Project Gutenberg's Fissure of the Anus and Fistula in Ano, by Lewis H. Adler This eBook is for the use of anyone anywhere in the United States and most other parts of the world at no cost and with almost no restrictions whatsoever. You may copy it, give it away or re-use it under the terms of the Project Gutenberg License included with this eBook or online at www.gutenberg.org. If you are not located in the United States, you'll have to check the laws of the country where you are located before using this ebook. Title: Fissure of the Anus and Fistula in Ano Author: Lewis H. Adler Release Date: November 17, 2014 [EBook #47387] Language: English Character set encoding: UTF-8 *** START OF THIS PROJECT GUTENBERG EBOOK FISSURE OF THE ANUS *** Produced by Mark C. Orton, Elizabeth Oscanyan and the Online Distributed Proofreading Team at http://www.pgdp.net (This file was produced from images generously made available by The Internet Archive)
In the following pages I have endeavored to give a concise yet thorough account of the two affections Fissure of the Anus and Fistula in Ano, in respect to their etiology, symptomatology, diagnosis, and treatment. It has not been my object to write upon rectal fistulæ in general.
While the two subjects treated in this volume have been ably written on at various times and by different authorities, it is undeniable that no organ of the body is more neglected by both the laity and the profession than is the rectum.
The neglect upon the part of the laity is largely attributable to carelessness in regard to regularity of habit and to want of cleanliness in this portion of the body. This neglect is the prime factor in the causation of many of the rectal maladies frequently encountered by the specialist. Furthermore, patients suffering from rectal diseases, especially women, often from a false sense of modesty defer their visit to a physician as long as possible, allowing their trouble to proceed from bad to worse, and when their suffering finally becomes almost unbearable and a doctor is consulted they refuse to allow him to make a rectal examination; in this way error in diagnosis occurs, and consequently relief is not obtained. The use of improper paper for toilet purposes often occasions the production of rectal diseases.
The profession as a body find other fields of labor more inviting than the study and treatment of rectal diseases, the diagnosis of which to be complete and satisfactory must in every case be based upon an ocular and thorough digital examination. As a result of this unattractiveness, even amounting to repulsiveness, to the general practitioner, most of the affections of the lower bowel are treated by him as "piles," the diagnosis being usually made by the patient, and accepted by the physician without question or personal examination. Such being the case, it is no wonder that when the surgeon prescribes equal parts of ung. acid. tannici et ung. belladonnæ, or a similar salve, to every patient complaining of rectal trouble, a cure does not often result.
A knowledge of these facts has led me to hope that a brochure upon the subjects herein treated might excite a deeper professional interest in rectal maladies if issued as a volume of the Physician's Leisure Library Series, which by its moderate price permits of a wide circulation.
I desire to express my obligations to the publisher, Mr. George S. Davis, for the attractive style in which the work has been issued, and to Dr. B. W. Palmer, of Detroit, Mich., for valuable suggestions while the work was passing through the press; also to my friend Dr. G. G. Davis, of Philadelphia, for the original drawings furnished, from which a number of the illustrations have been executed, and to Messrs. Chas. Lentz & Sons, surgical cutlers of Philadelphia, for the use of various cuts of instruments.
1610 Arch Street, Philadelphia, Pa.
Fissure.—The domain of surgery includes few diseases which produce such intense suffering to the patient as does the affection under consideration, and none in which proper treatment is followed by more prompt relief and more certain ultimate success.
Fissure, although so simple in extent and character and so readily curable, exercises a most potent influence in undermining the patient's health and strength, the constant pain and irritation to the nervous system being more than the majority of persons can endure.
Definition.—We may define a fissure, or irritable ulcer of the rectum, as a superficial breach of the mucous membrane in the anal region, of a highly sensitive nature, giving rise to spasmodic contraction and paroxysmal pain of a peculiar character. According to Bodenhamer,[1] its shape may be linear, oblong, or circular.
Location.—Its position is usually just within the verge of the anus, beginning at the muco-cutaneous junction or Hilton's line, and extending upward toward the rectum for a distance seldom exceeding half an inch. It may occupy any portion of the circumference of the anal region, but its usual site is at its posterior or coccygeal side.
Multiple Character.—Although this lesion is usually solitary, we sometimes find it multiple, especially when it is of syphilitic origin.
Age and Sex Affected.—Anal fissure is a disease of adult life, and is said to be more common among women than among men. Very young children, however, are not exempt, as many reported cases show. The late Dr. D. Hayes Agnew[2] mentions having seen it occur in infants not over two months old. Dr. A. Jacobi[3] is of the opinion that this affection is a more common one than is generally supposed, and believes that many of the fretful children who sleep badly and cry constantly, and often present symptoms simulating those of vesical calculus, suffer from fissure of the anus. He quotes Kjellberg, who at the Dispensary at Stockholm among 9098 children found 128 cases of fissure of the anus, of which number 60 were boys and 68 were girls; the majority were less than one year old, and in 73 cases the age was less than four months.
Etiology.—The explanation of the very intense pain by which this disease is characterized is to be found upon study of the structural arrangement of the termination of the bowel, with especial attention to the nerve-supply of the part. Therefore it will be in order to review at this point the more important anatomical features of the lower portion of the rectum.
The outlet of the intestine is closed by two sphincter muscles, the external being immediately beneath the skin surrounding the margin of the anus. It is elliptical in form, about half an inch in breadth on each side of the anus, and is attached posteriorly by a small tendon to the tip and back of the coccyx; anteriorly it becomes blended with the transverse and bulbo-cavernosus muscles at the central point of the perineum. The internal sphincter consists of the normal circular fibers of the rectum, considerably increased in number; its thickness is about two lines, and its vertical measurement from half an inch to an inch. It is situated immediately above and partly within the deeper portion of the external sphincter, being separated from it by a layer of fatty connective tissue.
These muscles—the two sphincters—are separated on the outer side by the attachment of the levator ani, some of the fibers of which are internally connected with the external sphincter; on the inner side the muscles are in contact, the line of union corresponding accurately with the junction of the skin and the mucous membrane. In most cases this junction of the sphincters is marked by a line of condensed connective tissue.[4] This line is known as "Hilton's white line."
Hilton has pointed out an important anatomical fact in connection with this line—to wit, that it is the point of exit of the nerves, principally branches of the pudic, which descend between the two sphincter muscles, becoming superficial in this situation, and are there distributed to the papillæ and mucous membrane of the anus (Fig. 1).
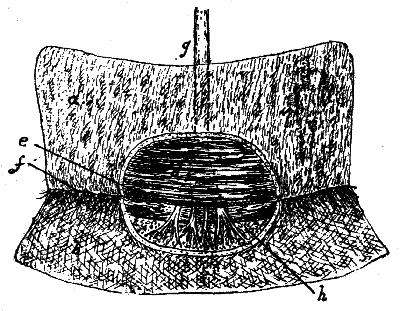
Fig. 1—Nervous Supply of the Anus (Hilton). a, mucous membrane of the rectum; b, skin near the anus; c, external sphincter muscle; d, internal sphincter muscle; e, line of separation of the two sphincters; f, the overlying white line marking the junction of the two sphincters; g, nerve supplying the skin near the anus, which it reaches by passing first externally to the rectum and then through the interval between the two sphincters; h, flap of mucous membrane and skin reflected back.
These nerves are very numerous, which accounts not only for the extreme sensitiveness of the part, but also, as stated by Andrews,[5] for its very abundant reflex communications with other organs. They play a very important part in the etiology of irritable ulcers. The exposure of one of their filaments, either in the floor or at the edge of the ulcer, is an essential condition of its existence.[6]
The upper portion of the rectum possesses very little sensibility, as the chief nerve-supply of the organ is at its termination and around the anus; hence it is that such grave diseases as cancer or ulceration may exist in the higher parts of the bowel and not manifest their presence by pain.
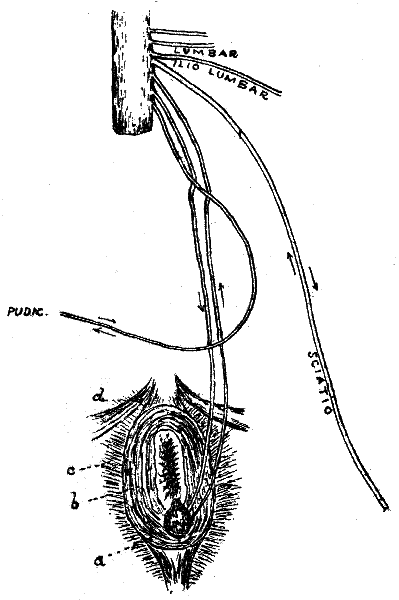
Fig. 2—Diagram of the Nervous Relations of Irritable Ulcer of the Anus (Hilton). a, ulcer on sphincter ani; b, filaments of two nerves are exposed on the ulcer, the one a nerve of sensation, the other of motion, both attached to the spinal cord, thus constituting an excito-motor apparatus; c, levator ani muscle; d, transversus perinæi muscle.
Andrews[7] directs attention to Hilton's diagram (Fig. 2), as showing that impressions from a fissure are carried to that part of the cord which supplies the pudic nerves and the ilio-lumbar, lumbar, and sciatics, which include the motor supply of the external sphincters as well as of the bladder and the lower extremities.
From these general considerations we can understand why reflex spasm of the sphincter is so constant and important a sign of this malady, and how other and more general reflexes are to be accounted for,—such as symptoms of bladder and urethral diseases, radiating pains, etc.
We also find in the nervous mechanism of the part an explanation of the predisposing causes, important symptoms, and pathology of this peculiar affection.
As to the immediate origin of this lesion, it may be said to arise from a variety of causes, such as atony of the rectum, or other conditions leading to constipated habits. In these cases the bowel becomes impacted with hardened feces, which when discharged overstretch the delicate mucous membrane, and thus, either by irritation or by direct abrasion, the ulcer is formed.[8]
In consequence of spasmodic or organic contraction of the external sphincter ani, fecal matter or some other foreign body lodges in the fossa between the two anal sphincters, and by its long-continued presence in this pent-up situation becomes highly irritating and gives rise to an obstinate fissure.[9]
Anal fissure sometimes results from the excoriations produced by vitiated and acrid discharges, such as occur in dysentery, chronic diarrhœa, cholera, leucorrhœa, etc. Hemorrhoids are frequently a predisposing cause and a complication of this affection.[10] They narrow the outlet of the bowel, and through the successive inflammatory attacks to which they are subject the neighboring tissue loses its elasticity, is rendered brittle, and is easily lacerated.
Polypi are not uncommon causes of this lesion.[11] The polypus is usually situated at the upper or internal end of the fissure, but it may be on the opposite side of the rectum, as in several cases coming under the author's observation.
Allingham[12] states that ulcer of the rectum may result from a congenital narrowness of the anal orifice, being then usually seen in children; or it may be caused by an hypertrophied condition of the sphincters, which has arisen from severe constipation or some rectal affection.
Anal fissure is sometimes produced by a superficial excoriation or ulceration of the outlet of the bowel, analogous to that so frequently observed upon the inside of the lips, the tongue, and other parts of the mouth. Bodenhamer[13] mentions having seen several severe cases of this disease produced by a kind of aphthous ulceration in nursing mothers, and one in a child. They were attended with extreme burning pain and more or less anal spasm. He also states that in these cases the ulcerations of the anus were contemporaneous with similar ulcerations of the mouth; their coexistence and the exact similarity of their appearance left little doubt as to their identity.
Harrison Cripps[14] states that a source from which these ulcers sometimes take their origin is a little marginal abscess which has led to the destruction of the portion of the muco-cutaneous surface lying over it.
The anus is liable to a species of chapping resembling that of the lips in winter, which sometimes results in extremely painful fissures. Such a condition is supposed to be induced by the influence of a dry atmosphere or by some slight disturbance in the general health, rendering the parts friable and liable to crack from the slightest violence.
Fissure is sometimes of syphilitic origin. Finally, it may be due to mechanical injuries, such as uterine displacement, the severe straining efforts made in parturition, the careless use of the enema syringe, the awkward employment of instruments by the surgeon in the diagnosis and treatment of rectal diseases, etc.
1. "Anal Fissure," 1868, p. 45.
2. "Principles and Practice of Surgery," vol. i, p. 416.
3. "Intestinal Diseases of Children," p. 295.
4. Andrews, "Rectal and Anal Surgery," Chicago, 1889, p. 69.
5. Op. cit., p. 69.
6. Ball, "The Rectum and Anus," Philadelphia, 1887, pp. 128-129.
7. Op. cit., pp. 69-70.
8. Bodendamer (op. cit., p. 58) calls attention to a fact of some importance as bearing upon this point—to wit, that in some cases of constipation, while the diaphragm and other abdominal muscles act with considerable energy, the anal sphincters remain more or less contracted, and yield but slowly, so that the indurated feces contuse and abrade the surface of one or more points of the mucous membrane, which abrasions, if they do not heal, lay the foundation of the disease.
9. Instances of this condition as the cause of anal fissures are mentioned by T. B. Curling in his "Observations on the Diseases of the Rectum," second edition, London, 1855.
10. T. J. Ashton, "Diseases of the Rectum," second American from the fourth English edition, 1865, p. 46.
11. Allingham, "Diseases of the Rectum," fifth edition, London, 1888, p. 208.
12. Op. cit., p. 209.
13. Op. cit., p. 59.
14. "Diseases of the Rectum and Anus," second edition, London, 1890, p. 185.
Symptoms.—The symptoms in the early stage of this disease are not usually severe, and are generally experienced during defecation, when at some point or other there will be an uneasy sensation, consisting of an itching, pricking, slight smarting, or a feeling of heat about the circumference of the anus. As the disease progresses, the discomfort attending the movements of the bowel is greatly augmented, and at a variable period of time gives place to a severe pain, of a burning or lancinating character, which is followed by throbbing and excruciating aching, attended by violent spasmodic contraction of the sphincter muscles, continuing from half an hour to several hours.
