the first mode, are much more frequently met with in practice, than those produced in the second, doubtless because, in the latter, the motion is weakened by the extent of parts through which it is distributed, previously to its arrival at the neck of the os femoris. Out of thirty observations made by Desault, on fractures of this description, twenty-four of them were produced by falls on the side. All those recorded by Sabatier, in his interesting memoir, appear to have been produced by similar falls.
§ XIII.
82. Fractures of the neck of the os femoris may occur, 1st, in the middle part of it, where it is smallest, and where nature has not thrown together, as she does in the middle of the long bones so often exposed to fractures, a great quantity of compact substance: 2dly, at its upper end, where it is united to the head of the bone: 3dly, at its junction with the great trochanter, where the solution of continuity may be outside of the joint, a circumstance which doubtless happens much more frequently than has been hitherto suspected.
83. The division, rarely oblique, is almost always transverse: sometimes, in the latter case, the neck remains enclosed or imbedded, as it were, in the body of the bone, being fractured in such a way, as to present a hollow or notch of greater or less depth. Several cases of this kind occurred to Desault; one of them, modelled in wax, is deposited in the collection of the School of Health, and the original preparation is in my possession. The fracture, though frequently simple, is sometimes complicated with that of the great trochanter.
Case V. A man having received a kick from a horse, on the external and upper part of the left thigh, fell down, and, not being able to move, was carried home. Desault being called to him, discovered, 1st, that the great trochanter, separated from the bone, yielded readily to every impression it received: 2dly, that the limb was perceptibly shortened; that the least effort was sufficient to restore to it its natural length; and, that the foot was turned outwards, all which are characteristic signs of a fracture of the neck.
§ XIV.
84. Whatever may be the mode and place of the fracture, its diagnosis presents difficulties which experience and habit may doubtless overcome, but which too frequently puzzle and embarrass the most enlightened practitioner. Let us endeavour to diminish them somewhat, by tracing, in their order of succession, the symptoms which characterize the accident.
85. At the time of the fall, a sharp pain is felt; sometimes a report is plainly heard; a sudden inability to move the limb occurs; the patient cannot rise, a circumstance, however, which does not always take place. A case is recorded in the fourth volume of the Memoirs of the Academy of Surgery, where the patient walked home after the fall, and even rose up on the following day. Some examples of a similar nature fell under the notice of Desault, one of which he has recorded. The interlocking of the two fragments formerly mentioned (83), may serve to explain this fact, which is, however, in general, very rare.
86. A shortening almost always occurs in the broken limb, but this is more or less perceptible, according as the extremity of the fragments is retained by the capsule, or as, the division being without the cavity, no resistance is made to their displacement. The muscular action, drawing the lower fragment upwards, and the weight of the trunk, pushing the pelvis and the superior fragment downwards, furnish here, as in fractures of the body of the bone, the two-fold cause of this shortening. I will not repeat what has been already said on this subject (10...14); I will only observe, that, in the present case, the influence of the muscles is even more considerable, because, the lower fragment being much longer, is of course attached to a greater mass of muscular fibres. A slight effort is sufficient, in general, to remove this shortening, which, however, soon returns, when the effort ceases. This circumstance Goursault and Sabatier have observed, not to occur in certain cases, till some time after the accident. A tumefaction appears in the anterior and upper part of the thigh, almost always proportioned to its shortening, of which it appears to be the effect.
87. The projection of the great trochanter is almost entirely removed. That protuberance, being directed upward and backward, is approximated to the spine of the ilium. But if it be pushed in the opposite direction, it readily yields, and then, returning to its proper level, allows the patient to move the thigh.
88. The knee is a little bent. A severe pain always accompanies the motions of abduction, when they are communicated to the limb. If, while the hand is applied to the great trochanter, the limb be made to rotate on its axis, this bony protuberance is perceived to turn on itself as on a pivot, instead of describing, as it does in its natural state, the arch of a circle, of which the neck of the os femoris is the radius. This sign, which was first observed by Desault, is very perceptible, when the fracture is at the root of the neck, less, when it is in the middle, and very little, when it exists towards the head of the bone; these are circumstances, the cause of which it is unnecessary to unfold. In rotatory motions, the lower fragment, rubbing against the upper one, produces a distinct crepitation, a phenomenon which does not however always occur.
89. The point of the foot is usually turned outwards; a position which Sabatier, Bruninghausen, and most other practitioners regard as a necessary effect of the fracture, although Ambrose Pare and Petit have borne witness that it does not always exist. Two cases, reported on this subject by celebrated surgeons, have been thought unfounded by Louis, who has attributed them either to an error in language, or a mistake of the transcriber. But the practice of Desault has fully confirmed their possibility. The first patient whom he had under his care, at the hospital of Charity, after he was appointed surgeon in chief, laboured under a fracture which presented this phenomenon. Many other examples occurred to him afterwards, and he believed it might be laid down as an established principle, that, in fractures of the neck of the os femoris, the direction of the foot outwards is to that inwards as 8 to 2.
90. The common opinion is, that this direction outwards is to be attributed to the muscles that perform rotation. But, were that the case, 1st, it is evident that it would always exist: 2dly, all the muscles running from the pelvis towards the trochanter, except the quadratus, are in a state of relaxation, in consequence of the approximation of the os femoris to their points of insertion: 3dly, muscles in a state of contraction would not allow the point of the foot to be drawn so easily inwards. Is it not more probable, that the weight of the part draws it in the direction in which it is usually found.
91. From the foregoing considerations, it follows, that none of the signs of a fracture of the neck of the os femoris, is exclusively characteristic, that the whole of them, taken separately, would be insufficient, and that it is their assemblage alone which can throw on the diagnosis that light which is oftentimes wanting to it, even in the view of able practitioners. But after all, in the present case, as in every other one, should any doubt exist, it is right to take the safe side, and apply the apparatus, which is indeed useless but not dangerous if the disease does not exist, but indispensably necessary if it does.
§ XV.
92. The existence of a fracture being ascertained, what prognosis is to be formed respecting it? In answer to this general question, it will be sufficient, I think, to resolve the following particular ones. What accidents accompany the fracture in the first instance? What phenomena make their appearance during its reunion? In what manner does it affect the patient, as to his power of walking, after reunion has taken place.
93. If we attend to the opinion of authors, on this fracture, we will find that they represent it in very dismal colours, as if it were necessarily productive of the most serious effects. Inflammation of the parts adjacent to the neck of the os femoris, numerous and repeated abscesses arising from this inflammation, propagating themselves externally and communicating with the interior of the joint, gangrene itself, as Morgagni remarks in a particular case, convulsions of the limb, an œdema occurring in it, and a slow fever destroying the patient by degrees; such is the dismal catalogue of misfortunes, generally considered as necessarily attendant on the kind of fracture under consideration. Bruninghausen remonstrated against this fatal prognosis of authors, and Siebold, one of the most celebrated German practitioners, among a great number of cases that fell under his care, had no such accidents to encounter. Desault never experienced them. Doubtless they are prevented by our more exact and more skilful modes of treatment. It is thus that under a more judicious treatment, fractures of the olecranon and of the rotula, are no longer marked with those terrible consequences formerly attributed to them.
94. In as much as the organization of the os femoris, is nearly the same in its neck and in its body, it is difficult to conceive how the progress of nature can be different in fractures of these two parts; why the first, in being denied the power of healing or reunion should be, in this respect, distinguished from all other living parts of animals, which are particularly characterized by that power, when they have sustained a solution of continuity. Many practitioners, even at the present day, advocate this doctrine, which is built, one while, on the circumstance of the periosteum not being continued along the neck of the os femoris; another while, on a belief that the head of this bone cannot receive a sufficiency of nourishment for the work of consolidation, in consequence of being attached to the rest of the system, only by the round ligament, and again, on an opinion, that the synovial fluid, by wetting the divided surfaces, prevents their reunion.
95. But is the periosteum the only agent in the formation of callus? Modern experience has refuted this opinion, which, like many others, will therefore in a short time exist only in the history of our errors. Were it even true that the periosteum is here indispensably necessary, is not its place supplied by the fold of the capsule, which surrounds both the head and neck of the os femoris? Besides, why cannot callus be formed by that part which has had sufficient power to accomplish ossification, since it is universally acknowledged, that, in these two processes, the labour of nature is nearly the same.
96. The head of the bone, separated from the soft parts, and attached to the acetabulum by the round ligament, always receives through that ligament a sufficiency of nutriment to enable it to live in that cavity; for, there is no instance of its having suffered mortification in consequence of a fracture. Why, then, should it not partake of the properties of life, and particularly of the faculty of reunion when placed in regular apposition with the body of the bone?
97. What shall we say respecting the idea of the synovia wetting the divided surfaces, and by that means preventing their reunion? The history of fractures communicating with joints, better known at the present day, answers this objection, which is indeed nothing but the offspring of mere hypothesis. To these considerations, which are dictated by reason, and to which many more might be added, let us unite the proofs derived from experience, and we will find numerous examples of cures actually performed, particularly in latter times; the truth of this is attested by many cases collected by Desault, both at the hospital of Charity and the Hotel-Dieu. Bruninghausen and Siebold, have had equal success. Many analogous facts have been presented to the Academy of Surgery. In the cabinet of the School of Health, are deposited some preparations obtained from the cabinet of Desault, calculated to remove all difficulties and doubts from this subject.
98. We must acknowledge, however, that in persons advanced in years, the cure is always difficult, often very tedious, and sometimes impracticable, however carefully the treatment may be conducted. But this is only a necessary consequence of the laws of ossification, which, constantly accumulating in the bones too great a quantity of calcareous matter, seems to deprive them by degrees both of life and all its properties. Yet Lesne laid before the academy a case of reunion obtained in a subject at the advanced age of eighty-four.
99. The observations of some modern practitioners seem to prove, that the reunion here is not produced by a substance similar to common callus, but by a kind of ligamento-cartilaginous tissue, in like manner as in the rotula, and the olecranon. But why need we inquire after the means employed by nature? those of art must be the same. It will be always necessary to favour the reunion, by bringing the fragments into contact, and maintaining them so. Without this contact, either a cure will never be obtained, or the substance destined to effect a reunion, becoming deformed and too bulky, will impede motion.
100. Lameness has been long considered as the inevitable consequence of fractures of the neck of the os femoris. Ludwig, professor of surgery at Leipsick, has particularly advocated this opinion, which is supported by Sabatier, and Louis, who considered the total destruction of the neck of the bone, as the cause of the lameness. But few such examples are to be found on record. Ruisk has given an engraving of one. Lameness when it does take place, depends, as it does in oblique fractures of the body of the bone, on the overlapping of the fragments, to which no opposition has been made; so that the insufficiency of our means, and not the nature of the disease, gives rise to this accident, which Desault seldom experienced in his practice.
101. From what has been said, it appears, that, in all respects, authors have given a much more unfavourable prognosis in fractures of the neck of the os femoris than facts and the nature of the affection will justify, that the progress of these fractures is the same with that of all others, and that, when treated with equal skill, there is no reason why their termination should not be equally favourable.
§ XVI.
102. Reduction, in this case, is attended in general with but little difficulty. The patient, lying on his back, is held under the arm-pits, and by the upper part of the pelvis, by assistants who make counter-extension in this way, without being obliged to pass, as recommended by the Academy of Surgery, a strap under the affected thigh (30). Another assistant makes extension, according to the method formerly described (29), drawing the point of the fragment very gradually in the direction opposite to that which it has taken in becoming displaced, and making the thigh at the same time rotate a little on its own axis. This gentle rotation renders success more certain.
103. If things be properly arranged, a slight effort is sufficient to bring the separated fragments into contact and to restore to the limb its natural form; for, as I have already observed (86), a facility of reduction is even one of the characters of this fracture. But it is very difficult for art to maintain permanently what she easily effects at the time of reduction, and on this account, our curative processes are oftentimes insufficient.
104. These processes may be considered under three classes, according as they relate 1st, to position; 2dly, to bandages; 3dly, to the forms of apparatus for making permanent extension.
In the first class must be included the method of Foubert, employed in ancient times, according to Louis, and which consists in placing the patient on a horizontal plain, while the limb is secured by simple splints, and the foot by a kind of shoe. But in a short time the muscular action, to which no resistance whatever is made, draws the lower fragment upwards, while the weight of the body pushes the pelvis downwards, and along with it the superior fragment. Hence a new reduction, the effect of which is again immediately destroyed as at first. Thus are new displacements succeeded by new replacements throughout the whole course of the treatment.
105. This method, almost universally adopted in latter times, and approved of by Louis, was in vogue at the hospital of Charity, when Desault entered it. Ought we then to be surprised, that the fracture was considered as incurable? Here indeed the plainest and most important indication is evidently disregarded. Nothing to retain the fragments in apposition, nothing to prevent them from being constantly moved. Does not the method of Foubert very closely resemble those experiments, in which, the bone of an animal is broken intentionally, and then to prevent a reunion and form an artificial joint, the fragments are kept in constant motion?
106. Will any better success attend the method of securing the leg, as Dalechamp recommends, to the foot of the bed? In such a case the trunk and the pelvis glide down along the inclined plain made by the pressure of the nates (14), and hence a constant cause of the shortening of the limb.
107. The second class of curative means, includes different forms of apparatus simply retentive. Pare, Petit, and Heister, recommend, as most useful, the Spica of the groin.26 But what effect can this produce? What force applied in that part can keep the lower fragment down, and the pelvis up, secure the immobility of the limb, and prevent its rotation outwards? If the bandage be tight, it will compress the muscles unequally, make them contract, and thus become the cause of a contraction or shortening of the limb. In some respects, there is more advantage to be derived from the tin case lined with cloth on its inside, which Fabricius of Hilden applied to the external part of the thigh; a method which has been renewed since his time, by certain celebrated practitioners of Germany; from the pasteboard case proposed by Duverney as a substitute for that of tin; from the retentive plaster27 of Buffle employed likewise by Arnaud; and from the splints adopted by most practitioners. But can these means, (so differently varied in form, yet still the same in their action), while they prevent displacement laterally or in the cross-direction of the bone, prevent it also in the longitudinal direction, which latter ought to be the principal object in view? Will they make any resistance to the muscular action? See what has been already said on splints, bandages, &c. (89...95).
108. The insufficiency of these forms of apparatus, arises from their not being constructed with a proper view or reference to the general principle that ought to be observed in the treatment of every fracture; namely, that the means intended to prevent displacement, ought to be founded on the causes that produce it. But, these causes here, are, 1st, The action of the muscles which draw the lower fragment upwards: 2dly, The weight of the body which pushes the pelvis downwards: 3dly, The weight and direction of the foot and leg, which tend to carry the toes outwards by a rotatory motion. Hence, the threefold indication or end of every apparatus, is, 1st, To keep the body of the bone down: 2dly, To retain the pelvis up: and 3dly, To secure the foot nearly in a right line with the leg.
109. The first consideration leads us naturally to the second. The means destined to fulfil this three-fold indication, must be constant in their action, since the causes which they have to combat act without remission. Hence the necessity of an apparatus for permanent extension. See what has been said on the nature of this expedient (46...51), on the different modes of effecting it (52...57), and particularly on the mode pursued by Desault (58...70).
110. The mechanism of his apparatus for permanent extension is the same here as in fractures of the body of the bone. The limb is secured against a strong splint, to the two ends of which two rollers, running one from the pelvis, and the other from the foot, are firmly tied. The first of these rollers holds the pelvis up, and the second draws the foot down: hence the two first indications are fulfilled. The third is also fulfilled by the extension of the limb, which prevents its rotation outwards, by means of the outside splint, which passing beyond the sole of the foot keeps it immoveable.
111. The bandage of strips and compresses, which in fractures of the body of the bone, are previously applied round the limb, and oppose in some measure its motions laterally, are here entirely useless. Being all indeed applied on the lower fragment, what purpose could they answer towards fixing it against the upper one? They could do nothing but compress the muscles, and by that means diminish their power of contraction: but extension alone produces this effect. Desault rejected the bandage altogether, and contented himself with the use of splints and bolsters, as appears from the following case reported by Couteau.
Case VI. Maria Nof, as she was running on the ice, in the severe winter of 1788, slipped, and falling on the great trochanter, fractured the neck of the os femoris. She was immediately carried to the Hotel-Dieu, where the signs formerly mentioned (60...66) disclosed at once the nature of her disease. The shortening of the limb was less than in ordinary cases.
The apparatus was applied in the following manner. The junk-cloth, the body-bandage, and the bits of tape, were laid on the bed, in the order already mentioned (60): the patient was then placed in such a manner that the affected thigh corresponded exactly to the middle of them. The reduction being effected, the two splints were applied, one on the external and the other on the internal side of the limb; on each side, and along the anterior part of the thigh, the bolsters were laid: three bits of tape for the leg, four for the thigh, and the body-bandage for the pelvis, served to secure the splints. One end of a roller, which had been previously fixed on the upper side of the foot, passing through the mortise on the external splint, and being tied to the other end which passed through the hollow or notch, produced extension, while counter-extension was made by means of another roller directed obliquely from the tuberosity of the ischium over the superior part of the same splint, which it drew downwards. This was the same apparatus formerly described (60...66), except as to the bandage of strips, the compresses, and the anterior splint, which running only from the fold of the groin, had no effect in retaining the fragments.
The treatment was simple. No general disease of the system existing, the patient returned, in a few days, to her usual regimen. Being visited every day, the apparatus was frequently tightened; and was renewed six times at different intervals.
A bilious disposition shewed itself on the seventeenth day. This was removed by an emetic given in solution, and after this nothing remarkable occurred. On the fifty-second day the state of the parts was examined. The consolidation was almost accomplished; by the sixtieth day it was complete, and the patient was discharged a few days afterwards, experiencing only a slight degree of lameness.
§ XVII.
112. It is more essential here than in fractures of the body of the os femoris, to keep up extension with the utmost exactness, because, in the present case, a much greater number of muscles being attached to the lower fragment, very greatly augment the powers tending to displace it. Hence the necessity of examining the apparatus every day, to see whether or not any shortening of the limb has occurred, to tighten, if they be relaxed, the rollers that make extension, and to renew the application of the whole, if it be in any measure deranged.
113. The proper treatment here, as well as in most other fractures, consists more in these attentions, taken collectively, than in the use of internal means. It is to the want or neglect of such attentions, that we ought to attribute the little success obtained by many surgeons from the bandage of Desault.
Case VII. A man, having fractured his thigh by a fall, called in a surgeon, who, reducing the fracture, and retaining it by this bandage, examined the state of the parts every day, and finding no derangement of the splints, neglected attending to the rollers destined for making extension. Seventh day, a shortening of two inches; a new reduction, and a new application of the bandage; the same want of attention as before; the same shortening at the expiration of a few days; the means were then rejected, and declared, in a publication, to be insufficient. How often do processes and modes of practice of great utility, by being transmitted from person to person, or from book to book, lose at length, that credit they are entitled to, and that approbation which they ought to command!
114. Serious accidents so seldom accompany fractures of the neck of the os femoris, that there is no necessity of employing numerous means to remove them. A diet somewhat strict for a few days, diluting drinks, and then a return to the patient’s usual mode of living, unless something besides the fracture should forbid it, constituted the simple treatment pursued by Desault in common cases. Any varieties resulting from accidental circumstances, must fall under the general treatment of fractures.
115. The period necessary for the healing of fractures of the neck of the os femoris, is represented by most authors as being longer than the term required in other similar affections. We read, in the Memoirs of the Academy of Surgery, that oftentimes the cure is not complete in less than three or four months. The reason of this will be evident, if we consider, on the one hand, that the reunion is always more tedious, in proportion as the contact of the fragments is more frequently interrupted: and, on the other, that, in the means formerly employed, there was nothing opposed to the powers of displacement. Hence it follows, that, if skilfully treated, this fracture ought to follow nearly the same course with others. It is this that confirmed the superior excellence of the practice of Desault, who almost always obtained a cure, all other things being equal, such as age, strength of constitution, &c. in the space of forty-five or fifty-five days.
116. We discover, in general, that the cure is complete, from a disappearance of the signs of the fracture, more particularly from the motions of the great trochanter, in which circumduction28 succeeds to rotation on its own axis, when the limb is made to move on itself, that is, to rotate outwards or inwards. The power of standing and walking is an infallible evidence of this reunion; nor are these exertions practicable, till the expiration of some time after it is completed; this circumstance is owing to a stiffness remaining in the parts around the joint, occasioned by long extension and a want of motion, and which exercise alone can effectually remove. (See what has been already said on this subject, in several parts of this work.)
117. Numerous cases may be adduced in favour of the doctrine laid down in this memoir. But a sufficient number have been already published in the Journal of Surgery. I shall subjoin only two, drawn up by Manoury and Seveille.
Case VIII. Maria ***, aged forty, falling on the great trochanter, experienced a sudden pain, and heard a considerable report: she rose, however, and with difficulty made her way home. On the day following, a shortening of an inch was perceived in her thigh: the great trochanter was drawn backward and upward: walking was now impracticable, the foot remained turned inwards. Notwithstanding this latter circumstance, Desault, being called to the patient, declared that a fracture existed, which was evidenced in particular by a rotatory motion of the great trochanter on its own axis. The necessary apparatus being applied, was carefully examined every day by Manoury, to whom the patient was intrusted. No shortening of the limb occurred, nor did any unfavourable accident supervene, and, by the thirty-ninth day, the fracture was exactly and firmly united; on the forty-third, the splints were removed; and on the fiftieth, the patient could walk without assistance.
Case IX. John Rignal fractured the neck of the os femoris by falling, not as in the preceding case, on the great trochanter, but on the knee, which was bent at the time of the fall, while the shoulder of the same side supported a heavy load. He was brought to the Hotel-Dieu, where the same signs, as in the preceding case, (except that here the foot was turned inwards) furnishing ground for the same diagnosis, gave rise to the same treatment, which, in fifty days, was followed by a result equally favourable.
118. The lower extremity of the os femoris, being thicker than the rest of the bone, and protected from the action of external bodies by a thinner covering of soft parts, is yet better secured from fractures than the other parts, for the following reasons: 1st, because counter-strokes, so frequently the cause of fractures of the body and neck of the bone, can affect this part but rarely: 2dly, because the os femoris, being more moveable at a distance from the centre of its motions, yields more easily to whatever strokes and impressions it there receives: 3dly, because motion, when distributed through a greater bulk of matter, has less power to destroy its continuity.
§ XVIII.
119. The fractures which occur in the lower extremity of the os femoris, are of two kinds very different from each other. Sometimes situated above the condyls, they only separate these from the body of the bone: at other times, affecting the condyls themselves, they extend into the very joint. My attention shall at present be confined exclusively to the latter kind, as the other may, in almost every respect, be classed with the fractures which have been already considered. Most authors have neglected to treat of fractures of this kind, under a distinct head, from a persuasion, that, owing to their communication with the joint, they ought to be ranked among complicated fractures, which are known to require a mode of treatment very different from that employed in such as are simple. But I shall presently show what regard ought to be paid to this ancient opinion.
120. The division presents itself, in general, under two different forms: 1st, running obliquely from above downwards, and from within outwards or from without inwards, it may separate a greater or smaller portion of one of the condyls from the rest of the bone: 2dly, these two bony protuberances may be divided from each other by a longitudinal fracture, meeting another transverse or oblique fracture, which by either passing through the whole thickness of the bone, separates both condyls from it, or extending only half way through it, separates but one of them. The fracture is single in the first case, but double in the second. The latter occurs in practice more frequently than the former. Both are usually produced directly, that is, by the immediate action of external bodies. Yet the following fact seems to evince that the accident may, possibly at least, arise from a counter stroke.
