The Project Gutenberg EBook of A System of Practical Medicine By American
Authors, Vol. II, by Various
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
Title: A System of Practical Medicine By American Authors, Vol. II
General Diseases (Continued) and Diseases of the Digestive System
Author: Various
Editor: William Pepper
Louis Starr
Release Date: April 3, 2014 [EBook #45313]
Language: English
Character set encoding: ISO-8859-1
*** START OF THIS PROJECT GUTENBERG EBOOK SYSTEM OF PRACTICAL MEDICINE, VOL II ***
Produced by Ron Swanson
|
|
RHEUMATISM. By R. PALMER HOWARD, M.D.
GOUT. By W. H. DRAPER, M.D.
RACHITIS. By ABRAHAM JACOBI, M.D.
SCURVY. By PHILIP S. WALES, M.D.
PURPURA. By I. EDMONDSON ATKINSON, M.D.
DIABETES MELLITUS. By JAMES TYSON, A.M., M.D.
SCROFULA. By JOHN S. LYNCH, M.D.
HEREDITARY SYPHILIS. By J. WILLIAM WHITE, M.D.
DISEASES OF THE MOUTH AND TONGUE. By J. SOLIS COHEN, M.D.
DISEASES OF THE TONSILS. By J. SOLIS COHEN, M.D.
DISEASES OF THE PHARYNX. By J. SOLIS COHEN, M.D.
DISEASES OF THE OESOPHAGUS. By J. SOLIS COHEN, M.D.
FUNCTIONAL AND INFLAMMATORY DISEASES OF THE STOMACH. By SAMUEL G. ARMOR, M.D., LL.D.
SIMPLE ULCER OF THE STOMACH. By W. H. WELCH, M.D.
CANCER OF THE STOMACH. By W. H. WELCH, M.D.
HEMORRHAGE FROM THE STOMACH. By W. H. WELCH, M.D.
DILATATION OF THE STOMACH. By W. H. WELCH, M.D.
MINOR ORGANIC AFFECTIONS OF THE STOMACH (Cirrhosis; Hypertrophic Stenosis of Pylorus; Atrophy; Anomalies in the Form and the Position of the Stomach; Rupture; Gastromalacia). By W. H. WELCH, M.D.
INTESTINAL INDIGESTION. By W. W. JOHNSTON, M.D.
CONSTIPATION. By W. W. JOHNSTON, M.D.
ENTERALGIA (INTESTINAL COLIC). By W. W. JOHNSTON, M.D.
ACUTE INTESTINAL CATARRH (DUODENITIS, JEJUNITIS, ILEITIS, COLITIS, PROCTITIS). By W. W. JOHNSTON, M.D.
CHRONIC INTESTINAL CATARRH. By W. W. JOHNSTON, M.D.
CHOLERA MORBUS. By W. W. JOHNSTON, M.D.
INTESTINAL AFFECTIONS OF CHILDREN IN HOT WEATHER. By J. LEWIS SMITH, M.D.
PSEUDO-MEMBRANOUS ENTERITIS. By PHILIP S. WALES, M.D.
DYSENTERY. By JAMES T. WHITTAKER, A.M., M.D.
TYPHLITIS, PERITYPHLITIS, AND PARATYPHLITIS. By JAMES T. WHITTAKER, A.M., M.D.
INTESTINAL ULCER. By JAMES T. WHITTAKER, A.M., M.D.
HEMORRHAGE OF THE BOWELS. By JAMES T. WHITTAKER, A.M., M.D.
INTESTINAL OBSTRUCTION. By HUNTER MCGUIRE, M.D.
CANCER AND LARDACEOUS DEGENERATION OF THE INTESTINES. By I. EDMONSON ATKINSON, M.D.
DISEASES OF THE RECTUM AND ANUS. By THOMAS G. MORTON, M.D., and HENRY M. WETHERILL, JR., M.D., PH.G.
INTESTINAL WORMS. By JOSEPH LEIDY, M.D., LL.D.
DISEASES OF THE LIVER. By ROBERTS BARTHOLOW, A.M., M.D., LL.D.
DISEASES OF THE PANCREAS. By LOUIS STARR, M.D.
PERITONITIS. By ALONZO CLARK, M.D., LL.D.
DISEASES OF THE ABDOMINAL GLANDS (TABES MESENTERICA). By SAMUEL C. BUSEY, M.D.
ARMOR, SAMUEL G., M.D., LL.D.,
Brooklyn.
ATKINSON, I. EDMONDSON, M.D.,
Professor of Pathology and Clinical Medicine and Clinical Professor of Dermatology in the University of Maryland, Baltimore.
BARTHOLOW, ROBERTS, A.M., M.D., LL.D.,
Professor of Materia Medica, General Therapeutics, and Hygiene in the Jefferson Medical College, Philadelphia.
BUSEY, SAMUEL C., M.D.,
An Attending Physician and Chairman of the Board of Hospital Administration of the Children's Hospital, Washington, D.C.
CLARK, ALONZO, M.D., LL.D.,
Late Professor of Pathology and Practical Medicine in the College of Physicians and Surgeons, New York.
COHEN, J. SOLIS, M.D.,
Professor in Diseases of the Throat and Chest in the Philadelphia Polyclinic; Physician to the German Hospital, Philadelphia.
DRAPER, W. H., M.D.,
Attending Physician to the New York and Roosevelt Hospitals, New York.
HOWARD, R. PALMER, M.D.,
Professor of Theory and Practice of Medicine in McGill University, Montreal; Consulting Physician to Montreal General Hospital, Canada.
JACOBI, ABRAHAM, M.D.,
Clinical Professor of Diseases of Children in the College of Physicians and Surgeons, New York, etc.
JOHNSTON, W. W., M.D.,
Professor of Theory and Practice of Medicine in the Columbian University, Washington.
LEIDY, JOSEPH, M.D., LL.D.,
Professor of Anatomy in the University of Pennsylvania, Philadelphia.
LYNCH, JOHN S., M.D.,
Professor of Principles and Practice of Medicine in the College of Physicians and Surgeons, Baltimore.
MORTON, THOMAS G., M.D.,
Surgeon to the Pennsylvania Hospital, Philadelphia.
MCGUIRE, HUNTER, M.D.,
Richmond, Va.
SMITH, J. LEWIS, M.D.,
Clinical Professor of Diseases of Children in the Bellevue Hospital Medical College, New York.
STARR, LOUIS, M.D.,
Clinical Professor of Diseases of Children in the Hospital of the University of Pennsylvania, Philadelphia.
TYSON, JAMES, A.M., M.D.,
Professor of General Pathology and Morbid Anatomy in the University of Pennsylvania, Philadelphia.
WALES, PHILIP S., M.D.,
Washington.
WELCH, WILLIAM H., M.D.,
Professor of Pathology in Johns Hopkins University, Baltimore.
WETHERILL, HENRY M., JR., M.D.,
Assistant Physician to the Pennsylvania Hospital for the Insane, Philadelphia.
WHITE, J. WILLIAM, M.D.,
Surgeon to the Philadelphia Hospital; Assistant Surgeon to the University Hospital; Demonstrator of Surgery and Lecturer on Venereal Diseases and Operative Surgery in the University of Pennsylvania, Philadelphia.
WHITTAKER, JAMES T., M.D.,
Professor of Theory and Practice of Medicine in the Medical College of Ohio, Cincinnati.
| FIGURE | |
| 1. | POSITION OF PUNCTURES IN DIABETIC AREA OF MEDULLA OBLONGATA NECESSARY TO PRODUCE GLYCOSURIA |
| 2. | THE LAST CERVICAL AND FIRST THORACIC GANGLIA, WITH CIRCLE OF VIEUSSENS, IN THE RABBIT, LEFT SIDE |
| 3. | DIAGRAM SHOWING COURSE OF THE VASO-MOTOR NERVES OF THE LIVER, ACCORDING TO CYON AND ALADOFF |
| 4. | DIAGRAM SHOWING ANOTHER COURSE WHICH THE VASO-MOTOR NERVES OF THE LIVER MAY TAKE |
| 5. | JOHNSON'S PICRO-SACCHARIMETER |
| 6. | PEMPHIGUS BULLA FROM A NEW-BORN SYPHILITIC CHILD |
| 7. | SECTION OF RETE MUCOSUM AND PAPILLÆ FROM SAME CASE OF PEMPHIGUS AS FIG. 6 |
| 8. | SECTION OF AN OLD GUMMA OF THE LIVER |
| 9. | SYPHILITIC DACTYLITIS, FROM BUMSTEAD |
| 10. | THE SAME AS FIG. 9 |
| 11. | SERRATIONS OF NORMAL INCISOR TEETH |
| 12. | NOTCHING OF SYPHILITIC INCISOR TEETH |
| 13. | OÏDIUM ALBICANS FROM THE MOUTH IN A CASE OF THRUSH |
| 14. | CHRONIC INTUMESCENCE OF THE TONGUE (HARRIS) |
| 15. | HYPERTROPHY OF TONGUE (HARRIS), BEFORE OPERATION AND AFTER |
| 16. | GLOSSITIS (LISTON) |
| 17. | INCISION FOR A CUSPID TOOTH (WHITE) |
| 18. | INCISION FOR A MOLAR TOOTH (WHITE) |
| 19. | FUSIFORM DILATATION OF OESOPHAGUS (LUSCHKA) |
| 20. | FAUCHER'S TUBE FOR WASHING OUT THE STOMACH |
| 21. | FAUCHER'S TUBE FOR WASHING OUT THE STOMACH |
| 22. | ROSENTHAL'S METHOD OF WASHING OUT THE STOMACH |
| 23. | ANTERIOR VIEW OF A STRANGLUATED INTESTINE AND STRICTURE |
| 24. | POSTERIOR VIEW OF A STRANGULATED INTESTINE AND STRICTURE |
| 25. | APPEARANCE OF THE NATURAL RELATIONS OF THE DIVERTICULUM TO THE INTESTINE |
| 26. | SIMPLE INVAGINATION OF THE ILEUM |
| 27. | SIMPLE INVAGINATION, WITH OCCLUSION OF BOWEL, FROM INFLAMMATORY CHANGES |
| RHEUMATISM. | PURPURA. |
| GOUT. | DIABETES MELLITUS. |
| RACHITIS. | SCROFULA. |
| SCURVY. | HEREDITARY SYPHILIS. |
SYNONYMS AND DEFINITION.—Acute Rheumatism, Acute Rheumatic Polyarthritis, Rheumarthritis, Rheumatic Fever, Polyarthritis Synovialis Acuta (Heuter).
Acute articular rheumatism is a general non-contagious, febrile affection, attended with multiple inflammations, pre-eminently of the large joints and very frequently of the heart, but also of many other organs; these inflammations observing no order in their invasion, succession, or localization, but when affecting the articulations tending to be temporary, erratic, and non-suppurating; when involving the internal organs proving more abiding, and often producing suppuration in serous membranes. It is probably connected with a diathesis—the arthritic—which may be inherited or acquired. It may present such modifications of its ordinary characters as to justify being called (2d) subacute articular rheumatism, and it may sometimes pass into the (3d) chronic form.
ETIOLOGY.—There is a general consensus of opinion that acute articular rheumatism belongs especially to temperate climates, and that it is exceedingly rare in polar regions; but respecting its prevalence in the tropics contradictory statements are made. Saint-Vel declares that it is not a disease of hot climates; Rufz de Levison saw only four cases of acute articular rheumatism, and not one of chorea, in Martinique during twenty years' practice; while Pruner Bey says it is common in Egypt, and Webb remarks the same for the East Indies. Even in temperate climates, like those of the Isle of Wight, Guernsey, Cornwall, some parts of Belgium (Hirsch), the disease is very rare—a circumstance not to be satisfactorily explained at present.
Acute articular rheumatism is never absent; it occurs at all seasons of the year, although subject to moderate variations depending mainly upon atmospheric conditions. It is the general opinion that it prevails most during the cold and variable months of spring, but this is not true of every place, nor invariably of the same place. Indeed, Besnier,1 after a long and special observation of the disease in Paris, concludes that there it is most frequent in summer and in spring. In Montreal, during ten years, the largest number of cases of acute rheumatism admitted to the General Hospital obtained in the spring months (March to June [p. 20]inclusive), when they averaged 51 a month; 33 was the average for all the other months, except October and November, when 26½ was the average. The statistics of Copenhagen, Berlin, and Zurich show a minimum prevalence in summer or in summer and autumn.
1 Dictionnaire Encyclopédique des Sciences Méd., Troisième Serie, t. iv.
Occupations involving muscular fatigue or exposure to sudden and extreme changes of temperature, especially during active bodily exertion, predispose to acute articular rheumatism; hence its frequency amongst cooks, maid-servants, washerwomen, smiths, coachmen, bakers, soldiers, sailors, and laborers generally.
While no age is exempt from acute articular rheumatism, it is, par excellence, an affection of early adult life, the largest number of cases occurring between fifteen and twenty-five years of age, and the next probably between twenty-five and thirty-five. A marked decline in its frequency takes place after the age of thirty-five, and a still greater after forty-five. It is not uncommon in children between five and ten, and especially between ten and fifteen, but is very rare under five, although now and then one meets with an example of the disease in children three or four years of age. While the acute articular affections observed in sucklings are, as a general rule, either syphilitic or pyæmic, some authentic instances of rheumatic polyarthritis are recorded. Kauchfuss's two cases among 15,000 infants at the breast, Widerhofer's case, only twenty-three days old, Stager's, four weeks old, and others, are cited by Senator.2
2 Ziemssen's Cyclop. of Pract. Med., xvi. 17.
An analysis of 4908 cases of acute rheumatism admitted to St. Bartholomew's Hospital, London,3 during fifteen years, and of 456 treated in the Montreal General Hospital during ten years,4 gives the following percentages at given periods of life:
| London. | Montreal. | ||
| Under 10 years | 1.79 per cent. | ||
| From 10 to 15 years | 8.1 per cent. | Under 15 years | 4.38 per cent. |
| From 15 to 25 years | 41.8 per cent. | From 15 to 25 years | 48.68 per cent. |
| From 25 to 35 years | 24.5 per cent. | From 25 to 35 years | 25.87 per cent. |
| From 35 to 45 years | 14.2 per cent. | From 35 to 45 years | 13.6 per cent. |
| Above 45 years | 9.5 per cent. | Above 45 years | 7.4 per cent. |
The close correspondence existing in the two tables for all the periods of life above fifteen is very striking: the disparity between them below the age of fifteen may, I believe, be explained by the circumstance that the pauper population of Montreal is, when compared with that of London, relatively very small, and by the further fact that the practice of sending children into hospitals hardly obtains here.
3 St. Bartholomew's Hospital Reports, xiv. 4.
4 Dr. James Bell, in Montreal General Hospital Reports, i. 350.
No doubt the above tables do not correctly represent the liability of children to acute articular rheumatism, but they are probably a fair statement of the relative frequency of the disease in the adult hospital populations of London and Montreal. If primary attacks of the disease only were tabulated, the influence of youth would be more evident, for it is scarcely possible to find on record an authentic instance of the disease showing itself for the first time after sixty. Dr. Pye-Smith5 has done [p. 21]this in 365 cases, and the results prove the great proclivity of very young persons to acute rheumatism: Between five and ten years, 6 per cent. occurred; between eleven and twenty, 49 per cent.; from twenty-one to thirty, 32.3 per cent.; from thirty-one to forty, 9.5 per cent.; from forty-one to fifty, 2.2 per cent.; and from fifty-one to sixty-one, 1.1 per cent. The same author has also shown that secondary attacks are most common in the young; so that advancing age not only renders a first attack of the disease improbable, but lessens the risk of a recurrence of it. The influence of age upon acute rheumatism is further shown in the fact that the disease is less severe, and less apt to invade the heart, in elderly than in young persons.
5 Guy's Hospital Reports, 3d Series, xix. 317.
The general opinion that sex exercises no direct influence beyond exposing males more than females to some of the predisposing and exciting causes of acute rheumatism is perhaps true if the statement be confined to adults, to whom, indeed, most of the available statistics apply; but it should be borne in mind that a larger proportion of men than of women resort to hospitals, and there is some reason to believe that in childhood the greater liability to the disease is on the part of the female sex. Thus, the number of cases of rheumatism treated at the Children's Hospital in London from 1852 to 1868 was 478, of whom 226 were males and 252 females.6 Of Goodhardt's 44 cases of acute rheumatism in children, 26 were girls and 18 were boys.7 Of 57 examples of rheumatism in connection with chorea observed by Roger in children under fourteen, 33 were girls and 24 were boys.8
6 Vide Dr. Tuckwell's "Contributions to the Pathology of Chorea," in St. Bartholomew's Hospital Reports, v. 102.
7 Guy's Hospital Reports, 3d Series, xxv. 106.
8 Arch. Gén., vol. ii. 641, 1866, and vol. i. 54, 1867, quoted by Tuckwell.
That heredity predisposes to acute articular rheumatism is admitted by nearly all modern authorities, even Senator, while speaking of it as "a traditional belief," not venturing to deny it. The frequency of the inherited predisposition Fuller placed at 34 per cent.; Beneke, quoted by Homolle,9 at 34.6 per cent; Pye-Smith at 23 per cent.10 Such predisposition favors the occurrence of the disease in early life, but does not necessarily determine an attack of acute rheumatism in the absence of the other predisposing or exciting causes. That the inherited bias or mode of vital action or condition of tissue-health may be so great as, per se, to induce an attack of the disease, is held by some authorities. It is probable that not only acute articular rheumatism in the parents, but simple chronic articular rheumatism and those forms grouped under the epithet rheumatoid arthritis, may impart a predisposition to the acute as well as to the chronic varieties of articular disease just mentioned. But owing to the obscurity which still surrounds the relations existing between acute articular rheumatism and rheumatoid arthritis this point needs further investigation. In what the inherited predisposition to acute articular rheumatism consists we are ignorant; to say that it imparts to the tissues or organs a disposition to react or act according to a fixed morbid type, or that some of the nutritive processes are perverted by it, is merely to state a theory, not to explain the nature of the predisposition.
9 Nouv. Dict. de Méd. et de Chir., t. 31, 557.
10 Guy's Hospital Reports, 3d Series, xix. 320.
No type of bodily conformation or temperament can be described that [p. 22]certainly indicates a proclivity to acute articular rheumatism; nor is there any change in the constitution of the tissues or fluids of the body by which the proclivity may be recognized. We infer the existence of the inherited predisposition—the innate bias—when rheumatism is found in the family history; when acute rheumatism or cardiac disease, or chorea not produced by mental causes, occurs in childhood; when the first attack of acute articular rheumatism is succeeded by subsequent attacks; and especially when the intervals between the attacks are short. Goodhardt has recently furnished valuable, but not conclusive, evidence to prove that in children obstinate headaches, night-terrors, severe anæmia, various neuro-muscular derangements, such as torticollis, tetany, muscular tremors, stammering, incontinence of urine, recurring attacks of abdominal pain, with looseness of the bowels quickly succeeding a meal, the cutaneous affection erythema nodosum, are indications of a rheumatic bias or predisposition.11
11 Guy's Hospital Reports, 3d Series, xxv.
There is some basis for the opinion that residence in damp, cold dwellings predisposes somewhat to acute articular rheumatism, although not at all to the same degree that it does to the chronic articular and muscular forms. Chomel and Jaccoud especially have insisted that it will gradually create a predisposition to the disease, even if it has not been inherited. All pathologists agree that cold is the most frequent exciting cause of acute articular rheumatism, and that it is especially effective when applied while the body is perspiring freely or is overheated or fatigued by exercise. There is no necessary ratio between the degree of cold or its duration and the severity of the resulting rheumatism. A slight chilling or a momentary exposure to a current of cold air will in some act as powerfully and as certainly as a prolonged immersion in cold water or a night spent sleeping on the damp grass. This circumstance, together with the fact that cold applied in the same way may also produce a pharyngitis or a bronchitis, a pneumonia or a nephritis, etc., is held to indicate that the cold acts according to individual predisposition; and Jaccoud, Flint, and others maintain that unless a rheumatic proclivity exists cold will not produce an attack of the disease under consideration. I doubt that we are yet in a position to assert that absolutely, although the weight of argument is in its favor. Let it suffice to say, that while a prolonged residence in a cold, damp dwelling may gradually develop a predisposition to rheumatism, a short exposure to cold will be likely to induce an attack of rheumatism if the predisposition exist.
There are other influences which may be regarded as auxiliaries to cold in exciting an attack, as they seem to increase the susceptibility of the patient to its operation: they establish what has been felicitously called a state of morbid opportunity. Such are all influences that reduce the resisting powers of the organs and organism, as bodily fatigue, mental exhaustion, the depressing passions, excessive venery, prolonged lactation, losses of blood, etc. It is probably in such a manner that local injuries (traumatism) sometimes appear to induce an attack of rheumatism. A blow on a finger (Cotain), the extraction of a tooth (Homolle), a hypodermic injection (ibid.), etc., may act powerfully in some persons upon and through the nervous system, and by lessening their resisting power [p. 23]may favor the overt manifestation of the rheumatic predisposition. But doubtless some such cases have been examples of mere coincidence.
There are certain pathological and even physiological conditions during or after which an inflammatory affection of one or several joints closely resembling acute articular rheumatism more or less frequently arises. Thus, during the early desquamating stage of scarlatina a mild inflammation of the joints of the hands and feet, and frequently of the large articulations as well, is very often seen, and it is attended with profuse perspiration, with a condition of urine like that of ordinary acute rheumatism, and occasionally with inflammation of the heart or pleura. During convalescence from dysentery an affection of a single or of several articulations resembling rheumatism has been noticed, and the two affections have even alternated in the same patient. That singular epidemic disease dengue is attended with a polyarticular affection closely resembling acute articular rheumatism, occasionally pursuing a protracted course, and not seldom leaving after it a cardiac lesion. In hæmophilia polyarticular and muscular disorders frequently arise which closely resemble, and appear to be sometimes identical with, ordinary acute articular and muscular rheumatism. Gonorrhoea too is often associated with a febrile polyarthritis, and rarely with an endocarditis at the same time. In the puerperal state an inflammation of one or several articulations is not unfrequently observed (puerperal rheumatism).
Respecting the real nature of these polyarticular inflammations very much has to be made out; and it must suffice at present to say that while many of them are of a pyæmic nature, as some examples of puerperal and scarlatinal arthritis, in which pus forms in or about the joints and in the serous cavities and viscera, some of them are no doubt examples of genuine rheumatism occurring in persons of rheumatic predisposition, which have either been induced by the lowering influence of the disease upon which they have supervened, or by the accidental coincidence of some of the other causes of acute rheumatism. There remains, however, the ordinary form of scarlatinal arthritis, which so closely resembles true acute articular rheumatism in its symptoms, course, visceral complications, and morbid anatomy that it cannot be said that the two affections are distinct and different. And much the same appears to be true of the articular affection of dengue. Yet so frequently does the articular affection accompany scarlatina and dengue respectively that it cannot logically be referred to a coexisting rheumatic predisposition, and must be a consequence of the disturbing influences of the specific poison of those zymotic affections per se.
PATHOLOGY.—The pathology of acute articular rheumatism is a very much debated question, and is not at all satisfactorily known. Hence a mere statement of the most prominent theories now held by different pathologists will be given.12
12 The reader may consult with advantage Dr. Morris Longstreth's fourth chapter in his recent excellent monograph upon Rheumatism, Gout, and some Allied Disorders, New York, 1882.
The latest modification of the lactic-acid theory of Prout is founded upon the modern physiological teaching that during muscular exercise sarcolactic acid and acid phosphate of potassium are formed, and carbon dioxide set free, in the muscular tissue, and that cold, acting on [p. 24]the surface under such circumstances, may check the elimination of these substances and cause their accumulation in the system. This view, it is held, explains why the muscles and their associated organs, the joints and tendons, suffer first and chiefly, because the morbific influence is exerted upon them when exhausted by functional activity; and it further accounts for the visceral manifestations and the apparent excess of acid eliminated during the course of the disease. The circumstance that in three cases of diabetes (Foster,13 Kuelz14) the administration of lactic acid appeared to induce polyarticular rheumatism favors the idea that acid is the materies morbi in rheumatism.
13 Brit. Med, Jour., ii. 1871.
14 Beiträge zur Path. und Therapie des Diabetes, u. s. w., ii. 1875.
Now it must be admitted that, as yet, no sufficient proof is forthcoming that a considerable excess of lactic acid exists in the fluids or solids of the body or in the excretions in rheumatism (it is true the point has not been sufficiently investigated). On the other hand, that acid has been found in the urine of rickets, and its excess in the system is regarded by Heitzmann and Senator15 as the cause of the peculiar osteoplastic disturbances of that disease—an affection altogether different from rheumatism. It is quite improbable that the amount of sarcolactic acid produced by over-prolonged muscular exertion, and whose elimination has been prevented by a chill or a mental emotion, is sufficient to maintain the excessive acidity of the urine and other fluids during a long rheumatic fever; and arguments can be adduced favorable to the view that excessive formation of acid is an effect rather than the cause of rheumatism: cases of that disease occur in which neither excessive muscular exertion nor exposure to chill have preceded the rheumatic outbreak. Lastly, lactic acid is not the only principle retained when the functions of the skin are arrested by cold, the usual exciting cause of rheumatism; why should not the retained acetic, formic, butyric, and other acids, for example, play their rôle in the production of the symptoms observed under such conditions?
15 Ziemssen's Cyclop., xvi. p. 177.
The same objections apply to Latham's16 hypothesis that hyperoxidation of the muscular tissue is the starting-point of acute rheumatism. He assumes, with other physiologists, the existence of a nervous centre which inhibits the chemical changes that would take place if the tissues were out of the body. If this centre be changed or weakened, the muscle, instead of absorbing and fixing the oxygen and giving out carbonic acid, disintegrates; lactic acid is formed, and, passing into the blood, may be there oxidized and produce the pyrexia of acute rheumatism. It need hardly be remarked that the existence of a chemical inhibitory centre has yet to be proved, although much may be advanced in its favor; and, secondly, the recent investigations of Zuntz render it highly probable that in all febrile affections it is the muscles chiefly, if not solely, which suffer increased oxidation, and that this is due to increased innervation—views not easily reconciled with Latham's theory.
16 Brit. Med. Jour., ii. 1880, p. 977.
The nervous theory of rheumatism and of articular diseases originated with Dr. J. K. Mitchell of Philadelphia17 in 1831, and was afterward elaborated by Froriep in 1843,18 Scott Alison19 in 1846, Constatt in 1847,20 [p. 25]Gull in 1858, Weir Mitchell in 1864,21 Charcot in 1872, and by very many others since. According to present physiological doctrine, the exciting cause of rheumatism, cold, either acts directly upon the vaso-motor or the trophic (?) nerves of the articulations, and excites inflammation of them, or else it irritates the peripheral ends of the centripetal nerves, and through these excites actively the vaso-motor and trophic nerve-centres. The local lesions, on this hypothesis, are of trophic origin; the fever is due to hyperactivity of the centres supposed to control the chemical changes going on in the tissues; the excessive perspiration to stimulation of the sweat-centres; and so on. It is not held that a definite centric lesion of the nervous system exists in rheumatism, analogous to the lesions which in myelitis or locomotor ataxia develop the arthropathies of those affections, but rather a functional disturbance. One of the latest and ablest advocates of the neurosal theory of rheumatism in all its forms (simple, rheumatoid, gonorrhoeal, urethral, etc.), Jonathan Hutchinson, calls it "a catarrhal neurosis, the exposure of some tract of skin or mucous membrane to cold or irritation acting as the incident excitor influence."22
17 Am. Jour. Med. Sci., 1831; ib., 1833.
18 Die Rheumatische Schwiele, Weimar, 1843.
19 Lancet, 1846, i. 227.
20 Spec. Pathologie und Therapie, 1847, ii. p. 609.
21 Vide Am. Jour. Med. Sciences, April, 1875, vol. lxix. 339-348.
22 Trans. International Med. Congress, 1881, ii. 93.
In order that peripheral irritation shall thus induce inflammation of the joints and the other affections of muscles, tendons, fasciæ, etc. which are called rheumatic, he holds with the French School that the arthritic diathesis must exist, or that state of tissue-health which involves a tendency to temporary inflammation of many joints or fibrous structures at once, or to repeatedly recurrent attacks of inflammation of one joint or fibrous structure. If I understand Mr. Hutchinson correctly, he also holds that a nerve-tissue peculiarity exists which renders persons liable to rheumatism. He does not indicate either the cause or the nature of the nerve-tissue peculiarity. But modern pathology teaches that the functional conditions of the nervous centres known as neuroses, whether inherited or acquired, reveal themselves as morbid manifestations of nerve-function on the part of special portions of or the entire nervous system, and, as Dr. Dyce Duckworth has well pointed out, these neuroses may be originated, when not inherited, in various ways, as by excessive activity of the nervous system, by prolonged or habitual excesses, etc. "Thus, undue mental labor, gluttony, alcoholic intemperance, debauchery, and other indulged evil propensities in the parent come to be developed into definite neurotic taint and tendency in the offspring."
But is there nothing more in acute articular rheumatism than an inflammation of certain structures, articular and visceral, lighted up in an individual of a neuro-arthritic diathesis? What do we learn from that closely-allied affection, gout, which involves especially the same organs as rheumatism, and is held by many of the ablest pathologists to belong to the same basic diathesis as it? Duckworth23 has very ably advocated a neurotic theory of gout, but it is admitted on all hands—and by Duckworth himself—that in gout a large part of the phenomena is due to perverted relations of uric acid and sodium and to the presence of urate of soda in the blood. May we not from analogy, as well as from other evidence, infer that in that so-called other neurosis, rheumatism, a considerable part of the phenomena is due to perversions of [p. 26]the processes of assimilation and excretion, and to the presence of some unknown intermediate product of destructive metamorphosis—lactic or other acid? This is admitted by Maclagan and strongly advocated by Senator; and in this way the pathology of the disease may be said to embrace the humoral as well as the solidist doctrines—the resulting theory being a neuro-humoral one. No doubt pathological chemistry and clinical investigation will ere long make important discoveries respecting the pathology of acute rheumatism which shall maintain the close alliance believed to exist between that affection and gout.
23 Brain, April, 1880.
The miasmatic theory, so ably advocated by Maclagan,24 assumes that rheumatism is due to the entrance into the system from without of a miasm closely allied to, but quite distinct from, malaria. His argument on this topic is ingenious and elaborate, yet has not been favorably received by pathologists. Opposed to it are the following amongst other considerations: Heredity exercises a marked influence upon the occurrence of rheumatism; unlike malarial disease, no climate or locality is immune from rheumatism; the many indications that a diathesis plays a chief rôle in rheumatism; the remarkable influence exerted by cold and dampness in the etiology of the disease.
24 Rheumatism: its Nature, Path., etc., London, 1881, pp. 60-95.
Heuter's25 infective-germ theory, like the miasmatic, refers rheumatism to a principle not generated in the system, but introduced from without. A micrococcus enters the dilated orifices of the sweat-glands, and, reaching the blood, first sets up an endocarditis, and then capillary emboli produce the articular inflammations. This is a reversal of what really happens, so far as the time of invasion of the endocardium and the synovial membranes is concerned; and Fleischauer's case, in which miliary abscesses were found in the heart, lungs, and kidneys, was probably one of ulcerative endocarditis, which, after all, is a rare complication of acute articular rheumatism. Moreover, it is a gratuitous assertion to say that endocarditis exists in all cases of the disease. If, however, Heuter were content to say that acute articular rheumatism was produced by a specific germ, as held by Recklinghausen and Klebs, which on entering the system acted specially upon the joints and the fibro-serous tissues, as the poison of small-pox does upon the skin, while at the same time it sets up general disturbances of the entire economy as other zymotic poisons do, there would be nothing opposed to general pathological laws. Even the existence of a diathesis capable of favoring the action of the specific germ would be analogous to the tuberculous diathesis, which favors the action of the bacillus of tubercle; and cold, its ordinary exciting cause, might be regarded simply as a condition which renders the system more susceptible to the action of the germ, and the modus operandi of cold in doing this might be variously explained.
25 Klinik der Gelenkkrankheiten, Leipzig, 1871.
SYMPTOMS.—The disease has no uniform mode of invasion. (a) Very frequently slight disorder of health, such as debility, pallor, failure of appetite, unusual sensibility to atmospheric changes, grumbling pains in the joints or limbs, or even in some muscle or fascia, precedes by one or more days the fever and general disturbance. (b) Not infrequently a mild rigor or repeated chilliness, accompanied or soon followed by moderate or high fever, ushers in the illness, and in from a few hours to one [p. 27]or at most two days the characteristic articular symptoms ensue. (c) In very rare cases febrile disturbance, ushered in by chills, may be followed by inflammation of the endo- or pericardium or pleura before the joints become affected.
Whatever the mode of invasion, the symptoms of the established disease are well defined, and marked febrile disturbance, transient inflammation of several of the larger articulations, excessive activity of the cutaneous functions, and a great proclivity to inflammation of the endo- and pericardium constitute the stereotyped features of the disease.
As a very general rule, the temperature early in the disease promptly attains its maximum of 102° F. to 104° F., yet the surface does not feel very hot; the pulse ranges from 90 to 100 or 110, and is regular, large, and often bounding; the tongue is moist, but thickly coated with a white fur; there are marked thirst, impaired appetite, and constipation; the stools are usually dark; the urine scanty, high colored, very acid, of great density, and holding in solution an excess of uric acid and urates, which are frequently deposited when the urine cools. The general surface is covered with a profuse sour-smelling perspiration, whose natural acid reaction, as a general rule, is markedly increased; indeed, the naturally alkaline saliva is also acid. Beyond a little wandering during sleep, occasionally observed in irritable, nervous patients, there is very rarely any delirium, and this notwithstanding that sleep is frequently much disturbed by the pain in the joints and the excessive sweating.
If the local articular symptoms have not set in almost simultaneously with the pyrexia, or even preceded it, they will follow it in from a few to twenty-four or forty-eight hours. At first one or more joints, usually the knees or ankles, become painful, sensitive to pressure, hot, more or less swollen, and exhibiting a slight blush of redness or none at all. The swelling may consist of a mere puffiness, due to slight infiltration of the soft parts external to the joint, or of a more or less considerable tumefaction, caused by effusion into the synovial capsule. In the knees, elbows, shoulders, and hips the swelling is usually confined to the articulations, and there is but little redness of the integument, but in the wrists and ankles the inflammatory process is often more severe, and may invade the whole dorsum of the hand or foot, rendering the integument tense, tumid red, and shining. Pitting of the swollen parts, although quite exceptional in acute articular rheumatism, will exist under the conditions just mentioned. The metacarpo-phalangeal articulations are likewise often a good deal swollen and of a bright-red color.
The pain in the affected articulations varies from a trifling uneasiness or dull ache to excruciating anguish; sometimes the pain is felt only on moving or pressing the joint; pressure always aggravates it; even the weight of the bed-clothes may be intolerable; and in severe cases the slightest movement of the joint or a jar of the bed produces great suffering. The pain, like the swelling, sometimes extends beyond the affected joints to the tendinous sheaths, the tendons, and muscles, and even to the nerves of the neighborhood.
It is a striking peculiarity of acute rheumatism that the inflammation tends to invade fresh joints from day to day, the inflammation usually, but not invariably, declining in those first affected; and sometimes this retrocession of the inflammation in a joint is so sudden, and so coincident [p. 28]with the invasion of a different one, that it is often regarded as a true metastasis. Exceptionally, however, one or several joints remain painful and swollen, although this occurs chiefly in subacute attacks. In this way most of the large joints may successively suffer once, twice, or oftener during an attack of acute rheumatism. And as the inflammation commonly lasts in each articulation from two to four or more days, it is usual to have six or eight of the joints affected by the end of the first week. While the ankles and knees, wrists, elbows, and shoulders, are especially liable to be affected, and with a frequency pretty closely corresponding to the above order, the joints of the hands occasionally, and the hips even more frequently, escape. The intervertebral and tempero-maxillary articulations have very rarely suffered in the writer's experience.
If the ear be applied to the cardiac region in acute rheumarthritis, another local inflammation than the articular will very frequently be detected, which otherwise would probably be unrecognized, and yet it is the most important feature of the disease. In the first or second, or even as late as the fourth, week of the fever the signs of endocarditis of the mitral valve, occasionally of the aortic, and sometimes of both, will exist in an uncertain but large proportion of cases, or those of pericarditis, but in a less proportion, will obtain. Indeed, the cardiac inflammation may even precede the articular, and some believe it may be the only local evidence of rheumatic fever. As a general rule, the implication of the endo- or pericardium in acute rheumarthritis gives rise to no marked symptoms or abrupt modification of the clinical features of the case, and a careful physical examination must be instituted to discover its existence. But the recurrence of pain or tightness either in the precordial or sternal region, of marked anxiety or pallor of the face, of sudden increase in the weakness or frequency of the pulse, or of irregularity in its rhythm, of restlessness or delirium, of oppression of breathing, or of short, dry cough,—may indicate the invasion of the endo- or peri- or myocardium, and a physical examination will be needed to detect the cardiac disease and to exclude the presence of pleuritis, pneumonia, or bronchitis. Sometimes, however, especially in severe cases, an extensive pericarditis, with or without myocarditis, will produce grave constitutional disturbance, in which sleeplessness, delirium, stupor, generally associated with a very high temperature and marked prostration, will, as it were, mask both the articular and the cardiac affection.26
26 See Stanley's case, Med.-Chir. Trans., 1816, vol. vii. 323, and Andral's Clinique Médicale, t. i. 34.
As regards the murmurs which arise in acute rheumatic endo- or pericarditis, while they are usually present and quite typical, this is not always so. The only alteration of the cardiac sounds may be at first and for some time a loss of clearness and sharpness, passing into a prolongation of the sound, which usually develops into a distinct murmur, or the sounds may be simply muffled. In pericarditis limited to that portion of the membrane which covers the great vessels no friction murmur may be audible, or it may be heard and be with difficulty distinguished from an endocardial murmur. On the other hand, a systolic basic murmur not due to endo- or pericarditis frequently exists, sometimes in the early, but usually in the later, stages of rheumatic fever.
[p. 29]Other local inflammations occasionally arise in the course of acute rheumatism: pneumonia is one of the most frequent; left pleuritis is not infrequent, and is doubtless often caused by the extension of a pericarditis; but both pneumonia and pleurisy are occasionally double in rheumatic fever. Severe bronchitis is observed now and then, and very rarely peritonitis, and even meningitis. These several affections, together with delirium, coma, convulsions, chorea, and hyperpyrexia, which are likewise occasional incidents of the disease, will be considered under the head of non-articular manifestations and complications of acute articular rheumatism.27
27 See observations of W. S. Cheesman, M.D., New York Medical Record, Feb. 25, 1882, 202.
Some of the symptoms of acute articular rheumatism need individual notice.
The temperature in acute articular rheumatism maintains no typical course, and usually exhibits a series of exacerbations and remissions, which correspond closely in time and degree with the period, duration, and severity of the local inflammatory attacks. As a very general rule in average cases, the temperature attains by the end of the first or second day to 102° F., and while the subsequent evening exacerbations may reach 104°, 104.4°, or very rarely 105°, yet in the great majority of cases the maximum temperature does not exceed 103° F., and in a very considerable number falls short of 102°. An analysis of one of Dr. Southey's tables28 shows that in 84 cases of acute rheumatism 1 attained the temperature of 105.8°; 8, that of 104° to 105°; 15, that of 103° to 104°; 32, that of 102° to 103°; 17, that of 101° to 102°; 10, that of 100° to 101°; and 1, that of 99.8°; that is, the temperature was below 103° in five-sevenths, and below 104° in about ten-twelfths, of the whole. In very mild cases, in which but a few joints are inflamed, and only to a slight degree, the temperature may not reach 100° at any time, and there may be intervals of complete apyrexia. On the other hand, in a few rare severe cases of rheumatic fever, especially when complicated with pericarditis, pneumonia, or delirium, or other disturbance of the cerebral functions, the temperature attains to 106°, 108°,29 109.4°,30 110.2°,31 or even 111°,32 or 112°. Such cases are now spoken of as examples of rheumatic hyperpyrexia.
28 St. Bartholomew's Hospital Reports, xiv. p. 12.
29 Weber, Clinical Society's Trans., vol. v. p. 136.
30 Th. Simon, quoted by Senator, Ziemssen's Cyclop. of Prac. Med., xvi. p. 46.
31 Murchison and Burdon-Sanderson, two cases, Clinical Society's Trans., vol. i. pp. 32-34.
32 Ringer, Med. Times and Gaz., vol. ii., 1867, p. 378.
There is no rule about the mode of invasion of this high temperature. It may ensue gradually or suddenly, the previous range having been low, moderate, or high, steady or oscillating.
Defervescence in rheumatic fever takes place, as a very general rule, gradually—i.e. by lysis—but exceptionally it is completed in forty-eight or even twenty-four hours. An interesting observation, which will be of much prognostic value if it be confirmed hereafter, has been made by Reginald Southey,33 to the effect "that a short period of defervescence, or a sudden remission and an early remission, betokens the relapsing form of the disease, and the likelihood of frequent relapses, as well as of slow ultimate recovery, in the direct ratio as this defervescence has been early and abrupt."
33 St. Bartholomew's Hospital Reports, xiv. p. 16.
[p. 30]The characters of the urine in acute rheumatism are tolerably uniform, but far from constantly so. Its quantity in the majority of cases is reduced, frequently not exceeding twenty-four ounces per diem, and occasionally not exceeding fourteen. This is owing in some degree to profuse sweating, but also, as in other febrile affections, to retention of water. Its density is usually high—1020 to 1030, or even 1035—which is due chiefly to its concentration, and not, as has been generally supposed, mainly to an increase in the total solids excreted.34 Its color is a very dark red or deep reddish-yellow, partly from concentration; but it is yet not known whether the deep hue is partly from increase of the normal pigments or of one of them (urobilin),35 or from the presence of some abnormal coloring matter. Its reaction is generally highly acid, and continues so for many hours after its discharge, unless in subacute cases, when it is occasionally neutral or sometimes alkaline at the time of its escape, or becomes so in a very short time afterward. It is commonly toward the decline of the attack that the urine becomes neutral or alkaline. As a very general rule, the amount of urea and of uric acid excreted during the febrile stage exceeds what is physiological, and begins to decline when convalescence commences; but this may be reversed (Parkes,36 Lede,37 Marrot38). The sulphuric acid is notably increased (Parkes), the chlorides often diminished and sometimes absent, and the phosphoric acid very variable (Beneke, Brattler39), but usually lessened (Marrot).
34 See Guy's Hospital Reports, 3d Series, vol. xii. 441.
35 Jaffe, Virchow's Archiv, xlvii. 405, quoted in Ziemssen's Cyclopæd. Prac. Med., xvi. 41.
36 On Urine, p. 286.
37 Recherches sur l'Urine dans le Rheumatisme Artic. Aigue, Paris, 1879.
38 Contribution à l'Étude du Rheumatisme Artic., etc., Paris, 1879, 41.
39 Quoted by Parkes, op. cit., 290.
During convalescence the urine increases in quantity, while, as a general rule, the urea and uric acid lessen relatively and absolutely, and the chlorides resume their normal proportions to the other ingredients. The reaction frequently becomes alkaline, and the specific gravity falls considerably, although not always as soon as the articular inflammation subsides. Temporary albuminuria occurs very frequently in the febrile and occasionally in the declining stage, but generally disappears when convalescence is completed. It obtained on admission in 8 out of 43 cases lately reported by Dr. Greenhow.40 A more abiding albuminuria, due very rarely to acute parenchymatous nephritis, may be met with (Johnson, Bartels, Hartmann, Corm). Blood, even in considerable amounts, has also rarely appeared in the urine,41 sometimes in connection with embolic nephritis and endocarditis, for such appear to have been the nature of Rayer's nephrite rheumatismale.42
40 Lancet, 1882, i. 913.
41 Clinical Lectures, R. B. Todd, edited by Beale, 1861, p. 346.
42 Traité des Maladies Reins. See also Dr. Weber, Path. Trans. of London, xvi. p. 166.
The saliva, which is normally alkaline, has usually a decidedly acid reaction in acute articular rheumatism, and Dr. Bedford Fenwick states that it always in this disease contains a great excess of the sulpho-cyanides, and that these slowly and steadily diminish, till at the end of the third week or so they become normal in amount.
A profuse, very acid, sour-smelling perspiration is one of the striking symptoms occurring in the course of acute articular rheumatism, and [p. 31]until very lately it has been generally held to indicate an excessive formation in, and elimination of acid from, the system, either lactic acid or some of the acids normal to the perspiration, as acetic, butyric, and formic. However, not only have chemists failed to detect lactic acid in the perspiration of acute rheumatism, but late research tends to show that the excessive acidity of the perspiration in this disease is but very partially due to the perspiration itself, and is chiefly owing to chemical changes taking place in the overheated and macerated surface of the skin and its epidermis, and to the retention of solid products accumulated on that surface. Besnier says that if in acute articular rheumatism or other disease attended with much perspiration the surface be kept well washed, the sweat will be found in the greater number of cases at the moment of its secretion to be nearly neutral as soon as actual diaphoresis occurs, more decidedly acid when the perspiration is less abundant or begins to flow, and exceptionally alkaline. Most physicians are aware that the profuse perspiration of acute rheumatism is non-alleviating; it is not a real critical discharge of noxious materials from the system, nor is it followed by prompt reduction of the temperature and other symptoms. It is but a symptom of the disease, and occurs especially in severe cases, and when it continues long after the reduction of the temperature it is a source of exhaustion, and may be checked with advantage.
The blood is deficient in red globules, Malassez finding in men from 2,850,000 to 3,700,000 per cubic millimeter instead of 4,500,000 to 5,000,000, and in women 2,300,000 to 2,570,000 instead of 3,500,000 to 4,000,000. The hæmoglobin and the oxidizing power of the blood are also considerably reduced; the fibrin is largely increased (6 to 10 parts in 1000 instead of 3); the albumen and albuminates are lessened, the extractives increased; the proportion of urea is normal, and no excess of uric acid is found in the blood. Instead of that fluid being less alkaline than normal, Lepine and Conard have recently stated that its alkalinity is increased in acute rheumatism, but constantly diminished in chronic rheumatism,43 and no excess of lactic acid has been proved to exist in the blood in either acute or chronic rheumatism. A condition of excessive coagulability of the fibrin, independently of its excessive amount (inopexia), is an habitual character of acute rheumatism; however, in very bad cases, especially those attended with hyperpyrexia and grave cerebral symptoms, the blood after death has been black and coagulated and the fluid in the serous cavities has given an acid reaction. The above alterations in the blood usually are proportionate to the intensity of the fever and the number of the joints and viscera involved.
43 Lepine, "Note sur la determination de l'Alcalinité du Sang," Gaz. Méd. de Paris, 1878, 149; Conard, Essai sur l'Alcalinité du Sang dans l'État de Sante, etc., Thèse, Paris, 1878.
The manifestations of acute articular rheumatism other than the articular are various, and some of them, more especially those observed in the heart, may be regarded as integral elements of the disease, for they occur in a large proportion of the cases, often coincidentally with the articular affection, and may even precede it, and probably may be the sole local manifestation of acute rheumatism, although under the last-mentioned circumstances it is difficult to prove the rheumatic nature of the ailment.
The cardiac affections may be divided into inflammatory and [p. 32] non-inflammatory. The former consist of pericarditis, endocarditis, and myocarditis; the latter embrace deposition of fibrin on the valves, temporary incompetence of the mitral or tricuspid valves, and the formation of thrombi in the cavities of the heart. For practical purposes hæmic murmurs may be included in the latter group.
No reliable conclusions can be drawn respecting the gross frequency of recent cardiac affections in rheumatic fever, for not only do authors differ widely on this point, but they do not all distinguish recent from old disease, nor inflammatory from non-inflammatory affections, nor hæmic from organic murmurs. Nor does it appear probable, from the published statistics, that these differences are owing to peculiarities of country or race. The gross proportion of heart disease of recent origin in acute and subacute articular rheumatism was in Fuller's44 cases 34.3 per cent.; in Peacock's,45 32.7 per cent.; in Sibson's46 (omitting his threatened or probable cases), 52.3 per cent.;47 in 3552 St. Bartholomew's Hospital cases analyzed by Southey,48 29.8 per cent.; in Bouilland's cases, quoted by Fuller,49 5.7 per cent.; in Lebert's,50 23.6 per cent.; in Vogel's,50 50 per cent.; in Wunderlich's,50 26.3 per cent. I am not aware of any analysis, published in this country, of a large number of cases of rheumatism with reference to cardiac complications, but Dr. Austin Flint,51 after quoting Sibson's percentage of cases of pericarditis, which was (63 in 326 or) 19 to the 100, remarks, "I am sure that this proportion is considerably higher than in my experience."
44 On Rheumatism, Rheumatic Gout, etc., 3d ed., p. 280.
45 St. Thomas's Hospital Reports, vol. x. p. 19.
46 Reynolds's Syst. of Med., Eng. ed., vol. iv. 186.
47 Those familiar with the accuracy and diagnostic skill of the lamented Sibson will not hesitate to add his 13 cases of very probable endocarditis to his 170 positive cases of cardiac inflammation in 325 examples of acute rheumatism, which will raise his percentage to 56.3.
48 Lib. cit., vol. xiv. 6.
49 Lib. cit., 264.
50 See Senator in Ziemssen's Cyclopæd. Pract. of Med., xvi. 49.
51 Pract. Med., 5th ed., 314.
The frequency of cardiac complications in rheumatism is influenced by several circumstances. Some unexplained influence, such as is implied in the terms epidemic and endemic constitution, appears to obtain. Peacock found the proportion of cardiac complications in rheumatism to range from 16 to 40 per cent. during the five years from 1872 to 1876, and a similar variability is shown in Southey's statistical table52 covering the eleven years from 1867 to 1877. Be it observed that these variations occurred in the same hospitals and under, it may be presumed, very similar conditions of hygiene and therapeusis. Youth predisposes to rheumatic inflammation of the heart, so that it may still be said that the younger the patient the greater the proclivity. Of Fuller's cases, 58 per cent. were under twenty-one, and the liability diminished very markedly after thirty. Of Sibson's cases, 62 per cent. were under twenty-one. In infancy and early childhood the liability is very great, and at those periods of life the heart, and more especially the endocardium, rarely escapes; and the cardiac inflammation often precedes by one or two days the articular. The careful observations of Sibson confirm the spirit, but not the letter, of Bouilland's original statement, and proves that the danger of heart disease is greater in severe than in mild cases of acute rheumatism, and that this is especially true of pericarditis. (It may be remarked here, en parenthese, that the number of joints affected is [p. 33]very generally in proportion to the severity of the attacks.) However, the mildest case of subacute rheumatism is not immune from cardiac inflammation, and it has occasionally been observed even in primary chronic rheumatism.53 Occupations involving hard bodily labor or fatigue, whether in indoor or outdoor service, render the heart very obnoxious to rheumatic inflammation. Existing valvular disease, the result of a previous attack of rheumatism, favors the occurrence of endocarditis in that disease. Some authorities maintain that treatment modifies the liability to rheumatic affection of the heart, and this will be spoken of hereafter. The period of the rheumatic fever at which cardiac inflammation sets in varies very much, but it may be confidently stated that it occurs most frequently in the first and second weeks, not infrequently in the third week, seldom in the fourth, and very exceptionally after that, although it has happened in the seventh. An analysis of Fuller's experience54 in 22 cases of rheumatic fever and 56 of endocarditis—a total of 78—shows that the disease declared itself under the sixth day in 8; from the sixth to the tenth in 29; from the tenth to the fifteenth in 17; from the fifteenth to the twenty-fifth in 18; and after the twenty-fifth in 6. The friction sound was audible in Sibson's 63 cases of rheumatic pericarditis—from the third to the sixth day in 10, and before the eleventh day in 30, or nearly one-half of the whole. That observer concludes "that in a certain small proportion of the cases, amounting to one-eighth of the whole," the cardiac inflammation took place at the very commencement of the disease, and simultaneously with the invasion of the joints.55
52 Lib. cit.
53 Raynaud, Nouveau Dict. de Méd. et de Chir., t. viii. 367.
54 Lib. cit., pp. 77-278.
55 Lib. cit., p. 209. See also Dickinson in Lancet, i., 1869, 254; Bauer in Ziemssen's Cyclopæd., vi. 557.
Of the several forms of rheumatic cardiac inflammation, endocarditis is the most frequent, and in a large proportion of cases it may exist alone; pericarditis is also very often observed, but it seldom is found per se, being in the vast majority of cases combined with endo- and occasionally with myocarditis. It is generally the ordinary verrucose endocarditis that obtains. The ulcerative form occurs sometimes, and should be suspected if in a mild or protracted case of acute rheumatism endocarditis sets in with, or is accompanied by, rigors, and the general symptoms are of pyæmic or typhoid character or both, even although an endocardial murmur is not present, for extensive vegetating ulcerative endocarditis frequently exists without audible murmur. It is remarkable, as Osler has shown,56 how few instances of ulcerative endocarditis developing during the course of acute rheumatism are reported; and I would add that by no means all of these were examples of first attacks, chronic valvular lesions, the consequence of former illness, existing in many of them at the time of the final acute attack. Southey's57 patient, and both of Bristowe's,58 had had previous rheumatic seizures. However, Peabody's case,59 one of Ross's three cases,60 and Pollock's61 case appear to have been examples of ulcerative [p. 34]endocarditis occurring during a first attack of acute articular rheumatism. The united and thickened condition of two segments of the aortic valve in one of Ross's cases indicates old-standing disease, although no history of former rheumatism is given. Goodhardt62 has lately insisted upon the tendency of ulcerative endocarditis to appear in groups or epidemics, but the evidence is not conclusive.
56 Archives Médecine, vol. v., 1881; Trans. International Med. Cong., vol. i. 341.
57 Clin. Soc. Trans., xiii. 227.
58 Brit. Med. Jour., i., 1880, 798.
59 Medical Record N.Y., 24th Sept., 1881, 361.
60 Canada Med. and Surg. Journ., vol. xi., 1882, 1, and ib., vol. ix., 1881, 673.
61 Lancet, ii., 1882, 976.
62 Trans. Path. Soc. London, xxxiii. 52.
Space will not permit any detailed description of the symptoms and signs of endo- or pericarditis: these will be found in their proper places in this work, but a few observations are needed upon myocarditis, which occasionally occurs in combination with rheumatic pericarditis, and is a source of much more danger than the latter is, per se. Dr. Maclagan63 is almost the only authority who recognizes the occurrence of rheumatic myocarditis independently of inflammation of the membranes of the heart. He maintains that the rheumatic poison probably and not infrequently acts directly on the cardiac muscle; in which case the resulting inflammation is apt to be diffused over the left ventricle and to produce grave symptoms, while in other instances the inflammatory process begins in the fibrous rings which surround the orifices of the heart (especially the mitral), extends to the substance at the base of the heart, and is there localized. As in this latter form the inflammation usually extends also to the valves, "any symptoms to which the myocarditis gives rise are lost in the more obvious indications of the valvulitis." However, this limited inflammation of the myocardium is not dangerous. Dr. Maclagan asserts that the more diffused and dangerous inflammation of the walls of the left ventricle, while always difficult, and sometimes impossible, of diagnosis, can be determined with tolerable certainty in some cases. In this view, however, he has been preceded by Dr. Hayden,64 who states that the diagnosis of myocarditis is quite practicable irrespective of the accompanying inflammation of the membranes of the heart.
63 Rheumatism: its Nature, Pathology, and Successful Treatment, 1881.
64 Diseases of the Heart and Aorta, 1875, 746.
From the observations of the author just named, as well as of many others, it may be inferred that acute diffused myocarditis of the left ventricle exists in rheumatic fever when either with or without coexisting pericarditis there are marked smallness, weakness, and frequency of pulse, anguish or pain or great oppression at the præcordia, severe dyspnoea, the respiration being gasping and suspirious, feeble, rapid, and irregular action of the heart, great weakness of the cardiac sounds, and almost extinction of the impulse, evidence of deficient aëration of the blood combined with coldness of surface, tendency to deliquium, and when these symptoms and signs cannot be fairly attributed to extensive pericardial effusion or to pulmonary disease, or to obstructed circulation in the heart consequent upon endocarditis with intra-cardiac thrombosis or upon rupture of a valve. It might, however, be impossible to exclude endocarditis complicated with thrombosis, conditions which do occur in rheumatic endocarditis, or a ruptured valve, which, although rarely, has been occasionally observed. Grave cerebral symptoms, delirium, convulsions, coma, though frequently present, are not peculiar to acute myocarditis.65 [p. 35]Hence, even with the above group of clinical facts, the diagnosis at best can be but probable. The disease, too, may be latent, or, like Stanley's66 celebrated case, produce disturbances of the cerebral system rather than of the circulatory.
65 In illustration see case by Southey in which the symptoms and signs agree very well with the above description, and yet, although the heart's substance was of dirty-brown color and the striation of its fibre lost, Southey did not believe these appearances due to carditis. (Clin. Trans., xiii. p. 29.)
66 Med.-Chir. Trans., vol. vii.
Dr. Maclagan has advanced the opinion that a subacute myocarditis is not of uncommon occurrence in acute articular rheumatism, and may be unattended by endo- or pericarditis. Such a condition, he says, may be diagnosed when early in the course of the case the heart's sounds quickly become muffled rather than feeble. As he quotes but one case67 in which an autopsy revealed alterations in the walls of the heart, and as endocarditis and a little effusion in the pericardium coexisted, it is premature to accept the evidence as final, and the great importance of the subject demands further investigation.
67 Lib. cit., p. 175.
Admitting with Fuller the occasional deposition of fibrin upon the valves and endocardium in rheumatic fever independently of endocarditis, the murmur resulting therefrom could not be reliably distinguished from that of inflammatory origin. It remains to speak briefly of temporary incompetence of the mitral and tricuspid valves and their dynamic murmurs, and of hæmic murmurs. Occasionally, in severe cases of rheumatic fever, more especially in the advanced stage, there may be heard a systolic murmur of maximum intensity either in the mitral area or over the body of the left ventricle, unaccompanied by accentuation of the second sound, or, as a general rule, by evidence of pulmonary obstruction. Such murmurs are apt to be intermittent, and as they disappear on the return of health, they have been satisfactorily referred to temporary weakness of the walls of the heart, so that the auriculo-ventricular orifices are not sufficiently contracted during the ventricular systole for their valves to close them, and regurgitation follows. Yet, inasmuch as Stokes distinctly mentions the absence of murmur in many cases of softening of the heart in typhus, it is probable that an excessive weakness of the ventricular wall is incompatible with the production of murmur, and that the presence of murmur in such circumstances is evidence of some remaining power in the heart.
Dr. D. West68 has published some cases of acute dilatation of the heart in rheumatic fever which strongly corroborate these views. The murmur in one of them became appreciable only as the heart's sounds increased in loudness and the dilatation lessened. One ended fatally, and acute fatty degeneration of the heart's fibres was found in patches.69 I believe that some of these temporary mitral murmurs in acute rheumatism depend upon a moderate degree of valvulitis quite capable of complete resolution. Sibson70 has lately stated that he has met with the murmur of tricuspid regurgitation without a mitral murmur in 13 out of 107 cases of rheumatic endocarditis, and with a recent mitral murmur in 27 out of 50 [p. 36]cases. "The tricuspid murmur generally comes into play about the tenth or twelfth day of the primary attack, along with symptoms of great general illness;" it appears earlier, as a rule, in those cases in which it is associated with mitral regurgitation than when it exists alone; it is of variable duration, but usually short—from one to nineteen days or more. He regards it as of non-inflammatory origin, and dependent upon regurgitation due to the so-called safety-valve function of the tricuspid valve; and when limited to the region of the right ventricle he infers that it is usually the effect and the evidence of endocarditis affecting the left side of the heart. These novel statements are confirmed by the observations of Parrot, Balfour, and William Russell,71 which go to prove that tricuspid regurgitation occurs frequently in the more advanced stages of debility. No other authority than Sibson, however, insists upon its frequent occurrence in acute rheumatism.
68 Barth. Hosp. Repts., xiv. 228.
69 On this subject see Stokes, Dis. Heart and Aorta, pp. 423, 435, 502; Stark, Archives générales de Méd., 1866; DaCosta, American Journal Med. Sci., July, 1869; Hayden, Dis. Heart and Aorta, 1875; Balfour, Clin. Lects. on Heart and Aorta, 1876; Cuming, Dublin Quart. Jour. Med. Sci., May, 1869; Nixon, ib., June, 1873. I. A. Fothergill has seen several cases in which such mitral murmurs have followed sustained effort in boys, and have disappeared after a time: The Heart and its Diseases, 2d ed., 1879, p. 177.
70 Reynolds's System. Med., Eng. ed., vol. iv. 463.
71 See Brit. Med. Jour., i. 1883, 1053.
The anæmia which is so striking a symptom of rheumatic fever, especially when several joints are severely inflamed, coexists very frequently with a systolic basic murmur, which is most often louder over the pulmonary artery (in second left intercostal space and more or less to left of sternum) than over the aorta. The murmur may appear early in the disease, but sets in most frequently when the disease is subsiding. When thus appearing late in a case accompanied by endocarditis and pulmonary congestion, it is of favorable omen and indicates improvement in the thoracic affection. The growing opinion, however, respecting so-called anæmic murmurs is, that they depend chiefly upon regurgitation through the tricuspid orifice, although Dr. W. Russell refers them to pressure of a distended left auricle upon the pulmonary artery.72
72 Ib., 1065.
Pulmonary affections in form of pleuritis, pneumonia, or bronchitis are common complications of rheumatic fever. Adding Latham's,73 Fuller's,74 Southey's,75 Gull and Sutton's,76 Pye-Smith's,77 and Peacock's78 cases together, we have a total of 920 in which some one or more of the above pulmonary affections obtained in 109 instances, or 11.8 per centum. A further analysis of Latham's and Fuller's cases shows that it is especially when rheumatic fever is complicated with cardiac disease that the lungs suffer; thus, pulmonary affections obtained in 26.5 per cent. of cases complicated with heart disease, and in only 7 per cent. of cases free from that disease. It is more especially when pericarditis complicates rheumatic polyarthritis that pulmonary affections occur. Thus, these were found in only 10.5 per cent. of cases of recent rheumatic endocarditis, in 58 per cent. of cases of pericarditis, and in 71 per cent. of cases of endo-pericarditis. The tendency which inflammation of the pericardium has to extend to the pleura probably partially accounts for the more frequent association of the pulmonary affections with rheumatic peri- than with rheumatic endocarditis. (Sibson found pleuritic pain in the side twice as frequent in pericarditis, usually accompanied with endocarditis (31 in 63), as in simple endocarditis, 26 in 108.79) But the greater severity of those cases of rheumatic fever complicated with peri- or endo-pericarditis must also have a decided influence in developing the pulmonary affections. [p. 37]Pneumonia and pleuritis are very frequently double in rheumatic fever, and are often latent, requiring a careful physical examination for their detection. So suddenly does the exudation take place in some cases of rheumatic pneumonia that the first stage is not to be detected either by symptoms or signs. On the other hand, in some cases the absence of the typical signs of hepatization, the want of persistence in the physical signs, and their rapid removal, and even in rare instances an obvious alternation between the pulmonary and the articular symptoms, suggest that the process often stops short of true hepatization, and partakes rather of congestion and splenization, with or without pulmonary apoplexy—a view which has been occasionally confirmed by the autopsy.80
73 Latham's Works, Syd. Soc., i. 98 et seq.
74 Lib. cit., 317.
75 Bartholomew Hospital Reports, xv. 14.
76 Guy's Hosp. Reports, 3d Series, xi. 434.
77 Ib. xix. 324.
78 St. Thomas's Hospital Reports, x. 12-17.
79 Reynolds's System Med., iv. 233.
80 Vide Sturges, Natural History and Relations of Pneumonia, 1876, pp. 70-78; T. Vasquez, Thèse, Des complications Pleuro-pulmonaires du Rheumatisme Artic. Aigue, Paris, 1878, pp. 25-31; M. Duveau, Dictionnaire de Méd. et de Chir., t. xxviii. p. 443.
Active general congestion of the lungs has occasionally been observed in this disease, and has proved fatal in five minutes81 and in an hour and a half82 from the invasion of the symptoms. The rheumatic poison frequently excites pleuritis, some of the characters of which are—the suddenness with which free effusion occurs; the promptness with which it is removed, only perhaps to invade the other pleura, and then to reappear in the cavity first affected; the diffusion of the pain over the side and its persistence during the effusion; and its frequent concurrence with pericarditis, and in children with endocarditis; its little tendency to become chronic, and its marked proclivity to become double. It is often latent and unattended with pain. Sibson asserts that if in rheumatic pericarditis "pain over the heart is increased or excited by pressure over the region of the organ, it may with an approach to certainty be attributed to inflammation of the pleura," etc. The product of the inflammation is commonly serous, but occasionally purulent.
81 Thèse d'Aigue pleur., 1866, par B. Ball.
82 M. Aran, quoted by Vasquez, lib. cit., p. 14.
The disturbances of the nervous system are amongst the most important complications of acute rheumatism, and are due either to functional disorder or very rarely to obvious organic lesions of the nerve-centres or their membranes. The dominant functional disturbance may be delirium, which is greatly the most frequent; or coma, which is rare; or chorea, very frequently observed in children; or tetaniform convulsions, which occur very seldom per se. As a rule, two or more of these forms coexist or alternate with or succeed one another, and the grouping, as well as the variety, of the symptoms may be greatly diversified. In 127 observations there were 37 of delirium only, 7 of convulsions, 17 of coma and convulsions, 54 of delirium, convulsions, and coma, 3 of other varieties (Ollivier et R., cited by Besnier).
Rheumatic Delirium.—Either with or without subsidence of the articular inflammation, about from the eighth to the fourteenth day of the illness, but occasionally at its beginning, or sometimes on the eve of apparent convalescence, the patient becomes restless, irritable, excited, and talkative; sleep is wanting or disturbed; some excessive discharge from the bowels or kidneys occasionally occurs; profuse perspiration is usually present, and may continue, but frequently lessens or altogether ceases; the skin becomes pungently hot, the temperature generally—not always, however—rising rapidly toward a hyperpyrexial point, and ranging from [p. 38]104° to 111°; and transient severe headache and disturbances of special sense sometimes obtain. At a later period, or from the outset in hyperacute cases, flightiness of manner or incoherence in ideas is quickly succeeded either by a low muttering delirium, twitchings of the muscles, violent tetaniform movements and general tremors, and a condition perhaps of coma-vigil, or by an active, noisy, even furious, delirium. The articular pains are no longer complained of, and sometimes the local signs of arthritis also quickly disappear; but neither statement is uniformly true. The pulse becomes rapid; prostration extreme; semi-consciousness or marked stupor gradually or rapidly supervenes; the temperature continues to rise; the face, previously pale or flushed, becomes cyanotic; and very frequently death ensues, either by gradual asthenia or rapid collapse, often preceded by profound coma or rarely by convulsions. Deep sleep often precedes prompt recovery.
The duration of the nervous symptoms varies from one or two, or more usually six or seven, hours in very severe cases, to three or four days in moderate ones, or occasionally seven, eight, or sixteen83 or twenty-nine days84 in unusually protracted cases. In the last-mentioned, however, the delirium is not usually constant, and frequently disappears as the temperature falls, and recurs when its rises. Moreover, a rapid and extreme elevation of temperature is frequently altogether wanting.
83 Southey's case, Clin. Soc. Trans., xiii. p. 25. Sleeplessness preceded it for four days, and there was no hyperpyrexia.
84 Graham's case, ib., vi. p. 7. Delirium set in on the seventh day of illness, and three days after invasion of joints. Temperature 104.8° early in disease; never exceeded 106°, probably owing to repeated use of cold baths. Temperature at death, 104.2°.
No real distinction can be established between these protracted cases of rheumatic delirium and so-called rheumatic insanity, in which occur prolonged melancholia, with stupor, mania, hallucinations, illusions, etc., often associated with choreiform attacks. This variety may be of short duration or continue until convalescence is established, or may rarely persist after complete recovery from the articular affection.
Coma may occur in acute rheumatism without having been preceded or followed by delirium or convulsions, although it is very rare; and, like delirium, it may obtain without as well as with peri- or endocarditis or hyperpyrexia. It usually proves very rapidly fatal. In Priestly's case, an anæmic woman of twenty-seven, during a mild attack of acute rheumatism, one night became restless; at 3 A.M. the pain suddenly left the joints; apparent sleep proved to be profound coma, and at 6 A.M. she was in articulo mortis.85 Southey relates the history of a girl of twenty who, without previous delirium or high temperature, suddenly became unconscious, and died in half an hour.86 One of Wilson Fox's cases had become completely comatose, and was apparently dying nine hours after the temperature had rapidly risen to 109.1°, when she was restored to consciousness by a cold bath and ice to her chest and spine.87
85 Lancet, ii., 1870, 467.
86 Clin. Soc. Trans., xiii. p. 29.
87 The Treatment of Hyperpyrexia, 1871, 4.
Convulsions of epileptiform, choreiform, or tetaniform character frequently succeed the delirium, but in exceptional cases they occur independently of it, and may even prove fatal.
Besides the choreiform disturbances which occur in connection with delirium, stupor, tremor, etc. in cerebral rheumatism, simple chorea is [p. 39]frequently observed as a complication or a sequence, or even as an antecedent, of acute articular rheumatism, and they occasionally alternate in the same patient and in the same family. Chorea is perhaps most frequently seen in mild cases and in the declining and convalescent stages of rheumatic fever, and, while very common in childhood and adolescence (five to twenty), it is very rare later in life.
Such are the chief functional disturbances of the brain met with in rheumatic fever, and the post-mortem examination reveals in them either quite normal naked-eye appearances, or more frequently, especially in rapidly fatal cases, general congestion of the pia mater, and to a less degree of the cerebral substance, or in more protracted cases a greater or less increase of transparent or opalescent serum in the subarachnoid space and ventricles. The serum may be slightly or deeply tinged with blood. If the serous or sero-sanguinolent effusion be considerable, the encephalic mass or portions of it may be anæmic. But besides these conditions, which are also commonly observed in many other febrile diseases, and which are probably only concomitants of the functional disturbance arising in the advanced stage of acute articular rheumatism, certain organic affections of the nervous centres or their membranes occasionally occur in this disease, and are plainly the cause of the cerebral disturbance observed during life. Cerebral meningitis, although very rare as a complication of acute articular rheumatism, except in certain hot climates, like that of Turkey,88 does occur, and lymph or pus is found, usually over the convexity of the brain, but sometimes at the base and down the cord.89 The symptoms of rheumatic cerebral meningitis are very like those of rheumatic delirium; vomiting, and even, but less frequently, pain in the head, may be absent, while hyperpyrexia may coexist (Foster's case), although not necessarily present. Should the pulse from being frequent become slow and irregular, and any paralytic symptoms ensue, meningitis may be suspected. In some of these cases the meningitis is a consequence of ulcerative endocarditis and embolism of the cerebral vessels,90 but in others it obtains without endocarditis or any purulent formation elsewhere than in the meninges, as there is probably a true rheumatic localization like pericarditis. The articular inflammation may continue after the invasion of the meningitis, or the latter may promptly follow the disappearance of the former, as though a metastasis of morbid action had taken place.91 In many instances, according to Ollivier, Ranvier, Behier, and others, although the macroscopic signs of meningitis are absent, the microscope detects proof of its presence in the existence of an increased number of vessels, fatty granulations on their walls, proliferation of nuclei and capillary extravasations—histological conditions identical with those found in the mild degrees of rheumatic inflammation of the joints.
88 Senator, in Ziemssen, xvi. 50.
89 Watson's Prac. Physic, 1872, Am. ed. vii. 335; Fyfe, Med. Gazette, vol. xxix. 703; Fuller, lib. cit., 302; Leudet, Clin. Médicale, 139; Dowse, London Lancet, ii. 1872, 9; Foster, ib., ii. 1868, 115; Hicks, New York Medical Record, Nov., 1878, 404.
90 That ulcerative endocarditis frequently produces meningitis is illustrated by Osler's cases, 4 out of 7 of which were complicated with purulent meningitis: Transactions of International Med. Congress, 1881, i. 344.
91 See a case reported by W. L. Ramsey in New York Medical Record, i., 1881, p. 9.
Embolism of the cerebral arteries, producing meningitis, or more frequently softening of the cerebral substance or hemorrhage, or proving [p. 40]fatal before necrobiosis has time to set in, is an occasional complication of acute articular rheumatism. A young lady, while under my care suffering from her first attack of articular rheumatism complicated with endocarditis, became suddenly hemiplegic and aphasic, and died twelve hours later. In a girl of thirteen, the subject of acute articular rheumatism complicated with ulcerative endocarditis, right hemiplegia suddenly occurred, and at the autopsy Bristowe found an embolon in the left middle cerebral artery and a softened area in the left corpus striatum. Bradbury reports a primary acute rheumatism with endocarditis, delirium, and coma, but without paralysis, in which a plug was found in the right middle cerebral artery, but the brain was quite healthy.92
92 Lancet, ii., 1870, 148; also a case in Lancet, i., 1882, p. 605: in eighth week of subacute articular rheumatism; embolism; right hemiplegia. Autopsy: large vegetations on valves; obstruction in middle cerebral artery.
Very much the same observations are applicable to the disturbances of the spinal cord and its envelopes in rheumatic fever as have been made in reference to those of the cerebrum and its coverings. They may exist with or without any alteration of the cord or membranes to which they can be reliably referred; that is to say, they may be simply functional in the peculiar sense in which that word is now understood, or they may be connected with obvious structural changes, and chiefly with those indicating inflammation of the membranes or substance of the cord. The spinal symptoms may precede the articular affection, but generally appear after it. They sometimes closely resemble those of idiopathic tetanus,93 or of spinal meningitis, or of myelitis, or of meningo-myelitis; and in the last case, along with severe rachialgia, muscular rigidity, cutaneous and muscular hyperæsthesia, and neuralgic pains, there will occur numbness and more or less paralysis of the lower extremities,94 bladder, and rectum (paraplegia). These spinal disturbances may or may not be accompanied by hyperpyrexia, and when simply functional they are usually less severe and persistent, have a greater tendency to alternate with one another and with the articular affection, and are more amenable to treatment, than when due to those very rare complications of rheumatic fever, spinal meningitis or meningo-myelitis. The inflammation may involve both the cerebral and spinal membranes at the same time.
93 Bright's case, 2, Med.-Chirurgical Transactions, xxii. 4; Dr. E. C. Mann, N.Y. Medical Record, 1875, 38; Bouilland, Traité sur les Maladies du Coeur, t. i. p. 33.
94 Leudet, lib. cit., p. 139; Dowse, Lancet, i., 1872, 9.
The causes of these disturbances of the nervous system, when not attributable to appreciable lesions, such as congestion, inflammation, hemorrhage, embolism, thrombosis, and softening, are not established. The following appear to be reasonable conclusions from the facts at present known:
The most constant condition, and without which these cerebral symptoms very rarely arise, appears to be some susceptibility or vulnerability of the nervous system, inherited or acquired, rendering it apt to be disturbed by influences which less susceptible centres would successfully resist. Trousseau, who has especially advocated this view,95 considered intemperance in the use of spirits to be a frequent source of this nervous predisposition. Accepting this neurotic predisposition as the factor generally present when acute articular rheumatism is complicated [p. 41]with disturbances of the nerve-centres, we may inquire what are the circumstances in the disease capable of developing into activity the predisposition.
95 Clin.-Med., Syd. ed., i. 513 et seq.
Unquestionably, the existence of acute pericarditis, or of endocarditis, or of inflammation of the lungs or pleura, is one of those conditions.
Probably hyperpyrexia acts in some cases as an exciting cause of the nervous phenomena, for while the delirium preceded the hyperpyrexia in 6 cases, it accompanied it in 19 and followed it in 10;96 and the nervous symptoms disappear when the hyperthermia is removed by the employment of cold, and recur with the return of high temperature. The phenomena of sunstroke and heat-apoplexy prove that a high temperature is capable of producing convulsions and coma. That these grave cerebral disturbances are so infrequent in acute rheumatism (obtaining in about 3 or 4 per cent. only) is probably owing to the usual moderate range of temperature and the rarity of hyperpyrexia in the disease. Still, while hyperpyrexia is a disturber of cerebro-spinal function, too much importance must not be attached to it, for not only does such disturbance very frequently precede the hyperpyrexia, but there are many facts indicating that the hyperpyrexia is itself very frequently, like the delirium, tremor, and coma which precede or accompany it, but a consequence of disorder, usually of a paralyzing kind, of the nerve-centres. It has been met with in lesions of the pons, in tetanus, in injuries of the cord, in some cases of non-inflammatory softening of the brain and of cerebral hemorrhage; that is, in a class of affections not belonging to the specific fevers, but to those directly disturbing or destroying the functions of the nerve-centres. And cases of acute rheumatism do rarely occur in which a very high temperature is not accompanied by cerebral disturbances. Sibson quotes two such,97 one of which, with a temperature of 110.8°, was only restless and talked when asleep, and the other, with a temperature of 106.3°, presented only vomiting and dyspnoea. Cardiac inflammation was absent in both. DaCosta relates one in his valuable paper upon cerebral rheumatism in which, although the temperature was 110°, no cerebral symptoms nor cardiac affection existed.98
96 "Abstract Report upon Hyperpyrexia in Ac. Rheum.," Brit. Med. Jour., 1882, p. 807.
97 Lib. cit., p. 264.
98 This essay contains a record of 11 cases of cerebral rheumatism and several autopsies: Am. Jour. Med. Sci., 69, 1845, p. 36, case xi.
The goodly number of instances lately published in which grave cerebral symptoms have obtained in acute articular rheumatism at ordinary febrile temperatures, while they prove that hyperthermia is not an essential condition productive of such symptoms, require to be explained. Some such, no doubt, have been instances of marked predisposition, so that a moderate febrile temperature or some complication sufficed to disturb the brain, as we see in typhoid and other fevers, in pneumonia, etc. If there be a rheumatic poison—which has not yet been proved—it may, in predisposed persons, produce the cerebral symptoms. The argument99 that such poison should produce inflammation of the nervous centres if it acted directly on them is not convincing. It need not necessarily produce similar alterations in serous or synovial membranes and in nervous tissues. Many toxic agents disturb, and even suspend, the [p. 42]cerebro-spinal functions, and leave no appreciable changes in them. Do these cases prove that there is something peculiar to rheumatic fever which tends to disturb the nervous centres? Hardly; for while such disturbance is comparatively rare in that disease, it is observed frequently in many other febrile affections, notably in typhus, scarlatina, and small-pox; and as in these, so in rheumatic fever, it is more often observed in the severe than in the mild cases, as though it were a part of the systemic disturbance incident to the febrile affection and largely proportionate to its severity.
99 Maclagan, Rheumatism: Its Nature, Pathology, etc., 1881, 287.
Yet there is something special in acute rheumatism which perhaps has to do with the occurrence as well as the severity of the cerebro-spinal symptoms and of the hyperpyrexia; viz. the long duration and severity of the pain, and the number and importance of the parts, in addition to the articulations, which are one after the other or simultaneously involved in severe inflammation—peri-, endo-, myocardium, lungs, pleura, etc. Perhaps in no other acute febrile disease are so many distinct and important organs involved in inflammation at the same time or in rapid succession; and it is no wonder that the functions of the nervous system should in consequence become greatly depressed, exhausted, or disturbed.
The kidneys appear very rarely to suffer serious disease in acute rheumatism, if we except embolism of their arteries due to endocarditis; and it is very doubtful whether the rare instances100 in which an acute parenchymatous nephritis has been observed in acute rheumatism can be referred to direct rheumatic inflammation, or not, rather, to the operation of the exposure which induced the rheumatism. Further investigation is needed to determine whether interstitial nephritis is even very exceptionally an indirect consequence of rheumatism, as Lancereaux admits.
100 See DaCosta's cases 1 and 2, Cerebral Rheumatism, lib. cit.; case 1 certainly favors the view that either the rheumatic poison, if there be such, or the constitutional disturbance incident to acute polyarticular rheumatism, may sometimes produce nephritis. See also a case by A. Deroye, Thèse, Doctorat, Paris, 1874, quoted by P. Coubere in Contribution à l'Étude des Complications Renales du Rheumatisme Artic. Aigue, Paris, 1877.
The other complications, being of less importance, must be but barely alluded to. A pharyngitis attended with severe dysphagia and high fever occasionally precedes the other symptoms or occurs in the early stage of the disease. Gastralgia, enteralgia, simple serous diarrhoea, and dysentery also rarely occur in acute rheumatism. That they are sometimes, at least, truly rheumatic appears probable from the circumstance that they may precede, follow, or alternate with the articular affection, and are all intensely painful. I have but once met with acute peritonitis as a complication of acute rheumatism; the immunity of this serous membrane from rheumatic inflammation is an inexplicable anomaly in view of the proclivity of the pericardium and pleura to that process. Cystitis and orchitis are rare.
Several cutaneous affections are not unfrequently observed in relation with acute rheumatism. Besides sudamina and miliaria rubra, which are very common as consequences of the excessive perspiration,101 there [p. 43]are others which may be themselves rheumatic manifestations. Such are especially erythema marginatum,102 e. papulatum, and e. nodosum. A well-marked urticaria frequently precedes acute rheumatism in a friend of the writer's; it may occur during its course or soon after the cessation of the pains. Scarlatiniform eruptions are occasionally observed, and very rarely punctiform hemorrhages—peliosis rheumatica or rheumatic purpura. The purpuric symptom may be accompanied by erythema or urticaria, and may precede, accompany, or alternate with other rheumatic manifestations. Unlike purpura variolosa and idiopathic purpura hæmorrhagica, this variety appears to be free from danger.
101 Dr. J. T. Metcalfe of New York many years ago showed me a case of rheumatic fever in which the sweat-vesicles had run together, forming, instead of the usual pearly globular vesicles, irregular flat blebs, some of them equal in area to seven or nine primary vesicles, filled with transparent fluid, and this fluid could be displaced by pressure to adjacent parts, as though it lay simply under the superficial epidermic layer. I have seen several similar cases since.
102 Dr. Palmer relates a case complicated with erysipelas and peritonitis in Boston Med. and Surg. Journal, 1868.
Besides a slight local oedema affecting the malleoli, scrotum, eyelids, etc., or accompanying the cutaneous eruptions just mentioned, a more decided infiltration of the subcutaneous cellular tissue occasionally exists in the vicinity of the inflamed joints and tendinous sheaths, and more rarely extends to an entire limb, which may not only be considerably enlarged and painful and resemble a milk leg, but may be red, hot, and tender, and excite suspicion of phlegmonous erysipelas. Phlebitis, although infinitely less frequent than in gout, has been observed in acute articular rheumatism.103 Jaccoud in 1871104 mentioned the exceptional occurrence of subcutaneous nodosities in rheumatism, which he says Froriep first pointed out;105 but Homolle states that they had been previously mentioned by Sauvage and Chomel.106 Since then several independent observers have met with this affection, and Drs. Thomas Barlow and Francis Warner of London have lately written a short valuable paper upon the subject based upon 27 cases which they had separately or conjointly investigated. From their paper the following account is chiefly derived:107 These nodules may vary in number from one to fifty, and in size from that of a pin's head to the volume of an almond, and are quite subcutaneous, firm and elastic, painless, and freely movable. They are not usually attached to the skin, but to the tendons, deep fasciæ, pericranium, periosteum, etc.; the integument over them is free from heat, redness, and infiltration, although exceptionally tenderness on pressure and slight redness may exist over them. They are found most frequently on the back of the elbow, the malleoli, and margins of the patella, but occur occasionally on the extensor tendons of the hand and foot, the scapular spine and iliac crest, the temporal ridge and superior occipital curved line, the ear, etc. These nodules occur singly or in clusters, and are often symmetrical; they are very rapidly developed in crops or in succession, and last sometimes for a few hours, more frequently from three or four days to four or five months, or even eighteen to thirty months. The original formations may disappear, and be succeeded by fresh ones; and sometimes, when no longer perceptible by touch, they may be found post-mortem. Their development is unattended by pyrexia, unless pleuritis, pericarditis, or other condition coexist to which the pyrexia might [p. 44]be referred. These nodosities do not appear to suppurate or ossify or become infiltrated with urate of soda, and histologically they resemble organizing granulative tissue. As regards their pathological associations, Drs. Barlow and Warner found evidences of rheumatism in 25 out of 27 cases; a morbid condition of the heart existed in all of them, and chorea in 10 of them. Two of the conclusions formulated by the authors just mentioned are of great importance: that these subcutaneous nodosities "may be considered as in themselves indicative of rheumatism, even in the absence of pain;" that, while unimportant in themselves, they are "of serious import, because in several cases the associated heart disease has been found actively progressive." Dr. Dyce Duckworth has reported two cases in which these nodules occurred in adults, lasted eighteen months in one, and were still present in the other case after thirty months, and were attached to the skin and periosteum. In one of them the nodules were very painful and ached more in cold weather, and the patient had no history of rheumatism or of chorea, although her mother and one sister had.108 In Dr. Stephen Mackenzie's case the woman was the subject of tertiary syphilis, and had no personal history of rheumatism or chorea, and she was free from heart disease; but her family history was not given.109
103 Phlebite Rheumatismale Aigue, Paris, 1869, par M. Lelong. In Revue de Méd., t. i. 492-499, 1881, a case by Dr. Launois.
104 Pathologie Interne, ii. 546, 1871.
105 Die Rheumatische Schwiele, Weimar, 1843.
106 Lib. cit., p. 628.
107 Trans. International Medical Congress, London, vol. iv. pp. 116-128, 1881. In this paper, and in an article by MM. E. Troisier and L. Brock, to be found in Revue de Médecine, t. i. 297-308, 1881, are references to the authors who had written upon it.
108 Brit. Med. Journ., i., 1883, 868.
109 Ibid., i., 1883, 867.
The course and duration of acute polyarticular rheumatism vary very much, and are apparently influenced by several circumstances, such as the severity or the mildness of the articular affection, as well as of the constitutional disturbance; the presence or not of complications; the state of health of the patient about the time of the attack, and, probably, the existence or not of a proclivity to the disease; and whether the disease present the continued or the relapsing type. As a tolerably general rule, when the constitutional symptoms are acute, the skin hot, the perspiration free and very acid, the urine of high density, color, and acidity, and several of the articulations are swollen and very painful—when no serious complication, and especially no severe cardiac affection, exists, and when the patient is endowed with a fair constitution and with organs not damaged by previous disease, the course of the fever is tolerably short and continuous, and the recovery more or less prompt. Amongst the most reliable evidences of approaching recovery in such cases is the tongue becoming clean and losing its red color and the urine increasing considerably in quantity, but containing a large proportion of solid matter, as indicated by a high density.
On the other hand, a large proportion of cases run a more irregular and protracted course, and more or less marked relapses succeed real but temporary improvements, the local disturbance affecting fresh joints or reappearing in those previously attacked, and the general symptoms resuming renewed activity. The duration of the active symptoms in these cases is considerable, seldom under six weeks, and frequently occupying seven, eight, or more. In these protracted cases the symptoms, as a rule, are usually rather milder, the perspiration not as profuse or sour, the urine of less density and acidity, the articulations less hot and painful, than in the previously described group. Sometimes, indeed, the perspiration and the urine are of neutral or even faintly alkaline reaction. It is not only the unexplained tendency to relapse which protracts these [p. 45]cases, but sometimes in addition an established proclivity to the disease—the rheumatic habit—or a condition of previous unsound or frail health.
Such cases occasionally pass into the subacute form, or the mild febrile symptoms gradually and finally decline, and the joints may either remain tender, swollen, and stiff some time longer, or these signs of recent inflammation may soon disappear and leave the articulations merely weak.
Many cases of acute rheumatism embody several of the features of the two groups just described, and no definite course or duration of acute articular rheumatism can be accurately laid down.
The course and duration of acute polyarticular rheumatism have received a good deal of attention of late years. But Dr. Austin Flint110 was one of the first to study the natural history of the disease uninfluenced by active treatment, and he was followed in 1865,111 1866,112 and 1869113 by Sir William Gull and Dr. Sutton, who treated a series of cases without medicine, unless mint-water be so regarded. The mean duration of Flint's 13 cases from the date of attack to convalescence, excluding one in which pericarditis and pneumonia occurred, was a fraction under twenty-six days. It is unfortunate that the number of cases was so small, and that 11 of the patients were females, who appear to be especially subject to the milder and more protracted attacks of the disease. A larger number, with an equal proportion of the sexes, would probably have given a different result.
110 American Journal of Med. Sciences, July, 1863.
111 Ib., vol. xii.
112 Medico-Chirurgical Transactions, vol. lii.
113 Guy's Hospital Reports, 2d Series, vol. xi.
Gull and Sutton have published the natural histories of 62 cases—viz. of 41 in their first series, of 8 more in their second, and of 13 more in their third. The average duration of the acute symptoms was, in the first series, 8.5 days, in the second, 9 days, and in the third, 10 days, giving an average of 9.1 days for the duration, after admission to hospital, of the acute symptoms of acute polyarticular rheumatism when there is no very severe cardiac disease. In their third paper, based upon 13 new cases and 12 of those published in their two previous communications, they conclude "that rheumatic fever uncomplicated with any very severe heart affection tends to run its course in nineteen days, calculating from the time the rheumatic symptoms first set in to their termination."114 Yet an analysis of the 23 of the 41 cases contained in their first series115 respecting which the duration of the rheumatic symptoms before admission and from admission to complete convalescence is given, shows that the period occupied from the setting in of the rheumatic symptoms to convalescence was in the 13 male subjects 25.8 days, and in the 10 female 42 days, or, including both sexes, the average duration was 32.8 days—i.e. 6.8 days longer than Flint's result.
114 Med.-Chir. Trans., lii. 82.
115 Guy's Hospital Reports, xi. 435.
As Gull and Sutton had especially pointed out the class that tends to assume acute characters and recover more quickly than any other, and the class that runs a protracted course and tends to relapse, it is somewhat remarkable that they did not tabulate the cases belonging to those classes separately, and show distinctly their differences in duration and [p. 46]modes of convalescence. This has been attempted by Southey,116 but, unfortunately, his conclusions, as will hereafter appear, have not been confirmed by other observers.
116 St. Bartholomew's Hospital Reports, xiv., and ib., xv.
Finally, in this connection, after carefully weighing ten subjects of acute articular rheumatism during their illness and until they had regained their usual weight, A. Roussel117 found that the time during convalescence occupied in regaining the weight previously lost was inversely proportional to the duration of the attack.
117 Essai sur la Convalescence du Rheumatisme Artic. Aigue, Paris, 1881, 66.
Under this head Charcot, Besnier, and Homolle describe an affection which corresponds closely with one variety of the disease commonly called rheumatoid arthritis, but the writer employs the term with the same significance as most modern English authors (Garrod, Sutton, Flint, Maclagan). It is milder yet more enduring than the acute form, but their symptoms are identical in kind. It is usually subacute from the outset, although occasionally succeeding the acute type. The febrile disturbance is but slight, rarely reaching 101°, and the perspiration is less abundant; there is less pain, heat, and tenderness in the joints, and only a few of them are involved together; but although the articular affection moves from joint to joint, it persists for weeks or months in several of them or in one only, improving and relapsing generally without apparent reason. However, it does not seriously damage the articulations, and they ultimately quite recover. Mild cardiac affections also occur, but less frequently, and the serious disturbances of the cerebral and respiratory systems are very seldom met with. The gradations between subacute articular rheumatism and the acute form on the one hand, and the simple chronic form on the other, are almost innumerable. Marked anæmia is as much a feature of subacute as of acute articular rheumatism, and its victims are often of unhealthy or asthenic constitution, and subject to recurring attacks of the disease on but slight provocation. The return of warm weather often relieves such cases.
THE MORBID ANATOMY OF ACUTE AND SUBACUTE ARTICULAR RHEUMATISM.—Although opportunities of ascertaining the conditions of the articulations in acute articular rheumatism are rare, yet it is now established that the process is an inflammation involving chiefly the synovial membrane, and to a less degree the cartilages, ligaments, tendinous sheaths, and in some cases even the bones and periarticular soft parts. The synovial membrane is more or less injected and reddened diffusely or in patches, especially where it forms fringe-like folds and at its line of union with the cartilage. It is somewhat thickened, opaque, and devoid of its satin-like lustre, and in somewhat protracted cases covered here and there with a thin, easily detached neo-membranous formation. Within the articulations will be found from a few drops to one or two ounces of a viscid, pale, citron- or reddish-colored fluid, like synovia, but more fluid, and generally turbid and containing transparent or semi-opaque gelatinous masses or albumino-fibrinous flocculi. The [p. 47]microscope reveals in the effusion large detached spherical epithelial cells in various stages of germination or of fatty degeneration, and a variable number of red blood-corpuscles and pus-cells. Very exceptionally, the effusion is mixed with more or less true pus. In two out of the eight fatal cases reported by Fuller, in which the joints were examined, pus in moderate quantity was found along with other products in some, but not in all, of the inflamed articulations, and one of them was complicated with erysipelas, the other with sloughs over both trochanters. In very severe forms complicated with hemorrhagic tendencies the inflammatory products have contained a large proportion of blood. Cornil et Ranvier118 insist that even in slight cases of rheumatic arthritis the diarthrodial cartilage constantly suffers changes arising from nutritive irritation and proliferation of the cartilage-cells. At first the cartilage loses here and there some of its polished hyaline appearance, and the microscope reveals a finely-striated condition of its structure which gives it a velvety aspect. When the inflammation has been more severe and of longer duration, so that the deeper layers have been involved, the unaided eye will perceive local swellings in which the natural elasticity and resistance of the cartilage are impaired, and its surface is fissured or villous-like in appearance. "In certain rare cases of mono-articular acute arthritis true ulcerations of the cartilage are observed."
118 Manual d'Histologie pathologique, Paris, 1869, 406.
The soft parts in the immediate vicinity of the inflamed joints may be in some cases more or less congested and oedematous, and the tendinous sheaths, and even the bursæ mucosæ, inflamed and distended with inflammatory products like those in the articulations. Charcot,119 holding the opinion that arthritis deformans is but a chronic variety of articular rheumatism, quotes Gurlt's statement that in acute articular rheumatism "the medullary tissue of the ends of the bones undergoes a great increase of vascularity, with proliferation of its corpuscles," and remarks that Hasse and Kussmaul have also referred to lesions of the bone and periosteum in that disease. But the condition of the osseous parts of the joints in acute articular rheumatism can hardly be said to be known, and it is premature to speak positively respecting it.
119 Clinical Lectures on Acute and Chronic Diseases, Sydenham Soc., 1881, p. 148.
Finally, in subacute rheumatism the alterations in the synovial membrane, and especially in the cartilages just described, are likely to be more marked than in the acute form.
The DIAGNOSIS of acute polyarticular rheumatism is seldom difficult in adults, but when acute rheumatism localizes itself in one joint or occurs in infancy or early childhood, a diagnosis, especially an early one, sometimes cannot be easily established. The considerations by which acute polyarticular rheumatism may be distinguished from acute gout, subacute rheumatoid arthritis, and gonorrhoeal rheumatism will be given in connection with those topics.
Pyæmia has perhaps been confounded with acute articular rheumatism more than any other disease, but the rheumatic affection, unlike the pyæmic, is not necessarily connected with any pre-existing condition capable of causing purulent infection of the blood or system, such as a wound, fracture, abscess, or a local inflammation of bone, periosteum, vein, pelvic organ, or a specific fever (variola, relapsing, typhoid, [p. 48]glanders, etc.); it does not present severe rigors, which recur at irregular intervals and are attended with teeth-chattering and a high temperature, 104° to 105°, rapidly attained; its type of fever is not so intermittent or markedly remittent as that of pyæmia; its profuse sweating continues although the temperature remains febrile, but that of pyæmia coincides with the decline of the temperature; unlike pyæmia, it only very rarely produces profound constitutional disturbance of a typhoid character, and has no tendency to run a rapidly fatal course in eight to ten days or in two or three weeks; its visceral inflammations are chiefly cardiac, pleural, and pulmonary, and tend to resolve; those of pyæmia are especially pulmonary, pleural, and hepatic, although frequently cardiac also, and generally produce suppuration and destruction of tissue. Multiple subcutaneous abscesses and cutaneous blebs and pustules do not occur in acute articular rheumatism, and its articular affection differs in many respects from that of pyæmia; many more joints are involved; the inflammation is erratic, very rarely fixed, and generally resolves without damage to the articulation; the affected joint is usually hotter, redder, more painful, and more sensitive, and the swelling is less diffused, and its outline corresponds more accurately with that of the synovial capsule. Sometimes acute articular rheumatism is complicated with the phenomena of pyæmia, as when so-called ulcerative endocarditis obtains.
The acute inflammations which are occasionally observed in one or several articulations of newly-born infants are generally pyæmic. It is only in the early stage of acute glanders that the severe muscular and articular pains sometimes present in that very rare disease in man might lead to its being confounded with acute articular rheumatism; but the patient's occupation and history, the early and severe prostration, the absence, as a rule, of redness and swelling around the painful articulations, and, in some instances, the early appearance of pustules and blebs on the skin and of abscesses in the deeper tissues, will suggest the real nature of the case.
Acute periostitis frequently occurs in children in close proximity either to one joint, or less frequently to more than one, and may readily be confounded with acute articular rheumatism. But the constitutional disturbance in acute periostitis is prompt and severe at the outset; the swelling increases rapidly, is firmer than that of arthritis, does not involve the joint proper and its capsule, but, like the tenderness on pressure, exists above or below the articulations, especially around the head of the bone; there are no visceral complications, provided pyæmia has not supervened; the constitutional symptoms early assume a typhoid character, and unless an early incision be made a fatal issue soon ensues.
The enlarged ends of the long bones and the pains in the limbs of rickets might lead to a suspicion of acute articular rheumatism, but the early age of such children, the absence of pain and swelling in the joints, the beaded condition of the sternal ends of the ribs, the late dentition and locomotion, the peculiarly shaped head, and other evidences of that affection, would prevent a careful observer from making a mistake. Inherited syphilis in infants, like rickets, may produce fusiform swelling and thickening at the ends of the long bones, especially the humerus and femur, and sometimes pain in the joints on movement; but at first the swelling [p. 49]is confined to the epiphyseal line, and only later extends to the joint; there is a pseudo-paralysis of the limb, and but little pain or fever; bony osteophytes may often be felt under the skin at the line of union of the epiphysis with the shaft; the epiphysis often becomes separated from the shaft, and suppuration may ensue around the bone and in the articulation; sometimes adhesions and perforation of the integument take place, allowing of the escape of disintegrating osseous and cartilaginous tissue; and there will coexist either on the skin or mucous membrane some of the ordinary evidences of inherited syphilis.120 The acute and subacute articular inflammations occasionally observed in cerebral softening and hemorrhage, in injuries and inflammation of the spinal cord and caries of the vertebræ, may be distinguished from acute and subacute articular rheumatism by the following circumstances: the existence of some one of these diseases of the brain or cord, the articular affection being usually confined to the paralyzed limbs; its invasion about the time of the setting in of the late rigidity, or even still later; the absence of cardiac complications and the presence of other trophic or neuro-paralytic lesions, such as acute sloughings, rapid atrophy of the palsied muscles, cystitis, ammoniacal urine, etc.121
120 Vide Parrot, Archives de Physiol. Norm. et Path., 1872 and 1876; R. W. Taylor, Bone Syphilis in Children, New York, 1875.
121 See J. K. Mitchell, Am. Jour. Med. Science, vol. viii., 1831, and ib., 1833; Scott Alison, Lancet, i., 1846, 276; Brown-Séquard, Lancet, i., 1861; Gull, Guy's Hosp. Repts., 1858; Charcot, Archives de Physiologie, t. i. p. 396, 1868, and many others.
Acute articular rheumatism in children presents peculiarities. It often affects but one joint, and has little tendency to become general; the joints of the lower extremity, ankle, and knee are most obnoxious; the local signs of inflammation, redness, swelling, and pain, are feebly developed, and the child may walk as if nothing were wrong; the disease is usually subacute; the temperature rarely very high; the perspiration not profuse; the urine not scanty, and not often loaded with lithic acid. Cardiac and the other internal complications, except the cerebral, are more frequent than in adults; endocarditis is especially frequent, pericarditis and pleuritis not rare. It is almost exclusively in childhood that acute articular rheumatism becomes associated with or followed by chorea, and yet the delirium, coma, and convulsions frequently observed during rheumatic fever in the adult are very rarely seen in the child. Muscular rheumatism, however, in the form of torticollis, frequently coexists, and so do erythema nodosum and the subcutaneous fibrous nodules previously described.
It is very rarely indeed that acute rheumatism invades a single joint to the exclusion of the rest; and it is perhaps impossible to be certain that such an arthritis is rheumatic unless some of the other symptoms or complications of articular rheumatism supervene, or unless it have succeeded a polyarticular rheumatism, which it very rarely does. Mono-articular rheumatism is very generally of the subacute type, and unattended with fever from the outset, or only a moderate pyrexia obtains for a few days; there is generally considerable effusion into the joint, with [p. 50]swelling, pain, and moderate local heat; visceral complications very rarely arise, but the local inflammation persists most obstinately for six or eight weeks or three or four months, and often leaves the joint tender, stiffs, and weak for a long time or even permanently. In both the acute and subacute forms, before concluding that the uni-arthritis is rheumatic, we must exclude the probability of its being traumatic, strumous, syphilitic, gonorrhoeal, neurotic, or, above all, of the nature of rheumatoid arthritis, which many such cases really are.
PROGNOSIS.—The disease is rarely directly fatal during the attack, yet as the frequency of the complications varies unaccountably from time to time, so the mortality may be exceptionally large or small for even prolonged periods. It may be said that the average mortality ranges between 1.16 and 4 per cent. in the experience of modern authors. The average mortality in the Paris hospitals for four years (1868-69, 1872-73) Besnier fixes at 1.65 per cent.;122 in St. Bartholomew's, London, Southey found it for fifteen years (1861-75) to be 1.16 per cent.;123 Pye-Smith fixes the rate at 4 per cent. in 400 cases treated in Guy's;124 W. Carter gives 2.5 per cent. as the rate during ten years at the Southern and Royal Southern Hospitals of Liverpool.125 The death-rate appears to vary remarkably with age, as Southey's figures show:126 under ten years, 3.40 per cent.; between ten and fifteen, 1.5 per cent.; between fifteen and twenty-five, 1.4 per cent.; between twenty-five and thirty-five, 0.9 per cent.; between thirty-five and forty-five, 0.8 per cent., the mortality declining very greatly after the tenth, after the twenty-fifth, and after the forty-fifth year of life.
122 Dictionnaire Encyclopédique, Troisième serie, t. iv., p. 463.
123 Barth. Hospital Reports, vol. xiv., p. 4.
124 Guy's Hospital Reports, xix. p. 327.
125 The Liverpool Medico-Chirurgical Journal, July, 1881, p. 88.
126 Lib. cit., p. 4.
The danger of the case is usually proportionate to the youth of the patient, the degree of the pyrexia, the number of the joints involved, and the number and the character of the complications, the habits, and previous health of the patient. A fatal issue is most frequently observed in connection with hyperpyrexia alone, or in combination with delirium or coma. A rapid rise of temperature and a temperature over 105°, especially if cerebral disturbance coexist, indicate danger; and so does arrested perspiration while the temperature is high. In a much smaller number of cases death is due to some other complication, especially to purulent pericarditis or to that combined with pleuritis or pneumonia; in not a few cases the prior existence of chronic valvular disease, with fibroid induration of liver and kidneys, renders a fresh rheumatic endo- or pericarditis, occurring as part of acute articular rheumatism, fatal. There is good if not conclusive evidence that rather sudden death in acute articular rheumatism is occasionally due either to diffuse myocarditis or to fatty degeneration of the muscle of the heart. In Greenhow's 2 deaths out of 50 cases treated by sodium salicylate the pericardium was universally adherent and the heart's fibre fatty in one and pale and flabby in the other. Sudden death in this disease is very rarely due to embolism of the pulmonary artery or of the cerebral vessels, while ulcerative endocarditis is very exceptionally one of the sources of a fatal issue.127 But although acute articular rheumatism rarely kills [p. 51] directly, it frequently lays the foundation of subsequent ill-health, and ultimately proves fatal through organic disease of the heart and its many consequences. However, it is an interesting circumstance that while acute rheumatic inflammation is prone to damage the heart permanently, it very rarely, quite exceptionally, impairs the structure or functions of the articulations. It is almost solely the subacute form that now and then becomes chronic or renders a joint for a long time painful, swollen, and crippled in its movements. Whether acute rheumatism, however intense per se, ever ends in destructive suppuration and ulceration of a joint is doubted by some authorities, notwithstanding the cases published by Fuller and others. No doubt some of the cases were really pyæmic, or perhaps gonorrhoeal; and it must be borne in mind that acute articular rheumatism occasionally develops pyæmia, and then an arthritis might be considered rheumatic when truly pyæmic. The question of acute rheumatic arthritis exciting a chronic rheumatoid affection will arise hereafter.
127 See an article on the mortality among rheumatic risks by A. Huntingdon, M.D., in N.Y. Medical Record, 1875, p. 195.
TREATMENT.—Owing to our imperfect knowledge of the real nature of acute articular rheumatism, its treatment is still largely either empirical or intended to combat certain prominent symptoms or complications of the disease. Of the various methods of treatment which have been employed space will not permit a description; even of those advocated by authorities of the present hour only very few will be considered.
The method which is now unquestionably the favorite one in both Europe and America, and which in its power of promptly relieving the articular and muscular pains and reducing the fever of acute rheumatic polyarthritis may without exaggeration be compared to that exercised by quinia over the paroxysms of ague, is that in which salicylic acid or salicylate of sodium is given in repeated and full doses. It was in July, 1875,128 that Buss first asserted that salicylic acid was a specific for rheumatism, and in March, 1876,129 Maclagan, after having employed salicine from 1874, published his experience of it as a valuable remedy in the treatment of acute rheumatism, its beneficial action being "generally apparent within twenty-four, always within forty-eight, hours of its administration in sufficient dose." Perhaps a sufficient time has now elapsed to permit of a just opinion of the power of these new remedies, the salicyl compounds, over acute articular rheumatism. The facts presented at the discussion recently held at the Medical Society of London130 are sufficiently numerous and authoritative to justify, at least provisionally, some definite conclusions as to the remedial relations of the salicylates to acute articular rheumatism.
128 "Die Antepyr. Wirkung der Salycylsäure," Centralbl. f. d. Medic. Wissenschr., 1875, 276.
129 The Lancet, March 4 and 11, 1876.
130 The Lancet, Dec. 17, 24, 31, 1881; Jan. 7, 14, 28, 1882.
1. The articular pain and the fever of acute rheumatic polyarthritis are more or less speedily removed by the salicyl remedies (salicylic acid, sodium salicylate, and salicine); the pains very frequently persist after the temperature has become normal. Both symptoms were removed by five days' use of such agents in 50 per cent., and by eleven days' use in 80 per cent., of 355 cases treated at Guy's Hospital, and tabulated by Fagge,131 and by five days' use in 60 per cent., and by eleven days' use [p. 52]in 66 per cent., of the 60 severe cases treated and severely criticised by Greenhow.132
131 Ibid., ii., 1881, 1031.
132 Clinical Society's Transactions, vol. xiii., 1880. See Dr. Fagge's table iv., Lancet, ii., 1881, 1032.
Again, in 190 cases of acute and subacute rheumatism the average duration, under salicyl remedies, of pyrexia was 5.5 days and of joint disease, 5.3 days (Warner133); in 156 cases at St. George's Hospital the average duration of pyrexia was 3.66 days, of pain 4 days (Owen134); in 82 at the Middlesex the average duration of pyrexia was 5 days, of pain 5.6 days (Coupland135); and in 55 at the Westminster the average duration of pyrexia was 7 days, of pain 7.25 days136—that is, a general average duration in the whole series for the pain and pyrexia of 5.4 days.
133 Ibid., p. 1080.
134 Ibid., p. 1081.
135 Ibid., i., 1882, 10.
136 Ibid., ii., 1881, p. 1080.
Further, 36 per cent. of Fagge's cases and 58 per cent. of Greenhow's were relieved of both the above symptoms on the fourth day; 24.8 per cent. of Fagge's and 50 per cent. of Greenhow's on the third day; and 13.5 per cent. of Fagge's and 26.6 per cent. of Greenhow's on the second day. In Clouston's 27 cases, treated in private, 66.6 per cent. were free from pain and 59 per cent. from fever within three days, and 85.2 per cent. were devoid of pain and 72.7 per cent. of fever within four days.137 Finally, all who have had much experience of this method of treating acute rheumatism will agree that the first or second dose frequently relieves the articular pains like a charm, and the local swelling then frequently subsides in from sixteen to forty-eight hours.
137 The Practitioner, i., 1882.
2. Relapses are more frequent—probably considerably more frequent—under treatment by salicylates than under other methods. Thus, the average of relapses in eight different tables of cases treated by the salicyl remedies ranged from 16.6 per cent. to 35 per cent., giving a general average of 26 per cent.;138 while under other methods in three different tables the average ranged from 5.4 per cent. to 27.6 (this last under the full alkaline), giving a general average of 16 per cent.139 Relapses appeared to recur less frequently in those cases which yielded to the salicylates within five days than in those which took from six to eleven days to yield, in the ratio, according to Fagge's figures, of 26.6 per cent. for the first, and 29.4 per cent. for the second day; and, according to Hood's, as 18.4 per cent. to 24.4 per cent. There does not appear to be any regularity in the order of occurrence or recurrence of relapses, nor is Southey's definite statement that in "relapsing cases the temperature is nearly or quite normal on the eighth evening, and a slight relapse occurs on the thirteenth morning," borne out by the statistics produced at the London Medical Society. Moreover, W. Carter's cases140 have not confirmed Southey's precise statement respecting the gradual remission of the temperature on the eighth and ninth days of illness in the continued or non-relapsing, uncomplicated forms. Irregularity and inconstancy are the typical features of articular rheumatism. The relapses under the treatment by the salicylates have been referred to the premature disuse of those remedies, but they do occur notwithstanding [p. 53]the continued employment of them. It is a general opinion that exposure to cold, errors in diet, and an early return to work are frequent causes of relapse; and Broadbent refers the increased liability to relapse under the salicyl compounds to the rapidity with which those remedies relieve the acute symptoms of articular rheumatism, in consequence of which sufficient care is not observed either by the patients or their nurses, and they are exposed to some of the above exciting causes of relapse. All the above causes do probably play their part so long as the materies morbi (if that really exist either as a chemical principle or as a germ) has not been wholly eliminated or destroyed. Indeed, the short intervals which frequently obtain between the primary invasion of the so-called relapses, and the failure of the salicyl compounds to prevent peri- and endocarditis, render it probable that what are commonly spoken of as relapses are not due to a new infection, as in the case of the relapse of typhoid fever, but to the recrudescences of a disease not yet terminated, but over some of the manifestations of which—the articular inflammation and the pyrexia—the salicylates exercise some control.
138 Fagge's, 26.2 per cent.; Greenhow's, 35; Warner's, 33.6; Owen's, 30.2; Hood's, 18.8; Coupland's, 35.3; Broadbent's, 16.6; Powell's, 18.7; total, 214 ÷ 8 = 26 per cent.
139 Hood's, 5.4; Warner's, 14.9; Owen's, 27.6; total, 47.9 ÷ 3 = 16 per cent.
140 The Liverpool Med.-Chirurgical Journal, July, 1881, p. 101.
3. Authorities are generally agreed that the salicyl compounds do not arrest or control rheumatic inflammation of the endo- or pericardium or pleura, or subdue the pyrexia, if these complications in well-marked degree exist; and there is strong evidence to show that they do not at all constantly prevent the disease from involving those organs, even after the articular affection has subsided under their use. Inestimable as is the benefit conferred by these remedies in promptly relieving the articular pain and fever, they do not secure the great desideratum in the treatment of acute articular rheumatism—protection of the heart.
In 352 cases treated with salicylate of soda at the Westminster Hospital, heart disease developed in 13.6 per cent.; in 267 treated without the salicylate, heart disease developed in 14.2 per cent. (Warner's cases).141 In 350 cases treated with salicylates at Guy's, heart complications obtained in 68 per cent., while in 850 treated without them, the cardiac complications occurred in 58.8 per cent. (Hood).142 Gilbart-Smith collected a large number of cases from several of the London hospitals, and analyzed them with the following results: Of 1727 cases of acute rheumatism treated before the introduction of the salicyl compounds, the proportion of cardiac complications was 54.4 per cent.; in 1748 cases treated subsequently to their introduction, the cardiac affections obtained in 63.4 per cent.; and in 533 cases treated by the salicyl compounds, those affections obtained in 68.4 per cent.143
141 The Lancet, ii., 1881, 1080.
142 Ibid., ii., 1881, 1120.
143 Ibid., i., 1882, 136.
These facts certainly seem to prove that the salicyl compounds do not prevent the occurrence of the visceral complications or manifestations of acute articular rheumatism; and if space permitted instances might be quoted from many authors in which either endo- or pericarditis or pleuritis or pneumonia or other visceral manifestation had set in after the patient had been taking the salicylates long enough to have produced their usual physiological effects; some of these will be mentioned under the next section.
It may be objected that in the above estimates sufficient attention has not been paid to the period of the disease at which the treatment by the [p. 54]salicylates was begun, the time it was continued, the doses given, the age of the patient, the severity and other characters of the illness, such as whether acute or subacute, first or second attack, complicated or not.
4. It must be admitted that there are a few facts which render it very probable that the salicyl compounds do really reduce the frequency of these complications, and thus give some protection to the heart in rheumatism. Of Powell's 32 cases, 19 = 60 per cent. had heart disease when admitted; and of the remaining 13, 6 = 46 per cent. developed cardiac disease after admission and while under the salicylates.144 Of Dr. Jacobi's145 150 cases, 78 = 52 per cent. were admitted with unsound hearts, and of the other 72, only 5 = 6.9 per cent. developed cardiac disease after beginning salicylate treatment. Of Southey's 51 cases, 24 = 47 per cent. were admitted with diseased hearts; and of the remaining 27, only 4 = 14.8 per cent. developed a cardiac affection subsequent to beginning treatment by the salicylates.146 Of the Boston Hospital cases, 38 per cent. were affected with heart disease at entrance, and only 4.76 per cent. afterward. No heart affection was developed in any of Clouston's 27 private cases—a result he attributes to the early period at which the remedies are given in private practice. But the number is too small to permit of any conclusion being drawn, and 4 of the cases were examples of recurrence of the disease at short intervals (three and four weeks) in the same patient, in whom there appears to have existed no proclivity to cardiac complication, for he had had four attacks before he came under Clouston's care. Moreover, his cases were mild, but 16 of them being acute, and of these only 3 attaining a temperature of 103° and upward. Finally, Herman147 estimates the percentage of heart affections that developed after beginning the salicylates in the London Hospital at 18.7 per cent., and after other treatment at 30 per cent. Omitting Clouston's, the general average of the above results is, that in 49.2 per cent. cardiac disease existed before the patients began the salicyl treatment, and that in 18.2 per cent. it developed after that, while 30 per cent. of cardiac disease developed after other methods of treatment were begun.
144 Lancet, i., 1882, 134.
145 St. Thomas's Hospital Reports, New Series, viii. 252.
146 St. Bartholomew's Hospital Reports, xvi. 10.
147 Quoted by T. G. Smith, Lancet, i., 1882, 137.
The subject is one beset with difficulties, and still needs investigation. It is reasonable to infer that as the salicylates promptly arrest the articular inflammation and allay the fever of uncomplicated acute rheumarthritis, they will prevent the visceral inflammations so apt to develop when the disease runs its course uninfluenced by treatment; but experience has shown that they do not control or arrest rheumatic inflammation of the heart or pleura or the attending pyrexia, although capable of subduing the articular inflammation and the pyrexia that accompanies it. The most eminent therapeutists are divided on the subject. Maclagan, while admitting that the salicyl compounds do not ward off cardiac complications, or cure them when they exist, maintains that their existence is an additional reason for giving those remedies freely and in large doses.148 Broadbent,149 while believing in the protective influence of the salicylates "when brought to bear upon the fever in the first days of its existence," finds in the presence of any cardiac inflammation a reason for at once discontinuing those remedies. Flint150 believes that rheumatic endo- and [p. 55]pericarditis are more common since the introduction of the salicyl treatment than when the alkaline method was relied upon almost entirely, and advises151 the administration of alkalies with the salicylates to protect the heart. Vulpian152 thinks the protective power in question probable, but not established; while the latest French authority, Homolle, is of opinion that "cardiac affections are really less frequent in patients treated by salicylate of sodium than in others."153
148 Lib. cit., pp. 266, 275.
149 Lancet, i., 1882, 138.
150 New York Med. Record, 1882, 66.
151 Pract. Med., 5th ed., 1098.
152 Du Mode d'Action du Salicylate du Soude dans le Traitement du Rheum. Artic. Aigue, Paris, 1881, 11.
153 Nouveau Dict. de Méd. et de Chir., xxxi., 1882, 648.
5. The occurrence of hyperpyrexia is not always prevented by the salicyl remedies, even when they have produced their full physiological effects. Fagge endeavors to explain away the two cases of hyperpyrexia which occurred under Greenhow and the other two which happened amongst the cases tabulated by himself, and remarks that if the temperature should begin to fall under the use of salicylic acid, and then should change its course and rapidly attain a dangerous height, that would really show that the drug is sometimes incapable of preventing the occurrence of hyperpyrexia. This actually happened in one of Powell's two cases,154 and the patient died suddenly at a temperature of 107°. In Greenhow's first case the patient had been taking the salicylate for four days, and was deaf and delirious when the temperature became 105.8°.155 Finney reports a case in which drachm iss of salicine were given daily for two days, and drachm ij on the third day, when pericarditis set in, and on the fourth day hyperpyrexia supervened.156 Haviland Hall records an instance in which the temperature fell from 103.5° to 100.6° after twenty-grain doses of salicylate soda, every three hours, taken for two days; on the third day the medicine was given every four hours; the temperature rose in the evening to 103.4°, and on the next day it rose rapidly to 108.7°, and the patient became delirious. Patient recovered rapidly after two baths.157
154 Lancet, i., 1882, 135.
155 Clin. Soc. Trans., xiii. 264.
156 Brit. Med. Journ., ii., 1881, 932.
157 Lancet, ii., 1881, 1082. See also two cases in Med. Times and Gaz., ii., 1876, 383.
Pericarditis is not always present when hyperpyrexia arises during the administration of salicylic acid; it was absent in Powell's cases, is not mentioned in Hall's, and did not ensue in one of Greenhow's until two days after the temperature had reached 105.4° F. However, either pericarditis or pneumonia is very frequently present when the temperature is excessive. It is generally admitted that the salicylates do not control rheumatic hyperpyrexia once it exists.
6. Notwithstanding the prompt removal of the pain and reduction of the fever by the salicyl compounds, the average duration of acute articular rheumatism is not very considerably lessened by those remedies. Thus, of Hood's158 350 cases treated by salicylates the average duration of the illness was 35.95 days as against 38.75 under other methods. The average time spent in bed by Warner's 342 cases was 19.5 days under the salicylates, and by 352 patients under other remedies 23.5 days. Both estimates show a curtailment of the duration of the disease by the new treatment of three to four days only; which is not a very material improvement.
158 Calculation from Dr. Hood's Tables 1 and 1a, Lancet, ii., 1881, 1119.
[p. 56]7. Nor do the salicylates materially alter the time spent in hospital by rheumatic patients; some evidence indicates that they actually prolong that period. The following are the average residences in hospital under the salicylates, according to several recent authors, and they are remarkably uniform with two exceptions: Coupland, 36 days; Warner, 34.9; Hall, 34; Southey, 32.5; Broadbent, 31.2; Powell, 31; Finlay and Lucas, 29.7;159 Owen, 23; Brown, 21.9;160 or a general average of 30.4 days for the salicyl remedies. Under full alkaline treatment: Owen, 26 days; Dickinson, 25;161 Fuller, 22.2;162 Blakes, 24;163 or a general average of 24.3 days for full alkaline treatment. And if to these we add Finlay and Lucas's results, 27.7 days, under but two to three drachms of alkaline salts in the twenty-four hours—a quantity only the fourth of that given under the full alkaline method—the general average residence in hospital under alkaline treatment was but 25.4 days; that is, five less than under the salicylate.
159 Lancet, ii., 1879, 420.
160 Boston Med. and Surg. Journ., Feb., 1877. The four cases excluded by the reports are included in this calculation, that it may more fairly be compared with other reports.
161 Lancet, i., 1869.
162 The Practitioner, i., 1869, p. 137.
163 Boston City Hospital Reports, 1st Series.
These several estimates of the time spent in hospital under the salicylates, with the exception of Owen's and Brown's, correspond closely with that of the time spent by Gull's and Sutton's patients under mint-water—32.8 days—although the general average of them falls short of the latter by 2.4 days.
The following table (iii.) of Hood's164 shows that under the salicylate method 45.7 per cent. remained in hospital beyond forty days, and 39 per cent. under other methods, and that about 50 per cent. more were discharged within twenty days under the other methods than under the salicylate:
| 350 cases treated with salicylates: | ||||
| Days. | ||||
| Under 10. | Under 20. | Under 30. | Under 40. | Ill longer. |
| 3 = 0.84%. | 31 = 8.88%. | 76 = 21.7%. | 84 = 24%. | 160 = 45.7%. |
| 850 without salicylates: | ||||
| Days. | ||||
| Under 10. | Under 20. | Under 30. | Under 40. | Ill longer. |
| 12 = 1.4%. | 105 = 12.35%. | 175 = 20.1%. | 182 = 21.4%. | 331 = 39%. |
164 The Lancet, ii., 1881, 1120.
These statistics favor Greenhow's opinion that patients treated with salicylate of sodium regain their strength slowly, and are long in becoming able to resume their ordinary occupations. Some allowance, however, must be made for the precautions against relapse under salicylates observed in hospitals since the great tendency thereto has been recognized.
8. Certain unpleasant or toxic effects are produced by salicylic acid and salicylate of sodium; such are nausea, vomiting, abdominal pain, frontal headache, tinnitus, incomplete deafness, vertigo, tremor, quickened respiration, very rarely amblyopia and even temporary amaurosis, and not unfrequently delirium. A feeling of prostration and general misery is not uncommon. These phenomena of salicylism are in great measure proportionate to the dose employed, but they have followed moderate [p. 57]doses, owing sometimes to idiosyncrasy, and perhaps frequently to retarded elimination consequent upon previous disease of the kidneys or disturbance of their function by the salicylic acid or its salt. Those agents are usually completely excreted in forty-eight hours, but in one of Powell's165 cases elimination was not completed before the fifth day, and not before the eighth in Byanow's case.166 Possibly uræmia may in some cases cause the delirium.167 The delirium, which may be violent or not, is often preceded by dryness of the tongue, restlessness, and rapid breathing. Impurities in the acid may account for the inconstancy with which delirium has been noticed by different observers. While but 2 instances in 82 cases were met with by Coupland, 3 out of 90 cases by Broadbent, and 3 out of 109 by Brown,168 Charles Barrows169 encountered 8 instances in 28 cases. In one of these a boy of eleven became delirious in eighteen hours, having taken 10 grs. of salicylate of sodium every three hours. In another instance the drug had been in full use for five days before the delirium manifested itself. These phenomena of salicylism rapidly disappear when the medicine is stopped, and delirium has not always recurred on its resumption. They are less frequent in children, in whom elimination by the kidneys takes place very rapidly and a marked tolerance of salicyl compounds exists. Occasionally more serious effects appear to be produced by the salicylates, owing to their direct action on the heart, impairing its power, as evidenced by feeble impulse and sounds, increased frequency of the pulse, and diminution of the arterial pressure.170 But, notwithstanding the very large number of cases of acute rheumatism that have been treated by the salicyl compounds, very few clear instances of their toxic action on the heart have been recorded, and even in some of these there were other conditions present that may have played some part, perhaps a chief part, in the production of cardiac failure. In Greenhow's case171 the autopsy revealed a dilated fatty heart and slightly granular kidneys, and the cardiac failure coincided with a fall of temperature to 97° F. Goodhardt's172 patient died in nine hours after beginning the salicylic acid, of which she took but one drachm, in divided doses, every three hours. The pulse rose rapidly to 160; she was restless and moaning, but died quietly and suddenly. Recent pericarditis, with one or two points of fatty degeneration of the heart's substance, and sound kidneys were found. The reporter of the case inclines to the opinion that the acid produced sudden collapse and cardiac failure, while Bristowe referred them to the rheumatic poison itself. I have not been able to refer to Hoppe Seyler's paper,173 in which he relates that having given 5 grammes of salicylic acid to a child of seven and a half years affected with articular rheumatism, shortly afterward there occurred deafness, agitation, profuse sweating, dyspnoea, and finally fatal collapse. The condition of the heart and kidneys before and after death is not given. Weber [p. 58]published174 an instance in which 15-gr. doses of salicin given to a woman of twenty-seven produced in thirty-four hours a rapid fall of temperature from 103° to 96° F., accompanied by delirium and serious but not fatal collapse. It is well to remember that a similar failure of cardiac power is occasionally observed in other fevers when rapid defervescence occurs, although the salicyl compounds have not been taken; and it is certainly necessary to give these remedies cautiously, and often to administer alcohol with them, when the heart's action is at all enfeebled by protracted pyrexia and pain, or by disease (inflammatory or degenerative) of its substance or envelope. Indeed, if severe cardiac inflammation obtain in rheumatism, the remedies are powerless and perhaps unsafe. The sudden reduction of the temperature when much exhaustion obtains, even in the hyperpyrexia of rheumatic and other fevers, whether by salicylic acid or quinia or the cold bath, may be attended with fatal collapse of the heart.
165 Lancet, i., 1882, 135.
166 Quoted by Wood in his Therapeutics and Mat. Med., 1880, from Centralb. für Chir., 1877, 809.
167 See DaCosta's observations in Am. Med. Journal, vol. lxix., and Ackland's in B. Med. Journal, i., 1881, 337.
168 Boston Med. and Surg. Journal.
169 N.Y. Med. Record, April 29, 1882, 456.
170 Köhler, Centralb. f. Med. Wissensch., 1876, and Dunowsky, Arbeiter Pharm. Labor., Moskau, i. p. 190, quoted by H. C. Wood, Therapeutics, Mat. Med., etc., 3d ed., p. 639.
171 Clin. Soc. Trans., xiii. p. 266, c. iii.
172 Ibid., p. 123.
173 Quoted by D. Seille, Thèse, De la Méd. Salicylée dans le Rheumatism, Paris, 1879, p. 54.
174 Clin. Soc. Trans., x. p. 70, 1877.
Instead of the frequent weak pulse above mentioned, I have many times found salicylate of sodium render the pulse very slow, labored, and compressible in typhoid fever, and generally at the same time the temperature has been considerably reduced below what it had been.
A temporary albuminuria is not infrequent; excluding mere traces, it obtained in 52 per cent. of cases treated by the salicylates alone or in conjunction with full doses of alkali, and in but 25 per cent. of those in which full doses of alkali, with or without quinia, were employed.175
175 Isambard Owen, Lancet, ii., 1881, p. 1081.
Very rarely hæmaturia and even nephritis have occurred. The active principle is chiefly eliminated by the kidneys, which may account for a local irritating influence upon those organs.
Salicine is much preferred by Maclagan to salicylic acid and to salicylate of sodium, on the grounds that it is a bitter tonic and produces less debility and more rapid convalescence than those agents, and that it never produces delirium nor depresses the heart's action. Ringer176 and Charteris177 state that they have never seen salicine, even in large doses, cause delirium; and Prof. Gairdner has not found it produce any unfavorable symptoms.178 On the other hand, Greenhow179 found that marked depression of the heart's power ensued in 4 out of 10 cases whilst the patients were taking salicine, and entirely subsided after it was discontinued. Further careful and extended observation is needed before the relative value of salicine and salicylate of sodium can be reliably stated. It is probable that the salt is more active and prompt than the bitter principle; and this, with the greater cheapness of the former, may perhaps account for the more general employment in hospitals of the salicylate than of salicine. The latter, moreover, is often tolerated when the former is not.
176 Handbook Therapeutics, 8th ed., 1880, 587.
177 Brit. Med. Jour., i., 1881, 229.
178 Lancet, i., 1882, in table giving experience of British hospitals, prepared by Maclagan.
179 Trans. Path. Soc., xiii. 262.
As regards the doses of these agents required in acute rheumatic arthritis, practitioners are not agreed; Maclagan, Stricker, Fagge, Broadbent, Ringer, Flint, Sée, recommend large doses at short intervals at the outset, with the view of getting the patient rapidly under the influence of the drug. Maclagan gives salicine scruple i-ij at first hourly, then every two hours [p. 59]as the acute symptoms begin to decline; after the second day he allows 20 to 30 grs. every four hours for two or three days; "and for a week or ten days more that quantity should be taken three times a day." Stricker, Fagge, Broadbent, and Sée recommend about 20 to 30 grs. of salicylate of sodium every hour or two for six doses (= drachm ij-iij in the day), and Ringer would employ 10 grs. hourly, and if in twenty-four hours this dose has not either modified the disease or produced its characteristic symptoms, he would increase it to 15 and then to 20 grains hourly. On the other hand, Owen's180 results show practically no difference in the duration of pain and pyrexia and in the average duration of illness from the commencement, whether drachm iij or drachm ij or drachm iss were given every twenty-four hours; and C. G. Young181 found that 10 to 15 grs. every one, two, or three hours are sufficient.
180 Lancet, ii., 1881.
181 Dub. Journ. Med. Sci., Sept., 1880, 193.
Indeed, exceptionally good and exceptionally indifferent results are reported under similar doses. No such good results are reported as those of the Boston City Hospital under doses of drachm ij to drachm iv per diem, the average residence in hospital being only eighteen days if four cases which became chronic are excluded, or 21.9 days if they are included.
The plan in vogue at our hospital here and in my own private practice is to give about 15 grains every two or three hours, according to the severity of the case and until the articular pain and pyrexia are relieved. After the pain and pyrexia have yielded, the remedy should be continued in smaller doses, say 10 to 15 grs., three or four times a day, according to the severity of the case, for eight to ten days longer, to prevent relapse, and during this period exposure, exercise, and dietetic excesses must be carefully guarded against.
The salicine may be given dissolved in milk or enclosed in wafers; the salicylate of soda, in a solution of any aromatic water, to which extract of liquorice or syrup of lemon and a few drops of spirits of chloroform may be added. The French add a little rum to flavor the mixture. Should severe cardiac inflammation exist, and, even although not severe, should there exist signs of failure of cardiac power, salicylates and salicine had better be avoided. If the secretion of urine diminish considerably under their use, or hæmaturia supervene, or organic disease of the kidneys exist, they must be employed cautiously, and may require prompt suspension. If marked debility exist, stimulants, especially the alcoholic, should be combined with them.
The oil of wintergreen has recently been well spoken of by F. P. Kinnicutt of St. Luke's Hospital, New York,182 as a substitute for salicylate sodium. It is itself a methyl salicylate 90 per cent., plus terebene 10 per cent. Its officinal name is oleum gaultheria, and it is given in doses of minim x-xv every two hours except during sleep, and in severe cases of articular rheumatism during the twenty-four hours, either by floating the oil upon a wineglass of water or milk or in capsules or upon lumps of white sugar. It resembles in its influence upon acute rheumatism very closely the sodium salicylate, for which it may perhaps be substituted, and Kinnicutt maintains that it is quite as effectual, pleasanter to take, and free from the intoxicating properties of the salt and the salicylic acid. It requires to be continued during convalescence just like the salicylate.
182 Med. Record of New York, Nov., 1882, 505.
[p. 60]The alkalies—in this country at least—were the favorite remedies in the treatment of acute articular rheumatism before the powers of salicine and salicylic acid became generally known, and there are still authorities who maintain their excellence, if not their superiority over the salicylates, in protecting the heart against the recurrence of rheumatic inflammation (Flint, Dickinson, Sinclair, Stillé).
Under the term the alkaline treatment unfortunately are included two distinct methods of administering the salts composed of potash and soda and the vegetable acids, carbonic, tartaric, citric, etc.—viz.: that in which about half a drachm of one of these salts is given three or four times a day; and the other known as Fuller's method, in which large doses are prescribed, so that from an ounce to an ounce and a half is given in the first twenty-four hours, with the view of rapidly rendering the urine alkaline, and if possible the perspiration also; for I have frequently produced the former effect in less than twelve hours, yet have found the perspiration still redden litmus on the second, and even the third, day and later. A disregard of the essential differences existing between these two methods of employing alkalies in acute rheumatism may partially account for the differences of opinion existing as to the value of the alkaline treatment, and for the differences in the statistical results thereof published by various observers—a remark applicable to other methods and statistics also. Fuller commonly ordered every three or four hours bicarb. sodium drachm iss and acetate of potassium drachm ss dissolved in ounce iij of water and rendered effervescing at the moment of administration by the addition of an ounce of lemon-juice or drachm ss of citric acid. As soon as the urine presents an alkaline reaction—which is usually the case in twelve to twenty-four hours—the quantity of the alkali is reduced by one-half, or to about 8 drachms, during the succeeding twenty-four hours, and provided the urine continues alkaline to 3 drachms on the third day. On the fourth day and subsequently only a scruple to half a drachm of alkali is given three times a day, sufficient to keep the urine alkaline, and to each dose are added 3 grains of quinia dissolved in lemon-juice; and this combination is continued till convalescence sets in. An aperient pill is given whenever needed, but is administered "only under conditions of extreme nervous irritation." The method is not an exclusively alkaline one.
Space will not allow of a lengthened analysis of the statistics that have been published on this subject, and I will give only some of the more important statistical results. While, as we have seen, the average duration of pyrexia and articular pain under salicylate treatment is about 5.4 days, under moderate alkaline treatment, according to the recent statistics of Finlay and Lucas,183 the average duration of pyrexia was 10.3 days and of articular pain 12.2 days, and of Owen184 6.5 days for the first and 8 days for the second, or a general average for the pain and pyrexia together of 9.25 days, or about 3.85 days longer than under the salicylate treatment. Nor can it be said even of the full alkaline plan that the first or second dose frequently relieves the articular pains like a charm. On the other hand, it has been already shown that the average time spent in hospital was five days less under the full alkaline than under the salicylate treatment.
183 Lancet, ii. 1879, 420.
184 Ibid., ii., 1881, 1081.
As regards the relative power of the salicylates and of full alkaline [p. 61]treatment in protecting the heart, the following analysis and calculation deserve attention. The percentage of cases in which cardiac disease set in after the salicylate treatment began was, according to Powell, 18.75; according to Haviland Hall, 37.1; according to Finlay and Lucas, 11.60; Southey, 8; Brown, 4.76; Jacobi, 3.35, or a general average of 14 per cent.; whereas cardiac disease developed after the alkaline treatment had commenced in 13.6 per centum according to Blake;185 in 10.7 per cent. according to Dickinson;186 in 7 per cent. according to Owen; in 6.6 per cent. according to Finlay and Lucas; and in 2 per cent. according to Fuller; making a general average of only 7.8 per cent.
185 Med. and Surg. Reports of Boston City Hospital, 1st Series, 1870.
186 This percentage is obtained by adding together all the cases treated by alkalies given by Dickinson in his IX., X., XI., and XII. tables. Their total was 65 cases in which the heart was affected seven times. In table IX. from drachm ii-iv of alkaline salts were given daily, and in table X. about drachm iij daily.—Lancet, i., 1869.
Judging from these statistics, it is not improbable that a combination of sodium salicylate, with full doses of bicarbonate of sodium or chlorate of potassium, will give better results in the treatment of acute rheumatism than either of those classes of remedies singly. Indeed, Flint and others have advised such combinations, and Bedford Fenwick has recently stated, as a result of his experience in 30 cases, that if, after giving a free purge, followed by scruple doses of sodium salicylate hourly for six hours, that salt be stopped, and in twelve hours afterward half-drachm doses of citrate of potassium be administered every four or six hours until the saliva becomes alkaline, relapses will be extremely rare, and that this is the safest and most successful method of treating acute and subacute articular rheumatism.187
187 Lancet, i., 1882.
Having spoken somewhat fully upon the remedies of which I have most personal experience, and which have the largest number of advocates at the present time, and having advised the combination of these remedies, I shall only glance at some of the other remedies or methods of treating the disease still more or less employed.
Quinia, given in divided doses to the extent of 15 to 30 grains in the day, is still highly thought of in France in the early stages, during the course of and on the occurrence of relapses, in acute (especially febrile poly-) articular rheumatism. It is claimed by Briquet, Monneret,188 Legroux, and others that although not a specific for the disease it moderates the general disturbance, diminishes the local affections, and even retards the development or lessens the gravity of the cerebral symptoms—that, although it does not control the cardiac inflammations, it is not contraindicated by them. The only recent English authority who has strongly advocated full doses of quinia in this disease is Garrod,189 but he mixed the drug, in five-grain doses, with half a drachm of bicarbonate of potassium, a little mucilage, and spirits of chloroform, and gave it every four hours until the fever and articular affection had completely abated. Sufficient facts have not been published to permit of the formation of a reliable judgment as to the actual or the comparative value of either the simple quinia or the quino-alkaline treatment of acute and subacute articular rheumatism. There can be no doubt as to the value of quinia to meet certain conditions incident to the disease, such as debility, lingering [p. 62]convalescence, periodical relapse, excessive perspiration, failure of appetite, and perhaps, in some instances, high temperature. Barclay has found quinia of much service when depression has followed the long continuance of the alkaline treatment and is attended with alkaline urine and a deposit of the earthy phosphates.190 It may be given by the rectum if not tolerated by the stomach or if the alkalines are being taken.
188 La Goutte et le Rheumatisme, Paris, 1857.
189 Reynolds's Syst. Med., 1870, p. 951.
190 St. George's Hospital Reports, vol. vi. p. 111 et seq.
Greenhow191 has treated 43 cases with iodide of potassium and quinine, and says that his experience of this method contrasts favorably with that of salicine and salicylate of soda. However, pneumonia supervened in 3 cases while under treatment; cardiac inflammation arose in 6 cases (= 14 per cent.) after admission; single relapses of short duration occurred in 21 per cent.; and, excluding two cases in which the treatment was soon discontinued and 7 very mild cases, the remaining 34 cases were on the average each thirty-six days in hospital. Under this method relapses were less frequent (21 per cent. instead of 26 per cent.), and stay in hospital longer (36 instead of 30.4 days), than under that by the salicylates; but the number of cases treated is too small to base a final opinion upon. He prescribed 5 grains each of iodide of potassium and carbonate of ammonia three or four times a day, and 2 grains of quinia with three of extract of hyoscyamus in pill as often. This method, in principle at least, resembles that recommended by DaCosta, who administers in uncomplicated cases bromide of ammonium in 15- to 20-grain doses every three hours, and as soon as the acute symptoms have disappeared follows it by quinia in fair doses. It has not come into general use in this country, although its eminent proposer published his cases in 1869.192
191 The Lancet, i., 1882, 913.
192 Pennsylvania Hospital Reports, vol. ii., 1869; New York Medical Record, September, 1874, p. 481.
Notwithstanding the encomiums passed upon propylamine—or, more correctly, trimethylamine—as a remedy for acute and chronic rheumatism by Awenarius of St. Petersburg in 1856, by Gaston of Indiana in 1872, by Dujardin-Beaumetz in 1873, and Peltier in 1874 (both of France), and Spencer of England in 1875, it has not been much employed, especially since the salicylates have attracted attention. It appears that in a considerable proportion of cases the articular pains have subsided in two or three days under its employment, and then the temperature has declined, but the visceral complications have not been prevented. From 4 to 8 minims of trimethylamine in an ounce of peppermint-water, with a drachm of syrup of ginger, may be given every hour or two, the intervals to be increased as the pains diminish. When pain has quite ceased the drug may be stopped and quinia given its place. It merits further study in this disease,193 and Dr. Shapter of the Exeter Hospital has very recently stated that he is so convinced or the value of propylamine that salicylic acid has not fully commended itself194 to him. Senator has recently recommended benzoic acid or its sodium salt in large doses (about ounce ss in the day) in those cases of acute rheumatic arthritis in which [p. 63]the salicylates have failed, although he admits that it scarcely rivals them.195 His 22 patients were relieved in 4.4 days as the average, and no complications occurred in any of them. Benzoic acid is said not to produce the nausea, depression, or unpleasant head phenomena of salicylic acid, to which it is closely related in chemical composition.
193 On this subject see Farier-Lagrange's Essai sur la Trimethylamine, Strasbourg, 1870; Journal de Méd. et de Chirurgie, 1873, No. 2; Medico-Chir. Rev., i., 1873, 497; Lancet, ii., 1875, 675; The Practitioner, London, i., 1875; Le Progrès Médicale, Jan. 10, 1874; ibid., Aug. 9, 1879.
194 The Brit. Med. Jour., 1881, p. 1012. See also Tyson, Philadelphia Med. Times, 1879, vol. x. 359.
195 Centralb. f. d. Med. Wiss., 1st May, 1880, quoted in Practitioner, Sept., 1880. See also McEwan's experience, Brit. Med. Journ., i., 1881, 336; F. A. Flint, M.D., N.Y. Med. Gazette, 1880.
Space will not permit of any notice of lemon-juice, perchloride of iron, the mineral acids, or the blistering treatment. Of this last my experience enables me to say that it frequently relieves the pains promptly, but does not at all always protect the heart. In my opinion it deserves an extended employment in conjunction with early and full doses of the sodium salicylate. As Andrews has not by any communication made since the publication of his paper in 1874196 maintained the value of the treatment of the disease by an exclusively non-nitrogenous diet of arrowroot, and as he had then treated but eight cases in that way, it is hardly necessary to consider it as a method of treatment.
196 St. Barth. Hospital Reports, vol. x. 359.
Having spoken of the treatment of the general disease acute articular rheumatism, it remains to speak of the treatment of its visceral manifestations and of some of its more important incidental symptoms and complications. As the treatment of the various forms of cardiac inflammation will be given in extenso in the articles specially devoted to those topics, I will be very brief in my notice of them.
In every case of rheumatic fever it is our primary duty to employ those measures as early and deftly as possible which in the present state of knowledge appear to promptly relieve the pyrexia and articular symptoms, and lessen the tendency to, but do not altogether prevent, the visceral complications. Such measures have been already said to be the administration of the salicylates and alkaline salts together in full doses, and the observance of certain dietetic and hygienic details to be given hereafter. If, notwithstanding, peri- or endocarditis, or both, supervene, as it frequently happens, what is to be done? I reply that even in pericarditis active interference is seldom necessary; the general treatment previously employed may be continued in the hope that it may mitigate the cardiac inflammation by reducing the pyrexia and subduing the polyarthritis, even although it be incapable of directly controlling the pericardial inflammation. If the pain in pericarditis be really severe and the heart's action much disturbed, a dozen leeches may be applied over the heart, and be followed by anodyne fomentations or hot poultices applied, as Lauder Brunton advised, over several layers of flannel interposed between the skin and them. Leeching, however, is seldom needed, a hypodermic injection of morphia generally sufficing to relieve the pain. Should these measures not relieve the pain and allay the cardiac excitement, small and repeated doses of chloral, which Balfour observes "is not more useful as a sedative than as an antiphlogistic," may be given. If there be, as so frequently happens, but little pain or cardiac disturbance, there being only a friction sound revealing the inflammation, the hot poultices or anodyne fomentations, or even covering the front of the chest with wadding or a belladonna plaster, which I prefer, will suffice. Should pericardial effusion ensue, the diet must be improved, and if much [p. 64]debility exists, the salicylate and alkalies should be stopped, and wine may be given along with quinine alone or with pretty full doses of muriate of iron. As the strength returns absorption commonly takes place; but if it is delayed, either the iodide of potassium or the infusion of digitalis may be employed along with the quinia; or, if no special contraindication exist, a pill containing a grain each of blue mass, digitalis, squill, and quinia may be given three times a day and its effects carefully watched. Much difference of opinion obtains as to the value of flying blisters on the præcordia. Although not often required, they appear to be more useful than iodine applications. In those comparatively rare instances in which the effusion is abundant and remains unabsorbed, either because it is largely sero-purulent or purulent, it is proper to aspirate the pericardial sac, which should certainly be done if marked signs of cardiac oppression and failure coexist. Having once hesitated to aspirate in recent rheumatic pericarditis with copious effusion in a lad, and found a large amount of pus in the sac after death, I would warn against hesitancy under such circumstances. Careful employment of the instrument can hardly do harm if even no large amount of effusion exist.
Active treatment is quite uncalled for, as a rule, in acute rheumatic endocarditis unattended by pericarditis. If the valvulitis occur notwithstanding the employment of the anti-rheumatic remedies, it is very doubtful if we have any others capable of directly controlling that inflammation. Inasmuch, however, as, owing to the inflamed surface being in constant contact with the fluid, many of our remedies may be applied directly to the diseased part, it is well neither to be dogmatic on the point nor to abandon hope that agents may yet be found that will prove directly useful. While carefully treating the rheumatic fever, the main indications remaining to be filled appear to be to quiet the cardiac excitement and secure as much rest to the inflamed valves as possible. The alkaline salts, salicine, and the salicylate of sodium do usually greatly reduce the frequency of the heart, and, pro tanto, secure rest. The tincture of aconite given hourly, so as to slacken the heart's speed, is useful in the sthenic stage of endo- and of pericarditis; and the benefit of absolute rest of the body in bed and of the joints in splints during the entire course of rheumatic fever, in preventing cardiac inflammations and in treating them, has been shown by Sibson.197 When signs and symptoms of cardiac weakness arise, whether from the pressure of pericardial effusion or from myocarditis or any other cause, the employment of salicylates, alkalies, aconite, and chloral should be at once stopped and alcoholic stimulants and tonics (strychnia, quinia, iron) and good food should be freely administered. The most valuable point made of late in the therapeutics of acute inflammations of the valves is Fothergill's development of Sibson's principle—viz. that "general quietude for weeks after an attack of acute endocarditis is indicated," as the cell-growth in the valve may not be quite over in a less time,198 and the work of repair, we may add, not completed. The same principle is specially applicable in myocarditis.
197 Reynolds's System of Med., vol. iv. p. 527, Eng. ed.
198 Diseases of Heart, with their Treatment, 2d Series, 1879, 149.
The disturbances of the nervous system were divided into those [p. 65] dependent upon gross organic alterations of the nervous centres and their envelopes, and those not so related, but which we commonly speak of as functional. Were it possible generally—which it is not—to diagnosticate rheumatic meningitis from the merely functional form of so-called cerebral rheumatism, then its treatment would resolve itself into a vigorous use of the anti-rheumatic remedies, salicylates, alkalies, etc., and the active employment of ice and leeches to the scalp, purgatives, full doses of the iodide and bromide of potassium, ergot, etc. If, together with the symptoms of that often obscure and comparatively rare complication of rheumatic fever, ulcerative endocarditis, there occurred severe headache, delirium, or paralysis, we might find great difficulty in determining the cause of the cerebral disturbance, and would naturally vary our measures according as we suspected meningitis, embolism, or simple functional disturbance, and the treatment adapted to these several conditions will be found under their respective heads in this work.
Coming now to the functional disturbances of the nervous centres, which are the ordinary forms met with in acute articular rheumatism, they may be divided, for therapeutical reasons, into two groups: (1) Those unattended by hyperpyrexia, and (2) those preceded, accompanied, or followed by hyperpyrexia.
(1) When any sign of disturbance of the nervous system, delirium, restlessness, taciturnity or talkativeness, insomnia or somnolence, deafness, tremulousness, vacancy, stupor, or what not, occurs in rheumatism with but a moderate temperature, 101° to 103°, while we anxiously watch the temperature from hour to hour, prepared to combat any tendency to hyperthermia the moment it is discovered, we endeavor to control the cerebral disturbance as in other febrile affections, but with greater diligence, knowing that in this disease these nervous symptoms very often precede hyperpyrexia. We persist with the salicylates to reduce the rheumatic element of the affection, employ remedies to control the cardiac or pulmonary inflammations which are so frequent in such circumstances, sustain the general powers by food, wine, and quinia, if, as frequently happens, there are evidences of failing strength, and meet any other special indication that may arise. For example, we procure sleep and allay motor and mental excitement by opium or chloral and by evaporating lotions or the ice-cap to the head. We reduce temperature, allay restlessness, preserve the strength, and promote sleep by lightening the bed-clothes, drying frequently the entire surface of the body if it is perspiring freely, or by sponging it with tepid water hourly if dry and hot. We act on the kidneys, bowels, and if necessary the skin, if from the scantiness of the urine or other evidence we suspect uræmia. Should these means fail and the delirium and other symptoms which occur in cerebral rheumatism continue, and especially should they be severe, it would be, in the writer's opinion, proper to employ the methods that are now resorted to when hyperpyrexia accompanies those symptoms; for patients suffering from cerebro-spinal disturbance or rheumatic fever, although unattended by hyperthermia, do die if those symptoms continue. Moreover, the hyperthermia may at any moment supervene; it is itself perhaps as much a nervous disturbance as delirium, and apt to succeed the latter. It was in these very cases in which the delirium preceded the hyperpyrexia that the London committee to be presently mentioned found the highest [p. 66]mortality. If along with these nervous symptoms the articular pain or the sweating disappear suddenly, or if the pulse suddenly increase in frequency without demonstrable increase of cardiac mischief, there is reason to anticipate the supervention of hyperpyrexia.
(2) When the cerebro-spinal disturbance of rheumatic fever is followed, preceded, or accompanied by hyperpyrexia, there is one indication for treatment which dominates all others, and that is the prompt reduction of the hyperthermia. The terrible danger of this condition in rheumatic fever is known to all persons who have had much experience of the disease. Wilson Fox in 1871 had not known a case recover after a temperature of 106° unless under the use of cold, yet that is not an alarming temperature in intermittent or relapsing fever, and is often recovered from in typhoid fever. Thanks to Wilson Fox,199 Meding,200 H. Thompson,201 H. Weber,202 I. Andrew,203 Maurice Raynaud,204 Black,205 Fereol,206 and many others since, it has been established that when the hyperthermia is removed by external cold the nervous disturbances also usually at once disappear or lessen very much. And thus we are brought to the treatment of the hyperpyrexia of acute articular rheumatism. On this important topic it will be most satisfactory and convincing to give some of the conclusions arrived at respecting hyperpyrexia in acute rheumatism by a committee of the Clinical Society of London.207 I will condense some of them.
199 Treatment of Hyperpyrexia, 1871, and Lancet, ii., 1871.
200 Archiv für Heilkunde, 1870, xi. 467.
201 Brit. Med. Jour., ii., 1872; Lancet, ii., 1872; and Clinical Lectures, 1880.
202 Clin. Soc. Transactions, v. 136.
203 St. Bartholomew's Hosp. Repts., x. 337.
204 Journal de Thérap., No. 22, 1874.
205 Gaz. Hebdomad. de Méd. Sci., 1875.
206 Soc. Méd. des Hôpitaux, 8 Juin, 1877.
207 Brit. Med. Jour., i. 82, 807.
1. "Cases of hyperpyrexia in acute rheumatism prevail at certain periods;" "such excess corresponds in a certain degree, but not in actual proportion, to a similar excessive prevalence of acute rheumatism generally. The largest number of cases of hyperpyrexia arise in the spring and summer months, whereas rheumatism is relatively more common in the autumn and winter." 2. "Whilst very little difference obtains between the two sexes in regard to proclivity to rheumatism, the proportion of males to females exhibiting hyperpyrexial manifestations is 1.8 to 1." (3 omitted.) 4. "The cases of hyperpyrexia preponderate in first attacks of rheumatic fever." 5. "Hyperpyrexia is not necessarily accompanied by any visceral complications, but may itself be fatal. The complications with which it is most frequently associated are pericarditis and pneumonia." 6. "The mortality of these cases is very considerable, hyperpyrexia being one of the chief causes of death in acute rheumatism." 7. "Although present in a certain number of cases, and these of much value from their prodromal significance, neither the abrupt disappearance of articular affection, nor the similarly abrupt cessation of sweating, is an invariable antecedent of the hyperpyrexial outburst." (8, 9, 10 omitted.) 11. "The post-mortem examinations in a certain proportion elicited no distinct visceral lesions, and when present the lesions were not necessarily extensive." 12. "The prompt and early application of cold to the surface is a most valuable mode of treatment of hyperpyrexia. The chances of its efficacy are greater the earlier it is had recourse to. The temperature cannot safely be allowed to rise above 105° F. Failing the most [p. 67]certain measure—viz. the cold bath—cold may be applied in various ways: by the application of ice, by cold affusions, ice-bags, wet sheets, and iced injections."
Whatever differences of opinion may obtain as to the value of cold in the treatment of the hyperthermia of typhoid fever, there is a tolerable consensus of opinion that it is our most reliable and promptest resource in those formidable cases of rheumatic fever attended with hyperpyrexia, both when alarming delirium and coma coexist and when they are absent.208 Space will not allow of details here in the employment of cold to reduce hyperpyrexia—a subject discussed elsewhere in this work. Suffice it to say, that besides the cold bath (70° or 60°) which the committee regards as the most certain, the tepid bath (96° to 86°) is employed by Fox and regarded as the best by Andrews; it may be cooled down to 70° by adding ice or cold water to it (Ziemssen). The cold wet sheet-pack is still thought much of, like the last, in old and feeble people. Kibbie's method deserves more attention than it has received. He pours tepid water (95° to 80°) over the patient's body, covered from the axillæ to the thighs with a wet sheet and laid upon a cot, through the open canvas of which the water passes and is caught on a rubber cloth beneath the cot, and conveyed into a bucket at the foot of the bed.
208 The powerful depressing effects of high temperature on the human body, and the remarkable opposite influences of a cool temperature, have been personally experienced by the writer in the last three days. For two or three days the weather has been very hot, and he has experienced the usual feeling of exhaustion, incapacity for thought and action. After a thunderstorm last evening the temperature fell 25°, and this morning, twelve hours later, he feels vigorous, refreshed, and capable of intellectual and physical labor. The change is remarkable.
The existence of polyarthritis, of peri- or endocarditis, of pneumonia or pleurisy, does not contraindicate the cold bathing. If much weakness of the heart obtains, it is well to give some wine or brandy before employing the bath, and perhaps while in it, and the patient should not be kept in the bath until the temperature reaches the norm, for it continues to fall for some time after his removal from the bath. If the temperature fall rapidly 2° to 3° in five or six minutes, remove the patient from it as soon as the temperature recedes to 102° or 101° F. If it fall very slowly, the bath may be continued till the temperature declines to 99.5°, when he should be taken out. Should marked symptoms of exhaustion or of cyanosis arise, the bathing should be at once stopped. After it has been found necessary to employ cold in this way, the thermometer should be used every hour, and if the temperature tend to rise rapidly again, the diligent application of a succession of towels wrung out of iced water and applied to the body and limbs, or of Kibbie's method, may suffice; but should they not, and a temperature of 103° or 104° be rapidly attained again, the cold or tepid bath should be at once resumed. In severe cases of this kind a liberal administration of alcohol and liquid food is generally needed, and it is well to try antipyretic doses of quinia by mouth or rectum, although they are usually very disappointing in these cases. It is admitted that cold baths have in a few rare instances caused congestion of the mucous membrane, pneumonia, pleurisy, and even fatal syncope. This is a reason for the exercise of care and constant oversight on the part of the physician, but hardly an excuse for permitting a person to die in rheumatic hyperpyrexia without affording [p. 68]him at least the chance of recovery by the use of the cold or tepid bath.
If delirium and deafness supervene during the employment of the salicylates, it is prudent to suspend their use and take the temperature every couple of hours, as one cannot feel confident that hyperpyrexia may not be impending. Both Caton and Carter have found that the addition of bromohydric acid to the sodium salicylate mitigated or controlled the tinnitus and deafness produced by full doses of that salt.
SUMMARY OF TREATMENT OF ACUTE RHEUMATIC POLYARTHRITIS.—As a general rule, commence at once with a combination of sodium salicylate, say 10 grains, and citrate of potass. gr. xv, every hour for twelve doses, after which give the citrate alone every two hours during the rest of the day. Repeat these medicines in the same way daily until the temperature and pain have subsided, when only half the above quantities of the drugs are to be given every twenty-four hours for about a week longer, after which three 15-gr. doses of the salicylate, with a like quantity of the citrate, are to be administered every day for another week or ten days, to prevent relapses. It is in this third week that quinia is most likely to be required, and as a general rule it may be given with benefit at this period in doses of 2 grains three times a day between the doses of the salicylate. Should the above dose of salicylate not relieve the pains sensibly in twenty-four hours, increase next day the hourly dose to 15 or 20 grains; and if this free administration of the medicine afford no relief after four or five days' use, substitute for the salicylate salt the benzoate of ammonia in 15- to 20-grain doses hourly, continuing the citrate of potassium and conducting the treatment in the manner first advised. Should the benzoate likewise fail after four or five days' trial, omit it, and employ the full alkaline method together with the quinia, of which about 10 to 15 grains may be given in the day between the doses of the alkaline salt.
For the local treatment no uniform method is invariably applicable. In many cases simply painting the joints with iodine daily, or enveloping them in cotton wool, with or without the addition of belladonna or laudanum, and securing it by the smooth and gentle pressure of a flannel roller, proves sufficient. Hot linseed poultices containing a teaspoonful of nitre or of carbonate of soda often afford relief, and so does Fuller's lotion, applied to the articulations by means of spongio-piline, or lint covered with oiled silk. It consists of liq. opii. sed. fl. ounce j, potass. carb. drachm iv to drachm vj, glycerinum fl. ounce ij, aqua fl. ounce ix. It must be plentifully applied. If the articular affection be very severe and not relieved by the above measures, absolute immobility of the joints, secured by means of starch and plaster-of-Paris bandages, has been shown to be very useful, relieving the pain, shortening the duration of the local and the general disturbance, and protecting neighboring joints from invasion.209
209 See Heubner in Archiv der Heilkunde, vol. xii., and Oehme in ibid., vol. xiv., and a striking case in St. Barth. Hosp. Reports, 1876, p. 174, by R. Bridges, M.D.
We have little experience in this country of ice continuously applied to the joints until all the symptoms of acute rheumatism have disappeared (Esmarch and Stromeyer).
Circlets of blistering fluid applied above all the affected joints [p. 69]simultaneously, as practised especially by Herbert Davies,210 often afford prompt relief to the pain, but they do not invariably protect the heart, in my experience.
210 London Hospital Reports, vol. i., 1864, 292.
The hygienic and dietetic management of acute articular rheumatism demands careful attention. While the room should be well supplied with fresh air and sunlight, it should be kept at a uniform temperature and free from draughts. Feather and other very soft beds should be prohibited. Many authorities put the patient between heavy blankets, which I regard as a mistake. The bed-clothing should be light and just sufficient to keep the patient agreeably warm; the night-gown may be of thin flannel and the sheets of cotton. The excess of perspiration should be removed by gentle rubbing with a warm towel at regular intervals, and the sheets should be changed frequently before they become almost saturated with the perspiration. Fatigue and exposure of the patient's person when taking food, attending to his natural calls, or having his personal or bed-clothing changed should be specially guarded against.
The diet in the early actively febrile stage should consist of panada, corn-meal or oat-meal gruel, milk, and barley-water, or even pure milk. Where persons will not take milk the various thin animal broths to which good barley-water or arrowroot or well-boiled rice has been added, jellies, sago and other starchy puddings, may be allowed. Suitable drinks are—plain water, Seltzer and Apollinaris water, carbonic-acid water, lemonade. This low, unstimulating diet should be observed until all fever and articular inflammation have subsided, the tongue become clean, and the visceral inflammations declined, and a return to solid food, and especially to animal food, should be made cautiously. Eggs are to be regarded as of very doubtful safety in this disease. As a very general rule, ales, wines, and the stronger alcoholic liquids are objectionable, but they may be required under the same conditions as in other fevers. Should the salicylates depress the heart, old wine or whiskey may be given with advantage.
During convalescence the patient should not be permitted to leave his bed for several days after complete removal of the fever and articular pain, and for the first four days he should occupy a sofa or easy-chair. Premature walking may induce relapse. An occasional alkaline or sulphur bath, if cautiously taken, sometimes appears to complete the recovery. If endocarditis have existed, a longer rest is desirable, more especially in severe cases, in order that the reparative process going on in the lately inflamed valves may not be in the least disturbed.
synonymous with rheumarthritis chronica, rheumatisme articulaire chronique simple (Besnier), polyarthritis synovialis chronica (Heuter), is defined here as a chronic idiopathic inflammation of one or a few articulations, which is more prone to become fixed than the acute form, and which, notwithstanding its protracted duration, produces no profound structural alterations in the joints.
ETIOLOGY.—It may be the direct sequel of a single attack or more [p. 70] commonly of several attacks, of acute, or more especially of subacute, articular rheumatism. But it is generally a primary affection, occurring in persons who have not had either acute or subacute rheumarthritis, yet owning the same causation as these, and occasionally in its course exhibiting acute or subacute symptoms. The specially predisposing conditions are inheritance; repeated attacks of subacute or acute articular rheumatism, which in accordance with general laws impair the resisting power of the affected joints; prolonged residence or employment in cold, damp, or wet rooms or localities; repeated exposure to bleak, cold currents of air or to frequent wettings of the body or lower limbs. For these reasons it is most common amongst the poor, who are especially exposed to the influences just mentioned; and amongst them cellar-men and sailors, washerwomen and maid-servants, are very liable to the disease. It is chiefly an affection of advanced life, or at least of mid-age, and is rare in youth. The first attacks, and especially exacerbations, are apt to be induced by the direct action of a draught of cold air or by unusual exposure to cold and damp air, especially when the body has been fatigued or overheated. In many cases no distinct exciting cause can be traced.
The morbid anatomy of simple chronic articular rheumatism will vary with the severity and duration of the disease. The alterations are such as chronic inflammation of a non-suppurative character might be expected to produce in the joints by one who had learned those characteristic of acute rheumarthritis. In the simple chronic form the proliferating process involves chiefly the synovial membrane, the capsular and other ligaments, and the periarticular tissues; to a less degree the cartilages, and to a much less degree, and exceptionally, the osseous surfaces. The synovial membrane is thickened, slightly injected, and its fringes hypertrophied and more vascular than normally. Little fluid usually exists in the joint unless during an exacerbation, when a moderate amount of thin, cloudy serum may be present; generally only a trace of thick, turbid fluid, containing oil-globules, and in severe cases débris of the cartilages, but no pus, is found. The fibrous capsule and ligaments become thickened, dense, and stiffened by hyperplasia; and sometimes the adjacent tendons and their sheaths, the fasciæ and aponeuroses, undergo similar alterations, so that the movements of the joints become seriously interfered with. In some cases this irritative hyperplasia specially involves these periarticular fibrous structures, and these, undergoing retraction, produce marked deviations, subluxations, and deformities of the articulations very like those observed in rheumatoid arthritis, although the osseous components of the joints are unaffected. Jaccoud gave to such cases the title of chronic fibrous rheumatism.211 It is worth noting that Jaccoud's, Charcot's,212 and Rinquet's213 cases of so-called "chronic fibrous rheumatism" developed out of acute articular rheumatism, while Besnier's was primarily chronic. In simple chronic rheumatism, if protracted, the cartilages also proliferate, lose their semi-transparency and polish, and become opaque and white; they are often rough and traversed by fissures, and occasionally present erosions; and these erosions [p. 71]are either naked or covered with a layer of newly-formed connective tissue, which may occasionally produce fibrous adhesions between the articular surfaces. Points of calcification occur in the cartilages and tendons in very chronic cases. Instances are observed in which the bones exhibit, to a slight degree, the alterations found in rheumatoid arthritis, and are probably transitional between the two affections. The muscles which move the affected articulations in severe cases are often atrophied, and the wasting imparts to the joints an appearance of considerable enlargement.
211 Vide Jaccoud, Clin. Méd. de la Charité, 23e Leçon, Paris, 1867.
212 Besnier, Dictionnaire Encyclopéd., etc., t. iv., p. 680 et seq.
213 Du Rheum. Artic. Chronique, etc., par Martial Rinquet, Thèse, Paris, 1879, pp. 28-33.
SYMPTOMS AND COURSE.—Simple chronic articular rheumatism presents many varieties. In the milder forms the patient experiences trifling or severe pain in one, or less frequently in two or more, joints, more especially in the knee or shoulder, or both, attended with want of power in the member or with stiffness in the affected articulation. The pain frequently is likewise felt in the soft parts, muscular and tendinous, near the joints, and is usually increased by active or passive movement; it is not always accompanied by tenderness, and rarely with local elevation of temperature or swelling. The wearying aching in the joint is of an abiding character, but is very liable to exacerbations, especially at night; and these come on just before atmospheric changes, such as a considerable fall of temperature, the approach of rain, variations in the direction of the wind, etc., and they usually continue as long as the weather remains cold and wet. A very common symptom is a creaking or a grating which may be felt and heard during the movements of the joint.
The above symptoms may rarely prove more or less constant by night and day for years, but far more frequently, at least at first, they last an indefinite period and disappear to recur again and again, especially in the cold and changeable seasons of the year. Although in the earlier attacks, and often for a long time, no alteration of structure is perceptible in the painful joints, yet in some instances slight effusion into the articulation may be observed during the exacerbations, or the capsule and ligaments may at length become slightly thickened, or the muscles may waste and produce an apparent enlargement of the joint; and this prominence of the articular surfaces may be increased by retraction of the tendons and aponeuroses—a condition which causes real deformities (deviations, subluxations, etc.) of the articulation and impairs more or less its movements. In very chronic cases a fibrous ankylosis may be established.
These last-mentioned conditions often entail great and long-continued suffering, and may even cause some anæmia and general debility; but very frequently the general health and vigor continue good, notwithstanding the permanent impairment of the functions of one or several of the large articulations, and the liability to exacerbations often amounting to attacks of subacute rheumarthritis from changes in the weather, fatigue, or exposure.
Besides the above varieties may be mentioned a not infrequent one consisting of a series of attacks of subacute articular rheumatism recurring at short intervals, involving the same joints, and attended with slight elevation of temperature, febrile urine, perspiration, and moderate local evidences of synovitis, heat, pain, tenderness, swelling, and effusion into the affected joints. This is an obstinate variety, and is often associated with rheumatic pain in the muscles and fibrous tissues of the affected member.
[p. 72]Simple chronic articular rheumatism, like the acute form, is most apt to affect the larger articulations, knees, shoulders, etc., but it frequently also involves the smaller ones of the hands and feet. Although usually polyarticular, it is prone to become fixed in a single joint, but even then it may attack several other articulations, and may migrate from one to another without damaging any.
The course of the disease is usually one of deterioration during persistent or recurring attacks, and in many cases the intervals of relief become shorter and less marked; the joints become weaker and stiffer; and although the pain may not increase and the general health may not be seriously impaired, yet the patients may continue for many years or the rest of their lives severe sufferers, unable to work, and often hardly able to walk even with the aid of a stick. Occasionally, after several years of pain and weakness, a sudden or slow improvement may set in and the patient become free from pain and lameness, and only experience some stiffness in the movements of the joints after several hours of rest, and slight thickening of the ligaments and capsule of one or more articulations. The duration of the disease is indefinite; the danger to life trifling.
The complications of simple chronic articular rheumatism are held by many, and especially by those who regard the disease as constitutional or diathetic, to be the same as those of the acute form, and that they may precede, follow, alternate, or occur simultaneously with the articular affection. All admit that they are observed much less frequently in the former than in the latter. Other pathologists either deny the occurrence of the visceral complications (Senator, Flint) or do not mention them (Niemeyer). It is not denied that cardiac disease may be found in chronic articular rheumatism which has succeeded the acute form, and which may then be referred to the acute attack. The tissue-changes then set up may not have produced at the time the murmurs indicative of endocarditis, but these tissue-changes may have ultimately roughened the endocardium, puckered a valve, or shortened its cords, so that cases of chronic articular rheumatism having a history of an acute attack cannot be safely included when inquiring into the influence of the chronic form upon the heart or other internal organ. Attention has not been sufficiently given to ascertain the frequency of the occurrence of these complications in primary chronic articular rheumatism, and reliable evidence is not at hand. It is not unlikely that the chronic form may slowly develop cardiac changes, as the acute form rapidly does; but when the advanced age of the persons most liable to chronic rheumatism is borne in mind, it must be admitted that valvular and arterial lesions (endarteritis) are observed at such periods of life independently of rheumatism, and referable to such causes as repeated muscular effort, strain, chronic Bright's disease, senile degeneration, etc. Somewhat similar observations are applicable to the attacks of asthma, of subacute bronchitis, of neuralgia, and of dyspepsia, which are frequently complained of by sufferers from simple chronic rheumarthritis. Such affections are common in elderly people in cold and damp climates; they may be mere complications rather than manifestations of rheumatism, or outcomes of the confinement and its attendant evils incident to chronic articular rheumatism, as is probably the relationship of the dyspepsia. There is [p. 73]no doubt of the frequent coexistence of muscular rheumatism with this variety.
DIAGNOSIS.—Simple chronic articular rheumatism may be confounded with rheumatoid arthritis, with the articular affections of locomotor ataxia and other spinal diseases, with chronic articular gout, with syphilitic and with strumous disease of the joints. The reader may consult the observations made on four of these affections in connection with the diagnosis of rheumatoid arthritis. A few additional remarks are called for in distinguishing chronic articular rheumatism from chronic articular gout, which is often a very difficult problem. Both are apt to be asymmetrical in distribution, to have paroxysmal exacerbations, to recur frequently without damaging the articulations, to have been preceded by acute attacks of their respective affections, and to be uncomplicated by endo- or pericarditis. But chronic rheumarthritis has no special tendency to attack the great toe; it is more persistent than gouty arthritis; it does not, even when of long standing, produce the peculiar deformities of the articulations or the visible chalk-like deposits in the ears or fingers observed in chronic gout. The etiology of the two diseases is dissimilar. There is no special liability to interstitial nephritis in articular rheumatism, nor is urate of soda present in the blood in that disease.
In chronic strumous or tubercular disease of a joint the youth, the personal and family history, and sometimes the evident defective nutrition, of the patient; the moderate degree of local pain compared with the considerable progressive and uniform enlargement of the joint; the evident marked thickening of the synovial membrane, either early or late according as the disease has originated in the synovial membrane or in the bones; the continuous course, without marked remissions or exacerbations, of the disease; the rarity with which more than one joint is affected; and the tendency to suppuration, ulceration, marked deformity, and final destruction of the joint,—will prevent the disease from being mistaken for chronic rheumatism.
The PROGNOSIS in simple chronic rheumarthritis is unfavorable as regards complete recovery, and it is chiefly while comparatively recent, and when the sufferer can be removed from the conditions productive of the disease, that permanent improvement, and sometimes cure, may be expected. As a rule, the disease once established recurs. It does not, however, endanger life.
TREATMENT.—All are agreed that hygienic treatment constitutes an essential, if not the most valuable, part of the curative and palliative management of chronic rheumarthritis. A dry and uniform climate is the most suitable, and there is much evidence in favor of a dry and warm rather than a dry and cold climate. Protection of the body against cold and damp by means of flannel next the skin, sufficient clothing, residence in dry and warm houses, etc., is of prime importance. In fact, all the known or suspected causes of the disease should be as far as possible removed.
The direct treatment of the disease resolves itself into general and local, and is essentially the same as that recommended for rheumatoid arthritis, to which subject the reader is referred. A few observations only need be made here. Although, like everything else in chronic rheumarthritis, it often fails, no single remedy has in the writer's [p. 74]experience afforded so much relief to the pain and stiffness of the joints as the sodium salicylate; and he cites with pleasure the confirmatory testimony of J. T. Eskridge of Philadelphia,214 of whose 28 cases 75 per cent. were decidedly benefited. Jacob of Leeds also reports some benefit in 75 per cent. out of 87 cases treated by the same agent.215 It must be given in full doses, and be persevered with. Salicylate of quinia should be tried if there be much debility or if the sodium salt fail. Propylamine or trimethylamine is deserving of further trial in this disease. From 100 to 200 grains are given in the day in peppermint-water. Iodide of potassium, cod-liver oil, arsenic, iodide of iron, and quinia are all and several remedies from which more or less benefit is derived in chronic articular rheumatism. The combination of iodide of potassium with guiaiac resin—gr. ij-iij of each three times a day in syrup and cinnamon-water—is sometimes very useful. The writer has no experience of the bromide of lithium (Bartholow). When the skin is habitually dry and harsh a dose of pilocarpine every other night for a few times will often prove very useful.
214 Phila. Med. Times, vol. ix. pp. 75-77, 1878, and The Medical Bulletin, Phila., July, 1879, pp. 44-48.
215 Brit. Med. Jour., ii., 1879, 171.
Cod-liver oil, iron, quinia, etc., the various forms of baths and mineral waters, electricity, and the several local measures recommended for the treatment of rheumatoid arthritis, are all occasionally very useful in, and constitute the appropriate treatment of, simple chronic articular rheumatism. The dietetic management of the two affections should be the same.
SYNONYMS.—Myalgia rheumatica or myopathia; Fr. Rheumatisme musculaire; Ger. Muskelrheumatismus.
DEFINITION.—The affections included under this term are certain painful disorders of fibro-muscular structures. They are commonly found in persons the subjects of the rheumatic diathesis, and are characterized by pain and often spasm, and sometimes a slight degree of fever. No doubt as our knowledge increases so many attacks connected with painful states of muscles and fasciæ are eliminated from the somewhat uncertain group of muscular rheumatism. True inflammation is not believed to exist, and pathological investigation has rarely shown any morbid changes in the affected parts. The symptoms, therefore, have been attributed to some temporary hyperæmia, slight serous exudation, or neuralgic state of the sensory nerve-filaments. The strongest support is given to this statement from the absence of any marked tenderness in such affected muscles as can be sufficiently examined. In certain cases, undistinguishable clinically, it is quite probable that a periarthritis is in reality the principal factor in the case. In others, again, a subacute rheumatism affecting a joint seems to spread to the adjoining tendinous sheaths, and thus secondarily to attack the muscles themselves, the affection of which may ultimately remain the only condition present.
ETIOLOGY.—Muscular rheumatism is a very common affection. All ages are liable to its occurrence, but the part affected varies with the time [p. 75]of life, children and young adults being much more subject to torticollis, and older persons to lumbago and general rheumatism of the limbs. Amongst hospital patients the disease prevails more amongst men than women, owing doubtless to the greater exposure of the former to the cold; but amongst other classes the same difference is not seen. It is observed in all countries, but according to some writers it is unusually frequent in tropical climates, although there acute rheumatism is very uncommon. The causes of muscular rheumatism are mainly exposure to cold and strain or fatigue of muscles. If these two conditions coexist—e.g. standing in a draught of cold air or lying on the ground when fatigued—the chances of the affection coming are greatly enhanced. Strain, a twist of the body, or a false step can actively start an attack of this kind, and by the sufferers themselves it is constantly attributed to this cause. The part played by this element is difficult to determine, a very slight strain being often followed by great pain and distress from the subsequent rheumatic affection. Some individuals are specially prone to attacks, the slightest current of air, change of clothing, etc. being sufficient to determine its occurrence. These persons are often found to have suffered from rheumatism in some other form, and thus in them we must consider that the rheumatic diathesis furnishes the reason for their unusual susceptibility. It only remains to mention the fact that a disposition to gout seems to favor the development of muscular rheumatism. In gouty families, therefore, it has been observed to be common.
SYMPTOMS.—In all cases pain is the prominent, and in many cases the only, symptom present. In all except the more aggravated attacks pain is felt only when the affected part is disturbed. In such when complete rest or fixed immobility is maintained there is comfort, or at most a somewhat dull, uneasy sensation, but when any contraction of the muscles in question is produced, whether voluntary or otherwise, severe often excruciating pain is at once experienced, often giving rise to a sudden cry or causing the features to be contracted in a grimace. The suffering ceases almost at once when the muscular contraction is relaxed. In more aggravated attacks the pain is more severe, and besides persists, though to a less degree, even when there is no contraction. In rare cases when the maximum degree has been attained there is continuous pain, but the affected muscles are persistently maintained in a relaxed condition by means of true spasm in the surrounding muscles. Slow passive movement affects the subject of muscular rheumatism, and may often be accomplished with a little management without causing pain. If, at the same time, these muscles be handled by pinching and slight pressure, it will be found that they are very sensitive to the touch. When some tenderness does exist, it is slight and is not located in the district of the lower nerve-trunks. Pressure even sometimes allays pain. The constant effort to avoid pain gives rise to a feeling and appearance of stiffness, and thus characteristic attitudes and positions of the head, trunk, or limbs are voluntarily and persistently maintained. There is no spasm of the affected muscles; the distortion is the result of stiff contraction of the associated muscles, which thus forcibly fix the faulty one and hold it in a state of relaxation. Cramp or spasmodic contraction of a single muscle of a painful character does, however, sometimes occur in rheumatic subjects, and much resembles the condition above described. In [p. 76]the same persons also muscular rheumatism may occur in a much more fugitive or erratic form, frequently being nothing more than a slightly painful condition of some group of muscles which have in some way been exposed to cold. This may last but a short time, and either spontaneously disappear or be readily removed by exercise or friction. Muscular rheumatism is generally confined to one muscle or a single group of muscles. Those most liable to it are the very superficial and those easily exposed to cold (e.g. the deltoid and trapezius), powerful muscles often subjected to violent strain (e.g. the lumbar muscles), and those aiding in the formation of the parietes of the great cavities.
This affection very commonly exists without any constitutional disturbances, but sometimes there are present the symptoms of pyrexia—slight elevation of temperature and temporary disorder of the digestive organs—loss of appetite, constipation, and general malaise.
The acute forms generally last but a few days, terminating by gradual subsidence and final disappearance of the pain. The fugitive kind, already alluded to, may, however, be present more or less during several weeks.
DIAGNOSIS.—Errors of diagnosis between muscular rheumatism and a variety of other disorders are common. Laymen especially are only too apt to attribute pain felt in muscles at once to rheumatism of these muscles—a term which is badly abused. Some of these errors are of no great interest, but others are of the highest importance, for they may cause the onset of a serious disease to be overlooked. The principal affections to be borne in mind with reference to diagnosis are the following: organic diseases of the spinal cord (notably tabes dorsalis), causing peripheral pains as an early symptom; functional disorder of the same part, as hysteria or spinal irritation; intra-thoracic inflammation; the onset of an exanthem; the pains produced by the chronic poisoning of lead and mercury; neuralgia; painful spasm of muscle from deep-seated inflammation or suppuration. It is sufficient to indicate these various sources of fallacy, which, if remembered, can generally be guarded against by a consideration of the special features characteristic of each one.
TREATMENT.—The indications for the treatment are mainly two—viz. to relieve the pain and to counteract the diathetic condition generally present. The relief of the pain is accomplished in various ways, according to the seat of the trouble. In severe cases it is proper to resort to the hypodermic use of morphia, to which may be advantageously added some atropia. When the pain is seated in large muscles, the injection will produce better results if thrown not merely under the skin, but into the substance of the muscle. Sometimes perfect rest in bed is necessary to secure the required immobility; in other cases this can better be secured by plaster or firm bandages. Soothing anodynes are extremely useful locally, and counter-irritants also may be used with benefit. Liniments give us a convenient form of application. The best are those containing a considerable proportion of chloroform with either aconite or belladonna, or both. The repeated application of tincture of iodine often gives great relief. Galvanism sometimes proves a rapid cure. Continuous heat is nearly always grateful, and may be applied either in the dry form or by means of soft warm linseed poultices with or without a [p. 77]percentage of mustard. When these are discontinued, care should be taken to protect the affected muscles from cold by keeping them enveloped in flannel or woollen coverings.
Whilst these local measures are being adopted the constitutional disorder should also receive attention. A diaphoretic action should be set up. For this purpose the hot-air or Turkish bath at the outset would seem to be sometimes really abortive. Of medicinal means amongst the most reliable are liquor ammonii acetatis and Dover's powder. Pilocarpine occasionally proves useful. The fixed alkaline salts are also sometimes beneficial, such as the acetate and citrate of potassium and, at a later stage, the iodide of potassium. In a certain number of cases of muscular rheumatism the sodium salicylate acts promptly and well. This drug will succeed well in proportion as the evidence of the rheumatic constitution is well marked, as shown by the tendency on other occasions to attacks of acute articular rheumatism.
Persons who are subject to muscular rheumatism should be made to wear warm clothing, avoid draughts, guard against strains and twists, and in other respects to be careful of their general hygiene. Obstinately recurring cases will very often receive benefit from a visit to some of the natural springs known to possess antirheumatic qualities.
The chief varieties of muscular rheumatism, divided according to the locality affected, require some separate description.
1. Lumbago, or myalgia lumbalis, is that common form which attacks the lumbar muscles and the strong aponeurotic structures in connection with these. It is more frequently than any other form attributed to some effort of lifting or sudden twist of the trunk, but in many cases it owes its origin directly to exposure to cold. The pain comes on suddenly and renders the person helpless, the body, if he is able to go about, being held stiffly to prevent any movement or bending; if severe, he is absolutely compelled to observe complete rest in bed. The muscles, when handled, appear slightly sore, but no local point of acute tenderness can be found. This fact, with the characteristic shrinking from any movement, distinguishes lumbago from neuralgia and from abscess. Pain in the loins, more or less severe, is such a frequent accompaniment of disorder of several organs and parts that careful examination should always be instituted lest some serious organic disease with lumbar pain as a symptom be mistaken for a simple lumbago. The most important of these are perinephritis, lumbar abscess, spinal disease, abdominal abscess, and disease of the rectum and uterus.
2. Pleurodynia, myalgia pectoralis or intercostalis. Here the affected muscles are the intercostals, and in some cases the pectorals as well. Spasmodic pain is felt in one or other side of the chest, and is especially aggravated by the movements of respiration; it is rendered intense by the efforts of coughing or sneezing. Pleurodynia may be confounded with pleurisy, the distinguishing features being the absence of fever and the friction sound of pleurisy. Intercostal neuralgia is sometimes with difficulty known from pleurodynia, but in the former the pain is more circumscribed, more paroxysmal, and more easily aggravated by pressure than in pleurodynia, and when severe there are tender points in the course of the nerve a little outside of the middle line posteriorly (dorsal point) and anteriorly (sternal point). Now and then the hyperæsthetic [p. 78]areas become anæsthetic, and even patches of herpes may form in the course of the nerve, when doubt can no longer remain. From periostitis of a rib pleurodynia may be known by the fact that in the one the tenderness is marked in the intercostal space, and in the other in the rib itself. Pleurodynia is a frequent accompaniment of thoracic affections, causing cough, the frequent paroxysms of coughing tending to induce a painful state of the overworked muscles. The pain, which may be very great, can often be controlled by fixing the chest with imbricated plaster or a firm bandage. Dry cups sometimes answer very well; if more active measures are necessary, then hypodermic injections of morphia must be resorted to.
3. Torticollis, myalgia cervicalis, stiff neck or wry neck, caput obstipum. This term includes those cases of rheumatic idiopathic affection of one or more of the muscles of the side and nape of the neck, which fixes the head firmly in the median line or else in a twisted fashion, with the face turned toward the sound side. The disease can be recognized at a glance by the peculiar manner in which a person will turn his whole body round instead of rotating his head alone. It is much more common in children than in adults. The sterno-mastoid is the muscle chiefly affected, but any of the muscles of the neck may become rheumatic in the same way, and frequently several of them suffer at the same time. The most important point at the outset of an attack of wry neck is to determine whether we have to do with a true rheumatic (idiopathic) disorder, or whether the muscular stiffness is secondary to some spinal or vertebral lesion. The diagnosis is usually founded upon the suddenness of the onset, the absence of other symptoms of nerve disease, and the rapid course of the case, terminating in a cure in a few days. There is nothing special in the treatment of torticollis beyond what has been already said under the general heading.
Other forms of muscular rheumatism which have received special names and have been separately described are the following: myalgia scapularis or omalgia, when the surroundings of the shoulder are affected; myalgia cephalica or cephalodynia, an affection of the occipito-frontalis; and abdominal rheumatism, when the external muscles of the abdomen are involved.
SYNONYMS.—Nodosity of the joints (Haygarth); Chronic rheumatic arthritis, or rheumatic gout (Adams); Arthritis, rheumatismo superveniens (Musgrove); Goutte asthénique primitive; Arthritis pauperum; A. sicca; Usure des cartilages articulaires (Cruveilhier); Arthrite chronique (Lute); Progressive chronic articular rheumatism; General and partial chronic osteo-arthritis;216 Arthritis deformans.
216 Nomenclature of Diseases R. C. Physicians, London.
Neither my space nor time will permit of a history of this disease; it must suffice to say that Sydenham in 1766-69 appears to have first tersely described it and distinguished it from gout; that in 1800, Landré-Beauvais in his inaugural thesis made some observations upon the disease under the title of primary asthenic gout; that in 1804, Heberden, and [p. 79]more especially Haygarth, in 1805, pointed out some of the more striking clinical features of this disease, and distinguished it from both gout and chronic rheumatism under the title nodosity of the joints. The latter author, in the work mentioned, claims to have written a paper upon the subject twenty-six years previously, although it was not published; and to him belongs the merit of having so described the disease as to have given it a place in nosology. Incidental allusions were made to the affection in 1813 by Chomel, in 1818 by Brodie, and by Aston-Key in 1835; in 1833, Lobstein, and about the same time Cruveilhier, pointed out some of the more striking characters of the morbid anatomy of the affection. But it is to Adams of Dublin that we are indebted for the most complete account of the anatomy and of many of the clinical features of the disease—first in a paper read before the British Association in 1836, next in his article on "The Abnormal Conditions of the Elbow, Hand, Hip, etc.,"217 and finally in his able monogram "On Rheumatic Gout" in 1857. The contributions to this subject since that date have been very numerous as well as valuable from the leading countries of Europe, and I must not here attempt to assign to each investigator his proper portion of the work.
217 Todd's Cyclop. of Anat. and Phys. (1836-39).
It may be here remarked that Landré-Beauvais and Haygarth described more particularly that form of the disease which, beginning in the small joints of the extremities, tends to extend to the larger joints in a centripetal way, and to involve many of them—peculiarities which have given rise to the epithets progressive polyarticular chronic rheumatism, peripheral arthritis deformans, and which is the form of the disease usually described by physicians as rheumatic gout, rheumatoid arthritis, nodular rheumatism, and by the other names just mentioned. On the other hand, Key, Colles, Adams in his earlier paper, and R. W. Smith described the disease as it affects the larger joints, hip, shoulder, or knee, to one or two only of which it may be confined; and as this variety is frequently observed in elderly persons, and in them often involves the hip, it is often spoken of as senile arthritis, malum senile articulorum, morbus coxe senilis, mono-articular arthritis deformans, partial chronic rheumatism, and has been described by surgeons rather than by physicians. However, even when beginning in the hip or shoulder, the disease is apt to involve several of the intervertebral articulations, and not unfrequently to extend to other joints than the one first affected, and even to the peripheral joints. Its progressive and general nature is thus evidenced, whether it invade from the beginning a single large joint or several symmetrical small articulations. Finally, on this topic Charcot has insisted that Heberden's nodi digitorum contributes a special form of the disease under consideration, and proposes to call it Heberden's rheumatism or nodosities.218
218 Lectures on Senile Diseases, Syd. ed., 1881, p. 137.
Rheumatoid arthritis presents the clinical varieties or groupings of phenomena just mentioned, at times quite distinctly appreciable from one another, but sometimes more or less blended, yet even then manifesting in their periods of invasion and early stages an adhesion to all of these typical groupings. Charcot has especially dwelt upon these: 1st, the general or polyarticular and progressive form; 2d, the partial or oligo- or mono-articular form; 3d, Heberden's nodosities.
[p. 80]1st. The symptoms and clinical history of general or polyarticular and progressive rheumatoid arthritis. This is the most common form of so-called chronic rheumatic arthritis, the classical rheumatic gout, or rheumatisme noueux, and it may declare itself, as Garrod and Fuller pointed out, very rarely in an active or acute form, or, as it usually does, in a chronic and insidious form.
The acute form of rheumatoid arthritis closely resembles the milder varieties of acute articular rheumatism or the best marked examples of the subacute form of that disease. But it presents the following particulars, by which it may generally perhaps, but not always, be distinguished: while the temperature, the thirst, the furring of the tongue, the frequency of the pulse, the articular pains and tenderness, etc., are less developed than in acute articular rheumatism, there is wanting the profuse and continued perspiration, the early involvement of the endo- or pericardium in the inflammation, and the prompt prostration of the strength so commonly witnessed in that disease. On the other hand, while the rheumatoid affection may involve the larger joints—knees, ankles, elbows, and wrists—it almost certainly implicates the smaller joints of the fingers, and often of the toes. There is apt to be greater effusion into the synovial capsules (McLeod's capsular rheumatism) and into the synovial sheaths and bursæ about the affected joints than in ordinary acute or subacute rheumatism; further, the inflammation does not migrate from joint to joint, but obstinately persists in several of them, and more especially in the wrist and in the metacarpo-phalangeal joints of the index and middle finger, perhaps also in the ankles and in the metatarso-phalangeal articulation of the great toe. Instead of disappearing in four to six weeks, the articular inflammation continues, although the pain may abate very much, and the capsules of the joints continue swollen and rather tense. The muscles of the extremities waste, and are the seat of painful reflex spasms which interfere with the movements of the joints; and although the patient is capable of moving about, and is free from all febrile disturbance, one or several of his joints remain permanently swollen, painful, and crippled. Perfect restoration of all the affected joints seldom if ever occurs. In common with other observers, I have met with this acute form most frequently in young women twenty to thirty years of age—several times in connection with recent delivery or rapid child-bearing, or lactation; once after what was regarded by the medical attendant as an attack of acute rheumatism occurring not long after labor. It has been observed in children, and is not uncommon after forty. These patients usually suffer in their general health—become weak, pale, depressed in spirits, and lose flesh. In several cases of this form marked intervals of improvement have occurred; the local disease has ceased to progress, and tolerable comfort has been experienced, perhaps, till pregnancy, delivery, or lactation again determined a fresh outbreak of the disease. Sometimes, however, this acute form steadily advances, and in a year or two establishes changes in the cartilaginous and osseous structure of the affected joints. Such a case I met in a lady of twenty-one who had had a good deal of anxiety as a mathematical teacher, and whose illness set in during vacation while at the seaside. It proved obstinately progressive for several years, until several of the larger joints, as well as the smaller, were badly crippled.
[p. 81]The primary chronic form is much the more frequent, although between it and the acute variety there are many intermediate grades. For weeks or months the patient may experience numbness or formication and rheumatic pains in the limbs, perhaps with a sense of stiffness in the joints, especially felt after rest or the day after unusual fatigue. Then one or more joints—most frequently the metacarpo-phalangeal of the fingers—become painful, swollen, tender when touched, and inordinately hot; these symptoms may subside under rest or treatment, and after weeks or months recur, either without known cause or from exposure, fatigue, or some impairment of the health. Usually, the original joint is again affected, but frequently one or two more of the same on the other hand suffer likewise. More or less complete remissions of the pain and local inflammation now tend to take place from time to time and alternate with exacerbations or fresh attacks of the local disturbance, and the disease extends, as it were, centripetally and more or less symmetrically to the wrists, then to the elbows, and then to the shoulders, or from the toes to the ankles and thence to the knees—although there is no invariable sequence of this kind—and next to the hands; the knees are specially liable to invasion. Of Haygarth's 34 cases, in 2 the knees alone suffered, and "in all or nearly all the rest the hands, chiefly the fingers, were probably affected." In Charcot's 45 cases the début took place in the small joints of the hands and feet 29 times; in the hands, feet, and one large articulation, 7 times; in one large joint, and later in the fingers, 9 times. Even in this primary chronic form there is usually in the earlier stages some effusion into the joints; the soft parts of the articulation are thickened and swollen; obscure fluctuation in the smaller and very distinct fluctuation in the larger joints may be felt. The pain may be severe, especially at night, and during the exacerbations of the disease it varies greatly in its degree and persistency. The position and shape of the joints are altered, partly by spasmodic retraction of the muscles, and more or less by the effusion into the capsules and adjacent bursæ and sheaths, and the thickening of the soft parts covering the articulations. As the disease progresses further deformities ensue from the growth of new bone around the heads of the bones, the absorption of the articular cartilage, the development of masses of cartilage in the hypertrophied synovial processes and beneath the synovial membrane at the margin of the bones; the relaxation of the articular ligaments; and the displacements and subluxations of the unshapely bones composing the joint. The great wasting of the muscles of the member affected has some share in producing its unnatural appearance. In the advanced stage there is more or less abiding pain, soreness, and stiffness in the affected articulations, violent cramps are experienced in the course of the adjacent muscles, and pains either along the nerves or vaguely down the limbs. Crackings or creakings are to be heard, and grating is to be felt during the movements of the joints; these movements become more and more restricted, so that an immobility almost equal to that of true bony ankylosis is established, this result seldom occurring except amongst the carpal, tarsal, tibio-tarsal, and the vertebral articulations. Interlocking of the osteophites formed on and around the articular surfaces, and in other cases union of these surfaces by the interposition of newly-formed fibrous tissue, produce a spurious ankylosis [p. 82]destructive of the articular functions. In the very advanced stages the feet, ankles, and legs are often considerably enlarged and the integument thickened by a chronic oedematous infiltration, or the bones and soft parts are atrophied and the integument is pale, smooth, and attenuated, resembling parchment or the condition seen in certain stages of scleroderma and tightly drawn over the wasted rigid fingers. This primary chronic form is especially apt to progress steadily for many years, the joints earliest affected becoming gradually more distorted and crippled, and fresh joints becoming invaded until there may hardly remain a single sound articulation in the limbs, or even in the body; and at length the patient may be unable to feed himself or masticate or raise his chin from his sternum or rotate his head or stand.
The deformities of the several joints, being largely the result of muscular contraction, observe certain general types, which, however, are not peculiar to the disease, but occur in various affections of the nerve-centres, involving paralysis or spasm or both. Charcot has carefully described those met with in the hands, and I must refer to his masterly article upon chronic articular rheumatism for his account of them.
(1) It must suffice to say here that the predominant features of the hand in chronic rheumatoid arthritis are the following: The first phalanx of the fingers is either flexed upon the metacarpus or extended, and the terminal phalanx in like manner is either markedly flexed or extended upon the second, or these two phalanges are maintained in a straight line, while the first phalanx is, as usual, decidedly flexed upon the metacarpus.219 In all these varieties the hand is pronated; there is a great tendency to deviation of the fingers toward the ulnar border of the hand, although sometimes the deformed fingers stand out, not unlike a bunch of parsnips. The thumb escapes longer than the other fingers, and its metacarpo-phalangeal joint is usually flexed, rarely extended.
219 Lectures on Senile Diseases, Syd. ed., trans. 1881. Figs. 1 and 2, Pl. II., on the hand, give good illustrations of these deformities.
(2) The great toe, enlarged at the metacarpo-phalangeal articulation, is usually drawn to the outer border of the foot, across and above, but rarely below, the other toes, and the foot is usually abducted and flattened, the prominent internal border resting on the ground. The wrist, elbow, and knee-joints are generally flexed; the distal ends of the ulna and radius, more or less enlarged, project backward; the semi-flexed tibia is drawn backward on the femur and rotated outward, thus rendering the internal condyle of the femur prominent and displacing the patella toward the external condyle, and foreign bodies may frequently be felt in the enlarged knee- and elbow-joints. Finally, the extremities of the affected bones will, as a rule, be found enlarged and misshapen, and nodosities, rims, tips, ridges, and stalactiform growths of new bone may be felt on them.220
220 Figs. 12 to 18 and 22 in Adams's Treatise on Rheumatic Gout are nice illustrations of these deformities.
The general condition in this chronic form varies in different individuals, and there is no characteristic disturbance of the functions, such as obtains in chronic gout. There is no elevation of temperature, unless to a slight degree during an active crisis of the disease; the tongue may be clean, the pulse tranquil, the appetite and digestion satisfactory, and [p. 83]the urine normal or perhaps pale and of low density. Fuller, however, says that "more generally the complexion is sallow and the skin sluggish, and evidence of mischief is furnished by yellowishness of the conjunctivæ, constipation of the bowels, a pale and unhealthy character of the dejections, excessive flatulence after meals, turbidity of the urine, and fulness of the pulse." My own experience hardly harmonizes with this, and I have seen many persons suffering for years from the general and partial form in the enjoyment of excellent general health. Should, however, the disease develop in a person the subject of menorrhagia or other uterine disorder, or of repeated child-bearing, or after prolonged mental anxiety, some disturbance of the general health fairly referable to such disturbing conditions may be certainly looked for. In the advanced stages the prolonged suffering and confinement often induce anæmia, dyspepsia, and failing health.
More numerous and exhaustive analyses of the perspiration, urine, and blood in the disease are needed. There is no uniform condition of the skin; general perspirations, chiefly at night, often obtain, but I know of no authoritative report as to the chemical reaction of the sweat in this disease; Garrod221 and Charcot222 vouch for an absence of uric acid in the blood, while Marrot223 found both this acid and the urea below the normal quantity in the urine, although the acid increased notably under baths of high temperature.
221 Reynolds's Syst. Med., i. 918.
222 Loc. cit., p. 190.
223 Contribution à l'Étude des Rheum. Artic., Examen de l'Urine et du Sang, Paris, 1879, p. 42.
Certain affections other than the articular have been occasionally observed in persons suffering from rheumatoid arthritis, but many even of those authors who regard the disease as a form of rheumatism speak of these affections as coincidences, and not as essential manifestations of the disease. Charcot and Besnier, however, maintain the latter to be their true relation to the articular affection which they regard as chronic rheumatism. The two authors just named allege that all the visceral localizations that occur in acute articular rheumatism may obtain in the nodular form, but that such localizations are infinitely less frequent and serious than in the acute, subacute, or simple chronic forms of articular rheumatism—that endo- and pericarditis undoubtedly do occur in nodular rheumatism, and appear especially where there is an exacerbation of the disease and where there is some approach to the acute state.224 As Charcot has adduced these cardiac affections in proof of the rheumatic nature of rheumatoid arthritis, it is deserving of mention that he had personally met with but two instances of endocarditis and five of pericarditis, four of the latter having been discovered not during life, but in nine autopsies, and that he cites only eight other cases of endo- or pericarditis which had been either published or reported to him. He admits too that there had generally been in these cases, at some former period, an attack of acute rheumatism. Besnier, Homolle, Malherbe, Vidal, and Colombel, in their articles upon the disease under consideration, do not cite a single case in which they have seen cardiac disease in rheumatoid arthritis. On the other hand, McLeod, Garrod, Fuller, Flint, Senator, and Pye-Smith either deny or ignore the occurrence of cardiac disease as a manifestation or complication of this disease. My personal [p. 84]experience coincides with that of those authorities last cited, except in one instance, and that is open to the objection that the patient's father had had acute articular rheumatism, the mother was the subject of chronic deforming arthritis, and the patient had experienced during many winters an affection which began in the smaller joints and permanently damaged them; when first seen by me he had chronic disease of the aortic valves. He may have had true articular rheumatism as well as rheumatoid arthritis. His father had experienced the one, his mother the other. If those instances be excluded in which a former attack of acute rheumatism might be adduced in explanation of the supervention of cardiac disease, but few cases will remain to suggest that rheumatoid arthritis may develop endo- or pericarditis; and when it is borne in mind that in several ways the cardiac affections may have arisen as mere coincidences of the rheumatoid affection, it is well to wait for further evidence before accepting as proved the occurrence of cardiac affections as local manifestations of rheumatoid arthritis. Garrod's observation is still pertinent: "The form of the disease in which acute cardiac inflammation has occurred may be rather that of true articular rheumatism of a very subacute character."
224 Loc. cit., 172-175; Besnier, loc. cit., 699.
Nor is the evidence at all satisfactory in favor of any special tendency to the following affections, much less of their being local manifestations of rheumatoid arthritis: viz. pleuritis (McLeod, Fuller), asthma (Charcot), chronic laryngitis (Garrod), grave cerebral or spinal disturbances (McLeod, Fuller, Vidal), paralysis agitans, locomotor ataxia, sciatica, trifacial neuralgia, and albuminous nephritis.225
225 To mention only some of the many sources of cardiac disease other than rheumatism may be adduced scarlet and other fevers, extension of inflammation from the pleura or lung and other sources of local irritation, powerful or oft-repeated muscular efforts, Bright's disease, senile degeneration, etc.
Among the more frequent complications may be mentioned migraine, certain cutaneous affections, more especially psoriasis, prurigo, lichen, and some diseases of the eye, chiefly iritis, which is apt to be relapsing, and sometimes episcleritis. It is remarkable that iritis very seldom occurs as a complication of acute articular rheumatism.
The so-called rheumatic nodules occur also in chronic rheumatoid arthritis. It is not yet established that they are peculiar to rheumatism and to rheumatoid arthritis. Dr. Stephen Mackenzie has seen them in one instance in tertiary syphilis, the patient not having had arthritis, rheumatism, or chorea.
2d. The partial or oligo-articular form of rheumatoid arthritis, like the general or polyarticular variety, is usually a primarily chronic affection, insidious in its invasion and slow in its progress. It is chiefly observed in old persons, especially men (senile arthritis), affects frequently a single joint, and chiefly the hip, but occasionally the knee, shoulder, or spinal column, either as a consequence of special injury or of the wear and tear of life, or exposure to cold and wet, or even of what seemed to be simple acute or subacute articular rheumatism or gonorrhoeal rheumatism. When not the result of injury, two or three joints may suffer, both hips or knees, or hip and some of the vertebræ, hip, knee, and ankle of the same limb, and so on. Even in those cases in which the disease for a long time is confined to a single joint and may have been caused by an injury,226 other joints, finally, are apt to become [p. 85]affected, often in a symmetrical order. So that it may seem almost general, or at least polyarticular, just as the converse sometimes happens in the general rheumatoid arthritis of long standing, where the disease becomes greatly aggravated in one articulation and produces great deformity and destruction of it, the others remaining as they were.
226 See Ord's case, II., Brit. Med. Journal, i., 1880, 158.
The symptoms of this partial chronic form are very much those of the general form already described, but there is usually in the early stages less heat, tenderness, and swelling of the affected joint; the pain is less acute, but more abiding, and, with the exception of more or less stiffness or impeded movement in the joint, it may be the only sign of disease present, so that at this stage of the affection it may be taken for simple chronic articular rheumatism. But the disease persists; the voluntary movements become more painful and difficult; slight exercise of the joint is followed promptly by fatigue and aggravation of the pain, and yet the articular surfaces may be pressed together, and flexion and extension be practised, without causing much suffering. Slowly and continuously alterations take place in the affected articulation; with but little heat or redness it enlarges steadily, the soft parts becoming infiltrated and thickened, or effusion taking place into the capsule; the articular surfaces become irregularly depressed by the growth of osteo-cartilaginous rings, osseous nodosities, and stalactiform processes upon them, and these irregularities, together with one or several loose bodies, may be felt in the joint. The enlargement of the articulation becomes more apparent, owing to the wasting of the muscles of the limb; its movements become more and more restricted and difficult, although perhaps not more painful, and are attended with creakings and gratings perceptible to the ear and hand; and at last nearly all movement of the joint may be prevented by the alterations in the shape of the epiphyses, or by the interlocking of the osseous outgrowths, or in rare cases by actual union of the bones. This form constitutes, par excellence, arthritis deformans. In many instances there is little effusion throughout the process, notwithstanding the grave deformity in progress; hence the term dry arthritis. Even the partial form is sometimes more active in its invasion, as when it very rarely succeeds acute or subacute articular or gonorrhoeal rheumatism, or, more frequently, follows an injury.
The duration of the partial form is usually very protracted; it may be ten or twenty years. Exacerbations of the disease occur from time to time, in the intervals of which the patient may be free from pain, although the affected joints are seriously crippled.
The affection is not in itself fatal; the patient may attain an advanced age and die of some intercurrent disease, such as dysentery, pneumonia, cerebral hemorrhage, or other affection incident to old age.
A description of the features presented by partial rheumatoid arthritis affecting the hip (morbus coxa senilis), the shoulder, and other joints rather appertains to works on surgery, and only a glance at the evidences of the disease in the vertebral column (spondylitis deformans) will here be given. When the cervical vertebræ are implicated the power of rotating the head from side to side is usually preserved and is attended with a crackling noise, while the rest of the cervical region is stiff and the head cannot be bent forward; when the dorsal or lumbar vertebræ suffer the back becomes bent, the patient stoops greatly and cannot stand [p. 86]erect, and his body is shortened and more or less twisted. A careful examination will discover not only the great rigidity of the spine, and as it were fusion en masse of its joints, but in these persons the bony outgrowths may be felt. Occasionally the alteration in the vertebræ by compressing the cord or its membranes, or the spinal nerves and ganglia, may produce neuralgic pains in the cervical, dorsal, lumbar, or sciatic nerves, wasting of the muscles, more or less paralysis, and even vasomotor disturbances.
3d. Heberden's nodosities are certainly sometimes the effect of rheumatoid arthritis, implicating chiefly, often solely, the distal joints of the fingers, where it slowly forms two little hard nodules about the size of dried peas upon the side of the articulations. These are notably enlarged and their movements impaired, but pain is seldom experienced, and were it not for deviation of the end of the finger to one side or the knob-like excrescences upon the joints—appearances which much disfigure the hand—patients would not speak of the affection. In many cases these alterations likewise involve, but in a minimum degree, the first phalangeal articulations, and less frequently the metacarpo-phalangeal, and even some of the larger joints—the wrist, knee, or hip, etc. Like the other varieties of rheumatoid arthritis, this form occasionally has a more active invasion than is above mentioned, and may be attended by local pain, heat, and redness, or such symptoms may occur as exacerbations of the chronic disease.
Gout may precede these nodosities, or, as in the case of Charcot's,227 the latter may precede the former by several years. Finally, Charcot remarks that Heberden's nodosities are "often accompanied by asthma, migraine, neuralgia, especially of the sciatic nerve, and muscular rheumatism, and that these manifestations may alternate with the exacerbations of the disease."
227 Loc. cit., 198.
MORBID ANATOMY.—Every component tissue of the articulations exhibits signs of a chronic inflammatory process. In the chronic form affecting the larger joints the synovial membrane is found more or less congested, opaque, and thickened; at the point of its reflection upon the bones its fringes are thickened and injected and their villosities greatly increased in number, length, and thickness, and in extreme instances have been aptly compared to the wool on a sheep's back. The cartilage-cells normally existing in the synovial fringes likewise proliferate and develop into cartilaginous growths, many of which become infiltrated with lime salts, or even ossified, and in this way originate some of the foreign bodies, pedunculated or sessile, which are found in the joints. These may be attached to the synovial fringes, or imbedded in the membrane itself, or set free by rupture of their pedicles. In some examples these neoplasms resemble in size small melon-seeds; in others they form irregular masses, many of which are as large as hazel-nuts.
At the outset there is frequently an increase of synovial fluid, richer in mucine than natural, which lessens considerably in the later stages and becomes a turbid, viscid fluid of a dirty white or reddish-yellow color, containing no pus, but degenerating epithelium and fragments of villosities and cartilage. In many cases, more especially of the partial [p. 87]form, very little effusion into the articulations takes place (arthrite sèche).
The inflammatory irritation excites proliferating and degenerating processes in the cells and basis-substance of the cartilage covering the bones, and the changes described in connection with acute rheumatic arthritis ensue. Those parts of the cartilage covering the bones which suffer pressure in locomotion fibrillate on their surface, and either undergo mucous degeneration, resulting in ulceration and complete absorption, or are thinned and worn away by attrition. In either way the ends of the bones become laid bare. Those portions of the cartilage at the periphery of the joints which escape compression in the erect posture likewise proliferate, but, according to Cornil and Ranvier, in consequence of being covered by the synovial membrane the proliferating elements are retained in situ, instead of escaping into the articular cavity, and develop into actual cartilage, and may ultimately ossify. In this way irregular masses of cartilage (enchondromata) and bone (osteophytes) form around the heads of the bones, enlarging them considerably, altering their shape, encroaching upon the articular cavity as well as extending up the shafts of the bones, and displacing the capsules of the articulations. Similar productions of cartilage sometimes form in the thickened capsules and ligaments, especially in very protracted cases, or these parts become infiltrated with lime salts.
While these processes are going on at the periphery and the centre of the cartilages, in its deeper layers the proliferating cells are undergoing ossification and rendering the ends of the bones very dense and compact, so that under the attrition to which they are exposed by the articular movements they acquire the smoothness, polish, and white aspect of ivory (eburnated). It is probable that the articular ends of the bones participate in this proliferation and development of bone, which increases their compactness and is followed by eburnation. That the bone itself does sometimes play a part in the hyperostosis which is in progress is shown by an increase of an inch in the length of the right ramus of the maxilla over that of the left in Adams's first plate.228 Forster's229 and Ziegler's230 later investigations confirm this view. Nor is the periosteum exempted from the proliferating process which may have long existed in the several articular tissues, as is shown by the considerable enlargement of the diameter of the shaft of the long bones and by the osteophytes which form on the exterior of the vertebræ and often unite several of them together by a series of osseous splints, interfering with the mobility of the spine. Notwithstanding this development of cartilage and bone upon the exterior of the articular extremities, the interior, especially in old people or in very chronic examples of the general form of the disease, or rarely in the partial form, undergoes degeneration and atrophy. The spongy substance becomes rarefied, thinned, and friable (osteoporosis), so that it has been easily cut or crushed, and it is frequently loaded with fat. True ankylosis of the diseased joints is rare, except in the very small articulations when kept at rest; even under this condition fibrous ankylosis is not of frequent occurrence.
228 Illustrations of the Effects of Rheumatic Gout, London, 1857.
229 Forster, Handbuch der Path. Anat., p. 1000.
230 Virchow's Archiv, 1877.
Finally, the interarticular fibro-cartilages and ligaments and the long [p. 88]tendon of the biceps degenerate and are absorbed. The muscles in protracted cases suffer simple atrophy, but are sometimes the seat of an interstitial accumulation of fat. Thus far, no lesions of the nerves supplying the diseased joints nor of the spinal cord have been discovered.
ETIOLOGY.—The causation of rheumatoid arthritis is involved in much obscurity—in part, because sufficient attention has not been paid to its clinical varieties. We will examine first the general progressive form which is the more common.
In women it prevails during the child-bearing period. It is probably oftenest developed between twenty and thirty, and continues to occur frequently up to the period of the menopause, fifty, after which it develops comparatively seldom. Of Ord's 33 cases, 10 were between twenty and thirty years; 11 between thirty and forty; 9 between forty and fifty; and 3 between fifty and sixty.231 Children are not exempt. E. C. Seguin saw three children of the same family suffering from the disease at ages from two and a half to four years.232 Moncorvo233 met with an example at two years and a half, Laborde at four, and Charcot at ten. It occasionally begins in both sexes after sixty.
231 Brit. Med. Jour., 1880, 156.
232 The Med. Record, London, 1877, 797.
233 Du Rheumatisme Chronique Noueux des Enfans, Paris, 1880.
It is pre-eminently a disease of females up at least to fifty; after that it is not infrequent in men, and is then often only partial, at least at first. The most frequent progressive form, however, does often occur even in boys.
It is probably more frequently observed in cold and damp climates than in those of opposite qualities, for cold is regarded as its most common cause. However, it is met with in India and other hot climates. Besnier asserts it is almost unknown in the tropics, but new investigations are needed on this point.
Direct hereditary predisposition exercises but little influence, according to Garrod, and we certainly often see the disease confined to a single member of a large family, although Seguin saw three young children of one family affected with it, their parents being free from any disease. Trastour three times saw the children of women who were afflicted with nodular rheumatism already suffering from articular rheumatism; and Charcot once saw the grandmother, the mother, and the granddaughter successively attacked. At present I have a patient whose mother at fifty-five and maternal grandmother at sixty became subjects of a crippling polyarticular affection; another of my patients informed me that his mother and a young sister were like himself victims of the disease. This direct transmission appears to be rare, judging from my own experience and from the few instances of it mentioned by writers. But very many authorities maintain that simple acute and chronic rheumatism and gout in the parents predispose to rheumatoid arthritis in the offspring (Charcot, Trastour, Besnier). Now, the facts given in support of this opinion are not numerous. Trastour found that out of 45 cases of nodular rheumatism the father or mother were rheumatic in 10 instances, but the form of the rheumatic affection is not stated. Charcot, Besnier, and Homolle, although believers in the doctrine, do not cite an example in proof. However, in Pye-Smith's 27 cases of osteo-arthritis, five stated that rheumatism had occurred in their families. Thus, two fathers [p. 89]had had rheumatic fever, and one was rheumatic, and two sisters of different families had had rheumatic fever. Besides, the father of a sixth and the grandmother of a seventh had had gout.234
234 Guy's Hospital Reports, 3d Series, xix. 348.
The evidence in favor of the doctrine that true articular rheumatism transmits an hereditary tendency to rheumatoid arthritis does not appear to be conclusive, although it is highly thought of by those who regard the latter disease as a variety of rheumatism. Some considerations of an opposing character deserve mention. Acute articular rheumatism has very rarely passed continuously into rheumatoid arthritis, and very rarely has been followed at short interval by that disease; and in such exceptional cases the antecedent affection may have been really the acute form of rheumatoid arthritis, which closely resembles acute articular rheumatism. Trastour,235 Vidal,236 Charcot,237 and others admit that acute rheumatism can hardly be placed amongst the antecedents of the rheumatoid affection. Garrod238 with some others states that now and then acute rheumatism acts as an exciting cause of it, which appears to have been Fuller's view;239 he had repeatedly known it to commence apparently as a sequel of acute rheumatism. However, Ord met with a case in which the lesions of rheumatoid arthritis were present in a typical form in a patient who had mitral disease as a result of acute rheumatism, the arthritis having begun as a continuation of the acute attack.240
235 Thèse de Paris, 1853, p. 41.
236 Ibid., 1855, p. 9.
237 Leçons Cliniques, p. 214.
238 Reynolds's Syst. Med., 1870, i. 920.
239 Lib. cit., 333.
240 Brit. Med. Jour., 1880, i., 158.
That so common an affection as articular rheumatism should occur in the family or personal history of a patient the subject of the rheumatoid arthritis is not improbable; nasal catarrh and many other very common diseases must be frequent antecedents of the rheumatoid affection, yet are not causes of it. Much the same remarks apply to the view that gout in the parents may transmit a tendency to rheumatoid arthritis in the offspring. The experience of English physicians in this matter is hardly reliable, owing to the great prevalence of gout in England. In Canada and many parts of the United States, however, while gout is a rare disease, rheumatoid arthritis is a common one, and the writer has not found an intimate relationship to obtain between the two affections. It is not intended to deny that when the children of rheumatic or gouty parents fail in health owing to their inherited constitutional disease, they become liable to rheumatoid arthritis, for feeble health predisposes to that affection.
Finally, many of the difficulties connected with this subject are reasonably met by Hutchinson's241 doctrine that there exists a state of tissue-health which is transmissible by inheritance, which involves liability to inflammations of joints and fibrous structures, and upon this arthritic diathesis as a foundation may be built up, under the influence of special causes, a tendency to gout, rheumatism, or any one of their various modifications or combinations.
241 Trans. International Med. Congress, ii. 95; Guéneau de Mussy's chap., "De la Diathèse Arthritique," Clin. Méd., 1874, t. i. 317-338.
Hutchinson has demonstrated that gout is often followed by rheumatoid arthritis, the lesions characteristic of both affections coexisting in the same joint. Charcot and Cornil had previously observed the same [p. 90]thing.242 Acute and perhaps chronic rheumarthritis have sometimes preceded rheumatoid arthritis. If a predisposition, inherited or acquired, to rheumatoid arthritis exist, the occurrence of gouty or rheumatic irritation in the joints may suffice to induce the peculiar form of disturbance characteristic of the rheumatoid affection, just as injuries sometimes develop the partial form.
242 Mémoires de la Société de Biologie, 1864.
There is a group of conditions affecting the sexual functions and organs of women which appear to be specially connected with the general peripheral form of rheumatoid arthritis. The disease follows pregnancy, and specially frequent pregnancies, protracted lactation, and various disorders of menstruation. The latter influence obtained in ten out of eleven instances of the disease met with in girls under eighteen by Fuller.243 The frequency of the disease about the period of the menopause has been already mentioned. Todd noticed its coincidence with dysmenorrhoea. Ord in an able and original paper244 has lately dwelt upon ovario-uterine disorder or irritation as a frequent active cause of the disease, having in his opinion met with 33 instances of the kind. The relationship between these various conditions of the functions and organs of generation and rheumatoid arthritis cannot be regarded as settled. Garrod supposed that such conditions, by causing debility, predisposed to the articular disease. Todd, an ardent humoralist, held the nexus between the two to be unhealthy secretions of the uterus, leading to blood impurity; while Ord has ably defended Remak's view that a direct influence of the nervous system is the real link of relationship. It seems necessary to remark that mere coincidence may play a large rôle in the explanation of many of these cases. In 17 at least of Ord's 33 cases the conditions stated by that author cannot safely be adduced as anything more; and it is probable that they would be found present in much the same proportion in any other chronic painful disease of women.
243 Loc. cit., 335.
244 Brit. Med. Jour., i., 1880, 151-153.
Scrofula and phthisis are regarded by Charcot, Cornil, and Garrod as frequent antecedents of rheumatoid arthritis: the first had several times seen white swelling in youth, followed by nodular rheumatism in later life;245 and Fuller found that 23 out of 119 victims of rheumatic gout had lost a parent or one or more brothers and sisters by consumption.246 Chlorosis has several times preceded rheumatoid arthritis. When the prevalence of scrofula, phthisis, and chlorosis is borne in mind, it will not appear strange that they should frequently be found amongst the antecedents of rheumatoid arthritis, without inferring any other relationship between them. Gonorrhoeal rheumatism has also occasionally preceded rheumatoid arthritis, but Ord and Hutchinson are probably correct in regarding that affection as a variety of rheumatoid arthritis.247
245 Loc. cit., p. 208, foot-note.
246 Loc. cit., p. 334, foot-note.
247 Trans. International Med. Congress, vol. ii. p. 92; Brit. Med. Jour., 1881, p. 158.
Cold, especially when prolonged and associated with dampness, is commonly held to be the most common cause of general rheumatoid arthritis. A protracted residence in low, damp dwellings, deprived of the sun's rays and of a free circulation of air, is a condition thought most favorable to the provocation of this disease, perhaps years after the condition has been done away with.
[p. 91]Poverty and all that it implies are at least frequent antecedents of the disease (hence one of its epithets, arthritis pauperum), as are other debilitating influences, such as night-watching, insufficient food, mental worry, grief, anxiety, etc. Be it remembered, however, that the disease is frequently observed in the well-to-do, who live in dry climates and warm houses, are well fed, and want for nothing; so that the external conditions first mentioned are not essential causes of the disease, and many of them may act merely as adjuvants.
Direct injury of a joint from a blow, a fracture, a whitlow, etc. may sometimes induce a local rheumatoid arthritis, which may subsequently become multiple and involve several articulations more or less symmetrically.248
248 Vide Charcot's and Ord's cases, loc. cit.
The partial form presents some peculiarities of causation—thus: it occurs chiefly in advanced life (senile arthritis), much less frequently in middle life, very exceptionally in the very young. Men are much more liable to it than women. It is chiefly this variety which follows injuries, blows, dislocations, pressure, etc., and the disease may then be limited to the injured joint and be monoarticular, or it may extend and become polyarticular, or rarely, as in Ord's case, even general. This monoarticular form appears to be sometimes induced by other local irritations of the articular structures than those following traumatic influences; and as foreign growths in joints and gouty irritation may respectively induce the lesions indicative of rheumatoid arthritis, so, it is probable, may simple chronic rheumatism; and this may be the true relationship existing between these several affections. It is doubtful at present whether purely local irritation or injury of a joint can originate the alterations belonging to rheumatoid arthritis—that is, in the absence of all predisposition to that disease or of the arthritic diathesis. Cold and dampness are generally admitted to be causes of the partial form, but the evidence on this point is not altogether satisfactory. It may be that chronic articular rheumatism is induced by the prolonged operation of damp cold, and that the prolonged rheumatic irritation, aggravated by constant use of the joint and by occasional violence, ultimately superinduces the profounder alterations characteristic of arthritis deformans. It appears highly probable that if the predisposition exist, any long-abiding irritation of a joint, whether the result of violence or disease, may ultimately originate the alterations of the cartilages and bones which obtain in rheumatoid arthritis.
As regards the etiology of Heberden's nodosities, and their relation to other affections of the joints, the following summary must suffice: They obtain chiefly in advanced life, but do occur rarely in the young; they are probably somewhat more frequent in women than in men; although more frequently seen in the upper classes, the poor are not exempt from them, no doubt because they are specially exposed to slight but oft-recurring injuries of their digits, such traumatism being an exciting cause of the disease, especially when confined to a single joint. The affection is sometimes hereditary; both it and the general or the partial forms of rheumatoid arthritis may coexist in the same family and even in the same person. The alterations in the joints are identical with those found in the general variety of rheumatoid arthritis, and exist without [p. 92]deposits of urate of soda (Charcot). It resembles the general form of the disease just mentioned in its tendency to involve many symmetrical articulations at the same time, and the partial form in the rarity with which it extends beyond the joints first attacked. While Heberden's nodosities, as Haygarth taught, do occur independently of gout and the gouty habit, I believe with Begbie249 and Duckworth250 that in some persons they are evidences of gout or the gouty diathesis.
249 Contributions to Practical Med., 1802, p. 29.
250 "On Unequivocal Gouty Diseases," St. Bartholomew's Hospital Reports, vol. xvi., 1880, p. 190.
Quite recently a woman aged forty-eight consulted me with these nodosities beginning upon the last joint of the fingers, while she was the subject of vesico-renal irritation and was passing free uric acid in the urine. Hutchinson has twice seen them in combination with a peculiar insidious and painless inflammation of the iris and vitreous body, which occurs in the children of the gouty, yet such children have no deposits of lithates in their joints, nor any lithiasis, nor acute paroxysms of true gout, and he considers that "the last joint arthritis is to be regarded as in part gouty, and in part a kind of articular chilblain."251
251 Trans. International Med. Cong., ii. p. 96.
Lastly, in some instances they are no doubt the hybrid offspring of an inherited tendency to both gout and rheumatoid arthritis.
No more important principle in pathology exists than has been of late years insisted upon, especially by Jonathan Hutchinson and in his recent lecture by Sir James Paget252—to wit, that "by inherited dispositions, accumulating and combining or converging in definite proportions, new diseases may be developed and old ones be variously modified."
252 Lancet, ii., 1882, 1017-1021.
The pathogenesis of rheumatoid arthritis is the subject of differences of opinion very like those existing in regard to acute articular rheumatism. The weight of evidence is in favor of its diathetic relationship to rheumatism; and the doctrine of an arthritic diathesis and of the operation of the causes of the disease through the nervous system appears to be specially applicable to it, with less difficulty than to acute rheumatism, and the probability of a specific germ being its true cause is very remote. What seems to be necessary in addition to the preceding is, that the causes shall be more persisting and oft-recurring, so as to maintain a prolonged local irritation of the articular tissues, or that the neuro-arthritic diathesis shall be highly developed. Under these conditions the prolonged or oft-repeated application of cold and damp to the peripheral nerves, severe or oft-repeated slight injuries to joints, urethral or ovario-uterine irritation, chronic gout or rheumatism, or even, exceptionally, an attack of the acute form of these diseases, may originate rheumatoid arthritis; and all wearing influences, such as anæmia, excessive menstruation, prolonged lactation, innutrition, failing health, mental anxiety, or shock, etc., act as adjuvants in the development, aggravation, and maintenance of the articular disease.
DIAGNOSIS.—It is perhaps not possible to distinguish with certainty either the acute or the chronic form of rheumatoid arthritis from subacute or chronic rheumarthritis respectively before the characteristic deformities of the former affections have appeared. Acute rheumatoid arthritis, which is comparatively rare, may be said to exist, rather than subacute [p. 93]articular rheumatism, if the disease affect early and chiefly the smaller joints of the hands and feet alone or along with some of the larger articulations, especially the sterno-clavicular or the temporo-maxillary; if the effusion into the joints be abundant; if inflammation persist in the articulations first involved, notwithstanding the invasion of other joints; if the heart escape; if the patient be a female who is constitutionally delicate, or has borne children rapidly, or is the subject of disordered menstruation, or has been attacked soon after childbirth or during lactation;—finally, if, on cessation of the attack, one or more of the joints remain swollen and permanently enlarged and impaired in function. The coexistence of iritis, or a history of a previous attack of that disease not attributable to syphilis or gout, would strengthen the above view.
Precisely the same considerations serve to distinguish chronic general or polyarticular rheumatoid arthritis from chronic articular rheumatism, with the following qualifications: endo- or pericarditis is not of frequent occurrence in chronic rheumatism, so that this distinction is not available, and chronic rheumarthritis of long standing does sometimes impair the movements of the joints, and even produce slight alterations in them. However, it does not, as a rule, involve so many joints as rheumatoid arthritis; it is less symmetrical in its distribution, and much less prone to implicate the sterno-clavicular, the temporo-maxillary, or the vertebral articulations. Nor does it cause removal of the articular cartilage, enlargement of the heads of the bones, and the formation of osteophytes around them, and of loose bodies in the articulations, together with marked deformities and luxations of the joints. A history of a remote or recent attack of acute rheumarthritis or of chorea, or the presence of chronic valvular disease, would strongly indicate the simple rheumatic nature of the case.
The partial form of rheumatoid arthritis can with even less certainty than the general be distinguished from chronic articular rheumatism before the characteristic alterations of the joints have been developed, more especially as it is sometimes a consequence of gouty irritation and probably of chronic rheumatism. Chronic arthritis following a traumatic cause, and persisting obstinately in the injured joint is probably rheumatoid, if not strumous, gouty, or periarthritic.
But before definitely deciding it will be prudent to await the development of some of the characteristic alterations of structure appertaining to rheumatoid arthritis. An affection of the shoulder frequently occurs which resembles in many respects rheumatoid arthritis, and has been well described by Simon Duplay253 and W. Pepper.254 It usually follows an injury, such as contusion, sprain, etc., of the joint, but may be spontaneous; it is unattended by swelling or deformity. Its early symptoms are pain on pressure of the shoulder a little below the outer border of the acromion, and especially behind it and at the coracoid process, also about the insertion of the deltoid and below the acromion during movements of the joint, especially when the arm is raised from the side or rotated inwardly; early restriction of these movements, which increases till a fibrous ankylosis becomes established and scapula and humerus move together as one piece, motion between those bones no longer existing, and forcible attempts to produce it giving great pain, and sometimes producing [p. 94]crepitus in or about the articulation; sometimes early numbness and pain down the member to the hand in the course of the ulnar, internal cutaneous, or the radial nerve; vicious and painful semiflexion of the elbow; after a time wasting of the group of muscles which move the shoulder-joint. Although usually monoarticular and of traumatic origin, I have seen it affect first one and then the other shoulder in the absence of any known injury, and beginning like a neuritis or a neuralgia of the scapulo-humeral nerves. Duplay, however, regards it as a periarthritis. It may be distinguished from the rheumatoid arthritis by the absence of effusion into or enlargement of the articulation, and of deformity of the bones; by the early restriction of the movements and the rapid development of adhesions which fix the articulation; and by the curability of the disease.
253 Archives Générales de Méd., Nov., 1872, pp. 512-542.
254 Archives of Med., Oct., 1880.
The articular affection of locomotor ataxia sometimes closely resembles monoarticular rheumatoid arthritis,255 but may be distinguished by its sudden invasion, often without pain or fever; the prompt development of a general and often enormous tumefaction of the entire member, with copious effusion into the joint; the early destruction of the articular cartilages, the rapid wearing away of the heads of the bones, and the proneness to spontaneous fracture of their brittle shafts; the prompt absorption of the articular effusion, followed by a relaxed state of the ligaments and a facility of dislocation; the early occurrence of the articular affection, when motor inco-ordination is scarcely developed, and its frequent association with the crises of ataxia or the presence of some of the other symptoms of that disease. The importance of these facts will be especially evident in those examples of ataxic articular disease in which, at an advanced stage, eburnation and deformity of the articular surfaces, with the formation of loose bodies and osteophytes, are observed, just as they are in arthritis deformans.
255 Charcot's Lectures on Diseases of the Nervous System, Syd. Soc., 1877; Archives de Physiologie, t. i., p. 161, 1868; ibid., xi., 1869.
Articular disease closely allied to what occurs in locomotor ataxia is now and then observed in the early stages of progressive muscular atrophy,256 but while the large joints, more particularly the knee and the shoulder, suffer in the former affection, the phalangeal chiefly and the larger articulations more rarely are attacked in the latter. Of course the peculiar symptoms of progressive muscular atrophy coexisting with those of the articular affection would serve to distinguish the latter from rheumatoid arthritis.
256 Remak, Allgem. Med. Central. Zeitung, March, 1862; Rosenthal, Clinical Treatise on Diseases of the Nervous System, translated by L. Putzel, M.D., 1879, p. 286.
It is often very difficult to say whether a given case is one of chronic rheumatoid arthritis or of chronic gout; and there is no doubt that in England, where gout prevails, it is not unfrequently associated with rheumatoid arthritis, sometimes preceding and even causing it, much more often following it, for the one does not exclude the other.
While rheumatoid arthritis most frequently begins in the hand, and is usually symmetrical and bilateral, gout commonly begins in the lower extremities, and especially in the metatarsal joint of the great toe, and of one foot only. Chronic gout is far more frequently preceded by attacks of acute gout than chronic rheumatoid arthritis is by the acute form of that affection; a history of inherited predisposition, of indulgence in the [p. 95]use of wine, ale, porter, and of animal food, of deficient bodily exercise, with perhaps great mental occupation or anxiety, of recurring gouty dyspepsia or of a tendency to lithiasis, would indicate gout, while the absence of these and a history of frequent exposure to cold and wet, of injury to the joint, of previous exhausting disease or drain, of impaired health, debility, or poverty, would strongly imply rheumatoid arthritis. Gout is especially observed in males over thirty, and very rarely in children; general rheumatoid arthritis is chiefly a disease of females during menstrual life, and occasionally occurs in children of either sex.
The partial form is, like gout, chiefly a disease of men, but occurs generally at a more advanced age than gout. Even chronic gout is more or less paroxysmal, with distinct intermissions; chronic rheumatoid arthritis is more or less abiding and progressive, with only remissions in its course and severity; the former is frequently associated with chronic renal disease, the latter is not. The urate-of-soda deposits about the articulations in gout appear as more or less round or ovoid swellings in the close vicinity of the joints, but not observing their exact level or their general form; softish when recent, they never acquire a bony hardness, and are nearly always capable of slight lateral movement. The skin covering them is frequently stretched and glossy, and may exhibit white spots of urate of soda. The articular nodosities in chronic rheumatoid arthritis are actual osseous enlargements of, or outgrowths from, the articular surfaces, forming part of them, immovable and conserving more or less their form. The integument covering the nodosities is not glossy or dotted with chalk-like specks. The several types of deformity of the fingers previously described, and mainly produced in rheumatoid arthritis by muscular contractions and altered shape of the articular surfaces, are not seen in gout. Finally, if chalk-like concretions are visible in the ears, joints, or finger-ends, or if the blood contain uric acid, gout is present. While rheumatoid arthritis and chronic gout occasionally coexist in the same patient in England, in Canada, where the latter disease is comparatively rare and the former quite common, the writer does not remember to have observed such coexistence.
Besides the acute syphilitic disease of the joints already alluded to as occurring in children (inherited), a chronic arthritis is observed in the adult amongst the very late lesions of syphilis. It is usually monoarticular, affects the larger joints, especially the knee, and may originate either in the synovial membrane or in the bone and periosteum. In syphilitic synovitis the history of the case, the existence occasionally of soft gummy tumors in the periarticular tissues and of hydrarthrosis, the trivial degree of pain and tenderness, the insidious invasion and chronic course of the affection, and its prompt relief by antisyphilitic remedies, will indicate the nature of the case.
When it originates in the bone and periosteum, although the invasion may be prompt and the pain at first severe, the latter usually moderates greatly and becomes nocturnal, and the articular surfaces present localized rather than general enlargement (hyperostosis); nodes often coexist; effusion is moderate, unless the synovial membrane is also involved, and full doses of iodide of potassium will soon afford relief.
PROGNOSIS.—In the polyarticular form the course varies much more than is commonly believed, and the disease must not be regarded as necessarily [p. 96]progressive and incurable. When it occurs in young persons, and in children more especially, although it may suffer exacerbations and remissions for a few years, yet arrest of the disease and recovery of the functions of the joints, sometimes with very little deformity, now and then take place under suitable management. Quite recently a man of thirty-two consulted me about a vesical affection who from the age of eight had suffered every winter for twenty years from rheumatoid arthritis in his hands and feet, and finally in the knees. Yet when seen by me he had been free from pain in his joints for three years, and, although they were somewhat deformed, their movements were remarkably free and painless.
Several of my younger patients while bearing children rapidly and nursing them have had the disease in their hands or hands and wrists; exacerbations have recurred during subsequent lactations, and yet the disease has either become arrested or progressed very slowly and at long intervals. It is admitted, however, that these are all exceptional cases, and that the tendency both of polyarticular and of the monoarticular forms is to progress, and, either steadily or at intervals and by recurring attacks, to permanently deform the joints and impair their movements. Even under these circumstances, however, the patients may suffer little pain unless when forcible movements of the articulations are attempted.
On the other hand, while the disease cannot be regarded as curable under the employment of drugs, very much can frequently be done, especially in the polyarticular form, to relieve the suffering and to retard, if not arrest, the progress of the disease, and even to restore sometimes very considerably the functions of the joints. Neither of these forms of rheumatoid arthritis can be said to be dangerous to life, and they often exist ten or twenty years and more without seriously injuring the general health. Heberden's nodosities are incurable, but they are little more than deformities.
TREATMENT.—The treatment of rheumatoid arthritis is, as a rule, disappointing, and perhaps no affection requires more perseverence and self-reliance on the part of the physician or more hopeful resolution on that of the patient. Our first duty is to make an exhaustive search as to the probable cause of the disease, as its removal is an important step in the treatment of the affection, although such search is frequently futile, and many of the alleged causes may, after all, be mere antecedents or coincidences. However, inasmuch as the pathology of the disease is very obscure, any abnormal condition of organ or function that may be discovered should receive strict and prompt attention, lest it should, either through disturbed innervation or malassimilation or impaired nutrition or defective excretion, be the predisposing or exciting cause of the disease. In women the most careful inquiry should be made into the state of the ovario-uterine organs and functions, and the least departure from their norm should be at once treated. Deficient, excessive, or painful menstruation, leucorrhoea, ovarian irritations, or pain, even displacements of the uterus or ovary, should be corrected as soon as possible. Repeated pregnancy and prolonged lactation, recurring mental anxiety and physical fatigue, defects of diet, want of food, of sunlight, and of good air, residence in damp dwellings, occupations involving exposure to cold and wet, are conditions supplying important indications which too often are [p. 97]beyond the control of the physician, although they peremptorily require his attention. The general form is often met with in anæmic persons and in those of impaired health and vigor, and probably very rarely occurs under opposite circumstances; and there is a consensus of opinion that a lowering system of treatment is contraindicated in rheumatoid arthritis.
Having efficiently set about correcting or removing these various predisposing or determining causes of the disease, we next direct our care to the disease itself. The remedies which had been found most useful in rheumatoid arthritis before the introduction of salicylic acid were cod-liver oil, quinia, iodine, iron, arsenic, and various mineral waters, employed either externally or internally, usually in both ways. Judging from my own late experience and from the results obtained by Sée257 and other French physicians, as communicated by Jules Compagnon,258 sodium salicylate, given in sufficient doses, promises to be more generally useful in the more acute forms or in the actively inflammatory periods and exacerbations of the disease than any of those agents. Including Sée's cases, Compagnon has related 17 examples of rheumatoid arthritis, most of them of the general progressive form, in which great improvement as regards pain, stiffness, swelling, and even deformity, followed promptly the employment of that salt, even after the failure of other remedies. It proved signally useful recently in a rebellious chronic case of my own. Pollock has lately published an instance in which 5 grains of salicylate of quinia three times a day were in three or four days followed by great relief.259 The testimony already given of Dr. J. T. Eskridge as to the great value of this salt in chronic rheumatism will be held by some to be corroborative of its value in rheumatoid arthritis. It is hardly necessary to say that it often fails in this intractable disease, but it has frequently relieved the pain and swelling and arrested the progress of it, at least for the time, even when alkalies, iodine, arsenic, baths, etc. had failed.
257 Bullétin de l'Académie de Méd., Paris, t. v., 2d Serie, 1877.
258 De l'Utilite du Salicylate de Soude dans le Traitement du Rheumatisme, par Jules Compagnon, Paris, 1880.
259 The Lancet, ii., 1882, 141.
It is probable that less than 45 grains per diem of the sodium salt is of little value in even the most chronic forms, and that the quantity requires to be increased in proportion as the febrile symptoms are active, so that a drachm and a half or two drachms may need to be administered in the day to some persons. It should be given in divided doses at intervals of two hours, and, what is of primary importance, it should be continued for a long time, even after much improvement has resulted, and should be resorted to from time to time, especially during recurrences of the pain, heat, or swelling. It is of consequence, especially in elderly patients, to ascertain that the medicine is being promptly eliminated by the kidneys and to watch its effect upon the heart. The administration along with it of a little old rye whiskey or brandy will sometimes be necessary in feeble people. In those rather common cases in which the skin is inactive and perhaps harsh the salicylate often improves that important organ of oxidation and elimination, and should it not do so the addition of the ammonium carbonate may be tried, especially in feeble persons with weak hearts.
[p. 98]Moreover, the other drugs which sometimes prove serviceable in this disease may be given at the same time or alternately with the salicylate, or instead of it if it is not found to be of use or is not tolerated. In chronic cases a prolonged course of cod-liver oil, alone or along with malt extract, often seems to be of real service, especially when nutrition is much impaired or when the patient is the subject of acquired or inherited struma. Iodide of potassium, in combination with quinia or other tonic, will often prove signally useful in chronic cases unaccompanied by pyrexia, in which the pains are worst at night. It should be first tried in moderate doses (5 to 8 grains), and be continued for a long time with occasional intermissions, and before discarding it from disappointment—which often arises—15- to 20-grain doses may be given tentatively for a short period. Milk or coffee or Vichy water are good vehicles for its administration. Whether free iodine in the form of the tincture, so highly spoken of by Laségue,260 acts as well or better than the iodide of potassium is doubtful. He gave it at meals, in doses progressively increased from 10 drops to 5 or 6 grammes twice a day, in sherry or sweetened water, and persevered with it for a long period. Garrod has had many restorations to health in severe forms of this disease from the persevering employment of the syrup of the iodide of iron. The iron in these preparations may deserve as much commendation as the iodine, for it has often proved signally useful in this disease, not alone on account of the anæmia which so frequently attends it, but through its beneficial influence upon the nutritive functions and the circulation.
260 Arch. Gén. de Méd., 1856.
The usual rules regulating the employment of iron are to be observed, and the condition of the digestive organs will demand special attention during its employment. Although the influence of arsenic upon rheumatoid arthritis is not uniform, yet as it sometimes proves really useful261 it should be tried. Like iron, it may prove beneficial in several ways—by improving the quality of the blood, promoting the circulation in the superficial layers of the skin, or exerting some influence upon either the nerve-centres or perhaps upon the vaso-motor nerves of the cutaneous or articular tissues. The last-mentioned suggestion is favored by the circumstance noted by Charcot—viz. that the first effects of arsenic in nodular rheumatism are often intensification of the articular pains, and sometimes the production of redness and swelling where they did not exist before. That author found arsenic without effect or injurious in very inveterate cases and when the disease had appeared at an advanced age. Five to ten minims of Fowler's solution, or of the solution of the arseniate of sodium, which is perhaps less irritating than the former, should be given immediately after meals, and its effects upon the gastric and hepatic functions carefully watched. De Mussy has highly recommended arsenical baths (drachm ss-ij of arseniate of soda to 30 gallons of water), but as the arsenic is not absorbed by the unbroken skin, any improvement which may follow its employment is probably owing to the temperature of the bath or the bath itself.
261 As to the value of arsenic in rheumatoid arthritis, see Bardsley's Medical Reports, London, 1807; Begbie, Edin. Med. and Surg. Jour., 1858; Fuller, lib. cit., p. 362; Garrod, lib. cit., 3d ed., p. 534; Guéneau de Mussy, Bull. de Thérapeutique, t. lxvii., 1864, p. 24; Charcot, lib. cit., p. 222.
A similar remark has been made respecting the value of the various [p. 99]thermal mineral baths, natural and artificial, so much employed in this disease.262 It is neither the nature nor proportion of their mineral ingredients, but the degree of temperature, which constitutes the essential point in the action of a bath. This, if true, explains the almost equal reputation of the many varieties of thermal mineral springs in the treatment of rheumatoid arthritis and chronic rheumatism. It is this that permits the physician to promise the poor patient as much benefit from the employment of hot baths of simple water as of those of New Zealand, Plombières, or Arkansas.
262 Vide Niemeyer, Text-Book Pract. Med., N.Y., 1867, p. 488; Traitement du Rheum. par les bains à haute temperature, par Ch. Aug. Bouther, Paris, 1878.
The time for a resort to hot baths in rheumatoid arthritis is when the very violent pains have subsided sufficiently to allow of their employment; and while they may be hopefully used in the most chronic and advanced cases, the earlier they are employed the more curative they are. The temperature of these hot baths need not, as a rule, exceed 95 to 100° F., although some authorities approve of raising the temperature to 110° or 112° while the patient is in the water. A series of twenty to thirty such baths, taken every second day for ten to twenty minutes, is sufficient for one trial, and often effects very great improvement in the disease. The aggravation or return of pain in the joints which often follows the employment of warm baths will cease after the fifth or sixth bath. Garrod's experience of the Turkish bath is not favorable; it very often does much mischief by causing debility, and its excessive use has induced rheumatoid arthritis in persons previously free from the disease.
Now, while it may be true that simple hot-water baths employed at home are as good as mineral thermal baths taken at their source, it is generally admitted that it is best to send persons who can afford the expense to the springs themselves, where they may drink the waters as well as employ them externally, and at the same time secure all the advantages arising from change of habits, scene, and climate, from restriction to a proper diet, and from the systematic employment of the waters and baths under the direction of persons experienced in their administration, etc. No reliable rules can be laid down for the selection of the mineral waters best adapted to each case: the stronger alkaline waters perhaps had better be used with great care, such as those of Carlsbad, Vichy, Mont Doré, Weisbaden, and after a course of thermal mineral baths at such places as Aix-les-Bains, Wildbad, Bath, Aix-la-Chapelle, etc., Garrod advises resort to some place where the air is bracing and the waters tonic or chalybeate, as Buxton, Spa, Schwalbach, or St. Moritz. In this country good results are often obtained at the Hot Springs of Arkansas and the Hot Sulphur and the Lithia Springs of Virginia. The use internally and in the form of hot baths of the mineral springs of Saratoga, of Michigan, of the Licks of Kentucky, and of California, of St. Leon and St. Catherine's (Canada), is frequently very beneficial. In the selection of the mineral waters to be drunk, and of the temperature and other qualities of the baths to be employed, careful attention must be paid to the condition of the functions of the skin, liver, kidneys, and nervous system; but space cannot be afforded here for the consideration of this extensive topic. Moreover, it occasionally happens that after failure of [p. 100]sulphur or alkaline baths some other form may succeed, as the vapor or hot-air, or tepid or very hot-water bath. If decided benefit follow the first series of baths, recourse should be had from time to time to a fresh series, even for several years, in obstinate cases. Mud and peat baths are much valued in Germany, although they do not always agree with weakly or aged people.
The local treatment is of equal importance with the general, and it is not unfrequently more effective in restoring the functions of the articulations. In that rare variety, acute rheumatoid arthritis, attended with much pain and heat in the joints, perfect rest in bed is called for, together with other measures adapted to subdue the inflammation and allay the pain. Compresses wet with warm water, rendered anodyne by the addition of laudanum or belladonna, or both, and covered with oiled silk, suit some cases—light linseed poultices, applied moderately warm and extending considerably beyond the limits of the articulation and covered with gutta-percha or oiled silk, in others. As the pain and local heat subside, the tincture of iodine may be applied extensively, or blistering-fluid over limited areas above and below the affected joints, but not on them until the inflammation has very much abated and is becoming chronic. These simple methods should be employed assiduously and be aided by appliances to secure actual rest of the inflamed joints. In the chronic variety complete rest is not needed unless during the acute exacerbations, but the movements should be at first somewhat restrained and be regulated by the effects produced. But the severe pain experienced during the movements must be borne; it will subside promptly. Decided increase of pain and heat in the part, lasting many hours, would indicate more reserve in the use of the joints. It is frequently very difficult to determine when and to what extent movement may be permitted in this disease. No fixed rule can be laid down of universal application, but it may be stated that in proportion as the local disease becomes indolent and inactive may pressure and active movements of the joints be resorted to, for they then have a beneficial influence in preventing stiffness, contraction, and deformity. Indeed, in my opinion it is not wise to delay these movements long even in subacute cases. The editor of this work has especially insisted upon the importance of systematic daily movements of the affected joints as the most essential part of the treatment,263 "combined with thorough massage of all the muscles whose functional activity is impeded and impaired."
263 "Some Practical Remarks on Chronic Rheumatism," by Wm. Pepper, M.D., Archives of Medicine, Oct., 1880.
The abiding chronic inflammation indicated by local heat, swelling, and inflammation of the affected tissues may be variously treated. The joints may be thoroughly fomented with tolerably hot water or by means of the local vapor bath for half an hour, morning and night, and then be gently rubbed for ten or fifteen minutes with iodine or weak mercurial ointment or with the compound camphor or acetic turpentine liniment, or, if these are too stimulating, with some bland oil, such as cod-liver or neats' foot or cocoa oil, after which should be applied hot-water compresses or linseed poultices or a wrap of soft cotton wool covered with oiled silk and secured by an elastic, moderately tight roller. If these means prove inefficient and the inflammatory process grow more [p. 101]indolent, counter-irritants may be conjoined with or substituted for them. Small fly blisters or strong iodine paint may be applied close to the joints, or the ordinary iodine tincture may be brushed over them, or the above ointments or liniments and one of the bland oils may be more forcibly rubbed in. The prolonged rubbing of these stiff, swollen joints with oil is not valued as much as it deserves.
Compression of the thickened tissues by means of a thick envelope of cotton wool and thin flannel or rubber bandage sometimes acts very well, probably by reducing the amount of blood and interfering with cell-growth or promoting cell-degeneration. Hot sand-baths to the affected joints are sometimes useful.
These several measures should be perseveringly applied, and in proportion as chronicity prevails the active and passive movements of the articulations and massage of the muscles and adjacent tissues should be daily and efficiently practised.
Electricity will often be found an important adjuvant in this as well as in an earlier stage, not only in improving the nutrition of the muscles, but in promoting absorption, allaying pain, and subduing excitability of the peripheral structures, removing muscular contractions, and probably modifying the local inflammatory processes. It appears also in some cases to improve the general health. The constant current is generally the most useful, and should have an intensity of about ten to fifteen milliampères, and be applied daily for ten or fifteen minutes. The positive pole, terminating in a large flat moistened sponge, is applied to the spinal origin of the brachial or lumbar plexus, according as the superior or inferior members suffer, while the negative pole is immersed in a vessel of warm salt water in which the hands or feet are placed. Some apply the negative electrode to the joints and the positive to the limb higher up.264 The faradic current may also be employed on account of its action upon the muscles and small vessels. In the advanced stage attended with marked thickening of the articular and periarticular tissues, with contractions of the muscles and greater or less impairment of movement, the above measures are still our chief resources; but they may be employed more vigorously. We have little fear now of lighting up inflammation; we indeed desire to excite a more active circulation in the part with a view of removing the congested state of the capillaries and venules, so favorable to the development of fibroid growths. In this stage especially vigorous active and passive movements of the affected joints, and massage of the muscles which move them, and gymnastics, are imperatively needed, and it is sometimes almost marvellous what an amount of mobility and usefulness may thereby be restored to apparently helplessly crippled and deformed articulations and members. Persons who have not walked for years are frequently so much improved as to be able to leave their sofa or bed, and with or without crutches or mechanical aids walk about, while their abiding pains depart, and this notwithstanding the permanent deformity of the articular surfaces. (For the various mechanical appliances that are sometimes necessary in this advanced stage works upon surgery may be consulted.)
264 Homolle, lib. cit., p. 710.
The hygienic measures to be observed are probably very much the [p. 102] same as those indicated in the article upon simple chronic articular rheumatism—some of them at least—and are such as may be inferred from a review of the exciting causes of rheumatoid arthritis. Be it remembered also that acute and chronic articular rheumatism appear amongst the causes of that disease. We are hardly justified in promising arrest of the disease on removal to a warm, dry, and even climate; yet wealthy patients need not be dissuaded from trying the experiment. The use of flannel underclothing and the employment of tepid or even moderately cool baths, followed by the use of the flesh-brush or rough towel, are important means of protecting persons predisposed to this disease. The ordinary hygienic laws adapted to maintain a healthy state of all the functions, mental as well as physical, are to be observed, for in this disease the influence of the mind over the body is shown by the frequency with which rheumatoid arthritis follows closely upon mental shocks, worry, etc.
The diet, it is generally admitted, should be of a nutritious character, yet plain and digestible, and, unless specially required to meet certain indications, should not include heavy wines or fermented liquors. However, Garrod affirms that uncomplicated rheumatoid arthritis is not aggravated by the use of porter, ale, or sound wines; and his rule is to give sufficient of these alcoholic beverages to support the tone of the whole system, but not enough to excite the circulation and thereby produce subsequent reaction.
Finally, the above system of treatment must be persisted in year by year with the object of securing arrest when cure has not been effected.
SYNONYMS.—Arthrite ou Arthropathie blennorrhagique, Tripper-rheumatismus, Gonocele, Urethral Rheumatism, Urethral Synovitis.
ETIOLOGY.—As its name implies, the cause, par excellence, of the disease is gonorrhoea, as was perhaps first indicated by Selle265 and Swediaur,266 although, no doubt, an affection apparently identical is rarely observed associated with non-contagious urethral discharge and with the urethral irritation incident to catheterism and to stricture. I have seen it associated with a simple mucous urethral discharge in a man of gouty habit, married and free from the suspicion of specific infection. Such discharge has been attributed to gouty irritation, to dietetic and venereal excesses, and to the contact of non-specific vaginal secretion; and such origin is well established. More than one observer has noticed a susceptibility to urethritis on the part of persons who have had gonorrhoeal rheumatism. A gouty taint is undoubtedly often present in urethral rheumatism. These non-gonorrhoeal cases require more close investigation than they have received.267 Fournier has not met with them.268
265 Chr. Th. Selle, Medicina Clinica, oder Handbuch der Medicin, Berlin, 1781.
266 Swediaur, London Med. Gaz., 1781.
267 See Elliotson, "Non-contagious Urethral Rheum.," Med. Times, i. 60, p. 613.
268 Fournier, Nouv. Dict. de Méd. et de Chir., t. v. p. 228.
The stage of the gonorrhoea at which the articular affection may appear varies very much. It frequently sets in from the sixth to the sixteenth day of the discharge; it is common enough between the third and sixth or twelfth weeks, and may be delayed as late as the twelfth month. There [p. 103]is no constant relation between the severity of the urethral inflammation and the frequency with which, or the time at which, the articular symptoms arise; and these, once established, appear to be largely independent of the state of the urethra. On the advent of the joint affection the discharge usually continues as it was, although it often abates somewhat. Fresh attacks of gonorrhoea, even when very mild, often develop new invasions of the articular affection, as though an idiosyncrasy existed.
While the ordinary exciting causes of simple acute articular rheumatism are not necessary to the production of gonorrhoeal rheumatism, they do now and then act as adjuvants. Such are cold, fatigue, and injuries of the joints, and a severe acute arthritis is not infrequently developed during gonorrhoea under such circumstances. Other predisposing influences probably exist, the absence of which in some measure explains the infrequency of gonorrhoeal rheumatism as compared with the prevalence of gonorrhoea. Besnier holds that constitutional rheumatism, the arthritic habit, or l'héredité arthritique, is not infrequently present in the victims of gonorrhoeal rheumatism as a predisposition; Nolen269 found an inherited rheumatic predisposition in 6 out of 88 cases, and that 4 others had had rheumatism before contracting gonorrhoea; and Hutchinson maintains that it is the existence of the arthritic diathesis which enables urethral inflammation to produce gonorrhoeal rheumatism. He says: "From statistics that I have carefully collected I have no hesitation in believing that the predisposing cause of it usually is the inheritance of arthritic tendencies;" and adds, "Very often the subject of gonorrhoeal rheumatism will give a family history of gout." However, the disease often occurs in the absence of any discoverable tendency, hereditary or acquired, to simple articular rheumatism. On the other hand, persons have had one or several attacks of gonorrhoea previously that did not give rise to rheumatism. Nolen's table of 88 cases contains 12 instances of this kind. It is probable that by reducing the resisting force of the organism, scrofula, the so-called lymphatic diathesis, anæmia, and debility favor the development of the disease.
269 "Rheumatismus gonorrhoicus," Deutsches Archiv für klin. Med., Bd. xxxii., 1883.
Gonorrhoeal rheumatism, like gonorrhoea, is proportionally as well as actually much more frequent in men than in women (111 men, 7 women, Nolen); and the greater proclivity of the former has been attributed to the greater delicacy, sensibility, and complexity of the structures involved in them than in women by gonorrhoea.
MORBID ANATOMY.—The lesions of gonorrhoeal rheumatism in the early stage resemble closely those of acute articular rheumatism; and it is probable, for opportunities of ascertaining by actual dissection are very rare, that the synovial membrane chiefly suffers. In more advanced stages the joints contain serous fluid in which fibrinous flakes and numerous leucocytes are found; the cartilages may be eroded and softened; and in some protracted cases even the bones may participate in the inflammation, and the changes found in polyarticular rheumatoid arthritis may be developed. Ultimately fibrous adhesions, resulting in ankylosis, may occur. Suppuration very rarely takes place, and it is probable that in such cases pyæmia is added to gonorrhoeal arthritis.
[p. 104]SYMPTOMS.—Gonorrhoeal rheumatism may attack any of the joints; it most commonly invades the larger at first, more especially the knee; the ankle is next in order of frequency, and then succeeds the shoulder, closely followed by the smaller joints of the hands and feet, which are very seldom affected primarily and antecedently to the larger joints. The temporo-maxillary, the sacro-iliac, the sterno-clavicular, the intervertebral, do not escape gonorrhoeal rheumatism more than they do rheumatoid or pyæmic arthritis.270 The disease most frequently invades several joints simultaneously or successively, but, soon declining in many of them, it finally becomes localized in a few or rarely in a single articulation. It is monoarticular from the first in about 20 per cent. of cases, especially in the knees.
270 Vide Fournier, Nouv. Dict. de Méd. et de Chir. Prat., t. v. p. 230: in 119 cases, knee, 83; ankle, 32; fingers and toes, 23; hip, 16; wrist, 14; shoulder, 12; elbow, 11; temp.-maxillary, 6; etc.
Gonorrhoeal rheumatism presents several clinical forms: First, Arthralgic: pains of greater or less severity, sometimes increased by movement, but unaccompanied by redness or swelling, affect one or frequently several joints; they wander from joint to joint, are liable to exacerbations, and sometimes resist treatment. This form occurs either in a chronic state in the course of an old gonorrhoea, and without other rheumatic symptoms, or as an acute affection along with other rheumatic symptoms, as in the second form. Second: Rheumatic: in this the symptoms are almost identical with those of subacute articular rheumatism or the more active forms of polyarticular rheumatoid arthritis. Several joints are usually implicated, perhaps suddenly, either quite spontaneously or after chill, exertion, or strain, or rheumatic-like pains having been felt for two or three days in the soles, ankles, or loins, the painful joints become moderately swollen, tender, and hot; pyrexia supervenes with its early chilliness, malaise, and anorexia; the temperature is not high; the profuse acid sweating and the very acid, high-colored urine of acute articular rheumatism are not observed or but transiently and to a very slight degree. In a few days the moderate febrile disturbance subsides, but the local inflammation persists, and extends to other joints, without promptly leaving those first invaded; while lingering in all it often fixes itself in one or more joints, and is apt to produce a copious and rebellious intra-articular effusion. Still, it very rarely involves as many articulations as primary acute rheumatism. The periarticular tissues usually are more involved than in subacute or even chronic primary articular rheumatism. Hence the considerable swelling from oedema on the back of the hand or foot, around the knee, behind the elbow, and the copious effusion into the adjoining bursæ and tendinous sheaths, and in the case more especially of the small joints of the fingers and toes the fusiform enlargement and deformities resulting from periostitis of the articular extremities. The pain, deformity, pseudo-ankylosis, etc. produced by these periarticular processes are very persistent and rebellious, and, although they do usually disappear at last, occasionally the inflammatory irritation extends to the cartilaginous and osseous structures, and rheumatoid arthritis with its permanent deformities results. It is perhaps chiefly in this polyarticular form of gonorrhoeal rheumatism that cerebral, spinal, cardiac, pleural, and ocular complications most frequently occur. [p. 105]In the Third form, or Acute Gonorrhoeal Arthritis, after two or three days of pain wandering from joint to joint, a single articulation suddenly, and frequently about the middle of the night, becomes the seat of atrocious and abiding pain, followed in a few hours by very considerable swelling of the articulation, not due chiefly to articular effusion, but to periarticular oedema and enlargement of the bones. The pain and tenderness are most severe at the line of junction of the articular surface; the swelling begins at that point, and extends widely, especially over the dorsal aspects of the wrists and elbows, the joints most liable to this form, although any articulation may suffer. The joint is also hot, it may be pale, but is usually more or less red, and occasionally presents the appearances of severe phlegmonous inflammation, and excites a sensation of pseudo-fluctuation.271 The affection may resolve, or fibrous ankylosis may ensue, or very rarely suppurative destruction of the articulation may occur, although such issue has been denied (by Fournier, Rollet, Voelker). It is remarkable that, like the other forms of gonorrhoeal rheumatism, the acute inflammatory form is not accompanied by a general febrile disturbance at all proportionate to the severity of the local disease. A Fourth form occurs as a Chronic Hydrarthrosis. Although occasionally accompanying the polyarticular variety, it is frequently observed independently, and is then often monoarticular, and affects especially the knee; however, both knees sometimes are involved. The ankle- and elbow-joints suffer much less commonly than the knee. The effusion into the articulation takes place insidiously, although rapidly producing considerable enlargement of and fluctuation in the joint, without local heat, redness, or tenderness, and often with but little or no pain or pyrexia. It is not as often associated with inflammation of the tendinous sheaths and bursæ or of the eye as the polyarticular form, but it is apt to be very slow in resolving, and may last for two or three months, a year, or several years, and in scrofulous patients may degenerate into white swelling. The formation of pus in the joint is very rare. It occurred twice in 96 cases tabulated by Nolen; hydrarthrosis obtained 12 times; and serous synovitis 64 times; chronic rheumatism or arthritis deformans 5 times; tumor albus once.272 A Fifth form of gonorrhoeal rheumatism, like other varieties of so-called secondary rheumatism, involves predominantly the tendons and tendinous sheaths, the bursæ and periosteum, sometimes without, but far more frequently in association with, affection of the joints. Pain, sometimes severe and increased by movement and pressure and aggravated at night, with local swelling and tenderness, are the symptoms. In their fixity and persistence, their tendency to relapse, and their chronic course these periarticular affections resemble gonorrhoeal inflammation of the joints. Gonorrhoeal bursitis is often severe enough to resemble phlegmon, but it does not end in suppuration; it is most common in the bursæ covering the patella, the olecranon, and especially in that under the tendo Achillis and the deep one covering the inferior tuberosity of the os calcis; but any of the bursæ may suffer from gonorrhoeal rheumatism. The periosteum in the vicinity of the affected articulation and over the most prominent parts of the bones is sometimes the seat of small circumscribed firm nodes which [p. 106]are painful and tender, and may either resolve rapidly or very slowly (Fournier).
271 De l'Arthrite aigue d'origine blennorrhagique, par le Dr. André Felix Bieur, Paris, 1881.
272 Loc. cit., p. 133.
Along chiefly with the third form of gonorrhoeal rheumatism, or independently, the various muscles and nerves may be the seat of myalgia and neuralgia. The sciatic nerve is specially liable. In the same form are often met those ocular affections observed not infrequently in rheumatoid arthritis and very rarely in acute articular rheumatism—viz. conjunctivitis and iritis. Aqua capsulitis is more common than the others, according to Fournier. The ocular affections may precede, accompany, or alternate with the articular, and, not being due to direct introduction of the urethral contagium into the eye, are regarded as manifestations or localizations of gonorrhoeal rheumatism. The varieties of erythema sometimes present in primary acute articular rheumatism have been observed in gonorrhoeal rheumatism.
Much difference of opinion obtains as to whether inflammations of the heart, lungs, and serous membranes occur as manifestations or localizations of true gonorrhoeal rheumatism. Even those who, like Besnier, contend for the rheumatic nature of gonorrhoeal rheumatism admit that they are quite exceptional in that affection. Endocarditis is probably more frequent than pericarditis, and the aortic are more liable than the other valves to suffer. Gonorrhoeal endocarditis has been observed without the articular affection, although it is especially when several joints are involved and the pyrexia is well marked in gonorrhoeal rheumatism that the above visceral complications occur. While admitting that Morel,273 Marty,274 Pfuhl,275 and others have reported what appear to have been authentic cases of gonorrhoeal endocarditis, I would remark that it must be almost impossible at times to distinguish a polyarticular acute gonorrhoeal rheumatism from ordinary acute articular rheumatism, and that in other instances the possibility of pyæmia developing in gonorrhoea, and producing both the articular and the visceral lesions, or the latter only, cannot be denied. And the same remarks are applicable to the cerebral and spinal disturbances that Vidart and others have recorded as occurring in gonorrhoeal rheumatism.
273 Rev. des Sciences Méd.
274 Archives générales de Méd., Dec., 1876.
275 Deutsche Zeitschrift für pract. Med., No. 50, 1878.
The course, termination, duration, and prognosis need not be insisted upon after what has gone before. The duration is very variable. Many recover in four to eight weeks, many not for three to six months and longer; relapses are of frequent occurrence; complete and tolerably prompt recovery is not uncommon in first attacks and in young and healthy subjects; rebellious persistency, and even deformity, with impairment of the articular movements, and not infrequently even fibrous ankylosis of one or many joints, sometimes including the vertebral, may be observed. Indeed, the most formidable examples of spondylitis are associated with gonorrhoeal rheumatism as its exciting cause.276 These unfavorable issues are most apt to follow repeated attacks in unhealthy and especially scrofulous persons. Both rheumatoid arthritis and strumous articular disease have appeared as sequels of gonorrhoeal rheumatism. Life is not endangered, except in very rare instances in which cardiac or cerebral [p. 107]complications obtain; and to stiffened enlarged joints the functions may often be restored by efficient treatment.
276 Brodfurst cites two such cases: Reynolds's System of Med., i. 980. So does Nolen in an elaborate article upon rheumatismus gonorrhoicus in Deutsches Archiv für klin. Med., Bd. xxxii., 1883. I had not seen it before this paper was written.
DIAGNOSIS.—In some instances no doubt what appears to be ordinary gonorrhoeal rheumatism, owing to the coexistence of urethral discharge and articular inflammation, is really pyæmic arthritis. The intermediate link in the causation may be suppuration in the prostate or its veins or in the testicle or the penis or in its dorsal vein, or the urethral pus may undergo changes and become septic and be absorbed. In other instances it is highly probable that true primary acute articular rheumatism sometimes occurs coincidentally with gonorrhoea. If in addition to the presence or recent existence of gonorrhoea the case present several of the following features, gonorrhoeal rheumatism may be said to exist: moderate or mild pyrexia and articular pain; the number of joints attacked being few, with a tendency to concentration in one, either from the first or secondarily; no migration from one joint to another; no delitescence, but marked chronicity and indolence, with a tendency to hydrarthrosis and to implication of the synovial sheaths and bursæ; an absence of cardiac complications; the frequent and often early coincidence of special ophthalmic affections.
TREATMENT.—The patient should be confined to bed, so as to secure rest to the inflamed articulations, and when severe arthritis (third form) exists an efficient splint is peremptorily required, and its application is often followed by prompt relief to the pain. It should be retained until not only all pain, but all tenderness on pressing the articulation, has disappeared. In short, the principles and details of local treatment suited to gonorrhoeal rheumatism are the same as those recommended for rheumatoid arthritis, which it so closely resembles; and the reader is referred to that article for information. Although there is a greater proclivity to copious effusion into the joints in gonorrhoeal rheumatism than in rheumatoid arthritis, there is less to those deeper lesions which affect the bones, and complete recovery is usually more certain and more prompt in the former than in the latter. Measures to prevent stiffness and even ankylosis of the articulations are often an urgent indication. In the general treatment, also, almost the same remedies are indicated as have been recommended for rheumatoid arthritis. The salicylate of sodium, given freely, is sometimes signally useful, more especially when several joints are acutely inflamed. In the more chronic stages, when much articular effusion exists, a prolonged course of potassium iodide is occasionally beneficial. The local measures, however, simultaneously employed, doubtless co-operate efficiently. Iron and quinia will frequently be demanded by general debility, anæmia, and impaired nutrition; and the same may be said of cod-liver oil, extract of malt, etc. The circumstances under which the various baths are likely to be useful have been mentioned in connection with the treatment of rheumatoid arthritis.
The gonorrhoea should be treated in the same way that it ought to be if no arthritis existed. The rest, the moderate diet, and even the salicylate of sodium, favor its removal, but the frequent employment of mild astringent injections should not be omitted.
DEFINITION.—Gout, as a disease, in the traditional acceptation of the term, is a specific arthritis, characterized by the deposit of the salts of uric acid in the affected joints. Gout, as a diathesis, is a blood crasis in which there is an accumulation in the blood serum of the uric acid salts, the consequence either of the increased formation or of the defective excretion of these products of proteid metamorphosis. The manifold irritations of the different tissues, and the accompanying subjective and objective symptoms provoked by this dyscrasia, are termed gouty.
SYNONYMS.—(a) Eng., Gout; Lat., Gutta; Fr., Goutte; Sp., Gota; Ger., Gicht—derived from the nomenclature of humoral pathology and descriptive of the distillation (goutte à goutte) of the poisonous humor into the joints—arthritis uratica. (b) Gouty diathesis; constitutional gout; irregular gout.
CLASSIFICATION.—(a) Gout as a specific form of articular inflammation is classified according to its location—cheiragra, onagra, podagra, gonagra, etc. (b) Gout as a constitutional disease is classified, 1st, according to the structures affected—e.g. articular gout; tegumentary gout, embracing mucous as well as cutaneous affections of gouty origin; nervous gout; parenchymatous or visceral gout; 2d, according to the degree of the inflammatory process—acute, subacute, and chronic; 3d, according to certain irregularities manifested in the development and progress of gouty lesions as metastatic, retrocedent, and suppressed gout. This classification of constitutional gout is based upon the well-recognized clinical observation in the history of gouty persons and gouty families, that the characteristic lesions of the joint-structures are often correlated with lesions of the skin, mucous and serous membranes, vessels, nerves, and parenchymatous organs, which are marked by the same blood dyscrasia that exists in articular gout, and which are most successfully treated by the same measures which experience has suggested in the management of the arthritic disease.
Musgrave in his work1 treats of a great number of varieties of gout, as follows: De arthritide anomala; de colica arthritica; de diarrhoea arthritica; de dysenteria arthritica; de abscesse intestinorum arthritica; de melancholia arthritica; de syncope arthritica; de calculo renum arthritico; de asthmate arthritico; de catarrho, tussi, et peripneumonia arthritica; de phthise arthritica; de angina arthritica; de capito dolore et [p. 109]vertigine arthritica; de apoplexia arthritica; de paralysi arthritica; de doloribus in corpore vagis, fixis; de ophthalmia, de erysipelate et achoribus arthriticis; etc.
1 De Arthritide Anomala, sive Interna, Dissertatio, Geneva, 1715.
HISTORY.—The records of medicine furnish simple evidence of the prevalence of gout in all ancient as well as in modern civilized communities. Its origin in the perversion of physiological functions was as clearly recognized by the prophets of the old testament of the medical art as it is by the founders of the gospel of modern science. The refined processes of animal chemistry have simply revealed the materies morbi which was foreshadowed in the "peccant matters" of the humoralists, which were supposed to be distilled into the joints and other structures, provoking inflammation and tophous deposits. This is the most notable and interesting fact in the history of gout, that it has from the earliest times been regarded as a specific form of arthritis and dependent upon the circulation in the blood of peccant matter. It was not, however, until the latter part of the eighteenth century, when Murray Forbes, and a few years later Wollaston, called attention to the fact that uric acid was the chief ingredient in urinary calculi and in tophous deposits, that our knowledge of the pathology of gout may be said to have had its beginning. The demonstration by Garrod, in 1848, of the presence of lithate of soda in the blood of gouty persons, also marks an era in the history of the pathology of gout.
While the humoralistic theory of gout has prevailed almost to the exclusion of all others, it is historically interesting to note that the views of the solidists, as represented by Cullen, who maintained that "gout was an affection of the nervous system in which the primary moving powers of the whole system are lodged," have been recently revived and are attracting considerable attention.
ETIOLOGY: PREDISPOSING CAUSES.—Heredity may be regarded as the most prominent of the predisposing causes of gout. Statistics of arthritic gout show this tendency in a varying but always large proportion of cases. Scudamore observed it in nearly 60 per cent. of his cases; Garrod, in 50 per cent. of his hospital cases and, in a much larger proportion, in his private practice; Gairdner found it in 140 out of 156 cases. If all the manifestations of the gouty vice were taken into consideration in determining the influence of heredity, it would doubtless be shown in a still larger percentage of cases.
It is generally supposed that there is a greater frequency of inheritance from the male ancestors and in the male descendants. This may be explained by the fact that men are more exposed to the other predisposing and to the exciting causes of gout. My own experience leads me to suspect that if we took into consideration the irregular manifestations of this morbid inheritance, we should find it as frequently in the female, both in the ascending and descending line; of the greater frequency of acute articular gout, however, in the male, there can be no question. While it is true that acute attacks are comparatively rare in women, both before and after the menopause, it is undeniable that the subacute and chronic forms of gouty arthritis are by no means rare in them, both before and after the cessation of menstruation. The Hippocratic proposition that women enjoy immunity from gout by reason of the menstrual flux can hardly be entitled to much consideration in view [p. 110]of the fact that they are commonly less exposed to the exciting causes of the disease, and that when they subject themselves to the same vicious habits which entail the disease in men they suffer like men.
Statistics as to the age at which articular gout is most often developed show that the larger proportion of cases occurs in the decade from thirty or forty. It is rare before twenty, and the frequency diminishes rapidly after sixty. Some well-authenticated cases have been observed before puberty in children in whom the hereditary taint was strongly developed. Gairdner claims to have seen several cases in infants at the breast. Trousseau saw a case in a boy aged six, and Garrod in a youth of sixteen. At the other extreme Garrod reports a first attack at the age of eighty, and another in the ninetieth year. The cases at the extremes of age are certainly rare, and other causes of arthritic inflammation might easily be invoked to explain them. It is a significant fact that the largest proportion of attacks of acute articular gout occurs after the period of complete development is ended and before the period of degenerative changes has begun, when the necessities of growth have ceased and food is required only for the nutrition of the tissues, the maintenance of vital energies, and the demands of work.
Much stress was laid by the earlier writers on the effect of temperament as a predisposing cause of gout. The vague ideas involved in the classification of mankind according to temperament may be said to have lost their influence in the scientific conceptions of modern pathology. Gout is observed in persons exhibiting the most diverse peculiarities in physical conformation and physical disposition. The true interpretation of the facts in regard to the relations of temperament to gout, so far as those relations exist, would seem to be that the conditions which give rise to gout are responsible also for the physical and moral idiosyncrasies of gouty subjects.
A vicious hygiene may be regarded as one of the chief predisposing causes of gout. The disease is essentially one of advanced civilization, and is alike the product of the luxury and the misery which a high civilization entails. It is a common error to suppose that gout is the consequence only of luxurious living. If the essential cause of the disease is the circulation of imperfectly oxidized plasma, then there are two ways in which this defective oxidation may be brought about: either there is an excess of food ingested beyond the capacity of the individual, under the most favorable conditions, to consume, or the conditions of oxidation may be so impaired that the complete combustion of even a moderate supply of food is impossible. Perfect oxidation requires an even balance between the amount of food ingested and the oxygen inhaled. A consideration of this axiom explains several circumstances in the history of gout. As has been remarked, the disease is rare during the period of growth and development, when the processes of nutrition are active and the consumption of food in excessive quantities is rendered possible by the large demands for the needs of the growing body and for the development of active energy. It is common in adult life when the processes of nutrition are less active, when growth is complete, and when the supply of food must be regulated according to the amount of energy to be developed. It must also be observed that while the disease is most frequently caused by excesses in the consumption of [p. 111]food, it is also often the consequence of an insufficient supply of pure air; hence we find it often among those who cannot be accused of gluttony, but whose occupations or poverty compel them to live and work in a vitiated atmosphere.
The influence of alcoholic liquors in the production of gouty dyscrasia is generally acknowledged. There seems to be a striking difference, however, in the effects of the distilled and fermented preparations of alcohol in this respect. Gout is certainly more prevalent in countries where large amounts of fermented liquors are used than in those where distilled spirits are chiefly consumed. The disease is more prevalent, for example, in England than in Scotland or Ireland, especially among the lower classes; it is said also that it is rare in Russia and Poland, where spirits are more exclusively used. There is a difference also in the predisposing influence of the different varieties of fermented liquors in the production of gouty dyscrasia. The heavier wines, sherry, madeira, and port, are known to be more mischievous in this respect than the lighter wines of France and Germany, though there is abundant clinical evidence of the fact that even these wines, and especially the richer clarets. Burgundies, and Rhine wines, frequently give rise to acute gout and the gouty habit. There can be no question as to the pernicious effects of the malt liquors as gout-producers. The great frequency of gouty diseases particularly among the lower classes who consume these beverages in large quantities is undeniable. This is true especially of the stronger English and Scotch ales, and to a less degree of the lighter English, American, and German beers. The effect of cider and perry as gout-producers is also well recognized. It has been observed in certain districts of England where cider is largely consumed, and, though acute articular gout is said not to be a common disease in New England, where cider has always been much used, there can be no question that it often leads to the development of the irregular forms of gout. As one of the forms of fermented alcoholic beverages containing, in its fresh state especially, a large amount of sugar, it favors the production of the acid dyspepsia which is a common antecedent in the formation of a gouty dyscrasia.
In 1854, Garrod called attention to the fact that a considerable proportion of the gouty patients in hospital practice—at least 30 per cent.—was represented by painters and other workers in lead. This statement has since been confirmed by other observers, and the association of the characteristic symptoms of this form of metallic poisoning, such as the blue line on the gums, colic, and the different forms of paralysis, with both articular and visceral gout, especially the contracted kidney, is certainly frequent. The relation, however, of saturnine poisoning to gout in this association is not easy to determine, Garrod himself pointing out that while the women in the lead-works frequently had the colic, they but rarely had gout. The difference in susceptibility of different individuals to all forms of metallic poisoning is well recognized. It is more strikingly observed perhaps in mercurial and arsenical poisoning than in that of lead. It is well known that the internal use of lead as an astringent in cases of hemorrhage and intestinal catarrh is occasionally, though very rarely, followed by the evidences of lead-poisoning. This difference in susceptibility is perhaps explicable on the theory that persons inclined to gout have less power in eliminating the [p. 112]metal than those who are not gouty, so that it is possible that plumbism is the effect rather than the cause of gout, as has been commonly supposed.
Tanquerel des Planches found none of those changes in the kidneys as the result of plumbism such as are frequently met with in gout, and Rosenstein, who was able to produce saturnine epilepsy in dogs, found no renal changes to have occurred. Charcot and Gombault in recent experiments of feeding guinea-pigs with lead found changes in the kidneys similar to those produced by tying the ureters.
EXCITING CAUSES.—Paroxysms of acute or subacute gouty inflammation of the joints, skin, or mucous membranes, as well as the neuroses of gouty origin, are excited by a variety of causes: errors in diet, both as to quantity and as to specific articles; excesses in the use of fermented liquors—even moderate indulgence, in persons with strong gouty tendencies—are perhaps the most common exciting causes. Sudden changes in temperature, and especially sudden changes in barometrical pressure, sometimes excite and often aggravate the sufferings of gouty persons. Blows, contusions, and mechanical strain frequently determine arthritic attacks; the large proportion of paroxysms affecting the metatarso-phalangeal joint of the great toe is explained by the fact that this joint is more exposed than any other to strain and injury. Finally, nervous exhaustion, from any cause, from overwork or sexual excesses, from grief, anger, or shock, may provoke any of the inflammatory or neurotic consequences of this disease.
PATHOLOGY.—It would be impossible in the limits of this article to review the many theories that have prevailed in regard to the pathology of gout, or even to discuss fully those that may be said to divide professional opinion at the present day. Since the discovery, by Garrod, of the salts of uric acid in the blood-serum of gouty patients, the humoral pathology of gout has certainly had the largest number of adherents.
The lithæmic pathology may be said to be based primarily upon the chemical theory of digestion or food-transformation. This theory proceeds upon the idea that every atom of albuminous or carbonaceous food that enters the body, whether it goes to the construction of tissue or is destined for the direct conversion of potential into active energy, is finally eliminated, for the most part, as urea, carbonic acid, and water. This transformation, of course, is supposed to be effected by a process of oxidation, but neither the exact mode of transformation nor the share which the different organs and tissues take in its accomplishment can be said to be certainly known. Recent investigations seem to indicate that the liver is chiefly concerned, not only in the metamorphosis of the carbohydrates, but also in the formation of urea, so that the arrest in the conversion of starches and sugars which results in glycosuria, and the check in the metabolism of the proteids which give rise to lithæmia, may both have their origin in hepatic derangement. The not infrequent association of glycosuria and lithæmia in the same patient, and the frequent alternation of gout and saccharine diabetes in gouty families, are significant facts in support of the common origin of these diseases.
The purely chemical theory of gout and diabetes, that they are diseases of suboxidation—a theory most ably advocated by Bence Jones2—has [p. 113]much to commend it from the valuable suggestions which it affords in the clinical management of these maladies; but it must be acknowledged that while a defective oxidation seems to be an essential factor in the production of gout and diabetes, it is impossible to reduce the process to the simplicity of a chemical equation. It cannot be claimed that the complex chain of transformations which organic chemistry has demonstrated in the destructive metamorphosis of albumen and starch in the laboratory is represented in the vital chemistry of the body. All that can be said in the present state of knowledge is, that the metabolism of food is in its nature a chemical analysis, modified and regulated by vital force, and resulting in the building up of tissues and in the conversion of potential into active energy. Imperfect blood-elaboration must depend upon much besides a disturbance of the balance between the amount of food ingested and the oxygen inhaled, though this must unquestionably be an important factor in its production. Heredity and the mysterious influence of the nervous system complicate the problem of the malnutrition which leads to gout, in such a way that while the general proposition may be maintained that gout is a disease in which suboxidation occurs, it is not possible to affirm whether suboxidation is the essence of the disease or only one of its phenomena.
2 Lectures on Some of the Applications of Chemistry and Mechanics to Pathology and Therapeutics, H. Bence Jones, London, 1867.
It is probable, however, that the pathogenesis of the gouty dyscrasia involves a much more complex process than the simple accumulation of uric acid salts in the blood. Uric acid, like urea, is one of the normal results of the metamorphosis of the albuminous foods and tissues. In birds and reptiles it takes the place of urea as the final issue of this metabolism. It has been supposed, as one atom of uric acid can be split by oxidation into two atoms of urea and one of mesoxalic acid, that uric acid was the penultimate of urea, the result of a lower degree of oxidation. It is by no means certain, however, that it is a necessary antecedent of urea. In birds, who consume by their rapid breathing an enormous proportion of oxygen, as well as in the slow-breathing reptilia, the nitrogenous excrements are in the form of urates; and under such divergent conditions it is impossible to explain the variations in the proteid metabolism by varying degrees of oxidation. The only reason that can be assigned for the elimination of the nitrogenous waste in some animals in the form of urea and in others in that of urates is the teleological one that the urea is destined for a fluid and the urates for a solid excretion.
But apart from these physiological objections to the theory that uric acid is necessarily the offending substance in gout, it is well known that uric acid salts accumulate in the blood in febrile diseases, in disorders of digestion, and in anæmia—notably in splenic anæmia—and do not produce either the symptoms or lesions of gout. Todd maintained that gout might occur without an excess of uric acid in the blood; and it is certain that in the atonic and irregular forms of the disease uric acid may not be found in excess in the blood or appear in excess in the urine. Another significant circumstance in the history of gouty persons tending to show that uric acid may be, after all, only an epiphenomenon in the disease, and not its exciting cause, is that the power of digesting farinaceous and saccharine foods in this disease is markedly diminished. To such a degree is this true that sufferers from the gouty dyscrasia are most [p. 114]promptly relieved of their symptoms of primary indigestion by restricting their diet very largely to albuminous foods; and not only does such a diet diminish the dyspeptic symptoms, but I am persuaded by a considerable experience that it is one of the surest prophylactics against the recurrence of gouty lesions. It is well known that the fermented preparations of alcohol are among the most frequent exciting causes of acute gout, and cases are by no means infrequent in which indulgence in sweet foods and in fruits will provoke many of the well-recognized local lesions of the disease.
The explanation of this anomaly in the uric acid pathology of gout may possibly be found in the suggestion of Garrod, that the deposition of the urates is caused by their insolubility, and, as this insolubility is increased by the diminished alkalinity of the serum, that the evolution of the acids in the digestion of the carbohydrates so diminishes the normal alkaline state of the blood that the uric acid salts are more readily precipitated. But even if we accept this explanation, the fact remains that as efficient factors in the production of the gouty diathesis the carbonaceous foods may play as large and perhaps a larger part than the albuminous foods. It would seem, therefore, in view of the conflicting evidence in regard to the theory of the uric acid origin of gout, that the chemical pathology of this dyscrasia is still involved in considerable obscurity.
The recent advances in neuropathology have revived of late years the views of Cullen on the pathology of gout. Dyce Duckworth3 has lately advocated the theory that gout is a trophoneurosis. This theory grows out of the recognition of the protean manifestations of this disease, and especially of the neurotic element which is so prominently developed in its evolution. The frequency of purely nervous symptoms in gouty persons is a fact which is daily brought to the notice of those who have much opportunity to study the disease. These symptoms may be said to affect all the functions of the nervous system; among these we may mention psychical disturbances, such as hypochondriasis and hysteria; derangements of sensation, such as neuralgias and dysæsthesias of every variety; and spasms of voluntary and involuntary muscles, such as cramps, grinding of the teeth, asthma, and vesical tenesmus. Another fact which arrests attention in the history of gouty persons is the frequency with which purely nervous influences determine attacks of gout; the effect of nervous exhaustion, whether provoked by overwork or mental anxiety, or the more explosive discharges of nerve-force in rage and great emotional excitement of any kind, is well recognized as a frequent precursor of gouty lesions. The influence of certain diseases of the nervous centres also, such as cerebro-spinal meningitis, Pott's disease, and tabes dorsalis, in determining arthropathies and lesions of the skin and mucous membranes, furnishes a striking analogical argument in favor of the possible nervous origin of the lesions in gout. The recognition of these facts, however, does not necessarily militate against the commonly accepted humoral pathology of gout. The healthy action of the nervous centres must depend primarily upon a normal nutrition, and a normal nutrition depends on healthy blood-elaboration. That perverted innervation may be an important factor [p. 115]in the development of malnutrition through the accident of inheritance is doubtless true, but in the acquired disease it seems more probable that the lithæmic condition is the primary source of disturbed innervation. It may be that gouty lesions are determined as reflex phenomena through the medium of the trophic centres—if such centres there be—rather than by the direct irritation of the affected tissues by the gouty blood; and it is not unreasonable to suppose that nervous exhaustion from any cause may produce in these centres greater reflex excitability.4
3 Brit. Med. Jour., March 26, 1881.
4 Edward Liveing, in his work On Megrim, Sick Headache, and Some Allied Disorders, p. 404, thus expresses his conviction as to the neurotic theory of gout: "The view which is commonly entertained is, that the excessive generation or retention of uric acid in the system, which is regarded as the fundamental fact in the pathology of gout, exerts a toxic influence upon the nervous centres, while the particular character of the disorder is determined by the territory involved. This limited operation of a cause so general in its nature is a real obstacle to this view; on the other hand, there is much in the history of gout—its hereditary character, limitation to particular ages and sexes, periodicity, explosive character, sudden translations, and remarkable metamorphic relations with nervous disorders—which seems to stamp the malady as a pure neurosis; and even the fit itself, with its sudden nocturnal invasion, the late Dr. Todd was accustomed to compare to one of epilepsy or of asthma."
PATHOLOGICAL ANATOMY.—Blood-Changes.—Garrod's demonstration of the excess of uric acid in the blood of gouty persons constitutes the chief recognized hæmic change in this disease. That this is a constant change, and one that is essential to the existence of gout, cannot be said to be proved. The presence of uric acid in the blood is not always productive of gout, since it has often been found in the blood of healthy persons, and its temporary excess during pyrexia, and especially in the fevers and other morbid states in which spleen is congested, has already been noted. The excess of uric acid, however, in gouty blood may reach, according to Garrod, as much as 0.11 grain in 1000 grains of serum. It is probable that other excrementitious substances exist in the blood in gout which bear a closer etiological relation to this disease than uric acid, but they have not been demonstrated. The other blood-changes which are noted by Garrod—the diminished specific gravity of the serum from loss of albumen, the diminished alkalinity, and the increase of the fibrin in the inflammatory forms of the disease—are probably inconstant. In chronic gout the objective signs of anæmia which are often present would indicate a marked diminution in the red blood-corpuscles.
The tissues which are the chief seat of gouty lesions are the connective tissues. In the evolution of the disease the joints, where the connective tissue is most dense and the least vascular, suffer earliest; at a later period the connective tissue of the blood-vessels, nerves, and viscera becomes subject to gouty changes.
According to Garrod, the exudations in articular gout are rich in the urates of soda, lime, magnesia, and ammonia; they also contain some phosphate of lime and traces of organic matter. The watery portion is absorbed and the salts are deposited in crystalline forms. The location of these deposits varies: they are found on the synovial surfaces, in the cartilage-cells, and in the intercellular substance; in the tendons, ligaments, and bursæ, and in the subcutaneous connective tissue. The urate of soda occurs not on the free surface of the cartilage, and replacing [p. 116]the latter, as was formerly generally supposed, but as an infiltration into the substance of that tissue; and Garrod found that there is always a thin layer of unaffected cartilage lying between the deposit and the free articular surface—an observation which has been confirmed by Budd and quite recently by Ebstein.5
5 W. Ebstein, Die Natur und Behandlung der Gicht, Wiesbaden, 1882.
Very important are the recent investigations of the latter. After making numerous observations on the cartilages and other affected tissues of gouty subjects, besides studying the disease artificially produced in fowls, he has shown that those portions of cartilage and other tissues in which the deposit occurs are in a state of necrosis, as is evident from the fact that when the urates are dissolved out by warm water the area in which the deposit occurred, though apparently normal to the eye, refuses to be stained with aniline dyes, and lies plainly visible as a light spot in the midst of stained tissue. Since the work of Weigert we know that this is a sure sign of that peculiar form of death of a tissue to which the name of coagulation necrosis has been given. Ebstein regards this necrosis as primary and the deposition of the uratic salt as secondary. According to him, the urates circulating in the blood give rise to necrosis in parts where the circulation is sluggish (as the articular cartilages, the ears, and the extremities generally), and where, consequently, they remain a greater length of time in contact with the tissues. The necrotic portion has, however, an acid reaction, which causes a deposition, from the soluble neutral salt, of an acid urate in a crystalline form. Ebstein claims that this necrotic area, in which there is deposited a crystalline urate of soda, and around which there is a secondary inflammatory zone, is characteristic solely of gout. "I have never seen," he says, "in gout a crystalline deposit of urates occurring in normal tissue."
In addition to these so-called specific changes we find a hyperplasia of the connective tissue in the fibrous structures of the affected joints. The thickening thus induced, with the contraction of the new tissue and the atrophic changes resulting from pressure and disuse, are the causes of the deformities, subluxations, and impaired movements of gouty joints. Occasionally, the local irritation provoked by the pressure of the tophous deposits results in abscesses from which a mixture of pus and pasty urates may be discharged. These abscesses in feeble and anæmic subjects are sometimes difficult to heal. More frequently the skin undergoes gradual absorption and the chalk-like deposits are exposed.
The frequency with which the metatarso-phalangeal joint of the great toes is affected in gouty persons has always been noted. In Scudamore's tables the proportion of the first attacks in this joint was 72 per cent., and in 66 per cent. one or both great joints were affected to the exclusion of other joints. This frequency is due to the fact that this joint is the most vulnerable one in the body, bearing as it does the weight of the body and being exposed to most frequent shock. The phalangeal joints of the hands and the wrist-joints are also often the seat of acute gout, though these joints are more frequently affected by the subacute form of the disease. The larger joints may also be the seat of true gouty inflammation; indeed, no joint, not even the intervertebral, can be said to enjoy immunity, and the hip and shoulder are occasionally attacked to [p. 117]the exclusion of others. The cartilages of the ear and the arytenoid cartilages are sometimes the seat of gouty deposits.
The great frequency of arterial sclerosis, and the subsequent fatty and chalky metamorphosis in persons who have suffered from chronic gout, are well recognized. Next to syphilis, gout seems to be the most common cause of these arterial changes. The influence of these lesions in the arteries and capillaries in determining cardiac hypertrophy and cerebral hemorrhage is often seen in the accidents which terminate the lives of gouty patients.
In the heart a gouty endocarditis is of not uncommon occurrence, according to Ebstein, who cites Lancereaux as having found uric acid in concretions on the valves. Garrod, however, after examining a number of cases in which cardiac disease existed with gout, states that in his opinion the valvular changes are not due to a gouty deposit, he never having been able to demonstrate the presence of uric acid in them.
Some years ago Sir James Paget called attention to the frequency of adhesive phlebitis as a gouty lesion. This is observed in connection with articular gout, but may also occur independently of joint-lesion. It is observed most frequently in the lower limbs, is generally symmetrical, and shows a disposition to metastasis.
Neuritis and sclerotic lesions of the nerve-centres are not uncommon in the history of acquired and inherited gout. The neuralgias and other temporary dysæsthesias which constitute a considerable category in the symptoms of gouty persons are doubtless due to transient central and peripheral lesions.
The so-called gouty kidney is the most striking illustration of the effect of the gouty dyscrasia in the production of a characteristic visceral lesion. The changes which occur in the kidney as a result of gout are—a contraction of the organ, the result of interstitial inflammatory processes, and a deposition of uratic salts, occurring mainly in the papillary portion. The views as to the exact locality where these deposits occur still differ considerably. Garrod is of opinion that it occurs in the fibrous interstitial tissue. Virchow, on the other hand, regards the lumen of the tubuli as the seat of the deposit, and in this he is supported by Charcot and Cornil and Ranvier, Lancereaux and Wagner. Dickinson inclines to the view of Garrod, and believes that it is the deposition of the urates in the interstitial tissue which gives rise to the chronic inflammation which results in cirrhosis of the kidney—the granular kidney of gout. Ebstein seems to think that the interstitial connective tissue, having previously undergone a state of necrosis, as in cartilage and other connective tissues, is the seat of the deposit. As in cartilage, he regards this necrotic state as typical of gouty deposits. About the necrotic area in which the deposit has occurred a secondary inflammation takes place, leading ultimately to contraction of the new fibrous tissue formed. He calls attention to the fact that (1) the kidneys may be perfectly sound in gout; (2) the kidneys may be the seat of chronic interstitial inflammatory changes, with cirrhosis, without any urate deposits of any kind being demonstrable; (3) there may be chronic interstitial nephritis, with crystallized urates in the urinary tubules.
As regards changes in the liver, few satisfactory accounts exist. [p. 118]Portal originally called attention to the fact that in gout and rheumatism indurations of the liver caused by the deposit of a phosphatic earth occurred, and Charcot has recently referred to the fact. Ebstein cites a case in which in a gouty patient he was able to make a diagnosis of moderate hypertrophic hepatic cirrhosis, but so far he had not been able to confirm it by post-mortem examination.6
6 Gout in Animals.—Of the occurrence of gout in animals not many reliable reports exist; Ebstein has collected a few. Thus, he cites a case where in an old hunting-dog uratic concretions were found in the articular ligaments and in the periosteum of the epiphyses of many joints, but especially those connecting the ribs with their cartilages. In the toes of falcons and of parrots kept in confinement deposits of urates have been observed, and in an alligator dying in captivity deposits were found in the muscles as well as the joints which consisted of free uric acid together with sodium urate.
Experimentally, Ebstein was able to produce gouty lesions having all the characteristics of those occurring spontaneously in man by injecting subcutaneously small quantities of the neutral chromate of potash into the blood of cocks for a considerable period of time. By this method changes in the epithelial elements of the kidney were produced, preventing the elimination of the urates from the blood and causing their consequent accumulation in the system. He obtained in this way typical deposits of urates in the joints, tendons, muscular sheaths, heart, and other organs, while the birds emaciated and finally died. But these experiments, which are extremely valuable and interesting, still need confirmation.
The experiment of tying the ureters of fowls is an old one. Galvani who was perhaps the first to perform it, employed it in his investigations on the kidney, and since then Zalesky, Pawlinoff, Von Schroeder, Colosanti, and others have made use of it in their experimented studies on the site of origin of uric acid. As a result of this operation deposits of urates occur in various organs. Ebstein, however, does not regard them as analogous to the gouty deposit in human beings, as they lack the feature of necrosis, which, as mentioned above, he considers as alone characteristic of the true gouty lesion.
SYMPTOMATOLOGY.—The development of true gouty lesions, whether of the acute or subacute form, is usually preceded by a period, more or less protracted, in which characteristic derangements of the health present themselves. These derangements may be conveniently classified as disturbances of primary digestion and as manifestations of malnutrition.
The disturbances of primary digestion are repeated attacks of flatulent dyspepsia, with pyrosis, colicky pains, alternate constipation and diarrhoea, and a scanty, high-colored, and heavy urine with uratic sediments. This dyspepsia may be accompanied with a variety of reflex nervous symptoms, such as pain in the nape of the neck and occiput, insomnia, palpitation, sighing respiration, singultus, and nausea. These symptoms are commonly described as due to biliousness, and are provoked by excesses in diet, and not unfrequently by moderate indulgence in certain common articles of food, such as sweets, fruits, farinaceous foods, and the fermented preparations of alcohol.
Derangements of nutrition are shown by a disposition to erythematous and catarrhal affections of the skin and mucous membranes, to affections of the sebaceous glands, and to premature falling of the hair. There is often a more or less marked tendency to obesity. Accompanying these derangements there may be a loss of energy, both physical and mental, manifesting itself in indolence and fatigue on slight exertion, in irritability of temper, with diminished intellectual activity and hypochondriasis. Neither the primary indigestion nor the nutritive derangements invariably precede the development of acute gouty lesions, nor are they necessarily followed when they exist by the articular signs [p. 119]of gout; but they are so commonly associated with the evolution of what are regarded as the specific lesions of gout that they may fairly be described as constituting its prodromal period.
ACUTE ARTICULAR GOUT.—A typical attack of acute gout is usually sudden. It seizes its victim without warning, and often rouses him from sleep with a vicious agonizing pain in the joint assailed. Examination will reveal a slight redness, heat, and puffiness of the part affected altogether disproportioned to the intensity of the pain; the tenderness is exquisite, and the torture is often aggravated by the occurrence of reflex spasms of neighboring muscles. There is usually moderate fever, and if the surface be exposed there may be a chill. Sleep is impossible and the restlessness uncontrollable. As the morning advances slight perspiration occurs, and sleep may become possible. With the abatement of pain there is coincident increase in the signs of inflammation: the joint swells, the skin becomes red and oedematous around the joint, and the superficial veins are distended. But, though the pain subsides with the occurrence of swelling, and usually in proportion to its degree, the tenderness and pain on any attempt to move the joint continue to be extreme. The day is passed in comparative ease, but the evening generally brings an exacerbation of pain and fever, and the night another paroxysm of agony—not as severe as the first, but severe enough to make the daylight a benison. The progress of the disease after the second day, provided it is confined to one joint, is usually marked by a steady and regular decline in the severity of the symptoms. If the attack is confined to a single joint, a week may elapse before the inflammatory signs subside, and it may be a fortnight before pressure can be borne or the mobility of the joint is restored. Occasionally the sufferings of an acute attack of gout may be protracted by successive seizures for several weeks. The fever during the attack is distinctly remittent, the evening exacerbation rarely exceeding 103° F.
The urinary symptoms before, during, and after an acute paroxysm of gout are interesting and important in their bearing upon the uric-acid theory of the disease. Garrod's statements upon this point are generally accepted, and have been confirmed by other observers. He says that previous to the attack the amount of uric acid in the urine is below the average—that during the paroxysm the proportion grows smaller, and only rises to the normal standard with the termination of the seizure. The reaction of the urine is strongly acid during the paroxysm. This is due probably to the increased excretion of acid phosphates. The quantity of the urine is generally diminished, the specific gravity increased, and the color deepened.
Attacks of acute gout are generally followed by improved health and capacity for physical and mental work and enjoyment. The blood seems to be purified, the processes of digestion and assimilation are once more normally performed, the equilibrium of the nervous centres is restored, and the evolution of all the vital energies proceeds with ease and vigor. This state of well-being may continue for a year or two years, or even a longer period, after the first attack, the immunity varying according to the intensity of the inheritance or the habits of life. The subsequent attacks are apt to occur at increasingly shorter intervals, and, as a rule, the acuteness of them tends to diminish. Gradually the dyscrasia becomes more [p. 120] profound, and the constitutional symptoms and structural changes which belong to the atonic and irregular forms of the disease are developed.
ATONIC GOUT.—Though subacute, irregular, or atonic gout is often the sequence of repeated attacks of the acute disease, it is not necessarily preceded by them, nor is acute gout invariably followed by a marked gouty dyscrasia. It is not uncommon for a well-characterized gouty habit to exist, manifesting itself by many and varied gouty phenomena, without the occurrence of any acute lesions, and repeated attacks of acute articular gout may occur without the development of the progressive impairment of health and the tissue-changes which distinguish the chronic malady. The recognition of this fact is important, inasmuch as the occurrence of acute gout is commonly regarded as an essential element in the diagnosis of the gouty dyscrasia. Acute articular attacks, as already noted, are very rare in women, in whom the subacute and irregular forms of the disease are by no means infrequent. So far as acute articular gout is of value in the diagnosis of the constitutional vice, it is perhaps as significant if established in the history of a near relative as in the individual in whom the disease is suspected.
The general symptoms of atonic gout—or, as it may more properly be called, the gouty dyscrasia—are similar to those which sometimes precede the development of the acute form. The difference lies in their persistence, in the subacute character of the local lesions, and in the absence of the relief to the constitutional symptoms which follows acute attacks.
The dyspeptic symptoms are perhaps the most pronounced and uniform in the history of the evolution of chronic gout. These symptoms have been already described, but the fact which seems especially to distinguish them is that they are chiefly provoked by the acid fermentation of the carbohydric elements of the food, the sugar and starches, and especially by the fermented preparations of alcohol; the ability to digest these articles of diet appears to be deficient in the gouty dyspeptic.
The changes in the urine in the gouty dyscrasia are especially important. In the formative stages of the gouty vice the amount of urine may not vary much from the normal quantity, but the proportion of solid constituents, especially of the urea, is increased, so that the specific gravity may rise to 1.030 or 1.035. The acid reaction is intensified by the excess of the acid urates and phosphates upon which the normal acidity depends. Sometimes crystalline deposits of uric acid, urates, and oxalates take place in the tubuli of the kidney and in the bladder, and lead to the nephritic and vesical irritations which are often the source of much inconvenience and pain. Where the urine is free from these crystalline constituents as it comes from the bladder it may deposit them within a few hours after its passage. At a later stage in the development of the gouty dyscrasia the quantity and quality of the urine undergo marked changes. The quantity is increased; the color is pale, partly in consequence of dilution and partly through a diminution in the amount of coloring-matter. The quantity may be so considerable as to constitute a polyuria. The reaction is neutral or only feebly acid; crystalline sediments of uric acid and calcium oxalate may occasionally appear, and the specific gravity may be so low as to indicate not only a relative but an absolute diminution in the daily excretion of urinary solids. Traces of albumen and of sugar are not infrequently observed.
[p. 121]The articular symptoms of chronic gout are subacute. They affect the joints, as a rule, which are most exposed to strain and injury, and hence are most common in the hands and feet, but they may involve the knee and the hips, the elbow and the shoulder, and even the intervertebral joints. The pain is less severe, because the tension is never so considerable; the tenderness is often a source of great discomfort; the swelling varies with the acuteness of the inflammatory process, the joints being more or less permanently enlarged by hypertrophic changes affecting the articular structures and by tophous deposits. The deformities are increased by ankylosis, by contractions, by absorption of the cartilages, by partial luxations, and by the atrophy of disused muscles. Crepitations are often observed in the affected joints. Exacerbations of the local symptoms are often provoked by movements, by imprudence in diet, by changes in temperature or in barometric and hygrometric conditions, and not infrequently by psychical disturbances.
The frequency with which tegumentary affections, mucous as well as cutaneous, are observed as correlative phenomena of arthritic lesions in gouty persons and in gouty families justifies the inference that the same lithæmic vice which determines articular inflammations is often responsible for derangements of nutrition in the skin and mucous membranes. The French school of dermatology, which has always maintained the humoral origin of many cutaneous diseases, has long recognized the arthritic nature of a large class of affections of the skin. Bazin7 has given the most precise description of the arthritides, as he terms them. He insists upon certain functional derangements of the skin as characteristic of the gouty diathesis, such as excessive perspiration, especially in certain regions, as the head, the axillæ, the hands and feet, and the sexual organs, and also affections of the sebaceous glands, causing the different forms of seborrhoea and the premature falling of the hair. He notes the liability in gouty persons to certain neurotic affections, such as pruritus, general or localized, about the arms and genital organs. Erythematous affections, especially urticaria, erythema nodosum, and the fugitive erythema which occurs about the face, causing sudden and evanescent swelling of the eyelids, cheeks, lips, and even the tongue and soft palate, are recognized by him and other observers as arthritic in their origin. Among the erythemata which are observed in gouty persons the peliosis rheumatica should be mentioned.
7 Affections génériques de la Peau, Paris, 1862.
The more persistent inflammatory lesions of the skin, such as eczema and psoriasis, which are characterized by long-continued hyperæmia with hyperplasia, are now recognized as among the possible transformations of gout. They are certainly often observed alternating with arthritic lesions, and associated with all the characteristic derangements of nutrition which belong to the gouty habit. The frequency of the various forms of acne, the inflammatory, as well as those which result from excessive function of the glands, in persons having a strong gouty inheritance, is recognized by many dermatologists. I have noticed these lesions especially in young women belonging to gouty families. They are generally accompanied by marked dyspeptic symptoms, and not infrequently by neurotic derangements.
Garrod, in a paper read at the International Medical Congress in 1881 [p. 122]on "Eczema and Albuminuria in Relation to Gout," affirms that each year strengthens his conviction that gout and eczema are most closely allied. Since his attention was first called to this relation in 1860, he has found a gradually increasing percentage of eczema in the cases of gout that have come under his observation. Dividing all the cases from 1860 to 1881 into ten groups, he found the percentage rose from 10 in the first group to 47 in the tenth. He accounts for this rapid increase in the percentage in the fact that in the first few years the eczema was only observed when it was very patent; during the past two or three years he has had made more careful inquiries as to the presence of eczema or other skin eruption in every case of gout, and by these means has frequently discovered its presence when it might otherwise have been overlooked. Garrod believes that eczema is the special skin-lesion of gouty subjects, and does not regard psoriasis as having anything more than an accidental connection with gout. He admits that the latter is often associated with rheumatoid arthritis. It must be remembered, however, that Garrod does not admit that gout ever exists without lithatic deposits.
In regard to the location of gouty eczema, it appears to affect by preference the more tender and vascular regions of the skin. The eyelids, ears, the scalp, and back of the neck, the fingers and toes, particularly the dorsal and lateral surfaces, and in old people the legs, are especially liable to be attacked. The subjective symptoms of gouty eczema are often the source of great suffering; the burning and itching are sometimes intolerable. This is especially true of persons of highly neurotic constitution.
It is not possible to affirm that there are lesions of the mucous membranes which are strictly analogous in their transient character to the erythematous affections of the skin, but it is not unreasonable to suppose that many of the temporary disturbances of indigestion to which gouty patients are subject are caused by an evanescent hyperæmia corresponding to the vaso-motor derangements which are observed in the external integument. In regard, however, to the more persistent catarrhal lesions, there can be no question as to their analogy with those which affect the skin. The continuity of these lesions at the orifices of the mucous tracts, and the frequent association of external eczemas with catarrhs of mucous membranes, are facts of common experience. Greenhow8 of London first called attention to the frequency with which chronic bronchitis is associated with the gouty dyscrasia. In an analysis of 96 cases of chronic bronchitis he elicited the fact that in 34 out of the 96 a distinct gouty history attached either to the patients themselves or to some of their immediate relatives. In 14 of the cases the patients were subject to attacks of acute regular gout as well as to bronchitis. He also noted the association in a number of cases of bronchitis and psoriasis with gravel and gout. My own experience confirms these observations, and also the alternations of catarrhal and parenchymatous tonsillitis, of pharyngeal and laryngeal catarrh, and of asthma and chronic bronchitis, with the more common manifestations of regular and irregular gout.
8 On Chronic Bronchitis, E. Headlam Greenhow, M.D., London, 1869.
The occurrence of subacute gastro-duodenal and intestinal catarrhs [p. 123]with hemorrhoidal complications is even more common that the catarrhal affections of the respiratory tract. The lesion, in fact, which gives rise to the manifold dyspeptic symptoms in gouty subjects is doubtless a catarrhal one.
The genito-urinary tract exhibits also the tendency to catarrhal affections in sufferers from the gouty dyscrasia. It is certain that gouty persons are especially liable to vesical catarrh, and it is generally admitted that rheumatic and gouty persons are particularly susceptible to gonorrhoea. My own experience leads me to suspect that chronic urethral discharge resulting from acute urethritis is more common in rheumatic persons than in those not having this taint. The etiological relations of gonorrhoeal rheumatism and kerato-iritis are still involved in obscurity, though I am inclined to believe that a careful examination of the personal and family history in cases of these diseases would establish the opinion that has been maintained as to their gouty origin.
The presence of albumen in the urine of persons suffering from acute gout is occasionally observed. Under these circumstances it is transient, and has probably no more significance than is usually attached to this symptom in the course of any acute febrile disease. In chronic gout it is by no means infrequently observed as a more or less persistent symptom. It is associated under these circumstances with a copious discharge of urine of pale color and low density, and with the general signs of what Rayer first described as the néphrite goutteuse.
The importance of this symptom is very great when we consider the insidious development of this form of disease and the difficulty of its early diagnosis. Recent investigations point to the value of the changes in the urine in the progress of the gouty dyscrasia as bearing upon this question. It has already been noted that in the early history of gouty persons the urine is often scanty, high-colored, excessively acid, of high specific gravity, occasionally albuminous and saccharine, and frequently depositing sediments of urates and calcium oxalate. McBride of New York9 has recently called attention to this condition of the urine and its association with high arterial tension as the functional stage of the granular kidney—as the stage, that is to say, during which the necessity of eliminating large amounts of imperfectly oxidized nitrogenous material maintains a constant state of renal hyperæmia, which finally induces the changes in the tubular and intertubular structures which constitute the anatomical features of this form of disease.
9 The Early Diagnosis of Chronic Bright's Disease, T. A. McBride, M.D., New York, 1882.
The occasional presence of sugar in the urine of gouty persons has already been noted. I have repeatedly observed this symptom in the urine of gouty dyspepsia. It occurs more commonly in obese subjects, and is usually intermittent and easily controlled by dietetic restrictions. In these cases it is not necessarily associated with a very large amount of urine. In chronic gout and in connection with the granular kidney a more serious form of glycosuria is occasionally observed. Under these circumstances it increases largely the polyuria which is characteristic of gouty nephritis, and is sometimes overlooked because it occurs in a urine of a low density, often not more than 1.010. It is not controlled by diet [p. 124]to the same extent that it is in the cases previously described, and is in my experience a prognostic sign of bad import.