From reflex irritation, pains are often experienced in other parts, simulating sciatica or rheumatism; the urinary organs, as has already been mentioned, are liable to be sympathetically deranged, causing attention to be diverted from the real seat of the disease.
The ulcer being fully established, the suffering usually comes on with intensity shortly after the actual passage of the motion, and frequently it lasts for many hours, completely incapacitating the patient for work while it continues. I have known persons affected with this malady who for hours were obliged to maintain one position, or to assume the recumbent posture, for fear that the slightest movement would aggravate the pain.
After an indefinite period the pain subsides or entirely disappears, the patient feeling fairly comfortable, or even perfectly well, and to all outward appearance he would continue so were it not for the knowledge that the subsequent passage of fecal matter will bring with it a recurrence of agony. In consequence of this dread, the act of defecation is postponed as long as possible, with the result that when the evacuation does take place the pain is greatly increased.
The feces, when solid, will be passed streaked with purulent matter,—possibly also with blood,—and when more soft will be figured and of small size; sometimes they are flattened and tape-like, due to the incomplete relaxation of the sphincters during defecation. Not infrequently the appearance of such a stool leads the inexperienced to make a diagnosis of stricture of the rectum. In this connection it may be well to state that a fissure is sometimes found associated with a stricture, which latter is due to a congenital contracted state of the anus. Serremone, quoted by Ball,[15] believes that the stricture is the cause and not the result of the fissure, the narrow outlet being more liable to injury from over-stretching.
When a fissure is of long duration, the constitution becomes greatly impaired as a result of the constant pain, the constipation, and the frequent resort to narcotics, and the patient is liable to fall into a state of melancholy and extreme nervous irritability; the countenance, expressive of pain, grows care-worn and sallow; the appetite is poor; and there is more or less emaciation, associated with the general appearance of a person suffering from serious organic disease.
Flatulence is another annoying symptom that generally attends severe cases of anal fissure.[16] It is not only troublesome, but also painful, the disengagement of gas being almost certain to bring on a paroxysm of pain.
Such are the rational symptoms of anal fissure. If, then, a patient comes to a physician, complaining of severe pain lasting for some time after defecation, the presumption is strong that a fissure exists, since no other rectal disease produces this characteristic distress. But in this as in all other affections of the inferior extremity of the intestinal tract we must supplement our investigation by an actual exploration of the parts, in order to determine the true character of the trouble and to exclude the presence of coexisting lesions.
Ocular and Digital Examination.—Previous to making the rectal examination, the bowels should be thoroughly emptied by an enema,—the subsequent pain and anal spasm being prevented by a preliminary local application of a four-per-cent. solution of the hydrochlorate of cocaine to the mucous membrane of the anus, the drug being applied on a pledget of cotton and left in situ for five or ten minutes. Care must be exercised not to use the solution too freely, as otherwise toxic symptoms are apt to ensue when the drug is employed in this region. The rich lymphatic and vascular supply of the part probably accounts for this fact.
Fig. 3—Head Mirror.
The rectum and the bladder being completely evacuated, the patient should be placed on the side in a good light, with the knees drawn up and one hand supporting the uppermost buttock. To condense the light on the parts to be examined the head mirror may be employed (Fig. 3).
Upon inspection, the first thing that attracts our notice, frequently, is a red, somewhat edematous prominence (Fig. 4) close to the verge of the anus, looking not unlike a small hemorrhoid. This excrescence has been termed the "sentinel pile." Upon placing a finger on each side of the tumor and pressing down and out, as recommended by Bodenhamer,[17] the fissure will be seen.
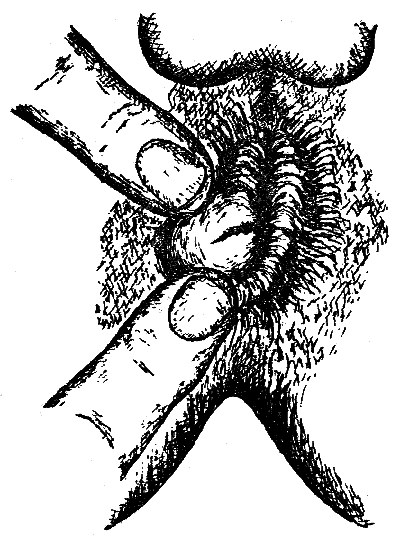
Fig. 4—Anal Fissure associated with the so-called "sentinel pile" (Bodenhamer).
An important point, to which Bodenhamer calls attention, is the external appearance of the anus itself, which in these cases is usually in a highly contracted state and more or less infundibuliform; the observer being struck by the very considerable depth to which the anus is retracted, and its unnatural look.
The fissure is sometimes difficult to find, and must be searched for in the folds of the anus. This can be accomplished by drawing the mucous membrane away on each side, by which means we shall usually be able to see just within the orifice an elongated, club-shaped ulcer, the floor of which may be very red and inflamed, or, if the disease is of long standing, of a grayish color, with the edges well defined and indurated. Sometimes the ulcer is quite superficial, while in other instances it extends completely through the muco-cutaneous surface, exposing the subjacent muscular coat. Cripps[18] states that these ulcers are sometimes undermined, so that a probe may be passed for a short distance beneath them, while occasionally a little fistulous channel will run some distance up the anus.
A fact to which special attention should be directed here is that small ulcerations may exist in the sinuses of Morgagni. Kelsey[19] and Vance[20] have met with such cases, the ulceration being completely hidden from sight, and detectable only by the sharp pain caused by the introduction of a small bent probe. This condition is no doubt a rare one, but is none the less important on this account, for its situation is such that it may be readily overlooked.
The next step in the examination of a case of fissure is the introduction of the finger into the rectum,[21] and it should be conducted in the following manner.[22] If the lesion be situated dorsally, pressure should be made by the finger toward the perineum, thus avoiding the fissure and rendering the introduction of the digit as painless as possible. If the fissure be situated anteriorly or laterally, the finger should be pressed toward the opposite side of the bowel.
In cases of fissure the speculum ani is seldom required by those accustomed to making rectal examinations. In the majority of instances the possession of the tactus eruditus—education of the sense of touch—will enable the surgeon to form a correct diagnosis without the aid of this instrument, and thus save the patient much pain. If a speculum should be required, the instrument of Aloe (Fig. 5) or of Sims (Fig. 6) may be employed.
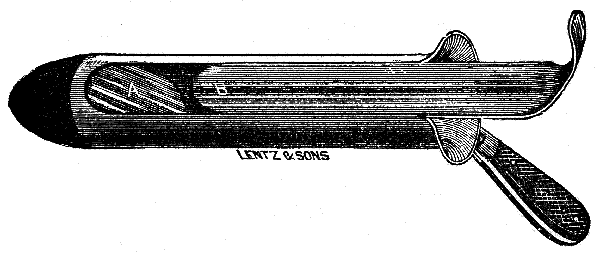
Fig. 5—Aloe's Speculum.
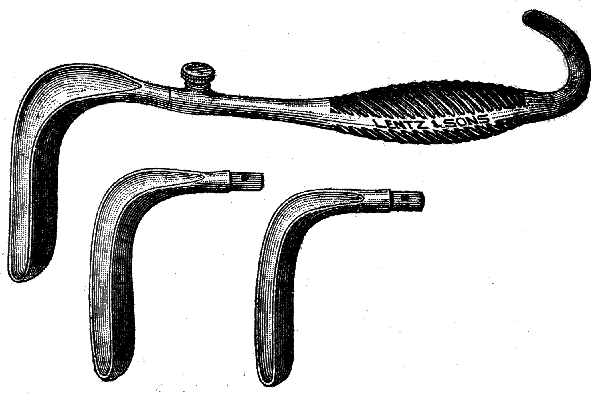
Fig. 6—Sims' Speculum (detachable handle).
It is not an uncommon occurrence, according to Allingham,[23] to find a polypus associated with fissure, it being situated at the upper end of the ulcer, or lying against it on the opposite side of the wall of the rectum. I have met with several such instances. If the polypus be undiscovered, treatment of the fissure will prove useless, for it will not heal until the polypoid growth is removed. In searching for a polypus, it is important to remember that the investigation should be conducted by passing the finger from above downward, as otherwise the tumor may be pushed up out of reach, the pedicle in these cases often being of considerable length.
Diagnosis.—The manifestations of this disease are so characteristic of the lesion that it seems almost impossible for an error to be made in its diagnosis. The peculiar nature of the pain, the time of its occurrence (either during or some time after an evacuation of the bowels), its continued increase until it becomes almost unbearable, and its gradual decline and entire subsidence until the next evacuation, are symptoms clearly pointing to fissure, and in most instances should be sufficient evidence to establish a diagnosis; yet in a number of well-authenticated cases mistakes have been made, and patients suffering from this disease have been treated for neuralgia, uterine or vesical trouble, stricture, and even hemorrhoids.
Anal fissure is very readily distinguished from neuralgia by the absence in the latter of any breach of surface or of any other disease of the mucous membrane of the rectum; by the entire want of connection between the pain and the alvine evacuations; and by the constant suffering. In neuralgia the pain caused by pressure with the finger in the anus is not confined to one spot, as it is in fissure, but all portions of the bowel are alike tender. It is true that the morbid sensibility of the rectum and anus caused by a fissure and that caused by neuralgia are often so intimately blended that it is sometimes no easy matter to distinguish between them; nothing but the detection itself, in some cases, of the fissure, which can always be discovered by a thorough examination, will clear up the diagnosis.[24]
The symptoms of anal fissure often simulate so closely those of uterine disease and bladder affections that the surgeon is led astray and overlooks the real seat and true nature of the malady. Occasionally the spasmodic condition of the sphincter in these cases simulates the symptoms of stricture; but a thorough examination will dispel all uncertainty by revealing the presence of the ulcer.
Frequently uterine trouble or hemorrhoids are found associated with the fissure, and in this event the case is treated for either one or the other of the first two complaints, the presence of the other lesion being unsuspected and consequently neglected. In all such instances a careful inspection of all the parts concerned will at once remove all errors in diagnosis and dispel all doubts.
In children, the fact must always be borne in mind that fissures and other erosions about the anal orifice may be due to the scratching induced by the irritation of pin-worms.
Course and Prognosis.—Anal fissure is not an immediately dangerous disease; nor can it be said that it has any tendency toward recovery if let alone. An indefinite time may elapse without any other change than the gradual wearing down of the patient's vitality from continued suffering and nervous strain. With proper treatment, however, this disease can be promptly cured, and practically without risk, the operation usually practiced being one of the simplest of surgical procedures.
15. Op. cit., p. 132.
16. Bodenhamer, op. cit., p. 81.
17. Op. cit., p. 92.
18. Op. cit., p. 187.
19. "Diseases of the Rectum and Anus," third edition, New York, 1890, p. 294.
20. Medical and Surgical Reporter, August 14, 1880.
21. In some cases of fissure the irritable condition of the sphincter will cause such contraction of the anus when an examination is attempted that it will be impossible for the surgeon to pass his finger into the rectum without etherization of the patient. In these instances it is best to advise the patient to submit to such operative measures as may be deemed necessary at the same time that the examination is made under ether.
22. Allingham, op. cit., p. 212.
23. Op. cit., p. 212.
24. Bodenhamer, op. cit., p. 100.
It is highly important to the success of any plan of treatment directed toward the cure of anal fissure, that attention be paid to the condition of the bowels. Regularity of habit should be established, and the evacuations rendered semi-fluid—as figured or hard stools generally aggravate the symptoms.
To accomplish these purposes, enemata or mild aperients should be employed, and the diet must be regulated, the use of bland and unirritating food being enjoined.
All drastic purges should be avoided, as they are more or less irritating to the extremity of the rectum.
In order to establish a daily evacuation of the bowels and to render the movement as painless as possible, I am in the habit of ordering an enema of warm water, or one of rich flaxseed tea, say from half a pint to a pint, to be administered every evening; preference being given to the night-time, as then the patient can assume the recumbent posture, which, combined with the rest, affords the most relief from subsequent pain.
If the first enema should prove ineffective, it should be repeated in half an hour. In order to relieve the pain and spasm of the sphincters attending the evacuation, it is well to use a suppository about half an hour before the enema is employed, consisting of:
| ℞ | Ext. belladonnæ | gr. 1/8 ad 1/2. |
| Cocain. hydrochloratis | gr. 1/4 ad 1/2. | |
| Ol. theobromæ | gr. x. | |
| Misce, | et fiat suppositoria j. |
Or an ointment of extract of conium may be used, as recommended by Harrison Cripps:[25]
| ℞ | Ext. conii | ℨ ij. |
| Olei ricini | ℨ iij. | |
| Ung. lanolini ad | ℥ ij. |
A small quantity of this ointment should be smeared on the part five minutes before expecting a motion, and again after the motion has passed.
All ointments used in the treatment of rectal disease may be applied by means of a hard-rubber pipe (Fig. 7).
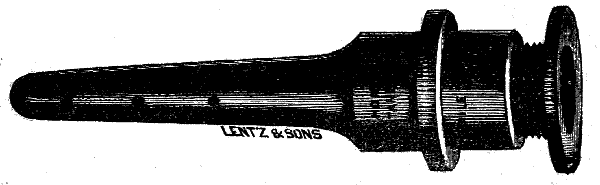
Fig. 7—Hard-rubber Ointment-Applicator.
The various methods of treating anal fissure may be divided, for the sake of convenience, into the palliative and the operative.
Palliative Measures.—Palliative treatment will meet with success in a considerable proportion of cases, especially when there is no great hypertrophy of the sphincter muscles. Allingham[26] states that the curability of this lesion does not depend upon the length of time during which it has existed, but rather upon the pathological changes it has wrought. He asserts that he has cured fissures of months' standing by means of local applications, where the ulcers were uncomplicated with polypi or hemorrhoids, and where there was not very marked spasm or thickening of the sphincters.
It is essential to the success of the treatment of fissure, especially by local applications, that rigid cleanliness of the parts be maintained; for this purpose the anus and the adjacent portions of the body should be carefully sponged night and morning and after each stool with hot or cold water, the temperature being regulated to suit the patient's comfort.
An excellent instrument for irrigating the rectum is the one devised by Dr. Edward Martin, of Philadelphia (Fig. 8). I have also employed Bodenhamer's instrument for this purpose (Fig. 9).
In applying the various local remedies it is necessary first to expose the ulcer to view, and to anæsthetize its surface with a four-per-cent. solution of hydrochlorate of cocaine, well brushed in with a camel's-hair pencil. The application of the cocaine may have to be repeated once or twice, at intervals of three or four minutes, in order to obtain the desired anæsthetic effect.