Case X. The corpse of a man of forty, was brought into the amphitheatre of Desault, soon after he became a public teacher. One of the pupils, on preparing to dissect the body, discovered a preternatural mobility in one of the condyls. The knee was examined. A double fracture was found, accompanied by a separation of the two condyls. On inquiry it was ascertained that the corpse came from the Hotel-Dieu. It was further discovered, with certainty, that the injured subject, in jumping through a window, had alighted on his feet, and that he experienced instantly a severe pain in his knee, and fell on the ground, unable to support himself.
Here, no doubt but the condyls, by being violently pressed between the weight of the body and the articulating surfaces of the tibia, had been fractured by a counter-stroke.
§ XIX.
121. But whatever may be the precise form and figure of the fracture, its signs are easily comprehended: a very perceptible separation oftentimes exists between the two condyls, increasing the transverse diameter of the knee. The rotula, sinking into this chasm between the condyls, renders the part more flat from before backwards, than it is in its natural state. If the rotula be pressed in a backward direction, the condyls are separated still further from each other. If, on the other hand, pressure be made on each side of the lower part of the os femoris, the condyls are brought together, and the knee resumes its usual shape. If we take hold of a condyl in each hand, it will be easy, by moving them alternately backward and forward, to make them rub against each other, and produce a crepitation which characterizes the fracture beyond a doubt.
122. If the upper fracture be oblique, a shortening of the limb more or less perceptible is always the effect of it: this appears to be principally owing to the weight of the body which pushes the upper fragment down, and to the action of the muscles which draws the lower ones up (10...14). In this case, the superior fragment, being forcibly pushed against the integuments, has sometimes lacerated, and even passed through them, giving rise to consequences of a serious nature. Desault has published a case of this kind. A similar effect has been produced, though more rarely, by the inferior fragment, in which case much mischief has arisen from the admission of air into the joint.
123. Sometimes when the upper fracture extends through the whole thickness of the os femoris, the extremity of the bone is turned round, so that the external condyl lies behind, the internal before, and the rotula on the outside, while the foot points in the same direction. A case of this kind is recorded in the Journal of Surgery. The body of the bone, being pressed into the chasm or interval between the two condyls, may prevent their reunion, by pushing them asunder, and thus give rise to various accidents.
124. Most of these phenomena will fail to occur, if the upper division, passing only half way through the bone, break off but one of the condyls, or if, passing through even the whole of the bone, it be perfectly transverse; but cases of this description are seldom met with.
§ XX.
125. I have little to add to the observations already made on the prognosis in fractures of the condyls of the os humeri. All that I have there said is applicable to the os femoris. As is the case with regard to the former fractures, so also here, the apprehensions of authors have been greatly exaggerated by their visionary doctrine respecting injuries of the joints: both reason and experience unite in showing such apprehensions to be unfounded.
I shall only observe, that in the present case, even more particularly than in fractures of the condyls of the os humeri, most of the unfortunate events that take place, are owing to the insufficiency of the means employed for effecting a cure. Indeed, as I have already observed (45), all those means can have no effect in opposing the continual tendency of the fragments to become displaced, if the upper fracture29 of the os femoris be oblique. And in most cases, this fracture is oblique: hence it follows, 1st, that the bony points of the fragments being constantly pushed, during their displacement, against the ligaments that surround the joint, will perpetuate in them the irritation first produced by the fracture, and thus give rise to swelling, inflammation, and all the other morbid affections of the part, so much dreaded by authors, and attributed by them to the mere communication of the fracture with the joint: 2dly, that the best expedient to prevent such affections, is an apparatus that shall retain the divided surfaces in perfect contact with each other by means of permanent extension.
126. It is obvious that this extension will be less necessary, if the upper division of the os femoris be transverse, because, then, the condyls and the body of the bone will find a mutual point of support against each other.
§ XXI.
127. Since the same causes, as in the preceding cases, tend here to destroy this contact, when the superior fracture is oblique (122), the apparatus ought, therefore, to be so constructed as to counteract these causes, that is, it ought, 1st, to draw the two condyls down; 2dly, to retain the pelvis up, and with it the superior fragment. This twofold indication relates only to the upper division of the bone, without any reference to that which separates the condyls; 3dly, it is necessary to counteract the tendency which the condyls may have to separate from each other.
128. Permanent extension, made in the manner already mentioned (60...63), fulfils the two first indications; while two lateral splints, and the bandage of strips fulfils the third. Desault, therefore, applied to this particular case his apparatus for permanent extension, modified only in such a way, that, instead of terminating at the knee, the bandage of strips was continued to a distance down the leg, in order that its action might be the more efficacious. For, it is well known, that it is at its middle part that the firmness and retentive power of a bandage are greatest, because the casts of the roller at the upper and lower ends, serve to secure those in the middle. The upper splint being altogether useless, was not employed.
129. If the superior fracture be transverse, the condyls, as I have already said, meet with resistance against the body of the bone, while they, on the other hand, support it in such a manner, as to prevent it from descending, though pushed by the weight of the body along the inclined plain made by the pressure of the nates. Here, then, permanent extension is generally useless, and all that is necessary is, to retain the condyls and prevent their separation by means of lateral pressure. The same apparatus may still be employed, provided the two rollers for extension be laid aside.
130. If a wound in the soft parts accompany the fracture, whether it be produced by the same cause, or by the subsequent passage of the fragments through the integuments, and whether it communicate with the articulation or not, it is necessary, as soon as suppuration has taken place, to renew the dressings every day or every other day, taking care, in the mean time, to supply, by the hands of an assistant, the want of extension by means of the apparatus. The following case, extracted from the Journal, exhibits a specimen of the treatment that ought to be adopted in similar cases.
Case XI. Claudius Legrange, aged thirty-one, and of a sound constitution, was wounded by the kick of a horse, on the internal condyl of the left os femoris. The violence of the pain obliged him to throw himself on a heap of straw, that lay at a little distance, and which he reached by hopping on his right foot. The pains were augmented by this, for at each step, the thigh being alternately bent or extended at the injured part, was moved sometimes backward and sometimes forward. The patient was brought to the Hotel-Dieu, a few hours after the accident.
The signs already specified (121 and 122) announced to Desault, a longitudinal fracture separating the two condyls, and terminated above by another fracture of the body of the bone, which descended obliquely from about five inches above the external condyl, to within two inches of the internal one.
The muscles of the thigh, by means of violent contraction, had drawn that portion of the os femoris attached to the external condyl upwards, and the superior fragment downwards. The sharp point of the latter had passed through the skin, and produced a wound of an inch and a half in extent, on the inside of the thigh, and a little above the condyl.
The patient being undressed, was placed on a bed nearly horizontal, on which had been previously spread the necessary pieces of apparatus, disposed in proper order. Desault then examined the wound, extracted a splinter of the bone, covered the wound with lint, and then proceeded to the application of the apparatus which he usually employed in such cases (128).
The extension was accompanied by no pain: on the other hand, it gave immediate relief: diluting drinks were prescribed. Next day, no pain; pulse a little raised; no dryness, nor any alteration of the skin; diet the same as on the preceding day; the apparatus wet with vegeto-mineral water. Fourth day, a new application of the apparatus, which had become relaxed; appearances of suppuration.
From this time the dressing was renewed every other day, till the sixteenth, when the wound was cicatrized. After this the apparatus was not touched except when deranged; it was only wet from time to time with vegeto-mineral water, and great pains were taken to keep up the extension. The apparatus was not laid aside till the sixty-fourth day, although the callus appeared to have acquired a state of solidity somewhat sooner.
The patient was soon in a situation to take exercise. The stiffness then disappeared rapidly, and, in about three weeks, he left the hospital, able to bend the leg to a right angle with the thigh, and under a full confidence that he would in a short time regain all the motions of the limb.
§ XXII.
131. As soon as the consolidation is complete, the motions of the limb must commence. These, at first gentle and confined, must be afterwards, increased in extent, and more frequently repeated, till, at length, the limb should be exercised every day for two or three hours without intermission. The position and direction of the leg ought to be constantly changed. One while, the thigh should be elevated by a bolster, so as to flex the leg; at another time, the bolster should be fixed under the leg to keep it extended. The rotula must be moved in every direction, and, as soon as the patient can leave his bed, he should take exercise himself. These precautions are more necessary here than in any other fracture, because a stiffness of the parts adjacent to the joint, is always the inevitable consequence of a long state of rest. Certainly writers would not have considered anchylosis as the most favourable termination of such fractures, had they been acquainted with the effect of exercise and rest in that now under consideration.
132. Provided the mode of treatment here laid down be faithfully pursued, the affection is seldom accompanied by those numerous accidents, of which so much has been said. The callus is formed in the usual manner: and, on some occasions, where the patients have died at the Hotel-Dieu, in consequence of some affection not connected with the fracture, the two condyls have been found perfectly united together and to the body of the bone. An instance of this kind is recorded in the Journal of Surgery.
133. Let us, in the mean time, not speak too favourably of that, respecting which the ancients were accustomed to speak too unfavourably. Even the practice of Desault would expose our error. Sometimes the most assiduous attention, and the most careful application of the apparatus, have not been sufficient to prevent abscesses around the knee, and an anchylosis of the joint. Desault related a case where even a caries of the articulating surfaces occurred. But some extraneous circumstances appeared to have an influence in these instances: and it may be laid down as a general rule, that fractures of the lower extremity of the os femoris, require the same treatment with fractures of its other parts.
This figure represents the apparatus for permanent extension, employed by Desault in oblique fractures of the os femoris.
AA. The external splint, with a notch and a mortise in it at the lower end to fix the inferior extending roller.
BB. A bandage passing round the body, intended to secure this splint against the pelvis.
CC. The anterior splint, reaching only to the knee.
d d d d. The anterior bolster, extending along the whole limb, and secured by pieces of strong tape.
EE. A portion of the bandage of strips, seen between the anterior and the external lateral bolsters.
FF. The junk-cloth intended to be folded round the two lateral splints.
g g. The superior extending roller, passing round the end of the external splint, and fixed underneath on the tuberosity of the ischium.
H. The sub-femoral roller or strap, intended to prevent the bandage BB, which passes round the body, from slipping upwards.
K k. A roller usually passed round the foot, to prevent it from turning.
L. The inferior extending roller, fixed in the mortise and the notch of the external splint.
1. Few kinds of luxation of the os femoris occur in practice more rarely than this. Practitioners who have seen it, and those who, on the authority of others, have described it, without having seen it, have all given an unfavourable prognosis respecting it, for the following reasons: 1st, on account of the inevitable rupture of the round ligament: 2dly, on account of the distension, and even laceration of the capsule, and of the compression and overstretching of the nerves and blood-vessels: 3dly, on account of the great difficulty of reduction. The following case will prove, that in all these respects, the apprehensions of authors have been exaggerated, that the obstacles to reduction arise less from the nature of the displacement, than from the nature of the means employed to remedy it; and that, if properly directed, art would here be as successful as in other cases.
Case. (Collected by C***). About the close of the winter which preceded the death of Desault, a porter was brought to the Hotel-Dieu, in consequence of a fall which he had received about two hours before, in the following manner. As he was carrying on his shoulders a heavy burden, his foot slipped, while his leg and thigh were directed backwards: he fell on his knee, his thigh maintaining still the same direction; so that the conjoined weight of his own body and of the burden which he carried, aided by the velocity of the fall, forcing the head of the os femoris, which pointed at the time forward and upward, against the distended capsule, lacerated it and drove the articulating end through the opening. Continuing still to act, it ruptured the ligament, which connects the extremity of the bone to the articulating cavity, and forced the head in front of the os pubis, where it could be easily felt.
At the moment of the fall, an acute pain was felt in the part; and the power of moving the limb was suddenly lost; the patient was carried home, where a surgeon who visited him, considered the accident as a fracture of the neck of the os femoris, and sent him to the Hotel-Dieu, to undergo the necessary treatment.
Desault having examined the parts, discovered, from the following appearances, not a fracture, but a luxation upward and forward. The limb was nearly an inch shorter31 than natural; the point of the foot was turned outwards; the thigh being in a state of painful extension, could not be flexed on the body; adduction and abduction were alike painful; the great trochanter, being more approximated than usual to the anterior and superior spine of the os ilium, was also too far forward; finally, the projecting head of the bone could be felt, as I have already said, in the groin.
The reduction was effected in the following manner. The patient being laid on a firm table, spread with a mattress, a strap was fastened above the ancle, for the purpose of extension; another, intended for counter-extension was placed between the scrotum and the thigh of the sound side, and brought up the back and front of the pelvis, along the body, till it passed over the shoulder, where it was twisted together and secured.
Extension was then begun, precisely in the direction in which the thigh pointed; and, during the execution of it, a rotatory motion inwards was given to the limb. At the expiration of a few minutes, the head of the bone remaining almost immoveable, notwithstanding the efforts to dislodge it, Desault directed extension to be discontinued, and, taking hold of the thigh, moved it in every direction, with a view to enlarge the opening in the capsule, the narrowness of which he suspected to be the cause that prevented the reduction.
Extension was then resumed, and varied in every direction, while the surgeon endeavoured to give assistance by pushing the head of the bone forcibly downwards, with his thumbs, and the palms of his hands. Useless efforts; the displaced bone remained stationary.
Desault ordering extension to be again discontinued, recommenced the motions of the os femoris, and even increased their force, changing them in every direction, for the purpose of lacerating the capsule. After this, extension was again renewed, with better success than before. Indeed, on the very first effort, the head resumed, of itself, its natural situation, without any further assistance on the part of the surgeon.
The sufferings of the patient ceased almost instantaneously; towards evening a slight swelling appeared around the joint, over which an emollient cataplasm was applied. On the day following, all the unfavourable symptoms were gone, and in about a fortnight the patient was able to return to his usual exercises, which, however, he was directed to pursue, for some time, with moderation.
2. There are, in this case, two circumstances, on which the practitioner should fix his attention, and which may throw great light on the reduction of all luxations of the os femoris, as they will be found applicable to most accidents of the kind. These are, 1st, The narrowness of the opening in the capsule. 2dly, The inutility of the motion or process of conformation, when that opening has been enlarged.
3. We formerly observed, when treating of luxations of the humerus, that one of the obstacles to reduction was, the narrowness of the opening in the capsule; the same circumstance occurs here. That membrane, lacerated at the time when the head of the os femoris is driven against it, is dilated sufficiently to let the head escape: but, the edges of the lacerated membrane, coming together again, and being thus drawn tight around the neck of the bone, retain it in that position, and prevent the head from re-entering the acetabulum. Thus, in a fracture, where one of the extremities of the bone is protruded through the integuments, the opening in the skin, by closing tightly round that extremity, sometimes prevents its reduction.
4. In such a case, what is the first and most obvious indication? It is necessary to increase the extent of the opening in the capsule, by moving the limb in every direction. Some persons have deemed it impossible to tear this membrane anew. But, if we recollect, that the neck of the os femoris, being placed between the edges of the opening, must necessarily draw them asunder by the motions impressed on it, it is easy to conceive, that the angles, where these edges unite, will be torn, if the motions be carried to an inordinate degree: besides, experience proves here, as well as with regard to the humerus, the truth of the doctrine contended for. Are we to apprehend, as these same persons will have it, that serious accidents may be produced by such violent motions? Experience again answers in the negative. Nothing, then, can be more certain, than that this observation, respecting the opening in the capsule, is a great stride towards perfection in the treatment of luxations in general, and particularly of that now under consideration.
5. When this obstacle to reduction has been removed, it is then very readily effected, and that without the process of conformation. Indeed that process is almost always unnecessary. For what purpose should it be employed? Is it to increase the effect of extension, and thus disengage the head of the bone from the place which it accidentally occupies? In this point of view, it is nothing but a very feeble force, added to a very powerful one, which receives from it, therefore, but little assistance: it is much better, if necessary, to augment the extending forces themselves. Is it to push the head of the bone into its cavity, after the extensions have dislodged it? It is to the muscles, and not to the efforts of the surgeon, that the performance of this office belongs. Indeed, the surgeon must act altogether in the dark in this respect, as he cannot possibly ascertain the precise point where the opening in the capsule exists: he may, therefore, even push the head of the bone against a sound part of the capsule, and thus himself create an obstacle to the reduction, which he is attempting to favour.
6. The muscles, on the other hand, by their contraction, naturally draw the head of the bone into its place, because the direction of their fibres is such as obliges them to do it. The great art of managing luxations, then, consists, in ascertaining clearly the obstacles that prevent reduction, in removing them, and, then, committing the rest to extension, and the powers of nature properly directed.
1. Our modern treatises on diseases are little else than fabrics artfully constructed of materials confusedly scattered through the writings of the ancients. Many of those materials oftentimes escape our notice, and we find them only, after practice has disclosed them to us, in the chambers of the sick. Thus, Hippocrates had an accurate knowledge of spontaneous luxations of the os femoris, and has even left an aphorism expressly on that subject. Yet this disease appeared to be unknown to the physicians who came after him, till John Louis Petit, having met with it in his practice, drew the attention of practitioners to it, by a memoir respecting it, published among those of the Academy of Sciences, in the year 1722.
2. The history of this affection, which was considered afterwards, ex professo, in his course on diseases of the bones, has been sanctioned by the assent of all practitioners, to whom it has since very frequently occurred, and who have generally admitted as Louis observes, the doctrine of Petit, respecting the cause on which it seems to depend.
3. Experience bears witness, that usually a fall on the great trochanter, more rarely on the knee, or the sole of the foot, precedes it, and has doubtless some share in producing it. But what is the nature of the primary affection which, rising immediately from this occasional cause, becomes the immediate cause of the luxation? Petit, and with him the practitioners of the present day, have conceived, that the different parts of the joint, being irritated and contused, pour out, in consequence of the injury received, a superabundant quantity of synovial fluid, which, not being absorbed with the same rapidity, accumulates in the articular cavity, distends the capsule, and, by degrees, forces the head of the os femoris from its natural cavity. Hence astringent and tonic remedies, with alum, spirit of wine, &c. are directed to be applied externally to the upper part of the diseased thigh.
4. But this doctrine, and the practice which results from it, seem by no means to accord with our knowledge of anatomy. The truth of this was deeply impressed on the mind of Desault, who had frequent opportunities of witnessing the disease.
Case I. A young woman walking hastily along the street, slipped and made a false step, in which the left thigh, being violently twisted, supported for a moment the whole weight of the body.
A severe pain experienced at the moment, obliged her to stop at first, but becoming easier afterwards, permitted her to proceed on her way, and soon ceased entirely. A sensation of weight occurring in the part about fifteen days afterwards, was at first troublesome to the patient in walking. This sensation was afterwards succeeded by a dull, deep-seated pain, accompanied by a swelling in the parts around the joint.
During six or seven months the limb was observed to increase in length gradually, but very slowly. At the expiration of that time, a contraction took place suddenly, and, in one night, the diseased thigh became shorter than the other by nearly two inches. The patient was then admitted into the hospital, where, after some time, she sunk under her disease. On opening the body the following appearances were presented to Desault, who was then consulting surgeon to the institution.
The cartilage of the acetabulum swollen to such a degree as to fill up the whole extent of that cavity, was yellowish and inorganic, somewhat resembling bacon, both in colour and consistence. A soft, spongy, whitish substance projected in the middle of it, the remains no doubt of the round ligament. The head of the os femoris, situated where it is usually found in luxations outward and upward, was surrounded by a cartilage equally tumefied.
5. Here the cause of the displacement of the os femoris was evident. The cartilages becoming tumefied, in consequence of the contusion and violence done to them, had by degrees, filled up the acetabulum, forcing out in the same gradual manner the head of the bone. Hence arose the original lengthening of the limb. But as soon as the head had escaped from the lacerated capsule, the limb was drawn upwards and consequently shortened, by the action of the muscles, and the weight of the body pushing the pelvis downward.
Case II. Some years afterwards, Desault had occasion to witness again the same disease, in the person of a man aged thirty-seven, who put himself under his care, but, being obliged to leave Paris, a short time afterwards, retired into the country, where he died in about six months, enfeebled and consumed by a hectic fever.
On opening the body, the surgeon of the place discovering the same phenomenon as in the preceding case, made a preparation of the part, and sent it to Desault, whose pupil he had been.
6. In this case the shortening was not so sudden as in the preceding one. It appeared at first to be coming on, during five days, in an imperceptible manner, when, fatigued with lying in bed, and having on that day drank a little, the patient attempted to walk, supported only by a cane. By evening, a shortening of two inches and a half had taken place, an effect evidently produced by the weight of the body on the diseased thigh. Hence the necessity of confining the patient to a state of perfect rest, of preventing, in particular, standing and walking, and all positions in which the diseased thigh would have to sustain the weight of the body.
Case III. Maria Genette was received into the Hotel-Dieu, in consequence of a fall on the great trochanter. She had been attacked by a pain in the joint of the thigh of the same side. Walking, which was performed with difficulty, augmented the pain, and standing, though more tolerable, could not be long continued. The thigh was evidently longer than the other. To leave the disease to nature, and confine the patient to a state of rest, constituted the practice of Desault. What effect could the external use of astringents, recommended by Petit, produce in such a disease? Some time after her admission, the patient was attacked by dysentery, in consequence of which she was removed to the medical ward, where she died.
On opening the body, the parts in the neighbourhood of the joint were evidently tumefied, and the capsule was stretched from above downwards. The head of the os femoris was situated on the external edge of the acetabulum. The capsule, though greatly elongated was still in a state of tension; and the articular cartilage was swollen to such a degree, as nearly to fill up the cavity. The quantity of synovial fluid was less than natural.
7. This case, taken at a period of the disease not far advanced, fully confirms the inference deducible from the two preceding ones, respecting the cause of spontaneous luxations. Here, indeed, the capsule not having given way, the swelling having only just commenced, and the synovia existing in but small quantity, the progress of nature was evident. Here, also, occurred a sign not noticed by Petit; namely, the elongation of the limb, which always, in such cases, precedes its contraction.
From what we have said, it appears, 1st, that the efficient cause of spontaneous luxations of the os femoris, is a swelling of the articular cartilages, which alters and destroys their organization: 2dly, that the presence of this swelling must necessarily render fruitless all attempts that might be made to replace the head of the bone in its cavity: 3dly, that the change in the organization of the cartilages, renders astringents, discutients, and other external means applied for the purpose of removing the tumefaction, entirely useless: 4thly, that here, as in many other cases, art ought to confine itself to the palliation of effects, and not attempt the removal of causes.
§ I.
1. The rotula, a sort of bony production of the sesamoid kind, attached to the tendon common to the extensors of the leg, represents a moveable pulley, intended to slide on that formed by the separation of the condyls of the os femoris. It protects the joint which it covers, and, in point of structure, use, and situation, greatly resembles the olecranon, from which it differs only in this, that, instead of being a continuation or process of the tibia as the olecranon is of the ulna, it is only attached to that bone by a strong and thick ligament which is inserted into its tuberosity. Hence it follows, that between the injuries of the one and the other, there must be a great analogy: and indeed most of the signs characteristic of fractures of the olecranon, are characteristic also of those of the rotula, and the treatment which, in such cases, is suitable for the former, differs but little from that required by the latter.
§ II.
2. Fractures of the rotula may, in general, assume any direction, transverse, longitudinal, or oblique: but the first kind occurs in practice much more frequently than the others; and so great indeed is the disproportion, that it has almost exclusively attracted the attention of authors, in the numerous forms of apparatus invented to retain the fragments.