Some of the most distressing symptoms to which gouty persons are especially liable are those connected with the passage of gravel from the kidney to the bladder. Where gravel alone passes, it may cause little uneasiness, and the fact is only recognized through the discovery of blood in the urine in connection with uric acid or calcium oxalate crystals. When, however, the sand forms concretions in the pelvis of the kidney, their dislodgment and passage through the ureter are accompanied by the well-known agonies of renal colic.
Dysuria is a symptom from which gouty persons often experience much inconvenience and suffering. It is usually associated with extremely acid urine of high density containing crystalline sediments. It may manifest itself only in frequent and painful micturition, or it may be associated with such a degree of vesical tenesmus as to cause retention and necessitate the use of the catheter.
DIAGNOSIS.—If the term gout be restricted to that form of arthritis in which an excess of urates is found in the blood with tophous deposits in the affected joints, the cartilages of the ear and nose, and in the subcutaneous connective tissue, then the diagnosis of this disease is a simple one. It is a disease with a pathognomonic sign. But if the pathology of gout consists rather in a more complex morbid condition of the blood, of which an excess of urates in the serum is only one of a number of phenomena, and not necessarily the sole and essential cause of the local lesions, then the question of diagnosis involves a consideration of all the correlated morbid conditions which are so frequently associated in gouty persons and gouty families as to justify the inference that they have a common origin in a perverted nutrition, the essential nature of which is imperfectly understood.
The very existence of the terms gouty rheumatism and rheumatic gout which are in common use shows that what is regarded by many excellent authorities as the confounding of distinct entities must have some foundation in clinical experience. If we consider gout, in its strictest pathological sense, acute inflammatory rheumatism, rheumatoid arthritis, or gouty rheumatism, and senile arthritis or the arthritis deformans and gonorrhoeal rheumatism as separate and distinct diseases, we shall find ourselves compelled to ignore certain common clinical facts which indicate a bond of union between them. Heredity, for example, is common to them all, and more than this, there appears to be a tendency to a differentiation of the taint in families. It is well known, for instance, that the children of gouty parents are especially liable to acute rheumatism, and acute rheumatism in youth is often followed by gout in later years. It is also a fact of common experience that while the men in gouty families are the victims of true gout, the women are apt to be the subjects of rheumatoid arthritis. The arthritis deformans which develops with the degenerations of advancing years is not infrequently associated with a family history of genuine gout. Gonorrhoeal rheumatism also, according to the experience of many trustworthy observers, often recognizes an inheritance to gouty lesions. But it is not alone in heredity and the differentiation of the type of the disease in families that the unity of these affections displays itself. The same disturbances of digestion which [p. 125]characterize the history of true gout are observed in those who are liable to acute rheumatism, to rheumatoid arthritis, and to arthritis deformans. It is true that excesses in food and fermented liquors do not determine, as in gout, attacks of acute rheumatism nor of the chronic forms of arthritis, for these latter diseases are commonly due to causes operating upon the nervous system, as exposure to cold and dampness or to physical or emotional shock of some kind; still, there is in the subjects of these diseases a more or less marked tendency to the same dyspeptic disorders, and especially to the diminished capacity in digesting the carbohydrates, which the subjects of true gout exhibit. In the diagnosis of gout, therefore, it would seem that the question of differentiating this disease from those which simulate it is not one in which we are called upon to distinguish one morbid entity from another, as typhus from typhoid fever or syphilis from cancer, but rather to determine, first, the presence of a recognized constitutional vice; and, secondly, to differentiate the variety of the lesions by which this vice manifests itself.
In the diagnosis of the gouty dyscrasia the first point to determine is that of heredity. This requires a careful inquiry into collateral as well as direct descent, and does not necessarily involve the discovery of arthritic diseases in the ancestors, though these are doubtless the most striking and trustworthy proofs; but the tradition in the family of persistent dyspepsia, or what is commonly called biliousness, of chronic catarrhal affections of the skin and mucous membranes, and of the chronic forms of renal disease, are significant indications of this dyscrasia. In the personal history the evidences of the lithæmic tendency, as indicated by the characteristic dyspeptic symptoms which have been described, and especially by the feeble capacity for the digestion of carbohydrates, are of great diagnostic value.
The diagnosis of gouty joint-lesions, whether acute or chronic, depends partly upon the determination of the gouty dyscrasia, and partly upon the differential distinctions which separate gouty inflammations from acute rheumatism, rheumatoid arthritis, and from the arthropathies which result from traumatism and from lesions of nerves and nerve-centres.
Gouty arthritis may be distinguished from acute rheumatism by the fact that it is more often hereditary—that it occurs in older subjects, attacking generally the smaller joints, and, as a rule, in the acute form, localizing itself in one or two joints. It is also noteworthy that the constitutional symptoms are not as severe as in rheumatism. Gout deforms the joints, while acute rheumatism leaves no traces of the inflammatory process. In addition to these distinctions there is, according to Garrod, the crucial test of an excess of urates in the blood-serum.
From rheumatoid arthritis or rheumatic gout, gout in its acute and regular form is distinguished by the more acute local and constitutional symptoms. Gout is periodical in its attacks, while rheumatoid arthritis is progressive. It attacks the smaller joints or those most exposed to strain, while rheumatoid arthritis occurs in the large as well as the small joints, and appears to be more independent of traumatism as an exciting cause. Gout is more common in men, rheumatoid arthritis in women. According to Garrod and other excellent authorities, deposits of urates are never found in the joints in rheumatoid arthritis, and there is no excess [p. 126]of urates in the blood. This statement is denied by Hutchinson. Ulcerations of cartilages, contractions of tendons, atrophies of muscles with subluxations of joints, are more common in rheumatoid arthritis than in gout.
While these local distinctions are undeniable, it is proper to observe that in rheumatoid arthritis the constitutional symptoms of the gouty dyscrasia, especially the dyspeptic derangements and the nervous disturbances, are often well marked; and it should also be noted that the principal distinction, the absence of urates in the blood and in the diseased joints, is one that is based on the exclusive theory that uric acid is the materies morbi of true gout. If, as is still maintained by some excellent authorities, uric acid is not essential to gout, then it must be confessed that the other distinctions are purely lesional, and that the common constitutional symptoms suggest that these diseases are divergent branches of a single trunk.
Gouty arthritis is not always easily distinguishable from traumatic inflammation of the joints, inasmuch as traumatism plays so important a part as an exciting cause of gouty attacks. The history of previous seizures and the presence of predisposing causes of gout are the points upon which the determination of the gouty nature of the inflammation would depend. A termination in suppuration would exclude the idea of the gouty nature of an arthritis.
With the arthropathies of purely nervous origin, such as occur in paralyzed limbs, in Pott's disease, and in tabes dorsalis, gout can hardly be confounded, although the arthritic complications in these diseases have been used to illustrate the neurotic theory of both gout and rheumatism.
The diagnosis of irregular gout—i.e. of gouty affections of the skin and mucous membranes, of the structures of the eye, and of the parenchymatous organs—must be based more upon the hereditary history and upon the correlated phenomena recognized in the personal history than upon any specific character in the lesions themselves. In the gouty form of nephritis there are, it is true, in the urinary symptoms, in the anæmia, in the arterial fibrosis, and in the cardiac hypertrophy, diagnostic signs of great value.
PROGNOSIS.—Acute, regular, articular gout is probably never a fatal disease where it occurs in a robust person without visceral complications. In rare instances the first attack may never be repeated, or only two or three attacks may occur in the course of a long life. In the majority of instances, however, frequent repetitions are the rule, the intervals between the attacks growing progressively shorter; occasionally repeated seizures go on through a long life, the attacks becoming milder with advancing years, and, save the crippling effects of the disease, the patient may enjoy in the intervals a fair degree of health. This, however, is the exception. With the increased frequency of the arthritic attacks the signs of the constitutional vice become more marked. The dyspeptic disorders become more persistent and rebellious to treatment, various transformations of the disease manifest themselves, and tissue-changes make insidious and inevitable progress. When this stage of the gouty disease is reached, the prognosis becomes more grave because of the complications and accidents to which the sufferer is liable. These complications and accidents are the result of the nervous, vascular, and visceral lesions which have been [p. 127]described. Vaso-motor instability gives rise to a great variety of painful functional derangements resulting from serious cerebral, pulmonary, gastric, and renal congestions. Glycosuria is not an uncommon complication in chronic gout, and seriously affects the question of prognosis. Arterial degenerations may cause thrombotic accidents, and the formation of miliary aneurisms in the brain may determine a fatal issue by softening or hemorrhage. Anginal attacks due to cardiac muscular degeneration may also imperil life.
The principal visceral lesion which leads directly or indirectly to a fatal issue in gout is that of the kidney. This involves danger either through the induction of a hopeless anæmia and its consequences in dropsical effusions, or by determining inflammatory accidents of the gravest nature.
That gout shortens life in the majority of cases is unquestionable—a fact which is sufficiently attested by the care with which life-insurance companies exclude risks in which a well-pronounced inherited tendency or existing manifestation of the disease can be substantiated.
The prognosis varies of course with the rapidity with which the constitutional dyscrasia is developed, and this rapidity will depend on the intensity of the inheritance and the mode of life. Some gouty subjects escape the vascular and visceral complications of the disease for a long period, although crippled and deformed by its articular ravages, and attain advanced age; others may succumb in comparative youth to its most profound lesions. It is a happy circumstance that under wise hygienic management and judicious medication acquired gout may be checked in its progress, and even a strong inherited tendency may be largely controlled.
TREATMENT.—A logical consideration of the treatment of gout embraces, first, the treatment of the constitutional vice, based, as far as possible, on the nature and causes of the disease; and, secondly, the treatment of the lesions which the disease determines. If we regard the accumulation in the blood-serum of the salts of uric acid as the essential cause of the gouty lesions, then the origin of the constitutional vice is in the conditions which bring about this accumulation. As we have urged, none of the theories of the production of the lithæmic state harmonize all its phenomena. It is impossible to represent the complex processes of nutrition by chemical formulæ, and equally impossible to divorce chemical reactions from a share in their production. We can trace the metabolism of the azotized and carbonaceous foods through many changes to their ultimate disintegration into urea, carbonic acid, and water, but we do not know all the steps by which this conversion is effected, nor the organs or tissues in which it is accomplished. We may reasonably assume that the agent through which the potential energy of the food is evolved is oxygen, and that the process of nutrition is hence partly, at least, a process of oxidation. This chemical view of the digestion and assimilation of food may be said to be the rational basis of the treatment of the lithæmic state. To control the accumulation of azotized matters in the blood, and to secure their thorough combustion and conversion into urea, carbonic acid, and water are the recognized aims of the treatment of the vice upon which gout depends.
DIET.—The prevention of the accumulation of azotized matters in the [p. 128]blood involves, first, a consideration of the question of the diet appropriate to the gouty dyscrasia. The almost uniform counsel upon this point of all the authorities from Sydenham to the present time is, that albuminous foods should be sparingly allowed in the diet of the gouty patient, and that vegetable foods, especially the farinaceous, should constitute the principal aliment. This counsel is based upon the theory that uric acid is the offending substance, and, this being the outcome of a nitrogenous diet, the nitrogenous element in diet must be reduced. My own observation has led me to believe that while this may be a legitimate deduction from the uric-acid theory of gout, it is not supported by the results of clinical experience. If there is one signal peculiarity in the digestive derangements of gouty persons, it is their limited power to digest the carbohydrates, the sugars and starches. In whatever form these foods are used, they are more commonly the source of the dyspeptic troubles of sufferers from gout than the albuminous foods. They provoke the acid and flatulent dyspepsia which so generally precedes the explosion of the gouty paroxysm; and it must have attracted the attention of every observer who has studied the dyspeptic disorders of sufferers from inherited gout, who have sought to control their unhappy heritage by abstemious habits, that these disorders are especially provoked by over-indulgence in saccharine and amylaceous foods.
It is not possible to explain satisfactorily why the lithæmic condition should be induced by the carbonaceous aliments, but we believe there can be no question as to the fact. If, as modern physiological investigations tend to show, the liver is the organ in which urea as well as glycogen is formed, it may be that the overtaxing of its functions manifests itself more readily in the conversion of the albuminous than in that of the carbonaceous foods; or it is possible that the carbonaceous foods are destined chiefly for the evolution of mechanical energy, and that when this destiny is not fulfilled through indolence and imperfect oxygen-supply, they escape complete combustion, and so vitiate the blood. But whatever may be the cause of this anomaly, the clinical fact remains that in gouty persons the conversion of the azotized foods is more complete with a minimum of carbohydrates than it is with an excess of them—in other words, that one of the best means of avoiding an accumulation of lithates in the blood is to diminish the carbohydrates rather than the azotized foods.
The diet which a considerable experience has led me to adopt in the treatment of the gouty dyscrasia is very similar to that which glycosuria requires. The exclusion of the carbohydrates is of course not so strict. Abstinence from all the fermented preparations of alcohol is perhaps the most important restriction, on account of the unfermented dextrin and sugar which they contain. This restriction accords with the common experience respecting the part which wine and beer play as predisposing causes of the gouty disease and as occasional exciting causes of gouty lesions.
Next to the fermented liquors, the use of saccharine food in the diet of gouty persons needs to be restricted. This limitation also is one which common experience confirms. Sweet foods cannot be said to be as provocative of the dyspeptic derangements of the lithæmic subjects as wine and beer, but they are certainly often responsible for the formation of [p. 129]the dyscrasia and for perpetuating many most distressing ailments. Their more or less strict prohibition may constitute the essential point of treatment not only in controlling the progress of the constitutional vice, but in subduing some of the most rebellious lesions. It is important to observe that this prohibition sometimes involves abstinence from sweet and subacid fruits, in the raw as well as in the preserved state. Paroxysms of articular gout have been known to follow indulgence in strawberries, apples, watermelons, and grapes, and the cutaneous and mucous irritations which follow even the most moderate use of these fruits in some gouty persons are certainly not uncommon.
Next in order to the saccharine foods as the source of indigestion in gouty persons come the amylaceous aliments. These constitute, necessarily, so large an element in ordinary diet that the limitation of them in the dietary of gouty persons applies, in the majority of cases, only to their excessive use. This excessive use, however, is often observed. There is a popular prejudice in favor of this class of foods, and a corresponding prejudice against the too free indulgence in animal foods. The purely starchy aliments, such as potatoes and the preparations of corn and rice, and even those which contain a considerable portion of gluten, like wheat, oatmeal, and barley, often provoke in gouty subjects a great deal of mischievous and painful indigestion. This feeble capacity for the digestion of farinaceous foods is most frequently observed in the children of gouty parents, and especially in persons inclined to obesity, and in those whose occupations are sedentary and whose lives are passed for the most part in-doors, and they are least common in those whom necessity or pleasure leads to much active muscular exercise in the open air.
The fats are as a rule easily digested by gouty dyspeptics. This is a fortunate circumstance, for the reason that in the anæmia which is frequently one of the consequences of chronic gout the fatty foods are of inestimable value. In cases of persistent and rebellious lithæmia an exclusively milk diet constitutes a precious resource.
The succulent vegetables, such as tomatoes, cucumbers, cauliflower, cabbage, and the different varieties of salads, constitute for the gouty as well as the diabetic subject agreeable and wholesome additions to a diet from which the starchy and saccharine vegetables have to be largely excluded.
The quantity of food proper for gouty persons to consume can only be determined in individual cases by the age, the habits, and the occupation. It is fair to assume that in adults, in whom there is no longer any provision to be made for growth, the daily quantity of food must be regulated according to the amount of energy which is expended. In this energy must be reckoned the amount necessary for the maintenance of animal heat and the other vital functions, and the amount which is necessary for the operation of every variety of nervous force. In other words, the potential energy latent in the food must correspond to the active energy exhibited in the daily evolution of vital, intellectual, and mechanical work. The more nearly this balance is maintained the more closely the physiological standard of health is preserved. That an excess of food is a most frequent cause of the gouty dyscrasia among the well-to-do classes is undeniable, and it is possible that regulation of the quantity according to the rule above mentioned [p. 130]may, after all, be the most important point in the management of many gouty patients. It may be, also, that the reason why the withdrawal of the carbohydrates produces its good effects upon these patients is that we thereby exclude a large amount of force-producing foods which do mischief because they are imperfectly consumed.
EXERCISE.—Next in importance to diet as a hygienic regulation in the management of gouty patients is enforced exercise. The axiom of Abernethy, "to live on a shilling a day, and earn it," comprises the philosophy of the true relations of food to work, and of both to the highest development of physical health. Exercise is to be enforced not simply as a means of securing an active respiration, and thereby an abundant supply of oxygen, but also as a means of converting the potential energy of the food consumed into vital energy. The essential condition, moreover, of healthy nutrition in every organ and in every tissue is the maintenance of a vigorous functional activity. Over-use is not more productive of tissue-degeneration than disuse. Hence the question of exercise in its largest sense involves not only muscular work, but work of all kinds, which tends to promote a healthy activity of the psychical as well as the physical functions. Muscular exercise in the open air has a special value for the victims of this gouty dyscrasia by equalizing the circulation, quickening the respiratory movements, and stimulating the elimination of effete matters from the skin and lungs, but mental work and wholesome diversions are not less important as antagonizing the evil effects of indolence and over-feeding, which are among the common predisposing causes of acquired gout. In persons who are incapacitated by neuræsthenia or by excessive corpulence, the result of long indulgence in indolent and luxurious habits, it may be necessary to resort to passive exercise by rubbing, massage, and electrical excitation in order to secure the good effects of voluntary work.
BATHING.—Another hygienic regulation of great value in the treatment of gouty dyscrasia is the promotion by bathing and friction of the eliminative function of the skin. Daily sponging with cold water, where it is not contraindicated by a feeble circulation and a slow reaction from the shock, is a practice to be commended. Where, for the reasons mentioned, it is not practicable, tepid baths and frictions may be substituted. In cases where the arthritic lesions are progressive and advanced much benefit may be derived from hot baths. It is doubtful whether the thermal alkaline and sulphur spas owe their renown in the treatment of chronic gout so much to the mineral ingredients of their springs as to their high temperature. The Russian and Turkish baths furnish most efficient means for increasing the functional activity of the skin, but they often have a depressing effect on the action of the heart, producing faintness and dyspnoea, and should always be advised with caution.
CLIMATE.—In rebellious forms of the gouty dyscrasia a warm climate is unquestionably a hygienic condition of great value. The geographical distribution of gout, which shows that the disease is much less common in warm than in temperate and cold climates, while it may not perhaps be wholly explained by temperature alone, is very certainly largely due to it. The possibility of out-door life and the increased functional activity of the skin which warm climates favor are circumstances more or less antagonistic to the development of the gouty diathesis.
[p. 131]MEDICINAL TREATMENT.—The objects to be aimed at in medicinal treatment of the gouty dyscrasia are—
1st, the improvement of the primary digestion.
2d, the relief of the gastro-intestinal catarrh, which is the cause of the direct and reflex dyspeptic symptoms which belong to this diathesis.
3d, the augmentation of food-oxidation, so as to secure its thorough combustion.
4th, the promotion of the elimination of the waste products of nutrition.
1. The improvement of primary digestion—or, as it has been aptly called, exterior digestion—often requires very strict attention beyond the proper selection of alimentary substances. The distressing symptoms that indicate primary gastric and intestinal indigestion are certainly often relieved by the rigid exclusion of certain articles of diet, but in many cases it is necessary to assist the preparatory processes which are essential to perfect food-absorption by artificial methods based upon the knowledge derived from physiological experiment. To no one is the knowledge of these methods more largely due than to Roberts of Manchester. Preparations of pepsin and pancreatin, by which the proteids and starches are peptonized and the fats emulsified, are often of inestimable value in the treatment of gouty dyspepsia. Pancreatin, especially, which by means of its trypsin, diastase, and emulsive ferment possesses the threefold property of aiding the digestion of the azotized, amylaceous, and fatty elements of food, is certainly the most valuable of the artificial means for augmenting the efficiency of primary digestion.
2. The relief of the gastro-intestinal catarrh in gouty dyspeptics may often be accomplished solely by dietetic restrictions and by the aid which may be given to primary digestion. It is often necessary, however, to direct some special medication toward the relief of the catarrhal lesion. The circumstances which demand this special medication are the existence of portal congestion, the result of functional derangement, or of chronic atrophy of the liver, or of chronic diffuse or interstitial nephritis, or of cardiac disease. The hydragogues, such as calomel, podophyllin, colocynth, and other vegetable cathartics, with the salts of sodium and magnesium, constitute the most common and efficient means of relieving portal congestion, whether it arise from temporary functional derangement or from organic disease. The renown of some of the more famous mineral springs in relieving the miseries of gouty sufferers is due mainly to the relief of portal congestion and the washing away of the catarrhal mucus which obstructs the process of primary food transformation and absorption. This is especially true of the sulphate of sodium waters, like those of Carlsbad, Marienbad, Friedrichshall, Pullna, and Hunyadi János. While the value of these waters in chronic gout is unquestionable where their use is properly regulated, there is good reason to believe that their long-continued employment is often harmful by relaxing the mucous membrane, and thereby tending to aggravate the condition they are given to relieve. This is markedly true of their use in weak and anæmic persons. For these the milder magnesian waters, such as those of Kissengen, Hombourg, Wiesbaden, and Saratoga, are to be preferred.
3. The augmentation of food-oxidation may be accomplished in a large degree by regulation of the diet and by out-door exercise. The [p. 132] regulation of the diet according to the occupation and habits of life is a point of primary importance in securing proper blood-elaboration. My experience leads me to believe that the evil consequences of in-door occupations and sedentary habits are most common in those who live upon a diet composed largely of starchy and saccharine foods, and that a diet in which animal foods and fats predominate is best suited to indoor workers, whether they be engaged in mechanical or intellectual labor.
The medicines which help to promote the oxidation of the food-elements, especially the carbohydrates, are alkalies and iron. Clinical observation establishes this fact as strongly in the treatment of gout as in that of glycosuria. The relative power of the salts of potassium and sodium in augmenting oxidation is not clearly determined. The salts of sodium appear to be most useful in aiding the process of primary digestion, and the potassium salts in improving the process of sanguification. It is well known that potash predominates in the corpuscles and soda in the serum of the blood. The efficacy of the combinations of iron with the salts of potassium, as in Blaud's pills and in the citrate and tartrate of iron and potassium, in the treatment of anæmia, is well known. In the most renowned ferruginous springs, however, such as those of Schwalbach, Spa, Pyrmont, and St. Moritz, the iron is combined with salts of sodium, calcium, and magnesium. It would appear, therefore, that the increased energy of iron in augmenting hæmatosis, when combined with alkalies, is not relatively greater with potash than with either of the other alkaline bases.
4. The promotion of the elimination of the waste products of nutrition is to be accomplished by remedies which act as solvents of uric acid and as diuretics. As solvents of uric acid the salts of lithia and potash have been shown to be superior to those of soda. The urate of lithia is the most soluble of the uric-acid salts, and the low chemical equivalent of the metal lithium makes the neutralizing power of the oxide much greater than that of equal proportions of the other alkalies. It is used in the forms of carbonate and citrate, and is generally combined with potash and soda. It exists in some of the mineral springs of Europe and of this country, but in such minute proportion as probably to be of little value. In administering the salts of potash and soda it is generally admitted that the carbonates and the neutral salts of the organic acids are to be preferred to solutions of the caustic alkalies. They have less power in neutralizing the acid of the gastric juice, and enter the circulation as neutral salts, where they are decomposed into alkaline carbonates by the oxidation of the organic acids, increasing the alkalinity of the serum and acting as diuretics. The combinations of the alkalies with sulphur, with iodine, and with mineral acids, as in the alkaline springs, are frequently used in the treatment of gouty lesions of the subacute variety. The sulphur salts probably owe their chief value to their alkaline bases when they are used internally; and in sulphuretted baths, as before remarked, the good effects are probably due to the high temperature at which the bath is usually administered.
The salts of iodine are generally supposed to have a special action in removing the consequences of chronic fibrous inflammation in gout and rheumatism. They often disturb the digestion and provoke troublesome irritations of the skin and mucous membranes. In removing the sclerotic [p. 133]effects of gouty inflammation they do not exhibit the same sorbefacient power which they show in their action upon the granulation tissue of syphilitic origin. It must be admitted, however, that in certain catarrhal affections of a gouty nature the iodides of potassium and sodium are almost specific in their good effects. In the pharyngeal, laryngeal, and bronchial catarrhs from which some gouty persons suffer, where there is a dryness and irritability of the mucous membrane, the administration of these salts produces the most prompt and beneficial result. As solvents of uric acid they do not appear to equal the salts of the organic acids.
As to the mode of administering salines in the treatment of the gouty dyscrasia, it is hardly necessary to observe that it must vary with the effect desired. As antacids in acid dyspepsia they should be given soon after meals, and for this purpose the salts of soda are to be preferred, for the reason that they not only neutralize excessive acidity, but they increase the efficiency of the peptonizing process. Where it is desired to introduce these salts into the circulation for their solvent action, as diuretics or to assist the process of sanguification, they should be given three or four hours after meals and largely diluted with water.
Before concluding the consideration of the treatment of the gouty dyscrasia it should be remarked that the ability of water as a solvent, as a means of stimulating tissue-changes and eliminating waste, is not generally estimated at its true value. The use of copious libations of hot water in the treatment of gout, recommended by Cadet de Vaux in 1825, has been revived from time to time, and is at present attracting considerable attention.
TREATMENT OF ACUTE ARTICULAR GOUT.—There are three distinct methods of managing an attack of acute gout—the antiphlogistic, the expectant, and the abortive.
The antiphlogistic method, in the strict application of the term, is practically obsolete. Bloodletting, both general and local, brisk catharsis and diaphoresis, with low diet, were formerly advocated as the natural and imperative antagonists of gout as well as of all other acute inflammatory affections. Carried to its extreme degree, this method was deprecated by Sydenham and his disciples as tending often to prolong the attack and precipitate the manifestations of atonic gout. The natural reaction from the vigorous antiphlogistic practice was what has been termed the expectant method.
The expectant method may be said to be founded upon the aphorism of Mead that "gout is the cure of gout." The discovery of the salts of uric acid in the blood-serum and in the affected tissues gave a scientific basis to the humoral pathology of gout and led to the formulation of definite principles in the application of the expectant method of treatment. These principles are the prevention of the further accumulation of the urates in the blood and the promotion of their oxidation and elimination. The first principle involves restriction to a rigid diet during the attack, excluding albuminous foods and the fermented preparations of alcohol, and allowing only milk and farinaceous gruels. The oxidation of the urates is encouraged by the administration of alkalies and by an abundant supply of air, the inhalation of oxygen even having been recommended. The elimination of the urates is accomplished chiefly [p. 134]by diuretics and moderate catharsis. The local treatment commonly used with this medication consists in the application of alkaline and anodyne fomentations or of dry flannel or cotton. Local bloodletting and blistering are now rarely commended. Under this treatment the intensity of the inflammatory process is abated, the suffering is allayed, but the progress and duration of the disease are not materially modified. The recovery, however, is satisfactory, and it is claimed that the chances of early recurrence of the attack are diminished. This method has many advocates, though it cannot be said to represent the common practice of the present day. It is becoming traditional, and may be said to be gradually giving place to the specific or abortive method.
The abortive method consists in cutting short the attack by the administration of colchicum, veratria, or the salicin compounds.
The value of colchicum in joint affections is a tradition of the earliest records of medicine. It shares its curative effects in acute gout with veratria, and, though the active principle of the meadow saffron and the veratrum album are not isomeric, their effects are similar. They constitute the basis of the famous nostrums so extensively patronized by sufferers from gout. Colchicum is the active agent in the eau médicinale de Husson, in Wilson's and Reynolds's specifics, and in the pills of Lartigue and Blair, while veratria is supposed to be that of Laville's remedy. The action of these substances is not understood. The physiological action of colchicum is that of a local irritant and a cardiac depressant of great energy. It purges violently when given in large doses, causes nausea and vomiting, and may produce collapse. In therapeutical doses in a gouty paroxysm it acts as a diuretic and an antipyretic, and allays, sometimes in a most magical manner, the objective and subjective symptoms of the disease. As simple purging by other cathartics does not abort the gouty seizure, the value of colchicum cannot be ascribed to its purging effect, and, besides, purging is by no means necessary to its efficiency. Nor can its utility be ascribed to its diuretic property. There is some question in regard to its claims as a diuretic, and there seems to be no doubt that it often does good where this effect is not observed. Its influence upon the heart does not explain its marvellous action upon the local process, for the same influence obtained by other drugs has no such result. We are driven, therefore, to the conclusion that colchicum has a specific action in gout as certain and as inexplicable as that of quinia in malarial fever, or iodide of potassium in constitutional syphilis. For those who accept the theory that gout is a tropho-neurosis the therapeutical action of colchicum is a strong confirmation of its neurotic origin, for the reasons that colchicum has no influence upon arthritic lesions which are not gouty, and that its physiological effects point to its action on the nervous system.
It is useless, however, to speculate on the way in which colchicum and allied substances affect gouty inflammation; the practical question to be determined is: Are they the best and safest remedies to control it? Upon this point there is a wide diversity of opinion. The objections to the colchicum treatment are based upon humoral pathology, and upon the idea that the attack is an effort of nature to cast out the poison and purify the blood. Colchicum, it is claimed, arrests this process; the poison is retained, diffuses itself through the tissues, and lays the [p. 135]foundation of vascular and visceral lesions. It shortens the intervals between the attacks, and tempts the patient to continued indulgence in the habits which perpetuate and exaggerate the disease. The advocates of the abortive treatment, on the other hand, claim that these arguments have no real force as applied to its therapeutical value. The cure accomplished is, to all appearances, complete, and the patient is saved the suffering and exhaustion which result from the expectant method. The fact that he is so easily and speedily cured, and that he resumes his vicious habits and suffers recurring attacks in consequence, proves only that the treatment lacks the quality of moral discipline which belongs to prolonged suffering and the penance of vigorous medication. It is an acknowledged fact that the great majority of sufferers from acute gout decide sooner or later in favor of the abortive treatment; and as professional opinion has heretofore generally advocated the expectant or eliminative treatment, they commonly resort to the use of some one of the quack remedies which contain colchicum or veratria.
In view of the present uncertainty of our knowledge of the true pathology of the acute gouty arthritis, as to whether it is a tropho-neurosis or the result of the local irritation caused by the salts of uric acid, the specific treatment seems to be justified by a regard for the comfort of the patient and as a means of protecting him against falling into the reckless use of quack remedies. A speedy relief of the acute symptoms, followed by the treatment appropriate to the gouty habit, would seem to be the most rational and safest mode of managing the acute articular attacks of gout.
The selection of the preparation of colchicum in the treatment of an acute paroxysm is a matter of individual experience and preference. The acetous extract and the wine of the seeds are most commonly used, and many practitioners are not scrupulous in prescribing the proprietary preparations of Reynolds, Laville, and Blair. The wine of colchicum may be given in doses varying from 20 to 40 minims, alone or combined with Epsom salts in drachm doses, with small quantities of opium, every six or eight hours. Under this medication the pain, tenderness, and swelling rapidly abate, and sometimes with an abruptness that is magical. As soon as the acute symptoms subside, the colchicum should be continued in smaller and less frequent doses until the fever and local tenderness subside. The use of quinia with small doses of colocynth after the colchicum has been discontinued helps to re-establish the strength and regulate the digestive functions. The patient should always be warned against the possible demoralizing effects of a speedy recovery from a serious disease. Recurrence after the colchicum treatment is certainly more common than after the expectant method, but this should not be ascribed so much to a defective cure as to the temptation which the antidote offers to trifling with the poison. The accidents which have been ascribed to colchicum through its causing heart-failure are probably to be explained by its injudicious administration in large doses where acute gout is complicated with cardiac or renal degeneration.
Next in importance and value to colchicum in the abortive treatment of gout are salicin, salicylic acid, the sodium salicylate, and the oil of wintergreen. Unlike colchicum, which has no marked effect upon acute rheumatism, these medicines appear to act with similar energy on [p. 136]gout and rheumatism. The rapidity and the almost uniform way with which they allay the inflammatory symptoms in rheumatic fever are well known; their value as specific remedies in both acute and subacute gout is not so generally appreciated. Whether the specific action of colchicum in gout differentiates this disease from rheumatism, or whether the similar action of the salicin compounds indicates that these diseases are allied in their etiology, are questions yet to be solved. The good effects of salicin and the sodium salicylate in many of the forms of irregular gout, and notably in the dyspeptic disorders and the erythematous tegumentary lesions, are especially worthy of notice. In acute attacks of articular gout the salicylic acid or the sodium salicylate, in 15 or 20 grain doses repeated every three or four hours, will often cut short the attack, and will very certainly allay within twenty-four hours the acuteness of the symptoms. As in rheumatism, the medicine should be continued in smaller doses after the acute symptoms have subsided for several days, the tendency to relapse being marked if the drug be discontinued too soon. In subacute articular gout and in the irregular forms of the disease, where the medicine has to be continued for some time, salicin and the oil of wintergreen are to be preferred to salicylic acid and the sodium salicylate. They are less liable to disturb the stomach and to produce toxic effects.
It is unnecessary to describe the treatment of the different forms of irregular gout, inasmuch as the general principles described in the treatment of the gouty dyscrasia involve the most important considerations in the management of these affections.
1 There is a difference of opinion as to the correct spelling of this word, and strong reasons exist to regard the form rhachitis as the proper one. It is true that this spelling of the word has been remarked upon as unorthographical by many, mostly modern, authors. Even Virchow writes "Rachitis," claiming that Glisson took the term from "the then popular rickets." This is a mistake, as H. Rohlffs points out (Deutsches Arch. f. Gesch. d. Med., 1883, p. 294). Rachitis is a Greek word, and was used in the classical time of Hellenism. It has, however, seemed best to preserve here the usual spelling, rachitis, which has become sanctioned by general usage.
DEFINITION.—Rachitis is a general nutritive disorder, almost always of long duration, usually with an introductory stage of weeks or months and a course mostly extending over months or years. Its beginning is mostly gradual, its final recovery slow. It is complicated with or dependent on disorders of the digestive or respiratory apparatuses, which are preceded by a disposition probably created by an undue width of the arteries. It exhibits amongst its prominent symptoms muscular debility; perspiration; anomalies of the subcutaneous tissue, which is either very much infiltrated with fat or deprived of it; disturbances of the intellectual and moral functions, and of those of the large thoracic and abdominal viscera and lymphatic glands; changes in the latter may outlive all others. Its most perceptible symptom, however, consists in an inflammatory disease of the primordial cartilage of the epiphyses, a copious deposit in that region and also under the periosteum of the bones; curvature of the diaphyses, and, while absorption remains intact, softening and retarded ossification of the bone. Without these affections of the osseous system the diagnosis of rachitis is not complete.
ETIOLOGY AND PATHOLOGY.—The nature of rachitis has been considered to be inflammatory by F. A. Walter.2 Renard looked for that inflammation in the periosteum. Guérin emphasizes the vascular increase in periosteum, bone, and marrow; Trousseau and Lasègue the congestive character of the local tumefaction, besides fever and pain. Virchow also3 inclines to the opinion that the rachitical process is of an inflammatory nature, though it be impossible to state the exact cause of the process. Still, he claims that we are no better off in regard to other inflammations of unknown character—for instance, those of the skin—and that we have to look for a future increase of our knowledge of such constitutional predisposition of the organism and of such specific qualities of the blood as will produce the local irritation of the osseous tissue in rachitis. Last, and mainly, it is Kassowitz who seeks the [p. 138]essence of the rachitical process in a chronic inflammation originating in the points of apposition of the growing bones of the foetus or infant. During the chronic inflammation blood-vessels are formed in large numbers, and a morbid congestion takes place in all blood-vessels, but mainly in those of the localities in which new bone is forming; thus in the chondro-epiphyses, in the perichondrium and periosteum, and the sutural substances. Faulty introduction or elimination of lime has nothing to do with this process. It cannot be deposited in the current of a copious circulation; in fact, it is not deposited in the immediate neighborhood of blood-vessels to any extent. Even in otherwise normal bone hyperæmia produced by the experimenter softens the bone, which was fully formed before. If the relative percentage of lime were of any account in the etiology of rachitis, the periosteal and cartilaginous proliferations would find no explanation. But why is it that this peculiar process takes place at an early age only? and in the bone only? Kassowitz urges the fact that the growth of the bone differs in this from the development of all other tissues: that the latter grow uniformly through their whole mass; that the circulation in them is more uniform and carries material through and into every particle simultaneously, while in the bones the only places in which the whole circulation can contribute to their growth—the few blood-vessels distributed in the interior not adding to their growth at all—are the periosteum and the places of apposition between epiphysis and diaphysis. Every morbid irritation, whether resulting from bad air, habitation, and food, or from either chronic or acute ailment, acts on the whole mass of other tissues and organs, but in the bones only on the growing ends or surface.
2 Anatom. Museum, Berlin, 1796, vol. ii.
3 Arch. f. Path. Anat., vol. v.
The results of the pathologists and experimenters are confirmed by chemical analyses. Fat has been generally found somewhat increased in the rachitical bones, and water largely so; chondrin is diminished according to Marchand and Lehmann, but was found unaltered in the later analyses of A. Baginsky. The latter found, after having deprived the bone of fat, the organic and inorganic material to be in a proportion of 100 to 563 in the normal, and of 100 to 160 in the rachitical osseous tissue; and in 100 parts of dry bone, Gorup-Besanez found in the
| Ossein. | Phosphoric Acid. | Lime. | Manganese Oxide. | |
| Healthy adult | 34 | 26 | 34 | 0.3 |
| Infant of six months | 34.9 | 27 | 35 | 0.5 |
| Rachitical femur | 72 | 7 | 9 | 0.3 |
| Rachitical tibia | 60 | 12.9 | 17 | 0.3 |
Defective calcification of the forming bone is one of the principal characteristics of rachitis. In it lime cannot either enter into the composition of the osseous tissue or remain in it. Its elimination must take place either through the kidneys or the intestinal tract. In the feces Ad. Baginsky, and many before him, have found an abnormal quantity. In regard to the urine, modern investigations do not agree with former analyses. Thus, Baginsky concludes that there is no increase of lime in the urine of rachitical as compared with that of healthy children; Seemann found even a diminution of the percentage of lime. Amongst modern writers only Rehn found an occasional increase of lime in the urine of rachitis.
[p. 139]In regard to the elimination of phosphoric acid, the analyses of different periods do not agree any better. The conclusions of previous researches, pointing to a quadruple elimination of phosphoric acid in the urine of rachitis, are refuted by Seemann, who found no increase, and by Baginsky, according to whose researches the phosphoric acid of the healthy urine compares with that of rachitical urine as 40:12-37.
As far as the elimination of nitrogen is concerned, there appears to be but little difference between normal and rachitical urine. Chlorine was found to be diminished in rachitis by Baginsky. Lehmann and Von Gorup found lactic acid several times. Several times albumen was met with; in a case of Ritchie's, blood; in one of Von Gorup's, fat.4
4 E. Salkowski und W. Leube, Die Lehre vom Harn, 1882, p. 536.
The etiology of rachitis must be studied from two points of view. It has its predisposition and its direct and proximate causes. The former has been studied by F. W. Beneke5 upon an anatomical basis. He finds that the arteries of rachitical patients are large all through the body. This is so particularly in the carotids; it seems probable that the changes taking place in the head are due to this anomaly in the size of the arteries. Three cases in which the width of the arteries of the neck was unusually large terminated fatally—one by hydrocephalus, one with a very large skull, and one suddenly. This width of the arteries is most marked, under ordinary circumstances, from the second to the fourth year; that is, the exact time in which (except the cases of early rachitis) the rachitical process is at its height. It is considered by Beneke to be the cause of the local increase of vascular irritation, particularly in the epiphyses with their retarded circulation; and also of the increase of nutritive development which is so often noticed during recovery from rachitis; and, finally, of the many pulmonary complications of an inflammatory nature.
5 Die Anatomischen Grundlagen der Constitutions Anomalien des Menschen, 1878, p. 75, etc.
There is another interesting consideration in regard to the effect of wide arteries on the relations between the blood and tissues. A great many more blood-cells are required to fill the arteries when wide than when narrow. Now, the formation of blood-cells is hindered by any disease of the digestive and blood-preparing organs, so that the tissues are liable to show the relative increase in the percentage of water, which is uniformly confirmed for rachitis by the biochemists.
The pulmonary artery of the healthy infant is larger than the aorta by not more than four millimeters. In the majority of cases of rachitis examined by Beneke this difference in size was very much more favorable to the pulmonary artery; it is abnormally large in rachitis. This anatomical fact is suggestive of the pathological processes so frequently found in the lungs and in the neighboring lymphatic and large abdominal glands. For, while the amount of blood introduced into the lungs through its wide artery is unusually large, particularly so in a chest which is contracted in consequence of the rachitical process in the bones, the exit from the lungs is relatively impeded. Not only, however, the narrowness of the chest is a cause of this disproportion. For even in rather normal chests the lungs of rachitical children are relatively small.
The liver of almost all rachitical children is large. In but one-half [p. 140]of the cases this enlargement is accompanied with a large heart. In pure cases of scrofula, on the contrary, Beneke found a small heart, rather narrow arteries, and usually a small liver, the size of the lungs offering but few anomalies.
The spleen also is large in the majority of cases. Its size is not dependent on the large size of the liver or the small size of the lungs. For these conditions are found in the majority of cases only, not in all of them, and the large spleen is not always found with a large liver and small lungs. The variability of the anatomical conditions permits of various degrees of combination; so that varying combinations of rachitis with other constitutional disorders may correspond with the different sizes of the principal organs. After all, as there is a great deal of independence of these organs, as to size, of each other, the conclusion is justified that those differences are not the result of the disease, but that they are congenital and stand in some causal relation with it.
The kidneys are large in the majority of cases, like the spleen and liver, while the lungs are small. This disproportion is apt to result in a hyperæmic condition of all the organs of the abdominal cavity, and especially of the kidneys. To what extent this undue amount of volume interferes with, or increases, renal secretion, it is difficult to say. The amount of urine secreted by rachitical children is about normal, though, as already stated, the percentage of lime in it is rather diminished, contrary to the opinions held formerly.
For the direct cause of rachitis Glisson looked to the inequality of nutrition by the arterial blood, and for that of the curvature of the long bones to their superabundant vascularization. He found the disease mainly amongst the well-to-do classes, not unlike a modern American writer, who declares infantile paralysis to be the result of the nervousness of the better classes of the American people! John Mayow (1761) held a disturbance of the innervation responsible; Zeviani (in the same year), improper food in general, and particularly prolonged lactation; and Selle (1791), a peculiar diathesis (acrimonia rachitica). About that time a defective nutrition with abnormal function of the lymph-ducts was looked upon as the cause of rachitis by many—by others, an undue production of acid, and the softening of the osseous tissue thereby. This result was attributed by some to the influence of milk (Veirac, De Krzowitz). Attention was directed at an early time to phosphoric acid and lime, with the view that variations in the elimination of these substances might explain the occurrence of rachitis. A large quantity of both was found in some urines (Malfatti); a superabundance of phosphoric acid was presumed to prevail in the whole system (Wendt, Fourcroy); while symptoms resembling rachitis were found in animals fed upon small doses of phosphoric acid by Caspari (1824). Chossat fed young animals on food deprived of lime, and claimed to produce softening of the bones and death, a result which was denied by Friedleben. Guérin claimed to produce rachitis by feeding young animals on meat in place of their mother's milk, a result equally denied by Tripier, who, like Friedleben, found the bones under such circumstances more liable to fractures, but not rachitical. Wildt and Weiske found the bones uninfluenced by withholding lime from food; Forster, however, and Roloff claimed to notice a marked influence, and the latter [p. 141] stated that animals, after having been rendered sick by depriving them of lime, recovered when they were again supplied with it. Wegner, in his numerous experiments with phosphorus, found that in growing animals it increases the growth and firmness of both long and flat bones; after the growth of the animal has been completed it renders epiphyses and vertebræ denser. There is no change, however, in the relative chemical composition of those parts. He found at the same time that results similar to those caused by the administration of phosphorus were obtained when food deprived of its phosphate of lime was given. But he met with no rachitical changes proper during these several procedures. Teissier having found an increase in the urine of rachitis after the administration of lactic acid, and lactic acid having been frequently found in the urine of rachitical patients by Ragsky, Morehead, Simon, and Lehmann, C. Heitzmann fed with lactic acid both carnivorous and herbivorous animals, found the cortical layer of the bones softened and the medullary substance hyperæmic, and claimed to produce rachitis in the former and osteomalacia in the latter. Both of these assertions were denied by Tripier and Toussaint, who insist upon Heitzmann's having selected animals which have a peculiar disposition to suffer from rachitis. Again, Milne Edwards and Boussaingault found the bones softened when they withdrew both phosphoric acid and lime from the food, without restoring the bone's consistency by administering powdered bone. But, lately, Ad. Baginsky states that he produced rachitis by withholding lime, and increased the effect by introducing lactic acid. By so doing, however, he changed only the relation of the mineral to the organic substances, without interfering with the normal proportions to each other of the constituents of the ashes. Beneke, finding oxalic acid in the urine in many cases of rachitis, attributes to it the want of calcification in rachitis, and Senator suggests that what impedes the deposition of bone might be formic, acetic, and lactic acids, which are also found in the young osseous tissue.6
6 L. Fürth, Path u. Ther. d. Rachitis, Wiener Klinik, 1882.
Of these statements many are uniform, others contradictory. Thus far, they are not convincing except in one way—viz. that both withholding and introducing certain ingredients, mainly lime, influence the growth of the bone considerably. This may prove nothing else but that lime is of paramount importance in the building up of bone, and that bone in the period of rapid development is amenable to a great many influences.
It is in the period of rapid development that rachitis is observed. Thus it occurs in every stage of intra-uterine and infant life. It is met with in the foetus in very early intra-uterine life; it is found as a congenital affection, continuing to develop after birth when it has originated in the latter half of foetal existence; there is, thirdly, the rachitis of early infancy; and, lastly, that of advanced infancy and childhood. Of 624 cases of rachitis enumerated by A. Baginsky, there were 256 less than a year old, 313 in the second, and 63 in the third year. After this time rachitis is rare, as far as the active symptoms of the disease are concerned. But still, a retarded form of rachitis (r. tardiva) has been described by some authors. It is said to occur about puberty, and to exhibit local changes in the bones of genuine rachitical character, but to be wanting in all the other symptoms required for the diagnosis of general rachitis. Such cases have been described [p. 142]by C. Lucas.7 He found it complicated, now and then, with albuminuria. The occurrence of the latter at that time of life had been referred to by Moxon.8 The principal symptoms described by Lucas are scoliosis, talipes valgus, and genu valgum. The epiphyses were slightly thickened; there were pain in the limbs, languor, and pallor. In some of the cases there were also rachitical deformities dating from infancy. He believes rachitis of adolescence to exhibit more symptoms belonging to relaxation of the ligaments than to softening of the bones.
7 Lancet, June 9, 1883.
8 Guy's Hosp. Rep., 1878.
A case of rachitis of undoubtedly congenital nature has been reported by Chiari. There were but twelve teeth. There were no other alveoli, nor was there any intimation of the formation of alveoli in the shape of the jaw, which resembled very much the usual senile form of retrograde metamorphosis.
Twenty years ago I described the lesions in part of a rachitical cranium removed from an infant who lived up to her eleventh day. She was born at full term with hernia of the brain, about one-sixth of which protruded through the small fontanel. Only the cranium could be studied with regard to rachitis, and but small portions of the frontal and the anterior half of the parietal bones surrounding the large fontanel could be removed. In these few square inches of bone there were between twenty-five and thirty openings of the usual craniotabic nature, nothing but a transparent membrane being left. The bony edges of these thin portions were partly sloping off gradually, partly very steeply, and somewhat thickened. They were distributed over the whole part of the skull removed; some were found in the immediate neighborhood of the points of ossification. No recent deposits of soft rachitical bone had taken place under the periosteum. Thus, evidently, the process was of rather an early date of intra-uterine life, and had at birth run the full course of its usual development without having had an opportunity to terminate in the restitution of the normal bone.9
9 Amer. Jour. Obst., Nov., 1870.
In a case reported by Dr. F. A. Burrall10 the infant (female) was cyanosed at birth, and had a small head and feeble general development. The respiration was shrill and piping from birth, as though from congenital laryngismus; in a few days it became raucous. The post-mortem examination proved the larynx normal, with no obstructive growths. She was pigeon-breasted, and the last phalanx of her right finger wanting.
10 Trans. N.Y. Path. Soc., vol. i. p. 81.
In the meeting of June 27, 1883, of the Société de Chirurgie of Paris, Guéniot presented a newly-born baby with well-pronounced rachitis of the extremities which had healed at the time of birth. The bones had recovered their firmness, and the characteristic deformities remained. In the meeting of December 19th he could report that the child had exhibited neither symptoms of rachitis nor of syphilis since. In regard to the latter, a very rigorous examination of the baby's whole family, made by Guéniot and Fournier, resulted in the existence of no trace of syphilis.11
11 Rev. Mens. des Mal. de l'Enfance, Janv., 1884.
Kassowitz has examined many still-born infants, and also children dying at an early age, at the foundling hospital of Vienna. In a large majority of the cases he found rachitical changes in the ends of the bones. In [p. 143]many of those who lived several weeks he found rachitis developed to such an extent that the presumption of its intra-uterine origin became conclusive. Here nothing is left but the conclusion that the cause of congenital rachitis has to be looked for in the condition of the maternal blood.
Thus, the foetal and congenital occurrence of rachitis cannot be doubted. Both forms are represented in literature. Neither requires the presence of rachitis in one or both of the parents. But the cause of the intra-uterine disease has not been found. Perhaps a disease of the mother with considerable nutritive disorders or a defective placentar supply may be found responsible. The foetal form runs its course long before the normal termination of pregnancy; the congenital may have run its full course at birth or complete it afterward. The bones are found of characteristic nature, the diaphyses suffering more than the epiphyses; even a rachitical pelvis has been met with by Fischer. Early foetal rachitis is probably dependent upon a defective development of the very first cartilaginous deposits and the first osseous nuclei; thus, many of the congenital synostoses find a ready explanation. Besides these, abnormal circulation is accounted for. For periosteal proliferation at that early period contracts the foramina carrying the blood-vessels, and, while interfering with the size of the bones, the foramen magnum also. Thus, a certain class of cretinism appears to be due to foetal rachitis, mainly of the base of the cranium, which results in early ossification of the synchondroses, particularly of the sphenoid bone. But lately I have seen a case of this description, which, however, had not terminated at the time of birth. For after birth the rachitical process developed further, and in addition to the rachitical deformity of the base of the cranium there were afterward thickening of the epiphyses, pigeon breast, and thoracic grooving and flattening.
Rachitis is found in city and country, less on mountains than in valleys. Still, it is met with at elevations of two thousand feet. In the tropical regions it is almost unknown. Why it should have been considered quite a new disease in England but a few centuries ago, or whether it did not exist before that time, it is difficult to say. It is certain, however, that deformities have been described in antiquity which we are accustomed to attribute to rachitis.
As the disease is one that occurs during the period of rapid growth, and is a developmental disease, everything that interferes with normal growth and development is apt to change physiological functions into pathological conditions and to produce rachitis. In the pregnant mother her ill-nutrition and the defective cell-material used in the building up of the embryo and foetus, or a defective placenta, may come in for the explanation of foetal and congenital rachitis, although the case of Klein's, who reports twins, of which one was normal and one rachitic, is rather difficult to explain on that basis only. Even rachitis of early infancy is not easily accounted for otherwise, for its first symptoms show themselves at a very early period; thus constipation, adiposity, and afterward craniotabes and thoracic grooving.
The common form, and that which is the usual subject of the text-books and monographs, has, however, in most cases a well-marked preparatory stage in the shape of diseases or ailments reducing sanguification [p. 144]and nutrition. Some cases are ushered in by, or follow the course of, acute exanthems or acute gastric disorders or the presence of entozoa. A larger number appear to result from insufficient oxygenation resulting from lung diseases, with a long chronic ailment following the acute stage. Even acute pneumonia, with its direct influence on general nutrition, stands often for the proximate cause of rachitis. Bad air alone, even swamp air, does not appear to be a sufficient cause. When it seems so, it is complicated with the main cause of rachitis; that is, bad, insufficient, improper food, with its immediate result—viz. intestinal catarrh. Cow's milk, particularly when acid, starchy food administered too early or in too large quantity or too exclusively, early weaning followed by improper artificial food, insufficient mother's milk or such as is either too thin or too caseinous, lactation protracted beyond the normal limit,—may all alike be causes of intestinal disturbances and rachitis.
Is rachitis hereditary? A number of women who were rachitical themselves have been known to have rachitical children. But it has been said that the process runs its full course during infancy, and that therefore a direct inheritance of rachitis from mother to child is an impossibility. Still, we must not forget that the consecutive conditions of the parents may, or will, influence the general condition of the infant and result in similar disturbances. No rule, however, exists. Dyscrasic parents may have healthy children, and healthy parents sickly or dyscrasic ones. But the probability is greater that diseased children should come from dyscrasic parents than from healthy ones. Tuberculosis in the parents has frequently been accused of being the cause of rachitis in the infant—not directly, but in consequence of general impairment of the tissues. Gout has also been accused of being the cause of rachitis, but it is a peculiar fact that the poor have but little gout and a great deal of rachitis. In all of these cases it is better to look upon rachitis as only one of the forms of general mal-nutrition, and to speak of inheritance of the disposition rather than of the disease. Thus it was that about the end of the eighteenth century Portal spoke of scrofulous, syphilitic, scorbutic, rheumatic, arthritic, and exanthematic rachitis. Particularly has syphilis been accused of being the main cause of rachitis by some, and even the only cause by others. Thus it was looked upon by Boerhaave. In modern times Parrot maintained, from 1872 up to the time of his death, which occurred recently, that every case of rachitis is of syphilitic origin. As his proof he relied mainly on the condition of the teeth and the bones. But those appearances in the teeth, the thin and ragged edges, the friability and the grooving, either horizontal or vertical, which have been considered characteristic of syphilis by Hutchinson and others, have no such dignity, and moreover they are not observed in the temporary teeth at all, but in the permanent only; the rachitical softening of the bones also is not found in syphilis at all. Particularly are there no curvatures in syphilis and no infractions. It is true that marasmus is found in both rachitis and syphilis, but it is met with in all sorts of diseases. The changes in the bones of syphilis are found at birth; in rachitis they usually develop in later months. When a baby is syphilitic and rachitic at the same time, the syphilis may last very much longer than the rachitis, which meanwhile has healed. The internal organs in rachitis do not exhibit any such [p. 145]changes as are known to occur in very many cases of syphilis. No gummata are ever found in rachitis, and the interstitial inflammation of the internal organs in syphilis is not met with to the same degree in rachitis. What Parrot claimed as a desquamative syphilide of the tongue—that is, red insulated spots, denuded of their epithelium, small in the beginning, later extending backward and increasing in size—is by no means always syphilitic, but is found in a great many cases where there is no suspicion of syphilis. It is mainly Kassowitz and Bouchut who have taken the stand against Parrot. The former, taking rachitis for a peculiar inflammatory process, admits that syphilis can be one of the causes. The latter directs attention mainly to the fact that by changing food in certain ways rachitis may be produced in dogs, but that they cannot be made syphilitic. There is no doubt, however, that syphilis may give rise to rachitis by its general influence on nutrition, and in this fact lies the key to the connection of great nutritive disorders with each other. Syphilis will undoubtedly change nutrition to such an extent as to result in rachitis. Rachitis will affect the glands; the caseous and suppurative degeneration of the glands will lead to metastatic processes, to acute tuberculosis, and so on.
Malaria been claimed as the main cause of rachitis by Z. Oppenheimer,12 or, rather, rachitis is presumed by him to be the form in which malaria makes its appearance in young infants. After disposing of other alleged causes of rachitis, none of which is proved to give rise to every case, and referring to the anatomical belief that the peculiar hyperæmia and inflammation of rachitical bones is created by the embryonic condition of the growing osseous tissue, he points to the prodromi, amongst which he emphasizes chronic diarrhoea and the nocturnal crying. The latter, with its perspiration and subsequent sleep, he claims as evidence of malaria, and as a substitute for the intermittent neuralgia of adults, the more so as he believes he finds the spleen tumefied. The persistent diarrhoea of these infants is said to be paroxysmal—to take place in the morning, contrary to what is seen in the usual form of intestinal catarrh; the discharges are said to be serous, not tinged with bile; the appetite to be good through the rest of the day; the weight of the body not to be lessened, but anæmia to develop gradually, and fever to occur occasionally. In other cases infants have cold hands and feet and blue lips toward evening; the skin is pale, the spleen enlarged; otherwise there are perhaps no symptoms, but the infants try to get uncovered, and have an increase of temperature of from 1° to nearly 3° F., and a perspiring head in the morning. After a while the rachitical symptoms belonging to the bones and the general system become apparent. After all of the author's ingenious and emphatic assertions and deductions, it becomes evident that malaria—in the severe forms in which it has been found by Arnstein, Browicz, and Henck to cause bone diseases—may give rise to rachitis, but it is also clear that he tries to prove too much. The long series of attempts at proving that every form and case of rachitis depends upon a single and uniform cause have proved futile. The physiological hyperæmia of the bones and the rapid growth of all the infant tissues are shaped into the complex ailment which we call rachitis by more than a single disease or a single nutritive disturbance.
12 D. Arch. f. klin. Med., xxx., 1881.
[p. 146]SYMPTOMS.—Before entering upon a more accurate and elaborate enumeration of the symptoms of rachitis, I mean to dwell upon peculiar differences which take place according to the age in which the disease makes its appearance. Very young babies—that is, infants of a month or two—develop rachitis in such a manner that many cases are overlooked until it is too late to relieve them in time. This occurrence takes place when there are no prominent causes, such as diarrhoea or other nutritive disorders, nor any premonitory symptoms. Such infants appear to be perfectly well; they have the average weight, and even more; they have plenty of adipose tissue, and look well. The only anomaly appears to be an undue degree of paleness. Without pain or flatulency they are constipated. This constipation is not congenital, as it always is when the colon is unusually long even for an infant, and when the sigmoid flexure is of double or even treble length, but makes its first appearance about the end of the first or the beginning of the second month. It is relieved only when the increasing muscular power of the intestine results in more effective peristalsis. The second symptom is the thoracic groove, to which I shall allude later, and a gradual thickening of the costo-cartilaginous junctures, with or without periosteal pain on pressure. About the same time the cranial softening, craniotabes, with its hyperæmia and perspiration of the entire scalp, and baldness, and the first symptoms of maxillary rachitis, become perceptible. During all this time the epiphysial swellings and the diaphysial curvatures develop but very slowly; but at a very early time chronic bronchial catarrh, with a loose cough, begins to be troublesome. When rachitis begins at a late period—say, about the sixth or eighth month—the aspect of the case is different. The infant has suffered before either from bronchitis and broncho-pneumonia, or in most cases from indigestion and intestinal catarrh. There is some degree of emaciation; the skin does not fit the limbs, as it were—is loose, thin, flabby, and rather dry. The tendency to diarrhoea continues to prevail. The epiphyses, particularly of the lower extremities, are thickened at an early time, curvatures of the tibiæ become apparent, and all the rest of the bones participate in the process, with the exception, sometimes, of those of the head.
The head, however, is liable to exhibit symptoms of rachitis at a very early period of life. It is large, or appears to be so,13 mostly for the reason that the face is proportionately small. The forehead is large, the frontal protuberances very prominent, as are also those of the parietal bones. Thus, the head is more or less square. Dilated veins are visible in and through the pale skin; there is but little hair, on the occiput less than on the rest of the head. Sometimes the occiput is quite bald, the hair having been rubbed off on the pillow. The scalp feels warm, except during perspiration. The latter is very copious, particularly on the occiput—to such an extent, indeed, that the pillow is drenched—and will remain so for months. The sebaceous follicles are often still larger and more numerous than they normally are at that age, and seborrhoea is [p. 147]often, though not always, met with. The sutures are wide, sometimes one or two centimeters; the posterior fontanel remains open; the large anterior fontanel is very large, being sometimes several inches long and wide. The pulse is felt very distinctly through it. The systolic cerebral murmur, which was first found by Fisher of Boston in 1833, and considered to be a positive symptom of rachitis (which certainly it is not, as it is found in almost every healthy baby with a patent fontanel), is very audible. The fontanel and sutures remain open for a long period. Instead of closing, as they do normally at the fourteenth or fifteenth month, the former ossifies about the end of the second or third year, or later. Gerhardt reports a case in which it persisted to the ninth year. The cranial bones appear to be thin, and give way under the pressure of the finger. Ordinarily, it is true, the cranial bones of every baby, even if perfectly healthy, are movable under pressure, but they are so only along the sutures, where they may retain this mobility, in some instances, a long time. Indeed, it appears that sometimes about the middle of the first year the occipital bone becomes thinned out in apparently quite healthy children. Moreover, even in the skulls of infants who were taken to be in good health small defects in the bones were found (Friedleben), with no uncomfortable symptoms at all. Therefore it is rather difficult to draw the exact boundary-line between the healthy and the morbid condition; thus it is possible that some of those cases which exhibited apparently morbid local changes without morbid symptoms may not have been diseased after all. In those, however, in which rachitis is really developed in the cranium a peculiar condition is found. In the posterior half or third of the parietal bones, either the right or the left side being more marked, there are in the tissue of the bone distinct spots in which the osseous material is not only thinned out, but has entirely disappeared. In fact, the bone is perforated, the edges of the holes being rather steep, sometimes slightly thickened, and the scalp separated from the brain only by a thin, transparent membrane, the remnant of the periosteum. These holes can be easily found through the integument. The finger, though ever so gently pressing down upon it, moves the cranium, if any be left, before it; the bone feels like paper, and the sensation as if it could be easily broken through is quite distinct and embarrassing. Such perforations are usually quite numerous; from five to twenty or more can often be counted. They are surrounded by normally hard bone, and thereby can be recognized from the flexible part of the cranium extending along the sagittal and lambdoid sutures. Where these results of rachitical softening, craniotabes, are most prominent—that is, on the part on which the infant is mostly reclining—the bone is flattened, and may remain so for life, though in the majority of cases the asymmetry will disappear. The flattening and perforations result from the same causes—viz. softening of the bones and pressure upon the bone between the pillow outside and the brain inside. With it go, hand in hand, thick rachitical deposits under the hyperæmic periosteum of other portions of the skull. Where craniotabes is largely developed on the occipital portion, the frontal and the parietal bones (in their anterior halves) are usually thus thickened. A cross-section with a knife will reveal a diameter of the new osteoid material between the periosteum and bone of one-half to one centimeter in thickness. It is very hyperæmic—even more so than the bone itself, [p. 148]which, when cut into, exhibits an unusual amount of blood. Sometimes the deposits are still larger, and are apt to change the appearance and weight of the skull considerably after recovery has taken place and eburnation and sclerosis have taken the place of the normal osseous tissue.
13 Boötius (1649), quoted by Haller (Bibl. Med. pract., 1779): "Infantibus caput grandescit, reliquum corpus contabescit, ossa in articulis tument, dextrum hypochondrium tumore æquali prominet; hoc malum multis millibus infantum molestum est" ("The infant head grows large, the rest of the body emaciates, the articular bones swell, the right hypochondrium is raised by a uniform tumor; this malady is a sore affection in many thousands of infants").
Such a case of rachitical cranial sclerosis I have described in the Amer. Med. Monthly of 1861. It was, however, by no means a mate of the case related by E. Huschke. The latter skull was that of a girl of seventeen years, and weighed 4117 grammes instead of the normal weight of 600 grammes. The medullary (Havers') canaliculi were large and very numerous on the surface, narrow and very few in the interior of the sclerotic bones, and the osseous canaliculi were more spherical and irregular in site and shape. The chemical composition was also abnormal, phosphate of lime being 65.59, carbonate of lime 11.12, sulphate of magnesia 1.14, cartilage and fat (very little), etc. 22.15 per cent. No fluorate of lime was found. Most of the bones were exceedingly hard, but fragile when tried in small pieces; very white inside, yellowish on the surface, the latter color being the remnant of extravasated blood or other pigmentous matter. Another skull, in Huschke's possession, and moderately sclerotic, weighed (lower jaw excluded) 1075 grammes; a third, in the museum of the University of Jena, is that of a young baboon,14 in which all the bones covering the hemispheres had become sclerotic.
14 Baboons suffer from rachitis very extensively. In the Transactions of the Pathological Society of London (xxxiv., 1883, pp. 310, 312) I. B. Sutton gives the description of two baboons, one of which was six months, the other one year and six months old, when they died. The careful description of the specimens exhibited leaves no doubt as to the rachitical nature of the changes in both the periosteum and the tissue of all the bones of the body.
Of undoubted total cranio-sclerosis Huschke reports but ten cases—those of Malpighi (1697), Cuvier (1822), Ribalt (1828), J. Forster and Bojanus (1826), Ilg (1822), Kilian (1822), Otto (1822), Vrolik (1848), Albers (1851), Huschke (1858). The disease does not affect the auditory bones, the condyles of the maxillary and occipital bones, nor the styloid process of the temporal bone. It is recognizable in the posterior part of the cranium and basis cranii, but affects mostly the bones of the face and the frontal, parietal, and cribroid bones. Thus, the disease takes its origin in the anterior portion of the skull, particularly in the superior maxilla, and proceeds upward and backward, terminating in the basis cranii in the neighborhood of the infundibulum and appendices. But two of all the cases were observed during life. In all the disease was traced back to early life. The chemical composition of the bones was greatly changed in all. Instead of the normal proportion of earthy to organic material = 2.1 (or 1.5):1, it was from 3.5 to 4.4:1. Particularly the carbonate of lime was greatly increased.
The brain and its meninges participate, in many respects, in the changes worked by rachitis, and mainly in the abnormal vascularization of the bones. They are very much congested, and succulent. A section through the brain shows a great many large and small blood-points. This hyperæmia may give rise to over-nutrition, which assumes the character of real hypertrophy of the brain. When that hyperæmia, however, becomes excessive, effusion will take place into the cavities, the tissue of the arachnoid, and the substance of the cerebrum, which latter looks [p. 149]peculiarly brilliant, elastic, and sometimes white, in consequence of the blood-vessels being emptied by the pressure on the part of the enlarged mass of the cerebrum upon the blood-vessels. Thus, instead of cerebral hyperæmia there may be anæmia. Every form of hydrocephalus may follow the rachitical process. Afterward, when the craniotabes has healed, the secondary effusions will generally also disappear, but not a few cases of hydrocephalus may be traced to rachitis occurring during the first half year of life. When that occurs, the intellectual faculties may suffer, while, on the contrary, complete recovery not infrequently exhibits an unusual degree of mental development, for the same reason which improves the chances of the development of the bone. The degrees of physiological and pathological nutrition and over-nutrition are very variable in their nature and results.
This condition of the cranial contents is not the only one brought about by rachitis. The softness of the cranial bones permits a direct pressure on the brain. The side on which the infant for the most part reposes gets flattened, and the brain is also compressed. The skull consequently bulges out in the opposite direction. This anomaly, as stated above, is sometimes visible through life, though in the large majority of cases after recovery from rachitis has taken place this asymmetry will gradually disappear. Before that can occur, however, the infant is liable to suffer from the rachitical changes. Convulsions are by no means rare. Vogel has, however, been able to produce an attack of convulsions by pressing upon the softened spots of the cranium. Permanent or temporary contractures of the fingers and toes I have seen in several instances. Gerhardt looks upon rachitis as one of the causes of tetany.
A frequent symptom of the cerebral changes which take place during, and in consequence of, craniotabes is the crowing inspiration, or laryngismus stridulus, of infants. It may be mild or severe. The mild form is very frequent, and consists in the occurrence of a shrill inspiratory sound while the baby is either quite placid or excited or crying. It is frequently overlooked entirely, is usually overcome after a number of months, and gives rise to serious trouble in but very few instances. The severe form is of a different nature. While the baby is awake or asleep, without any premonitory symptoms, while playing or crying, placid or excited, all at once respiration will cease. This will take place, usually, after expiration. The limbs are hanging down, as it were lifeless, the face turns pale, then purple, and slight convulsive twitching may set in for ten or twenty seconds. There appears to be a complete paralysis, and death from apnoea seems to be imminent. All at once, a long, deep crowing inspiration will be heard, respiration will commence again, and the whole terrible attack is overcome. It may return a number of times every day, or sometimes not for several days, during a period of many weeks or several months. The attacks which set in after inspiration are apt to be more dangerous. In such an one, but also in the other kind which sets in after the expiratory movement, death may occur suddenly, or the attack may be followed by a convulsion which may terminate fatally like any other eclamptic seizure. In this manner it is that the majority of cases of rachitis perish which terminate fatally during the active progress of the morbid process. In this connection, however, it may be well to add that craniotabes is not the only cause of laryngismus, particularly when the [p. 150]latter is found in the second year of life, or even later. But almost every case, without any exception, which is observed during the first eight or nine months is due to that very cause; and a good many cases occurring later, when the craniotabic bones have become normal, arise from the effects, either meningeal or encephalic, of the rachitic process. Still, complications of craniotabes with a large size of the thymus gland may occur, and enlargements of the tracheal and bronchial lymphatic glands are quite frequent, as we shall see below.15
15 Z. Oppenheimer prefers the name rachitic asthma in place of laryngismus, and suggests an explanation of the symptoms from a strictly anatomical point of view. If not correct, it is at all events interesting, as everything this ingenious writer proposes. He points to the ligament situated between the spinæ intrajugulares of the temporal and occipital bones, which, as long as it is of normal consistency, separates the jugular vein from the pneumogastric nerve. As it is covered with periosteum and dura, it is apt to ossify, and forms an osseous partition in the foramen jugulare, which participates in all the changes taking place in the periosteum. As this becomes softened and succulent, so will the ligament, either on both sides or on either. Its influence on the neighborhood depends on its size or succulence (as also on the difference in width of the foramen jugulare or lacerum, which corresponds with the difference in size of the transverse sinuses). The irritation of the pneumogastric is perhaps easily explained thereby, but in very exceptional cases only the accessory nerve would be affected. As, however, the latter controls the sterno-cleido mastoid and trapezius, and also the laryngeal muscles, and is apt to provoke cardiac paralysis during diastole, the occurrence of sudden death would be best accounted for.
While the size of the cranium is normal, or sometimes more than normal, the face undergoes some changes which result in absolute or relative diminution of size. These depend mostly on a reduction in the volume of the jaws. Glisson knew of it, and therefore looked for the cause of rachitis in the process of dentition. Now, both maxillæ are liable to become rachitical at an early date, as early indeed as the bones of the cranium. Rachitical deposits and softening take place in them very generally. The lower maxilla is flat anteriorly, it loses its rounded outline, is shorter in longitudinal direction, while the rami are thick and clumsy; the whole bone is shorter than normal, and sometimes asymmetric. Its changed appearance is greatly due to the effect the muscles, with their powerful insertions, produce on the softened bone; mainly the masseter, also the mylohyoid, which draws the lateral portions inward, and the geniohyoid, which pulls at the central portion. Of the latter, the lower portion is drawn out, the inner and the alveolar part inward. Thus, the teeth, mainly the incisors, of the lower jaw are turned inward to such an extent that, as those of the upper look outward, the two rows of teeth do not touch but cover each other. Besides, the periosteal proliferation around the alveoli is excessive, sometimes so much so as not only to crowd the teeth into irregular positions, but even to absorb and annihilate alveolar processes in the course of the morbid changes. The cases in which the number of teeth are actually diminished by rachitis are not at all rare. In the superior maxilla the last-described anomaly is also observed. Periosteal thickening is mainly noticed about the intermaxillary bone—sometimes to such an extent that above and behind it a considerable impression takes place. The shape of the upper jaw is more spherical than normal, and the cheek-bones become very prominent.
The belief that maxillary rachitis is now and then met without any other symptom of rachitis I do not share. What I said of craniotabes is also valid in regard to this form.
[p. 151]Irregular teething is a constant companion of maxillary rachitis, but is also present where the latter is not well, or not at all, marked. As a rule, the first teeth protrude late, about the ninth or tenth or twelfth month. That the first year and more should elapse without any tooth is of frequent occurrence in rachitis. Cases in which the first teeth do not come before the second year is completed are not very uncommon; in some there are none even when the child is much older. In most cases the retardation of dentition goes hand in hand with very marked retardation in the development of the rest of the bones and in the closure of the cranial fontanel. But not in every case of rachitis is there a retardation in the process of teething. In some a few teeth appear at the regular period (at the completion of the seventh or eighth month), or even at a very early age (in the fourth or fifth month); after which there is an interruption in the protrusion of teeth for an indefinite period. Evidently, the period in which rachitis is developed exerts its influence on the teething process. When it exists at a very early age, it will retard teething until recovery takes place. Still, it is possible that a moderate amount of periosteal and osteal hyperæmia and over-irritation matures the teeth abnormally. In all those cases, however, in which rachitis does not occur before the second half of the first year, the first teeth will appear at the normal time, and a long period will follow in which no teeth at all will make their appearance. Then, again, when the whole process comes to a standstill, and recovery takes place with solidification of the bones, and even eburnation, the teeth will come in rapid succession. Whether they will, as is frequent, decay almost as soon as formed, or whether they will be unusually hard, solid, and yellowish, depends on the stage of the disease in which they made their appearance, and on the complications aggravating the case. Of very grave import in this respect are digestive disorders before and during the course of the disease.
The vertebral column suffers also. In the normal infant it is straight, but in the rachitic it exhibits a kyphotic deformity very soon. When such a baby of three or six months is sitting up, the middle portion of the back is protruding, as in Pott's disease. In almost every case, however, this kyphosis is but apparent and the result of muscular debility. In order to arrive at a diagnosis at once, it is sufficient to place the patient on his face and support the head, and raise the lower extremities and pelvis in the air. If the kyphosis is but functional, the prominence disappears at once. By nothing can the muscular insufficiency of early rachitis be better demonstrated than by this little experiment. But actual deformity is also found in rachitis. It softens both the vertebræ and intervertebral cartilages, and either their anterior or posterior portion may be irregularly developed, and be either too high or too low. Besides, the articulating surfaces are sometimes too convex. Thus the causes of both kyphosis and scoliosis are amply furnished, and complications of the two are quite frequent, and the deformities resulting therefrom quite formidable. Scoliosis is mostly to the left; kyphosis generally complicated with lordosis, and sometimes the vertebral column exhibits a spiral shape.
The ribs of the convex half are prominent and divergent, those of the concave side flattened and parallel. The two halves of the chest are therefore very unequal indeed. Muscular traction, atmospheric pressure, [p. 152]the elastic traction of the lungs, the presence of pulmonary complications, and the pressure from below on the part of the enlarged viscera of the abdominal cavity, come also in for a considerable share in the completion of the deformity.
The ribs and the sternum aggravate it considerably. Even without any affection of the vertebral column they suffer seriously from the general affection. The manubrium is thickened and drawn inward, the ensiform process protuberant, the sternum often swelled and painful to the touch. The ribs are sensitive to the touch on one or both sides. The child cries when taken up or when fearing to be taken up. The costo-cartilaginous junctures are thickened, mainly so from the fourth to the eighth ribs. The insertion of the diaphragm becomes soon perceptible by a deep groove around the chest. The anterior portion of the ribs is flattened, posteriorly they are inserted at acute angles. Thus the intrathoracic space becomes narrow, the sternum with the costal cartilages is pressed forward (pigeon breast, pectus carinatum), the thorax is deprived of its elliptical shape and becomes triangular, the dorsal aspect being flattened, and the distance between the vertebral column and the sternum increased. Below the diaphragmatic groove the thorax expands, the liver and other abdominal organs crowding the ribs outward. All sorts of changes are experienced by the ribs in these conditions. Parts of them are flattened, parts undergo infraction, parts are even concave; they are bent and twisted, now and then to such an extent as to turn the concave side out, the convex surface in. In addition to all this, the scapula is big and clumsy and protuberant, the clavicle considerably bent and frequently infracted, and not rarely covered with genuine callus.
That the respiratory and circulatory organs must suffer from such anomalies, though they be not excessive, is certain. The heart is crowded by the flattening of the ribs and the contraction of the thoracic cavity. Its beat is visible over a large surface, and its percussion dulness is extended over its normal space, though no enlargement have taken place. This, however, is very apt to occur after some time by overexertion. The latter is increased by the condition of the respiratory organs. The ribs being flexible, the chest contracted and compressed, the diaphragm raised, the respiratory muscles feeble, respiration is insufficient, even without the presence of any further complications; thus dyspnoea and a certain amount of cyanosis are frequently met with in consequence of the anatomical changes only. In addition to this, there is from the beginning a tendency to catarrhal and inflammatory conditions. Even without any deformity the rachitical process is accompanied from an early time with bronchial and tracheal catarrh. A chronic cough in an infant, with very little or no fever, disappearing and returning, mostly with copious secretion—which, however, is swallowed as soon as it reaches the pharynx—rouses the suspicion of general rachitis. It is often complicated with extensive dulness over the manubrium sterni, due (to rachitical thickening of this bone and) mostly to the persistence of a large size of the thymus gland; and also with enlargement of the bronchial and tracheal glands, the latter of which are often accessible to recognition by percussion. They are to be looked upon as a frequent occurrence in rachitis, though no associated diseases leading to their enlargement have been noticed. They and the chronic tracheo-bronchial [p. 153]catarrh are closely dependent upon each other. They are each other's both cause and effect. Neither of them, however, remain uncomplicated. Catarrh grows into broncho-pneumonia, with frequent returns. Atelectasis, interstitial pneumonia, dilatation of bronchi, and pulmonary consumption are often traceable to such apparently slight catarrhs, which, when not recognized as depending on their constitutional cause, cannot be removed. Nor are the cases of miliary tuberculosis, resulting from caseous degeneration of rachitical glands, very exceptional.
The anatomical changes in the abdominal viscera may be due to the preparatory diseases or the complications of rachitis; but, at all events, the abdomen yields a number of changes visible through the whole duration of rachitis. It is very large; its size is due to the contraction of the thoracic cavity and the downward pressure of the chest-wall upon the contents of the abdominal cavity. It is also due to the changes wrought by rachitis in the pelvis. Softening of bones and synchondroses, torsion, the weight of the trunk, and the pressure of the femora from below produce the change of the pelvis so well known and much feared in the parturient female. The promontory and sacrum are pushed in, the arcus pubis is large, the pelvis asymmetric; the small pelvis is contracted, the large pelvis broader. Thus, the small pelvis has no room for viscera, which, then, are crowded upward. The digestive disorders which gave rise to, or formed the first stage of, rachitis result in the accumulation of gas; the scrobiculus cordis is greatly expanded. The liver16 is large, congested, and in fatty degeneration. The latter is the more frequent the more a certain degree of fatty condition is a normal attribute of every infant liver. When the liver is found but small in post-mortem examination, it is so because of the general anæmia and emaciation. Sometimes it is amyloid, as are also the spleen (mostly hyperplastic only), the kidneys, and the arteries of the intestines in many instances.
16 Dr. Norman Moore presented a cast and drawing to the Pathological Society of London (Trans., vol. xxxiv., 1883, p. 185) showing how considerable may be the digressions of the diaphragm and local pressure upon the liver in a case of rickets. Three large beads caused as many projections from the under side of the diaphragm, and corresponded with local thickenings of the capsule of the liver, probably produced by the continued pressure through the diaphragm of the beads, which were on the seventh, eighth, and ninth ribs, and the largest of which was equal in size to a hazel-nut.
The alimentary tract is the seat of many changes recognizable during life. The tonsils are often large. The tongue is seldom coated to an unusual degree. On it are found little islands, red, marginated, deprived of epithelium. They will increase in size and number and extend backward. They will heal and reappear. They are by no means syphilitic, as Parrot would have it, and correspond exactly with the erosions near the solitary glands and those of Lieberkühn in the intestinal part, which mean nothing else but a nutritive disorder of the epithelia, and give rise to nothing worse than incompetency of absorption in that locality and abnormal secretion. The stomach is in a condition of chronic catarrh, sometimes dilated. Acid dyspepsia is frequent. Anorexia and bulimia will alternate. Feces contain an abnormally large amount of lime. Diarrhoea and constipation will follow each other in short intervals. The former owes its origin to faulty ingesta or chronic catarrh; the latter, sometimes to improper food, but more generally to muscular insufficiency. [p. 154]This condition has not been estimated at its proper value. Besides myself,17 nobody but Bohn has paid the attention to it which it deserves. Here, again, I have to insist that rachitis is a disease of the whole system, and not exclusively of the bones. Indeed, the muscular system is amongst the first to suffer. In the same way in which the voluntary muscles are not competent to raise and support the head or to allow a baby to sit up without a functional kyphosis, the involuntary muscles of the intestine are too feeble for normal peristalsis. The infant of a month or two months of age may have had normal and sufficiently numerous evacuations; gradually, however, constipation sets in; the feces become dry, but are perhaps not much changed otherwise. If no other cause be apparent, the suspicion of rachitical constipation is justified. Seldom, however, after it has lasted some time—and only after some time has elapsed relief will be sought—it will remain alone. Other symptoms of rachitis will turn up and the case be easily recognized. This constipation is an early symptom, as early as thoracic grooving or craniotabes. Very often it precedes both—is, in fact, the very first symptom—and ought therefore be known and recognized in time.
17 Jour. Obst., etc., Aug., 1869.
The kidneys have been mentioned above. They are often found rather large. Though the fact has been alluded to before, I will here again state that it has always been the general impression that the amount of lime eliminated in the urine of rachitic children is excessive. The reverse of that is true. Seemann and Lander have proved beyond dispute that in most stages of rachitis there is less than the normal amount of lime in the urine. Thus, the theory that lime is eliminated by an excess of acids in the blood is proven to be incorrect. But it is a fact that the rachitical bone contains a proportionately small amount of lime. The conclusion is, then, that its introduction must have been diminished. On the other hand, every article of food contains a large amount of lime, which might be introduced into the circulation if digestion be not at fault. The fact is, that a large amount of lime introduced is not utilized, and is eliminated with the feces.
In connection with these facts the following will be found very interesting. It has been found by Bunge that when potassium, with the exception of chloride of potassium, meets chloride of sodium, the two will exchange their acids, so as to form chloride of potassium and phosphate of sodium. They will be found in the blood also, will be eliminated as such, and result in a comparative absence of chloride of sodium from the serum of the blood. Now, comparative absence of chloride of sodium diminishes the possibility of the development of hydrochloric acid. Thus, it is not a surplus of acid, but a lack of hydrochloric acid, which results from such chemical combinations. If such be the case, calcium salts are not absorbed sufficiently. Thus, they will appear in the feces, and not even be absorbed in the intestines, because of the alkalinity of the intestinal secretion, by which the lime cannot be dissolved. The more lime, then, is introduced under these circumstances, the greater the incumbrance to digestion.
The correct proportion between chlorine, phosphorus, potassium, and sodium is certainly exhibited in woman's milk. There is lime enough in even the poorest article of that kind. But indigestion brought on by [p. 155]woman's milk in a disordered condition or by any other cause will prevent the absorption of lime when a superabundance of phosphorus and potassium disturbs the formation of hydrochloric acid. In these cases not only the development of the bones, but also that of the muscles, is disturbed. The latter is of great importance in regard to circulation, because a large part of the circulation depends on the pressure on the part of the muscular fibres exerted on the small blood-vessels. These facts have been the reason why I insist upon the addition of chloride of sodium to the food of infants and children, particularly those who are fed on cow's milk; for cow's milk and vegetables contain a relative superabundance of potassium compared with sodium. Even adults will find cow's milk very much more digestible by adding table-salt to it.
The extremities begin to suffer at a later period than the ribs and cranium. The opinion of Guérin, that the rachitical process begins in the lower extremities and ascends gradually, is erroneous. It cannot even be stated that the lower extremities are affected sooner than the upper. There is no regularity at all; it is not even necessary that all the osseous tissue should fall sick. But this can be taken as a fact, that hands and feet, and particularly the phalanges, are the latest to undergo the rachitical change. First in the line of morbid alteration of the bones are the epiphyses, mainly of the tibia, fibula, radius, and ulna. Their integument appears to be thin; now and then the cutaneous veins are dilated. The periosteum of the diaphysis becomes thick, softened, and painful to the touch and pressure, its compact layer thin, the medullary space large, the whole bone flexible, at the same time that the ligamentous apparatus of the joint becomes softened and flabby. At this time babies are greatly admired and applauded for the facility with which they introduce their feet into their mouths. For at the same time the bones begin to curve under the influence of the flexor muscles, which are always stronger, as they do in later months under the weight of the body when the child begins to walk. The curvature is not always a mere arching, but sometimes the result of infraction (green-stick fracture), a complete fracture not being accomplished because both of the softness of the osseous tissue and the resistance on the part of the thickened and softened periosteum. Both the legs and forearm bend on the external side, the resulting concavity looking inward. The humerus bends in a direction opposite to that of the forearm; the thigh, usually outward and forward.
The attempts at locomotion are often the causes of quite preposterous anomalies; creeping, sliding, walking, turn the extremities in such unexpected directions that talipes valgus, genu valgum, and now and then double curvatures, are the results. These, however, may not always be very marked, but there is one change in the rachitical bone which is constant—viz. the impairment of longitudinal growth. In every case the diaphyses remain abnormally short, and the proportion of the several parts of the body are thereby disturbed. Chiari measured parts of the skeleton of a rachitical woman of twenty-six years who was nine years old before she could walk. Her height was 116 centimeters, the length of the lower extremities 42, femur 23, tibia 15, fibula 20, humerus 16, right radius 12.5, left radius 11, right ulna 15, left ulna 14 centimeters. In a second case the parts of the skeleton were measured after they had [p. 156]been extended with great care. The right arm from the acromion to the middle finger (incl.) was 39 centimeters, the left 38; the right lower extremity from the trochanter to large toe (incl.) 39, the left 41.
The skin participates in the general nutritive disorder. It is soft and flabby. In those infants who become rachitical gradually while proving their malnutrition by the accumulation of large quantities of fat, it exhibits a certain degree of consistency. When rachitis develops in the second half of the first year or later, with the general emaciation the skin appears very thin, flabby, unelastic. The veins are generally large. Complications with eczema and impetigo are very frequent; where they are found the glandular swellings of the neck and below are still more marked than in uncomplicated cases. Circumscribed alopecia is sometimes found (not to speak of the extensive baldness of the occiput). It is not attended with or depending on the microsporon Audouini, but the result of a tropho-neurosis. In the hair Rindfleisch found fat-globules between its inferior and central third. Then it would break, the axial evolution would cease, and the end become bulbous by the new formation of cells.
There is a form of rachitis which may be, and has been, called multiple epiphysitis or multiple periostitis of the articular ends of the long bones. The changes which in the usual form of rachitis require months to develop take place in a very short time. Not infrequently the children were quite well before they were taken with this peculiar affection. Cases have been known to occur between the fourth and twenty-fourth months of life, and to last from two to six weeks, or just as many months. They have been known to get well, or a few of them terminate fatally. They are accompanied with fever and rapid pulse, perspiration, now and then with diarrhoea, with eager or reduced appetites. At the same time the epiphyses swell very rapidly, and are painful. The same is true of the diaphyses and the flat bones of the head. Many authors do not recognize this form as an independent variety. Some call it an acute initial stage of certain cases of rachitis, as they are not infrequently found in infants which exhibit a very rapid growth. Some have taken it as an independent disease, developed on the basis of a constitutional disposition; some look upon it as a very intense acute form of rachitis; others, as an intense growth of the osseous tissue only. Others call it an inflammation of the bone. Some refer it to hereditary syphilis, and a few to the influence of malaria. That the disease is epiphysitis and periostitis there is no doubt. I do not hesitate to claim it as rachitis, for epiphysitis and periostitis of early age not of rachitical basis are not apt to run such a favorable course as this form frequently does. The cases complicated with subperiosteal hemorrhages are claimed as scurvy by Th. Barlow.
The differences of opinion would probably not have been so great if every author had seen all the cases of the other observers. It will not do to judge of unobserved cases by the light shed by a single case under one's own observation. I have seen cases of acute rachitis which were [p. 157]the initial stages of general rachitis, and have observed those of local or multiple epiphysitis, mainly after infectious fevers, which were diagnosticated as such. They are, however, very uncommon. But even without a preceding infectious fever, such as scarlatina or more frequently typhoid fever, there are unexplained cases of rachitis and deformity. Thus, R. Barwell had some before the Pathological Society of London,18 which are positive proofs that some forms of ostitis may occur and result in the most formidable deformities without being rachitical. A girl of seventeen years was perfectly well formed up to the age of two and a half or three years. After that time the deformities began to develop, and did not change after she was thirteen, at which time the author saw her the first time.
| Her | left humerus measured | 7¾ inches | from shoulder to elbow; | distance 6¼ |
| right humerus measured | 7½ inches | from shoulder to elbow; | distance 4¼ | |
| left tibia measured | 10 inches | from knee to ankle; | distance 7¼ | |
| right tibia measured | 9½ inches | from knee to ankle; | distance 4½ |
Her bones were always very brittle. When she was between nine and thirteen she broke her arms four times and her lower limbs on several occasions. A male patient of twenty-two years, who was born healthy and well formed, continued thus until five years of age, when he was attacked with a fever, after which his bones became soft and bent. Osteotomy was performed on him, and the femora were found to be mere thin shells of bones surrounding cavities containing great quantities of medulla, which flowed out of the wound as oil; five ounces were discharged at once. In both cases there appeared to be a hypertrophy of the medulla at the expense of the bone-substance—a condition which Barwell proposes to call eccentric atrophy. "While these subjects are still youthful very little bone-earth is deposited, or at least remains in the very thin layer of osseous tissue that subsists. The relationship between infantile ostitis and extreme development of the intraosseous fat, though well known, is still occult; neither should we lose sight of the possibility that the softening process of ostitis may be due to a fatty acid. Now, fatty ostitis usually occurs in epiphyses. In these cases the shafts were affected."
18 Trans., xxxiv., 1883, pp. 203-208.
PROGNOSIS.—The course and the prognosis of rachitis are, as a rule, favorable, but they change according to the degree and locality of the affection and the age of the patient. Generally there is neither fever nor rapid exhaustion. But the process lasts for months and even years. In favorable cases, when recovery takes place the teeth will grow faster, the bones become firmer, the epiphyses will diminish in relative size, the bowels become regular. But the length of the bones is, and remains, reduced, and the head remains large as compared with the length of the body. Not only are the bones of normal firmness, but the compact substance undergoes a process of hardening called eburnation by Guérin. The internal organs also become very active, perhaps because the total amount of blood has to supply only a body less extended in length. Nor does the brain suffer after complete recovery has taken place. On the contrary, it appears that the somewhat more than normal vascular dilatation, which under unfavorable circumstances leads to effusion, is [p. 158]frequently apt to nourish the organ of intellect up to a higher standard. In all cases of rachitis, however, the curvatures of the extremities will not disappear altogether, while mild ones, it is true, are hardly recognizable in advanced age. Curvature of the ribs and of the vertebral column, however, will remain, and interfere with the expansion and the normal functions of the lungs and heart. In regard to the lungs, it appears that in many cases they do not find sufficient space to expand. As far as the heart is concerned, it touches the flattened, no longer elliptic, chest-wall over a larger surface, and is very apt to give rise to the suspicion of enlargement in consequence of extended dulness on percussion. The rachitic pelvis is well known to the obstetrician for the difficulties it gives rise to during parturition.
Thus, the prognosis would, as a general thing, be sufficiently favorable if it were not for the number of complications or severe symptoms. The chronic catarrh of the lungs accompanying rachitis, the enlargement of the tracheal and bronchial glands and the lymphatic glands in general, are apt to lead to inflammatory disease of the lungs, which, after having returned several times, leads to infiltration of the lungs with caseous deposits, and not infrequently results in phthisis. The nervous symptoms accompanying craniotabes may prove very dangerous. Spasm of the larynx and laryngismus stridulus may prove fatal in a single attack by suffocation, or general convulsion may set in during an attack of laryngismus or without it, in which the child may perish. Therefore the prognosis in every case of laryngismus and in every case of craniotabes has to be very guarded. It is my rule to wait from six to eight weeks before giving expression to a decided prognosis, because during that time medicinal and dietetic treatment will probably have resulted in such an improvement of the symptoms and condition as to render the prognosis more favorable. Under no circumstances, however, ought we to lose sight of the fact that, though rachitis may disappear, the causes leading to it may still linger on. Defective nutrition, diseases of the lungs, and intestinal affections which gave rise to or accompanied rachitis will complicate the prognosis, though rachitis itself, as far as the bones were concerned, be no longer in existence.
TREATMENT.—To meet the cause of a disease by preventive measures is the main object and duty of the physician. He thus either obviates a malady or relieves and shortens it. Now, if the original disposition to rachitis, as has been suggested, is to be looked for in early intra-uterine life, when the blood-vessels begin to form and to develop, we know of no treatment directed to the pregnant woman or uterus which promises any favorable result. But the more we recognize an anatomical cause of the chronic disorder, the more we can appreciate the influence upon the child of previous rachitis in the mother, and are justified in emphasizing the necessity on the part of the woman to be healthy when she gets married, and to remain so while she is pregnant. After the child is born the most frequent cause of rachitis is found within the diet or the digestion of the patient. To attend to the former is in almost every instance equal to preventing disorders of the latter; for most of the digestive disturbances during infancy and childhood are the direct consequences of errors in diet. It is, however, impossible to write an essay on infant diet in connection with our subject. I have elaborated the subject in my [p. 159] Infant Diet (2d ed. 1876), in the first volume of Buck's Hygiene, and of C. Gerhardt's Handbuch d. Kinderk. (2d ed. 1882). Still, the importance of the subject requires that some points should be given, be they ever so aphoristic.
The best food for an infant, under ordinary circumstances, is the milk of its mother. The best substitute for the mother is a wet-nurse. Woman's milk ought not to be dispensed with when there is the slightest opportunity to obtain it, particularly when the family history is not good and nutritive disorders are known to exist, or to have existed, in any of its members. When it cannot be had, artificial food must take its place, and it is in the selection of it where most mistakes are constantly made. This much is certain, that without animal's milk no infant can or ought to be brought up; as ass's milk can be had only exceptionally, and dog's milk, which has been said to cure rachitis, is still less available, the milk of either goat or cow must be utilized. The former ought not to be selected if the latter is within reach, mainly for the reason that it contains, besides other objectionable features which it possesses in common with cow's milk, an enormous percentage of fat. Cow's milk differs in this from woman's milk, that it contains more fat, more casein, more potassium, and less sugar than the latter, and that its very casein is not only different in quantity, but also in chemical properties. Even the reaction of the two milks is not the same, woman's milk being always alkaline, cow's milk often either neutral or amphoteric, and liable to acidulate within a short time. Thus, the dilution of cow's milk with water alone yields no equivalent at all of woman's milk, though the dilution be large enough to reduce the amount of casein in the mixture to the requisite percentage of one, and one only, in a hundred. The addition of sugar (loaf-sugar) and of table-salt, and sometimes alkali (bicarbonate of sodium or lime-water, according to special circumstances), is the least that can be insisted upon. Besides, the cow's milk must be boiled to prevent its turning sour too rapidly, and this process may be repeated to advantage several times in the course of the day. Instead of water, some glutinous substance must be used for the purpose of diluting cow's milk. As its casein coagulates in hard, bulky curds, while woman's milk coagulates in small and soft flakes, some substance ought to be selected which keeps its casein in suspension and prevents it from curdling in firm and large masses. Such substances are gum-arabic, gelatin, and the farinacea. Of the latter, all such must be avoided which contain a large percentage of amylum. The younger the baby, the less is it in a fit condition to digest starch; thus arrowroot, rice, and potatoes ought to be shunned. The very best of all farinacea to be used in diluting cow's milk are barley and oatmeal. A thin decoction of either contains a great deal of both nutritious and glutinous elements, the former to be employed under ordinary circumstances, the latter to take its place where there is, on the part of the baby, an unusual tendency to constipation. The decoction may be made of from one to three teaspoonfuls of either in a pint of water; boil with a little salt, and stir, from twelve to twenty minutes, and strain through a coarse cloth. It ought to be thin and transparent. Then mix with cow's milk in different proportions according to the age of the baby. Four parts of the decoction, quite thin, and one of milk (always with loaf-sugar), for a newly-born, equal parts for an infant of six months, [p. 160]and gradual changes between these two periods, will be found satisfactory. Whenever there is a prevalence of curd in the passage the percentage in the food of cow's milk must be reduced, and now and then such medicinal correctives resorted to as will improve a disturbed digestion. Care ought to be taken lest for the newly-born or quite young the preparations of barley offered for sale contain too much starch. The whiter they are, the more unfit for the use of the very young, for the centre of the grain contains the white and soft amylum in preference to the nitrogenous substances which are found near the husk. Thus, it is safest to grind, on one's own coffee-grinder, the whole barley, but little deprived of its husk, and thus secure the most nutritious part of the grain, which is thrown out by the manufacturer of the ornamental and tidy packages offered for sale. But very few cases will ever occur in which the mixtures I recommend will not be tolerated. In a few of them, in very young infants, the composition recommended by Meigs19 has proved successful. It consists of three parts of a solution of milk-sugar (drachm xvij¾ in pint j of water), two parts of cream, two of lime-water, and one part of milk. For each feeding he recommends three tablespoonfuls of the sugar solution, two of lime-water, two of cream, and one of milk: mix and warm. The baby may take all of it, or one-half, or three-fourths.
19 In Med. News, Nov. 28, 1882.
The recommendations given above are based on a long experience, and the simplicity, cheapness, and facility of preparation of the articles. The substitutes offered for sale under the title of infant foods are in part worthless, all of them expensive when compared with the simple articles recommended by me, and not recognizable as to their uniformity and compounds. But no matter how appropriate my mixture may be, it is always for the young infant to be considered as a makeshift. It is to be used as a representative of mother's milk only when this cannot be had. Therefore it is better to alternate with breast-milk when this is secreted in but an insufficient quantity. Some good breast-milk is better than none at all; but with this proviso, that it is good. There are some milks either too watery or too dense and white. The former will produce diarrhoea, the latter hard and dense curd. The former may be improved by feeding and strengthening an anæmic and overworked mother; the latter, by giving the baby, before each nursing, a tablespoonful of a mixture of barley-water and lime-water, or, when it produces constipation, lime-water and thoroughly sweetened oatmeal-water. The cases in which breast-milk, such as can be had, is not digested by the infant are rare, but they will occur. In them the proper substitute will yield a better result than mother's milk; for mother's milk will not always be a boon, and must then be dispensed with. Particularly is this so when it is too old. Weaning ought to take place when the first group or the first two groups of teeth have made their appearance. After that time mother's milk is no longer the proper food, and instead of preventing indigestion and sickness it is a frequent cause of them and of rachitis. Instead of muscle, it will then give fat, and the large fontanels and big head, the paleness of the rotund cheeks, the flabbiness of the soft abdomen and thighs, will tell the story of rachitical disease slowly engendered by the persistent employment of an improper article of food. I cannot insist too often on this, that rachitis may develop with increasing weight, [p. 161]and that the use of the scales alone is no means of ascertaining the healthy condition of a baby. As much harm, therefore, can be done by weaning too late as by so doing too early or too abruptly.
At that early age we treat of here, digestive disorders are more frequently the results of improper diet than of a primary gastric disturbance. But when the latter is once established it furnishes its own indications. A frequent occurrence, together with a general gastric catarrh, is the presence of fat acids in the stomach, such as an improper amount of lactic, acetic, butyric, etc. acids. Before digestion can be anything like normal they must be neutralized. For that purpose calcined magnesia, carbonate and bicarbonate of sodium, prepared chalk, and lime-water have been found useful. The latter, as it contains but a trifle of lime, in order to neutralize must be given in larger doses than is usually done; a tablespoonful contains but a quarter of a grain of lime. And all of the alkalies must not be given in the food only, but also between meals. For when given in the former way alone it neutralizes the abnormal and injurious acids, together with the normal digestive secretion, the lactic and muriatic. Not infrequently, when the infants have suffered for some time, general anæmia will set in, and result in diminishing the normal secretions of the mucous membranes (and glands). In those cases which do not produce their own gastric juice in sufficient quantity or quality pepsin and muriatic acid may be given to advantage. In these cases the plan suggested by me is particularly favorable—viz. to add a fair amount of chloride of sodium (one-half to one drachm daily) to the infant's food. Also that of I. Rudisch referred to by me previously,20 who mixes one part of dilute muriatic acid with two hundred and fifty of water and five hundred of milk, and then boils (one-half teaspoonful of dil. mur. acid, one pint of water, one quart of milk). Again, there are the cases in which wine and the bitter tinctures, which are known to increase the secretion of gastric juice, render valuable service. The addition of bismuth to any of the proposed plans is quite welcome. As a disinfectant and a mild cover on sore and eroded mucous membranes it has an equally good effect.
20 Am. Jour. Obstet., July, 1879.
Under the head of roborants we subsume such substances, either dietetic or remedial, which are known or believed to add to the ingredients of the organism in a form not requiring a great deal of change. Rachitical infants require them at an early period. Meat-soups, mainly of beef, and of mutton in complications with diarrhoea, ought to be given at once when the diagnosis of rachitis becomes clear or probable. Any mode of preparation will prove beneficial; the best way, however, is to utilize the method used by Liebig in making what he called beef-tea. A quarter of a pound of beef or more, tender and lean, cut up finely, is mixed with a cup or a tumbler of water and from five to seven drops of dilute muriatic acid. Allow it to stand two hours and macerate, while stirring up now and then. This beef-tea can be much improved upon by boiling it a few minutes. It may be given by itself or mixed with sweetened and salted barley-water or the usual mess of barley-water and milk which the infant has been taking before. Older infants, particularly those suffering from diarrhoea, take a teaspoonful of raw beef, cut very fine, several times a day. It ought not to be forgotten, however, [p. 162]that the danger of developing tænia medio-canellata from eating raw beef is rather great. Peptonized beef preparations are valuable in urgent cases.
Iron must not be given during any attack of catarrhal or inflammatory fever. The carbonate (cum saccharo) combines very well with bismuth; a grain three times a day, or less, will answer well. The citrate of iron and quinine (a few grains daily) can be given a long time in succession. The syrup of the iodide of iron (three times a day as many drops as the baby has months up to eight or ten), in sweetened water or in sherry or malaga, or in cod-liver oil, acts very favorably when the case is, as so frequently, complicated with glandular swelling.
Cod-liver oil, one-half to one teaspoonful or more, three times a day, is a trusted roborant in rachitis, and will remain so. Animal oils are so much more homogeneous to the animal mucous membrane than vegetable oil that they have but little of the purgative effect observed when the latter are given. The former are readily absorbed, and thus permit the nitrogenous ingesta to remain in store for the formation of new tissue, but still affect the intestinal canal sufficiently to counteract constipation. As the latter is an early symptom in a peculiarly dangerous form of rachitis, cod-liver oil ought to be given in time (in craniotabes). Diarrhoea is but seldom produced by it; if so, the addition of a grain or two of bismuth or a few doses of phosphate of lime (one to four grains each) daily, may suffice to render the movements more normal. There are but few cases which will not tolerate cod-liver oil at all. The pure cod-liver oil—no mixtures, no emulsions—ought to be given; the large quantities of lime added to it in the nostrums of the wholesale apothecaries embarrass digestion and bring on distressing cases of constipation. These mixtures have been prepared and are eulogized on the plea of their furnishing to the bones the wanting phosphate of lime. The bones, however, as we have seen before, are not grateful enough to accept the service offered. But only a certain amount of phosphate of lime is useful in rachitis and in digestive disturbances. In small doses it neutralizes acids like other alkalies; its phosphoric acid combines with sodium very easily, and gives rise to the formation of glyco-phosphoric acid, which is of very great importance in the digestive qualities of the upper portion of the small intestines.
Plain malt extracts will be well tolerated by some older children. The preparations which are mixed with a goodly part of the pharmacopoeia by generous manufacturers are to be condemned.
Craniotabes requires some special care in regard to the head. The pillow ought to be soft, but not hot; no feather pillow is permitted. The copious perspiration of the scalp requires that it should be kept cool, the perspiration wiped off frequently to avoid its condensing into water, and the flattening side of the head may be imbedded in a pillow with a corresponding depression. Copious perspiration indicates the frequent washing with vinegar and water (1:5-6). The muscular debility commands great caution. The baby must not be carried on the arm, but on a pillow which supports both back and head, or in a little carriage. No sitting must be allowed until the back will no longer bend to an unusual degree. No walking must be encouraged at any time. The patients will walk when their time has come. The bones are so fragile that great care [p. 163]is needed sometimes not to fracture or to infract them and to avoid periosteal pain in lifting. The skin must undergo some training by gradually accustoming the little patient to cool water. It can be readily, but gradually, reduced to 70° for a bath at any season. The addition of rock- or table-salt to the bath is a welcome stimulant. And fresh air ought to be granted freely.
Laryngismus stridulus shares the indications for treatment furnished by craniotabes. The general treatment remains the same. Prominent symptoms and complications ought to be treated besides; constipation requires the more attention the more convulsive attacks of any description may arise from reflex action. The general nervous irritability may be relieved by bromide of potassium, sodium, or ammonium. One gramme daily (15 grains) of either, in three doses, is well tolerated for a long period. When there are symptoms of an imminent convulsion, or to soothe the convulsibility which may break out any moment, chloral hydrate, eight or ten grains in from one hour to four hours, two grains in a dose, will be convenient. If the stomach refuses or is to be spared, from four to eight grains may be given in an enema of warm water. A severe attack of convulsions ought to be checked with inhalations of chloroform. When a warm bath is to be had, care should be taken that the child be not tossed about. Hold the baby in a small sheet or a large napkin, and immerge it thus into the water, raising the head and cooling it with cold cloths or an ice-bag. Genuine attacks of laryngismus with well-developed stages—the first paralytic, the second spasmodic—give but little time for any treatment. The proposition to apply the electrical current is well meant, but the attack has passed by, or terminated fatally, or resulted in a general convulsion, before the apparatus can possibly be in operation. I can imagine, however, that a Leyden flask kept ready might be used to advantage during the stage of apnoea for the purpose of bringing on inspiration. Sprinkling with cold water, beating with a wet towel, shaking by the shoulders, may certainly contribute to awake respiratory movements. The advice to wait quietly until the attack has passed by is more easily given than carried out. Marshall Hall's direction to perform tracheotomy will, I hope, soon be forgotten.
Nothing is more gratefully appreciated by the little patients than air. May it never be forgotten that night-air is better than foul air, and that furnace-air means air greatly modified by injurious additions. More than twenty years ago I was in occasional attendance upon a male baby—now a medical man of some promise—with craniotabes and a number of general convulsions. No treatment would remove, or even relieve, the attacks, until, without the physician's advice, the father took the baby into the street in the hardest winter weather. After the first long absence from his furnace the baby was well of his convulsions, and the physicians profited by their involuntary experience.
In the same way that salt-bathing is beneficial, so is sea-air. A summer at the seaside is a great blessing to rachitical children. Sea-baths have been arranged for them in France (Berx-sur-mer), in Italy (San Ilario di Nervi, Viarreggio, Livorno, Volti, Fano), in England (Margate), in Germany (German Sea, by Prof. Beneke), and for some little time past in the neighborhood of our own large cities.
[p. 164]Complications command great attention in rachitis, particularly where there is danger from the affection of the nerve-centres, for the slightest irritation in some distant part of the body may give rise to an outbreak. Thus, in craniotabes it is desirable to watch even the gums. Not sharing the etiological superstition which attributes so many diseases of infancy to dentition, I still know that a slight irritation of the gums may suffice to exhaust the slim resisting power of the infant. If there be local swelling and congestion of the gums over a growing tooth, it may become necessary, or at least advisable, to lance. An otitis which under ordinary circumstances would give rise to no symptoms at all besides some inconvenience or slight pain will prove the source of great danger in a rachitical (craniotabic) infant. The chronic bronchial catarrh and frequent broncho-pneumonia of such patients require early attention, for they and the neighboring lymphatic glands stand too much in the relation of a vicious circle of cause and effect.
Rachitical constipation, depending on incompetency of the intestinal muscle, must not be treated with purgative medicines. Now and then, when a great deal of abnormal acid is formed in the stomach, calcined magnesia, a grain or two given before each meal, will control that disorder and at the same time keep the bowels open. But, as a rule, every purgative after it has taken effect will leave the intestinal muscular layer less fitted to perform its functions than before. Its place may be taken by a daily enema of tepid water. Further indications are—such a change in the food as will contribute to keep the bowels moist and slippery, but principally such a modification of food and such medical treatment as are known to prove beneficial when all the symptoms of rachitis are fully developed. When the cause of the infant's rachitis can be traced back to the mother or to an insufficient quality of her milk, she must give way to a wet-nurse, or the nurse must be changed for similar reasons. When neither mother nor wet-nurse prove competent, or either be dangerous, artificial food will take their place to advantage in the manner I have stated above. Beef-soup or beef-peptone is to be added to the baby's food daily. Of the two best farinacea, barley- and oat-meal, the latter is preferable as an addition to cow's milk, because of its greatly laxative effect. The percentage of cow's milk in the food ought to be more carefully watched than in other conditions. Pure cow's milk or cow's milk mixed with water only is borne worse in no other condition. Half a drachm or more of table-salt and a few drachms of sugar ought to be added to the daily mess. The general indications require the administration of iron, which has no constipating effect in this ailment. Particularly is that the case with the iodide of iron. Cod-liver oil, in three half-teaspoonful or teaspoonful doses daily, acts very satisfactorily both for its general rachitical and for its local effect on the mucous membranes. Now and then massage, repeated many times a day a few minutes each time, practised with the palm of the hand only, or gentle friction, with the dry or oiled hand, of the abdominal surface, will prove effective in bringing about peristalsis and strengthening the intestinal muscle. An obstinate case may also require two daily doses of one one-hundred-and-fiftieth or one one-hundred-and-twentieth of a grain of strychnia for the same purpose, or such other improvements on the above detailed plan as the judgment of the attending physician may direct. At all events, the diagnosis of [p. 165]any case, and the appreciation of the cause of any ailment, are, to a well-balanced and educated mind, of infinitely greater value than any number of specified rules and prescriptions.21
21 Jour. Obstetr., Aug., 1869.
It is not impossible that phosphorus, in substance, not in any of its compounds, may prove of great utility in the treatment of rachitis. Minimal doses of phosphorus render the newly-formed tissue at the points of apposition of the bones more compact in a very brief time. The new formation of blood-vessels in the osteogenous tissue gets retarded by it. Larger doses of phosphorus, however, increase vascularization, and osseous tissue is either less rapidly formed or even softened. When the doses are still larger, vascularization and softening may rise to such a point as to separate the epiphysis from the diaphysis. Thus the administration of the drug results in an irritation which, according to the doses employed, may give rise either to normal condensation or to inflammatory disintegration. This experience, arrived at by Wegner in a great many experiments made on animals, Kassowitz has confirmed. For its therapeutic effect he tried phosphorus in 560 cases of rachitis. Employing doses of one-half milligramme (one one-hundred-and-twentieth of a grain) several times daily (less will suffice), he soon found the skull to become harder, the fontanel smaller, the softening of the bones of the thorax and extremities to disappear, and all the other symptoms of rachitis to improve. This result was obtained though no particular change in the feeding of the patients was resorted to. To what extent this experience will be verified by others we shall soon learn. My own is already sufficiently extensive to base upon it a strong recommendation of the plan of treatment I have detailed. My therapeutical results in other diseases of the bones also encourage me to believe that phosphorus will accomplish much in the treatment of rachitis. Ever since Wegner's publications—viz. these thirteen or fourteen years—I have utilized phosphorus in cases of chronic and subacute inflammations of the bones, mainly of the vertebral column and the ankle-joint and tarsus. After having taught the method for many years in my clinic and otherwise, I made a brief communication on the subject to the Medical Society of the State of New York.22 Since that time, again, I have followed the same plan in many cases of the same description, and feel sure that the prognosis in this serious class of bone diseases has become more favorable and recovery speedier. Infants of a year or more were given a dose of one-eightieth or one one-hundredth of a grain of phosphorus daily. One grain, dissolved in an ounce of oil or cod-liver oil, is a convenient mixture, four or six drops of which may be administered daily in two or three doses.
22 Trans., 1880.
From what I have seen of phosphorus in bone disease, and what is thus far known by experience in rachitis, it appears to me that it will be of decided advantage in that form of acute rachitis which is apt to destroy rapidly with the symptoms of acute epiphysitis, rapid pulse, diarrhoea, rapid diminution of strength, and scorbutic gum. In the few cases I have seen these last years it appeared to me to act satisfactorily, together with immobilization of the whole body.
Rachitical curvatures are very apt to become less marked while growth is increasing and the limbs extending. But many of them are so marked [p. 166]that they remain for life. Many of these might have been benefited by timely orthopædic interference. That the application of Sayre's jacket is indicated in every form and stage of spondylitis, though it be not equally valuable in all forms, goes without saying; and that infractions ought to be straightened and supported by splints when observed and when practicable, is self-evident. But, as a rule, while the chronic rachitical process is developing in the long bones the use of mechanical apparatuses is of doubtful merit; they ought not to be resorted to before the healing has at least commenced. Nor is it advisable to postpone mechanical interference so long that eburnation of the bones has time to take place. Surgical operations for the purpose of removing the curvature are of different nature according to the different types to be treated. Mere straightening of the curvatures is indicated, and successful with children under two years. Osteoklasy—that is, fracturing of the curvature while the periosteum is left intact—is successful in children of three (or four, according to Volkmann) years. The fracture does not injure the periosteum, and is always transverse. In later years osteotomy has proved successful to an almost unexpected degree, and is one of the happiest achievements of modern surgery.
Partly as a preventive, partly as a curative measure, Gramba of Turin and Pini of Milan point to well-directed gymnastics as a requisite in the treatment of rachitis. For older children they have established schools in which systematic exercises are brought to bear on chronic deformities.
SYNONYMS.—French, Scorbut; Spanish, Escorbuto; Italian, Scorbuto, are the various terms in the Romance languages used to designate this disease, derived from the Middle-Latin word scorbutus, which is evidently an offspring of one of the early Gotho-Teutonic dialects, perhaps of the Low German word Schärbunk, Danish Scorbuck, or the Old Dutch Scheurbuyck, from scheren, to separate or tear, and bunk, the belly. These terms originally denoted rupture of the belly, and afterward scurvy, or scorvy, as it is found in the English dialect. It has also been traced to the Sclavonic word scorb, disease. The first is now believed to be the true etymology.
DEFINITION.—Scurvy is an acquired condition of the body whose essential feature is a perversion of nutrition, which gradually arises from prolonged employment of food deficient in succulent or fresh vegetable matter, and progresses uniformly to a fatal issue, in a longer or shorter time, if the dietetic errors remain uncorrected. This condition becomes manifest by a change in the complexion to a dull yellowish or earthy tint, lassitude, marked decrease in the muscular power, depression of spirits and mental hebetude, breathlessness on the slightest exertion, minute flecks at the roots of the hairs, especially those of the legs; and, later, hemorrhagic effusion into the skin, forming blotches and spots of varying sizes and aspects, which may finally slough and lead to obstinate ulceration; sponginess of the gums, which bleed easily and break down into a detritus that impresses a malodorous taint upon the breath; ecchymotic staining of mucous and serous surfaces, and, in advanced stages of the disease, effusions of bloody serum or of blood into the cavities and tissues of the body.
HISTORY.—Obscure passages in certain of the ancient medical classics (Hippocrates, Celsus) and historical works (Pliny, Strabo) have been considered as descriptive of scurvy, but the earliest trustworthy accounts are to be found in the writings of the thirteenth century. Jacob de Vitry describes an epidemic which occurred among the troops of Count Saarbrücken besieging Damietta in 1218, and Sire de Joinville another epidemic among the troops of Louis IX. lying before the same town in 1249. On both occasions the sufferings of the men were inexpressible and the mortality fearful. The disease was directly traceable to defective supplies of fresh vegetable food, aided by exposure to wet and cold weather, fatigue, and mental depression.
[p. 168]The almost total neglect of horticulture in Europe during the Middle Ages, especially in its more sterile northern portions, the habitual diet of salted, smoked, and dried flesh and fish, and the prolonged spells of cold and damp weather of this region, were conditions most favorable to the development of scurvy, and these regions were the very first in which its devastating effects were early observed and recorded. In the first half of the fifteenth century it prevailed epidemically in the north of Europe and almost everywhere endemically, more especially in the countries bordering on the Baltic and North Seas, although the largest and richest cities were frequently afflicted in the severest manner in consequence of imperfect food-supplies and the wretched sanitary conditions under which the inhabitants lived (Fabricius). The long voyages and imperfect diet of crews of ships furnished a large quota of harrowing nautical experiences with the scurvy, commencing with Vasco da Gama's voyage to India in 1497, and running up to 1812. In this interval it was all but universal on long voyages, both on single ships and in fleets, in the mercantile marine and in the navy.
In 1798, through the better insight into the causes of the disease, and especially through the exertions of Dr. James Lind in ameliorating the dietary of British sailors, it was practically stamped out of the navy or restricted to isolated occurrences. The influence of the success thus achieved was not lost upon the navies of other nations nor upon the growing fleets engaged in commerce, as the disease has become less and less frequent, constituting at present but a very trifling proportion of the diseases incident to seafaring people. This remarkable result is in part attributable to the fact that the chief maritime nations have enacted beneficent laws intended to compel the owners and masters of merchant vessels to observe certain sanitary and hygienic measures that protect the crews from scurvy. The number of cases returned in the English navy for 1881, in an aggregate of 52,487 cases of all diseases, was 4; in the Prussian navy, 3 in 8659; in the Austrian navy, 27 in 8096; in the U.S. navy, none in 13,387. Thus, in a grand total of all diseases in the chief naval services of the world of 82,629 there were only 34 cases of scurvy—a ratio of .41 per 1000. In the mercantile marine 62 cases occurred in 32,613 cases of all diseases, of which 43 were on the Pacific coast: this gives a ratio of 1.9 per 1000. Altogether, the 115,242 cases produced only 96 of scurvy—a ratio of .83 per 1000. The difference in favor of the naval over the marine service is accounted for by the greater attention paid to the health and comfort of the men in the former.
The U.S. steamer Jeannette spent two winters in the Arctic region, and had a single case of scurvy. The U.S. steamer Rodgers was wrecked, and the crew, during its sojourn of six months among the Siberian tribes, suffered severely.
The operations of armies in recent times have not furnished the frightful mortality which, from neglect of sanitary precautions, formerly afflicted them. During the rebellion of 1861-64, out of 807,000 cases there were but 47,000 of scurvy, or 5.8 per cent., with a death-rate of 16 per cent. The French army1 of 103,770 men during the Crimean struggle had 27,000 cases of scurvy, or 26.0 per cent., with a death-rate of 1.5 per [p. 169]cent. In the Bulgarian campaign of 1877-78, in an army of 300,000 strong, there were, according to Pirigoff,2 87,989 cases of disease, of which 4234, or 4.8 per cent., were frankly-expressed cases of scurvy. This gave a proportion of only 1.4 per cent. of the entire force—a result entirely due to the maintenance, both before and during the war, of a high standard of health.
1 Scrive, Rélation Médico-Chirurgicale de la Campagne de l'Orient, Paris, 1857.
2 Krieg Sanitäts-Wesen, Leipzig, 1882.
ETIOLOGY.—Perhaps no disease has furnished a more fertile field for etiological conjectures than scurvy. The father of medicine ranked the disease in one place among those presenting enlarged spleens, and in another with the twisted bowels. He recognized a putrescence of the humors as the underlying factor—a theory that held sway until the beginning of the nineteenth century. The disease attracted wide attention in the seventeenth and eighteenth centuries from its frequent epidemic and endemic occurrence in various parts of the north of Europe, and was believed to be restricted to cold and particularly wet districts—a view that has been long since abandoned with a better knowledge of its habitats. It has been encountered alike in high latitudes north and south, amidst sterile wastes covered with eternal snows and ice, in the temperate zones and in the burning plains of the equatorial regions of America and Africa.
Sex has no predisposing influence, and the fact that more males than females are affected during an epidemic simply indicates that the former are more exposed to the ordinary determining causes. During the siege of Paris, according to the tables of Lasègue and Legroux, there was a very large excess of male cases, and Hayem's figures show only 6 women in 26 cases.
Scurvy has been observed at all ages from infancy to advanced periods of life; it is believed by certain writers that adolescence is less predisposed than adult age.
The epidemic feature of the disease led many to the opinion that it was contagious—a view that retained its hold for many years. It was also considered to be of a miasmatic character, which, with the previous feature, seemed to assimilate it in nature with typhus fever and other diseases of the miasmatic contagious group. This view had a vigorous advocate in Villemin, who in 1874 read a lengthy paper before the Royal Academy of Medicine in its support. His arguments were specious, inconclusive, and inaccurate, the weight both of facts and authority being decisively against his view. Its occurrence among members of the same family led a few to regard it as hereditary, and it was thought to be transmissible from the mother to the recently-born as well as to nursing infants. The depressing influence of certain emotions, fear, anxiety, and nostalgia, upon the functions of nutrition has, as might have been anticipated, been noted as contributing indirectly to the manifestation of epidemics of scurvy in the presence of the essential determining dietetic causes.
Scurvy cannot be regarded, as Lhéridon-Cremorne3 has argued, as the last term of nostalgia, the other alleged causes being secondary; nor as the immediate result of mental depression, as Gueit4 believed from his experience in the ship Henry IV. during his service on the blockade in the Black [p. 170]Sea in 1858, because the disease first invaded those laboring under nostalgia. The currency of such opinions may be readily explained by the fact that ordinarily depressing mental influences occur under the same conditions as those associated with scurvy—viz. during sieges, after defeat, in prisons, and in workhouses; and, further, the mental phenomena ordinarily occur as prodromes of the disease long before the pathognomonic phenomena present themselves. Out of these facts grew the mistake of regarding the mental change as causative instead of consecutive. Murray went farther and regarded mental despondency as at once cause and effect, and long ago scurvy was compared to hypochondriacal diseases.5 It may be concluded from the recorded epidemics that no degree of mental exhilaration could ward off the disease in presence of the determining causes, nor any degree of mental despondency induce it with proper alimentation.
3 Thèse de Paris.
4 Thèse de Montpellier, 1858.
5 Dolée, 1684.
The various qualities or changes in the atmosphere were regarded individually or collectively at various times as the determining causes. It was supposed that the air might become impregnated with putrid exhalations from various sources, as the holds of ships, or rendered impure by the vapors of the sea. The foul air of crowded habitations, vessels, or cities was appealed to, or the common cause was sought either in its temperature or humidity, or in both. The earlier observers gave prominence to cold as a determining cause of scurvy, and especially when combined with dampness, and hence its frequency in the north of Holland, Brabant, Belgium, Russia, and Germany. This was the current view in the seventeenth century. On the other hand, with equal confidence the disease has been supposed to be determined by excessively high temperatures, and its occurrence in India, South Africa, and the equatorial regions has been alleged in support.
Personal habits have been in the eyes of earlier observers an all-sufficient cause, and thus excessive exertion attended with fatigue and exhaustion has been considered the cause of several severe outbreaks on shore and at sea. In contrast with this opinion we find the English physicians placing great stress upon indolent habits and lack of exercise as a predisposing if not a powerfully determining cause.
The use of tobacco was inveighed against by Maynwaring and Harvey as a powerfully morbific cause, while to the lack of the same narcotic its occurrence was ascribed by Van der Mye. More recently it has been referred by Fabre6 to vaso-motor disturbance due to a miasm.
6 Des Rélations Pathogéniques des Troubles Nerveux, etc., Paris, 1880.
In the drink and food, however, most observers have sought the exciting causes of scurvy. Instances have been reported where the disease seems to have depended upon the use of impure water, etc. The imagination has been tortured to seek in some quality or sort of food the specific origin of scurvy. With regard to quantity, it may be stated that in severe famines scurvy may or may not occur according as the food, though scant, is in due proportions of animal and vegetable, though it is true that the ordinary conditions of a famine preclude the procurement of succulent vegetables. The quality of the food has nothing further to do with the production of scurvy than by impairing the general health, for it has often happened that putrid food has been long used without scorbutic symptoms arising. The kind of food is equally [p. 171]innocent, although various special articles have been charged with specific activity. The frequency of scurvy in Brabant was attributed by Ronseus to the use of aquatic birds; Sherwin and Nitsch assigned the same peculiarity to a free use of fish; and Henry Ellis to the too free use of spirits. Even the generally widespread and much-esteemed article of diet sugar was in disrepute with Willis. The too free use of salted meats has been often accused of causing the trouble. The fat rising on water in which salt provisions were boiled was considered by Cook and Vancouver to be of particular pernicious effect, and even the copper vessels in which they were cooked were condemned by Travis as able to communicate the scorbutic poison to the food. To the milk of animals browsing on verdure upon which pernicious dew had fallen was referred an epidemic which occurred in Silesia in 1591. Diseased potatoes were considered sufficient to determine scurvy in Ireland and Scotland by O'Brien.
The scurvy occurring on land was deemed to be different from that occurring at sea, and its frequency afloat brought into unmerited disrepute the sailor's salt diet, and its saline materials were even considered the chief offending cause. This idea was rejected by numerous observers, who assigned as the chief causative rôle in scurvy deficiency in vegetable food, especially of the fresh, succulent variety. The particular constituent of this sort of food, so powerful in warding off scurvy and of curing it when prevention has failed, has baffled discovery. Dr. Aldridge attributed it to mineral elements generally. Dr. Garrod singled out the potassic salts as the particular one to which the specific action must be attributed; but neither of these views has gained in credit. From all the facts, both positive and negative, we may reasonably assume that the essential dietetic error leading to the development of scurvy, in the immense majority if not in all cases, consists in a deficiency in the variety of food; that is to say, there is not the requisite proportion of animal matter with a diversity of vegetable substances. No single natural order contains plants that supply all the elements essential to the nutrition of the body and the right composition of the blood. The graminaceous and leguminous articles of food, for instance, are numerous, but not various; they all afford the same or analogous albuminous elements, which have about the same nutrient value as the corresponding substances in animal food, and hence health and vigor cannot be sustained on a diet of flesh, combined with wheat, rice, and oatmeal or with beans and peas, or with all of them together. Outbreaks of scurvy have occurred on shipboard, where the ration is made up principally of these articles; as in Anson's ship, when supplied with an abundance of fresh animal, farinaceous, and leguminous foods. It is clear, therefore, that in order to obtain a variety of materials required in nutrition, we must resort to several of the natural groups, those particularly which comprise the succulent vegetables and fruits.
MORBID ANATOMY.—The bodies of persons dead of scurvy are, in most cases, much emaciated, because the quantity as well as the quality of the food has usually been defective. When the food-supply is abundant and only lacking in the elements indispensable in warding off scurvy, the bodily weight is not noticeably decreased, although the characteristic tissue-changes of scurvy are present. This was noticeable in the cases recorded by Trotter of negro slaves dying of scurvy while their bodies [p. 172]presented a fat and sleek appearance. Rigor mortis usually sets in early, and chemical decomposition invades the tissues speedily. The skin presents the discolorations and blotchings observed during life. The subcutaneous connective tissues are soaked with serous exudations, especially in the lower extremities, and in various localities are infiltrated with bloody or fibrinous extravasations. The same changes occasionally affect the muscles, the infiltration occurring beneath the fibrous sheaths and into the intermuscular spaces, and the fibres are more or less torn. These effusions occur most frequently about the knees, the elbows, and the pterygoid muscles of the jaw.
The bones are sometimes necrosed by the mechanical influence of copious effusion beneath the periosteum, forming nodes of varying sizes and obstructing the supply of blood. The joints are occupied by serous or bloody transudations; their synovial investment is destroyed in part, so that the cartilage is exposed; and the latter not infrequently is softened, and even separated from the subjacent osseous connections. Sometimes the morbid changes occurring in the joints are the results of disease in the subcutaneous connective tissues surrounding them.
The muscular system presents marked changes. The muscles undergo fatty degeneration in a remarkable degree. The changes begin first in the lumbar muscles, the fibres losing their striations and sarcolemma, and finally being replaced by granular and fatty matter.
The brain has been found in rare instances the seat of softening and infiltration, and the ventricles may contain serous or bloody fluid. Similar effusions have also been noted in the arachnoid. Most frequently, however, the brain and its membranes present an anæmic appearance, there is less blood than natural in the vessels, and the tissues are pale. Very often no changes whatever are observed.
The heart is smaller than normal, relaxed, and flabby, its fibres easily broken, and a cut surface presents the yellowish aspect of fatty degeneration in certain parts, with occasional extravasations located in the cardiac walls. The valves of the heart are relaxed and illy adapted to accurate closure. In certain recent cases soft coagula or dark fluid blood, and in others firmly coagulated blood, are found in the cavities; in those which have been prolonged the blood is more likely to be found fluid and the coagula diffluent. The endocardium is often blotched to a greater or less extent by sanguineous imbibition. The pericardium often contains serum, and in the worst cases is inflamed, lacerable, and contains bloody effusions. The inner surface of the great vessels at the base of the heart is stained by imbibition.
The respiratory organs are variously affected. The mucous membrane lining the nose, larynx, and trachea is generally pale and flecked with extravasations of a dark-red color; more or less frothy fluid, tinged with blood, is present in these passages, and occasionally oedema of the glottis is encountered. The lungs are, as a rule, infiltrated with a bloody serosity, particularly in those cases with renal complication, or with a fibrinous or bloody exudation. The posterior portions of the lobes often present evidences of hypostatic congestion, or even of gangrene, and in the latter case the tissue is easily friable and emits a disagreeable odor. Their surfaces are mottled with superficial discolored patches of varying size and outline. The lungs may, on the other hand, be found pale, [p. 173]with empty collapsed vessels and with little or no effusion. The pleural cavities commonly contain a serous fluid, or, in rare cases, a copious effusion of blood. Traces of inflammation and discoloration by sanguineous staining are traceable on the pleural surfaces.
The digestive organs furnish strongly marked lesions. The mouth presents the most constant scorbutic feature, a stomatitis in which the gums are infiltrated, spongy, livid, and the seat of fatty degeneration; the teeth are loosened or have already fallen out. The stomach and small intestines are thin-walled, and the mucous membrane is often softened, and in places ulcerated; similar changes have been noted in the solitary glands. Follicular ulceration of the large intestine occurs, with softening and infiltration of the mucous membrane. Hemorrhagic effusions into the mucous membrane, forming stippling, flecks, or patches, occur in various degrees along the whole extent of the alimentary canal. The pancreas is occasionally found softened and containing hemorrhagic effusions.
The kidneys are, as a rule, found in the normal condition in cases in which albumen has been observed in the urine. Occasionally they are engorged, with infarction of the cortical substance, and the mucous lining softened and thickened and covered with blood-tinged mucus, or they may present various degrees of parenchymatous degeneration. The ureters and bladder sometimes present ecchymotic spots, and the contained urine is mingled with blood.
The liver is always more or less altered by fatty degeneration, and at times replete with blood and softened, and its surface ecchymotic. The spleen is occasionally greatly enlarged, and its tissues very lacerable, laden with blood, and infarcted.
PATHOLOGY.—The essential character of scurvy consists in perverted nutrition, in which the blood undergoes such peculiar and profound changes that its fitness for the maintenance and renewal of the various tissues and organs is impaired; hence the nervous depression, loss of muscular power and tonicity of tissues, and the transudation of the blood or of its constituent parts.
The processes of secondary assimilation are chiefly at fault, leading to the blood-changes, and through these to the textural lesions. Primary assimilation remains intact, as the bodily weight is little altered as long as the food is in sufficient quantity. This loss of nutritive balance between the blood and tissue is due to the absence of certain elements furnished by fresh vegetable matter. What these are, and how their absence acts in inducing this disturbance, have not yet been determined; we only know that the mysterious harmony of the vital, chemical, and physical relations which exist between the blood and tissues in health is deranged by their absence.
Endless explanatory surmises and assumptions have been proffered. The earlier explanations involve either the Galenical theory of putrefaction of the fluids and humors, a breaking down of the blood-corpuscles, or the later chemical theories of superabundance or absence of certain salts, sulphur, etc., and hence there were an acid scurvy, an alkaline scurvy, a muriatic scurvy, etc.
The frequent effusions of blood in scurvy led Andral to suspect that the chief peculiarity in scorbutic blood was the decrease of fibrin; which was [p. 174]in perfect accord with a theory that he had formed that this change was the uniform cause of passive hemorrhage. Magendie had already given experimental support to this conjecture by inducing in animals phenomena analogous to those of scurvy by the injection into the veins of defibrinated blood or of alkaline solutions. Andral7 believed his views confirmed when in 1841 he analyzed on two occasions the blood of scorbutic patients and found the fibrin reduced to 1.6 parts per 1000. Similar results were obtained by Eckstein and Frémy. On the other hand, the blood was analyzed by Busk, about the same time, in three well-marked cases of scurvy that occurred on the Dreadnaught hospital-ship, and in all of them the fibrin was in excess of the normal amount, the least being 4.5 and the greatest 6.5 parts per 1000. In perfect accord with Busk's results were the analyses of the blood of five scorbutic females, communicated in a note to the Academy of Sciences in 1847 by Becquerel and Rodier. In no case was the fibrin diminished, but in some it was sensibly increased. In a subsequent case Andral found that the fibrin, instead of being less, exceeded the physiological mean, reaching 4.4 parts, and he concluded that a diminution of this element was not a necessary and common occurrence, but only an effect—a result of prior morbid modifications, and a consequence which was produced more or less frequently according to the severity and duration of the disease. Parmentier and Déyeux found the blood of three scorbutics to resemble inflammatory blood in respect to fibrin, while Frick obtained in one analysis 7.6 parts of fibrin and Leven 4.3 parts.
7 Essai d'hématologie pathologique.
In mild cases of scurvy neither the color, the alkalinity, nor the coagulability of the blood differs from that of blood in health, though Wood alleges that the clot is loose and cotton-like, and Canstatt that its coagulability, in consequence of the large proportion of saline matters, is diminished. In Busk's cases the separation of the clot and serum was as perfect, and took place as rapidly, as in healthy blood, and in two of them the blood was both buffed and cupped, as it was also in Leven's cases. In two of the most severe of Becquerel's cases the blood coagulated firmly, and in a slight case the clot was dark and loose. The albumen of the blood shows no marked change as regards its quantity. The five analyses of Becquerel and Rodier showed the average amount of organic matters of the serum to be 64.3 parts in 1000, the smallest being 56.2 and the largest 69.2 parts. 1000 parts of the serum of the same cases gave an average of 72.1 parts of organic matter. Frick's single case gave 87.045 parts per 1000, and the average of Busk's was 78.2 parts, while Chotin and Bouvier obtained only 62.3 parts. The last-mentioned writers have recorded a fact in connection with the physical characters of scorbutic blood that deserves notice: the blood in one case did not coagulate at the usual temperature (about 158° F.), but required a temperature some degrees higher for that purpose. The red corpuscles in all the foregoing cases were notably diminished, the largest amount given being 117.078 parts per 1000, while the lowest was 47.8 parts. In Andral's second case the globules had decreased to 44.4 parts per 1000, the lowest amount yet recorded.
The alkalinity of the blood seems not to be changed, although Chotin and Bouvier noticed a slight increase. The saline constituents do not [p. 175]vary greatly from the normal standard. The average amount in the cases of Becquerel and Rodier and Busk was 8.1 per 1000, the smallest being 5.5 parts and the largest 11.5. In Ritchie's two analyses the proportion of saline matters is given as 6.44 and 6.82 parts per 1000. Opitz and Schneider have found less than the physiological mean. In Frick's case the amount was 8.8, the iron being 0.721 parts per 1000, and 0.782 to 127 parts of globules; lime 0.110, chlorides 6.846, and phosphates 1.116 parts per 1000. The iron was in excess of that in the normal blood, but in Becquerel's cases the mean was 0.381—less than the normal. The proportion of iron in Duchet's cases was respectively 0.393, 0.402, and 0.476 parts, giving a mean of 0.423 parts per 1000, which nearly approximates the normal. Garrod in one analysis of the blood found a deficiency of the potassium salts, upon which he erected his well-known theory of the etiology of the disease. It is an interesting fact that in the physiological state the quantity of sodium chloride is not subject to variation, any excess introduced with the food being thrown off by the kidneys. The quantity in the urine bears a relation to the amount introduced as food, but the proportion in the blood is constant.
The quantity of water in the blood has been found to be increased in all the analyses which have been made. Chotin and Bouvier estimated water and loss at 831.1; in Frick's case it was 791.69 parts per 1000; and in Becquerel's five cases it was put at 807.7, 810.9, 811, 813.7, and 854.0 parts per 1000, respectively. In Busk's three cases the lowest amount was 835.9 and the highest 849.9 parts per 1000. The specific gravity of the defibrinated blood was in all cases low in comparison with the normal standard (1057), the average in Becquerel and Rodier's cases being 1047.2, the lowest 1083.3, and the highest 1051.7. In the single observation of Chotin and Bouvier it was 1060. The specific gravity of the serum was also less than normal (1027), the average of four of Becquerel's analyses giving 1023.8, the lowest 1020.8, and the highest 1025.5. Busk gives 1025 in one case and 1028 in another.
The results of the most recent analyses, those of Chalvet, are shown in the following table, in which scorbutic blood is contrasted with that of a healthy, robust female:
| Scorbutic blood. | Healthy blood. | |
| Water | 848.492 | 772.225 |
| Solid matters | 151.508 | 220.775 |
| Dry clot | 140.194 | 209.000 |
| Albumen | 72.304 | 68.717 |
| Fibrin | 4.342 | 2.162 |
| Globules | 63.548 | 138.121 |
| Extractive matter—by absolute alcohol | 10.312 | 8.013 |
| Extractive matter—by ether | 1.002 | 1.300 |
| Ashes of clot | 3.000 | 5.691 |
| Peroxide of iron of globules | 1.060 | 2.259 |
| Potassium of globules | 0.329 | 0.625 |
From the conflicting statements of various observers the following conclusions may be drawn: that in scorbutic blood water is in excess; that there is, on the one hand, a marked increase of the fibrin, and in a less degree of the albumen and extractive matters, while on the other hand there is a marked decrease of the globules and in a less degree of the mineral matters. On the authority of Chalvet it may be also stated [p. 176]that demineralization of the muscular tissue is a notable chemical feature in scurvy.
So far, microscopic examination has been entirely negative. Hayem8 found no appreciable alteration from healthy blood, and in this view Leven9 concurs; while Laboulbène10 notes the occurrence of an unusual number of white globules.
8 Mém. de la Société de Biologie.
9 Communication to the Académie des Sciences, 1871.
10 Epidemie de Scorbut.
Petrone Luigi11 injected scorbutic blood into the connective tissue of rabbits. In three instances the animals died, presenting on the ears distinct evidences of the formation of petechial extravasations. The viscera revealed everywhere bloody effusions of larger or smaller size. The spleen was enlarged and its parenchyma and capsule distended. In the blood were found oval, shining, spontaneously-moving corpuscles, which he regarded as the bearers of the specific poison of scurvy.
11 Annali Univers. di Med. c. Chir., 10, 1880.
SYMPTOMS.—The symptoms of scurvy are insidiously and usually slowly developed under the influence of the efficient causes, and the disease runs a chronic course, often extending over five or six months, especially in cases in which the hygienic surroundings of the patient have been imperfectly or not at all rectified. In light cases the course is much shorter. A gradual alteration of the nutritive processes first occurs, until what might be called a scorbutic cachexia is established in a period varying from a few weeks to several months. The initial symptoms consist in the skin losing its color and tone and assuming a yellowish or earthy hue: it is relaxed, dry, unperspiring, and rough; in the legs particularly this roughness is very marked, and the skin, when rubbed, sheds an abundance of furfuraceous scales. The cutaneous follicles, markedly on the extensor aspect of the lower extremities, are prominent, similar in appearance and feel to the condition known as goose-flesh. Rouppe12 calls this the signum primum pathognomonicum. Dark-red or brownish flecks, of a circular outline and of varying but small size, not unlike flea-bites, appear on the face and limbs. The cutaneous circulation is feeble and the superficial warmth less than natural; slight depression of the atmospheric temperature produces a sensation of chilliness, and the feet and hands are cold. On assuming the erect posture the patient complains of headache and dizziness. The muscles are relaxed and soft to the feel, and a corresponding loss of vigor and strength is experienced by the patient, who is indisposed to exert himself in the performance of his customary duties and seeks repose and freedom from feelings of fatigue and languor in recumbency. This prostration is occasionally so extreme that the slightest efforts in attempting to stand or walk are attended with rapid action of the heart, accelerated respiratory movements, and a sense of suffocation and breathlessness. The general circulation is impaired; the heart acts feebly; the arteries are contracted; and the pulse is slow, small, and compressible.
12 De morbis navigantium.
The mental powers are equally impaired. The face wears a haggard appearance and depressed expression; gloomy forebodings of evil and disinclination to turn the attention to the usual mental pursuits are markedly present—a disinclination that may subsequently merge into complete apathy or indifference to passing events, or even into somnolency.
[p. 177]Pains in the legs, joints, and loins are early manifestations: they closely resemble those of rheumatism, for which they are often mistaken. The pains are not exacerbated at night, but, on the contrary, are often more severe by day. Not unfrequently lancinating pains in the muscles of the chest are complained of. The sleep is not disturbed until the disease has made some advance, when it becomes broken and is no longer refreshing.
The appetite is usually unimpaired in the early periods of the disease, and even throughout its course the condition of the mouth alone prevents the patient from indulging his desire for food, even, as is occasionally noticed, to voracity. There may be a yearning for certain articles of diet, principally those of an acid character; but, on the other hand, some cases present exactly the reverse condition—a disgust for food in general or for particular varieties; or the appetite may be vacillating, at one time craving and at another repelling nourishment. There is no noticeable change in the normal thirst, except on the occurrence of febrile complications, when it is increased. The gums do not, at this stage of the disease, present the livid, swollen appearance of fully-developed scurvy, but, on the contrary, are generally paler than usual, with a slight tumid or everted line on their free margins, and are slightly tender on pressure. The breath is commonly offensive, and the patient complains of a bad taste in the mouth. The tongue is flabby and large, though clean and pale, and the bowels are inclined to be sluggish.
This preliminary stage is followed, after varying intervals of time, by certain local phenomena which are quite characteristic of the disease. There is a marked tendency to extravasation of blood into the tissues, either causelessly or upon the infliction of slight injuries or wounds. Fibrinous exudations occur sooner or later into the gums, which become darkened in color, inflamed, swollen, spongy, and bleed upon the slightest touch or even spontaneously, and finally separate from the teeth. These results are due, in part, to the considerable amount of pressure to which these parts are subject in mastication, and it is a conspicuous fact that the gums of edentulous jaws remain free from these changes. In a few cases the gums are but slightly altered, perhaps oedematous only or pitting upon pressure, or they become the site of bloody extravasations. In severer examples, in later stages of the disease, these various alterations progress to an extreme degree, and the extravasation is so voluminous that the gums present great, fungous, lacerable excrescences, which may finally break down into a suppurating, brownish, and very fetid mass, communicating to the breath an odor of a most offensive character. In certain epidemics of scurvy, notably in that of Florence described by Cipriani, the lesions of the gums were absent. The rest of the mucous membrane of the mouth remains unaltered, or at most slightly ecchymotic. Samson and Charpentier13 in a large number of cases saw this but once, and in one of Leven's14 cases the fungous growth invaded the palatal mucous membrane, extending to the anterior pillars of the fauces. The salivary glands are enlarged and swollen; the tongue is imprinted with the form of the teeth, while the latter become encrusted with tartar and more or less concealed by the exuberant gums, or, becoming gradually loosened from the alveoli, finally drop out. The morbid process may extend to the bone itself, and necrosis and extensive [p. 178]exfoliation follow. Mastication is more or less painful, and often impossible, so that the patient is reduced to the necessity of prolonging life by the use of fluid or semi-solid food. Under the influence of appropriate treatment it is remarkable how rapidly (in from two to four weeks) these marked changes recede and the parts resume their normal condition, yet it occasionally occurs that permanent, callous thickening of the gums results.
13 Étude sur le Scorbut, 1871.
14 Une épidémie de Scorbut, p. 28, 1872.
In the progress of the disease effusions of blood under the skin are of early occurrence. They are at first located in the superficial stratum of the cutis or just beneath the epidermis, especially around the roots of the hair, and present themselves as roundish, bluish-red flecks, varying in size from that of a pin's head to that of a split pea, not effaceable by pressure with the tip of the finger, but slightly, if at all, elevated above the surface, and enduring for weeks together. The nutrition of the hair-follicles is impaired, so that the hairs are often either lost, broken, or distorted. These petechiæ fade in color with progressive improvement in the case, and finally disappear, leaving brownish-yellow discolorations. They first appear on the extremities, particularly the lower limbs, then on the face, and lastly on the trunk. At a later period extravasations of a larger size and more irregular form occur in the deeper layers of the derma. They vary in size from that of a finger-nail to blotches two or three inches in diameter; at first reddish in color and subsequently of a bluish red. When recession occurs under appropriate treatment, the color passes through various shades of violet, blue, green, and yellow, as in ordinary traumatic ecchymosis. Outpourings of blood also occur into the subcutaneous connective tissue, notably that of the legs, and in localities where connective tissue is particularly abundant and loose, as in the ham and axilla. The dispersion of blood in this tissue may be so considerable as to cause the legs from the knees down to present a uniform dark-blue coloration that in form may not inaptly be compared to a stocking. The upper extremities also suffer, usually on their inner side from the armpit down, the extravasation rarely reaching, however, to the hand. These extravasations may take place after the infliction of very slight injuries, as from blows or the pressure of hard bodies, or even from the mechanical effects of prolonged dependency of the limbs, as in riding on horseback. Extravasations of a similar nature are occasionally present in the connective tissues of the muscles themselves or between them, giving rise to swellings of various forms and dimensions. Nearly always along with the sanguineous effusions there is more or less oedema, usually beginning at the ankles and gradually extending upward; in some cases there are puffiness of the face and general anasarca, so that deep pits remain on pressure.
This profound impairment of nutrition of the skin continuing, in the worst cases blood is effused beneath the cuticle, forming blebs of varying size, which finally break and leave superficial ulcerated surfaces, that ultimately become covered with flabby, exuberant granulations, pouring out a purulent often offensive sanies and bleeding upon the slightest touch.
In some cases the ulceration begins in the petechiæ at the hair-roots, and a number of these, running together, form a large ulcer. The destruction of tissue by ulceration is disposed to spread more widely and deeply, and is often of a most intractable character. Old cicatrices [p. 179]are the first tissues in these cases to take on the ulcerative action. Certain muscles, chiefly those of the legs, and notably the gastrocnemii, the abdominal and pectoral muscles, the psoas magnus, and pterygoids, may become the seat of fibrinous extravasations, which finally change, by lapse of time, into hard, firm tumors, impairing the functions of those parts and leading to contractions of the limbs.
The symptoms in certain epidemics of extraordinary severity have displayed alterations in still deeper structures. Effusions occur between the periosteum and the bone, forming painful, hard, and resisting nodes of varying dimensions, especially along the course of the tibiæ, upon the scapulæ, and upon the maxillæ. In young persons the epiphyses are separated from the shaft of the long bones, and in other cases the ribs become necrosed and disarticulated from the sternum, producing a creaking noise during respiratory movements, as related by Poupart.15 This occurs mostly on one side and about the middle of the series, yet it has been noted to occur on both sides, so that the sternum and attached cartilages, deprived of support, were perceptibly sunken. Oserctzkowski16 reports two fatal cases of scurvy attended with spontaneous fracture of the ribs. There was extravasation into and beneath the periosteum, and subsequent destruction of the continuity of the bone. In one case the ribs on both sides were affected, so that the anterior wall of the thorax sunk in and embarrassed the respiration, which was chiefly maintained by the diaphragm. Inflammation of the lungs succeeded, and the patient died in agony.
15 Mémoires de l'Académie des Sciences, p. 237, 1699, and Philosophical Transactions, vol. xv.
16 Wratsel, No. 51, 1881.
Recently-repaired fractures have been known to recur under the influence of scurvy from the destruction of the callus.17
17 Anson's Voyage Around the World, edited by Walter.
The articulations as well as the bones in very severe cases of scurvy present evidences of disease, consisting in periostitic effusions which involve the surrounding soft parts, producing impairment of motion, enlargement, and false ankylosis, and even destroying the normal anatomical relation of the osseous surfaces, so as to determine deformities. These changes are usually attended with severe pain, and most commonly occur in the ankle-, knee-, shoulder-, and hip-joints, and disappear tardily, requiring perhaps months for their recession, if indeed this takes place at all.
The symptoms manifested by the circulatory organs are prominent from an early period of the disease. The pulsations of the heart are slower, feebler, irregular, and often intermittent; its impulse is decreased or becomes quite imperceptible; and when the associated anæmia has progressed to a certain extent a systolic murmur may be audible. The arterial and venous channels are of diminished calibre; the pulse becomes soft, of less volume, and tardier; and a venous murmur may sometimes be heard in the cervical veins. The remarkable nutritive changes in the capillary walls in part account for the numerous hemorrhages which occur both by rhexis and diapedesis. The most frequent is epistaxis; the slightest blows, sneezing, or blowing the nose will often determine it, or it may occur spontaneously, and in severer cases with such profuseness as to threaten impending dissolution, requiring nothing less than timeous introduction of the tampon to rescue the victim. Hemorrhage from the [p. 180]lungs is of rare occurrence, and when it does happen is rather indicative of pre-existing pulmonary disease, such as phthisis, or of the approach of a complication, such as infarction or gangrene, than a constituent feature of scurvy. Hæmatemesis is less uncommon, but is by no means frequent; the blood ejected from the stomach is usually small in quantity, but in isolated examples the bleeding is profuse, producing great exhaustion and a sense of cardiac depression which preludes speedy death. Hemorrhage from the bowels is also an ill-omened feature, completely blanching the patient and presaging early exhaustion and death. Blood may also appear as a product of a complicating dysentery which determines abundant, offensive discharges that may run on for several weeks before the patient is finally exhausted. Hæmaturia sometimes occurs, especially in broken-down and cachectic subjects and in an advanced stage of scurvy. All of these forms of hemorrhagic effusion, now mentioned as localized in the mucous membranes, are to be deprecated as exercising a pernicious influence, seriously aggravating ordinary cases and fatally jeopardizing the issue of severe ones.
Effusive and inflammatory complications are also encountered in the serous structures, and usually in cases of great severity, though they occasionally present themselves when the more common localized phenomena of scurvy are not particularly prominent. These complications may be marked by a gradual accession, or they may rapidly arise and involve the patient, just before in apparent security, in the greatest peril. These incursions are almost always attended by febrile exacerbations and the usual grouping of clinical characters denotive of the same pathological conditions arising under ordinary circumstances. The local complications may either affect the pleura or pericardium, or both. In Karairajew's18 60 autopsic examinations pericardial effusions were noticed in 30, pleural in 30, pericardial and pleural in 6, peritoneal in 7, and arachnoidal in only 1. The exudations are sero-sanguinolent or fibrinous in character, and sometimes reach the inordinate quantity of four or five pounds, occasioning the patient the utmost distress and embarrassing the respiratory and circulatory functions. Although these augment in a high degree the risk to life, yet under prompt and appropriate treatment recovery may take place and the effusions vanish with surprising rapidity.
18 Himmelstiern, Beobachtungen über den Scorbut, S. 50, Berlin, 1843.
Hemorrhagic extravasation into the nervous centres is a very rare occurrence. It has not been as yet recorded as having occurred in the brain-substance itself, but has in several instances been noted between the meninges, producing headache, dizziness, vertigo, and sometimes somnolence, delirium, and coma. Opitz19 relates an interesting case in which convulsions suddenly occurred with unconsciousness, followed by hemiplegia of the left side of the body and the corresponding side of the face. After twenty-four hours consciousness returned and the paralysis disappeared. There were, however, headache and hyperæsthesia of the upper extremities present; twelve days later these also receded, and the patient finally recovered. The same author records paralysis as occurring in one case from extravasation into the spinal meninges. Samson observed an instance in which a fibrinous effusion formed upon the sciatic nerve, with consequent pain.
19 Prag. Vierteljahrschrift, S. 153, 1861.
[p. 181]In the circulatory system symptoms always of threatening and often of fatal import may arise: embolism may occur at various points, particularly in the lungs and spleen, occasioning hemorrhagic infarctions, which have undoubtedly been the occasion of the sudden deaths sometimes observed in scorbutic cases not apparently of a very dangerous form nor attended with an excessive degree of exhaustion.
The urinary system supplies no prominent symptoms; the statements as to the condition of the kidneys and the composition of the urine are contradictory. The urine not infrequently contains albumen, particularly in severe cases, but this is by no means indicative of corresponding changes in the renal structure: on the contrary, this may be found after death to be apparently free from disease.
The conclusions that would seem to be authorized by the statements of various authorities are that the quantity of urine passed is decreased, as well as that of the urea, while the amounts of the albuminoid and mineral matters are increased.
Physical examination will reveal the frequent occurrence of enlargement of the spleen, independent of malarial influences, and Krebel has encountered one case in which the liver was involved in inflammation.
Some derangement of the visual organs is present in many cases. Foltz, in the epidemic on the Raritan, reported four cases of nyctalopia and two of hemeralopia, and other affections of the eye, such as conjunctivitis, induration and irritation of the ciliary margins of the lids, with a copious and acrimonious discharge, these conditions being obviously due to the scorbutic diathesis. Medical Director J. Y. Taylor, U.S. Navy, in a private communication to me states that hemeralopia was a frequent premonitory symptom of scurvy that occurred in the U.S. sloop-of-war Decatur in 1854 during a laborious and tedious passage of three months through the Straits of Magellan. The men were overworked and much exposed to cold and wet, and part of the time were on diminished rations. The hemeralopia was at first erroneously attributed to the reflection from the snow and glaciers—a species of snow-blindness—but other phenomena speedily appeared in a majority of the causes: a subacute inflammation, with considerable pain and swelling of the small joints, especially those of the toes; sore and tender gums, although only a few progressed so far as to exhibit sponginess or bleeding; and debility, depression, anxiety, and insomnia. In a few cases the blindness was so complete as to render their subjects almost helpless after sunset. This was the most pronounced and remarkable symptom and the one most complained of. These incipient scorbutic symptoms were promptly arrested by the free use of wild celery (Apium graveolens), which was found growing abundantly in sheltered places. The short rations were also supplemented advantageously by mussels (Mytilus edulis) whenever they could be obtained. A few weeks later the crew appeared to be in ordinary health.
Hemorrhage may occur under the conjunctiva, raising it into small pouches; into the anterior chamber, causing iritis and adhesions; and, finally, into the choroid and vitreous humor, exciting a general inflammation of the entire organ.
Dulness of hearing and buzzing in the ears have also been signalized as occasional symptoms of scurvy.
[p. 182]The phenomena of fever are always absent during the course of uncomplicated scurvy, the temperature of the mouth sometimes falling as low as 92° F., and being always one or two degrees lower than normal. It is only in the later periods of the disease, when pathological processes most often supervene in the internal organs, that an elevated temperature and the other ordinary symptoms of fever are manifested. The lowered vital resistance of scorbutic subjects particularly disposes them to the incursions of fevers, especially those of malarial and typhoid types: hence in the low, marshy districts of Northern Europe and in sections of country afflicted by famine and overcrowded dwellings these complications are very common.
DIAGNOSIS.—Little or no difficulty will be encountered in discriminating scurvy from other diseases under the circumstances that usually surround its development and prevalence. These circumstances are altogether peculiar and characteristic, and involve the absence of succulent vegetable food as the prime factor, and exposure to cold, fatigue, mental despondency, or other depressing influences as accessory in its production. This combination of causes has been usually witnessed in all the outbreaks of scurvy in camps, besieged towns, on shipboard, particularly on ships in Arctic service.
Sporadic cases may escape immediate identification in the absence of some of these circumstances, but a close attention to the symptoms will surely lead to a correct conclusion. The scorbutic cachexia denoted by the sallow or earthy hue of the skin; the spongy gums; the discoloration of the surface; pains in the limbs and joints; the sense of weariness, and, later, the exhaustion, dyspnoea on the slightest exertion; the bloody and fibrinous effusions into the connective tissues and muscles about the joints, and into the pleuræ, pericardium, and peritoneum; the stiffness and contraction of the legs,—furnish a complexus of phenomena not met with in any other disease than scurvy. The discoloration of the skin in purpura, leucocythæmia, anæmia, chlorosis, and hæmatophilia, or other conditions involving hemorrhagic extravasation, are easily discriminated from those of scurvy when taken in connection with the other symptoms and the history of those diseases. In the beginning of scurvy the pains in the back and limbs might divert the attention to rheumatism, but an examination at this early stage will, in all likelihood, disclose the peculiar gingival and cutaneous lesions of scurvy.
The rapid improvement of scorbutic cases under a fruit and vegetable diet is also a noticeable feature not witnessed in any of the foregoing diseases.
PROGNOSIS.—The prognosis of scurvy is always favorable in the early stages, and even in the very worst recovery occurs under improved hygienic surroundings with remarkable promptness and certainty. It must not be overlooked, however, that sudden death may occur in seemingly light cases from failure of the heart's action or from embolism. There is a ready disposition to the recurrence of the disease under slight causes, and it may so impair the health as to lead to the development of other fatal maladies. The gravity of the case is to be gauged not so much by its seeming severity as by the accessibility of proper food-supplies, for without these the worst results may be expected. Where the case is embarrassed with complications of the respiratory and circulatory [p. 183]organs, involvement of the bones, and intercurrent diseases, the outlook becomes correspondingly grave.
Throughout the world, in recent times, greater areas of territory are devoted to agriculture and horticulture, and the products are distributed over wide extents of country by the increased facilities of communication by the highways and railroads, so that it would now be impossible for an epidemic of scurvy to devastate a region of country so provided as it did a century ago, or might do and has done in regions of country where tillage is neglected and communications are cut off by an absence of roads from more productive centres, as in Southern and Eastern Russia.
Hygienic improvements that have almost stamped out scurvy on shore have also done good service for mariners, and thousands of ships now cross the ocean on long cruises with perfect security from the disease. In the naval services of the world, as has been already shown, the disease is rarely encountered, and it is greatly diminished in the merchant marine, from which, it is hoped, in a few years, by a more rigid enforcement of existing laws for the protection of sailors, it may also entirely disappear. Even in exceptionally long and arduous cruises, as in the Arctic regions, the disease may be arrested, as was the case with the Jeannette, which was drifted about, locked up in ice, for sixteen months, yet only a single case of scurvy appeared.
It is of the first importance to enlist a healthy crew for long voyages, free from previous syphilitic, scorbutic, or other constitutional taint; then, by observing proper hygienic precautions, to maintain their health. One of the prime factors in securing this result is a suitable dietary. The improved methods of preserving food afford facilities for storing up adequate quantities of both kinds, animal and vegetable, to last the cruise. To economize these stores it will be well to start with a stock of live animals and recent vegetables, such as can be now had in almost any quantity in any considerable maritime city, and not until these are consumed are the canned and preserved supplies to be opened. All the ordinary meats, as beef, mutton, veal, and lamb; most vegetable products, as asparagus, beans, peas, potatoes, and a great variety of fruits, as peaches, plums, berries, etc., are obtainable at moderate expense, and should form an integral portion of the ration. Eggs can be easily preserved so as to keep for months by simply packing them in plaster or in salt, and they furnish a valuable and acceptable article of diet. Among articles of great nutritive value milk takes high rank, and it can be preserved sweet and pure indefinitely. Sauer-kraut is an antiscorbutic of considerable virtue, and should not be overlooked in laying in stores for a distant cruise. Cheese and oatmeal will be found useful additions to the ordinary ration.
It may be proper to state in the event of the occurrence of scurvy and the exhaustion of the fresh vegetable stores that various quickly-growing vegetables, such as mustard, radishes, turnips, and cresses, could be cultivated on shipboard if seeds are provided.
With such a varied dietary, comprehended in the above enumeration, it would be impossible for scurvy to invade the ship's company, especially when aided by other wholesome agencies, as cleanliness, well-ventilated and dry sleeping rooms, and clothing adapted to the weather. The antiscorbutic virtues of lime-juice were known long ago, being mentioned by [p. 184]Albertus in 1593, but it was not until many years later that it became an integral part of the English navy-ration. The law requires it to be carried on board all merchant vessels, and to be served out ten days after the crew has been living on salt rations. The juice keeps well if properly prepared and preserved from contact with air, especially when fortified with a small quantity of alcohol, the usual strength being about 10 per cent. It should be carried in vessels containing just enough to furnish a few days' rations to the whole crew, by which plan only a small amount need be exposed to the decomposing influence of the air. The juice can be reduced by evaporation to a very small bulk. This method was adopted in supplying the Arctic cruiser Rodgers.20 The juice was reduced to a paste, each pound of which represented one gallon of the solution of the ordinary strength. It has also been used in the form of lozenges and biscuit. It may be stated that great reliance has been placed upon malt, the acid wines, and cider as good antiscorbutics.
20 Report of the Surgeon-General of the Navy for 1880.
In connection with the food-supplies it is proper to mention those influences of a depressing character which have a tendency to favor the development of scurvy. The first is dampness in the sleeping apartments of the men. This should be prevented by ventilation, drying stoves, and taking care that no wet garments are permitted to remain in the apartments. They should be taken off immediately and hung outside to dry, and under no circumstances should the men be permitted to sleep in them, as is sometimes done.
Exposure to cold is unavoidable under certain conditions, and the men should then be protected by proper clothing adapted to the weather. Protracted fatigue is a third favoring circumstance, and the crew should be spared all the strain of hard work possible, especially in high latitudes. The apartments should also be kept well ventilated and scrupulously clean; and, lastly, depressing mental emotions, which are so apt to arise from exposure to danger and want, should be dispelled by cheering assurances, constant occupation, and whatever amusements can be had. These are the chief influences which are to be considered in adopting measures to prevent the occurrence of scurvy in communities, armies, on shipboard, or in persons confined in houses of detention.
The therapeusis of scurvy presents no intricate problems for solution. Its origin in dietetic errors is admitted by almost common consent, and it is surprising with what rapidity patients apparently beyond hope of recovery gather health and strength with a change in the character of the food. This is indispensable in the treatment, as drugs have little or no curative influence without it; and, therefore, the first object should be to supply the patient with lemon-juice or acescent fruits and fresh vegetables, as garlic, mustard, cresses, sorrel, nasturtium, taraxacum among the wild plants, and potatoes, onions, turnips, beets, radishes, etc. among the domesticated plants. And in conjunction with these fresh meats, in the form of soups if the solids cannot be masticated, may be used with advantage. Ordinarily, the dietetic treatment alone will suffice to re-establish the health. Should, however, convalescence be delayed, the vegetable bitters with the mineral acids and ferruginous tonics and quinia will furnish useful adjuvants. These are the standard remedies; others have been recommended at various times, as the juice [p. 185]of the maguey, a Mexican plant, potassium nitrate alone or combined with vinegar, tincture of cantharides, etc.
Attention will often be required to the various scorbutic complications, especially stomatitis, which is always a source of discomfort and suffering. One of the best local applications for this is pencilling the parts with a solution of nitrate of silver, which often affords marked relief. Mouth-washes, composed of solutions of chlorinated lime, potassium permanganate, carbolic acid, are beneficial by suppressing foul odors, exercising local stimulative action upon the gums, and promoting healing. Should ulceration attack the legs, as is often the case, the application of mild astringents and stimulative ointments will be all that is required. The parts should, of course, be kept clean and protected from irritation by protective dressings.
Hemorrhages from the nose, gums, stomach, bowels, or into the serous cavities should be treated upon the general principles applicable to their character, as the local use of cold, astringents, and the internal administration of hæmostatic agents—lead acetate, ergot, tincture of iron, and other remedies, vegetable and mineral, of this class. In desperate cases effusions into the chest, threatening death by interfering with the respiratory and circulatory organs, may render operation necessary as the last resort for their removal.
During the treatment it is important to obviate any sudden or severe strain upon the heart by premature movements or exercises, as this is fraught with danger.
It has been customary with authors to describe under the general heading Purpura a number of affections presenting as a common symptom the extravasation of blood into the tissues, more especially of the skin and mucous membranes, quite irrespective of etiological or pathological considerations. Thus, the tiny ecchymoses caused by the bites of fleas have been denominated purpura pulicosa; the larger bruises resulting from external violence, purpura traumatica; the extravasations occurring in the course of scurvy, purpura scorbutica; those encountered in malignant small-pox, purpura variolosa; and so on. These affections, differing widely in nature, possess as a common symptom the escape of blood from the vessels into the tissues. It is evident, therefore, that in the sense often employed the term purpura is used to describe a symptom or symptoms common to a variety of non-related maladies.
If there be a peculiar morbid process having for its constant and characteristic symptom the spontaneous escape of the blood from the blood-vessels, it is plain that interstitial hemorrhage from external violence or from the action of a definite poison circulating in the blood and disorganizing it and its containing vessels, as in phosphorus-poisoning, or from the influence of certain zymotic diseases, should not be designated by the title properly belonging to a substantive malady. The question, therefore, is: Are there groups of symptoms indicating morbid action of definite character, but of varying intensity, to which the name purpura may with propriety be applied?
In the present light of pathological science it is impossible to answer this question in the affirmative without considerable qualification. It must be confessed that we do not possess a knowledge of any definite chain of morbid processes constituting a distinct disease that may be designated as purpura. And yet we are able to recognize a set of symptoms varying greatly in intensity, from the most trivial petechial eruption to profuse and fatal hemorrhages, accompanied by a train of manifestations which we are unable to connect with any of the causes already spoken of, and which, indeed, depend upon no fixed exciting cause with which we are acquainted. It may be eventually proven that purpura, even as we understand it, is merely a set of phenomena due to widely-differing influences acting upon the blood and blood-vessels, and that the term will disappear from our nomenclature as indicating a disease, but will be preserved as denoting a symptom. For the present, [p. 187]purpura is understood to be a group of symptoms characterized by the effusion of blood into the tissues of the body, or upon its free surfaces, or into its serous cavities, which seem to arise spontaneously, and for which we are unable to assign a definite cause. With this view of the nature of purpura it becomes necessary to exclude from present consideration blood-extravasations from internal or external violence, the action of the specific principles of contagious or infectious fevers, the dyscrasia of scurvy, the influence of poisonous substances, and, in a word, any of those affections of which the escape of blood from the vessels constitutes an epi-phenomenon.
Purpura may be conveniently considered as presenting three varieties: 1, purpura simplex; 2, purpura hæmorrhagica; 3, purpura rheumatica.
These three forms of the disease are not distinguished by sharply-outlined differences, but merge the one into the other, now one, now another set of symptoms predominating. To these may be added, likewise for convenience, three sub-varieties—purpura urticans, purpura papulosa, and purpura nervosa. The difference between these forms of purpura should not be considered as of more than clinical import. Whatever variations present themselves may with probable propriety be ascribed to complicating influences.
PURPURA SIMPLEX.—This is the mildest form of purpura, and may in many cases readily escape observation. It may begin abruptly, in the midst of health, without the slightest subjective symptom, or the extravasations may be preceded for several days by some discomfort, aching of limbs, sluggishness, anorexia, even a small amount of fever. The eruption usually appears first upon the lower extremities, preferably the flexor surfaces of the thighs (Duhring), but frequently upon the legs. It extends from these points to the upper extremities and trunk, usually sparing the face. The lesions vary in size from that of a pin-head to that of a fingernail (petechiæ), or they may be linear (vibices). They remain discrete, and do not increase in size throughout their course. Each spot of hemorrhage will endure for from one to two weeks. At first the lesions are of a livid red color, and declare their extra-vascular nature by remaining unaltered when subjected to pressure. The color of these spots changes, as in ordinary ecchymosis, in consequence of the metamorphoses of the hæmatin preparatory to its final absorption, from crimson to purple, to blue, to green, to yellow, and finally fades away. When recent, the spots appear sharply outlined, with sometimes a faint encircling zone of hyperæmia, but as they become older their margins grow indistinct. While the early lesions slowly disappear, others continue to develop, and the affection may thus be protracted for weeks. At times the petechiæ appear in crops, recurring every few days, the patient at one time apparently nearly well, at another time worse than ever. Finally, the symptoms definitely disappear, to return no more, or they pass into those of other forms of purpura. During the course of purpura simplex the blood-vessels of the skin alone are affected, the deeper tissues and mucous membranes probably remaining unchanged.
Throughout the attack the general health may—usually does—remain good. As an occasional symptom there will be observed a few vesicles or blebs, containing blood, upon the skin. The extent of the general eruption may vary from a few scattered petechiæ to a copious and startling [p. 188]number of purpuric spots. The maintenance of the upright position tends to perpetuate the evolution of the lesions.
In elderly persons purpura simplex is sometimes observed, and has been described by many writers as purpura senilis. Hillier, following Bateman, describes it as occurring in old women "upon the outside of the forearms in successive dark, purple blotches of an irregular form and various magnitude."1 Aged men as well as women are liable to the affection, which may quite as well appear upon the lower extremities of either sex. It is altogether likely, however, that in such cases degenerations of the vascular walls alone may cause the extravasations.
1 Reynolds's System of Medicine, vol. i. p. 792.
PURPURA HÆMORRHAGICA (MORBUS MACULOSUS WERLHOFII).—In this form of purpura there are added to the symptoms of purpura simplex hemorrhages into and from the various mucous tracts, the nasal, faucial, pharyngeal, gastric, intestinal, renal, uterine, rarely the pulmonary mucous membranes, and exceptionally into the various serous membranes and cavities. It may begin abruptly, in the midst of apparently vigorous health, or after premonitory symptoms extending over several days, vague sensations of discomfort—headache, pains, anorexia, indisposition to exertion, and the like—or it may occur as a transition from other forms of purpura. Usually there is no fever.
The hemorrhagic spots upon the skin appear much as in purpura simplex, though the lesions are larger, acquiring the size of coins or even of the palm of the hand. Spots soon appear upon the visible mucous membranes, and free hemorrhages occur; indeed, the latter may be the first symptom observed. Epistaxis is of most common occurrence, but bleeding from the mouth, stomach, and intestines almost as frequently results. The gums are almost constantly affected, and upon inspection these may be found covered with blackish scabs, upon removal of which the mucous membrane will be found pale and not swollen—an important point in diagnosticating this affection from scurvy. Vesicles and blebs filled with blood form both on the skin and mucous membranes. They quickly rupture and discharge their contents. Bleeding from the stomach and intestines is revealed—in the former case by the vomiting of a brownish material resembling coffee-grounds; in the latter case by the passage of black, tar-like evacuations. Pulmonary hemorrhage is to be distinguished from hæmatemesis by the frothy and arterial character of the blood. Hæmaturia may proceed from any part of the urinary tract. Bleeding from several parts may occur at the same time, and may be very copious.
In the mucous membranes extravasations of greater or less extent may occur, as in the derma. Into the serous membranes they may take place with or without effusion into serous cavities. It is only, however, in cases that will almost certainly end fatally that the effusions into these cavities are encountered. Hemorrhages into the substance of the lungs, into the brain and other viscera, as well as into the tissues generally, are occasionally observed.
At the outset of these bleedings the general health of the patient may appear unimpaired, and if they be few in number and moderate in extent but slight evidences of debility may be shown throughout the attack; but it is often the case that the loss of blood is excessive and long continued, and symptoms of profound anæmia supervene. The [p. 189] patient becomes greatly exhausted; intense pallor is developed, shortly followed by general oedema. Attacks of syncope appear, and in fatal cases—which are not common—death results from asthenia. This result may occur after a few days from the profuseness of the hemorrhage; usually, however, only after several weeks. Throughout the attack the cutaneous lesions continue to develop, either irregularly or in successive outbreaks, scattered over the general surface, involving the face less frequently than other parts. These spots undergo the color-changes peculiar to extravasated blood, and may be seen in all the stages of involution in the same patient. Fever, usually absent throughout the attack, may appear at the height of the affection, but does not run high. Local inflammations are exceedingly rare. In favorable cases recovery follows the gradual mitigation and disappearance of the symptoms, but relapses frequently occur, and convalescence may be retarded for months.
PURPURA RHEUMATICA (PELIOSIS RHEUMATICA).—Schoenlein in 1829 described as peliosis rheumatica an affection in which the symptoms of purpura simplex were associated with pain and often with effusion into the joints, especially those of the knee and ankle. He considered it as an independent malady. This opinion has been shared by Fuchs, Hebra, Kaposi, Neumann, and many others. Kaposi2 regards it as related to erythema nodosum, with which affection, indeed, it possesses some features in common. It probably, however, constitutes a complication of ordinary purpura. That it is not primarily rheumatic is shown by the almost invariable absence of many of the symptoms characteristic of rheumatism; that it cannot be an independent affection appears from its intimate relations with other forms of purpura.
2 Hautkrankheiten, 1880, p. 277.
Purpura rheumatica commonly begins with malaise, anorexia, debility, sometimes with mild fever. The patient is soon attacked with pains, of a more or less acute character, in the joints, especially the knees and ankles. There may be some effusion into the joint and cutaneous oedema. After a few days the nature of the complaint will be revealed by an eruption of petechiæ, first near the painful joints, but soon extending, involving in many cases even the head and trunk. The eruption may be at first slightly elevated and surrounded by a fine halo of hyperæmic injection.
The pains usually subside upon the appearance of the eruption, and the malady may be completed after a single outbreak. More commonly new joint-pains are experienced, fresh crops of petechiæ appear, and the trouble may be prolonged for weeks, even months, the patient meanwhile suffering not very greatly in general health. The lesions may be cutaneous only; rarely bleeding from mucous surfaces will occur (Scheby-Buch). Albuminuria may be present (Kaposi). An annual type is said by Kaposi, Neumann, and others to be sometimes observed, the spring and autumn being the usual seasons for the outbreaks. This is supposed to indicate a relationship with erythema nodosum and multiforme. Cardiac murmurs have been detected in the course of purpura rheumatica,3 but these were probably anæmic or antedated the purpuric symptoms. Purpura rheumatica never seems to result in endo- or pericarditis.
3 Kinnicutt, Archives of Dermatology, i. p. 193; Mollière, Ann. de Dermatol., v. p. 44.
SUB-VARIETIES.—Henoch4 and Couty5 have described a form of [p. 190] purpura mostly observed in children, in whom rheumatoid pains occur along with colic and vomiting of greenish or bilious matter, tenesmus, and sometimes with loss of blood from the bowels. The disease may be protracted throughout months by relapses. Cutaneous oedema frequently occurs. Couty regards it as a form whose peculiarities justify its assignment to a position of its own. The cause of the associated train of symptoms is supposed (Couty) to reside in the sympathetic system, and the name purpura nervosa is proposed for it. So many features of ordinary purpura are manifested in these cases that it seems better to consider them as examples of ordinary purpura complicated with gastro-intestinal derangement. It has been suggested that the nausea, vomiting, and abdominal pains may result from extravasation of blood into the peritoneal tissue.6
4 Berl. Klin. Wochenschr., 51, 1874.
5 Gaz. Hebd., 36 et seq., 1876.
6 Immermann, Ziemssen's Cyclopæd., vol. xvii. p. 265.
In the course of purpura there is frequently observed, more especially in purpura simplex, a wheal-like arrangement of the eruption—such, indeed, as occurs in urticaria. The term purpura urticans has been given to this sub-variety, which may or may not be accompanied by itching. Scheby-Buch has suggested that the urticaria may, with more propriety, be attributed to the gastric disturbances that so often accompany the forms of purpura presenting it.7 The wheals are usually seen upon the lower extremities, but may appear elsewhere. A considerable degree of oedema may be present, particularly in lax tissue, such as that of the scrotum, eyelids, etc.
7 Deutsche Arch. f. Klin. Med., B. xiv. p. 490.
Purpura papulosa (lichen lividus, Willan) is a form of purpura where, in the midst of ecchymoses, livid papules appear. These probably depend upon a large amount of hemorrhage occurring within a limited space, most often surrounding the orifices of hair-follicles, because these are supplied with a capillary network that comes directly from the deeper layer.8 They are formed most abundantly on the legs of scrofulous, cachectic persons who have purpura. Care must be taken to distinguish this form of purpura from erythema multiforme and erythema nodosum, where blood is usually extravasated secondarily into the tissues. Those cases only where the purpura is primary should be recognized as purpura papulosa.
8 Hebra, Skin Diseases, New Syd. Soc. Transact., ii. p. 425.
The purpuric effusion appears to act as an irritant upon the tissues, and to excite inflammation. Gangrene of the mucous coat of the intestines has resulted from extensive hemorrhagic extravasations, and from a similar cause cutaneous gangrene has been known. These complications, however, are rare.
ETIOLOGY.—The immediate causes of purpura are quite unknown. Both sexes and persons of every age are affected by it. While it is most often seen in debilitated subjects, those in vigorous health possess no immunity. It has often been observed during convalescence from other maladies. It cannot be said that those who are miserably clothed, fed, and lodged are especially predisposed to attacks of purpura. Between purpura and hæmophilia, etiologically, there are many points of difference. Purpura is not hereditary, nor is there a purpuric diathesis in the strict sense of the term. Some persons, indeed, seem to possess a [p. 191]predisposition to the disease, and some authors claim for purpura rheumatica a distinct annual type. This, however, is not at all certain.
Recently it has been claimed that purpura hæmorrhagica depends upon the presence of a minute organism in the blood. Petrone9 injected blood drawn from patients with this disease under the skin of rabbits, producing widely-distributed hemorrhages. In the blood of these individuals and of the injected rabbits micrococci and bacilli were detected. Watson Cheyne10 also describes a plugging of the capillaries with bacilli. These were 1/7700 of an inch in length and 1/20000 of an inch in diameter, and were arranged in colonies. In another case there were found micrococci arranged in chains. These swarmed in the capillaries and some larger vessels, and sometimes completely blocked them. Although an origin in infection has thus been claimed for purpura hæmorrhagica, the fact that more than one variety of micro-organism was observed cannot fail to excite suspicion of, possibly, erroneous observation.
9 Lo Sperimentale, 51, 1883.
10 Lancet, i., 1884, 344.
PATHOLOGY.—In the foregoing description those extravasations of blood due to simple mechanical violence, as from flea-bite, and sudden increase of blood-pressure, as in the effort of coughing in whooping cough, also from the deleterious influence exerted upon the blood-vessels and blood by certain drugs, the specific fevers, Bright's disease, and the like, have been excluded. Only those have been considered where the effusion of blood seemed to occur spontaneously, and the symptoms to result from some peculiar but not understood morbid process. The hemorrhage is but a symptom; the process by which it is brought about depends upon some change in the blood or blood-vessels. We do not know what these subtle changes are. The blood of purpuric patients has been carefully examined, but, with the exception above mentioned, no definite changes have been discovered. Immermann11 found during the first stage of the disease the blood-corpuscles perfectly normal in appearance, the white corpuscles subsequently slightly exceeding the red in number—a simple result of copious hemorrhage. No stated chemical changes in the blood are known in purpura, nor is it known how the blood escapes from the vessels. It undoubtedly escapes through alterations in the vascular wall, but it is also true that red blood-corpuscles, as well as the pale ones, may find their way in considerable numbers through the unruptured wall of the vessels, per diapedesin, as was first suggested by Velpeau, but definitely determined by Stricker. The causes of this migration are obscure. Immermann12 asserts that a fatty degeneration of the vascular tissues and of the muscles takes place. This, however, is manifestly a result of the loss of blood, and not its cause. Dr. Wilson Fox13 found extensive albuminoid disease of the muscles and capillaries of the skin; but the albuminoid degeneration involved several organs of a patient with syphilis, and the purpura was certainly secondary to the morbid conditions. Rigal and Cornil14 think that the hemorrhages are a result either of sympathetic irritation or of diminished action of the vaso-motor centre. It is indeed altogether likely that the cause will ultimately be found to reside in the vaso-motor system.
11 Ziemssen's Cyclop., xvii. p. 258.
12 Loc. cit.
13 Brit. and Foreign Med.-Chir. Review, Oct., 1865.
14 L'Union Méd., 5, 6, 7, 1880.
[p. 192]DIAGNOSIS.—The affection bearing the closest resemblance to spontaneous purpura is scurvy; indeed, its supposed relationship to this disease has given purpura one of its synonyms, land scurvy. The two affections, however, are probably without the slightest relationship. They possess in common the hemorrhagic symptoms, both in the tissues and from free surfaces, but the resemblance does not extend much beyond this. Scurvy depends upon deprivation of fresh vegetable food and the use of unsuitable and insufficient food generally, and upon bad hygienic surroundings. Purpura may—frequently does—appear in broken-down constitutions, but it equally attacks the strong and vigorous, while the character of food exerts no special influence on its production. Scurvy only follows long-continued privations and as a culmination of a train of distressing symptoms. Purpura appears in the midst of health, or after brief premonition, or during convalescence from totally unrelated diseases. In scurvy there is a decided tendency toward ulceration, which is absent in purpura. In scurvy the mouth and gums inflame and ulcerate, the latter becoming swollen, spongy, and of a bluish-red color. In purpura, ulceration of the buccal mucous membrane does not occur, and the gums are pale and intact. The curative influence of fresh vegetables, lime-juice, etc. in the treatment of scurvy is not observed in purpura. It has been claimed that purpura is but a mild degree of scurvy: this cannot be so, for we may have a mild scurvy or a severe, even fatal, purpura.
The hemorrhagic diathesis, or hæmophilia, presents points of analogy with purpura. Here, however, is found the almost constant history of heredity and the implication only of persons of the male sex. The disposition to bleed at all times upon the receipt of the smallest injury is quite unlike the suddenly-developed and transitory hemorrhages of purpura, which are also more generally distributed.
With the secondary hemorrhagic effusions and ecchymoses that occur in conditions of profound alterations of the blood and blood-vessels in cases of malignant small-pox, scarlatina, typhus fever, etc., and in some cases of poisoning, as from phosphorus, spontaneous purpura presents identities, but the history of the complaint and the condition of the patient will prevent error. A knowledge of the circumstances will serve to distinguish purpura simplex from the petechiæ and small ecchymoses produced by fleas, by diminished atmospheric pressure, by coughing, in the course of Bright's disease, etc.
Purpura rheumatica presents, as has been shown, many points of resemblance to erythema multiforme and erythema nodosum. The mild fever, the joint-pains, the extravasations of the latter affections, are much like the symptoms of this form of purpura. The nodular, inflamed, tender condition of the lesions, their location—frequently upon the extensor surfaces of the extremities—their course and duration, usually serve to identify erythema nodosum, while with erythema multiforme it is usually not difficult to observe its essentially inflammatory character. Scheby-Buch has shown the difficulties often opposed to the differentiation of purpuric lesions and ecchymoses due to violence.15 Where the petechial eruption of purpura simplex is well marked, where the internal hemorrhages of purpura hæmorrhagica are copious, the inquiries of the observer will usually lead him to correct conclusions. Where the [p. 193]ecchymoses are larger and upon exposed parts of the body, the diagnosis from the lesions alone becomes impossible, and due consideration of all concomitant circumstances is essential. It should be remembered that in purpura very slight violence may call forth extensive ecchymosis. This circumstance has important medico-legal bearings.
15 Viertelj. f. Dermatol. und Syph., 1879, p. 99.
PROGNOSIS.—Purpura usually terminates favorably. Its course runs from two to six weeks, rarely longer. Relapses and remissions are frequent. Purpura simplex is of very little gravity, and need excite little apprehension. Purpura rheumatica almost always ends in recovery; fatal terminations, however, have been known. Purpura hæmorrhagica is of much more serious import. Even here, however, though the patient may fall into profound debility from loss of blood, recovery is the rule, the symptoms gradually diminishing in severity until health becomes re-established. In fatal cases death ensues after prolonged and profuse losses of blood. Purpura may subside after a single outbreak or many relapses, and recrudescences may occur extending through months. Anæmia may persist long after the disappearance of purpuric symptoms. A tendency to purpura may be shown at irregular intervals for years, and even throughout life.
TREATMENT.—Very mild cases of purpura simplex require no treatment, not even confinement within doors. The patient is often first made aware of his disease by accident; doubtless it frequently escapes detection altogether. It has been observed that purpura often appears upon the lower limbs of convalescents from other diseases when they first essay the upright position. Relapses of purpura also frequently appear as the patient leaves his bed. We have here an important indication for treatment—viz. the maintenance of the recumbent posture in cases of any degree of severity. Fresh vegetables and vegetable acids do not have the same happy influence as in scurvy. It is manifestly important that appropriate food should be administered in sufficient quantity, both to improve the general health and to repair the exhausting losses of blood. Milk is an exceedingly valuable article of diet in these cases, being but little apt to irritate the mucous membrane of the alimentary canal.
The patient should be guarded against violence. Injuries that may be of no consequence to healthy persons may excite in the purpuric profuse hemorrhage, free or interstitial. Violent emotions and physical efforts should be avoided, as in stimulating the heart's action a condition of increased blood-pressure ensues that may readily result in extravasation.
There are no remedies that exert a specific influence over purpura, and yet quite a number have enjoyed, and still enjoy, high reputation in controlling the symptoms. Probably the most frequently employed remedy against purpura is sulphuric acid, preferably the aromatic sulphuric acid, in doses of from 15 to 20 drops, diluted well with water and administered every third or fourth hour. It is certainly an agent of value, though some authors maintain that it has no efficacy (Immermann). Acetate of lead undoubtedly exercises an influence over the course of the disease. More recently, ergot has been employed. Its use has been highly extolled by Buckley and others. Very large doses may be given. The hypodermic use of ergotin has been followed by results most gratifying to those employing it. Oil of turpentine has enjoyed considerable reputation. A remedy that undoubtedly has a good effect is iron, both as [p. 194]exercising a controlling action over the bleeding and as assisting to repair the resulting anæmia. The tincture of the chloride is the most suitable preparation, and may be given in large doses (from minim xx to fluidrachm ss), well diluted, every fourth hour. Care must be exercised to avoid irritating the digestive organs with it. Formerly, venesection was employed to prevent the occurrence of hemorrhage, but its efficacy in this direction is at least doubtful, and cannot but help to intensify the disastrous consequences of severe and protracted attacks.
The various complications that may arise, as well as the general results of purpura, must be treated symptomatically. For the mucous membranes astringent washes should be used, and in favorable situations the tampon may sometimes be employed with profit. In purpura rheumatica the arthritic pains will be alleviated by anodyne liniments and plasters, and the often accompanying abdominal pains and colic by anodynes internally administered. Hæmatemesis, hæmaturia, etc. must be treated upon general principles. The results of profuse hemorrhage must be combated with stimulants. Transfusion of blood has been proposed and practised for the extreme anæmia that sometimes occurs, but without encouraging results. If necessary, the bowels may be kept free by mild aperients. In severe cases rest in bed should be rigidly enforced until after the establishment of convalescence. Quinia, iron, and nux vomica are indicated above all other remedies for the anæmia resulting from an attack of purpura.
Diabetes mellitus is a term applied to a group of symptoms more or less complex, of which the most conspicuous is an increased flow of saccharine urine—whence the symptomatic title. It is associated with a derangement of the sugar-assimilating office of the liver, as the result of which an abnormally large quantity of glucose is passed into the hepatic vein and thence into the systemic blood, from which it is secreted by the kidneys. The condition is sometimes associated with alterations in the nervous system, at others with changes in the liver or pancreas, while at others, still, it is impossible to discover any structural alterations accompanying it.
| FIG. 1. |
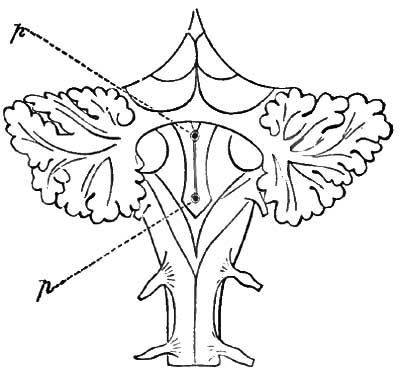
|
| To show the position of the punctures required to produce glycosuria, the lobes of the cerebellum are separated. Below are seen the restiform bodies, the divergence of which circumscribes the apex of the calamus scriptorius and the fourth ventricle. The puncture p' produces glycosuria; the puncture p, glycosuria with polyuria; and a puncture a little higher up than p, albuminuria. |
PATHOLOGY AND PATHOGENESIS.—Notwithstanding that this disease has been recognized for two centuries and a half, that abundant opportunity has been furnished for its post-mortem investigation, and that experimental physiology has contributed much information bearing upon the subject, its pathology is still undetermined. Experiment has, however, rendered it very likely that all cases of essential glycosuria—that is, all cases in which saccharine urine is not the direct result of over-ingestion of sugar or sugar-producing food—are accompanied by a hyperæmia of the liver. This hyperæmia, with its consequent glycosuria, can be induced by puncturing or irritating the so-called diabetic area1 in the medulla oblongata. This area corresponds with the vaso-motor centre, and with the roots of the pneumogastric or vagus nerve in the floor of the fourth ventricle; whence it was at first inferred that this nerve is the excitor nerve of glycosuria. It was soon ascertained, however, that when the pneumogastric was cut, glycosuria ensued only when the central end was stimulated, while [p. 196]stimulation of the peripheral portion was without effect. Whence it became evident that this nerve is not the excitor, but the sensory nerve concerned in glycogenesis.
1 The diabetic area, as marked out by Eckhard, and which corresponds with the vaso-motor area, as defined by Owsjannikow (Ludwig's Arbeiten, 1871, p. 21), is bounded by a line drawn four or five mm. above the nib of the calamus scriptorius, and another about four mm. higher up.
It was also learned in the course of continued experiment that glycosuria resulted upon transverse section of the medulla oblongata, of the spinal cord above the second dorsal vertebra, of the filaments of the sympathetic accompanying the vertebral artery, upon destruction or extirpation of the superior cervical ganglion, and sometimes, but not always, after division of the sympathetic in the chest (Pavy); also after section or careful extirpation of the last cervical ganglion, section of the two nerve-filaments passing from the lower cervical to the upper thoracic ganglion around the subclavian artery, forming thus the annulus of Vieussens,2 and after section or removal of the upper thoracic ganglion.
2 Cyon and Aladoff, reprint from the Mélanges biolgiques and Bullétin de l'Académie Impériale de Petersbourg, vol. xiii. p. 91; cited by Dr. Brunton in the Lectures named in note on p. 198; also British Medical Journal, Dec. 23, 1871, p. 731.
| FIG. 2. |
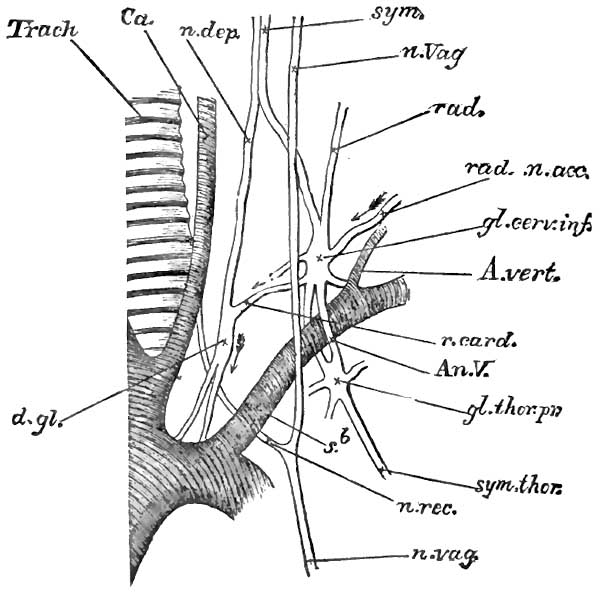
|
|
The last cervical and first thoracic ganglia,
with circle of Vieussens, in the rabbit, left side. (Somewhat
diagrammatic, many of the various branches being omitted.) Trach., trachea; Ca., carotid artery; n. vag., the vagus trunk; n. rec., the recurrent laryngeal; sym., the cervical sympathetic nerve ending in the inferior cervical ganglia, gl. cerv. inf. Two roots of the ganglion are shown—rad., the lower of the two accompanying the vertebral artery, A. vert., and being the one generally possessing accelerator properties; gl. thor. pr., the first thoracic ganglion. Its two branches, communicating with the cervical ganglion, surround the subclavian artery, forming the annulus of Vieussens. sym. thor., the thoracic sympathetic chain; n. dep., depressor nerve. This is joined in its course by a branch from the lower cervical ganglion, there being a small ganglion at their junction, from which proceed nerves to form a plexus over the arch of the aorta. It is this branch from the lower cervical ganglion which possesses accelerator properties, hence the course of the accelerator fibre is indicated in the figure by the arrows. (Modified from Foster's Physiology.) |
All these operations paralyze the vaso-motor nerves by which, in health, the blood-vessels of the liver are kept in a state of tonic contraction; hence these vessels dilate when the nerves are cut. From the facts named we also learn the path of the glycogenic influence, which must be from the medulla oblongata into the spinal cord, thence by the filaments of the [p. 197]sympathetic which accompany the vertebral artery into the lower cervical ganglion; thence through the annulus of Vieussens into the first dorsal ganglion; and thence through the prevertebral cord of the sympathetic, and branches not precisely determined, to the hepatic blood-vessels as shown by the dotted line in Fig. 3.
| FIG. 3. |
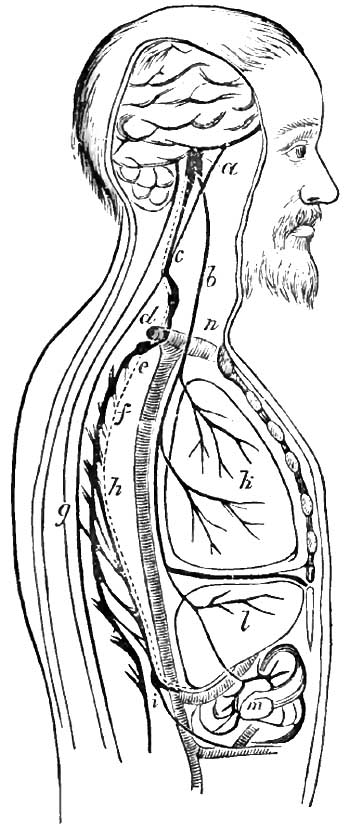
|
| Diagram showing the course of the vaso-motor nerves of the liver, according to Cyon and Aladoff. These nerves are indicated by the dotted line which accompanies them: a, vaso-motor centre; b, trunk of the vagus; c, passage of the hepatic vaso-motor nerves from the cord along the vertebral artery; d, fibres going on each side of the subclavian artery and forming the annulus of Vieussens; e, first dorsal ganglion; f, ganglionated cord of the sympathetic; g, the spinal cord; h, the splanchnic nerves; i, coeliac ganglion, from which vaso-motor nerves pass to the hepatic and intestinal vessels; k, the lungs, to which fibres of the vagus are seen distributed; l, the liver; m, the intestine; n, the arch of the aorta. |
I say, by branches of the sympathetic not precisely determined, because our power to produce artificial diabetes fails below the first thoracic ganglion; for section of the sympathetic between the tenth and twelfth ribs, and of the splanchnics, is not followed by glycosuria, although the vaso-motor nerves to the liver are known to pass through them.
According to Eckhard,3 the phenomena of artificial glycosuria are irritative and not paralytic. This view he believes sustained by his own experiments, according to which if the splanchnics, through which [p. 198]the vaso-motor nerves of the liver pass, are cut prior to the diabetic puncture, not only does this operation fail to produce glycosuria, but it even renders ineffectual the puncture itself as well as the section higher up. But Cyon and Aladoff remind us that it is not mere dilatation of the hepatic vessels, but increased velocity in the movement of the blood, which deranges the sugar-assimilating function and causes glucose to appear in the urine. The vaso-motor nerves of the intestinal blood-vessels also pass through the lower part of the sympathetic and the splanchnics, and section of the latter must cause these blood-vessels to dilate. Now, in rabbits, in which this experiment is usually performed, the digestive canal is very long, and the blood-vessels so capacious that when dilated they hold as much blood as all the rest of the vascular system together, so that when the lower sympathetic and splanchnics are cut, so much blood goes into the intestines that the increased velocity required in the blood-vessels of the liver to produce glycosuria is impossible. But if the vessels of the liver be first dilated by puncturing the floor of the fourth ventricle, section of the sympathetic or of the splanchnics may then be made without arresting the formation of sugar; whence it would appear that the glycogenic influence may still pass through the lower sympathetic and splanchnics.
3 Beiträge zur Anat. und Physiologie, iv., 1859, p. 1; vii., 1873.
In view of the fact that Eckhard4 has failed to confirm the results of Cyon and Aladoff, but has traced the glycogenic influence down the spinal cord as far as the fourth dorsal vertebra in rabbits, and even a little lower, and that Schiff5 has shown that diabetes sometimes results after section of the anterior columns of the cord between the medulla and the fourth cervical vertebra, Dr. Brunton6 suggests that the vaso-motor nerves of the liver may not always leave the spinal cord to join the sympathetic by the branches accompanying the vertebral artery, but sometimes pass farther down the cord, leaving it by the communicating branches to some of the dorsal ganglia, as indicated in Fig. 4.
4 Beiträge zur Anat. u. Physiologie, viii., 1877, p. 79.
5 Untersuchungen über Zuckerbildung in der Leber, 1859, S. 108.
6 Lectures on the Pathology and Treatment of Diabetes Mellitus; reprinted from the British Medical Journal, 1874, p. 12.
| FIG. 4. |
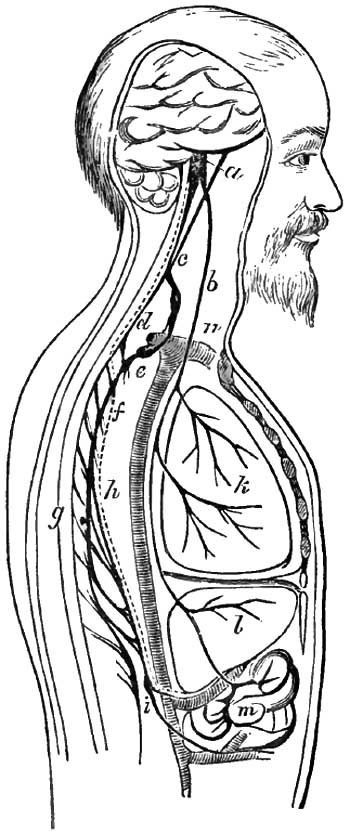
|
| Diagram showing another course which the vaso-motor nerves of the liver may take. The letters indicate the same parts as in Fig. 3. The hepatic vaso-motor nerves are here represented as passing lower down the cord than in Fig. 3, and leaving it by communicating branches to the second dorsal ganglion. It is possible that they may sometimes leave by the branches to the first, and sometimes by those going to a lower, ganglion. In such cases any irritation to the third or one of the other cervical ganglia may cause diabetes by being conveyed along the vertebral artery and up the cord, as indicated by the dark line, to the vaso-motor centre, where it may cause reflex inhibition in the same way as any irritation to the vagus. |
It is evident that an agency involving any part of this tract in such a way as to paralyze the vaso-motor nerves of the liver is capable of producing glycosuria. Such cause may operate upon the central ganglia whence the nerves emanate, as the vicinity of the oblongata and upper parts of the spinal cord or the coeliac ganglion and its branches, including those to the pancreas. Or the irritation may be peripheral and its effects reflex. We have seen that irritation of the central end of the cut vagus will produce glycosuria. Any irritation, therefore, involving the peripheral distribution of this nerve may produce it. Hence embarrassed respiration, whether due to disease of the respiratory passages, strangulation, or inhalation of irrespirable gases and anæsthetics, produces glycosuria in dogs and rabbits; and this symptom has been known to attend these conditions in the human subject. So, too, glycosuria may be produced by such substances as woorara, strychnia, morphia, and phosphoric acid, introduced into the blood and irritating the terminal filaments of the pneumogastrics, or it may be brought about secondarily through the embarrassed respiration these drugs produce. Such peripheral [p. 199]irritation may reside also in the stomach, intestines, liver, or any organ to which the pneumogastric is distributed.
It is not unlikely that irritation of the extremities of sensory nerves other than the pneumogastric may become the cause of reflex glycosuria. Even puncture of the floor of the fourth ventricle itself may be reflex in its operation, the roots of the pneumogastric being thus irritated. The effect of the irritation conveyed to the glycogenic centre is to inhibit the usual tonic influence of the vaso-motor nerve upon the vessel walls. Among the experimental irritations, in addition to puncture of the floor of the fourth ventricle, which produce glycosuria by reflex action, are injuries of the cerebral lobes and cerebellum, optic thalami, cerebral peduncles, pons varolii, middle cerebellar peduncles, and even of the sciatic nerve and brachial plexus; whence it may be inferred that pathological irritation in the same situations may result in a glycosuria, which is temporary or permanent according as the irritation is temporary or permanent.
Finally, there is no reason why an inhibitory reflex action should not originate in the sympathetic itself. When we remember that this nerve is both sensory and motor in function, and that the inhibitory influence to which the heart's action is subject is accomplished through the sympathetic as a sensory nerve and the pneumogastric as a motor, there is no reason why similar results may not be brought about by the sympathetic alone. This being the case, we need not ascribe glycogenic phenomena to irritation in Eckhard's sense—that is, to a direct stimulant action of the irritant upon the vaso-motor nerves of the liver—but may suppose a sensory influence to ascend one set of sympathetic filaments and an inhibitory influence to descend through another.
Dr. Pavy has recently put forward some chemical theories which explain the action of the hyperæmia in producing glycosuria, but they do not account for the hyperæmia itself. In healthy digestion the carbohydrates (starch and sugar) are converted, not into glucose, but into maltose, C12H22O11, dextrin being intermediate in composition. Maltose is absorbed and assimilated, converted into glycogen. So, too, when glucose is ingested as such, it is converted by the glucose ferment into maltose in the stomach and intestines. For the proper production of maltose and its assimilation a good venous blood, producing a maltose-forming ferment, is necessary. In diabetes, in consequence of the dilatation of the arteries of the chylopoëtic viscera, the blood enters the liver too little deoxygenated, and a glucose-forming ferment is produced. The glucose thus formed is not assimilable, but passes off into the circulation and the urine.
MORBID ANATOMY.—Such are some of the facts bearing upon the pathology of diabetes mellitus. Throwing out the milder type of cases, in which glycosuria is the result of an over-ingestion of saccharine and sugar-producing food—and these can scarcely be called instances of essential diabetes—it is evident that glycosuria may be produced in a variety of ways operating through the nervous system; and accordingly we may infer that there is scarcely an organ in close relation with the sympathetic system derangement of which is not capable of producing it. Among these we would naturally expect to find conspicuous alterations in the nervous centres, and yet I have never found changes in these centres after death. At the same time, others have noted meningitis, tubercular [p. 200]and traumatic, apoplectic effusions, and tumors of the brain, especially in the neighborhood of the medulla oblongata. The alterations in the nerve-centres described by Dickinson as the essential morbid anatomy of diabetes I have looked for in vain. These changes are described as a cribriform or porous condition of the white nervous matter, said to be visible to the naked eye. The spaces thus produced are partially occupied by dilated blood-vessels, which, in turn, are surrounded by dilated perivascular sheaths and broken-down nervous matter, into which extravasations of blood have taken place, as evidenced by the presence of pigment-granules. The changes are found in the white matter of the convolutions of the brain, but fewer and larger in the central portions. The corpora striata, optic thalami, pons, medulla, and cerebellum are favorite seats for the largest and most striking holes. In rapidly-fatal cases the cavities are sometimes filled with a translucent, gelatinous substance, containing, besides vascular elements, the globular products of nervous disintegration. In the more chronic forms of the disease, as it occurs in elderly persons, the excavations are usually empty, although the elements of nervous decay are still to be found fringing the margins or collected as an irregular sheath upon the dilated or shrunken artery. There are changes in the cord similar to those in the brain, but less decided. But the most striking alteration in the cord, according to Dickinson, although not always present, is dilatation of the central canal, which in the dorsal and lumbar regions is sometimes expanded to many times its normal diameter, and forms a conspicuous object immediately after the cord is divided.
These alterations have eluded the vigilance of other pathologists who have sought for them in well-determined cases of diabetes mellitus, while they have been found, on the other hand, in the nervous centres when no diabetes was present. In the recent discussion on diabetes at the Pathological Society of London, Douglas Powell7 seemed to be the only one who was convinced that most of Dickinson's specimens were examples of positive lesions.
7 London Lancet, May 5, 1883, p. 776.
A hyaloid thickening of the blood-vessels of the brain has been noted by Stephen Mackenzie8 and Seymour Taylor9 in some cases, and miliary aneurisms of the retina in one.
8 Discussion on Diabetes, Path. Soc. of London, London Lancet, April 7, 1883, p. 593.
9 Ibid., Lancet, May 5, 1883, p. 774.
Of other organs, one of the most frequently found diseased is the pancreas, and, according to Senator, it is fair to assume that disease of the pancreas is present in about one-half of all cases of diabetes. As the result of increased experience, I am inclined to attach much more importance to pancreatic disease as a cause of diabetes than I did a few years ago. Among the changes found is a pseudo-hypertrophy, which consists chiefly in a hyperplasia of the connective tissue, fatty degeneration of the gland-cells, and atrophy of the glandular structure; cancerous disease; calculous concretions in the ducts with or without obstruction; and cystic dilatation.
Facts bearing upon the relation of pancreatic disease to diabetes have been accumulating since Cowley first discovered calculi in the pancreas of a diabetic, and Bright pancreatic cancer in a similar case. Since then [p. 201]instances have multiplied to such extent that it would be unprofitable to enumerate them. But in 1877, Lancereaux10 communicated to the French Academy of Medicine specimens of profound lesion of the pancreas from cases dying of diabetes mellitus. This, he alleged, constitutes a special and distinctive variety of diabetes, characterized by sudden onset, emaciation, polydipsia, polyphagia, and peculiar alvine dejections. More recently, Depierre11 has confirmed these observations, apparently establishing this variety of diabetes mellitus, of which a very rapid course—six months to three years—and the habitual presence of diarrhoea are characteristic; while the presence of greasy or creamy stools, and the appearance in them of undigested nitrogenous substances, may aid in the diagnosis. Precisely such a case, running the same rapid course—less than one year—with emaciation, uncontrollable diarrhoea, creamy stools, jaundice, and pancreatic disease, came under the writer's care in 1882. At the autopsy the pancreas was found enlarged, and numerous gritty particles were disseminated through it.
10 "Notes et réflexions à propos de deux cas de diabète sucre avec altération du pancréas," Bull. Acad. de Méd., Paris, 1877, 2d Serie, vi. 1215-1240.
11 Med. News and Abstract, vol. xxxix., June, 1881, p. 344, from Jour. de Méd. et de Chir. pratiques, Dec, 1880.
Supposing such pancreatic disease to be primary, it is evident that it must operate through the coeliac plexus, which, with its ganglion, is gradually encroached upon. On the other hand, it is also possible that the disease of the coeliac plexus may be primary, and the coexisting pancreatic disease and diabetes mellitus both secondarily dependent upon it. This can only be settled by more careful study of the coeliac plexus after death from diabetes, but up to the present time facts would seem to support the view of primary pancreatic disease.
The liver is frequently enlarged—sometimes but slightly, at others decidedly. It has been known to reach three times the size of the normal organ. Again, it may be darker and harder—hyperæmic. By minute examination the acini are found enlarged, the capillaries dilated and distended; the liver-cells are enlarged, distinctly nucleated, rounded, and indistinct as to their outline, appearing to fuse into each other. A weak solution of iodine strikes a wine-red color, which, according to Rindfleisch, is confined to the nucleus, but, according to Senator, may extend to the whole cell. This reaction Klebs ascribes to post-mortem changes in the glycogenic substance. They are more striking in the portal or peripheral zone of the lobule, while the intermediate or hepatic artery zone is often fatty, and the central part, surrounded by the rootlets of the hepatic vein, is nearly normal. Stockvis and Frerichs ascribe the enlargement of the liver partially to a new formation of liver-cells—in other words, to a true hypertrophy. At other times the organ has been found reduced in size.
Dickinson, Trousseau, and Budd describe an overgrowth of connective tissue, as well as of the cells of the liver, producing a hypertrophic cirrhosis.
According to Beale, Frerichs, and Folwarczny, the fat which is found in small proportion in the liver-cells in health is often diminished, and even absent, and quantitative12 analysis by the last-named observer [p. 202]confirms this view. Such diminution may be the forerunner of an atrophy of liver-cells which has been noted, and which, as the disease continues, leads to the atrophy referred to as occasionally present. On the other hand, intense fatty degeneration of the entire organ, similar to that found in phosphorus-poisoning, has been met by Gamgee, associated with a lipæmic state of the blood and symptoms of acute acetonæmia.
12 Folwarczny, "Leberanalysen bei Diabetes Mellitus," Wiener Zeitschr., N. F., 1859, ii. 6.
The kidneys, in cases which have continued some time, are apt to be hyperæmic and enlarged, although primarily they are uninvolved. It would seem that the long-continued hyperæmia which is a necessary condition of the copious secretion of urine, results, sooner or later, in an over-nutrition of the renal epithelium, a widening of the tubules, and consequent enlargement of the whole organ. The changes are mainly of a parenchymatous or catarrhal rather than an interstitial nature, the epithelium being disposed to shed. These changes may reach a more advanced stage of cellular degeneration, and may be attended by albuminuria. The cells may become very large, present a yellowish-brown color, their nuclei indistinct and non-responsive to ordinary staining solutions, but may take a red stain with a weak solution of iodine, similar to that described in the case of the liver-cells. Mackenzie describes a hyaline degeneration of the intima of the arterioles and a skeleton condition of the epithelium of the collecting tubes.13 There may also be a catarrh of the pelves of the kidneys and ureters, due to irritation of the saccharine urine.
13 Loc. cit.
Atrophy of the testes has been noted by Romberg and Seegen in young men, and recently Hofmeier14 has reported the case of a young diabetic woman, aged twenty, who came under observation for pruritus vulvæ, in whom the uterus was found small, scarcely 5 cm. (2 inches) long, and the ovaries very much atrophied. As this young woman had no other ailment, the atrophy was ascribed to the diabetes.
14 Berliner klin. Wochenschr., 1883, No. 42.
Among the most constant secondary lesions is the aggregate of changes known as those of pulmonary phthisis. But a few years ago, when our ideas on this subject were more definite than they are to-day, and when it was thought we had three distinct varieties of phthisis—the tubercular, the catarrhal, and the fibroid—the phthisis of diabetes was regarded as typically catarrhal.15 At the present time, however, when the tendency at least is to regard all phthisis as tubercular, diabetic phthisis must be consigned to the same category. At the same time, if the tubercle bacillus is to be regarded as the essential criterion of tuberculosis, it must be stated that the diabetic patient is subject to two different lung processes—at least if the observations of Riegel of Giessen16 are to be regarded as correct. In two cases of diabetic phthisis studied at his clinic, the sputum of one contained numerous bacilli, while the other, although the case presented the most distinct signs of infiltration of the apex, and although more than fifty preparations were investigated, revealed none. The sputum was also said to present some unusual physical characters. So far as I know, no autopsies of cases showing these clinical differences have been reported, although there have been found in diabetes, distinct from the usual cheesy foci, fibroid changes with small smooth-walled cavities. In such cases [p. 203] tubercle bacilli would be absent, while the physical signs of consolidation would be present.
15 See the writer's work on Bright's Disease and Diabetes, Philada., 1881, p. 256.
16 Medical News, Philada., May 19, 1883, from Centralblatt f. klin. Med., Mar. 31, 1883.
As a part of the phthisical process in diabetes, cavities of various sizes are found and gangrene of the lungs has been observed.
ETIOLOGY.—The problem of the etiology of diabetes mellitus is as unsatisfactorily solved as is that of its pathogenesis. Certainly, a majority of cases of diabetes cannot be accounted for. A certain number may be ascribed to nervous shock, emotion, or mental anxiety; a few to overwork; some to injury and disease of the nervous system; others to abuses in eating and drinking. Among the injuries said to have caused diabetes are blows upon the skull and concussions communicated to the brain, spinal cord, or vaso-motor centres through other parts of the body. Hereditation is held responsible for a certain number of cases. Malarial and continued fevers, gout, rheumatism, cold, and sexual indulgence have all been charged with producing diabetes.
Diabetes mellitus is most common in adult life, although Dickinson reports a case at six years which was fatal, Bence Jones a case aged three and a half, and Roberts another three years old; and in the reports of the Registrar-General of England for the years 1851-60 ten deaths under the age of one and thirty-two under the age of three are included. This statement, in view of the experience of the difficulties of diagnosis in children so young, seems almost incredible. I have never myself met a case in a child under twelve years. At this age I have known two, of which one, a boy, passed from under my notice, while the second, a girl, recovered completely. The disease is most common between the ages of thirty and sixty. The oldest patient I have ever had died of the disease at seventy-two years, having been under my observation for three and a half years.
It is decidedly more frequent in men than in women, carefully prepared statistics of deaths in Philadelphia during the eleven years from 1870 to 1880, inclusive, giving a total of 206 deaths, of which 124, or three-fifths, were males, and 82, or two-fifths, females. This is the experience of all.
My own experience has been singular and interesting. Up to April, 1881, I had never met a case in a woman. Of 18 cases outside of hospital practice which I have noted since that date, 9 were men and 9 women. But I still do not recall an instance of a woman in hospital practice, although I have constantly cases among men.
Not much that is accurate can be said of the geographical distribution of the disease. It seems to be more common in England and Scotland than in this country, at least if the statistics of New York and Philadelphia are considered. In the former city, statistics extending over three and a fourth years show that out of 1379 deaths, 1 was caused by diabetes; in Philadelphia, in eleven years, 1 out of 875; in England and Wales, according to Dickinson from observations extending over ten years, 1 out of 632; and in Scotland, 1 out of 916. According to the same authority, the disease is more prevalent in the agricultural counties of England, and of these the cooler ones, Norfolk, Suffolk, Berkshire, and Huntingdon. According to Senator, it is more common in Normandy in France; rare, statistically, in Holland, Russia, Brazil, and the West Indies, while it is common in India, especially in Ceylon, and relatively very frequent in modern times in Wurtemberg and Thuringia. Seegen says it is more [p. 204]frequent among Jews than among Christians, but I have never seen a case in a Hebrew.
SYMPTOMS, COURSE, AND DURATION.—The earliest symptom commonly noted by the diabetic is a frequency of micturition and the passage of larger amounts of urine than is natural. Coincident with or immediately succeeding this is an undue thirst and dryness of the mouth, which soon becomes the most annoying symptom the patient has, the freest draughts of water giving but partial or temporary relief. To this succeeds dryness, and sometimes itching, of the skin and absence of perspiration. A good appetite with fair digestion accompanies this stage of the disease, but notwithstanding this the patient loses in weight. If a male, his attention is sometimes called to his urine by the white spot left after the evaporation of a drop of urine on his boot or clothing or by the stiffness of his linen due to the same cause. To these symptoms are sometimes added an intolerable itching of the end of the urethra in males and of the vulva in females, probably due to the irritation caused by the saccharine urine in passing over and drying upon these parts.
As the disease progresses muscular weakness supervenes. This, however, comes on at varying periods after the incipient symptoms make their appearance. Sexual inclination grows less. The muscular weakness gradually increases, if the disease is not checked, until the patient can barely walk: he totters in his gait, and reminds one of a case of Duchenne's disease. Even before this he sometimes gives up and goes to bed. Often harassing cough ensues, adding its exhausting effect to that of the essential disease. Percussion and auscultation discover consolidation at one apex or over larger areas of the lungs. Dyspepsia and indigestion replace the good appetite which attended the onset of the symptoms, and all efforts to increase the latter are unavailing. The heart begins to flag, and its action is irregular. It finally ceases to act, and the patient dies suddenly, sometimes unexpectedly. Or coma may supervene before death. This coma, known as diabetic coma, is generally ascribed to the accumulation of acetone or acetone-producing substance in the blood. It is supposed to be a product of the decomposition of the sugar in the blood, and the phenomena resulting from its presence are known as those of acetonæmia. Some further account of it will be given in the section on changes in the urine. It is sometimes recognizable by a fruity odor of the breath, which may even pervade the atmosphere of the room in which the patient lies, and may be recognized on entering. It has been compared to the odor of a room in which apples have been kept, again to sour beer, and again to chloroform.
During all this time the thirst and discomfort arising therefrom, continue, although it sometimes happens that toward the end the quantity of urine and its contained sugar diminish and the urine becomes darker in hue.
Such is the course of a typical case of diabetes mellitus. Other symptoms, less conspicuous, are a lowered temperature of the body, from 1° to 2½° F. or even more; cataract, dilatation of the retinal vessels, intraocular lipæmia, functional derangements of vision, including amblyopia, presbyopia, and loss of accommodating power; and occasionally total blindness from atrophy of the retina may be present. I have known almost total blindness to appear very early in the disease, and [p. 205]subsequently to disappear. Derangements of the other special senses, as impairment of hearing, roaring in the ears, and disorders of smell and taste, also occur. Boils and carbuncles are occasional symptoms; although usually late in occurrence, the former are said to be sometimes the first symptoms recognized. Numerous skin affections may occur. Ulcerated surfaces are slow to heal, and gangrene supervenes sometimes spontaneously, but more often as the result of some trifling injury. It may start from a blister produced by cantharides, although such instances are scarcely frequent enough to justify interference with treatment demanding blisters. More frequently surgical operations do badly. Allied to this tendency is a spongy state of the gums, with recession and excavation, resulting, in asthenic cases, in absorption of the alveolar processes and falling out of the teeth. Eczema of the labia and vicinity in females, and a similar irritation about the meatus urinarius in males, are annoying symptoms. A purulent-looking discharge has been seen issuing from the urethra, in which the spores of penicilium glaucum have been recognized by the microscope.
The term diabetic coma is applied to a form of coma which is apt to occur late in the disease, indeed most frequently to terminate it; while it is also used to indicate a train of nervous symptoms of which coma is the terminal one. To this train of symptoms the word acetonæmia is also applied, and should alone be used, while the term diabetic coma should be restricted to the terminal symptom. The coma, as well as the previous nervous symptoms, is considered due to the accumulation in the blood of a product of the decomposition of sugar, formerly believed to be acetone, but now thought to be an acetone-producing substance, probably aceto-acetic acid. It is likely that in all cases of diabetes a small quantity of this substance exists in the blood, from which it is separated by the kidneys and lungs, while it is only when these channels are insufficient for its removal that it accumulates and produces the symptoms described.
Usually, the coma comes on gradually, deepening until it terminates in death. In other instances it is preceded by various symptoms, including dizziness, drowsiness, cephalalgia, delirium, mania, muscular pains, gastric and intestinal symptoms, including epigastric pain, vomiting—sometimes of blood—and even purging; also dyspnoea, with short, panting respiration like that of an animal with both vagi cut, and a fluctuating pulse-rate which continues until coma is established, after which it remains rapid and small. Both the breath and urine may exhale the peculiar odor of acetone, or it may be absent, and the urine strikes the peculiar burgundy-red reaction with perchloride of iron to be again referred to.
These symptoms may be sudden in their occurrence, whence acute acetonæmia, or they may ensue slowly. Ralfe,17 who has studied the subject of acetonæmia very thoroughly, has called attention to the parallelism between the phenomena of acute acetonæmia and those of acute yellow atrophy of the liver and of phosphorus-poisoning. The sudden, sharp epigastric pain, with gastric disturbance and vomiting, often of blood; the peculiar panting dyspnoea referred to; the short, [p. 206]noisy delirium, followed almost suddenly by deep coma; the fall in temperature as the nervous symptoms develop; the irregular, and finally rapid, pulse,—are all symptoms common to the two conditions.
17 Clinical Chemistry, 1883, p. 98; also Discussion on Diabetes before Pathological Society of London, Lancet, April 7, 1883, p. 592.
Although acknowledged to be a grave complication, and the most frequent cause of death in diabetes,18 yet it does not follow that a fatal termination is inevitable when diabetic coma sets in. I have now a patient, a woman, who considers herself in perfect health, but in whom there remains a trifling glycosuria, who at one time was supposed to be dying of diabetic coma.
18 Of 400 cases of diabetes which passed under the observation of Frerichs, the majority died of acetonæmia (Frerich's "Ueber den plötzlichen Tod und über das Coma bei Diabetes," Zeitschr. für klin. Med., 1883, vi. 3-53). Of 53 persons dying of diabetes at Guy's Hospital, London, during the last ten years, 33 died comatose (Dr. Fred. Taylor, Discussion on Diabetes, Pathological Society of London, Lancet, May 5, 1883). In my own experience acetonæmia has not been so frequent a cause of death as phthisis, acute pneumonia, and heart-failure.
Crampy pains in the legs and facial paralysis are among the nervous symptoms sometimes present, and the term diabetic neuralgia has been applied to a special form of neuralgia peculiar to this disease. It is characterized by its acuteness, stubbornness, and symmetry. Its favorite seats are the inferior dental nerves and the sciatics. Greisinger referred to the frequency of sciatica in 1859, Braun again in 1868, and others still later; but Worms in 1881 established the close relation between the two conditions and the features described. Most recently (1884), Cornillon19 collected 22 cases of diabetic neuralgia, and has further elaborated the study. Believing that diabetes affects particularly those persons who have had serious attacks of rheumatism and gout, he is inclined to think the neuralgia as much due to uricæmia as to hyperglycosuria, and that these conditions cause, not neuritis, but transitory lesions in the nerve-centres, but whether in the membranes or gray or white matter is undetermined.
19 "Des nevralgies diabétiques," Revue de Médecine, 1884, iv. 213-230.
That the phenomena of acetonæmia are those of a toxic agent or agents in the blood derived from the sugar there present is generally conceded, although Sanders and Hamilton,20 after a study of the clinical histories and the result of autopsies in several cases, are disposed to ascribe diabetic coma to slow carbonic-acid poisoning due to fat embolism of the pulmonary vessels. So far as I know, these conclusions have not been reached by any other observers. R. H. Fitz21 and Louis Starr22 have each reported cases of diabetic coma with lipæmia, carefully studied with this point in view, without finding any facts to sustain the carbonic-acid theory.
20 Edinburgh Med. Journal, July, 1872.
21 "Diabetic Coma; its relations to Acetonæmia and Fat Embolism," Boston Medical and Surgical Journal, vol. cvi. p. 24, Feb. 10, 1881.
22 "Lipæmia and Fat Embolism in Diabetes Mellitus," New York Medical Record, vol. xvii., 1880, p. 477.
Alterations in the Blood.—The blood of diabetics is variously charged with sugar, which may be in such quantity as to impart a viscidity and higher specific gravity to the plasma, which has reached 1033, the normal being 1028. On the other hand, analyses have sometimes failed to discover sugar in the blood after death, the result, probably, of the tendency of the sugar to rapid disintegration. Alcohol and acetone, or [p. 207]acetone-producing substance (aceto-acetic acid), are occasionally present as the products of such decomposition, to which are ascribed the symptoms of acetonæmia already discussed.
The presence of fat in the blood of diabetics was noted by the earliest students of the disease. It is sometimes sufficient in amount to produce a milky appearance of the serum, while the analyses of Simon revealed a quantity of 2 to 2.4 per cent., the normal being 1.6 to 1.9 per cent. The fat thus present is said to be sometimes sufficient to cause fat embolism in the capillaries of the lungs, and cases of this condition have been reported by Sanders and Hamilton,23 Louis Starr,24 and Rickards.25 Ralfe ascribes the lactescent appearance of the blood to the action of the aceto-acetic acid, since acetic will give a milky appearance when agitated with a dilute and slightly alkaline mixture of fatty matter at 100°, and the injection of acids into the blood of animals leads to the increase of fatty matter in the blood and fatty infiltration of tissues.
23 Loc. cit.
24 Loc. cit.
25 Birmingham Med. Review, Jan., 1882.
It must be admitted that the mode in which this lipæmic state of the blood is brought about is imperfectly understood, and whether it be by some chemical agency of the kind described by Ralfe, or by rapid absorption of the subcutaneous fat, or from an imperfect oxidation of absorbed fat, is undetermined. Possibly all may contribute.
Albert G. Heyl26 has described an altered appearance of the retinal vessels recognizable by the ophthalmoscope, which he ascribes to the fatty blood-plasma at the periphery of the blood-current, the normal plasma being invisible on account of its transparency.
26 For a detailed description of this appearance, with a colored lithograph depicting it, see the author's work on Bright's Disease and Diabetes, p. 262.
The red blood-discs are diminished and their ratio to the white corpuscles altered. In a count by F. P. Henry, in Louis Starr's case, the number of red discs was 4,205,000 to a cubic millimeter, the normal being at least 5,000,000; the white were 50,000 to a cubic millimeter, or 1 white to 84 red, instead of 1 to 350 or 500.
Changes in the Urine.—The most important changes in the urine are its increase in quantity and the presence of sugar. The variations in the former are extreme, being from an amount which but slightly exceeds the normal to as much as 50 pints (23.65 liters) in twenty-four hours, and even more. The quantity is of course limited by the fluid ingested, and although it may exceed this amount for a day or more, it cannot do so for any length of time. It is generally a little less. The more usual quantity in the twenty-four hours is from 70 to 100 ounces (210 to 300 cc.).
The quantity of sugar varies greatly in different cases and at different times in the same case. The maximum quantity reported by Dickinson was 50 ounces, or 1500 grammes, in twenty-four hours. The proportion may reach as much as 15 per cent., but the more usual amounts are from 1 to 8 per cent., or from 5 to 50 grains (.324 to 3.24 grams) to the fluidounce, or from 300 to 4000 grains (19.44 to 260 grams) in the twenty-four hours.
It is important to know that intercurrent febrile disease may produce a decided diminution in the daily quantity of urine, and of the sugar contained in it. A similar decrease, and even disappearance, is said to take place sometimes toward the fatal termination of a case.
[p. 208]The effect of exercise upon the sugar secretion is not uniform. Bouchardat and Kuelz have noted a diminution, and even disappearance, of sugar from urine as its result, and it is reasonable to suppose that judicious exercise is at least without harmful effect, while it is certain too that muscular exercise, if excessive, will increase glycosuria.
Changes in diet of course modify the secretion of sugar, starches and saccharine foods increasing it, while nitrogenous and oily foods diminish it. So, too, the urine secreted on rising in the morning has almost always less sugar in it than that passed on retiring; and it is not rare to find no sugar in urine passed on rising, when that passed on retiring at night may contain a small amount of sugar—from ¼ to 1 per cent. On the other hand, I have found a small amount of sugar in the morning urine when the evening urine contained none. Anxiety and excitement both increase the proportion of sugar.
Inosite, or muscle-sugar, is sometimes associated in urine with diabetic sugar, and occasionally replaces it. So, too, in experiments upon animals puncture of the fourth ventricle is sometimes followed by inosuria instead of glycosuria, and in corresponding organic disease of the brain the same thing is observed. The substitution of grape-sugar by inosite in the course of diabetes is considered by Laboulbène27 a favorable change.
27 "Note sur l'Inosurie, succédant au diabète glycosurique, et paraissant avoir une action favorable," L'Union Médicale, Oct. 14, 1883.
As would be expected, the specific gravity of saccharine urine is usually high—most frequently from 1025 to 1040—and Bouchardat noted a specific gravity of 1074 in one instance. On the other hand, I have found sugar easily detectable in urine with a specific gravity as low as 1010. Pavy records an instance of the same specific gravity, and Dickinson one in which the specific gravity was as low as 1008. It is to be remembered that the sugar is rapidly destroyed when fermentation sets in. A coincident diminution in the urea and other solids of the urine will reduce the specific gravity of a saccharine urine otherwise heavier.
The depth of color of diabetic urine is inversely as the quantity passed. Hence, when this is very large the urine is pale, and even almost colorless, but it may still contain considerable amounts of sugar and possess a decided color, quite as deep as that of urine passed in smaller quantity. When exposed to the air, diabetic urine becomes rapidly turbid from the growth of fungi, including the yeast fungus and penicilium glaucum.
The odor of diabetic urine just passed is usually in no way peculiar, but as fermentation progresses an acetous odor is developed, which is ascribed to acetic acid. At other times the odor is quite peculiar, being spoken of as vinous or compared to that of sour beer, stale fruit, alcohol, chloroform, or, as by one of my patients, to sweetbrier.
Diabetic urine has almost invariably an acid reaction, which becomes more decided as fermentation progresses. As a consequence of this increased acidity, and sometimes independent of fermentation-changes, the urine deposits a sediment of uric acid, but with this exception diabetic urine is generally free from sediment. Diabetic patients on a meat diet sometimes have a good deal of uric acid from this source.
Albuminuria may coexist with glycosuria, but is not generally found until late in the disease, after changes in the kidney begin to make their [p. 209]appearance, unless, as may happen, glycosuria supervenes upon primary renal disease.
Alcohol and acetone, or an acetone-yielding substance—aceto-acetic acid—are sometimes found in diabetic urine. They are products of the breaking up of sugar, but chemists do not explicitly agree as to the exact method in which acetone originates in the organism. First recognized in the distillate of urine and blood of a diabetic patient by Petters28 through its physical properties, odor, combustibility, etc., rather than by actual isolation, it was further investigated by Kaulich,29 Gerhardt,30 Rupstein,31 and Markownikoff,32 who obtained it in an impure state from urine; by Deichmüller and Tollens,33 whose isolated substance was pure, and finally most recently by Jaksch34 and Penzoldt.35 The former found it not only in diabetic urine, but also in that of fever, and even of carcinoma. The latter found it by the indigo test in but 18 out of 22 diabetics, and by the iodoform test, either decidedly or feebly, in 20 out of 20; in 3 out of 11 cases of typhoid fever, in 6 out of 7 cases of pneumonia, in none of 6 cases of phthisis, in 1 out of 3 cases of measles, and in 1 case of cerebro-spinal meningitis. Finally, v. Jaksch has been led to believe, from his extensive investigations, that acetone is a constant and normal product of tissue-change, although Penzoldt considers such conclusion scarcely justified.
28 Prager Vierteljahrschrift, xiv. 3, 1857, S. 88.
29 Ibid., xvii. 3, 1860, S. 59.
30 Wiener Med. Presse, No. 28, 1865.
31 Centralbl. für d. med. Wiss., No. 55, 1874.
32 Liebig's Annalen, Bd. 182, S. 362.
33 Ibid., Bd. 209, S. 25.
34 Zeitschrift für physiol. Chemie, vi. 6.
35 "Beiträge zur Lehre von der Acetonurie und von verwandten Erscheinungen," Deutsch. Archiv für klin. Med., xxxiv., 2 Oct., 1883, S. 127.
Gerhardt early discovered a substance in the urine of diabetics and habitual drinkers which struck a deep-red reaction with chloride of iron. This he considered was the source of acetone, and was probably ethyl diacetate or diacetic ether, which by decomposition yields equal molecules of acetone and alcohol; thus:
This view is still held by some, but others, in view of the recent discovery of Deichmüller and Tollens,36 that diabetic urine when distilled yields decidedly more acetone than alcohol, have suggested that the substance is derived from aceto-acetic acid.
36 Loc. cit.
The first test suggested for acetone was Gerhardt's chloride-of-iron test. A solution of chloride of iron added to urine containing acetone strikes a burgundy-red color. But this reaction occurs with so many substances that it cannot be considered entirely reliable. Ralfe's modification of Lieben's iodoform test37 is made as follows: About a fluidrachm (3.7 c.c.) of liquor potassæ, containing 20 grains (1.2 grams) of iodide of potassium, is placed in a test-tube and boiled; a drachm (3.7 c.c.) of the suspected urine is then carefully floated upon the surface. When the urine comes in contact with the hot alkaline solution a ring of phosphates is formed, and after a few minutes, if acetone or its allies are present, the ring will become yellow and studded with yellow dots of iodoform, which, in turn, will sink through the ring of phosphates and deposit itself at the bottom of the test-tube. A number of other substances [p. 210]produce the iodoform reaction, but only one of these, lactic acid, is likely to be met in urine.
37 Clinical Chemistry, Philadelphia, 1884, p. 100.
The perspiration, saliva, exudations, and effusions in diabetic cases have all been found, at times, to contain sugar.
DURATION.—Diabetes is a disease of which the duration is measured by months and years, and although cases are reported in which death supervened in from six days to six weeks after the recognition of the disease, it is evident that such periods do not necessarily measure its actual duration. The disease may have existed some time before coming under observation. On the other hand, a case is reported by Lebert which lasted eighteen years; another, under the successive observation of Prout and Bence Jones, sixteen years; and a third, under Bence Jones and Dickinson, fifteen years. The younger the patient the shorter usually is the course run and the earlier the fatal termination. Yet I have known a girl of twelve recover completely. After middle age the disease is usually so easily controlled by suitable dietetic measures, if the patient is willing to submit to them, that its duration is only limited by that of an ordinary life, while carelessness in this respect is apt to be followed by early grave consequences.
COMPLICATIONS.—The almost sole complication of diabetes mellitus is the tubercular phthisis which so often terminates it. Indeed, it is doubtful whether this complication should not be regarded as a consequence, as should also the boils, gangrenous processes, and ophthalmic conditions which have been mentioned under Symptomatology. Jaundice has occurred three times in my experience up to the present time. Senator says that when not an accidental complication due to a catarrh of the duodenum it may result from compression of the biliary capillaries by the overloaded blood-vessels and enlarged gland-cells of the liver. In one of my cases, in which jaundice appeared to be the initial symptom, but which disappeared some months before death, the autopsy revealed atrophy of the liver. It is well known that pancreatic disease, especially cancer, is apt to be accompanied by jaundice, and as pancreatic disease is often at the bottom of diabetes, it will similarly account for the jaundice, while the presence of jaundice may also suggest a pancreatic diabetes.
DIAGNOSIS, INCLUDING THE TESTS FOR SUGAR IN THE URINE.—The diagnosis of diabetes mellitus, the disease being once suspected, is easy. The passage of large amounts of pale urine of high specific gravity, the presence of thirst, dryness of the mouth, fauces, and skin, and progressive emaciation even while the appetite is good, can scarcely be misinterpreted. In the urine from such a case the application of any of the tests for sugar will produce prompt response. The urine is not always so much increased as to attract attention, while its color is also sometimes but slightly changed; but the symptoms of thirst and dryness or clamminess of the mouth are seldom wanting. On the other hand, the discovery of a glycosuria without these symptoms is, as a rule, accidental. It is a question how far such degrees of glycosuria as do not produce the usual symptoms of diabetes in an appreciable degree are signs of positive disease. At the same time, its detection is important, in that there is always danger of the simple glycosuria becoming a diabetes—a danger which its recognition and suitable treatment may avert. Accordingly, the urine of all persons having unusual appetites without evident cause, [p. 211]and of those who are fond of eating and drinking, should be tested for sugar. This should also be done for those who have passed through severe mental or physical strain, have suffered shock or concussion of the nervous system, blows upon the abdomen, etc.
Testing for Sugar.—Under the head of Diagnosis I prefer to include the testing for sugar, which requires some detailed consideration. Unless it be that the indigo test recently revived by George Oliver of London prove more delicate, that form of cupric test known as Fehling's solution is, with suitable precautions, all things considered, the most satisfactory for general use.
Fehling's volumetric solution, suitable for both qualitative and quantitative purposes, is made as follows: Dissolve 34.639 grams of pure crystallized cupric sulphate in about 200 cubic centimeters of distilled water; 173 grams of chemically pure crystallized neutral sodio-potassic tartrate and 80 grams of potassium hydrate in 500 or 600 c.c. of distilled water. To the latter add the copper solution slowly, and dilute the clear mixed fluid to 1 liter. One cubic centimeter of this solution will be decolorized by 0.005 grm. of sugar, or 200 grains will be decolorized by 1 grain of sugar. Or the copper may be dissolved in 1 liter of water, and the tartrate and potassium hydrate in another, and a cubic centimeter of each mixed at the moment they are to be used.
For qualitative testing, put a cubic centimeter of Fehling's solution into a test-tube (or if the copper and the alkaline sodio-potassium tartrate solutions are kept separate, a cubic centimeter of each), and dilute with distilled water to 5 c.c. Boil, and if, after the lapse of a couple of minutes, the solution remain unchanged, it is fit for testing. If it becomes turbid or a red sediment falls, it is spoiled, and a new solution should be obtained.38 A cubic centimeter of the suspected urine is then measured out and added drop by drop to the solution kept hot. If there is much sugar, the first drop will throw down a yellow precipitate of suboxide of copper, which becomes rapidly red. If no reaction takes place after adding the entire cubic centimeter of urine, the addition should be continued until 4 c.c. are added, when, if, after the mixture has cooled, there be no response, it may be concluded that the urine is free from sugar. By operating with a cubic centimeter of the test-fluid and the same quantity of urine or multiples thereof, we may roughly estimate the proportion of sugar. Thus, if the cubic centimeter of undiluted urine just decolorizes the cubic centimeter of Fehling's solution, sugar is present in the proportion of one-half of 1 per cent.; or if a half cubic centimeter of the urine removes all the color, the quantity is 1 per cent. If the urine is highly charged with sugar, it may be diluted, and the degree of dilution being remembered, a rough quantitative estimation may be similarly made.
38 Should this not be possible, a little more soda may be added and the fluid filtered, when it is again ready for use.
If the urine contains very minute quantities of sugar, the reaction is less satisfactory. The copper is reduced, but the suboxide is so small in quantity that it is obscured by the excess of copper solution, and a mixture results which is greenish or greenish-yellow or yellow or milky, and on standing a small yellow sediment falls to the bottom. Now, it dare not be said that it is sugar which produces such reaction. It may be [p. 212]sugar, but it may also be uric acid. Uric acid is really more frequently a source of error than is commonly supposed. I have myself seen the reaction due to it so vivid that I did not suspect it could be due to any reducing agent excepting sugar; but, noting the next day a copious sediment of uric acid which had fallen during the night, a testing of the supernatant fluid then revealed no reaction whatever. Such a urine, after being treated by the lead process to get rid of the uric acid, fails also to respond. But this process is very tedious,39 and cannot be conveniently carried out by the busy practitioner. The same thing is, however, accomplished by treating the urine with hydrochloric acid, which in twenty-four hours precipitates all of the uric acid. Simple precipitation by lead acetate solution and filtration does not answer, because all of the uric acid is not thus removed. Other substances, as hippuric acid, urates, hypoxanthin, etc., are said to act similarly, but they produce no practical interference with the test. On the other hand, a small amount of sugar may be present and yet fail to show the reaction, because the cuprous oxide is held in solution by certain substances. Such are ammonia and nitrogenous matters, including albumen, creatinin, pepsin, peptones, urinary coloring matters, etc. The latter probably produce their effect through the ammonia which is given off while heating them in the presence of an alkali. Hence all albumen should be precipitated and filtered out of urines suspected to contain sugar, and the heat applied should not be too great. Finally, excess of glucose will also hold in solution cuprous oxide, so that the suspected urine should not be added in too large a quantity at a time, but rather drop by drop.
39 The details of this process will be found in the writer's work on the Practical Examination of Urine, 5th ed., 1883, p. 63.
But qualitative testing is not sufficient during the treatment of a case of diabetes. The percentage of sugar and the quantity discharged in twenty-four hours should be determined occasionally. The process is done as follows: Place 10 cubic centimeters of Fehling's solution in a porcelain capsule, and dilute it with 40 c.c. of distilled water. Fill a Mohr's burette with the urine, which, if it contain more than 1 per cent. of sugar, should be diluted with nine times its bulk of distilled water. Slowly heat the contents of the capsule to boiling, and then allow a little of the diluted urine to run in from the burette; continue the cautious addition of urine and the gentle heating until the blue color is completely removed from the Fehling's solution. To determine the exact moment at which this takes place requires a little experience, but its recognition is facilitated by carefully tilting the capsule after each addition and stirring, so that its clear white surface may be seen through the edge of the fluid and contrasted with the latter. The number of cubic centimeters of urine used should now be read off from the burette, the number of c.c. of undiluted urine calculated therefrom, and each c.c. multiplied by .005 grm. The result indicates the quantity of sugar in grams in the urine employed, whence the percentage of sugar is determined, and also the twenty-four hours' quantity, the amount of urine passed in that period being known.
The Fermentation Test.—A very simple and easy method of determining the proportion of sugar is by Roberts's fermentation method, which, although not so precise as the volumetric process, is still [p. 213] sufficiently so for clinical purposes. A small piece of German yeast or a teaspoonful of liquid yeast is added to about four ounces (120 c.c.) of the urine, which is kept lightly stopped, at a temperature of 20° to 30° C. (68° to 80° F.), for about twelve hours; at the end of this time the sugar will have been converted into alcohol and carbonic acid. The latter will have passed off, and the urine lost in weight because of the destruction of sugar; while the difference between the specific gravity before and after the fermentation indicates the number of grains of sugar per fluidounce. Thus, suppose the specific gravity before fermentation to have been 1040, and afterward 1025; there will have been 15 grains of sugar to the fluidounce, whence, again, the twenty-four hours' quantity can be calculated. If the metric system is used, each degree of specific gravity lost will correspond to .2196 grams of sugar in every 100 c.c. of urine.
The specific gravity of the fermented urine should be compared with that of the urine soon after it is passed, because saccharine urine under suitable circumstances undergoes fermentation without the addition of yeast; and, the specific gravity being thus lowered spontaneously, the reduction in the urine fermented by yeast would appear less than it actually is. At the same time, care should be taken that the urine is of the same temperature when the specific gravity is taken before and after fermentation.
The Picric Acid and Potash Test.—Although attention was called in 1865 by C. D. Braun,40 a German chemist, to a reaction between grape-sugar and picric acid, as the result of which the latter is converted into picramic acid, very little attention seems to have been paid to this announcement. Quite ignorant of it, George Johnson rediscovered this reaction in 1882, and published it in 1883.41 It is applicable to both qualitative and quantitative purposes. In order to make use of it, a standard comparison-solution is made as follows: Take 1 fluidrachm of a solution of grape-sugar, 1 grain to the fluidounce; mix it in a long test-tube with half a drachm of liquor potassæ (U. S. P. or B. P.) and ten minims of a saturated solution of picric acid; dilute the mixture to 4 fluidrachms with distilled water, to facilitate which a tube used for the purpose may be marked at 4 fluidrachms. Raise the mixture to the boiling-point, and continue the boiling for sixty seconds, to ensure complete reaction between the sugar and picric acid. During the boiling the pale-yellow color of the liquid is changed to a vivid claret-red. Cool the liquid by cautiously immersing the tube in cold water, and if it is not then at the level of the 4-drachm mark, raise it to this by adding distilled water. The standard color thus obtained is that which results from the decomposition of picric acid by a grain of sugar to the ounce, four times diluted, or by a solution of sugar containing one-quarter of a grain per ounce. But the picramic solution rapidly becomes pale on exposure, so it becomes necessary to make a more permanent solution to use as a standard. This may be accomplished by combining liquor ferri perchloridi drachm j, liquor ammonii acetatis drachms iv, acidum aceticum (glacial) drachms iv, and water enough to make ounces iiss. The color of this is identical with that of the picric acid reduced by a one-grain solution diluted four times, and, [p. 214]according to Johnson, it will retain its color unchanged for at least six months. At the same time, whenever a new solution is made it should be compared with that of the one-quarter grain per ounce solution of sugar, boiled with picric acid and potash.
40 "Ueber die Umwandlung der Pikrinsaüre in Pikramminsaüre, und Ueber die Nachweisung der Traubenzucker," Zeitschrift für Chemie, 1865.
41 British Medical Journal, March, 1883.
For qualitative testing Johnson directs: To a drachm of urine in a test-tube add a few drops, enough to give a distinct yellow color, of a saturated solution of picric acid. Add about 10 drops of liquor potassæ and boil. If sugar is present, the mixture becomes promptly red in hue.
| FIG. 5. |

|
| Johnson's Picro-Saccharimeter. |
| The shading of the side tube indicates the ferric-acetate standard. The darker shading at the bottom of the graduated tube shows the saccharine fluid, darkened by boiling with picric acid and potash, and occupying ten divisions between dilution. |
The quantitative estimation is based upon an accurate approximation, by dilution, of the color of the tested fluid with that of the standard solution. Johnson recommends the picro-saccharimeter figured in the text. This is a stoppered tube twelve inches long and three-quarters of an inch in diameter, graduated into ten, and each of these again into ten other equal divisions. By the side of this tube, and held in position by an S-shaped band of metal, is a stoppered tube of equal diameter and about six inches long, containing the standard solution corresponding to the reaction of the one grain of grape-sugar with picric acid and potash diluted four times.
It has been found that ten minims of a cold saturated solution of picric acid are rather more than sufficient for decomposition by one drachm of a solution of grape-sugar in the proportion of one grain to the ounce. A drachm of the solution will therefore contain one-eighth of a grain of sugar, which is the strength of the solution used in making the standard-color liquid. In making the analysis, while the quantity of liquor potassæ used is always the same and the dilution is always to four drachms, the picric acid must be added in proportion to the amount of sugar present, so that if the urine contains as much as six grains to the fluidounce, sixty drops or a fluidrachm of the picric-acid solution would have to be used; and when the proportion of sugar is higher than this, the urine should be diluted with distilled water five or ten times before commencing the analysis, and the degree of dilution remembered in the computation.
If, now, a drachm of a solution of grape-sugar, containing two grains to the ounce, be mixed with the same quantity of liquor potassæ and picric acid and increased by the addition of distilled water to four drachms in the boiling tube, and boiled as before for sixty seconds, the result will be a mixture of much darker color than will be produced by the one-grain solution; but if the dark liquid be diluted with its own volume of water, the color will be the same as that of the one-grain solution or the standard.
It is plain, then, that if a given quantity of the dark saccharine fluid produced by boiling—say, enough to cover ten divisions of the graduated tube, as shown in the figure—has to have added to it an equal bulk of distilled water in order to produce [p. 215]the color of the standard solution, the tested fluid will be of the strength of two grains to the ounce; if three times, three grains; and so on; while fractional additions, as indicated by the graduated markings, would show fractional additions to the proportion of sugar.42
42 A more exact comparison of the saccharine liquid with the standard is made by pouring into a flat-bottomed colorless tube six inches long and an inch in diameter as much of the standard solution as will form a column about an inch in height, and an exactly equal column of the saccharine fluid in a precisely similar tube. The operator then looks down through the two tubes at once, one being held in each hand, upon the surface of a white porcelain slab or piece of white paper. In this way slight differences of tint are easily recognized; and if the liquid to be analyzed is found darker than the standard, it is returned to the graduated tube and diluted until the two liquids are found to be identical in color, when the final reading is made.
The presence of albumen, even in considerable amount, has but little effect upon the test, nor does the coloring matter of normal urine, according to Johnson; but he says there is a coloring matter associated with ser-albumen in albuminous urine, and with egg-albumen as well, which has a reducing action on picric acid. This is partly separated by filtering off the precipitated albumen, and entirely removed by repeated filtration through animal charcoal. So, too, the albumen removed by coagulation and filtration, if thoroughly washed, does not give any red reaction if boiled with picric acid and potash diluted in the same proportion as when testing for sugar. Neither do any other unoxidized sulphur compounds found in urine decompose the picric acid and render the test fallacious.
Johnson and his son, G. Stillingfleet Johnson, claim that the picric-acid test is as accurate as any other, and that it is even more accurate than either Fehling's or Pavy's process, because the picric acid is not acted upon by uric acid or urates, which do reduce the oxide of copper. The method of analysis by the picro-saccharimeter, they claim, is at least as speedy and as easy as any other. The materials and apparatus required are easily prepared, inexpensive, and not, like Fehling's copper solution, liable to undergo rapid changes.
But while Johnson claims that neither coloring matters of normal urine nor uric acid reduce the picric acid, he admits that he has tested with picric acid and potash a large number of specimens of normal urine with the almost uniform result of a depth of color indicating the proportion of .6 of a grain of sugar to the fluidounce, the indication varying between the limits of .5 to .7 grain. The ammonio-cupric method used at the same time gave results of from .7 to .9 grain to the fluidounce, or an excess of .1 to .3 grain. Now, if my own views, the grounds for which are announced elsewhere,43 are correct, strictly normal urine contains no sugar, and any reducing action upon oxide of copper is due to uric acid, either picric acid is reduced to a degree by uric acid or by some other constituent of normal urine. This, in the light of Oliver's44 recent investigations, may be kreatinin. For he has shown that kreatinin strikes in a few seconds a red color with the cold alkaline picric solution, which is quickened by heat. From this it would seem that the exact value of the picric-acid test has as yet to be determined.
43 Tyson, Practical Examination of Urine, 4th ed., Philadelphia, 1884.
44 On Bedside Urine-Testing, including Qualitative Albumen and Sugar, by Geo. Oliver, M.D., London, Member of the Royal College of Physicians of Lond., etc., 2d ed., London, 1884.
[p. 216]The Indigo-Carmine Test.—The fact that indigotine, the coloring matter of commercial indigo, is converted into indigo when heated with an alkali in the presence of glucose and certain carbohydrates, has recently been applied by George Oliver of London in the construction of a test-paper. Carmine of indigo is the sulph-indigotate of sodium, an intensely blue salt, soluble in 120 parts of water. Sulph-indigotic acid is made by heating indigo with sulphuric acid, and when combined with a base, sodium, produces indigo-carmine. When sodium carbonate is mixed with a solution of indigo-carmine, the latter is precipitated in a minute state of division, but is redissolved on heating, when there results a greenish-blue solution. A freshly-made mixture of the indigo solution and sodium carbonate furnishes a fluid not unlike Fehling's solution, which gives the reaction to be described with glucose. Unfortunately, such a mixture will not keep, and the reagent would be useless but for the happy idea of Oliver of making the test-paper. In doing this bibulous paper is immersed in a solution of indigo-carmine with carbonate of sodium.45 The paper is then cut into strips an inch long and one-quarter of an inch wide.
45 No more precise directions than this are given by Oliver, either in his papers in the Lancet for 1883 or in his little book just published, On Bedside Urine-Testing. The sugar test-papers, as well as the entire series of albumen test-papers, suggested by Oliver, are now made by Parke, Davis & Co. of New York, and by Wilson & Son, Harrogate, London.
Mode of Testing.—One of the test-papers and a sodium carbonate paper46 are dropped into a half-inch test-tube, and water added until the upper end is just covered; a column of fluid one inch in height and half an inch in diameter will thus be produced, so that the solution of carmine obtained on boiling will always acquire the same concentration. Heat is now applied, the tube being gently shaken, and boiling kept up for a second or two. A beautiful blue solution will result. The test-paper may now be removed or allowed to remain.
46 Test-papers of the same size, charged with a saturated solution of sodium carbonate.
Not more than one drop of the suspected urine is let fall into the tube from a pipette held in an upright position. Drops of equal size are thus secured. The contents of the tube are again freely boiled for a few seconds, after which the tube should be raised an inch or more from the flame and held without shaking, while the solution is kept quite hot, but not boiling, for exactly one minute. If glucose be present in abnormal amount, the soft rich blue will be seen first of all to darken into violet; then, according to the quantity of sugar, there will appear in succession, purple, red, reddish-yellow, and finally straw-yellow. When the last-named color has been developed the slightest shaking of the tube will cause red streaks to fall from the surface and mingle with the pale yellowness of the solution, while further agitation will cause the return of purple and violet and the restoration of the original blue.
The time required for the commencement of the reaction after the boiling of the test liquid is in inverse proportion to the amount of glucose present. When the latter is large, over 20 grains to the ounce, it will be but a few seconds; but when small, 2 or 3 grains, from thirty to sixty seconds may elapse. If the urine do not contain more than the normal amount of sugar47—i.e. under half a grain to the ounce—the color of the solution [p. 217]at the end of the heating for one minute will be unchanged. The test is available by artificial light as well as by daylight.
47 It will be noted from this that Oliver accepts the view that there is a small amount of sugar in normal urine.
Precautions.—1. Care should be taken during the testing not to shake the tube or to permit free ebullition. 2. While keeping the contents of the tube hot, the latter should not be held up between the eye and the sky, for then the early color-changes will probably escape observation. The tube should be kept below the eye-level and its contents viewed by the reflected light of some bright object, such as a sheet of white paper propped up an inch or two beyond the tube as a background. 3. Oliver is not aware that the presence of earthy carbonates will prevent the carmine reaction, but as a precautionary measure he suggests the use of a soda-paper whenever the water is exceptionally hard. 4. The acids of the urine rob the carmine-paper of much alkali, so that the addition of more than a certain number of drops of urine—varying of course with the degree of acidity—will at first retard and then prevent the reaction. The addition of the soda-paper will prevent any such interference, although Oliver says that by invariably submitting only one drop of saccharine urine to the test-paper, and keeping up the heating for not less than two minutes, he has never failed to obtain the characteristic reaction without using a soda-paper. It is well to remember, however, that an excessively acid urine may thus interfere, and that the soda-paper will prevent it. 5. The blue color of the carmine is discharged by caustic alkali—liquor potassæ or sodæ. The only chance of being misled by this reaction lies in using an imperfectly cleansed test-tube which may have contained Fehling's solution or the alkaline picric solution. The caustic alkali converts the blue carmine into a green solution, which, on heating, disappears; nor does it return by again shaking the contents of the tube.
Critical comparison of this test with Fehling's solution and picric acid by Oliver has shown that of sixty-four substances experimented upon, normal and abnormal constituents of urine or medicines which after ingestion are eliminated in the urine, Fehling's was reduced by fifteen, picric acid by eleven, and indigo-carmine by eight. The only substances producing the characteristic play of colors with indigo-carmine test-papers reacted with both picric acid and Fehling's solution. They were unoxidized phosphorus, ammonium sulphide, milk-sugar, dextrin, inosit, gallic acid, tannic acid, and iron sulphate. Both the carmine and picric acid were reduced by inosit, which merely turned Fehling's solution green. On the other hand, uric acid and urates, which reduce Fehling's solution, do not react with the carmine test, while kreatinin, which reacts with picric acid also, does not respond to the carmine. Albumen, if abundant, interferes with Fehling, but not with the indigo-carmine.
Detection of Inosit.—It has been said that inosit sometimes accompanies, and even substitutes, grape-sugar in the course of diabetes. It has been mentioned that it does not reduce Fehling's solution, but turns it olive-green. It reduces the carmine and alkaline picric acid solution, and is therefore not recognizable by these. The methods recommended for its recognition in the books are troublesome, and as its presence in the absence of sugar indicates a favorable change, it is not likely that a more precise recognition than is furnished by the olive-green reaction will be needed for clinical purposes.
PROGNOSIS.—The prognosis in diabetes depends upon the organ whose [p. 218]involvement is responsible for the symptoms, upon the stage at which the condition comes under observation, and upon the age of the patient. It has appeared to me that the cases of diabetes depending upon pancreatic disease are the most intractable, that their progress is scarcely checked by treatment, and that they are comparatively rapidly fatal in their termination. In the others, where the symptom is one of a central nervous lesion, it has always seemed to me to be of secondary importance that the glycosuria is itself less marked, that it is unattended by the other distinctive symptoms of diabetes, and that its issue is that of the nervous malady.
Again, it is well known that the later in life diabetes occurs the more amenable it is to treatment, and that if a proper diabetic diet be adhered to by the patient his life need scarcely be shortened. On the other hand, diabetes mellitus is a disease in which the expectant plan is dangerous. If it does not improve it usually gets worse; and many a patient has fallen a victim to his own indifference and indisposition to adhere to a regimen under which he could have lived his natural term of life. This is especially the case when the disease appears after middle life.
If, on the other hand, the condition becomes thoroughly established before twenty-five years of age, it is less amenable to treatment; but even in such cases a promptly vigorous treatment is sometimes followed by recovery. I have already mentioned the case of a child twelve years old in which complete recovery took place.
If tubercular phthisis supervenes, recovery is not to be expected, while intercurrent disease, as pneumonia, which is rather prone to occur, is very much more serious and apt to terminate fatally.
TREATMENT.—The treatment of the aggregate of symptoms known as diabetes mellitus is conveniently divided into the dietetic, the medicinal, and the hygienic, of which the first is by far the most important. The efficiency of this treatment depends upon the successful elimination from the diet of all articles containing grape-sugar, cane-sugar, beetroot-sugar, and starch, it being universally recognized that in the early stages of the disease these foods are the sole source of the glucose in the urine. The normal assimilative action of the liver, by which the carbohydrates are first stored up as glycogen, and then gradually given out as glucose or maltose to be oxidized, being deranged, such foods not only become useless as aliments, but if continued seem to aggravate the glycosuria, and the excretion of sugar steadily increases. There is, therefore, a double reason for excluding them from the food. This is easiest accomplished by an exclusive milk diet. The exclusive milk treatment of diabetes was suggested by A. Scott Donkin in 1868. That he is correct in his assertion that in the early stages of diabetes lactin or sugar of milk is quite assimilable, and does not in the slightest degree contribute to the production of glycosuria, I cannot doubt; that it is in this respect even superior to casein, as claimed by Donkin, I am not prepared to state from actual knowledge; but that casein itself resists the sugar-forming progress immeasurably greater than any other albuminous substance, so that in all but the most sure and advanced or complicated cases its arrest is complete, I am also satisfied. Certain it is that in a large number of diabetics the use of a pure skim-milk regimen results in a total disappearance of the sugar from the urine. That in a certain proportion of these cases a [p. 219]gradual substitution of the articles of a mixed diet may be resumed without a return of the symptoms is also true. In other more confirmed cases the use of skim-milk results in a decided reduction in the amount of sugar, with an abatement of other symptoms, which continues as long as the diet is rigidly observed. In still other cases, while the skim-milk treatment makes a decided impression upon the quantity of sugar, it still remains present in considerable amount, while the disease progresses gradually to an unfavorable issue. These three classes of cases represent, ordinarily, different stages of the disease, so that it may be said that as a rule cases recognized sufficiently early may be successfully treated with skim-milk, although it may occasionally happen that cases pursue a downward course from the very beginning despite all treatment. Yet I have never seen a case which, when taken in hand when a few grains of sugar only to the ounce were present, failed to yield to this treatment.
As to the method of administration, my practice with adults is to give eight ounces (an ordinary tumblerful) every two hours, beginning at seven or eight o'clock in the morning, and continuing to the same hour in the evening. Sometimes it is well to begin with half as much at first, but rapidly to increase to the required amount. This method ensures the ingestion of three to four quarts daily—a quantity generally sufficient to maintain the body-weight of an adult person of average size and taking moderate exercise, although a slight reduction may take place at first. But if the individual is very active or of large size, it will not be found sufficient. In such event the quantity must be increased as demanded by a feeling of unsatisfied hunger. I have known fourteen pints to be taken in twenty-four hours. But when the quantity becomes thus large, the inconvenience in ingesting it is very great, and it is much more convenient to coagulate the casein of a part of the milk and use the curd thus obtained, while the second part is drunk. Curd may be seasoned with salt to make it more palatable, and should be thoroughly masticated before it is swallowed.
The milk should not be taken too cold, especially if the amount ingested is large, else it is likely to reduce the temperature of the stomach below the point necessary for gastric digestion. The temperature should not be less than 60° F., nor much over 100°. Something depends upon the idiosyncrasies of the patient, which must be the guide as to temperatures intermediate between those named.
The chief advantage of the skim-milk over the unskimmed is simply that it is more easy of digestion. Many persons who cannot take unskimmed milk for any length of time without its deranging the digestion, or, as is commonly said, making them bilious, can take with impunity milk from which the cream is removed. Although Salomon48 claims to have shown that glycogen is produced in the liver of rabbits fed upon pure olive oil, it is at least probable that fat is among the last of the substances undergoing this conversion, and in ordinary cases of diabetes it is rather its indigestible nature which renders it prudent to remove from milk the greater proportion of fat by skimming it off.
48 Virchow's Archiv, Bd. 61, Heft 3, 1874, 18.
Still more easily assimilable is the peptonized milk, in which the casein is at least partially digested, and it should be employed where there is any [p. 220]difficulty in the way of using the ordinary milks. Either skimmed or unskimmed milk may be used for peptonizing, the latter peptonized being quite as easy of digestion as the former unpeptonized. I have found the extractum pancreatis of Fairchild Brothers & Foster most successful in the peptonizing of milk, and according to the following directions: Into a clean quart bottle put 5 grains of extractum pancreatis, 15 of bicarbonate of sodium, and a gill of cool water; shake, and add a pint of fresh cool milk. Place the bottle in a pitcher of hot water or set the bottle aside in a warm place, usually for three-quarters of an hour. When the milk has acquired a slightly bitter taste, it has been completely peptonized—that is, the casein has been completely converted into peptone. After the process is complete the milk must be immediately put on ice.
It is not always necessary to completely peptonize the milk, and if the bitter taste is unpleasant the process may be stopped short of this by putting the milk on ice, the degree of digestion depending upon the length of time the milk is kept warm.
While I am confident that the promptest and most effectual method of eliminating sugar from the urine is by a milk diet, it occasionally happens that a patient cannot or will not submit to so strict a regimen. In other instances, again, it is not necessary to resort to it, because a less restricted diet answers every purpose.
A suitable diabetic diet would also be obtained by eliminating from the bill of fare all saccharine and amylaceous and other sugar-producing substances. Such a diet is, strictly speaking, impossible. For, apart from the fact just mentioned that even fats, as well as albuminous substances to a degree, are capable of producing glycogen, the monotony of a pure meat diet soon becomes unbearable, to say nothing of other derangements it may produce. Fortunately, it is not necessary that such an exclusive diet should be maintained, for certain saccharine foods seem capable of resisting the conversion into sugar more than others. Sugar of milk, or lactin, has already been mentioned as one of these, and to it may be added the sugar of some fruits, and probably also inosit or muscle-sugar, mannite or sugar of manna, and inulin, a starchy principle abundant in Iceland moss. It is found also that there are many vegetable substances containing small quantities of sugar and sugar-producing principles which may be used with impunity in at least the milder forms of diabetes. This being the case, a bill of fare for diabetics may be constructed quite liberal enough to satisfy the palate of most reasonable persons by whom it is attainable.
FOOD AND DRINK ADMISSIBLE.—Shell-fish.—Oysters and clams, raw and cooked in any way, without the addition of flour.
Fish of all kinds, fresh or salted, including lobsters, crabs, sardines, and other fish in oil.
Meats of every variety except livers, including beef, mutton, chipped dried beef, tripe, ham, tongue, bacon, and sausages; also poultry and game of all kinds, with which, however, sweetened jellies and sauces should not be used.
Soup.—All made without flour, rice, vermicelli, or other starchy substances, or without the vegetables named below as inadmissible. Animal soups not thickened with flour, beef-tea, and broths.
Vegetables.—Cabbage, cauliflower, brussels-sprouts, broccoli, green [p. 221]string-beans, the green ends of asparagus, spinach, dandelion, mushrooms, lettuce, endive, coldslaw, olives, cucumbers fresh or pickled, radishes, young onions, water-cresses, mustard and cress, turnip-tops, celery-tops, or any other green vegetables.
Fruits.—Cranberries, plums, cherries, gooseberries, red currants, strawberries, apples, without sugar. Or they may be stewed with the addition of bicarbonate of sodium instead of sugar. (See below.)
Bread and cakes made of gluten, bran, or almond flour, or inulin, with or without eggs and butter. Griddle-cakes, pancakes, biscuit, porridges, etc. made of these flours. Where especial stringency is required these should be altogether omitted.
Eggs in any quantity and prepared in all possible ways, without sugar or ordinary flours.
Nuts.—All except chestnuts, including almonds, walnuts, Brazil-nuts, hazel-nuts, filberts, pecan-nuts, butternuts, cocoanuts.
Condiments.—Salt, vinegar, and pepper in moderate quantities.
Jellies.—None except those unsweetened. They may be made of calf's-foot or gelatin and flavored with wine.
Drinks.—Coffee, tea, and cocoa-nibs, with milk or cream, but without sugar; also milk, cream, soda- (carbonated) water, and all mineral waters freely; acid wines, including claret, Rhine, and still Moselle wines, very dry sherry; unsweetened brandy, whiskey, and gin. No malt liquors, except those ales and beers which have been long bottled, and in which the sugar has all been converted into carbonic acid and alcohol.
Vegetables to be especially Avoided.—Potatoes, white and sweet, rice, beets, carrots, turnips, parsnips, peas, and beans; all vegetables containing starch or sugar in any quantity.
The following list, including essentially the same articles, but arranged in the shape of a true bill of fare, by Austin Flint, Jr.,49 will be found very convenient:
BILL OF FARE FOR DIABETES.—Breakfast.—Oysters stewed, without flour; clams stewed, without flour. Beefsteak, beefsteak with fried onions, broiled chicken, mutton or lamb chops; kidneys, broiled, stewed, or devilled; tripe, pigs' feet, game, ham, bacon, devilled turkey or chicken, sausage, corned-beef hash without potato, minced beef, turkey, chicken, or game with poached eggs. All kinds of fish, fish-roe, fish-balls, without potato. Eggs cooked in any way except with flour or sugar, scrambled eggs with chipped smoked beef, picked salt codfish with eggs, omelets plain or with ham, with smoked beef, kidneys, asparagus-points, fine herbs, parsley, truffles, or mushrooms. Radishes, cucumbers, water-cresses, butter, pot-cheese. Tea or coffee, with a little cream and no sugar. (Glycerin may be used instead of sugar if desired.) Light red wine for those who are in the habit of taking wine at breakfast.
Lunch or Tea.—Oysters or clams cooked in any way except with flour; chicken, lobster, or any kind of salad except potato; fish of all kinds; chops, steaks, ham, tongue, eggs, crabs, or any kind of meat; head-cheese. Red wine, dry sherry, or Bass's ale.
[p. 222]Dinner.—Raw oysters, raw clams.
Soups.—Consommé of beef, of veal, of chicken, or of turtle; consommé with asparagus-points; consommé with okra, ox-tail, turtle, terrapin, oyster, or clam, without flour; chowder, without potatoes, mock turtle, mullagatawny, tomato, gumbo filet.
Fish, etc.—All kinds of fish, lobsters, oysters, clams, terrapin, shrimps, crawfish, hard-shell crabs, soft-shell crabs, (No sauces containing flour.)
Relishes.—Pickles, radishes, celery, sardines, anchovies, olives.
Meats.—All kinds of meat cooked in any way except with flour; all kinds of poultry without dressings containing bread or flour; calf's head, kidneys, sweetbreads, lamb-fries, ham, tongue; all kinds of game; veal, fowl, sweetbreads, etc., with curry, but not thickened with flour. (No liver.)
Vegetables.—Truffles, lettuce, romaine, chicory, endive, cucumbers, spinach, sorrel, beet-tops, cauliflower, cabbage, brussels-sprouts, dandelions, tomatoes, radishes, oyster-plant, celery, onions, string-beans, water-cresses, asparagus, artichoke, Jerusalem artichokes, parsley, mushrooms, all kinds of herbs.
Substitutes for Sweets.—Peaches preserved in brandy without sugar; wine-jelly without sugar, gelée au kirsch without sugar, omelette au rhum without sugar; omelette à la vanille without sugar; gelée au rhum without sugar; gelée au café without sugar.
Miscellaneous.—Butter, cheese of all kinds, eggs cooked in all ways except with flour or sugar, sauces without sugar or flour. Almonds, hazel-nuts, walnuts, cocoanuts. Tea or coffee with a little cream and without sugar. (Glycerin may be used instead of sugar if desired.) Moderately palatable ice-creams and wine-jellies may be made, sweetened with pure glycerin; but although these may be quite satisfactory for a time, they soon become distasteful.
Alcoholic Beverages.—Claret, burgundy, dry sherry, Bass's ale or bitter beer. (No sweet wines.)
Prohibited.—Ordinary bread; cake, etc. made with flour or sugar; desserts made with flour or sugar; vegetables, except those mentioned above; sweet fruits.
49 "On the Treatment of Diabetes Mellitus," a paper read before the American Medical Association at its meeting in Washington, May, 1884, and published in the Journal of the association July 12, 1884. I have so far modified the bill of fare as to permit the use of milk, which Flint excludes.
One of the foods the omission of which is most illy borne by the diabetic, however great his previous indifference to it, is wheaten bread, while the substitutes which have been at different times suggested for it very imperfectly supply its place. Perhaps the best known of these is the bread made of gluten flour. It was suggested by Bouchardat in 1841, and is made by washing the ordinary wheat flour to free it from starch.50
50 The Health Food Company, of 74 Fourth Avenue, N.Y., prepare a gluten flour by first removing the five bran-coats, pulverizing the cleaned berry by the cold-blast process, stirring the powder into iced water, and precipitating the gluten, cellulose, and mineral matters, siphoning off the water holding in suspension the starch, and drying out the precipitate. In this manner the salts of the wheat are retained. A purified gluten made by the Health Food Company is deprived of the cellulose walls of the cells in which the gluten granules are held. Directions for making gluten bread and cakes of various kinds are furnished by the company on application.
Gluten flour, however prepared, contains some starch, as indeed it must if bread is to be made out of it; and I confess to having been a good deal disappointed in its use. I have known the sugar absent in a [p. 223]selected diet to return when gluten bread was permitted, and again disappear on its withdrawal. Of course gluten flour contains less starch than the ordinary wheat flour, and there may be cases where the starch in the former can be assimilated when the quantity in the latter cannot be. The gluten may be made into porridge.51
51 Gluten porridge is made by stirring the gluten into boiling water until thick enough, and then keeping up the boiling process for fifteen minutes. A little salt and butter are added at the close to improve the flavor, and it may be eaten with milk or cream.
A method of getting rid of the starch and sugar in bread, suggested by Liebig and tried by Vogel, consists in converting the starch into sugar by the action of diastase and dissolving out the sugar thus produced. This is accomplished by treating thin slices of bread with an infusion of malt. The bread is then washed, dried, and slightly toasted.
Another substitute for wheaten flour is the bran flour whence the starch is removed by washing.52 The bran itself, according to Parkes,53 sometimes contains as much as 15 per cent. of nitrogenous matter, 3.5 per cent. of fats, and 5.7 per cent. of salts. It is therefore not wholly innutritious, although the salts are washed out in removing the starch. It is considered especially useful when there is constipation, the slightly irritant properties of the bran aiding in maintaining a proper peristalsis and action of the bowels. These irritant properties are, however, inversely as the degree of comminution. The bran flour may be made with milk and eggs into a variety of cakes, of which the best known are those made according to Camplin's directions.54
52 A very carefully prepared bran flour, as well as a wheat-gluten flour, is prepared by John W. Sheddon, pharmacist, corner of Broadway and Thirty-fourth street, New York City.
53 Practical Hygiene, 5th ed., Philadelphia, 1878, p. 222.
54 The following are Camplin's directions for making biscuit of bran flour: To one quarter of a pound of flour add three or four fresh eggs, one and a half ounces of butter, and half a pint of milk; mix the eggs with a little of the milk, and warm the butter with the other portion; then stir the whole together well; add a little nutmeg or ginger or other agreeable flavoring, and bake in small forms or patterns. The cake, when baked, should be about the thickness of an ordinary captain's biscuit. The pans must be well buttered. Bake in rather a quick oven for half an hour. These cakes or biscuits may be eaten by the diabetic with meat or cheese for breakfast, dinner, or supper; at tea they require rather a free allowance of butter, or they may be eaten with curd or any soft cheese.
Where extreme restriction of diet is not required the ordinary bran bread of the bakers may be used. The unbolted flour of which this is made of course contains the starchy principles, but in consequence of the retention of the bran the proportion of starch is less. The cold-blast flour of the Health Food Company is said to contain the nutritious, but not the innutritious, parts of the bran.55
55 It is made by pulverizing the carefully cleaned wheat by a compressed, cold air blast, which strikes the wheat and dashes it to atoms.
The almond food suggested by Pavy is another substitute for bread. The almond is composed of 54 per cent. of oil, 24 per cent. of nitrogenized matter known as emulsin, 6 per cent. of sugar, and 3 per cent. of gum, but no starch enters into its composition. Theoretically, therefore, the food should be everything that can be desired if the gum and sugar can be removed. The latter is done by treating the powdered almonds with boiling water slightly acidulated with tartaric acid, or soaking the almonds in a boiling acidulated liquid which may form a part of the process for blanching. The boiling and acid are necessary to precipitate [p. 224]the emulsin, which would otherwise emulsify the oil of the almond. Pavy speaks well of biscuit made of almond flour and eggs, which he says go very well with a little sherry or other wine, although he admits they are found too rich by some for ordinary consumption. One person only under my observation has used the almond food, and found it unpalatable.
Seegen recommends an almond food made as follows: Beat a quarter of a pound of blanched sweet almonds in a stone mortar for about three-quarters of an hour, making the flour as fine as possible; put the flour thus obtained into a linen bag, which is then immersed for an hour and a quarter in boiling water acidulated with a few drops of vinegar. The mass is thoroughly mixed with three ounces of butter and two eggs; the yolks of three eggs and a little salt are added, and the whole is to be stirred briskly for a long time. A fine froth made by beating the white of the three eggs is added. The whole paste is now put into a form smeared with melted butter and baked by a gentle fire.
Biscuits made of inulin, the starchy principle largely contained in Iceland moss, were suggested by Kuelz. Although a starch, it is one of the assimilable ones alluded to, of which small quantities at least may be taken as food without appearing in the urine as sugar. The biscuits are made with the addition of milk, eggs, and salt, and are inexpensive.
To some persons sugar is almost as imperative a necessity as bread, although to many it is not a very great sacrifice to omit it from ordinary cooking, if not from tea and coffee. For the latter it is just as well to dispense with sugar altogether. But where patients feel that they must have some substitute for sugar, glycerin has been suggested for this purpose, at least for sweetening tea and coffee. But Pavy has noted56 that under the use of glycerin the urine increased from three and three and three-fourth pints to between five and six pints, and the sugar from 1100 grains to 3000 grains per diem, in the course of three days. Its withdrawal was followed by a prompt fall in both the urine and sugar, a return to it by a second increase, and subsequent withdrawal by another decline. Along with the increase of urine and sugar came also more thirst and discomfort. An examination of the chemical composition of glycerin would seem to confirm these results of experience. Glycerin is represented by C3H8O3, sugar by C6H12O3, and glycogen by C6H10O5; whence it is evident that a conversion of glycerin into sugar may take place in the liver. These facts seem to show conclusively that glycerin is no suitable substitute for sugar. I therefore do not use it.
56 On Diabetes, London, 1869, p. 259.
From what has been said it may be inferred that sugar of milk, mannite, and lævulose, or fruit-sugar, are admissible where sugar is demanded. They may be tried, but the urine should be carefully examined under their use, and if glycosuria occur or be increased they should be promptly omitted.
Almost every purpose of sugar in the cooking of acid vegetables is served by bicarbonate of sodium or potassium. As much bicarbonate of potassium to the pound as will lie upon a quarter of a dollar will neutralize the acidity of most fruits which require a large amount of sugar to mask this property. In this manner cranberries, plums, cherries, gooseberries, red currants, strawberries, apples, peaches, and indeed [p. 225]all fruits to which sugar is usually added in the cooking, become available to the diabetic.
In the matter of drinks, where the patient is not on a skim-milk diet, which usually affords as much liquid as is required by the economy, little restraint need be placed upon the consumption of water, which is demanded to replace that secreted with the sugar. Instead of water, Apollinaris water, Vichy, or the ordinary carbonated water may be used if preferred, and to many they are much more refreshing by reason of the carbonic acid they hold in suspension. Apollinaris water is particularly so, and one of my patients, who recovered completely under a suitable selected diet with which this mineral water was permitted, insists that it was that which cured her.
Where a simple selected diet is adopted, tea and coffee without sugar are usually permitted. The propriety of the substitutes for sugar already referred to must be determined by circumstances.
Of distilled and fermented liquors, moderate quantities of whiskey and brandy, dry sherry and madeira, the acid German and French wines—in fact, any non-saccharine wines—may be permitted. A medical friend who reports himself about cured of diabetes writes me that he has consumed eighty gallons of Rhine wine since he began to adhere closely to a diabetic diet. On the other hand, the free use of the stronger alcoholic drinks has been charged with causing diabetes, and I have known such use to produce a recurrence of sugar. No malt liquors, except those in which the sugar has been completely converted into carbonic acid and alcohol, should be used. Bass's ale may be allowed where no especial stringency is required.
HYGIENIC TREATMENT.—The patient should be surrounded by the most favorable hygienic influences. He should sleep in well-ventilated rooms; pass much time in the open air; bathe regularly, but not in water that is very cold, and especially the body should not be long submerged in cold water, as the liver must share the general internal hyperæmia incident to prolonged cooling of the skin, and increased glycosuria may result. I have known sugar to reappear after a prolonged drenching of the skin of patients overtaken by a rainstorm. Perhaps the most suitable time for the hot or tepid bath is on retiring in winter, but in summer it may be taken on rising. Thorough friction of the entire body should be practised after the bath or independently of it. An ounce or two of sodium carbonate may be added to it with advantage, as it softens the skin and facilitates the removal of the effete epithelium. The bowels should be kept regularly open, as the effect of their confinement is to produce torpor and congestion of the liver.
Certain natural mineral waters have always enjoyed a reputation for the cure of diabetes, and notably those of Vichy and Carlsbad. The former is an alkaline water with a slight laxative tendency, and the latter a decided aperient alkaline-saline water; and it is not unlikely that they owe a part of their good effects to an action upon the liver and upper bowel. This seems the more likely because Carlsbad, which enjoys the highest reputation, contains a far larger proportion of chlorides and sulphates, which are purgative. Vichy water contains 35 grains of carbonates to the pint, and Carlsbad 11, but the latter contains twice the proportion of chlorides, or 8 grains to the pint, and ten times as much sodium [p. 226]sulphate, or 19 grains to the pint. They may be used as adjuvants to the treatment, a pint of Vichy or half as much Carlsbad in the morning. Being imported waters, they are comparatively expensive, and I know of no American waters which closely approach them in composition.
Of American waters, the Saratoga Vichy contains twice as much chlorides as the Carlsbad, 17.7 grains to the pint, but no sulphates. It contains about the same amount of carbonates as Vichy. It is therefore a saline-alkaline water, and may be expected to serve the purposes of Vichy and some of those of Carlsbad, for which it may be substituted. Most of the American mineral waters vaunted as useful in diabetes will be found, on comparison with these waters, to be chemically indifferent, and therefore about as useful as so much ordinary spring-water. Of the Crab Orchard Springs in Kentucky, the Sowder's spring contains 25 grains of sulphate of sodium and magnesium and 7 grains of sodium chloride to the pint, therefore about the same proportion of the two substances combined as Carlsbad; yet I am not aware that these waters have any reputation in diabetes. The waters of Bedford Springs, Pennsylvania, also approximate them in the proportion of sulphates of sodium and magnesium.
Other Saratoga waters have an undoubted action on the liver through their chlorides, and may be used in lieu of the European waters above referred to, and of the Saratoga Vichy, when these cannot be obtained; such are the Geyser spring, which contains 70 grains of chlorides to the pint, and the Hathorn, containing 63 grains.
MEDICINAL TREATMENT.—While the dietetic treatment, and especially the skim-milk treatment, of diabetes mellitus is much to be preferred for its results over an exclusively medicinal treatment, and is of itself sufficient to control, if not to cure, a large number of cases, yet instances arise in which it is insufficient to complete the removal of sugar from the urine, and there are others in which it is impossible for various causes to carry out such treatment.
In my book on Bright's Disease and Diabetes, published three years ago, I gave the preference of drugs to ergot; but since then extended opportunities have convinced me that codeia is a far more efficient remedy. Repeated comparative trials of this drug in the wards of the Philadelphia Hospital and elsewhere have satisfied me of this. The trials have been made while the patients were upon a mixed diet, which I hold to be the only fair way of arriving at a knowledge of the true value of a drug in the disease. Codeia was first suggested by Pavy in lieu of opium and morphia, which had long been used, his reason being that it did not produce the same narcotic effect. Favorable reports upon its use have been made by Foster, Image, Brunton, R. Shingleton Smith, Cavafy, Austin Flint, Sr., Harvey L. Byrd, and others. It may be given in pill or solution. One should begin with ¼ of a grain three times a day, increasing ¼ of a grain daily until the sugar disappears or the remedy ceases to have any effect, or until drowsiness is produced. Thus gradually increasing, I have reached as high as 47 grains in a day. Cavafy has given 15 grains three times daily.
Opium—which is said to have been used by Aetius for this disease—or morphia might be used if codeia cannot be obtained, but they are less efficient, more dangerous, and more apt to produce the troublesome [p. 227]symptom of constipation. MacGregor57 gave in one case 60 grains of opium, and in another 90 grains, in the twenty-four hours.
57 London Medical Gazette, 1837.
While I have seen the most striking results upon the quantity both of sugar and urine during the administration of codeia, and at the same time have noted a gain in flesh and strength, I cannot say that I have ever seen a case totally recover under its use. Such cases are, however, reported by others. I have always used it in the very worst cases, where dietetic measures had also failed to remove the sugar. As to the mode of action of codeine, we can only speculate. It may be said that it quiets the irritation of the vaso-motor centre, whence result the glycosuria and other symptoms of diabetes.
Next to codeine in efficiency, of drugs, is ergot. The favorable results of its use are more easily explained by its physiological action—contraction upon the muscular walls of blood-vessels—than those of codeine, but it is not so efficient a remedy. It may be used by beginning with half a drachm, and increasing to a drachm, four times a day. Larger doses than this, as much as half an ounce four times a day, have been given, but the stomach rarely permits their continuation for any length of time.
Bromide of potassium, an old remedy for diabetes, has recently been revived and much lauded by the French physicians, but I have never found any results from its use. I can understand, however, how in certain cases of nervous origin it may be useful.
Comparatively recently, Clemens of Frankfort-on-the-Main has recommended the use of what he terms brom-arsen or bromide of arsenic. The dose is one-forty-eighth of a grain three times a day, gradually increased by this same amount until one-sixth or one-fifth of a grain is given daily.58 Clemens, however, unites with its use a dietetic treatment. I have used it in connection with an unselected diet, and have not found the results claimed by Clemens. It is, however, both tonic and sedative, and as such is to be recommended in conjunction with other measures.
58 The late Mr. R. F. Fairthorne, with Mr. James T. Shinn, apothecary, cor. Broad and Spruce streets, Philadelphia, prepared for me a solution of bromide of arsenic in the following manner: 77 grains of metallic arsenic in powder are added in small portions to 240 grains of bromine, the latter being placed in a long test-tube immersed in ice-water to control the otherwise violent reaction. One hundred grains of the tribromide thus obtained are dissolved in sufficient distilled water to make ten fluidounces. One minim will then contain one-forty-eighth of a grain.
Arsenic itself has some reputation in the treatment of diabetes, based upon the observation of Salkowsky that glycogen diminishes in the livers of animals poisoned with arsenic. It is at least a good adjuvant tonic. Leube gave it in diabetes in doses of one-third of a grain three times a day.
Strychnia is also very useful as a tonic, and may be used either alone or in the shape of the sulphate, or combined with arsenic and iron, or it may be given, perhaps preferably, in solution in combination with an acid. Given in combination with phosphoric acid, I believe it the most valuable tonic available in this disease.
To supply the phosphates, in which gluten bread is deficient, as well as for their tonic effect, the various preparations of phosphates are useful. [p. 228]The well-known compound syrup of the phosphates, or Parrish's chemical food, may be considered a type of these preparations. Every fluidrachm, which is a dose, contains 2½ grains of calcium phosphate, 1 grain of ferric phosphate, with fractions of a grain of sodium and potassium phosphate with free phosphoric acid. Similar is the solution of phosphates and phosphoric acid59 known in this country as solution of phosphoric acid with iron, or the latter may be omitted.
| 59 Rx. | Calcii phosphat. | gr. iij; |
| Magnesii phosphat. | gr. ss; | |
| Potassii phosphat. | gr. iv; | |
| Ferri phosphat. | gr. ss; | |
| Ac. phosphoric | minim vj; | |
| Aquæ q. s. ad. | fluidrachm i, which is a dose. |
Iodide of potassium has been used in some cases with satisfactory results, and may be expected to be useful where syphilitic disease of the nervous system is suspected.
Seegen has seen sugar disappear from the urine under a dosage of 20 to 30 drops of tincture of iodine daily, but the sugar reappeared after the remedy was discontinued.
Lactic acid was recommended by Cantani on theoretical grounds as a substitute for sugar. He supposes that in health the sugar ingested is converted by the liver into lactic acid, and he would furnish the latter already formed, and thus spare the liver this function. Senator also favors the use of this acid for a similar purpose, but reasons that in health sugar is converted into lactic acid in the small intestine, while in diabetes this conversion is interfered with. Hence, too, it should be given fully formed. Patients under its use are said to gain in weight and to become stronger, while it is not claimed that it alone diminishes the glycosuria; this must be brought about by a selected diet. The lactic acid is simply an important force-producer not otherwise obtainable, because sugar fails to undergo its usual conversion. Cantani recommends that from 75 to 150 grains of the acid should be taken daily in from 8 to 10 fluidounces of water. Diarrhoea and pains in the joints are said to follow the use of large quantities of the drug, but these again disappear on its omission. My experience is limited to a single case, which recovered while taking 30 drops three times a day in conjunction with Carlsbad water and a pill of iron, quinia, and arsenic.
Senator suggested that the fatty acids—oleic, palmitic, stearic, and butyric—be used on the same principle that lactic acid is given, that their force-producing power may be availed of. To this end he prescribed, with partially satisfactory results, soap in pills containing 21/3 grains each, of which four were taken daily.
Cod-liver oil is especially suitable as a food where debility is to be combated. Even those who claim that fats are convertible into sugar in the liver admit that it is only in the most advanced stages of diabetes that such conversion takes place. Cod-liver oil, therefore, in common with other fats, may form part of a diabetic diet, and is especially indicated where phthisis is present, as it so often is, in the latter stages of the disease, or indeed whenever a good tonic is indicated.
In 1882, Moleschott60 suggested the use of iodoform in diabetes. He reported the effect of its use in five cases, giving .1 to .3 grm. (1.5 to [p. 229]4.5 grs.) in pill with extract of lactucarium and cumarin, the purpose of the latter being to disguise the odor. His formula was as follows: Iodoform, 1 gram (15 grs.); ext. lactuc. sat., .1 gram (15 grs.); cumarin, .1 gram (1.5 grs.), to be made into twenty pills. In one case the sugar disappeared in twelve days; in the second, at the end of six months; in the third case it had diminished from 14.4 to 1.6 grams in three months; in the fourth, from 28 grams to 1.6 in four months; and in the fifth case, from 9.2 to 6.1 grams.
60 Wiener Med. Wochenschr., Nos. 17, 18, 19.
The use of the remedy in Moleschott's hands produced no unpleasant results, but Drasch,61 who used the same treatment after Moleschott's method in three cases, with the effect of diminishing the thirst, the quantity of urine, and the proportion of sugar, found excessive itching of the skin, diminished appetite, and diarrhoea to result in such degree as to demand its disuse in the majority of cases. Iodoform has been used by the Italian physicians De Renzi,62 Bozzolo,63 and Silvestrini,64 and by Sara E. Post65 of New York, with varying but generally favorable results, except in Silvestrini's case. These results included diminution in thirst, quantity of sugar and urea, with increase in weight. The drug deserves a trial in doses of from 1 to 2 grams (15 to 30 grains) a day, but due regard should be had to possible toxic effects; and to this end the administration should be interrupted at the end of one or two weeks, and the interruption continued for a like period. It may be given in pill or in capsule, and in divided doses or in a single dose at bedtime. The latter course is recommended by Post, and is said to avoid eructations and anorexia. Theories of its action based upon experimental use of poisonous doses ascribe its effect to a primary stimulating and ultimately fatally degenerative effect upon the protoplasm of cells, and especially those of the liver and nervous system.
61 Wiener Med. Presse, 1882, xxiii. 1487.
62 "Tre Storie di Diabete." Gior. internaz. d. sc. med., Nap., 1882, N. S. iv. 913-917.
63 "Sur l'action du iodoforme dans la diabète sucre," Arch. ital. de biol., Turin, Feb., 1883, iii. 317-321.
64 "Iodoforme dans le diabète," La France Méd., October, 1883, ii. 567.
65 Archives of Medicine, April, 1884, p. 116.
Transfusion of blood has been recommended by Dieulafoy,66 and is approved of by Ralfe,67 especially to combat the symptoms of acetonæmia, which, if due to a toxic agent, as seems most likely, should be met by altering the percentage composition of the blood with relation to the toxic agent.
66 "Étude sur la Transfusion du Sang dans le diabète sucre," Bullétin et Mém. Soc. Méd. de Hôp. de Paris, 1884, 4, S. 1, 38, 41.
67 "Discussion before the Path. Soc. of London," Lancet, Apr. 7, 1883, p. 592.
Diabetic neuralgia yields generally to the treatment of the disease in general correspondingly to the reduction in the quantity of sugar, and at times to salicylate of sodium, while it does not respond to morphia or other remedies for ordinary neuralgia.
The alkalies, which attained some reputation after Mialhe claimed for them the power of destroying sugar in the blood and of neutralizing the fatty acids which were thought to accumulate there in consequence of the deficient action of the skin, are not often used at the present day. Potassium carbonate was the favorite preparation, and in the hands of Pavy its use seems to have been followed by good results. He gave it in 10, 15, and 20 grain doses in combination with aromatic spirit of [p. 230]ammonia. Sodium bicarbonate was less satisfactory, as were also potassium acetate, potassium citrate, and Rochelle salts. These were given in doses of from four drachms to an ounce daily. In Germany, too, the alkaline treatment has been used to some extent.
As is the case with so many diseases which are incurable by any special treatment, a large number of remedies have at different times been suggested for diabetes, mostly on a foundation which does not admit of close analysis. One of these was the nitrate of uranium, suggested by Dale of Lemont, Pennsylvania, who gave it in doses of 1 grain three times daily, increased to 3 if necessary, in pill, powder, or solution, by aid of a few drops of nitric acid. He appears, however, to have used it in connection with a selected diet. I have tried it both with and without a selected diet; in the latter case there was no effect, and in the former there was none which the diet alone would not have produced.
Sodium phosphate, salicylic acid, salicylate of sodium, have all been used, it is claimed, with good results, and the late Dr. Dougherty of Newark, New Jersey, used with apparent advantage a mixture into which all of these, together with sodium carbonate, entered, made up with glycerin, tincture of cardamom, and water, the doses being 2½, 2½, 4½, and 8½ grains respectively. Moleschott has also obtained good results with salicylic acid.
SYNONYMS.—Scrophula, Scrofulosis, Morbus scrophulosus, Struma, King's evil, The evil, Quince, Cruels and Crewels (Scotice).
DEFINITION.—A morbid condition of the system manifested by a peculiar liability to certain forms of nutritive disorders of the skin, mucous membranes, joints, bones, organs of special sense, and especially the lymphatic glands.
There is probably no disease of which it is more difficult to give an exact and satisfactory definition than scrofula. The general tendency of medical opinion within the last few decades has been to narrow the significance of the term, and even to restrict it to those slow and indolent inflammations and over-growths of lymphatic tissue which end in caseation and finally imperfect suppuration. Formerly almost every deviation from healthy functional activity in the young, as well as every disorder of nutrition which could not be assigned to any definite cause, was called struma; and thus, as Heule well remarks,1 "Scrofula became the receptacle into which one vaguely casts all the ailments which afflict children under fourteen years, and of which we do not know the cause."
1 Handbuch der Rationellen Pathologie.
Before hereditary syphilis was understood all its manifestations were classed as scrofulous, and at least one eminent authority in the United States2 has expressed the opinion that scrofula is only a manifestation of the syphilitic poison in the second or third generation. Rickets, chronic hydrocephalus, favus, lice, and worms (Lugol), diabetes (Carmichael), and even scirrhus and cancer (R. Hamilton), have all been classed as scrofulous diseases. Then there is a large class of unhealthy persons whose morbid state can be no more definitely expressed than by saying that they are "delicate" or of "feeble health" or of "frail constitution," and by some all these are included under the term scrofulous. But as knowledge advances, and pathological knowledge as well as diagnostic acumen becomes larger and keener, many of these affections and morbid conditions can be eliminated from scrofula and assigned their true pathological and nosological position.
2 S. D. Gross, Transactions American Medical Association, 1878.
To many who have been educated in the more modern schools of medical thought, therefore, our definition will appear much too broad, while to others it may appear too narrow.
Scrofula is essentially and purely a diathetic, not a cachectic, disease. [p. 232]It is true that what may be called the manifestations or lesions of the disease are often excited by some preceding dyscrasia, and also that the long persistence of these lesions may excite a cachectic condition which we might call the scrofulous cachexia; still, as many children suffer from the lesions of scrofula who have never exhibited any evidence of a precedent dyscrasia, but on the contrary appear to be in perfect health, and many others, on the other hand, show unmistakable evidence of ill-health and are decidedly dyscrasic, yet are never attacked by scrofula, it is believed that every subject of scrofula becomes so not because of any pre-existing dyscrasia or cachexia, but because of some peculiar condition of the system—innate or acquired—which constitutes a diathesis.
"The hypothesis," says Niemeyer,3 "that scrofula depends upon a faulty composition of the blood (dyscrasia), and that the lesions found in scrofulous persons were due to a deposit in the tissues of a matter circulated by the blood and called a scrofulous material, is almost universally abandoned."
3 Textbook of Practical Medicine, vol. ii.
But while insisting upon the peculiar and, so to say, specific origin of the disease in some special condition of the system, without which it will never exist, it is admitted that the lesions of scrofula do not differ essentially from other similar lesions of the same tissues of a non-scrofulous origin. They are mostly of an inflammatory nature, and are only to be distinguished by the often trivial character of their exciting causes—often, indeed, by the total absence of any known exciting cause—and by their tediousness and intractability.
ETIOLOGY.—We believe, as already stated above, that the essential cause of scrofula is some peculiarity in the constitution of the tissues of the scrofulous subject; and we think it highly probable that H. F. Formad of Philadelphia has pointed out what constitutes this peculiarity. He declares—and the correctness of his observation has been abundantly verified—that microscopic examination of the tissues of certain animals characterized by their extreme aptness to be affected by scrofula and tuberculosis, as well as of children known to have been scrofulous or tuberculous, discloses the fact that the lymph-spaces in these subjects are always more numerous, larger, and more crowded with cells than in non-scrofulous subjects. The tissues of the scrofulous are therefore coarser, less compact and solid, and there is a greater tendency to undue cell-growth, than in the non-scrofulous. And these are precisely the characteristics which they present clinically, and such as we might have, a priori, expected to find.
This peculiarity of anatomical structure is in a large number of cases undoubtedly inherited from the parents, but while heredity plays, as is well known, an important part in the etiology of struma, it is not the essential factor. Bad hygienic surroundings, overcrowding, and consequent want of fresh air, improper food, consisting of a too great proportion of starch, during the early months or years of life, will cause the growing tissues to assume the peculiar anatomical arrangement alluded to above. "A coarse diet, containing but little nourishment in comparison with its bulk, is especially held in evil repute. The earlier this injudicious feeding of an infant commences, so much the greater danger that it will become scrofulous; hence the children fed on pap furnish a very important contingent to the army of scrofulous persons."4 The [p. 233]well-known fact that few children at the breast suffer from scrofulous lesions, but that a large number do so within the first two or three years after weaning, certainly tells in favor of the belief that too much starch and an insufficiency of animal food favor, if they do not actually produce, that faulty nutrition and construction of tissues which we believe lies at the foundation of the scrofulous diathesis. Independent, however, of improper food and the other predisposing causes mentioned, it is quite probable that faulty nutrition caused by accidental disease of the digestive or assimilative organs during infancy may create a predisposition. How else can we account for those not very rare cases in which from parents perfectly free from any scrofulous taint a large family of children may be reared, of which only one will suffer from any scrofulous lesions? Two such instances have been brought to my notice, and as the children in these cases lived upon a farm on the water-side, and enjoyed an abundance of pure air and salt-water bathing, and were certainly not stinted in food of proper quality, it is difficult to account for the acquired diathesis except upon the hypothesis above. Among the general predisposing causes of scrofula in addition to the special ones I have mentioned may be added—
4 Niemeyer, loc. cit.
1. Locality and Climate.—It has long been believed that scrofula is more common in the temperate zone than in the extreme north or in the tropics. While this is probably true, it must be stated that a sufficient amount of reliable statistics bearing upon this point have not yet been collected to prove the fact beyond cavil. That we should find that the disease prevails more extensively in cold and damp situations than in warmer and drier ones is to be expected, since the former conditions involve a greater confinement within dwellings, and consequently a diminished supply of fresh air, which, as we have seen, constitutes one of the predisposing causes of scrofula. Moreover, it is in these situations we would encounter a greater number of catarrhs, which, as we shall see, are known to be among the most active of the exciting causes of the glandular affections of scrofula.
2. Season.—For the same reason we find that a large number of cases of scrofula make their appearance in the early spring months, the results of catarrh contracted during the previous winter or of the sudden changes of temperature which accompany the transition of winter to summer.
3. Age.—Scrofula is essentially a disease of early life, but not exclusively so. As the diathesis can only be acquired directly from the parent, or fortuitously by malnutrition during the period of active growth, it follows that it becomes established, if at all, before the age of twenty years. And as the predisposition seems to be quite strong in most cases, and as the exciting causes are more apt to be applied during the earlier years of life, it is not surprising that a very large majority of the cases occur between the ages of three and fifteen years. A few, however, escape during childhood, and only suffer from it between twenty and thirty, while a small number only develop the disease in old age. Rindfleisch mentions the period between twenty and thirty as a common one for the development of hereditary scrofula; and senile scrofula was first pointed out by Sir James Paget.5 In all these cases of deferred [p. 234]manifestation of the scrofulous diathesis—and they are not very numerous—it is to be presumed that they have escaped the most active of the exciting causes of the disease. Indeed, it is natural that a person having inherited the predisposition should be more sedulously guarded—at first by his parents, and afterward by himself—against the exciting causes of scrofula during infancy and adolescence.
5 Clinical Lectures and Essays, London, 1875.
4. Sex.—There is no reason to believe that sex plays any part in the predisposition to this disease. Both sexes seem to be affected in about equal proportions, but from the statistics bearing upon this point it does seem to have some influence in determining the variety of its lesions. Thus, females seem to be more frequently affected with glandular disease, while males suffer from diseases of the joints in the form of coxalgia, white swelling of the knee, and Pott's disease.
5. Condition in Life: Social Position.—If what we have said about the predisposing influence of improper or insufficient food, overcrowding, etc. be true, it will naturally be inferred that a large proportion of the cases of scrofula will be found in the lower strata of society; and this is true. Especially in cities, where the disease prevails most extensively, we always find that the denizens of narrow streets, lanes, and alleys furnish the largest contingent to the deaths as well as the deformities from scrofula. It is here that the poor congregate to avail themselves of the cheaper rents, and here will be found combined all those predisposing causes which may be briefly summed up in one word—poverty. It is true that cases of scrofula are quite numerous in the country, and in a note to Sir Thomas Watson's Practice of Physic (1851) D. Francis Condie quotes from a work on The Nature and Causes of Scrofula, by Phillips, statistics which showed a greater preponderance of deaths from scrofula in a given number of the rural population than a nearly equal urban one. But at the time these statistics were gathered in England (and perhaps now) it is probable that there was a comparatively greater number of abjectly poor people among the rural population than in London, where was congregated such a large number of small tradesmen, artisans, and laborers, who, though not well-to-do, were better paid, and consequently lived better, than the agricultural laborers. Of course, a certain number of cases of scrofula are found in the United States, and perhaps in all other countries, among the children of the wealthy. These, however, are almost invariably caused either by direct transmission from parents or by some accidental injury to the digestive and assimilative organs in early childhood, as we have already pointed out. When it is remembered that in the constantly changing fortunes which are so frequently witnessed in this age of excessive activities, and that in the grand opportunities for obtaining wealth furnished by the liberal institutions and rapidly-growing industries of the United States the descendant of the pauper of the last generation may be the millionaire of the present, it is not surprising that so many who are now wealthy may possess the strumous diathesis as an inheritance from their parents or grandparents, and which they in turn transmit to their offspring.
6. Consanguineous Marriage.—It has long been a popular belief that the offspring of parents closely related by blood are more apt to be scrofulous than when no such relation has existed. Indeed, not only scrofula, but numerous other diseases, deformities, and imperfections have been [p. 235]ascribed to such unions. Idiocy or feeble-mindedness has also been especially accredited to the production of such marriages. But a thorough investigation of this point in England some years ago demonstrated positively that no more idiotic, feeble-minded, or insane children are born of such marriages than of an equal number of marriages contracted between persons not related by blood to each other. There is, however, this amount of truth in the popular belief: if persons closely related to each other possess the scrofulous diathesis, there will be a greater probability—almost certainty—that the diathesis will be transmitted to their offspring. If one parent only is tainted with scrofula, and the other is entirely free from it, there is a possibility—even a probability—that some or all of the children may escape.
7. Complexion and Temperament.—It has been stated by some observers that scrofula occurred principally in the fair-haired, and with equal positiveness by others that it was in the dark-haired that the disease found the most of its victims. Such statistics as have been furnished, however, upon this subject seem to show that there is no connection whatever between scrofula and complexion. It will generally be found that whenever in any country or locality more cases of scrofula occur in persons of one or the other of the complexions, it is only because that particular complexion is the predominant type among the inhabitants of that locality.
8. Race and Nationality.—While it would seem that no race or nation is entirely free from struma, yet there are certainly in the United States two peoples who furnish an enormously disproportionate number of scrofulous cases: these are the Irish and Jews. Among the first of these both scrofula and tuberculosis abound with exceeding frequency, while among the latter it is scrofula alone which seems to predominate. The last, however, are not exempt from tuberculosis, but only exhibit about an equal predisposition to it with their fellow-citizens. It is not difficult to explain the special predisposition of these peoples to scrofula when their past history is taken into account in connection with what has been said about the bad influence of food and surroundings in producing the scrofulous diathesis. The principal food of the Irish peasantry—oppressed and ground into poverty by their Anglo-Saxon conquerors for hundreds of years—have been bread and potatoes, often potatoes alone. It cannot be surprising, therefore, that Irish children fed upon this diet and reared in ill-ventilated hovels should develop the scrofulous diathesis in legions. The Jews, too, oppressed by all nations through ages, have been during many generations reared in poverty and squalor. Even those of them who in not very remote times had acquired by thrift the means of securing both the comforts and luxuries of life dared not live according to their means, lest a show of wealth should attract the unpleasant, often fatal, attention of their rapacious and unscrupulous Christian or Mohammedan neighbors. This condition, this mode of life, has existed among them for many hundreds of years, and has so intensified the strumous diathesis among them that almost the whole race may be said to be patently or latently scrofulous. The negro or African race, however, as observed by the writer in the Southern States of the American Union, do not seem to have developed any special predisposition to struma, notwithstanding their servile condition. This, at first sight, would seem to [p. 236]be contrary to our expectation based on what has been said about Jews and Irishmen. But as my remark has been predicated only on observation of the African in the Southern States, where the climate is not favorable for the development of scrofula, the fact is not so surprising. Besides, the food of these people consisted largely of bacon or pork, fish, milk, and the succulent fruits and vegetables, with a moderate quantity of corn bread, and very rarely potatoes. As the rude cabins in which they dwelt were usually constructed of unhewn logs and covered with rough boards, and cost almost nothing except labor, overcrowding was unknown and ventilation always perfect. The waiter practised medicine fourteen years in Wilcox county (S. W.), Alabama, containing a population in 1870 of 28,377, of whom 21,610 were colored, and during this time saw only two cases of genuine scrofula and one of tuberculosis among the colored population.
Pork as an article of food has often been accused of producing a tendency to scrofula, but evidently with great injustice, for we have seen that the Jews, who never eat it, are almost universally scrofulous, while the Southern negroes, whose staple animal food it was, were conspicuously free from it.
9. Acquired Scrofula.—Although in perhaps a majority of all scrofulous cases the diathesis has been inherited from the parents, the fact cannot be too strongly emphasized that in a large number of cases the disease may be developed de novo, independent of such heredity. To scrofula developed from the influence of bad ventilation and overcrowding, absence of sunlight, insufficient, bad, or unsuitable food, cold and damp, imperfect clothing—in short, all those conditions associated with poverty, squalor, and ignorance—Grancher has well applied the term la scrofula a miseria. And it is only by a clear comprehension that scrofula may be, and often is, developed under these conditions that the medical profession in general, and municipal health authorities in particular, may be induced to teach and enforce upon the poor both the knowledge and the practice which may prevent it. Even in the open country, where there is at least no lack of pure air and light, the lesson can be enforced with equal profit; for the children of the farm-laborer are likely to be imperfectly and improperly fed, and lodged in apartments at night that in the matter of foul air and filth could not be well surpassed in the purlieus of the dirtiest and most overcrowded city.
EXCITING CAUSES.—The actual exciting causes of scrofula when the diathesis already exists are too numerous to be mentioned in detail. Indeed, almost any trivial injury or inflammation, any disease which has produced a temporary cachexia, may rouse into activity the perhaps hitherto latent tendency. How often do we see a slight blow upon the knee-joint produce a white swelling which lames for life the heretofore healthy and active boy or girl! A fall upon the hip which was almost unnoticed at the time excites a coxalgia which either destroys life or renders the child for life a cripple; or a slight jar of the spine induces a disease of the vertebræ which, if recovered from at all, produces a terrible deformity. A slight eczema of the face or scalp or a catarrh of the mouth or throat will excite that slow and generally painless enlargement and induration of a neighboring lymphatic gland which always ends in its caseation and final destruction by suppuration. A slight injury to the [p. 237] periosteum may excite a destructive caries or necrosis of the underlying bone, and a temporary catarrh of the intestines a tabes mesenterica with all its fatal consequences.
Speaking generally, it may be said that anything that produces a local disorder of nutrition or impairs the health generally of a person predisposed to scrofula is sufficient to bring about some manifestations of the disease. They are especially apt to follow the eruptive fevers. Measles and scarlatina are very commonly arousers of the scrofulous process, not only by the temporary impairment of health which follows them, but also through the catarrhs which are usually present in both diseases. Vaccination has often been accused of imparting scrofula; and, although this is untrue, since scrofula cannot be imparted in the sense of transference from one person to another, there can be no doubt that the predisposition may be roused into activity by the slight impairment of health associated with vaccination or by the slight injury inflicted at the point of introduction of the vaccinal virus. In some cases the disease has manifested itself for the first time during pregnancy or lactation, and there is no doubt that in cases where the disease has existed in childhood these conditions often cause it to reappear. In conclusion, it must be said that many cases apparently occur spontaneously—"the disease came on of itself"—or if there are any exciting causes they were so trivial as to have escaped notice altogether.
Finally, it must be remembered that the eczemas, catarrhs, ophthalmias, otitis, chilblains, erysipelas, and numerous other local disorders of nutrition which are often the causes of graver manifestations of the disease, are themselves very prone to run a peculiar course characterized by chronicity and intractableness; and many regard these disorders as themselves manifestations of scrofula. Indeed, Virchow, basing his argument upon the fact "that scrofulous enlargement of the lymphatic glands of the neck often follows upon certain diseases affecting the throat, such as mumps, diphtheria, and scarlet fever, maintains that scrofulous proliferation of these glands, like ordinary inflammatory hyperplasia of the same organs, is always secondary to some peculiar process going on at the mucous surface or other part which is in direct relation with them by means of the lymphatic vessels; that scrofulous disease of the glands of the neck is traceable to some inflammatory condition of the throat, fauces, or contiguous parts; of the bronchial and mediastinal glands, to pulmonary or bronchial inflammation; and of the mesenteric and retro-peritoneal glands, to similar conditions of the alimentary canal. But he considers that there may be some special element or quality in the primary inflammation, and a tendency in its products to undergo rapid decay similar to that which characterizes the morbid products of the diseased lymphatic glands, but that generally they are not recognizable, from the fact that in this case the cells are mostly developed at a free surface, and are speedily shed from it." He admits, however, "that there may be some special aptitude or weakness, congenital or acquired, in the lymphatic glands of certain persons, or of certain parts of them, which makes their inflammations, induced by indifferent causes, assume the scrofulous character."6 From the last of these propositions no one will be likely to dissent, but that there is "some specific quality or [p. 238]element in the primary inflammation," etc. few will be inclined to agree. There is nothing peculiar in the eczemas, ophthalmias, catarrhs, etc. spoken of, except that they occur in persons possessing the scrofulous diathesis; and it is this alone that gives them their special characters, if there are any. In other words, we cannot say that these disorders occur in certain children because they are scrofulous, but that they are specially intractable on account of the scrofulous diathesis upon which they are engrafted. Millions of children have catarrh and ophthalmia (indeed, few escape these disorders throughout the first ten or twelve years of life) who never show any other evidence of the scrofulous taint; and nearly all have measles and scarlatina, but it is only the scrofulous who usually suffer severely from the secondary effects of these diseases. But they do not have measles or scarlatina because they are scrofulous, and we can with no more justice say that they have catarrhs or other inflammations because they are so. We do not believe, therefore, that strumous children have cutaneous and catarrhal inflammations simply because they are strumous; and if we speak of scrofulous catarrh or ophthalmia or eczema, we use the terms in the same sense as when we would speak of a scrofulous measle, scarlatina, or whooping cough.