Fig. 8—Martin's Rectal Irrigator.
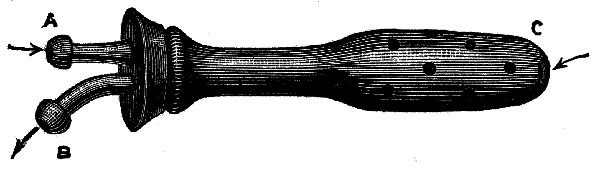
Fig. 9—Bodenhamer's Irrigator.
If any ointment has been used about the fissure, the anus should be subjected to a hot-water douche before using the cocaine, as cocaine will not exert its anæsthetic influence on a greasy surface.[27] For this purpose Martin's irrigator (Fig. 8) answers admirably. The parts should subsequently be dried thoroughly with cotton or a sponge. A convenient sponge or cotton mop holder is shown in Fig. 10.

Fig. 10—Rectal Sponge-Mop Holder.
Among the different remedies that have been used for the local treatment of fissure of the anus may be mentioned the following: Nitrate of silver; acid nitrate of mercury; fuming nitric acid; carbolic acid; sulphate of copper; the actual cautery, etc.
Of these topical applications, the nitrate of silver is the best. Its effects are various: it lessens or entirely calms the nervous irritation which is so important a factor in producing spasmodic contraction of the sphincters; it shields the raw and exposed mucous surface, by forming an insoluble albuminate of silver; it destroys the hard and callous edges of the ulcer, and tends to remove the diseased and morbid action of the parts.
The form in which I usually employ this salt is in solution (from ten to thirty grains to the ounce). To attain the best results, the solution should be used once in twenty-four or forty-eight hours, according to circumstances. It may be applied by means of cotton attached to a silver applicator or cotton-holder (Fig. 11), or to a piece of wood. The application is made by separating the margins of the anal orifice with the thumb and index finger of the left hand, and introducing into the anus the probe charged with the solution.

Fig. 11—Cotton-Applicator.
According to Bodenhamer,[28] if the ulcer is more than one-third of an inch above the margin of the anus it will be necessary to use the speculum.
The solution is to be applied to the fissure only; a few drops are all that will be required. If thorough local anæsthesia has been induced by the use of cocaine, the application of the silver salt produces little if any suffering; for by the time the anæsthetic has lost its effect the acute pain caused by the nitrate of silver will have passed away.
After each application the part should be well smeared with an ointment of iodoform (thirty grains to the ounce). The odor of the iodoform may be disguised by the addition of a few drops of otto of roses. Iodol may be used instead of iodoform, and in the same way.
After the ulcer has been touched once or twice with the silver solution, the effect will be, in those cases which are benefited by this treatment, a considerable mitigation of the severe pain which has troubled the patient when at the closet and afterwards; and the sore will present a healthy granulating appearance, and slowly contract in size.
In children and in young persons, unless the fissure be complicated with some other affection, this lesion is almost always curable by adopting the foregoing mode of treatment.
Some authorities speak highly of the use of the acid nitrate of mercury, fuming nitric acid, carbolic acid, the actual cautery, etc., but in my experience their employment is attended with more suffering than follows the employment of the nitrate of silver or the simple operative treatment which will presently be described. Furthermore, the application of these remedies is not so certain to effect a cure as either of the two procedures just mentioned, so that I rarely resort to their use.
The daily introduction of a full-sized bougie, made of wax or tallow, will sometimes act beneficially in cases of fissure, by distending the sphincter and producing such an amount of irritation as will set up a healing process in the ulcer. An application of cocaine or of belladonna ointment should be made to the part prior to the employment of the bougie.
Allingham[29] strongly advocates the local use of the following ointment:
| ℞ | Hydrarg. subchlor | gr. iv. |
| Pulv. opii | gr. ij. | |
| Ext. belladonnæ | gr. ij. | |
| Ung. sambuci | ℨ j. | |
| M. | Sig.: To be applied frequently. |
This authority states that he has cured many cases with this ointment alone.
Another excellent ointment recommended by Mr. Allingham[30] is the following:
| ℞ | Plumbi acetatis } __ | |
| Zinci oxidi } aa | gr. x. | |
| Pulv. calaminæ | gr. xx. | |
| Adipis benzoatis | ℥ ss. | |
| M. |
An ointment of red oxide of mercury, thirty grains to the ounce, has also cured many cases.
The "Brinkerhoff System," as applied to fissures of the anus, is thus described by Dr. Edmund Andrews:[31]
"Once or twice a month, as the itinerant doctor comes around on his circuit, he inserts his little speculum, cleans out the ulcer, and applies to it a solution of nitrate of silver, forty grains to the ounce. Between the applications the patient uses a morning and evening treatment himself. Each morning he is to evacuate the bowels, then inject the rectum with lukewarm water, and finally insert into it a little ointment, consisting of three grains of carbolic acid and eight grains of sulphur to the ounce of vaseline or lard.
"For evening treatment he uses 'Brinkerhoff's Ulcer Remedy,' having the following composition:
| ℞ | Extract of hamamelis dist | f ℨ v. |
| Solution of persulph. of iron | f ℨ j. | |
| Cryst. carbolic acid | gr. ij. | |
| Glycerine | f ℨ ij. |
M. Sig.: Add half a teaspoonful of this to the same quantity of starch, and about an ounce and a half of water. Inject into the rectum every evening."
Operative Treatment.—In the more severe cases local treatment will fail to effect a cure, and operative interference will be necessary. There are three methods of repute to be considered in this connection: (1) forcible dilatation; (2) incision; (3) a combination of these two procedures, dilatation and incision.
Forcible Dilatation.—This is the operation recommended by Récamier, Van Buren, and others. It consists in introducing the two thumbs into the bowel, back to back, and then forcibly separating them from each other until the sides of the bowel can be stretched as far out as the tuberosities of the ischia. It is essential to place the ball of one thumb over the fissure, and that of the other directly opposite to it, in order to prevent the fissure from being torn through and the mucous membrane being stripped off. As pointed out by Allingham,[32] it is well to repeat the stretching in other directions until the entire circumference of the anus has been gone over. In this manner, by careful and thorough kneading and pulling of the muscles, the sphincters will be made to give way, and will be rendered soft and pliable. This procedure should always be done with the patient thoroughly under the influence of an anæsthetic, and should occupy at least five or six minutes.
This operation is perfectly safe, but, as it is no less severe than the operation by incision, and as in some cases it fails to effect a cure, I can see no advantage in adopting it instead of the more satisfactory and always successful plan of treatment by combined dilatation and incision. It may be found preferable in some cases on account of the prejudice of patients against the use of the knife.
Incision.—A fissure can be cured by this method, by making an incision through the base of the ulcer and a little longer than the fissure itself, so as to make sure of severing all the exposed nerve-filaments. The cut should divide the muscular fibers along the floor of the ulcer.
In a fair proportion of cases this operation will meet with success, but it is not so certain and radical as the operation next to be described.
It has the advantage over the other operations, however, of being nearly or entirely painless under local anæsthesia produced by cocaine, and therefore, when general anæsthesia is contra-indicated, or is refused by the patient, this method is worthy of a trial.
Dilatation and Incision.—This operation, if skillfully and carefully performed, I believe to be a radical and unfailing cure for the disease. The bowels should be cleared out by a dose of castor-oil and an injection; after which, under ether-anæsthesia, the sphincters should be dilated in the manner previously described. This being accomplished, and the ulcer properly exposed, a straight blunt-pointed bistoury (Fig. 12) should be drawn deeply across the surface, making a cut about an inch in length and a third of an inch in depth. Instead of the blunt bistoury, a sharp-pointed scalpel may be used (Fig. 13). It should be entered at the margin of the anus, passed under the ulcer, and made to protrude above the ulcer, the overlying structure being then divided from without inward.