3. A shattering of the bone, the effect of a violent blow; a contusion; an echymosis; an effusion of blood into the adjacent soft parts; one or more wounds of the soft parts, with or without an opening into the joint; a swelling, the degree of which varies greatly, according to the state of the fracture, and the disposition of the subject, but which is constantly present; a double division of the bone, one of which, being longitudinal, forms an angle with the other, which is transverse; and a concomitant fracture of the condyls of the os femoris, or of the tibia: such are the varieties and complications, of which the fracture under consideration is susceptible.
4. But this fracture may be produced in two modes. 1st, by the action of external bodies: 2dly, by that of the extensor muscles. The first mode of division takes place in falls on the knee, or when a body in motion strikes against it, and, in this case, there is no counter-stroke, the rotula being too small for such an occurrence, and always sustaining the fracture where it receives the blow. In the second, the fall is only subsequent to the fracture, and, as Camper has well observed, is most frequently the effect of it. For instance, the line of gravity of the body is, by some cause, removed behind it; the anterior muscles contract themselves to bring it forward again; the extensors act on the rotula; it is broken, and a fall ensues. Again, the leg is suddenly thrown into a state of violent extension; the extensors act with great force; a fracture is the consequence, and the patient falls. A soldier once fractured his rotula in kicking at his serjeant; thus the olecranon, in like manner, has been broken by throwing a stone. A man, in the Hotel-Dieu, fractured the rotula of each knee, in the operating room, by means of convulsive motions, produced by the operation of lithotomy.
5. The action of external bodies, can alone produce a longitudinal fracture, as when a person falls on a sharp projecting piece of timber: but this may also produce a transverse fracture. On the other hand, muscular action can never give rise to any but the latter kind, since the direction of this fracture is at a right angle with that of the extensors. A fracture resulting from the action of external bodies, is oftentimes accompanied by a wound, a contusion, or a shattering of the part (2); a fracture, arising from muscular action, is always simple, except as to a swelling around the joint. The latter cause may, instead of fracturing the rotula, rupture the common tendon of the muscles, or, what is more common, the inferior ligament. Desault has seen many examples of this: Petit has also observed several, and Sabatier has sometimes met with them. External violence seldom produces this double accident.
§ III.
6. In longitudinal fractures the diagnosis is always accompanied with more or less difficulty, because the extensor muscles, drawing by their contractions the two fragments equally upwards, and the inferior ligament holding them equally down, tend to keep them in apposition, and to prevent them from separating. Sometimes also the ligamentous production which covers the rotula, remains entire and serves to keep the fragments together. It will be necessary, therefore, should the existence of such a fracture be suspected, to move the two sides of the rotula in opposite directions, by pressing them to the right and to the left, in order to arrive at certainty on the subject. Should a wound exist, as is oftentimes the case (5) the diagnosis is less difficult.
7. If the division be transverse, the diagnosis becomes then as plain and easy, as it is difficult and obscure in cases where it is longitudinal. In such a case, a considerable separation or space exists between the two fragments, sensible to the touch, when the hand is placed on the knee. In this separation, the fragments are not displaced by the same means. The superior fragment being attached to the extensors, is drawn upwards with great force by these muscles, the action of which the rotula no longer resists. The lower fragment, on the other hand, being attached only to the inferior ligament, is not moved by any muscle, and cannot be displaced in any other way than by the motions of the leg with which it is still connected.
8. Hence it follows, 1st, that, in a state of extension, the separation is the least possible, because it is then produced on the part of the superior fragment only; 2dly, that in a state of flexion it is greatest, because then both fragments concur alike in producing it; 3dly, that it may be increased or diminished by varying the degrees of flexion.
9. This fracture is further characterized by the following circumstances, namely, a practicability of moving the fragments transversely in opposite directions, and of producing, by that means, some degree of crepitation, provided they be first brought close together; by the pain which accompanies these motions; by the swelling common to every kind of fracture of the rotula, and which, if very great, may involve the other signs in more or less uncertainty; by a difficulty of standing; and an almost entire loss of the power of walking, in consequence of the extensors being no longer able to communicate motion to the leg, unless when the fracture exists very low down, near to the inferior ligament.
10. The touch will always discover in what part of the bone the fracture is situated, which, if it be oblique, will partake more or less of the characters of the longitudinal or the transverse, accordingly as it approaches to the one or the other.
§ IV.
11. Many authors have pretended that fractures of the rotula cannot be cured, and it even appears that the Academy of Surgery adopted this opinion, on receiving a memoir from a Flemish physician, which contained several facts tending to establish that principle. But what do these facts prove? That in some particular cases, reunion did not take place, but they do not show that this was owing to the nature of the fracture.
12. But, what, in such cases, could prevent a cure from taking place? The structure of the rotula differs, say they, from that of the other bones. Now, admitting this difference of structure to be real, it certainly approaches to the structure of tendons to which indeed it bears a strong affinity. But, who does not know, that, when tendons are divided, they unite as readily as bones? Besides, is not the power of reunion common to every part endowed with life? I have already shown, when treating of other fractures that communicate with joints, what credit is due to those hypotheses so often revived but never confirmed, nay even clearly proved to be unfounded, such as, an effusion of callus into the joint, a failure of reunion from a want of periosteum on the posterior part of the bone, the synovia diluting the matter of callus, and thus preventing it from being duly prepared, &c.
13. The inflammation of the articulating surfaces and of the ligaments around the joint, ought to have more influence in constituting an unfavourable prognosis, than any circumstance that authors have mentioned. But experience proves, that, when judiciously treated, these fractures are not accompanied by that accident, and even that the swelling, which for the most part attends them, always yields more or less speedily, when a bandage, uniformly applied, presses equally on all parts around the joint, and thus forms a kind of discutient, while at the same time it retains the fragments.
14. Pare, Fabricius of Hilden, and a number of other writers, have pretended, that some degree of lameness must always be the consequence of this fracture. But, from what causes must this lameness so certainly arise? Is it from a want of reunion in the part? I have already shown (11 and 12) that this apprehension is wholly unfounded. Is it from an anchylosis? This accident cannot take place, except either in consequence of inflammation occurring in the articulating surfaces, (and I have already shown how that may be avoided, 13) or of a stiffness in the ligaments, and I shall hereafter make it appear that that may be readily prevented by motion. Is it from the fragments being drawn asunder, and in that state united by an intermediate substance of too great an extent? I shall prove, that a bandage properly constructed, is always sufficient to keep these fragments in contact.
From these considerations it appears, that writers have, in general, without sufficient cause, given an unfavourable prognosis, in relation to fractures of the rotula, which have, indeed, a great affinity to other affections of the same kind.
§ V.
15. I have already observed (7), that the causes of the separation of the fragments are, as far as respects the upper one, the contraction of the extensor muscles; and, in relation to the lower one, the flexion of the leg; whence it follows, that the means of preserving contact between these fragments are 1st, all those that are calculated for the prevention of muscular action; 2dly, such as may keep the limb in a state of permanent extension. Hence two leading curative indications must be fulfilled by the bandage constructed for fractures of the rotula: the last of these indications presents in general but little difficulty; but, with regard to the other, the case is different. To fulfil the latter, it is necessary first, to weaken the contractile force of the muscles, and by that means diminish the effort which they make to draw the superior fragment upwards; and then, to oppose to them a proper mechanical resistance, which, by acting in a direction the very reverse of that in which they act, may countervail their efforts.
16. But the force of contraction is diminished, 1st, by throwing the muscular fibres into a state of relaxation; this end is best attained by bending the thigh on the pelvis: 2dly, by making compression over the whole limb, by means of a circular bandage, which, by confining the muscles, tends to restrain and weaken their action. Thus it is known that the advantage of the bandage employed to unite transverse wounds, consists chiefly in that compression which, by diminishing muscular action, prevents the retraction of their edges. Another advantage resulting from the bandage in this case is, that it prevents the swelling of the limb.
17. As to the mechanical resistance, which must act in a direction opposite to that of the contraction of the muscles, and, by that means, prevent the displacement of the superior fragment, it cannot, in the present case, be of the same nature as in fractures of the thigh, the clavicle, &c. where permanent extension is practised. The superior fragment offers too small a purchase for any extending forces to act on. This resistance must be made, then, by placing some body above this fragment, and retaining it in that situation with a force sufficient to hinder the fragment from rising upwards: such as a few turns of a roller drawn tight, a bit of leather, some hollow compresses, &c.
18. It is evident from the foregoing principles, that every bandage intended to retain a transverse fracture of the rotula, ought to be calculated to maintain the following state of things: 1st, the extension of the leg on the thigh; 2dly, the flexion of the thigh on the pelvis; 3dly, a uniform compression over the whole limb; and, 4thly, some mechanical resistance properly secured above the superior fragment: the three last expedients relate to the displacement of that fragment alone; while the first has a relation to that of the lower one. Let us examine whether or not the bandages, hitherto employed by different authors, be calculated for these purposes.
19. M. Valentin, believing that position alone was sufficient to retain the fragments in contact, neglected the application of apparatus entirely, which he even considered as hurtful, in consequence of the swelling it produced; but experience soon proved the insufficiency of this method. The slightest movement, or the least effort on the part of the patient, made the extensor muscles contract, which, drawing the superior fragment upwards, separated it from the lower one; and, as the time of reunion is in direct proportion to the distance of the fragments from each other, it must, under such treatment, have been necessarily tedious, and sometimes must have even failed altogether.
20. As to a swelling being produced by the bandage, this never occurs, unless when some openings are left, through which the integuments protruding become tumefied: but, when the pressure is uniform throughout, when the fluids find throughout an equal resistance, this accident is not to be apprehended, as is proved by the practice of Desault, who never met with it; on the contrary, a bandage properly constructed and applied, is calculated to prevent swelling (16).
Mere position, then, though always of service in this affection, is not alone sufficient, because it fulfils only the first of the indications or principles laid down with respect to every form of apparatus for transverse fractures (18), namely, that which relates only to the lower fragment; while those that relate to the upper one, remain still to be fulfilled.
21. Most authors have employed, with a view to these, a kind of figure of 8 bandage, known in art by the name of Kiastre,32 and approved of by Petit, Heister, &c. This is made of a roller formed into two balls, which are brought across each other alternately under the ham, passing over two hollow or forked compresses, that enclose the two fragments of the rotula.
But the unequal pressure which this makes on the unequally projecting parts of the knee, renders its application extremely painful, particularly below, where the pasteboard covering applied by Louis, immediately on the skin, afforded but a feeble protection to the tendons of the flexors. Besides, it did not prevent the swelling, which is indeed a necessary consequence both of this unequal pressure, and of the openings left between the casts of the bandage. This swelling is taken notice of by all writers, and is, according to them, one of the troublesome circumstances attending the fracture. The third indication is not all fulfilled (18).
22. The extensor muscles, not being at all compressed, will act with their whole force on the upper fragment, and, on the slightest effort of the patient, overcome the resistance of the bandage, the action of which, being oblique with respect to the fragment, is inconsiderable, unless it be drawn very tight, and thus a displacement will again occur. This obliquity of the turns of the roller obliges the surgeon, either to draw it very tight, in which case a swelling is inevitable, or to make it but moderately tight, and then the apparatus will be insufficient to resist the action of the muscles.
23. Most of the objections to the ancient apparatus for fractures of the rotula, apply also both to that proposed by Ravaton in his surgery, and to that which Bell employs in his practice. Both of these, while they fail in making sufficient resistance to muscular action, as well as in fulfilling the third condition laid down as necessary to every bandage (18), contribute to the swelling, and can rarely produce a perfect contact between the fragments. Thus Bell has well observed, that the reunion is rarely perfect, and that there is always a separation more or less perceptible.
24. The complication, the intricacy, the expense, and other more weighty inconveniences of the machine described by Garengeot in his treatise on instruments, and employed, for the first time, by Arnaud, and also of that which was proposed and used by Solingen, have, long since, entirely banished them from among the means of reduction.
25. Some practitioners have advised the uniting bandage used in cases of transverse wounds, which is formed, as is well known, of two small rollers or strips placed in the longitudinal direction of the limb, one of them having holes in it, to which the divisions of the other are fastened. Both of these are first secured by circular turns; being then drawn in opposite directions so as to meet, they draw the parts on which they are applied in the same directions. But the action of this bandage is confined to the integuments, and would have of course but a feeble influence on the fragments beneath. It is also attended with this further inconvenience, that by wrinkling the integuments, and throwing them into folds, it might press them down between the fragments, and thus prevent their contact. Besides, it is liable to most of the objections urged against the preceding one.
26. This view of the means employed by different practitioners, to counteract the causes of displacement in this fracture, are sufficient to convince us, that the difficulties hitherto experienced in the treatment of it, have arisen from the feebleness of the former, and the strength of the latter. So great indeed have been these difficulties, that some authors, conceiving a reunion impossible, have, in conformity to such an opinion, though contrary to all the rules and principles of the profession, advised us to abandon the patient to himself. But I have already exposed the fallacy of that opinion, respecting the want of a healing power in the rotula (12), an opinion which, if generally adopted, would give rise to consequences of the most serious nature. In the present case, as in all other fractures, the contact of the fragments ought to be the chief object of the surgeon’s efforts.
27. But ought this contact to be perfect and exact? Several authors, particularly Bell, have conceived, that the motions of the limb can be performed as well with a slight separation of the fragments. Pott even declares that such a separation will enable the patient, after his recovery, to walk with more ease. Flajani advances the same opinion in a dissertation on the subject.
From this doctrine arose a new mode of treatment, which consisted in not suffering the fragments to be at rest. They were accordingly, during the cure, put frequently in motion, the more effectually to prevent an anchylosis, which is sometimes the consequence of this fracture.
28. But, on the one hand, it is difficult to conceive, on what this opinion of these authors can be founded; while, on the other, reason declares, in the plainest and most forcible terms, that the more the state of a bone, after it has been broken, differs from its natural state, the less free will be the exercise of its functions, and, that the perfection of the treatment of fractures consists, in leaving behind it no vestige of the accident.
29. This truth was frequently confirmed in the experience of Desault, who had an opportunity of seeing numerous fractures of the rotula, both in the Hotel-Dieu, and in his private practice. He always observed, that, when the separation of the fragments was considerable, and the ligamento-cartilaginous substance uniting them was of some extent, standing and walking were performed with much difficulty; that the patient was exposed to frequent falls, from the want of a proper correspondence, in point of strength and motion, between the two limbs; and that, on the contrary, the less extensive the separation and the substance that filled it up were, the more free and easy were the motions of the part, which still remained, however, somewhat defective and imperfect, unless every vestige of the division was obliterated.
Paul of Egina long since observed, that, when no means of reduction were employed, though the patient might walk tolerably well on a level surface, he could not, without difficulty go up an ascent.
30. From what has been said, it follows, 1st, that in the treatment of this fracture, the perfect contact of the fragments ought to be the principal object of the practitioner; 2dly, that the kinds of apparatus employed by different authors, are but ill calculated for the attainment of this end, because they fulfil but imperfectly the indications formerly laid down (18). Let us see whether or not the apparatus of Desault be any better suited to this purpose.
31. The bandage, which he employed in this case, analogous to that for fractures of the olecranon, is composed, 1st, of one splint, two inches broad, and long enough to reach from the tuberosity of the ischium, to a little above the heel; 2dly, of two rollers, five or six yards long, and nearly three inches wide; 3dly, of another single roller, with two holes about the middle of it, a little longer than the injured limb of the patient, along the fore part of which it must be extended.
32. Every thing being arranged for the application of the apparatus,
1st, One assistant secures the pelvis, in the same manner as in fractures of the lower extremities; while another keeps the leg in a state of perfect extension on the thigh, and the thigh on the pelvis.
2dly, The surgeon, then, standing by the side of the fractured limb, extends along the anterior part of the leg and thigh the roller with holes in it, having previously wet it with vegeto-mineral water, taking care to make the two openings correspond to the lateral parts of the rotula, that, by being thus better adapted to its shape, it may not be thrown into wrinkles.
3dly, He then secures it on the top of the foot, by three circular casts of a roller placed one over the other, three or four inches above its lower end which must next be turned up over the three first casts, and made fast by two other ones. Then, while the compress roller33 is secured above by an assistant, he passes up along the leg by oblique and reverse turns, according to the inequalities of the limb.
4thly, Having arrived at the lower part of the knee, he pushes the lower fragment upwards, and makes below it two or three circular turns to secure it. He then gives the roller into the hands of an assistant, and directing him who holds the long compress roller, to draw it forcibly upwards, pushes the integuments of the knee in the same direction, lest, by becoming interposed between the fragments, they might prove an obstacle to their reunion. Passing then the fingers of his left hand through the holes in the compress-roller he places them behind the superior fragment and pushes it forcibly downwards.
5thly, When the reunion of the fragments is exact, without any space intervening, he resumes the roller, and passing it obliquely under the ham, and bringing it up again behind the superior fragment, withdraws his fingers which held this fragment down. In place of his fingers, he then applies two or three tight circular casts, covers the knee with several oblique casts in form of the figure of 8, so as to leave no opening between them, and, then, continues the bandage up along the thigh, securing by it the compress-roller extended along the fore part of the limb.
6thly, When he has arrived at the upper part of the limb, the assistant who holds the compress-roller, drawing it forcibly upwards, doubles down its end over the circular casts. The surgeon next fixing this end by several additional casts, descends again along the thigh, covers the knee by a few more oblique turns, and finishes with the roller on the leg.
33. This first part of the bandage evidently fulfils the third and fourth indications (18). The compression of the roller on the muscles weakening their action and impeding their motions prevents their tendency to draw the superior fragment upwards: while the circular casts passed behind this fragment, acting in opposition to the muscular contractions, prevents it from moving upwards in obedience to them. The long compress-roller, stretched on the fore part of the limb, being first secured below, and then drawn forcibly upwards, presses the casts of the roller against each other, and prevents those that correspond to the thigh from slipping upwards, and thus abandoning the superior fragment, and prevents also those on the leg from slipping down and withdrawing their support from the inferior fragment. As there remains no vacant space between the circular turns, their pressure is uniform throughout: no swelling can consequently supervene (20).
34. But the first and second indications remain still to be fulfilled (18): it is necessary to prevent the separation of the lower fragment, by the extension of the leg on the thigh, and to throw the muscles into a state of relaxation by extending the thigh on the pelvis, and to maintain permanently, by the apparatus, that double position, which the assistant maintains only during the operation.
35. To obtain the first effect different means have been employed; but none answers so well, to extend the limb and retain it immoveably in that state, as a long and strong splint, placed, as Desault did it, subsequently to the application of the first part of the bandage, along the posterior part of the limb. An assistant must hold the end of this splint, while the surgeon secures it in its place by the second roller (31): in this way the extension of the leg is effected.
36. To obtain the extension of the thigh, it is necessary to place on the top of each other, two or three bolsters or little bags filled with chaff, so disposed as to form an inclined plain, considerably elevated towards the heel above the level of the bed, but which, gradually descending to the same level towards the tuberosity of the ischium, forms a supporting basis on which the whole limb may rest in a uniform manner. By this twofold extension of the leg and of the thigh, the lower fragment is kept up immoveably, and the muscles are kept in a state of relaxation.
Hence it follows, that this bandage fulfils extremely well the conditions laid down (18), and that it ought to be preferred to all the others (19...25), which answered the indications only in part.
37. Whatever may be the advantages of this bandage over the others, it must still be acknowledged to have its inconveniences. The rollers become relaxed in a short time; their compression is less active; the muscles, being less confined, contract more readily; hence the necessity of frequently repeating the application of the apparatus, a circumstance which is very troublesome, on account of the roller which composes it, and covers the whole limb. The resistance of it even when it is recently applied, is not always equal to the power of the muscles, whence the most assiduous attention is necessary, to obtain such a consolidation as to leave no trace of the fracture behind. Few persons ever possessed, like Desault, the art of overlooking nothing that might in any way contribute to the success of his treatment: from this, no less than from the excellence of his processes, arose the number of his cures. Let us confirm, by a few examples selected from among a great many, the doctrine here laid down. The following cases were collected by Julian and Bezard.
Case I. Francis Leclert, of a sanguine temperament, fell on the 7th of October, 1790, on his right knee, and produced a transverse fracture of the rotula. He was not able to rise; he was carried home, where a surgeon, on discovering the nature of his disease, advised him to be taken to the Hotel-Dieu.
He was conveyed thither on the day following, and, in the interval, a considerable swelling had occurred around the joint. The usual bandage was employed; the pains ceased immediately after its application; a copious blood-letting was directed, and a low diet was prescribed.
The whole apparatus was wet with vegeto-mineral water, two or three times a day. On the next day some light food was allowed, and the quantity increased by degrees, till in a short time the patient returned to his usual regimen. Eighth day, the swelling being almost gone, the bandage had become relaxed it was therefore reapplied. Every day the inclined plain formed by the bolsters was carefully examined, and put in order again as often as it became deranged.
Fifteenth day, a new application of the apparatus: twentieth day, an evacuation in consequence of a bilious disposition. Nothing particular occurred from this time till the completion of the cure, which took place on the sixty-seventh day after the accident: no depression existed at the place of the fracture: the motions were perfectly free; these were aided, by daily exercising the knee joint for some time.
Case II. Vincent Grenier, aged thirty-eight, making a false step, fell on the rotula, and fractured it, on the 6th of June, 1791: he was brought to the Hotel-Dieu, where Desault demonstrated to his pupils, by the usual signs the existence of the disease: a considerable swelling had already taken place. The bandage formerly described was applied: the same precaution as in the preceding case; apparatus examined every day; renewed as often as relaxed; extension maintained with great exactness. On the forty-fifth day, the consolidation was nearly effected; on the fifty-second it was complete, the joint was exercised for some time, and on the seventy-seventh day the cure being in all respects complete, the patient was discharged.
1. The history of foreign bodies divides itself naturally into two great sections; the one includes those that are introduced from without; the other such as are formed within our own systems. This latter section may be again divided into two classes; to the first class belong bodies altogether inorganic, such as the different kinds of stones; to the second, those which are truly organic, and become foreign only by being situated in places where they impede the functions, such as cartilaginous or bony productions, existing accidentally within the joints.
On the subject of the latter class, art is much more deficient than she is with regard to the former. Let us endeavour to assist her a little, by giving a sketch of the opinions and practice of Desault with respect to these productions.
2. Before his time, the surgery of France appears to have contained scarcely a record of this affection. Described only in some ancient works, such as the writings of Pare, it had been forgotten by the moderns, when numerous instances of it were suddenly met with by English and German surgeons, and soon afterwards by Desault, who illustrated and confirmed the practice of his predecessors in it, and even added something of his own.
3. All the joints may become the seat of these concretions; Haller found many of them in that of the lower jaw; Bell mentions, as a very rare occurrence, their existence at the junction of the foot with the leg. Some authors have met with them in the wrist; but none are more common, or merit more particular attention, than those that exist in the joint of the knee. To these alone shall the following observations be confined, because these alone have fallen under the notice of Desault.
§ II.
4. Concretions of the joints do not always assume the same aspect. They vary greatly as to number, size, figure, structure, &c. In general, these bodies exist singly; sometimes, however, two of them are found in the same joint, and then they may be extracted either at the same time, or in succession, as was once done by Desault. Some English surgeons have also met with two concretions, and Morgagni has found even twenty-five, in the same joint.
5. They vary also in size. The largest ever met with by Desault, was fourteen lines in its longest, and ten in its shortest diameter. Six lines diameter in every direction, was the measure of the smallest one that occurred in his practice.