6 The Theory and Practice of Medicine, by Jno. Syer Bristowe, M.D., 1879, pp. 80, 81.
Although we have few reliable statistics bearing upon the question, it can scarcely be doubted, judged by the results of casual observation, that scrofula is much less frequent in America than in Europe, and that in the latter there is less of it than formerly. The cheapness of land in America has prevented that excessive overcrowding that exists in the older and more densely populated countries, and the abundance and cheapness of animal food has prevented that excessive feeding on bread and potatoes which constitutes such an important factor in the production of the scrofulous diathesis in some other countries.
PATHOLOGY AND MORBID ANATOMY.—The most important and central anatomical and pathological facts both in the causation and progressive development of struma, according to the writer's views, are—
1st. That faulty anatomical—or rather histological—construction of the tissues of the scrofulous individual already alluded to as having been first brought to the notice of the profession by Formad of Philadelphia, which consist of an unusually large number of lymph-spaces (which are also unusually large), and consequently an excessive number of lymph-vessels and lymph-glands.
2d. Excessive production of rudimentary lymphoid cells, and probably also of lymphatic tissue.
3d. Diminished and insufficient number of the capillary blood-vessels; and, as a necessary consequence of these,
4th. Diminished nutritive activity of all those processes, both physiological and pathological, which depend upon a full supply of nutritive blood.
The most striking feature in all scrofulous inflammation is excessive cell-growth, but these cells show little tendency to differentiation and organization, probably for two reasons: 1st, because they are derived from the blood-vessels principally, and not from proliferation of the proper connective-tissue cells of the part; and 2d, because they are insufficiently supplied with nutrition from the scanty blood-vascular [p. 239]network, and this supply is too rapidly absorbed into the lymph-spaces, and is carried off by the too numerous lymph-vessels. The cells, therefore, speedily perish, undergo partial or imperfect fatty degeneration, and finally caseation, unless the process is going on at a free surface, in which case, of course, they are shed and thus gotten rid of.
Virchow some time ago called attention to the predominant cellular character of the scrofulous exudation and the low vitality of the cells which compose it. Rindfleisch declares that the fresh scrofulous exudations contain relatively large cells with glistening protoplasm, and that the white blood-corpuscles have a tendency in scrofulous persons to grow larger on their way through the connective tissue. He adds that they swell up by the imbibition of albuminous substances, and by this very swelling die and slowly degenerate.
It seems to the writer, however, that it is probable that herein lies the reason why swelling and apparent hyperplasia of the lymphatic glands in the neighborhood of a local inflammation occurring in a scrofulous person always takes place. The swollen cells become arrested at the first gland they reach, and block the channels through the gland. Successive additions of cells continue to block these channels, and finally the passage of lymph through the gland becomes impossible, and then begins that secondary increase of the lymph-cells in the gland resulting from their inflammatory proliferation.
"In scrofulous inflammation," say Cornil and Ranvier,7 "there is a remarkable tendency to permanent infiltration of the affected tissue. In simple inflammation (i.e. inflammation in non-scrofulous persons) the infiltration is a temporary condition which terminates in suppuration, in organization, or in resolution." Now, the several steps in this process of resolution are—contraction of the distended blood-vessels, thus cutting off the excessive supply of blood which has caused the exudation and cell-proliferation; fatty degeneration of the new cell-formation; liquefaction of this fat by union with the alkaline blood-plasma, converting it into a dialyzable (saponaceous) liquid which can now be readily absorbed by the veins. In scrofulous infiltration the cells are speedily attacked by fatty degeneration (which seems to be strictly a physiological process), but instead of becoming liquefied, it (the fat) remains, slowly dries and hardens, and finally becomes converted into the so-called cheesy mass or cheesy infiltration. It does not liquefy, because it does not receive a sufficiently abundant supply of the alkaline blood-plasma from the scanty blood-vessels, and that which is supplied too rapidly flows into the numerous large lymph-spaces and is carried off by the lymph-vessels. In the case of the infiltrated gland the supply of this plasma is cut off in both directions. The passage of lymph through the gland is blocked, when, of course, none can then reach it through the lymph-vessel leading to it, while the swelling of the gland itself from accumulated cells compresses the neighboring nutrient vessels and cuts off the supply from this direction also. Hence the speedy death, fatty degeneration, and caseation (not liquefaction) of the cells.
7 Ed. 1880, p. 114.
"The newly-formed material not only interrupts the lymph-passages of the gland, but also compresses the blood-capillaries in such manner that the circulation completely stagnates. It is impossible by any [p. 240]method of injection to penetrate into the most swollen parts of the gland. With the supply of blood the nutrition also self-evidently ceases; the gland falls into caseous degeneration. Where this enters in the gray mass first becomes opaque, then whitish-yellow, non-transparent, dry, friable. If the whole gland has passed into the caseous condition, it appears upon a section as a fresh potato, only not quite so moist, but just as homogenously yellowish-white."8
8 Rindfleisch, Textbook of Pathological Histology, 1870, p. 202.
The subsequent fate of these glands seems to depend somewhat upon their situation. In the mesenteric and bronchial glands almost always the caseous mass is attacked by calcareous infiltration, and finally dries into a solid chalky concretion. The writer counted seven of these chalky masses around the primary bronchi of a boy about fifteen years old whose body was brought into a dissecting-room in Baltimore City. But the more common result of the caseous process in the glands of the neck is softening. "The caseous dépôt melts from within outward into a whitish-yellow, whey-like fluid, which holds a fatty granular detritus suspended in smaller or larger fragments. If all the caseous material has softened, the neighborhood of the gland is wont to inflame; this inflammation facilitates the way for the scrofulous pus outward. This is evacuated, and we have the scrofulous ulcer, with its overhanging, bluish, hyperæmic, flabby edges. At length this opening also closes, and a drawn-in, radiated cicatrix marks the place where the evacuation took place."9
9 Ibid., loc. cit.
But it must be borne in mind that all so-called scrofulous hyperplasias of lymphatic glands do not run this destructive course. Undoubtedly, in a few cases there remains a sufficient nutritive supply to carry on the liquefactive process which normally follows fatty degeneration, and thus resolution of the affected gland takes place. We are, however, of the opinion that Virchow was mistaken when he asserted that complete resolution of the cheesy material could take place; and from what we know of the dangerous and usually fatal consequences of the absorption of this cheesy detritus, Rindfleisch is certainly in error in describing this as the most desirable possibility of decomposition.
We have heretofore purposely avoided any mention of tubercle or tuberculosis as a part of the scrofulous process. In the views of many physicians the relations between the two processes are so close that to them tuberculosis and scrofulosis mean one and the same thing. While medical opinion as to the true meaning of the word tubercle was so discordant and unsettled, while so many products of diverse pathological processes were included in that term, and while many, following the view of Burdon-Sanderson of England, believed that tubercle always takes its origin in small, even microscopic, collections of lymphatic tissue, such a belief in the identity of the two processes was not only possible, but reasonable. But since, by very many good authorities, the term tubercle is now limited to the miliary or submiliary tubercle, since numerous inoculation experiments have shown that tuberculosis can be induced in non-scrofulous animals, and Koch of Germany has proved that there exists in decaying tubercle a peculiar and distinctive bacillus which even when cultivated out of the body of a tuberculous person will excite tuberculosis also if inoculated upon a non-scrofulous animal,—a belief in the identity of the two diseases seems to be no longer tenable. Certainly, it [p. 241] would seem that to Sanderson's view that tubercle always takes its origin in lymphatic tissue it is only necessary to reply that the subjects of miliary tuberculosis do not more frequently than those suffering from other non-scrofulous diseases present those larger glandular hyperplasiæ which are so distinctly characteristic of scrofula, and to which many persons limit the term scrofulosis. It may be said, perhaps, that the converse of this is not true, and that scrofulous persons are more frequently attacked by miliary tuberculosis than an equal number of non-scrofulous persons. But the extreme susceptibility or liability of the scrofulous to be attacked by numerous and even diverse morbid processes, and the profound cachexias and dyscrasias which the scrofulous processes engender, amply account for the apparent susceptibility of the scrofulous to be attacked by miliary tuberculosis. The strumous are more susceptible to the exciting causes of tuberculosis undoubtedly, but perhaps the same may be said in regard to measles, scarlatina, and the various other exanthemata. It is undoubtedly true also that among the lower animals (and probably also in the higher ones) the introduction into the circulation of the semi-purulent fluid resulting from the breaking down of a cheesy scrofulous gland will produce that peculiar (perhaps specific) dyscrasia which results in miliary tuberculosis. But as it has also been abundantly proved that a similar fluid derived from a cheesy pneumonia, or from the inflammatory products of any other disease which have undergone the cheesy degeneration, will also excite tuberculosis, the fact does not seem to tell in favor of the identity of, or even of any close relationship between, the two processes. Still, as the scrofulous more frequently than other people are the subjects of this cheesy process, it is not surprising that they should more frequently be poisoned by the entrance into their blood of the cheesy detritus.
We do not deem it necessary to adduce all the evidence or to state authorities upon this subject, but we think we are justified in stating the following doctrine in regard to the relation of scrofula to tuberculosis as best supported by facts and by the consensus of medical opinion:
Scrofula is a purely diathetic disease inherent in the individual.
Tuberculosis is a cachectic (possibly a purely dyscratic) one, not inherent in the individual, but always caused by some morbid influence from without. Tuberculosis may therefore occur in the non-scrofulous as well as in the scrofulous.
But the scrofulous are more likely than others to have tuberculosis—1st, because of their greater susceptibility to all morbid influences; 2d, because the scrofulous processes are apt to produce some cachectic condition which is always a condition precedent to tuberculosis; and, lastly, because the products of decay resulting from scrofulous processes may enter the circulation and directly produce the tuberculous dyscrasia. These remarks of course apply only to primary tuberculosis.
But while we thus deny anything else than a purely incidental relation of scrofula to tuberculosis, we believe that there exists the very strongest possible relationship of scrofula to pulmonary consumption. We think we are justified in stating that fully 95 per cent. of all cases of pulmonary consumption are of inflammatory origin, and of that variety miscalled catarrhal pneumonia. Broncho-pneumonia or catarrho-pneumonia more exactly describes the process. It begins as a catarrh, [p. 242]sometimes in the nasal passages or post-nasal fossæ, sometimes in the pharynx, but most frequently in the trachea and large bronchial tubes, and sometimes rapidly, but oftener more slowly, travels downward and invades the lining membrane of the air-sacs, which soon become packed with cells derived partly from emigration of leucocytes, partly from proliferation of the epithelium lining the sacs. These cells soon undergo the cheesy degeneration, and, finally breaking up, as in the case of the scrofulous gland, cause the formation of vomicæ attended with the familiar signs of pulmonary consumption. Every step in this process is attended with that abundant cell-production, and the process itself is marked by that inveteracy and intractableness, which always characterize scrofulous inflammations, or rather inflammations in the scrofulous. Occurring as they most frequently do in young adults, these cases are often mistaken for pulmonary tuberculosis; and as post-mortem examination generally reveals a more or less abundant secondary tubercular eruption caused by absorption of infective material from the centres of cheesy degeneration and softening, the diagnosis is claimed to be confirmed. But they are for the most part, nevertheless, cases of genuine scrofulous inflammation of the bronchial membrane and lining membrane of the alveoli, and should be called scrofulous pneumonia. It is true that Mr. Phillips, Mr. Kiener, Villemin, Grancher, Mr. Treves, and others have collected numerous statistics which would show that comparatively few of those who had died of pulmonary phthisis bore any evidence of previous scrofulous disorder. But as the principal evidence relied upon to prove this fact was an absence of scars resulting from suppurating glands, their statistics are inconclusive. Besides, it is a well-known fact that there is a decided antagonism between scrofulous diseases of all kinds, and a patient who has one severe or well-marked manifestation of scrofula is not likely to develop another strumous disease at the same time. The records of the Margate Infirmary for Scrofula show this fact very strongly, and numerous writers—among whom may be mentioned Holmes, Birch-Hirschfeld, Walsh, Mr. Treves, and others—strongly express the same opinion. Indeed, some of them go so far as to maintain that one form of the scrofulous manifestation confers protection against others. The question may perhaps be more clearly stated by saying that the scrofulous, like the non-scrofulous, have their special predispositions and indispositions to certain morbid affections, and while one scrofulous child may be specially predisposed to affections of the bones, joints, skin, or other tissues, it may have no predisposition whatever to affections of the lungs or lymphatic glands, etc. This difference in vulnerability or invulnerability of certain tissues or organs in individuals, whether scrofulous or not, is so distinctly recognized as a controlling factor in determining the special form of disease resulting from a given irritant that its discussion is entirely unnecessary. It is argued against the identity of scrofula and pulmonary consumption that the commoner manifestations of the former occur in childhood for the most part, while consumption is a disease of adult life. But this is readily accounted for by the different morbid tendencies and exposures in the two periods of life. "Scrofula tends to appear in early life on account of the unusual activity of the lymphatic system at that period, and phthisis somewhat later—at a time, indeed, when the lungs are in more active use, when [p. 243]sedentary and perhaps unhealthy pursuits are assumed in exchange for the liberty of childhood, when the modifying influences of puberty are active, and the structural responsibilities of adult life press heavily on an organization never other perhaps than frail.... I would, on the contrary, assert that scrofula and phthisis are as much manifestations of the same morbid change as acute bubo, acute orchitis, and acute pneumonia are outcomes of one single process—acute inflammation."10
10 Scrofula and its Gland Diseases, by Frederick Treves, F.R.C.S., Eng.; New York, 1882, p. 62.
It is entirely unnecessary—and indeed it would be too tedious—to describe the anatomical appearances of the almost innumerable lesions met with in the scrofulous. Holding as we do that scrofula is not a disease per se, but merely a condition resulting from malnutrition and consequent faulty construction of the tissues during the early years of childhood, no peculiar or distinct anatomical lesion can be ascribed to it; and yet every lesion of nutrition as well as of function may have certain specific characteristics impressed upon it by the scrofulous diathesis. These may be briefly summed up as great slowness in evolution, intractableness, incurability, and chronicity of all pathological processes, and in all inflammatory processes abundant cell-production and tendency to caseation.
SYMPTOMS, COURSE, DURATION, AND TERMINATIONS.—A great deal of fine writing has been expended in describing the physiognomy of scrofula, and for ages writers exercised their descriptive powers upon the type of face and form supposed to be indicative of the disease. It is almost needless to say that much of this has been evolved from the imaginations of the writers, while many of these descriptions are not pictures of those liable to suffer from scrofulous processes, but of those who are already the subjects of these, and are simply types, not of the scrofulous diathesis, but only of the scrofulous cachexia. Many of these pictures, too, were drawn not from the scrofulous, but the tuberculous patient, because they were considered identical. Scrofula is not confined to the dark or the fair, the dull or vivacious, nor even to the weak and puny or the strong and robust; but all these may have this faulty and often fatal construction. Nor do we believe that scrofulous children are either more brilliant or more stupid than other children. At most we can only say that the scrofulous habit is marked by a deficiency of blood and a bad nutritive state of the more important and more highly organized tissues. In some an abundance of fat is found, giving to the individual a certain amount of plumpness, which might be thought to be inconsistent with a state of bad health; in others there is an imperfect development not only of the subcutaneous fat, but of the skin and muscles also, so that they appear tender and delicate. In the first of these conditions there is supposed to be an indolent state of the processes of constructive and destructive assimilation; in the second, an unnatural activity of these processes. These differences have led to a classification of scrofula into the phlegmatic or torpid and the sanguine or erethistic forms, which Canstatt has thus described: "An unusually large head, coarse features, a thick chin, a swollen abdomen, enlarged cervical glands, and flabby, spongy flesh." The erethistic form is said to possess "a skin of remarkable whiteness, with a tendency to redden easily, and through which the [p. 244]rose-pink or bluish subcutaneous veins are visible, a deep redness of the cheeks and lips, blueness of the thin and transparent sclerotica, which imparts a swimming and languishing look to the eyes. The muscles of such persons are thin and soft, and their weight is light in proportion to their stature, indicating a slightness of their bones. The teeth are handsome and of a bluish lustre, though long and narrow; the hair is soft."11 Although this description may be characterized as diagrammatic, since it describes rather the extremes and not the mean of the general appearance of the scrofulous, and numerous cases will be met with that cannot be assigned to either of the above categories, yet as quite a large number of cases will be seen that obviously belong to one or the other of these types, and as, moreover, we shall see that by this classification we shall obtain valuable data for therapeutic indications, it may be well to preserve this division of the scrofulous into the lymphatic and sanguine types.
11 Niemeyer's Text-book of Practical Med., vol. ii. p. 741.
The leading points in the physiognomies of each of these types were admirably shown in the composite photographs exhibited by Dr. Mohamed at the last International Congress in England. By some special process a composite photograph of many faces was, as it were, condensed into a single picture, in which all that is common remains, all that is individual disappears. And although Mohamed's pictures were all of phthisical patients, it must be admitted that the two types of coarse struma and sanguine struma were strikingly illustrated, and were very suggestive of Canstatt's descriptions as given above. But it must be borne in mind that a large number of the strumous belong strictly to neither of these types, but rather to a medium between the two. "Such a type would include what is known as pretty struma. The general features of the individuals so termed belong to the so-called phlegmatic type, but the coarseness of the features is toned down; the lips would be called full, not tumid; and a coarse flabbiness would subside into a pretty, plump condition of the body. The limbs, if not actually graceful, are at least prettily rounded. The skin may not be thin and fine, but it is soft, white, and clear. The general expression is not absolutely apathetic, but would be termed gentle and eminently feminine. Excellent representations of this type of pretty struma were also shown in the photographic series above mentioned."12
12 Treves, Scrofula and its Gland Diseases, p. 84.
This matter of physiognomy of the scrofulous has this much at least of practical importance—viz. that to the sanguine or erethistic type belong those cases that show distinct heredity, while the phlegmatic or torpid is usually the type assumed in the acquired forms. While there are doubtless numerous exceptions, it will generally be found that scrofula in the rich assumes the first, and in the poor the second, of these forms. It has been asserted that the erethistic form is more apt to develop tuberculosis or phthisis; and to a certain extent this is doubtless true, but the torpid are by no means exempt from this grave accident. The first are undeniably more liable to the more severe and fatal forms of the disease, which run a more rapid course and are less amenable to treatment, while in the second phthisis is more apt to be chronic and incomplete recoveries are by no means rare. The first form is said to [p. 245]be more frequent in women, while the second is more frequent in males; and this accords with my own observation and experience.
There are certain features more or less peculiar to scrofula, besides those appertaining to the general physiognomy already discussed, which it may be well to call attention to, since these may aid us in detecting the scrofulous diathesis even before the grosser manifestations have declared themselves.
Allusion has already been made to the defective blood-vascular capillary network in the scrofulous as a necessary consequence of the excessive predominance of lymph-spaces and lymphatic vessels. Indeed, there can scarcely be a doubt that the slowness of evolution of various pathological processes, their chronicity, and the absence of tendency to resolution and cure of inflammatory lesions, so prominent a feature in all scrofulous manifestations, is due to this very condition. It is especially in the coarser type of struma that these defects in the circulation are most conspicuous. In these the pulse is often below the average, soft, and wanting in vigor. The cheeks and limbs often assume a bluish and mottled aspect, due perhaps to a tendency to stagnation of the blood in exposed parts. The extremities appear swollen as if from cold, and in the winter generally appear chapped. They are particularly liable to chilblains, which persist far into the summer and often take on a very unhealthy action. This last feature is so common as to constitute an important symptom in scrofula. These defects in the circulation also probably explain the frequent catarrhs and eczemas with which such persons are affected, and account also for their intractableness as well as the unwholesome character of their wounds.
For the same reason (deficient circulation) the temperature is generally found to be a little lower in the coarsely strumous than in healthy children, and even in their fevers a very high temperature is rarely met with. Acute sthenic inflammations are rarely seen, and hence these persons seldom have acute croupous pneumonias; it is rather the catarrhal variety, and of this the subacute and chronic forms, which they suffer from.
Opinions are completely at variance as to the influence of the scrofulous habit in delaying or hastening menstruation. Lugol referred to the frequency of dysmenorrhoea among the strumous, and there is no doubt that the scrofulous as a rule often suffer from suppressed or scanty menstruation. But it is improbable that the diathesis exerts any influence whatever in determining the period of puberty in either sex.
We have already stated our belief that the strumous are neither more intelligent nor stupid mentally than other people. An exception ought perhaps to be made to this in the case of the exaggerated type of the coarsely strumous. In these extreme cases we must confess that we have generally found associated great slowness and dulness of the mental faculties. If great intelligence and precocity are sometimes met with, it is only in the erethistic or pretty struma, who, because it is the delicate one of the family, is petted, has more notice taken of it, and afforded every facility for the development of the points that make up the precocious infant. The prettiness of these children, moreover, attracts more attention to them than to other children or than the bulk of the sickly would receive.
In young scrofulous children we often observe a considerable amount [p. 246]of close-lying downy hair upon the forehead, more abundant upon the sides of the forehead. Upon the arms and back from the occiput to below the shoulders also a like condition is often seen. Later the eyelashes appear thicker and longer, and the eyebrows more abundant, coarser, and longer, than in the non-scrofulous. The color of these is also apt to be darker than the rest of the hair.
Constantine Paul, as quoted by Treves, has drawn attention to certain changes in the ears, after they have been pierced for earrings, that he considers to be diagnostic of scrofula. The mere weight of the earring seems to cause the puncture to slowly ulcerate, and the ring thus cuts its way out, either leaving behind it a linear scar or a slit in the lobule. If the lobule be repaired the ring may cut its way out again, and this may occur three or four times. These changes seem not so frequently to be observed in England and America, and may be due in part to the fact that earrings of greater weight, and more frequently of base metal, are worn in France than in the countries named. But still, from what has been said concerning the histology and minute anatomy of the scrofulous, and the consequent less resistance of the tissues, this cutting-out process by earrings is just what we would be led to expect in strumous persons.
The thick upper lip is never absent from the older descriptions of the physiognomy of the strumous. This is almost invariably present in the coarse type of struma, and seldom absent even in the erethistic. It is not always due to irritation from acrid discharges from the nose, as is maintained by Treves, though doubtless the eczematous and herpetic eruptions are often caused and maintained by these discharges, and these may in time cause and increase this thickening.
The teeth in scrofula show nothing that is distinctive, though there is undoubtedly a tendency to early decay. As this tendency to decay is, however, so common in many persons who have at least shown no other evidences of the scrofulous diathesis, no positive conclusions can be drawn from this fact.
Clubbed fingers, too, so common in persons who have become cachectic from the long persistence of scrofulous disorders, are not characteristic. Clubbed fingers and incurvated nails will generally be found in persons suffering from any disease characterized by slow wasting. They are seen in phthisis of all varieties, as well as in cancer, heart disease, aneurism, Bright's disease, empyema. They therefore have no significance as far as struma is concerned.
GENERAL MANIFESTATIONS OF SCROFULA.—As, according to our view, there is no such disease per se as scrofula, but simply a diathesis which impresses its own malign influence upon every other disease with which the strumous individual may happen to be afflicted, increasing perhaps the general predisposition to be injuriously affected by all morbific influences, or impairing the powers of resistance to these, and especially intensifying any special predisposition which age, sex, personal peculiarities, occupation, habits, mode of life, or heredity may have created, we cannot describe any morbid processes as specifically scrofulous. At most, we can only say that struma is more apt to impress its malign influence upon certain diseases or upon inflammations and injuries of certain tissues, that some diseases in the scrofulous are more apt to be [p. 247]attended by certain complications and followed by certain sequelæ, and that all of these are characterized by chronicity and incurability, by slowness of evolution of pathological processes, and, in the case of inflammations, by a tendency to profuse cell-production and to rapid caseation. Thus, measles is apt to be complicated with or followed by otorrhoea, chronic bronchitis, caseation of bronchial glands, phthisis, and even tuberculosis; scarlatina by otitis, hyperplasia of the tonsils, caseation or suppuration of the submaxillary and other lymphatic glands about the neck, and by chronic catarrh of the renal mucous membranes, causing dropsy and finally death; eczemas about the face or catarrhs of the mouth and throat by hyperplasiæ and caseation of lymphatic glands in the neighborhood. Boils and other subcutaneous inflammations of the areolar tissue, so common in childhood and adolescence, do not run their usual rapid course, ending in suppurations and cicatrization, but become in the one case the scrofulous gumma, degenerating into the scrofulous ulcer, or if more deeply seated become a cold abscess. A single injury of a joint, whether mechanical or rheumatic, will "sometimes take the form of a simple hydrarthrosis, sometimes that of a so-called tumor albus, while at others it assumes the nature of a malignant arthrocace, accompanied by suppuration, caries of the articular surfaces, burrowing of pus, and the establishment of fistulæ."13 A slight injury inflicted in the sports of childhood and soon forgotten—the prick of a pin perhaps—is followed by a disease sometimes beginning in the periosteum, sometimes in the bone itself, and presenting at one time the character of periostitis and ostitis, and at another that of caries or necrosis, or of the two combined.
13 Niemeyer, loc. cit.
"As long as the existence of cheesy masses," says Niemeyer, "was regarded as characteristic of the tuberculous nature of a disease, it was of course necessary to ascribe many of the inflammations of the joints and bones of scrofulous persons to a complication of scrofulosis with tuberculosis."14
14 It is a well-established fact, however, that true miliary tubercles are often found in the neighborhood of bone and joint affections in the scrofulous, as well as in lupus, in cold abscess, and in softening caseous glands, which last are considered by many as specifically scrofulous diseases. It is suggested that an explanation of this may be found in the probable fact that caseous pus may be capable not only of producing a general tuberculosis when carried by veins or lymphatics into the blood, but that it may also set up a local tuberculosis by a morbid influence exerted upon the neighboring lymphatics and blood-vessels with which it may come in contact. We are aware that Wilson Fox (according to the Medical Times and Gazette), captivated by the theory of Koch, has recently recanted his belief in the inoculability of tuberculosis with anything except tubercle. But we are afraid that Dr. Fox (who we believe was one among the first to confirm Ferdinand Cohn's experiments in producing tuberculosis in rabbits and guinea-pigs by inoculating them with caseous pus) is suffering from that most active and virulent of all contagions, the contagion of popular belief. Just now a belief in specific bacilli and micrococci may be said to be riding upon the crest of a very high wave of popularity, and we are afraid that many of those who are rushing forward to mount this wave also will ultimately find themselves stranded upon that shore which has been strewn with so many wrecks in the past.
A simple bronchitis, possessing nothing specific in its origin at least, will persist and extend to the lobuli of the lung and excite a catarrho-pneumonia which ends in consumption and death; a simple intestinal catarrh will result in inflammation and caseation of the mesenteric glands—a tabes mesenterica; or a simple dysentery, persisting in spite of the most [p. 248]approved treatment, causes proliferation and caseation of the endothelial cells of the follicles, terminating in that obstinate and intractable follicular ulceration which wastes the strength and wears out the life of the little patient.
A simple conjunctivitis of the globe often will be followed by ulceration of the cornea, giving rise to intense photophobia, and leave behind it opacities of that organ which remain a perpetual evidence of the scrofulous diathesis, if they do not shut out for ever the light from the eye. Or if it is the palpebral conjunctiva that is affected, the meibomian glands and follicles of the ciliæ become involved, destroying the lashes and leaving the lids raw and everted or inverted—a perpetual deformity. In short, there is no conceivable disease or injury occurring in what we may call the intensely scrofulous that does not have impressed upon it some one or more of the malign characteristics which we have spoken of as indicative of the scrofulous diathesis. But it is not probable that there is ever any special disorder or lesion which can be said to be caused exclusively by scrofula; or, in other words, there is no such disease as a specifically scrofulous one. Lupus, cold abscess, and particularly caseous glands, are especially attributed to struma, because they are often thought to make their appearance independent of any assignable cause; but as boils, eczema, impetigo, and numerous other affections of the skin and areolar tissue affect children who are not scrofulous, and equally independent of any known causes, the argument is not conclusive. Besides, all these affections occur sometimes in the non-scrofulous; and even caseation of a single inflamed gland quite often occurs in children who are weak or in ill-health, but who show no other evidences at that or at any other time of the scrofulous habit.
DIAGNOSIS.—The only affection likely to be mistaken for scrofula is congenital or acquired syphilis in its later manifestations. In this disease we see the same tendency to increased cell-production, the same tedious, slow, and intractable inflammations and ulcerations, which are characteristic of scrofula. And this apparent similarity has induced many persons to believe that scrofula is nothing else than syphilis in the second or third generations. But in congenital syphilis the lesions usually make their appearance soon after birth or are present at birth, and long before even hereditary scrofula begins to show its malign influence. In most cases, too, a history of syphilis can be obtained, and even when this is not obtainable a few inunctions or fumigations with mercury, in connection with a few large doses of iodide of potassium, will very quickly decide the question of diagnosis for us.
In the case of lupus, in which Erichsen admits there is no means of positively distinguishing the syphilitic from the so-called scrofulous varieties, the diagnosis is more difficult. But as this disease appears later in life than the more ordinary scrofulous manifestations—when, therefore, a history of syphilis can generally be obtained if there is one, and when there would almost certainly be also a history of scrofula if it existed—it would seem that the diagnosis even in this case cannot be so difficult. Diagnosis here, however, is of little consequence, since the treatment recommended for both forms is the same.
PROGNOSIS.—This of course depends upon the nature of the special lesion. The simpler lesions incident to childhood, such as glandular [p. 249]hyperplasiæ, catarrhs, eczemas, impetigoes, etc., usually do well under appropriate treatment and proper hygienic conditions. Diseases of joints, bones, mesenteric glands, etc. often terminate fatally or result in serious deformities and permanent impairment of function. Not infrequently diseases of the bones and articulations, attended with profuse and protracted suppuration, cause amyloid degeneration of the liver, kidneys, spleen, or other glandular organs, and, as a consequence, death. Catarrho-pneumonia in a scrofulous subject almost invariably causes phthisis sooner or later. Occasionally the caseated cellular exudation in the air-sacs remains quiescent for months, and even years, the patient remaining quite well except for a harassing cough during the winter months; but sooner or later the caseous mass will soften, the symptoms of active consumption ensue, with fever and wasting, and death closes the scene. Far more frequently, however, softening and suppuration follow swiftly upon the caseous degeneration, and the whole process occupies a period of only a few months. Tuberculosis especially runs a rapid course in these subjects, and while a few perhaps only develop tuberculosis of the lungs—in which case the duration of the disease may be a little longer—in by far the larger number there is a generalization of the tubercular process which puts a speedy end to their existence.
TREATMENT.—This may be most profitably discussed under two heads—prophylactic and therapeutic.
Prophylactic.—Scrofulous persons who are closely related by blood should be earnestly advised not to intermarry. We have so often seen the deplorable results upon offspring of such marriages that we cannot too strongly urge this upon the profession. Such persons should be frankly and clearly told what are most likely to be the consequences of such marriage, and all possible moral influences should be exerted to prevent them. The canons of the Church wisely interdict such marriages, but, unfortunately, its ministers seldom attempt to enforce them, or if they do their efforts are made ineffectual by the facility with which the marriage-rite can be obtained from civil officers in most of the States of the American Union. The medical profession can do more than any other class to diffuse knowledge and create a correct public opinion upon this subject, but, unfortunately, it too often neglects this important mission.
The children of scrofulous parents should be nursed (at the breast) longer than other children, so as to ensure an abundance of animal food during the first two years of life. Some advise scrofulous mothers not to nurse their children, lest they should imbibe the scrofulous taint through the milk. This fear is entirely groundless. We know of no reason why such a mother should not nurse her offspring, unless it be that it injures her. The child receives its scrofulous inheritance not through the mother's milk, but from the ovarian or spermatic cell. Milk can convey no disease or diathesis except on account of its deficiency in nutritive properties. If, therefore, there is any special reason why the mother should not nurse her infant on her own account, it may be well to turn it over to a healthy wet-nurse; but the temptation to give an infant raised on the bottle starchy foods prematurely is too strong generally to be resisted. The numerous infant foods advertised consist principally of starch, and young infants would infallibly starve on any or all of them [p. 250]if their venders did not always direct that they should be taken with a large quantity of cow's milk. If the circumstances of the parents do not enable them to obtain a wet-nurse, then good cow's milk constitutes the best food for infants until they have cut their canine and anterior molar teeth. The custom of weaning infants at a certain age in every case is a pernicious one. Some infants are as well developed as to their digestive organs at fifteen months as others are at thirty, and the eruption of the teeth may generally be taken as a safe guide as to that question. A moderate amount of food containing starch after the period indicated may be allowed, but always with a preponderance of animal food. It is not so much the starch that acts injuriously upon the nutrition of children as the excess of that substance; and if the food contains but little nutrition in proportion to its bulk, it is so much the worse. Even milk containing too little casein and fat in proportion to the watery elements may be perhaps quite as injurious as potatoes. And hence if the mother's milk should be poor in these elements, it ought to be supplemented with cod-liver oil or other animal fat in small doses.
A practice existed among the Southern slaves (and to some extent also among the whites) before emancipation which at first I was inclined to condemn until I saw the excellent effects resulting from it. Within an hour or so after birth a piece of fat salt pork or bacon was placed between the child's lips, and it was permitted to suck this at all times when not nursing. Tied to its wrist by a short string, so as to prevent swallowing it, this piece of pork furnished both nutrition and amusement to the infant for many hours while the mother was at work in field or garden. The children throve well on it, and thus treated we found them to be as well developed at twelve months as most other children were at twenty. It was doubtless due in part to this practice that there was so little scrofula among them.
An abundance of pure air is also a valuable factor in preventing the establishment of the strumous diathesis. Strict regard, therefore, should be had to ventilation, and overcrowding should if possible be avoided. Children over twelve months of age should not even be permitted to sleep with their parents, but should have in cold weather a crib, cradle, or other bed to themselves; and in warm weather they should be put to sleep in a net hammock, which is now so cheap as to be within the means of almost everybody. This will not only secure to them a better supply of air, but it will also prevent them from suffering so much from the heat, which is so potent a factor in the production of cholera infantum.
Bathing in proper season is also useful as a prophylactic. Sea-bathing especially has long enjoyed great credit as a remedy for scrofula, but we think this is often resorted to too soon and practised at improper times. In warm countries a bath of cold water may be taken every day in the year, but it should be given at the warmest hour of the day, not early in the morning. In all climates due regard should be had to the powers of resistance to cold and the promptness of reaction after the bath. If children remain cold and pale for a long time after the cold bath, the practice should be discontinued and tepid water substituted. In colder climates tepid bathing should be practised once or twice a day during the winter, and in summer a little lower temperature may be used. Bathing children under three or four years in the sea at any time is pernicious, [p. 251]both because the temperature is too low and on account of the fright which it always causes in these young children. After four years a child will take to the water almost as instinctively as a young duck.
Therapeutic.—Almost all of the so-called scrofulous manifestations belong to the surgeon, dermatologist, or oculist and aurist, and we shall therefore say nothing about the special and local treatment of these manifestations, but refer the reader to works upon these several departments of medicine. But as little success will be had in the treatment of these special disorders unless due regard is had to the general condition, and unless the local treatment is supplemented by constitutional measures, we shall briefly give some directions for this constitutional treatment of the scrofulous individual.
It is important in determining upon the proper treatment in any given case to bear in mind the division of the scrofulous into the two types of torpid or lymphatic and sanguine or erethistic already described. It is true that in many cases it is not easy to determine to which class a patient belongs, and many possessing some of the characteristics of both certainly cannot be referred to either. Still, in many cases the discrimination is easy, and then furnishes very clear and valuable indications as to treatment. Iodine (and its preparations) has since the time of Lugol, who first brought it into prominent notice, been regarded as a useful remedy in scrofula. But burnt sponge (spongia usta), which contained the iodides of sodium and potassium, had been used to dissipate goitrous and scrofulous swellings many hundreds of years before the time of Lugol. It is a valuable remedy in certain cases, and if it is falling into disuse it is probably for the want of proper discrimination in the selection of cases. In all cases in which there seems to be an abundant production of fat, and therefore in nearly all the cases of coarse struma where there is an indolent process of assimilation and disassimilation, iodine and its preparations will be found useful. Indeed, in the form of syrup of iodide of iron we have rarely failed with it to cause strumous enlargements of glands to disappear when the remedy was used soon after their first appearance. Of course, neither iodine nor any other medicine can have any effect in removing these enlargements after the glands have become caseous. While good results may be obtained with the syrup in all forms of scrofula, it is unquestionably in the sanguine and neutral types that it is most useful. It should be given in doses of 10 to 30 drops to children under five years of age, and to older ones ½ to 1 fluidrachm three or four times a day may be administered. We have given the latter dose to children four or five years of age for a long time, with the best effect upon their scrofulous manifestations, and without any injury whatever to their digestive organs.
In the torpid types preparations stronger in iodine should be used. Here Lugol's solution or iodide of potassium or sodium will be found very useful, either alone or in connection with the iron preparation above mentioned. Indeed, as in these cases it seems to be disassimilation that appears to be specially faulty, even very small doses of mercury in the form of bichloride or biniodide will be found useful. Donovan's solution may be prescribed in these cases along with the active preparations of iodine with good effect, or if the arsenic in that preparation is objectionable, one-fiftieth of a grain of bichloride or biniodide of [p. 252]mercury may be substituted. The mercurial should not, however, be continued longer than one or at most two weeks at a time, after which it should be suspended and the iodine continued.
Cod-liver oil, which is too indiscriminately prescribed in all cases, will be found to be of little use in the lymphatic types, if indeed it is not actually injurious; but in those cases with pale, thin skin, with deficient development of fat, and with small muscles—in short, those in which emaciation or delicacy is prominent—it is a most valuable remedy. It is almost surprising to see how rapidly ulcerations, caries, eczemas, catarrhs, etc. occurring in this class of subjects will disappear under the use of this medicine alone.
The hypophosphites and lactophosphates are also useful in this class of cases, especially where there is disease of bone or joints, in connection with the cod-liver oil. We have long been in the habit of using the following formula, which we have found very useful:
| Rx. | Pulv. Acaciæ, | drachm ij; |
| Ol. Amygdal. amar., | gtt. vj; | |
| Syr. Calcii hypophosphit., vel Syr. Calcii lactophos., |
fluidounce iv; | |
| Ol. Morrhuæ, Ft. mist. |
fluidounce iv; |
S. Teaspoonful to tablespoonful three times a day according to age. Syrup of iodide of iron may be added if desirable, though we prefer to give this by itself.
Gentle exercise, passive or active, pure air, well-ventilated sleeping apartments, a generous diet—in which wholesome animal food should predominate—and bathing are of course as necessary and as useful in the treatment as in the prevention of the scrofulous diathesis.
Alkalies should be given in all cases in which we are trying to dissipate enlarged lymphatic glands, for the reason that caseation of these glands occurs because of insufficient alkalinity of the blood to effect reduction of fat, and because also the strumous almost always suffer from excessive acidity of the gastric and other secretions. When the iodides of potash or soda or the hypophosphites of lime and soda are given, the additional administration of alkalies may not be necessary; but if not, bicarbonate of sodium or potassium (which have long enjoyed a good reputation in the treatment of struma) should be added to the other remedies.
Since the appearance of Niemeyer's Handbook of Clinical Medicine the proper treatment of scrofulous glands that have undergone the caseous degeneration has been a moot question. Some recommend the ablation of these glands by the knife, some advise spooning out the caseous matter through a small opening, while others prefer to await the natural process of softening and the discharge of the caseous matter by suppuration. There can be no question that the removal of these glands by the knife, when this can be done without serious risk, will leave behind a less unsightly scar, and will be attended with less fever and consequent deterioration of the general health, than usually attends suppuration. Spooning out the caseous matter will perhaps leave no extensive cicatrix, but we can never be sure that by this operation we have removed all the caseous matter, and it must certainly be more painful than the knife. Mothers will generally object to either of these [p. 253]operations, and as the risks of infection by absorption of the caseous pus during the suppurating process do not seem to be very great, it is perhaps best to leave these glands to nature, unless the vitality of the patient is so low as to give reasonable ground for fear that the child may succumb to the effects of the natural process. If any surgical interference is deemed necessary, we are decidedly in favor of removing the caseous gland entire by the knife.
About a half century ago Mr. Abraham Colles, who had just resigned the professorship of the Theory and Practice of Surgery in the Royal College of Surgeons in Ireland, the duties of which, in the opinion of the college, he had discharged for thirty-two years in an "exemplary and efficient manner," wrote the following introductory paragraph to his remarkable chapter on "Syphilis in Infants:" "Perhaps there is not in the entire range of surgical diseases any one the contemplation of which is more calculated to arrest our attention or to excite our interest than syphilis infantum."
Although it was not then, and is not at the present day, strictly relegated to the domain of surgery, hereditary syphilis, like its parent disease, was generally treated of by the practitioner of that branch of medicine. And yet in the great majority of instances the management of such cases, especially as regards their family relations, the relations of husband and wife, the management of the latter during pregnancy, the delivery and subsequent care of the child, the necessary attention to the safety of other members of the family—in fact, all of the most weighty responsibility—falls upon the ordinary medical attendant. It is therefore in every way proper that the condition should receive some notice in a system of general medicine.
A proper presentation of the subject of hereditary syphilis involves a consideration of the vexed question as to the mode by which the disease is conveyed from parent to offspring. That it may be so transmitted has been generally believed since the doctrine was first announced by Torella at the end of the fifteenth century; and the facts in its support are so numerous and convincing that, in spite of a few distinguished opponents—among whom John Hunter was the most conspicuous1—it has been unhesitatingly accepted by the profession down to the present day. As regards the manner of transmission, however, controversy has been and still is rife. Opposing theories have been constructed and ardently supported, differing radically as to essential points, often resting upon exceptional or anomalous, and still oftener upon imperfectly observed, cases.2
1 Works of John Hunter, vol. ii. p. 383.
2 Parrot, in a clinical lecture on syphilitic abortion (Le Progrès Médicale, Nov. 3, 1877, p. 798), says: "The infection of children was known, but its true origin was not suspected. The belief of Gaspard Torella (1498) and Matthioli (1536) that it came from the nurses through the milk was generally accepted."[p. 255]
According to Diday, Paracelsus (1529) was the first to plainly state the heredity of syphilis: "Fit morbus hereditarius et transit a patre ad filium."
Others attribute the original announcement to Augier Ferrier (1553), and it seems certain that he was first to specify the three modes of infection of the product of conception: "La semence du père, celle de la mère, et la contamination de la mère durant la grossesse."
Fallopius in a posthumous treatise on the Mal Français (1566) adds the authority of his name to this view: "Præterea videbitis puerulos nascentes ex foemina infecta, ut ferant peccata parentum, qui vedentur semi cocti."
Ambroise Paré also acquiesced in the theory, saying, "Souvent on voir sortir les petits enfants hors le ventré de leur mère, ayant ceste maladie, et tost après avoir plusieurs pustules sur leur corps; lesquels étant ainsi infectés, baillent la vérolle à autant de nourrices qui les allaictent."
Subsequently, Mauriceau, Boerhaave, and Astruc sustained the same view, which, with the single exception of Hunter, had no prominent antagonist.
It was not, however, until the eighteenth century that it was described with any attempt at detail or exactness by Rosenstein, and his essay is loaded with errors. It was in the foundling hospitals of Paris at the end of the last century, in the wards of Salpétrière and Bicêtre, and in the hospitals of Vaugirard and in the Capucin convents of the Rue Saint Jacques, where pregnant women and nurses attacked with syphilis were admitted, that methodical and trustworthy observations were made (1780-1810) by Colombier, Despenières, Doublet, Mahon, Cullerier, and Bertin. Since then the history of the disease has been the history of syphilis itself.
A full consideration of these, or even a recapitulation of the respective arguments pro and con, would far exceed the limits allotted to the present article, and we will confine ourselves simply to stating the questions which most nearly concern the practical physician, and the conclusions which the accumulated observation and experience of the profession seem to justify. The points bearing upon the general subject of hereditary syphilis which exercise an important influence upon advice or opinions of the utmost gravity as regards the happiness and well-being of the individual or family may be enumerated as follows:
1. Is syphilis in all its stages transmissible (a) to the wife or husband, (b) to the offspring? Or, in other words, is it ever proper to consent to the marriage of a person who has had syphilis? If so, under what circumstances?
2. By what means or through what channels can the disease of the parents reach the child?
3. What are the pathology and symptoms of hereditary syphilis?
4. What is the treatment—(a) prophylactic, applied to the parents, and (b) curative? We may now take these up seriatim.
No more important questions can be submitted to a medical man than those pertaining to the marriage of syphilitics. Involving as it does the welfare of many individuals, modifying or fixing the conditions or circumstances of one or more lives, his opinion should be exceptionally definite and well grounded. The responsibility of advising or consenting to the marriage of a person who has once had syphilis is undoubtedly great; the responsibility of prohibiting it is, however, no less so. Matrimony is the natural condition for the majority of people. Enforced celibacy, especially in males, brings with it not infrequently a long train of attendant evils, moral and physical. It will not do to assume that professional duty is properly discharged by telling all patients to be on the safe side and to remain single for fear of inoculating wife or offspring, unless it can be clearly shown that there is a definite and unavoidable risk in every case, which continues throughout life.3
3 "The surgeon who, on account of past syphilis, forbids marriage to an otherwise [p. 256] eligible man must remember that he forbids it at the same time to some woman, who, possibly, if well informed as to her risks, would willingly encounter them.... Respecting a malady so common as syphilis, while it is often our duty to warn, it is also not unfrequently our duty to encourage" (Mr. Hutchinson, preface to the English translation of Fournier's Syphilis and Marriage, p. vii.)
There are two distinct methods of arriving at an answer to the question under discussion: first, by considering the probabilities in regard to the essential nature of syphilis; and, second, by carefully weighing the clinical evidence in the matter. It seems evident that belief in any particular theory of syphilis assigning it to this or that class of disease must have an important influence in determining the opinion which is held as to its curability, or at least as to its indefinite transmissibility.
If the late symptoms, the so-called tertiary outbreaks of the disease, are held to be evidences of the presence in the system of the specific virus, which has simply remained for a long period, perhaps for many years, latent or quiescent, and which is thus again manifesting its power; if syphilis is believed, accordingly, to be a practically unlimited disease, conforming to no known law as regards its duration, corresponding to no other infectious or contagious malady in having a period of termination—more or less delayed perhaps, or more or less indefinite, but still invariably present—at which time either the particular poison or the susceptibility of the system to its influence has become exhausted;—if tertiary syphilis, in other words, is regarded as simply a continuance or recurrence of the disease, differing in no essential respect, except as to the particular tissues involved, from the same disease in its early stages, it is difficult to see how marriage can ever be conscientiously recommended to a person who has once contracted it.
It is unfortunately true that in no given instance is it safe to assure a patient of further complete immunity from the disease. In any case, however mild in its course or under whatever treatment, there is always an element of doubt as to the development of subsequent symptoms. The probability of their appearance may be reduced to a minimum, the character of the case and the thoroughness of the treatment may both seem to give assurance that a cure has been completed, and yet both patient and physician may be mortified and annoyed by an outbreak of tertiary lesions. This, I think, would be admitted by every one of large experience with the disease, and indeed furnishes the chief argument to those who deny or are sceptical as to its curability. If, then, it were impossible to predict with any sort of certainty that the contagious and highly transmissible stage of syphilis would terminate during the life of the individual, it would manifestly be unwise to permit marriage, with its risk of inoculating the innocent partner and the consequent double risk to the offspring.
If, however, syphilis is, as taught by Mr. Hutchinson,4 one of the exanthemata, having, like them, a period of outbreak, a period of efflorescence or eruption, and a period of subsidence, and followed, like them, by certain non-contagious sequelæ, which we call the tertiary symptoms, but which are merely relapses or degenerations of parts affected during the secondary stage, it becomes evident that the risk of transmission to wife or husband or children after the lapse of a certain interval becomes greatly reduced or almost nil. No one thinks of forbidding marriage on [p. 257]account of a previous attack of small-pox or scarlet fever or typhoid fever, even although there are unpleasant consequences which sometimes follow these diseases.
4 The London Lancet, Feb. 5, 1876; Reynolds's System of Medicine, Am. ed., p. 423.
Or if another and still more plausible theory of syphilis is adopted, and we look on the tertiary period as one of contraction or obliteration of lymphatics due to long-continued irritation by the new cell-growths of the secondary stage, which from the very onset affect those vessels, our views will be materially modified. During the primary period, then, when the new cells, which either constitute the poison of syphilis or are its carriers, are accumulating at the site of original inoculation, constituting the induration of the chancre, or are slowly finding their way into the general system through the lymphatic vessels, proliferating in their walls and thickening and hardening them, or during the secondary period, when they are rapidly multiplying in all the tissues of the body, the risk of inoculation or transmission would be manifestly great. When, however, by destructive metamorphosis and degeneration, either with or without the aid of drugs, they have been eliminated from the body, the contagious element disappears with them; and although here and there throughout the body some important lymphatic trunk may have undergone irreparable injury, and may have been contracted or obliterated, permitting of the accumulation of waste products until the node or gumma or tubercle which we call a tertiary symptom makes its appearance, yet the disease has lost much of its terror, and has become dangerous only to the patient himself.5
5 Clinical Lectures on the Physiological Pathology and Treatment of Syphilis, by F. N. Otis, M.D.; Syphilis, by V. Cornil, Am. ed., 1882, pp. 17-27.
These theories are only alluded to by way of elucidation of the statement that belief in one or the other of them has an important bearing on the relation of syphilis to marriage, and because, whichever is thought to be the most plausible, they equally lessen or altogether do away with a certain proportion of the danger formerly thought to surround the marriage of a syphilitic even after a most protracted interval. It is not necessary to accept either the one or the other implicitly. The essential point is the recognition of the fact that modern syphilographers, as a rule, regard the tertiary or late symptoms as indicative of damage done during the active period—as relapses or sequelæ, and not as fresh outbreaks, of a highly contagious and transmissible disease. Their time of appearance, their entire want of symmetry, their non-contagiousness, their non-inoculability, all favor this view, and we may now see what evidence corroborative of it may be obtained from clinical facts.
It will be necessary, in the first place, to admit that there seems to be but little doubt in the minds of most syphilographers that in rare instances syphilitic children have been born to parents who had long passed the limits of the secondary period. At least the great majority of writers upon this subject speak confidently of the exceptional occurrence of such cases, and assert that syphilis may be transmitted during any of its stages.6 If, however, we come to look for positive evidence in this respect, we will find very little that is entirely satisfactory. Cases are reported, to be sure, in which eight, ten, twelve, or even fifteen or twenty, years after the primary sore, syphilitic patients have become the parents [p. 258]of children who showed unmistakable indications of the disease. When we examine the history of the cases, we find usually that many important points are omitted without which it is impossible to be certain of its true character. Were both parents originally infected? If not, has a recent case of syphilis occurred in the one who at first escaped? If they were both diseased originally, has either been subsequently re-infected?—a much more frequent accident than has been commonly supposed.7 On applying these tests to the cases in question it will be found that few if any of them are thoroughly convincing. Kassowitz's observations,8 made, it must be remembered, upon persons with whom no mercurial treatment had been employed, seemed to show that the average limit of transmissibility was about ten years, after which time healthy children began to be born. His observations were, however, incomplete in many respects, and, like all such investigations, are of course open to the suspicion of intentional deception on the part of the patients.9 Even these cases, however, show unequivocally, as do all which have ever been recorded, the steady diminution of the transmissive power under the influence of time alone.
6 Belhomme et Martin, Traité de la Syphilis, p. 413.
7 Cornil, op. cit., p. 20.
8 Die Vererbung der Syphilis, Wien, 1876.
9 See also Hutchinson, British and Foreign Med.-Chir. Rev., Oct., 1877.
I have said that the majority of writers seem to have no doubt of the long continuance of this transmissive power in rare cases. There are, however, a few notable exceptions. Fournier, whose immense experience and acuteness of observation entitle his opinion to the utmost consideration, says that in cases of paternal heredity the duration of the force of transmission never exceeds at the maximum three or four years.10 In no case of the many hundreds he has observed has he known a syphilitic father to infect a child—the mother being healthy—at a later period than the one mentioned. And he is equally positive that the gradual diminution and final extinction of the syphilitic reaction of the parents upon the children is a veritable pathological law, "absolutely demonstrated."11
10 Syphilis and Marriage, Am. ed., p. 87.
11 Op. cit., p. 88. Of course when both parents are diseased a somewhat longer period of activity is to be expected for the poison.
M. Mireur, a careful and accurate observer, records12 a striking instance in which in the history of a couple, both syphilitic and untreated, eight pregnancies occurred. The first resulted in abortion at fifth month; the second, in abortion at seventh month; the third, in a stillbirth; the fourth, a syphilitic child dying in one month; the fifth, in a syphilitic child dying in forty-five days; the sixth, seventh, and eighth, in living, healthy children. To me the most interesting fact in the whole relation is that during a portion of the time, and immediately after the last three pregnancies, which resulted in the birth of healthy children, both husband and wife manifested grave tertiary syphilitic symptoms—gummata, tubercles, ulcers, etc. This is direct evidence of the strongest kind in favor of the view that syphilis ceases to be transmissible by heredity at the end of a certain period, as we know that it ceases to be contagious or inoculable.
12 Essai sur l'Hérédité de la Syphilis, Thèse de Paris, 1867, p. 91.
M. Ricord long ago,13 and even before him Astruc and Doublet,14 had [p. 259]promulgated the same theory, Ricord asserting that in the tertiary stages the only effect of the disease upon the children was so to modify their organization and temperament as to expose them to developments of a scrofulous character—a view of the relation between syphilis and struma which has been so ably supported in our own day by Professor Gross.
13 Traité pratique des Maladies vénériennes Paris, 1838, p. 644.
14 Legendre, Nouvelles Recherches sur les Syphilides, 1841 (quoted by Belhomme et Martin).
M. Bazin also15 denies absolutely that tertiary syphilis is any more transmissible than it is communicable in other ways, although he fails to give his reasons for this belief.
15 Leçons sur les Syphilides, 1859, p. 35.
Hill and Cooper state16 that the transmissive power continues as long as the secondary eruptions are present, but usually ceases when the tertiary stage is reached.
16 Syphilis and Local Contagious Disorders, London, 1881, p. 62.
Van Buren and Keyes17 believe that fathers with tertiary syphilis certainly, as a rule, procreate non-syphilitic children; and in speaking of the fact that when the mother has syphilis the child is generally infected, they except the later tertiary stages.
17 Genito-urinary Disease and Syphilis, 1874, p. 521.
Bumstead18 and Taylor say that without mercurial treatment the danger of transmitting the disease to offspring usually persists up to the fourth year of syphilitic contagion.
18 Venereal Diseases, 1879, p. 739.
Mr. Lane says:19 "It is certainly the rule that when the parents have fully reached the tertiary stage the children born to them are free from all signs of syphilis."
19 Lectures on Syphilis, London, 1881, p. 65.
Mr. Hutchinson says:20 "It is almost an acknowledged law that parents in the late tertiary stages do not transmit taint."
20 The Med. Press and Circular, Aug. 2, 1882, p. 85.
It will be seen from the foregoing extracts, which might be greatly multiplied,21 that there is a strong tendency on the part of many authors to limit more or less strictly the period of transmissibility of syphilis even when the disease is allowed to progress without treatment. As to the facts that it becomes milder with time, both in parents and offspring, that it ceases to be conveyed from husband to wife or vice versâ, that with each succeeding year after the termination of the secondary period the chances of escape of the product of conception increase in a rapidly augmenting ratio,—there is no difference of opinion whatever. Neither is it seriously disputed that the length of time during which the disease remains active, as well as the degree of its activity, may be markedly and beneficially influenced by the administration of mercurial treatment. Under proper medication patients who have rashly or disobediently married in the height of the secondary period have been enabled to escape the danger of transmission either to spouse or offspring—have, in fact, had children born healthy and who never subsequently manifested any symptoms of the disease.
21 M. Diday, Traité de la Syphilis des Nouveau-nés, Paris, 1854, p. 183; M. Bertin, Traité de la Maladie vénérienne chez les Nouveau-nés, Paris, 1870, p. 142; M. Bazin, op. cit., p. 164; M. Roger, L'Union Médicale, 1865, t. i. p. 147 (quoted by Fournier).
I may add that my own experience seems to confirm the views which have thus been set forth. I have notes of all my cases occurring in private practice in a large city—some of them, I regret to say, among personal friends or acquaintances, some of them in our own profession—and have repeatedly [p. 260]given permission to men to marry or to resume marital relations after three years or three years and a half of mild mercurial treatment, to which during the last six months or a year had been added iodide of potassium. In many instances healthy children have been born: in none, so far as I know, has the wife or mother been directly infected. There have been a few doubtful cases in which premature deliveries or stillbirths have occurred, but in nearly every such instance there seemed to be other and entirely competent causes for the accident; and in none of them, as I learned from the father or from the obstetrician in attendance, were the children the subjects of unmistakable syphilitic symptoms.
As to the exact time at which it is safe to permit marriage, and as to the proper treatment before and after that event, it is hardly possible in an essay like this to enter into many details. Yet so much is involved in the answer to our first question that it may not be altogether out of place here to indicate briefly the views of the writer as to general methods of treatment. This is the more proper because in every case of suspected syphilis in a new-born child, in every case of threatened or actual abortion or miscarriage in the wife of a man who has at some time in his life had syphilis, these questions will present themselves, and the answers to them will greatly influence not only the diagnosis and prognosis, but even the treatment, of such cases.
1. In the first place, then, the diagnosis of syphilis should have been assured. No venereal sore can with certainty be pronounced to be syphilitic before the occurrence of general constitutional symptoms, either the early cutaneous eruptions or at least the general glandular involvement. Treatment begun prior to these developments leaves the whole case open to the suspicion of mistaken diagnosis.22
22 "It is unsafe to predict confidently that any venereal ulcer, even a soft sore attended with suppurating bubo, will entail no further consequences. There is a strong probability that an indurated sore will prove infecting; and there is a probability, though not nearly so strong, that a soft suppurating sore will not; but exceptions to both these general rules will be met with, and there is really no absolute proof of the infecting nature of any given sore but the fact of infection itself" (Lectures on Syphilis, James S. Lane, London, 1881, p. 23).
2. The drug which should at once be begun when the character of the case is fully recognized is mercury in one of its various forms. It may be given by the mouth, by inunction, by vaporization, by hypodermic injection, according to the preferences of the physician or patient; but, however administered, it should be given in sufficient quantity—i.e. in each case the full physiological dose of that particular patient should be employed. To ascertain this the amount used should have been gradually increased until commencing symptoms of salivation are produced, when it should be diminished about one-half.
3. The quantity which has been thus determined should be given continuously, or stopping only for the management of intercurrent complications, for at least eighteen months. If during this time new syphilitic symptoms make their appearance, the dose should be temporarily raised until they have vanished, when it should be brought down again to the original amount.
4. At the end of eighteen months or two years small doses of iodide of potassium should be added to the mercurial, and this mixed treatment should be persevered in for six months or a year longer, or should be [p. 261]still further prolonged if during that time any evidence of syphilis is seen.
5. At the end, then, of from two to three years, if no symptom has been seen for six months or a year, treatment may be stopped and the patient kept under observation for a year; and if during that time no symptom develops he may consider himself as in all probability cured. Any course of treatment less thorough than this should be set down as insufficient to afford any reasonable presumption of further immunity from the disease.
There is evidence to prove, on the other hand, that this plan of treatment, rigidly carried out, results in the majority of cases in curing the disease, or at any rate in putting the patient in such condition that he may with safety marry and may expect to have healthy children.
To recapitulate: Syphilis after a certain period, not extending much over four years where the disease is allowed to run its own course, and probably much reduced by treatment, ceases to be a contagious disease; and at about the same time or some time after loses, in the majority of cases, its capability of being transmitted.
As there are probably exceptions to the rule that this power of transmission disappears spontaneously within any specified time, it is never safe to trust altogether to the unaided efforts of nature, but a vigorous and sufficient specific treatment must be employed.
Given, however, the lapse of a sufficient time—say from three to four years as a minimum—the history of a proper and continuous plan of treatment, and the absence for a year or more of any specific symptoms whatever, and the risks of marriage are so reduced as probably to warrant a careful physician in permitting it.23 And conversely, of course—and this constitutes the reason for introducing the foregoing matter into a paper on hereditary syphilis—in any doubtful case where such a history can be elicited, and where all these precautions have been observed, it is improbable that any taint of syphilis has been transmitted.
23 This refers, of course, to an ordinary case of syphilis. If the symptoms have been unusually grave, if the deeper tissues or the viscera have been seriously involved, if cerebral or spinal complications have occurred, the situation is of course much more grave, and no step should be taken without the most thoughtful deliberation. The work of Fournier already alluded to (Syphilis and Marriage) furnishes an admirable guide under these circumstances.
Mr. Frederick Lowndes, surgeon to the Liverpool Dock Hospital (Lancet, July 8, 1882), says: "Each case must be judged on its own merits. When the constitution is good, and there has been sufficient specific treatment, marriage may be permitted within a much shorter period than M. Fournier suggests, and with safety. Syphilis alone and syphilis combined with scrofula are two very different foes to contend with, and if our patient be of a scrofulous temperament a delay even longer than M. Fournier's may be desirable."
He quotes Dr. Thomas Edward Beatty in an address at the annual meeting of the British Medical Association at Leeds in 1869: "Mercury given to the man when first diseased would, I firmly believe, have prevented this terrible calamity—i.e. the syphilitic infection of the wife; and I would now humbly suggest to all who undertake the treatment of venereal disease that if they have a certainty that their patients will remain celibate all their lives, they may heal up their sores and dispel their eruptions and sore throats in any manner they like, but that they have no right to expose the pure, innocent, high-minded females of society to contamination by marrying men treated without mercury."
Beyond this in positiveness of assertion it is not safe to go. There may be exceptions to these as to most other hygienic or therapeutic rules, but they will surely be of excessive rarity.
[p. 262]Before considering the methods by which syphilis can reach the child from one or the other of its parents, it may be well to mention the modes in which they can infect each other.
The father can derive syphilis from the mother only in the usual way—i.e. by contagion through a breach of surface permitting of the direct absorption of the poison, the development of the disease being attended by the usual phenomena—chancre, lymphatic enlargement, skin eruptions, etc. The woman may—and in the vast majority of cases does—acquire the disease from the husband in a similar manner. But there seems to be good reason for believing that she may also become infected through the medium of the child, who receives its syphilis directly from the father, the mother up to the time of conception having escaped contagion. More than this, it appears to be highly probable24 that no woman ever bears a syphilitic child and remains herself absolutely free from the disease.
24 The strongest argument against the theory that every woman who has had a syphilitic child has herself been infected lies in the existence of cases like the following, several of which have been observed: The wife of a man having active but untreated syphilis gives birth to one or two syphilitic children, she herself developing no symptoms. Later, the husband is placed on mercurial treatment. She then conceives and gives birth to a healthy child. He stops treatment, and she again bears a syphilitic child, which on his resuming his mercurial course is followed by another healthy infant. Such cases certainly indicate that the syphilis of the mother, if any exists, is incapable of transmission to the child, as the effect of the treatment of the father is too direct and unvarying to admit of doubt.
The existence of this form of infection—syphilis by conception—has been vehemently denied by many authors25—by some on the theoretical grounds that as the essential elements or carriers of the syphilitic virus have been shown to be cells or protoplasmic particles, and as, after conception, the embryo is supplied with serum, but not with cells of any kind, it is impossible that syphilis can be conveyed either to or from it;26 by others on reported observations of numerous cases in which mothers who have been delivered of syphilitic children have shown no evidences of the disease.
25 Kassowitz, Von Baerensprung, Bidenkap, and others.
26 Bumstead and Taylor, op. cit., p. 742.
It would appear, however, that, setting aside arguments based on theoretical considerations, the weight of clinical evidence is altogether in favor of the frequent, if not the invariable, contamination of the mother through the medium of the foetus. No physician of large experience in this class of cases can fail to have seen some in which the husband, having had syphilis and having married after an insufficient interval or an imperfect course of treatment, has infected his wife with the disease, although at the time no discoverable symptom is to be found upon his body—no abrasion, sore, mucous patch, no lesion of continuity or suspicious point of any description. An equally careful inspection of the woman will also in such cases be attended by negative results—no initial lesion, no spot of induration, no adenopathy being at all discoverable—and yet she will be found with unmistakable evidences of constitutional syphilis.27 There is a clue to all such cases which will immediately resolve the difficulty. In every instance, providing that no mistake has [p. 263]been made and that both husband and wife are really free—the one from any contagious lesion, the other from any evidence of a present or previous primary sore—it will be found that pregnancy has occurred; that the woman has either been delivered of a syphilitic child or has had an abortion or miscarriage at some time before the outbreak of the symptoms of syphilis. Although I am firmly convinced that this is a statement of facts based upon careful clinical observation, and although this view has received the unqualified endorsement of no less an authority than Fournier,28 it is yet strongly combated by many excellent authorities. They say in reply to the above arguments that the reported cases are open to just criticism, that trifling and unnoticed lesions of the father—chafes or abrasions almost microscopic—suffice to transmit it on his part; while as an explanation of the supposed absence of the primary lesion in the mother they plead the well-known difficulty of discovering it in women under any circumstances.
27 For a typical case see Colles's Works, New Sydenham Society, London, 1881, p. 253. From that date to this hundreds of such cases have been observed, and it would be idle to refer to them.
28 Op. cit., pp. 26-30. He confesses to complete ignorance as to the precise method by which this contagion takes place, whether by poisoning of the fecundated ovule at the moment of conception (the theory of Von Baerensprung) or by exchanges of the utero-placental circulation, and regards the various hypotheses upon these points as without practical value.
Another argument, however, which seems to me to be unanswerable lies in the application to the case in question of the well-known "law of Colles," which from the date of its first enunciation by its distinguished expounder in 1837 down to the present day has been found to be absolutely without exception. I know of no other statement in reference to disease which is at once so sweeping and comprehensive in its bearings and so completely substantiated by clinical experience. It may be given in his own words: "One fact well deserving our attention is this: that a child born of a mother who is without obvious venereal symptoms, and which, without being exposed to any infection subsequent to its birth, shows this disease when a few weeks old,—this child will infect the most healthy nurse, whether she suckle it or merely handle and dress it; and yet this child is never known to infect its own mother, even though she suckle it while it has venereal ulcers of the lips and tongue."29
29 The Works of Abraham Colles, edited by Robert McDonnell, the New Sydenham Society, London, 1881, chap. xiii. p. 287.
As to the absolute and unvarying truth of this law there is no excuse for a shadow of doubt. To quote Mr. Hutchinson: "It has received the assent of every authority who has written on the subject since it was announced. It has attracted attention both at home and abroad, and I am not aware that a single exception to it has been recorded.30 We have all of us seen chancres on the nipples of wet-nurses. They are, indeed, not very infrequent. We have, however, none of us seen such on those of the mothers of infected children. Let us remember that it is very unusual to put a syphilitic infant out to wet-nurse—a thing which no prudent physician would ever permit—and that, probably, for one so nursed a hundred are suckled by their mothers, and we can appreciate the weight which this entire absence of proof that mothers ever suffer [p. 264]bears. It amounts, I think, to all but proof that they are absolutely insusceptible."31
30 The cases of Cazenave (1847), Cocchi (1858), Müller (1861), Ranke (1878), Guibout (1879), Scarenzio (1880), and Zingalès (1882), are defective in important particulars, the first two so much so as to render them valueless. Ranke's case is by far the strongest yet recorded, but lacks fulness and rests upon his unsupported testimony. (See Hill and Cooper, op. cit., p. 55, and Nouveau Dict. de Méd. et de Chir., vol. xxxiv. p. 687.)
31 Dr. J. N. Hyde suggests (Archives of Dermatology, April, 1878, p. 103) that "the full weight of Colles's law is to be estimated in connection with the question whether the child whose hereditary syphilis is derived from the mother exclusively is capable of infecting its healthy father; and if no instance of this latter can be adduced a higher law becomes defined—viz. that the child whose hereditary syphilis is transmitted by one parent only is incapable of infecting either." He explains this hypothetical immunity, in which he seems to believe, by saying that "it is probably due to the fact that the syphilis-bearing cell-element cannot readily be implanted upon the soil from which it sprang—a fact illustrated by the infecundity of consanguineous marriages and the non-auto-inoculability in general of the primary lesion of syphilis." When, however, we exclude the large number of cases in which the father is already syphilitic, and remember that in the others the contact between him and the child is slight, infrequent, and fleeting—being usually limited to an occasional kiss or caress—it does not seem strange that no instances of such infection have been reported; nor does the fact seem at all worthy of being made the foundation of a general law.
There can be but one rational explanation of these facts—viz. that the mothers who have thus acquired an immunity have done so by first acquiring the disease. It may, in those cases where no secondary symptoms appear, be in a modified form, due, as suggested by Mr. Hutchinson, to some heteromorphism or alternation of generations on the part of a specific fungus, or to the excessively small quantity of the poison which finds its way from child to mother, or to some other obscure cause with which we need not now concern ourselves. It is, at any rate, no more mysterious than the protective influence of vaccine in small-pox, and when one is rationally explained doubtless the other will be found to be closely allied in its mode of action. The fact which interests us at present is that it is in the highest degree improbable that anything but some form of syphilis itself could afford this entire protection, and that it is not in the least unreasonable, but, on the contrary, logical and consistent with all the known facts, to suppose that while in some cases no observable symptoms might be produced, in others where the cause was the same, but more active, or the powers of resistance less, the usual constitutional phenomena would be developed.
We may conclude, then, that the husband may infect his wife—(1) In the usual manner or by direct contagion; (2) through the medium of the child, or at any rate by the production of conception.
The theory upheld by Von Baerensprung, that the syphilis of the mother is imparted to her at the moment of impregnation, the disease being impressed upon the fecundated ovule, does not materially conflict with the above views, conception being in either case the essential factor, but in the latter instance the intervention of the foetus itself not being necessary. It has to support it the clinical fact that in those cases where syphilis appears during pregnancy the outbreak of symptoms occurs at about the ninth or tenth week after the date of conception, or a period which closely corresponds to that of the appearance of general symptoms after exposure to ordinary contagion—allowing about three weeks for the so-called incubation of the chancre and six weeks for the secondary incubation.32
32 This has been shown not only by Von Baerensprung (Die Hereditäre Syphilis), but also by Diday, whose observations were intended to prove the possibility of syphilis being derived from the child by the mother—"choc en retour." In 24 cases the period at which the first eruption appeared in the mother averaged sixty-five days after conception; only once did the first signs appear after the fourth month of pregnancy.
[p. 265]It may also be said to be rendered probable by the following line of argument:
Colles's law, which is without exception, demonstrates that every woman who has had a syphilitic child has been herself infected, even if she has had no observable symptoms;33
Cases are recorded, however, in which a woman having given birth to one or more syphilitic children, and therefore herself syphilitic, bears healthy ones in consequence of specific treatment administered to the father before and during the period of conception, she remaining untreated;34
The determining cause, therefore, of the syphilis of the child is not the syphilis of the mother, but the condition of the fecundating germ of the father; and, as a corollary,
The determining cause of the syphilis of mothers in whom the disease follows conception is not by infection from the foetus through the utero-placental circulation35 or otherwise, but is the diseased male procreative cell which becomes blended with the female ovule.36
33 It is obviously no explanation of the law of Colles to say that "it would seem to indicate that the escape of the mother is due to some occult, undiscernible change in her system" (Bumstead and Taylor, op. cit., p. 745).
34 See foot-note, p. 262.
35 On account of the absence of cellular elements in the fluid interchanged.
36 An elaborate paper by Fraenkel (Archiv für Gynaekologie, 1873, vol. v. p. 1), based on twenty-one cases of childbirth, was written to prove by the condition of the placenta that direct infection of the child by the father was possible without the participation of the mother, and that when the latter became infected it was through the medium of the child (choc en retour). In fourteen of his cases the specific change in the placenta began in the foetal portion or affected it exclusively. These cases, however, as analyzed by Hill and Cooper (op. cit., p. 57), are altogether defective in important particulars. Of course to sustain his theory there should be indubitable evidence that the fathers were syphilitic, and that the mothers were not so. So far from this being the case, but one of the fathers was known to be syphilitic, while two of the mothers had evidences of constitutional syphilis at the date of childbirth, and nine others had markedly suspicious histories. The lesions of the placenta which are thought to be syphilitic consist in the development of papular or gummatous growths which give rise secondarily to inflammatory troubles affecting either the placenta itself or the placenta and the uterine mucous membrane.
If the premises are admitted the conclusions seem irresistibly to follow.
There is no proof whatever that the semen of a syphilitic man is contagious or can transmit the disease in any but the way above discussed. On the contrary, it has been shown experimentally37 that it is entirely innocuous and non-inoculable.
37 Mireur, Annales de Derm. et Syph., 1876, p. 77.
All other theories as to methods of contagion are so entirely hypothetical and unsupported by trustworthy evidence that we can afford to disregard them.
We may now consider the ways by which syphilis reaches the child, and they may be broadly classified into—
1. By descent from the father.
2. By descent from the mother.
3. By direct infection.
As a matter of course, the influence of the father upon the child, so far as regards heredity, ceases at the moment of conception; or, to be more exact, no subsequent condition of the male parent, no development or acquirement of disease, can exert any further effect. That the existence of active syphilis in the father may result in the transmission of the malady to the child can hardly be doubted. To be sure, there are numerous [p. 266]examples of cases where both wife and child have escaped though the husband showed at the time of conception very active secondary lesions. These, however, are exceptions, and do not in the least invalidate the rule that it is possible for a father to hand the disease directly to his child. There is no other possible interpretation of the cases already alluded to in which successive pregnancies in the same woman alternately resulted in healthy or in syphilitic children according as the father was or was not kept under specific treatment. Other arguments might be advanced, but that seems to me conclusive.
The relative effect of paternal as compared with maternal influence may be considered after we have described the latter.
Descent from the mother may occur theoretically in consequence of—
1. Infection of the mother previous to conception.
2. Infection of the mother at the moment of conception.
3. Infection of the mother during the period of utero-gestation.
As to the first of these methods of transmitting the disease there is little if any difference of opinion. Even those who claim the most for paternal influence38 include among the conditions which may give rise to syphilis in the child disease of the ovule, and it may be stated as incontrovertible that recent or active syphilis in the mother at the time of conception will almost certainly be followed by syphilis in the child. As a rule, women who have borne syphilitic children, even when they do not give unmistakable evidence of the disease, fail in health, become anæmic, and often develop glandular or osseous swellings which, according to Zeissl,39 are only relieved by antisyphilitic treatment. The bearing of Colles's law upon the alleged immunity in many instances of the mothers of syphilitic children has already been shown (p. 264); and there is other evidence, not perhaps so conclusive, but strongly corroborative, of the same view—viz. that their escape is only apparent, and that syphilis, either latent or active, always affects such mothers.40 There can be no manner of doubt that in every instance at or about the time of childbirth there are not to be found pathognomonic lesions of syphilis, nor do such lesions always make their appearance in cases where the period of observation is a short one; but it is claimed with much show of truth that prolonged and patient inspection of such patients will in time result in the discovery of some symptom which betrays the presence of the disease.
38 Bumstead and Taylor, op. cit., p. 745. Hutchinson in Reynolds's System of Medicine, Am. ed., vol. i. p. 431: "In a large proportion of the cases met with in practice the taint is derived from the father only." (On this point see foot-note to p. 270.) If there were any doubt as to the fact that syphilis in the mother only may be transmitted to the child, it would be removed by the cases of Bardicet and others mentioned in Nouv. Dict. de Méd. et Chir., vol. xxxiv. p. 688. In these cases nurses who had contracted the disease from their sucklings subsequently became pregnant (without having infected their husbands) and gave birth to syphilitic children.
39 Jahrbuch, vol. ii. p. 303, 1872.
40 Zeissl, Sigmund, Oewre, Flindt, Woodman, and others are quoted by Hill and Cooper to this effect. Woodman, for other purposes, gave the histories of 200 cases of infantile syphilis. In all of these the mothers had suffered from typical secondary lesions.
The cases in which treatment of the father has resulted in healthy children, whereas without treatment he procreated only syphilitic children, the mother being without either symptom or treatment, have been urged as evidence of the direct descent of syphilis from the father to the child without the intervention or participation of the mother. Doubt [p. 267]has been thrown upon them by those who uphold the contrary view;41 but after looking into them carefully I am constrained to admit that some of them, notably those of Kassowitz42 and R. W. Taylor,43 are convincing of the facts—(1) that treatment of the father controlled the condition of the child, and (2) that there was no evidence that the mother had syphilis. But we have seen that the only proof of the universal infection of mothers of syphilitic children is the law of Colles, and that in many cases the disease is for a long time latent or unrecognizable. Let us admit that this was the condition in the cases in question; it does not at all follow, necessarily, that because the mother has latent or hidden syphilis she must infect her child. Every case even of active syphilis in the parents is not handed down to the children, a certain proportion of whom escape even when both parents are in the height of the secondary stage at the time of conception.44 But the activity of the disease in the children, and even more the likelihood of its reaching them, are in direct proportion to its activity in the parents.45 A mother, therefore, who under the influence of active syphilis in her husband has given birth to two or three syphilitic children, and has herself shown no symptoms of the disease, may nevertheless have it in the latent form and have no strong tendency to transmit it. Consequently, treatment of the father will result in the procreation of healthy children, because it removes the active and efficient cause of their infection. To take any other view of these cases is to assume that every syphilitic parent must hand down the disease to the children—an assumption which is not in consonance with numerous well-attested clinical facts.
41 Hill and Cooper, op. cit., pp. 52, 53.
42 "Die Vererbung der Syphilis," Stricker's Med. Jahrb., 1875, p. 391.
43 Archives of Clinical Surgery, New York, Sept., 1876.
44 Fournier, op. cit., pp. 35-37.
45 Hutchinson, op. cit., p. 431.
Leaving this interesting question, however, we may consider the other methods by which syphilis descends from the mother to the child, having seen already that it is beyond doubt that it may be handed down by disease of the ovule due to syphilis acquired previous to conception, and having seen that there is a high degree of probability that the mother herself rarely, if ever, escapes the disease. The second method, or that in which the mother becomes syphilitic at the moment of conception, has already been sufficiently discussed. It is really, strictly speaking, an example of paternal heredity, as the resulting germ is syphilitic—not because the ovule of the mother was infected, but on account of the disease of the spermatozoid of the father.
There remains for consideration the influence upon the child of a syphilis acquired by the mother during some period of utero-gestation. That under these circumstances the child can become infected has been and is still absolutely denied by some very respectable authorities.46 All that is [p. 268]necessary for proof of its occurrence is, however, (1) freedom of both parents from syphilis at the time of conception, or, in other words, syphilis must have been acquired by both—not alone by the mother—after the beginning of pregnancy; (2) that the syphilis of the child be unmistakably pre-natal—that is, not acquired by some accident during or after birth.
46 Bumstead and Taylor, op. cit., pp. 742, 744. They base their denial, first, on the physiological fact (?) that no interchange of cellular elements between mother and father is possible, and next on the absence of satisfactory evidence of the occurrence of infection during pregnancy. Zeissl's case seems sufficient answer to the last assertion, and there is strong evidence that the first is without good foundation. "The placenta is penetrated by the virus, and does not play the part of a filter for the elementary particles of matter which, so far as we know, represent the true active contagion of the disease. In the absence of direct experiments, which it would be almost impossible to institute, we may argue from the facts known to exist in certain acute infectious diseases in which there are very interesting points of resemblance.
"It has been known for a long time that small-pox occurring in the mother may be transmitted to the product of conception enclosed in the uterus, and it is supposed that the virulent particles traverse the walls of the maternal vessels in order to penetrate the circulating apparatus of the foetus. But what is only a supposition in the case of small-pox seems to have been actually demonstrated in symptomatic charbon (Arloing, Cornevin, and Thomas), bacteridian charbon, and recurrent fever, in which the poisonous element is easily recognized. The recent experiences of Strauss and Chamberland (1882) have shown that the foetus participates in the 'infection charbonneux' of the mother. Albrecht has shown (1880) the presence of numerous spirochoetæ in the blood of the heart of a child born at seven months of a woman with a second attack of relapsing fever. It may be supposed, therefore, though not demonstrated, that the transmission of syphilis takes place by the same method as that of relapsing typhus or of charbon" (Nouveau Dict. de Méd. et de Chir., pp. 682, 683).
The following case,47 reported by a most accurate observer, seems to combine both these requisites. Zeissl the younger reports that O. X., thirty-six years old, never having had syphilis, left his wife, to whom he had been married two years, to go a journey on July 15, 1877. The wife was then in the second month of her first pregnancy. On July 24th O. X. had extra-marital intercourse. About twenty-one days after this coitus he observed a small lump on the inner surface of the foreskin, and on Aug. 22d he consulted Zeissl the elder. On Sept. 23d a maculo-papular eruption of the skin with erythema faucium appeared. Under treatment these symptoms completely disappeared. On Oct. 29th he went home to fetch his wife to Vienna for her lying-in, and had intercourse with her soon after his return, notwithstanding Zeissl's strict prohibition. At the beginning of December a hard sore developed on the left nympha of the wife, who was then in the seventh calendar month of her pregnancy. At the end of December a maculo-papular eruption spread over the body and was treated with mercury. On Feb. 14, 1878, a well-grown and apparently healthy female child was born at full term. When eleven days old48 a pustulo-scaly eruption came out on the child's soles and toes, and soon afterward a maculo-papular eruption over the body generally. A few days later the child died. No post-mortem examination was permitted. In July, 1878, the wife had iritis, and after that gummata on the leg. She miscarried in July, 1878, at the third month, and again in February, 1879, at the second month.
47 Quoted by Hill and Cooper, op. cit., p. 60.
48 Of course much too early for constitutional symptoms if the disease had been acquired during or after birth.
There seems to be no reasonable escape, after reading this carefully, from the conclusion that in some manner the poison of syphilis found its way from the mother to the child. The old idea that the latter was directly infected in utero from the semen of the father is altogether without foundation. Other cases equally satisfactory and complete have been reported, and, unless the intelligence or the truthfulness of the observers be impugned, establish without doubt the possibility of infection during utero-gestation.
In the above case the contagion of the mother occurred in the seventh [p. 269]month of pregnancy; and this, I believe, is as late as it has ever been known to be communicated to the child. The exact date at which it becomes impossible so to transmit it is unknown, but as a general rule it may be said that the earlier a mother is infected during gestation the less likely is it that the child will escape. Treatment of the mother—as of the father in cases where he is at fault—very greatly modifies the whole problem and adds immensely to the chances that the child will not be infected.
Direct infection of the child during birth could not properly come under the head of hereditary syphilis. There is no possible reason why, when the mother has contagious lesions of the genitals, acquired too late to infect the child in utero, this should not occur, but as a matter of fact no such case has ever been recorded. One explanation of this circumstance may be found in the protective covering of vernix and mucus which coats the infant's body and lessens greatly the risk of absorption. This hardly accounts satisfactorily, however, for the entire absence of such cases from medical literature, and it is fair to suppose that in all but those cases in which the primary sore is acquired during the last month of gestation—which for obvious reasons are excessively rare—the infant acquires some immunity which protects it from its mother, and is similar to that which, under Colles's law, operates in her favor. In other words, even though apparently free from syphilis at birth—a not uncommon event, as we shall see—it has a latent or modified syphilis which protects it from contagion.
We may now briefly restate the conclusions at which we have thus far arrived:
1. After a certain interval, not less than four years, and after thorough specific treatment, a person who has contracted a syphilis not especially severe or malignant in its type may be permitted to marry. The assent to marriage will then be based on a belief in the curability of syphilis or the cessation of its contagiousness, its inoculability, and, in the vast majority of cases, its transmissive power at the end of the secondary stage.
2. It may be inherited from either parent or from both, and the probability that this will occur increases in a direct ratio with the nearness of the time of conception to the date of their infection with the disease. The severity of the inherited disease in the child increases in the same proportion.
3. It is undoubted that, the father being healthy and the mother syphilitic, the child may, and in all probability will, have the disease.49
49 Dr. Sturgis, who disbelieves altogether in the possibility of paternal heredity, concludes, after examining the subject carefully, that (1) a mother begets non-syphilitic children as long as she is not infected, even though the father is syphilitic; and (2) the moment she is diseased the children are inevitably so (Paper on "The Etiology of Hereditary Syphilis," New York Medical Journal, July, 1871). This doctrine was previously supported by M. Cullerier, whose views gave rise to the remarks of M. Voillemier (quoted by Fournier) that if they were accepted "the father would be only the accidental occasion of a child; one would be, in reality, the child of his mother only." Cullerier's cases are invalidated by the fact that the syphilitic fathers who had healthy children had been subjected to mercurial treatment (Mém. de la Société de Chirurgie, Paris, 1854, quoted by Taylor in Archives of Clin. Surg., vol. i. p. 83). The theory is a very old one. Vassal has sustained this idea as long ago as the end of the last century. Kostum (1804), and after him Hufeland, were of the same opinion. Cullerier (1857) wrote: "In order that a child acquire syphilis hereditarily it is necessary that the mother is or has been [p. 270] syphilitic." Notta, Follin, Charrier, Mireur (1867), and Langlebert (1873) support this theory more or less earnestly. Oewre wrote (1873): "Paternal influence is nil as regards hereditary syphilis." Isseff (1879) wrote: "Where a man suffers or has suffered from syphilis he cannot transmit the disease to his descendants without infecting his wife; that is to say, in fewer words, there is no infection from the father." Sigmund says: "The heredity of syphilis is derived in its last analysis from the mother" (Nouveau Dict. de Méd. et Chir., vol. xxxiv. p. 689).
4. It is probable, but less so,50 that, the mother being healthy and the father syphilitic, the child will be infected.
50 This refers simply to the comparative probability of infection, and does not conflict with the statistical fact expressed by Hutchinson (Reynolds's System of Medicine, vol. i. p. 431) in his words: "In the large proportion of cases met with in practice the taint is derived from the father only." This numerical predominance of paternal influence is very readily explained. There are many more syphilitic men than syphilitic women, and especially among the couples who contract fertile marriages the number of women who are infected before becoming mothers is inconsiderable. On the other hand, it frequently happens that men who have had syphilis, but have been without symptoms for a longer or shorter interval, marry and transmit to a series of children a disease which has ceased to be directly contagious to their wives, the transmissive power continuing after the possibility of ordinary contagion has disappeared. As in the majority of such women the disease is latent, and may be only displayed in their immunity from infection, it becomes evident that, history and symptoms both being wanting on their part, the conditions justify the assertion of Mr. Hutchinson. (See Nouveau Dict. de Médecine et Chirurgie, p. 684.)
That assertion (quoted above) has, however, been thought by several writers to indicate his belief in the escape of the mother. That I have not misinterpreted him is evident from the following extract from an article on "The Transmission of Syphilis," written by him (Brit. and For. Med.-Chir. Rev., Oct., 1877): "I take it for granted (although I know that there are still some who doubt) that it is possible for a father to transmit the taint, the mother being at the time of conception wholly free. I believe, indeed, that in practice this is by far the most common way in which syphilis is transmitted. Whether in these cases it is correct to speak of the inheritance being paternal only is, as we have just seen, another matter, since it is possible that in every instance the mother derives an infection from the father, and may thus in turn influence it."
5. It is highly probable, though it can hardly be considered as proven, that in all cases where a child becomes syphilitic through paternal influence the mother is also the subject of syphilis, which may, however, assume a latent form, the only evidence of its presence in a few cases being the protection which it affords against contagion through the medium of the child.
6. Syphilis may be transmitted from mother to child even when it is acquired by the former as late as the seventh month of utero-gestation.
Since writing the above the thirty-fourth volume of the Nouveau Dictionnaire de Médecine et de Chirurgie has been published. In the article on syphilis seventeen pages are devoted to the question of heredity, which is reviewed in a most thorough manner and finally summed up as follows (p. 698):
"The most definite views which we possess on the subject of the hereditary transmission of syphilis may be thus expressed:
"Children may be infected by heredity, not only when the two parents are syphilitic, but also when only one, either the father or mother, is diseased at the time of conception.
"When both parents are diseased at that time there is more certainty that the child will be infected, and infected gravely, than if only one of them has the pox.
"The hereditary disease is not always fatal, even when both progenitors have actual specific symptoms. The more recent the disease of the parents the greater the chances of their transmitting the disease and of its assuming [p. 271]a serious form. There is no proof that inherited syphilis is more grave when derived from the father than when coming from the mother.
"It is altogether exceptional for the mother, healthy at the moment of conception, not to participate in the disease transmitted by the father to the child. If she escapes direct contagion—which is rare when the disease of the father is active—she undergoes a species of infection from contact with the contaminated foetus.
"Syphilis by conception, which is thus transmitted from the foetus to the mother, may present the usual characters and evolutions of the acquired disease; frequently, also, it is latent, and is betrayed only by the existence of immunity from further contagion on the part of the mother. It may finally manifest itself by tertiary symptoms or by systemic troubles without specific characters.51
51 "This form of syphilis shows itself in the mother in three ways:
"1st. By the usual signs of syphilis by contagion, with the exception of the primary sore, appearing about the sixty-fifth day after conception.
"2d. Appearing at a later date as secondary or even as tertiary symptoms, and preceded merely by a little disturbance of the general health, unhealthy appearance of skin, falling of hair, etc., but nothing truly specific.
"3d. Showing itself some years afterward in a tertiary form, having in the mean while given no indication of its existence save only in the protection it afforded against contagion from the child" (Nouveau Dict. de Méd. et Chir., vol. xxxiv. p. 696).
"The power of transmitting syphilis hereditarily decreases spontaneously as the disease of the parent becomes older. The influence of treatment is no less certain than that of time. When the two progenitors are at the moment of conception free from syphilis, the foetus may still be infected if the mother acquire the disease during her pregnancy."
Syphilis of the placenta is of especial interest in its relation to the abortions and stillbirths so frequent in syphilis. Until the elaborate paper of Fraenkel upon this subject (see foot-note, p. 265) almost nothing was known about it. He describes52 the macroscopic changes as consisting of increased size and weight of the placenta, closer and firmer texture of the placental tissue, the presence of old and recent extravasations of blood in all stages, opacity and thickening of the decidual covering and of the amnion and chorion, which are in places adherent to each other. Microscopically, it was found that the placental villi were filled with small nucleated cells, which were especially abundant in the centre of the villous spaces along the axis where the vessels usually take their course. The ends of the villi were enlarged with knob-like processes.
52 I condense here from the translation of Fraenkel's paper, which constitutes the bulk of chap. xxvii. of Bumstead and Taylor's excellent work.
Fraenkel's explanation of these changes is as follows: Under the influence of syphilis53 cell-proliferation begins in the villi, which are, normally, only sparingly supplied with cells. These new cells excite proliferation of the cells of the connective-tissue stroma and of the epithelium. This proceeds to such an extent that it leads to compression of the vessels,54 interfering with the circulation, and finally obliterates them. The [p. 272]vascular spaces into which the villi dip become filled up and narrowed, and often disappear. In this way, and also by reason of the thickening of the epithelium, the interchange between the maternal and foetal blood is interfered with, and at last is prevented.
53 Fraenkel took as his criterion of syphilis the presence of the osteo-chondritis described by Wegner (see p. 286).
54 "Hennig was the first who called attention to the intimate relation of the cell-growths to the vessels. The obliteration or compression of numerous vessels of the villi interferes with the mutual interchange of gases between the maternal and foetal blood, causing fatty degeneration of the villi and, if the process is extensive, the death of the foetus" (article "Syphilis," Ziemssen's Cyclopædia, vol. iii. p. 237).
If this process is spread over the whole placenta, the foetus perishes before it is complete. If it is limited to circumscribed areas, it may continue to live for a shorter or longer period.
These observations require to be repeated and confirmed, but they have served to open up a most interesting branch of syphilitic pathology.
Syphilis in the parents will manifest itself in the children in one of several ways, which are determined chiefly by two factors—viz. first, the length of the interval between the infection of the parent and the date of conception; and, second, the thoroughness of the treatment of the parents during that interval. To these may be added as subsidiary, but still of definite importance, a third, the type of disease which has affected the father or mother, whether mild or severe, benign or malignant.
From what has already been said in reference to the question of marriage, it will be at once understood that the danger to the offspring in untreated cases, and in those where conception has occurred during the early secondary period of the disease, is of the most extreme gravity.55 In such cases the usual result of pregnancy is abortion at from the first to the fifth or sixth month,56 the foetus sometimes exhibiting the evidences of the disease in the shape of large bullæ upon the palms and soles, or in the presence of characteristic visceral lesions, but quite as often showing nothing distinctive. It has generally undergone more or less maceration, and the skin, which is readily detachable, is of a congested, purplish color.
55 According to Kassowitz, in women who are not treated all pregnancies occurring within the first three years of their infection terminate either in abortion or in the birth of children who survive for only a few weeks or months.
Weber (quoted by Parrot, Le Progrès Médicale, Nov. 24, 1877, p. 882) treated thirty-five pregnant women by mercurial inunction, and they all went to full term under normal conditions. Among those treated with mercury and iodide of potassium, but who, by reason of intolerance of the former drug, took chiefly the latter, 20 per cent. aborted; when the mixed treatment was carried out regularly 15 per cent. aborted; and when only iodide of potassium was given 36 per cent. aborted. His studies were made on 109 syphilitic pregnant women. Parrot himself says (ibid.) that "abortion occurs in about one-third of all syphilitic women. Syphilis should always be suspected when this accident occurs several times successively." "The date of abortion depends on the age of the syphilis of the woman. It is most to be feared during the evolution of secondary symptoms, particularly when they are grave. There is more probability that it will occur when infection has preceded pregnancy than when it occurs during its course. Nothing is so much to be feared as contamination of the ovule. The nearer the date of infection of the mother approaches to full term, the fewer the chances of abortion. It is not likely to occur even when the mother is infected at five months."
56 Many observers think that abortion results directly from the death of the foetus. Babington (notes to Hunter's Treatise on Venereal), Trousseau, and Von Baerensprung were of this opinion.
Dr. Cory thinks that in many cases it is possible that the effect of syphilis may be to effect so early an abortion that the case is simply regarded as one of delayed menstruation or of menorrhagia. Such a conception would, however, be competent to infect the mother, and might seem to explain cases otherwise involved in obscurity.57 At least one-third [p. 273]of all syphilitic children are dead born.58 As time goes on, however, and the intensity of the parental disease is lessened, or in cases where appropriate treatment has been applied, either the abortion occurs at a later period of pregnancy or the children are brought alive into the world. Even then, however, and although at birth they may show no evidences of the disease, their chance of escape is but small. One-fourth of them die within the first six months. If they survive that period, the chances for life are slightly in their favor, but those for health or freedom from deformity and disease are still overwhelmingly against them.
57 As, for instance, when a woman married to a syphilitic man, but without issue, remarries a man with no history of syphilis, and yet gives birth to a syphilitic child. In such a case there would be no history of direct infection and none of pregnancy, the only two modes by which she could have contracted the disease, and the father—the second husband—might be unjustly suspected.
58 Kassowitz, op. cit.
The course of inherited syphilis differs strikingly from that of the acquired disease. It will hardly be necessary to do more than remind the reader of the ordinary stages of the latter affection—the primary, which includes the period of the chancre and of lymphatic engorgement, lasting about sixty to seventy days; the secondary, or exanthematic, characterized by copious cutaneous eruptions and extensive involvement of mucous surfaces, lasting from one to three years; the intermediate,59 or the stage of latency and relapses, lasting for a very variable period, from three to ten years, but under proper treatment very much reduced or altogether abolished; and finally, the tertiary period, beginning four or five years after contagion, extending indefinitely throughout life, but often in cases properly treated absent altogether.
59 So designated by Mr. Hutchinson, and for clinical purposes a very valuable addition to the periods of syphilis. He describes it as follows: The patient may be either wholly free from symptoms and in good health, or he may remain pale and rather feeble, and liable from time to time to slight returns of eruption on the skin, sores on the mucous membranes, condylomata, etc. He is protected as regards fresh contagion, and should he beget children they are almost certain to suffer. The relapses during this stage are usually easy to be distinguished from true secondary symptoms. There is little or no febrile disturbance, the rash is not copious, and often not symmetrical. Acute iritis, retinitis, etc. never occur for the first time, though they may do so in the form of relapses.
For purposes of description and of contrast we may similarly divide the whole period of evolution of a case of inherited syphilis,60 omitting the primary stage, which has never been found to exist in true cases of hereditary syphilis. Of course in congenital or infantile syphilis, in which by direct contagion, either from the mother or from any one else, the disease was acquired by the child, the course would not differ materially from that observed in the adult. But as this stage in all probability corresponds to the period during which the poison is already finding its way into the system through the lymphatics, of course it is not found in the child who is infected from the moment of conception or who receives the poison from the mother directly into the circulation.61 For from one to three weeks the infants often show no symptoms of the disease. In 158 cases collected by Diday, 86 manifested symptoms of the disease before the expiration of the first month, and 60 of the remainder before the end of the third month.62 When to these are added the [p. 274]statistics of Roger, we find that of a total of 172 cases, 159 showed syphilitic symptoms before the end of the third month.63 When the symptoms are present at birth, they consist largely in a general withered, atrophied, weazened appearance of the child; a hoarse cry, due to swelling, with subacute inflammation, or even ulceration, of the laryngeal mucous membrane; a coryza,64 due to a similar condition of the Schneiderian membrane; and certain cutaneous eruptions, the most common of which at this early date is the large vesicular or bullous eruption known as syphilitic pemphigus.
60 The idea that the character of the symptoms which first appeared depended upon and corresponded with the stage of the disease in the parent has now, I believe, no supporters. It was once thought, at least by some syphilographers, that if the parents were in the tertiary stage at the time of conception the child would develop tertiary symptoms, omitting the other stages.
61 If chancre were the first symptom of constitutional syphilis, why should it not appear in cases of hereditary syphilis?
62 Infantile Syphilis, p. 101
63 About 1823, from 16,000 to 17,000 children were admitted annually to the wards devoted to foundlings at Lyons. Clièt, recording his experience with this disease, says that syphilis is one of the most common of their maladies, but that "it exceedingly seldom shows itself at birth by evident signs" (Compte-Rendu Méd. Chir. des Observations à l'Hôpital général de la Charité de Lyon, 1823). Cristoferi, physician to the foundling hospital at Bologna, says that syphilis generally manifests itself between the ages of one and three months. Never once, he states, was a newly-born infant admitted with the disease unquestionably developed (Gazette Medica di Milano, 1844). Trousseau says that it "rarely appears before the second week, and very exceptionally after the eighth month" (Lectures on Clin. Med., vol. iv. p. 331, London, 1871, ed. of New Sydenham Society).
64 Usually appears later, but exceptionally at birth.
Pemphigus.—With regard to the specific or non-specific character of this eruption there has been much difference of opinion, and, as it is often the earliest distinctive expression of syphilis, a diagnosis of which could hardly be founded on the general appearance of the child, or even on the hoarse cry and the coryza, it becomes important to have definite ideas upon the subject. Nearly a century ago (in 1794) it was denied65 that this eruption was a manifestation of venereal disease; and this view has been supported by many able and accurate observers down to the present day. In 1851 a discussion upon the subject took place in the French Academy of Medicine, which elicited the opinions of the majority of those members who were entitled to speak with authority in the matter, and which has since been referred to by most writers. Cazeaux upheld the non-syphilitic hypothesis on the ground (1st) that the so-called syphilitic pemphigus of children does not differ from the simple pemphigus of adults, presenting none of the physical characters which distinguish the specific cutaneous eruptions; (2d) that it appears at birth or immediately after, while the symptoms of hereditary syphilis generally show themselves later;66 and (3d) that at that time there had been seen no cases of pemphigus at the Lourcine Hospital, where so many syphilitic children were born.67 In this view he was supported by Trousseau, Lasègue, Gibert, Bazin, and other obstetricians and syphilographers of note.68
65 Ariander, Mémoires de Méd. et d'Accouch., quoted by Diday.
66 This is now known to be an unreliable distinction, expressing perhaps a general rule, but one with so many exceptions as to render it void of diagnostic significance.
67 This may have been true at that time, but has certainly not continued to be so. Cornil says: "We often see at the Lourcine children born prematurely or at the full term with pemphigus, either fully developed at the moment of birth or appearing a few days afterward, and who commonly die with syphilitic cachexia, the sad heritage derived from their maternal parents."
68 Pemphigus may indeed be a specific affection, but no characteristic sign has been discovered sufficient to distinguish it from the ordinary form of pemphigus. "On the other hand, there is no inconsistency in admitting that syphilis, which so deeply impairs the constitution of the parent, may act like any other common cause and excite non-specific pemphigus; for an infant is badly lodged and poorly nourished in the womb of an enfeebled mother, apart from the influence of the virus" (Ricord, note to John Hunter's Works, 1853).
On the other hand, Dubois claimed a specific character for the affection [p. 275]on the ground (1st) of the fact that in the majority of cases there was a syphilitic history in the parents; and (2d) that the eruption often coexists with well-known syphilitic lesions. This was supported by Cazenave, Danyan, Bouchut, Vidal, Ollivier, and others.69 Diday, who devotes several pages of his interesting work on Infantile Syphilis to this subject, regards the eruption as simply a manifestation of a cachexia produced by syphilis,70 founding this opinion on (1st) the absence of specific characters in the eruption; and (2d) that syphilitic pemphigus is a rare affection in the adult, if it occurs at all, so that to recognize it in the child would be to make a single exception to the general rule that "all the syphilitic eruptions of new-born children have their equivalents in those of adults." He explained the two cases which were then (1858) recorded of cures of pemphigus by mercury71 by saying that it was the treatment of the diathesis, not of the disease, which caused the improvement. He acknowledges, however, the very frequent association of pemphigus in the child with syphilis in the parent, and says that it springs from the latter affection, "specially, but not specifically"—a rather wire-drawn distinction.72
69 Jullien (op. cit., p. 1005), after considering the opposing views as to the character of this eruption, says: "We have no hesitation in declaring ourselves in accord with Roger, Ollivier, Ranvier, Parrot, and others, and in distinctly separating from the specific affection the rare eruption known as simple pemphigus, sometimes epidemic, occasionally febrile, and appearing most frequently about three months after birth. We consider likewise that an evidence of congenital syphilis which is by no means doubtful is found in the bullous eruption seen at birth or within the first two weeks, comparatively frequent, and involving by preference the palms and soles. This opinion is based upon (1st) its appearance in children whose parents are known to be syphilitic; (2d) its association with syphilitic lesions of the lungs, liver, kidneys, thymus gland, etc.; (3d) its partial disappearance under mercurial treatment, and its reappearance when that treatment is discontinued."
70 Op. cit., pp. 70-77.
71 Depaul, Gaz. Méd. de Paris, 1851, p. 472, and Galligo, Gaz. Med. Toscana, 1852, p. 123.
72 Trousseau (Clinical Lecture on Syphilis in Infants), after detailing a case in which there was some doubt as to the existence of hereditary syphilis in a child born alive, and in which case the previous pregnancy had resulted in a stillborn child at seven months, the body of the latter having been preserved in alcohol and exhibiting numerous traces of pemphigus, says: "So far as I was concerned, this demonstration did not amount to more than the establishing of a probability, and several physicians who participated in this indecision finally accepted a compromise. They considered that maternal syphilis had determined a sort of cachexia in the foetus which had led to an eruption of bullæ which was not specific. By accepting this too-facile hypothesis you will imprudently open a door which you will with difficulty be able to close."
As these differences of opinion have been perpetuated to the present day, it has seemed to me proper to make this reference to their history, although I am strongly convinced that the progress of clinical and pathological knowledge enables us now to assert that although, as an exception, bullæ may be due to a profound cachexia not dependent on syphilis, yet that in the large majority of cases they are specific in their character.
The argument which always seemed to me the strongest, the fact that a similar eruption is almost—or quite—unknown in the adult, has been removed by the observations of Cornil, who has shown that it belongs properly with the papular rather than with the bullous eruptions, and should be classed with the roseola and papules of early syphilis—just where, from its clinical history, we should expect to find it. The raising of the epidermic layers is due chiefly to their delicacy, their slight resistance, and their previous immersion in the amniotic fluid—i.e. to [p. 276]conditions which are peculiar to the skin shortly after birth.73 He founds these very important opinions upon the autopsy of a child stillborn a little before full term, the mother being in the height of secondary syphilis. The child presented characteristic bullæ on the soles and palms. After hardening these were found to consist of the two layers of epidermis placed one above the other. Fig. 6 represents a bulla about one centimeter in diameter which was situated on the plantar surface of the great toe.
73 Cornil, op. cit., p. 203.
| FIG. 6. |
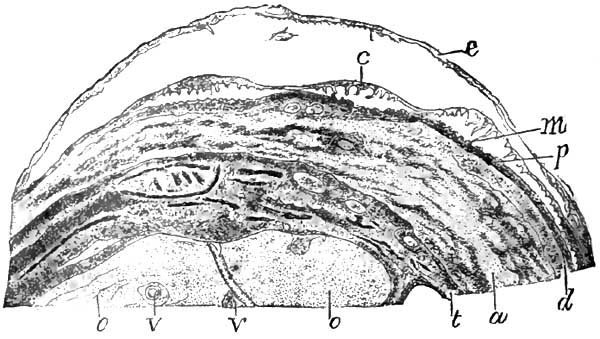
|
| Pemphigus bulla from a new-born syphilitic child. The superficial epidermic layer e is elevated by a fluid exuded between it and the rete mucosum. The rete mucosum, c, is also partly raised, so that there exists a space filled with fluid between it and the papillæ, p. The epithelial prolongations and the ducts of the sudorific glands m, placed between the papillæ, and which run between them into the derm, are broken and suspended from the rete mucosum. d. Derm. a. Fibrous and muscular layers. t. Tendons and fibrous tissue. o. Cartilage of ossification of the first phalanx. v. Vessels. X 8. |
| FIG. 7. |
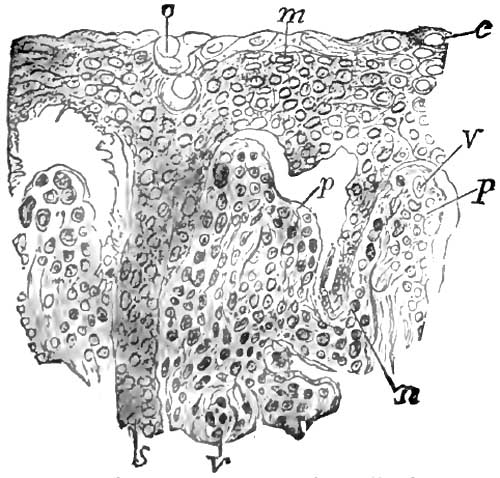
|
| Section of the rete mucosum and papillæ from the same case of pemphigus as Fig. 6. o. Orifice of a sudorific gland. m. Cells of the rete mucosum, some of which are excavated, c. p. Papillæ. v. Their vessels. n. Prolongations of the rete mucosum between the papillæ. X 200. |
If, then, we find an infant at birth or immediately after74 presenting on the soles, the palms, the fingers and toes, or on the limbs, an eruption consisting of blebs more or less perfectly distended with a liquid which may be clear, cloudy, or bloody, circular or oval in shape, sometimes irregular, seated on inflamed, reddish skin, and surrounded by trifling areolæ, we may strongly suspect the presence of syphilis in an active and most menacing form. And this suspicion becomes a certainty if, in combination with such an eruption, the general cutaneous surface is yellowish or muddy in hue, is hard, dry, wrinkled, without elasticity or softness—owing to the absence of subcutaneous fat—and, for the same reason, is furrowed and wrinkled about the face, imparting an appearance of senility; if the child has a hoarse cry, a discharge from the [p. 277]nostrils; and, of course, if there are at the same time other and unmistakable syphilodermata. This eruption is specially important, however, because upon the recognition of its specific character in cases of stillbirth, or in those in which the child survives only a few days—not long enough for the development of further symptoms—will depend the opinion as to the cause of death, which, whether expressed or not, will determine the future treatment of both parents during the interval and of the mother during the next pregnancy.
74 Non-syphilitic pemphigus is said to be never present at birth, nor until the child has become considerably exhausted by wasting from some defect of nutrition. It therefore does not appear until it is several weeks old. It then attacks the trunk in preference to the palms and soles.
We may now consider the other symptoms of the secondary period in the child.
Coryza is one of the most characteristic, and at the same time one of the most important, of these in its influence on the health of the child. It is due to the same condition of the mucous membrane lining the nasal fossæ as manifests itself simultaneously or soon afterward on the skin in the shape of erythema, roseola, or papules; in other words, it is a hyperæmia with papillary infiltration. Now, on the skin this condition, except in so far as it indicates the presence of a grave constitutional disease, is of no special importance. In the nostrils of a sucking infant, already debilitated and impoverished by the anæmia of syphilis, and depending upon its nutrition for the continuance of the miserable flickering life which was its original endowment, the same condition assumes the gravest significance.
The excessive supply of blood to the parts induces a catarrhal condition which shows itself in a thin, watery discharge, which, as the child during sucking is compelled to breathe through the nose, is rapidly dried into crusts. These become adherent, fill up and lessen the channel for the passage of air, and in so doing add to the rapidity and force of the respiration through the nose, and thus increase the tendency to the deposit of these crusts. The peculiar nasal, noisy respiration of the child has given the affection the popular name of snuffles. As the child can no longer breathe, or can breathe only with great difficulty, while sucking, it takes the breast only to drop it again immediately on account of impending suffocation.75 As the disease progresses ulceration occurs beneath the crusts, and often involves the entire thickness of the delicate mucous and periosteal layers underlying the thin bones of the nose; perforation of these bones results, sometimes with caries to such an extent as to cause an entire loss of the nasal septum, with flattening of the nose—a symptom comparable to one which sometimes occurs in the tertiary period of adults, but produced, as we have seen, by other causes. In adults syphilitic caries and necrosis are usually due to lesions seated primarily in the osseous or subperiosteal tissues; in the child, at least in this instance, these tissues are involved secondarily.
75 For an admirable description of the mechanism of this and other symptoms of coryza see Diday, op. cit., pp. 78-83.
Erythema, or roseola as it is differently called, is apt to present itself about the second or third week76 after birth. As in the adult, it begins upon the abdomen in the form of little oval, circular, or irregular spots, dull red in color and disappearing upon pressure. Later the color becomes deeper, the eruption extends to the trunk and limbs, and, as exudation and cell-proliferation succeed to simple capillary stains, it [p. 278]ceases to disappear when pressed upon. It is often moist, owing to the thinness of the epidermis, sometimes excoriated. Occasionally it is confluent, and covers large areas with an almost unbroken sheet of deep-red color.
76 Bassereau gives an instance of its occurrence within three days.
The diagnosis in the early stage is often difficult on account of the resemblance to the simple erythema of infancy. As the disease progresses, however, maculæ form here and there; the cell-infiltration involves the papillæ, several of which coalesce, forming flat papules; the nutrition of the superficial layers of the epiderm is interfered with, especially where it is thick, as on the palms and soles, and the eruption in those regions becomes scaly, and then the diagnosis is not difficult.
Papules and Mucous Patches.—In the ordinary evolution of the disease the next manifestation is usually the development of papules upon the general cutaneous surface and of mucous patches on the tongue, lips, and cheeks—probably also on other mucous membranes not exposed to examination. The papules are apt, for the reason already mentioned—the thinness and moisture of the skin—to be of the broad, flat kind, especially, as in the adult, in those regions where the elements of warmth and friction are superadded to the moisture, as in the folds of the skin about the genitalia, the neck, the flexures of the joints, etc. They are then moist, covered with a grayish secretion or a thin crust, and are in reality mucous patches. Occasionally they take on a little hypertrophy and develop condylomatous excrescences which closely resemble the simple acute condylomata of infants. In syphilis, however, the growth springs from a previously existing papule, which is not apt to be solitary, there being others in the neighborhood which will probably establish the diagnosis. The syphilitic condylomata also have a peculiar fetid discharge, resembling that of mucous patches and more or less characteristic.77
77 Van Harlingen, article "Syphilis" in the International Encyclopædia of Surgery, vol. ii. p. 560.
Mucous patches in the infant are among the most important of the early syphilitic lesions—not to the child itself, because they do not materially affect its health, save in those exceptional instances where they are accompanied by a marked degree of stomatitis, and thus interfere with its nursing. Their importance is due to the fact that they are almost constantly present, and they are thus by far the most frequent vehicle of contagion from the child to its nurse or to others with whom it may come in contact. At times they do not differ materially from the same lesion occurring in the adult, but lose much sooner their epithelial investment (on account of the delicacy and comparatively slight attachment of the epithelium at this stage), and they then appear as oval or irregular red, slightly depressed spots, distinct or coalescing, ulcerating or oftener covered by a false membrane. They especially affect the angles of the mouth and the sides and dorsum of the tongue; and indeed their disposition to select the former situation constitutes a diagnostic difference between them and non-specific stomatitis which is to be found in the sulci between the gums and cheeks and on the gums themselves—locations rarely invaded by mucous patches.78 When the latter are ulcerating or are concealed by diphtheritic membrane, and are situated on the tongue, they may be mistaken for either simple or parasitic stomatitis. The [p. 279] diagnosis can often be made by the presence of other syphilitic symptoms—coryza, erythema, and especially papules. In their absence, however, it must be remembered that in simple stomatitis, the inflammation not being limited to special areas, the whole tongue is apt to be involved or a much larger portion of the buccal mucous membrane; and as there is no marked tendency to cell-proliferation in these cases, the accompanying exudation is apt to be serous or watery and to result in vesiculation—a condition never seen in syphilitic stomatitis. In the parasitic disease, too, the inflammation is less localized, there is more swelling and congestion, and the false membrane is said to be of a whiter color.
78 Bumstead and Taylor, op. cit., p. 750.
No child that has even been suspected of having a taint of hereditary syphilis should be permitted to nurse at the breast of any one but the mother, to share its cup or nursing-bottle with other children, to receive the caresses of relatives or friends; and in this last restriction we would include the father, even if the suggestion79 be true, that in the case of syphilitic children the protection from contagion probably extends to the male as well as the female parent. Paternity is sometimes a more doubtful problem than would seem probable, and even if the father were protected the husband might not be. The mucous patches, if any are found to exist, should be actively treated both locally and constitutionally, and during their demonstrable presence a most rigorous quarantine should be observed.
79 Hyde, op. cit. See p. 264.
Syphilitic condylomata are due to hypertrophic changes in the papules, which under the influence of heat and moisture in certain regions coalesce and become more elevated. They vary in size from an eighth of an inch to a quarter or even a half of an inch in diameter. Their surface is flat and covered by a crust or by an offensive secretion. They are found most commonly about the anus or at the angles of the mouth.
Pustular Syphilides.—A little later in the secondary period, usually at about the sixth week, but sometimes much earlier, the papules become transformed into pustules, the change taking place slowly, so that if examined at any time after it has begun the child will present an eruption which is markedly polymorphic, showing here and there yellowish or reddish-yellow maculæ left after the absorption of the cell-element of certain papules, at other places beefy-red papules at the height of their development, or papules crowned by a ring of desiccated and desquamating epidermic scales, and in still other regions pustules in various stages of formation. Or the various formative stages of the pustules may be passed through so quickly that the eruption will be almost entirely pustular, few if any unmodified papules being discovered. The pustules may remain distended with pus for a considerable time, after which they may wither and slowly disappear or may rupture and leave ulcerated surfaces. A number of these ulcers sometimes run together and make extensive patches covered with thick, dark-colored crusts. These patches may resemble areas of impetigo or of impetiginous eczema, but in those affections the crusts are usually thinner and of a lighter color, and the skin beneath them is generally on a level with the surrounding surface, bright red and glazed; while under the crusts of the syphilide will be found a more or less depressed or excavated ulcer, often covered with pus. The diagnosis may indeed often be made by gently detaching and [p. 280] raising one of the crusts and noting the character of the surface beneath. The erosion under the crusts of eczema heals over more readily and without leaving a cicatrix.
A so-called furuncular eruption80 is said to appear at variable periods between the sixth month and the third year, but does not appear to me to be clearly differentiated from the large pustular syphilides with thickened and elevated bases on the one hand, or the ulcerating tubercular eruption on the other.81 They are all so rare in hereditary syphilis, at any rate, as to have little clinical importance.
80 Bumstead and Taylor, op. cit., p. 750.
81 The distinction between the two forms is usually manifest if the development of the lesions has been observed; but even this fails in regard to the tubercular eruption. They both occur at the same period; they both begin similarly, the furuncles as "small nodules in the corium," the tubercles as "deeply-seated papules or nodules;" they both run on to ulceration and pursue a chronic course (Van Harlingen, op. cit., p. 561).
Iritis.—Another symptom of the secondary period, but of later development and of rarer occurrence than the syphilodermata which have been described, is iritis. In spite of its rarity this is extremely important, because it is frequently overlooked until it has reached such a stage that occlusion of the pupil results, and also because when it is recognized it constitutes an almost pathognomonic sign of syphilis.82 This statement may now be made unhesitatingly, although for many years it was contended that iritis, and even the still more characteristic symptom keratitis, were only associated with syphilis as coincidences, the constitutional disease, when hereditary, having no causative relation to the local condition.
82 "When primary iritis occurs in syphilis in young children it is almost always due to syphilis" (Soelberg Wells, Treatise on Diseases of the Eye, Philada., 1873, p. 173).
To Mr. Hutchinson belongs the credit of having first clearly developed the specific character of this trouble,83 which, on account of the mildness of the attendant symptoms, is often overlooked. The sclerotic zone of congestion so marked in the adult, and therefore so valuable a diagnostic sign to the general practitioner, is very slight, sometimes absent; and as a consequence the attention of neither parent nor physician is attracted to the condition until in the more serious cases it has done irreparable mischief. In milder cases, particularly where the child is under mercurial treatment for concomitant symptoms of syphilis, it may run its course and escape notice altogether;84 and it is possible that owing to this fact the rarity of the affection has been overestimated. It is also possible that in such cases changes occurring at this time may in some instances lay the foundation for some of the deeper-seated ocular troubles of later life.
83 Med. Times and Gazette, 1860, July 14; Ophthalmic Hospital Reports, vol. i. pp. 191, 226; A Clinical Memoir on Certain Diseases of the Eye and Ear consequent on Inherited Syphilis, London, 1863. In the introduction to this volume Mr. Hutchinson states that acute iritis dependent on hereditary syphilis was first described in connection with its true cause by Mr. Lawrence, but, as from the date of that gentleman's first case (1830) up to 1863 but six cases had been recorded, the announcement had made but little impression on the profession.
84 "In the cases of this form of iritis which are seen in ordinary eye-practice much damage has often been done by occlusion of the pupil and deeper mischief. Probably many of the slighter cases escape the notice of the parents and are not brought to the surgeon" (Mr. Edward Nettleship. See Hill and Cooper, p. 271).
If, however, attention has been attracted to the eyes, the diagnosis is not usually difficult. The pupil is irregular, especially under atropia; [p. 281]there are streaks of lymph, dulness, swelling, change of color, and on very careful inspection a faint pink zone may be seen in the sclerotic. The conjunctiva and cornea are generally clear.
Mr. Hutchinson's analysis of the twenty-three cases reported by him is still of interest as furnishing reliable data for prognosis. The average age at the time the iritis commenced was five months and a half. The oldest was sixteen months at the time of the outbreak, the youngest six weeks. In twelve cases but one eye suffered; in eleven both were affected. In seven cases (ten eyes) the cure was complete; in two or three other cases very slender adhesions remained; in twelve cases, in nearly all of which the patients came under care only at a late period of the disease, one pupil was permanently occluded by organized false membrane. In nearly all, coincident symptoms of syphilis of the skin or mucous membranes were present. Of the thirteen cases in which alone a history of the family is recorded, the affected infant was the only living child of his parents in twelve instances. In the only case in the whole series in which it is stated that there were other living children the mother had lost four infants out of seven live births.
The prognosis depends on the stage at which they come under treatment. The lymph if recent, no matter in what quantity, will probably be absorbed under mercurial treatment, which will often be of great benefit even in those cases in which a certain amount of organization has occurred.85
85 It will not be uninteresting, perhaps, to append the aphorisms regarding iritis in infants which Mr. Hutchinson at that time enunciated: 1. The subjects of infantile iritis are much more frequently of the female than the male sex. 2. The age of five months is the period of life at or about which syphilitic infants are most liable to suffer from iritis. 3. Syphilitic iritis in infants is often symmetrical, but quite as frequently not so. (In his article in Reynolds's System of Medicine, written in 1866, three years later, but revised in 1870, he describes it as "usually symmetrical," vol. i. p. 444.) 4. Iritis, as it occurs in infants, is seldom complicated, and is attended by but few of the more severe symptoms which characterize the disease in the adult. 5. Notwithstanding the absence of phenomena of acute inflammation, the effusion of lymph and the danger of occlusion of the pupil are usually very great. 6. Mercurial treatment is most signally efficacious in curing the disease, and, if recent, in procuring the complete absorption of the effused lymph. 7. Mercurial treatment previously adopted does not prevent the occurrence of this form of iritis. 8. The subjects of infantile iritis, though often puny and cachectic, are also often apparently in good condition. 9. Infants suffering from iritis should always show one or other of the well-recognized symptoms of hereditary taint. 10. Most of those who suffer from syphilitic iritis are infants born within a short period of the date of the primary disease in their parents.
We have now a group of symptoms characteristic of the secondary period of syphilis, or that extending from birth, or much more commonly from the age of three or four weeks to about the end of the first year. The syphilitic child during this time has several or all of the following symptoms: Coryza with snuffles; an erythematous, papular, or pustular eruption on the skin; mucous patches on the lips, tongue, cheeks, etc.; a marked tendency to general wasting; a hoarse cry or cough; senility of aspect; iritis. The majority of syphilitic children born alive die during this stage.
Before its termination, sometimes even at birth, other lesions have been noticed (especially those affecting the liver), which, however, may better be described in connection with the special organ or organs involved.
Succeeding this stage—i.e. beginning in about a year or eighteen [p. 282]months—comes an intermediate period, which extends to second dentition, to puberty, or even much later, and which is characterized rather negatively—that is, by the absence of symptoms—than otherwise. The evidence of the general diathesis will of course be present in the shape possibly of malnutrition, stunted growth, or retarded development, perhaps shown in the weazened or withered face, the sunken nose, the pallor of the skin, the premature loss of the upper incisor teeth or the malformation of the others if they have erupted.
There is but little tendency to recurrence or relapse of any of the secondary symptoms; and in certain cases, not a very small proportion, in which these symptoms have been light and have been well and thoroughly treated, this stage extends throughout life; or, in other words, as is frequently the case with the adult who has followed a proper course of treatment, the disease appears to terminate with the secondary stage. In other cases, however, it recurs, and the symptoms which it then presents may be taken up in connection with the different organs or tissues involved.
Syphilis of the ear is for obvious reasons not often discoverable until the patient has reached an age at which interference with the function of hearing becomes a noticeable phenomena. The only symptom likely to attract attention during the stage of inherited syphilis which we are now considering is a catarrh of the middle ear, which may have for its starting-point some inflammation, ulceration, or mucous patch of the pharynx, causing a temporary or permanent occlusion of the orifices of the Eustachian tubes.86 This may lead to perforation of the membrana tympani, purulent infiltration of the mastoid cells, etc., and when accompanied by an otorrhoea which attracts attention to the ear will be easily discovered by the physician. These cases are, however, exceptional, otorrhoea only being present in nine out of Hutchinson and Jackson's87 one hundred cases of inherited syphilis, and consequently but little is known about the frequency or gravity of lesions of the auditory apparatus in the secondary stage of this form of syphilis.88 The changes which occur later on are chiefly those which involve either the nerves themselves or their distribution in the labyrinth.
86 Bäumler, Ziemssen's Cyclopædia, vol. iii. p. 226.
87 Hutchinson and Hughlings Jackson, Med. Times and Gaz., Nov. 23, 1861.
88 Schwartze (quoted by Hill and Cooper) found also that otorrhoea was a rare complication in deafness from syphilis.
The affections of the middle ear and Eustachian tube are said to be contemporaneous with the keratitis which appears in the neighborhood of puberty,89 while those of the nerve are somewhat later in point of time, and are almost always conjoined with retinitis, choroiditis, and optic neuritis. As usual when investigating or describing any subject relating to syphilis, Mr. Hutchinson's opinion and observation must be detailed. In 1863 he wrote90 that it was only recently that he had thought of specially investigating the disorders of hearing in reference to hereditary taint, having had his attention called to a peculiar form of deafness, usually symmetrical, passing rapidly through its different stages and [p. 283]unaccompanied by any marked degree of pain or any external disease. He then reported eighteen cases of which he had notes. The oldest of these patients was twenty-seven, the youngest eight—the average time of development of the deafness from twelve to fifteen. Although the membrana tympani was in no instance quite normal, in none were there found adequate changes to account for the deafness. In all the Eustachian tubes were pervious. In nearly all the disease was symmetrical. This fact, together with the absence of discoverable lesions of the external or middle ear, seems to point conclusively to disease of the nerves themselves, or at least to a central cause.91 He adds: "With regard to the prognosis of heredito-syphilitic deafness, I believe that it is very unfavorable. When the disease was progressive I have rarely witnessed any permanent improvement or arrest. In most it has gone on to total loss of hearing, and this in several instances in spite of the cautious use of specific remedies almost from the beginning. From six months to a year would appear to be the usual time required for the completion of the process and the entire abolition of the function."92
89 Purves, Guy's Hospital Reports, 1875, p. 564; Pritchard, British Medical Journal, April 21, 1877.
90 Clinical Memoirs on Certain Diseases of the Eye and Ear consequent on Inherited Syphilis, London, 1863, pp. 182, 183.
91 In the Lancet for Jan. 16, 1875, he reports a case of total deafness in a young woman of seventeen which had come on in ten months without pain or otorrhoea. He believes the disease of the organ of hearing to be parallel with those cases of choroiditis disseminata or of optic neuritis in which blindness is produced without pain or any external evidence of inflammation, and which are distinctly and positively associated with inherited syphilis.
92 Mr. Hinton, in his edition of Toynbee's work on Diseases of the Ear, states that at Guy's Hospital, of his aural patients, one in twenty is affected with deafness due to heredito-syphilis; that it usually makes its appearance between the tenth and sixteenth years; and that the great majority of the cases which he has seen have been females. He adds: "Patients suffering from this disease may, as a rule, at least when young, be at once distinguished by the amount of deafness which they exhibit. I know no other affection except fever which in a person under twenty brings on a deafness so rapidly and so nearly complete. In the course of a few weeks a girl previously hearing well will, without pain or known cause, become unable to distinguish words." In one of Dalby's cases total deafness came on in three weeks, previous to which hearing was normal. According to Pierce, the deafness is most apt to manifest itself between eleven and eighteen years of age. Troeltsch says that "l'audition du diapason par le vertex" is lost at an early date after the beginning of the disease, and that there are also often concomitant affections of the nose and pharynx.
Dalby93 is said to regard syphilis as, next to scarlatina, the most fruitful cause of deaf-mutism as it occurs in children born with good hearing powers. "The patient usually becomes deaf in early childhood—after he begins to talk—or between this period and puberty."94
93 The Lancet, Jan. 22, 1876.
94 Bumstead, op. cit., p. 734.
Syphilis of the Liver.—In 1852, Gubler published an account of the general appearances in syphilitic disease of the liver in new-born children, which was distinguished especially by increase in size and weight. This increase depended, as might be expected in this stage—that of general cell-proliferation—upon a proliferation of cells from the connective tissue between the acini, or from the adventitia of the interlobular vessels, this growth becoming transformed into connective tissue.95 The change is quite analogous to what is taking place at the same time in the skin, the mucous membranes, and other tissues. Wilks has also described96 a form of syphilitic disease of the liver which corresponds to that of Gubler, and in which the whole organ is infiltrated by a new fibrous tissue, producing a uniform and general hardening.
95 Bäumler, op. cit., p. 186.
96 Trans. Path. Soc., vol. xvii., 1866.[p. 284]
| FIG. 8. |
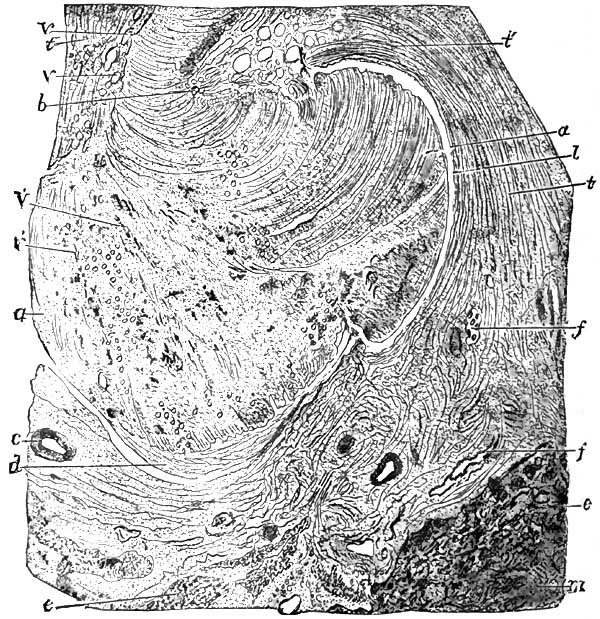
|
| Section of an old gumma of the liver. a, a. Central caseous tissue of the gumma. v', v'. Its vessels. l. Boundary between the central portion and fibrous zone; this line of demarcation is marked in places by an opening or cleft. t, t. Connective tissue of the fibrous zone which entirely surrounds the central part. v, v. Small vessels of this zone. c. An arteriole of the fibrous zone. f, f. Quite large biliary vessels included in the fibrous zone. t'. Fasciculi of connective-tissue fibres running parallel with the surface of the caseous part. At b and d the fasciculi of fibres of the fibrous zone penetrate into the central caseous part. e, e. Tissue of hepatic cells interrupted by bands of fibrous tissue, m, m. X 12. |
As described by Gubler,97 the liver in such children is hypertrophied; hard, resistant to pressure, so that it cannot be indented; elastic, so that it rebounds; creaks, but does not bleed, when it is cut into, and presents the yellow color and the semi-transparence of flint. There are seen on a yellowish ground a number of small white granulations like grains of wheat, which a histological examination shows to be formed by an accumulation of embryonic cells in the spaces which separate the hepatic acini. Injections reveal the fact that the vascular network has become almost impenetrable, the capillaries obliterated, the larger vessels diminished in calibre. Fibro-plastic matter is found throughout the organ in large quantity. In consequence of these conditions—the compression of the hepatic cells and the destruction of the vessels—the secretion of bile is stopped, and the gall-bladder is found after death to contain a pale-yellow liquid consisting of bile mixed with an excess of mucus. This form of hepatitis has thus far been observed almost exclusively in infants. Cornil [p. 285]says98 that he has had frequent occasion to examine such cases of hepatic syphilis, and describes them as follows: "The hepatic acini, in the normal state, are in contact except at the prismatic spaces which are formed by their union—spaces in which the capsule of Glisson forms an envelope to the afferent portal vessels of the lobuli. It is in these spaces that the round lymph-cells form and collect into small nodules representing microscopic gummata. The cells at the centre of the new formation are sometimes granular. This neoplasm is seated about the ramifications of the portal veins, which in consequence also present thickened walls with newly-formed cells in their external tissues. The small granules above mentioned are not always visible to the naked eye, and in their places are only seen, about the perilobular capillaries of the portal vein, an excessive number of embryonic cells." In addition to this interstitial sclerosis or interstitial infiltrating hepatitis there is an inflammation of the liver depending upon the presence of gummata—gummous hepatitis—which occurs in two forms: one in which very small and very numerous nodules are present, situated along the course of the fibrous seams, the prolongation of the capsule, and another in which there are two or three large circumscribed tumors. This form of hepatitis is always accompanied by the interstitial form, although the latter may be only slightly developed.99 The gummata, though not infrequently found in the liver of new-born children, are more likely to develop later, at from about the eighth to the twelfth year.
97 Mémoires sur une nouvelle Affection de Foie, and Gaz. Méd. de Paris, 1852.
98 Op. cit., Am. ed., p. 370.
99 It does not differ essentially, either pathologically or clinically, from the same lesion in adults.
Rochebonne100 describes the following symptoms of syphilitic hepatitis in infants: A deep wine-colored venous stain and oedema of the lower extremities, often accompanied by pemphigus; ascites due to mechanical obstruction of the circulation, as in cirrhosis; a more or less pronounced chloro-anæmic appearance of the face; and the presence in the urine of albumen and hæmato-globulin. Vomiting may occur, and constipation alternating with diarrhoea has been observed. Icterus, symptomatic of the affection, has not been observed.
100 Quoted by Bumstead and Taylor, p. 758.
Bäumler says:101 Implication of the peritoneal coating of the liver may be recognized by the pain in the hepatic region. In new-born children—unless, possibly, there may be some enlargement of the liver—the only local symptoms, often, are those due to peritonitis—screaming, drawing up of the legs, vomiting. In those cases it is not rare for the peritonitis to become diffuse.102
101 Op. cit., p. 194.
102 In an article on "Inherited Syphilis" in the British and For. Medico-Chirurgical Review, 1875, p. 28, it is said: "Of the liver the lesion consists in enlargement and induration of the organ in whole or in part, due to the development of fibro-plastic material between the cells of the acini, with obliteration of the vessels and interference with the secretion of bile. This condition is generally doubtful during uterine life, and is rapidly fatal. The symptoms are vomiting, diarrhoea, and tympanitis, but, strange to say, no jaundice. The enlarged and indurated organ may be felt by palpation. It is probably in this connection that the peritonitis described by Simpson as occurring in inherited syphilis is found."
Hill says:103 "The symptoms are mainly those of functional derangement of the organ, with alteration of its bulk."
103 Op. cit., p. 163.
Hutchinson104 has described cases in which in young persons the subjects [p. 286]of hereditary syphilis there has been great hepatic enlargement which has subsequently wholly disappeared. He finds it difficult to believe that there is any kind of gummous growth in such cases, and feels obliged rather to fall back upon the hypothesis of mere vascular turgescence. In one such case the liver occasionally was so large as to be visible as the patient lay on his back in bed.105
104 Path. Transactions, 1877, p. 309.
105 Illustrative cases of this condition may be found in the Med. Times and Gazette, Dec. 22, 1877.
It seems much more likely that the enlargement is due to an exceptionally active cell-proliferation, which does not, however, go on to organization, but may be just as susceptible of absorption and resolution as are the papules or maculæ of the skin. A portion of the enlargement may be due to a passive congestion caused by the presence of this cell-accumulation.106
106 Barlow (Path. Trans., 1877, p. 355) has suggested that the engorgement is only a preliminary stage of the fibrous thickening, and may disappear either with or without leaving permanent contractions or adhesions in its wake.
As to the diagnosis of hepatic syphilis in infants, I am disposed to agree with Cornil, who says:107 "The symptoms are null, or they are identical with those of local and general troubles so often observed in children who have poor or insufficient nourishment. The only physical sign which properly belongs to hepatic syphilis is, when it exists at all, increase in the size of the liver."
107 Op. cit.
Syphilis of the Bones.—Until the publication in 1870 of the researches of S. Wegner,108 an assistant of Prof. Virchow, diseases of the osseous system due to hereditary syphilis were either ignored or denied by the various writers upon this subject.109 Valleix, Bargione, Ranvier, and Guéniot had indeed recorded cases of bone disease occurring at the points of junction between the epiphyses and diaphyses and in the costal cartilages, but it remained for Wegner first fully to describe the pathological changes which occurred there, and to differentiate them from those due to rickets or scrofula. His memoirs recognized three stages of alteration in the long bones:110 1st. While in the normal state the boundary of the hyaline cartilage is distinctly marked by a line which indicates the direct transformation of the cartilaginous tissue into a spongy tissue, the unaided eye being unable to distinguish a spongio-calcareous layer, in new-born syphilitic children, on the contrary, the bones are seen to have a spongio-calcareous layer interposed between the bone and cartilage, measuring two millimeters in thickness. This is a zone of calcifying cartilaginous material more extensive than in the normal state. 2d. These same changes become more distinct and more extensive. The unnaturally thick layer of calcareous material continues to grow. There is proliferation of the cartilaginous trabeculæ, abundant calcification of the cartilage, too early and irregular ossification of the intercellular substance [p. 287]of the cartilage, and at the same time an arrest of the normal formation of bone which should be going on from the epiphysial cartilage. 3d. There is now added, by extension of these processes, a thickening of the perichondrium and periosteum at the extremities of the long bones and at the junction of the ribs with the costal cartilages. In consequence of the interference with nutrition occasioned by these changes atrophy and fatty degeneration of the cartilage-cells occur, and they form between the epiphysis and diaphysis a necrosed mass which irritates the living bone. This causes osteo-myelitis, which frequently results in a separation of the epiphyses. Occasionally pus is produced in such quantity as to perforate the periosteum, escape into the surrounding tissues, and become superficial. He terms the entire process an osteo-chondritis.
108 Virchow's Archiv, 1870, B. 50, S. 305: "Ueber hereditäre knochen Syphilis bei jungen Kindern."
109 Diday says: "Affections of the bones are so rare in children with inherited syphilis that the annals of medicine scarcely offer five or six well-authenticated cases of caries or periostitis" (op. cit., p. 83). Referring to this statement, Mr. Hutchinson remarks: "So different has been my own experience from this that I may say that we are scarcely ever without a severe example of it in the wards of the London Hospital" (Illustrations of Clinical Surgery, London, 1875, p. 47).
110 Cornil, op. cit., p. 282 et seq.
Waldeyer and Köhner,111 after examining twelve cases, confirm in the main these investigations of Wegner, but interpret the changes as arising rather from the formation of a gummous tissue between the epiphysis and diaphysis than from an osteo-chondritis. The tissue-death which occurs later, the atrophy of the cells, etc., they compare with the same modifications observed in syphilomata.
111 "Beiträge zur Kenntwiss der hereditäre knochen Syphilis," Virchow's Archiv, B. 55, S. 367.
Parrot112 in a number of exceedingly valuable papers has repeated and greatly extended these observations. He places especial importance upon the formation of osteophytes, which, he says, in the first stage envelop the diaphyses of the long bones, especially at their inferior extremities. In the succeeding stage the new bony layers are more porous; a gelatinous degeneration affects the epiphysial cartilage and the spongy bones at a point where they are in contact; the epiphyses tend to separate from the diaphyses. This solution of continuity results in a characteristic pseudo-paralysis, with curvatures, abnormal twistings, and preternatural mobility of the bones, with loss of the power of locomotion. Then the osteophytes increase in size by the formation of several layers, thus enlarging the inferior extremities of the long bones. He describes the general process as consisting, first, of a periosteo-genesis—a formation of osseous tissue from the periosteum; next of a chondro-calcosis—a calcareous incrustation of cartilage; and finally of a gelatiniform degeneration and softening of the bone, with diaphyso-epiphysial disjunction.113
112 Société de Biologie, June 1, 1872; Société anatomique, 1873, p. 92; Archives de Physiologie, 1876, vol. iii. pp. 138, 139; Revue mensuelle de Médecine et de Chirurgie, 1877; Pathological Trans., 1871, vol. xxx. p. 339, etc., etc.
113 Cornil (op. cit.) coincides in the main with this description.
Taylor114 sums up the results of his observations as follows: "In the first stage we have a simple hyperplasia of cells with irregular deposition of lime salts; in the second, an intensification of this condition; and in the third, a new element—namely, the abnormal proliferation of all the elements of the tissues, with an infiltration of granulation-tissue into the medullary spaces following the vessels."115
114 Syphilitic Lesions of the Osseous System in Infants and Young Children, New York, 1875, p. 134.
115 Verraguth (Archiv für Path. Anat.) describes the first step as an excessive formation of vessels in the cartilage and a corresponding overgrowth of the cellular elements. This becomes inflammatory, and constitutes a primary syphilitic chondritis, the changes in the medulla of the bone being degenerative and secondary to the affection of the cartilage. Still other observers have described the process, each with minor modifications; but as they are of no clinical importance, it does not seem worth while to quote them.
[p. 288]We see, then, that, setting aside minor points of difference, these observers all coincide in describing this condition as one essentially of the nature of syphilitic bone troubles with which we are familiar in the acquired form of the disease, consisting primarily and throughout of an unnatural accumulation of cell-elements, which in the later stages by their pressure produce various degenerations of surrounding structures, and which, as they occur during the process of bone-formation, are accompanied by irregular and abnormal deposition of lime salts. They especially affect the regions mentioned—the junctions of the epiphyses and diaphyses—because at that time those points are the seat of great physiological activity. Syphilis, indeed, throughout its entire course is notably subject to similar influences, as one example of which I may instance the preference displayed by the periostitis which results in nodes or in caries for the subcutaneous bones, the tibia, clavicle, cranium, etc.; or, in other words, for those which are subject to frequent traumatisms—trifling, perhaps, but sufficient to determine a slight hyperæmia, which is followed by abnormal cell-proliferation or accumulation.
The symptoms which obtain in this condition of syphilitic osteo-chondritis are as follows: The child may be attacked during intra-uterine life, and in that event the osseous lesions will probably be coincident with other syphilomata and with placental disease of sufficient gravity to destroy life.116 If the child is born alive, the first development of the disease will probably be noticed as a swelling at the diaphyso-epiphysial junction of one of the long bones, which in the emaciated subjects of hereditary syphilis is often visible, and can always be discovered by palpation. The bones most frequently attacked are the humerus, radius and ulna, tibia and femur, but the clavicle, ribs, sternum, and bones of the metatarsus and metacarpus are also often involved, and much more rarely the frontal and parietal. The more pronounced the syphilis of the parents, or the nearer the date of conception to the time at which their infection occurred, the more probable is it that several bones will be affected, and the more unfavorable the prognosis as respects the life of the child. Indeed, it has been noticed that "in stillborn infants and in those dying soon after birth the majority, or even all, of the long bones are affected."117
116 Pollnow found osteo-chondritis in 35 out of 50 syphilitic foetuses (Der Hydrops Sanguinolentes foetus, Berlin, 1874, quoted by Hill and Cooper, op. cit., p. 352).
117 Bumstead and Taylor, op. cit., p. 767.
The swelling is found to consist of a ring or collar which more or less completely surrounds the bone, is apt to be smooth rather than irregular, and when two bones situated near to each other are simultaneously affected may conjoin them. This condition persists during the first stage of pathologists, and passes with greater or less rapidity into the second stage, in which the swelling, the cell-proliferation, reaches its height. This may take, in cases uninfluenced by treatment, several weeks or even months. Under the use of mercurials and iodide of potassium they usually subside rapidly. During this second stage, however, owing to the proximity of the swellings to the joints, a moderate amount of synovitis is often present. This affects chiefly the elbow and the knee, but may appear in any joint. It is also readily influenced by specific treatment and well-regulated pressure.
[p. 289]When the third stage is reached, or that of the formation of granulation-tissue, with degenerative changes of the cartilages and of the bones themselves, deformity often becomes more marked. There are unnatural curves or angles in the bones, with more or less complete separation at the point of junction. Where many bones are affected in this way, the resulting deformity is extreme and the patient may be absolutely powerless, a condition of pseudo-paralysis supervening in which the limbs lie motionless or swing about like the arms or legs of a doll when the child is carried.
When the swelling does not undergo absorption, the superjacent tissues sometimes become involved, abscesses form and make their appearance externally, extensive necrosis of the shaft of the affected bone takes place, and the little patient usually dies of hectic, pyæmia, or exhaustion. When the cranial bones are involved, the disease is apt to limit itself chiefly to the stage of osteophytic formation, the immovability of the bones probably favoring the organization of the new cell-growth rather than the production in it of inflammatory changes. The growths are met with chiefly in older children than those affected with the form of osteo-chondritis just described; they affect the periphery of the liver, and are found most usually around the anterior fontanel, and later on the parietal and frontal eminences. The sutures are sometimes completely soldered together.118 The osteophytes vary in thickness from a quarter of an inch to an inch, or are even larger.119
118 In a case reported by Barlow it was not possible at the autopsy to discover the point of union (Path. Transactions, 1879, p. 339).
119 These conditions may all result in a child the subject of acquired syphilis, but are apt to be milder, to involve fewer bones, and to yield more readily to treatment. This would of course be expected, inasmuch as the same difference in favor of the acquired form, as compared with that which is inherited, extends to all the lesions. As Diday succinctly expresses it: "In the one case the poison vitiates only the elements of nutrition; in the other it vitiates at the same time those of formation and those of nutrition." It would exceed the limits of the present article to describe acquired syphilis in children.
The most important differential diagnosis to be made in these cases is between the rachitis of young children and the form of syphilis in question. Much difference of opinion still exists as to the relation between these diseases, syphilis being claimed, on the one hand, as having in the majority of cases a definite causative influence, while, on the other, the existence of this relation is denied. When we come to contrast the pathology of the two diseases, we can readily understand why they should be confounded, the minuter changes which occur being essentially the same—viz. cell-proliferation and accumulation, with subsequent inflammatory changes, associated with irregular deposits of lime salts.
Compare, for example, the description of the pathology of bone diseases in inherited syphilis already given (pp. 287, 288) with the following terse summary of the changes which take place in rickets in cases where no suspicion of syphilis exists, either ancestral or acquired: "The changes are more distinctly noticed at the epiphyses than in the diaphyses. Instead of the regular stages and distinct boundaries observed in the normal development of bone, there is a singular disorderly commingling of the exaggerated cartilage-proliferation and transition substance, with calcification. The cartilage-cells, stimulated to excessive multiplication, are transformed, some into bone-corpuscles, some into medullary cells, [p. 290]and others into connective-tissue forms. The same process is in active operation in the deep periosteal layers, the material accumulating to such a degree as to add much to the thickness of the shaft."120
120 Agnew's Surgery, vol. i. p. 1030.
The points of resemblance are manifest, just as they are between a syphilitic and a variolous pustule, but they end in both cases when we come to study the evolution of the phenomena either from an anatomical or from a clinical standpoint. They may be expressed as follows in tabular form:
| OSSEOUS LESIONS DUE TO INHERITED SYPHILIS. | RICKETS. |
| The swellings, particularly those of the long bones, show themselves at or soon after birth. | Rarely appear before six months, generally still later. |
| A history of syphilis or evidence of existing syphilis in one or both parents. | No such history necessarily. |
| Preceded or accompanied by snuffles, coryza, and cutaneous and mucous lesions. | No such prodromata. |
| No such prodromata in most cases. | Pallor, restlessness, sweating, nausea, diarrhoea, etc. constitute a combination of symptoms which often precede the bone disease. |
| Cachexia absent or moderate. | Cachexia marked. |
| Physiognomical peculiarities of syphilis present.121 | Not present as a group. |
| Circumscribed tumors on frontal and parietal bones, rarely on occiput. | Cranial bones thickened in spots, usually upon the occiput. |
| Ribs not markedly affected. | All or nearly all involved. |
| Swellings on long bones or extremities irregular. | Extremities symmetrically enlarged. |
| Disease of ribs, when existent, not ordinarily coincident with that of other bones. | Nearly always so. |
| Fontanels close at usual period. | Closure delayed. |
| Other syphilitic symptoms present; enlargement of phalanges, metatarsal bones, etc. | Syphilitic symptoms absent. |
| Often accompanied by sinuses, synovitis, abscesses, cutaneous ulcers, etc. | Little external or surrounding involvement. |
| Generally disappears by resolution, without leaving any permanent change. | Usually leaves some bending of shaft and distortion of the neighboring joint. |
| Mortality among children in whom many bones are involved is very great. | Much less. |
| Specific treatment useful. | Of no benefit. |
| In the first stage there is an exuberant calcification of the ossifying cartilage, causing necrosis of the new-formed tissue and a consecutive inflammation, which terminates in the separation of the epiphyses.122 | This is less marked. There is formed, instead, a soft and non-calcified osteoid tissue. |
121 See p. 313.
122 This table is founded on one which I added to the translation of Cornil made by Dr. Simes and myself, and is compiled chiefly from the excellent work of Dr. Taylor already alluded to.
The diagnosis of the bone lesions of hereditary exostosis can readily be recognized in a short time by noting the fact that they are stationary, [p. 291]even if their later appearance, larger size, the absence of syphilitic history or symptoms, and the resistance to specific treatment left us in doubt.
The diagnosis from accidental separation of the epiphysis, or from fractures, may be made from the history of the case.
In cases of separation of the epiphysis, complicated with suppuration, sinuses, etc., the trouble may be mistaken for a similar condition due to non-specific inflammation. In all the recorded instances, however, the latter has occurred much later in life, is attended with much more acute inflammatory symptoms, lymphangitis, etc., and is of course without concomitant symptoms of syphilis. In both these cases there is a decided osteo-periostitis, and as so much depends on the early and vigorous use of specific treatment, it may be worth while to contrast the two forms of the disease.
| SYPHILITIC OSTEO-PERIOSTITIS. | NON-SPECIFIC OSTEO-PERIOSTITIS. |
| Occurs in infants under three months of age. | No instance of its occurrence in children under one year of age. |
| History of syphilis in child and its parents. | No history of syphilis; sometimes a history of traumatism. |
| Implication of other bones. | Usually confined to one bone. |
| Coincident with the development of the shaft of the bone. | Coexists with the ossification of the epiphyses. |
| Other lesions of syphilis: nodes, skin eruptions, etc. | No such symptoms. |
| All the local symptoms comparatively mild. | Pain, redness, and swelling very marked. |
| Disease sharply localized. | Involves neighboring parts. |
| Lymphatics of limb unaffected. | Lymphangitis present. |
| Beneficial effect of specific treatment if employed early.123 | No such effect. |
123 Cornil, op. cit., p. 274.
Syphilitic dactylitis in the inherited variety of the disease, as in the acquired, consists of two varieties. The one of these which usually appears earlier involves chiefly the periosteum and the fibrous and integumentary structures surrounding a joint, usually a metacarpo- or metatarso-phalangeal articulation, involving a phalanx, and is characterized by slow, almost painless, swelling and discoloration of the affected member. (Fig. 9.) This is due to a gummous infiltration which, after absorption under proper treatment, leaves the toe or finger temporarily stiff, but not permanently disabled.
The second form is a specific osteo-myelitis, with periostitis, coming on later, and often destroying the bone or the articulation involved. (Fig. 10.)
| FIG. 9. |
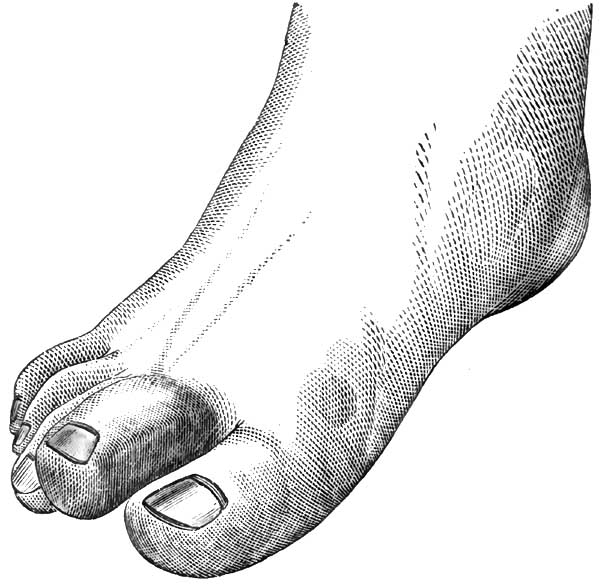
|
| FIG. 10. |
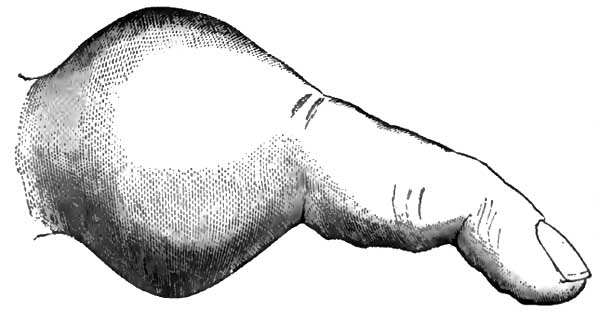
|
| From Bumstead on Venereal Diseases, illustrating Syphilitic Dactylitis. |
The absence of acute inflammatory symptoms in the first variety distinguishes it from paronychia, whitlow, and gout. Rheumatoid arthritis begins in the joints, is associated with other symptoms; deformity of the fingers comes early in the disease, and there is a teno-synovitis with contraction.
The second variety might be taken for enchondroma or exostosis, but these growths increase much more slowly, involve only a limited portion of the bone, are of greater density, and are much more strictly circumscribed.
As a rule, especially in cases which are recognized early and treated [p. 292]actively, the prognosis is good. Iodide of potassium should be used in combination with mercury.
Syphilis of the Teeth.—Syphilis of the teeth has its chief interest to the general practitioner from its very important bearing on diagnosis. As manifesting itself at an age when the child is not apt to present the active and unmistakable cutaneous and mucous lesions of the disease, and when, consequently, its recognition is often extremely difficult, this diagnostic importance is greatly increased.
The teeth of the first dentition, although exhibiting the usual signs of interference with nutrition in their irregular development, opaque and chalky enamel deficient in quantity and unevenly distributed, soft and friable dentine, incongruity of size individually and relatively, and proneness to decay, do not often display any distinctive evidence of syphilis. [p. 293]The same conditions may, and often do, depend on other causes, and are commonly associated with various cachexiæ—the strumous, gouty, rheumatic, rachitic, etc.—and even with other slighter ailments tending to produce imperfect assimilation and malnutrition.
In the permanent teeth, likewise, the same condition may be due to the same causes. Stomatitis, however produced—by mercury, by gastro-intestinal derangements, by local irritation of any kind—is apt to result in imperfectly organized dental structures. Mercurial teeth, for example, are usually irregularly aligned, horizontally seamed, honeycombed, craggy, malformed, of an unhealthy dirty yellow color, separated too widely, and deficient in enamel.124 The diseases of childhood, especially the eruptive fevers, eclampsia, typhoid fever, etc., by temporarily arresting or greatly interfering with nutrition during the developmental period of the teeth, often cause horizontal furrows across their crowns, which are, of course, persistent throughout life, and mark indelibly the influence of such disorders on all the formative processes.
124 The latter defect is particularly noticeable on the cusps of the sixth-year molars. (See note on "Syphilis of the Teeth," by Dr. James W. White, in Am. ed. of Cornil, pp. 287-290.) The discussion as to the effect of mercury in producing the condition of the teeth known as honeycombed is still going on, but the evidence seems to point clearly to a direct connection with the administration of mercury in infancy, either for syphilis or in excessive doses as a purge, or in some of the teething powders, which often consist of calomel and opium. Mr. Hutchinson, at a meeting of the Odontological Society (see Proceedings for 1877, p. 249), gave an interesting description of the way in which the supposition was arrived at. Lamellar cataract is a disease which affects the eyes of children who have suffered from convulsions: it was noticed that in cases of that form of catarrh there were also honeycombed teeth, and it was thought that the convulsions, the cataract, and the honeycombed teeth were all due to the same unknown cause. At last a few exceptions were found—patients with cataract, but with good teeth, and then some who had had convulsions only, and yet had honeycombed teeth; lastly, it was noticed that most of the patients had been treated with mercury. So it came to be recognized that the honeycombed teeth were only accidentally associated with the cataract, and that they were, in fact, the result of the mercury which had been given to cure the convulsions. The same gentleman figures a case of this disease in his Illustrations of Clinical Surgery (London, 1875), and thus describes it (p. 55): "The present state of his permanent teeth is so characteristic as to deserve more detailed description. The change about to be mentioned affects all the incisors, canines, and first molars of both upper and lower jaws, the bicuspid being scarcely implicated at all; the second molars are also quite healthy. In the first molars the alterations consist of deficiency of enamel on the upper surface of the crown and the presence of spines of uncovered dentine. In the case of the incisors a considerable portion of the crown of each tooth is totally devoid of enamel, and its dentine is also deficient to some extent, so that the teeth are thin, sharp-edged, and of a dirty yellowish color. The transition from the enamel-covered to the diseased part occurs suddenly in a horizontal line at some little distance from the crown of each tooth; the position of this line or step being in each tooth nearly at the same distance from the gum. The general effect when all the teeth are seen together is as if a string had been tied around them when soft and the distal part had withered."
None of these conditions, however, are in the least degree characteristic of syphilis, the special expression of which in the mouth is to be found only in the permanent upper median incisors. For the recognition and description of the peculiarities of these teeth in the subjects of inherited syphilis we are indebted, as we are for so much else of inestimable value in the study of the disease, to Mr. Hutchinson. In 1863, in a memoir on Syphilitic Diseases of the Eye and Ear, he wrote as follows125 [p. 294]concerning the symptoms which, in a suspected case, would aid in determining the diagnosis: "By far the most reliable amongst the objective symptoms is the state of the permanent teeth if the patient be of age to show them. Although the temporary teeth often, indeed usually, present some peculiarities in syphilitic children of which a trained observer may avail himself, yet they show nothing which is pathognomonic, and nothing which I dare describe as worthy of general reliance.126 The central upper incisors of the second set are the test teeth, and the surgeon not thoroughly conversant with the various and very common forms of dental malformation will avoid much risk of error if he restricts his attention to this pair. In syphilitic patients these teeth are usually short and narrow, with a broad vertical notch in their edges and their corners rounded off. Horizontal notches or furrows are often seen, but they, as a rule, have nothing to do with syphilis. If the question be put, Are teeth of the type described pathognomonic of syphilis? I answer unreservedly that when well characterized I believe they are. I have met with many cases in which the type in question was so slightly marked that it served only to suggest suspicion, and by no means to remove doubt; but I have never seen it well characterized without having reason to believe that the inference to which it pointed was well founded."
125 Chapter on "The Means of Recognition of the Subjects of Hereditary Syphilis during the Tertiary Stage," p. 204. Before this, however, he had called attention to the same peculiarities in a paper on "The Means of Recognizing the Subjects of Inherited Syphilis in Adult Life," Medical Times and Gazette, London, Sept. 11, 1858, p. 265.
126 So far as I know, the only recorded instances by reliable observers of the temporary teeth presenting the peculiar characteristics of syphilis are as follows: In the Transactions of the Odontological Society of Great Britain, vol. ix., 1877, p. 258, Mr. Oakley Coles described a case—without, unfortunately, giving details—in which the "peg-shaped temporary teeth were very characteristic of syphilis." Mr. Coles's abilities are well known, and the fact that at the previous meeting the society had been addressed by Mr. Hutchinson on this very subject would seem to indicate that he was quite familiar with the importance of his statement.
M. Fournier calls attention (Archives de Derm. et Syph., Sept. 25, 1883) to a cast (No. 48) to be found in the collection of M. Parrot in the museum of the Foundling Hospital at Paris. This displays the dentition of a child twenty-seven months old, in which the two upper median incisors are typical Hutchinson teeth. M. Fournier adds that later researches show unmistakably that the temporary teeth may be affected by hereditary syphilis in the same manner as those of the second dentition, although not more than one case of the former is recognized to fifteen or twenty of the latter. He thinks, however, that this proportion would be greatly modified if in the autopsies of young children the alveoli were opened to examine the embryonic teeth. M. Parrot by this means claims to have often discovered lesions of the milk teeth.
As a matter of course, so positive a statement in a matter of such gravity and importance excited considerable criticism, and the views of Mr. Hutchinson have never been without earnest and often able opponents; but it is safe to say that time has only served to place them on a surer foundation and to enhance their value in the eyes of the profession. That they have undergone no material change in the mind of their distinguished author is shown by his expressions of opinion during the debate on syphilis in the London Pathological Society in 1876,127 and still later by the following memoranda which he gives as a guide in diagnosis:128
"1. No special peculiarities are to be looked for in the first set of teeth.
"2. There can be no more serious blunder than to imagine that bad teeth in proportion to their badness of form are to be suspected of syphilis.
[p. 295]"3. The upper central incisors are the only teeth which are positively characteristic. The others may afford corroborative testimony, but are not to be relied upon alone.
"4. The chief peculiarity is a general dwarfing of the tooth, which is both too short and too narrow, and, from its sides slanting together, presents a tendency to become pointed. This tendency to pointing is always defeated by the cutting off of the end, the truncation being usually effected in a line curved upward, so as to produce a single shallow notch. At the bottom of this notch the enamel is deficient and the dentine exposed, but there is no irregular pitting, as in stomatitis teeth.
"5. The malformations are unusually symmetrical and affect pairs of teeth. The two central incisors resemble each other, and the two laterals are also alike. If any defect passes horizontally across all the incisors at the same level, and affects them all alike, it is probably not due to syphilis.
"6. In syphilis the lateral incisors usually show little or no malformation.
"7. The occurrence of the peculiarities due to syphilis and those due to mercury in the same mouth are exceedingly common."
127 London Lancet, 1876, pp. 56 and 535.
128 Illustrations of Clinical Surgery, fasciculus xi., London, 1878.
The great importance of the subject seems to me to justify one more quotation, as showing the opinion at a very recent date of men well qualified to judge of the correctness or inaccuracy of these statements. Mr. C. Macnamara and Dr. Thomas Barlow129 say: "The characters of the teeth are so valuable when present that it is important to have them clearly noted—the more so that, in spite of Mr. Hutchinson's clear description, they have been much misrepresented. It may be pointed out—(1) That only the upper median permanent incisors are characteristic, and sometimes only one of them is typical, of the disease; (2) that these teeth are generally a little apart, instead of being in apposition, and are more or less dwarfed; (3) that in a typical specimen the width of the cutting edge is narrower than the width of the tooth as it emerges from the gum; (4) that a typical syphilitic tooth presents a single notch, not a serrated margin; and that occasionally, if the notch has not been actually scooped out, there is a little lunula-shaped area which may readily become a notch; (5) finally, that although such teeth, when present, are absolutely pathognomonic, the existence of normal permanent upper median incisors by no means excludes the existence of hereditary syphilis."
129 On behalf of the Collective Investigation Committee, who have issued a circular designed to elicit information as to the effect of syphilis on the civil population of Great Britain. This circular has been sent to physicians, and contains queries as to various points relating to the symptoms of inherited syphilis; among others as to the existence in any given case of "notched, dwarfed upper median incisors," which, with or without other symptoms, would establish the diagnosis of that case. The observations above quoted are explanatory of this question (The British Medical Journal, Dec. 16, 1882).
I believe this may fairly be taken to represent the general belief at the present day among those best qualified to pronounce upon the merits of the case; and I may say that it is unqualifiedly my own opinion, arrived at after some experience and considerable investigation into the literature of the subject. It is not uncommon, however, to hear doubts expressed as to the value of this sign in the diagnosis of syphilis, and at intervals articles are written or papers read to prove that it is not of the uniform and distinctively conclusive significance that has been attributed to it.130
130 "I cannot say more in favor of the diagnostic values of these teeth than that, when [p. 296] present in typical form, they have a certain weight in favor of the existence of hereditary syphilis in the given subject" (Van Harlingen, article "Syphilis" in Internat. Encyc. of Surgery, vol. ii. p. 565). "It has been the custom from time to time since Mr. Hutchinson made his observation to question the validity of his views, both as to the fact of interstitial keratitis being due to hereditary syphilis, and as to the diagnostic values of the so-called characteristic teeth. Thus, it has been asserted, not only in England, but on the Continent, and especially in Germany, that the disease may be the result of malnutrition in scrofulous and rickety subjects; and it has been maintained that the malformation of the teeth is the simple arrest of development in a perverted constitution from other causes than syphilis" (Bumstead and Taylor, op. cit., p. 701). Garretson says (Oral Surgery, p. 316): "Observations will be found to greatly vary concerning the existence of any constancy in phenomenal expressions of the teeth in this relation."
M. Magitot, who has for some years been supposed to pay especial attention to this subject, has recently written an elaborate paper (Gazette des Hôpitaux, Sept. 29, Oct. 4, 11, and 18, 1881) to prove (1st) that dental erosions, as he calls them, are not due to syphilis; and (2d) that they are due to, or are almost invariably associated with, infantile convulsions. He has collected a number of interesting facts, but a very careful study of his article and inspection of his diagrams have convinced me that he does not recognize at all the special peculiarities of the Hutchinson teeth, but includes under his title of "erosion" a variety of widely-differing conditions. He has altogether misinterpreted Mr. Hutchinson's views as stated in his Memoirs on Certain Diseases of the Eye and Ear due to Inherited Syphilis, and represents him as at that time (1863) believing that the cause of the change in the incisors was a mercurial stomatitis. The quotation on p. 294 sufficiently refutes this absurdity. Of course the paper as an argument against the syphilitic origin of these teeth is without the slightest value.
Corroborative evidence—which, to my mind, is very strong as coming from men whose opportunities for observation of dental peculiarities are almost unlimited—is found in the writings of those gentlemen who have devoted themselves to dental and oral surgery exclusively. Mr. Henry Moon131 says:132 "My observations on this subject extend over some twelve years, and include some hundreds of cases; and although, in some details as to the manner of causation, I may differ from the view published by Mr. Hutchinson (before knowledge on tooth-development was advanced as it is at present), yet I must coincide entirely with his general conclusions." "The question really is this: Is there one peculiar conformation of the teeth due to inherited syphilis and not produced by any other cause? The evidence in favor of an affirmative answer to this question appears to me to be so strong that I think the onus of disproof rests with the sceptics."133 These views were coincided in by the majority of the gentlemen to whom they were addressed, all of them dentists and surgeons of experience and repute, and who included men so well known to the profession as Mr. Oakley Coles, Mr. Samuel Cartwright, Mr. Charles Tomes, and others.
131 Author of the section on "Surgery of the Teeth" incorporated in Bryant's Surgery.
132 Proceedings of the Odontological Society of Great Britain, vol. ix., 1877, pp. 238, 239. In the same journal for 1875, vol. vii. p. 17, Langdon Down says that whenever he has discovered syphilitic teeth he has "never failed to find confirmatory evidence of the syphilitic history of the case."
133 He says elsewhere (Bryant's Surgery, 3d Am. ed., p. 429) that the most characteristic change in these teeth is "the lessened breadth of the cutting edge as compared with that of the neck, the vertical groove on their anterior face being often absent, and the notch on their cutting edge not being an absolutely constant feature, and being also subject to obliteration through wear."
It may be considered as well established, then, that these peculiar teeth—stunted, abnormally narrow at the cutting edge, crescentically rounded with the convexity upward, and the surface inclined upward and forward instead of backward as in normal teeth, widely separated, but converging at their lower edges—are pathognomonic of hereditary syphilis.134 They are [p. 297]often described as pegged, having been likened to a row of pegs stuck in the gums. This appearance is due to the fact that they are shortened, often projecting not more than half the normal distance from the gum, and are also widely separated; which abnormalities often affect the adjoining teeth as well, and sometimes the entire dentine. It has been asserted that other specific peculiarities are to be found associated with those of the incisors, and Mr. Moon describes as characteristic, and figures135 small dome-shaped first molars with suppressed angles and absence of enamel from the masticatory surfaces. He believes also that when the upper incisors are typical it is exceedingly rare for the lower incisors to be altogether unaffected.
134 Mr. Hutchinson stated in 1877 that in spite of the fact that many years previously he had challenged any one to bring forward a patient with well-marked syphilitic teeth in whose history no evidence of syphilis could be found, none had come.
135 Proc. of Odont. Soc. of Great Brit., vol. ix. pp. 241, 242; Bryant's Surgery, Am. ed., p. 429.
| FIG. 11. |
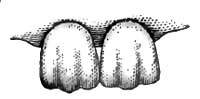
|
| Serrations of Normal Incisors. |
| FIG. 12. |

|
| Syphilitic Incisors. |
A mistake which I know, from observation, to be frequently made is the confusing of the normal serrations of the cutting edges of recently-erupted normal incisors with the peculiar crescentic edges of the syphilitic teeth. It seems worth while to call especial attention to this, on account of the unpleasant consequences which often follow injudicious questioning based on such supposed syphilitic phenomena. Indeed, the space which has been devoted to this subject of syphilis of the teeth is well warranted, I am sure, by the fact that not only do diagnosis, prognosis, and treatment in cases of great severity, and in both children and parents, often depend upon a recognition of these peculiarities, but that in addition to the clinical and therapeutic problems there are others the solution of which is dependent upon the same knowledge on the part of the practitioner, and which may involve reputation, marital relations, and personal honor and happiness.
The approximate cause of these peculiarities in the incisors can hardly be said to have been demonstrated. Mr. Hutchinson thought at one time136 that they were due to a stomatitis or an alveolar periostitis, but he has since changed his mind as to that point, believing now137 that the syphilitic tooth is the result of an arrest of development in the central or first-formed portion of the dentine. The incisors being made up of these lobes or denticles, and dwarfing of the middle one taking place, the two lateral ones fall together. This accounts at once for the small size of the tooth, its shape of an inverted truncated cone, and its crescentic edge.138 If it were due to stomatitis, it would be more likely to be equally [p. 298] distributed, syphilis in its late manifestations being notably unsymmetrical; there would be no rational explanation of the involvement of one or two teeth while those on either side so frequently escaped; if it were mercurial stomatitis, the enamel too would be involved, as is not usually the case in the syphilitic teeth. It is possible that the central incisors are chiefly affected because they, with the first molars—also affected according to Mr. Moon—and the lower incisors—not infrequently involved—are the first-formed teeth.
136 "The physiognomonical, dental, and other peculiarities by which we recognize the subject of inherited taint when advanced beyond the period of infancy are all of them the direct consequences of special inflammations from which the patient has suffered at former periods; e.g. the synechiæ and lustreless iris of iritis; the malformed teeth of periostitis of the alveolus and dental sacs; the protuberant forehead of hydrocephalus; the flattened nose of snuffles; the pale, earthy, opaque skin of cutaneous inflammation and eruption" (Aphorisms respecting Constitutional Syphilis, 1863).
137 Proc. of Odont. Soc. of Great Britain, vol. ix., p. 248. See also ibid., pp. 241, 242, remarks of Mr. Moon; also Monthly Review of Dental Surgery, June 15, 1877.
138 The denticle theory of formation is not necessarily opposed by the fact that there is only a single undivided pulp-cavity in these incisors. Instances of the separate formation of processes of dentinal pulp while others are being used and worn away, all of them finally to unite in a common pulp-chamber, have been observed in lower animals, as in the molar of the elephant.
The most elaborate article upon syphilitic teeth which has appeared since Mr. Hutchinson's original memoir is one by Fournier,139 in which, after a very broad and comprehensive consideration of the subject, he arrives at the following conclusions: The hereditary influence of syphilis shows itself in the dental system in two ways, very unequal in point of diagnostic value—viz. first, by a retardation of evolution; second, by the arrest of growth and modifications of structure. The phenomena belonging to the second class may be grouped as follows: First, dental erosion. This is due to imperfect formation of the tooth, the result of a temporary stoppage in its development; but as it produces an appearance like that of worm-eaten wood, it has been called erosion, though in so far as the word conveys the idea of the wearing of a surface which has been previously normal, it is incorrect. The tooth affected with syphilitic erosion has never been normal. The different forms of erosion can be subdivided into groups according as they affect the face or the free edge or grinding surface of the tooth. Of those involving the face there are four types: Erosions en cupule, consisting of small excavations or cups in the surface of the crown; erosions en facettes, in which the surface presents a series of small planes, as though they had been filed; erosions en sillon when there is a linear excavation in the crown of the tooth in the shape of a transverse groove; and erosions en nappe, in which the whole surface is discolored, disorganized, and honeycombed.
139 Archives de Derm. et Syph., Sept. 25, Oct. 2, Oct. 9, 1883. A translation made by the writer may be found in the Dental Cosmos for January and February, 1884.
A second group of erosions affects the free edge of the tooth, and includes the Hutchinson teeth, with several less important varieties. Dental erosions are multiple, symmetrical, maintain the same level on the crowns of corresponding teeth, and are situated at different heights on the crowns of teeth of different classes. It is evident, therefore, that they are the result of a morbid influence of a general character. There are three theories as to their etiology: (a) that they have no relation to syphilis,140 but are always connected with infantile eclampsia; (b) that they are exclusively the result of hereditary syphilitic influence; and (c) that they are simply ordinary lesions originating from syphilis with marked frequency, and even in one form—the Hutchinson tooth—appearing to originate only from it. This latter view is the one adopted by Fournier himself. Continuing to group the symptoms due to arrest of growth and modification of structure, we have, second, microdontism, or dwarfing and stunting of the teeth—pegged teeth; third, dental amorphism, in [p. 299]which the teeth are strangely distorted or even transformed in type; fourth, dental vulnerability, or extreme susceptibility to all traumatic or disintegrating influences.
140 M. Magitot, Treatise on the Anomalies of the Dental System, Paris, 1877; Clinical Studies on Erosion of the Teeth considered as a Retrospective Sign of Infantile Convulsions, Paris, 1881; Castanié, Paris, 1879, Thesis No. 384; Rattier, Paris, 1879, Thesis 569; and others.
Interstitial Keratitis.—The frequency of this form of diffuse inflammation of the cornea, and the diagnostic significance which has been so positively attributed to it—and has been as positively denied—render it of special interest to the general practitioner, who is almost certain to meet with occasional cases, and should be prepared to recognize its possible relation with other, and often graver, conditions.
It begins, commonly, as a slight, diffused haziness situated in the substance of the cornea itself, usually not far from the centre, and at first affecting only one eye. This depends at this stage on the presence of a number of little distinct dots of inflammation, limited to circumscribed, almost microscopic, areas, but later, in a few days, these coalesce, and at the end of a few weeks the whole cornea will probably have become nearly or quite opaque, looking like ground glass. There is no ulceration, and but little congestion as compared with that seen in other inflammatory diseases of the eye, although in the majority of cases there is a fulness of the ciliary vessels and a little photophobia with pains around the orbit. This condition may persist for one or two months, after which the other cornea is nearly always attacked,141 and is similarly affected, although the disease is apt to pass through its different stages rather faster than in the first eye.
141 In 91 out of 102 cases in Mr. Hutchinson's series—in 6, the left alone; in 5, the right alone (op. cit., p. 123).
When the height of the disease is reached the corneæ are nearly opaque, a bare perception of light remaining, so that the patient is just aware of the difference between its presence and absolute darkness. Then the cornea which was first involved begins to clear; this is soon followed by improvement in the other one, which in the course of a year or two results in a return to fairly good sight, although in most cases there remain a slight haziness and an abnormal expansion of the cornea.
This favorable result is much influenced by the character of the case, which is sometimes very mild from the outset, and by the thoroughness of the treatment. It is sometimes complicated with iritis, kerato-iritis, cyclitis, posterior choroiditis, secondary glaucoma, etc., in which cases of course the prognosis is most unfavorable. Even in ordinary cases it should be guarded in respect to perfect restoration of function, as clearing of the corneæ may reveal adhesions from iritis or spots of choroiditis disseminata, which could not, of course, have been previously detected. In very mild cases, however, without much evidence of involvement of the other tunics, and which have been submitted to treatment early, it is not uncommon for the cornea to regain almost perfect transparency.
The diagnosis of this condition may generally be made with ease. The ground-glass appearance in the earlier stages and the dull pink or salmon color in the more vascular stage are very characteristic. The vascularity differs from that attending other chronic forms of keratitis, granular lids, etc., in which the vessels are large and superficial, in that in the syphilitic keratitis they are much deeper and very closely interwoven, so that the effect is almost that of an ecchymosis. In other cases both eyes are not so apt to be affected, nor is the tendency to spontaneous cure [p. 300]so marked. The absence of ulceration and the very slight degree of accompanying sclerotic or ciliary congestion are also valuable features.
The conditions which Mr. Hutchinson has known to be most frequently mistaken for it142 are certain forms of inflammation following small-pox and very superficial ulcers in a healing stage, together with cases of vascular conjunctiva.
142 Op. cit., p. 128.
There is also said143 to be some difficulty in distinguishing it from a form of non-syphilitic relapsing cyclitis with corneal opacities and iritis. This, however, is a disease of adults, often limited to one eye, with a strong tendency to relapse, the opacities being more abruptly defined and limited to the region near the circumference.
143 Edward Nettleship in Hill and Cooper, op. cit., p. 267.
The chief point of interest, however, in the diagnosis of interstitial keratitis is its association with other symptoms of syphilis, upon which, for the general practitioner at least, the diagnosis will usually depend.144 Mr. Hutchinson's conclusions, drawn from an analysis of 102 cases of interstitial keratitis, bear strongly upon this point, and are as follows:145 A large proportion of all cases occur in patients between the ages of eight and fifteen, the disease being comparatively rare in early childhood, and still more so after adult age has been reached. He never saw it begin after the age of twenty-six. The patients presented the physiognomical peculiarities of inherited syphilis (see p. 313). In more than half the cases the previous history, especially as regards infancy, was one of hereditary syphilis, and in many instances there was a clear history of infantile syphilis in brothers or sisters. In half the cases no questions were asked as to the existence of venereal disease in the parents prior to the birth of the child. In 29 out of the other half such disease was freely admitted. All the patients had lost in early life nearly half their brothers and sisters. Omitting miscarriages and premature births, it was found that 77 mothers had borne 547 children, of whom only 284 remained alive—an excessive rate of mortality. It appeared in the large proportion of cases in the eldest children in their respective families—a circumstance to be expected in view of the usual behavior of hereditary syphilis in families. Undoubted syphilitic lesions, such as nodes, ulceration of the palate, etc., are not infrequently associated with the keratitis.
144 "To those who have not had opportunities for observation at an ophthalmic hospital I would recommend that the diagnosis should be held to be doubtful if the patient does not present the peculiarities of teeth and physiognomy which I have described, since we find that the latter are the almost invariable concomitants of the true disease" (Mr. Hutchinson, op. cit., p. 128).
145 Op. cit., pp. 109-129.
Examination of large numbers of cases has, I believe, established the general accuracy of these statements; and although there is still much difference of opinion as to the exact relation between syphilis and this form of keratitis—whether, for example, it is a symptom of syphilis itself or of a cachexia frequently produced by syphilis, but often by other systemic diseases affecting nutrition—yet, on the whole, so far as I am able to judge of the question outside of its purely technical and ophthalmological relations, I think the weight of modern authority is chiefly on the side of a distinct and practically invariable relation of cause and effect between inherited syphilis and the corneal inflammation.
[p. 301]Mr. James Dixon,146 for example, proposes to call the disease syphilitic keratitis, and says it is met with exclusively as a sequel of an inherited taint. He adds: "We may meet with some syphilitic keratitis in patients with healthy physiognomy and deformed teeth, or, still more rarely, in those with faultless teeth and the syphilitic cast of features; but to find the true form of keratitis in connection with both good teeth and good complexion is, I think, next to impossible." Many other ophthalmologists express themselves to the same effect more or less strongly. Nettleship,147 Noyes,148 Förster,149 Macnamara,150 De Wecker,151 and Carter152 may be mentioned as having ranged themselves upon this side. On the other hand we have Schweiger,153 Maunther,154 Sæmisch,155 Soelberg Wells,156 and others who are not convinced that syphilis is the sole nor even, in the opinion of some of them, the principal cause of this disease.
146 Article on "Diseases of the Eye," Holmes's System of Surgery, Am. ed., vol. ii. p. 71.
147 Op. cit.
148 Text-book of Ophthalmology.
149 Handbuch der gesam. Augenheilkunde, vol. vii. p. 186, 1876.
150 Op. cit.
151 Ocular Therapeutics, trans. of Forbes, 1879, p. 124.
152 He even asserts the converse to be true, which is going beyond what I believe can be established in regard to the invariable connection between the two diseases. He says: "The subjects of what we call simply inherited syphilis are liable—nay, are almost sure—to suffer from a peculiar form of interstitial keratitis."
153 "Hutchinson's view, that this form of keratitis is to be regarded as the direct consequence of congenital syphilis, has not been generally accepted in Germany" (Handbook of Ophthalmology, p. 298).
154 Zeissl's Jahrbuch der Syphilis, 1875, p. 288.
155 Graefe and S.'s Handbuch d. Augenheilkunde, 1875, vol. iv. p. 264.
156 Diseases of the Eye, p. 138.
Probably the conclusions of Jullien157 most nearly express the views of those who do not accept in its entirety the syphilitic theory of the disease. He concludes—(1st) that interstitial keratitis coincides frequently, but not invariably, with syphilitic derangement of the dental apparatus; (2) that it is associated with a feeble constitution and with malnutrition, and is thus produced indirectly by scrofula, rheumatism, or syphilis, each of which by its debilitating influence may give rise to a diathesis which favors such morbid developments.
157 Op. cit., p. 1013.
As a specimen of the evidence which is produced by observers other than Mr. Hutchinson—who, as he himself observes, may be suspected of "that bias which almost necessarily warps more or less the judgment of one who supposes himself to have noted something new"158—the statistics of Förster,159 who apparently takes an unbiassed view of the question, may be noted: In a total of 214 cases of interstitial keratitis evidence of hereditary syphilis other than the corneal disease was noted in 146 (68 per cent.). This number was made up as follows: a, evidence of syphilis in parent, 17; b, evidence of hereditary syphilis in other members of the family, 14; c, evidence in the patient other than keratitis, 115; characteristic teeth, 69; evidences in physiognomy, bones, skin, palate, or choroid, 46. In the remaining 68 cases (32 per cent.), though inheritance of syphilis was not proved, there was, almost without exception, strong suspicion of that disease apart from the keratitis.
158 Op. cit., Preface, p. x.
159 Graefe and Sæmisch's Handbuch, vii., Part I.
The condition of the permanent central upper incisors was noted in 138 of the cases; of these they were typical in 73 (53 per cent.); suspicious in 34 (24 per cent.); normal in 31 (23 per cent.). In 15 cases [p. 302]the permanent teeth had not been cut, and in the remaining 61 the state of the teeth was not recorded.160
160 Note by Mr. Nettleship, Hill and Cooper, op. cit., pp. 263, 264.
This seems to me such direct and such unequivocal clinical evidence that it is safe to say, as of the question of syphilitic teeth, that the burden of disproof rests with the doubters, and that we may venture the assertion that interstitial, diffuse, or parenchymatous keratitis is a symptom of inherited syphilis, and that the unmistakable presence of the former disease is sufficient proof of the existence of the latter.
Syphilis of the Nerve-Centres and Nerves.—Until a comparatively recent period our only guide to the course and progress of the nerve diseases of inherited syphilis was to be found in analogy. We knew, for instance, that in acquired syphilis three forms of cerebral disease could be recognized in a general way—one characterized by sudden attack of paralysis, in which the lesion was usually thrombosis from specific endo-arteritis; one in which the symptoms of brain tumor were present, and in which gummata were the cause of the difficulty; and one in which pain, headache, and various functional or convulsive disturbances—chorea, epilepsy, paralysis of single nerves, etc.—were the customary phenomena, and in which periosteal, meningeal, or neuroglial thickenings constituted the pathological basis. The last two are often intermingled both symptomatically and histologically.
Heubner161 divides cerebral syphilis into three groups, two of which very closely resemble those I have described. In one, however, he includes both the general physical disturbances, incomplete paralysis, and final coma characteristic of tumor and the epileptiform attacks so often due to peripheral or meningeal irritation. This combination is explained by the results of his autopsies, which disclosed in 26 cases in which these symptoms were conjoined a gummous growth in the pia mater of the convexity of one of the cerebral hemispheres, either limited and superficial or involving more or less of the cortex and forming a distinct tumor. The epileptiform attacks were present in 19 out of these 26 cases, while in 20 other cases where the growth was limited to the white substance at the base of the brain they were present only twice. This second form is the apoplectic, followed by general hemiplegia, and depending on disease of the cerebral arteries. His third division is a very ill-defined one, depends much for its limitations upon subjective symptoms, and is of no special interest as applied to the subject of inherited syphilis.
161 Ziemssen, vol. xii.
Althaus162 also makes three divisions, two of which are as follows: (1) Cerebral tumor—a gumma either hard or soft. There are then nocturnal headache, sleeplessness, epileptiform attacks, the various phenomena produced by involvement of the cerebral nerves, etc. (2) Disease of the arteries, apoplexy, or softening, followed by hemiplegia.
162 Medical Times and Gazette, Nov. 10, 1877.
Hutchinson makes a similar division of lesions and symptoms,163 and the observations of Jaksch, Wilks, and Hughlings Jackson more or less closely coincide with this general classification.
163 Ibid., Feb. 17, 1877.
Now, in spite of certain striking differences—more apparent than real, however—between inherited and acquired syphilis as regards cause, [p. 303]duration of stages, etc., the essential pathological changes are the same. When syphilis in its later periods attacks the brain or spinal cord or nerve-trunks or vessels of a foetus, it proceeds just as in the adult, the same characteristic accumulation of cells taking place and setting up an arteritis or a meningitis, thickening the sheaths of nerves, or constituting a pericranial node or a gumma according to their number and their situation. We would accordingly expect to find in subjects of inherited syphilis manifestations closely allied to those observed in the adult; and the observations of Barlow,164 Graefe,165 Jackson,166 Heubner,167 Dowse,168 and Hutchinson,169 though comparatively few in number, have already demonstrated the correctness of this supposition.
164 Trans. of Path. Soc. of London, vol. xxviii., 1877.
165 Archiv für Ophthalmologie, Bd. 1, Ab. i.
166 Journal of Mental Science, Jan., 1875.
167 Ziemssen, vol. xii.
168 Syphilis of the Brain and Spinal Cord, London, 1879, chapter on "Hered. Syph.," p. 67.
169 Med. Times and Gazette (? Feb. 17, 1877).
We find, thus, that in these patients meningitis, growths, and arterial disease constitute the three clinical divisions of the disease which have thus far been distinctly differentiated, and the reported cases, with or without autopsy, fall naturally into these classes.
These cases are naturally few, and to make them absolutely reliable it is necessary to have unmistakable evidence of hereditary syphilis in some other form and the demonstration of syphilitic lesions at an autopsy. The case of Dowse, however,170 includes these requirements. A child twelve years of age, of syphilitic parents, with a history of coryza, sore eyes, and a tubercular syphilide, was attacked with epilepsy, diplopia, facial paralysis, etc., and finally died. At the autopsy three gummatous growths of the surface of the brain were found, and the vessels of the base were found to have undergone the special changes described by Heubner. Their lumen was in some places nearly occluded by an accumulation of spindle-shaped cells between the tunica fenestra and the epithelial lining; and interspersed with them, but particularly in the muscular and adventitious coats, were to be seen enormous quantities of round cells which in many parts seemed actually to replace the normal structures. Dowse's other cases are not at all conclusive in their clinical histories; even the diagnosis was not established by autopsy.
170 Op cit., pp. 71-75.
Barlow's two cases were both very young children, and are extremely convincing.171 A child four months old, with snuffles, serpiginous ulcers, etc., and with a syphilitic father, had epileptiform attacks, followed by laryngismus, carpo-pedal contraction, and changes in the choroid. She died aged about fifteen months, and the autopsy disclosed thickening of the pia mater, evidently not tubercular, and changes in the arteries, which in the gradual narrowing of the lumen of the vessel, the absence of ulceration or disintegration or calcification, and the continuity and extent of the cell-proliferation are as different as possible from ordinary atheroma, but correspond precisely with the description of Heubner's cases, which were undoubtedly the subjects of acquired syphilis.
171 Transactions of the Pathological Society of London, 1877, vol. xxviii. pp. 287-291.
In the second case the symptoms were associated chiefly with the cranial nerves. These were nystagmus, paresis of facial muscles, laryngeal spasms, etc. He died at the age of fifteen months. The vessels of the base were extensively diseased as in the other case, and the fourth, [p. 304]fifth, sixth, seventh, and eighth pairs of nerves were smaller by a new growth of a gummatous nature which had produced almost entire atrophy of the nerve-cylinders. There were cicatrices of the liver and spleen. Cases in which the diagnosis rested upon the history, upon the co-existence of undoubted syphilitic symptoms, and upon improvement under specific treatment are by no means rare.
Berkely Hill reports172 a typical case of syphilitic epilepsy. A girl aged nine was the first child of the family that had lived, two having previously been born dead. She presented characteristic teeth, traces of choroiditis, and, while under treatment, suffered from both keratitis and iritis. Her first fit was when she was four years of age, and the attacks had recurred frequently since that time. The convulsion was confined to the left side. The left arm was very weak, the weakness having come on gradually, and being especially great in the extensors of the wrist. Under specific treatment the attacks ceased entirely. In this case there was certainly organic disease, probably a gumma on the surface of the right hemisphere.
172 Op. cit., p. 253.
Other cases reported by the same author, numerous instances of nervous troubles in inherited syphilis reported by Hughlings Jackson,173 Fournier,174 Henoch,175 and Hutchinson,176 warrant the statement, then, that the nervous diseases of inherited syphilis fall into the same general category as those of the acquired disease; that they may appear at any age, from three or four months to that of puberty; that they depend for their production upon a cell-proliferation which, according to its locality, results in the development of new growths, the production of localized meningeal inflammations, or the obstruction and inflammation of arteries; and that the symptoms are those usually associated with such pathological changes, the diagnosis of syphilis depending chiefly on the history and the presence of other specific phenomena.
173 Journal of Mental Science, Jan. 8, 1875; Transactions of St. Andrew's Med. Graduates' Ass., vol. i., 1868.
174 Annales des Derm. et Syph.
175 Nouveau Dict. de Méd. et Chirurgie, p. 885.
176 Op. cit.
The prognosis is more unfavorable than in similar cases in acquired syphilis, the meningeal and vascular lesions being the most frequent and showing themselves very obstinate even under careful treatment. Spinal troubles, chorea, and idiocy have been attributed to inherited syphilis, but must occur with great rarity.
Hill177 reports a case of a child aged five years who had been hemiplegic since he was two and a half years old, and who developed paralysis of the flexors of the ankle in each leg.
177 Op. cit., p. 254.
Keyes reports a case of a boy five years of age, with nodes on tibiæ and other signs of inherited syphilis, who had two attacks of paraplegia.
Hill reports a case of imbecility associated with inherited syphilis, but there is no evidence that it was other than a coincidence.
Fletcher Beach found not more than 1 per cent. of syphilitic children in the Dareult Asylum, and Mr. Mercier could only trace syphilis in 5 out of 220 female idiots, probably imbecile from birth.178
178 Ibid., p. 255.
Hughlings Jackson only found 1 case of inherited syphilis among 80 [p. 305]cases of chorea. The most carefully recorded cases of the latter affection associated with hereditary syphilis are two reported by Alison.179
179 American Journal of the Medical Sciences, July, 1877.
Syphilis of the Spleen.—Disease of this organ in inherited syphilis is especially important from two points of view. It is a valuable aid to diagnosis, and by its size and the degree of persistence of the swelling gives an approximate indication of the severity of the case.
Attention was first called to the frequency and importance of enlargement of the spleen in early hereditary syphilis by Gee in a paper read before the Royal Medical and Chirurgical Society in 1867.180 He gave the histories of thirteen children in support of the statement that such enlargement occurred in almost one-fourth of all cases of hereditary syphilis, sometimes with, sometimes without, enlargement of the liver and lymphatic glands. According to him, the degree of splenic enlargement may be taken as a sort of index of the severity of the cachexia; the majority of cases with great enlargement die, but sometimes such children survive, the spleen gradually diminishing in size as the health improves—not diminishing, however, pari passu with such improvement, but remaining for a long time "a monument of past cachexia."
180 British Medical Journal, 1867, vol. i. p. 435.
Barlow,181 ten years later, thought Gee had rather understated the proportion of cases in which splenic enlargement occurs, he having found it in 22 out of 28 children with definite hereditary syphilis. Birch-Hirschfeld, Eisenschitz, and Tepel182 corroborate these observations, finding that the enlargement is almost invariable and that the spleen is often double its normal size.
181 Trans. of Path. Soc. of London, Jan. 20, 1877.
182 Quoted by Hill and Cooper, op. cit., pp. 164, 165.
Mr. W. J. Tyson has reported183 a cure of a child born of syphilitic parents, in whom, at two years of age, the spleen extended downward three and a half inches, reaching the crest of the ilium and approaching closely to the umbilicus. The liver was not enlarged; the urine was not albuminous. He ordered mercury with chalk, one grain every morning and evening, and one grain of iodide of potassium, with ten minims of syrup of iodide of iron to an ounce of water, three times a day. Sixteen months later the spleen had become imperceptible, and three years afterward the child was in excellent health.
183 The Lancet, Oct. 23, 1880.
The diminution of the liver under treatment appears to take place before there is any diminution in the size of the spleen.184 This persistence of the latter renders it, as has been stated, a valuable diagnostic sign. In the paper already quoted from,185 Macnamara and Barlow allude to this as follows: Enlargement of the liver, although it ought to be noted because it is often present in hereditary syphilis, has but little value as a confirmatory symptom—first, because the liver is proportionally large in infancy, and it is difficult to state the limit of what is actually normal; and, secondly, because other causes besides congenital syphilis lead to its enlargement.
184 Barlow, British Medical Journal, Jan. 20, 1877.
185 British Medical Journal, Dec. 16, 1882.
With regard to enlargement of the spleen the case is different. Gee's observation, that in the early stage of infantile syphilis some enlargement of the spleen occurs in a large number of cases, has been abundantly [p. 306]confirmed. Although with the subsidence of the other symptoms this enlargement often disappears, so that on post-mortem examination two or three months after there may be no trace of it, yet in a few cases it persists, and indeed sometimes increases, so as to be considerable when the other signs have quite vanished. The importance of this sign is greatest when noted early; as, for example, when the child is from two to three months old, for at that period the enlargement of the spleen due to rickets can hardly come into question.
The condition of the spleen during this period of enlargement seems to be simply that of hyperæmia, or at the most of hyperplasia, Gee's, Barlow's, and Birch-Hirschfeld's autopsies showing no evidence of new growth or of amyloid or other changes.186
186 Parrot reports (Le Mouvement méd., Paris, Nov. 23, 1872) two forms of splenic disease produced by inherited syphilis: 1. A simple hypertrophy, which he thinks is secondary to diffuse infiltration of the liver, obstructing the portal circulation and causing the spleen to act as a reservoir; 2. An inflammatory condition resulting in the formation of false membranes around the capsule. His explanation of the first condition is unsatisfactory, because there are numerous cases in which the spleen is enlarged without any involvement of the liver. His other observations have never been confirmed.
The cause seems to me to be in all probability the well-known effect of syphilis on the glandular system in general, and the lymphatic system in particular, to which I believe the spleen is now generally assigned. The analogy between this slow, persistent, painless enlargement preceding the cutaneous symptoms,187 unaccompanied by inflammatory symptoms, unattended by any breaking down of tissue, subsiding slowly but evenly under specific treatment, and the behavior of the buboes of acquired syphilis, is certainly very striking.188
187 Eisenschitz, Wiener med. Wochenschrift, Nos. 48 and 49.
188 A similar enlargement occurs, but much more rarely, in the secondary period of acquired syphilis. Weaver noted it in 3 out of 79 soldiers suffering from early syphilis. Wilks and Moxon report cases in which the average weight was 19 oz.
In most cases of hereditary syphilis there are evidences of disturbance of the gastro-intestinal tract. Vomiting, diarrhoea, colic, anorexia, and emaciation are well-known, but of course not at all characteristic, symptoms.
It has been supposed that the mucous membrane of the entire tract was probably, during the early period at least, and coincidently with the cutaneous eruption, in a condition of hyperæmia and irritation comparable to that of the skin.189 Whether this be so, or whether it is due to associated involvement of the glandular apparatus, has not yet been determined.
189 "There is surely no a priori probability that a blood disease so severe as syphilis should produce lesions on the skin, in the mouth, and in the eye only—that it should, in fact, affect all the visible parts and avoid all the concealed ones" (Mr. Hutchinson, The Lancet, Feb. 6, 1876).
Förster190 has found fibroid degeneration of Peyer's patches in a syphilitic infant who died six days after birth, the glandular structure having been replaced by elevated grayish-red masses of nuclei, cells, and connective-tissue fibre. Ulcers of the intestines have been described, but appear to have had no specific characters.
190 Quoted by Bumstead and Taylor, op. cit., p. 757. His observations were confirmed by Eberth, Roth, and Oser.
The pancreas has been most extensively studied by Birch-Hirschfeld, who examined seventy-three syphilitic foetuses. In thirteen of them he [p. 307]found enlargement of the pancreas with increased weight and density, proliferation of connective tissue, and in some cases compression—almost obliteration—of the lobules, with atrophy and fatty degeneration of their epithelium.191
191 Klebs discovered a gumma in the pancreas of a six-months' foetus.
The peritoneum has been described by Simpson, Von Baerensprung, and others as occasionally invaded in early hereditary syphilis. There seems to be no evidence that it is ever directly affected, the cases in which death occurs from peritonitis being due usually to trouble connected with the liver or spleen.
Syphilis of the lung, originally described by Depaul and Virchow, has been carefully studied also by Förster, Robin, Lorain, and Cornil, from whose description192 of the pathology of the condition I condense the following: In the syphilitic foetus born before term, in the syphilitic child born dead at full term, and in the syphilitic children who live a few days, there are found at the autopsy, in the lungs, nodules or tumors, usually superficial, sometimes deep, hard, isolated or in groups, pink, gray, or red in color, with scattered whitish or yellowish points. Their size varies from a pea to a small walnut. They represent a portion of the lung more or less considerable in a state of special lobular hepatization. Sometimes a whole lobe is involved. The affected portion is very dense and covered with thickened inflamed pleura. The lesions are those of chronic pneumonia. The interlobular connective tissue enters into proliferation and presents a large quantity of embryonal cells; the alveolar walls are thick, while the narrow alveoli are livid, and even filled by epithelial cells, which are of the pavement form in contact with the walls, round in the centre of the alveoli. As the process progresses the epithelial cells become fatty, degenerated, and subsequently broken down and absorbed, while the embryonal interalveolar tissue rapidly organizes into fibrous tissue. Thus results a small fibrous tumor, in which a gumma may ultimately develop.193
192 Syphilis, trans. of Simes and White, Philada., 1882, p. 404.
193 Cornil and Ranvier's Path. Histology, Am. ed., 1880.
It is impossible to confound this syphilitic pneumonia with tuberculosis. The granulations of tubercle are never congenital.
The fact that in syphilitic interstitial hyperplasia the change begins in the interlobular connective tissue and around the interlobular vessels, at first consisting of small spindle-shaped and roundish cells which quickly develop into connective tissue, and the fact that blood-vessels are freely produced among the fibres of this new tissue, seemed, in the estimation of those pathologists who took part in the discussion on visceral syphilis in 1877, to constitute its most distinctive feature.194
194 Trans. of Lond. Path. Soc., vol. xxviii.—views of Green, Jones, Greenfield, Moxon, and others.
Gummata in the lungs of children suffering from inherited syphilis have been described by a number of writers. They appear likewise to begin in the walls of the blood-vessels or the bronchioles. They differ from tubercular nodules in being few in number—not more than half a dozen usually—and are generally confined to one lung.
The condition of the arteries in the few cases in which they have been noticed as affected by inherited syphilis was precisely similar to that found by Heubner in the arteries of adults.195
195 See Cornil, op. cit., p. 305.
[p. 308]The symptoms are very variable; new-born children often die asphyxiated in a few days. If they live longer, the disease develops into a more generalized broncho-pneumonia.
Syphilis of the Larynx.—The hoarse cry of the new-born infant so characteristic of hereditary syphilis depends upon the presence of hyperæmia, of mucous patches, or even of extensive ulceration. I am inclined to think that the first is the more common, as if it were otherwise cases of death from oedema glottidis or other forms of laryngeal obstruction would be oftener met with. When ulceration does exist it is generally, but not invariably, secondary to pharyngeal ulcers.196
196 See synopsis of six cases of George M. Lefferts, reported in Bumstead and Taylor, op. cit., p. 754.
Bronchial catarrh, giving rise to cough, and sometimes to considerable embarrassment of respiration, is a not infrequent complication of laryngeal syphilis.197
197 Schnitzler, Die Lungen Syphilis, etc., 1880, S. 41.
Later troubles of the larynx in connection with inherited syphilis have not yet been carefully enough studied to warrant us in drawing any distinction between them and the usual symptoms seen in the acquired disease.
Syphilis of the testicles has been studied by Henoch,198 Cornil,199 Parrot,200 Hutinel,201 North,202 Bryant,203 and others. It is found to consist of a true interstitial orchitis, very closely resembling that seen in the syphilitic testicles of adults. Hutinel's investigations, based on ten cases, showed the testicles slightly enlarged and harder than normal, the scrotum pendent, the epididymis normal, the tension of the tunica vaginalis and tunica albuginea slight. The basis of the lesion is in a collection of small round embryonal cells resembling lymph-cells, arranged in the connective tissue around the arterioles which come from the tunica albuginea. This may be accompanied by a more or less marked diffused interstitial orchitis, or there may be only a thickening from the new formation of small round cells on the connective tissues of the testicles. Cornil found the seminal ducts separated by numerous round or fusiform cells. The disease usually occurs at from two months to three years of age; both testicles are generally involved, and are enlarged, hard, inelastic, and frequently nodulated. Mercurial treatment generally causes a marked improvement unless the inflammation has already resulted in the development of a new fibroid formation, in which case it would be likely to remain unaffected by any form of treatment. Inunctions with diluted mercurial ointment, iodoform, etc. are useful adjuvants.
198 Schmidt's Jahrbuch, 178, No. 4.
199 Op. cit., p. 420.
200 Rev. mens. de Méd. et de Chir., Paris, Feb., 1878.
201 Ibid.
202 Med. Times and Gaz., Lond., 1862, vol. i. p. 403.
203 Ibid., Dec., 1863.
The kidneys are not infrequently involved in inherited syphilis. Parrot reports the pathological change to consist of a proliferation of small round cells in the intertubular connective tissue, followed by contraction, obliteration of the tubules, and degeneration of their epithelium.
Bradley has reported204 the case of a child aged four months in whom a well-marked syphilitic eruption and an attack of acute Bright's disease were coincident. Mercurial treatment for three weeks cured both.
204 British Med. Journ., Feb. 4, 1876.
Coupland has reported two cases of parenchymatous nephritis associated with inherited syphilis, but advances no proof that it was not an accident. [p. 309]Gummata have been from time to time found in the kidneys of very young children who have died from their effects and from other visceral lesions due to syphilis.205 Cases of enlargement, of fibroid, fatty, and gelatinous degenerations of the suprarenal capsules, have been recorded.
205 See discussion in Clinical Soc. of London, Jan., 1880; "Remarks on Visceral, and especially on Renal, Syphilis," by Barthelémy, Annales de Derm. et Syph., April, 1881.
The thymus gland is occasionally found in syphilis to have undergone alterations claimed by Dubois, Depaul, and others to be syphilitic in their nature, but ascribed by Parrot simply to degenerative changes due to malnutrition. The gland does not appear to undergo any marked alteration in size, color, or consistency, but is found after death to contain a small quantity of purulent matter.
The tendency of syphilis is certainly not, as a rule, to the formation of pus. Nearly all the lesions we have studied with the exception of breaking-down gummata have consisted in various forms of cell-proliferation or accumulation, and not in the formation of abscesses, and it is not probable that this is an exception. I doubt very much the syphilitic character of these changes.206
206 Lancereaux believed that it was due to the breaking down of a gummy deposit, but that seems to be entirely hypothetical, none having been discovered. Weisflag (quoted by Bumstead) arrives at the following conclusions after studying the lesion and the literature of the subject: 1. This thymus abscess does exist. 2. When associated with other signs of congenital syphilis it indicates that the father or mother of an infant suffers or has suffered from syphilis. 3. It is possible, but not proved, that this affection may exist in children in whom there are no symptoms of syphilis, but its existence renders the diagnosis of hereditary syphilis probable, even if the disease of the parent is not proved. 4. Such is the great similarity in the appearance of pus and of the secretion of the thymus that they cannot always be distinguished.
THE DIAGNOSIS AND PROGNOSIS OF INHERITED SYPHILIS.—In reviewing the general course of a case of inherited syphilis it seems evident that the differences between it and the acquired disease which have been so much dwelt upon are apparent rather than real.207 The primary stage is of course missing, and on any theory of the essential nature of syphilis this is readily comprehensible. Whether the chancre is the first symptom of a constitutional disease, or, as I believe to be the case, is the simple accumulation at the point of original inoculation of the cells which constitute the syphilitic virus—or are at any rate its carriers—it would naturally be in the first case undiscoverable, in the second nonexistent.
207 "That the noteworthy differences between chancre-syphilis and the inherited disease are to be interpreted by considerations of the tissues of the growing child and the adult, is made very probable by what is observed when a mother near the end of pregnancy becomes infected with primary disease. In such a case the foetus nearly full grown acquires the disease, without a chancre, directly from the maternal blood. It is acquisition, not inheritance, for at the date of conception both the paternal and maternal elements were free from taint, and during the first six, seven, or even eight months of intra-uterine life the foetus remained healthy. Yet, as I have proved elsewhere by citation of cases, syphilis obtained in this peculiar method resembles exactly that which comes by true inheritance, and not that which follows a chancre. This important fact goes, with many others, in support of the belief that the poison of syphilis remains identical, however obtained, and that the differences which are so patent in its manifestations are due to differences in the state of its recipient" (Mr. Hutchinson, article on "Transmission of Syphilis," Brit. and For. Med.-Chir. Rev., Oct., 1877, p. 475).
"It is not true that the diversity of symptoms presented by infants authorizes us to admit a congenital and an hereditary syphilis. Whatever the mode of infection, it is impossible to make this distinction" (Ricord, note to John Hunter's Works, 1883).
The secondary stage, characterized in the acquired form chiefly by [p. 310]lymphatic engorgement and symmetrical, widely-spread, polymorphic cutaneous and mucous eruptions, and pathologically by a marked tendency to the proliferation of certain new small round nucleated cells, upon the presence of which depend all the manifestations of the disease, is in inherited syphilis strictly analogous. Eruptions of the same character make their appearance, differing only in minor points, as in a greater tendency to become moist or ulcerated, due to the more delicate texture of the infantile epidermis. To the same cause must be assigned the macroscopic peculiarities of the only syphiloderm said to be peculiar to infantile syphilis—pemphigus—which has been shown, however, to have a papular basis, and in that way to conform to all the other secondary eruptions.
The lymphatic engorgement either exists in the infant as in the adult or has its analogue in the enlargement of the spleen and liver—especially the former, which is almost as constant a phenomenon as is general glandular enlargement in acquired syphilis. The same pathological changes occur, the same infiltration of cells producing, according to their situation, papular, pustular, or mucous patches, or inflammation of such structures as the iris, choroid, or retina.
The tertiary stage, except in the fact that its phenomena may appear unusually early and may be commingled with those of the secondary period,208 does not widely differ in the hereditary from that of the acquired disease. It affects the same tissues, results in the same pathological formations, and is preceded by the same period of latency or quiescence of variable duration. There is no reliable evidence with which I am familiar to show that in this stage inherited syphilis is either contagious or transmissible—another point of close resemblance between the two varieties under consideration.
208 This is by no means unknown even in the acquired form; frequent examples of it have been recorded, and it can be readily explained either on the theory of relapses in parts previously diseased (Hutchinson), or on that of obliteration of lymphatic trunks and accumulation of nutritive waste (Otis).
In considering the question of diagnosis, therefore, we have an excellent guide in the fact that the disease conforms in most respects to the general laws of acquired syphilis, and that our knowledge of the latter affection will be a valuable aid to recognition of the former.
The chief elements of diagnosis and prognosis of inherited syphilis in its various stages may then be summarized as follows:
A history of syphilis in either parent is important just in proportion to the shortness of the interval between the time of infection and the date of conception. In other words, the shorter that interval the more likely (a) that the child will have syphilis, (b) that it will have it in a severe or fatal form. If the mother has been syphilitic and the father healthy—which is rare—it is perhaps more likely that the child will be diseased than when the reverse is the case. If both parents were syphilitic at or before the time of conception, the probability that the disease will be transmitted, and in a severe form, is much increased. There is no evidence to show that inheritance from one parent results in a graver variety of the disease than when it is derived from the other.
A history of abortion or miscarriage on the part of the mother should have weight in the determination of any given case, and if such accidents [p. 311]have been very frequent their diagnostic importance is greatly increased. The loss of elder brothers or sisters and the causes of death, with the precedent symptoms, should be carefully inquired into. The nearer either of these occurrences—abortion or death of elder children, if there is a fair presumption that they were due to syphilis—has been to the birth of the patient in question, the greater the likelihood that the latter has been infected.
Upon examining the product of abortion or stillbirth the most easily observable symptoms will be those of the skin. Maceration and elevation of the epidermis into bullæ are in themselves hardly characteristic, though they may—especially the latter—be regarded as suspicious. If the cutaneous lesions are, however, distinctly papular or pustular or ulcerative, or if the bullæ have all the characteristics of syphilitic pemphigus, the diagnosis is assured.209
209 "It is probable that very early abortions are less rare than statistics indicate, but are often unsuspected."
"It is impossible to demonstrate the existence of syphilitic lesions in foetuses expelled during the first months of pregnancy. Later, the signs which have the greatest value are the lesions of the epiphyses of the long bones. When the foetus has nearly arrived at full term, and is not macerated, visceral and cutaneous lesions may be observed. According to Mewis, the skin eruptions cannot be seen before the eighth month, and are only recognizable on foetuses whose death has been very recent or who are born living. Pulmonary lesions may be determined at the end of the sixth month. Those of the pancreas are met with in about half the foetuses which perish a little before or a little after birth. The lesions of the liver, the spleen, and the bones may be recognized even in macerated foetuses, this frequency increasing from month to month" (Nouv. Dict. de Méd. et Chir., vol. xxxiv. p. 864).
The most distinctive symptom—one which may really be considered as pathognomonic, is, however, the inflammation of the diaphyso-epiphysial articulations, with or without their disjunction. Distinct enlargement of the spleen or liver, and arachnitis with hydrocephalus, are valuable diagnostic points, and the presence of gummata—not very infrequent—would of course be conclusive.
At birth the syphilitic child may be small, stunted, emaciated, weazened, senile in appearance; this would properly give rise to suspicion, but may be associated with any disorder of nutrition on the part of child or mother. It may also disclose cutaneous or mucous eruptions evidently specific in character. The most common of these at this early date is the bullous eruption affecting the palms and soles, sometimes distributed over the whole body, and, as it indicates a feeble resistance of the tissues to the tendency to exudation and cell-growth, is usually a precursor of an early and fatal termination. In any event, marked symptoms at time of birth render the prognosis highly unfavorable.
It is quite as common, however—perhaps more so—for the subject of hereditary syphilis to give no evidence of the disease at birth, but even to appear healthy and well-nourished. In such cases the first symptoms of the disease appear, on an average, in from six weeks to two or three months, and consist principally of coryza (snuffles), hoarseness of voice, and syphilodermata. The latter may be macular, papular, pustular, or bullous. They are usually polymorphous, irregular in shape, dark coppery-red in color, with sometimes a glazed or crusted, but oftener a moist or ulcerating, surface, with a strong tendency to coalesce into large patches, or to form irregular serpiginous ulcers, or to take on hypertrophic growth [p. 312]and develop into condylomata. Eruptions which are squamous and are situated about the mouth and chin and on the body, the legs, or the soles of the feet, though exceptional, are of more value than those on the nates, where the results of irritation from urine and feces may closely simulate syphilodermata.
Mucous patches on the tongue, cheeks, tonsils, and pharynx are common, often extending to the larynx, increasing the hoarseness, and to the nasal cavities, aggravating the snuffles. Both of these occurrences, by interfering with the respiration of the child and rendering its nursing interrupted and insufficient, greatly add to the gravity of the case. Enlargement of the spleen (common), enlargement of the liver (less so), and iritis (rare), may be mentioned among the phenomena of this stage, often associated with the skin eruptions.
About the time of the subsidence of the rash there may be developed the specific inflammation at the junction of epiphyses and diaphyses which produces a swelling of the long bones near their ends. The child will be noticed to cry a little when, for example, the wrist or elbow on one side is washed, and not to use these joints as much as the corresponding ones on the other side. The parts are not hot, only slightly tender, and as yet there is but little swelling. Later, the droop and the disuse of the affected limb become more noticeable and simulate infantile paralysis. There is, however, no wasting, no alteration of reaction by faradism, no real loss of power, so that the term pseudo-paralysis is an appropriate one. In a week or two similar symptoms will occur in the bone on the opposite side, and finally the ends of all the long bones may be affected; ordinarily the elbows, wrists, knees, and shoulders are the joints involved. Suppuration is rare, disjunction of the epiphysis from the diaphysis common. Recovery is apt to take place spontaneously within a month. The associated changes are chiefly endosteal at the junction of the shaft with the epiphysis, but there is also a little periostitis or perichondritis, which is the principal cause of the external swelling. Moderate deformity may ensue.210
210 For the diagnosis from rickets see p. 290.
Similar changes occurring in the cranial bones give rise to what has been called the natiform skull. During the first year it is very common for syphilitic children to develop a number of lenticular swellings on the cranium, which appear symmetrically around the anterior fontanel, but at a little distance from it; i.e. one on each frontal and one on each parietal bone. These are said to be "bossed." They are at first circumscribed, and in a child nine or ten months old often measure three-quarters of an inch to an inch in diameter. They are at first circular, afterward more irregular, and finally tend to organize, becoming diffused and massive and causing a permanent thickening of the skull.
These symptoms which have been described are the prominent ones occurring during the first six or eight or twelve months of life. If they do not manifest themselves before the eighth month, it is highly probable, even in a case with a syphilitic parental history, that the child will either escape altogether or that the secondary stage has been very slight and altogether intra-uterine and unattended with noticeable phenomena. If during this first year the child's cachexia is marked, if there are any intercurrent diseases, if the symptoms show themselves early, if the nasal or laryngeal affection is severe, if the eruptions are markedly bullar or [p. 313]pustular or ulcerative, if the enlargement of the spleen is great or the osseous lesions precocious or grave, and if, especially, there is any intermingling of tertiary symptoms, gummata, nodes, etc.,—the prognosis will be unfavorable.
From adolescence on through adult life the diagnosis of inherited syphilis will depend on the following points: First, of course, the history of parental or of infantile syphilis, or of both. Then a group of physical and physiognomical peculiarities, which are not definitely characteristic, and are of little value when taken separately, but are of considerable importance when all or a majority are present in any given case. These are low stature or puny development proportionate to the severity of the intra-uterine and infantile symptoms; a pasty, leaden, or earthy complexion,211 a relic of previous syphilodermata, probably also a result of malnutrition; a prominent forehead, bulging in the middle line at and within the frontal eminence, and due either to thickening of the skull or to a previous arachnitis and hydrocephalus before the ossification of the fontanels; a flat, sunken bridge to the nose, due to the coryza of infancy extending to the periosteum of the delicate nasal bones, and either interfering with their nutrition or partially destroying them; dryness and thinness of the hair, with brittleness and splitting of the nails; synechiæ and dulness of the iris (rare); ulcerations of the hard palate;212 and periosteal thickenings or enlargements of the shafts of the long bones near the ends, or slight angular deformity, results of the osteo-chondritis of infancy.
211 Trousseau (Clinical Lectures, vol. ii. p. 588, Philada., 1873), after calling attention to this peculiar hue of the face, says: "It not unfrequently happens that the physician, taught by long familiarity with this appearance, will almost at once diagnose syphilis after having simply seen the child's face, although the peculiar hue can be but vaguely described in words. The visage presents a special shade of bistre; it looks as if it had been lightly smeared with coffee-grounds or a very dilute aqueous solution of soot. There is neither the pallor, the icteric hue, nor the straw-yellow tinge of skin seen in other cachectic affections; the tinge is not nearly so deep, but is almost like that of the countenance of a recently-delivered woman, and either does not extend at all, or only partially, to the rest of the body. I know no disease except syphilis in which a child's skin has this peculiar color; and consequently, when it is well marked, it has more diagnostic value than any other symptom."
212 Mr. Oakley Coles reports (Proc. of Path. Society of Great Britain, vol. vii. p. 5) several cases of inherited syphilis in which there was wide separation of the jaws in the median line. In one family one member had typical teeth and wide separation; three others had the same separation, but not the characteristic teeth. It was suggested that in such cases the teeth were in size far below the average, and that the condition was that often observed where the jaws are in development in excess of the teeth which they contain. I. E. Atkinson details some interesting cases of this lesion in late hereditary syphilis, and attributes to it considerable diagnostic importance (American Journal of the Medical Sciences, New Series, vol. lxxvii., Jan., 1879, p. 71).
A much more valuable group of symptoms, however, are the following, which are mentioned in the order of their importance, any one of the first three being almost or quite conclusive:
Dwarfed permanent median upper incisors, broader at the top than at the cutting edge, which is crescentically notched, separated by an undue interval and converging toward each other.
Evidence of past or present interstitial keratitis—a dusky and thin sclerotic in the ciliary region and slight clouds here and there in the corneal substance, there being no scars on its surface—or of disseminated choroiditis; patches of absorption especially around the periphery.
[p. 314]A radiating series of narrow cicatricial scars extending right across the mucous membrane of the lips, or a network of linear cicatrices on the upper lip and around the nostrils, as well as at the corners of the mouth and on the lower lip.
Periosteal nodes on one or many of the long bones; sudden, symmetrical, and complete deafness, without otorrhoea and unattended by pain or other subjective symptoms.213
213 In a few instances there has been noticed an arrest of sexual development; in one case of Hughlings Jackson's there was such an entire absence of all sexual characteristics that it was supposed that the ovaries had been destroyed by syphilitic inflammation in early life.
Late or tardy hereditary syphilis is rarely dangerous to life. The prognosis is almost unvaryingly favorable unless some grave visceral complication, such as interstitial pneumonia, gummata of the brain, liver, or kidney, or meningeal and periosteal inflammation within the cranium, should occur.
TREATMENT.—The prophylactic treatment, or that directed to the health and sexual relations of the parents previous to conception, has already been sufficiently considered. That of the mother during pregnancy, after having conceived from a syphilitic husband, or having had antecedent syphilis, or having contracted it by direct contagion subsequent to impregnation, is simply that of acquired syphilis in either adult or child. Mercury in its full physiological dose is the drug indicated. It may not be amiss to combine with it iodide of potassium in moderate doses, but the practice of employing the latter to the exclusion of the former is both theoretically and clinically unsound. Care should especially be taken to give it in such a manner, either by inunction or vaporization or so guarded with opium, that it will not produce any irritating effect on the intestinal canal, the sympathy between which and the uterus may, in the event of a strong purgative action being set up, lead to an abortion.214
214 "In respect to prophylaxis as applied to infants, all chances of infection should be entirely removed whenever constitutional symptoms exist or the nature of the primary symptoms renders them probable. Our caution should be carried still farther, and in the absence of all appreciable symptoms we should assure ourselves by the antecedents, so far as possible, that the parents are not under the influence of a syphilitic diathesis; in which case they may give birth to infected infants until appropriate treatment shields the latter from infection. With still stronger reasons, when the mother during pregnancy is affected with primary syphilitic symptoms of such a character as to give rise to secondary symptoms, or if the latter already exist, we should hasten to cope with them, and, far from regarding pregnancy as a contra-indication to treatment, should recollect that it generally prevents the disease in the infant, and when skilfully administered obviates the frequent abortions which syphilis excites. When primary symptoms have been contracted by the mother a short time before delivery, since the infant may be infected in its passage into the world, the same course should be followed with it as with a person who has just exposed himself to an impure connection" (Ricord, note on prophylaxis of venereal disease appended to his edition of John Hunter's Treatise on Venereal, Philada., 1853, p. 481).
As we have seen that the pathology, the stages, and the general course of hereditary syphilis are all closely related to or identical with the same phenomena in the acquired disease, and so know that they both depend upon the same ultimate cause, whatever that may be—a virus, a fungus, or a degraded cell—it follows that the same principles should govern us in the treatment of the one as in that of the other.
We know from clinical experience that mercury exercises an almost [p. 315]controlling influence over the secondary manifestations of acquired syphilis, whether by acting as a true antidote or as a tonic, or by virtue of its property of hastening destructive metamorphosis and thereby facilitating the absorption or elimination of new cell-growths. We know also that iodide of potassium, probably by virtue of its powerful stimulating influence on the lymphatic system, has an equal power over the tertiary growths, which by their pressure upon or situation in important tissues or organs may be so destructive. There is no reason, therefore, by analogy why these drugs should not, comparatively speaking, be equally beneficial in hereditary syphilis; and such is, indeed, found to be the case. In the latter affection, however, there are two elements which should modify the treatment somewhat, and must be taken into consideration. These are—1st. The existence of a more or less profound cachexia influencing all the nutritive and formative processes, and in itself, entirely apart from any definite specific involvement of vital organs, threatening life. 2d. The not infrequent occurrence during the secondary period of symptoms—notably gummata—belonging to the tertiary stage.
The first indication is met by making the treatment from first to last not only antisyphilitic, but also supporting or even stimulating; and with this object in view especial attention should be paid to nutrition. It may be stated, axiomatically, that for every reason, whenever it is within the bounds of possibility, the nurse of a syphilitic child should be its mother. To her it is harmless—to every other woman, not already syphilized, it is in the highest degree dangerous. Space will not permit me here to discuss the medico-legal aspect of the interesting question as to relations between such children and the outside world, especially as represented in their nurses. It will suffice to say that it is criminal and legally punishable to induce any healthy woman to act as wet-nurse to a syphilitic child unless she does so with a full knowledge of the risks she runs in undertaking that function. In the rare cases where with such information she still consents to suckle the child a written statement of the facts of the case should be signed by her, with the proper legal formalities, for the protection of the physician and the family.
If the mother has died or on account of ill-health is unable to nurse her child, and if no wet-nurse willing to enter the above agreement can be obtained, the possibility and propriety of obtaining one who has already had syphilis must next be considered. This idea to many parents seems revolting, but will naturally be less so to those who have themselves had the disease, and is, besides, so almost vitally important to the child that no hesitation should be felt about making the suggestion. If it is accepted, and if there is any opportunity for making a selection, it may be said that the more robust the present condition of such a nurse, and the more remote the date of her syphilis, the better will be the chances of the child.
If neither mother nor wet-nurse can be had to suckle the child, it must be fed by cow's, goat's, or ass's milk or by artificial alimentation; but its prospect of life will be greatly, immeasurably, reduced. In addition to careful feeding a little careful tonic treatment should from the first be employed in conjunction with the specific remedies, iodide of iron, cod-liver oil, and preparations of the phosphates being the most useful drugs.
The existence of the second condition, which, as I have stated, exercises a modifying influence upon treatment—the early appearance of tertiary [p. 316]symptoms—is probably due in many cases at least to an overwhelming of the lymphatic system by the new cell-growth, which not only greatly increases the amount of material to be transported by the lymphatics, but at the same time, by invading their walls and diminishing their lumen, greatly cripples them. Accumulations of nutritive matter and of these new cells then take place, forming the characteristic new growths or deposits which we call gummata. This leads us to combine with the mercury from the beginning, at least in all cases where bony or periosteal involvement, suppuration, or the existence of gummata points to this condition, small doses of iodide of potassium or of some other soluble and easily decomposed iodine salt.
The principle of treatment being thus recognized, the routine procedure may be thus described: Give mercury as soon as the diagnosis of syphilis is assured—preferably by inunction. Sir Benjamin Brodie's opinion, expressed many years ago, still represents that of the profession:215 "I have tried different ways of treating such cases. I have given the child gray powder internally and given mercury to the wet-nurse. But mercury exhibited to a child by the mouth generally gripes and purges, seldom doing any good, and given to the wet-nurse it does not answer very well, and certainly is a very cruel practice.216 The mode in which I have treated cases for some years past has been this: I have spread mercurial ointment, made in the proportion of a drachm to an ounce, over a flannel roller and bound it around the child once a day. The child kicks about, and, the cuticle being thin, the mercury is absorbed. It does not either gripe or purge, nor does it make the gums sore, but it cures the disease. I have adopted this practice in a great many cases with signal success. Very few children recover in whom mercury is given internally, but I have not seen a case where this method of treatment has failed."
215 Clinical Lectures on Surgery, Philada., 1846, p. 230.
216 This, the so-called indirect method, is altogether unreliable, and should only be employed as a forlorn hope in those cases where in every other way mercury sets up gastro-intestinal irritation.
When, for any reason, as irritation of the skin, this cannot be employed, probably the best form of giving mercury by the mouth is in the following formula:
| Rx. | Hydrarg. cum Creta, | gr. j to vj. |
| Sacch. alb. | gr. xij. | |
| In M. ft. chart No. xij. | ||
S. One powder three times a day, to be taken soon after nursing.
Iodide of potassium may be given separately in a syrupy solution in doses of a half-grain to a grain, or if there are any marked tertiary symptoms even in much larger doses, three or four times daily.217 [p. 317]Treatment should, of course, be continued long after the disappearance of syphilitic symptoms, and it would probably be well to continue the mixed treatment intermittently until after puberty.
217 Wm. Campbell of Edinburgh was in the habit of commencing with doses of a quarter of a grain of calomel and two grains of creta præparata, once daily for the first ten days. He afterward progressively increased the calomel to a quarter of a grain twice each day. Sir John Rose Cormack says (Clinical Studies, vol. ii. pp. 423, 424, London, 1876) that an infant six weeks old will generally bear these doses well. In cases where they do not, he was in the habit of ordering a solution of half a grain of the bichloride in three ounces of distilled water and one ounce of syrup—one to two teaspoonfuls every six, eight, or twelve hours. When he used mercurial "swabbing" he employed from one to four drachms of unguent, hydrargyri to the ounce of lard. He alternated this treatment with short courses of the syrup of the iodide of iron, and continued the treatment up to the period of dentition. He says he has generally obtained excellent results by these methods.
With the treatment of special symptoms the general practitioner has little concern. The cases of visceral syphilis in very young children are generally fatal. Those that recover do so in response to the active use of the above remedies. Later, the prognosis is more favorable, the treatment the same. Of course moist eruptions should be dusted with some astringent or absorbent powder; mucous patches should be cauterized; and great attention should be paid to avoidance of sources of cutaneous irritation—frequent changing of diapers, etc.—but the general methods are the same as in the adult.
DEFINITION.—Inflammation of the interior of the mouth.
The term Stomatitis is used to designate inflammatory affections of the mucous membranes of the structures of the interior of the mouth, including thus the mucous membrane of the lips, gums, tongue, cheek, palate, and anatomical adnexes. Inflammatory affections of the mucous membrane of the palate, palatine folds, and tonsils are usually described more particularly under the heads of angina, sore throat, and tonsillitis.
Stomatitis occurs idiopathically, deuteropathically, and traumatically.
Several varieties of stomatitis occur, sufficiently characteristic to require separate description: viz. erythematous or catarrhal, aphthous or vesicular, folliculous or glandular, pseudo-membranous or diphtheritic, ulcerous, gangrenous, cryptogamous or parasitic, and toxic.
Simple, superficial, erythematous, or catarrhal stomatitis; pultaceous stomatitis.
DEFINITION.—A simple inflammation or erythema, general or partial, of the mucous membrane of the interior of the mouth.
It occurs both in adults and in children, and may be primary or secondary, acute or chronic. In adults and adolescents it accompanies catarrhal and ulcerous affections of the throat, and is described, therefore, to a certain extent, in connection with these affections.
SYNONYMS.—Ordinary or common diffuse Inflammation of the mouth; Erythema of the mouth; Oral catarrh.
ETIOLOGY.—In many cases of catarrhal stomatitis, both in adults and in children, the affection is of obscure origin and the cause eludes detection. In the great majority of instances the cause lies in some irritation of the alimentary tract, whether local or at a distance.
The local causes, which are by far the more frequent, include every variety of topical irritation to which the oral mucous membrane is in itself liable or to which it may be subjected. Thus, irritating foreign substances taken into the mouth; unduly heated, unduly iced, or unduly spiced food and drink; the excessive use or abuse of tobacco and of stimulants; contact of acrid and corrosive acid and alkaline mixtures; [p. 322]the constitutional action of certain medicines, particularly mercury, but likewise bromine, iodine, arsenic, antimony, and, to a slighter extent, other medicinal substances also; inspiration of irritating dust, gases, vapors, steam, and smoke; even hare-lip, cleft palate, and congenital or acquired deformities of the mouth generally,—may all be included in this category.
In the newly-born a special hyperæmia of the mucous membrane has been cited (Billard) as the cause.
Morbid dentition is the most frequent local cause of catarrhal stomatitis in children, but it is an occasional cause in adults likewise. Hence it is frequent from the sixth to the thirtieth month of life; again, between the ages of six and fifteen years, the period of second dentition; and likewise between the eighteenth and twenty-second years, the period for the eruption of the last molars. Deformed, carious, and broken teeth, improper dentistry, wounds and ulcerations of the gums, negligence in cleansing the teeth,—all these contribute their quota as exciting causes. Nurslings occasionally contract the affection from the sore nipples of their nurses. In some instances they acquire it by protracted sucking at an exhausted breast. Protracted crying, from whatever cause, sometimes induces catarrhal stomatitis, not only in nursing children, but in older ones. Prolonged or too frequent use of the voice, whether in talking, reading, singing, or shouting, may be the exciting cause.
Distant irritations of the alimentary tract, exciting catarrhal stomatitis, include stomachic and intestinal derangements of all sorts. Poor food and lack of hygiene on the one hand, and over-feeding, excess of spices, alcohol, and tobacco on the other, are not infrequent exciting causes. Undue excitement, excessive mental emotion, unrestrained passion, deranged menstruation, normal and abnormal pregnancy and lactation, sometimes incite the affection. Slight colds from cold feet or wet clothing give rise to catarrhal stomatitis. It likewise presents as an extension from coryza, sore throat, glossitis, tonsillitis, pharyngitis, and laryngitis.
Deuteropathic or secondary catarrhal stomatitis occurs in various febrile diseases, especially the acute exanthemata—measles, scarlet fever, small-pox; in syphilis, in pulmonary tuberculosis, and in long-continued chronic pneumonia.
Infantile stomatitis is most frequent between the ages of two and twelve months; the stomatitis of adolescents at the periods of dentition; and that of adults when local sources of irritation predominate.
SYMPTOMATOLOGY.—The symptoms in catarrhal stomatitis vary in severity with the intensity and extent of the inflammatory processes.
In the infant the subjective symptoms usually commence with restlessness, fretfulness, and crying. Unwillingness to nurse or inability to do so soon becomes manifest. The child may seize the nipple eagerly with a firm grasp of the lips, but at the first suction lets it drop away with a cry of pain and disappointment. The cause of the pain is made evident on inspection and palpation of the interior of the mouth. The parts are dry, glazed, hot, and tender. So hot is the mouth at times that its heat, conveyed to the nipple in suckling, is sometimes the first intimation of the existence of the malady. Similar conditions often prompt an older [p. 323]child to refuse the teaspoon. This sensitiveness is observed in the tongue and on the inner surface of the cheeks. It increases during movements of the tongue and jaw. Deglutition becomes painful, especially when the food tendered is rather hot or rather cold. There is a grayish-white accumulation of partially detached epithelium on the tongue, sometimes in longitudinal strips, sometimes in a continuous layer. Should the stomatitis be due to dentition, the affected gums will be swollen, hot, and painful. There is usually an augmentation of the secretions in the mouth. Sometimes they flow from the mouth in great quantity, inflaming the lips. These secretions acquire an increased viscidity, so that they become adherent in clammy masses to the tongue, the gums, and the lips. Taste thus becomes impaired, while decomposition of these masses in sitû imparts fetor to the breath; the odor being especially pronounced when the child awakens from a night's sleep, the secretions having accumulated meanwhile more rapidly than they could be discharged. When the secretions of the mouth are not excessive there may be merely a faint mawkish odor to the breath, sweetish in some instances, sour in others. Loss of appetite is usual. Diarrhoea sometimes exists to a moderate degree, attended at times by gaseous distension of the intestines.
In severe cases dependent on morbid dentition swelling of the submaxillary glands and infiltration of the connective tissue may take place. More or less pyrexia becomes evident. In some instances convulsions supervene; either directly from cerebral hyperæmia, or in reflex manner from irritation of the sensitive gingival nerves.
In the adult impairment of taste is one of the earliest subjective symptoms. This symptom is usually accompanied or else closely followed by peculiar viscid and sticky sensations about the tongue, gums, and palate—sensations that excite vermicular motions of the lips and tongue to get rid of the foreign material by expectoration or by deglutition. The taste is usually a bitter one, and the viscid sensations are usually due to accumulations of desquamated epithelium upon the tongue and other structures. An unpleasant odor is sometimes exhaled, the result of decomposition of the excessive secretions.
In the chronic form of the affection, especially as it occurs in the adult, the alterations of taste, the saburral coatings of the tongue, and the fetor of the breath are more marked than in the acute form.
The mucus accumulating during sleep often awakens the patient in efforts at hawking and spitting to detach and expectorate it. These movements are occasionally so violent as to provoke emesis. The disagreeable odor from the mouth is almost continuous.
In uncomplicated cases there is no loss of appetite or impairment of digestion. The presence of these symptoms is presumptively indicative of gastric disease, usually ulcerous or carcinomatous.
The course of the disease varies according to the causes which have given rise to it. When these subside, the stomatitis soon ceases; when they are irremediable, the stomatitis remains incurable. No special period can be mentioned, therefore, for its duration. It terminates, when cured, in complete restoration of the parts to their normal condition. There are no special complications or sequelæ.
PATHOLOGY AND MORBID ANATOMY.—The hyperæmia of the [p. 324]tissues, physiological during the entire process of dentition, is readily provoked into a pathological hyperæmia. Whatever the origin, however, acute catarrhal stomatitis begins, usually, with congestion and tumefaction of the oral mucous membrane. The congestion is sometimes preceded by pallor, as though anæmia from constriction of the capillaries were the initial step in the phenomena. The congestion and swelling are more rarely diffuse than circumscribed; i.e. confined to certain portions of the tissues, especially the gums, which become swollen and painful to contact. The surface is dry and glistening, and the secretion diminished. The mucous membrane is raised in patches here and there where the submucous tissues are the most lax. These patches, irregular in size and configuration, are seen on the tips and edges of the tongue, on the inner surface of the cheeks, at the gingival junctions of the jaws, around the dental margins of the gums, about the angle of the mouth, and on the palate. Sometimes the patches coalesce—to such an extent in rare instances as to cover the entire mucous membrane even of the palate and the gums. Their margins are bright red, their centres yellowish. These elevated patches are due to local accumulation of new-formed cellular elements, perhaps determined by the distribution of capillaries or lymphatics. Intensification of the inflammatory process around or upon them, giving rise to a more abundant cell-proliferation, sometimes occurs; the results presenting macroscopically in ridges or welts of a vivid red, surrounding the patches or traversing them.
The tongue undergoes engorgement, and becomes increased in bulk; exhibiting dentated facets along its edges and around its tip, due to the pressure sustained from the adjoining teeth. Opposite the lines of junction of the two rows of teeth the impression is double. The dividing lines separating the facets project a little, and are opalescent, grayish, or whitish, owing to increased proliferation of epithelium. Similar dentate impressions from a like cause may be seen on the inner surfaces of the cheeks.
The hyperæmia of the parts is soon followed by excessive production of new cellular elements, rendering the now increased secretions turbid; so that the surfaces of the tongue and cheeks become moist again, and covered with a grayish-white, pultaceous form of desquamated epithelium, but slightly adherent, and therefore readily detached by movements of the tongue, lips, and cheeks. In some instances the epithelium becomes raised into minute vesicles, and chiefly on the edges of the tongue, thus presenting a sort of lingual herpes. Excoriations, and even shallow ulcerations, may follow.
Isolated lesions occur. There may be congestion of the palate without tumefaction, its epithelium undergoing detachment in shreds. The congested patches at the dental margins of the gums may become overlaid by opalescent masses of desquamated epithelium, followed by their actual ulceration, and even by detachment of the teeth.
In children the lips may be swollen and excoriated or surrounded by an eruption of herpes. Profuse salivation may occur in a child a few months old when the affection becomes protracted. Febrile movement is rare before the fifth or sixth month.
In chronic stomatitis the tumefaction is usually greater, with distension of the capillaries and hypertrophy of some of the mucous follicles, [p. 325]especially those upon the cheeks and palate. There is also hypertrophy of the lingual papillæ, especially those at the tip of the tongue. Adherent to the gums and the tongue is a yellowish tenacious mucus, composed of squamous epithelia, fat-globules, bacteria, and the usual débris of disorganization. The saliva is secreted in unusual quantities, and sometimes dribbles more or less continuously.
DIAGNOSIS.—Recognition of the conditions described under the head of Pathology and Morbid Anatomy, in the presence of the symptoms described under Symptomatology, renders the diagnosis easy.
Chronic stomatitis may be mistaken for mere indication of gastric catarrh, which is likewise attended with loss of appetite, fetor of breath, and coating of the tongue.
PROGNOSIS.—The prognosis is favorable in almost every instance, recovery being almost universal in the acute form. Stomatitis of dentition subsides with the physiological completion of that process; stomatitis of exanthematic origin ceases with the evolution of the eruptive disorder. In the chronic form ultimate recovery will depend upon the permanency of the existing cause and the extent of the inflammatory new formations.
TREATMENT.—The first indication, as a matter of course, is to obviate the cause, whatever that may be. This, when practicable, usually suffices to bring the malady promptly to a favorable termination.
Intestinal disturbances, whether causative or incidental, must be duly corrected, and the administration of a saline purge is almost always desirable. In addition, resort is made to frequent ablutions with fresh water, warm or tepid, in sprays, gargles, or washes, as may be most convenient or practicable. Emollients (gum-water, barley-water, quinceseed-water), astringents (alum, tannin), and detergents (borax, sodium bicarbonate), may be added, with opiates to relieve pain if need be.
Frequent or continuous suction of fragments of ice usually affords prompt relief to local pain and heat. The anæsthetic properties of salicylic acid have been utilized,1 one part to two hundred and fifty of water containing sufficient alcohol for its solution.
1 Berthold, cited by Ringer, Handbook of Therapeutics, 10th ed., London, 1883, p. 612.
DEFINITION.—Inflammation of the mucous membrane of the interior of the mouth, characterized by small superficial ulcers. These ulcers are irregularly circular or oval, are not depressed below the general surface of the mucous membrane, and support a creamy sebum or exudation. They occupy positions known to be normally supplied with mucous glands.
The classical description of this affection includes the initial eruption of vesicles or groups of vesicles which rupture within a day or two of their appearance, leaving, upon discharge of their contents, the little superficial characteristic ulcers. Modern investigation, however, casts some doubt upon the vesicular character of the initial lesion, and renders it extremely probable that the reiterated expression of this opinion has [p. 326]been a simple deference by writer after writer to the descriptions given by his predecessors. This subject will receive further elucidation more appropriately in describing the pathology and morbid anatomy of the disease.
Aphthous stomatitis may be either idiopathic or symptomatic, discrete or confluent. It is often recurrent, and is sometimes epidemic.
SYNONYMS.—Aphthæ; Vesicular stomatitis; Follicular stomatitis (Billard); Canker sore mouth.
ETIOLOGY.—Aphthous stomatitis occurs at all ages, and is most prevalent during summer heat. In children it is most frequent from the period of the commencement of dentition to the completion of the eruption of the temporary teeth. It is infrequent during the fourth year of life, and is rare after the fifth. It is most apt to appear in pale, delicate, and scrofulous children, especially in such as are predisposed to catarrhal and cutaneous diseases (Billard, Barthez and Rilliet). Sometimes it seems to be hereditary (Barthez). Some individuals are subject to frequent recurrences. Poor food, insufficient clothing, want of due ventilation, lack of cleanliness, and similar deprivations act as predisposing causes. Hence the disease is apt to occur in the crowded wards of hospitals and asylums for children.
Anything that exhausts the physical forces of the adult, such as excessive heat, overwork, anxiety, hardship and privation as in shipwreck, and the drains of menstruation, pregnancy, and lactation, excessive sexual intercourse, etc., may predispose to the disease.
Long-continued debility from severe constitutional maladies, with chronic febrile conditions, such as chronic phthisis, chronic syphilis, chronic enteritis, chronic gastritis, and from diabetes and carcinoma, likewise acts as a predisposing cause, giving rise, during the final stages of the systemic disease, to symptomatic aphthæ, often of the confluent variety. Aphthous stomatitis sometimes accompanies certain of the continued fevers, exanthematous and non-exanthematous.
As exciting causes the following may be cited: gingivitis, from morbid dentition in children, and from neglect of the teeth, dental caries, and dental necrosis in adults; tobacco-smoking; the local contact of acrid substances in food or otherwise; acute gastro-intestinal disorder from improper or tainted food. Excessive humidity of the atmosphere is assigned as a prominent exciting cause of the disease in some countries. This is especially the case in Holland, where it often exists epidemically. The confluent form at these times is said to attack parturient women principally (Ketslaer). Inundations, not only in Holland, but in Hayti, Porto Rico, and in the United States, are sometimes followed by an endemic of aphthous stomatitis. It is believed that the emanations from decayed animal and vegetable matters left ashore on the reflux of the water, produce the morbid conditions which constitute the predisposing cause under such circumstances.
The use of certain drugs—preparations of antimony, for example—sometimes produces a vesicular stomatitis sufficiently analogous to aphthæ to be mentioned in this connection, and only to be distinguished therefrom by the history of the case.
PATHOLOGY AND MORBID ANATOMY.—As has been intimated, the morbid anatomy of aphthæ has long been described as a series of initial [p. 327] vesicles2 upon the buccal, labial, gingival, or lingual mucous membrane. Their variance from analogous cutaneous vesicles—herpes, for instance—is attributed to anatomical differences in the constitution of the mucous membrane and the skin. The rarity of their detection has been accounted for by the rapid maceration of the epithelium.
2 Tardieu, Hardy and Behier, Barthez and Rilliet, Meigs and Pepper, and many others.
The general opinion at present, however, is that the apparent vesicle is an inflamed mucous follicle.3 Some observers contend that it is an inflammation of the mucous membrane pure and simple (Taupin); others consider it an inflammation, sometimes in a follicle, sometimes in the mucous membrane (Grisolle); others, a fibrinous exudation in the uppermost layer of the mucous membrane (Henoch). Some have described it as the analogue of a miliary eruption (Van Swieten, Sauvage, Willan and Bateman); others, of herpes (Gubler, Simonet, Hardy and Behier); others, of ecthyma (Trousseau) and of acne (Worms).
3 Bichat, Callisen and Plenck, Billard, Worms, and others.
The vesicle of the primary stage, though generally vouched for, is rarely seen by the practitioner, so rapid is the metamorphosis into the aphthous ulcer. Its very existence is positively denied by several authorities (Vogel, Henoch), and Vogel states that he has never, even upon the most careful examination, discovered a real vesicle upon the mucous membrane of the mouth—one which, upon puncture, discharged thin fluid contents and then collapsed.
Beginning in a few instances, only, in a simple stomatitis, the initial anatomical lesion presents as a red, hemispherical elevation of epithelium one to two millimeters in diameter, and barely perceptible to the touch of the finger, though described by the patient as positively appreciable to the touch of the tongue. Believed to have been transparent or semi-transparent at first, its summit is usually opaque when first seen by the medical attendant, appearing as a little white papule. Billard describes a central dark spot or depression—the orifice of the duct of the inflamed follicle, as he considers it. Worms and others, however, who likewise attribute the little tumor to an inflamed follicle, have failed to recognize any such central depression. There may be but four or five of these papules; rarely are there more than twenty. Diffuse inflammation between them is rare. A few new papules are seen on the second day, perhaps a few fresh ones on the third day. Eventually, contiguous desquamations coalesce into an irregular excoriated or ulcerated surface. These appearances and processes may be summed up as hyperæmia, increased cell-proliferation into circumscribed portions of the mucous structures, with distension of the epithelium (dropsical degeneration?), rupture, and ulceration.
This is the stage at which the local lesion usually comes under professional notice as a superficial circular or ovoidal ulceration or patch, with irregularly rounded edges and an undermined border of shreddy epithelium. It is level with the surface or but slightly tumefied, and is usually surrounded by an inflammatory areola that gives it a slightly excavated aspect. Sometimes this is a narrow red rim, and sometimes it is a delicate radiating arborescence of several millimeters. Adjacent ulcerations coalesce and produce irregularly elongated losses of substance. The floor [p. 328]of the ulcer is covered with an adherent semi-opaque or opaque lardaceous mass, sometimes grayish-white, sometimes creamy or yellowish-white when unadmixed with other matters; the color depending more or less upon the number of oil-globules present, the result of fatty degeneration of the epithelium.
For a few days, three to five or more, the surface of the ulcer increases slightly by detachment of its ragged edges, eventually leaving a clean-cut sore, gradually reddening in color, with an inflammatory margin indicative of the reparative process. Repair steadily progresses by the reproduction of healthy epithelium from periphery to centre, so that within a day or two the size of the ulcer becomes diminished to that of a pinhead; and this is promptly covered over, leaving a red spot to mark its site, until, in a few days more, the color fades in its turn, and no trace of the lesion remains. The period of ulceration is prolonged to one or more weeks in some subjects, chiefly those of depraved constitution.
It was the uniform configuration of the initial lesions, their invariable seat, and the central depression which he detected, that led Billard to the opinion that the so-called eruption or vesicle was an inflamed mucous follicle. This view was further supported by the fact that the disease does not occur in the new-born subject, in whom the lymphatic glands and follicles of the digestive tract are barely developed, while it does occur after the fifth or sixth month of life, up to which time these structures are growing rapidly, and thus predisposing the infant to this peculiar disease by reason of the physiological nutritive hyperæmia.
Discrete aphthæ are found principally in the sides of the frenum and on the tip and sides of the tongue; on the internal face of the lips, the lower lip particularly, near their junction with the gums; on the internal face of the cheeks, far back, near the ramus of the jaw; upon the sides of the gums, externally and internally; on the summit of the gums of edentulous children (Billard); exceptionally upon the soft palate; in rare instances upon the pharynx.
Confluent aphthæ appear in the same localities as are mentioned above, and are much more frequent in the pharynx and oesophagus than are discrete aphthæ. They are said to be found occasionally in the stomach and in the intestinal canal.
In the confluent form of the disease the aphthæ are much more numerous, and the individual ulcerations run into each other; coalescing into elongated ulcers, especially upon the lower lip and at the tip of the tongue.
SYMPTOMATOLOGY, COURSE, DURATION, TERMINATIONS, COMPLICATIONS, AND SEQUELÆ.—The discrete form of the affection is rarely attended by constitutional disturbance of any gravity, and such disturbance, slight as it may be, is much more frequent in children than in adults. The local manifestation gradually wanes from periphery to centre in from eight to ten days, the patches changing in color from grayish to yellow, becoming translucent, and losing their red areola, until nothing but dark-red spots remain to mark their site. These spots fade in time, removing all trace of lesion.
Aphthous stomatitis of secondary origin attends conditions of serious constitutional disturbance—circumstances under which it is incidental and not causal.
The confluent form, unless exceedingly mild, is attended by symptoms [p. 329]of gastric or intestinal derangement—viz. coated tongue, thirst, salivation, acid or acrid eructations, nausea, perhaps vomiting, indigestion, and constipation or diarrhoea, as may be. The vomiting in these instances is usually attributed to the presence of aphthæ in the oesophagus and stomach, and the diarrhoea to their presence in the intestines.
Severer cases present, in addition, febrile phenomena, restlessness, loss of appetite, and unhealthy fecal discharges.
The constitutional symptoms precede the local manifestations in some instances by a number of days.
Confluent epidemic aphthous stomatitis, as it occurs in parturient women, is described (Guersant) as commencing with rigors, headache, and fever. The local symptoms are very severe. Pustules form upon the palate and pharynx. Deglutition becomes painful and difficult. Vomiting and painful diarrhoea occur, indicating extension of the disease to the stomach and the intestines. Typhoid conditions may supervene, and continue as long as three weeks, even terminating fatally.
The earliest local symptoms consist in some degree of discomfort and heat, to which severe smarting becomes added at the period of ulceration. The little sores, no matter how minute they may be, are exceedingly painful to the touch, even to the contact of the tongue. Mastication thus becomes painful, and even impracticable, in the adult; and suction at the breast or the bottle difficult and painful in the infant. The mouth of the infant is so hot that its heat is imparted to the nipple of the nurse, whose sensations in nursing sometimes furnish the earliest indication of the disease. Indeed, the heat of the child's mouth at this time, and the acridity of the buccal secretions, are often sufficient to irritate and inflame the nipple, and even to produce superficial excoriation. The general mucous secretions of the mouth are usually augmented. Hypersalivation is much less frequent.
The course of the disease is mild as a rule. The chief inconvenience is the difficulty in alimentation consequent on the pain in mastication and in swallowing.
The duration of the affection in idiopathic cases varies, as the rule, from four to seven days, counting from the first appearance of the local lesion to the complete repair of the succeeding ulceration. Individual cases are often more protracted. Successive crops of aphthæ may prolong the disease for many days. In confluent aphthæ the course is slower and the disease less amenable to treatment; ulceration often continuing longer than a week, and recovery requiring twelve or fifteen days. The duration in consecutive cases varies with the nature of the underlying malady. In individuals seriously debilitated by protracted constitutional disease, as in the subjects of phthisis, the affection may continue, with intermissions and exacerbations, as long as the patient lives. The termination of the individual ulcerations is in repair.
There are no special complications. The accompanying stomatitis is usually a gingivitis simply, and is apt to be circumscribed when more extensive.
There are no sequelæ. Sometimes labial herpes or similar ulcerations follow, which are likewise sore and painful.
DIAGNOSIS.—The isolated patches of the discrete form are usually sufficiently characteristic to establish the diagnosis.
[p. 330]In children the gums are usually seen to be congested, swollen, moist, and glistening. Sometimes they are even sanious. This condition is deemed of great importance in cases of small, solitary aphthæ concealed in the sinus between gums and lips (Rilliet).
Confluent aphthæ may be mistaken for ulcerative or ulcero-membranous stomatitis, especially when the emanations from a coated tongue exhale a disagreeable or fetorous odor.
From thrush—with which it is most frequently confounded—it is to be discriminated by the absence, upon naked-eye inspection, of the peculiar curdy-like exudations to be described under the appropriate section, and under microscopic inspection by the lack of the peculiar thrush-fungus (Oïdium albicans).
PROGNOSIS.—Recovery is usually prompt in discrete cases, but relapses are not infrequent. In confluent cases recovery is dependent upon the character of the constitutional disorder by which the local disease has been caused or with which it is associated, and is therefore much slower.
The disease is grave in certain epidemic confluent forms, such as are described as occurring in Holland and elsewhere under conditions alluded to. Parturient women under such circumstances occasionally succumb to the typhoid condition into which they are thrown. When following measles there is some danger of laryngitis, and the case becomes grave. Oedema of the larynx is sometimes produced.
TREATMENT.—Very simple treatment suffices in the discrete form of the disease. A mild antacid, or even an emetic, may be indicated when there is gastric derangement or disturbance; or a mild laxative when the patient is costive. Castor oil, rhubarb, or magnesia may be given, followed, if need be, by an astringent if diarrhoea should occur. A little opium may be administered if requisite. The diet should be quite simple and unirritating. Cold milk is often the very best diet, especially while the mouth remains quite sore.
Topical treatment in the milder cases may be limited to simple ablutions, by rinsing or by spray, with water, cold or tepid as may be most agreeable to the patient. A little opium may be added when the parts are painful or tender. In severer cases an antiseptic wash may be substituted, as the sodium sulphite or hyposulphite, thirty grains to the ounce, creasote-water, or the like.
Demulcent washes of elm, sassafras-pith, or flaxseed are often more soothing than simple water. Pellets of ice from time to time are quite refreshing and agreeable. Occasional topical use of borax or alum, applied several times a day by means of a hair pencil, soft cotton wad, or the like, is often useful, care being taken to touch the sores lightly, and not to rub them. If the course toward repair is retarded, the parts may be touched lightly with silver nitrate in stick or in strong solution (60 grains), or washed more freely, two or three times a day, with a weaker solution, five or ten grains to the ounce of distilled water. Cupric sulphate, ten grains to the ounce, zinc sulphate, twenty grains to the ounce, mercuric chloride, one grain to the ounce, or potassium chlorate, twenty grains to the ounce, may be used as local applications, repeated at intervals of four or five hours. Iodoform has been highly recommended of late.
[p. 331]The confluent variety requires constitutional treatment adapted to the underlying malady. Nutritious diet is often demanded, together with tonics, such as iron and quinia, or even stimulants, wine or brandy. Topically, cauterization with silver nitrate is more apt to be indicated, and to be indicated more promptly than in the discrete form. Potassium chlorate in doses of one or more grains may often be given with advantage, at intervals of from four to two hours.
DEFINITION.—An exudative inflammation of the interior of the mouth, due to the development upon the mucous membrane of a parasitic vegetable confervoid growth, the Oïdium albicans (Robin).
SYNONYMS.—Stomatitis cremosa; Stomatitis pseudo-membranosa; Thrush; Muguet of the French; Schwämmchen of the Germans.
HISTORY.—Thrush was long regarded as a pseudo-membranous variety of stomatitis, and was likewise confounded with other varieties of stomatitis, especially aphthæ, its differentiation from which will be rendered apparent by a study of its etiology and morbid anatomy.
The microscopic researches of Berg4 of Stockholm upon the minute structure of the supposed pseudo-membrane developed the fact that it was largely composed of certain cryptogams. This growth was named Oïdium albicans by Prof. Ch. Robin,5 by whom it had been subjected to minute study.
4 Ueber die Schwämmchen bei Kindern, 1842—Van der Busch's translation from the Swedish, Bremen, 1848.
5 Histoire naturelle des Végétaux parasites, Paris, 1853.
Later observers consider the oïdia in general simply transitional forms in the life-history of fungi otherwise classified. According to Grawitz, the O. albicans is a stage of the Mycoderma vini, his experiments having shown that on cultivation the filaments germinate like Torula and Mycoderma, and that the latter can be grown in the epithelium of the mucous membrane.6
6 Ziegler, A Text-book of Pathological Anatomy and Pathogenesis, translated by Macalister, vol. i. p. 319, London, 1883.
| FIG. 13. |
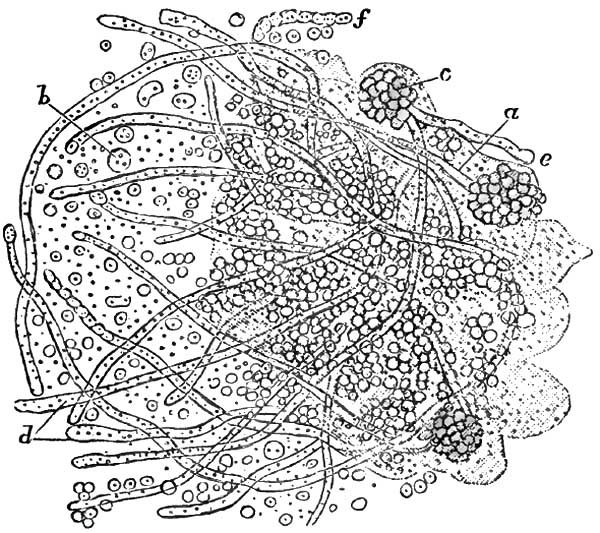
|
| Oïdium albicans, from the Mouth in a case of Thrush (Küchenmeister). a, fragment of a separated thrush-layer implanted in a mass of epithelium; b, spores; d, thallus-threads with partition walls; e, free end of a thallus somewhat swollen; f, thallus with constriction, without partition walls. |
ETIOLOGY.—Thrush is usually a symptomatic disease, secondary to an [p. 332]acid condition of the fluids of the mouth. Athrepsia (Parrot, Meigs and Pepper), or innutrition, is the presumable predisposing cause. Negligence in maintaining cleanliness of the mouth and of the articles which are placed in it is regarded as the main exciting cause. It occurs both in the adult and in the infant, but it is much more frequent in infancy and in early childhood. It is most frequently encountered in asylums and hospitals for children, being often transmitted from child to child by the nurse or by means of the feeding-bottle. The poor health of the child seeming less accountable for the disease than the unsanitary condition of the wards, buildings, and surroundings, it is consequently much less frequent in private than in public practice. It is more frequent in the first two weeks of life than later. Seux observed it within the first eight days in 394 cases out of 402 (Simon). It is much more frequent during summer than at any other season, more than half the cases (Valleix) occurring at that portion of the year.
In senile subjects, in adults, and in children more than two years of age it is cachectic, and observed chiefly toward the close of some fatal and exhausting disease, such as diabetes, carcinoma, tuberculosis, chronic pneumonia, enteric fever, puerperal fever, erysipelas, chronic entero-colitis and recto-colitis, and pseudo-membranous sore throat. It is sometimes observed in the early stage of enteric fever.
Meigs and Pepper, apparently following Parrot, deem the central cause to lie in a certain failure of nutrition under which the general vitality slowly ebbs away. They are inclined7 to recognize a causal factor in a deficiency in the supply of water in much of the artificial food administered to young subjects. The normal acidity of the fluids of the mouth of the newly-born (Guillot, Seux) is not sufficiently counteracted until saliva becomes abundant. Premature weaning, entailing, as it often does, the use of improper foods, renders the child liable to gastro-intestinal disorders. To this add want of care of the bottle and nipples, of the teaspoon or pap-boat, and of the mouth itself, and the conditions are fulfilled in fermentations of remnants of milk taking place without and within, which produce the acid condition of the fluids and secretions of the mouth said always to accompany and precede the development of the disease (Gubler).
7 A Practical Treatise on the Diseases of Children, 7th ed., Philada., 1882.
The theory of contagiousness seems established (Guillot, Berg, Gubler, Robin, Trousseau). This has been further demonstrated by experiments upon sheep (Delafeud), in which thrush has been implanted whenever the animals were unhealthy, but not otherwise.
PATHOLOGY AND MORBID ANATOMY.—The mucous membrane of the mouth within a few hours after its invasion by thrush is seen to be covered to some extent by minute masses of a granular curdy substance adherent to the tissues, which often bleed slightly when the substance is forcibly removed.
In children much reduced by inanition or severe disease, much of the deposit soon coalesces into a membraniform product, grayish or yellowish from rarefaction by the air, or even brownish from admixture of blood. By the same time the general congestion of the mucous membrane will have subsided into the pallor of anæmia. Though tolerably adherent when fresh, the deposit when older often becomes loosened [p. 333]spontaneously, so that it may be removed by the finger in large flakes without producing any hemorrhage whatever.
The characteristic masses present both as delicate roundish flakes, isolated, not larger than a pinhead, and as confluent patches several times as large and more irregular in outline. These masses under microscopic inspection are seen to be composed of the filaments and spores of a confervoid parasitic plant, the Oïdium albicans, enclosing altered epithelia in various conditions. This parasitic growth does not become developed upon healthy mucous membrane with normal secretory products. Acidity of the fluids and exuberance of epithelium are the requisites for its production, whatever be the cause. The acidity of the fluids irritates the mucous membrane upon which they lie. This irritation induces abnormal proliferation of epithelium, upon which the spores of the cryptogam then germinate. Dissociated epithelial cells become proliferated at the surface of the mucous membrane, between which and upon which both free and agglutinated spores accumulate. From these spores sprout out simple and ramified filaments in compartments containing moving granular elements. (For the minute detailed anatomy of these filaments and spores the reader is best referred to Robin's work on Vegetable Parasites.)
It may suffice here to mention that the filaments are sharply-defined tubercles, slightly amber-tinted, of a mean diameter of between four and three millimeters, simple while immature and branched when fully developed. These tubules are filled with link-like groups of elongated cells in compartments, giving them an appearance of regular constriction at the junctions of adjoining groups of cells. Surrounding these tubules are groups of spheroid or slightly ovoid spores from five to four millimeters in diameter. Each spore contains one or two granules and a quantity of fine dust. This cryptogamic growth is developed in the proliferated cells of epithelium. The filaments in their further growth separate the epithelia, and even penetrate them. Thence they penetrate the mucous membrane and the submucosa (Parrot).
The mucous membrane beneath the growth is red, smooth, and glistening. Papillæ are sometimes prominent. It is not excoriated unless the growth has been removed with some violence, when, as noted, it may bleed slightly. Duguet and Damaschino have recently encountered cases associated with a special ulceration of one of the palatine folds; the former in enteric fever, the latter in a primitive case. The growth is quickly reproduced after removal—even within a few minutes when the secretions are very acid.
The glossal mucous membrane is usually the tissue first involved, the specks being more numerous at the tip and edges of the tongue than at its central portion. The glands at the base of the tongue may become invaded. From the tongue extension takes place to the lips, the cheeks, the gums, and the palate, hard and soft. The growth is especially prolific in the folds between lips and gums and between cheeks and gums. Sometimes the parts mentioned become involved successively without actual extension. In several recently reported instances occurring during enteric fever,8 the affection began on the soft palate, tonsils, and pharynx, and then progressed anteriorly toward the tongue, the cheeks, and the lips.
8 Duguet, Soc. Méd. des. Hôp., Mai 11, 1883; Rev. mens., Juin 1, 1883, p. 187.
[p. 334]But there is no limitation of the disease to these structures. The growth may cover the entire mucous membrane of the mouth. From the mouth it may reach the lateral walls of the pharynx, and in rare instances the posterior wall of the pharynx. The product is said to be more adherent on the pharynx (Reubold) than in the mouth. From the pharynx it may reach the epiglottis, and even the larynx (Lelut), in which organ it has been seen upon the vocal bands (Parrot). It has never been observed in the posterior nares or at the pharyngeal orifice of the Eustachian tube. It flourishes best, therefore, upon squamous epithelium. In infants much reduced, Parrot has seen ulceration in the neighborhood of the pterygoid apophyses, but attributable to the cachectic state of the child, and not to the disease in the mouth.
In many cases—in as large a proportion as two-thirds, according to some observers—the oesophagus becomes invaded, either in irregular longitudinal strips or in rings, in all instances (Simon) terminating a little above the cardia. In exceptional cases the entire mucous surface of the oesophagus may be covered with the product (Seux). It has been seen in the stomach (Lelut, Valleix), and is even said to be developed there (Parrot), presenting as little yellow projections, isolated or contiguous, from the size of millet-seeds to that of peas, and usually located along the curvatures, especially the smaller curvature and cardia (Simon).
In instances still more rare it is found in the intestinal canal (Seux), even at the anus (Bouchut, Robin), and thence upon the genitalia. In a child thirteen days old, Parrot found it in the pulmonary parenchyma at the summit of the right lung, where it had probably been drawn by efforts of inspiration.
The nipple of the nurse often becomes covered with the growth (Gubler, Robin, Trousseau, Simon).
SYMPTOMATOLOGY.—In infants the earliest symptom is distress during nursing, the nipple being seized repeatedly, and as frequently released with cries of pain and disappointment. This cry is hoarse when the vocal bands are involved.
The constitutional symptoms depend upon the underlying malady, and may of course vary with its character. Thus we may have the symptoms of simple diarrhoea, gastro-enteritis, or entero-colitis on the one hand, and of tuberculosis and other diseases elsewhere enumerated on the other. Cachectic children, especially in asylum and hospital practice, lose flesh, and their skins become harsh, dry, and inelastic from loss of fluids (Meigs and Pepper). The genitalia, the anus, and the adjacent parts become eroded by the acridity of the discharges, and then become covered with the growth.
The disease rarely lasts longer than eight days in strong children that can be well cared for. It may continue indefinitely, on the other hand, in cachectic children; that is to say, for several months or until the patient succumbs, as may be. Death occurs usually from the causal disease, and not as a result of the morbid condition of the mouth.
DIAGNOSIS.—In the Infant.—Examination of its mouth to detect the cause of the child's inability to nurse reveals congestion of the mucous membrane, intense and often livid in severe cases. It is first noticed at the extremity of the tongue. When the congestion is general it is darkest in the tongue. This livid congestion may extend over the entire [p. 335]visible mucous membrane, save upon the hard palate, where it is tightly adherent to the periosteum, and upon the gums, where it is rendered tense by the approach of erupting teeth. The papillæ at the tip and sides of the tongue are very prominent. Sometimes the organ is quite dry, even sanious, while it is painful to the touch. The reaction of the secretions of the mouth is acid instead of alkaline, and the parts are hot and very sensitive.
Two or three days later the circular milky-white or curdy spots or slightly prominent and irregularly-shaped flakes or patches may be seen on the upper surface of the tongue toward the tip and inside the lips and the cheeks, especially in the grooves connecting gums and lips and gums and cheeks. The surrounding mucous membrane is unaltered in mild cases, and there is no evidence of other local disorder or of any constitutional involvement. In severe cases the entire mucous membrane is dry and deeply congested.
The affection can be positively discriminated from all others by microscopic examination of the deposit, which reveals the presence of the cryptogam described.
TREATMENT.—In infants, artificial nourishment, whether with milk of the lower animals or prepared food of whatever composition, should be given up, if possible, and a wet-nurse be supplied. If this procedure be impracticable, the least objectionable mode of preparation of cow's milk should be employed (and this will vary with the practice of the physician), and the utmost circumspection should be maintained in securing the cleanliness of the vessels in which it is prepared, the bottle from which it is given, and the nipple which is placed in the child's mouth. Should the sugar and casein in the milk appear to keep up the disease, weak soups may be substituted for the milk diet until it has subsided. Weiderhofer advises artificial nourishment, by way of a funnel inserted in the nasal passages, in case the child should refuse to swallow. Deglutition is excited in a reflex manner when the milk or other fluid reaches the pharynx.9
9 Journ. de Méd. Bordeaux, Juin 10, 1883.
The local treatment should consist in careful removal of the patches from time to time—say every two or three hours—with a moistened soft rag. This must be done without roughness of manipulation. In addition to this, the parts may be washed or painted every hour or so with an alkaline solution for the purpose of neutralizing the acidity of the fluids of the mouth. For this purpose borax is most generally used, in the proportion of twenty grains to the ounce of water or the half ounce of glycerin. Sodium bicarbonate or sodium salicylate may be substituted for the sodium borate. The use of honey in connection with the drug is calculated to promote acidity by fermentation of its glucose, and is therefore, theoretically, contraindicated.
Adults may use washes, gargles, or sprays of solutions of sodium borate or of sodium bicarbonate.
The constitutional treatment in each case must be adapted to the nature of the underlying malady which has favored the local disease, with resort in addition to the use of quinia, iron, wine, spirit, and beef-essence. The hygienic surroundings should be made as sanitary as possible.
DEFINITION.—Inflammation of the interior of the mouth, usually unilateral, eventuating in multiple ulcerations of the mucous membrane.
SYNONYMS.—Fetid stomatitis, Phlegmonous stomatitis, Putrid sore mouth, Stomacace, are synonymous terms for idiopathic ulcerous stomatitis. Ulcero-membranous stomatitis, Mercurial stomatitis (Vogel), are synonymous terms for the deuteropathic variety of the disease.
ETIOLOGY.—The principal predisposing cause of the disease is to be found in ochlesis; the contaminating atmosphere of crowded dwellings and apartments insufficiently ventilated; uncleanliness; insufficiency of proper clothing; unhealthy food, and the like. It prevails epidemically in crowded tenements, schools, prisons, asylums, and hospitals; in garrisons and in camps; in transports and men-of-war. It is often propagated by contagion, but whether by infection or actual inoculation seems undetermined. Measles is an active predisposing cause. Feeble individuals are the most liable to the disease. It occurs at all ages. In civil life it is most frequent between the ages of four and ten years. Sometimes more girls are affected than boys (Meigs), and sometimes it is the more prevalent among boys (Squarrey). Autumn is the season of greatest prevalence.
Carious teeth, fracture and necrosis of the jaw (Meigs), and protracted catarrhal stomatitis are among the chief exciting causes. Irregular dentition is sometimes the exciting cause; and this may occur at the first and second dentition or at the period of eruption of the last molars.
PATHOLOGY.—The anatomical lesion is the destructive inflammation of portions of the mucous membrane of the mouth, leaving ulceration on detachment of the eschars. It usually commences as a gingivitis. At two periods of life—namely, from the fourth to the eighth year of life, and from the eighteenth to the twenty-fifth year—it is apt to be ulcero-membranous, a condition asserted to be altogether exceptional at other periods (Chauffard).
A diffuse fibro-purulent infiltration of the lymph-spaces of the mucosa is regarded as the first step in the pathological process. This infiltration is sufficiently abundant to compress the capillary vessels of the tissues, and thus arrest the circulation (Cornil et Ranvier). All those localized portions of mucous membrane from which the circulation is cut off perish and are discharged in fragments. The ulcers thus left are grayish, granular, and sanious, with thin, irregularly dentated borders a little undermined, through which pus can be expressed on pressure. The usual cryptogams of the oral cavity, in various stages of development, are in great abundance in the grayish detritus, which likewise contains altered red and white blood-corpuscles.
According to some observers (Caffort, Bergeron), the first evidence of the disease is an intensely congested erythematous patch, upon which one or more pustules present, point, and rupture promptly, leaving the characteristic ulcerations.
For some indeterminate reason, the ulcerations are mostly unilateral, and occur much the more frequently on the left side. The principal [p. 337]primal points of ulceration are upon the external borders of the gums, more frequently those of the lower jaw, and upon the corresponding surface of the cheek and lip—the cheek much oftener than the lip. Thence ulceration may extend to the tongue, less frequently to the palate. The ulcerative process follows the outline of the gums, baring the bases of the teeth to a variable extent, so that they seem elongated. On the cheek the patch of inflammation is generally oval, the longest diameter being antero-posterior, and the most frequent position is opposite to the last molar.
Each ulcer is surrounded by an intensely red areola, beyond which the tissues are succulent and tumid from collateral inflammatory oedema, often giving the ulcers an appearance of great depth; but when the detritus is discharged they are seen to have been superficial. Detachment of the necrosed segments of mucous membrane takes place by gradual exfoliation from periphery to centre. Sometimes detachment occurs in mass, usually in consequence of friction or suction. The ulcers, gingival and buccal, bleed easily when disturbed. They may remain separate, or may coalesce by confluence of interposing ulcerations extending across the furrow between gum and cheek or lip. The adjoining side of the tongue sometimes undergoes similar ulceration from behind forward, inoculated, most likely, by contact with adjoining ulceration. In rare instances, neglected cases most probably, the ulceration may extend to the palatine folds, the tonsils, and the soft palate.
SYMPTOMATOLOGY.—The affection usually begins without any constitutional symptoms. Young infants sometimes present slight febrile symptoms, with impairment of appetite and general languor. Fetid breath, salivation, and difficulty in deglutition are usually the first manifestations of the disease to attract attention. The mouth will be found to be hot, painful, and sensitive to the contact of food. Infants often refuse food altogether, though usually they can be coaxed to take liquid aliment. Larger children and adults complain of scalding sensations. They find mastication painful, and cannot chew at all on the affected side. The salivation is excessive, the saliva bloody and often extremely fetid. When swallowed, this fetid saliva causes diarrhoea. The cheeks sometimes become swollen, and the submaxillary connective tissue oedematous. Adenitis takes place in the submaxillary, retro-maxillary, and sublingual glands of the affected side. Sometimes the other side becomes affected likewise, but to a less extent. The glands do not suppurate, but the adenitis may remain as a chronic manifestation in scrofulous subjects.
The disease, left to itself, will often continue for a number of weeks, or even months as may be, unmodified even by intercurrent maladies (Bergeron). Long continuance may result in partial or complete disruption of the teeth, or in local gangrene, or even in necrosis of the alveoli (Damaschino). Properly managed, the ulcers become cleansed of their detritus, and within a few days heal by granulation, their position long remaining marked by delicate red cicatrices upon a hard and thickened substratum. Repeated recurrences are sometimes observed.
DIAGNOSIS.—The appearances of the gums and adjoining structures described under the head of Pathology establish the diagnosis. The usually unilateral manifestation and the peculiar fetid odor distinguish it from severe forms of catarrhal stomatitis. From cancrum oris it is [p. 338]distinguished by the absence of induration of the skin of the cheek over the swollen membrane, and by the succulence and diffuseness of the tumefaction. From mercurial stomatitis it is discriminated by the history, and by the absence of the peculiar manifestations to be discussed under the head of that disease.
PROGNOSIS.—The prognosis is good, the disease being susceptible of cure in from eight to ten days in ordinary cases. When due nutrition is prevented by the pain in mastication and deglutition, and in much-reduced subjects, the disease may continue for several weeks. It is in these cases that detachment of the teeth takes place, with periostitis and necrosis of the alveoli. Protracted suppuration and failure in nutrition may lead to a fatal result, but such a termination is uncommon.
TREATMENT.—Fresh air, unirritating and easily digestible food, the best hygienic surroundings practicable, attention to secretions from skin and bowels by moderate and judicious use of ablutions, diaphoretics, and laxatives, with the internal administration of cinchona or its derivatives, with iron and cod-liver oil, comprise the indications for constitutional treatment.
Locally, demulcent mouth-washes are called for, containing astringents, detergents, or antiseptics. Acidulated washes are more agreeable in some instances. For antiseptic purposes, however, sprays and douches may be used of solutions of potassium permanganate, boric acid, carbolic acid, or salicylic acid. Gargles of potassium chlorate, ten or twenty grains to the ounce, are highly recommended, as well as the internal administration of the same salt in doses of from two to five grains three times a day for children, and of ten to twenty grains for adults.
If the sores are slow to heal, the ulcerated surfaces may be touched once or twice daily with some astringent, such as solution of silver nitrate (ten grains to the ounce), or, if that be objectionable, with alum, tincture of iodine, or iodoform.
Prompt extraction of loose teeth and of loose fragments of necrosed bone is requisite.
DEFINITION.—A non-contagious, deuteropathic inflammation of the interior of the mouth, almost invariably unilateral, and characterized by a peculiar gangrenous destruction of all the tissues of the cheek from within outward.
SYNONYMS.—Gangrenous stomatitis; Gangrena oris; Grangrenopsis; Cancrum oris; Stomato-necrosis; Necrosis infantilis; Gangrene of the mouth; Gangrenous erosion of the cheek; Noma; Buccal anthrax; Aquatic cancer; Water cancer; Scorbutic cancer; Sloughing phagedæna of the mouth.
HISTORY.—The most important work upon the subject was published in 1828, from the pen of Dr. A. L. Richter,10 whose accurate historical account of the disease was in great part reproduced, with additions thereto, by Barthez and Rilliet in their Treatise on the Diseases of Infants, Paris, 1843, and quoted by nearly all subsequent writers on the [p. 339]theme. From these records it appears that the first accurate description of the affection was given in 1620 by Dr. Battus, a Dutch physician, in his Manual of Surgery. The term aquatic cancer, water-kanker, bestowed on it by van de Voorde, has been generally followed by the physicians of Holland, although van Swieten (1699) properly designated it as gangrene. J. van Lil termed it noma, as well as stomacace and water-kanker, and cited a number of Dutch physicians who had observed its epidemic prevalence. The majority of more recent observers, however, deny its epidemic character.
10 Der Wasserkrebs der Kinder, Berlin, 1828; further, Beiträg zur Lehre vom Wasserkrebs, Berlin, 1832; Bemerkungen über den Brand der Kinder, Berlin, 1834.
Of Swedish writers, Lund described it as gangrene of the mouth; Leutin, under the name of ulocace. In England, Boot was the first to write of gangrene of the mouth, and was followed by Underwood, Symmonds, Pearson, S. Cooper, West, and others.
In France it has received great attention. Berthe11 described it as gangrenous scorbutis of the gums; Sauvages (1816) as necrosis infantilis. Baron in 1816 published12 a short but excellent account of a gangrenous affection of the mouth peculiar to children; and Isnard presented in 1818 his inaugural thesis on a gangrenous affection peculiar to children, in which he described, simultaneously, gangrene of the mouth and gangrene of the vulva. Then followed Rey, Destrees (1821), Billard (1833), Murdoch, Taupin (1839), and others, until we reach the admirable description by Barthez et Rilliet, from which the present historical record has been chiefly abstracted.
11 Mémoires de l'Académie royale de Chirurgie, Paris, 1774, t. v. p. 381.
12 Bullétins de la Faculté de Médecine de Paris, 1816, t. v. p. 161.
German physicians likewise have largely studied the subject. De Hilden, A. G. Richter, C. F. Fischer, Seibert, and many others preceded A. L. Richter, whose important contribution to the literature and description of the disease has been so highly extolled by Barthez and Rilliet.
In America the disease has been best described by Coates, Gerhard, and Meigs and Pepper, all of Philadelphia.
(For extensive bibliographies the following sources should be consulted in addition to those cited: J. Tourdes, Du Noma ou du Sphacèle de la Bouche chez les Enfants, Thèse, Strasbourg, 1848: A. Le Dentu, Nouveau Dictionnaire de Médecine et de Chirurgie pratique, article "Face," Paris, 1871.)
ETIOLOGY.—Almost exclusively a disease of childhood, gangrenous stomatitis is exceedingly rare in private practice, and very infrequent at the present day even in hospital and dispensary practice. Lack of hygienic essentials of various kinds, impoverishment, long illnesses, and debilitating maladies in general are the predisposing causes. It is sometimes endemic in hospitals and public institutions, but rarely, if at all, epidemic. It is not generally deemed contagious, though so considered by some writers. It appears to have been more frequent in Holland than elsewhere, to be more frequent in Europe generally than in the United States, and now much less frequent in the United States than formerly. To recognition of the predisposing causes and to their abolition and avoidance may probably be attributed its diminished frequency all over the world. Though attacking children only as a rule, it has been observed in adults (Barthez et Rilliet, Tourdes, Vogel). Nurslings are not liable to the disease. Though occurring occasionally earlier in life, the greatest period of prevalence is [p. 340]from the third to the fifth or sixth year of age, and thence, with diminishing frequency, to the twelfth and thirteenth years. It is probably equally frequent in the two sexes, though the majority of authors have described it as more frequent in females.
Healthy children are not attacked. Even in delicate children it is so rarely idiopathic that this character is utterly denied it by many observers. The disease which it follows, or with which it becomes associated, may be acute or chronic. According to most writers, it occurs with greatest frequency after measles. It follows scarlatina and variola much less often. It is observed likewise after whooping cough, typhus fever, malarial fever, entero-colitis, pneumonitis, and tuberculosis. Excessive administration of mercury has been recognized as an exciting cause, some cases of mercurial stomatitis progressing to gangrene.
According to Barthez et Rilliet, acute pulmonary diseases, and especially pneumonia, are the most frequent concomitant affections, and are usually consecutive.
SYMPTOMATOLOGY, COURSE, DURATION, TERMINATIONS, COMPLICATIONS, AND SEQUELÆ.—The disease usually becoming manifested during other disease, acute or chronic, or during convalescence therefrom, there are no special constitutional symptoms indicating its onset. Hence considerable progress may be made before its detection. The earliest local characteristic symptom distinguishing gangrenous stomatitis is a tense tumefaction of one cheek, usually in proximity to the mouth. The lower lip is generally involved, thus rendering it a matter of difficulty to open the mouth. This tumefaction in some instances progresses over the entire side of the face up to the nose, the lower eyelid, and even out to the ear in one direction, and down to the chin, and even to the neck, in the other. Before the parts become swollen externally, ulceration will have taken place to some extent in the mucous membrane, but usually without having attracted special attention, the subjective symptoms having been slight. A gangrenous odor from the mouth, however, is almost always constant. Its presence, therefore, should lead to careful investigation as to its seat and cause. The gums opposite the internal ulcer become similarly affected in most instances, and undergo destruction, so that the teeth may become denuded and loosened, and even detached, exposing their alveoli. The bodies of the maxillary bones suffer in addition in some instances, and undergo partial necrosis and exfoliation.
It is maintained (Löschner, Henoch) that in some instances there is no involvement of the mucous membrane until the ulcerative process has reached it from the exterior.
The tumefied portions of the check and lip are pale, hard, unctuous, and glistening. They are rarely very painful, and often painless. On palpation a hard and rounded nodule one or two centimeters in diameter can be detected deep in the central portion of the swollen cheek.
From the third to the sixth day a small, black, dry eschar, circular or oval, becomes formed at the most prominent and most livid portion of the swelling, whether cheek or lip. This gradually extends in circumference for a few days or for a fortnight, sometimes taking in almost the entire side of the face or even extending down to the neck. As it enlarges the tissues around become circumscribed with a zone intensely red. The internal eschar extends equally with the external one. Eventually, the [p. 341]eschar separates, in part or in whole, and becomes detached, leaving a hole in the cheek through which are seen the loosened teeth and their denuded and blackened sockets.
During this time the patient's strength remains tolerably well maintained, as a rule, until the gangrene has become well advanced. Intelligence usually remains good. Many children sit up in bed and manifest interest in their surroundings. Others lie indifferent to efforts made for their amusement. Some exhibit insomnia and delirium. The pulse is small and moderately frequent, rarely exceeding 120 beats to the minute until near the fatal close, when it often becomes imperceptible. Appetite is often well preserved, unless pneumonia or other complications supervene, but thirst is often intense, even though the tongue remain moist. The desire for food sometimes continues until within a few hours of death. Toward the last the skin becomes dry and cold, diarrhoea sets in, emaciation proceeds rapidly, collapse ensues and death.
Death usually occurs during the second week, often before the complete detachment of the eschar—in many instances by pneumonia, pulmonary gangrene, or entero-colitis. Some die in collapse, which is sometimes preceded by convulsions. When the eschars have become detached, suppuration exhausts the forces of the patient, and death takes place by asthenia.
The complication most frequent is pneumonia, and the next entero-colitis. Gangrene of the lungs, of the palate, pharynx, or oesophagus, of the anus, and of the vulva, may supervene. Hemorrhage from the facial artery or its branches has been noted as an exceptional mode of death (Hueber), the rule being that the arteries in the gangrenous area become plugged by thrombi, and thus prevent hemorrhage.
Recovery may take place before the local disease has penetrated the cheek—indeed, while the mucous membrane alone is involved. In recent instances, however, the disease does not subside until after the loss of considerable portions of the cheek, and the child recovers with great deformity, not only from loss of tissue in the cheek and nose, but from adhesions between the jaws and the cheek.
PATHOLOGY AND MORBID ANATOMY.—Gangrenous stomatitis always involves the cheek, almost always that portion in proximity to the mouth. It is almost invariably unilateral. Either side seems to be equally liable. Both sides suffer only, it is contended, when the gangrene is limited in extent, confined to the mucous membrane, and occupies the sides of the frenums of the lips (Barthez et Rilliet). It usually if not invariably begins in the mucous membrane, as a phlyctenular inflammation, which undergoes ulceration, followed by gangrene, immediately or not for several days, and then becomes covered with a more or less brownish-gray eschar. The ulceration of the mucous membrane is occasionally preceded by an oedematous condition of the cheek externally, similar to that sometimes observed in ordinary ulcerous stomatitis; but this is not the characteristic circumscribed, tense infiltration observed later. This ulceration is situated most frequently opposite the junction of the upper and lower teeth. Sometimes it proceeds from the gingivo-buccal sulcus of the lower jaw, sometimes from the alveolar border of the gums. It extends in all directions, and often reaches the lower lip. From three to sixteen days may be consumed in these extensions. The [p. 342]surrounding mucous membrane becomes oedematous. The ulceration soon becomes followed by gangrene, sometimes within twenty-four hours, sometimes not for two or three days, and exceptionally not for several days. The ulcerated surfaces bleed readily, change from gray to black, and become covered with a semi-liquid or liquid putrescent detritus. They are sometimes surrounded by a projecting livid areola, which soon becomes gangrenous in its turn. The shreds of mortified membrane, though clinging a while to the sound tissues, are easily detached, and often drop spontaneously into the mouth. Meanwhile, there is abundant salivation, the products of which pour from the mouth, at first sanguinolent, and subsequently dark and putrescent and mixed with detritus of the tissues. Large portions of the gums, and even of the mucous membrane of the palate, may undergo destruction within a few (three to six) days. The gangrenous destruction of the gums soon exposes the teeth, which become loose and are sometimes spontaneously detached. Thence the periosteum and bone become implicated and undergo partial denudation and necrosis, and portions of necrosed bone become detached if the patient survives. The characteristic implication of the exterior of the cheek becomes manifest from the first to the third day, but occasionally not until a day or two later. A hard, circumscribed swelling of the cheek or cheek and lip occurs, sometimes preceded, as already intimated, by general oedematous infiltration. The surface is tense and unctuous, often discolored. In its central portion is an especially hard nucleus, one to two centimeters or more in diameter. Gangrene often takes place at this point from within outward at a period varying from the third to the seventh day or later. The skin becomes livid, then black; a pustule is formed at the summit of the swelling, which bursts and discloses a blackened gangrenous eschar from less than a line in thickness to the entire thickness of the cheek beneath. The area of gangrene gradually extends. The dead tissues become detached, and a perforation is left right through the cheek, through which are discharged saliva and detritus. Meanwhile, the submaxillary glands become swollen and the surrounding connective tissue becomes oedematous. In some instances, however, no change is noticeable in these glands.
Examinations after death have shown that thrombosis exists for some distance around the gangrenous mass. Hence the rarity of hemorrhage during the detachment of the eschar.
DIAGNOSIS.—In the early stage of the disease the main point of differential diagnosis rests in the locality of the primitive lesion, the mucous membrane of the inside of one cheek. Subsequently there is the gangrenous odor from the mouth; the rapid peripheric extension of the local lesion, which acquires a peculiar grayish-black color; its rapid extension toward the exterior of the cheek or lip; the tumefaction of the cheek, discolored, greasy, hard, surrounded by oedematous infiltration, and presenting a central nodule of especial hardness; then the profuse salivation, soon sanguinolent, subsequently purulent and mingled with detritus of the mortified tissues. Finally, the eschar on the exterior of the swollen cheek or lip leaves no doubt as to the character of the lesion. From malignant pustule it is distinguished by not beginning on the exterior, as that lesion always does (Baron).
PROGNOSIS.—The prognosis is bad unless the lesion be quite limited [p. 343]and complications absent. At least three-fourths of those attacked perish; according to some authorities fully five-sixths die. The objective symptoms of the local disease are much more important in estimating the prognosis than are the constitutional manifestations, the vigor of the patient, and the hygienic surroundings, although, as a matter of course, the better these latter the more favorable the prognosis. Prognosis would be more favorable in private practice than in hospital or asylum service.
TREATMENT.—Active treatment is required, both locally and constitutionally. Local treatment is of paramount importance, and alone capable of arresting the extension of the process of mortification. The topical measure in greatest repute is energetic cauterization with the most powerful agents, chemical and mechanical—hydrochloric acid, nitric acid, acid solution of mercuric nitrate, and the actual cautery, whether hot iron, thermo-, or electric cautery. The application of acids is usually made with a firm wad or piece of sponge upon a stick or quill, care being taken to protect the healthy tissues as far as practicable with a spoon or spatula. After the application the mouth is to be thoroughly syringed with water to remove or dilute the superfluous acid. Hydrochloric acid has been preferred by most observers.
As these cauterizations must be energetic to prove effective, anæsthesia ought to be induced. Should ether be employed for this purpose, hydrochloric acid or the acid solution of mercuric nitrate would be selected of course.
In the early stages these agents are to be applied to the inside of the cheek, so as to destroy all the tissue diseased, if practicable, and expose a healthy surface for granulation. Should the exterior of the cheek become implicated before cauterization has been performed or in spite of it, it is customary to destroy the tissues from the exterior, including a zone of apparently healthy surrounding tissue. As the gangrene extends, the cauterization is to be repeated twice daily or even more frequently. After cauterization the parts are dressed with antiseptic lotions, and antiseptic injections or douches are to be used frequently during day and night to wash out the mouth and keep it as clear as possible from detritus.
Meigs and Pepper report beneficial results from the topical use of undiluted carbolic acid, followed by a solution of the same, one part in fifty of water, frequently employed as a mouth-wash. The progress of the sloughing was checked and the putridity of the unseparated dead tissue completely destroyed in the two cases mentioned by them, one of which recovered quickly without perforation of the cheek. Gerhard preferred undiluted tincture of the chloride of iron; Condie, cupric sulphate, thirty grains to the ounce. Bismuth subnitrate has recently been lauded as a topical remedial agent.13
13 Maguire, Medical Record N.Y., Feb. 3, 1883.
The mouth should be frequently cleansed by syringing, douching, spraying, or washing with disinfectant solutions, such as chlorinated soda liquor, one part to ten; carbolic acid, one to twenty. Lemon-juice is sometimes an agreeable application, as in some other varieties of stomatitis. Constitutionally, tonic and supporting treatment is demanded, even in those instances where the appetite is well maintained and the [p. 344]general health apparently well conserved. Soups, milk, semi-solid food, egg-nog, egg and wine, wine whey, milk punch, finely-minced meat, should be administered as freely as the state of the digestive functions will permit. If necessary, resort should be had to nutritive enemata. Quinia and tincture of chloride of iron are the medicines indicated. When sufficient alcohol cannot be given with the food, it should be freely exhibited in the most available form by the mouth or by the rectum. The apartment should be well ventilated, the linen frequently changed, the discharges promptly removed.
DEFINITION.—An inflammation of the interior of the mouth due to poisoning, especially by drugs, and chiefly by mercury, copper, and phosphorus.
DEFINITION.—An inflammation of the mucous membrane of the mouth, eventually ulcerating, the result of systemic poisoning by the absorption of mercury.
SYNONYMS.—Stomatitis mercurialis; Mercurial ptyalism, Ptyalismus mercurialis; Mercurial salivation, Salivatio mercurialis.
ETIOLOGY—Predisposing and Exciting Causes.—Special vulnerability to the toxic influence of mercury, and special proclivity to inflammatory affections of the mouth and the organs contained therein, are the predisposing causes of mercurial stomatitis. The exciting cause is the absorption of mercury into the tissues of the organism. The susceptibility of healthy adults is much greater than that of healthy children. The susceptibility of adults varies very greatly. Constitutions deteriorated by prolonged disease, undue exposure, and the like are much more promptly influenced in consequence. Tuberculous subjects do not bear mercury well.
Idiosyncratic susceptibility to toxæmia by mercurial preparations is now and then encountered in practice, and instances have been published14 in which fatal results have ensued, after prolonged suffering, from the incautious administration of a single moderate dose of a mercurial drug.
14 For example, see in Watson's Practice of Physic a case of furious salivation following one administration of two grains of calomel as a purgative, the patient dying at the end of two years, worn out by the effects of the mercury and having lost portions of the jaw-bone by necrosis.
Until comparatively recent years the most common cause of mercurial poisoning was the excessive employment of mercurial medicines, whether by ingestion, inunction, or vapor bath. Topical cauterization with acid solution of mercuric nitrate is likewise an infrequent, and usually an accidental, cause of the affection. Elimination of the mercury by way of the mucous glands of mouth and the salivary glands proper excites the stomatitis in these instances. An entirely different series of cases occur in artisans exposed to handling the metal and its preparations or to breathing its vapor or its dust. In these instances the poison may gain [p. 345]entrance into the absorbent system by the skin, the mucous membranes of the nose, mouth, and throat, the stomach, or the lungs. No matter what care may be exercised in cleansing the hands, it is often impossible to prevent occasional transference of the noxious material from fingers to throat, or to thoroughly free the finger-tips under the nails. The avocations entailing the risks of mercurial stomatitis comprise quicksilver-mining, ore-separating, barometer- and thermometer-making, gilding, hat-making, manufacturing of chemicals, and exhausting the globes employed in certain forms of electric illumination.15 The slow absorption of mercury into the bodies of artisans induces in addition serious constitutional nervous disturbances—tremors, palsy, etc.
15 Med. and Surg. Reporter, Philada., Dec. 30, 1883, p. 734.
SYMPTOMATOLOGY, COURSE, DURATION, TERMINATIONS, COMPLICATIONS, AND SEQUELÆ.—The principal subjective symptoms of mercurial stomatitis are—characteristic fetor of the breath, sore gums and mouth, continuous nauseous metallic brassy or coppery taste, and profuse salivation.
At first the mouth feels parched and painful, the gums tender, the teeth, the lower incisors especially, set on edge. Soon the gums become swollen, and when touched with the tongue seem to have receded from the necks of the teeth, which thereby appear to be longer than usual. The gums feel quite sore when pressed upon with the finger or when put on the stretch by clashing the rows of teeth against each other. This sort of soreness is often watched for in the therapeutic administration of mercurials purposely given to "touch the gums," as an indication that the system is under the influence of the drug. It is, therefore, one of the earliest indications of mercurial poisoning, but if not sought for it may elude attention until after the mouth has become sore a little later. The pain in the mouth is augmented by efforts of mastication and expectoration, and may be associated with pains at the angle of the lower jaw or extending along the domain of the third or of the third and second divisions of the distribution of the fifth cerebral nerve. Mastication of solid food is often unendurable. Constitutional manifestations become evident about this time in increased heat of skin, acceleration of pulse, furred tongue, dry mouth, great thirst, and loss of appetite. The dryness of the mouth does not last long, but is soon followed by hypersalivation, one of the characteristic phenomena of the disorder. The saliva secreted, often acid in reaction, varies greatly in quantity, which is usually proportionate to the severity of the case. It is secreted night and day, sometimes to the amount of several pints in the twenty-four hours—in moderately severe cases to the amount of from one to two pints in that space of time. It is limpid or grayish, mawkish or somewhat fetid, and reacts readily to the simplest tests for mercury. The salivation is almost continuous, sometimes quite so. The patient soon becomes unable to endure the fatigue of constant expectoration, and the fluid then dribbles from his mouth or runs off in an unimpeded slobber. When excessive, the patient's strength becomes rapidly exhausted—in part by impoverishment of the fluids, in great measure from the lack of refreshing sleep.
Meanwhile, the local inflammatory process extends from the gums to the floor of the mouth and to the lips, and thence to the tongue and the [p. 346]cheeks. The salivary glands are in a state of inflammation likewise, but rather in consequence of direct irritation in the elimination of the poison through their channels than by extension of the stomatitis along their ducts. The lymphatic glands of the lower jaw become engorged and tender. Mastication, deglutition, and articulation all become impeded mechanically by tumefaction of the tissues.
In some instances the glossitis is so great that the tongue protrudes, thereby impeding respiration and even threatening suffocation. In some cases oedema of the larynx has been noted, threatening suffocation from that cause. Should the inflammatory process extend along the pharynx to the Eustachian tubes, deafness and pains in the ears will become additional symptoms.
The subsequent progress of unarrested mercurial stomatitis is that of ulcerous stomatitis.
Should gangrene of the mucous membrane take place, there will be great fetor from the mouth, and some danger of hemorrhage on detachment of the sloughs should the process be taking place in the direction of vessels of some calibre. Necrosis of the inferior maxilla entails continuance of the disagreeable local symptoms until the discharge in fragments or in mass of the dead portions of bone.
In the earlier stages of the attack the constitutional symptoms may be sthenic. Fever, cephalalgia, and the usual concomitants of pyrexia, however, soon give way to the opposite condition of asthenia. Exhausted by the excessive salivation, and unable to repair waste by eating or sleeping, the sufferer soon passes into a condition of hopeless cachexia. Those who survive remain cachectic and feeble for a long time—some of them disfigured for life by various cicatrices between cheeks and jaw, by loss of teeth or of portions of the jaw-bone.
The duration of mercurial stomatitis varies with the susceptibility of the patient, the intensity of the toxæmia, and the character of the treatment. Mild cases may get well in a week or two; severe cases may continue for weeks, and even months; extreme cases have persisted for years. Even moderate cases occasionally resist treatment for weeks.
Under the improved therapeutics of the present day mercurial stomatitis almost always terminates in recovery, especially if it receive early and prompt attention. Neglected or improperly managed, it may terminate in serious losses of tissue in gums, cheeks, teeth, and bone, leaving the parts much deformed and the patient in a permanently enfeebled condition.
Erysipelas, metastatic abscesses, inflammations, pyæmia, or colliquative diarrhoea may be mentioned as complications which may prove sufficiently serious to produce death, independently of the virulence of the primary stomatitis.
PATHOLOGY AND MORBID ANATOMY.—Mercurial stomatitis is an ulcerative process attended with an excessive flow of saliva containing mercury. It has a tendency to terminate in destruction and exfoliation of the mucous membrane of the gums and other tissues attacked, and eventually in necrosis of the jaw-bone. The detritus is found, microscopically, to consist of granular masses of broken-down tissue, swarming with bacteria and micrococci, and containing some blood-cells and many pus-cells. In some instances micrococci have been detected in the blood.
The disease usually begins in the gums of the lower incisors, and [p. 347]extends backward, often being confined to one side of the jaw. The gums, first swollen and then livid, become separated from the necks of the teeth. Their edges undergo ulceration. The ulcers are surrounded by fungous margins, pale or red, which bleed on the slightest contact, and some become covered with grayish-yellow detritus. The ulceration extends in depth, destroying the supports of the teeth, so that they become loosened and even detached. The inflammatory process extends to the lips, the cheek, and the tongue, which undergo tumefaction and exhibit the impressions of the teeth in grayish opalescent lines or festoons of thickened epithelium at the points of pressure. The glossitis may become intense. It is almost always present, to some extent, as a superficial or mucous glossitis. Occasionally acute oedematous glossitis has ensued, and such cases sometimes terminate fatally. Ulceration takes place in these structures similar to that which has taken place in the gums. If not arrested, gangrenous destruction ensues, not only in these tissues, but beneath them. Thus, the teeth become loosened, and even detached; the jaw-bones themselves may become bared, necrosed, and in part exfoliated; and the cheeks undergo partial destruction by gangrene. Sometimes the inflammation descends to the larynx, and this may produce oedematous infiltration of the loose connective tissue of that structure. Sometimes it mounts the pharynx and reaches the orifices of the Eustachian tubes. The salivary glands become swollen and discharge great quantities of fluid, as detailed under Symptomatology. The retro-maxillary and submaxillary lymphatic glands become enlarged by inflammatory action.
DIAGNOSIS.—In the earliest stages the inflammation of the gums in mercurial stomatitis cannot be distinguished from that which takes place in other forms of ulcerative stomatitis. The fetor of the breath, however, the profuse salivation, and the chemical reaction of the saliva, together with the history of exposure to mercury, soon place the nature of the case beyond doubt. Similar results following poisonings by copper salts and by phosphorus are differentiated by the history of the special exposure.
PROGNOSIS.—In mild cases the prognosis is favorable, provided further exposure to the cause can be avoided. This holds good almost invariably in cases due to over-medication with mercurials, but is far less applicable to cases in artisans, the result of prolonged exposure to the poisonous influences of mercury and its slow absorption. On the whole, the affection is much less serious than formerly, both because it can, in great measure, be guarded against by proper prophylaxis in risky vocations, and because its treatment has been made much more efficient. In severe cases serious results may ensue despite the most judicious treatment, and convalescence is usually very slow, weeks often elapsing before solid food can be chewed without pain or without injury to the gums.
When death ensues, it may be by asthenia, erysipelas, pneumonia, pyæmia, or colliquative diarrhoea.
TREATMENT.—Mercurial stomatitis may sometimes be prevented by the administration of potassium chlorate during exposure. Mild cases following the administration of mercurials often subside upon mere withdrawal of the drug. Should spontaneous subsidence not take place, the administration of potassium chlorate every few hours, in doses of [p. 348]from thirty to sixty grains or more in the twenty-four hours, soon effects amelioration, which promptly terminates in recovery. The characteristic fetor often ceases within twelve hours' use of this drug. Should the inflammatory manifestations be severe, a few leeches applied beneath the edge of the lower jaw, followed by a poultice enveloping the neck to promote further flow of blood, often affords prompt relief (Watson). Lead acetate (ten grains to the ounce of water) and iodine (half a fluidrachm of the compound tincture to the ounce of water) are useful as gargles and washes. When the result of slow poisoning, elimination of the mercury by sulphur vapor baths and the administration of small doses of potassium iodide are recommended.
Cauterization of the ulcerated surfaces is sometimes serviceable, silver nitrate or hydrochloric acid (Ricord), or chromic acid 1:5 (Butlin, Canquil), being used for the purpose.
Opium in decided doses is indicated for the relief of pain. It may be added with advantage to detergent and disinfective mouth-washes (potassium chlorate, sodium borate, creasote-water, saponified emulsion of coal-tar, tincture of cinchona, tincture of myrrh, etc.), the use of which should form an important part of the treatment. Watson highly recommended a wash of gargle of brandy and water, 1:4 or 5. In severe cases difficulty is encountered in maintaining effective alimentation. When mastication is not impracticable, soft-boiled egg and finely-chopped raw beef may be given. When the patient cannot chew at all, resort is confined to milk, soups, and the juice of beef. Nourishing enemata should be administered, as in all affections where it becomes impracticable to sustain the patient by way of the mouth. Tonics and stimulants are indicated to avoid debility from the excessive salivation and its sequelæ—quinia, coffee, wine, and alcohol, the first, if required, by hypodermatic injection, all of them by enema if necessary.
Glossitis and oedema of the larynx may require the surgical procedures often necessary when they occur under other circumstances.
Other forms of toxic stomatitis hardly require special elucidation.
Apart from the anomalies presented in monsters, there are a few congenital abnormalities of the tongue with which it becomes the accoucheur at least to be familiar, as their presence may interfere materially with the nutrition of the infant, whether nursed or spoon-fed.
CONGENITAL DEFICIENCY OF THE TONGUE.—A considerable portion of the tongue may be wanting anteriorly, comprising, in some instances, the entire free portion of the organ. The stump then presents as a single or a bifid protuberance of variable size. In some instances considerable power of movement exists, and even conservation of taste. Suction and deglutition are both practicable. When the child grows it can speak, though with a certain amount of difficulty. A few cases are on record, however, of ability to speak without any evidence of a tongue above the floor of the mouth.
An instance of lateral deficiency has been observed by Chollet,16 the [p. 349]deficient half being represented merely by the two layers of the lingual mucous membrane, without any intervening muscular substance.
16 Demarquay, Dict. de Méd. et de Chir. prat., xx. p. 130.
BIFID TONGUE, separate investment of the two sides, has been occasionally observed in connection with similar arrest of development in the lower jaw and other organs.
DEFINITION.—An abnormal attachment or adhesion of some portion of the tongue to some portion of the surrounding structures of the mouth.
SYNONYM.—Tongue-tie.
PATHOLOGY AND MORBID ANATOMY.—The ordinary form of tongue-tie consists in an abnormal development of the frenum of the tongue, the anterior vertical portion of the duplicature of mucous membrane which connects the lower surface of the raphé of the tongue with the floor of the mouth. The tongue cannot be extended beyond the lips. Suction is interfered with in some cases. If not remedied spontaneously or by surgical interference, mastication and articulation may become seriously impeded.
Other forms of ankyloglossia, congenital and acquired, possess special interest from surgical points of view mainly.
DIAGNOSIS.—Inspection and digital exploration readily reveal the nature of the restriction in the movements of the tongue and the size of the frenum.
PROGNOSIS.—The prognosis is good, the difficulty being susceptible of relief by division of a portion of the constricting frenum. Accidents have been reported following the operation, the occasional occurrence of which should be borne in mind. These are hemorrhage, which is not dangerous except in the prolonged absence of some one competent to restrain it should it be extreme; and retroversion of the tongue, an accident which has been known to prove fatal by occluding the orifice of the larynx (Petit).
TREATMENT.—Slight cases rarely need operation; but when the movements of the tongue are restricted by a very short and deep frenum its division becomes necessary. The operation is usually performed with scissors, the ranine arteries being protected by means of a fissured plate of metal (Petit), such as has long been used as a handle to the ordinary grooved director of the physician's pocket-case. The cut should be more extensive in the lateral directions of the fold than antero-posteriorly. After-treatment is rarely necessary, unless annoying hemorrhage is produced by movements of suction. Compression between the fingers, maintained for a number of minutes, suffices to restrain the hemorrhage in most instances. When this fails, recourse may be had to cauterization with the point of a heated iron or some other form of actual cautery.
DEFINITION.—Hypertrophy of the tongue.
SYNONYMS.—Megaloglossia, Glossoptosis, Prolapsus linguæ, Lingua [p. 350] propendula, Chronic prolapse of the tongue, Chronic intumescence of the tongue.
HISTORY.—This rare affection has been long known, the first cases on record being in the works of Galen. Other cases have been recorded by Celsus and Avicenna. Among more modern recorders may be mentioned Scaliger (1570), Bartholin (1680), Benedict and Pencer; among recent recorders, Lassus,17 Percy,18 Harris,19 Humphrey,20 Gayraud,21 W. Fairlie Clarke,22 Bryant,23 and the French dictionaries in present process of publication; to all of which the reader is referred for bibliographic, descriptive, and illustrative details.
17 Mémoire de l'Institut National, 18—, an VI. t. i.
18 Dict. Sci. Méd., t. xxvii.
19 Am. Journ. Med. Sci., vol. vii., 1830, p. 17; vol. xx., 1837, p. 15—both illustrated.
20 Trans. Med.-Chir. Soc. London, 1853, p. 113.
21 Thèse de Montpellier, No. 68, 1865.
22 Diseases of the Tongue, London, 1873.
23 "Surgical Affections of the Tongue," Guy's Hosp. Reports, 1883, p. 102 et seq.
ETIOLOGY.—This affection is usually congenital, at least to a certain extent, and augments with the growth of the child. It has been attributed, on apparently insufficient grounds, to injury received during parturition. It is probably intra-uterine in origin. Though encountered in both sexes, the majority of recorded cases have been in females. In summing up these observations, it appears that the affection often attracts little or no attention until dentition is in progress. The hypertrophy begins to augment rapidly during the second or third year of age, or a year or two later in some cases.
The gradual increase of the congenital deformity during infancy has been attributed to hypernutrition from local irritation produced by habits of sucking on the organ, induced, in some subjects, by forcible efforts at suction from a short nipple. Similarly, the rapid augmentation of volume noted as occurring during the period of dentition or a little later has been attributed to hypernutrition excited by irritation suffered by the protruding organ from the lower row of teeth. Cases commencing at this age have been supposed to be due exclusively to tongue-sucking. In some instances, due to this cause apparently, the deformity is associated with idiocy (Lawson24). Convulsions, epileptic seizures, and whooping cough have been regarded by some writers as occasional causes of the deformity. Indeed, idiocy and cretinism are not infrequent co-associates with the deformity (Parrot25). It has been observed likewise in anencephalous monsters (Brissot, idem).
24 Trans. Clin. Soc. London, vol. v. p. 158.
25 Gaz. Méd. Paris, Dec. 10 and 17, 1881; Lond. Med. Record, Mar. 15, 1882, p. 113.
SYMPTOMS, COURSE, DURATION, TERMINATIONS, COMPLICATIONS, AND SEQUELÆ.—The prominent symptom of macroglossia is the enlarged tongue protruding beyond the mouth. The resemblance of the protruding tongue of a child with macroglossia to the tongue hanging from the mouth of a calf gave rise to the name lingua vitulina by which it has sometimes been designated. In some instances, where the enlargement is but moderate, the organ can be retained within the mouth. When bilateral, the enlargement may be symmetrical, or may interest one side of the tongue more than the other. When the enlargement is confined to the free portion of the tongue, it interferes little with respiration and with movements of suction. When occupying the base of the organ, it may seriously embarrass respiration, and even produce suffocation in [p. 351]some instances (Clarke). The mouth being maintained open, saliva dribbles away constantly except during alimentation. Thirst is often very great in consequence of this, and of the desiccation of the tongue and of the walls of the mouth by the unmodified air to which they are continuously exposed. The tongue is usually free from pain.
In some subjects, although the tongue, left to itself, protruded considerably, it has been found quite practicable to maintain it within the cavity of the mouth by means of bandages or other appliances secured to the back and top of the head. These bandages are removed from time to time to give relief from the restraint and to permit food and drink to be taken. Systematic compression, indeed, has been induced in this way in some instances, and has produced considerable diminution in the size of the organ—sufficient to maintain its concealment without the aid of an appliance. When the tongue cannot be retained within the mouth the patient becomes unable to close the jaws. Hence saliva dribbles constantly, save when food or drink is being taken. The protruded portion of the tongue undergoes a livid discoloration, sometimes diffuse, sometimes disseminated. Though sometimes remaining comparatively soft in texture, it usually becomes hard, dry, rough, fissured, ulcerated and sanious, covered with desiccating layers of mucus and epithelium, and marked by indentations made by the edges of the teeth, which sometimes seem almost to strangle it. Mastication, deglutition, and articulation often become very difficult, and respiration also, but less frequently. The lower lip becomes much everted. The larynx and hyoid bone become drawn upward and forward by the weight of the organ. The configuration of the lower jaw undergoes considerable change, and the teeth become pressed out of position. Dislocation of the jaw from this cause has been noticed (Chalk26).