Fig. 12—Blunt-pointed Bistoury.
Fig. 13—Sharp-pointed Scalpels.
The subsequent treatment consists in keeping the patient in the recumbent position, and in the use of a little opium to confine the bowels. After three or four days a laxative may be given, from which time daily alvine movements should be secured. In seven or eight days the patient can begin to move about; but for at least two weeks he should avoid standing long on the feet. No dressing is required further than bathing the parts with a little warm water and carbolic acid soap, to remove any offensive discharges. For the same purpose, peroxide of hydrogen may be employed.
The subcutaneous division of the sphincters, as recommended by some authors for the cure of fissure, is not a satisfactory method, and is mentioned here solely to condemn it. It is not only uncertain in its results, but is also painful, and in more than one instance has been followed by abscesses.
25. Op. cit., p. 189.
26. Op. cit., p. 215.
27. W. P. Agnew, M.D., "Diagnosis and Treatment of Rectal Diseases," second edition, 1891, p. 97.
28. Op. cit., p. 111.
29. Op. cit., p. 214.
30. Op. cit., p. 215.
31. Op. cit., pp. 75-76.
32. Op. cit., p. 221.
Fistula in Ano which is not due to ulceration and perforation of the rectal wall from within is the result of a previous abscess. Such an abscess forms in the ischio-rectal fossa, and, although opened early by a free incision even before the cavity becomes distended with pus, it frequently fails to heal. It may fill up and contract to a certain extent, but it does not become entirely obliterated; a narrow track remains, which constitutes the affection designated fistula in ano.
There are several reasons why rectal abscesses so frequently degenerate into fistulæ. One is, that, owing to an internal opening within the bowel, small particles of fecal matter find their way into the sinus, and, acting as foreign bodies, prevent the healing; another, that, owing to the frequent movement of the parts by the sphincter muscles, sufficient rest is not obtained for the completion of the reparative process; and, finally, the vessels near the rectum are not well supported, and the veins have no valves, hence there is a tendency to stasis, which is unfavorable to rapid granulation.
According to the authority of Mr. Harrison Cripps,[33] if the fistula be divided its surface will be seen to be lined with a smooth, gelatinous membrane, which when examined under the microscope is found to consist of granulation-tissue exactly analogous to that which lines the interior of a chronic abscess. The leucocytes constituting the outer wall of this membrane are but loosely adherent, and constantly becoming free they form the chief part of the pus which drains from the fistula.
Relative Frequency of this Affection.—In point of frequency, compared with other rectal diseases, fistula is next to hemorrhoids. This statement is contrary to the showing made by the published statistics of St. Mark's Hospital, as quoted by Allingham.[34] This table shows that out of four thousand cases taken consecutively from the out-patient department of the hospital there were one thousand and fifty-seven persons suffering from fistula and one hundred and ninety-six from abscess, of which latter number one hundred and fifty-one subsequently became fistulæ, so that more than one-fourth of the whole number of cases treated were fistulæ. Allingham also states that a recent examination of the records of the in-patients of the same institution, covering a period of several years, shows that two-thirds of those operated upon were cases of fistula.
Mr. Allingham[35] justly calls attention to one source of error in drawing conclusions from statistics—namely, the fact that many patients suffer from more than one malady. He states that it constantly happens that a fistula is found in connection with hemorrhoids, either as the substantive disease or as a complication. Again, a fissure or circular ulcer often has a sinus running from it, so that it may fairly be considered as the opening of an internal fistula, and the case called a fistula; or the sinus is not detected, and the case is called ulcer or fissure.
Another fallacious element in the statistics of Mr. Allingham, which should not be overlooked, is pointed out by Mr. Chas. B. Ball.[36] St. Mark's has a special reputation for the cure of fistula, so that many persons suffering from this disease go there, and in this way the records show an apparent greater frequency of fistula. Mr. Ball also states[37] that at the Dublin General Hospital, although fistula is common, it is by no means the commonest of rectal diseases; and in his own practice this affection has not furnished more than one-sixth of rectal operative cases.
Age and Sex Affected.—This disease is commonly met with during middle age, but it is by no means restricted to that period of life. Allingham states[38] that he has operated upon an infant in arms, and upon a man over eighty years old. Dr. Henry R. Wharton[39] mentions having seen a number of cases at the Children's Hospital, Philadelphia, among which he records one of complete fistula in a child a few months old.
Causes.—Fistula in ano may originate in ulceration and perforation of the mucous membrane of the bowel—the result of the irritation produced by fecal accumulations (arising from any cause, such as atony of the intestines, irregularity of habits, rectal stricture, etc.), or by foreign bodies, such as fish- or rabbit-bones, grape- or fig-seeds, etc.; more frequently it owes its origin to an abscess caused by injuries, such as blows or kicks upon the anus, or by exposure to cold, as from sitting upon damp seats—especially after exercise, when the parts are hot and perspiring; it may also arise from excessive irritation of the rectum occasioned by the presence of any of the forms of parasites which infest the anus and its immediate neighborhood. Other predisposing causes are thrombosed veins and suppurating hemorrhoids. Abscess, and then fistula, may likewise supervene in fevers and certain depressed conditions of the blood, such as frequently give rise to boils or carbuncles.[40]
"The late Dr. W. E. Horner, Professor of Anatomy in the University of Pennsylvania, used to describe an arrangement of pouches opening upward, in the mucous membrane of the rectum, by which the entanglement of seeds, bits of bone, etc., contained in the feces was favored. His account may be found in his 'Special Anatomy and Histology,' vol. ii, p. 46 (edition of 1851), where he quotes a paper on Fistula in Ano, by Ribes. He says, also, that Glisson and Ruysch had described them as valves, and that Winslow was acquainted with them. The latter author (Douglas's Transl., 1743, vol. ii, p. 149) says, 'They form little bags or semilunar lacunæ.' Another American writer, Bushe ('Malformations, Diseases, and Injuries of the Rectum and Anus,' 1837, p. 15), speaks of these pouches, and confirms Winslow's description. They are also mentioned in the treatises of Leidy and S. G. Morton. Hyrtl (Handb. der Topogr. Anatomie, 1871, bd. ii, p. 142) describes them quite fully, and speaks of their agency in the development of fistulæ.
"Mr. W. T. Clegg, of Liverpool, says (Lancet, Feb. 5, 1881) that Mr. Bickersteth has for four years been describing these anal pouches, which 'are not mentioned in any of the books he has consulted.'
"It is certainly strange that this arrangement, so clearly pointed out, should have been passed over in silence, not only by many anatomists, but by late writers on rectal surgery; yet it is undoubtedly a frequent cause of fistula. In Fig. 14 these pouches are shown, with a fistula, probably formed by a foreign body lodging in one of them. Over the fistula the mucous membrane has been removed, and a bougie has been passed through the canal."[41]
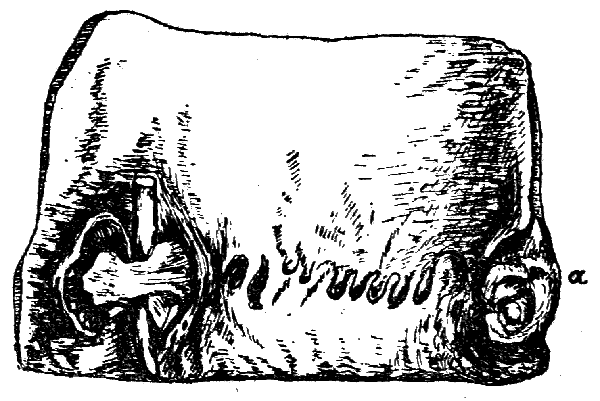
Fig. 14—Section of the Rectum, showing the rectal pouches, and a fistula with a bougie passed through it, the mucous membrane dissected off. At a is a small external pile, cut in half.—St. George's Hospital Museum, ser. ix, No. 42 (Holmes, Princ. and Pract. of Surgery, vol. ii, p. 643).
Finally, a tubercular or strumous diathesis seems to be as potent a factor in the causation of fistula as it is in other suppurative troubles. The appearance of a fistula in a tubercular subject is characteristic of the constitutional malady. It is thus described by Messrs. Alfred Cooper and F. Swinford Edwards:[42] "The part is, as a rule, unusually hirsute; the ischio-rectal fossæ are drawn in, owing to absence of fat; the sphincter is weak and offers no resistance to the introduction of the finger. The skin around the orifice is bluish and often considerably undermined, and the discharge is thin and watery. The internal orifice is often large, and the mucous membrane around it is also undermined."
The tendency to the occurrence of abscess and fistula in phthisical patients has long been recognized, and has given rise to some doubts as to the propriety of resorting to operative measures in such cases. This point will be considered in the chapter on Treatment. According to Messrs. Cooper and Edwards,[43] about five per cent. of phthisical subjects also suffer from fistula, and about twelve per cent. of fistulous patients are the subjects of tuberculosis.
Varieties.—For all practical purposes we may divide fistulæ into the following four forms: (1) the complete fistula, in which there are two openings, one in the rectum and one on the skin more or less remote from the anus (Fig. 15); (2) the incomplete internal fistula, in which there is a communication with the cavity of the rectum by means of an opening in the mucous membrane, but none with the external surface of the body (Fig. 16); (3) the incomplete external fistula, in which there is an external opening through the skin, but no communication with the bowel (Fig. 17); and (4) the complex fistula, in which there are many sinuses and numerous external openings (Figs. 18 and 19). Some of these tracks run outward; some extend up the bowel beneath the mucous membrane; whilst others travel round the bowel and open in the other buttock, giving rise to the so-called horseshoe fistula. The second and third varieties named are often spoken of as blind fistulæ.
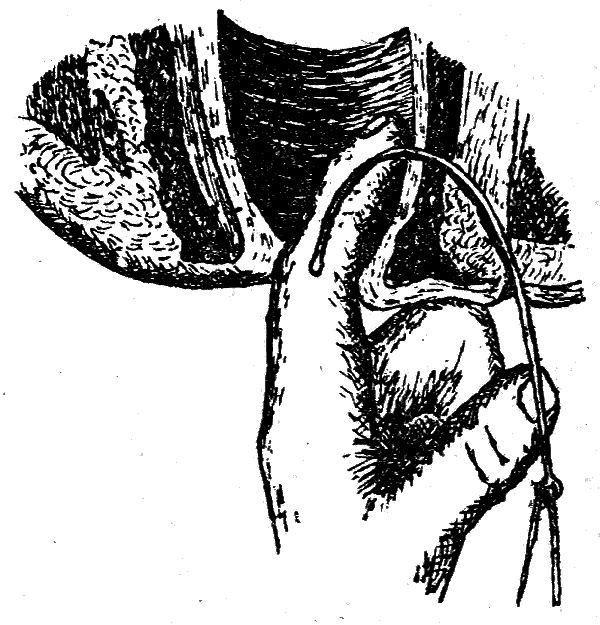
Fig. 15—Complete Fistula traversed by Probe (Esmarch).
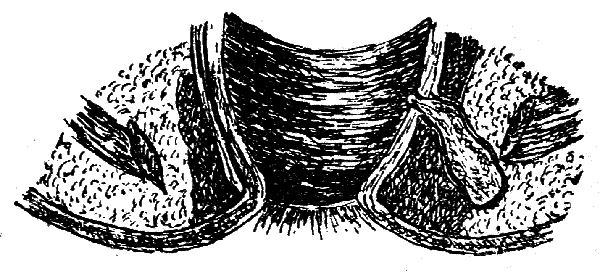
Fig. 16—Internal Incomplete Fistula (Esmarch).
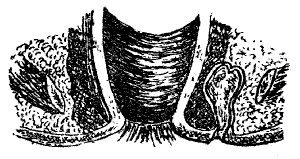
Fig. 17—External Incomplete Fistula (Esmarch).

Fig. 18.
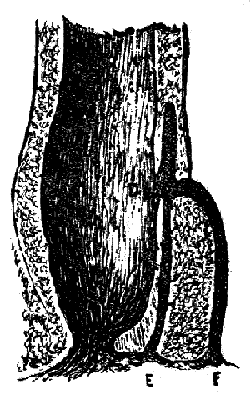
Fig. 19.
Fig. 18—A, B, deep submuscular track resulting from an ischio-rectal abscess; A, I, submucous track running up and down the bowel.
Fig. 19—D, E, subtegumentary and submucous fistula with internal and external opening; D, F, deep submuscular track, having same internal but separate external opening.
33. Op. cit., p. 152.
34. Op. cit., p. 13.
35. Op. cit., p. 13.
36. Op. cit., p. 66.
37. Op. cit., p. 67.
38. Op. cit., p. 13.
39. Keating's "Cyclopædia of the Diseases of Children," vol. iii, p. 341.
40. Allingham, op. cit., p. 14.
41. Article on Diseases of the Rectum, by Henry Smith, Esq., revised by John H. Packard, M.D., in Holmes' "System of Surgery" (Packard, editor of American edition), vol. ii, pp. 643-644.
42. "Diseases of the Rectum and Anus," second edition, London, 1892, p. 126.
43. Op. cit., p. 126.
Symptoms.—The symptoms of fistula are not easily overlooked. Occasionally there is considerable pain present, but more frequently only a feeling of uneasiness about the anus is experienced. When a fistula originates, as I believe it most commonly does, from a preëxisting abscess, there is a sensation of weight about the anus, with swelling of the integument, considerable tenderness upon pressure, pain in defecation, and a constitutional disturbance associated with rigors. These symptoms are relieved after the matter is discharged. The exploring needle (Fig. 20) is often useful in determining the presence of pus in such abscesses in which it is impossible to obtain fluctuation. In complete fistula in ano, and in the incomplete internal variety, the evacuations are streaked or covered with pus and mucus, perhaps also slightly tinged with blood.