6. Their figure is sometimes lenticular and smooth on both sides, sometimes unequal, rough in one part, even in another, concave on one side, convex on the opposite, sometimes marked around the circumference and sometimes not with reddish points, and having occasionally a stem of a cellular texture and of some length, as may be seen in a paper by Theden. They usually consist of a single mass, but are in some cases divided into several lobules united by a kind of ligaments, as in the fourth case related in the Journal of Surgery. Though most frequently detached and floating in the interior of the joint, they have yet been found adhering by means of small portions of cellular substance, loose and capable of being stretched, or tight, hard, and even of a ligamentous nature.
7. If, from the external figure, we pass to the structure of these bodies, we will find them existing in three different states. Sometimes purely cartilaginous, sometimes completely bony, they at other times partake of both these states, in which case a bony nucleus is covered with a cartilaginous crust. Out of five cases, recorded by Desault, three are of the first, and two of the third kind. Many authors have met with the second kind, particularly Morgagni, who has even found in the same joint, some bodies of a bony and others of a cartilaginous nature. Hence it appears, that this variety of structure is to be attributed to the longer or shorter standing of the disease, that every concretion must pass successively through these three states, and that there is a great analogy between the formation of such bodies and natural ossification.
8. If we examine a body of the third kind cut in two through the middle, we will find it red and vascular in the centre, like an epiphysis, even when it is floating in the joint perfectly loose and free from adhesion.
9. Bell, in his treatise on surgery, speaks of a kind of tumour, at first soft, membranous, and adhering to the internal surface of the capsule, but which, according to him, may become afterwards hard and solid, and be detached so as to float loose in the joint. But are not these tumours different in their nature from those destined to be converted into bone? Do they, in fact, ever undergo the changes mentioned by Bell? Desault having never met with any of them, was unable to offer an opinion on the subject. In the mean time, an observation made by Monro, may serve to throw some light on the question: he once saw, in one of these productions, a cellular nucleus surrounded by a covering of bone.
10. Though usually simple and free from complication, this affection may, according to some authors, give rise occasionally to a dropsy in the joint. Pare is the first who has made mention of this: he found one of these bodies in a patient’s knee, into which he had made an incision for the purpose of drawing off a collection of water. Simson, on extracting a similar body, gave vent to four ounces of water. But, as on the one hand, a dropsy of a joint oftentimes exists without these foreign bodies; so, on the other, these bodies are almost always found disconnected from dropsy. Nor is there any affinity between the acknowledged causes of an accumulation of synovia, and the presence of these bodies; so that when the two diseases do exist together, it is altogether probable, that they are independent of each other.
§ III.
11. The formation of articular concretions succeeds frequently to blows or falls received on the joint, in which case, a swelling more or less considerable in the surrounding soft parts, showing itself from the first, and remaining for some time, at length allows the foreign body to be perceived, and does not, in general, disappear during the continuance of the body in the part.
12. Sometimes no external injury contributes to the formation of the body, and then, a spontaneous swelling precedes its detection, as Desault observed in two patients, where nothing was known to have concurred in the production of the disease. Constant rest increases this swelling, while exercise and a temperate mode of life diminish it.
13. But what can be the immediate cause of these tumours? Are they, as some allege, an aggregation or crystallization of particles of matter conveyed into the interior of the joint by the synovia, in the same manner as the rudiments of a stone are conveyed into the bladder by the urine? Their organic appearance and the vessels that pervade them, are unfavourable to such an opinion. Can they be, agreeably to the conjecture of Theden, articular glands bruised by means of strokes or falls? Or are they, as some authors will have it, portions of the cartilage of the joint, detached by the same causes? How then will their spontaneous formation be explained?
But why trouble ourselves about the cause, provided we can remedy the effects? Nature conceals from us the means, and discloses to us nothing but the results. Theories are fluctuating; but experience is still the same: let us search, then, by an attention to facts, for that which we cannot learn from first principles.
§ IV.
14. The phenomena which announce the presence of foreign bodies in the joint of the knee, are sometimes clothed in a character of such evidence, that they cannot be mistaken; at other times, the nature of the disease eludes the most accurate researches: the cause of this variety may be easily perceived.
As the joint presents different depressions and eminences, and as the bodies, being usually loose and detached, may travel through its whole extent, they produce different effects, according to the particular situations which they occupy. If lodged in a depression, they are not compressed, and cannot, of course, give rise to any troublesome affection. If they bear on an eminence, such as the condyls, or the posterior part of the rotula, they are forcibly compressed, and must derange, in some measure, the functions of the joint. Hence the precise nature of the affection cannot be at all times derived from the state of the symptoms.
15. Sometimes the patient can stand and walk with perfect freedom and ease, while, at other times, a sudden pain seizing him, obliges him to sit down, or even causes him to fall, if there be nothing at hand to support him. This pain subsists for a longer or shorter time. One motion produces it, and sometimes another, made in an opposite direction, removes it. But in common it is of some continuance, and then the patient is obliged to keep his bed.
16. If the state of the joint be examined, it will be found more or less swollen, when the pain is very acute. When the pain ceases, the swelling in part disappears. It is never sufficient to prevent the fingers, when drawn along the external surface of the joint, from discovering the presence of the foreign body, when it forms a protuberance under the integuments. It is then found sometimes above the rotula, by the side of the tendon of the extensor muscles, and that is the place where it usually produces least pain; at other times, it is lower down, in front of the condyls, and by the side of the rotula. It is occasionally found immediately behind the tendon of the extensor muscles; in this case so acute is the pain, that the patient is generally unable to stand. But it is when it is situated behind the rotula, near to the projecting ridge which runs across its posterior surface, that it gives rise to the most serious affections.
17. The body passes from one place to another, on the least motion, and sometimes, as Bell observes, the patient, on changing his position during sleep, is awakened by severe pain, in consequence of the foreign body being moved by this change. It happens, in certain cases, that it disappears, and lies concealed for some time, in the back part of the joint. During this period the joint performs all its functions with freedom and ease. Desault made this remark, in the case of a captain of dragoons, from whom, for the first time in his practice, he extracted one of these bodies, and who, for six months previously, had been able to perform all the motions of the joint freely, without pain. This person, experiencing no uneasiness, considered himself perfectly cured, when the body suddenly reappeared, in consequence of a hasty extension of the leg.
18. If the body, when projecting under the integuments, be gently compressed, it yields to the pressure, changes its situation, and, according to the impression it has received, moves either to the internal or the external side of the joint, or reciprocally from one side to the other, passing also behind the rotula, behind the inferior ligament, or sometimes behind the tendon of the extensor muscles. In these alternate displacements, it may in some cases be turned round, in such a manner that its anterior surface will take the place of its posterior one, and then resume its primitive situation. Desault met with an instance, in which the patient himself was in the habit of turning the body round in this manner.
19. Bell, in conformity to the distinction of articular concretions into cellular and solid, attributes to each division its peculiar signs. In the first case, the pains, being rather obtuse than sharp, are constant; in the second, they are extremely acute, but disappear and return at intervals. Supposing the division to be a real one, cases of the last description certainly occur much more frequently than those of the first.
§ V.
20. From what has been said it follows, 1st, that these cartilages floating through the joints, do mischief mechanically (14), by coming into contact with the articular surfaces: 2dly, that to obviate this mischief, it is necessary either to prevent their contact, by fixing the bodies in a spacious part of the joint, and thus doing constantly what nature does on certain occasions, or to extract them through an opening made into the articular cavity.
21. Hence, art can have recourse to but two methods of cure, all hope of discussing these tumours by external applications being, as Bell observes, entirely extinguished.
22. The first method was proposed by Middleton and Gooch, who having brought the foreign body into a situation where it produced no pain, endeavoured to confine it there a length of time sufficient to make it form adhesions with the corresponding part of the capsule. As we are not informed of the result of the experiments of these two physicians, we are left to our own conjectures on the subject.
23. Are these foreign bodies capable of forming adhesions? Supposing they are, will the internal surface of the capsule attach itself to them at the pleasure of the surgeon? Even admitting the existence of both these conditions, by what means can the bodies be kept stationary for a length of time sufficient for the formation of these adhesions? Will they not be displaced by the slightest motion? Besides, experience seems to be unfavourable to the expedient. I have already said (17) that, in a certain case, the foreign body disappeared for six months, remaining, no doubt, during that whole time, in the same place: but, if it could not, on that occasion, form adhesions, if a motion was sufficient to produce its reappearance, can we expect that art will be more fortunate in her attempts?
24. But, even admitting that the foreign body does form these adhesions with the capsule, if it should increase in size in the part of the joint which it occupies, becoming in a short time disproportioned to its extent, it will impede motion as before, and produce, by degrees, nearly the same affections.
25. From these considerations it follows, that the only expedient which can promise a radical cure is, the extraction of the foreign body. In the performance of this extraction, an incision must first be made through the integuments and the capsule.
26. This operation, simple and easy in itself, has given rise to apprehensions as to its consequences, which have long prevented practitioners from undertaking it.
It was in former times a maxim in surgery, that wounds of the joints are, if not mortal, at least extremely dangerous, in consequence of their admitting air into contact with the articulating surfaces. But observation has demonstrated the fallacy of this doctrine, and Desault in particular, has thrown great light on the subject, as I have frequently had occasion to mention in the course of this work: so that, at the present day, it is clearly ascertained, that, if judiciously treated, these wounds are seldom productive of serious consequences.
27. Hence it follows, that the operation we are considering, when skilfully performed, never gives rise to any dangerous or disagreeable affections. Experience has proved the truth of this assertion in the practice of Theden, Simson, Gooch, Broomfield, Bell, and Desault, the latter of whom performed the operation five times with complete success. The only case in which he was less fortunate, was that of a man, in whom the wound of the integuments closed up at first without any accident, but which was succeeded by two abscesses, one in the thigh, and the other in the leg, but without any affection of the interior of the joint. This patient was subject to a wandering rheumatism, which oftentimes attacked the lower extremities, and was perhaps in the present case the chief cause of the unfavourable occurrences.
28. It is to the English that we are indebted for the first operation performed for the extraction of these bodies. An account of this is given in the Transactions of a society in Edinburgh. Since that, the operation has been frequently repeated, and more than ten instances of it were already on record, when Desault first performed it in France. His method, somewhat different from that of others, was as follows.
1st, The patient must be laid on a bed, or seated on a high chair. The first position, however, is to be preferred, because when it is adopted, the patient need not be moved after the operation.
2dly, The leg is extended on the thigh, in order to relax the anterior part of the capsule of the joint.
3dly, The surgeon then searches for the foreign body, moves it to the internal side of the joint, against the attachment of the capsule, and secures it between his thumb and the fore-finger of his left hand, while an assistant draws the skin over the fore part of the rotula.
4thly, Taking then a common bistoury, he makes, on the protuberance formed by the body, a longitudinal incision of an extent proportioned to its size, through both the integuments and the capsule, so as to lay the body bare at the first stroke.
5thly, Sometimes the body escapes immediately of its own accord, in consequence of the compression made on it by the fingers. If its passage out be not spontaneous, a small scoop or a taper-pointed spatula passed under it, answers the purpose of extracting it. But, in the introduction of these instruments, it is necessary to avoid touching the articulating surfaces with their ends, lest, by being irritated, they might swell, and give rise to troublesome accidents.
6. If any resistance be met with, enlarge the opening and the extraction will become easy. Without this precaution, the edges of the wound, being bruised and irritated by the passage of the body, will swell, inflame, and unite again with difficulty.
7. When the extraction is finished, the assistant who draws the skin towards the inside of the joint, suddenly lets it go, when it returns to its natural situation. This causes the two incisions, which corresponded, at the time of the operation, to change their relative situation, the one remaining internal and the other becoming external.
8. Hence arises a twofold advantage; the entrance of air into the interior of the joint is prevented, and the external and loose portion of the capsule, being drawn inwards with the skin, unites with the condyl, if it be not brought into exact apposition with the other portion of the capsule, divided near its attachment.
9. The extraction being finished, it is then necessary to examine carefully, in order to ascertain whether or not the joint contain any more of these foreign bodies. On some occasions, when this is even the case, they cannot at the time be discovered. Desault himself was once deceived on this score, in consequence of which his patient was obliged to submit to a second operation.
10. The incision in the integuments is now united by means of adhesive plaster. Over this are laid compresses and a little lint, and the whole secured by a few turns of a roller drawn moderately tight.
11. The leg being then placed on a pillow, is kept in a state of extension, by means of a splint applied, for a few days, behind the joint.
29. If we examine but for a moment the process in this operation, we must perceive, that an incision made through the skin and capsule at a single stroke, is, in no respect, less advantageous than one made at two strokes, as recommended by all practitioners, and that, it is in the following respects greatly preferable to it: 1st, it shortens the operation very considerably: 2dly, it diminishes the pain: 3dly, it exposes the joint a much shorter time to the contact of the air.
30. The object of the operator is better answered by drawing the skin outward and towards the rotula, than by either depressing it, as Broomfield did, or raising it, as Bell does. Being more loose and more easily stretched in this direction, the opening in it is removed farther from that in the capsule, which prevents more certainly the access of air to the joint, and also favours the examination of the capsule.
31. In the mean time, the operation may succeed, even although the openings in the integuments and the capsule correspond to each other. Many English and German practitioners, without previously stretching and changing the natural situation of the skin, make a common incision, which they dress afterwards like a simple wound, and are yet no less successful than others in the result of their operations. This is a further proof of the fallacy of the ancient surgical doctrine, respecting the admission of air into the cavities of joints. Perhaps Desault might have omitted this precaution, had any operations of the kind occurred in his practice during the last years of his life.
32. The operation is seldom attended with much pain. Only one patient manifested signs of this in the practice of Desault. Nor have those operations of the kind performed in England been more painful, so that it may be laid down as a principle, that in most cases no primitive accident is to be dreaded.
33. With regard to hemorrhagy, as there is no large artery near the place of the incision, there is nothing to be apprehended on that score. Oftentimes there is scarcely any loss of blood at all, as may be seen in the first case published in the Journal of Surgery. But, even admitting that a small articular branch be divided, the reunion of the edges of the wound will be sufficient to check the hemorrhagy, in the same manner as in the operation for the hare-lip, the contact of the divided integuments of the lip, puts an end to the hemorrhagy from the small arteries of the part.
§ XIV.
34. I have already said that but little is to be apprehended on the score of accidents subsequent to the operation (26). Out of the numerous operations of the kind performed lately in Europe, but few cases have proved troublesome in their consequences, and even these were influenced by some foreign circumstances. Thus, for example, one of the patients of Simson rode out on horseback a few hours after the operation, on a cold and stormy day, and thus produced a troublesome affection of the part. A similar remark may be made respecting the case formerly mentioned (27).
35. The apparatus or dressing remains untouched for the two or three first days, during which time it is necessary to wet it frequently with vegeto-mineral water. It is a certain truth, that the use of this liquid retards the suppuration of wounds, and that, when continued a due length of time, it keeps inflammation at that degree most proper for the process of healing.
36. On the removal of the dressing, the wound is sometimes so perfectly healed up, as not to exhibit the least discharge. At other times a slight suppuration takes place; but, at the end of a few days, the cure is complete. Under the care of Desault, it was always effected in eight or ten days.
37. Let us bring the doctrine just laid down to the test of experience. Five cases have been published on this point. I have selected two of them, both which occurred in the same subject, where we find the same operation twice performed with equal success.
Case I. M. Vielle, aged nineteen, was attacked about the beginning of the year 1790, by a spontaneous swelling in the joint of the knee. Inconsiderable at first, but increased afterwards by a laborious journey, it disappeared at the end of two months, discovering to the touch, near the internal edge of the rotula, a foreign body, which was hard and moveable, and which somewhat impeded the motions of the joint.
About a month afterwards, the swelling returned, and, having continued for three months, disappeared again, when the body was found at the external side of the rotula, increased in size. Sundry external applications were tried for six months without success.
Weary of this unavailing practice, the patient came, in March, 1791, to consult Desault, who discovered a cartilaginous substance of a flat and circular figure. Its usual situation was at the external side of the joint, but it could be easily moved to the internal side, and could be turned on its own axis within the joint, nor did it occasion any pain, when suffered to remain at rest by the side of the rotula. But, when it passed behind the tendon of the extensor muscles, the patient was unable to stand, and he experienced severe pains when it made its way under the condyls or behind the rotula.
The indication was evident. Before the operation Desault prepared the patient by a proper regimen, and then, in the method already described (28), extracted a foreign body, whitish, and oval, fourteen lines in length, ten in breadth, and two and a half in thickness at its middle. It consisted of three pieces, united by a ligamentous substance, and was smooth on the side next the joint, but rough with irregular tubercles on the opposite side, and on its circumference. There was no loss of blood during the operation: the usual dressing was applied, after the most attentive examination, as to the existence of a second body.
Neither pain nor swelling supervened, and by the fourth day, the reunion was complete. In a short time motion was performed with as much ease as before the occurrence of the complaint. In the mean while, a degree of uneasiness remained in the joint; but barely perceptible at first, this uneasiness continued to increase; in about four months, symptoms of the existence of another foreign body made their appearance.
M. Vielle being now a distance from Desault, put himself under the care of his brother, who extracted a second body, in the manner already described, except that the incision was made at two strokes.
Dressing the same as in the preceding case, with this additional precaution, that the thigh and leg were covered by a roller, for the purpose of moderating the action of the muscles.
No fever, no pain; the reunion completed on the eighth day, except a small point in the centre of the wound, which suppurated slightly till the fourteenth. There was now neither difficulty in walking, nor the least sensation of pain. Since that time, M. Vielle has enjoyed the entire use of his limb.
§ I.
1. Case I. (Reported by Levacher). Catharine Belet, aged fifty-five, of a strong and vigorous constitution, fractured her leg in the middle, by a false step in alighting from a carriage. Being carried home, in a careless manner, she was visited by a surgeon, who merely reducing the fracture, but applying nothing to retain the reduction, sent the patient to the Hotel-Dieu. She was conveyed on the same day to the amphitheatre, where Desault discovered the existence of the affection by the following signs.
Pain in the middle of the leg, less severe when the limb was at rest, more so when it was suddenly moved; the patient absolutely unable to support herself on it so as either to stand or walk since the accident; inequalities sensible to the touch on the anterior surface of the tibia; a shortening or contraction of about half an inch; a preternatural mobility at the place of the fracture; evident crepitation, produced by the rubbing of the fragments against each other, when moved in contrary directions: a change in the direction of the lower fragment, which was bent somewhat outwards. These signs, added to the circumstance of the fall, evidently announced a simple fracture of both bones. The reduction was effected in the following manner.
One assistant made counter-extension by grasping the lower part of the thigh with both his hands, the fingers being placed behind it, and his thumbs corresponding to its anterior surface. Another made extension, not as writers recommend, at the lower part of the leg, but on the foot itself, which was taken hold of in such a manner that the fingers met on its upper side, while the thumbs crossed each other on its sole. In this way a lever of the first kind was formed, the resistance to which was the fragment to be replaced, while its centre of motion was in the joint.
Extension being directed at first in the course or line of the displacement, till the limb had attained its usual length, was then directed in such a way as to restore to the leg its natural form. By this, the fragments being brought into apposition, united exactly without the process of coaptation being employed.34 The apparatus, usually employed by Desault in such cases, was applied to maintain the reduction: the different pieces of it had been previously arranged on a pillow in the following order: 1st, four strong pieces of tape placed at equal distances from each other; 2dly, a junk-cloth,35 long enough to reach from the knee beyond the sole of the foot; 3dly, a bandage of strips, similar to that described for the thigh (page 246), arranged in the usual mode; 4thly, two long compresses, the lower one of which being the longest was turned back on the other; three bolsters had also been prepared; these, being formed of several pieces of linen joined together, were about one inch and a half thick: the broadest of these was designed to be placed on the anterior part of the leg; the two other lateral ones, though narrower, were a little longer, in order that, by folding back on themselves, they might be accommodated to the inequalities of the limb; 6thly, lastly, there were also prepared two splints, an inch broad, three lines thick, and of the same length with the junk-cloth.
Every thing being ready, the assistants still keeping up extension raised the leg a little, while a pillow was slipped under it, to support it equally and uniformly throughout its whole length. The leg was placed on this pillow in such a way as to correspond exactly to the middle of the apparatus which was arranged in order on it, and was previously wet with vegeto-mineral water.
On the anterior part of the leg was then applied a long compress, extending from the knee to the upper part of the foot. Over this were lapped the other two compresses, which had been previously placed in order as part of the apparatus. These were then secured by the bandage of strips, the application of which was begun at the lower strip next to the foot, and continued successively upwards with the rest, making them cross each other at the anterior part of the leg.
On the sides were placed the bolsters which were doubled at the ancle to protect that part from the pressure it might otherwise sustain. The splints were then applied along the external surfaces of the bolsters, the edges of the junk-cloth having been previously folded round them, in order to render their pressure the more close and steady. Along the fore part of the leg was laid the largest of the bolsters, and the whole was then secured by the four pieces of tape tied on the external splint, with a degree of tightness sufficient to keep the fragments immoveable.
A compress wet with vegeto-mineral water covered the foot, and was secured by a roller, applied in such a manner, that its two ends, crossing on the back of the foot, were fastened laterally to the two splints.
The leg, being firmly fixed by this apparatus, and gently flexed by means of a pillow placed under it, was protected by hoops from the pressure of the bedcloaths. The fragments being now in complete apposition irritated the parts no longer, in consequence of which the pain ceased.
The patient being properly disposed in bed, remained tranquil and easy throughout the remainder of the day. Diluting drinks and light nourishment were prescribed.
Next day, no pain; patient composed; a slight swelling on the back of the foot; the apparatus wet anew with vegeto-mineral water. Fourth day, the bandages a little relaxed; the point of the foot turned somewhat outwards; a new application of the apparatus. Seventh day, bilious symptoms appear, loathing of food, nausea, and bitterness of the mouth. Eighth day, tongue furred, inclination to vomit; loss of appetite; a grain of tartar emetic given in solution; copious dejections; evidently better: next day, appetite returned, tongue clean. Tenth day, a third application of the apparatus, which had become too loose. Fifteenth day, fresh bilious symptoms; further evacuations; success the same. Twentieth day, consolidation evidently advancing; no deformity of the limb; fourth application of the apparatus. Thirty-second day, consolidation almost complete; the apparatus still kept on till the forty-second day, when the patient was discharged perfectly cured.
2. This case, which is in no respect different from those that most frequently occur in practice, presents us with a view of the mode of reduction, the means of retention, and the subsequent treatment, employed by Desault, in cases of the kind. The advantage of the bandage of strips, which allows the limb to be uncovered without being disturbed, is now generally acknowledged in fractures of the lower extremities. In the treatment of these, practitioners reject entirely, at present, the roller bandage, which was recommended by Petit, Heister, and all the authors who preceded them, and which, by producing a new displacement, at each time of reapplication, may entirely prevent the fragments from uniting. The bandage of Scultet, brought into use again by Desault, the form of which has been just described, is also preferable to the eighteen-tailed bandage, which some practitioners still employ.
3. The strips which compose the former bandage, being narrower than the tails of the latter, can be more neatly applied to the leg, as they more readily mould themselves to its inequalities; the compression made by them is, therefore, more exact, more uniform, and consequently less inconvenient. If one of the strips become soiled, it can be changed without deranging the bandage. (Respecting this point, see what was said on fractures of the thigh.) This bandage being less bulky than the eighteen-tailed one, is therefore less troublesome to the patient.