26 Trans. Path. Soc. London, vol. viii. p. 305.
These symptoms undergo aggravation with the growth of the subject, and, while presenting general features of resemblance in all cases, vary considerably in individual instances. Great difficulty is encountered, as a rule, in taking food, and mastication has to be performed very slowly. In some instances mastication can be performed satisfactorily by the molars, owing to a compensatory curvature of the lower jaw, even though the anterior portions of the jaw may remain permanently separated (Harris). Some patients get along by using their fingers to push the bolus far [p. 352]enough back to permit of its deglutition. Some have used a cup with a long tube slightly curved to convey fluids to the back part of the mouth for a similar purpose. Some have been systematically fed by means of a catheter passed through a nasal passage and thus on into the oesophagus. The difficulties in nourishing patients reduce some of them to extreme emaciation.
Notwithstanding all these drawbacks, quite a number of cases are on record where the patients have reached well into adult life before being submitted to radical measures for relief. One patient is recorded as having reached the age of eighty, having worn for some sixty-five years a silver shield to conceal her deformity (Clarke).
PATHOLOGY AND PATHOLOGICAL ANATOMY.—The hypertrophy may involve all the structures of the tongue, but usually implicates the muscular tissue especially (Sédillot, Paget, Bouisson). In a case published by W. Fairlie Clarke it was found on microscopic examination that the papillæ as well as the mucous and submucous tissues were somewhat enlarged and thickened, while the bundles of muscular fibre were slightly coarser than natural. Maas reports a unilateral case of macroglossia in a male child two months of age associated with hyperdevelopment of the entire left side of the body.27 In some instances the blood-vessels and lymphatics are chiefly involved (Virchow, Billroth, Maas), two cases of which have been described by Virchow as cavernous lymphatic tumors.
27 Arch. klin. Chir., p. 413, Bd. xiii. Heft 3.
Hilliard reports28 a congenital case from vicious growth, removed at fourteen months of age. Microscopic sections showed the large lacunæ filled with corpuscles, blood-pigment in different stages of degeneration, [p. 353]and the papillæ much hypertrophied. Winiwarter29 reports a congenital macroglossia associated with congenital cysts of the neck.
28 Brit. Med. Journ., Nov. 26, 1870, p. 591.
29 Arch. klin. Chir., 1874, Bd. xvi. Heft 3.
Sometimes there is very little true muscular hypertrophy, as in a case quoted by Bryant which was presented to the Pathological Society of London in 1872 by M. H. Arnott. In this specimen the epithelial covering was very thick and the papillæ enlarged. The blood-vessels were larger than usual, and there were large irregular spaces, thin-walled and filled with blood or clear fluid. "A few vesicular bodies which may have been enlarged lymphatics were also present"—probably cross-sections of lymphatic vessels.
The size that may be attained even in young children seems incredible, three and four inches protruding from the mouth in some instances. The free portion is more bulky than the intra-oral portion. One case reported "as thick as an arm" probably refers to the arm of the child. As a rule, both sides of the tongue are involved; exceptionally, the affection is unilateral.
In most instances the hypertrophy occupied the free portion of the tongue chiefly, the base of the organ having been implicated in but a few.
| FIG. 14. |

|
| Chronic Intumescence of the Tongue (Harris). |
| FIG. 15. |

|
| Hypertrophy of the Tongue (Harris), before operation and after. A, odontolith. |
DIAGNOSIS.—The presence of the tongue outside of the mouth speaks for itself (Figs. 14 and 15). The age of the patient, usually a young child, the history of the case if it present in the adult, suffice to differentiate macroglossia from the tumefaction of glossitis on the one hand and from certain protruding tumors and malignant diseases on the other. Hypertrophy of the tongue following chronic glossitis, syphilitic or non-specific, must not be confounded with the congenital or idiopathic affection under consideration.
PROGNOSIS.—The prognosis is good as to relief from the deformity, provided the patient is submitted to surgical interference, and the prognosis of the operation depends upon the procedure selected. Sometimes additional operations are requisite to remedy the defects the lower jaw has sustained by prolonged depression. In comparatively young adults restoration of its position, configuration, and function seems likely to result spontaneously after the protruding portion of the tongue has been removed.
TREATMENT.—It has been maintained (Lassus) that the hypertrophy can be overcome by systematic compression of the tongue, by leeching the tongue, bandaging or strapping it, and forcibly maintaining it in the mouth by suitable retentive appliances. While it has been admitted that this plan may prove successful in cases of moderate enlargement of but few years' duration and unaccompanied with change in the shape of the lower jaw, the experience of more recent observers has been recorded as unfavorable, at least in pronounced cases. Clanny30 succeeded in this way with a child five years of age whose tongue protruded three inches. This plan is said to be very painful and irritating. It requires close watching on account of the difficulty of respiration which may ensue from thus blocking up the pharynx. It has been advised as a useful and sometimes an essential preliminary (Syme) to a radical procedure consisting in the excision of a V-shaped segment. This latter operation (Boyer) has been successfully performed by Howe, Harris, Humphry, Syme, and others. [p. 354]Frederici31 extended the incisions to the very base of the tongue. It has been performed both with knife and with scissors, the cut surfaces being united with sutures after ligation or torsion of the bleeding vessels. Re-enlargement ensued in one of Syme's cases operated upon in this way,32 and likewise in a case of Gies,33 requiring subsequent excision of the exuberant portions. Operations with the ligature, though sometimes successful (Fergusson,34 Hodgson35), may be followed by fatal septicæmia during the slough (Liston36), or, failing to strangulate the tongue sufficiently, may require the application of the knife, after all, to affect the separation (Harris37).
30 Edinb. Med. and Surg. Journ., 1805, vol. i., cited by Clarke.
31 Arch. gén. de Méd., 1844; Edinb. Med. and Surg. Journ., p. 528, vol. lxiv., 1845.
32 Edinb. Med. Journ., 1857, vol. ii. p. 1057.
33 Arch. klin. Chir., 1873, p. 640.
34 Practical Surgery, London, 5th ed., p. 518.
35 Trans. Med.-Chir. Soc. London, 1858, p. 129.
36 Elements of Surgery, p. 334, Philada., 1842.
37 Am. Journ. Med. Sci., vol. vii. p. 17.
Excision with the incandescent loop of the galvano-cautery seems to be the most suitable procedure. Valerani38 operated in this manner without the loss of a drop of blood upon a congenital macroglossia in a child seven months of age. Maas39 operated in this way on a child two months of age. Fairlie Clarke, who removed a congenital macroglossia with the écraseur in a child five months of age, recommends operation before dentition begins40—an opinion which appears to be justified by the belief that the pressure of the teeth contributes to the subsequent rapid enlargement of the organ. Nevertheless, the operation may be undertaken at any age. Several of those already cited were performed upon adults, and Stephen O'Sullivan41 excised the hypertrophied tongue of a female sixty-five years of age.
38 Giornale della Reale Accademia di Turino, fasc. 1518; London Med. Record, Sept. 15, 1876, p. 408.
39 Loc. cit.
40 Lancet, March 30, 1872, p. 432.
41 Dublin Journ. Med. Sci., Aug., 1875, p. 178.
Ignipuncture with the thermo-cautery of Paquelin has been successfully used of late by Helferich and by von Bruns of Tübingen.42 In the latter instance the subject was five years of age. Fourteen punctures were made from above downward at intervals of about one centimeter, and five were made transversely. Not a drop of blood was lost. On the third day secondary hemorrhage occurred from the intercommunication of three of the punctures; this was restrained by ferric chloride, and the case went on to a favorable conclusion. Surgical procedures must constitute our sole therapeutic reliance. The temporary subsidence of enlargement under the influence of mercury and the iodides seems sure to be followed, sooner or later, by reproduction of the deformity. It is therefore a waste of time to attempt cures by medication.
42 Centbl. f. Chir.; Med. Times and Gaz., Sept. 23, 1883.
DEFINITION.—Inflammation of the tongue.
The term glossitis is usually applied to inflammation of the tissues of the tongue as a whole (parenchymatous glossitis), and not to those superficial inflammations which exist associated with the different varieties of [p. 355]stomatitis and with other affections, and which implicate the mucous membrane and its glands and papillæ only (superficial glossitis). Superficial glossitis, however, sometimes terminates in parenchymatous glossitis. Papillæ and glands are usually affected together in superficial glossitis. When the inflammation predominates in the papillæ the disease is often designated as papillary glossitis; when in the glands, it is often termed follicular glossitis. Superficial glossitis, again, is sometimes manifested by the eruption of vesicles on the tongue, under which circumstance it is often denominated vesicular glossitis, sometimes herpetic glossitis. Glossitis is sometimes restricted to a portion of the tongue (circumscribed glossitis), and it sometimes involves the whole of the tongue (diffuse glossitis). Either form may be unilateral (hemiglossitis), though both forms are more frequently bilateral. Either form may be acute or chronic.
DEFINITION.—An inflammation of the mucous membrane of the tongue, usually involving likewise both papillæ and glands.
SYNONYMS.—Catarrhal glossitis, Angina lingualis. Varieties: Papillary, follicular, vesicular (herpetic and eczematous), psoriatic, ichthyotic.
ETIOLOGY.—Predisposing and Exciting Causes.—It is rarely idiopathic, is most frequently deuteropathic, and sometimes traumatic. Superficial deuteropathic glossitis usually occurs in connection with gastric and gastro-enteric affections. It occurs likewise in association with stomatitis, tonsillitis, pharyngitis, many febrile affections, scorbutus, tuberculosis, syphilis, so-called psoriasis and ichthyosis of the tongue, carcinoma of the tongue, and the various neoplasms of the organ. Irregular and sharp-cornered or jagged teeth often induce traumatic superficial glossitis. Pungent vapors, such as those of chloride of ammonium, so much used of late years in the treatment of nasal catarrhs, sometimes produce a superficial traumatic glossitis, usually localized on the superior surface of the anterior portion of the tongue. Tobacco-smoking, especially from a short-stemmed pipe, will likewise produce it occasionally at the point where the concentrated smoke strikes the organ. Attempts to drink liquids too hot, too acrid, or too caustic may be mentioned as other occasional causes. Nervous irritation, such as of the chorda-tympani nerve, is attributed as a causal influence of unilateral vesicular glossitis, herpetic or otherwise, and as a probable factor in other varieties of unilateral glossitis. Eczema of the tongue may ensue as a sequel of prolonged cutaneous eczema (De Mussy43).
43 Gaz. hebd., June 22, 1883; Med. News, Aug. 11, 1883, p. 151.
PATHOLOGY AND MORBID ANATOMY.—Superficial glossitis, as indicated, involves the mucous membrane, glands, papillæ, and epithelium. It is hardly necessary to dwell upon the pathological conditions of the lingual mucous membrane and its epithelium in gastro-intestinal and febrile disorders, as these are described in connection with the various diseases. Ordinarily, the epithelium increases in thickness, and when detached, spontaneously or otherwise, exposes a red and swollen membrane with erect papillæ. Sometimes the condensed stratified layer of epithelium becomes dry and very hard. Under some illy-defined [p. 356]conditions, the papillæ of the tongue undergo great hypertrophy. The filiform papillæ become elongated to several times their normal length, and feel and look like so many hairs on the tongue. Like many other lingual affections, this is often unilateral. It is quite marked in some cases of influenza and other febrile disorders, producing great annoyance in the mouth. It occurs likewise in gastro-intestinal disorders and in disorders of the mouth and teeth. It is evidently a deuteropathic phenomenon. In other cases the glands of the tongue, especially at its base, become involved, forming the follicular glossitis of some writers. In another class of cases, most frequently syphilitic or at least quasi-syphilitic, one or more whitish circumscribed patches are seen on the tongue, resembling such as are left after superficial cauterization with nitrate of silver. This condition is described as psoriasis linguæ. It is due to condensation of layers of epithelium, which may become detached in a few days in mass or in fragments, leaving the denuded mucous membrane red and the papillæ erect and somewhat swollen.
When psoriasis of the tongue has existed for a long time, a further change, and a more permanent one, takes place in the papillæ and epithelium. This condition has been denominated ichthyosis linguæ. Superficial ulceration takes place at the psoriatic patches, and the repair eventually excites such a proliferation of epithelium that it becomes quite horny to the sight and to the touch. It spreads over a much larger extent of surface than the original psoriasis, but, like it, leaves the unaffected portions of the tongue in an apparently normal condition. Both affections are usually bilateral, and the patches or series of patches most frequently symmetrical or engaging analogous vascular territory upon the two sides.
In a case reported by Mr. Hulke44 portions of the horny substance were habitually sliced off with a razor. Microscopic examination "showed colossal papillæ; the indurated portion of the mass was altogether epithelial, the lower cells being clear, transparent, and natural, the middle ones granular, and the superficial layer felted together into a dense opaque mass" (Clarke).
44 Medical Times, Nov. 30, 1861, p. 556.
Both of these affections are liable in about one-third of the cases to terminate in epithelioma. Although the opinion generally entertained classes all cases of psoriasis and ichthyosis linguæ in the category of syphilitic affections, there is reason to doubt its accuracy. Sangster45 has drawn up a tabular statement of 44 cases, of which 1 only occurred in a female; 23 occurred in smokers, 12 being inveterate smokers. In but 12 instances (81/3 per cent.) was there positive proof or strong evidence of syphilis; 30 per cent. of the whole number eventuated in epithelioma.
45 Med. Times and Gaz., London, April 8, 1882, p. 370.
Vesicular glossitis, usually unilateral and most frequently right-sided, has been described by Paget,46 Stoker,47 Barker,48 Hill,49 and De Mussy,50 and doubtless by others.
46 Lancet, March 11, 1865; Clarke, op. cit., p. 88.
47 Dub. Journ. Med. Sci., May 1, 1876, p. 401, illustrated.
48 Lancet, Nov. 22, 1879, p. 764.
49 Brit. Med. Journ., Oct. 7, 1882, p. 683.
50 Gaz. hebd., June 22, 1883; Med. News, Aug. 11, 1883, p. 151.
[p. 357]SYMPTOMATOLOGY, COURSE, DURATION, TERMINATIONS, COMPLICATIONS, AND SEQUELÆ.—Dryness of the tongue, stiffness, heat, and pain—the latter especially during movements of the organ in deglutition and in articulation—are the prominent subjective symptoms of acute superficial glossitis. There are rarely any marked symptoms of febrile disturbance unless the disorder is about to undergo extension into parenchymatous glossitis.
DIAGNOSIS.—Redness of the tongue, prominence of the papillæ, slight enlargement, perhaps bearing impressions made by the teeth, and pain or sense of impediment on movement, are the main diagnostic features of superficial glossitis.
Vesicles indicate the vesicular variety of superficial glossitis; irregular whitish patches, the psoriatic variety; and hard, horny patches with intervening fissures, the ichthyotic variety. A superficial circumscribed glossitis attending the local ulcerations of syphilis, tubercle, and epithelioma is differentiated by the clinical history of the case.
TREATMENT.—In ordinary cases the treatment described under catarrhal stomatitis suffices, so far as local measures are concerned. The gastritis or gastro-enteritis requires appropriate attention, as does any systemic malady under which the patient may be laboring. Demulcent and astringent lotions may be applied by douche, spray, or gargle. Local applications of weak solutions of iodine have been recommended. In cases of considerable severity, and especially when there is reason to expect extension into the deeper tissues, superficial scarification of the dorsum of the tongue is advisable.
Ulcers are perhaps best treated locally by touching the edges daily with the pencil of sulphate of copper. Any imperfect teeth in their immediate vicinity to which the ulceration may be attributable should be extracted or put in repair. De Mussy's case of eczema was cured after five months' daily use of a large quantity of water-cress.
DEFINITION.—An inflammation of the tongue said to be due to parasitic vegetation.
SYNONYMS.—Nigrities, Glossophytia, Black tongue.
Under the term black tongue two different affections have been described, the one an epidemic erysipelatous disorder to be mentioned under parenchymatous glossitis, and the other, now to be mentioned, a peculiar black pigmentation due to parasitic disease seated upon and around the hypertrophied filiform papillæ. The ordinary parasitic vegetations found upon the tongue do not produce the affection in question.
HISTORY.—First described by H. Hyde Salter,51 and then by Eulenburg, it has been made the subject of observation by Raynaud,52 Fereol and others,53 Lanceraux,54 Dessois,55 Hirz,56 Pasquier,57 Moure,58 and a few [p. 358]others. Outside of French literature, little had been written of it until very recently.
51 Article "Tongue," Encyclopedia of Anatomy and Physiology, London, 1849-52, vol. iv. pp. 1159, 1160.
52 Gaz. hebd., 1869, No. 14, p. 221.
53 Gaz. des Hôp., June 29, 1875.
54 Union Méd., March 20, 1877.
55 De la Langue noire [Glossophytie], Paris, 1878, 8vo, p. 38, illustrated.
56 Gaz. Méd., Strasbourg, 1879.
57 Bull. Méd. du Nord, 1883.
58 Revue mensuelle de Laryngologie, etc., Sept., 1883, p. 276.
ETIOLOGY.—The affection appears to be due to some fault of nutrition, but the cause has not been determined. The fluids of the mouth always exhibit an acid reaction. It has been seen chiefly in dyspeptics and hypochondriacs, and has seemed in one instance (Moure) to have followed the use of chlorate-of-potash lozenges. A case has been recorded by Solomon Solis Cohen59 in a negro child the subject of congenital syphilis. Mr. George Stoker60 and G. Y. Broatch61 have each reported a case of long duration occurring in a painter.
59 The Polyclinic, Philada., July, 1884, p. 10.
60 Brit. Med. Journ., March 29, 1884, p. 602—said to be first case recorded in England.
61 Ibid., April 19, 1884.
PATHOLOGY AND MORBID ANATOMY.—The disease is characterized by a grayish-black or fully black discoloration on the upper surface of the tongue, which gives it an aspect which recalls the normal appearance of the tongue of the parrot and the giraffe, and an occasional appearance of the organ in the ox, sheep, dog, cat, and some other animals. The filiform papillæ are enormously elongated, so that they closely resemble hairs, and they are described by some writers as lying upon the surface of the tongue in confusion like that of a field of wheat thrown down by the wind. The individual papillæ are surrounded with a parasitic vegetable growth. Raynaud compared the microscopic spores in his case to the microphyte of tinea tonsurans or that of herpes circinatus. According to Malassez, they do not differ from those found in the saburral tongue of the dyspeptic, and he considers that their development is favored by their very arrest by the hypertrophied papillæ. Nevertheless, the subjects of this disease are not all dyspeptics by any means. Dessois made culture-efforts to reproduce the disease upon his own tongue, but failed to inoculate it. For detailed description of the disease we cannot do better than refer the interested reader to Dessois' monograph, from whose observations, chiefly, it appears that the discoloration begins at the central portion of the tongue, increases gradually in extent and intensity for three or four days, and then gradually disappears by desquamation. The tongue is very dry while the affection is at its height. Close examination of the parts and microscopic inspection of papillæ removed for the purpose are said to show that the spores of the cryptogam are first developed at the base of the papillæ, separating them from each other. The irritation produced by the parasite causes longitudinal hypertrophy of the papilla, and the continued growth of the parasite produces a muff-like envelopment of the papilla; the spores at the same time becoming insinuated between the most superficial epithelial cells and dislocating them, so that they maintain their position around the axis of the papilla only by means of the intervening parasitic masses. The papilla continues to elongate and the cryptogam to increase, until finally it invades nearly the entire length of the papilla. This entire parasitic mass soon becomes detached, carrying with it the epithelial cells under which it has become insinuated, and leaves the papilla naked, save for a few cells remaining attached by their superior borders. In the case observed by my brother, as in Mr. Stoker's and Broatch's cases, microscopical examination of the black filaments showed them to be composed of closely-packed epithelial cells, overlapping one another, stained [p. 359]brown, and decreasing in intensity of color from the apex toward the base of the filament. In some cells the nucleus was darker, and in others lighter, than the surrounding protoplasm. The cryptogam, therefore, cannot always be detected. Indeed, there seems reason to believe that the affection may not be parasitic,62 although the prominence given to this feature by French writers apparently warrants its being so considered. There may be two kinds of black tongue—one non-parasitic.
62 Hutchinson, The Medical Press, p. 20, July 11, 1883.
SYMPTOMS.—There are no special subjective symptoms. The objective symptoms are the peculiar dark or black discoloration of the upper surface of the tongue and the excessively elongated filiform papillæ.
DIAGNOSIS.—The chief diagnostic feature is the black discoloration of the tongue which has given the name black tongue to the disease. Discrimination is requisite from discoloration by food or medicine.
PROGNOSIS.—This is favorable, the condition subsiding under treatment, and sometimes spontaneously, though liable to recurrence. In some instances the condition becomes chronic.
TREATMENT.—The indication is to endeavor to favor desquamation of the papilla by means of potassium chloride or sodium borate, and to administer alkalines, so as to render the saliva alkaline and unfavorable for the development of the parasite. It is recommended, in addition, to scrape the tongue with a spatula, and to douche it with a spray of mercuric chloride, 1:500. Attention to the general health is requisite, especially in dyspeptics and hypochondriacs. In the case of the negro child above alluded to the discoloration of the tongue finally disappeared under the systemic use of potassium iodide, without topical treatment, although repeated recurrences took place at varying intervals.
DEFINITION.—An inflammation of the tongue involving its substance as well as the mucous membrane.
SYNONYMS.—Idiopathic glossitis. Interstitial glossitis. Erectile glossitis (Salter), Glossomegistus (Sauvages), Paraglossia.
HISTORY.—Albeit a comparatively infrequent disease, especially at the present day, numerous cases and collections of cases are on record from very early times; and the affection seems to have attracted the attention of medical writers ever since. Hippocrates, Galen, Aretæus, Celsus, Aëtius, Avicenna, Forestus, Rivière, Schenkins, Sauvages, Vogel, van Swieten, are referred to by more modern writers as having described the disease. Louis, De la Malle, Lassus, J. P. Frank, Jn. Frank, Fleming,63 Clarke, and Bryant may be cited as the most prominent recent observers.
63 Dublin Journ. Med. Sci., 1850, vol. x.
ETIOLOGY.—Predisposing and Exciting Causes.—Glossitis is sometimes idiopathic, sometimes deuteropathic, and sometimes traumatic. Impaired health from over-fatigue or from exhaustive disease may be regarded as a predisposing cause in the presence of the causes which more frequently give rise to traumatic glossitis. Sudden or prolonged exposure to atmospheric changes, to cold and moisture, as when working in damp and wet localities, is often the apparent determining cause in [p. 360]both the idiopathic and deuteropathic varieties. In many instances occurring in this way it is found that the tongue has long been subjected to mechanical irritation from jagged teeth.
Idiopathic glossitis occurs at all ages, but has been supposed by some observers to be more frequent in scrofulous subjects. It occurs in the apparently healthy only after severe exposure to wet and cold, and in convalescents from acute febrile diseases usually after some moderate exposure to a draught of air or change of temperature. It appears to be more imminent after influenza (Möller, Smee, Graves, Salter) than after other febrile disorders. It has occasionally been caused by chewing acrid plants, some of them food-plants, some of them medicinal. In the list have been included celery, bilberries, Daphne mezereum and Daphne laureola, aconite, and tobacco. It has been known to follow the eating of shellfish (Watson, Salter).
Deuteropathic glossitis has occurred during the course of scarlatina, variola, epidemic erysipelas (black tongue), scorbutus, enteric fever, glanders, septicæmia from various causes, rheumatism, diffuse inflammation of the connective tissue of the cervico-mental region, herpes, syphilis, ptyalism, mercurial and other varieties of toxæmic stomatitis, tonsillitis, pharyngitis, gastritis, and epithelioma of the tongue. It appears to be occasionally endemic (Fleming64), and is occasionally epidemic (Reil65). In the United States it prevailed extensively during an epidemic of erysipelas that overran the country from 1842 to 1846, inclusive, and was frequently reported in the American medical journals of that period under the name of black tongue. In some localities more than half the cases terminated fatally, sometimes within two or three days, more frequently about the eighth or tenth day, and occasionally still later. Traumatic glossitis arises from a number of causes. Among these may be mentioned the irritation of jagged edges of broken and carious teeth; wounds from firearms and other weapons; wounds from splinters of toothpicks, spiculæ of bone, broken pipe-stems, pins, needles, nails, slate-pencils, and other pointed things inadvertently placed in the mouth; wounds from the teeth during epileptic seizures and other convulsive paroxysms; contact of the tongue with cold iron in cold weather; the inspiration of very hot air, as in burning buildings; burns, scalds, scalding beverages; acrid and corrosive substances introduced by design or accident; incautious use of tobacco in bulk, and of ammonia; incautious cauterization; concealed calculi in the tongue; concealed bulbs of teeth; rupture of the lingual frenum; the bites and stings of venomous insects, as the wasp, the hornet, and the bee. For many years writers have referred to a case reported by Dupont to the Parisian Academy of Medicine which followed a young man's attempt to win a wager that he would bite into the body of a living toad, and to two fatal cases reported by Ambrose Paré from drinking a vinous infusion of sage which was subsequently found to have been impregnated with the saliva of the toad.
64 Dub. Journ. Med. Sci., 1850, vol. x. p. 88.
65 Memorabilia Clinica (Dict. Sciences méd.), vol. xviii.
SYMPTOMS, COURSE, DURATION, TERMINATIONS, COMPLICATIONS, AND SEQUELÆ.—In acute parenchymatous glossitis the local symptoms often appear quite suddenly, usually unilaterally, even when they become bilateral subsequently, and they increase in severity with great rapidity. [p. 361]These symptoms are, at first, distinct sensations of heat and tumefaction in the tongue, quickly followed by stiffness and considerable impediment in its movements, as though it were numb and weighted down. In cases where the glossitis is an extension from tonsillitis, these sensations begin in the root of the organ. They commence at the root likewise, in most instances following exposure to severe cold and moisture. In other instances the extremity of the organ is affected first. In cases resulting from local injury the symptoms commence at the injured portion. The local symptoms are sometimes preceded by rigor, followed by fever, cephalalgia, and pains in the neck and occiput. Examined at this time, the tongue is seen to be swollen and studded with indentations due to the pressure sustained from the teeth. At first the surface is punctated and red; subsequently it becomes brownish or decidedly brown. Although the organ may remain moist for several hours, it eventually becomes excessively dry, and supports a thick adhesive coating of mucus and epithelium.
| FIG. 16. |
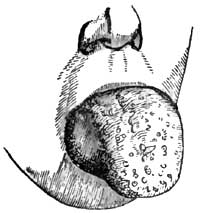
|
| Glossitis (Liston). |
In a few hours, sometimes as few as two or three, the entire organ may become involved in the inflammation, enlarging to such an extent as to keep the lower jaw depressed, to fill almost the entire oral cavity or to quite fill it, and to project like a tumor beyond the teeth and the lips (Fig. 16). In exceptional cases the enlargement of the tongue has been so great as to produce dislocation of the lower jaw. The soft palate is lifted up and the epiglottis often pressed down. The latter condition has been known to threaten suffocation. In this condition the patient cannot breathe through the mouth, widely as it may be forced open, and has great difficulty in breathing through the nose. Respiration is therefore laborious. Articulation is impeded or impossible, and deglutition difficult or impracticable. The tumefaction and congestion are often continuous into the floor of the mouth and the parts adjacent. The sublingual and submaxillary glands often become swollen, tense, and painful; and the entire neck is sometimes swollen to such a degree as to exert injurious pressure on the jugular veins. The tongue is very hard to the touch, almost or quite immovable, and is the seat of burning heat and pain. The pain often extends from the root of the tongue along the glosso-pharyngeal folds into the pharynx, and thence by way of the Eustachian tubes into the ears, the folds just named being very much upon the stretch. When the tongue protrudes far out of the mouth it becomes excessively dry, fissured, sanious, and excoriated, or even ulcerated at points where it is subjected to the pressure of the teeth. It is covered with dark viscid secretions, which often extend beyond it and over the entire aperture of the mouth. The epithelial coating often undergoes desquamation, and then the organ becomes exquisitely sensitive to the contact of food, water, or even the air. This desquamation is sometimes in mass, in sheets peeling off like a pseudo-membrane. The general symptoms vary in individual cases. As a rule, the face is turgid and its expression anxious; the conjunctiva suffused, respiration impeded, and sleep disturbed or impracticable. Saliva dribbles externally, often in considerable quantity. The [p. 362]odor from the mouth becomes quite fetid from decomposition of the retained products of secretion. Thirst is usually intense, though immoderate only in some cases. Cough is more or less constant and quite exhausting. This and the dribbling of saliva contribute with the dyspnoea to prevent sleep. Pyrexia is often intense. The pulse is strong and quick at first, 100-120 per minute, and there is often marked throbbing of the temporal and carotid arteries. The skin is hot and dry at first, but cold sweat subsequently accumulates upon the face and neck as the dyspnoea increases. The bowels are constipated. The urine is scanty and high colored. The impediment to the return of blood to the heart from the head causes cerebral congestion, drowsiness, and even threatens asphyxia. In other cases there is intense cephalalgia, nervous irritability, restlessness, and even delirium.
The symptoms sometimes reach their acme in rather less than forty-eight hours, and then gradually subside. More frequently they continue on into the third or fourth day. Occasionally they are protracted as long as the fifth or sixth or even the eighth day, rarely longer. Resolution occasionally takes place within twenty-four hours, however (van Swieten), though more frequently occurring from the fifth to the seventh day. In some instances remittance or intermittence has been noted, the cause therefor not being apparent, although attributed to malaria.
Resolution of the inflammatory process is usually indicated by the gradual return of moisture on the tongue and progressive detumescence of the organ, accompanied by subsidence of the redness, heat, and pain. Increased secretion of saliva, general perspiration, or diuresis sometimes marks the cessation of the pyrexia.
Should the process be going to terminate in suppuration, the local distress increases, markedly about the end of the week. The pains become lancinating, and associated with throbbing of the lingual blood-vessels. The swelling becomes prominent and softer at some one point, although the sense of fluctuation is not very perceptible on palpation, and finally the abscess bursts through the surface, unless previously incised, and discharges a fetid pus. Suppuration always involves a prolonged duration of the attack.
In rare instances glossitis terminates in gangrene of the tongue, circumscribed or diffuse. This result is indicated by adynamic symptoms on the part of the constitution, and by the livid appearance of the parts undergoing mortification. The hemorrhage following extensive sloughs from gangrene has been fatal in some instances.
Fleming66 calls prominent attention to a complication of glossitis, of which he alludes to several examples. This is "an inflammation, circumscribed or diffused, originating in the loose areolar tissue between the genio-hyo-glossi muscles, and first manifesting itself by a train of symptoms identical with those of ordinary glossitis, but soon characterized by peculiar features." These features comprise fulness under the chin like that dubbed double chin, pressure upon which, especially near the hyoid bone, being very painful; and suppuration, which, circumscribed or diffuse, burrows most freely toward the base of the tongue.
66 Loc. cit., p. 91.
Chronic induration of the tongue sometimes remains unilateral, although the acute disease has not been unilateral.
[p. 363]PATHOLOGY AND MORBID ANATOMY.—It has been advanced that in idiopathic glossitis from cold the engorgement of the vessels is probably a consequence of vaso-dilator influence of the glosso-pharyngeal nerve for the base of the organ, and of the chorda-tympani for the anterior portion. An instance of herpetic glossitis from probable irritation of the chorda-tympani nerve by an aural polypus (Berkely Hill67) seems to lend some force to this opinion. However engendered, there is a rapid distension of the organ by blood, followed by infiltration of fibrin and serum into the intermuscular connective tissue and into the planes of the connective tissue separating the muscular fasciculi. In some instances degeneration of muscular fibre has been observed. There is great increase in the thickness of the coats of epithelium, beneath which the mucous membrane is red and its papillæ erect. This coating sometimes peels off like a false membrane. In cases extending from tonsillitis the base of the tongue suffers most.
67 Brit. Med. Journ., Oct. 7, 1882, p. 683.
The disease usually terminates by resolution, although a slight amount of hypertrophy, unilateral or bilateral, sometimes persists, and occasionally to a marked degree (Wells). In instances much less frequent suppuration ensues, usually in debilitated subjects or in cases due to traumatism or in cases inefficiently treated. The suppurative process is usually circumscribed and unilateral, and the abscess points most frequently just beneath the side of the tongue; sometimes, however, the pointing takes place at the dorsum, sometimes at the tip. The pressure of the teeth seems to be the provocative cause of the disposition to point at the edge of the tongue. The pus is usually quite fetid. Sometimes the abscess is gangrenous.
Gangrene is an infrequent result of glossitis. The pressure of the teeth, strangulating the organ at the oral outlet, seems to occasion the failure of nutrition in instances where it occurs. The losses are ordinarily insignificant, though appearing quite extensive while the tongue remains swollen. Sometimes large portions drop off, and fatal hemorrhage has resulted (Frank) in consequence. From the nature of the organ the parts separate more readily than in almost any other instance. Gangrenous abscess, ensuing even from very slight causes, such as a wound with the head of a barleycorn (Ranking68), sometimes proves fatal.
68 Provincial Med. and Surg. Journ., 1844.
In those cases of diffuse inflammation of the interconnective tissue of the genio-hyo-glossi muscles Fleming states that the suppuration—which, whether circumscribed or diffuse, burrows toward the root of the tongue—absolutely dissects its extrinsic muscles and destroys their functions; ultimately injuring the periosteum and laying bare the inside of the inferior maxilla in the vicinity of their attachments. When an incision is made to the parts through the integument, the muscles will be found on palpation flabby and detached, and their interstices filled with purulent matter, sometimes very fetid.
DIAGNOSIS.—These is no difficulty in the diagnosis, except in the early stage of such examples as are attributed to metastatic gout and rheumatism. The subsidence of the peculiar pains elsewhere, and the onset of pain in the tongue, would lead to the inference that a glossitis of this kind [p. 364]was in progress. The acuteness of the tumefaction would distinguish it from hypertrophy of the tongue on the one hand, and from the tumefaction attending malignant disease on the other.
Cystoma of the tongue has sometimes been mistaken for abscess due to glossitis; but even here the history of the case should serve in most instances as a satisfactory factor for the differential diagnosis.
PROGNOSIS.—The prognosis depends upon the gravity of the local symptoms and the activity of the treatment. A case left to itself will be likely to terminate fatally within five or six days. Death, indeed, has been known to take place within forty-eight hours, even in cases submitted to treatment. On the whole, however, the prognosis should be regarded as favorable in the absence of specially lethal complications. Even suppuration adds little gravity to the prognosis, the structure of the organ being but little favorable to accumulations of purulent material. Should an abscess become gangrenous, however, the prognosis becomes grave at once, as it in the presence of gangrene from pressure or other cause. Should the patient survive losses by gangrene, there may be permanent impairment in articulation.
TREATMENT.—Superficial glossitis, as a rule, merely requires active purgation, with the topical use of cold emollient mouth-washes containing mucilage of slippery elm, quince-seed, or the like, to which detergents, such as alum and borax, may be advantageously added in the proportion of five grains to the ounce. In cases resisting this mild treatment topical applications of glycerite of tannin twice or thrice a day are often serviceable.
Parenchymatous glossitis demands the most active antiphlogistic treatment. If the case be seen at an early stage of the process, before the tumefaction of the tongue has become so great as to fill the mouth and interfere with swallowing, a saline purge—say salts and senna—containing some tartar emetic can be advantageously administered to begin with. Following this, tartar emetic may be continued in small doses every two or three hours, associated with small doses of tincture of aconite-root (minim j-iij), according to the condition of the pulse and the effect of medication. Should this treatment fail to produce prompt amelioration in the local symptoms, or should the tongue be considerably swollen when the case comes under care, free leeching should be applied from the hyoid bone to the angle of the jaw on each side, including the region of the hyoid bone (fifteen to twenty-five Spanish leeches). This should be followed by emollient cataplasms, reaching from ear to ear, to favor continuous hemorrhagic oozings from the leech-bites. The internal antiphlogistic treatment is indicated just the same, and if not administrable by the mouth may be administered by the bowel; the nauseant and depressent effects of the tartar emetic and aconite being maintained by hypodermatic injection. Leeching the inflamed tongue itself is said to be often prompter in producing detumescence of the organ than leeching exteriorly, but the leech-bites are apt to add to the local irritation; besides which, the mouth is so filled by the swollen tongue as to leave little more than the tip accessible to the leeches without danger of losing control of them. Venesection from the arm, the jugular vein, or from vessels elsewhere is no longer much in vogue, it being doubtful whether general venesection is more useful than local bleedings. Debility, whether presenting originally or as the result of withdrawal of blood and other [p. 365]antiphlogistic measures, may be met by the systematic use of tincture of chloride of iron and of quinia.
Severe cases demand one or more longitudinal incisions on each side of the raphé of the tongue, deep enough to reach nearly halfway into the substance of the organ and carried from base to tip. Cases are on record in which the patients themselves had in their despair cut into their tongues in order to obtain relief from their local sufferings, and had in this way rescued their own lives by the means most appropriate for the purpose (Camerarius, Lusitanus69). When the mouth is filled by the tongue, it is necessary to insert the knife on the flat until the base of the tongue is reached, and then to turn it and make the cuts as indicated. Copious bleeding usually follows these incisions, often followed by marked diminution in the volume of the organ. Deep as these cuts appear when made, they become quite shallow before the organ has shrunk to its normal volume. Bleeding from the ranular veins, recommended by some practitioners in preference to incisions into the organ, is often impracticable on account of the tumefaction preventing access to them.
69 Dict. Sciences méd., vol. xviii.
If severe hemorrhage takes place from divided vessels, the vessels may be subjected to torsion, which is the preferable mode of management, or to searing with some form of the incandescent cautery (hot iron, electric cautery, Paquelin's thermo-cautery). Astringent and chemical styptics are of little use. The method of searing is open to the objection that secondary hemorrhage may ensue on detachment of the eschars, but this accident is not likely to happen under circumstances at all favorable.
In localized or circumscribed glossitis the incision to be made should interest the swollen portion only.
Should the tongue swell again, the incisions may be repeated. Whether the tongue require incision or not, it is good treatment to have the patient inhale vapor from hot vinegar, alcohol, or cologne spirits to render the parts more comfortable. Washes of weak detergent solutions containing potassium nitrate, sodium borate, or ammonium chloride may be used by syringe or spray to cleanse the parts and promote detachment of the epithelial coatings on the tongue and interior of the mouth, the accumulations of which are sometimes matters of great annoyance. The drug last mentioned exerts in addition a special action on the inflammatory process which is often quite serviceable. I have seen good results follow the prolonged use of sprays of an aqueous solution of ammonium chloride (Stuver), one drachm to the ounce, from the steam-spray apparatus, continued for fifteen to twenty minutes at a time and repeated every two or three hours.
In many instances the patient is unable to take food by the mouth. The best plan under such circumstances is to pass a catheter into the stomach through the larger of the two nasal passages, and retain it in position unless its presence interferes too much with respiration. Milk and stimulus can then be poured into the stomach from time to time with the aid of a funnel passed into the outer opening of the tube, which should be kept corked during the intervals when retained in position. This failing or impracticable, it will be necessary to nourish the patient with enemata.
On the appearance of abscess the same should be freely laid open. In cases of hesitation, the true nature of the presumable abscess can be [p. 366]determined beforehand with the exploring-needle. The pus from an abscess of this kind is rarely copious and is usually fetid. It would be good practice to distend the sac after discharge of pus by injecting into it a solution of carbolic acid.
In resisting or advanced cases of suppurative inflammation of the planes of connective tissue between the muscles at the lower portion of the root of the tongue, Fleming recommends a free incision under the chin in the middle line, through skin and fasciæ and on through the raphé of the muscles themselves.
In cases of gangrene, washes, douches, or sprays of carbolic acid, chlorinated soda, hydrogen peroxide, or potassium permanganate are indicated to relieve fetor; while the most supporting treatment by mouth or otherwise is requisite on general principles.
Chronic glossitis, like acute glossitis, may be superficial or parenchymatous.
Superficial chronic glossitis is usually confined to the papillæ of the tongue, territories of which, so to speak, are mapped out on the surface of the tongue, separated by furrows reaching to the basement mucous membrane. In pronounced cases the dividing furrows are quite deep, giving the organ a mamelonnated appearance, and they penetrate into the mucous membrane (dissecting glossitis, Wunderlich), which becomes subjected to great irritation by the retention of articles of food in the fissures. Demarquay70 has recorded a case of this kind in which, to relieve the intense sufferings with which the patient had been plagued for a number of years, he had been forced to amputate the anterior half of the organ—an operation which succeeded thoroughly.
70 Loc. cit., p. 142.
In another group of cases the surface of the swollen tongue is mapped out in small ovoid patches, smooth, red, and glossy, from which the papillæ have become separated without regeneration. Sometimes chronic glossitis presents as an aphthous inflammation. Sometimes superficial ulcers occur upon the dorsum of the tongue, irritable, indolent, and indurated.
ETIOLOGY.—Chronic superficial glossitis is in rare instances a sequel of the acute form of the disease. Usually, however, it is encountered as a chronic affection from the outset, so to speak, generally as a result of long-continued irritation in connection with dyspepsia and other gastric and gastro-intestinal disorders. It is frequently encountered in subjects of chronic alcoholism.
The superficial ulcerations often occur at the sides of the organ, usually in some of the depressions formed by the contact of the teeth.
SYMPTOMATOLOGY.—The symptoms are those due to a consciousness that the tongue is too large, with occasional pain in taking acid and succulent food.
[p. 367]PATHOLOGY.—The pathology does not differ from that of chronic inflammations elsewhere. The apparent obliteration of the papillæ in some cases is due to a filling up of the intervening furrows by permanent deposit of new-formed cells. The excoriations and superficial ulcerations are most frequently due to disturbance of nutrition by pressure.
DIAGNOSIS.—The affection may be confounded with syphilitic disease of the tongue or with papillary epithelioma, but the history of the case, the resistance to antisyphilitic treatment, and the negative results from microscopic examination of fragments of tissue removed for the purpose, serve to establish the diagnosis in cases of doubt. It must not be forgotten, however, that many cases of epithelioma begin in chronic glossitis, non-specific as well as syphilitic.
PROGNOSIS.—Though not threatening to life, the prognosis of the disease itself is bad. It resists treatment, being, in fact, a complication of some obstinate or intractable gastric or gastro-intestinal disorder, or an evidence of constitutional dyscrasia. Cure may be expected in recent cases, following cure of the dyspepsia or other malady upon which the chronic glossitis may be dependent.
TREATMENT.—Care to cleanse the tongue by washes, douches, or wet cloths after each meal, in order to remove particles of food which may have become impacted in the anfractuosities of the organ, is important in order to avoid additional sources of irritation.
Astringents and caustics of various kinds have been extensively employed, carefully applied to the floors of the fissures, but it is very rarely that any benefit ensues. Demarquay71 reports good results in one case of dissecting papillary glossitis from biweekly applications of equal parts of chromic acid and water. Butlin reports good results from chromic acid (1:10).
71 Loc. cit., p. 143.
Careful attention to the gastro-intestinal functions, and a thorough change of diet, such as the adoption of the milk cure and the like, with due attention to bathing and outdoor exercise, comprise the most rational method of constitutional treatment. Should the secretions of the mouth give an acid reaction with litmus-paper, alkalies are strongly indicated, topically and systemically. Avoidance of alcohol in all forms is often absolutely essential.
The chronic parenchymatous form of glossitis is usually circumscribed. When diffuse or general it has usually been a sequel of acute parenchymatous glossitis. It is not a painful disorder, and as a rule is not associated with constitutional manifestations. The circumscribed tumefaction usually presents as an induration upon some portion of the side of the tongue, being most frequently directly or indirectly due to irritation sustained from a jagged tooth. Ordinary sensibility is much diminished, and sometimes the sense of taste likewise. Sometimes the indurated mass is ulcerated superficially. The enlargement of the organ is not sufficient to keep it outside the mouth. Sometimes, indeed, the tongue, [p. 368]as a whole, has undergone atrophy, unilateral or bilateral. Chronic abscess of the tongue sometimes supervenes, chiefly in scrofulous subjects.
PATHOLOGY AND MORBID ANATOMY.—This consists merely in interstitial connective-tissue hyperplasia, with atrophy of muscular fibres from compression.
SYMPTOMS.—In addition to the objective symptoms of induration or circumscribed tumefaction, the subjective symptoms may be summed up as general hypersensitiveness to sapid and acrid substances; diminished tactile sensibility at the part affected; slight stinging sensations while the parts are at rest; occasional or continuous local pains; and a sense of impediment in the movements of the tongue in articulation and even in deglutition.
DIAGNOSIS.—Inspection reveals the swelling, and palpation its induration. In addition, the adjacent source of irritation, a jagged tooth or two, is seen. Abscess is recognized by special prominence at one point of the swelling and by indistinct sense of fluctuation.
Cystic tumor is liable to be mistaken for abscess, but the exploring-needle will solve the difficulty. Circumscribed induration may be confounded with tumor or with epithelioma.
PROGNOSIS.—This is good, provided the source of irritation can be removed or suppressed.
TREATMENT.—The first element in the treatment is the removal or repair of any offending tooth, and next attention to any underlying malady, constitutional or local. Weak solutions of iodine locally are said to be of service. Abscesses require incision and evacuation. Their walls should be distended with solutions of carbolic acid or be touched with solutions of iodine, silver nitrate, or cupric sulphate, to promote reparative inflammation.
This is a special variety of gangrenous ulcerative glossitis, presenting as an integral phenomenon of a disease peculiar to slaughterers, who become infected from diseased cattle, usually by means of the knife, which they are sometimes in the habit of holding in the mouth (Heyfelder and others). It has been described chiefly by Heyfelder,72 Duhamel, Chavarrien d'Audebert, Felix Plata, Breschet et Finot, and Maisonneuve.73
72 Med. Vereins Zeitung, 1834.
73 Des Tumeurs de la Langue, Paris, 1848, Thèse de Concours.
The period of incubation occupies about one day. The tongue then undergoes rapid tumefaction and becomes the seat of intense pain. The points of inoculation become hard, covered with vesicles containing bloody serum, which blacken, rupture, and leave dark, livid, gangrenous patches of ulceration. Profound cachexia rapidly ensues under typhoid manifestations, and death may result in less than twenty-four hours, though usually not until sixty hours. The prognosis, therefore, is of the gravest character.
The chief treatment consists in thorough cauterization of the inoculated [p. 369]points by means of the actual cautery, followed by deep incisions into the body of the tongue if the glossitis be severe.
Apart from the ulcerations of the tongue incidentally mentioned in the foregoing pages, there are two forms of ulcer, both of sufficiently frequent occurrence in ordinary practice to require special description: these are the tuberculous ulcer and the syphilitic ulcer.
Tuberculous Ulcer of the Tongue.—Tuberculous ulceration of the tongue occurs in a certain number of cases of advanced tuberculosis of the lungs or of the lungs and larynx. It has even been asserted to precede pulmonary tuberculosis. It is most frequently observed upon the upper surface of one side of the organ, sometimes at the tip, sometimes farther back, and usually on the same side upon which the disease is most advanced in the lungs or the larynx. It is often associated with previous or subsequent tuberculous ulcerations of the palate or of the pharynx or contiguous structures. It gradually extends, and rarely if ever heals. It is characterized by a superficial excavation, and by being covered with a grayish detritus entirely different from the purulent layers seen on other kinds of ulcers. When of long standing its base is indurated, and this may give rise at first to suspicion of squamous-celled carcinoma. Small yellowish elevations are sometimes observed in the reddened mucous membrane around the ulcer—an appearance deemed sometimes characteristic of the tuberculous nature of the lesion (Trélat74).
74 Bull. de l'Acad. de Méd., 1869, or Arch. gén. de Méd., 1870.
PATHOLOGY AND MORBID ANATOMY.—Nodular tuberculous infiltration takes place beneath the mucous membrane, which becomes elevated in small, semiglobular, yellow protuberances of one or more millimeters in diameter, around which the mucous membrane is red and swollen. The epithelium becomes shed without undergoing renewal, and thus a little point of superficial ulceration remains. When several such points are sufficiently contiguous they coalesce into a single ulcer of irregular contour, which gradually spreads without much other change. Practically, it never heals.
SYMPTOMS.—In addition to the superficial ulceration described, and in addition to the constitutional and local symptoms of advanced tuberculosis of the lungs or lungs and larynx, as may be, there are no special symptoms attending the tuberculous ulcer of the tongue. Saliva is sometimes secreted in excess, but that is not characteristic. There is little pain and little impediment to the movements of the tongue until the disease has advanced.
DIAGNOSIS.—The presence in a tuberculous subject of a unilateral, irregular ulcer of the tongue surmounted with grayish detritus and surrounded by reddened edges, should suffice for the recognition of its presumptive tuberculous character. It is most difficult perhaps to differentiate from a small ulcerated squamous-celled carcinoma, and the two indeed sometimes coexist, rendering the discrimination extremely difficult until the advanced progress of the carcinoma places the diagnosis beyond doubt.
[p. 370]In the early stages, however, it is distinguished by lack of the peculiar lancinating pains of carcinoma, which, however, are not invariably attendant, and by lack of secondary involvements of the cervical lymphatic glands. At all times it should be distinguishable from the carcinomatous ulcer by lack of the fungus-like appearance of the bed of the ulcer which is usual in carcinoma.
From syphilitic ulcer it is distinguishable by the history of the case, its tendency to be unilateral, and its failure to respond to antisyphilitic treatment. Syphilitic ulceration of the tongue may represent the primary, the secondary, or the tertiary manifestation of the specific disease. The former will not be discussed in this connection.
Secondary ulcers occur on the upper surface of the tongue, most frequently at the anterior portion, as fissures, usually longitudinal, the floors of which are ulcerated. They occur likewise at the sides, tip, and even lower surface of the organ. They are often associated with secondary ulceration in the mucous membrane of some portion of the mouth. They are quite painful, especially to the contact of pungent articles of food. Some ulcers occur as simple superficial excoriations at some portion of the edge or tip of the tongue, giving little evidence of any specific character.
Tertiary ulcers are usually sequelæ of gummata. They are much deeper than secondary ulcers, sanious at bottom, often serpiginous in configuration, and apt to extend in depth as well as in superficies, sometimes penetrating through and through the organ. They are most frequent in the very central portion of the tongue, or are symmetrically disposed on either side of it.
PROGNOSIS.—The prognosis of tuberculous ulceration is bad, both as regards tongue and patient.
TREATMENT.—The only topical treatment offering any prospect of local cure is the bodily destruction of the ulcer and the surrounding tissue with caustics, the best of which are the incandescent metals, or else the excision, with the incandescent knife, of a portion of the tongue comprising all the affected tissue. In the former case the tuberculous process often reappears about the cicatrix; in the latter, at some more distant point.
Tincture of iodine locally, detergent washes, and the like, often secure a certain amount of comfort as palliatives. The same indications prevail as in simple chronic glossitis, superficial and deep-seated. Iodoform locally is of benefit, inasmuch as it relieves pain and reduces collateral inflammation, but it is powerless to arrest the onward march of the ulcerative process.
DEFINITION.—A loss of blood from the mouth.
SYNONYM.—Stomatorrhagia.
ETIOLOGY.—Hemorrhage from the mouth is usually a symptom of some disease or injury of the mouth, tongue, gums, palate, pharynx, or nose. It may, however, occur as one of the phenomena of scorbutus or of hæmophilia. It is said to occur occasionally as a vicarious [p. 371] menstruation. It may be slight, so as barely to tinge the saliva, or it may be profuse enough to terminate fatally. Between these extremes there is an infinity of gradations. As a result of disease it may be caused by simple hyperæmia of the mucous membrane, by rupture of dilated blood-vessels, by ulceration, by gangrene. As a result of injury it may arise from wounds of various kinds, accidental or self-inflicted.
The gums are the most frequent source of slight hemorrhage from the mouth. The pharynx, probably, is the next most frequent seat. Hemorrhage from the tongue, cheeks, lips, and palate is usually traumatic or the result of ulceration.
SYMPTOMATOLOGY, COURSE, DURATION, COMPLICATIONS, TERMINATIONS, AND SEQUELÆ.—The symptoms of hemorrhage from the mouth are the presence of blood in the saliva or in the mouth itself, or in the expelled products of expectoration, emesis, or catharsis, for sometimes the blood is swallowed, and occasionally inhaled into the air-passages. The course, duration, complications, and terminations of stomatorrhagia depend upon its cause. Prolonged hemorrhage will entail anæmia; profuse hemorrhage may terminate fatally.
DIAGNOSIS.—Careful examination of the mouth, tongue, pharynx, and posterior nares, both by direct and by reflected light, may be necessary to discover the source of the hemorrhage and discriminate it from hæmoptysis and hæmatemesis.
PROGNOSIS.—The prognosis will depend upon the nature of the cause, its susceptibility of arrest, the quantity of blood lost, and the general health of the patient. It is grave, as a rule, in the subjects of hæmophilia, as there is a constitutional malnutrition of the blood-vessel system which cannot be counteracted.
TREATMENT.—Ergot or oil of turpentine internally, astringent mouth-washes, and recumbency constitute the main features in treatment.
DEFINITION.—Departure from the physiological processes concerned in the eruption of teeth, entailing certain local and systemic disorders.
SYNONYMS.—Dentitio difficilis, Pathological dentition, Odontitis infantum.
The correct comprehension of the subject will be facilitated by considering its etiology, pathology, and symptomatology in connection. Indeed, morbid dentition has been assigned so prominent a part in the etiology of various affections elsewhere discussed that a satisfactory consideration of its own causation would require the repetition of much that belongs more appropriately under other titles. While in some infants the teeth erupt so quietly that the parents are astonished by the accidental discovery of their presence above the gum, few children escape a greater or less amount of local and constitutional disturbance while passing through the process of dentition. So severe may these disturbances become that, according to the mortality-tables of London, as cited by West,75 teething was assigned as the cause of death of 4.8 per cent. of all children dying under one year old, and of 7.3 per cent. of those who died between the [p. 372]ages of twelve months and three years. It is furthermore well recognized that the period of greatest mortality among children is that of the first dentition. Associating these facts, we see, on the one hand, that while disorders of dentition may act a causative part in the production of systemic diseases or aggravate morbid processes due to ordinary causes, on the other hand they may be but one expression of some profound constitutional disturbance; or both aberration in the eruption of the teeth and systemic disease may be dependent upon the influence of dyscrasia. The period is one of active organic processes; the child is becoming fitted for a new manner of existence; and change and development are going on throughout nervous, vascular, respiratory, and alimentary systems. Hence there exists peculiar susceptibility to morbid influences; and any process, physiological or pathological, once started, goes through its stages with excessive energy.
75 Lectures on the Diseases of Infancy and Childhood, Philada., 1860, p. 425.
Although the periods of normal eruption of the deciduous teeth vary within extensive limits, and an invariable order in eruption is not observed in all subjects, it may be stated as a rule that the lower central incisors are cut in quick succession about the seventh month. Some infants get these teeth during the fourth month (Vogel), and others have to wait until the tenth or eleventh month, some even longer. A few weeks after the appearance of these lower incisors—within fourteen days in some subjects, not until nine or more weeks in others—the central incisors of the upper jaw are cut, and its lateral incisors shortly afterward, followed in their turn by the lateral incisors of the lower jaw. In some instances—the majority, according to Vogel—the eruption of the inferior lateral incisors is delayed until the anterior molars are about to become exposed, usually from the twelfth to the fifteenth month. Sometimes the upper molars are cut before the lower, sometimes after them. From the sixteenth to the twentieth, or even the twenty-fourth, month the canine teeth are cut, and the four posterior molars follow between the twentieth and thirtieth months, rarely delayed until the thirty-sixth month,—completing the process of the first dentition.
From this it will be seen that the teeth erupt as a rule in pairs, and that a longer or shorter interval of repose takes place between the eruption of successive pairs.
Variations from the usual order beyond the limits noted above may be considered abnormal. Numerous cases are on record both of precipitate and of tardy dentition. Tanner cites from Haller nineteen examples in which one or more of the central incisors have been found through the gums at birth, and have had to be removed to prevent injury to the mother's nipple; from Crump, a case of full dentition at birth, reported to the Virginia Society of Dentists; and from Ashburner, a case of a child beginning to cut its first tooth, an incisor in the upper jaw, during its twenty-third month, the infant being very delicate, with a large head, tumid abdomen, and peculiarly small-sized extremities. The same author quotes from Serres cases of persons passing through several years of life—in one instance seven—before cutting their first teeth, and mentions on the authority of Tomes that Boxalli and Baumes have each recorded an instance in which the patient reached old age without a single tooth having ever appeared.
Rachitis is often the cause of tardy dentition, and in the subjects of this [p. 373]diathesis not alone are the teeth retarded in development, but they decay early and even fall from their sockets.
The first indication of approaching dentition is the markedly increased production of saliva. For some little time after birth the salivary glands seem to remain wholly inactive, and until the fourth or fifth month of extra-uterine life they furnish very little secretion. At this period a decided change occurs. The mouth is constantly filled with saliva, which dribbles from its corners. To this continual slobbering, wetting the garments covering the chest, has been attributed the bronchial catarrh which attends some infants; and diarrhoea has likewise been referred to the swallowing of large quantities of saliva, acting as a mild laxative by virtue of its saline constituents.
There may be no further manifestation until the seventh month, beyond the broadening of the dental ridge. The exact position of each tooth is usually indicated by greater prominence of the gum above it for some time before it comes through, its entire outline being very distinct in the upper central incisors. As the tooth approaches the surface the gum becomes hot, shining, tense, and tumid, often painful. A slight amount of catarrhal stomatitis is almost invariable. There is some elevation of temperature; flushing of the cheek may occur; the child is restless, peevish, and fretful; its sleep may be broken; it may cry out with pain; its thumb, its fingers, any hard substance it can obtain, are thrust into its mouth to allay the irritation of the gums. Otalgia is not uncommon, and its occurrence may be inferred from the fact that the child pokes its thumb or finger into the auditory canal or firmly presses the tragus down over the external meatus. These may comprise all the disordered manifestations, local or constitutional, or there may be in addition loss of appetite, diarrhoea, vomiting, and the various disturbances of reflex nervous origin to be alluded to later; or, in the not common yet not rare instances already mentioned, there may be absolutely no appreciable disturbance whatever.
Sometimes a disposition exists to the formation of small aphthous ulcerations on the tongue or elsewhere in the mouth, particularly at the duplicature of the lip and the outer surface of the alveoli. Ulceration occurs most frequently at the tip of the tongue, probably occasioned by friction from the new teeth. Usually there is a single flat, round ulcer, its edges somewhat infiltrated, its bed covered with a yellow lardaceous substance. It is extremely painful to the touch, and thus every movement of the tongue occasions distress. It may heal within a few days or continue for weeks. Ulcers in other situations are less obstinate.
Occasionally—and more frequently in debilitated subjects or those exposed to unhygienic surroundings—there is an unusual amount of heat and swelling of the gum, which becomes excessively tender, usually over the summit of a particular tooth—in which case there will be a little tumor-like elevation—or around a tooth which has partially pierced through it. Small sloughy ulcerations form in this situation. There is great pain, and usually high fever and severe gastro-intestinal disorder. This affection, often difficult of cure, is termed by some writers odontitis infantum. So severe is the pain, and so great its tendency to aggravate constitutional disturbances, that life may be placed in jeopardy, and even fatal results ensue.
[p. 374]Less severe than either of the forms just described, and yet far more intense than the mild stomatitis which many authors regard as physiological, is an aggravated form of catarrhal stomatitis sometimes attendant upon morbid dentition, in which there is swelling of the submaxillary glands and infiltration of the adjacent connective tissue. In this case there is usually considerable pyrexia.
The constitutional disturbances of reflex nervous origin occasioned by morbid dentition are of the most varied character, both in their degree of gravity and in the manner and locality of their manifestation. Doubtless the extensive ramifications of the great vagus nerve, and its connections both of origin and distribution with the exquisitely sensitive fifth nerve, as well as with the facial nerve and with the sympathetic system, will explain why the irritation should now be seated in the gastro-intestinal tract, giving rise to vomiting and diarrhoea (gastritis, gastro-enteritis, enteritis, entero-colitis, cholera infantum); now in the respiratory tract, provoking cough more or less severe, or even a well-marked bronchitis; now manifest itself in various cutaneous eruptions (urticaria, eczema, impetigo, lichen, prurigo, herpes); and now accumulate in the cerebro-spinal axis, manifesting its presence by slight spasms (dysuria, muscular twitchings), or discharging with terrific force in some of those convulsive seizures which are the dread of mothers and the cause of much anxiety to physicians.
The mechanical causation of diarrhoea and bronchitis, insisted upon particularly by Vogel, has already been alluded to. While this may be one element, most certainly the nervous factor is too important to be disregarded. Bronchitis, not attributable to ordinary exposure, occurs coincidently with teething even in children who have been protected against wetting of the chest; and the fact that more purely nervous phenomena, and especially the dreaded brain symptoms, are usually absent in children who have an excessive flow of saliva, and particularly if there be also a moderate diarrhoea, would conduce to the belief that nervous irritation, discharging itself in this manner, does not accumulate in the centres.
Doubts have been expressed whether dentition can give rise to convulsions in perfectly healthy children, although its rôle as an exciting cause in predisposed subjects is admitted (Hillier). That dentition alone, in the absence of any other predisposing or exciting influence, will provoke any of the disorders with which it is associated may be doubted in view of the fact already cited, that in some infants there are no untoward occurrences. But there seems to be no valid reason for separating the disturbances purely in the domain of the nervous system from the other pathological processes originated or aggravated by morbid dentition. Doubtless predisposition often determines the direction and severity of the reflected phenomena; and in the same manner reflected irritation may bring an organ within the influence of the ordinary disease-producing cause.
The convulsive phenomena associated with dentition may take the form of general eclampsia or spasms of particular groups of muscles. These latter are very common—according to Vogel, universal—and vary in intensity from that slight contraction of the facial muscles which sends the mother into raptures of delight over the heavenly smile of her [p. 375]sleeping babe to the distressing seizure of laryngismus stridulus. Sometimes the child may sleep with its eyes half open, the eyeballs directed upward, and only the white sclerotic to be seen through the gap between the lids, "producing an appearance which is unnatural and alarming to the laity."
The attacks of general eclampsia are usually sudden. The child has been to all appearances perfectly healthy, when, without warning, there occurs a series of tetanic spasms like a succession of electric shocks. The individual eclamptic shock cannot be distinguished from an epileptic seizure. These convulsions sometimes continue for several days, but frequently they cease after a few minutes. They may pass off and leave nothing to testify to their occurrence; very frequently they occasion permanent distressing lesions. Partial, so-called essential paralyses, squint, or even idiocy, are cited among their sequelæ; infants subject to repeated convulsions while cutting successive teeth have eventually perished from cerebro-spinal meningitis; death has not infrequently been an immediate result. In these graver cases teething is probably but one of the morbid influences at work.
Purulent otitis media follows dentition in some infants, usually, if not invariably, of a scrofulous diathesis. At the clinic of the Jefferson Medical College Hospital fully one-third of all the cases of otorrhoea in children are said to be so occasioned.
Blennorrhoeal conjunctivitis is a rare complication of teething, and when it occurs usually accompanies the eruption of the upper molars and canines (eye teeth). It is attributed to direct extension of the gingival inflammation by continuity through the antrum of Highmore and the nasal passages. By some it is said to occur only in strumous subjects. It is unilateral, and is not contagious, so that there is no cause for alarm concerning the unaffected eye. The lids soon swell enormously and the eyeball is exposed with difficulty. There is considerable pain. The secretion is more mucous, translucent, and stringy than in genuine blennorrhoea. The eyeball always remains intact and the prognosis is always favorable (Vogel). Milder forms of catarrhal conjunctivitis are not very uncommon.
Thus far, we have considered only the process of the first dentition. Before the shedding of any of the deciduous teeth, the first permanent molars inaugurate the second dentition, appearing in position at about the sixth year. Next, displacing their temporary predecessors, come the central incisors, between the sixth and eighth years, the inferior pair generally preceding the superior ones. The lateral incisors are cut between the seventh and ninth years; the anterior bicuspids between the ninth and tenth years; the posterior bicuspids between the tenth and eleventh years; the canines between the eleventh and thirteenth years; the second molars between the twelfth and fourteenth years; the third molars, or wisdom teeth, between the seventeenth and twenty-first years as a rule, occasionally much earlier, sometimes later.
The eruption of the permanent teeth does not usually occasion any very great amount of distress; nevertheless, it sometimes acts both as a predisposing and as an exciting cause of various disorders, local and systemic. The various forms of stomatitis, tonsillitis, sore throat, gastro-intestinal derangements, febrile disturbances, bronchitis, internal rhinitis, [p. 376]diseases of the eye, of the ear, of the skin, chorea, epilepsy, etc., have all been noted as accompanying, if not occasioned by, the second dentition. Ashburner76 records, among other similar instances, that of a lad twelve years old who presented a marked case of chorea, and after three months' continuance of the twitchings fell into a violent epileptic fit, from difficulty in the eruption of the second pair of permanent molars of the upper jaw. The use of the gum lancet relieved the convulsion, and there was no return of the chorea.
76 On Dentition and some Coincident Disorders, London, 1834, cited by Tanner.
Quite frequently, the eruption of the inferior dentes sapientiæ occasions great and protracted suffering, especially when they appear very close to or partially under the coronoid processes. Considerable irritation is occasioned, in which the gums and adjacent tissues participate. Inflammation may result and extend to the fauces; mastication becomes impossible; severe odynphagia is excited. Suppuration may ensue, and then the pus burrows in various directions, finding exit at points more or less remote, internal or external. Among the consequences of the eruption of a wisdom tooth into a crowded arch, White77 cites fistulæ, necrosis, exostosis, ulceration and sloughing of the soft tissues, cystic and other tumors, ankylosis of the jaw, amaurosis, otalgia, otorrhoea, deafness, facial paralysis, hemicrania, oesophagismus, tonsillitis, erysipelas, aphonia, hysteria, neuralgia, chorea, epilepsy, tetanus, death.
77 "Pathological Dentition," extract from annual supplement to the Obstet. Journ. of Great Britain and Ireland, April, 1878.
DIAGNOSIS.—The age of the child and the appearances already described will afford a basis for diagnosis so far as the local manifestations in the mouth are concerned. The diagnosis of local disorders at a distance, or of systemic disturbances of whatever character, can be made out only by careful consideration of all the attending circumstances; and it is always to be borne in mind that while the process of dentition is to be recognized as one of the causative factors, grave injustice might be done the little patient, and its life perhaps endangered, by failure to recognize the presence of other and perhaps more potent morbid influences.
In cases of chorea or epilepsy, of eye or ear troubles, or of any morbid condition not otherwise accounted for, occurring during the period of the second dentition, especially at the sixth, twelfth, and seventeenth years, or until the wisdom teeth are fully erupted, it is well to inspect the mouth and to think of dentition as the possible cause.
PROGNOSIS.—The prognosis will depend upon the character and gravity of the associated symptoms, the presence or absence of diathesis, and the etiological importance attached to dentition. It is impossible to lay down a general law.
TREATMENT.—The treatment of the deuteropathic or associated disorders is to be conducted on the general principles applicable to those diseases; for a consideration of which the reader is referred to the appropriate articles of this work. We have here to consider general prophylaxis and local measures. The proper management of the child during the period of the first dentition is a matter of great importance, and may avert serious complications. The child should be as much as possible in the open air whenever the weather is favorable. The head may be daily sponged with cold water, and caps and warm head-coverings of all kinds should [p. 377]be forbidden.78 Frequent rubbing of the gums with a crust or other hard substance, or with the finger, is advisable; and something for the child to bite on, preferably a silver piece, should be provided. Orris-root, calamus, and other vegetable substances frequently given to children for this purpose are objectionable; their fermentation is apt to lead to thrush. The secretions must be kept active. The diet should be carefully regulated, and cooling drinks be freely given in order that the child may not overload its stomach by too frequent suckling in its efforts to relieve the local heat by moisture. The mother should be warned not to put it too frequently to the breast. Weaned children will often be found unable to digest their ordinary food, and in that case still greater care will be required. Slight diarrhoea does not call for interference, and is often beneficial in relieving nervous tension and thus averting a tendency to convulsions. Indeed, when the bowels are not relaxed gentle aperients should be given, especially in plethoric subjects or in those with cutaneous eruptions (Clarke). Cutaneous eruptions do not call for treatment, and there seems to be ground for the popular fear that they may be driven inward; at least, cases are on record in which their disappearance under treatment, and even spontaneously, has been followed by more or less severe convulsions.
78 Tanner after Clarke.
In cases where bronchitis can be traced wholly or in part to soaking of the clothing, due protection of the chest by an oil-cloth or waterproof bib may be prophylactic against future attacks. In children who have suffered from any special set of morbid manifestations during the eruption of one pair of teeth, similar disturbances may be expected, and should be guarded against, in the future.
Aphthous ulcerations are usually associated with disorders of digestion, the relief of which must be the main object of treatment. Locally, the treatment does not differ from that of aphthous stomatitis in general. Obstinate ulceration of the tongue may require the use of silver nitrate. In that form of ulceration called odontitis infantum, in addition to proper attention to the diet and secretions and mild antiphlogistic medication, local depletion by leeches, preferably at the angle of the jaw, is often beneficial. Some writers advise the application of leeches directly to the gum. Potassium chlorate internally, two grains every four hours to a child twelve months old, is curative in the majority of cases. It may be given dissolved in sweetened water. Solutions of borax, and, in severe cases, of silver nitrate, may be applied locally. The use of the lancet is contraindicated, for the cut surfaces would be liable to ulceration.
| FIG. 17. |

|
| Incision for a cuspid (White). |
| FIG. 18. |
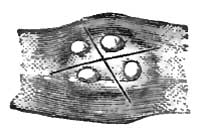
|
| Incision for a molar (White). |
The propriety of resort to the lancet for cure of systemic disturbances by obviating the source of local irritation is one which deserves consideration. It can only be decided upon the indications presented by the individual case. The knife is not a panacea for all the disorders of childhood occurring during dentition, and its indiscriminate use is to be discountenanced. Nevertheless, there can be no doubt that engorged and inflamed gums demand incision for their relief, on the same general principles of surgery applicable to similar conditions elsewhere. Where it is probable that systemic disease, even if not solely caused, is aggravated by the irritation and pain of a tooth unable to make its way to the surface unaided, it is clearly the duty of the physician to give his little patient that modicum of relief, if not of cure, which will be afforded by a proper incision of [p. 378]the gum. It will not do merely to score the gums, but cuts should be made deep enough to reach the presenting surface and extend even beyond its boundaries. The developing enamel cannot be injured unless undue force be exerted. The best instrument to employ is a curved double-edged bistoury, so wrapped as to prevent injury to tongue, cheek, or lips. The child should be firmly held by another person, and in such a position that the parts may be well illuminated. The jaws can be separated by the operator's left hand, and the fingers so disposed as to protect the tongue and lips. Sometimes the insertion of a small cork between the jaws will be of advantage. The cuts should be made with special reference to the form of the presenting tooth. James W. White79 recommends for the incisors and cuspids a division of the gum in the line of the arch; for the molars a crucial incision, thus X, the centre of the crown as near as can be determined indicating the point of decussation. A cuspid partially erupted needs severance of the fibrous ring on the anterior and posterior as well as on the lateral surfaces (Fig. 17). All the cups of a molar may have erupted, and yet strong fibrous bands maintain a decided resistance. In this case White thinks that all the boundaries of the tooth should be traced by the lancet and all such bands completely severed, or else a crucial incision, as in the figure (Fig. 18), should be made so as to ensure perfect release from pressure. The only contraindication to the use of the lancet, except in ulcerative odontitis, as before mentioned, is the existence of a hemorrhagic diathesis.
79 Op. cit.
DEFINITION.—An acute inflammation of the tonsil or tonsils; or inflammation of the tonsil or tonsils, with inflammation of the peritonsillar connective tissue and of the palatine folds.
VARIETIES.—When the inflammatory process is confined to the mucous membrane the disease is erythematous, superficial, or catarrhal tonsillitis; when it involves the lacunæ it constitutes lacunal or follicular tonsillitis; when it involves the gland as a whole it constitutes parenchymatous, phlegmonous, or suppurative tonsillitis. The two latter varieties may present in combination. When the superficial inflammatory process is a vesicular one, eventually sheathing the surface of the organ in whole or in part with a membranous envelope, it constitutes herpetic or membranous tonsillitis. This variety may complicate superficial tonsillitis. When the inflammation of the tonsil, usually superficial, is due to the presence of a cryptogamic growth, it is a mycotic or parasitic tonsillitis, benign or malignant (diphtheria), as may be. When the inflammation of the tonsil is due to rheumatism, it is rheumatic or constitutional tonsillitis.
SYNONYMS.—Inflammation of the tonsils, Amygdalitis, Quinsy, Angina tonsillaris, Angina phlegmonosa, Phlegmonous sore throat, Cynanche tonsillaris. Lacunal tonsillitis is more generally known as folliculous tonsillitis (tonsillitis follicularis). Common membranous or pseudo-membranous sore throat (angina membranosa communis) is used as a synonym for herpetic or membranous tonsillitis (tonsillitis herpetica seu membranosa). Mycosis tonsillaris is a synonym for mycotic tonsillitis (tonsillitis mycotica benigna or tonsillitis parasitica). The tonsillitis of diphtheria is sometimes termed tonsillitis diphtheritica, tonsillitis mycotica maligna; that of rheumatism, tonsillitis rheumatica, angina rheumatica, rheumatic sore throat.
HISTORY.—Tonsillitis was described by Hippocrates. Of recent authors, Sauvages, Cullen, Louis for researches on the effects of blood-letting; Bell on the specific value of guaiacum; Velpeau as to the use of powdered alum and nitrate of silver; Bourgeoise on the use of tartar emetic; Maingault on paralytic sequelæ; Hering on mycosis; and the authors of the various encyclopædias and dictionaries,—may be mentioned as chief among the numerous observers whose contributions have been of most value. The bibliographical references appended to the [p. 380]compilations last cited will guide the student in gaining access to the more important special observations of anomalous cases.
ETIOLOGY.—Predisposing and Exciting Causes.—Tonsillitis may be idiopathic, deuteropathic or symptomatic, or traumatic.
The predisposing cause of idiopathic tonsillitis is usually diathetic, and is associated with congenital or inherited vulnerability of the organ. Of diathetic causes, scrofula is undoubtedly the most provocative, but even rheumatism and gout are likewise so considered, though in a far more limited degree. Acute articular rheumatism is, in fact, sometimes preceded by rather a sharp attack of tonsillitis (rheumatic tonsillitis), which subsides spontaneously in a very few days, sometimes within one day, sometimes suddenly and synchronously with the onset of the ordinary manifestations of rheumatism, though the latter are often slight and transient, as if the force of the attack had been spent on the tonsils. Tonsillitis, non-specific in character, is apt to be prevalent during epidemics of scarlatina, diphtheria, rubeola, and variola. Membranous tonsillitis is common before and after epidemics of diphtheria. Epidemics of tonsillitis have been recorded, but in the face of their extreme rarity it becomes questionable whether they were not extensive examples of the proclivity just alluded to.
Tonsillitis is more frequent in individuals with chronically diseased tonsils than in individuals in whom these glands are healthy. Such individuals, too, are more liable to recurrences; and such recurrences often follow very slight provocations.
Idiopathic tonsillitis is rare in infancy. At the period of eruption of the permanent teeth it is much more liable to occur than before that period, and the liability increases progressively until the second dentition has been completed. It is most frequent during the decennium immediately following puberty—that is to say, in adolescents and young adults—or from the fifteenth to the twenty-fifth year. The disposition or predisposition to renewed attacks continues marked during the decennium immediately succeeding; after which attacks are more and more infrequent. Certain anatomical changes occurring in the tonsils, as the rule about the fortieth year, may diminish their proclivity to inflammation. Nevertheless, the disease occasionally occurs in advanced age.1
1 Solomon Solis Cohen, "Abscess of the Tonsil in an Octogenarian," Med. News, Philada., Feb. 16, 1884, p. 186.
Deuteropathic tonsillitis is quite frequent in infancy, being excited by the infection of scarlet fever, diphtheria, measles, and small-pox, as discussed under these headings respectively. Under similar circumstances it occurs in the adolescent and the adult likewise. It is also produced in carcinoma and sarcoma of the tonsil.
Rheumatic tonsillitis, a deuteropathic variety, is most prevalent during atmospheric changes.
Herpetic tonsillitis, often a deuteropathic variety, seems sometimes of nervous origin exclusively. It is sometimes traceable to defective drainage. It is sometimes prevalent during epidemics of diphtheria, when its membranous character renders it extremely liable to be mistaken for the tonsillitis of diphtheria.
Traumatic tonsillitis occurs occasionally. The causes are—inspiration of irritant gases, the deglutition of chemically acrid substances, the [p. 381]accumulation of calcareous concretions in the crypts or in the lacunæ, direct and indirect gunshot and other wounds, the impaction of fish-bones, fragments of toothpicks, cherry-stones, and other foreign bodies, and the like.
Mycotic tonsillitis is due to the development of a cryptogam upon tonsils probably already in a state of catarrhal inflammation in individuals with health impaired by previous disease or unfavorable hygienic influences.
SYMPTOMATOLOGY, COURSE, DURATION, TERMINATIONS, COMPLICATIONS, AND SEQUELÆ.—The onset of tonsillitis, sometimes preceded by headache and general malaise, is often accompanied by a chill, pyrexia following within twenty-four hours. The temperature may reach 105° F., being at its maximum, as a rule, about the third day. It is rarely below 101° F. The pulse is accelerated to 120 beats per minute. Simultaneously with the constitutional symptoms local distress is usually manifested, but either set of disturbances may precede the other by several hours or by an entire day. Heat and soreness of the throat are early complained of, gradually increasing in severity to actual pain. The pain may become intense, especially during deglutition. When the posterior palatine fold is put upon the stretch, additional pain is referred to the ear, for this fold encloses the staphylo-salpingeus muscle, which runs from the palate to the pharyngeal orifice of the Eustachian tube. This pain in the ear, sometimes the principal cause of complaint, is often premonitory of suppuration. Noises in the ears on the one hand, and impairment of hearing on the other, often attend extension of the inflammation in this direction, the enlarged tonsil sometimes pressing the posterior palatine fold against the pharyngeal orifice of the Eustachian tube.
On inspecting the throat early in the disease, one of the tonsils will be seen to be swollen into an irregularly tumid, much-inflamed mass, usually of a vivid red color. Occasionally both tonsils are involved simultaneously, but this is far less frequent than involvement of the second tonsil a few days later or after subsidence of the process in its fellow. In many instances the inflammation affects one tonsil only.
The inflammatory process is seldom confined to the tonsil. All the structures of the throat, even to the base of the tongue, are often involved, and it is rarely indeed that the anterior palatine fold, distended over the surface of the tumefied gland, escapes inflammation. It is this stretching of the anterior palatine fold which occasions much of the exquisite pain that forms so prominent a subjective symptom in severe cases. The soft palate, hanging forward in the cavity of the pharynx, is often inflamed or intensely congested, and the uvula tumefied, elongated, and oedematous. It may be flaccid upon the posterior part of the tongue or hang immediately over the epiglottis or upon it, and induce painful and tiresome efforts at deglutition and expectoration to relieve the consequent titillation. Sometimes it adheres by viscid secretion to the side of the swollen tonsil.
The inflamed tonsil or the tonsil and its coverings project far into the cavity of the pharynx, often as far as the middle line, touching its fellow when both are involved, so that ulceration sometimes ensues at the points of contact. The posterior surface of the anterior palatine fold sometimes becomes unfolded, as it were, in the tumefaction of the gland, and remains [p. 382]stretched over it in a thin continuous layer without any line of demarcation. The swollen palate projects upon the enlarged tonsil like a shelf, from which depends the uvula, the latter being often oedematous, usually anteriorly, but sometimes posteriorly.
Inflammation of the connective tissue about the lower jaw, especially when at or near the articulation, often renders it difficult or even impracticable to open the mouth sufficiently to permit direct inspection of the parts; but it is rarely that sufficient space cannot be made to allow partial protrusion of the tongue on the one hand, and the introduction of a fore finger for exploratory purposes on the other, though both of these acts are sometimes impossible. The tumefaction of the parts impairs the freedom and ease of deglutition, which may become so painful as to prevent the swallowing of the saliva, which then may dribble from the mouth.
The pain experienced in swallowing is often manifested by convulsive action of the muscles of deglutition and of the muscles of the face. The swollen tonsils prevent the soft palate from being applied to the surface of the pharynx, as usual in deglutition; and as the upper or retro-nasal portion of the pharynx thus fails to be shut off from the lower oesophageal portion, liquids are often forced up into the nasal passages posteriorly, and are regurgitated through the nostrils, thus rendering it impracticable, for the time, to slake thirst or to swallow liquid nourishment.
At first sensations of dryness and pastiness in the throat are complained of, but in a few hours these symptoms become relieved by a more copious secretion of mucus or mucus and saliva. This secretion soon becomes viscid, and so adherent to the parts as to be detached only with difficulty, thus causing harassing efforts for its dislodgment by hawking and expectoration, or equally distressing efforts to swallow it. Should the inflammatory process extend to the salivary glands, as is not infrequently the case, secondary ptyalism often results, with increased distress from this source, and the patient lies or sits with his head inclined upon the diseased or most diseased side to favor the uninterrupted flow of saliva from the mouth.
Extension of the inflammatory process to the submaxillary glands, or to the parotid, or to the connective tissue surrounding them, is indicated by tumefaction externally, which is often exquisitively sensitive to pressure.
The timbre or quality of the voice is often impaired in a peculiar manner by the tumefaction of the throat and the immobility of the soft palate. The voice is thick, throaty, or guttural, having a characteristic harsh, rasping aspiration in enunciation, while articulation is much impeded by impairment in the movements of the jaw, palate, tongue, and lips. At times it is also painful. Speech is sometimes indistinguishable or impossible, and the voice may even become suppressed, so that signs and writing remain the sole means of communication.
Impairment of respiration, at least to any considerable degree, does not occur, unless both tonsils are involved and swollen to an intense degree—conditions under which dyspnoea may become pronounced, severe, and even urgent, and suffocation become imminent. Painful respiration is not uncommon in rheumatic tonsillitis.
The fever is sthenic in type. There are often severe aching pains in [p. 383]the limbs. Headache, restlessness, insomnia, nausea, and even vomiting, may occur. The tongue is heavily coated, the breath is fetid, appetite is impaired, and the bowels are constipated. The urine is diminished in quantity, high-colored, and of high specific gravity. It usually shows slight increase of urea and great diminution of chlorides. Albuminuria occurs in rare instances.
The symptoms are proportionate to the severity of the attack. A first attack is usually much severer than subsequent ones, and suppurative cases more severe than those terminating by resolution. Resolution is the usual termination, and the parts are restored to a normal condition at the end of ten to fourteen days, sometimes earlier; in exceptional cases not until three or four weeks. Sometimes permanent hypertrophy of the tonsil remains.
Where the inflammatory process fails to subside, suddenly at the end of five or six days, or a little later, or not until ten days to a fortnight have passed, slight rigors supervene, announcing suppuration, and the local distress is very great, with pulsation and lancinating pains in the tonsils, until all at once the abscess bursts and its contents are discharged with immediate relief. Sometimes the pus or much of it is involuntarily swallowed; sometimes it is expectorated. In exceptional instances the pus has escaped into the larynx and suffocated the patient, usually during sleep.2 In rare instances the abscess, having burrowed beneath the pharyngeal muscles, may open at the external angle of the jaw or behind the sterno-mastoid muscle. It may discharge into the epiglotto-pharyngeal fold, and thence reach and distend the epiglottis. It has been known to descend along the planes of connective tissue into the mediastinum or into the lungs. Even ulceration into the maxillary and carotid arteries has occurred, usually with fatal result, occasionally with an opportunity to save life by ligating the carotid (Erhmann).3
2 Stokes, Med. Times and Gaz., Aug. 29, 1874, p. 251; Littlejohn, Brit. Med. Journ., Jan. 2, 1875, p. 16.
3 Gaz. méd., Paris, 1878, p. 42.
The most frequent point of spontaneous rupture externally is at the upper portion of the gland anteriorly, just beneath the anterior palatine fold. Sometimes internal rupture occurs into the lacunæ.
Termination by gangrene is exceptional, and is confined to individuals with debilitated constitutions. It is much less frequent than formerly—as a result, perhaps, of better methods of treatment.
Metastasis is one of the methods of termination as to joints or muscles in rheumatic tonsillitis—to lungs, brain, or gastro-intestinal tract—as formerly occurred with much more frequency under direct depletory treatment.
In rare cases extension of the inflammation occurs to the epiglottis, even to the larynx, and the laryngitis may be so severe as to threaten life from the occurrence of oedema. Diffuse inflammation of the retro-pharyngeal connective tissue or of the connective tissue of the neck may constitute an unpleasant complication of the disease.
In a few instances paralysis of the palate occurs as a sequel of tonsillitis, and in exceptional cases the paralysis may also affect the arytenoid muscles of the larynx, and even the accommodator muscles of the eyes.
PATHOLOGY AND MORBID ANATOMY.—Tonsillitis is almost always [p. 384] associated with inflammation of the tissues surrounding the tonsil and those contiguous to it, even in the mildest and most frequent manifestations of the affection. Thus, inflammation of the palate (staphyllitis) and uvula, and even of the pharynx (pharyngitis), are anatomically included with tonsillitis in angina or sore throat.
The mildest form of the malady is a catarrhal inflammation of the mucous membrane covering the gland, and does not extend along the lacunæ which dip inward from the surface and divaricate toward the interior of the organ. It is termed catarrhal tonsillitis, and, as has been intimated, is almost always associated with catarrhal sore throat. It is attributed to hyperæmia, with passive engorgement of the vessels, following retrocession of blood from the cutaneous surface after undue exposure to cold and moisture. A severer form of the malady involves the lacunæ in addition—several or all of them. This should be termed lacunar tonsillitis, as suggested by Wagner. Primarily, at least, it does not involve the follicles of the tonsils which open into the lacunæ, and is therefore incorrectly denominated follicular tonsillitis, although it is most generally so described. The lacunæ are involutions of the mucous membrane, and in health furnish a slightly turbid mucoid secretion which serves to lubricate the parts and, as is generally believed, to facilitate deglutition. When the lacunæ are inflamed these products become pent up in them to a certain extent, accumulate, and project in part at their orifices in turbid creamy or curdy masses, plastered over the parts when thin in consistence, or tightly imbedded when thick or desiccated. These masses are usually white, but sometimes, owing to various admixtures, they are more or less yellowish or gray or brown. They consist of epithelium chiefly, with more or less pus and accumulation of cells similar to those of which the follicles are composed—whether from follicles which have become distended by proliferation of their constituents, and have then burst, is not known. This epithelium has often undergone fatty degeneration in part. Cholesterin is an occasional constituent, and swarms of micrococci and bacteria abound when the masses are not recent, especially if the inflammation is occurring in a tonsil long the seat of chronic disease of the lacunæ.
The tonsil itself is moderately swollen and its mucous membrane hyperæmic. If the parenchyma of the tonsil be involved likewise, as often occurs, the swelling will be much greater, so that the gland will project a considerable distance beyond the margins of the palatine folds. When a hypertrophied tonsil is the seat of the inflammation the tumefaction will be much greater than when the inflamed tonsil has been normal.
Acute inflammation of the palatine folds often coexists, especially of the anterior fold. The soft palate may also be engaged in the morbid process, which may involve the uvula likewise. Pharyngitis is an occasional accompaniment, and stomatitis quite a rare one.
Lacunar tonsillitis sometimes subsides by spontaneous evacuation of the pent-up contents of secretion and desquamation, the parts returning to their normal condition. More frequently a desiccation of some of these products ensues, with permanent chronic inflammation. Decomposition then often takes place, fouling the breath by the escape of the gases. Butyric acid has been recognized as one of the most prominent of these fetid [p. 385]gases. Calcareous change occurs in these contents of the lacunæ in some instances. Lacunar or follicular tonsillitis is often associated with severe inflammation of the peritonsillar connective tissue and the contiguous palatine fold, with serous or cellular infiltration into these structures almost always terminating in suppuration. This form of tonsillitis is very frequent, and is often confounded with parenchymatous tonsillitis or with tonsillar abscess. In these cases the abscess is in the peritonsillar tissue or in the posterior leaflet of the anterior palatine fold. It bursts above the tonsil at the angle between the two folds in the greater number of cases. In some instances the suppurative inflammation affects the anterior surface of the posterior palatine fold, sometimes contiguously to the antero-tonsillar abscess, sometimes independently, constituting a retro-tonsillar abscess. The follicles in the posterior palatine fold are sometimes involved, the thickened anterior surface of this structure becoming studded with small projections the size of ordinary pinheads or larger, distended with whitish-yellow contents.
In another class of cases of tonsillitis the inflammatory process may be chiefly parenchymatous, for rarely is it wholly so. That is to say, it may involve the glandular structure of the organ wholly or in main part. The disease is then an adenitis, an inflammation of gland-tissue—tonsillitis per se. It is associated with superficial inflammation of the surrounding mucous membrane, secondarily if not primarily, and often with inflammation of the lacunæ. In many instances the parenchymatous inflammation is a direct extension of the lacunar inflammation.
Parenchymatous tonsillitis may subside by resolution, or, as is quite frequent, terminate by suppuration. A number of small abscesses may be formed, which usually become confluent and rarely remain discrete. Sometimes a single large abscess is formed. The confluent abscess may discharge by several points. It is always associated with a severe inflammation of the palatine folds and palate, especially the anterior fold; sometimes of the adjoining half of the soft palate and the uvula; sometimes of the entire velum and uvula. Sometimes these parts become oedematous; sometimes suppuration ensues. Severe pharyngitis is not uncommon. Glossitis, involving the posterior portion of the tongue especially or exclusively, is an occasional accompaniment of parenchymatous tonsillitis. (See GLOSSITIS.) Occasionally oedema takes place in the epiglottis and upper margin of the larynx.
The character of the secretions varies. Sometimes these are semifluid; sometimes soft, caseous, or pultaceous; sometimes fibrinous and arranged in pseudo-membranes; sometimes hemorrhagic; sometimes moist and viscid, sometimes very dry; often adherent, and always containing cryptogams (leptothrix, Oïdium albicans, bacteria, and micrococci). Collections of caseous products accumulate not only in the crypts of the tonsils and in their overlying mucous membrane, but likewise in the follicles of the palatine folds below the tonsil, and thence toward the base of the tongue.
The submaxillary glands often undergo engorgement, and become so tender that external manipulation is painful, and sometimes they undergo suppuration. The tumefaction due to the swollen glands and infiltrated connective tissue around it is frequently incorrectly referred to the tonsil itself, rather than to the accompanying inflamed palate, with the [p. 386]lymphatics of which these glands are in more direct anatomical connection. The tonsil is at a considerable distance from the inflamed glands, and cannot be felt from the exterior except under unusual circumstances.
Herpetic tonsillitis is a rare form of inflammation of the tonsil, or rather of its investing mucous membrane, characterized by the eruption of herpetic vesicles on its surface. The vesicles soon undergo rupture, and the resulting ulcers coalesce and become covered with a fibrinous exudation. The disease is usually associated with similar vesicles upon the palatine folds and upon the soft palate, and exceptionally with vesicles on the pharynx. (See Herpetic Pharyngitis.) It is by some fortuitous circumstance only that it is observed in the vesicular stage. It is confined to one side of the throat in most instances, but may be bilateral also.
Mycosis tonsillaris has been described by a few observers. B. Fraenkel4 has recorded three cases, E. Fraenkel5 one, and Bayer6 two. In these cases the disease was not confined to the tonsils, but implicated the calciform papillæ of the tongue also, and one of Bayer's cases some pharyngeal follicles in addition. E. Fraenkel's case was in a male, and occupied but the right tonsil and base of tongue. The white masses in this case were formed of spores and filaments (Bacillus fasciculatus, Sadebeck), which are described as penetrating some millimeters into the gland-tissue. These masses were tenacious, and were reproduced rapidly after removal. In Bayer's cases, both females, the same microphyte was recognized. In a female patient observed at the Philadelphia Polyclinic7 this affection followed rheumatic tonsillitis, diphtheria being prevalent near her residence, which was in a very unsalubrious locality. The deposit, confined to the left tonsil, was so firmly adherent to the mucous membrane that the implicated portion had to be torn away to get rid of the growth, which was twice reproduced. The fungus was in its mycelial state, a few spores and conidiferous filaments being recognized microscopically.
4 Berlin. klin. Woch., 1873, S. 94; ibid., 1880, No. 18.
5 Zeitschrift für klin. Med., iv., 1882.
6 Rev. mens. de Laryngologie, etc., Nov., 1882, p. 329.
7 S. Solis-Cohen, The Polyclinic, March, 1884, p. 133.
Quite recently, and since the above was written, the results of an elaborate study of this affection by Theodor Hering of Warsaw have been published in a paper entitled "Pharynxmycosis leptothricia,"8 read before the Society of German Naturalists and Physicians. The author collates fourteen cases, six of which were observed by himself. He claims that the microphyte is simply the Leptothrix buccalis.
8 Zeitschrift für klinische Medicin, Bd. vii. H. 4, 1884.
The local subjective symptoms as collated by Hering vary from the merest sense of discomfort in chronic cases to intense pain, difficulty in speech and in deglutition, and various grades of cough in acute ones. In some cases they are altogether wanting. Constitutional disturbance may be entirely absent or may be presented in various febrile or sub-febrile manifestations.
DIAGNOSIS.—The history of the attack, the appearances described, and the symptoms narrated should ordinarily suffice for a correct diagnosis. Still, mistakes do occur. An unsuspected tumor of the tonsil observed for the first time during an ordinary sore throat might be taken for an inflamed tonsil, but the progress of the case would soon lead to its due [p. 387]recognition. While tonsillitis is infrequent after the fourth decennium, it occasionally occurs late in life, and has been observed even in the ninth decennium; and reserve is proper as to the cause of enlarged tonsils in the sore throats of those advanced in life.
The deposit in follicular or lacunar tonsillitis or angina is pulpy and not membraniform. It can be wiped from the surface with a fragment of sponge, and does not tear from the surface in strips, as is the case with the pseudo-membrane of diphtheria or of common membranous sore throat. There is no abrasion of the mucous membrane beneath the deposit. The patches are more prominent, usually more circumscribed, and dip down into the lacunæ, or rather project from the crypts upon the surface of the tonsil. In its physical aspect the deposit more closely resembles that observed in the sore throats accompanying cachectic conditions, as in chronic tuberculosis, advanced syphilis, some forms of scarlatina, typhus and typhoid fever, extreme old age (agine pultacée, Fr.; cachectic angina); but the existence of previous constitutional disease and actual debility should prevent the mistake in diagnosis. In susceptible subjects the oncoming of an attack of rheumatic tonsillitis may often be inferred, previous to the manifestation of local symptoms, from the existence of otherwise inexplicable odynphagia, the pain being especially intense upon attempts to swallow saliva. Sometimes laryngoscopic inspection at this early stage of the disease will reveal vivid redness of the mucous membrane in the neighborhood of the crico-arytenoid articulations.9 The value of this early diagnosis lies in the opportunity it affords to try abortive treatment.
9 S. Solis Cohen, The Medical News, Aug. 11, 1883, p. 146.
PROGNOSIS.—The prognosis of catarrhal tonsillitis is almost invariably favorable, except under very obviously unfavorable conditions, the inflammatory process subsiding spontaneously within a few days. It is favorable, as a rule, in phlegmonous tonsillitis subsiding within ten or twelve days in most instances, even though all the stages be completed to suppuration and discharge of the abscess. Sometimes two or three weeks are consumed in the process. A certain amount of reserve is requisite, nevertheless, in severe cases, in view of the possible complications which may prevent recovery. If both tonsils are affected to such an extent as to interfere seriously with respiration, death by suffocation may ensue should the obstruction be not relieved by excision of portions of the swollen glands or an artificial opening be not made into the air-passage. Suppuration may perforate the internal carotid or the external maxillary artery and produce sudden fatal hemorrhage. The remembrance of such occurrences should screen a surgeon from the imputation of carelessness should he be unfortunate enough to incise an abscess under similar conditions. Some cases are on record of fatal hemorrhage but a short period before a proposed operation could have been performed.
Suffocation has ensued from discharge of the abscess into the air-passage, usually during sleep; but it has occurred even during the moment of speaking (Stokes).10 Such results are accidental and exceptional.
10 Med. Times and Gaz., Aug. 29, 1874, p. 251.
Recurrences are frequent, especially in scrofulous subjects, and such recurrences are apt to result in permanent hypertrophy and induration.
TREATMENT.—Mild cases of tonsillitis require no treatment except to [p. 388]keep the patient protected from exposure to abrupt changes of temperature. The course of the affection both in mild cases and in severe ones may often be materially shortened by prompt resort to the use of guaiacum, both internally and topically. A gargle containing an ounce each of ammoniated tincture of guaiacum and compound tincture of cinchona to the pint, with the addition of three ounces of clarified honey, and saturated with potassium chlorate (twenty grains to the ounce), may be used, a drachm at a time, every two hours, hour, or half hour, according to the urgency of the symptoms, and may likewise be administered internally in drachm doses for an adult every two or more hours. The beneficial effects will often be manifested within less than twelve hours. Pellets of ice held in the mouth from time to time often relieve pain and repress inflammation. Sodium bicarbonate locally, in powder, affords great relief in some instances. In the presence of marked pyrexia tincture of aconite may be given in drop doses every hour until an impression has been made upon the heart, when its continuance at intervals of four or more hours will be a matter for consideration.
Guaiacum and aconite may be given with equal benefit in any form preferred by the prescriber. At the same time saline laxatives may be required from time to time. Regulation of the diet is often necessary.
When the tonsils are very much swollen, gargling of all kinds becomes too painful, and therefore sprays of sedative and emollient mixtures are to be substituted, or steam from water impregnated with volatile substances, as benzoin, paregoric, hops, chamomile, and sage. When the cervical glands are swollen, continuous hot and moist applications externally afford great relief. If the suffering from the inflamed tonsil be intense, scarification should be practised and the bleeding be encouraged by warm water. When suppuration exists, the abscess should be promptly evacuated by incision at the most prominent accessible point.
Special symptoms require appropriate management on general principles. The pain in swallowing can often be diminished by pulling on the lobe of the ear at the moment of deglutition (Grewcock).11 In debilitated subjects, or during epidemics of diphtheria, quinia, iron, and supporting measures are indicated.
11 Lancet, Nov., 1882, N.Y. reprint, p. 399.
The rheumatic cases are best treated with sodium salicylate, ten to fifteen grains every hour or two until relieved. Instituted in the formative stage above alluded to, this treatment frequently seems to be veritably abortive, especially when preceded by a full dose of an alkaline purgative—say one ounce of Rochelle salts. Oil of gaultheria may be used in small doses as an agreeable flavor to the mixture, or in doses of ten to twenty minims, well diluted, as an adjuvant to the salicylate, or even as a substitute for it. After subsidence of the acute symptoms cinchonidine salicylate may be continued for a few days in appropriate doses.
Herpetic tonsillitis requires the ordinary treatment for erythematous tonsillitis, with additional topical treatment by sprays of alkaline solutions, such as sodium borate or bicarbonate, five grains to the ounce, or lime-water. Internally, small doses of mercuric chloride will be of service, the dose varying, according to the age and size of the patient, from one-forty-eighth to one-sixteenth of a grain every two hours, until the stomach shows signs of irritation therefrom. In cases of doubt as to [p. 389]diagnosis from diphtheria the treatment for diphtheria will be indicated as the safer measure. Here, again, the mercuric chloride is sometimes equally valuable.
Mycosis of the tonsil does not seem amenable to medicinal treatment. Thorough removal of the fungus with forceps or sharp spoons is required, even though mucous membrane be detached with it. When this is impracticable, ablation of the tonsil may be necessary. Raw or cut surfaces left by any of these manipulations should be subjected to thorough cauterization, electric cauterization being the most feasible method.
DEFINITION.—An acute inflammation of the mucous membrane of the pharynx, whether implicating the glandular structures or not, and usually associated with inflammation of contiguous structures.1 Acute pharyngitis may be catarrhal or erythematous, phlegmonous or suppurative, ulcerative, herpetic or membranous, gangrenous, and erysipelatous.
1 In deference to the plan suggested by the editor of this work, separate articles have been prepared under the heads of Pharyngitis and Tonsillitis respectively. The two processes, however, are so frequently associated that they should be studied together, the more that both of them are likewise associated with extensions of the inflammatory process to the palate, palatine folds, base of the tongue, and other contiguous structures. The writer has always preferred to describe these diseases under the head of sore throat, which does not presuppose any limitation to individual anatomical structures.
SYNONYMS.—Sore throat; Angina.
ETIOLOGY.—Acute pharyngitis may be idiopathic, deuteropathic, traumatic, toxic, or parasitic. The predisposing cause may be diathetic, as scrofula, rheumatism, gout, and syphilis; it may be a depression of the vital powers from any cause, such as continued exposure to foul air or impure water, improper diet or sedentary occupations. There exists in some individuals a predisposition to "catching cold," independent of any cachexia. Pharyngitis may occur at any age, but is more frequent in the young. One attack increases subsequent liability to the disease.
The exciting cause is usually exposure to cold and damp. Hence the disease is more frequent at the seasons when these conditions prevail or when sudden changes of temperature are taking place. Sudden chilling of the body when overheated may occasion it in warm weather; for instance, a plunge into the ocean while covered with perspiration. The ulcerative variety, when not due to syphilis or tuberculosis, is usually of septic origin, and is apt to occur in the debilitated especially. The gangrenous form, which is rare, results from profound blood-poisoning. The herpetic or membranous variety may be due to disturbance of the trophic nervous system, and has been attributed to mental emotion (Feron), to uterine disturbances (Bertholle), to the contact of irritating substances and to miasmatic or fetid exhalations (Peter). It prevails principally during epidemics of diphtheria or of scarlet fever, and may be of cryptogamic origin. The cryptogam of thrush is sometimes developed on the mucous membrane of the pharynx, either primitively or as an extension of the disease from the oral cavity. Certain conditions of the [p. 391]atmosphere give rise at times to so-called epidemic pharyngitis. Paludal or malarial pharyngitis may arise from the same causes as malarial fevers. Pharyngitis occurs in the various exanthemata as an essential part of the morbid process, and is always more or less prevalent during epidemics of measles or scarlet fever. It occurs not rarely in typhoid fever, and is an occasional complication of pneumonia, rheumatism, herpes, pemphigus, and other acute affections. It is one of the complications of facial erysipelas, but erysipelatous pharyngitis may occur primarily. Pharyngitis may be excited by the inhalation of deleterious solid, fluid, and gaseous substances in the atmosphere which act mechanically or chemically on the mucous membrane. Many drugs administered in poisonous or even in medicinal doses may give rise to an attack of inflammation of the pharynx; among them may be cited preparations of mercury, antimony, iodine, arsenic, copper, lead, zinc, silver, stramonium, belladonna, and most of the Solanaceæ. Traumatic pharyngitis results from deglutition of boiling water or of acrid or caustic substances; from inhalation of hot air, of steam, or of flame, and is most usually associated with traumatic oesophagitis or with laryngitis.
PATHOLOGY AND MORBID ANATOMY.—Acute pharyngitis, as most commonly encountered, is a simple erythematous inflammation of the mucous membrane; the palate and tonsils being likewise involved. In most instances there is simply an active hyperæmia which may subside in a day or two. When more intense than this the mucous membrane of the palate, tonsils, and pharynx becomes congested and swollen, uniformly or in circumscribed areas. In some instances the submucous tissue of the pharynx is greatly relaxed, and the mucous membrane lies upon the substructure in thick folds. In others there is more or less oedema. The mucous follicles, especially those of the posterior palatine folds, are frequently swollen. There is an abnormal though not excessive secretion of viscid mucus, clear or turbid. The uvula is often swollen or distended with serum, and its mucous membrane is relaxed. Sometimes it appears as though pasted to one of the folds of the palate by viscid secretion. The posterior palatine folds may be distended with serum, and their arched appearance thus become obliterated. Resolution occurs gradually in some instances, quickly in others.
Phlegmonous pharyngitis exhibits a still higher grade of inflammation. It involves the submucous structures as well as the mucous membrane, including at times the fibrous sheaths of the muscles. It may, in addition, involve the palate, the tonsils, the base of the tongue, and contiguous structures. Suppuration is common, usually circumscribed, but not infrequently diffuse in patients of enfeebled constitution.
One variety of the disease is essentially a deep-seated pharyngitis; and this form almost always progresses to suppuration (suppurative pharyngitis). The process becomes then, not infrequently, a diffuse suppurative inflammation of the subpharyngeal connective tissue, extending sometimes downward along the oesophagus, into which the pus may be discharged by spontaneous rupture, with a result of permanent stricture from irregular cicatrization. Sometimes the suppurative process extends anteriorly beneath the cervical fascia, and the pus may gravitate so as to occlude the air-passages, partly or completely, by direct pressure; or in other instances the entrance of [p. 392]the larynx may become blocked by the tumefaction of the pharynx. When phlegmonous pharyngitis is of traumatic origin, there will be more or less destruction of the mucous membrane according to the nature of the injury, whether accidental or designed, whether due to burn, scald, inhalation of hot air or steam, or to deglutition of alkaline, acid, or other corrosive substances. In these cases the morbid process is rarely confined to the pharynx, but the larynx, the oesophagus, and even the stomach, are liable to be involved. If regurgitation of hot air or of caustic fluids takes place through the nasal passages, the injury will of course involve those regions.
Ulcerative pharyngitis is a low form of inflammation present in sore throat, probably dependent upon septicæmia. The tonsils are somewhat congested and swollen, and one or more white superficial ulcers form on their surface, or on the palate, or on the pharynx. These ulcers are generally round or oval, and vary greatly in size. When two or more ulcers exist, they exhibit no tendency to confluence. Healing takes place rapidly, usually without leaving any traces of the lesion.
Membranous pharyngitis, or herpes of the pharynx, is one of the infrequent phenomena of a not uncommon sore throat, which exhibits at first a collection of small vesicles the size of millet-seeds or larger, isolated here and there or clustered in groups on the palate and uvula, less frequently on the tonsils. Herpes of the mouth and lips sometimes coexists. These vesicles are surrounded by inflammatory areolæ. Their contents are more or less turbid. In rare instances they disappear without trace after a day or two. Usually they soon undergo rupture, sometimes within a few hours, so that small ulcers are left, which almost immediately become covered with a grayish-white exudation. A number of patches will coalesce, forming limited sheets of false membrane not unlike those of diphtheria. The disease is usually confined to one side of the throat, the corresponding submaxillary or cervical glands being affected moderately when at all involved. The tonsil is swollen, and the mucous membrane of the palate and the palatine folds is congested and often tumefied. There is an abnormal secretion of viscid, ropy, turbid mucus. In a few days the ulcers heal beneath the exudation, which becomes disintegrated and detached, the inflammatory process subsiding by gradual resolution. Sometimes the ulcers cicatrize without previous deposit of false membrane. Occasionally there are at longer or shorter intervals successive crops of vesicles, which may or may not undergo ulceration.
Gangrenous pharyngitis may supervene upon any form of pharyngitis, but in the majority of instances its malignant character is inevitable from the outset; so that some authors have even restricted the term gangrenous to a form of sore throat characterized by primitive gangrene of the pharyngeal mucous membrane originating independently of any other malady. Whether an idiopathic disease, or whether it follows scarlatina, measles, small-pox, dysentery, or enteric fever, it is associated with that depraved condition of the system denominated typhoid. At times it occurs in tuberculous phthisis. The initial manifestations may be simply those of intense inflammation. The tongue is covered with a dark creamy, pultaceous deposit consisting of broken-down epithelium, pus-cells, bacteria, and molecular débris, while similar masses are occasionally seen upon other mucous surfaces of the mouth and throat. The tonsils, [p. 393] palate, and pharynx are livid and swollen, and sometimes oedematous. At an early period the tonsils, the palatine folds, and the posterior wall of the pharynx become covered with dark, ashy-colored ulcers with excavated edges. Sometimes these spots are black from the first, and appear slightly elevated. These soon slough out with more or less of the surrounding tissues, and the ulcers left are covered with sanious, ichorous, fetid secretion. In some instances a delicate pseudo-membrane has been found in the bed of the ulcer after death (Mackenzie). The destructive process rapidly extends—sometimes to the oesophagus in one direction or to the nares in the other. The larynx is less frequently implicated; should it be attacked, oedema is liable to occur. Occasionally the process is limited to the tonsil, and there is no pharyngitis at all. Erosion of the blood-vessels may give rise to fatal hemorrhage. In those instances where the gangrene is circumscribed there are found, post-mortem, depressed oval or circular patches from one-twentieth to one-half an inch in diameter, varying in color from dark gray to absolute black. The edges are of a brownish color and are perpendicular. The bundles of muscular fibre are laid bare by destruction of the mucous membrane and submucous connective tissue, but as a rule escape implication of their substance. Similar patches have been noted in the epiglottis and the upper part of the larynx as well as in the mouth and pharynx—in some cases, indeed, in the trachea, the lungs, the oesophagus, the stomach, and the intestines.
Erysipelatous pharyngitis is usually an extension of erysipelas from the facial integument, which may take place by the lips and mucous membrane of the mouth, by the nasal fossæ, by the Eustachian tube from the tympanum and external ear, or by the nasal fossæ from the conjunctiva and eyelids through the lachrymal duct. When the disease begins in the pharynx the order of communication may be reversed. The pathological processes are the same as in cutaneous erysipelas. The mucous membrane of the pharynx will be diffusely red or purplish and shiny. Sometimes little bullæ are formed and become ruptured, leaving a patch of softened whitish-yellow tissue, which is sometimes torn from the surface beneath by the act of coughing or of deglutition. The inability to swallow is not due to swelling of the tissues, but to actual paresis of the muscles, probably from interstitial infiltration, but perhaps from implication of their substance. The cervical and submaxillary glands are rarely involved. Erysipelatous pharyngitis usually terminates by resolution, desquamation of the greater part of the epithelium of the mucous membrane often taking place; but it may be followed by abscess or by gangrene. Extension may take place to the larynx, and oedema may follow.
Exanthematous pharyngitis accompanies some cases of cutaneous exanthemata. The pharyngitis of small-pox is occasioned by an eruption upon the mucous membrane similar to that which appears on the skin. Often in advance of the cutaneous eruption it occupies the inside of the cheeks, the palate, uvula, and pharynx; sometimes the larynx as well. Maturation occurs more rapidly than upon the skin, and there is more or less purulent infiltration of the submucous connective tissues. Ulceration of the larynx or trachea may ensue so severe in character as to cause fatal termination by the local lesion.
[p. 394]In measles an eruption similar to the cutaneous manifestation occupies the air-tract from nostril to bronchi rather than the food-passages. The Eustachian tubes may be involved, and the inflammation is sometimes propagated along the lachrymal duct. The throat may be affected a day or two before the external integument. Small red points the size of a millet-seed or larger appear on the palate, the tonsils, the posterior palatine folds, and the wall of the pharynx. These disappear in a few days, though sometimes in bad cases fibrinous exudation may accumulate. In other instances abscess or ulceration takes place, chiefly in the larynx.
The pharyngitis of scarlatina develops a day or two prior to the cutaneous eruption, the mucous membrane of the palate, tonsils, and pharynx being deeply congested, uniformly or in patches, with slight papulous elevations here and there. In the course of a day or two an opalescent or milky deposit, consisting chiefly of detached epithelium and viscid mucus, is observed on the swollen palate and tonsils. In the anginose variety the hue of the inflamed structures is more dusky. There is a pseudo-membranous deposit of a dirty-white, ash, or even yellow color. It is not limited to the tonsils, but accumulates rather on the palate, palatine folds, and posterior wall of the pharynx. The mucous membrane beneath the patches is often ulcerated, and sometimes gangrenous. There is much greater tumefaction of all the parts than in simple scarlatina, the enlargement of the cervical and submaxillary glands and the infiltration of contiguous connective tissue being so great in some instances as to prevent the mouth from being opened. A viscid and turbid secretion accumulates in the mouth. The nasal secretions sometimes desiccate into firm crusts. Suppuration may occur. Sometimes otitis media results from extension along the Eustachian tube, and sometimes suppuration of the membrana tympani, suppurative external otitis, or disease of the internal ear with extension to the cerebrum. In malignant cases all the processes are aggravated. Ulceration or gangrene soon ensues, the pseudo-membranous deposit being dark, almost black, from extravasated blood. Oedema of the uvula and soft palate is liable to occur, and if the larynx be involved there may be oedema of the epiglottis and ary-epiglottic folds.
SYMPTOMATOLOGY.—Simple pharyngitis very often gives rise to but little discomfort. There is usually more or less heat and dryness in the parts, especially at first. There is some dysphagia, principally from pain in swallowing, but in part from actual debility in the muscles of deglutition. Hoarseness is not usual, and cough is infrequent if there be no elongation of the uvula. Speech may be embarrassed by difficulty of articulation. There is usually some febrile movement, with acceleration of pulse and respiration. Some cases exhibit more intense inflammatory action, with a corresponding aggravation of the constitutional symptoms. The skin becomes markedly heated, the body-temperature rises to 101° F. or higher, the pulse reaching 100-120, in some instances 140, beats per minute, even in the adult.
In that variety known as rheumatic sore throat there will be in addition pain and soreness in the neck, back, and limbs, often severe, and increased by motion. There will be great accumulation of saliva in the mouth because of the intense pain in swallowing it. Speech, and even respiration, may become painful. These manifestations are frequently [p. 395]followed by the ordinary phenomena of acute articular rheumatism, but they may subside in a few days, leaving only a general feeling of muscular soreness or slight stiffness in one or more of the joints. Sometimes a temporary torticollis follows.
In some cases of pharyngitis the cervical glands become swollen and painful, but this is not common. In children the constitutional disturbance is much greater than in adults. In malarial districts or in subjects of malarial poisoning the manifestations may assume a periodic character. Recovery takes place, as a rule, in from three to ten days.
In many instances the local phenomena are most prominently manifested on one side of the throat. There will then exist great liability to similar involvement of the other side after convalescence of a day or two, and without care and avoidance of exposure the second attack may be far more severe than the first.
The severe variety of pharyngitis denominated phlegmonous is often ushered in with a decided chill, the phenomena of fever following within twenty-four hours. The symptoms, both local and general, are of much greater severity than in catarrhal pharyngitis, especially in cases proceeding to suppuration.
Paralysis of the palate and other paralyses may follow either of the forms of sore throat just described. Albuminuria sometimes results. In extremely rare cases it is an accompaniment of the disease.
Superficial ulceration of the mucous membrane may occur in almost any form of pharyngitis or of sore throat. Some authors have separated a special form of ulcerative sore throat occurring in those enfeebled from long exposure to unwholesome influences, such as nurses, hospital attendants, etc., in whom the first symptom is pain in deglutition, especially of saliva. The tongue is furred and the breath is offensive. There is loss of appetite, with general lassitude, feebleness of circulation, and more or less elevation of temperature. Intense headache is often present. Under suitable treatment recovery is rapid.
The ulcerative sore throats of syphilis and of tuberculosis require separate consideration.
Common membranous pharyngitis frequently gives rise to but slight symptoms, differing very little from those of other forms of pharyngitis; but there may be high fever of sthenic or of asthenic type, very often preceded by general malaise, sometimes by a decided chill. The pain in deglutition and the local heat and dryness are sometimes much greater than in the more ordinary forms of pharyngitis. The distress may extend into the ear, sometimes to the nasal passages, in rare instances to the larynx. The disease lasts for a week or ten days, usually terminating in recovery. In occasional instances, chiefly in children, it terminates fatally by apnoea from extension of the membrane into the larynx. Paralytic sequelæ are not rare.
The advent of gangrenous pharyngitis is sometimes indicated by sthenic phenomena, but usually from the first it is marked by extreme prostration, comparable in some instances to the collapse of cholera. There is a low type of fever. The pulse is feeble and infrequent. The skin, especially of the extremities, is cold and blue. The eye is glassy, the countenance haggard. The pain, as a rule, is not severe, sensation being benumbed. The disease is often accompanied by an irregular erythematous cutaneous [p. 396]eruption. The secretions and excretions escape by the mouth and nose, and they are extremely fetid. There is indeed a peculiar odor, which once encountered can scarcely be mistaken. If the lungs become affected there will be copious hæmoptysis. In some cases the tendency to hemorrhage is general, blood oozing or gushing simultaneously from lungs, bowels, nose, and mouth, and sometimes extravasating beneath the skin. Sphacelus ultimately takes place at the points of ecchymosis. Diarrhoea, abundant and fetid, due to invasion of the alimentary tract, often sets in before the close, and may be regarded as a sure precursor of death. Death usually takes place from syncope, intelligence often remaining unaffected to the last. When these cases recover a horrible amount of deformity often remains to mark the ravages of the disease. During cicatrization the positions of contiguous parts become very much altered. The palate may become adherent by its sides, and by more or less of its posterior surface, to the pharynx, sometimes resulting in complete occlusion of the nasal portion of the pharynx.
The constitutional symptoms of erysipelas of the pharynx are those that attend the usual manifestations of external erysipelas, the febrile phenomena, epigastric pain, nausea, and so on, being increased in severity. There will be great pain and difficulty of deglutition. If there be serious oedema, symptoms of suffocation will occur. Laryngitis will be indicated by pain referred to the larynx. The duration of the disease varies from forty-eight hours to a week, rarely longer. Death may occur within two or three days from oedema of the larynx or from other causes frequently indiscernible. Resolution usually takes place in those cases which recover. Occasionally abscess occurs.
DIAGNOSIS.—The diagnosis rests upon the conditions already described under the heads of Pathology and Symptomatology. Under ordinary circumstances it presents no difficulty, but during the prevalence of epidemics of scarlatina or diphtheria even the mildest sore throat demands careful attention and frequent inspection until the exclusion of the graver maladies may be positively determined. The greatest difficulty will present in cases of common membranous sore throat, for it is sometimes impossible to make the differentiation from diphtheria, especially as the vesicular stage is rarely seen. Sometimes, it is said, it is possible to detect one or more of the small ulcers left by the rupture of the vesicles; sometimes small isolated spots of false membrane will by their transparency indicate recent formation, and by their circular shape the previous existence of a vesicle (Peter, cited by Mackenzie). The coexistence of cutaneous herpes is corroborative of the diagnosis, but by no means an infallible sign. It must not be forgotten in this connection that membranous sore throat may predispose to an attack of diphtheria. In gangrenous sore throat the grayish-black patches may be mistaken for the pseudo-membranes of diphtheria, but their color is dark from the outset, while in diphtheria they become dark only as the disease progresses. They always represent actual death of the tissues, which is not an essential lesion of diphtheria. Swelling of the cervical glands is unusual. Finally, the characteristic odor of gangrene is almost unmistakable.
PROGNOSIS.—The prognosis is favorable in catarrhal pharyngitis and in the milder forms of the phlegmonous, non-specific, ulcerative, and [p. 397]common membranous varieties. It is unfavorable in intense suppurative pharyngitis, though cases often get well. In gangrenous pharyngitis the prognosis is extremely grave, but recovery is not impossible. In traumatic pharyngitis the prognosis will of course depend upon the nature and extent of the injury, being not unfavorable if this be confined to the pharynx, though even in limited cases there may be stenosis or other ill results from cicatrization. Erysipelatous pharyngitis is of grave prognosis when the result of extension of the disease from the face, but recovery is frequent when the pharyngeal disease is primary.
TREATMENT.—The treatment of superficial pharyngitis is very simple. Unless the case be so light that no special medicinal treatment seems advisable, the patient should be confined to a bed or lounge to secure rest, a light coverlid being thrown over the body to equalize the heat of the surface. If a meal has recently been taken, a mild emetic is often of service to empty the stomach and save the labors of digestion. A gentle laxative or, if the patient be of costive habit, a saline purge is indicated to facilitate the passage of matters already in the intestinal canal. In cases of actual constipation a drastic cathartic may be required. If there be considerable pain a small dose of morphine may be advantageously combined with the aperient. If frequent pulse or high temperature exist, especially in severe cases, tincture of aconite, in doses of one or two drops every hour or two hours at first, will be useful. As soon as any marked effect has been produced the aconite may be discontinued or the intervals between administrations lengthened. Locally, the free use of demulcent drinks, and of pellets of ice when cold is agreeable, will relieve the pain in the throat and sometimes repress excessive secretion. Cold compresses to the neck anteriorly are often soothing, and sponging the entire surface of the body with tepid water, acidulated or alcoholized, will allay the intense heat of the skin. The diet should be light and nutritious. Very often the emetic, rest, and regulation of diet will constitute the entire treatment required.
When the local distress is very great, astringent lozenges (catechu, krameria) may be allowed to dissolve in the mouth, or sprays of weak solutions of alum or of carbolic acid may be propelled upon the mucous membrane. Tannin, potassium chlorate, and cupric sulphate are often used for this purpose. When the uvula is elongated or oedematous it is often a constant source of irritation and discomfort. Scarification to give vent to pent-up blood or puncture to allow the escape of effused serum will afford prompt relief. Excision is never necessary.
In phlegmonous pharyngitis the treatment will necessarily be more active. Here an early emetic is of great service. A saline laxative may be administered every three or four hours for a day or two, each dose containing a drop or two of the tincture of aconite, with the addition of morphine if indicated by pain. Drop-doses of aconite at more frequent intervals sometimes serve a better purpose. Inhalation of steam, or of steam from water impregnated with hops, chamomile-flowers, paregoric, compound tincture of benzoin, juice of conium, or the aqueous extract of opium, belladonna, or conium, will afford great relief, as will the frequent projection of sprays of warm water, simple or slightly aromatized with cologne-water or with toilet vinegar. Warm and moist applications externally are often very soothing. Gargling entails too much pain to be of [p. 398]service, but medicated sprays may be used of aqueous solutions (twenty grains to the ounce) of tannin, alum, zinc sulphate, or cupric sulphate, care being taken to guard against the swallowing of any of these drugs. Powders of alum, tannin, krameria, etc., diluted with liquorice, acacia, bismuth, lycopodium, and the like, may be blown upon the parts, and are often efficient. Sodium bicarbonate frequently affords relief. The topical application of silver nitrate is rarely practicable and generally unnecessary.
When the inflammatory process is of a higher grade and not likely to yield to purely medicinal treatment, leeching or venesection may be employed, but should not be resorted to without urgent reason. The recognition of abscess is an indication for its immediate discharge by incision or aspiration. In suppurative cases quinia and iron should be given in large doses. The general treatment is like that of simple sore throat. When liquid food cannot be swallowed, nourishment by enema is requisite. Efforts at deglutition should be spared as much as possible, and with this view medicines which can be administered by inhalation, by enema, or by hypodermatic injection are to be preferred.
In pharyngeal sore throat, whether catarrhal or phlegmonous, depending on rheumatic or gouty diathesis, salicylic acid or the salicylates will prove useful, either alone or in conjunction with other measures.
The treatment of ulcerative pharyngitis is practically the same as that recommended for phlegmonous pharyngitis. Antiseptic gargles may be used locally, but as a rule the pain is so great that inhalations of soothing vapors, as before recommended, will answer a better purpose. When the process is very acute fragments of ice will be most useful. Ice to the head will afford relief to pain. A little good wine, with quinia and iron, comprises the medicinal measure requisite.
Gangrenous pharyngitis calls for the most active and supporting treatment. Eggs, milk, cream, nutritious soups (up to the limits of the patient's capacity for swallowing, and by enema when necessary), quinia, tincture of the chloride of iron, and alcohol in large doses, are indicated. Local treatment is of high importance. Agents to destroy diseased tissue promptly and prevent the extension of the gangrenous process, such as bromine, strong nitric or hydrochloric acid, acid solution of mercuric nitrate, or caustic potassa, are to be thoroughly applied, in the hope of exposing a healthy surface beneath which will heal by granulation. When this treatment is unsuccessful or too hazardous, as in cases where the blood-vessels are probably involved, we can only palliate the symptoms by applying weak solutions of acids and astringents, to which opium may be added, relying on constitutional measures for restraining the destructive process. Washes and sprays of potassium chlorate, eucalyptol, thymol, hydrogen peroxide, etc., or the agents employed in common sore throat, are often agreeable to the patient, and may be useful in restraining fetor, but they have no direct therapeutic influence on the progress of the disease. If the ulceration is extending into the vicinity of the great vessels of the neck, measures for compression should be at hand, in the use of which the nurse should be instructed, and preparations be made to facilitate ligation of the carotid artery in an emergency. Tracheotomy may be necessitated by oedema of the larynx. The deformities resulting from gangrenous sore throat in cases that recover usually require surgical treatment.
[p. 399]Traumatic pharyngitis must be treated on general principles. When due to contact of caustic or corrosive substances, an attempt may be made to neutralize the effects by a chemical antidote, but the physician is usually summoned too late to accomplish much in this manner. Morphine should be given in full doses, hypodermatically. Insufflations of morphine in powder, soothing inhalations, fragments of ice in the mouth, cold compresses, and, where possible, oleaginous drinks, are indicated to relieve topical distress. Rectal alimentation should be resorted to where the difficulties of deglutition are at all great. If symptoms of suffocation occur, tracheotomy must be performed. The results of traumatic pharyngitis require treatment according to their special indications.
Erysipelatous pharyngitis is to be treated by the administration, by enema if necessary, of large doses of quinia, tincture of the chloride of iron, brandy, and diffusible stimulants. Alimentation is to be kept up by mouth or rectum, as may be necessary, with as much food as can be given containing the most nutrition in the smallest bulk possible. Locally, a strong solution of silver nitrate (sixty grains to the ounce) should be so applied as to cover a margin of unaffected structures. Sedative inhalations are of service. Extension to the larynx demands scarification or tracheotomy.
When the diagnosis of common membranous sore throat can be made out with certainty, there is nothing calling for special treatment, but the treatment pursued in ordinary sore throat may be generally followed with advantage. When fetor exists, as during the detachment of patches of exudation, antiseptic and detergent sprays may be employed. Solutions of borax, boric acid, carbolic acid, potassium chlorate, potassium permanganate, etc. are appropriate. In some individuals, especially strumous and tuberculous subjects, there is a constitutional proclivity to chronicity or to the recurrence of the peculiar manifestations. More active measures will be required in these cases. Locally, frequent application of the dilute acids (i.e. every day or two) affords the most satisfactory results. Internally, iron and cinchona preparations should be administered. Opium in small doses has a special application—not as a narcotic, but as a gentle stimulant or nervous tonic. Nux vomica or arsenic may be employed for a similar purpose. The diet should be highly nutritious and easily assimilable. Unnecessary exposure should be avoided, and supporting measures generally, hygienic, as well as medicinal, should be persisted in. Membranous pharyngitis sometimes exhibits a tendency to phagedæna. The treatment for gangrenous sore throat is then indicated. It may invite an attack of diphtheria or the diagnosis may be in doubt. In that case the prudent course is to treat it as diphtheria, but to avoid the recommendation for diphtheria of some indifferent remedy, during the exhibition of which a case of membranous sore throat has recovered. When extension to the larynx occurs threatening suffocation, tracheotomy to avert death should be performed, as in croup or diphtheria.
The sore throats of the exanthemata, of typhoid fever, etc., are to be treated on the general principles applicable to catarrhal or phlegmonous pharyngitis. Oedema or tumefaction, as in malignant scarlatina, of a sufficient extent to obstruct respiration, is to be relieved by scarification, and when this is inefficient resort must be had to tracheotomy. The sore [p. 400]throats caused by drugs are to be treated first by removal of the cause, and afterward according to the special indications.
DEFINITION.—An acute ulcerative pharyngitis due to infiltration with miliary and granular tubercle and the consequent destructive metamorphosis.
SYNONYMS.—Acute tuberculous sore throat, Acute tuberculous pharyngitis, Tuberculosis of the pharynx, Phthisis of the pharynx.
HISTORY.—Only of late years has tuberculosis of the pharynx been distinctly recognized as a tuberculous disease. The tubercular sore throat or pharyngitis described by Green of New York, and other authors following him, is an affection of entirely different character, and not tuberculosis at all. The chronic tuberculous sore throat of advanced tuberculosis is likewise a different affection clinically, though of the same histological character.
To the late Isambert2 of Paris belongs the credit of definitively recognizing the specificity of acute tuberculous sore throat or pharyngitis, and to him likewise the credit of indicating its differentiation from syphilitic sore throat, with which it had long been confounded. To B. Fraenkel of Berlin3 is likewise due the credit of an accurate comprehension and elucidation of the clinical and histological pathology of this disease.
2 Annales des Maladies de l'Oreille, du Larynx, etc., vol. xi., 1875, p. 162; Conférences cliniques sur les Maladies du Larynx et des premières Voices, Paris, 1877, p. 219.
3 Berlin. klin. Woch., Nov., 1876; London Med. Record, Jan. 15, Feb. 15, 1877.
ETIOLOGY.—Acute tuberculous pharyngitis is quite a rare disease. Its predisposing causes, in all probability, are identical with those of acute tuberculosis. Its exciting cause, in some cases at least, is some unusual exposure to cold and wet. It is not certain that the throat is affected before the lungs; but if this be the case, it is certain that the lungs become affected soon afterward. The disease occurs in young children, Isambert having recorded a case at four and a half years of age, but it is much more frequent in adolescents and young adults. It is impossible, as yet, to assign the reason why the pharynx rather than other structures undergoes tubercularization in these exceptional cases of pharyngitis. Syphilis sometimes coexists in the adult certainly, and it may be questioned whether hereditary taint may not be an important factor in determining tuberculosis in a region so frequently ravaged by syphilis.
PATHOLOGY AND MORBID ANATOMY.—The local disease is essentially an ulcerative pharyngitis or pharyngo-laryngitis, as may be, extremely rapid in its progress, and terminating fatally within a few weeks, or a few months at farthest. The ulcerative process usually begins on the palatine folds or else on the lateral wall of the pharynx, thence extending to the palatine folds, soft palate, uvula, and hard palate in one direction, and toward the posterior wall of the pharynx in the other. The uvula sometimes becomes thickened into a club-shaped, gelatinous-looking mass, somewhat characteristic. Previous to ulceration the mucous membrane is subjected to abundant infiltration with miliary and granular tubercle just beneath the epithelial layer. Macroscopically, these infiltrated portions of [p. 401]tissue present as irregular chagrinated groups of patches, generally confluent, which when abundant or prominent are liable to be confounded with syphilitic patches. Just beneath the surface the collections of tubercle project as little semi-transparent grayish nodules, in size and form recalling the appearance of vermicelli-seeds or fish-eggs. They steadily increase in volume and in number, lose their translucency, and finally undergo disintegration into lenticular ulcers with caseous bottoms and undermined hyperæmic edges. The ulcers extend steadily in periphery and in depth, and coalesce by necrosis of intervening mucous membrane. Polypoid excrescences springing from the beds of the ulcers have been described (Fraenkel). Collateral tumefaction takes place in some instances, due, it is stated (Isambert), to infiltration of the tissues by a gelatinous material, possibly a mucoid degeneration of the connective tissue. The usual tendency of the disease, however, is to incite atrophic metamorphosis of the adjacent tissues not undergoing actual tubercularization. In many instances extension to the upper portion of the larynx takes place; in some, extension to the vault of the pharynx. Extension to the oesophagus, as has been remarked by Mackenzie, and to the posterior nasal outlets, has not been noticed. Enlargement of the cervical lymphatic glands is quite common.
Microscopic examination of the tissues of the pharynx has revealed profuse infiltration with round cells—most frequently in the mucous membrane and submucous connective tissue only, occasionally in the muscular fibres likewise. The muscles sometimes undergo the fatty degeneration, and the mucous glands both fatty and colloid degeneration.
SYMPTOMATOLOGY.—The chief and characteristic subjective symptom is extreme pain in swallowing (odynphagia)—pain much more intense than in other morbid processes in the same locality, and inexplicable by the extent of the visible disease merely. This pain often extends toward the ears. Cough, adynamic fever, rapid emaciation, and so on are present, as in acute tuberculosis generally.
DIAGNOSIS.—It cannot be stated that the diagnosis is easy. The two distinguishing characteristics are the exquisite pain in swallowing and the absence of pus from the surface of the ulcers. The aspect of the ulcers differs, furthermore, from that of syphilitic ulcers by the lack of opalescence and of inflammatory areolæ. The gray nodules in the affected mucous membrane are different from what is observed in any other disease. These points, with the history of the attack, the family history, and the probable evidence of tuberculosis in the lungs, will usually serve to discriminate the disease from syphilis, for which it is most likely to be mistaken. In cases of doubt ophthalmoscopic examination of the choroid and iris may reveal tubercle. The bacillus tuberculosis has been found in the detritus from the ulcers (Guttman, Gurovitch). The fact must not be ignored that syphilitic and tuberculous pharyngitis may exist together. Febrile symptoms, typhoidal in type, in a case of supposed syphilitic sore throat will most likely be indicative of tuberculosis.
PROGNOSIS.—The disease is rapidly fatal, apparently inevitably so. An exceptional case has been recorded, however (Cadier4), living [p. 402] several years after the diagnosis had been made by Isambert and many others.
4 Annales des Maladies de l'Oreille, du Larynx, etc., July, 1883, p. 136.
Death takes place by asthenia in from six weeks to six months; occasionally within a fortnight from the apparent onset.
TREATMENT.—The little that can be accomplished in the way of treatment is limited to improving the diet and hygienic surroundings, with the administration of such constitutional remedial agents as are given in acute tuberculosis, and palliative treatment of the local suffering. For the latter purpose insufflations of iodoform and morphine are to be recommended, two or three grains of the former with one-fourth to one-half grain of the latter, once a day or oftener. Such insufflations should be preceded by douches or sprays of sodium borate or bicarbonate, to rid the parts of mucus and detritus. A drop or two of carbolic acid, of eucalyptol, or of a solution of thymol may be advantageously added for purposes of disinfection. Solution of hydrogen peroxide (2 per cent. or weaker) is a very valuable agent for use in spray or douche. It may be rendered more agreeable by the addition of a few drops of some balsamic.
When swallowing is impracticable, nourishment by enema is indicated, with forced feeding by means of a catheter passed through the larger of the two nasal passages into the oesophagus.
DEFINITION.—A chronic inflammation of the mucous membrane of the pharynx, whether implicating the glandular structures or not, and commonly associated with similar chronic inflammation of contiguous structures.
SYNONYMS.—Chronic sore throat, Chronic angina.
Chronic pharyngitis presents in two varieties: 1, simple chronic pharyngitis (chronic catarrhal pharyngitis, chronic catarrhal sore throat), in which the disease does not affect, or affects but slightly, the glandular structures of the mucous membrane; and 2, follicular pharyngitis (granular pharyngitis, clergyman's sore throat), in which groups of the follicular glands of the mucous membrane are enlarged, and sometimes inflamed.
ETIOLOGY.—The predisposing causes of chronic catarrhal pharyngitis are those enumerated under the head of the acute form of the affection, and the exciting causes are repeated attacks of the acute malady.
The predisposing causes of chronic follicular pharyngitis are overcrowding, and sedentary occupations; and the exciting causes are chiefly improper use of the voice and exposure to local irritations, mechanical and chemical, including too free use of condiments, tobacco, and alcohol, gormandizing, and the alternations of hot food, cold drinks, ices, and hot drinks at meals. It is not so often a direct sequel of attacks of acute sore throat as a result of prolonged catarrhal pharyngitis; and sometimes it appears to be chronic, so to speak, from the outset.
Both forms of chronic pharyngitis are frequently associated with chronic inflammations of the mucous membranes elsewhere, particularly of the nasal passages and of the stomach, and, to a less extent, of the genito-urinary apparatus; the entire train of phenomena, in some instances, [p. 403]being due to passive congestion dependent upon impaired cardiac power. Similarly, it presents at times as one of the accompaniments of exophthalmic goitre. It is often associated with phthisis, and is sometimes found in phthisical subjects prior to the detection of the pulmonary disease. It is sometimes coincident with chronic cutaneous eruptions, and may depend on the same causes, whether dietetic or nervous.
Uterine disturbances may give rise to chronic pharyngitis, probably by reflex nervous influence, and so do other chronic and dispiriting complaints. In like manner, depression of spirits and impairment of bodily vigor from domestic, financial, and social chagrin provoke a train of phenomena in which chronic pharyngitis may be a prominent manifestation.
PATHOLOGY AND MORBID ANATOMY.—Simple chronic pharyngitis is a chronic catarrhal inflammation of the mucous membrane and submucous connective tissue of the pharynx, with irregular hyperplasia of all the histological elements, chiefly affecting the epithelial layers and the most superficial strata of the submucosa. The pharynx, the posterior surface of the palate, and the pharyngo-palatine folds are the structures most generally implicated, but the glosso-palatine folds, the base of the tongue, and even the anterior surface of the palate, are sometimes involved. At an advanced stage of the affection extension may take place to the vault of the pharynx and the posterior nasal outlets, and in occasional instances to the larynx.
The initial hyperæmia of diffuse congestion finally leads to permanent dilatation of tracts of capillaries varying in area and mode of distribution, sometimes recalling the territorial outlines upon a map. The mucous membrane is bright red in color and irregularly thickened, sometimes into prominent welts or folds. The palate is often relaxed. Hypersecretion takes place over the entire diseased surface, and there is considerable desquamation of turbid epithelium, which sometimes accumulates in masses. Glands are dilated and hypertrophied here and there, but not in every instance, or if so indiscernibly, at least, to the naked eye.
In some cases enlarged follicles are very prominent in the infra-tonsillar space, between the anterior and posterior palatine folds, and along the lateral walls of the pharynx down toward the base of the tongue. The circumvallate papillæ may also be enlarged, and the fungiform papillæ are sometimes very prominent and deeply congested.
In the folliculous variety of the disease the hyperplasia affects chiefly the mucous glands and follicles, isolated or in groups, together with zones of connective tissue surrounding them and the epithelial investment of the mucous membrane in their immediate neighborhood. A number of small projections, from the size of pinheads to that of peas, mostly somewhat hemispheroidal, sometimes ellipsoidal or quite irregular in configuration, stud the pharynx irregularly. When clustered they are more apt to occupy the lateral angles of the pharynx. In this locality indeed the chains of glands and their enveloping mucous membrane sometimes present in longitudinal ridges which simulate additional or adventitious post-palatine folds. The projections are usually opaque, deeper in color than the surrounding congested mucous membrane, and velvety from loss of squamous epithelium. Sometimes they are translucent, as if filled with colloid material, probably retained and degenerated secretion. [p. 404]Very often their contents undergo caseous degeneration, and sometimes even calcification—a variety designated tubercular by Green, Gibb, and others, but far different histologically from true tuberculosis of the pharyngeal glands, which does occur occasionally in phthisical patients.
Delicate red lines of engorged capillaries usually surround the base of these projections. There is great disposition to the accumulation of viscid, discolored mucus on the surface of the mucous membrane. As the disease progresses all the processes become more widely extended, until finally nearly the entire pharyngeal and oral mucous membrane becomes involved. The soft palate becomes relaxed and the uvula thickened and elongated, sometimes to an extreme degree. Chronic folliculous tonsillitis exists in many cases.
When either form of chronic pharyngitis continues for a long while unchecked, there may result atrophy of the glandular structures and epithelial elements generally, giving rise to pharyngitis sicca or atrophic pharyngitis (so-called dry catarrh). There is then but scanty secretion, and this dries rapidly upon the surface of the thin mucous membrane, which becomes rough, inflexible, and glazed.
SYMPTOMATOLOGY.—Cough, expectoration, impairment of voice, dysphagia, and uncomfortable sensations in the throat present in various degrees according to the stage of the disease and the temperament of the patient. Hemming and hawking to clear the throat often become habitual, especially in cases associated with chronic internal rhinitis, being provoked in many instances by secretory products which drop into the pharynx or glide along its walls. It is sometimes important to distinguish this habit from the cough of laryngeal or bronchial irritation.
In cases associated with chronic gastritis the loss of appetite and consequent emaciation accompanying the symptoms of pharyngitis sometimes lead friends of the patient to a mistaken diagnosis of consumption; and when, as is not infrequent, chronic bronchitis also coexists, even the physician may be misled.
In many instances of chronic folliculous pharyngitis evidently of long standing, and accidentally discovered at times to the surprise of the patient, no history of the classical group of symptoms can be obtained.
DIAGNOSIS.—The diffuse congestion of the mucous membrane and the absence of marked involvement of the follicles are, with the history of the case, the main discriminative features in the diagnosis of chronic catarrhal pharyngitis. The regular or irregular masses of tissue projecting beyond the general surface of the mucous membrane are the distinguishing characteristics of chronic folliculous pharyngitis. The vascular network of dilated capillaries mapping the surface into numerous irregular small areas of different sizes is not peculiar to either variety.
PROGNOSIS.—The prognosis of chronic catarrhal pharyngitis is favorable when no irremediable malady of body or mind exists. Much depends on the practicability of improving the dietetic and hygienic environment of the patient. The prognosis is likewise good in chronic folliculous pharyngitis under favorable surroundings, so far as relief from suffering is concerned; but the follicles, when long hypertrophied, so rarely undergo absorption under any treatment that their destruction becomes necessary—quite a different thing from their cure. The enlarged follicles once destroyed, the collateral irritative inflammation caused by [p. 405]them usually subsides. Impairment of voice, a result of the disease, may be remedied in young subjects, who will learn to use the voice with the abdomen in distension; but much improvement cannot be expected in old subjects and in those in whom the disease has been produced by improper methods of declamation, which are beyond correction.
TREATMENT.—In chronic catarrhal pharyngitis constitutional treatment adapted to the diathetic condition is required in the first instance. Alkaline laxatives are usually indicated by the irregularly coated tongue and the tendency to costiveness. These may be advantageously administered in half a pint of hot water one hour or so before meals, with a view of washing the stomach free from accumulations of mucus, epithelium, and retained products of digestion and decomposition, so that its condition may be improved for the reception and digestion of the ensuing meal. Topical medication of the throat is likewise requisite. This should be of a soothing character. Mild astringents are applicable, but strong astringents are often actually injurious. Silver nitrate and cupric sulphate in stick or strong solution should not be used; but sprays of dilute solutions (one or two grains to the ounce of distilled water), twice or thrice a day, are often of service. Zinc sulphate (five grains to the ounce) may be used in the same manner. Zinc chloride (ten grains to the ounce), carefully applied to the surface daily with a broad brush or soft cotton wad, is a useful remedy. Tannin in ether sometimes answers admirably, a delicate film being left for some time on the surface. Solutions of bismuth nitrate or borate in glycerin applied locally often relieve uneasiness. A broad flat brush is the best instrument for making these applications, placed low in the pharynx so as to paint the entire posterior wall by a single movement from below upward.
For home use, sprays, three or four times a day, of tar-water, containing five or ten grains to the ounce, of sodium borate or bicarbonate, or sodium, potassium, or ammonium chloride, or sodium, potassium, or ammonium iodide, are soothing and efficacious, and much superior to gargles. They are often preferred warm. Demulcent lozenges (gelatin, acacia, althæa, glycyrrhiza) slowly dissolved in the mouth often relieve topical discomfort.
Much more active treatment is required in chronic folliculous pharyngitis. Judicious constitutional treatment is of great importance. Topical medication is of equal importance. In recent cases of moderate intensity the ordinary treatment for the catarrhal variety sometimes suffices. In cases of long standing strong solutions of silver nitrate (sixty to one hundred and twenty grains to the ounce), carefully applied with the broad flat brush twice or thrice a week, are often of great remedial effect. Iodine (one drachm to the ounce of glycerin), alone or in combination with equal parts of carbolic acid, applied daily, may be serviceable in cases unimproved by the silver nitrate. Dilatation of the capillaries may sometimes be benefited by applications of ergot (fluid extract) or ergotin (grs. x-xx to the ounce). Enlarged follicles of long standing are rarely amenable to astringent and alterant topical treatment. They require destruction. The agent to be used is a matter of indifference as a rule, and, according to the taste or resources of the practitioner, may be the solid silver nitrate, caustic potash, London paste, zinc chloride, [p. 406]or the incandescent cautery, whether heated by fire, hot naphtha, or electricity.
The sprays and lozenges already mentioned are useful in this variety of pharyngitis also. They may be medicated with sedative ingredients according to indications for the relief of pain and discomfort.
In cases resisting the plan of treatment suggested mercuric chloride may be successfully used, both internally (gr. 1/16 two or three times a day) and in spray, a drachm or less night and morning (one grain to four ounces). External counter-irritation by repeated blistering over the larynx and under the angles of the jaws is useful in some instances. During treatment the voice should be used as sparingly as practicable.
In chronic atrophic pharyngitis the treatment, constitutional and local, should be such as favors secretion from mucous membranes—internally, cubeb, pyrethrum, calamus, xanthoxylum, jaborandi, ammonium chloride; topically, sprays, four or more times a day, of hot water, glycerin and water, ammonium chloride. Patients sleeping with the mouth open should wear an apparatus, extemporized or made to order, to keep the lower jaw closed in sleep.
DEFINITION.—A specific inflammation of the mucous membrane of the pharynx or of the mucous membrane and submucous tissues, the result of syphilis, and often associated with like disease in contiguous structures.
SYNONYMS.—Pharyngitis syphilitica, Pharyngitis specifica, Syphilitic sore throat, Syphilis of the pharynx.
ETIOLOGY.—Contamination by syphilitic virus is the sole cause, whether by direct inoculation or by systemic poisoning, hereditary or acquired. Direct inoculation proceeds from primary sores on the lips, tongue, cheek, and hard palate, themselves the result of actual contact with sores in other individuals. Initial sores have been seen upon the tonsils, palatine folds, pharynx, and even the epiglottis. Direct inoculation from secondary sores may be communicated by the tooth-brush, blow-pipe, pipe-stem, trumpet, mouth-piece of feeding-bottle, pap-boat, or similar article previously used by an infected individual. Uncleansed surgical instruments convey the disease in like manner.
PATHOLOGY AND MORBID ANATOMY.—Syphilitic pharyngitis—or, more strictly speaking, syphilitic sore throat—occurs in all varieties, primary, secondary, tertiary, and hereditary. Secondary manifestations are the most frequent, and primary sores the most infrequent. The primary sore is soft in some instances, and hard in others. Phagedænic ulceration may ensue. Secondary manifestations are usually bilateral, and often symmetric in configuration and distribution. They appear from a few weeks to a few months after infection, and are among the most frequent early manifestations of secondary syphilis. The inflammatory process begins in erythema, usually diffuse, often punctated, sometimes in patches. It extends from above downward more frequently than in the reverse direction, but may spread in any direction. The lesion commences upon the soft palate and tonsils more frequently than [p. 407]on the pharynx, but may commence in any portion of the oro-guttural cavity. Tumefaction ensues, with lividity of the surface. The epithelial cells become distended; the resulting opalescence, somewhat characteristic, eventually subsides into a central opacity, the true mucous patch or condyloma latum. Mucous patches vary in size from mere specks to large irregular surfaces, often the result of coalescences. They sometimes become red and granular and covered with purulent products. Microscopically (Cornil), they consist of thickened epithelium upon a base of proliferated lymphoid cells, which often infiltrate the deeper tissues extensively. They may disappear in the course of a few weeks by resolution and absorption. Sometimes suppuration occurs in small superficial abscesses which discharge upon the surface. Several abscesses discharging simultaneously in coalescence, an extensive ulcer may result, which, in repair, leaves a cicatricial trace of its site. Flat and circular bluish-white patches, due to thickening of epithelium, appear after the first year of constitutional syphilis, and may exist in association with the true mucous patch. They bleed readily on rough handling, but rarely undergo ulceration.
Tertiary manifestations may present within a few months after infection or not until many years. Gummatous infiltration of the connective tissue, diffused or circumscribed (syphiloma), follows diffuse or localized erythema, and then the gummata break down, discharge by ulceration, and leave deep-seated irregular ulcers with undermined edges and surrounded with inflammatory areolæ. These manifestations are much more frequent in the palate than in the pharynx, and the ulcerative process often destroys the uvula and large portions of the palate and palatine folds. When the pharynx and posterior surface of the palate are both ulcerated, cicatricial adhesions are sometimes inevitable, and thus serious stricture of the suprapalatine pharyngeal canal may ensue. The lesion may be quite limited in extent or may involve the entire pharynx. The ravages may become sufficiently extensive to involve the vertebra and the skull or to perforate the large blood-vessels. Cicatrization in the pharynx is vertical or stellate as the rule, and the peculiar pallid lustre of the cicatrices is quite characteristic of the syphilitic lesion. In many instances secondary and tertiary manifestations commingle. Ulceration is then more likely to extend superficially than in depth.
Hereditary manifestations pursue much the same course as tertiary manifestations. They usually occur before puberty, but are occasionally delayed until after maturity. Deferred tertiary and late hereditary manifestations sometimes present the characteristic ulceration of the commingled secondary and tertiary disease; and this form of ulceration is often incorrectly attributed to scrofulosis and to lupus.
SYMPTOMATOLOGY, COURSE, DURATION, COMPLICATIONS, AND SEQUELÆ.—The subjective symptoms of syphilitic pharyngitis are those of erythematous and ulcerative pharyngitis of like grade, except that there is very little pain. The course is chronic unless specific treatment be instituted, when prompt repair may be expected unless the general health has been much undermined. The duration is indefinite. The manifestations subside under treatment, and recur if it is not sufficiently prolonged. Complications occur with similar manifestations of syphilis in adjacent or contiguous or distant structures, as may be. The most frequent sequel in neglected cases is cicatricial stricture.
[p. 408] DIAGNOSIS.—Bilateral inflammation in symmetric distribution is very characteristic of syphilis. Irregular ulcers with undermined borders and surrounded by inflammatory areolæ are similarly characteristic. Acknowledged history of syphilis or the detection of syphilitic manifestations elsewhere serves to confirm the diagnosis. In cases of doubt a few days' treatment with specific remedies in large doses will almost invariably serve to clear up the diagnosis.
PROGNOSIS.—The prognosis as to life is good unless the ulcerations have become so extensive as to threaten perforation into blood-vessels or the patient has become greatly debilitated. The prognosis as to freedom from cicatricial adhesions and stricture is not good in the presence of lesions which have destroyed large territories of tissue, even under very careful management.
TREATMENT.—Specific medicines in positive doses constitute the most effectual treatment. Mercury is indicated in secondary lesions. Extensive ulcerative tertiary and hereditary lesions are peculiarly susceptible to large doses (30 to 90 or more grains daily) of potassium iodide, under the influence of which they often heal without any local applications whatever. As soon as a positive impression has been produced the dose may be diminished. The parts should be kept clean and comfortable by periodic douching with sprays of alkaline solutions, or, what is still more serviceable, with a ten-volume solution of hydrogen peroxide diluted with one or more parts of distilled water. The best local application to the edges of the pharyngeal syphilitic ulcers is the solid cupric sulphate. Chromic acid (1:8) is a serviceable local stimulant to indolent ulcers. Necrosed fragments of bone should be removed. Should any impediment to respiration take place during administration of the iodides, oedema of the larynx may be suspected, and should be looked for. Professional supervision is requisite for many months after the lesions have healed. Cicatricial sequelæ of stricture require surgical interference.
DEFINITION.—Inflammation of the oesophagus.
SYNONYMS.—Inflammatory dysphagia, Inflammation of the gullet.
Oesophagitis may be acute or chronic. Either form may be idiopathic, deuteropathic, or traumatic.
DEFINITION.—Acute inflammation of the gullet.
SYNONYM.—Oesophagitis acuta.
HISTORY.—Until the publication in 1829 of a thesis by J. T. Mondière entitled Recherches sur l'Inflammation de l'Oesophage, et sur quelques points de l'anatomie pathologique de cet organ, little study had been devoted to acute inflammation of the oesophagus; and since that time Mondière's researches have been largely utilized by subsequent writers. It has been taken for granted that Galen's mention of pain in the oesophagus1 has indicated his recognition of the disease. Fernel2 mentions phlegmon of the oesophagus; Honkoop3 describes inflammation of the oesophagus; J. P. Frank4 describes an oesophageal angina; and Joseph Frank5 seems to have been the first author to use the term oesophagitis. Since the publication of Mondière's monograph the principal systematic descriptions have been those of Hamburger6 Von Oppolzer7 Zenker and Ziemssen8 Luton,9 and Bernheim.10
1 De locis affectis, lib. iv. cap. iii.; lib. v. cap. v.
2 De partium mortis et sympt., lib. vi. p. 277.
3 Specimen inaugurale de morbo oesophagi inflammatorie, Lugd. Batav., 1774.
4 De curandis hominem morbis, Epitome prælectionibus academicis dicata, Mannheim, Stuttgardt, and Vienna, 1792-1820.
5 Praxeous medica præcepta universa, Lipsiæ, 1826-32.
6 Klinik der Oesophaguskrankheiten, Erlangen, 1871.
7 Vorlesungen über specielle Pathologie und Therapie, Erlangen, 1872; Englished in abstract by the writer in Philada. Med. Times, 1872.
8 Handbuch der speciellen Pathologie und Therapie, 1877; English translation, New York, 1878, vol. viii.
9 Dictionnaire de Médecine et de Chirurgie pratiques, Paris, 1877, vol. xxiv.
10 Dict. Encyclopediques des Sciences médicales, Paris, 1880, vol. xiv.
ETIOLOGY.—Acute oesophagitis is quite a rare disease. It occurs idiopathically, deuteropathically, and traumatically—traumatically far the most [p. 410]frequently, and idiopathically least frequently. It is doubtful whether any special predisposing causes of oesophagitis can be indicated. Nevertheless, infancy has been so cited by some authors (Mondière, Billard, Behier, and Steffan). Slight idiopathic catarrhal—or rather erythematous—oesophagitis occasionally ensues in the adult from sudden or prolonged exposure to cold and moisture, and under such circumstances may sometimes be regarded as rheumatic in origin, subsiding after a few hours' continuance, to be immediately succeeded by manifestations of articular rheumatism, acute or subacute, as in some analogous examples of rheumatic pharyngitis. Exceptionally, severe oesophagitis may follow a simple cold (Noveene, cited by Bernheim), or presents as an extension of sore throat, the result of cold (Graves11). It is induced also by the habitual use of very hot drinks and food, and occasionally by the opposite extremes, the use of very cold articles of food and drink (Mondière, Bourguet, Hamburger). The abuse of tobacco and alcohol is alleged as quite a frequent cause of mild oesophagitis, usually occurring, however, in association with pharyngitis from the same causes.
11 Lon. Med. and Surg. Journ., 1836-37, No. 172, and Clinical Lectures, Dublin, 1864, p. 592.
Oesophagitis sometimes follows the deglutition of irritating medicines or moderately caustic poisonous substances not sufficiently acid to produce veritable traumatic oesophagitis. Mercury, codeina, and particularly tartar emetic, are cited as capable of exciting oesophagitis.
Large doses of tartar emetic, as formerly administered in pneumonia (Laennec12), sometimes produced a peculiar form of pustulous oesophagitis, not unlike the pustulous oesophagitis sometimes occurring as part of the local manifestations of small-pox.
12 Traité de l'Auscultation médicale, etc., Paris, 1837, vol. iii. p. 560, illustrated; Laboulbène, Anatomie pathologique, and Nouveau Dict. de Méd. et de Chir., vol. xxiv. p. 370, illustrated; Von Oppolzer, op. cit., p. 109.
Deuteropathic catarrhal oesophagitis occurs sometimes as an extension of catarrhal pharyngitis on the one hand, and of catarrhal gastritis on the other. It also occurs in scarlet fever, measles, and typhus fever. It is likewise consecutive to the various diseases and surgical lesions of the tube itself. Parasitic oesophagitis occurs as an extension of parasitic stomatitis or thrush. Deuteropathic circumscribed phlegmonous oesophagitis is sometimes produced by extension of inflammation from softened caseous bronchial glands at the bifurcation of the trachea, and by pressure from mediastinal tumors, aneurism of the aorta, etc.
Pseudo-membranous oesophagitis is almost always deuteropathic. It has been encountered chiefly in association with pseudo-membranous pharyngitis or diphtheria, and with croupous pneumonia, but likewise in enteric and typhus fever, in cholera and in dysentery, in measles, scarlatina, and small-pox, in nephritis, tuberculosis, carcinoma, and pyæmia.
In a case of hysteria, to be mentioned later, the entire epithelial coat of two-thirds of the oesophagus was discharged by emesis. In this respect the local disease—in that instance at least—resembles pseudo-membranous enteritis.
Traumatic oesophagitis is produced by the deglutition of corrosive substances, which destroy portions of the mucous membrane in their passage or excite a suppurative inflammatory process, or is produced by the [p. 411]passage of foreign bodies of sharp and irregular contour, or by the passage of surgical appliances, whether used for actual operations or for explorations merely.
In rare cases traumatic oesophagitis is the result of wounds with firearms or other weapons.
Phlegmonous oesophagitis may be the result of disease or injury of the interior of the oesophagus, or of its external coat by extension of disease from tissues surrounding it. Foreign bodies, arrested in the oesophagus or wounding it in their passage to the stomach; injuries from surgical appliances, exploratory or operative, employed in treatment for foreign bodies in the tube or in cases of stricture and morbid growth; and chemical irritants swallowed by accident or design,—are the chief causes in the former class of cases; but pustulous and pseudo-membranous oesophagitis must likewise be regarded as occasional causes. The causes operating upon the exterior of the tube primarily are suppurative laryngitis and tracheitis, tumefaction and softening of bronchial and tracheal lymphatic glands, and caries of the spine. Isolated cases have been attributed to emboli in connection with valvular diseases of the heart (Parenski, cited by Daton), and to fits of anger (J. Frank and Rigal, cited by Daton). In certain cases the cause is unassignable, and is then usually attributed to some dyscrasia, syphilis in particular.
PATHOLOGY AND MORBID ANATOMY.—Acute oesophagitis presents both as a diffused inflammation and a circumscribed process, annular or irregular in contour. It does not appear from the post-mortem records consulted that any special portion of the tube is particularly liable to circumscribed inflammation, though the lower fourth appears most frequently affected. The inflammatory process may be simply superficial or erythematous, catarrhal or desquamative (Zenker and Ziemssen), or it may be phlegmonous, and thus interest the submucous tissues as well as the mucous membrane. This may terminate in abscess or in diffuse suppuration with ulcerations. In occasional instances gangrene ensues. Both in diphtheria and in croupous pneumonia, pseudo-membranous oesophagitis is an occasional complication; and the same process is said to have been observed in typhus fever, measles, scarlatina, cholera, pyæmia, dysentery, tuberculosis, and carcinoma (Von Oppolzer and others).
Pustulous oesophagitis occurs in small-pox, and occasionally follows the use of tartar emetic in large doses.
The morbid anatomy of acute idiopathic oesophagitis, though usually detailed in descriptions of the disease, must be known by theory much more than by demonstration, few examples coming under the inspection of the pathologist in time to distinguish the progressive stages of the inflammatory process, and still fewer being revealed by oesophagoscopy during life. The lesions most frequently observed post-mortem are thickening, softening, and desquamation of the epithelium, with very scanty accumulations of viscid mucus here and there upon the mucous membrane. The mucous membrane is seen to have suffered numbers of pinhead or slightly larger superficial circumscribed erosions, rounded or longitudinal, and likewise a few actual ulcerations. The follicles of the mucous membrane are often both swollen and hypertrophied, reaching the size of peas, especially in the upper portion of the tube.
The desquamation of the epithelium usually takes place in small [p. 412] patches. One case, however, has been recorded (Birch-Hirschfeld13) in which a young hysterical woman, after suffering three days with acute oesophagitis without assignable cause, ejected by emesis a membranous tube two-thirds of the entire length of the oesophagus, and shown under examination to have been the completely detached epithelial coat of the oesophagus, wholly normal in its upper layers and infiltrated with agglomerated round cells in its lower layers. It was supposed that the mass had been detached in consequence of acute subepithelial suppuration.
13 Lehrbuch der pathologische Anatomie, Ziemssen, 1877, p. 818; English translation, vol. viii. p. 140.
In addition to swollen and hypertrophied follicles there may be some evidence of ulcerative destruction of these follicles. Mondière and others declare that this folliculous inflammation and ulceration may exist without any other change whatever in the remaining constituents of the mucous membrane; and therefore this form of oesophagitis was termed folliculeuse by Mondière (folliculous oesophagitis). This form of the disease has been observed in typhus fever, in croup (Mondière), and in tuberculosis. Ulceration of the oesophagus occurs, likewise, in carcinoma and in oesophagitis from corrosive fluids, wounds, and other injuries.
In pseudo-membranous oesophagitis the exudation occurs usually in small circumscribed gray-yellow or brownish flakes or stripes distributed over different portions of the surface, more closely, however, at the upper portion of the tube. Superficial erosions are sometimes observed beneath these deposits, and occasionally ulcerations, at times sufficient to give rise to severe hemorrhage (Zenker and Ziemssen). Usually the mucous membrane is but slightly hyperæmic. In some instances pseudo-membrane is so massed in plugs as to occlude the cavity of the tube, as with obturators. In cases associated with pseudo-membranous gastritis the oesophageal manifestations are greatest in the vicinity of the cardiac extremity. Somewhat allied to pseudo-membranous oesophagitis, and apt to be confounded therewith, is the parasitic deposit of the Oïdium albicans in cases of thrush; in connection with which subject this point has already received attention.
The pustules of small-pox may interest any portion of the mucous membrane, but are most numerous at the upper portion of the tube. They may be discrete or confluent. The pustules from tartar-emetic poisoning are most numerous at the two extremities of the canal. It is contended that the so-called pustules of variolous oesophagitis are really superficial variolous ulcers, the antecedent specific lesions having been lenticular papules merely, with abrasion of the softened epithelial layer.14 Variolous oesophagitis may excite an accompanying catarrhal or pseudo-membranous oesophagitis. The local lesions, be they pustular or ulcerous, heal without cicatrices.
14 Virchow's Deutsche Klinik, 1858, No. 31, p. 306; Zenker and Ziemssen, op. cit., p. 146.
Phlegmonous oesophagitis presents both as a diffuse and as a circumscribed inflammation. Examined after death, there is abundant purulent infiltration into the submucous connective tissue, which has undergone destruction in portions of its extent. The infiltration pushes the folds of mucous membrane outward to the interior of the tube, and thus diminishes its calibre considerably when the infiltration is annular. [p. 413]The mucous membrane is congested, ecchymosed, and covered with mucus, and has usually suffered desquamation of portions of its epithelium. Ulcerations through the mucous membrane will have taken place in some instances. Cicatrices mark the location of ulcers which have healed.
In the diffuse variety the oesophagus is inflamed and swollen, as a whole, in proportion to the extent of the disease. In the circumscribed variety the morbid appearances are circumscribed. It has been known to continue into the stomach (Belfrage and Hederius, cited by Zenker and Ziemssen), and to extend therefrom (Ackermann, idem).
As described by Zenker and Ziemssen, chiefly from ten autopsies by themselves and one by Belfrage and Hederius, phlegmonous oesophagitis begins with a submucous purulent infiltration, transforming the areolar tissue into an apparent layer of pus, although microscopic examination shows the bundles of connective tissue to be intact at first. At a later period they become really destroyed, leaving mere crevices filled with pus. The mucous membrane, but little involved, may remain normal or may present the evidence of catarrhal inflammation, desquamation of epithelium, congestion, and slight deposits of mucus. The muscular coat, intact to the unaided eye, under the microscope gives some evidence of purulent infiltrations. The pus may finally escape through the mucous membrane, in extensive infiltrations, at several points, which give the parts a sieve-like appearance when the perforations are closely grouped.
Gangrene sometimes occurs as a result of intense phlegmonous oesophagitis, but this is far more rare than the gangrene supervening after injuries by caustic substances. Sometimes it results from capillary embolism (Rokitansky, Virchow, cited by Luton, op. cit.).
SYMPTOMATOLOGY, COURSE, DURATION, TERMINATION, COMPLICATIONS, AND SEQUELÆ.—The main subjective symptoms of oesophagitis are pain and difficulty in swallowing, with febrile phenomena superadded in severe cases. In simple oesophagitis of mild character these symptoms may be so slight as to be attributed to other causes or be disregarded altogether. In most instances there is a dull, steady pain beneath the sternum, some sense of impediment to deglutition or absolute pain in swallowing (odynphagia), and occasional regurgitation of viscid, glairy mucus, food, or acid products from the stomach. In severe cases the substernal pain is more acute and more diffused, and is frequently associated with pain between the scapulæ and to the left side. This latter pain may be attributable to acid from the stomach. Sometimes the pain is described as acute, especially during the passage of large boluses, particularly if they are very hot, or even very cold. The seat of pain, however, does not always indicate the seat of inflammation, even though the pain be always referred to the same locality. When the cervical portion of the tube is implicated, tenderness may sometimes be detected by external pressure or by special movements of the head and vertebræ.
The amount and character of the dysphagia vary greatly. Sometimes there is a sense of impediment to the passage of food, solid or liquid, or solid only, through and beyond the painful region. This sensation may be accompanied or be followed at a brief interval by regurgitation of food or mucus, or food enveloped with mucus, the latter in some instances tinged with blood. The deglutition or the regurgitation may be [p. 414] accompanied by spasm of the muscular coat of the oesophagus. The dysphagia is not always due to tumefaction of the mucous membrane, but usually in part to coexisting inflammation of the muscular coat or infiltration between the sheaths of muscular fibres, paralyzing their efforts at contraction.
There are no subjective symptoms which permit discrimination between desquamative catarrhal oesophagitis and folliculous oesophagitis. The only symptom particularly indicating pseudo-membranous oesophagitis is the expulsion of shreds of the membrane by hawking or by emesis; but a strong inference is justifiable when the ordinary symptoms of oesophagitis occur in cases of pseudo-membranous pharyngitis or croupous pneumonia.
Phlegmonous oesophagitis is indicated by the presence of pus or of dead mucous membrane in the matter regurgitated or vomited. In severe cases there is considerable febrile reaction. In children, convulsions may supervene from reflex irritation conveyed along the pneumogastric nerve.
The course of acute catarrhal oesophagitis is, as a rule, short, the pain and dysphagia usually subsiding in a few days, with complete resolution and no unfavorable sequelæ. When due to obstruction, the course is indefinitely prolonged. Sometimes it subsides into a mild or unsuspected chronic oesophagitis. In the symptomatic oesophagitis of febrile diseases, the course is longer and unequal. In severer forms and in phlegmonous oesophagitis, the disease may be protracted by suppuration, abscess, gangrene, perforation of the oesophagus, and other complications. It often terminates fatally—in three or four days in some cases—sometimes under symptoms of collapse. Cases may recover without important sequelæ, but stricture very often results from cicatricial complications. Chronic oesophagitis is a more frequent sequel of the phlegmonous variety than of the catarrhal. It, in its turn, may give rise to dilatation of the oesophagus, annular or diverticular, from detention of food and consequent pressure.
DIAGNOSIS.—The diagnosis will rest upon the interpretation of the coexistence of a certain number of the symptoms mentioned. Idiopathic phlegmonous oesophagitis may readily be mistaken for dorsal myelitis by the location of the pain—the more so that the spinal disease is occasionally attended with spasm of the oesophagus, and the myelitis by difficulty in deglutition; but the differentiation may be determined by the inability to produce oesophageal pain by pressure made along the dorsal vertebræ. In deuteropathic or traumatic phlegmonous oesophagitis, the history of the attack will indicate the probable nature of the malady, and prevent the mistake. Diffused oesophagitis is suspected when the general pain or the painful dysphagia appears to extend along the entire tract of the oesophagus, or at least a large portion of it.
Circumscribed oesophagitis is usually indicated by odynphagia at a certain point of the tube after completing the act of deglutition. The location of the inflammation can sometimes be determined by auscultation of the descent of the alimentary bolus or of a swallow of water (Hamburger), which may yield evidence to the ear of arrest or impediment to its passage. Auscultation of the oesophagus, however, is less useful in acute oesophagitis than in stenosis, stricture, and mechanical obstruction. When available in oesophagitis, the normal sound of the passage of water down [p. 415] the gullet becomes masked, and accompanied by that of regurgitative ascent of small bubbles of air. Sometimes there is a slight friction sound during the act of deglutition itself. In circumscribed oesophagitis, especially when annular, as is most frequently the case, sounds are heard attributable to marked obstruction to the descent of the bolus. Abscess cannot be positively diagnosticated until after its rupture and the appearance of pus in the matters regurgitated or otherwise expelled from the oesophagus.
Catheterism of the oesophagus is hardly justifiable as a method of diagnosticating oesophagitis, though proper enough when it becomes important to determine the locality of attendant obstruction.
It is important that inflammation of the oesophagus be differentiated from spasm, stricture, stenosis, carcinoma, and other oesophageal maladies; nearly all of which present the same main subjective symptoms—pain and impediment to deglutition. The history of the case is in itself a guide of great diagnostic value, often quite sufficient for the purpose; but in its absence or retention other data must be gathered.
Spasm of the oesophagus is most frequent in neurotic subjects. Its manifestations are often sudden. It is evanescent or intermittent. It is not a febrile affection. It is often overcome in a moment by catheterization.
Stricture presents often an additional symptom of oesophagitis, the regurgitation of mucus and food. The differentiation is made, in cases of doubt, by the passage of the bougie or catheter.
Carcinoma of the oesophagus, while recent, may present much similitude to oesophagitis, but as the case advances, the glandular involvements, the cachexia, the expulsion of cancerous fragments, and the vomiting of blood seem sufficient to prevent further confusion.
PROGNOSIS.—The prognosis is favorable in acute catarrhal oesophagitis, the manifestations often subsiding within a few days; sometimes, indeed, within a few hours, and that, too, without special medication. It is therefore largely dependent on the cause of the oesophagitis and the severity and extent of the malady. The only unfavorable prognostications arise from the impediment to nourishment and the complications which may ensue.
In presumptive pustulous oesophagitis from the use of preparations of antimony, the manifestations usually subside within a few days upon suspension of the remedy. Sometimes, however, these cases terminate fatally.
Pseudo-membranous oesophagitis is usually fatal in its significance, and the same may be said of the pustulous or ulcero-papular oesophagitis of small-pox.
Phlegmonous oesophagitis is of grave augury, though many cases recover. It may prove fatal within two or three days, though life is usually prolonged for several days, even in fatal cases. When not fatal, abscesses are apt to form, which, discharging internally or externally, are followed by stricture or fistulæ.
Both ulcerative oesophagitis and intense catarrhal oesophagitis may terminate in chronic thickening of the walls of the oesophagus and in cicatricial adhesions more or less extensive.
TREATMENT.—Mild oesophagitis requires no special treatment. The patient should be kept within doors, and be fed on rice-water, [p. 416] barley-water, and other mucilaginous articles of diet, so as to avoid all sources of local irritation. These drinks are usually better borne hot than cold, but sometimes cold is quite agreeable. When cold can be well borne the frequent deglutition of pellets of ice is useful as well as agreeable, and ice-cream becomes a medicinal article of diet.
In severe cases the measures indicated become still more requisite, and the use of the voice should be restrained in addition. All unnecessary efforts at deglutition should be avoided, and anodyne medicaments (opium, hyoscyamus, belladonna) should be added to the demulcent food or beverages. When swallowing is impracticable or very painful, nutriment should be given by the bowel, and medicines by the bowel or by the skin. Thirst may be allayed by retaining fragments of ice in the mouth from time to time, by rinsing the mouth with simple or acidulated water, by sucking the juice of acid fruits, or by allowing compressed effervescent lozenges to dissolve slowly in the mouth.
The external application of cold compresses, continuously or in frequent renewals, is also indicated.
Febrile phenomena require ordinary antiphlogistic medication. When this is impracticable, the indications may be met by using the cold bath or the wet sheet, and by administering antipyretics hypodermatically. Traumatic oesophagitis from a foreign body requires removal of the object if still in the oesophagus; that from swallowing alkalies is met by the use of acidulated beverages (vinegar and water, Orfila); that from swallowing acids, by the use of alkaline drinks, of which the handiest is usually soap and water. As soon as they can be procured this may be changed for lime-water and calcined magnesia. Theoretically, the carbonates of the alkalies are indicated likewise, but it is contended (Hamburger, Oppolzer) that the extrication of the carbonic acid gas renders mechanical rupture of the corroded oesophagus imminent. Subsequently, fresh water should be freely drunk, or be injected into the oesophagus when swallowing is impracticable. The subsequent treatment is to be instituted upon general principles.
DEFINITION.—A chronic inflammation of some of the tissues of the oesophagus.
SYNONYM.—Oesophagitis chronica.
ETIOLOGY.—Chronic oesophagitis is sometimes a sequel of the acute affection. More frequently it is the result of excessive use of strong alcoholic beverages or of very hot drinks. It is said to be sometimes the result of passive congestion in chronic pulmonary and cardiac diseases. It follows the prolonged sojourn of foreign bodies in the oesophagus. It exists in connection with carcinoma of the oesophagus, with dilatation, and with stricture of the oesophagus, and with other diseases obstructing the tube externally or internally. It is sometimes produced by caries of the vertebræ, both scrofulous and syphilitic, and by the pressure of aneurismal and other tumors.
PATHOLOGY AND MORBID ANATOMY.—Hypertrophy of the mucous membrane of the oesophagus, of the submucous connective tissue, and [p. 417]even of the muscular coat, are the processes which take place in chronic oesophagitis, especially when it has been of long continuance. This hypertrophy, when at or near the cardiac extremity, may produce stricture (Rokitansky and others), with subsequent dilatation of the oesophagus from its frequent and prolonged distension by food which should have passed on at once into the stomach.
On post-mortem examination the main evidences of disease are most frequent in the lower third of the organ. Its folds of mucous membrane are thick and prominent, dirty red, brownish-red, or gray, as may be, abraded here and there, and covered with viscid muco-purulent secretions. Abscesses and ulceration are not uncommon in cases due to prolonged pressure or extension of disease from outside the tube. Such ulceration has not uncommonly been the source of serious hemorrhage.
Diffuse inflammation of the peri- or retro-oesophageal connective tissue has been noted as an occasional sequel to the inflammatory process in the walls of the oesophagus.
SYMPTOMATOLOGY, ETC.—The symptoms of simple chronic oesophagitis are similar in the main to those of mild acute oesophagitis, but are often still more moderate, and therefore likely to be overlooked. In severe cases the symptoms are chiefly those of the disease, usually stenotic, which has excited the chronic inflammatory process. The course is prolonged and the duration indefinite. Stricture is a frequent sequel.
DIAGNOSIS.—The diagnosis rests on the same principles and inferences as in acute oesophagitis, the symptoms, however, being of longer duration. The auscultatory signs of arrest or impediment in the descent of the solid or liquid bolus are usually more definite than in acute oesophagitis. The same differentiations are available in excluding spasm, stricture, and malignant diseases. The use of the sound or catheter is much more justifiable than in the acute variety.
PROGNOSIS.—The prognosis is usually unfavorable, on account of the great liability to stricture and occlusion from organization of inflammatory products.
TREATMENT.—Chronic oesophagitis may require both local and constitutional treatment. The constitutional treatment will have to be adapted to the cause of the disease. If due to obstructed circulation in consequence of valvular disease of the heart, digitalis and remedies of its class will be indicated. If due to obstructive pulmonic disease, chloride of ammonium and alkaline remedies will be indicated. Syphilitic inflammation requires the mixed treatment, with mercuric chloride and potassium iodide or their equivalent. Iodides, indeed, are often required in non-specific cases, and are useful particularly in ordinary circumscribed oesophagitis. Under all conditions alcoholic beverages should be interdicted, and so should the deglutition of all irritating food and drink. Mild, bland, and mucilaginous substances should be largely employed in food and drink. The copious use of carbonic-acid waters is also recommended (Oppolzer). Sinapisms and revulsives to the side of the cervical and dorsal vertebræ are also recommended by some writers (Oppolzer).
The topical treatment consists in the systematic use every few days of aqueous solutions of astringents (alum, tannin, ten to thirty grains to the ounce) or alterants (compound solution of iodine, twenty minims to the [p. 418] ounce) passed gently over the diseased surfaces by means of a piece of soft surgical sponge securely attached to a flexible staff.
Severe pain of rather sudden occurrence is usually attributable to circumscribed ulceration, and is best treated by superficial cauterization, as above, with a dilute solution of silver nitrate (ten grains to the ounce). These remedies may be used in the form of ointments of the same strength smeared upon a rather large flexible bougie. To relieve pain and sense of constriction belladonna or stramonium ointment, applied in the same manner, sometimes fulfils a useful indication. Before making these applications attempts should be made by auscultation to locate the seat of disease or obstruction. After subsidence of the disease, occasional catheterization may be practised at intervals of several weeks, in order to detect any recommencing stenosis.
DEFINITION.—Circumscribed destruction of portions of the mucous membrane of the oesophagus, the result of inflammatory processes.
ETIOLOGY.—Ulceration of the oesophagus occurs as a result of inflammation of the organ, as discussed in connection with Oesophagitis, and the cause varies with the character of the oesophagitis, whether idiopathic, traumatic, or symptomatic of disease elsewhere. Diseases, constitutional or local, provocative of ulceration of the oesophagus, usually implicate some portion of either the alimentary or the respiratory tract.
SYMPTOMATOLOGY.—The symptoms are in the main those described under Acute Oesophagitis, particularly the expulsion of sanguinolent products or of unmixed blood. Perforation into the trachea is indicated by expectoration of food or drink; perforation into the great vessels, by hæmatemesis, usually fatal; and perforation into the mediastinum, by emphysema and purulent cellulitis. When large or extensive ulcerations have cicatrized they occasion symptoms of organic stricture.
PATHOLOGY AND MORBID ANATOMY.—Referring to the corresponding section under Oesophagitis, attention may be directed here to the liability of deep-seated ulcers of the oesophagus to perforate the gullet and establish fistulæ with the trachea, bronchi, mediastinum, aorta, and carotid artery, according to the locality of the lesion. These lesions are usually necessarily fatal.
DIAGNOSIS.—The presence of blood in matters regurgitated or vomited forms the chief diagnostic indication of ulceration of the oesophagus, taken in connection with the usual symptoms of acute or chronic oesophagitis.
PROGNOSIS.—The prognosis is altogether dependent on the nature of the disease which has given rise to the ulceration.
TREATMENT.—The constitutional treatment will depend on the nature of the disease which has occasioned ulceration. Ergot and turpentine are administered in case of hemorrhage—the former best, perhaps, hypodermatically. Attempts are sometimes made to cauterize the ulcer or ulcers with nitrate-of-silver stick conveyed in a covered slotted canula, to be exposed when the fenestrum reaches the ulcerated locality, previously [p. 419] determined by catheterization, or inferred to be reached by the sensations of the patient. The practice is uncertain in its manipulation and questionable in its results.
DEFINITION.—A constriction of the calibre of the oesophagus, whether spasmodic or organic in character. This definition excludes stenosis due to pressure from without.
DEFINITION.—A contraction of the muscles of the oesophagus, of variable duration, causing partial or complete stenosis of the gullet and interfering with the passage of food or of food and drink to the stomach.
SYNONYMS.—Oesophagismus, Spasm of the oesophagus, Cramp of the oesophagus, Convulsive dysphagia, Spasmodic dysphagia, Spasmodic stenosis of the oesophagus, Spastic stricture of the oesophagus.
HISTORY.—On this subject there is little of importance in medical annals previous to the observations of Frederick Hoffmann,15 and little of importance subsequently save the observations of Mondière,16 though numerous personal observations are on record, as well as a number of excellent compilations in various monographs, text-books, encyclopædias, and dictionaries.
15 De spasmo gulæ inferioris, Halæ, 1733; De morbis oesophagi spasmodicis, Opera omnia, vol. iii., Geneva, 1761.
16 "Recherches sur l'Oesophagisme ou Spasme de l'Oesophage," Arch. gén. de Méd., April, 1833.
ETIOLOGY.—Spasmodic stricture of the oesophagus is a neurosis often hysterical. It is much more frequent in females than in males, and, although observed in young subjects and less frequently in old ones, is most common between the ages of twenty and fifty. It is sometimes observed in several members of a neurotic family. It is often associated with other evidences of neurosis, but sometimes constitutes the sole manifestation. Sometimes the cause defies detection. Sometimes it can be traced to a fear of strangulation, induced primarily by some accidental impediment to deglutition or the entrance of a foreign body. Strong mental emotion, such as the dread of hydrophobia after having been bitten by a dog, sometimes produces the affection.
It occurs in connection with organic lesions of the oesophagus, organic lesions of the stomach, organic lesions of the larynx and trachea, and organic lesions of the lungs, heart, large blood-vessels, and perioesophageal tissues, but likewise as a reflex disorder, with lesions of distant organs, as the genito-urinary tract, the intestines, the brain and spinal cord. Even pregnancy may produce reflex oesophagismus. It sometimes occurs as a direct or reflex manifestation of gout and of rheumatism. In a few instances it occurs as one of the manifestations of tetanus and of hydrophobia.
SYMPTOMATOLOGY, COURSE, DURATION, ETC.—The spasm may affect [p. 420]the oesophagus only, or may be associated with spasm of the muscles of the pharynx. It is usually manifested in a sudden inability to swallow or to complete the acts of deglutition. This may be transitory or may continue for a number of hours. The relaxation of the spasm is sometimes followed by the discharge of flatus and the copious secretion of pale urine. The spasm may recur at irregular intervals or be more or less distinctly intermittent. Sometimes it precedes every effort at deglutition. In some instances it occurs only upon attempts to swallow certain kinds of food, and the articles of food vary with different patients. Cold viands sometimes produce spasm when warm and hot food is tolerated. Consciousness of a liability to spasm increases the dysphagia for the time being, or brings it on suddenly when this liability had been forgotten. The spasm is sometimes painless and sometimes painful. In some instances it is associated with partial regurgitation of a mass of air (the globus hystericus).
The dysphagia is rarely complete, instances in which no liquids can be swallowed being infrequent. The aliment swallowed usually passes on into the stomach, upon relaxation of the spasm, after a certain period of detention varying from a number of seconds to many minutes. In cases of prolonged or persistent spasm the aliment is usually rejected, either at once or after a time, according as the contraction takes place at the pharyngeal extremity of the oesophagus or lower down. When rejected after some detention in the gullet, the aliments are usually enveloped with mucus or followed by expulsion of mucus and of flatus.
In some subjects the pain in swallowing is severe. Sometimes it is associated with spasm of the diaphragm (hiccough), spasm of the air-passages, palpitation of the heart, and syncope.
The liability to spasm sometimes continues for years. Sometimes it ceases permanently as suddenly and as unexpectedly as it began.
The seat of the spasm is referred by the patient to different regions, which in their totality comprise the entire extent of the oesophagus. In some patients the seat varies on different occasions. The actual seat of any individual spasm is best determined by exploration with the oesophageal bougie or by auscultating the oesophagus during the passage of a bolus. It is most frequent perhaps at the upper extremity, and then perhaps at the cardiac extremity. When habitually low down, there is some liability to permanent distension of the oesophagus from repeated retentions of food at the same place for hours together. In some instances food is regurgitated from the oesophagus after its retention for a day or even longer. When the spasm is high up, the regurgitation may follow the act of deglutition almost immediately.
PATHOLOGY AND MORBID ANATOMY.—The affection being usually a pure neurosis, there is no oesophageal lesion to be cited. In some of the few autopsies recorded, constriction has been noted without lesion of tissue.
DIAGNOSIS.—The diagnosis is based on the sudden onset of the spasm without assignable cause, its intermittent or recurrent character, its manifestation in advance of the effort at deglutition, the symptoms of regurgitation, the coexistence of some of the affections mentioned in connection with its etiology, and on the satisfactory result of exploration with the oesophageal bougie; which differentiates the affection from organic stricture or mechanical obstruction. In catheterization of the oesophagus [p. 421]in cases of pure spasm, although the sound is usually arrested at the seat of constriction, it passes onward after a few moments by sudden relaxation of the spasm. Sometimes, indeed, the very first manipulation of this kind overcomes the spasm permanently.
In the absence of other indications the differentiation from spasm of organic origin rests, in great measure, on the conservation of nutrition, cases being few in which the spasm is persistent enough to interfere so materially with the ingestion of aliment as to produce emaciation.
PROGNOSIS.—The prognosis is usually favorable in spasm of the oesophagus, except in cases where the underlying malady is itself a grave one. Patients do not die of neurotic spasm of the oesophagus. In the majority of cases it is susceptible of cure within a few weeks, sometimes much more promptly. Even when it continues for months or for years there is little fear of permanent injury to the general health, inasmuch as sufficient nutriment of some kind or other can be ingested to sustain the patient.
The duration of the affection depends upon the surroundings of the patient, his amenability to treatment, and the existence or absence of disease in the oesophagus or elsewhere. In cases dependent upon diseased conditions in the oesophagus or elsewhere the character of the disease controls the prognosis, both immediate and ultimate. Thus, aneurism of the aorta, tuberculosis, ulceration of the larynx and trachea, carcinoma of the stomach, tetanus, and hydrophobia present the highest unfavorable indications. Purely neurotic cases are extremely prone to recurrence.
TREATMENT.—The treatment to be pursued will depend upon the nature of the case. If due to organic lesion in the oesophagus or in some other organ, the treatment will be directed to that affection, whatever it may be. If due to emotional disturbance, therapeutic efforts will be directed to their suppression or removal. If purely hysterical, appropriate constitutional remedies for that condition will be prescribed. These comprise asafoetida, valerian, camphor, musk, oxide of zinc, bromides, belladonna, conium, and so on, best administered in small doses at frequent intervals.
Local treatment is almost always necessary, both for its beneficial mechanical effects and for its emotional influence. This consists in the systematic passage of the bougie; and it is by far the best practice to insist upon the patient's submission to it without an anæsthetic. In cases of intense hyperæsthesia, which are rare, and in the initial exploratory passage of the instrument in highly excitable or uncontrollable subjects, anæsthesia may be resorted to if there be no contraindication. The mere passage of the bougie will often effect immediate relaxation of the spasm. When required, the manipulation may be repeated a few times at intervals of several days. Should the passage of the bougie determine the stricture to be purely spasmodic, the patient should be made to partake of food in the physician's presence at first, and afterward under the supervision of an efficient attendant, until it becomes evident that there is no absolute impediment to the passage of food. The presence of the physician during early attempts at taking ordinary food imparts such confidence in the patient that he soon overcomes his dread of strangling and learns to eat again as he should do. Meantime, it may be necessary from time to time to pass the bougie just before food is taken. [p. 422] In such cases it is well to smear the instrument with ointment of belladonna, so as to deposit it more or less along the entire tract of the oesophagus. Failing by these methods, success may follow the occasional passage, at intervals of a few days, of a sponge probang saturated with a very weak solution of iodine or of silver nitrate.
Counter-irritation along the course of the pneumogastric nerve or along the spine is sometimes useful.
Electricity is sometimes employed to overcome the spasm; but intra-oesophageal electrization of every kind is risky from the danger of exciting fatal syncope from irritation of the pneumogastric nerve. This objection is not applicable to percutaneous electrization, save in a much more limited degree. Caution is requisite even with external manipulations along the tract of the pneumogastric nerve; and such manipulations, therefore, should not be undertaken without sufficient familiarity with the effects of electric currents in that situation.
Taken all in all, the best results seem to follow the systematic use of the bougie and enforced deglutition under the eye of an attendant in whom the patient feels reliance can be placed in case the food should "go the wrong way" or become impacted in the gullet.
DEFINITION.—Diminution in the calibre of the oesophagus in consequence of organic alterations in its walls, whether interstitial, cicatricial, or malignant.
SYNONYM.—Stenosis of the oesophagus.
HISTORY.—As mentioned in connection with other affections of the oesophagus, so with organic stricture: though much more has been written on the subject, it is to the observations and publications of Mondière, so frequently cited, that we must credit medical literature with a due appreciation of this topic. The last thirty years especially have been prolific in the record of cases, and their study has been further stimulated by the attention directed to the operation of gastrostomy as a means of prolonging life in cases otherwise hopelessly fatal.
ETIOLOGY.—Organic stricture of the oesophagus is occasionally congenital. As a rule, life is rarely prolonged under such conditions, but cases are on record in which it has been preserved to quite advanced age. Thus, in a female who died from inanition at fifty-nine years of age, after lifelong symptoms of stricture (Everard Homes17), there was an annular stricture behind the first ring of the trachea; and in a male subject who died with pneumonia at seventy-four years of age, after lifelong symptoms of stricture,18 the stricture was found at the cardiac extremity of the oesophagus, which was enormously dilated its entire length above the constriction.
17 Biblioth. méd., t. viii. p. 260; Michel, Dict. Encyclopedique, t. xiv. p. 466.
18 Wilks, Path. Trans. London, xvii. p. 130; Holmes, The Surgical Treatment of the Diseases of Infancy and Childhood, 2d ed., p. 137.
In the majority of cases the stricture is due to cicatricial obliteration of more or less of the calibre of the oesophagus, the result of losses of substance following scalds produced by caustic substances swallowed, mostly by accident and sometimes by design. Wounds of all kinds, [p. 423] whether from the interior, as in the case of foreign bodies and instruments of extraction, or from the exterior, as in the case of surgical operations, wounds from firearms, and the like, are apt in their cicatrization to give rise to this form of stricture.
Though denied by some authorities, syphilitic disease of the oesophagus is an undoubted cause of stricture. Setting aside disputed records of older authorities, we may cite recent cases reported by Lancereaux, West,19 Wilks, Virchow, and Lublinski,20 the latter-named going deeply into the bibliography, pathology, and therapeutics of stricture from syphilis. The author could add his personal testimony were it requisite.
19 The Lancet, 1872.
20 Berlin. klin. Woch., Aug. 20, 1883; London Medical Record, Nov. 15, 1883, p. 489.
Stricture of the oesophagus is likewise occasioned by the presence of papillomatous, fibroid, and other morbid growths. Carcinoma is quite a frequent cause.
The frequent deglutition of undiluted spirituous liquors is said to give occasion at times to stricture of the oesophagus, but in these instances this result is usually due to precedent chronic oesophagitis thereby excited, and terminating in infiltration and hyperplasia of the submucous connective tissue, and sometimes great thickening of the epithelium as well.
Males are more frequently the subjects of stricture of the oesophagus, and early adult life the most frequent period for its occurrence, though it may present at any age.
SYMPTOMATOLOGY.—Except in traumatic cases, the earliest symptoms, preceded in some instances by indications of mild oesophagitis, perhaps unnoticed or unrecognized, are occasional impediments to deglutition of large and firm boluses, or rather a mechanical obstacle to completion of the act of glutition occurring at intervals of a few meals or a few days. After a while the swallowing of a large solid bolus becomes permanently impracticable. Then, sometimes, repeated efforts become necessary to swallow small masses of solid food; and even to do this may require external manipulation, or at least the additional pressure of liquids swallowed immediately after the solid bolus. These efforts are sometimes attended with spasm, regurgitation, and pain, and may be accompanied in addition with tracheal dyspnoea, and with nervousness in consequence. As the disease progresses it becomes impossible to swallow solid food, and subsequently even fluid food in extreme cases. The bolus is then often regurgitated immediately after its deglutition, and may be covered with mucus, blood, pus, or fragments or detritus of ulcerated malignant growth, according to the nature of the case. Pain and sensations of rawness are often felt at the point of constriction, whence the pain often radiates toward one or both scapulæ. If the tube is much dilated above the stricture, the food may be detained in the sac for several hours, and then be regurgitated in a softened, partially-decomposed condition. Should the mass be so situated as to compress the trachea, suffocative symptoms may be produced.
In stricture due to organic disease there may be dysphonia from pressure or injury to the recurrent laryngeal nerve producing paralysis of the vocal band. The anatomical relations of the left recurrent nerve renders it the much more liable of the two to become implicated. Moderate dyspnoea may result from this paralysis by reason of the reduced space of the glottis.
[p. 424] PATHOLOGY AND MORBID ANATOMY.—Organic stricture of the oesophagus is usually due to disease or structural change involving the mucous membrane and submucous connective tissue; but the muscular structure may become involved likewise. It may, however, be due to abnormal laxity of the mucous membrane, permitting a fold to occupy a position impeding the passage of the bolus.
In cases which are not carcinomatous the diminution in the actual calibre of the tube is usually due to submucous proliferation of connective tissue and to thickening of the mucous membrane. The encroachment on the calibre of the tube may be quite slight, or may be so great as to amount to almost complete occlusion.
The seat of stricture is at the upper portion of the oesophagus most frequently, then at the cardiac extremity, at the point of crossing by the left bronchus, and at the point of passage through the diaphragm—all localities slightly constricted normally—but it may occur at any portion.
In most instances the stricture is single. There may, however, be two, three, or even four strictures. Multiple strictures are most common after deglutition of caustic substances which have made their way clear down into the stomach.
Syphilitic strictures are usually single, and so, as a rule, are strictures of malignant origin. The latter are much larger in extent.
Cicatricial strictures from caustic substances may be in the form of bands, rings, or longitudinal stripes or folds. Sometimes they are quite extensive, and have been known to interest fully one-third of the length of the oesophagus. The circumference, length, calibre, and thickness of the stricture, however, vary within the most extreme limits. Occasionally occlusion of the tube is complete.
The detention of food above the stricture usually dilates the oesophagus, producing hypertrophy of the mucous membrane and submucous connective tissue, followed in its turn by fatty degeneration. Atrophy of the oesophagus may ensue below the stricture if at all tight, and the mucous membrane becomes thrown into longitudinal folds.
DIAGNOSIS.—The diagnosis of organic stricture of the oesophagus rarely presents difficulty. Dysphagia, spasm, and regurgitation are quite characteristic of stricture. When the constriction is high up, the vomiting or regurgitation of food may closely follow its deglutition; when low down, this act may be delayed ten or fifteen minutes, in some cases for hours. Alkaline reaction of the vomited matters is indicative of their having failed to reach the stomach. The presence of blood-cells, pus-cells, and cancer-cells indicates ulceration, suppuration, and malignant disease, respectively.
Auscultation of the oesophagus during deglutition of water will indicate the seat of stricture by revealing the ascent of consecutive air-bubbles even when palpation with bougies fails. The passage of oesophageal bougies or the stomach-tube into the oesophagus will often reveal the point of stricture. Its length is estimated by the distance of the resistance offered to the passage of the instrument; its diameter, by the size of the largest instrument which can be passed through it; and its consistence, by the character of the resistance. Care is requisite in manipulating with these instruments, lest by undue exertion of force they be passed through an ulcerated portion of the wall of the tube or [p. 425] a diverticulum. The character of the resistance is sometimes the sole means of differentiating stricture from stenosis due to compression of the oesophageal wall from its outside.
It sometimes happens, in individuals with impaired sensitiveness of the epiglottis or vestibule of the larynx, that the exploratory bougie is introduced into the air-passage instead of the gullet. The usual premonitory phenomena of suffocation will indicate the mistake. There is some likelihood, too, of entering the larynx in individuals with unusually prominent cervical vertebræ and in cases of stricture at the extreme upper portion of the oesophagus. In introducing these instruments into the oesophagus, therefore, it is well that they be guided along the fore finger of the disengaged hand, and passed deeply into the throat, either to the side of the larynx or behind it. By keeping to the side and reaching the oesophagus by way of the laryngo-pharyngeal sinus the risk of entering the larynx may be avoided. Before introducing the tube the case should be carefully examined for aneurism, which by pressure sometimes gives rise to the ordinary subjective symptoms of stricture. Should aneurism be detected, passage of the tube would be hazardous.
PROGNOSIS.—The prognosis is in most instances unfavorable. It is comparatively favorable in cases of moderate stricture due to causes apparently remediable. The extent and volume of the stricture progress more or less slowly according to the nature of its cause, and in non-malignant cases, such as are due to the action of caustic substances, it may last for years before the patient, if not relieved, succumbs, as he does, from gradual inanition. In the earlier stages, before the hypertrophied muscles above the stricture undergo fatty metamorphosis, the increased muscular power is sufficient to force nourishment through the stricture; but when this becomes no longer possible progressive marasmus must ensue. Meantime, abscess may become developed in consequence of the pressure of retained food, and tuberculous degeneration of the lung and local gangrene may take place in consequence of the malnutrition.
TREATMENT.—The treatment of organic stricture of the oesophagus resolves itself into maintenance of the general health, the administration of the iodides to promote absorption of effusions into the connective tissue or the muscles, mechanical and operative measures for removal of the causes of the constriction or the strictured tissues themselves, and operations for securing artificial openings below the point of stricture for the introduction of nourishment (oesophagostomy and gastrostomy). Nourishment by enema is of great value.
In carcinomatous stricture local measures are in the main unjustifiable, as they usually entail injury which may prove very serious. Arsenic internally is thought to retard the progress of malignant disease when administered early and persistently. Morphine is used hypodermically to assuage pain.
In cancerous and tuberculous disease great caution is requisite in determining upon mechanical or surgical procedures. In cicatricial stenosis from the effects of caustic substances, such measures may be undertaken with much less consideration.
The local treatment consists in systematic mechanical dilatation with bougies or mechanical dilators properly constructed. These are employed [p. 426] daily, every other day, or at more prolonged intervals, according to the tolerance of the parts and the progressive improvement. They are retained several moments at each introduction, and followed by the passage and immediate withdrawal of an instrument of larger size. It is often advisable that the final dilatation of each series be made with a stomach-tube, so that liquid food may be poured through it from a syphon or a small-lipped vessel, that there may be no necessity for swallowing food for some hours thereafter. This method is continued until it becomes evident that nothing further is to be gained by its continuance. In cases that have been at all successful, the introduction of the instrument should be repeated every week or two for a long time, to prevent or retard recurrence of the constriction, which is very liable to take place. M. Krishaber has reported21 cases in which a tube passed through the nose was retained from forty to three hundred and five days; and from this success he deduces the practicability of continuous dilatation in this manner. Billroth and Rokitansky have encountered cases in which frequent dilatation had set up inflammation of the surrounding connective tissue, which had caused fatal pleurisy by continuity.
21 Trans. Internat. Med. Congress, London, 1881, vol. ii.
Forcible dilatation by mechanical separation of the sides of a double metallic sound has been employed with success in some instances. It is a risky procedure.
Destruction of cicatricial tissue by caustics has been attempted, and, though successes occasionally attend the practice, it is hardly considered sufficiently promising.
Division of the stricture by internal oesophagotomy, with subsequent dilatation, has been practised of late years, and offers some chances of success. Oesophagostomy and gastrostomy have been performed in some cases of impassable stricture, and the latter operation is gaining in favor. For surgical details, however, we must refer to works on surgery.
DEFINITION.—Carcinomatous degeneration of the oesophagus, whatever the variety.
SYNONYM.—Cancer of the oesophagus.
ETIOLOGY.—Carcinoma is the most frequent disease of the oesophagus that comes under professional observation. The most frequent variety is the squamous-celled (53 out of 57, Butlin). Spheroidal-celled and glandular-celled varieties are much less frequent. In some instances the morbid product is a combination of the two. Colloid degeneration is occasionally met with. Carcinoma is usually primitive. Its cause is undetermined, but, as it is most frequent at the constricted portions of the tube, pressure is supposed to be the exciting cause. It does not always give rise to secondary infection. Sometimes it is an extension from the tongue, epiglottis, or larynx, or from the stomach. It is most frequent in males, and more so in the intemperate than in the abstinent.
The immediate exciting cause is often attributed to local injury from retention of foreign bodies or the deglutition of hot, acrid, or indigestible substances.
[p. 427] There appears to be some disposition to carcinoma of the oesophagus in tuberculous subjects (Hamburger), while the children of tuberculous parents may have carcinoma of the oesophagus, and their offspring, again, tuberculosis.
SYMPTOMS.—The earliest local symptom is slight dysphagia, with impediment to completion of the act of glutition—an evidence of commencing stricture. Subsequently, inverted peristaltic action is added, an evidence of dilatation above the stricture, with partial retention of food. At a later stage vomiting will occur, with admixtures of pus and sanguinolent fragments of cancerous tissue.
Progressive emaciation and impaired physical endurance usually precede these local symptoms, but actual cachectic depression may come on quite tardily. At first there is no pain; subsequently there comes on considerable uneasiness at some portion of the tube. Finally, there may be severe local burning or lancinating pains, particularly after meals. If the disease be high up, there may be pain between the shoulders, along the neck, and even in the head, with radiating pains toward either shoulder and along the arm. If low down, there may be intense cardialgia and even cardiac spasm. If the trachea or larynx be compressed or displaced, dyspnoea will be produced. If the recurrent laryngeal nerve be compressed, there will be dysphonia or aphonia. Perforation of the larynx will be indicated by cough, expectoration, hoarseness, or loss of voice; of the trachea, by paroxysmal cough, dyspnoea, or suffocative spasm; of the lungs, by acute pneumonitis, especially if food shall have escaped, and expectoration of blood, pus, and matters swallowed, as may be; of the pleura, by pneumothorax; of the mediastinum, by emphysema; of the pericardium, by pericarditis; of the large vessels, by hemorrhage. Perforation of the aorta or pulmonary artery is often followed by sudden death from hemorrhage, and of the lungs by rapid death from pneumonitis.
PATHOLOGY AND MORBID ANATOMY.—Primitive carcinoma is usually circumscribed. It is most frequent at the cardiac extremity, but often occurs where the oesophagus is crossed by the left bronchus, and sometimes occupies the entire length of the tube. The greater proclivity of the lower third of the oesophagus has been attributed to mechanical pressure where it passes through the diaphragm; that of the middle third, to pressure of its anterior wall against the left bronchus by the bolus. It begins, either nodulated or diffuse, in the submucous connective tissue, implicates the mucous membrane, encroaches upon the calibre of the tube, undergoes softening and ulceration, and becomes covered with exuberant granulations. When the entire circumference of the oesophagus is involved stricture results, sometimes amounting eventually to complete obstruction. Ulceration taking place, the calibre again becomes permeable. The oesophagus becomes dilated above the constriction and collapsed below it.
As the disease progresses the adjoining tissues become involved. Adhesions may take place with trachea, bronchi, bronchial glands, lungs, diaphragm, or even the spinal column (Newman22). Perforation may take place into the trachea, usually just above the bifurcation, or into the lungs, pleura, mediastinum, pericardium, aorta, or pulmonary artery. Abscesses are formed, the contents of which undergo putrefaction. There [p. 428] may be involvement of the pneumogastric nerve, with reflex influence on the spinal nerves and the sympathetic (Gurmay23).
22 N.Y. Med. Journ., Aug., 1879, p. 158.
23 Bull. méd. de l'Aisne, 1869; Gaz. méd. Paris, April, 1872.
DIAGNOSIS.—The diagnosis will rest on due appreciation of the symptoms enumerated and the ultimate evidence of the cancerous cachexia. Auscultation will often reveal the location of the disease. This may be further confirmed by palpation with the bougie, but the manipulation should be made without using any appreciable force. Laryngoscopic inspection and digital exploration are sufficient when the entrance into the oesophagus is involved.
Differential diagnosis is difficult at an early stage, and often to be based solely on negative phenomena. At a later stage it is easy, especially when cancerous fragments are expelled. In some instances a tumor can be felt externally. Such a tumor, however, has been known to have been the head of the pancreas (Reid24).
24 N.Y. Med. Journ., Oct., 1877, p. 404.
Cancer of the oesophagus is liable to be confounded with chronic oesophagitis, cicatricial stenosis, diverticulum, extraneous compression, abscess, and non-malignant morbid growths.
PROGNOSIS.—The prognosis is unfavorable, the disease incurable. Death may be expected in from one to two years, though sometimes delayed for longer periods. Inanition or marasmus is the usual cause of death in uncomplicated cases. Sometimes it takes place by hæmatemesis, sometimes following involvement of the stomach, and sometimes wholly unassociated with any direct disease of the walls of the stomach. Death takes place not infrequently from perforation into adjoining organs, and sometimes from secondary inflammation of other vital organs, as the brain and the lungs.
TREATMENT.—There is little to be done in the way of treatment apart from the constitutional measures indicated in carcinoma generally and in chronic diseases of the oesophagus. The cautious use of the stomach-tube to convey nourishment into the stomach is allowable during the earlier stages of the disease only. It is dangerous after ulceration has taken place, from the risk of perforating the walls of the oesophagus, and thus hurrying on the fatal issue by injury to the intrathoracic tissues.
When deglutition becomes impracticable or the passage of the oesophagus absolutely impermeable to nutriment, food and alcoholic stimuli should be administered by enema. Indeed, it is good practice to begin to give nourishment occasionally by the bowel before it becomes absolutely necessary, so as to accustom the part and the patient to the manipulation. Narcotics to relieve pain are best administered hypodermatically, so as to avoid unnecessary irritation of the rectum.
The passage of dilators, as in stricture of cicatricial origin, is very hazardous. They produce irritation, which hastens the softening of the tissues, and are open to the risk of penetrating the softened tissues and passing through the walls of the oesophagus into the pleura, lung, or mediastinum. Fatal accidents of this nature are on record.
Gastrostomy is sometimes performed to prolong life.
DEFINITION.—Loss of motive-force in the muscular tissue of the oesophagus, whether intrinsic or reflex in origin.
SYNONYMS.—Gulæ imbecillitas, Paralytic dysphagia, Atonic dysphagia.
ETIOLOGY.—Paralysis of the oesophagus may be caused by impairment of function in one or more of the nervous tracts distributed to the muscles concerned in dilating the upper orifice of the gullet or in those concerned in the peristaltic movements which propel the bolus to the stomach. These impairments of function may be nutritive in origin, as in softening and atrophy of the nerve-trunk, or, as is more frequent, they may be pressure-phenomena from extravasations of blood, purulent accumulations, exostoses, tumors, and the like.
The paralysis may be due to disease or wounds of the nerves themselves or of their motor roots, or of the cerebro-spinal axis, implicating their origin, or to pressure and atrophy of a trunk-nerve in some portion of its tract. It is likewise due to neurasthenia from hemorrhage or from protracted disease (enteric fever, yellow fever, cholera), or to systemic poisoning in diphtheria, syphilis, and plumbism. It may be due to muscular atrophy or intermuscular proliferations of connective tissue, to dilatation of the oesophagus, and to disease in the tube. It may be due to mechanical restraint from external adhesions of the oesophagus to intrathoracic tumors (Finny25). It may result from sudden shock or fright. It may follow the sudden reaction of cold upon the overheated body. It is one of the manifestations of hysteria and of the hysteria of pregnancy.
25 Dub. Journ. Med. Sci., Oct., 1877.
SYMPTOMS.—Partial paralysis may give rise to no symptoms at all. The earliest manifestations are those of impediment to the prompt passage of the bolus to the stomach, repeated acts of deglutition or additional swallows of food or drink being necessary. Large masses are swallowed and propelled onward more readily than small ones, and solids more readily than fluids. There is often a characteristic gurgling attending the passage of fluids along the tube. Swallowing is best performed in the erect posture. These symptoms increase in severity as the paralysis increases. There is little pain or none at all. In some cases there is no regurgitation of food; in others, this is more or less frequent. When the paralysis is complete, deglutition becomes impossible, and the food attempted to be swallowed is expelled from the mouth and nose in a paroxysm of cough. Sometimes the food enters the larynx and produces paroxysms of suffocation or threatens asphyxia.
There is more or less flow of saliva from the mouth in consequence of the inability to swallow it; and in some cases the losses of material from the blood are so great as to reduce the patient very rapidly.
PATHOLOGY AND MORBID ANATOMY.—Paralysis of the oesophagus may be partial or complete. It may be associated with paralysis of the pharynx, palate, tongue, epiglottis, or larynx; with so-called bulbar paralysis; with general paralysis; with cerebro-spinal disseminated sclerosis.
DIAGNOSIS.—The diagnosis rests mainly on the symptoms of dysphagia, especially when associated with paralyses elsewhere. It is differentiated [p. 430] from paralysis of the pharynx by the ability to swallow the bolus and the apparent arrest of the bolus at some portion of the tube. Auscultation of the oesophagus will determine the locality of the arrest. It likewise affords presumptive evidence of an alteration in the usual form of the bolus, which, being subjected to compression at its upper portion only, assumes the form of an inverted cone. The remaining auscultatory indications are similar to those of dilatation.
There is no impediment to the passage of the stomach-tube or oesophageal sound, or to its free manipulation when within the oesophagus.
When the symptoms quickly reach a maximum, they indicate a paralysis due to apoplexy, and so they do when the symptoms are sudden, hysteria being eliminated. Paralysis due to gumma or other cerebral tumor is much slower in its course.
PROGNOSIS.—In idiopathic paralysis, the local or special affection to which it is due being curable, the prognosis is favorable, especially if the paralysis be confined to the oesophagus. Recovery, however, is often slow, even in curable cases. In hysterical paralysis the prognosis is good. In deuteropathic paralysis the prognosis is much less favorable, and will depend upon the nature of the causal disease—apoplexy, insanity, cerebral tumor, syphilis, etc.
TREATMENT.—The treatment varies with the nature of the cause as far as combating the origin of the disease is concerned. With regard to the intrinsic paralysis of the oesophagus itself, strychnine and its congeners are indicated, and may be administered hypodermatically if the difficulty in swallowing be very great. If the paralysis be partial, it is better to give nux vomica or Ignatia amara by the mouth, in hopes of getting some beneficial astringent influence on the walls of the oesophagus.
In all instances the feeding of the patient is an important element in treatment. Masses of food arrested in the tube should be forced onward with the sound. In some cases nourishment must be habitually introduced through the stomach-tube and nutritive enemata be resorted to.
Electricity, though sometimes successful, is a risky agent to employ, because, as announced by Duchenne, the use of an oesophageal electrode is attended with some risk of unduly exciting the pneumogastric nerve and thereby inducing syncope.
DEFINITION.—An abnormal distension of a portion of the oesophagus or of the entire tube, whether general, annular, or pouched.
SYNONYMS.—Oesophagocele, Hernia of the oesophagus, Diverticulum of the oesophagus.
ETIOLOGY.—Dilatation of the oesophagus is occasionally met as a congenital affection (Hanney,26 Grisolle,27 and others). The cause under these circumstances is obscure. Usually, however, dilatation of the oesophagus is of mechanical origin, due to distension by food or water above a stricture or an impacted foreign body. Presumptive paralysis of the muscular coat in chronic oesophagitis is alleged as a source of similar distension.
26 Edinb. Med. and Surg. Journ., July, 1883.
27 Traité Élément. de Path. int., Paris, 1883, ii. p. 358.
[p. 431] General dilatation is presumed to be the mechanical result of constriction of the cardiac extremity, leading to distension of the oesophagus by the accumulation of large quantities of liquids. Sometimes it is due to paralysis of the muscular coat, permitting its distension by food.
Annular dilatation is sometimes due to distension just above the seat of a stricture. Sometimes it is due to impaction of a foreign body; sometimes there is no mechanical impediment; occasionally it is observed as a congenital anomaly.
Pouched dilatation (diverticulum) is usually due to retention of food immediately above an impacted foreign body or some obstruction of another character. Some of the muscular fibres of the oesophageal wall become separated and spread asunder, allowing the mucous membrane to be gradually forced through them by repeated efforts of deglutition upon retained masses of food or drink, until finally a pouch is formed, hernia-like, outside of the tube. Another mode of production is said (Rokitansky28) to consist in the subsidence of tumefied glands outside the oesophagus, after adhesions had been contracted with the oesophagus during the inflammatory process. The shrinking of these enlarged glands to their normal volume sometimes draws the tube outward into a funnel-shaped sac constricted at its margin by the muscular coat, which has receded from the pouch or has been stripped loose. The same form of dilatation is likewise an occasional result of rupture of the muscular coat sustained in blows or falls. It occasionally exists, too, as a congenital defect, and this has been attributed (Bardeleben and Billroth29) to partial closing of one of the branchial fissures externally, while the internal opening has remained patent.
28 Archiv. gén. de Méd., 1840, p. 329.
29 Trans. Clin. Soc. London, 1881, p. 130.
SYMPTOMATOLOGY.—The symptoms, at first, are usually those of obstruction to the passage of food, but before this obstruction occurs dilatation may have existed without symptoms. In some cases of diverticulum high up, there is a tumor, usually on the left side of the neck. Rokitansky has reported one the size of the fist situated on the right side of the neck, and Hankel30 and others a tumor upon each side. The tumor varies in bulk from time to time according as it may be empty or may be distended with food, drink, or gas.
30 Rust's Mag., 1833; Dict. Encycl., loc. cit.
Food caught in the pouch can often be forced out into the pharynx by external pressure over the tumor in the neck. The retention of food above a constriction or in a sac is usually accompanied by some distress after indulgence in too much food. This uneasiness becomes relieved upon regurgitation or vomiting. Deglutition is impeded to a less extent when the disease does not implicate the upper portion of the gut.
Complete dilatation is sometimes indicated by long addiction to habits of rumination. In some instances this rumination is an agreeable sensuous process. In pouched dilatation it is very often disagreeable, the regurgitated matters being acrid, owing to acid fermentation of the contents of the sac.
While the dilatation remains moderate there may be little dysphagia or none at all, the muscles continuing sufficiently vigorous to propel the food; but after the muscles become paralyzed by distension the dysphagia gradually increases and may culminate in complete aphagia. One [p. 432] of the special indications of diverticulum is that the regurgitation does not take place until several hours after a meal. As the sac enlarges there may be less and less complaint of dysphagia, because it becomes able to contain larger quantities of food. At the same time it may so compress the main tube as to occlude its calibre and prevent access of food to the stomach.
The symptoms of annular dilatation are similar to those of stricture with retention of food above it, the regurgitation usually following deglutition more quickly.
In some cases of dilatation, circumscribed and general, food is sometimes retained for an entire day or more before it is ejected. The decomposition of the retained food usually produces a more or less continuous foul odor from the mouth.
The course of the affection is progressively from bad to worse, and entails ultimate emaciation. Some patients succumb early, and some live to advanced age. Perforation of the oesophagus ensues in some instances, and death results in consequence of the injuries sustained by perioesophageal structures by the escape of the contents of the oesophagus. Perforation is indicated by sudden collapse and by emphysema from swallowed air.
PATHOLOGY AND MORBID ANATOMY.—Dilatation of the oesophagus is either general or partial, according as it takes place in the whole or greater portion of the oesophagus or in a circumscribed portion. Partial dilatation may involve the entire circumference of the canal (annular dilatation), or it may implicate but a portion of the wall, which becomes pouched into a sac externally (diverticulum or saccular dilatation).
| FIG. 19. |
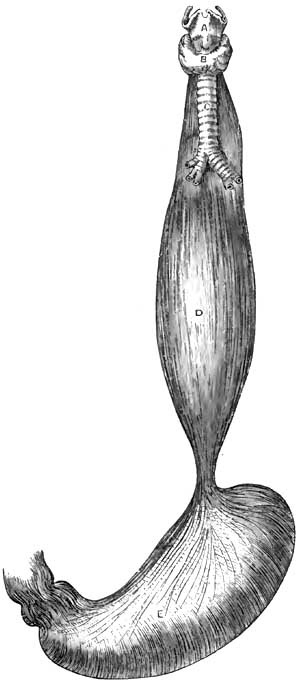
|
| Fusiform Dilatation of Oesophagus (Luschka). A, Larynx; B, Thyroid gland; C, Trachea; D, Oesophagus; E, Stomach. |
General dilatation, though sometimes congenital, is, as mentioned under Etiology, more frequently the mechanical result of distension of the oesophagus by food or drink prevented from ready entrance into the stomach by a constriction at the cardiac orifice. This form of dilatation is sometimes discovered as a post-mortem curiosity. The muscles have usually undergone great hypertrophy, and the mucous membrane some thickening and congestion, with erosions and sometimes ulcerations, indicative of chronic oesophagitis. In some instances all the coats of the oesophagus have undergone hypertrophy. The dilatation may vary from slight enlargement to the thickness of an ordinary man's arm or larger (Rokitansky31); in rare cases, even a capacity nearly equal to that of the stomach (Luschka32 and others). (See Fig. 19.)
31 Path. Anat.
32 Arch. für Anat., etc., March, 1868, p. 473.
The oesophagus is usually fusiform or spindle-shaped, being constricted at those portions at which it is normally slightly constricted. Sometimes the dilatation takes place between the lobes of the lungs (Raymond33).
33 Gaz. méd. de Paris, 1869, No. 7, p. 91.
Annular dilatation is usually due to circumferential distension just above a stricture. When not due to stricture its seat is usually just above the diaphragm, where the oesophagus is normally liable to constriction. The upper portion of the dilatation is larger than the lower portion, and the muscular walls are usually hypertrophied.
Pouched dilatation (diverticulum) is usually formed chiefly of mucous membrane and submucous tissue pushed through gaps in the fibres of the [p. 433] muscular coat, produced by distension. It sometimes involves the entire coat in cases in which the oesophageal wall has become adherent to enlarged lymphatic glands, which subsequently undergo subsidence in volume and drag the adherent portion of the wall after them (Rokitansky). The muscular walls are then usually hypertrophied, the mucous membrane sometimes hypertrophied, sometimes atrophied. The diverticulum is usually located in the upper portion of the oesophagus, just below the inferior constrictor muscle of the pharynx. It may thus be, in part, a pharyngocele also. It may be located behind the point of bifurcation of the trachea or where the oesophagus is crossed by the left bronchus. Its direction may be to the left side in the upper portion of the oesophagus, to the right side, or upon both sides; but when situated lower down it is usually directed backward, between the posterior wall of the tube and the spinal column. Hence its distension with food completely blocks up the calibre of the oesophagus. The orifice by which the oesophageal wall remains in communication with the pouch is round or elliptic in shape and variable in size, sometimes being about an inch in its long diameter, sometimes much smaller. The size of the diverticulum varies; a common size is that of a duck egg, but the size of a fist has been attained. Sometimes the diverticulum drags the oesophagus out of position and forms a sort of blind pouch in the direct line of its axis, so that it becomes filled with food which fails to reach the stomach. Sometimes there are several dilatations.
The dilatations become enlarged by retention of food, and are liable to undergo inflammation, ulceration, and perforation.
DIAGNOSIS.—The diagnosis will depend upon the symptoms of dysphagia, regurgitation, and so on, and upon the evidence furnished by auscultatory indications, palpation with the oesophageal sound, and, in some instances, the existence of a tumor in the neck, enlarging after meals, and [p. 434] from which food or mucus can be forced up into the pharynx by pressure externally.
Stethoscopic auscultation of the oesophagus during the deglutition of water indicates an alteration in the usual form of the gulp, which seems to trickle rapidly in a larger or smaller stream according to the degree of dilatation. If the dilatation be annular and located high up, auscultation is said to give the impression of a general sprinkling of fluid deflected from its course. The peculiar gurgle is often audible without the aid of stethoscopy. Palpation with the oesophageal bougie is competent to reveal the existence of a large sac by the facility with which the terminal extremity of the sound can be moved in the cavity. In the case of a diverticulum, however, the sound may glide past the mouth of the pouch without entering it, although arrested at the bottom of the sac in most instances.
In annular dilatation any constriction below it is usually perceptible to the touch through the sound; but, on the other hand, the ready passage of the bougie into the stomach, while excluding stricture, does not positively disprove the existence of a circumscribed dilatation. If high up, the dilatation may be detected externally by its enlargement when filled with food after a meal, and the subsidence of tumefaction when the sac is emptied by pressure from without, or by regurgitation. If the dilatation occupy a position which exercises compression of the trachea, dyspnoea will ensue when it is distended. The intermittence of the tumefaction serves to differentiate the swelling from abscess or morbid growth. From aneurism of the aorta, which it may simulate (Davy34), it is to be discriminated by absence of the usual stethoscopic and circulatory manifestations. The diagnosis of congenital dilatation is based upon a history of difficulty in deglutition dating from the earliest period of recollection.
34 Irish Hosp. Gaz., 1874, p. 129; Med. Press and Circular, May, 1874.
PROGNOSIS.—The prognosis is not favorable in any given case unless the cause can be removed, and not even then unless food can be prevented from accumulating in the distended portion of the tube. Nevertheless, cases sometimes go on into advanced age. On the other hand, they may terminate fatally within a year (Lindau35). The danger of perforation adds additional gravity to the prognosis, for life may be suddenly lost by this accident. Death usually takes place by inanition. A case of death by suffocation has been recorded, attributed to the pressure of the distended oesophagus upon the intrathoracic vessels (Hannay36).
35 Casper's Wochenschrift, 1840, No. 22; Arch. gén. de Méd., 1841, p. 498; Dict. de Méd et de Chir., xxiv. p. 410.
36 Edinb. Med. and Surg. Journ., July 1, 1833.
TREATMENT.—If the dilatation be due to stricture or to an impacted foreign body, the treatment should be directed to overcoming the one and removing the other.
General dilatation from chronic oesophagitis requires treatment for that disease.
Much depends upon preventing the accumulation of food in a sac or diverticle; the best means of accomplishing which is the systematic administration of all nutriment by means of the stomach-tube. When this is not advisable, care must be exercised in the selection of such food as is least likely to irritate the parts if detained in the pouch.
[p. 435] As far as general treatment is concerned, stimulants are usually indicated, as the patients become much reduced. If paralysis of the muscular coat of the oesophagus is believed to exist, the administration of preparations of phosphorus and of strychnine are indicated on general principles of therapeutics. Stimulation of muscular contractility by the oesophageal electrode has been recommended, but the prospects of success hardly justify the risks of serious injury in the domain of the pneumogastric nerve.
It has not yet been determined whether surgical procedures are competent to relieve dilatation. In cases of pouched dilatation high up it would not be difficult, as suggested by Michel,37 to expose the sac and excise it in such a manner that the sutures uniting the walls of the oesophagus shall occupy the site of the mouth of the diverticulum, and, thus obliterating it by cicatrization, restore the normal path of the food from the pharynx to the oesophagus. Gastrostomy, too, should hold out some hope of rescue, no matter what portion of the oesophagus be dilated.
37 Dict. Encyclop., xiv. p. 465.
To difficulty in the physiological process of digestion the familiar name of dyspepsia has been given, while to a merely disturbed condition of the function the term indigestion is more frequently applied. This distinction, difficult at all times to make, may appear more arbitrary than real; and inasmuch as it involves no important practical point, the author of the present article will use the terms interchangeably as indicating functional disturbance of the stomach—i.e. disturbance of the digestive process not associated with changes of an inflammatory character, so far as we know.
Since it is one of the most common of all complaints from its association with various other morbid conditions, the term is not unfrequently vaguely employed. It is difficult, of course, to define a disease whose etiology is so directly related to so many distinct morbid conditions. Indeed, there are few diseases, general or local, which are not at some time in their history associated with more or less derangement of the digestive process. For purposes of limitation, therefore, it will be understood that we now refer to chronic functional forms of indigestion which depend largely, at least, on a purely nervous element, and for this reason are not infrequently described as sympathetic dyspepsia. Doubt has been expressed as to whether such forms of disease ever exist, but that we encounter purely functional forms of dyspepsia, corresponding to the dyspepsia apyretica of Broussais, would appear to be a well-recognized clinical fact.
What the precise relation is between digestive disturbances and the nervous system we may not fully understand, no more than we understand how a healthy condition of nervous endowment is essential to all vital processes. Even lesions of nutrition are now known to depend upon primary disturbance of nervous influence. This is seen in certain skin diseases, such as herpes zoster, which closely follows the destruction of certain nerves. And it is well known that injury of nerve-trunks is not unfrequently followed by impaired nutrition and failure in reparative power in the parts to which such nerves are distributed. Indeed, so marked is the influence of the nervous system over the nutritive operations that the question has been considered as to whether there are [p. 437] trophic nerves distributed to tissue-elements themselves whose special function is to keep these elements in a healthy state of nutrition. The proof, at least, that the digestive process is, in some unexplained way, under the immediate influence of the nervous system, either cerebro-spinal or trophic, is both varied and abundant. The digestive secretions are known to be the products of living cells which are abundantly supplied with nerve-fibres, and we can readily believe that the potential energy of this cell-force is probably vital and trophic. At any rate, it is unknown in the domain of ordinary chemistry. The digestive ferments, as clearly pointed out by Roberts, are the direct products of living cells. Their mode of action, he claims, bears no resemblance to that of ordinary chemical affinity. It has a distinctly physiological character. Nor do they derive their vital endowments from material substances. "They give nothing material to, and take nothing from, the substances acted on. The albuminoid matter which constitutes their mass is evidently no more than the material substance of a special kind of energy—just as the steel of a magnet is the material substratum of the magnetic energy, but is not itself that energy" (Roberts). That this living cell-force is partly, at least, derived from the nervous system is clear from the well-known effects of mental emotion, such as acute grief, despair, etc., in putting an immediate stop to the digestive process. Experiments on the lower animals have also shown the direct influence of the nervous system over gastric secretion. Wilson Philip showed by various experiments on rabbits and other animals that if the eighth pair of nerves be divided in the neck, any food which the creatures may afterward eat remains in the stomach undigested, and after death, when the nerve has been divided, the coats of the stomach are not found digested, however long the animal may have been dead. Bernard also excited a copious secretion by galvanization of the pneumogastric, and by section of the same nerve stopped the process of digestion and produced "pallor and flaccidity of the stomach." Recently doubt has been thrown on these statements of Bernard and Frerichs. Goltz concludes, from observations made on frogs, that nerve-ganglia, connected by numerous intercommunicating bundles of nerve-fibres, exist in the walls of the stomach, the irritation of which gives rise to local contractions and peristaltic movements of the stomach, and that these ganglia influence the gastric secretion. However this may be, it still remains true that these gastric ganglia are in connection, through the vagi, with the medulla oblongata, and are thus influenced by the cerebro-spinal nerve-centres. And clinical observation confirms what theoretical considerations would suggest. Thus, strong mental impressions are known to produce sudden arrest of secretion, and that which arrests secretion may, if continued, lead to perversion of the same.
Impressions made upon the nerves of special sense are also known to affect the salivary and gastric secretions. The flow of saliva is stimulated by the sight, the smell, the taste, and even thought, of food. Bidder and Schmidt made interesting experiments on dogs bearing upon this point. They ascertained by placing meat before dogs that had been kept fasting that gastric juice was copiously effused into the stomach. Other secretions are known to be similarly affected. Carpenter by a series of well-observed cases has shown the direct influence of mental conditions on the [p. 438]mammary secretion. The nervous association of diabetes and chronic Bright's disease is interesting in this connection, and the direct nervous connection betwixt the brain and the liver has been shown by numerous experiments. It is maintained by modern physiologists that "the liver—indeed each of the viscera—has its representative area in the brain, just as much as the arm or leg is represented in a distant localized area" (Hughlings Jackson). And in harmony with this view Carpenter long since pointed out the fact that if the volitional direction of the consciousness to a part be automatically kept up for a length of time, both the functional action and the nutrition of the part may suffer. It has been described by him as expectant attention, and it has, as we shall see, important practical bearings on the management of gastric affections. Sympathetic disturbance of the stomach is also connected with direct disease of the brain. This is seen in cases of concussion. The almost immediate effects of a blow are nausea and vomiting, and the same thing is observed in local inflammation of the meninges of the brain.
Many forms of functional dyspepsia due to nervous disturbance of a reflex character will be pointed out when discussing the etiology of the disease.
ETIOLOGY.—Among the agencies affecting the digestive process in atonic forms of dyspepsia may be mentioned—
First, predisposing causes;
Second, exciting causes.
In general terms it may be said that all conditions of depressed vitality predispose to the varied forms of atonic dyspepsia. These conditions range through an endless combination of causes, both predisposing and exciting. There is not a disturbed condition of life, extrinsic or intrinsic, that may not contribute to this end. In some cases it may be the effects of hot and enervating climates; in others the alterations in the elementary constituents of the blood may be apparent; while in still others the cause may be exhausting discharges, hemorrhages, profuse suppuration, venereal excesses, sedentary occupations, and long-continued mental and moral emotions.
Heredity may also predispose to functional dyspepsia. Certain faulty states of the nervous system are specially liable to be transmitted from parent to offspring—not always in the exact form in which they appeared in the parent, but in forms determined by the individual life of the offspring. For obvious reasons, growing out of our modern American civilization, the inheritance of a faulty nervous organization is apt to spend itself upon the digestive apparatus. The inordinate mental activity, the active competitions of life, the struggle for existence, the haste to get rich, the disappointments of failure,—all contribute to this end. The general tendency of American life is also in the direction of a highly-developed and morbidly sensitive nervous system, and functional dyspepsia is a natural sequence of this. The symptoms of dyspepsia thus caused usually manifest themselves at an early period of life.
Age also predisposes to weak digestion. The stomach becomes weak as age advances, in common with all the functions of the body, and consequent upon this weakness there is diminished excitability of the gastric nerves, with diminished muscular action of the walls of the stomach and deficient secretion of the gastric juice. Chronic structural changes are [p. 439] also apt to occur in advanced life. The gastric glands become atrophied and the arteries become atheromatous, so that with symptoms of indigestion there are often associated loss of consciousness at times, vertigo, irregular action of the heart, etc. These general facts have an important bearing upon the hygienic management of dyspepsia in the aged. They require, as a rule, less food than the young and vigorous. In times when famine was more frequent than now it was found that the older a human being was, the better deficiency of food was borne. Hippocrates tells us, in his Aphorisms, that old men suffer least from abstinence. Their food should be such, both in quantity and quality, as the enfeebled stomach can digest. There is less demand for the materials of growth, and consequently for animal food. Moderate quantities of alcohol, judiciously used, are also specially adapted to the indigestion of the aged. It has the double effect of stimulating the digestive process and at the same time checking the activity of destructive assimilation, which in old age exhausts the vital force. And in order to more effectively arrest destructive metamorphosis great caution should be taken against excessive muscular fatigue, as well as against sudden extremes of temperature. Loss of appetite from deficient formation of gastric juice is a common symptom in old age. This is not often successfully treated by drugs, and yet medicines are not without value. The sesquicarbonate of ammonium acts as a stimulant to the mucous membrane and to the vaso-motor nerve, and in this way becomes a valuable addition to the simple vegetable bitters. Dilute hydrochloric acid with the vegetable bitters may also be tried. Condiments with the food directly stimulate the action of the enfeebled stomach. The old remedy of mustard-seed is not unfrequently useful, and pepper, cayenne, horseradish, and curries act in a similar manner in torpid digestion. And in cases of great exhaustion associated with anæmia benefit may be derived from small doses of iron added to tincture of columbo or gentian.
Nor should it be forgotten that in the opposite extreme of life the digestive capacity is extremely limited. The infant's digestion is readily disturbed by unsuitable alimentation. For obvious reasons it does not easily digest starchy substances. The diastasic ferment does not exist in the saliva of young sucking animals, at least to any extent. No food is so suitable for early infantile life as the mother's milk, provided the mother herself is healthy. It contains in an easily digestible form all the constituents necessary to the rapidly-growing young animal. Van Helmont's substitute of bread boiled in beer and honey for milk, or Baron Liebig's food for infants, cannot take the place of nature's type of food, which we find in milk. If a substitute has to be selected, there is nothing so good as cow's milk diluted with an equal quantity of soft water, or, what in many cases is better, barley-water, to which may be added a teaspoonful of powdered sugar of milk and a pinch of table-salt and phosphate of lime. Lime-water may be added with advantage. Dilution of alimentary substances is an important condition of absorption in the infant stomach.
Anæmia is a common predisposing cause of indigestion. Indeed, as a widely-prevailing pathological condition few causes stand out so prominent. It affects at once the great nutritive processes, and these in turn disturb the functional activity of all the organs of the body. Not only are the gastric and intestinal glands diminished in their [p. 440] functional activity by impoverished or altered blood, but the movements of the stomach are retarded by weakened muscular action. It is impossible to separate altered blood from perverted tissue-structure and altered secretion. Indigestion produced by anæmia is difficult of treatment, on account of the complexity of the pathological conditions usually present, the anæmia itself being generally a secondary condition. Careful inquiry should be made, therefore, into the probable cause of the anæmia, and this should, if possible, be removed as an important part of the treatment of the dyspepsia. Nothing will more promptly restore the digestive capacity in such cases than good, healthy, well-oxidized blood. Indeed, healthy blood is a condition precedent to the normal functional activity of the stomach.
To these general predisposing causes may be added indigestion occurring in febrile states of the system. The cause here is obvious. In all general febrile conditions the secretions are markedly disturbed; the tongue is dry and furred; the urine is scanty; the excretions lessened; the bowels constipated; and the appetite gone. The nervous system also participates in the general disturbance. In this condition the gastric juice is changed both quantitatively and qualitatively, and digestion, as a consequence, becomes weak and imperfect—a fact that should be taken into account in regulating the diet of febrile patients. From mere theoretical considerations there can be no doubt that fever patients are often overfed. To counteract the relatively increased tissue-metamorphosis known to exist, and the consequent excessive waste, forced nutrition is frequently resorted to. Then the traditional saying of the justly-celebrated Graves, that he fed fevers, has also rendered popular the practice. Within certain bounds alimentation is undoubtedly an important part of the treatment of all the essential forms of fever. But if more food is crowded upon the stomach than can be digested and assimilated, it merely imposes a burden instead of supplying a want. The excess of food beyond the digestive capacity decomposes, giving rise to fetid gases, and often to troublesome intestinal complications. The true mode of restoring strength in such cases is to administer only such quantities of food as the patient is capable of digesting and assimilating. To this end resort has been had to food in a partially predigested state, such as peptonized milk, milk gruel, soups, jellies, and beef-tea; and clinical experience has thus far shown encouraging results from such nutrition in the management of general fevers. In these febrile conditions, and in all cases of general debility, the weak digestion does not necessarily involve positive disease of the stomach, for by regulating the diet according to the digestive capacity healthy digestion may be obtained for an indefinite time.
Exhaustion of the nerves of organic life strongly predisposes to the atonic forms of dyspepsia. We have already seen how markedly the digestive process is influenced by certain mental states, and it is a well-recognized fact that the sympathetic system of nerves is intimately associated with all the vegetative functions of the body. Without a certain amount of nervous energy derived from this portion of the nervous system, there is failure of the two most important conditions of digestion—viz. muscular movements of the stomach and healthy secretion of gastric juice. This form of indigestion is peculiar to [p. 441] the ill-fed and badly-nourished. It follows in the wake of privation and want, and is often seen in the peculiarly careworn and sallow classes who throng our public dispensaries. In this dyspepsia of exhaustion the solvent power of the stomach is so diminished that if food is forced upon the patient it is apt to be followed by flatulence, headache, uneasy or painful sensations in the stomach, and sometimes by nausea and diarrhoea. It is best treated by improving in every possible way the general system of nutrition, and by adapting the food, both in quantity and quality, to the enfeebled condition of the digestive powers. Hygienic measures are also of great importance in the management of this form of dyspepsia, and especially such as restore the lost energy of the nervous system. If it occur in badly-nourished persons who take little outdoor exercise, the food should be adapted to the feeble digestive power. It should consist for a time largely of milk and eggs, oatmeal, peptonized milk gruels, stale bread; to which should be added digestible nitrogenous meat diet in proportion to increased muscular exercise. Systematic outdoor exercise should be insisted upon as a sine quâ non. Much benefit may be derived from the employment of electric currents, and hydrotherapy has also given excellent results. If the indigestion occur in the badly-fed outdoor day-laborer, his food should be more generous and mixed. It should consist largely, however, of digestible nitrogenous food, and meat, par excellence, should be increased in proportion to the exercise taken. Medicinally, such cases should be treated on general principles. Benefit may be derived from the mineral acids added to simple bitters, or in cases of extreme nervous prostration small doses of nux vomica are a valuable addition to dilute hydrochloric acid. The not unfrequent resort to phosphorus in such cases is of more than doubtful utility. Some interesting contributions have been recently made to this subject of gastric neuroses by Buchard, Sée, and Mathieu. Buchard claims that atonic dilatation of the stomach is a very frequent result of an adynamic state of the general system. He compares it to certain forms of cardiac dilatation—both expressions of myasthenia. It may result from profound anæmia or from psychical causes. Mathieu regards mental depression as only second in frequency. Much stress is laid upon poisons generated by fermenting food in the stomach in such cases. It may cause a true toxæmia, just as renal diseases give rise to uræmia. Of course treatment in such cases must be addressed principally to the general constitution.
But of all predisposing causes of dyspepsia, deficient gastric secretion, with resulting fermentation of food, is perhaps the most prevalent. It is true this deficient secretion may be, and often is, a secondary condition; many causes contribute to its production; but still, the practical fact remains that the immediate cause of the indigestion is disproportion between the quantity of gastric juice secreted and the amount of food taken into the stomach. In all such cases we have what is popularly known as torpidity of digestion, and the condition described is that of atony of the stomach. The two main constituents of gastric juice—namely, acid and pepsin—may be deficient in quantity or disturbed in their relative proportions. A certain amount of acid is absolutely essential to the digestive process, while a small amount of pepsin may be sufficient to digest a large amount of albuminoid food. [p. 442] Pure unmixed gastric juice was first analyzed by Bidder and Schmidt. The mean analyses of ten specimens free from saliva, procured from dogs, gave the following results:
| Water | 973.06 | |||
| Solids | 26.94 | |||
| Containing— | Peptone and pepsin | 17.19 | ||
| Free hydrochloric acid | 3.05 | |||
| Alkaline chlorides | 4.26 | |||
| Ammonium chloride | 0.47 | |||
| Chlorine | 5.06 | |||
| Phosphates— | Lime | 1.73 | ||
| Magnesia | 0.23 | |||
| Iron | 0.08 | |||
They proved by the most careful analyses that fresh gastric juice contains only one mineral acid—namely, hydrochloric; since which time Richet has been able to prove that "this acid does not exist in a free state, but in loose combination with an organic substance known as lucin," the chloride of lucin. And just here the curious and puzzling question arises as to the secretion of a mineral acid from alkaline blood. Ewald, the distinguished lecturer in the Royal University of Berlin, tells us that "a brilliant experiment of Maly's has thrown unexpected light upon this. There are fluids of alkaline reaction which may contain two acid and alkaline mutually inoffensive salts, but still have an alkaline reaction, because the acid reaction is to a certain extent eclipsed; for instance, a solution of neutral phosphate of soda (Na2HPO4) and acid phosphate of soda (NaH2PO4) is alkaline. Such a solution placed in a dialyzer after a short time gives up its acid salt to the surrounding distilled water, and one has in the dialyzer an alkaline fluid outside an acid fluid." He thus proved that the acid phosphate of sodium is present in the blood in spite of its alkaline reaction.
Lack of the normal amount of the gastric secretion must be met by restoring the physiological conditions upon which the secretion depends. In the mean time, hydrochloric and lactic acids may be tried for the purpose of strengthening the solvent powers of the gastric secretion.
EXCITING CAUSES.—The immediate causes of dyspepsia are such as act more directly on the stomach. They embrace all causes which produce conditions of gastric catarrh, such as excess in eating and drinking, imperfect mastication and insalivation, the use of indigestible or unwholesome food and of alcohol, the imperfect arrangement of meals, over-drugging, etc.
Of exciting causes, errors of diet are amongst the most constantly operative, and of these errors excess of food is doubtless the most common. The influence of this as an etiological factor in derangement of digestion can scarcely be exaggerated. In very many instances more food is taken into the stomach than is actually required to restore tissue-waste, and the effects of such excess upon the organism are as numerous as they are hurtful. Indeed, few elements of disease are more constantly operative in a great variety of ailments. In the first place, if food be introduced into the stomach beyond tissue-requirements, symptoms of indigestion at once manifest themselves. The natural balance betwixt [p. 443]supply and demand is disturbed; the general nutrition of the body is interfered with; local disturbances of nutrition follow; and mal-products of digestion find their way into the blood. Especially is this the case when the excessive amount of food contains a disproportionate amount of nitrogenous matter. All proteid principles require a considerable amount of chemical alteration before they are fitted for the metabolic changes of the organism; the processes of assimilative conversion are more complex than those undergone by fats and amyloids; and it follows that there is proportional danger of disturbance of these processes from overwork. Moreover, if nitrogenous food is in excess of tissue-requirement, it undergoes certain oxidation changes in the blood without becoming previously woven into tissue, with resulting compounds which become positive poisons in the economy. The kidneys and skin are largely concerned in the elimination of these compounds, and the frequency with which these organs become diseased is largely due, no doubt, to the excessive use of unassimilated nitrogenous food. Then, again, if food be introduced in excess of the digestive capacity, the undigested portion acts directly upon the stomach as a foreign body, and in undergoing decomposition and putrefying changes frets and irritates the mucous membrane. It can scarcely be a matter of doubt that large groups of diseases have for their principal causes excess of alimentation beyond the actual requirements of the system. All such patients suffer from symptoms of catarrhal indigestion, such as gastric uneasiness, headache, vertigo, a general feeling of lassitude, constipation, and high-colored urine with abundant urates, together with varied skin eruptions. Such cases are greatly relieved by reducing the amount of food taken, especially nitrogenous food, and by a systematic and somewhat prolonged course of purgative mineral waters. Europe is especially rich in these springs. The waters of Carlsbad, Ems, Seltzer, Friedrichshall, and Marienbad, and many of the alkaline purgative waters of our own country, not unfrequently prove valuable to those who can afford to try them, and their value shows how often deranged primary assimilation is at the foundation of many human ailments. The absurd height to which so-called restorative medicine has attained within the last twenty years or more has contributed largely to the production of inflammatory forms of indigestion, with all the evil consequences growing out of general deranged nutrition.
The use of indigestible and unwholesome food entails somewhat the same consequences. This may consist in the use of food essentially unhealthy or indigestible, or made so by imperfect preparation (cooking, etc.). Certain substances taken as food cannot be dissolved by the gastric or intestinal secretions: the seeds, the skins, and rinds of fruit, the husks of corn and bran, and gristle and elastic tissue, as well as hairs in animal food, are thrown off as they are swallowed, and if taken in excess they mechanically irritate the gastro-intestinal mucous membrane and excite symptoms of acute dyspepsia, and not unfrequently give rise to pain of a griping character accompanied by diarrhoea. Symptoms of acute dyspepsia also frequently follow the ingestion of special kinds of food, such as mushrooms, shellfish, or indeed fish of any kind; and food not adapted to the individual organism is apt to excite dyspeptic symptoms. Appetite and digestion are also very much influenced by the life and [p. 444] habits of the individual. The diet, for instance, of bodily labor should consist largely of digestible nitrogenous food, and meat, par excellence, should be increased in proportion as muscular exercise is increased. For all sorts of muscular laborers a mixed diet is best in which animal food enters as a prominent ingredient. Thus, it has been found, according to the researches of Chambers, that in forced military marches meat extract has greater sustaining properties than any other kind of food. But with those who do not take much outdoor exercise the error is apt to be, as already pointed out, in the direction of over-feeding. It cannot be doubted at the present time that over-eating (gluttony) is one of our popular vices. Hufeland says: "In general we find that men who live sparingly attain to the greatest age." While preventive medicine in the way of improved hygiene—better drainage, better ventilation, etc.—is contributing largely to the longevity of the race, we unfortunately encounter in more recent times an antagonizing influence in the elegant art of cookery. Every conceivable ingenuity is resorted to to tempt men to eat more than their stomachs can properly or easily digest or tissue-changes require. The injurious consequences of such over-feeding may finally correct itself by destroying the capacity of the stomach to digest the food.
But, on the other hand, in many nervous forms of dyspepsia the weak stomach is not unfrequently made weaker by severely restricted regimen, and especially is this the case with mental workers. Theoretical and fanciful considerations sometimes lead to physical starvation. This is apt to be the case with dyspeptics. Men who toil with their brain rather than their muscles, whether dyspeptic or not, require good, easily-digested mixed diet. It is a popular error to suppose that drugs can take the place of such food, especially drugs which are supposed to have a reconstructive influence over the nervous system, such as iron and phosphorus. The expression of Büchner, "No thinking without phosphorus," captivating to theoretical minds, has gained much notoriety, and has doubtless led to the excessive use of that drug in nervous forms of indigestion. There never was a period when phosphorus was so universally prescribed as the present. It enters into endless combinations with so-called nerve-tonics. Of the injurious influence of the drug in many cases of functional indigestion there can be no doubt; and the statement itself, so often quoted, that "the amount of phosphorus in the blood passing through the brain bears an exact proportion to the intensity of thought," is calculated to mislead. T. K. Chambers, author of the excellent Manual of Diet, makes the statement that "a captive lion, tiger, leopard, or hare assimilates and parts with a greater amount of phosphorus than a hard-thinking man; while the beaver, noted for its power of contrivance, excretes so little phosphorus that chemical analysis cannot find it in its excreta." In the wonderful adaptations and regulative mechanisms of nature we may trust largely to the natural law of supply and demand in maintaining a proper equilibrium. It may be doubted, indeed, whether we require at any time more phosphorus for brain- and nerve-tissue than can be found in such food as contains digestible phosphatic salts. The natural demand for food grows out of healthy tissue-change. An appetite to be healthy should commence in processes outside of the stomach.
Food may also be introduced into the stomach in an undigestible form [p. 445] from defects of cookery. The process of cooking food produces certain well-known chemical changes in alimentary substances which render them more digestible than in the uncooked state. By the use of fire in cooking his food new sources of strength have been opened up to man which have doubtless contributed immeasurably to his physical development, and has led to his classification as the cooking animal. With regard to most articles the practice of cooking his food beforehand is wellnigh universal; and especially is this the case with all farinaceous articles of food. The gluten of wheat is almost indigestible in the uncooked state. By the process of cooking the starchy matter of the grain is not only liberated from its protecting envelopes, but it is converted into a gelatinous condition which readily yields to the diastasic ferments. Roberts, in his lectures on the Digestive Ferments, points out the fact that when men under the stress of circumstances have been compelled to subsist on uncooked grains of the cereals, they soon fell into a state of inanition and disease.
Animal diet is also more easily digested in the cooked than in the raw state. The advantage consists chiefly in the effects of heat on the connective tissue and in the separation of the muscular fibre. In this respect cooking aids the digestive process. The gastric juice cannot get at the albumen-containing fibrillæ until the connective tissue is broken up, removed, or dissolved. Hot water softens and removes this connective tissue. Hence raw meat is less easily digestible. Carnivorous animals, that get their food at long intervals, digest it slowly. By cutting, bruising, and scraping meat we to a certain extent imitate the process of cooking. In many cases, indeed, ill-nourished children and dyspeptics digest raw beef thus comminuted better than cooked, and it is a matter of observation that steamed and underdone roast meats are more digestible than when submitted to greater heat.
Some interesting observations have been made by Roberts on the effects of the digestive ferments on cooked and uncooked albuminoids. He employed in his experiments a solution of egg albumen made by mixing white of egg with nine times its volume of water. "This solution," says Roberts, "when boiled in the water-bath does not coagulate nor sensibly change its appearance, but its behavior with the digestive ferments is completely altered. In the raw state this solution is attacked very slowly by pepsin and acid, and pancreatic extract has no effect on it; but after being cooked in the water-bath the albumen is rapidly and entirely digested by artificial gastric juice, and a moiety of it is rapidly digested by pancreatic extract."
It is a mistake, however, to suppose that cooking is equally necessary for all kinds of albuminoids. The oyster, at least, is quite exceptional, for it contains a digestive ferment—the hepatic diastase—which is wholly destroyed by cooking. Milk may be indifferently used either in the cooked or uncooked state, and fruits, which owe their value chiefly to sugar, are not altered by cooking.
The object in introducing here these remarks on cooking food is to show that it forms an important integral part of the work of digestion, and has a direct bearing on the management of all forms of dyspepsia.
Haste in eating, with imperfect mastication, is a common cause of indigestion in this country. Mastication is the first step in the digestive [p. 446] process. It is important, therefore, that we have good teeth and that we take time to thoroughly masticate our food, for by so doing we prepare it for being acted upon by the juices of the stomach. Time is also necessary in order that the salivary secretion may be incorporated with the alimentary substances. By the salivary diastase starch is converted into sugar and albuminoids are prepared for the action of the gastric juice. If these changes take place imperfectly, the stomach can scarcely regain in gastric digestion what was lost in imperfect mastication and insalivation. Haste in eating is one of the American vices. It grows out of the temperament of our people. We are jealous of lost time, and unfortunately this time is too often taken from the stomach. We bolt our food with unseemly haste, and pay the penalty in ruined stomachs. Many cases of indigestion are greatly relieved, if not permanently cured, by simply doubling or quadrupling the time occupied in eating.
Irregularity in the intervals between meals, such as taking one meal only in twenty-four hours or taking food before the preceding supply has been digested, is another fruitful source of indigestion. The digestive process, in the natural order of change, is confused; changes which should take place are delayed; and the results are such as arise from excessive eating. Moreover, the stomach lacks the rest so essential to digestion. The necessary interval, however, between meals varies with the nature of the food taken. "Between the extremes of the carnivoræ," says Ewald, "which feed once in twenty-four hours, and the herbivoræ, which never have done with the business of feeding, man holds a middle place, but not without permitting the recognition in the course of his life of a sort of transition from the herbivora to the carnivora. Infants should have the breast during the first three weeks as often as they wake; after that every two hours to the third month; then up to dentition every three hours; and later there should be five meals in twenty-four hours." But to this general statement there are, of course, many exceptions. Under certain pathological conditions food should be taken in small quantities at short intervals. This is especially the case in chronic gastric catarrh and in feeble digestion of nervous subjects. Such patients are not unfrequently improved by becoming again infants or herbivoræ. By the use of an exclusive milk diet or peptonized milk gruels, given in small quantities at comparatively short intervals of time, the stomach may be so accommodated that it will digest without discomfort a large amount of nourishment within a given time. To S. Weir Mitchell of Philadelphia we are indebted for some valuable observations bearing upon this point of forced alimentation.
To the causes of indigestion already alluded to may be added the habit of spirit-drinking, especially the habit of taking alcohol undiluted on an empty stomach, which rarely fails after a time to engender dyspeptic symptoms. It is a prominent factor in the production of chronic gastric catarrh—a condition more frequently present in painful indigestion than any that have been named. It is one of the most common diseases met with in practice. Indeed, all causes already alluded to involve, sooner or later, if they are constantly operative, irritative and catarrhal conditions of the mucous membrane of the stomach, so that we find it difficult at times—indeed impossible—to separate purely functional from subacute inflammatory forms of dyspepsia. Practically, we simply study the [p. 447]subject in the relative degrees of prominence of the one condition or the other.
But, in a still more comprehensive sense, indigestion is caused by disturbance of organs directly associated with the stomach in the digestive process. All organs closely associated with each other in their physiological functions are apt to become associated in morbid action. The clinical recognition of this is a matter of great importance in the management of gastric affections. And first in the order of importance in such association is the liver. So closely, indeed, are the liver and stomach functionally associated in the process of primary assimilation that they may be considered parts of the same great digestive apparatus. Hence disturbance of the liver—either in the formation of glycogen, the destruction of albuminoid matter, or the secretion of bile—is immediately communicated to the stomach. It may be difficult to say which of these separate and distinct functions of the liver is most at fault; that can only be a matter of physiological inference. In the one case, for instance, the dyspeptic may be fairly well nourished, yet his elimination may be bad. In the other there is no failure of the destructive and excreting functions, but those concerned in the assimilation of fat and peptones are disordered, so that the patient is not well nourished, so far as the fatty element is concerned. This is the more common form, and a form not unfrequently associated with pulmonary consumption. The liver finally becomes fatty—a condition usually found associated with the constitutional forms of phthisis.
The pancreas is also closely associated with the stomach, and its secretion is of essential value in the digestive process. It is to be regretted that our precise knowledge of its diseases is in such striking contrast with its importance in the animal economy, and yet it can scarcely be doubted that in dyspeptic symptoms associated with failure of digestion of starchy, albuminous, and fatty elements of food there is disorder of the secretion of the pancreas. Hence in the treatment of the early stages of pulmonary consumption and other disorders associated with deficient digestion and assimilation of fatty substances the importance of directing our attention to the condition of the liver and pancreas, as well as to the stomach.
That morbid states of the intestinal track occupy a prominent place in the etiology of dyspepsia is also a well-recognized clinical fact. Indeed, constipation of the bowels is an almost universal accompaniment of deranged digestion, and when persistent for years it is apt to lead to the most disastrous consequences. These are mainly in the direction of lessened elimination from the intestinal glandulæ. The general symptomatology of deficient excretion from these glandulæ is closely analogous to the same condition of the liver: there is impairment of the general health; the clear florid complexion disappears; the patient becomes of a greenish or sallow hue; the blood is altered in quality; fatigue is experienced after the slightest exertion; the nights are restless; and there is great tendency to mental despondency. Moreover, constipation often precedes the gastric symptoms. The diminished muscular activity of the intestinal track extends to the stomach; its movements are diminished; food is not properly mixed with the gastric juice, and by being too long retained in the stomach in a comparatively undigested state acetous fermentation in the saccharine and starchy articles of diet is set [p. 448] up, acid eructations and a sour taste in the mouth being commonly complained of. Dyspepsia associated with this condition of the intestinal track cannot be relieved until the constipation is relieved, and by overcoming the constipation the dyspeptic symptoms often disappear.
Mention has been made of the baneful influence of certain mental states in the production of dyspeptic symptoms. But there are forms of indigestion due to local nervous disturbance existing elsewhere than in the nerve-centres. This was ascribed by the older writers to what they termed consensus nervorum, or sympathy, by which "the operation of a stimulus is not limited to the nerves immediately irritated, but is extended to distant parts in known or unknown connection with the irritated nerves." An intimate acquaintance with this law of sympathy is of the utmost importance in the study of the functional forms of dyspepsia, for no other organ of the body is subjected to such a wide range of reflected nervous disturbance as the stomach. Morbid sympathetic impressions are transmitted mainly through branches of the vaso-motor nerve of the semilunar ganglia of the abdomen, and from the pneumogastric to the stomach. Thus, a pregnant uterus not unfrequently produces very troublesome vomiting; some females suffer from nausea and indigestion during each menstrual period; and the more chronic forms of pelvic irritation, such as a flexed uterus, and endometritis, cervicitis, or tender ovary, may be the continuous exciting cause of most troublesome forms of nervous dyspepsia. There is also close sympathy of the stomach with the lungs and heart through the distribution of the pneumogastric. So also may fixed points of irritation in any part of the nervous system be reflexly transmitted to the stomach, giving rise to most pronounced symptoms of indigestion. And it is evident that in all such cases but little can be accomplished in the way of relieving the dyspeptic symptoms until the cause upon which they depend is removed. The treatment must have reference mainly to the removal of such cause.
Lastly, all the causes mentioned finally concur in producing irregularities of the mechanism of digestion; and this may be done by disturbing either the muscular movements of the stomach or in suspending or perverting the gastric solvents, or in these two conditions combined.
SYMPTOMS.—1st. Referable to the Stomach.—The symptoms which attend and indicate the presence of functional dyspepsia are such as accompany in a greater or less degree almost all cases of chronic gastritis. Clinically, so far as the direct gastric symptoms are concerned, it is difficult to separate them. The more prominent of the local symptoms are—a sense of fulness and distension after meals, discomfort during the digestive process, derangement of appetite, acid eructations, flatulence, regurgitations of food, and sometimes nausea and vomiting. There is seldom severe pain; the sensation is rather that of uneasiness. Exceptionally, however, there may be pain, which radiates from the stomach to the shoulders, and may pass down the left arm so as to simulate angina pectoris. But it may be readily distinguished from that complaint by coming on after food, and not after exertion. In other cases a sense of constriction may be accompanied by dyspnoea, arising from impeded movements of the diaphragm from being pushed upward by the distended stomach, or there may be heartburn, with an ill-defined sense of burning felt in the epigastrium; [p. 449] but thirst, so frequently present in chronic gastritis, is, as a rule, absent in functional dyspepsia. These symptoms are manifested in varying degrees of prominence in individual cases, and some of them are rarely found present. Thus, nausea and vomiting are not characteristic features of the chronic forms of functional dyspepsia, and as a rule epigastric tenderness is entirely absent. In markedly hysterical subjects or in persons whose nervous system has been unduly excited by alcohol there may be shrinking from the slightest touch upon pressure; but in these cases the tenderness is not confined to the stomach, nor is it increased by deep pressure. In some cases there is an unnatural craving for food—a symptom rarely if ever observed in structural lesions of the stomach—and now and then it happens that the appetite becomes depraved, especially with hysterical patients. They crave indigestible and unnatural substances, such as earth, chalk, and substances wholly devoid of alimentary properties. Impairment of appetite, however, is the more common feature of this form of indigestion.
Flatulence and eructations are generally complained of, the flatulence being accompanied by a painful sense of fulness, affecting in equal degree the stomach and small intestines. It is derived principally from putrefactive or fermentative changes of the ingesta, which are imperfectly elaborated in the stomach. The gases consist of carbonic acid, sulphuretted hydrogen, hydrogen, nitrogen, and the hydrocarbons, the butyric and acetic fermentations furnishing the hydrogen and carbonic acid gas. In addition to these marsh gas is formed by a special fermentation, the basis of which exists in the cellulose taken with vegetable food. In excessive meteorism from paralysis of the intestines the gas is principally nitrogen; the marsh-gas fermentation results from the ingestion of certain easily-fermentable vegetables, such as cabbage, cauliflower, etc.
In a certain proportion of cases regurgitation occurs from the stomach. The liquor regurgitated may be intensely acid from the presence of some of the fatty acids, probably butyric, lactic, or acetic. Exceptionally, it may be insipid or brackish, constituting what is known as pyrosis, or water-brash. The fluid is usually tasteless and without smell, and in reaction it is neutral to test-paper. It contains sulphocyanuret of potassium, and it has been supposed therefore to be only saliva. The quantity thrown up may vary from a spoonful to a pint or more. It affects females more than males, and especially those who subsist upon coarse and indigestible food. It is best treated by astringents—such as kino, krameria, logwood, or tannin—administered in the intervals between digestion, so that they may act directly on the mucous membrane. The oxide and nitrate of silver are thought by some to be superior to the vegetable astringents.
Cardialgia is a painful condition of the stomach, usually referred to its cardiac orifice, and is popularly known as heartburn. It is met with in both functional and organic disease of the stomach. It is very constantly present in chronic catarrhal gastritis, and evidently depends upon the presence of an acid, for it is usually promptly relieved by alkalies, such as chalk, magnesia, soda, or alkaline saline waters. Food containing much fat, starch, or sugar should be avoided.
Nausea and vomiting are only occasional symptoms of functional dyspepsia. When vomiting does occur it may take place at different times [p. 450] and with varying degrees of severity, differing in this respect from the nausea and vomiting of subacute gastritis, which takes place, if at all, soon after the ingestion of food. The time of vomiting and the character of the matter ejected are liable to great variation in functional dyspepsia. It may be the result of direct irritation of morbidly sensitive gastric nerves, or it may be a reflex phenomenon; it may follow soon after the ingestion of food, or it may come on when the stomach is empty; the material vomited may be simply food but little altered or an alkaline ropy mucus; it may consist in the acid juices of the stomach or in a neutral watery fluid; or the ingesta may have undergone fermentative and putrefactive changes from either insufficient amount of the gastric solvent or from narrowing (constriction) of the pyloric extremity, in which case the yeast fungus (Torula cerevisiæ) or the Sarcina ventriculi may be found in great abundance in the vomited matter. Vomiting of this kind usually occurs some time after eating. The gastric juice itself checks putrefaction; so also does the admixture of bile. In the absence of these natural antiseptics fermentation takes place. But it would be erroneous to suppose that the fermentative dyspepsia is the primary disease; it is a symptom which can be permanently corrected only by correcting the condition upon which it depends.
Among the most noticeable of the phenomena referable to other organs than the stomach are those connected with the liver and the alimentary canal. The tongue in dyspeptic troubles varies much in character. In reflex sympathetic indigestion it is not unfrequently clean; in hepatic dyspepsia it is generally thickly coated with a white or yellow fur. The symptoms are such as pertain more especially to chronic gastro-duodenal catarrh, such as nausea, epigastric oppression, furred tongue, heartburn, acid eructations, flatulent distension of the stomach and bowels, unpleasant taste in the mouth, offensive breath, loaded urine, frontal headache, irritability, and hypochondriasis.
Constipation, as we have seen, is an almost universal accompaniment of functional dyspepsia, sustaining to it not unfrequently a causative relation. It is undoubtedly one of the most common of the slighter ailments of civilized life, and exerts a wide influence in deranging the general health. "It is quite extraordinary how many different derangements of health may result from imperfect action or a torpid state of the secreting and expelling structures of the large bowel. There may be violent and persistent nerve-pains, referred to the back, or hip, or groin, and certain other symptoms which lead pessimist practitioners, excelling in the discovery of neuroses, to diagnose structural changes in some part of the spinal cord or the antecedent state which is supposed to lead to them" (Beale). Pains in the loins and thighs, violent lumbar pain, and certain remediable forms of sciatica are sometimes due to imperfect excretion of the lower part of the alimentary canal. And it is even possible that a condition of hypochondria bordering on insanity may be brought about by long-continued defective action of the bowels. In exceptional cases of dyspepsia diarrhoea may be present. This is more frequently the case when indigestion is associated with a congested state of the liver, in which case the symptom should be regarded as curative. Excessive irritability of the muscular walls of the stomach, superadded to weak digestion, may also be followed by lienteric forms of diarrhoea. Undigested [p. 451] food hastily finds its way into the intestinal track, and not unfrequently appears in the fecal evacuations.
Functional derangements of the stomach are often accompanied by pale urate deposits in the urine. It may contain an excess of phosphates, and in microscopical examination crystals of the oxalate of lime are frequently found, constituting a special affection described by Golding-Bird as oxaluria. He associated it with irritative dyspepsia, hypochondriasis, and exhaustion of nerve-power. This form of dyspepsia is best managed by the mineral, vegetable, and acid tonics, to which may be added small doses of nux vomica, with the usual adjuvants of good air and exercise, freedom from anxiety and care, cold sea-water baths, and well-selected, generous animal diet.
Another form of dyspepsia is sometimes associated with a peculiar form of dizziness—gastric vertigo. German writers speak of it as abdominal dizziness, and Trousseau calls it vertigo stomicale. It is usually an acute symptom, begins without any premonition, and is liable to be confounded with disease of the brain. It sometimes occurs soon after a meal, but more often when the stomach is empty (Trousseau). It perhaps, in a majority of cases, depends upon dyspepsia, but it has to be differentiated from organic brain disease, from cerebral anæmia, cerebral hyperæmia, the slighter forms of epilepsy, Minière's disease, and general nervous exhaustion and depression. But in many cases it will be found that treatment directed against the dyspepsia cures the vertigo.
Dyspeptic patients are also liable to skin diseases, and especially is this observed in the gastro-duodenal forms of indigestion. Disorders of the skin, such as urticaria, erythema, lichen, eczema, and other allied conditions, are well-recognized external indications at times of disordered conditions of the gastro-intestinal mucous membrane. Thus, it is a matter of common observation that the gastric symptoms increase when the eruption on the surface disappears.
The general influence of the nervous system over the function of digestion is perhaps the most remarkable feature of the disease, so that disturbed innervation becomes conspicuous in its symptomatology. The phenomenon varies in individual cases. Languor, drowsiness after taking food, depression of spirits, irritability, hypochondriasis, sleeplessness, palpitation, dry cough, dyspnoea, are all of common occurrence; and the mental disturbance—the anxiety, gloom, and sadness—is to many dyspeptics more distressing than absolute pain.
It is impossible, however, to present, in this connection, a complete clinical history of functional dyspepsia, for the reason that it is associated with so many separate and distinct affections, the dyspepsia itself being symptomatic of these affections.
PATHOLOGY.—But little is known of the pathology of the purely functional forms of dyspepsia beyond what is expressed by the terms atony and asthenia. These express simply certain states of the system with which atonic dyspepsia is so frequently found associated. Pathological anatomy has shown, however, that some cases are dependent upon, or associated with, certain appreciable alterations of the stomach, such as atrophy of the mucous membrane or fatty degeneration of its walls; and not unfrequently it is the seat of the so-called amyloid or lardaceous degeneration, although this albuminoid infiltration or cloudy [p. 452] swelling is more frequently the accompaniment of chronic inflammatory process. But Jones and Fenwick have shown that these conditions may occur independently of inflammation. However, upon this point we are compelled to speak with caution. The boundary-line between functional and structural diseases is not always clearly defined. Functional and structural troubles of the stomach are certainly very intimately associated. Moreover, symptoms of purely functional dyspepsia are so frequently associated with the subacute forms of gastritis that the pathology of the disease becomes, from necessity, doubtful and complex. It can only be studied in connection with certain states or conditions of which functional derangement of the stomach is a symptom readily recognized during life. In the light of more advanced physiological and pathological researches we may expect the limits of purely functional dyspepsia to be much restricted.
DIAGNOSIS.—The diagnosis of atonic dyspepsia must have special reference to its etiology. It is usually a chronic disease, and has to be discriminated from subacute or chronic inflammation of the stomach. This is the more difficult because many symptoms exist in common in both varieties of indigestion. But in functional or atonic dyspepsia the symptoms are not so continuous; there is less epigastric uneasiness, less tenderness, less nausea or loathing of food, less thirst, and less acidity and heartburn, less emaciation, less cerebral and nervous disturbance, and the constitutional symptoms are also less severe. The tongue, as a rule, is not so thickly coated, is not so red or broad and flabby, the papillæ are less marked, the breath less offensive, and the urine, instead of showing a condition of lithæmia, is not unfrequently pale and sometimes neutral, depositing oxalates and phosphates, especially in feeble, broken-down conditions of the nervous system.
With other painful affections of the stomach, such as ulcer and cancer, it is not likely to be confounded, especially when in these affections pain, vomiting, and hæmatemesis are present.
TREATMENT.—The first and leading indication is to remove, as far as possible, all causes of the disease, and this requires patient research and much diagnostic skill. Suggestive hints of treatment may be found in connection with the discussion of the varied etiology of the disease. We can, in conclusion, only allude to the matter in a very general way. Special cases must furnish their own indications of treatment.
In many cases a condition of nervous asthenia will be found prominently present. A leading indication, therefore, irrespective of the special determining cause, is to improve the general health of the patient; and this is accomplished by all means which invigorate the system generally. And first in the order of importance are diet and regimen. It is evident that if a patient eat too much or too often, or if he eat indigestible or unwholesome food, or lead an indolent and luxurious life, nothing can be accomplished by way of drugs in the relief of the disease. Excessive alimentation is, as we have seen, a most prolific source of the disease. Tempted to excess by great variety and by the ingenuity of culinary refinements, the stomach is burdened beyond its capacity of digestion and beyond the actual requirements of the system; and especially is this the case with those who live sedentary, indoor lives. In all such cases it is absolutely essential that the digestive organs have rest. [p. 453]Better even in cases of doubt reduce the diet for a time below the actual wants of the system until waste products are thoroughly removed and appetite is revived. The benefit derived in some instances from the protracted use of purgative mineral waters is largely attributable to the restricted regimen enforced and to the washing out of the system the waste products.
On the other hand, too great or too protracted abstemiousness may equally impair the digestive process. In ordinary forms of atonic dyspepsia we should seek rather, by appropriate treatment, to raise the digestive capacity to the level of digesting good, healthy, nutritious food, than to reduce the food to the low standard of feeble digestion. But it is a mistake to suppose that this can be accomplished by simply forcing food upon a stomach that lacks capacity of digestion.
As to the kind of diet, no precise rule is suited to all cases. Within certain limits individual experience must be consulted. But these experiences are not always reliable. Dyspeptic patients, more than any others, are apt to have fancies. Certain general rules, therefore, should be insisted upon. The food should be wholesome and digestible; it should be well cooked, well masticated, and taken at regular and not too long intervals. The intervals of time between meals depend upon circumstances already referred to. In some cases small quantities of easily-digested food should be taken at short intervals. In cases of feeble digestion of nervous subjects milk diluted in Seltzer water, or milk and lime-water, or peptonized milk, may be taken in liberal quantities at comparatively short intervals of time. Sometimes isinglass, arrowroot, or ground rice may be advantageously combined with the milk, to which tender, undone meats may be added.
Peptonized Food.—Recently the attention of the profession has been attracted to artificially digested food. The essential acts of digestion are known to be chemical transmutations. Albuminoid substances are changed into peptones and starchy matters are changed into dextrin and sugar. To Roberts, in his excellent lectures delivered in the Lumleian course before the Royal College of Physicians of London in 1880, we are indebted for valuable information on the digestive ferments and in the preparation and use of artificially-digested food; and from these lectures we shall derive most of the information we possess at present. It has been demonstrated that an extract of the stomach or pancreas, in water, has to a certain extent the same powers as the natural secretions of these organs. Hence, says Roberts, it is possible for us to subject articles of food beforehand to complete or partial digestion. Heat approximatively accomplishes the same thing. In the practice of cookery we have, as it were, a foreshadowing of this art of artificial digestion. Heat and digestive ferments alike aid gastric digestion. In case of the lower animals the whole process has to be accomplished by the labor of their own digestive organs.
Artificially digested food may be prepared in two ways—either by following the gastric method with pepsin and hydrochloric acid, or by following the intestinal method and using extract of pancreas. Both of these plans have had special advocates. Roberts claims that the latter yields by far the better results. "The pancreas not only acts upon albuminous substances, but also upon starch. Pepsin, on the other hand, is [p. 454] quite inert in regard to starch. Moreover, the products of artificial digestion with pepsin and acid are much less agreeable to the taste and smell than those produced by pancreatic extract." The pancreas of the pig, according to Roberts, yields the most active preparation, but the pancreas of the ox or the sheep may be employed. The pancreas of the calf is not active on starchy materials. A very active extract of pancreas is now prepared, and is easily obtainable, with directions for making peptonized milk, milk gruel, milk punch, soups, jellies, blanc-manges, beef-tea, enemata, etc. It is important to remember that peptonized foods do not keep well, especially in warm weather. If a quantity sufficient for twenty-four hours be prepared at any one time, the quantity which remains over twelve hours should be reboiled before using. Food thus peptonized is indicated in feeble conditions of digestion and when the derangement of digestion results from causes pertaining to the condition of the stomach itself—i.e. catarrhal forms of dyspepsia.
As a rule, the food should be such as will require the least possible exertion on the part of the stomach. Raw vegetables should be forbidden; pastries, fried dishes, and all rich and greasy compounds should be eschewed; and whatever food be taken should be eaten slowly and well masticated. Many patients digest animal better than vegetable food. Tender brown meats, plainly but well cooked, such as beef, mutton, and game, are to be preferred. Lightly-cooked mutton is more digestible than beef, pork, or lamb, and roast beef is more digestible than boiled. Pork and veal and salted and preserved meats are comparatively indigestible. Bread should never be eaten hot or fresh—better be slightly stale—and bread made from the whole meal is better than that made from the mere starchy part of the grain. Milk and eggs and well-boiled rice are of special value.
But to all these general dietetic rules there may be exceptions growing out of the peculiarities of individual cases. These should be carefully studied. The aged, for obvious reasons, require less food than the young; the middle-aged, inclined to obesity and troubled with feeble digestion, should avoid potatoes, sweets, and fatty substances and spirituous liquors; persons suffering from functional derangements of the liver should be put, for a time, on the most restricted regimen; while, on the contrary, the illy fed and badly-nourished require the most nutritious food that can be digested with comfort to the patient.
The general regimen should be tonic and invigorating. The patient should have the benefit of the best possible hygiene. Under this head may be mentioned suitable clothing, fresh air, moderate exercise, sunlight, baths, rest, regular hours, and the abandonment of all bad habits. No single measure has such marked influence on the digestive powers of the stomach as systematic, well-regulated muscular exercise in the open air, and especially if the exercise be accompanied by a cheerful mental state. For this reason outdoor sports are of benefit. Hunting, fishing, boating, are known to excite the keenest appetite for food, and the stomach will digest substances that would distress it under other circumstances. Exhaustion, however, is to be carefully avoided. Horseback exercise is a remedy of much value, especially in the hepatic forms of indigestion.
The mental and moral treatment of the purely functional forms of [p. 455] indigestion are amongst the most powerful means we possess. As an etiological factor certain morbid mental states rank first, as we have seen, in the order of importance. Grief, despondency, and despair are effectual barriers to digestion, and in a less degree mental worry seriously interferes with the process. It is a matter of prime importance, therefore, that the patient's mind be pleasantly occupied, that he should be free from all care and mental worry, and that he especially be kept from dwelling, if possible, upon his own bodily ailments. This is often best accomplished by travel, when practicable, in foreign countries, where everything will be novel and new and calculated to lead him away from himself. Get him to travel, says Watson, in search of his health, and the chances are in favor of his finding it. We have the authority of Sir James Johnson also for saying that no case of purely functional dyspepsia can resist a pedestrian tour over the Alps.
We come now to discuss the medical treatment of dyspepsia, which, though not unimportant, is subordinate to the general hygienic measures already referred to. General hints of treatment have been made in connection with special causes mentioned in the text. We seek, in a general way, by therapeutic measures—
1st. To stimulate the secreting and muscular coats of the stomach;
2d. To supply materials in which it is supposed the gastric juice is defective;
3d. To lessen abnormal irritability;
4th. To combat special symptoms or conditions which may hinder the digestive process.
To meet these indications innumerable remedies have been recommended, but they are of benefit only as they counteract the conditions upon which the dyspepsia depends. For loss of appetite, if there are no contraindications to their use, the vegetable bitters are often useful, such as quassia, gentian, and columbo. Of these columbo is the simplest of its class, but none more generally useful than mistura gentianæ with soda. The Hydrastis canadensis has also peculiar claims as a bitter stomachic. It, perhaps more than any of the bitters, promotes gastric secretion in feeble digestion, and has at the same time peculiar salutary effects on the enfeebled condition of the chronically inflamed gastric mucous membrane. It is supposed also to have a stimulating effect on the pancreatic secretion. It may be given in the form of a fluid extract combined with glycerin and small doses of nux vomica.
Among the specific stimulating nerve-tonics, nux vomica, or its alkaloid, strychnia, deserves special mention. In small tonic doses it is specially indicated in conditions of general nervous prostration associated with a tendency to hypochondriasis. In such cases we frequently observe pale urine, containing an excess of the phosphates. The mineral acids are valuable additions to the bitter tonics in all broken-down conditions of the nervous system. In administering nux vomica care should be taken as to limitation of time and dose. The excessive or prolonged use of the drug is apt to produce serious general nervous disturbance, the secondary condition being often the opposite to that for which it was prescribed. Temporary saccharine diabetes is not unfrequently one of the results.
In atony of the mucous membrane, with morbid sensibility and slow [p. 456] digestion, ipecacuanha is a remedy of much value. It was first brought into prominent notice in connection with gastric affections by Budd, since which time it has been more or less used by the profession. In torpid, slow digestion, with depraved or lessened gastric secretion, it is of undoubted value. It should be given on an empty stomach at least half an hour before meals. The dose should be short of producing nausea. We may commence with two to four drops of the tincture or wine of ipecac, and gradually increase until we find the point of tolerance; or it may be given in the form of pill in doses of a quarter or a half grain before meals, combining it with rhubarb in three- or four-grain doses. Ipecacuanha may be administered at the same time we are giving the mineral acids, or mineral acids with pepsin.
Adjuvants to Digestion.—In atony of the stomach the gastric mucous membrane responds feebly to the stimulus of food. There is failure in both muscular movement and gastric secretion, with slowness of digestion as a result. To meet this condition we seek to increase the digestive power by the addition of certain principles natural to the digestive process—viz. the mineral acids, pepsin, and pancreatin. Of these acids, the hydrochloric should be preferred, because it is the natural acid of the gastric juice. Lactic, nitro-hydrochloric, and phosphoric acids have also been used with benefit. There can be no doubt of the efficacy of either of these preparations. They are best given when the stomach is empty, so that they may directly act on the relaxed atonic mucous membrane. Half an hour before or two hours after a meal is the best time for their administration, and to be of benefit they should be administered for a length of time. From fifteen to twenty minims of the dilute hydrochloric or nitro-hydrochloric acid may be given in some bitter tincture or infusion for months. An elegant preparation may be made by adding the acid to tincture of orange-peel and syrup of lemon. Aromatic tincture, tincture of ginger, or glycerin may be added in some cases. It is important that remedies administered in gastric affections should be made pleasant as possible to the patient.
Metallic preparations are of use in some cases. If for any reason they are preferred, the perchloride of iron is one of the very best preparations. Arsenic and zinc may also be tried in small doses.
Pepsin and its Uses.—Of the efficacy of pepsin as an artificial substitute for the normal solvent of the food adverse opinions have been expressed, but in spite of the most critical scepticism as to its action its use since first introduced into medicine has steadily increased. It has been shown to be the natural constituent of the gastric juice and glands, and as a natural ferment, when combined with hydrochloric acid, it constitutes the most important solvent of the nitrogenous portions of our diet (Habershon). There is a vast number of different preparations of pepsin in the market, and some of them are doubtless of little value. We ought to be quite sure that the article is what it purports to be. The pepsina porce is the best preparation, one grain of which, says Beale, ought to thoroughly digest one hundred grains of boiled white of egg in three or four hours at a temperature of 100° F. His test as to the value of pepsin is as follows: "One hundred grains of hard-boiled white of egg, cut into thin slices, may be placed in a wide-mouthed bottle or flask with one ounce of water and twenty drops of dilute hydrochloric acid. One [p. 457] grain of pepsin powder is to be added, and the mixture placed before a fire at a temperature of about 100° F. The flask is to be shaken from time to time. In about an hour the white of egg begins to look transparent at the edges, and in about four hours it will be completely dissolved if the pepsin is good." In cases of feeble digestion from deficiency of gastric juice pepsin is a valuable adjuvant to the digestive power, and may be given with advantage in connection with the mineral acids or with ipecacuanha or capsicum before meals.
Special Remedies.—There are certain symptoms characteristic of the different forms and complications of dyspepsia that require special remedies. Bismuth is often useful. It is especially indicated where there is a morbid painful condition of the gastric nerves. The subnitrate or carbonate of bismuth may be given in ten- or twenty-grain doses, suspended in water by means of mucilage of acacia, and flavored with ginger or peppermint. It should always be given on an empty stomach. Other elegant preparations supposed to be improvements upon these have been recommended, and may be tried.
In cases of anæmia, if there are no contraindications, iron may be tried. If digested and assimilated, it improves the blood, and this is often the first step in the direction of restoring functional activity. Of the preparations of iron, none is perhaps superior to the perchloride. The saccharo-carbonate and the ammonio-citrate are also valuable and unirritating salts of iron, and may be given with other tonics. Ferruginous mineral waters slightly charged with carbonic acid are well tolerated in small doses. The free dilution favors the action, and is frequently more acceptable to the stomach than the more concentrated forms. From one-half to one glassful may be taken at a time; and the use of iron in this form may be preceded or accompanied by the administration of small doses of quinia and of the bitter tonics. But it is a mistake to commence the treatment by the indiscriminate use of iron, quinine, and nerve-tonics. The contraindications to the use of iron are irritable and inflammatory states of the mucous membrane, or dyspepsia associated with deranged conditions of secretion, as manifested by dirty tongue and loaded urine.
When the nervous system is prominently at fault, nux vomica, arsenic, and the nitrate and oxide of silver often prove to be valuable remedies. Here also benefit may be derived from the lighter ferruginous preparations; indeed, few combinations have greater influence over the nervous system than the joint action of arsenic and iron. Much benefit may also be derived, in special cases, from methodical hydro-therapeutic treatment. If judiciously used it strengthens the nervous system, stimulates the organic functions, and increases the power of vital resistance. And in some cases of nervous dyspepsia electricity gives good results. In all cases of nervous prostration as much wholesome food should be taken as the stomach can easily digest.
In hepatic forms of indigestion there is no substitute for an occasional mercurial cathartic, for, notwithstanding adverse criticism, clinical experience has taught the great value of this drug upon the upper portion of the intestinal track. The mode of operation may be doubtful, but the result is unquestionable. In functional disturbance of the liver or morbid conditions of the upper portion of the intestinal track, as indicated [p. 458]by the loaded tongue, sallow complexion, want of appetite, and lithæmia, no remedy will give so much relief as a few broken doses of calomel, followed by a saline aperient; or eight or ten grains of blue mass, with a grain of ipecacuanha, may be administered at bedtime, followed by a saline draught in the morning. After the bowels are thoroughly unloaded by a mercurial, great advantage may be derived from a systematic course of the aperient mineral waters—the Friedrichshall, the Hunyadi, Carlsbad, or some of the mineral waters of our own country. The hepatic form of indigestion cannot be relieved until we relieve the congested hepatic portal system, and this is best accomplished by the general line of treatment here indicated. The simple vegetable bitters, with or without alkalies, may be used at the same time or subsequent to this treatment; but they are often worse than useless until we secure freedom of abdominal circulation. The diet should be light and nourishing, and the patient should spend most of his time out of doors. Horseback exercise is peculiarly advantageous.
But in many cases of the more chronic forms of dyspepsia the colon is as atonic as the stomach, and therefore the bowels require special attention. In colonic dyspepsia all active purgation should be avoided, and salines, such as sulphate of magnesia, the Hunyadi and other saline mineral waters, should be specially prohibited. The most useful aperients in such cases are rhubarb, aloes, senna, colocynth, or podophyllin. Few laxatives answer a better purpose than the ordinary compound rhubarb pill. It may be improved, in special cases, by combining with it extract of nux vomica or belladonna. When there is no affection of the rectum to forbid its use, the watery extract of aloes answers very well, and, unlike many cathartic substances, the dose need not be increased, nor does it disturb the digestive process. It may be given in one-sixth of a grain up to a grain or more, and its purgative action may be improved by being reduced to a state of very minute division and combining with it small doses of belladonna. Belladonna itself is a useful remedy. According to the observations of Harley, it "tones and tightens the longitudinal fibre, while it relaxes the circular;" and long before this theory of its action was suggested, Trousseau called attention to its singular efficacy in producing easy and natural evacuations from the bowels. It is important to observe its mode of use. It should be given in sixth of a grain doses of the extract in the morning a half hour or hour before breakfast. Its efficacy may be increased by combining with it small doses of the watery extract of aloes. In colicky conditions of the bowels two- or three-drop doses of tincture of colocynth sometimes act wonderfully well. In obstinate constipation the free use of diluents at the termination of digestion is often attended with excellent results. But the hygienic and dietetic treatment of constipation is even more important than the medicinal, such as outdoor exercise, the cold bath, rubbing, kneading the bowels, and the use of bread made of whole meal, oatmeal, and an abundant supply of fresh vegetables and fruits.
Nausea and vomiting, occasional symptoms of functional dyspepsia, may be relieved by various agents, such as effervescing draughts, lime-water, oxalate of cerium, hydrocyanic acid, creasote, ice, and alkalies.
When vomiting is dependent on fermentation or putrid action of the contents of the stomach with development of sarcinæ, it may be checked [p. 459] by carbolic acid or by creasote, or by the sulphite of soda or sulphurous acid; and in irritable conditions of the stomach bismuth is a valuable remedy. It may be given with alkalies or with finely-triturated animal charcoal.
Gastric pain needs treatment appropriate to the circumstances under which it arises. Sometimes it is relieved by regulating the ingesta or the intervals at which it is taken; sometimes by warm carminative stimulants or by chloric ether, ginger, or brandy. If the pain is more constant, approaching a condition of gastralgia, hydrocyanic acid and bismuth are more effective remedies. But it cannot be too strongly stated, in conclusion, that in the management of the atonic forms of dyspepsia hygienic treatment is of prime importance. The hopeful future of medicine lies in the direction of promoting healthy nutrition, and this is best accomplished by the careful adaptation of food and exercise and modes of living to individual cases of disease.
Under the head of neuroses of the stomach have been variously described the conditions indicated in the heading of this section; and a certain amount of confusion has arisen in the use of these terms from the fact that they represent subjective sensations common alike to organic and functional forms of indigestion: pain, for instance, is felt in gastritis, cancer of the stomach, and ulcer of the stomach. Indeed, it rarely occurs independently of some disorder of digestion or structural lesion of the stomach.
By gastralgia, considered as a distinct affection, however, we mean a purely neuralgic condition of the sensory fibres of the stomach, excluding inflammatory and structural changes on the one hand and chronic forms of atonic dyspepsia on the other. The attacks are usually periodical in character, with constricting pain in the pit of the stomach, and the intervals are not necessarily associated with symptoms of dyspepsia. It chiefly occurs in females of nervous temperament at the catamenial periods.
Two forms of the disease have been described—one depending on hyperæsthesia of the sensory fibres of the pneumogastric, the other on hyperæsthesia of the solar plexus. This may be correct in theory, but practically it can be of little importance to make the discrimination, even if it were possible to do so.
Clinically, the disease is presented to us in two forms. In one the pain is agonizing, comes on without premonition, is sometimes intermittent or remittent in character, and conveys to the sufferer the idea of spasm; hence it has often been described as colic of the stomach. If not relieved by appropriate remedies, the pain may last for hours or days. This is the acute form. In the other the pain is more of a neuralgic character and is not so severe. There may be varying exacerbations which may last for months or years. This is not an unfrequent form, and may consist simply in the more acute form becoming chronic.
ETIOLOGY.—With the limitation indicated, we have naturally to seek the causes of the affection, says Ziemssen, in two directions: either in the abnormal nature of the irritants to which the gastric nerves are subjected, [p. 460] or in an altered condition of the nerves themselves, which therefore react abnormally with the normal degree of irritation. This briefly covers the whole ground of the etiological relations of the disease.
The predisposing causes are such as produce general depressed vitality, embracing at the same time special conditions of extreme nervous excitability. Some of these general conditions were pointed out while speaking of atonic forms of dyspepsia. Indeed, the two conditions are often associated, and practically it may be difficult to separate them, although the connection between them is not necessarily an invariable one. Like atonic dyspepsia, gastralgia is apt to affect anæmic persons, and notably anæmic females at menstrual periods. Thus, the association between gastralgia, chlorosis, and hysteria is a matter of common observation. Of 350 cases noted by Briquet, only 30 had no signs of gastralgia; and this observation is a fair average expression of the experience of others.
Certain blood-poisons are also known to give rise to the disease. Infection of the blood by malaria was observed by Niemeyer to produce spasm of the stomach instead of the paroxysms of intermittent fever; and in malarious regions of the United States the same observation has been made. Gout and rheumatism are also known to sustain causative relations to the disease. Certain idiosyncrasies also enter as a factor into the somewhat complex etiology of the disease. Thus, some persons suffer immediately from eating certain kinds of food and fruits, such as shellfish, strawberries, honey, and even milk and coffee. The pain and spasm are produced by direct contact with the sensory fibres of the stomach; i.e. they react abnormally to normal stimulation. But disease of the nerve-centres may enter into the causation. This is seen by the effects of morbid growths impinging upon nerve-trunks; their terminal branches often become extremely irritable and painful, and this condition may be intensified by idiosyncrasy. Excessive acidity of the stomach, seeds of fruit, certain articles of food, the presence of worms in the stomach, and draughts of ice-water may simply act as exciting causes to a centric predisposition.
Of the more direct causes operating upon nerve-centres, all the depressing passions and emotions deserve special mention; so do all causes which produce an exhausted state of innervation, such as venereal excesses, onanism, the abuse of narcotics, etc.
But chief among the causes are those of a reflex kind. Painful affections of the kidneys, irritable conditions of the bladder, diseases of the liver, and, above all, morbid conditions of the female genital organs, sustain a direct and close relation to painful and spasmodic conditions of the stomach. It is a common accompaniment of versions, flexions, prolapses, inflammations, erosions of the os, as well as diseased conditions of the ovaries. When such local conditions are associated with anæmia and hysteria, patients rarely fail to have painful gastric complications.
SYMPTOMS.—The symptoms of gastralgia, like most of the neuroses, are characterized by severe pain occurring in paroxysms, followed by remissions, and sometimes by complete intermissions, again to recur with varying degrees of severity. The pain in the acute variety is of a violent, spasmodic character, and is referred to the epigastrium immediately beneath the ensiform cartilage. Frequently it extends from the epigastrium to the back and chest and into the right and left hypochondrium. [p. 461] No one has so briefly and so accurately described the immediate attack of gastralgia as Romberg: "Suddenly, or after a precedent feeling of pressure, there is severe griping pain in the pit of the stomach, usually extending into the back, with a feeling of faintness, shrunken countenance, cold hands and feet, and small, intermittent pulse. The pain becomes so excessive that the patient cries out. The epigastrium is either puffed out like a ball, or, as is more frequently the case, retracted, with tension of the abdominal walls. There is often pulsation in the epigastrium. External pressure is well borne, and not unfrequently the patient presses the pit of the stomach against some firm substance or compresses it with his hands. Sympathetic pains often occur in the thorax under the sternum, in the oesophageal branches of the pneumogastric, while they are rare on the exterior of the body. The attack lasts from a few minutes to half an hour; then the pain gradually subsides, leaving the patient much exhausted, or else it ceases suddenly with eructation of gas or watery fluid, with vomiting, with a gentle soft perspiration, or with the passage of reddish urine."
Besides the violent paroxysmal pain referred to the stomach, symptoms of derangement of other organs are often present. Prominent among these are hysterical phenomena which are protean in their manifestations, and if not recognized they are liable to mislead. Thus, with gastric pain there may be violent palpitation of the heart, with shortness of breath, cough, globus, hiccough, and convulsive affections, and in a certain proportion of cases there is marked melancholia or hypochondriasis.
The stomach is variously modified in its function. In many cases it is entirely unaffected. The desire for food may be indeed increased, and its ingestion may give a sense of relief. In others vomiting may be severe, while in still others there may be merely a condition of anorexia. The tongue is, as a rule, clean, the skin cool, the temperature undisturbed, and there is absence of tenderness over the epigastrium. Generally pressure relieves the pain.
DIAGNOSIS.—Functional and structural troubles of the stomach very markedly simulate each other; therefore the diagnosis requires to be made with great caution, and this is best done by a most rigid and careful exclusion; and this becomes difficult because the symptoms are mainly subjective.
It is a matter of great moment in differentiating the disease to take into account all constitutional states which predispose to nervous asthenia. Thus in conditions of chlorosis and hysteria the presumption is strong that the pain is neurotic or spasmodic in character; and this presumption is intensified if there be no accompanying constitutional symptoms which indicate inflammatory action. We exclude inflammatory conditions of the stomach by the frequent and complete intermissions, by the absence of thirst, tenderness, and all febrile movement. Moreover, the pain of inflammatory affections, unless produced by corrosive poisons, is rarely so severe as in neuralgic affections; nor are nausea and vomiting so uniformly present in neurotic affections. Then the time at which the pain is experienced is a matter of importance. In inflammatory affections it is felt immediately on taking food. In neurotic affections it may occur when the stomach is empty, and it is not unfrequently relieved by food. In ulcer and cancer of the stomach pain is a common element, and, as in [p. 462] gastralgia, it is referred to the epigastrium. But in gastric ulcer the pain is rarely absent; it is of a dull, gnawing character, is strictly localized in the centre of the epigastrium, and is aggravated by pressure and by food. Moreover, the vomited matter often contains blood. In cancer of the stomach the pain is not as severe and spasmodic in character as in gastralgia, the vomiting is a more prominent symptom, and the material vomited has the characteristic cancerous look. Cancer is more apt to occur too in advanced life, and it is characterized by a steady progressive emaciation.
Gastralgia may also be confounded with rheumatism of the abdominal muscles as well as neuralgia of the inferior intercostal nerves, and it is liable to be confounded with colic resulting from biliary calculi. Colicky pains in the transverse portions of the colon may also be mistaken for pains in the stomach. "It is no exaggeration to say," says Trousseau, "that in perhaps half the cases which are called gastralgia the affection is nothing more than cholalgia." The more fixed the pain is to one spot, and the nearer it is to the median line, the greater is the probability of its being gastric.
PROGNOSIS.—Notwithstanding the severe and apparently alarming nature of the symptoms, the prognosis of gastralgia is in the main favorable, although the prospect of a permanent and speedy cure is small. The duration of the disease depends on the nature and persistence of the exciting causes, and these are so often associated with an exhausted state of innervation that speedy recovery from the disease cannot be promised. In the simpler varieties, caused by improper food, the disease will disappear by removing the cause, and the hysterical forms are liable to disappear with advancing life. So also cases arising from malaria, anæmia, chlorosis, uterine disease, rheumatism, and gout may be relieved by removing the cause. But there are cases produced by unknown causes, and especially cases associated with a general and unexplained cachexia, in which the prognosis is not good.
TREATMENT.—This is both radical and palliative. The radical treatment must have reference to the diseases which have given rise to it. If, for instance, the gastralgia can be traced to sympathetic disturbances of the uterine organs, no remedy can be permanently effective until the cause is removed. Since chlorosis and anæmia are so often found associated with it, benefit may be expected from the ferruginous preparations in some form. Iron occupies a prominent place as a remedial agent. The precipitated carbonate is to be preferred on account of its peculiar influence over the nervous system, and especially over painful neuralgic conditions. It may be given in drachm doses, or even larger, combined with ginger or aromatic powder. If the stomach will not tolerate it, other preparations may be tried.
Quinia is a valuable addition to iron, and it is specially valuable in cases of suspected malarious origin. Sometimes a few large doses will break up the paroxysmal pains as no other agent will.
In the more chronic forms of the disease arsenic is one of the most reliable remedies we possess. It has a well-deserved reputation in the treatment of a great variety of nervous affections, and in none more than in the disease now under consideration. It should be given for a length of time—three or four minims of Fowler's solution, gradually increased and [p. 463] given immediately after food—and in cases of anæmia it should be associated with iron.
In irritable, broken-down conditions of the nervous system nux vomica, or its alkaloid strychnia, is a useful remedy. But it is a powerful stimulant to the spinal nerve-centre, and care should be used in the too protracted use of the remedy or in its administration in too large doses. It may be combined with the phosphate or the valerianate of zinc, or either may be given separately. The nitrate and oxide of silver have also been used with asserted success. Nitrate of silver may be given in pill form with opium.
If there is a strong hysterical element, the bromides and antispasmodics may be tried in connection with remedies calculated to strengthen the nervous system. The judicious employment in such cases of hydro-therapeutic measures is of great value. Good results are also obtained from electricity. The constant current should be preferred.
Among palliative remedies—i.e. remedies that act directly on the painful gastric nerves—the subnitrate of bismuth has long been regarded with great favor. Its action is mainly local; it may be given, therefore, in drachm doses or more three or four times a day. If there is nothing to contraindicate its use, aconite or dilute hydrocyanic acid may be given with the bismuth.
For the immediate relief of pain, however, there is no substitute for opium. The subcutaneous injection of morphia will generally give immediate relief. But there are many reasons why we should try other palliative remedies. In a disease so painful in character a remedy that gives such prompt relief is liable to abuse. The formation of the opium habit should be carefully guarded against. Spirits of chloroform may be tried, therefore, as a substitute for opium, followed by large draughts of hot water—hot as the patient can possibly sip it. Hot water of itself often gives immediate relief.
An important part of the treatment consists in well-regulated hygiene. Change of air, travel, pleasant mental surroundings, together with carefully regulated diet, are in a majority of cases more efficacious than drugs.
Reasoning from the great functional activity of the stomach, from its daily periodical change of blood-supply, from its extensive glandular arrangement, and from its important relations to the functions of vegetative and animal life, we might readily infer that it would be frequently the seat of acute and destructive inflammation. But it is remarkable, all things considered, how seldom that is the case. Indeed, acute spontaneous inflammation of the stomach is almost unknown. When it occurs it most frequently results from toxic causes. In less severe forms, however, not attended with immediate danger to life, it is undoubtedly a disease of frequent occurrence, and in this more comprehensive sense the subject will be considered in the present section.
The mucous membrane alone is usually the seat of the disease, and for this reason it has become the custom of late years to describe it as gastric [p. 464] catarrh. This may be objectionable, for the reason that it does not include gastric inflammation of every grade of intensity. The term catarrh is generally applied to much more simple anatomical structures than those pertaining to the stomach. We shall consider the subject therefore under two forms—namely, (1) Catarrhal; (2) Erythematous gastritis.
ETIOLOGY.—Certain conditions predispose to the disease. Acute catarrhal gastritis is specially liable to occur in those who habitually suffer from a disordered stomach. This may arise from functional disturbance of the digestive process on the one hand, or mechanical obstruction on the other. Mechanical causes are widespread in their influence. Thus, weak heart-action from any cause tends to disturb the normal adjustment between the two sides of the circulation—arterial and venous. An abnormal amount of blood accumulates on the venous side of the circulation, and chronic passive hyperæmia of the abdominal viscera is the result. The effect of this upon the stomach is to lower its functional activity and to invite inflammatory action. The same condition results from structural diseases of the heart, lungs, or liver. Persons suffering from valvular diseases of the heart, emphysema of the lungs, or cirrhosis of the liver are strongly predisposed to diseases of the stomach. Gastric troubles are also apt to supervene during the progress of various diseases.
Gouty and rheumatic persons are specially prone to suffer from gastric catarrh; and eruptive disorders, such as scarlatina, diphtheria, etc., tend to erythematous forms of gastric inflammation. Catarrhal gastritis is also a very common sequence of the whole class of malarious fevers, including yellow fever, intermittents, and remittents. In its more acute form gastric inflammation supervenes in the course of yellow fever; and what is observed here in an extreme degree exists in a minor degree in all the so-called malarious fevers. Intermittent and remittent fevers are always attended with gastro-duodenitis and gastro-hepatitis. The degree of this inflammatory complication determines the continued character of the fever. Upon this point the writer has very decided views based upon a wide field of observation in malarious regions of country. We have lost ground in the treatment of these diseases by directing our attention almost exclusively to the febrile and malarious, to the exclusion of the inflammatory, elements. Quinia is inoperative in the cure of these troublesome and often fatal complications. Indeed, it is more than that: it is often positively injurious. Arrest the local phlegmasia and secure freedom of abdominal circulation, and we at once get the action of the specific remedy. It may be going too far to affirm, as did Broussais, that gastritis sustains a causative relation to all forms of fever, but that gastro-duodenitis is an important secondary condition in all forms of malarious fever, complicating and perpetuating the febrile state, there can be no doubt; and it is equally clear that it constitutes one of the most dangerous complications. Excessive alimentation, with the injudicious use of tonics and stimulants, so often resorted to in the treatment of these fevers in their early stages, only serves to intensify the local inflammation. Abolish the congestive and inflammatory element of a remittent, and it at once becomes an intermittent.
Mention has been made of weak heart-action as a factor in catarrhal [p. 465] gastritis; also mechanical impediments to the return of blood from the stomach to the heart. The stomach is thereby kept in a constant state of congestion, the nutrition of the mucous membrane is less active than in health, and its solvent juices are more sparingly secreted. Thus in long-continued congestion produced by mitral disease of the heart Samuel Fenwick found the formation of pepsin impaired. He made artificial gastric juice from the mucous membrane of three males dying of heart disease, and he found, on the average, only 2-9 grs. of albumen were dissolved, whereas the amount digested by the mucous membrane of persons who had died of other maladies was 4 grains. In the cases of three females a still smaller amount of solvent power was displayed. These facts have important bearings upon the question of alimentation in fevers and the conditions in which there is chronic congestion on the venous side of the circulation. Long-continued passive hyperæmia of the stomach from any cause not only impairs its functional activity, but strongly predisposes to inflammatory complication.
Acute erythematous gastritis is most frequently met with in children. It is a very common form of disease in early life, and the local nature of the malady is frequently overlooked. Few questions in practical medicine are more embarrassing to the physician. It has been known and described as gastric and remittent fever, as continued typhoid, and even as acute hydrocephalus. Writers and teachers describe and dogmatize, while practical men hesitate at the bedside. There is little doubt but in the background of these febrile manifestations in children there is often an acute erythematous gastritis, which is more successfully treated by a rigid milk diet, small doses of calomel and bismuth, mucilaginous drinks, cooling saline laxatives, and sometimes leeches applied to the epigastrium, than by the heroic doses of quinia so frequently resorted to.
We must not, in this connection, lose sight of the fact, so clearly pointed out by Broussais, that inflammation of the stomach is often secondarily repeated in the brain. The whole field of clinical observation abounds in illustrations of this. How often, for instance, we can trace the sick headache, the delirium, and even convulsive movements of the voluntary muscles, to primary gastro-intestinal irritation! In the play of the sympathies morbid irritative action is transmitted from the organic to the cerebro-spinal nerves; and of all portions of the abdominal viscera the stomach and upper portion of the intestinal track are the most frequent seat of these intense morbid sympathies. Remedies which cool the stomach and lessen inflammatory action diminish the excitement of the brain, and vice versâ.
EXCITING CAUSES.—Among the direct exciting causes of gastric inflammation—exclusive of acrid or corrosive poisons—the most frequent in this country is the excessive use of alcohol. It acts most injuriously when it is but slightly diluted and taken on an empty stomach. And next to this pernicious habit, in the order of importance, is the use of large quantities of food—more than the stomach has capacity to digest, and more than is necessary for the wants of the system. Excessive alimentation is a prolific source of gastric inflammation. It generally manifests itself, however, in a chronic or subacute form.
Acute erythematous gastritis, so frequently met with in children, is [p. 466] often present in scarlatina. It is evidently not catarrhal in character, for in the earlier stages there is no increased secretion of mucus and but little injection of the mucous membrane. The changes are observed in the deeper structures of the stomach, and principally in the gastric tubules. They are much distended by granular, fatty, and albuminous matter; and in this respect it is analogous to erythematous affections of the skin with which it is associated in scarlatina.
Finally, acute gastric catarrh may be excited by all causes that weaken the digestive power either by weakening the gastric juice or by retarding the movements of the stomach.
ANATOMICAL CHARACTERS.—No disease requires more knowledge and caution in determining post-mortem changes than those of the stomach. In the first place, it presents in inflammatory conditions markedly different degrees of intensity, with corresponding differences in anatomical changes. Its diseases also present many special forms, and changes take place after death which simulate morbid processes during life. Moreover, intense vascular injections are apt to disappear in the small superficial vessels after death. This applies to all mucous membranes, but specially to the mucous membrane of the stomach, which is the seat of varying amounts of blood in their physiological limits during life. For this reason the observations of Beaumont made upon a living subject are invested with peculiar interest. It will be remembered that in the case of Alexis St. Martin the appearances noted were such as belong to the milder forms of inflammation. Beaumont noticed in this case, after indiscretions in eating or abuse of ardent spirits, a livid erythematous redness of the gastric mucous membrane, with, at the same time, dryness of the mouth, thirst, accelerated pulse, and, at the height of the injection, an entire absence of gastric secretion. At other times there was considerable muco-purulent matter, with oozing of grumous blood, "resembling the discharge from the bowels in cases of chronic dysentery." The fluid taken out through the fistulous opening consisted mostly, however, of mucus and muco-pus which showed an alkaline reaction. He describes also a condition of ecchymosis and oozing of blood from certain red spots of the gastric mucous membrane, and when thus limited the constitutional symptoms experienced by the patient were correspondingly slight. Ecchymoses may be present in large number, with exudates of false membrane, which Beaumont describes as aphthous. Brinton also describes a severe form of gastritis which he terms ulcerative, in which he observed hemorrhagic erosions.
In the catarrhal form of gastritis the mucous membrane is covered with a thick, tenacious, stringy mucus; it is softer than usual, and generally thickened. It presents at the same time a dead-white appearance, corresponding to Virchow's cloudy swelling—a condition analogous to that which is observed in acute Bright's disease. Even casts of the tubes are sometimes met with.
This inflammatory change in the substance of the mucous membrane is especially observed in the acute erythematous form of gastritis complicating scarlatina. In the early stage there is no increased secretion of mucus, and at a more advanced stage the membrane may be even paler than usual.
In cases of acute toxic gastritis intense redness is seen over the entire [p. 467] surface of the mucous membrane, followed by rapid exudations and sloughing of portions of the membrane.
In all forms of the disease there is a tendency to extension of the inflammation into the duodenum and small intestines. In the more chronic forms we almost invariably encounter the condition of gastro-duodenitis.
SYMPTOMS.—The symptoms of inflammation of the stomach present wide differences in their intensity, depending upon the degree of severity in different cases. In acute inflammation caused by the direct action of poisonous irritants they are pronounced and highly diagnostic. The patient immediately complains of burning pain, referred to the epigastrium, followed by intense thirst and vomiting. The thirst is apt to be very great and the act of vomiting painful. The vomited matters contain mucus, saliva, sometimes bile, and not unfrequently, in fatal cases, black, grumous, coffee-ground material. There is marked tenderness on pressure, the pulse is frequent and small, coldness of the surface is marked, and hiccough is apt to occur. The expression of the patient is anxious, the abdominal muscles rigid, and, in fatal cases, the prostration becomes rapidly extreme. The patient dies by asthenia. These symptoms apply to acute cases of marked severity, usually of toxic origin.
In the milder forms of catarrhal gastritis more frequently met with there is seldom complaint of pain. The sensation is rather that of fulness, uneasiness, with more or less tenderness on pressure. The symptoms are such as belong to acute indigestion and the embarras gastrique of French authors. The phenomena may be those of a slight bilious attack. The tongue is foul, the breath offensive, the bowels confined, and the urine high-colored and scanty. There is also generally a sense of fatigue, and soon secondary cerebral symptoms supervene, such as cerebral hyperæmia, headache, vertigo, noises in the ears, palpitation, sighing, yawning, dyspnoea, faintness, and in severe cases marked physical and mental depression. Nausea and vomiting are common, and if the inflammation extends to the duodenum and liver, symptoms of gastro-hepatic catarrh manifest themselves. If fever supervenes, urticaria sometimes complicates these attacks.
In young children the inflammation is apt to involve a general catarrh of the whole intestinal track. Thirst is excessive, followed by vomiting and diarrhoea. The discharges are liquid, watery, offensive, acid, and out of all proportion to the amount of fluid absorbed by the stomach. The pulse becomes weak and fluttering, the skin pale, the features pinched, the eyes sunken, and the extremities cold. The tendency is toward rapid collapse and fatal issue. The symptoms describe what is usually known as cholera infantum. It has its analogue in the cholera morbus of adults.
In erythematous gastritis nausea and vomiting are as general as in the catarrhal form, but, unlike the catarrhal, pain at the epigastrium is a prominent symptom. It comes on directly after taking food. In phthisical cases the sensation is rather that of rawness of the oesophagus and stomach. Thirst is a troublesome symptom; the tongue is red or dry and glazed; tenderness of the epigastrium is marked; diarrhoea is generally present; and, as in the catarrhal form, the stools are fetid and unhealthy. The disease shows a marked tendency to become chronic.
[p. 468] DIAGNOSIS.—In the more acute forms of the disease the symptoms are all highly diagnostic. Vomiting, burning pain of the stomach, tenderness on pressure, intense thirst, with frequent and small pulse, point with almost unerring certainty to acute gastric inflammation. But vomiting of itself, however persistent, is not evidence of gastritis, for it may be present from many other causes. If the vomiting be attended by headache, it may be confounded with gastric irritability from brain disease. Thus, chronic meningitis with persistent vomiting strongly simulates gastritis, and in the case of children it is liable to be mistaken for it. In gastritis the nausea is from the first a pronounced feature of the disease. Vomiting in affections of the brain is often unattended by nausea. In gastritis the tongue is more frequently coated or red and glazed. Diarrhoea is also more frequently present, especially in early life. In affections of the brain the tongue may be clean and the bowels are usually obstinately confined. When there is much fever, gastritis may be confounded with remittent or typhoid fever. In periods of childhood this mistake is specially liable to occur, for there are many symptoms in common. In all such cases the early history of the case ought to be carefully inquired into. In gastritis we may be able to detect the cause in any particular case. The gastric symptoms are apt to occur suddenly, and, as already stated, are prominent from the first. In meningitis the skin is more frequently dry; in gastric catarrh perspirations are common. The more prominent and characteristic symptoms of typhoid should also be carefully excluded, such as the gradual invasion, peculiar eruption, bronchial catarrh, enlargement of the spleen, gurgling in the right iliac fossæ, with tympanitic abdomen. Peritonitis, with vomiting, may be mistaken for gastritis, but the diffuse tenderness, the fixedness of position, the rigidity of the abdominal muscles, and the tympanitic distension serve to guide us in our diagnosis.
PROGNOSIS.—The prognosis must have reference to the cause. The more violent forms of the disease resulting from corrosive poisons are generally fatal. Death is apt to take place in a few hours from a condition of collapse. The immediate cause of death is failure of heart-action. It is also a dangerous disease in the extremes of life. In its acute form in children it is apt to terminate fatally, especially if it is not recognized early and judiciously treated. The complications of the disease may also render the prognosis unfavorable. Milder cases tend to recovery.