Fig. 20—Small Trocar and Acupuncture or Exploring Needle (for testing the character of ambiguous swellings or fluid collections about the rectum).
The chief discomfort to a patient with fistula is the discharge, in greater or less quantity, of purulent or muco-purulent matter which is kept up from the sinus so long as it remains unhealed, soiling the linen and making it wet and uncomfortable, and producing an excoriation of the nates. The discharge is not of itself sufficient to be a source of great exhaustion, and does not interfere with ordinary occupations, so that many patients have had fistula for a considerable length of time without being conscious of any serious ailment. The escape of flatus and mucus from the bowel in complete fistula will often prove a source of annoyance, as will also the passage of feculent matter which will be expelled through the sinus should the fistulous channel be very free.
An attack of secondary suppuration is always liable to complicate the presence of a fistula, and is usually due to a stoppage of the track by small particles of feces or by exuberant growth of the granulations. Such a sequela, of course, is attended with pain, until a new opening forms or one is made by the surgeon. In some cases the original fistulous track becomes reëstablished. Fistula in some persons, particularly those of a nervous temperament, produces an impression of physical imperfection and weakness in their organization, which renders them miserable. As in other affections of the rectum, various reflex or sympathetic pains are experienced in cases of fistula; they are referred to the back, to the loins, and to the bottom of the abdomen. When such pains extend down the leg and to the foot, they are likely to be attributed to sciatica unless the history of the case is carefully studied and a critical examination made.
Ocular and Digital Examination.—Immediately before an examination is made in cases of fistula, as well as in all other investigations connected with the diagnosis of rectal diseases, the bowels should be emptied by an enema. This procedure not only renders the exploration of the parts easier and cleaner, but also, in women especially, serves to quiet the patient's fears of any untoward accident occurring, and therefore facilitates the thoroughness of the surgeon's examination by securing the coöperation of the patient, as in extruding the parts, etc.
In order to examine a patient with supposed fistula, he should be placed in a recumbent position on a table or an examining-chair, preferably on the side on which the external opening is situated, with the legs well drawn up toward the abdomen, and the buttocks brought to the edge of the couch.

Fig. 21—Silver Probe attached to handle.
The anus and the surrounding parts should be carefully examined to detect any apparent lesion. If the external orifice of the sinus is prominent, or if there is a sentinel granulation present, the outlet of the fistula will be obvious; but when it is small and located between folds of the skin, its situation may be demonstrated by making pressure with the top of the finger in the suspected locality, which will usually cause a little drop of matter to exude. The site of a fistula may often be detected by feeling gently all around the anus with the forefinger and finding an induration which feels like a pipe-stem beneath the skin. A flexible silver probe (Fig. 21) should now be passed along the fistulous track. In doing this, considerable care is requisite, and the utmost gentleness should be observed, bearing in mind that the probe is to be directed by its own weight through the sinus, and not by force applied by the hand of the surgeon. If it does not pass easily, bend it and see if it cannot be coaxed along the channel. In many cases it will pass directly into the bowel. When the probe has been passed as far as it will go without the use of any force, introduce the finger gently into the rectum. This should be subsequent to the passage of the probe, as otherwise the introduction of the finger into the bowel will set up a spasm of the sphincter muscles, which will greatly interfere with the passage of the probe. When the finger is in the bowel it will frequently come in contact with the probe, which fact demonstrates the presence of a complete fistulous track; in other cases the mucous membrane is felt to intervene between the digit and the probe. In such cases the internal opening generally exists, but is difficult to discover,—sometimes because the examiner searches for it too high in the bowel. Palpation with the sensitive tip of the finger will often render the presence of the inner orifice obvious, by coming in contact with an indurated mass of tissue. If such a spot be felt, the finger should be placed upon it and the probe passed toward the finger. Make sure that the fistula is a complete one, by feeling the probe touch the finger. There may not be an internal opening; if not, see how near the probe comes to the surface of the bowel.
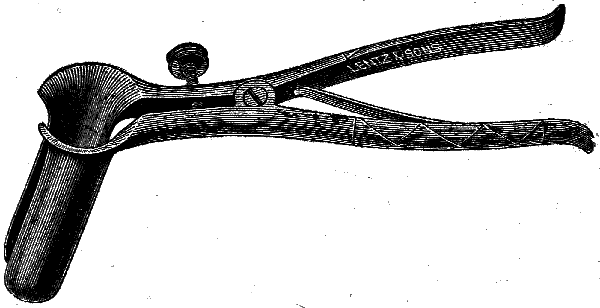
Fig. 22—Pratt's Speculum.
If a doubt still exists as to the completeness of the track, one of a variety of specula (Figs. 22, 23, 24) may be introduced into the rectum, and the outer orifice of the sinus injected with either milk or a solution of iodine, when if there be an internal opening the appearance of the colored fluid within the bowel will set the question at rest.
If the inner opening be not discovered by these methods, the case must be looked upon as one of external rectal fistula.
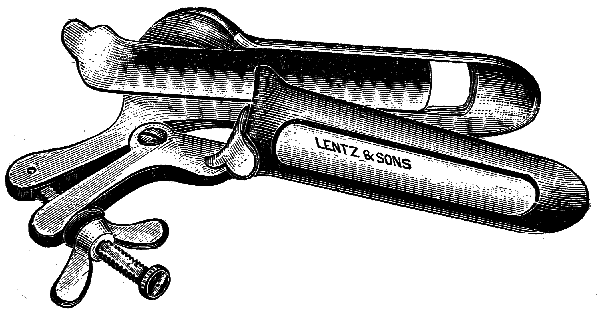
Fig. 23—O'Neil's Speculum.
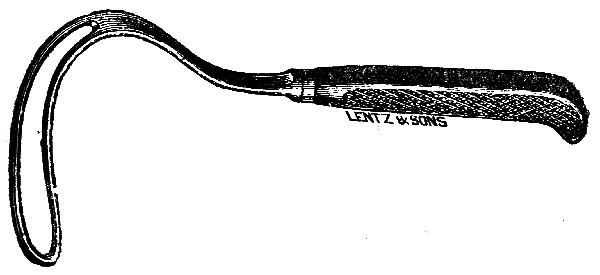
Fig. 24—Kelsey's Rectal Retractor.
According to Ball,[44] in cases where the probe passes away from the rectum and is directed along the anal fascia to the upper portion of the ischio-rectal fossa, or where the entire substance of the rectal wall separates the finger and the probe, the case is one either of external rectal sinus, or of fistula originating in the superior pelvi-rectal space. In such cases, Mr. Ball states, "we must go farther and try and find the cause, such as diseased bone, etc.; and in the female a vaginal examination may show us a uterine or ovarian origin. Where there are numerous external openings it is necessary to carefully probe all of them, so as to determine whether they are all connected, and the direction which they take. The upper limit of the separation of the mucous membrane should also be made out, and search should be made for the presence of more than one internal orifice, if such is likely to be present."
The presence of incomplete internal rectal fistula is more difficult to determine than the other varieties of this lesion which have just been considered. It is the most painful form, but, fortunately, it is of infrequent occurrence. Its orifice may be located anywhere in the rectum, but is generally found between the internal and external sphincters. According to Allingham,[45] the circumference of this opening is often as large as an English threepenny piece, its edges being sometimes indurated, at other times undermined. The feces, when liquid, pass into the sinus and create great suffering—a burning pain often lasting all day after the bowels have acted.
In this variety of fistula the feces are coated more or less with pus or blood, and a boggy swelling is noted at some portion of the circumference of the anus. A peculiar feature of this swelling is often noted—viz., its presence one day and its disappearance in a day or two, followed by an increased discharge of pus from the bowel. This fact is explainable by the closure of the outlet of the fistula, caused either by a plug of feces or as a result of inflammatory swelling, which allows the collection of a quantity of pus and the consequent formation of a boggy tumor. The swelling disappears upon the reëstablishment of the communication between the bowel and the sinus, and is attended by the profuse discharge of matter previously mentioned. This phenomenon is repeated over and over again, and indicates the nature of the disease.
In other cases of blind internal fistula, if the orifice can be felt, or if it can be seen through a speculum, a bent probe may be introduced into it and made to protrude near to the cutaneous surface of the body, where its point can be felt.
Diagnosis.—The method of diagnosing fistula has already been sufficiently detailed. A few words, however, as to differential diagnosis may prove useful. Fistulæ frequently coexist with other rectal diseases; it is therefore important that an examination should be carefully made, so as to exclude such lesions—for instance, the presence of stricture, malignant disease, hemorrhoids and other tumors, etc. A thorough physical examination of the chest should also be made, to ascertain the presence or absence of phthisis, which so frequently complicates fistula in ano. Serious kidney disease should be excluded before recommending operation, for obvious reasons. In cases of caries of the vertebræ, of the sacrum, or of the pelvis, fistulous tracks may form and simulate anal fistula. In such instances a careful investigation will reveal the true origin of the trouble, and will show that the case is not one of ordinary fistula in ano.
Course and Prognosis.—This disease untreated has a tendency to increase. The longer its duration the more tortuous and complicated does it become. Hence the earlier the patient submits to treatment the more favorable will be the prognosis, and the time and extent of the treatment necessary to effect a permanent cure will be correspondingly diminished.
44. Op. cit., p. 77.
45. Op. cit., p. 21.
Treatment of Abscess.—Preliminary to a consideration of the treatment for the disease when the fistulous track has been formed, some attention must be devoted to the importance of dealing promptly with the inflammatory and suppurative process which leads to abscess, and which usually forms the first stage of the affection known as fistula in ano.
When a patient presents the symptoms of a threatened abscess in the vicinity of the rectum, he should be directed to go to bed, or at least to avoid all undue exercise; the bowels should be thoroughly evacuated, preferably by the use of a saline cathartic; the diet should be nutritious; and, if the case be seen early, hot fomentations and poultices may be applied to the parts. The early adoption of these measures may abort the threatened abscess.
If, however, there be reason to suspect that matter has formed or is forming, it will be advisable to make a free incision into the center of the affected site with a sharp curved bistoury, if the trouble is superficial, or, if it is deep, with a narrow straight knife. When pus is present and is deeply seated, the evacuation of the abscess will be aided by the introduction of the forefinger into the bowel, by which means the swelling may be pushed forward, rendered tense, and hence made more apparent.
In opening these abscesses, if possible, ether should be given. The patient should lie on the side on which the threatened abscess is situated; the upper leg should be bent forward upon the abdomen. When pus is present, the operator should stand out of the line of its exit, for when the cavity is opened it often squirts out a considerable distance. After the matter has been discharged, the forefinger should be introduced into the abscess-cavity for the purpose of breaking down any secondary cavities or loculi that may exist. When this has been accomplished, the abscess should be thoroughly washed out with peroxide of hydrogen (Marchand's, undiluted, or some other reliable preparation), after which a rubber drainage-tube should be inserted, or a piece of iodoform gauze should be lightly placed between the lips of the incision, to prevent its closing too rapidly, and also to allow free drainage. Careful daily attention should be paid to the wound while the cavity of the abscess is contracting, as it is important to maintain a free and dependent outlet for the matter which continues to be secreted; but stuffing and distention of the cavity should be avoided. If a drainage-tube be used, it should be shortened from day to day as the wall of the abscess contracts.
After an operation for rectal abscess, the patient should be kept quiet for several days; and if great care be taken, both with the subsequent drainage and in keeping the orifice open, the part may heal without the formation of a fistula.
Treatment of Fistula in Ano.—The treatment of fistula, like that of fissure, may be either palliative or operative.
Palliative Treatment.—This method of treatment will be required in cases where there is a positive refusal on the part of the patient to submit to an operation, and in persons whose constitutions are broken down by disease and in whom the reparative powers of the body are not equal to the task of restoring it to health. Chronic alcoholism, albuminuria, diabetes, malignant diseases, etc., are conditions in which operative procedures are attended with risk, and in which palliative measures should be tried. Phthisis is not an absolute contra-indication to operative measures. The rule which I observe is to operate in those cases of tubercular subjects in which the disease is quiescent, but to avoid such interference if the lung-mischief is at all active.
Incomplete external fistulæ, and even complete fistulæ of somewhat recent origin and not extensively indurated, may be cured by non-operative measures; but such treatment requires constant attention on the part of the practitioner, as well as a willingness on the part of the patient to give sufficient time to the treatment. Even under such circumstances the process of repair is slow, and in many cases the result will not be perfectly satisfactory. It is true that fistulæ sometimes recover spontaneously, or are cured by simple means, such as the mere passage of a probe used in examining the fistulous track, but instances of this kind are rare.
In certain selected cases of fistulæ I am in the habit of endeavoring to effect a cure by stimulating the sinus and allowing free drainage of the secretions, so as to avoid the use of the knife. To accomplish satisfactory results with this mode of treatment, the following indications should be borne in mind: 1, that the external orifice be perfectly free; 2, that the sinus be kept clean, so as to prevent putrefactive changes; 3, that an effort be made to excite a healthy action in the fistulous channel; and 4, that the parts be kept as quiet as possible.
To meet the first indication, it is necessary to dilate the outer opening of the fistula with sponge or sea-tangle tents: but better still for this purpose are the Lee's Antiseptic Slippery-Elm Tents (Fig. 25).[46] These are made of selected slippery-elm bark, and compressed under high pressure. Owing to their non-irritant and demulcent properties, I find them superior to other tents.