4. The broad and strong splints which form a part of this apparatus, have the following advantages over those previously used both by the ancients and the moderns; 1st, they come in contact with and bear on a larger extent of the surface of the limb; 2dly, they consequently maintain the fragments in apposition with greater firmness and effect; 3dly, they prevent the rotation of the foot outwards, an accident which very frequently occurs when the fracture is complete, that is, when both bones are broken; 4thly, they remain constantly in their place, without slipping either forward or backward, an inconvenience necessarily attendant on the other splints, which, from their roundish form, touch the limb in only one point or line.
5. To sustain the foot, Petit recommends a piece of a board to be applied immediately to its sole, and supported by two bits of tape fastened to the splints. This practice is adopted to some extent even at present: but a simple roller, applied in the manner already mentioned, is sufficient for the purpose; the tendency of the foot to turn outwards is never so strong as not to be effectually resisted by this expedient: besides, should the piece of board be placed ever so little too vertically, it retains the foot in a state of inconvenient and painful flexion.
6. The situation of the leg, gently flexed by means of a thick cushion or pillow placed between it and the mattress, is, in all respects to be preferred to the method of Pott, which is exclusively adopted by Bell. What, indeed, can be the object of this latter method? To relax, say they, the muscles, that tend to make the lower fragment overlap the upper one. But is it not evident, that most of these muscles, not being attached to the os femoris at all, cannot be influenced by this position? To obtain the relaxation of the posterior muscles, it is necessary to flex the foot; but, in such a case, the anterior muscles are necessarily in a state of tension: this completely counter-balances the relaxation of the others, and, therefore, there is nothing whatever gained. It is certainly much best to allow the leg to be in a state of moderate flexion, such as we assume when asleep, and which appears to be the most natural.
7. The apparatus just described, produces on the fragments a twofold action: 1st, by a kind of side walls formed by the splints, it prevents their displacement laterally, and from this circumstance alone, is fully sufficient for the retention of transverse fractures: 2dly, the pressure of the rollers, splints, and bolsters, if these be applied with sufficient tightness, prevents the lower fragment from mounting on the upper one, and thus preserves the natural length of the limb. Hence its advantages in oblique fractures; and, as the powers of displacement are weaker here than in the thigh, this apparatus, is in general, sufficient to counteract them.
8. It is true that cases do sometimes though rarely occur, where, in consequence, of being irritated by splinters, or the points of the fractured bone, or acted on by some other causes which make them contract, the muscles overcome the resistance of the apparatus, and make the fragments overlap. Under such circumstances, permanent extension affords here the same advantages as in fractures of the thigh.
9. Most authors, to obtain the desired end in such cases, recommend means calculated to act on the thigh. Thus, Manne proposes the use of his glaussocome. Desault, under such circumstances, effected his purpose by the apparatus described in the following case.
§ II.
10. Case II. Pierre Bejol, aged thirty-seven, of a strong and vigorous constitution, fell, as he was carrying a heavy load, over a beam which lay in his way. His leg was fractured towards its lower part; he was lifted up and carried home, where a surgeon, by making unskilful efforts at reduction, gave him extreme pain.
A roller and a kind of round splint applied to each side of the limb, forming the whole of the apparatus, and not being sufficient to retain the fragments, soon allowed them to overlap each other nearly two inches. The pains continue; a considerable swelling appears around the fracture; the patient is greatly agitated; he is brought to the Hotel-Dieu, where, from the deformity of the limb, Desault was satisfied, at first sight, of the existence of a fracture; on a more attentive examination, it was discovered to be complete and very oblique.
The muscles being tense and in a state of violent contraction, drew the inferior fragments very forcibly upwards; these were finally, however, by means of well directed efforts, brought into perfect contact, with the superior fragments: the difficulty now lay in maintaining this contact. The age of the patient, his strength, and the almost convulsive state of the muscles, gave reason to apprehend that a displacement was about to occur. An attempt was made to prevent this in the following manner.
The patient being laid on a bed properly prepared,
1st, The foot and the leg above the ancle, were covered by a bolster or compress, round which was passed a strong roller intended for the purpose of making extension. The ends of this roller, being left free, were carried, one on the outside, and the other on the inside of the limb.
2dly, Below the tubercle of the tibia was placed another bolster, surrounding the leg, and on this, was secured another roller for the purpose of counter-extension. The ends of this roller, after crossing under the knee, were left hanging loose one on each side of the limb.
3dly, The two rollers being thus arranged, while the assistants, still continued to make extension, the surgeon applied successively, and in the order already mentioned, the compresses, the bandage of strips, and the bolsters.
4thly, He then took two splints with notches in their lower ends, of the same breadth with the splints already described, but long enough to reach, each of them, from four inches above the knee to the distance of four inches beyond the sole of the foot. One of these was applied on the outside and the other on the inside of the leg.
5thly, The surgeon then taking hold of the two ends of the upper roller, drew them over the upper ends of the corresponding splints, while an assistant crossing the two ends of the lower roller under the sole of the foot, drew the external end over the lower extremity of the internal splint, and the internal end over the lower extremity of the external splint. Carrying them, then, up along each side, he brought them, at the middle of each splint, to meet the ends of the upper roller, to which they were firmly secured by knots, so as to make extension at the foot, and counter-extension at the knee. The two fragments, being drawn by this apparatus, the one down and the other up, could not again overlap.36
On the same day the patient was bled copiously; a low diet was prescribed; some diluting drinks were administered; and the whole apparatus was frequently wet with vegeto-mineral water.
Next day, fever; restlessness; blood-letting repeated; the extending rollers, having become relaxed, were tightened. Third day, evidently better. Fifth day, a new application of the apparatus; some swelling of the foot; a few small blisters on the leg; these were opened and dressed with cerate spread on linen. Eighth day, the patient easy and tranquil; a little shortening of the limb; a third application of the bandage. Twelfth day, bilious symptoms appear. Thirteenth day, an emetic given in solution; symptoms decline. Twentieth day, the fractured limb in a favourable state; the roller for extension laid aside; that formerly described employed in its place. Thirtieth day, an appearance of consolidation. Thirty-fourth day, bilious symptoms recur; further evacuations. Forty-third day, consolidation perfect; scarcely a vestige of the fracture remains. Exercise is repeated for several days. Fiftieth day the natural strength and motion of the part completely restored.
11. The general end to be answered by every bandage intended to retain a very oblique fracture of the leg, is evidently, 1st, to hold the knee up, and with it the superior fragments; 2dly, to draw the lower fragment down: from this twofold effect arises a twofold resistance diametrically opposed to the powers of displacement, which are; 1st, the slipping down of the trunk, which pushes the thigh before it, and with it the upper fragments of the leg; 2dly, the action of the muscles of the leg, drawing the foot upwards, and the lower fragment along with it.
12. But, if to these indications we compare the bandage described in the foregoing case, we will perceive that they are perfectly fulfilled by it. Indeed the splints forming a kind of pullies which change the direction of the rollers, we must count on the action of these rollers only from the part of the limb which they surround, to the ends of the splints over which they are reflected: whence it follows, that the two ends of the upper roller, reflected over the superior extremities of the splints, cannot be drawn down along each of these splints, without that part of the rollers, which reaches from the leg to these extremities, being drawn up, and with it the knee and the upper fragment. In like manner, the ends of the lower roller cannot be drawn up towards the ends of the upper one, without those portions of them which run from the sole of the foot, being drawn down and pulling the foot and the inferior fragments along with them.
13. Hence it follows, that by tying on each side, one end of the upper roller to the corresponding end of the lower one with sufficient tightness, the two indications above laid down (12) are accurately fulfilled.
14. But, in general, the common bandage is sufficient, as I have already mentioned, even in cases of oblique fractures, to prevent the ascent of the lower fragments on the upper ones. Desault never employed any others in the last years of his practice, and it was only in cases of extraordinary disposition to muscular contraction, that he ever had recourse to the second kind. By means of the common apparatus, he was able to prevent the overlapping of the fragments from forming any protuberance on the anterior and internal part of the leg.
15. We must acknowledge, however, that this apparatus is liable to the same objection with most others intended for permanent extension. The roller placed below the knee, for the purpose of counter-extension, surrounds almost all the muscles, which tend to make the inferior fragments overlap the superior ones, by drawing the foot upwards. By pressing on and irritating these, it favours, and even excites their contractions, and, by that means, gives rise to a shortening of the limb, the very accident which the apparatus is intended to prevent. This inconvenience induced Desault, in a particular case, to substitute to the preceding apparatus, that used for permanent extension in fractures of the thigh.
1. It might be supposed that a work on diseases of the soft parts, would be a more proper place for this article, than the present one, where my express object is to treat of affections of the hard parts. What induces me to insert it here is, the analogy which exists between a division of the tendo Achillis and a fracture of the os calcis, the light which the treatment of the one throws on that of the other, and the example of the celebrated Petit, who, in his work on diseases of the bones, speaks also of this division.
§ I.
2. The division of the tendo Achillis is the result, either, 1st, of the action of a cutting instrument; or, 2dly, of muscular action: hence two very different modes of its production, the one by a wound, the other by a rupture. The first is not a very rare accident, because the projection of the tendon exposes it oftentimes to the stroke of external bodies: the second, though but little noticed by the ancients, has been frequently observed by the moderns, since their attention was called to it by Petit.
3. The manner in which the division is produced by a wound, has nothing particular in it; that by a rupture, takes place in the following manner. A man leaps over a ditch, but his spring or exertion is too weak; he reaches the opposite bank only with the ends of his feet: the line of gravity not falling on the ground, the weight of the body throws the feet into a state of violent flexion, the muscles contract with great force, to prevent a fall backwards, and, at that instant, the tendon is ruptured, in consequence of being drawn downwards by the violent flexion of the foot, and upwards by the effort of the muscles: hence it appears that Petit was deceived with regard to the mechanical cause of the rupture, which he considered as taking place at the moment of the patient’s alighting on his feet, when, as he said, the tendons were surprised, so to speak, into a state of too great tension. It is easy to apply the principles of this particular case to others that may happen, and where the position may not be the same; such as, when we leap on a table, &c. Sometimes slighter efforts have produced the effect; and, as Louis observes, dancers have sometimes ruptured the tendo Achillis by making a powerful exertion on the point of the foot, as well as by other motions.
4. Divisions produced in the first mode, may be situated in any part of the tendon. Those produced in the second, occur more particularly about its middle: to that part the effort or strain is most forcibly determined, and there the resistance is the weakest. The rupture of the tendon may, according to Petit, be either complete or incomplete; but, if we consider the simultaneous contraction of the gastrocnemii and soleus muscles, and the intimate manner in which their two tendons are united at a considerable distance above the heel, it will be difficult to conceive how these tendons can be ruptured separately. With regard to divisions produced by cutting instruments, the case is different: there, the weapon may pass half way through the tendon either from behind or laterally; and perhaps divisions of this kind are much more frequently incomplete than otherwise, in consequence of the great resistance of the tendinous fibres.
§ II.
5. The superficial situation of the tendo Achillis, always renders the diagnosis of its division easy. It can be rendered difficult only by the occurrence of a considerable swelling, an accident that rarely happens. If there be an external wound, the depth to which the instrument has penetrated, and the possibility of sometimes feeling the ends of the tendon between the edges of the wound, are the first evidences of its division. If, on the other hand, the tendon be only ruptured, then at the moment when the rupture happens, a report is heard by the patient, not sharp, and like the crack of a whip, as is said to take place when the plantaris muscle is ruptured, but more dull and flat, according to the account given to Desault by a patient, whom he interrogated on the subject.
6. In either case, there occurs suddenly, if not an entire inability, at least, an extreme difficulty in either standing or walking: hence the patient falls, and is unable to rise again; but, in divisions that are only partial or incomplete (4), this sign does not occur. Between the divided ends of the tendon there exists a depression sensible to the touch. This depression is increased by the flexion of the foot, but diminished and even entirely removed by its extension.
7. The patient can spontaneously flex the foot, none of the flexor muscles being affected, and this flexion may be carried even beyond what is natural, because the divided tendon forms no obstacle to it behind. Spontaneous extension is also practicable, in as much as the peroneus longus, tibialis posticus, &c. which remain uninjured, are capable of producing that motion. Some have alleged that the calf of the leg must be increased in size by the swelling of the gastrocnemii and soleus muscles, in consequence of their state of contraction; but modern experience has shown, that there is but little reliance to be placed on that appearance.
§ III.
8. Divisions of the tendons are not in general dangerous. These organs, being insensible in their nature, are not painful when ruptured, as is proved both by experiments on living animals, and by the observations of surgeons who have had such affections under their care, more particularly of Monro, who experienced the accident in his own person. No inflammation supervenes, and if a swelling be sometimes the consequence, it is in general soon dispersed, leaving behind it nothing serious.
9. Whence arose then the exaggerated fears of the ancients respecting injuries of this kind? Doubtless from an opinion which was then entertained, that tendons and nerves were of the same nature. Hence the severe pains, the convulsions, and even death itself, which, according to them, frequently happened, and was always to be apprehended, as the consequence of injuries done to these organs. Lamotte, among the moderns, still entertained these prejudices, when, in speaking of affections of the tendo Achillis, he said, “So dangerous are they in their consequences, that they can seldom be brought to a favourable termination.”
10. Doubtless the unskilful treatment, employed by the ancients, in cases of this kind, the use of the bloody suture without proper means to retain the parts in a suitable situation, the abuse of irritating remedies applied externally, the imprudent administration of oily substances, and, still more, the motions of the patient, contributed not a little to the production of those accidents, which no longer occur in the practice of the moderns, since the nature and treatment of the disease is better understood. It has been proved, by late observations, that the division of the tendo Achillis is apt to produce some diminution in the size of the affected leg. But this soon disappears, nor does it, indeed, even occur, if, by a proper application of the bandage, a speedy union of the divided part be obtained. The patients of Desault never experienced it.
§ IV.
11. That I may present, in order, what I have to offer on the treatment of the division of the tendo Achillis, 1st, I will lay down, with precision, the indications of cure that arise out of this division: 2dly, with these indications I will compare the means used by different authors, by which the insufficiency of almost all of them will be demonstrated: 3dly, by showing the relation or correspondence that subsists between these indications, and the apparatus employed by Desault, I will prove that it fulfils them sufficiently, and is, therefore, to be preferred to every other.
12. To bring the edges of the division into contact, and to retain them so, are here, as in other simple wounds, the two general principles of treatment. The first of the principles presents an easy indication; it is only to extend the foot forcibly on the leg. The indications that arise out of the other, are more difficult to be fulfilled.
13. To form a proper idea of these, let us call to mind what it is that prevents the contact of the divided ends. As far as relates to the lower end, it is the flexion of the foot on the leg, and with respect to the upper one, the contractions of the gastrocnemii and soleus muscles, which are not now opposed by the continuity of the tendon. Therefore, 1st, to keep the foot permanently extended; and 2dly, to oppose the action of these muscles, are the two general indications or objects of every apparatus destined to retain the two ends of the tendon in contact.
14. But, the action of the muscles may be opposed in different ways; 1st, by keeping the muscles themselves in a state of relaxation. This relaxation may be easily effected, as far as relates to the gastrocnemii, in consequence of their insertion into the posterior part of the condyls of the os femoris: it is sufficient, for this purpose, to keep the leg half-bent on the thigh: 2dly, by a judicious and well directed compression made on the muscles. I say judicious and well directed, because it ought to bear chiefly on the fleshy portion, and not on the tendon, otherwise it will depress its divided ends, destroy their contact, and make them unite, not with each other, but with the adjacent parts, and thus produce considerable lameness. At the same time that care is taken not to depress the divided ends, these ends must not be permitted to move from side to side, a kind of displacement which may readily occur, in consequence of the hollow or depression situated on each side of the tendon. But, the only expedient to attain this twofold purpose, is, to place in these hollows, some soft substance, lint, for example, which may project sufficiently to protect the tendon behind, and to retain it laterally.
15. This compression, that ought to be made by the bandage, appears to have escaped all writers, as none of them have given it a place among their means of cure. Yet, do we not plainly perceive, that, by confining the muscles, impeding their contractions, and reducing their irritability by its long continued use, it must tend to prevent the superior end from being drawn upwards and thus separated from the inferior one? Will not compression, in this case, be similar to the effect of the uniting bandage, in transverse wounds, where the great number of circular casts which cover the limb, are particularly intended to weaken muscular action, analogous to what takes place in hare-lip, where the compresses do as much good by compressing the muscles, as by bringing together the edges of the divided lip? But further, besides reducing the force of the muscles, does not this compression serve to prevent the swelling of the limb, an effect almost inevitably resulting from its state of rest and deficiency of action? So far, then, from being, as Louis says, one of the inconveniencies of the first bandage of Petit, it constitutes one of its principal titles to a preference among practitioners.
16. It appears from what has been just advanced (13...15), that the following are the three ends to be attained by every bandage, intended to retain the divided ends of the tendo Achillis in contact; 1st, the immobility of the foot in a state of permanent extension on the leg; 2dly, the immobility of the leg, in a state of semiflexion, on the thigh; 3dly, a judicious and well directed compression made on the whole leg and foot, but bearing on the tendon with only sufficient force, to keep it from moving backward or laterally. Let us compare the methods of authors with these indications.
§ V.
17. The treatment recommended by authors may be reduced to three general methods. The first consists in rejecting all artificial aid, and leaving the cure to nature and the position of the limb. To the second belongs the use of sutures, intended to retain the edges of the division together. The third includes the different kinds of apparatus employed for the same purpose.
18. First method. Chronological order places this method after the others. But this order must be disregarded by him, whose object is things rather than time. The history of the sciences calls sometimes for the approximation of distant periods, and, at other times, for the separation of those already approximated.
19. Several practitioners, in France and England, have lately proscribed the use of all external means. Pibrac and Dupouy were of opinion, that the mere precaution of the patient not to flex the foot, assisted by constant rest, was sufficient. Hoin and Gauthier mention many cases in confirmation of this doctrine. M. J. Rodbard, surgeon at Ipswich, having ruptured his own tendon about three inches above the heel in leaping over a little rivulet, instead of confining himself to bed, continued in the exercise of his profession. He walked every day, without any other precaution than that of not flexing the foot, and five years afterwards, he was able, as he mentions, “to walk, run, mount or alight from his horse, without pain, in a word, the affected leg performed its functions as well as the other one.” We have an account of a patient who was cured without a bandage by A. Petit.
20. Was there indeed a true rupture of the tendon, in all these cases, particularly in those where the patients continued to walk as before the accident? Most of the cases which we have seen prove the impossibility of either standing or walking (6). But, admitting that they were ruptures, are we authorized to pursue the mode of treatment there adopted? Certainly we are not. None of the indications formerly mentioned (16) is there fulfilled. What is there, under such circumstances, to prevent an involuntary motion from destroying the contact of the divided ends, by forcibly flexing the foot and extending the leg? The limb is not subject to any compression. Should such an accident happen, the cure must necessarily be tedious. Besides, if the ends be separated, a reunion cannot take place, except by an intermediate substance, which, by filling up the vacant interval between them, must lengthen the tendon. In consequence of this, the muscles will be impeded in their contractions, and the foot in its motions, as Desault has oftentimes observed in animals, which he left to themselves, after having divided the tendo Achillis. Thus, in a fracture of the rotula, the motion of the limb is very much impaired, when the ligamento-cartilaginous substance which unites the fragments is too long.
21. Hence it follows, that here, in like manner as in other ruptures of the tendons, art must assist nature, because without the former the powers of the latter will be insufficient.
22. Second method. The ancients pursued a course not less uncertain, and much more dangerous. Sutures, sanctioned by general custom, were extended to wounds in the tendons, and were even more especially employed in such cases, because the tendinous end being drawn forcibly and greatly displaced by the contraction of the fleshy portion in which it terminates, it was deemed necessary to oppose to this force a greater resistance.
23. What useful end was attained by this practice? Muscular action was left perfectly free; and the only thing done was an attempt made to resist its effect. But, in a short time the tendinous ends, in consequence of being forcibly stretched by the contractions of the muscles, either gave way at the points where the stitches were introduced, or, in case they did not give way, became swollen, painful, and inflamed, in consequence of the violent distension which they suffered: hence the serious affections produced by such treatment (9 and 10).
24. The ancients, then, were mistaken, with respect to the indications in this disease, which are, not to resist muscular contraction left free and unimpeded, but to check and prevent this contraction, by the means formerly pointed out (16). It is a principle generally acknowledged at the present day, that sutures ought not to be used as a mean of approximating divided parts, but only to keep the edges of parts already approximated in perfect contact. But, in the present case, the means of approximation being sufficient for the purpose of exact contact, sutures are altogether unnecessary. This, however, does not hold true in every case, though certain practitioners, who have too generally rejected the use of sutures, contend that it does. Finally, however, these means have been excluded from the treatment of the division of the tendo Achillis, and the doctrine of the Academy of Surgery, though erroneous in many other cases, has established, with regard to the present one, the true practice.
25. Third method. It is to the celebrated Petit that we are indebted for that method of treating the division of the tendo Achillis, which consists merely in position maintained by apparatus. Having ascertained that the extension of the foot brought the fragments into contact, he conceived the idea of continuing this extension throughout the whole treatment, for the purpose of continuing the contact also. This was a happy idea, the simplicity of which recommended it to practitioners, and which, being once discovered, has formed the common basis of all the numerous processes devised since by different authors.
26. When we consider the action of these several processes, and compare it with the indications formerly laid down (16), we may divide the processes themselves into three general classes. Thus, some of them fulfil only the first and third of these indications, namely, the permanent extension of the foot, and a regular compression made on the leg; others fulfil only the first and second, the latter of which consists in keeping the leg constantly flexed on the thigh; while those of the third and last class, fulfil the first indication only. This manner of classing the processes, will shorten the consideration of each of them individually, since it is evident that each class is chargeable with one general inconvenience, namely, that of being deficient with respect to one or two of the leading indications. I shall examine nothing, therefore, but the disadvantages peculiar to each.
27. To the first class belongs, almost exclusively, the first bandage invented by Petit. It is formed by a long compress, placed longitudinally behind the leg and foot, and secured by a roller applied regularly on these parts. The two ends of the compress, being reflected back, are then knotted together behind the leg so as to extend the foot. This expedient is simple and ingenious, and would be preferable to all others, were it not that, besides the charge of not fulfilling the second general indication (16), it is further liable to the following objections: 1st, the compression which it makes is injudicious and ill directed, because it bears not only on the fleshy portion of the leg, but also on the divided tendon, which being more projecting and therefore more exposed, has its two ends pressed down and separated: 2dly, in some cases, it does not maintain the extension of the foot with sufficient certainty: 3dly, it does not prevent displacement in a lateral direction.
28. To the second class belong, 1st, the celebrated slipper of Petit, substituted by that author for his first bandage; this machine was composed of a slipper fixed to the foot, of a knee-piece37 secured on the lower part of the thigh, and of a strap running from the one and fastened to the other, to extend at pleasure the foot on the leg, and to flex the leg on the thigh: 2dly, the bandage of Duchanoy, made in imitation of the preceding apparatus, and consisting of a simple sock surmounted by a roller, which running along the back part of the leg, was fastened to another roller applied round the lower part of the thigh. Besides the general objection of not at all fulfilling the third indication (16), these processes are liable also to the following ones; 1st, they fatigue the toes by the constant pressure of the slipper and the sock, as Monro experienced in his own person, to such an extent that he was unable to support their use; 2dly, the slipper is quite too complicated, and is therefore seldom at hand when wanted. The apparatus of Duchanoy, does not possess sufficient solidity and steadiness.