TREATMENT.—The most important indication of treatment, applicable to all forms of gastric inflammation, is to secure complete or partial rest for the inflamed organ. In dangerous cases no food should be taken into the stomach. The patient should be nourished exclusively by nutrient enemata. If food is permitted, it should be restricted to milk and lime-water, administered in small quantities at short intervals. In acute and dangerous cases, suddenly manifesting themselves, the exciting cause should be carefully inquired into, and speedily removed, if possible, by an emetic, or, if need be, by the stomach-pump, if the poison be one which can be ejected; and following this antidotes are to be administered according to the nature of the poison.
To allay the intense thirst small pieces of ice should be swallowed at frequent intervals, or, what is often more grateful to the patient, iced [p. 469] effervescing drinks in small doses oft repeated. Injections of water may also tend to relieve thirst. To allay vomiting the physician is often tempted to try a great variety of remedies which are usually worse than useless, for they aggravate rather than relieve the distressing symptom. For the purpose of quieting the stomach opium is the most reliable remedy we possess. It is best administered hypodermically. Fomentations may be applied over the epigastrium. Stimulants are, of course, contraindicated on account of their irritating action on the inflamed membrane, but in case of rapid tendency to death by failure of heart-action they should be administered by the rectum or hypodermically.
In milder cases—which are much the more common—physiological rest of the organ is also a cardinal principle of treatment. Rest of the body is equally essential. In cases of any severity the patient should be kept quiet in bed. For the condition of acute indigestion known as embarras gastrique ipecacuanha in six- or eight-grain doses, given three times within twenty-four hours, will often produce healthy bilious stools, and in this manner accomplish the cure. One or two grains of calomel may be added to each dose of ipecacuanha with benefit. In all forms of catarrhal gastritis, especially if symptoms of portal congestion are present, mild mercurial cathartics are attended with benefit. Six or eight grains of calomel may be rubbed up with sugar of milk and placed dry on the tongue, followed by a cooling saline aperient. When diarrhoea is present in such cases, it should be regarded as conservative, and encouraged by the administration of half-grain or grain doses of calomel, combined with bismuth and bicarbonate of soda. The diet should be restricted to milk and lime-water or milk mixed with Vichy or Seltzer water. Demulcent drinks should be freely given. In the slighter attacks effervescing drinks are grateful to the patient; and if there be excessive formation of acid in the stomach, antacids and sedatives should be administered.
Bismuth has a peculiar sedative and antiseptic effect in the milder forms of inflammatory action of mucous membranes. It is especially valuable in gastro-intestinal troubles of children. Its action is mainly local surface action, and may therefore be given in liberal doses if necessary. Children may take from five to ten grains, and adults twenty grains or more. Hydrocyanic acid adds to its sedative qualities, or when pain is present, with diarrhoea, opium in some form may be added. The salicylate of bismuth is specially indicated when we want to add to the antiseptic qualities of bismuth.
The general principles of treatment indicated here are applicable to the so-called remittent fevers of children—namely, calomel in small doses, combined with bismuth and bicarbonate of soda, followed by occasional cool saline laxatives. Ipecacuanha is also a valuable agent in correcting morbid gastro-intestinal secretions. When there is early epigastric tenderness, with hot skin and elevation of temperature, two or three leeches should be applied to the epigastrium, followed by warm poultices of linseed meal. Dry cupping may also be used with benefit; and if decided remissions occur, with suspicions of a complicating malarious element, a few liberal doses of quinia may be tried. In many such cases, however, it will be found unnecessary, and not unfrequently hurtful. In acute gastro-intestinal inflammations of children—the [p. 470] temperature reaching 105° or more—no febrifuge, in the opinion of the writer, is equal to the cool or cold bath, repeated from time to time until there is a decided reduction of temperature. But the gastric inflammation, rather than the fever, should mainly claim our attention.
Great care is necessary during convalescence from acute gastric disease, particularly as regards the hygienic management. The apparent debility of the patient too often tempts the physician to the early and injudicious use of tonics, stimulants, and excessive alimentation, which, if persisted in, can scarcely fail to perpetuate a chronic form of inflammatory action.
There is perhaps no malady more frequently met with than chronic gastric catarrh, and none more frequently misunderstood. It comprises many different forms of gastric derangement, which are grouped under the general head of inflammatory dyspepsia, with many symptoms strongly simulating ordinary functional dyspepsia. It includes, in the author's opinion, a large number of cases of obstinate chronic dyspepsia, which are badly managed because not recognized as of inflammatory origin.
ETIOLOGY.—In a more or less chronic form it is frequently met with as a result of the acute affections. Hence the etiology is mainly that of acute gastric catarrh. It may be caused—
1. By functional disorders of the stomach.
2. By mechanical causes which interfere with the portal circulation.
3. In connection with certain constitutional states, such as gout, rheumatism, phthisis, renal disease, certain eruptive diseases, and as a sequence of malarious fevers.
4. By the excessive use of alcohol and other gastric irritants.
5. By errors of diet, especially excessive alimentation.
6. By decomposition of ingested aliment owing to deficiency of gastric juice.
7. By all causes that weaken the digestive power and lower the general tone of the system.
Of all these causes, errors of diet are most apt to produce it, and to perpetuate it when once established. And next to this, in the order of importance, is the immoderate use of alcohol, especially by persons whose general health and digestive power are below a healthy standard. Such persons are apt to suffer from irritative and inflammatory forms of dyspepsia, which, in various degrees of intensity, alternate with the acuter forms of embarras gastrique.
The injudicious use of drugs may also be mentioned. There can be no doubt that many transient and functional forms of indigestion merge into the more chronic inflammatory forms of dyspepsia from the abuse of stimulants, tonics, and purgatives. Anxious for relief, and urged on by hope of recovery, the victims of functional dyspepsia are apt to have recourse to every grade of quacks and to be subjected to every form of harassing and mischievous treatment. Indeed, the use of potential and irritating drugs, administered for all kinds of ailments, real or imaginary, enters largely into the etiology of chronic gastric catarrh.
Mechanical causes deserve also special consideration. These are mainly [p. 471] such as offer impediment to the return of blood from the stomach to the heart. In acute cases the congestion may be very intense. Congestion of the same kind, but more gradual in its occurrence and less in degree, may be present from all conditions affecting the circulation of venous blood through the liver. General anæmia, by producing weak heart-action, disturbs the normal adjustment between the arterial and venous sides of the circulation. Blood accumulates in the veins and capillaries, and morbid action propagates itself in a direction contrary to the circulation. Hence in all conditions of general anæmia there is tendency to dyspnoea, pulmonary oedema, bronchorrhoea, special forms of liver disease, gastric catarrh, and even temporary albuminuria. All mechanical obstructions to the free transit of blood through the heart, lungs, or liver are followed by the same results. A free secretion of mucus into the stomach is one of the most commonly recognized. It is often vomited in large quantities. This alkaline mucus, while it dilutes the digestive juices of the stomach, furnishes favorable conditions for the development of low micro-organisms, which contribute to the fermentative process. We may not duly estimate the effects of these organisms on a mucous membrane softened by long-continued passive hyperæmia.
Malarious fevers, from their congestive tendency, give rise to the more acute forms of gastro-enteric inflammation. In the more chronic forms of intermittent and remittent fevers more or less gastric inflammation is invariably present. Indeed, in all forms of fever gastric inflammation is a complicating element, and the recognition of the fact has an important bearing on the treatment.
Certain constitutional diseases appear to involve special liability to this affection, such as scrofula, phthisis, gout, rheumatism, syphilis, and many chronic forms of skin disease; and in many cases the cause is not apparent.
ANATOMICAL CHARACTERS.—The gross appearance of the stomach in chronic gastritis is thus admirably described by Broussais, who faithfully recorded what he "observed during many years in the bodies of those who have long suffered from distaste for food, nausea, and vomiting." These observations were made long before morbid anatomy had thrown much light on the more minute structural changes of organs, and the general picture will be recognized as faithful to-day: "Softening, friability, and the reduction into a kind of gelatinous mass commonly occurs in the region of the lower part of the larger curvature of the stomach; and when closely examined it is perceived that it is not only the mucous membrane that has undergone that species of decomposition, but that the muscular has participated in it, and that the whole of the cellular tissue which united the three membranes has entirely disappeared. The parietes of the viscus are then reduced to a very thin lamina of serous membrane, commonly so fragile as to tear on the slightest handling, or even already perforated without any effort on the part of the anatomist. The pyloric region, on the contrary, has manifestly acquired more consistence and thickness; the mucous membrane there presents large folds, the muscular appears more developed, and the cellular and vascular are injected; sometimes even a true scirrhous state is observed there. The portion of the mucous membrane which covers this scirrhus is sometimes [p. 472]ulcerated, but that in the surrounding parts and at the border of the ulcer, far from being softened, is, on the contrary, tumefied, indurated, and injected. Finally, though there may or may not be ulceration of the pylorus, it is always manifestly hypertrophied, whilst the lower part of the great curvature is the seat of softening and atrophy."
These were the observations of the great anatomist apparent to the naked eye. At the present time we can only confirm them by stating that structural changes are particularly noticed in the pyloric region of the stomach. The mucous membrane generally is vascular and covered with a grayish, tough, transparent mucus. It is more opaque and thicker than natural. The surface is usually changed in color: it may be red, brown, ash-gray, slate-colored, or even black in spots. The darkened spots are due to pigmented matter, and this is generally most marked in the pyloric half of the stomach. It is most commonly met with in cases of prolonged passive congestion of the stomach from portal obstruction, and requires for its production the rupture of capillaries in the superficial layers of the membrane and the transformation of the hæmatin into pigment. The same condition often produces ecchymoses and hemorrhagic erosions in spots. In other cases the mucous membrane is strikingly uneven, being studded with numerous little prominences separated from each other by shallow depressions or furrows. This condition, which has been compared to granulations upon wounds, is called mammillation. It is the état mamelonne of Louis, and is considered by him as a sure and constant sign of inflammatory action. Like many other structural changes, it is usually found in the neighborhood of the pylorus. More rarely polypoid growths project from the membrane, and little cysts also frequently appear in the mucous membrane.
Chronic inflammation tends to thickening of the mucous membrane. It sometimes is not only greatly thickened, but acquires an extreme degree of toughness. Exceptionally, however, the membrane, either entire or in spots, may be abnormally thin. The thickening of the walls of the stomach, when it involves the pylorus, gives rise to constriction of the orifice and consequent dilatation of the stomach.
When the disease has been of long standing the interstitial tissue between the tubules becomes thickened, the stomach is changed in its normal structure, and the tubules themselves become confused, compressed, and much less straight and parallel than in the normal state. Or they may in some cases be enlarged, according to Flint, in consequence of swelling and parenchymatous or fatty degeneration of their epithelial cells. Microscopic examination often shows changes such as occur in other glandular organs. The glands and tubules become the seat of degenerative changes, such as are observed in Bright's disease of the kidney, and they are frequently found associated in the same case. The mouths of the gastric tubules become blocked up, while deeper parts are dilated into cysts; and at times they are atrophied or filled with granular fatty matter.
Many cases of persistent anæmia may be traced, according to Flint, to this degenerative process of the gastric tubules.
The SYMPTOMS of chronic gastritis are mainly those of difficult digestion of an aggravated kind, and are liable to be mistaken for those of [p. 473] ordinary functional dyspepsia. Some points of distinction were referred to in the section treating of functional dyspepsia; and while there are many symptoms in common, it is vastly important that the two forms of the disease should be early recognized, for they are radically distinct in their pathology and treatment.
We now speak of what is usually known as inflammatory, irritative, or gastric dyspepsia—a persistent and aggravated form of indigestion which has its origin in the stomach itself, in contradistinction to dyspepsia which originates largely from causes outside of the stomach and transmitted to it through nervous impression. The one is functional and indirect; the other is inflammatory and direct.
The symptoms referable directly to the stomach are mainly those of difficult and painful digestion, and are alike characteristic of all forms of indigestion, such as loss of appetite, sense of weight and fulness of the epigastrium, distress after taking food, acidity, eructations of gas, etc. But chronic gastritis is more frequently accompanied by a burning sensation in the epigastric region, accompanied by tenderness on pressure, which is generally increased after meals. Sometimes this tenderness amounts to actual pain, which is increased after meals. But we are liable to be misled by pain: gastric pain is not a characteristic symptom; subacute forms of the disease may exist without any fixed pain; the sensation is rather that of burning, uneasiness, and oppression of the epigastric region. The appetite, as a rule, is greatly impaired—indeed, the sense of hunger is rarely experienced—and nausea and vomiting frequently follow the ingestion of food. This is especially the case when catarrh of the stomach is associated with renal disease, portal congestion, or chronic alcoholism. Large quantities of mucus are brought up, the vomiting taking place usually in the morning, and on examination of the mucus it will frequently be found to contain sarcinæ and large numbers of bacterial organisms. When stricture of the pylorus is present the vomiting of putrid, half-digested food usually takes place about the termination of the digestive process.
The tongue presents characteristics peculiar to chronic inflammation of the stomach. In some cases it is small and red, with enlarged and red papillæ; in others, it is broad and flabby and somewhat pale; but in either case, on close inspection, the papillæ will be found red and enlarged, this being more apparent on the tip and edges. In children of scrofulous habits and in older persons of tubercular tendency the whole organ is redder than natural, the papillæ standing out as vivid red spots.
In other cases the catarrh of the stomach extends to the mucous membrane of the mouth. In all cases of oral catarrh the tongue, instead of being red and pointed, is large and apparently oedematous. It is uniformly covered with a white or dirty brownish coat, and frequently shows the impression of the teeth upon its edges. The secretions of the mouth are depraved, the breath heavy and offensive, and the gums spongy and unhealthy in appearance. Acidity is also common.
Thirst is a common symptom. It is rarely absent either in the acute or chronic form of the disease. It is most marked in the intervals between meals and in the evenings.
It is rare in gastric catarrh of long standing that it does not extend to the intestines, and occasionally from the duodenum to the ductus [p. 474] choledochus; in which case we have the combined symptoms of gastro-intestinal catarrh associated with jaundice. The nutritive system becomes implicated, and patients are especially prone to develop any diathesis to which they may be liable.
There remains a group of symptoms of great interest in the study of gastric inflammation—important because liable to mislead as to the real nature of the difficulty—namely, morbid conditions of the nervous system. Few diseases have such a wide range of morbid sympathies, and few, it may be added, are so generally misunderstood and misinterpreted. Two main facts, as formulated by Broussais, deserve to be restudied by the profession:
First, that irritations of the visceral parenchyma which do not implicate their serous membranes only give rise to ill-defined sensations, and they not painful;
Second, that most of the acute pains arising from visceral irritation are rather referred to external parts than to the viscera themselves.
Unless the seat of very acute inflammation, mucous membranes are remarkably free from pain, and yet the gastric mucous membrane is the seat of a most exquisite internal visceral sense and has a wide range of morbid sympathetic disturbances. These sympathetic phenomena are often treated for primary neuralgias. No fact in the clinical study of disease deserves more careful consideration than this. Absence of pain, then, is calculated to mislead. It is often only the sensation of uneasiness, depression and melancholy, want of appetite, thirst, nausea, loathing of food, and derangement of the bilious and gastric secretions, that directs our attention to the stomach. Moreover, in gastro-enteric inflammations pain is more frequently felt in parts sympathetically affected than in the stomach itself. "It is only when irritations of mucous membranes are in the vicinity of the openings of cavities that the irritations are distinctly perceptible in the seat they occupy" (Broussais). Morbid irritative action commencing in the stomach repeats itself in the cerebro-spinal system of nerves, and the secondary irritation may develop a more immediately dangerous inflammation than the primary. This is frequently observed in children, who are specially prone to irritation of the visceral apparatus. Many cases of primary gastric irritation terminate in acute cerebral inflammation. Indeed, the greater number of phlegmasiæ of the brain are only sympathetic irritations issuing from primary inflammation of the stomach. Short of inflammation, the transmitted irritation may merely give rise to reflex convulsions, and in adults to sick headache, or, if long continued, to conditions of hypochondria. Headache is a prominent symptom of gastric irritation. It is not usually acute, but rather a sense of fulness and pressure, sometimes felt in the frontal, at other times in the occipital, region. Many cases commonly called cerebral hyperæmia and cerebral anæmia are nothing more than malassimilation from chronic gastric catarrh. This fact deserves to be specially emphasized at present, for we are apt to consider the cerebral the primary lesion. Vertigo, as in functional dyspepsia, is also an occasional symptom, and very commonly patients complain of extreme degrees of sleeplessness and disturbed dreams and nightmare.
The heart's action is often disturbed in its rhythm, and sympathetic dyspnoea leads to suspicion of disease of the lungs. And to all these [p. 475] nervous phenomena may be added unusual languor, lassitude, irritability of temper, and a feeling of inability for either mental or physical exertion.
But in the play of morbid sympathies it must be borne in mind that the stomach may be secondarily affected. Irritations of all organs are constantly transmitted to the stomach from their very commencement. Hence the frequent loss of appetite, the thirst, the embarrassed digestion, the deranged gastric secretion, and the altered color of the tongue. This is markedly the case in all the malarious and essential forms of fever. Gastric complication in these fevers is rarely, if ever, absent, and if aggravated by the too early use of tonics and stimulants and by harsh irritating cathartics, it becomes too often a fatal complication.
Gastric symptoms are also associated with other constitutional disorders, such as phthisis, renal disease, rheumatism, gout, and almost all forms of chronic eruptive diseases.
Intestinal symptoms are rarely absent. Constipation is often obstinate, and especially is this the case if the catarrhal condition is confined to the duodenum. The lower down the inflammation the greater the probability of diarrhoea, and when present the stools are offensive and frothy; sometimes they are dry and scybalous and coated with a tough, tenacious mucus which may form casts of portions of the intestinal track. In other cases patients suffer from distressing intestinal flatulence and a sense of general discomfort. Piles is a complication frequently present without reference to complication of the liver.
The urine is more frequently disordered than in any other form of disturbance of digestion. The most common changes consist in an abundant deposit of the urates; exceptionally, however—especially in cases of long standing in which there are marked nervous symptoms associated with defective secretion of the liver and pancreas—it may be of low specific gravity and pale in color from the presence of phosphates. Slight febrile movement is not uncommon.
Finally, in all cases of chronic gastric catarrh the nutritive system becomes deeply implicated—much more so than in functional disturbances of the stomach. Emaciation is almost constantly present, the patient often showing signs of premature decay.
DIAGNOSIS.—The disease with which chronic gastritis is most liable to be confounded is atonic dyspepsia, the chief points of distinction from which have been already alluded to. In general terms it may be said that in chronic gastritis there is more epigastric tenderness, more burning sensation and feeling of heat in the stomach, more thirst, more nausea, more persistent loss of appetite, more steady and progressive loss of flesh, more acidity, more eructations of gas, more general appearance of premature decay, and greater tendency to hypochondriasis. And yet all these symptoms, in varying degrees of prominence, may be present in all forms of indigestion. To the points of distinction already mentioned, then, a few circumstances may be added which will afford considerable assistance in coming to a correct diagnosis:
1. The length of time the disease has uninterruptedly lasted. It is essentially a chronic disease.
2. The local symptoms are never entirely absent, as is not infrequently the case in functional dyspepsia.
[p. 476] 3. The uneasy sensations, nausea, oppression, or pain, as the case may be, follow the ingestion of food. They are not so prominently present when the stomach is empty.
4. The result of treatment. In chronic gastritis it will be found that all the local symptoms are exasperated by the usual treatment of functional dyspepsia.
5. Stimulants and stimulating food are not well borne. Alcohol, especially on an empty stomach, produces gastric distress. There is also frequently slight febrile disturbance.
Chronic gastritis, with nausea, vomiting, hæmatemesis, general pallor, and loss of flesh, may be mistaken for cancer of the stomach. But in cancer vomiting is about as apt to take place when the stomach is empty as during the ingestion of food; pain is usually greater, especially when the orifices of the stomach are involved; the tenderness is more marked; the emaciation and pallor more steadily progressive; the vomiting of coffee-ground material takes place more frequently; and the disease is more rapid in its progress. The age and sex of the patient may also aid us in our diagnosis. Cancer is more frequently a disease of middle and advanced life, and localizes itself oftener in the stomach of males than females. Finally, the discovery of a tumor would remove all doubts. Hæmatemesis in chronic catarrh of the stomach is almost invariably associated with obstruction to venous circulation in the liver, heart, or lungs.
In rare cases it may be difficult to distinguish chronic gastric catarrh from ulcer of the stomach. In ulcer of the stomach pain is a more prominent and constant symptom; it is more centrally located; the vomiting after taking food is more immediate and persistent; the tongue may be clean; flatulence is not a constant symptom; the appetite is seldom much affected; the bowels are generally confined; and there is nothing characteristic about the urine.
TREATMENT.—In this, as in the more acute forms of the disease, rest of the stomach is important. From mistaken notions of disease we are prone to over-feed our patients, and thus seriously impair the digestive and assimilative processes. In chronic inflammation of the stomach a restricted diet is of prime importance. The physician should most carefully select the patient's food, and urgently insist on its exclusive use. This of itself, if faithfully persevered in, will often effect a cure.
The exclusive use of a milk diet—especially skim-milk—should be thoroughly tested. In testing it we should allow two or three weeks to elapse before any other food is taken. At the end of that time soft-boiled eggs, stale bread, and well-cooked rice may be added, with an occasional chop once a day. Some patients do not tolerate raw milk well. In such cases we should thoroughly test the peptonized or pancreatized milk or the peptonized milk-gruel, as suggested by Roberts. This artificially-digested milk agrees wonderfully well with many stomachs that cannot digest plain milk. Milk, in whatever form administered, should be given at comparatively short intervals of time, and never in quantity beyond the digestive capacity. Better err on the side of under- than over-feeding. Nothing should be left to the fancy or caprice of the patient. The food should be carefully selected by the medical adviser, and given in definite quantities at definite times. Even the moral [p. 477] effect of such discipline is healthful for the patient. After testing milk diet for a time, we may gradually add small quantities of rare and thoroughly minced meat. Milk, eggs, and rare meat are more easily digested, as a rule, than starchy substances. Farinaceous food is apt to give rise to excessive acidity. But stale bread may be added to the milk, and, if there is tendency to acidity, better have it toasted thoroughly brown.
In addition to the dietetic treatment of the disease, diluents, timeously administered, are of essential service. As a rule, patients are too much restricted from their use, under the supposition that they dilute the gastric juice and thereby impair the digestive power. This restriction is proper at, and for some time after, the ingestion of food. But at the end of the first hour after taking food several ounces of gum-water, or some mucilaginous fluid sweetened and rendered palatable by a few drops of dilute muriatic acid, should be administered, and repeated every hour during the digestive process. Diluents, thus administered, are not only grateful in allaying the thirst of the patient, but are at the same time an essential part of the treatment. The free use of demulcents at the termination of digestion in the stomach is especially useful.
Beyond these general principles of treatment, applicable to all varieties of gastric catarrh, we must have reference to the varied etiology of the disease. This, we have seen, is most complicated. Hence the difficulty in prescribing any rules of treatment applicable to all cases. We should seek here, as in all cases, to generalize the disease and individualize our patient.
Chief among remedial agents may be mentioned the alkaline carbonates. When combined with purgative salines they are specially valuable in gastro-duodenal catarrhs associated with disease of the liver. These are a very numerous class of cases, especially in malarious regions of country, and when present in a chronic form lay the foundation of widespread disorders of nutrition. No treatment in such cases is effective until we diminish engorgements of the liver and spleen, and nothing accomplishes this so well as the use of alkaline saline laxatives. These may be assisted in their action by small doses of mercurials. It was a cardinal principle among the older practitioners, in the absence of more minute means of diagnosis, to look well to the secretions; and what was their strength is, I fear, our weakness.
Wonderful results often follow a course of the Carlsbad, Pullna, or Marienbad waters, taken on an empty stomach, fasting, in the morning. While taking the waters a rigid and restricted diet is enforced. This is an important part of the treatment. And the fact that so many varied ailments are cured by a course of these mineral waters with enforced dietetic regulations only shows the prevalence of gastro-duodenal catarrhs and their relation to a great variety of human ailments. To a certain extent the potassio-tartrate of sodium and other saline laxatives may take the place of these waters if perseveringly used and taken in the same way. In feebler subjects minute doses of strychnia or some of the simple vegetable bitters may be used in conjunction with the laxative salines.
In chronic inflammatory conditions of the gastric mucous membrane, which frequently follow acute attacks, the protracted use of hot water is often followed by excellent results. There can be no doubt of the value [p. 478] of hot water in subacute inflammation of mucous membranes in any locality; and it is specially valuable in gastro-intestinal catarrh associated with lithæmia. Hot water, laxative salines, combined with restricted diet and healthful regimen, accomplish much in correcting morbid conditions of primary assimilation; and by accomplishing this many secondary ailments promptly disappear. A pint of water, hot as the patient can drink it, should be taken on an empty stomach on first rising in the morning, and it may be repeated again an hour before each meal and at bedtime. A few grains of the bicarbonate of sodium and a little table-salt may be added. In some cases three or four drops of tincture of nux vomica or some of the simple bitters may be taken at the same time with benefit. Alkaline bitters are natural to the upper portion of the digestive track. No food should be taken for a half hour or an hour after the hot water. This treatment, to be effective, must be persevered in for a length of time. A most rigid system of dietetics suited to individual cases should be enforced at the same time. This is an important part of the treatment.
In irritable and morbidly sensitive conditions of the mucous membrane the sedative plan of treatment is not unfrequently followed by good results; and of remedies belonging to this class bismuth is the most effective. It is specially indicated in the more irritable forms of gastric disturbance in which there is a sense of uneasiness and pain at the epigastrium after taking food. If there is much acidity present, it may be combined with magnesia or a few grains of finely-pulverized animal charcoal.
Chronic cases of long-continued inflammatory action, with intestinal complication, are often much benefited by the use of mercurials in small doses. The one-fifth of a grain of calomel, combined with bismuth or the bicarbonate of sodium, may be given for weeks without danger of salivation. Excellent results sometimes follow this treatment. In small doses calomel is undoubtedly sedative to the mucous membrane of the upper portion of the digestive track. In cases of long standing that have resisted other modes of treatment the more direct astringents have been found of great value. Of these, nitrate of silver is to be preferred, alike for its sedative, astringent, and alterative properties. It may be given in pill form in from one-quarter to one-grain doses, combined with opium, a half hour before each meal. The writer of this article can speak from much experience of the value of this drug. It proves in many cases a valuable addition to the hot-water and dietetic course already alluded to.
If large quantities of mucus are vomited from time to time, especially in the morning, we may resort with benefit to the use of other astringents, such as bismuth, oxalate of cerium, kino, and opium; and if we have reason to suspect stricture of the pylorus in connection with a catarrhal condition of the mucous membrane, the stomach-pump gives the patient great relief. It should be used about three hours after a meal, injecting tepid water, and then reversing the syringe until the water comes out perfectly clear. Niemeyer speaks highly of it in such cases. He says: "Even the first application of the pump generally gives the patients such relief that, so far from dreading a repetition of this by no means pleasant operation, they clamorously beg for it."
The gastric catarrh of phthisis is difficult to relieve. Artificial digestives may be tried, with dilute muriatic acid, as already indicated; and [p. 479] for the relief of pain and irritation there is no remedy so efficacious as hydrocyanic acid, which may be combined with bismuth and opium in case there is diarrhoea. Hot water may be also tried, with restricted animal food.
Habitual constipation must be overcome by suitable laxatives and by enemata. Castor oil is mild and efficient in these cases, or in cases of unusual torpor of the muscular coat of the bowels small doses of aloes and strychnia may be tried. The free use of diluents toward the close of digestion favors free action of the bowels. All harsh and irritating cathartics are to be carefully avoided.
When there is much tenderness of the epigastrium, benefit may be derived from counter-irritation, and nothing is so effectual as the repeated application of small blisters.
General hygienic measures are in all cases to be insisted upon. In morbid conditions of the liver and the upper portion of the digestive track the free supply of oxygen to the lungs is a remedy of much power. Hence patients should live as much as possible in the open air. They should be warmly clad, and, if not too feeble, frequent cold baths should be resorted to.
After local irritation has been subdued by appropriate treatment, tonics may be tried to counteract the enfeebled state of the stomach. They are such as are appropriate for functional diseases of the stomach. But they should be used with caution and judgment in irritable and inflammatory forms of dyspepsia. If we attempt to force an appetite by their use, and to crowd upon the stomach more food than it has capacity to digest, we may intensify the trouble and thereby add to the patient's general debility. Food and tonics fail to impart strength because the stomach is not in a condition to digest them.
One thing should be mentioned, in conclusion, as an important item in the treatment—namely, patience. Chronic gastric catarrh, it should be remembered, is essentially a chronic disease, and time becomes an important element in its cure.
DEFINITION.—Simple ulcer of the stomach is usually round or oval. When of recent formation it has smooth, clean-cut, or rounded borders, without evidence of acute inflammation in its floor or in its borders. When of long duration it usually has thickened and indurated margins. The formation of the ulcer is usually attributed, in part at least, to a disturbance in nutrition and to a subsequent solution by the gastric juice of a circumscribed part of the wall of the stomach. The ulcer may be latent in its course, but it is generally characterized by one or more of the following symptoms: pain, vomiting, dyspepsia, hemorrhage from the stomach, and loss of flesh and strength. It ends frequently in recovery, but it may end in death by perforation of the stomach, by hemorrhage, or by gradual exhaustion.
SYNONYMS.—The following epithets have been employed to designate this form of ulcer: simple, chronic, round, perforating, corrosive, digestive, peptic; ulcus ventriculi simplex, s. chronicum, s. rotundum, s. perforans, s. corrosivum, s. ex digestione, s. pepticum.
HISTORY.—It is only since the description of gastric ulcer by Cruveilhier in the year 1830 that especial attention has been paid to this disease.
In the writings of the ancients only vague and doubtful references to ulcer of the stomach are found (Galen, Celsus). It is probable that cases of this disease were described under such names as passio cardiaca, gastrodynia, hæmatemesis, and melæna.
After the revival of medicine in the sixteenth century, as post-mortem examination of human bodies was made with greater frequency, the existence of ulcers and of cicatrices in the stomach could not escape attention. But only isolated and curious observations of gastric ulcer are recorded up to near the end of the eighteenth century. One of the earliest recorded unmistakable cases of perforating ulcer was observed by John Bauhin, and is described in the Sepulchretum of Bonetus, published in 1679. Other cases belonging to this period were described by Donatus, Courtial, Littré, Schenck, and Margagni.1
1 References to these and to other cases may be found in Lebert's Krankheiten des Magens, Tübingen, 1878, p. 180 et seq.
To Matthew Baillie unquestionably belongs the credit of having first accurately described, in 1793, the anatomical peculiarities of simple gastric ulcer.2 At a later date he published three good engravings of [p. 481] this disease.3 Baillie's concise and admirable description of the morbid anatomy of gastric ulcer was unaccompanied by clinical data, and seems to have had little or no influence in directing increased attention to this disease.
2 The Morbid Anatomy of Some of the Most Important Parts of the Human Body, London, 1793, p. 87.
3 A Series of Engravings, accompanied with Explanations, etc., London, 1799.
A valuable account of the symptoms of gastric ulcer was given by John Abercrombie in 1824.4 Nearly all of the symptoms now recognized as belonging to this affection may be found in his article. He knew the latent causes of the disease, the great diversity of symptoms in different cases, and the modes of death by hemorrhage, by perforation, and by asthenia. He regarded ulcer simply as a localized chronic inflammation of the stomach, and did not distinguish carefully between simple and cancerous ulceration.
4 "Contributions to the Pathology of the Stomach, the Pancreas, and the Spleen," Edinburgh Med. and Surg. Journ., vol. xxi. p. 1, Jan. 1, 1824. See also, by the same author, Pathological and Practical Researches on Diseases of the Stomach, etc.—an excellent work which passed through several editions.
Cruveilhier,5 in the first volume of his great work on Pathological Anatomy, published between the years 1829 and 1835, for the first time clearly distinguished ulcer of the stomach from cancer of the stomach and from ordinary gastritis. He gave an authoritative and full description of gastric ulcer from the anatomical, the clinical, and the therapeutical points of view.
5 J. Cruveilhier, Anatomie pathologique du Corps humain, tome i., Paris, 1829-35, livr. x. and livr. xx.; and tome ii., Paris, 1835-42, livr. xxx. and livr. xxxi.
Next to Cruveilhier, Rokitansky has had the greatest influence upon the modern conception of gastric ulcer. In 1839 this pathologist gave a description of the disease based upon an analysis of 79 cases.6 The anatomical part of his description has served as the model for all subsequent writers upon this subject.
6 Rokitansky, Oesterreich. med. Jahrb., 1839, Bd. xviii. (abstract in Schmidt's Jahrb., Bd. 25, p. 40).
Since the ushering in by Cruveilhier and by Rokitansky of the modern era in the history of gastric ulcer, medical literature abounds in articles upon this disease. But it cannot be said that the importance of these works is at all commensurate with their number or that they have added very materially to the classical descriptions given by Cruveilhier and by Rokitansky. Perhaps most worthy of mention of the works of this later era are the article by Jaksch relating to symptomatology and diagnosis, that of Virchow pertaining to etiology, the statistical analyses by Brinton, and the contributions to the treatment of the disease by Ziemssen and by Leube.7 In 1860, Ludwig Müller published an extensive monograph upon gastric ulcer.8
7 Jaksch, Prager Vierteljahrschr., Bd. 3, 1844; Virchow, Arch. f. path. Anat., Bd. v. p. 362, 1853, and A. Beer, "Aus dem path. anatom., Curse des Prof. R. Virchow in Berlin, Das einfache duodenische (corrosive) Magengeschwür," Wiener med. Wochenschr., Nos. 26, 27, 1857; Brinton, On the Pathology, Symptoms, and Treatment of Ulcer of the Stomach, London, 1857; V. Ziemssen, Volkmann's Samml. klin. Vorträge, No. 15, 1871; Leube, Ziemssen's Handb. d. spec. Path. u. Therap., Bd. vii., Leipzig, 1878.
8 Das corrosive Geschwür im Magen und Darmkanal, Erlangen, 1860. Good descriptions of gastric ulcer are to be found in the well-known works on diseases of the stomach by the English writers, Budd, Chambers, Brinton, Habershon, Fenwick, and Wilson Fox.
ETIOLOGY.—We have no means of determining accurately the average frequency of simple gastric ulcer. The method usually adopted is to observe the number of cases in which open ulcers and cicatrices are found [p. 482] in the stomach in a large number of autopsies. But this method is open to two objections. The first objection is, that scars in the stomach, particularly if they are small, are liable to be overlooked or not to be noted in the record of the autopsy unless special attention is directed to their search. The second objection is, that it is not proven that all of the cicatrices found in the stomach are the scars of healed simple ulcers, and that, in fact, it is probable that many are not. In consequence of these defects (and others might be mentioned) this method is of very limited value, although it is perhaps the best which we have at our disposal.
In 32,052 autopsies made in Prague, Berlin, Dresden, Erlangen, and Kiel,9 there were found 1522 cases of open ulcer or of cicatrix in the stomach. If all the scars be reckoned as healed ulcers, according to these statistics gastric ulcer, either cicatrized or open, is found in about 5 per cent. of persons dying from all causes.
9 The Prague statistics embrace 11,888 autopsies, compiled from the following sources: 1, Jaksch, Prager Vierteljahrschr., vol. iii.; 2, Dittrich, ibid., vols. vii., viii., ix., x., xii., xiv.; 3, Willigk, ibid., vol. li.; 4, Eppinger, ibid., vol. cxvi.
The Berlin statistics are to be found in dissertations by Plange (abstract in Virchow's Archiv, vol. xviii.), by Steiner, and by Wollmann (abstracts in Virchow und Hirsch's Jahresbericht, 1868), and by Berthold (1883).
The Dresden statistics are in a dissertation by Stachelhausen (Würzburg, 1874), referred to by Birch-Hirschfeld, Lehrb. d. path. Anat., Bd. ii. p. 837, Leipzig, 1877.
The Erlangen statistics are reported by Ziemssen in Volkmann's Samml. klin. Vorträge, No. 15.
The Kiel report is in an inaugural dissertation by Greiss (Kiel, 1879), referred to in the Deutsche med. Wochenschr., Feb. 4, 1882, p. 79.
So far as possible, duodenal ulcers have been excluded. Only those reports have been admitted which include both open ulcers and cicatrices.
It is important to note the relative frequency of open ulcers as compared with that of cicatrices. In 11,888 bodies examined in Prague, there were found 164, or 1.4 per cent., with open ulcers, and 373, or 3.1 per cent., with cicatrices. Here scars were found about two and one-fourth times as frequently as open ulcers. The observations of Grünfeld in Copenhagen show that when especial attention is given to searching for cicatrices in the stomach, they are found much more frequently than the figures here given would indicate.10 It would be a moderate estimate to place the ratio of cicatrices to open ulcers at 3 to 1.
10 Grünfeld (abstract in Schmidt's Jahrb., Bd. 198, p. 141, 1883) in 1150 autopsies found 124 cicatrices in the stomach, or 11 per cent., but in only 450 of these cases was his attention especially directed to their search, and in these he found 92 cases, or 20 per cent., with scars. Grünfeld's statistics relate only to persons over fifty years of age. Gastric ulcer, moreover, is extraordinarily common in Copenhagen.
The inexact nature of the ordinary statistics relating to cicatrices is also evident from the fact that in the four collections of cases which comprise the Prague statistics the percentage of open ulcers varies only between 0.81 and 2.44, while the percentage of cicatrices varies between 0.89 and 5.42.
The statistics concerning the average frequency of open ulcers are much more exact and trustworthy than those relating to cicatrices. It may be considered reasonably certain that, at least in Europe, open gastric ulcers are found on the average in from 1 to 2 per cent. of persons dying from all causes.11
11 If in this estimate were included infants dying during the first days of life, the percentage would be much smaller.
It is manifestly impossible to form an accurate estimate of the frequency of gastric ulcer from the number of cases diagnosed as such [p. 483] during life, because the diagnosis is in many cases uncertain. Nevertheless, estimates upon this basis have practical clinical value. In 41,688 cases constituting the clinical material of Lebert12 in Zurich and in Breslau between the years 1853 and 1873, the diagnosis of gastric ulcer was made in 252 cases, or about 2/3 per cent.
12 Lebert, op. cit., p. 196.
Of 1699 cases of gastric ulcer collected from various hospital statistics13 and examined post-mortem, 692, or 40 per cent., were in males, and 1007, or 60 per cent., were in females. The result of this analysis makes the ratio 2 males to 3 females.
13 These statistics include the previously-cited Prague, Berlin, Dresden, and Erlangen cases so far as the sex is given, and in addition the returns of Rokitansky, op. cit.; Starcke (Jena), Deutsche Klinik, 1870, Nos. 26-29; Lebert, op. cit.; Chambers, London Journ. of Med., July, 1852; Habershon, Dis. of the Abdomen, 3d ed.; Moore, Trans. of London Path. Soc., 1880; and the Munich Hospital, Annalen d. städt. Allg. Krankenh. zu München, vols. i. and ii.
Only series of cases from the post-examinations of a number of years have been admitted. It is an error to include isolated cases from journals, as Brinton has done, because an undue number of these are cases of perforation, which is a more common event in females than in males. Thus, of 43 cases of gastric ulcer presented to the London Pathological Society since its foundation up to 1882, 19, or 44 per cent., were cases of perforation. In my cases are included a few duodenal ulcers not easily separated from the gastric ulcers in the compilation.
In order to determine from post-mortem records the age at which gastric ulcer most frequently occurs, all cases in which only cicatrices are found should be excluded, because a cicatrix gives no evidence as to the age at which the ulcer existed.
The following table gives the age in 607 cases of open ulcer collected from hospital statistics14 (post-mortem material):
| Age. | 1-10. | 10-20. | 20-30. | 30-40. | 40-50. | 50-60. | 60-70. | 70-80. | 80-90. | 90-100. | Over 100. |
| No. of cases. | 1 | 32 | 119 | 107 | 114 | 108 | 84 | 35 | 6 | ... | 1 |
| Totals. | 33 | 226 | 222 | 119 | 7 | ||||||
From this table it is apparent that three-fourths of the cases are found between the ages of twenty and sixty, and that the cases are distributed with tolerable uniformity between these four decades. The largest number of cases is found between twenty and thirty. The frequency of gastric ulcer after sixty years diminishes, although it remains quite considerable, especially in view of the comparatively small number of those living after that period.
14 The sources of these statistics are the same as those of the statistics relating to sex in the preceding foot-note. The age in the Erlangen cases of open ulcer is given by Hauser (Das chronische Magengeschwür, p. 191, Leipzig, 1883). It is evident that only about two-fifths of the cases could be utilized, partly because in some the age was not stated, but mainly on account of the necessity of excluding scars—a self-evident precaution which Brinton did not take.
The probability that many cases of ulcer included in the above table existed for several years before death makes it desirable that estimates as to the occurrence of the disease at different ages should be made also from cases carefully diagnosed during life, although the diagnosis must necessarily be less certain than that in the post-mortem records. The best [p. 484] statistics of this character which we possess are those of Lebert, from whose work the following table has been compiled:
| Age. | 5-10. | 11-20. | 21-30. | 31-40. | 41-50. | 51-60. | 61-70. |
| No. of cases. | 1 | 24 | 87 | 84 | 34 | 17 | 5 |
| Totals. | 25 | 171 | 51 | 5 | |||
| Per cent. | 9.92 | 67.85 | 20.24 | 1.99 | |||
Of these cases, nearly seven-tenths were between twenty and forty years of age—a preponderance sufficiently great to be of diagnostic value.16
15 Op. cit., p. 199. Of these cases, 19 were fatal, and the diagnosis was confirmed after death. All of the cases were studied by Lebert in hospitals in Zurich and Breslau.
16 In my opinion, clinical experience is more valuable than are post-mortem records in determining the age at which gastric ulcer most frequently develops. In support of this opinion are the following facts: In many cases no positive conclusions as to the age of the ulcer can be drawn from the post-mortem appearances, and sufficient clinical history is often wanting; a considerable proportion of the cases of gastric ulcer do not terminate fatally with the first attack, but are subject to relapses which may prove fatal in advanced life; in most general hospitals the number of patients in advanced life is relatively in excess of those in youth and middle age. By his faulty method of investigating this question, Brinton came to the erroneous conclusion that the liability to gastric ulcer is greatest in old age—a conclusion which is opposed to clinical experience.
The oldest case on record is the one mentioned by Eppinger,17 of an old beggar whose age is stated at one hundred and twenty years.
17 Prager Vierteljahrschrift, Bd. 116.
The occurrence of simple ulcer of the stomach under ten years of age is extremely rare. Rokitansky, with his enormous experience, said that he had never seen a case under fourteen years.18 There are recorded, however, a number of cases of gastric ulcer in infancy and childhood, but there is doubt as to how many of these are genuine examples of simple ulcer. Rehn in 1874 analyzed a number, although by no means all, of the reputed cases, and found only six, or at the most seven, which would stand criticism.19 The age in these seven cases varied between seven days and thirteen years. In one case (Donné) a cicatrix was found in the stomach of a child three years old. Since the publication of Rehn's article at least four apparently genuine cases have been reported—namely, one by Reimer in a child three and a half years old; one by Goodhart in an infant thirty hours after birth; one by Eröss in a girl twelve years old suffering from acute miliary tuberculosis, in whom the ulcer perforated into the omental sac; and one by Malinowski in a girl ten years of age.20
18 Communication to Von Gunz in Jahrbuch d. Kinderheilkunde, Bd. 5, p. 161, 1862.
19 Jahrb. d. Kinderheilk., N. F., Bd. 7, p. 19, 1874.
20 Reimer, ibid., Bd. x. p. 289, 1876; Goodhart, Trans. London Path. Soc., vol. xxxii. p. 79, 1881; Eröss, Jahrb. f. Kinderheilk., Bd. xix. p. 331, 1883; Malinowski, Index Medicus, vol. v. p. 575, New York, 1883.
Rehn does not mention Buzzard's case of perforating ulcer in a girl nine years old (Trans. London Path. Soc., vol. xii. p. 84, 1861). See also Chvostek's case of round ulcer in a boy (Arch. f. Kinderheilk., 1881-82) and Wertheimber's case of recovery from gastric ulcer in a girl ten years old (Jahrb. f. Kinderheilk., Bd. xix. p. 79).
The mean age at which gastric ulcer develops is somewhat higher in [p. 485] the male than in the female. This is apparent from the following collection of 332 cases of open ulcer in which both age and sex are given:21
| Age. | 10-20. | 20-30. | 30-40. | 40-50. | 50-60. | 60-70. | 70-80. | 80-90. | 90-100. | Over 100. | Total. |
| Males. | 9 | 33 | 44 | 39 | 37 | 20 | 5 | 1 | ... | 1 | 189 |
| Females. | 13 | 35 | 25 | 25 | 18 | 18 | 9 | ... | ... | ... | 143 |
In males the largest number of cases is found between thirty and forty years, and in females between twenty and thirty. In males 54½ per cent. of the cases occur after forty years of age, and in females 48.9 per cent.
21 These cases are obtained from the same sources as those of the first table (page 483).
The relation between age and perforation of gastric ulcer will be discussed in connection with this symptom.
The conclusions concerning the age of occurrence of gastric ulcer may be recapitulated as follows: Simple ulcer of the stomach most frequently develops in the female between twenty and thirty, and in the male between thirty and forty. At the post-mortem table it is found with almost equal frequency in the four decades between twenty and sixty, but clinically it appears with greatly diminished frequency after forty years of age. In infancy and early childhood simple ulcer of the stomach is a curiosity.
We have no positive information as to the influence of climate upon the production of gastric ulcer. The disease seems to be somewhat unequal in its geographical distribution, but the data bearing upon this point are altogether insufficient.
According to the returns of Dahlerup and of Grünfeld, gastric ulcer is unusually common in Copenhagen.22 According to Starcke's report23—which, however, is not based upon a large number of cases—the percentage is also unusually high in Jena. Sperk says that gastric ulcer is very common in Eastern Siberia.24 Palgrave gives a high percentage of its occurrence in Arabia.25 The disease is less common in France than in England or in Germany,26 and in general appears to be more common in northern than in southern countries. The statement of DaCosta27 coincides with my own impression that gastric ulcer is less common in this country than in England or in Germany. I have found 6 cases of open ulcer of the stomach in about 800 autopsies made by me in New York.
22 Dahlerup in Copenhagen (abstract in Canstatt's Jahresbericht, 1842) found 26 cases in 200 autopsies (13 per cent.) made in the course of a year and a half. Grünfeld (loc. cit.) found 124 cicatrices in 1150 autopsies (11 per cent.).
23 Starke (loc. cit.) found 39 cases in 384 autopsies (10 per cent.); cf. also Müller, Jenaische Zeitschr., v. 1870.
24 Deutsche Klinik, 1867.
25 Narrative of a Year's Journey through Central and Eastern Arabia, London, 1865.
26 Laveran and Teissier, Nouveaux Éléments de Path. et de Clin. méd., t. ii. p. 1060, Paris, 1879; and Godin, Essai sur l'Ulcère de l'Estomac, Thèse, Paris, 1877, p. 8.
27 Medical Diagnosis, 5th ed., Philada., 1881. Keating expresses the same opinion in the Proc. of Path. Soc. of Philadelphia, vol. i. p. 142.
In 444,564 deaths in New York City from 1868 to 1882, inclusive, ulcer of the stomach was assigned as the cause of death only in 410 cases. Little value can be assigned to these statistics as regards a disease so difficult of diagnosis.
[p. 486] Gastric ulcer is more common among the poor than among the rich. Anxiety, mental depression, scanty food, damp dwellings, insufficient exercise, and exposure to extreme cold are among the depressing influences which have been assigned as predisposing causes of gastric ulcer, but without sufficient proof.
The comparative frequency of gastric ulcer among needlewomen, maidservants, and female cooks has attracted the attention of all who have had large opportunity for clinical observation.
Pressure upon the pit of the stomach, either by wearing tight belts or in the pursuit of certain occupations, such as those of shoemaking, of tailoring, and of weaving, is thought by Habershon and others to predispose to ulcer of the stomach.28
28 Bernutz found gastric ulcer in a turner in porcelain, and learned that other workmen in the same factory had vomited blood. He thinks that in this and in similar occupations heavy particles of dust collecting in the mouth and throat may be swallowed with the saliva, and by their irritation cause gastric ulcer (Gaz. des Hôpitaux, June 18, 1881).
Vomiting of blood has been known in several instances to affect a number of members of the same family, but beyond this unsatisfactory evidence there is nothing to show hereditary influence in the origin of gastric ulcer.
In a few cases injury of the region of the stomach, as by a fall or a blow, has been assigned as the cause of ulcer. The efficacy of this cause has been accepted by Gerhardt,29 Lebert, Ziemssen, and others. In many of the cases in which this cause has been assigned the symptoms of ulcer appeared so long after the injury that it is doubtful whether there was any connection between the two.
29 "Zur Aetiologie u. Therapie d. runden Magengeschwürz," Wiener med. Presse, No. 1, 1868.
That loss of substance in the mucous membrane of the stomach may be the result of injury directly or indirectly applied to this organ cannot admit of question. But it is characteristic of these traumatic ulcers that they rapidly heal unless the injury is so severe as to prove speedily fatal. Thus, Duplay30 relates three cases in which pain, vomiting, repeated vomiting of blood, and dyspepsia followed contusions of the region of the stomach. But these traumatic cases, which for a time gave the symptoms of gastric ulcer, recovered in from two weeks to two months, whereas the persistence of the symptoms is a characteristic of simple ulcer.31
30 "Contusions de l'Estomac," Arch. gén. de Méd., Sept., 1881.
31 In a case reported by Potain, however, the symptoms of ulcer appeared immediately after injury to the stomach, and continued up to the time of death (Gaz. hebdom., Sept. 12, 1856).
In the same way, ulcers of the stomach produced by corrosive poisons as a rule soon cicatrize, unless death follows after a short time the action of the poison. That corrosive ulcers may, however, be closely allied to simple ulcers is shown by an interesting case reported by Wilson Fox,32 in which the immediate effects of swallowing hydrochloric acid were recovered from in about four days, but death resulted from vomiting of blood two weeks after. At the autopsy the source of the hemorrhage was found in an ulcer of the pyloric region of the stomach. An equally striking case is reported by Williams.33 A boy who suffered severely for three or four days after drinking some strong mineral acid recovered, so that he [p. 487]ate and drank as usual. Two months afterward he died suddenly from perforation of a gastric ulcer.
32 Trans. of the Path. Soc., vol. xix. p. 239, London, 1868.
33 The Lancet, April 9, 1842.
While, then, it would be a great error to identify traumatic and corrosive ulcers of the stomach with simple ulcer, it is possible that either may become chronic if associated with those conditions of the stomach or of the constitution, for the most part unknown to us, which prevent the ready healing of simple ulcer.
Gastric ulcer is often associated with other diseases, but it occurs also uncomplicated in a large number of cases. Most of the diseases with which it has been found associated are to be regarded simply as coincident or complicating affections; but as some of them have been thought to cause the ulcer, they demand consideration in this connection.
The large share taken by pulmonary phthisis in deaths from all causes renders this disease a frequent associate of gastric ulcer. It is probable that the lowered vitality of phthisical patients increases somewhat their liability to gastric ulcer. Moreover, it would not be strange if gastric ulcer, as well as other exhausting diseases, such as diabetes and cancer, diminished the power of resisting tuberculous infection. Genuine tuberculous ulcers occur rarely in the stomach, but they are not to be identified with simple ulcer.
There is no proof that amenorrhoea or other disorders of menstruation exert any direct influence in the production of gastric ulcer, although Crisp went so far as to designate certain cases of gastric ulcer as the menstrual ulcer.34 Nevertheless, amenorrhoea is a very common symptom or associated condition in the gastric ulcer of females between sixteen and thirty years of age.
34 The Lancet, Aug. 5, 1843.
Chlorosis and anæmia, especially in young women, favor the development of gastric ulcer, but that there is no necessary relation between the two is shown by the occurrence of ulcer in those previously robust. Moreover, it is probable that in some cases in which the anæmia has been thought to precede the ulcer it has, in fact, been a result rather than a cause of the ulcer.
Especial interest attaches to the relation between gastric ulcer and diseases of the heart and of the blood-vessels, because to disturbances in the circulation in the stomach the largest share in the pathenogenesis of ulcer has been assigned by Virchow. As might be expected, valvular lesions of the heart and atheroma of the arteries are not infrequently found in elderly people who are the subjects of gastric ulcer. A small proportion of cases of ulcer has been associated also with other diseases in which the arteries are often abnormal, such as with chronic diffuse nephritis, syphilis, amyloid degeneration, and endarteritis obliterans. But, after making the most generous allowance for the influence of these diseases in the causation of ulcer of the stomach, there remains a large number of cases of ulcer in which no disease of the heart or of the arteries has been found.35 Gastric ulcer develops most frequently between fifteen and forty years of age, a period when arterial diseases are not common. Changes in the [p. 488] blood-vessels of the stomach will be described in connection with the morbid anatomy of gastric ulcer.
35 From Berlin are reported the largest number of cases of gastric ulcer associated with diseases of the circulatory apparatus; thus, by Berthold 170 out of 294 cases, and by Steiner 71 out of 110 cases of ulcer. Endocarditis and arterial atheroma (present in one-third of Berthold's cases of ulcer) form the largest proportion of these diseases.
Chronic passive congestion of the stomach in cases of cirrhosis of the liver, direct injury to the mucous membrane of the stomach by parasites in trichinosis, hemorrhage into the coats of the stomach in scorbutus and in dementia paralytica, persistent vomiting in pregnancy, and anæmia induced by prolonged lactation, have each been assigned as causes in a few cases of gastric ulcer, but they are not associated with gastric ulcer in enough cases to make their causative influence at all certain.
Galliard assigns diabetes mellitus as the cause in one case of gastric ulcer.36
36 Clin. méd. de la Pitié, Paris, 1877, p. 77.
Rokitansky attributed some cases of gastric ulcer to intermittent fever.
Those who believe in the inflammatory origin of ulcer of the stomach think that chronic gastritis is an important predisposing cause.
The abuse of alcohol is admitted as an indirect cause of gastric ulcer by the majority of writers.
Lastly, burns of the skin, which are an important factor in the etiology of duodenal ulcers, have been followed only in a very few instances by ulcer of the stomach.
The direct causes of ulcer of the stomach, concerning which our positive knowledge is very limited, will be considered under the pathenogenesis of the disease.
SYMPTOMATOLOGY.—The following classes of cases of gastric ulcer may be distinguished:
First: Gastric ulcer may give rise to no symptoms pointing to its existence, and be found accidentally at the autopsy when death has occurred from some other disease. This latent course is most frequent with gastric ulcers complicating chronic wasting diseases, such as tuberculosis, and with gastric ulcers in elderly people.
Second: Gastric ulcer may give rise to no marked symptoms before profuse hemorrhage from the stomach or perforation of the stomach, resulting speedily in death, occurs. Acute ulcers in anæmic females from fifteen to thirty years of age are those most liable to perforate without previous symptoms.
Third: Gastric ulcer may occasion only the symptoms of chronic gastritis, or of functional dyspepsia, or of purely nervous gastralgia, so that its diagnosis is impossible. In this class of cases after a time characteristic symptoms may develop. Here, too, sudden death may occur from hemorrhage or from perforation.
Fourth: In typical cases characteristic symptoms are present, so that the diagnosis can be made more or less positively. These symptoms are pain, and hemorrhage from the stomach, associated usually with vomiting and disturbances of digestion.
The different symptoms of gastric ulcer will now be described.
Of all the symptoms, pain is the most constant and is often the first to attract attention. It is absent throughout the disease only in exceptional cases. In different cases, and often in the same case at different times, the pain varies in its quality, its intensity, its situation, its duration, and in other characteristics.
The kind of pain which is most characteristic of gastric ulcer is severe [p. 489] paroxysmal pain strictly localized in a circumscribed spot in the epigastrium, coming on soon after eating, and disappearing as soon as the stomach is relieved of its contents.
More common, although less characteristic, than the strictly localized pain are paroxysms of severe pain, usually called cardialgic37 or gastralgic, diffused over the epigastrium and often spreading into the surrounding regions. This is like the neuralgic pain of nervous gastralgia, which is not infrequent in chlorotic and hysterical females. The pain may be so intense as to induce syncope, or even convulsions, in very sensitive patients.
37 There is much confusion as to the meaning of the term cardialgia. With most English and American writers it signifies heartburn, while continental writers understand by cardialgia the severe paroxysms of epigastric pain which we more frequently call gastralgia.
The strictly localized pain is probably caused by direct irritation confined to the nerves in the floor of the ulcer. In the diffuse gastralgic attacks the irritation radiates or is reflected to the neighboring nerves, and sometimes to those at a distance.
In most cases of gastric ulcer localized epigastric pain and diffuse gastralgic paroxysms are combined.
The painful sense of oppression and fulness in the epigastrium which is felt in many cases of gastric ulcer after eating is simply a dyspeptic symptom, and is probably referable to an associated chronic catarrhal gastritis. This dyspeptic pain is of little value in diagnosis.
Most subjects of gastric ulcer feel in the intervals between the paroxysms a more or less constant dull pain, or it may be only a sense of uneasiness, in the epigastrium. When sharp epigastric pain is felt continuously, it is usually inferred that the ulcer has extended to the peritoneum and has caused a circumscribed peritonitis, but this inference is not altogether trustworthy.
The quality of the pain caused by gastric ulcer is described variously as burning, gnawing, boring, less frequently as lancinating.
More important than the quality is the situation of the pain. The situation of the localized pain is usually at or a little below the ensiform cartilage. It may, however, be felt as low as the umbilicus or it may deviate to the hypochondria. In addition to pain in the epigastrium (point épigastrique), Cruveilhier called attention to the frequent presence of pain in the dorsal region (point rachidien). The dorsal pain, which may be more severe than the epigastric, is sometimes interscapular, and sometimes corresponds to the lowest dorsal or to the upper lumbar vertebræ. It is usually a little to the left of the spine. The pain is often described as extending from the pit of the stomach through to the back.
According to Brinton, the situation of the localized pain gives a clue to the situation of the ulcer, pain near the left border of the ensiform cartilage indicating ulcer near the cardiac orifice, pain in the median line and to the right of this indicating ulcer of the pyloric region, and pain in the left hypochondrium indicating ulcer of the fundus. It does not often happen that the pain remains so sharply localized as to make possible this diagnosis, even if the situation of the pain were a safe guide.
Of the various circumstances which influence the severity of the pain in gastric ulcer, the most important is the effect of food. Pain usually [p. 490] comes on within a few minutes to half an hour after taking food, although it may appear immediately after ingestion or be delayed for an hour or more. The pain continues until the stomach is relieved of its contents by vomiting or by their passage into the duodenum. It is unsafe to attempt to diagnose the position of the ulcer merely from the length of time which elapses between the ingestion of food and the onset of pain. It has sometimes been noticed that as improvement progresses pain comes on later and later after eating. As might naturally be expected, coarse, indigestible, imperfectly-masticated food, sour and spirituous liquids, and hot substances are more irritating than bland articles of diet. In some exceptional cases the ingestion of even coarse food, instead of aggravating, has had no effect upon the pain, or at least for the time being has even relieved it.
External pressure usually increases the intensity of the pain of gastric ulcer; in rare instances pressure relieves the pain.
Rest and the recumbent posture as a rule alleviate the pain of ulcer of the stomach. The position of the patient may affect the severity of the pain in a more striking way. It may naturally be supposed that that posture is most agreeable which removes from the ulcer the weight of the food during digestion. Hence it was claimed by Osborne38 that the site of the ulcer could often be inferred from the effect of posture on the pain. Thus, relief in the prone position would indicate ulcer of the posterior wall; relief in the supine position, ulcer of the anterior wall; relief on the left or on the right side, ulcer of the pyloric or of the cardiac region respectively. As ulcer of the posterior wall is the most frequent, relief should be obtained oftener by bending forward or by lying on the face than in the supine position. Experience has shown that the influence of posture on the pain is not a safe guide in diagnosing the location of the ulcer.
38 Jonathan Osborne, Dublin Journal of Medical Science, vol. xxvii. p. 357, 1845.
Mental emotions—particularly anxiety and anger—fatigue, even moderate exercise, exposure to cold, and the menstrual molimen may each cause exacerbations of pain in some cases of gastric ulcer.
Tenderness on pressure is a common symptom of gastric ulcer. A localized point of tenderness may be discovered even when the subjective pain is not localized. Pain sometimes follows pressure not immediately, but after a brief interval. A fixed point of tenderness can often be determined when the stomach is empty more accurately than when it is full. The tender spot can sometimes be covered by the finger's end. In searching for a point of tenderness it should be remembered that many persons are very sensitive to pressure in the epigastrium, and also that pressure is not without danger to those who are the subjects of gastric ulcer. Not only may pressure induce paroxysms of pain, but it may cause even rupture of the ulcerated walls of the stomach.39 Hence pressure should be cautiously employed and should not be often repeated.
39 Dalton has reported a case in which perforation of a gastric ulcer occurred while the patient was subjected in a water-cure establishment to kneading of the abdomen to relieve his flatulence (Trans. N.Y. Path. Soc., vol. i. p. 263.)
In some cases of gastric ulcer pain is felt in regions at a distance from the stomach. The most frequent of these so-called radiation neuralgias are—neuralgia of the lower intercostal spaces, combined sometimes with [p. 491] hyperæsthesia or with analgesia of the affected region, pain in the right shoulder (perhaps due to adhesions between the stomach and the liver or the diaphragm), pain in the left shoulder, and pain in the loins. In a case of ulcer reported by Traube terminating in perforation the sole complaint, besides loss of appetite and retching, had been difficulty in breathing and oppression in the chest. These symptoms, which may be combined with gastralgic paroxysms, are referred by Traube to transference of the irritation from the gastric to the pulmonary filaments of the pneumogastric nerve.40
40 Deutsche Klinik, 1861, No. 10. These symptoms evidently correspond to the vagus neurosis described by Rosenbach, in which, as the result of reflex irritation of the pneumogastric nerve in the stomach, occur difficulty in breathing, oppression in the chest, palpitation, arhythmical action of the heart, and epigastric pulsation (Deutsche med. Wochenschr., 1879, Nos. 42, 43).
Sometimes the pain of gastric ulcer intermits for days or even weeks. When the intermission is of considerable duration it is probable that cicatrization has been in progress. It should, however, be remembered that gastralgic attacks may continue even after cicatrization of the ulcer is completed, probably in consequence of compression of nerve-filaments by the cicatricial tissue. Once in a while the pain exhibits a marked periodicity in its appearance. Thus in a case of ulcer ending fatally from hemorrhage the pain came on but once a day, and that with considerable regularity at the same hour. In this case the pain was relieved by taking food.41 The pain of gastric ulcer may be temporarily relieved by hemorrhage from the stomach, and perhaps by division of the irritated nerve by sloughing (Habershon).
41 Case reported by Peacock, Rep. of Proceedings of London Path. Soc., vol. i. p. 253, 1847.
The causes of the pain of gastric ulcer are not far to seek. Foremost is the irritation of nerve-filaments exposed by the ulcerative process. The irritation may be by mechanical, chemical, or thermic agencies. With our present imperfect knowledge it is profitless to discuss whether the pneumogastric or the sympathetic nerves are the chief carriers of the abnormal sensations.42 In the next place, we may have radiation of the irritation from these nerves to neighboring and even to remote nerves. Furthermore, the extension of the inflammation to the peritoneum and the surrounding parts, and the formation of adhesions, are additional factors in some cases in causing pain. Finally, the great differences in susceptibility to pain manifested by different individuals is to be borne in mind.
42 Leven, without sufficient reason, distinguishes two kinds of gastralgic attacks—the one having its point of departure in the pneumogastric, the other in the sympathetic nerve; in the former the pain is associated with dyspnoea and palpitation of the heart; in the latter the pain is deeper, and is accompanied by vaso-motor (?) troubles on one side of the body.
Next to pain, vomiting is the most frequent symptom of gastric ulcer. There is, however, little which is characteristic of ulcer in this symptom, unless the vomited material contains blood. In some cases of gastric ulcer vomiting is the most marked and most distressing symptom of the disease. It may, however, be absent during the whole course of gastric ulcer.
Vomiting occurs most frequently after taking food, and is greatly aggravated by an unregulated diet. Sometimes nearly everything which is taken into the stomach is vomited. The vomiting of mucus or of a [p. 492] thin fluid unmixed with food is indicative only of chronic catarrhal gastritis. Alimentary vomiting, which is more indicative of gastric ulcer, usually occurs not immediately after taking food, but at the acme of a gastralgic attack caused by the food. Soon after the stomach is emptied by one or more acts of vomiting the pain is relieved. The act of vomiting is usually easy, and at times is hardly more than regurgitation of the food. Sometimes the patient experiences an excessively sour taste from the vomit.
Vomiting exhausts the patient by withdrawing nutriment, and when persistent may even cause death from inanition. But in some cases of gastric ulcer, especially in women, the vomiting seems to be mainly a nervous symptom, and even when long continued may be attended by little or no loss of flesh. Evidently, more food is retained in these cases than might be supposed.
There are two evident causes of vomiting in gastric ulcer—namely, chronic catarrhal gastritis, which is a frequent complication, and direct irritation of the nerves in the ulcer. Vomiting due to dilatation of the stomach is oftener a sequel than an immediate symptom of gastric ulcer.
For the diagnosis of gastric ulcer hemorrhage from the stomach is the most important symptom.
The frequency of only the larger hemorrhages can be determined with any degree of exactness. If the blood be effused in small quantity or slowly, it may be discharged solely with the stools and escape detection. Such slight hemorrhages doubtless occur in most cases of gastric ulcer. It is probable that easily-recognized hemorrhages from the stomach occur in about one-third of the cases of gastric ulcer.43 Hemorrhage is absent as a rule in the acute perforating ulcer of the stomach.
43 In consequence of the uncertainty of the diagnosis in cases of gastric ulcer which recover without hemorrhage, the estimates of the frequency of this symptom have a very limited value, and will vary with different observers according to their standard of diagnosis of this disease. Lebert observed gastric hemorrhage in four-fifths of his carefully-studied cases, and in three-fifths of his cases there was profuse hæmatemesis. Brinton estimates that the larger hemorrhages occur in about one-third of the cases. Müller found them in one-fourth of the cases which he analyzed.
In most cases hemorrhage from gastric ulcer is preceded by pain, vomiting, and disturbances of digestion. Antecedent symptoms may, however, be absent, or may be so obscure that no suspicion of ulcer exists until the hemorrhage occurs.
The hemorrhage may be slight, moderate, or excessive in amount (Cruveilhier). The larger hemorrhages are those which are most distinctive of gastric ulcer.
The blood may be vomited, or voided with the stools, or retained in the stomach and the intestines.
As has been remarked, when the hemorrhage is scanty all the blood may escape by the bowel. Sometimes, although much less frequently, blood effused in large quantity is entirely evacuated with the stools. After hæmatemesis more or less blood is discharged by the bowel, sometimes for several days after the vomiting of blood has ceased. Blood which has traversed the whole length of the intestinal canal acquires a tarry consistence and a black or brownish color in consequence of the production of dark-brown hæmatin by the action of the digestive juices [p. 493] upon the hæmoglobin, and in consequence of the formation of black sulphide of iron by the union of hydrogen sulphide in the lower part of the intestine with the iron of the hæmatin. The passage of these black viscid stools is called melæna. Inasmuch as we cannot presume gastric hemorrhage to be absent simply because no blood has been vomited, it is evidently important to examine the stools for blood when the diagnosis of gastric ulcer is obscure, and also in cases of gastric ulcer where there are symptoms of internal hemorrhage not accounted for by blood vomited. It should be remembered that certain drugs, particularly iron and bismuth, may blacken the feces.
In very exceptional cases of gastric ulcer the effusion of a large volume of blood causes sudden death before any of the blood has been vomited. The autopsy shows the stomach and more or less of the small intestine distended with coagulated blood.
Hemorrhage from gastric ulcer is usually made manifest by the vomiting of blood. The quantity of the vomited blood varies from mere traces to several pounds. The color and the consistence of the blood depend upon the quantity effused and the length of time that the blood has remained in the stomach. Blood which has been acted upon by the gastric juice is coagulated, has a grumous consistence, and acquires by the formation of hæmatin out of hæmoglobin a dark-brown color, often compared to that of coffee-grounds. Blood effused in small quantity is usually vomited only with the food, and has usually the coffee-grounds appearance. The patient's condition is not appreciably influenced by this slight loss of blood. A little blood expelled after repeated acts of vomiting has no diagnostic importance. Vomiting usually occurs soon after a large gastric hemorrhage. It is the mechanical distension of the stomach rather than any irritating quality of the blood which causes the vomiting. Blood which is rejected immediately after a large gastric hemorrhage is alkaline, fluid, and of an arterial (rarely of a venous) hue. Often, however, even with large hemorrhages, the blood remains sufficiently long in the stomach to be partly coagulated and to be darkened in color. Ulcer more frequently than any other disease of the stomach causes the vomiting of unaltered blood in large quantity. But this kind of hæmatemesis is not peculiar to simple ulcer. It may occur in other diseases, such as gastric cancer, and coffee-ground vomiting may be associated with ulcer.
Copious hæmatemesis in cases of gastric ulcer appears usually without premonition, or it may be preceded for a day or two by increased pain. Its occurrence is somewhat more common during the digestion of food than in the intervals, but there have been cases of ulcer where the bleeding was favored by an empty stomach and was checked by the distension of the organ with food. The free use of stimulants and violent physical or mental exertion may excite hemorrhage. With the onset of the hemorrhage the patient experiences a sense of warmth and of oppression at the epigastrium, followed by faintness, nausea, and the vomiting of a large quantity of blood. An attack of syncope often causes, at least temporarily, cessation of the hemorrhage. But the thrombus which closes the eroded vessel may easily be washed away, so that the hemorrhage often recurs and continues at intervals for several days, thereby greatly increasing the danger to the patient. Thus, the tendency is for [p. 494] the hemorrhage from gastric ulcer to appear in phases or periods occupying several days.
A single hemorrhage is rarely so profuse as to cause immediate death. More frequently the patient dies after successive hemorrhages. In the majority of cases the hemorrhage is not immediately dangerous to life, but is followed by symptoms of anæmia, more or less profound according to the strength of the patient and the amount of blood lost. Prostration and pallor follow the larger hemorrhages. Dizziness, ringing in the ears, and dimness of vision appear when the patient attempts to leave the recumbent posture. Thirst is often a marked symptom. The pulse is feeble and more frequent than normal. There is often a moderate elevation of temperature (anæmic fever) after profuse hemorrhage. The urine is pale, abundant, and sometimes contains albumen (Quincke). After a few days anæmic cardiac murmurs can often be heard. Under favorable circumstances these symptoms of anæmia disappear in the course of a few weeks.
The other symptoms of ulcer, particularly the pain, are sometimes notably relieved, and may even disappear, after an abundant hemorrhage. They usually, however, return sooner or later. After a variable interval one attack of hæmatemesis is likely to be followed by others. There is much diversity in different cases as regards the frequency of these attacks and the character of the symptoms in the intervals. In a few cases recovery follows a single attack of gastric hemorrhage; in other cases the hemorrhage recurs frequently after intervals of only a few days, weeks, or months; in still other cases hemorrhage recurs only after long intervals, perhaps of years, although other symptoms of ulcer continue. Sometimes the disappearance of symptoms indicates only an apparent cure, and later the patient dies suddenly while in apparent health by a profuse gastric hemorrhage. In the rare cases of this last variety Cruveilhier has found sometimes that the ulcer has cicatrized except just over the eroded blood-vessel.
The sources of the hemorrhage in gastric ulcer will be described in connection with the morbid anatomy.
The symptoms of gastric indigestion are commonly, although not constantly, present in gastric ulcer. They may constitute the sole symptoms, in which case the diagnosis of the lesion is impossible. The most important local symptoms of gastric dyspepsia are diminution, less frequently perversion or increase, of the appetite; increased thirst; during digestion, and sometimes independent of digestion, a feeling of discomfort merely or of painful oppression, or even of sharp pain, in the epigastrium; nausea; vomiting of undigested food, of mucus, and of bile; regurgitation of thin fluids; often acid, sometimes neutral or alkaline, flatulence, with belching of gas, and constipation. In many cases of gastric ulcer the appetite is not disturbed, but the patient refrains from eating on account of the pain caused by taking food. Among the so-called sympathetic symptoms of dyspepsia are headache, dizziness, depression of spirits, oppression in the chest, and irregularity of the heart's action. Dyspepsia contributes its share to the production of the anæmia and of the loss of flesh and strength which are present in some degree in most cases of chronic gastric ulcer.
[p. 495] In many cases of acute perforating ulcer, as well as in some cases of chronic ulcer, the symptoms are either absent or they are but slightly marked. It has been demonstrated that in many cases of gastric ulcer the resorptive power of the mucous membrane of the stomach is unimpaired.44
44 This is shown by the experiments of Pentzoldt and Faber, who determined the length of time which elapsed between swallowing gelatin capsules containing iodide of potassium and the appearance of the iodide in the saliva (Berl. klin. Wochenschr., No. 21, 1882). Quetsch observed rapid absorption from the stomach in two cases of gastric ulcer (ibid., 1884, No. 23). It is believed that also the duration of the digestive process in the stomach is often within normal limits in cases of gastric ulcer, although exact experiments upon this point, as they require the use of the stomach-pump, have not been made in this disease (Leube).
The most common cause of dyspepsia in gastric ulcer is the chronic catarrhal gastritis which usually accompanies this disease. It is probable that the movements of the stomach may be seriously interfered with by destruction of the muscular coat of the stomach when the ulcer is of considerable size and is seated in the pyloric region. Adhesions of the stomach to surrounding parts may likewise impair the normal movements of the stomach. It is possible that ulcers, especially those which are very painful, may cause reflex disturbance of the peristaltic movements of the stomach and alterations in the quality or the quantity of the gastric juice. The serious digestive disturbances which are caused by distortions and dilatation of the stomach resulting from cicatricial contraction of gastric ulcer are not considered in this article.
Although Niemeyer emphasized the frequency in gastric ulcer of a strikingly red tongue with smooth or furrowed surface, it does not appear that any especial importance is to be attached to this or to any other condition of the tongue as a symptom of the disease.
Increased flow of saliva is a rare symptom, which, when it occurs, is usually associated with dyspepsia.
Constipation is the rule in gastric ulcer. The most important of the various circumstances which combine to produce this condition is the small amount of solid food taken and retained by the patient. The restraint caused by gastric ulcer and gastric catarrh in the normal movements of the stomach may diminish by reflex action the peristalsis of the intestines (Traube and Radziejewski). The passage of large quantities of blood along the intestinal canal is often associated with colicky pains and diarrhoea.
Amenorrhoea is a symptom which was formerly thought to be characteristic of gastric ulcer, although there was much discussion as to whether it was the cause or the result of the ulcer. Amenorrhoea is indeed common in the gastric ulcer of young women, but there is nothing strange in this when one considers the frequency of amenorrhoea in general, and its causation by various debilitating and depressing influences such as are to be found in gastric ulcer. Notwithstanding a few striking cases which have been recorded, it has not been demonstrated that hemorrhages vicarious of menstruation take place from gastric ulcer.
Gastric ulcer is not a febrile disease. Temporary elevation of temperature may follow profuse gastrorrhagia and may attend various complications, of which the most important are gastritis and peritonitis. It has been recently claimed by Peter that the surface-temperature of the [p. 496] epigastrium is elevated in gastric ulcer, but the observations upon this point are as yet too few for any positive conclusions.45
45 According to Peter, the normal surface-temperature of the epigastrium is from 95½° to 96° F. (35.3° to 35.5° C.), while in gastric ulcer the temperature may equal or even exceed by one or two degrees the axillary temperature. It is said to register the highest during attacks of pain and of vomiting and after hemorrhages (Gaz. des Hôpitaux, June 23 and 30, 1883). See also Beaurieux (Essai sur la Pseudo-gastralgie, etc., Thèse, Paris, 1879).
The general health of the patient remains sometimes surprisingly good, even in cases of gastric ulcer with symptoms sufficiently marked to establish the diagnosis. But in most cases of chronic gastric ulcer the general nutrition sooner or later becomes impaired. This cannot well be otherwise when dyspepsia, vomiting, paroxysms of severe pain, and hemorrhage are present, separately or in combination, for any great length of time. In proportion to the severity and the continuance of these symptoms the patient becomes pale, weak, and emaciated. The face, thin, anxious, of a grayish-white color, and marked with sharp lines of suffering, presents the appearance which the older writers called facies abdominalis, to which even so recent an author as Brinton attaches exaggerated diagnostic importance. A little cachectic dropsy may appear about the ankles. While it is true that the general nutrition is less rapidly, less continuously, and, as a rule, less deeply, impaired in gastric ulcer than in gastric cancer, nevertheless sometimes a cachexia develops in the former which is not to be distinguished from that of cancer. Litten46 relates a case of gastric ulcer which simulated for a time pernicious anæmia. In this case the profound anæmia could not be explained by vomiting, hemorrhage, or other symptoms of ulcer.
46 Berliner klin. Wochenschrift, Dec. 6, 1880.
Beyond determining the existence of a fixed point of epigastric tenderness, physical examination of the region of the stomach is usually only of negative value in the diagnosis of gastric ulcer. In some cases of ulcer of the stomach epigastric pulsation is very marked, and sometimes most marked during gastralgic attacks. In these cases there may be dilatation of the aorta from paralysis of vaso-motor nerves analogous to the dilatation of the carotid and temporal arteries in certain forms of migraine (Rosenbach). When the diagnosis lies between gastric ulcer and gastric cancer, the presence of epigastric tumor is justly considered to weigh against ulcer; but it is important to know that tumor may be associated with ulcer. Thickening of the tissues around old ulcers and the presence of adhesions may give rise to a tumor. A thickened portion of omentum which had become adherent over an old gastric ulcer produced a tumor which led to a mistake in the diagnosis.47 Rosenbach48 calls attention to the occasional production of false tumors by spasm of the muscular coat of the stomach around a gastric ulcer. These tumors disappear spontaneously or yield to the artificial distension of the stomach by Seidlitz powders—a procedure which one would not venture to adopt if he suspected gastric ulcer. Fenwick thinks that in some cases of gastric ulcer fixation of the stomach by adhesions can be made out by physical exploration.
47 A. Beer, Wiener med. Wochenschrift, No. 26, 1857.
48 Deutsche med. Wochenschrift, 1882, p. 22.
The gravest symptom which can occur in gastric ulcer is the perforation of the ulcer into the general peritoneal cavity.
[p. 497] Only rough estimates can be made of the frequency of this symptom. These estimates vary from 2 to 25 per cent. From the data which I have collected I infer that perforation into the general peritoneal cavity occurs in about 6½ per cent. of all cases of gastric ulcer.49
49 Miquel (Schmidt's Jahrb., Bd. 125, p. 65, 1864) reckons the frequency of perforation at 2 per cent. Brinton's estimate of 13½ per cent. is the one generally accepted. He found 69 cases of perforation in 257 open ulcers collected from various sources. He doubles the number of open ulcers, as he considers cicatrized ulcers twice as frequent as the open. The statistics of some of the authors to whom he refers should not be used in this computation, either because they do not give accurately the number of cases of perforation, or because they include under perforation all cases of ulcer which have penetrated all of the coats of the stomach, whereas of course only perforation into the general peritoneal cavity should be here included. Valuable and laborious as are Brinton's researches, his statistics upon this point, as upon many others, are inaccurate.
In 249 fatal cases of open ulcer taken from the statistics of Jaksch, Dittrich, Willigk, Wrany (Prager Vierteljahr., vols. xcv. and xcix.), Eppinger, Starcke, Chambers, Moore, and Lebert (loc. cit.), I find 50 cases of perforation into the peritoneal cavity. This makes the percentage of perforations 6½ if the open ulcers be multiplied by 3, the number of cicatrized ulcers being taken as three times that of open ulcers (p. 482). This method of computation, which is adopted by Brinton, is defective on account of the uncertainty as to the proper proportion between cicatrized and open ulcers.
Lebert observed 9 cases of perforation with fatal peritonitis in his 252 cases studied clinically. He places the frequency of perforation with peritonitis at 3 to 5 per cent., which corresponds to Engel's estimate of 5½ per cent. (Prager Vierteljahrschrift, 1853, ii.).
As regards sex, perforation occurs two to three times oftener in the female than in the male. This increased liability is referable mainly to the preponderance of the acute perforating ulcer in young women.50
50 The liability to perforation in females seems to be not only absolutely, but also relatively, to the number of ulcers greater than in males, although, on the contrary, Brinton holds that the excess of perforations in females is not greater than that of ulcers. Berthold found perforation in 3.1 per cent. of the cases of gastric ulcer in males, and in 9.7 per cent. of the cases in females (op. cit., p. 28).
In the female the liability to perforation of gastric ulcer is greatest between fourteen and thirty years of age. In the male there seems to be no greater liability to perforation at one age than at another.51
51 Of 139 cases of perforated ulcer in females, Brinton found that four-fifths occurred before the age of thirty-five. He calculates the average age at which perforation occurs in the female as twenty-seven, and in the male as forty-two. He thinks that the average liability to perforation in both sexes decreases as life advances, although he holds that the liability to ulcer itself constantly increases with age.
As will be explained in considering the morbid anatomy, ulcers of the anterior wall of the stomach perforate more frequently than those in other situations.
As regards the symptoms which may have preceded perforation three groups of cases can be distinguished:
In the first there has been no complaint of gastric disturbance. In the midst of apparent health perforation may occur and cause death within a few hours. This is the ulcère foudroyante of French writers. It is met with more commonly in chlorotic young women than in any other class.
In the second group of cases, which are more frequent, gastric symptoms have been present for a longer or shorter time, but have been so ambiguous that the diagnosis of gastric ulcer is not clear until perforation occurs. Then, unfortunately, the diagnosis is of little more than retrospective interest.
In the third group of cases perforation takes place in the course of gastric ulcer, the existence of which has been made evident by characteristic symptoms, such as localized pain and profuse hemorrhage.
[p. 498] The immediate cause of perforation of gastric ulcer is often some agency which produces mechanical tension of the stomach, such as distension of the organ with food or with gas, vomiting, straining at stool, coughing, sneezing, pressure on the epigastrium, violent exertion, and jolting of the body.
With the escape of the solid, the fluid, and the gaseous contents of the stomach into the peritoneal cavity at the moment of perforation, an agonizing pain is felt, beginning in the epigastrium and extending rapidly over the abdomen, which becomes very sensitive to pressure. The pain sometimes radiates to the shoulders. Symptoms of collapse often appear immediately or they may develop gradually. The pulse becomes small, rapid, and feeble. The face is pale, anxious, and drawn (facies hippocratica). The surface of the body, particularly of the extremities, is cold and covered with clammy sweat. The internal temperature may be subnormal, normal, or elevated; after the development of peritonitis it is usually, but not always, elevated. Consciousness is usually retained to the last, although the patient is apathetic. Vomiting is sometimes absent—a circumstance which may be of value in diagnosis, and which Traube attributes to the readiness with which the contents of the stomach can be discharged through the abnormal opening into the peritoneal cavity. There is usually constipation. The respirations become more and more frequent and costal in type. Thirst is often urgent. Suppression of urine is not an uncommon symptom, although there may be frequent and painful attempts at micturition. Albumen and casts may appear temporarily in the urine. Retraction of one testicle, like that in renal colic, has been observed (Blomfield). The patient usually lies on his back with the knees drawn up. The abdomen is often at first hard and retracted from spasmodic contraction of the abdominal muscles, but later it usually becomes tympanitic, sometimes to an extreme degree. The presence of tympanitic resonance replacing hepatic dulness in front is usually considered the most important physical sign of gas free in the peritoneal cavity, but this sign is equivocal. On the one hand, the presence of adhesions over the anterior surface of the liver may prevent the gas from getting between the liver and the diaphragm;52 and on the other hand, in cases of meteorism coils of intestine may make their way between the liver and the diaphragm, or the liver may be pushed upward and backward, so that its anterior surface becomes superior and the hepatic dulness in front disappears. Physical examination may reveal in the dependent parts of the peritoneal cavity an accumulation of fluid partly escaped from the stomach and partly an inflammatory exudate.53 For humane reasons one should not submit the patient to the pain of movement in order to elicit a succussion sound or to determine change in the position of the fluid upon changing the position of the patient.54 There is sometimes relief from pain for some hours before death.
52 Even without these adhesions liver dulness may persist after perforation of the stomach, as in a case of Nothnägel's in which for twenty-four hours after a large perforation from gastric ulcer the abdomen was retracted and hepatic dulness was well marked (Garmise, Ulcus Ventriculi cum peritonitide perforativa, Inaug. Diss., Jena, 1879).
53 In a case of peritonitis resulting from perforation of a latent ulcer of the duodenum, Concato found in the acid fluid withdrawn by aspiration from the peritoneal cavity Sarcina ventriculi (Giorn. internaz. delle Scienze Med., 1879, No. 9).
54 Other symptoms which have been thought to be diagnostic of pneumo-peritoneum in [p. 499] distinction from meteorism, but the value of which is doubtful, are these: In pneumo-peritoneum the respiratory murmur can be heard by auscultation over the entire abdomen, while in meteorism it does not extend beyond the region of the stomach (Cantani); in the former amphoric sounds synchronous with respiration can sometimes be heard over the abdomen (Larghi); borborygmi are heard, if at all, distantly and feebly; the percussion note of gas free over the liver is different from that of tympanitic intestine (Traube); the percussion note is of the same character over the whole anterior wall of the abdomen; the epigastric region is more elastic to the feel than in tympanites; the distension of the abdomen is more uniform than in tympanites; and coils of distended intestine, sometimes showing peristaltic movement, cannot be seen or felt as in some cases of meteorism (Howitz).
There are exceptional cases of perforation in which some of the most important of the enumerated symptoms, such as pain, tenderness of the abdomen on pressure, tympanites, and the symptoms of collapse, are absent.
Death sometimes occurs from shock within six or eight hours after perforation. More frequently life is prolonged from eighteen to thirty-six hours, it may be even for three or four days, and, very rarely, even longer.55 When life is prolonged more than twelve hours an acute diffuse peritonitis is usually but not always developed.
55 In the Descriptive Catalogue of the Warren Anatomical Museum, by Dr. J. B. S. Jackson, p. 448, Boston, 1870, is described a case of gastric ulcer in which, so far as can be judged by the symptoms and the post-mortem appearances, the patient lived nineteen days after perforation.
The contents of the stomach, instead of being diffused throughout the peritoneal cavity, may be confined by a rapidly-developed circumscribed peritonitis to a space near the stomach, or perforation may occur into a space previously shut off from the general peritoneal sac by adhesions. In this way circumscribed peritoneal abscesses form in the neighborhood of the stomach. Diffuse peritonitis may be caused either by an extension of the inflammation or by the rupture of these abscesses into the general peritoneal cavity. The cases of circumscribed peritonitis following perforation of gastric ulcer, with escape of the contents of the stomach, although more protracted than those in which the whole peritoneal surface is at once involved, generally terminate fatally sooner or later. The symptoms are often very obscure.
The most interesting of these peritoneal abscesses is the variety to which Leyden has given the name of pyo-pneumothorax subphrenicus (false pneumothorax of Cossy), the diagnostic features of which first were recognized by G. W. Barlow and Wilks in 1845.56 Here there is a cavity, circumscribed by adhesions, just beneath the diaphragm, containing pus and gas and communicating with either the stomach or the intestine. By the encroachment of this cavity upon the thoracic space the symptoms and signs of pyo-pneumothorax are simulated. Barlow and Leyden have diagnosed during life this affection when resulting from perforated gastric ulcer. The points in diagnosis from genuine pyo-pneumothorax are the presence of respiratory murmur from the clavicle to the third rib, the extension of the respiratory murmur downward by deep inspiration, history of preceding gastric disturbance with circumscribed peritonitis, absence of preceding pulmonary symptoms, rapid variations in the limits of dulness with changes in the position of the body, absence or only slight evidence of increased intrapleural pressure (such as bulging of the [p. 500]thorax as a whole, and of the intercostal spaces), displacement of the heart, displacement of the liver downward, and, if necessary, the determination by means of a manometer that the pressure in the abscess cavity rises during inspiration and falls during expiration, the reverse being true in genuine pneumothorax.57
56 Barlow and Wilks, London Med. Gazette, May, 1845; Leyden, Zeitschr. f. klin. Med., i. Heft 2; Cossy, Arch. gén. de Méd., Nov., 1879; Tillmanns, Arch. f. klin. Chirurg., Bd. 27, p. 103, 1881.
57 Schreiber has shown that this last diagnostic point, which was given by Leyden, is not without exceptions, for the pressure in the peritoneal cavity may sink during inspiration and rise during expiration (as in the pleural cavity), especially when the diaphragm takes little or no part in respiration ("Ueber Pleural- und Peritonealdruck," Deutsches Arch. f. klin. Med., July 31, 1883).
Through the medium of subphrenic abscess, or directly through adhesions between the stomach and the diaphragm, gastric ulcer may perforate into one of the pleural cavities (generally the left) and cause empyema or pneumo-pyothorax. Adhesions may form between the diaphragm and the pulmonary pleura, so that the ulcer perforates directly into the lung; in which case pulmonary gangrene or pulmonary abscess is usually developed. The diagnosis of the perforation into the lung has been made by recognizing a sour odor and sour reaction of the expectoration, and by finding in the sputum particles of food derived from the stomach. Sudden death from suffocation has followed perforation of the stomach into the lung.58
58 Tillmanns (loc. cit.) has collected 12 cases of communication between the stomach and the thoracic cavity from perforation of gastric ulcer; all proved fatal. In Sturges's case of recovery from pneumothorax supposed to be produced by perforation of a gastric ulcer the diagnosis of the cause of the pneumothorax was very doubtful (The Lancet, Feb. 7, 1874).
Perforation of gastric ulcer into the transverse colon has been followed by the vomiting of formed feces and by the passage of undigested food by the bowel (Abercrombie). Enemata may be vomited, so that, as suggested by Murchison, the introduction of colored enemata may aid in the diagnosis.
Gastro-cutaneous fistulæ are among the rare results of perforation of gastric ulcer. In these cases food, sometimes only in liquid form, escapes through the fistula.
The opening of gastric ulcer into the pericardium is one of the rare causes of pneumo-pericardium.
Other varieties of perforation which are of pathological rather than of clinical interest will be mentioned under the morbid anatomy of gastric ulcer.
COURSE.—Few diseases are more variable in their course and duration than is simple gastric ulcer. It is customary to distinguish between acute and chronic forms of gastric ulcer, but this is a distinction which cannot be sharply drawn. Those cases are called acute in which, with absence or short duration of antecedent gastric symptoms, perforation or gastrorrhagia suddenly causes death. But in some of these cases the thickened and indurated margins of the ulcer found at the autopsy show that the disease has been of much longer duration than the clinical history would indicate. Still, there is reason to believe that within the course of a few days ulcers may form and perforate all of the coats of the stomach.
In the great majority of cases of gastric ulcer the tendency is to assume a chronic course, so that the often-used term chronic gastric ulcer is generally applicable.
[p. 501] The great diversity of the symptoms in different cases makes it impossible to give a generally applicable description of the course of gastric ulcer. It is, however, useful to designate the main clinical forms of the disease. Thus we may distinguish—
1. Latent ulcers, with entire absence of symptoms, and revealed as open ulcers or as cicatrices at the autopsy.
2. Acute perforating ulcers. With or without a period of brief gastric disturbance perforation occurs and causes speedy death.
3. Acute hemorrhagic form of gastric ulcer. After a latent or a brief course of the ulcer profuse gastrorrhagia occurs, which may terminate fatally or may be followed by the symptoms of chronic ulcer.
4. Gastralgic-dyspeptic form. In this, which is the most common form of gastric ulcer gastralgia, dyspepsia and vomiting are the symptoms. Sometimes one of the symptoms predominates greatly over the others, so that Lebert distinguishes separately a gastralgic, a dyspeptic, and a vomitive variety. Gastralgia is the most frequent symptom.
5. Chronic hemorrhagic form. Gastrorrhagia is a marked symptom, and occurs usually in combination with the symptoms just mentioned.
6. Cachectic form. This usually corresponds only to the final stage of one of the preceding forms, but the cachexia may develop so rapidly and become so marked that the course of the disease closely resembles that of gastric cancer.
7. Recurrent form. In this the symptoms of gastric ulcer disappear, and then follow intervals, often of considerable duration, in which there is apparent cure, but the symptoms return, especially after some indiscretion in the mode of living. This intermittent course may continue for many years. In these cases it is probable either that fresh ulcers form or that the cicatrix of an old ulcer becomes ulcerated.
8. Stenotic form. By the formation of cicatricial tissue in and around the ulcer the pyloric orifice becomes obstructed and the symptoms of dilatation of the stomach develop.
DURATION.—The average duration of gastric ulcer may be said to be from three to five years, but this estimate is not of great value, on account of the absence of any regularity in the course and duration of the disease. In cases of very protracted duration, such as forty years in a case of Habershon's and thirty-five in one of Brinton's, it is uncertain whether the symptoms are referable to the persistence of one ulcer or to the formation of new ulcers, or to sequels resulting from cicatrization.
In 110 cases (44 fatal) analyzed by Lebert59 the course was latent until the occurrence of perforation or of profuse hemorrhage in 15 per cent., the duration was less than one year in 18 per cent., from one to six years in 46½ per cent., from six to twenty years in 18 per cent., from twenty to thirty-five years in 2½ per cent.
59 Op. cit., p. 235.
TERMINATIONS.—In the majority of cases gastric ulcer terminates in recovery. The recovery is often complete. Various gastric disturbances may, however, follow the cicatrization of gastric ulcer, especially if the ulcer was large and of long duration. These sequential disturbances are due to the contraction of the cicatrix, to adhesions between the stomach and surrounding parts, to deformity of the stomach, and especially to dilatation of the stomach by cicatricial stenosis of the pylorus. Hence, [p. 502]gastralgia, dyspepsia, and vomiting may continue after the ulcer has healed, so that anatomical cure of the ulcer is not always recovery in the clinical sense. Relapses may occur after recovery, as those who have once had gastric ulcer are more prone to the disease than are others. Not infrequently the patient recovers so far as to be able to attend to the active duties of life, but to avoid renewed attacks he is always obliged to be very careful as regards his mode of living.
How often gastric ulcer ends in death it is impossible to say. It is certain that Brinton under-estimates the number of recoveries when he computes that only one-half of the ulcers cicatrize. Lebert reckons the mortality from gastric ulcer as 10 per cent., which appears to be too low an estimate. Perhaps 15 per cent. would be a more correct estimate of the mortality.
The causes of death are perforation, hemorrhage, exhaustion, and complicating diseases.
About 6½ per cent. of the cases of gastric ulcer terminate fatally by perforation into the peritoneal cavity. Although this estimate can be considered only approximative, there is little doubt but that the much larger percentages given by most writers are excessive, and are referable to the undue frequency with which cases of perforation of gastric ulcer have been published. Such cases naturally make a strong impression upon the observer, and are more likely to be published than those which terminate in other ways.
Death from hemorrhage occurs probably in from 3 to 5 per cent. of the cases of gastric ulcer.60 In many more cases hemorrhage is an indirect cause of death by inducing anæmia. Unlike perforation, fatal hemorrhage from gastric ulcer is more common in males than in females—more common after than before forty years of age. The average age at which fatal hemorrhage occurs is given by Brinton as forty-three and a half years both for males and females.
60 In 270 fatal cases of open ulcer from the statistics of Jaksch, Dittrich, Eppinger, Starcke, Chambers, Habershon, Moore, and Lebert, I find 27 deaths by hemorrhage. Reckoning three cicatrices to one ulcer, this would give a percentage of 31/3.
In a considerable proportion of the fatal cases exhaustion is the cause of death. According to Lebert, death from exhaustion occurs in about 4 per cent. of the cases of gastric ulcer. The causes of exhaustion are the pain, hemorrhage, dyspepsia, and vomiting which constitute the leading symptoms of the disease.
Finally, death may be due to some of the complications or sequels of gastric ulcer.
COMPLICATIONS.—Some of the complications of gastric ulcer are directly referable to the ulcer, others are only remotely related to it, and others are merely accidental.
Pylephlebitis is among the most important of the complications directly referable to the ulcer. This pylephlebitis is usually of the infectious variety, and leads to abscesses in the liver, sometimes to abscesses in the spleen and other organs.
As has already been mentioned, chronic catarrhal gastritis stands in close relationship to gastric ulcer. Chronic peritonitis is a rare complication of gastric ulcer (Moore, Vierordt). Chronic interstitial gastritis, with contraction of the stomach and thickening of its walls, was [p. 503] associated with ulcer in a case under my observation. In a case of ulcer under the care of Owen Rees61 this condition of the stomach was associated with chronic deforming peritonitis (thickening, induration, and contraction of the peritoneum) and ascites, so that the symptoms during life and the gross appearances after death resembled cancerous diseases of the peritoneum. Simple ulcer and cancer may occur together in the same stomach, or cancer may develop in an ulcer or its cicatrix. Glässer reports a case of phlegmonous gastritis with gastric ulcer.62 Extension of inflammation to the pleura without perforation of the diaphragm sometimes occurs. Fatty degeneration of the heart may be the result of profound anæmia induced by gastric ulcer.63 Embolic pneumonia and broncho-pneumonia are occasional complications. A moderate degree of cachectic dropsy is not very infrequent in the late stages of gastric ulcer.
61 Med. Times and Gaz., April 24, 1869.
62 Berlin. klin. Wochenschrift, 1883, No. 51.
63 Shattuck, Boston Med. and Surg. Journ., June, 1880, vol. ciii.
Other complications, such as pulmonary tuberculosis, valvular disease of the heart, general atheroma of the arteries, cirrhosis of the liver, syphilis, chronic Bright's disease, waxy degenerations, and malaria, have been considered under the Etiology, and some of them will be referred to again in connection with the Pathology, of gastric ulcer. In most instances when ulcer is associated with these diseases the ulcer is secondary.
SEQUELÆ.—The most important sequelæ of gastric ulcer are changes in the form of the stomach in consequence of adhesions and in consequence of the formation and contraction of cicatrices. These lesions are most conveniently described under the Morbid Anatomy. The symptoms of the most important of these sequels—namely, stenosis of the pylorus with dilatation of the stomach—will be described in another article.
MORBID ANATOMY.—As regards number, simple ulcer of the stomach is usually single, but occasionally two or more ulcers are present. It is not uncommon to meet in the same stomach open ulcers and the scars of healed ulcers. According to Brinton, multiple ulcers are found in about one-fifth of the cases. In one case O'Rorke found six ulcers on the anterior wall of the stomach.64 Berthold mentions a case in which thirty-four ulcers were found in the same stomach.65
64 Trans. of the New York Path. Soc., vol. i. p. 241. Wollmann mentions the occurrence of over eight simple ulcers in the same stomach (Virchow und Hirsch's Jahresb., 1868, Bd. ii. p. 126).
65 Op. cit., p. 21. It is expressly stated that these were not hemorrhagic erosions, but deep corrosive ulcers.
The usual position of simple gastric ulcer is the posterior wall of the pyloric portion of the stomach on or near the lesser curvature. Ulcers of the anterior wall are rare, but they carry a special danger from their liability to perforate without protective adhesions. The least frequent seats of ulcer are the greater curvature and the fundus.
The table on page 504 gives the situation of 793 ulcers recorded in hospital statistics:66 [p. 504]
| Lesser curvature | 288 | (36.3 per cent.) |
| Posterior wall | 235 | (29.6 per cent.) |
| Pylorus | 95 | (12 per cent.) |
| Anterior wall | 69 | (8.7 per cent.) |
| Cardia | 50 | (6.3 per cent.) |
| Fundus | 29 | (3.7 per cent.) |
| Greater curvature | 27 | (3.4 per cent.) |
From this table it is apparent that ulcers occupy the lesser curvature, the posterior wall, and the pyloric region three and a half times more frequently than they do the remaining larger segment of the stomach.
66 These statistics are collected from the previously-cited works of Rokitansky, Jaksch, Wrany, Eppinger, Chambers, Habershon, Steiner, Wollmann, Berthold, Starcke, Lebert, and Moore. They represent 566 cases. So far as noted, most of the ulcers on the posterior wall were nearer to the lesser curvature than to the greater; those on the lesser curvature extended more frequently to the posterior than to the anterior wall. Although not apparent from the table, most of the ulcers of the lesser curvature and of the posterior wall were in the pyloric region. So far as possible, cicatrices were excluded. Pylorus and cardia in the table indicate on or near those parts.
Occasionally two ulcers are seated directly opposite to each other, the one on the anterior, the other on the posterior, wall of the stomach. The most plausible explanation of this is that the ulcers are caused by a simultaneous affection of corresponding branches which are given off symmetrically from the same arterial trunk as it runs along one of the curvatures of the stomach (Virchow).67
67 A. Beer, "Aus dem path. Anatom. Curse et. Prof. R. Virchow, etc.," Wiener med. Wochenschr., Nos. 26, 27, 1857.
The ordinary size of the ulcer varies from a half inch to two inches in diameter. The ulcer may be very minute, as in two cases reported by Murchison, in each of which a pore-like hole was found leading into a perforated artery from which fatal hemorrhage had occurred.68 On the other hand, the ulcer may attain an enormous size, extending sometimes from the cardiac to the pyloric orifice and measuring five or six inches in diameter.69
68 Murchison, Trans. of the Path. Soc., vol. xxi. p. 162, London, 1870.
69 In one of Cruveilhier's cases the ulcer was 6½ inches long and 31/3 inches wide. Law describes an ulcer measuring 6 inches by 3 inches (Dublin Hosp. Gaz., ii. p. 51).
The ulcer is usually round or oval in shape. The outline of the ulcer may become irregular by unequal extension in the periphery, or by the coalescence of two or more ulcers, or by partial cicatrization. Simple ulcers, especially when seated near the lesser curvature, have a tendency to extend transversely to the long axis of the stomach, thus following the course of the blood-vessels. By this mode of extension, or more frequently by the coalescence of several ulcers, are formed girdle ulcers, which more or less completely surround the circumference of the stomach, oftener in the pyloric region than elsewhere.
As the ulcer extends in depth it often destroys each successive layer of the stomach in less extent than the preceding one, so that the form of the ulcer is conical or funnel-shaped, with a terrace-like appearance in its sloping edges. The apex of the truncated cone, which is directed toward the peritoneum, is often not directly opposite to the centre of the base or superior surface which occupies the mucous membrane, so that one side of the cone may be vertical and the other sloping. In the half of the stomach nearer the lesser curvature the cone slopes upward, and in the lower half of the stomach it slopes downward. The usual explanation of its conical shape is that the ulcer exactly corresponds to the territory supplied by an artery with its branches. Virchow finds an explanation for the oblique direction of the funnel in the arrangement of the arteries of the stomach. These, coming from different sources, run along the curvatures of the stomach, and there give off symmetrically branches which run obliquely toward the mucous membrane, so that one of these [p. 505]branches with its distributive twigs (arterial tree) would supply a part shaped like an oblique funnel. One of the chief supports of the theory which refers the origin of simple gastric ulcer to an arrest of the circulation is this correspondence in shape of the ulcer to the area of distribution of the branches of the arteries supplying the stomach.
All ulcers do not present the conical form and terraced edges which have been described. These appearances are far from constant in fresh ulcers, and they are usually absent in those of long duration.
The most characteristic anatomical feature of simple ulcer of the stomach is the appearance of the edges and of the floor of the ulcer. The edges of recently-formed ulcers (acute ulcers) are clean-cut, smooth, and not swollen. To use Rokitansky's well-known comparison, the hole in the mucous coat looks as if it had been punched out by an instrument. The floor of the ulcer may be smooth and firm or soft and pulpy. The floor and edges of fresh ulcers are often infiltrated with blood, but they may be of a pale-grayish color. Usually no granulations and no pus are to be seen on the surface of the ulcer.70 In ulcers of longer duration the margins become thickened, indurated, and abrupt; the floor acquires a dense fibrous structure.
70 In rare instances granulations may be present, as in a case of W. Müller's, in which their presence rendered difficult the diagnosis of simple ulcer from carcinoma (Jenaische Zeitschrift, v., 1870). The microscope may also be required to distinguish the irregularly thickened margins of old ulcers from scirrhous cancer.
The floor of the ulcer may be the submucous, the muscular, or the serous coat, or, if the whole thickness of the stomach be perforated, it may be some adjacent organ to which the stomach has become adherent, this organ being usually the pancreas or the left lobe of the liver or neighboring lymphatic glands.
The microscopic examination of recently-formed ulcers shows that the tissue immediately surrounding the ulcer is composed of granular material, disintegrated red blood-corpuscles, pale and swollen fragments of connective-tissue fibres, and cells unaffected by nuclear-staining dyes. The red blood-corpuscles are sometimes broken into fragments of various sizes in about the same way as by the action of heat. The gastric tubules are separated from each other and compressed by infiltrated blood, and contain cells which do not stain. Around this margin of molecular disintegration, which has evidently been produced by the action of the gastric juice, there is often, although not constantly, a zone of infiltration with small round cells, probably emigrated white blood-corpuscles. These cells are most abundant near the muscularis mucosæ and in the submucosa. Extravasated red blood-corpuscles extend a variable distance around the ulcer, farthest as a rule in the submucous coat. Many of the blood-vessels in the immediate neighborhood of the ulcer appear normal; others, particularly the arterioles and the capillaries, may be filled with hyaline thrombi. Clumps of hyaline material may also be seen in the meshes of the tissue around the ulcer. Fine fatty granules may be seen in the tissue near the ulcer. The interstices of the loose submucous tissue and the lymphatic vessels are often filled with fibrillated fibrin and scattered blood-corpuscles for a considerable distance around the ulcer.
In the margins of old gastric ulcers there is also a zone of molecular necrosis. The induration and the thickening of the edges of these ulcers [p. 506] are caused by a new growth of fibrillated connective tissue, which blends together all of the coats invaded by the ulcer. This new tissue is usually rich in lymphoid cells, which are often most abundant in the lymphatic channels. In the fibrous edges and base of old ulcers are arteries which are the seat of an obliterating endarteritis, and which may be completely obliterated by this process. An interstitial neuritis may affect the nerve-trunks involved in the fibrous growth. Blood-pigment may be present as an evidence of an old hemorrhagic infiltration.71
71 The histological changes here described are based upon the examination of typical specimens both of recent and of old gastric ulcers which have come under my observation.
Cicatrization is accomplished by the development of fibrous tissue in the floor and borders of the ulcer. By the contraction of this new-formed tissue the edges of the mucous membrane are united to the floor of the ulcer, and may be drawn together so as to close completely the defect in the mucous membrane. The result is a white stellate cicatrix, which is usually somewhat depressed and surrounded by puckered mucous membrane. It is probable that small, superficial ulcers may be closed so that the scar cannot be detected. The mucous membrane which has been drawn over the cicatrix is intimately blended with the fibrous substratum, and is usually itself invaded by fibrous tissue which compresses and distorts the gastric tubules. Hauser72 has shown that the tubular glands grow down into the cicatricial tissue, where they may branch in all directions. These new-formed tubules are lined by clear cylindrical or cutical epithelial cells, and may undergo cystic dilatation. Very irregular cicatrices may result from the healing of large and irregular ulcers. When the ulcer is large and deep and the stomach is adherent to surrounding parts, the edges of the mucous membrane making the border of the ulcer cannot be united by the contraction of the fibrous tissue in the floor of the ulcer. The cicatrix of such ulcers consists of fibrous tissue uncovered by mucous membrane. The closure of the ulcer is incomplete. Such cicatrices are liable to be the seat of renewed ulceration.
72 Das chronische Magengeschwür, etc., Leipzig, 1883. In the rare instances of carcinoma developing in the borders or in the cicatrix of gastric ulcer, Hauser believes that the cancerous growth starts from these glandular growths, which in general have only the significance of Friedländer's atypical proliferation of epithelial cells.
The formation and contraction of the cicatrix may cause various deformities of the stomach. The character of these deformities depends upon the situation, the size, and the depth of the ulcer which is cicatrized. Among the most important of these distortions are stenosis of the pyloric orifice, followed by dilatation of the stomach, more rarely stenosis of the cardiac orifice, with contraction of the stomach, approximation of the cardiac and of the pyloric orifices by the healing of ulcers on the lesser curvature, and an hour-glass form of the stomach, produced by the cicatrization of girdle ulcers or of a series of ulcers extending around the stomach. These abnormalities in form of the stomach, particularly the constriction of the orifices, may be attended by more serious symptoms than the original ulcer.
As the ulcer extends in depth a circumscribed peritonitis, resulting in the formation of adhesions between the stomach and surrounding parts, is usually excited before the serous coat is perforated, so that the gravest of all possible accidents in the course of gastric ulcer—namely, perforation [p. 507]into the peritoneal sac—is permanently or temporarily averted. It has been estimated that adhesions form in about two-fifths of all cases of gastric ulcer (Jaksch). On account of the usual position of the ulcer on the lesser curvature or on the posterior wall of the stomach, the adhesions are most frequently with the pancreas (in about one-half of all cases of adhesion); next in frequency with the left lobe of the liver; rarely with other parts, such as the lymphatic glands, the diaphragm, the spleen, the kidney, the suprarenal capsule, the omentum, the colon, and other parts of the intestine, the gall-bladder, the sternum, and the anterior abdominal wall. Adhesions cannot readily form between the anterior surface of the stomach and the anterior abdominal wall, on account of the constant movement of these parts, so that ulcers of the anterior gastric wall are those most liable to perforate into the peritoneal cavity.
It is difficult to include in any description all of the various and complicated lesions which may result from perforation by gastric ulcer of all of the coats of the stomach. The consequences of perforation may be conveniently classified as follows:
1. Some solid organ, usually the pancreas, the liver, or the lymphatic glands, may close the hole in the stomach.
2. An intra-peritoneal sac shut in by adhesions may communicate through the ulcer with the cavity of the stomach.
3. A fistulous communication may form either between the stomach and the exterior (external gastric fistula) or between the stomach and some hollow viscus (internal gastric fistula).
4. The ulcer may perforate into the general peritoneal cavity.
These lesions may be variously combined with each other. It is to be noted that in the first three varieties protective adhesions are present, and that in the last these adhesions are either absent or ruptured.
When the pancreas, the liver, or the spleen form the floor of the ulcer, they may be protected from extension of the ulcerative process by a new growth of fibrous tissue extending from the floor of the ulcer a variable depth into these organs. Sometimes, however, the ulcerative process, aided doubtless by the corroding action of the gastric juice, eats out large excavations in these organs. These excavations communicate with the cavity of the stomach, and are usually filled with ichorous pus. The pancreas, unlike the spleen and the liver, possesses comparative immunity against this invasion by the ulcerative process.
The situation, the form, and the extent of circumscribed peritoneal abscesses resulting from perforation of gastric ulcer depend upon the parts with which the stomach has contracted adhesions. Should an ulcer on the posterior wall of the stomach perforate before the formation of adhesions, the perforation would of course be directly into the lesser peritoneal cavity. An interesting example of this rare occurrence has been communicated by Chiari.73 In this case, the foramen of Winslow being closed by adhesions, the lesser peritoneal cavity which communicated with a gastric ulcer was filled with ichorous pus, and in this floated the pancreas, which had necrosed in mass and had separated as a sequestrum. That form of intra-peritoneal abscess known as subphrenic pneumo-pyothorax has been already described under Symptomatology. Peritoneal abscesses communicating with the stomach may open into various places, [p. 508]as into the general peritoneal cavity, into the pleural cavity, into the retro-peritoneal tissue, through the abdominal or thoracic walls, etc.
73 Wiener med. Wochenschr., 1876, No. 13.
Gastro-cutaneous fistulæ are a rare result of the perforation of gastric ulcer.74 The external opening is most frequently in the umbilical region, but it may be in the epigastric or in the left hypochondriac region or between the ribs. Fistulous communications resulting from the perforation of gastric ulcer have been formed between the stomach and one or more of the following hollow viscera or cavities: the colon, the duodenum and other parts of the small intestine, the gall-bladder, the common bile-duct, the pancreatic duct, the pleura, the lung, the left bronchus, the pericardium, and the left ventricle. Gastro-colic fistulæ, in contrast to gastro-cutaneous fistulæ, are more frequently produced by cancer than by ulcer of the stomach.75 In rare instances the peritoneum over ulcers of the lesser curvature has contracted adhesions with the pyloric portion of the stomach or with the first part of the duodenum. To accomplish this it is necessary that a sharp bend in the lesser curvature should take place. By extension of the ulcerative process abnormal communication is established between the left and the right half of the stomach or between the stomach and the duodenum. In either case the right half of the stomach is often converted into a large blind diverticulum, the digested food passing through the abnormal opening.76 Gastro-duodenal fistulæ are more frequently with the third than with the first part of the duodenum. In one of Starcke's cases the stomach communicated with the colon and through the medium of a subphrenic abscess with the left lung.77
74 Of the 25 cases of gastro-cutaneous fistula collected by Murchison, 18 were the result of disease. In 12 of these cases the probable cause was simple gastric ulcer (Med.-Chir. Trans., vol. xli. p. 11, London, 1858). Middeldorpf says that among the internal causes of the 47 cases of external gastric fistula which he tabulated, simple ulcer of the stomach played an important rôle (Wiener med. Wochenschr., 1860).
75 Of 33 cases of gastro-colic fistula collected by Murchison, 21 were from gastric cancer and 9 or 10 probably from simple ulcer. On the other hand, gastro-cutaneous fistulæ are twice as frequently the result of simple ulcer as of cancer (Edinb. Med. Journ., vol. iii. 1857).
76 Thierfelder has made the best study of the complicated relations existing in these cases (Deutsches Arch. f. klin. Med., Bd. iv. p. 33, 1868).
77 Deutsche Klinik, 1870, No. 39. Habershon also reports a case in which a subphrenic abscess communicated with the lung, the stomach, and the colon, but he believes that the ulceration was primary in the colon (Guy's Hosp. Rep., Ser. 3, vol. i. p. 109).
Four cases of perforation of gastric ulcer into the pericardium,78 with the production of pneumo-pericardium, have been reported, and two cases of perforation into the left ventricle.79 Müller found lumbricoid worms in a pleural cavity which had been perforated by gastric ulcer.80 Diaphragmatic hernia may result from perforation of the pleural cavity by gastric ulcer.81 In one instance the greater part of the small intestines [p. 509]passed through a hole in the transverse meso-colon which had been caused by a gastric ulcer.
78 Hallin, Schmidt's Jahrb., cxix. S. 37; Säxinger, Prager med. Wochenschr., 1865; Guttmann, Berl. klin. Wochenschr., 1880, No. 23. Murchison mentions a specimen in the museum of King's College, London, of a simple gastric ulcer opening into the pericardium (Edinb. Med. Journ., vol. iii. p. 6). In a case reported by Graves a liver abscess burst into the stomach and into the pericardium (Clin. Lect., ii. p. 237, Dublin, 1848).
79 Oser, Wiener med. Blätter, 1880, No. 52; Brenner, Wiener med. Wochenschr., 1881, No. 47.
80 Müller, Memorabilien, xvii., Oct., 1872.
81 Needon, Wiener med. Presse, 1869, No. 42. In a case of Günsburg's the hole in the diaphragm was as large as the hand, and the left pleural cavity contained the upper half of the stomach and the spleen (Arch. f. phys. Heilk., xi. 3, 1852).
The various fistulæ which have been mentioned may be either direct or through the medium of an abscess. While some of them are only pathological curiosities, others, particularly the communications of the stomach with the pleural cavity and with the lung, are sufficiently frequent to be of practical clinical interest.
As has already been explained, ulcers of the anterior wall are the ones most liable to perforate into the general peritoneal cavity,82 but on account of their comparative infrequency perforation occurs oftener in other situations, particularly in the lesser curvature and near the pylorus. Except on the anterior wall the perforation is often brought about by the rupture of adhesions which for a time had prevented this accident. In a considerable number of cases, particularly of ulcers on the anterior wall, the ulcer looks as if recently formed (acute perforating ulcer); in other cases its thickened and indurated margins indicate long duration. Chiari83 describes a case in which rupture into the peritoneal cavity took place through the cicatrix of an old ulcer, probably in consequence of the distension of the stomach with gas. The hole in the peritoneum is usually circular, smaller than the inner surface of the ulcer, and has sharp, well-defined edges. Less frequently the edges are ragged. Post-mortem digestion may, however, so change the borders of the opening as to make it difficult or impossible to tell from their post-mortem appearances alone whether perforation has occurred before or after death. The peritoneal cavity after death from perforation is found to contain gas and substances from the stomach. Usually within a few hours after perforation septic peritonitis is excited, but in exceptional cases no inflammation of the peritoneum has occurred even when life has been prolonged twenty-four hours after perforation.
82 According to Brinton, "the proportion of perforations to ulcers is such that of every 100 ulcers in each of the following situations, the numbers which perforate are—on the posterior surface, about 2; the pyloric sac, 10; the middle of the organ, 13; the lesser curvature, 18; the anterior and posterior surface at once, 28; the cardiac extremity, 40; and the anterior surface, 85."
83 Wiener med. Blätter, 1881, No. 3.
Emphysema of the subcutaneous, subperitoneal, and other loose areolar tissue of the body is a rare but remarkable result of the perforation of gastric ulcer. The emphysema is sometimes observed shortly before death, but it attains its maximum development after death, when it may spread rapidly over the greater part of the body. The gas consists in part of hydrogen, as it burns with a blue flame. It is generated, at least in great part, by fermentation of the contents of the stomach. The gas may enter the subserous tissue at the edges of the ulcer and thence spread, or, after perforation of the stomach, it may make its way from the peritoneal cavity into the loose subserous connective tissue through some place in the parietal peritoneum which has been macerated, perhaps by the digestive action of the gastric juice.84
84 Roger (Arch. gén. de Méd., 1862) and Demarquay (Essai de Pneumatologie médicale, Paris, 1866) deserve the credit of first calling general attention to the occurrence of subcutaneous emphysema after rupture of the digestive tract. The following writers have each reported a case of emphysema following the perforation of gastric ulcers: Cruveilhier, Anat. Path., t. i. livr. xx.; Bell, Edinb. Med. Journ., vol. vi. p. 783; Thierfelder, Deutsches Arch. f. klin. Med., iv., 1868, p. 33; Newman, The Lancet, 1868, vol. ii. p. 728; Poensgen, Das subcutane Emphysem nach continuitätstrennungen des Digestionstractus, etc., Inaug. Diss., Strassburg, 1879, p. 40; Korach, Deutsche med. Wochenschr., 1880 p. 275; [p. 510]Jürgensen, Deutsches Arch. f. klin. Med., Bd. 31, p. 441, 1882. Doubtful cases are reported by Lefèvre, W. Mayer, and Burggraeve. The fullest consideration of the subject is to be found in the dissertation of Poensgen.
In two cases of sudden death from gastric ulcer Jürgensen found gas in the veins and arteries of various parts of the body. He believes that this gas, which certainly was not the result of putrefaction after death, was derived from the stomach, and that it entered during life the circulation through vessels exposed in the borders of the ulcer, thus causing death. In one of the cases a profuse hemorrhage preceded death, and in the other the ulcer had perforated into the peritoneal cavity.85
85 Jürgensen does not consider whether this gas may not have made its way into the blood-vessels after death in a manner similar to its extension through the cellular tissue of the body in the cases of emphysema just mentioned. In the case which he has reported in full interstitial and subserous emphysema could be traced from the ulcer ("Luft im Blute," Deutsches Arch. f. klin. Med., Bd. 31, p. 441, 1882).
The source of hemorrhage from gastric ulcer is from blood-vessels either in the stomach itself or in the neighborhood of the stomach. Hemorrhages slight or of moderate severity occur from the capillaries and small arteries and veins in the mucous and submucous coats. Sometimes profuse and even fatal hemorrhage comes from arteries or from veins in the submucous coat, especially when these vessels are dilated. Quickly-fatal hemorrhages take place from the large vessels between the muscular and the serous coats, particularly from the main trunks on the curvatures. After the formation of adhesions, followed by the perforation of all of the coats of the stomach, profuse bleeding may proceed from the erosion of large vessels near the stomach, such as the splenic, the hepatic, the pancreatico-duodenal arteries, the portal and the splenic veins, and the mesenteric vessels. Bleeding may also occur from vessels in the parenchyma of organs invaded by the ulcer. The most common source of fatal hemorrhage is from the splenic artery, which from its position is peculiarly exposed to invasion by ulcers of the posterior wall of the stomach. The hemorrhage is usually arterial in origin. It may come from miliary aneurisms of the gastric arteries or from varicose veins in the wall of the stomach. As Cruveilhier has pointed out, an ulcer may cicatrize except over one spot corresponding to an artery from which fatal hemorrhage may occur. Ulcers which give rise to large hemorrhages are usually chronic in their course. Those seated on the middle of the anterior wall, although peculiarly liable to perforate, are comparatively exempt from hemorrhage on account of the small size of the blood-vessels there.
Changes in the blood-vessels of the stomach have been seen in a considerable number of cases of gastric ulcer. Instances have been recorded of the association with gastric ulcer of most of the diseases to which blood-vessels are subject. An example in all respects convincing of embolism of the artery supplying the ulcerated region of the stomach has not been published. Probably the best case belonging here is one of perforating ulcer of the stomach with hemorrhagic infiltration in its walls, presented by Janeway to the New York Pathological Society in 1871.86 In this case there was in the gastro-epiploic artery an ante-mortem fibrinous plug which was continued into the nutrient artery of the ulcerated piece of the stomach. No source for an embolus could be found. In one case Merkel found an embolus in a small artery leading to an ulcer [p. 511]of the duodenum.87 The arch of the aorta was atheromatous and contained a thrombus. Patches of hemorrhagic infiltration existed in the stomach.
86 Trans. of the N.Y. Path. Soc., vol. ii. p. 1.
87 Wiener med. Presse, vii. p. 30, 1866.
In many cases thrombosis of the arteries, and especially of the veins involved in the diseased tissue around an ulcer, has been observed, and in some the thrombus was prolonged in the vessels for a considerable distance from the ulcer. It is probable that in most of these cases the thrombus was secondary to the ulcer. Hyaline thrombosis of the capillaries near the ulcer is also to be mentioned.
In a certain, but not large, number of cases atheroma with calcification or with fatty degeneration of the arteries of the stomach has been found associated with gastric ulcer.88 Reference has already been made to the occurrence of obliterating endarteritis in the thickened edges and floor of gastric ulcer, where it is doubtless secondary. In one case of gastric ulcer I found a widespread obliterating endarteritis affecting small and medium-sized arteries in many parts of the body, including the stomach.89
88 For cases in point see Norman Moore, Trans. of the Path. Soc. of London, vol. xxxiv. p. 94.
89 On the posterior wall of the stomach, midway between the greater and the lesser curvature and five inches to the right of the cardiac orifice, was a round ulcer half an inch in diameter, with smooth, sharp edges. In the floor of the ulcer, which extended to the muscular coat, was a small perforated aneurism of a branch of the coronary artery. In addition there were small, granular kidneys, hypertrophied heart without valvular lesion, and chronic interstitial splenitis. Small and medium-sized arteries in the kidneys, spleen, heart, lymphatic glands, and stomach were the seat of a typical endarteritis obliterans, resulting in some instances in complete closure of the lumen of the vessel. The patient, who was attended by Sassdorf, was seized during the night with vomiting of blood, which continued at intervals for twenty-four hours until his death. The patient was a man about fifty years of age, without previous history of gastric ulcer or of syphilis.
In one case Powell90 found a small aneurism of the coronary artery in an ulcer of the lesser curvature of the stomach. Hauser91 found an aneurismal dilatation of an atheromatous and thrombosed arterial twig in the floor of a recent ulcer. In my case of obliterating endarteritis just referred to there was a small aneurism in the floor of the ulcer. These miliary aneurisms in the floor of gastric ulcers seem to be analogous to those in the walls of phthisical cavities. Miliary aneurisms occur in the stomach independently of gastric ulcer, and may give rise to fatal hæmatemesis, as in four cases reported by Galliard.92
90 Trans. of the Path. Soc. of London, vol. xxix.
91 Das chronische Magengeschwür, etc., p. 11, Leipzig, 1883.
92 L'Union méd., Feb. 26, 1884. Curtis reported a case of fatal hæmatemesis from an aneurism, not larger than a small pea, seated in the cicatrix of an old ulcer (Med. Annals of Albany, Aug., 1880).
Gastric ulcer is occasionally associated with waxy degeneration of the arteries of the stomach.93 In most of these cases there were multiple shallow ulcers. Hæmatemesis is generally absent in gastric ulcer resulting from waxy disease of the gastric blood-vessels. As is well known, the amyloid material itself resists the action of the gastric juice.
93 Hauser (op. cit.) alludes to a case in which, with waxy degeneration of the stomach, over one hundred small ulcers were found in different stages of development, from hemorrhagic infiltrations to complete ulcers. Cases belonging here are reported by Fehr, Ueber die Amyloide Degeneration, Inaug. Diss., Bern, 1866; Merkel, Wiener med. Presse, 1869; Edinger, Deutsches Arch. f. klin. Med., Bd. 29, p. 568; Marchiafava, Atti del Accad. Med. di Roma, iii. p. 114; and Mattei, Deutsche med. Zeitung, July 5, 1883.
Finally, varicosities of the veins of the stomach have been once in a [p. 512] while found with gastric ulcer. In a large number, probably in the majority, of cases of gastric ulcer no changes have been found in the blood-vessels of the stomach except such as were manifestly secondary to the ulcer.
That gastric ulcer is frequently complicated with chronic catarrhal gastritis has been repeatedly mentioned in the course of this article.
PATHOGENESIS.—Without doubt, the most obscure chapter in the history of gastric ulcer is that relating to its origin and to its persistence. Notwithstanding a vast amount of investigation and of discussion, unanimity of opinion upon these subjects has not been reached. In view of this uncertainty it is desirable in this article to do little more than to summarize the leading theories as to the development of gastric ulcer.
Most observers are agreed that the digestive action of the gastric juice has some share in the development and the progress of the ulcer, but as to the first cause of the ulcer there are various hypotheses.
The earliest theory refers the origin of simple ulcer of the stomach to inflammation. Since its advocacy by Abercrombie and by Cruveilhier this theory has always had its adherents, particularly among French writers. It is true that in stomachs which are the seat of simple ulcer evidences of inflammation can often be found both in the neighborhood of the ulcer and elsewhere. In recent times the supporters of the inflammatory origin of gastric ulcer lay especial stress upon the presence of foci of infiltration with small round cells in the mucous and the submucous coats.94 But it is difficult to explain by the inflammatory theory the usually solitary occurrence and the funnel-like shape of gastric ulcer.
94 Laveran, Arch. de Phys. norm. et path., 1876, p. 443; Galliard, Essai sur la Pathogenie de l'Ulcère simple de l'Estomac, Thèse de Paris, 1882; Colombo, Annali univ. di Med., 1877.
The theory that gastric ulcer is of neurotic origin has also been advocated. Some refer the origin to the secretion of an excessively acid gastric juice under abnormal nervous influence (Günsburg), others to vaso-motor disturbances, and others to trophic disturbances. Wilks and Moxon compare simple gastric ulcer to ulcers of the cornea resulting from paralysis of the trigeminus. The neurotic theory of the origin of gastric ulcer is altogether speculative and has never gained wide acceptance.95
95 The first to attribute gastric ulcer to nervous influence was Siebert (Casper's Wochenschr. f. d. Heilk., 1842, No. 29, and Deutsche Klinik, 1852). Cf. also Günsburg, Arch. f. phys. Heilk., xi., 1852; Wilks and Moxon, Lect. on Path. Anat., 2d ed., Philada., 1875, p. 386. Osborne in 1845 attributed gastric ulcer to the secretion of an abnormally acid juice by a circular group of the gastric glands (Dublin Journ. of Med. Sci., vol. xxvii. p. 357).
The view which has met with the greatest favor is that which attributes the origin of gastric ulcer to impairment or arrest of the circulation in a circumscribed part of the wall of the stomach, and to a subsequent solution by the gastric juice of the part thus affected. Rokitansky first suggested this view by assigning hemorrhagic necrosis of the mucous membrane as the first step in the formation of the ulcer; but it is Virchow who has most fully developed this view and has given it its main support. The first cause of gastric ulcer, according to Virchow, is a hemorrhagic infiltration of the coats of the stomach induced by local disturbances in the circulation. The part the nutrition of which is thus impaired or destroyed is dissolved by the gastric juice.
[p. 513] The affections of the gastric blood-vessels to which importance has been attached are (a) embolism and thrombosis; (b) diseases of the coats of the vessels, as atheroma, obliterating endarteritis, fatty degeneration, amyloid degeneration, and aneurismal and varicose dilatations; (c) compression of the veins by spasm of the muscular coats of the stomach in vomiting and in gastralgia; (d) passive congestion of the stomach by obstruction in the portal circulation.
In support of this view are urged the following facts: First, it has been proven by the experiments of Pavy that parts of the gastric wall from which the circulation has been shut off undergo digestion; second, hemorrhagic infarctions have been observed in the stomach, both alone (Von Recklinghausen, Hedenius) and associated with gastric ulcer (Key, Rindfleisch); third, the hemorrhagic infiltration in the walls of recently-formed ulcers indicates a hemorrhagic origin; fourth, the funnel-like shape of the ulcer resembles the funnel-shaped area of distribution of an artery; fifth, gastric ulcers have been experimentally produced by injecting emboli into the gastric arteries (Panum, Cohnheim).96
96 Pavy, Philosoph. Trans., 1763, p. 161; V. Recklinghausen, Virchow's Archiv, Bd. 30, p. 368; Axel Key, Virchow und Hirsch's Jahresb., 1870, Bd. ii. p. 155; Rindfleisch, Lehrb. d. path. Gewebelehre, 5te Aufl., Leipzig, 1878; Panum, Virchow's Archiv, Bd. 25, p. 491; Cohnheim, Vorles. über allgem. Path., Bd. ii. p. 53, Berlin, 1880.
The main objections to this view are the infrequency with which the assumed changes in the blood-vessels have been demonstrated, the common occurrence of gastric ulcer at an age earlier than that at which diseases of the blood-vessels are usually present, and the absence of gastric ulcer in the vast majority of cases of heart disease, with widespread embolism of different organs of the body. To meet some of these objections, Klebs97 presupposes in many cases a local spasmodic contraction of the gastric arteries, causing temporary interruption of the circulation; Rindfleisch and Axel Key, compression of the gastric veins, with resulting hemorrhagic infiltration by spasm of the muscular coat of the stomach in vomiting and in gastralgic attacks. But these are pure hypotheses.
97 Handb. d. path. Anat., Bd. i. p. 185, Berlin, 1869.
What is actually known concerning diseases of the gastric blood-vessels in ulcer of the stomach has already been stated under the morbid anatomy. From this it may be inferred that the origin of gastric ulcer in diseased conditions of the blood-vessels has been established only for a comparatively small group of cases.
Böttcher's98 view that gastric ulcer is of mycotic origin, being produced by micrococci, has thus far met with no confirmation.
98 Dorpater med. Zeitschr., Bd. v. p. 148, 1874.
There are those who hold an eclectic view concerning the origin of gastric ulcer. They believe that ulcer of the stomach may be produced by a variety of causes, such as inflammation, circulatory disturbances, irritating substances introduced into the stomach, traumatism, etc. The peculiarities of the ulcer are due not to any specific cause, but to the solvent action of the gastric juice, which keeps clean the floor and the sides of the ulcer. These clean edges and floor, which are incident to all ulcers of the stomach, justify no conclusion as to the cause of the ulcer. Engel99 over thirty years ago held that gastric ulcer might [p. 514]originate in various ways—that there was nothing specific about it. Brinton was also of similar opinion.
99 Prager Vierteljahrschr., 1853, ii.
Gastric ulcers have been produced experimentally in animals in a variety of ways, but these experiments have not materially elucidated the pathenogenesis of ulcer in man. Schiff by lesions of various parts of the brain, and later Ebstein by lesions of many parts of the central and peripheral nervous system by injections of strychnine—in fact, apparently by any means which greatly increased the blood-pressure—produced in the stomachs of animals ecchymoses and ulcers. Müller by ligation of the portal vein, Pavy by ligation of arteries supplying the stomach, likewise produced hemorrhages and ulcers. The results of Pavy could not be confirmed by Roth and others. Panum, and afterward Cohnheim, produced gastric ulcers by introducing multiple emboli into the gastric arteries. Daettwyler under Quincke's direction caused, in dogs with gastric fistulæ, ulcers of the stomach by various mechanical, chemical, and thermic irritants applied to the inner surface of the stomach. Aufrecht observed hemorrhages and ulcers in the stomachs of rabbits after subcutaneous injections of cantharidin.100
100 Schiff, De vi motorea baseos encephali, 1845, p. 41; Ebstein, Arch f. exp. Path. u. Pharm., 1874, p. 183; Müller, Das corrosive Geschwür im Magen, etc., p. 273, Erlangen, 1860; Pavy, Guy's Hosp. Rep., vol. xiii., 1867; Roth, Virchow's Archiv, Bd. 45, p. 300, 1869; Panum, loc. cit.; Cohnheim, op. cit.; Daettwyler, Quincke, Deutsche med. Wochenschr., 1882, p. 79; Aufrecht, Centralbl. f. d. med. Wiss., 1882, No. 31.
The most interesting of these experiments are those of Cohnheim and of Daettwyler, who demonstrated that in one essential point all of these experimental ulcers differ from simple gastric ulcer in man—namely, in the readiness with which they heal. To this ready healing the gastric juice, much as it has been accused of causing the spread of gastric ulcers in man, seems to have offered no obstacle. We know that similar losses of substance in the human stomach heal equally well.101 Hence it has been maintained throughout this article that it is unjustifiable to regard all of the scars found in the human stomach as the result of simple ulcer.
101 Portions of the mucous membrane of the stomach, sometimes with some of the submucous coat, have been in several instances removed with the stomach-pump, but thus far no bad effects have followed.
It appears from these experiments, as well as from observations on man, that it is more difficult to explain why ulcers in the stomach do not heal than it is to understand how they may be produced. From this point of view the observation of Daettwyler is of interest, that in dogs which had been rendered anæmic by repeated abstraction of blood not only did slighter irritants suffice to produce ulcers of the stomach, but the ulcers healed much more slowly. Practically, it is important to learn what are the obstacles to the repair of gastric ulcers, but our positive knowledge of these is slight. It is probable that such obstacles are to be found in constitutional causes, such as anæmia and chlorosis, in abnormal states of the blood-vessels around the ulcer, in catarrhal affections of the stomach, in irritating articles of food, in improper modes of living, and in increased acidity of the gastric juice.
DIAGNOSIS.—In many cases the diagnosis of gastric ulcer can be made with reasonable certainty; in other cases the diagnosis amounts only to a suspicion more or less strong, and in still other cases the diagnosis is impossible.
[p. 515] The diagnostic symptoms are epigastric pain, vomiting, and gastric hemorrhage. The characteristics of the pain which aid in the diagnosis are its fixation in one spot in the epigastric region, its onset soon after eating, its dependence upon the quantity and the quality of the food, its relief upon the complete expulsion of the contents of the stomach, its alleviation by changes in posture, and its increase by pressure. That the pain of gastric ulcer has not always these characteristics has been mentioned under the Symptomatology. Vomiting without hæmatemesis is the least characteristic of these symptoms. It aids in the diagnosis when it occurs after eating at the acme of a gastralgic attack and is followed by the relief of pain. Hæmatemesis is the most valuable symptom in diagnosis. The more profuse the hemorrhage and the younger the individual in whom it occurs, the greater is the probability of gastric ulcer. It should not be forgotten that the blood is sometimes discharged solely by the stools.
The simultaneous occurrence of all these symptoms renders the diagnosis of gastric ulcer easy.102 In all cases in which gastrorrhagia is absent the diagnosis is uncertain; but gastric ulcer should be suspected whenever the ingestion of food is followed persistently by severe epigastric pain and other causes of the pain have not been positively determined. When the course of the ulcer is latent and when the symptoms are only those of dyspepsia, the diagnosis is of course impossible. In cases previously obscure a diagnosis in extremis is sometimes made possible by the occurrence of perforation of the stomach.
102 That even under the most favorable circumstances absolute certainty in the diagnosis of gastric ulcer is not reached is illustrated by a case reported with great precision and fulness by Banti: A female servant, twenty-one years old, had every symptom of gastric ulcer, including repeated hæmatemesis and the characteristic epigastric pain. She was nourished by enemata. She died from an ulcerative proctitis four days after the last hemorrhage from the stomach. Only a slight catarrhal inflammation of the stomach was found at the autopsy, without trace of ulcer, cicatrix, or ecchymosis ("Di un Caso d'Ematemesi," La Sperimentale, Feb., 1880, p. 168). It would seem as if there must have been an ulcer which had healed so completely as to leave no recognizable scar.
In making a differential diagnosis of gastric ulcer, as well as of any disease, reliance should be placed more upon the whole complexion of the case than upon any fancied pathognomonic symptoms.
The diseases which are most difficult to distinguish from gastric ulcer are nervous affections of the stomach. Like gastric ulcer, most of these are more common in women than in men, and especially in chlorotic women with disordered menstruation and with hysterical manifestations. These nervous affections are manifold and their leading characteristics are not yet well defined. The most important of these affections are nervous dyspepsia, nervous vomiting, nervous gastralgia, and gastric crises.
The leading symptoms of nervous dyspepsia, as described by Leube,103 are the ordinary symptoms of dyspepsia without evidence of anatomical alteration of the stomach, and with the proof by washing out the stomach that the process of digestion is not delayed. Nervous dyspepsia is often associated with other nervous affections, and is caused especially by influences which depress the nervous system. Epigastric pain, and especially tenderness on pressure over the stomach, are not common symptoms in nervous dyspepsia. Only those rare cases of gastric ulcer in which hemorrhage from the stomach is absent and epigastric pain is not prominent [p. 516]are likely to be confounded with nervous dyspepsia. In such cases, although the diagnosis of nervous dyspepsia is by far the most probable, the patient may be confined to bed and put upon the strict regimen for gastric ulcer. If in the course of ten days or two weeks essential relief is not obtained, ulcer may be excluded, and the proper treatment for nervous dyspepsia with tonics and electricity may be adopted (Leube).
103 Deutches Arch. f. klin. Med., Dec. 18, 1878.
In nervous vomiting, which occurs most frequently in hysterical women, other nervous manifestations are present; there are usually less epigastric pain and tenderness than in ulcer; the nutrition is better preserved; the vomiting is less dependent upon the ingestion of food and more dependent on mental states; and there are longer intervals of relief than in ulcer. Still, it may be necessary to resort to the therapeutical diagnosis as in the preceding instance.
In this connection attention may be called to the importance of searching for reflex causes of vomiting, such as beginning phthisis, ovarian or uterine disease, cerebral disease, and pregnancy; also to certain cases of chronic Bright's disease in which gastric disturbances are the main symptoms.
Of all the nervous affections of the stomach, nervous gastralgia is the one which presents the greatest similarity to gastric ulcer. Its diagnosis from gastric ulcer is often extremely difficult, and may be impossible. The points of difference given in the following table may aid in the diagnosis:
| NERVOUS GASTRALGIA. | ULCER OF THE STOMACH. |
| 1. Pain is often independent of the ingestion of food, and may even be relieved by taking food. | 1. Pain is mostly dependent upon taking food, and its intensity varies with the quality and the quantity of the food. |
| 2. Pain is often relieved by firm pressure. | 2. Pain is increased by pressure. |
| 3. Pain is rarely relieved by vomiting. | 3. Pain after a meal is usually relieved by vomiting. |
| 4. Fixed point of tenderness and of subjective pain not generally present. | 4. These are often present. |
| 5. Relief is usually complete between the paroxysms. | 5. Some pain often continues between the paroxysms. |
| 6. Nutrition frequently well preserved. | 6. Nutrition usually affected. |
| 7. Usually associated with other nervous affections, such as hysteria, neuralgia in other places, ovarian tenderness, etc. | 7. Neuropathic states less constantly present. |
| 8. Benefited less by regulation of diet than by electricity and tonic treatment. | 8. Benefited not by electricity, but by regulation of diet. |
| 9. Not followed by dilatation of stomach. | 9. Dilatation of stomach may supervene. |
According to Peter,104 the surface temperature of the epigastrium is elevated in gastric ulcer, but not in nervous gastralgia.
104 Gaz. des Hôp., June, 1883.
Probably not a single one of the points mentioned in the table is without exception. Nervous gastralgia may be associated with gastric ulcer, and if the ulcer is otherwise latent the diagnosis is manifestly impossible. A diagnosis of purely functional gastralgia has been repeatedly overthrown by the occurrence of profuse hæmatemesis. There is no symptom [p. 517] upon which it is more unsatisfactory to base a diagnosis than upon pain. There is much difference among physicians as regards the frequency with which they diagnose gastric ulcer in the class of cases here described. It is probable that the error is oftenest a too frequent diagnosis of gastric ulcer than the reverse. Nevertheless, when there is doubt it is well to submit the patient for a time to the proper treatment for gastric ulcer.
In several instances gastric crises have been mistaken for gastric ulcer. These gastric or gastralgic crises, as they are called by Charcot, by whom they have been best described,105 are most frequently associated with locomotor ataxia, but they may occur in connection with other diseases of the spinal cord (subacute myelitis, general spinal paralysis, and disseminated sclerosis), and an analogous affection has been described by Leyden106 as an independent disease under the name of periodical vomiting with severe gastralgic attacks. Gastric crises have been most carefully studied as a symptom in the prodromic stage of locomotor ataxia. The distinguishing features of these crises are the sudden onset and the atrocious severity of the gastric pain; the simultaneous occurrence of almost incessant vomiting; the habitual continuance of the paroxysms, almost without remission, for two or three days; the normal performance of the gastric functions in the intervals between the paroxysms, which may be months apart; the frequent association with other prodromic symptoms of locomotor ataxia, such as ocular disorders and fulgurating pains in the extremities; and the development after a time of ataxia. Leyden has observed during the attacks retraction of the abdomen without tension of the abdominal walls, obstinate constipation, scanty, dark-colored urine, even anuria for twenty-four hours, and increased frequency of the pulse (also noted by Charcot). Vulpian107 mentions a case in which there was vomiting of dark-colored blood, and in which naturally the diagnosis of gastric ulcer had been made. In the autopsies of Leyden and of Charcot no lesions of the stomach have been found.
105 Leç. sur les Maladies du Syst. nerveux, t. ii. p. 32, Paris, 1877.
106 Zeitschr. f. klin. Med., iv. p. 605, 1882.
107 Maladies du Syst. nerveux, p. 273, Paris, 1879.
The differential diagnosis of gastric ulcer from gastric cancer will be considered in the article on GASTRIC CANCER.
It has already been said that a part of the symptoms of gastric ulcer are due to an associated chronic catarrhal gastritis. Usually other symptoms are present which render possible the diagnosis of the ulcer. There is usually some apparent external or internal cause of chronic catarrhal gastritis, whereas the etiology of ulcer is obscure; in chronic gastritis gastralgic paroxysms and the peculiar fixed epigastric pain of gastric ulcer are usually absent; in chronic gastritis profuse hæmatemesis is a rare occurrence; and in gastritis the relief obtained by rest and proper regulation of the diet, although manifest, is usually less immediate and striking than in most cases of gastric ulcer.
The passage of gall-stones is usually sufficiently distinguished from gastric ulcer by the sudden onset and the sudden termination of the pain, by the situation of the pain to the right of the median line, by the complete relief in the intervals between the attacks, by the occurrence of jaundice, by the recognition sometimes of enlargement of the liver and of the gall-bladder, and by the detection of gall-stones in the feces.
[p. 518] There is not much danger of confounding abdominal aneurism and lead colic with gastric ulcer, and the points in their differential diagnosis are sufficiently apparent to require no description here. The diagnosis of duodenal ulcer from gastric ulcer will be discussed elsewhere. The different causes of gastric hemorrhage, a knowledge of which is essential to the diagnosis of gastric ulcer, will be considered in the article on HEMORRHAGE FROM THE STOMACH.
PROGNOSIS.—Although a decided majority of simple ulcers of the stomach cicatrize, nevertheless, in view of the frequently insidious course of the disease, the sudden perforations, the grave hemorrhages, the relapses, and the sequels of the disease, the prognosis must be pronounced serious.
The earlier the ulcer comes under treatment the better the prognosis. Old ulcers with thickened indurated margins containing altered blood-vessels naturally heal with greater difficulty than recently-formed ulcers.
Profuse hemorrhage adds to the gravity of the diagnosis. It usually indicates that the ulcer has penetrated to the serous coat of the stomach. A hemorrhage may exert a favorable influence, in so far as to convince the patient of the necessity of submitting to the repose and the strict dietetic regimen which the physician prescribes.
The severity of the pain is of little value as a prognostic sign. Vomiting and dyspepsia, if uncontrolled by regulation of the diet, lead to a cachectic state which often ends in death.
Little basis as there is to hope for recovery after perforation into the general peritoneal cavity, there nevertheless have been a very few cases in which there is reason to believe that recovery has actually taken place after this occurrence.108
108 The most convincing case of recovery after perforation of gastric ulcer is one reported by Hughes, Ray, and Hilton in Guy's Hosp. Rep., 1846, p. 332. A servant-girl was suddenly seized with all of the symptoms of perforation. Fortunately, she had eaten nothing for four hours before the attack, and then only gruel. She was placed at once under the influence of opium, was kept in the recumbent posture, and was fed by the rectum. She was discharged apparently cured after fifty-two days. Two months afterward she was again suddenly seized with the same symptoms, and she died in fourteen hours. Shortly before the second perforation she had eaten cherries, strawberries, and gooseberries, which were found in the peritoneal cavity. The autopsy showed, in addition to a recent peritonitis, evidences of an old peritonitis. There were adhesions of the coils of the intestines with each other and between the stomach and adjacent viscera. In the stomach were found a cicatrix and two open ulcers, one of which had perforated.
Other cases in which recovery followed after all of the symptoms of perforation of gastric ulcer were present, but in which no subsequent autopsy proved the correctness of the diagnosis, have been reported by Redwood (Lancet, May 7, 1870); Ross (ibid., Jan. 21, 1871); Tinley (ibid., April 15, 1871); Mancini (La Sperimentale, 1876, pp. 551, 665); and G. Johnson (Brit. Med. Journ., March 26, 1870).
Frazer's two cases, reported in the Dublin Hosp. Gaz., April 15, 1861, are not convincing. The case reported by Aufrecht (Berl. kl. Wochenschr., 1870, No. 21) and the one by Starcke (Deutsche Klinik, 1870, No. 39), which are sometimes quoted as examples of recovery, were cases of circumscribed peritonitis following perforation.
In an interesting case from Nothnägel's clinic reported by Lüderitz, the patient lived sixteen days after perforation into the peritoneal cavity, followed by all of the symptoms of diffuse perforative peritonitis. Death resulted from pneumonia secondary to the peritonitis. At the autopsy were found adhesions over the whole peritoneal surface and streaks of thickened pus between the coils of intestine. The perforation in the stomach was closed by the left lobe of the liver (Berl. kl. Wochenschr., 1879, No. 33).
In estimating the prognosis one should bear in mind the possibility of relapses; of a continuance of gastric disorders, particularly of gastralgia, after cicatrization; of the formation of cicatricial stenosis of [p. 519] the orifices of the stomach; and of the development of dilatation of the stomach.
After the worst has been said concerning the unfavorable issues of gastric ulcer, it yet remains true that the essential tendency of the ulcer when placed under favorable conditions is toward recovery, and that in many cases the treatment of the disease affords most excellent results, and is therefore a thankful undertaking for the physician.
TREATMENT.—In the absence of any agent which exerts a direct curative influence upon gastric ulcer the main indication for treatment is the removal of all sources of irritation from the ulcer, so that the process of repair may be impeded as little as possible.
Theoretically, this is best accomplished by giving to the stomach complete rest and by nourishing the patient by rectal alimentation. Practically, this method of administering food is attended with many difficulties, and, moreover, the nutrition of the patient eventually suffers by persistence in its employment. In most cases the patient can be more satisfactorily nourished by the stomach, and by proper selection of the diet, without causing injurious irritation of the ulcer.
At the beginning of the course of treatment it is often well to withhold for two or three days all food from the stomach and to resort to exclusive rectal feeding. In some cases with uncontrollable vomiting and after-hemorrhage from the stomach it is necessary to feed the patient exclusively by the rectum.
The substances best adapted for nutritive enemata are artificially-digested foods, such as Leube's pancreatic meat-emulsion, his beef-solution, and peptonized milk-gruel as recommended by Roberts.109 Beef-tea and eggs, which are often used for this purpose, are not to be recommended, as the former has very little nutritive value, and egg albumen is absorbed in but slight amount from the rectum. Expressed beef-juice may also be used for rectal alimentation. The peptones, although physiologically best adapted for nutritive enemata, often irritate the mucous membrane of the rectum, so that they cannot be retained. It has been proven that it is impossible to completely nourish a human being by the rectum.110 Rectal alimentation can sometimes be advantageously combined with feeding by the mouth.
109 Leube's pancreatic meat-emulsion is prepared by adding to 4-8 ounces of scraped and finely-chopped beef l-2½ ounces of fresh finely-chopped oxen's or pig's pancreas freed from fat. To the mixture is added a little lukewarm water until the consistence after stirring is that of thick gruel. The syringe used to inject this mixture should have a wide opening in the nozzle; Leube has constructed one for the purpose (Leube, Deutsches Arch. f. klin. Med., Bd. x. p. 11).
The milk-gruel is prepared by adding a thick, well-boiled gruel made from wheaten flour, arrowroot, or some other farinaceous article to an equal quantity of milk. Just before administration a dessertspoonful of liquor pancreaticus (Benger) or 5 grains of extractum pancreatis (Fairchild Bros.), with 20 grains of bicarbonate of soda, are added to the enema. This may be combined with peptonized beef-tea made according to Roberts's formula (Roberts, On the Digestive Ferments, p. 74, London, 1881).
Preparatory to beginning the treatment the bowels should be emptied by a clyster, and this should be occasionally repeated. About three to six ounces of the tepid nutritive fluid should be slowly injected into the rectum. The injections may be repeated at intervals of from three to six hours. If necessary, a few drops of laudanum may be occasionally added to the enema.
110 Voit u. Bauer, Zeitschrift f. Biologie, Bd. v.
There is universal agreement that the dietetic treatment of gastric ulcer is of much greater importance than the medicinal treatment. There is [p. 520] hardly another disease in which the beneficial effects of proper regulation of the diet are so apparent as in gastric ulcer. Those articles of food are most suitable which call into action least vigorously the secretion of gastric juice and the peristaltic movements of the stomach, which do not cause abnormal fermentations, which do not remain a long time in the stomach, and which do not mechanically irritate the surface of the ulcer. These requirements are met only by a fluid diet, and are met most satisfactorily by milk and by Leube's beef-solution.
The efficacy of a milk diet in this disease has been attested by long and manifold experience. By its adoption in many cases the pain and the vomiting are relieved, and finally disappear, and the ulcer heals. In general, fresh milk is well borne. If not, skimmed milk may be employed. If the digestion of the milk causes acidity, then a small quantity of bicarbonate of soda or some lime-water (one-fourth to one-half in bulk) may be added to the milk. Large quantities should not be taken at once. Four ounces of milk taken every two hours are generally well borne. Sometimes not more than a tablespoonful can be taken at a time without causing vomiting, and then of course the milk should be given at shorter intervals. It is desirable that the patient should receive at least a quart, and if possible two quarts, during the twenty-four hours. The milk should be slightly warmed, but in some cases cold milk may be better retained. In some instances buttermilk agrees with the patient better than sweet milk. Although many suppose that they have some idiosyncrasy as regards the digestion of milk, this idiosyncrasy is more frequently imaginary than real. Still, there are cases in which milk cannot be retained, even in small quantity.
For such cases peptonized milk often proves serviceable.111 The artificial digestion of milk as well as of other articles of food is a method generally applicable to the treatment of gastric ulcer. The main objection to peptonized milk is the aversion to it that many patients acquire on account of its bitter taste. The peptonization should not be carried beyond a slightly bitter taste. The disagreeable taste may be improved by the addition of a little Vichy or soda-water. Peptonized milk has proved to be most valuable in the treatment of gastric ulcer.
111 Milk may be peptonized by adding to a pint of fresh milk, warmed to a temperature of 100° F., 5 grs. of extract pancreatis (Fairchild Bros. and Foster) and 20 grs. of bicarb. sodii dissolved in 4 ounces of tepid water. The mixture is allowed to digest for about an hour at a temperature of 100° F., which may be conveniently done by placing the milk in a bowl in a pan of water maintained at this temperature. It is then boiled, strained, and placed on ice, or when the milk is to be taken immediately it is better not to boil it, in order that the partial digestion may continue for a while under the influence of the pancreatic ferment in the stomach. The milk without boiling may be kept on ice without further digestion; and this procedure has the advantage that the pancreatic ferments, although inactive at a temperature near that of ice, are not destroyed. The degree of digestion aimed at is indicated by the production of a slightly, but not unpleasantly, bitter taste. When the digestion is carried to completion, milk has a very bitter and disagreeable flavor. Peptonized milk-gruel, mentioned on page 519, may also be employed.
Leube's beef-solution112 is a nutritious, unirritating, and easily-digested article of diet. It can often be taken when milk is not easily or [p. 521] completely digested, or when milk becomes tiresome and disagreeable to the patient. It is relied upon mainly by Leube in his very successful treatment of gastric ulcer. A pot of the beef-solution (corresponding to a half pound of beef) is to be taken during the twenty-four hours. A tablespoonful or more may be given at a time in unsalted or but slightly salted bouillon, to which, if desired, a little of Liebig's beef-extract may be added to improve the taste. The bouillon should be absolutely free from fat. Unfortunately, not a few patients acquire such a distaste for the beef-solution that they cannot be persuaded to continue its use for any considerable length of time.
112 By means of a high temperature and of hydrochloric acid the meat enclosed in an air-tight vessel is converted into a fine emulsion and is partly digested. Its soft consistence, highly nutritious quality, and easy digestibility render this preparation of the greatest value. The beef-solution is prepared in New York satisfactorily by Mettenheimer, druggist, Sixth Avenue and Forty-fifth street, and by Dr. Rudisch, whose preparation is sold by several druggists.
Freshly-expressed beef-juice is also a fairly nutritious food, which can sometimes be employed with advantage. The juice is rendered more palatable if it is pressed from scraped or finely-chopped beef which has been slightly broiled with a little fresh butter and salt. The meat should, however, remain very rare, and the fat should be carefully removed from the juice.
To the articles of diet which have been mentioned can sometimes be added raw or soft-boiled egg in small quantity, and as an addition to the milk crumbled biscuit or wheaten bread which may be toasted, or possibly powdered rice or arrowroot or some of the infant farinaceous foods, such as Nestle's. Milk thickened with powdered cracker does not coagulate in large masses in the stomach, and is therefore sometimes better borne than ordinary milk.
For the first two or three weeks at least the patient should be confined strictly to the bill of fare here given. Nothing should be left to the discretion of the patient or of his friends. The treatment should be methodic. It is not enough to direct the patient simply to take easily-digested food, but precise directions should be given as to what kind of food is to be taken, how much is to be taken at a time, how often it is to be taken, and how it is to be prepared.
In all cases of any severity the patient should be treated in bed in the recumbent posture, and warm fomentations should be kept over the region of the stomach. Mental and physical fatigue should be avoided.
Usually, at the end of two or three weeks of this diet the patient's condition is sufficiently improved to allow greater variety in his food. Meat-broths may be given. Boiled white meat of a young fowl can now usually be taken, and agreeable dishes can be prepared with milk, beaten eggs, and farinaceous substances, such as arrowroot, rice, corn-starch, tapioca, and sago. Boiled sweetbread is also admissible. Boiled calf's brain and calf's feet are allowed by Leube at this stage of the treatment.
To these articles can soon be added a very rare beefsteak made from the soft mass scraped by a blunt instrument from a tenderloin of beef, so that all coarse and tough fibres are left behind. This may be superficially broiled with a little fresh butter. Boiled white fish, particularly cod, may also be tried.
It is especially important to avoid all coarse, mechanically-irritating food, such as brown bread, wheaten grits, oatmeal, etc.; also fatty substances, pastry, acids, highly-seasoned food, vegetables, fruit, and all kinds of spirituous liquor. The juice of oranges and of lemons can usually be taken. The food should not be taken very hot or very cold.
For at least two or three months the patient should be confined to the [p. 522] easily-digested articles of diet mentioned. These afford sufficient variety, and no license should be given to exceed the dietary prescribed by the physician. Transgression in this respect is liable to be severely punished by return of the symptoms. When there is reason to believe that the ulcer is cicatrized, the patient may gradually resume his usual diet, but often for a long time, and perhaps for life, he may be compelled to guard his diet very carefully, lest there should be a return of the disease. Should there be symptoms of a relapse, the patient should resume at once the easily-digested diet described above.
Medicinal treatment of gastric ulcer, although less efficacious than the dietetic treatment, is not to be discarded. Since its advocacy by Ziemssen the administration of Carlsbad salts or of similarly composed salts belongs to the systematic treatment of gastric ulcer. The objects intended to be accomplished by the use of these salts are the daily evacuation of the contents of the stomach into the intestine by gentle stimulation of the gastric peristaltic movements, the neutralization of the acid of the stomach, and the prevention of acid fermentations in the stomach. Of these objects the most important is the prevention of stagnation of the contents of the stomach. The chief ingredients of the Carlsbad waters are sulphate of sodium, carbonate of sodium, and chloride of sodium. The most important of these ingredients is sulphate of sodium (Glauber's salts), which by exciting peristalsis propels the gastric contents into the intestine, and thus relieves the stomach of its burden, prevents fermentation, and removes from the surface of the ulcer an important source of irritation. The carbonate of sodium neutralizes the acids of the stomach, but the main value of this ingredient and of the chloride of sodium is that in some way they correct the action of the Glauber's salts, so that the latter may be taken in smaller quantity and without the usual unpleasant effects of pure Glauber's salts.113 The artificial Carlsbad salts are to be preferred to the natural or the artificial Carlsbad water. The natural Carlsbad salts and much of those sold as artificial Carlsbad salts consist almost wholly of sulphate of sodium. It is therefore best to prescribe in proper proportion the leading ingredients of these salts. A suitable combination is sulphate of sodium five ounces, bicarbonate of sodium two ounces, and chloride of sodium one ounce (Leichtenstern114). The relative proportion of the ingredients may of course be varied somewhat to suit individual cases. The salts are to be taken daily before breakfast dissolved in a considerable quantity of warm water. One or two heaping teaspoonfuls of the salts are dissolved in one-half to one pint of water warmed to a [p. 523] temperature of 95° F. One-fourth of this is to be drunk at a time at intervals of ten minutes. Breakfast is taken half an hour after the last draught. After breakfast there should follow one or two loose movements of the bowels. If this is not the case, the next day the quantity of the salts is to be increased, or if more movements are produced the quantity is to be diminished until the desired result is obtained. In case the salts do not operate, an enema may be used. Usually, to obtain the same effect, the quantity of salts may be gradually diminished to a teaspoonful.
113 Water from the Sprudel spring contains in 16 ounces 18.2 grains of sulphate of sodium, 14.6 grains of bicarbonate of sodium, and 7.9 grains of chloride of sodium, and 11.8 cubic inches of carbonic acid. Its natural temperature is 158° F. The other Carlsbad springs have the same fixed composition and vary only in temperature and amount of CO2.
114 The second edition of the German Pharmacopoeia contains a formula for making artificial Carlsbad salts, so that the ingredients are in about the same proportion as in the natural water. The formula is as follows: Dried sulphate of sodium 44 parts, sulphate of potassium 2 parts, chloride of sodium 18 parts, bicarbonate of sodium 36 parts. These should be mixed so as to make a white dry powder. The Carlsbad water is imitated by dissolving 6 grammes of this salt in 1 liter of water (Pharmacopoeia Germanica, editio altera, Berlin, 1882, p. 232).
According to a prescription very commonly used in Germany, the Carlsbad salts are made by taking sulphate of sodium 50 parts, bicarbonate of sodium 6 parts, chloride of sodium 3 parts. Dose, a teaspoonful dissolved in one or two tumblers of warm water (Ewald u. Lüdecke, Handb. d. Allg. u. spec. Arzneiverordnungslehre, Berlin, 1883, p. 480).
The Carlsbad salts are directed especially against the chronic gastric catarrh which complicates the majority of cases of ulcer of the stomach. It is well known that the most effective method of treating this morbid condition is the washing out of the stomach by means of the stomach-tube. The propriety of adopting this procedure in gastric ulcer comes, therefore, under consideration. Although the use of the stomach-tube in gastric ulcer is discarded by Leube and by Sée on account of its possible danger, nevertheless this instrument has been employed with great benefit in many instances of this disease by Schliep, Debore, and others.115 No instance of perforation of an ulcer by means of the stomach-tube has been reported, and in general no evil effects have resulted; but Duguet cites a case of fatal hemorrhage following washing out of the stomach.116 In view of the great benefit to be secured by washing out the stomach, and of the comparatively slight danger which attends the process, it seems justifiable to adopt this procedure cautiously and occasionally in cases of gastric ulcer with severe gastric catarrh. Of course only the soft rubber tube should be used, and the siphon process should be adopted.117 The stomach may be washed out with pure warm water or with water containing a little bicarbonate of sodium (one-half drachm to a quart of water). The occasional cleansing of the stomach in this way can hardly fail to promote the healing of the ulcer. Recent or threatened hemorrhage from the stomach would contraindicate the use of the stomach-tube.
115 Schliep, Deutsch. Arch. f. klin. Med., Bd. 13; Debore, L'Union méd., Dec. 30, 1882; Bianchi, Gaz. degli Ospitali, March 26, 1884.
116 Gaz. des Hôp., Apr. 29, 1884. In a case of gastric ulcer of Cornillon severe hemorrhage followed washing out the stomach (Le Prog. méd., Apr. 28, 1883).
117 Soft rubber stomach-tubes are made by Tiemann & Co. in New York, and are sold by most medical instrument-makers. A description of the appropriate tube and of the method of its use is given by W. B. Platt ("The Mechanical Treatment of Diseases of the Stomach," Maryland Medical Journal, March 8, 1884).
Beyond the measures indicated there is little more to do in the way of treatment directed toward the repair of the ulcer. Not much, if anything, is to be expected from the employment of drugs which have been claimed to exert a specific curative action on the ulcer. Of these drugs those which have been held in the greatest repute are bismuth and nitrate of silver. Trousseau118 devised a somewhat complicated plan for administering bismuth and nitrate of silver in succession for several months in the treatment of gastric ulcer. There are few who any longer cherish any faith in these drugs as curative of gastric ulcer. The same may be said of other drugs which have been thought to have similar specific virtue in the treatment of gastric ulcer, such as acetate of lead, arsenic, chloral hydrate, iodoform, etc.
118 Clinique médicale, t. iii. p. 95, Paris, 1865.
[p. 524] It remains to consider therapeutic measures which may be necessary to combat individual symptoms of gastric ulcer.
The pain of gastric ulcer is generally relieved in a few days by strict adherence to the dietetic regimen which has been laid down. When this is not the case, it may be best to withhold all food from the stomach and to nourish by the rectum. But this cannot be continued long without weakening the patient, and sometimes the pain persists in spite of the rest afforded the stomach. Undoubtedly, the most effective means of quieting the pain of gastric ulcer is the administration of opium in some form. Opium should not, however, be resorted to without full consideration of the possible consequences. When the use of this drug is once begun, the patient is liable to become dependent upon it, and may be inclined, consciously or unconsciously, to exaggerate the pain in order to obtain the narcotic. When prescribing opium in this disease the physician should have in mind the danger of establishing the opium habit. Moreover, opium retards digestion, and is anything but an aid to the proper dietetic regimen, which is all-important. If it is decided to give opium, it does not matter much in what form it is administered, but the dose should be as small as will answer the purpose. Hypodermic injections of morphine over the region of the stomach may be recommended. Codeia often produces less disturbance than opium or morphine. A useful powder for the relief of pain is one containing 8 or 10 grains of subnitrate of bismuth, 1/12 grain of sulphate of morphia, and 1/5 grain of extract of belladonna. Much of the beneficial effect attributed to bismuth is in reality due to its customary combination with a small quantity of morphine. Before resorting to opium in cases of severe pain it will be well to try some of the other means for relieving the pain of gastric ulcer, although they are less effective. Gerhardt thinks that astringents are better than narcotics to relieve the pain of ulcer, and he recommends for the purpose three or four drops of solution of chloride of iron diluted with a wineglassful of water, to be taken several times daily. Although this recommendation is from high authority and is often quoted, sufficient confirmatory evidence of its value is lacking. Other medicines recommended are hyoscyamus, belladonna, choral hydrate, chloric ether, hydrocyanic acid, bismuth, nitrate of silver, and compound kino powder. Sometimes warm fomentations, at other times a light ice-bag over the epigastrium, afford marked relief of the pain. Counter-irritation over the region of the stomach has also given relief. This may be effected with a mustard plaster or by croton oil. I have known the establishment of a small nitric-acid issue in the pit of the stomach to relieve the pain, but such severe measures of counter-irritation are generally unnecessary. The application of a few leeches over the epigastrium has been highly recommended, but this should be done without much loss of blood. The effect of position of the body upon the relief of pain should be determined. When the pain is due to flatulence or to acid fermentation in the stomach, the treatment should be directed to those states.
The most effective means of controlling the vomiting in gastric ulcer are the regulation of the diet and, if necessary, the resort to rectal alimentation. Absolute rest should be enjoined. Whenever small quantities of milk, peptonized or in any other form, cannot be retained, then exclusive rectal feeding may be tried for a while. There have been cases of gastric [p. 525] ulcer when both the stomach and the rectum have been intolerant of food. In such desperate cases the attempt may be made to introduce food into the stomach by means of the stomach-tube, for it is a singular fact that food introduced in this way is sometimes retained when everything taken by the mouth is vomited.119 The cautious washing out of the stomach by the stomach-tube may prove beneficial. In these cases the attempt has also been made to nourish by subcutaneous injections of food. In a case of gastric ulcer where no food could be retained either by the stomach or by the rectum Whittaker120 injected subcutaneously milk, beef-extract, and warmed cod-liver oil. The oil was best borne. The injections were continued for four days without food by the mouth or rectum. The patient recovered. At the best, hypodermic alimentation can afford but slight nourishment, and is to be regarded only as a last refuge. If there is danger of death by exhaustion, transfusion may be resorted to.
119 Debore, L'Union médicale, Dec. 30, 1882, and Gaz. des Hôp., April 29, 1884. For this reason Debore makes extensive use of the stomach-tube in general in feeding patients affected with gastric ulcer. He objects to an exclusive milk diet on account of the quantity of fluid necessary to nourish the patient, which he says amounts to three to four quarts of milk daily. To avoid these inconveniences, he gives three times daily drachm viss of meat-powder and drachm iiss of bicarbonate of sodium (or equal parts of calcined magnesia and bicarb. sod.), well stirred into milk. This is to be introduced by the stomach-tube on account of its disagreeable taste. He believes that the addition of the large quantity of alkali prevents digestion from beginning until the food has reached the intestine. He also gives daily a quart of milk containing grs. xv of saccharate of lime. Debore's method of preparing the meat-powder is described in L'Union médicale, July 29, 1882, p. 160. He also uses a milk-powder (ibid., Dec. 30, 1882; see also Le Progrès méd., July 12, 1884).
120 J. T. Whittaker, "Hypodermic Alimentation," The Clinic, Jan. 22, 1876.
Bernutz practised successfully in two cases the hypodermic injection of fresh dog's blood (Gaz. des Hôp., 1882, No. 64).
Krueg (Wiener med. Wochenschr., 1875, No. 34) injected 15 cc. of olive oil twice a day subcutaneously without causing abscesses.
Menzel and Porco were the first to employ hypodermic alimentation (ibid., 1869, No. 31).
Of remedies to check vomiting, first in importance are ice swallowed in small fragments and morphine administered hypodermically. Effervescent drinks, such as Vichy, soda-water, and iced champagne, may bring relief. Other remedies which have been recommended are bismuth, hydrocyanic acid, oxalate of cerium, creasote, iodine, bromide of potash, calomel in small doses, and ingluvin. But in general it is best to forego the use of drugs and to rely upon proper regulation of the diet, such as iced milk taken in teaspoonful doses, and upon repose for the stomach.
Hemorrhage from the stomach is best treated by absolute rest, the administration of bits of ice by the mouth, and the application of a flat, not too heavy, ice-bag over the stomach. The patient should lie as quietly as possible in the supine position, with light coverings and in a cool atmosphere. He should be cautioned to make no exertion. His apprehensions should be quieted so far as possible. All food should be withheld from the stomach, and for four or five days after the cessation of profuse hemorrhage aliment should be given only by the rectum. There is no proof that styptics administered by the mouth have any control over the hemorrhage, and as they are liable to excite vomiting they may do harm. Ergotin, dissolved in water (1 part to 10), may be injected hypodermically in grain doses several times repeated if necessary. If internal styptics [p. 526]are to be used, perhaps the best are alum-whey and a combination of gallic acid 10 grains and dilute sulphuric acid 10 drops diluted with water. Fox praises acetate of lead, and others ergot, tannin, and Monsell's solution. If there is vomiting or much restlessness, morphine should be given hypodermically. If the bleeding is profuse, elastic ligatures may be applied for a short time around the upper part of one or more extremities, so as to shut out temporarily from the circulation the blood contained in the extremity. If syncope threatens, ammonia or a little ether may be inhaled, or ether may be given hypodermically. Brandy, if administered, should be given either by the rectum or hypodermically. Caution should be exercised not to excite too vigorously the force of the circulation, as the diminished force of the heart is an important agent in checking hemorrhage. When life is threatened in consequence of the loss of blood, then recourse may be had to transfusion, but experience has shown that this act is liable to cause renewed hemorrhage in consequence of the elevation of the blood-pressure which follows it. Transfusion is therefore indicated more for the acute anæmia after the hemorrhage has ceased and is not likely to be renewed. It should not be employed immediately after profuse hæmatemesis, unless it is probable that otherwise the patient will die from the loss of blood, and then it is well to transfuse only a small quantity.121
121 Michel transfused successfully in a case of extreme anæmia following gastrorrhagia (Berl. klin. Wochenschr., 1870, No. 49). In a case of profuse and repeated hæmatemesis which followed washing out the stomach Michaelis infused into the veins 350 cc. of solution of common salt. Reaction gradually followed, and the patient recovered. This case, which was one of probable ulcer, illustrates the advantages of infusing a small quantity (ibid., June 23, 1884). The dangers are illustrated by a case reported by V. Hacker, who infused 1500 cc. of salt solution in a patient in a state of extreme collapse resulting from hemorrhage from gastric ulcer. The patient rallied, but he died three hours after the infusion from renewed hemorrhage (Wiener med. Wochenschr., 1883, No. 37). In Légroux's case of gastric ulcer renewed hemorrhage and death followed the transfusion of only 80 grammes of blood (Arch. gén. de Méd., Nov., 1880). In a case quoted by Roussel, Leroy transfused 130 grammes of blood in a girl twenty years old who lay at the point of death from repeated hemorrhages from a gastric ulcer. In the following night occurred renewed hemorrhage and death (Gaz. des Hôp., Sept. 22, 1883). According to the experiments of Schwartz and V. Ott, the transfusion, or rather infusion, of physiological salt solution is as useful as that of blood, and it is simpler and unattended with some of the dangers of blood-transfusion. The formula is chloride of sodium 6 parts, distilled water 1000.
Schilling recommends, when the bleeding is so profuse that the patient's life is threatened, to tampon the stomach by means of a rubber balloon attached to the end of a soft-rubber stomach-tube.122 The external surface of the balloon is slightly oiled. It is introduced into the stomach in a collapsed state, and after its introduction it is moderately distended with air. When the balloon is to be withdrawn the air should be allowed slowly to escape. Schilling tried this procedure in one case of hemorrhage from gastric ulcer, allowing the inflated bag to remain in the stomach twelve minutes. The hemorrhage ceased and was not renewed. Experience only can determine whether this device, to which there are manifest objections, will prove a valuable addition to our meagre means of controlling hemorrhage from the stomach.
122 F. Schilling, Aerztl. Intelligenzbl., Jan. 8, 1884. Schreiber, in order to determine the position of the stomach, was the first to introduce and inflate in this organ a rubber balloon (Deutsches Arch. f. klin. Med., June 5, 1877). Uhler recommends in case of profuse gastric hemorrhage to pass a rubber bag into the stomach and fill it with liquid (Maryland Med. Journ., Aug. 30, 1884, p. 347).
[p. 527] The boldest suggestion ever made for stopping gastric hemorrhage is that of Rydygier, who advocates in case hemorrhage from an ulcer threatens to be fatal to cut down upon the stomach, search for the bleeding ulcer, and then resect it.123 Notwithstanding the great advances made in gastric surgery during the last few years, Rydygier's suggestion seems extravagant and unwarrantable.
123 Berl. klin. Wochenschr., Jan. 16, 1882.
The most effectual treatment of the dyspepsia which is present in many cases of gastric ulcer is adherence to the dietetic rules which have been laid down, aided by the administration of Carlsbad salts and perhaps in extreme cases the occasional and cautious use of the stomach-tube. If eructations of gas and heartburn are troublesome, antacids may be employed, but they should be given in small doses and not frequently, as the ultimate effect of alkalies is to increase the acid secretion of the stomach and to impair digestion. The best alkali to use is bicarbonate of sodium, of which a few grains may be taken dry upon the tongue or dissolved in a little water.
If perforation into the peritoneal cavity occur, then opium or hypodermic injections of morphine should be given in large doses, as in peritonitis. Bran poultices sprinkled with laudanum or other warm fomentations should be applied over the abdomen, although in Germany ice-bags are preferred. Food should be administered only by the rectum. The chances of recovery are extremely slight, but the patient's sufferings are thus relieved. In view of the almost certainly fatal prognosis of perforation of gastric ulcer into the general peritoneal cavity, and in view of the success attending various operations requiring laparotomy, it would seem justifiable in these cases, after arousing, if possible, the patient from collapse by the administration of stimulants per rectum or hypodermically, to open the peritoneal cavity and cleanse it with some tepid antiseptic solution, and then to treat the perforation in the stomach and the case generally according to established surgical methods.124 This would be the more indicated if it is known that the contents of the stomach at the time of perforation are not of a bland nature.
124 Mikulicz has successfully treated by laparotomy a case of purulent peritonitis resulting from perforation of the intestine with extravasation of the intestinal contents. He says that the operation is not contraindicated by existing peritonitis if the patient is not already in a state of collapse or sepsis. The perforation is closed by sutures after freshening the edges of the opening (abstract in the Medical News, Philada., Sept. 6, 1884). Both Kuh and Rydygier recommend opening the abdomen after perforation of gastric ulcer. The borders of the ulcer are to be resected and the opening closed by sutures (Volkmann's Samml. klin. Vorträge, No. 220, p. 12).
It is important to maintain and to improve the patient's nutrition, which often becomes greatly impaired from the effects of the ulcer. This indication is not altogether compatible with the all-important one of reducing to a minimum the digestive work of the stomach. Nevertheless, some of the easily-digested articles of food which have been mentioned are highly nutritious. By means of these and by good hygienic management the physician should endeavor, without violating the dietetic laws which have been laid down, to increase, so far as possible, the strength of his patient. Starvation treatment in itself is never indicated in gastric ulcer. Inunction of the body with oil is useful in cases of gastric ulcer, as recommended by Pepper.125
125 North Carolina Medical Journal, 1880, vol. v. p. 5.
[p. 528] In view of Daettwyler's experiments, mentioned on page 514, it is manifestly important to counteract the anæmia of gastric ulcer. Iron, however, administered by the mouth, disturbs the stomach and is decidedly contraindicated during the active stage of gastric ulcer. During convalescence, only the blandest preparations of iron should be given, and these not too soon, lest they cause a relapse. When the indication to remove the anæmia is urgent, and especially when the chlorotic form of anæmia exists, it may be well to try the hypodermic method of administering iron, although this method has not yet been made thoroughly satisfactory. Especially for the anæmia of gastric ulcer would an efficient and unirritating preparation of iron for hypodermic administration prove a great boon. Probably at present the best preparation for hypodermic use is the citrate of iron, given in one- to two-grain doses in a 10 per cent. aqueous solution, which when used must be clear and not over a month old. The syringe and needle shortly before using should be washed with carbolic acid. The injections are best borne when made into the long muscles of the back or into the nates, as recommended by Lewin for injections of corrosive sublimate. A slight burning pain is felt for ten minutes after the injection. This is the method employed by Quincke with good result and without inflammatory reaction.126 It is well to remember that Kobert127 has found by experiment on animals that large doses of iron injected subcutaneously cause nephritis. Other preparations of iron which have been recommended for hypodermic use are ferrum dialysatum (DaCosta), ferrum pyrophosphoricum cum natr. citrico (Neuss), ferrum pyrophosphoricum cum ammon. citr. (Huguenin), ferrum peptonatum and ferrum oleinicum (Rosenthal).128 When it becomes safe to administer iron by the stomach, then the blander preparations should be used, such as the pyrophosphate, lactate, effervescing citrate, ferrum redactum. Leube recommends the following prescription: Ferr. redact. gr. 80, Pulv. althææ gr. 60, Gelatin q. s.; make 90 pills: at first one, and afterward as many as three, of these pills may be taken three times a day. When carefully prepared the pills are about as soft as butter.
126 Quincke, Deutsch. Arch. f. klin. Med., Bd. xx. p. 27; Glaenecke, Arch. f. exper. Path. u. Pharm., Bd. 17, p. 466.
127 Arch. f. exper. Path. u. Pharm., Bd. 16.
128 DaCosta, N.Y. Med. Record, vol. xiii. p. 290; Neuss, Zeitschrift f. klin. Med., Bd. 3, p. 1; Huguenin, Correspondenzbl. f. Schweiz. Aerzte, 1876, No. 11; Rosenthal, Wiener med. Presse, 1878, Nos. 45-49, and 1884, Jan. 20.
Various sequels of gastric ulcer may require treatment. Cicatrization of the ulcer is by no means always cure in the clinical sense. As the result of adhesions and the formation and contraction of cicatricial tissue very serious disturbances of the functions of the stomach may follow the repair of gastric ulcer. The most important of these sequels is stenosis of the orifices of the stomach, particularly of the pyloric orifice. Very considerable stenosis of the pylorus may be produced before the ulcer is completely cicatrized. In three instances a stenosing ulcer of the pylorus has been successfully extirpated.129 The most important of these sequels [p. 529]of gastric ulcer will be treated of hereafter. Here it need only be said that during convalescence from gastric ulcer attention to diet is all-important. For a long time the diet should be restricted to easily-digested food. The first symptoms of relapse are to be met by prompt return to bland diet, or, if necessary, to rectal alimentation.
129 The successful operators were Rydygier (Berl. klin. Wochenschr., Jan. 16, 1882), Czerny (Arch. f. klin. Chir., Bd. xxx. p. 1), and Van Kleef (Virchow u. Hirsch's Jahresbericht, 1882, Bd. ii. p. 383). Cavazzani cut out by an elliptical incision an old indurated ulcer of the stomach adherent to the anterior abdominal walls. The patient died three years afterward of phthisis (Centralbl. f. Chir., 1879, p. 711). Lauenstein resected the pylorus unsuccessfully for what appears to have been an ulcer of the pylorus with fibroid induration around it (ibid., 1882, No. 9). These four cases (three successful) are all which I have found recorded of resection of gastric ulcer. In my opinion the resection of gastric ulcers which resist all other methods of treatment, and especially those which cause progressive stricture of the pylorus, is a justifiable operation.
Ulcers of the stomach which do not belong to the category of simple ulcer are for the most part of pathological rather than of clinical interest.
Although miliary tubercles in the walls of the stomach are more frequent than is generally supposed, genuine tuberculous ulcers of the stomach are not common. The most important criterion of these ulcers is the presence of tuberculous lymphatic glands in the neighborhood, and of miliary tubercles upon the peritoneum corresponding to the ulcer. Sometimes miliary tubercles can be discovered in the floor and sides of the ulcer. Tuberculous gastric ulcers, when they occur, are usually associated with tuberculous ulceration of the intestine. In an undoubted case of tuberculous ulcer of the stomach reported by Litten, however, this was the only ulcer to be found in the digestive tract.130 Tuberculous gastric ulcers generally produce no symptoms, but they have been known to cause perforation of the stomach and hæmatemesis. Many cases which have been recorded as tuberculous ulcers of the stomach were in reality simple ulcers. Cheesy tubercles as large as a pea, both ulcerated and non-ulcerated, have been found in the stomach, but they are very rare.
130 Litten, Virchow's Archiv, Bd. 67, p. 615.
Typhoid ulcers may also occur in the stomach, but they are infrequent. Both perforation of the stomach and gastrorrhagia have been caused by typhoid ulcers, which, as a rule, however, produce no symptoms distinctly referable to the ulcer.
Syphilitic ulcers and syphilitic cicatrices of the stomach have been described, without sufficient proof as to their being syphilitic in origin.
Necrotic ulcers, probably mycotic in origin, may be found in the stomach in cases of splenic fever, erysipelas, pyæmia, etc.
Ulceration occurring in toxic, in diphtheritic, and in phlegmonous gastritis need not be discussed here.
Follicular and catarrhal ulcers of the stomach have been described, but without sufficient ground for separating them from hemorrhagic erosion on the one hand and simple ulcer on the other.
Hemorrhagic erosions of the stomach, to which formerly so much importance was attached, are now believed to be without clinical significance. They are found very frequently, and often very abundantly, after death from a great variety of causes.
DEFINITION.—Cancer of the stomach is characterized anatomically by the formation in this organ of a new growth, composed of a connective-tissue stroma so arranged as to enclose alveoli or spaces containing cells resembling epithelial cells. The growth extends by invading the tissues surrounding it, and frequently gives rise to secondary cancerous deposits in other organs of the body. The forms of cancer which occur primarily in the stomach are scirrhous, medullary, colloid, and cylindrical epithelial cancer. The disease develops usually in advanced life. Rarely latent, occasionally without symptoms pointing to the stomach as the seat of disease, gastric cancer is usually attended by the following symptoms: loss of appetite, indigestion, vomiting with or without admixture with blood, pain, a tumor in or near the epigastric region, progressive loss of flesh and strength, and the development of the so-called cancerous cachexia. The disease is not curable. After its recognition it rarely lasts longer than from twelve to fifteen months.
SYNONYMS.—Carcinoma ventriculi; Malignant disease of the stomach. Of the many synonyms for the special forms of cancer, the most common are—for scirrhous, hard, fibrous; for medullary, encephaloid, soft, fungoid; for colloid, gelatinous, mucoid, alveolar; and for cylindrical epithelial, cylindrical-celled or cylindrical or columnar epithelioma, cylindrical-celled cancroid, destructive adenoma.
HISTORY.—Cancer of the stomach was known to the ancients only by certain disturbances of the gastric functions which it produces. The disease itself was not clearly appreciated until its recognition by post-mortem examinations, which began to be made with some frequency after the revival of medicine in the sixteenth century. During the seventeenth and eighteenth centuries several instances of gastric cancer are recorded, the best described being those observed and collected by Morgagni (1761). During this period scirrhus was regarded as the type of cancerous disease. It was a common custom to call only the ulcerated scirrhous tumors cancerous.
With the awakened interest in pathological anatomy which marked the beginning of the present century, the gross anatomical characters of cancer and the main forms of the disease came to be more clearly recognized. After the description of encephaloid cancer by Laennec1 in 1812, [p. 531] and the first clear recognition of colloid cancer by Otto2 in 1816, these two forms of cancer took rank with scirrhus as constituting the varieties of cancer of the stomach as well as of cancer elsewhere. All that it was possible to accomplish in the description of cancer of the stomach from a purely gross anatomical point of view reached its culmination in the great pathological works of Cruveilhier (1829-35) and of Carswell (1838), both of whom admirably delineated several specimens of gastric cancer.
1 Dict. des Sciences méd., t. i. and t. xii., Paris, 1812-15.
2 Otto, Seltens Beobachtungen, etc., 1816.
During this period of active anatomical research the symptomatology of gastric cancer was not neglected. The article on cancer by Bayle and Cayol in the Dictionnaire des Sciences médicales, published in 1812, shows how well the clinical history of gastric cancer was understood at that period.
Cylindrical-celled epithelioma of the stomach could not be recognized as a separate form of tumor until the application of the microscope to the study and classification of tumors—an era introduced by Müller in 1838.3 Cylindrical-celled epithelioma of the stomach was first recognized by Reinhardt in 1851, was subsequently described by Bidder and by Virchow, and received a full and accurate description from Förster in 1858.4
3 Ueber den feineren Ban, etc., der krankh. Geschwülste, Berlin, 1838.
4 Reinhardt, Annalen d. Charité, ii. 1, 1851; Bidder, Müller's Archiv, 1852, p. 178; Virchow, Gaz. méd. de Paris, April 7, 1855; Förster, Virchow's Archiv, Bd. 14, p. 91, 1858.
Until the publication by Waldeyer5 in 1867 of his memorable article on the development of cancers, it was generally accepted that gastric cancer originated in the submucous coat of the stomach, and that the cells in the cancerous alveoli were derived from connective-tissue cells. Waldeyer attempted to establish for the stomach his doctrine that all cancers are of epithelial origin. In all varieties of gastric cancer he believed that he could demonstrate the origin of the cancer-cells from epithelial cells of the gastric tubules—a mode of origin which had previously been advocated for cylindrical epithelioma by Cornil6 (1864). Waldeyer's view has met with marked favor since its publication, but there are eminent pathologists who have not given adherence to it in the exclusive form advocated by its author.
5 Virchow's Archiv, Bd. 41.
6 Journ. de l'Anat. et de la Phys., 1864.
It is somewhat remarkable that although in the early part of the present century several monographs on gastric cancer appeared,7 all the more recent contributions to the subject are to be found in theses, scattered journal articles, and text-books. Of the more recent careful and extensive articles on cancer of the stomach, those of Lebert and of Brinton are perhaps most worthy of mention.8
7 Chardel, Benech, Daniel, Germain, Prus, Sharpey, Barras, etc.
8 Lebert, Die Krankheiten des Magens, Tübingen, 1878; Brinton, Brit. and For. Med.-Chir. Rev., 1857.
ETIOLOGY.—The data for estimating the frequency of gastric cancer are the clinical statistics of hospitals, series of recorded autopsies, and mortuary registration reports.
Statistics with reference to this point based exclusively upon the clinical material of hospitals have only relative value, as they do not [p. 532] represent in proper proportion both sexes, all ages, all classes in life, and all diseases. Statistics based upon autopsies surpass all others in certainty of diagnosis, but they possess in even greater degree the defects urged against hospital statistics. Not all the fatal cases in hospitals are examined post-mortem, and gastric cancer is among the diseases most likely to receive such examination. Hence estimates of frequency based exclusively upon autopsies are liable to be excessive. Estimates from mortuary registration reports, and therefore from the diagnoses given in death-certificates, rest manifestly upon a very untrustworthy basis as regards diagnosis, but in other respects they represent the ideal point of view, including, as these reports do, all causes of death among all classes of persons. It is evident that in all methods of estimating the frequency of gastric cancer inhere important sources of error. In general, the larger the number of cases upon which the estimates rest the less prominent are the errors. Such estimates as we possess are to be regarded only as approximate, and subject to revision.
From mortuary statistics Tanchou estimates the frequency of gastric cancer as compared with that of all causes of death at 0.6 per cent.; Virchow, at 1.9 per cent.; Wyss, at 2 per cent.; and D'Espine, at 2½ per cent.9
9 Tanchou, Rech. sur le Traitement méd. des Tumeurs du Sein, Paris, 1844. These statistics, which are based upon an analysis of 382,851 deaths in the department of the Seine, are necessarily subject to sources of error, but they do not seem to me to deserve the harsh criticisms of Lebert and others.
Virchow, Verhandl. d. phys.-med. Gesellsch. Würzburg, 1860, vol. x. p. 49—analysis of 3390 deaths in Würzburg during the years 1852-55.
Wyss, quoted by Ebstein in Volkmann's Samml. klin. Vorträge, No. 87—analysis of 4800 deaths in Zurich from 1872-74.
D'Espine, Echo médical, 1858, vol. ii.—mortuary statistics of the canton of Geneva, considered to be particularly accurate.
In 8468 autopsies, chiefly from English hospitals, Brinton10 found gastric cancer recorded in 1 per cent. of the cases. Gussenbauer and Von Winiwarter11 found gastric cancer recorded in 1½ per cent. of the 61,287 autopsies in the Pathological Anatomical Institute of the Vienna University. From an analysis of 11,175 autopsies in Prague, I find gastric cancer in 3½ per cent. of the cases.12
10 Loc. cit.
11 Arch. f. klin. Chirurg., Bd. xix. p. 372.
12 Statistics of Dittrich, Engel, Willigk, Wrany, and Eppinger, in Prager Vierteljahrschr., vols. vii., viii., ix., x., xii., xiv., xxvii., l., xciv., xcix., and cxiv. Grünfeld found in 1150 autopsies in the general hospital for aged persons in Copenhagen 102 cancers of the stomach, or 9 per cent. (Schmidt's Jahrb., Bd. 198, p. 141).
I have collected and analyzed with reference to this point the statistics of death from all causes in the city of New York for the fifteen years from 1868 to 1882, inclusive.13 I find that of the 444,564 deaths during this period, cancer of the stomach was assigned as the cause in 1548 cases and cancer of the liver in 867 cases. Probably at least one-third of the primary cancers of the liver are to be reckoned as gastric cancers. This would make the ratio of gastric cancer to all causes of death about 0.4 per cent. This ratio becomes about 1 per cent. (0.93) if only the deaths from twenty years of age upward be taken: gastric cancer hardly ever occurs under that age. It is probably fair to conclude that in New York not over 1 in 200 of the deaths occurring at all ages and from all causes [p. 533]is due to cancer of the stomach, and that about 1 in 100 of the deaths from twenty years of age upward is due to this cause.
13 These statistics are obtained from the records of the Board of Health of the city of New York. These records are kept with great care and system.
The organs most frequently affected with primary cancer are the uterus and stomach. In order to determine the relative frequency of cancer in these situations, I have compiled the following table of statistics from various sources:14
| Primary Cancers. | Stomach. | Uterus. | |
| 11,131 | in Vienna | 10 per cent. | 31 per cent. |
| 7,150 | in New York | 25.7 per cent. | 24.2 per cent. |
| 9,118 | in Paris (Tanchou) | 25.2 per cent. | 32.8 per cent. |
| 1,378 | in Paris (Salle) | 31.9 per cent. | 32 per cent. |
| 587 | in Berlin | 35.8 per cent. | 25 per cent. |
| 183 | in Würzburg | 34.9 per cent. | 19 per cent. |
| 1,046 | in Prague | 37.6 per cent. | 33.3 per cent. |
| 889 | in Geneva | 45 per cent. | 15.6 per cent. |
| 31,482 | total | 21.4 per cent. | 29.5 per cent. |
From this table it appears that in some collections of cases the uterus is the most frequent seat of primary cancer, while in other collections the stomach takes the first rank. If the sum-total of all the cases be taken, the conclusion would be that about one-fifth of all primary cancers are seated in the stomach, and somewhat less than one-third in the uterus. Even if allowance be made for the apparently too low percentage of cases of gastric cancer in the large Vienna statistics,15 I should still be inclined to place the uterus first in the list of organs most frequently affected with primary cancer, and to estimate the frequency of gastric cancer compared with that of primary cancer elsewhere as not over 25 per cent.
14 Vienna cases: Gurlt, Arch. f. klin. Chir., Bd. xxv. p. 421—statistical analysis of 16,637 tumors observed in the three large hospitals of Vienna from 1855 to 1878. New York cases: see preceding foot-note. Paris cases: Tanchou, op. cit., and Salle, Étiologie de la Carcinose, Thèse, Paris, 1877, p. 145 et seq.—fatal cases in Paris hospitals, 1861-63. Berlin cases: Lange, Ueber den Magenkrebs, Inaug. Diss., Berlin, 1877—post-mortem material. Würzburg cases: Virchow, loc. cit., and Virchow's Archiv, Bd. 27, p. 430. Prague cases: reference given above—post-mortem material. Geneva cases: D'Espine, loc. cit.
15 That this percentage is too low is apparent from the fact that the number of cases of gastric cancer is only twice that of primary cancer of liver in Gurlt's statistics.
The liability to gastric cancer seems to be the same in both sexes. Of 2214 cases of gastric cancer which I have collected from hospital statistics, and which were nearly all confirmed by autopsy, 1233 were in males and 981 in females.16 This makes the ratio of males to females about 5 to 4. This difference is so slight that no importance can be attached to it, especially in view of the fact that in most hospitals the males are in excess of the females.
16 My statistics regarding sex are obtained from Prager Vierteljahrschr., vols. xvii., l., xciv., xcix., cxiv.; Lange, op. cit.; Katzenellenbogen, Beitr. zur Statistik d. Magencarcinoms, Jena, 1878; Leudet, Bull. de l'Acad., t. 29, p. 564; Gussenbauer and V. Winiwarter, loc. cit.; Lebert, op. cit.; Habershon, Diseases of Abdomen, Philada., 1879; and Ann. d. Städt. Allg. Krankenh. zu München, Bd. i. and ii.
If to these accurate statistics be added collections of cases from heterogeneous sources, including mortuary statistics (Brinton, Louis, D'Espine, Virchow, Gurlt, Welch), there results a total of 5426 cases, with 2843 males and 2583 females, the two sexes being more evenly represented than in the more exact statistics given in the text. In this collection of cases Gussenbauer and V. Winiwarter's cases only up to the year 1855 are included, as the subsequent ones are doubtless in great part included in Gurlt's statistics. According to Brinton, gastric cancer is twice as frequent in males as in females.
[p. 534] The following table gives the age in 2038 cases of gastric cancer obtained from trustworthy sources and arranged according to decades:17
| Age. | 10-20. | 20-30. | 30-40. | 40-50. | 50-60. | 60-70. | 70-80. | 80-90. | 90-100. | Over 100. |
| Number of cases. | 2 | 55 | 271 | 499 | 620 | 428 | 140 | 20 | 2 | 1 |
| Per cent. | 0.1 | 2.7 | 13.3 | 24.5 | 30.4 | 21 | 6.85 | 1 | 0.1 | 0.05 |
From this analysis we may conclude that three-fourths of all gastric cancers occur between forty and seventy years of age. The absolutely largest number is found between fifty and sixty years, but, taking into consideration the number of those living, the liability to gastric cancer is as great between sixty and seventy years of age. Nevertheless, the number of cases between thirty and forty years is considerable, and the occurrence of gastric cancer even between twenty and thirty is not so exceptional as is often represented, and is by no means to be ignored. The liability to gastric cancer seems to lessen after seventy years of age, but here the number of cases and the number of those living are so small that it is hazardous to draw positive conclusions.
17 The sources of the statistics for age are—Dittrich (160), Prager Vierteljahrschr., vol. xvii.; D'Espine (117), loc. cit.; Virchow (63), Virchow's Archiv, Bd. 27, p. 429; Leudet (69), loc. cit.; Lange (147), op. cit.; Katzenellenbogen (60), op. cit.; Gussenbauer and Von Winiwarter (493 cases up to 1855), loc. cit.; Lebert (314), op. cit.; Habershon (76), op. cit.; Gurlt (455), loc. cit.; Trans. N.Y. Path. Soc., vol. i. (41); and Trans. London Path. Soc., vols. i.-xxxiv. (43). The results correspond closely to those of the smaller statistics of Brinton and of Lebert.
Cancer of the stomach in childhood is among the rarest of diseases. Steiner and Neureutter18 failed to find a single gastric cancer in 2000 autopsies on children. Cullingworth19 has reported with microscopical examination a case of cylindrical-celled epithelioma in a male infant dying at the age of five weeks; it is probable that the tumor was congenital. It is not certain whether Wilkinson's20 often-quoted case of congenital scirrhus of the pylorus in an infant five weeks old was a cancer or an instance of simple hypertrophy. Kaulich21 cites a case of colloid cancer affecting the stomach, together with nearly all the abdominal organs, in a child a year and a half old, but whether the growth in the stomach was primary or secondary is not mentioned. The case which Widerhofer22 has reported as one of cancer of the stomach secondary to cancer of the retro-peritoneal glands in an infant sixteen days old seems from the description to be sarcoma. Scheffer23 has reported a case of large ulcerated encephaloid cancer of the fundus, involving the spleen, in a boy fourteen years old. Jackson24 has reported an interesting case of encephaloid cancer in a boy fifteen years old in whom no evidence of disease existed up [p. 535] to ten weeks before death. These cases, which are all that I have been able to find in children, are to be regarded as pathological curiosities.25
18 Prager Vierteljahrschr., vol. lxxxix. p. 77.
19 British Med. Journ., Aug. 25, 1877, p. 253.
20 London and Edinburgh Month. Journ. of Med., 1841, vol. i. p. 23.
21 Prager med. Wochenschr., 1864, No. 34.
22 Jahrb. f. Kinderheilk. Alt. Reihe, Bd. ii. Heft 4, p. 194.
23 Jahrb. f. Kinderheilk., xv. p. 425, 1880.
24 J. B. S. Jackson, Extracts from the Records of the Boston Society for Medical Improvement, vol. v., Appendix, p. 109, Boston, 1867.
25 Mathien (Du Cancer précoce de l'Estomac, Paris, 1884) has recently analyzed, chiefly from a clinical point of view, 27 cases of gastric cancer occurring under thirty-four years of age. Of these, 3 were under twenty and 14 were between twenty and thirty years. He also emphasizes the error of considering cancer of the stomach as exclusively a disease of advanced life.
Such statistics as we possess would make it appear that gastric cancer, as well as cancer in general, is somewhat less common in the United States than in the greater part of Europe.26 These statistics, however, are too inaccurate, and the problems involved in their interpretation are too complex, to justify us in drawing any positive conclusions as to this point. It is certain that cancer is not a rare disease in the United States.
26 Of 1000 deaths in New York in 1882, 19.3 were from cancer. The statistics on this point from some of the large European cities are—Geneva, 53 deaths from cancer per mille; Frankfort, 47.6; Copenhagen, 33.2; Christiania, 29; London, 28.7; Paris, 27; Edinburgh, 25.4; Berlin, 22.4; St. Petersburg, 15; Amsterdam, 12. These statistics are obtained from the Forty-fourth Annual Report of the Registrar-General (for 1881), London, 1883; from Preussische Statistik, Heft lxiii., Berlin, 1882; and from Traité de la Climatologie médicale, Paris, 1877-80, by Lombard, in whose excellent work will be found much information on this subject.
To judge from statistics in this country and in England, the death-rate from cancer is undergoing a rapid annual increase. Whereas in New York in 1868 this death-rate was only 12.6 per mille, in 1882 it was 19.3. In England and Wales in 1858 the deaths from cancer per 1,000,000 persons living were 329, and in 1881 they were 520. It seems probable, as suggested in the above report of the Registrar-General, that this apparently increasing large death-rate is due to increased accuracy in diagnosis. It may be also that decrease in infant mortality and prolongation of life by improved sanitary regulations may account in part for this increase. From this point of view Dunn makes the paradoxical statement that the cancer-rate of a country may be accepted as an index of its healthfulness (Brit. Med. Journ., 1883, i.).
It is said on good authority that in Egypt and Turkey gastric cancer and other forms of cancer are infrequent.27 A similar infrequency has been claimed for South America, the Indies, and in general for tropical and subtropical countries; but all of these statements as to the geographical distribution of cancer are to be accepted with great reserve, as they do not rest upon sufficient statistical information.
27 Hirsch, Handb. d. Historisch-geographische Pathologie, Bd. ii. p. 379, Erlangen, 1862-64.
I have analyzed the frequency of gastric cancer among negroes upon a basis of 7518 deaths among this race in New York, and I find the proportion of deaths from this cause about one-third less than among white persons.28 It has been stated that cancer is an extremely rare disease among negroes in Africa.29 The admixture with white blood makes it difficult to determine to what degree pure negroes in this country are subject to cancer.
28 According to the Ninth Census Report of the United States, in the census year 1870 the deaths from cancer among white persons were 13.7 per mille, and among colored persons only 5.7 per mille; but it is well known that the registration returns upon which the vital statistics in these reports are based are very incomplete and unsatisfactory.
29 Bordier, La Geographie médicale, Paris, 1884, p. 464. Livingstone speaks of the infrequency of cancer among the negroes in Africa.
The question as to what rôle is played by heredity in the causation of gastric cancer belongs to the etiological study of cancer in general. Probably in about 14 per cent. of the cases of cancer it can be determined that other members of the family are or have been affected with the disease.30 [p. 536]The influence of inheritance, therefore, is apparent only in a comparatively small minority of the cases. As suggested long ago by Matthew Baillie, this hereditary influence is better interpreted as in favor of a local predisposition (embryonic abnormality?) in the organ or part affected than in favor of the inheritance of a cancerous diathesis. It has been claimed by D'Espine, Paget, and others that cancer develops at an earlier age when there is a family history of the disease than when such history is absent.
30 This statement is based upon the collection of 1744 cases of cancer analyzed with reference to this question. Of these, a family history of cancer was determined in 243 cases. The cases are obtained from statistics of Paget and Baker, Sibley, Moore, Cooke, Lebert, Lafond, Hess, Leichtenstern, Von Winiwarter, and Oldekop. There is extraordinary variation in the conclusions of different observers upon this point. Velpeau asserted that he could trace hereditary taint in 1 in 3 cancerous subjects; Paget, in 1 in 4; Cripps, in 1 in 28. My conclusions agree with those obtained at the London Cancer Hospital (Cooke, On Cancer, p. 11, London, 1865).
The most remarkable instance of inherited cancer on record is reported by Broca (Traité des Tumeurs, vol. i. p. 151, Paris, 1866): 15 out of 26 descendants over thirty years of age of a woman who died in 1788 of cancer of the breast were likewise affected with cancer. As is well known, Napoleon the First, his father, and his sister died of cancer of the stomach.
It may be considered established that cancer sometimes develops in a simple ulcer of the stomach, either open or cicatrized. It is most likely to develop in large and deep ulcers with thickened edges, where complete closure by cicatrization is very difficult or impossible. It is difficult to prove anatomically that a gastric cancer has developed from an ulcer, and hence such statements as that of Eppinger, that in 11.4 per cent. of cancers of the stomach this mode of development existed, are of no especial value.31 No etiological importance can be attached to the occasional association of cancer with open or cicatrized simple ulcers in different parts of the same stomach. Of the comparatively few cases in which strict anatomical proof has been brought of the origin of cancer in simple gastric ulcer, probably the most carefully investigated and conclusive is one studied and reported by Hauser.32 It is, however, by no means proven that Hauser's view is correct, that cancer develops from the atypical epithelial growths often to be found in the cicatricial tissue of gastric ulcer. In a few instances both the clinical history and the anatomical appearances speak decisively for the development of cancer in a simple gastric ulcer;33 and the establishment of this fact is of clinical importance.
31 Prager Vierteljahrschr., vol. cxiv.
32 Das chronische Maqengeschwür, Leipzig, 1883, p. 61. See also Heitler, "Entwicklung von Krebs auf narbigen Grunde in Magen," Wien. med. Wochenschr., 1883, p. 961. It seems to me that at present there is a tendency to exaggerate the frequency with which cancer develops from gastric ulcer.
33 A particularly satisfactory case of this kind is reported by Lebert, op. cit., p. 503.
Many other factors in the causation of gastric cancer have been alleged, but without proof of their efficacy. This is true of chronic gastritis, which was once thought to be an important cause of gastric cancer, and is even recently admitted by Leube to be of influence.34 Certainly the majority of cases of cancer of the stomach are not preceded by symptoms of chronic gastritis. Although in a few instances gastric cancer has followed an injury in the region of the stomach, there is no reason to suppose that this was more than a coincidence.
34 In Ziemssen's Handb. d. spec. Path. u. Therap., Bd. vii. p. 134, Leipzig, 1878.
Few, if any, at present believe that depressing emotions, such as grief, anxiety, disappointment, which were once considered important causes of cancer, exert any such influence. Cancer of the stomach occurs as [p. 537] frequently in those of strong as in those of weak constitution—as often among the temperate as among the intemperate. If, as has been claimed (D'Espine), gastric cancer is relatively more frequent among the rich than among the poor, this is probably due only to the fact that a larger number of those in favorable conditions of life attain the age at which there is greatest liability to this disease. No previous condition of constitution, no previous disease, no occupation, no station in life, can be said to exert any causative influence in the production of gastric cancer.
It will be observed that the obscurity which surrounds the ultimate causation of gastric cancer is in no way cleared up by the points which have been here considered and which are usually considered under the head of etiology. It is impossible to avoid the assumption of an individual—and in my opinion a local—predisposition to gastric cancer, vague as this assumption appears. All other supposed causes are at the most merely occasional or exciting causes. The attempts to explain in what this predisposition consists are of a speculative nature, and will be briefly considered in connection with the pathenogenesis of gastric cancer.
SYMPTOMATOLOGY.—We may distinguish the following groups of cases of gastric cancer:
First: Latent cases, in which the cancer of the stomach has produced no symptoms up to the time of death. Many secondary cancers of the stomach belong to this class. Here also belong cases in which a cancer is found unexpectedly in the stomach when death has resulted from other causes. I have found a medullary cancer, slightly ulcerated, as large as a hen's egg, seated upon the posterior wall and lesser curvature of the stomach of a laboring man suddenly killed while in apparent health and without previous complaint of gastric disturbance. These cases, in which life is cut short before any manifestation of the disease, are without clinical significance, save to indicate how fallacious it is to estimate the duration of the cancerous growth from the first appearance of the symptoms.
Second: Cases in which gastric symptoms are absent or insignificant, whereas symptoms of general marasmus or of progressive anæmia or of cachectic dropsy are prominent. Cases of this class are frequently mistaken for pernicious anæmia, and occasionally for Bright's disease, heart disease, or phthisis. It is difficult to explain in these cases the tolerance of the stomach for the cancerous growth, but this tolerance is most frequently manifested when the tumor does not invade the orifices of the organ.
Third: Cases in which the symptoms of the primary gastric cancer are insignificant, but the symptoms of secondary cancer, particularly of cancer of the liver or of the peritoneum, predominate. In some, but not in all, of these cases the primary growth is small or has spared the orifices of the stomach.
Fourth: Cases in which the symptoms point to some disease of the stomach, or at least to some abdominal disease; but the absence of characteristic symptoms renders the diagnosis of gastric cancer impossible or only conjectural.
Fifth: Typical cases in which symptoms sufficiently characteristic of [p. 538] gastric cancer are present, so that the diagnosis can be made with reasonable positiveness.
It is not to be understood that these groups represent sharply-drawn types of the disease. It often happens that the same case may present at one period the features of one group, and at another period those of another group. Nor is it supposed that every exceptional and erratic case of gastric cancer can be classified in any of the groups which have been mentioned.35
35 In the thesis of Chesnel may be found many curious clinical disguises which may be assumed by cancer of the stomach, such as simulation of Bright's disease, heart disease, phthisis, chronic bronchitis, cirrhosis of the liver, etc. (Étude clinique sur le Cancer latent de l'Estomac, Paris, 1877). Layman (Med. Annals Albany, 1883, p. 207) reports a case of gastric cancer in which extra-uterine foetation was suspected.
A typical case of gastric cancer runs a course about as follows: A person, usually beyond middle age, begins to suffer from disordered digestion. His appetite is impaired, and a sense of uneasiness, increasing in course of time to actual pain, is felt in the stomach. These symptoms of dyspepsia are in no way peculiar, and probably at first occasion little anxiety. It is, however, soon observed that the patient is losing flesh and strength more rapidly than can be explained by simple indigestion. He becomes depressed in spirits. The bowels are constipated. Vomiting, which was usually absent at first, makes its appearance and becomes more and more frequent. After a while it may be that, without any improvement, the vomiting becomes less frequent, comes on longer after a meal, but is more copious. In the later periods of the disease a substance resembling coffee-grounds and consisting of altered blood is often mingled with the vomit. By this time the patient has assumed a cachectic look. He is wasted, and his complexion has the peculiar pale yellowish tint of malignant disease. Perhaps there is a little oedematous pitting about the ankles. During the progress of the disease in the majority of cases an irregular hard tumor can be felt in the epigastrium. While one or another of the symptoms may abate in severity, the general progress of the disease is relentlessly downward. Within six months to two years of the onset of the symptoms the patient dies of exhaustion.
Too much stress should not be laid upon any so-called typical course of gastric cancer. This course is modified by many circumstances, such as the situation of the cancer, its size, its rapidity of growth, the presence or absence of ulceration, the existence or non-existence of secondary tumors, the presence of complications, and the individuality of the patient. It is necessary, therefore, to consider in detail each of the important symptoms of gastric cancer. But in thus fixing attention upon individual symptoms one must not lose sight of the clinical picture as a whole. It is not any single symptom which is decisive; it is rather the combination, the mode of onset, and the course of the symptoms, which are of most importance in diagnosis.
Impairment of the appetite is the rule in gastric cancer. Anorexia is sometimes a marked symptom before pain, vomiting, and other evidences of gastric indigestion are noted. There is often a special distaste for meat. The appetite may be capricious; it is very rarely even increased. There are exceptional cases in which the appetite is preserved throughout the greater part or even the whole course of the disease. This seems to [p. 539] be more frequent with cancer of the cardia than with cancer of other parts of the stomach. Loss of appetite is a much more common symptom in gastric cancer than in gastric ulcer. In cancer, as well as in ulcer, the patient sometimes refrains from food less on account of disrelish for it than on account of the distress which it causes him.
Pain is one of the most frequent symptoms of cancer of the stomach. If the pain begins early in the disease, and continues, as it often does, with increasing severity, it renders gastric cancer one of the most distressing affections. The pain is usually felt in the epigastrium, but it may be more intense in the hypochondria. It is sometimes felt in the interscapular region, the shoulders, or even in the loins.36 With cancer of the cardia it is often referred to the point of the xiphoid cartilage or behind the sternum. In general, however, there is so little correspondence between the site of the cancer and the exact locality of the pain that no weight can be attached to the situation of the pain in diagnosing the region of the stomach involved in the growth. Nor does any import attach to the quality of the pain, whether it is described as burning, gnawing, dull, lancinating, etc. Severe gastralgic paroxysms occur, although less frequently than in gastric ulcer.
36 The pain in cases of gastric cancer may be felt in parts of the body remote from the stomach. Thus, in a case of cancer of the cardia reported by Minot the pain was felt, not in the epigastrium, but in the left shoulder, the back of the neck, and the pharynx. In several instances the pain has been interpreted as of renal origin. In a case of gastric cancer reported by Palmer each attack of vomiting was invariably preceded by pain in the middle of the shaft of the left humerus (Extr. fr. the Records of the Boston Soc. for Med. Improvement, vol. iv. p. 217).
The pain is usually aggravated by ingestion of food, although it may not become severe until the process of digestion is far advanced. Pain, however, occurs independently of taking food, and is occasionally a marked symptom when there are no evidences of dyspepsia. There can be no doubt that the cancer, as such, produces pain by involvement of the nerves of the stomach, but there is no specific cancerous pain, such as has been described by Brinton and other writers. There is usually tenderness on pressure over the stomach, and this tenderness is often over the tumor, if such can be felt.
In general, it may be said that the pain of gastric cancer, as contrasted with that of simple gastric ulcer, is often less dependent upon taking food, less intense, less circumscribed, less paroxysmal, less often relieved by vomiting; but there is so little constancy about any of these points that no reliance is to be placed upon any peculiarity of the pain in the diagnosis of gastric cancer.
The observation of several cases of gastric cancer without pain as a marked symptom leads me to emphasize the fact that absence or trifling severity of pain throughout the greater part or the whole of the disease, although exceptional, is not extremely rare. The frequency of painless gastric cancers is given by Lebert as 25 per cent., and by Brinton as 8 per cent., of the whole number. For many reasons, numerical computations as to the frequency of this and of other symptoms of gastric cancer are of very limited value.37 Absence of pain is more common in [p. 540] gastric cancers of old persons and in cancers not involving the orifices of the stomach than it is at an earlier period of life or when the gastric orifices are obstructed.
37 Gastric cancer cannot be considered as a disease with uniform characters. It is irrational to group together cancers of the pylorus, of the cardia, of the fundus, of the curvatures, cancers hard and soft, ulcerated and not ulcerated, infiltrating and circumscribed, and to say that pain or vomiting is present in so-and-so many cases of cancer of the stomach. There is not a sufficient number of recorded cases in which the symptoms are fully described with reference to the peculiarities of the growth to enable us to apply to gastric cancer the numerical method of clinical study with valuable results. The great discrepancy between Lebert's and Brinton's statistics as to the frequency of painless cancers of the stomach illustrates the present inadequacy of the numerical method, which is misleading in so far as it gives a false appearance of exactness.
The functions of the stomach are almost invariably disordered in gastric cancer. Sometimes, especially in the early stages, this disorder is only moderate, and is manifested by the milder symptoms of indigestion, such as uneasy sensations of weight and fulness after a meal, nausea, flatulent distension of the stomach relieved by eructation of gases, and heartburn. With the progress of the disease the uneasy sensations become actually painful; watery fluids, and sometimes offensive acrid fluids and gases, are regurgitated; and nausea culminates in vomiting. The breath is often very fetid. The eructation of inflammable gases has been observed in a few cases.
The most troublesome symptoms of indigestion occur with those cancers which by obstructing the pyloric orifice lead to dilatation of the stomach. Cases of gastric cancer in which the distressing symptoms of dilatation of the stomach dominate the clinical history are frequent. These symptoms are in no way peculiar to cancer of the stomach, but belong to dilatation produced by pyloric stenosis from whatever cause, and will be described in the article on DILATATION OF THE STOMACH.
Various causes combine to impair the normal performance of the gastric functions in cancer of the stomach. Chronic catarrhal gastritis is a factor in not a few cases. The destruction by the cancer of a certain amount of secreting surface can be adduced as a sufficient cause only in exceptional cases of extensive cancerous infiltration. Of more importance is interference with the peristaltic movements of the stomach, particularly in the pyloric region, where the cancer is most frequently situated. As already mentioned, dilatation of the stomach is a most important cause of indigestion in many cases. Of great interest in this connection is the discovery by Von den Velden38 that as a rule (to which there are exceptions) the gastric juice in cases of dilatation of the stomach due to cancer contains no free hydrochloric acid, and that this gastric juice has comparatively feeble digestive power, as proven by experiments. As this alteration of the gastric juice interferes particularly with the digestion of albuminous substances, it is explicable why many patients with gastric cancer have an especial abhorrence for meat.
38 Deutsches Arch. f. kl. Med., Bd. 23, p. 369.
During the progress of the disease the dyspeptic symptoms may improve, but this improvement is usually only temporary. In exceptional cases of gastric cancer dyspeptic symptoms, as well as other gastric symptoms, may be absent or not sufficiently marked to attract attention.
Hiccough, sometimes very troublesome, has been observed not very infrequently during the later periods of the disease.
There is nothing noteworthy about the appearance of the tongue, which is often clean and moist, but may be furred or abnormally red and dry. In the cachectic stage, toward the end of the disease, aphthous patches [p. 541] often appear on the tongue and buccal mucous membrane. An increased flow of saliva has been occasionally observed in gastric cancer as well as in other diseases of the stomach. Thirst is present when there is profuse vomiting.
Vomiting usually appears after other symptoms of indigestion have been present for some time. It may, however, be one of the earliest symptoms of the disease. At first of occasional occurrence, it increases in frequency until in some cases it becomes the most prominent of all symptoms. Vomiting may occur in paroxysms which last for several days or weeks, and then this symptom may improve, perhaps to be renewed again and again, with remissions of comparative comfort. There are rare cases of gastric cancer in which the first symptom to attract attention is uncontrollable vomiting, accompanied often with pain and rapid emaciation. Such cases may run so acute a course that a fatal termination is reached within one to two months.39 In these cases, which have been interpreted as acutely-developed gastric cancers, it is probable that the cancer has remained latent for weeks or months before it gave rise to marked symptoms.
39 For example, Andral relates a case in which death took place thirty-seven days after the onset of the symptoms, these being obstinate vomiting, severe gastralgic paroxysms, marasmus, and, about ten days before death, profuse black vomit. There was found a fungoid tumor the size of a hen's egg projecting into the cavity of the stomach near the pylorus. In this situation the walls of the stomach were greatly thickened by colloid growth (Arch. gén. de Méd., June, 1823). Here may also be mentioned the fact that in several instances pregnancy has been complicated with gastric cancer. Here the uncontrollable vomiting which often exists has been referred to the pregnancy, and has led to the production of premature labor.
The situation of the cancer exerts great influence upon the frequency of vomiting and the time of its occurrence after meals. When the cancer involves the pyloric orifice, vomiting is rarely absent, and generally occurs an hour or more after a meal. As this is the most frequent situation of the cancer, it has been accepted as a general rule that vomiting occurs at a longer interval after eating in cases of gastric cancer than in cases of simple ulcer. But even with pyloric cancer the vomiting may come on almost immediately after taking food, so that it is not safe to diagnose the position of the cancer by the length of time between eating and the occurrence of vomiting. As the cancer in its growth obstructs more and more the pyloric orifice, the vomiting acquires the peculiarities of that accompanying dilatation of the stomach. The vomiting comes on longer after a meal—sometimes not until twelve or twenty hours or even more have elapsed. It may be that several days elapse between the acts of vomiting, which then present a certain periodicity. The patient then vomits enormous quantities containing undigested food, mucus, sarcinæ, and gaseous and other products of fermentation. Sometimes, especially toward the end of the disease, the vomiting ceases altogether. This cessation has been attributed to reopening of the pyloric orifice by sloughing of the growth. It is not necessary to assume such an occurrence, as a similar cessation of vomiting sometimes occurs in dilatation of the stomach due to persistent stenosis of the pylorus. Cessation of vomiting in these cases is by no means always a favorable symptom.
Next to pyloric cancer, it is cancer involving the cardiac orifice which is most frequently accompanied by vomiting. Here the vomiting occurs often immediately after taking food, but there are exceptions to this rule. [p. 542] If in consequence of stenosis of the cardiac orifice the food does not enter the stomach, it is shortly regurgitated unchanged or mingled simply with mucus. It is this regurgitation rather than actual vomiting which in most common and characteristic of cardiac cancer. Even in cases in which the passage of an oesophageal sound reveals no obstruction at the cardiac orifice it sometimes happens that food, including even liquids, is regurgitated almost immediately, as in a case reported by Ebstein in which cold water was returned at once after swallowing.40 In these cases Ebstein with great plausibility refers the regurgitation to reflex spasm of the oesophagus induced by irritation of a cancer at or near the cardia through contact of food or liquids, especially when cold, with its surface.
40 "Ueber den Magenkrebs," Volkmann's Samml. klin. Vorträge, No. 87, p. 21.
When the cancer is seated in other parts of the stomach and it does not obstruct the orifices, vomiting is more frequently absent or of only rare occurrence. Vomiting is absent, according to Lebert, in one-fifth, according to Brinton in about one-eighth, of the cases of gastric cancer. Absence of vomiting is sufficiently frequent in gastric cancer to guard one against excluding the diagnosis of this disease on this ground alone.
Although in many cases the vomiting of gastric cancer can be explained on mechanical grounds by stenosis of the orifices, this is an explanation not applicable to all cases. Mention has already been made of spasm of the oesophagus as a cause of regurgitation of food in some cases of cardiac cancer. A similar spasm of the muscle in the pyloric region may explain the vomiting in certain cases in which during life there were symptoms of pyloric stenosis, but after death no or slight stenosis can be found. There is reason also to believe that atony of the muscular coats of the stomach may cause stagnation of the contents of the stomach and dilatation of the organ. In exceptional cases of gastric cancer in which the stomach is so intolerant as to reject food almost immediately after its entrance a special irritability of the nerves of the stomach must be assumed. It is customary to refer this form of vomiting to irritation of the ulcerated surface of the cancer by analogy with a similar irritability of the stomach observed in some cases of simple gastric ulcer. But there is little analogy between the ulcerated surface of a cancer in which tissues of little vitality and irritability are exposed and the surface of a simple ulcer in which the normal or slightly altered tissues of the stomach are laid bare. Finally, in the existence of chronic catarrhal gastritis is to be found another cause of vomiting in many cases of gastric cancer.
The presence of fragments of the cancer in the contents removed by washing out the stomach with the stomach-tube has been observed by Rosenbach41 in three cases of gastric cancer, and utilized for diagnostic purposes. A cancerous structure could be made out in these fragments by the aid of the microscope. Hitherto, the presence of particles of the tumor in the vomited matter has been considered as hardly more than a curiosity, and I have not been able to find a well-authenticated instance in which such particles in the vomit have been recognized by microscopical examination. According to Rosenbach, the fragments of the tumor in the washings from the stomach can be recognized by the naked eye by the red, reddish-brown, or black specks on their surface, due to recent or old hemorrhages which have aided in the detachment of the fragments. [p. 543] By this means such particles are distinguished macroscopically from bits of food. By employing soft-rubber tubes and the syphon process there is no danger, in washing out of the stomach, of detaching pieces of the normal mucous membrane, which, moreover, can be distinguished from the fragments of the tumor by the aid of the microscope and usually by the naked eye. It remains to be seen how frequently such fragments of the tumor are to be found in the fluids obtained by washing out the stomach. It is not probable that they will be found so often as Rosenbach anticipates. According to the experience of most observers, they are very rarely present. They would naturally be most readily detached from soft, fungoid, and ulcerating cancerous growths. In this connection may also be mentioned the occasional separation of bits of the tumor by the passage of the stomach-tube in cases of cancer of the cardia. The eye of the tube as well as the washings from the stomach should be carefully examined for such particles.
41 Deutsche med. Wochenschr., 1882, p. 452.
The habitual absence of free hydrochloric acid in the gastric fluids in dilatation of the stomach due to carcinoma of this organ was noted by Von der Velden.42 He found in eight cases of dilatation due to cancer of the pylorus that the fluids removed by the stomach-pump were free from hydrochloric acid, whereas in ten cases of dilatation due to other causes, such as cicatrized simple ulcer of the pylorus, free hydrochloric acid was only temporarily absent from the gastric juice. Von der Velden therefore attributes to the presence or the absence of free hydrochloric acid in the gastric juice in these cases great diagnostic importance. The observations which have followed Von der Velden's publication are not yet sufficient to justify us in drawing positive conclusions in this matter. Recently, Kredel43 has reported from Riegel's clinic seventeen cases of simple dilatation in which free hydrochloric acid was only exceptionally and temporarily absent from the gastric fluids, and nineteen cases of cancerous dilatation in which, with very rare exceptions, free hydrochloric acid was continuously absent. Cases, however, have been observed by Ewald, Seeman, and others in which free hydrochloric acid has been found in stomachs dilated from gastric cancer. It is to be noted that free hydrochloric acid is absent from the stomach in other conditions than in gastrectasia due to cancer; of which conditions the most important are fever, amyloid degeneration of the stomach (Edinger), and some cases of gastric catarrh. Free hydrochloric acid is also usually absent during the first twenty minutes to an hour after a meal. We have not sufficient information as to the presence or absence of free hydrochloric acid in cases of gastric cancer without dilatation of the stomach. To Von der Velden's symptom no pathognomonic value can be attached, but it may prove, in connection with other symptoms, an aid in diagnosis. The presumption is against gastric cancer if free hydrochloric acid be found continuously in a dilated stomach. Less importance can be attached to the absence of free hydrochloric acid unless the observations extend over several weeks and fever and amyloid degeneration are excluded.
42 Deutsches Arch. f. klin. Med., Bd. 23, p. 369, 1879.
43 Zeitschrift f. klin. Med., Bd. 6, p. 592, 1884.
The tests for free hydrochloric acid are most satisfactorily applied to the fluids withdrawn by the stomach-pump. After a sufficient quantity for examination has been withdrawn the syphon process may be [p. 544] substituted. Tests may also be applied to vomited material, although here the admixture of secretions from the nose, mouth, and throat may render the results less conclusive. Edinger's method of swallowing bits of sponge enclosed in gelatin capsules and attached to a string, by which they can be withdrawn, may also be employed. The sponge should be free from sand, deprived of alkaline carbonates by hydrochloric acid, and rendered perfectly neutral by washing in distilled water.
For clinical purposes the most convenient tests are those which depend upon certain changes in color produced in reagents which enable us to distinguish inorganic from organic acids. In the gastric juice the only inorganic acid which comes into consideration is hydrochloric acid, and the most important organic acid is lactic.
1. Saturated aqueous solutions of tropæolin, marked in the trade OO (Von Miller, V. d. Velden). The solution should be perfectly clear and of a lemon-yellow color. This solution is colored red by the addition of hydrochloric acid even in very dilute solution (0.01 per cent.). A similar change in color is produced by lactic acid in somewhat less dilute solution (0.06 per cent.), but the red color produced by lactic acid disappears upon shaking with ether, while that produced by hydrochloric acid remains, unless the acid was present in very minute quantity. Tropæolin is therefore a very delicate test for free acid in general, but it does not distinguish so well as some other tests hydrochloric from lactic acid.
2. Aqueous solution of methyl-violet (an aniline dye) in the strength of 0.025 per cent. (Witz, Maly). The solution should be of a violet color, and in a test-tube should allow the light to pass readily through it. The addition of hydrochloric acid in dilute solution changes the violet to a blue color, in stronger solution to a greenish tint. With lactic acid in stronger solution methyl-violet gives a similar but less distinct reaction. Methyl-violet, while a less delicate test than tropæolin, is better adapted for distinguishing hydrochloric from lactic acid.
3. Ferric chloride and carbolic acid test (Uffelmann). Mix 3 drops of liquor ferri chloridi (German Pharmacopoeia, specific gravity 1482), 3 drops of very concentrated solution of carbolic acid, and 20 ccm. of distilled water. The addition of even very dilute solutions of lactic acid (0.05 per cent.) changes the amethyst-blue color of this test-fluid to a yellow color, with a shade of green. Dilute solutions of hydrochloric acid produce a steel-gray, and stronger solutions a complete decolorization of the fluid. When both hydrochloric and lactic acids are present the effect of the lactic acid predominates unless only a mere trace of it is present. This is therefore a good test for lactic acid. It is necessary to prepare the test-fluid fresh each time before using.
4. It is well to test the digestive power of the filtered fluid from the stomach by suspending in the fluid a floccule of washed fibrin and keeping the fluid at a temperature of about 100° F. If free hydrochloric acid be present in moderate quantity, in a short time the fibrin will begin to be dissolved, but if the acidity be due to organic acid the fibrin will be dissolved very slowly or not at all.
In applying these various tests the fluids from the stomach should be filtered and the filtrate used. It is best not to rely upon a single test, but to employ them in combination. The fluids may be mixed in a test-tube. The reaction is sometimes most distinct when the fluids are allowed [p. 545] to mingle upon a white porcelain dish. It is sometimes of advantage to concentrate the mingled fluids by evaporation. The fluid obtained by the stomach-pump five or six hours after a meal is the most suitable for diagnostic tests. The presence of peptones and of dissolved albumen makes the tests less delicate for the gastric fluids than for simple aqueous solutions of the acids.44
44 For further information on this subject consult Von der Velden, loc. cit.; Uffelmann, Deutsches Arch. f. klin. Med., Bd. 26, p. 431; Edinger, ibid., Bd. 29, p. 555; and Kredel, loc. cit.
It is important to distinguish between the slight and the copious hemorrhages of gastric cancer.
The admixture of a small quantity of blood with the vomit, giving to the latter the so-called coffee-grounds appearance, is a very common occurrence in gastric cancer. Melænamesis, as the vomiting of brown or black substance resembling coffee-grounds is called, is estimated to occur in about one-half of the cases of cancer of the stomach. It is observed particularly in the cachectic stage, in which it is not rare for some brown or black sediment to be almost constantly present in the vomit. The brown or black color is due to the conversion by the acids of the stomach of the normal blood-coloring matter into dark-brown hæmatin.
The presence of blood in the vomited matter can generally be recognized by the naked eye. By the aid of the microscope red blood-corpuscles, more or less changed, especially decolorized red blood-corpuscles (the so-called shadows), can usually be detected. Sometimes only amorphous masses of altered blood-pigment can be seen. The spectroscope may also be employed, in which alkaline solutions of hæmatin produce an absorption-band between C and D, usually reaching or passing D. The presence of blood-coloring matter can also be readily detected by the production of hæmin crystals.45 The slight hemorrhages are in most cases the result of ulceration of the cancer, by which process a little oozing of blood from the capillaries is produced.
45 Hæmin crystals may be produced by boiling in a test-tube a little of the suspected fluid or sediment with an excess of glacial acetic acid and a few particles of common salt. After cooling, a drop from the lower layers will show under the microscope the dark-brown rhombic crystals of hæmin in case blood-coloring matter was present in not too minute quantity.
Copious hemorrhages from the stomach are not common in gastric cancer. They occur probably in not over 12 per cent. of the cases (Lebert). According to Lebert, they are more liable to occur in males than in females. Blood vomited in large quantity is either bright red or more or less darkened in color according to the length of its sojourn in the stomach. Following profuse hæmatemesis, some dark, tarry blood is usually passed by the stools, constituting the symptom called melæna. Copious hemorrhages from the stomach hasten the fatal termination and may be its immediate forerunner. Cases of gastric cancer have been reported in which death has occurred from gastrorrhagia before there has been time for any blood to be either vomited or voided by stool. As might naturally be expected, patients with gastric cancer do not usually rally as readily from the effects of gastric hemorrhage as do most patients with simple ulcer. Profuse gastric hemorrhage, if it occur, is most common in the late stage of gastric cancer, but I have known a [p. 546] case of cancer of the stomach in which copious hæmatemesis was the first symptom, with the exception of slight dyspepsia.46
46 In a case of cancer of the lesser curvature observed by Laborie fatal hæmatemesis occurred before there had been any distinct symptoms of gastric cancer (Bouchut, Nouv. Éléments de la Path. gén., ed. 3, p. 288).
Profuse hæmatemesis is more common with soft cancers than with other forms. The source of profuse hemorrhage is in some large vessel eroded by the ulcerative process. The same vessels may be the source of the bleeding as have been enumerated in connection with gastric ulcer. Cancers situated near the pylorus or on the lesser curvature are the most likely to cause severe hemorrhage.
While it is true that coffee-grounds vomiting is most common in cancer, and profuse hæmatemesis is most common in ulcer of the stomach, it is important to remember that either disease may be attended by that form of hemorrhage which is most common in the other.
Dysphagia is one of the most important symptoms of cancer of the cardia. Dysphagia is sometimes one of the first symptoms to attract attention, but it may not appear until late in the disease. It is usually accompanied with painful sensations near the xiphoid cartilage or behind the sternum, or sometimes in the pharynx. The sensation of stoppage of the food is usually felt lower down than in ordinary cases of stenosis of the oesophagus. Stenosis of the cardia can be appreciated by the passage of an oesophageal bougie, but it is important to bear in mind that dysphagia may exist in cases of cancer of the cardia in which the oesophageal bougie does not reveal evidence of stenosis. Dysphagia may be a prominent symptom in cancer occupying parts of the stomach remote from the cardia.47 The dysphagia here considered is not likely to be confounded with the difficulty in swallowing which is due to weakness or to aphthous inflammation of the throat and gullet, which often attends the last days of gastric cancer.
47 A case in point has been reported by J. B. S. Jackson. The cancer occupied the pyloric region (American Journ. of Med. Sci., April, 1852, p. 364).
From a diagnostic point of view the presence of a tumor is the most important symptom of gastric cancer. In the absence of tumor the diagnosis of gastric cancer can rarely be made with positiveness. A tumor of the stomach can be felt in about 80 per cent. of the cases of cancer of the stomach (Brinton, Lebert). With all of its importance, it is nevertheless possible to exaggerate the diagnostic value of this symptom. It is by no means always easy to determine whether an existing tumor belongs to the stomach or not, and even if there is proved to be a tumor of the stomach, there may be difficulty in deciding whether or not it is a cancer. Many instances might be cited in which errors in these respects have been made by experienced diagnosticians. The value of tumor as a diagnostic symptom is somewhat lessened by the fact that it often does not appear until comparatively late in the disease, so that the diagnosis remains in doubt for a long time. It is to be remembered also that tumor is absent in no less than one-fifth of the cases of gastric cancer.
In order to understand in what situations cancers of the stomach are likely to produce palpable tumors, it is necessary to have in mind certain points concerning the situation and the relations of this organ.
The stomach is placed obliquely in the left hypochondrium and the epigastric regions of the abdomen, approaching the vertical more nearly [p. 547] than the horizontal position. The mesial plane of the body passes through the pyloric portion of the stomach, so that, according to Luschka, five-sixths of the stomach lie to the left of this plane. The most fixed part of the stomach is the cardiac orifice, which lies behind the left seventh costal cartilage, near the sternum, and is overlapped by the left extremity of the liver. The pyloric orifice lies usually in the sagittal plane passing through the right margin of the sternum, and on a level with the inner extremity of the right eighth costal cartilage. The pylorus is less fixed than the cardia. When the stomach is empty the pylorus is to be found in the median line of the body; when the stomach is greatly distended the pylorus may be pushed two and a half to three inches to the right of the median line. The pylorus is overlapped by a part of the liver, usually the lobus quadratus or the umbilical fissure. About two-thirds of the stomach lie in the left hypochondrium covered in by the ribs, and to the left and posteriorly by the spleen. The highest point of the stomach is the top of the fundus, which usually reaches to the left fifth rib. The lowest point of the stomach is in the convexity of the greater curvature to the left of the median line. The lower border of the stomach varies in position more than any other part of the organ. In the median line this border is situated on the average about midway between the base of the xiphoid cartilage and the umbilicus, but within the limits of health it may extend nearly to the umbilicus. The lesser curvature in the greater part of its course extends from the cardia downward to the left of the vertebral column and nearly parallel with it. The lesser curvature then crosses to the right side on a level with the inner extremity of the eighth rib, and in the median line lies about two and a half fingers' breadth above the lower margin of the stomach. The lesser curvature and the adjacent part of the anterior surface of the stomach are covered by the left lobe of the liver.
It follows from this description that only the lower part of the anterior surface of the stomach is in contact with the anterior abdominal walls. This part in contact with the anterior abdominal walls corresponds to a part of the body and of the pyloric region of the stomach, and belongs to the epigastric region. The remainder of the stomach is covered either by the liver or by the ribs, so that in the normal condition it cannot be explored by palpation.
It is now evident that tumors in certain parts of the stomach can be readily detected by palpation, whereas tumors in other parts of the organ can be detected only with difficulty or not at all. Cancer of the cardia cannot be felt by palpation of the abdomen unless the tumor extends down upon the body of the stomach. Cancers of the fundus, the lesser curvature, and the posterior wall of the stomach often escape detection by palpation, but if they are of large size or if the stomach becomes displaced by their growth, they may be felt. Cancerous tumors of the anterior wall or of the greater curvature are rare, but they can be detected even when of small size, unless there are special obstacles to the physical examination of the abdomen. Cancerous tumors of the pylorus can be made out by palpation in the majority of cases notwithstanding the overlapping of this part by the liver. The pyloric tumor may be so large as to project from beneath the border of the liver, or the hand may be pressed beneath this border so that the tumor can be felt, or, what is most frequently the [p. 548]case, the weight of the tumor or the distension of the stomach drags the pylorus downward. The pylorus may, however, be so fixed by adhesions underneath the liver, or the liver may be so enlarged, that tumors of this part cannot be reached by palpation.
The situation in which cancerous tumors of the pylorus can be felt varies considerably. The usual situation is in the lower part of the epigastric region, a little to the right of the median line, but it is almost as common for these tumors to be felt in the umbilical region, and it is not rare for them to appear to the left of the median line.48 Brinton states that the tumor is in the umbilical region more frequently in the female sex than in the male, in consequence of the compression exercised by corsets. Occasionally pyloric cancers produce tumors in the right hypochondrium. Exceptionally, pyloric tumors have been felt as low as the iliac crest or even in the hypogastric region.
48 According to Jackson and Tyson, pyloric cancers are felt more frequently to the left than to the right of the median line.
Cancers of the stomach do not usually attain a very large size. Sometimes they form visible protuberances. An important criterion of cancerous tumors of the stomach is their gradual increase in size by progressive growth.
The consistence of cancerous tumors of the stomach is nearly always hard, as appreciated by palpation through the abdominal walls. The surface of the tumor is usually nodulated or irregular, but exceptionally it is smooth. The tumor may be movable or not, but in the majority of cases it is rendered immovable by adhesions. Mobility of the tumor, however, does not exclude the presence of adhesions. The tumor sometimes follows the respiratory movements of the diaphragm, especially when it is adherent to this structure or to the liver, but more frequently the tumor is not affected or but slightly affected by the movements of the diaphragm. If the tumor is not fixed by adhesions, it may change its position somewhat according to the varying degrees of distension of the stomach or in consequence of pressure of intestine distended with gas or feces. In consequence of these movements or of an overlying distended colon the tumor may even disappear temporarily. It is possible that the tumor may lessen or disappear in consequence of sloughing of the growth.49 It is not rare for a certain amount of pulsation to be communicated to the growth by the subjacent aorta. This pulsation is most common with pyloric tumors.
49 Symptoms which have been considered as diagnostic of sloughing of stenosing cancers of the pylorus are diminution in the size of the tumor, alleviation of the vomiting, hemorrhage, replacement of obstinate constipation by diarrhoeal stools which often contain blood, increased pain after eating, and rapid progress of cachexia.
The percussion note over the tumor is usually tympanitic dulness. Sometimes there is very little alteration over the tumor of the normal tympanitic note belonging to the stomach; on the other hand, exceptionally there is absolute flatness over the tumor.
It is often of assistance in determining that a tumor belongs to the pylorus to find dilatation of the stomach. An abnormal fulness of the epigastric and umbilical regions may then be observed, and through the abdominal walls, if thin, may be seen the peristaltic movements of the stomach. Other signs and symptoms aid in the diagnosis of dilatation of the stomach, and will be described in connection with this disease.
[p. 549] It is to be noted that what one takes to be the primary tumor of the stomach is not so very rarely a secondary cancerous mass in the stomach or in adjacent lymph-glands or in the peritoneum. Such nodules may also increase the apparent size of the original tumor. As has been pointed out by Rosenbach,50 spasm of the muscular coat near a cancer or an ulcer of the stomach may produce a false tumor or enlarge a real tumor.
50 Deutsche med. Wochenschr., 1882, p. 22.
The cancer, instead of appearing as a circumscribed tumor, may infiltrate diffusely the gastric walls, and so escape detection. When the greater part or the whole of the stomach is the seat of this diffuse cancerous infiltration, a sense of abnormal resistance may be appreciated by palpation in the epigastric region. In these cases the stomach is often much shrunken in size. The outlines of the thickened organ can sometimes be made out, but the physical signs do not suffice for the diagnosis of cancer.
With cancer of the cardia there is usually more or less atrophy of the stomach, which is manifested by sinking in of the epigastric region.
Sometimes the tumor eludes discovery on account of special obstacles to the physical examination of the abdomen, such as a thick layer of fat in the abdominal walls or a large quantity of ascitic fluid. Every aid in the physical examination of the abdomen should be resorted to. The patient should be examined while lying on his back with the utmost possible relaxation of the abdominal walls. If necessary, he should also be examined while standing or in the knee-elbow position. Sometimes a deep inspiration will force down a previously concealed tumor. The emptying of a dilated stomach by means of a stomach-tube will sometimes bring to prominence a gastric tumor.
The inflation of the stomach by the development in it of carbonic acid gas may render valuable assistance in the diagnosis of tumors of this organ and of surrounding parts. This method has been recommended by W. Ph. H. Wagner among others, and especially by Rosenbach.51 From 20 to 30 grains of bicarbonate of soda and from 15 to 20 grains of tartaric acid may be introduced into the stomach. The soda, dissolved in lukewarm water, may be given first and followed by the acid in solution, or, better, the mixed powders may be swallowed in the dry state and followed by a tumblerful of water. Some persons require a larger quantity of the powder in order to inflate the stomach. Occasionally the introduction of the effervescing powder fails to produce any appreciable distension of the stomach. This negative result may be due to the escape of the gas into the intestine in consequence of incontinence of the pylorus—a condition which Ebstein52 has observed and described especially in connection with pyloric cancer. When this pyloric insufficiency exists the resulting tympanitic distension of the intestine is a hindrance to palpation of tumors of the stomach. Failure to secure distension of the stomach is not always due to this cause. It may be necessary to make repeated trials of the effervescing mixture. It is well to have a stomach-tube at hand to evacuate the gas if this should cause much distress.
51 W. Ph. H. Wagner, Ueber die Percussion des Magens nach Auftreibung mit Kohlensäure, Marburg, 1869; O. Rosenbach, Deutsche med. Wochenschr., 1882, p. 22.
52 W. Ebstein, Volkmann's Samml. klin. Vorträge, No. 155.
In some respects simpler and more easily controlled is the method of [p. 550] distending the stomach by injecting air into it through a stomach-tube, as recommended by Runeberg.53 For this purpose the balloon of a Richardson's spray apparatus may be attached to a soft-rubber stomach-tube. In this way the desired quantity of air can be introduced and at any time allowed to escape through the tube.
53 J. W. Runeberg, Deutsches Arch. f. kl. Med., Bd. 34, p. 460, 1884.
When the stomach has been inflated the contours of tumors of the pylorus often become surprisingly distinct in consequence of the changes in the position and the shape of the stomach. When the tumor is fixed by adhesions, it may be possible to follow the contours of the stomach into those of the tumor. False tumors produced by spasm of the muscular walls of the stomach may be made to disappear by this distension of the organ. This procedure enables one to distinguish between tumors behind and those in front of the stomach, as the former become indistinct or disappear when the stomach is inflated. By bringing out the contours of the stomach the relations of the tumor to surrounding organs may be rendered for the first time clear. Assistance in diagnosis may also be afforded by distension of the colon with water or with gas or with air, per rectum, in order to determine the course of the colon and its relations to abdominal tumors (Mader, Ziemssen, Runeberg). A manifest contraindication to distension of the stomach or of the colon with gas exists if there is a suspicion that the coats of these parts are so thinned by ulceration that they might rupture from the distending force of the gas. There have been no cases recorded where such an accident has happened.
Only in exceptional cases are the bowels regular throughout the course of gastric cancer. Constipation is the rule, and not infrequently there is obstinate constipation. This is to be expected when the patient eats little and vomits a great deal, or when there is stenosis of the pylorus. In cancer, as in many other diseases of the stomach, the peristaltic movements of the intestine are inclined to be sluggish.
Occasional diarrhoea is also common in gastric cancer, being present, according to Tripier,54 at some period or other in over one-half the cases. Constipation often gives place to diarrhoea during the last months or during the last days of life. In other periods of the disease diarrhoea not infrequently alternates with constipation. In rare cases diarrhoea is an early symptom, and it may be present exceptionally throughout the greater part of the disease. The irritation of undigested food sometimes explains the diarrhoea. When diarrhoea is persistent there probably exists catarrhal inflammation of the large intestine, or in some instances there may be diphtheritic and ulcerative inflammation of the colon, causing dysenteric symptoms during the last stages of cancer of the stomach.
54 "Étude clinique sur la Diarrhée dans le Cancer de l'Estomac," Lyon Méd., 1881, Nos. 40, 41, 42.
Black stools containing altered blood occur for some days after profuse gastric hemorrhage. It is important to examine the stools for blood, as bleeding may occur from cancer of the stomach without any vomiting of blood.
There is no change in the urine characteristic of gastric cancer. Deposits of urates are not uncommon. If there be profuse vomiting or frequent washing out of the stomach, the urine often becomes alkaline from fixed [p. 551] alkali.55 The amount of urea is diminished in consequence of the slight activity of the nutritive processes of the body. Rommelaere attaches unmerited diagnostic importance to this diminution of urea. A similar diminution of urea occurs in other like states of depressed nutrition.
55 According to Quincke, when the acid in the stomach is not hydrochloric acid, but organic acid resulting from fermentation, then vomiting and washing out the stomach do not reduce the acidity of the urine (Zeitschrift f. klin. Med., Bd. 7, Suppl. Heft, p. 25).
Albuminuria does not belong to the history of gastric cancer, although a small quantity of albumen may be present in the urine as in other anæmic and cachectic conditions. A larger quantity of albumen may be due to parenchymatous and fatty degeneration of the kidney or to chronic diffuse nephritis, which are infrequent but recognized complications of gastric cancer. There is often an excess of indican in the urine, to which, however, no diagnostic significance can be attached.
The urine in gastric cancer sometimes contains an excess of aceton, or at least of some substance which yields aceton upon the application of various tests. This so-called acetonuria is present without any symptoms referable to it, so far as we know. Allied to this so-called acetonuria is that condition of the urine in which it is colored burgundy-red upon the addition of ferric chloride in solution (Gerhardt's reaction). It is not positively known what substance imparts this last reaction to the urine. V. Jaksch, who has studied the subject industriously, believes that the red coloring substance is diacetic acid, and he proposes to call the condition diaceturia. Fresh urine, which shows in a marked degree Gerhardt's reaction, often has a peculiar aromatic, fruity odor, as has also the expired air. Gerhardt's reaction has been studied mostly in diabetic urine, but it occurs sometimes in cases of gastric cancer and in a variety of diseases. This so-called diaceturia may be associated with a peculiar form of coma, but it is oftener observed without any symptoms referable to it56 (see page 555).
56 The various tests for aceton in the urine are not altogether satisfactory. They are to be found in an article by Von Jaksch in the Zeitschrift f. klin. Med., Bd. viii. p. 115. For English readers a good abstract of an article by Penzoldt on these tests and on acetonæmia in general is to be found in The Medical News of Philadelphia, Aug. 9, 1884, p. 162, but this does not consider the corrections and additions to be found in V. Jaksch's article cited above. Acetonuria has been observed especially in diabetes mellitus, fevers, carcinoma, and dyspepsia.
The substance which produces Gerhardt's reaction is to be distinguished from other substances which may be present in the urine and give a red color with ferric chloride—first, by the fact that boiling the urine in a test-tube for five or six minutes destroys the first-named substance, or causes the red color to disappear in case this has been produced by ferric chloride; and, secondly, by the fact that ether extracts the substance from acidified urine, and that the red color produced in the ether extract by ferric chloride (it may be necessary to first neutralize the acid) fades away in the course of a few days (V. Jaksch, Zeitschrift f. Heilkunde, Bd. iii. p. 17). Urines which respond to Gerhardt's reaction in a marked degree yield aceton on distillation, but aceton or an aceton-yielding substance may be present in considerable quantity without response of the urine to Gerhardt's test.
Disorders of nutrition embrace an important group of symptoms, such as loss of flesh and strength, impoverished blood, and cachectic color of the skin. Emaciation and debility are sometimes the first symptoms of gastric cancer to attract attention, and often the first symptoms to arouse anxiety. More frequently these symptoms of disordered nutrition first appear after dyspeptic ailments or pain have existed for several weeks or months. It may aid in the diagnosis of gastric cancer to weigh the patient [p. 552] from time to time, as carcinoma is generally attended by progressive loss of weight.
The patient frequently becomes morose and depressed in spirits. His strength fails, sometimes disproportionately to the loss of flesh. There is no disease in which emaciation becomes more extreme than in cases of gastric cancer.
In many cases profound anæmia develops, and sometimes in such a degree that this symptom cannot be regarded always as simply co-ordinate with the other disorders of nutrition, but is to be regarded rather as an evidence of some special disturbance of the blood-forming organs. The blood may present the same changes as are observed in pernicious anæmia, such as extreme reduction in the number of red blood-corpuscles (to one million or even half that number in a cubic millimeter) and manifold deformed shapes of the corpuscles (poikilocytosis). In extreme cases the proportion of hæmoglobin in the blood may be reduced to 50 or 60 per cent. of the normal quantity.57 There is occasionally a moderate increase in the number of white blood-corpuscles. In one case of gastric cancer I observed a leucocytosis in which there was one white to twenty red blood-corpuscles without enlargement of the spleen.58
57 The granular disintegrating corpuscles (Zerfallskörperchen of Riess) may also be found in the blood in considerable number. Leichtenstern has observed that toward the end of life the relative proportion of hæmoglobin in the blood may be increased, sometimes rapidly, and may even exceed the normal limit. This is due to concentration of the blood in consequence of the loss of water. In such cases the tissues appear abnormally dry and the blood thick and tarry at the autopsy (Ziemssen's Handb. d. spec. Path. u. Therap., Bd. viii. 1te Hälfte, p. 344).
It seems to me proper to distinguish two kinds of anæmia in gastric cancer—a simple anæmia, which is present in the majority of cases, and can be explained by the development of the cancer and the disturbance of the gastric functions; and a pernicious anæmia, which is present only in exceptional cases, and has the typical symptoms of progressive pernicious anæmia.
58 In a case of large medullary cancer of the stomach reported by H. Mayer there was one white to fifty red blood-corpuscles. The spleen was not enlarged (Bayer, Aerztl. Intelligenzblatt, 1870, No. 21). A similar case is related by Lebert, in which, however, the spleen was enlarged (op. cit., p. 481).
To the pallor of anæmia is added often a faded yellowish tint of the skin which is considered characteristic of the cancerous cachexia. At the same time, the skin is frequently dry and harsh, and may present brownish spots (chloasma cachecticorum). The pallid lips, the pale greenish-yellow color of the face, the furrowed lines, and the pinched and despondent expression make up a characteristic physiognomy, which, however, is neither peculiar to gastric cancer nor present in all cases of the disease. There is no cachectic appearance which is pathognomonic of cancer; and in this connection it is well to note that there are cases of gastric ulcer, and particularly of non-cancerous stenosis of the pylorus, in which all of the symptoms described as peculiar to the cancerous cachexia are met with. Nevertheless, the weight of these symptoms in the diagnosis of gastric cancer should not be underestimated. There is no disease in which profound cachectic symptoms so frequently and so rapidly develop as in gastric cancer.
The profound nutritive disturbances of gastric cancer are referable partly to the cancer as such, and partly to the impairment of the functions of the stomach. It is impossible to separate the effects of these two sets of causes, and distinguish, as some have done, a cachexia of cancer [p. 553] and a cachexia of inanition. It is the combination of these causes which renders the cachexia of cancer of the stomach so common, so rapid in its development, and so profound as compared with that of cancer in other situations. The relation of cancer in general to cachexia need not here be discussed, save to say that there is the best ground for believing that the cachexia is directly dependent upon the growth and metamorphoses of the primary cancer and its metastases, and that there is not reason to assume any dyscrasia antedating the cancerous formation.
While the failure of the general health and the gastric symptoms in general develop side by side, it is especially significant of gastric cancer when the symptoms of impaired nutrition are more pronounced than can be explained by the local gastric disturbance. When, however, as sometimes happens, gastric symptoms are absent or no more than can be explained by anæmia and marasmus, then in the absence of tumor a positive diagnosis is impossible. Such cases of gastric cancer during life often pass for essential or pernicious anæmia. Otherwise, unexplained symptoms of anæmia with emaciation and debility, particularly in elderly people, should lead to a careful search for gastric cancer.
Finally, it is necessary to add that there are exceptional cases of gastric cancer in which there is no emaciation, and in which the general health appears to be astonishingly well preserved. In most of these cases death occurs either from some accident of the disease or from some complication.
Slight or moderate oedema about the ankles is a common symptom during the cachectic stage of gastric cancer. This oedema is due to hydræmia. This cachectic dropsy in rare cases becomes excessive and leads to anasarca, with serous effusion in the peritoneal, pleural, and pericardial sacs. Such cases are liable to be mistaken for heart disease, particularly as a hæmic murmur often coexists, or for Bright's disease. Ascites may be the result not only of hydræmia, but also of cancerous peritonitis or of pressure on the portal vein by cancer. Many cases of gastric cancer associated with ascites have been falsely diagnosed as cirrhosis of the liver, and sometimes the distinction is extremely difficult or impossible.
During the greater part of the disease the pulse is usually normal; toward the end it is not infrequently rapid, small, and compressible. In consequence of weakness and anæmia any exertion may suffice to increase the frequency of the pulse, and may induce palpitation of the heart and syncope.
As might be expected as the result of anæmia, hæmic murmurs in the heart and blood-vessels are not rare in gastric cancer.
Epigastric pulsation is often very prominent in cases of gastric cancer, as it may be in various other conditions. This pulsation is sometimes of a paroxysmal nature.
Venous thrombosis is not a rare complication in the last stages of gastric cancer. It is most common in the femoral and saphenous veins, and is rapidly followed by painful oedematous swelling of the affected extremity. Thrombosis of the subclavian and axillary veins is much less frequent. When it occurs there are the same symptoms of phlegmasia alba dolens in the upper extremity as have been mentioned for the lower. Lebert has recorded a case of thrombosis of the right external jugular [p. 554] vein.59 The thrombosis is the result of marasmus, and therefore may occur in other gastric diseases besides gastric cancer, so that this symptom has not all the diagnostic importance for gastric cancer claimed by Trousseau. Being an evidence of great weakness of the circulation, marantic thrombosis in cancer of the stomach is of grave prognostic import.
59 Op. cit., p. 394.
The temperature is often normal throughout the course of gastric cancer. Febrile attacks, however, are not uncommon in this disease. Elevation of temperature may occur without any complication to explain it. During the second half of the disease there may be either irregular febrile attacks or a more continuous fever, which is, however, usually of a light grade, the temperature not generally exceeding 102°. Slight chills may be experienced. Lebert describes a light and a hectic carcinomatous fever.
There may be subnormal temperature with collapse during the last days of life, and in general anæmia and inactivity of nutritive processes tend to produce a low temperature.
Dyspnoea on slight exertion may be present in gastric cancer as a result of anæmia or of fatty heart. In a few cases of gastric cancer have been observed symptoms pointing to a reflex vagus neurosis, such as paroxysms of dyspnoea, oppression in the chest, and palpitation of the heart, but these symptoms are less common in gastric cancer than in some other diseases of the stomach. Watson60 relates a case of gastric cancer in which increasing dyspnoea and palpitation were such prominent symptoms that he was led to diagnose fatty heart with portal congestion as the sole trouble. At the autopsy the heart and lungs were found healthy, but there was extensive cancer of the greater curvature of the stomach. He subsequently ascertained that there had been symptoms pointing to gastric disease.
60 Sir T. Watson, Lectures on the Principles and Practice of Physic, vol. ii. p. 471, Philada., 1872.
The various complications of gastric cancer which affect the respiratory organs will be considered later.
Depression of spirits, lack of energy, headache, neuralgia, sleeplessness, and vertigo are functional nervous disturbances which are often the result of disordered digestion from whatever cause, and are therefore not uncommon in gastric cancer. The theory that these symptoms are due to the absorption of noxious substances produced in the stomach and intestine by abnormal digestive processes is plausible,61 and more intelligible than reference to some undefined sympathy between the digestive organs and the nervous system.
61 This theory is elaborated by Senator ("Ueber Selbstinfection durch abnorme Zersetzungsvorgänge, etc.," Zeitschrift f. klin. Med., Bd. 7, p. 235).
The intelligence is generally not impaired in the course of gastric cancer.
Considerable interest belongs to coma as a symptom of cancer of the stomach, and more particularly to the occurrence of coma with the peculiar characters which have been described by Kussmaul as distinguishing diabetic coma.62 The most distinctive feature in Kussmaul's group of symptoms is the accompaniment of the coma by a peculiar [p. 555] dyspnoea in which, without evidence of disease of the lungs or air-passages, the respirations are strong and deep and often attended with a groaning sound in expiration. The breathing is either normal in frequency or oftener moderately increased. The pulse is usually small and frequent. The temperature is not much elevated, and sometimes is much below the normal. Sometimes the coma is preceded by a period of excitement, with restlessness, and perhaps with screaming. Gerhardt's reaction in the urine may or may not be present. When it is present in a marked degree there is often an aromatic, chloroform-like odor to the breath and to the fresh urine. The patient may come out of the coma, but in the vast majority of cases the coma terminates fatally.
62 Deutsches Arch. f. klin. Med., Bd. 14, p. 1.
It is now known that this dyspnoeic coma is not confined to diabetes mellitus, but that it occurs also in gastric cancer and in various other diseases.63 Its occurrence in gastric cancer is rare. In this disease it does not usually appear until anæmia is far advanced, but it may occur in cases of cancer in which the patient's general health and nutrition are still fairly good. I recently made the post-mortem examination of an elderly man, fairly well nourished, who was found in the streets comatose and brought in this condition to Bellevue Hospital, where he died in about twelve hours. While in the hospital his breathing was increased in frequency, forcible, and deep. His temperature was normal. The urine contained a small quantity of albumen, but no sugar. No previous history could be obtained. Uræmic coma was suspected. At the autopsy was found a large, soft, ulcerated cancer of the lesser curvature and posterior wall of the stomach near the pylorus. The kidneys, brain, heart, and other organs were essentially healthy.
63 Von Jaksch was the first to describe this form of coma in cancer of the stomach (Wien. med. Wochenschr., 1883, pp. 473, 512). He adopted the term coma carcinomatosum, and more recently coma diaceticum. L. Riess has reported seventeen cases of this coma occurring in a variety of diseases, such as pernicious anæmia, gastric cancer, gastric ulcer, tuberculosis, which all had in common profound anæmia. He proposes the term dyspnoeic coma (Zeitschrift f. klin. Med., Bd. 7, Suppl. Heft, p. 34, 1884). Senator has described two cases of gastric cancer with this coma. He uses the terms dyscrasic coma and Kussmaul's group of symptoms (ibid., Bd. 7, p. 235). In the cases described by Litten under the name coma dyspepticum, dyspnoea was absent, but Gerhardt's reaction in the urine was present. In Litten's cases structural disease of the stomach was not supposed to be present. The patients recovered from the coma (ibid., Suppl. Heft, p. 81).
We possess no satisfactory explanation of this form of coma. In diabetes it is considered to be due to the presence in the blood of some intoxicating agent. For a time this agent was thought to be aceton; it is now believed by Von Jaksch to be diacetic acid. Much stress has been laid upon the aromatic, fruity odor of the breath and of the fresh urine, and upon the presence of some substance in the urine which imparts to it a burgundy-red color upon the addition of liquor ferri chloridi (Gerhardt's reaction. See changes in the urine, page 551). Although the whole aceton question is at present in a very confused state, there is no proof that aceton or its allies possesses the toxic properties assumed by this theory;64 and it is certain that dyspnoeic coma may occur in diabetes and in other diseases without the presence of Gerhardt's reaction in the urine. It is also true that this reaction often occurs without any clinical symptoms referable to it. Riess and Senator believe that in non-diabetic [p. 556] cases anæmia is the most important factor in the production of this coma.65
64 Frerichs, Zeitschrift f. klin. Med., Bd. 6, p. 3.
65 Riess refers the coma to the anæmia as such, whereas Senator thinks that, in consequence of the depraved nutrition of the body resulting from the anæmia, some toxic substance is developed which enters the circulation.
Coma, probably belonging to this same variety, may occur in gastric cancer without the peculiar dyspnoea which has been described. There is reason to believe that this dyspnoea is not a necessary symptom of the so-called diabetic coma.
Chronic Bright's disease terminating with uræmic coma is an occasional but not frequent complication of gastric cancer.
Coma and other cerebral symptoms may be produced by secondary cancerous tumors in the brain.
Stupor deepening into coma may develop during the often-prolonged death-agony of gastric cancer.
The distribution, origin, and frequency of cancerous growths secondary to gastric cancer are most conveniently considered under Pathological Anatomy. Symptoms referable to certain localizations of these secondary cancerous deposits, however, are so common, and so interwoven with the clinical history of cancer of the stomach, that it is desirable to consider some of these symptoms in the present connection.
Cancer of the liver is the most important of these secondary cancerous growths. It is estimated to be present in nearly one-third of the cases of gastric cancer, but by no means in all these cases does it produce symptoms. As a rule, the earlier hepatic cancer forms in the course of gastric cancer the more likely is it to be attended by symptoms. The most important symptoms of secondary cancer of the liver are enlargement of the liver, peritoneal exudation, and persistent icterus. When nodular growths can be felt in the free border or surface of the liver, the diagnosis is generally easily established. Sometimes the liver remains of normal size or is even contracted, and then the diagnosis is difficult or impossible. Ascites or exudative peritonitis is present in about one-half of the cases of cancer of the liver. Jaundice is less frequently present. It is only persistent jaundice which aids in the diagnosis of hepatic cancer.
The various combinations of gastric cancer with secondary hepatic cancer may be clinically grouped as follows:
1. Symptoms of gastric cancer with latent hepatic cancer.
2. Symptoms of gastric cancer followed by symptoms of hepatic cancer.
3. Symptoms both of gastric cancer and of hepatic cancer present when the case comes under observation.
4. Symptoms of hepatic cancer with latent gastric cancer.
5. Symptoms of hepatic cancer followed by symptoms of gastric cancer.
6. Both hepatic and gastric cancer latent. Symptoms of anæmia and marasmus, or of chronic exudative peritonitis, or of chronic pleurisy.
From this grouping it is evident that the existence of secondary hepatic cancer may aid in the diagnosis of cancer of the stomach, or may mislead, or may be without influence. The greatest assistance in diagnosis is rendered when the physical signs and the symptoms of hepatic [p. 557] cancer develop some time after the appearance of gastric symptoms which may previously have been equivocal. Much more difficult to diagnosticate are the cases of hepatic cancer accompanied or followed by gastric symptoms, inasmuch as cancer of the liver, whether primary or secondary, may be attended with marked disturbance of the gastric functions, including hæmatemesis. In these cases, unless a tumor of the stomach can be discovered, a positive diagnosis of gastric cancer is impossible. In view of the infrequency of primary cancer of the liver, however, there will be in many of these cases a strong probability in favor of primary cancer of the stomach. When it is remembered that over one-third of the cancers of the liver are secondary to cancer of the stomach, it is evident that in cases which appear to be primary hepatic cancer very careful attention should be given to the exploration of the stomach. But even then diagnostic errors will often be unavoidable.
Cancer of the peritoneum secondary to cancer of the stomach may produce no symptoms, and so pass unrecognized. The diagnosis of peritoneal cancer is readily made when, after the recognition of gastric cancer, secondary cancerous nodules in the peritoneum can be felt through the abdominal walls or through the vagina. There are cases of gastric cancer in which the symptoms are all referable to secondary cancer of the peritoneum. Cancer of the peritoneum is usually attended with fluid exudation in the peritoneal cavity. The chemical and the microscopical examination of this fluid withdrawn by paracentesis may aid in the diagnosis of cancerous peritonitis. Whereas in dropsical accumulations in the peritoneal cavity the quantity of albumen in the fluid is usually less than 2½ per cent., in cancerous peritonitis there is usually from 3 to 4 per cent. of albumen, the percentage rarely falling as low as 2½ per cent., but sometimes being as high as from 5 to 6 per cent. The percentage of albumen in ordinary peritonitis is usually over 4.66 Clumps of cancer-cells are sometimes to be found by microscopical examination of the fluid. These cells are large, epithelioid in shape, and often contain vacuoles and fatty granules. It is only when these cells are arranged in clumps or as so-called budding cells, and when they are present in abundance, that they are diagnostic. They are to be sought especially in fibrinous coagula. They are present only when the cancerous alveoli actually communicate with the peritoneal cavity.67 The development of cancerous nodules in the margins of an opening made in the abdominal walls by a trocar is also evidence of cancerous disease of the peritoneum. The same thickening and retraction of the mesentery and omentum may occur in cancerous as in tuberculous peritonitis. In both the exudation is often hemorrhagic.
66 The conditions under which the estimation of the quantity of albumen in the peritoneal exudation may prove of diagnostic aid are fully considered by Runeberg (Deutsches Arch. f. klin. Med., Bd. 34, p. 1). Here also are given methods for making this analysis for clinical purposes.
67 The literature on this subject is as follows: Foulis, Brit. Med. Journ., July 20, Nov. 2, 1878; Thornton, ibid., Sept. 7, 1878; Quincke, Deutsches Arch. f. klin. Med., Bd. 30, p. 580; Ehrlich, Charité Annalen, vii. p. 226; Brieger, ibid., viii.
Importance has been attached to enlargement of the supraclavicular lymphatic glands in the diagnosis of cancer of the stomach, but there are so many causes of enlargement of these glands that not much significance can be attached to this symptom, which, moreover, is absent in most [p. 558] cases. Still, under certain circumstances this glandular enlargement may aid in the diagnosis. The same remarks apply to enlargement of the inguinal glands, which is a common occurrence in case cancer involves the peritoneum. One must not mistake abnormal prominence of the lymphatic glands in consequence of emaciation for actual enlargement.
Gastric cancer much less frequently than gastric ulcer causes perforation of the stomach. Of 507 cases of gastric cancer collected by Brinton, perforation into the general peritoneal cavity occurred in 17 (31/3 per cent.).68 In two cases of gastric cancer reported by Ellis perforative peritonitis was preceded by symptoms supposed to be only those of ordinary dyspepsia, hemorrhage and vomiting being absent.69 Various fistulous communications like those described under gastric ulcer may be the result of perforation of gastric cancer, but with the exception of gastro-colic fistula they are much more frequently produced by ulcer than by cancer. In 160 cases of gastric cancer collected by Dittrich, gastro-colic fistula existed in 6 (3¾ per cent.).70 In 507 cases collected by Brinton this fistula existed in 11 (2.17 per cent.). In Lange's 210 cases gastro-colic fistula existed in 8 (3.8 per cent.). Of 33 cases of gastro-colic fistula collected by Murchison, 21 were caused by cancerous ulceration.71 The symptoms characteristic of fistulous communication between the stomach and the colon are the vomiting of fecal matter and the passage of undigested food by the stools. These symptoms are not present in all cases, so that a diagnosis is not always possible. Fecal vomiting is influenced by the size of the opening between the stomach and the colon. With great obstruction at the pylorus, fecal vomiting, as might be expected, is absent or infrequent, while the passage of undigested food by the bowels is common. Under these circumstances vomiting is sometimes relieved after the establishment of the fistula. Aid may be afforded in the diagnosis of gastro-colic fistula by the introduction into the rectum or into the stomach of colored or other easily recognizable substances, and determining their presence in the vomit or in the stools in consequence of their escape by the unnatural outlet. V. Ziemssen has determined in a case of gastro-colic fistula due to cancer the escape into the stomach of carbonic acid gas artificially generated in the rectum, with failure to obtain distension of the colon.72 A number of instances of gastro-cutaneous fistula due to gastric cancer have been recorded, but this form of fistula is much less common than gastro-colic fistula, and much less frequently the result of cancer than of ulcer of the stomach. Subcutaneous emphysema may precede the formation of the fistula. Other gastric fistulous communications resulting from cancer, such as with the pleura, the lungs, the small intestine, are too infrequent to merit consideration under the symptomatology of the disease.
68 Loc. cit. Lange (op. cit.) records in 210 cases of gastric cancer 12 perforations into the peritoneal cavity (5.7 per cent.).
69 Extr. fr. the Rec. of the Boston Soc. for Med. Improvement, vol. iii. p. 116, and vol. iv. p. 109.
70 Prager Vierteljahrsch., vol. xvii.
71 Edinb. Med. Journ., vol. iii. p. 4, 1857.
72 Deutsches Arch. f. kl. Med., Bd. 33, p. 237. He recommends for extreme distension of the colon in an adult the introduction, by means of a tube passed up the rectum, of a solution of about 5 drachms of sodii bicarb. and 4½ drachms of tartaric acid—injected not all at once, but in three or four doses at intervals of a few minutes, the tube being cleaned in the intervals by the injection of three ounces of water, so as to avoid generation of gas in the tube. The generation of a smaller quantity of gas would suffice for the purpose here in view.
[p. 559] As a rule, patients with gastric cancer die from gradual exhaustion. In a condition of extreme emaciation and feebleness the patient sinks into a state of collapse, accompanied often with stupor, sometimes with mild delirium. The death-agony is prolonged frequently from twelve to twenty-four hours, and sometimes even longer. On the other hand, death may occur somewhat suddenly in the last stages of gastric cancer, and without satisfactory explanation.
Death from copious gastric hemorrhage does not occur probably in more than 1 per cent. of the cases of cancer of the stomach.
In the rare cases of death from perforation of the stomach the patient is sometimes so exhausted at the time of perforation that the occurrence of this accident remains unrecognized in the absence of any complaint of characteristic symptoms.
The coma which sometimes leads to the fatal termination of gastric cancer has already been sufficiently considered.
Finally, death may be the result of certain complications more or less dependent upon the cancer. Of these the most important are suppurative peritonitis and pulmonary complications, particularly oedema, terminal pneumonia, and embolism of the pulmonary artery.
DURATION.—It is evidently impossible to determine the exact duration of a cancer of the stomach. Doubtless in all cases there is a period of growth of the tumor before it produces symptoms, and the duration of this latent period can never be determined. When symptoms appear they are often at first so mild as to be readily overlooked, and so ambiguous that even if recognized they are not clearly referable to the cancer. Gastric symptoms may have preceded, perhaps for years, the development of the cancer, so as to lead to the assumption of a longer duration of the cancer than is really the case. Estimates, therefore, of the duration of gastric cancer can be only of limited value.
From 198 cases Brinton73 estimates the average duration of gastric cancer as about twelve and a half months, the maximum duration as about thirty-six months, and the minimum as one month. From 36 cases Katzenellenbogen74 estimates the average duration as eighteen months, the maximum as five years and five months, the minimum as one month. From 112 cases Lebert75 makes the average duration fifteen months and the maximum four years. In 4 per cent. of the cases Lebert found the duration less than three months, in 62 per cent. between six and eighteen months, in 42 per cent. between six and twelve months, in 17 per cent. between three and six months, and in the same number of cases between eighteen months and four years.
73 Loc. cit.
74 Op. cit.
75 Op. cit.
Estimates of several years' duration (such as nine years in the case of Napoleon) are to be received with scepticism. In these cases symptoms of gastralgia or of dyspepsia or of gastric ulcer have preceded the development of the cancer. It has already been mentioned that cancer may develop in a simple ulcer of the stomach.
Mathieu,76 from an analysis of 27 cases of gastric cancer occurring under thirty-four years, found the average duration in early life to be only three months. In only 2 out of 19 cases did the duration exceed one year. Although this analysis is based upon too small a number of cases, there [p. 560] seems to be no doubt that gastric cancer pursues a more rapid course in early life than it does in old people.
76 Du Cancer précoce de l'Estomac, Paris, 1884, p. 40.
COMPLICATIONS.—Some of the complications of gastric cancer have been mentioned under Symptomatology. Jaundice may appear in the course of gastric cancer from a variety of causes, such as catarrhal gastro-duodenitis, impaction of gall-stones in the common bile-duct, and pressure on the bile-duct by cancerous growths in the pancreas, in the portal lymphatic glands, or in the liver itself. Pylethrombosis, which is likely to be suppurative, is a rare complication. In a case of cancer of the anterior wall and greater curvature of the stomach reported by Wickham Legg77 the symptoms seem to have been mostly referable to a complicating suppurative pylethrombosis. Simple and cancerous pylethromboses also occur. Other forms of peritonitis than the cancerous may complicate gastric cancer, such as suppurative, sero-fibrinous, and chronic proliferative peritonitis. Catarrhal enteritis, and particularly diphtheritic colitis, are not infrequent complications, especially in the later stages of the disease. Chronic diffuse nephritis, both in the form of the large and of the small kidney, is a rare complication of cancer of the stomach. Hydrothorax, sero-fibrinous pleurisy, and emphysema may develop either with or without cancerous invasion of the pleura. Pericarditis is much less common; it is most likely to occur with cancer of the cardia. Pyo-pneumothorax, abscess, and gangrene of the lung may result from perforation of the pleura or of the lung by gastric cancer. Oedema of the lungs, splenization, and pneumonia, involving usually the lower lobes, are common in the last days of gastric cancer. Emboli derived from venous thrombi are sometimes carried into the pulmonary artery or its branches. Although much has been written as to the exclusion of tuberculosis by cancer, no such law exists. Both old and fresh tubercles have been repeatedly observed in cases of gastric cancer. Reference has already been made to the frequent development of aphthæ in the mouth, pharynx, and oesophagus in the final stage of gastric cancer. Fatty degeneration of the heart may develop in gastric cancer as in other anæmic states. Phlegmasia alba dolens has already been mentioned. It is not probable that insanity is to be regarded as more than an accidental complication of gastric cancer; still, it has been noticed in several cases—for instance, of Dittrich's 160 cases, 5 patients were insane, 2 with violent mania. Amyloid degeneration has been present in some cases. Purpura hæmorrhagica has been present in a few instances in the later stages (cachectic purpura). Chronic catarrhal gastritis and dilatation of the stomach are less complications than a part of the disease. The relation of cancer to simple ulcer of the stomach has already been considered. The various secondary cancerous deposits are most conveniently considered under the Morbid Anatomy. It is to be remarked that many of the complications of gastric cancer—as, for instance, pneumonia and peritonitis—may have a very obscure clinical history, as they often occur when the patient is greatly prostrated.
77 St. Bartholomew's Hosp. Rep., vol. x. p. 236.
MORBID ANATOMY.—The following table gives the situation of the tumor in 1300 cases of cancer of the stomach:78 [p. 561]
| Pyloric region. | Lesser curvature. | Cardia. | Posterior wall. | The whole or the greater part of the stomach. | Multiple tumors. | Greater curvature. | Anterior wall. | Fundus. |
| 791 | 148 | 104 | 68 | 61 | 45 | 34 | 30 | 19 |
| 60.8% | 11.4% | 8% | 5.2% | 4.7% | 3.5% | 2.6% | 2.3% | 1.5% |
From this table it appears that three-fifths of all gastric cancers occupy the pyloric region, but it is not to be understood that in all of these cases the pylorus itself is involved. In four-fifths of the cases the comparatively small segment of the stomach represented by the cardia, the lesser curvature, and the pyloric region is the part affected by gastric cancer. The lesser curvature and the anterior and the posterior walls are involved more frequently than appears from the table, inasmuch as many cancers assigned to the pyloric region extend to these parts. The fundus is the least frequent seat of cancer. In the cases classified as involving the greater part of the stomach the fundus often escapes.
78 These cases are collected from the following sources: Lebert, op. cit.; Prague statistics of Dittrich, Engel, Wrany, and Eppinger, loc. cit.; Habershon, op. cit.; Katzenellenbogen, op. cit.; and Gussenbauer and V. Winiwarter, loc. cit. Gussenbauer and V. Winiwarter assign to the class of cancers involving the whole stomach all cases which they found designated simply as carcinoma ventriculi without further description. This produces in their statistics an excessive number of cancers under this class. I have preferred, therefore, to estimate in their collection of cases the number of cancers involving the whole stomach, according to the percentage for this class obtained from the other authors above cited.
As was shown by Rokitansky, it is the exception for cancer of the pylorus to extend into the duodenum, whereas cancer of the cardia usually invades for a certain distance the oesophagus.
The varieties of carcinoma which develop primarily in the stomach are scirrhous, medullary, colloid, and cylindrical epithelial carcinoma.79 The distinction between scirrhous and medullary cancer is based upon the difference in consistence, the former being hard and the latter soft. Cylindrical-celled epithelioma cannot be recognized as such by the naked eye. It presents usually the gross appearances of medullary cancer. Soft cancer (including both cylindrical-celled epithelioma and medullary carcinoma) is the most frequent form of gastric cancer. Next in frequency is scirrhous cancer, and then comes colloid cancer, which, although not rare, is much less frequent than the other varieties.
79 I have not been able to find an authentic instance of primary melanotic cancer of the stomach, although this form is included by most authors in the list of primary gastric cancers. It is known that most cases formerly described as melanotic cancers are melanotic sarcomata, which originate usually in the skin or the eye and are accompanied frequently with abundant metastases. Secondary melanotic tumors have been several times found in the stomach. They were present in 7 out of 50 cases of melanotic cancer (or sarcoma) analyzed by Eiselt, although out of 104 cases not a single primary melanotic cancer occurred in the stomach (Prager Viertaljahrschr., vol. lxxvi. p. 54). The list of secondary melanotic sarcomata of the stomach might be still further increased. Of course gastric cancers colored by pigment from old blood-extravasations should not be confounded with melanotic tumors.
As all degrees of combination and of transition exist between the different forms of cancer, and as a large number of cancers of the stomach are of a medium consistence and would be classified by some observers as scirrhous and by others as medullary, statistics as to the relative frequency of the different varieties have very little value. Moreover, in most statistics upon this point there is no evidence that simple fibrous growths have not been confounded with scirrhous cancer, and as a rule [p. 562] little or no account is taken of cylindrical-celled epithelioma, which is a common form of gastric cancer—according to Cornil and Ranvier, the most common.80
80 For any who may be interested in such statistics I have collected 1221 cases of gastric cancer, of which 791 (64.8 per cent.) were medullary, 399 (32.7 per cent.) scirrhous, and 31 (2.5 per cent.) colloid. 22 cases described as epithelial have been included with the medullary; 29 cases described as fibro-medullary, and 1 as fasciculated, have been included with the scirrhous. The cases are from the previously-cited statistics of Lebert, Dittrich, Wrany, Eppinger, Gussenbauer, and V. Winiwarter, and from Fenger (Virchow u. Hirsch's Jahresbericht, 1874, Bd. i. p. 312).
Cancer of the stomach may grow in the form of a more or less complete ring around the circumference of the stomach, or as a circumscribed tumor projecting into the cavity of the stomach, or as a diffuse infiltration of the walls of the stomach. The annular form of growth is observed most frequently in the pyloric region. Cancerous tumors which project into the interior of the stomach are sometimes broad and flattened, sometimes fungoid in shape, but most frequently they appear as round or oval, more rarely irregular, crater-like ulcers, with thickened, prominent walls and ragged floor. The free surface of the tumor presents sometimes a cauliflower-like or dendritic appearance, which characterizes the so-called villous cancer. Diffuse cancerous infiltration is seated oftenest in the right half of the stomach, but it may occupy the cardiac region or even the entire stomach.
The relation of the cancerous growth to the coats of the stomach varies in different cases. The tumor usually begins in the mucous membrane and rapidly extends through the muscularis mucosæ into the submucous coat. In this lax connective-tissue coat the tumor spreads often more rapidly than in the mucous membrane, so that it may appear as if the cancer originated in the submucosa. The mucous membrane, however, is usually invaded, sooner or later, over the whole extent of the tumor. The dense muscular coat offers more resistance to the invasion of the tumor. Cancerous masses, however, penetrate along the connective-tissue septa between the muscular bundles, which often increase in number and size. In the muscular coat thus thickened can be seen the opaque white fibrous and cancerous septa enclosing the grayish, translucent bundles of smooth muscular tissue. Often, however, the whole muscular coat beneath the tumor is replaced by the cancerous growth, and can no longer be recognized. The serous and subserous connective tissue, like the submucous coat, offers a favorable soil for the growth of the tumor, which here appears usually in the form of large and small nodules projecting from the peritoneum. Adhesions now form between the stomach and surrounding parts, and opportunity is offered for the continuous growth of the cancer into these parts. In the manner described the tumor grows in all directions, sometimes more in depth, sometimes more laterally, sometimes more into the interior of the stomach.
Ulceration occurs in all forms of gastric cancer.81 The ulceration is caused either by fatty degeneration and molecular disintegration of the surface of the tumor or by the separation of sloughy masses. Doubtless the solvent action of the gastric juice aids in the process. The softer and [p. 563] the more rapid the growth of the cancer, the more extensive is likely to be the ulcer. Such ulcers are usually round or oval in shape, but their contours may be irregular from the coalescence of two or more ulcers or from serpiginous growth. The edges are usually high, soft in consistence, and often beset with polypoid excrescences. The floor is generally sloughy and soft, and often presents warty outgrowths. The edges and floor may, however, be hard and smooth. In the more slowly-growing scirrhous and colloid cancers the ulcers are more likely to be superficial. Partial cicatrization of cancerous ulcers may take place. The development of cicatricial tissue may destroy the cancerous elements to such an extent that only by careful microscopical examination can the distinction be made between cancer and simple ulcer or fibroid induration. The examination of secondary cancerous deposits in adjacent lymphatic glands or other parts becomes, then, an important aid in the diagnosis.
81 Ulceration was present in 60 per cent. of Lebert's cases, and in 66½ per cent. of Gussenbauer and V. Winiwarter's pyloric cancers.
Suppuration has been known to occur in gastric cancers, but it is extremely rare.
Each form of gastric cancer has certain peculiarities which require separate consideration.
Medullary carcinoma grows more rapidly than the other varieties of cancer. It forms usually soft masses, which project into the stomach and are prone to break down in the centre and develop into the crater-like ulcers already described. All of the coats of the stomach are rapidly invaded by the growth. The consistence of the tumor is soft, the color upon section whitish or reddish-gray, sometimes over a considerable extent hemorrhagic. Milky juice can be freely scraped from the cut surface of the tumor. The so-called villous cancer and the hæmatodes fungus are varieties of medullary carcinoma. Medullary carcinoma is more frequently accompanied by metastases than the other forms. In consequence of its tendency to deep ulceration medullary cancer is more liable to give rise to hemorrhage and to perforation than is scirrhous or colloid cancer. The continuous new formation of cancerous tissue in the floor of the ulcer and the formation of adhesions, however, greatly lessen the danger of perforation into the peritoneal cavity.
Histologically, medullary cancer is composed of a scanty stroma of connective tissue enclosing an abundance of cancerous alveoli filled with polyhedrical or cylindrical epithelial cells. The stroma is often richly infiltrated with lymphoid cells, and contains blood-vessels which often present irregular dilatations of their lumen.
Waldeyer describes with much detail, for this as for the other forms of gastric cancer, the origin of the tumor from the gastric tubules. According to his description, a group of gastric tubules, ten to twenty in number, sends prolongations downward into the submucous coat. These tubular prolongations are filled with proliferating epithelial cells, which make their way into the lymphatic spaces of the surrounding tissue and give origin to the cells in the cancerous alveoli. A small-celled infiltration of the surrounding connective tissue accompanies this growth of the tubules.
The tissue beneath and at the margins of medullary cancer may be predominantly fibrous in texture and contain comparatively few cancerous alveoli. This scirrhous base is often exposed after the destruction of the greater part of the soft cancer by ulceration and sloughing. It is [p. 564] probable that many of the scirrhous cancers are formed in this way secondarily to medullary cancer (Ziegler).
Cylindrical-celled epithelioma presents the same gross appearances and the same tendency to ulceration and to the formation of metastases which characterize medullary cancer. The consistence of cylindrical epithelioma may, however, be firm like that of scirrhus. Not infrequently the alveoli are distended with mucus secreted by the lining epithelium, and then the tumor presents in whole or in part appearances similar to colloid cancer.
Upon microscopical examination are seen spaces resembling more or less closely sections of tubular glands. These spaces are lined with columnar epithelium. Often in certain parts of the tumor the alveolar spaces are filled with cells, so that the structure is a combination of that of ordinary cancer and of epithelioma. The stroma is generally scanty and rich in cells, but it may be abundant. Cysts may be present in this form of tumor, and in one case I have found such cysts nearly filled with papillary growths covered with cylindrical epithelium, so that the appearance resembled closely that of the so-called proliferous cysto-sarcoma of the breast.
The origin of cylindrical epithelioma from the gastric tubules is generally accepted, and is more readily demonstrable than the similar origin claimed for the other forms of gastric cancer.
Scirrhous cancer assumes often the form of a diffuse thickening and induration of the gastric walls, particularly in the pyloric region, where it causes stenosis of the pyloric orifice. Scirrhus may, however, appear as a circumscribed tumor. Irregular hard nodules frequently project from diffuse scirrhous growths into the interior of the stomach. Scirrhous cancer and medullary cancer are often combined with each other.
The dense consistence of scirrhous cancer is due to the predominance of the fibrous stroma, the cancerous alveoli being relatively small in size and few in number.
Colloid cancer generally appears as a more or less uniform thickening of the gastric walls. All of the coats of the stomach are converted into the colloid growth. Nearly the whole of the stomach may be invaded by the new growth.82 The tumor has a tendency to spread to the omenta and to the rest of the peritoneum, where it may form enormous masses, but it rarely gives rise to metastases in the interior of organs. Colloid cancer may, however, form a circumscribed projecting tumor in the stomach, and in rare instances it causes abundant secondary colloid deposits in the liver, the lungs, and other parts.
82 In a case reported by Storer the whole stomach, except a little of the left extremity over an extent of about an inch, was converted into a colloid mass in which no trace of the normal coats of the stomach could be made out. The colloid growth replacing the gastric wall measured seven-eighths of an inch in thickness in the pyloric region. Digestion was less disturbed in this case than in most cases of gastric cancer (Boston Med. and Surg. Journ., Oct. 10, 1872). In Amidon's case (reported in the Trans. of the N.Y. Path. Soc., vol. iii. p. 38) there seems to have been an equally extensive colloid metamorphosis of the stomach.
Colloid cancer presents, even to the naked eye, an exquisite alveolar structure, whence the name alveolar cancer as a designation of this tumor. Bands of opaque white or gray connective tissue enclose alveolar meshes which are filled with the gelatinous, pellucid colloid [p. 565] substance. This colloid material is thought to be produced by a colloid transformation of the epithelial cells in the alveoli, but the same transformation seems to occur also in the stroma. Few or no intact epithelial cells may be found in the alveoli. Colloid metamorphosis may take place in all forms of gastric cancer, but it is particularly common in cylindrical epithelioma. Colloid cancer may originate in the peritoneum unconnected with any glandular structures. It occurs often at an earlier age than other forms of cancer. Deep ulceration rarely attacks colloid cancer.
Flat-celled epithelioma is found at the cardiac orifice and as a metastatic growth in other parts of the stomach. Originating in the oesophagus, it may extend downward into the stomach. By noting whether the structure is that of squamous or of cylindrical epithelioma it is often possible to determine whether a tumor at the cardiac orifice originates in the oesophagus or in the stomach.
Secondary cancer of the stomach, although rare, is not such a curiosity as is often represented. Without aiming at completeness, I have been able to collect 37 cases of secondary cancer of the stomach, of which the larger number will stand critical examination.83 Of these cases, 17 were secondary to cancer of the breast, 8 to cancer of the oesophagus, 3 to cancer of the mouth or nose, and the remainder to cancer of other parts of the body. The large number of cases secondary to cancer of the breast is explained by the large statistics relating to mammary cancer which were consulted. Gastric cancer is more frequently secondary to cancer of the oesophagus than to cancer of any other part. In this category of course are not included cases of continuous growth of oesophageal cancer into the stomach, but only metastatic cancers of the stomach. A part at least of the gastric cancers secondary to cancer of the alimentary tract above the stomach I refer, with Klebs, to implantation in the mucous membrane of the stomach of cancerous particles detached from the primary growth in the oesophagus, pharynx, or mouth. This view is supported by the absence in some cases of any involvement of the lymphatic glands. The secondary deposits in the stomach conform in structure to the primary growth. They are usually situated in the submucous coat, where they form one or often several distinctly circumscribed tumors. The secondary tumors may or may not ulcerate. They rarely produce symptoms.
83 These cases are from Dittrich, 2 (the remainder of his cases I rejected); Cohnheim, 1; Petri, 2; Klebs, 3; Lücke, 1; Weigert, 1; Coupland, 1; Cruse, 1; Hausmann, 1; Bartholow, 1; Oldekop, 5; Edes, 1; V. Török and V. Wittelshöfer, 8; Grawitz, 4; Haren Noman, 5. So-called melanotic cancers, cancers involving only the serous coat of the stomach, and those extending by continuous growth into the stomach, are not included in this list.
Primary cancers may be present at the same time in different organs of the body; for instance, in the uterus and in the stomach.84 The possibility of multiple primary cancers is to be borne in mind in considering some of the apparently secondary cancers of the stomach, as well as in determining whether certain cancers are secondary to gastric cancer or not. Here the microscopical examination is often decisive.85
84 Case of A. Clark's (Trans. N.Y. Path. Soc., vol. i. p. 260), and a similar one reported by J. B. S. Jackson in Extr. from Records of the Boston Soc. for Med. Improvement, vol. i. p. 335.
85 The subject of multiple primary cancers is considered by Kauffmann (Virchow's Arch., Bd. 75, p. 317), and by Beck (Prager med. Wochenschr., 1883, Nos. 18 and 19). V. Winiwarter reports a cancer of the stomach in a patient who died one year seven and a half months after extirpation of a cancer of the nose. He regards the case as one of multiple primary cancer.
[p. 566] Gastric cancer often causes important secondary changes in the coats and the lumen of the stomach. In the neighborhood of the tumor are often found hypertrophy of the muscular coat and fibrous thickening of the submucous coat. Polypoid hypertrophy of the mucous membrane near the cancer is not rare. Not only near the tumor, but over the whole stomach, chronic catarrhal gastritis usually exists.
The most important alterations are those dependent upon obstruction of the orifices of the stomach. This obstruction may be caused either by a tumor encroaching upon the orifice or by an annular thickening of the walls of the orifices. Even without apparent stenosis, destruction of the muscular layer at or near the pylorus may be an obstacle to the propulsion of the gastric contents into the duodenum. As a result of obstruction of the pyloric orifice the stomach becomes dilated, sometimes enormously, so as to occupy most of the abdominal cavity. The walls of the dilated stomach, particularly the muscular coat, are usually thickened, but exceptionally they are thinned. Sometimes with pyloric stenosis the stomach is reduced in size. This occurs particularly when a scirrhous growth extends diffusely from the pyloric region over a considerable part of the stomach. Obstruction of the cardiac orifice or in the oesophagus leads to atrophy of the stomach, although here also there are exceptions. Above the obstruction the oesophagus is often dilated. An existing obstruction may be reduced or removed by ulceration or sloughing of the tumor.
Both dilatation and contraction of the stomach may attend gastric cancer without any involvement of the orifices of the stomach in the cancerous growth. The cavity of the stomach may be so shrunken by scirrhous thickening and contraction of the gastric walls that it will hardly contain a hen's egg. Irregular deformities in the shape of the stomach, such as an hour-glass shape and diverticular recesses, may be caused by gastric cancer.
Changes in the shape of the stomach and the weight of the tumor may cause displacements of pyloric cancers, so that these tumors have been found in nearly all regions of the abdomen, and even in the true pelvis.86 Such displaced cancers usually contract adhesions with surrounding parts.
86 Lebert, op. cit., p. 420.
It is not necessary to dwell upon the formation of adhesions which may bind the stomach to nearly all of the abdominal organs, most frequently to the liver, the pancreas, the intestine, and the anterior abdominal wall. Adhesions of pyloric cancers are found in at least two-thirds of the cases, and probably oftener.87
87 Gussenbauer and V. Winiwarter found adhesions recorded in 370 out of 542 pyloric cancers. In considering the propriety of resection of gastric cancers it has become a matter of importance to know in what proportion of cases adhesions are present. I agree with Ledderhose and with Rydygier in believing that adhesions are present oftener than appears from Gussenbauer and V. Winiwarter's statistics. The fact that adhesions are not noted in post-mortem records of gastric cancer cannot be considered proof of their absence. Little has been done in the study of gastric cancer from a surgical point of view. Metastases and adhesions were absent in only 5 out of 52 cases of pyloric cancer in which either pylorectomy or exploratory laparotomy was performed (Rydygier).
Cancer of the stomach in the majority of cases is accompanied with [p. 567] metastases in other parts of the body. In 1120 cases of gastric cancer secondary cancers were present in 710, or 63.4 per cent., and absent in 410, or 36.6 per cent.88 In about two-thirds of the cases, therefore, secondary deposits were present.
88 These cases are from Habershon, op. cit.; Lebert, op. cit.; Trans. N.Y. Path. Soc., vol. i.; and Gussenbauer and Von Winiwarter, loc. cit.
In order to determine the relative frequency of the secondary deposits in various organs of the body, I have constructed the following table, based upon an analysis of 1574 cases of cancer of the stomach in which the situation of the metastases were given:89
| Lymphatic glands. | Liver. | Peritoneum, omentum, and intestine. | Pancreas. | Pleura and lung. | Spleen. | Brain and meninges. | Other parts of the body. |
| 551 | 475 | 357 | 122 | 98 | 26 | 9 | 92 |
| 35% | 30.2% | 22.7% | 7.8% | 6.2% | 1.7% | 0.6% | 5.8% |
89 These cases include, in addition to those cited in the preceding foot-note, those of Dittrich (Prager Vierteljahrschr., vol. xvii.), Wrany (ibid., vols. xciv. and xcix.), Katzenellenbogen (op. cit.), and Lange (op. cit.). Metastases in the intestine formed only a small number of those under the heading peritoneum, omentum, and intestine, but as they were all included together in Gussenbauer's large statistics, the intestinal metastases could not well be placed separately. In 673 cases the peritoneum and omentum were cancerous in 21.7 per cent.
Secondary cancerous deposits are probably even more frequent in the lymphatic glands than appears from the table. In 1153 cases of gastric cancer in which the situation of the affected lymphatic glands is specified, the abdominal glands, and chiefly those near the stomach, were the seat of cancer in 32½ per cent. In Lange's 210 cases the cervical glands were affected in 4.3 per cent. In other statistics this percentage is much smaller. In nearly one-third of the cases there are secondary cancers in the liver. These may attain an enormous size in comparison with the tumor of the stomach. Cancer of the peritoneum and of the omentum is found in about one-fifth of the cases of gastric cancer. The spleen is rarely involved, except by continuous growth of a cancer of the fundus or in cases of widespread distribution of cancer through the aortic circulation. Cancer of the liver increases the liability to metastases in the lungs, but the latter may be present without any cancerous deposits in the liver. Secondary cancers may be present in the suprarenal capsules, the kidneys, the ovaries, the heart, the thoracic duct, the bones, the skin, etc. In an interesting case reported by Finlay90 the subcutaneous tissue of the trunk was thickly studded with small nodules, of which two were excised during life and found to be cylindrical epitheliomata. This led to the diagnosis of a primary tumor of the same nature in the stomach or in the intestine. At the autopsy was found a cylindrical epithelioma of the stomach which had not given rise to characteristic symptoms. Secondary cancer of the intestine is rare if the deposits in the peritoneal coat be [p. 568] excepted. Several cancerous ulcers or multiple cancerous nodules may be found along the intestinal tract, involving the mucous and the submucous coats.91 These metastases seem best explained by the theory of implantation of cancerous elements which have been carried from the primary growth in the stomach into the intestine. In some of the cases the idea of multiple primary cancers may also be entertained.
90 Trans. Path. Soc. London, vol. xxxiv. p. 102. Unfortunately, in Röseler's case of multiple skin-cancers with an ulcerated cancer of the stomach no microscopical examination of the skin-nodules was made. The interpretation of this case is therefore doubtful (Virchow's Archiv, Bd. 77, p. 372).
91 Cases in point are recorded by Wrany (loc. cit.), Blix (Virchow u. Hirsch's Jahresbericht, 1876, ii. p. 207), Lange, Katzenellenbogen, and Lebert.
It is not rare for gastric cancer to cause secondary deposits in the stomach itself. Sometimes it is difficult to decide which of two or more cancers in the stomach is the primary growth, as in Ripley's case of ulcerated cancer of the cardiac orifice with a similar growth around the pyloric orifice.92 It is probable that in very rare instances multiple primary cancers may develop in the stomach.
92 J. H. Ripley, Trans. N.Y. Path. Soc., vol. iv. p. 121. Maurizio has also reported a case of scirrhous cancer of the cardia with scirrhous cancer of the pylorus (Annal. univ. di Medicina, Oct., 1869). A similar case was observed by Barth (Gaz. hebdom., 1856, No. 24, p. 424).
Cancerous metastases are produced by the transportation of cancerous elements by the lymphatic current or by the blood-current. In a number of instances the portal vein or some of the branches which help to form it have been found plugged with a cancerous mass which may or may not be organized.93 The cancer in these cases has burst through the walls of the vessel into the lumen, where it may grow both in the direction and against the direction of the current. On serous surfaces, and probably also, although rarely, on mucous surfaces, secondary cancers may develop from cancerous particles detached from a parent tumor and scattered over the surface as a kind of seminium.
93 Cases of this kind have been reported with especial fulness by Spaeth (Virchow's Archiv, Bd. 35, p. 432), Acker (Deutsches Arch. f. kl. Med., Bd. 11, p. 173), and Audibert (De la Généralisation du Cancer de l'Estomac, Paris, Thesis, 1877).
Mention has already been made of the invasion of parts adjacent to the stomach by the continuous growth of gastric cancer. In this way lymphatic glands, the liver, the pancreas, the omenta, the transverse colon, the spleen, the diaphragm, the anterior abdominal wall, the vertebræ, the spinal cord and membranes, and other parts may be involved in the cancerous growth.
Under the head of Complications reference has already been made to various lesions which may be associated with gastric cancer. As regards the manifold complications caused by perforation of gastric cancer, in addition to what has already been said the article on gastric ulcer may be consulted. In general, the various fistulous communications caused by gastric cancer are less direct than those produced by gastric ulcer. The wasting of various organs of the body in cases of gastric cancer may be found on post-mortem examination to be extreme. Habershon mentions a case in which the heart of a woman forty years old weighed only 3½ ounces after death from cancer of the pylorus. As in other profoundly anæmic states, the embryonic or lymphoid alteration of the marrow of the bones is often present in gastric cancer.
PATHENOGENESIS.—The problems relating to the ultimate causation and origin of gastric cancer belong to the pathenogenesis of cancer in general. Our knowledge with reference to these points is purely hypothetical. It will suffice in this connection simply to call attention to [p. 569] Virchow's doctrine, that cancer develops most frequently as the result of abnormal or of physiological irritation, hence in the stomach most frequently at the orifices; and to Cohnheim's theory, that cancer as well as other non-infectious tumors originate in abnormalities in development, more specifically in persistent embryonic cells. According to the latter view, gastric cancer develops only in those whose stomachs from the time of birth contain such embryonic remnants. These unused embryonic cells may lie dormant throughout life or they may be incited to cancerous growth by irritation, senile changes, etc. According to Cohnheim's theory, the orifices of the stomach are the most frequent seat of cancer on account of complexity in the development of these parts.
For a full consideration of these theories the reader is referred to the section of this work on General Pathology.
DIAGNOSIS.—The presence of a recognizable tumor in the region of the stomach outweighs in diagnostic value all other symptoms of gastric cancer. The detection of fragments of cancer in the vomit or in washings from the stomach is of equal diagnostic significance, but of rare applicability. The discovery of secondary cancers in the liver, in the peritoneum, or in lymphatic glands may render valuable aid in diagnosis. Of the local gastric symptoms, coffee-ground vomiting is the most important. The relation between the local and the general symptoms may shed much light upon the case. While anorexia, indigestion, vomiting, and epigastric pain and tenderness point to the existence of a gastric affection, the malignant character of the affection may be surmised by the development of anæmia, emaciation, and cachexia more rapid and more profound than can be explained solely by the local gastric symptoms. The value to be attached in the diagnosis of gastric cancer to the absence of free hydrochloric acid from the contents of the stomach must still be left sub judice. The age of the patient, the duration, and the course of the disease are circumstances which are also to be considered in making the diagnosis of gastric cancer. These symptoms of gastric cancer have already been fully considered with reference to their presence and absence and to their diagnostic features.
It remains to call attention to the differential diagnosis between gastric cancer and certain diseases with which it is likely to be confounded. The points of contrast which are to be adduced relate mostly to the intensity and the frequency of certain symptoms. There is not a symptom or any combination of symptoms of gastric cancer which may not occur in other diseases. Hence the diagnosis is reached by a balancing of probabilities, and not by any positive proof. Notwithstanding these difficulties, gastric cancer is diagnosed correctly in the great majority of cases, although often not until a late stage of the disease. Errors in diagnosis, however, are unavoidable, not only in cases in which the symptoms are ambiguous or misleading, but also in cases in which all the symptoms of gastric cancer, including gastric hemorrhage and tumor, are present, and still no gastric cancer exists. Cases of the latter variety are of course rare.
In the absence of tumor the diseases for which gastric cancer is most liable to be mistaken are gastric ulcer and chronic gastric catarrh. In the following table are given the main points of contrast between these three diseases:[p. 570]
| GASTRIC CANCER. | GASTRIC ULCER. | CHRONIC CATARRHAL GASTRITIS. |
| 1. Tumor is present in three-fourths of the cases. | 1. Tumor rare. | 1. No tumor. |
| 2. Rare under forty years of age. | 2. May occur at any age after childhood. Over one-half of the cases under forty years of age. | 2. May occur at any age. |
| 3. Average duration about one year, rarely over two years. | 3. Duration indefinite; may be for several years. | 3. Duration indefinite. |
| 4. Gastric hemorrhage frequent, but rarely profuse; most common in the cachectic stage. | 4. Gastric hemorrhage less frequent than in cancer, but oftener profuse; not uncommon when the general health is but little impaired. | 4. Gastric hemorrhage rare. |
| 5. Vomiting often has the peculiarities of that of dilatation of the stomach. | 5. Vomiting rarely referable to dilatation of the stomach, and then only in a late stage of the disease. | 5. Vomiting may or may not be present. |
| 6. Free hydrochloric acid usually absent from the gastric contents in cancerous dilatation of the stomach. | 6. Free hydrochloric acid usually present in the gastric contents. | 6. Free hydrochloric acid may be present or absent. |
| 7. Cancerous fragments may be found in the washings from the stomach or in the vomit (rare). | 7. Absent. | 7. Absent. |
| 8. Secondary cancers may be recognized in the liver, the peritoneum, the lymphatic glands, and rarely in other parts of the body. | 8. Absent. | 8. Absent. |
| 9. Loss of flesh and strength and development of cachexia usually more marked and more rapid than in ulcer or in gastritis, and less explicable by the gastric symptoms. | 9. Cachectic appearance usually less marked and of later occurrence than in cancer; and more manifestly dependent upon the gastric disorders. | 9. When uncomplicated, usually no appearance of cachexia. |
| 10. Epigastric pain is often more continuous, less dependent upon taking food, less relieved by vomiting, and less localized, than in ulcer. | 10. Pain is often more paroxysmal, more influenced by taking food, oftener relieved by vomiting, and more sharply localized, than in cancer. | 10. The pain or distress induced by taking food is usually less severe than in cancer or in ulcer. Fixed point of tenderness usually absent. |
| 11. Causation not known. | 11. Causation not known. | 11. Often referable to some known cause, such as abuse of alcohol, gormandizing, and certain diseases, as phthisis, Bright's disease, cirrhosis of the liver, etc. |
| 12. No improvement or only temporary improvement in the course of the disease. | 12. Sometimes a history of one or more previous similar attacks. The course may be irregular and intermittent. Usually marked improvement by regulation of diet. | 12. May be a history of previous similar attacks. More amenable to regulation of diet than is cancer. |
[p. 571] The diagnosis between gastric cancer and gastric ulcer is more difficult than that between cancer and gastritis, and sometimes the diagnosis is impossible. The differential points mentioned in the table are of very unequal value. An age under thirty, profuse hemorrhage, and absence of tumor are the most important points in favor of ulcer; tumor, advanced age, and coffee-ground vomiting continued for weeks are the most important points in favor of cancer. As cancer may have been preceded by ulcer or chronic gastritis for years, it is evidently unsafe to trust too much to the duration of the illness. As has already been said, it is best to place no reliance in the differential diagnosis upon the character of the pain. Any peculiarities of the vomiting, the appetite, or the digestion are of little importance in the differential diagnosis. Cachexia is of more importance, but it is to be remembered that ulcer, and even chronic gastritis in rare instances, may be attended by a cachexia indistinguishable from that of cancer. Cases might be cited in which very decided temporary improvement in the symptoms has been brought about in the course of gastric cancer, so that too much stress should not be laid upon this point. Enough has been said under the Symptomatology with reference to the diagnostic bearings of the absence of free hydrochloric acid from the stomach, of the presence of cancerous fragments in fluids from the stomach, and of secondary cancers in different parts of the body.
One must not lose sight of the fact that the whole complex of symptoms, the order of their occurrence, and the general aspect of the case, make an impression which cannot be conveyed in any diagnostic table, but which leads the experienced physician to a correct diagnosis more surely than reliance upon any single symptom.
In the early part of the disease there may be danger of confounding gastric cancer with nervous dyspepsia or with gastralgia, but with the progress of the disease the error usually becomes apparent. What has already been said concerning the symptomatology and the diagnosis of gastric cancer furnishes a sufficient basis for the differential diagnosis between this disease and nervous affections of the stomach.
Chronic interstitial gastritis or fibroid induration of the stomach cannot be distinguished with any certainty from cancer of the stomach. Fibroid induration of the stomach is of longer duration than gastric cancer, and it is less frequently attended by severe pain and hemorrhage. Sometimes a hard, smooth tumor presenting the contours of the stomach can be felt, but this cannot be distinguished from diffuse cancerous infiltration of the stomach.
Non-malignant stenosis of the pylorus is of longer duration than cancer of the pylorus. The symptoms of dilatation of the stomach are common to both diseases. Cicatricial stenosis is the most common form of non-malignant pyloric stenosis. This is usually preceded by symptoms of gastric ulcer which may date back for many years. Non-malignant stenosis more frequently occurs under forty years of age than does cancer. The diagnosis between malignant and non-malignant stenosis of the pylorus is in some cases impossible.
Although the surest ground for the diagnosis of gastric cancer is the appearance of tumor, there are cases in which it is difficult to decide whether the tumor really belongs to the stomach, and even should it be [p. 572] established that the tumor is of the stomach, there may still be doubt whether or not it is cancerous.
The diagnosis between cancerous and non-cancerous tumors of the stomach, such as sarcoma, fibroma, myoma, etc., hardly comes into consideration. The latter group of tumors rarely produces symptoms unless the tumor is so situated as to obstruct one of the orifices of the stomach. Even in this case a positive diagnosis of the nature of the tumor is impossible.
Of greater importance is the distinction between cancerous tumors of the stomach and tumors produced by thickening of the tissues and by adhesions around old ulcers of the stomach. Besides the non-progressive character of the small and usually indistinct tumors occasionally caused by ulcers or their cicatrices, the main points in diagnosis are the age of the patient and the existence, often for years, of symptoms of gastric ulcer antedating the discovery of the tumor. The long duration of symptoms of chronic catarrhal gastritis and of dilatation of the stomach is also the main ground for distinguishing from cancer a tumor produced by hypertrophic stenosis of the pylorus.
Tumors of organs near the stomach are liable to be mistaken for cancer of the stomach. The differential diagnosis between gastric cancer on the one hand, and tumors of the left lobe of the liver and tumors of the pancreas on the other hand, is often one of great difficulty.
Tumors of the liver are generally depressed by inspiration, whereas tumors of the stomach are much less frequently affected by the respiratory movements. The percussion note over tumors of the liver is flat, while a tympanitic quality is usually associated with the dulness over tumors of the stomach. Light percussion will often bring out a zone of tympanitic resonance between the hepatic flatness and the dulness of gastric tumors. Gastric tumors are usually more movable than hepatic tumors. By palpation the lower border of the liver can perhaps be felt and separated from the tumor in case this belongs to the stomach. Most of the points of distinction based upon these physical signs fail in cases in which a gastric cancer becomes firmly adherent to the liver. The basis for a diagnosis must then be sought in the presence or the absence of marked disturbance of the gastric functions, particularly of hæmatemesis, vomiting, and dilatation of the stomach. On the other hand, ascites and persistent jaundice would speak in favor of hepatic cancer. There are cases in which the diagnosis between hepatic cancer and gastric cancer cannot be made. This is especially true of tumors of the left lobe of the liver, which grow down over the stomach and compress it, and which are accompanied by marked derangement of the gastric functions. The frequency with which cancer of the stomach is associated with secondary cancer of the liver should be borne in mind in considering the diagnosis.
There are certain symptoms which in many cases justify a probable diagnosis of cancer of the pancreas, but this disease can rarely be distinguished with any certainty from cancer of the stomach. The situation of the tumor is the same in both diseases. With pancreatic cancer the pain is less influenced by taking food, the vomiting is less prominent as a symptom, and anorexia, hæmatemesis, and dilatation of the stomach are less common than with gastric cancer. Of the positive symptoms in [p. 573] favor of cancer of the pancreas, the most important are jaundice, fatty stools, and sugar in the urine. Of these symptoms jaundice is the most common.
Should there be any suspicion that the tumor is caused by impaction of feces, a positive opinion should be withheld until laxatives have been given.