Fig. 25—Slippery-Elm Tent (large size).
The second indication (that the sinus be kept clean, so as to prevent putrefactive changes) is best carried out by the use of peroxide of hydrogen. I have cured some cases of fistula in ano by means of injections into the sinus of peroxide of hydrogen alone, being careful to keep the external opening free, and treating the patient daily until healing occurred. I am in the habit of using Marchand's preparation, undiluted. It is injected into the sinus by means of a long, flexible silver canula (Fig. 26) attached to a hypodermatic syringe.

Fig. 26—Flexible Silver Canula.
Other antiseptics may be employed for the same purpose, such as bichloride of mercury (1 to 2000), or carbolic acid (1 to 80), but I much prefer the peroxide of hydrogen.
The third indication (to excite a healthy action in the sinus) can be met in one of a number of ways. In the first place, before applying such remedies it will be well to obtund the sensibility of the channel by an injection into the sinus of a four-per-cent. solution of cocaine. This may be accomplished by using the same syringe and canula that are used for cleansing the fistula.
If the wall of the sinus is somewhat indurated, it is better to insert a small, flexible curette (Fig. 27) and scrape the wall of the fistula along its entire length. The sinus is now prepared for some one of the various stimulating substances which have been recommended for this purpose. Among these may be mentioned peroxide of hydrogen; nitrate of silver, fused, or in solution (thirty to sixty grains to the ounce); sulphate of copper in solution (ten grains to the ounce); carbolic acid mixed with equal parts of glycerine and water.

Fig. 27—Flexible Curette.
These substances may be applied to the fistulous track by means of cotton attached to a silver probe or to an applicator (Fig. 11, p. 26); or they may be injected into the sinus by means of the syringe and silver canula (Fig. 26, p. 57).
If the fistula is a complete one and the substance used be applied as an injection, the finger should be passed into the rectum and made to cover the internal orifice of the sinus, so as to prevent the escape of any of the fluid into the bowel.
Regarding the fourth point (keeping the parts at rest), the patient, whilst under treatment, should be confined to the horizontal position, either in bed or on a sofa. Congestion of the parts is thereby lessened. A firm pad placed over the anus and well supported by a T-bandage is useful in limiting the motions of the anus due to the alternate contraction and relaxation of the levator ani muscle.
The chance of success in the palliative treatment of fistula in ano will be greatly increased if due attention be paid to the general state of health of the patient, and when circumstances render it possible he should be advised to seek the benefits of a change of air.
46. Made by J. Elwood Lee Co., Conshohocken, Pa.
In all cases of fistula in ano, before undertaking operative interference it is essential for the surgeon to examine the patient carefully, not only locally, but also as to the general state of health; for this disease is not infrequently complicated with other lesions—as has been previously mentioned—which may render operative procedures inadvisable.
Thus, when a fistula is associated with a stricture of the rectum of a malignant nature, any operative interference on the former lesion will be out of the question. If it is a simple stricture and its existence be not recognized, or if it be left untreated, any operation performed on the fistula will fail to effect a cure.
Treatment by Incision.—In a large majority of cases of fistula in ano, the operation which is sanctioned by experience as the most prompt and certain at the same time that it is the safest in its results is to lay open the sinus into the rectum, dividing with the knife all the tissues intervening between its cavity and that of the bowel. Figs. 28, 29, 30 and 31 represent useful forms of knives for incising a fistula.
The preparation of the patient consists in having the bowels moved by means of castor oil or some other mild cathartic on the day preceding the operation, and on the morning of the operation the lower bowel should be evacuated by means of an enema.

Fig. 28—Blunt-pointed Knife.

Fig. 29—Curved Knife, useful in certain fistulous cases.
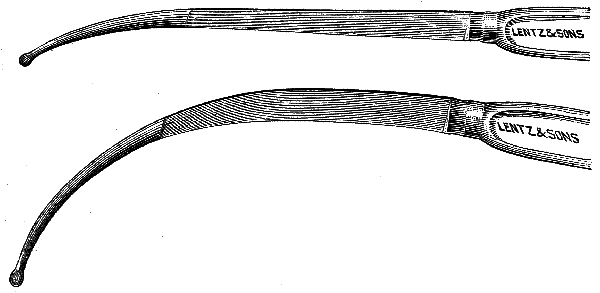
Fig. 30—Gowlland's Bistouries.
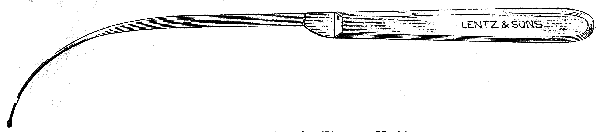
Fig. 31—Kelsey's Fistula-Knife.
After etherization the patient should be placed on the side on which the fistula exists, the buttock being brought to the edge of the operating-table. Occasionally the lithotomy posture is preferable, as in cases in which there is a complex fistula.
The first step in the operation is to dilate the sphincter muscles, which is to be done in a slow but steady manner by introducing the thumbs into the rectum, back to back, and making gradual pressure around the anal orifice until muscular contraction is overcome.

Fig. 32—Probe-pointed Director.

Fig. 33—Kelsey's Fistula-Director.
In dealing with COMPLETE FISTULÆ a flexible probe-pointed director (Figs. 32, 33) is passed through the sinus, and is then brought out of the anus by means of the forefinger of the left hand introduced into the bowel. The tissues lying upon the director are then to be divided with a sharp bistoury. A careful search is now to be made for any diverticula, which if found should be divided. If none exist, the granulations lining the track should be scraped away with a Volkmann's spoon (Fig. 34). The healing process will be facilitated by removing with scissors all overtopping edges of skin and mucous membrane.