29. In the third class are included, 1st, the first machine of Monro, formed of a slipper similar to that of Petit, surmounted by a strap of leather, which was to be fastened by a buckle to a kind of guetre or spatterdash, fixed on the upper part of the leg; 2dly, the second apparatus of the same author, subject, like the other, to several inconveniences; 3dly, the simple apparatus of Schneider, who rested satisfied with maintaining the extension of the foot, by a splint placed anteriorly. Besides various other objections to them, these are all chargeable, alike, with the radical fault, of not fulfilling the second and third indications (16).
30. From this comparison of the indications (16) with the means destined to fulfil them, it appears that there were material defects on the part of the latter. Let us examine whether or not that of Desault was better calculated for the purpose. It is, so to speak, nothing but a modification of the apparatus of Petit (27), but such a modification as amounts to an improvement in principle, and entitles it to be called the apparatus of Desault.
31. The pieces which compose it are; a compress two inches broad, and long enough to reach from the lower part of the thigh to the distance of four inches beyond the foot; a roller five or six yards long and two inches wide; a sufficient quantity of lint; and two long graduated compresses.
32. Every thing being ready;
1st, An assistant supports the foot and leg, the former in a state of great extension, and the latter half-flexed: another assistant supports the thigh, grasping it about its middle.
2dly, If there be a wound of the integuments, a little lint wet with vegeto-mineral water is laid directly over the division of the tendon; if it be a simple rupture, this precaution is unnecessary. Under the foot, up behind the leg, and the lower part of the thigh, is then extended the long compress, which is to be secured in that situation by the hands of the assistants.
3dly, The hollows situated at the sides of the tendo Achillis, are then filled up with pledgets of dry lint, surmounted by the two long graduated compresses, which retain the pledgets, and must project a little beyond the tendon, because they are liable to be rendered flat by pressure.
4thly, The surgeon now taking the roller, makes at first several circular turns round the toes, fixing the long compress there, the end of which, being reflected over these first casts, is secured by a few additional ones which cover the whole foot, and are afterwards directed obliquely above and below the division, round which is formed a kind of figure of 8, that brings the edges of the wound into perfect contact. If there be no wound of the integuments, it is necessary to take care, lest the skin interposing between the divided ends of the tendon, should separate them, and thus prevent their reunion. Ascending, then, by circular casts, along the whole leg, and even to the lower part of the thigh, the surgeon there turns down the upper end of the long compress, and securing it by a few more circular casts, finishes the application of the roller.
5thly, The apparatus being thus applied, and the extension of the foot and the flexion of the leg firmly secured by it, the leg is then placed on a pillow or bolster, one side of which corresponding to the angle which the leg forms with the thigh, assists in keeping it half-flexed.
6thly, Should the long compress prove insufficient to keep the foot extended, or should it, by becoming relaxed too soon, render frequent reapplications of the apparatus necessary, (circumstances which rarely happen when the bandage is well applied), a splint placed anteriorly, as was the case in Schneider’s apparatus (29), completely remedies the defect.
33. On comparing this apparatus with the indications formerly laid down, in the present disease (16), we find it evidently calculated to fulfil them with great exactness. 1st, The extension of the foot is permanently secured, both by the long compress, and by the splint when it is employed: 2dly, the same compress, aided by the bolster or pillow placed under the leg, maintains the flexion of the leg on the thigh: 3dly, The muscles are effectually compressed; their action is impeded in part by the compression of the circular bandage, which does not bear on the tendon, in consequence of the bolsters of lint placed on each side of it: these bolsters prevent the tendon both from moving laterally, and from being depressed: hence it follows, that the action of the circular bandage is precisely conformable to the principles already established (14 and 15); and that the whole of the apparatus, taken together, fulfils perfectly all the indications (16); this is an advantage not to be derived from any of the forms of apparatus used by preceding authors.
34. This apparatus is in no degree complex or troublesome. Simple and easy, it requires nothing for its construction but what the surgeon can easily obtain, and what he can even himself prepare. There exists a great analogy between it and the bandages which Desault used for the reunion of transverse wounds, and for fractures of the rotula and the olecranon. A truly great man does not estimate his merit, by the number of processes which he invents; he well knows that the perfection of art consists in producing numerous effects by few and simple means.
35. We will confirm, by two cases, the principles laid down in this memoir. One of these relates to a division of the tendon, connected with a wound, and was reported by Bezard; the other by Manouri, and relates to a simple rupture of the tendon.
Case I. J. B. Lavigne, aged thirty, as he was going down into a cellar without light, struck his leg against the edge of a sharp saw, which completely divided the tendo Achillis. The patient was immediately carried to the Hotel-Dieu. The wound of the integuments was transverse, two inches long, and had its edges but slightly separated from each other. The ends of the tendon, in contact during the extension of the foot, were separated two inches when it was flexed.
The usual apparatus was applied (32), and the limb placed on a bolster, in a position favourable for the relaxation of the posterior muscles.
In the evening, wound painful; pulse raised; a copious blood-letting; low diet. Next day, more blood taken away; antiphlogistic regimen, which was continued for several days, till the symptoms were gone: no troublesome accident occurred. Tenth day, the apparatus taken off; the wound partly healed; the apparatus reapplied, and continued till the twentieth day, when the perfect reunion of the parts rendered its further use unnecessary. From this time the patient began to walk on crutches. Thirty-sixth day, could walk well without his crutches. At this period, a small abscess occurring in his heel, induced him to remain in the Hotel-Dieu two weeks longer, when he was discharged perfectly cured.
Case II. M. Delp, leaping with some of his young companions, ruptured the tendo Achillis, about two inches above the os calcis. Both standing and walking became instantly impracticable: the patient falling down, was taken up, carried home, and from thence to Paris, where he arrived in the evening. Desault being immediately called to him, found him affected with all the signs of a division of the tendon; such as, a hollow between its divided ends, which was increased by the flexion of the foot, diminished by its extension, &c. The usual apparatus was immediately applied, and as the patient felt but little pain, only a moderate blood-letting was prescribed. Next day, no alteration in the treatment; antiphlogistic regimen; low diet continued for some days, when the patient was permitted to return to his usual mode of living. Ninth day, apparatus removed for the first time: a slight separation of the ends of the tendon; and a wrinkle in the skin interposed between them: a new application of the bandage, taking care to free the integuments from wrinkles. Twelfth day, a relaxation of the rollers; a third application of the bandage: every thing found in a good state; but, the patient being, from sprightliness, too much inclined to exert himself, a splint was applied anteriorly to prevent the extension of the foot. Seventeenth day, a fourth application of the apparatus, which was not moved again till the thirtieth. At this period, the reunion was somewhat advanced: fortieth day, almost complete. Fiftieth day, the patient was permitted to leave his bed, and take very gentle exercise, which he continued to increase gradually, till the sixtieth day, when he was discharged cured. Doubtless the tediousness of this case was owing to the slight separation which existed for some time between the fragments.
§ I.
1. The os calcis, being a short and thick bone, has such a power of resistance, that it is but seldom fractured. Such an accident does, however, sometimes occur, and may arise from two causes, 1st, the action of external bodies, which is rare: 2dly, the contraction of the gastrocnemii and soleus muscles, from which it almost always proceeds. Thus, the rotula is more frequently broken by the action of the extensor muscles, than by blows received on the bone from without: there is, however, this difference between the effects of muscular contraction in these two cases, namely, that in the former, the rupture of the tendo Achillis is common, and the fracture of the os calcis very rare; whereas in the latter, on the contrary, the rotula is oftentimes broken, while the tendon of the extensors remains almost always sound. This phenomenon is explained by the difference between the thickness of the two bones, between the length of the two tendons, and between the power of the causes.
2. Be the cause of the fracture what it may, it generally occurs in that portion of the os calcis, called its great tuberosity, which projects behind the astragulus, which corresponds above and below to a large quantity of cellular membrane, inwardly to the great groove of the bone, externally to some ligamentous attachments, and behind to the insertion of the tendo Achillis.
3. It is known, 1st, by an evident inequality under the heel: 2dly, by an elevation, sensible to the touch, of the posterior fragment above its usual level: 3dly, by an almost entire inability either to stand or walk: 4thly, by severe pain being the inevitable consequence of moving the foot: 5thly, by its being practicable to increase the displacement by flexing, and to diminish it by extending the foot: 6thly, by the facility with which the posterior fragment may be moved in every direction by taking hold of it with one hand, and steadying the foot with the other: 7thly, by a swelling more or less considerable, which frequently appears around the divided surfaces.
4. The ancients gave in general an unfavourable prognosis respecting this kind of fracture. Hippocrates was apprehensive of some injury being done to the surrounding parts. Pare considered the case mortal, on account of the laceration of numerous vessels which are connected with the bone. Most of the moderns adopt these principles, not for the foregoing reasons, but on account of the vicinity of the accident to the joint of the foot. The practice of Desault cannot throw much light on this subject, as he never had more than one or two such cases of fracture under his care; but the analogy of other fractures, situated in the neighbourhood of joints and even extending into them, induces us to believe, that, if properly treated, fractures of the os calcis will terminate as favourably as those of other bones.
§ II.
5. If we attend to the signs just mentioned (3), we will perceive that they almost all result from the displacement of the fragments. But, whence arises this displacement? As far as the anterior fragment is concerned in it, it arises from, and is increased by, the flexion of the foot; and, as far as relates to the posterior one, it is to be attributed to the contraction of the muscles attached to the tendo Achillis, which is itself inserted in that fragment. Hence it follows, that the apparatus intended to prevent this displacement, ought, 1st, to keep the foot permanently extended on the leg: 2dly, to prevent the action of the muscles, by keeping them in a state of habitual relaxation by means of the constant flexion of the leg on the thigh, by making on those whose contractions are dreaded, such a regular and well directed compression as may disqualify them for contracting; and, lastly, by placing behind the posterior fragment some resisting substance, to prevent it from rising upwards.
6. If to these indications we compare Desault’s apparatus for a rupture of the tendo Achillis, as described in the preceding memoir, we will readily perceive 1st, that it perfectly fulfils that indication which relates to the anterior fragment; 2dly, that that one which relates to the posterior fragment will be equally well fulfilled by the half flexed state of the leg, by the compression made on the muscles, and by a thick compress, not very broad, laid transversely above the fragment, secured by the long roller, and afterwards by a circular bandage, which must form here, as in the case of a fractured rotula, a kind of figure of 8 around the fracture. This compress is the only modification of the apparatus requisite to accommodate it to the particular case now under consideration.
7. In applying the figure of 8 bandage here, as well as in the case of a fractured rotula, to prevent the ascent of the fragment, it is necessary to use the utmost care to free the integuments from wrinkles both above and below the fracture, lest by getting between the fragments, they might keep them asunder, and thus impede their reunion.
8. Desault used to relate in his lectures, the case of a woman whom he had formerly seen receiving a fracture of the os calcis, by falling from a great height. I cannot state the case fully, because I am not in possession of all the facts. The following one however drawn up during the first years of Desault’s practice in the Hotel-Dieu, will furnish an example of his mode of treatment.
Case. A man, likely to be arrested by some one who pursued him, leapt from a window nearly twelve feet high. In lighting, his feet struck on a beam which lay in his way, in such a manner, that the fore part of them only was supported. He made an effort to recover his equilibrium, but as the line of gravity of his body had nothing to rest on, he fell backwards, rose in order to make his escape, but fell a second time unable to rise again.
When assistance came to him, he complained of a severe pain in his heel, and said, that on falling, he had heard a considerable report. He was taken up, and assisted in walking to the Hotel-Dieu, where he did not arrive without pain, being able to bear only on the point of the diseased foot, and suffering greatly if he attempted to put his heel to the ground.
From the signs mentioned (3), Desault perceiving that there existed a fracture of the os calcis, made arrangements for reducing it. This he did by extending the foot on the leg, and drawing down the exterior fragment from the elevation to which muscular contraction had raised it, so as to bring it into perfect contact with the body of the bone. He then applied the common apparatus for a rupture of the tendo Achillis, with the modification already pointed out (6).
In the evening venesection was prescribed: the patient experienced sharp pains at the place of the fracture; a slight swelling occurred at the ends of the toes; an anodyne was prescribed. Next day, evidently better: venesection again. Fourth day, the patient is allowed to return to his usual regimen. Eighth day, apparatus removed for the first time; fragments in contact. Fifteenth day, a second application of the bandage. Nineteenth day, bilious symptoms. Twenty-first, an emetic given in solution. Thirty-second day, further evacuations: apparatus renewed. Forty-seventh day, consolidation complete. A stiffness remained in the part for some time, but this was gradually removed by exercise.
§ I.
1. Complicated luxations of the foot, like complicated fractures, show themselves under such a variety of forms, are accompanied by so many peculiar affections, and so many different circumstances are connected with them, that it would be difficult to lay down rules applicable to their treatment in all cases. On this subject, indeed, art is in possession of certain general principles, liable however to numerous exceptions and modifications. In the treatment of such cases, who can fix the limits between reduction, and amputation or extirpation? Who can point out, with precision, where the one ceases to be useful and becomes hazardous; while the others constitute the only resources of art? Experience and talents alone are capable of deciding on these points, and that only in the chambers of the sick. It is, therefore, less by precept than example that practitioners ought to be instructed here.
2. To furnish suitable examples on this head constitutes my only object in the present memoir, which will consist of the histories of a few cases, with such inferences and remarks as the occasion may seem most naturally to suggest. Here the practice of a great master, varying his means with the varying forms of disease, will serve as models to those who may meet with similar cases. Our experience is composed of the facts which we receive from reading, as well as of those derived from observation. Who would have a right to call himself a surgeon, if he had no other title to that name, but such as resulted exclusively from his own personal observation?
3. However difficult it may be, as already observed, to speak in general terms, on the present subject, we may yet assert with safety, that authors have greatly exaggerated the danger of complicated luxations of the foot. Terrified at the extent and unpromising appearance of the accidents, these writers have lost that confidence in the powers of nature which we never ought to abandon. They have taken up an opinion, that luxations of the foot, differing in their symptoms from other luxations, require also a different mode of treatment; that reduction, by perpetuating the accidents of the case, must prove fatal, and that amputation ought to be adopted as the only resource. Cases do certainly at times occur, where a doctrine different from this would be fatal in its effects: such are those terrible lacerations, where the foot is entirely separated from the leg, except some shreds of flesh with a few tendons among them that still retain it.
4. But, provided the blood-vessels have escaped, and any hope of circulation and life in the part still remain, the success of reduction should always be first tried; and the following examples will show, what ought to be expected from this practice, when accompanied by skilful treatment.
§ II.
Case I. (The following case was collected by Leveille.) Abraham Genty, aged forty-three, a dealer in wine, as he was running along the street, slipped, and made a false step on his left foot, which turned with its external edge under him, and its internal edge upwards. He fell, luxated his foot, and fractured the fibula.
The patient was carried home, where a surgeon who was ignorant of his profession being called, did nothing but apply a cataplasm to the foot. In the evening the parts began to swell, and were extremely painful; fever supervened, accompanied with great restlessness. Third day, to a rapid increase of all the symptoms was added a delirium; blood-letting from the jugular vein was prescribed to no purpose; things continued to grow worse till the sixth day, when the patient was brought to the Hotel-Dieu, in extreme danger.
The following was then the state of the parts. A considerable swelling around the joint; a projection of the malleolus internus, with a depression underneath it; a preternatural direction of the tibia before, and of the os calcis, behind; a depression near the lower end of the fibula; a crepitation readily perceived, on moving the fragments; a large tumour on the outside of the foot: with a depression and mobility of the malleolus externus.
The luxation was immediately reduced. Extension made on the foot and leg brought the parts into their proper situations, where they were retained by means of the bandage for fractures of the leg, and four compresses well secured by the bandage. One of these compresses, being placed on the malleolus internus, another on the outside of the foot, a third on the anterior and lower part of the tibia, and the fourth under the os calcis, prevented these different parts from being again displaced.
As soon as the apparatus was applied, the pupils remarked with astonishment, that the restlessness of the patient ceased, that his pains were relieved, and his delirium disappeared; he expressed his surprise at the state from which he had just recovered, and was now able to give an accurate account of his fall. He was scarcely put to bed, when he fell into a tranquil sleep, which lasted three hours. For six days previously he had not slept a moment.
In the evening, the patient was free from pain, and perfectly tranquil. Diluting drinks were prescribed, with twenty-five drops of Hoffman’s anodyne liquor: the apparatus was wet from time to time with vegeto-mineral water: the patient slept well throughout the night.
Next day, the apparatus renewed: the parts perfectly in place: swelling diminished; same means continued. Sixth day, the anodyne discontinued. Tenth day, swelling still less; echymosis gone; a yellow colour in the skin, an evidence that resolution is going forward. Twentieth day, swelling gone.
Thirtieth day, the fracture of the fibula healed; that bone slightly separated from the tibia: the circular roller drawn tighter; and a thick compress placed on the external malleolus, to bring it to its proper place. Forty-fifth day, the apparatus for a fractured leg removed, and a simple roller substituted in its place: the motions of the foot painful and contracted; a small gangrenous spot appeared on the heel. Fifty-fifth day, the ulcer which proceeded from this spot healed: motions of the part more free and extensive. Sixty-first day, the patient able to walk without assistance, though not without pain.
5. It is difficult to find an instance where the advantages of reduction have been more remarkable than in the preceding one. The patient had passed six days in pain, extreme agitation, and uninterrupted delirium: the foot was reduced, and these unfavourable appearances instantly vanished, and were succeeded by a state of tranquillity. Alarmed by such a state of things, the ancients would doubtless have proceeded to amputation. Let us examine into the motives which led Desault to an opposite line of practice, and then inquire into the cause of the success with which that practice was crowned.
6. Had amputation been performed here, it must have been for one of the two following reasons; 1st, for fear of gangrene; or 2dly, to remove the unfavourable symptoms that existed. The first apprehension would have been quite visionary, in as much as all the blood-vessels were sound. Would the second consideration have been any better founded? It was perfectly obvious, that the unfavourable symptoms which existed arose from the tension and overstretching of the parts, in consequence of the preternatural position of the bones of the foot. The indication was evident. Replace these bones in their natural situations, the strained parts will then necessarily become relaxed, and all the troublesome and alarming symptoms cease with the cause that produced them. Experience confirmed the justness of this reasoning.
7. But the mere replacement of the parts would be of very little avail, if it were not permanently maintained, and followed up by a judicious mode of treatment. Without such treatment there would doubtless be reason to apprehend all that train of troublesome consequences, of which authors speak in such frightful terms, and which arise, not from the nature of the luxation, but from the manner in which the patient is treated. A loose apparatus, incapable of preventing displacement, would allow the bones to be deranged anew, and to produce again an overstraining of the parts, accompanied with pain, swelling, &c. Irritating local applications, such as camphorated spirits of wine, &c. would increase these pains; emollients which are employed in other cases would keep up the swelling.
8. It follows from what has just been said, that an opposite mode of treatment ought to succeed the reduction, and this we see was the case in the preceding instance. There, when the bones were once reduced, all new displacement was prevented, because the apparatus was so constructed, as to counteract the tendency of the bones to be displaced. The external edge of the foot, which had been turned outwards, was now pushed inwards by a thick compress; the same means served to push outwards the internal malleolus, which had received by the accident an inclination inwards, and to push the anterior part of the tibia backward, and the os calcis forward, both of which were displaced, as has been remarked, in contrary directions. Two strong splints fixed the lateral compresses, while the anterior and posterior ones were firmly secured by rollers. In the midst of all these resistances, the foot being necessarily immoveable, no new displacement could occur.
9. A suitable and judicious position, in which the foot, raised a little higher than the leg, was placed on a pillow forming an inclined plain, prevented swelling, while gentle compression, made by a bandage, contributed to the same end. This end was also further attained by the external topical applications. To relieve pain and remove congestion, were here, as in sprains, the two indications to be fulfilled. To these indications the spirituous and the relaxing applications formerly in use, are alike opposed. Vegeto-mineral water, on the contrary, fulfils them extremely well. Hence the necessity of keeping the apparatus constantly wet with that liquid.
10. Regimen influences not a little the success of the treatment. A strict diet is necessary during the time of the inflammatory and unfavourable symptoms. Any excess might then prove fatal. Desault gave, in his lectures, an account of a woman, who had her foot luxated outward, and the astragulus forward. Her fever was considerable, her pains excruciating, and the swelling wore an alarming aspect. The luxations were reduced: all the threatening appearances vanished, and every thing seemed to promise a favourable termination of the disease. But, on the fiftieth day, the patient, having procured strong food, ate largely of it: in the evening all the unfavourable symptoms returned; the swelling became great, and a few days afterwards she died.
But if strong food be prejudicial during the time in which bad symptoms are to be dreaded, a diet too strict would be equally injurious when that time is passed. The weakened powers of the system would not be adequate to the purposes of a cure, particularly to the consolidation of the bone, should the case be a fracture. Desault, therefore, permitted the patient to increase his diet by degrees, and at length to return to his usual regimen.
11. The following case, reported by Giraud, proves still further the advantages of this simple mode of treatment, which, should it even fail, always allows the surgeon to avail himself of amputation, which is indeed the last resource of art, and should never be employed till rendered indispensable by the failure of all other means.
Case II. Maria Constant, aged forty-six, descending a flight of stairs in haste, fell, and luxated her right foot outwards, the tibia inwards, and fractured the fibula near to the lower end.
Her cries brought assistance to her, and she was carried to the Hotel-Dieu. Giraud, who then officiated as surgeon in chief, visited her, and discovered that there existed both a luxation and a fracture, though most of the signs were rendered obscure by a considerable swelling: a slight echymosis occupied the back of the foot, and severe pains were experienced.
Extension on the foot, and counter-extension on the leg, dislodged the parts by degrees from their accidental situations, while, by the process of conformation, the surgeon endeavoured to bring them into their natural ones. This was soon effected without much violence: the unfavourable appearances soon vanished; the pain ceased; an apparatus similar to the former one was applied, and kept wet with a strong solution of common salt, instead of the vegeto-mineral water.
In the evening, the pulse being full, and somewhat raised, a moderate blood-letting was deemed necessary. Next day, the apparatus was kept constantly moist, and some part of it which had become relaxed was tightened. The pulse continuing full, a low diet was prescribed.
Fifth day, the apparatus taken off; contact between the bones perfect: a yellowish tinge bespoke an incipient resolution of the echymosis: a slight swelling of the leg: vesications formed on the part: these are opened and a quantity of acrid water discharged from them. Sixth day, light nourishment allowed; a small excoriation of the heel, which is dressed with cerate spread on a linen rag. Seventh day, regimen less strict; no bad symptoms supervene. Eighth day, the excoriation enlarged; same dressing. Tenth day, the excoriation become fungous: caustic is applied to remove it.
Twenty-eighth day, the discharge from the leg decreased; from this time the dressings are renewed only every other day. Thirty-second day, the ulcer is cicatrized: no pains in the leg. Thirty-ninth day, fracture of the fibula firmly united: no deformity remaining; the apparatus is laid aside: the joint remains stiff: motions performed by the limb difficult at first, but become gradually more free. Forty-sixth day, symptoms of bile; gentle evacuants. Fifty-fourth day, the patient is discharged cured, except a slight impediment in walking, which exercise will soon remove.