Mistakes may occur as to the diagnosis between gastric cancer and tumors of the omenta, the mesentery, the transverse colon, the lymphatic glands, and even the spleen or the kidney. Encapsulated peritoneal exudations near the stomach have been mistaken for gastric cancer. Where a mistake is likely to occur each individual case presents its own peculiarities, which it is impossible to deal with in a general way. Of the utmost importance is a careful physical exploration of the characters and relations of the tumor, aided, if necessary, by artificial distension of the stomach or of the colon by gas (see page 549). No less important is the attentive observance of the symptoms of each case. In doubtful cases fluids withdrawn from the stomach by the stomach-tube should be carefully examined for cancerous fragments, and the gastric fluids may be tested for free hydrochloric acid by methods already described.
Pyloric cancers which receive a marked pulsation from the aorta sometimes raise a suspicion of aneurism, but the differential diagnosis is not usually one of great difficulty. Gastric cancer when it presses upon the aorta may simulate aneurism, not only by the presence of pulsation, but also by the existence of a bruit over the tumor. The tumor produced by aneurism is generally smoother and rounder than that caused by cancer. The pulsation of an aneurism is expansile, but the impulse of a tumor resting upon an artery is lifting and generally without lateral expansion. The impulse transmitted to a tumor resting upon the abdominal aorta may be lessened by placing the patient upon his hands and knees. Sometimes the tumor can be moved with the hands off from the artery, so that the pulsation momentarily ceases. A severe boring pain in the back, shooting down into the loins and the lower extremities, and not dependent upon the condition of the stomach, characterizes abdominal aneurism, but is not to be expected in gastric cancer. With aneurism gastric disorders and constitutional disturbance are much less prominent than with cancer of the stomach.94
94 In a case of pulsating pyloric cancer observed by Bierner the symptoms were much more in favor of aneurism than of cancer. The cancer had extended to the retro-peritoneal glands, which partially surrounded and compressed the aorta. There were marked lateral pulsation of the tumor, distinct systolic bruit, diminution of the femoral pulse, and severe lancinating pain in the back and sacral region. With the exception of vomiting, the gastric symptoms were insignificant. The patient was only thirty-three years old (Ott, Zur Path. des Magencarcinoms, Zurich, 1867, p. 71).
Spasm of the upper part of the rectus abdominis muscle may simulate a tumor in the epigastric region. The diagnosis is made by noting the correspondence in shape and position between the tumor and a division of the rectus muscle, the superficial character of the tumor, the effect of different positions of the body upon the distinctness of the tumor, the tympanitic resonance over the tumor, and, should there still be any doubt, by anæsthetizing the patient, when the phantom tumor will disappear. Spasm of the rectus muscle has been observed in cases of cancer of the stomach.
[p. 574] Attention is also called to the possibility of mistaking in emaciated persons the head of the normal pancreas, or less frequently the mesentery and lymphatic glands, for a tumor.95 As emaciation progresses the at first doubtful tumor may even appear to increase in size and distinctness.
95 In the case of the late Comte de Chambord the diagnosis of gastric cancer was made upon what appeared to be very good grounds. No cancer, however, existed, and the ill-defined tumor which was felt during life in the epigastric region proved to be the mesentery containing considerable fat (Vulpian, "La dérnière Maladie de M. le Comte de Chambord." Gaz. hebd. de Méd. et de Chir., Sept. 14, 1883).
It is sufficient to call attention to the danger of mistaking, in cases where the gastric symptoms are not prominent and no tumor exists, gastric cancer for pernicious anæmia, senile marasmus, or the chronic phthisis of old age. In some of these cases the diagnosis is impossible, but the physician should bear in mind the possibility of gastric cancer in the class of cases here considered, and should search carefully for a tumor or other symptom which may aid in the diagnosis.
The possibility of mistaking gastric cancer accompanied with peritoneal exudation for cirrhosis of the liver or for tubercular peritonitis is also to be borne in mind.
The diagnosis of the position of the cancer in the stomach can usually be made in cases of cancer of the cardia or of the pylorus. The symptoms diagnostic of cancer of the cardia are dysphagia, regurgitation of food, obstruction in the passage of the oesophageal bougie, and sinking in of the epigastric region in consequence of atrophy of the stomach. It has already been said that catheterization of the oesophagus does not always afford the evidence of obstruction which one would expect. Cancerous stenosis of the cardia is to be distinguished from cicatricial stenosis in this situation. The diagnosis is based upon the history of the case, which is generally decisive, and upon finding fragments of cancer in the tube passed down the oesophagus.
That the cancer is seated at the pylorus is made evident by the situation of the tumor (see p. 561) and by the existence of dilatation of the stomach. There are many more causes of stenosis of the pylorus than of stenosis of the cardia, so that, notwithstanding the absence of tumor, cancer of the cardia is often more readily diagnosticated than cancer of the pylorus.
The greatest difficulty in diagnosis is presented by cancers which do not obstruct the orifices of the stomach. Many of these cancers run an almost latent course so far as the gastric symptoms are concerned, and in case they produce no recognizable tumor and are unattended with hemorrhage, the difficulties in their diagnosis are almost insurmountable.
In general, a diagnosis of the particular form of cancer which is present cannot be made, nor is such a diagnosis of any practical value. In very exceptional cases such a diagnosis might be made by the examination of secondary subcutaneous cancers96 or of fragments found in the fluids obtained from the stomach.
96 As for example, in Finlay's case, already referred to (p. 567). It is not safe to trust implicitly in this criterion, as the subcutaneous tumors may be of a different nature from the tumor of the stomach, as in an interesting case observed by Leube (op. cit., p. 125).
Although the diagnosis of gastric cancer can generally be made before the death of the patient, unfortunately a positive diagnosis in the early stages of the disease is usually impossible. Should resection of cancer [p. 575] of the stomach become a legitimate operation in surgery, it will be of the utmost importance to make the diagnosis in an early stage of the disease. Only those cases are suitable for resection in which there are no secondary deposits, the general health of the patient is in fair condition, and extensive adhesions have not been formed. It was to be hoped that the ingenious instrument devised by Mikulicz for exploring the interior of the stomach by electrical illumination would prove a valuable aid in diagnosis. The gastroscope in its present construction, however, has proved of little value.97 It is, moreover, difficult to manipulate, and is not free from danger to the patient. We may be permitted, however, to hope for improvement in this direction.
97 Mikulicz has observed with the gastroscope in a case of pyloric cancer immobility of the pylorus and absence of rugæ in the mucous membrane of the pyloric region (Wiener med. Wochenschr., 1883, No. 24). It does not seem probable that there can be anything peculiar to cancer in these appearances.
In cases in which there is reasonable suspicion of the existence of gastric cancer, and in which there is proper ground to contemplate resection of the tumor, it is justifiable to make an exploratory incision into the abdomen. It can then be decided whether or not cancer exists, and whether the case is suitable for operation. When this incision is made with all of the precautions known to modern surgery, it is attended with little or no danger,98 and it should not be made except by surgeons who are practically familiar with these precautions.
98 Of 20 exploratory incisions for tumor of the stomach performed by Billroth, not one had ended fatally (Deutsche med. Wochenschrift, 1882, ii.).
PROGNOSIS.—There is no proof that cancer of the stomach has ever ended in recovery. It may be admitted that partial cicatrization of gastric cancer may occur. We have, however, no sufficient reason to believe that cancer of the stomach has ever been completely destroyed by any process of nature or by any medicinal treatment.
A successful resection of a cancer of the pylorus by Billroth in January, 1881, made a great sensation in the medical world. Since that time the operation has been performed successfully ten times, and with fatal issue twenty-seven times. A radical cure has not, however, been effected, although life has been prolonged for a year and a half after the operation.99 The possibility of permanent cure of gastric cancer by extirpation must be admitted. Enthusiasm over this possibility, however, is seriously lessened by the fact that a radical cure is not to be expected unless the operation is undertaken when the tumor is of small size, has produced no distant metastases, is free from many adhesions, and the patient is not greatly prostrated. In view of the difficulty of diagnosis in the early stages it is not likely that these favorable conditions can be fulfilled except in the rarest instances. Metastases may already exist when the tumor is small and before it has given rise to any symptoms.100 Pylorectomy, moreover, will probably be successful in the hands of only comparatively few surgeons. It is therefore but a feeble glimmer of hope [p. 576]which is now admitted to the hitherto relentlessly fatal forecast of this disease.
99 Several of the patients are still living (1884), but, so far as I can learn, no patient has survived the operation more than a year and a half.
100 Birch-Hirschfeld relates a case in which a non-ulcerated cancerous tumor not larger than a silver half-dollar was found in the pyloric region of the stomach of a woman who died from injury. The tumor had given rise to no symptoms. Nevertheless, numerous metastases existed in the lymphatic glands of the omentum and of the lesser curvature (Jahresb. d. gesellschaft f. Natur u. Heilk. im Dresden [1882-83], 1883, p. 37).
TREATMENT.—Even up to the present time various drugs have been vaunted as effecting a radical cure of cancer of the stomach. Some of these, such as mercury, are positively harmful; others, such as conium, belladonna, and condurango, are often palliative; but not one has been proven to be curative. Since its recommendation by Friedreich in 1874, condurango has enjoyed the greatest vogue. The few observations in which, under the use of this agent, tumors, real or apparent, of the stomach have lessened in size or disappeared, admit of other interpretations than as cures of gastric cancer. There is, however, considerable testimony as to the virtues of condurango as a stomachic. In some cases it relieves the pain, vomiting, and indigestion of gastric cancer, but in many cases it is employed without benefit. The drug which passes by the name of condurango in the market is a very variable preparation. According to Friedreich's directions, decoction of condurango is prepared as follows: Macerate oz. ss of cort. condurango for twelve hours with fluidounce xij of water; then boil down to fluidounce vj and strain. The dose is a tablespoonful two or three times daily. The decoction of condurango may be combined with syr. aurantii cort.
While all specific treatment of gastric cancer is to be abandoned, much can be done for the relief and comfort of the patient. The treatment is symptomatic.
In general, the indications are similar to those in gastric ulcer. It is not necessary, however, to restrict the diet to the same extent as in gastric ulcer. The patient's tastes may be consulted to a considerable extent. Still, it will be found, as a rule, that the patient is most comfortable when his diet is confined to easily-digestible substances, such as milk, beef-juice, Leube's beef-solution, rare beefsteak, and other articles mentioned under the treatment of gastric ulcer.
The pain of gastric cancer will usually require the administration of opium in some form. There is manifestly not the same objection to the employment of narcotics in a necessarily fatal disease like cancer as in ulcer of the stomach. Opium may be given in pill form or as the tincture or deodorized tincture, or often most advantageously as hypodermic injections of morphia, to which atropia may be added.
Vomiting is sometimes controlled by regulation of the diet, particularly by iced milk. For this symptom also opium or morphia is often necessary. In addition, the customary remedies for relief of vomiting, such as bits of ice, iced champagne, soda-water, hydrocyanic acid, oxalate of cerium, creasote, may be tried. Cold or hot applications to the abdomen and mild counter-irritants, such as mustard plaster or turpentine stupes, sometimes afford relief. If the vomiting be incoercible, it may be well to administer food for a short time exclusively by the rectum, and in case of stenosing cancer of the cardia this method of administering food may be the only one possible.
Acid eructations and heartburn are often relieved by the antacids, as bicarbonate of sodium, lime-water, or calcined magnesia. Against fermentative processes in the stomach have been recommended salicylate of sodium, creasote, carbolic acid, and the alkaline hyposulphites. Charcoal tablets are as useful as, and less likely to disagree than, other antifermentatives. [p. 577] In view of V. d. Velden's investigations, already mentioned, the administration of dilute hydrochloric acid in an hour after a meal is indicated.
Excellent results have been obtained by regularly washing out the stomach in cases of gastric cancer, particularly in pyloric cancer with dilatation of the stomach. By this procedure pain, indigestion, and vomiting are often greatly relieved, and the patient experiences a renewed sense of well-being. Unfortunately, the benefit is only temporary. The syphon process is most conveniently employed. Contraindications to the use of the stomach-tube are copious gastrorrhagia and great weakness of the patient.
When constipation is not relieved by washing out the stomach, enemata should be employed. Drastic purgatives should not be given.
For diarrhoea opium may be given, particularly in the form of small enemata of starch and laudanum.
Scanty hemorrhage in the form of coffee-grounds vomiting requires no treatment. Copious hæmatemesis is to be treated according to the principles laid down under the treatment of hemorrhage from gastric ulcer.
Discussion of the surgical treatment of gastric cancer of course does not belong to this work. The opinion entertained by the physician as to the propriety of surgical interference in gastric cancer is not, however, a matter of indifference, for cases of gastric cancer come first into the hands of the physician, and generally only by his recommendation into those of the surgeon. So long as the physician stands absolutely powerless before this disease, his general attitude as to the propriety of surgical interference should not be one of hostility. Experience only can determine the justification of surgical operation in cases of gastric cancer. As yet, it is too soon to express a positive opinion as to the value of resection of gastric cancer. Of 37 published resections of cancer of the pylorus, 27 died from the effects of the operation, and of the fatal cases 18 within the first twenty-four hours. These results are certainly not calculated to awaken much enthusiasm for the operation. Still, it would be wrong to draw definite conclusions from the existing statistics of resection of the cancerous pylorus, partly because the number of operations is as yet too small, partly because the operation has been done when it was certainly unwarrantable according to the best judges (Billroth, Czerny), and chiefly because the number of operators in proportion to the number of operations is too great. For the 37 published operations there have been 27 operators. Ovariotomy was not considered a justifiable operation until the excellent results of individual operators were obtained. It is probable that to an even greater extent resection of the pylorus will become the specialty of certain operators. Therefore, before concluding as to the value of resection of cancer of the stomach it is necessary to await the results of individual surgeons in a series of cases.101
101 Already, from this point of view, the operation appears more hopeful. Czerny has performed 6 resections of the stomach with only 2 fatal results; 4 of the operations were pylorectomies for cancer. Billroth has performed the operation 8 times with 3 fatal results (Wiener med. Wochenschrift, 1884, Nos. 17 and 29).
So much, however, is now certain, that with our present means of diagnosis the number of cases suitable for extirpation is very small.102 A [p. 578]radical cure is to be expected only in the rarest instances, so that the value of the operation will depend chiefly upon the condition of the patient after its performance. As regards this point, the results in the successful cases have been encouraging. In several instances the terrible sufferings of the patient have given place to months of comparative health and comfort.
102 Billroth at the eleventh session of the Congress of German Surgeons said that he was amazed at the number of resections of the pylorus which had been performed. Out of 50 to 60 cases of gastric cancer, only 1 appeared to him suitable for operation.
In cases of extreme cancerous stenosis of the pylorus which are not suitable for resection Wölfler proposed forming a fistulous communication between the stomach and the small intestine (gastro-enterostomy). The results of the operation have not been encouraging. Out of six cases in which this operation has been performed, only two patients lived after the operation.
For the same condition Schede proposed making a duodenal fistula (duodenostomy), but I am not aware that the operation has been performed.
The results of gastrostomy for relief of cancerous stenosis of the cardia or of the oesophagus have not been encouraging.103
103 Of 76 cases of gastrostomy for the relief of cancer of the oesophagus or of the cardia, only 14 lived over thirty days (Leisrink and Alsberg, Arch. f. klin. Chir., Bd. 28, p. 760, 1882).
Little clinical interest attaches to non-cancerous tumors of the stomach. They are comparatively rare and usually unattended by symptoms. Even should a tumor be discovered, there are no means of determining the nature of the tumor; and if symptoms are produced by the tumor, the case will probably be diagnosticated as one of cancer. It is necessary, therefore, in the present work to do little more than enumerate the different forms of non-cancerous tumor of the stomach.
The most common of benign gastric tumors are polypi projecting into the interior of the stomach. These are usually so-called mucous or adenomatous polypi, being composed of hypertrophied or hyperplastic elements of the mucous membrane with or without new growth of submucous tissue. They may be present in large number (one hundred and fifty to two hundred in a case of Leudet's). Their development is usually attributed to a chronic catarrhal gastritis, so that a gastritis polypora has been distinguished. These polyps are important only when they obstruct one of the orifices of the stomach, in which case they may cause even fatal stenosis. This occurrence is very rare.
Benign adenomata appear less frequently as growths in the submucous coat of the stomach (Winiwarter).
Myomata and myosarcomata, projecting sometimes as polyps either into the gastric or the peritoneal cavity, may attain a very large size, as in a case reported by Brodowski in which a cystic myosarcoma of the stomach weighed twelve pounds.104
104 Virchow's Archiv, Bd. 67.
Sarcoma, either as a primary or a secondary tumor of the stomach, is rare. Two cases of secondary lympho-sarcoma of the stomach (primary of the retro-peritoneal glands) without gastric symptoms have come under my observation. In a similar case reported by Coupland the symptoms resembled those of gastric cancer.105
105 Trans. London Path. Soc., vol. xxviii. p. 126.
[p. 579] In connection with gastric ulcer mention has already been made of the occurrence of miliary aneurisms in the stomach, which may be the cause of fatal hæmatemesis.
Sometimes the mucous membrane is studded with little cysts, as in a case reported by Harris.106
106 Am. Journ. Med. Sci., April, 1869.
Fibromata and lipomata are very rare.
Foreign bodies in the stomach, particularly balls of hair, have been sometimes mistaken for tumors, particularly cancer, of this organ. Schönborn removed successfully a ball of hair from the stomach by gastrotomy.107 Before the operation the tumor was considered to be a movable kidney.
107 Arch. f. kl. Chirurg., Bd. xxix. p. 609.
Hemorrhage from the stomach is a symptom, and not a disease. It is a result of a great variety of morbid conditions in the description of which it receives more or less consideration. Already the symptomatology and treatment of hemorrhage from the stomach have been considered in connection with its two most important causes—namely, gastric ulcer and gastric cancer. It remains to give a summary of the etiology and diagnosis of gastric hemorrhage.
Hemorrhage from the stomach is also called gastrorrhagia. The term hæmatemesis is not synonymous with gastric hemorrhage, for blood may be vomited which has simply been swallowed or has passed from the intestine into the stomach.
ETIOLOGY.—The causes of gastric hemorrhage are as follows:
1. Ulcer of the Stomach.—Simple gastric ulcer is the most frequent cause of abundant hemorrhage from the stomach. Tuberculous gastric ulcers, typhoid gastric ulcers, and the ulcers of phlegmonous gastritis are extremely rare causes of hemorrhage. Hemorrhagic erosion of the stomach, which by many writers is assigned an important place in the etiology of gastric hemorrhage, is not an independent affection, and in my opinion is without any clinical significance.
2. Cancer of the Stomach.—(Non-cancerous tumors of the stomach hardly deserve mention in this connection, so infrequently are they the cause of gastric hemorrhage.)
3. Traumatism (mechanical, chemical, thermic).—a. Acting from without the stomach: severe injury to the abdomen, as by a blow or a fall; penetrating wounds of the stomach.
b. Acting from within the stomach: foreign bodies, particularly sharp-pointed ones; corrosive poisons, as acids and alkalies; other toxic inflammatory irritants; and very hot substances. Here should also be mentioned injury from an inflexible stomach-tube and aspiration of mucous membrane with the stomach-pump.
4. Diseases of the Gastric Blood-vessels.—a. Aneurism of the arteries of the stomach. Miliary aneurisms have been found by Galliard and others as a cause of profuse and even fatal hemorrhage from the stomach. Especially in obscure cases should careful search be made for miliary aneurisms.
b. Varices of the veins are a not unimportant cause of gastric hemorrhage. They are most frequently associated with chronic passive [p. 581] congestion of the stomach, but they may be found without any apparent disturbance of the circulation.
c. Degenerations of the vessels, particularly fatty and atheromatous degeneration of the arteries. Probably gastric hemorrhage in phosphorus-poisoning is to be attributed to fatty degeneration of the arteries. Amyloid degeneration of the blood-vessels is a doubtful cause of hemorrhage.
5. Active Congestion of the Stomach.—Here is usually placed gastric hemorrhage as a result of severe inflammation of the stomach (as acute catarrhal gastritis), although in these cases the inflammatory alteration of the vascular walls is an equally important factor.
With more probability the so-called vicarious hemorrhages from the stomach are to be assigned to active congestion. Sceptical as one is inclined to be as regards vicarious hemorrhages of the menses, the occurrence of such hemorrhages, although rare, must be admitted. Doubtful, however, are alleged cases of gastric hemorrhage taking the place of suppressed hemorrhoidal bleeding or of epistaxis.
6. Passive Congestion of the Stomach.—This embraces an important group of causes of gastric hemorrhage. This hemorrhage is the result of venous congestion caused by some obstruction to the portal circulation. The obstruction may be—
a. In the portal vein itself or its branches within the liver, as in pylethrombosis, cirrhosis of the liver, tumors, such as cancer or echinococcus cysts, compressing the portal vein, occlusion of capillaries in the liver by pigment-deposits in melanæmia, and dilatation of the bile-ducts in the liver from obstruction to the flow of bile. Next to ulcer and to cancer of the stomach, cirrhosis of the liver is the most frequent and important cause of gastrorrhagia.
b. In the pulmonary blood-vessels, as in pulmonary emphysema, chronic pleurisy, and fibroid induration of the lungs.
c. In the heart in consequence of uncompensated valvular and other diseases of the heart.
For evident reasons, obstruction of the pulmonary or of the cardiac circulation is much less likely to cause gastric hemorrhage than is obstruction in the portal vein or the liver.
Possibly, gastric hemorrhage which is caused by violent acts of vomiting may be caused by venous congestion of the mucous membrane of the stomach. In support of this view, Rindfleisch advances the idea that the veins in the muscular layers of the stomach, in consequence of the thinness of their coats, are much more likely than the arteries to suffer from the compression of the muscle during its contraction.
The occasional occurrence of gastric hemorrhage during pregnancy has also been attributed to passive congestion of the stomach.
7. Acute Infectious Diseases—namely, yellow fever, acute yellow atrophy of the liver, relapsing fever; less frequently cholera, typhoid fever, typhus fever, diphtheria, erysipelas, and the exanthematous fevers, small-pox, measles, and scarlet fever.
The cause of gastric hemorrhage in these diseases is not understood. The usual explanation attributes the hemorrhage to dissolution of the blood-corpuscles and secondary alteration of the walls of the blood-vessels. Plugging of the vessels with micro-organisms has been found [p. 582] in only a few instances. The gastrorrhagia of acute yellow atrophy of the liver has been attributed to dissolution of the blood, not only by some infectious agent, but also by constituents of the bile, and also to obstruction of the portal circulation by destruction and occlusion of capillaries in the liver.
8. Other Constitutional Affections.—a. Hemorrhagic diatheses—namely, scorbutus, purpura, and hæmatophilia. Strictly speaking, a hemorrhagic diathesis exists in other affections of this class.
b. Malaria. Here we may distinguish, first, periodical malarial hemorrhages from the stomach which are cured by quinia; second, pernicious gastric malarial fever, of very grave prognosis; and third, hemorrhages in malarial cachexia due to extreme anæmia. Cases which have been described as malaria with scorbutic complications belong mostly to the last variety. Mention has already been made of gastric hemorrhages attributed to malarial pigmentation of the liver.
c. Profound Anæmias. The most important affections in this category are progressive pernicious anæmia, leucocythæmia, and pseudo-leucocythæmia, including the so-called splenic anæmia.
d. Cholæmia. The hemorrhage is attributed to dissolution of the blood-corpuscles by the action of the biliary salts.
Gastric hemorrhage is a rare event in Bright's disease, occurring more especially with small kidneys. In one such case I found that the fatal hemorrhage was due to the bursting of a miliary aneurism of a small artery in the submucous coat. Probably in all similar cases the hemorrhage is referable to disease of the vascular walls.
9. Neuropathic Conditions.—Although ecchymoses in the mucous membrane of the stomach can be experimentally produced by injury of various parts of the brain and spinal cord, there is no proof that gastric hemorrhage which is of any clinical importance is referable to structural diseases of the nervous system. The occasional occurrence of gastric hemorrhage in progressive paralysis of the insane, in tuberculous meningitis, in epilepsy, is to be attributed to other causes.
In lack of a better explanation, however, the gastric hemorrhages which have been occasionally observed in hysterical women may be classified here. These constitute not the least important class of gastric hemorrhages. The hemorrhages from the stomach in chlorosis belong partly here and partly to anæmia.
10. Melæna Neonatorum.—Although in some cases ulcers have been found in the stomach or duodenum, and in others a general hemorrhagic diathesis exists, it must be said that the etiology of this grave disease is still very obscure.
11. Bursting of Aneurisms or of Abscesses from without into the Stomach.
12. Idiopathic Causes.—Under this unsatisfactory designation are included cases which are aptly described by Flint1 in the following words: "Hemorrhage sometimes occurs from the stomach, as from the bronchial tubes, the Schneiderian membrane, and in other situations, without any apparent pathological connections, neither following nor preceding any appreciable morbid conditions. It is then to be considered [p. 583] as idiopathic." A person in apparent health has suddenly a hemorrhage, often profuse, from the stomach, which is followed only by symptoms immediately referable to the hemorrhage. The hemorrhage is naturally the source of great anxiety. Ulcer or cancer of the stomach or some other grave disease is usually suspected. But the patient develops no further symptoms, and often never has another hemorrhage. Whatever hypotheses one may construct for these cases of so-called idiopathic hemorrhage, the recognition of the clinical fact of their occurrence is important.
1 Austin Flint, A Treatise on the Principles and Practice of Medicine, 5th ed., p. 513, Philada., 1881.
Inasmuch as hemorrhage from the stomach is usually made manifest by the vomiting of blood, it is important to bear in mind that gastric hemorrhage is not the only cause of hæmatemesis. Blood may gain access to the stomach by being swallowed in cases of hemorrhages from the nose, mouth, throat, bronchi, lungs, and oesophagus. Blood may also enter the stomach from the duodenum in cases of simple ulcer of the duodenum or of typhoid ulcers situated in the upper part of the intestine.
The SYMPTOMS of hemorrhage from the stomach have already been described in connection with ULCER OF THE STOMACH.
MORBID ANATOMY.—As is evident from the enumeration of the causes of gastric hemorrhage, the lesions found after death are manifold. A description of these lesions, however, does not belong here. It is necessary, however, to say a few words concerning the demonstration of the source of the hemorrhage.
The hemorrhage is arterial, venous, or capillary in origin. Ulcerations from the stomach into the heart, which have been mentioned in connection with gastric ulcer, are too infrequent to come into consideration in this connection. If the bleeding is from a large artery or vein or from a medium-sized aneurism or varix, the demonstration of its source is not difficult. Often, however, in cases of fatal gastric hemorrhage the search for the source of the hemorrhage has proved fruitless. It is supposed that in many such cases the hemorrhage is due to diapedesis, and not to rupture of a blood-vessel (rhexis). Doubtless, small gastric hemorrhages, particularly those into the tissues of the stomach, are often the result of diapedesis, but in cases of profuse hemorrhages from the stomach where the source of the hemorrhage is not demonstrable after death, the convenient assumption of hemorrhage by diapedesis, in my opinion, plays too important a rôle. In most cases of profuse gastrorrhagia the symptoms point to a sudden outpouring of blood into the stomach; and our knowledge of diapedesis does not warrant the belief that the red blood-corpuscles can escape through the unsuffused walls of the vessels with that combined rapidity and abundance which would be necessary to explain the sudden and profuse hemorrhage. In these cases hemorrhage by rhexis is altogether more probable even when ruptured vessels cannot be demonstrated. It often requires a long-continued and careful search to find a small vessel which is ruptured. In the case above mentioned of fatal hæmatemesis from miliary aneurism over an hour of continuous searching was required to find the pinhole perforation in the mucous membrane in the bottom of which lay the small aneurism. Chiari2 has reported a fatal gastric hemorrhage due to rupture of a submucous vein. The erosion of the mucous membrane was not larger than a hempseed. The examination of the mucous membrane is often much impeded by the [p. 584]closely-adherent mucus and blood, which have to be carefully removed. Injection of the vessels of the stomach with fluid may aid in finding a ruptured vessel. It is not intended to assert that in all cases of fatal gastric hemorrhage a painstaking search would reveal the source of the hemorrhage, but it is believed that cases of fatal gastric hemorrhage would less frequently be reported with negative anatomical result as hemorrhages by diapedesis, or by exhalation, or as parenchymatous or capillary hemorrhages, if such a search were made.
2 Prag. med. Wochenschr., 1882, No. 50.
DIAGNOSIS.—Undoubtedly, small hemorrhages into the stomach often occur which are not recognized, and in the absence of vomiting even larger hemorrhages may escape detection unless a careful examination of the stools be made. The patient may die from abundant gastric hemorrhage before any blood has been vomited or has passed by the bowels.
When there is doubt whether the black color of the stools is due to blood or to the administration of iron or of bismuth, it generally suffices to add water to the stools. If blood be present, the water will acquire a reddish color. Should doubt still remain, then the microscope, the spectroscope, or the test for hæmin crystals may be called into requisition (see p. 545).
Whether black, tarry stools are produced by hemorrhage from the stomach or by hemorrhage in the upper part of the intestine can be decided only by the clinical history. If hæmatemesis be likewise present, the presumption is strongly in favor of gastric hemorrhage. The diagnosis, however, between hemorrhage from duodenal ulcer and that from gastric ulcer is very difficult, and can rarely be positively made.
The mere inspection of the vomit is generally sufficient to determine whether it contain blood or not. Color more or less resembling that of altered blood may be produced in the vomit by iron, bismuth, red wine, various fruits, such as cranberries, and by bile. When a careful inspection by the physician leaves doubt as to the presence of blood—which will rarely be the case—then here also recourse may be had to the microscope, spectroscope, and test for hæmin crystals.
Sometimes blood is swallowed and then vomited by hysterical females or by malingering soldiers or prisoners for purpose of deceit. In such cases there are generally no evidences of acute anæmia or of gastric disease. The blood of some animals can be distinguished by the microscope from human blood. When suspicion of deceit exists, there are generally various ways of entrapping the patient.
When blood is vomited by nursing infants the possibility of its coming from the breast of the mother is to be thought of.
Sometimes blood from the nose or throat is swallowed, particularly when the bleeding occurs during the night. This blood may subsequently be vomited. The inspection of the nose or throat will generally reveal the source of the hemorrhage in such cases.
The diagnosis between hemorrhage from the oesophagus and that from the stomach must be based upon the clinical history. The oesophagoscope, however, has been successfully employed for diagnostic purposes. Several cases have been reported of fatal hemorrhage from varices of the oesophagus. Such hemorrhage cannot be distinguished from gastric hemorrhage.
Much more frequently arises the question whether the hemorrhage is from the stomach or from the lungs. Sometimes the decision of this point [p. 585] is very difficult, and it may even be impossible, especially when the physician is obliged to trust only to the statements of the patient or his friends. Difficulty in the diagnosis results mainly from the fact that coughing and vomiting of blood are often associated with each other. With hæmoptysis blood may be swallowed and then vomited, and with hæmatemesis more or less coughing occurs. The diagnosis is to be based upon the points contained in the following table:
| HÆMOPTYSIS. | HÆMATEMESIS. |
| 1. Usually preceded by symptoms of pulmonary or of cardiac disease. Bronchial hemorrhage, however, without evidence of preceding disease, is not rare. | 1. Usually preceded by symptoms of gastric or of hepatic disease, less frequently by other diseases (see Etiology). |
| 2. The attack begins with a tickling sensation in the throat or behind the sternum. The blood is raised by coughing. Vomiting, if it occurs at all, follows the act of coughing. | 2. The attack begins with a feeling of fulness in the stomach, followed by nausea. The blood is expelled by vomiting, to which cough, if it occurs, is secondary. |
| 3. The blood is bright red, fluid or but slightly coagulated, alkaline, frothy, and frequently mixed with muco-pus. | 3. The blood is dark, often black and grumous, sometimes acid, and usually mingled with the food and other contents of the stomach. |
| If the blood has remained some time in the bronchi or a cavity, it becomes dark and coagulated. | If the blood is vomited at once after its effusion, it is bright red and alkaline, or it may be alkaline if it is effused into an empty stomach. |
| 4. The attack is usually accompanied and followed by localized moist râles in the chest, and there may be other physical signs of pulmonary or of cardiac disease. | 4. After the attack the physical examination of the lungs is usually negative, but there are generally symptoms and signs of gastric or hepatic disease. |
| Bloody sputum continues for some time, often for days, after the profuse hemorrhage ceases. | Black stools follow profuse hæmatemesis. |
As it is important that the patient should be as quiet as possible during and for some time after the hemorrhage, any physical examination which disturbs the patient, such as percussing the posterior part of the chest or palpating the abdomen, should be avoided.
The diagnosis of the many causes of gastric hemorrhage belongs to the description of the various diseases which have been enumerated under the etiology.
PROGNOSIS.—It is exceptional for gastric hemorrhage to prove immediately fatal. According to Fox, such an occurrence is more frequent with cirrhosis of the liver than with ulcer or cancer of the stomach. The ultimate result of the hemorrhage depends greatly upon the previous condition of the patient. If this condition was good, he often rallies from the most desperate prostration immediately following the hemorrhage. A previously enfeebled patient is of course more likely to yield to the further anæmia and exhaustion caused by profuse hemorrhage. Although the symptoms of gastric ulcer and of cirrhosis of the liver are sometimes improved after hemorrhage from the stomach, nevertheless this hemorrhage can never be regarded as a welcome event.
For the treatment of gastric hemorrhage see ULCER OF THE STOMACH.
DEFINITION.—By dilatation of the stomach is understood a condition in which the stomach is abnormally large and is unequal to the performance of its normal functions. It will be observed that this definition of dilatation of the stomach includes an anatomical disturbance and a physiological disturbance. A stomach which, although unusually large, performs its functions perfectly well is not, in the clinical sense, a dilated stomach. The most characteristic functional disturbance in dilatation of the stomach is delay in the propulsion of the gastric contents into the intestine in consequence of inability of the muscular coat of the stomach to perform the work imposed upon it. This muscular insufficiency, whether primary or secondary, necessarily involves disorder of the digestive and absorptive powers of the stomach.
SYNONYMS.—Dilatatio ventriculi; Gastrectasia. It has been proposed to call the early stages of the disease insufficiency of the stomach (Rosenbach). The condition described by Chomel as dyspepsia of liquids is undoubtedly dilatation of the stomach.
HISTORY.—Dilatation as a disease of the stomach is not mentioned by writers of antiquity. Fabricius ab Aquapendente in 1623 was among the first to record an observation of dilatation of the stomach. During the following century cases of dilatation of the stomach were recorded more as curiosities than as of clinical interest. Most cases were attributed to eating or drinking inordinate quantities. In 1743, Widman clearly recognized stenosis of the pylorus as a cause of gastric dilatation. In the works of Van Swieten, Morgagni, Lieutaud, and J. P. Frank, during the latter half of the last century, different causes of dilatation of the stomach are recognized. The last writer especially distinguishes clearly between dilatation due to stenosis and that due to atony. The data as to the symptoms of the disease were still very imperfect. In 1833, Duplay1 published an important article in which the main points in the causation and symptomatology of dilatation of the stomach are clearly described. After this time the important works on the practice of medicine or on diseases of the stomach contain, in the main, correct descriptions of the disease under consideration. Since the publication in 1869 of Kussmaul's memorable article2 on the treatment of dilatation of the stomach by the [p. 587] stomach-pump, much greater attention has been paid to this disease than ever before, so that the literature upon this subject during the last fifteen years is very considerable. In 1875, Penzoldt published an excellent monograph upon dilatation of the stomach.3
1 Arch. gén. de Méd., Ser. 2, t. iii. pp. 165, 523.
2 Deutsches Arch. f. kl. Med., Bd. vi., 1869. Kussmaul first employed the stomach-pump in dilatation of the stomach in 1867, and in that year he reported a successful result (Schmidt's Jahrb., Bd. 136, p. 386).
3 Die Magenerweiterung, Erlangen, 1875. To this work I am indebted for most of the historical data in the text.
ETIOLOGY.—Dilatation of the stomach is the result of inability of this organ to propel its contents into the intestine within the normal space of time. In the performance of this mechanical work three factors are involved—namely, the muscular force of the stomach, the quantity and quality of the gastric contents, and the size of the opening between the stomach and the intestine. All causes of dilatation of the stomach may be referred to abnormalities of one or more of these factors.
The most important group of causes is represented by stenosis of the pyloric orifice or of the adjacent part of the stomach or of the intestine.4 Most cases of hypertrophic dilatation of the stomach—that is, dilatation with hypertrophy of the muscular walls of the stomach—are produced by causes belonging to this group.
4 Dilatation of the stomach in consequence of intestinal obstruction below the duodenum is so rare that no further attention is given to the subject in the present article. The term pyloric stenosis is often used in the course of the article to include any obstruction to the passage of the contents of the stomach into the intestine, whether the obstruction be in the duodenum, the pyloric orifice, or the pyloric region.
The most frequent cause of pyloric stenosis is carcinoma, either in the form of a diffuse infiltration of the gastric walls in this region or as a tumor projecting into the cavity of the pyloric portion of the stomach. Next in frequency are cicatricial growths resulting from simple ulcer involving the pyloric region. Much less frequent are similar cicatricial stenoses of the pylorus resulting from ulcers produced by swallowing corrosive poisons. Simple hypertrophy of the coats of the stomach in the pyloric region, particularly of the fibrous and muscular coats, is an occasional cause of dilatation. Obstruction of the pylorus by mucous polypi or by hypertrophic folds of mucous membrane is so rare as to have little practical interest. Likewise, stenosis caused by sarcomata, fibromata, myomata, lipomata, and cysts need be mentioned only for the sake of completeness.
Narrowing of the pyloric orifice may be caused also by pressure from outside of the stomach, as by tumors, particularly cancer, of the liver and of the pancreas, and by the contraction of fibrous adhesions and thickenings resulting from perigastritis. Obstruction of the duodenum by tumors growing in its walls, by cicatrices resulting from ulcers, and by external pressure may also cause dilatation of the stomach. According to Barker, compression of the duodenum by a wandering right kidney may induce dilatation of the stomach. The mere association of dilatation of the stomach and movable right kidney, however, cannot be considered proof that the former is caused by the latter, for the subjects of movable kidney (most frequently women with flabby abdominal walls who have borne many children) are often also favorable subjects for atonic dilatation of the stomach.
Sometimes with dilatation of the stomach the pyloric orifice is found abnormally small, without any thickening or other appreciable change in the walls of the pylorus. These cases in adults have been described by [p. 588] Landerer under the name of congenital stenosis of the pylorus, but his conclusions are not free from doubt.5 Congenital stenosis, and even complete occlusion of the pylorus, has been observed in infants.6
5 Ueber angeborene Stenose des Pylorus, Inaug. Diss., Tübingen, 1879. In the ten cases studied by Landerer the patients were all adults, mostly in advanced life. In only one case is it mentioned that indigestion existed from childhood; the clinical history in all is incomplete. With the exception of one case there was no marked hypertrophy of the muscular coat of the stomach, such as is usually found with benign pyloric stenosis and would naturally be expected with a stenosis existing since birth. The pyloric orifice varied from 1½ cm. to 2 mm. in diameter. Some of the specimens had been in alcohol for a considerable time. In my opinion, Landerer has not brought forward sufficient proof that in these cases stenosis of the pylorus existed since birth.
6 Wünsche, Jahrb. d. Kinderheilk., viii. 3, p. 367. Andral, Förster, and Bull have found congenital stenosis and atresia of the pylorus.
Spasm of the pyloric muscle, which, according to Kussmaul, may be referable to erosions, ulcers, and inflammations of the adjacent mucous membrane, can be admitted only as a hypothetical explanation of some cases of dilatation of the stomach.
Somewhat problematical, although not improbable, is the production of stenosis of the pylorus or of the duodenum by torsion and by displacement of these parts. Dilatation of the stomach is sometimes associated with scrotal hernia, particularly with that containing omentum or transverse colon. This dilatation Kussmaul explains by the production of a sharp bend between the movable first part and comparatively fixed second part of the duodenum, in consequence of the dragging downward of the stomach by the displaced omentum or transverse colon. In a similar way Kussmaul believes that the weight of an over-distended stomach may produce stenosis, and by this mechanism he explains the occasional occurrence of symptoms of complete pyloric obstruction when a large quantity of material has accumulated in an already dilated stomach, and the prompt relief of these symptoms when the burden of the stomach is removed either by vomiting or by the stomach-tube.7
7 Another explanation given by Kussmaul, and likewise based upon experiments on the cadaver, is that when the stomach is over-distended it may rotate upon its own axis, so that the pylorus acquires a sagittal direction and impinges against the first part of the duodenum. This rotation of the stomach, however, can occur only when the abdominal walls are flabby (Kussmaul, "Die Peristaltische Unruhe des Magens," Volkmann's Samml. klin. Vortr., No. 181).
The manner in which stenosis of the pylorus causes dilatation of the stomach is sufficiently obvious to require no especial explanation. It is, however, important to know that stenosis of the pylorus may be compensated, so that even a very considerable degree of obstruction of this orifice may exist without any dilatation of the stomach. The obstruction may be completely counteracted by hypertrophy of the muscular coat of the stomach, particularly of that in the right half of the organ. Leube suggests that this increased muscular force, by increasing the peristaltic movements, may also hasten the digestion and absorption of the food, so far as these processes take place in the stomach.8 The timely removal of the contents of the stomach by vomiting may also prevent over-distension of the organ. Another compensatory circumstance may be the reduction of the quantity of solid and liquid food taken by the patient. Conditions are often present, however, which oppose the development of these [p. 589] compensatory circumstances. Such conditions are feebleness of the patient, degeneration of the muscular coat of the stomach, chronic catarrhal gastritis, insufficient secretion of gastric juice, and delayed absorption, causing stagnation and fermentation of the food in the stomach.
8 Leube, in V. Ziemssen's Handb. d. spec. Path. u. Ther., Bd. vii. 2te Hälfte, p. 211, Leipzig, 1878.
Dilatation of the stomach may occur without any obstacle to the evacuation of the gastric contents into the intestine. The cases of so-called atonic dilatation of the stomach belong to this class. The degree of dilatation in these cases is rarely so great as when the dilatation is caused by stenosis. The cause of gastric dilatation in the absence of stenosis is not always clear, so that a variety of hypotheses, more or less probable, have been broached to explain these obscure cases.
Dilatation with unobstructed outlet of the stomach must be referable either to abnormalities in the quantity or quality of the contents of the stomach or to weakness of the muscular walls of the stomach. In most cases both of these causes are combined, and it is not easy to separate their action.
Abnormal gastric contents may be the result of improper ingesta or of disturbances in gastric digestion. Although in former times the frequency of excessive eating and drinking as a cause of dilatation of the stomach was doubtless exaggerated, nevertheless the efficacy of this cause cannot be doubted. Dilatation of the stomach is said to be common in people who live almost exclusively upon a vegetable diet and therefore require large quantities of food. The habitual drinking of large quantities of beer may cause dilatation of the stomach. The occasional association of a dilated stomach with diabetes is referred to the inordinate appetite and thirst which characterize this disease. If the food reaches the stomach imperfectly masticated, the process of digestion is delayed, and as a result the stomach may become dilated. Indigestible food, particularly that which readily ferments in the stomach, may be an indirect cause of the disease under consideration. A similar rôle may be played by swallowing foreign substances either by accident or by design. It is not proven that dilatation of the stomach may be referable to exhaustion of its muscular power by the abuse of agents which at first excite peristalsis, such as emetics, purgatives, alcoholics, tobacco, spices, etc. Equally doubtful is the production of dilatation by the misuse of narcotics, such as opium, which restrain peristalsis.
Of great importance in the production and continuance of gastrectasia are all circumstances which cause stagnation and fermentation of the contents of the stomach. These abnormalities of the gastric contents are referable both to muscular and to chemical insufficiency of the stomach, but in this connection it is desired to call attention especially to chemical insufficiency, although in the production of gastric dilatation this becomes always associated with muscular insufficiency. In this way chronic catarrhal gastritis is operative in the causation of gastric dilatation. In consequence of insufficient secretion of normal gastric juice and of delayed absorption, the food remains abnormally long undigested in the stomach, and fermentative changes, with the development of gas, occur. No less important, however, is the impairment of the muscular power of the stomach in chronic gastritis. Stagnation and fermentation of the contents of the stomach occur also in functional or atonic dyspepsia, which is to be reckoned as a cause of dilatation of the stomach. [p. 590] Naunyn9 emphasizes especially the importance of abnormal fermentations in the stomach (alcoholic, butyric acid, lactic acid, acetic acid fermentations) both as a cause and as a result of dilatation of the stomach. Ulcer and cancer of the stomach may cause dilatation by interfering with the normal digestive processes.
9 Deutsches Arch. f. kl. Med., Bd. 31.
We come now to the third and final group of causes of dilatation of the stomach—namely, those included under weakness of the muscular walls of the stomach. In the last analysis all causes of gastric dilatation come under this heading, for even with pyloric stenosis and with excessive contents a stomach will not dilate so long as its muscular power is equal to the proper performance of the work which is demanded. In this connection, however, reference is had especially to those cases in which impairment or restraint of the muscular movements of the stomach may be regarded more or less directly as the primary cause of dilatation of the stomach.
Clearest of comprehension are those cases in which the muscular power of the stomach is impaired by organic changes in the muscular coat. Here may be mentioned partial destruction of the muscular coat, particularly of that in the pyloric region, by ulcers and by cancers. Thus, ulcers and cancers which in no way obstruct the outlet of the stomach may cause dilatation of the organ. Inflammatory infiltration (inflammatory oedema) of the muscular coat has been adduced as a cause of its weakness in chronic catarrhal gastritis and in peritonitis. Whether this is the proper explanation or not, there is no doubt that the muscular coat of the stomach may become paretic in cases of chronic catarrhal gastritis, as well as the subjacent muscle in inflammations of other mucous membranes, as in laryngitis or in cystitis. Our knowledge of the relation between degeneration of the muscular coat of the stomach and gastrectasia is very imperfect. Fatty and colloid degeneration of the muscle of dilated stomachs is probably to be interpreted as a secondary change. It is probable that amyloid degeneration may be a cause of atonic dilatation of the stomach.10 Oedematous infiltration of the coats of the stomach in cases of cirrhosis of the liver, pulmonary emphysema, cardiac disease, and Bright's disease has been assigned as a cause of gastric dilatation, but without satisfactory evidence. Chronic interstitial gastritis (cirrhosis of the stomach) is more frequently a cause of contraction than of dilatation of the stomach.
10 Edinger, ibid., Bd. 29.
The restraint of the muscular movements of the stomach by adhesions and by dragging downward of the organ in hernia may cause dilatation. Relaxation of the abdominal walls, as in women who have borne many children, by removing the normal support of the stomach, has been thought to cause dilatation.
Atony of the muscular walls of the stomach may be a part of general muscular weakness and impaired nutrition. Here belong cases of adynamic dilatation of the stomach secondary to typhoid fever, cholera, tuberculosis, anæmia, chlorosis, cachexia, senile marasmus, neurasthenia.
Whether primary paralysis of the stomach can occur or not is wholly uncertain. We have no positive knowledge as to the occurrence of paresis of the stomach in consequence of organic or functional changes [p. 591] in the peripheral or central nervous system. Nor does our meagre information as to the relation between the nervous system and the muscular movements of the stomach justify the construction of any hypotheses as to this point.
For the sake of clearness the various causes of dilatation of the stomach according to the foregoing classification may be recapitulated as follows. Some of the more doubtful and of the rarer causes are omitted:
A. Stenosis of the Pylorus or of the Duodenum.
1. Cancerous;
2. Cicatricial;
3. Hypertrophic (of pylorus);
4. From external pressure;
5. Congenital (of pylorus)?;
6. From torsion of duodenum?
B. Abnormalities in Contents of Stomach.
1. Ingesta:
a. Excessive;
b. Imperfectly masticated;
c. Indigestible.
2. Stagnation and fermentation in consequence of chemical
insufficiency of the stomach, as in chronic catarrhal gastritis and functional dyspepsia.
C. Impairment of Muscular Force of Stomach.
1. Organic changes in muscular coat:
a. Partial destruction by ulcers and cancers;
b. Inflammation, as in chronic catarrhal gastritis and peritonitis;
c. Degenerations (fatty, colloid, amyloid);
d. Oedema?;
e. Cirrhosis of stomach.
2. Mechanical Restraint:
a. By adhesions;
b. By weight of herniæ.
3. Impaired Nutrition and General Muscular Weakness, Adynamic
dilatation from typhoid fever, tuberculosis, anæmia, etc.
4. Paresis from neuropathic causes?
As a rule, not a single one, but several, of the above-mentioned causes are operative in the production of dilatation of the stomach, and it is often impossible to say which is the primary cause. The various gastric functions are so dependent upon each other that if one is disturbed the others also suffer. If, for instance, atony of the muscular coat of the stomach exists, then in consequence of enfeebled peristalsis the secretion of gastric juice is insufficient, the food is not thoroughly mingled with the gastric juice, and the absorption of the products of digestion in the stomach is interfered with; in consequence of which the accumulating peptones still further hinder the digestive process. The pylorus remains contracted for an abnormal length of time, as it naturally is closed until the process of chymification in the stomach is far advanced, and this process is now delayed. The stagnating contents of the stomach readily ferment, and the irritating products of fermentation induce a chronic [p. 592] catarrhal gastritis, which further impairs the functions of the mucous and muscular coats of the stomach. Thus, in a vicious circle one cause of dilatation induces another. To assign to each cause its appropriate share in the production of the final result is a matter of difficulty, and often of impossibility. From this point of view the dispute as to whether in atonic dilatation the most important factor in causation is chemical insufficiency of the stomach (impaired secretion of gastric juice, fermentations) or mechanical insufficiency (weakened muscular action, stagnation), appears of little practical importance.
Of the causes of non-stenotic dilatation of the stomach, the first place is to be assigned to chronic catarrhal gastritis and to atonic dyspepsia, as this term is understood by most English and American writers.
As regards frequency, gastric dilatation is a common result of cancer of the pylorus. It is less frequently caused by simple ulcer. Other forms of pyloric stenosis than the cancerous and the cicatricial are rare.
Opinions differ as to the frequency of non-stenotic or atonic dilatation of the stomach according to the manner in which one interprets the cases. Non-stenotic dilatations which are comparable in degree to those produced by stenosis are rare. The lesser grades of atonic dilatation, however, are not rare; but here arises the difficulty of distinguishing these cases from mere chemical or mechanical insufficiency of the stomach, which often represents the early stage of the process. Hence it has been proposed to discard altogether the term dilatation, and to substitute that of insufficiency of the stomach. But this latter term is applicable to many affections of the stomach other than dilatation. A typical case of atonic dilatation of the stomach is a well-defined disease, and because it is difficult to diagnosticate its early stages is not sufficient reason for discarding altogether the designation.
Gastrectasia may develop at any age. It is most frequent in middle and advanced life. The largest number of cases of atonic dilatation is met with between thirty and forty years of age. The disease is rare in childhood.11 The disease occurs in all classes of life. Atonic dilatation seems to be comparatively more frequent in private practice and among the favorably situated than in hospitals and among the poor. Kussmaul says that the largest contingent of patients is furnished by persons who lead a sedentary life and eat and drink a great deal.
11 Kundrat and Widerhofer mention no case of stenotic dilatation of the stomach in children. They say, however, that atonic dilatation due to over-feeding, and particularly to rachitis, is not infrequent in children. Widerhofer reports a case of very large dilatation of the stomach in a girl twelve years old. The cause of the dilatation was not apparent, and the clinical history was imperfect (Gerhardt's Handb. d. Kinderkrankh., Bd. iv. Abth. 2). Lafage (Thèse, Paris, 1881) reports a case of gastric dilatation at ten years, and another at sixteen years of age. R. Demme (abstract in Berl. kl. Wochenschr., 1883, No. 1) reports a case of large dilatation of the stomach in a boy six and a half years old. Cicatricial stenosis was suspected. Pauli (De Ventriculi Dilatatione, Frankfurt, 1839) reports an enormous dilatation of the stomach, believed to be due to congenital stenosis.
SYMPTOMATOLOGY.—Inasmuch as dilatation of the stomach is usually secondary to some other disease, the symptoms of the primary disease have often existed a long time before those of dilatation appear.
The subjective symptoms of gastric dilatation are for the most part directly referable to disturbances of the functions of the stomach. These [p. 593] subjective symptoms alone do not suffice for a positive diagnosis of the disease. Of the greatest diagnostic importance are an examination of the vomit and a careful physical exploration of the stomach.
The appetite with dilatation of the stomach may be normal, diminished, increased, or perverted. In the majority of cases the appetite is diminished, and there may be complete anorexia. Sometimes the appetite is increased even to voracity, which is explicable by the small amount of nutriment which is absorbed. Polyphagia may therefore be a result as well as a cause of dilatation of the stomach.
Often there is excessive thirst in consequence of the small quantity of fluid absorbed.
Dilatation of the stomach in itself does not usually cause sharp epigastric pain, although it is often associated with painful diseases of the stomach.
There is usually in the region of the stomach a sense of fulness and weight, which is often distressing and may be accompanied with dull pain.
Heartburn and eructations of gas and of bitter or of acid fluids are frequently present. The gas is often odorless, but sometimes it is very offensive. It may contain sulphuretted hydrogen. In a number of cases—which, however, are exceptional—the gas has been found inflammable, burning usually with a colorless flame (hydrogen), but rarely, as in a case from Frerichs' clinic, with a bright yellowish-white flame (hydrocarbons). Detonation upon setting fire to the gas has been noted. The analysis of the inflammable gas has shown oxygen and nitrogen in approximately the same proportion as in the atmosphere, in addition to large quantities of carbonic acid and of hydrogen, also marsh gas, and in Frerichs' case olefiant gas in small amount.12 The oxygen and nitrogen are doubtless simply swallowed, but the carbonic acid and hydrogen are the result of abnormal fermentations in the stomach. The origin of the hydrocarbons in the gas is not clear, but they are probably also produced by fermentation within the stomach.
12 One of the analyses in Frerichs' case gave carbonic acid, 17.40; hydrogen, 21.52; marsh gas, 2.71; olefiant gas, traces; oxygen, 11.91; nitrogen, 46.44. In another analysis were found marsh gas, 10.75, and olefiant gas, 0.20. Sulphuretted hydrogen was also present (Ewald, in Reichert und Du Bois-Reymond's Archiv, 1874, p. 222).
One of the most frequent symptoms, although not a constant one, of dilatation of the stomach is vomiting. This symptom often presents characters which, if not pathognomonic of dilatation, at least raise a strong presumption in favor of its presence. The act of vomiting is sometimes accomplished with such ease that it is hardly more than regurgitation; at other times the act is accompanied with violent and exhausting retching. A feature particularly characteristic of dilatation of the stomach is the abundance of the vomited material. In no other disease is such an enormous quantity evacuated from the stomach at one time. Blumenthal relates a case in which the vomited material amounted to sixteen pounds. Such large quantities can accumulate in the stomach of course only when a considerable time intervenes between the acts of vomiting. The vomiting of gastric dilatation does not generally occur until some hours after a meal. It often presents a certain periodicity, occurring, for instance, at intervals of two or three days, and followed usually by temporary relief. It is often observed that as the stomach [p. 594]becomes larger and larger the vomiting becomes less and less frequent, but at the same time more abundant. Especially toward a fatal termination of the disease the walls of the stomach may become so paralyzed and insensible, and the patient so feeble, that the vomiting ceases altogether. Another valuable diagnostic sign furnished by the vomit is the presence of undigested food which has been taken a considerable time, it may be many days, previously.13 If the morning vomit habitually contains undigested food which has been eaten the previous day, gastric dilatation either exists or is almost sure to develop.
13 Ritter relates the case of a man who vomited cherry-pits, although he had not eaten cherries for over a year (Canstatt's Jahresbericht, 1851, iii. p. 260)!
The vomited matter is almost always in a condition of fermentation. If the vomit be allowed to stand in a vessel, it will separate into three layers—an upper, frothy; a middle, of turbid fluid, usually yellowish or brownish in color; and a lower layer, composed of solid particles, mostly alimentary débris. The vomit often emits an extremely offensive odor. The reaction is nearly always acid. Different kinds of fermentation—alcoholic, acetous, lactic acid, and butyric acid—are present, usually in combination with each other. The microscope reveals, besides undigested and partly-digested food, crystals of fatty acids, sarcinæ ventriculi, fungus-spores, and various forms of bacteria, particularly rod-shaped ones. The connection between sarcinæ and fermentative processes is not understood. There is no evidence that sarcinæ are capable of causing fermentation. Of greater importance is the recognition by the microscope of the spores of the yeast-fungus (Torula cerevisiæ). These spores are rarely absent, and their constant presence is evidence that fermentation is in progress. Fermentation often exists in undilated stomachs, but, as has already been mentioned, it is an important factor in the production of dilatation, so that its early recognition, if followed by proper treatment (washing out the stomach especially), may ward off the development of dilatation. The article on GASTRIC CANCER is to be consulted with reference to the habitual absence of free hydrochloric acid from the stomach in cases of cancerous dilatation. If cancer or ulcer of the stomach exists, blood is frequently present in the vomit, but even in the absence of ulcer or cancer or other demonstrable source of hemorrhage the vomit in cases of dilatation of the stomach may exceptionally contain blood, even for a considerable length of time. If the dilatation be due to pyloric stenosis, bile is not often found in the vomited material.
It has already been mentioned that vomiting is not a constant symptom of dilatation of the stomach. It remains to add that vomiting may be present without any of the distinctive features which have been described. Gastric dilatation, especially in its early stages, is often accompanied by attacks of acute indigestion (embarras gastrique) after some indiscretion in diet.
Constipation is an almost constant symptom of dilatation of the stomach. This is naturally to be expected when so little substance passes from the stomach into the intestine. The constipation is also to be explained in part by the absence of the usual reflex stimulus which the stomach during digestion normally exerts upon intestinal peristalsis, for the constipation is usually much relieved when the overweighted stomach is systematically washed out.
[p. 595] Occasionally, attacks of diarrhoea occur in cases of dilatation of the stomach. The diarrhoea may perhaps be explained by the sudden discharge of a large quantity of fermenting material from the stomach into the intestine.
With marked dilatation of the stomach, especially when there is profuse vomiting, the urine is often considerably diminished in quantity. Particularly in cases treated by systematic washing out of the stomach, but also in other cases, especially with abundant vomiting, the acidity of the urine is often much reduced. The reaction may be even continuously alkaline (Quincke). Crystals of phosphate of magnesium have been occasionally found in the alkaline urine of gastrectasia (Ebstein). The urine is prone to deposit abundant sediments. It often contains an excess of indican.
The patient may suffer from attacks of dyspnoea and of palpitation of the heart in consequence of flatulent distension of the stomach.
The general condition of the patient will of course depend chiefly upon the character of the primary disease and upon the severity of the gastric symptoms. A moderate degree of dilatation may exist without much disturbance of the general health of the patient. But as the disease progresses and the food stagnates more and more in the stomach, finally to be rejected by vomiting, the patient cannot fail to lose flesh and strength. In extreme cases of gastrectasia, even without organic obstruction, the patient may be reduced to a degree of emaciation and of cachexia indistinguishable from that of cancer. As in so many other gastric diseases, the patient is usually mentally depressed and hypochondriacal. His sleep is disturbed. He suffers much from headache and vertigo. He feels incapable of physical or mental exertion. The skin is dry and harsh; the extremities are cold. Toward the last, cachectic oedema about the ankles can often be recognized.
Kussmaul was the first to call attention to the occurrence of tetanic spasms in cases of dilatation of the stomach.14 This symptom has been observed almost exclusively in an advanced stage of the disease when the patient has become anæmic and weak. The spasms come on chiefly after attacks of profuse vomiting or after evacuating large quantities by the stomach-tube. The spasms may be preceded by a sense of pain or distress in the region of the stomach, by dyspnoea, by numbness of the extremities, or by great prostration. The tetanic spasms affect especially the flexor muscles of the hand and forearm, the muscles of the calves of the legs, and the abdominal muscles. The spasm may be confined to one or more of these groups of muscles, or there may be general tetanic contraction of the muscles of the body. Sometimes typical epileptiform convulsions with loss of consciousness occur. With general tetanic spasms the pupils are usually contracted, and often irresponsive to light. Sometimes there is abnormal sensitiveness upon pressure over the contracted muscles. The spasms may last for only a few minutes, or they may continue for several hours, or even for days. After their disappearance the patient is left extremely prostrated. Although tetanic spasms increase the gravity of the prognosis, they are not necessarily fatal.
14 Deutsches Arch. f. kl. Med., Bd. vi. p. 481.
Kussmaul considers that these spasms are analogous to those occurring in cholera, and are referable to abnormal dryness of the tissues in consequence of the extraction of fluid. This view is supported by the usual [p. 596] occurrence of the spasms after profuse vomiting or after washing out the stomach. Another explanation, which is perhaps more applicable to the epileptiform attacks, refers the convulsions to auto-infection by toxic substances produced in the stomach by abnormal fermentative and putrefactive changes (Bouchard).15
15 Laprevotte, Des Accidents tétaniformes dans la Dilatation de l'Estomac, Thèse, Paris, 1884, p. 48.
Coma, with or without the peculiar dyspnoea of diabetic coma, is a rare occurrence in gastrectasia. (For a description of this form of coma see page 205.)
The temperature in gastric dilatation is generally unaffected. Penzoldt, however, saw two cases with moderate rise of temperature in the evening, which could not be explained by any complication. On the other hand, abnormally low temperature with slow pulse has been observed (Wagner).
Essential to the diagnosis of gastric dilatation is the physical examination of the stomach.
If the stomach be markedly dilated, inspection may reveal an abnormal prominence of the abdominal walls in the epigastric region and extending a variable distance below the level of the umbilicus. This prominence is most marked on the left side. When the abdominal walls are sufficiently thin and relaxed, sometimes the outline of the greater curvature between the umbilicus and pubes, less frequently that of the lesser curvature, can be made out. Sometimes the peristaltic waves of the stomach can be perceived through the thin abdominal walls. By pressure or by passing the hand across the abdomen gastric peristalsis may sometimes be excited. The peristaltic movements of the stomach, however, are rarely perceived except when the dilatation is due to stenosis and the muscular coat of the stomach is hypertrophied. The peristaltic waves generally pass from left to right, rarely in the opposite direction as well. Careful attention to the situation, direction, and extent of these waves is necessary to distinguish them from similar peristaltic movements of the intestine.16 The diminution in size of the abdominal prominence caused by a dilated stomach after profuse vomiting or after washing out the stomach may aid in the diagnosis.
16 Kussmaul says that vigorous peristaltic movements of the stomach may be perceptible through the abdominal walls even when there is no dilatation of the stomach. Under these circumstances he attributes the peristaltic commotion to an independent neurosis of the stomach ("Die Peristaltische Unruhe des Magens," Volkmann's Samml. klin. Vorträge, No. 181).
An important aid in bringing out the contours of the stomach is the artificial distension of the organ by the generation within it of carbonic acid gas, as first suggested by Frerichs. For this purpose 20-30 grains of bicarbonate of sodium and 15-20 grains of tartaric acid, each dissolved in a little lukewarm water, may be given one after the other. If the stomach be much dilated and relaxed, it may be necessary to give much larger quantities of the powders (up to 2-2½ drachms of the soda and a corresponding quantity of the acid). It is well to have a stomach-tube at hand in order to withdraw the gas in case unpleasant symptoms develop. Sometimes the stomach fails to become distended by this procedure. This is due in some cases to the escape of the gas through the pyloric orifice into the intestine—a condition designated by Ebstein as incontinence of the pylorus. It may be that sometimes the gas produces such firm [p. 597]contraction of the gastric walls that the stomach does not expand by the pressure of the gas. Instead of generating gas, a similar result may be produced by simply injecting air into the stomach through a stomach-tube, as recommended by Oser and by Runeberg. The air may, however, escape along the side of the tube.
Palpation of the distended stomach yields an elastic resistance which has been compared to that of an air-cushion. By palpating carefully from above downward the greater curvature can sometimes be appreciated, but in general it is difficult to distinguish it from the transverse colon. Peristaltic movements may perhaps be appreciated by palpation when they are not evident on inspection. If a dilated stomach contains considerable fluid and the abdominal walls are yielding, fluctuation may be perceived by palpation. The lowest level at which this fluctuation can be felt may afford a clue as to the position of the lower border of the stomach, but not much dependence can be placed upon this sense of fluctuation unless many sources of error in its interpretation are excluded.
By pressing gently and repeatedly against the abdominal walls a splashing sound can usually be heard in cases of well-marked dilatation of the stomach (bruit de clapotement). This sound can best be brought out when the patient is in the recumbent position, with relaxed abdominal walls, by palpating near the left border of the ribs. The same sound can be produced by shaking the patient (bruit de glou-glou). This sound may be heard at a considerable distance from the patient, to whom it may be a source of much annoyance. In itself this splashing sound is without diagnostic significance, as the condition for its production—namely, the simultaneous presence of gas and liquid in the stomach—exists often in healthy persons. By paying attention, however, to the time at which this sound can be produced after eating or drinking, and to its greater or less constancy, some diagnostic importance can be attached to this sign. If the splashing sound can be usually produced two hours or longer after the ingestion of liquid or six hours after an ordinary meal, it generally indicates that dilatation of the stomach exists.17 It is necessary to exclude somewhat similar sounds which may be produced in the intestines, particularly in the transverse colon and cæcum. The series of gurgling sounds which may sometimes be produced in the intestine by palpation are not likely to be confounded with the single splashing sound produced in the stomach, but under certain circumstances a splashing sound may be produced in the transverse colon which cannot be distinguished from the gastric sound. If a dilated stomach contains a very large quantity of fluid, the splashing sound cannot readily be produced.
17 Baradat, Étude sur le Bruit de Clapotement stomacal, Thèse, Paris, 1884. Baradat says that this bruit is also diagnostic of dilatation when it can be produced by palpating below a horizontal line passing through the junction of the ninth and tenth ribs, but it is evident that motion might be transmitted to the stomach even when its greater curvature is above this line by palpating below the level of the umbilicus.
Leube has pointed out that the end of the stomach-tube (of course the hard tube), after it has been inserted into the stomach, can often be felt through the abdominal walls.18 He says that if the tube can be felt below a horizontal line passing through the anterior superior spinous processes of the ileum, dilatation of the stomach may be positively diagnosed, [p. 598] and the existence of dilatation is probable if the tube can be felt much below the umbilicus. No force should be used in trying to make the end of the tube palpable. Of course if the abdominal walls are thick or very tense the tube cannot be felt. Leube's method is simple and convenient, and applicable to many cases. As will be explained hereafter, a position of the lower border of the stomach even quite as low as Leube's rule demands cannot be considered by itself positive evidence of dilatation.19
18 Deutsches Arch. f. kl. Med., Bd. xv. p. 394.
19 According to Oser, there is a possible source of error in Leube's method—namely, that the sound may slide along the greater curvature of the stomach, and even reach the pylorus, so that the end may be felt higher than the lowest point of the stomach. Considerable objection has been made to Leube's method on the ground of its danger, but this objection is based on the assumption that greater energy is employed in pressing forward the sound than Leube recommends (Oser, article "Magenerweiterung" in Eulenburg's Real Encyclopädie, Bd. viii., 1881).
The length to which the stomach-tube can be inserted before meeting resistance may evidently give some idea as to the size of the stomach. The attempt, however, to establish any general law with reference to this point has not proven successful.
In many cases valuable information as to the size of the stomach is afforded by percussion. Over the greater part of the stomach the percussion note is tympanitic, sometimes with a metallic quality. Over the most dependent part of the stomach a dull sound is produced on percussion in case a sufficient quantity of fluid or solid material is contained in the viscus. In the upright position, therefore, in percussing over the stomach from above downward, the tympanitic note gives place to a dull sound, and this zone of dulness will change with the position of the patient, so that in the recumbent posture the dulness may entirely disappear. In order to prove that the region of dulness belongs to the stomach, Piorry caused the patient to drink a large quantity of water (a pint to a quart). In a healthy empty stomach this quantity of water suffices to produce a zone of dulness which does not descend below the level of the umbilicus. If, however, the dulness be produced below the level of the umbilicus, it is inferred that dilatation exists. Penzoldt's modification of Piorry's method gives more certain results.20 By withdrawing the fluid from the stomach by the stomach-tube the dulness may be made to disappear, and by injecting more fluid the dulness may be made to reappear at will. By noting the lower limit of the dulness thus produced the position of the lower border of the stomach may be determined. The farther this lies below the umbilicus the greater, presumptively, is the degree of dilatation. The artificial distension of the stomach with gas may also aid in determining its limits by percussion. It must be said that in general the separation of the lower limits of the stomach from the transverse colon by means of percussion is a matter of great difficulty, and sometimes is impossible.
20 Penzoldt, op. cit., p. 48.
Upon auscultation over a dilated stomach sometimes a fine crackling or sizzling sound, like that audible upon first uncorking a bottle of soda-water, can be heard.21 This is referable to the fermentation which is in progress in the stomach. Eichhorst says that a similar but finer crackling sound can be heard over a stomach in which carbonic acid gas is [p. 599] being artificially generated, and that this sound abruptly ceases when the ear passes below the limits of the greater curvature.22
21 Pauli was the first to record this phenomenon (De Ventriculi Dilatatione, Frankfurt, 1839).
22 Handb. d. spec. Path. u. Ther., Bd. i. p. 750, 1883.
The displacement of neighboring organs by a dilated stomach does not generally give rise to important physical signs. As the tendency of a dilated stomach is to sink down in the abdomen, there is not usually much displacement of the thoracic viscera. If, however, the fundus of the stomach be distended with gas, the heart may be pushed upward, and, being pressed against the chest-wall, its apex-beat may be more forcible and diffused than normal. The tympanitic stomach may impart a metallic quality to the cardiac sounds.
MORBID ANATOMY.—Considerable degrees of dilatation of the stomach are easily recognized by post-mortem examination. In extreme cases the stomach occupies all of the anterior region of the abdomen, covering over the intestines and extending down to the pubes or even into the true pelvis. Many cases are recorded in which the stomach was capable of holding six to twelve pints. Godon23 describes under the name ventriculi hydrops a hardly credible case in which it is said that the stomach contained ninety pounds of fluid! In the ordinary cases of gastrectasia the lower border of the stomach is found somewhere between the umbilicus and the pubes, frequently about a hand's breadth below the level of the umbilicus.
23 Diss. de Hydrops Ventriculi, London, 1646. This celebrated case is described with much detail. For three years the abdomen was enormously distended, but the patient, a woman, never vomited. The affection was supposed to be dropsy of the peritoneum. Death occurred in a condition of extreme marasmus. The pylorus was the seat of a hydatid cyst which extended into the duodenum. The stomach, which was enormously distended, contained ninety pounds of fluid, in which floated a great number of hydatid cysts, some of which were ruptured. The anterior wall of the stomach was adherent to the parietal peritoneum. The two orifices of the stomach were drawn close to each other. The length of the stomach equalled a Paris ell.
The fundus, being the most dilatable part of the stomach, is in most cases disproportionately dilated in comparison with the pyloric region. This excessive dilatation of the fundus is most noticeable in gastrectasia due to stenosis. In most cases of dilatation the pylorus sinks down somewhat in the abdomen, but in consequence of the distension of the lower segment of the stomach the long axis of the organ is more nearly transverse than normal. If the pylorus be fixed, the lesser curvature may be drawn down in its middle so as to acquire a hooked shape. The lesser curvature, which should be covered by the liver, may be found considerably below its normal level. The dilated fundus may extend from the left hypochondrium into the left iliac region.24
24 Fogt reports a case in which an enormously dilated stomach occupied a scrotal hernia of the left side. He refers to two other similar cases (Aerztl. Intelligenzbl., 1884, No. 26).
More or less dilatation of the oesophagus is associated with marked dilatation of the stomach. If dilatation of the stomach be due to obstruction in the upper part of the intestine, then the pyloric orifice and the intestine on the proximal side of the obstruction will be found dilated.
The walls of a dilated stomach may be hypertrophied, and such cases are called hypertrophic dilatation; or the walls may be of normal thickness or may be thinned, and these cases are called atrophic or atonic dilatation. In general, the thickness of the gastric walls in gastrectasia [p. 600] depends upon that of the muscular coat. As a rule, in cases of pyloric stenosis the muscular coat of the stomach is hypertrophied. This hypertrophy affects chiefly the muscle of the pyloric region. The gastric walls in stenotic dilatation may, however, be of normal thickness or even atrophied. In non-stenotic dilatation the muscular coat may be either hypertrophied or atrophied, but it rarely attains the thickness observed in cases of gastrectasia due to obstruction. Maier and others have repeatedly observed fatty and colloid degeneration of the muscular fibres of dilated stomachs.25 More frequently, however, no degenerative change has been found in the muscle.
25 Deutsches Archiv f. klin. Med., Bd. vi. p. 480; Landerer, op. cit. Maier designates as colloid degeneration a peculiar homogeneous, glistening appearance of the muscular fibres. This change is not such as would usually be called colloid, but this term is loosely used to designate a great variety of pathological changes. The form of muscular hypertrophy in gastrectasia is chiefly the numerical.
The mucous membrane in dilatation of the stomach is usually in the condition of chronic catarrhal gastritis. Although there are various statements as to atrophy of the gastric tubules and degeneration of the epithelial cells in the tubes in cases of gastric dilatation, satisfactory histological investigations of the mucous membrane of the stomach in this disease are wanting.26
26 For satisfactory studies of this nature it is desirable that alcohol or some preservative fluid should be injected into the stomach immediately after death.
Atrophy of various abdominal viscera—particularly of the spleen, which is usually small in this disease—has been attributed to the pressure of a dilated stomach. This atrophy, however, is probably in many cases only a part of the general emaciation and anæmia.
While well-marked cases of dilatation of the stomach cannot be mistaken on post-mortem examination, it is important to add that the pathological anatomist cannot always decide whether or not dilatation of the stomach exists in the clinical sense. The following considerations will make this evident: In the first place, the stomach is a very variable organ as regards its size, so that it is impossible to set definite limits, and say that a stomach exceeding these is necessarily dilated, while a stomach not exceeding these limits is normal. In the second place, it belongs to the clinical definition of dilatation of the stomach that the organ is insufficient for the performance of its normal functions. This insufficiency cannot be determined at the post-mortem table. To determine, therefore, whether stomachs which fall within certain not easily definable limits of size are pathologically dilated or not, it is necessary to correct and complete the results of the post-mortem examination by a knowledge of the clinical history.27
27 To deny all value to post-mortem examination in the determination of dilatation of the stomach, as has been done, is absurd. In the majority of cases this examination affords satisfactory evidence, but for some cases a reservation like that in the text must be made. Rosenbach in an able article shows the error of regarding dilatation of the stomach too exclusively from the anatomical point of view ("Der Mechanismus und die Diagnose der Mageninsufficienz," Volkmann's Samml. klin. Vorträge, No. 153).
DIAGNOSIS.—A considerable degree of dilatation of the stomach can generally be diagnosticated without difficulty by means of the symptoms and physical signs which have been described. The most important diagnostic features relate to the character of the vomiting and to the physical signs, together with the information afforded by the use of the [p. 601] stomach-tube. The diagnostic characters of the vomiting are the large quantity rejected, its occurrence several hours after a meal, its periodicity with long intervals, the temporary relief afforded, the presence of undigested food taken a considerable time previously, and the existence of fermentation. Washing out the stomach will also afford evidence of stagnation of food. The time generally occupied in the digestion of an ordinary meal is not over six to seven hours, so that in health the contents of the stomach removed by the stomach-tube at the end of this time should usually be free from undigested food. There are of course individual idiosyncrasies with reference to the time occupied in digestion, so that implicit reliance cannot be placed on this diagnostic test. Delayed digestion is in itself no evidence of the existence of dilatation, but the establishment of the presence of this symptom may confirm other points in the diagnosis.
Simple inspection, palpation, and percussion of the abdomen are sometimes, although rarely, sufficient for the diagnosis of dilatation of the stomach. Various devices have already been described which aid in the physical examination of the stomach, such as the administration of effervescing powders, the introduction of the stomach-tube, and Piorry's and Penzoldt's methods of determining the lower border of the stomach.28 It [p. 602]is not necessary to repeat here the diagnostic evidence afforded by physical examination. Excellent service as these devices often perform, it must be confessed that they do not always answer the purpose intended. The artificial distension of the stomach with gas does not enable us always to distinguish intestine from stomach. If the abdominal walls are thick or very rigid, this method, like most of the others, is of little or no assistance. Then, as already mentioned, the administration of the powders may fail to produce any distension of the stomach, and may possibly mislead by causing distension of intestine. Moreover, the artificial tympanites may cause the patient much discomfort. The method of determining the lower border of the stomach by Piorry's or Penzoldt's method is not always conclusive. If the stomach be much dilated, it may take a very large quantity of water to produce an appreciable zone of dulness. If the transverse colon be distended with feces, it will not be easy to separate the dulness of the stomach from that of the colon. Moreover, loops of intestine containing feces or gas may lie over the anterior surface of the stomach. The use of the stomach-tube simply for diagnostic purposes is, for various reasons, not always practicable. With due recognition of the important additions during the last few years to our means of exploring the stomach, it must be admitted that we are still far from any positive and universally applicable method of determining the size and position of this organ during life. This admission is the more necessary in view of the extravagant claims which have been made for various more or less complicated contrivances for physical exploration of the stomach.
28 Several other methods have been suggested for determining the size and position of the stomach, but they have not found general acceptance. Thus, Schreiber attaches a soft rubber balloon to the end of a stomach-tube, and after its insertion in the stomach inflates it (Deutsches Arch. f. kl. Med., Bd. 19). In Neubauer's method the long end of a syphon-tube communicating with the stomach is bent upward, and a glass tube is placed in the bent portion. The fluid will evidently stand at the same level in the tube as in the stomach in case the atmospheric pressure in both is the same. The atmospheric pressure in the stomach is produced by using a double tube or by passing a second tube into the stomach (Prager med. Wochenschr., 1879). Purjesz attached a manometer to a stomach-tube, and thought that he could fix the position of the cardia by noting the moment when in the passage downward of the tube the negative pressure changed to positive, but Schreiber has shown that the manometer may indicate negative pressure even after the tube has entered the stomach (Deutsches Arch. f. kl. Med., Bd. 33, p. 425). It has been asserted that by means of auscultatory percussion of a stomach artificially distended with gas the boundaries of the organ can be determined. Leichtenstern considers the metallic quality of the tone heard over the stomach under these circumstances more or less characteristic, while Skamper compares the characteristic tone to that produced by tapping with the finger on the dorsal surface of the hand of which the valar surface is placed against the external ear (Inaug. Diss., Berlin, 1879, p. 30). It has been claimed that the sound as of water dropping into a large cavity, which can be heard when the patient is drinking, can no longer be heard when the auscultating ear passes beyond the greater curvature (V. Bamberger). Wunderlich suggests the possibility of feeling the arteries of the greater curvature through the abdominal walls. Ferber calls attention in cases of gastrectasia to a strip of dulness, with absent vocal and respiratory sounds, corresponding to the posterior inferior border of the left lung. This dulness, which is produced by material in the most dependent part of the dilated stomach, disappears when the patient assumes the knee-elbow position (Deutsche Zeitschr. f. prakt. Med., 1876, No. 42). When it is impossible by other methods to distinguish the lower portion of the stomach from the transverse colon, it has been proposed to distend the colon with water, with gas, or with air injected through a tube passed into the rectum. Penzoldt (op. cit.) found that the length of a tube (hard) or bougie reaching the bottom of the stomach, estimating from the upper incisor teeth, should be in a normal stomach at least 5 cm. less than that of the vertebral column (occiput to coccyx), and at the most not much more than one-third of the length of the body (1:2.8-1:3.3). In three cases of gastrectasia he found the length of the tube inserted into the stomach considerably more than one-third of the length of the body (1:2.4); in one of the cases this length even exceeded that of the vertebral column, and in the others it nearly equalled the length of the vertebral column. Rosenbach's method of determining the elastic and contractile power of the stomach is ingenious, but hardly of practical utility. By injecting air into the stomach through a bulb apparatus attached to the end of a stomach-tube, he is able to tell when the point of the tube passes beneath the surface of fluid in the stomach by hearing on auscultation a characteristic moist bubbling sound. Elevation or depression of the level of the fluid can be determined by withdrawing or by pushing forward the tube. That quantity of fluid which, introduced into an empty stomach, causes no elevation, or perhaps causes a depression, of the level of the food in the stomach, indicates the utmost limit of the elastic and contractile forces of the stomach (Rosenbach, Volkmann's Samml. klin. Vorträge, No. 153).
The determination of the position of the lower border of the stomach does not in itself enable us to infer positively the size of the organ. It may be taken as a general rule that if the lower border of the stomach be found persistently below the level of the umbilicus, the stomach is dilated; but there are many exceptions to this rule. Sometimes an otherwise normal stomach preserves in adult life the vertical position which it had in the foetus, so that its lowest point may be below the umbilicus. According to Kussmaul, a vertical position of the stomach is a predisposing cause of dilatation. Occasionally a stomach has a looped shape, so that without any dilatation of the organ the lowest point may fall below the level of the umbilicus. It is, moreover, a clinical fact established by the experience of many observers that the lower border of the stomach may be found below the level of the umbilicus without the existence of any symptoms of dilatation.
The uncertainty of the anatomical diagnosis of dilatation of the stomach in some cases makes it all the more necessary, as has been repeatedly urged in the course of this article, to make a careful study of the evidences of disordered gastric functions. The symptoms of most importance in determining whether the condition called insufficiency of the stomach is present or not are fermentation of the gastric contents and the [p. 603] persistent presence of undigested food in the stomach beyond the limits of normal digestion. It is true that these symptoms may be present without any dilatation of the stomach, but they are likely to lead to dilatation if unchecked, and, what is of practical importance, they require essentially the same treatment as dilatation.
A differential diagnosis between chronic catarrhal gastritis and atonic dyspepsia on the one hand, and the early stages of dilatation of the stomach on the other, cannot be made with any positiveness.
Of course, with our present means of diagnosis the confounding of dilated stomachs with ascites, ovarian cysts, pregnancy, hydatid cysts (of each of these errors there are recorded instances), is inexcusable.
PROGNOSIS AND COURSE.—The prognosis of dilatation of the stomach depends first of all upon the nature of the primary disease causing the dilatation. The prognosis of cancerous dilatation is as unfavorable as possible. In dilatation due to non-cancerous stenosis the prognosis is in general more favorable. Life may be prolonged sometimes for many years, and the patient's condition greatly benefited by proper treatment. A permanent cure of stenotic dilatation is not impossible, but it is rarely to be expected. Even if temporarily relieved, the symptoms of dilatation are likely sooner or later to return and to lead to a fatal termination. The progress of the disease depends upon the degree and the stationary or advancing character of the stenosis. In the article on GASTRIC ULCER mention has been made of the cure of a few cases of desperate gastric dilatation due to cicatricial pyloric stenosis by means of resection of the diseased pylorus.
In general, the prognosis is more favorable in dilatation without stenosis. If the degree of dilatation be only moderate, a permanent cure may often be effected by proper treatment. If, however, the dilatation be considerable, while the symptoms may be relieved or even made to disappear for a time, relapses are prone to occur, and a permanent cure is rarely obtained. Undoubtedly, Kussmaul's publication in 1869, in giving to us a most valuable method of treatment, at the same time raised extravagant expectations of the frequency with which dilatation of the stomach can be cured. Too often the treatment with the stomach-tube proves only palliative and not curative.
The course of dilatation of the stomach is chronic. The mode of death is usually by inanition, very rarely from rupture of the stomach.
TREATMENT.—Reference to the causation of dilatation of the stomach will show that there is considerable scope for the prophylactic treatment of dilatation not referable to stenosis or incurable organic disease. Thus, the correction of the habits of eating or drinking inordinate quantities, or of imperfectly masticating the food in consequence of haste or bad teeth or vicious custom, may avert the development of gastric dilatation. Of especial importance is the timely treatment of cases of dyspepsia or of chronic catarrhal gastritis which are accompanied with fermentation or delayed digestion—conditions in which the stomach-tube is of great service.
Of the means at our disposal for meeting the causal and the symptomatic indications of dilatation of the stomach, the most important by far is the use of the stomach-tube for the purpose of emptying and of washing out the stomach. The introduction of this procedure by Kussmaul in 1867 marked a new era in the treatment of gastric disorders.
[p. 604] By washing out the stomach we accomplish three important things: first, we remove the weight which helps to distend the organ; secondly, we remove mucus and stagnating and fermenting material which irritates and often inflames the stomach and impedes digestion; and, thirdly, we cleanse the inner surface of the stomach and obtain the beneficial influence of the direct application of water, to which various medicinal substances can be added. It is probable that in removing the fermenting contents of the stomach we also remove a possible source of self-infection of the system (see page 596).
By accomplishing these things we may possibly also enable the stomach to regain its lost elasticity and muscular contractility. But unless the normal elastic and contractile powers of the stomach are restored, the treatment with the stomach-tube, indispensable as it is for the relief of symptoms, is only palliative and not curative. Whether or not this restoration of the stomach to its normal functional activity is to be expected depends chiefly upon the cause and the degree of the dilatation. Unfortunately, as has already been stated under Prognosis, the permanent cure of dilatation of the stomach due to organic stenosis, although possible, is not to be expected, and the number of cases in which largely dilated stomachs can be restored to their normal volume or made to perform permanently their normal functions is small. There remains, however, a considerable number of curable cases—to be sure, not always easily diagnosticated—in which the muscular coat of the stomach has not been seriously damaged and in which the dilatation is generally only moderate. Furthermore, excellent results are obtained by the use of the stomach-tube in the cases which have been designated insufficiency of the stomach, and which are closely allied to dilatation—in fact, often represent its early stage. As has already been mentioned, the most important criteria of this so-called insufficiency are the fermentation of the contents of the stomach and the presence therein of undigested food after the period required for normal digestion (six to seven hours for an ordinary meal).
There are two principal methods of washing out the stomach—one by the stomach-pump, the other by the siphon process. The stomach-pump is the older method, and still has its advocates. The pump used by Kussmaul is the Wyman pump, described by Bowditch in the American Journal of Medical Sciences, vol. xxiii. p. 320, 1852. This (which is also called the Weiss pump), as well as other forms of stomach-pump, consists in principle simply of an aspirating syringe having at its anterior extremity two openings communicating with the barrel of the syringe. These openings can be alternately opened and closed by means of an arrangement of valves. Through one opening, which is made to communicate with an incompressible tube inserted into the stomach (the other opening being now closed), the gastric contents are drawn into the barrel of the syringe. This opening is now closed, and through the other opening the contents of the syringe are discharged through a tube externally. In a similar way fluid can be drawn into the syringe and pumped into the stomach.
In the siphon process the outer end of the tube inserted into the stomach is connected with a piece of elastic tubing about three and a half feet long, in the free end of which is inserted the extremity of a medium-sized glass funnel. A single elastic tube about six feet long may also be used. [p. 605] When the funnel is elevated, water which has been poured into it will run into the stomach. If now, before the water has all run out, the funnel be depressed below the level of the stomach, the fluid contents of the stomach will flow out through the tube according to the principle of the siphon. Figs. 20 and 21 will make clear the mode of operation of this process. (The tube shown in these figures is the Faucher tube, commonly used in France, and consisting, with the funnel, of one piece. A longer tube than that shown in the figure should be used.)
| FIG. 20.29 | FIG. 21.29 |
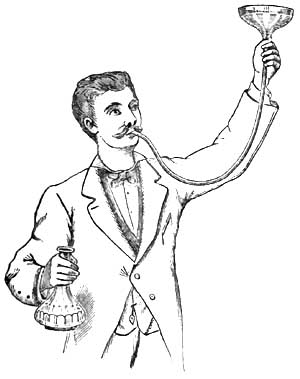
|

|
29 From Souligoux, De la Dilatation de l'Estomac, Paris, 1883.
Another convenient but somewhat more complicated method of employing the siphon process is according to Rosenthal's principle, and is represented in Fig. 22. To the outer end of the stomach-tube is attached a Y-shaped glass tube, one arm of which is connected with an elastic tube running to an irrigator, while the other arm is connected with the discharging tube. Through the irrigating tube water runs into the stomach, the discharging tube being compressed. If the discharging tube be opened while the fluid is flowing from the irrigator, and if then, after the establishment of a column of water in the discharging tube, the irrigating tube be compressed or the stopcock of the irrigator be closed, a siphon communicating with the stomach is formed and empties this organ of its fluid contents.
| FIG. 22.30 |
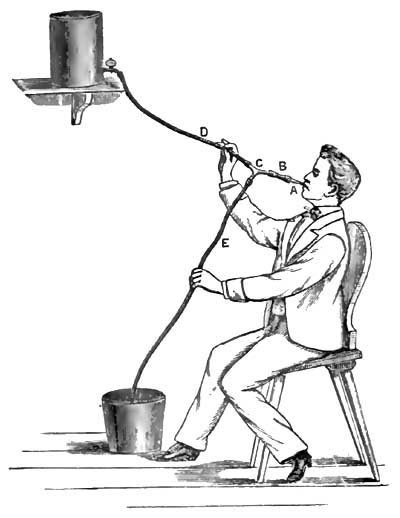
|
30 From Leube, in Ziemssen's Handb. d. spec. Path. u. Therap., Bd. vii.
In the siphon process the tube inserted into the stomach may be an incompressible hard-rubber tube like that employed with the stomach-pump, but by far the simplest, most convenient, and safest form of stomach-tube is the soft, flexible, red rubber tube, resembling the Jacques catheter, but of course larger and longer.31 This soft tube can inflict no [p. 606] injury, and in most cases it is readily introduced. Generally, the patient himself can best manipulate the introduction of the tube. After the tube is introduced into the pharynx, the patient, who should be in a sitting posture, makes repeated acts of swallowing, by means of which, accompanied by directing and gently pushing the tube with the fingers, the tube passes along the oesophagus into the stomach. Often at first the nervousness and inexperience of the patient occasion some trouble, but after a little practice he generally succeeds in introducing the tube without discomfort or difficulty. Before its introduction the tube should be anointed with a little vaseline or some similar substance. In an adult the tube is introduced for a length of at least 20 to 25 inches, and in cases of dilatation of the stomach of course for a greater distance. Whatever form of stomach-tube be used, it is important that the tube should be at least 30 inches long, and should be provided with one, and preferably with two, large eyes at its distal extremity.
31 Such a tube (marked 19 A) is made by Tieman & Co. of New York, and is to be had of most surgical instrument-makers. (For a fuller description of the tube and the mode of its employment see article by W. B. Platt, "The Mechanical Treatment of Diseases of the Stomach," Maryland Medical Journal, March 8, 1884.)
Oser's tube is 2 meters long, and is made of mineralized rubber. There are two sizes. The smaller has a lumen of 8 mm. The thickness of the wall is 2½ mm. In the larger tube the lumen is 10 mm., and the thickness of the wall 3 mm. He generally uses the smaller tube.
Faucher's tube is 1½ meters long. The external diameter of the tube is 10 to 12 mm. The walls are of such thickness that the tube can be bent without effacing its lumen. At one extremity is a lateral eye with two orifices. To the other extremity is adapted a funnel with a capacity of about 500 grammes.
Although the stomach-pump has the advantage of more completely evacuating the stomach and of removing coarser solid particles than is possible with the siphon, nevertheless its disadvantages—namely, the possibility of inflicting injury to the mucous membrane of the stomach,32 the expense and greater complexity of the instrument, and the circumstance that it should be used only by the physician—in contrast with the advantages of the siphon—namely, its cheapness, simplicity, safety, and possible employment by the patient or his attendants—have led to the general adoption of the latter process. Only the soft-rubber stomach-tube should be left to the employment of the patient.
32 A number of cases have been recorded in which pieces of the mucous membrane of the stomach have been detached by the stomach-pump. Although as yet no serious effects have followed this accident, the possibility of its occurrence can certainly not be regarded with equanimity.
Sometimes the flow through the siphon is interrupted by occlusion of the eye of the stomach-tube by a solid mass or by some cause not always clear. As already mentioned, it is desirable that there should be two openings at the gastric extremity of the tube. When the flow is [p. 607] interrupted the position of the tube in the stomach may be changed, or the patient may be directed to cough or to exert the pressure of the abdominal muscles, or more water may be allowed to run into the stomach in order to displace an occluding mass in the tube. It is, however, well for such cases to have, if possible, a stomach-pump and an incompressible tube in reserve. Moreover, as is apparent from the foregoing statement of the advantages of the stomach-pump, there are cases in which this instrument is much more useful than the siphon, so that one cannot decide unconditionally in favor of one instrument over the other.
The stomach-tube should be secured so that there can be no possibility of its being swallowed entirely. A string may be attached to the distal end of the tube. Leube33 has reported an instance in which the whole tube disappeared into the stomach, and Jackson34 has also narrated a case in which an insane patient swallowed the stomach-tube. In both cases the tube was subsequently rejected by vomiting.
33 Deutsches Arch. f. klin. Med., Bd. 33, p. 6.
34 Extracts from the Records of the Boston Society for Medical Improvement, vol. vi. p. 261.
For washing out the stomach after the greater part of the contents have been withdrawn, about a pint of tepid fluid is allowed to slowly run into the stomach, and is then siphoned out. This process is to be repeated several times. In general, tepid water suffices for washing out the stomach, but it is often better to use, at least a part of the time, a 1 to 2 per cent. solution of bicarbonate of sodium, which facilitates the removal of mucus. The artificial and the natural Vichy and Carlsbad waters are also excellent for this purpose. Various additions are also made to the water with the view of counteracting fermentative changes in the stomach. For this purpose perhaps the best agents are salicylate of sodium (1 per cent. solution) or resorcin (2 per cent. solution). Other substances which have also been recommended are carbolic acid, permanganate of potassium, hyposulphite of sodium, creasote, benzine. Simple water, however, accomplishes about all that is possible, and many are satisfied to use it without any medication.
As regards the frequency with which the stomach is to be washed out, one is to be guided by the symptoms and the effect obtained by the use of the stomach-tube. As a general rule, it suffices to wash out the stomach once a day, and often the process need be repeated only every second or third day.
Opinions are divided as to the best time of day to select for washing out the stomach. Kussmaul recommends the morning before breakfast, and the majority have followed his advice; others prefer the evening. There is much, however, in favor of washing out the stomach about half an hour before the principal meal of the day. The best opportunity has been offered for the digestion and absorption of the food taken at the previous main meal, and the stomach is placed in the best possible condition for the reception of more food.
The habitual washing out of the stomach is not without its drawbacks. We often remove, as has been pointed out especially by Leube, not only noxious substances from the stomach, but also the completed products of digestion. To withdraw from the nourishment of the body this chyme which the stomach has laboriously manufactured cannot be a matter of indifference. Still, with the weakened absorptive powers of the stomach, [p. 608] and its inability to properly propel its contents into the intestine, it is a question how much of this chyme would eventually be utilized for nutrition. Another point is worthy of attention. The relief which the patient experiences when his overloaded stomach is freed of its burden, and the knowledge that this method of relief is always at hand, may make him careless in the observance of the dietetic rules which are of great importance in the treatment of this disease. It is well, therefore, not to wash out the stomach oftener than is necessary, nor to continue the habitual use of the stomach-tube longer than is required.
There are contraindications to the use of the stomach-tube. In very rare instances the attempt to introduce the tube causes the patient so much distress, produces such violent spasm of the pharyngeal and adjacent muscles, or induces so much retching and vomiting, or is attended with such prostration or even syncope, that this method of treatment has to be abandoned. Great weakness, recent gastric hemorrhage, ulcer of the stomach in most cases (see page 523), often cancer of the cardia or of the oesophagus, and aneurism of the aorta, are contraindications to the use of the stomach-tube.
If we group together the results obtained by the use of the stomach-tube in gastric dilatation, we shall find cases in which no benefit results; cases which are benefited, but are obliged to continue the use of the stomach-tube throughout life; cases in which recovery is slow and gradual; cases with more or less speedy relief or apparent cure, but followed by relapses; and cases of prompt relief and permanent cure.
The regulation of the diet is never to be neglected in cases of dilatation of the stomach. Here the guiding principles are that little fluid should be taken, and that the food should be small in bulk, nutritious, easily digestible, and not readily undergoing fermentation. The patient should drink as little water as possible, and should therefore avoid whatever occasions thirst. It is hardly practicable to carry out the plan of giving water mostly by the rectum, as has been proposed. In most cases milk is useful, but an exclusively milk diet is not generally well borne on account of the quantity of fluid required. Leube's beef-solution is often serviceable. Soft-boiled eggs and tender meats are to be allowed, particularly the white meat of fowl and rare beefsteak, especially that prepared from scraped and finely-chopped beef, as recommended in the treatment of gastric ulcer (page 521). Fatty, saccharine, and amylaceous articles of food—hence most vegetables and fruits—are to be avoided on account of their tendency to undergo fermentation in the stomach. Alcohol in any form is usually detrimental. If gastric symptoms, particularly vomiting, be very urgent, or if food introduced into the stomach affords little or no nourishment, as in some cases of tight pyloric stricture, then rectal alimentation is to be resorted to.
An important indication is to restore the tone and contractile power of the muscular coat of the stomach. For this purpose electricity, in the form both of the constant and of the faradic current, has been beneficially employed. The best results are reported from the use of the faradic current. Both poles may be applied over the region of the stomach. The application of electricity to the inside of the stomach by means of electrodes attached to stomach-tubes or bougies is a more [p. 609] difficult procedure, but has its advocates. Uniformly good results are not obtained by the use of electricity in gastric dilatation, but there can be no doubt that in some cases decided benefit follows this method of treatment.
Nux vomica, particularly its alkaloid strychnia, has been much employed with the view of stimulating the muscular power of the stomach. Strychnia is given either internally or hypodermically. Hypodermic injections of ergotin have also been used for the same purpose. It has been hoped to increase the contraction of the stomach by cold applications to the abdomen, as by ice-bags applied immediately after washing out the stomach. The benefit derived from these various attempts to increase the tonicity of the gastric muscle is not very apparent.
A belt or bandage around the abdomen in order to support the stomach sometimes makes the patient feel more comfortable; in other cases it aggravates the symptoms.
In many cases digestion is promoted by giving dilute hydrochloric acid with or without pepsin. About ten drops of dilute hydrochloric acid may be given half an hour to an hour after each meal.
When the stomach is systematically washed out, the individual symptoms of dilatation of the stomach will rarely require special treatment. The sensation of fulness and weight in the stomach, the eructations, the vomiting, and the constipation are generally relieved, at least temporarily, by washing out the stomach. The appetite is improved, and an increase in weight is usually soon noticeable.
If heartburn and eructations of gas continue troublesome, an antacid, such as bicarbonate of sodium or prepared chalk, will be found useful.
Leube, in order to relieve constipation and to increase the peristalsis of the stomach, administers Carlsbad water (see page 522). Not more than five or six ounces of the water need be given, and this should be taken slowly in divided doses. A laxative pill containing rhubarb may be given occasionally.
If anæmia be the cause or a prominent accompaniment of dilatation of the stomach, iron may be administered in a form as little disturbing the digestion as possible, as the effervescing citrate or the lactate, or arsenic in the form of Fowler's solution may be tried. In general, however, all drugs which impair the appetite or digestion are to be withheld. The digestion and the general condition of the patient are often benefited by massage.
Resection of the pylorus in cases of cancerous and of cicatricial stenosis of this orifice has been performed in several instances. The subject, as regards its medical in distinction from its surgical bearings, has already been discussed in connection with cancer of the stomach (see page 577). Here it may be added that the propriety of resection is less open for dispute in cases of non-cancerous pyloric stenosis than it is in cancer of the pylorus.
Remarkable results have been reported by Loreta in cases of cicatricial stenosis of the pylorus. After performing gastrotomy he inserts his fingers through the constricted pyloric orifice and forcibly dilates the stricture.35 To judge from experience in divulsing strictures in other parts of [p. 610] the body, it does not seem probable that a permanent cure can be often effected by this bold and dangerous procedure.
35 Loreta has performed this operation successfully no less than nine times (The Lancet, April 26, 1884).
Under the name acute dilatation of the stomach36 have been described cases in which it has been supposed that a more or less suddenly developed paralysis of the muscular coat of the stomach exists. But the propriety of the term acute dilatation, and the very existence of an acute paralysis of the stomach, are, to say the least, questionable.
36 The literature pertaining to the subject of acute dilatation of the stomach is to be found in Poensgen, Die Motorischen Verrichtungen des Menschlichen Magens, Strasburg, 1882, p. 95.
As causes of this so-called acute dilatation of the stomach have been assigned injuries, particularly those affecting the abdomen, surgical operations involving the peritoneum, acute inflammations of the mucous and of the peritoneal coats of the stomach, acute fevers, especially during convalescence, and overloading the stomach with food or with liquids.
The symptoms which have been chiefly emphasized are severe abdominal pain, tympanitic distension of the stomach, and absence or cessation of vomiting if this has previously existed. It will be noted that inability to vomit under these circumstances implies not only paralysis of the stomach, but also that of the abdominal muscles.
The prognosis depends on the character of the primary disease causing the alleged paralysis.
If there be acute distension of the stomach with inability of the organ to expel its contents either externally or into the intestine, the stomach-tube may be employed to evacuate the gas and other material present.
In a case described by Hilton Fagge37 as acute dilatation of the stomach the symptoms of dilatation appeared suddenly and ran an acute course, but the autopsy showed that the dilatation was doubtless of much longer development than the symptoms indicated. In a case reported by Nauwerk38 of extreme dilatation in consequence of hypertrophic stenosis of the pylorus, after ten months of insignificant dyspeptic symptoms there suddenly appeared, after excess in eating, symptoms of dilatation of great severity, which continued until a fatal termination at the end of three months. Thus it appears that chronic dilatation of the stomach may cause little disturbance for a considerable time and then run a rapid course.
37 "On Acute Dilatation of the Stomach," Guy's Hosp. Rep., xviii. p. 4, 1873.
38 Deutsches Arch. f. kl. Med., Bd. xxi. p. 573.
DEFINITION.—Cirrhosis of the stomach is characterized by thickening of the walls of the greater part or of the whole of the stomach in consequence of a new growth of fibrous tissue, combined usually with hypertrophy of the muscular layers of the stomach. The cavity of the stomach is usually contracted, but sometimes it is of normal size or even dilated.
SYNONYMS.—Fibroid induration of the stomach; Hypertrophy of the walls of the stomach; Chronic interstitial gastritis; Sclerosis of the stomach; Plastic linitis.
HISTORY.—The writings of the seventeenth and eighteenth centuries contain many records of extremely contracted stomachs with uniformly and greatly thickened walls (Butzen, Löseke, Storck, Portal, Lieutaud, Pohl, etc.). In the works of Lieutaud and of Voigtel may be found references to many such cases.1 Doubtless, some of these cases were examples of cirrhosis of the stomach, but in the absence of microscopical examination it is not possible to separate these from cancer.
1 Lieutaud, Historia anat.-med., t. i. p. 8, Venet., 1779; Voigtel, Handb. d. Path. Anat., Bd. ii. p. 450, Halle, 1804. Here it may be mentioned that Diemerbroeck's case, which is so often quoted to prove that polyphagia instead of causing gastric dilatation may produce hypertrophy of the muscular coat of the stomach, with contraction, was probably an instance of cirrhosis of the stomach.
Andral2 was the first to describe fully and systematically hypertrophy of the walls of the stomach. He attributed the lesion to chronic inflammation. He erroneously supposed that scirrhus of the stomach was only hypertrophy of the gastric walls. Cruveilhier3 distinguished between scirrhous induration and hypertrophy, which he considered to be a final result of the irritation accompanying chronic diseases of the stomach. Rokitansky's4 description of fibroid induration of the stomach, although brief, is accurate. He says that the process usually involves the whole [p. 612]stomach, and that it originates in an inflammation of the submucous connective tissue. This inflammation may occur either independently or in combination with gastritis mucosa. Rokitansky emphasizes the error of confounding the disease with scirrhous cancer. Bruch5 made an elaborate study of hypertrophy of the walls of the stomach, which he considered to be the final stage of various chronic diseases of the stomach. Fibrous or scirrhous cancer he considered to be nothing but this hypertrophy.
2 Précis d'Anat. path., Paris, 1829.
3 Anatomie pathologique, Paris, 1830-42.
4 Lehrb. d. Path. Anat., Wien, 1855-61.
5 Zeitschr. f. rat. Med., Bd. vii., 1849.
The best descriptions of cirrhosis of the stomach have been furnished by English writers, by most of whom it is properly regarded as an independent disease. Brinton6 first employed the names cirrhosis of the stomach and plastic linitis. Excellent descriptions of the disease have been given by Hodgkin, Budd, Brinton, Habershon, H. Jones, Wilks, Quain, and Smith.
6 Diseases of the Stomach.
While in former times cirrhosis of the stomach was confounded with cancer, in recent times it has not been separated by many from chronic catarrhal gastritis. In German systematic works the disease receives, as a rule, only passing mention in connection with chronic catarrhal gastritis.
ETIOLOGY.—Cirrhosis of the stomach is rare, but it is not so exceptional as to be without any clinical importance. I have met with three cases at post-mortem examination.
The disease is more frequent in men than in women. A considerable number of cases have occurred between thirty and forty years of age, but the greatest frequency is after forty. At an earlier age than twenty the disease is very rare.
The causation of cirrhosis of the stomach is obscure. Nearly all writers upon the subject have emphasized the abuse of alcohol as an important cause in this as in other diseases of the stomach. Intemperance cannot, however, be the only cause; and here, as elsewhere, it is not easy to say what importance is to be attached to it as an etiological factor. In only one of the three cases which I examined post-mortem could it be determined that the patient was an immoderate drinker, and in one case intemperance could be positively excluded. Other cases have been recorded in which the abuse of spirits could be positively excluded. In one of my cases syphilis existed, as was established by the presence of gummata in the liver. In some cases the disease has been attributed to cicatrization of a gastric ulcer. In a case reported by Snellen the disease followed an injury to the epigastric region.7
7 Canstatt's Jahresbericht, 1856, iii. 302.
Cirrhosis of the stomach, as well as cancer, ulcer, and most other chronic structural diseases of this organ, is usually associated with chronic catarrhal gastritis. There is, however, no proof of the prevalent idea that chronic catarrhal gastritis is the cause of the enormous new growth of fibrous tissue which characterizes typical cases of this disease.
SYMPTOMATOLOGY AND DIAGNOSIS.—The symptoms of cirrhosis of the stomach are not sufficiently characteristic to warrant a positive diagnosis. Sometimes the disease pursues a latent course. Like cancer of the stomach, it may put on various disguises. Thus, in a case of cirrhosis of the stomach reported by Nothnägel8 the symptoms were [p. 613] typically those of progressive pernicious anæmia. Association with ascites or with chronic peritonitis may lead to a false diagnosis. Thus, in one of the cases which I examined after death, and in which there was chronic peritonitis with abundant fluid exudation, the disease during life was diagnosticated as cirrhosis of the liver. Most frequently, however, cirrhosis of the stomach is mistaken for gastric cancer, from which, in fact, it can rarely be positively diagnosticated.
8 Deutsches Arch. f. kl. Med., Bd. 24, p. 353.
The symptoms are usually those of chronic dyspepsia, which sooner or later assumes a severity which leads to the diagnosis of some grave structural disease of the stomach, usually of cancer.
Indigestion, loss of appetite, oppression in the epigastrium, vomiting, are the common but in no way characteristic symptoms of cirrhosis of the stomach. There may be severe gastralgia, but in general the disease is less painful than either ulcer or cancer of the stomach. The inability to take more than a small quantity of food or of drink at a time, with the sense of fulness which even this small quantity occasions, has been considered somewhat characteristic of cirrhosis of the stomach, but this symptom is too inconstant, and occurs in too many other affections of the stomach, to be of much service in diagnosis. The symptoms of dyspepsia are often of much longer duration than in cancer, existing sometimes for many years (up to fifteen years), but on the other hand there have been cases in which the clinical history of gastric cirrhosis was as rapid in its progress as cancer. Moreover, cancer may be preceded by dyspeptic symptoms of long duration, but long duration is the exception with cancer and the rule with cirrhosis of the stomach.
As the disease progresses the patient loses flesh and strength, and usually dies in a condition of marasmus. Blood is rarely present in the vomit, but in a few cases the vomiting of coffee-ground material has been noted.
By physical examination sometimes a tumor in the region of the stomach can be felt. Under favorable circumstances it can sometimes be determined that this tumor is smooth, elastic, tympanitic on percussion, and presents more or less distinctly the contours of the stomach. By administering effervescing powder it may be possible to obtain further evidence that the tumor corresponds in its form to the stomach. The diagnosis of contraction of the cavity of the stomach is not easy. Some information may be afforded by noting the length to which the inflexible stomach-tube can be passed. The quantity of water which can be poured into the stomach until it begins to run out of the stomach-tube may also bring some confirmatory evidence as to the existence of contraction of the stomach.
Even should the physical signs suffice to determine that the tumor is the thickened and contracted stomach, still cancer cannot be excluded, for this also may grow diffusely in the gastric walls and may cause contraction of the cavity of the stomach. With our present means of diagnosis, therefore, the most which can be said is, that a special combination of favorable circumstances may render probable the diagnosis of cirrhosis of the stomach, but a positive diagnosis is impossible.
MORBID ANATOMY.—In most cases of cirrhosis of the stomach the stomach is contracted. The cavity of the stomach has been found not larger than would suffice to contain a hen's egg, but such extreme [p. 614] contraction is very rare. When the stomach in this disease is found dilated, either the thickening involves only or chiefly the walls of the pyloric portion, or the morbid process probably began there and was followed by dilatation.
In typical cases the walls of the entire stomach are thickened, but frequently the thickening is most marked in the pyloric region. The walls may measure an inch and even more in thickness. The thickened walls are dense and firm, so that often upon incision the stomach does not collapse.
Upon transverse section the different coats of the stomach can be distinguished. The mucous membrane is least affected, being sometimes thickened, sometimes normal or atrophied. The muscularis mucosæ is hypertrophied, and is evident to the naked eye as a grayish band. The submucous coat is of all the layers the most thickened, being sometimes ten to fifteen times thicker than normal. It appears as a dense white mass of fibrous tissue. The main muscular coat is also, as a rule, greatly hypertrophied; the grayish, translucent muscular tissue is pervaded with streaks of white fibrous tissue prolonged from the submucous and subserous coats. This last coat resembles in appearance the submucous coat, which, however, it does not equal in thickness, although it is, proportionately to its normal thickness, much hypertrophied. The free peritoneal surface usually appears opaque and dense.
To the naked eye it is apparent that the new growth of fibrous tissue is most extensive in the submucous coat, which it is probably correct to regard as the starting-point of the disease. The hypertrophy of the muscular layers is also in most cases an important element in the increased thickness of the gastric walls.
Microscopical examination9 shows sometimes a nearly normal mucous membrane. The tubules, however, are usually more or less atrophied. In the case reported by Nothnägel tubules could be found only in the pyloric region of the stomach. The essential lesion is the new growth of fibrillated connective tissue pervading all of the coats of the stomach. In an interesting case reported by Marcy and Griffith,10 which was believed to be caused by an extensive cicatrized ulcer, a new formation of smooth muscular tissue was found not only in the main muscular tunic and the muscularis mucosæ, but also throughout the submucosa. This peculiarity was probably referable to the cicatrization of the ulcer.
9 Microscopical examination is always necessary for a positive diagnosis of cirrhosis of the stomach. In a case which I examined post-mortem of double ovarian cancer, with multiple secondary deposits in the peritoneum and with chronic peritonitis, the stomach presented the typical gross appearances of cirrhosis, but here and there were to be found nests of cancer-cells in the prevailing new growth of fibrous tissue in the walls of the stomach.
10 Am. Journ. of the Med. Sci., July, 1884, p. 182.
Not infrequently adhesions exist between the stomach and surrounding organs. Exceptionally, a diffuse growth of fibrous tissue may invade the greater part of the peritoneum, particularly the visceral layer, and cause a thickening similar to that existing in the stomach. In such cases ascites is usually a marked symptom.
PROGNOSIS.—The prognosis of cirrhosis of the stomach is grave. The disease runs a chronic course, and usually terminates in death by asthenia. There is no reason to believe that the stomach can ever be restored to its [p. 615] normal condition. Still, cases have been reported in which it has been supposed that cirrhosis of the stomach has terminated in recovery.11 The diagnosis, however, in such cases must remain doubtful.
11 Lesser, Cirrhosis Ventriculi, Inaug. Diss., Berlin, 1876; Smith, "Cirrhosis of the Stomach," Edinb. Med. Journ., 1872, p. 521.
TREATMENT.—The treatment is symptomatic, and is to be guided by the general principles developed in previous articles concerning the regulation of the diet and the administration of remedies.
The various causes of stenosis of the pylorus have already been mentioned under DILATATION OF THE STOMACH, and the most important of these causes have received full consideration in connection with ULCER and with CANCER OF THE STOMACH.
Only one of the varieties of pyloric stenosis can claim consideration as an independent disease. This variety is the so-called hypertrophic stenosis of the pylorus (Lebert) or fibroid degeneration of the pylorus (Habershon12). Under the name of hypertrophic stenosis have been described cases in which the stenosis was due to hypertrophy of only one of the coats of the stomach, usually either the submucous or the muscular coat, sometimes only the mucous coat. In most cases, however, all of the coats of the stomach are involved, and the lesion is similar to that of cirrhosis of the stomach, but it is confined to the pylorus or to the pyloric region. In such cases there is new growth of fibrous tissue, most marked in the submucous coat, and hypertrophy of the muscular coat. The appearance of the pylorus in some instances of hypertrophic stenosis has been not inappropriately compared to that of the cervix uteri.
12 Habershon, On Diseases of the Abdomen, London, 1862; Lebert, Die Krankh. d. Magens, Tübingen, 1878; Nauwerk, Deutsches Arch. f. klin. Med., Bd. 21, 1878.
In the majority of cases the change here described is the result of cicatrization of a gastric ulcer, and some believe that all cases of so-called hypertrophic stenosis or fibroid degeneration of the pylorus are referable to ulcer, although it may be very difficult to discover the cicatrix of the ulcer. It is certainly not always possible to detect either ulcer or cicatrix, so that it seems proper to regard the hypertrophic stenosis in such cases as constituting an independent affection.
The symptoms are those of dilatation of the stomach, sometimes preceded by evidences of chronic catarrhal gastritis. The thickened pylorus can sometimes be felt during life as a small, cylindrical, usually movable tumor, either stationary in progress or of very slow growth.
In most cases the diagnosis of organic stenosis of the pylorus can be made. Cancer may sometimes be excluded by the long duration of the symptoms and the stationary character of the tumor if a tumor can be felt. The exclusion of ulcer is more difficult and hardly possible, for ulcer may have existed without producing characteristic symptoms.
The prognosis and treatment have been considered under DILATATION OF THE STOMACH.
Atrophy of the stomach may be the result of stenosis of the cardia or of the oesophagus. The stomach may participate with other organs in the general atrophy attending inanition and marasmus. The walls of a dilated stomach may be very thin.
Especial importance has been attached in recent years to degeneration and atrophy of the gastric tubules. The glands of the stomach may undergo degeneration and atrophy in various diseases of the stomach, such as chronic catarrhal gastritis, phlegmonous gastritis, cirrhosis of the stomach, and cancer of the stomach. Parenchymatous and fatty degeneration of the glandular cells of the stomach occurs in acute infectious diseases, as typhoid fever and yellow fever, also as a result of poisoning with phosphorus, arsenic, and the mineral acids.
It is claimed by Fenwick that atrophy of the stomach may occur not only as a secondary change, but also as a primary disease attended by grave symptoms. Fenwick has described a number of cases in which the gastric tubules were atrophied without thickening of the walls of the stomach and without diminution in the size of the cavity of the stomach—cases, therefore, which cannot be classified with cirrhosis of the stomach.13 He attributes in many cases the atrophy of the tubules to an increase in the connective tissue of the mucous membrane, and draws a comparison between atrophy of the stomach and the atrophic form of chronic Bright's disease.
13 The Lancet, 1877, July 7 et seq.
In 1860, Flint14 called attention to the relation between anæmia and atrophy of the gastric glands. He expressed the opinion that some cases of obscure and profound anæmia are dependent upon degeneration and atrophy of the glands of the stomach. Since Flint's publication cases have been reported by Fenwick, Quincke, Brabazon, and Nothnägel, in which lesions supposed to be due to pernicious anæmia have been found after death associated with atrophy of the gastric tubules.15 Nothnägel's case, which has already been mentioned, was one of cirrhosis of the stomach.
14 A. Flint, American Medical Times, 1860. Further contributions of Flint to this subject are to be found in the New York Medical Journal, March, 1871, and in his Treatise on the Principles and Practice of Medicine, p. 477, Philada., 1881.
15 Fenwick, loc. cit.; Quincke, Volkmann's Samml. klin. Vorträge, No. 100 (case b); Brabazon, British Med. Journ., 1878, July 27 (without microscopical examination!); Nothnägel, Deutsches Arch. f. kl. Med., Bd. 24, p. 353.
The symptoms which have been referred to primary atrophy of the stomach are severe anæmia and disturbances of digestion, such as anorexia, eructations, and vomiting. The digestive disturbances are often not greater than are frequently observed in cases of severe anæmia.
In my opinion, the existence of atrophy of the stomach as a primary and independent disease has not been established. In many cases which have been described as primary atrophy the histological investigation of the stomach has been very defective. Degeneration and atrophy of the gastric tubules secondary to various diseases of the stomach and to certain general diseases is an important lesion when it is extensive, and must seriously impair the digestion, and consequently the nutrition, of the patient.
These anomalies, so far as they have not received consideration in previous articles, are of more anatomical than clinical interest, and therefore here require only brief mention.
The stomach may have an hour-glass shape in consequence of a constriction separating the cardiac from the pyloric half of the organ. This constriction is sometimes congenital,16 sometimes caused by cicatrization of a gastric ulcer, and sometimes caused by spasmodic contraction of the muscle, which may persist after death, but disappears when the stomach is artificially distended. Hour-glass shape of the stomach has been diagnosed during life by administering an effervescing powder according to Frerichs' method.
16 A careful study of the congenital form of hour-glass contraction of the stomach has been made by W. R. Williams ("Ten Cases of Congenital Contraction of the Stomach," Journ. of Anat. and Physiology, 1882-83, p. 460).
Foreign substances of hard consistence which have been swallowed sometimes cause diverticula of the stomach.
Sometimes the fundus of the stomach is but little developed, so that the organ is long and narrow like a piece of intestine.
The stomach may be variously distorted by external pressure, as from tumors and by adhesions.
The loop-shaped stomach and vertical position of the stomach have been already considered in connection with DILATATION OF THE STOMACH (page 602).
In transposition of the viscera the stomach is also transposed. In such a case difficulties may arise in the diagnosis of pyloric cancer, as in a case described by Légroux.
The stomach may be found in hernial sacs. Mention has already been made of the presence of dilated stomachs in scrotal hernia. More frequently the stomach is found in umbilical hernias. In diaphragmatic hernia the stomach is found more frequently in the thorax than is any other abdominal viscus. In 266 diaphragmatic hernias collected by Lascher17 the stomach was found either wholly or partly in the thorax in 161 cases. The clinical consideration of diaphragmatic hernia, however, does not belong here.
17 Deutsches Arch. f. kl. Med., Bd. 27.
Furthermore, the stomach may be displaced by tumors, enlargement of neighboring organs, tight-lacing, adhesions, and the weight of hernias. These displacements, however, are generally inconsiderable and of little importance.
In a case described by Mazotti18 the stomach, of which the pyloric portion was fixed by adhesions, was twisted around its long axis. Death was caused by uncontrollable vomiting.
18 Virchow und Hirsch's Jahresbericht, 1874, ii. p. 249.
Sufficient attention has already been given to perforation of the stomach in consequence of diseases of its walls, such as ulcer, cancer, abscesses, and toxic gastritis.
A healthy stomach may be ruptured by violent injury to the abdomen even when no external wound is produced. An example of rupture of the stomach from this cause is that sometimes produced when a person has been run over by a heavy vehicle.
It has been claimed that a stomach with healthy walls may burst in consequence of over-distension of the organ with solids or with gas. The older literature is especially rich in reports of so-called spontaneous rupture of the stomach. Most of these cases were examples of perforation of gastric ulcer. In a case of apparently spontaneous rupture of a stomach which had become abnormally distended with gas, Chiari19 found that the rupture was through the cicatrix of a simple ulcer in the lesser curvature. It is hardly conceivable that rupture of the healthy stomach from over-distension can occur so long as the orifices of the organ are unobstructed.
19 Wiener med. Blätter, 1881, No. 3.
Lautschner20 reports a case of spontaneous rupture of the stomach in a woman seventy years old with an enormous umbilical hernia which contained the pyloric portion of the stomach. After drinking eight glasses of water and two cups of tea and eating meat, she was seized with vomiting, during which the stomach burst with a report which was audible to the patient and to those around her. She passed into a state of collapse and died in thirteen hours. A rent several centimeters long was found in the posterior wall of the stomach. Lautschner thinks that the pylorus was bent in the hernial sac so as to be obstructed. In the walls of the stomach he found no evidence of pre-existing disease.
20 Virchow und Hirsch's Jahresbericht, 1881, ii.
There is no satisfactory proof of the possibility of the occurrence of rupture of a stomach with healthy walls except as a result of external violence.
The symptoms and treatment of rupture of the stomach are those of perforation of the stomach, and have already been described. The prognosis is fatal.
That the subject of gastromalacia should still occupy so much space in medical works the purpose of which is mainly clinical proves that many physicians still cling to the belief that this process may occur during life. It is, nevertheless, certain that the condition which, according to the ordinary and traditional use of the term, is designated gastromalacia, is always a post-mortem process and is without the slightest clinical significance. So long as the circulation of the blood in the walls of the stomach is undisturbed, self-digestion of this organ cannot occur. No one doubts [p. 619]that parts of the gastric walls in which the circulation has been arrested, and which are exposed to the gastric juice, undergo self-digestion, as has already been set forth in the article on GASTRIC ULCER. To describe cases of this nature under the name of gastromalacia, however, is misleading, and can cause only confusion, for the long-continued discussion as to whether gastromalacia is a vital or a cadaveric process applied certainly to a different conception of the term. In some of the cases which have been published, even in recent years, in support of the vitalistic theory of gastromalacia, and in which it has been proven that perforation of the stomach occurred during life, the solution of continuity took place through parts of the gastric walls in which the circulation had already been obstructed, particularly by extensive hemorrhagic infiltration. Some of these cases are probably also examples of perforation of gastric ulcer or of rupture of cicatrices from over-distension of the stomach, in which post-mortem digestion of the edges of the ulcer or of the cicatrix obscured the real nature of the process. The subject of gastromalacia should be relegated wholly to works on physiology and on pathological anatomy.
NATURE.—The term indigestion in its most common meaning refers to gastric indigestion only. This limitation has arisen from the fact that gastric digestion has been more thoroughly understood than intestinal digestion, and because the symptoms, flatulence, acidity, eructations of gas, pyrosis, and vomiting of unaltered food, are readily referred to the stomach as their source. Intestinal digestion has not been well known until within a recent date, and its phenomena in disease have been mistaken for other pathological conditions.
From the important and complex function of the intestinal juices, and the very great share they take in the solution of food, there must be many phases of departure from the normal state. The processes of intestinal digestion are more intricate than those of gastric digestion, of a higher grade, and the chemical reactions are more numerous, depending upon the participation of the bile, the pancreatic juice, and the succus entericus; while intestinal absorption is a more complex act than that of gastric absorption.
A brief review of the physiology of intestinal digestion will be of aid in making clear its pathology.
The object of all digestion is to make such a solution of the ingesta that they may pass through animal membrane and so enter the system. Mechanical disintegration and simple solution do something toward this, but for substances insoluble in water a more thorough change is brought about by ferments which convert insoluble into soluble compounds.
The process of digestion begins in the mouth. Mastication breaks up the masses of food; the saliva softens them, dissolves soluble substances, as salt and sugar, and thus the pleasures of the palate are enhanced. The ferment ptyalin acts upon starch (boiled starch being more rapidly altered than unboiled), and changes it to dextrin and grape-sugar, both of which are diffusible through animal membrane, entering lymph-spaces and blood-vessels. The greater part of the saliva secreted is swallowed with the food or in the intervals of eating. The amount formed in twenty-four hours varies from 1500 gm. (Bidder and Schmidt) to 700 gm. (Tuczek). It must therefore serve some ulterior purpose in the stomach. Ewald1 says that saliva converts starch into sugar in acid as well as in alkaline and neutral solutions. But Langley2 asserts that the ferment of [p. 621]saliva is destroyed by the hydrochloric acid of the gastric juice. The longer food is subjected to mastication and insalivation, the more thorough is the mouth digestion and the better prepared is the mass for the action of the gastric and intestinal juices. It is asserted that fatty matters are emulsified to a certain extent by the alkaline ferments of the saliva.
1 Lectures on Digestion, New York, 1881, p. 37.
2 "On the Destruction of Ferments in the Alimentary Canal," Journal of Physiology, London, Jan., 1882, p. 246.
When the food enters the stomach the nitrogenous (albuminoid) elements are attacked by the gastric juice, the bundles of muscular fibre are broken up, the fibrillæ are reduced to a granular mass, but not completely dissolved (Frerichs), the fat-globules are freed from their envelopes of connective tissue, milk is coagulated, and the casein is dissolved.
"The tangible, practical object of this change is to form out of a little-diffusible body (albumen) one easily diffusible (peptone), which is capable of absorption through animal membrane in a higher degree than ordinary albumen" (Ewald). Peptone is formed out of ordinary albumen, as grape-sugar is formed out of starch, by taking up water; it is therefore the hydrate of albumen.
The more tardy the digestion in the stomach the more highly charged with acid is the gastric juice. According to Wright, the degree of alkalinity of the saliva is in proportion to the acidity of the stomach fluids, and Bence Jones has observed that during the excretion of acid in the stomach the total alkalinity of all alkaline digestive fluids is increased. The lesson is thus learned that a too careful preparation of food, so as to shorten and lessen gastric labor, diminishes the activity of the gastric juice as well as that of all other digestive fluids.
Intestinal digestion begins when the softened mass passes through the pylorus. This mass (chyme) is composed of (1) the products of gastric digestion which have not been absorbed—peptone, dextrose, levulose, peptonized gelatin, with mucus and gastric juice; (2) all matters which have escaped digestion—the starch of vegetable substances, dissolved gelatin and albumen which have not been peptonized, and some unaltered muscle-structure; and (3) fat, fatty acids, and cellulose upon which neither saliva nor gastric juice has had any influence (Ewald).
This complex semi-fluid mass with an acid reaction enters the duodenum and comes in contact with fluids and ferments destined to work remarkable changes in its composition. The first of these fluids is the bile, which is alkaline and composed of the glycocholate and taurocholate of sodium, cholesterin, soaps, etc., phosphates and carbonates of lime and sodium, chlorides of potassium and sodium, bile-pigment, etc. The outflow of bile is excited by the contact of the chyme with the orifice of the bile-duct. When the alkaline bile is mingled with the acid mass in the duodenum, it neutralizes its acidity, precipitates the peptones, and therefore stops all further action of the gastric juice. Fats containing free fatty acids are emulsified, soaps being formed by a combination of the alkalies of the bile with the fatty acids. Lastly, bile hinders fermentation in the intestine and acts as a purgative by exciting peristalsis. Absorption is probably also favored by bile, as it has been found that emulsified fats pass more readily through an animal membrane which has been wet with bile.3
3 Ewald thinks this result is doubtful: in animals killed during digestion he has found an acid reaction in the contents of the intestine beyond the opening of the bile-duct, with no precipitation of the albumen (op. cit., p. 82).
[p. 622] As far as we now know, the function of the bile is to neutralize the acidity of the duodenal contents, and thus pave the way for the action of a digesting fluid of much greater potency and of much higher function.4
4 In order still further to demonstrate the necessity of bile-action as a preparation for pancreatic digestion, it may be mentioned that in artificial experiments, with a heat equal to that of the body, if antiseptics analogous to gastric juice and bile are not used, there is a too rapid change from alkalinity to acidity, and consequently all of the starch is not converted into sugar before it develops lactic acid with putrefactive disorganization. A deficiency of bile, therefore, is a cause of intestinal indigestion (Bartlett, op. cit., pp. 12, 13).
This fluid, the pancreatic juice, is composed of inorganic salts, albuminoids, and certain specific ferments, and has an alkaline reaction. It has a threefold operation upon the softened mass with which it now comes in contact: 1. The starch of vegetable matter, which has been only slightly acted on up to this time, is now rapidly converted into grape-sugar by a peculiar diastatic ferment more active than any other known ferment. 2. Albuminous matters (proteids) which have escaped digestion in the stomach are changed into a soluble and absorbable pancreas—peptone. Trypsin is the active ferment in this case (Kühne), and it is only in alkaline or neutral solutions that the albuminoids are readily dissolved. The necessity of neutralization by the alkaline bile is thus demonstrated. 3. A ferment distinct from the others splits the fats into fatty acids and glycerin, and emulsifies them so that they can be taken up by the lacteals lower down.
Experiments made by mixing albuminates with pancreatic gland-extract, under favorable conditions, show after a certain time the presence of leucin, tyrosin, hypoxanthin, and asparaginic acid. In a feebly alkaline or neutral solution a faint putrefactive odor is soon noticed, with the development of bacteria; ammonia, sulphuretted hydrogen, hydrogen, and carbonic acid—evidences of the putrefaction of albumen—are also detected.
It is difficult to tell when normal digestion in the intestines ends and putrefaction begins. The conclusion is, that the normal action of pancreatic juice (trypsin) gives origin to bodies met with in the ordinary putrefaction of albumen.5 This thin border-line between normal intestinal digestion and the decomposition of the intestinal contents has an important bearing on the facts of intestinal indigestion.
5 Ewald, op. cit., p. 92.
The intestinal juice performs a minor but independent part in digestion. It converts albuminous matter into peptone, and hydrated starch into sugar. Its function is therefore supplementary to that of the gastric and pancreatic secretions.6
6 Ewald, op. cit., p. 103; also, "The Functions of the Intestinal Juice," Charles L. Dana, Med. News, Philada., July 15, 1882, p. 59.
When food enters the mouth the process of digestion begins, and all the activities of the glands concerned in digestion are probably at once set in motion. Mastication excites, by reflex action, pancreatic secretion; the acid chyme touches the orifice of the common bile-duct and stimulates the outflow of bile; the neutralized chyme next invites pancreatic digestion. For the integrity of intestinal digestion it is required that mastication and stomach digestion should be normally performed.
The intestinal movements which are so necessary to digestion by making successive changes in the position of the intestinal contents are [p. 623] controlled by nervous arrangements, but may occur independently of the central nervous system. The ganglia of Auerbach and of Meissner in the intestinal wall are sufficient for the development of peristaltic waves. The irritation of the mucous membrane by food, hyperæmia, and the pouring out of digestive juices, and intestinal movements, are parts of one process. Paralysis by section of the splanchnic leads to hyperæmia of the intestinal vessels and increased peristalsis; stimulation of the splanchnic causes anæmia of the intestinal wall and arrest of movement. Local cold by producing anæmia brings about the same result.
The products of digestion as they pass toward the jejunum consist of diffusible peptones, sugar, emulsified fats and oils, and substances which have escaped digestion, as fragments of muscular fibre, starch-corpuscles, connective tissue, hairs, or other foreign matters. The bowel contains also carbonic acid, hydrogen, nitrogen, sulphuretted hydrogen, and marsh gas. The mass, alkaline or neutral in the duodenum and jejunum, becomes acid in the ileum from the putrefaction of albumen and fermentation. The peptones and sugar pass by osmosis into the blood-vessels of the portal system and thence to the liver. In the liver the sugar is converted into glycogen (carbohydrate), and stored in the liver-cells until needed for the maintenance of animal heat and for the nutrition of the tissues. The peptones are used in part to supply the nitrogenous waste of tissue, but much of the albuminoid matter is broken up in the liver into glycogen and urea, the latter of which is excreted by the kidneys as waste matter.
The minute granules of oil in emulsion are taken up by the epithelial cells covering the villi; thence they enter the adenoid tissue of the villi on their way to the lymphatic radicles, the lacteals. From here the passage is open to the underlying lymphatic vessels and to the larger abdominal lymph-vessels and the thoracic duct beyond.
Intestinal digestion is not completed and the body does not receive its pabulum until the products of digestion have reached the liver and the thoracic duct.
ETIOLOGY.—It is usually said that intestinal dyspepsia is more common in women than in men, but the contrary is the rule. Some of its most common causes—over-eating and the eating of indigestible food—are especially vices of men.
It is more frequent between the ages of forty and fifty, but no age is exempt. Infants at the breast, children of any age, adults, and old men and women are alike subject to it. Men in middle life begin to suffer from the imprudence and carelessness of youth and from the anxiety and cares of business. The indulged children of rich parents and improperly bottle-fed infants frequently suffer.
Heredity and idiosyncrasy have a certain influence in determining the prevalence of intestinal dyspepsia. The distaste for and inability to digest vegetables, fruits, and fats are often peculiarities of family history. The occurrence of cases in the same family is often explained by improper food, bad cooking, and irregular hours, to the evil influences of which all the members are similarly subjected.
All conditions of the organism which result in a depraved or altered blood-supply, as anæmia, primary and secondary rachitis, chronic syphilis, and continued febrile diseases, are causes of intestinal indigestion. [p. 624] The connection of the indigestion of fats with the strumous diathesis and with phthisis is undisputed. J. Hughes Bennett traced the origin of phthisis to defective fat-digestion; strumous indigestion and the indigestion of fat are synonymous terms.
Debilitating influences, such as bad air, want of cleanliness and outdoor exercise, impair functional activity in the intestines as elsewhere. Sexual excesses, but especially masturbation, have a special influence for evil in this direction.
The influence of the mind upon the digestion of starch and fats is even greater than upon gastric digestion, for no other reason perhaps than that the former is a more complex function and less easily relieved than the latter. Prolonged or excessive mental labor does not do so much harm as mental worry, over-anxiety, and the strain and overwork of business. Professional men—lawyers, physicians, and clergymen—who become over-burdened with responsibilities, and who sympathize too much with the distresses of others, are very prone to suffer. The careworn face with lines about the mouth and forehead is one of the plainest signs of duodenal defect. The proper secretion of the juices of the intestine and normal peristalsis are impossible where brain and nerves get no rest. The too rapid mental development of the children of the present day is a fruitful source of weakened fat-and-starch digestion and of impaired development. So long as children are sent to the public school at four and six years of age, there will continue to grow up a precocious race with active brains in feeble bodies.7 This injurious result is largely brought about by the direct interference of premature brain-development with the complex intestinal processes of digestion and absorption.
7 In eight of the States and Territories the minimum age for entering the public school is fixed at four years; in seventeen States at five years; in the others, except two, at six years. The two notable exceptions are Alabama and New Mexico, where children do not enter school until the age of seven.
Wealth, with ease and inactivity, and sedentary occupations, contribute to the same end by lessening the need of food, and thus debilitating the organs of digestion by inaction. Sedentary pursuits, especially those in which the body is bent forward and constricted or compressed at the waist, interfere with active function in the intestine. This is the case in tailors, shoemakers, etc. Tight-lacing in women and a too tight trouser-band in men are injurious.
Hot climates, especially when combined with dampness, lead to disorder in the intestine and liver. This effect is most marked among persons coming from colder climates, as among the English in India, who keep up the habits of eating to which they have been accustomed at home. The lessened demand destroys the appetite, and stimulants and condiments are resorted to to whip up the inactive functions. The intestine is loaded with a mass of crude, unaltered matter which can with difficulty be disposed of. Chronic indigestion results, varied with acute attacks of diarrhoea or dysentery. The portal system is filled with an excess of albuminoid material which the liver is unable to store away. The excess is got rid of by conversion into uric acid. Lithæmia and chronic congestion and enlargement of the overloaded liver result, with their many attendant evils.
Over-eating occasions first gastric and then intestinal indigestion by the [p. 625] entrance of unaltered food into the duodenum. Eating without hunger often involves the taking of food which the body does not need and which the stomach cannot digest. Diners-out rarely go through a season without one or more internal revolts. A too-varied diet, a dinner of many dishes, is faulty in variety as well as in excess. On the other hand, a too great sameness in diet and the prolonged use of one or two articles of food which are not easy of digestion, and which have a great deal of waste, fatigue and then disorder intestinal digestion. This is a fault into which children are often allowed to fall.
Indigestible food and an excess of starchy or fatty food conduce to disorder of duodenal digestion. In conditions of debility and anæmia and in the convalescence of fevers the deficiency of saliva involves an inability to digest starch in the mouth and points to a corresponding want in the duodenal secretions. The improper use of alcoholic liquors, taking them on an empty stomach between meals and in excess, tends to direct irritation of the mucous tract. Condiments in large quantity have the same effect.
Irregularity in the hours of eating and a faulty distribution of the amount of food disturb the perfect working of the mechanism of digestion. Very light breakfasts and very late and large dinners are injurious. The habit, now quite general in cities, of deferring the breakfast proper until midday, leaves the system too long—fifteen to sixteen hours—without proper food and weakens digestive activity. Intestinal indigestion is very common among Americans who have lived abroad and adopted European customs.
Another cause which is unfortunately very common is the imperfect mastication and insalivation of food, due to too great haste in eating, to defects in the teeth or gums, or to a deficiency of saliva. The saliva no doubt sometimes possesses a feeble diastatic power, although abundant in amount. Carnivorous animals bolt their food, but vegetable-eaters must masticate. Slow mastication transforms starch into sugar, and at the same time excites secretive activity in the glands of the digestive tract, especially in the pancreas. The more thoroughly this preliminary function is performed the better preparation is there for the subsequent acts of digestion.8
8 "The familiar act of chewing is seldom a subject of reflection, yet it throws into motion a more complicated system of levers, accompanied by a drain of fluids from more curiously adapted apparatus, than the arts can parallel" (Leared, On Indigestion, London, 1863, p. 3).
The chewing of tobacco, a wretched habit which is much less common now than formerly, and to a less extent the habit of smoking, are causes of deficient, altered, or depraved saliva, and secondarily of altered pancreatic secretion. The thin smoker grows fat when he abandons the weed.
The normal functions of the intestines are interfered with and indigestion is set up by constipation. Every one has felt the activity in digestion which accompanies the regular habit of defecation, and the torpor and oppression which depend upon an unemptied colon. "There is a concert of action in virtue of which the whole muscular apparatus of the digestive tube sympathizes with that of the large intestine. This concert of action, which induces pathological states, is the reason why in the [p. 626] physiological state a regular contraction of the whole intestinal tube, including the stomach, is the consequence of the regular contraction of the large intestine."9
9 Trousseau, "Les Dyspepsies," L'Union médicale, tome xi., 1857, p. 313.
An excess of acid in the stomach would enfeeble the solvent power of the intestinal fluids by antagonizing neutralization by the alkaline bile; the same effect follows any cause which prevents the outflow of the bile, as the plugging of the common bile-duct by mucus and epithelium in catarrh or by an impacted gall-stone. The emulsification of fats is incomplete and decomposition in the intestine follows. The antagonism of the saliva and the gastric juice, of the gastric juice (or the chyme) and the bile, must preserve their delicate and nice adjustment in order for digestion to be properly performed.
Diseases of the pancreas seriously embarrass digestion in the intestine. Lesions of this organ, as catarrh of the duct, cancer, fatty degeneration, etc., may result in impaired emulsification of fats, fatty diarrhoea, and wasting.
Intestinal indigestion accompanies hyperæmia and catarrh of the intestinal mucous membrane, diseases of the heart, lungs, and liver, and all other causes which impede portal circulation.
SYMPTOMS.—Intestinal indigestion cannot be so clearly pictured as that of gastric dyspepsia. This is owing to the frequent concurrence of the two conditions, the gastric symptoms taking precedence of the others. The more complex nature of the intestinal function is another reason, intestinal indigestion having more modifications in its phenomena. In the stomach there is only one active secretion; in the intestine there are three, all participants in the act of solution. An alteration in the quality or quantity of one of these—the bile, for example—would lead to different symptomatic results than would follow another defective secretion, as that of the pancreas, for instance. Clinical study has not yet fully differentiated the forms of indigestion due to these several deficiencies. But there are certain well-defined symptoms associated with intestinal disorders which are distinguished by their seat, time of their appearance, and their character from analogous symptoms connected with the stomach.
Intestinal indigestion may be acute or chronic. The latter is the more typical and more common form.
When a sudden attack of indigestion in the intestine results from the entrance into the duodenum of food in such a state that it cannot be digested, the result is the rapid development of pain, flatulence, borborygmi, and frequently of fever, ending in diarrhoea, with the escape perhaps of the offending matter: a condition then exists which may be called acute or subacute intestinal catarrh or acute intestinal indigestion. One name would be as correct as the other. Slight acute forms are marked by a coated tongue, loss of appetite, headache, pains in the limbs, distress in the epigastrium or right hypochondrium, flatulence, and constipation. These might be accompanied by symptoms indicating a disorder of the liver functions—light-colored stools, slight jaundice, lithates in the urine. But intestinal indigestion alone can cause these symptoms without the condition of so-called biliousness being present. The local symptoms are due to the presence in the intestine of an [p. 627] imperfectly-altered mass and the development of gas; some of the general symptoms are reflex; others, as headache and lassitude and pain in the limbs, come from the absorption into the blood of the gases, particularly sulphuretted hydrogen. The participation of the stomach in acute attacks of this sort modifies the symptoms as here described. Such attacks are apt to recur at intervals.
If the causes which bring about acute disorder in the intestine are allowed to continue, the intervals between the acute or subacute attacks diminish, and there is in time a fixed state of chronic intestinal dyspepsia in which the partly-altered food coming from the stomach is not properly prepared for absorption. Instead of digestion there is decomposition; the transition is easy from the one to the other of these states. The symptoms connected in this case with the digestive organs are pain, occurring from two to six hours after eating, in the right hypochondrium, the epigastrium, or the umbilical region, due to distension of the intestine with gas. This pain is dull, not always fixed, lasts from one to three hours, and is accompanied by tenderness on pressure over its seat.
Tympanites, borborygmi, and a sensation of fulness in the abdomen accompany the pain or may exist without it. Gaseous accumulations in the intestine, the cause of these symptoms, have an independent source, being produced by decomposition in the gut itself, and are not due to the descent of gases from the stomach through the pylorus. What is a physiological and temporary condition becomes in disease a distressing symptom of long duration. In intestinal indigestion the gut is nearly always inflated with gas, which in its movement produces rumbling noises. In acute indigestion it is rapidly formed in large amount, and by the stretching of the wall of the bowel and pressure on nerve-filaments causes intense pain—colic. In the chronic form the distension excites uneasy sensations, prevents sleep, and may be so great as to cause dyspnoea by pushing the diaphragm upward. When the small intestine is distended the greatest swelling may be about the umbilicus, or the abdomen may be evenly rounded. When the colon is chiefly or solely inflated, its outline across the upper part or at the sides of the abdomen can be easily made out.
Constipation is a common feature. It is produced by a loss of contractility of the intestinal wall. The more direct causes are over-distension of the gut and disturbance in the circulation and innervation of its walls. The stools are hard and dry, and are expelled with difficulty. Sometimes they are coated with shreds or films of mucus, the product of a chronic catarrh of the mucous membrane of the colon, or mucus from the small intestine is intimately mixed with the mass. Diarrhoea may alternate with constipation. The passage of unaltered food, as fragments of meat, vegetables, or fruit, clearly shows the extent to which indigestion exists. By the microscope particles of food which have escaped complete disintegration may be detected. The stools vary in color. Very dark-green or black discharges show an excess of bile; light-yellow or gray slate-colored, a deficiency. Stools of the latter character are highly offensive in odor.
Hemorrhoids are often present, being due to the sluggish portal circulation and to the pressure of hard fecal masses in the rectum. The appetite is not impaired, as a rule, but it may be fitful or irregular. A bad [p. 628] taste in the mouth, and a swollen, relaxed, and coated tongue may exist without any decided gastric disease.
The symptoms of disorder of the nervous system are more marked than in gastric dyspepsia. This results not so much from the depressing influences of pain as from the peculiar malnutrition of the nerve-tissue. In order to have furnished to the blood the pabulum out of which the nerve-elements are reconstructed the digestion of fat must be normally performed. Lecithin, which is found conspicuously in the brain and nerves, is a complex fat containing phosphorus and nitrogen.10 Anæmia and waste follow directly from interference with the digestion and absorption of fats and starch in the intestine, but the most delicate, the most easily-disorganized solid of the body, the nerve-tissue, is the first to feel and to manifest its want of natural supply. And so the dyspeptic whose intestine is at fault becomes depressed in spirits, hypochondriacal, absorbed in the contemplation of his sufferings, analyzing them and referring them to the most serious organic changes. There are sleeplessness, disturbing dreams, the habit of waking at a fixed hour, dizziness, uneasy sensations or pain in the head, and disturbances of the special senses, as buzzing in the ears, muscæ volitantes, and attacks of blindness. Headache assumes often the form of hemicrania; it may be in the forehead or about the eyes. Attacks of vertigo and sensations as if the ground were rising beneath the feet accompany intestinal flatulence. Confusion of thought, loss of the power of application, and mental inertia are frequent sources of anxiety. Paralysis has been noted as following indigestion. Epileptiform convulsions and milder epileptic attacks can be traced to undigested matter in the intestine.11 Various modifications of general sensibility also happen: there are pains in the back and limbs, hyperæsthesia, and anæsthesia. An inaptitude for exertion, especially for mental labor, forces the boy to give up school and college life. Successful careers are abandoned by men who at the cost of neglecting all the rules of health have succeeded for a brief period in passing their fellows in the race. Sudden attacks of fainting have been noted, with very grave collapse. These are the effect upon the nervous centres of the absorption of sulphuretted hydrogen which has been evolved in large quantities in the intestine.12 The daily occurrence of vertiginous and other morbid sensations, with melancholia, may be due to the daily toxic absorption of gas from the intestine.
10 Fothergill, Indigestion and Biliousness, New York, 1881, p. 76.
11 Chambers, The Indigestions, London, 1867, pp. 305-307.
12 Tyrell, case of a man with eructations smelling of sulphuretted hydrogen who had vertigo and sudden collapse; symptoms relieved by purgative (Pacific Med. and Surg. Journ., May, 1882, p. 539).
The action of the heart is disturbed as in stomach indigestion. Irritability of the heart and palpitation are in part due to anæmia and in part to mechanical pressure and reflex influences. The nervous, anæmic, thin dyspeptic has among his chief troubles a throbbing heart, which keeps him awake at night and fixes his attention upon this organ as the seat of his disease. The general circulation is languid; cold hands and feet and cold sweats testify to this, and the irregularity or suppression of catamenia follows upon the irregular blood-supply.
The urine is usually high-colored, has an abnormally high density, is acid, and on cooling deposits lithates, uric acid, and oxalate-of-lime [p. 629] crystals. The urine is most heavily loaded with sediment when digestion has been recently completed. Therefore, the morning urine after a heavy dinner of the night before contains the largest amount of lithates. Albuminuria is occasionally a symptom of indigestion in the bowel. The eating of cheese or pastry in excess may cause it.13 Seminal emissions at night frequently occur. The action and reaction upon each other of this perversion of the sexual function, the indigestion, and the mental disorder, reduce the poor sufferer to a most pitiable condition of despondency and prostration.14
13 Warburton Begbie's Works, Sydenham Society's Publications, 1882, p. 359.
14 The writer has observed cases in which an exaggeration of the sexual instinct in men of middle age was associated with intestinal indigestion.
Anæmia is one of the earliest indications of impaired nutrition. It precedes loss of flesh and the wrinkled and dry condition of the skin which may be a marked symptom in cases of long standing. Various eruptions appear on the skin. In the strumous dyspepsia of children the white, almost waxy, skin is covered with dry scales, which may be seen over the whole body from head to foot. No symptom is more characteristic of intestinal indigestion and of imperfect fat digestion and absorption than this. Eczema and psoriasis, pityriasis, impetigo, and porrigo decalvans are forms of skin eruption seen.
Closely allied to the symptoms caused by indigestion in the intestine are those due to functional disorder of the liver. The liver completes the work which the intestine has begun. It receives directly from the intestine blood laden with the products of digestion, and further transforms them into substances to be used in the economy. The symptoms which result from disturbances in the performance of these functions are, as has been said, closely connected with the symptoms of intestinal indigestion. This association is shown by the tendency among older writers to trace all such symptoms to the liver, the terms bilious and biliousness including all the phenomena of derangement of the function of digestion in the intestine, as well of the function of the liver. Later writers excluded the part of the liver to a great extent in giving rise to the so-called bilious symptoms. Recent physiological study has shown how closely the intestine and the liver are associated in health and in disease. When the liver is implicated in indigestion the symptoms which follow are due either to a deficiency of the secretion of bile, and the resultant disturbance of digestion in the intestine, or to a derangement in the transformation in the liver of the products of albuminoid digestion. When the disorganization of the peptones is imperfectly performed in the liver, instead of urea there is a production of lithates and lithic acid, constituting the condition called lithæmia. The lithates pass into the urine and are deposited. The occurrence of this urinary sediment after excesses and imprudences in diet is well known. The continuance of lithæmia leads to the development of symptoms more or less characteristic. These are a loss of appetite and coated tongue, flatulence, oppression after eating, and constipation. The nervous system is soon disturbed, and often to a marked extent. Vertigo, headache, disturbances of the special senses, sleeplessness at night, drowsiness during the day, annoy the patient and induce extreme hypochondria. He is worried, moreover, with numbness and tingling in one or both arms or in the [p. 630] legs, and hence spring fears of paralysis. The heart is disturbed in action, and is irregular and feeble. Emaciation in previously corpulent persons is not unfrequent.
COURSE, TERMINATION, AND SEQUELÆ.—Acute dyspepsia in the bowel lasts from a few hours to a day or two, and ends in leaving the patient as well as before. A diarrhoea of indefinite duration may follow.
Chronic intestinal indigestion in infants and young children often continues until the diet is changed to one suited to the powers of digestion. In adults interference with so important a function cannot but have the most serious results. While the progress is slow, lasting many years, there is a steady march from bad to worse.
The character and conduct are so altered by the disease that a man may be said to be just what his digestion makes him. Amiability under the daily goad of intestinal dyspepsia is an impossibility. The irreconcilables, the men out of joint with the world, are living witnesses of the antagonism and disaffection within their intestines. The deterioration in health paves the way for many diseases, and there is hardly an organ in the body which may not ultimately become the seat of organic change.
In the young, phthisis is frequently the ultimate result of the malassimilation and malnutrition; in men beyond middle life degenerative changes in the intestine, liver, and kidneys close the series of morbid changes which began in the intestine. Thomas N. Reynolds attributes bronchitis and phthisis in part to the local influence of septic matter carried by the portal and lacteal vessels to the lungs in cases of intestinal dyspepsia, with constipation and septic fermentation of the ingesta.15
15 Paper read before section of Practical Medicine at meeting of Am. Med. Assoc. in 1883.
In many cases business and professions are abandoned, and men become, under the influence of despair and complete absorption in their symptoms, intellectual and moral wrecks, burdens to themselves and to all around them. In this stage the primary cause, the dyspepsia, is lost in the exaggerated prominence of the nervous symptoms.
DIAGNOSIS.—The acute variety is known by the seat of the abdominal symptoms, the pain, distension, and movement of gas not being in the stomach, but in the intestines. The pain is like colic; the abdomen is sensitive to the touch; tympanites is general and may be very great. If vomiting occurs, the symptoms continue after the stomach is empty. Diarrhoea may quickly come on, and is followed by relief. The fever may be quite high. There is no sleep, but restlessness, and in children delirium. They may also have convulsions.
In the chronic form the history of the case and the study of the causes are of great value in formulating an opinion. The persistent abuse of the pleasures of the table sooner or later develops intestinal indigestion. Inquiry into the mode of life, hours of eating, manner of eating, kinds of food taken, etc. gives important information. The teeth are defective, and mastication and insalivation are neglected. There is distress in the pit of the stomach or in the right hypochondrium, beginning about two hours after eating and lasting from four to six hours; intestinal distension with gas, either in the small intestine or colon, with borborygmi and constipation, is generally present. The nervous symptoms are characteristic: they are depression of spirits, irritability, sleeplessness, vertigo, and [p. 631] headache. The man is more completely altered mentally than in gastric dyspepsia. The urine contains lithates in excess; anæmia and emaciation progress rapidly. Seminal emissions and weight and heaviness about the loins are present.
The following symptoms distinguish gastric dyspepsia, and do not occur in intestinal indigestion unless the stomach is at the same time involved: pain or weight in the epigastrium immediately after eating, vomiting of unaltered food, of food in a state of acid fermentation, eructations of ill-tasting or bad-smelling gas or of acid fluid, water-brash, and heartburn. Loss of flesh may not take place to any extent even in very bad forms.
The diagnosis of differences in the forms of indigestion due to defects in the pancreatic, biliary, or intestinal secretions is not at present a matter of precise knowledge. A pancreatic indigestion would be followed, it might be supposed invariably, by fatty stools; but such is not the case, since degeneration of the pancreas and closure of the duct have occurred without fatty evacuations from the bowels.16 Moreover, ulceration of the duodenum is followed sometimes by fat in the stools. Still, if the symptoms of intestinal indigestion include rapid wasting and fatty diarrhoea, we may conclude that the pancreas is at fault. The fat varies in appearance and amount. It may be seen as oil-drops passed alone or with fecal matter, or as lumps of fat, pale yellow and tallow-like. Glycosuria17 bears some relation to pancreatic diseases, and therefore may be an aid in diagnosis.
16 Ewald, op. cit., p. 95; D. S. Haldane, "Cancer of Pancreas," Edin. Monthly Journ. of Med. Sci., xix. 1854, p. 77; J. S. Bartrum, "Scirrhus of Pancreas and Stomach," Assoc. Med. Journ., 1855, p. 564; DaCosta, "Primary Cancer of Pancreas," Proc. Path. Soc. Philada., 1857, vol. i., 1860, p. 8; S. W. Gross, "Primary Cancer of Head of Pancreas," ibid., vol. iii., 1871, p. 94.
17 Bright, "Cases and Observation connected with Diseases of the Pancreas," Med.-Chir. Trans., vol. xviii. p. 1.
A deficient excretion of bile is indicated by a whitish or yellowish coating of the tongue, with loss of appetite and bad taste in the mouth. The stools are scanty, dry, slate-colored or white, and offensive in smell. The urine contains lithates. The complexion is pale or muddy. The nervous system is much deranged. The patient is languid, often irritable and hypochondriacal. He complains of headache, and is dull and drowsy after eating. The heart's action is unsteady, intermittent, or frequent. It is impossible to recognize indigestion due solely to a deficiency of the intestinal juice or to feeble peristalsis, granting that such forms exist.
PROGNOSIS.—A fatal result does not follow directly from intestinal indigestion. Its complications and results are frequently the causes of death. Treated early and with decision, a cure can be expected. Everything depends upon the extent to which the patient submits to the strict directions of his physician; his whole life must be made subordinate to the plan of treatment.
When the general health has become profoundly altered there is less chance to do good. Discouraging symptoms are anæmia, debility, coexisting gastric dyspepsia, an inherited hypochondriacal tendency, or the strumous diathesis in children.
When the disease has so far progressed that the patient is unable to [p. 632] rouse himself to the point of wishing to be well, only the most severe measures directed to the control of an irresponsible person can save him from ruin. In organic disease of the pancreas, intestine, liver, or heart the result will depend upon the nature and curability of the lesion.
TREATMENT.—Acute intestinal indigestion due to the presence of undigested food and gas in the intestine is treated by relieving present distress and procuring a free movement from the bowels. A large enema or a quick cathartic followed by an opiate—hypodermic injection of morphia, paregoric, or other preparation—may give early relief. A strict diet, warm poultices over the abdomen, and an anodyne may be needed for several days after.
The integrity of intestinal digestion depends upon the normal performance of all the preceding stages of digestion. Perfect insalivation, mastication, and gastric digestion are necessary to a proper action of the intestinal juices. The first rule of treatment in the chronic form is to examine into the condition of the mouth and teeth—to insist upon a slow and thorough mastication of food, especially of starchy food. Mastication is under the control of the individual, and he refuses to exercise this salutary means of prevention and cure at his own risk. The habit of chewing on both sides should be cultivated. All habits which waste and weaken the saliva should be given up, as smoking, chewing, and needless expectoration. Where the teeth are imperfect they should be attended to; false teeth should replace absent ones. All means should be used for improving gastric digestion: complete solution of food here means easier work for the intestine, and sometimes the cure of intestinal indigestion by removal of its cause. The rules which more directly bear upon the subject of intestinal dyspepsia are these: All the causes which have acted to bring about the disease should be removed. A change from a hot climate to a cooler and dry one will sometimes have an immediate good effect. Especially is this the case if travel is combined with change of scene. The substitution of exercise for inertia, of fresh for confined air, and the abandoning of occupations and habits of dress which hinder the freedom of movement of the abdominal muscles are of the highest importance. The patient should be made to cultivate pleasure instead of work if his mind has been overtaxed in his profession or business. Relaxation of the strained energies is indispensable to recovery. This rule is as applicable to school-children as it is to the overworked adult, man or woman. The benefits of travel, with change of scene and air, cannot be overestimated. Pedestrian tours in the mountains for young men, a trip to Europe for men and women in middle life, will secure the best results. For men who work much with their brains nothing is more conducive to aiding intestinal digestion than manual labor in the garden or workshop as a recreation. Exercise on horseback is pleasurable and improves a sluggish abdominal circulation. Rowing is good for younger men if it is confined to the field of pleasure, and is not made a task. For very feeble persons, especially for women, massage serves the purpose of exercise. The Swedish movement cure expands the thorax and abdomen, hastens the circulation, and quickens all the functions of nutrition and secretion.
A course of treatment would be incomplete without suggestions as to bathing. Life at the seashore would be of little service without the daily plunge in the surf. Still salt-water bathing is better for children and [p. 633] delicate women. The reaction should be thorough to secure the best results. It is much to be regretted that hydrotherapy is not available and is not made use of more generally. A well-managed establishment where appropriate regimen and good and sufficient food could be combined with the renewal of the tissues by bathing would be of great advantage in all forms of indigestion. Nearly all of the benefit derived from the Hot Springs of Arkansas in chronic cachectic diseases follows upon the immediate improvement of the digestion and nutrition. The Warm and Hot Springs of Virginia have an equally good effect upon torpid abdominal functions. The Russian bath, the very hot bath, the cold plunge, the cold douche to the back or abdomen, and the cold pack to the abdomen, are means which may be employed at home for inducing a revolution ending in reform in the state of the digestive organs.
Irregularity in the hours of eating is of so much injury that rules must be given to enforce uniform habits. Instead of the light breakfast and heavy dinner, a good breakfast, a midday dinner, and a light tea are to be preferred. It is of much value to regulate the appetite according to the needs of the body and to avoid excess in everything. In this disease eating too little or starvation to a moderate degree gives that rest to the intestine which is necessary to its restoration to health.
The selection of the food should not be left to the patient; the dietary should be chosen for him with a view to lessening intestinal labor. In general terms, this should consist of a moderate amount of albuminoid food of the most digestible kind, and of farinaceous food and fats in an acceptable and digestible form. In other words, as the intestine digests proteids, starch, and fats, no exclusive diet can be devised which will secure a perfect result. In each case the examination of the stools and experience with different articles of diet must be made the means for determining upon a suitable regimen.
The exclusive milk diet is the best starting-point in feeding a patient suffering from acute or chronic indigestion. In addition to the fact that milk has all the elements of a perfect food, it contains sugar and fat in the most favorable condition for absorption; the casein of milk alone requires transformation into peptone. The pancreatic juice has the greatest activity in its effect upon milk, as is easily demonstrated by the artificial digestion of milk by pancreatic extract. In milk, therefore, we find a most easily digestible and most highly nutritious food for such cases. Instead of milk with cream, skimmed milk will be found sometimes to serve better the purpose of an exclusive diet, because it has less fat and because larger quantities can be taken without distaste or a sense of repletion. Koumiss may be added to the milk diet; it is digestible, palatable, and nutritious.
The peculiar and very active diastatic ferment of pancreatic juice converts starch into sugar very readily. Farinaceous articles of diet can be added to milk with advantage. Digestion takes place more slowly and more thoroughly in consequence, and an additional article of nutriment is obtained. Thus, milk can be diluted with a thick gruel of barley or oatmeal, or some of the best of the various artificial foods can be stirred in. To the milk diet may be added animal broths or soups prepared with vegetables, animal jellies, or some of the ready-prepared beef-essences. They may not in themselves be highly nutritious, but they contain at least [p. 634]the salts of meat, and act as stimulants to the appetite and to the secreting glands.
Such a rigid diet cannot be kept up for a very long time without change; the appetite craves variety. Therefore solid albuminoid food in small quantity may be added to milk and farinaceous diet. Sweetbread boiled in milk, without dressing of any kind, is well suited for a beginning of animal diet. Oysters for some palates make an agreeable variety without putting much strain upon the digestive powers. They should be eaten uncooked, as cooking in any way renders them less digestible, and for greater precaution the hard part, or the adductor muscle which serves to keep the two shells together, should be removed. Fish boiled or plainly cooked and eaten without sauce is very easily digested. White-fleshed fish which has but little fat incorporated with the muscle-fibre is to be preferred. The patient may have eggs uncooked or slightly boiled, but one to two daily will be as much as he can well digest. The meat of poultry and game, especially that from the wings and breast, may be given even in a very feeble state of the digestive organs. When a more solid or satisfying diet is craved the patient may have beef or mutton cooked rare. Tripe and rabbit are suitable to some cases.
Bread, one day old and made light and porous, need not be denied the patient. Toast disagrees with some. To many, well-made biscuits or crackers are agreeable.
Vegetables should be given in small quantities, as the intestine is almost solely the seat of their digestion, and excess will tax too much a function which should be allowed as much rest as possible. The green vegetables contain less starch, and are therefore to be preferred. Lettuce, cabbage, kale, spinach, and celery come under this class, but even these are to be given to patients under treatment in moderation, with the intention of pleasing the palate rather than for purposes of nutrition. Macaroni and rice are easily digested.
Fruit contains very little nitrogenous matter and much water, and therefore has but little nutritive value, but it may be given to relieve the tedium of a restricted diet of milk or broths. Grapes, oranges, figs, strawberries, blackberries, raspberries, and peaches are the most digestible. But fruit should never be given as food. Fruit-juices, especially if acid and fresh, are unobjectionable. Coffee should not be allowed; its effect upon the nervous system is sufficient objection to its use. Tea can be given diluted largely with milk; cocoa, racahout, and broma are nutrient and make pleasant drinks. Sugar need not be excluded if used sparingly, and butter and oil in moderation may be permitted.
If the stomach is not disturbed thereby, wine may be taken with food to excite appetite. But except in the case of those who have always taken it, and cannot do without it, it is better to dispense with alcohol altogether. A red wine well diluted with water is a pleasant addition to the meal. Old wine is to be preferred to new, as being softer and less alcoholic. Good pure American wine from California or Virginia will answer the purpose when reliable French wine cannot be secured.
The value of mineral waters in the treatment of indigestion is great, but without proper dietetic regimen they can accomplish but little. The good results following a visit to Saratoga, Bedford, or other watering-place are due to other causes than the waters. In combination, however, [p. 635]with the advantages of change of scene, air, good hours, and a simple diet the mineral waters aid in bringing about a cure. They are especially useful in men who drink too little water at home, in gouty and plethoric subjects, and in states of acid stomach digestion and chronic constipation. The alkaline and saline waters are the best, the former containing a notable proportion of the carbonate or bicarbonate of sodium, potassium, or lithium—the latter having neutral salts in considerable quantity.
The articles of food to be avoided are pastry, cheese, much butter or fat, meat richly dressed or over-cooked, pork, veal, lobsters, crabs, vegetable matter in excess, very cold or very hot fluids or solids.
All of the methods so far described are designed to accelerate the circulation in the abdominal organs and in the tissues generally, to quicken the secretory and nutritive processes, and to give to the intestinal secretions the foods which they can most readily digest. In the event of such means failing to accomplish the desired end, is there any direct stimulus which can be brought to bear on the intestinal glands concerned in digestion? The pancreas being the most active and most important of these, it would be desirable to have some agent which could excite its gland-structure to greater activity. Sulphuric ether has been found to have this effect; it may be given before meals. The salivary secretion begins pancreatic digestion (the digestion of starch), and therefore its outflow should be stimulated at the same time; but thorough mastication does this usually without need of further aid.
When all plans fail to secure a thorough digestion in the intestine, and unaltered food and fat are passed, while the patient grows thinner and feebler daily, artificially-digested food may be given. The intestine is thus relieved of labor, and time is given for a restoration of activity by rest and an improved tone of all the tissues and organs. Rice, bread, baked flour, potatoes, or barley may be given in combination with malt extract, which converts starch into grape-sugar and dextrin.
As pancreatic juice acts both upon proteids and starch, an extract of the pancreas has a more general application than an extract of the stomach—pepsin. Roberts of Manchester has given full directions for the method of digesting food by pancreatic extract. Beef, milk, and the farinacea may be digested, the albuminoid substances being changed into peptones, the starchy matters into dextrin and sugar, capable of being absorbed readily with but little or no further alteration in the digestive tract.18 Pancreatic emulsion (Dobell) is another method of giving fat emulsified.
18 Fresh pancreatic extract is made by cutting into small pieces the pancreas of the pig (which is the best), the ox, or sheep. The pancreas of the calf yields an extract which acts only on albuminous substances, but not on starchy matters. The divided pieces of the pancreas, well freed from fat, are put in a well-corked, wide-mouthed bottle with four times their weight of dilute alcohol (one part of rectified spirit to three parts of water). The mixture should be agitated once daily: at the end of a week the mixture is filtered through paper until it is clear. A well-made liquid extract of pancreas is made and sold by Metcalfe of Boston, and a solid extract by Fairchild Bros. & Foster of New York. No doubt improvements will be made in the processes of manufacture of these extracts, and better results will in time be obtained from their use.
A less successful way of gaining the same object is by administering the pancreatic extract internally. The difficulty lies in conveying the extract (the ferment of which is destroyed by the acid gastric juice) through the stomach in safety. This chemical danger is thought to be obviated by giving the extract one to two hours after eating with a [p. 636] protecting guard of an alkali, the bicarbonate of sodium; but the mechanical difficulty of securing direct transit through the stomach to the intestine early enough and in quantity enough to digest the duodenal contents is as great as the chemical obstacle. It is very doubtful whether this method of use can be of any real service.
In those cases in which the form of indigestion is due to, or is associated with, a deficient hepatic secretion—a condition indicated by offensive and light-colored stools and other symptoms—it is advisable to stimulate the liver to increased secretion. It is probable that the same remedies which excite a flow of bile do at the same time stimulate the pancreas. The best of these are euonymin, sanguinarin, iridin, ipecacuanha, colocynth, jalap, podophyllin, sodium sulphate, and potassium sulphate. Sodium benzoate, ammonium benzoate, and the salicylate of sodium are also powerful hepatic stimulants. As one of the purposes of the bile is to create the alkaline medium necessary for pancreatic digestion, the administration of an alkaline19 solution in full doses, as in the form of mineral water, when gastric digestion is finished, may make amends for the lack of bile. A combination of an antiseptic and the alkali may to some extent supply the deficiency still better, as the bile is the antiseptic of the intestinal canal.
19 The waters of Ems, Vichy (Grande Ville or Hôpital Springs), Vals, or Bilin may be used for this purpose.
Atony of the intestinal wall leads to flatulence, colics, and constipation, and would be a cause of indigestion if none other existed. It is to be treated by the general rules already given, by electrical stimulation of the abdominal muscles with the faradic current, or by the effort to stimulate the intestinal wall more effectively with the galvanic current. Strychnia in small doses should be given for some time. In women of relaxed muscular fibre with enlarged abdomens an elastic belt may be worn with advantage.
After the special aids to the parts concerned in digestion, tonics are called for to combat the general want of tone and anæmia. The saccharated iron, the carbonate, potassio-tartrate, lactate, pyrophosphate, or the ferrum redactum may be given. The syrup of the iodide of iron is the best form for children. The bitter tonics are inadvisable except for loss of appetite in cases where the stomach is not disordered. Quinia is available in a large number of cases in which malarial influence plays a part. Strychnia is a good general tonic, and may be prescribed combined with mineral acids, particularly with the dilute hydrochloric acid.
The special symptoms which call for treatment are flatulence, abdominal pains, and constipation. All the remedies already described are directed toward their relief. But sometimes they appear in so exaggerated a form as to need immediate attention. The many remedies for colic and tympanitic distension which have the property of relieving spasm and absorbing gas find application in these conditions. Constipation is not to be treated by laxatives if it can be avoided. But the bitter waters, Friedrichshall, Pullna, Hunyadi Jânos, and Rakoczy, by exciting bile outflow, are sometimes of undoubted curative value.
The form of dyspepsia called strumous, as it occurs in children of anæmic appearance with dry skin covered with minute scales, and with bad breath and light ill-smelling stools, demands a very thorough and [p. 637] persevering treatment. The advantages of climate must be sought—seashore in summer with bathing, dry and moderately warm air in winter. Outdoor life in the sun, with active exercise, is to be had at the expense of education within-doors. Study is not good for children of this class except when health is made paramount to it. Cod-liver oil, either pure, in phosphatic emulsion, or in the pancreatic emulsion, is a necessity. Malt extract with the hypophosphites is beneficial. The food must be carefully selected, and the child educated to a varied diet, including fats. The skin should be anointed daily with cocoanut oil, olive, cottonseed oil, or cod-liver oil.
SYNONYMS.—Costiveness, Fecal retention, Fecal accumulation, Alvine obstruction, Obstipation. Ger. Koprostase, Stuhlverstopfung, Hartleibigkeit, Kothstanung. Fr. Constipation, Paresse du ventre, Échauffement. It. Constipazione. Older synonyms: Constipatio vel obstipatio alvi; Alvus tarda, dura, adstricta; Tarda alvi dejectio; Obstipatio alvarina; Stypsis; Coprostasis (Good).
NATURE AND DEFINITION.—The act of defecation is almost wholly due to the working of an involuntary mechanism which may be set in play by the will, and is in part dominated by it, but which is frequently independent and uncontrolled by volition. Deep inspiration, closure of the glottis, downward pressure of the diaphragm, and contraction of the abdominal muscles are accessory, but not essential, to the expulsion of feces from the rectum. In certain persons, and occasionally in all persons, especially in diseases where the fecal mass is in a semi-fluid or fluid form, the strongest effort of the will cannot resist the expulsive contractions of the rectal muscle. The sphincter is kept in a state of tonic contraction by a nervous centre situated in the lumbar portion of the spinal cord. The fecal mass, supported by the bladder and the rectum, does not at first touch the sphincter; the rectum is usually empty; but when the column has been well driven into the rectum peristaltic action is excited in the rectal walls and the sphincter is firmly pressed upon. The lumbar sphincter centre is now inhibited, and the ring of muscle opens, the accessory and voluntary muscles contract, and the expulsive act is completed. In the well-ordered and healthy individual the rectal walls and the sphincter do not receive the maximum of irritation from pressure of the advancing column but once in twenty-four hours. The habit of having one movement in each day is, it may be believed, in accordance with the natural and physiological demand, although both the number and the hours of evacuating are fixed to a great extent by education. The habit once established, the mechanism of expulsion recurs at the same hour and entirely without the direction of the will. If the desire be resisted, it will be most apt not to return until the same hour on the next day.
Defecation depends for its normal character upon the healthy functioning of the organism, but especially upon the normal processes of digestion. The character of the rectal contents as to composition and consistence, and the time of the arrival of the mass at the sphincter, are [p. 639] regulated by the taking of food at stated hours and by its normal digestion and absorption. Unaltered or partly-changed remains of the ingesta pass down the bowel, mingling with the secretion from the intestinal glands and with mucus and epithelium. As this mass passes into and through the colon, being propelled by regular peristaltic waves, it acquires odor from the development of a substance which is a final product of the putrefaction of albumen.1 Gradually the more fluid elements are absorbed, and in the descending colon a less fluid or semi-solid consistence of the feces is reached. A healthy digestion and assimilation, with active and regular contractile movements of the muscular walls of the small and large intestines, are essential to normal defecation.
1 Ewald, Lectures on Digestion, New York, 1881, p. 106.
Constipation may be defined to be that condition in which there is a prolonged retention of the feces or in which they are habitually expelled with difficulty or in insufficient quantity.2 While there are individual peculiarities due to habit or nature, the custom with most persons of having one movement in the twenty-four hours would cause any longer retention of the rectal contents to be considered constipation. The limits between health and disease are not well defined, and a failure to evacuate the bowels for several days need not be considered pathological nor require medical interference. In persons otherwise in good health such an occurrence due to neglect, change of habit or diet, as in travelling, would cause no interruption to health or comfort. Nature brings relief sooner or later and re-establishes order and regularity. In many cases constipation is a primary disease and the cause of many secondary disturbances, but it is often the effect or the symptom of various acute and chronic diseases. It may be acute or chronic.
2 Cases of constipation due to mechanical obstruction from changes in the wall of the intestine or to exterior pressure will not be considered in this article.
In long-continued constipation the intestinal contents are so retarded in their progression along the canal that they undergo a too early and too complete absorption of their fluid portion. In time there are an accumulation and impaction of dry fecal masses in the rectum, sigmoid flexure, descending transverse colon, or cæcum. An obstacle is thus created which may ultimately close the tube entirely and cause intestinal obstruction.
ETIOLOGY.—1. Constipation occurs most frequently in advanced life. It is the effect of loss of peristaltic force and of a diminution of sensibility in the lower bowel, and is associated with general functional inactivity and with muscular degeneration and obesity. Infants are more subject to constipation than children of one year and over. In many instances this is due to artificial feeding with cow's milk, condensed milk, and the patent foods so largely used, or with any diet unsuited to the digestive organs. Imperfect digestion of casein or other food, the filling of the bowel with a dry mass difficult to propel, and the consequent catarrhal state of the mucous membrane, are causes of both constipation and diarrhoea. Feeble, delicate children with imperfect muscular development, and children born rachitic, scrofulous, or syphilitic, are generally constipated.
2. Women are prone to constipation much more than men. False modesty, which imposes restraint upon young girls, and their ignorance [p. 640]of the necessity of regularity, their habits of indoor life, and avoidance of exercise, are largely the causes of this. But the anatomical structure and physiological life of the woman offer another explanation. At every menstrual period the uterus enlarges and exercises a greater compression upon the rectum. A tender and enlarged ovary (and at the menstrual epoch the ovary is always tender and enlarged) exercises an inhibiting action upon the muscles which bring the feces in contact with it in their downward passage. In the married woman recurring pregnancies lead to the habit of constipation from the long-continued pressure upon the colon, sigmoid flexure, and rectum, from the extreme stretching of the abdominal muscles, and from the paralyzing effect of compression during labor. The relaxed condition of the pelvic and abdominal organs after labor offers no resistance to the distension of the rectum and sigmoid flexure. The cessation of the catamenia is accompanied with constipation, nervousness, and a feeling of ill-defined apprehension when the bowels are moved, or abdominal pains deter many persons, chiefly women, from habits of regularity. All uterine and ovarian derangements by mechanical or reflex means bring about the same result. Chlorosis and anæmia in girls are almost invariably associated with constipation.
3. Hereditary influence shows itself very markedly in the tendency to constipation which is seen in many members of the same family. This is probably more often apparent than real, and is the result of neglect of the proper attention to the wants of children and of the perpetuation of vicious habits of taking purgatives.
4. The habits of life and the occupation of the individual have much to do with the causation of constipation. Those who lead active outdoor lives are generally regular in their daily movements, but persons of sedentary pursuits or who work in constrained attitudes—lawyers, clerks, tailors, shoemakers, and seamstresses—are predisposed to constipation. Intellectual work, not only from the muscular inactivity which it entails, but from the diversion of energy to the nerve-centres, develops the constipated habit as well as indigestion. Men who are overworked in business, employés in banks, government offices, shops, etc., bring on the habit from the hurry incident to their occupations. Luxurious and enervating habits of life, over-eating and sloth, with the over-indulgence in alcohol and tobacco, have the same effect. All the influences which deteriorate health, such as bad ventilation and over-heating of rooms, foul air, want of cleanliness of the person, indigestible food, imperfect mastication, tight-lacing in women, compression of the abdominal organs in men, can be said to share in bringing it about. Servants, especially women, are constipated more frequently than their masters. This is due to ignorance and neglect, and sometimes to excessive tea-drinking and irregularity in eating.
5. Neglect to establish or continue a habit of daily regularity in defecation leads to the accumulation in the rectum of masses of feces. Resisting the desire to empty the bowel interrupts the necessary reflex acts, and finally the muscular excitability and response to the presence of feces are entirely wanting. The continued contact of fecal matter with the mucous membrane wears out its susceptibility; the over-distension of the rectum enfeebles the power of its muscular wall, as is the case when all hollow muscular organs—stomach, heart, bladder—are overstretched. Thus a [p. 641]neglect to answer the demand for a daily movement and the failure to completely empty the rectum will gradually develop constipation in a person who has before been perfectly well regulated. In childhood failure to teach and to insist upon good habits is the cause of much of the trouble of after-life.
6. Acute and chronic diseases of the brain and spinal cord bring about constipation. Meningitis, encephalitis, and myelitis, senile dementia and softening, have it as a symptom at some time or other. In encephalitis and myelitis there is an interruption of motor nerve-currents. In meningitis and tetanus the muscular walls of the bowel and the abdominal muscles are in a state of tonic contraction.
7. The use of aperients is an important agent in developing the constipated habit by over-stimulating and wearing out muscular activity. The idea that a daily movement is a necessity, and that an occasional purgative is useful in relieving the system of morbid matter which would otherwise induce disease, is the chief source of this hurtful custom. The traditional meaning attached to the term biliousness implied the resort to cathartics for its relief, and it is much to be regretted that with our more advanced knowledge the effort should be made to revive the use of this term, which was wellnigh abandoned. More ignorance and erroneous treatment has hung upon the theory of biliousness than upon any other doctrine of medicine within the past thirty years: it is well for physicians to condemn it and to resist its reintroduction into scientific phraseology.3 If the term bilious as applied to diseases were abandoned, much good would come of it. The general use of purgative mineral waters has added to this evil. Among the better classes these waters play the same part as the liver regulators and vegetable pills do among laborers and servant-maids. Both gratify the innate love for self-medication by a resort to cathartics for the slightest ailment. At first the injurious effects are not apparent, but in time the reflex function is not brought into activity except by artificial aids. The intestinal and rectal muscles must be whipped into action, their normal contractile power being lost.
3 For an excellent and dispassionate statement of the reasons for abandoning the theory of the influences of bile as a cause of disease, and the use of the term bilious, consult The Bile, Jaundice, and Bilious Diseases, by J. Wickham Legg, chaps. viii. and xxix. The Hippocratic and Galenical belief has been transmitted with but little alteration through Stoll, Andrie, Abernethy, and Copland to the writers of to-day on biliousness.
8. Certain vegetable and mineral substances taken either intentionally or by accident constipate the bowels. Chief among these stand opium and its preparations. All opium-eaters are constipated. Lead which is accidentally taken into the system by workers in metals, painters, etc. invariably produces obstinate constipation. The use of tobacco in excess has the effect of deranging digestion and causing constipation in many persons, but this result is occasional only.
9. Chronic diseases of the lungs and heart, by enfeebling the muscular movements which take part in defecation, as well as by the general feebleness and the chronic intestinal catarrh and indigestion which they create, are causes of constipation. Chronic diseases of the liver, especially cirrhosis, are also causes. Constipation accompanies obesity, for in very fat persons the abdominal walls have but little power of contraction; the [p. 642] muscle-layer is thin and flaccid. There is also in such persons in advanced life an accumulation of fat in the mesentery and around the colon. The muscle of the bowel is in a state of fatty degeneration, and atony and dilatation of the gut follow.
10. Painful affections about the rectum and anus deter persons from yielding to the desire for defecation. Fissure of the anus is the principal one of these, but fistula, hemorrhoids, and local eczema have a similar influence. A simple rigidity or spasmodic stricture of the anal sphincter creates constipation.4
4 Kunemann, De la Constipation compliqués de Contraction du Sphincter anal, et de son Traitement par la Dilatation de l'Anus, Paris, 1851.
11. Constipation is a symptom in chronic cachexiæ and wasting diseases, in the convalescence of acute exhausting illness, as typhoid fever and pneumonia, or in persons bedridden from any cause. Defective nutrition and degeneration of the muscle-fibre of the intestine explain these cases. In some of them, with improved nutrition, regeneration takes place with a return of contractility.
12. Disorders of the digestive system have constipation as a consequence and a symptom. The reflex sympathy between the movements of the stomach and of the intestines brings this about in gastric diseases.5 It occurs in gastric cancer and ulcer, in acute and chronic gastritis, in dilatation of the stomach, and in pyloric stricture. The small amount of ingesta entering the duodenum in these diseases diminishes the bulk of fecal matter. In acute intestinal catarrh diarrhoea is the rule, but the bowels may be constipated in intense inflammation and ulceration of the mucous membrane, as is often the case in typhoid fever. In chronic intestinal catarrh constipation is more common in the mild forms than diarrhoea. The thickening and irritation of the mucous membrane lead to a diminution of reflex excitability and loss of elasticity and contractility in the muscular coat. Hence, except in cases where the inflammation is low down or where ulcers have formed, constipation is a more frequent symptom than diarrhoea. The alteration in the quantity and character of the intestinal secretions in chronic catarrh is stated to be an important element. This is to some extent true. Mucus, which is the chief product of this condition, leads to indigestion and fermentation of the intestinal contents and to increased irritation of the mucous membrane. The evolved gas distends the bowel and weakens its contractile power. The fecal mass when it reaches the rectum has an excess of mucus within it or around it which makes its expulsion more difficult. But the diminution or absence of bile does not constipate. In simple jaundice diarrhoea is not uncommon, and an excess of bile does not of necessity cause diarrhoea.6
5 Leube, in Ziemssen's Cyclopædia, vol. vii. p. 211.
6 Legg, op. cit., p. 271.
The effects of the modifications of the pancreatic secretion are not well known. Pancreatitis is attended by constipation. Fatty diarrhoea is believed to follow occlusion of the pancreatic duct by pancreatic calculi and chronic catarrh of the duct. Peristalsis is lost in peritonitis from the muscular coat being infiltrated with serum and paralyzed, but tuberculous peritonitis is frequently accompanied by diarrhoea.
13. Loss of fluids by abundant perspiration, by diuresis, diabetes and lactation, increases the dryness of the bowel contents and hinders free [p. 643] evacuations. This is observed as a result of the arrival in a tropical climate and in very hot weather in any climate. The profuse sweats accompanying phthisis, acute rheumatism, intermittent fever, and unusual exercise cause constipation. Another explanation which applies to this has been offered by Good and Eberle, who ascribe constipation to the excessive action of the absorbents in the small intestine, by which the fluid portion is too rapidly and too thoroughly removed.7 Exercise by promoting activity of the functions in general may induce constipation in this way. In spermatorrhoea the stools are infrequent. An insufficient amount of water taken with food is another cause.
7 Dick, Braithwaite's Retrospect, xvii. p. 152.
14. Food which has but little waste to be got rid of—as milk or beef—leaves a small residuum to be propelled along the intestine, and therefore in one sense is constipating. Insufficient food acts in the same way. An indigestible diet in excess, especially vegetable food, a large part of which is insoluble, constipates by filling the bowel with matter which cannot be got rid of, and chronic catarrh results. The stones and seeds of fruits, as cherry- and plum-stones, raspberry- and currant-seeds, husks of corn and oats, produce acute or chronic constipation with serious symptoms. Intestinal worms (generally lumbricoids) when in large numbers cause obstruction of the bowel;8 and various foreign substances taken by caprice or to take the place of food have produced the same result: among these stick cinnamon,9 sawdust,10 and clay (among the clay-eaters of the South) have been mentioned. Magnesia, insoluble pills, and other medicines sometimes form concretions in the bowel. Enteroliths and accidental concretions form in the intestinal canal and are sources of obstruction. Any foreign body is a nucleus around which concentric layers of phosphate of lime are deposited, and thus a hard calculus is formed. Gall-stones may pass into the canal and there accumulate in such numbers as to interfere with the passage of the fecal matter.
8 Copland, Medical Repository, vol. xvii. p. 243.
9 Ware, Boston Med. and Surgical Journal, 1858, vol. lviii. p. 501.
10 Bonney, ibid., 1859, vol. lix. p. 39.
PATHOLOGICAL ANATOMY.—In cases where constipation has lasted many years no alteration of the parts involved may be found. When lesions do occur the pathological anatomy includes changes in the position,11 calibre, and in the walls and contents of the intestines. The most common displacement is that of the transverse colon, which is depressed in its centre; the acute angle of the descending part may reach as far down as the hypogastrium. The cæcum sometimes lies in the centre of the abdomen. Dislocations of the intestines are congenital, due to anomalies of intra-uterine development, in which case they become causes of death in newly-born children from obstruction, or if insufficient to cause death they establish habitual and incurable constipation; or constipation may bring about displacement by the greater weight of a portion of the bowel constantly loaded with fecal matter.
11 Vötsch, Koprostase, Erlangen, 1874.
The sigmoid flexure is usually the seat of the greatest dilatation; its expansion may be a cause or a consequence of constipation.12 It may reach a maximum of distension when it fills the entire abdominal cavity, compressing all the abdominal organs and pushing the stomach, liver, [p. 644] and intestines into the thorax. In a case of this kind the circumference of the dilated part was twenty-seven inches.13 The descending colon may be distended with the sigmoid flexure, or the whole colon may be dilated from the upper part of the rectum to the cæcum;14 the same thing happens rarely in the small intestine. In one case, in which there was an accumulation of feces in the sigmoid flexure, the large intestine presented itself as two immense cylinders lying side by side, extending from the epigastrium to the pelvis.15 Each was about five and a half inches in diameter, and together they filled the abdominal cavity. The circumference of the stretched colon varies from ten to thirty inches. Pouches forming little rounded tumors are seen on the outer surface of the colon; they are sometimes hernial protrusions of the mucous membrane through the muscular coat (Wilks and Moxon), or if large they are dilatations of the pouches of the colon.16
12 Trastour, "De la Dilatation passive de l'Iliaque, et de ses conséquences," Journal de Méd. de l'Ouest, 1878-79, tome xii. p. 165.
13 Dupleix, Le Progrès médicale, Paris, 1877, tome v. p. 953.
14 Peacock, "Fatal Constipation, with Excessive Dilatation of the Colon," Tr. Path. Soc. London, vol. xxiii. p. 104.
15 Lewitt, Chicago Med. Journ., vol. xxiv., 1867, p. 359.
16 Gay, "Sacculated Colon, Prolonged Constipation," Tr. Path. Soc. London, vol. v. p. 174.
The colon is sometimes much lengthened. But little weight can be attached to this anomaly, as there is a difference in the length of the colon in different nations and individuals, depending upon the character of the food, being longer in those who eat largely of vegetable food.17
17 Ziemssen's Cyclopædia, vol. vii. p. 606.
The mucous membrane is normal or hyperæmic, or is in various stages of chronic catarrh. Proctitis may exist with follicular ulcers; ulcers form in the cæcum, sigmoid flexure, and in the bends of the colon; perforations and peritonitis rarely occur. Chronic peritonitis has resulted from the stretching of the bowel from retained and hardened feces; adhesions may form which ultimately cause death by obstructing the canal. The walls of the intestines are in long-standing cases much thinned. There are many reasons to believe that fatty degeneration of the smooth muscular fibre takes place, in consequence of which it loses its contractile power and atrophies. This lesion is most common in advanced life, and accompanies fatty accumulation and degeneration elsewhere. Its results would be constipation, distension of the bowel with gas, and sometimes symptoms of intestinal obstruction.18 A thinned and dilated bowel may easily be lacerated under unusual stimulation, as from a purgative. In a case recently seen by the writer such an accident, rupture of the colon and death from peritonitis, occurred from the effects of an active purge taken to bring on abortion. Hypertrophy of the wall, especially of the muscular coat, coexists with dilatation, and is most common in the upper part of the rectum and sigmoid flexure. It is caused by overwork in expelling fecal accumulations. The walls never become as much thickened as in constipation from organic stricture.
18 Cases are recorded of death with symptoms of intestinal obstruction in which no lesion was found beyond a dilated colon; as, for example, in British Medical Journal, April, 1879, p. 621.
Collections of fecal matter may be found in any portion of the colon, but more frequently in the rectum, sigmoid flexure, descending or [p. 645] transverse colon, or cæcum. They lie within the intestinal tube, partly or wholly occluding it, or within lateral pouches, forming tumors which are sometimes quite large. In this last form there is no obstacle to the free passage of feces along the canal. Fecal accumulations occur as small round, oval, or irregularly-shaped lumps (scybalæ), and are often covered with layers of transparent semi-fluid mucus, puriform mucus, or mucus in filaments. The small concretions vary in density; they may be so hard as to resist the knife, and may be mistaken for gall-stones; larger masses, semi-solid or solid, are most commonly seen in the rectum and sigmoid flexure. Here the collection may reach an immense size. In one case fifteen quarts of semi-solid, greenish-colored fecal matter were removed at the autopsy.19 In two other cases the weight of the feces found in the bowel was thirteen and a half20 and twenty-six pounds21 respectively. The whole colon from the anus to the cæcum may be filled with such a mass, as in a case mentioned by Bristowe, where the colon "was completely full of semi-solid olive-green colored feces. The small intestines were also considerably distended, ... and were filled throughout with semi-fluid olive-green contents."22
19 Peacock, Tr. Path. Soc. London, vol. xxiii. p. 104.
20 Lamazurier, Archives générales, Paris, 1824, t. iv. p. 410.
21 Chelius, Heidelberg Med. Ann., 1838, vol. iv. p. 55.
22 Bristowe, "Diseases of Intestines and Peritoneum," Wood's Library, New York, 1879, p. 21.
The color of these collections is black, reddish, deep green, or yellow. In composition the scybalæ, concretions, and larger masses consist of fecal matter, with unaltered vegetable fibre; they may be composed partly of skins of grapes, cherry-stones, biliary calculi, hair, woody fibre, magnesia, or other foreign substances. Where fecal concretions long remain in the intestine they acquire a hardness like stone, and can with the microscope only be distinguished from mineral matter.23 Hemorrhoidal tumors, anal fissures, perirectal abscesses, fistulæ communicating externally or with the gut, are found in connection with constipation. Abscess of the iliac fossa has been observed in the same relationship.24
23 A remarkable case is recorded (Dictionnaire de Médecine, Paris, 1834, t. viii. p. 435) in which an ulcerating cancer of the fundus of the uterus had opened communication and formed adhesions with the small intestine, from whence the feces passed into the uterus and out through the vagina. The large intestine, totally occluded, contained petrified fecal matter.
24 Richet, "Abscess of Iliac Fossa," Revue de Thérapeutique médico-chirurgicale, 1876, p. 563.
SYMPTOMS.—In persons who have a daily movement an occasional interruption of two to four days may take place without local or general signs of inconvenience. It is often asserted by patients that one day's omission induces suffering, and recourse is immediately had to laxatives. This may be justified sometimes, but in the majority of cases no actual suffering follows a very rare and short constipation.25 If, however, symptoms do occur after a constipation of one to three days, there is a sense of fulness and heat about the rectum which is greater after stool; when the bowels are moved, it is with effort (provided that no enema or purgative has been taken), and the bulk of the expelled mass is much greater [p. 646]than usual, being moulded and hardened from its longer retention in the rectum. The margins of the anus are tender, and the unsatisfied feeling after stool is due to distension of the hemorrhoidal veins and oedema of the tissues around them—a condition which ends in painful or bleeding hemorrhoids. There are signs of impaired digestion, loss of appetite, a coated tongue, oppression after eating and flatulence, and distension of the abdomen. Headache is apt to be present, with flushing of the face and general discomfort or irritability of temper. These phenomena may all disappear within two or three days by a spontaneous stool or by the use of a purgative.
25 Some interesting remarks in connection with the idea that constipation is not necessarily hurtful, and is in some cases beneficial, may be found in a pamphlet by C. I. Harris, Is our Physiology of the Large Intestine correct, and is Constipation in certain cases as Injurious as is supposed? London, 1878.
Acute symptoms of a violent nature are sometimes developed in persons who have been constipated a long or short time, in consequence of attempts at purgation or from the accumulation of indigestible food. Violent paroxysmal pains in the abdomen and efforts at stool are soon followed by symptoms of intestinal obstruction and serious collapse. Quick relief follows a free movement from the bowels obtained by an enema, or if not so relieved the case may terminate fatally.
A frequent recurrence of fecal retention from the causes mentioned will in time develop the constipated habit. Distension of the rectum increases its capacity and destroys its sensibility and expulsive power. The colon above the point of stoppage is distended with gas and weakened. The bowels are rarely moved spontaneously, and finally are never emptied without artificial aid. The literature of medicine contains many extraordinary records of prolonged fecal retention, ranging from a few weeks to many months.26
26 Am. Journ. Med. Sci., Philada., 1846, p. 260 (three months and twenty-two days); Renaudin, Dict. des Sci. méd., t. vi. p. 257 (four months); Strong, Am. Journ. Med. Sci., Oct., 1874, p. 440 (eight months and sixteen days); Valentin, Bull. des Sci. méd., t. x. p. 74 (nine months); Staniland, London Med. Gaz., vol. xi. p. 245 (seven months); Dublin Hosp. Reports, vol. iv. p. 303 (eight months); Inman, Half-Yearly Abst. Med. Sci., vol. xxxi. p. 275 (two years); Devilliers, Journ. de Méd., 1756, t. iv. p. 257 (two years); J. Chalmers, Med. Gaz., London, 1843, vol. xxi. p. 20 (three years); Philada. Med. Museum, 1805, vol. i. p. 304 (fourteen years).
The evacuations in chronic constipation are harder and more dry than they should be; they are passed in masses of various sizes, and in color are brown, black, dark-green, or yellow. Sometimes a coating of mucus is on the outside, and sometimes streaks of blood, or there is an intimate admixture of mucus, giving a slimy, gelatinous appearance to the mass. Semi-digested food, as partly-altered milk, meat, or vegetable matter, is seen, and quite frequently there is an intercurrent diarrhoea which alternates with costiveness.
The local symptoms about the pelvis and anal opening and in the lower extremities come from the pressure of accumulations of feces. Thus, compression of the iliac veins delays circulation in the lower extremities; cold feet or oedema of the feet and ankles and varicose veins follow. If the pressure is on the ilio-hypogastric and ilio-inguinal nerves, there are neuralgic pains in the groin and over the crest of the ilium. The sciatic and crural nerves may be the seats of pain. Varicocele is the effect of weight upon the spermatic veins. Erections and seminal emissions in men follow pressure on the pubic veins and prostatic portion of the urethra. Retention of urine also may come from the latter cause. If the kidneys and ureters are compressed by fecal tumors in the descending or transverse [p. 647] colon, nephritic pain, albuminuria, or retraction of the testicle, with delay in the escape of urine, may happen. Icterus and its consequences are owing to pressure on the common bile-duct; the liver and other organs may be displaced and the aortic circulation obstructed by fecal compression. In women the retention of fecal matter in the rectum is the source of special symptoms; it contributes largely to the occurrence of cervical anti-flexion in the soft, pliable, growing uterus of girlhood (Thomas), and unites with retroversion in women who have borne children to produce great suffering.
An unnatural state of the digestive system, as a cause or result, is the invariable accompaniment of chronic constipation. The appetite is wanting; the tongue is coated, and may be pale, soft, and indented by the teeth. Distress follows eating; the abdomen is distended with gas and is hard; all the evidences of gastric or intestinal indigestion may be found. Nutrition is imperfect, as is shown in loss of flesh and in the signs of functional disorder to be next described.
The nervous system is soon deranged; sleep is unrefreshing, restless, and disturbed by dreams. There are headache and mental and physical indolence. The patient speaks of being giddy, faint, and nervous. Disturbance of vision (muscæ volitantes), of hearing (tinnitus aurium), and alarming attacks of dyspnoea and cardialgia may occur.27 Heart-palpitations and profuse perspirations are the effect of excitement or effort of any kind. Chilliness or violent chills can be traced to this cause also. In women hysteria, disturbed menses, anæmia, and chlorosis accompany constipation.
27 C. C. Melhose, Hufeland's Journal, 1841, xcii., Stuch iv. p. 105.
Nervous symptoms are very common in the young, and it is doubtful whether they are consequences of constipation or whether they form a part of a general state of malnutrition and anæmia. Hypochondria is undoubtedly closely connected with the constipated habit, and the failure to secure a daily movement becomes the subject of unceasing thought and anxiety. Hallucinations and sudden loss of consciousness, aphasia,28 and delirium, have been found to depend upon fecal accumulation.29 The absorption of fluids and gases from too-long-retained and decomposing feces may explain such cases. The nerve-centres soon show the effect of the supply of altered or contaminated blood.30 It is probable that the marked nervous symptoms are more due to this cause than to reflex influences.
28 Mattei, "Aphasia cured by relieving Constipation," Bull. de l'Acad. de Méd., Paris, t. xxx., 1864-65, p. 870.
29 Pulitzer, Wien. med. Presse, 1866, x. p. 439. Case.—A man æt. 42, with sleeplessness, hypochondriasis, hallucinations, and one attack of sudden loss of consciousness; symptoms relieved by removing a large quantity of fetid fecal matter from bowels. Also Dujardin-Beaumetz, serious nervous symptoms due to constipation (Bullétin de Thérap., Paris, t. 89, 1875, p. 179).
30 Bell, Lancet, London, 1880, i. 243-283.
A coincidence exists between dislocation of the colon and various states of mental disturbance. Ten cases of suicide were seen by Vötsch in which there were displacements of the colon. Laudenberger of Stuttgart found that in ninety-four autopsies of insane persons there were anomalies of position of the transverse colon in one-seventh of the number (Vötsch).
Fever is not infrequently due to constipation. During the course of typhoid and other fevers an unusual elevation of temperature is often [p. 648] traced to a neglect to have the bowels emptied. But very high temperature sometimes depends upon constipation alone, and is at once reduced by removing the cause. This may occur in the course of chronic diseases or in health, especially in children.31 The temperature rises from normal to 104° F., and even higher, and immediately drops to normal when the bowels are moved. When a sudden rise in temperature comes with acute constipation, the influence must be a reflected one from the mucous surface to the heat-centre.
31 F. Barnes, "On the Pyrexial Effects of Constipation," Med. Press and Circular, 1879, N. S. xxviii. p. 477. Also, C. H. Jones, Lancet, London, 1879, ii. p. 229—a case in which there was a temperature of 104.1°, pulse 180, and delirium due to scybalæ in bowel; Cabot and Warren, "High Temperature from Constipation," Boston Med. and Surg. Journ., 1880, ciii. p. 1571.
The urine is dark-colored and scanty, loaded often with urates, or it may be limpid and of a very low specific gravity. The escape from the bladder and through the ureters may be obstructed by compression, as already mentioned. Suppression of urine has occurred, and been relieved by removing large fecal collections.32 In women catamenial irregularity and dysuria are generally associated with constipation. Disturbances in pelvic circulation and local pressure of a distended rectum explain these conditions.
32 Barnwell, Cincin. Med. News, 1875, vol. viii. p. 353—female æt. 45. Had no movement for five days; suffered with tympanites; severe pain in right iliac region, with persistent vomiting; tumor in same region; complete suppression of urine. At the end fifth day passed large quantity of apple-peelings and fecal matter. Return of flow of urine; passed two gallons in ten hours.
The skin is often parched, sallow, and is sometimes covered with eruptions, as acne, psoriasis, eczema, erythema, or prurigo. Injuries, wounds, and cracks of the skin heal slowly.
RESULTS AND COMPLICATIONS.—The lateral pouches of the colon, most commonly at the sigmoid flexure, become distended, and deeper pouches are formed, where fecal matter is retained.33 This need not interfere with the regular daily movements. Fecal tumors are thus formed, the nature of which is often not recognized. The colon may be distended so as to fill a large part of the abdomen. The pressure of hardened feces brings about ulceration of the mucous membrane, perforation and extravasation of the contents into the abdominal cavity, with fatal peritonitis. Abscesses in the perirectal tissues, with fistulæ,34 anal fissures, hemorrhoids, prolapse of the rectum, varices of the prostate gland and bladder, owe their origin to fecal collections, especially in advanced life.
33 Long, Med. Times and Gazette, 1856, vol. ii. p. 286.
34 Bannerot, C., Du Phlegmon pelvi-rectal inférieure et de la Fistule de l'Anus consécutive causées par la Constipation, Paris, 1880.
Intussusception has been attributed to the weight of a mass of feces. Typhlitis and perityphlitis may come from retention in the cæcum. Pressure upon the viscera brings about derangements in their functions, many of which have already been described. From straining at stool a hernia, hæmoptysis, or cerebral hemorrhage may happen. Cases have been reported of death from rupture of an aneurism of the aorta while at stool, and J. F. Hartigan met with a case of spontaneous rupture of the aorta, where the vessel was apparently but little diseased, occurring in a man aged sixty during the act of defecation.35
35 Hartigan, Tr. Med. Soc. District of Columbia, vol. i. No. 3, 1874, p. 55. See also same number for a valuable paper on spontaneous rupture of aorta, by J. J. Woodward.
[p. 649] The effects upon the general system are those connected with malnutrition. The health may be profoundly altered and death occur from secondary diseases. Many general symptoms are due to the retention in the blood of excrementitious matters or to their reabsorption.36
36 Sterk, "Ueber den schudlichen einfluss der chronischen Stuhlverhatten auf den Gesamur organismus," Wien. med. Presse, xxii., 1881, p. 330 et seq.
DIAGNOSIS.—The diagnosis of constipation is not difficult except in hysterical women, who select this as one of their subjects of deception. Primary must be distinguished from secondary constipation, the last being a symptom of some general or local disease. The history of the case and the predominating symptoms will be guides to a decision, but constipation should be regarded as a symptom until it is proved to be otherwise. The tendency is to look upon it and to treat it as a distinct malady; important organic changes elsewhere may thus be overlooked. Simple habitual constipation may be mistaken for constipation due to lesions in the wall of the intestine or to closure from the external pressure of tumors.
Slowly-developed symptoms of obstruction may come from polypoid growths or benign tumors in the rectum, colon, cæcum, duodenum, and ileum. They are usually found in the rectum. The diagnosis can only be made when the growth is in the rectum or when the tumor is expelled from the bowel. Cancerous obstruction is accompanied by cachectic changes, by the presence of an abdominal or rectal tumor, the passage of blood and mucus, and violent rectal or abdominal pain. Primary cancer in the small intestine appears in the form of lymphoma; it readily ulcerates, and rather widens than narrows the channel of the bowel.37
37 Wilks and Moxon, Path. Anat., Philada., 1875, p. 417.
Stricture of the bowel is most commonly found low down in the rectum or sigmoid flexure, within reach of the finger or exploring bougie. If high up, it can only be diagnosed by exclusion and by its slow progression from bad to worse. Syphilis or dysentery has nearly always preceded the development of stricture.
Tumors in the abdomen or pelvis compress the colon, and while they are small they may be overlooked; sooner or later they grow so as to be recognized.
The presence of gall-stones as obstructions may not be detected until they are passed. The previous occurrence of attacks of hepatic colic, followed by jaundice, gives rise to the suspicion that gall-stones are in the intestine if they have been carefully looked for in the stool but never found.38 Enteroliths give no indication by which they could be known to be in the bowel.
38 In a case seen by the author three separate attacks of typhlitis occurred in a young woman suffering from chronic constipation. After the last attack she passed from the bowel several dark, irregularly-shaped concretions. The largest of these was a gall-stone covered with fecal matter. Since this time—two years ago—there has been no recurrence of inflammation and the constipation is much better.
All forms of constipation from organic modification of the walls grow worse and have no remissions; some rapidly progress toward a fatal termination. Simple constipation is subject to improvement and relapses due to the character of the food, climate, exercise, etc. The etiology is an important guide.
Stercoral tumors may be known by their position and character as [p. 650] ascertained by physical examinations and by their history. They are found in the iliac, lumbar, or hypochondric regions, and sometimes in other parts of the abdomen. The most common seat is in the sigmoid flexure and descending colon. They are nodulated, movable, painless, can be made to change shape or are indented by pressure, and have a doughy feel. Exploration of the rectum, by detecting impaction, will make the diagnosis clear when the obstruction is low down. The distension of the abdomen above the point of obstruction is limited at first to the region of the colon; but if the colon is much dilated with gas or is displaced, the enlargement becomes more central and more general. On percussion the sound is of a dull tympanitic quality, and never absolutely dull even in cases of great fecal accumulation.39
39 Case referred to by Guttmann (Physical Diagnosis, Sydenham ed., p. 360), in which the sound was dull tympanitic over two large fecal tumors which weighed when removed at the post-mortem six kilogrammes (sixteen pounds).
Fecal tumors40 are preceded by habitual constipation, and are most common in elderly people; they are changed in position and size or made to disappear by cathartics or rectal injections. Persistent treatment will bring away scybalæ which by their color and consistence show that they have long been in the canal. But the free movement of the bowels and the non-disappearance of the tumors are no proof that they are not fecal.
40 Tumeurs stercorales, Paris, Thèsis No. 240, 1878.
Fecal accumulations have been mistaken for ovarian tumors,41 cancerous tumors of the mesentery, uterine fibroids, and retro-uterine hæmatocele. Fecal tumors in the transverse colon have been taken for enlargement of the liver and spleen. In one instance obstruction of the bowel from fecal impaction was supposed to be a strangulated gut in a patient suffering from hernia: an operation was performed, the patient dying in sixteen hours afterward.42 Ovarian tumors in their early stages are sometimes thought to be fecal.43
41 Jas. Y. Simpson, Med. Times and Gazette, London, 1859, vol. ii. p. 549.
42 Thomas Bryant, Med. Times and Gazette, London, vol. i., 1872, p. 303.
43 J. B. Brown, Lancet, London, 1850, vol. ii. p. 48.
Fecal impaction in the rectum, with ulceration and bloody and mucous stools, may for a time be called cancerous ulceration. Sacculated scybalæ cannot be distinguished from submucous tumors even by the hand pressing on them in the rectum.44
44 H. R. Storer, Gynæcological Journ., 1869, vol. i. p. 80.
The history of each individual case, a full knowledge of etiological factors, and a careful physical examination will in most instances lead to a proper diagnosis.
PROGNOSIS.—The result of treatment depends upon the age. Although in infancy constipation is very common, cure is the usual result where a mixed diet begins to be taken in childhood. At from one to fourteen years of age regular movements can usually be secured, unless there is a radical defect in the organization of the child. In young girls at puberty and after, if constipation once is established it is apt to become inveterate, associated as it is with imperfect development and with uterine displacements. In middle life in men the result depends upon the cause and upon attention to the physician's counsel. If intestinal catarrh or atony is the cause, a persistent subordination of the life of the individual to the object in view will generally end in cure. In women who have borne [p. 651] children the hope of relief depends upon the duration of the malady before treatment. It is a dispiriting task to attack a constipation of many years' standing in women with relaxed abdomens, uterine prolapsus or retroversion, and general debility. In old age the causes are generally such as cannot be removed. The bowels can be moved when the occasions demand, but there is very little expectation of establishing a spontaneous habit of regular fecal movements.
At every age and from whatever cause perseverance and hope on the part of the patient and doctor are the chief elements of success. In neglected cases the worst results may happen: dilatation of the colon, ulceration, fecal impaction and obstruction, perforation; or in milder cases chronic indigestion, hypochondria, etc.
TREATMENT.—The physician can render great service by giving to parents advice which will prevent constipation in children. He should insist upon the importance of habits of regularity in defecation. At the period of puberty in young girls this is of even greater moment, and no opportunity should be lost for pointing out the danger of neglect. As a prophylactic measure in adults counsel should be given suited to the occupation. To persons leading sedentary lives the necessity of exercise ought to be made clear. In the trades little can be done, but in the case of literary men and those who read or write for many hours prevention is easier than cure. Daily exercise, walking or riding, frequent bathing with active sponging and friction of the surface, especially over the abdomen, will be of much service. Avoiding constrained positions where pressure is brought to bear upon the abdomen, as in bending forward to write, is quite an important item. Among ignorant people advice of this kind is rarely attended to, but even here the doctrine of regularity should never cease to be preached. Active business-men, especially young men, need emphatic teaching. They cannot plead ignorance for the habitual and persistent neglect of the simplest rules of health of which they are in this country so often guilty. The symptoms of indigestion which are precursors of constipation should receive due attention, and a mode of life and dietary suited to a complete digestion of the food will favor the timely and proper expulsion of waste matter.
Acute constipation in a previously healthy person, lasting for one to three days, does better without interference. No harm attends temporary inaction of the bowel, and if a spontaneous stool takes place at the end of this time it is a sign of a healthful and vigorous condition. After this the normal regularity is restored. The habitual clearing out of the bowel by a purgative pill or dose of mineral water whenever such a state of matters occurs creates the necessity for the interference. The man who never lets himself go over a day without an action is miserable if he misses his purgative and its effects.
In the onset of acute diseases the custom of giving a preliminary purgative is generally unnecessary, often injurious. It disturbs the rest which such cases need; it produces exhaustion in some diseases, as pneumonia, pleurisy, and rheumatism; it irritates the mucous membrane when irritation involves danger, as in intestinal catarrh and typhoid fever.
When it is desirable to empty the bowel in acute constipation a warm-water enema for adults and children is the best means. When a laxative is necessary in case of a failure of the enema, one mild in its operation [p. 652] should be chosen—a compound rhubarb pill, one to five grains of calomel, a teaspoonful of Rochelle salts, or half a bottle to a bottle of the solution of the citrate of magnesia or the tartro-citrate of sodium. For children calomel, in doses of one-third of a grain to one grain, is one of the most certain and least objectionable. One grain of powdered rhubarb can be added to this for a more active effect.
Under such circumstances as a blocking up of the bowel with a mass of partially digested or undigested food, fruit-stones, skins, or other foreign bodies, where the symptoms are violent pain, tympanites, and vomiting, the best method is to give large enemata of warm water through a long rectal tube passed as high up as possible, and to administer calomel in doses of one to three grains, repeated every two to three hours until the bowels are moved. Cold can be applied to the abdomen to diminish tympanites and prevent inflammation. Should the constipation not yield and the pain, vomiting, and tympanites augment, the case will then be considered one of intestinal obstruction, and be treated as such.
When called upon to treat chronic constipation, the physician should remember that it is not the symptom, but its causes, to which he should direct attention. Constipation is so often a symptom, a complication, of other diseased states that its management is a matter of secondary importance. Moreover, its causes are so peculiar to the individual and depend upon so many variable habits of life that each case asks for special study. The cure is only to be found by learning the particular cause—the habit of neglect, hurried eating, the use of aperients, uterine displacement, or any of the many causes enumerated.
The digestion and all that concerns it is of primary importance, and to it attention should be at once directed. The stomach and intestinal digestion should be examined separately, and the relative power to digest different articles of food determined. A diet, then, should be selected, not with a view to correcting the constipation, but as to its suitability to the digestive capacity of the patient. No system of diet can be fixed upon as suited to every case: the aim is to secure normal digestion and absorption and normal peristalsis. Many trials may have to be made before a proper dietary can be chosen. When there is indigestion of fats and malnutrition, with pale offensive stools containing much mucus, an exclusive nitrogenous and easily digestible diet—such as is advised in the article on INTESTINAL INDIGESTION—should be prescribed. In constipation connected with membranous enteritis a similar system of diet is proper. The drugs given should be those which aid intestinal digestion, and reference must be made again to this subject, already treated of. Many cases of constipation can only be cured by this treatment; the routine treatment by purgatives and a diet of vegetables and fruits would aggravate and not relieve. A course of exclusive milk or skim-milk diet, if persevered in for some weeks, will cure cases of constipation of this kind without the use of laxatives. Of course a purgative must sometimes be given if enemata fail, but the least irritating one should be selected.
The mineral waters best suited to constipation depending upon intestinal catarrh are in this country those of the Rockbridge Alum Springs and Capon Springs (Va.), the California Seltzer Springs, and the milder [p. 653] waters of Saratoga. The most suitable from Europe are the waters of Apollinaris, Vichy, Buda, Vals, Ems, Salzbrunn, Selters, Mt. Doré, and Kissengen. The warm baths of Virginia (Warm Springs, Hot Springs) are useful in increasing the activity of the skin and in giving relief to the catarrhal state. A month spent at the Warm Springs, with a daily bath the natural heat of which is 98°, will work a complete transformation in the abdominal circulation. This should be conjoined, of course, with a properly-regulated diet and exercise. Another month spent at the Rockbridge Alum Springs will complete the restoration of the bowel to a normal state. It is much to be regretted that the really valuable mineral springs of Virginia lack so many of the comforts which the invalid requires. In cases where it is more convenient a stay at the Arkansas Hot Springs is to be suggested, and for obstinate cases of intestinal catarrh with sluggish circulation, obesity, and gouty tendencies these springs are to be preferred. A season at some of the mineral baths of Europe, as Aix-la-Chapelle, followed by the strict regimen of the grape cure (as at Bingen, Durkheim, Vevay, Montreux, or Meran), is a rational mode of treatment which offers an almost certain prospect of cure.
If the case is one of atony of the colon due to impaction of the rectum and dilatation of the rectum and colon, without gastric or intestinal indigestion, a quite different regimen is required. The constitution and mode of life are the guides to the general plan to be followed. Sedentary pursuits are to be given up as far as possible. Long vacations and travel must be insisted on, with active exercise by walking and riding; also cold bathing or sponging, with brisk friction of the whole body. Sea-bathing is useful both as an exercise and for the effect upon the sluggish peripheral circulation, but the slothful life at the seashore, with over-indulgence in eating and drinking, is a source of more harm than good. Warm baths, and cold douches to the abdomen, compresses of cold water or of alcohol, the cold douche to the spine while in the hot bath, are all beneficial. Massage for women, children, and feeble persons takes the place of exercise. The kneading of the muscles over the abdomen can be combined advantageously with an effort to accelerate the passage of the contents of the colon by manipulation in the direction of movement.
The interrupted electrical current, used for the purpose of developing the feeble abdominal muscles, is a source of much advantage.45 But to be of service it should be persevered in for months, the patient himself making the application under the direction of the physician. In addition, the introduction of one insulated electrode into the rectum, while the other is in contact with the abdominal muscles or along the line of the large intestine, has been advised. The Swedish movement cure may be a useful aid in some cases. The movements exercise the muscles of expulsion. These are deep inspiration, flexion and extension of thighs or trunk, twisting the trunk, pressure on the abdomen and colon, stroking in the direction of fecal movement.
45 S. T. Stern, "Die faradische Behandlung der Obstipation und der nervosen Enteropathie," Centralblatt für Newenheil, 5 Jahrg., Mai, 1882, p. 201; also, I. Althaus, "Treatment of Obstinate Constipation by Faradization of the Bowel," Lancet, London, 1867, ii. 606.
In the relaxed condition of the abdomen in women who have borne [p. 654] children or in old persons the wearing of an abdominal support sometimes gives help and comfort.
The best diet for cases of atony of the colon and rectum is one which is easily digested and has a moderate amount of waste, as a full colon will stimulate muscular action. Various articles are suggested with a view to excite peristalsis by irritation of the mucous surface, but as such substances are in themselves insoluble and innutritious, it is unwise to resort to them. The following list includes the foods suitable to such cases: Fresh vegetables, as spinach, raw or stewed tomatoes, lettuce, kale, salsify, peas, asparagus, kohlrabi, and other summer vegetables; in winter canned vegetables, if well prepared, take their place. Among fruits, fresh fruit in general, especially grapes, peaches, and oranges; dried fruit, as figs, raisins in small quantity, stewed prunes, and baked or stewed apples, can be tried.
Too much vegetable matter is harmful, as the bowel is filled with an excess of waste, much of which is undigested food; the quantity must be regulated by the appearance of the stools and by the success of the regimen. If the blockade continues obstinately, the vegetable diet should be reduced. The microscope in many cases can alone decide the amount of undigested vegetable matter. Meats are all advisable in moderation. The least digestible, as ham and veal, are to be avoided. Graham-flour bread, brown bread, or bran bread are better than bread made of the best bolted flour. The first is more digestible, and bran bread46 is thought to increase peristalsis, but this is a doubtful effect. Oatmeal well boiled, fine hominy, corn meal, or cracked wheat with milk are pleasant and digestible. A cup of café au lait at breakfast or before breakfast is the best morning drink;47 it has a laxative influence. Tea is thought to have the opposite effect. Milk at breakfast answers well for those who take it with relish. An orange on rising in the morning is a pleasant remedy.
46 "The Efficacy of Bran Bread in relieving Despondency ... dependent on an Irregular and Constipated State of the Bowels," Journ. Ment. Sci., London, 1858-59, v. 408-411.
47 "Treatment by Café au Lait," Gaz. des Médecins prat., 1840, No. 4, p. 13.
Certain drugs are called for to aid these measures in giving tone directly or indirectly to the weakened bowel muscles. Strychnia stands first, but it woefully disappoints one who trusts much in the theoretical arguments for its use. In fact, it may be said of all drugs given for constipation that they stand in a very subordinate rank to the measures already discussed. They should be thought of last, not first, and but little confidence should be put in the vaunted value of new drugs. Strychnia can be combined in anæmia and debility with the dried sulphate or carbonate of iron, and with quinia or arsenic,48 or in feeble digestion with dilute hydrochloric acid and pepsin. Belladonna was advised by Trousseau as a stimulant to unstriped muscular fibre, and it can well be given with strychnia; ipecacuanha and atropia are approved of in conjunction.49 A pill of ergot, belladonna, and strychnia would answer the indication of a feeble peristalsis. DaCosta has suggested giving one drop [p. 655]of the fluid extract of belladonna with compound tincture of gentian or cinchona three times daily after meals. The sulphate or valerianate of zinc, oxide of zinc, extract of valerian or gentian, capsicum, or black pepper can be tried in pill form with belladonna and strychnia.
48 Bartholow thinks arsenic overcomes constipation when due to deficient secretion and dryness of the feces (Mat. Med., New York, 1879, p. 129).
49 Legros and Onimus, Journal de l'Anat. et de la Phys., t. vi. pp. 37 et 163. Ringer says one grain of ipecacuanha taken while fasting each morning will relieve constipation from torpor (Therapeutics, New York, 1882, p. 438).
These remedies are slow-acting, and in the mean while the bowels must be moved artificially, methodically, and taught to act at stated hours. For this purpose a small enema of cool or cold water at the same hour every day after breakfast does well. It is irrational to distend the bowel, already weakened by distension, with large enemata of warm water. Recourse should not be had to this until all hopes of effecting a cure are gone, or only as an occasional remedy in impacted accumulations where the mass must be softened before it can be removed. If the enema does not in time empty the colon sufficiently, laxatives will have to be taken with some regularity until the habit is created. A tumblerful of water with or without a teaspoonful of salt, or a tumblerful of any alkaline water charged with carbonic acid, taken on rising in the morning, may prove effective. A tablespoonful of sweet oil at night acts well as a lubricator and softens the feces. If these more simple means fail, it becomes unfortunately necessary to give a purgative drug: any one of this class can be combined with strychnia, belladonna, vegetable tonics, and iron. Those to be preferred are aloes, colocynth,50 and podophyllin. The compound podophyllin pill or a pill of one-sixth of a grain of belladonna and podophyllin at night or three times daily, the pill of aloes and myrrh, or the Lady Webster pill, are well-approved forms of administration. A compound rhubarb pill acts well if taken after dinner.
50 A few drops of the Prussian tincture of colocynth several times daily is advised by Ringer (Therapeutics, New York, 1882, p. 642).
If one desires to select a purgative which will probably increase the outflow of bile, selection can be made from the following drugs: podophyllin, aloes, rhubarb, colchicum, euonymin, colocynth, calomel, jalap, sodium sulphate, potassium sulphate, cream of tartar; and among the rarer alkaloids iridin, sanguinarin, physostigma, and juglandin. These, according to Rutherford, Vignal, and Dodds, increase the secretion of bile in fasting animals. Ox-gall and pig-gall are laxatives only; they have no effect on the liver, but can be added to other purgatives in pill forms.
Salines largely diluted may be given to strong adults: Epsom or Rochelle salts quite early in the morning, a solution of sulphate of magnesia with dilute sulphuric acid, to which dried sulphate of iron may be added, are quite popular; and of the bitter waters, Hunyadi Jânos, Friedrichshall, or Pullna water serves the purpose. One grain of sulphate of quinia added to a saline will increase its effect. The milder laxative waters are to be preferred to the bitter waters. The Saratoga waters, Congress, Geyser, Hathorn, answer the purpose taken early in the morning, or among the European springs those of Kissengen, Plombières, Marienbad, Homburg, Seltzer, or Leamington in England, are not too active in their effects. In atonic constipation, the form now under consideration, the laxative chalybeate waters are indicated where there is anæmia or debility. These are represented by the Columbian, Pavilion, Eureka, and Excelsior Rock among the Saratoga waters, and by the Bedford Springs water.
[p. 656] It is well to administer a number of drugs in rotation in habitual constipation, as the susceptibility to a particular drug is lost after continued use. Increase of the dose is the usual method to offset this result, but it is irrational to meet exhaustion by over-stimulation. Rest of the part stimulated by using a remedy which brings about the result in a different way is the wiser course. The dose should be gradually reduced, tempting the bowel to act more and more without aid. Among the laxatives which can be borne in mind in alternating treatment the following list includes some which can be used with advantage: the fluid extracts of rhamnus (buckthorn) and cascara sagrada; alum, which is called for in certain forms of atony; sulphur in the form of confection or sulphur with guaiacum51 (half a drachm of each in powder at night); the wine of colchicum (five drops or more three times daily), advantageously used in gouty or rheumatic persons; the infusion or tincture of euonymus; the tincture of benzoin; senna in fluid extract and in the compound powder of liquorice.
51 Fuller, Lancet, London, April 23, 1864, p. 459.
Infants and children should be cured of constipation without purgatives if possible. Attention to the diet of the infant, and close inspection of the stools to see the effect of the food given, will guide to a proper system of feeding. Breast-milk is the best remedy; next, a food which most nearly resembles mother's milk—cow's milk properly diluted with barley-water, oatmeal-water, or rice-water—stands first. Condensed milk, given in barley- or oatmeal-water, is a second and excellent substitute in cities. Antacids prevent a too rapid coagulation of the casein and the formation of curdy lumps. Lime-water with milk or bicarbonate of potassium or of sodium may be administered with the food or before it. The quantity of food must be lessened until the child can digest all it takes.
The infant should be taught to empty the bowel at the same hour daily by always placing it at this hour in a position favorable to and suggestive of defecation. Dilating the sphincter at the same time with the soap suppository or the small end of a Davidson's syringe, or just touching the margins of the anus, will excite the necessary reflex movement. If defecation is painful, examine the inner edge of the anus for small cracks or for eczema ani.52 Over-stretching the sphincter with the finger in cases of rigid or spasmodic contractions will sometimes produce permanent relief.
52 Betz, "Eczematous Proctitis," Memorabilien, iv., Dec. 28, 1859, S. 190.
In children the question of diet is equally important. Most cases of constipation in them originate in intestinal catarrh from improper diet and over-feeding. Strict rules of diet should be rigidly enforced, and each case receive special study in order to determine upon the best dietary. The minutest details of the child's life, its habits and surroundings, are to be controlled so as to secure the best possible influences for health. Feeble development and muscular inertia must be remedied by change of climate and tonics—iron, strychnia, and cod-liver oil. When other methods fail to give early relief, a purgative may be needed. Rhubarb, magnesia, calomel, Friedrichshall or Hunyadi water, given in milk, the compound liquorice powder, the compound anise [p. 657] powder, are better than the more active cathartics.53 Habitual administration of laxatives to children ought to be regarded as a confession that the case is incurable; it is a last resort, for which necessity is the only argument.
53 The compound anise powder, a non-officinal preparation in use in Washington, is a convenient form of administration: heavy calcined magnesia, 360 grs.; rhubarb powdered, 180 grs.; oil of anise, 40 minims; stronger alcohol, one fluidrachm. The bicarbonate or fluid magnesia is also a good preparation. Ringer knows nothing so effectual in bringing back the proper consistence and yellow color to the motions of children as podophyllin. Dissolve one grain of the resin in one drachm of alcohol, and of this give one or two drops on a lump of sugar twice or three times a day (op. cit., p. 458). Bouchut suggests the same solution, with simple syrup as a menstruum.
In old persons tonics should be combined with the laxatives, as strychnia, iron, quinia, gentian with aloes, colocynth, rhubarb, or podophyllin. The rectum should always be examined, as impacted fecal masses will often be found there.
SYNONYMS.—Enterodynia, Tormina, Colicodynia, Colalgia, Dolor colicus, Passio colica, Spasmus intestinorum, Ileus spasmodicus, Spasmus ventriculi, Neuralgia mesenterica; Spasm of the bowels, Cholick or Cholick Colic, and Pain in the Belly; Ger., Das Banchgrimmem, Die Kolik; Fr., La colique.
HISTORY.—Colic is described by Hippocrates.1 He recommended the use of emetics and gave other sound advice regarding the treatment of the affection. Galen2 administered sedatives, as opium and henbane, and he advised them to be combined with carminatives. Aretæus3 speaks of the pain of colic extending to the back, limbs, and testicles, and also states that when affecting the sides of the body it may be confounded with pleurisy, hepatitis, or splenitis. Alexander4 points out the differential diagnosis of the disease and directs a proper course of treatment. Cupping, friction of the extremities, and dry fomentations were recommended by Celsus;5 and internally he advocated a mixture of poppy, anise, pepper, etc. Aëtius6 describes the affection. Serapion7 and Avicenna8 treated of colic more clearly than any previous writers had done, and advised narcotics administered by the mouth and rectum. Atony of the bowels is given as a cause of the disease by Haly Abbas,9 and Alsaharavius adds10 to the etiology a hot intemperament, indurated feces, and poisonous medicines. Rhazes11 directs the administration of emetics when the colic is due to indigestion.
1 De Affect., xv.
2 De Med. Sec., loc. ix.; iv., de loc. Affect., vi. 2.
3 Morb. Acut., ii. 6; Chron., ii. 8.
4 Lib. x. 1.
5 Medicina, Libri octo, iv. 14.
6 Lib. iii. 1, 29.
7 iii. 32.
8 iii. 16, 4.
9 Pract., vii. 28.
10 Ibid., xvii. 2, 12.
11 Divis. 69.
NATURE AND DEFINITION.—Enteralgia is the name given to intestinal pain which is independent of indigestion and of inflammation or other organic change in the wall of the bowel, and corresponds to gastralgia and other visceral neuralgias. It involves the nerves which pass to the intestine along the line of attachment of the mesentery, and which are derived from the superior mesenteric plexus, with a prolongation from the junction of the right pneumogastric nerve with the coeliac plexus.12
12 The very extensive distribution of terminal nerve-filaments in the intestine is an explanation of the frequency and severity of attacks of intestinal pain. "We may form some estimate of the extent to which the nervous system of the intestines is developed from the fact that about one hundred ganglia belonging to the submucous and over two thousand to the myenteric plexus are to be found in one square inch of the intestine of the rabbit" (Frey, Histology, New York, 1875, p. 493).
[p. 659] The pain of enteralgia is not spasmodic, and is not accompanied by flatulence, borborygmi, or other signs of indigestion and gaseous distension of the bowels.
Colic, on the other hand, applies to intestinal pain accompanied by indigestion, distension of the bowel with gas, or the contact of irritating ingesta. The pain is spasmodic, and is relieved by the passage of gas and other contents from the bowel. The pain is due to the local irritation of the richly-gangliated plexus of nerves seated in the submucous layer and which extends from the pylorus to the anus.
At present enteralgia must be considered from its symptoms and from post-mortem examinations as a pure neurosis of the sympathetic system. Opportunities are rarely offered for studying the post-mortem appearances of the disease, from the fact that when idiopathic it seldom ends fatally. Out of forty-nine autopsies on patients who had suffered from colic due to lead-poisoning, only one was found with any change of the abdominal ganglia of the sympathetic. Ségoud found the ganglia and some of the fibres of the sympathetic hypertrophied and indurated,13 and "in recent times Kussmaul and Maier have published an example of sclerosis of the coeliac and superior cervical ganglia."14
13 Ségoud, Essai sur la Névralgie du Grand Sympathique, Paris, 1837.
14 M. Rosenthal, "Diseases of the Nervous System," Wood's Library, New York, 1879, vol. ii. p. 265.
The pathology of enteralgia due to a vitiated state of the system, a morbid condition of the tissues of the intestines, the presence of irritating ingesta, or to reflexion from other organs, differs in no wise from a neuralgia of other parts arising from constitutional, local, or reflex causes. Pain will likewise manifest itself here in consequence of deleterious substances circulating in the blood, as in Bright's disease, rheumatism, gout, or lead-poisoning. The terminal nerve-fibres of the intestines are irritated in attacks of colic by substances or food within the alimentary canal; gases are generated from the decomposition of the ingesta. The consequent dilatation of the gut produces loss of tone and abolition of the contractile power of the muscular coat. Constipation and pain from pressure exercised on the neighboring nerves will be the result.
Obstinate constipation, and even symptoms resembling ileus, may arise from a portion of the intestine thus distended becoming bent upon itself, the sharp angular flexure interrupting or completely obstructing the passage of the feces.15
15 F. H. Hamilton, Med. Gaz., New York, 1880, vii. p. 3.
ETIOLOGY.—Enteralgia may be either idiopathic or symptomatic. The causes can best be considered by dividing them into general and reflex.
Under the head of general causes may be mentioned an inherited neurotic temperament, particularly in individuals of a hypochondriacal tendency. Females are far more apt to suffer from this affection than males, on account of their more impressionable nature and greater liability to nervous diseases in general. Hereditary tendencies, overtaxing the mental powers during the developmental period of youth, and later in life excessive mental labor and anxiety of business affairs, are causes. It may occur in the cachexia developed during the course of many chronic diseases, as diarrhoea, rheumatism, gout, phthisis, cancer, Bright's disease, etc. Various morbid conditions of the blood are followed by [p. 660] enteralgia, as anæmia arising from prolonged lactation, masturbation, or venereal excesses, and the presence of various blood-poisons, as syphilis, malaria, lead, copper, and arsenic. Other causes are living in cold, damp climates, with sudden changes of temperature and chilling of the body. Persons addicted to the use of tobacco or alcohol and to dissipations of various kinds may become predisposed to enteralgia. Idiosyncrasy is a predisposing cause.
Enteralgia is often secondary to ovarian, uterine, or other distant disease. Also, owing to intimate sympathetic relations, pain is often felt in the bowels as a result of disease situated in some of the solid abdominal viscera, as the liver, spleen, and pancreas. In the same way, organic affections of the brain and spinal cord, especially acute myelitis and spinal sclerosis and lesions of the vertebral bones, excite intestinal pain. Emotion may also bring it about. The application of cold to the feet or catching cold in general is followed by pain which is due to reflex influence.
There may be a predisposition to colic from hereditary influence and the neurotic temperament. A feeble digestion is a source of constant risk. Much of the pain occurring in the course of dysentery, catarrh of the bowel, invagination, fecal impaction, and other structural affections is of the nature of colic. The most frequent by far of the local causes is the direct irritation of the terminal nerve-fibrils by substances within the alimentary canal and by over-distension of the bowel with contained gas. Some of these irritants are partly-digested and indigestible articles of food; food taken cold or in excessive quantity; the decomposition of food and consequent distension of the bowel by gas. Acid drinks and alcohol have the same effect. Constipation with scybalæ may produce colic in an otherwise healthy person. A morbid state of the intestinal secretions, either as regards quantity or quality, is said to have a like result, but this is a doubtful cause. Foreign bodies within the canal, as fruit-stones, various concretions, worms, and gall-stones if of large size, may produce pain during their passage through the bowel. Cathartic medicines may be enumerated as among the local causes, and also various poisonous drugs. Lesions of any sort seated in the intestinal wall, as ulcers and neoplasms, induce paroxysmal pains.
SYMPTOMS.—The pain of enteralgia occurs in attacks which come on slowly and continue for a variable time—some hours or days. The pain is situated about the umbilicus, and is relieved by deep pressure, although at the same time there may be hyperæsthesia of the skin. The intensity of suffering ranges from a dull heavy pain to one which is acute and lancinating. Retraction of the abdomen is common, but there may be tympanites. No signs of indigestion may appear, but eructations of tasteless gas, or even borborygmi, may be complained of.
The duration of an attack of enteralgia is variable and depends to a great extent upon the cause. Usually, when the symptoms are severe, the duration is short. It may pass off in less than an hour, or a succession of paroxysms continue to recur, and the attack will be kept up for several days, weeks, or even a month. One seizure predisposes to another, and each is liable to be more severe than its predecessor.
The malady may end gradually or as rapidly as it was ushered in. Attacks are often mitigated, or even terminated, by the occurrence of some other morbid condition—by a profuse sweat, the discharge of lochia, [p. 661] the menses, or some secretion which has been checked. The development of rheumatism or gout may relieve it. Attacks often terminate with vomiting, belching, and more especially with movements of the bowels and discharge of flatus. A free emission of pale, colorless urine is sometimes followed by relief. This occurs in hysterical cases, and the disease is generally accompanied with some uterine disorder and with tenderness along the spine.
The attack of intestinal colic may be developed suddenly and with full intensity, or it may be preceded a short time, usually a few hours, and rarely much longer, by prodromic symptoms. These are nausea, a sensation of weight in the epigastrium, anorexia, eructations, tympanites, rumbling, and slight griping pains. The patient is irritable and restless, his bowels are usually confined, and urination is often rendered painful by the distended bowels pressing upon the bladder.
These symptoms, which are in truth but a part of the attack, being only of a lower grade, increase in severity and the pain becomes more acute and distinctly paroxysmal. It is of a sharp cutting, twisting, or most frequently griping character, and is in the earlier part of the attack usually referred to the umbilicus or to one of the iliac fossæ, and sometimes radiating thence in different directions. Generally it becomes concentrated about the umbilicus. The exacerbations of pain vary in degree of severity, in duration, and in frequency of recurrence, while the intervals may afford complete relief or merely a remission of the acute suffering. The sufferer either lies quietly upon his abdomen or upon one side or the other, with his body bent forward and thighs flexed, or he is restless and writhes in pain, groaning and crying out from the intensity of suffering. He may seek relief by trying a variety of positions and by pressure applied with the hands or some solid object against the abdomen. Anxiety and pain are depicted in his features. His face and extremities are cool and covered with a clammy sweat. The pulse is small, hard, and generally slower than normal. Breathing is sometimes oppressed, as a result of spasmodic contraction of the abdominal and thoracic muscles. Often the muscles of the hands, calves of the legs, and the feet are similarly affected. The tongue is moist and as a rule clean. The bowels are constipated—at times so much so as to amount to obstruction—or, again, diarrhoea and tenesmus may be present.
Other abdominal symptoms are nausea or vomiting, eructation of gas, and borborygmi. Micturition is at times urgent and painful, and the testicles are frequently retracted.
The abdomen is occasionally tender, but pressure generally affords relief. It is distended with gas, especially over the large bowel. Palpation often reveals lumps or knots situated within the abdominal walls and due to spasmodic contraction of its muscles, particularly of the recti. In thin persons the constricted and dilated coils of the intestines can also be distinguished as nodular masses which rapidly alter in shape and position.
The severity of attacks of colic varies from a few slight griping pains felt at intervals to a seizure of such intensity that the patient suffers agony and presents symptoms of an alarming nature. Fortunately, these grave cases are comparatively seldom observed. In them the local and general symptoms are aggravated. Pain is more intense and [p. 662] constant, having less marked intervals of relief, and the patient may pass into collapse, with a small, rapid, and wavering pulse, restricted respiration, shivering and chilliness, and a cool, clammy skin. The abdomen is greatly distended; hiccough comes on, also stercoraceous vomiting, tenesmus, and in the worst cases involuntary stools and suppression of urine. Nervous symptoms have been observed, as dizziness or fainting, and finally delirium and convulsions may end the scene.
VARIETIES.—Attention has been called to a distinct form of enteralgia due to the effects of alcohol.16 It affects steady drinkers, and is, as a rule, met with only during the hot months. The presence of undigested food within the alimentary canal or exposure to cold may act as exciting causes of the disease. The development is usually gradual. Dull pains, felt at first over the abdomen, become later more continuous and fixed about the epigastrium or umbilicus. Sometimes they are complained of more over the bladder. Bilious vomiting and hiccough are prominent symptoms; the patient is thirsty, and the liquids taken only promote vomiting; and the bowels are constipated. There is restlessness, and sleep is obtained with difficulty. Paralysis at times supervenes, and affects the lower as well as upper extremities. In the worst cases delirium and even convulsions occur. The disease nearly always ends in recovery in from three to ten days. Severe intestinal and gastric pain occurs in opium-eaters, but especially in women who use morphia in excess. The suffering is always greater when the opiate is reduced, but can only be cured by breaking up the bad habit.
16 Colica bacchanalium, J. H. Claiborne, Med. Monthly, New York, 1855, p. 227.
A variety of colic which occurs epidemically17 in some of the inter-tropical countries has been studied and described by different observers. It is known by various names, such as colique sèche; colique végétale; rachialgie végétal; colic of Poitou, of Devonshire, of Madrid, of Java, of Surinam; colique nérveuse; endémique des Pays Chauds (Fonssagrives); endemic colic, dry colic, bilious colic, nervous colic; girafy; dandy, etc. Ségoud called it a neurosis of the great sympathetic, and attributed the disease to the effect of cold.18 The symptoms resemble, in many respects, those of lead colic, and at one time they were erroneously considered identical with it.19 Thompson and Chisholm,20 after an [p. 663]experience with the disease in the West Indies, assert that such is not the case. Epidemics which occurred in Madrid and several of the Spanish provinces, and many hundred cases witnessed among the French soldiers by other observers, were ascertained not to be due to lead-poisoning.
17 Colique végétale, or endemic and epidemic colic, did not escape the notice of the older writers. It is mentioned by Aretæus; Paulus Ægineta describes an epidemic of the disease which extended through Italy and a large part of the Roman empire, and he states that attacks were often followed by paralysis. François Citois gives an account of an epidemic which raged at Poitou in 1616. Monson Smith described the disease in 1717. In 1724 it appeared in Devonshire, England, and presented the characteristic symptoms and sequelæ. In more recent times epidemics of the disease have occurred in nearly all the countries of Europe. It prevailed in the northern part of France and in Belgium from 1853 to 1859, inclusive. It has likewise visited the Caribbee Isles, Cayenne, Guadaloupe, Madagascar, India, the West Indies, some of the provinces of Spain, Java, the west coast of Africa, the Antilles, Senegal, New Zealand, Brazil, and various other localities. The disease occurs in all seasons, but is more prevalent in summer and in the commencement of autumn.
18 Ségoud, Essai sur la Névralgie du Grand Sympathique, Paris, 1837.
19 The disease frequently appeared on board of French war-vessels, and was regarded by Lefèvre (Recherches sur les Causes de la Colique sèche) as due to lead-poisoning. He asserts that lead is more used in French ships than in those of other nations, and accounts for its being epidemic in tropical countries because a warm climate aids in developing the affection, and because there men drink more freely of water. (See also Dutrouleau, Arch. gén., 1855, "Mal des Européens dans les Pays Chauds.")
20 Quoted by Oppolzer, Wien. med. Woch., Bd. xvi., 1867, p. 724.
The affection is not accompanied with any constant lesion. Pascal21 made post-mortem examinations in six cases and found the mucous membrane of the duodenum a little reddened: the gall-bladder contained thick bile, and in a few cases there was congestion of the sympathetic ganglia. The attack is usually marked by certain prodromic symptoms. The patient complains of malaise, loss of appetite, a load in the epigastrium, embarras gastrique, dull pains in the colon, borborygmi, and cramps or tingling in the limbs. For the first few days the bowels generally move several times daily. The stools are difficult, painful, and of a black or dark-green color, offensive odor, and accompanied with the discharge of flatus. As the disease progresses the bowels become constipated and the discharge of gas ceases. After a few days the pain is more severe and radiates to the lumbar region, the testicles, or the thighs. It is seated principally in the epigastrium, in the line of the transverse colon, or it may involve the whole abdomen. Movement aggravates the pain, while pressure often relieves it. The tongue is large, trembling, and coated white or yellow; the breath is fetid, the saliva viscid, and mouth sticky. Anorexia is complete; there are hiccough, nausea, vomiting of undigested food and mucous or bilious matters, and constipation with hard black stools. The patient is restless and sleepless. The abdomen may be distended or retracted, and micturition is often painful and the urine high-colored. The pulse is generally slower than in health, but becomes accelerated when the attack is over. The skin is pale, the conjunctiva often stained with bile, and in the later stages oedema of the lids and emaciation come on. The effect upon the nervous system may manifest itself by amaurosis, deafness, delirium, mania, coma, epileptiform convulsions, or paralysis. The paralysis affects the extensors of the hand, arm, and leg, or it may become general and end in death.
21 "Recherches anatomico-pathologique sur la Colique dite de Madrid," Rec. de Mém. de Méd. mil., Paris, 1826, xix. pp. 98-113.
The duration of the disease is from eight to fifteen days, but in some cases it becomes chronic. Relapses frequently occur. At times intermittent or remittent symptoms develop, and occasionally the affection is complicated with enteritis or peritonitis. The prognosis depends very much upon the character of the epidemic, and the most serious cases are those accompanied with either cerebral symptoms or peritonitis.
The paralysis sometimes passes off in a few days, but oftener lasts indefinitely. Emetics, purgatives, and anodynes are recommended in the treatment of the disease, and frequently a change of climate is necessary in order to recover fully from the affection.
DIAGNOSIS.—The diagnosis of enteralgia usually presents some difficulty even when the symptoms are well marked. That the disease is a true neuralgia is apparent from the periodical recurrence of the pain, its sharp and darting character, from the sudden cessation followed by complete relief, and from the absence of symptoms of indigestion. Affections bearing a certain resemblance to enteralgia are to be excluded.
In lumbo-abdominal neuralgia the pain is unilateral and extends around [p. 664] to the back. Tender spots can usually be detected by pressure on the umbilical or hypogastric regions or on the spinous processes of the vertebræ. In dermalgia the soreness is superficial, and light pressure gives more pain than deep compression, while nervous and hysterical symptoms are constantly associated with this form. Gastralgia is more frequent than enteralgia, and the pain is located about the ensiform cartilage. In myalgia of the abdominal parietes pressure causes pain, as do also movements of the body, coughing, sneezing, etc. Rheumatic pains would likely be felt in other muscles. In ileus the pain is more continuous, the tenderness localized; there is constipation of a most obstinate character, and vomiting of stercoraceous matter. The patient has an anxious expression and a rapid, feeble pulse. In renal calculus the pain is situated in the course of the ureter and shoots down to the pubes and thighs. There is frequent desire to urinate, accompanied by a scanty discharge of urine, and a copious flow of urine is followed by cessation of pain. The maximum of pain in hepatic colic is situated in the right hypochondrium, and is often reflected into the shoulder of the same side. Icterus may also be expected. Colic arising from lead-poisoning is usually associated with sufficiently characteristic symptoms to render the diagnosis easy. When syphilitic the pain is apt to be most severe at night.
In catarrh of the bowel the skin is hot and dry, the pulse accelerated, and other indications of a symptomatic fever are presented. The pain is more constant, more localized, and pressure causes it to be increased. Tenderness on pressure is not invariably met with, but the rule holds good that when deep pressure increases the pain inflammation rather than enteralgia is indicated.
If colic is due to indigestible food, a sensation of weight will be complained of at the epigastrium, griping pains occur at short intervals, with flatulence, vomiting, and later diarrhoea. If the attack be wind colic, the abdomen is enlarged by tympanitic distension; borborygmi and belching occur. If it is the result of accumulation of feces, there would be a previous history of constipation, and the lump of feculent matter can be located by palpation and percussion.
PROGNOSIS.—The prognosis of idiopathic enteralgia is favorable, the disease generally terminating after a variable period. Attacks are very apt to recur, and each one will, in all probability, prove more severe than the preceding. In symptomatic enteralgia the prognosis will depend upon the nature of the fundamental disease.
Colic terminates favorably in nearly every case. Death has rarely occurred from complications, as convulsions, and rupture of the bowel has been observed from great distension.
TREATMENT.—If attacks of enteralgia are associated with hysterical symptoms, it would be proper to employ antispasmodic sedatives. The compound spirit of ether is very useful in these cases, especially if they are accompanied with flatulence. Rubbing the spine with stimulating or anodyne liniments frequently promises well. The hypodermic dose of morphia gives relief more quickly than can be got in any other way, but in pure enteralgia with frequently recurring paroxysms care must be taken not to create the demand for the remedy by giving it often. The radical cure of the disease is a more important matter than the treatment of the acute attacks.
[p. 665] If the cause of enteralgia be located in some of the solid viscera or in the nervous system, remedies should be addressed to these parts, and the reflex nervous impressions allayed by the bromides or other nervous sedatives. The valerianate of zinc in doses of one grain three or four times a day is extremely useful in neuralgia from reflex irritation of the female pelvic organs. Constitutional remedies are indicated in the cases due to a morbid condition of the blood—iodide of potassium and mercury if a syphilitic poison or if of a rheumatic or plumbic origin; colchicum if gouty; quinia if malarial; and iron when an anæmic state is presented. H. C. Wood states that alum is used with success; being of service when there is no lead in the primæ viæ, it must act in some other way than as a chemical antidote. Arsenic is very highly recommended in idiopathic enteralgia. Excellent results have been reported from the use of nitrate of silver,22 hydrocyanic acid, belladonna,23 and iodoform. Change of climate and travel may have to be resorted to in obstinate cases.
22 Nauman, Deutsche Klinik, Bd. iii., 1851, p. 388.
23 Lancet, vol. i., 1867, p. 81.
The objects of treatment in colic are to relieve suffering and terminate the attack as soon as possible. For this purpose the various anodyne and antispasmodic remedies, as opium, hyoscyamus, chloral, ether, chloroform, Indian hemp, and camphor, may be employed. Carminatives are most useful, alone or combined with anodynes and cathartics. Oleum cajuputi often affords immediate relief. Warm teas of chamomile, ginger, valerian, or peppermint sometimes do good. When the suffering is very acute nothing acts so promptly as a hypodermic injection of morphia, either alone or combined with atropia.
The surface of the body should be kept warm, and hot applications to the abdomen assist in relieving pain. The heat may be conveniently applied by means of poultices, hot salt- or sand-bags, or rubber bottles filled with hot water. Cold,24 used externally, is more grateful in some cases, and is preferable if there be much tympanites. Sinapisms, turpentine stupes, and stimulating and rubefacient liniments answer well in some cases, and should be tried. Anodyne applications to the spine occasionally do good, and cold, applied by means of the spinal ice-bag, is recommended by Ringer.
24 Roux, Journal de Médecine, Paris, 1765, p. 48.
In order to treat the disease successfully and bring the attack to an end, its cause should be ascertained if possible, and remedies directed to its removal. If it be the result of indigestion, the contents of the stomach should be removed by emetics. Drastic or powerful cathartics will only tend to aggravate the disease, and on that account mild laxatives are to be preferred in all cases. Castor oil, calomel, pil. rhei comp., senna, etc. may very properly be prescribed.
In flatulent colic means should be directed to expel the gas. Anodynes—preferably chloroform—and carminatives should be administered by the mouth, and enemata containing turpentine or asafoetida injected into the rectum. In severe cases a clyster with ten or fifteen drops of liquor ammoniæ is said to do good. If distension of the bowel be so great as to threaten rupture, it may with propriety and safety be relieved by puncturing the colon with an exploring-needle or a fine trocar. In cases of flatulent colic where the gas arises from the decomposition of food [p. 666]remedies to check fermentation, such as alkalies, creasote, carbolic acid, or the sulphites, would be indicated. Good sometimes results from pressure and massage of the abdomen. Rubbing with etherized oils and electricity have also been used successfully. If the attack be from fecal impaction, it may be possible to liquefy and remove the mass by using saline cathartics, as sulphate of magnesium, aided by large oily or mucilaginous clysters, which in obstinate cases should be injected through a flexible rubber tube passed up the rectum as far as possible. Injections of an infusion of tobacco are now seldom used for this purpose, on account of the dangerous symptoms which often supervene. If pain or tenderness be present at the seat of impaction, cathartics should be used very cautiously or not at all, and opium given instead. The administration of this drug, by relieving pain and allaying spasmodic action, is often followed by free catharsis.
Persons subject to attacks of colic may diminish the intensity, or even prevent the recurrence, of the disease by employing during the intervals such remedies as would be indicated in their individual cases. Phosphate of sodium has been highly recommended for preventing the recurrence of attacks of colic. R. N. Taylor states25 that his experience with the use of the drug is quite extensive, and he found the treatment uniformly successful. Thirty grains dissolved in a glassful of water may be taken three times a day—preferably before meals—and this quantity should be reduced if it causes any irritation of the stomach. The bowels should be regulated and strict attention given to diet. A milk diet is of course best in obstinate cases. Any article of food known to disagree must be excluded, and tea, coffee, and alcoholic drinks should also be prohibited.
25 Med. Herald, Louisville, 1880-81, ii. p. 348.
SYNONYMS.—Enteritis, Catarrhal enteritis, Mucous enteritis, Endo-enteritis, Ileo-colitis, Entero-colitis, Diarrhoea. Older synonyms: Chordapsus, Cauma enteritis, Enterophlogia, Enterophlogosis, Colica acuta seu inflammatoria, Ileus inflammatorius, Enteralgia inflammatoria, Febris intestinorum seu Iliaca inflammatoria, Colique inflammatoire.
HISTORY.—It is interesting to start at the fountain-head of the two streams of inquiry—the clinical and the anatomical—and to follow each in its widely-diverging wanderings until they unite to give to the phenomena of intestinal inflammation a just interpretation.
The symptom diarrhoea was fully described by the earliest writers in medicine.1 The symptomatic differences between diarrhoea, dysentery, and lientery and the different forms of diarrhoea (bilious, watery, etc.) were given in detail by the Greek and Roman physicians. The Arabians had a much more elaborate classification of the fluxes. Avicenna made seven varieties of simple diarrhoea. European writers followed closely in these footsteps. Sennert made twelve and Sauvages twenty-one varieties of diarrhoea, depending upon as many different causes, as undigested food, worms, the bile, etc. Many recent writers have adhered closely to the older authors in their method of treating of diarrhoea, regarding it as a disease and dividing it into varieties based on the causes or on the appearances of the stools. Among them may be mentioned Cullen (1789), Good (1825), Tweedie (1841), G. B. Wood (1852), Trousseau (1865), and Habershon (1879).
1 J. J. Woodward, Med. and Surg. Hist. of the War, Part 2, Medical Volume, foot-note, p. 273 et seq.
It was only after many years of laborious investigation that the appropriate lesion was affixed to a symptom so well understood and described in its clinical aspects. The first conception of abdominal and intestinal inflammation had no relation to diarrhoea. Under the name [Greek: eileos], Hippocrates described abdominal symptoms of intestinal obstruction and inflammation. For Sennert (1641) inflammation of the intestines meant peritonitis. Bonet (1679), Hoffman (1710), and Boerhaave (1758) included under this head peritonitis, ileus, and all febrile and painful abdominal affections. Sauvages (1763) and Morgagni (1779) gave in detail the symptoms of peritonitis and called the disease intestinal inflammation—enteritis. In 1784, Cullen made an advance in subdividing [p. 668]enteritis into e. phlegmonodoea and e. erythematica—the one involving the entire wall of the intestine and the peritoneum, the other the mucous membrane lining the intestine. John Hunter (1794) first fixed the place of peritonitis as a distinct affection from inflammation of the mucous membrane of the intestines.2
2 J. Hunter, A Treatise on the Blood, Inflammation, and Gun-shot Wounds, London, 1794, p. 284.
Up to this time constipation was the chief symptom of enteritis. The meeting of the streams, the affixing the symptom diarrhoea to its appropriate lesion, was brought about hypothetically at first by J. Carmichael Smith in these words: "I think it is probable (for we can have no positive evidence of the fact) that in diarrhoeas from catching cold the villous or interior coat of the stomach is sometimes slightly inflamed."3
3 Paper read Jan. 8, 1788, Med. Communications, London, vol. ii., 1790, p. 168.
On the Continent enteritis soon after this was limited in its meaning by Pinel (1798) to inflammation of the mucous membrane of any part of the intestines. He gave the name catarrhal diarrhoea to the same condition. A still further restriction of its meaning was made by Broussais (1821), who defined enteritis to be an inflammation of the mucous membrane of the small intestine; he gave the name colitis to the same disease in the colon. This distinction was adopted by Rostan (1826), Andral (1836), C. H. Fuchs (1846), G. B. Wood (1852), Wunderlich (1856), Grisolle (1865), Flint (1866), and Aitkin (1868). According to the views of some authors, chiefly English, as Copland (1844), Bristowe (1871), Roberts (1874), Habershon (1879), enteritis includes inflammation of the serous as well as of the mucous coat of the intestines.
Niemeyer (1864), Jaccoud (1869), Leube (1875), Bartholow (1880), and most German and French authors prefer the name intestinal catarrh as applied to inflammation of the mucous coat; inflammation of the serous coat is peritonitis; the word enteritis is abandoned as involving a pathological error.
NATURE AND CLASSIFICATION.—Catarrh of the intestines is an inflammation of the mucous membrane of the intestinal tract. There are various peculiarities of the catarrhal process due to the anatomical structure of the parts involved, the presence of open glands, lymphatic follicles, etc. This disease is to be distinguished from inflammation of the serous coat of the intestine (peritonitis). The two are quite distinct in their etiology, pathological anatomy, and symptomatology, although they have been often confounded under the same name, enteritis.4 As so much confusion prevails as to the proper meaning of enteritis, it is best to abandon the word altogether.
4 For cases called enteritis in which the lesions of peritonitis were found, see Hamilton, Edin. Med. Journ., vol. ii., 1857, p. 304; also Breed, Chicago Med. Examiner, Oct., 1869, p. 579.
Diarrhoea is still regarded by some authors (J. J. Woodward) as synonymous with intestinal catarrh; by others it is considered separately as a disease distinct from catarrh. Habershon describes the lesions of catarrhal diarrhoea and mucous enteritis almost in the same words.5 It is an unscientific method to take one symptom of a pathological state, to [p. 669] erect it into a disease, subdividing it into varieties which are but differences in the intensity of its manifestation, and to assign to it no fixed lesion. Diarrhoea is in reality but a sequence and symptom of hyperæmia or inflammation of the intestinal mucous membrane.
5 Such a method of treating the subject involves a repetition, with an inversion, of the same description. Thus, catarrhal diarrhoea has as its lesion mucous enteritis; mucous enteritis has for its symptom (catarrhal) diarrhoea.
ETIOLOGY.—Intestinal inflammation is more prevalent in the Northern, Middle, and Western than in the Southern States. There is no relation between the distribution of malarial and intestinal diseases: in some regions where malarial disease is rife there is very little disease of the intestines. Limited areas in Lower Mississippi, Eastern Kentucky, Eastern North Carolina, etc. have a special predisposition to diseases of this class.6
6 F. A. Walker, Statistical Atlas, 1874, table v. p. 3; also plates xlii. and xlv.
During the Civil War diarrhoea and dysentery were more frequent and fatal in the central region than in the Atlantic and Pacific regions.
It is difficult to compare the relative liabilibity of the native and foreign-born populations in the United States to intestinal disease. Inasmuch as children, among whom the bulk of such cases occur, bear such a small proportion to the adult foreign population, allowing for differences due to this cause, statistics show that the foreign-born race has a very distinct predisposition to these forms of disease.7 The Swedes, Norwegians, and Danes have a marked susceptibility to intestinal diseases; the English and Welsh have the same tendency; but the Irish have a comparative immunity. The colored race is more prone to intestinal than to malarial diseases in the Middle States, but there is the reverse susceptibility in the Northern and Southern States.
7 The number of children under ten to 1000 native population is 306; number of children under ten in 1000 foreign population, 47 (F. A. Walker, "Relations of Race and Nationality to Mortality in the United States," Statistical Atlas, 1874, p. 213).
Under ten years more males than females have enteritis, in the proportion represented by the figures 362 and 299. After ten the predisposition of the two sexes is about the same.
The summer is the season when diarrhoea is most prevalent and most fatal. June, July, and August are the months in which the greatest number of cases occur and in which there is the highest mortality. The extraordinary death-rate in these months in cities is of course due to the influence of summer heat on children, and the death-rate from diarrhoea and entero-colitis is chiefly among infants under one year. But among adults the same rule holds. The highest monthly mortality from acute diarrhoea among the U.S. troops (white) between 1861 and 1866 was 147, in July, 1862; the next highest was 114, in August, 1862. June and September were after these the most fatal months. According to the census of 1870, the most fatal month is August.
Elevation of temperature in the summer months is the cause of the prevalence of intestinal catarrh and of its great mortality among infants and children. The number of deaths bears a direct ratio to the degree of heat, the highest death-rate occurring in seasons of unusual high temperature.8 The effect of excessive or prolonged heat is to arrest or weaken the digestive processes; undigested masses in the stomach or the intestines act as foreign bodies and produce inflammation.
8 Among the numerous publications bearing on this subject, those contained in The Sanitary Care and Treatment of Children and their Diseases (Boston, 1881) are of especial value. S. C. Busey's article contains much valuable matter on the relation of summer heat to illness and mortality among children.
[p. 670] Sudden changes of temperature from cold to heat or from heat to cold develop diarrhoea. If the air is at the same time saturated with moisture, the effect of a change in temperature is greatly intensified. In the first hot days of June there is on the Atlantic coast, especially in cities, a rapid increase in the number of cases of gastro-intestinal disturbance. A larger number of children are taken ill in June than in August. The child in time becomes habituated to heat, and if not attacked early runs less risk of illness in the later months. A sudden or unusual exposure to low temperature, as in lying on damp ground, leads to the same result. The check to perspiration after violent exercise is especially provocative of diarrhoea. In these instances the congestion and consequent inflammation of the mucous membrane are brought about through the effect of heat or cold upon the peripheral nervous system. Cold may act more directly by the driving of suddenly-cooled blood from the surface of the body to the interior. External burns belong to the same category, as they lead to extensive inflammation, sometimes to ulceration, of the duodenal mucous membrane through reflex influence. A case is reported of a boy aged twelve years who after an external superficial burn of the left thigh was taken with profuse diarrhoea which ended fatally in three hours (Ziemssen).
Contamination of the atmosphere with emanations the result of the overcrowding of many human beings together, as in prisons, camps, or asylums, especially where decomposition of organic matter is going on, is of great influence in causing diarrhoea. Persons living in badly-ventilated houses, or in houses improperly drained where the air is vitiated by escaping gas from sewer-pipes, are especially prone to be attacked. But sewer-gas, per se, does not cause diarrhoea any more than it causes diphtheria or scarlatina.9 It is a step backward to hang upon this ready explanation all our doubts and our ignorance of the origin of disease. The specific germ of the zymotic diseases may be conveyed in the gases from sewers, but there are other and more direct modes of communication which should receive equal attention.
9 Longstaff (Brit. Med. Journ., London, 1880, vol. i. p. 519) believes that summer diarrhoea has a specific poison which is intimately connected with the process of putrefaction, and that the infective material has its source in the public sewers.
Children are much more liable to intestinal inflammation than adults. This is due to the greater susceptibility of the mucous membrane in them to congestion and catarrh from external influences and from direct irritation. In infants fed upon an unsuitable diet—cow's milk or other substitutes for mother's milk—this susceptibility is much increased. The age most liable to attack is under one year, or from the first to the second year, when, in consequence of dentition, weaning, and a change from a diet chiefly or almost wholly liquid to one of solids, there is a great liability to a disturbance of the normal equilibrium. Intestinal catarrh forms almost one-third of the total number of the affections of childhood. According to the census of 1870, 761 out of every 1000 deaths from diarrhoea, dysentery, and enteritis occurred under the tenth year. In old age a similar predisposition exists, and a mild attack will in old persons induce more serious symptoms than in middle life. Epidemics of diarrhoea among the aged in asylums and hospitals are not uncommon.
[p. 671] Temperament and idiosyncrasy are causes of differences in predisposition. Many persons in consequence of taking cold invariably have diarrhoea, while others as invariably have nasal catarrh or bronchitis. Certain articles of food, as oysters and eggs, lead always in some persons to intestinal disturbance. An exaggerated sensibility of the mucous membrane to particular impressions is the cause of this peculiarity.
Previous attacks of intestinal inflammation render the individual liable to recurrences from very slight causes. The suppression of the menses and of hemorrhoidal discharges and the healing of eruptions are said to be followed by serious diarrhoea, but such an occurrence is probably more often a coincidence than a result.
Sedentary life, by enfeebling muscular movement and by inducing indigestion and constipation, brings on diarrhoea. Constipation impairs the muscular tone of the bowel, and hardened fecal accumulations act as irritants which sometimes provoke acute catarrhal processes—diarrhoea and dysentery. Insufficient clothing in children and in adults makes the skin more susceptible to changes of temperature and conduces to intestinal congestion. Smoking in excess and the use of narcotics and stimulants are mentioned as debilitating causes which pave the way for disease in the intestine; the habitual use of the stronger liquors, by keeping up chronic engorgement of the mucous membrane, is undoubtedly a potent cause. Occupations which involve deprivation of fresh air and sunlight, and all trades which enfeeble the individual, make him liable to all digestive disorders. A feeble constitution, debility from disease, from over-fatigue, or from loss of sleep, or any perturbing influence, puts the body in a state favorable to indigestion and diarrhoea.
The eruptive fevers are accompanied more or less by gastro-enteric catarrh. In scarlet fever, measles, and variola there is a state of equilibrium between the skin and the intestinal mucous membrane. When the morbid manifestation does not normally appear upon the skin there is a transference of irritation to the intestine. The administration of purgatives in the early periods of scarlet fever and measles delays, sometimes prevents, the outburst of the eruption on the skin. The intestinal catarrh of the eruptive fevers has sometimes the significance of an exanthem and sometimes of a secondary complication. In measles it is more frequently the former; in scarlatina and variola it comes later as a complication.
Uræmia, malarial infection, chronic suppuration, pyæmia and septicæmia, cancerous and strumous disease of the mesenteric glands, scurvy, tuberculosis, Bright's disease, and chronic wasting diseases in general, are conditions in which diarrhoea appears as a result of the defective nutrition of the vessels of the intestinal wall and their liability to dilatation and hyperæmia, or from the presence in the blood of septic matter.10
10 For experiments relating to the production of intestinal catarrh by injections of irritating or putrid matter into the blood consult Traité clinique et expérimentelle des Fièvres dites essentielles, Gaspard et Bouillaud; also, Path. anat., Lebert, tome ii., Texte, Paris, 1861, p. 205.
The ingestion of a larger quantity of food than the stomach and intestines are able to soften, and the taking of food essentially indigestible or improperly prepared by cooking, are causes of the passage of masses of food more or less unaltered along the intestinal tract. Hyperæmia [p. 672] follows the mechanical irritation of the mucous surface. When articles of food are in a partial state of putrefaction, so that the antiseptic properties of the gastric juice cannot be quickly enough brought into play, there is a rapid fermentation in the stomach, with the development of symptoms of gastric and subsequently of intestinal catarrh. Unripe fruit, vegetables composed of hard tissue, as early potatoes, cucumbers, pineapples, and cherries, by their indigestible nature, are frequent causes. Oysters, crabs, fish, and lobsters often occasion acute diarrhoea in consequence of being in an unfit condition for food. Cheese has been known to produce violent illness with symptoms of intense intestinal irritation; these effects are due to some poisonous substance, hitherto undiscovered, developed in the course of putrefaction. New coffee causes diarrhoea; six months is usually the time before coffee grown in Ceylon reaches the European and American markets; by this time it does not have this effect.11
11 J. Stevenson, "Medical Notes from Ceylon," Edin. Med. Journ., Feb., 1862, p. 693.
The irritant and caustic poisons, as mineral acids, caustic alkalies, corrosive sublimate, arsenic, oxalic acid, tartar emetic, and carbolic acid, kindle an intense inflammation of the mucous membrane of the stomach, duodenum, and of the lower portion of the intestinal canal. Softening of the coats of the intestines from corrosion, with perforation, is not an infrequent result.
Drastic purgatives act as irritant poisons in producing acute hyperæmia of the mucous coat with excessive transudation of serum; or, in other words, an acute catarrh. A discharge of vitiated bile or an excess of bile is given by recent12 as well as by older writers as a provoking cause of diarrhoea. The proper relationship is the reverse of this: an intestinal catarrh the result of irritant action upon the mucous surface entails a more active outflow of bile, just as some cathartics by irritating the duodenum excite the gall-bladder to empty itself.13 Impacted fecal masses are direct irritants, exciting inflammation (typhlitis, dysentery); putrefactive changes in long-retained fecal collections have an additional power of irritation. Foreign bodies accidentally or purposely swallowed, intestinal parasites, the pus from an abscess which bursts into the intestine, likewise are excitants of disease. Tubercle nodules, typhoid ulcers, cancer, or other neoplasms in the wall are surrounded by areas of inflammation.
12 Roberts, Th. and Pract. Medicine, Am. ed., Philada., 1880, p. 160.
13 "The propositions which are the foundation of the whole theory that bile can cause diarrhoea, and that its absence leads to costiveness, cannot be looked upon as proved" (J. Wickham Legg, On the Bile, Jaundice, and Bilious Diseases, New York, 1880, p. 661).
Alcohol taken in excess, as in a debauch, leads to acute gastro-intestinal catarrh. The stomach symptoms are the earliest to develop and are the most prominent. Habitual alcoholic indulgence is a more common source of chronic than of acute intestinal catarrh.
The influence of unwholesome drinking-water as a cause of diarrhoea has been carefully examined by Woodward.14 Turbid or muddy water holding inorganic matters in suspension, he concludes from the evidence, is not a source of disease, and the injurious effects of such waters have been grossly exaggerated. Water containing inorganic substances in solution produce diarrhoea, and are purgative if the dissolved matters have purgative properties. Limestone-water may produce [p. 673] temporary disturbance of the bowels, but is wholesome. Carbonate and sulphate of lime and magnesium in solution are more cathartic, but not as much so as selenitic waters which contain an excess of sulphate of lime. The salts of sodium and potassium in the waters of Colorado, New Mexico, and Utah are still more liable to produce diarrhoea.
14 Med. and Surg. History of the War, Part 2, Medical Volume, p. 599 et seq.
Water contaminated with organic matters of vegetable origin, which are found in states of decomposition in marshes and stagnant pools, does not, in the opinion of Woodward and Parkes, have very great influence in the production of diarrhoea or dysentery. Impurities from decomposition of animal matters are unhealthful. This is especially true of water impregnated with soakage from privies and sewers; and yet epidemics of diarrhoea cannot as often be clearly traced to this source as can outbreaks of typhoid fever. Parkes says water contaminated with three to ten grains per gallon of putrescent animal matter may be hurtful.
Contusions and injuries of the bowel by sudden pressure or shock to the abdominal wall may lead to intestinal inflammation. The large intestine is more exposed from its size and position to such injuries. Pressure upon the bowel by a tumor, as an enlarged or retroverted uterus, may cause diarrhoea, the source of which may be overlooked. Early-morning diarrhoea from a displaced womb is of frequent occurrence.
Emotional influence, as sudden fright or grief, will produce sudden diarrhoea. Lesions of nerve-centres—corona radiata, optic thalamus, or corpus callosum—induce hyperæmia, softening, and ulceration of the mucous membrane of the small intestine.15
15 Rosenthal, "Diseases of the Nervous System," Wood's Library, New York, 1879, vol. ii. p. 266.
Minute organisms (bacteria) are thought by some observers to be the cause of diarrhoea, especially of a zymotic form, which prevails in the summer months. In accordance with this theory, the dejecta from infected persons are the vehicle of the contagious poison which by air- and water-contamination infects others.16
16 Wm. Johnston, Lancet, London, 1878, vol. ii. p. 397; also, Brit. Med. Journ., London, 1879, p. 81; also, G. E. Paget, "On the Etiology of Zymotic Diarrhoea," Brit. Med. Journ., Nov. 19, 1881, p. 819.
PATHOLOGICAL ANATOMY.—A description of the morbid anatomy of acute intestinal catarrh includes the changes which are observed (1) in the exterior appearances of the intestines, (2) in their contents, and (3) in the condition of their mucous lining.
1. The external appearances of the intestines depend upon the degree of distension of the tube, the character of the contents, and the presence or absence of inflammation of the serous coat. Great distension of the colon, of the cæcum, and of the small intestines is met with in acute intestinal catarrh of some duration, and is due to relaxation of the muscular coat. The colon usually presents the greatest distension. The calibre of the tube may be lessened by strong contraction of the muscular layer in acute intestinal inflammation of great intensity with early and fatal termination. The color of the exterior varies with the tension of the wall, the color of the contents, and the amount of vascular injection. If the bowel is much distended with gas, the color is pale; the mingling of bile with the feces causes a yellowish or brownish color; if blood is in the tube a dull red hue is given to the walls. If the intestine is congested or inflamed, the vessels are outlined distinctly and can be seen in [p. 674] different layers. The areas of external redness generally correspond to internal hyperæmic patches. The serous membrane shows arborescent congestion at the mesenteric attachment or is inflamed from perforation; the signs of peritonitis are most marked in the neighborhood of the irregularly-shaped, round, oval, or pin-point openings in the gut. The abdominal cavity may contain fecal matter, food, medicines, or worms which have passed through the perforation.
2. The intestinal contents, instead of being homogeneous, of pale-yellow color, and pea-soup-like appearance in the small intestine, brown and more condensed in the lower part of the large intestine, may present various changes. The fluid is usually increased in quantity, and is thinner than normal in the colon: the color is greenish from the bile, very pale from the closure of the bile-duct, red or black from blood. The odor is absent from excess of serum, or very offensive from decomposition due sometimes to the closure of the common bile-duct and the want of bile. Shreds or masses of mucus may float in the liquid. Undissolved pills or drugs, as bismuth, accumulated seeds, skins of fruits or vegetables, parasites, or foreign bodies are seen. Epithelial cells, the débris of digestion, micrococci, and bacteria are visible under the microscope.
3. Inflammation involving the mucous membrane of the whole intestinal canal is rarely or never met with. The nearest approach to generalized catarrh of the bowel is found in eruptive fevers, especially measles. Inflammation extending throughout the whole length of either the small or large intestine alone, and affecting all parts equally, is also rare. The ileum is the part of the small intestine most frequently the seat of disease, but the ileum is rarely affected alone. Inflammation is more frequently limited to the colon than to the small intestine. The most common form of intestinal inflammation is ileo-colitis, where the lower part of the ileum and a part of the colon, sometimes of considerable extent, are inflamed. The duodenum is sometimes the seat of a local inflammation, but this rarely happens except in the case of external burns; duodenitis is most frequently an extension of catarrh from the stomach, but the pathological anatomy of the duodenum presents some peculiarities which will be described hereafter.
(a) Hyperæmia of the intestinal mucous membrane may exist without inflammation. The engorgement of the veins by mechanical retardation in disease of the liver, heart, or lungs does not constitute catarrh, although it is sooner or later followed by catarrhal processes, usually of a chronic nature. Gravitation of blood to the most dependent parts in cases of long illness distends the vessels, and post-mortem hypostasis leads to the passage of serum and coloring matter into the meshes of the mucous and submucous tissue. In fatal cases of acute diarrhoea sometimes no lesion has been observed. The hyperæmic membrane pales after death, as does the skin in scarlatina and erysipelas.17 The presence or absence of hyperæmia is therefore no positive proof of the previous existence or non-existence of inflammation. To constitute inflammation there must be other changes besides hyperæmia, as oedema, softening, and infiltration with cell-elements.
17 It is difficult to recognize post-mortem hyperæmia in the mucous membrane of the mouth or throat where intense inflammation has been seen in life.
[p. 675] A degree of vascular turgescence visible to the naked eye is nearly always present in the mucous and submucous tissues which have been the seat of catarrh. It is usually found in the lower part of the ileum, the cæcum, sigmoid flexure, and other parts of the colon. The redness is diffused over a surface of several feet in length or is circumscribed in patches of varying size. When vessels of small size are distended with blood, red branching lines are seen (arborescent or ramiform injection) which have their starting-point in the insertion of the mesentery. When the capillary system is engorged a fine interlacing network can be discovered, which gives to the membrane a more uniform red color. Parallel lines or bands of redness extend in a transverse direction across the axis of the canal corresponding to the folds of mucous membrane in the small and large intestine.
The shades of color depend upon the intensity and duration of the congestion. In acute mild forms the color is light red; in more intense grades the membrane is more vivid or purplish. Brown and slate-colored tints show a passage into the chronic stage. A black hue occurs in gangrenous inflammation. Minute dots (speckled redness) are due to minute extravasations, and ecchymotic irregular patches are sometimes seen.
Bile-staining of the mucous surface is met with; this cannot be removed by washing. In metallic poisoning the redness is more vivid and the mucous membrane is eroded.18
18 For colored plates illustrating hyperæmia and inflammation of the intestines see Carswell, Path. Anat., London, 1838, plate ii. figs. 1 and 2. These are beautiful representations of (1) ramiform vascular injection passing into (2) capilliform injection, which becomes (3) uniformly red, or from its intensity (4) ecchymotic or hemorrhagic. See also Annesley, Morbid Anatomy, London, 1828, plates x. (Fig. 2), xiii., xxii., xxiv., and xxv. Many of these are illustrations of peritonitis as a complication of enteritis. See also Kupferlafelnzer, Lesser, Ueber die entzundung und Verschwarung der Schleimhaut des Verdauungskals, Berlin, 1830, tab. iv. fr. 3; also J. Hope, Illustrations of Morbid Anatomy, London, 1834, figs. 116, 118, 124, and 125. These plates are wonderful in their truthfulness and execution.
(b) Acute oedema and increase in the cell-elements in the inflamed parts give rise to swelling and to softening, so that the mucous membrane seems to be easily scraped off. This is not always the case, as no loss of firmness of the reddened tissue is often found. In the small intestine the villi, which in health are not seen, become enlarged, giving a "plush-like" or velvety appearance to the mucous membrane; they are sometimes club-shaped from epithelial accumulations on their free extremities.
(c) When the small intestine is examined the solitary glands, which in the normal state are barely visible, are so enlarged that they appear as rounded prominences. They are described as looking like grains of mustard-seed on a red ground, and are the size of pinheads. When they are distinctly seen it may be concluded that they are enlarged. In children the glands are enlarged when there has been slight or no diarrhoea.
Peyer's patches are also tumefied, and are more distinct from being elevated above the surface, but they have not in intestinal catarrh as great a relative enlargement when compared with the solitary glands as in typhoid fever. The interfollicular substance of the patch may hypertrophy without any increase in the size of the follicles; a reticulated [p. 676] appearance is then given to the gland. The color of the swollen follicles in recent inflammation is translucent from oedema; later they are gray and opaque. These changes are more marked at the lower end of the ileum, because the isolated follicles and Peyer's patches are more numerous there.
(d) Catarrhal ulcers—erosions—are produced by the loss of epithelium or from a process of vesicle-forming and rupture, as in stomatitis. They may enlarge, undermine, and coalesce, thus reaching quite a large size. They may deepen and perforate the wall of the bowel, causing peritonitis, or they may heal, forming cicatrices which in contracting may narrow the canal.
Small follicular ulcers are found on the mucous surface. They result from the breaking down of the exposed wall of the closed follicle from over-distension. The ulcer is either on the apex of the dome of an isolated follicle or is within the area of a Peyer's patch. Sometimes several ulcers may be seen on the surface of the swollen patch.19 The ulcerative process is sometimes very rapid. In the case of a child aged eight years, with no previous intestinal disease, who died in the Children's Hospital, Washington, in June, 1882, after a two days' illness with watery discharges and rapid prostration, the solitary glands throughout the ileum were many of them enlarged. As many as a dozen small ulcers were seen at the apices of the enlarged follicles.
19 See photograph facing page 302 of Med. and Surg. History of the War.
In the large intestine the same lesions are found, but in a more advanced stage, especially in the cæcum and descending colon. Enlarged solitary glands of the size of a pinhead or small bird-shot are scattered along the canal.
Follicular ulcers20 are found in the large intestine, occupying the summit of the enlarged follicles and involving a large extent of mucous surface. Pigment-deposits are seen which give rise to the appearances described as occurring in chronic intestinal catarrh.
20 For description of the mode of formation and growth of follicular ulcers see article on CHRONIC INTESTINAL CATARRH.
(e) The mucous surface is covered, especially in the areas of redness, with an adhesive, opaque mucus of neutral or alkaline reaction and of yellow, red, or brown hue, depending upon the relative amount of bile or blood. It is composed of mucus-corpuscles, epithelium-cells of cylindrical and prismatic form, pus-cells, and sometimes blood-corpuscles. Vibrios and bacteria also are seen.
The chief distinction between the lesions of acute intestinal catarrh and typhoid fever are these: In typhoid fever the number of Peyer's patches involved is larger; there will be a chain of enlarged glands from the ileo-cæcal valve throughout the ileum, those nearest the ileum being the most altered. Near the valve there is usually some ulceration, so that the gland acquires a ragged appearance. In catarrh of the bowel there is a more irregular distribution of enlarged glands; they project less above the surface, and if ulcerated have one or two spots of erosion. In typhoid fever the Peyer's patch has the most prominence. In catarrh of the bowel the solitary glands are the most enlarged. In catarrh the large intestine may be the seat of the most advanced lesion; in typhoid fever, except with rare exceptions, the lesions in the ileum are most advanced.
[p. 677] (f) The mesenteric glands are enlarged, but not so uniformly so or to the same extent as in typhoid fever. The stomach is sometimes found inflamed, the mucous membrane being reddened, thickened, or softened. The liver, spleen, and kidneys are normal or present accidental conditions of disease. In the respiratory organs pulmonary congestion, pleurisy, and pneumonia are found. The heart contains clots which are fibrinous or soft and red; they are found on both sides, but when one cavity alone is filled the right is the common seat. The brain is usually normal; fluid may be in the subarachnoid space, and thrombi in the cerebral sinuses.
PATHOLOGICAL HISTOLOGY.—In the genesis of catarrh of the intestinal mucous membrane the first effect of the exciting cause is an over-distension of the capillaries and small vessels; this congestion is most marked in the meshwork of vessels around the closed follicles. A transudation of serum takes place into the mucous layer, and in more marked congestion into the submucous layer also; these tissues become more or less oedematous and swollen. Transudation of serum into the intestinal tube follows. From over-stretching the walls of minute vessels may rupture and small extravasations take place, staining the tissue red. These subsequently become black pigment-spots. Post-mortem extravasations are due to decomposition of the wall of the vessel. Rupture of vessels on the surface leads to escape of blood into the bowel, which is mixed with the transuded serum. The proper secretion, intestinal juice, is diminished as a result of these changes, but an excess of the mucus with which the mucous membrane is always coated immediately follows. The origin of the mucus is not to be sought for in the activity of the glands alone, but in the transformation of the protoplasm of the epithelial cells.21 The varying proportions of serum, mucus, and blood cause the stools to be serous, mucous, slimy, or bloody, hence the terms serous, mucous, and bloody diarrhoea.
21 Rindfleisch, Path. Histology, Sydenham ed., vol. i. p. 412.
Hypernutrition, swift life of the mucous membrane, the result of continued excess of blood, entails the increase of the cell-elements. Lymphoid cells accumulate in the submucous layer, especially where these cells are normally most numerous. There is a saturation of the membrane with an excess of plasma. Cells also appear in increasing numbers in the interfibrillary spaces of the mucous membrane, which increase its bulk, and the follicles of Lieberkühn appear as if pushed apart. Lymph-corpuscles accumulate in the meshes of the closed follicles, which are distended and project above the surface as described. Multiplication of the cells within the follicle (follicular suppuration) causes over-stretching and the wall bursts, forming the first stage of the follicular ulcer. The appearance upon the epithelial surface of an increased number of loosened cells, which are sometimes epithelial in character and at other times resembling pus-cells (epithelial and purulent catarrh), is believed to be due to a rapid manufacture and exfoliation of epithelial elements, and to constitute one of the essential features of catarrh. Desquamation of the epithelium in catarrh of the bowel, even in that of Asiatic cholera, has been called in question by Woodward, who thinks that the stripping off of epithelium is cadaveric.
SYMPTOMS.—Owing to the difference in the intensity and extent of [p. 678] the catarrhal process there is every possible variation in the symptoms of intestinal inflammation. No one symptomatic picture will properly represent all cases, and with a view to greater convenience and exactitude of illustration a division may be made into mild and severer forms.
Under the head of mild forms can be included all cases of intestinal catarrh which by their short duration and benignant character point to a mild degree of inflammation. They correspond to the following anatomical states: hyperæmia of the mucous membrane of parts of the small or large intestine, or of parts of both simultaneously; slight or moderate swelling of the membrane from serous saturation; transudation of serum into the canal; increase of lymphoid cells in the mucous and submucous tissues; and increased manufacture of epithelial cells, but without any marked tumefaction or ulceration of the closed follicles. The termination is by resolution, which is reached in a few days usually, and the membrane is rapidly and entirely restored to the normal state. Between the normal condition of the mucous membrane, with its recurring periods of physiological hyperæmia, and the hyperæmia with exaggerated secretion and peristalsis which leads to diarrhoea, there is no well-defined border-line. Diarrhoea may be regarded as the most certain sign of the catarrhal process. Whenever the frequency and fluidity of the stools are such as to be regarded as pathological, some stage or other of catarrhal inflammation may be assumed to exist.
In a large number of mild forms the onset is sudden. After a meal of indigestible food or an unusual excess pain will be felt in the abdomen, recurring in paroxysms, which start in the neighborhood of the umbilicus and radiate throughout the abdomen. The pain is accompanied by borborygmi, and is succeeded sooner or later by a desire to go to stool. The first one or two movements, which follow each other in quick succession, are more or less consistent or moulded, but in a short time diarrhoea is established by frequent discharges of watery fluid, containing perhaps some undigested fragments of food, which may have been the exciting cause of the illness by mechanical irritation. Each stool is preceded by colics, griping pains in the abdomen, which are relieved by the evacuation. An attack beginning in this way and from such causes may cease in a few hours, and be unattended by any general symptoms if proper precautions are taken. A slight dryness and coating of the tongue, with loss of appetite and occasional griping pains or a tendency to looseness of the stools, may continue for a day or two. Indiscretions in diet or other imprudences, as fatigue, may prolong the mildest attack during one or more weeks, but the character of the illness is here due not to the nature of the disease, but to the addition of fresh causes which delay the natural progress toward recovery.
Severer forms either begin suddenly, as in the milder forms just described, or are preceded for a time by symptoms of gastric or intestinal indigestion. The patient may have complained of distress after eating, flatulence, colicky pains, distension of the abdomen and tenderness on pressure, loss of appetite, with a general feeling of ill-health—symptoms which point to the existence of a condition of the mucous membrane of the gastro-intestinal canal favorable to the action of an exciting cause.
A feeling of chilliness ushers in the attack. This is accompanied by fever, which at first, and sometimes throughout, is of a marked remittent type. [p. 679] The griping pains, colics, which at first are infrequent and dull, now recur at short intervals and become sharper. They are sometimes attended with vomiting of food or of a greenish fluid. The intensity of suffering may be so great as to cause pallor of the countenance, a feeling of faintness, and coldness of the surface with sweating. The paroxysm usually precedes a movement. The more severe pains extend to the lower extremities and the scrotum.
Movement of gas in the intestines produces rumbling, gurgling, or splashing sounds, called borborygmi. They are paroxysmal, lasting a few moments, or are coincident with pain, and frequently are the immediate precursors of an evacuation. The cause for their production is the quick propulsion of the fluids by strong peristaltic action from one part of the bowel to the other or the rapid movement of gas within the bowel. Relief is obtained both from the pain and from the sense of distension by expulsion of flatus.
Tympanites is closely connected with the symptoms just described. An excess of gases within the bowel is not primarily a result of the inflammation of the mucous membrane, but is an early phenomenon due to the decomposition of indigestible food in its transit through the intestine. Later, the gases are developed very readily by the decomposition of even the most digestible articles of food, the mucus, which is the product of the catarrh, acting as a ferment.
The distension of the intestinal canal produces an intumescence of the abdomen which is commonly uniform, but may be greater in some portions of the tract than in others. Thus the transverse and descending colon are more projecting and more distinctly outlined than other portions of the canal.
Sensibility of the abdomen to pressure exists along the line of the colon or over a considerable area. But no defined limitation of the affected part can usually be made by the location of pain to the touch. If there is any local tenderness, it is over the descending colon. In one form of enteritis—typhlitis—the localization of the inflammation in the cæcum produces subjective pain and pain on pressure in a restricted region—a peculiarity which results no doubt from the early intensity of the inflammation and the implication of the connective tissue behind the bowel. But this is not true of inflammation of any other part of the intestinal canal.
A sensation of soreness on movement, as in turning in bed, standing, or walking, is not uncommon, even when the attack is of no great gravity. The patient on standing bends forward to relieve tension, and he may feel nervous when the bed is shaken.
Diarrhoea is the most important symptom, as it is directly related to catarrh. The number of evacuations varies from one or two to twenty or more in the day. In cases of medium intensity there are from six to ten in twenty-four hours, the interval between the movements being two to three hours during the day and somewhat longer at night. The matters passed in quantity range from two ounces to a pint; the average is about four fluidounces. This, however, is subject to great variations, depending upon the intensity of the disease; the more choleriform the attack the greater the amount of fluid passed. The weight of the evacuations varies from five ounces to forty pounds in twenty-four hours; this increase does not depend upon the greater quantity of water only, but the solid constituents are in greater amount.
[p. 680] The normal brown color, which is due to hydrobilirubin, changes as the movements become thinner to yellowish-brown or pale yellow from dilution of the fecal matter with water. An excess of serum or mucus renders them colorless. A greenish-brown, greenish-yellow, or green hue is due to the presence of bile. The rapid descent of the contents of the bowel delays or prevents the reabsorption of bile,22 or the fluid is expelled before the usual transformations in color take place.23 The bile-pigment is also absent in duodenal catarrh from closure of the opening of the ductus choledochus.
22 L. Brunton, "On the Action of Purgative Medicines," The Practitioner, London, June, 1874, p. 403.
23 The reaction of bile-pigment with nitric acid, which does not take place in the contents of the colon or in normal feces, is seen in the green stools of acute intestinal catarrh, especially in children.
The coloration of the stools further depends upon the character of the food and drink and upon the drugs given. From an exclusive milk diet the discharges are pale or contain undigested whitish lumps of casein. The preparations of bismuth and iron give a black color and the sulphate of copper a dark-green hue. A green or greenish-brown tint is observed after the use of calomel, and while the experiments of the Edinburgh committee demonstrated that no increase of bile follows its administration in dogs, yet the opinion is still general that the green stools contain an excess of bile.
Blood appears in three forms in the stools: as a coffee-ground or black powder from hemorrhage in the stomach or upper bowel; as a reddish fluid with small coagula in flakes, which come from intense congestion or ulceration of the intestine; or an abundant hemorrhage may result from deep ulceration in the duodenum or elsewhere.
The characteristic odor of the feces is altered in several ways. As the movements become less solid they acquire a nauseous or sour smell, due essentially to the volatile products formed in connection with the decomposition of fatty matters.24 When very thin and containing little or no feculent matter the discharges lose odor, as in cholera, or they become excessively offensive—cadaveric—in intense and fatal inflammation and in ulceration of the bowels. After exposure to the air the stools of diarrhoea undergo decomposition and develop offensive smells more rapidly than in health. The absence of bile, whether there is diarrhoea or not, gives rise to a peculiar and unpleasant odor, showing that this secretion is to some extent an antiseptic. The escape of fetid gas from the anus is rarely an accompaniment of a decomposed state of the rectal contents. In children the stools are more variable in quantity, color, and odor than in adults, and are more readily affected by the ingesta.
24 Guttmann, Physical Diagnosis, Sydenham Soc. ed., p. 404. The odor of normal feces is due to a substance isolated by Briequer, called scatol, which is a final product of the putrefaction of albumen (Ewald, Lectures on Digestion, New York, 1881, p. 106).
In the diarrhoea of old persons the discharges are thin, yellow, offensive, and often frothy.
The disorder of the digestive apparatus is attended with other symptoms. The tongue is normal in some cases; in others red at the point and edges with a central whitish coat, or the surface is red, polished, and dry. Marked change in the appearance of the tongue is due to a complicating gastric catarrh. There is thirst, with loss of appetite, and a tendency to [p. 681] nausea and vomiting in children and feeble persons. The breath has a peculiarly offensive odor (spoken of as fecal) in some instances.
Fever is not always present. In cases of moderate severity it occurs in the beginning of the illness, but declines rapidly under treatment by rest and diet. The course of fever does not conform to any type even in severe cases, although it so nearly resembles that of typhoid fever in its first week as to lead to mistakes in diagnosis. The height of the fever and its duration are measures of the extent of the lesions and their gravity. Sudden outbursts of fever point to some complication. In catarrh of the bowel due to cold the fever is higher than when indigestion is the cause. In very feeble persons, in children, and in any case from neglect and improper feeding the body-heat may be very high.
The urine is diminished and high-colored. Very little disturbance of the nervous system is seen except in young and old patients; some headache and restlessness are all that may be observed. Moderate delirium at night accompanies very acute attacks. In children convulsions are not unusual in the onset and at the end of the attack. In the aged exhaustion from the illness soon lapses into stupor or coma.
Paraplegia and contraction of the muscles of the extremities are referred by some observers to gastro-intestinal inflammation.25
25 Potain, Le Praticien, Paris, 1879-80, p. 88.
In uncomplicated mild cases of intestinal catarrh there is a movement toward recovery after a few days' illness. The stools become less frequent, smaller, and more consistent. In a week to ten days the tongue cleans, the thirst ceases, the appetite returns, the tympanites and pain diminish. The fever declines, and ceases before the diarrhoea is completely arrested. There are always more or less emaciation and loss of strength from the fever and arrest of nutrition. The liability to relapse is great, and the patient by indiscretions reproduces the same symptoms, thus prolonging the attack for several weeks. Acute intestinal catarrh may pass into the chronic form by a disappearance of fever and amelioration of all the abdominal symptoms. The patient begins to take solid food, gains strength and flesh, but complete recovery does not come. The diarrhoea recurs at variable intervals as the result of indulgences in a mixed diet, over-exercise, or exposure to cold, and in time we have some degree of chronic catarrh permanently established.
Very mild cases may be prolonged by the neglect of the patient to consider his painless diarrhoea of sufficient moment to need attention.
In inflammation of the more intense kind the picture is somewhat different. The prodromes are longer and the general symptoms more severe. Restlessness, a sense of prostration, delirium, and high fever mark the early stages and continue for a longer time. The patient loses flesh and strength quickly. The features express anxiety and illness, the skin is hot and dry, and the thirst great. Vomiting is repeated. Borborygmi, the tension of the abdomen, pain, and sensibility to pressure are all intensified. The stools are at first yellow and thin, but change much from day to day. They may be green or very thin and dark or grayish, and are sometimes very offensive in odor. Blood and mucus may be seen in them, being slimy or grumous and bloody. When the patient is very weak the discharges are involuntary; the tongue is coated white, with bright red tip and edges, and is often dry.
[p. 682] The severer forms last from three to six weeks. After a tedious period of alternate improvement and relapse the illness becomes chronic or the patient dies from asthenia, perforation and peritonitis, or some other complication.
In the most intense varieties which find examples among Europeans and Americans in intertropical countries, or result from acute mineral poisoning and from rapidly-progressing cases of acute ulceration of the intestinal wall, especially in children, there is a sharper and more violent invasion. The strength is reduced in a very short time, and there is rapid emaciation; the features assume an anxious expression; the complexion is leaden or livid; the skin is cold and clammy; the pulse is small, weak, and rapid; the breath comes quick and short, and is frequently complicated with hiccough. In the early stages vomiting occurs, due to a concurrent gastritis; in cases of poisoning vomiting is incessant.
The pain in the abdomen is intense, and less paroxysmal than in other forms. The abdomen is tympanitic and excessively tender to the touch, and the knees are drawn up to relieve the tension of the abdominal muscles. Thin, black, or reddish stools are passed every few moments. As the attack progresses the urine is suppressed, the voice becomes whispering, and collapse is developed. This is marked by cold extremities, dyspnoea, feeble and finally imperceptible pulse. Death may end the scene in a few hours or the patient may rally and recover slowly.
Choleriform diarrhoea occurs chiefly in children during hot weather.
VARIETIES DUE TO SEAT.—The symptoms and progress of acute catarrh of the intestines present numerous differences depending upon the seat of the inflammation. The symptomatology already given is that of the most common form (ileo-colitis), in which the lower part of the ileum and a considerable portion of the colon are simultaneously involved. Many cases no doubt occur in which the disease is limited and in which early recovery is the rule. The pathological anatomy of cases of generalized catarrh is better known, as they form the bulk of the fatal cases.
I. Acute Duodenitis.—The most common form of duodenitis is that in which the inflammation spreads by continuity of tissue from the stomach to the duodenum, as in acute gastric catarrh after a debauch. The prominence of the gastric symptoms disguises the intestinal lesion, unless the catarrh, as is frequently the case, extends into and obstructs the common bile-duct and its branches, and suddenly develops icterus with clayey stools and altered urine. Besides icterus, a careful isolation of symptoms will show that some cannot be attributed to the stomach: there is a dull pain seated in the right hypochondrium, extending to the right shoulder or shoulder-blade, which is increased by pressure upon the region of the duodenum. As the gastric symptoms improve there is no change in the icterus, which continues for some days or weeks longer. The connection between burns of the integument and ulcer of the duodenum is well known. Symptoms of perforation, with death, may be the first sign of this lesion, but vomiting of blood, icterus, purging of blood, indigestion, and cardialgia occur from duodenal ulcers.
The typical acute duodenitis described by authors as an independent [p. 683] affection is of rare occurrence. An epidemic of duodenitis26 has been reported where many persons were simultaneously attacked, all the cases having had the same traits—headache, pain in the line of the duodenum at the left edge of the right hypochondrium, pain in the first and second lumbar vertebræ, constipation, jaundice, slow pulse, and mental depression. Gangrenous inflammation of the duodenum27 has been once seen, and produced a chill, a severe sense of weight and pain in the epigastrium, retching and eructations of gas, tenderness on pressure, frequent pulse, and high temperature. There was obstinate constipation, with dyspnoea, death ensuing in a few days. At the autopsy gangrenous inflammation of the duodenum was found, which ended abruptly twelve inches from the pylorus. There was a large gall-stone in the gall-bladder.
26 McGaughey, Philada. Med. Times, Aug. 1, 1872, ii. p. 407; also, T. N. Reynolds, Detroit Clinic, June 7, 1882, p. 181.
27 Eskridge, Philada. Med. Times, Feb. 15, 1879, ix. p. 239.
A fatal case of duodenitis is recorded28 in which the following symptoms were observed: sudden and severe pain in the right hypochondrium, increased by pressure; rigors, vomiting and purging of a green flocculent fluid, and later of blood; jaundice, fever, delirium, collapse, and death. The pylorus and two-thirds of the duodenal mucous membrane were much inflamed and the orifice of the bile-duct closed.
28 Die Krankheiten des Duodenums, Mayer, quoted by Leube in Ziemssen's Cyclopædia, Am. ed., vol. vii. p. 373.
II. Acute Ileitis, Acute Jejunitis.—When the ileum, with or without the jejunum, is the seat of catarrh, diarrhoea may not be present, provided the inflammation is slight and there is no increase of colon peristalsis. The symptoms then are borborygmi, pain and fulness about and below the umbilicus or between it and the right ileum, especially after eating, and the general symptoms arising from indigestion and malnutrition. Fever is slight or absent; there are malaise and loss of strength. The feces give important indications. They contain unaltered bile and fragments of muscular fibre and starch-granules in excess of the quantity found in health. An increased quantity of mucus, diffused evenly in a fluid evacuation, or globules of mucus stained with bile, or bile-stained epithelium, denote inflammation confined to the small intestine. A larger amount of indican in the urine than is normally present is a sign of the same lesion.29
29 These conclusions are based upon the results of one thousand examinations of feces made by H. Nothnägel, and reported in Zur Klinik der Darmkrankheiten; Zeitschrift für klin. Medicin, iv., 1882, p. 223.
Intense inflammation of the small intestine may exist without diarrhoea or other symptoms betokening the real nature of the attack. Flint30 mentions having met with three such instances, and Goodhart31 records thirteen cases of enteritis with marked lesions in which no diagnosis had been made before death. Rilliet and Barthez report twenty-four autopsies in children with intestinal lesions in which no symptoms had been observed.32
30 Clinical Medicine, Philada., 1879, p. 280.
31 Guy's Hospital Gazette, Sept., 1878, p. 98 et seq.
32 Maladies des Enfants, Paris, 1861, tome i. p. 748.
III. Acute Colitis.—Fifty years ago colitis was synonymous with enteritis, and not with dysentery, as at a more recent date.33 The older [p. 684] signification expressed the fact that inflammation in the colon is essential to diarrhoea. Later the term was used synonymously with dysentery.34
33 Journal général de Médecine, Paris, 1825, t. xci. p. 18.
34 Tweedie, System of the Practice of Medicine, 1841.
The colon is a conducting tube; the contents are composed of matters unabsorbed in the small intestines. At first the mass entering the colon is fluid, but by the gradual absorption of its watery part it approaches solidity. The discharge from the rectum of a fluid shows that the propulsion through the large intestine is so rapid that the process of drying does not take place, or that from inflammation of the colon there is an excess of fluid transudation from the intestinal wall. The superficial position of the colon, its great size and length, expose it to the action of external cold, to blows, etc.
In catarrh limited to the colon there are essentially the same symptoms as in ileo-colitis, inasmuch as the inflammation of the colon gives to that form its characteristic features—borborygmi, diarrhoea, and tympanites. When the disease in the colon preponderates or exists alone, the pain and tenderness are more superficial and confined to the line of the large intestine. The distended colon projects and the abdominal swelling is not so uniform. If the attack is subacute or mild, the stools contain normal feces mixed with a great deal of mucus; when the inflammation is in the sigmoid flexure, pure mucus is passed. Blood mixed with mucus and tenesmus accompany inflammation low down. Blood may, however, come from intense inflammation of the ascending and transverse colon without disease of the lower bowel.35
35 In a case seen by the writer of colitis terminating fatally from perforation of the transverse colon this point was illustrated. A woman aged fifty was taken with diarrhoea in August, 1873. In November the symptoms became worse: tongue dry and red; abdominal pain; tympanites; frequent stools, ten to seventeen in twenty-four hours; quantity large, of a yellow or brownish-red color with floating flakes. General symptoms grew worse; blood in stools from time to time. November 24, sudden cessation of discharges from the bowels, and the following day sudden collapse and death. Autopsy: Descending colon and sigmoid flexure comparatively healthy. Transverse colon adherent to stomach; deposits of lymph on colon and small intestines; fluid and feces in the peritoneal cavity. The mucous membrane of the ascending and transverse colon in a state of black pulpy disintegration. In the transverse colon the walls were thinned by ulceration and easily torn; gangrenous appearance of mucous coat; perforation of the colon wall below greater curvature of the stomach.
IV. Proctitis.—The rectum may be the seat of simple catarrh, which differs in its symptoms from catarrh of other portions of the canal. By many this form is called simple, non-infective dysentery. But as it is a form of intestinal catarrh, it is right that it should be considered in connection with colitis. The first indication of its onset is a frequent desire to go to stool, with an unsatisfied feeling after each effort. Normal fecal matter is first expelled in solid form, coated with mucus which may be streaked with blood. Soon, however, the discharges consist of jelly-like mucus, alone or mixed with blood. A small quantity of this is passed with tenesmus at short intervals. The patient complains of a burning feeling in the rectum and a constant and irresistible desire to strain. The same spasmodic contraction may involve the bladder.
This affection rarely assumes a serious form. It usually ends in recovery spontaneously or under treatment by the cessation of the mucus and blood and the discharge of normal fecal matter.
DIAGNOSIS.—A combination of the symptoms described as belonging to inflammation of the small and large intestine gives the most common [p. 685] form of intestinal catarrh, ileo-colitis. This union is diagnosed by the following symptoms: fever; general distension of the abdomen; paroxysmal pains starting from the umbilicus, but having a general distribution; noisy movements of gas; diarrhoea, the stools being large, thin, stained more or less with bile, containing more or less mucus intimately mixed with fluid matter and with particles of partially-digested or unaltered food. It is possible in many cases to recognize the part of the intestinal canal which is the seat of disease from differences in symptoms which have already been described. But great care in observation is needed, combined with a minute inspection and microscopical examination of the stools, to arrive at accurate and well-founded conclusions.
Acute follicular ulceration may be thought to have begun if after a week or more of illness thin and sometimes putrescent stools are passed containing small blood-coagula, with mucus and pus.36 This opinion would be confirmed by an increase in abdominal tenderness and the persistence of the diarrhoea or tendency to relapse notwithstanding careful treatment and diet. The transition of the disease into the chronic form would give additional support to this view of the nature of the lesion.37
36 "The intestinal mucous membrane, especially that of the small intestine, scarcely ever produces pus without ulceration" (Virchow's Cellular Pathology, Philada., 1863, p. 492).
37 For a more detailed account of the symptoms and diagnosis of follicular ulceration see article on CHRONIC INTESTINAL CATARRH.
Some or all of the symptoms of acute intestinal catarrh are, however, found in other diseases. It is well, therefore, to devote some attention to differential diagnosis, giving a résumé of the salient points of distinction.
Typhoid fever in many of its features resembles intestinal catarrh, and in many cases is confounded with it. Until within quite recent times the symptoms of typhoid fever were grouped under the names gastro-enteritis and follicular enteritis. In the first week of the illness there is reasonable ground for delay in making a positive diagnosis. Etiological data are here of great help. The occurrence of the symptoms in children under two years and in adults beyond fifty years points strongly to intestinal catarrh. Spring and early summer are the seasons for diarrhoea; typhoid belongs to late summer and to autumn. A sudden onset after errors in diet or exposure to cold, with the early development of pain in the bowels, rumbling of gas, diarrhoea, would be easily recognized as a local disorder. In typhoid fever there is a less sudden onset, with prodromal debility, anæmia, indigestion, and nocturnal fever. To these symptoms the diarrhoea, which is attended with little or no pain, plays a very subordinate part. In many cases of mild typhoid the development is sudden, with rigors. A week's study of the temperature, if no rose-spots appear, will be needed before the diagnosis can be made. There is not much difficulty in making the distinction when the attack has reached its second week. At this period in catarrh of the bowel the high fever, with regular morning remissions and evening exacerbations, is not constant, as in typhoid fever; there is tenderness on pressure over the abdomen and gurgling, but no great meteorism; sibilant râles are not heard in the chest; there are no rose-spots; rarely cerebral symptoms except insomnia; and delirium is uncommon. The spleen is not enlarged. The prostration is proportioned to the diarrhoea, and is by no means as [p. 686] great as at the same period in enteric fever. The colicky pains preceding and accompanying the stools are a more marked feature of intestinal catarrh; they are absent in enteric fever or have a feeble intensity.
In children between the ages of two and seven years there are certain peculiarities which augment the difficulties of diagnosis. Intestinal catarrh in them is accompanied by an abundant, frequently painless diarrhoea, by tympanites, cerebral disturbances, a dry and coated tongue, with sordes on the lips and gums, and by a rapidly-developed anæmia, emaciation, and exhaustion. Typhoid fever in children of this age is generally benignant; vomiting is more common than in adults; high grades of meteorism are infrequent; tenderness of the cæcal region is determined with greater difficulty; and severe nervous phenomena and fatal intestinal complications rarely occur.38 In other words, in young children intestinal catarrh by its severity and enteric fever by its benignity more nearly approach each other than in adults; in many instances the diagnosis must be undecided until late in the attack.
38 Consult "Diseases of Children," Henoch, Wood's Library, New York, 1882, p. 300.
Typhoid fever can of course be known if rose-spots, a splenic tumor, or the characteristic delirium are manifested, or if the fever-curve conforms to the type; but in children all these symptoms may be negative; even the fever has great variability. If fever is continued beyond ten days, and is accompanied by progressive anæmia and emaciation and debility, the attack is enteric fever if all local causes of fever can be excluded. There is no minimum limit to the temperature in typhoid fever, and no matter how low the maxima of the fastigium may be, typhoid fever cannot be excluded.39
39 Johnston, "On the Diagnosis of Mild Cases of Typhoid Fever," Am. Journ. Med. Sci., Oct., 1875, p. 372; also, "On the Mild Forms of Continued Fever in Washington," Am. Journ. Med. Sci., Oct., 1882, p. 387.
The large watery stools and the absence of tenesmus mark the difference between diarrhoea and dysentery. Blood may be present in colitis, owing to a high grade of inflammation and to ulceration. Simple catarrh of the rectum, proctitis, is not readily distinguished from infective dysentery. Small mucous and bloody stools may be catarrhal. In the present state of our knowledge dysentery would be known by marked tenesmus, by the grave general symptoms, the reddish fluid stools with flocculi, and by its occurrence in epidemic form.
Enteralgia presents the following features which distinguish it from intestinal catarrh: The tongue in enteralgia is clean or coated white, but with no red tip and edges; the appetite is capricious, but not lost; the bowels are constipated; the pain bears no relation to the ingestion of food or drink, as in enteritis. Fever is accidental, and there are other nervous phenomena. In lead colic there is no fever, tympanites, nor diarrhoea. In rheumatism of the abdominal walls the pain is superficial and sharp, not griping, and is increased by movements of the trunk. The digestive system is in no way disordered. From peritonitis intestinal catarrh is distinguished by a less degree of illness and by its usually favorable result, by diarrhoea, a greater freedom in movement, and by a less degree of suffering on palpating the abdomen. Tympanites, constipation, great tenderness on pressure over the abdomen, and a small, quick pulse, point to peritonitis.
[p. 687] PROGNOSIS.—A simple intestinal catarrh of the form first described involves no danger, and if treated by rest and diet soon recovers. The more severe form, beginning as a primary disease, when rationally treated ends in recovery in most instances.
Unfavorable predisposing causes are—a hot climate (India, the West Indies, and intertropical climates in general); very hot weather of the summer and autumn months; a very early or very advanced age; the contaminated atmosphere of prisons, camps, etc.; all bad hygienic influences; and previous or coexisting illness. When diarrhoea occurs as a complication of the acute infectious diseases it has a special gravity. In typhoid fever, scarlatina, measles, acute tuberculosis, etc. it adds another element of illness and danger. During the progress of chronic general diseases (malaria, scurvy, tuberculosis) it becomes an obstinate and sometimes a fatal complication. Among the exciting causes mineral poisons induce the most dangerous form of intestinal catarrh. Unfavorable symptoms occurring during the course of acute diarrhoea are the early development of high temperature, cerebral disturbance, great sensibility to pressure over the abdomen, thin and bloody or highly offensive stools, involuntary discharges, and very rapid emaciation and loss of strength.
TREATMENT.—There have been many fluctuations of opinion as to the relative value of modes of treatment in this disease. Various therapeutic measures have been suggested which, after enjoying favor for a time, have been abandoned, and revived after long periods of disfavor. Venesection was alternately recommended and forbidden. Emetics and evacuants, mercurials, diuretics, diaphoretics, have been in turn warmly supported and vigorously opposed. Opium, belladonna, the various astringents, and cinchona-bark have run through many changes of favor. Individual drugs give curious evidence of inconstancy. Oxide of zinc, suggested by James Adair in 1785 and by Hendy in 1784, after a hundred years of weak approval is commended highly by Penrose (1863), Brakenridge, and Mackey (1873),40 and by more recent writers. Acetate of lead, which dates back to Paracelsus, had varying fortunes of repute and disrepute. In the end of the seventeenth century it had a name for curing diarrhoea, but in the following century it was spoken of by Boerhaave as a deceitful and destructive poison, and Cullen in 1789 said that hardly any one then thought of using lead internally.41 In 1799 it had warm advocates in this country; among them, Thomas Ewall of Washington, who wrote in 1808. Since then it has come into very general use and favor, which it still holds.
40 J. J. Woodward, op. cit., p. 776.
41 Ibid., op. cit., p. 780 et seq.
In view of the many changes of faith in systems of treatment and in drugs, we have no right to assume that we have as yet reached the perfection of treatment. In fact, experience brings the conviction that our systems are quite imperfect and that drugs fail in our hands when they are most needed.