Fig. 34—Volkmann's Spoon.
If the internal opening is more than an inch from the anus, a probe-pointed bistoury (Figs. 28, 30, p. 61) should be introduced into the fistula upon a director, and its point made to impinge upon a finger in the rectum. As the finger and the instrument are withdrawn, the necessary incision is made. Or the director can be passed through the sinus, and a wooden gorget (Fig. 35) inserted into the bowel, after which the track can be divided with an ordinary bistoury. The gorget prevents the opposite side of the bowel from being injured should the knife slip. (Fig. 36).
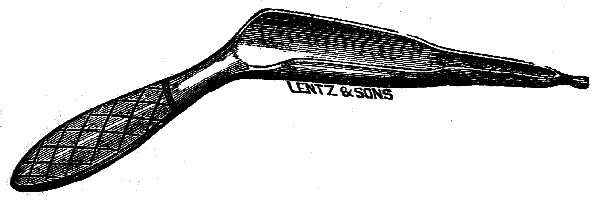
Fig. 35—Gorget.
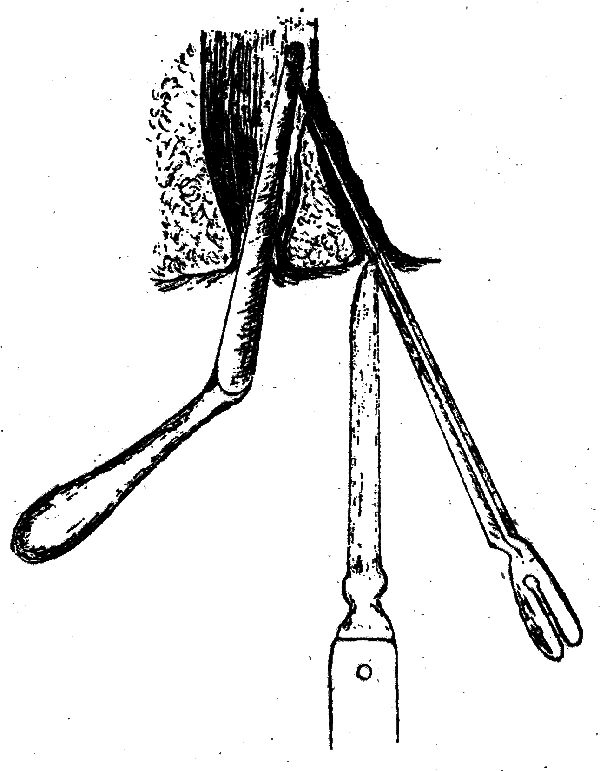
Fig. 36—Operation for Fistula with Gorget (Bernard and Huette).
When the track of the fistula is much indurated, and considerable force is therefore required to make the incision, it will be better to perform the operation by means of Mr. Allingham's spring-scissors and special director (Fig. 37). With this instrument, fistulæ running high up in the bowel may be divided, no matter how dense they may be. The director is made with a deep groove, the transverse section of which is more than three-quarters of a circle; in this the globe-shaped probe-point of one blade of the scissors runs. When placed in the groove the blade cannot slip out; so, the director having been passed through the sinus, the forefinger of the left hand is introduced into the bowel, and then the probe-pointed blade of the scissors is inserted into the groove of the instrument, and run along it, cutting its way through the diseased tissue as it goes, the finger in the bowel preventing the healthy structure from being wounded.
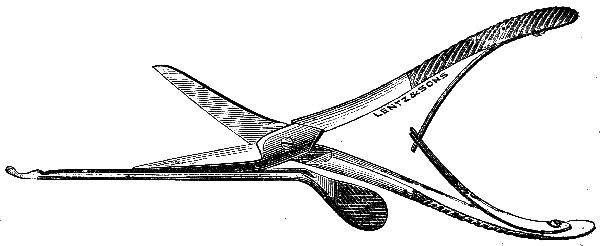
Fig. 37—Allingham's Spring-Scissors and Director.
A frequent error in operating on fistulous cases consists in not keeping to the sinus, the director being pushed through the track-wall, and then being free to roam about in the cellular tissue of the part, at the operator's will. In this manner a portion of the fistulous channel is left, and an unnecessary amount of the tissues (skin and subcutaneous structures) is divided. Such a mistake can always be avoided by taking plenty of time in performing the operation, and by careful sponging of the sinus as it is laid open, in order to follow the track of the granulation-tissue lining it, which by this simple means is freely exposed to view.
The method of treating EXTERNAL RECTAL FISTULÆ must vary according to the direction and extent of the track. If the mucous membrane alone intervenes between the finger introduced into the bowel and a probe passed along the sinus, the channel should be transformed into a complete fistula by perforating the mucous membrane with the probe, or with a director, at the uppermost limits of the fistulous channel. The regular operation for complete fistula is then to be performed by dividing the intervening septum between the fistula and the bowel.
In cases in which the sinus is directed away from the rectum, the proper course is not to divide the sphincters, but freely to enlarge the external orifice and to maintain free drainage.
The treatment of INCOMPLETE INTERNAL RECTAL FISTULÆ invariably demands operative interference at the earliest possible moment after a diagnosis is made; for if left alone its tendency is to burrow.
The operation for a blind internal fistula consists in making it a complete fistula and in dividing the intervening structures between the bowel and the sinus. This is best performed by introducing a probe-pointed director, bent at an acute angle, into the bowel, and passing the bent portion through the internal opening. This done, the point of the probe can be felt subcutaneously and cut down upon, and the remainder of the operation completed.
In dealing with COMPLEX FISTULÆ the surgeon must be guided by the peculiarities of each case. In operating upon a horseshoe fistula it is essential to recognize the true condition of affairs; for a careless or an inexperienced observer might think that he had two separate fistulæ to deal with, and operate accordingly. Even were he to recognize that he was dealing with a horseshoe fistula, if he followed the usual plan he would slit up first one sinus and then the other, dividing the sphincter in two places obliquely through its fibers, thus endangering the patient's future power of controlling the movements of the bowel. (Fig. 38.)
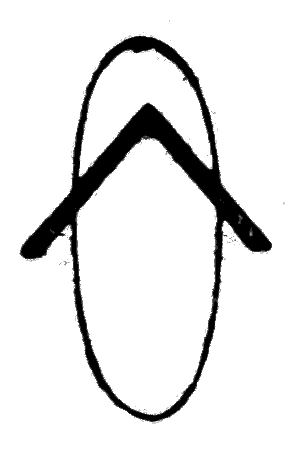
Fig. 38.—Diagram showing wrong method of operating in horseshoe fistula.
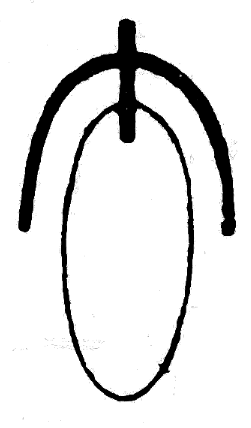
Fig. 39.—Diagram showing the method recommended in operating upon horseshoe fistula.
According to Messrs. Cooper and Edwards,[47] "If this fistula can be laid open in such a way as to entail only one division of the sphincter, and that at right angles to its fibers, there will be a minimum amount of risk of subsequent incontinence." The operation can be done in this way (Figs. 39, 41, 43). First pass a probe-pointed director through the internal aperture, and on its point incise the skin in the middle line behind; now push the director through, and slit up. Secondly, slit up the lateral sinuses on directors passed in at the external openings and brought out at the dorsal incision. These lateral sinuses may take a straight, a curved, or even a rectangular direction. Fistulæ taking these different courses are illustrated in Figs. 40 and 42.
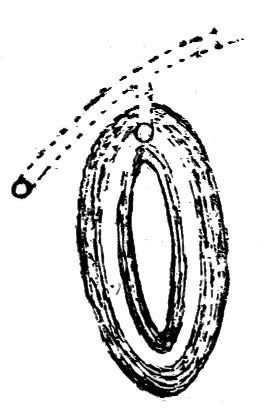
Fig. 40.—A diagram of one variety of horseshoe fistula.
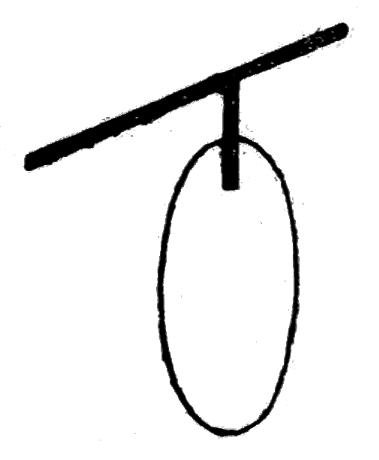
Fig. 41.—Diagram of incisions necessary.
"The first incision will have divided the sphincter, but the other two will only have divided tissue external to it. Should the external apertures be so placed that a straight line drawn from the one to the other would pass behind the anus (Fig. 40), the steps of the operation could be reversed, and a director be passed in at one external orifice and out at the other, and the tissues divided. Now pass the director from the wound in the middle line into the bowel, through the internal opening, and slit up the tissue with the included sphincter. In this way the incisions will be found to be more or less T-shaped, the stem corresponding to the dorsal cut."
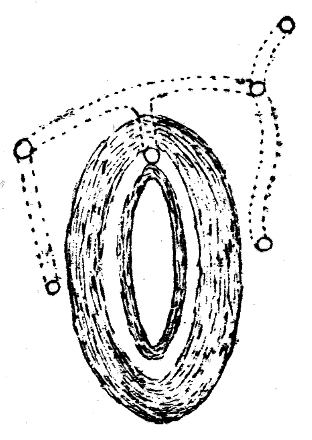
Fig. 42.—A diagram of severe horseshoe fistula, with five external openings.
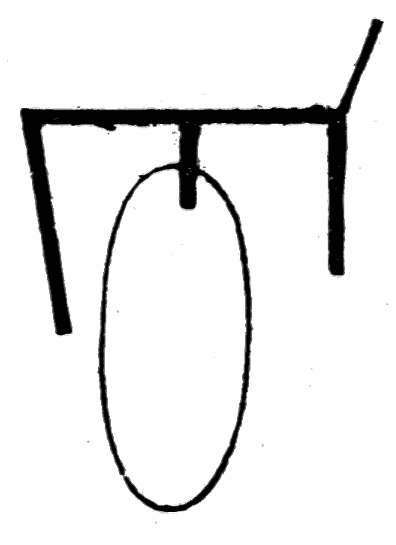
Fig. 43.—Diagram showing incisions necessary for the cure of foregoing with one division of sphincter.
Treatment of Hemorrhage.—There is seldom much hemorrhage after an operation for fistula, but in some cases it may be necessary to ligate a large vessel which has been divided. If there should be a profuse general oozing, the sinus may be packed with iodoform gauze, or, if necessary, the rectum may be plugged; for this purpose Allingham ties a double string into the center of a large bell-shaped sponge, which is passed into the bowel so as to prevent the blood from escaping upward into the colon. He then firmly packs the parts below with cotton dusted with powdered alum or persulphate of iron. In order to allow the escape of flatus, a catheter may be passed through the sponge. As a rule, all hemorrhages following rectal operations are easily controlled by mild measures, such as the local application of hot water, of ice, or of some mild astringent.
The After-Treatment.—After the operation for fistula in ano, the wound should be packed with iodoform gauze, which is left undisturbed for twenty-four hours. This is done to prevent subsequent hemorrhage. A pad of gauze and cotton and a T-bandage are next applied.
The subsequent dressing of the case should be daily attended to by the surgeon himself. The parts should be kept perfectly clean, and the wound syringed with peroxide of hydrogen, carbolic acid solution, etc., after which a single piece of iodoform gauze laid between the cut surfaces of the wound will be all the dressing required.
In the after-treatment of these cases I have seen the healing process greatly retarded by excessive packing of the wound with the lint, or delayed by the undue use of the probe. Such interference is to be avoided.
If the granulations are sluggish, and the discharge is thin and serous, it will be well to apply some stimulating lotion, such as peroxide of hydrogen or a weak solution of copper sulphate (two grains to the ounce).
The surgeon should be on the watch during the healing process to avoid any burrowing or the formation of fresh sinuses. Should the discharge from the surface of the wound suddenly become excessive, it is evidence that a sinus has formed, and a careful search should be made for it. Sometimes it begins under the edges of the wound, at other times at the upper or lower ends of the cut surface, and occasionally it seems to branch off from the base of the main fistula.
Pain in or near the seat of the healing fistula is another symptom of burrowing, and when complained of the surgeon should carefully investigate its cause.
After an operation for fistula, the patient's bowels should be confined for three or four days, for which purpose opium is usually given. At the end of this time the bowels may be opened by the administration of a dose of castor-oil, and so soon as the patient feels a desire to go to stool an enema of warm water should be injected, which will tend to render the feces soft and fluid and hence make their passage easier. The patient should be kept in a recumbent posture until the fistula is healed; and until the bowels are moved the diet should be liquid—such as milk, beef-tea, and broths. The time required for a patient to recover after an operation for fistula in ano varies with the extent of the disease. In an average case it will be necessary to keep the patient in bed for two or three weeks, and confined to the house for a couple of weeks longer.
Fig. 44—Set of three Cautery Irons to fit one handle.
Fig. 45—Paquelin's Thermo-Cautery.
Incontinence of feces is an unpleasant sequela to the operation for fistula. It is, happily, of rare occurrence, and follows only extensive operations, such as those in which the sphincter has been divided more than once, etc. When it exists to any extent it is productive of great annoyance to the patient, possibly more so than the original fistula. The application of the old-fashioned cautery-iron (Fig. 44), heated to the proper degree, or the small point of Paquelin's thermo-cautery (Fig. 45), applied to the cicatrix of the operation wound, will often suffice to relieve this trouble, by causing contraction of the anal outlet and giving tone and increased power to the sphincter muscle.
Mr. H. W. Allingham, Jr.,[48] recommends for this condition freeing the ends of the muscle by a deep incision through the old cicatrix and allowing the wound once more to heal from the bottom by granulation.
Dr. Chas. B. Kelsey[49] advocates in these cases the complete excision of such a cicatrix, exposing freely the divided ends of the sphincter and bringing them together by deep sutures, exactly as in cases of lacerated perineum.
In dealing with a fistula situated anteriorly in a female subject, Messrs. Cooper and Edwards[50] recommend that after a free division of the sinus the track be scraped thoroughly with a Volkmann's spoon, and then deep sutures inserted as in the case of rupture of the perineum, in the hope by this means of getting union by first intention.
Treatment by Immediate Suture.—In otherwise healthy subjects, affected with fistula in ano, a method of operating which has met with success, especially in this country, consists in the immediate suture of the wound after the fistula has been excised. The steps of the operation are as follows. The septum between the fistula and the bowel is divided; the entire fistulous channel, and all lateral sinuses, are excised; buried sutures of catgut or of silk are then passed around the wound, at intervals of a quarter of an inch, and tied so as to bring the deep tissues together. The sutures are inserted very much in the same manner as in the ordinary operation for ruptured perineum. The advantage of this plan of treatment is that primary union is secured and the patient recovers in a shorter time than would have been the case after one of the operations which aims to secure union by granulation.
Treatment by Ligature.—There are two methods of using the ligature, which we may term the immediate and the mediate.
The IMMEDIATE OPERATION has little to recommend it. It consists in passing a silk thread through the fistula and drawing it backward and forward so as to cut its way through. The same object may be accomplished by the use of the galvanic écraseur, or of the wire écraseur of Chassaignac.
Mediate Operation by Ligature.—In this method either the silk ligature or an elastic one may be employed.
Silk Ligature.—If silk be used, it may be employed in one of two ways. In both methods a short piece of silk is threaded to a silver probe bent to a curve, which is passed through the fistula and drawn out at the anus. The thread is passed through the track, so that one end hangs out of the bowel and the other at the external orifice of the fistula. It is at this point that the methods diverge. One plan consists in knotting the ends loosely together and allowing the patient to go about. After a time, ranging from two to four weeks, the ligature comes away, having slowly cut through the included tissue. According to Mr. Harrison Cripps,[51] the pathological process by which this is accomplished appears to be a gradual destruction or disintegration of the included tissue, due to the ulcerative action of the thread. The other plan is to tie the silk so tightly that it will completely cut its way through and strangulate all the tissue requiring division in an ordinary case of fistula. This method causes considerable suffering to the patient, and has therefore been discarded in favor of the operation next to be described.
Operation by Elastic Ligature.—The advocates for the use of the elastic ligature maintain that with it there is no hemorrhage. This is a matter of considerable importance when the fistula penetrates deeply, and also in those rare cases of hemorrhagic diathesis where severe bleeding is apt to follow a trivial incision.
For the introduction of the elastic ligature we are indebted chiefly to Dittel, of Vienna. This ligature causes strangulation of the parts by the firm pressure it constantly exerts upon the included structures; it cuts its way out in a week's time or less.
It is stated by those who have an extended experience with this plan of treatment, that, contrary to what might be expected, the pain attending the ulceration of the band through the tissues is slight, especially after the first twelve hours. Consequently, this method would prove an excellent way of treating fistula if it were always to be relied upon to effect a cure. Unfortunately, this is not the case, for it often happens that after the ligature has cut its way through, and the superficial parts have healed, the fistula remains uncured. The reason for this is to be found in the fact that the ligature has dealt with the main track, only, of a fistula in which exist one or more secondary channels and diverticula. I therefore resort to this method of treatment only in that class of patients who have an insuperable dread of any cutting operation; when the fistula is uncomplicated with sinuses; in cases of deep fistula where there is danger of wounding large vessels; in cases in which the patients are debilitated by means of some chronic disease; and, finally, in patients of known hemorrhagic tendency. It is a valuable adjunct to the use of the knife in dealing with cases in which a sinus runs for some distance along the bowel.
The method of employing this ligature is as follows. A solid cord of india-rubber, about one-tenth of an inch in diameter, may be threaded to a probe having at one end a rounded opening, or eye, through which the ligature is passed. The probe enters the fistula from the external to the internal opening, and passes out through the anus. To facilitate the passage of the cord, the rubber should be put on the stretch. After the ligature is passed, a soft metallic ring is slipped over the two ends of the cord; the cord is then tightly stretched and the ring slipped up as high as possible and clamped.
Fig. 46.—Allingham's Ligature-Carrier.
If the internal opening be any distance up the bowel, Allingham's instrument (Fig. 46) facilitates the passage of the ligature. In using it, remember that it is intended to draw the cord from the bowel out of the external orifice, and not vice versa. This instrument has been modified and improved by Helmuth, of New York. (Fig. 47.)
Fig. 47—Helmuth's Ligature-Carrier.
Little after-treatment is required when the elastic ligature has been used. It will frequently be found that by the time the cord separates the wound has become superficial.