12. To this example, I might add many others, where similar displacements, properly treated, terminated with equal success: no pain; no swelling; no inflammation; and therefore, of course, no mortification. Yet these are occurrences of which authors speak, as if they were the usual consequences of such luxations, where, to a violent injury done to the soft parts, is added a fracture near to, or even communicating with, a joint. The erroneous opinions of the ancients and most of the moderns, respecting the dangers arising from such vicinity or communication, have contributed not a little to their unfavourable prognosis in the cases under consideration. Should the patient survive the disease, his inevitable lot, according to them, must be, a complete anchylosis of the leg with the foot. But, the preceding cases fully prove, that this apprehension is unfounded. A considerable time is doubtless necessary, for the recovery of motion, on account of the distension and rupture of the ligaments, the long continued inactivity of the parts, and the swelling which they have undergone. But this recovery can always be effected by means of exercise, gentle at first, increased afterwards, and regulated according to the principles so frequently laid down in the course of this work. Much more to be relied on is such exercise, than the long catalogue of discutient means, such as pumping of water on the parts, alkaline baths, mineral waters, and all other external applications, so often extolled as efficacious, and so often found entirely useless.
§ III.
Case III. (The following case was reported by Thevenot). I. Joseph Schneider, an ebonist, aged thirty-six, as he was walking in haste, on the 23d of March, 1792, fell forward, his foot being forced backward and outward. He experienced at the instant severe pains in the joint: he was unable to rise, and was therefore carried home, where a surgeon, after making a slight extension, applied a roller on the limb, and did nothing further. The patient experienced no relief. The pains increased; a swelling supervened; convulsive motions began to occur; and the patient was brought to the Hotel-Dieu, six days after the accident.
From the deformity of the foot, Desault immediately discovered that it was luxated. Its point was directed outwards, while its sole was turned in the same direction: beneath the malleolus internus, which was too prominent, was a tumour formed by the astragulus. The crepitation of the bones which was easily heard, the preternatural distance between the tibia and the fibula, the mobility of this latter bone, and the absence of the signs of a fracture, plainly showed that a separation of the two bones of the leg had taken place.
A reduction was immediately effected by means of extension and counter-extension, and was announced when it took place by a report distinctly heard. It was then retained by a bandage, calculated to answer a twofold purpose; 1st, to approximate, and keep together, the two bones of the leg: 2dly, to secure the contact and immobility of the bones of the foot.
Blood-letting was prescribed: an anodyne mixture administered; low diet; in the night severe pains were felt; next day, they were increased; on dressing the limb, nothing amiss discovered; all the parts in perfect contact: no vestige of separation between the tibia and the fibula: a new apparatus applied; and kept constantly moist. Third day, the patient better: fifth day, the fibula a little separated from the tibia: the circular bandage drawn tighter to reduce it to its place again. Tenth day, every thing in its natural state: no pains: swelling gone. Fifteenth day, a simple roller substituted in place of the bandage for a fracture of the leg. Nineteenth day, the patient began to walk, with the assistance of a stick: twenty-third day, walks easily: twenty-eighth day, is dismissed perfectly cured, and nearly free in all his motions.
13. The separation of the bones of the leg, at their lower end, does not constitute a very serious complication of luxations of the foot, although the contrary is asserted by several authors. Desault met with this accident several times in the course of his practice, but never saw it terminate otherwise than favourably. But here, as in all other cases, the most minute attention is necessary to ensure success, the want of which is more frequently owing to the negligence of the surgeon, than to the deficiencies of the art. The bandage employed after reduction ought to act principally from without inwards, and in a direction perpendicular to the axis of the lower part of the leg, in order to approximate the two bones. It will be of some service, in this respect, to place on each bone a compress, which, projecting more than the rest of the circumference of the limb, will be more compressed, and on that account, contribute to the end in view.
§ IV.
14. Petit never met with more than two instances of that displacement of the astragulus, now under consideration. His general prognosis on the subject is more favourable than that respecting other luxations of the foot, with which he never saw the present luxation of the astragulus complicated, as occurred in the following cases. Had such complex cases fallen under his notice, there can be little doubt, but he would have declared amputation to be the only recourse of art on the occasion.
But the experience of Desault demonstrates to us here, as well as in the preceding cases, the great extent to which we ought to carry our confidence in the powers of nature, when skilfully guided by the hand of art. The following case was communicated to me by Leveille.
Case IV. John Baptist Landrin, a postilion, aged thirty-six, was brought to the Hotel-Dieu, on the 19th of February, 1791.
On the morning of the same day, a horse on which he was mounted having fallen, his foot was caught under the belly of the animal. As soon as he was disencumbered of the vast weight, he endeavoured to rise, but in vain. The pains which he experienced in his foot were extreme. He was carried home, where some surgeons, having ascertained that his foot was luxated, but being unable to reduce it, sent him to the Hotel-Dieu.
Desault on examining him, found the bones of his foot to be situated as follows. The internal part of the os calcis corresponded to the lower extremity of the tibia: the back of the foot was directed outwards, and its external edge downwards: under the skin and in front of the tibia was the astragulus, resting on the scaphoide and first of the cuneiform bones, where it formed a considerable projection: on the back of the leg, the fibula corresponded to the tendo Achillis. The pains had been inconceivably great from the moment of the accident.
Imboldened by numerous instances of success in similar cases, Desault, notwithstanding the extent of the disease, attempted the reduction. One assistant took hold of the superior part of the leg to make counter-extension, and another, for the purpose of extension, grasped the metatarsus with one hand, and the heel with the other. While these were pulling in different directions, the surgeon applying his thumb on the astragulus, endeavoured to force it into its place. His efforts were ineffectual: the opening through the capsule of the astragulus being too narrow, would not suffer it to pass. Desault perceiving this, cut through the integuments which covered the bone, and having laid bare the capsule and the ligaments which strengthen it, made an incision into them of a sufficient extent, taking care to avoid the tendon of the tibialis anticus, which was brought into view. The openings being thus enlarged, admitted of an easy reduction, and all the parts resumed, without difficulty, their natural situation.
The reduction being effected, the wound was closed, and covered with some lint. A square compress was then placed on the back of the foot, while a long one was applied to its sole, and the whole secured by an apparatus similar to that described in the preceding case. The patient was confined to a very strict diet, and ordered to use diluting drinks.
Next day, a slight bilious diathesis; an emetic in solution given; apparatus renewed. Fourth day, an abscess on the malleolus externus opened; a copious discharge of pus. Eighth day, the parts in perfect contact; a favourable discharge from the wounds; dressings applied twice a day. Fifteenth day, a general œdema; aperient ptisans ordered. Twentieth day, the œdema gone: a bilious diathesis returned: in consequence of this, the wounds became pale: another emetic given. Twenty-seventh day, a very painful excoriation occurred on the heel: care taken not to let the foot rest on that part, as the sore appeared to be the effect of compression. Thirtieth day, the wounds in a favourable way: all the bones in exact contact. Fortieth day, apparatus laid aside, and a simple roller substituted in its place: wounds already cicatrizing. Fiftieth day, the limb put in gentle motion, which is gradually increased every day. Same dressing continued till the eightieth day: wounds not yet cicatrized. Hundred and twenty-seventh day, a considerable swelling around the joint: a splinter made its way out, and was followed in a few days by several more. In the fifth month an abscess formed on the heel, from which, when opened, another splinter escaped. In the mean time, the patient left the Hotel-Dieu. During his absence more splinters were discharged. Returning about a year afterwards with a small ulcer, he was dismissed again in a short time, perfectly cured, except a slight stiffness of the joint.
15. The reduction of this luxation of the foot presents a difficulty worthy of the attention of practitioners, as well on account of its own nature, as in consideration of the process which was employed on the occasion: I allude to the narrowness of the opening in the capsule. I mentioned, on a former occasion, the obstacles sometimes created by this circumstance to the reduction of luxations of the os humeri and the os femoris. It was impracticable in the present to enlarge the opening in the capsule, as could be done in those cases, by moving the head of the bone in all directions; because the bone was too small to afford any purchase to the surgeon. The only resource was, the use of the knife; and the operation was the more easily performed, on account of the capsule being situated immediately beneath the integuments, from which circumstance it could be the more speedily brought into view.
16. The apprehension of mischief resulting from the admission of air to the articulating surfaces, would no doubt, in this case, have restrained most practitioners: but, even supposing this apprehension to be well founded, ought it to deter the surgeon from adopting the only possible mean of effecting a reduction, and of thus putting an end to the alarming state of things arising from the displacement of the bones? Desault proved in numerous instances, that the apprehensions of authors respecting such cases have been greatly exaggerated, and that it is practicable to cure wounds that penetrate into the cavities of joints, in the same manner as if they were simple wounds, and with but very little more danger to the patient. Yet it would seem, that the tediousness of the cure and the exfoliation of the bones, arose, in the present case, from the opening made into the joint, and perhaps also, in part, from the disposition and habit of the patient. Finally, in those alarming injuries of the joints, unconnected with external wounds, where practitioners have looked to no resource but that of amputation, Desault has, in a short time, and without any dangerous occurrence, restored to the subjects the free use of their limbs. The following case, drawn up by Plaignault, is a proof of this.
Case V. Pierre Phipe, aged twenty-four, fell, on the 20th of February, 1788, from an elevation of more than twenty feet: lighting on his foot, he turned it outwards, sunk instantly to the ground, and was unable to rise again. He was carried home, and from thence to the Hotel-Dieu.
Desault examining him on his arrival, discovered a luxation of the foot outwards, and of the astragulus forward and upward: the patient’s sufferings were great. Convinced that the most effectual method to relieve these was to reduce the luxation, the surgeon undertook it immediately, pushed the astragulus into its place without difficulty, and with a report which was heard by every one present, while the bones of the foot were brought into their proper situation by means of extension. In an instant the pains vanished and the motions of the foot became easy. The necessary apparatus was applied. The activity of the pulse called for blood-letting, which was immediately performed. A low diet was prescribed.
On the two following days blood-letting was repeated, both on account of the active state of the pulse, and of a considerable swelling which took place in the joint. The apparatus was kept constantly wet with vegeto-mineral water. Eighth day, somewhat better: echymosis gone. Fifteenth day, the apparatus laid aside. From this time the foot was gently moved every day. Eighteenth day, the patient able to stand on the affected foot without pain. Twenty-sixth day, walks with the assistance of a staff. Thirty-ninth, walks without limping, and enjoys all the motions of the foot. Discharged.
§ V.
17. When, in a luxation of the foot, the integuments, capsule, and ligaments are so lacerated, as to suffer the astragulus to escape, it would oftentimes be imprudent to attempt its reduction, as was done in the preceding cases. The violence already done to the parts around the joint is excessive; but this would be increased by the extension, and other efforts necessary in reduction. Whatever care might be taken, it would be difficult to prevent a vast swelling, long continued pains, and perhaps even a caries of the bone exposed to the air, with all those sufferings and dangers, to which such an accident gives origin. In such a case all the bones of the foot have been known to become carious, a state of things, which calls for the ultimate resources of art, and draws after it a train of evils, which it is always of the utmost importance to prevent.
18. What means are then to be employed? Two expedients only remain. 1st, the amputation of the foot; 2dly, the extirpation of the astragulus. The first is a cruel resource, which should never be adopted but in the last extremity, because it deprives the patient of a portion of himself, necessary to the performance of his functions. But the measure is forbidden by a reason still more powerful. Amidst the general disorder of the system, the severe pains experienced by the patient, the convulsions, and the delirium which oftentimes exists, what ground has the surgeon to hope for success? Will not the operation add to the number of these alarming appearances? Will it not aggravate them? May it not render them fatal? Both reason and experience reply in the affirmative.
19. In such a case, then, the extirpation of the astragulus is the expedient to be preferred. What, indeed, are its inconveniences? 1st, An inevitable anchylosis of the foot and leg: 2dly, a shortening of the affected limb. But a leg even in this state, is still better than a wooden leg, which is the necessary consequence of amputation: besides, a leg of the former description occasions no great inconvenience in either walking or standing, whereas one of the latter, produces extreme lameness: in the first case, a heel on the affected side somewhat higher than that on the other, is an easy method of removing the deformity. What, then, are such trifling disadvantages, when compared with the evils which they ward off? The extirpation of the astragulus is accompanied with but little pain. The want of this intermediate body between the leg and the foot, by producing a relaxation of the surrounding soft parts, prevents pain and swelling in such cases: should abscesses supervene, they will not, if properly treated, greatly retard the cure. In a word, experience coincides with this doctrine. Desault has seen it twice verified in the practice of other surgeons, and three times in his own. I have known of but one case of the kind, in which the termination was fatal, and there, a malignant fever, induced by the contaminated air of the hospital, certainly contributed to the death of the patient, which did not occur till two months after the reduction.
Case VI. Desault usually gave in his lectures, the history of a case where the success of this practice was remarkable. A man was brought to the Hotel-Dieu, with a luxation of the foot, complicated with a fracture of the lower part of the leg, and a laceration of the ligaments and capsule, through which the astragulus had escaped by a luxation forward and upward, so as to have half of its anterior surface exposed. The extent of the injury seemed to call for amputation. But the youth, the vigour, and sound constitution of the patient, gave ground to hope that a process less desperate might succeed. The astragulus, already separated anteriorly, was extracted by dividing the attachments which held it to the os calcis, and the bones of the leg: the reduction was then effected without difficulty. The parts being replaced more readily in consequence of the removal of this bone, were retained so by means of a bandage similar to that for fractures of the leg, but modified so as to suit the particular case. The patient lost blood once or twice: the apparatus was kept constantly wet; a very strict regimen was prescribed for some days; but few troublesome symptoms occurred; a slight swelling took place, but was soon removed; a favourable suppuration came on; the dressing was renewed twice a day; some splinters escaped occasionally; several abscesses formed successively were opened, and healed up again: the wounds themselves closed, and the patient finally recovered, with an anchylosis, indeed, between the foot and leg, and a limb a little shorter than natural, but which still served the purposes of walking and standing.
20. To this example, I might add those of other patients treated at the Hotel-Dieu, in the same manner and with equal success. But what purpose would such an accumulation of facts answer? It would only fatigue the reader without adding to his conviction.
21. If the injury accompanying the luxation be so extensive, as to destroy the principal blood-vessels, and leave no hope of saving the limb, amputation becomes then the only resource, and the case assumes a resemblance to those where the limbs are shattered by cannon balls: the success then depends very much on the strength or weakness of the patient.
Case VII. A man fell from a carriage: his foot becoming entangled between the spokes of the wheel, was almost separated from the leg. It adhered only by a small portion of skin behind, and by the tendons of the muscles which run to the toes both above and below.
Desault was called to the patient, whom he found in a most deplorable state: the pains which he suffered were excruciating: the parts around the wound were greatly swollen; a general spasm affected the system: amputation was judged necessary, but was deferred till the symptoms should be mitigated. The limb was dressed: next day, a gangrene began to affect the foot, which was then separated from the leg by cutting the tendons: the ends of the tibia and fibula exfoliated; the wound healed, and the patient now enjoys, in part, the functions and uses of the leg, by means of an artificial foot, framed and fitted on by an ingenious mechanic. Had the limb been too hastily amputated while the patient was affected with general spasms, fatal consequences would probably have ensued.
The following interesting paper, extracted from the Medical Repository, Hexad: ii. vol. i. p. 122 . . . 124, will give the reader a better idea, than he can receive from any other source, of Dr. Physick’s new and successful method of treating an old and obstinate fracture of the os humeri.
A Case of Fracture of the Os Humeri, in which the broken ends of the bone not uniting in the usual manner, a cure was effected by means of a seton. Communicated to Dr. Miller by Philip S. Physick, M. D.
“Isaac Patterson, a seaman, twenty-eight years of age, applied to me in May, 1802, in consequence of a fracture of his left arm, above the elbow joint, which had taken place several months before; but the ends of the bone not having united, rendered his arm nearly useless to him.
“The history he gave me was, that on the 11th of April, 1801, after having been at sea seven months, his arm was fractured by a heavy sea breaking over the ship. Nothing was done for his relief until next day, when the captain and mate bound it up, and applied splints over it. No swelling supervened, nor did he suffer any pain, Three weeks after this accident, he arrived at Alexandria, when the state of the arm was examined by a physician, who told him, that the ends of the bone were not in a proper situation. After making an extension, the splints and bandages were again applied. He remained in Alexandria four months, when, finding his arm no stronger, he left off all dressings, and went on board the New-York frigate as steward: in this capacity he remained near the Federal City six months, and by being under the necessity of using his arm as much as possible, he found the connexion between the ends of the bones became looser and looser, till, at length, the arm bent as easily as if a new joint had been formed at the place of the fracture. From the frigate he went to Baltimore, where an attempt was made by machinery to extend the arm, and keep the ends of the bone in apposition, by continuing the extension. Under this treatment he remained two months, but experiencing no benefit, he was advised to come to Philadelphia.
“On examining the arm, I found that the humerus had been fractured about two inches and a half above the elbow joint, and that the ends of the bone had passed each other, about an inch: the lower fragment, or that nearest the elbow, was situated over, and on the outside of the upper portion of the bone. The connexion that existed between the ends of the humerus was so flexible, as to allow of motion in every direction, and by forcible extension, the lower end might be pulled down considerably, but never so low as to be on a line with the end of the upper extremity. He was admitted into the Pennsylvania hospital, the latter end of May; but the weather becoming very hot, it was judged best to defer any operation that might be necessary, until the fall of the year. Unfortunately he then contracted a bilious fever, of which he was so ill, that his life was despaired of for some days. From this fever his recovery was so slow, that it was not thought proper to perform any operation until December. It still remained to decide, by what means a bony union of the humerus, might most probably be effected. In the year 1785, when a student, I had seen a case in our hospital, similar to this in every essential circumstance, in which an incision was made down to the extremities of the fractured bone, which were then sawed off, thereby putting the parts into the condition of a recent compound fracture. No benefit, however, was derived from this painful operation, and some months afterward the arm was amputated. This case had made a strong impression on my mind, and rendered me unwilling to perform a similar operation. I therefore proposed to some of the medical gentlemen of the hospital, who attended in consultation, that a seton-needle, armed with a skein of silk, should be passed through the arm, and between the fractured extremities of the bone, and that the seton should be left in this situation, until by exciting inflammation and suppuration, granulations should rise on the ends of the bone, which uniting and afterwards ossifying, would form the bony union that was wanting. This operation being agreed to, it was performed on the 18th of December, 1802, twenty months after the accident happened. Before passing the needle, I desired the assistants to make some extension of the arm, in order that the seton might be introduced as much as possible between the ends of the bone. Some lint and a pledget were applied to the orifices made by the seton-needle, and secured by a roller. The patient suffered very little pain from the operation. After a few days the inflammation (which was not greater than what is commonly excited by a similar operation through the flesh, in any other part) was succeeded by a moderate suppuration. The arm was now again extended, and splints applied. The dressings were renewed daily for twelve weeks, during which time no amendment was perceived; but soon afterwards the bending of the arm at the fracture was observed to be not so easy as it had been, and the patient complained of much more pain than usual whenever an attempt was made to bend it at that place. From this time, the formation of the new bony union went on rapidly, and, on the fourth of May, 1803, was so perfectly completed, that the patient could move his arm, in all directions, as well as before the accident happened. The seton was now removed, and the small sores occasioned by it, healed up entirely in a few days. On the 28th May, 1803, he was discharged from the hospital; perfectly well, and he has since repeatedly told me that his arm is as strong as it ever was.”
To the preceding paper it is unnecessary to add, that the mode of treatment there stated might be adopted in similar fractures of other bones, provided a seton-needle could be passed near to the ends of the fragments, without any risque of wounding blood-vessels, nerves, or other parts of importance. It is thus that solitary facts minutely detailed and well substantiated, oftentimes grow into principles of extensive application.
An account of Dr. Physick’s improvement of Desault’s apparatus for making permanent extension in oblique fractures of the os femoris.
Dr. Physick having observed that in the application of Desault’s apparatus, the patient was sometimes injured by the pressure of the strap or roller g g (plate 2) which passes under the tuberosity of the ischium for the purpose of making counter-extension, devised the following method of remedying this inconvenience, in which he succeeded to his wishes.
He directed the upper end of the long external splint to be formed like the head of a crutch, and the splint itself to be lengthened so as to reach and bear against the axilla of the affected side, which must be well defended from pressure by a bolster of flannel or some other soft material. By this expedient the Dr. evidently formed two points of counter-extension, instead of one, as is the case in the apparatus of Desault. Between these two points, namely, the axilla and the perineum, the same quantity and force of pressure is, by Dr. Physick’s improvement, divided, which, in the original apparatus of Desault, is borne by the perineum alone. The risque of excoriation and injury to the patient, then, in the former case, is to that which he runs in the latter, only as one to two, or nearly so. As it is no less the duty of the surgeon to prevent suffering than it is to remove deformity or to save life, Dr. Physick has certainly in this respect made an important step in the advancement of his profession.
But there is still another advantage derived from the lengthening of the external splint. In the original apparatus of Desault, the strap gg intended for counter-extension, by passing no higher up than the spine of the ilium, runs too much across, and therefore acts too much on, the upper part of the thigh. By this it not only irritates the muscles of the part, and induces them to contract, but also tends to draw the upper fragment of the os femoris a little outward, and thus to render the thigh in some measure deformed. But, in the improvement of Dr. Physick, the strap gg is secured in a mortise cut in the external splint, about midway between the spine of the ilium and the axilla. This strap, by being thus carried higher up on the body, does not run across the thigh at all. It consequently presses on and irritates the muscles much less, acts more in the direction of the os femoris, and has no tendency to draw the superior fragment outward.
Hence this improvement not only diminishes the patient’s sufferings, but gives him, perhaps, the best possible chance of having his limb preserved free from deformity.
Another improvement made on the lower end of the external splint by Dr. James Hutchinson deserves also to be mentioned. It was found that in the original apparatus of Desault, the strap or roller L (plate 2) used for the purpose of extension, had a tendency to draw the foot too much outward. This fault Dr. Hutchinson very ingeniously remedied, by attaching to the lower part of the external splint, a little above the mortise, a small block extending inwardly, at a right angle with the splint, so far as to be on a line with the middle of the sole of the foot. Over the end of this block, in which a notch is cut to receive them, the ends of the strap L are carried, previously to their being secured to the external splint. By means of this expedient extension is made precisely in the direction of the limb, and the inconvenience of drawing the foot outward is completely obviated.
Thus improved by Drs. Physick and Hutchinson, the apparatus of Desault for oblique fractures of the os femoris, leaves, perhaps, scarcely a remaining desideratum on the subject.
This plate gives a full view of an apparatus for making permanent extension, in oblique fractures of the leg, when both bones are broken. This apparatus was first devised and constructed several years ago, by Dr. James Hutchinson, then a pupil in the Pennsylvania hospital, and is now in general use among the practitioners of Philadelphia.
Fig. 1. Represents the leg and foot, with the apparatus applied.
A. A common roller, passed several times round the leg a little below the knee, on which counter-extension is made.
B. A silk handkerchief folded, or a strong roller made of soft muslin, passed once round the leg, just above the ancle, from behind forward. C. The place where its two ends cross each other to pass down along each side of the foot, as seen at b, to D, where they are secured by a knot drawn but moderately tight. a a. The same ends continued to E where they are again secured by a firm knot over the cross piece F, which passes between the two strong splints G G, that run on each side of the leg from a little above the knee, to the distance of four or five inches beyond the sole of the foot. This is the bandage by which extension is made, as will be mentioned hereafter.
H. Two bits of strong tape, each about two feet long, placed in the longitudinal direction of the leg, and firmly secured by the roller A, which passes over their middle. Two such bits of tape, are thus applied on each side of the leg, and their four ends, passing through four holes in the upper end of each of the splints G G, are secured on their outsides by firm knots as represented at H.