The prophylactic treatment is of importance, especially in children, delicate persons, and in those suffering from disease or predisposed by idiosyncrasy to intestinal catarrh. Directions must be given by the physician as to the food for children appropriate to their age and digestive capacity. Summer heat and city life being so fatal to them, they should [p. 688] be sent to the cool climate of the seashore or mountains during the first and second years of life. In warm weather laxatives should not be given to children, except with precautions against their acting too freely; the same rule applies to the aged. Too great care in diet in older children predisposes to indigestion and diarrhoea. Variety in food is of service, therefore. It is not well to give children food prepared so as to do away with the necessity for mastication and for active gastric movements. The stomach gains strength by exercise. All reasonable care should be used not to take food in excess of the individual's power of digestion. Unripe fruit, stale vegetables or fruits, cheese, pork, shellfish which are not absolutely fresh, are among the aliments which may produce diarrhoea, and are to be avoided. Many people have to be told what food is unsuited to them, and certain articles of food in individual cases invariably excite diarrhoea. Alcohol is often to be blamed for diarrhoeas which are attributed to indigestible food, and frequent recurrences of intestinal catarrh can only be prevented by abandoning stimulants altogether. The bad effects of sudden changes in temperature are warded off by wearing flannel next to the body. This is an important rule for adults as for children. Even in summer thin flannel or gauze gives protection. Well-ventilated rooms, good house-drainage, personal cleanliness, with all other hygienic aids, are means of prevention. Persistent disinfection of sources of air- and water-contamination should be practised, especially in hot weather. In the country the open privies and wells need frequent clearing out. Cases of fatal diarrhoea are met with in elevated regions where the continued low temperature renders it improbable that heat could have anything to do with their causation.42 Water should not be used which could in any way be tainted with soakage from privies, barnyards, or other places where animal decomposition is going on.43 Avoiding the use of cathartics in the onset of acute illness, the nature of which is not known, is a useful prophylactic measure. A fatal diarrhoea may result from injudicious purging in such cases. Care in the use of laxatives should be observed in the chronic wasting diseases—tuberculosis, rachitis, cancer, etc.
42 The yearly occurrence of typhoid fever and diarrhoea at seashore hotels shows that there is great danger in crowding persons together and saturating the soil with the excreta. In the summer of 1882 in a boarding-house in the mountains of Maryland, where the temperature was never above 75°, there were three fatal cases of diarrhoea in children, and several others of diarrhoea and dysentery which recovered.
43 The drinking-water supplying a country boarding-house visited by the writer passed through iron pipes imbedded in the manure-heap of a barnyard.
The selection of a plan of treatment for intestinal catarrh will depend upon the nature and cause of the symptoms. The diagnosis of the case is incomplete and the treatment irrational until the indications furnished by etiology have been obtained.
If cold has been the exciting cause, the patient should be confined to bed. In the beginning a full dose of pilocarpin, hypodermically,44 or of the fluid extract of jaborandi by the mouth, may cause a powerful diversion from the bowel to the skin. A hot-water or vapor bath has the same object in view. Hot fomentations or mustard poultices can be next applied to the abdomen. This should be succeeded by a febrifuge [p. 689] mixture containing the tincture of aconite-root, to which an opiate (the deodorized tincture of opium or morphia) is to be added if there is much pain or diarrhoea. A hypodermic injection of morphia given on the first day of the attack immediately after a hot bath will give a quiet night and diminish the intensity of the illness. The subsequent treatment is that common to all the acute forms.
44 Atropia can be given with pilocarpin to diminish its effect on the heart; atropia is the antidote for pilocarpin. (See Schuk, Centralb. f. d. med. Wissen., Bd. 20, 1882, p. 357; also, Frohnmüller, Med.-Chir. Centralb., July 14, 1882.)
If summer heat has been the cause in adults or children, artificial cooling of the temperature of the room by the evaporation of ice-water or by one of the refrigerating machines yet to be perfected meet the indication. If there is much body-heat (thermic fever), cold sponging, the application of cold to the head, or the giving of pounded ice to satisfy the intense thirst, are all advisable. Such cases are benefited by a change of climate when the acute symptoms subside. The form of diarrhoea due to malaria is to be treated by quinia and change of air to a more healthful climate. Iron, with quinia or arsenic, is needed in obstinate cases.
Intestinal catarrh which proceeds from the presence of undigested food or hard fecal lumps in the bowel is benefited by early removal of the irritating cause. It is not often that substances of this kind are retained when the stools are large and frequent. The peristalsis is here as active as it need be, and no good, but only harm, can come from over-stimulating the contractile muscles. In those instances where there is a distinct history of the taking of indigestible food, especially fruit with seeds or skins, and where the efforts at stool are frequent, ineffectual, and accompanied by colic and borborygmi, or where scybalæ are found floating in the fluid passed, a large enema of warm water given slowly will excite the bowel to successful expulsive efforts. If this does not give a certain amount of prompt relief, a moderate dose of castor oil, calomel, Rochelle or Epsom salts ought to be prescribed, and repeated after some hours until a free fluid or semi-fluid stool results; one or two doses will usually suffice. If the inflammation is localized in the cæcum (typhlitis), as indicated by local pain, tenderness on pressure in the right iliac or right lumbar regions, constipation, flexing of the right thigh on the trunk, and vomiting, a purgative should not be given, nor should prolonged efforts be made to empty the bowel by injection through long rectal tubes. If there is doubt as to whether typhlitis or undigested food and fecal impaction is the cause of the local pain, it is better to err on the safe side, and not to give a purgative unless the case is seen in the onset before the more pronounced symptoms appear; then calomel or castor oil may be tried once, but not repeated in case of failure.
As the diarrhoea of Bright's disease is salutary, no effort should be made to arrest it. Its periodical recurrence prolongs life. In tuberculosis the special character of the diarrhoea must be considered, and every effort must be made to control it. In the eruptive fevers an early diarrhoea, as in scarlet fever, does harm; it delays or prevents the normal development of the eruption. In the later stages it is of service sometimes, as in measles, when it leads to a rapid fall of temperature. The course of action depends upon the nature of the specific disease and upon the time of the appearance of diarrhoea.
There are certain principles, founded on the knowledge derived from pathological study and from the experience of the past in the treatment [p. 690] of intestinal catarrh, which guide us to a treatment which is more or less rational in all cases.
Rest is essential to the cure of the inflamed intestine, but absolute inertia of the bowel is undesirable, even injurious. The retention of fluids, transuded serum, bile, intestinal juices, and partly-altered food is hurtful. Decomposition sets in and gas is developed, which by distending the bowel causes great suffering and increases the inflammation. The movements of the intestine are not entirely under control; the patient must be fed; digestion and assimilation involve the activity of inflamed parts. The stomach can be made to do most of the work, but the sympathy of action is so close between the stomach and intestines that one cannot function without the other being excited into activity.
The first rule of treatment is to put the patient to bed and to keep him in a horizontal position. Even in mild cases time will be saved by resorting to absolute rest at once. If the attack is at all severe, the bed-pan should be used; the effort to rise and the straining at stool exaggerate peristaltic movement, increasing the frequency of the evacuations. Additional rest can be given to the intestines by applying a flannel binder around the trunk, compressing the abdomen; broad strips of adhesive plaster could be used for the same purpose. In cases where the diarrhoea, tympanites, and griping pain are not relieved by other measures this suggestion may be of service.
In order to lessen intestinal hyperæmia and allay suffering, counter-irritants and soothing external applications are employed. Local blood-letting, although in vogue during more than two centuries, has fallen into disuse. Recent authors still continue to advise the application of leeches to the anus in order to deplete the portal circulation,45 but it is a decided objection to this remedy that the fluid stools irritate the leech-bites and cause much discomfort. Sinapisms or turpentine stupes may be of some service apart from the relief which they give to pain. Blisters might be more generally used than they are when the tenderness on pressure is confined to the colon. In intense inflammation they should always be tried. Hot poultices of flaxseed meal or hot fomentations of any sort applied over the entire abdomen have a soothing and beneficial effect. A flannel compress saturated with alcohol and covered with gutta-percha cloth makes a most agreeable application.
45 Niemeyer, Practice of Medicine, Intestinal Catarrh.
The directions for diet should be carefully and explicitly given. In the onset of the attack entire deprivation of all food for twenty-four or forty-eight hours is expedient. To relieve thirst, cracked ice, carbonic-acid water, Apollinaris, Seltzer, or Deep Rock water can be ordered; barley- or rice-water is slightly nourishing and relieves thirst, but all liquids should be given in moderation. When it becomes necessary to give food, the stomach must be made to do the work of digestion, and, as far as possible, of absorption also. Such substances are to be chosen as are converted in the stomach into peptones, and which do not require contact with the intestinal juices for their absorption.
The peptones transformed in the stomach from nitrogenous alimentary principles are highly soluble and diffusible. Milk is better suited to the conditions of intestinal catarrh than any other nitrogenous food. It is palatable, relieves the thirst, and can be taken for a long time without [p. 691] aversion. By removing the cream, the fat, which would require intestinal digestion, is partly got rid of. Skimmed milk does not produce a feeling of distaste and what is called biliousness, as does milk unskimmed. In cases where there is gastric catarrh the milk can be made more digestible by adding an equal quantity of barley-water or rice-water. The casein is then more slowly acted on by the gastric juice and more thoroughly digested. Milk should be given in small quantities at short intervals, as in this way the stomach performs the entire work more thoroughly. If a large quantity is given, a portion of it passes into the intestine unaltered. Buttermilk contains less fatty matter than skimmed milk, and is a pleasant substitute for it. Koumiss, if it could be properly prepared, would be an excellent food for diarrhoea. Even the imperfect imitations are retained and digested when other aliments fail. The whey of milk contains lactin, salts, a little casein, and fatty matter. It may be made by adding to milk rennet, sherry or other wine, cream of tartar, tamarind-juice, or alum. Milk-whey is slightly nourishing, and is said to be sudorific; when prepared with wine it is a mild stimulant well suited to the cases of children.
Where it is desired to give as little work to the digestive organs as is possible, milk and other foods can be given already partly digested, as peptonized milk prepared according to the formulæ of Roberts and Fothergill.46 Eggs are changed quickly in the stomach. Egg albumen is more easily digested by artificial gastric juice than by pancreatic extract (Roberts). A solution of egg albumen boiled in the water-bath is swiftly and entirely transformed by pepsin and hydrochloric acid. Raw eggs have been thought to be the most digestible, but Roberts found that a solution of egg albumen when raw was very slowly acted on by pepsin and acid, but after being cooked it was rapidly and entirely digested. Eggs are best given, therefore, boiled slightly at a slow heat; when an egg is plunged in boiling water the white sets hard, leaving the yelk soft. The albumen of the white and the yelk should be equally cooked throughout.
46 J. M. Fothergill, Indigestion and Biliousness, New York, 1881, p. 63 et seq. See also quote to article on CHRONIC INTESTINAL CATARRH.
Beef-tea is said by the chemist to possess little nutritive value; practical experience convinces the physician that it supports life. Peptonized beef-tea may be substituted when thought best. Animal broths thickened with rice, barley, or with peptonized gruel, as advised by Fothergill, or with the addition of vermicelli, are valuable aids when the palate is capricious. Raw beef is not as digestible as when the tendinous and aponeurotic structures of the muscular fibre have been softened, disintegrated, and converted into the soluble and easily-digested form of gelatin by cooking.47 Scraped raw beef, when the pulp is removed from much of the connective tissue, is easily digested by children as well as by adults.
47 Ibid., op. cit., p. 47.
In most cases of acute intestinal catarrh the patient can be well sustained by a diet consisting of one or other of the aliments described. For the largest number milk alone—that is, skimmed milk or milk diluted with barley-water, rice-water, or Seltzer water—is all that is necessary to support strength during the attack. Although starch after deglutition is [p. 692] acted on in the intestine only, it becomes desirable sometimes to give farinaceous food in some form or other; milk may be undigested and animal broths may become distasteful; the palate craves some change. In this case a blanc mange made after the formula of Meigs and Pepper is as well suited to adults as to children,48 the proportion of cream and arrowroot being made larger for adults. Sago49 and tapioca50 can be tried to tempt the palate. The flour of the Egyptian lentil51 is made into a gruel also. Most of the patent foods for infants and invalids contain starch in some form or other. Racahout is one of the pleasantest and best of these. Nestle's food contains baked biscuits of wheat flour ground to a powder. Liebig's food is made of wheat flour, malt flour, and a little bicarbonate of potassium. Revalenta Arabica is an attractive name for the flour of Arabian lentil with barley flour. Any of these may be advantageously employed in cases of some duration and in the later stages of convalescence.
48 Meigs and Pepper, Diseases of Children, Philada., 1870, p. 304.
49 Put half an ounce of sago into an enamelled saucepan with three-quarters of a pint of cold water, and boil gently for an hour and a quarter. Skim when it comes to the boil, and stir frequently. Sweeten with a dessertspoonful of sifted loaf sugar. If wine be ordered, two dessertspoonfuls; and if brandy, one dessertspoonful.
50 Half an ounce of the best tapioca to a pint and a quarter of new milk. Simmer gently for two hours and a quarter, stirring frequently; sweeten with a dessertspoonful of sifted sugar.
51 Take three tablespoonfuls of lentil flour, a salt-spoonful of salt, and one pint of water. Mix the flour and salt into a paste with the water and boil ten minutes, stirring (Food for the Invalid, Fothergill and Wood, New York, 1880).
The diet for convalescence should be controlled by the physician until the patient has been well for at least two weeks. Liquid preparations give place to fine hominy, corn meal or oatmeal porridge, with milk. Then bread or crackers may be given, the intervals between the meals increasing to three or four hours. Raw oysters, sweetbreads, tender rare steak or mutton finely divided and well masticated, rice, and ripe peaches, succeed the simpler diet. Much saccharine, starchy, or fatty food is to be avoided for at least two weeks after entire recovery.
When the indications derived from the study of the cause have been acted on, and the patient has been placed under a rigid discipline of rest and diet, the treatment of symptoms comes next in order.
In mild cases, where the cause has been irritating ingesta, diet may relieve the symptoms in a short time without medicine. If diarrhoea with slight colicky pains and flatulence continue after a few hours, a mixture holding in suspension subnitrate of bismuth, with five drops of the deodorized tincture of opium in each dose, or a pill of lead and opium, will suffice in a short time to give relief. In severer attacks the fever heat may mount to a high point, giving great distress to the patient. If a temperature of 103° to 104° F. is reached—which is not unusual in children—a warm bath is a sedative and antipyretic remedy, or a bath of 95° can be gradually cooled down to 75° or 65° F.—a procedure which will bring down the body-heat two or three degrees. A substitution for the bath is sponging with cool or cold water, to which vinegar or bay rum may be added; or towels wrung out of cold water can be applied to the trunk and extremities (Ringer) with a very happy effect.
Quinia can be used antipyretically in full doses, dissolved in dilute hydrochloric acid. Pills, especially the sugar- or gelatin-coated pills, [p. 693] should not be given, as they irritate the mucous membrane whether they are dissolved or not. In diarrhoea quinia pills often pass unaltered.
Flatulence, eructations of gas, and borborygmi are controlled by strict diet according to the rules given. Bismuth subnitrate or subcarbonate unites with sulphuretted hydrogen and absorbs it. The alkalies, sodium and potassium bicarbonate, sodium hyposulphite, the aromatic spirits of ammonia, either relieve acidity or prevent fermentation and the development of gas. A satisfactory formula for the early stages of intestinal catarrh is one containing bismuth subcarbonate, sodium bicarbonate, aromatic spirits of ammonia in water or cinnamon-water. When the abdominal distension is great enough to be a cause of distress, external cold—dry cold—is the best, applied with a rubber bag filled with cracked ice or ice-water; it causes absorption of gas. Abdominal compression with a bandage may be of some service also. Mineral acids, especially the dilute hydrochloric acid, by affording aid to the digestion prevent acid fermentation.
Diarrhoea is the central symptom and the best standard by which to measure the intensity of the catarrh and its progress. But it is only a symptom, and the mind ought to be directed to the lesion and not to it. Having the cause in view, the object in all cases is to allay the inflammation. This done, the diarrhoea decreases, then ceases. Shall the effort be made to check the discharges, or shall they be allowed to continue? The evacuant plan of treatment has been advocated, on the ground that the purgative, by increasing intestinal secretion, relieves the congestion of the intestinal blood-vessels and leaves the membrane in a better state than before.52 But inasmuch as a purgative only acts by bringing about an intestinal hyperæmia and catarrh, there is no good reason for, and many reasons against, treatment by evacuation.
52 Woodward, op. cit., pp. 727, 728.
A preliminary purgative, as has already been stated, is necessary to expel undigested food and scybalæ, but for the purpose of increasing intestinal or biliary secretion and diminishing engorgement of the vessels this method is unsuccessful and unnecessary. When irritating substances have been removed (and this is done usually without the physician's aid by the spontaneous expulsive movements of the bowel) the effort to check the discharge and to give rest is one and the same. Opium is the one invaluable remedy which we cannot do without.53 As little of it should be given as is necessary to relieve the intensity of the symptoms. The aim should not be to stop the pain and check diarrhoea, but to take the edge off the sharp agony and to lengthen the interval between the stools. Thus gradually the spasms of peristalsis cease, and there is a diminution, and finally cessation, of the fluid accumulation in the bowel. The diarrhoea is relieved entirely in a period ranging from an hour after the giving of the first dose to one week, according to the severity of the attack. Opium is given in pill form, in the deodorized tincture, Dover's powder, or one of the salts of morphia may be preferred. Any of these may be combined with antacid and antifermentative mixtures, relieving the colic, gaseous distension, and diarrhoea. If opium is combined with, [p. 694] or followed by, evacuants, its effects are thwarted, and it might as well not be given at all.
53 The objections urged against opium, that it increases thirst and nervousness, causes a retention of fermenting products, produces opium intoxication, and that it is a routine practice to give it, and does not cure the inflammation, may be valid, but we cannot do without opium, nevertheless.
It is the custom to combine astringents with opium, but in acute cases of short duration it is a question whether astringents do not do more harm than good. When good does come from the combination, it is the opium which acts promptly and decidedly. The astringent lags behind, and in cases of some duration and severity supplements the work of the active partner. Bismuth is classed under this head, although it is not an astringent. Its action is mechanical; much that is taken is passed from the bowel as the black sulphide, which appears as a black granular powder in the fluid stool. This is no proof that it may not have been of service in its transit.54 After death, when large doses have been given, it has been found lining the whole intestinal canal.55 The subnitrate or subcarbonate can be given in powder on an empty stomach in doses of five to twenty grains alone or in combination with opium, or it can be dispensed with alkalies in water. The enormous doses (one hundred and fifty to nine hundred grains daily), as given by Monneret, are useless or hurtful. The value of bismuth is based on empirical grounds only, but it is irrational to load the bowel with an insoluble powder which if retained must cause irritation. As the discoloration of the stools is an objection to bismuth when it is desired to study their character for diagnosis, oxide of zinc may be substituted for it, as the latter is an absorbent of acids and gases.56 Gubler has insisted upon combining it with bicarbonate of sodium to prevent the formation of the irritating chloride of zinc in the stomach.57 One of the oldest and most popular remedies tor diarrhoea is lime in the form of the carbonate or lime-water. The officinal mistura cretæ is perhaps more generally used for children than any other remedy. Lime-water is added with advantage to milk when given to adults as well as children. Carrara-water, made by dissolving the bicarbonate of lime with an excess of carbonic acid, is less nauseous than liquor calcis, and may be mixed with an equal part of milk.58 Chalk and its preparations are less beneficial than bismuth as astringents, but may be used merely for their antacid effect.
54 Headland asserted that bismuth was insoluble, but it has been detected in the liver, in milk, in urine, and in the serum of dropsy by Orfila, Sewald, Bergeret, and Mayençon (Materia Med., Phillips, vol. ii. p. 81).
55 Levick, Am. Journ. Med. Sci., July, 1858, p. 101.
56 Bonamy, "Du Traitement des Diarrhées rébelles par l'Oxyde de Zinc," Bull. gén. de Thér., t. xcii., 1877, p. 251; also, J. Jacquier, De l'Emploi de l'Oxyde de Zinc dans la Diarrhée, Paris, Thèsis, 1878, No. 118.
57 Gubler, Principles of Therapeutics, Philada., 1881, p. 25.
58 Phillips, Materia Medica, vol. ii. p. 105.
The sugar of lead is a valuable astringent, because unirritating and sedative to the mucous membrane. With opium in pill form, in doses of one to three grains, it checks diarrhoea if the inflammation has not lasted long and is not extensive. If there are cases where the bile is passed in quantity, it is especially called for, as it is the only astringent which diminishes the flow of bile.
The mineral acids—dilute hydrochloric, nitric, and sulphuric acids—are given with some success. The first aids gastric digestion, and in small doses with pepsin can be directed after food irrespective of other treatment. The great repute which it has enjoyed in the diarrhoea of typhoid is no doubt due to the improved digestion and assimilation [p. 695] which follow its use. The acid principle is what is lacking in the gastric juice in fever and debility.59 In all cases of intestinal catarrh rapidity of gastric digestion should be sought for. Nitric acid is of doubtful utility. Without an opiate in combination there is little reason to hope for any result from its use; all the suggested formulæ contain opiates.60 Dilute sulphuric acid is thought to be more astringent than the others. If it has any efficacy, it is due to the local astringent or alterative effect by contact with the inflamed surface. Much testimony is to be found in its support in cases tending to become chronic and where astringents combined with opiates have failed after some days' trial. It should be administered in doses of five to twenty drops in the form of mixture with mucilage or some aromatic, as lavender and cardamom. An opiate should not be combined with it if it is desired to test it fairly. It would be called for when the stools are pale, abundant, watery, and alkaline.
59 Manassein, Virchow's Archiv, lv., 1872, p. 451.
60 The favor in which nitric acid is held is due to the advocacy of nitrous acid by Hope ("Observations on the Powerful Effects of a Mixture containing Nitrous Acid and Opium in curing Dysentery, Cholera, and Diarrhoea," Edin. Med. and Surg. Journ., vol. xxvi., 1826, p. 35). Nitrous acid, the same as the fuming nitric acid of the shops, is a reddish-yellow fluid highly charged with nitrogen trioxide. Hope said that ordinary nitric acid did not produce the same effects, and yet nitric acid is now given with the belief that it is of service.
Calomel is of ancient repute as a remedy in the early stages of diarrhoea. According to recent views, it acts as a sedative to the gastro-intestinal mucous membrane and checks fermentation. It should be given in small doses (one-twelfth to one-eighth of a grain to children, one-fourth to one-half of a grain to adults); it should not be continued for more than two or three days. In combination with Dover's powder it acts well, but it is doubtful which of the two remedies should receive the greater praise for the resulting improvement. A very small dose of the bichloride of mercury has been found beneficial by Ringer for clayey, pasty stools or straining stools containing slime and blood. His formula is—Hydrarg. bichloridi gr. j; Aquæ fluidounce x; a teaspoonful frequently during the day. The gray powder is not as much thought of now as formerly; it is not so good for the early stages of diarrhoea as calomel, but may be tried as an alterative when the stools are green and offensive.
In the vegetable materia medica there are many and ancient remedies. Tannin represents a large class, and there is nothing more than fancy in preferring to it kino, catechu, hæmatoxylon, or blackberry-root. Tannin is precipitated in the stomach as an inert tannate; gallic acid is to be preferred for this reason, and also for its pleasant taste and less irritating effect on the mucous membrane. It is well borne by children, even in large doses, when given with water and syrup. It is to be hoped that the unsightly and unsavory combinations of the astringent tinctures with chalk mixture will be soon given up. They are given chiefly to children, who are repelled by the sight, and still more by the taste, of such compounds. The syrup of krameria is the least objectionable, and catechu and krameria are made into troches which are sometimes available.
Ipecacuanha is said by Bartholow to be extremely serviceable in the diarrhoea of teething children with greenish stools containing mucus or blood. He prescribes it with bismuth and pepsin.
[p. 696] Recently some favor has been paid to coto-bark and its active principle, cotoin. The latter is advised to be given in the following formula:
| Rx. | Cotoinæ, | gr. j; |
| Aquæ distillat. | fluidounce iv; | |
| Alcohol, | gtt. x; | |
| Syrupi, | fluidounce j. |
A tablespoonful every hour. Five to eight drops of the fluid extract of coto are given. It is said to have a speedy and certain effect in acute diarrhoea.61
61 Coto-bark was imported into Europe from Bolivia in 1873, and was called quinquina coto. Wittstein of Munich and Julius Jobst of Stuttgart made the first analyses (Neues Repertorium für Pharmacie, xxiv. and xxv.). Von Gietl (idem, xxv.) first concluded from experiments that it was of use in diarrhoea. Cotoin and paracotoin were separated by Jobst. It has been found successful in the treatment of diarrhoea in Germany and of cholera in Japan (Baelz, Centralb. f. d. med. Wissen., 1878, xvi. p. 482). Cotoin sometimes disturbs the digestion to a marked degree. Paracotoin may be used hypodermically.
Salicin,62 ergot, guarana, have all been spoken of by enthusiasts as possessing valuable properties in diarrhoea.
62 Lawson, "Diarrhoea and its Treatment at the London Hospitals," Med. Times and Gaz., vol. ii., 1868, p. 122; Bishop, "Salicin in Diarrhoea and Dysentery," Southern Med. Rec., vol. iv., 1874, p. 585; "Comparative Value of Opium and Salicin in Diarrhoea and Dysentery," Detroit Review of Med. and Pharm., vol. x., 1875, p. 387.
Alum is not often prescribed. Sulphate of copper is fitted for cases in danger of passing into the chronic stage. Sulphate of zinc might be more generally ordered than is the case. The sulphate of iron and the fluid preparations of iron—tincture of the chloride, solution of the pernitrite, and persulphate—are astringents, and could be tried if other remedies fail. The effect of nitrate of silver is to constrict vessels, to coagulate and disinfect excretions, and to form an adherent protecting membrane (Phillips). It occupies the next place to lead, and is suited to a subacute stage when acute symptoms have subsided. It is warmly recommended by William Pepper and others.63 The oxide of silver has been preferred by some writers.64 For the protracted diarrhoea of children, in whom follicular ulcers form so rapidly, the nitrate of silver is of special value. To adults it is administered in a pill freshly made in doses of one-eighth to one grain. A solution in distilled water with syrup answers well for children, the dose varying from one-twentieth to one-fourth of a grain.
63 J. Maggregor, "On the Internal Use of Nitrate of Silver in Inflammation of the Intestines," Lancet, 1841, vol. ii. p. 937.
64 Lane, Med.-Chir. Rev., July, 1840, p. 289 et seq.; Eyre, The Stomach and its Difficulties, London, 1852.
The theory of the germ origin of diarrhoea has naturally brought into notice antiseptic remedies. Carbolic acid,65 creasote,66 naphtha,67 sulpho-carbolate of calcium,68 salicylic acid,69 and chlorine-water have each been advocated. Practice does not support their claim to be considered remedies for intestinal inflammation.
65 Habershon, Lancet, London, 1868, vol. i. p. 7; C. G. Rothe, Berliner klin. Wochenschrift, 1871, p. 527.
66 Southern Med. and Surg. Journ., vol. ii., 1846, p. 583; ibid., vol. iii., 1847, p. 147; London Med. Gaz., vol. ix., 1849, p. 254; ibid., vol. xii., 1851, p. 235.
67 Gaz. des Hôpitaux, 1849, p. 46.
68 Tr. Obstet. Soc. Lond., vol. xii., 1870, p. 12.
69 W. Wagner, Kolbe's Journ. für prakt. Chemie, Bd. xi., 1875, S. 60.
[p. 697] Treatment by the rectum may be employed when medicines are rejected by the stomach or when it is desired to bring the drugs into more direct contact with the inflamed colon. Opiates, astringents, and alteratives are employed in this way. Laudanum in two to four ounces of warm water or in warm milk or starch-water can be thrown into the rectum, the fluid being allowed to remain. The injections are to be given often enough to relieve pain and lessen the number of discharges. With the laudanum, or without it, the mineral astringents can be used by enema. Acetate of lead or sulphate of zinc is to be preferred. The objection that but a small portion of the inflamed surface is reached by the fluid is a valid one, and therefore those cases are most benefited where the catarrh is in the lower colon and rectum. Ringer70 says that it is not at all necessary for the fluid to reach that part of the intestine which is the seat of the catarrh; the impression made on one part is communicated to the other by sympathy. It was the practice with O'Beirne,71 Hare,72 and others to inject fluid by a long flexible tube passed beyond the sigmoid flexure. This method is advocated and employed in Europe by Mosler, Winterinz, and Monti. Quite recently Dulles has drawn attention to irrigation of the large intestine as a means of treating inflammation of the colon, according to the plan of Alois Monti of Vienna.73 Henoch has tried with partial success in children the throwing into the rectum of a large quantity of water holding in solution acetate of lead, alum, or tannin. His method contemplates medication above the sigmoid flexure; a part of the fluid escapes, while the rest remains five or ten minutes in the bowel.74 Monti says as much as two pints can be injected into the bowel of a nursing child—for older children twice this quantity.
70 Therapeutics, New York, 1882, p. 99.
71 New Views of the Process of Defecation, Washington, 1834, p. 85.
72 E. Hare, "On the Treatment of Tropical Dysentery by means of Enemata of Tepid Water," Edin. Med. and Surg. Journ., vol. lxxii., 1849, p. 40.
73 Dulles, "Irrigation of the Colon," Philada. Med. News, Aug. 19, 1882, p. 199. The patient is placed on the side, back, or on belly, with the hips elevated. A large flexible catheter if a child, a stomach-tube if an adult, is inserted into the rectum. The tube is connected with a reservoir of water elevated above the patient. The rectum is first distended with water, and the tube is gradually made to follow the course of the bowel until it finds its way into the descending colon. Thus the water may be made to distend the whole of the colon to the cæcum. The fluid remains from a few minutes to half an hour.
74 Henoch, Diseases of Children, Am. ed., New York, 1882, p. 206.
Messemer75 reported three cases (one child and two adults) treated in this way with the most striking success. His object at first was to cleanse the rectum, but warm water did not check the diarrhoea. Cold water was tried, and (probably by reflex influences) diminished rapidly the number of the discharges. And Ewald76 has imitated Messemer's method with results which are surprisingly good. He injected 200 and 300 cc. of cold water, which was expelled by pressure on the abdomen; 50 cc. were then thrown in and allowed to remain. He has used the treatment in a large number of cases in children. The question as to the ability to force water thrown into the rectum through the sigmoid flexure and distend the colon has been settled by the experiment of Mosler in a case where there was a cæcal fistula. Water injected into the [p. 698] rectum traversed the colon and escaped through the fistula in two minutes.77
75 J. B. Messemer, "Cold-Water Enemata as a Therapeutic Agent in Chronic Diarrhoea," American Journal of the Med. Sci., vol. lxxvi., 1878, p. 133.
76 Lectures on Digestion, New York, 1881, p. 149.
77 Berlin. klin. Woch., No. 45, 1873, p. 533. Woodward, in discussing the claims of Battey of Georgia to priority in the discovery of the permeability of the entire alimentary canal by enema (see paper by Battey in Virginia Med. Monthly, vol. v., 1878, p. 551), quotes from A. Guaynerius, who lived in the fifteenth century, from J. M. de Gradibus (1502), Sennertus (1626), and from others among the older writers to show that it was well known that suppositories and enemata introduced into the rectum are sometimes thrown up by the mouth. He mentions experiments by Alfred Hall (1845), G. Simon (1873), and F. Köster (1874) which demonstrated that large quantities of water may be forced from the rectum into the stomach. (See Woodward, op. cit., foot-note, p. 836.)
When ulcers are thought to be present, the remedies of particular value are nitrate of silver, bismuth or turpentine, and the mineral acids, given in conjunction with a rigid system of diet.
In hemorrhagic diarrhoea ice externally or ice-water injections, opium, acetate of lead in large doses (ten to fifteen grains), gallic or tannic acid, and ergot are the appropriate remedies.
Some modifications of treatment are required for the choleraic form (in children, cholera infantum); the danger here is imminent from the drain of water and collapse. For the vomiting of the early stages, pounded ice eaten freely, potassium or sodium bromide in ice-water, and counter-irritants over the abdomen, with cold sponging or cold baths and ice to the head if there is much body-heat. Brandy, whiskey, or coffee in full doses is called for early. Iced coffee can be given to children. Spirit of camphor in five-drop doses every ten minutes aids in averting collapse. Small doses of calomel every hour or two may benefit nausea and vomiting. Arsenic is said to do well for vomiting and profuse watery diarrhoea. For adults, morphia hypodermically is perhaps the best remedy for the vomiting and purging; even for children, minute doses given in this way are best for alarming illness. Hypodermic injections of ether have also been suggested.
For the relief of duodenitis means are used to relieve the digestion of the want of the biliary and pancreatic secretions. Nitrogenous food is to be taken, but no fats or starch. Counter-irritation over the epigastrium and right hypochondrium by a blister or iodine is of direct service. If icterus accompany duodenitis and catarrh of the bile-ducts, all treatment must be directed to the duodenum. For ileo-colitis and colitis the rules already given apply.
ETIOLOGY.—Chronic intestinal catarrh has many of the same causes as the acute form; it is the expression of a large number of different pathological states and complicates many general and local diseases.
It is very common in children under two years of age, and is associated with change in diet in weaning and with the irritability of all the tissues during dentition. It is also a frequent disease in old persons, being due to imperfect mastication, the weakness of digestion, portal congestion, the gouty diathesis, and other causes.1 Men have the disease more frequently than women. Hereditary influence and idiosyncrasy predispose to chronic catarrh of the bowel as to catarrh of the bronchi. Bad hygiene, want of cleanliness with an unhealthy condition of the skin, constant breathing of foul air due to want of proper ventilation, animal decomposition, or overcrowding predisposes to chronic diarrhoea. The chronic diarrhoeas among soldiers in camps,2 among the inmates of prisons, workhouses, and asylums, are examples of these influences. Overwork, especially mental overwork with anxiety, and privation of sleep act in the same direction. In the chronic constitutional diseases and in many chronic diseases of organs diarrhoea sooner or later appears, and very generally is the immediate cause of death. In phthisis pulmonum, whether tubercular or not, simple catarrh of the bowel is nearly always present.
1 La Diarrhée chez les Viellards, Paris, Thèsis, 1865, No. 112. See also works of Durand-Fardel and Charcot and Loomis.
2 According to the statistics prepared in 1871 by T. B. Hood of the U.S. Pension Office, chronic diarrhoea was the disease for which a pension was granted in 20 per cent. of all cases of disability from disease and in 75 per cent. of all the diseases of the digestive system (Report of Commissioner of Pensions, 1871).
During the course of chronic Bright's disease, more frequently in the cirrhotic form, lesions are developed in the intestine which cause obstinate diarrhoea. The discharge of urea into the intestine, and its conversion into carbonate of ammonium, which acts as an irritant to the mucous membrane, is the reason of the diarrhoea in this disease, according to Luton and Treitz;3 and in so far as the discharge represents the escape of urea by the bowel, it may be regarded as salutary. In gout, especially in old persons, periodical diarrhoea gives relief. Chronic gouty subjects assert that they are not benefited by colchicum until it has purged them. The [p. 700]lithic-acid diathesis, pyæmia, septicæmia, scurvy,4 diabetes, leucocythæmia, Addison's disease, and syphilis5 have diarrhoea during some part of their progress. The malarial cachexia is often attended with a diarrhoea which quinia alone will relieve; this symptom may occur periodically or be constant.
3 A. Luton, Des Séries morbides, Affections urémiques de l'Intestin, Paris, Thèsis, 1859, No. 38, p. 45; also, Treitz, "Ueber urämische Darmaffectionen," Prager Vierteljahrschrift, Bd. 64, 1859, S. 143.
4 See testimony as to the influence of scurvy in promoting diarrhoea (Woodward, Med. and Surg. History of the War, Part 2, Medical Volume, p. 638).
5 A. Trousseau, "Comments on a Case of Syphilitic Diarrhoea cured by Mercury," Clinique méd., Paris, 1868, t. iii. p. 123.
Disease of the liver, heart, or lungs, by retarding the circulation in the portal system, causes venous stasis and catarrh in the gastro-intestinal mucous membrane. The chief conditions which bring this about are tumors compressing the mesenteric veins, cirrhosis of the liver, tumors pressing on the ascending vena cava, valvular disease of the right and left heart, fatty degeneration or dilatation of the heart, cardiac debility from chronic exhausting diseases, fibroid phthisis, chronic pneumonic phthisis, chronic pleurisy, and pulmonary emphysema.
An unsuitable diet may not set up an acute catarrh, but may slowly induce changes of a chronic nature in the mucous membrane. This is the case in infants fed upon artificial food instead of breast-milk, or when the digestion is overtaxed after weaning. In adults food difficult of digestion and over-eating bring about the same result. Alcohol, spices, and condiments, if taken in excess, and the habitual use of purgatives, lead to chronic inflammation of the intestine.
Foreign bodies, such as fecal concretions, gall-stones, stones of fruit, bones, coins, and pins, by remaining in contact with the mucous membrane for a length of time, determine inflammation and ulceration.6
6 Lothrop, "Case of a Child in whom seventeen plum-stones, three cherry-stones, and seven small bones were impacted In the cæcum and ileum for a year. Inflammation, ulceration, and perforation of the bowel resulted" (Buffalo Med. and Surg. Journ., March, 1882, p. 346).
Neglect in the treatment of acute catarrh, the prolongation of an acute attack, from its intensity and the incurability of the lesions, establish chronic disease.
All chronic lesions of the bowel are complicated with chronic catarrh, as chronic tubercular ulcer, neoplasms in the wall, pressure of a tumor from without, etc.
PATHOLOGICAL ANATOMY.—The alterations in the intestines in chronic catarrh involve the walls to a much greater extent than in the acute form.
The intestinal tube is dilated, contracted, or irregularly dilated and contracted. When the calibre is increased the walls are thinned. Hypertrophy and hardening of the tunics, chiefly of the muscular and submucous tissue, are accompanied by a narrowing of the canal, and this change, most common in the rectum and sigmoid flexure, sometimes involves a very considerable extent of the colon. Lebert records the case of a woman who had diarrhoea for six weeks; constipation and vomiting with abdominal tenderness ensued. There was hypertrophy of all the coats of the stomach and of the ascending colon and rectum. The rectum was so narrowed by the thickening of its wall that a female catheter could not be passed through it.7 In chronic catarrh the mucous membrane [p. 701] of the colon and of the lower part of the ileum is the seat of the most characteristic lesions. The colon was alone the seat of disease in 9 out of 99 cases analyzed by Woodward; in the remaining 90 the two were involved together. In these the lesions in the colon (especially in the rectum and sigmoid flexure) were always more advanced and more serious than in the small intestine.
7 Lebert, Path. Anat., t. ii. pp. 247, 248; another case, Laboulbène, Anat. path., Paris, 1879, p. 194.
Gastric catarrh may by extension become duodenal catarrh, and from the duodenum the disease may extend into the common bile-duct and its branches. The duodenitis and catarrh of the ducts may persist, and become chronic after the stomach lesion is gone.
The mucous lining of the intestine is changed in color, form, thickness, consistence, and in the appearance of its glandular structures. The shades of color in chronic inflammation are dark red, livid, brown, drab, or slate-color, light blue, and greenish. The coloration is not uniform. Dark-red and gray spots are seen on a pale and uniform red ground; grayish streaks and patches are mingled with red or whitish areas, giving rise to a mottled or marbled appearance.8 In some cases red predominates, in others the slate-color.9 Dark-brown, almost black, patches are also seen. These different tints depend upon the intensity and character of the inflammation and the stage which it has reached. Diffused bright-red discolorations belong to acute inflammation, and are rarely seen in the chronic form. Acute hyperæmic patches appearing in the midst of a slate-colored membrane indicate intercurrent acute attacks. Dark-red streaks or spots are caused by extravasations. Brown and slate-colored areas represent the changes in old extravasations or pigment-deposits where inflammation or ulceration has existed. Where the inflammation is progressing toward the destruction of tissue the membrane is dark-purplish or black in color, mottled with patches of dull reddish hue and minute spots of bright red. Black dots are seen in the small and large intestine isolated or in close proximity. They are due to minute specks of black pigment deposited in the apices of the villi, in the centres of solitary glands, in rings around them, or in the glands of a Peyer's patch. The juxtaposition of pinhead black points gives rise to the shaven-beard appearance10 of the mucous membrane. Dark streaks or wavy lines of pigment are also seen.11
8 For illustration of color of mucous membrane in chronic inflammation see the following illustrations in color: Med. and Surg. Hist. of the War, Part 2, Medical Volume—plates facing pp. 308, 518, and 520; also, Illustrations of Morbid Anatomy, J. Hope, London, 1834, figs. 128, 129.
9 For an excellent illustration of slate-color of chronic inflammation, with supervening acute inflammation and hemorrhagic patches, see Carswell, Path. Anat., Plate ii. fig. 4; also, Lebert, Path. Anat., t. ii. Pl. cxiv. fig. 7.
10 For an excellent illustration of this change see Med. and Surg. Hist. of the War, volume cited, plates facing pp. 298, 304; also, Atlas d'Anatomie path., Lancereaux, Paris, 1871, Pl. iii. figs. 3 and 4.
11 See colored plates Med. and Surg. History of the War, volume cited, facing p. 308.
In the ileum the mucous folds are obliterated or swollen and thickened. Obliteration of the folds occurs in connection with a dilated intestine; when the intestine is contracted they are elevated, tortuous, and close together. The villi are hypertrophied, looking often like minute polypi. The mucous coat is usually thickened, measuring from one-fifth to one-fourth of an inch. It is softened, and more easily scraped off,12 but quite [p. 702]frequently there is induration instead of softening. The solitary glands of the ileum are hypertrophied and appear scattered over the mucous surface as small rounded elevations. They are quite numerous or a few only may be seen. A ring of vascular injection usually surrounds each enlarged follicle. Peyer's patches may be unchanged or from swelling of the follicles are more prominent than is normal, but relatively the enlargement of the solitary glands is greater. In chronic catarrh the follicles acquire greater size than in the acute form. The apices of the solitary glands in the small intestine may be broken down, leaving small follicular ulcers, with swollen rings around them formed of the undestroyed and hypertrophied gland-structure. Here and there one or two of the follicles in the Peyer's patch may have its centre indented by ulceration. These changes are usually in the lower part of the ileum near the cæcum.
12 The mucous membrane is often tumefied and softened in cases where there are thickening and contraction of the intestine with great reduction of its calibre (Elliot Coues, Med. and Surg. Rep., Philada., 1863, vol. x. p. 207).
In the colon the enlarged solitary glands are in greater number, and are dotted about more closely in the descending colon and sigmoid flexure.13 When there is ulceration the large intestine has many more ulcers than the ileum, and they are more numerous in the lower part of the colon. They appear as sharply-punched openings, and give to the mucous surface a honeycombed look; their diameter varies from one-tenth to one-fourth of an inch. Large ulcers formed by the confluence of smaller ones measure from one-fourth to one inch in diameter; they may be so deep as to have the muscular tunic for their base, and quite often the bottom of the ulcers is black. A ragged or uneven appearance is given to the surface by the ulcers being close together. Such extensive destruction sometimes takes place that no normal mucous membrane seems to be left. Perforating ulcers are occasionally seen in the large intestine or ileum. Perforation occurred in two of Woodward's ninety-nine cases. Healing ulcers14 are found by the side of others which are growing. Healed follicular ulcers are known by a puckered, stellated appearance15 of the mucous membrane, which is pigmented and of a slate-gray or marbled-brown color16 if the process has been long completed. Larger dense cicatrices, pigmented also, mark the site of more extensive ulcerations.
13 Illustration, Kupfertafeln zu DR. LESSER über die Entzündung und Verschwärung du Schleimhaut des Verdauungskanales, Berlin, 1830, Bei Enslin, Tab. ii. fig. 4.
14 Illustration, J. Hope, Illustrations of Morbid Anatomy, figs. 168, 169.
15 Illustration, Med. and Surg. Hist. of the War, tom. cit., p. 528.
16 Illustration, Cruveilhier, Anat. path., xxx. livraison, Pl. iii.; also, J. Hope, Illustrations of Morbid Anatomy, figs. 128, 129.
Besides follicular ulcers the mucous membrane is disorganized by ulcers which have their origin in a loss of epithelium and superficial erosion. These deepen and may attain considerable size.
In addition to the lesions already described, the inflamed and ulcerated surface is sometimes covered with a pseudo-membranous layer of greenish-yellow color.
Chronic catarrh of the duodenum is the cause of dilatation of the vessels and thickening of the coats. A varicose condition of the veins may give rise to hemorrhage without ulceration.17 The orifice of the common bile-duct and the ducts for some distance are narrowed by swelling of their lining membrane.18 Ulcer of the upper part of the duodenum [p. 703] is found rarely in connection with external burns and chronic Bright's disease. It is more common in men between thirty and forty years of age. An embolized artery is the starting-point of the lesion. The mucous layer, deprived of its nutrition in a limited area, dies or is destroyed by the acid gastric juice; a round ulcer with terraced edges is left, its base being the muscular or serous coat. Adhesions may form between the peritoneum near the ulcer and the liver, gall-bladder, or pancreas, or an opening may take place posteriorly in the right seventh intercostal space or into the peritoneal cavity. Cicatrization of the ulcer may lead to narrowing of the canal of the bowel or of the pancreatic and common bile-ducts.19
17 G. Coulon, Bull. de la Soc. Anat. de Paris, 1879, p. 690.
18 Duodenitis was made much of by Broussais and his followers, and a great deal has been written about it. (See Boudin, Paris, Thèsis, 1837, No. 76, Essai sur la Duodenite chronique.)
19 Ziemssen's Cyclopædia, Amer. ed., vol. vii. p. 404.
Suppuration in the wall of the duodenum is still rarer. One case only is on record of pus being found in the intestinal wall.20
20 Picard, Bull. de la Soc. Anat. Paris, t. xv., 1840-41, p. 393. See also microscopic view of suppuration in wall of duodenum, Thierfelder, Atlas d. path. Histologie, 2 lief., Tab. x. fig. 6.
Chronic proctitis or inflammation of the rectum may exist by itself. The mucous membrane is swollen, hyperæmic, and the walls may be indurated and thickened so as to reduce the calibre of the tube. Superficial erosions or deep ulcers and perforation are due to the retention of hard fecal matter in the distended pouches of the rectum. Inflammation in the tissue around the rectum (periproctitis) is excited by inflammation of the wall without perforation; abscesses form and burst externally or into the bowel, thus establishing fistulæ.
PATHOLOGICAL HISTOLOGY.—The essential primary feature of chronic catarrh is the increase and persistence of cell-accumulation in the reticular connective tissue of the mucous and submucous layer. After an acute or subacute attack some time elapses before the large number of cell-elements are disintegrated or absorbed. By remaining they offer a constant invitation to causes of irritation, hence the necessity for prolonged care in diet after acute attacks. Fresh causes—imprudence in eating, etc.—induce additions to the number of cells, and the tissue becomes overcharged with active elements of growth. Hypertrophy of tissues results, the mucous and submucous tissues thicken, and the glandular structures are stimulated to a condition of morbid activity. The glands of Lieberkühn elongate, the number of acini increases, and the contained cells multiply. Accidental closure of the gland-openings from outside pressure or over-accumulation of the contents leads to cyst-formations. The lymph-cells in the reticular tissue of the closed follicles undergo rapid increase; the follicle is over-distended, projects above the surface, bursts, and a small ulcerating cavity is left. This is now enlarged by the breaking down of the remaining tissue of the follicle, then of the submucosa. The overhanging roof of mucous membrane, deprived of its nutrition, sloughs off at the edges and the exposed ulcerated surface is increased. By the confluence of two or more burrowing ulcers more extensive destruction of the mucous and submucous layers is brought about. The large deepened ulcers have the mucous layer for their base. Cicatrization of the ulcers takes place by the formation of cicatricial tissue at their base; the excavation is filled up partially, by contraction the edges are brought together, and the tissue solidifies. No villi or epithelium covers these cicatrices.
[p. 704] There are rarer pathological changes. In catarrh of long duration cysts are found, especially in the large intestine. They are about the size of a small pea, projecting above the mucous surface. They have a yellow or amber color, and contain a jelly-like yellow fluid which can be pressed out. They originate in the distension of the dilating glands of Lieberkühn; according to Woodward, they find a favorable nidus for their growth in the softening tissue of the solitary glands; hence the cystic forms are seen occupying the interior of follicles undergoing disintegration.21 The presence of the glands of Lieberkühn in the interior of the closed follicles has been observed by other pathologists, some of whom are unable to explain so remarkable a lesion.22 Around the edges or in the midst of healing ulcers in the intestine granulation-like excrescences or polypoid growths are observed as a rare lesion. These seem to be projections from undestroyed islands of mucous membrane, being surrounded by the ulcerated surface. The minute polypi originate in a process of growth of the undestroyed mucous tissue. Cicatricial contractions around their bases give them peculiar forms; they are club-shaped, simple, or branched. This lesion has been described by Johann Wagner,23 Carl Rokitansky,24 and J. J. Woodward25 from original specimens. According to Woodward, the growths (pseudo-polypi he calls them) are composed of a central portion of connective tissue continuous with the submucous connective tissue of the intestine and a peripheral portion of diseased mucous membrane. The central connective tissue was filled with large and numerous cells, and the glands of Lieberkühn in the mucous covering were elongated and branched and showed evidences of an active hyperplasia.
21 J. J. Woodward, op. cit., pp. 570, 571.
22 A. Laboulbène, Anat. path., Paris, 1879, p. 186.
23 "Einige Formen von Darmgeschwüren; iii., die Dysenterische Darmverschwärung," Med. Jahrb. des k. k. öst. Staates, Bd. xi., 1832, S. 274.
24 "Der dysenterische Prozess auf dem Dickdarme und der ihm gleiche am Uterus, vom anatomischen Gesichtspuncte, beleuchtet," ibid., Bd. xxix., 1839, S. 88.
25 "Pseudo-polypi of the Colon," Am. Journ. Med. Sci., Jan., 1881, p. 142.
Polypi of the colon have been seen and figured by other pathologists, but they were not connected with ulceration and cicatrization of ulcers. Luschka26 saw the mucous membrane from the ileo-cæcal valve to the end of the rectum covered with polypi, club-shaped, the size of a hempseed or bean, and made up of glandular tubes simple or branched. Other cases have been described by Lebert, Heuriet, and others,27 in which polypi were distributed in the rectum, colon, cæcum, or about the ileo-cæcal valve. This is the condition described by Virchow as colitis polyposa.
26 Virchow's Archiv, vol. xx. p. 133.
27 Heuriet, Bull. de la Soc. Anat. Paris, t. xlviii., 1873, p. 250; Tr. N.Y. Path. Soc., vol. ii., 1877, p. 172. For illustration of multiple polypi of colon and rectum, Lebert, Path. Anat., tome ii., Pl. cxxii. figs. 1 and 2; granular elevations in ileum, idem, Pl. cxxi. fig. 1. Also, mucous polypi of rectum, Thierfelder, Tab. xiii. figs. 3, 3a, 3c; also, intestinal polypi of rectum, Lancereaux, Atlas Path. anat., 1871, Paris, Pl. iv. fig. 4. Polypi are rarely seen in the small intestine; see Böttcher, "Polypöses Myom des Ileums," Archiv der Heilkunde, xi. Jahrgang, 1870, p. 125.
Atrophy of the wall of the intestine, chiefly of the mucous layer, supervenes upon catarrh. It is confined to certain areas, the rest being normal or in a state of chronic catarrh. It is found in 80 per cent. of the cases examined either in the large or small intestine. The cæcum is the most frequent seat; next in the order of frequency it is seen in the ascending [p. 705] colon, the lower part of the ileum, the other parts of the colon, and is least common in the upper part of the ileum. In children the lesion is more common in the small intestine than in adults. The changes in the mucous membrane of the colon are a diminution in its thickness and disappearance of the glands of Lieberkühn. The mucous layer is reduced to one-fifth of its normal size, and no trace of the glands may be left; a layer of connective tissue with imbedded round cells is all that remains. The surface of the membrane is irregular and colored with yellowish pigment. In the ileum the villi are shrunken, with few cells; in some cases they disappear altogether. The muscular tunic may share in the atrophy.28
28 Nothnägel, "Zur Klinik der Darmkrankheiten," iii. Abtheilung, Darmatrophie, Zeitschr. f. klin. Med., Berlin, 1882, iv. p. 422; Virchow, "Ueber den Gang der amyloiden Degenerationen," Virchow's Archiv, Bd. viii. S. 364; E. Neumann, "Neue Beobachtungen über amyloide Degeneration," Deutsche Klinik, Bd. xii., 1860, S. 337, 353, and 373; Lambl, "Ueber amyloide und colloide Degeneration im Allgemeinen und die des Darmsinsbesondere," Beob. und Studien (aus dem Prager Kinder-Spitale), Prag., 1860, S. 319; Frerichs, "Diseases of the Liver," New York, 1879 (Wood's Library), vol. ii. p. 180; M. G. Hayem, "Note sur la Dégénérescence amyloide du Tube digestif," Compte Rend. des Séances de la Soc. de Biologie, Nov., 1865, 4me Série, t. ii. p. 191; also, Gaz. méd. de Paris, t. xxi. p. 99.
Lardaceous (amyloid or waxy) degeneration of the intestinal mucous membrane is met with in chronic catarrh. The small arteries of the villi and submucous layer, the muscular and other tissues, are infiltrated with a new material allied to fibrin. The membrane to the eye is paler than normal. When iodine is applied, a characteristic red staining of the infiltrated parts is noticed. This lesion is a cause of diarrhoea and of hemorrhage,29 from the greater permeability and greater fragility of the arteries. It is also associated with follicular ulceration, and is probably a cause of disintegration of the mucous membrane.30
29 T. Grainger Stewart, "On Hemorrhage from Waxy or Amyloid Degeneration," Br. and Foreign Med.-Chir. Rev., vol. xli. p. 201.
30 Frerichs, "Diseases of the Liver," New York, 1859 (Wood's Library), vol. ii. p. 180; also, E. Aufrecht, Berl. klin. Woch., 1869, p. 315.
The abdominal organs present other lesions in chronic intestinal catarrh, few of which have any distinctive character. The peritoneum shows signs of old or recent inflammation. The former is subacute or chronic, and is recognized by the adhesions of opposed surfaces in a limited area, frequently corresponding to the seat of intense intestinal inflammation. Fatal perforations are delayed or prevented by these adhesions. General peritonitis with soft lymph or sero-purulent effusion is found with perforation. The mesenteric glands may be enlarged. The liver is larger or sometimes smaller than normal, and its tissue is softened and may be fatty. Abscess of the liver31 is a very rare result of chronic intestinal catarrh, with ulceration. The gall-bladder is usually filled with bile. The spleen is small and firm in texture; less commonly it is soft and friable. The pancreas is healthy. The kidneys are large and pale; the cortical substance is relatively increased and the tubules contain granular epithelium.
31 It occurred in 4 per cent. of Woodward's cases of chronic follicular ulceration. See case reported by the writer in which the ulcers healed before the death of the patient from hepatic abscess (Maryland Med. Journ., March 15, 1883, p. 562).
In the thorax the heart is flabby, pale, and small; clots are found in the right and left side extending into the pulmonary artery and aorta. Sudden death has been attributed to cardiac thrombosis. That coagula [p. 706] do form in the heart during life is shown by the sudden occurrence of cerebral embolism with aphasia.32
32 The writer has seen one case of this kind occurring during the effort at stool in a patient who was very feeble and very anæmic from chronic intestinal inflammation with ulceration.
Pneumonia is the most frequent pulmonary lesion; it may be single or double. It was found in 18 of the 99 cases of Woodward, and in 21 out of H. A. Allen's 41 cases. Inflammation of the pleura is not infrequent. The brain and its membranes may be congested, and fluid is found in the subarachnoid space, in some instances in cases which have had a sudden termination. The cornea is ulcerated, and the eye destroyed by opening of the anterior chamber in a small proportion of cases. The sloughing process begins in the lower part of the cornea and in the sclerotic.
SYMPTOMS.—When chronic intestinal catarrh succeeds the acute form, the transition is marked by the disappearance of fever and an amelioration of all the symptoms, with apparent recovery. The patient begins to go about, but diarrhoea returns whenever there is any unusual fatigue or excess in eating. In some cases there is no improvement in the diarrhoea, but in the general symptoms only. When the malady is chronic from the beginning, the onset is characterized by symptoms of indigestion and occasional diarrhoea, which become more and more pronounced according to the severity of the illness.
Mild forms of catarrh have constipation, or diarrhoea alternates with a normal or constipated state of the bowels. The form in which constipation is continuous is associated with mechanical stasis from liver and heart lesions and with the gouty and uric-acid diathesis. The mucous membrane is in a state of passive hyperæmia, an excess of mucus being the product of the inflammatory process. Mucus coats the lining tunic, lessens its irritability, interferes with digestion and absorption, and acts as a ferment, exciting decomposition in the food. The bowel is atonic and is distended with contained gas; there is great feebleness of peristaltic contractions.
Intestinal indigestion and constipation are therefore the symptoms of this form. The signs of indigestion occur one to three hours after eating, according to the location of the maximum of catarrh and the time taken by the food to reach this point. They are a sense of fulness or distress in the abdomen from gaseous distension, slight colicky pains, and a rumbling of gas, which may be prolonged during several hours after a meal. The constipation is indicated by the spontaneous passage of dry masses or scybalæ coated with layers of mucus which are clear or cloudy, or the mucus may be intimately mixed with solid matter. Pure mucus is also expelled without fecal matter. There may be no stool without a purgative, and then softened matter with scybalæ and mucus is passed. Altered mucus in the form of membraniform shreds or cylinders occasionally pass in the so-called membranous enteritis.
The abdomen is full and not sensitive to pressure. The tongue is coated and usually pale and flabby. In appearance the patient exhibits a general want of tone; the skin is white or muddy, the muscles are soft, and the expression indicates the depression of spirits, the lassitude, and the inertia which he feels. Hemorrhoids are very likely to [p. 707] exist. Such a condition may last for months or years without much change. Under proper treatment recovery may take place, but if entirely neglected or improperly treated the disease inevitably becomes worse.
In a second mild form there is no permanent disease, only an impressionability of the mucous membrane of the bowel to causes which induce hyperæmia and excessive secretion ending in diarrhoea. Exposure to cold, fatigue, or slight indiscretions in diet may bring it on; even an emotional cause may do it. The attacks last one or several days, and may at times assume some gravity. This predisposition to diarrhoea lasting through a lifetime is analogous to the tendency to inflammation of the nasal and other mucous membranes.
In severer and typical forms the symptoms point to permanent lesions. The tongue is smooth, shining, or glazed, sometimes with a central brown streak, but it may be also pale and covered with a white coat. The appetite is diminished or lost, or it is capricious, craving unsuitable food. If there is no gastric catarrh, the chief distress does not come until some hours after eating, but the taking of food sometimes excites pain and brings on an evacuation of the bowels through reflex influence.
There may be slight tympanites or a retracted abdomen. The imperfect digestion of food and the fermentation of the intestinal contents develop gas which keeps the abdomen distended and causes slight pains and borborygmi. Pain may, however, be entirely absent. A feeling of abdominal soreness is not unusual; it is increased by coughing, sneezing, or any sudden movement. Sensibility to pressure is usually wanting; when it exists it is found along the line of the colon in most cases.
The diarrhoea is the characteristic symptom. The number of the stools varies from one to eight in twenty-four hours; four is about the average number. They occur usually in the early morning hours, from two to six o'clock, but food may at any time bring on peristaltic contraction, so that a motion after every meal is not uncommon. In quantity there is much variability; two to four ounces of fluid matter is the rule perhaps, but a very much larger amount than this is often passed with each evacuation. As a rule, the larger the quantity of fluid the more extensive is the catarrh and the more advanced are the lesions. The matters passed are composed chiefly of fecal matter varying in consistence from a solid or semi-solid mass to a watery fluid. In the soft stool, like thickened gruel, the consistence is due to the presence of mucus; in the thinner evacuation water is the chief element. Liquid stools are sometimes frothy. In color the dejecta are brown, yellow, red, green, slate-color, or white. They may be colored dark by medicines, as iron or bismuth, or by blood. The presence of blood gives a pinkish, bright-red, dark-brown, or black color, depending upon the amount of blood and the changes it has undergone in the bowel from a longer or shorter retention. Blood, when it comes from the rectum, is in bright-red streaks or small coagula. When its source is higher up, it is much altered, being dark and granular. Coffee-ground sediment in a fluid stool is blood from the upper part of the intestine or stomach. The spreading of an ulcer may open a vessel of some size, and a fatal hemorrhage follow. A yellow tint like that of a child's movement may arise from a mixture of pus and fecal matter. Pus, as a milky or creamy fluid which may be [p. 708]streaked with blood, is a frequent appearance in disease of the rectum and sigmoid flexure. The odor of the stools is fecal, sour, or sickening from fermentation or offensive from decomposition. In bad forms of chronic diarrhoea in children the black watery stools have a most offensive odor.
Mucus is the most constant ingredient of the diarrhoeal stool, and is in itself a sufficient evidence of catarrh, as it is not seen in normal stools except as a temporary phenomenon. It is present in flakes in watery evacuations, giving a jelly-like character to the fluid if it is in excess, or it is mixed with semi-solid feces. Pure mucus may be passed, if the catarrh is low down, in clear, glairy, or opaque masses. The frog's-egg or boiled-sago particles supposed by Niemeyer and others to point to follicular ulceration, and by Traube to be the swallowed bronchial secretion, are said by Virchow to be partly-digested starch, and also by Nothnägel to be of vegetable nature.33 The stools may contain small yellow or brownish masses which are mucoid in nature, being yellow from bile-staining. Pavement epithelial cells are found in the coating of mucus around a hard fecal lump. Cylindrical epithelium is passed uncolored or stained with bile. These cells are separated, and are deformed and shrunken, with a granular protoplasm and indistinct nucleus. Goblet-cells are also seen. Round cells in the form of mucus-corpuscles or giant-cells are mixed with shreds of mucus or float in the thin stools. Crystals of triple phosphate, of neutral phosphate, oxalate of lime, and other lime salts, and of cholesterin, are also seen.
33 Virchow's Archiv, v. S. 329; Nothnägel, "Zur Klinik der Darmkrankheiten," Zeitschrift für klin. Med., iii., 1881, p. 241.
Micrococci and bacteria have no pathological importance; they are seen in different diseases and in health.
Unaltered food may be expelled (lientery) by rapid peristaltic movements. But the microscope will detect what cannot be seen by the eye—unaltered starch-granules, filaments of meat-fibre, or fat in drops or in needle-shaped or feathery crystals.
The nervous system is disturbed after a certain time. There is languor, with depression of spirits, mental weariness, and inaptitude for work of any kind. The patient is querulous, morose; his sleep is restless, but sometimes profound until disturbed by the demand to empty the bowel. Melancholia is attributed to this as to other diseases of the abdomen, but their influence in producing insanity is doubtful.34
34 Griesinger, Mental Path. and Therap., Am. ed., New York, 1882, pp. 137, 138.
No decided symptoms are exhibited in the respiratory and circulatory systems. Even slight exertion will cause shortness of breath and increased frequency or palpitation of the heart. This irritability of the heart is a marked feature of the disease.35
35 DaCosta found that of 200 cases of irritable heart, 61 were in patients who had suffered from or still had diarrhoea (Am. Journ. Med. Sci., vol. lxi., 1871, p. 37).
The appearance of the urine is normal; it may be abundant, with phosphatic deposit, or it is scanty and high-colored. In bad cases albumen and casts have been found.36
36 Alonzo Clark, "Proc. of New York Path. Soc.," Med. and Surg. Reports, vol. ix., 1862-63, p. 312.
The symptom indicative of atrophy of the mucous membrane is believed by Nothnägel to be the persistent passage of one soft, unformed stool daily. Mucus and fat, which diminish the consistence of the stool, are [p. 709] excluded by microscopical examination. One stool daily shows that there is no exaggerated peristalsis which hurries the food along so rapidly that water cannot be absorbed.37
37 Nothnägel, "Zur Klinik der Darmkrankheiten," Zeitschrift für klin. Med., iv., 1882, p. 422.
PROGRESS AND TERMINATION.—As the disease advances it is marked by progressive emaciation and debility. The skin gradually acquires great pallor, indicating profound anæmia. The loss of flesh is very rapid. An exacerbation of the disease will in a few days cause the cheeks to grow hollow, the eyes to appear sunken with dark rings around them. In all cases of long duration the progress is intermittent; frequent relapses occur from which the patient may rally and regain a moderate degree of flesh. Recovery may take place in weeks or months—eighteen months is the average duration38—but in most instances a tendency to a recurrence of the diarrhoea from cold, fatigue, or indiscretions in diet will continue throughout life. An incomplete recovery may take place by the cessation of the diarrhoea and formation of a stricture from the healing of an intestinal ulcer. In the worst cases there is no rule as to the rapidity or regularity of the march of the disease.
38 C. H. Ralfe, Seamen's Hospital, London: see Aitken's Handbook of Treatment, New York, 1882, p. 116.
When the advance is toward a fatal issue the emaciation progresses until it becomes extreme; nothing but skin and bone are left. The cuticle is hard and dry, pale or brownish in color. The muscular strength is so reduced that the patient is unable to move from bed. The voice may sink to a whisper. The nervous depression and moroseness assumes a more marked character. Among the soldiers during the Civil War who had undergone great privations with insufficient or improper diet the mental phenomena were those of dementia.39 In them the disease was modified also by the symptoms of scurvy and malarial poisoning.
39 W. Kempler, "Entero-Colitis," Am. Journ. of Med. Sci., vol. lii., 1866, p. 337.
Fever is seen in the late stages; it is nocturnal at first, and later assumes the features of hectic. The pulse grows more frequent and thready; aphthous deposits appear on the inside of the mouth and pharynx. Toward the end the discharges may become more frequent and very abundant; they are more fluid, lighter colored or black, with floating particles of blood and mucus. There may be a loss of odor or they may have a cadaveric smell.
Death takes place in a few weeks or after years of alternate suffering and relief. The immediate causes of death are exhaustion, marasmus from starvation, collapse from perforation of an intestinal ulcer and consecutive peritonitis, syncope from sudden exertion, pneumonia, or acute pulmonary congestion, pleurisy, or subarachnoid effusion in the brain, with coma and convulsions.
COMPLICATIONS.—General dropsy results from the hydræmia and languid circulation of the late period of the disease. Other causes of this symptom are coincident diseases of the liver, kidney, or the malarial cachexia. Oedema of one extremity follows a thrombus in the crural vein. Chronic bronchitis and pulmonary phthisis are sometimes met with. Acute pneumonia40 and acute pulmonary congestion are occasional [p. 710] causes of death. Peritonitis may occur with and without perforation. The latter variety begins as a local inflammation of subacute or chronic nature, and spreads slowly until it becomes general. Extensive adhesions and abundant accumulations of serous, sero-purulent, or purulent fluid in the abdominal cavity result.
40 Pneumonia (8 double and 12 single) occurred in 20 out of 41 fatal cases reported by Harrison Allen, Tr. Path. Soc. Philada., 1867, vol. ii. p. 161.
The causal conditions which have been enumerated may be considered as complications. They are tuberculosis, Bright's disease, cirrhosis of the liver, abdominal tumors, scurvy, tubercular and other neoplasms in the wall of the intestine; attacks of intercurrent, intermittent, or remittent fever arise from the malarial influence to which the intestinal catarrh is due. These fevers and rheumatism and pseudo-rheumatism are complications in soldiers from the exposure to malarial influences and to cold and dampness.41
41 Woodward, op. cit., p. 495.
Ulceration of the cornea, escape of the aqueous humor, and collapse of the eye were observed in quite a number of cases occurring among soldiers.42
42 Elliot Coues, Med. and Surg. Reporter, Philada., 1863, vol. x. p. 207, and H. Allen, Tr. Path. Soc. Philada., 1867, vol. ii. p. 161.
SEQUELÆ.—The alteration of structure from long-standing inflammation leaves the mucous membrane prone to recurrence of inflammation. Chronic intestinal indigestion and permanent malnutrition come from the same cause. The glandular and lymphatic structures of the intestine and the mesenteric glands are so changed by disease that they imperfectly perform their function. Tabes mesenterica is the ultimate phase of this change. Constipation succeeds chronic diarrhoea, and is due to atony of the muscular wall from long-continued distension, and probably from degeneration of the muscular structure. A more serious cause of constipation, and sometimes of intestinal obstruction, is found in stenosis of the bowel from the healing of the ulcers of long-standing chronic catarrh. Stricture is more common in the colon, sigmoid flexure, and rectum. How frequently such a result follows the cicatrization of intestinal ulcers is not definitely known. Woodward concludes from a careful search of books and pathological museums that stenosis from this cause is very rare.43 Syphilis is the most common cause of ulcer. Local or general peritonitis leads to the formation of adhesions or fibrous bands uniting neighboring links of intestine. By the contracting of these narrowing of the intestinal canal may result. Paralysis, hemiplegia, paraplegia, etc. have been found to follow upon diarrhoea of long standing.44
43 Woodward, op. cit., p. 504.
44 Potain, "Parésie des Membres inférieurs ayant succedé à un Catarrhe gastro-intestinal," Rev. de thérap. Med.-Chir., Paris, 1880, xlvii. p. 562; "Paralysis spinale sécondaire à une Diarrhée chronique," Journ. des Conn. méd. Prat., Paris, 1880, 3, S. ii. p. 57.
DIAGNOSIS.—The mild form of chronic catarrh of the intestines associated with constipation has been confounded with hepatic disorders, and the obscure symptoms attending it have been attributed to excess or diminution of bile, and medicines to regulate the liver have been given accordingly. In the absence of lesions in the liver, in cases where symptoms such as have been described have preceded death, the opinion is not justified that disease of this organ has existed. On the contrary, alteration in the mucous membrane is almost always found, which points to the true nature of the disease. The diagnosis is based upon the accompanying [p. 711]gastric catarrh and upon the symptoms of intestinal indigestion and malnutrition. Greater sensibility to pressure over the right hypochondrium and along the line of the colon, pain one to two hours after eating, with distension of the abdomen, the passage of well-formed and somewhat indurated feces mixed or coated with mucus, are symptoms peculiar to these mild forms.
The tendency to diarrhoea from cold, indigestible food, etc. which marks the second form of mild catarrh is easily recognized.
The characteristic symptom of the severe form is the persistent diarrhoea. Paroxysmal pains, tympanites and rumbling of gas, tenderness on pressure over the colon, the alternate periods of improvement and relapse, with the constitutional signs of impaired nutrition and progressive anæmia and debility, point out the nature and the seat of the lesion with sufficient clearness. It is futile to attempt to distinguish chronic intestinal diarrhoea from chronic dysentery. The lesions of the two conditions are essentially the same; it depends upon the fancy as to which name is given to the lesions described here under the title chronic intestinal catarrh. A greater amount of blood and mucus in the stool with tenesmus would more properly be called dysenteric, but the same case may present at one time diarrhoeal, at another dysenteric, symptoms.
Primary must be distinguished from secondary diarrhoea. Therefore the liver, heart, and lungs must be examined to discover diseases which might cause portal congestion. Any constitutional malady may be a cause and an explanation: tuberculosis or pulmonary phthisis stands first in its influence; next, chronic Bright's disease, septicæmia, scurvy, syphilis, and gout are attended by intercurrent diarrhoea. If all general disease can be excluded and the morbid process be located in the intestine alone, its cause may be known by studying the habits, occupation, and diet of the patient. Foreign bodies—hardened feces, gall-stones, fruit-stones, etc.—are possible causes which the history of the case may point to.
Having located the disease in the intestine and decided upon its primary or secondary nature, it remains to determine more precisely (a) the locality of the lesion, and (b) the stage of the inflammatory process.
(a) In what part of the intestinal canal is the disease located? It must be remembered that in typical and fatal cases the large intestine is the home par excellence of the lesions of chronic catarrh, and that the lower part of the ileum is often associated in the morbid processes, but limited areas of the small or large intestine are affected in mild forms which yield readily to treatment.
Icterus, clay-colored stools, and bile in the urine show that the catarrh is in the duodenum and involves the opening of the common bile-duct. The absence of diarrhoea, with flatulence and colics, limits the area of inflammation to the duodenum. Symptoms of duodenal indigestion accompany this form of catarrh; the failure of bile to neutralize the acid chyme impairs the effect of the pancreatic secretion. Fats are not digested and there is fatty diarrhoea. To this may be added tenderness in the right hypochondrium, and pain and oppression in the epigastrium and to the right one hour after eating. There may be wasting and hypochondriasis.
[p. 712] The lower part of the duodenum below the opening of the bile-duct, the jejunum, and the ileum can be taken together as forming the small intestine. Chronic catarrh of the small intestine is attended with pain about the umbilicus, which comes on immediately or in one hour after taking food. Tympanitic distension gives a full, rounded prominence to the abdomen, which is more central than lateral, and greater below the umbilicus than above it. It is accompanied by a sense of oppression, which is greater after eating. Inability to digest food consisting largely of starch or sugar, as well as tardiness in the digestion of all foods, with resulting loss of flesh, are signs of intestinal indigestion. There may be no diarrhoea; if there is, important help to diagnosis can be gained by examining the stools. They contain undigested or partly-altered meat-fibre and starch-granules, discoverable only by the microscope. The discharges are soft and pulpy from an intimate admixture of mucus. To the naked eye no mucus is visible, but a thin layer under the microscope shows clear islets of pure mucus, or mucus may only be detected by the adhesion of the covering-glass to the slide. Bile-stained epithelium and globules of stained mucus are seen in the liquid stools from catarrh of the small intestine and of the ascending colon. There is the characteristic reaction and play of color on testing for bile-pigment. These are evidences that the stool with the bile has been hurried along the ileum and colon, and expelled before the transformation in the coloring matter has had time to take place.45
45 "II. Abtheilung, Diagnostische Bemerkungen zur Localisation der Catarrhe," Zeitschrift für klinische Medicin, Berlin, 1882, iv. p. 223.
In catarrh of the large intestine there is sensitiveness to pressure along the line of the colon; the distension of the abdomen is not uniform, depending upon the prominence of the transverse or descending colon. The pains are more severe and precede the stools, which are more frequent and larger than in catarrh of the ileum. The discharges are pulpy or watery. Globules of mucus are visible to the naked eye, and mucus is intimately mixed with fecal matter.
If the lower half of the colon is chiefly the seat of the disease, pure mucus coats the more solid stool and is in its substance. With catarrh limited to the descending colon scybalæ are imbedded in mucus. From the sigmoid flexure and rectum larger masses of mucus, without fecal matter or with it, are expelled. Pure lumps of mucus, mixed or stained with red blood and without fecal matter, indicate catarrh of the rectum—proctitis.
(b) The stage of the process of inflammation is diagnosed by the condition of the patient, the course of the disease, and the character of the stools. As long as there is a pulpy fecal diarrhoea, with no blood, pus, or fragments of tissue and no marked emaciation or fever, and with a tendency to improvement under favorable conditions, there is every reason to believe that there is no ulceration.
In follicular ulceration the course of the disease is essentially chronic, and is marked by periods of improvement under careful treatment, with exacerbations and relapses from slight causes of irritation. There is progressive emaciation and debility, with fever of hectic character, which is worse in the later stages. The abdomen may be retracted. The movements are frequent and liquid, and are without odor or fetid. They [p. 713] contain mucus, glassy-gray or green, pus-cells imbedded in masses of mucus, blood in small amount, but sometimes abundant, and shreds of the tissue of the mucous membrane. This last is an important aid to diagnosis.
The higher the ulcer the less marked is the diarrhoea. The lower its situation the greater is the frequency of the stools and the more liable are they to be accompanied by tenesmus and to contain blood and pus. Toward the last, ulceration is accompanied by rapid emaciation, fever, sweats, a feeble circulation, a dry tongue, great thirst, and oedema of the feet and ankles. Death takes place by gradual exhaustion, more rarely from perforation and peritonitis or from intestinal hemorrhage.46
46 Nothnägel, "Die Symptomatologie der Darmgeschwüre," Klinische Vorträge Volkmann, No. 200, Aug. 24, 1881.
Duodenal ulcer is with difficulty recognized during life.47 The following are the symptoms which have preceded death from this lesion: Profuse hemorrhage from the bowel, vomiting of food as well as blood, icterus, dysphagia, hiccough, oppression in the epigastrium after eating, attacks of cardialgia with tenderness on pressure in the right hypochondrium, and sudden death with symptoms of collapse. If these symptoms follow an extensive burn of the skin, they are easily referred to a duodenal ulcer.
47 W. L. Loomis, "Perforating Ulcer of Duodenum and Sudden Death." For two years the patient had suffered with dyspepsia and epigastric pain after eating, was gouty, and had lost flesh. Autopsy: atheroma of arteries, beginning cirrhosis of kidneys, walls of stomach thickened, perforated ulcer one inch below pylorus (Med. Record New York, 1879, vol. xv. p. 188; also Boston City Hospital Report, 1882, p. 374).
Tuberculous ulcers are distinguished from follicular ulcers by the history of hereditary predisposition, the existence of pulmonary tuberculosis, higher fever, and more rapid emaciation and debility.
A cancerous ulcer may be the cause of bloody stools; it is usually within reach of the finger in the rectum; the mass exercises pressure upon the prostate, and at times occludes the bowel, causing obstruction. The cachexia and rapid decline are not seen in catarrhal ulceration.
PROGNOSIS.—Chronic catarrh of the intestine is most fatal in children. Among infants artificially fed, when the illness develops and continues during hot weather, the mortality is very great. Recovery in the young is rendered less probable if chronic diarrhoea is associated with rickets, scrofula, or tuberculosis.
If the catarrh in adults is a complication of some previously existing constitutional disease, as Bright's disease or scurvy, or is connected with lesions of the liver, spleen, heart, or lungs, there is less hope of cure. In old persons this disease has a special gravity.
The longer the disease has lasted before treatment is begun, and the longer it continues without being influenced by treatment, the more unfavorable will be the prognosis. Discouraging symptoms are an uninterrupted loss of flesh and strength, lientery, hectic fever, relapses notwithstanding care in diet, and the signs of ulceration—blood, pus, and tissue-shreds in the stools, with an odor of decomposition.
Favorable promises may be based upon a hearty willingness of the patient to submit to the strictest regimen and to subordinate his life to the plans of treatment, the absence of other diseases, early improvement in his general condition and local symptoms under rest and diet. A [p. 714] complete cure cannot be assumed to exist unless the patient has passed one or more years without a relapse.
TREATMENT.—As chronic intestinal catarrh is a complication of so many conditions, the prevention of it becomes a matter of great importance and of very general application. All rules for preserving health—temperance in eating and drinking, bathing, exercise, good ventilation, the avoidance of overwork, both mental and physical—are so many means for escaping an intestinal catarrh which may present itself as an indigestion with constipation or as a diarrhoea.
The special liability of infants and children, and to a less extent of very old persons, and the greater dangers they run, call for the most careful selection of appropriate diet at these periods of life.
Where there is hereditary predisposition, idiosyncrasy, chronic diseases of organs, or constitutional diseases, an easily-digested dietary should be supplemented by precautions against chilling of the surface by the wearing of flannel underclothing and woollen socks.
The etiology of each case may at once suggest a line of treatment. Among the causes which point to appropriate measures are—the continued presence in the bowel of indigestible or undigested food, constant exposure to cold or to changes of temperature, chronic cardiac disease and portal congestion from any cause, chronic cachexiæ, as syphilis, malaria, tuberculosis, or Bright's disease, the crowding together of individuals in prisons, asylums, etc.
1. The mildest form of intestinal catarrh characterized by intestinal indigestion and constipation or by the passage of fecal matter more or less solid, mixed or coated with mucus, is best treated by a diet such as is advised for intestinal indigestion, bathing with friction, outdoor life, exercise on horseback or by walking, pleasurable occupations, and travel. Iron if there is anæmia, and strychnia if there is a sluggish capillary circulation, with cold hands and feet, are available and useful in many cases. Massage and the Swedish movement treatment find useful application in feeble men and in women who are not strong enough for outdoor exercise. To aid the digestion the liquor pancreaticus as advised by Roberts, a teaspoonful one hour and a half to two hours after each meal, with ten to twenty grains of the bicarbonate of sodium, is, theoretically at least, to be warmly recommended. The Rockbridge alum water, a small glass three times daily between meals, has astringency enough for the hyperæmic membrane and is of good service without increasing constipation.
Purgatives should be avoided as much as possible. An enema of cool water, not more than a tumblerful, taken each morning after breakfast if persevered in, may do all that is needed in this direction. If it fails to empty the bowel completely, a larger enema of warm water—one pint—holding in solution sulphate of zinc or alum in the strength of one grain to three or four ounces, can be thrown high up with a rubber tube once daily. This acts upon the mucous surface, constringes mildly the congested vessels, and when expelled brings away the retained fecal matter. These astringent rectal injections offer promise of cure in many obstinate cases where the colon is chiefly the seat of disease. Belladonna is advised for cases of this kind in combination with strychnia for the constipation. Mild laxatives are often necessary. Bedford mineral water, Hunyadi water, or other salines and the less active vegetable [p. 715] cathartics, can be given alternately. Ipecacuanha has had quite a reputation in combination with purgatives in intestinal catarrh. Aloin pills empty the bowel without much attendant irritation.
2. The form of catarrh which shows itself in a tendency to diarrhoea from indiscretions in diet or from exposure to cold must receive prophylactic treatment. Especially in this form is it important to improve the activity of the skin by bathing and friction, and to lead a temperate life in all things, regulating the diet according to the rules already stated. Tonics are called for in such cases. Fowler's solution of arsenic (one drop before each meal, Ringer), the potassio-tartrate or the tincture of the chloride of iron, dilute sulphuric acid, nitro-muriatic or hydrochloric acid, are efficient in improving digestive activity or in opposing the anæmia which is nearly always present. Quinia is indicated in malarial anæmia with a disposition to loose bowels. Quassia or other vegetable bitters can be given if the appetite is languid; the bitters are, as a rule, of little benefit, and may do harm if diarrhoea exists. Strychnia with quassia or columbo stimulates the appetite and the gastric digestion. When intercurrent attacks of diarrhoea come on with coated tongue, flatulence, distress about the umbilicus after eating, bismuth given on an empty stomach in full doses is serviceable. Small doses of morphia or of opium in some form can be added to the bismuth if there is much pain or when the stools are frequent.
In this and in other forms of intestinal catarrh mineral waters are profitably employed. They are best taken at their sources; and here, as in the case of sea-bathing, the benefit is largely due to the change of air and scene and to the more simple mode of life. Any of the watering-places where alkaline-saline waters or ferruginous waters are found may be of benefit. A trip to Europe and a stay at Carlsbad will break up many an obstinate case of chronic abdominal disorder; but other beneficial waters in Europe are Tarosp, Rohitsch, Marienbad, Kissengen, and Plombières.
In this country the comfort and conveniences of the summer hotels and climate are as much to be considered as the chemical composition of the waters. For milder forms of catarrh with constipation a season at Saratoga, with a life of temperance there, is a wise procedure. Bedford Springs, Pa., offer the same advantages in part, but the waters are best suited to catarrh with constipation. Many of the Virginia springs benefit health-seekers who do not place too much reliance upon the virtues of the waters, and who trust to the value of pure air, exercise, diversion, and rest.
3. All plans of treatment for the more severe form of catarrh with chronic diarrhoea (follicular enteritis) must be based upon a knowledge of the lesions. Bearing in mind the alterations in the mucous and submucous tissues, it is clear that no treatment can be successful which is not carried out with the most careful attention to details, and which is not continued for some time after all the symptoms of the disease have ceased. The complete resolution of hypertrophied glandular tissue, the scattering of cell-accumulations, and the healing of ulcers can only be secured in this way. It is best to present the whole case before the patient, so as to enlist in the task his intelligent co-operation.
Directions for the guidance of cases of this kind must include every [p. 716] detail of the patient's life. The question of residence is of importance to begin with. A cool and dry climate is better than a wet and warm one, and where other means fail change of climate is sometimes the only cure. A sea-voyage, a residence in a mountain-region, will oftentimes promptly and effectually cure an obstinate diarrhoea. House-drainage and ventilation should be examined into and improved. The occupation may have developed the disease; in overwork may lie the origin and the cause of its continuance. Rest from work is therefore in some instances the one thing needed. In all cases the energies and the brain should not be overtaxed. The bath to keep the skin active can be combined with friction. The hot bath, as hot as can be borne, is the best. It is a stimulant, not a depressant, as is the tepid bath, and it is safer than the cold bath.
The cold sitz bath or the application of cold compresses diminishes abdominal plethora, and is wisely advised in strong persons who are not depressed or chilled by external cold. Sea-bathing is another hydro-therapeutic measure which is of unquestioned advantage in all forms of intestinal catarrh.
Permanent baths have been found very serviceable in many chronic diseases, and there are many reasons for advising them in obstinate diarrhoeas. There can be no better means for bringing to bear a strong and continued influence upon the intestinal mucous membrane. The patient should be kept in the warm bath for one, two, or three weeks, according to his strength and the effect upon the disease. Systematic hot bathing under the direction of a physician at Richfield, Sharon, the Hot Springs of Virginia or Arkansas, is an invaluable aid.
Rest in the recumbent position for cases where the symptoms indicate marked tissue-alteration is very often the most important part of the treatment. Rest and diet are alone necessary to cure many cases, and without these combined means relief is often impossible. The rest should be absolute, the patient using a bed-pan and lying down all the time. The contraindications for this method are a slight diarrhoea which yields to other treatment, and loss of strength and appetite from the deprivation of air and exercise.
If rest is not advisable, or does no good after a fair trial of two to four weeks, outdoor life in fair weather by driving or walking slowly can be suggested. A long drive will bring back a diarrhoea which has taken many weeks to relieve.
The rules for diet must be clearly given and strictly enforced. An exclusive milk diet should have a trial in every case. Skimmed milk can be taken in larger quantities and with less repulsion, and is therefore to be preferred. The exclusive milk diet can be varied with buttermilk, koumiss, or wine-whey; and fruit-juices, as orange-juice, lime-juice, or tamarind-water, please the patient without doing harm. In the case of adults as well as children the milk is made more digestible by diluting it with barley- or rice-water or by adding transformed farinaceous food to milk in the form of Mellin's food and other foods of this class.
Animal broths, as chicken-soup and beef-tea, are well digested if properly made and given in small quantities. Raw meat scraped, beef or mutton rare and thoroughly masticated, the breast of poultry, game, broiled fish, raw oysters, raw or very slightly boiled eggs, or sweetbread, are foods from which selection can be made to add variety to the dietary. [p. 717] Saccharine, starchy, and fatty foods are to be given as little as possible. Vegetables may be added to the list as the condition improves. Rice and fine hominy (grits) are to be thought of first, as being easily digested and nourishing. Good wine in moderation is not hurtful; the red wines diluted with water are the best, but good port, tokay, and whiskey well diluted find application in particular cases.
Whatever food be given, it should be taken in the quantities and at hours prescribed by the physician, who by careful inspection of the stools judges of the necessity of changes in his regulations and of the success of his treatment.
The further treatment of chronic diarrhoea has for its object by the aid of drugs to change the anatomical state of the mucous membrane. Manifestly, the choice depends upon the state of this tissue. In the earlier stages the increased vascularity and hypersecretion call for mild astringents or for medicines which are believed empirically to oppose these conditions. When drugs can be dispensed with, it is better to do so; they should always be made subordinate to the careful regimen already described.
Bismuth in large doses (ten to thirty grains) is a safe and efficacious remedy in this stage. Nitrate of silver in pill form (one-sixth to one-fourth of a grain) has the endorsement of Wm. Pepper and many other practitioners. It should be continued for two or three weeks at least, but it may be given in small doses during several months, with intermissions, without danger of silver staining.48
48 A case is recorded of silver staining of the skin after four weeks' administration (Woodward, op. cit., p. 780).
A routine administration of any drug or class of drugs is reprehensible, and from the numerous remedies which are advocated in chronic diarrhoea selection can be made for trial in the course of intractable cases. The list would include sulphate of copper (one-fourth to one-half a grain), the liquid preparations of iron (liquor ferri nitratis, tinct. ferri chloridi), dilute nitric and sulphuric acids, gallic acid and other vegetable astringents, oxide or sulphate of zinc, alum, precipitated phosphate of calcium, salicin, corrosive sublimate (1/100 gr. every hour), the Indian bael-fruit, etc. No remedy should be abandoned until it has been continuously given for one or more weeks.
The Rockbridge (Va.) alum water is markedly astringent, is not unpleasant, and may be used as a substitute for water with advantage. In fact, there is no better way of introducing in quantity a mild astringent into the intestine than by the drinking of this water.
Cold-water rectal irrigation has a sedative and astringent influence, and when properly used is of great advantage to both children and adults.49 The patient should be placed in the proper position, and the water made to enter the rectum as high up as possible. The number of stools lessens almost immediately after this treatment, peristalsis being inhibited thereby.
49 A long rectal rubber tube, such as advised by Surgeon-General Wales, U.S.N., serves this purpose well.
To the water used in irrigation astringents may be added in small doses. Sulphate of zinc, sugar of lead, or alum may be given in this way in the strength of one grain to four or six ounces of water. This [p. 718] method of treatment promises more and is more rational than the internal administration of drugs.
Opium and its preparations should be avoided except to control frequent or watery discharges or to relieve pain, but it is not often that this is called for if wiser measures are first employed. Any of the remedies spoken of may be given in the form of suppositories with greater advantage often than by the mouth.
In that more severe class of cases called follicular ulceration, in which the follicles are known to be ulcerated from a prolongation of the illness, the obstinacy of the diarrhoea, the character of the discharges, and the effect upon the general health, other measures are to be adopted. The diet should be most strictly regulated and the digestive power of the patient carefully studied. Cod-liver oil is added with advantage to other foods if there is a lack of nutrition. Aids to gastric digestion are called for.
The intestinal lesion is to be reached through the stomach or the rectum. Nitrate of silver in small doses is more especially applicable, and is to be preferred to all other drugs in this stage. It is to be given in small doses and for several weeks.
Turpentine and copaiba have something in their favor in ulceration. Ergot has been suggested, and where there is much hemorrhage from the bowel may be prescribed.
Irrigations with solutions of nitrate of silver seem to be a direct and certain remedy in cases where ulceration has existed for a long time. Two and a half to three pints of distilled water, holding in solution five grains of nitrate of silver, should be thrown up the rectum as high as possible with a rubber tube; the effort should be made to secure immediate exit to the fluid. This procedure is to be repeated after the bowels are moved—once every day or every other day if the rectum becomes irritable.50
50 See case reported by the writer to the Medical Society of the District of Columbia, and published in the Maryland Medical Journal, March 15, 1883, p. 562.
SYNONYMS.—Cholera nostras, Sporadic cholera, European or English cholera, Spasmodic cholera, Cholera biliosa, Passio cholerica, Cholerhagia, Trousse-galant, Die Gallenruhr, Brechruhr.
DEFINITION.—An affection of the gastro-intestinal mucous membrane characterized by violent abdominal pain, nausea, and sudden, violent, and incessant vomiting, and by purging of a watery fluid containing little albumen and bile; attended with spasms of the muscles of the abdomen and extremities, a pinched and sunken countenance, pallor, cyanosis, and coldness of the surface of the body; a feeble and rapid pulse, oppressed respiration, and great restlessness; dryness of the tongue, great thirst, and diminished or suppressed urinary secretion and a state approaching collapse, which may rarely prove fatal, but is, as a rule, followed by reaction.
HISTORY.—The term cholera has been in use since the time of Hippocrates, but he confounded with it every disease which seemed to him to come from acridity or corruption of humors, as colics and meteorism with constipation.1 He well described cholera morbus in saying that "it is a disease which appears in summer, due to imprudence in eating, at the same time as intermittent fever."2 If Celsus be correct in deriving the name from [Greek: cholê] "bile," and [Greek: reô] "I flow," it is more applicable to the disease now under consideration than to the Asiatic disease, as it is the bile which is absent in the colorless rice-water discharges of Asiatic cholera. Trallian and Ruysch, however, ascribe it to [Greek: cholêra] the rain-gutter of a house.
1 Append. au Traité du reg. les Maladies aigues, 19, ii. p. 495, ed. Littré.
2 Epidémies, lib. v., ed. Littré, 71, p. 247.
In the Old Testament mention is made of a disease resembling cholera morbus.3 Its true pathogeny was known to Galen, and it was accurately described by Celsus,4 and Aretæus5 mentions the nature of the discharges and its frequency among young people and children.
3 Hist. Méd. des Maladies epidémiques, Paris, 1825.
4 Lib. iv. cap. 2.
5 Lib. ii. cap. 5.
The first mention of epidemics was in the sixteenth century. Various epidemics in 1695, 1717, and 1718 in Germany were probably cholera morbus. Forestus6 reports seven observations from 1559 to 1565 of attacks due to indigestible food or drastic medicines. F. Hoffman,7 [p. 720] J. Frank,8 and L. Rivière speak of the benignity of the disease as contrasting it with its apparently dangerous symptoms.
6 Opera Omnia, Rothomagi, 1633, "De stomachi affectibus," lib. xxviii.
7 Medicina rationalis systemica, t. iv. pt. 3, 1734.
8 Praxeos medicæ universæ præcepta, Leipzig, 1826, p. 43.
Sydenham's9 description of the epidemics in England in 1669-72 is the earliest account of the disease in modern literature, and it was he who gave it the name cholera morbus.
9 Sydenham Soc. edition, vol. i. p. 163.
NATURE.—There prevails at the present time a great diversity of opinion in regard to its nature; the want of uniformity in the appearances presented by post-mortem examinations may in some measure account for this. The present state of our knowledge, derived both from pathological anatomy and a study of the symptoms, will not warrant a positive opinion in regard to it.
Niemeyer,10 in common with most German and some French authors, considers cholera morbus to be a variety of gastro-intestinal catarrh. Leube11 thinks it a variety of gastric catarrh with simultaneous inflammation of the intestines and running a peculiar course. It is certainly not identical with the specific Asiatic disease, although in some cases the symptoms and morbid anatomy are exactly similar, and any differentiation is impossible. By some it is believed that cholera morbus is due to surviving germs implanted by previous epidemics of Asiatic cholera.
10 Pract. Med., 1879, vol. i. p. 480.
11 Ziemssen's Cyclopædia, New York, 1876, vol. vii. p. 146.
The slight changes found in some fatal cases would lead to the belief that the effect of the exciting cause is something more than a mechanical irritation of the gastro-intestinal mucous membrane.
The sudden onset, rapid development of symptoms, and dangerous collapse justify the theory that there must be some previous change in the individual or some peculiar result of food-decomposition. The nervous system may be so enfeebled by prolonged heat that an irritant quickly destroys its equilibrium and brings about vaso-motor paralysis of the intestinal vessels and abundant serum transudation. Or the irritation may be specific, depending upon the development of poison germs in food which has been subjected to heat influences. There is a close relationship between cholera morbus and cholera infantum in their etiology, symptoms, and pathology.
ETIOLOGY.—Predisposing Causes.—The disease is more common in the tropics, but is not confined to any climate. In temperate latitudes it is more likely to occur in July and August, when the variation of temperature between day and night is great, although the other months of summer and autumn are not entirely exempt. It is said to be more frequent and fatal in Southern Europe than in the northern and temperate climates. In periods immediately preceding and following epidemics of Asiatic cholera many persons are attacked, although there is great liability to errors in diagnosis at these times.
It occurs more frequently in youth and adolescence than in advanced life, and males seem to be more liable to attacks than females, but difference in occupation may assist in this predisposition. Persons endowed with an extreme sensibility of the nervous system and who are subject to frequent attacks of intestinal catarrh are much more liable to the disease. The exhaustion of the nervous system by heat, which is the [p. 721] probable explanation of the phenomena of cholera infantum, has no doubt much to do with the development of cholera morbus. Mental anxiety or overwork in summer increases this nerve-exhaustion and renders the termini of nerves and the centres very susceptible to peculiar irritation.
Exciting Causes.—It is probable that the cause of most attacks is a septic material generated in the fermentation and decomposition of food. This poison acts as an irritant upon the gastric and intestinal nerves and gives rise to excessive peristaltic movements and vomiting. Hence the quality of the food is an element of more importance in the causation than the mere quantity ingested; and herein may reside the chief difference between cholera morbus and Asiatic cholera, the latter being due to a specific, imported, or acclimated poison which invariably produces the same specific form in those exposed to its action.12 Unripe fruits, partially cooked or decaying meats and vegetables, shellfish and fish some time from the water, may produce the disease in those predisposed to it. The intemperate use of ice-water and other cold drinks after a full meal or when the body is exhausted by heat and fatigue, exposure to showers at the close of a hot day, or passing from a heated room into damp cellars and outbuildings, are frequent exciting causes.
12 "Bias the pugilist, naturally a great eater, had a sudden choleraic attack after having eaten of succulent food" (Hippocrates, lib. v. p. 247, ed. Littré).
At times there exists a certain condition of inactivity of the digestive organs when the gastric juice is not secreted in sufficient quantity, and perfectly sound food may undergo fermentation and set up an attack.
The offensive exhalation from a filthy alley which had been recently cleaned was the exciting cause of a fatal epidemic in a London school,13 and Levier recounts an epidemic caused by the drinking-water during the winter in Berne.14
13 Lond. Med. and Surg. Gaz., 1829, iv. p. 375.
14 Schweiz. Zeitschr. f. Heilk., iii., 1864, p. 140.
Nervous disturbance from other diseases may act as a cause. Leube reports a case of intermittent fever which was followed by an annual attack of cholera morbus preceded by febrile symptoms.15
15 Leube, Ziemssen, 1876, vol. vii. p. 148.
Malaria, sewer-gas, and sudden and powerful mental emotions are credited with the causation of some attacks.
PATHOLOGICAL ANATOMY.—In a few cases an examination of the body has revealed no phenomena sufficient to account for the symptoms, even when they have been the most severe during life. In these cases either the inflammation has not passed the first stage of development and the resulting hyperæmia has disappeared after death, or the irritation of the gastro-intestinal nerves has been sufficiently intense to cause death before the alimentary tract has undergone any consequent structural change.
Usually, however, there are evidences of a general gastro-intestinal catarrh: the mucous membrane is congested throughout and denuded of epithelium. The solitary glands are enlarged and Peyer's patches swollen and prominent. The blood is thickened and dark in color, and the serous membranes dry, sticky, and covered with desquamated epithelium. Indeed, the appearances may be identical with those observed in true Asiatic [p. 722] cholera. The kidneys are congested, sometimes enlarged, and the tubules devoid of epithelium. In protracted cases the general muscular system shows a beginning of granular degeneration.
In no case, however, can a positive diagnosis between Asiatic cholera and cholera morbus be made from post-mortem appearances.
SYMPTOMS.—The attack is usually sudden in its onset, but in some cases is preceded by nausea, thirst, loss of appetite, and slight general distress for some hours, or it may come on in the course of some gastro-intestinal disturbance. Frequently it is developed during sleep, particularly after midnight, the patient being aroused by a feeling of pressure at the pit of the stomach, which is followed by nausea and violent and incessant vomiting with intense pain, the contents of the stomach being ejected with great force.
The matters first vomited consist mainly of the food last eaten, little altered or mixed with gastric mucus and tinged with bile. In a certain proportion of cases the amount of bile is increased, although it is difficult to judge of the relative proportion by the color and taste of the vomited liquid. The general belief that the liver is implicated and the bile secreted in morbid quantity rests upon conjecture alone, and has no solid basis. After a time only yellow, brown, or greenish mucus, with more or less bile, is ejected, and in protracted cases hiccough is most distressing.
Following the vomiting or at the same time with it purging comes on, and it is usually preceded by borborygmi. In rare cases there is no vomiting, but only intense pain in the bowels and copious alvine discharges from the beginning to the end of the attack. The stools in the beginning are normal in color, but soon become pulpy or semi-fluid. As they increase in quantity they become watery, consisting of blood-serum with mucus, cast-off epithelium and pus-cells, and are nearly odorless, and sometimes resemble very closely the discharges of Asiatic cholera, but almost invariably retain the yellow or green color of the bile. Colorless rice-water discharges are observed in undoubted cases of cholera morbus outside of any epidemic influence. The discharges are acrid and irritating, and the neighboring parts become red and excoriated.
At the same time there is intense burning or tearing pain in the abdomen, generally centring at the umbilicus, great thirst and painful contractions of the muscles of the abdomen and extremities, particularly in the calves of the legs, and of the flexors of the thighs, forearms, fingers, and toes. In the beginning there may be tympanites, but this soon disappears, and the abdomen becomes retracted and the muscles drawn up into knots. The cramps usually come on after each act of vomiting and purging, but they may appear spontaneously. Abdominal tenderness is either wanting or slight. As the transudation continues the thirst becomes intense, the tongue cold, dry, and coated, and the tissues shrivelled from loss of water. The skin is cold, clammy, or covered with a viscid sweat, and the surface of the body is cyanosed, violet, or in the extremities it may have a marbled appearance. The nose is pointed, the eyes dark and sunken, and there is a general appearance of collapse.
The mind may be clear throughout, but in protracted cases there is great nervous prostration. The patient becomes dull and lethargic, passing into stupor after great restlessness and jactitation. The voice is faint [p. 723] or whispering, the breath cold, and the respiration sighing. The pulse in the beginning may be depressed, but soon becomes rapid and often imperceptible, and there is great præcordial anxiety.
As the blood becomes thickened the urine is highly colored, small in quantity, and it may be suppressed. An examination shows traces of albumen, casts and desquamated epithelium, and a decrease in the amount of urea and salts. In the last stages there may be a slight rise in temperature, but it has no definite course and it is usually absent. In collapse the temperature of the surface of the body sinks below normal, but the temperature of the interior may rise as high as 101° or 102° F., as shown by the thermometer in the rectum or vagina.16
16 London Hosp. Reports, 1856, vol. iii. p. 457.
PROGRESS AND TERMINATION.—But, fortunately, the course of the disease tends toward recovery in the large majority of cases. The discharges gradually decrease in quantity, the intervals are longer, the appearance becomes more natural, and a profuse perspiration is followed by a refreshing sleep. The surface becomes warmer, the pulse slower and more full, and the skin regains its normal color.
If the case has been a severe one or if it occurs in a person much enfeebled by disease, it pursues a different course. The discharges become almost uninterrupted, and at last are passed involuntarily. The cramps are almost continuous or are convulsive, the pulse grows rapidly weaker and is finally lost, coma succeeds stupor, and death follows in collapse.
The duration of the disease varies from a few hours to two or three days; death has occurred within twelve hours.
Recovery is generally complete after a few hours; and this rapid return to the normal condition shows that there have been no textural change of organs. Sometimes great emaciation, irritability of the stomach, and slight diarrhoea persist for a few days, or symptoms of a general gastro-enteritis may supervene.
DIAGNOSIS.—In making the diagnosis of cholera morbus it is necessary to carefully differentiate it from epidemic cholera and the effects produced by irritant poisons, such as the metallic salts, poisonous fungi, etc.
Occurring during an epidemic of Asiatic cholera, it is not possible to make a diagnosis, as the symptoms of cholera morbus and of mild cases of the Asiatic disease are identical. From severe cases it is to be distinguished by the absence of antecedent diarrhoea, by the presence of bile in the vomited matters, and by the color and fecal odor of the stools. The nausea and abdominal pain are more marked, while the dyspnoea, cyanosis, and shrunken condition of the skin are less marked. The mortality of cholera morbus is slight, whilst about one-half of those attacked with epidemic cholera die.
In irritant poisoning the vomiting follows quickly after the ingestion of a meal or poisonous matter; it continues for some time before purging begins, and is out of all proportion to the diarrhoea. The vomited matters contain blood and mucus and are never serous in character. Corrosive poisons may cause redness, charring, or ulceration of the mouth and throat and a burning sensation in the stomach. The pain over the stomach is more constant and severe, particularly in the intervals of [p. 724]vomiting, and there may be abdominal tenderness and bloody discharges. The expression is more anxious and the pulse rapid and weak.
Elaterium and tartar emetic will bring on vomiting and purging which resemble the symptoms of cholera morbus. Choleriform attacks due to uræmia simulate cholera morbus. The distinction is to be made by the previous history—pain and purging being relatively less prominent in uræmia—by the presence of albumen and casts in the urine, and by the early tendency to coma.
Acute peritonitis, attended by copious vomiting and purging, has been mistaken for cholera morbus, and the true nature of the affection only revealed by the autopsy.
PROGNOSIS.—As a rule, cholera morbus occurring in persons otherwise healthy ends favorably in a few hours. Cases of secondary fever, with gastro-intestinal catarrh, may prolong the attack from a few days to two weeks. Should treatment have no effect in lessening the vomiting and purging, and should the evidences of heart-failure become apparent, a fatal result may be feared. Death has occurred within twelve hours, and the mortality is 3 per cent. of uncomplicated cases.17
17 Bartholow, Pract. Med., New York, 1880, p. 58.
Cases occurring in the course of other diseases possess a special gravity.
TREATMENT.—During the summer months, and particularly in August and September, when the hot days are succeeded by cool nights, iced drinks should be used in moderate quantities; the diet should be light, nutritious, and easy of digestion. Unripe fruits and articles of food liable to fermentative changes should not be indulged in.
Exposure to the night air, particularly after a full meal, should be especially avoided, and the clothing ought to be so arranged that additions may be made as night approaches. Slight attacks of indigestion should not be neglected, and any irregularity of the bowels must receive immediate attention.
The period when the physician is called upon to prescribe for an attack of cholera morbus is usually when the stomach has been emptied of food and the patient is vomiting incessantly, purging, and writhing in pain. If vomiting has not occurred and violent epigastric pain is the only symptom, the stomach should be emptied by an emetic of hot water and mustard repeated until the overcharged organ is completely emptied. Partially-digested food in a state of acid fermentation will thus be got rid of, and the sufferings may be immediately but not wholly relieved.
If spontaneous vomiting has expelled the food, and the matters vomited are green and watery, while pain and frequent stools with muscular cramps, heart feebleness, and threatening collapse are the symptoms presented, the remedy par excellence is a hypodermic injection of sulphate of morphia (gr. 1/8 to 1/3) with sulphate of atropia (gr. 1/120 to 1/100). If one dose is not followed by decided mitigation of suffering, the injection is to be repeated in a half hour or an hour, not giving above one grain of morphia in divided doses. At the same time, and while waiting for the full effect of the narcotic, efforts can be directed to giving ease to the muscular spasms and pain by brisk friction with stimulating lotions or by mustard poultices to the abdomen and extremities. The morphia will be the best and quickest stimulant which can be used; it will therefore be useless in most cases to administer brandy, camphor, chloroform, [p. 725]or other remedies of that sort. Waiting and giving nothing by the mouth is the wiser course. In twenty minutes to half an hour the most perfect bien être succeeds to the previous agony and exhaustion. In some cases the vomiting, purging, and cramps cease more gradually, and six hours will pass before the patient is at ease. The intense thirst is best treated by the giving of cracked ice sparingly at first, more freely later.
Nothing substitutes morphia hypodermically with success, but in some instances or when the stomach is not very irritable it may be necessary to give medicine by the mouth. In this case chloroform (xv to xxx drops), chlorodyne (x to xx drops), or spirits of camphor (v to x drops) every quarter or half hour in ice-water may be directed. Chloroform and camphor can be combined with the deodorized tincture of opium in ten- to twenty-drop doses. Time is wasted in expecting relief from remedies which are inevitably rejected as soon as taken; it is only when the stomach is very tolerant that it is judicious to begin with them.
The weakness of the heart's action must be combated by brandy or whiskey, given by the mouth with pounded ice or administered hypodermically. A considerable quantity of brandy or diluted alcohol may be introduced by repeated injections beneath the skin. Iced champagne may be tried with good effect. H. C. Wood quotes Hall18 as recommending hypodermic injections of chloral in the cold stage of cholera. Five to eight grains in twenty minims of distilled water can be thus given, and repeated at intervals of fifteen to twenty minutes until some effect is perceived.
18 Lancet, May 2, 1874.
If vomiting persists after the other symptoms—pain and muscular spasms—are relieved, it is due to the intense gastric hyperæmia; giving nothing which is not necessary is the wiser plan. Carbolic acid, hydrocyanic acid, bismuth, bromide of sodium, or small doses of calomel are remedies which meet the indication. Food should be withheld as long as possible; then iced barley-water, followed by milk and lime-water in very small quantities at short intervals, will test the power of the stomach to retain and digest food.
The summer affections of the intestines in children are chiefly of a diarrhoeal character. Diarrhoeal attacks, as is well known, are much more frequent and severe in the summer months than in other portions of the year. Moreover, the diarrhoea of the summer season occurs chiefly among children under the age of two and a half years, and is much more common and fatal in the cities than in the country. In the large cities this malady has heretofore been the annually-recurring scourge of infancy, but of late years its prevalence has been in some degree diminished and its severity controlled by the establishment of health boards and the enforcement of sanitary regulations. Still, it remains an important disease in all our cities, and one that largely increases the aggregate mortality. The truth of this statement is shown by the statistics of deaths taken at random from the mortuary records of any large city. Thus, in New York City during 1882 the deaths from diarrhoea reported to the Health Board, tabulated in months, were as follows:
| Jan. | Feb. | Mar. | Apr. | May. | June. | July. | Aug. | Sept. | Oct. | Nov. | Dec. | |
| Under five years. | 34 | 32 | 50 | 50 | 72 | 231 | 1533 | 817 | 362 | 195 | 68 | 35 |
| Over five years. | 14 | 15 | 14 | 20 | 15 | 19 | 131 | 149 | 84 | 55 | 31 | 24 |
Therefore, in 1882—and the statistics of other years correspond in this particular—it is seen that nine times as many deaths of children under the age of five years occurred from diarrhoea during the five months from June 1st to October 31st as in the remaining seven months of the year. It is also seen, in corroboration of the statement that diarrhoea due to hot weather is chiefly a disease of infancy and early childhood, that during these same five months, which embrace the summer season, the number of deaths from diarrhoea under the age of five years was seven and a half times greater than the number over that age. These statistics agree with the general experience of physicians in city practice. The summer diarrhoea would indeed be comparatively unimportant were its death-rate as low in the first five years of life as subsequently.
The following statistics show how great a destruction of life this malady causes even under the surveillance of an energetic health board; and before this board was established it was much greater, as I had abundant opportunities to observe. The last annual report of the New York Board of Health was made in 1875, since which time weekly bulletins have been [p. 727] issued. The deaths from diarrhoea at all ages in the three last years in which annual reports were issued were as follows:
| 1873. | 1874. | 1875. | |
| January | 94 | 43 | 46 |
| February | 84 | 34 | 52 |
| March | 97 | 40 | 58 |
| April | 114 | 47 | 45 |
| May | 95 | 61 | 89 |
| June | 220 | 144 | 157 |
| July | 1514 | 1205 | 1387 |
| August | 967 | 1007 | 1012 |
| September | 424 | 587 | 608 |
| October | 213 | 255 | 185 |
| November | 87 | 105 | 57 |
| December | 53 | 56 | 50 |
Thus, in these three years the aggregate deaths from diarrhoea during the months from June to October inclusive, in which months the summer diarrhoea prevails, were 9885, while in the remaining seven months the number was only 1407. How large a proportion of these deaths in the warm season occurred in children we may infer from remarks made by the Health Board in regard to another year. In their annual report for 1870 the board state: "The mortality from the diarrhoeal affections amounted to 2789, or 33 per cent. of the total deaths; and of these deaths 95 per cent. occurred in children less than five years old, 92 per cent. in children less than two years old, and 67 per cent. in those less than a year old." Every year the reports of the Health Board furnish similar statistics, but enough have been given to show how great a sacrifice of life the summer complaint produces annually in this city.
What we observe in New York in reference to this disease is true also, to a greater or less extent, in other cities of this country and Europe, so far as we have reports. Not in every city is there the same proportionate mortality from this cause as in New York, but the frequency of the summer diarrhoea and the mortality which attends it render it an important disease in, I believe, most cities of both continents. In country towns, whether in villages or farm-houses, this disease is comparatively unimportant, inasmuch as few cases occur in them, and the few that do occur are of mild type, and consequently much less fatal than in the cities.
The comparative immunity of the rural districts has an important relation, as we will see, to the hygienic management of these cases.
ETIOLOGY.—In the causation of this disease two distinct factors are recognized—the one atmospheric, the other dietetic.
The prevalence and severity of the summer diarrhoea correspond closely with the degree of atmospheric heat, as may be inferred from the foregoing statistics. In New York this disease begins in the month of May—earlier in some years than in others—in a few scattered cases, commonly of a mild type. Cases become more and more numerous and severe as the weather grows warmer until July and August, when the diarrhoea attains its maximum prevalence and severity. In these two months it is by far the most frequent and fatal of all the diseases in cities. In the middle of September new patients begin to be less common, and in the latter part of this month and subsequently new cases do not occur, unless under unusual circumstances which favor the development of this malady. In New York a considerable number of deaths [p. 728] of infants occur from the diarrhoea in October. October is not a hot month in our latitude—its average temperature is lower than that of May—and yet the mortality from this disease is considerably larger in the former than in the latter month. This fact, which seems to show that the prevalence of the summer diarrhoea does not correspond with the degree of atmospheric heat, is readily explained. The mortality in October, and indeed in the latter part of September, is not that of new cases, but is mainly of infants, as I have observed every year, who contract the disease in July or August or earlier, and linger in a state of emaciation and increasing weakness till they finally succumb, some even in cool weather.
The fact is therefore undisputed, and is universally admitted, that the summer season, stated in a general way, is the cause of this annually-recurring diarrhoeal epidemic, but it is not so easy to determine what are the exact causative conditions or agents which the summer weather brings into activity. That atmospheric heat does not in itself cause the diarrhoea is evident from the fact that in the rural districts there is the same intensity of heat as in the cities, and yet the summer complaint does not occur. The cause must be looked for in that state of the atmosphere engendered by heat where unsanitary conditions exist, as in large cities. Moreover, observations show that the noxious effluvia with which the air becomes polluted under such circumstances constitute or contain the morbific agent. Thus, in one of the institutions of this city a few years since, on May 10, which happened to be an unusually warm day for this month, an offensive odor was noticed in the wards, which was traced to a large manure-heap that was being upturned in an adjacent garden. On this day four young children were severely attacked by diarrhoea, and one died. Many other examples might be cited showing how the foul air of the city during the hot months, when animal and vegetable decomposition is most active, causes diarrhoea. Several years since, while serving as sanitary inspector for the Citizens' Association in one of the city districts, my attention was particularly called to one of the streets, in which a house-to-house visitation disclosed the fact that nearly every infant between two avenues had the diarrhoea, and usually in a severe form, not a few dying. This street was compactly built with wooden tenement-houses on each side, and contained a dense population, mainly foreign, poor, ignorant, and filthy in their habits. It had no sewer, and the refuse of the kitchens and bed-chambers was thrown into the street, where it accumulated in heaps. Water trickled down over the sidewalks from the houses into the gutters or was thrown out as slops, so that it kept up a constant moisture of the refuse matter which covered the street, and promoted the decay of the animal and vegetable substances which it contained. The air in the domicils and street under such conditions of impurity was necessarily foul in the extreme, and stifling during the hot days and nights of July and August; and it was evidently the important factor in producing the numerous and severe diarrhoeal cases which were in these domicils.
In another locality, occupied by tripe-dealers and a low class of butchers who carried on fat- and bone-boiling at night, the air was so foul after dark that the peculiar impurity which tainted it could be distinctly noticed in the mouth for a considerable time after a night visit. In the street where [p. 729]these nuisances existed and in adjacent streets the summer diarrhoea was very prevalent and destructive to human life. Murchison states that twenty out of twenty-five boys were affected with purging and vomiting from inhaling the effluvia from the contents of an old drain near their school-room. Physicians are familiar with a similar fact showing this purgative effect of impure air—that the atmosphere of a dissecting-room often causes diarrhoea in those otherwise healthy.
The exact nature of the deleterious agent or agents in foul air which cause the diarrhoea, whether they be gases or organisms, has not been fully determined; but at a recent meeting of the Berliner Med. Gesellschaft, A. Baginsky made a report on the bacilli of cholera infantum, which he states he has found both in the dejections and in the intestinal mucous membrane in the bodies of those who have perished with this disease. In the stools, along with numerous other organisms, Baginsky states that he found masses of zoögloea, and the same organisms he detected on the surface of the small intestines, and could trace their wanderings as far as the submucous tissue.1 But it is evidently very difficult to determine whether such organisms sustain a causative relation to diarrhoea or spring into existence in consequence of the foul secretions and decomposing fecal matters which are present.
1 Allegem. Wien. Mediz. Zeitung, Nov. 6, 1883.
The impurities in the air of a large city are very numerous. Among those of a gaseous nature are sulphurous acid, sulphuric acid, sulphuretted hydrogen; various gases of the carbon group, as carbonic acid, carburetted hydrogen, and carbonic oxide; gases of the nitrogen group, as the acetate, sulphide, and carbonate of ammonium, nitrous and nitric acids; and at times compounds of phosphorus and chlorine (Parkes). A theory deserving consideration is that certain gaseous impurities found in the air form purgative combinations. D. F. Lincoln, in his interesting paper on the atmosphere in the Cyclopædia of Medicine, writes in regard to sulphuretted hydrogen: "When in the air, freely exposed to the contact of oxygen, it becomes sulphuric acid. Sulphide of ammonium in the same circumstances becomes a sulphate, which, encountering common salt (chloride of sodium), produces sulphate of sodium and chloride of ammonium. The sulphates form a characteristic ingredient of the air in manufacturing districts." The sulphates, we know, are for the most part purgatives, but whether they or other chemical agents exist in the respired air in sufficient quantity to disturb the action of the intestines, even where atmospheric impurities are most abundant, is problematical and uncertain.
Again, the solid impurities in the air of a large city are very numerous, as any one may observe by viewing a sunbeam in a darkened room, which is made visible by the numerous particles floating in it. These particles consist largely of organic matter, which sometimes has been carried a long distance by the wind. The remarkable statement has been made that in the air of Berlin organic forms have been found of African production. Ehrenberg discovered fragments of insects of various kinds—rhizopods, tardigrades, polygastrica, etc.—which, existing in considerable quantity and inhaled in hot weather, when decomposition and fermentation are most active, may be deleterious to the system. Monads, bacteria, vibriones, amorphous dust containing spores which [p. 730] retain their vitality for months, are among the substances found in the air of cities. The well-known hazy appearance of the atmosphere resting over a large city like New York when viewed from a distance is due to the gaseous and solid impurities with which the air is so abundantly supplied—impurities which assume importance in pathological studies, since minute organisms are now believed to cause so many diseases the etiology of which has heretofore been obscure. With our present knowledge we must be content with the general statement that impure air is one of the two important factors which cause summer diarrhoea, without being able to state positively which of the elements in the air are most instrumental in causing this result. But the theory is plausible that minute organisms rather than chemical products are the chief cause. Henoch of Berlin, writing upon this subject, calls attention to the disease known as intestinal mycosis, its prominent symptom being a severe diarrhoea produced by eating diseased meat containing a fungus. He believes that "a portion of the fungus not destroyed by the gastric juice settles upon different parts of the intestine, and there produces its effects;" and he adds, "At present, however, we can regard the mykotic theory of cholera infantum only as a very probable hypothesis. There is no doubt that high atmospheric temperature increases the tendency to fermentation dyspepsias which is present in imperfectly-nourished children at all seasons, and causes them to appear not only epidemically, but also in an extremely acute form which is not frequent under ordinary circumstances. This would lead to the conclusion that, in addition to the heat, infectious germs are present, which, being developed in great masses by the former, enter the stomach with the food." The fungus theory of the causative relation of atmospheric heat to the diarrhoea of the summer season as thus explained by Henoch commands the readier assent since it comports with the well-known facts relating to the etiology of the summer complaint. This disease, as we have seen, is most prevalent and fatal under precisely those conditions of dense population, filthy domicils and streets, and atmospheric heat which are favorable for the development of low organisms.
In those portions of our cities which are occupied by the poor, more than anywhere else, those conditions prevail which render the atmosphere deleterious. One accustomed to the pure air of the country would scarcely believe how stifling and poisonous the atmosphere becomes during the hot summer days and close summer nights in and around the domicils in the poor quarters of the city. Among the causes of this foul air may be mentioned too dense a population, the occupancy of small rooms by large families, rigid economy and ceaseless endeavor to make ends meet, so that in the absorbing interest sanitary requirements are sadly neglected. Adults of such families, and children of both sexes as soon as they are old enough, engage in laborious and often filthy occupations. Many of them seldom bathe, and they often wear for days the same undergarments, foul with perspiration and dirt. The intemperate, vicious, and indolent, who always abound in the quarters of the city poor, are notoriously filthy in their habits and add to the insalubrity by their presence. Children old enough to be in the streets and adults away at their occupations escape to a great extent the evil effects of impure air, but the infantile population always suffer severely.
Every physician who has witnessed the summer diarrhoea of infants is [p. 731] aware of the fact that the mode of feeding has much to do with its occurrence. A large proportion of those who each summer fall victims to it would doubtless escape if the feeding were exactly proper. In New York City facts like the following are of common occurrence in the practice of all physicians: Infants under the age of eight months, if bottle-fed, nearly always contract diarrhoea, and usually of an obstinate character, during the summer months. The younger the infant, the less able is it to digest any other food than breast-milk, and the more liable is it therefore to suffer from diarrhoea if bottle-fed. In the institutions nearly every bottle-fed infant under the age of four or even six months dies in the hot months with symptoms of indigestion and intestinal catarrh, while the wet-nursed of the same ages remain well. Sudden weaning, the sudden substitution of cow's milk or any artificially-prepared food in place of breast-milk in hot weather, almost always produces diarrhoea, often of a severe and fatal nature. Feeding an infant in the hot months with indigestible and improper food, as fruits with seeds or the ordinary table-food prepared in such a way that it overtaxes the digestive function of the infant, causes diarrhoea, and not infrequently that severe form of it which will be described under the term cholera infantum. Many obstinate cases of the summer complaint begin to improve under change of diet, as by the substitution of one kind of milk for another or the return of the infant to the breast after it has been temporarily withdrawn from it. It is a common remark in the families of the city poor that the second summer is the period of greatest danger to infants. This increased liability of infants to contract diarrhoea in the second summer is due to the fact that most infants in their second year are table-fed, while in the first year they are wet-nursed. Such facts, with which all physicians are familiar, show how important the diet is as a factor in causing the summer complaint.
Occasionally, from continued ill-health, the milk of the mother or wet-nurse does not agree with the nursling. Examined with the microscope, it is found to contain colostrum. Under such circumstances if a healthy wet-nurse be employed the diarrhoea ceases. It is very important that any woman furnishing breast-milk to an infant should lead a quiet and regular life, with regular meals and sleep. In the Louisville Med. Journal, Aug. 19, 1882, R. B. Gilbert relates striking cases in which venereal excesses on the part of wet-nurses were immediately followed by fatal diarrhoea in the infants which they suckled.
One not a resident would scarcely be able to appreciate the difficulty which is experienced in a large city in obtaining proper diet for young children, especially those of such an age that they require milk as the basis of their food. Milk from cows stabled in the city or having a limited pasturage near the city, and fed upon a mixture of hay with garden and distillery products, the latter often largely predominating, is unsuitable. It is deficient in nutritive properties, prone to fermentation, and from microscopical and chemical examinations which have been made it appears that it often contains deleterious ingredients. If milk be obtained from distant farms where pasturage is fresh and abundant—and in New York City this is the usual source of the supply—considerable time elapses before it is served to customers, so that, particularly in the hot months of July and August, it frequently has begun to undergo [p. 732]lactic-acid fermentation when the infants receive it. That dispensed to families in the morning is the milking of the previous morning and evening. The common result of the use of this milk in midsummer by infants under the age of ten months is more or less diarrhoea.
The ill-success of feeding with cow's milk has led to the preparation of various kinds of food which the shops contain, but no dietetic preparation has yet appeared which agrees so well with the digestive function of the infant as breast-milk, and is at the same time sufficiently nutritive.
In New York City improper diet, unaided by the conditions which hot weather produces, is a common cause of diarrhoea in young infants, for we meet with this diarrhoea in infants who are bottle-fed at all seasons; but when the atmospheric conditions of hot weather and the use of food unsuitable for the age of the infant are both present and operative, this diarrhoea so increases in frequency and severity that it is proper to designate it the summer epidemic of the cities. Several years since, before the New York Foundling Asylum was established, the foundlings of New York, more than a thousand annually, were taken to the almshouse on Blackwell's Island and consigned to the care of the pauper-women, who were mostly old, infirm, and filthy in their habits and apparel. Their beds, in which the foundlings were also placed alongside of them, were seldom clean, not properly aired and washed, and under the beds were various garments and utensils which these pauper-women had brought with them as their sole property from their miserable abodes in the city. With such surroundings, the air which these infants breathed day and night manifestly contained poisonous emanations; while their diet was equally improper, for it was prepared by these women from such milk and farinaceous food as were furnished the almshouse. When assigned to duty in the almshouse, this service being at that time a branch of Charity Hospital, I was informed that all the foundlings died before the age of two months; one only was pointed out as a curiosity which had been an exception to the rule. The disease of which they perished was diarrhoea, and this malady in the summer months was especially severe and rapidly fatal. The unpleasant experiences in this institution furnished additional evidence, were any wanting, that foul air and improper diet are the two important factors in causing the summer diarrhoea of infants. Since that beneficial charity, the New York Foundling Asylum, in East Sixty-eighth street, came into existence, providing pure air and, for a considerable proportion of the foundlings, breast-milk, many of these waifs have been rescued from death.
I have already stated that this disease occurs, with an occasional exception, under the age of two and a half years. The following table embraces all the cases that came to one of the city dispensaries during my service between the months of May and October, inclusive:
| Age. | Cases. |
| 5 months or under | 58 |
| 5 months to 12 months | 212 |
| 12 months to 18 months | 174 |
| 18 months to 24 months | 93 |
| 24 months to 36 months | 36 |
| Total | 573 |
After the third year the liability to the summer complaint so rapidly [p. 733] diminishes that comparatively few are affected by it. It is seen from the above statistics that by far the largest number of cases occur during the period of first dentition; hence the prevalent opinion among families that dentition causes the diarrhoea. It is the common belief among the poor of New York that diarrhoea occurring during dentition is conservative, and should not be checked. They believe that an infant cutting its teeth suffers less, and may be saved from serious illness, if it have frequent stools. Every summer I see infants reduced to a state of imminent danger through the continuance of diarrhoea during several weeks, nothing having been done to check it in consequence of this absurd belief. The progressive loss of flesh and strength and wasting of the features do not excite alarm, under the blinding influence of this theory, till the diarrhoea has continued so long and become so severe that it is with difficulty controlled, and the patient is in a state of real danger when the physician is first summoned. The following statistics, which comprise cases occurring during my service in one of the city dispensaries, show the preponderance of cases during the age when dental evolution is occurring:
| Cases. | |
| No teeth and no marked turgescence of gums | 47 |
| Cutting incisors | 106 |
| Cutting anterior molars | 41 |
| Cutting canines | 40 |
| Cutting last molars | 20 |
| All the teeth cut | 28 |
| Total | 282 |
It so happens that the period of dental evolution corresponds with that of the most rapid development and the greatest functional activity of the gastric and intestinal follicles, and the predisposition which exists to diarrhoeal maladies at this age must be attributed to this cause rather than to dentition.
SYMPTOMS.—The summer diarrhoea of infants commonly begins gradually with languor, fretfulness, and slight febrile movement. The diarrhoea at first usually attracts little attention from its mildness. The stools, while they are thinner than natural, vary in appearance, being yellow, brown, or green. Infants with milk diet are apt to pass green and acid stools containing particles of undigested casein. The tongue in the commencement of the attack is moist and covered with a slight fur. At a more advanced stage it may be moist, but is often dry, and in dangerous forms of the malady, accompanied by prostration, the buccal surface is red and the gums more or less swollen and sometimes ulcerated. Vomiting is common. It may commence simultaneously with the diarrhoea, especially when food that is unusually indigestible and irritating to the stomach has been given, but more frequently this symptom does not appear until the diarrhoea has continued a few days. I preserved memoranda of the date when vomiting began in the cases treated in two consecutive summers, and found that ordinarily it was toward the close of the first week. When it is an early and prominent symptom it appears to be due to the presence in the stomach of imperfectly digested or fermented and acid food, which, when ejected, gives a decidedly acid reaction with appropriate tests. It contains coagulated casein and undigested particles of whatever food has been given. In many patients the progressive loss of flesh and [p. 734] strength is largely due to the indigestion and vomiting by which the food, which is so much required for proper nourishment, is lost.
Emesis occurring at a late stage of the summer complaint is often due to commencing spurious hydrocephalus, which is not an infrequent complication, as we will see, of protracted cases. Perhaps when a late symptom it may sometimes have an uræmic origin, for the urine is usually quite scanty in advanced cases. It seems probable, however, that deleterious effects from non-elimination of urea are to a considerable extent prevented by the diarrhoea.
The fecal evacuations may remain nearly uniform in appearance during the disease, but in many patients they vary in color and consistence at different periods. In the same case they may be brown and offensive at one time, green at another, and again they may contain masses of a putty-like appearance, the partly-digested casein or altered epithelial cells. The stools sometimes consist largely of mucus, with or without occasional streaks of blood, indicating the predominance of inflammation in the colon. This is the mucous diarrhoea of Barrier. The stools are sometimes yellow when passed, but become green on exposure to the air from chemical reaction due to admixture with the urine.
The character of the alvine discharges is interesting. In addition to undigested casein I have found epithelial cells, single or in clusters (sometimes regularly arranged as if detached in mass from the villi), fibres of meat, crystalline formations, mucus, and occasionally blood, as stated above. In one instance I observed an appearance resembling three or four crypts of Lieberkühn united, probably thrown off by ulceration. If the stools are green, colored masses of various sizes, but mostly small, are also seen under the microscope.
The pulse is accelerated according to the severity of the attack. The heat of the surface is at first apt to be increased, though but slightly in ordinary cases; but when the vital powers begin to fail from the continuance of the diarrhoea the warmth of the surface diminishes. In advanced cases approaching a fatal termination the face and extremities are pallid and cool, and the pulse gradually becomes more frequent and feeble. The skin is usually dry, and, as already stated, the urinary secretion diminished. In severe cases attended by frequent alvine discharges the infant does not pass urine oftener than once or twice daily. The imperfect action of the skin and kidneys is noteworthy.
Protracted cases of the summer complaint are apt to be complicated by two cutaneous eruptions—erythema extending over the perineum and frequently as far as the thighs and lower part of the abdomen, due to the acid and irritating character of the stools; and boils upon the forehead and scalp. The latter sometimes extend to the pericranium, and in case of recovery leave permanent cicatrices. This furuncular affection of the scalp has seemed to me useful in consequence of the external irritation which it causes, since it occurs at a time when, on account of the feeble heart's action and languid circulation, passive congestion of the vessels of the brain and meninges is liable to be present.
Patients who are weak and wasted in consequence of protracted diarrhoea, remaining almost constantly in the recumbent position, often have an occasional dry cough which continues till the close of life. It is due to hypostatic congestion in the lungs, usually limited to the posterior and [p. 735] inferior portions of the lobes, extending but a little way into the lungs. It is the result of prolonged recumbency with feeble heart's action and feeble pulmonary circulation. Infants reduced by chronic diseases, lying day after day in their cribs with little movement of their bodies, are very liable to this passive congestion of depending portions of their lungs, toward which the blood gravitates, and into which but little air enters in consequence of their distance and position and the feeble respirations. The hyperæmia which results is of a passive character, a venous congestion, and the affected lobules have a dusky-red color. This congestion, continuing, soon results in pneumonitis of the catarrhal form, subacute and of a low grade, for pulmonary lobules in which the blood remains stagnant soon exhibit augmented cell-proliferation, perhaps from the irritating effects of the elements of the blood now withdrawn from the circulation.
I have made or procured a considerable number of microscopic examinations in these cases of hypostatic pneumonia, and the solidification of the pulmonary lobules has been found to be due to the exaggerated development of the epithelial cells in the alveoli, together with venous congestion. The affected lobules, whether in the stage of hypostatic congestion or the more advanced stage of hypostatic pneumonitis, when examined at the autopsy, were somewhat softer than in health, of dark color, and many of the lobules could be inflated by strong force of the breath; but in protracted cases the alveoli in central parts of the inflamed area resisted insufflation. The lung in hypostatic pneumonia, even when it is inflated, still feels firmer between the fingers than normal lung.
Hypostatic pneumonia is so common in hospitals for infants that some physicians whose observations have been chiefly in such institutions have almost ignored other forms of pulmonary inflammation. Billard, many years ago, wrote: "... The pneumonia of young children is evidently the result of stagnation of blood in their lungs. Under these circumstances the blood may be regarded as a kind of foreign body." Of all the chronic and exhausting diseases of infancy, no one has, according to my observations, been so frequently complicated by hypostatic pneumonia as the disease which we are considering, although it does not usually give rise to any more prominent symptom than an occasional cough. Limited to a small and almost immovable part of the lung, it does not ordinarily accelerate respiration or render it painful, and the cough is also apparently painless.
When progressive loss of flesh and strength has continued several weeks, and the patient is much exhausted, another complication is apt to occur, known as spurious hydrocephalus or the hydrocephaloid disease, the anatomical characters of which will be described in the proper place. The commencement of spurious hydrocephalus is announced by gradually increasing drowsiness, perhaps preceded by a period of unusual fretfulness. Vomiting and rolling the head are occasional early symptoms of this complication. As the drowsiness increases the pupils become less sensitive to light than in their normal state, and are usually contracted. When the drowsiness becomes profound and constant, the pupils remain contracted as in sound sleep or in opium narcotism. The functional activity of the organs is now also diminished, the vomiting ceases, the stools become less frequent, the buccal surface dry, and the urine more [p. 736]scanty, while the pulse is more frequent and feeble. Spurious hydrocephalus either continues till death, or by stimulation the patient may emerge from it. When profound the usual result is death.
Although the summer complaint in its commencement may be promptly arrested by proper hygienic and medicinal treatment, if it continue a few weeks the anatomical changes which occur are such that recovery, if it take place, is necessarily slow and gradual. Improvement is shown by better digestion, fewer stools and of better appearance, less frequent vomiting, a more cheerful countenance, and the absence of symptoms which indicate a complication. Many recover after days of anxious watching and perhaps after many fluctuations.
Death may occur early from a sudden aggravation of symptoms and rapid sinking, or the attack may be so violent from the first that the infant quickly succumbs; but more frequently death takes place after a prolonged sickness. Little by little the patient loses flesh and strength, till a state of marked emaciation is reached. The eyes and cheeks are sunken, the bony projections of the face, trunk, and limbs become prominent, and the skin lies in wrinkles from the wasting. The altered expression of the face makes the patient look older than the actual age. The joints in contrast with the wasted extremities seem enlarged and the fingers and toes elongated. The stools diminish in frequency from diminished peristaltic and vermicular action, and vomiting, if previously present, now ceases. A feeble, quick, and scarcely appreciable pulse, slow respiration, and diminished inflation of the lungs, sightless and contracted pupils, over which the eyelids no longer close, announce the near approach of death. The drowsiness increases and the limbs become cool, while perhaps the head is hot. The infant no longer has the ability to nurse, or if bottle-fed the food placed in the mouth flows back or is swallowed with apparent indifference. So low is its vitality that it lies pallid and almost motionless for hours or even days before death, and death occurs so quietly that the moment of its occurrence is scarcely appreciable.
ANATOMICAL CHARACTERS.—Since the prominent and essential symptoms of the disease which we are considering pertain to the digestive apparatus, it is evident that the lesions which attend and characterize it are to be found in this part of the system. Lesions elsewhere, so far as they are appreciable to us, are secondary and not essential. I have witnessed a large number of autopsies of infants who have perished from the summer complaint, chiefly in institutions, and they have been sufficiently marked and uniform to enable us to designate it an entero-colitis. Several years since I preserved records of the autopsical appearances in the intestinal catarrh of infants, most of the cases being of summer diarrhoea. The number aggregated eighty-two. Since then I have each summer witnessed autopsies in the institutions in cases of this disease, and the lesions observed were the same as in the eighty-two cases.
The question may properly be asked: Can inflammatory hyperæmia of the intestinal mucous membrane be distinguished from simple congestion if there be no ulceration and no appreciable thickening of the intestine? It is possible that occasionally I have recorded as inflammatory what was simply a congestive lesion, but I do not think I have incorporated a [p. 737] sufficient number of such cases to vitiate the statistics. In a large proportion of the cases there was evident thickening of the intestinal mucous membrane or other unequivocal evidence of inflammation. The following is an analysis of the eighty-two cases:
The duodenum and jejunum presented the appearance of inflammatory hyperæmia in 12 cases. The hyperæmia was usually in patches of variable extent or of that form described by the term arborescent. In 51 cases the duodenal and jejunal mucous membrane was pale and without any other appearance characteristic of catarrh or inflammation. In the remaining 19 cases the appearance of the duodenum and jejunum was not recorded, so that it was probably normal. On the other hand, in the ileum inflammatory lesions were present as a rule. In 49 cases I found the surface of the ileum distinctly hyperæmic, and in that portion of it nearest the ileo-cæcal valve, including the valve itself, the inflammation had evidently been the most intense, since in this portion the hyperæmia and thickening of the mucous membrane were most marked. In 16 cases the surface of the ileum appeared nearly or quite normal; in 14 hyperæmia in the small intestines in patches, streaks, or arborescence was recorded, but the records do not state in which division of the intestines they were observed.
Billard, with other observers, has noticed the frequency and intensity of the inflammatory lesions in entero-colitis in the terminal portion of the small intestines, and the thickening in many cases of the ileo-cæcal valve, and he asks whether the vomiting which is so common and often obstinate in this disease may not be sometimes due to obstruction to the passage of fecal matter at the valve in consequence of the hyperæmia and swelling, but has not observed any retained fecal matter above it, such as we find in any part of the colon, or any other appearance which indicated sufficient obstruction to cause symptoms. Still, it seems not improbable that the reason why the inflammatory lesions are more pronounced at and immediately above the valve than in other parts of the small intestine is that the fecal matter, so commonly acid and irritating in this disease, is somewhat delayed in its passage downward at this point.
Small superficial circular or oval ulcers were observed in the ileum in 4 cases, in 2 of which they were found also in the lower part of the jejunum. In 1 case the records state that ulcers were in the jejunum, but do not mention whether they were also in the ileum. In 1 case, in which there was much thickening of the ileum next to the ileo-cæcal valve, many small granulations had sprouted up from the submucous connective tissue, so that the mucous surface appeared as if studded with small warts.
Softening of the mucous membrane was also apparent in certain cases. The firmness of its attachment to the parts underneath varied considerably in different specimens. I was able in cases in which there was considerable softening to detach readily the mucous membrane with the nail or handle of the scalpel within so short a period after death that it was probable that the change of consistence was not cadaveric. In some cases the vessels of the submucous tissue were injected and this tissue infiltrated.
In all the cases except one lesions were present indicating inflammation [p. 738] of the mucous membrane of the colon. In 39 hyperæmia, thickening, and other signs of inflammation extended over nearly or quite the entire colon; in 14 the colitis was confined to the descending portion entirely or almost entirely; in 28 cases the records state that inflammatory lesions were found in the colon, but their exact location is not mentioned. In 18 of the autopsies the mucous membrane of the colon was found ulcerated.
Therefore, according to these statistics—and autopsies which I have witnessed that are not embraced in them disclosed similar lesions—colitis is present, almost without exception, in cases of summer diarrhoea, associated with more or less ileitis. The portion of the colon which presents the most marked inflammatory lesions is that in and immediately above the sigmoid flexure—that portion, therefore, in which any fermenting fecal matter has reached its greatest degree of fermentation, and consequently contains the most irritating elements, and where, next to the caput coli, it is longest delayed in its passage downward.
The solitary glands of both the large and small intestines and Peyer's patches undergo hyperplasia. In cases of short duration, and in parts of the intestine where the inflammatory action has been mild, the solitary glands present a vascular appearance, like the surrounding membrane, and are slightly enlarged. The enlargement is most apparent if the intestine be viewed by transmitted light, when not only are the glands seen to be swollen, but their central dark points are distinct. If a higher grade of intestinal catarrh or a catarrh more protracted have occurred, the volume of these follicles is so increased that they rise above the common level and present a papillary appearance. Peyer's patches are also distinct and punctate. The enlargement of Peyer's patches, like that of the solitary glands, is due to hyperplasia, the elementary cells being largely increased in number.
The small ulcers which, as we have seen from the above statistics, are present in a certain proportion of cases in the mucous membrane of the colon, and more rarely in that of the small intestine when the inflammation has been protracted and of a severe type, appear to occur in the solitary glands and in the mucous membrane surrounding them. While some of these glands in a specimen are simply tumefied, others are slightly ulcerated, and others still nearly or quite destroyed. The ulcers are usually from one to three lines in diameter, circular or oval, with edges slightly raised from infiltration. Rarely, I have seen minute coagula of blood in one or more ulcers, and I have also observed ulcers which have evidently been larger and have partially healed. The ulcers are more frequently found in the descending colon than in other portions of the intestines. When ulcers are present they commonly occur in the descending colon, or if occurring elsewhere they are most abundant in this situation.
According to my observations, these ulcers are found chiefly in infants over the age of six months—during the time, therefore, when there is greatest functional activity and most rapid development of the solitary glands. Peyer's patches, though frequently prominent and distinct, have not been ulcerated in any of the cases observed by me.
The appendix vermiformis participates in the catarrh when it occurs in the caput coli, its mucous membrane being hyperæmic and thickened. In [p. 739] certain rare cases the inflammation is so intense that a thin film of fibrin is exuded in places upon the surface of the colon. It is apt to be overlooked or to be washed away in the examination. The rectum usually presents no inflammatory lesions, or but slight lesions in comparison with those in the colon. It usually remains of the normal pale color, or but slightly vascular even when there is almost general colitis. Hence the infrequency of tenesmus.
As might be expected from the nature of the disease, the secretion of mucus from the intestinal surface is augmented. It is often seen forming a layer upon the intestinal surface, and it appears in the stools mixed with epithelial cells and sometimes with blood and pus.
The mesenteric glands in cases which have run the most protracted course and end fatally are found more or less enlarged from hyperplasia. They are frequently as large as a pea or larger, and of a light color, the color being due not only to the hyperplasia, but in part to the anæmia. Occasionally, when patients have been much reduced from the long continuance of the diarrhoea, and are in a state of marked cachexia at death, we find certain of these glands caseous.
The condition of the stomach is interesting, since indigestion and vomiting are so commonly present. I have records of its appearance in 59 cases, in 42 of which it seemed normal, having the usual pale color and exhibiting only such changes as occur in the cadaver. In the remaining 17 cases the stomach was more or less hyperæmic, and in 3 of them points of ulceration were observed in the mucous membrane.
All physicians familiar with this disease have remarked the frequency of stomatitis. In protracted and grave cases it is a common complication. The buccal surface in these cases is more vascular than natural, and if the vital powers are much reduced superficial ulcerations are not infrequent, oftener upon the gums than elsewhere. The gums are apt to be spongy, more or less swollen, bleeding readily when rubbed or pressed upon. Thrush is a common complication of the summer complaint in infants under the age of three or four months, but is infrequent in older infants. Occurring in those over the age of six or eight months, it has an unfavorable prognostic significance, indicating a form of summer diarrhoea which commonly eventuates in death.
The belief has long been prevalent in the past that the liver is also in fault. The green color of the stools was supposed to be due to vitiated bile. But usually in the post-mortem examinations which I have made I have found that the green coloration of the fecal matter did not appear at the point where the bile enters the intestines, but at some point below the ductus communis choledochus in the jejunum or ileum. The green tinge, at first slight, becomes more and more distinct on tracing it downward in the intestine. It appears to be due to admixture of the intestinal secretions with the fecal matter.
I have notes of the appearance and state of the liver in 32 fatal cases. Nothing could be seen in these examinations which indicated any anatomical change in this organ that could be attributed to the diarrhoeal malady. The size and weight of the liver varied considerably in infants of the same age, but probably there was no greater difference than usually obtains among glandular organs in a state of health. The following was the weight of this organ in 20 cases:[p. 740]
| Age. | Weight. | Age. | Weight. | |
| 4 weeks | 5 ounces. | 10 months | 6¾ ounces. | |
| 2 months | 3½ ounces. | 13 months | 6 ounces. | |
| 2 months | 3½ ounces. | 14 months | 9 ounces. | |
| 4 months | 5 ounces. | 15 months | 6 ounces. | |
| 5 months | 6½ ounces. | 15 months | 7½ ounces. | |
| 5 months | 9 ounces. | 15 months | 9½ ounces. | |
| 7 months | 4½ ounces. | 16 months | 6 ounces. | |
| 7 months | 6 ounces. | 19 months | 4½ ounces. | |
| 7 months | 6¼ ounces. | 20 months | 9¼ ounces. | |
| 9 months | 8 ounces. | 23 months | 15 ounces. |
In none of these cases did the size, weight, or appearance of this organ seem to be different from that in health or in other diseases, except in one in which fatty degeneration had occurred, but this was probably due to tuberculosis, which was also present. In most of these cases the liver was examined microscopically, and the only noteworthy appearance observed was the variable amount of oil-globules in the hepatic cells. In some specimens the oil-globules were in excess, in others deficient, and in others still they were more abundant in one part of the organ than in another. Little importance was attached to these differences in the quantity of oily matter.
Hypostatic congestion of the posterior portions of the lungs, ending if it continue in a form of subacute catarrhal pneumonia and giving rise to an occasional painless cough, has been described in the preceding pages. The character of the cough in connection with the wasting might excite suspicions of the presence of tubercles in the lungs; but tubercles are rare in this disease, and when present I should suspect a strong hereditary predisposition. They occurred in only 1 of the 82 cases.
The state of the encephalon in those patients in whom spurious hydrocephalus occurs is interesting. In protracted cases of the diarrhoea the brain wastes like the body and limbs. In the young infant, in whom the cranial bones are still ununited, the occipital and sometimes the frontal bones become depressed and overlapped by the parietal, the depression being of course proportionate to the diminution in size of the encephalon. The cranium becomes quite uneven. In older children, with the cranial bones consolidated, serous effusion occurs according to the degree of waste, thus preserving the size of the encephalon. The effusion is chiefly external to the brain, lying over the convolutions from the base to the vertex. Its quantity varies from one or two drachms to an ounce or more. Along with this serous effusion, and antedating it, passive congestion of the cerebral veins and sinuses is also present. This congestion is the obvious and necessary result of the feebleness of the heart's action and the loss of brain substance.
DIAGNOSIS.—The occurrence and continuance of diarrhoea in the warm months, without any apparent cause except the agencies which hot weather produces, indicate this disease. The exciting cause of the attack may be the use of some indigestible and irritating substance, dietetic or medicinal, as fruits with their seeds or a purgative medicine; but if it continue after the immediate effects of the agent have passed off, it is proper to attribute the diarrhoea to the summer season.
In the adult abdominal tenderness is an important diagnostic symptom of intestinal catarrh, but in the infant this symptom is lacking or is not in general appreciable, so that it does not aid in diagnosis. When the [p. 741] diagnosis of the disease is established, the symptoms do not usually indicate what part of the intestinal surface is chiefly involved, but it may be assumed that it is the lower part of the ileum and the colon. The presence of mucus or of mucus tinged with blood in the stools shows the predominance of colitis.
PROGNOSIS.—Although this disease every summer largely increases the death-rate of young children, most cases can be cured if the proper hygienic and medicinal measures be early applied. It is obvious, from what has been stated in the foregoing pages, that cholera infantum is the form of this malady which involves greatest danger. Except in such cases there is sufficient forewarning of a fatal result, for if death occur it is after a lingering sickness, with fluctuations and gradual loss of flesh and strength. Patients often recover from a state of great prostration and emaciation, provided that no fatal complications arise. The eyes may be sunken, the skin lie in folds from the wasting, the strength may be so exhausted that any other than the recumbent position is impossible, and yet the patient may recover by removal to the country, by change of weather, or by the use of better diet and remedies. Therefore an absolutely unfavorable prognosis should not be made except in cases that are complicated or that border on collapse. The most dangerous symptoms, except those which indicate commencing or actual collapse, arise from the state of the brain. Rolling the head, squinting, feeble action or permanent contraction of the pupils, spasmodic or irregular movements of the limbs, indicate the near approach of death, as do also coldness of face and extremities and inability to swallow. It is obvious also that in making the prognosis in ordinary cases we should consider the age of the patient, the state of the weather, the time in the summer, whether in the beginning or near its close, and the surroundings, especially in reference to the impurity of the air, as well as the patient's condition.
This is the most severe form of the summer complaint. It receives the name which designates it from the violence of its symptoms, which closely resemble those of Asiatic cholera. It is, however, quite distinct from that disease. It is characterized by frequent stools, vomiting, great elevation of temperature, and rapid and great emaciation and loss of strength. It commonly occurs under the age of two years. It sometimes begins abruptly, the previous health having been good; in other cases it is preceded by the ordinary form of summer diarrhoea. The stools have been thinner than natural and somewhat more frequent, but not such as to excite alarm, when suddenly they become more frequent and watery, and the parents are surprised and frightened by the rapid sinking and real danger of the infant.
The first evacuations, unless there have been previous diarrhoea, may contain fecal matter, but subsequently they are so thin that they soak into the diaper like urine, and in some cases they scarcely produce more of a stain than does this secretion. Their odor is peculiar—not fecal, but musty and offensive, and occasionally almost odorless. Commencing simultaneously with the watery evacuations or soon after is another [p. 742] symptom, irritability of the stomach, which increases greatly the prostration and danger. Whatever drinks are swallowed by the infant are rejected immediately or after a few moments, or retching may occur without vomiting. The appetite is lost and the thirst is intense. Cold water is taken with avidity, and if the infant nurse it eagerly seizes the breast in order to relieve the thirst. The tongue is moist at first, and clean or covered with a light fur, pulse accelerated, respiration either natural or somewhat increased in frequency, and the surface warm, but the temperature is speedily reduced in severe cases. The internal temperature or that of the blood is always very high. In ordinary cases of cholera infantum the thermometer introduced into the rectum rises to or above 105°, and I have seen it indicate 107°. Although the infant may be restless at first, it does not appear to have any abdominal pain or tenderness. The restlessness is apparently due to thirst or to that unpleasant sensation which the sick feel when the vital powers are rapidly reduced. The urine is scanty in proportion to the gravity of the attack, as it ordinarily is when the stools are frequent and watery.
The emaciation and loss of strength are more rapid than in any other disease which I can recall to mind, unless in Asiatic cholera. In a few hours the parents scarcely recognize in the changed and melancholy aspect of the infant any resemblance to the features which it exhibited a day or two before. The eyes are sunken, the eyelids and lips are permanently open from the feeble contractile power of the muscles which close them, while the loss of the fluids from the tissues and the emaciation are such that the bony angles become more prominent and the skin in places lies in folds.
As the disease approaches a fatal termination, which often occurs in two or three days, the infant remains quiet, not disturbed even by the flies which alight upon its face. The limbs and face become cool, the eyes bleared, pupils contracted, and the urine scanty or suppressed. In some instances, when the patient is near death, the respiration becomes accelerated, either from the effect of the disease upon the respiratory centres or from pulmonary congestion resulting from the feeble circulation. As the vital powers fail the pulse becomes progressively more feeble, the surface has a clammy coldness, the contracted pupils no longer respond to light, and the stupor deepens, from which it is impossible to arouse the infant.
In the most favorable cases cholera infantum is checked before the occurrence of these grave symptoms, and often in cases which are ultimately fatal there is not such a speedy termination of the malady as is indicated in the above description. The choleriform diarrhoea abates and the case becomes one of ordinary summer complaint.
ANATOMICAL CHARACTERS.—Rilliet and Barthez, who of foreign writers treat of cholera infantum at greatest length, describe it under the name of gastro-intestinal choleriform catarrh. "The perusal," they remark, "of anatomico-pathological descriptions, and especially the study of the facts, show that the gastro-intestinal tube in subjects who succumb to this disease may be in four different states: (a) either the stomach is softened without any lesion of the digestive tube; (b) or the stomach is softened at the same time that the mucous membrane of the intestine, and especially its follicular apparatus, is diseased; (c) or the stomach is healthy, [p. 743]while the follicular apparatus or the mucous membrane is diseased; (d) or, finally, the gastro-intestinal tube is not the seat of any lesion appreciable to our senses in the present state of our knowledge, or it presents lesions so insignificant that they are not sufficient to explain the gravity of the symptoms.
"So far, the disease resembles all the catarrhs, but what is special is the abundance of serous secretion and the disturbance of the great sympathetic nerve.
"The serous secretion, which appears to be produced by a perspiration (analogous to that of the respiratory passages and of the skin) rather than by a follicular secretion, shows, perhaps, that the elimination of substances is effected by other organs than the follicles; perhaps, also, we ought to see a proof that the materials to eliminate are not the same as in simple catarrh. Upon all these points we are constrained to remain in doubt. We content ourselves with pointing out the fact."2
2 Maladies des Enfants.
On the 1st of August, 1861, I made the autopsy of an infant sixteen months old who died of cholera infantum with a sickness of less than one day. The examination was made thirty hours after death. Nothing unusual was observed in the brain, unless perhaps a little more than the ordinary injection of vessels at the vertex. No marked anatomical change was observed in the stomach and intestines, except enlargement of the patches of Peyer as well as of the solitary and mesenteric glands. Mucous membrane pale. In this and the following cases there was apparently slight softening of the intestinal mucous membrane, but whether it was pathological or cadaveric was uncertain, as the weather was very warm. The liver seemed healthy. Examined by the microscope, it was found to contain about the normal number of oil-globules.
The second case was that of an infant seven months old, wet-nursed, who died July 26, 1862, after a sickness also of about one day. He was previously emaciated, but without any marked ailment. The post-mortem examination was made on the 28th. The brain was somewhat softer than natural, but otherwise healthy. There was no abnormal vascularity of the membranes of the brain, and no serous effusion within the cranium. The mucous membrane of the intestines had nearly the normal color throughout, but it seemed somewhat thickened and softened; the solitary glands of the colon were prominent. The patches of Peyer were not distinct.
In the New York Protestant Episcopal Orphan Asylum an infant twenty months old, previously healthy, was seized with cholera infantum on the 25th of June, 1864. The alvine evacuations, as is usual with this disease, were frequent and watery, and attended by obstinate vomiting. Death occurred in slight spasms in thirty-six hours. The exciting cause was probably the use of a few currants which were eaten in a cake the day before, some of which fruit was contained in the first evacuations. The brain was not examined. The only pathological changes which were observed in the stomach and intestines were slightly vascular patches in the small intestines and an unusual prominence of the solitary glands in the colon. The glands resembled small beads imbedded in the mucous membrane. The lungs in the above cases were healthy, excepting hypostatic congestion.
[p. 744] Since the date of these autopsies I have made others in cases which terminated fatally after a brief duration, and have uniformly found similar lesions—namely, the gastro-intestinal surface either without vascularity or scantily vascular in streaks or patches, sometimes presenting a whitish or soggy appearance and somewhat softened, while the solitary glands were enlarged so as to be prominent upon the surface. In cases which continue longer evident inflammatory lesions soon appear which are identical with those which have already been described in our remarks on the ordinary form of the summer diarrhoea.
During my term of service in the New York Foundling Asylum in the summer of 1884, an infant died after a brief illness with all the symptoms of cholera infantum, and the intestines were sent to William H. Welch, now of Johns Hopkins Hospital, for microscopic examination. His report was as follows: "I found undoubted evidence of acute inflammation. There was an increased number of small, round cells (leucocytes) in the mucous and submucous coats. This accumulation of new cells was most abundant in and around the solitary follicles, which were greatly swollen. Clumps of lymphoid cells were found extending even a little into the muscular coat. The epithelial lining of the intestine was not demonstrable, but this is usually the case with post-mortem specimens of human intestine, and justifies no inferences as to pathological changes. The glands of Lieberkühn were rich in the so-called goblet-cells, and some of the glands were distended with mucus and desquamated epithelium, so as to present sometimes the appearance of little cysts. This was observed especially in the neighborhood of the solitary follicles. The blood-vessels, especially the veins of the submucous coat, were abnormally distended with blood. I searched for micro-organisms, and found them in abundance upon the free surface of the intestine in the mucous accumulations there, and also in the mouths of the glands of Lieberkühn. Both rod-shaped and small round bacteria were found. I attach no especial importance to finding bacteria upon the surface of the intestine. The general result of the examination is to confirm the view that cholera infantum is characterized by an acute intestinal inflammation."
NATURE.—Cholera infantum appears from its symptoms and lesions to be the most severe form of intestinal catarrh to which infants are liable. The alvine discharges, to which the rapid prostration is largely due, probably consist in part of intestinal secretions and in part of serum which has transuded from the capillaries of the intestines. That the intestinal mucous membrane sometimes presents a pale appearance at the autopsy of an infant who, previously well, has died of cholera infantum after a sickness of twenty-four or forty-eight hours, is perhaps due to the great amount of liquid secretion and transudation in which the inflamed surface is bathed. Moreover, it is, I believe, a recognized fact that the hyperæmia of an acutely-inflamed surface when of short duration frequently disappears in the cadaver, as that of scarlet fever and erysipelas. The early hyperplasia of the solitary and mesenteric glands, and the hyperæmia and thickening of the surface of the ileum and colon in those who have survived a few days, indicate the inflammatory character of the malady.
The opinion has been expressed by certain observers that cholera [p. 745] infantum is identical with thermic fever or sunstroke. There is indeed a resemblance to thermic fever as regards certain important symptoms. In cholera infantum the temperature is from 105° to 108°; in sunstroke it is also very high, often running above 108°. Great heat of head, contracted pupils, thin fecal evacuations, embarrassed respiration, scanty urine, and cerebral symptoms are common toward the close of cholera infantum, and they are the prominent symptoms in sunstroke. Nevertheless, I cannot accept the theory which regards these maladies as identical, and which removes cholera infantum from the list of intestinal diseases. In cholera infantum the gastro-intestinal symptoms always take the precedence, and are, except in advanced cases, always more prominent than other symptoms. It does not commence as by a stroke like coup de soleil, but it comes on more gradually, though rapidly, and it often supervenes upon a diarrhoea or some error of diet. In the commencement of cholera infantum the infant is not apt to be drowsy, and it is often wide awake and restless from the thirst. Contrast this with the alarming stupor of sunstroke. Sunstroke only occurs during the hours of excessive heat, but cholera infantum may occur at any hour or in any day during the hot weather, provided that there be sufficient dietetic cause. Again, intestinal inflammation is not common in sunstroke, while it is the common or, as I believe, the essential lesion of cholera infantum. These facts show, in my opinion, that the two maladies are essentially and entirely distinct. Nevertheless, cases of apparent sunstroke sometimes occur in the infant, and if the bowels are at the same time relaxed the disease is apt to be regarded as cholera infantum, and if fatal is usually reported as such to the health authorities. Cases of this kind I have occasionally observed or they have been reported to me, although they are not common.
With the exception of the organs of digestion no uniform lesions are observed in any of the viscera in cholera infantum, except such as are due to change in the quantity and fluidity of the blood and its circulation. Writers describe an anæmic appearance of the thoracic and abdominal viscera, and occasionally passive congestion of the cerebral vessels. The cerebral symptoms often present toward the close of life in unfavorable cases of cholera infantum are often due to spurious hydrocephalus, which we have described above; but as the urinary secretion is scanty or suppressed, cerebral symptoms may in certain cases be due to uræmia.
DIAGNOSIS.—This form of the summer diarrhoea is diagnosticated by the symptoms, and especially by the frequency and character of the stools. The stools have already been described as frequent, often passed with considerable force, deficient in fecal matter, and thin, so as to soak into the diaper almost like urine. The vomiting, thirst, rapid sinking, and emaciation serve to distinguish cholera infantum from other diarrhoeal maladies.
When Asiatic cholera is prevalent the differential diagnosis between the two is difficult if not impossible.
PROGNOSIS.—Cholera infantum is one of those diseases in regard to which physicians often injure their reputation by not giving sufficient notice of the danger, or even by expressing a favorable opinion when the case soon after ends fatally. A favorable prognosis should seldom be expressed without qualification. If the urgent symptoms be relieved, [p. 746] still the disease may continue as an ordinary intestinal inflammation, which in hot weather is formidable and often fatal. If the stools become more consistent and less frequent without the occurrence of cerebral symptoms, while the limbs are warm and the pulse good, we may confidently express the opinion that there is no present danger.
The duration of true cholera infantum is short. It either ends fatally, or it begins soon to abate and ceases, or it continues, and is not to be distinguished in its subsequent course from an attack of summer diarrhoea beginning in the ordinary manner.
TREATMENT.—Preventive Measures.—Obviously, efficient preventive measures consist in the removal of infants so far as practicable from the operation of the causes which produce the disease. Weaning just before or in the hot weather should, if possible, be avoided, and removal to the country should be recommended, especially for those who are deprived of the breast-milk during the age when such nutriment is required. If for any reason it is necessary to employ artificial feeding for infants under the age of ten months, that food should obviously be used which most closely resembles human milk in digestibility and in nutritive properties. Care should be taken to prevent fermentation in the food before its use, since much harm is done by the employment of milk or other food in which fermentative changes have occurred and which occur quickly in dietetic mixtures in the hot months.
It is also very important that the infant receive its food in proper quantity and at proper intervals, for if the mother or nurse in her anxiety to have it thrive feed it too often or in too large quantity, the surplus food which it cannot digest if not vomited undergoes fermentation, and consequently becomes irritating to the gastro-intestinal surface. The physician should be able to give advice not only in reference to the frequency of feeding, but also in regard to the quantity of food which the infant requires at each feeding. Correct knowledge and advice in this matter aid in the prevention and cure of the dyspeptic and diarrhoeal maladies of infancy.
Chadbourne of this city and myself made some observations in order to ascertain how much food well-nourished infants receive daily. We selected infants that had an abundance of breast-milk, and weighed them before and after each nursing, so as to determine how much each infant took during twenty-four hours. The avoirdupois ounce contains 437.5 grains, and we ascertained by careful weight and measurement, employing the metric system for its greater accuracy, that one fluidounce of human milk, with a specific gravity of 1.031, weighed 451.9 grains. With these data it was easy to determine the quantity of milk in fluidounces from its weight. Our first observations related to 12 infants under the age of five weeks, 8 of which nursed twelve times, and the remaining 4 eight, nine, nine, and eleven times respectively, in the twenty-four hours. The quantity of milk received by them in twenty-four hours varied considerably in the different cases, but the average was 12.41 fluidounces. Therefore if a baby in the first five weeks nurse every two hours, it receives only a little more than one fluidounce at each nursing.
The next observations were made upon 15 infants between the ages of five weeks and ten months: 8 of the 15 were under the age of six [p. 747] months, and the remaining 7 were between the ages of six months and ten months. The weighing showed that the younger took nearly the same quantity per day, on the average, as the older infants in this group. The average quantity received by each was twenty-four and six-tenths fluidounces. Hence if the nursings were eight in the twenty-four hours, three ounces were taken at each nursing; if the nursings were twelve, the quantity each time was two ounces.
Biedert of Germany has also made similar observations in order to determine the amount of nutriment required by infants. The results of his weight-studies, as he designates them, were published in the Jahrbuch für Kinderheilkunde, xix. B., 3 H. His weighing showed that infants during their first month, if fed on cow's milk, required from 160 to 200 grammes of milk daily, and in the third month 300 grammes. These quantities in fluid measure are 5.44 to 6.83 ounces, the quantity required each day in the first month, and 10.22 ounces, the quantity required daily the second month. Therefore, both my weights and Biedert's show that infants under the age of two months assimilate a smaller quantity of milk than is usually supposed. For infants older than two months he estimates the quantity of milk required by infants by their weight. He believes that the greater the weight the greater is the amount of food which the infant needs. The method pursued by Chadbourne and myself is more simple, and it seems to indicate with sufficient exactness the amount of food required.
Some infants, like adults, need more food than others, so that there can be no exact schedule of the quantity which they require at each feeding; but while in the first and second months they do not need more than from one to one and a half fluidounces at each feeding, whether of breast-milk, or of cow's milk prepared so as to resemble as closely as possible human milk, infants as they grow older and their stomachs enlarge can take food in larger quantity, and therefore require less frequent feeding. Under the age of two months the stomach is so small that it cannot receive much more than one or one and a half fluidounces without undue distension. At the age of six months it can probably receive and digest without discomfort three ounces, and in the last half of the first year even four ounces. Infants nourished at the breast should be allowed to nurse every two hours in the daytime, whatever the age, after the second month, but less frequently at night, for frequent nursing promotes the secretion of milk, and the milk is of better quality than when it is long retained in the breast. If by the fifth or sixth month mothers or wet-nurses find, as is frequently the case, that they do not have sufficient milk, other food should be given in addition, perhaps after each second nursing or every fourth hour. The kind of food which it is best to employ to supplement the nursing will be mentioned under the head of curative measures. By knowledge on the part of the mother and nurse of the dietetic needs of the infant, and by consequent judicious alimentation, and by measures also to procure the utmost purity of the air, there can be no doubt that the summer diarrhoea may to a great extent be prevented.
Curative Treatment.—The indications for treatment are—1st, to provide the best possible food; 2d, to procure pure air; 3d, to aid the digestive function of the infant; 4th, to employ such medicinal agents as can be safely given to check the diarrhoea and cure the intestinal catarrh.
[p. 748] The infant with this disease is thirsty, and is therefore apt to take more nutriment in the liquid form than it requires for its sustenance. If nursing, it craves the breast, or if weaned, craves the bottle, at short intervals to relieve the thirst. No more nutriment should be allowed than is required for nutrition, for the reason stated above, and the thirst may best be relieved by a little cold water, gum-water, or barley-water, to which a few drops of brandy or whiskey are added.
Since one of the two important factors in producing the summer diarrhoea is the use of improper food, it is obviously very important for the successful treatment of this disease that the food should be of the right kind, properly prepared, and given in proper quantity. I need not repeat that for infants under the age of one year no food is so suitable as breast-milk, and one affected with the diarrhoea and remaining in the city should, if possible, at least if under the age of ten months, be provided with breast-milk. It can be more satisfactorily treated and the chances of its recovery are much greater if it be nourished with human milk than by any other kind of diet. If, however, the mother's milk fail or become unsuitable from ill-health or pregnancy, and on account of family circumstances a wet-nurse cannot be procured, the important and difficult duty devolves upon the physician of deciding how the infant should be fed. In order to solve this problem it will be well to recall to mind the part performed in the digestive function by the different secretions which digest food:
1st. The saliva is alkaline in health. It converts starch into glucose or grape-sugar. It has no effect upon fat or the protein group. It is the secretion of the parotid, submaxillary, and sublingual glands, which in infants under the age of three months are very small, almost rudimentary. The two parotid glands at the age of one month weigh only thirty-four grains. The power to convert starch into sugar possessed by saliva is due to a ferment which it contains called ptyalin.
2d. The gastric juice is a thin, nearly transparent, and colorless fluid, acid from the presence of a little hydrochloric acid. It produces no change in starch, grape-sugar, or the fats, except that it dissolves the covering of the fat-cells. Its function is to convert the proteids into peptone, which is effected by its active principle, termed pepsin.
3d. The bile is alkaline and neutralizes the acid product of gastric digestion. It has no effect on the proteids. It forms soaps with the fatty acids and has a slight emulsifying action on fat. The soaps are said to promote the emulsion of fat. Their emulsifying power is believed to be increased by admixture with the pancreatic secretion. Moreover, the absorption of oil is facilitated by the presence of bile upon the surface through which it passes.
4th. The pancreatic juice appears to have the function of digesting whatever alimentary substance has escaped digestion by the saliva, gastric juice, and bile. It is a clear, viscid liquid of alkaline reaction. It rapidly changes starch into glucose. It converts proteids into peptones and emulsifies fats. While the gastric juice requires an acid medium for the performance of its digestive function, the pancreatic juice requires one that is alkaline. This important fact should be borne in mind, that such a mistake as presenting pepsin with chalk mixture, or the extractum pancreatis with dilute muriatic acid, may be avoided.
[p. 749] 5th. The intestinal secretions are mainly from the crypts of Lieberkühn, and their action in the digestive process is probably comparatively unimportant, but in some animals they have been found to digest starch. It will be observed that of all these secretions that which digests the largest number of nutritive principles is the pancreatic. It digests all those which are essential to the maintenance of life except fat, and it aids the bile in emulsifying fat.
One of the most important conferences in pædiatrics ever held convened at Salzburg in 1881 for the purpose of considering the diet of infants. Among those who participated in the discussion were men known throughout the world as authorities in children's diseases, such as Demme, Biedert, Gerhardt, Henoch, Steffen, Thomas, and Soltmann. None of the physicians present dissented from the following proposition of the chairman: That "all the advances made in physiology in respect to the digestive organs of children only go to prove that the mother's milk is the only true material which is quantitatively and qualitatively suited to the development of the child, which preserves the physiological functions of the organs of digestion, and under favorable circumstances of growth unfolds the whole organism in its completeness." All agreed that when the breast-milk fails animal milk is the best substitute. Henoch, who was one of the conference, expresses the same opinion in his well-known treatise on diseases of children, as follows: "Cow's milk is the best substitute for mother's milk during the entire period of infancy. I consider the administration of other substances advisable only when good cow's milk cannot be obtained or when it gives rise to constant vomiting and diarrhoea."
The many infants' foods contained in the shops were considered by the conference, and, in the words of the chairman, "Now and evermore it is unanimously agreed that these preparations can in no way be substituted for mother's milk, and as exclusive food during the first year are to be entirely and completely rejected." But, unfortunately, we soon learn by experience that animal milk, although it is the best of the substitutes for human milk, is, especially as dispensed in the cities, faulty. It is digested with difficulty by young infants, and is apt to cause in them diarrhoea and intestinal catarrh. Therefore in the hot months its use is very apt to act as one of the dietetic causes of the summer diarrhoea in infants exclusively fed upon it, unless it be specially prepared so as to more closely resemble human milk. The frequent unsatisfactory results of its use have led to the preparation of the many proprietary substitutes for human milk which the shops contain, and which have been so summarily discarded by the German conference.
Woman's milk in health is always alkaline. It has a specific gravity of 1.0317; cow's milk has a specific gravity of 1.029. That of cows stabled and fed upon other fodder than hay or grass is usually decidedly acid. That from cows in the country with good pasturage is said to be alkaline, but in two dairies in Central New York a hundred miles apart, in midsummer, with an abundant pasturage, two competent persons whom I requested to make the examinations found the milk slightly acid immediately after the milking in all the cows.
The following results of a large number of analyses of woman's and cow's milk, made by König and quoted by Leeds, and of several of the [p. 750] best known and most used preparations designed by their inventors to be substitutes for human milk, show how far these substitutes resemble the natural aliment in their chemical characters:
| Woman's Milk. | Cow's Milk. | |||||
| Mean. | Minimum. | Maximum. | Mean. | Minimum. | Maximum. | |
| Water | 87.09 | 83.69 | 90.90 | 87.41 | 80.32 | 91.50 |
| Total solids | 12.91 | 9.10 | 16.31 | 12.59 | 8.50 | 19.68 |
| Fat | 3.90 | 1.71 | 7.60 | 3.66 | 1.15 | 7.09 |
| Milk-sugar | 6.04 | 4.11 | 7.80 | 4.92 | 3.20 | 5.67 |
| Casein | 0.63 | 0.18 | 1.90 | 3.01 | 1.17 | 7.40 |
| Albumen | 1.31 | 0.39 | 2.35 | 0.75 | 0.21 | 5.04 |
| Albuminoids | 1.94 | 0.57 | 4.25 | 3.76 | 1.38 | 12.44 |
| Ash | 0.49 | 0.14 | ... | 0.70 | 0.50 | 0.87 |
The following analyses of the foods for infants found in the shops, and which are in common use, were made by Leeds of Stevens's Institute:
| 1. Blair's Wheat Food. |
2. Hubbell's Wheat Food. |
3. Imperial Granum. |
4. Ridge's Food. |
5. "A.B.C." Cereal Milk. |
6. Robinson's Patent Barley. |
|
| Water | 9.85 | 7.78 | 5.49 | 9.23 | 9.33 | 10.10 |
| Fat | 1.56 | 0.41 | 1.01 | 0.63 | 1.01 | 0.97 |
| Grape-sugar | 1.75 | 7.56 | Trace. | 2.40 | 4.60 | 3.08 |
| Cane-sugar | 1.71 | 4.87 | Trace. | 2.20 | 15.40 | 0.90 |
| Starch | 64.80 | 67.60 | 78.93 | 77.96 | 58.42 | 77.76 |
| Soluble carbohydrates | 13.69 | 14.29 | 3.56 | 5.19 | 20.00 | 4.11 |
| Albuminoids | 7.16 | 10.13 | 10.51 | 9.24 | 11.08 | 5.13 |
| Gum, cellulose, etc. | 2.94 | Undeterm'd. | 0.50 | ... | 1.16 | 1.93 |
| Ash | 1.06 | 1.00 | 1.16 | 0.60 | ... | 1.93 |
| Mellin's. | Hawley's. | Horlick's. | Keasbey and Mattison's. | Savory and Moore's. | Baby Sup No. 1. | Baby Sup No. 2. | |
| Water | 5.00 | 6.60 | 3.39 | 27.95 | 8.34 | 5.54 | 11.48 |
| Fat | 0.15 | 0.61 | 0.08 | None. | 0.40 | 1.28 | 0.62 |
| Grape-sugar | 44.69 | 40.57 | 34.99 | 36.75 | 20.41 | 2.20 | 2.44 |
| Cane-sugar | 3.51 | 3.44 | 12.45 | 7.58 | 9.08 | 11.70 | 2.48 |
| Starch | None. | 10.97 | None. | None. | 36.36 | 61.99 | 51.95 |
| Soluble carbohydrates | 85.44 | 76.54 | 87.20 | 71.50 | 44.83 | 14.35 | 22.79 |
| Albuminoids | 5.95 | 5.38 | 6.71 | None. | 9.63 | 9.75 | 7.92 |
| Gum, cellulose, etc. | ... | ... | ... | ... | 0.44 | 7.09 | 5.24 |
| Ash | 1.89 | 1.50 | 1.28 | 0.93 | 0.89 | Undeterm'd. | 1.59 |
| Nestle's. | Anglo-Swiss. | Gerber's. | American-Swiss | |
| Water | 4.72 | 6.54 | 6.78 | 5.68 |
| Fat | 1.91 | 2.72 | 2.21 | 6.81 |
| Grape-sugar and Milk-sugar | 6.92 | 23.29 | 6.06 | 5.78 |
| Cane-sugar | 32.93 | 21.40 | 30.50 | 36.43 |
| Starch | 40.10 | 34.55 | 38.48 | 30.85 |
| Soluble carbohydrates | 44.88 | 46.43 | 44.76 | 45.35 |
| Albuminoids | 8.23 | 10.26 | 9.56 | 10.54 |
| Ash | 1.59 | 1.20 | 1.21 | 1.21 |
It is seen by examination of the analyses of the above foods that all except such as consist largely or wholly of cow's milk differ widely from human milk in their composition, and although some of them—as the Liebig preparations, in which starch is converted into glucose by the action of the diastase of malt—may aid in the nutrition and be useful as adjuncts to milk, physicians of experience and close observation will, I think, agree with the German conference that when breast-milk fails or is insufficient our main reliance for the successful nutrition of the infant must be on animal milk. Nestle's Food, which consists of wheat flour, the yelk of egg, condensed milk, and sugar, and which has been so largely used in this country and in Europe, is probably beneficial mainly from the large amount of Swiss condensed milk which it contains.
Although the preference is to be given to animal milk over any other kind of food as a substitute for human milk, yet even when obtained fresh and from the best dairies and properly diluted it is very apt to disagree with infants under the age of one year, producing indigestion and diarrhoea. The close resemblance in chemical character of cow's, ass's, and goat's milk to human milk would lead us to expect that either would be a good substitute for the latter. The fact that the milk of these animals is apt to cause indigestion and intestinal catarrh, especially in the hot months, when the digestive function of the infant is enfeebled from the heat, must be due to the quality rather than quantity of its constituents. The difference in quality of the casein of human and animal milk is well known, since that of human milk coagulates in the stomach in flakes, and that of animal milk in firm and large masses. The German conference saw at once the importance of the problem which confronted them—i.e. how to modify cow's milk so that it bears the closest possible resemblance to human milk. They even discussed the difference of the milk of different breeds of cows, and the proper feeding and care of cows, but the most important suggestion made—and one which has already produced good results in this country and in Europe, and promises to be instrumental in saving the lives of many infants who by the old method of feeding would inevitably perish—was made by Pfeiffer of Wiesbaden. I allude to the peptonizing of milk. The pancreatic secretion digests milk that is rendered alkaline at a temperature between 100° and 150° F. Milk thus treated becomes in from twenty minutes to one hour thinner, resembling human milk in appearance, and if the peptonizing be continued beyond a certain point, and is more complete, its taste is decidedly [p. 752] bitter. The process should be watched and the peptonizing suspended as soon as the bitterness becomes appreciable, for, although more advanced peptonizing so changes the milk that it is more easily digested by the infant than when the peptonizing is partial, yet the bitterness which is imparted to it renders it very disagreeable as a dietetic preparation. Milk thus prepared closely resembles human milk in appearance, and its casein is so digested that it is either not precipitated by acids or is precipitated, like that of human milk, in flakes. By this process a digested or an easily-digested casein is produced, instead of the casein of ordinary cow's milk, which produces large and firm masses in the stomach—masses that the digestive ferments penetrate with such difficulty that they cause indigestion, and occur in the stools in coagula of greater or less size. Pfeiffer pointed out that when peptonized milk is employed "the feces showed absolutely no trace of the white cheesiness." Milk thus prepared quickly spoils, and it is necessary to peptonize it in small quantity and often during the twenty-four hours.
In New York City during the last year peptonized milk has been employed largely as recommended by Pfeiffer, and with such results as to encourage its further use. It is now used in the New York Infant Asylum and New York Foundling Asylum. Five grains of extractum pancreatis (Fairchild & Co.'s) and ten grains of sodium bicarbonate are added to one gill of warm water. This is mixed with one pint of warm milk, and the mixture, in some convenient vessel, is placed in water kept at a temperature of 100° F. for one hour, when it is placed upon ice to prevent further digestion. It should be tasted frequently during the peptonizing process, and if the least bitterness be observed the process should be suspended before the expiration of the hour. With some specimens of milk, especially at a temperature of 115° to 120°, a half hour or even less is sufficient. This artificial digestion is arrested either by boiling the peptonized milk, which destroys the ferment, or by reducing its temperature to near the freezing-point, which renders it latent and inactive, but does not destroy it. I need not add that placing the peptonized milk on ice is preferable to boiling it, since we wish the ferment to continue to act in the stomach of the infant. In the present state of our knowledge of infant feeding, therefore, we can recommend no better substitute for human milk than peptonized cow's milk.
Leeds recommended the following formula for peptonizing milk in his very instructive remarks made before the New York County Medical Association, July 16, 1884. In order that no mistake might be made, I wrote to him for his formula, which he kindly sent me. The following is an extract from his letter: "The formula which I ventured to suggest for the preparation of humanized cow's milk was as follows: 1 gill of cow's milk, fresh and unskimmed; 1 gill of water; 2 tablespoonfuls of rich cream; 200 grains of milk-sugar; 1½ grains of extractum pancreatis; 4 grains of sodium bicarbonate. Put this in a nursing-bottle; place the bottle in water made so warm that the whole hand cannot be held in it without pain longer than one minute. Keep the milk at this temperature for exactly twenty minutes. The milk should be prepared just before using."
The object is of course to provide from cow's milk a food which will be the nearest possible approximation to healthy human milk; and this [p. 753] appears to be achieved by the peptonizing process. Certainly, what physicians have long been desiring—namely, some mode of preparing cow's milk so that its casein will coagulate in flakes like that of human milk—has been obtained by peptonizing.
It is a common error to expect too much of a new remedy which has a real value, and we must not expect that all patients not in an utterly hopeless state will begin to improve as soon as peptonized milk is prepared for them, or that it is a full and exact substitute for human milk, so that wet-nurses may be dispensed with. Healthy human milk is the best of all food for infants under the age of twelve months, and should always be preferred when it can be obtained, but we claim that peptonized milk is a most useful addition to the dietetic preparations for infants, probably surpassing in value the best of those in the shops. We employ it in the belief that it affords important aid in curing the dyspeptic and diarrhoeal maladies of infancy. Who first formulated and recommended the process of peptonizing milk I am not able to state, but I am informed that Roberts of Great Britain called attention to it as a means of improving milk at a time antedating the German conference.
Milk from healthy, properly-fed cows may be prepared without peptonizing, so as to agree with many infants except in the warmest weather, but is obviously less easily digested than peptonized milk. It should be diluted as follows with water boiled so as to free it from germs: In the first week after birth one-fourth milk with the addition of a little sugar. The milk should be gradually increased, so that it is one-third by the end of the fourth week, one-half by the end of the third month, and two-thirds to three-fourths by the end of the sixth month. After the sixth month it is still proper to add one-fourth water, but pure milk may be given. Water increases the urination.
Before peptonizing—which, as we have seen, digests the casein to a great extent, and changes that which is not digested so that it coagulates in flakes in the stomach like breast-milk—was resorted to, it was customary to use a thin barley- or oat-water in place of the water used for diluting the milk. One heaped teaspoonful of barley flour to two tablespoonfuls of water make a gruel of proper consistence. A little farinaceous substance added to the milk by mechanically separating the particles of casein tends to prevent their coagulation in large and firm masses. This was the theory which explained the beneficial action of the admixture. If for any reason peptonized milk be not employed, milk prepared in the way I have mentioned, by admixture with a farinaceous substance, is probably the next best substitute for human milk.
It is very important to determine when and how farinaceous foods shall be given in this disease. It is well known that infants under the age of three months digest starch with difficulty and only in small quantity, since the salivary and pancreatic glands which secrete the ferments which digest starch are almost rudimentary at that age. The artificial digestion of starch is, however, easily accomplished. Among the last labors of the renowned chemist Baron Liebig was the preparation of a food for infants in which the starch is digested and transformed into grape-sugar, and thus infants at any age who are fed with it are relieved of the burden of digesting it. The baron led the way which has been so successfully followed since in the artificial digestion of foods. A considerable part of the starch [p. 754]in wheat flour is converted into grape-sugar by the prolonged action of heat. I frequently recommend that from three to five pounds of wheat flour be packed dry in a firm muslin bag, so as to form a ball, and be placed in water sufficient to cover it constantly and the bag kept over the fire three or four days. During the nights the fire may go out for a few hours. At the expiration of this time the external part, which is wet, being peeled off, the remainder resembles a lump of yellowish chalk. The flour grated from it gives a decided reaction of sugar by Fehling's test. Starch is also quickly transformed into glucose by the action of the diastase of malt, which indeed Liebig employed. If to a gruel of barley flour, oatmeal, or other farinaceous substance, when hot, a little of a good preparation of extract of malt, such as that prepared by Trommer & Co. at Fremont, Ohio, which acts promptly, or by Reed & Carnrick, be added, it becomes thinner. It is claimed that the starch is thus quickly converted into glucose; which seems doubtful. It is, however, so modified that it is apparently more readily digested and assimilated. Farinaceous substances thus prepared may be employed with peptonized or other milk. Infants frequently do better with this admixture than when either the milk or gruel is used separately.
Of the foods contained in the shops which have been most prescribed, and which have apparently been useful in certain cases, I may mention those which have been prepared according to Liebig's formula, of which there are several, the analyses of which I have given, and Nestle's farina. In the use of those foods which contain no milk, as Ridge's food, Imperial granum, etc., it is recommended that milk be added, while for such as contain condensed milk, as Nestle's and the Anglo-Swiss food, only water should be employed. The Anglo-Swiss food contains about 60 per cent. condensed milk and about 20 per cent. each of oatmeal and Russian wheat flour. It gives an acid reaction, unlike Nestle's, which is alkaline. When Biedert's cream conserve was announced great expectations were awakened from the fact that the inventor is an authority in pædiatrics, but, unfortunately, they have not been realized in this country. Much of Biedert's conserve when it reaches us is spoiled, and the directions for its use are too complicated for ordinary family use, since a different mixture is required for each month of the infant's age. I have employed this food, but, with Henoch, "could not convince myself that it is more efficacious than cow's milk." I am informed that the sale of it in this country has ceased.
Condensed milk is largely used in the feeding of infants. The milk is condensed in vacuo to one-third or one-fifth its volume, heated to 100° C. (212° F.) to kill any fungus which it contains, and 38 to 40 per cent. of cane-sugar is added to preserve it. In the first month one part of milk should be added to sixteen of water, and the proportion of water should be gradually reduced as the infant becomes older. The large amount of sugar which condensed milk, preserved in cans, contains renders it unsuitable in the dietetic rôle of the summer diarrhoea of infants. The sugar is apt to produce acid fermentation and diarrhoea in hot weather. Borden's condensed milk, freshly prepared, as dispensed from the wagons, contains, I am informed by the agent, no cane-sugar or other foreign substance, and on this account is to be preferred to that in the cans. It is cow's milk of good quality, from which 75 to 79 per cent. of the water [p. 755] has been removed under vacuum. The sole advantage which it possesses—and it is an important one—is that it resists fermentation longer than the ordinary milk.
To select the best food for the infant from this considerable number of dietetic preparations is one of the most important duties of the physician. If called to an infant unfortunately deprived of wholesome breast-milk, and suffering in consequence from indigestion and diarrhoea, what diet shall we recommend? My recommendation would be as follows: Use cow's milk of the best possible quality and peptonized in the manner stated above, and peptonized in small quantity at a time, such as a pint, or, better, half a pint. This may be the sole food till the age of five or six months. Unfortunately, in the cities the milk that is delivered in the morning is the milking of the preceding evening, mixed with that of the preceding morning, brought often many miles from the farms where it is produced. Milk twelve and twenty-four hours old, notwithstanding the use of ice around the milk-cans, is apt to undergo some fermentative change before it reaches the nursery. This prevents the preparation of the best quality of peptonized milk, so that in some instances during the heated term I have found that the peptonized milk did not agree as well as the condensed milks, like Borden's or Nestle's food. Not a few infants suffering from diarrhoeal maladies seem to do better if some farinaceous food properly prepared be added to the peptonized milk than when the milk is used alone. It is better, I think, that the starch, or a considerable part of the starch, be converted into glucose before the admixture. This can be done if a few pounds of wheat flour be pressed dry in a bag, so as to form a ball, and boiled three or four days, as I have elsewhere recommended. The flour grated from the mass gives a decided sugar reaction to Fehling's test. For infants under the age of six months one tablespoonful of the flour thus prepared should be mixed with twelve tablespoonfuls of water and boiled. When it has been removed from the fire and become tepid, a small quantity of a good extract of malt, as Trommer's or Reed & Carnrick's, may advantageously be added to the gruel to increase the transformation of starch and render it more digestible. To avoid the time and trouble of preparing the food in this manner, one of the foods contained in the shops, in which the starch has been transformed into glucose by the employment of Baron Liebig's formula, may be used, as Mellin's or Horlick's, instead of the wheat flour prepared by long boiling. The older the child, the thicker should be the gruel.
Beef-, mutton-, or chicken-tea should not be employed, at least as it is ordinarily made, since it is too laxative. Occasionally, for the older infants, we may allow the expressed juice of beef, raw scraped beef, or beef-tea prepared by adding half a pound of lean beef, finely minced, to one pint of cold water, and after allowing it to stand for half an hour warming it to a temperature not exceeding 110° for another half hour. By this process the albumen is preserved. Salt should be added to it, and I am in the habit of adding to it also about seven drops of dilute muriatic acid to facilitate its digestion. It is chiefly for infants over the age of ten months that the meat-juices are proper. A concentrated nutriment, prepared, it is stated, from beef, mutton, and fruits, has lately been introduced in the shops under the name Murdoch's Liquid Food. Young [p. 756]infants with dyspeptic and diarrhoeal symptoms can take it, and it appears to be readily assimilated, as the quantity given at each feeding is small. It has its advocates, and it appears to be of some service in cases of weak and irritable stomach.
But since one of the two important factors in producing the summer diarrhoea of infants is foul air, it is obvious that measures should be employed to render the atmosphere in which the infant lives as free as possible from noxious effluvia. Cleanliness of the person, of the bedding, and of the house in which the patient resides, the prompt removal of all refuse animal or vegetable matter, whether within or around the premises, and allowing the infant to remain a considerable part of the day in shaded localities where the air is pure, as in the parks or suburbs of the city, are important measures. In New York great benefit has resulted from the floating hospital which every second day during the heated term carries a thousand sick children from the stifling air of the tenement-houses down the bay and out to the fresh air of the ocean.
But it is difficult to obtain an atmosphere that is entirely pure in a large city with its many sources of insalubrity; and all physicians of experience agree in the propriety of sending infants affected with the summer diarrhoea to localities in the country which are free from malaria and sparsely inhabited, in order that they may obtain the benefits of a purer air. Many are the instances each summer in New York City of infants removed to the country with intestinal inflammation, with features haggard and shrunken, with limbs shrivelled and the skin lying in folds, too weak to raise, or at least hold, their heads from the pillow, vomiting nearly all the nutriment taken, stools frequent and thin, resulting in great part from molecular disintegration of the tissues—presenting, indeed, an appearance seldom observed in any other disease except in the last stages of phthisis—and returning in late autumn with the cheerfulness, vigor, and rotundity of health. The localities usually preferred by the physicians of this city are the elevated portions of New Jersey and Northern Pennsylvania, the Highlands of the Hudson, the central and northern parts of New York State, and Northern New England. Taken to a salubrious locality and properly fed, the infant soon begins to improve if the disease be still recent, unless it be exceptionally severe. If the disease have continued several weeks at the time of the removal, little benefit may be observed from the country residence until two or more weeks have elapsed.
An infant weakened and wasted by the summer diarrhoea, removed to a cool locality in the country, should be warmly dressed and kept indoor when the heavy night dew is falling. Patients sometimes become worse from injudicious exposure of this kind, the intestinal catarrh from which they are suffering being aggravated by taking cold, and perhaps rendered dysenteric.
Sometimes parents, not noticing the immediate improvement which they have been led to expect, return to the city without giving the country fair trial, and the life of the infant is then, as a rule, sacrificed. Returned to the foul air of the city while the weather is still warm, it sinks rapidly from an aggravation of the malady. Occasionally, the change from one rural locality to another, like the change from one wet-nurse to another, has a salutary effect. The infant, although it [p. 757] has recovered, should not be brought back while the weather is still warm. One attack of the disease does not diminish, but increases, the liability to a second seizure.
Medicinal Treatment.—The summer diarrhoea of infants requires, to some extent, different treatment in its early and later stages. We have seen that acids, especially the lactic and butyric, the results of faulty digestion, are produced abundantly, causing acid stools. In a few days the inflammatory irritation of the mucous follicles causes such an exaggerated secretion of mucus which is alkaline that the acid is nearly or quite neutralized. In the commencement of the attack these acid and irritating products should be as quickly as possible neutralized, while we endeavor to prevent their production by improving the diet and assisting the digestion. In the second stage, when the fecal matter is less acid and irritating from the large admixture of mucus, medicines are required to improve digestion and check the diarrhoea, while the indication for antacids is less urgent. Therefore it is convenient to consider separately the treatment which is proper in the commencement or first stage, and that which is required in the subsequent course of the disease.
First stage, or during the first three or four days, perhaps the first week.—Occasionally, it is proper to commence the treatment by the employment of some gentle purgative, especially when the disease begins abruptly after the use of indigestible and irritating food. A single dose of castor oil or syrup of rhubarb, or the two mixed, will remove the irritating substance, and afterward opiates or the remedies designed to control the disease can be more successfully employed. Ordinarily, such preliminary treatment is not required. Diarrhoea has generally continued a few days when the physician is summoned, and no irritating substance remains save the acid which is so abundantly generated in the intestines in this disease, and which we have the means of removing without purgation.
The same general plan of medicinal treatment is appropriate for the summer diarrhoea of infants as for diarrhoea from other causes; but the acid fermentation commonly present indicates the need of antacids, which should be employed in most of the mixtures used in the first stage as long as the stools have a decidedly acid reaction.
Those who accept the theory that this disease is produced by micro-organisms which lodge on the gastro-intestinal surface and produce diarrhoea by their irritating effect are naturally led to employ antiseptic remedies. Guaita administered for this purpose sodium benzoate. One drachm or a drachm and a half dissolved in three ounces of water were administered in twenty-four hours with, it is stated, good results.3 I have no experience in the use of antiseptic remedies.
3 N.Y. Med. Rec., May 31, 1884.
If by the appearance of the stools or the substance ejected from the stomach, or by the usual test of litmus-paper, the presence of an acid in an irritating quantity be ascertained or suspected, lime-water or a little sodium bicarbonate may be added to the food. The creta præparata of the Pharmacopoeia administered every two hours, or, which is more convenient, the mistura cretæ, is a useful antacid for such a case. The chalk should be finely triturated. By the alkalies alone, aided by the judicious use of stimulants, the disease is sometimes arrested, but, unless [p. 758] circumstances are favorable and the case be mild, other remedies are required.
Opium has long been used, and it retains its place as one of the important remedies in this disease. For the treatment of a young infant paregoric is a convenient opiate preparation. For the age of one to two months the dose is from three to five drops; for the age of six months, twelve drops, repeated every three hours or at longer intervals according to the state of the patient. After the age of six months the stronger preparations of opium are more commonly used. The tinctura opii deodorata or Squibb's liquor opii compositus may be given in doses of one drop at the age of one year. Dover's powder in doses of three-fourths of a grain, or the pulvis cretæ comp. cum opio in three-grain doses every third hour, may be given to an infant of one year.
Opium is, however, in general best given in mixtures which will be mentioned hereafter. It quiets the action of the intestines and diminishes the number of the evacuations. It is contraindicated or should be used with caution if cerebral symptoms are present. Sometimes in the commencement of the disease, when it begins abruptly from some error in diet, with high temperature, drowsiness, twitching of the limbs—symptoms which threaten eclampsia—opiates should be given cautiously before free evacuations occur from the bowels and the offending substance is expelled. Under such circumstances a few doses of the bromide of potassium are preferable. In the advanced stage of the disease also, when symptoms of spurious hydrocephalus occur, opium should be withheld or cautiously administered, since it might tend to increase the fatal stupor in which severe cases are apt to terminate.
The vegetable astringents, although they have been largely employed in the treatment of this as well as other forms of infantile diarrhoea, are, I think, much less frequently prescribed than formerly. I have entirely discarded them, since they are apt to be vomited and have not proved efficient in my practice. As a substitute for them the subnitrate of bismuth has come into use, and in much larger doses than were formerly employed. While it aids in checking the diarrhoea, it is an efficient antiemetic and antiseptic. It should be prescribed in ten or twelve grains for an infant of twelve months; larger doses produce no ill effect, for its action is almost entirely local and soothing to the inflamed surface with which it comes in contact. It undergoes a chemical change in the stomach and intestines, becoming black, being converted into the bismuth sulphide, and it causes dark stools. Rarely it gives rise in the infant to the well-known garlicky odor, like that occasionally observed in adult patients, and which Squibb thinks may be due to tellurium accidentally associated with the bismuth in its natural state. For those cases in which the symptoms are chiefly due to colitis, and the stools contain blood with a large proportion of mucus, it has been customary to prescribe laudanum or some other form of opium with castor oil. I prefer, however, the bismuth and opium for such cases as are more decidedly dysenteric, as well as for cases of the usual form of intestinal catarrh. In ordering bismuth in these large doses it is important that a pure article be dispensed.
The following are convenient and useful formulæ for a child of one year:[p. 759]
| Rx. | Tinct. opii deodorat. | minim xvj; |
| Bismuth. subnitrat. | drachm ij; | |
| Syrupi, | fluidrachm ij; | |
| Misturæ cretæ, | fluidrachm xiv. Misce. |
Shake thoroughly and give one teaspoonful every two to four hours.
| Rx. | Tinct. opii deodorat. | minim xvj; |
| Bismuth. subnitrat. | drachm ij; | |
| Syrupi, | fluidounce ss; | |
| Aq. cinnamomi, | fluidounce iss. Misce. |
Shake bottle; give one teaspoonful every two to four hours.
| Rx. | Bismuth. subnitrat. | drachm ij; |
| Pulv. cret. comp. c. opio, | drachm ss. Misce. |
Divid in Chart No. X. Dose, one powder every three hours.
| Rx. | Bismuth. subnitrat. | drachm ij; |
| Pulv. ipecac. comp. | gr. ix. Misce. |
Divid in Chart No. XII. Dose, one powder every three hours.
Cholera infantum requires similar treatment to that which is proper for the ordinary form of the summer diarrhoea, but there is no disease, unless it is pseudo-membranous croup, in which early and appropriate treatment is more urgently required, since the tendency is to rapid sinking and death. As early as possible, therefore, proper instructions should be given in regard to the feeding, and for an infant between the ages of eight and twelve months either one of the above prescriptions should be given or the following:
| Rx. | Tinct. opii deodorat. | minim xvj; |
| Spts. ammon. aromat. | fluidrachm j; | |
| Bismuth. subnitrat. | drachm ij; | |
| Syrupi, | fluidounce ss; | |
| Misturæ cretæ, | fluidounce iss. Misce. |
Shake bottle. Give one teaspoonful every two or three hours.
An infant of six months can take one-half the dose, and one of three or four months one-third or one-fourth the dose, of either of the above mixtures.
If cerebral symptoms appear, as rolling the head, drowsiness, etc., I usually write the prescription without the opiate; and with this omission it may be given more frequently if the case require it, while the opiate prescribed alone or with bromide of potassium is given guardedly and at longer intervals. Although every day during the summer months I have written the above prescriptions, it has been several years since any case has occurred in my practice which led me to regret the use of the opiate; but it must not be forgotten that there is danger in the summer complaint, and especially in cholera infantum, of the sudden supervention of stupor, amounting even to coma, and ending fatally. A few instances have come to my knowledge in which, when death occurred in this way, the friends believed that the melancholy result was hastened by the medicine. But injury to the patient in this respect can only occur, in my opinion, through carelessness in not giving proper attention to his condition. It is chiefly in advanced cases, when the vital powers are beginning to fail, when the innervation is deficient, and the cerebral circulation sluggish, that the use of opiates may involve danger. Explicit and positive directions should [p. 760]be given to omit the opiate or give it less frequently whenever the evacuations are checked wholly or partially and signs of stupor appear.
Second Stage.—The summer complaint in a large proportion of cases begins in such a gradual way that the treatment which we are about to recommend is proper in many instances at the first visit of the physician, who is frequently not summoned till the attack has continued one or two weeks. The alkaline treatment recommended above for the diarrhoea in its commencement does not aid digestion sufficiently to justify its continuance as the main remedy after the first few days. In a large number of instances, however, one of the above alkaline mixtures may be given with advantage midway between the nursings or feedings, while those remedies, presently to be mentioned, which facilitate digestion and assimilation are given at the time of the reception of food.
Some physicians of large experience, as Henoch of Berlin, recommend small doses of calomel, as the twelfth or twentieth of a grain, three or four times daily for infants with faulty digestion and diarrhoea. To me, this seems an uncertain remedy, without sufficient indications for its use, and I have therefore no experience with it. The following are formulæ which I employ in my own practice, and which have been employed with apparent good results in the institutions of New York:
| Rx. | Acid. muriat. dilut. | minim xvj; |
| Pepsinæ saccharat. (Hawley's or other good pepsin), | drachm j; | |
| Bismuth. subnitrat. | drachm ij; | |
| Syrupi, | fluidrachm ij; | |
| Aquæ, | fluidrachm xiv. M. |
Shake bottle; give one teaspoonful before each feeding or nursing to an infant of one year; half a teaspoonful to one of six months.
| Rx. | Tinct. opii deodorat. | minim xvj; |
| Acid. muriat. dilut. | minim xvj; | |
| Pepsinæ saccharat. | drachm j; | |
| Bismuth. subnitrat. | drachm ij; | |
| Syrupi, | fluidrachm ij; | |
| Aquæ, | fluidrachm xiv. Misce. |
Shake bottle; give one teaspoonful every three hours to a child of one year; half a teaspoonful to one of six months.
| Rx. | Pepsinæ saccharat. | drachm j-ij; |
| Bismuth. subnitrat. | drachm ij. Misce. |
Divid in Chart No. XII. One powder every three hours to a child of one year; half a powder to one of six months.
I have also obtained apparent benefit from lactopeptin, given as a substitute for one of the above mixtures before each feeding or nursing. In several instances which I recall to mind I have ordered as much as could be placed on a ten-cent piece to be given every second or third hour, while midway between the feedings in some instances of considerable diarrhoea one of the mixtures of bismuth and chalk recommended above was employed, and the result has been good.
Enemata.—It will be recollected, from our remarks on the anatomical characters, that inflammatory lesions are commonly present in the entire length of the colon, and that at the sigmoid flexure, where acid and irritating fecal matter is probably longest delayed in its passage downward, the colitis is usually most severe. Aware of this fact, I was [p. 761] led to prescribe at my first visit a large clyster of warm water, given with the fountain or Davidson's rubber syringe, especially in cases in which the stools showed mucus or mucus tinged with blood. This, given with the lower part of the body raised a little above the level of the shoulders, washes out the large intestine and has a soothing effect upon its surface. The benzoate of sodium may be added to the water for its antiseptic effect, as in the following formula:
| Rx. | Sodii benzoat. | drachm j; |
| Aquæ, | pint j. Misce. |
In occasional cases in which the stomach is very irritable, so that medicines given by the mouth are in great part rejected, our reliance must be largely on rectal medication, and especially on clysters containing an opiate. Laudanum may be given in this manner with marked benefit. It may be given mixed with a little starch-water, and the best instrument for administering it is a small glass or gutta-percha syringe, the nurse retaining the enema for a time by means of a compress. Beck in his Infant Therapeutics advises to give by the clyster twice as much of the opiate as would be required by the mouth. A somewhat larger proportion may, however, be safely employed. The following formula for a clyster has given me more satisfaction than any other medicated enema which I have employed:
| Rx. | Argent. nitrat. | gr. iv; |
| Bismuth. subnitrat. | oz. ss; | |
| Mucilag. acaciæ, | ||
| Aquæ, aa | fluidounce ij. Misce. |
One-quarter to one half of this should be given at a time, with the addition of as much laudanum as is thought proper; and it should be retained by the compress. It is especially useful when from the large amount of mucus or mucus tinged with blood it is probable that the descending colon is chiefly involved.
Alcoholic stimulants are required almost from the commencement of the disease, and they should be employed in all protracted cases. Whiskey or brandy is the best of these stimulants, and it should be given in small doses at intervals of two hours. I usually order three or four drops for an infant of one month, and an additional drop or two drops for each additional month. The stimulant is not only useful in sustaining the vital powers, but it also aids in relieving the irritability of the stomach and in preventing hypostasis in depending portions of the lung and brain, which, as we have seen, is so frequent in advanced cases.
The vomiting which is so common a symptom in many cases greatly increases the prostration, and should be immediately relieved if possible. The following formulæ will be found useful for it:
| Rx. | Bismuth. subnitrat. | drachm ij; |
| Spts. ammon. aromat. | fluidrachm ss-fluidrachm j; | |
| Syrupi, | ||
| Aquæ, aa | fluidounce j. Misce. |
Shake bottle. Dose, one teaspoonful half-hourly or hourly if required, made cold by a piece of ice.
| Rx. | Acid. carbolic. | gtt. ij; |
| Liquor. calcis, | fluidounce ij. Misce. |
Dose, one teaspoonful, with a teaspoonful of milk (breast-milk if the baby nurse), to be repeated according to the nausea.
[p. 762] Lime-water with an equal quantity of milk often relieves the nausea when it is due to acids in the stomach, but it is rendered more effectual in certain cases by the addition of carbolic acid, which tends to check any fermentative process. Perhaps also some of the recent antiseptic medicines introduced into our Pharmacopoeia, as the benzoate of sodium, may be found useful for the vomiting. A minute dose of tincture of ipecacuanha, as one-eighth of a drop in a teaspoonful of ice-water, frequently repeated, has also been employed with alleged benefit.
Of these various antiemetics, my preference is for the bismuth in large doses, with the aromatic spirits of ammonia, properly diluted, that the ammonia do not irritate the stomach. Nevertheless, in certain patients the nausea is very obstinate, and all these remedies fail. In such cases absolute quiet of the infant on its back, the administration of but little nutriment at a time, mustard over the epigastrium, and the use of an occasional small piece of ice or the use of carbonic acid water with ice in it, may relieve this symptom.
In protracted cases, when the vital powers begin to fail, as indicated by pallor, more or less emaciation, and loss of strength, the following is the best tonic mixture with which I am acquainted. It aids in restraining the diarrhoea, while it increases the appetite and strength. It should not be prescribed until the inflammation has assumed a subacute or chronic character:
| Rx. | Tinct. calumbæ, | fluidrachm iij; |
| Liq. ferri nitratis, | minim xxvij; | |
| Syrupi, | fluidounce iij. Misce. |
Dose, one teaspoonful every three or four hours to an infant of one year.
SYNONYMS.—Membranous enteritis; Infarctus (Kaempf); Diarrhoea tubularis, Tubular looseness (Good); Follicular colonic dyspepsia, Follicular duodenal dyspepsia (Todd); Pellicular enteritis (Simpson); Pseudo-membranous enteritis (Cruveilhier); Pseudo-membraneuse entérite (Laboulbène); Painful affection of the intestinal canal (Powell); Mucous disease (Whitehead); Hypochondriasis pituitosa (Fracassini); Fibrinous diarrhoea (Grantham); Mucous disease of the colon (Clark); Chronic, catarrhal, or mucous diarrhoea; Colique glaireuse (of the French); Chronic exudative enteritis (Hutchinson); Diarrhoea febrilis (Van Swieten); Paraplexia rheumatica, Chlorosis pituitosis, Diarrhoea pituitosa (Sauvages); Arthritis chlorotica (Musgrave); Colica pituitosa (Sennertus); Scelotyrbe pituitosa (Perywinger); Mucositas intestinalis colloides, Concretiones gelatiniformes intestinales (Laboulbène); Tubular exudation-casts of the intestines (Hutchinson).
DEFINITION.—The disease is a non-febrile affection, consisting in a peculiar, and usually persistent, morbid condition of the intestinal mucous membrane, marked by the periodical formation of viscous, shreddy, or tubular exudates composed chiefly of mucin, on the discharge of which temporary amelioration of the accompanying acute digestive and nervous symptoms occurs.
HISTORY.—Although no distinct and separate accounts of pseudo-membranous enteritis occur in the medical writings of the ancients, nor even in those dating up to the eighteenth century, yet there may occasionally be detected in some of the descriptions of certain pathological conditions grouped under such titles as colic, passage of gall-stones, tenesmus, coeliac and pituitous affections, diarrhoea, dysentery, etc., the peculiar features of the disease under consideration. This confusion ruled up to a comparatively recent time. J. Mason Good,1 writing in the first quarter of the nineteenth century, groups the disease as a species of diarrhoea—diarrhoea tubularis—and remarks that he had "never hitherto seen this species classified, and not often described, although it occurred frequently in practice."
1 Study of Medicine, 1822.
Aretæus,2 in the second century, in discussing the subject of dysentery, speaks of alvine discharges sometimes occurring of a substance of considerable length, in many respects not to be distinguished from a sound piece of intestine, which he regarded as the inner coating of the bowel. [p. 764] This false interpretation of a fact arose from the circumstance that the membranous exudate occasionally assumes a tubular form, bearing the impress of the inner surface of the bowel upon which it is formed, and was perpetuated up to a comparatively recent period by successive authors. This error befell Simpson,3 Morgagni,4 Lancisi, and Spindler;5 the last of whom describes the material discharged as worked up into a "materia alba, longa, compacta."
2 Lib. ii. cap. ix.
3 Ed. Med. Essays, vol. v. p. 153, 1752.
4 31st Epistle.
5 Actis Nat. Cur., vol. v. p. 483.
Bauer6 under the title of "intestinal moles" describes in Haller's Disputations the discharges of this disease as "concreta fibrosa quædam pro parte pinguedine rara abducta, membranacea molarum ex utero muliebri rejectarum formam accurate sistentia."
6 "De Moles Intestinorum," Disputationes ad Morborum, Dresdæ, 1747, p. 463.
In the same volume Kaempf7 discourses on this subject under the title of "infarction of the intestinal vessels," and also in a separate treatise8 published somewhat later. In the latter he groups the disease with others of a far different nature, their only point of convergence being preternatural alvine discharges.
7 De Infarctu Vasorum Ventriculi, Basiliæ, 1751.
8 Abhandlungen von einer neuer methode der hartnackigsten Krankheiten die ihren Sitz im unterleibe haben, zu heilen, Leipzig, 1784.
Subsequent authors, as a rule, fell into the same error, and it was not until 1818 that membranous enteritis was discriminated by Powell9 from that condition in which we recognize the presence of gall-stones. Since then more correct views have prevailed, and the disease has now a recognized place in nosology.
9 Trans. of Col. of Phys. London, vol. vi. p. 106.
ETIOLOGY.—As in other diseases of obscure nature, so in this, there has been much divergence of opinion as to its cause.
The influence of age is striking, as it is rarely seen in childhood or in persons who have passed the forty-fifth year. Of my own cases, the youngest was forty, and the oldest fifty-four. Rilliet and Barthez10 state that membranous formations in the intestinal canal of children are very rare; that they always occupy the summits of the folds, rarely the intervals, of the mucous membrane; and that they are detached in layers of greater or less extent. They are not diphtheritic. Heyfelder11 has described similar exudations under the name of enteritis exudatoria.
10 Traité clinique pratique des Maladies des Enfants, t. i. p. 677, 1853.
11 Studien in Gabiete der Heilwissenschaft, p. 173.
Sex exerts as marked an influence as age, as the immense preponderance of cases occurs in females. In an analysis of 100 cases, 4 only occurred in males, 2 of which were children. All of my cases were women; with the exception of two cases occurring in males, the same experience is reported by Powell and by Copeland.
In regard to temperament, it is undoubted that the disease invades nervous and hypochondriacal subjects oftener than others, but all temperaments are liable in the presence of those enervative influences that degrade physical health and impair nerve-power. All of my patients belonged to the nervous type. Whitehead says that those of a phlegmatic temperament, not easily excited into action, or persons deficient in elasticity of fibre, compose all but a very small percentage of the sufferers from this [p. 765]complaint, and he had particularly noticed that a large proportion of the women have light flaxen hair, fair complexions, and white skins.
The determinative causes, whatever they may be, occasion perversion of nutrition and innervation of the gastro-intestinal canal, principally, I believe, by their action upon the ganglionic nerves presiding over those functions originating the peculiar exudatory phenomena of this disease. This condition of the nervous system once established, local irritation of any sort may precipitate an attack, and hence the multitudinous influences that have been assigned as exercising a causative agency, as exposure to wet and cold, coarse, bad food, fecal impaction, and the abuse of cathartic medicines, as alleged by Grantham,12 who asserts that the use of mercury, conjoined with a too frequent use of aperient agents, is the cause of the disease in every case.
12 Facts and Observations in Med. and Surg., 1849, p. 205.
Farr considered the irritation of the intestinal canal owing to a parasitic growth of a confervoid type (oscillatoria). This view is supported by no other authority than that of himself and Bennett, as nothing of this sort is recorded as occurring in the discharges of patients of other observers; certainly in mine there was no parasitic development. The presence of it in their cases may then be fairly regarded as accidental, or at least unessential.
Habershon regarded ovarian diseases and painful menstruation in the female, and prostatic diseases in the male, as exciting causes.
SYMPTOMS.—The most characteristic symptoms disclosing the presence of pseudo-membranous enteritis are those arising from derangements of the digestive organs. They are, in the beginning, vague and irregular in occurrence, or so over-veiled by associated disorders of the genito-urinary and nervous systems that their nature and import often escape recognition until, weeks, and even months, of fruitless medication addressed to these secondary phenomena having been expended, the disease assumes such severity and presents such a complex of peculiar symptoms that it no longer eludes identification.
The disease rarely starts as an acute affection; sometimes it is subacute, but in the great majority of cases its course is chronic. Its initiation is marked with symptoms of gastro-intestinal disturbances—irregularity of the bowels, constipation and diarrhoea alternately; and dyspeptic annoyance of one sort or another—capricious appetite, nausea or vomiting, and pyrosis, usually increased by liquid diet. In Dunhill's case there was almost daily vomiting of mucus and pus streaked with blood, and occasionally pure blood. This prominence of gastric derangement supplies an explanation why Todd conferred upon the disease the title of follicular dyspepsia.
There is a sense of discomfort, soreness, or rawness of the abdomen, especially along the line of the colon, and in two of my cases the rectum was tender and raw, which augmented to decided pain in sitting or riding, and the abdominal muscles were tense; a feeling of heat or burning in the bowels often occurs, and almost always more or less lassitude and mental depression. These symptoms aggravate, especially upon indiscretions in diet, exposure to wet, or indeed under any sort of enervative influences, at irregular intervals. Their persistence finally induces grave disorders of nutrition, marked by the blood becoming poor and thin, by sluggish [p. 766]circulation and local congestions in the pelvic and abdominal viscera, and loss of strength and flesh. Yet certain patients seem to retain their flesh for a long time, as I have seen, after suffering several years from the disease. The depression of vital powers is still further manifested in a small, slow, soft pulse and a temperature running below the normal standard. The tongue is usually moist, pale, and flabby, and coated with a pearl-white or yellowish-white coating; sometimes, however, it is raw, red, tender, and fissured, or patchy from exfoliation of the mucous coating. The gums and cheeks are usually pale and bloodless, and often the seat of small roundish painful ulcers, which occasionally invade the palate and throat. Grantham13 says that ulceration of a phagedænic kind sometimes forms on the tonsils. The complexion usually assumes a muddy or flavescent tint, which during the attack may deepen to a jaundiced hue. At other times it presents a transparent or waxy appearance.
13 Op. cit., p. 204.
The skin is dry and furfy, sometimes cold and clammy, or, from over-action of the sebaceous glands, greasy. There is a disposition, especially on the chest, neck, and face, to papular eruptions or even phlegmonous or carbuncular inflammation.
The urine is high-colored and loaded with abundant phosphates, which in cooling precipitate as a heavy deposit. The bladder is often irritable, and discharges more or less mucus. According to Grantham,14 patients occasionally pass urine with evident traces of albumen, and seldom containing a normal quantity of phosphates. On an increase in fever or mental excitement a larger quantity than natural of the lithate of ammonium is found; frequently the mucous membrane of the bladder is found thickened in these cases.
14 Op. cit., p. 204.
The characteristic symptom, however, of this disease is the periodical formation and discharge of mucous exudates varying in physical appearances and frequency. The discharge may occur daily, with every stool, or at irregular intervals—a week, month, or longer—but usually in from twelve to fifteen days. The recurrence may be precipitated by irregularity in diet, exposure to wet and cold, or by excesses of any sort. The paroxysm is marked by tormina or severe pain, which may resemble that of colic or that of the passage of a biliary calculus, extending down the thighs or to the bladder, in the latter case sometimes causing retention, requiring the use of the catheter. The pain is usually referred to some part of the large intestine. In certain cases the paroxysm is announced by chills radiating from some point in the abdomen or even from other parts of the body.
After the paroxysm has endured two, three, or more days—usually a week—membranous exudates, either with a spontaneous or with an artificial movement of the bowels, are voided; after which there is a gradual assuagement of the local and general symptoms, but the patient experiences a sense of exhaustion or lassitude, and the tenderness of the abdomen and the irregularity of the bowels usually persist.
During the attack there is anorexia, but in the intervals the appetite remains fairly good, and the alvine discharges may assume quite a natural condition.
In the course of the disease there is more or less disturbance in the functions of the nervous system. During the paroxysm, when the [p. 767] sufferings are severe, the cast of symptoms running through the case is of a decidedly hypochondriacal type. At times, with the expulsion of the exudates and succeeding respite from suffering, there often occurs a mental rebound which lifts the patient from the slough of despair to the most hopeful anticipations of future health and happiness. In one of my cases this transition was remarkable. This hysterical type is common enough, and the irritability of the nervous system is still further manifested in the occurrence of irregular contractions of various groups of the voluntary muscles, as shown in hysterical tetanus, general convulsions, or chorea in children, or by paralyses of motion.
Copeland15 reports a case of a lady in whom this disease was complicated with the severest symptoms of hysteria, occasionally amounting to catalepsy. The paroxysms of pain recurred at intervals between four and six weeks, followed or attended by the discharge of large quantities of false membrane in pieces, and sometimes in perfect tubes. The menstrual flow was painful and irregular, accompanied with shreds of false membrane—not, however, contemporaneous with those of the intestine. The sensory nerves are often deranged, for in some cases there is paræsthesia—anæsthesia or hyperæsthesia—in limited areas of the skin. There is more or less headache, neuralgic pains in this or that nerve, or in several at the same time.
15 Dictionary of Medicine, vol. ii. p. 669.
The special senses do not escape; they manifest various forms of functional derangement. In one of my cases there were constant buzzing in the ears and perversion of the sense of smell, and in another the vision was thought impaired and the services of an oculist sought.
The uterine functions are always involved in greater or less degree. The menstruation is difficult and painful, and occasionally accompanied with membranous discharges. In one of my cases there was a uterine exudate, though the menopause had occurred several years before. Leucorrhoea and cervical inflammation are common.
PATHOLOGY.—Despite the fact that the disease in question, without being very frequent, is far from rare, little light has been shed upon its pathology. Indeed, even its individuality as an independent and distinct affection has been contested, although it is marked by a complex of symptoms as peculiar and characteristic as those of any other disease in the nosology.
There are those who maintain that the disease consists essentially in an inflammatory condition of the intestinal mucous membrane, either of the ordinary or of some specific type, croupous or diphtheritic. Copeland says the formation of the membranes depends upon a latent and prolonged state of inflammation extending along a very large portion, sometimes the greater part, of the intestinal canal, as is evinced by the quantity thrown off. Valleix16 dismisses the subject summarily with the delivery of the oracular judgment that the greater number of cases of this disease are dysenteric, and the remainder diphtheritic. Habershon is in full accord with this view, having, as he says, seen these membranous exudates "follow severe disease of the intestines of a dysenteric character, and sometimes associated with a state of chronic congestion of the liver, and often perpetuated by the presence of hemorrhoids, polypoid [p. 768] growths, etc." Wilks and Clark,17 after a full examination of the enteric exudates submitted to them, concluded that they are true casts of the large intestines produced by chronic inflammatory action of the mucous membrane and subsequent exudation. Conjectures have been ventured as to the exact anatomical structure in which the process occurs. Thus, Todd18 says that the proximate cause of the disease is dependent upon a morbid condition of the intestinal mucous follicles. Golding-Bird19 holds similar language. He says: "It is probable that the follicles are the principal seat of the disease, for we know that they sometimes secrete a dense mucus differing little in physical qualities from coagulated albumen or even fibrin." Livedey20 attributed the process to a morbid secretion into the mucous crypts.
16 Guide du Médecine practicien, vol. iii. p. 10.
17 Trans. Path. Society, vol. ix. p. 230.
18 Cyclopædia of Practical Medicine, vol. ii. p. 279.
19 Guy's Hospital Reports.
20 L'Union médicale, 1868.
Among those believing in its croupous nature was Powell, who assumed the character of the inflammation to be specific, and the exudate of the same nature and formed in the same manner as that of ordinary croup. This was the view entertained by Cruveilhier and Trousseau and other French authors. Good was misled in a similar manner, as shown by his statement that the exudation bears a striking resemblance to the fibrous exudation thrown forth from the trachea in croup. He says, however, that it is discharged in longer, firmer, and more compact tubes. Serres,21 in a dissertation upon pseudo-membranous colitis, confounds the exudate with that of thrush, muguet, and infective dysentery. Laboulbène,22 a later writer, also remarks that there are found in many treatises and in periodical literature a great number of occurrences of false membranes in the dejecta. Most of these cases are referable to dysentery, to muguet, hydatids, etc., but there remain a certain number which are owing to different inflammatory and non-diphtheritic affections of the digestive tube.
21 Thèse de Paris, No. 39, 1836.
22 Recherches cliniques et anatomiques sur les Affections pseudo-membraneuse, Paris, 1861.
Whitehead, in summing up his conclusions respecting the nature of the disease, compares it with dermic inflammation. He says: "The mucous membrane (intestinal), like the skin (and is not the one looked upon as an inversion of the other?), is prone under certain conditions in certain constitutions to develop products unnatural to its functions. It is not natural for the skin to produce eczema, neither is it natural for mucous surfaces to produce mucus in a concrete form; that the proximate cause of the symptoms referable to this disease is the hypersecretion and accumulation of mucus on the free surface of mucous membranes; such accumulations sheathe and prevent the healthy performance of the functions natural to the part, and thus induce immediate and remote results, the effect of such suppressed functions; that this hypersecretion indicates a want of balance between nerve-force and germinal matter, and that the nerve-force is perverted by irritation."
Simpson held similar views, and regarded the disease as a chronic pellicular or eruptive inflammation of the mucous lining of the bowels.23 Other observers have been inclined to ignore the inflammatory nature of the disease, at least as a primary condition, and have sought the proximate cause in some as yet undefined derangement of the nervous [p. 769] system. Thus, Clark does not regard the membranous exudates as the products of inflammation, properly so called—that is, of capillary blood-stasis which has preceded their formation—as the characteristic of such exudates is that they contain fibrin. He says the abnormal cell-forms present arise in some other way than by free cell-development out of an exuded blastema. Good24 asserts its dependence upon what he calls a "peculiar irritability of the villous membranes of the large intestines, which in consequence secrete an effusion of coagulating fibrin—fibrin mixed with albumen—instead of secreting mucus, occasionally accompanied with some degree of chronic inflammation."
23 Obstet. Works, Am. ed., p. 279.
24 Study of Medicine, op. cit.
Also, DaCosta doubts whether the disease is originally inflammatory at all. "Where inflammation," he says, "occurs, is it not secondary rather than primary, the result rather than the cause?" "Is not the true trouble in the nervous system, in the nerves presiding over secretion and nutrition in the abdominal viscera?"
Bennett and Byford represent the opinions of a very small minority who regard the disease as simply an expression of uterine derangement.
MORBID ANATOMY.—As none of the cases coming under my observation terminated fatally, no opportunity was offered to me of making personal investigation into the anatomical changes occurring in membranous enteritis. Such opportunities have been so rarely met with that, indeed, it may be said that the nature of these changes is wholly unknown.
Simpson alludes to a case of phthisis in which the patient had passed large quantities of "membranous crusts or tubes," and in which the mucous membrane of the colon was covered with an immense number of small spots of a clear white color, or vesicles, which, when punctured, discharged a small quantity of clear fluid; and also refers to the case of Wright, in which the mucous membrane of the colon and of the lower portion of the small intestine was studded everywhere with a thickly-set papular eruption.
My endoscopic examinations revealed, in the living subject, the intestinal mucous membrane of a red, verging into a scarlet color, thickened, and denuded of epithelium in patches of varying extent. This condition does not always invade the ampulla of the rectum, but with the long tube I am in the habit of using it was possible in all my cases to reach a point where it existed. The extent of diseased surface can only be conjectured by an inspection of the exudates and by abdominal palpation.
In most cases the exudate is restricted to the large intestines—colon and rectum—and often to a circumscribed portion of them; but in rare cases its length and quantity would seem to indicate that extensive portions of the surface are covered. One of the most remarkable cases recorded is that of a woman forty years old who had been sick for five years with gastro-intestinal derangement. Suddenly the case became acute, and after much suffering she passed membranous exudates three millimeters in thickness and many centimeters long, weighing in all three kilograms.25
25 Recueil de Mémoires de Médecine, de Chirurgie, et de Pharmacie militaires, tome xxxvii. p. 297, 1855.
Kaempf26 gives another case, in which the length of the membranes [p. 770] discharged was sevenfold greater than the stature of the patient. In Dunhill's27 case the patient had suffered from this disease for a long period, and during two years passed many yards of perfect cylindrical shape, many of them several feet in length, and sufficiently coherent to permit of their being handled, held up, etc. In one of my cases a perfect cylinder three-quarters of a yard long was voided.
26 Op. cit., p. 232.
27 Trans. of Path. Society of London, vol. ix. p. 188.
Laboulbène28 describes the gastro-intestinal false membrane as thin, soft, and granular, of a more or less yellow color, slightly adherent to the mucous membrane, and when stripped off forming a yellow pultaceous mass. He says it is first deposited in small, irregular, sparsely-scattered patches, located on the summits of the intestinal folds; afterward these patches increase, and cover the folds entirely and almost the whole calibre of the intestinal canal. The mucous membrane, he remarks, beneath the deposit is greatly inflamed.
28 Op. cit., p. 105.
Powell believes that at times the deposit extends as high as the duodenum, his opinion being solely based upon the clinical features of the disease. In the first of his cases the membrane was found in perfect tubes, some of them full half a yard in length, and certainly sufficient in quantity, he says, to have lined the whole intestinal canal.
In examining the membranes it is always best to float them from the fecal or other foreign material by passing the discharges in a clean vessel containing water. Their physical characters can then be readily studied. They are best preserved in a 10 per cent. solution of alcohol. The exudate consists usually of a single lamina, but at various points in certain cases several superposed laminæ may be observed, enclosing between them particles of undigested food of various kinds. In most cases the superficial layers are more opaque, drier, less elastic, and friable than the deeper.
The configuration of the exudate varies greatly. The more common variety is that occurring in loose, transparent, jelly-like masses, like the white of an egg or glue, tinged often with various hues of yellow. In three of my cases I noticed also the frequent occurrence of a thin, serous, yellow discharge. In some cases the discharge resembles pieces of macaroni, tallow, or wax; in others it assumes a shreddy or ribbon-like form; and in a still rarer class it is tubular, being an exact reprint of the surfaces from which detached. These tubular pieces are, however, more or less torn and broken into smaller fragments of an inch or two in length when discharged.
Its thickness also varies: sometimes it does not exceed that of the thinnest film, and at others it is a quarter of an inch or more.
Its consistence ranges from that degree of loose aggregation that permits elongation into stringy, breaking masses when fished up from the water in which it floats, to a firmness and tenacity that will enable it to be handled without fear of breakage.
The color differs in different cases. It is usually yellowish-white, but this is often modified by tints dependent upon admixture with extraneous matters from the intestinal canal—biliary coloring, blood from the rupture of the vessels beneath the exudate, or with blood and pus. It exhales a feculent odor.
The surfaces of the membranes are ordinarily smooth and uniform, but sometimes reticulated. Certain observers have described the outer [p. 771] surface of the tubular exudate as uniformly smooth, and the inner as broken and flaky at some points, at others ragged and flocculent, and in many places thrown into shallow folds, lying in some situations across, but chiefly along, the axis of the gut.
The microscopic characters of the exudate are pretty uniform. Wilks and Clark29 describe the surface of the tubes, examined with a linear magnifying power of forty diameters, as exhibiting the appearance of a gelatinous membraniform matrix traversed by a coarse network of opaque yellow lines, studded at their points of intersection by similarly colored rounded masses. From the larger network proceeds a smaller secondary network, and in the recesses of this were found, at close and regular intervals, well-defined round or oval openings, with elevated margins, resembling in size and appearance the mouths of the follicles of the great gut. With higher powers the exudate was found in many cases to consist of a structureless basement membrane, which in certain points showed a fibrous appearance, owing doubtless to the presence of filaments of mucin. Numerous irregular granular cells, as well as granules from the breaking up of these cells, thickly studded the surface of the membrane. In the specimens of Wilks and Clark the surface, besides being marked by the opaque yellow lines and dots, presented various foreign matters, such as bile-pigment, earthy and fatty granules, portions of husks of seed, gritty tissues of a pear, a peculiar form of elastic tissue, stellate vegetable hairs, and a mucedinous fungus. Clark, in describing the fibres found between the layers of the exudates, says that they exhibited a very distinct and regular transverse striation, approaching in character that found in the ligamentum nuchæ of the giraffe. Quekett and Brooke have met with the same fibres in the feces. The transverse division depends probably upon beginning decay. The division is sometimes so distinct and complete as to lead, according to Beale,30 to their confounding with confervoid growths. Farre31 actually describes the formation as of a confervoid character.
29 Op. cit., p. 232.
30 The Microscope in Medicine, p. 194.
31 Trans. Microscopical Society.
Here and there, in my specimens, were observed scattered epithelial cells which were occasionally gathered in patches. Small colored masses of irregular shape, doubtless of fecal origin, were also noticed. The cells imbedded in the matrix, according to the above-quoted observers, consisted of two kinds—one more or less spherical, the other more or less cylindrical. In size the spherical cells varied from 1/2000 to 1/800 of an inch in diameter. The smaller cells had no distinct cell-walls. Some of the larger cells were filled with fat-granules, and represented granular cells; others had a single or double vesicular nucleus; a few were acuminated at two opposite points and somewhat compressed. All the other cells possessed demonstrable cell-walls. The cylindrical cells resembled in their general characters those which normally coat the mucous membrane of the larger gut, but they were much more elongated, compressed, and firmly matted together. Many of the more elongated cells were constricted in the middle, and exhibited a nucleus on each side of the constriction. The more or less spherical cells occupied the attached, and the cylindrical cells the free, surface of the membranous tubes.
The perforations in the matrix were of uniform size and appearance, [p. 772] surrounded by elevated margins formed of closely-grouped cylindrical cells, and led to two kinds of pits—one short and flask-shaped, the other long and uniformly cylindrical. The flask-shaped pits were about one-tenth of an inch in diameter and distinctly hollow. The wall of each pit was made up of one or two layers of subspheroidal cells, held together by an amorphous stroma. A few of these follicles contained a deposit which was opaque in situ, and which when broken up was found to consist of large flattened nuclear cells, analogous to those met with in epithelial growths.
The cylindrical pits were also for the most part hollow, about one-sixteenth of a line in length and one-thirty-first of a line in breadth. These walls, devoid of membrane, were composed of small, more or less spherical cells in various stages of development, imbedded in a gelatinous matrix.
In examining the chemical characters of the specimens obtained in my cases the membranes were thoroughly washed, when they were nearly as colorless as the water in which they floated. They were drained on a sieve, and presented a gelatinous appearance, much like the white of an egg. Their specific gravity was about that of distilled water. When treated with strong alcohol, the membranes shrank and assumed a striated appearance. Chemical tests of tincture of guaiacum, peroxide of hydrogen, and others failed to show the presence of fibrin or albumen. Treated with ether, globules of fatty matter were obtained, which were identified by their microscopical characters and by their reaction with osmic acid. By boiling the liquid in which the membranes had been soaked it became faintly hazy, indicating a trace only of albumen. Faint evidence of the presence of this body was also presented by picric acid and Mehu's test. Treated with a weak solution of caustic potassa and heat, the membrane dissolved, leaving a little haziness. The liquid was then filtered, and exactly neutralized with acetic acid, and plumbic acetate added, when a copious precipitate was formed. Mercuric chloride and potassic ferrocyanide failed to produce this effect. From these and other tests used the conclusion was reached that these membranes were composed essentially of mucin.
Both the microscopical and chemical characters of the exudates of the disease under consideration show that they are widely different in nature from those of other diseases. They are evidently a production of the muciparous glands (follicles of Lieberkühn) of the intestinal canal, and consist essentially of mucin. Perroud32 concluded from his analysis that they contain a small quantity of albumen, but are principally formed of the same substance as that which enters into the composition of the epidermis. The exudates of other diseases of the alimentary mucous membrane contain albumen and fibrin, as well as molecular or homogeneous filaments. The ordinary croupous exudate, according to Cornil and Ranvier, always contains filaments of fibrin, sometimes mucin and pus-corpuscles mingled with the cellular constituents, which vary in character with the locality of the inflammation. The filaments form a reticulum in the meshes of which are contained the other elements.
32 Journal de Médecine de Lyon, 1864.
Diphtheritic exudates, as shown by Lehmann,33 consist of fibrin, a large [p. 773] quantity of fatty matter, and 4 per cent. of earthy phosphates, while its structure is made up of epithelial cells united together, which, becoming infiltrated with an albuminous substance and gradually losing their nuclei and walls, are finally converted into homogeneous branching masses. The cells of these masses are liable to undergo fibrinous degeneration. The inflammation determining the exudate is not confined to the conglomerate glands, but involves all the textural elements of the part affected, and the material of the membrane originates from the capillary disturbance in them.
33 Lehrbuch der Physiolog. Chemie, Leipzig, 1855.
Andrew Clark34 states that he has observed in his studies of exuded blastema, the product of diseased action in mucous membranes, three varieties. The first is clear, jelly-like, and imperfectly membranous. The second is yellowish, semi-opaque, flaky, and usually membranous. The third is yellowish-white, dense, opaque, distinctly membranous, tough, and rather firmly adherent to the subjacent surface. The first contains only the merest trace of albumen, and no fibrin; the second contains an abundance of albumen, and no fibrin; the third contains both albumen and fibrin in abundance, the latter in a fibrillated form. They all contain the same cell-forms. Yet it is to be noticed that in the first variety there is no evidence of transudation or exudation; in the second, no evidence of a true exudation; and that in the third, in which the existence of a true inflammatory exudation is undeniable, the only additional structural element present is fibre.
34 Op. cit., p. 133.
DIAGNOSIS.—The diagnosis of membranous enteritis can never in its advance, and rarely in its early stages, present much difficulty. Its chronic course, irregular exacerbations, lack of febrile excitement, the persistent derangement of the intestinal canal, the mental depression, the gradual impairment of health, the various visceral complications, and, lastly and chiefly, the peculiar character of the alvine discharges,—stamp the disease with an individuality entirely its own.
The mucous discharges of certain forms of chronic diarrhoea and the membranous discharges of infective dysentery are all so different in physical character, and are associated with such a different complex of general symptoms, that they cannot be confounded with those of the diseases in question. The peculiar irritative quickness of the pulse of ordinary enteritis, according to Powell and Good, suffices to differentiate this disease from membranous enteritis. The peculiarities of the physical and chemical properties of these exudates, already fully dwelt upon, not only distinguish them from those of the above diseases, but also from such dejecta as may contain fragments of undigested connective tissue, of hydatids, or of worms. The flakes of mucus discharged from the bowels in protracted constipation, fissura ani, and in the later stages of cirrhosis of the liver are composed of mucus in which are found imbedded epithelial cells from the colon and mucus-corpuscles. The microscope will also reveal the character of the fatty discharges that may be associated with diseases of the pancreas, liver, and duodenum. The mucous flakes of cholera stools are composed of masses of intestinal epithelium mixed with amorphous and granular matter, crystals of different substances, and, according to Davaine, of parasitic forms, particularly the Circomonas hominis.
[p. 774] Membranous casts from the upper part of the digestive track are, in rare cases, passed by the bowels. One of the most curious instances of this sort is reported by Villermé:35 A woman swallowed a tablespoonful of nitric acid, and seventy days afterward a long membranous exudate, one or two lines thick and of a brown color, was discharged, which corresponded in form with the oesophagus and stomach. The patient died a few days later.
35 Dictionnaire des Sciences médicales, tome xxxii. p. 264.
PROGNOSIS.—The prognosis of the disease as regards life is not unfavorable, but as regards permanent restoration to health and strength the case is entirely different. Theden36 and Hoffman37 have, however, stated that the disease is not an unfrequent cause of sudden death.
36 Remarques et Experiences, tome ii.
37 Med. Ration., vol. v.
Abercrombie38 records a case of death from phthisis complicated with this disease, and Wright another case in which the patient died in an extreme state of marasmus. The acute and subacute forms are more amenable to treatment, and the chances are correspondingly greater of permanent recovery, though in all cases there is a strong tendency to relapse. The chronic forms may almost be enrolled among the opprobria medicorum when once they have made deep inroads upon nutrition and the vital powers, and produced that condition named by Todd the pituitous cachexia (cachexia pituitosa). These cases may, however, be alleviated by judicious treatment, diet, and climatic changes, but repeated relapses may be expected as the rule under slight exciting causes or even without apparent cause. Patients under these circumstances drag out a life of valetudinarianism, but it may be cut short at any time by the supervention of some intercurrent disease, as phthisis, renal degeneration, etc., or, according to Grantham, atrophy of the intestines. Broca39 records two cases of this disease, one of which lasted ten and the other fifteen years. Three of my cases have endured over six years.
38 Inflamm. Affec. of Mucous Memb. of Intestines, pp. 213, 279.
39 Bullétin de la Société Anat. de Paris, 1854.
TREATMENT.—The treatment of membranous enteritis embraces medical and hygienic measures. The medical means have for their object, first, the removal of the membranous exudation when it has once formed; and, second, to correct the conditions upon which its formation depends by improving nutrition and invigorating the nervous system. The severe sufferings of the paroxysms are greatly alleviated and the duration of this stage cut short by freely emptying the bowels. The best means to do this is by the injection of hot water with the long elastic bougie three or four times a day, and to assist this with laxatives. Instead of water, solutions of potassa, soda, and lime-water are preferred by some practitioners. As a rule, the enemata cause considerable discomfort, but in the end are followed by improvement in the condition of the bowels. The best laxative is emulsion of castor oil, but occasionally a mercurial, guarded by the extract of belladonna, will furnish more marked relief. Powell and Copeland say that they have employed with decided advantage a purgative consisting of the compound infusion of gentian and infusion of senna, to which were added ten or twenty minims of liquor potassæ. This was repeated, so that four stools in the twenty-four hours were obtained. Clark preferred to regulate the bowels, when needed, with rhubarb, soda, and [p. 775] ipecac, conjoined or not, as required, with mercury and chalk. Good recommends four grains of Plummer's pill every night, and the bowels kept open by two drachms of sublimed sulphur daily. It should always be borne in mind that all active or irritating purgatives are harmful. The bowels by this treatment will not only be disembarrassed of the membranous exudates, but also of any fecal collection the retention of which would surely cause irritation, as occasionally happens even when there is an apparent diarrhoea. This condition may be easily determined by abdominal palpation. The relief from pain procured by free evacuation of the intestine will be enhanced by the employment of hot fomentations to the abdomen. Despite these means, its severity may, however, demand the administration of narcotics. The best form will be a hypodermic injection of a sixth or a quarter of a grain of morphia; enemata of starch and laudanum are also beneficial. Burrows mentions a case in which he succeeded in allaying nervous irritation by the nightly use of thirty drops of laudanum. The patient noticed that the habitual constipation was increased when the accustomed narcotic was omitted. Bromide of potassium in large doses long continued will also be found useful for the same purpose.
During the intervals of the paroxysms local medication of the bowels and medical and hygienic measures should be had recourse to to prevent the re-formation of the exudates by modifying the vital activities of the intestinal mucous membrane and by restoring the general tone of the constitutional powers. For local treatment the nitrate of silver, sulphate of zinc, the sulphate of copper dissolved in glycerin, the tincture of iodine, and carbolic acid cannot be over-prized. From five to ten grains of the metallic salts, fifteen drops of tincture of iodine, ten of the acid, administered through the long rubber tube, are suitable doses to begin with. I am also in the habit of using stronger solutions by mopping it on to the bowel through the endoscopic tube. Kaempf made frequent and large injections of decoctions of various plants—saponaria, taraxacum, etc.—which he imagined possessed dissolvent and resolvent virtues. Cumming40 speaks highly of the efficacy of electricity.
40 Lond. Med. Gazette, 3d Series, vol. ix.
For the purpose of improving the general health the preparations of iron are advisable, of which the best are the tincture of the chloride, pernitrate, pyrophosphate, lactate, and potassio-tartrate. Habershon advises infusions of the bitter tonics with hydrocyanic and nitro-muriatic acid. I have found a combination of these acids with henbane and infusion of serpentaria useful. I also employ hot solutions of the latter acid as a local bath over the abdominal region, applied with a large sponge. Clark speaks favorably of the extract of nux vomica and astringent remedies. Simpson praises the oleo-resins under the form of pitch pills and tar, while Clark and others laud copaiba and turpentine. Good advises the copaiba to be given by enema when it cannot be borne by the stomach. Brodie used cubebs in small doses.
The alterative effects of small doses of arsenic, corrosive sublimate, sulphate of copper, etc. may be tried in obstinate cases. Grantham in the early stages of the complaint advises the use of ten grains of iodide of potassium combined with one-quarter of a grain of morphia at bed-time. He [p. 776] also strongly urges the use of cod-liver oil, which, he says, improves the strength and increases the flesh, lessens the spasmodic pains, but does not check the discharges.
Counter-irritation of the abdominal region with tincture of iodine, fly blisters, mustard, etc. has afforded little if any advantage. Dunhill kept a blister open for six months without any good results.
The mineral waters of Pyrmont, Harrogate, and Carlsbad have been found serviceable; the latter, Henoch41 says, should be preferred before all.
41 Klinik der Unterleub. Krankheiten, p. 668.
The case will amend more speedily and surely by the adoption of those sanitary measures, as regards clothing, diet, bathing, exercise, and change of climate, which have such important influences upon health. The healthy performance of the functions of the skin is of such paramount necessity in maintaining that of the intestinal canal that the patient should endeavor to avoid any exposure likely to lead to checked perspiration, and should use flannel underwear and stimulate the skin by friction with the hand or the flesh-brush. The diet should be graded to the ability of the stomach to digest and the body to assimilate. Our chief reliance will be upon milk, plain or peptonized, eggs, and beef given in the various forms of acceptable preparations, so as not to impair the tone of the stomach nor clog the appetite by sameness. Such vegetables and fruits as agree with the patient may be allowed. I have tried exclusive diets of milk, farinacea, and meat without marked benefit. All stimulants, tea, and coffee should as a rule be interdicted.
Systematic exercise in the open air and change of climate to a cool, dry, bracing atmosphere will contribute to comfortable existence, if not lead to recovery.
DEFINITION.—Dysentery is the clinical expression of a disease of the large intestine, of specific and non-specific (catarrhal) origin and form; characterized by hyperæmia, infiltration, and necrosis (ulceration) of its mucous membrane; distinguished by discharges of mucus, blood, pus, and tissue-débris; and attended with griping and expulsive pains (tormina and tenesmus).
ETYMOLOGY.—The name is compounded of the two Greek words [Greek: dys enteron], which, though untranslatable literally into English, have long since received the exact Latin equivalent, difficultas intestinorum. With appropriate alteration the same name is still employed in every civilized language in the common as well as the classical description of the disease. The French synonym, colite, locates the anatomical seat of the disease, while the German Ruhr and the English flux express one of its cardinal symptoms, the frequency (flow) of the evacuations.
HISTORY.—Ancient.—In its clinical history dysentery is one of the oldest known diseases, the name being found in common use before the time of Hippocrates, as in the often-quoted passage from Herodotus (443 B.C.), who relates that it and the plague reduced the army of Xerxes on the desert plains of Thessaly.
Fayrer informs us that in the ancient system of Hindoo medicine of the Ayur Veda, and in the commentaries of Dhanwantari, Charaka, and Sussutra, which carry us back nearly three thousand years, and in later Sanskrit writers, dysentery is described by the name of atisar, under two forms—amapake, or acute, and pakistar, or chronic; these again are subdivided into six varieties, ascribed by those ancient sages to changes in air, bile, phlegm, food, or to perturbations of the emotions and passions.
Hippocrates (430 B.C.) makes frequent reference to the disease, the nature of which he regards as a descent of the humors from the brain. "Men of a phlegmatic temperament are liable to have dysenteries," he says, "and women also, from the humidity of their bodies, the phlegm descending downward from the brain."
"The disease is caused," he says more exactly in another place, "by the overflow of phlegm and bile to the veins of the belly, producing ulceration and erosion of the intestine." In his country, at least, it seemed most to prevail in spring, but it was clearly connected with the heat and moisture of this season in Greece—prime factors everywhere in the genesis of the disease: "For when suffocating heat sets in all of a [p. 778] sudden while the earth is moistened by the vernal showers and by the south wind, the heat is necessarily doubled from the earth, which is thus soaked by the rain and heated by a burning sun, while at the same time men's bellies are not in an orderly state, nor is the brain properly dried." Of the prognosis he observes with great acumen, "Dysenteries when they set in with fever ... or with inflammation of the liver and hypochondrium or of the stomach, ... all these are bad. But such dysenteries as are of a beneficial nature and are attended with blood and scrapings of the bowels cease on the seventh or thirtieth day, or within that period. In such cases even a pregnant woman may recover and not suffer abortion;" whereas, "dysentery if it commence with black bile is mortal." Galen comments upon this statement that such a discharge is as incurable as cancer. The practitioner of our day will interpret this assertion, which was repeated with singular unanimity by all the writers of antiquity, with the belief that the black bile was blood, and that such cases really were cancers. Indeed, Paulus Ægineta distinctly says, "Dysentery arising from black bile is necessarily fatal, as indicating an ulcerated cancer."
Thus, although dysentery is among the oldest of the known maladies, and was recognized then as now by the same symptoms, the disease was by no means closely defined or differentiated in ancient times. As Ackermann long ago pointed out, many other affections were included under the term dysentery, and some of the symptoms of true dysentery, notably the tenesmus, were raised to the dignity of distinct diseases.
The gravity of the so-called lotura carnea, the fleshy stools, was fully appreciated by Hippocrates, as is evidenced by the remark that "if in a person ill of dysentery substances resembling flesh be discharged from the bowels, it is a mortal symptom." Fleshy masses, [Greek: xysmata], scrapings of the guts (originally epidermic exfoliations from the bodies of gladiators, used in pills as a tonic), were frequently alluded to by the older writers, more especially by Aretæus, in description of the discharges of dysentery. Hippocrates was also aware of the fact that dysentery may be a secondary as well as a primary malady. "One may expect," he says in speaking of the victims of gangrene, "that such patients will be attacked with dysentery; for dysentery usually supervenes in cases of mortification and of hemorrhage from wounds." Finally, Hippocrates recognized the effects of emesis in relief of the disease with the remark in one of his aphorisms that a spontaneous vomiting cures dysentery.
Celsus (25 B.C.-45 A.D.), the great encyclopædist, whose works "constitute the greatest literary monument since the days of Hippocrates," compiles all the information obtained up to his time; but it is plain as regards dysentery, though he defines it in terms that might stand in a modern text-book, that he has nothing new to add to the knowledge of the Hippocratic school. He named the disease from one of its most prominent symptoms, tormina (tenesmus he considered a separate affection), speaks of the stools as being mixed with mucus and fleshy masses, and in its treatment especially enjoins rest, "as all motion proves injurious to the ulcer."
Aretæus (50 A.D.), of all the authors of antiquity, wrote the most perfect and at the same time the most picturesque account of the morbid anatomy and symptomatology of this disease. The gross appearance of the ulcers in the intestine and the common character of the discharges he [p. 779] describes with the accuracy of the modern pathologist and the ardor of the true clinician. He speaks of the superficial, the deep-seated, the irritable, and the callous ulcer. There is, he says, "another larger species of ulcers, with thick edges, rough, unequal, callous, as we would call a knot of wood; these are difficult to cure, for they do not readily cicatrize, and the cicatrices are easily dissolved." Their tendency to arrest and renewal and their general and local effects he notices at length. "There may be a postponement of their spreading for a long time," he says, "various changes taking place in the ulcers, some subsiding and others swelling up like waves in the sea. Such is the course of the ulcers; but if nature stand out and the physician co-operate, the spreading may indeed be stopped, and a fatal termination is not apprehended, but the intestines remain hard and callous, and the recovery of such cases is protracted." Vivid descriptions he gives of the stools: "Sometimes they are like chopped tallow, sometimes merely mucus, prurient, small, round, pungent, causing frequent dejections and a desire not without a pleasurable sensation, but with very scanty evacuations." Again, they are "fetid like a mortification;" composed of "food now undigested, as if only masticated by voracious teeth, ... the dejection being discharged with much flatulence and noise; it has the appearance of being larger than its actual amount."
Galen (164 A.D.) attempted to correct the pathology of his contemporaries, who considered all bloody discharges dysenteric. There are four distinct varieties of bloody stools, he claims, only one of which, that due to ulceration of the intestine, deserves to be called dysentery. The bilious stool he derived from melancholy, and the fleshy stool from disease of the liver. But, though Galen regarded the presence of blood as a necessity, he was well aware of the fact that the stools contained ingredients other than blood. It was Galen who first used the word scybala ([Greek: schybala], feces) to express the small, solid masses of excrementitious matter often voided with the stools. In his treatment of the disease he made much use of the various drying earths, the Samian, Lemnian, Armenian, the sources of which he made long journeys to visit in order to become better acquainted with their properties, and which are better substituted in our day by bismuth, chalk, magnesia, and the carbonate of iron. It is the distinguished merit of Galen to have called special attention to the anatomical seat of the disease. Ulceration of the intestine he claimed as the very essence of the disease, and all the physicians of his day, he maintained, regarded as dysenteric only such cases as are attended with ulceration.
Galen was the exponent of the flower of Grecian, we might say of ancient, medicine. With very few exceptions, the later writers, if they do not obscure the original text with their speculations, are content to simply paraphrase the observations of their predecessors, and the subsequent contributions to the ancient history of dysentery may be briefly summed up in a few additional notes.
Coelius Aurelianus (400 A.D.) adopted the humoralistic doctrine of Hippocrates and regarded dysentery as an intestinal rheumatism (catarrh) with ulceration. He seems to have been the first author to recognize the cardinal fact that dysentery, notwithstanding the number of its stools, should be classed with the diseases which constipate the bowels, or, as it [p. 780] was centuries later aptly put by Stoll, "ut hanc morbis adnumeres alvum potius occludentibus," and he blames Erasistratus for using nothing but astringents, whereas many cases of dysentery require laxatives. It is worthy of note that Coelius Aurelianus ascribes the first use of opium in the treatment of dysentery to Diocles of Carystus (300 B.C.), who administered the juice of poppies combined with galls. By the time of Galen opium was so freely used in the treatment of the fluxes as to call for protest against its abuse.
Alexander of Tralles (575 A.D.) is often credited as having been the first to locate the disease in the large intestine. The truth is, he suggested various rules by which the seat of the disease, whether in the small or large intestine, might be definitely determined. But none of these rules—the seat of the pain, for instance, whether above or below the umbilicus, and the interval of time between the pain and discharges, whether long or short—possess the least diagnostic value or add to the attempts in this direction of previous writers—Aretæus, Archigenes, and Galen. Like these, his predecessors, he recognized an hepatic dysentery with discharges of bloody serum, which he attributed with them to atony of the liver, but more boldly than they, and with characteristic independence, he ventured to treat his patients with fresh vegetables and fruits, damsons and grapes.
Paul of Ægina (660 A.D.) locates the disease in the rectum, and gives a graphic account of its symptomatology. He made the mistake of many later practitioners in regarding as a separate disease a symptom, tenesmus, which he describes as an irresistible desire of evacuation, "discharging nothing but some bloody humor, which is the cause of the whole complaint, being an oedematous inflammation of the rectum which creates the impression of feces lodged in the intestine and a desire of evacuation." "Dysentery," he continues, "is an ulceration of the intestines, sometimes arising from the translation of tenesmus, and sometimes being of itself the primary affection; and is attended with evacuations at first bilious and of various colors, then accordingly bloody, and at last ichorous, like that which runs from dead bodies."
In curious contrast to these accurate observations is the absurd suggestion of an obsolete therapy (Galen), that the dried dung of dogs who had eaten bones, when drank in milk which has been curdled by having heated pebbles put into it, is of great service; but as an offset to this freak of fantasy is the renewed advocacy of warm milk, fallen somewhat into disuse since the days of Hippocrates and Galen: "And milk itself moderately boiled is an excellent thing"—a recommendation of the milk diet which now plays such an important rôle in the treatment of so many diseases of the alimentary canal.
Modern.—From this brief survey it is seen that the writers of antiquity left nothing in the symptomatology of dysentery for subsequent authors to describe. All further advance in our knowledge of this, as of all diseases, was now rendered impossible by the extinction of the light of science in the long night of the Middle Ages, whose gloom deepens with succeeding centuries and whose shadows fall close up to our own times.
The modern history of dysentery may be said to begin with Daniel Sennertus, whose first Tractatus de Dysenteria was published at [p. 781] Wittenberg in 1626. Sennert gave the deathblow to tenesmus as a distinct disease, or as even a pathognomonic sign of dysentery, showing that it is often present in purely local troubles, ulcers, fissures, hemorrhoids, etc., or is due to disease of other organs—stone in the bladder, tumors in the womb, etc. He recognized sporadic and epidemic attacks of the disease, and described under the terms fiens and facta forms which coarsely correspond to the catarrhal and diphtheritic varieties of modern pathologists. Improper food, unripe fruits, at least, cannot be the cause of dysentery, because, he shrewdly observes, the epidemic of 1624 began in May, before the fruits were ripe, and ceased in autumn, when they were ripe and in daily use. Moreover, sucklings at the breast suffered with the disease. Nor could moisture alone account for the disease, as this epidemic occurred after an unusually hot and dry spring and early summer. Some other cause must be invoked, and this other cause is perhaps the occult influence of the constellations and planets—an explanation which he afterward admits to be only an asylum of ignorance. In the treatment of the disease the indication should be to heal the abraded or ulcerated intestine; but since this cannot be done unless the cause is first removed, "the abrading, eroding humor should be evacuated and absterged, at the same time its acrimony mitigated and corrected; then the flux should be checked by astringents, and the pain, if vehement, lenified and removed." Purgatives should be repeated until all vicious humors are discharged.
Sydenham colored his descriptions of the epidemic which he witnessed in London in 1669-72 with the artistic touches of the master's hand. "The disease sets in," he says, "with chills and shivers. After these come the heat of the fever, then gripings of the belly, and lastly stools. Occasionally there is no fever; in which case the gripes lead the way, and the purging follows soon after. Great torment of the belly and sinking of the intestines whenever motions are passed are constant; and these motions are frequent as well as distressing, the bowels coming down as they take place. They are always more slimy than stercoraceous, feces being rarely present, and when present causing but little pain. With these slimy motions appear streaks of blood, though not always. Sometimes, indeed, there is no passage of any blood whatever from first to last. Notwithstanding, provided that the motions be frequent, slimy, and attended with griping, the disease is a true bloody flux or dysentery." The efficacy of opium in its treatment causes him to break out in praises of the great God who has vouchsafed us a remedy of so much power. But Sydenham was too good a practitioner not to know that all treatment must be prefaced with laxatives. For "after I had diligently and maturely weighed in my mind," he says, "the various symptoms which occur during this disease, I discovered that it was a fever—a fever, indeed, of a kind of its own—turned inwardly upon the bowels. By means of this fever the hot and acrid humors contained in the mass of the blood, and irritating it accordingly, are deposited in the aforesaid parts through the meseraic arteries." The indications then were plain—viz. "after revulsion by venesection to draw off the acrid humors by purging." It was the frequent and successful practice of Sydenham also to drench the patient with liquids, per os et per rectum—a mode of treatment which both he and the learned Butler, who accompanied the [p. 782]English ambassador to Morocco, where dysentery was always epidemic, hit upon, "neither of us borrowing our practice of the other." Butler declared that the method of deluging the dysentery by liquids was the best. But many attacks are cured almost on the expectant plan alone. This was the case with the excellent and learned Daniel Coxe, Doctor of Physic, in whom "the gripes and bloody motions ceased after the fourth clyster. He was kept to his bed, limited to milk diet; and this was all that was necessary in order to restore him to perfect health."
Zimmermann (1767) did not believe that improper food could be a cause of dysentery, as in the epidemic of 1765 fresh grapes were plentifully supplied to patients and proved an excellent remedy. He also noticed the muscular pains (rheumatism) which had been mentioned by Sydenham before him, and the paralyses first noticed by Fabricius in 1720, as occurring in the course of, or as sequelæ to, the disease. It was only contagious, he thought, in bad cases, when the stools have a cadaveric odor. But his main and most useful contributions were in the field of therapy. He discarded venesection entirely, was among the first to recognize the value of ipecacuanha, and objected strenuously to opium until the cause of the evil was expelled. Hence he was vehemently opposed to all astringents, to the use of which he ascribes the rheumatisms and dropsies which sometimes occur. Wines and spices were likewise put under ban; whey he permitted, but not milk, and water freely, but always warm. Barley-water and cream of tartar were sufficient food and medicine for ordinary cases, while camphor and cinchona best sustain the strength in bad cases.
Pringle (1772) observed the frequent occurrence of dysentery coincidently with malarial fever, and was a firm believer in the contagion of the disease. He claimed that the foul straw upon which the soldiers slept became infectious, but maintained that the chief source of infection were the privies "after they had received the dysenteric excrements of those who first sicken." It is spread in tents and in hospitals, and may be carried by bedding and clothing, as in the plague, small-pox, and measles. Neither food nor drink propagates the disease, he thinks, for, so far as the fruits are concerned, he too had seen it prevail before the fruits were ripe. The first cause of the disease is "a stoppage of the pores, checking the perspiration and turning inward of the humors upon the bowels." Antimony was his specific in its treatment. He was also fond of Dover's powder in its relief, and preferred fomentations to opium, which "only palliates and augments the cause." The best drink for patients with dysentery was lime-water (one-third) and milk.
This period of time is made memorable in the history of dysentery, as of nearly all internal diseases, by the contributions from direct observation upon the dead body by the father of pathological anatomy, John Baptist Morgagni (1779). From the days of Hippocrates down, the seat of the disease had been, as has been shown, pretty accurately determined, and the same acumen which enabled the clinicians to localize the affection had inspired them, as we have seen, to define and describe its nature. But any descriptions from actual post-mortem examinations were not put upon record until the beginning of the sixteenth century, when were published the posthumous contributions of Benivieni (1506-07). In his description of the lesions of the disease he says that "the viscera displayed [p. 783] internal erosion from which sanies was continually discharged." Nearly three centuries elapsed before Morgagni made his anatomical studies—an interval of time void of any contributions from pathological anatomy; and so little attention was paid to this branch of medical science that the descriptions of Morgagni and of his more immediate successors failed to excite any general interest or make any permanent impression. Morgagni himself, while he fully recognized their significance, did not consider the ulcerations of dysentery as absolutely essential to the disease, as many cases, even fatal ones, did not exhibit them at all. They were not liable to be mistaken for the lesions of typhoid fever, the ulceration of Peyer's glands, because, though they may, they only rarely, coexist in the same subject. As to the membranous fragments sometimes evacuated with the discharges of dysentery, Morgagni showed that they are occasionally true fragments or shreds of the intestinal coats, as has been maintained by the older writers, Tulpius and Laucisius, but are far more frequently nothing else than inspissated mucus—conceptions which subsequent studies with the microscope have fully confirmed.
In view of the general disregard of direct observations, it is therefore not surprising to learn that the nature of the intestinal lesions gradually fell into oblivion or at least became underrated in its import. But it is a matter of surprise that Stoll (1780) was able to declare as the result of autopsies made by himself that, although the colon is thickened and inflamed, ulcerations in dysenteries are very rare. This distinguished author did not at all believe in the contagion of the disease, as he had never seen it attack physicians or nurses. It developed, he thought with the older writers, as the result of exposure to cold during a perspiration. He emphatically insisted upon the frequency of rheumatism as complicating the disease, and describes in proof a number of cases of painful swollen joints during and subsequent to the attack. It was his especial merit to have succeeded in dispensing with the acrid bile as a cause of the disease, maintaining that hepatic derangements were only accidental complications, and thus disposed, but only for a time, of bilious dysentery in so far as it was supposed to depend upon defective or abnormal action of the liver.
But Annesley (1828) soon reinstated the liver in the pathology of dysentery, with the exhibition of colored plates displaying abscess of the liver in connection with the disease, as well as illustrating the displacements and constrictions of the colon which sometimes occur in its course.
The fourth decade of our century now brought in the anatomical contributions of Cruveilhier and Rokitansky, to be followed later by those of Virchow, upon which the modern morbid anatomy of the disease is based; while the labors of the Indian physicians and of Copeland, Parkes, and Vaidy put us in possession of the facts pertaining to its general pathology. Fayrer has quite recently published the results of his vast experience with dysentery in India, an important contribution to the practical study of the disease, and Hirsch has treated exhaustively of its medical geography. But the merit of publication of the most complete chapter or work upon dysentery that has ever been written anywhere belongs to, and is the especial pride of, our own country. It constitutes the bulk of the second volume of the Medical and Surgical History of the War of the Rebellion. It is a veritable encyclopædia of knowledge, not [p. 784]only upon the subject of which it treats, but upon all subjects immediately or even remotely collateral to it, and is a lasting monument to the labor and the learning of its author, Joseph J. Woodward, Surgeon of the United States Army.
GENERAL REMARKS.—Dysentery may be a primary or a secondary disease. As a primary disease it occurs in sporadic, endemic (often closely, sometimes curiously, circumscribed), or epidemic form, and is either acute or chronic, according to the nature of its symptoms and lesions. The ancient types of sthenic and asthenic or adynamic, typhoid, bilious, and malarial dysenteries belong rather to history than to modern medicine. The classification of cases in general use at present—viz. the catarrhal and croupous or diphtheritic forms—has reference rather exclusively to the nature of the lesion, and is hence extremely defective. Nor are the divisions (as in cholera) into sporadic and epidemic forms much more satisfactory, in that they indicate simply the range or extent of the disease, and by no means define a separate array of symptoms or lesions; precisely the same symptoms or lesions being encountered in individual cases of either form. None of these divisions clearly indicate differences in etiology, upon which factor alone can any acceptable division of cases be based. Perhaps less objection may be urged against the assumption of catarrhal and specific forms, including under the provisional term catarrhal all the cases which cannot as yet be accounted for by the action of a special or specific cause.
It will become apparent in the study of the etiology of dysentery that while any of the factors invoked may suffice to produce the catarrhal (sporadic) form, none will explain the specific (epidemic) form of the disease; both forms may be alike in their lesion and signs, but they differ widely in their cause. In other words, dysentery is only a clinical, and is in no way an etiological, expression of a disease. In this respect dysentery finds its analogue in a much grosser lesion of the bowels—namely, occlusion, acute or chronic, which, while it presents pretty much the same train of symptoms, may depend upon a great variety of causes, as impaction, strangulation, intussusception, etc. While any of the causes cited may be sufficient to excite the catarrhal form of the disease, the same causes may stand to the specific form only in the relation of predisposing agents. Or, as Maclean has better put it, "It appears that many of the so-called causes of dysentery must be regarded more as acute agents of propagation than of causation."
As a secondary disease dysentery occurs in the course of, or as a sequel to (not infrequently as the terminal affection of), pyæmia and septicæmia (puerperal fever), typhus and typhoid fevers, pneumonia, Bright's disease, variola, scarlatina, abscess of the liver (though the order of sequence is here oftener reversed), scorbutus, marasmus from any cause, tuberculosis, and cancer. It must not be forgotten, however, of these latter affections that each produces its own lesions in the large intestine, which are not to be confounded with those of genuine dysentery.
The view that dysentery shows a periodicity of recurrence at certain distinct intervals or cycles—three, five, or ten years—is entirely without foundation in fact; but there is strong ground for believing that the disease is gradually abating both in frequency and virulence with improvements in sanitation and hygiene. Thus, Heberden shows that the [p. 785] number of deaths set down in the seventeenth century under the titles of bloody flux and gripings of the guts was never less than 1000 annually, and in some years exceeded 4000, whereas during the last century the number gradually dwindled down to 20 (Watson)—a number which is certainly a misprint for 200; and Aitken states that as a cause of death it has been decreasing since 1852. Geissler also remarks1 that the variation in epidemics is nowhere so well illustrated as in the case of dysentery. A noticeable reduction in the number of cases in England began about 1850, and has continued almost without interruption to the present time, so that now (1880) six to eight times less cases occur than in the forties. The same diminution has been noticed in Bavaria and Sweden. In Sweden the cases treated by physicians in 1857 numbered no less than 37,000, with over 10,000 deaths; whereas now the number is reduced to 400-500 a year, and the mortality has experienced a corresponding reduction from 20-30 to 6-8 per cent.
1 Periodische Schwanderungen der wichtigsten Krankheiten.
At the same time, it is known of dysentery that it sometimes shows an almost freakish recurrence after long intervals of time, appearing in a place for many decades free from the disease, to establish itself there for years as a regular endemic malady, not to disappear again for a long series of years; in which respect, Hirsch remarks, it much resembles malaria.
Allusion has been already made to the occasional curious circumscription of the disease in definite localities. In fact, dysentery, even when late to assume the proportions of a widespread epidemic, begins, as a rule, and is confined for a time, in individual enclosed regions—prisons, barracks, hospitals, etc.; and in the process of dissemination it is rather characteristic of the disease to leap over or to spare intervening territory and appear in new foci at some distance from its original seat. A direct irradiation or linear transmission of the disease is the exception, and not the rule. The significance of this fact will become evident in the study of the etiology of the disease.
Dysentery is pre-eminently a disease of army life, its victims among soldiers numbering more than all other diseases together. Sir James MacGrigor, Medical Superintendent of the British army, called it the scourge of armies and the most fatal of all their diseases. Aitken says that "it has followed the tracks of all the great armies which have traversed Europe during the continental wars of the past two hundred years." It decimated the French, Prussian, and Austrian armies in 1792. In Cape Colony in 1804 every fourth man among the soldiers was attacked with the disease, and of those attacked every fifth man died. In Napoleon's campaign in Egypt dysentery numbered one-half more victims than the plague; Kinglake says that 5000 men died of dysentery alone in the war of the Crimea; and in our own country during our Civil War from 1861-65 chronic camp dysentery was the cause of more than one-fourth of all the diseases reported, the mortality being at the rate of 12.36 per 1000.
Woodward relates that the dysenteries, acute and chronic, with diarrhoeas, made their appearance in the new regiments at the beginning of the war, and, though mild at first, quickly assumed a formidable character. "Soon no army could move without leaving behind it a host of the victims. They crowded the ambulance-trains, the railroad-cars, the [p. 786] steamboats. In the general hospitals they were often more numerous than the sick from all other diseases, and rivalled the wounded in multitude. They abounded in the convalescent camps, and formed a large proportion of those discharged for disability." Most of the prisoners died of this disease, and great numbers succumbed to it on retirement to their homes after the cessation of the war. It is the story of many a campaign, Eichhorst says, that dysentery kills more men than the enemy's guns.
The fact that it sometimes shows itself in periodic form or with periodic exacerbation, that it is sometimes successfully treated with quinia, and that, as has been noticed from the days of Hippocrates down, it prevails in greatest intensity in malarial regions, has given rise to the view that dysentery is a malarial disease. This view, which was strongly advocated by many of the older writers, Senac, Fournier, Annesley, met with renewed support at the hands of many of the surgeons in our Civil War. But wider observation has shown the fallacy of such a view; for not only may the diseases prevail entirely independently of each other in malarial regions, but there are regions where one does and the other does not exist. Thus Huebner quotes from Rollo concerning St. Lucie (West Indies), a town situated on a mountain in the midst of a swampy country in which both dysentery and malaria abound, while the town itself is almost free from dysentery; and Dutrolan cites Réunion as a place where marsh fevers do not occur, while dysentery is very common. Bérenger-Féraud2 scouts the idea of any such connection. "Let us mention only St. Pierre de la Martinique," he says, "where there is not a piece of marsh as big as a hand, but where dysentery has made great ravage more than once. We might cite also Mauritius, Gibraltar, Malta, New Caledonia—places exempt, or almost exempt, from malaria, but often visited by dysentery."
2 Traité théorique et clinique de la Dysenterie, etc., Paris, 1883.
The view that dysentery is a form of typhus or typhoid fever (Eisenmann) or scurvy needs no refutation in the light of existing knowledge regarding the pathogenesis and pathology of these affections. These diseases may often complicate, but can never cause, dysentery.
Dysentery is a disease which spares no age, sex, or social condition, the seeming greater suffering of the poorer classes being due to the filth, food, darkness, dampness—in short, to the bad sanitation—of poverty.
Though the disease is often confined exclusively to soldiers in the midst of a civil population, examples are not wanting of an exclusive selection of civilians or of an indiscriminate attack in every direction. Lastly, dysentery is a disease which may recur repeatedly in the same individual, one attack rather predisposing to than preventing another.
ETIOLOGY.—Dysentery is an omnipresent disease. "Wherever man is," Ayres observed of it nearly a quarter of a century ago, "there will some of its forms appear." But the character of the form, and more especially the extent and severity of the disease, vary in extreme degree with the conditions surrounding the abode of man. No one of these conditions affects the disease so markedly as the climate. It is the testimony of Hirsch, based upon the study of seven hundred epidemics of the disease, that no other disease is so dependent upon the influence of the climate. The home of dysentery is the tropical zone. It prevails in greatest frequency [p. 787]and virulence in the tropics, and in those regions of the tropics where the characteristics of this zone are more pronounced, diminishes in intensity in the temperate regions, and occurs only in sporadic form farther north. At 40° latitude the line may be pretty sharply drawn; beyond it dysentery as an epidemic is almost unknown.3
3 Shakespeare (Troilus and Cressida) cites "griping of the guts" among the "rotten diseases of the south."
India has been from time immemorial the hotbed of this disease. Henderson says it is perhaps more fatal to natives than all other diseases put together, and Hutchinson, Hunter, and Tytler observe that it causes three-fourths of the deaths among the natives of Hindostan. In Egypt the disease is indigenous, and is, according to Frank, post pestem maxime timendus. Greisinger reports that one-half of all the autopsies made by him in Egypt showed dysentery as a primary or secondary affection. It is epidemic here at all times, Roser says, and all fatal cases of acute or chronic disease finally perish with it.
Similar testimony might be adduced from a large part of Africa, much of Asia, the Indian Archipelago, and the West Indies. It rages "murderously" in Peru, causing a mortality in some epidemics of 60 to 80 per cent., and occurs in this country not only in the valleys, but in cities and provinces at the lofty elevation of 8000 to 13,000 feet.
Heat, moisture, vegetable decomposition, and sudden atmospheric change are the distinguishing characteristics of southern climes, and the study of the etiology of a disease incident or indigenous to these conditions calls for an investigation of these various factors.
It is well established of dysentery that it occurs for the most part in the hottest season of the year. Of 546 epidemics tabulated by Hirsch, 404 prevailed in summer and fall, 113 in fall and winter, 16 in spring and summer, and only 13 in winter. Fourteen-fifteenths of the whole number of epidemics occurred in the months of June to September. And it is corroborative of these conclusions that of 1500 deaths from dysentery in the cities of Boston, New York, Philadelphia, and Baltimore from 1816 to 1827, 1100 occurred in the months of July, August, and September. In fact, the Census Reports (1860-70) of our country show the maximum mortality in August and September, and the minimum in January and February.
The prevalence of unusual heat may also call out an epidemic in places where the disease usually shows itself only in endemic or sporadic form. Thus, the severe epidemic of 1540 in England was preceded by a heat so intense as to dry up the wells and small streams, in consequence of which many cattle died of thirst; and the epidemics of 1583 in Germany, of 1758 in France, and of 1847 in our own country, were characterized in the same way. Interesting in this connection is the statement of Frick concerning the epidemic in Baltimore in 1849, who found the cases to increase and decrease almost in proportion to the elevation and depression of temperature. The epidemic of Weimar in 1868, where 12,000 people fell ill with the disease, illustrated the rule when it ceased suddenly on the approach of cool weather at the end of August.
But that heat alone is not sufficient to account for the genesis of the disease is apparent from the occasional occurrence of it in the tropics in the colder seasons of the year; in the colder climates, Russia, Sweden, [p. 788] and Canada; and in temperate regions during exceptionally cool seasons, as in Plymouth in 1769, London in 1808, Massachusetts in 1817. Moreover, the temperate zone is often characterized by seasons of unusual heat, during the prevalence of which dysentery may be almost unknown. Thus, during the summer of 1881, in Cincinnati, the thermometer scarcely fell below 95° F. for weeks at a time, and was often nearly 100° during the entire night, but the records at the Health Office show that while cases of heatstroke were alarmingly frequent, dysentery was unusually rare during the entire season.
That moisture cannot act more, at most, than as an occasional predisposing cause of dysentery is sufficiently clear from the statement of Hirsch, that of 119 epidemics, 62 commenced or were preceded by wet and 57 by dry weather. In truth, dryness long continued and excessive heat have already been invoked as remote causes of the disease. But moisture, as contributing to, or being a necessary element of, vegetable decomposition, the third characteristic of tropical regions, is entitled to further consideration. Annesley observed that among troops stationed in the vicinity of rivers, canals, and places abounding with emanations from the decay of animal and vegetable matters dysentery became extremely prevalent and assumed a more or less malignant nature; and Baly, who studied the disease in its famous outbreak in the Milbank Penitentiary, remarks that "it is greatest at those seasons and in those states of the atmosphere which most favor decomposition of organic matter in the soil."
In Africa it has been noticed that dysentery appears with the rainy season, to disappear only at its close; and the same observation has been made of Bengal, while in Lower Egypt the disease follows the inundations of the Nile. Burkhardt says of 10,000 cases that one-half occur in wet hot seasons, two-fifths in dry hot seasons, and but one-tenth in cold seasons. Moreover, the removal of camping-grounds to dry localities has often arrested the disease or checked its further dissemination. Thus, Mursinna states that the removal of the army of Prince Henry of Hesse from Nîmes, where the disease raged fearfully, to Leitmeritz was attended by its immediate cessation, notwithstanding the fact that the soldiers ate large quantities of fruit. A statement of Dillenius, quoted by Heubner, is in this connection exceedingly instructive: "Dillenius had to march with a dysentery hospital of more than 500 patients from July 26 to August 3, 1812, and it required four whole days to accomplish an ordinary nine or ten hours' march. The patients, extremely exhausted, were finally put into a sheep-shed. Here, in the fresh air and lying on hay, they all improved very quickly. By advice of the physician they ate for medicine the fresh whortleberries which they themselves had picked." Werneck attributes the exemption of the city of Halle since the end of the last century to the draining and drying of the neighboring marshes.
On the other hand, numerous observations go to prove that dysentery is likewise prevalent in dry sandy soils where the factors so necessary to the production of malaria are entirely unknown. Thus, Hirsch quotes from Harthill to the effect that dysentery never occurred among the English troops in Afghanistan until they entered upon its thoroughly dry and sandy plains; and from Lidell, who declared that the disease prevailed most in Panama in March, the dry season at this place. Again, a striking confirmation of exemption from dysentery in a marshy region [p. 789] is offered in the Antilles at Grande-Terre, "a wet, marshy plain severely visited by malaria, but used by patients attacked with chronic dysentery at Basse-Terre as the safest place of refuge and recovery."
The rôle of moisture and vegetable decomposition may be, then, summed up in the words of Annesley, that "all situations which furnish exhalations from the decay of animal or vegetable productions under the operation of a moist and hot state of the atmosphere will always occasion dysentery in the predisposed subject—circumstances which, with other causes [italics ours], combine to generate the disease."
Atmospheric vicissitudes, checking of perspiration, catching cold, are synonyms in the present popular as in the ancient professional conception of the genesis of dysentery. "Of the remote causes of dysentery," Johnson says, "I need say little; they are the same in all parts of the world—atmospheric vicissitudes." And in making this statement the author expresses the almost universal testimony of the Indian physicians. "Sudden change of temperature," observes Kaputschinsky of the Trans-Caucasus, where dysentery is rife, "is in this region no rarity. The sultry heat of noon often alternates with a cutting cold wind, and vice versâ. In the same place is now a warm, now a cold, now a glowing hot breeze, and such changes most predispose to dysentery." And McMullin says of the Barbadoes that "it is a curious fact that this disease is most prevalent where from the immediate contiguity of mountains sudden vicissitudes of temperature are experienced." Didelot says also of South France, "It is not the fruits, as people still believe to-day, which act as causes of dysentery, but the sudden variations of the air." Ruthay remarks of the dysentery of China that the most common cause is a chill caught by sleeping in a draught uncovered or in the open air. Metzler attributes the exemption of Stuttgart (since 1811) from any great epidemic to the fact that the city lies in a valley open only to the east, which permits no contrast of hot days and cold nights; and Seeger, in speaking of the epidemic which occurred in Ludwigsberg in 1872 (a city of twelve thousand population, where no epidemic of any kind had appeared since 1834, and where 870 were suddenly attacked with dysentery) that it first broke out in Kaffeeburg in two streets exposed to the wind, and thence spread to different parts of the city. Exposure of the body, especially the abdomen, during sleep or when perspiring, the sudden laying aside of flannel body-clothes, are proceedings, Fayrer says, pregnant with danger in dysenteric regions. A lamentable dysentery appeared, according to Trotter, on board H.M.S. Berwick Oct., 1780, "in consequence of the hurricane on the fifth of the month, by which the clothes and bedding of the seamen, and indeed all parts of the ship, were soaked in water, and many of the men slept for nights together on the wet decks overcome with fatigue and debilitated from want of food." Fayrer also quotes from Moseley the observation that "it often happens that hundreds of men in a camp have been seized with the dysentery almost at the same time after one shower of rain or from lying one night in the wet and cold."
As illustrating the conjoined operation of all these various causes, together with filth and foul effluvia, more especially exposure to cold, the story of dysentery was never better told than by Sir James MacGrigor, who, in speaking of the Peninsular campaign, remarks that "the army during June as well as July was traversing Castile, where it was [p. 790] exposed to the direct influence of a burning sun darting its rays through a sky without a single cloud, the troops marching and fighting during the day, and bivouacking during the night on arid, unsheltered plains. They felt at times every vicissitude of heat and cold. In the rapid advance they could not be regularly supplied with food or had not time to cook it, and not unfrequently indulged in bad wine and unripe fruit." ... The thousands of sick (chiefly from diarrhoea, dysentery, and remittent fever) were hurried off to Ciudad Rodrigo, the nearest hospital-station to the frontier of Portugal, a town "composed chiefly of ruins with very narrow streets," ... and from having been "so much the object of contest, and alternately the site of the hospitals of all the contending armies, nearly twenty thousand bodies were calculated to have been put into the earth either in the town or under its walls in the course of a few months." ... "It may easily be conceived," the author adds, "in what state cases of dysentery must have arrived after having sustained a journey in extent from four to twenty days, conveyed chiefly in bullock-carts or on the backs of mules, sometimes under incessant rain for several days together."
It is really quite superfluous to cite further opinions or examples in illustration of a fact which is so universally conceded as to be exaggerated in its general significance. Taking cold is the common idea of the cause of dysentery, and is always a satisfactory explanation in a case of obscure origin in this or any disease, even though the patient may be able to recall no possible exposure. The physician himself contents himself only too easily with resort to this refuge, and with further appeal to the locus minoris resistentiæ, as the explanation of the seat of the disease, which he hopes to cure with the aid of the vis medicatrix naturæ. But taking cold is only a popular paraphrase for contracting a disease, and will bear no scientific analysis of its meaning. Mere reduction of temperature will certainly not produce a disease whose habitat is the hottest zone, nor will a sudden chill of the surface be accepted as a sufficient cause so long as men daily remain exempt after a sudden plunge into cold water. Some other factor must be invoked to account for the outbreak of specific (epidemic) dysentery.
The influence of the nervous system, the mechanical and chemical or specific action of the ingesta and dejecta, remain to be especially considered in the etiology of the disease.
The influence of the nervous system is more directly seen in the production of diarrhoeas than dysenteries, but that sustained disturbances of the emotions play an important part in the production of dysentery is shown by the greater frequency of the disease among prisoners of war. In the Franco-Prussian war the French prisoners suffered more than the Germans, and the records of prison-life in our own war, at Andersonville, Libby, and Salisbury, furnish ghastly chapters in the history of this disease. Many other factors contribute to the development of the disease under such circumstances—in fact, all the cruelties of man's inhumanity to man—but the influence of the nervous system is too plain to be mistaken. The communication between the cervical ganglia and the sympathetic nerve-fibres which preside over the cerebral circulation and regulate intestinal peristalsis has been invoked (Glax) in explanation of the direct action of the brain upon the intestinal canal. Curious in this [p. 791]connection is the claim of Savignac, who considered dysentery a disease of the nervous system because in two cases he found spots of softening in the spinal cord.
The noxious action of irritating articles of diet has been recognized in the production of dysentery from the earliest times. Aretæus mentions acrid foods, and Aëtius crudities, as directly causing the disease; and unripe fruits have been especially stigmatized from the days of Galen down. Decomposing, fermenting food and drink cause diarrhoea much more frequently than dysentery, but if the irritation be severe or prolonged, or be superimposed upon a catarrhal state, a diarrhoea, it is claimed, may pass over into dysentery. Impurities in drinking-water were charged with causing dysentery by Hippocrates himself, with whom Avicenna fully coincided; and the view that epidemics of the disease are caused in this way has been abundantly advocated ever since. So far as running water is concerned, the researches of Pettenkofer have shown that all impurities are speedily destroyed, for even at the distance of a few rods from the reception of sewage the water is perfectly safe. Nor does standing water lack the means of purification, provided it be sufficiently exposed to the air. The observations of Roth and Lex have shown that the water of the wells of fifteen churchyards in Berlin contained nitrates in less quantity than the average wells in the city; and Fleck made a similar statement with regard to the wells of Dresden. But no one in our day would rely upon a mere chemical analysis in the detection of the organic poisons or particles of disease. It is the physiological test which remains the most conclusive, and the evidence in favor of the production of dysentery by the ingestion of drinking-water poisoned by the reception of excrementitious matter, especially the dejecta of disease, is as positive as in the case of typhoid fever. Thus, De Renzy found that the number of cases of dysentery "immediately decreased at Sibsagor (India) so soon as better drinking-water was obtained from wells deeply sunk and lined with earthenware glazed pipes;" and Payne found that the cases of dysentery (as well as diarrhoea and lumbrici) almost disappeared from the asylum at Calcutta as soon as the habit of drinking water from the latrines was stopped. In face of such facts, which might be infinitely multiplied, one would hesitate to subscribe to the statement of Fergusson that "true dysentery is the offspring of heat and moisture, of moist cold in any shape after excessive heat; but nothing that a man could put into him would ever give him a true dysentery."
The relation of the action of the dejecta must be studied from the double standpoint of the development and the dissemination of the disease, as originating the catarrhal form by mechanical or chemical irritation of the intestinal mucosa, and as spreading the specific form by direct or indirect infection.
By the time the contents of the alimentary canal have reached the colon they have become, through absorption of their fluids, more or less inspissated, and hence as hard, globular masses fill the sacculi of the large intestine. Mechanical irritations by crude, indigestible residue of any kind of food, more especially of vegetable food, or chemical irritations, as by fermenting food, accumulate in this region, fret the mucous membrane into a state of inflammation, even ulceration, and produce the anatomical picture and the clinical signs of dysentery. If there be a superadded or [p. 792]pre-existent catarrhal condition of the mucosa or a defective peristalsis of the muscular coat, which is sluggish enough at best, the development of a pathological state is much facilitated. And there is no doubt that the dysentery of the tropics is increased by the bulky, indigestible, feces-producing character of the food.
The anatomical construction of the colon may also favor these processes by its mere abnormal length or size or by duplicatures in its course. The protracted constipation of the insane, in whom the transverse colon is often found elongated or displaced—to assume the well-known M-form, for instance—may partially account for the frequency of dysentery in these cases (Virchow), though the neglect which comes of preoccupation of the mind, with the general inhibition of peristalsis, is a more frequent cause of the constipation.
Wernich (1879) sums up the action of the feces, independently of a specific cause, in attributing the dysentery of the tropics, aside from the great changes of temperature, to (1) bad aborts, the dejecta being deposited in all parts of the towns or into an opening made in the floor of the hut, with which is associated total lack of personal cleanliness; (2) to the diet, which causes a large amount of feces; and (3) to the relaxation of the intestine in general, permitting accumulations of infecting matter.
Upon the question of the propagation of the disease by the dejecta rest in great measure the all-important problems of a specific virus and of the contagiousness of the disease.
It is the almost universal opinion of those who have had the opportunity of widest observation that epidemic dysentery arises from, or is due to, a specific cause, a miasm, a malaria (in its wide etymologic sense, bad air), which emanates from the soil. The simultaneous sudden attack of great numbers under the most diverse surroundings admits of explanation in no other way. But the precise nature of the morbific agent is still unknown. The similarity of epidemic dysentery to malaria would indicate the existence of a low form of vegetable life, a schizomycete, as the direct cause of the disease. But the proof of the presence of a specific parasite or germ is still lacking, and though its speedy disclosure by means of the solid-culture soils may be confidently predicted, it cannot, in the light of existing knowledge, be declared as yet.
Especial difficulty is encountered in the study of micro-organisms in diseases of the alimentary canal because of the myriad variety in enormous numbers found in healthy stools. Decomposition and fermentation both begin in the large intestine, so that the feces swarm with the bacteria and torulæ productive of these processes. Woodward declares that his own observations have satisfied him that "a large part of the substance of the normal human feces is made up of these low forms in numbers which must be estimated by hundreds of millions in the feces of each day," bacteria, micrococci, and torulæ being found "floating in countless multitudes along with fragments of partly-digested muscular fibres and other débris from the food;" but while the torulæ are increased, the other micro-organisms, bacteria, etc., do not appear to be more numerous in the stools of dysentery than in healthy feces.
The doctrine that dysentery depends upon parasites is very old in medicine, and included animal as well as vegetable growths. Langius (1659) declared that swarms of worms could be found in dysenteric stools, and [p. 793] Nyander (1760) went so far as to call dysentery a scabies intestinorum interna; which extravagant conception would have speedily met with merited oblivion had not his preceptor, the great Linnæus, incorporated the Acarus dysenteriæ into his Systema Naturæ. Sydenham about this time (1670) expressed a much clearer conviction of the cause of the disease when he spoke of "particles mixed with the atmosphere which war against health and which determine epidemic constitutions."
Baly (1849) first proclaimed the idea of a vegetable fungus, similar to that described by Brittan and Swayne in cholera, as the parasite of the disease; and Salisbury (1865) described algoid cells and species of confervæ as occurring abundantly in all well-marked cases. Klebs (1867) found spore-heaps and rod-like bacteria in the stools of dysentery as in cholera, but maintained that those of dysentery were larger and thinner than those of cholera. Hallier (1869) maintained that although there was no morphological difference in the micro-organisms of the stools of dysentery, typhoid fever, and cholera, he was able by culture-experiments to develop the micrococcus of dysentery into a special fungus, which he called Leïosporium dysentericum. Busch (1868) demonstrated nests and colonies of micrococci, as well as mycelium, in the villi and among the glands of the mucous and submucous tissues in the cases of dysentery from Mexico which he examined, but Heubner (1870) was able to disclose them in equal numbers in preserved preparations or fresh contents of healthy intestines. Dyer4 (1870) believes that the parasites constituting the mildew or sweat which forms a viscous pellicle upon fruit is the agent which directly produces and propagates the disease. Mere immaturity of fruit gives rise only to diarrhoea. This parasite occurs in some years more than others, which accounts for the irregularity of occurrence of the disease. He avers that it is only necessary to clean fruit, more especially plums, to prevent the disease. This suggestion merits place only as a curiosity in the history of the mycology of dysentery.
4 Journal f. Kinderkrankheiten, No. 317.
More important are the results of the experiments of Rajewski (1875), who found the lymph-spaces filled with bacteria, and who was able to produce a diphtheritic exudation upon the surface and in the substance of the mucous membrane of the colon by the injection of fluids impregnated with bacteria into the bowels or blood of rabbits; but this result was only obtained when the mucous membrane had been previously irritated or brought into a catarrhal state by the introduction of dilute solutions of ammonia. It remains for subsequent investigation to confirm these highly significant conclusions, which, when properly interpreted, may explain the action of the predisposing and exciting causes of the disease. Rajewski's bacteria, it is needless to state, were simply the bacteria of common putrefaction. Lastly, Prior (1883) describes a micrococcus as the special micro-organism of dysentery, and Koch (1883), in prosecuting his studies of cholera in Egypt, remarks incidentally upon a special bacillus which he encountered in the intestinal canal in dysentery, though he is as yet by no means prepared to ascribe to it pathogenetic properties.
The question of contagion hinges upon the specificness of the disease, and cannot be definitely determined until this problem is finally solved. The old writers believed in the contagion of dysentery. Helidæus [p. 794] declared that he "had often seen it communicated by the use of clyster-pipes previously used in the treatment of those suffering with the disease, and not properly cleaned;" and Horstius and Hildanus speak of the communicability of the disease from the latrines contaminated by dysenteric excreta. Van Swieten maintained that washerwomen contract it, and that physicians and nurses might be affected. Degner saw the disease spread from street to street in Nimeguen, while every one who came in contact with the disease became affected. Pringle observed it spread from tent to tent in the same way; and Tissot went so far as to declare, "Sil ya une maladie veritablement contagieuse c'est celle ci." Ziemssen believed that the disease is only contagious when the element of crowd-poisoning is superadded; and Heubner states that trustworthy army surgeons in the Franco-Prussian War frequently saw infection occur when many severe cases were heaped together in a small space. Under these circumstances thorough disinfection of the privies checked the spread of the disease. But it was the universal testimony of these surgeons, as also of our own surgeons of the Civil War, that the disease was never transported to the civil population by any of the tens of thousands of cases on their return to their homes.
By most modern writers dysentery is given a place, in respect to contagion, between the exanthematous maladies, typhus and scarlatina, which are without doubt contagious, and the purely miasmatic diseases, malarial and yellow fevers, which are without doubt not contagious. Dysentery is ranked with typhoid fever, which is contagious, not by contact with the body, but with the discharges. It is not a question in dysentery of epithelial drift or pulmonary exhalations, but of ingestion or reception of the dejecta of the disease. By this observation it is intended to convey the impression that dysentery, like typhoid fever, is mostly spread in this way, but the reverse may be true; it may be spread, like yellow fever and malaria, by poisons in the air. But dysentery, as has been repeatedly remarked, is only a clinical expression of a disease which may be caused in many ways; and among these causes, least potent perhaps, but present nevertheless, is contagion. For, not to mention the epidemics which were undoubtedly spread in this way, as among the Allies at Valmy in 1792, among the French in Poland in 1807, and in the hospital at Metz in 1870, dysentery has been directly communicated by the use of clysters, bed-pans, and privies in a most unmistakable way.
According to Eichhorst, the poison of dysentery is endowed with extraordinary persistence of duration or tenacity of life in the stools; for "observations are recorded where dysenteric stools have been emptied into privies, and individuals employed to clean them out after the lapse of ten years have been infected with the disease. These observations go to prove, of this as of other similar affections (typhoid fever), that the virus or microbe of the disease finds its most favorable nidus in vaults, cesspools, sewers, etc. When the poison is exposed to the air it is much more speedily destroyed, but is in the mean time of course a possible conveyer of the disease." Fayrer quotes from an anonymous writer, "whose views are as remarkable for their force as for their originality," the rather extravagant assertion that "if human excrement be not exposed to the air there can be no dysentery."
[p. 795] Knoewenagel has recently5 opened up a new series of reflections in his suggestion of a possible direct infection of the large intestine per rectum, where the disease usually begins and is mostly best expressed. He calls attention to the fact that people who suffer with constipation indulge in longer sessions at stools and induce in straining efforts a degree of relaxation of the rectal mucosa. The mucous membrane at its orifice may become at the same time abraded by hardened fecal masses, to leave open surfaces or crevices upon which germs may lodge. Moreover, aspiration follows the efforts at expulsion, and the air with its particles is drawn directly into the rectum, thus affording all the conditions for immediate or direct infection.
5 Schmidt's Jahrbucher, Sept. 25, 1882.
At any rate, it must be admitted that the evidence in favor of contagion is in some cases too strong to be ignored. A single instance may suffice for illustration: Flügel reports that the towns of Nordhaben and Reichenbach, containing together twenty-two hundred inhabitants, were visited by dysentery in 1873, when nearly four hundred people were attacked. The visit of a relative carried the disease from Reichenbach to the daughter of an innkeeper at Tauchnitz, and from this house the disease spread over the whole place, so that in a short time more than one hundred people fell ill. Four to six, sometimes as many as eleven, members of one family were successively or simultaneously affected. The use of the same bed was the surest means of contagion.
The duration of the poison was proven in an exquisite case, which is, however, not entirely free from objection: Two children of an officer were severely affected in September and October, 1872. In January, 1873, the house was vacated and occupied by a successor in office, whereupon in April, six months after dysentery had disappeared from the place, the wife and child of the second officer were affected with the disease.
To sum up the etiology of dysentery in a few words, it may be said that few chapters in medicine are so thoroughly unsatisfactory, as the prospect of reconciling the accumulated discordant facts is very discouraging. Because of the singular uniformity in the symptoms and lesions the temptation is strong to look for a common cause, and to ascribe all cases to this cause, explaining differences by degree rather than by kind. Such a view would find solid support in the assumption of a specific germ, and would ally dysentery with typhoid fever, a disease which has likewise, in all cases, uniform symptoms and lesions, and which prevails in both sporadic and epidemic form. The advocates of this view would fix the poison of the disease in the air and alimentary canal (but not in the blood), and explain the existence of individual cases, as well as the prevalence of epidemics, by meteorological conditions as affecting the growth or dissemination of specific germs. Nor would the adoption of this view exclude the possibility of producing the catarrhal (sporadic) cases by many kinds of noxious germs, including those of common putrefaction. Hot air and wet air are notorious bearers and breeders of germs, and the law of gravity keeps them near the surface of the earth—conditions which coincide with the prevalence of the disease in the tropics and among individuals (soldiers) who sleep upon the ground. If the contagion of the disease be admitted, the existence of a [p. 796]contagium animatum is implied at once, for no chemical poison has the power of propagation.
But the germ of dysentery has not been found as yet, and until it has been found, cultivated in suitable soil, and inoculated to produce the disease, the evidence of its existence remains merely presumptive.
So that at the present time dysentery must be regarded as a malady which stands in closer relation to, or finds a better analogue in, cholera than typhoid fever; for cholera is a disease which has the same geography, has likewise nearly uniform symptoms and lesions, so far as it leaves any, and certainly has two distinct forms of origin—one clearly specific, cholera Asiatica, and the other catarrhal, cholera morbus.
PATHOLOGY.—Dysentery is a local malady, but, like every local malady if sufficiently severe, it may show constitutional effects. It is usually gradually ushered in from a lighter form of gastro-intestinal catarrh. After a stage of incubation which lasts from a few hours to a few days symptoms of dyspepsia and diarrhoea set in or increase, attended with anorexia, heartburn, nausea, eructation or borborygmi, pain in the abdomen, and copious fluid discharges. Hereupon ensue the pains and the discharges characteristic of the disease. Violent griping and colicky pains (tormina) traverse the abdomen, with sickening sensations of depression. The desire of evacuation of the bowels (tenesmus) becomes intense and more or less constant, and the discharge itself is attended with little or no relief. At the same time the region of the rectum, intensely inflamed, is the seat of intolerable burning pain, which becomes excruciating with the introduction of a speculum or the finger.
The discharges may be copious, dark-brown, thin, and highly offensive (bilious dysentery), may contain occasional hard round fecal casts of intestinal sacculi (scybalæ), or may become more and more scant, until with the most violent efforts only the minutest quantity is extruded of mucus, generally streaked or tinged with blood (rose mucus) like the rusty sputum of pneumonia. Later, all effort at emptying the alimentary canal may be futile (dysenteria sicca), or the mucus may be pure or commingled with pus to remain perfectly colorless (dysenteria alba), or with blood in larger quantity (dysenteria rubra). In other cases, or at other periods in the same case, the discharges consist of fleshy masses composed of inspissated mucus or pus, blood, and tissue-débris (lotura carnea). Sometimes, though rarely, the discharges consist of pure blood, but oftener of a copious turbid fluid, which on standing separates into a clear upper layer of serum and a sediment of disintegrated lotura carnea. Or, lastly, the sediment is composed of small round vitreous masses, evidently swollen by maceration to look like sago-grains, which have been erroneously supposed to represent the liberated contents of the intestinal follicles.
The general condition of the patient suffers correspondingly. There may be fever or there may be none throughout the whole course of the disease, but the pain and discharges quickly exhaust the strength of the patient, and in severe or long-continued cases lead to emaciation and profound prostration.
The skin is hot and dry; the tongue is heavily coated; the face wears an anxious expression. The abdomen is tumid with gases, or in more advanced cases sunken, discolored, and tender, especially in the course [p. 797] of the colon, whose thickened walls may often be felt beneath the emaciated surface. The anus is spasmodically constricted, or in the worst cases paralyzed, patulous, and livid or blue. Prolapse of the rectum is common in children, and excoriation of the perineum by the acrid discharges is not infrequent.
Finally, a typhoid state may set in or a pyæmia occur, when the discharges may become involuntary or unconscious, and brain symptoms—insomnia, stupor, delirium, and coma—supervene; or the patient may linger long enough to perish by simple exhaustion or marasmus.
Under favorable hygiene the great majority of cases of catarrhal dysentery recover without special treatment in the course of from three to ten days, but specific dysentery has no definite duration and but little tendency to spontaneous cure. The worst cases are often quickly controlled by appropriate interference, and the most surprising results may be sometimes obtained in cases of even years' duration. On the other hand, a certain percentage of cases is characterized by a defiance to every kind of treatment, including the last resort, a change of climate.
An acute case of catarrhal dysentery generally subsides without lesions, and the natural duration of the attack may be much abbreviated by proper treatment. Specific or epidemic dysentery lasts from two to four weeks, or, becoming chronic, continues for years or for life, with exacerbations and remissions.
Various complications are liable to occur in the course of the disease. Three deserve especial mention—viz. affection of the joints (rheumatism), paralysis, and abscess of the liver. Perforation and peritonitis, always possibilities, and deformities of the colon, thickenings, and constrictions, are not infrequently left.
MORBID ANATOMY.—The lesions of dysentery are the ordinary signs of inflammation of a mucous membrane and its subjacent structures. They do not differ in any essential way from those of any mucous surface in a state of inflammation, the minor variations being due to differences in the anatomy and physiology of the part affected. Thus, a description of the pathological process in inflammation of the pharynx, bronchi, or uterus would answer upon the post-mortem table for the same process in the large intestine, and the finer microscopic lesions could be differentiated in any case only by the histology of the part affected.
A slight lesion of any mucous membrane constitutes what is known as a catarrhal process; a more grave affection, a diphtheritic process; a more chronic inflammation, a hypertrophic or hyperplastic process. Hence an easy distinction between sporadic and epidemic cases might be based upon the character of the lesion found. But, as has been stated already, it is impossible to draw a line between catarrhal and specific cases, the same lesions being found in either form. The difference, so far as the morbid anatomy is concerned, is wholly in degree or stage, and not at all in kind, the specific (epidemic) form presenting the graver lesion as a rule. So most cases of sporadic dysentery show only catarrhal lesions, while most cases of epidemic dysentery show diphtheritic lesions.
Catarrhal dysentery shows as its first obvious alteration a hyperæmia of the mucous surface. It is limited exclusively to the large intestine in the vast majority of cases, and only in rare exceptions affects the small intestine, though cases have been mentioned as curiosities in which the [p. 798] process has reached the stomach in its upmost prolongation. The hyperæmia is most marked, as a rule, in the lowest parts of the large intestine, the rectum and descending colon, but there is, as Virchow has pointed out, a peculiar predisposition to affection at the seat of all the flexures, the iliac, hepatic, splenic, sigmoid, where the additional element of fecal arrest or impaction is superadded to the cause of the disease.
The catarrhal process occurs first in detached spots or streaks upon the projecting folds or duplicatures of the mucous membrane; which spots coalesce to form extensive surfaces. Examined by transmitted light, these surfaces show a distinct arborescence of the vessels. Or the disease may commence in the follicles in distinct areas of the large intestine, and may remain confined to these structures to constitute the variety known as follicular dysentery.
The hyperæmia of inflammation is attended with dilatation and paresis of the vessel-walls and retardation of the circulation. The whole process may be arrested at this stage, so that there escapes from the vessels, at most, only serum to develop the oedema which, with the defective nutrition from arrest of the circulation, gives rise to the softening of the epithelial cells. These cells may be thus lifted from their bed to constitute the process of desquamation, the fundamental anatomical characteristic of acute dysentery, by which process the submucous connective tissue is laid bare and the so-called catarrhal ulcer results. Or the epithelium, but partially detached, may remain upon the surface, "either raised in the shape of small vesicles which contain clear serum, or it forms a grayish-white layer resembling the mealy scurf of the epidermis—an appearance which probably induced Linnæus to term dysentery scabies intestinorum interna" (Rokitansky).
Kelsch maintains that the inflammatory process in dysentery commences in the delicate connective tissue between the follicles, the network of small spindle-shaped cells with multiple nuclei becoming speedily penetrated by a number of very small, newly-formed vessels. Where the epithelium is desquamated the surface is covered with granulations as after a wound. The disposition of the follicles is soon deranged, for, instead of standing in rows like gun-barrels, they are pushed asunder and uplifted, so as to remain at different heights. Their interior becomes blocked with mucus or their orifices occluded, so that retention-cysts are formed to give rise to the appearance of the bead necklace. Soon the walls of neighboring follicles coalesce, dissolve away, and communication is established between them. The interior of these communicating tubes or canals is filled with vitreous mucus; the walls are stripped of their lining cells, but their "blind extremities contain still adherent colossal epithelial cells." Moreover, the follicles break into each other under the proliferative budding process, so that the end of a distorted tube may be found in the interior of another. Where follicles are destroyed the mucous membrane above them or in their vicinity collapses—a condition observed and described by Colin as effrondement. The mucosa in these regions may appear perfectly uninjured, but by "blowing upon it with a tube it is lifted up like an ampulla to show an opening in its centre," though more frequently the mucous membrane collapses or sinks in at the region of destruction. The inner surface of the mucosa is rendered additionally uneven by the elevations or protuberances caused by the [p. 799] proliferations in the submucous connective tissue. The older writers (Pringle, Hewson) regarded these projections as tumors of the mucosa, and Rokitansky, who describes their true nature, speaks of them as warty, tubercular (nodular) swellings or fungoid excrescences—constituting a condition, he says, which Gély has termed hypertrophie mamelonné. The alternate elevations and depressions thus produced have been likened to the representations of bird's-eye views of mountain-chains.
As a rule, occasional red blood-corpuscles are also permitted to escape through the vessel walls in the process of diapedesis to give to the surface mucus its characteristic tinge, and punctate submucous hemorrhage is very frequently seen.
The pressure of the swollen, softened mucosa upon the sensitive nerves, and the irritation of the acrid intestinal contents, are often invoked to account for the constant desire of defecation (tenesmus) which constitutes such an essential symptom of the disease; but both the tenesmus and the colicky pains (tormina) precede the anatomical changes, and are much more rationally explained by the direct action upon the nerves of the cause of the disease, or by the derangement of innervation effected through changes in the circulation.
An acute case of catarrhal dysentery may exhibit no further lesions, and in the lightest cases even these may have entirely disappeared post-mortem, so that no change at all may be observed at the autopsy.
In a more severe or protracted case the other alterations which constitute the more complete cycle of the inflammatory process follow the stage of hyperæmia. The arrest of circulation becomes more or less complete, and the white corpuscles emigrate from the vessels to form the pus-cells. Fibrin, or the elements which compose it, also escapes to infiltrate the mucous membrane and remain upon its surface. The pseudo-membranous or diphtheritic process is now developed, and may vary in intensity from a mere frosting of the surface to dense infiltration of the entire thickness. The false membrane, as well as the mucous membrane, next suffers necrosis to form more or less extensive sloughs. These sloughs are grayish-white when fresh, dark-brown when stained by the intestinal contents, or greenish or black when undergoing gangrene. They may cover patches of the mucosa or the whole mucosa from the ileo-cæcal valve to the rectum. They soon become soft and pultaceous, hang in flaps or festoons in the interior of the intestinal tube, or, detached, are voided in fragments or shreds. One such fragment nine inches long is recorded in Woodward's exhaustive description of the pathology of this disease. Examined under the microscope, they are seen to consist of coagulated fibrin, red and white blood-corpuscles, epithelial cells and débris, necrotic pieces of mucosa, and myriads of micrococci and other micro-organisms.
The fall of the sloughs leaves the dysenteric ulcer. Its edges are irregular and ragged, its base uneven like a crater, and its surface is more or less covered with pultaceous débris. The submucous connective tissue may form its base, or, this structure having been also destroyed, the muscularis may be exposed, or in more extensive necrobiosis the peritoneum itself may be laid bare. Occasionally this last barrier is broken down, and perforation occurs. Or an acute peritonitis may be developed, in dysentery as in typhoid fever, by simple extension of the inflammatory [p. 800]process without perforation. Perforation is very rare in cases of follicular ulceration, and is by no means frequent in the diphtheritic process, but it is the most frequent cause of peritonitis in chronic dysentery. It may occur in any part of the colon, but does occur most frequently in the cæcum. The resulting peritonitis is fatal as a rule, but the danger is obviated sometimes, as in typhoid fever, by agglutination of the gut to a contiguous structure or viscus. Perforation usually occurs late in the disease, but it may occur very early. Thus Nägele reports from the Franco-Prussian War a case in which perforation took place on the fourth day, the diagnosis having been confirmed by an autopsy. In rare cases a perityphlitis may ensue, with its natural consequences, or periproctitis may be developed with perineal abscess, or, finally, fistulæ may form to burrow about and discharge themselves anywhere in or upon the surface of the abdomen, the lumbar region, or the thigh. Bamberger describes cases of perityphlitis attending dysentery, in some of which resorption occurred, while in others pus was discharged upon the surface of the abdomen; and the writer of this article once saw, in consultation with T. A. Reamy, a case of fistula which extended from the descending colon to the vagina. Through the opening made to discharge the pus from a fluctuating abscess pointing in the vaginal vault an india-rubber tube could be passed for six to eight inches. The patient finally died from marasmus.
Chronic dysentery is distinguished by the alterations which occur in inflammation developing more gradually and extending over a longer period of time. Under the irritative changes resulting from an altered circulation the connective tissue undergoes marked hyperplasia, so that the wall of the intestine becomes at times enormously thickened, and its calibre is often correspondingly diminished. Cornil observes that acute or subacute dysentery is characterized by infiltration of the submucous connective tissue, followed by destruction, while in chronic dysentery the predominant lesion is essentially a proliferation and thickening of the connective tissue of the large intestine. The muscular tissue also undergoes hypertrophy, and the peritoneum becomes thickened and opaque. Sometimes the peritoneum is covered with patches of false membrane, or agglutination occurs with other portions of the intestine to give rise to contortions or occlusions.
Ulceration shows itself in chronic dysentery in every grade and stage of the process, from the first denudations to old cicatrizations. In bad cases the whole course of the colon from the ileo-cæcal valve to the rectum may constitute one vast tract of suppuration. Blood-vessels may be opened by the necrotic process, and copious, even fatal, hemorrhage may ensue. When pure blood is discharged, the hemorrhage usually occurs in this way per rhexem, but the quantities of blood evacuated with other elements usually escape per diapedesem.
The cicatrization which results puckers the edges of the ulcers, and may in cases of extensive or circular ulceration lead to more or less stenosis of the intestinal tube. According to Rindfleisch, the scars of dysenteric ulcers are very prone to contract, so that "the liability of a subsequent stricture is directly proportionate to the extent of the previous ulceration." The danger in these cases may be immediate from entire, or more remote from partial, occlusion. Thus, Bamberger records a case of [p. 801] typhlitis due to impaction of feces above a stenosis gradually developed from a dysenteric ulcer.
Although dysentery is a disease of the large intestine, its lesions are not exclusively limited to this structure. It is always a purely local disease at first, and, strictly speaking, continues so throughout its course, yet it produces in severe or chronic cases widespread and general effects. Rapid emaciation sets in, and anæmia is soon pronounced in all the internal organs. The mesenteric glands show signs of irritation or of absorption of specific products in hyperæmic pigmentation and hyperplasia. The kidneys in acute cases exhibit venous stasis, and in chronic cases may undergo parenchymatous change. The joints are peculiarly liable to suffer in certain cases, and the nervous system may exhibit lesions—points to be described in the symptomatology of the disease. Should pyæmia occur, it superimposes its own particular lesions in the serous membranes and internal organs. All of these affections are to be regarded, however, rather as complications than essential effects.