47. Op. cit., p. 119.
48. Medical Press and Circular, May 23d.
49. Annual of the Universal Medical Sciences, 1889, vol. iii, p. 5, D.
50. Op. cit., p. 124.
51. Op. cit., p. 181.
A most excellent and agreeable tonic and appetizer. It nourishes and invigorates the tired brain and body, imparts renewed energy and vitality, and enlivens the functions.
Dr. Ephraim Bateman, Cedarville, N. J., says:
"I have used it for several years, not only in my practice, but in my own individual case, and consider it under all circumstances one of the best nerve tonics that we possess. For mental exhaustion or overwork it gives renewed strength and vigor to the entire system."
Descriptive pamphlet free.
WE supply Antiseptic Liquid, Tablets of Bichloride of Mercury, for easily preparing solutions of any desired strength; Labbaraque's Solution, Solution Aluminium Acetate, Sulphur Bricks.
We furnish Cocaine in the following packages: Cocaine alkaloid, pure in crystals; Cocaine citrate, 4 per cent. solution; Cocaine hydrobromate, pure in crystals; Cocaine hydrobromate, 4 per cent. solution; Cocaine muriate, pure in crystals; Cocaine muriate, 2 per cent. solution; Cocaine muriate, 4 per cent. solution; Cocaine oleate, containing 5 per cent. of the alkaloid; Cocaine salicylate, 4 per cent. solution; Cocainized oil, 5 per cent.
Cascara Cordial and Glycerin Suppositories are eligible and satisfactory laxatives after operations.
Mosquera's Beef-Meal, Beef-Cacao and Beef-Jelly are concentrated foods, highly nutritious, perfectly palatable, and may be administered in a variety of forms. They constitute ideal foods for those enfeebled by operative procedures.
Pepsin Cordial is an agreeable and efficient digestive and tonic.
Descriptive literature of our products sent to physicians on request.
DR. JOHN S. BILLINGS, Surgeon U.S.A.,
New subscribers taking more than one journal, and accompanying subscription by remittance, are entitled to the following special rates:
GAZETTE and AGE, $2.50; GAZETTE, AGE and LANCET, $4.00: LANCET and AGE, $2.50; WESTERN MEDICAL REPORTER or BULLETIN with any of the above at 20 per cent. less than regular rates.
Combined, these journals furnish a complete working library of current medical literature, all the medical news, and full reports of medical progress.
We have made a new departure in the publication of medical books. As you no doubt know, many of the large treatises published, which sell for four or five or more dollars, contain much irrelevant matter of no practical value to the physician, and their high price makes it often impossible for the average practitioner to purchase anything like a complete library.
Believing that short practical treatises, prepared by well known authors, containing the gist of what they had to say regarding the treatment of diseases commonly met with, and of which they had made a special study, sold at a small price, would be welcomed by the majority of the profession, we have arranged for the publication of such a series, calling it The Physicians' Leisure Library.
This series has met with the approval and appreciation of the medical profession, and we shall continue to issue in it books by eminent authors of this country and Europe, covering the best modern treatment of prevalent diseases.
The series will certainly afford practitioners and students an opportunity never before presented for obtaining a working library of books by the best authors at a price which places them within the reach of all. The books are amply illustrated, and issued in attractive form.
They may be had bound, either in durable paper covers at 25 Cts. per copy, or in cloth at 50 Cts. per copy. Complete series of 12 books in sets as announced, at $2.50, in paper, or cloth at $5.00, postage prepaid. See complete list.
(a) To be issued one a month during 1892.
| P. O. Box 470 | Detroit, Mich. |
| SEXUAL IMPOTENCE IN MALE AND FEMALE | $3.00 |
| By Wm. A. Hammond, M. D. | |
| PHYSICIANS' PERFECT VISITING LIST | 1.50 |
| By G. Archie Stockwell, M. D. | |
| A NEW TREATMENT OF CHRONIC METRITIS | .50 |
| By Dr. Georges Apostoli. | |
| CLINICAL THERAPEUTICS | 4.00 |
| By Dujardin-Beaumetz, M. D. | |
| MICROSCOPICAL DIAGNOSIS | 4.00 |
| By Prof. Chas. H. Stowell, M. S. | |
| PALATABLE PRESCRIBING | 1.00 |
| By B. W. Palmer, A. M., M. D. | |
| UNTOWARD EFFECTS OF DRUGS | 2.00 |
| By L. Lewin, M. D. | |
| SANITARY SUGGESTIONS (Paper) | .25 |
| By B. W. Palmer, M. D. | |
| SELECT EXTRA-TROPICAL PLANTS | 3.00 |
| By Baron Ferd. von Müller. | |
| THE PRINCIPLES AND PRACTICE OF BANDAGING | 3.00 |
| By Gwillym G. Davis, M. D., Universities | |
| of Pennsylvania and Göttingen. |
End of the Project Gutenberg EBook of Fissure of the Anus and Fistula in Ano, by
Lewis H. Adler
*** END OF THIS PROJECT GUTENBERG EBOOK FISSURE OF THE ANUS ***
***** This file should be named 47387-h.htm or 47387-h.zip *****
This and all associated files of various formats will be found in:
http://www.gutenberg.org/4/7/3/8/47387/
Produced by Mark C. Orton, Elizabeth Oscanyan and the
Online Distributed Proofreading Team at http://www.pgdp.net
(This file was produced from images generously made
available by The Internet Archive)
Updated editions will replace the previous one--the old editions will
be renamed.
Creating the works from print editions not protected by U.S. copyright
law means that no one owns a United States copyright in these works,
so the Foundation (and you!) can copy and distribute it in the United
States without permission and without paying copyright
royalties. Special rules, set forth in the General Terms of Use part
of this license, apply to copying and distributing Project
Gutenberg-tm electronic works to protect the PROJECT GUTENBERG-tm
concept and trademark. Project Gutenberg is a registered trademark,
and may not be used if you charge for the eBooks, unless you receive
specific permission. If you do not charge anything for copies of this
eBook, complying with the rules is very easy. You may use this eBook
for nearly any purpose such as creation of derivative works, reports,
performances and research. They may be modified and printed and given
away--you may do practically ANYTHING in the United States with eBooks
not protected by U.S. copyright law. Redistribution is subject to the
trademark license, especially commercial redistribution.
START: FULL LICENSE
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full
Project Gutenberg-tm License available with this file or online at
www.gutenberg.org/license.
Section 1. General Terms of Use and Redistributing Project
Gutenberg-tm electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or
destroy all copies of Project Gutenberg-tm electronic works in your
possession. If you paid a fee for obtaining a copy of or access to a
Project Gutenberg-tm electronic work and you do not agree to be bound
by the terms of this agreement, you may obtain a refund from the
person or entity to whom you paid the fee as set forth in paragraph
1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this
agreement and help preserve free future access to Project Gutenberg-tm
electronic works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the
Foundation" or PGLAF), owns a compilation copyright in the collection
of Project Gutenberg-tm electronic works. Nearly all the individual
works in the collection are in the public domain in the United
States. If an individual work is unprotected by copyright law in the
United States and you are located in the United States, we do not
claim a right to prevent you from copying, distributing, performing,
displaying or creating derivative works based on the work as long as
all references to Project Gutenberg are removed. Of course, we hope
that you will support the Project Gutenberg-tm mission of promoting
free access to electronic works by freely sharing Project Gutenberg-tm
works in compliance with the terms of this agreement for keeping the
Project Gutenberg-tm name associated with the work. You can easily
comply with the terms of this agreement by keeping this work in the
same format with its attached full Project Gutenberg-tm License when
you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are
in a constant state of change. If you are outside the United States,
check the laws of your country in addition to the terms of this
agreement before downloading, copying, displaying, performing,
distributing or creating derivative works based on this work or any
other Project Gutenberg-tm work. The Foundation makes no
representations concerning the copyright status of any work in any
country outside the United States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other
immediate access to, the full Project Gutenberg-tm License must appear
prominently whenever any copy of a Project Gutenberg-tm work (any work
on which the phrase "Project Gutenberg" appears, or with which the
phrase "Project Gutenberg" is associated) is accessed, displayed,
performed, viewed, copied or distributed:
This eBook is for the use of anyone anywhere in the United States and
most other parts of the world at no cost and with almost no
restrictions whatsoever. You may copy it, give it away or re-use it
under the terms of the Project Gutenberg License included with this
eBook or online at www.gutenberg.org. If you are not located in the
United States, you'll have to check the laws of the country where you
are located before using this ebook.
1.E.2. If an individual Project Gutenberg-tm electronic work is
derived from texts not protected by U.S. copyright law (does not
contain a notice indicating that it is posted with permission of the
copyright holder), the work can be copied and distributed to anyone in
the United States without paying any fees or charges. If you are
redistributing or providing access to a work with the phrase "Project
Gutenberg" associated with or appearing on the work, you must comply
either with the requirements of paragraphs 1.E.1 through 1.E.7 or
obtain permission for the use of the work and the Project Gutenberg-tm
trademark as set forth in paragraphs 1.E.8 or 1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any
additional terms imposed by the copyright holder. Additional terms
will be linked to the Project Gutenberg-tm License for all works
posted with the permission of the copyright holder found at the
beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including
any word processing or hypertext form. However, if you provide access
to or distribute copies of a Project Gutenberg-tm work in a format
other than "Plain Vanilla ASCII" or other format used in the official
version posted on the official Project Gutenberg-tm web site
(www.gutenberg.org), you must, at no additional cost, fee or expense
to the user, provide a copy, a means of exporting a copy, or a means
of obtaining a copy upon request, of the work in its original "Plain
Vanilla ASCII" or other form. Any alternate format must include the
full Project Gutenberg-tm License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works
provided that
* You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is owed
to the owner of the Project Gutenberg-tm trademark, but he has
agreed to donate royalties under this paragraph to the Project
Gutenberg Literary Archive Foundation. Royalty payments must be paid
within 60 days following each date on which you prepare (or are
legally required to prepare) your periodic tax returns. Royalty
payments should be clearly marked as such and sent to the Project
Gutenberg Literary Archive Foundation at the address specified in
Section 4, "Information about donations to the Project Gutenberg
Literary Archive Foundation."
* You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or destroy all
copies of the works possessed in a physical medium and discontinue
all use of and all access to other copies of Project Gutenberg-tm
works.
* You provide, in accordance with paragraph 1.F.3, a full refund of
any money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days of
receipt of the work.
* You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project
Gutenberg-tm electronic work or group of works on different terms than
are set forth in this agreement, you must obtain permission in writing
from both the Project Gutenberg Literary Archive Foundation and The
Project Gutenberg Trademark LLC, the owner of the Project Gutenberg-tm
trademark. Contact the Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
works not protected by U.S. copyright law in creating the Project
Gutenberg-tm collection. Despite these efforts, Project Gutenberg-tm
electronic works, and the medium on which they may be stored, may
contain "Defects," such as, but not limited to, incomplete, inaccurate
or corrupt data, transcription errors, a copyright or other
intellectual property infringement, a defective or damaged disk or
other medium, a computer virus, or computer codes that damage or
cannot be read by your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH 1.F.3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium
with your written explanation. The person or entity that provided you
with the defective work may elect to provide a replacement copy in
lieu of a refund. If you received the work electronically, the person
or entity providing it to you may choose to give you a second
opportunity to receive the work electronically in lieu of a refund. If
the second copy is also defective, you may demand a refund in writing
without further opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS', WITH NO
OTHER WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT
LIMITED TO WARRANTIES OF MERCHANTABILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of
damages. If any disclaimer or limitation set forth in this agreement
violates the law of the state applicable to this agreement, the
agreement shall be interpreted to make the maximum disclaimer or
limitation permitted by the applicable state law. The invalidity or
unenforceability of any provision of this agreement shall not void the
remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in
accordance with this agreement, and any volunteers associated with the
production, promotion and distribution of Project Gutenberg-tm
electronic works, harmless from all liability, costs and expenses,
including legal fees, that arise directly or indirectly from any of
the following which you do or cause to occur: (a) distribution of this
or any Project Gutenberg-tm work, (b) alteration, modification, or
additions or deletions to any Project Gutenberg-tm work, and (c) any
Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of
computers including obsolete, old, middle-aged and new computers. It
exists because of the efforts of hundreds of volunteers and donations
from people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need are critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future
generations. To learn more about the Project Gutenberg Literary
Archive Foundation and how your efforts and donations can help, see
Sections 3 and 4 and the Foundation information page at
www.gutenberg.org
Section 3. Information about the Project Gutenberg Literary Archive Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Contributions to the Project Gutenberg Literary
Archive Foundation are tax deductible to the full extent permitted by
U.S. federal laws and your state's laws.
The Foundation's principal office is in Fairbanks, Alaska, with the
mailing address: PO Box 750175, Fairbanks, AK 99775, but its
volunteers and employees are scattered throughout numerous
locations. Its business office is located at 809 North 1500 West, Salt
Lake City, UT 84116, (801) 596-1887. Email contact links and up to
date contact information can be found at the Foundation's web site and
official page at www.gutenberg.org/contact
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
[email protected]
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To SEND
DONATIONS or determine the status of compliance for any particular
state visit www.gutenberg.org/donate
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including checks, online payments and credit card donations. To
donate, please visit: www.gutenberg.org/donate
Section 5. General Information About Project Gutenberg-tm electronic works.
Professor Michael S. Hart was the originator of the Project
Gutenberg-tm concept of a library of electronic works that could be
freely shared with anyone. For forty years, he produced and
distributed Project Gutenberg-tm eBooks with only a loose network of
volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as not protected by copyright in
the U.S. unless a copyright notice is included. Thus, we do not
necessarily keep eBooks in compliance with any particular paper
edition.
Most people start at our Web site which has the main PG search
facility: www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.