Fig. 2. A view of one of the splints G G, separated from the leg.
a. The four holes in the upper end, through which the bits of tape H pass.
b. The mortise in the lower end, which receives the cross-piece F.
Fig. 3. A view of the cross-piece F, which must be firmly fixed in one of the splints G G, but moveable in the mortise of the other, so that the splints may be taken asunder at pleasure.
The following is the method of applying this apparatus.
While extension and counter-extension are made by two assistants, the surgeon placing the bits of tape H on each side of the leg, secures them firmly by the roller A applied round the limb, with a proper degree of tightness. He then applies the middle of the handkerchief or roller B on the tendo Achillis, brings its ends across each other, before the leg at C, and carrying them down along each side of the foot, secures them by a knot at D. Letting go the ends of the handkerchief B, he next places on each side of the leg the splints G G, connects them at the lower end by the cross-piece F and secures them at the upper end by the tapes H. He then resumes the ends of the handkerchief B, carries them downward as seen at a a and secures them by a firm knot at E round the cross-piece F.
From this view and explanation of the apparatus Fig. 1, I presume its construction, application, and mode of operation will be very easily understood. It is unnecessary therefore to add, that the extension and counter-extension made on the limb, will be directly proportioned to the degree of force with which the ends a a of the handkerchief B are drawn over the cross-piece F. As action and reaction, in this case, must, as in all others, be equal, the splints G G will be pushed upward by the ends of the handkerchief B with precisely the same force that is applied on these ends to draw the foot and lower fragments downward. Hence the counter-extension made above on the roller A will be exactly equal to the extension made below by the handkerchief B.
I ought to have observed, that it is necessary to defend the soft parts, both above and below, from the pressure of the extending and counter-extending straps, by means of soft compresses applied next to the skin. This is particularly necessary on the instep C where the ends of the handkerchief B cross each other. It requires some attention on the part of the surgeon to prevent this spot from being excoriated, especially if it be found necessary to make a forcible extension.
If the fracture be simple, a bandage of strips previously applied round the limb from the ancle to the knee is highly useful. It secures the fragments more effectually from lateral displacement, and prevents the swelling of the leg. A simple roller applied with a moderate degree of tightness round the foot, is also of service in preventing a swelling in that part, as well as in removing it if it has already occurred.
This apparatus is still more strikingly useful in compound fractures, on account of the facility with which it enables the surgeon to apply the necessary dressings. These can be renewed as often as may be requisite, without giving the patient the least pain, without discontinuing extension, or in any measure whatever deranging the fragments. The surgeon can also, in all cases, discover by a single glance of his eye, whether or not the fragments are in proper apposition. It is right to secure the whole apparatus by three bits of tape passed round it, similar to those tied round the leg in the apparatus for fractures of the thigh, as represented in plate 2.
I shall only add, that the surgeon must employ such bolsters and compresses as he may find necessary to support the limb, and protect it from undue pressure, and that he must be vigilant to prevent, by frequent examinations, the extending and counter-extending straps from becoming relaxed.
For a few further remarks on the subject of this apparatus, the reader is referred to a paper published by Dr. Hutchinson, in the second number of the Philadelphia Medical Museum.
FINIS.
Return to transcriber’s notes
Inconsistencies:
armpit/arm-pit
condyl/condyle
coracoid/corocoid
coronoid/coronoide
expence/expense
fixt/fixed
forearm/fore-arm/fore arm
inconveniencies/inconveniences
plane/plain
Scultel/Scultet
teres-major/teres major
Corrections:
aingly → singly
appplication → application
backwaad → backward
Bruningaushen → Bruninghausen
cataloginous → cartilaginous
ciscumstance → circumstance
considerasion → consideration
constanly → constantly
controuling → controlling
cotemporaries → contemporaries
croud → crowd
decieve → deceive
divison → division
examing → examining
exextremities → extremities
faciæ → fasciæ
follow → following
imitatators → imitators
make → makes
matrass → mattress
nect → neck
of of → of
passsive → passive
percieve → perceive
recieves → receives
resourse → recourse
the the → the
to to → to
whould → would
1303 → 1803 (date)
67 → 66 (para numbering error)
Return to transcriber’s notes
1
(Appareil.) I am fully sensible that the word Apparatus,
does not, according to the common acceptation of the term,
convey, in English, precisely the same ideas, that the word
“appareil” does, in French; but it certainly approaches much
nearer to it than any other term found in English works on surgery.
It signifies a collection or assemblage of means, used for
the attainment of a particular end; and this is, in substance,
what Desault meant by the term “appareil.” His “appareil”
(apparel) for a broken bone included splints, bandages, bolsters,
and every thing else necessary for retaining the fractured ends
in apposition. The English reader will naturally enough annex
the same ideas to the word Apparatus, as used throughout the
present work. I have, therefore, thought proper to adopt it, rather
than to introduce a new or uncommon term, and am sure,
that, for all practical purposes, it will be found sufficiently expressive
of the meaning of the original. And I am much more
solicitous to become instrumental in giving some aid to the surgeon
in the practice of his profession, than to escape the censure
of the fastidious critic.
Trans.
2
That form of lever, where the weight to be raised or the
resistance to be overcome, is at one end, the force at the other,
and the fulcrum or prop between them. This form is well represented
by the handle of a pump, where the piston is the weight
or resistance, the hand of the drawer of water the force, and
the iron pin, on which the handle works, the fulcrum or prop.
Trans.
3
This paragraph is so obscure in the original, that a translation
of it would be scarcely intelligible. Instead of a mere
translation, therefore, I have given rather a comment on what
I believe to be its true meaning.
Trans.
4
That process or operation in which the surgeon uses his
hands to effect the reduction and apposition of parts, which
cannot be accomplished by extension and counter-extension
alone. If a bone be broken into two or three pieces, mere
extension and counter-extension will not bring all the fragments
into their proper places, so as to restore the natural
form of the part. In such cases, the surgeon uses his hands to
aid the action of the extended muscles, and this is the process
which our author denominates conformation. The term occurs
in many places in the course of the work.
Trans.
5
I find in English books of anatomy no appropriate names
for these two ligaments. I am therefore obliged to translate
the French terms for them literally. The anatomist will have
no difficulty in recollecting their situation.
Trans.
6
I do not recollect any terms in English works of anatomy
equivalent to these.
Trans.
7
Compresses laid one upon another, of which the upper
one is still the smallest, not in relation to thickness, but as far
as regards length and breadth.
Trans.
8
The rupture in the capsule that surrounds the joint.
T.
9 Une pelotte.
10
For a very important improvement made by Dr. Physic
in the treatment of an old fracture of the os humeri, and which
may be applied also to similar fractures of other bones, see Article
I. of the Appendix.
Trans.
11
(* L’echelle, † la porte, ‡ le baton.) These pieces of machinery,
though formerly in use, are now, I believe, in all parts
of the world, laid aside. It would be superfluous, therefore, to
consume time in describing either them, or their mode of
operation.
Trans.
12
In this form of lever, the power is applied between the
fulcrum and the weight to be moved, or the resistance to be
overcome.
Trans.
13
(Bandage a bandalettes.) This is a most convenient form
of bandage, in fractures of the upper or lower extremities. It
is composed of strips of soft linen or muslin, from two to three
inches wide, and of a length accommodated to the size of the
limb, on which they are to be applied. These strips are not
sewed together, but merely laid along side of each other, or rather
spread in such a way that their adjoining edges may overlap
a little. Being thus arranged, on the bed or mattress, where
the patient is to lie, the broken limb is placed on them, when
the surgeon, taking them, one by one, folds them round it, so as
to form a very perfect and neat covering. The number of these
strips must be regulated by the extent of the limb, or, at least,
of that portion of the limb, which they are intended to cover.
Trans.
14
(La fosse sous-scapulaire). I know of no English anatomical
term for this. I therefore translate it literally. The same
is true with respect to “fossa sous-epineuse,” translated here,
fossa infra-spinata.
Trans.
15 (De mouffle de Petit.)
16
That is, to draw, or otherwise force the head of the os humeri,
with his hands, towards the glenoid cavity, while the assistants
are making extension and counter-extension. In doing
this, he must pull the head upwards, if it be lodged in the axilla,
backward if it be under the upper part of the pectoralis
major, &c. Desault, however, contends that this assistance
from the surgeon is unnecessary, and that extension and counter-extension
are alone sufficient to effect the reduction.
Trans.
17
With the particular mechanism and mode of action of
this bandage, I am unacquainted. Nor are these matters of
much moment, as the bandage is, I believe, entirely out of use.
Trans.
18
On this point Desault is certainly mistaken. Paste-board,
when of a proper thickness and well applied, makes an excellent
splint for fractures of the fore-arm. It moulds itself to the
form of the arm, sits easy, and retains the fracture extremely
well.
Trans.
19 Not generally named in English works of anatomy.
20 Echancrure sigmoide.
21
That deep depression in the os humeri, which, in a
natural state of the parts, receives the upper end of the olecranon
process.
Trans.
22
(La longueur, l’epaisseur, et la direction.) That is, the
thigh may be shorter than natural, owing to the ends of the
broken bone overlapping each other; it may have a protuberance
on one side, in consequence of these ends being separated
or displaced laterally; or the direction of the limb may be
changed, by a bend or angle being produced in the bone at the
place of the fracture.
Trans.
23
A term of nearly the same import with “conformation.”
Trans.
24
(Le lit d’Hippocrate.) As many of the machines mentioned
here have probably never been seen in this country,
and as there is, perhaps, scarcely one of them used, at present,
in any country, I shall not consume the time of the reader
by troubling him with descriptions of them.
Trans.
25
(Drap-fanon.) This is a piece of linen or muslin (Desault
appears to have used flannel, which is not however so
good) spread under the broken limb, reaching in length from
one end of it to the other, and wide enough to go about twice
round it. It is to be folded at its edges several times round the
internal and the long external splints, in order to retain them
the better, and make them bear with more steadiness and advantage
on the limb. The junk-cloth and these two splints,
when properly applied, form a kind of soft elastic case, in
which the limb rests. This case is of service in securing the
bolsters in their places. The junk-cloth is the outside piece of
the apparatus, except the bits of tape which go round and secure
the whole. In arranging the different pieces, therefore,
on the bed or mattress, where the patient is to lie, the surgeon
places the tapes first, the junk-cloth next, the bandage of strips
next, and so on, in an order the reverse of that in which he
afterwards applies them on the limb.
Trans.
26
Le Spica de l’aine.
Trans.
27
(L’ecusson.) The literal meaning of this word is an escutcheon,
or a coat of arms. But when used in surgical language,
it signifies a retentive or strengthening plaster. Such I
conceive its meaning to be in the present instance.
Trans.
28
A motion or sweep describing the arch of a circle.
Trans.
29
That which forms the superior boundary of the longitudinal
fracture by which the condyls are separated from each
other.
Trans.
30
For an account of an improvement of the splint, represented
in this plate, projected by Dr. Physick, and now used in
the Pennsylvania hospital, see Article II. of the Appendix.
Trans.
31 A case of luxation of the head of the os femoris in a forward direction, but differing in some respects from the above, occurred lately in the Pennsylvania hospital under the care of Dr. Physick. The doctor reduced this luxation in the amphitheatre, in the presence of his class, by a process which was also somewhat different from that adopted by Desault.
In the case of Desault’s patient the luxated limb was shorter than the sound one: in that of Dr. Physick’s it was evidently longer. This was no doubt owing to the head of the os femoris having, in the former case, passed farther up towards the superior rim of the os pubis than it had in the latter. In both cases the protuberance formed by the head of the bone in the groin could be readily felt.
For the purpose of making counter-extension, Desault passed a strap between the scrotum and the thigh of the sound side: Dr. Physick, for the same purpose, passed the strap between the scrotum and the affected thigh. He conceived that by this mode he could act with more effect on the pelvis, and more effectually prevent the acetabulum of the affected side from being drawn in any measure downward by the extending forces. It would seem, that by making counter-extension, in such a case, on the sound side, the pelvis is made to rotate, so to speak, on its own axis, in the direction in which the counter-extension is made. The necessary effect of this rotation must be, a slight descent of the acetabulum of the affected side. But to retain the acetabulum firmly up is the true and only end of counter-extension. Dr. Physick appears therefore to have availed himself of the greatest mechanical advantage of which the situation of the parts admitted.
Again: Desault placed the strap on which extension was made just above the ancle: Dr. Physick placed the strap intended for the same purpose above the knee. His object in this was, to have the leg free and unincumbered, in order that he might be able to use the limb with more advantage, as a lever of the first kind, to assist in moving the head of the os femoris towards the acetabulum. The fulcrum of the lever into which the limb was thus converted, was a strap passed round the affected thigh a few inches below the groin, and drawn laterally with great force in a direction opposite to that in which the bone was displaced.
In this case extension and counter-extension were made by means of powerful sets of pullies. Notwithstanding this, these forces were not alone sufficient to subdue the resistance of the muscles. The reduction was not completed till muscular contraction had been weakened, and the patient reduced almost to a state of syncope, by the loss of nearly two quarts of blood. This copious evacuation, co-operating with the fatigue which the muscles of the limb necessarily sustained, in consequence of the powerful extension to which they were for some time subjected by the action of the pullies, overcame all resistance and the head of the bone was finally replaced. To exhaust the energy of the resisting muscles by forcible and permanent extension, and to weaken the action of the system generally, by copious blood-letting, appear to be the two most effectual modes of ensuring success in the reduction of all obstinate cases of luxation.
Another point of difference between these two cases of
luxation remains yet to be mentioned. In Desault’s case the
head of the os femoris was, as he tells us, displaced in a direction
“upward and forward.” In Dr. Physick’s case, the direction
of the displacement was downward and forward. This was
proved beyond all doubt, by the circumstance of the affected
limb being longer than the sound one.
Trans.
32 I know not of any English term equivalent to this. T.
33
The roller or strip with holes in it, which is extended
along the fore part of the limb, serving, in some measure, the
purpose of a compress.
Trans.
34
That is, without any assistance from the hands of the
surgeon.
Trans.
35
Analogous in its form and uses to that employed in fractures
of the thigh. It may not be amiss, on this occasion to
mention, that in the form of apparatus for oblique fractures of
the leg, represented in the Appendix, plate III. no junk-cloth is
necessary.
Trans.
36
For a view and description of an excellent form of apparatus
for oblique fractures of the leg, constructed on the principles
of that here described, see article III. plate III. of the
Appendix.
Trans.
37
(Genouilliere.) I believe this was a piece of apparatus
made of leather, somewhat similar to the top of a boot, and
secured on the limb just above the knee.
Trans.
End of the Project Gutenberg EBook of A Treatise on Fractures, Luxations,
and other Affections of the Bones, by Pierre-Joseph Desault
*** END OF THIS PROJECT GUTENBERG EBOOK A TREATISE ON FRACTURES ***
***** This file should be named 58602-h.htm or 58602-h.zip *****
This and all associated files of various formats will be found in:
http://www.gutenberg.org/5/8/6/0/58602/
Produced by Thiers Halliwell, Sonya Schermann and the
Online Distributed Proofreading Team at http://www.pgdp.net
(This file was produced from images generously made
available by The Internet Archive)
Updated editions will replace the previous one--the old editions will
be renamed.
Creating the works from print editions not protected by U.S. copyright
law means that no one owns a United States copyright in these works,
so the Foundation (and you!) can copy and distribute it in the United
States without permission and without paying copyright
royalties. Special rules, set forth in the General Terms of Use part
of this license, apply to copying and distributing Project
Gutenberg-tm electronic works to protect the PROJECT GUTENBERG-tm
concept and trademark. Project Gutenberg is a registered trademark,
and may not be used if you charge for the eBooks, unless you receive
specific permission. If you do not charge anything for copies of this
eBook, complying with the rules is very easy. You may use this eBook
for nearly any purpose such as creation of derivative works, reports,
performances and research. They may be modified and printed and given
away--you may do practically ANYTHING in the United States with eBooks
not protected by U.S. copyright law. Redistribution is subject to the
trademark license, especially commercial redistribution.
START: FULL LICENSE
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full
Project Gutenberg-tm License available with this file or online at
www.gutenberg.org/license.
Section 1. General Terms of Use and Redistributing Project
Gutenberg-tm electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or
destroy all copies of Project Gutenberg-tm electronic works in your
possession. If you paid a fee for obtaining a copy of or access to a
Project Gutenberg-tm electronic work and you do not agree to be bound
by the terms of this agreement, you may obtain a refund from the
person or entity to whom you paid the fee as set forth in paragraph
1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this
agreement and help preserve free future access to Project Gutenberg-tm
electronic works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the
Foundation" or PGLAF), owns a compilation copyright in the collection
of Project Gutenberg-tm electronic works. Nearly all the individual
works in the collection are in the public domain in the United
States. If an individual work is unprotected by copyright law in the
United States and you are located in the United States, we do not
claim a right to prevent you from copying, distributing, performing,
displaying or creating derivative works based on the work as long as
all references to Project Gutenberg are removed. Of course, we hope
that you will support the Project Gutenberg-tm mission of promoting
free access to electronic works by freely sharing Project Gutenberg-tm
works in compliance with the terms of this agreement for keeping the
Project Gutenberg-tm name associated with the work. You can easily
comply with the terms of this agreement by keeping this work in the
same format with its attached full Project Gutenberg-tm License when
you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are
in a constant state of change. If you are outside the United States,
check the laws of your country in addition to the terms of this
agreement before downloading, copying, displaying, performing,
distributing or creating derivative works based on this work or any
other Project Gutenberg-tm work. The Foundation makes no
representations concerning the copyright status of any work in any
country outside the United States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other
immediate access to, the full Project Gutenberg-tm License must appear
prominently whenever any copy of a Project Gutenberg-tm work (any work
on which the phrase "Project Gutenberg" appears, or with which the
phrase "Project Gutenberg" is associated) is accessed, displayed,
performed, viewed, copied or distributed:
This eBook is for the use of anyone anywhere in the United States and
most other parts of the world at no cost and with almost no
restrictions whatsoever. You may copy it, give it away or re-use it
under the terms of the Project Gutenberg License included with this
eBook or online at www.gutenberg.org. If you are not located in the
United States, you'll have to check the laws of the country where you
are located before using this ebook.
1.E.2. If an individual Project Gutenberg-tm electronic work is
derived from texts not protected by U.S. copyright law (does not
contain a notice indicating that it is posted with permission of the
copyright holder), the work can be copied and distributed to anyone in
the United States without paying any fees or charges. If you are
redistributing or providing access to a work with the phrase "Project
Gutenberg" associated with or appearing on the work, you must comply
either with the requirements of paragraphs 1.E.1 through 1.E.7 or
obtain permission for the use of the work and the Project Gutenberg-tm
trademark as set forth in paragraphs 1.E.8 or 1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any
additional terms imposed by the copyright holder. Additional terms
will be linked to the Project Gutenberg-tm License for all works
posted with the permission of the copyright holder found at the
beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including
any word processing or hypertext form. However, if you provide access
to or distribute copies of a Project Gutenberg-tm work in a format
other than "Plain Vanilla ASCII" or other format used in the official
version posted on the official Project Gutenberg-tm web site
(www.gutenberg.org), you must, at no additional cost, fee or expense
to the user, provide a copy, a means of exporting a copy, or a means
of obtaining a copy upon request, of the work in its original "Plain
Vanilla ASCII" or other form. Any alternate format must include the
full Project Gutenberg-tm License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works
provided that
* You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is owed
to the owner of the Project Gutenberg-tm trademark, but he has
agreed to donate royalties under this paragraph to the Project
Gutenberg Literary Archive Foundation. Royalty payments must be paid
within 60 days following each date on which you prepare (or are
legally required to prepare) your periodic tax returns. Royalty
payments should be clearly marked as such and sent to the Project
Gutenberg Literary Archive Foundation at the address specified in
Section 4, "Information about donations to the Project Gutenberg
Literary Archive Foundation."
* You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or destroy all
copies of the works possessed in a physical medium and discontinue
all use of and all access to other copies of Project Gutenberg-tm
works.
* You provide, in accordance with paragraph 1.F.3, a full refund of
any money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days of
receipt of the work.
* You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project
Gutenberg-tm electronic work or group of works on different terms than
are set forth in this agreement, you must obtain permission in writing
from both the Project Gutenberg Literary Archive Foundation and The
Project Gutenberg Trademark LLC, the owner of the Project Gutenberg-tm
trademark. Contact the Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
works not protected by U.S. copyright law in creating the Project
Gutenberg-tm collection. Despite these efforts, Project Gutenberg-tm
electronic works, and the medium on which they may be stored, may
contain "Defects," such as, but not limited to, incomplete, inaccurate
or corrupt data, transcription errors, a copyright or other
intellectual property infringement, a defective or damaged disk or
other medium, a computer virus, or computer codes that damage or
cannot be read by your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH 1.F.3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium
with your written explanation. The person or entity that provided you
with the defective work may elect to provide a replacement copy in
lieu of a refund. If you received the work electronically, the person
or entity providing it to you may choose to give you a second
opportunity to receive the work electronically in lieu of a refund. If
the second copy is also defective, you may demand a refund in writing
without further opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS', WITH NO
OTHER WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT
LIMITED TO WARRANTIES OF MERCHANTABILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of
damages. If any disclaimer or limitation set forth in this agreement
violates the law of the state applicable to this agreement, the
agreement shall be interpreted to make the maximum disclaimer or
limitation permitted by the applicable state law. The invalidity or
unenforceability of any provision of this agreement shall not void the
remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in
accordance with this agreement, and any volunteers associated with the
production, promotion and distribution of Project Gutenberg-tm
electronic works, harmless from all liability, costs and expenses,
including legal fees, that arise directly or indirectly from any of
the following which you do or cause to occur: (a) distribution of this
or any Project Gutenberg-tm work, (b) alteration, modification, or
additions or deletions to any Project Gutenberg-tm work, and (c) any
Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of
computers including obsolete, old, middle-aged and new computers. It
exists because of the efforts of hundreds of volunteers and donations
from people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need are critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future
generations. To learn more about the Project Gutenberg Literary
Archive Foundation and how your efforts and donations can help, see
Sections 3 and 4 and the Foundation information page at
www.gutenberg.org
Section 3. Information about the Project Gutenberg Literary Archive Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Contributions to the Project Gutenberg Literary
Archive Foundation are tax deductible to the full extent permitted by
U.S. federal laws and your state's laws.
The Foundation's principal office is in Fairbanks, Alaska, with the
mailing address: PO Box 750175, Fairbanks, AK 99775, but its
volunteers and employees are scattered throughout numerous
locations. Its business office is located at 809 North 1500 West, Salt
Lake City, UT 84116, (801) 596-1887. Email contact links and up to
date contact information can be found at the Foundation's web site and
official page at www.gutenberg.org/contact
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
[email protected]
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To SEND
DONATIONS or determine the status of compliance for any particular
state visit www.gutenberg.org/donate
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including checks, online payments and credit card donations. To
donate, please visit: www.gutenberg.org/donate
Section 5. General Information About Project Gutenberg-tm electronic works.
Professor Michael S. Hart was the originator of the Project
Gutenberg-tm concept of a library of electronic works that could be
freely shared with anyone. For forty years, he produced and
distributed Project Gutenberg-tm eBooks with only a loose network of
volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as not protected by copyright in
the U.S. unless a copyright notice is included. Thus, we do not
necessarily keep eBooks in compliance with any particular paper
edition.
Most people start at our Web site which has the main PG search
facility: www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.