But the liver is found affected so frequently in dysentery as to constitute more than a mere coincidence. Schneider has recently (1873) reported of the results of his observations on 1400 cases of tropical dysentery that in the 395 post-mortem examinations the liver was found normal in but 10 cases. The abnormalities were as follows: hyperæmia of various grades, 160; fatty degeneration, 62; abscess, 57; nutmeg liver, 47; perihepatitis, 25; granular atrophy, 19; syphilitic atrophy, 8; cicatrices, 6; excavation with helminth, 1. Bérenger-Féraud (1883) reports of 411 fatal cases of dysentery observed at Senegal that the liver appeared sound to the naked eye 98 times (23 per cent.) and diseased "undeniably" 313 times (77 per cent.). Of the 313 cases of hepatic affection there were found—hypertrophy, softening, or hyperæmia, 123 times (39 per cent.); abscess, 143 times (46 per cent.); simple discoloration, 29 times (9 per cent.); atrophy or cirrhosis, 18 times (6 per cent.). Annesley found abscess of the liver 21 times in 29 cases of dysentery; Hospel, 13 times in 25 cases; and Budd found ulceration of the large intestine 10 times in 17 cases of hepatic abscess. Gluck had the opportunity of making 28 post-mortem examinations in 151 cases of dysentery in Bucharest, finding abscess of the liver 16 times. All these authors adopt the explanation first offered by Budd of direct transfer of diseased products through the mesenteric and portal veins.
But more extensive observation has developed the fact that the frequency of abscess of the liver in connection with dysentery is a peculiarity of tropical climates. In the temperate and colder regions of the North this complication is not by any means so frequent. Frerichs declares that of 16 observations collected by Louis and Andral, "ulcers were present in only 3, and in 2 of these cases the ulcers were tubercular; of his own 8 cases, there was intestinal affection in none." Gluck believes that the liver is more prone to show suppuration when already predisposed to it by a preceding amyloid or cirrhotic change of malarial origin. Eichhorst calls attention to the well-known fact that abscess of the liver is especially a disease of the tropics independently of dysentery, and the frequency of its occurrence here may be a mere coincidence. But it must be remembered that opportunity for post-mortem examination, upon the [p. 802]results of which these statistics are based, does not occur in the great majority of cases of dysentery, and abscess of the liver is very often overlooked. Thus, Schneider cites cases where persons with abscess of the liver of the size of the head were considered simulants up to twenty-four hours before death. Since the diagnosis of hepatic abscess has been made so easy by aspiration, cases begin to multiply; and it is doubtless the experience of most practitioners, in the temperate zone at least, that the decided majority of cases of hepatic abscess acknowledge an existing or previous attack of dysentery. Certainly, few authors would now venture to subscribe to the view of Annesley, that the abscess of the liver was the primary malady and was the cause of the dysentery.
SYMPTOMATOLOGY.—Dysentery, as stated, begins, as a rule, with the general signs of a gastro-intestinal catarrh. So frequent is this mode of inception, and so few are the exceptions, that it is impossible to resist the conclusion that the disease is caused by the introduction of a noxious element into the alimentary canal. The irritation thus induced begins at the stomach, and is rapidly propagated throughout the whole tract of the intestine. In the course of a few days the cause of the disease becomes strictly localized to the large intestine, whose greater capacity and more sluggish movement fit it for the easier reception and longer retention of noxious matter.
But specific dysentery and the more intense forms of catarrhal dysentery occasionally exhibit distinctive symptoms from the start, and in rarer cases the disease is suddenly announced with such tempestuous signs as to excite the suspicion of poisoning. Thus, a case (one of five lighter cases) is reported from the Rudolfstiftung in Vienna (1878) where the disease closely simulated Asiatic cholera, and where it rapidly ran a fatal course, in spite of laudanum, soda-water, ice pills, mustard plasters, injections of amyl nitrite, camphor, and ether, and faradization of the phrenic nerve to stimulate the failing respiration. Finger reports similar cases from the hospital at Prague.
Ordinarily, the peculiar pains of dysentery first proclaim the character of the disease. The severe grinding, twisting pains, tormina, are more or less localized in the course of the colon, and hence surround or traverse the entire abdomen, the pains at the epigastrium being due to spasmodic contractions of the transverse colon. The patient in vain adopts various postures in relief or sits with his hands firmly compressing the abdominal walls. The tormina are more or less intermittent or remittent, and are usually experienced in greatest severity toward evening. During their acme the face wears the aspect of the intense suffering, which is expressed in outcries and groans. At the same time there is upon pressure over the whole abdomen more or less tenderness, which soon comes to be especially localized at the cæcum or sigmoid flexure.
The tenesmus (cupiditas egerendi) is a more distressing, and certainly more distinctive, sign of dysentery. It is the feeling of heavy weight or oppression, of the presence of a foreign body in the rectum, which demands instant relief. At the same time intense heat is felt in the rectum, which the patient likens sometimes to the passage of a red-hot iron. The desire of evacuation becomes as frequent as urgent. In well-marked cases the patient sits at stool half an hour or an hour at a time, straining until faint [p. 803]and exhausted, leaving the commode with reluctance, only immediately or very soon to use it again.
Great depression is felt at the stomach at the same time, with nausea, occasionally with vomiting; and strangury, with the discharge of only a few drops of scalding urine or blood from the bladder, adds additional suffering to the disease. Retraction of the testicle and prolapsus ani, especially in children, are prone to occur in severe cases.
But neither the pain nor the prostration is so characteristic of dysentery as the stools, which, though of very varied nature, are nevertheless distinctive. After the discharge of the intestinal contents the first evacuations consist of mucus in the form of glairy, stringy matter, like the white of an egg, expressed as the result of the violent efforts at straining. The mucus may be pure or tinged with blood, but it is usually very scant in quantity, and stands in this regard in marked contrast with the violence of the efforts to secure its extrusion. It is the frequency of its discharge which constitutes an especial distress. Twenty to forty, even two hundred, times in the twenty-four hours the patient must go to stool. In the worst cases the patient sits at stool or lies upon the bed-pan the most of the day.
The mucus is sooner or later mingled with pus or stained with blood. The presence of pus by no means necessarily implies the existence of ulceration, as the apparently pure mucus always shows occasional white blood-corpuscles under the microscope, and even extensive suppurations occur without apparent solutions of continuity.
The presence of blood is equally characteristic of dysenteric stools. Usually it is intimately commingled with the mucus or pus or forms the chief element of the copious so-called bilious discharge. The evacuation of pure blood indicates erosion of vessels low in the colon, often in the rectum itself, though enormous quantities of blood are sometimes voided from unbroken surfaces. Thus Lécard reports the case of a soldier who "while sitting restless at stool lost one and a half quarts of blood." The patient died on the fifth day of the disease, and at the autopsy there was found "apoplectiform congestion from the ileo-cæcal valve to the anus, but no ulcers anywhere, nor any broken vessels."
Besides the mucus, pus, and blood, the dysenteric stools contain the sloughs which have been torn off by violent peristalsis in cases of the diphtheritic form. Usually they are separated in shreds and fragments, but occasionally large sheets, even casts of a section of the colon, are voided en masse. These were the cases considered by the older authors to be detachments of the mucous membrane itself. As already observed, these fragments consist for the most part of inspissated mucus, pus, blood, and tissue-débris; but there is no doubt that in some cases partially necrosed mucosa also enters into their construction. One enormous tubular cast fourteen inches long, preserved in our Army Medical Museum, was found to be "composed of pseudo-membranous lymph in which no traces of the structure of the mucous membrane could be detected" (Woodward).
There still remains to be mentioned the boiled-sago or frogs'-spawn matter whose origin has given rise to such a curious mistake. Not infrequently these vitreous-looking bodies compose the bulk of the sediment in the stools of dysentery, and even some of our modern authors, [p. 804] unacquainted with the more searching investigations of Virchow, have regarded them as expressed contents of intestinal follicles. Virchow found that under the application of iodine they always assumed a blue color, whereupon he ironically remarks that the sago-like mucus is really mucus-like sago. They are simply granules of starch ingested as food, to remain partially or wholly undigested.
The scybalæ, the composite matter known as the lotura carnea, and the micro-organisms found in the stools have already received mention elsewhere.
Although the stools of dysentery are scant, as a rule, they are so frequent as to discharge during the entire twenty-four hours a very large quantity of albuminous matter. Oesterlen has made the curious calculation to show that the mean daily loss of albuminates in dysentery of moderate intensity is from 50 to 60 grammes during the first fourteen days, and on an average about 20 grammes during the next eight days. The total loss experienced in an attack of three weeks' duration thus amounts to about 1000 grammes—in rough figures, two pounds avoirdupois. The rapidity with which emaciation, hydrops, and marasmus occur in severe cases is thus easily accounted for. Nägele speaks of cases where patients were reduced to skeletons in eight to fourteen days, so that the convalescence extended over six weeks to eight months.
The alteration in the character of the secretion in dysentery is not confined to the mucous membrane of the large intestine. On the contrary, all the digestive juices are changed, in some cases entirely checked. In the graver cases the saliva takes on an acid reaction and loses its glycogenic properties; the gastric juice in the same cases becomes alkaline and loses its peptonizing properties; while the secretion of the bile is wholly arrested. Uffelmann, who had the rare opportunity of studying the secretion of bile in a case of biliary fistula, relates that during an attack of dysentery the bile ceased entirely to flow, and only began to show itself again, at first greenish, then greenish-brown, finally brown, during the process of resolution on the ninth day of the disease. The anorexia, nausea, and vomiting which so often mark the access or attend the course of dysentery find thus easy explanation.
Should the disease continue, the general strength of the patient becomes so profoundly reduced as to resemble the status typhosus. The tongue, which has been hitherto thickly coated, now becomes black, shows fissures, and bleeds, while the gums are covered with sordes. The pulse becomes feeble, thready, or barely perceptible. The skin is dry and harsh or scaly. The abdomen is tumid or collapsed, the anus paralyzed, and the discharges continuously ooze out to excoriate the perineum. While the brain is usually clear throughout the disease, insomnia, stupor, or coma develop in the gravest cases from absorption of disease-products (Senator), or death suddenly ensues from heart-clot or from thrombus of the venous sinuses of the dura mater (Busey).
Pyæmia announces itself with a series of chills, followed by irregular temperature, by the speedy occurrence of multiple abscesses in distant organs, venous thromboses, affections of the serous membranes, pleuritis, pericarditis, and embolic pneumonia. Gangrene of the intestine, which may occur as early as the third day of the disease (Nägele), is evidenced by the signs of general collapse.
[p. 805] COMPLICATIONS AND SEQUELÆ.—The lighter cases of dysentery, as well as most of the grave cases, run their entire course without complication, and often without sequelæ. But a certain percentage of cases is attended with complications on the part of the joints (rheumatism), of the nervous system (paralysis), and on the part of the liver and the kidneys.
Arthritis, when it occurs, shows itself, as a rule, in the second week of the disease (Eichhorst), or after the disease has run its course, during the period of convalescence (Huelte). That it is not a mere coincidence is evidenced by the fact that it is present in a large number of cases in certain epidemics, while it is not present independently of dysentery. Thus, Braun of Stannenheim saw in the two epidemics of 1833-34 more than forty cases of rheumatism, and Huelte reports ten cases observed by himself in the epidemic at Montargis in 1854. Certain epidemics are distinguished by the rarity of this complication, while most are marked by its absence altogether. In the epidemic at Rahden (1872), 400 cases among 3800 inhabitants, Rapmund saw inflammation of the joints set in only six times; and the entire absence or extreme rarity of it in later epidemics have led most physicians to deny any connection between the diseases, or to regard the joint affection as incident to a complicating scorbutus or neuralgia. All authors who admit it describe the knee-joint as being the most frequent seat of the affection, but acknowledge that it is mostly polyarticular; while there is much difference of opinion whether it ever presents the general signs of true rheumatism—pyrexia, diaphoresis, or its complications on the part of the heart. Huelte maintains that it does not, and that it is allied to gonorrhoeal rheumatism in this respect, while Eichhorst states that it may not only show all these signs, but may be followed in exceptional cases by suppuration and ankylosis. It usually lasts four to six weeks, but neither its occurrence nor its severity stands in any relation to the intensity of the attack of dysentery. It is probably to be regarded as a manifestation of a light pyæmia or septicæmia, as it is a frequent manifestation of this condition in or after scarlatina, puerperal fever, and the septic fevers of surgery.
Paralysis has been observed to occur after dysentery ever since the days of Galen, and, disregarding the observations of ancient and of the older periods of modern times, we find occasional records of cases in our own days. Leyden,6 in reporting a case of paresis and rheumatic pains following an attack of dysentery, says that although post-dysenteric paralysis is now rarely mentioned, it was frequent in the older reports, and claims it as an admitted fact that it occurs not at all infrequently now. Joseph Frank quotes some observations of this kind, and refers especially to the dissertation of Fabricius.7 These paralyses, Fabricius observes, have been seen after the premature suppression of malignant epidemics of dysentery by opiates and astringents. Observations were afterward recorded by Graves in which paralysis occurred after colics and inflammation of the intestines; and English veterinary surgeons mention the fact that paralytic weakness of the posterior extremities of horses and cattle follow attacks of intestinal inflammation. The paralysis, when it occurs, is usually confined to the lower extremities, but may extend to [p. 806] and involve the upper extremities, by preference in the form of paralysis transversa (opposite arm and leg). Brown-Séquard attributes it to reflex contraction of the blood-vessels; Jaccoud, to exhaustion of the nerve-centres; and Röser, to the contact of the inflamed transverse colon with the solar plexus. Remak first suggested the idea of an ascending neuritis—a view which would seem to be corroborated by the paralysis observed after the experiments, by Lewisson, of crushing the uterus, kidneys, bladder, or loop of intestine, and which finds additional support, as Leyden remarks, in the length of time which lapses before it appears. Landouzy8 says that Finger found diffuse myelitis in a patient affected with paralysis supervening upon cancer of the intestine, and that Delioux and Savignac saw spots of softening in the cervical and lumbar region of the cord in the case of a man affected with post-dysenteric paralysis. Weir Mitchell suggests the possibility of other factors—long marches, malaria, bad diet, and injuries to the spine—in the genesis of the cases, mostly paraplegias, observed by him; and Woodward calls attention to lead-poisoning (as by treatment) in explanation of a certain number of cases.
6 "On Reflex Paralysis," Volkmann's Sammlungen.
7 Paralysis seu hemiplegia transversa resolutionem brachii unius et pedis alterius exhibet, Helmstedt, 1750.
8 Des Paralysies dans les Maladies aigues.
Abscess of the liver gives rise to few distinctive symptoms, and is mostly recognized or suspected, in the absence of positive signs, by the persistence or obstinacy of the dysentery. The ease and impunity with which aspiration may be performed in its recognition justifies the use of it in every doubtful case.
Regarding complications on the part of the kidneys, Zimmerman recognizes four classes of cases: (1) mild cases, showing no albumen and no casts; (2) severe, long-continued cases, with putrid stools, status nervosus, and collapse, showing albumen; (3) cases commencing with nervous symptoms, paralysis, scanty urine, showing kidneys filled with exudation-cells and detritus; and (4) cases of speedy renal complication and death. To these may be added the cases of protracted chronic dysentery with long-continued suppuration, entailing the possibility, of really rare actual occurrence, of amyloid degeneration and chronic parenchymatous change (Bartels).
Dysentery may be further complicated by parotitis; by venous thrombosis (phlegmasia dolens); by diphtheritic deposits on other mucous surfaces, which Virchow declares to be exceedingly rare; and by hydrops, which is oftener a concomitant of the period of convalescence.
Besides the deformities of the colon, which may ensue as a consequence of ulceration or peritonitis, a long attack of dysentery is apt to leave a hyperæsthetic or non-resistant state of the mucous surface, so that every imprudence in exposure or in diet begets an intestinal catarrh or a relapse of the disease.
DIAGNOSIS.—When dysentery presents itself with its whole train of symptoms the recognition of the disease is very easy. The tormina and tenesmus, the peculiar discharges, the rapid reduction of strength, leave no doubt as to the nature of the affection. The prevalence of an epidemic of the disease will often establish the character of a case even when all the signs are not present or when anomalies occur. Embarrassment in diagnosis only attends the recognition of catarrhal or isolated cases, and in these cases there may be a doubt as between dysentery and [p. 807] diarrhoea—if such a symptom can be called a disease—or typhoid fever, cholera, or some purely local affection of the rectum, cancer, hemorrhoids, etc. In children difficulty of diagnosis may arise as between dysentery and intussusception.
Dysentery is differentiated from that lighter form of intestinal catarrh whose main symptom is diarrhoea by the presence of tenesmus in dysentery, as well as by its mucous, muco-purulent, diphtheritic, and bloody discharges. Dysentery lasts longer than diarrhoea as a rule, and does not yield so readily to treatment.
Typhoid fever shows from the start brain symptoms, which are absent from dysentery; has a typical temperature-curve, whereas there may be no fever in dysentery, or, if any, of irregular remittent type; is often prefaced by epistaxis and attended with bronchitis, both of which are absent in dysentery; and exhibits ochre-colored pea-soup stools, altogether different from those of dysentery.
Cholera morbus distinguishes itself from dysentery by its sudden onset, its profuse vomiting and discharges, its violent cramps, and the speedy collapse.
Cancer of the rectum can be usually felt, and hemorrhoids can be always seen, so that no difficulty should be experienced in the recognition of these cases.
Intussusception occurs mostly in children, and has, in common with dysentery, vomiting, mucous or bloody stools, colic, tenesmus, nervous unrest, and prostration, so that a differential diagnosis may be impossible for a few days. The more strict localization of an intussusception, which may sometimes be felt as a sausage-like mass, most frequently in the right ileum and hypochondrium, the greater frequency and persistency of the vomiting and pain, the presence visibly or palpably of the invaginated gut at the anus or rectum, soon enable the careful examiner to recognize the case.
PROGNOSIS.—The prognosis of dysentery varies between extremes. Some cases are so mild as to merit the remark of Sydenham concerning certain cases of scarlet fever: "Vix nomen morbi merebantur." They terminate of themselves under favorable hygiene without especial treatment. On the other hand, no known disease has a more frightful mortality than dysentery in some of its epidemics, especially in army-life. It was this class of cases which Trousseau had in mind when he called dysentery the most murderous of all diseases. Sixty to eighty may be the appalling percentage of death in these cases.
Under favorable surroundings the average mortality of dysentery amounts to 5-10 per cent., but is much influenced by the age and the general condition of the patient, as well as by the complications which occur in its course. Thus, Sydenham said of it over two hundred years ago, "It is not infrequently fatal to adults, and still more so to old men, but is nevertheless exceedingly harmless to infants, who will bear it for months together without suffering, provided only Nature be left to herself." But dysentery is by no means always harmless to infants, for in some epidemics this period of life has been visited with the greatest severity. Thus, Pfeilstücker reports of Würtemberg (1873-74) that the greatest mortality, 39 per cent., occurred at the age of one to seven years, and the least, 4 per cent., at the age of thirty-one to fifty years; [p. 808]and Oesterlen says of England that dysentery causes 20 per cent. of deaths from all causes in the first year of life.
Nor does the prevalence of a greater number of cases necessarily imply a heavier mortality. For Bianchi reports of Rome that cases of dysentery constituted but 2.28 per cent. of all the admissions into the Ospedale di San Spirito in 1873, while in 1874 the percentage increased to 3.68; yet the mortality of 1873 was 17.02 per cent., while that of 1874 was but 9.09 per cent.
Complications on the part of the nervous system, the status typhosus, pyæmia, and great prostration, necessarily render the prognosis grave, yet even these cases are not necessarily fatal. Thus, Jules Aron reports from the epidemic at Joigny (1876) a case of recovery after complete paralysis of the sphincter ani. The recognition and discharge of an hepatic abscess relieves the patient from the dangers of this complication. Peritonitis alarmingly aggravates the prognosis, and perforation is almost of necessity fatal.
PROPHYLAXIS.—The improved sanitation of modern times has already diminished the frequency and mitigated the severity of epidemics of dysentery; and this fact, which is only an accidental observation as it were, gives the clue to the means of its further prevention.
The selection of proper sites for camping-grounds, barracks, and hospitals, the prevention of overcrowding in tenement-houses, ships, and jails, the regulation of sewage, the care for the food and drink, the observation of the strictest cleanliness by authoritative control,—all these are general measures which suggest themselves in the prophylaxis of this or any disease.
In the management of individual cases the first precaution is to prevent the dissemination of the disease. Whether it be really contagious or not, every case should be managed, as Bamberger suggests, as though it were contagious; and this protection of others secures for the individual patient the most favorable hygiene.
The bedding must be frequently changed; the windows kept open to secure free ventilation, which, in the light of existing knowledge, is the only true disinfectant; and all the furniture of the sick-room, especially including the receptacles for the discharges, must be kept perfectly clean. For this purpose the best purifier is very hot water. The temperature of the sick-chamber, if it be subject to regulation, should never be allowed to sink below or rise above 65-70° F.
The drinking-water should be secured, during an epidemic, from the purest possible source, and if good drinking-water cannot be had, what there is should be thoroughly boiled.
The discharges should properly be mixed with sawdust or some combustible substance and burned, or if this be impracticable should be buried in the soil a few feet below the surface, and not emptied into water-closets or privy-vaults used by others.
Such articles of food should be abjured as have a tendency to produce intestinal catarrh. So unripe fruits, vegetables which readily undergo fermentation—in short, all indigestible substances—should stand under ban. But no prohibition should be put upon ripe fruits or simple nutritious food of any kind.
Lastly, individuals should protect themselves from catching cold. The [p. 809] researches of Pasteur have disclosed the fact that certain germs of disease will grow and multiply in the body of an animal whose temperature is reduced, when they would not increase without it.
TREATMENT.—The first requisite in the treatment of an individual case is perfect rest. Patients with even the lighter forms of catarrhal dysentery should observe the recumbent posture, and cases of more serious illness should be put to bed. Rest in bed, an exclusive diet of milk—which should always have been boiled—and the time of a few days is sufficient treatment for the mildest cases. Where there is objection to milk, meat-soups, with or without farinaceous matters, rice, barley, etc., may take its place.
A case which is somewhat more severe will require perhaps a light saline laxative—a Seidlitz powder, a dose of Rochelle salts or Epsom salts in broken doses—or a tablespoonful of castor oil or five to ten grains of calomel, to effect a cure. For the relief of the pain of the lighter cases nothing is equal to tincture of opium, of which five to ten drops every three or four hours in a tablespoonful of camphor-water acidulated with a few drops of nitric acid will generally suffice; or Dover's powder in broken doses, one to three grains, with five to fifteen grains of bismuth or soda, or both, is a good substitute for a change.
The successful treatment of dysentery in any form depends upon a recognition of the fact that the disease is local as to its seat, and is probably specific as to its cause. The anodynes relieve the effects, but the laxatives remove the cause. Consequently, the most rational treatment of the severer cases is the irrigation of the large intestine and the thorough flushing out of its contents. The use of clysters in the treatment of dysentery dates from the most ancient times, with the object, however, rather of medicating than washing out the bowel. O'Beirne (1834) and Hare (1849) were the authors of the irrigation treatment, which they executed by means of a long tube introduced into and beyond the sigmoid flexure. Since Hegar has recently shown how the whole tract of the large intestine can be thoroughly inundated and flushed with a common funnel and rectal tube, the practice has continually gained ground, until it is now admitted as the most valuable method of treatment. H. C. Wood of Philadelphia, and later Stephen Mackenzie of London, have reported a number of cases in which irrigation of the bowel with large injections medicated with nitrate of silver, drachm j-pint j, was attended with the most surprising results—sometimes but a single injection effecting a cure; and the writer of this article has reported one case almost in articulo mortis where complete cure followed the irrigation of the bowel—on three occasions with three pints of water containing three drachms of common alum. This case was all the more instructive from the fact that a relapse had occurred after very striking but only temporary relief had been obtained with the nitrate of silver, the alum having been substituted simply on the ground of expense.
Salicylic acid has also been extensively employed in this way with the best effects, but carbolic acid has been discarded since the reports of several cases of poisoning have been published. Should it become a question of the necessity of a parasiticide, the bichloride of mercury in extremely dilute solution, 1 to 1000, would be the agent par excellence; but it is probable that the simple flushing of the bowel is the chief [p. 810] curative agent. The use of alum is not attended with the dangers which have ensued from the absorption of carbolic acid, and which might ensue from the bichloride of mercury. The water used in the injections should always be cold. Ice-water injections alone give at times the greatest relief. Wenzel uses injections of ice-water in all recent and acute cases, whether slight or severe—in bad cases every two hours. He seldom finds it necessary to use opium. The object is to introduce as much water as possible without producing too much pain. The large intestine of an adult holds, on an average, six imperial pints, but in the author's experience not more than three or four pints can be safely introduced. The patient should lie upon the back or the left side with the hips elevated and the head low, while the injection is slowly introduced from a funnel, fountain, or a bulb syringe whose nozzle is thoroughly anointed with vaseline. In the absence of a thoroughly competent assistant the operation should be performed by the physician himself, for the proper use of an irrigating enema is a practice which requires both judgment and skill. When pain is experienced, the further influx of the fluid should cease for a few minutes, when it may be resumed again and again until the largest possible quantity is introduced. It is impossible to over-estimate the value of this treatment in cleansing, disinfecting, and constringing the foul and flabby surface of the whole seat of the disease. As was said by Hare, "It changes a huge internal into an external abscess, and enables us to cleanse the bowel of its putrid contents."
Of all the remedies which have been recommended in the relief of dysentery besides the irrigation method, but one, ipecacuanha, deserves the name of a specific. This remedy was first introduced into practice in 1648 by the botanist Piso, who was led to adopt it from the popular praise he had heard of it while travelling in Brazil. He considered it the most exquisite gift of nature, and administered it in infusion according to the Brazilian (subsequently known as the French) method. Légros made three successive voyages to South America to import supplies of the drug to France, but neither he nor the French merchant Grènier, who had brought over more than one hundred and fifty pounds of it, could secure its general use. Thereupon, Grènier acquainted Adrian Helvetius, a Dutch physician practising in Paris at the time, with the wonderful virtues of the Radix dysenterica, who, having experimented with it first upon patients of the lower classes, was later successful in curing the Dauphin of France. The further use of it, by permission of the king, at the Hôtel Dieu, enabled him to secure a monopoly of its sale and secured for him a grant of a thousand pounds. Grènier hereupon put in his claim for a division of the profits, and upon the refusal of Helvetius instituted suit to obtain his rights. Justly indignant at the loss of his suit, he revealed the secret, and ipecacuanha became common property at once. Extravagant ideas were now entertained of its value, but in the extreme reaction which followed every virtue of it was disavowed, so that the drug came to be almost forgotten. From this temporary oblivion the remedy was rescued by an English army surgeon, E. Scott Docker, in 1858, who administered it, in combination with laudanum, in his regiment, on the island of Mauritius, in all cases and stages of the disease with such success that out of fifty cases he lost but one. Although such indiscriminate use and such almost unvaried success has not attended, and from the nature [p. 811]of different cases could not attend, its universal employment, there is no doubt of the inestimable value of the service rendered in the restoration of the remedy in the treatment of dysentery. Yet over twenty years elapsed before its author received from his country, at the urgent solicitation of the Director-General, in recognition of this service, a grant of four hundred pounds.
Remarkable testimony as to its efficiency soon began to appear. Ewart9 recommends ipecacuanha in every form and type of acute dysentery, as well as in the acute attacks supervening upon chronic cases. Its advantages are simplicity, safety, comparative certainty, promptitude of action, decrease of chronic cases and of complications, especially abscess of the liver, and great reduction of mortality. "It produces all the benefits that have been ascribed to bloodletting, without robbing the system of one drop of blood; all the advantages of mercurial and other purgatives, without their irritating action; all the good results of antimony and other sudorifics, without their uncertainty; all the benefits ascribed to opium, without irritating, if not aggravating or masking, the disease." To the objections urged against it he replies that the nausea is only temporary and evanescent—that vomiting is exceptional and of but short duration; moreover, it permits nourishment and assimilation and produces sleep. If uncontrollable sickness and vomiting occur, they are probably due to abscess of the liver, malaria, some other cachexia, Bright's disease, strumous mesenteric glands, hypertrophy of the spleen, peritonitis, or extensive sloughing.
9 Indian Annals Med. Science, April, 1863.
Cunningham prefaces the treatment by a sinapism to the epigastrium and half a drachm of the tincture of opium. Then from one to one and a half drachms of ipecacuanha are administered in powder. It causes considerable nausea, and vomiting occurs in one to two hours. During the nausea copious perspiration breaks out, the pulse becomes fuller, softer, and less frequent, the tenesmus and abdominal pains cease, and the patient has no more stools for twelve to twenty-four hours. The next evacuation is easy, fluid, but free from blood or mucus. Sometimes the dose of ipecacuanha may require to be repeated.
Malun reports the results of treatment of 436 cases occurring in twenty-one months. There were only 6 deaths, and in only 1 of these could the remedy be fairly said to have failed. Under all other plans of treatment the mortality has varied from 12 to 22.3 per cent.
Mr. Docker says that the mortality of dysentery in the British army during the ten years that followed the adoption of the ipecacuanha treatment fell from 11 to 5 per cent.
The remedy is best administered in large doses, 20 to 40 grains, and should be repeated every four to twelve hours until permanent good effects are secured. A dose of 15 to 30 drops of tincture of opium, or morphia, one-fourth grain hypodermically, will best protect the patient from too great exhaustion. The beneficial results are mostly obtained in the acute cases, though surprising results sometimes follow in cases of very long standing. Thus, Gayton records a case of severe chronic dysentery of eighteen months' duration which was entirely cured by ipecacuanha, and probably most physicians of large practice can recall cases where the continual relapses of the dysenteric habit have been completely broken up by [p. 812]one course of active treatment. Should the remedy fail to be of service in the course of forty-eight hours, it should be discontinued.
Batiator, the bark of the root of the Ailanthus glandulosa; mudar, the bark of the root of the Calotropis gigantea; and bael-fruit, more especially in chronic cases,—have been proposed by Roberts, Duval, Chuckerbutty, and others as substitutes for ipecacuanha, but are not likely to soon supplant it.
Materia medica is rich in drugs whose virtues have been vaunted in dysentery, and cases occur where the judicious physician will make his selection according to the indications in a given case. Turpentine internally, as well as externally in the form of a stupe (Copland), has had advocates from ancient times; astringents, tannic acid or the substances which contain it, kino, catechu, krameria; the acetate of lead, nitrate of silver, etc.; antiseptics, carbolic acid, salicylic acid, boracic acid; anodynes, opium and its preparations; and quinia,—are among the agents most frequently employed.
Bonjean (1870) had occasion to laud the efficacy of ergotin in checking hemorrhage and controlling the discharges in a report which substantiates the claim of Rilliet and Lombard in the epidemic at Geneva in 1853. Massolez had the same good results in the war of the Crimea, as had also Andrea in the Spanish hospitals of Ceuta and Tetuan.
Clysters of nitrate of silver, 4 grains to 5 ounces of water (Duchs), or with a few drops of tincture of opium (Berger); of ipecacuanha (Begbie and Duckworth); of laudanum and starch (Sydenham, Abercrombie); of the various astringents,—may be tried in obstinate, more especially chronic, cases.
Local inspection of the rectum by means of the speculum may possibly reveal an ulcer, which is the chief or sole cause of the tenesmus and bloody discharge. Maury reports such a case in which the ulcer was deep enough to hide a small sponge. In such cases topical treatment may effect a cure.
Dilatation may suffice to overcome a stricture in the rectum, the result of cicatricial contraction, or colotomy may be necessary in cases more refractory or situated higher in the bowel. Post10 reported a successful colotomy, with the formation of an artificial anus in the left lumbar region, in such a case.
10 New York Med. Record, 1879, xvi. 24, p. 260.
The food should be fluid, but nutritious, and milk best fulfils both these requisites. Where milk cannot be tolerated it may be substituted by soups, beef-tea, mutton-broths, chicken-soup, etc. But it should be known of these substitutes that they contain little or no nutritious matter on account of the insolubility of the albuminoids, and are really only stimulants. Soft-boiled egg, thin custards, sweetbreads, scraped or chopped raw beef—albumen thus in substance—constitute the best food. But during the intensity of an attack the patient should almost altogether abstain from food, both from lack of inclination for it and from lack of ability to digest it. During convalescence the food should be on the basis of animal diet, though ripe fruits and fresh succulent vegetables should not be altogether withheld.
In all cases of pronounced prostration stimulants are to be freely used, and of all stimulants alcohol is the best, as it has also nutritive and [p. 813] antiseptic properties. Alcohol is thus triply indicated in the treatment of dysentery, but the choice of the form and strength will be a matter of judgment in the individual case.
Where life is imperilled by hemorrhage or anæmia from any cause, a forlorn hope is offered in transfusion, which in the hands of C. Schmidt (1874) has proved successful in two cases.
Abscess of the liver is best treated by aspiration or hepatotomy; rheumatism, by the salicylates; and paralysis, by the constant current of electricity.
Obstinate cases of chronic or continually recurring dysentery are thoroughly cured only by a sea-voyage, a sojourn at the seashore, a mountain-excursion, or a permanent change of climate.
HISTORY.—Typhlitis ([Greek: typhlos], blind), inflammation of or about the head of the colon, more especially the vermiform process, is a disease of modern recognition. Individual cases had been reported as curiosities where foreign bodies or fecal accumulations had excited inflammation in this part of the intestine, but it is undoubtedly to Dupuytren1 that the credit is due of having first individualized this disease as a separate affection. About the same time (1827) Longer Villermay published his communications in the Archives gén., t. v. 246, on the diseases of the vermiform process, to be followed in the same year by Mêlier2 and Hussar and Dance with observations on inflammation of the connective tissue in the region of the cæcum. These affections, which had been hitherto described as inflammatory tumors in the right iliac region, now received from Puchelt3 the distinct name perityphlitis.
1 Leçons oral de Cliniq. chirurg., t. iii. art. xii.
2 Arch, gén., Sept., 1827.
3 Heidelberg klin. Annal., i. 571 and viii. 524.
Perhaps the most remarkable events in the history of these affections since this time are the contributions of Stokes and Petrequin (1837) on the value of opium in the treatment of perforation of the vermiform appendix, of Albers,4 who first distinguished the special form of typhlitis stercoralis, and of Oppolzer (1858-64), who set apart, perhaps as an unnecessary refinement in differential diagnosis, a paratyphlitis, an inflammation of the post-cæcal connective tissue. Matterstock5 (1880) deserves especial mention for having given such prominence to anomalies of the vermiform appendix in the etiology of the affection; and Kraussold6 (1881) has connected his name with the therapy of the disease by the boldness with which he expresses his convictions regarding the necessity of early evacuation, by incision, of inflammatory products, as first practised by Willard Parker in 1843.
4 Beobacht. aus dem Gebiete der Pathologie, ii. 1.
5 Handbuch d. Kinderkrank., Bd. iv. p. 893.
6 Volkmann's Sammlung., No. 191.
GENERAL REMARKS.—Typhlitis, strictly speaking, is limited to affections of the cæcum and its appendix vermiformis; perityphlitis is mostly due to extension of the inflammation to the peritoneal envelope of these organs; while paratyphlitis signifies an involvement of the extra-peritoneal and post-cæcal connective tissues. Both perityphlitis and paratyphlitis are therefore secondary processes, though they may, in exceptional cases, arise from affections of organs other than the cæcum, as from [p. 815] perinephritis, psoitis, vertebral caries, or as an expression of metastatic processes in pyæmia, septicæmia (puerperal fever), typhoid fever, etc.
ETIOLOGY.—Typhlitis and its allied affections or complications show especial predilection for the male sex and the period of adolescence. Nearly three-fourths (733) of the whole number (1030) of cases of perityphlitis collected from the literature by Matterstock were males, and this proportion holds good in infancy and early youth as well as in adolescence. The greatest number of cases, 33 per cent., occurred at the ages of 21-30; next, 30 per cent., at 11-20; while the ratio gradually decreases toward both extremes of life. So the opinion is expressed with singular unanimity by all authors that these diseases pre-eminently affect the bloom of life.
The observation that typhlitis has so often been found to arise from disease of the vermiform process has led to a closer study of its anatomical relations, and developed the fact that this organ is subject to great variation in size, shape, and situation.
Normally, the appendix vermiformis arises from the posterior interior aspect of the cæcum as a tube of the diameter of a goosequill and a length of three to six inches, with a general direction upward and inward behind the cæcum. It is commonly provided with a small mesentery, which retains it in its place. Its cavity communicates with the cavity of the cæcum by a small orifice which is at times guarded by a valvular fold of mucous membrane, while its free closed end terminates abruptly in a blunt point. It is commonly found filled with mucus throughout its entire length. The existence of this superfluous structure, which is found only in man and certain of the higher apes, has given rise to much speculation among the anatomists and physiologists, especially of the teleological school, as to its possible use. It is now, however, the generally acknowledged opinion that the appendix vermiformis is a relic or rudiment of a subsidiary stomach in lower forms of life. The head of the large intestine, which forms almost an additional stomach in the Gramnivora, and is three times the length of the whole body in the marsupial koala, is very much reduced in the Carnivora, whose food contains but little indigestible matter, and is greatly reduced in the Omnivora, as in man. The vermiform appendix is the shrivelled remnant of the great cæcal receptaculum of the lower animals. In the orang it is still a long convoluted tube, but in man it is reduced, as stated, to the size of a quill three or four inches in length, and is often entirely absent.
Kraussold, who complains that the vermiform process has hitherto received only step-motherly treatment at the hands of anatomists and clinicians, undertook a series of investigations which went to show how often and what extreme anomalies do occur. In some cases the appendix was disposed in an exactly opposite to the normal direction, its blind end being turned upward along the ascending colon. In one case it was found wound about the ileum; in another, spirally turned at its end and lightly adherent to a hernial sac. Sometimes it was abnormally long or short, open or closed with a valve, cylindrical, saccular, or bulbed, fixed or free, curved or bent upon itself at a sharp angle, provided with a short mesentery, and sometimes, as stated, it was entirely absent.
But by far the most interesting point connected with this organ was the frequency with which it was found the seat of ulceration or stricture [p. 816] from cicatrization somewhere in its course, the result of dysentery, typhoid fever, syphilis, and more especially of tuberculosis. Clinicians who have been struck with the frequency with which typhlitis has occurred in tuberculous subjects find in this discovery a satisfactory explanation of this very remarkable coincidence.
Normally, the vermiform appendix is found filled, as stated, with a tough vitreous mucus, but not infrequently masses of feces, foreign bodies, intestinal worms, etc. find their way into it, where they may remain innocuous or may excite a dangerous inflammation. This fact, in connection with the general uselessness or superfluousness of this structure, has led pathologists to characterize the vermiform process with the significant appellation of a death-trap.
Two anatomical factors deserve especial emphasis in explanation of the frequent origin of disease in the vermiform appendix. One is the existence of the valvular fold of mucous membrane, already mentioned, at or near the orifice of the tube in the cæcum, the clinical importance of which was first pointed out by Gerlach. This fold is most marked between the ages of three and twelve, and when pronounced narrows the orifice to one-half or one-third of the whole calibre of the tube. As a rule, this fold, and the consequent diminution in the size of the orifice, are but little marked in the first years of life and in old age, which accounts for the relative infrequency of typhlitis at these periods of life.
The second mechanical factor is the deformity caused by the abnormal anatomical position of the organ, either as a congenital defect or as a pathological change. Matterstock quotes from Züngel, who observed in 59 cases in the Hamburg hospital whole or partial obliteration 30 times, catarrh and old fecal concretions 43 times, abnormal adhesions 12 times, and tubercular ulceration (without perforation) 11 times. Toft claims as the result of 300 personal investigations that every third person between the ages of twenty and seventy showed the traces of present or past inflammation, and that actual ulceration existed in 5 per cent. of all bodies examined. Kraussold declares that this percentage is rather too low than too high, and adds that among his patients—who were, it should be stated, mostly phthisical—it was remarkable how extraordinarily often the whole vermiform appendix was the seat of an encroaching ulcer. In a number of cases cicatrices or cicatricial alterations were found where typhoid fever or dysentery had existed in the previous history.
Attention should at least be called to a last anatomical factor in explanation of the frequency of ulceration and inflammation of this structure, in that its walls are so sparsely endowed with muscular tissue as to render it unable to empty itself of the virus or germs of disease which enter it from the comparatively stagnant reservoir, the cæcum.
Constipation is usually invoked as a cardinal factor in the genesis of typhlitis (typhlitis stercoralis). Speck calls attention to the frequency of the disease in East Siberia, where the food, mostly vegetable, contains a large amount of indigestible residue. But that this condition cannot sufficiently account for the disease in most cases is proved by the fact that constipation is more frequent in advanced life and among females, in whom typhlitis with its associate lesions is more infrequent. For the same reason a sedentary mode of life loses force as an argument in its production. Perhaps the most efficient cause of the condition is a local [p. 817]paresis of the muscular tissue of the cæcum produced by the irritation of intestinal catarrh, of disease virus, of a fecal concretion or a foreign body—an irritation which may induce first a spasmodic action, and subsequently, as a result, a partial paralysis or a paresis. The same condition may be brought about more directly by the presence of a centre of irritation—viz. by reflex inhibition of innervation. Accumulation and impaction of feces must then necessarily ensue, and it is highly probable that this accumulation occurs in this way as a result more frequently than as a cause of the condition. For the symptoms of a simple accumulation of feces (coprostasis) are never so severe, at least at the start, as to mark the onset of a genuine typhlitis. Nor is there anything in healthy feces to induce the signs of a severe blood-poisoning which so commonly announces the advent or course of typhlitis.
Room is here open for the surmise that most cases of typhlitis pur et simple are due to the presence in the cæcum of the germs or virus of disease taken with the food or drink, and traversing innocuously the whole length of the alimentary tract, to finally bring up in this most stagnant part of the intestinal canal.
The rôle of pure mechanical causes cannot be ignored or underrated in perityphlitis, understanding by this division processes which commence in the vermiform appendix. For it is the rule to discover in the vermiform appendix in these cases either fecal concretions or foreign bodies. Haeckel and Buhl found concretions of meconium in a new-born child, and fecal concretions, intestinal stones, are far more frequently encountered than foreign bodies. In 146 accurately observed adult cases recorded by Matterstock, fecal concretions were met with 63 times, foreign bodies 9 times, while in the other cases nothing could be discovered; and in 49 cases among children, fecal concretions were discovered 27 times, foreign bodies 3 times, and nothing abnormal in the remaining cases. Not infrequently a small foreign body acts as a centre of crystallization for feces which become superimposed in successive layers. Hairs, as of the beard, sometimes officiate in this way. Among other foreign bodies met with in fatal cases of perforation, independently of feces, may be mentioned round-worms (Faber), cherry-stones (Paterson), needles (Payne), fish-bones (Züngel), gall-stones (Hallete), a mass of ascarides (Klebs), buttons (Gerhardt), etc., etc. As already intimated, supposed foreign bodies are often found on examination to be nothing else than intestinal concretions. As to cherry-stones, which are so often accused of producing typhlitis, Biermer and Bossard found it difficult or impossible to force them into the vermiform process.
MORBID ANATOMY.—The lesions revealed upon the post-mortem table show for the most part the ordinary picture of perforative peritonitis, which is by far the most frequent cause of death. The peritoneum in the vicinity of the perforation is found hyperæmic, swollen, necrosed, covered with flakes of soft fibrin, or partially agglutinated to contiguous structures. The wall of the bowel is very much thickened by catarrhal swelling of its mucosa, proliferation of its submucous tissue in more chronic cases, oedema of all its coats, or suppurative processes. Not infrequently the mucous tissue is the seat of extensive ulceration which may involve other structures of the gut or form an abscess, even as large as a man's head, in its immediate vicinity. The abscess may remain strictly localized or [p. 818]may wander to discharge itself into the ileum, cæcum, duodenum, and diaphragm (Bamberger) with resultant empyema (Duddenhausen), colon (Prudhomme), bladder (Bossard), in which case the fecal concretion became the nucleus for a vesical stone; acetabulum (Aubry), inferior vena cava (Demaux), or peritoneal cavity, the most frequent eventuality. Duddenhausen saw in one case a pylephlebitis result, Von Buhl a pylephlebitis and metastatic liver abscess, which condition, Matterstock says, is noted 11 times in 146 autopsies; and older writers speak of discharges into the pleural sac, into the lungs, pericardium, uterus, vagina, etc. A curious case was observed by Eichhorst in Frerichs' clinic, where pus found escape through the umbilicus. So cases of burrowing sinuses with abscesses at distant seats, as in the groin or lumbar region, fistulæ with continuous discharge, and other curiosities, may be found among the records by the curious.
In cases of more acute course the lesions are often found centred about the vermiform appendix. The most various contortions, adhesions, or erosions are observed in this structure. Occasionally a constriction occludes the course of the tube, while the distal end is dilated into a condition of hydrops. It may be found perforated in one or in several places. The cicatrices or agglutinations of old attacks may be encountered; it may be cut in two or three pieces (Matterstock), or have been entirely absorbed. Kraussold records a case of this kind in a colleague who died of typhlitis. Upon the post-mortem table no trace of the vermiform appendix could be encountered except a dimple on the mucous surface of the cæcum, indicating the site of its former orifice.
SYMPTOMATOLOGY.—Typhlitis announces itself in two ways—suddenly and insidiously. In adults the disease begins as a rule with violent signs; in children there is often a prodromatous stage which may last for days or for months before a positive diagnosis can be established. There are in these cases anorexia and vomiting, constipation and diarrhoea, colicky pains, mostly concentrated about the ileo-cæcal region. There are at this time a disinclination to stand or walk, a stooped posture or gait, occasionally a light icterus, a feeling of formication or paresis in the right leg, and lastly an increased resistance or a palpable tumor in the right ileum.
In the adult the disease is wont to begin with more tempestuous signs. Not infrequently it is ushered in with a well-marked chill, upon which immediately supervenes a sharp pain at the affected region. A general collapse of strength soon follows, with fever, thirst, a husky voice, a coated tongue, vomiting, singultus, and an expression of anxiety. The impression of serious illness becomes apparent at once. The case early bears the aspect of a grave infectious disease. A constant, dull, boring, gnawing, or lancinating pain in the right iliac region first excites the suspicion of the physician as to the real nature of the disease. In children the pain is sometimes felt first in the epigastrium; in three cases mentioned by Büchner, Herzfelder, and Traube it was first experienced in the left ileum. There may be at this time no tumor, but there is increased resistance to pressure and exquisite tenderness to touch in the neighborhood of the cæcum. The whole abdomen is more or less tender, and often tumid. If there should be also gurgling from displacement of gas, doubt is excited as to the possible existence of typhoid fever.
[p. 819] In the course of a few days the tumor takes shape. A typhlitis stercoralis shows a distension of the whole ascending colon, a sausage-shaped tumor, smooth or nodulated, along the entire right side of the abdomen, with increased resistance also in the transverse colon. More frequently in typhlitis—and, as a rule, in peri- and paratyphlitis—the tumor or tumefaction is more localized about the head of the colon. Frequently the swelling is so great as to be visible as a protrusion or bulging of the affected region. Percussion shows dulness, tanquam femoris, in cases of pure typhlitis, whereas in peri-, and more especially in paratyphlitis, there is tympanites on light and dulness only on deep percussion. Palpation or palpatory auscultation occasionally, though very rarely, reveals a peritoneal friction sound (Gerhardt).
The third cardinal symptom of the disease is the disturbance of digestion, which, as stated, often precedes or attends the first manifestation of the pain and the tumor. Anorexia, nausea, and vomiting—which is in the last stage of the disease often substituted by singultus—present themselves as occasional or constant signs of the disease. Constipation remains as a rule throughout the whole course of the disease with an obstinacy which sometimes excites apprehension of an intestinal occlusion; or the constipation may alternate with diarrhoea or dysenteric phenomena, more especially in the earlier stages. The tongue is, as a rule, heavily coated, or in typhoid states is dry, glazed, or fissured, and sordes covers the teeth and gums.
Fever is not a necessary factor in typhlitis, but when present distinguishes itself by its irregular range. The pulse is usually accelerated, full, and hard; the skin is dry and harsh; the urine is scanty and high-colored, and contains "almost without exception unusually large quantities of indican" (Eichhorst).
Perforation, when it occurs, is usually recognized at once by the signs of more or less immediate collapse, which quickly results in death.
The abdomen becomes suddenly distended, meteoric over its entire surface, the normal hepatic dulness giving place to a tympanitic resonance.
Not infrequently perforation occurs as the result of an accident, as after a push or blow upon the abdomen (Volz), heavy lifting (Volperling), riding in a wagon (Marsh), after dancing (Cless), mere turning of the body in bed (Langdon Downs), after emesis (Urban), purgation (Stokes), enema (Mêlier), etc., etc. That the slightest agitation may suffice at times to break down the last barrier of serous tissue separating the intestinal and peritoneal cavity is shown in the case recorded by With, where fatal perforative peritonitis occurred after a fit of immoderate laughter.
Paratyphlitis distinguishes itself from the other forms of the disease by its more insidious character. There is also in paratyphlitis, as a rule, less disturbance in the alimentary canal. The cæcum in paratyphlitis is mostly empty or is filled with gas, whose presence is recognized by tympanitic resonance on lighter percussion. On the other hand, paratyphlitis is characterized by the greater frequency of pressure signs in the right lower extremity. If the subjacent iliac and psoas muscles be implicated, the thigh is flexed upon the leg in decubitus. Various paræsthesiæ, formication, numbness, pain, and veritable paresis are experienced in the right leg. Dysuria, retraction of the testicle, and priapism may also occur in this form of the disease. Or pressure upon the iliac vein [p. 820]induces thrombosis, with oedema, milk leg. The long-continued process of suppuration in paratyphlitis leads also at times to hectic fever or pyæmia, with slow marasmus.
In all cases relapses are very frequent, as repeated occurrences of the disease constitute the rule. Eichhorst records the case of a court-officer who suffered five attacks of paratyphlitis in the short space of one and a half years.
DIAGNOSIS.—The recognition of the disease is mostly simple. The pain, the tumor, and the disturbances of digestion sufficiently, and for the most part sufficiently early, distinguish the affection.
Simple impaction of feces is differentiated by the history of constipation; by the feel of the hardened feces, which form an elongated, nodulated, sausage-shaped tumor along the entire ascending colon, and later in shifting along the transverse colon; by the comparatively slight tenderness; and by the entire relief which follows thorough irrigation of the bowel.
Cancer may be eliminated by regard of the age of the patient, the slow development and course of the symptoms, and the gradual manifestation of its cachexia.
Invagination is an affection for the most part of early childhood—is marked by the sudden appearance of violent symptoms of disturbance of digestion, vomiting, often stercoraceous, occlusion, diarrhoea, or dysentery, with straining and discharges of blood.
DURATION.—Typhlitis and its complications have no definite duration. A case may terminate fatally in the course of a few days or may extend itself over months, or with its effects over years or for life. The disease is, as a rule, much shorter in childhood than in adult life. According to Matterstock, nearly one-half (44 per cent.) of children succumb to the disease within the first three days. Wood records the case of a girl aged ten who died in nine hours. The average duration of cases of typhlitis without suppuration ranges from fourteen to twenty-one days. The early evacuation of inflammatory products by aspiration or incision may cut the disease short at any time, or exacerbations and remissions may manifest themselves for months or years—a condition especially liable to occur when burrowing sinuses or fistulæ develop, or when passive encapsulated abscesses are aroused into activity by some accident or indiscretion on the part of the patient.
PROGNOSIS.—A case of typhlitis stercoralis has no gravity, and should terminate or be terminated within twenty-four to forty-eight hours after its recognition. Neglected or unrecognized cases, however, are not infrequently fatal from the circumscribed or more especially diffuse peritonitis which may ensue.
Typhlitis independent of fecal impaction is always a grave affection, requiring in every instance a very guarded prognosis.
Every form of typhlitis is more fatal in childhood than in adult life, and any case of the disease may present grave complications or assume a dangerous form at any time. The greater danger of childhood lies in the greater liability to peritonitis. Most subsequent writers confirm this statement, first made by Willard Parker, who also remarked that suppurative processes, abscess formation, is more common in the adult. The mortality of perityphlitis alone in childhood is 70 per cent., in adult life 30 per [p. 821] cent., so that the proportion of recoveries is exactly the reverse of these figures at the different periods of life.
The general adoption of the opium treatment has, however, rendered the prognosis of typhlitis far more favorable—has, in fact, reduced the mortality in adult life from 80 per cent., the appalling figures of the older statistics (Volz), to 30 per cent., the ratio of modern times.
The means of earlier detection and readier relief of accumulated pus have also contributed much to reduce the mortality of typhlitis. In 1872, Bull of New York had to report of 67 cases of perityphlitic abscess collected by him, mostly treated without operation, a mortality of 47½ per cent., while ten years later (1882) Noyes of Providence was able to report of 100 cases treated by operation a mortality of only 15 percent. (Pepper7).
7 "Contribution to the Clinical Study of Typhlitis, etc.," Trans. Med. Soc. Penna., 1883.
The development of fistulæ or wandering abscess, the occurrence of pyæmia and peritonitis, necessarily aggravate the prognosis of a simple case. Perforation is fatal of necessity, yet cases are not wanting where recovery has occurred even after this gravest of all the accidents of the disease. Thus, Patschkrowski reports, from Frerichs' clinic, a case of recovery after perforation, and Pepper mentions the results of an autopsy made upon an old man who died of vesical hemorrhage, in whom he "found that there had, at some unknown previous time, been perforation of the appendix."
PROPHYLAXIS.—The prevention of typhlitis has reference more especially to cases of habitual recurrence of the disease in adults, or to the earliest, prodromatous, stage in childhood. The slightest manifestation of pain in the right iliac region should be looked upon with suspicion in these cases, and absolute rest enjoined at once. Since in childhood perforation has occurred in insidious cases after so slight an irritation as a laxative or an enema, or even after a bath, every provocation of this kind should be avoided. Injunction is to be put upon all solid food in all cases in the inception as well as throughout the course of the affection, that the element of coprostasis be not superadded to the irritation of the disease. Adults subject to frequent recurrences or relapses will thus avoid also the development or aggravation of an intestinal catarrh, which in other cases of trivial import may become dangerous to them. Many cases of typhlitis are doubtless aborted at the start by the observance of absolute rest and abstinence from food or rigid diet at the start.
TREATMENT.—Perhaps no disease requires such careful consideration of its cause or form, inasmuch as the different varieties call for entirely different treatment. A typhlitis stercoralis, for instance, requires an exclusive evacuant treatment, whereas a peri- or paratyphlitis demands a treatment that shall put the bowels at rest.
The safest and most effective method of emptying the cæcum of impacted feces is by irrigation of the bowels by means of the funnel syringe devised by Hegar. The patient is put in the knee, elbow, or chest posture, and warm water—which is the best solvent for hardened feces—is allowed to slowly inundate the whole tract of the colon, after the manner and with the precautions already pointed out in the article on dysentery. Feeble or reduced patients should be supported in this posture until as much water as possible is slowly introduced. As a rule, a single thorough irrigation will suffice, or one or several additional operations may be required [p. 822]to secure the desired effect. At the same time, broken doses, twenty grains, of sulphate of magnesia may be administered every hour or two, not so much for the purpose of exciting additional peristalsis as of turning water into the intestinal canal from above.
The other varieties of the affection call for opium at the start, with the double view of preventing the irregular, spasmodic, or tetanic contraction of the muscular coat and of obviating the danger of peritonitis. Opium is not contraindicated in these cases, even if the element of fecal impaction be superadded, as all clinicians are familiar with the fact that the bowels will move of themselves at times even under its full narcotic effects.
The remedy is best given in fluid form, as in the tincture, that the dose may be graduated in its repetition to secure its full effect without danger. When a quick action is required, morphia hypodermically may be preferred; yet it is to be remembered that opium with all its active principles is of more value in the relief of peritonitis than morphia alone. A careful watch should be kept upon all patients treated with large or frequently-repeated doses of opium, that its toxic effects be avoided. Not infrequently symptoms of poisoning have supervened after a sudden relief of pain, necessitating the use of means to keep the patient awake for a number of hours.
Hot embrocations, or poultices applied over large surfaces of the abdomen, give great comfort to the patient, though the very opposite treatment of an ice-bag, occasionally shifted or suspended, is more agreeable in some cases in the inception of the disease.
So soon as a distinct doughy sensation or a more marked fluctuation indicates the development of pus, steps should be undertaken at once to secure its evacuation. In cases of doubt it is best to make a tentative exploration with the needle of the aspirator, a large-sized needle being preferred on account of the liability of occlusion with tissue-shreds or other débris. It is quite surprising how rapidly a case clears up at times after the evacuation of even only a drachm or two of oedematous fluid. More frequently, however, the aspiration must be repeated until a quantity of pus is secured and the abscess completely discharged.
An abscess of more superficial situation, of larger size, or of continuous formation is best relieved by free incision. As to the time of the operation, the old rule, ubi pus ibi incisio, holds good here as elsewhere. An early evacuation of the products of inflammation prevents the supreme danger of perforative peritonitis or the formation of burrowing sinuses, fistulæ, amyloid degeneration, and marasmus.
Indurated tumors are sometimes made to soften under the long-continued use of cataplasms, and chronic thickenings of the walls of the intestine are relieved by general tonics, mild laxatives, mineral waters, and gentle frictions with iodine or mercurial ointments.
Perforative peritonitis calls for opium in maximum doses as a means of facilitating possible agglutinations or encapsulations, and a forlorn hope is offered in an early laparotomy, which the bolder surgeons are now undertaking in the equally desperate cases of perforation by gall- or kidney-stones, etc.
Under no circumstances should a patient affected with typhlitis leave the bed until the last trace of inflammation has subsided, as in no disease is there greater liability to recurrence or relapse.
Intestinal ulcer, Ulcus intestinorum entero-helcosis ([Greek: helchôsis], ulcer), represents a solution of continuity in the wall of the intestine, affecting first, as a rule, its mucous coat. Ulcer of the intestine, like ulcer of the stomach, its occasional congener and not infrequent associate, is the expression of an insult or injury offered to the intestinal coat in its inner exposed surface, or of a necrobiosis the result of a local occlusion in the general blood-supply. Hence, ulcer of the intestine may be a purely local disease, or be the local expression of a general, so-called constitutional, disease. While in many cases the lines differentiating these conditions may not be distinctly drawn, as many so-called constitutional conditions (tuberculosis, typhoid fever, etc.) are discovered to be—at first, at least—local processes, the toxic ulcer (arsenic, mineral acids) may be taken as a type of the local process, acting from within, and the syphilitic ulcer as the type of the general process, acting from without. At the same time, it must be recognized of syphilis that an ulcer may result from the dissolution or breaking down of a gummatous mass anywhere in the course of the intestine, or may be the effect of infection by extension into the rectum of syphilitic processes about the genital organs, or, lastly, of direct introduction of the disease in perverted intercourse (pederasty, coitus heterotopicus).
Ulcer of the intestine is occasionally, though comparatively very rarely, observed also as the result of pressure from within or without. Such an ulcer is properly considered of traumatic or mechanical origin, as it is induced as the direct effect of mechanical irritation or arrest of blood-supply. Thus, dense masses of inspissated feces, foreign bodies, indigestible residue of food, may fret the mucous surface into a condition of hyperæmia, and, later, absolute ulceration. Undue retention, as behind a cicatricial contraction, or an occlusion from whatever cause at places where the intestinal tube normally offers resistance (at the ileo-cæcal valve, sigmoid flexure, etc.), may lead to ulceration in the same way. Schönlein has called attention to the paralytic condition of the intestinal muscularis in age as a predisposing cause of mechanical intestinal ulcer; and Virchow has noticed the same condition among the insane, whose intense preoccupation leads to neglect of evacuation of the bowels. Certain intestinal parasites, more especially ascarides, are admitted as occasional causes of ulceration, and more superficial solutions of continuity in the rectum have been noticed as the result of too frequent or too careless use of enemata.
[p. 824] Curling was the first to call attention to the fact that extensive burns of the skin are sometimes followed by ulceration of the intestines. The ulcerative process is almost exclusively confined to the duodenum. Various attempts have been made to explain the intestinal ulcer consequent upon burning of the skin, but a satisfactory explanation is lacking as yet. Leube suggests an inhibition in the force of the circulation by reason of accumulation of waste products in the blood, while Billroth believes the ulcer to be the result of an embolic process. Whatever the cause, the frequency of its occurrence makes it more than a mere coincidence. According to Meyer, it is observed most frequently in women, and shows its first symptoms in seven to fourteen days after the initial burn.
Aside from toxic and traumatic causes, ulcer of the intestine occurs as the result of dysentery, typhoid fever, and tuberculosis—diseases mentioned in the order of frequency in the production of intestinal ulcer. The ulcers of dysentery in the large intestine, and of typhoid fever in the small intestine, assume such prominence in these affections—having even been erroneously considered at one time as the cause of these maladies—that their study belongs to the history of these diseases. The ulcer of tuberculosis is rather an accident in the course of this affection, and is now recognized as the occasional result of direct infection by the ingestion of tuberculous flesh, or, far more frequently, of the deglutition of tuberculous sputum. As a rule, the tuberculous ulcer shows itself late in the course of pulmonary phthisis, and is the cause of the obstinate and colliquative diarrhoea which speedily exhausts the patient. Yet cases are occasionally met in which numerous or extensive ulcers occur in the intestinal canal early in the history of phthisis, before any serious damage has been inflicted upon the lungs. The tuberculous ulcer affects, and for the most part is confined to, the same structures which form the seat of disease in typhoid fever—viz. the solitary and agminated glands of the ileum. When the bacilli tuberculosis are conveyed to the intestine by means of the lymph- and blood-supply through the mesenteric vessels, the resulting ulcer takes the shape of the vascular arrangement; that is, the long axis of the ulcer is at right angles to the course of the tube. Thus, if sufficiently extensive, the ulcer may be circular or form a girdle or ring entirely around the tube. With the tubercular ulcer or ulcers are usually found tubercular nodules or plaques in the serous coat, which are visible to the naked eye as opacities or milky deposits beneath the peritoneal coat. The glands of the mesentery may be at the same time so much increased in size as to form visible or palpable tumors in the abdomen.
The frequency with which tuberculosis affects the vermiform appendix has already been noticed in detail in the etiology of perityphlitis.
The ulcer of the intestine which is the result of a catarrhal process, so called, belongs to the history of chronic diarrhoea and dysentery.
The true intestinal ulcer, per se, which has its analogue in the stomach as the gastric ulcer, ulcus rotundum, is due to the same cause as in the stomach—viz. to arrest of circulation and erosion by the gastric juice. It is a well-established fact in physiology that gastric digestion is continued—is, indeed, mainly effected—in the small intestine; hence it is not surprising to learn that an arrest of circulation in the small intestine [p. 825] is attended by the same result. The fact that this so-called peptic ulcer is found almost exclusively in the duodenum speaks most emphatically for this origin of the disease. Arrest of the circulation in the intestinal wall may be due to embolus, which, according to the observations of Nothnägel and Parènski, is not infrequently found in the branches of the duodenal artery; to infarction, the condition so commonly encountered in pyæmia and septicæmia; or to thrombotic occlusion, as seen in amyloid degeneration—a disease process which selects by preference the vessels of the alimentary canal, along with those of the kidney and spleen.
The duodenal resembles the gastric ulcer in form as well as origin. It has the same appearance, in its recent stage at least, of having been cut out with a punch, shows no inflammation, induration, or thickening about its borders, and presents the same funnel-shape with terraced walls, its apex below eccentrically situated, as a rule corresponding to the situation of the artery. It is most frequently found in the upper horizontal portion of the duodenum, but is occasionally, though rarely, seen in the descending portion. In the further course of the duodenum the gastric juice becomes gradually neutralized, so that ulcers situated below the orifice of the gall-ducts are very great exceptions. In Krauss' collection of 47 cases but 2 were found in the lower sections of the duodenum. The intestinal like the gastric ulcer is usually found single or alone, but occasionally two, three, or even four ulcers are encountered. According to the tables of Morot, a single ulcer is found in 81.8 per cent. of cases, two in 9.2 per cent., and three and four in 4.5 per cent. each.
Duodenal like gastric ulcers are attended with the liability to hemorrhage and perforation in equal if not greater degree. There is also the same tendency to implication of contiguous structures. Stich records a case of perforation of the aorta; Eichenhorst mentions the formation of abnormal communication with the gall-bladder; and Frerichs, a thrombosis of the vena porta in consequence of duodenal ulcer. Lastly, the process of cicatrization may be followed by the same disasters as occur in pyloric ulcers in consequence of contraction and constriction. Thus, the orifices of the pancreatic or choledochus ducts may be narrowed or completely closed, or the whole lumen of the duodenum obliterated, with consecutive dilatation of the stomach and oesophagus, as in the case narrated by Biermer. A very nice question in differential diagnosis as between pyloric carcinoma and pyloric or duodenal ulcer is sometimes raised in this way. In the vast majority of cases it is safe, even in the absence of a palpable tumor and without regard to the age of the patient, to decide this question in favor of carcinoma. Cases of complete occlusion constitute the rule in carcinoma, and the very great exception in ulcer.
It remains to be said that duodenal is much more rare than gastric ulcer, in the ratio of 1 to 30, and that, unlike gastric ulcer, it chiefly affects males. According to the statistics of Krauss, already cited, the ratio of males to females is 9 to 1, and according to Trier the ratio is 5 to 1. It occurs in greatest frequency between the ages of thirty to forty, diminishing in frequency with advancing age.
SYMPTOMATOLOGY.—Ulcer of the intestines announces itself by symptoms which are, as a rule, much more vague and indefinite than the same process in the stomach. In a certain percentage of cases the symptoms [p. 826] may be entirely latent, and the cause of a sudden death be revealed only on the post-mortem table. In less severe cases the entire symptomatology of intestinal ulcer is grouped under the term dyspepsia, no characteristic phenomena being manifest throughout the course of the disease.
On the other hand, a very small ulcer may give rise to the most dangerous symptoms—hemorrhage and perforative peritonitis, which may be even fatal in the course of a few days or hours.
Among the symptoms that appear with prominence in the course of the disease is pain. Although cases are abundantly on record marked by the entire absence of pain, and although pain is by no means so universally present as in gastric ulcer, it occurs in the great majority of cases of ulcer of the intestine. The pain of intestinal ulcer distinguishes itself from gastric ulcer by being more independent of the character of the food or the time of taking it. For the most part, it occurs in attacks of colic, which are characterized at times by their extreme severity, long duration, and obstinacy to every means of relief. These attacks occur in paroxysms with complete or only incomplete remissions, and are ascribed, as in gastric ulcer, to the erosive action of the gastric juice upon exposed nerve-fibres, the intervals of relief corresponding to the periods of exhaustion of the nerve-centres. At the same time, in exceptional cases, a long-continued localized tenderness to pressure may indicate the seat of the disease.
Palpation may elicit, besides tenderness, points or regions of induration or intumescence. Such a condition is more especially encountered in cases of tuberculous disease, the so-called scrofula of the intestine or the tabes mesenterica of childhood. More localized enlargements are occasionally to be felt in the vicinity of the duodenal or other intestinal ulcer in consequence of circumscribed peritonitis, with its resultant agglutinations and adhesions. In this connection caution must be exercised not to confound masses of impacted feces with tumefactions. The history of constipation or the administration of a light laxative will generally suffice to remove this source of error.
Anorexia is a symptom of intestinal ulcer as a rule. The loss of appetite may amount to a complete aversion to all food or only to the more fatty articles of diet. A curious exception to this rule is not infrequently seen in the unappeasable hunger of children the victims of tuberculous ulceration. The contrast offered in the extreme emaciation of these patients has been made the subject of frequent comment.
With this loss or perversion of appetite and defective digestion of the food, the general condition soon begins to fail. Though cases are occasionally met in which a bien-être has been maintained for years, or a condition of obesity has been retained, these cases form the exception in the history of intestinal ulcer. More or less emaciation gradually develops as a rule, and a reduction of the general strength that is out of all proportion in its degree to the loss of flesh. At the same time the mental condition of the patient suffers a degradation to the level of the sufferer with chronic dyspepsia.
The disturbances of digestion which occur in intestinal ulcer present many varieties in degree and kind. Some patients show none or but few of the signs, while others run the gamut, so to speak, in the semeiology of dyspepsia. Heartburn, eructations, pyrosis, borborygmi, flatulence, gastralgias, pseudo-anginas, nausea, and vomiting, the familiar [p. 827] phenomena of gastric or intestinal catarrh, attend at some time or other in the course of the disease most of the cases of intestinal ulcer.
The condition of the discharges demands notice in detail, more especially as abnormalities in the evacuations belong among the few of the more constant symptoms of the disease.
Diarrhoea is the rule in intestinal ulcer. The discharges consist at first of the undigested food and the digestive juices, which have been hurried along the alimentary canal and prematurely evacuated on account of the increase of peristalsis caused by the irritation in the upper part of its tract. The arrest of the digestive process leads to early decomposition of the ingested matters, and thus imparts to the discharges an exceedingly offensive odor. While, in exceptional cases, constipation may be present, or even obstipation of the bowels, the discharges are usually so abundant as to constitute a diarrhoea, which in some cases is so frequent or profuse as to become colliquative and speedily exhaust the strength of the patient.
An ulceration situated in the colon or rectum would furnish the discharges characteristic of dysentery, already described in detail, while the same process in the ileum would show the evacuations characteristic of typhoid fever or tuberculosis.
The most characteristic ingredient of the true duodenal ulcer is blood. As stated in the article on HEMORRHAGE OF THE BOWELS, ulcer of the intestine constitutes the most frequent source of this accident, which is sometimes so grave as to destroy life in the course of a few days or hours. The blood from an intestinal ulcer may be evacuated both by the mouth and the anus, or may be retained in the alimentary canal and not appear at all. Such cases constitute the condition known and described under the heading of occult or concealed hemorrhage, which is recognized by the rapid general collapse of the patient. When the blood issues from a duodenal ulcer, it is intimately commingled with the contents of the alimentary canal. The discharges in such cases are usually black, tarry, and more or less fluid; whereas blood from the colon or rectum still preserves its fresh red color and is discharged separate from the feces or simply coats its exterior. Occasionally cases are met where the blood coagulates in the interior of the intestinal canal, to form a cast of its lumen or to accumulate in great mass in the sigmoid flexure or rectum. In one case in the experience of the author such an accumulation was the cause of a very severe tenesmus, which was only relieved by the digital evacuation of large masses of inspissated, coagulated blood.
The presence of pus would indicate lesion of the colon, as typically shown in dysentery, as suppuration, at least with any visible products, does not occur in ulcer of the duodenum.
DURATION.—Ulcer of the intestine has no definite duration. As in the case of its prototype, gastric ulcer, it may speedily be covered with cicatricial tissue and never appear again in the course of a long life. But such a course is as unusual as in gastric ulcer. Frequent recurrence constitutes the rule in intestinal ulcer, or a partial recovery with frequent relapses, as in the course of ulcer of the stomach. So ulcer of the intestine is not infrequently a lifetime malady, with exacerbations and remissions dependent largely upon the prudence or imprudence of the patient with regard to diet. It need hardly be stated that ulcer of the intestine [p. 828]may terminate fatally even in the course of a few days from hemorrhage, circumscribed and later diffuse peritonitis, or may drag out a slow length of years, to finally destroy the patient with the general symptoms of inanition, hydrops, and marasmus.
DIAGNOSIS.—From what has been already stated, it is seen that ulcer of the intestine is often entirely overlooked or may be readily confounded with other maladies of the digestive tract. Cases of traumatic or toxic origin are generally readily recognized by the history of the patient, and tuberculosis reveals itself by the youth of the individual, the existence of the disease elsewhere, the gradual emaciation, the premature senescence—in short, the general signs of the phthisical habitus, the meteorism, and perhaps the presence of nodular enlargements of the mesenteric glands.
The most characteristic symptom of the peptic ulcer is, as has been stated, hemorrhage. But hemorrhage is present in only the minority of cases, is, as a rule, occasional and transitory, and is at all times difficult of differentiation as to its source. Blood from a gastric ulcer may also be voided per rectum as well as per os, and the blood from a duodenal ulcer after regurgitation may be wholly discharged by vomiting. The absence of vomiting and the presence—more especially the persistence—of tarry evacuations from the bowels would speak for ulcer of the intestine. Dilatation of the duodenum, a condition of ectasia, closure of the bile-duct with consecutive jaundice, or the presence of fatty stools from occlusion of the pancreatic duct (a sign not now regarded of the same value as in the days of Bright), would also declare in favor of ulcer in the duodenum.
As between intestinal ulcer and catarrh or intestinal ulcer and carcinoma, precisely the same rules would hold as in the case of the stomach. A simple enteralgia would be recognized by its more frequent occurrence among females or individuals of neurotic temperament; by its connection with faults of diet, malaria, or exposure to cold; by the absence of hemorrhage, diarrhoea, or peritonitis.
PROGNOSIS.—Too much caution cannot be exercised in the prognosis of ulcer of the intestine; for even in the cases which run a perfectly mild course the gravest, even fatal, accidents are liable to occur. The danger of perforation in cases of typhoid fever from a single or from one of the few ulcers that may be present imparts one of the chief elements of gravity to this disease; and the same catastrophe may occur at any time in dysentery or tuberculosis. The duodenal ulcer may likewise have a sudden gravity imparted to a mild case by a copious hemorrhage or a peritonitis, and, even though the patient escape all possible complications, to recover with the surface of the ulcer healed so that the loss of substance is filled in with firm cicatricial tissue, the danger of contraction or stenosis still remains. The ulcers of dysentery in the colon and of syphilis in the rectum are especially liable to be followed by deformities of this kind, while the tuberculous ulcer in the ileum not infrequently results in a more or less complete stenosis. The ulcer of typhoid fever in its cicatrization almost never reduces the size of the intestinal canal.
TREATMENT.—The most valuable therapeutic means of relieving the pain and obviating the dangers of ulcer of the intestine consist in the [p. 829] regulation of the diet. The food should be light, easily digestible, and during the acute stage of the disease as nearly fluid in its consistency as may be. Milk would be the staple article of diet in all cases were it not for the fact that in some cases constipation attends its too exclusive use. The various soups, without solids, broths, preparations of starch (sago, arrowroot, tapioca, etc.), may sufficiently nourish the patient until the healing process shall have commenced. Raw beef, chopped up and made into an emulsion, is perhaps the most nutritious and least injurious of any kind of food. Bread, potatoes and other vegetables should be ruled out altogether, because of their liability to produce masses of feces whose inspissation may do mechanical damage to ulcers in process of cicatrization.
Where there is failure in the general strength early resort should be had to alcohol, which may be administered in the form of red wine (in preference to white, because of the tannin it contains), wine-whey, or, in more serious prostration, of sherry wine, milk punch, egg-nog made with good whiskey or brandy.
In the worst cases, where all food irritates, feeding by the mouth may be abandoned altogether for a time, and the strength of the patient sustained by nutritive enemata of beef or pancreatic emulsion.
The diarrhoea should be controlled rather than entirely checked, for fear of the greater evil of constipation. A little bismuth with bicarbonate of sodium or oxide of zinc may suffice for the milder cases, while in the more aggravated cases resort must be had sooner or later to opium.
Constipation is best relieved by careful injections of warm water or by the administration of the lighter laxatives—mineral waters, Seidlitz powders, citrate of magnesia, castor oil, etc.
Vomiting is combated by ice, soda-water, champagne, cherry-laurel water, and in graver cases morphia hypodermically.
Pain may be relieved by applications of hot water, cataplasms, injections of hot water, and, when necessary, by morphia with or without belladonna.
Hemorrhage is checked by ice internally and externally, turpentine, ergot or preferably ergotin by hypodermic injection, and opium.
Peritonitis, more especially perforative peritonitis, calls imperatively for the liberal use of opium.
Patients the victims of intestinal ulcer must maintain a guarded diet for months, often for years, after all signs of the disease have disappeared as the best prophylaxis against recurrence. Constant vigilance is also required to avoid constipation, and the greatest temperance exercised with regard to the use of alcohol. The author has at the present time a patient under treatment who presents all the symptoms of duodenal ulcer, including hemorrhage, with every indulgence in strong drink, and in whom all symptoms disappear under entire abstention. Sometimes a course of mineral waters, a sea-voyage, or other change of life or scene constitutes the best means of avoiding frequent relapse.
It need hardly be said that an ulcer in the rectum, which is readily recognized by its attending tenesmus, calls for local treatment; and it is equally plain that tuberculosis or syphilis requires appropriate internal means of relief.
GENERAL REMARKS.—Hemorrhage of the bowels occurs in both sexes, though more frequently in the male, and at all ages, though more frequently at the middle period of life. In the infant a form of it is sometimes considered as a distinct affection under the head of melæna neonatorum, and in age it sometimes shows itself as a distinct sign of a disease characteristic of age—namely, cancer. According to the tables of Bamberger, it is caused in the order of frequency by dysentery, typhus fever, cancer (of the colon), mechanical injury, poisons and foreign bodies, ulceration (tubercular, follicular), the round ulcer of the duodenum, and aneurism; last and least frequent is the so-called vicarious hemorrhage.
ETIOLOGY.—Hemorrhage from the intestinal canal arises from (1) anomalies in the contents of the bowel; (2) disease of the wall of the bowel; and (3) from general diseases.
(1) The inspissation of the natural contents of the bowel during long-standing or habitual constipation may convert the feces into dense masses which irritate and scratch the mucous membrane, and thus induce hemorrhage directly by simple solution of continuity, or indirectly as the result of extreme hyperæmia. Such hemorrhage is nearly always slight, streaking or coating the surface of the scybalous mass or being extruded from the anus as a small deposit of blood during the last act of defecation; in which latter case it is found mostly associated with hemorrhoids or fissure of the anus—conditions which require separate description. Independent of these conditions, the hemorrhage nearly always has its origin in the lowest regions of the large intestine, where condensation of the feces is naturally greatest.
Foreign bodies in the intestinal canal descended from the stomach may also be the cause of hemorrhage in the same way. Thus, stones of fruits, bones of fish, fragments of oyster-shell, or other substances in no way connected with aliments (false teeth, buttons, pins and needles, etc.), may be swallowed accidentally or purposely (as by children or the insane) to produce intestinal hemorrhage. Drastic cathartics (podophyllin, gamboge, etc.) and poisons (arsenic, mineral acids) occasionally act in the same way. Thus, Tardieu reports1 the case of a servant to whom was administered by a homoeopath veratrin with coffee, with fatal effect in six days. At the autopsy, made by Amussat and Reymond, the stomach and small [p. 831]intestine were found filled with a dark-brown or black bloody fluid, but there was no trace of perforation, ulceration, or organic disease.
1 Annales d'Hygiène, July, 1854.
Under this head mention should be made also of certain parasites whose habitat is the intestinal canal, the walls of which they perforate. Two varieties, the Anchylostoma duodenale and the Distoma hepaticum, are frequent causes of hemorrhage, the former from the duodenum and jejunum, the latter from the rectum, in hot climates, more especially in India and Egypt.
(2) Anomalies in the intestinal walls produce hemorrhage as the result of intense hyperæmia (per diapedesin) or of actual loss of substance (per rhexin). Copious, even fatal, hemorrhage has thus ensued from dysenteric and typhoid processes (and even without discoverable cause) where no ulceration or loss of substance could be discovered on autopsy; and this accident is so frequent as the result of ulceration in the diseases mentioned as to constitute a characteristic sign or complication. It must be said, however, that cases of alarming or fatal hemorrhage without apparent cause during life or lesion after death were more frequently reported in the literature of the times preceding our more accurate knowledge of pathology and pathogeny. Few clinicians or pathologists would now be content with reports made without full knowledge of the history of the case or microscopic examination of the intestinal walls. Thus, the report to the Société Médicale d'Emulation, April 2, 1834, by Dubois of a young man who quickly died of intestinal hemorrhage five days after a severe headache, and on the same occasion by Guillemot of several similar cases, would awaken the suspicion of masked typhoid fever; and the case of an old man aged seventy-four who died of intestinal hemorrhage after four days' diarrhoea, reported by Husson,2 would call for a close examination of the vessels in the intestinal walls. In fact, Bricheteau, who reported a case from the Hôpital Neckar, was able on autopsy to discover a rupture in a small artery of the intestines.
2 Proceedings of the Anatomical Society at Paris, 1835.
Embolic processes leading to the formation of ulceration (by predilection in the duodenum) are often attended with intestinal hemorrhage, which would be more constantly present were it not for the fact that, as in the stomach, the speedy establishment of collateral circulation prevents the consequences of complete infarction.
Besides dysentery and typhoid fever, tuberculosis and syphilis are occasional causes of ulceration and necrosis of the intestinal walls which may be attended with hemorrhage. Cancer of the intestine most frequently affects the rectum, but wherever situated may show hemorrhage as one of its signs.
The local hyperplasia of the mucous tissue which constitutes a polypus—and which in children, in whom it most frequently occurs, is mostly situated in the rectum—is suspected to exist or is recognized by the frequent discharge of blood from the bowels. A far more grave affection of the intestinal walls, likewise most frequent in childhood, is the peculiar dislocation known as intussusception or invagination. This condition is so commonly attended with distressing evacuations of blood and mucus as to simulate dysentery. The strangulation of the intussuscepted mesentery with its vessels easily accounts for the hemorrhage in such cases.
A more extensive compression is exercised at times by tumors in the [p. 832] abdominal cavity, as by pregnancy, ovarian growths, etc., occlusions in the course of the portal system (cirrhosis hepatis), interference with the general circulation, as in diseases of the heart or lungs, with intestinal hemorrhage as a consequence.
Diseases of the blood-vessels themselves, as amyloid degeneration, aneurism, should not be omitted from the list of factors possibly productive of this result.
(3) The general diseases attended with hemorrhage from the bowel are characterized for the most part by more or less general disintegration or dissolution of the blood, with the manifestation of hemorrhage in various parts of the body—kidneys, uterus, subcutaneous tissue, etc.; the enterorrhagia being an accidental localization, so to speak, of the effusion. The most prolific causes of this disorganization are the micro-organisms which "touch the life of the blood corruptibly;" and hence the various acute infectious diseases may show in the severer forms hemorrhage from the bowels. Under this head may be ranged variola, which boasts even of a hemorrhagic form; typhus, yellow, and malarial fevers; the forms of nephritis marked by uræmia, cholera, icterus gravis, erysipelas, etc. Disintegration of the blood or partial dissolution of its corpuscular elements occurs also in those obscure affections which constitute the group, or are included in the description, of the hemorrhagic diatheses, as hæmophilia, leuchæmia, pernicious anæmia, scurvy; of any of which enterorrhagia may be a distinct or dangerous sign.
Melæna neonatorum is the distinct name given to a hemorrhage from the bowels which occurs a few hours or days after birth, and which is often so profuse as to cause death at once or in a short time. In most cases no anatomical lesions can be discovered after death, save an intense hyperæmia of the intestinal mucosa, so that the etiology of this affection is involved in obscurity. The various causes assigned in its production—ulceration of the stomach or duodenum (Bohn), embolism (Landau), fatty degeneration (Steiner), premature ligature of the umbilical cord (Kiwisch)—answer only for individual cases. Betz reported a case in a family subject to hæmophilia, and Trousseau once saw twins thus affected; but that heredity cannot account for all cases is shown by the fact that it occurs mostly in healthy children from healthy parentage. Klebs is inclined to attribute the affection to the action of micro-organisms, introduced perhaps as the result of puerperal infection, but this cause can be assumed in only a small minority of cases; at least, but a small percentage of cases coincide with puerperal disease on the part of the mother.
The affection is fortunately rare. Eichhorst states that Hecker observed it but once in 500 births, and Gemich but once in 1000 births. According to Rilliet, the hemorrhage is oftener (8/14) intestinal, rarer (4/14) gastric, and rarest (2/14) both. It is almost always abundant and quickly repeated, the blood being mostly pure, in clots or masses and fluid, though it is sometimes commingled with meconium. It usually ceases within twenty-four hours, though it may continue for three, five, or more days. Of 23 cases reported by this author, 12 recovered and 11 died.
MORBID ANATOMY.—Hemorrhage from the bowels, being only a symptom of very many different conditions, is marked by lesions characteristic of the condition in an individual case. These lesions are more appropriately described in connection with the various diseases. Not [p. 833] infrequently in these cases the intestine is distinguished by the absence of any lesion at all; but, from whatever cause, hemorrhage from the bowels, like hemorrhage from any other source, shows a more or less profound anæmia of all the internal organs, and in more chronic and protracted cases leads to fatty degeneration, more especially of the heart.
SYMPTOMATOLOGY.—Hemorrhage from the bowels is usually readily recognized by the discharge of blood, either pure or mixed with the natural contents of the alimentary canal. The actual seat of the hemorrhage may, however, only rarely be recognized by the rectal speculum. The colicky pains, borborygmi, or sensations of fluids in the abdomen which are occasionally experienced may not be relied upon in fixing the seat of the effusion. Should the hemorrhage occur in quantity, or, more especially, should the seat of the effusion be low in the intestinal canal, the blood which escapes is more or less pure. When the hemorrhage is higher, or when the stay of the blood in the bowel is longer, it becomes more or less incorporated with the contents of the bowels or altered by the intestinal juices to present a discharge of mushy or semi-fluid consistence, of dark-brown or black color. So-called tarry stools are thus largely composed of blood.
But serious, even fatal, hemorrhage sometimes occurs without the escape of any blood at all. Such are the so-called cases of concealed, occult, or internal hemorrhage, in which the nature of the malady is only suspected or recognized by the general symptoms attending the profuse loss of blood. Should the hemorrhage be gradual, anæmia slowly supervenes, with hydræmia and subcutaneous dropsy. Traube reports a fatal case of oedema of the glottis from such a cause. Sudden hemorrhage announces itself by pallor and prostration, dyspnoea, vertigo, and syncope. Amaurosis, tinnitus aurium, formication, emesis, and, if the disease be high up in the intestinal canal, hæmatemesis, are the common attendants of serious hemorrhage. In the worst cases of sudden effusion the patient may present the appearance of complete collapse, and the intestinal canal be found on autopsy distended with blood throughout a great part of its course, while no blood whatever has escaped from the rectum. In such cases, or with more gradual loss of blood, the patient experiences a sense of increasing weakness, the skin becomes cold and bedewed with a clammy sweat, the pulse grows feebler, the temperature falls, and death from exhaustion more or less speedily ensues.
DIAGNOSIS.—The presence of blood in any quantity in the stools is readily recognized by its coarser characteristics. Ridiculous errors have been made by mistaking the coloration produced by bismuth, iron, logwood, etc. administered internally, or by coloring matters introduced into the discharges for purposes of deception. The microscope, Zeichmann's test for blood-crystals, and in extremely doubtful or medico-legal cases the spectroscope, furnish easy means of detecting blood in whatever quantity or character.
It is the cause and seat, rather than the existence, of the hemorrhage that mostly cause embarrassment in differential diagnosis. Hemorrhage from the lungs, nose, or stomach is usually readily excluded by the absence of any evidence of disease of these organs, and the presence of the other symptoms of any general disease attended with enterorrhagia makes a diagnosis in most cases easy enough. Alterations in the contents of the [p. 834] bowel, the presence of foreign bodies, are recognized by the history of the case and by careful local examination, while a diagnosis of anomalies in the walls of the bowel is usually reached by exclusion. In no doubtful case should local inspection or digital examination of the anus and rectum be omitted.
TREATMENT.—As in all cases of hemorrhage, the first requisite is absolute rest. The patient should be at once put to bed and kept perfectly quiet. Many a case of hemorrhage in typhoid fever is produced by arising from bed to go to stool. The bed-pan is an absolute necessity in the management of a case of typhoid fever after the second week of the disease. Rest is the chief agent in prophylaxis as well as therapy.
The most effective styptic in enterorrhagia is cold. An ice-bladder should be laid upon or suspended immediately above the abdomen during the whole duration of the flow. The injection of ice-water into the bowel should be practised only in cases where the hemorrhage is believed to come from the colon. Otherwise, the peristalsis it awakens may only aggravate the danger. Should rest and cold fail to quickly check the hemorrhage, resort should be had at once to ergot. This remedy, in the form of ergotin, is most effective when introduced beneath the skin. In cases of less imminent danger the practitioner may be content to give the remedy by the mouth.
Small doses of the simple or camphorated tincture of opium frequently repeated speedily arrest contractions of the bowel, and at the same time feed the brain in threatening syncope. The astringents proper—tannic acid or its preparations, acetate of lead, alum, the perchloride of iron—are seldom necessary or advisable, but may be called for in obstinate or protracted cases.
To turpentine has been ascribed, from time immemorial, specific virtues in relief of hemorrhage of the bowels, and its administration is still a routine system with many older practitioners. It is most effective in large doses—one drachm, with milk or in emulsion, every hour or two until the hemorrhage ceases.
In relief of collapse, alcohol, ether, and musk are imperatively indicated, with the external application of heat; and in the treatment of the anæmia and hydræmia the preparations of iron, including, later, the mineral waters which contain it. In the worst cases of sudden alarming hemorrhage the physician should not fail to practise the transfusion of blood or solutions of salt or soda.
Milk is the best food and drink during the attack, and after it for some days or weeks. Chopped or scraped raw beef may substitute it later, while all farinaceous foods are to be strictly avoided for some time.
When a mechanical impediment to the passage of the contents of the bowel along the intestinal canal exists, the condition is known as intestinal obstruction. The causes of this occurrence are numerous, the symptoms urgent, the diagnosis difficult, the treatment uncertain, and the termination, unless relieved by nature or art, speedily fatal. There is no class of cases to which the practitioner is called more important, or which demands on his part greater skill and judgment.
It is customary to divide the causes of obstruction of the bowels into two great classes—acute and chronic.
In acute cases the attack is sudden, the symptoms violent, and, unless the cause is speedily removed, life ends in a few hours or at most in a few days. In chronic cases the causes act comparatively more slowly, the symptoms are chronic and less urgent, and danger of death less imminent. In this class the cause is not uncommonly spontaneously relieved, and the individual restored to perfect health without the aid of medicine or the surgeon's art. This result may happen in apparently the most desperate cases.
This classification of acute and chronic obstruction is necessary for a proper clinical study of the subject, but it should be remembered that in practice there will be found some cases which partake of many of the symptoms of both acute and chronic obstruction, making it difficult to determine to which division the cases properly belong. It will also be seen that some, at first, well-marked acute cases subside and become chronic in character, and that (old) chronic cases of obstruction sometimes suddenly change their nature and become acute. Again, some of the causes mentioned as giving rise to acute obstruction of the bowel in rare instances produce symptoms of chronic obstruction, and some of the causes referred to as giving rise to symptoms of chronic obstruction in rare instances provoke signs of acute obstruction. These cases are exceptional. As a rule, the following list embraces conditions which produce symptoms of acute obstruction:
1. Congenital malformations.
2. Impaction of foreign bodies, gall-stones, enteroliths, etc.
3. Twisting of the bowel—volvulus.
4. Internal strangulation by loops, bands, false membranes, diverticula, mesenteric pouches, slipping of a portion of bowel into natural or unnatural openings, diaphragmatic hernia, etc.
[p. 836] 5. Invagination.
As a rule, the following causes produce symptoms of chronic intestinal obstruction:
1. Constipation and fecal accumulation.
2. Stricture of the bowel, sometimes cancerous.
3. Compression of the bowel from abdominal tumors.
4. Contraction of the bowel from inflammatory changes, often tuberculous.
A consideration of external hernia is, of course, not included in this paper, but the possibility of the symptoms of intestinal obstruction being due to this cause should never be overlooked.
Cases of congenital strictures and malformations are confined almost wholly to the rectum and anus, and come more properly under the province of the surgeon. Some of the cases, however, belong to the physician, the obstruction being so slight as not to require surgical assistance. With all of them, however, the physician should be familiar, that he may be able to distinguish between congenital malformation giving rise to immediate obstruction and other forms of intestinal occlusion. He should know, too, when to seek the aid of the surgeon. For these reasons, as well as to make the history of the causes of intestinal obstruction as complete as possible, it has been thought proper to include in the list congenital occlusion and malformation of the intestine. They will be treated, however, in the briefest possible way, and the reader is referred to works on surgery for a more detailed account of the pathology, symptoms, and treatment.
When congenital occlusion of the colon occurs, it is almost invariably found in the sigmoid flexure, and is due, as most congenital atresia of the intestine, to foetal peritonitis. Congenital occlusion may be found in any portion of the small bowel, but a frequent site is the lower part of the ileum and the ileo-cæcal opening. The following case1 gives an example of a form of stricture of the duodenum in infants, with the symptoms and pathological changes. The septum is supposed to be an unnaturally developed valve, or two valvulæ conniventes united: "A child when born presented no unusual symptoms for the first twenty-four hours. Vomiting then came on, and continued with short intermissions until death, which took place some thirty-eight hours after birth. The bowels were never relieved during life. The only disease found was stricture of the duodenum close to the entrance of the gall-duct, so that a probe passed down the latter entered the duodenum immediately below the constriction. There was nothing to indicate in what manner the constriction had occurred. On the gastric side of the latter the duodenum was immensely distended—so much so that at first sight it appeared like the pyloric end of the stomach itself, and only by a more careful examination was the distinction between the stomach and intestine detected by a ridge running around their place of junction."
1 Quoted by Mr. Pollock in Holmes's System of Surgery, from Pathological Transactions, vol. xii. p. 101.
[p. 837] Cases like this, a number of which are on record, are instructive and of pathological interest; when, however, congenital occlusion exists in the small intestines, no treatment can be suggested. If the sigmoid flexure is the part involved and diagnosis can be made, opening the intestine in the right groin and establishing an artificial anus should be attempted.
In the development of the foetus the anal part of the bowel, beginning below, develops upward, and the intestinal portion, commencing above, grows downward; both portions, advancing, finally unite, making one continuous tube. When, however, there is some interruption in the foetal development of the intestine, and the two portions of bowel fail to unite, we have malformation of the rectum and anus and intestinal obstruction; or the two portions of bowel may have been united and continuity of the intestinal track established, and subsequent intra-uterine inflammation may obliterate the canal. Under these circumstances a ligamentous cord represents the original tube. The cord descends from the cul-de-sac in which the upper part of the bowel ends to the skin about the anus, or is lost in the tissues about the neck of the bladder. In congenital malformations the following conditions may be found: 1st. The anal orifice may be so minute as not to allow the feces to escape; or the aperture may be occluded by a membrane, through which the meconium may be seen; or the anus may be entirely absent. 2d. The rectum may be occluded by a membranous septum, the presence of which is not suspected until symptoms of intestinal obstruction arise, and then it is discovered by introducing the finger or a probe; or the rectum may be entirely absent, the colon terminating in the iliac fossa in a dilated pouch, or ending at the top of the sacrum or stopping at any point between this and the normal anus, the place being determined by the period of arrest of foetal development; or, the anus being absent, the rectum may open into the vagina, bladder, urethra, and other places. These cases belong exclusively to the surgeon.
Intestinal obstruction may arise from the introduction, accidental or otherwise, of foreign bodies into the stomach and bowels. Coins, marbles, bullets, fruit-seeds, etc. are often swallowed by children, sometimes intentionally, and if the object is round and small it rarely gives rise to any serious trouble. The foreign body, however, if small, may drop into the appendix vermiformis or some other diverticulum and end in serious mischief, or if the individual has stricture of the bowel the foreign body may be arrested by it.
Foreign bodies which are pointed or irregular in shape, swallowed by accident or design, may give rise to dangerous and fatal symptoms, but not unfrequently they escape per vias naturales. Thus, pins, needles, pieces of bone, artificial plate and teeth, small pen-knives, and other pointed or irregular-shaped bodies, have passed in this way. Sharp-pointed bodies, as needles, sometimes make their way through the walls of the stomach and present themselves at other and more distant parts of the body. I have removed a needle from the calf of the leg which [p. 838] the patient had a month before accidentally swallowed. Jugglers accidentally, in practising their calling, and insane people, not unfrequently intentionally, introduce into the stomach all sorts of foreign bodies, such as buckles, forks, spoons, knives, pieces of wood, iron, bone, etc. Gross2 records the case of a juggler who let a bar of lead ten inches long and weighing a pound slip into his stomach. Bell of Iowa removed it by gastrotomy, and the man recovered. Agnew3 reports a post-mortem of an insane woman in whose intestinal canal he found three spools of cotton, two roller bandages, a number of skeins of thread, and a pair of suspenders.
2 System of Surgery, by S. D. Gross, 6th ed., vol. ii. p. 616.
3 Agnew's Surgery, vol. i. p. 393.
The morbid appetite of some people, particularly girls and pregnant women, sometimes induces them to swallow powdered chalk, magnesia, and other substances, and when this practice is continued for a long time the insoluble powder is deposited in the bowel and forms hard masses which more or less completely obstruct the intestines.
Stony concretions or enteroliths are found generally in the cæcum or in the sacculi of the colon, very rarely in the small intestines. They are round or oval, and when two or more are found together they have facets. They consist usually of carbonate of lime or magnesia or sesquioxide of iron. Other concretions are sometimes seen composed of starch or the felted husks of oats, called oat-stones (avenoliths), found particularly among the poorer classes of people in Scotland. Other vegetable remains of husks, fibres, etc. may produce the same thing. Young and middle-aged people more frequently suffer with these concretions than the old. Foreign bodies made up by the gradual accumulation of hair, string, and other substances are not unfrequently found in the stomach and intestines. The mass produced in this way is often very large. Sometimes the foreign body is arrested in the oesophagus. In a post-mortem reported to the writer by Fairfax a large copper coin, accidentally swallowed a few days before, was found lodged in the gullet. Ulceration followed, a neighboring artery was opened, and the patient died from hemorrhage.
Impaction of the bowel by gall-stones escaping from the gall-bladder into the bowel is by no means an unfrequent cause of fatal obstruction. Small gall-stones, after giving rise to intense pain and often grave symptoms during their passage through the bile-ducts, may escape into the duodenum and be discharged through the rectum, as any other small foreign body. If, however, there is constriction or stricture of the bowel at any point, the small gall-stone may lodge there, and if other stones follow and lodge, the collection may soon be great enough to produce obstruction. A very large single stone or a number of stones forming a coherent mass may collect in the gall-bladder, slowly distend the dilatable biliary passages, and escape into the bowel; or—and this is more common—an opening made by ulceration between the distended gall-bladder and the duodenum allows the concretion to escape into the small intestine. These stones or aggregation of stones are sometimes three, four, or five inches in circumference and from one to four inches long. They occur, as a rule, in people over fifty years of age, and more commonly in women. Brinton, in his excellent book on Intestinal Obstruction, makes the average age in these cases fifty-three and a half [p. 839]years, and from the statistics he has gathered it will be seen that their occurrence is four times as often in females as in males. In 41 cases collected by Leichtenstern, 32 were women and 9 men. The site of the impaction is always in the small intestines. In 32 cases observed by Leichtenstern, 17 were found in the lower part of the ileum, 10 occupied the duodenum and jejunum, and 5 the middle part of the ileum.
SYMPTOMS.—Foreign substances introduced into the stomach do not always immediately give rise to serious symptoms. It is wonderful sometimes to see how tolerant the stomach is of their presence. Many instances are recorded of foreign bodies remaining in the stomach for months without producing dangerous symptoms. The mass may be discharged by vomiting, or it may escape through the pyloric opening into the intestine, and ultimately be discharged through the rectum, or, lodging in the bowel, give rise to symptoms of inflammation and obstruction. If, however, the foreign mass remains in the stomach, and is not removed by the surgeon's art or spontaneously discharged by ulceration, as in several rare instances has been the case, it uniformly proves fatal.
Before the foreign body is discharged by ulceration through the walls of the abdomen, adhesive inflammation unites that portion of the alimentary canal, gastric or intestinal, in which the mass is lodged with some part of the abdominal wall. By this union the cavity of the peritoneum is protected, just as we see the peritoneal sac protected by an effusion of lymph in hepatic abscess opening into the small intestine. If the adhesion between the canal and abdominal wall is imperfect, or by an undue amount of inflammation is disunited, the foreign body or inflammatory products which surround it may escape into the peritoneal sac and produce fatal peritonitis. Instead of passing through the abdominal wall, the foreign substance may escape into the bladder or vagina, or from the small intestine into the colon or rectum. Dangerous peritonitis may follow the simple presence of the foreign body in the alimentary canal from the obstruction it produces when no attempt at discharge by ulceration has been made. If the size and shape of the body permit its passage into the small intestine, it makes its way very slowly along this tube, giving rise to occasional attacks of colicky pains and symptoms of partial impermeability of the bowel.
At any moment the foreign body may lodge, become impacted in the canal, and all the grave symptoms of enteritis and general peritonitis present themselves. Symptoms of inflammation may appear, and after a longer or shorter time suddenly disappear, as if the foreign body had glided over some point of obstruction and again begun its descent through the tube. Its course is always irregular, passing quite rapidly over a portion of the intestine, then going more slowly, then lodging for a time at some point where it is obstructed by a fold or the contents of the bowel or by spasmodic contraction of the muscular coat of the intestines. As the calibre of the small intestine gradually diminishes as it approaches the cæcum, the passage of the foreign body becomes more and more difficult as it is propelled onward toward the ileo-cæcal valve. After a time it may reach the cæcum, where, of all places, it is most apt to lodge; but it may continue its course to the rectum, where it gives rise to tenesmus and a constant desire to go to stool. Finally, spontaneously or aided by the finger of the physician or some instrument, it is [p. 840]evacuated per anum. Not unfrequently, the foreign body can be felt through the abdominal walls, and its course traced day after day as it makes its way along the canal.
It is a common practice with uninformed persons to give castor oil or some purgative medicine when a pin, needle, coin, or other foreign substance has accidentally passed from the mouth into the stomach. Such practice is irrational and hurtful. Experience has shown that the larger and more solid the alvine discharges, the more likely the foreign body is to escape by the natural outlet; and the physician should order such a regimen and diet as will probably secure this condition of the contents of the bowel.
Long residence of a foreign mass at any point in the intestinal canal is certain to produce some chronic enteritis and effusion of lymph and subsequent stricture of the bowel, or the presence of the foreign body may produce an ulcer; and when this is healed the resulting cicatrix may end in serious obstruction from the natural tendency of the new material to contract. Signs of constriction of the bowel may not be noticed for some time after the escape of the foreign body.
Obstruction from the presence of intestinal stones and concretions is almost invariably preceded by impaired health, emaciation, or cachectic appearance, signs of partial impermeability of the bowels, and repeated attacks of inflammation, especially in the region of the cæcum. It terminates sometimes by the concretion becoming encysted, by its spontaneous evacuation, or by ulceration and perforation, or sometimes by complete occlusion of the bowel, and death.
As occlusion of the bowel by the presence of gall-stones always occurs in the small intestines, the symptoms are at once of the most urgent and violent character. The signs are those of internal strangulation, and the termination is often rapid in the extreme. Colicky, griping pains are soon succeeded by violent agony; vomiting begins at once, and is constant; at first bile is thrown up, and afterward feculent matter; the pulse is small, wiry, and frequent; the belly is retracted; the features are pinched, the extremities cold, and prostration soon comes on, succeeded by collapse.
Evidences of disorder of the liver, symptoms of inflammation of the peritoneum in that region, or attacks of hepatic colic sometimes precede obstruction of the bowel by gall-stones; unfortunately, however, for the purposes of diagnosis, these premonitory symptoms are not invariably present.
When a portion of bowel within the abdomen is constricted, its circulation interfered with, and the passage of the contents of the bowel interrupted, it gives rise to acute internal strangulation. This condition is very similar to that of external strangulated hernia. The difference is, that one is inside and the other outside of the cavity of the abdomen.
Twisting of the gut upon its mesenteric axis, the passage of the bowel through some natural or unnatural opening, the encircling of one portion of bowel by another or by bands, false membranes, etc., may cause [p. 841] internal strangulation. It may happen at any age, and involves generally the small intestine or the more movable parts of the large bowel—viz. the sigmoid flexure and cæcum.
Twisting, or torsion, is not an unfrequent cause of intestinal obstruction, and may involve almost any portion of the intestinal tube. Its most common site is the sigmoid flexure, and next in point of frequency the cæcum. It sometimes, but rarely, involves the small intestines, and may occur as a simple twisting of one loop of intestines upon another. Several conditions are necessary for its production. First, the mesentery must be elongated. This change in the mesenteric root may have been caused by the dragging of an old and large hernia, or the mesentery may have been lengthened by relaxation of the abdominal walls from childbearing or by the disappearance of fat. However caused, before torsion of the gut takes place the mesentery is elongated, so that the two ends are approximated and something like a pedicle formed. Second, the portion of bowel attached to the lengthened mesentery may become filled with an enormous quantity of fecal matter and paralyzed by the great distension. In this paretic condition it may be displaced by the living, moving parts around it, and become bent and twisted, or the length of bowel belonging to the elongated portion of the mesentery may be the seat of inflammation, and, paralysis following, it becomes without resistance subject to the pressure and movements of the active vital parts surrounding it. A portion of bowel with its accumulated contents having a redundant mesentery and paralyzed by enormous distension or by inflammation, or by both, may readily be twisted more or less completely, and in some cases several times upon itself.
The weight of the bowel and its contents, along with the rapid distension of the intestine above, fixes the gut in this state of torsion and effectually prevents it from untwisting. A semi-rotation of the paretic and distended bowel about the mesenteric axis is sufficient to interfere with the supply and return of blood and provoke enteritis. Indeed, the rotation is rarely sufficiently great to produce complete obstruction, and the symptoms are frequently rather those of inflammation than of internal strangulation. For weeks before the final attack the patient usually has symptoms of intestinal disorder, such as flatulence, constipation, and spells of colic, due no doubt to the changes provoked by the elongated mesentery and bent or curved intestine. When torsion takes place the attack is sudden and the symptoms violent and urgent. Vomiting, meteorism, insuperable constipation, and frequently tenesmus, are soon followed by collapse and speedy death. The patient may die in twenty-four hours; he rarely lives beyond the fourth day. In some cases excessive tenesmus and bloody stools are seen in the early stages of torsion of the bowel. The condition may be mistaken for intussusception, but can usually be distinguished by the premonitory symptoms of twisting and by the more rapid course, the sudden meteorism, and quick collapse of the latter.
Still another way by which displacement of intestine may occasion obstruction to the passage of its contents is when a portion of the intestine has a long and narrow mesentery, and around this mesentery, which is like a pedicle, another portion of the bowel is thrown, encircling and compressing it. The accompanying figure, taken from Ziemssen's Cyclopædia, gives a good idea of this condition (Fig. 23). It represents a [p. 842] loop of the small intestine placed around the mesenteric pedicle of the sigmoid flexure. Leichtenstern calls this "intertwining or knotting of two intestinal loops."
| FIG. 23. | FIG. 24. |
 |
 |
| Anterior view of the strangulated intestine and stricture. a, gastric extremity; b, rectal extremity. | Posterior view of the strangulated intestine and stricture. a, gastric extremity; b, rectal extremity. |
In consequence of inflammation of the peritoneum and effusion of lymph, peritoneal surfaces are joined together, and before the lymph is fully organized these surfaces are separated by the constant movements of the organs and the change in the relationship of the parts, and strings and bands of various shapes and sizes are formed in which a portion of the intestine may become entangled and constricted. Sometimes the bowel accidentally becomes engaged in a loop or noose of false membrane, or becomes bound down under a band of fibrin; or, the peritoneal surfaces of some of the organs having been joined together or to the wall of the abdomen or pelvis, a loop of bowel may escape into a slit or opening and become incarcerated; or a fold of bowel may fall into a fissure in the omentum or mesentery or broad ligament of the uterus or suspensory ligament of the liver, and become constricted; or the appendix vermiformis may be twisted around the intestine in such a way as to cause ligation of the tube, or, by becoming attached to some neighboring part, it may form a loop through which the intestine may pass and become obstructed. In the same way the bowel may be constricted by a diverticulum. (This is well shown in Figs. 23, 24, and 25.) Bands entangling the bowel and causing strangulation may be attached to the fimbriated process of the Fallopian tube or the ovary or uterus. Indeed, it is impossible to describe in a limited space the almost infinite ways in which these bands and strings may engage and incarcerate the intestinal tube (Figs. 24, 25).
[p. 843]| FIG. 25. |
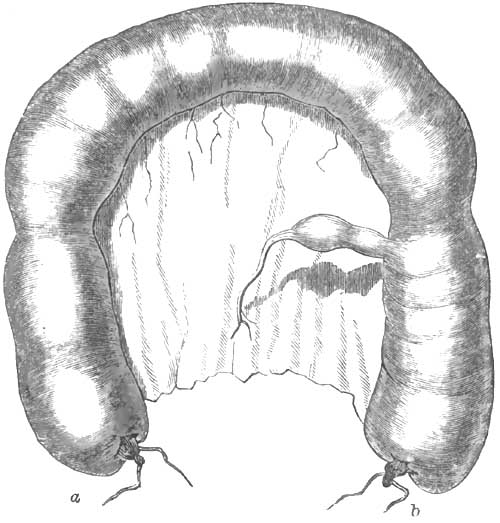 |
| An appearance of the natural relations of the diverticulum to the intestine. a, gastric extremity; b, rectal extremity. |
Internal strangulated hernia may result from the bowel falling into a pouch of the peritoneum and becoming ligated by the orifice of the pouch, or passing into the foramen of Winslow, of which there are three cases of strangulation recorded; or a retro-peritoneal hernia may be formed; or, more common still, a hernia of the intestine through the diaphragm.
In diaphragmatic hernia an opening is more frequently found in the posterior part of this muscle. Two hundred and fifty-two cases of this form of internal hernia have been collected by Leichtenstern, in which the diagnosis was made in only five cases. He found the oesophageal opening, a spot just behind the sternum, and a gap between the lumbar and costal parts of the muscle, the weakest points in the diaphragm.
Diaphragmatic and other forms of internal hernia may exist and not produce symptoms of strangulation either at the time of formation or subsequently, just as we so commonly see in cases of external hernia. When the bowel is constricted, however, and its circulation interfered with, symptoms of internal strangulation come on, and are exactly like the symptoms of external strangulated hernia. The attack is sudden, the symptoms acute and urgent, and the course and termination very rapid. Unless the constriction is relieved death may take place in twenty-four hours; life is rarely protracted beyond three or four days.
The patient has first eructations, soon succeeded by nausea and vomiting. The matter vomited consists of the contents of the stomach, then of gastric fluid, bile, and the contents of the intestines. When the last is ejected the vomiting is called fecal or stercoraceous. The patient complains of a sense of constriction about the abdomen, griping pains about the umbilicus, flatulence, tenesmus, and insuperable constipation. One or two free stools from the large intestine below the site of strangulation may be passed, but this should not deceive the practitioner. As a rule, peritonitis soon follows strangulation. The belly becomes tympanitic and tender, the pulse small and wiry, and the face anxious. When gangrene supervenes the pain subsides, the pulse becomes weak and intermittent, the surface cold and clammy, and the patient soon dies in a state of collapse. Slight delirium may precede death, or the mind remain unimpaired to the end. Very often, when gangrene sets in and pain disappears, the patient has a grateful sense of relief and is hopeful of recovery.
One of the most frequent and important causes of intestinal obstruction is intussusception or invagination of the bowel; by which term is meant the protrusion or slipping of one portion of bowel into a portion immediately adjoining.
This condition is sometimes found after death in persons old or young, but particularly the latter, in whom during life there were no symptoms of intestinal obstruction or intestinal trouble of any kind. The displaced intestine in these subjects is easily reduced, is unattended by any signs of inflammation, and is evidently the result of spasmodic contraction of the transverse muscular fibres of the bowel at one part, with distension and relaxation at another part, by which, just before death, one piece of the bowel is pushed into an adjacent piece. Not unfrequently two or more invaginations are seen in the same subject. Flint4 counted as many as fifteen in a child who died of typhoid fever. This invagination of the death-struggle almost invariably involves the small intestine, and may be the protrusion of a piece of the bowel above into a piece immediately below, or the reverse, a portion of bowel below being pushed into a portion above. It has been suggested that this slight and temporary intussusception may occur during life and give rise to temporary symptoms of intestinal obstruction, which disappear when reduction of the displacement spontaneously takes place.
4 Practice of Medicine.
| FIG. 26. | FIG. 27. |
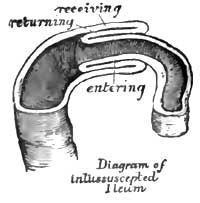 |
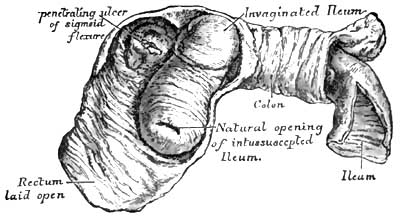 |
It will be seen by the diagrams that three successive portions of intestine enter into the formation of an intussusception—an entering, returning, and receiving portion. Two mucous surfaces and two serous surfaces are thus brought into apposition. The mesentery attached to the included lengths of bowel—viz. the entering and returning lengths—is necessarily pulled down with the bowel in its descent, and is also embraced by the receiving portion of the intestinal tube. The traction excited by this portion of mesentery, thus wedged in between the middle and inner layers of the bowel, materially alters what would otherwise be the relationship of the parts. Fig. 26 shows simple invagination of the ileum like the finger of a glove, in consequence of the traction exerted. The entering or invaginated portion does not always lie in the axis of the enveloping tube, but is more or less curved, until very often its lower orifice is in contact with the wall of the outer layer. The concavity of this curve looks [p. 845]toward the mesenteric edge of the invaginated portion of bowel, and the convexity toward the opposite side of the receiving portion. The convex side of the middle cylinder is often thrown into transverse folds or convolutions. Intussusception, which gives rise to symptoms characteristic of intestinal obstruction during life, is invariably from above downward. It is doubtful whether there is on record a single well-authenticated case of inflammatory invagination where the lower segment of bowel protruded into the upper.
Reference to the diagrams will show that the lumen of the bowel is diminished, and that more or less intestinal obstruction must follow invagination. This obstruction is increased by the inflammation which necessarily follows this condition. The large and numerous blood-vessels of that portion of the mesentery involved in the invagination are compressed and stretched; arterial supply, and especially venous return, are interfered with; congestion quickly follows, with copious inflammatory exudation; the layers of intestine become swollen, and blood, sometimes in abundance, is poured out from the mucous membrane. Peritonitis, limited sometimes to the invaginated part, more often spreading to the peritoneum covering neighboring structures, soon begins, and the contiguous serous surfaces are agglutinated and the intussusception rendered irreducible. Lymph and other inflammatory products are poured out freely; the coats of the intestine become distended and thicker, and the inner and middle layers of the invagination are separated by the deposit; the invaginated part becomes more and more curved toward the mesenteric border of the outer layer; and occlusion of the bowel, begun by the invagination, is made more or less complete by the changes wrought by inflammation (Fig. 27). That intestinal obstruction is not always complete in intussusception is shown by the fact that fecal matter, often in considerable quantity, is passed through the bent and narrowed tube, the intestine retaining, at least for a time, its contractile power. The changes produced by inflammation are chiefly seen in the inner and middle layers of intestine, the receiving or outer layer of the invagination often escaping any serious damage. These changes vary with the character and duration of the inflammation. Sometimes they are limited to an agglutination of the opposed serous membranes, an effusion of blood and serum from the mucous surfaces, and an enormous distension and swelling of all the invaginated parts; or the inflammation may end in mortification of the middle or both the inner and middle cylinders, the dead part coming away in shreds or in large fragments, or, if the patient lives long enough, the entire invaginated tube being discharged through the anus. If the inflammation involves the invaginated parts unequally, strips and shreds of the bowel are detached by ulceration and sloughing, and may escape in the discharge from the bowels in pieces so small as to be unnoticed; but if the intussuscepted part dies en masse, a circular line of demarcation is formed by ulceration, and the dead segment is detached and drops into the cavity of the bowel below, and escapes through the rectum. It is often so complete that the inner and middle cylinders can be recognized, and the part of the intestinal tube to which the expelled bowel belonged can be determined. In favorable cases the blood-vessels of the healthy bowel above and below the dead segment pour out a circular mass of coagulable lymph, which, becoming organized, closes the breach and [p. 846]completes the intestinal tube. To accomplish this it is necessary that the ends of the two portions of bowel should be accurately coaptated: if they are not, some opening may be left through which the contents of the gut may escape into the peritoneal cavity, producing fatal peritonitis; or the new formation may be imperfectly organized, and burst during some peristaltic movement of the bowel or from the pressure of gas accumulating in the gut; or the supply of lymph may be so redundant as to obstruct the calibre of the bowel, or end in cicatricial contraction, stricture, and obstruction. Aitken5 records four instances where the curved end of the invaginated portion of bowel by prolonged pressure caused ulceration and perforation of the coats of the enclosing bowel, the invaginated portion passing through the side of the enclosing segment and projecting into the cavity of the peritoneum.
5 Science and Practice of Medicine.
Gangrene and ulceration, however, do not always follow intussusception. The mesenteric injuries may be sufficient to produce congestion and exudation, and the patient survive the invagination for weeks, and death eventually occur without sloughing or ulceration; or spontaneous reduction of the invagination may take place and recovery of the patient follow. The last termination must be rare, and impossible when firm adhesion between the serous surfaces has taken place; but that it does exceptionally occur is proved by cases where the diagnosis of intussusception was undoubted, the invagination being felt in the rectum or seen prolapsed through the anus. The most common termination, if the patient survives, is mortification of the invaginated part and separation in mass or by shreds or fragments.
Intussusception may occur in any portion of the intestinal canal, but some points are more liable to it than others. 56 per cent. of the cases collected by Brinton were ileo-cæcal; in 32 per cent. the small intestine alone was involved; 28 iliac and 4 jejunal; in 12 per cent. the colon, including its sigmoid flexure, was the part implicated.
When the rectum is involved, it usually forms the outer layer of the invagination, the middle and inner layers being formed by the bowel which has passed from above into it; when prolapse of the rectum itself occurs, the mucous membrane is generally alone involved, but along with this the muscular coat may also descend and a true invagination of the rectum be found.
The most common variety of intussusception is the ileo-cæcal. It is in this form that we find the greatest length of bowel involved. This invagination begins generally at the ileo-cæcal valve, the lips of which at first turn toward, and descend into, the cavity of the cæcum, drawing with them the end of the ileum; in this case the valve forms the lowest point of the invagination. If the invagination continues, the end of the cæcum is next inverted; and if the process still goes on, more and more of the colon is invaginated, until in some rare cases it traverses the whole of the large intestine, appearing just above or even protruding through the anus. In this variety the vermiform appendix lies between the middle and inner layers of the intussusception, and its opening, usually stretched and enlarged by the inverted cæcum and inflammatory effusion, is found close to the ileo-cæcal orifice. In this intussusception the cæcum and colon are large and roomy, and the invaginated portion not so liable, [p. 847]as it is when the small intestine is alone implicated, to strangulation and sloughing; nor is there seen in ileo-cæcal intussusception, unless the portion of bowel involved is very short, the marked curvature of the invaginated portion so commonly found in the small intestine. In the ileo-cæcal form it is twisted or much convoluted rather than bent.
Another variety of ileo-cæcal invagination—very rare, however—is where the ileo-cæcal orifice does not descend into the cavity of the cæcum, but the lower end of the ileum passes through the valve into the large intestine. In this instance the invaginated portion is tightly compressed by the valve, and strangulation is speedy and complete. An invagination may occur in the lower part of the ileum, and the inner and middle layers pass on to the ileo-cæcal valve, and be arrested at that point, and afterward, in consequence of violent peristaltic action, the whole intussusception, inner, middle, and outer layers, be invaginated into the colon. In this way the invagination becomes doubled.
While intussusception may occur in either sex and at all periods of life, it happens nearly twice as often in males as in females, and is most frequently seen in childhood. Leichtenstern6 found in his statistics of 473 cases that one-half were seen in children under ten years old, and one-fourth of all intussusceptions occurred in children from four to twelve months old. Invagination of the small intestine is found almost exclusively in adults. Brinton from his records gives the mean age of its occurrence 34.6 years. According to the same author, the average age of ileo-cæcal invaginations is 18.57 years, and one-half of all cases of this form of intussusception observed by him were in children under seven years of age. Leichtenstern states that the lower part of the ileum is the most frequent site of invagination in the small intestine, and the descending colon and sigmoid flexure the most common portion involved in intussusception occurring in the large intestine.
6 Op. cit.
The mechanism of intussusception is probably not always the same. The following is thought to be the most frequent process: A segment of bowel becomes paralyzed by local peritonitis, some injury, diarrhoea, or colic, and while in this state a segment of bowel above is subjected to violent peristaltic action, and is forced into the unresisting portion below. In this case the paretic segment forms the outer or receiving layer of the intussusception. Leichtenstern believes that the paretic portion is turned in and invaginated into the normal bowel below, and that the clinical course of intussusception and post-mortem appearance correspond with this explanation. If such is the case, the paralyzed portion forms the inner layer, and the active bowel below the receiving layer. Another theory, which applies with much force to the most common of all invaginations—viz. the ileo-cæcal—is, that as violent anal tenesmus produces prolapse of the rectum, so prolonged and powerful tenesmus at the ileo-cæcal opening may cause prolapse of the lips of this orifice, and, eventually, invagination of the ileum, or of both this and the cæcum, into the colon. When we remember that the ileo-cæcal valve is furnished with a sphincter muscle, the analogy is complete. The idea so long entertained that intestinal worms may occasion invagination of the bowel has generally been abandoned. A polypoid tumor, by dragging down the portion of bowel to which it is attached, may produce invagination; and [p. 848] Brinton's statistics give 5 per cent. of cases of intussusception from this source. An examination of a larger number of cases would probably show a much smaller percentage due to this cause.
A majority of cases of intussusception, however, take place suddenly, without previous diarrhoea, colic, traumatism, or ill-health of any kind, and probably occur without any tenesmus or paresis of a portion of bowel. It may be that the longitudinal fibres of a segment of gut contract, dilating and shortening a portion of the bowel; while this part is distended a portion immediately above may be lengthened and narrowed by contraction of the circular fibres, and violent peristalsis going on at this moment, aided, possibly, by contraction of the muscular wall of the abdomen, forces the upper and narrow segment into the lower and dilated one.
At first the invagination involves a small portion of the bowel, but, active peristaltic action continuing, it rapidly increases in size. This increase is made at the expense of the sheath or outer layer, which turns in to form the middle layer. The length of the invagination varies from two or three inches to three, four, or five feet.
The symptoms of intussusception generally come on suddenly, and indicate both intestinal obstruction and inflammation. Pain resembling violent colic, and referred to the site of the invagination, is a prominent symptom. The pain is intense, paroxysmal in character, but after a time it becomes continuous. At first pressure gives relief, but in a few hours tenderness, denoting peritonitis, appears, limited to the invagination or spreading gradually over the whole abdomen. Vomiting soon follows, and, with rare exceptions, is persistent. After two or three days occasionally blood and sometimes fecal matter are ejected from the stomach. Diarrhoea, with bloody, mucoid stools, is rarely ever absent, and is characteristic of invagination. The patient has from fifteen to twenty passages a day. If the large intestine is involved, the diarrhoea is accompanied with tenesmus. Above the obstruction gas and ingesta accumulate, and produce abdominal distension, sometimes well marked. Generally the tumor formed by the invagination can be felt through the abdominal wall, and is a symptom of great importance. Meteorism and peritonitis may render the existence of the tumor obscure or altogether prevent its recognition, but in intussusception of the colon and at the ileo-cæcal valve the solid cylindrical mass can usually be found, and frequently, when the small bowel alone is implicated, a very careful and patient examination will enable the observer to detect it. Sometimes it changes its site, size, and shape; occasionally it can be felt in the rectum or is seen protruding through the anus.
The urgency of the symptoms of invagination depends upon the portion of bowel involved and the degree of constriction of the gut and its attached mesentery. When the bowel is tightly constricted the symptoms are acute, and the patient may die in a day or two; when the bowel is not constricted the symptoms are chronic in character, and in the early stages not urgent. The difference here is like that between strangulated and incarcerated hernia.
In acute cases the attack is sudden, obstruction complete, and the symptoms those of internal strangulation of the bowel, often followed by collapse, which may destroy life in a few hours. These cases are [p. 849] chiefly jejunal and iliac invaginations, and the higher up in the small intestine the seat of obstruction the more violent and urgent the symptoms. Constriction, being great, is followed by engorgement and inflammation of the invaginated bowel, and if the patient lives long enough gangrene ensues, by which the obstructing mass is separated and discharged en masse or in fragments through the anus. Not unfrequently life is saved in this way. That gangrene has taken place and separation of the invaginated segments is in progress are often known by the very fetid character of the evacuations and by their admixture with blood and shreds of necrosed bowel. When the sequestrum has been detached entire, it is often passed with difficulty. Frequently it lodges at some point in the bowel, producing temporary obstruction and giving rise to tenesmus and pain as it passes along the large intestine. There is no doubt that the continuity of the intestine above and below the neck of the invagination has been established, and complete cures effected in the way already mentioned. Usually, however, the patient dies from collapse, peritonitis, or perforation of the bowel before the obstructing mass can be removed by gangrene. Children almost invariably die before this can take place, and adults live from the seventh to the fourteenth day, according to the greater or less violence and acuteness of the symptoms. When the slough has been discharged and the continuity of intestine established, recovery is still uncertain, and death very often happens for reasons referred to in speaking of the separation of the sequestrum.
Separation of the invaginated portion and its expulsion, according to Leichtenstern, in the majority of cases takes place from the eleventh to the twenty-first day, but in chronic cases it is often delayed for months. According to Brinton, separation of the sequestrum occurs between the eighth and fifteenth in intussuscepted small intestine, and between the fifteenth and twenty-second days in acute cases of ileo-cæcal and colic invaginations.
In chronic cases of intussusception, which usually embrace the ileo-cæcal and colic varieties, strangulation is not common and the course of the disease is protracted. These cases often last for several months, and the symptoms are not always well defined. At first the pain is paroxysmal, with long intervals of ease. Vomiting succeeds, but is not persistent; discharge of the contents of the bowel below the seat of lesion takes place and afterward fecal matter from above this point, because the permeability of the bowel is not usually lost in chronic cases. Eventually the alvine discharges become bloody, mucoid, and characteristic of intussusception; the severity of the symptoms may gradually increase, the pain becoming greater, more constant, the vomiting more incessant, the discharges from the bowels more frequent, and in one, two, or three months the patient dies from asthenia. Several authentic cases are related where the disease lasted one or two years before terminating fatally. Very often some days before death the pain and tenderness cease, and the operations become free from blood and normal in character.
Constipation is a prominent symptom in all of the conditions which give rise to intestinal obstruction, and habitual constipation or loss of the powers provided for the advance of the contents of the intestines not unfrequently leads to permanent occlusion of the canal. It is impossible to fix any definite rule as a standard of health for the number and quantity of alvine evacuations. Some individuals have a passage from the bowels once every day; others, in the enjoyment of as good general health, suffer from the ordinary inconveniences of constipation if they have less than two or three daily fecal discharges; others, again, apparently equally as well, have a movement from their bowels once in two or three days or once a week, or even once in two weeks. Habershon7 records the case of a "woman sixty years old who from youth upward had had a passage from the bowels only every six or eight days, and whose health had been perfect." A lady under my own observation, for twenty years never had an alvine discharge oftener than once in two weeks, and three times in her life had passed two months without a movement of her bowels. This lady was the mother of several children, and, although not in perfect health, was able to attend to her ordinary household duties. Such cases are not very uncommon, and occur, as far as I have been able to ascertain, more frequently in women than in men.
7 On Diseases of the Abdomen, quoted by Leichtenstern in Ziemssen's Cyc. P. of Med., vol. vii. p. 588.
The number of fecal evacuations and the quantity discharged have been shown by Bischoff and Voit to depend, to some extent, upon the character of the food ingested, vegetable diet producing abundant, and animal diet scanty, stools. Doubtless, the quality of the food partly explains the quantity of the alvine evacuation, although, to some extent, this must depend upon the time that the feces remain in the colon, a long residence there taking away a greater part of the watery constituents and making the fecal mass thicker and harder; but the variations in the number of stools in persons living on the same diet can only be explained by the variations in the activity of the peristaltic action in different individuals, or in the same individual at different periods and under different surroundings.
The causes of habitual constipation are of the most varied and diversified character, and it is not always possible in an individual case to point out the original or primary one. Not unfrequently several causes are in operation at the same time to produce sluggishness of the intestinal canal and constipation. Very often it begins with change of scene and habits, by which the daily visit to the water-closet is interfered with, or after confinement to bed with some temporary indisposition. It is more likely to occur in men and women whose habits are sedentary and who are constitutionally lazy and indolent. The feces are allowed to remain in the rectum and colon, and every hour after the ordinary time for going to stool diminishes the watery parts of the fecal mass and makes it harder and more consistent. Many cases of chronic constipation, begun in this way, have ended in dilatation and thickening of the intestine, ulceration of the mucous membrane, and, eventually, perforation of the coats and escape of the contents of the gut into the peritoneal cavity. Rapid [p. 851] excretion of water by the kidneys, lungs, and skin produces constipation by withdrawing a large proportion of the water from the fecal mass, rendering it unnaturally dry and of diminished bulk. In diabetes, constipation arises from this cause unless the patient makes up the loss by drinking an unusually large quantity of water. Constipation in nursing-women is explained by the loss of water in the secretion of milk. The profuse sweating which attends malarial fever, phthisis, and other diseases readily accounts for the constipation which often accompanies these disorders.
Certain articles of food not necessary to mention here produce constipation. They fail to excite peristaltic action; or articles of diet which at first act as a stimulus to the bowels, and even provoke temporary diarrhoea, lose their power if kept up too long—just as certain purgative medicines lose their force if continued for too long a period. Gradually they cease to increase the peristaltic action, and rather add than otherwise to the inactivity of the intestines. Eating the same kind of food day after day is very apt, sooner or later, to result in diminished sensibility of the intestinal canal, a reduction of the peristaltic force, and deficiency in the secretion of the digestive juices, which in itself is a common cause of constipation. Frequent change of diet is generally needed to supply the stimulus necessary for that intestinal motion which relieves the bowels.
Bile is looked upon as one of the most powerful agents in stimulating peristaltic action, and when, from any cause, mechanical or otherwise, it is not poured into the bowel, constipation ensues. Unnatural flexures, congenital or acquired, of the large intestine are not unfrequently the source of chronic constipation. These flexures, normal or factitious, favor accumulation of feces, especially in subjects who have diminished sensibility of the bowel and a paretic state of the muscular coat. Certain injuries and diseases of the brain and spinal cord reduce, and sometimes altogether prevent, intestinal activity. Hysteria, if it exist for any length of time, is generally attended by sluggishness of the bowels, and great mental depression (melancholia) is sometimes preceded and sometimes followed by habitual constipation. In treating such a case it is important to make the distinction.
Temporary paralysis of the muscular coat of the bowel, followed by symptoms of intestinal constriction, with insuperable constipation, sometimes attends violent contusion of the abdomen. In some cases prolonged functional weakness of the muscular coat follows the injury. Many chronic diseases leave the bowel in a sluggish condition by the pathological changes produced in the intestine. The function of the muscular coat is frequently injured by the infiltration which accompanies peritonitis. The fibres are separated by the serous effusion which attends this inflammation; they become overstretched, and, losing their contractility, end in paralysis and obstinate constipation. Occlusion of the canal from this cause may last for days, and be accompanied with tympanitis, stercoraceous vomiting, and all the signs of internal strangulation, ending in death. Post-mortem examinations in such cases show no stricture or unnatural diminution in the size of the canal, but that the fatal occlusion was due to paralysis of the muscular coat of the bowel and arrest of its power.
The normal advance of the contents of the bowel is interfered with by any cause which lessens the contractility of the muscular coat. Chronic [p. 852] diseases which debilitate the general muscular system affect at the same time the contractile power of the muscular coat of the canal, and the debility and degeneration of old age are felt here, and sometimes occasion the constipation which often accompanies this period of life. Leichtenstern8 says that chronic intestinal catarrh is a common factor of constipation—that when this catarrh is of long standing it produces relaxation of the muscular coat and diminishes the elasticity of the intestinal walls. He believes that this pathological condition exists in a large proportion of the cases of habitual constipation attended with mental depression, that the hypochondriasis makes its appearance after the constipation has become chronic, and that it is a secondary symptom. This affection is located chiefly in the small intestine, and does not usually involve the colon.
8 Op. cit.
Probably the most common form of chronic constipation is that which accompanies loss of sensibility and muscular inactivity of the colon and rectum. The large bowel becomes sometimes so distended by the accumulated fecal masses that it has been found after death to measure ten or fifteen inches in circumference and to contain an astonishing quantity of feces. Any part of the canal, except the last two inches of the rectum, which is kept empty by the contraction of the sphincters, may be occupied by the mass, but the accumulation is greatest in the rectum, cæcum, and sigmoid flexure. At the last-named location the distension is so great that the mass can be readily felt through the abdominal walls. The tumor may be as large as a foetal head, and may be mistaken for a simple or malignant tumor of the omentum, stomach, or other organ, or for pregnancy or ovarian growth. The dilatation may be so enormous as to push the small intestines into the back part of the abdominal cavity and to interfere with the function of any organ upon which it encroaches. It may press upon the concave surface of the liver, and, arresting the flow of bile, produce jaundice or mechanically interfere with some portion of the track of the urinary organs and cripple their functions. When situated in a portion of the canal not tightly attached to the abdominal walls it is slightly movable, more or less hard and consistent, according to its duration, for it remains often for months unchanged, sometimes giving to the fingers the impression of a rather soft, easily-indented swelling with a uniform smooth surface—more often feeling like a hard, irregular, elongated, and corrugated mass of fecal balls. Contraction here and there of bundles of the circular muscular fibres of the gut produces the irregular, corrugated impression imparted to the fingers. Their shape and position may sometimes be changed by pressure through the abdominal wall. If the accumulation occurs in the rectum, the introduction of a tube or bougie is prevented by the impacted mass, which can be gotten away only by the fingers or by some instrument. The colon and rectum may be dilated to their utmost capacity with an enormous amount of feces, enough to fill a common-sized pail, and both the patient and medical attendant be deceived as to the sufferer's condition by the fact that he has his daily number of stools. The semi-fluid contents of the small intestines find their way through this mass by some irregular and uncertain track, undermining and breaking down sometimes a lump of the old fecal accumulation, which, if small in size or broken up, may pass on and [p. 853] escape by the anus, but if large and hard may drop into the irregular and uncertain passage and permanently close it; then sudden and complete intestinal occlusion takes place, with all of its fearful consequences. If this, however, should not occur, and the accumulation is not recognized and removed, the enormous dilatation may go on until complete paralysis of the muscular coat is produced, and entire stoppage of the current of feces, with permanent occlusion of the bowel; or before this takes place ulceration may set in, partly because of the great pressure of the fecal mass upon the mucous membrane, and partly from the irritating character of the contents of the bowel. Ulceration begins, most likely, at some point where resistance is greatest, and perforation of the bowel may ensue.
SYMPTOMS.—If the accumulation occupies only a portion of the colon, as the cæcum or sigmoid flexure, the distended part may become displaced and twisted on its long axis. This condition scarcely ever happens in the large intestines except at the parts mentioned. Torsion of the cæcum rarely takes place except in persons of from forty-five to sixty years of age, while twisting of the sigmoid flexure may happen at any period of life. When distended and very heavy from the weight of feces, with probably some congenital defect about its mesenteric attachment, the sigmoid flexure may become twisted and drop into the pelvis, producing at once symptoms of internal strangulation.
Individuals accustomed to having one or more alvine evacuations a day are made uncomfortable by two or three days of constipation. A feeling of distension about the abdomen, with flatulence and heat, follows this condition, and soon afterward headache, loss of appetite, and symptoms of indigestion supervene. If this state of the bowels continues unrelieved, pressure upon the hemorrhoidal veins takes place and interference with venous return, producing congestion in the lower end of the rectum. This is attended by straining, diarrhoea, evolution of gaseous matter, colicky pains, and possibly sympathetic disturbance of the genito-urinary organs. When at last the hardened and enlarged mass is discharged, it produces some pain and burning about the anus, with possibly rupture of the mucous membrane in that region. Fissure of the anus may thus originate. In the case of a lad aged about nine years under my care fissure of the anus began in this way, and after its formation the pain of defecation was so intense that he resisted for ten days every attempt of his bowels to move. After this time he passed every day or two one or more hardened fecal balls, but always with such atrocious pain that he looked forward to the next attempt with terror. This case ended in fecal impaction, which nearly proved fatal.
Not unfrequently persons who habitually go two or three days without having a passage from the bowels are not apparently inconvenienced, and after a time any of the discomforts ordinarily felt from constipation are not noticed, if indeed any exist.
Generally, however, chronic constipation leads to a host of troubles of the most varied character. There is not an organ in the body that is not more or less influenced by it. The generation of gas in the intestines produces a sense of fulness of the abdomen and elevation of the diaphragm which interferes with the action of the lungs and heart. The sufferer is oppressed, sighs, and has difficult respiration and attacks of [p. 854] palpitation of the heart. The influence of the abdominal pressure is conducted by the sympathetic nerves to the brain, and the patient frequently has vertigo, headache, ringing in the ears, faintness, etc., and in consequence of the pressure upon other nerves or of hyperæmia of the spinal cord and its membranes he has dull aching pains in his back, groins, genitals, or extremities. I have seen in several instances pain in the legs, coming on after the patient has retired and lasting until morning, violent enough to prevent sleep, at once permanently relieved by an active cathartic after antiperiodics, alteratives, and anodynes had failed to do any good.
A patient suffering from habitual constipation usually obtains temporary relief by the bowels acting either spontaneously or after a dose of medicine; but, the causes of constipation continuing, the physical discomforts and suffering continue, varied in every conceivable way. His digestion being disturbed, appetite poor, and assimilation imperfect, he gradually loses flesh and his complexion becomes sallow and unhealthy. In addition to this, he soon grows irritable and fretful, trifling affairs trouble him, he has fits of great mental depression, and soon settles down into hypochondriasis, his life becoming a burden to himself and a nuisance to his friends.
If the constipation ends in fecal accumulation, the worst symptoms of mechanical obstruction may present themselves at any time, and death of the individual follow. The practitioner should always keep this fact in mind in treating every case of intestinal obstruction, and search for fecal impaction by examining the rectum and the whole length of the large intestine through the anterior abdominal wall. Very often symptoms of impaction come on gradually in one who has been ailing for some weeks or months, but sometimes the onset is as sudden as in a case of acute occlusion of the intestines. The patient is seized with pain like that of colic and an urgent desire to empty his bowels, but all attempts to do this are futile, and the straining is followed by great exhaustion; borborygmus, nausea, vomiting, and possibly hiccough, soon come on, with tympanitic distension of the belly. If the impaction is not overcome, death by collapse or from peritonitis follows. Post-mortem examination shows enormous fecal accumulation, peritonitis as a consequence of the obstruction, perforating ulcer in some part of the large bowel, more often the sigmoid flexure, or, in some cases, absolute rupture of the cæcum itself, and escape of its contents into the peritoneal cavity.
In a report by George Pollock9 of 127 cases of intestinal obstruction, 77 belonged to the above class; and Brinton, in his analysis of the whole group of cases collected by him, says stricture constitutes about 73 per cent. In 124 cases of intestinal obstruction reported by Mr. Bryant10 from the post-mortem records of Guy's Hospital, 47 were found to be stricture of the bowel. The above statements show that stricture, or diminution of the calibre of the bowel, is the most frequent cause of [p. 855]intestinal obstruction, and the subject is worthy of our earnest consideration.
9 Medico-Chirurgical Review, 1853.
10 Practice of Surgery.
While stricture of the bowel may be found in any portion of the intestinal canal, it occurs most frequently in the sigmoid flexure and rectum. Brinton found in 100 fatal cases of stricture 30 in the rectum and 30 in the sigmoid flexure; only 8 cases in 100 were in the small intestine. Brinton's statistics correspond very nearly with those of other writers. The affection is more common in men than women, and the average age at death is about forty-four years.
The most common cause of stricture is contraction following cicatrization of ulcers of the mucous and submucous coats of the intestine. The ulcer may involve the circumference of the bowel, and the resulting cicatrix terminate in uniform constriction of its lumen, or the ulceration may extend several inches along the side of the intestine, ultimately causing contraction in the direction of its longitudinal axis, marked stenosis, and kinking of the gut. When ulceration, continuous or in patches, involves a large extent of bowel, it may reduce the gut to a mass of indistinguishable cicatricial tissue. Bristowe11 says he has seen the whole cæcum thus contracted "into a channel barely capable of admitting a goose's quill."
11 Reynolds's System of Medicine.
Stricture of the intestine often follows dysentery or tubercular and syphilitic ulceration of the bowel. Follicular or hemorrhoidal ulceration is sometimes the beginning of a stenosis which ends in stricture of the rectum. Stercoral ulcers of the colon are not unfrequently the starting-point of cicatricial contraction of the calibre of the bowel. Sometimes, but rarely, ulcers of typhoid fever end in constriction of the intestinal tube. The diameter of the gut is also contracted by the effects of caustic substances, by ulceration following the lodgment of foreign bodies, and by effusion of lymph or thickening attendant upon long-standing hernia. Very often after death it is impossible to determine what particular kind of inflammation and ulceration caused the stricture. Generally, the cause which provokes the ulceration sets up chronic peritonitis, which materially aids in producing the obstruction. Spasm of the circular muscular fibres usually accompanies these lesions, and materially contributes in many cases to fatal intestinal obstruction. Some authors assert that spasm without organic change can produce acute obstruction: such an occurrence, except possibly in the rectum, must be very rare, if indeed it ever happens.
The most common cause of stricture is cancer. This disease may originate in the bowel itself, or, beginning in some neighboring organ or tissue, gradually spreads and involves the gut. It may extend around the bowel or be infiltrated along the sides of the canal for several inches, and may be scirrhous, medullary, or epithelial in character. Eighty per cent. of the cases of cancer of the bowel are situated in the rectum. Usually, but not invariably, cancerous deposits are found in persons who have passed middle age.
An impediment to the passage of fecal matter is invariably produced in constriction of the intestine from the above causes, and it frequently continues until fatal occlusion occurs. The contents of the bowel accumulate above the block, producing distension of the gut and thickening of the muscular coats above the stricture, with contraction and atrophy [p. 856] of the portion of intestine below. Dilatation of the bowel above the seat of lesion is sometimes great enough to cause rupture and peritoneal extravasation, or distension and stretching of the coats of the canal may be sufficient to interfere with its circulation, and ulceration ensue.
Occasionally cases of stricture or well-marked circumscribed contraction of the bowel are seen which give rise to no marked symptoms of constriction during life. Such was the case in the instance related by Bristowe and referred to above. These instances are, however, exceptional in the large intestine.
Symptoms of stricture vary according to the site, cause, and extent of the lesion. They are gradually developed, and in this respect are unlike the symptoms of internal strangulation or of intussusception, which are generally acute and rapid in their course. When the obstruction in stricture is complete, progress toward death is comparatively slow. If the stricture is seated in the small intestine, the symptoms are often so obscure that for a long time the presence of the contraction may not be suspected; the contents of the small bowel are usually fluid, and in this state readily pass through the constricted part. The more solid the contents of the bowel, the greater the difficulty in passing a contracted and narrow orifice, and the more conclusive and characteristic the assemblage of symptoms of obstruction from stricture.
The history of a case of intestinal obstruction from stricture is often instructive. For weeks or months there have been colicky pains and intestinal disorder; possibly, in the early stages, diarrhoea, but later marked constipation, and probably previous attacks where constipation was for a time insuperable and death from obstruction imminent. Hemorrhage, except in cancer or when complicated with piles, is rare. The attack may come on suddenly, or constipation become more and more difficult to overcome; violent peristalsis presents itself, accompanied by pain and abdominal distension, and followed by nausea and vomiting, the latter often being stercoraceous. During the throes of pain—for it is paroxysmal—the outline of the distended gut can be felt and seen through the abdominal walls if they are thin and free from fat. Unless the stricture is relieved the patient gradually dies from asthenia. Inflammation is often absent throughout, but enteritis or peritonitis may come on, or perforation and peritoneal extravasation ensue and hasten the fatal termination.
When the obstruction is in the rectum it can be felt with the finger; if in the sigmoid flexure, it may be felt with a gum bougie or probe, but the use of the former is unreliable, and the latter, unless carefully employed, dangerous. Obstruction at this point, however, is attended with marked distension of the descending and transverse colon. If seated in the small bowel, the large intestine is flaccid and collapsed. Careful manual exploration often enables the practitioner to determine the site of the contraction. Weight, pain, dulness, and fulness are usually found about the stricture, but these signs may be of little value when the abdominal wall is thick and unyielding, or peritonitis or tumor is present, or the contracted portion of bowel is compressed or drawn out of its proper site. Brinton suggests that the site of stricture may be determined by the quantity of water which can be injected through the anus into the bowel. Such an estimation must often be erroneous, as stricture [p. 857] is rarely ever complete and fluid may be forced through the constricted part. Indeed, Battey of Georgia has demonstrated upon dead and living subjects that fluid may be made to pass through the entire canal from the anus to the stomach.
Obstruction due to cancer of the rectum can be determined by digital examination. When seated in the small intestine or higher up in the large bowel, the presence of a painful tumor, preceded for weeks by evidences of impaired nutrition, emaciation, and followed by lancinating pain, cancerous cachexia, etc., will indicate the character of the trouble.
Obstruction of the bowel is sometimes occasioned by compression or traction exerted on the intestine by abdominal tumors or cysts. Fibrous tumors of the uterus, ovarian cysts, hydatid growths, or indeed any form of abdominal tumor, may by pressure on some part of the intestinal track produce fatal obstruction. Several inches of bowel may thus be compressed and rendered impervious, or if traction is exerted by the tumor, which is often adherent to the bowel, the tube may be sharply bent or twisted and its action interfered with. A case is reported of compression of the bowel from a great accumulation of fat about the colon. Adhesions of intestinal coils from chronic peritoneal inflammatory changes constitute a large and important class of cases of intestinal obstruction. This condition is known as contraction of the bowels: 23 of the 124 cases reported by Bryant were of this character.
The usual site of stricture is the large bowel: contraction is far more frequently seen in the small intestine, and is caused by an effusion of lymph following simple peritonitis or the inflammation attending the formation of cancer or tubercle of the peritoneum. Coils of intestine are matted together or to neighboring parts in this way by bands of lymph or false membranes, and the action of the bowel interfered with or obstructed. Constriction of a length of bowel may be found after death, or a sharp, angular bend by which complete obstruction has been produced.
Circumscribed peritonitis may produce adhesion of a portion of bowel by bands of lymph to the uterus or its appendages, or to some part of the large intestine, or to the abdominal wall, and the action of the bowel become embarrassed by traction, constriction, or bending. In consequence of the irritation following this condition, spasmodic contraction may follow and add to the difficulty, or enteritis may ensue; and this will especially be the case if the circulation of the part is interfered with, and render complete what before was a partial obstruction. Distension and fulness of the bowel above the obstruction, with contraction and emptiness of the portion of the gut below, are found after death in cases of contraction, just as we see in fatal cases of stricture. The history of the case and presence of a tumor will generally enable the practitioner to determine when obstruction is due to the presence of some adventitious growth. When contraction is complicated with the presence of tubercle or cancer, symptoms attending these conditions will be present.
Obstruction of the intestines from contraction generally comes on [p. 858] insidiously. The patient may date the beginning of his trouble from an old attack of circumscribed peritonitis which probably took place weeks or months before. He has attacks of colicky pains, indigestion, and constipation. The last is difficult to overcome, continuing for hours before it is relieved by medicine or the efforts of nature. During the attack of almost insurmountable constipation violent peristaltic movement of the bowel above the impediment may be noticed. The patient may gradually become more and more feeble from suffering and interference with nutrition, and die from exhaustion, or fits of obstinate constipation may continue to recur, until finally one of them becomes insuperable and fatal.
The symptoms of contraction closely resemble those of stricture, but it is important to distinguish one from the other, as the treatment, especially if surgical interference is demanded, is very different. A rigid analysis of all of the signs will usually, but not invariably, enable the practitioner to make the distinction.
There is an important difference between the constipation of stricture and that of contraction. In the former the difficulty is in defecation, emptying the large bowel, the usual site of stricture; in the latter the difficulty is in the passage of the contents of the gut along the narrowed and contracted small intestine, the common site of contraction. In stricture the calibre of the bowel is diminished by some sharply-defined mechanical impediment seated in the cavity or in the walls of the tube; in contraction the bowel is bent or kinked by adhesions, or coils of intestine are matted and glued together and peristalsis interfered with. In stricture defecation is difficult and painful; in contraction the alvine discharges are painless. In the former blood and mucus are not unfrequently seen in the feces; in the latter the motions are healthy. In stricture constipation alternates with diarrhoea; in contraction looseness of the bowels is rarely seen. In stricture distension of the abdomen is lumbar and epigastric; in contraction the distension is less and is central and hypogastric. In both conditions violent distinct peristaltic action is seen during a fit of constipation, and in both the bowel above the constriction is distended and hypertrophied. In contraction the powerful, writhing peristalsis involves the small intestine above the impediment, and in stricture the large bowel above the obstruction. In both stricture and contraction inflammation of the bowel and peritoneum may supervene. In contraction, when inflammation sets in or when enteritis and peritonitis are absent and the attack of constipation is insurmountable, I have noticed that the symptoms are more urgent and rapid in their course, and danger of death from collapse greater, than when these conditions exist in stricture.
DIFFERENTIAL DIAGNOSIS.—In every case of intestinal obstruction a careful examination should be made for external strangulated hernia. All of the regions of the abdomen in which hernia may occur should be thoroughly inspected, as the symptoms of the two conditions are identical. A small or incomplete external strangulated hernia may easily be overlooked. An individual with an old hernia may suddenly have symptoms of intestinal obstruction, and it may be doubtful whether the obstruction is due to internal constriction or to the external hernia. Diagnosis is especially difficult when the chronic hernia is irreducible in character. If the cause [p. 859]of the impermeability is internal and below the external hernia, that portion of intestine in the hernial tumor becomes swollen, tense, and hard, and closely resembles the local symptoms of strangulated hernia. If the external hernia is reducible, reduction en masse may take place and a retro-peritoneal hernia be formed. When the case is doubtful and urgent, an operation for strangulated hernia should be performed.
Functional obstruction of the bowel is sometimes seen, closely simulating obstruction from one of the structural changes mentioned. Cases of functional obstruction are seen usually in hysterical or nervous women, and are generally recognized by the history, course, and termination of the malady. The fact that local enteritis, peritonitis, or typhlitis, by paralyzing a portion of the bowel, may produce all the signs of acute and complete obstruction, should not be lost sight of.
In cases of congenital stricture or malformation, or the presence of foreign bodies in the intestine, or acute internal strangulation, or twisting of a length of bowel, and generally in intussusception, symptoms of acute obstruction are present. The individual may have been in perfect health, and suddenly symptoms of the gravest character set in. Intense pain, referred to some special part of the belly, is the first sign of trouble. Nausea soon follows, and with it great prostration; the depression of vital power approaches, and sometimes reaches, syncope; the patient rolls and tosses in agony; his mental distress is equally great, and if old enough he is conscious of his danger and is anxious and despondent. Vomiting succeeds the nausea: at first the contents of the stomach, and then those of the small intestines, are thrown up; after a time the vomiting is stercoraceous. The belly becomes swollen, tympanitic, and exquisitely tender; the weight of the bed-clothes or the slightest touch of the finger upon his abdomen is intolerable; he keeps his head and shoulders raised and his lower limbs retracted to avoid pressure of the abdominal muscles. Constipation is complete and insuperable. If the abdominal wall is thin, the violent motion of the intestines can be seen and felt through it. These painful peristaltic movements of the bowel are paroxysmal and attended by loud rumbling or gurgling noises. The pain gradually increases; the patient is very restless and complains of great thirst; his pulse is small, hard, and frequent, his extremities cool and features pinched. If not soon relieved, exhaustion comes on; he has muttering delirium, cold clammy perspiration, hiccough, twitching of the tendons, and death soon follows from collapse or from peritonitis or gangrene, or from both. The average period of death is from six to eight days. It may occur in thirty-six or forty-eight hours, or the patient may last for two weeks.
In congenital occlusion and malformation the history of the case, the age of the patient, and the fact that the deformity in such cases is almost always confined to the anus and rectum, usually render the diagnosis sufficiently easy.
Obstruction caused by foreign bodies impacted in the intestines can generally be diagnosed. The history of the case may show that foreign bodies have been swallowed or that the patient has been subjected to some of the conditions which cause the formation of enteroliths. These stony concretions are usually found in the cæcum or colon, and frequently give rise for days and weeks to symptoms of indigestion, emaciation, [p. 860] constipation, and other evidences of bad health before complete occlusion of the intestine takes place. Not unfrequently, before the sudden attack of impermeability of the bowel the patient has had repeated attacks of typhlitis, and has been conscious for a long time of the presence of a tumor in the region of the cæcum or colon. Possibly he has passed on some former occasion pieces of the stony concretion.
Diagnosis of obstruction by gall-stones is often aided by the fact that the patient has recently suffered characteristic pains of hepatic colic and by the icterous condition of the skin. Possibly the individual has suffered repeated attacks of hepatic trouble and has previously passed a gall-stone. Obstruction from this cause is seen four times as often in women as in men, and always after the middle period of life.
In obstruction occasioned by internal hernia or the presence of membranous bands, loops, mesenteric pouches, the symptoms are often such as to baffle all attempts at accurate and certain diagnosis. The onset of the symptoms is sudden and the course of the disease rapid; prostration of vital power is extreme, sometimes amounting to syncope; vomiting incessant and persistent; pain constant and fixed. The most characteristic symptom of internal strangulation is the very great and prolonged depression of vital power; it occurs generally in early adult life.
Erichsen states that in twisting of the bowel the abdomen is unevenly distended, it being tympanitic on one side and flattened on the other. This condition of the bowel is usually seen after middle age. In intussusception the principal signs are, usually, the early age of the patient—obstruction from other causes in children being rare—the suddenness of the onset of symptoms, the frequent desire to go to stool, the tenesmus, and the characteristic bloody mucus discharges. By abdominal palpation frequently the sausage-like tumor can be recognized, and very often the intussuscepted part can be felt in the rectum or seen protruding through the anus. When invagination involves the upper part of the small intestine, diagnosis of the cause of occlusion is almost impracticable.
In obstruction of the bowel from fecal accumulation, inflamed and thickened intestine, stricture, compression and traction, and contraction of the gut from cancerous deposit, the symptoms are gradually presented and chronic in character. They are unlike the signs of acute obstruction, which occur in persons apparently in perfect health and are sudden and violent from the beginning. In chronic obstruction of the intestine the patient has probably been complaining for some time, with symptoms of abdominal trouble. He has been unwell for weeks, his appetite poor, digestion disordered, strength diminished, and bowels constipated. The last symptom is the most distressing of all. Purgatives do not give the relief ordinarily obtained, but add to the griping, colicky pains, nausea, and general depression. When his bowels do act, the stool is sometimes liquid, sometimes very hard (scybalous), or the form of the matter passed is tape-like or pipe-like. Sometimes, in his frequent attempts at stool, the only discharge is blood and mucus or pus. Attacks of eructation and vomiting often take place during the progress of the disease. Stercoraceous vomiting is, however, rare, and only seen in the later period of the attack. Abdominal distension is slow in making its appearance, but after a time is well marked, and due more to tympanitis than to [p. 861] constipation; the tympanitic distension is accompanied by loud rumbling and gurgling noises in the bowels. After a period which varies much in different cases, inflammation, suddenly or gradually, is set up, and all the symptoms of acute obstruction are presented, grafted on signs of chronic occlusion. We have pain, nausea, vomiting, great distension and tenderness of the abdomen, peristalsis plainly seen and felt if the abdominal wall is thin, the small, frequent, wiry pulse, clammy perspiration, prostration with hiccough, tendinous twitchings, and death, very like that following a case of external strangulated hernia.
Obstruction due to fecal accumulation generally happens in persons who have passed middle age, and can often be diagnosed by digital rectal examination and palpation of the abdomen, by the presence of fecal tumors, and the history of long-existing constipation with its manifold consequences; previous attacks of impermeability, and relief by discharge of enormous masses of feces.
Obstruction caused by the presence of some abdominal tumor is generally known by the history of the case, the fact of the existence of the tumor being known to the patient or discovered by the physician by an examination through the abdominal walls or through the vagina or rectum. The progress of such cases is essentially chronic, but acute symptoms may at any time come on. Diagnosis of obstruction due to stricture is frequently made by examination of the rectum and sigmoid flexure, the usual sites of constriction from this cause. Complete occlusion from stricture is almost always preceded by well-marked premonitory symptoms.
When the obstruction is situated in the lower part of the colon and rectum, its precise seat can be determined by digital or manual examination or the use of a bougie or tube. When the site of obstruction is above the sigmoid flexure, it is difficult, and occasionally impossible, to determine its exact locality. As a rule, when the constriction is in the small intestine the symptoms are acute and urgent; pain is intense, vomiting comes on soon, and prostration is early and extreme. When the large intestine is involved, except in volvulus, the symptoms are generally chronic. In twisting of the gut the symptoms are rapid and uncommonly severe. The higher up the obstruction, the earlier stercoraceous vomiting begins. Above the constriction the bowel is distended and tympanitic; below the constriction it is generally collapsed. In obstruction of the large intestine the outline of the tympanitic and distended gut may be traced with the eye and hand. In constriction of the small intestine the secretion of urine, as has been shown by Hilton, G. Bird, and Barlow, is less than where obstruction is seated in the large bowel. Besides rectal and vaginal examinations, which should never be neglected in any case of intestinal obstruction, abdominal palpation may also aid in determining the site of constriction. It should not be forgotten, however, when a tumor is found—as, for instance, in invagination—that the bowel may be displaced; a distended cæcum may be pushed into and occupy the left side of the belly. Cases are not uncommon where the symptoms are so combined and uncertain as to render accurate diagnosis of the site of obstruction impracticable.
Very little light is thrown upon the diagnosis by pain, constipation, or vomiting when these symptoms are considered separately. Pain is common to many diseases of the abdomen; obstinate constipation, lasting for [p. 862] days and weeks, is often seen where there is no mechanical obstruction; and vomiting attends many morbid conditions of the body. But when these symptoms are combined and examined along with the history of the case and mode of invasion, they are often characteristic of constriction of the intestine. Pain in acute obstruction is fixed, umbilical, and intermittent; in chronic cases it is more diffused and increases with the distension. In acute cases constipation is complete and insuperable; in chronic cases this symptom gradually increases; in intussusception we have frequent discharges of a dysenteric character, and hemorrhage, sometimes copious, when the small bowel is involved. The bowel below the seat of complete constriction may be full of fecal matter, and the discharge of this spontaneously or by the aid of enemata may induce the attendant not to regard the case as one of occlusion. Stercoraceous vomiting, as a rule, comes on early in acute and late in chronic cases of complete occlusion of the gut; in spasmodic ileus or impermeability not due to mechanical occlusion feculent vomiting is only occasionally seen.
The duration of life in acute intestinal obstruction varies very much in different cases: death may ensue in a few hours or not for ten or twelve days; the average period is six days. The duration depends upon the site of the constriction and the mechanical injury to the bowel; the nearer to the pylorus the constriction, the more rapid the progress. In volvulus involving the sigmoid flexure, when injury to the bowel is great, the symptoms are acute in the extreme. After peritonitis or enteritis begins, progress toward a fatal issue is very rapid, the patient rarely living more than three or four days. In occlusion from stricture, compression, fecal impaction, and chronic intussusception the patient may live for weeks or even months.
The statistics of Leichtenstern show that from 5 to 10 fatal cases of intestinal obstruction occur every year among every 100,000 inhabitants; and according to the mortuary records of England an average of 1 death from this cause is seen in every 260 deaths. Brinton reports 1 death from intestinal obstruction in every 280 deaths; his statement is based upon 12,000 promiscuous autopsies. The first author states that the statistical reports of the general hospital of Vienna inform us that out of 60 cases of ileus, 6 or 10 per cent. recovered. This report, however, is too meagre to be of much value. From Brinton's statistics of 500 deaths from obstruction we find that out of 100 cases, 43 are intussusception, 17 stricture, 4.8 impaction of gall-stones, 27.2 internal strangulation, and 8 torsion.
TREATMENT.—There are few conditions of the body which cause the practitioner more anxiety and embarrassment than cases of intestinal obstruction, and when the precise seat and nature of the occlusion are not known the treatment is almost entirely empirical. The distinction, however, between acute and chronic cases of obstruction of the bowels, or of acute supervening upon chronic symptoms, can almost always be made, and a patient investigation of the history of the case, the mode of invasion, and a rigid analysis of all the symptoms presented will generally enable the attendant to come to some positive conclusion as to the cause and site of the occlusion. One fact in the treatment which cannot be too strongly impressed upon the mind, especially of the young practitioner, is not to use purgatives and irritating enemata, formerly so much in vogue, [p. 863]in the hope of forcing a passage through the occluded bowel. The patient is urgently solicitous for medicine which will open his bowels, but the use of purgatives to overcome internal strangulation is as senseless and hurtful as when used to overcome the constipation of external strangulated hernia. These agents only add to the nausea, vomiting, pain, and peristalsis. The latter is violent enough already to render coils of intestine visible, and with every paroxysm is adding to the entanglement and impermeability. It is said that cathartics in some instances have unlocked the bowel in intestinal obstruction: these cases are exceptional, and many of them were probably functional and not structural in character. The only exception to the rule of avoiding purgatives is as stated by Jonathan Hutchinson: "In certain cases when impaction of feces is suspected, and in cases of stricture when fluidity of feces is desirable."
Formerly, some of the best practitioners resorted to the exhibition of one or two pounds of quicksilver, in the hope of overcoming intestinal obstruction by the weight of the metal. This plan has properly been almost if not quite abandoned. Crude mercury is very slow to reach the obstruction, is divided into small portions by the peristalsis, which its presence increases, and if it should finally arrive at the point of constriction in any considerable quantity, it is more liable to add to than overcome the difficulty.
The great remedy in intestinal constriction is opium, in large or small and repeated doses. Its use arrests the vomiting, stops the pain, and quiets the violent movements of the bowel. Very often by it the intestine is preserved and the life of the individual saved. No special dose can be prescribed: it should be administered until slight narcosis is obtained and pain and vomiting cease. Small doses of morphine, given hypodermically and quickly repeated, is the best plan of exhibiting it. It may be given by the stomach, but under such circumstances it is apt to be rejected, or if retained absorption goes on slowly, or possibly not at all. If for any reason its hypodermic use is impracticable, it had better be given by the rectum. Opium lessens the danger of death from collapse: it gives nature an opportunity to untwist the gut in volvulus, or to unroll it in intussusception, or to cut off the invaginated part by gangrene; and in internal hernia, morbid adhesions, strangulation by bands of lymph, stricture, and other forms of obstruction, it diminishes violent peristaltic action, postpones inflammatory infiltration, fixation of the strangulated portion, and keeps the parts in better condition for operative interference, which in many cases offers the only hope of relief. To carry it farther than slight narcosis and arrest of the most painful symptoms of obstruction is an abuse of the remedy. By such abuse the symptoms will be masked and both patient and practitioner deceived.
When obstruction is due to fecal impaction or spasm, the opium treatment is still often indicated. Not unfrequently, after pain and vomiting are relieved and slight narcosis kept up for some hours, the bowels relax and spontaneous evacuation takes place. If not, discharge of the contents of the bowel should be assisted by the administration of castor oil, calomel, or repeated enemata of warm water. These agents should not be used, however, as long as there is pain, tenderness of the belly, or any evidence of peritonitis, but the opium treatment continued until all signs of inflammation have disappeared. It has been proposed to give [p. 864] belladonna in place of opium; in small doses and carefully watched it may be added to the opium, but should not be substituted for it.
The local application of ice-water or pounded ice to the abdomen has been recommended; and it is asserted that the danger of general peritonitis is lessened, and that the strangulation itself has disappeared, under the influence of cold. If, however, cold increases pain and peristalsis, it should be abandoned. The local application of moist heat or fomentations will more probably do good and give a grateful sense of relief to the sufferer. General bleeding should never be resorted to, and the use of leeches, except to ward off or subdue some local inflammation, is of doubtful expediency. Blisters, ointments, and cups are useless in such an emergency. Cracked ice, strong coffee, and carbonated water in small quantities are valuable in allaying thirst and nausea.
Cases are reported where obstruction of the bowels has been overcome by the use of electricity; both the continuous and induced currents, but chiefly the former, have been used; its value in such cases is improbable.
Abdominal taxis or massage has been earnestly recommended and frequently practised in cases of constriction. Successful results from this procedure have been reported. It has been attempted while the patient was in a warm bath or under chloroform or while taking large enemata of warm water. Abdominal traction by the use of large cups to the belly has also been advised. We can only hope for success from these measures in the early stages of obstruction, before inflammatory action or fixation of the strangulation has taken place, and any attempt of this kind should be made with tact and gentleness. Inversion of the body has also been suggested.
The injection of large quantities of warm water into the bowels to overcome obstruction should never be omitted before resorting to operative interference. The author has seen this plan in five or six instances succeed after all other means had failed. Simple warm water should be used, introduced by means of the common Davidson or a fountain syringe. The injection should be made slowly, with occasional intervals of rest, to allow the fluid time to pass through the intestinal coils. During the operation the patient should be in the knee-elbow or Sims's left lateral position, and under the influence of an anæsthetic. One or two gallons of water may be used. In place of water, the bowel may be inflated with air, introduced by a pair of common bellows to the nozzle of which a piece of India-rubber tubing is attached. The addition of castor oil, turpentine, carbonic acid gas, and other irritants will more likely detract from than add to the efficacy of these measures. In chronic intussusception, or in acute cases when fixation of invagination is believed to have taken place, and especially when inflammation is great, gangrene threatening or in existence, injections of air or water should not, of course, be attempted.
In invagination, when the intussuscepted part is low down in the rectum or protruding from the anus, replacement by fingers or sound should be tried; reduction begun in this way may be completed by injections of air or water. The propriety of introducing the whole hand into the rectum is very questionable. In occlusion of the gut by compression and traction the cause should be found, and, if possible, removed. An abdominal or pelvic tumor may be pushed out of the way of the compressed bowel, a cyst punctured, a displaced womb replaced.
[p. 865] Great care should be taken to support the strength of the patient by concentrated and nutritious food, and in the later stages by stimulants. When the bowels are distended by gas an injection into the rectum of ten grains of sulphate of quinia will often give marked relief.
It has been proposed to tap the distended gut with a fine trocar when accumulation of gas is enormous, causing dyspnoea and great general distress; temporary relief is often obtained by this plan, which is an imitation of a common practice among veterinary surgeons. Something more than temporary relief may, however, follow the tapping. In twisting of the bowel, in internal strangulation by band or loop or ring, and in some cases of invagination, the constriction is kept up by the enormous gaseous distension. The obstruction is continued as much by causes within as without the intestine. When tapped and the gas drawn off, the bowel collapses, and may escape from its constriction and return to its natural condition. Tapping is not always certain or safe. The trocar or aspirating tube may pass between the convolutions and no escape of gas take place, or it may be followed by fecal extravasation into the peritoneal cavity. Notwithstanding the risk, the plan is a valuable one, and in suitable cases should be resorted to.
SURGICAL TREATMENT.—In cases of acute obstruction of the bowel from bands of lymph, diverticula, internal hernia, slipping of a portion of gut into some opening, or twisting, when the treatment suggested has been tried and fails, laparotomy should be performed; that is, the abdomen should be laid open, the cause of the obstruction searched for, and, if possible, removed. In acute cases a few hours, at most one day, may be spent in trying the medical means recommended. After that time, if the patient is not relieved, the sooner laparotomy is resorted to the better the chance to save life. Acute internal strangulation of the bowel from these causes has the same symptoms, course, and termination that acute external strangulated hernia has. It demands the same treatment—removal of the cause of the constriction. Delay in performing the operation in the former is as certain to be followed by peritonitis, gangrene, and death as it is in the latter; and the surgeon who hesitates to open the abdomen and attempt to remove the constriction in a case of acute obstruction after a fair trial and failure of medical measures, is as culpable as the one who delays the operation of herniotomy for unrelieved strangulated hernia.
In rare instances spontaneous self-reduction of external strangulated hernia takes place; the cases are exceptional, and the fact is no apology for postponing herniotomy. So in occasional instances acute internal strangulation is spontaneously relieved; here too the cases are exceptional, and the occurrence should be no excuse for delay in laparotomy. To justify the operation it is not necessary that the precise site and nature of the mechanical impediment should be determined, although this can usually be done. It is only necessary to know that the cause of the acute obstruction is not enteritis or peritonitis, but a constriction mechanical in character, which no medicine or manipulation or expectant treatment can relieve. When diagnosis is clear and laparotomy is indicated to save or prolong life in intestinal obstruction, the aid of the surgeon should at once be invoked. Delay is fatal. Peritonitis beginning or in actual existence makes abdominal section more dangerous and [p. 866]lessens materially the chances of recovery. To make the operation absolutely the last resort when the bowel is injured beyond repair, when peritonitis is in full progress, gangrene threatening, or the patient on the verge of collapse, is a useless cruelty to the sufferer and his friends, and only serves to bring surgery into disrepute. If the truth were known, many of the cases of death following laparotomy should be ascribed not to the fact that the knife was used, but to the fact that it was used too late.
In intussusception not relieved by medical means the propriety of abdominal section is questionable. The subjects of this condition are usually children. Dislodging the invaginated bowel is not always practicable, and the opium or expectant treatment may end in spontaneous cure by the bowel righting itself or by sloughing of the intussuscepted part. It is doubtless true that many of the so-called cures from the latter process subsequently die from contraction of the cicatrix at the site of the separation of the slough. In 43 cases collected by Ashhurst of laparotomy for invagination, 13 recovered and 30 died. The record is bad, and to some extent the heavy mortality is due to the fact that the operation was put off too long—delayed in acute cases until sloughing had taken place, and in chronic cases until adhesion of the invaginated parts had occurred. Indeed, some of the cases reported were moribund when the operation was undertaken. Recently many successful cases have been reported, and it is fair to presume that the percentage of recoveries in the future will be greater than they have been in the past.
In acute intestinal obstruction due to bands, internal hernia, volvulus, or the presence of foreign bodies, as gall-stones, there is no question that laparotomy should be performed after other measures for relief have been employed and failed. Death in such cases is inevitable and imminent, and operative interference should not be postponed until peritonitis has set in. After the abdominal cavity has been opened the distended gut can easily be found and the fingers of the operator carried on down until the site of the constriction is reached and the cause of the obstruction discovered. If the constriction is due to the presence of bands or adhesions, they should be cut or broken up and the gut relieved. If an internal hernia is found or a portion of bowel has slipped into some fissure or pocket, it should be withdrawn and the parts restored to their natural position. If the cause of the obstruction is a volvulus, the bowel should be untwisted. If a foreign body is felt impacted in the bowel and closing it, unless it can be readily and without danger of lacerating the coats of the gut pushed on by the fingers of the operator until it has passed the ileo-cæcal valve, the foreign body should be removed from the bowel by an incision and the wound in the bowel afterward closed by sutures. If the case is one of intussusception, the invaginated parts should be pulled out: this is practicable where adhesions are absent or slight, but if the adhesions are very firm, and it is impossible to restore the parts to their natural position, the gut should be laid open above the occlusion, the edges of the opening should be attached to the margin of the external wound, and a fecal fistula established. If the case of acute obstruction be due to stricture of the small intestine, which is exceedingly rare, the gut may be laid open, and the patient recover with fecal fistula, or entorectomy or resection of the diseased part of the gut be resorted to. The operation of entorectomy has been recommended by many [p. 867] surgeons, and a large proportion of the cases reported recovered. In one case by Koeberle six and a half feet of the gut were successfully excised.
The following table by Ashhurst12 shows the results of laparotomy. It will be seen that in 230 cases 68 recovered:
| Operations for— | Cases. | Result not ascertained. | Recovered. | Died. |
| Volvulus | 14 | 1 | 4 | 9 |
| Strangulation continuing after herniotomy or taxis | 18 | ... | 6 | 12 |
| Invagination | 43 | ... | 13 | 30 |
| Foreign bodies, impacted feces, gall-stones, etc. | 18 | 1 | 7 | 10 |
| Strangulation by bands, adhesions, or diverticula | 76 | 1 | 20 | 55 |
| Obstructions from tumors, strictures, ulcers, etc. | 28 | 2 | 7 | 19 |
| Internal hernia and ileus | 20 | 1 | 7 | 12 |
| Obstructions from other causes | 4 | ... | 1 | 3 |
| Causes of obstruction not ascertained | 9 | 1 | 3 | 5 |
| Aggregate | 230 | 7 | 68 | 155 |
12 Surgery, p. 835.
Enterotomy is an operation originally performed by Nélaton. It is done by making an incision, preferably in the right groin, above the crest of the ileum and parallel with Poupart's ligament. When the abdomen is opened a coil of intestine is found and carefully stitched to the walls of the incision. A very small opening is then made into the bowel, and a fecal fistula established. Enterotomy is less dangerous than laparotomy, as by it there is less interference with the peritoneum; but no relief could be afforded by this procedure in cases of intussusception or acute obstruction from bands, hernia, or volvulus. It is applicable to cases of intestinal constriction when the obstruction is about the lower part of the small or upper part of the large intestine. It may be resorted to as a palliative measure when exact diagnosis as to the character and site of the obstruction is not clear, the case being otherwise hopeless, or in cases of obstruction where severe symptoms persist and death is near, and yet for any reason laparotomy or colotomy is inapplicable; or it may be performed in cases of contractions after failure of patient and persistent medical treatment. Many successful cases of enterotomy have lately been reported, and the operation has been earnestly advocated by Trousseau, Maunders, Wagstaffe, Bryant, and others. In chronic constriction due to stricture or other mechanical obstructions, malignant or otherwise, not remediable by any medical measures, colotomy should be performed. By this operation the colon is opened and an artificial anus established. The sigmoid flexure in the left lumbar region is the part selected for the colotomy if the obstruction is situated in the gut below that point. When the obstruction is higher up in the colon or its exact site cannot be determined, the cæcum in the right lumbar region is the part chosen. In cases of obstruction from the mechanical pressure of tumors, the possibility of relieving the compressed bowel by treating the tumors should of course be considered before resorting to colotomy.
The term cancer of the intestines is used here in a clinical sense to designate new formations in the intestinal tract the tendency of which is to destroy life, and has no reference to the histological characters of the tumors, inasmuch as these are, during life, for the most part, concealed from the eye of the pathologist. It so happens, however, that in a histological as well as in a clinical sense the term is appropriately applied to all but a very few of the malignant new growths that develop in the parts under consideration, if we adopt, as seems proper, the opinion of most modern pathologists, that cancer or carcinoma should only include those tumors "consisting of cells of an epithelial type, without any intercellular substance, grouped together irregularly without the alveoli of a more or less dense fibroid stroma."
Carcinoma of the intestines appears either as cylindrical-cell cancer, as scirrhus, or as gelatinous or colloid cancer. Scirrhous cancer of the intestines may resemble in appearance and texture the ordinary medullary cancer, degrees of hardness or of softness depending upon the predominance of the stroma or of the cellular elements in the constitution of the tumor. Rarely, and in a purely clinical sense, cancer of the bowels may exist as a lympho-sarcoma in the small intestine, and then through progression from the glands of the mesentery or elsewhere. Primary intestinal sarcoma has, however, been observed. Similarly, melano-sarcoma has been detected in the intestine as secondary to this form of sarcoma, originating in the skin or in the eye.
Of the forms of carcinoma, cylinder-cell cancer is the most frequent. Carcinoma gelatinosum or colloid cancer is of great relative frequency, but it is altogether probable that here, as elsewhere, this represents a degenerative form of ordinary carcinoma. At all events, it is certain that it may be detected in many cases where the essential changes reveal the ordinary glandular or cylinder-cell variety. These forms of cancer may affect the bowel primarily or secondarily by extension from adjacent organs and textures, or by metastasis. Primary cancer occurs most frequently, metastatic cancer with great rarity. The relative frequency of the different forms of cancer is not definitely known. In the article on carcinoma in the Dictionnaire Encyclopédique des Sciences médicales (xii. pp. 576, 577) cancer of the bowels is said to constitute about 8 per centum of all carcinomatous new growths. Sibley1 found that primary [p. 869] carcinoma occurred in the alimentary canal (exclusive of the mouth, tongue, and the annexed organs) in 6 per centum of the cases collated by him. Tauchou's compilations of nine thousand fatal cases of carcinoma show that intestinal cancer was present in 4 per centum.2 These computations include cancer of the rectum. If statistics of cancer of the bowels exclusive of rectal cancer were available, they would show, doubtless, a much smaller proportion.
1 Medico-Chir. Transact., xlii., 1859.
2 Leube, Ziemssen's Cyclop., vii. p. 432.
Any portion of the intestinal tract is liable to be attacked by cancer, though undoubtedly some parts of it with much greater frequency than others. Köhler3 reported that in thirty-four cases the cancer was situated twenty-two times in the large intestine (the rectum excluded) and twelve times in the small intestine (nine times in the duodenum). It is not unlikely that in the cases of duodenal cancer the new growth extended from the pylorus. At all events, primary cancer is seated with far greater frequency in the large intestine, and, not including the rectum, usually in either the sigmoid flexure or the cæcum. Grisolle4 declares the large intestine to be four times more often affected with cancer than the small intestine; that the sigmoid flexure is attacked as often as all the rest of the colon taken together; and that the cæcum is still more often affected. Where the intestinal new growth is secondary to carcinoma elsewhere, it is usually so by extension from neighboring parts; thus, the ileum may become implicated by contact with uterine cancer, etc., and cancer of the stomach, liver, kidney, etc. may invade the colon.
3 Ibid., vii. p. 431.
4 Pathologie int., 1865, ii.
Cancer of the intestines usually begins after the middle period of life, and apparently irrespective of sex. Nevertheless, young persons are occasionally affected, and children sometimes develop malignant new growths of the bowels (usually sarcomatous), either primarily, which is rare, or secondarily, by extension from other parts. The influence of heredity seems not to be well established. There can be no doubt that chronic irritation may act as an exciting cause of cancer of the bowels, as it may in cancer of other parts. It has been impossible to recognize any specific influence from especial forms of irritation, and it is not likely that such exist. Indeed, the etiological relations of intestinal cancer remain exceedingly obscure.
SYMPTOMATOLOGY.—Up to a certain period of development cancer of the bowels will give no sign of its presence; indeed, cases have been observed where, death having occurred from other causes, the existence of the malady became apparent only at the necropsy. In all cases the symptoms are, at first, of an indefinite character and very inconstant. Vague abdominal pains are experienced; these gradually tend to become referable to a certain locality and to become associated with irregular action of the bowels. Constipation, alternating with short intervals of diarrhoea, supervenes, and a varying amount of meteorism is developed. These symptoms may be attended by the signs of failing nutrition. The body gradually shows the effects of chronic imperfect assimilation, and becomes emaciated. The complexion slowly assumes the peculiar hue of chloasma cachecticorum. Long before this occurs, however, the cancerous new formation usually becomes perceptible as a more or less distinct abdominal tumor, movable or fixed, as the part affected permits of free movement [p. 870] or is bound down to the neighboring parts either by normal attachments or by adhesions resulting from inflammatory processes or from the extension of the cancerous growth. When the tumor is movable, it is generally situated in the small intestine or transverse colon or sigmoid flexure, the other portions of the intestinal canal being comparatively fixed. It should be mentioned, however, that portions of the intestines normally freely movable may become adherent to contiguous parts, as the transverse colon, with the gall-bladder, liver, stomach, spleen, etc. etc.; the transverse colon and small intestine, drawn down by the weight of the new growth, with the pelvic organs, the bladder, uterus, uterine appendages, etc.; and that, finally, different portions of the bowels may become involved in one mass.
When the duodenum is the portion implicated the tumor may escape observation or may be indistinguishable from cancer of the pylorus. It occasionally happens that no tumor can be discovered until the malady is far advanced whatever part of the bowel is affected. In nearly all cases, however, before very long the tumor will be detected wherever situated, but it will often remain difficult, owing to its situation, to arrive at exact conclusions as to its precise character. Usually, it offers considerable resistance to the touch, but its features may readily be obscured by the fecal accumulation that forms above the constricted portion of the gut and by the gaseous distension of the bowel. This tumor will be slightly painful to pressure, and the patient will refer to it a spontaneous pain, usually of a dull aching, sometimes of a stabbing, character. Percussion yields a sound of muffled resonance, due to the tubular nature of the tumor. Cancerous neoplasms of the bowel, and of the duodenum especially, are apt to be associated with a distinct pulsation caused by the subjacent abdominal aorta. This may readily be distinguished from aneurismal pulsation by the absence of an expansile character, by the disappearance of the impulse that may sometimes be observed when the patient is made to kneel upon all fours, and by the occasional mobility of the cancerous tumor. By extension and by inflammatory infiltration the tumor frequently becomes converted into a conglomerate mass where all determination of locality becomes conjectural. The tumor is, with very rare exceptions, single.
The symptoms that accompany the development of these growths depend mostly upon their position in the alimentary tract. Pain alone seems independent of this, but is at best a most uncertain concomitant. When the duodenum is the part affected by extension from the pylorus, the symptoms are indistinguishable from ordinary pyloric cancer. Even primary cancer of this part may exactly simulate pyloric cancer. The localized pain and tumor, the vomiting after meals, the frequent presence of blood in the vomited matters, the progressive emaciation from starvation, the absence of abdominal distension (a result of the constriction of the gut at its upper extremity), the gastric dilatation,—all combine to make the diagnosis difficult.
Cancer of the duodenum in its descending part may be suspected when signs of hepatic and pancreatic obstructive difficulties point to implication of the ducts, through which are produced jaundice upon the one hand, and evidences of imperfect pancreatic digestion, in the presence of undigested fat in the stools, upon the other. In the lower portions of the [p. 871] intestines the cancer becomes more and more associated with meteorism and fecal accumulations. Constipation becomes steadily more obstinate, but there are occasional fluid evacuations containing blood, pus, and mucus, often stinking abominably. When the tumor is toward the end of the large intestine—in the sigmoid flexure, for example—fluid discharges occur with very great frequency at times; but these are scanty in amount and but slightly fecal in character. In these cases one does not usually observe the compressed, ribbon-like stools that are seen in rectal cancer. These symptoms may precede the appearance of the tumor, when the diagnosis will be less readily made. The constipation will at first be more amenable to the use of purgatives. (It is said to be due more to a loss of contractility of the bowel than to the narrowing of its lumen.) Gradually these will lose their efficacy, and finally complete obstruction of the lumen of the gut is effected; in which event the symptoms of ileus will develop, with cramps and vomiting, finally of a fecal character, and the fatal issue quickly follow. Not unfrequently peritonitis is developed, and may be of a chronic character or may destroy life within a day or two, or the patient may die from exhaustion before the obstruction becomes complete.
It may happen that the integument will become involved in the malignant process, or may become continuous with the tumor by adhesive inflammation. In such cases an opening may be formed by suppuration, or the lancet may secure the passage of feces through an artificial anus, and temporary respite be obtained. Sometimes a sudden disappearance of the symptoms of obstruction—a result due to the softening and breaking down of the cancerous mass, restoring temporarily the integrity of the intestinal tube—may give an unjustifiable hope to the patient; or the same effect may follow the establishment of a communication, by ulceration, between the bowel above the tumor and some portion nearer to the anal orifice. The progress of the new growth soon annuls the benefits thus gained.
Not uncommonly, particles of the cancerous mass may become detached, and, if diligently searched for, may be discovered in the feces. Microscopic examination may then definitely determine the nature of the disease. It has been claimed that colloid cancer may be diagnosticated in this manner even before the appearance of other symptoms.5 Death may be hastened by the occurrence of metastatic deposits in other and vital organs. Oedema of the lower extremities (of the left extremity in cancer of the sigmoid flexure) will often be observed as a result of the interference of the cancerous mass with the return of blood from the extremities by pressure upon the large veins. The combination of pain, tumor, constipation, tympanitis, progressive wasting, and the cachexia that sooner or later supervenes, stamps eventually most cases with unmistakable characters.
5 Charon and Ledegank, Journ. de Med.-Chir. et de Pharm., v. lxviii., 1879, p. 493.
The duration of intestinal cancer may extend from several months to one, rarely two, years, the latter age sometimes being attained by colloid cancer, the most chronic and least malignant form.
MORBID ANATOMY.—By far the most frequently encountered malignant new growth of the bowel is carcinoma, in one or another of its forms. The cylinder-cell epithelioma is probably the most common of [p. 872]these, and, as seen in the intestine, offers many naked-eye points of resemblance with ordinary encephaloid carcinoma. It is soft, filled with a milky juice, and may attain considerable size. The tumors appear as discoid prominences of varying size and number. Later, these may become fungoid and ulceration ensue. The growths early involve the whole intestinal wall, and by their increase tend to obstruct the passage of the intestinal contents. When ulcerated they present a nodular, uneven surface, situated upon a thickened base consisting of the infiltrated coats of the bowel. Villous prolongations (villous cancer; the undestroyed connective-tissue stroma) may project into the lumen of the bowel and give a peculiar tufted appearance to the part implicated. One or more points may be invaded by cancerous growth, and above each will be developed a dilatation of the gut (the result of distension) containing uncertain quantities of fecal matter, upon the removal of which the tumor will appear much smaller than it appeared during life.
Scirrhus usually implicates the gut in its entire circumference, so that a high degree of constriction may result from a small amount of cancerous infiltration. It begins as small nodules or plates upon the mucous membrane. As commonly observed, the lumen of the intestine is narrowed by an annular band of gristly hardness. All the coats of the bowel, with the peritoneum, become involved, and frequently the contiguous parts are included in the cancerous infiltration, forming an undefinable mass through which the contracted channel of the bowel may be traced, though often impervious to any but the smallest articles (a crow-quill, for example). The surface of the gut is generally ulcerated, irregular, and nodular. The walls of the ulcer are irregular and infiltrated. It will sometimes happen that the autopsy reveals permeability of the bowel where total obstruction prevailed during the latter days of life. This may be probably accounted for by the disappearance of the hyperæmia that doubtless existed during life and caused more or less turgidness of the growth. Sometimes the connective-tissue element is less predominant, and gives place to a more or less luxuriant cell-development; in a word, scirrhous carcinoma is replaced by soft or encephaloid cancer. This difference is simply one of degree, but is associated with greater rapidity and extent of growth. Ulceration is extensive, and one may here also often discover the villous, tufted appearance of villous cancer, caused by the fringe-like shreds of stroma entangling cellular elements not yet detached from the mass.
Colloid cancer, or carcinoma gelatinosum, may be associated with either of the above-described forms as a degenerative form, or may, apparently, develop as such from the beginning. It is a very frequent variety of the malady. In 27 cases of intestinal cancer, colloid cancer was present in 5, as reported by Lebert. It is most often observed in the sigmoid flexure and cæcum, as are the other forms of carcinoma. It is composed of a considerable mass extending around the bowel. Ulceration is less often found here than in the other forms, nor is there the same tendency to secondary infiltrations. By the unaided eye an alveolar structure may be detected, and when the mass is extensive a soft, jelly-like consistency is presented, together with "a bright, honey-yellow color." Small deposits of the colloid matter may be seen upon the surface. These have been described as resembling wheals of urticaria or herpetic or eczematous [p. 873] vesicles (Bristowe). The glairy fluid of colloid carcinoma oozes from the cut surface of the tumor, bathes it, and is to be found in the intestine.
These different forms of cancer sooner or later invade neighboring parts, as the peritoneum, mesenteric and retro-peritoneal glands, and adjacent organs. On the other hand, the intestines may become invaded by cancer of the peritoneum and other parts. It has even been observed, reversing the usual order of things, as secondary to cancer of the liver (Wilks and Moxon). Under these conditions the symptoms of intestinal cancer will have been associated with those due to the primary affection. Lympho-sarcoma will rarely be found as an extension from the lymphatic glands and involving the small intestine. Melanotic sarcoma may occur as metastatic from an original melano-sarcomatous tumor of the skin or eyeball.
DIAGNOSIS.—In its earlier stages it is impossible to recognize cancer of the intestines. After its symptoms have become established they may resemble those of several disorders. Cancer of the duodenum cannot be distinguished from that of the pylorus unless evidences of pancreatic or biliary disturbances indicate obstruction to the passage of the bile and pancreatic secretions. Previous to the appearance of a tumor one must often remain in doubt. The alternations of constipation and diarrhoea, the signs of partial obstruction, the localized pain usually present, the gradual wasting, will arouse suspicions of cancer, though chronic inflammatory affections of the bowels may induce symptoms not altogether unlike these. The presence of a tumor will supply the additional evidence necessary for a definite diagnosis. It will be necessary to exclude fecal enlargements of the bowels. The cancerous tumor will be somewhat painful, hard, nodulated. A tumor due to fecal accumulation may closely simulate it, and is, indeed, usually associated with it. By manipulation the fecal mass may be moulded, and even displaced, and by appropriate purgative treatment may be caused to entirely disappear. Foreign bodies, mesenteric tumors, and other abdominal enlargements may offer physical resemblances to intestinal cancer, but their symptomatology is usually so different that doubt may be easily dispelled. Syphilitic gummy infiltration, with resulting stricture, is more apt to occur in the rectum than in other parts of the alimentary tract.
The presence of fragments of the new growths may sometimes be detected in the stools, when microscopic examination will determine their nature. With cylinder-cell epithelioma and glandular cancer this is not common, but with colloid cancer much information may be gained by examining the evacuations. According to Charon and Ledegank,6 colloid cancer of the intestine may be detected before symptoms develop, by the presence of colloid matter in the feces. In the later stages, however, the gelatinous change of all the histological elements may occasion embarrassment, as at this stage the peculiarities of the cellular structure will have been destroyed.
6 Journ. de Med.-Chir. et de Pharm., lxviii., 1879.
PROGNOSIS.—Intestinal cancer always proves fatal. Death may result from the debility resulting from the cancerous cachexia or from intestinal occlusion or from peritonitis. The duration of the malady is usually not long. It runs its course in from several months to one, rarely to two, years.
[p. 874] TREATMENT.—Treatment must be directed to the alleviation of the distress caused by the disease. No curative treatment is known. When the cancer is situated in the colon, especially in the sigmoid flexure, the operation for artificial anus often affords great though temporary relief. The diet should consist of such articles in the digestion of which a large residue is not formed. Milk, eggs, soups, etc. should compose the principal articles of food. Mild laxatives will be required to secure the proper evacuation of the bowels, and to relieve pain and discomfort opium is invaluable and should be freely used. When obstruction is imminent nutrient enemata afford the most efficient means of administering nourishment.
SYNONYMS.—Albuminoid degeneration, Waxy degeneration, Amyloid degeneration, etc.
Lardaceous degeneration of the intestines is an affection of quite frequent occurrence in those persons who are the subjects of a like change elsewhere; for although it has been asserted that it may be present as a primary affection, it almost always succeeds the same form of degeneration in other organs. Since, for the most part, it only makes itself manifest at an advanced stage of the disease, its importance is usually masked by the grave constitutional condition of the patient, whose vital forces are wellnigh exhausted by the already advanced degenerations present elsewhere. The extensive implication of other organs and tissues in the same degenerative process also creates great obscurity in the symptomatology of intestinal lardaceous disease, and is doubtless the cause of the existing dearth of definite knowledge upon the subject.
That the intestines are comparatively frequently involved in lardaceous disease is shown by dead-house statistics. Thus, Charlewood Turner7 reported from the London Hospital that in 58 cases of lardaceous disease the intestines were affected 10 times; and Goodhart8 in 150 consecutive necropsies of lardaceous disease at Guy's Hospital reported implication of the intestines 63 times.
7 Transactions Path. Soc. London, 1879, p. 517.
8 Ibid., p. 533.
Although the bowels do not become affected as early as several other parts, they will almost certainly become involved should the patient's life be prolonged; and in those cases where death is a direct result of the degeneration the intestines share with the kidneys the chief responsibility. It is not, however, until an advanced stage of lardaceous degeneration that its presence in the alimentary canal is revealed by symptoms; indeed, many cases do not, throughout life, betray evidences of the pronounced alterations that are to be discovered after death. Even in extreme cases there are no symptoms that would, even with probability, be referred to lardaceous disease of the bowels in the absence of the same degeneration in other organs and parts. There are, then, no specific symptoms following lardaceous degeneration of the bowels.
Where the normal functions of the intestines can no longer be properly performed in consequences of the changes that have taken place in them, there results a moderate diarrhoea. At first the number of movements [p. 875] may not be increased; the evacuated matters are fluid and of a greenish or pale color. Usually, little or no pain is experienced, though at times and in certain individuals this may be severe and colicky. The diarrhoea is not always steadily progressive, but may from time to time disappear. With the progress of the disease it may become more free and persistent, and in the later stages hemorrhage from the bowels may be superadded. This may vary in amount, and where, as is often the case, the stomach participates in the degeneration, hæmatemesis may also appear. These hemorrhages may be insignificant, or may at once assume alarming proportions, and even bring to an unexpected termination the life of the individual. Already, at the outset of the intestinal symptoms, the general health will have shown evidences of profound alteration, but upon the supervention of the diarrhoea more rapid progress will be observed, consequent upon the increased nutritive disturbance. The use of remedies in temporarily controlling this diarrhoea may prolong for months the life they are powerless to save.
So far as concerns the intestinal affection, there is no special tendency toward febrile excitement. It must not be forgotten, however, that acute inflammatory attacks of various tissues and organs frequently arise in the course of lardaceous disease.
Though there seems to be reason to believe that mild degrees of lardaceous degeneration may sometimes be cured, especially when dependent on syphilis, there is but little hope of arresting its progress at the late stage when the bowels become implicated. Indeed, when pronounced degeneration of the bowels takes place the disease is usually nearing the end of its course; for it is a well-settled fact that in this degeneration extensive implications of organs may occur without markedly reducing the patient's general condition, so long as the kidneys and intestines remain unaffected. The cause of death is usually to be traced to these organs. Dickinson9 found that in 35 cases where death was apparently due to renal lardaceous disorder, the immediate result was brought about by diarrhoea in 13 cases. Presumably, in a large proportion of these lardaceous disease of the bowel was present.
9 Diseases of Kidney, Part ii., 1877, p. 496.
The degeneration usually affects the lower portion of the small and the upper part of the large intestine. Occasionally it will be found to have invaded the whole alimentary tract. As in lardaceous degeneration generally, the process begins in the small arteries and capillaries and veins, affecting primarily the arterial and venous muscular coats—not, however, according to the latest authorities, the muscular fibres themselves, but their perimysium and the cement substance, the degeneration being one limited to the connective tissues.10 In the mildest cases only some of the small vessels of the mucous membrane are involved, and no naked-eye changes can be detected. In more advanced stages the mucous membrane is pale and shows evidence of catarrh. Thickening occurs, and as the process advances a peculiar appearance is revealed which has been compared to that of wet wash-leather (Wilks). The iodine test now gives the mahogany-colored reaction of lardaceous matter, with the tissues affected, or, if the methyl-aniline-violet test of Cornil be employed, the lardaceous material will display a red-violet color, while [p. 876] normal structures will be tinged blue-violet. It is said to be better to make the test near a Peyer's patch, since the latter is seldom affected by the degeneration, and brings out, by contrast, the surrounding lardaceous material.11 This distribution of the material cannot be considered as constant, however, since Hayem found the patches of Peyer most frequently affected.
10 Cohnheim, Allgem. Path., 1882, p. 667.
11 Wilks and Moxon, Path. Anat., p. 404; Kyber, Virchow's Archiv, Bd. 81, H. 1 and 2.
In more advanced stages the surface may become irregular from glandular enlargement, and ulceration may occur. Microscopic examination shows the lardaceous material in the vessels, and also in the stroma of the mucous membrane and villi.12 The epithelium is not involved. The degeneration, at first confined to the mucous membrane, extends to the submucous tissue, the proper muscular coat of the intestines being often implicated—so far, at least, as concerns its connective tissue. In the more severe cases Hayem found the agminated and solitary glands extensively involved. Fine branches from affected vessels penetrate to the interior of the glands. In such cases the mesenteric glands will be found implicated. The degeneration of the vessels running through the gland structure causes disappearance of this substance by fatty degeneration, and occasions a reticulated arrangement of the lardaceous material, and, secondarily, ulceration. In a similar manner ulcers may arise in any part of the affected tract. Finally, the lardaceous material may involve the whole thickness of the gut.
12 Eberth, Virchow's Archiv, 80, S. 138.
The diagnosis of lardaceous disease of the bowels can only be made with certainty in the presence of pronounced albuminoid disease of other parts in association with the symptoms of intestinal disorder. It possesses no characteristic symptoms.
Inasmuch as the disorder invades the bowels only at a late stage of its existence, the prognosis acquires additional gravity. It is probable that advanced albuminoid disease is never cured; so much the more hopeless is it when affecting this tract. If unchecked, the diarrhoea rapidly saps the powers of life; if temporarily alleviated, the approach of death is more gradual.
Whatever attempts are to be made to cure the disease, they must be through the general system, and are identical with those directed toward the cure of lardaceous disease generally. Treatment directed to the intestines must be palliative. The diarrhoea must be combated by appropriate diet and the administration of such remedies as protect the surface of the mucous membrane and control the intestinal movement. Bismuth subnitrate in large doses is therefore indicated. Various astringents may be employed, while the use of opium often secures most gratifying relief. It should be given in generous doses. Preparations of the crude drug seem to answer better than its salts. The necessity of keeping the gut free from undigestible matters that may irritate the already badly-damaged mucous membrane is apparent. Patients with this form of lardaceous degeneration usually show the cachexia resulting from profound modifications of nutrition, and their intestinal symptoms can only be regarded as links in a long pathological chain. Hemorrhage will call for remedies that under ordinary circumstances are employed to control bleeding from the bowels.
Diseases of the inferior and terminal portion of the large intestine may be divided into primary and secondary—the former when the morbid cause is local and independent of disease elsewhere, the latter when it is consequent upon or incident to some other bodily affection. Among the primary lesions may be classed congenital malformations, prolapse of the rectum, hemorrhoids, and some varieties of new growths; also diseases caused by local irritations, infection, or traumatism, such as proctitis, ulceration, fissure, non-malignant stricture, chancroidal invasion and primary syphilis, including obstruction of the bowel by impacted feces and foreign bodies. Thread-worms and various cutaneous eruptions about the anus may also be included among the causes of the primary diseases of this portion of the alimentary canal.
The secondary affections are quite numerous, and may be caused by direct extension of disease from the colon, as in the dysentery following typhoid fever, and follicular enteritis, or entero-colitis of children; by contiguity, from diseases in neighboring organs—e.g. ischio-rectal abscess causing fistula—or by changes in the nervous or vascular supply, such as is seen in spasmodic contraction, paralysis, epidemic dysentery, cholera, and the action of certain remedies.
The rectum, the third or terminal portion of the large intestine, has no sharply-defined upper limits: it is usually understood to begin at the sigmoid flexure, opposite the left sacro-iliac symphysis; it is from six to eight inches in length and terminates in the anus. As the sigmoid flexure is the narrowest portion of the colon, so the calibre of the first part of the rectum is narrower than the portion below, where it gradually becomes more commodious, and near the anus presents a peculiar condition of the walls which gives it a capacity for remarkable distension. The rectum, which is somewhat cone-shaped, in its anatomical and pathological characters retains those of the large intestine with slight variation. Upon the upper or first part of the rectum the duplicature of the peritoneum is continued, forming the meso-rectum, which invests the bowel, attaching it to the sacrum. Below this the middle portion of the rectum (extending to the tip of the coccyx) is attached to the sacrum by connective tissue only, but also has a peritoneal investment on the upper portion of its anterior surface.
[p. 878] The third or terminal part of the rectum, which is only an inch and a half in length, and is entirely without peritoneal covering, terminates at the anus. The circular and transverse muscular fibres, mucous crypts, and appendages throughout the rectum are identical with those above, except that the general muscular tunic is thicker; but the longitudinal fibres are less distinctly aggregated into bands than in the colon, being disposed in a more uniform manner, except that, like the circular fibres, they are especially aggregated between the sacculi. The fact that the meso-rectum limits the mobility of the upper and more narrow part of the rectum has led some to locate a third sphincter at this point, but the existence of such an organ has not been generally admitted. Van Buren characterizes it as an organ which "anatomy and physiology had been equally unsuccessful in assigning either certainty of location or certainty of function."1
1 Kelsey, Diseases of the Rectum and Anus, New York, 1882, p. 20.
The anus guards the outlet of the bowel by its double sphincter muscle, which under normal circumstances affords voluntary control, within certain limits, over defecation. The well-known peculiarity of the vascular supply, a sort of erectile tissue being formed by the inferior hemorrhoidal plexus and the passage of some of the efferent veins through the sphincter muscle, by which they are subjected to pressure, is very favorable to the development of certain forms of disease which will be considered among the local disorders. As embryology has thrown considerable light upon the pathology of morbid growths by demonstrating relationships that were previously unsuspected, so a consideration of the development of the lower portion of the intestinal canal may lead to a better understanding of some of its diseases, especially those which are symptomatic or secondary. In early foetal life the third division of the primitive intestine, the pelvic portion, terminates in a cloaca in common with the urachus; subsequently, about the eighth week, a partition (the perineum) is formed which divides the cavity into two portions, the uro-genital sinus and the anal cavity. In the mean time, at an early period a depression occurs on the cutaneous surface at the site of the anus, which deepens progressively until it encounters the primitive intestine, with which it unites at the end of the fourth week, and the continuity of the tube becomes established. It therefore is seen that the rectum in its upper and middle portions is derived from the internal and middle layers of the blastodermic membrane, while its lower third, with the anus, like the buccal cavity, is formed by the external and middle layers.
In its diseases, then, the greater part of the rectum would seem to naturally participate in those of the large intestine, to which it structurally belongs, while its inferior portion and the anus would partake more in the disorders of the general cutaneous system. This peculiarity of development also explains the difference noticed in the vascular supply. The rectal veins are usually divided, like the rectal arteries, into three sets—superior, middle, and inferior. They are arranged so as to form two distinct venous systems, the rectal returning its blood through the inferior mesenteric veins into the portal system, the anal terminating in the internal iliac. The first system is made up of the superior hemorrhoidal, the second of the remaining veins.
The superior hemorrhoidal forms a venous plexus which surrounds the [p. 879] internal sphincter muscle; the inferior hemorrhoidal vein also forms a plexus, but it is subcutaneous and principally below the inferior border of the external sphincter.
There are, however, a number of communicating branches passing along the walls of the rectum from one plexus to the other. The internal hemorrhoidal veins also communicate freely with the branches of the internal iliac around the trigone of the urinary bladder by means of small vessels, which pass through the prostate gland and seminal vesicles. By this method of anastomosis some relief is afforded when there is an obstruction in the portal circulation, which is such a common cause of turgescence of these veins, often resulting in permanent dilatation or hemorrhoids.
At the lower part, or at the junction of the middle and lower third of the rectum, the internal circular fibres of the muscular coat of the intestine become quite numerous, forming what is called the internal sphincter muscle; it is nearly an inch in breadth, and completely surrounds the lowest part of the rectum. It is about an inch above the margin of the anus; its muscular fibres are of the involuntary or unstriped variety; in function it assists the external sphincter in closing the anus and preventing the involuntary escape of the contents of the bowel.
The external sphincter lies directly under the skin and upon the internal sphincter and the levator ani muscle; its fibres encircle the anus: arising from the coccyx, they are inserted into the tendinous centre of the perineum, joining the transversus perinæi, the levator ani, and accelerator urinæ muscles. The sphincter ani is constantly in a state of tonic contraction, but the force of its contraction may be voluntarily increased. In the skin and superficial fascia are found minute branches of the pudic and small sciatic nerves; in the ischio-rectal space the internal pudic nerve; crossing about the centre are the inferior hemorrhoidal nerves, which are distributed to the anus and the lower portion of the rectum; the perineal nerve is especially distributed to the anterior part of the anus.
Thus it is seen that the rectum and anus have vascular and nervous supplies of considerable diversity and importance.
The simplest form of congenital malformation in this region consists in an anus of insufficient size for the natural demands of the system, but in no other manner abnormal. The most frequent variety of imperforate anus is where complete occlusion is effected by the common integument or by two cutaneo-mucous flaps, which owing to defective development remain united without forming a raphé or perceptible line of union. The rectum is not involved, and when the child strains the contained meconium causes bulging of the part, which disappears under slight pressure, but reappears when again free. In other cases the occluding tissue is very firm, dense, with a disposition to pucker or form rugæ. The sphincter muscle is rarely perfect, and though an artificial anus may be made, years may elapse before the child can control the evacuation. In conjunction with an imperforate anus the colon may terminate in a cul-de-sac, or it may communicate with the urethra, the bladder, or the vagina.
[p. 880] An imperforate rectum has been known to discharge at the umbilicus, upon the face, under the scapula, upon the penis or the anterior part of the scrotum. Sometimes, though very rarely, a common cloaca has been found, as in fowls, common to the rectum and to the genito-urinary organs; and still more rarely the rectum has opened in abnormal sites upon the perineum and upon the buttocks.
The anus may be entirely absent. The rectum may be entirely absent or it may be incomplete, terminating at various distances from the anus. These malformations of the bowel may be associated with a perfect anus, or with any of its imperforate forms, or with a fecal fistula. In occlusion of the rectum the offending structure is in some cases a hymen-like fold of mucous membrane, which, during straining, can be recognized by the finger as a fluctuating protrusion; while in others it consists of a mass of dense fibrous tissue which extends upward from an inch to an inch and a half: in the former there is always found a normal anus; in the latter there is either no trace of anus or one in a more or less rudimentary state. In those cases where the rectum is entirely absent the intestine terminates either in a cul-de-sac or a fecal fistula; very rarely the rectum is replaced by a fibro-ligamentous cord or band which springs from the colon, and, descending toward the bladder, blends with the connective tissue of the part. In the latter the pelvis is always in an imperfect state of development, being much contracted in its lower diameters, and the anus is absent; and Rokitansky and Curling lay stress upon the non-development of the pelvis as a diagnostic guide in determining the absence of the rectum. The passage of a sound into the bladder or vagina is a procedure of some diagnostic value, as if its point impinges directly against the sacrum it may be presumed that no rectum exists. If the malformation is of such a character that the fecal matter can find no exit, a train of symptoms ensues analogous to those seen in the adult affected with intestinal obstruction: the infant cries and is constantly restless, refuses food, vomits, the abdomen distends, and death speedily ensues. A remarkable exception to this rule was the case mentioned by Bodenhamer of a child with absence of the rectum who was not operated on until three months after birth, and who was apparently in perfect health. At the operation the intestine was found three inches from the surface, and the child made a good recovery.
Although the statistics of this class of malformations are somewhat contradictory and confusing, it is safe to state that more male than female children are so afflicted.
The prognosis in the large majority of these cases is grave, for unless the operator can see or feel the fluctuating protrusion, or can recognize it after a very slight exploratory incision, he is working totally in the dark and in close proximity to the peritoneum. Hemorrhage, peritonitis, pelvic cellulitis, and septicæmia diminish the chances for recovery. Indeed, the majority of these cases are scarcely amenable to surgical treatment.
These conditions obtain most frequently at the two extremes of life, infancy and senility, but have a very different causation in each. Prolapse of the bowel may be partial or complete—partial when a portion of the mucous membrane is extruded, and complete when the entire rectum appears outside the anal orifice. A predisposing cause in infants is found in the mobility of the bowel—in the fact that it and the sacrum are much less curved than in the adult, and the abdominal viscera are more voluminous: this, associated with the undeveloped state of the muscular system, causes the weight and strain to act directly and forcibly upon the sphincters, and the extrusion takes place. It is often excited by allowing children to sit for a length of time upon the chamber-vessel. It is frequently caused among children by the presence of vesical calculi, by Oxyuris vermicularis, diarrhoea, constipation, dysentery, polypi, and by the long-continued acts of coughing and crying.
In adults and the aged it may be caused by loss of tone of the anus and rectum in chronic diarrhoea and dysentery, or from the energetic action of drastic cathartics, by urinary calculi, the long-continued use of enemata, chronic cough, diarrhoea alternating with constipation, stricture of the urethra, prostatic hypertrophy, tenesmus due to the presence of polypi, and by the pressure of a pelvic tumor. It may accompany procidentia uteri and hemorrhoids. An incomplete, reducible prolapse consists of two or more overlapping plications of normal-looking mucous membrane, sensitive but painless. In these cases there is provoked a hyperplasia of much-elongated connective tissue in the submucous space which undergoes serous infiltration and causes an oedematous condition of the part. In a complete prolapse the entire rectum—all of its component layers—is protruded through the anus. In a recent case the folds of the gut are well marked, but in one where the bowel has remained in this abnormal condition for some time the submucous tissue becomes charged with inflammatory deposit which effaces the plications and causes the bowel to become pale, hard, dry, and tough; and finally pigmentation occurs and the part assumes somewhat the character of true skin. These vary greatly in size, from the slightest protrusion of mucous membrane to a tumor the size of a melon. Usually they are reduced with ease, but their reappearance is occasioned by the slightest tenesmus.
In old age the soft parts of the floor of the pelvis and the anal sphincters lose to a great extent their tone and contractile vigor, and the rectum, also participating in this change, is often unable to withstand the increased thrust of the diaphragm and the compression of the abdominal muscles during defecation; which act frequently demands more exertion on account of a tendency to constipation in advanced life.
In these long-standing cases of senile procidentia it is a matter of experience, verified by post-mortem dissection, that the fibres of the sphincters and of the levatores ani muscles are flattened, pale, and stretched beyond the possibility of contraction, while the entire perineum is in a state of atrophy.
There are two varieties of these—the gelatinoid or soft, and the fibroid or firm. The latter is of rare, the former of common, occurrence, especially in children under the age of twelve years. The fibroid polypus is only found in adults, and is composed of dense connective-tissue elements and blood-vessels. The gelatinoid or soft polypi are also partly composed of connective tissue and vessels, but much finer than in the other: they contain hypertrophied follicles and are covered with spherical epithelium. They resemble nasal polypi, but are more dense. These growths are not malignant in character, but are very troublesome, as they are almost always pedunculated, the stem being from half an inch to four inches in length, which admits of the descent of the tumor within the grasp of the sphincters during defecation, and frequently admits of its escape from the anus. Their presence is not free from danger, as they are very vascular, bleed readily, and are sometimes detached by the breaking of the pedicle during defecation. They frequently bleed spontaneously. The presence of these abnormal growths teases the rectum and brings on tenesmus and frequent desire to go to stool; the feces are flattened, and with them escapes a quantity of glairy red mucus which has been compared to thin currant-jelly. When caught in the grasp of the sphincters they often bleed profusely, and especially is this the case with children so affected. The presence of these bodies is accompanied with a sense of weight and uneasiness in the bowel. They may be single or multiple; they may be round, reniform, oval, fusiform, or irregular; they may be smooth or villous. In size they vary from that of a marble or cherry to that of a small hen's egg, and they are usually found about three inches above the anus, but they vary in position from a point just within the sphincter to one six inches up the rectum. Their presence is usually diagnosticated without difficulty, or, if any is experienced, a digital exploration will reveal them. A child with functional disturbances of the bowels accompanied with frequent hemorrhages should be examined for polypus. One of these growths sometimes unpleasantly complicates a case of hemorrhoids.
A rectal polypus is an adenoma, consisting of dilated glands of Lieberkühn imbedded in connective tissue, also containing nerves and blood-vessels, and is covered with the epithelium of the bowel.
These are usually fibrous when situated below, or vascular when situated above, the sphincter ani muscle. They are conveniently known as external and internal piles, but in some instances it is impossible to say whether these tumors are external or internal. In either variety they are due to an abnormal state of the blood-vessels, and especially of the plexus of superior, middle, and inferior hemorrhoidal veins disposed around the lower extremity of the rectum immediately above the internal sphincter muscle. The inferior mesenteric and internal iliac veins receive a large portion of the blood from this plexus, so that a very free intercommunication exists, around the lower portion of the rectum, between the general [p. 883] venous system and that of the liver. It should be borne in mind that these veins are destitute of valves, and are situated in a very dependent part, which is normally in a high degree of functional activity.
External hemorrhoids are found at the very verge of the anus, and, when not irritated or inflamed, appear like movable, dependent plications of hypertrophied skin. They appear either singly or in groups, but it is nothing unusual to find five or six of them together, and they are not infrequently associated with the internal variety. These pendulous tabs of integument are very prone to inflammation, and they then become exquisitely tender, painful tumors, which vary in size from that of a small pea to that of a pigeon's egg. That portion of the tumor presenting toward the anus is covered with mucous membrane; the other is covered with integument; the former is dark-colored, due to engorgement of its vessels. These, being composed internally of tortuous, dilated veins which have totally lost their normal resiliency, bleed freely on section, but after a time they undergo the following changes: the over-distended vein, of which each is mainly composed, either becomes obliterated by the encroachment of inflammatory deposit or its walls give way and the contained blood escapes; its serum is absorbed, and the tumor now consists of a blood-clot, the remains of a vessel, inflammatory lymph, a hyperplasia of connective tissue, mucous membrane, and integument. It undergoes a still further change by absorption, and remains a permanent pendulous teat of cutaneous and connective tissue, bearing no trace of vascular channels.
On account of the extremely sensitive nature of the mucous membrane and skin of the anus, an inflamed condition of these tumors entails an amount of suffering very disproportionate to their size: there is torture in the act of defecation, constant tenesmus, spasm of the sphincters, a sense of weight and heat in the perineum, and sometimes a swollen, very painful, condition of the raphé, which stands out like a cord.
Occasionally there is a total inability to urinate, combined with a frequent desire to do so. When an attack such as this ends in suppuration of the tumor a radical cure is effected, but a marginal ulcer of the anus sometimes follows. An unclean and neglectful habit provoking constipation, sexual incontinence, over-indulgence in highly-seasoned food or in stimulating beverages, exposure to cold and wet, and the straining attendant upon dysuria, will provoke an attack. No age or sex is exempt from this affection (Gross). It is claimed that before puberty females are more subject to it than males; after that age the reverse obtains, except during pregnancy.
Internal hemorrhoids are round, oval, or sometimes cylindroid-shaped tumors covered by mucous membrane; they are smooth, granular, or rough to the touch, much less sensitive and painful than the inflamed external variety, and are situated within the rectum it may be an inch or two above the internal sphincter muscle. They occur in groups or scattered over the surface of the bowel. In structure they are soft, spongy, vascular tumors composed of dilated and tortuous blood-vessels, the veins predominating over the arteries, their interstices scantily supplied with connective tissue, and their covering is of mucous membrane. In color they are dark red, but when compressed and strangulated by the sphincters they assume a dusky purple hue. After long exposure they take on a pseudo-cutaneous appearance.
[p. 884] The columns of the rectum are the seat of the cylindroid pile, which is brighter in color and much more arterial in its structure than the ordinary variety, and bleeds very freely. Anything which causes stasis and accumulation of blood in the hemorrhoidal plexus of veins predisposes to this very common affection. Constipation is the usual cause; and among others may be named diseases of the liver which cause portal obstruction, pelvic tumors causing engorgement from pressure, the gravid uterus, labor, prostatic hypertrophy, urinary calculi, stricture of the urethra, stricture of the rectum, and rectal tumors. Among other causes are horseback-riding, the erect posture, violent cathartics, seat-worms, dysentery, diarrhoea, dyspepsia, and a sedentary life, with a diet of rich, stimulating food.
These piles do not usually cause much suffering; they vary in size from that of a pea to that of a pigeon's egg, and cause a sense of weight and stuffing in the bowel; but when they are large and numerous they cause severe pain, tenesmus, difficult defecation, spasm of the sphincters, and prolapse of the anus. When the patient is at stool the tumors are forced down and protrude in a bunch, surrounded and constricted by a collar of prolapsed mucous membrane: under these circumstances the tortuous and dilated vessels of which they are composed give way and free arterio-venous hemorrhage takes place. In some cases this happens at every stool, the patient losing from a few ounces to a half pint of blood almost daily until alarmingly depleted. Usually, the protruded piles are easily restored after a motion of the bowels, and so remain until the next one occurs; but in other cases of longer standing and of more gravity the sphincter loses all tone and the piles remain constantly prolapsed. This affection is very chronic, and the subject of it has to regulate his life with the greatest care, as the least unusual effort or excess may provoke an exacerbation. Excepting in the worst cases the general health is not materially impaired. They occasionally become so strangulated as to slough off, which effects a cure, but this is accompanied by grave constitutional disturbance. The disease is rather rare before the age of puberty, but is very common in both sexes in adult life, and is frequently associated with fistula, polypus, fissure, or carcinoma of this region. In females suffering with piles a free hemorrhage from them sometimes takes the place of the menstrual flow. The presence of internal piles causes a sense of weight and fulness and the sensation of a foreign body or of feces remaining in the rectum, with troublesome and obstinate itching about the anus. These symptoms, with the occurrence of hemorrhage from the rupture, erosion, ulceration, or abrasion of the dilated vessels, render the diagnosis easy. Should the piles not protrude, they can readily be made to do so by directing the patient to sit and strain over a vessel containing hot water. If the piles do not appear, a digital examination should be made. Indeed, it would be better to make one in every case of this kind.
About the margin of the anus the superficial veins are prone to great dilatation, and when presenting form masses of a bluish color, often very dark, covered partly by mucous membrane, partly by integument. These are also commonly known as piles.
This is an uncommon disease, generally occurring in those advanced in years, and consists of an hypertrophy, and sometimes of an inflammation, of the natural rectal sacs. These pouches are quite small in early life, and enlarge gradually as age advances, this condition being favored by the lodgment in them of extraneous substances, such as indurated fecal matter, inspissated mucus, the seeds of fruit, and other undigested masses. Constipation, so usual with the old, predisposes to this affection, as it keeps the bowel distended with hardened feces. The pouches vary much in size, the largest of them admitting the end of a finger. The disease is insidious and slow, but is capable of producing intense suffering should inflammation, suppuration, or ulceration attack them. Sometimes as many as a dozen are involved.
The symptoms, which are rather misleading than suggestive of the disorder, are a sensation of weight and uneasiness just within the anus and uneasy sensations in the rectum, distressing itching, and, after a time, pain following defecation and lasting often for hours. The pain, which is aching and burning in character, is not confined to the parts affected, but radiates down the thighs, toward the back, and into the perineum. An increased secretion of mucus always exists in these cases, but the discharge of purulent matter is uncommon, and its presence indicates the existence of very active inflammation.
It is said that even in the worst cases no spasm of the sphincters occurs. An exploration of the bowel with a blunt-pointed hook affords the only reliable guide to correct diagnosis: this, as it is moved about in the rectum, engages the rim of a sac, which may thus be drawn down through the anus and examined.
In the absence of ulceration or syphilitic infection this is an uncommon disease, and very many of the cases of so-called stricture of the rectum are caused by spasm which always disappears during anæsthesia.
The affection may be described as a narrowing of the lumen of the rectum, more or less circumscribed, by the deposition of inflammatory lymph or fibrous tissue in the mucous, submucous, or muscular tunic of the bowel. It may be due to traumatic causes, such as the introduction of foreign bodies, the frequent and careless use of enema-pipes, or the presence of sharp or irritating substances swallowed, as pieces of shell or bone. It is said to have been caused by indurated feces, but no cases have been published in which this causation is clearly shown. This condition has also been brought about by various operations upon the mucous coat of the bowel, such as the application of nitric acid and other escharotics and the removal of portions of mucous membrane and of hemorrhoids.
Stricture may be secondary and a result of extension of an inflammation outside the bowel, as pelvic cellulitis; and it is frequently caused by syphilitic deposition and by chancroidal invasion—in the former by [p. 886] infiltration, ulceration, and cicatrization, in the latter by unnatural sexual connection, or by infecting vaginal discharge running into the bowel.
When the stricture involves only the mucous tunic, it imparts to the finger the sensation of a ring-like elevation or a valve-like projection, into which the finger enters or beyond which it passes usually without much difficulty; but when it involves the submucous and muscular layers, as after the cicatrization of a large rectal ulcer, the finger encounters a dense fibrous mass which in some cases appears to have no lumen, but in others will admit only the end of the finger. In these grave cases of long standing there occurs considerable dilatation of the rectum above the stricture due to fecal detention and impaction at this point, and hypertrophy of the muscular coat of the bowel produced by long-continued straining and expulsive efforts.
Allingham2 speaks of chronic constipation as a cause, and says, "Straining to evacuate the contents of the bowel forces down the upper part of the rectum into the lower, causing an intussusception; it gets within the grasp of the sphincter muscles, and this may be the starting-point of the irritation." Stricture does not usually follow proctitis, even when the latter is very chronic. The long-continued pressure of the child's head in cases of delayed labor is said to have caused stricture of the rectum.
2 Diseases of the Rectum, p. 195.
This affection is a disease of adult life, and more cases of it occur among women than among men. "If stricture of the rectum is found in a young woman, it is probably due to chancre cicatrices; if it is met with in old women and men, the inference should be that it is either caused by cancer or by syphilitic infiltration and its consequences. Only in those cases in which no cicatricial tissue has been formed—that is, when the contraction is due to the infiltration alone—will the results of the antisyphilitic treatment contribute anything toward rendering the diagnosis more certain."
Stricture of the bowel may exist for months and years without being recognized and without causing the patient much uneasiness; more frequently, however, there is marked uneasiness, with an increased desire to go to stool and a sense of weight or of a foreign body in the bowel. Violent straining accompanies the act. It is given usually as one of the most common and reliable symptoms of this condition that the feces are flattened, ribbon-shaped, or triangular or wire-drawn: in true stricture, according to Allingham, this is not the case, but the characteristic stool consists of small, irregular, broken fecal fragments. When the contents of the bowel happen to be watery, the loose stool is spurted out with great force. In this disease diarrhoea alternates with constipation; the intestines become distended with quantities of gas and feces, which provoke frequent and severe attacks of colic; the appetite and digestion fail; the complexion becomes sallow; the patient emaciates; ulceration sets in, and the patient slowly sinks from exhaustion. Usually, these cases do not give rise to much pain, and what there is, is usually referred to the back, thighs, penis, or perineum. A discharge of mucus resembling white of egg immediately precedes each action of the bowels. Usually, these strictures are within two and a half or three inches of the anus, but sometimes they have been found high up in the sigmoid flexure, and rarely at a greater distance. A syphilitic stricture by direct inoculation [p. 887] is found just within the sphincter muscle, and consists of an infiltration of inflammatory lymph in a circumscribed portion of the submucous tissue. It is tight, highly sensitive, thickened, inflamed, and bathed in pus; there are also constitutional symptoms, as fever, anorexia, and mental irritability. The subjects of this variety are usually women. The tissues composing strictures of the rectum of a very chronic character are found to be gray or bluish-white in color, of very dense fibrous structure, and creaking under the knife when cut, as a piece of cork would do.
Besides the before-mentioned stricture, due to the contraction of a chancroidal ulcer, is another caused by submucous gummata of the ano-rectal region, which is very rare; and yet another, the diffuse gumma, or ano-syphiloma of Fournier, which is the most frequent of all causes of stricture of the rectum. The diffuse gumma is one of the later manifestations of syphilis, and consists in "an infiltration of the ano-rectal walls by a neoplasm of as yet undetermined structure originally, but susceptible of degenerating into a retractile fibrous tissue, and thus giving rise to narrowing of the intestinal calibre to a greater or less extent."
Inflammation and suppuration in the lower part of the rectum are even more common than the corresponding affections of the cæcum, and their causes are quite as various. In many cases, no doubt, this affection is traceable to ulceration (perforative or otherwise) of the mucous membrane; in others it probably originates in the connective tissue which surrounds the rectum (periproctitis). The rectum, still more frequently than the cæcum, becomes involved in inflammation and suppuration originating in the various pelvic, and even in distant, organs. Abscesses arising in the abdominal cavity or its parietes are peculiarly apt to gravitate into the pelvis and to communicate with the rectum.
Proctitis in its acute form has some symptoms in common with dysentery, but it differs from it by the absence of abdominal pain, tenderness, and severe constitutional symptoms. The pain in proctitis is usually referred to the sacrum and perineum, and there is frequently dysuria from sympathetic affection of the bladder. This disease may be acute or chronic; the latter form occurs in those advanced in life. Frequent attempts to evacuate the bowels, with great tenesmus, heat, weight, and fulness in the bowel, and a mucous and bloody discharge in the absence of impaction of the rectum, characterize the attack. Should it be protracted and severe, the discharge will become purulent. A digital exploration should always be made to ascertain if any foreign or irritating substance is exciting the inflammation.
The presence in large numbers of Oxyuris vermicularis may excite irritation and inflammation of the rectal mucous membrane, which is sometimes very intense.3
3 Curschmann, Ziem. Encyclop., Am. ed., vol. viii. p. 848.
Inflammation of the anus and buttocks, caused by the application of the leaves of Rhus toxicodendron after defecation, has extended into the [p. 888] rectum and produced proctitis and peritonitis.4 "In some cases of dysentery the pathological lesions are limited to the rectum, which would produce an apparently local inflammation very similar to proctitis. The irritation of unnatural sexual intercourse and the contact of gonorrhoeal poison have been known to excite intense inflammation of the mucous membrane of the rectum, with a copious discharge of pure pus, and accompanied by intense burning pain and great heat of the parts involved."5
4 Case of Dunmire, Philada. Med. Times, vol. xii.
5 Heubner, Ziemssen's Cyclopæd., vol. i. p. 552.
The painful ulcer of Allingham is quite a common affection, attacking women more frequently than men, and no age is exempt from it. Of 4000 consecutive cases of rectal and anal disease observed by Allingham, 446 presented fissure of the rectum. They are rarely multiple. Their usual position is dorsal, although they may be found at any part of the circumference of the anus, and just within the verge of the anus at the junction of the skin and mucous membrane, extending upward toward the rectum usually not more than half an inch, and appearing as a crack or fissure, often very trifling in appearance, or a club-shaped ulceration, the floor of which will be very red and inflamed if it is recent, but if chronic the floor will be grayish, with hard, well-defined margins. Sometimes there will be found at the external extremity of the fissure a small club-shaped papilla or muco-cutaneous polypoid growth; but this is not to be confounded with the ordinary polypus, nor is it the cause of the fissure, but the result of irritation caused by the latter. In other cases the external site of the fissure is indicated by a very tender and swollen flap of integument, which often becomes the seat of a small but very painful fistula. The club-shaped papilla is said to indicate invariably the existence of fissure.
Fissure of the rectum is often associated with anteversion and retroflexion of the womb. In many of these cases the fissure will heal spontaneously when the malposition is rectified. However treated, the result will not be satisfactory while the uterine trouble remains uncorrected.
Fissure is not infrequently caused by and accompanied with polypi: it may be caused by any accident whereby the verge of the anus is torn or superficially lacerated—by chronic diarrhoea, by violent expulsive, straining efforts, as in labor, by the passage of very hard, dry stools—and very frequently it is syphilitic in origin. The most prominent symptom of this disease is pain, and this is very severe and peculiar in character, coming on in most cases not during the act of defecation, but twenty minutes to half an hour afterward, and is preceded by a hot, burning, throbbing sensation at the anus: then comes on spasmodic contraction of the sphincters, and the patient endures agonizing pain, often for several hours, when relief is gradually experienced, and no pain is felt until defecation again becomes necessary. Now, it has been observed that in some cases where the local lesion is very trifling the pain and spasm are intense and long-continued; in other cases, where spasm and agonizing [p. 889]pain followed every act of defecation, no lesion of the anus or rectum could be found. This led Dolbeau to consider the essence of fissure of the anus neuralgic, and to define it as "a spasmodic neuralgia of the anus with or without fissure." The mental depression is so much out of proportion to the local disease that this may come within Curling's observation, that "mental causes may produce local disease in the rectum."
This is, fortunately, a rare disease, and is peculiar and distinct from any other form of ulceration in this region. It is not cancerous, although bearing some resemblance to epithelioma. As it first appears it is very like a syphilitic sore, and its situation and the character of the pain might lead to the supposition that fissure existed. Rodent ulcer is usually situated upon the mucous membrane, although it occasionally invades the integument about the anus; its shape is irregular, its edges sharp and well defined, and it does not undermine the neighboring tissues. There is no induration about this sore, as nature does not seem to attempt to limit it or to set up any reparative action, and its surface is red and dry. The surrounding tissues seem quite normal. It is very destructive, and seems to prefer mucous membrane, although sometimes it destroys deeply. It does not cause infiltration; it does not spread by the lymphatic system, forms no secondary deposits, nor does it produce stricture. It may remain in a quiescent state for some time, and a certain amount of cicatricial tissue may form; but it never heals spontaneously, and an exacerbation comes on which destroys in a very few hours the repair which may have been the work of many days. This form of ulceration of the rectum is usually considered incurable; the pain is intense, being compared to that produced by hot iron, and of course being much aggravated by the acts of defecation. Patients so affected die from exhaustion and pain, although recovery may take place, I have known one case entirely cured by complete excision. Spasm of the sphincters is a usual accompaniment, and greatly augments the suffering of the patient. Of the four thousand consecutive cases of rectal disease tabulated by Allingham, only two were cases of rodent ulcer.
This condition may be caused by foreign bodies introduced into the anus, by indigestible substances swallowed, by impaction of feces, by pressure of tumors external to the rectum, and by intestinal concretions. Any condition which causes loss of muscular and nervous tone in the large intestine favors its obstruction; thus, it is not uncommon in the aged of both sexes, but especially is this the case in women, and in them it often follows parturition. Hysterical, nervous, and debilitated persons are particularly prone to it. The insane, if not carefully watched and regulated, will become the subjects of it. Impaction of feces is a very common cause of obstruction of the rectum, and atony of this organ is usually the primary cause, the feces in these cases being [p. 890]either very hard and dry or clayey and tenacious. These masses are of a more or less globular shape, and, as they irritate the bowel and produce diarrhoea, the practitioner sometimes falls into the error of prescribing doses of opium and the astringents, misled by the appearance of feculent fluid which oozes around the impacting mass. The impaction occurs just above the internal sphincter. Habitual constipation soon stretches the rectum and robs it of expulsive force, and an accumulation of months of fecal matter is sometimes found. The appearance of persons so affected suggests malignant disease: they are cachectic, sallow, dyspeptic, irritable, and nervous. Vomiting, anorexia, thirst, cough, hectic, irregular and profuse sweating, are also among its symptoms. Cases of melancholia and of hypochondriasis have been cured simply by the discovery and removal of rectal impactions. This condition has been mistaken for cancer, phthisis, intermittent fever, and enlarged mesenteric glands. Accompanying impaction, and as a result, is spasmodic contraction of the sphincter ani, which causes the anus to protrude in a nipple shape and to firmly resist the introduction of the finger. Usually, there is no discharge from the anus in these cases. Tenesmus, a sense of weight and of a body present in the bowel, are experienced. Young people are not often subjects of impaction.
Concretions also cause obstruction of the rectum: these are more frequently cylindroid in shape, and sometimes have a nucleus consisting of some firm foreign body. Wetherill reports a case of a young adult, who had been accustomed to the daily ingestion of a substance known as hygienic bread (this substance is made from the husks of grain, and is very coarse: it is used to excite peristaltic action), from whose rectum he removed a very hard ball of this substance which was covered with mucus, but which contained no nucleus. He reports another case in which the offending substance was a globular mass of casein, stained with bile and covered with mucus, and which had for a nucleus a small mass of hardened fecal matter.
Guéneau de Mussy6 reports a case in which there was an occlusion of the rectum by a mass of magnesia, which was so firmly impacted that it had to be removed by a mallet and chisel. A similar case occurred in the practice of Dunlap of Norristown. Fendick7 relates an instance of impaction by a fish-bone near the anus, causing obstruction requiring surgical interference; which illustrates the importance of examining carefully all cases of acute piles and threatened abscess.
6 Medical Times and Gazette, 1879, vol. ii. p. 214.
7 Lancet, 1880, vol. ii. p. 239.
These concretions often consist of animal and vegetable fibres matted together about a nucleus, the latter consisting of the seeds of fruit, fragments of bone or gristle, hair, small coins, or pins. "Enteroliths may lodge in the rectal ampullæ" and cause obstruction. Indigestible substances swallowed with the food may be arrested in the rectum, such as grape-skins, fruit-pits, husks, and fibres, and where there already exists stenosis of the bowel a dangerous form of obstruction may be produced. Jones8 reports a case of chronic impaction of the rectum by plum-stones, which gave rise to trouble in defecation, and at the end of eighteen months produced symptoms of piles; at the end of two years impaction occurred, and the mass was removed by the surgeon. Hazelhurst relates [p. 891] a case of impaction in a negro where two hundred and eighty plum-stones were removed from the rectum after having been there for a week. The records of the Pennsylvania Hospital furnish the following interesting case of obstruction:9 "The patient (a male) stated that twenty years before he swallowed a peach-stone. Two years afterward he had symptoms of rectal irritation, tenesmus, constipation alternating with diarrhoea, and liquid stools, etc. These symptoms had continued ever since. His health had been markedly impaired. A digital examination revealed a hard, stony mass two and a half inches above the anus. Under ether Morton divided the external sphincter, and with a pair of bone-forceps removed, with considerable difficulty, a good-sized peach-stone which was lodged in the rectal tissues. The stone was very sharp at the ends, and had evidently lodged crosswise and become imbedded. The patient was discharged quite well and free from all symptoms."
8 Lancet, 1856, vol. ii. p. 278.
9 Surgery in the Pennsylvania Hospital, Phila., 1880, p. 335.
Gall-stones may cause impaction or they may form the nuclei of concretions. A case of impaction is related by Walker,10 who removed a gall-stone from the rectum which measured three and a half inches in its longest and one and a quarter inches in its shortest diameter; also one by Roberts,11 in which he removed a gall-stone measuring five inches in circumference from the rectum of a woman two weeks after confinement. Mischievous, revengeful, insane, or intoxicated persons sometimes force very curious foreign bodies into the rectum, among which may be mentioned hot iron, bottles, cups, bougies, pieces of wood, stones, a champagne flask, a goblet, slate-pencils, and the tail of a pig with the bristles cut short. Some foreign bodies introduced from below find their way through the sigmoid flexure and lodge in the colon, or they may remain for a long time in the rectum. The cæcum is the favorite resting-place of foreign bodies. Turgis12 removed by linear rectotomy a cup which had been forced into the bowel. These foreign substances, if not promptly removed, set up violent inflammation. Obstruction of the rectum may be caused by vast numbers of round- or thread-worms twining themselves together in a mass; and when this happens in children or in adults of very nervous organization a curious train of reflex symptoms may be developed, among which may be mentioned choreic movements, convulsions, pruritus ani, insomnia, irritability, melancholia, and hypochondriasis. Finally, the rectum may be obstructed mechanically by pressure exerted from without. Such an effect might be produced by morbid growths from the sacrum or ileum; by deposits in Douglas' cul-de-sac; by ovarian disease; by pelvic cellulitis causing stricture of the rectum; by vesical trouble; by ascites with hepatic disease; and by various abnormalities of the uterus, such as inflammation, morbid growths within or upon, simple retroversion or retroflexion, or retroflexion of this organ in a gravid state.
10 Flint, Prac. Phys., 460.
11 Bost. Med. Journ., 1879, vol. ii. p. 116.
12 Société de Chirug., 1878.
Impaction of feces under some circumstances may give rise to extensive sphacelus of the rectum and the contiguous parts from pressure. This is well illustrated in the following case of a woman aged sixty-five, who was found to have an immense distension of the abdomen from ascites, incident to a large omental scirrhus. The patient suffered greatly from the pressure caused by the accumulation of water, and she was tapped. Soon after this an impaction of feces was observed, which probably had been forming [p. 892] for some time prior to her coming under observation. A week or ten days after the tapping the impaction was detected, but not soon enough to prevent the formation of a large slough of the posterior and inferior part of the rectum immediately above the anus. The submucous tissues and the skin, owing to the greatly enfeebled condition of the patient, soon gave way, leaving a large opening which communicated with the bowel. The tissues adjacent were oedematous, red, and painful. The finger carried into the bowel through the anus discovered the slough to have involved a region of at least two and a half inches in diameter.
These are quite numerous, and they almost invariably produce much distress and excite painful pruritus, which is augmented rather than relieved by scratching or friction of any sort. The application of the leaves of Rhus toxicodendron after defecation is capable of exciting considerable inflammation upon and around the anus, accompanied by small pearly vesicles, which, when ruptured by scratching, seem to spread the disease wherever the contained serum flows. Eczema, when found in the anal region, is usually due to parasitic growth. Erythema intertrigo is caused by the friction of moist opposing surfaces, as between the nates of stout persons, who perspire freely, and infants. The abraded derma exudes a sero-purulent fluid which excites troublesome pruritus. When this condition exists about the anus it causes painful defecation and spasm of the sphincters. Erythema chronicum occurring in this locality is frequently a sequel to chronic eczema and chronic lichen: the skin cracks, is moist, thickens, and the epidermis exfoliates. The proximate cause in both of these conditions is congestion of the vascular rete of the derma. In prurigo podicis papules appear which itch intensely, and when scratched bleed, the summit of each papule bearing a small black scab. If not cured, in time a true psoriasis may develop. Herpes of the anus occurs similar to herpes at the other mucous outlets of the body, and is usually symptomatic of slight disorder of digestion. Wetherill has seen a case of herpes zoster, (var. proserpens,) in which the vesicles extended from the side of the scrotum along the perineum to the verge of the anus. This condition was accompanied with neuralgia of the rectum, painful defecation, and spasm of the sphincters. Furunculi sometimes form at the verge of the anus, causing spasm, pain at stool, and occasionally marginal fistulæ. Various syphilodermata also appear in this region. Gross was the first to describe a condition of trichiasis of the anus—a very irritating complication to fissure—due to a perverted recurvation of the hairs usually found in the anal region. Villermé states that hairs have been found growing from the mucous membrane of the rectum. The colonization of pediculus pubis about the anus occasions a certain amount of irritation. Sarcoptes hominis is sometimes found in this region, having been carried there by hands infested with this parasite. The result is very distressing. The peculiar tracks or burrows made by this little animal, and the use of the microscope, make the diagnosis certain. The Acarus autumnalis, or mower's mite, has been found in the skin of this part, and it is capable of causing great distress. These do not furrow the [p. 893] integument longitudinally, but burrow vertically, and may be picked out of the summits of the wheals, where they appear as small red points.
This is a condition very different from fissure or the painful ulcer of Allingham—much more grave, difficult to treat, and, in chronic cases, much less hopeful of cure. It is not an uncommon affection, Allingham's table of 4000 consecutive cases of diseases of the rectum and anus furnishing 190 of the disease under consideration. An ulcer of the rectum may be partly within, partly without, the internal sphincter, but in most instances is found above that muscle, from an inch and a half to two inches from the anus, situated dorsally.
The symptoms are unfortunately obscure and insidious, misleading not only the patient, but also too frequently his medical adviser, and gaining grave headway before a correct diagnosis is reached. Often the very first symptom is a slight diarrhoea every morning as soon as the patient rises, accompanied with a little discharge resembling coffee-grounds; or, again, the discharge is like the white of an egg; in some rare instances pus is formed. At this stage there is little or no pain, but the patient suffers from tenesmus—which is not followed by relief—and a sense of uneasiness in the part. Several stools of this nature or streaked with blood may be passed during the earlier part of the day, after which the patient feels partly relieved, and no more evacuations occur until the following morning, when he again experiences the same train of symptoms; and this repeats itself daily for a long time. Finally, these discharges occur in the evening as well as in the morning, then at various times during the day: his general health begins to give way; the discharge becomes augmented in amount and contains more blood and pus; and he suffers occasional pain from flatulent distension. Local pain in the rectum is now felt, which is not acute, but is very wearying, is augmented by much walking or by long standing, and which has been described as similar to a dull toothache. These ulcers may be multiple, and not infrequently lead to stricture of the rectum, which condition is indicated by the alternation of attacks of diarrhoea and constipation. As the ulcerative process proceeds, nature makes efforts to limit the process, which causes infiltration and thickening of the submucous and muscular tissues, and produces narrowing of the lumen of the intestine, which in time loses its tone and contractile power and becomes a passive tube, utterly unfit to perform its normal duties. The sphincters give way and the patient loses control over his evacuations. Finally, abscesses form, which, burrowing toward the surface, form fistulæ, and may perforate the bladder, the vagina, or the peritoneal cavity. If one of these ulcers be examined while yet in the acute stage, it will be found to be oval in shape, with well-defined edges: the base will be either grayish or very red and inflamed, the surrounding mucous membrane appearing normal. The rectal glands will be found to be enlarged. Should the ulcer be examined at a later stage, it will be found to be much deeper and more extensive, with great thickening and nodulation of the mucous membrane, and looking in places as though the latter [p. 894]had been torn off. At this stage the ulceration may be partial or may involve the entire lower portion of the rectum. The suffering is now intense, and a constant discharge of fetid pus and mucus takes place. The appearance of the anus at this time suggests malignant disease: it is covered with swollen, shiny, tender, club-shaped flaps of integument constantly bathed in an ichorous discharge. The entire rectum and sigmoid flexure have been involved in some cases, while in others necrosis of the sacrum has occurred. Patients suffering from ulceration and stricture are very liable to a low form of peritonitis, attended by intense abdominal pain.
The causation of these ulcers of the rectum is frequently very obscure: some are of syphilitic, others of strumous, origin. Some are of traumatic origin, but more often the patient was in apparent health up to the time of the appearance of the disease. The experience of Allingham would indicate that neither chronic constipation nor dysentery is a frequent forerunner of this malady. T. Claye Shaw,13 in an article entitled "On Some Intestinal Lesions of the Insane," says: "After death are found patches of ulceration sometimes so extensive as to resemble a honeycomb network. The edges are usually slightly raised, and perhaps hardened; but the ulcers are at other times mere local punchings out of the mucous membrane, and there is often a little loose gelatinous material." It is claimed that such disorders are not infrequent among the insane.
13 St. Bartholomew's Hospital Reports, 1880.
It is also claimed that the chronic mechanical irritation from foreign bodies, impacted feces, and the like exert a causative influence in the formation of ulcer of the rectum. Like typhlitis, this affection leads to chronic inflammatory changes in the immediate neighborhood (periproctitis), with the formation of fistulæ and crater-shaped ulcerations, and to the extensive destruction of the mucous membrane, followed by wasting and contraction of the rectum. The healing of these ulcers is much delayed by the fact that the ulcerated and undermined mucous membrane is irritated by the fecal masses which are especially apt to accumulate in the lower part of the bowel and around the anus. We find also hemorrhoidal swelling and ulcerations, which may be regarded as partly a cause, partly a result, of the ulcerative proctitis.
In this condition the most extensive ravages are found in the rectum and sigmoid flexure. The causes are identical with those of catarrh of the large intestine, if we except the follicular disease produced by dysenteric infection. In this form of the disease, at least in its earlier stage, the form of these ulcers is always round and funnel-shaped, with distinct thickening of the edges of the mucous membrane around the ulcers. These appearances may be explained by the mode in which the follicular ulcerations originate: "The solitary follicles become swollen, a result of catarrhal irritation, and the cellular elements accumulate in the reticulum, giving rise at first to nodules which project above the level of the mucous membrane: then the newly-formed tissue-elements become necrosed in consequence of the mutual pressure of the cells upon [p. 895] each other; finally, the apices of the follicular nodules give way and the ulcers are formed. The surrounding mucous membrane bends over downward toward the base of the ulcer, so that the orifices of the crypts look down into the same."14 As the suppurative process extends, particularly in the submucosa, and the tissue surrounding the follicles becomes destroyed, these small ulcers coalesce to form larger ones, and the undermined edges of the mucous membrane project over the base of the ulcers, bleed, and become necrosed. Healing is possible by cicatrization, the borders of mucous membrane becoming applied to the base of the ulcer and gradually drawn together by the cicatricial tissue. Still, this result is extremely rare if the ulcerative process has gained much headway. When, however, a follicular ulcer of some size does heal, cicatricial stenosis may result, followed by chronic constipation, just as in the case of simple catarrhal ulceration. The situation of follicular ulcerations is almost always in the large intestine, and they vary considerably in number: sometimes only a few follicles are thus affected, while in other cases the bowel is crowded with them.
14 Rokitansky, Path. Anat., iii. 1861, S. 226.
The anus and rectum may become the seat of chancroidal invasion. An ulcer of this character fairly within the rectum is very rarely met with, especially in this country, and could scarcely be produced except by unnatural intercourse. They are of not uncommon occurrence in the anal region, and are met with in this situation more frequently among females than among males. Occurring among the former, they no doubt often arise from accidental contact during normal sexual intercourse. When this condition is found in males, it rather indicates at least an attempt at unnatural intercourse. Of 1271 males affected with chancroids, only 3 were found with the disease in the anal region. Out of 388 females similarly affected, 33 were found with chancroid of the verge of the anus. The table of Debauge gives 23 cases among 206 females having chancroid in various other situations. The destruction of tissue in these cases may be very serious should the nature of the ulcer not be recognized, and stricture of the rectum or cicatricial stenosis of the anus might result. Ulceration of the rectum may occur during chronic proctitis; it may accompany advanced states of prolapse and procidentia of the bowel; it may attack a stricture of the rectum and cause peritonitis by erosion. Ulceration may accompany hemorrhoids, or it may attack them and cause dangerous hemorrhage. Finally, a very intractable form of ulceration may follow the clamp-and-cautery operation upon piles. When this untoward result is seen, it is usually due to the fact that the patient has been allowed to move about too soon. Allingham claims to have seen these ulcerated stumps of piles even ten days after operation.
The ischio-rectal fossa is peculiarly liable to attacks of inflammation resulting in abscess, as it is filled with much loose connective tissue which supports a considerable amount of fat, and is situated in a region which is constantly exposed to injury both from within and without. It is a very vascular part, being freely supplied by branches of the inferior [p. 896] hemorrhoidal arteries and veins; the latter, being large and destitute of valves, empty into the portal circulation. Abscess in this region is of very common occurrence, and may attack any one at any period of life. It occurs more frequently among men than among women, and usually during middle life.
Abscesses in this situation may be acute or chronic. The former variety may be caused by injury to the anus or to the surrounding parts; by exposure to cold and wet, and particularly by sitting upon damp seats while the body is overheated; by impaction of feces, constipation, and straining at stool. Irritating substances swallowed with the food, such as small pieces of bone, oyster-shell, or the stones of fruit, may excite abscess by their presence in the rectum. Among other causes are general debility, an impoverished state of the blood, the scrofulous and tuberculous diatheses. The disease sometimes occurs in quite young infants. Wetherill reports the case of an infant attacked by an enormous ischio-rectal abscess while nursing from the mother, who was at the time suffering from a succession of boils. Many cases have been traced to sitting upon the outside of damp omnibuses. Hepatic disorders, causing engorgement and stasis of the blood in the hemorrhoidal plexus, have frequently occasioned this condition. These abscesses are not always situated in the ischio-rectal fossa; frequently they are subcutaneous and just outside the anus: in other cases the starting-point may be ulceration of the mucous membrane of the rectum, with escape of fecal matter into the areolar tissue; they also originate in the submucous connective tissue of the rectum. The acute abscess is sudden and very severe in its onset; the pain is continuous, throbbing, and augmented during defecation; dysuria is almost always present, and in some cases there is total inability to pass water. There is local tenderness, dusky redness, and fluctuating prominence, and, if not interfered with, a rupture of the integument will take place and the pus will escape externally. Sometimes their formation is accompanied with a chill or with a succession of rigors: there is always considerable constitutional disturbance, febrile movement, loss of appetite, and malaise. This form of abscess is usually circumscribed and does not burrow irregularly, and sudden relief of pain and distress is coincident with their evacuation.
Chronic rectal abscess corresponds to the cold or chronic abscess in other situations: it is apt to occur among those who are much debilitated or among those of the scrofulous diathesis. These abscesses have little disposition to open spontaneously upon the surface, but they burrow extensively in all other directions—high up along the outside of the rectum, laterally into the tissues of the buttock, or downward and forward into the perineum. The process of formation may occupy many months, and sad havoc may be occasioned before their existence is suspected. They occasion no pain nor distress nor acute febrile movement, but may be accompanied with a hectic condition, erratic sweatings, and rapid loss of strength. Upon examination of the anal region in these cases a painless flat, boggy, crepitating enlargement is the only surface-indication of the probably extensive damage sustained by the deeper structures.
This form of abscess may be of traumatic origin, but more frequently the inflammatory process arises in the cellular tissue of the ischio-rectal fossa; in some cases the morbid action is due to ulceration of the rectum. [p. 897]In either case peri-rectal or peri-anal cellulitis will be induced. When these abscesses are of strumous origin the pus is thin, curdy, and offensive.
Both the acute and the chronic abscesses of this region are often difficult to heal, the external opening remaining permanently patulous, communication with the bowel resulting from internal burrowing and erosion, with the formation of extensive sinuses in all directions, resulting in fistulæ in ano.
This condition occurs more frequently than any other of the abnormalities of this region, Mr. Allingham finding 1208 out of his table of 4000 consecutive cases of diseases of the rectum and anus. He found also that fistulæ followed rectal abscess in 151 out of 196 cases, the abscesses which healed kindly and gave no further trouble being only 45 in number. A fistula in ano is a linear ulceration with a patulous orifice which discharges pus: it may or may not communicate with the bowel, and it may have more than one external opening. The great majority of fistulæ in this region are caused by abscess, either arising in the submucous areolar tissue of the bowel, or in the subcutaneous connective tissue in the immediate neighborhood of the anus, or in the ischio-rectal fossa, or in an ulcerated state of the mucous membrane of the rectum: in other cases it is congenital, or it may result from the presence of foreign bodies or worms in the bowel, or from puncture of the rectum by pins, scales of shell, fragments of bone, or other sharp substances swallowed with the food. Abscesses leading to fistulæ have followed kicks, blows, or wounds of the anal region: in short, anything which induces an abscess here may result in a fistula, and as in the former more cases occur in males than females, and more during middle age than at any other period, the same is true as to the latter. Fistula is quite common among the phthisical as a result of malnutrition and septicæmia, aided by the constant succussion of the perineum produced by efforts at coughing. Of the 4000 cases previously referred to, 1208 were cases of fistula; "of these, 172 presented more or less marked symptoms of lung trouble, hæmoptysis, cough, or impaired resonance in some portion of the chest."
A fistula may be complete or incomplete. To be complete, it must have two openings (it may have more)—one in the anus or rectum, and one upon the surface. There are two forms of the incomplete or blind fistula—one in which there exists an internal but no external opening, and the other in which there is an external but no internal opening. In complete fistula there may be more than one external opening, and this is in the majority of cases not far from the anus, but it may open in the perineum or upon any part of the gluteal region. When the openings are multiple they usually converge to form a common tract or sinus. The external opening presents nothing to the untutored eye to lead to the suspicion of grave internal trouble: frequently the vent is so minute and valvular or shielded by a thin pellicle as to be entirely overlooked; in other cases a little teat formed of superabundant granulations guards the entrance: there may or may not be discoloration, elevation, or depression of the surrounding integument, and erythema resulting from the [p. 898]irritating nature of the discharge. Inflamed and suppurating follicles in the integument about the anus are not to be mistaken for the orifices of fistulous tracts.
The internal opening in anal fistula is situated between the sphincter muscles, sometimes just within the anus, but oftener about half an inch above; in rectal fistula the internal opening or openings may be at any point above the internal sphincter. These sinuses may be very tortuous, with pockets, blind passages, or diverticulæ, and are known as horseshoe fistulæ when they commence at one side of the bowel and ulcerate around it to a point opposite before making an opening.
Of the two varieties of incomplete fistulæ, by far the least frequent is that where no internal opening exists, but where there are one or more external orifices: these do not invariably even run toward the bowel, but may extend off through the tissues in any direction. In the other variety, where there exists no external evidence of disease, considerable damage may be done before its recognition. Fistula may coexist with hemorrhoids, stricture, ulcer, or malignant growth: it may be a very trivial affair, with the internal but a fraction of an inch from the external opening, or it may be long, deep, and tortuous, with sinuses running in all directions through the buttock.
Usually, fistulæ become worse when not operated upon, but there are cases which have healed without surgical interference—others in which this condition has gone on for many years without getting any worse or without the discharge increasing in amount. The fluid discharged from a chronic fistula loses after a time much of its purulent character and becomes serous and watery; but fresh abscess and inflammation is apt to take place in these cases from feculent matter lodging in the sinus. Those which burrow most readily are the internal fistulæ with large openings, into which the feces are pushed, with the sinus running toward the anus, because of their funnel-shape.
The presence of fistula may be suspected if there are in the anal region abscesses which have not completely healed, or which, having apparently done so, break out from time to time and discharge pus; or from the existence of a circumscribed hardness or swelling unaccompanied by an opening which varies in size and is at times painful; or if there exist any ulcerated moist openings. To make a positive diagnosis the tract must be explored by a probe: enter the oiled, blunt-pointed probe gently into the external opening and let it find its way along without force, bending the probe if necessary, until it has traversed the sinus as far as it will go; then pass the finger into the rectum and feel about for an internal opening or for the point of the probe. If the finger be introduced first, the relations of the parts are interfered with and the internal opening, should one exist, might not readily be found. Sometimes the bottom of the tract does not correspond in situation to the internal opening, but extends beyond it. In those cases where no external opening exists, the rectal speculum, aided by judicious pressure, will discover an issue of pus from a sinus upon the mucous membrane of the rectum.
In order to illustrate the amount of damage which a small foreign body may cause when lodged in the rectum, Wetherill relates the following case, which occurred in his practice at the Pennsylvania Hospital for the Insane: The patient was a middle-aged man, intelligent, and an [p. 899] employé of the hospital. "Upon examination of the anal region I found a small, tender, firm swelling, which did not fluctuate, about an inch to the left of the anus: this had been forming for about a week, and there was no history of painful defecation, of exposure to damp and cold, nor of a blow or injury of the part. Without waiting for the development of fluctuation, I made a free and deep incision into the ischio-rectal space, and a large quantity of very fetid pus escaped: upon introducing a large probe I found that it passed up into the fossa to a depth of four and a quarter inches and turned but slightly toward the bowel. Remembering the experience of Allingham, that when the pus in these cases was very offensive there existed an opening in the bowel, I questioned the patient again as to pain in the bowel or painful defecation, which was answered in the negative. No communication could be found with the finger in the bowel and a probe in the wound, and poultices were applied, liquid diet ordered, and the man kept in bed. The cavity was loosely filled with absorbent cotton and the entire wound (apparently) healed slowly, but kindly, and in about ten days after operation the patient left the house to all appearance sound. About a week after the patient returned with the report that he felt uneasy throbbing in the part, and that there was a very slight discharge. Upon inspection I found in the surface-line of the cicatrix a pinhole opening which yielded upon pressure a drop or two of pus; upon entering a very fine probe it passed into a narrow sinus to a depth of three and a quarter inches, but no communication could be made with it with the finger in the bowel. Upon withdrawing the probe it grated over something which felt like dead bone, about two inches from the surface. I enlarged the opening, introduced a pair of fine dressing-forceps, and withdrew a piece of the rib of a chicken about half an inch in length and sharpened at one extremity to a fine point. Upon making inquiry I found that he had not eaten any chicken since the development of the abscess. He then suddenly remembered that while he was at stool a few days prior to the formation of the abscess he experienced a sudden pang of very acute pain in the rectum, which, however, soon passed off. This was no doubt the moment when the piece of chicken-bone pierced the rectum."
Hemorrhage from the rectum may be accidental, primary, or secondary—accidental when it follows the ulceration of internal piles or the erosion of large arterial or venous trunks during the progress of malignant disease, or when it occurs from the rupture of a rectum during defecation—a very rare and curious occurrence reported by M. E. Quénu;15 primary when it occurs during, and secondary when it occurs after, a surgical operation upon these parts.
15 Révue de Chirurg.; Practitioner, p. 29, Oct., 1882.
Hemorrhage from the rectum without any structural lesions is quite unusual, but occasionally copious losses of blood are seen in vicarious menstruation, and several instances have been reported.
When ligatures separate after operations upon those of broken-down constitution very copious and dangerous bleeding may occur without any symptoms save a "sensation of something trickling in the bowel," [p. 900] a feeling of weight and fulness in the part, with increasing weakness and syncope of the patient, until he expresses a desire to go to stool, when suddenly a large quantity of blood escapes.
This class of affections depends upon constitutional infection, direct extension of disease by contiguity, by contiguity from disease in neighboring organs, or by abnormal conditions excited by disease of remote origin; and are frequently due to changes in the nervous and vascular supply.
True primary syphilitic chancre of the rectum must be an extremely rare lesion, and could have been acquired only by unnatural intercourse. There are syphilographers who deny that the hard chancre has ever been found within the sphincter muscles; but it certainly is not uncommonly found in the anal region, and oftener among women than men. The table of Jullien gives 12 instances of this lesion in males, and 1 instance of chancre of the buttock, out of 77 cases, while among 82 cases occurring in the opposite sex, 21 were of the anus and perineum and 4 of the buttocks. The French authorities give the frequency of this condition in men as 1 case in every 119; in women, 1 case in every 12.
Anal chancres are easily overlooked, as they occupy the puckered folds of the anus, which when not opened out to the fullest extent afford perfect concealment: they may be either in the form of cracks or slight fissures, elongated ulcerations, or firm papules. It has been claimed that the initial lesion has provoked stricture of the rectum, but this is not probable.
The secondary manifestations of this disease which show themselves in the anal region are some of the syphilodermata, moist papules, mucous patches, and moist papillomatous excrescences or condylomata. The statistical tables of Davasse and Deville16 in regard to the occurrence of moist papules and mucous patches in women show that out of 186 cases they appeared about the anus in 59 and on the perineum in 40. Bassereau's17 statistics show that in men these lesions occurred in the anal region 110 times out of 130 cases. These are, of course, very contagious. Besides true syphilitic warts, which sometimes occur in this region, it is quite usual to see the anus surrounded and the entire gluteal cleft filled up with moist, offensive, papillomatous excrescences, which remain obstinately so long as these surfaces are permitted to rest in moist contact. Syphilitic stricture of the rectum is one of the results of a later stage of infection, and occurs oftener among women than men. It is stated by Jullien that of 60 cases only 7 were men, the remaining 53 women. They are invariably formed as follows: A gummatous deposit in the [p. 901]submucosa undergoes ulceration, and the subsequent cicatricial contraction gives rise to the stricture. Whether the stricture will be valvular or annular depends upon the extent of rectal mucous membrane involved in the ulcerative process. The diffuse gummatous infiltration of the ano-rectal tissues and the subsequent deposition of contractile tissue are the most usual causes of these specific strictures. The lower portion of the rectum is commonly the situation of specific ulcerations, usually of the secondary or tertiary stage, which lead to the formation of stricture: this occurs more frequently among women than men, and between the ages of seventeen and thirty years. Gosselin and Mason regard strictures as the result of chancres, and not as the result of constitutional infection; but it is known that ulcerations of secondary syphilis may extend upward from affections about the anus, and also that gummata do commonly give origin to this condition. Gummata, and strictures following them, may be distinguished from other affections on account of the greater distance from the anus at which they occur, chancres or chancroid ulcers being usually within four or five centimeters of the anal orifice. Strictures due to gummata are more apt to occur late in life, but may therefore be easily confounded with cancer. Condylomata at the anus are often associated with syphilitic disease of the rectum.
16 Internat. Encyclop. of Surgery, vol. ii. p. 508.
17 Loc. cit.
There are cases which yield abundant evidence of struma in the form of enlarged glands, chronic abscess in the neck, swelling and abscess in the vicinity of the articulations, and the like, in which ulceration of the mucous membrane of the rectum has been found: this condition may result in fistula in ano by erosion, permitting escape of flatus and excrementitious products into the cellular tissue. A similar result may follow by erosion of the bowel from a strumous abscess in the connective tissue around the rectum; both these forms tend to the production of that class of fistula which has no outlet at the surface, but which has one or more openings upon the mucous membrane of the rectum. Thus concealed (for often there is no marked surface indication of either abscess or fistula), they may remain for a long time unsuspected and acting as a serious drain upon the already impaired constitution. The pus in these cases is watery, curdy, and offensive. These chronic conditions are subject to intercurrent attacks of acute inflammation, due to the lodgment in the abscess cavity or the fistulous tract of fecal matter or indigestible solid substances. Any or all of the abnormalities of this region may be complicated by the existence of tubercular or scrofulous conditions of the system. Tubercular ulceration of the rectum is now a well-recognized condition. Rectal ulceration and tubercular disease of the lungs have not been found to coexist in any marked preponderating number of tabulated cases. The frequent association of fistula in ano and tubercular disease of the lungs has long been recognized, Allingham having found 172 such cases among 1208 cases of fistula in ano.
The pathology of tubercular ulceration of the rectum is graphically described in Ziemssen's Encyclopædia as follows: "These [ulcerations] begin in the follicular apparatus with swelling of the individual [p. 902] follicles and their vicinity from tuberculous deposit. The newly-formed cells become caseous, the superficial layer of the tubercle breaks down, and thus ulcerations arise of a round funnel shape. The enlargement of these ulcerations is probably produced by the constant formation in the base and edges of the ulcers of new nodules, which themselves caseate and ulcerate. This process of extension, to which these tuberculous ulcerations of the intestines exhibit a marked tendency, takes place chiefly in a transverse direction (girdle-shape), following the direction of the blood-vessels. The infiltration and necrosis may advance longitudinally, and, finally, the individual ulcerations coalesce with each other: in this way may be explained in part the dentate appearance of the edges of these ulcerations. The ulceration extends also in depth, although usually the muscular coat appears to be covered by a thick layer of connective tissue: the destruction advances slowly in the muscularis, but in the lymphatic vessels which pierce the muscularis less opposition is presented to the progress of the tuberculosis; and thus it is not uncommon to find tubercles ranged one after the other, like links in a chain, from the base of the ulcer directly down to the serosa. Healing is extremely rare. The most frequent situation is the lower end of the ileum, but the process may extend upward to the stomach, or downward, involving the rectum. There is almost invariably unmistakable signs of tuberculosis in other organs. It is possibly never primary, but this is a still-disputed point. It usually occurs with tuberculosis of the lungs, and when so occurring it is always secondary. The clinical symptoms of this state are by no means characteristic."
Dwelling upon the subject of intestinal tubercle, it has been suggested by Klebs18 that the intestinal disease is produced by swallowing morbid products derived from phthisical lungs—an hypothesis supported also by the fact that tubercle in the intestines tends so strongly to spread downward. "The seat of the deposit is the submucous tissue or the corium of the mucous membrane: it is certainly subjacent to the basement membrane, and not contained in the follicles, as Creswell taught."
18 Jones and Sieveking, London, pp. 593-595.
Woodward, in his article upon diarrhoea,19 says: "The lesions, whether mild or severe, are most generally seated in the cæcum and colon, but more or less extensive tracts of the small intestine, especially of the ileum, are often involved also." He continues: "Tubercular disease of the lung was noted in nearly one-sixth of the autopsies of fatal cases of forms of flux heretofore described. Possibly the frequency in chronic cases may be explained by the fact that protracted intestinal flux forms the development of lung phthisis in the predisposed."
19 Med. and Surg. History of the War of the Rebellion, p. 266.
The rectal fissure or painful ulcer may be connected with diathetic causes, as struma or scrofula: it is doubtful if syphilis should be included among its causes.
The forms of cancer met with in these regions are epitheliomatous, scirrhous, encephaloid, and colloid. Considerable diversity of opinion has [p. 903] existed as to which variety occurs most frequently; but it is now probably a matter of absolute knowledge that the epithelial form is the one most commonly observed, and next to that in frequency the scirrhous form. Encephaloid and colloid are of quite infrequent occurrence. Again, as to the sex in which this affection appears the most often, there is much disparity existing between surgical writers: it is usually thought to be much more prevalent among women than among men. This is not the experience of many of the authorities upon this subject, yet the statistics of the Hôtel Dieu, Paris, furnish overwhelming evidence in favor of its preponderance in women. Carcinoma of the rectum, occurring as a primary infiltration in the rectum, probably occurs oftener in men, but there are among females so many contiguous structures prone to cancerous degenerations, as the uterus, the vagina, the ovaries, the Fallopian tubes, tumors and cancerous masses occupying Douglas's cul-de-sac, that it would seem likely that they would be more frequently the victims of secondary cancerous deposit in the bowel or of erosion and extension of disease by contiguity or continuity. Epithelioma in other situations attacks men much more frequently than women. This form of disease usually occurs in middle life and in old age, but to this general rule there have been many exceptions; it has been seen in children. Allingham quotes its occurrence in a lad of seventeen, and Gowland in one of thirteen. It very rarely occurs as a secondary deposit of cancer in a remote region or organ. In the table of 4000 cases of rectal and anal disease, before referred to, cancer existed in 105. This disease is usually within easy reach of the finger, except when the growth is in the sigmoid flexure, being within an inch or two of the anus or from two and a half to three inches above it. The epithelial form, when it commences at the anus, is closely analogous to epithelioma of the lip: from the anal outlet it spreads upward into the bowel, or it may be primarily seated there. When occupying the junction of skin with mucous membrane it is sometimes sluggish, and a long time may elapse before it takes on aggressive action: induration, nodulation, obstinate fissure, or fungous growth marks its inception; as the condition proceeds, infiltration of surrounding structures takes place and large, hard, irregular masses form, which ulcerate, split, and form cauliflower excrescences. The rectum becomes blocked with fungoid growths: both these and the cancer proper are very vascular, and frequent hemorrhages occur, and an offensive muco-purulent discharge constantly oozes from the bowel.
Scirrhus of the rectum commences as an infiltration of the submucosa, which rapidly involves the other elements of the bowel, pushing hard nodules upward into the lumen of the intestinal tube: these break down and form ragged ulcers with indurated margins, and bleed profusely. Its situation is usually not higher than three inches above the anus. It has a tendency to invade all the neighboring organs and soft structures, to bind them to itself in a firm, dense mass, and to form communications with the vagina, bladder, uterus, perineum, and penis. Abscesses and fistulæ are common complications.
These neoplasms are insidious in their onset, and when seated at some little distance from the anus do not excite much pain at first. In the epithelial form the anus presents an abnormal appearance: it is inflamed and is covered with irritated, hypertrophied tags of integument bathed in [p. 904] a sanious, offensive fluid. Difficult defecation, of which the natural form is absent, with inordinate tenesmus, a sense of weight and fulness in the bowel, and an irritable condition of the bladder, are among the symptoms. The feces are passed in little, irregular lumps or broken fragments, or this state is accompanied by or alternates with small, liquid, offensive stools. As the diseased action proceeds, very severe local and general pain is endured: this is of a dull, lancinating character, and affects not only the diseased bowel, but involves the entire contents of the pelvis, shoots down the thighs, up the back, and into the penis: frequent and exhausting hemorrhages take place; the patient exhales a peculiar sickening odor; his complexion becomes cachectic; his strength fails; and death ensues, after a variable period of intense suffering, from a few months to two or three years after the first symptoms appeared. The modes of termination of life in these cases are—exhaustion, secondary deposition, septicæmia, peritonitis, and hemorrhage. Stricture of the bowel and very extensive ulceration attend all of these advanced cases of malignant rectal disease.
The encephaloid variety is prone to very sudden and rapid breaking down, and may destroy life within a few months. If the finger be passed into the bowel in a case of encephaloid degeneration, it will encounter a large soft tumor occluding the gut: this is a very different sensation from that imparted to the finger in a case of epithelioma or scirrhus. In the former there will be felt a crepitating, as though due to the giving way of a moist, friable substance; in the latter the touch will perceive dense, irregular nodulations and ragged ulcerations having very firm margins.
The rectum may also be involved and destroyed by any of these neoplasms in neighboring organs. A middle-aged woman who was admitted to the Pennsylvania Hospital in a very advanced stage of epithelioma of the cervix uteri died from hemorrhage from the rectum and uterus in eight minutes. At the autopsy it was found that the disease had almost separated the cervix from the body of the uterus, had involved the cul-de-sac of Douglas, and had eroded a large opening into the rectum. Numerous ends of large vessels were observed which had undergone erosion.
Carcinoma of distant organs does not seem to frequently involve the rectum by secondary deposition. "In 160 cases of gastric cancer examined at the Pathological Institution in Prague, Dittrich found secondary cancer of the rectum only twice."20
20 Leube, Ziemssen's Cyclopæd., vol. vii. p. 235.
In these cases of carcinomatous disease originating in the bowel the neighboring lymphatic glands are indurated and enlarged, and secondary deposition in neighboring and distant organs is the rule.
The lower portion of the intestinal tract may become involved in disease by direct extension from the colon, as in dysentery following enteritis or entero-colitis. Habersham says that diarrhoea arises generally from an irritated condition of the large intestine, catarrhal and mucous diarrhoea from slight inflammatory disease closely allied to ordinary coryza affecting the mucous membrane of the large intestine. "In the diarrhoea of soldiers the lesions of the large intestine have been either those of congestion with varying degree of extravasation or of ulceration more or less extensive. The colon in the former cases has invariably presented [p. 905]patches of intense congestion, and in numerous instances extravasation, the amount and intensity varying in different subjects, in a few the whole mucous surface of the intestine having a livid red color; in others tracts of more or less intense congestion at irregular intervals, as in the small intestines, would be noticed. The ileo-cæcal valve almost invariably presented intense congestion. The rectum has uniformly presented intense congestion, with more or less fibrinous exudation. Frequently the presence of fibrinous exudation was a question of doubt."21 The entero-colitis or ordinary summer complaint of infants not infrequently causes a very troublesome form of proctitis. Besides the ordinary causes of dysentery, Feyrer22 states that it is caused by irritation of the solar plexus of nerves, also by the inhalation of sewer emanations and by the ingestion of impure water.
21 Med. and Surg. History of the War of the Rebellion, vol. ii. p. 102.
22 Times and Gazette, 1881, p. 87.
"In dysentery the anus becomes bluish-red, and is even marked with cracks and rents; it is painful to the touch and tightly contracted. In the later stages of severe cases it becomes large and gaping; then the stools are generally discharged unconsciously, and the pain is slight, paralysis of the sphincter ani having occurred. These symptoms indicate generally that death is to be expected. In some of these cases the pathological lesions are limited to the rectum. Dysentery may succeed typhoid fever."23
23 Heubner, Ziemssen, vol. i. p. 552.
"Pigmentation is common after dysentery, and also after typhoid fever when dysentery has existed. Pigment-deposits are encountered in the large intestine in those who have suffered from repeated attacks of acute diarrhoea or from protracted flux. They may be seated as diffuse patches on the general surface of the mucous membrane or may be more especially localized in the closed glands. The diffuse form of these deposits is more frequently encountered in the large than in the small intestine, and is apt to be more intense in the former, producing darker and more extensive discoloration; hence the ash- and slate-colored, greenish, and blackish tracts which are so frequently observed in the cæcum, colon, and rectum."24 Follicular ulceration of the rectum sometimes follows chronic dysentery and typhoid fever. Woodward has observed that a catarrhal condition of the rectum commonly occurs in typhoid fever cases. Referring to typhoid fever lesions of the large intestine, Rokitansky25 says: "The ulcerative process is by no means confined to the small intestine; we have seen the mucous membrane of the large intestine riddled with ulcers. They were many of them of large size, and had clean-cut, non-thickened margins. This condition, indicating the absence of reparative action, is not nearly so frequent as that of thickening and induration, which generally took place to some extent in the edges of the ulcers. The bottoms of the ulcers are commonly formed by the submucous tissue. Sometimes the muscular fibres are completely exposed: this, however, is generally the result of secondary advance subsequent to the reception of the morbid action."
24 Med. and Surg. History of War of Rebellion, vol. ii. p. 308.
25 Jones and Sieveking, p. 590.
John Harley26 calls attention to the intestinal lesions of scarlatina as follows: "I know of no disease in which the morbid effects are more [p. 906] uniform. Scarlatina is essentially a disease of the lymphatic system. It is attended with inflammatory action of this system of glands, in which are included the agminated glands of the intestine. In 28 cases examined, 8 had the solitary glands of the large intestine enlarged and inflamed; in 1 there was acute desquamation of the mucous membrane of nearly the whole of the large intestine. In about half the cases the large intestine was found healthy."
26 Med.-Chir. Trans., vol. iv. p. 102.
The rectum and anus are frequently subject to attacks, by contiguity, from diseases in neighboring organs. The most frequent of these is doubtless that form of ischio-rectal abscess which invades the bowel, causing fistula in ano. Various neoplasms having their seat in the tissues or organs near the bowel may obstruct it by simple mechanical pressure, or may cause inflammation, infiltration, and ulcerative erosion. Mechanical encroachment by the pressure of a foreign body in the vagina may cause grave interference with the normal functions of the lower bowel. At the out-patient department of the Pennsylvania Hospital in 1880, Arthur V. Meigs, assisted by Wetherill, removed a large, hollow, glass ball-pessary from the upper end of the vagina of an aged woman, who declared the pessary had been so placed by a physician sixteen years before, and had remained ever since, despite her repeated efforts to remove it with an ordinary table-fork. Upon its extraction, which was accomplished with difficulty, a small portion of its surface was found covered with scratches. Its presence had caused constipation, impaction of feces, and atony of the rectum.
Interference with the rectal functions often follows tedious cases of labor where the child's head remains long in the perineum.
"In diseases of the spinal cord and its envelopes there is a great tendency to constipation, owing to impairment of the secretion of the intestinal juices. The intestinal movements are usually much affected, either in the way of increase or diminution, in the former of which the symptom is a frequent, watery, slimy diarrhoea; as a less common condition it is even capable of being produced reflexly. Thus in a patient with chronic myelitis I observed the regular evacuation of a mucous fluid mass from the intestine as often as his bed-sores were cleansed; and the like has been seen in dogs after division of the lumbar cord. Much more commonly there is habitual, even excessively obstinate, constipation, of which almost all chronic spinal patients complain. The stool is slowly discharged, dry and hard, and the evacuation occurs only at considerable intervals and after the application of energetic remedies. Several causes doubtless contribute to this: diminution of intestinal secretion and peristaltic contraction, and probably also weakness of the abdominal muscles of compression, which is often present. If there is an extreme degree of weakness, meteorism and accumulation of feces are other consequences. We do not know exactly from what portions of the cord these disturbances proceed."27
27 Erb, Ziemssen's Encyc., xiii. p. 138.
[p. 907] "There are also in many diseases of the cord disturbances of evacuation caused by paresis or paralysis of the sphincter ani. In mild cases simple difficulty in retaining stool for any length of time exists. There may be also great disturbance of sensibility, so that the patient does not feel the call, and even if he possess some voluntary control, he is surprised by the discharge, of which he feels nothing."28
28 Erb, loc. cit., p. 139.
The sphincter ani is affected in cases of myelitis, the usual symptoms being those of paralysis; the same is true in softening of the cord or myelo-malacia, and there is also diminished reflex excitability of the anus.
Paralysis of the bladder and rectum is often delayed in cases of slow compression of the cord; but if the compression exists to any considerable extent, involuntary discharges of urine and feces will be sure to occur. A pressure-myelitis of the lumbar portion of the cord causes paralysis of the bowel, and in the later stage of some cases of bulbar paralysis it also occurs.
Early in the course of spinal meningitis there exists a spasmodic condition of the sphincters: these muscles are also paralyzed in spinal and in meningeal hemorrhage, and from the pressure of tumors upon the cord giving rise to paraplegia. "In acute ascending paralysis the bladder and rectum are generally quite undisturbed in their functions. In hemiplegia and in hemi-paraplegia specialis disturbances in the evacuation of the bladder and bowels are almost always present, and in the acute traumatic cases it is especially common to find severe paralytic symptoms at the beginning of the attack (complete retention or complete incontinence, involuntary stools, etc.), which, however, generally soon recede and give place to lighter, more permanent trouble, as weakness of the sphincters. Sometimes these disturbances are very significant."29
29 Ibid., loc. cit., p. 740.
The following is an extract from Gower's Diagnosis and Diseases of the Spinal Cord:30 "The spinal cord possesses centres, situated in the lumbar enlargement, which preside over the action of the bladder and rectum. They are probably complex reflex centres: that for the sphincter ani is the more simple.... But if the volitional path in the cord is damaged above the lumbar centres, the will can no longer influence the reflex processes: as soon as the feces irritate the rectum they are expelled by the reflex mechanism.... If the damage to the cord involves also the sensory tract, the patient is unconscious of this process; if the sensory tract is unaffected, the patient is aware of the action of the bladder or bowel, but cannot control it. It is often said that there is permanent relaxation of the sphincters, but this is true only when the lumbar centres are inactive or destroyed. In this condition evacuation occurs as soon as feces or urine enter; the urine escapes continuously instead of being expelled at intervals.... We may, however, distinguish between the two states of the rectum by the introduction of the finger: if the lumbar centre is inactive, there is a momentary contraction due to local stimulation of the sphincter, and then permanent relaxation. If, however, the reflex centre and motor nerves from it are intact, the introduction of the finger is followed first by relaxation, and then by gentle, firm, tonic contraction."
30 London, 1880, p. 37.
[p. 908] Morton has at this time in his wards at the Pennsylvania Hospital two cases of rectal paresis following fracture of the vertebræ. The first, a lad aged nineteen years, while crossing the Atlantic was struck during a gale by a spar upon the back about the region of the lower dorsal vertebræ. From the deformity and from other symptoms there was undoubtedly a fracture destructive to the normal functions of the cord. Upon the arrival of the steamer, some ten days after the accident, the lad was brought to the hospital, where he has remained for the past eighteen months. Total palsy of sensation and motion has continued from the time of the accident to the present day, and extends from the navel downward: the sphincter ani is constantly but feebly contracted; the finger, when pressed into the anus, encounters slight resistance, which continues during and after the simple passage of the finger; very slight pressure, however, against the sphincter causes a very marked relaxation, which continues so long as this is kept up. With the removal of the finger the sphincter slowly and fairly contracts. The second case is also one of vertebral fracture which has been in the hospital about ten months. In this instance the sphincter is always found contracted, but it readily yields under finger pressure, and contracts quickly and regularly in the absence of this pressure. Constipation and rectal impaction readily occur, and the bowel requires to be regularly emptied. In another case, at the Episcopal Hospital, under the care of W. B. Hopkins, there is fracture of the spine, with total palsy below the seat of injury. The margins of the anus were found in apposition, but in no firm contraction: mere contact of the finger appeared to have little or no effect, but slight pressure upon the sphincter caused a contraction, and very moderate pressure upon the anus after the introduction of the finger produced excessive dilatation. The action of the sphincter was in all respects very tardy.
Two recent cases (August, 1883) of fracture of the dorsal vertebræ have been admitted into the Pennsylvania Hospital. One, a lad aged ten years, was struck by a bale of cotton which fell upon him; the other, a man aged thirty years, fell from a second-story window. In both cases total palsy occurred at once upon the receipt of injury, and in each the same conditions of the anus have obtained as before described.
In the convulsive attacks incident to epilepsy the sphincters of the bowel and urinary bladder are relaxed and the discharges are involuntary; probably, also, one of the first symptoms indicative of tumor of the base of the brain is recognized in involuntary rectal evacuations. Rectal incontinence may be also due to tabes, while atony and constipation are sometimes noticed as a result of excessive intellectual exertion (DaCosta). The same may be said of chronic lesions of the brain and spinal cord. Paresis of the rectum has been noticed as a result of chronic congestions of the heart and in hepatic disease. Allingham has observed failing nerve-power as a cause of rectal atony: the latter, with constipation, is one of the commonest troubles attendant upon melancholia and the chronic forms of insanity. Seeley of Ovid, New York, related to Morton a case of paraplegia with rectal paresis and dysenteric symptoms from malarial poisoning in a married lady aged thirty years. An examination revealed an immense rectal impaction. A free administration of quinia was followed by complete recovery in a few weeks.
Apart from those cases in which spasm is induced by the irritating stools of diarrhoea and dysentery, or by local ulcerations, fissures of the anus, and intestinal worms, there are those in which painful spasm occurs, due to the presence of a vesical calculus: it is also caused by urethral stricture, impaction of feces, irritations and inflammations involving the bladder or the adjacent organs. Spasm is also seen in nervous females, without constipation; also in the varied irritations of the female genito-urinary apparatus. In cases where spasm is due to rectal impaction retraction of the anus is frequently seen.
This most painful, distressing, and obstinate affection belongs to the class of neuroses, and is simply functional in character, without the least structural change in the skin or mucous membrane of the anus or rectum: the itching may be confined to the former or it may extend into the latter. It may be brought about by a constipated state of the bowels, but it is more often due to derangements of the digestive apparatus.
Sufferers from pruritus ani are generally dyspeptics, although the malady is observed in persons who are otherwise in most robust health. Overwork, mental and physical exhaustion, have been charged with producing pruritus, and in some instances spinal irritation seems to have been unquestionably the exciting cause: now and again, pruritus ani has been produced by the pregnant condition, and in some cases this malady has persisted during the entire period of utero-gestation. Intestinal worms, uterine maladies, rheumatism, and especially gout, have unquestionably been exciting causes. Some years since a gentleman having the most intense pruritus, which defied all treatment, was suddenly relieved of all former distressing symptoms by the passage of a small vesical calculus, the presence of which had never been suspected, as no vesical symptoms had at any time existed. Some of the most aggravated instances of anal pruritus are found in those far advanced in diabetes mellitus. The nerves of the lumbar plexus in rare instances have suffered from compression, more or less severe, from fecal accumulations; in one case of spinal curvature detailed by Portal31 the rectum at its upper part was so narrowed by the encroachment of the false ribs that excessive fecal accumulation occurred which gave rise to remote pain in the great toe.
31 Cours d'Anatomie médicale, tome iv. p. 276.
It seems to be unquestionable that there are instances of pure neuralgia of the rectum, for in such cases the most carefully conducted explorations have failed in demonstrating any evidences of disease. The pain is doubtless reflex, due to depressing causes, to atmospheric conditions, or to exposure to cold and wet. Neuralgia of the rectum has also been noticed in malarial [p. 910]poisoning, and especially in those who have long been victims of intermittent fever. Neuralgia in this region of the body is also due to general causes, as witnessed in cases of rheumatism and of the gouty diathesis. Patients now and again complain of "violent and painful pressure in the rectum, conjoined with active pains in the perineum and anus and in the sexual parts: these symptoms probably have a neuralgic character."32 In many nervous disorders, but especially in spinal irritations or inflammation, the rectum is invaded by pains of a neuralgic nature more or less severe, which are undoubtedly only functional in character. But 12 cases of neuralgia were observed out of 4000 cases of rectal disease. Anstie33 says: "It needs some very powerful irritant to set up neuralgia in any portion of the alimentary canal: ... this condition has been described by Ashton.... In one case the patient complained of acute, paroxysmal, cutting pain extending about an inch within the rectum.... The cause of this attack was his getting chilled from sitting in his wet clothes." Curling says that constantly directing the mind to this part of the body will excite congestion and disease, possibly by producing abnormal sensations, itching, and superficial inflammation.
32 Erb, Ziemssen's Cyclop., vol. xiii. p. 139.
33 Neuralgia and its Counterfeits, p. 130.
"In patients with piles hyperæmia of the spinal cord may become habitual, returning regularly and frequently, and this may lead by degrees to severer disturbance by the development of chronic inflammation and proliferation."34 Among some of the reflex troubles arising from rectal disease are—sterility in women, simulation of uterine disease, pruritus ani, pseudo-sciatica, pains in the legs and feet, and impairment of co-ordination in the muscles of defecation. There is a case reported35 of a curious pain in the sole of a foot caused by rectal disease; and another36 in which irritation of the eyes was caused by hemorrhoids.
34 Ziemssen's Cyclop., vol. xiii. p. 138.
35 Med. Times and Gazette, 1868, vol. ii. p. 175.
36 Cooper, Lancet, 1862, i. p. 625.
There are some cases occasionally met with of so-called irritable rectum. Now, a rectum may be irritable because irritated, but in some of these instances there is no apparent cause. There occur frequent, small stools expelled with force, but without pain: there must be abnormal peristaltic action to cause this condition.
After death from cholera there is found congestion and a swollen state of the mucous membrane of the rectum: in some cases the epithelium of the entire alimentary canal is almost absent. In slow poisoning by arsenic the bowels show ulceration, but more particularly the rectum. After phosphorus-poisoning the large intestine has been found inflamed and contracted to the calibre of a quill. Among the effects of copper have been seen ulceration and a peculiar green staining of the rectum; of lead, no marked change of the mucous membrane except, in some instances, hardening, but the muscularis was in an advanced state of hardening and contraction. The action of croton oil is to render the mucosa very soft and friable. Extensive destruction of the mucous membrane of the rectum has resulted [p. 911] from poisoning by bichromate of potassium. The mineral acids and the caustic alkalies, when not immediately fatal, cause corrosive ulceration of the rectum; the soluble salts of zinc, tin, bismuth, and antimony produce a like effect. Corrosive sublimate in its action upon the large intestine produces a dysenteric condition; similar in their effects are colocynth, jalap, elaterium, and cantharides. Strychnia causes a deep violet congestion; alcohol, congestion and thickening; and tobacco, redness of the mucous membrane with great engorgement of the vessels of the rectum. One of the results of the long-continued abuse of morphia is a catarrhal condition of the large intestine, accompanied with exfoliation of the intestinal epithelium. Some persons are very susceptible to the action of jaborandi, and in such its exhibition is followed by hyperæsthesia and dull pain in the rectum and the urethra.
It is interesting to note that an abnormal condition in the rectum may cause extensive disease in a remote organ; thus, a stricture of the rectum may cause abscess in the liver. Wilkes37 exhibited at the Pathological Society a specimen in which an abscess, a diffuse, purulent infiltration of the liver, and a gall-bladder filled with purulent bile were distinctly traceable to the suppuration arising from an ulcerating stricture of the rectum consisting of dense fibrous tissue situated about four inches from the anus of a man aged thirty-seven years. "Any form of suppurative intestinal disease seems capable of producing hepatic abscesses of a metastatic or pyæmic character."38 It has not been found, however, that tubercular ulceration of the intestines has ever given rise to hepatic abscess.
37 Soc. Trans., vol. ii.
38 Darley, On the Liver, 1883, p. 536.
Examinations and explorations of the abdominal viscera by the hand introduced into the rectum, having for their object the detection of tumors or morbid growths, are procedures which have fallen into merited disrepute, and are mentioned here in condemnation. However, some years since, Morton, in consultation with (J. Forsythe) Meigs, satisfactorily demonstrated the absence of a suspected renal calculus by this method.
The distension of the rectum with water, either free or contained in a rubber bag, in order to facilitate operations upon the pelvic viscera, has been lately brought into notice by Garson at a meeting of the British Medical Association. The most significant point brought out at the meeting was that the water-distended rectum displaced the distended urinary bladder upward and forward until it occupied a position quite outside of the pelvic cavity, carrying along with it the peritoneum both in front and behind. By this method of distension it was found possible so to raise the peritoneum in front of the bladder as to leave a clear working space of four centimeters between the upper border of the symphysis pubis and the edge of the peritoneum: this may prove useful in suprapubic lithotomy, as well as in operations upon the uterus and its appendages during laparotomy.
FISSURE OF THE ANUS, in its true sense, is not to be confounded with ulcerations either slight and superficial in extent, or with more grave ulcerations involving not only the anus, but the mucous membrane of the [p. 912] rectum also. The true fissure is a mere linear crack or abrasion or superficial ulceration. The pain accompanying this condition is out of proportion to the length and depth of the fissure, varying from slight uneasiness to as severe suffering as that caused by a deep and extensive ulceration.
The treatment to be adopted in such cases is first to regulate the bowels and to insist upon a scrupulous cleansing of the part after each evacuation. Much sitting is to be avoided and a sedentary mode of life is to be discouraged. Sometimes a few light topical applications of the solid nitrate of silver will bring about a cure, or a lotion of the same of the strength of from two to ten grains to the ounce of water should be applied with a camel's-hair brush every other morning. The ointment of the oxide of zinc, combined with any of the local anæsthetics, will be found useful. As a dernier ressort in obstinate cases an incision should be made through the fissure, together with a thorough dilatation of the anal sphincter.
ULCER OF THE RECTUM, OR THE GRAVER FORM OF FISSURE OF THE ANUS.—In the milder forms of this very common and painful affection the treatment consists in thorough cleanliness of the part; the ulcerated surface may be cauterized with nitrate of silver, and subsequently the application of the red precipitate ointment or the lotio nigra. Should a vaginal discharge exist, treatment should be instituted with a view to its arrest, as the irritating fluid coming in contact with the ulcer would prevent its healing. The treatment of that variety of ulceration where the disease is situated partly without the anus and partly within the rectum, besides the use of the means enumerated above, embraces the daily introduction of a full-sized bougie made of wax or of yellow soap. Henry Hartshorne says: "Experience leads me to have especial confidence in collodion, to which one-fiftieth of glycerin has been added to lessen its constricting effect." Glycerite of tannin and tinct. benzoin. comp. have been useful. J. C. Peters39 recommends the use of iodoform suppositories. Tarnier40 dusts the part with the same drug in fine powder. Créquy41 has had success with a dressing of charpie saturated in a solution of hydrate of chloral. For the more extensive and obstinate forms of ulceration the three methods of treatment mainly relied on are—by cauterization, by dilatation, and by incision. The caustics usually relied upon are the fuming nitric acid and the acid nitrate of mercury, one application of either of these often exciting healthy granulation. This application is to be followed by the use of an ointment consisting of thirty grains of calomel and three grains of morphia to one ounce of lard. If there is much spasm of the sphincters, extract of belladonna may be added.42 During this treatment the bowels should be kept rather loose by the use of compound licorice powder, and if much pain is experienced an opium suppository should be used. Dilatation, first practised by Récamier, consists of the introduction of the thumbs of the operator into the rectum, placing them back to back, and then forcibly separating them from each other until the sides of the bowel can be stretched out as far as the tuberosities of the ischia. On account of the fact that both cauterization and dilatation are not infrequently followed by relapse, the method of operation which includes both incision and dilatation can usually be relied [p. 913] upon. The bowels should be thoroughly emptied by a laxative, and an enema should be given three hours before the operation.
39 Philada. Med. Times, Nov. 8, 1879.
40 Bull. gén. de Thérap., Sept. 30, 1875.
41 Ashton, On the Rectum, p. 157.
42 Agnew's Surgery, vol. i. p. 418.
After full anæsthesia the ulcer may be readily exposed. The left index finger of the operator is then carried into the rectum, and a sharp-pointed curved bistoury is entered, three-quarters of an inch or more from the side of the anus, to the depth of an inch or less, and carried on toward the bowel until the point is felt by the finger within, when it is made to puncture the mucous membrane, and then to cut out to the surface. In some cases of deep fissure, before dividing the sphincter the ulcer may be scraped freely or the entire ulcer may be removed. The anus should now be well dilated with the fingers, after which an opium suppository should be introduced and a fragment of lint or linen well oiled be placed in the wound. The subsequent treatment consists in keeping the patient in a recumbent position and confining the bowels with opium. After three or four days a laxative may be given. No dressing is necessary save attention to cleanliness.
The subcutaneous division of the sphincter has been proposed, but is objected to on account of the liability of the extravasated blood retained in the very loose cellular tissue of the part to form abscess. In one case which Morton operated upon in this manner many years ago a large abscess formed very rapidly, with serious constitutional symptoms, which were relieved only after the freest opening and division of the sphincter.
Should any polypi be found, their removal by ligation or by the knife is an essential element of success in the operation; retention of urine is not infrequent after operations upon fissure. When fissure or ulceration makes its appearance in a syphilitic subject, it will usually disappear under appropriate constitutional treatment.
TUBERCULOUS ULCER OF THE ANUS is best treated by the topical use of a weak solution of chloral hydrate.
CHRONIC ULCER OF THE RECTUM.—In this condition the treatment should include the use of anodyne and astringent lotions, suppositories or enemata, and the internal administration of Ward's paste—i.e. confection of black pepper.
RODENT ULCER OF RECTUM.—In this rather rare, exceeding painful, and generally incurable malady the patient sometimes dies merely from the exhaustion of pain. Another mode of death is by diarrhoea; another by hemorrhage. To quote Allingham:43 "I have really nothing to offer as regards treatment; all the various sedatives will be required in their turn, and in the earlier stage I should recommend excision—not that I have much hope that you will eradicate the malady, but you will remove the pain, and for some time the sufferer will be comparatively comfortable. I think also the application of fuming nitric acid should be tried with the same object; one of my patients was fairly easy for three months after I had destroyed the ulcer with the acid." Morton accomplished the permanent healing of an undoubted rodent ulcer of the rectum by the complete divulsion of all the involved tissues.
43 Page 30.
CANCER OF THE RECTUM.—The medical treatment of this affection is necessarily restricted to efforts to alleviate suffering and to obtain sleep—anodynes in the form of suppositories of pil. saponis comp. or of morphine mixed with ext. hyoscyamus in the proportion of a half grain of the [p. 914] salt to ten grains of the extract. Enemata of warm water are useful. D'Arpene of Elba has suggested enemata of gastric juice. The profuse discharge of sanious pus must be met by weak injection of sulphate of copper and opium or a very dilute solution of chloride of zinc. Now, as to the use of bougies in these cases, it may be laid down as a general rule that their employment may be mischievous, yet in certain cases justifiable—indeed, absolutely necessary. When the disease is met with in its early stage, has not ulcerated, is within reach of the finger, and is producing much contraction of the calibre of the gut, a gum-elastic bougie, thoroughly lubricated, may be introduced through the contraction. In case this produces much suffering, the attempt must be abandoned; if not, once or twice a week is often enough. Where no extensive ulceration exists the patient can be much helped by this procedure. F. N. Otis44 has reported a case of malignant stricture in which he completely divided the recto-vaginal septum, sphincter ani, and perineum with great temporary relief to his patient. When large portions of a malignant mass protrude from the anus, they may be removed by the application of a paste of arsenite of copper or by the elastic ligature, the destruction being safe and rapid. The injection of acetic acid into these growths has been practised, but is useless and harmful.
44 Arch. Clin. Surg., 1877.
As to operative procedure, when the morbid growth is an epithelioma situated within a short distance of the anal opening an excision is not only justifiable, but may be recommended. The results show that its removal from this situation is as frequently successful as is its removal from the lip. When a cancer completely fills the lumen of the gut and plugs it so that the act of defecation becomes impossible, excision of the rectum and the establishment of an artificial anus are the two operative procedures open to the choice of the surgeon. A decided reaction of opinion has lately taken place among members of the profession relative to the latter of these; the few surgeons who did practise excision of the rectum in cases of cancer were looked upon as being rather unscientific and unsurgical. Billroth has excised the rectum 16 times, with 4 fatal cases; Dieffenbach performed it 30 times; Lisfranc had recourse to this operation as early as 1826; while the operation has been performed very frequently in this country, and with success.
Morton says: "In the spring of 1882, I was consulted in the case of a lady aged fifty-six who had suffered for two years from what were supposed to be internal hemorrhoids. An examination revealed the existence of a large scirrhous mass encircling about two-thirds of the gut, on the anterior part especially, and extending upward three inches. The patient was worn down by long suffering, but was otherwise in fair condition of health. With the assistance of Gross and Agnew, I excised the mass, which included the entire lower part of the rectum. The wound healed kindly, without an untoward symptom, and the patient was very soon enabled to leave her home for the seaside, where she passed the summer. The disease, however, resumed, but without any of the severe pains which she had had prior to the operation. Death occurred from gradual exhaustion seven months afterward."
He also relates the following case of excision of the rectum: The patient, a female aged thirty-five years, first noticed some rectal [p. 915] irritation about four years ago. This was followed by distressing pain during defecation and by hemorrhages; finally a tumor, which was described by her medical attendant as being like an opened umbrella, protruded, partly at first, then fully, through the anus. The growth seemed to be spongy in character, and was very vascular. It was removed by carrying a double-threaded needle through the mass, and thus ligating it. Upon the seventh day after the operation a hemorrhage occurred, which was controlled by plugging the rectum. Although the growth was removed, the patient did not make a good recovery; symptoms of rectal irritation continued. In September, 1884, the patient presented herself in a wretched condition, with bearing-down pains and frequent hemorrhages. Upon digital examination an elevated mass was readily detected upon the sacral aspect of the bowel. By carrying the fingers beyond this mass and making traction, it was brought down within working distance, and was excised along with the entire lower portion of the rectum. The freshly-cut edges of the gut were then drawn down and stitched to the mucous membrane just above the anus. The patient made a good recovery and has a serviceable anus.
R. J. Levis45 has operated upon two cases of cancerous growth in the rectum, removing the lower part of the bowel. The first case was that of a man aged sixty, who made a very good recovery from the successful operation, although three inches of the gut were removed. The second case was that of a man aged fifty-two, who had a carcinomatous tumor the size of a hen's egg at the right side of the rectum. The section of gut excised was about one and a half inches in length. The patient died of peritonitis upon the fourth day after operation. At the autopsy there was no wound found in the peritoneum, the lowest point of which was one inch above the end of the excised bowel.
45 Surgery in the Pennsylvania Hospital, pp. 81-83.
The etherized patient, his bladder having been emptied, should be placed in the lithotomy position. If a male, a sound should be passed into the bladder. An incision is then carried from the centre of the perineum along the raphé to the anterior margin of the anus, encircling the latter by two semicircular cuts and continuing the division directly back to the coccyx. In the female the incision should begin just posterior to the vagina. If the anus is not included in the diseased mass, the external sphincter may be spared by raising the skin and the muscle together and turning them on each side. When the lower end of the rectum is reached the dissection should be made entirely by the fingers or by the handle of the knife, tying vessels as they spring. Double ligatures should be introduced through the gut from its mucous surface outward, and, when possible, then stitched to the skin at the margins of the wound. The bowels should be controlled by opium for the following eight or ten days.
The other operative procedure is lumbar colotomy. This was first advocated by Amussat in 1839, when he appeared in a treatise upon the subject entitled On the Possibility of Establishing an Artificial Anus in the Lumbar Region. It is denied that he ever performed this operation. It has happened to sound surgeons and skilful operators, when the patient has been very muscular or very fat or when the colon has been collapsed, that they have been at length compelled to abandon the search for the gut [p. 916] and to stitch up the external wound. Allingham states that the cause of failure often is that the colon is searched for too far from the spine, resulting, in the opening of the peritoneum, in the starting up into the wound of a mass of small intestine which baffles the operator very seriously. He, having made more than fifty dissections, has come to this conclusion: "that the descending colon is always normally situated half an inch posterior to the centre of the crest of the ileum (the centre being the point midway between the anterior, superior, and posterior-superior spinous processes)." An incision four inches in length should be made midway between the last rib and the crest of the ileum. The incision may be made transverse, or, better, obliquely downward and forward, as suggested by Bryant. Allingham says that care should be taken to preserve the original length of the incision down through all structures, lest when the operator approaches the gut he finds himself working in the apex of a triangle the base of which is the line of the wound. If the surgeon has reason to expect the gut to be collapsed, an attempt should be made to distend it with some fluid. The intestine should be drawn well out through the wound, and a longitudinal opening an inch in length made in it. The edges of this are to be stitched to the edges of the skin. Fecal matter is much less likely to flow into the wound if the sutures are passed through the intestine previous to opening it. A weak carbolated wash is all that is required as a dressing. In one case of stricture of the rectum from a scirrhous mass, in which Morton performed colotomy, an immense cyst of the kidney, which was somewhat puzzling for a moment, protruded in the wound. After emptying the cyst the gut was readily discovered and opened.
DILATATION AND INFLAMMATION OF THE RECTAL POUCHES.—This is a comparatively rare condition of the rectum, called by Physick encysted rectum, which is treated by bending the end of a probe into a hook, passing it up into the bowel, and then withdrawing it with its extremity resting against the surface, so as to engage and draw down the pouches, the straining or bearing down of the patient assisting in their extrusion; they may then be incised or cut off with a pair of curved scissors.
LOSS OF CO-ORDINATION IN THE MUSCLES OF DEFECATION.—In those cases where it can be ascertained that this curious trouble is not symptomatic, sympathetic, nor reflex, the treatment must be directed to the building up of the general health, such as electricity, baths, asafoetida, and iron. Regular outdoor exercise should be enforced.
SPHINCTERISMUS.—This condition, though frequently attendant upon, may exist in the absence of, any fissure, crack, or ulcer of the anus. It is usually associated with constipation. In its treatment magnesia and rhubarb are to be used, and the diet must be simple, unstimulating, and taken at regular intervals. A hot hip-bath at night, with the use of a belladonna suppository, often proves effective. In more obstinate cases a bougie covered with ointment of belladonna should be used daily. In still more intractable cases the muscle must be forcibly stretched with the fingers. In the more obstinate cases which now and then occur it becomes necessary to completely divide the fibres of the sphincter muscle, followed by a thorough stretching of the parts.
[p. 917] PRURITUS ANI.—This distressing and vexatious complaint proceeds frequently from hemorrhoids. When caused by the presence of seat-worms, they must be dislodged by purgatives and enemata of quassia or of one composed of one part of carbolic acid to six parts of sweet oil, or of turpentine and flaxseed tea. An enema of milk of asafoetida answers a good purpose. If the pruritus is a result of the burrowing of the itch insect, any wash, ointment, or dressing that evolves sulphuretted hydrogen will rapidly bring relief. If caused by other parasites, an application of ung. hydrarg. or red precipitate ointment, followed by a warm bath, will be all that is necessary. In some it is a symptom of dyspepsia, in others of a disordered state of the nerves of the anus independent of local cause: in this case iron, quinia, and arsenic should be given, and the patient should live an outdoor life as much as possible. The remedies that have in turn been extolled and abandoned during the treatment of this distressing condition it would require too much space to even mention. The following are among the best: Sulphate of zinc and alum, equal parts, are to be placed in an earthen vessel and heated until a glassy mass is left, which is to be dissolved in a little water and thrown into the bowel; palm soap pressed into the anus, ointments of carbolic acid and morphia or of bromide of potassium and cosmoline, citrine and other mercurial ointments, and suppositories containing iodoform. Allingham uses a bone or a metallic plug of peculiar construction, so as to keep the anus upon the stretch at night without slipping into the bowel. The pressure which this exerts upon the nerves and vessels prevents the itching. Hot (not warm) water pressed against the anus with a sponge, or ten-drop doses internally of tincture of gelsemium, or washes of dilute hydrocyanic acid or of chloroform, or ointments of balsam of Peru or of veratria and aconitia, or the corrosive chloride of mercury in solution applied locally, are a few of the more reliable among this host.
STRICTURE OF THE RECTUM (NON-MALIGNANT).—The main modes of treatment of non-malignant stricture of the rectum are two—by dilatation or by linear incision (rectotomy). Dilatation may be practised by the finger alone or by the finger covered with hollow rubber covers of various sizes. These are open at the end, so that the guiding and recognizing sense of touch may be left to the end of the finger. When the stricture is out of reach of this method, either gum or metallic bougies must be used, beginning with the smaller sizes and deliberately and carefully adding sizes. When the lumen of a stricture is tortuous it is best to use a long rather flexible rubber bougie having an olive-shaped extremity. It is not necessary to leave these bougies standing for hours in a stricture, according to the practice of some; this merely excites inflammation. Should the stricture be irritable, every second or third day would be sufficiently often to attempt dilatation. In constrictions which are firm, but not sensitive, a good plan is to insert a Molesworth elastic tube and gradually distend it by hydrostatic pressure; Barnes's dilators have also been successfully used. When the stricture is elastic and re-forms itself at once after dilatation, incision should be practised. In those strictures which are low down, the constriction may be nicked in several places by a hernia knife, the blade of which is guided along a finger in the bowel; when high up, a long double-bladed knife must be employed. In syphilitic strictures, in addition to dilatation, proper alterative treatment is [p. 918] indispensable. As dilatation has often to be kept up for a long time, the patient may be taught to practise this for himself.
PERI-ANAL AND PERI-RECTAL ABSCESS.—When acute, and when the surgeon is called in time, the prompt application of leeches may abort the abscess, but usually, by the time the surgeon sees it, it is necessary to apply hot flaxseed poultices as fast as they become cool, keeping the patient in bed upon light diet. The rule is to open deeply and freely so soon as the least softening under the poultices indicates that pus is within reach. After lancing, the poultices should be continued for a few days: then the deep wound should be packed with a strip of oiled lint and allowed to granulate from the bottom. As the fetor of these abscesses is horrible, they should be injected with a solution of permanganate of potash or liq. sodii chlorinata. When the chronic variety of this abscess is discovered, it, with all its sinuses, diverticula, and pockets, should be laid freely open upon a director and packed with carbolized lint. It is often very necessary in these chronic cases to use tonic and alterative treatment, such as cod-liver oil and iodide of iron.
GONORRHOEA OF THE RECTUM.—Undoubted cases of gonorrhoea of the rectum in the persons of prostitutes have been observed. Burning heat and great pain are usually felt, with a free discharge of pure pus: the mucous membrane is always intensely inflamed. The treatment is simple; an injection of lead-water and laudanum or of sulphate of zinc answers a good purpose. Primary syphilitic disease of the anus and rectum is rarely seen, but of course the treatment indicated would be similar to that laid down for primary syphilis in its usual localities.
IMPACTION OF FECES.—This condition usually occurs among the aged and in women after parturition and in cases of paralysis. Those persons of sedentary habits who do not pay sufficient attention to the necessity of a daily alvine evacuation sometimes find themselves in this condition. Impaction occurs not infrequently among the insane, and more frequently among women than men. Allingham states that he has never seen a case of impaction in a young person; but Wetherill now has under his care a most obstinate case of this disorder in a young man whose system has been completely broken down by intemperance in drink.
In paralysis of the rectum of traumatic origin impaction is almost certain to take place unless great care is taken to prevent it. Diarrhoea is a very misleading element in these cases, and is a symptom which frequently deceives those who are not on their guard. The clayey mass of feculent matter forms a hard ball in the distended bowel, around which the small loose passages flow. Spasm of the sphincter ani is the usual accompaniment of impaction, and the muscle should be gently but thoroughly dilated before means can be used to free the canal. The finger or the handle of a tablespoon is best to use in the dislodgment of these masses, and should be oiled before introduction, the accumulation broken up, and then washed out by an enema of soap, turpentine, and warm water. Purgatives and hydragogue cathartics usually fail to give relief, and add much to the patient's discomfort. The bowel once freed, care must be taken to prevent a reaccumulation, which very readily takes place, as the bowel in these cases is distended and has lost tone. To this end frequent enemata of cold water should be used, and the patient should [p. 919]take a pill of dried sulphate of iron, sulphate of quinia, extract of nux vomica, extract of aloes, as recommended by Allingham. The diet should be restricted. An excellent adjunct to this treatment is the local use of the faradic galvanic current daily after breakfast. Let the patient lie upon a bed and apply one pole or electrode to the anus, while the other one is passed with pressure along the course of the large intestine. Not infrequently it happens after this has been continued for a few minutes that a very urgent desire is felt to go to stool. In the case mentioned of the young man affected with impaction this treatment answered admirably well, but before its use he had to take a small dose of croton oil daily to cause an action of the bowels, all milder measures having proved ineffectual. It is important in these cases to interdict a sedentary mode of life.
IRRITABLE RECTUM.—A rectum is said to be irritable when it shows an intolerance of the presence of feces or flatus, causing frequent desire to go to stool. From such abnormal activity of the part there arise a burning, uncomfortable impression of fulness and a soreness of the anus. If after examination it is found that there is no local exciting cause, a starch enema containing forty drops of laudanum should be given and retained. This plan of treatment will usually afford relief. Should the irritability prove to be obstinate, examine the rectum, and if a spot of redness or increased vascularity be found, touch the spot with strong nitric acid.
CONCRETIONS IN THE RECTUM.—These occur less frequently than do impactions, and differ from them in being cylindrical and nucleated, the nuclei being such bodies as balls or tangled masses of hair, or coins, buttons, biliary calculi, or the like. Covering these are matted animal or vegetable fibres or hardened fecal matter. They are not so readily dislodged as are impactions, and it is necessary to dilate the sphincter thoroughly and remove them with a scoop. Not infrequently these bodies are bathed in pus and are very fetid.
PROCTITIS, OR INFLAMMATION OF THE RECTUM.—This may be either acute or chronic, the latter being a disease of the aged. Allingham recommends in this variety small doses of Barbadoes aloes to stimulate the bowel, also such drugs as copaiba, turpentine, and black pepper. As an injection in the acute form starch and laudanum, or bismuth suspended in a mucilaginous vehicle, should be used. Probably the use of small, smooth fragments of ice in the rectum would allay the tenesmus and help to subdue the inflammation.
PROLAPSUS ANI AND PROCIDENTIA.—Prolapsus occurs much more frequently in children than in adults, making its appearance at every movement of the bowels. The child thus affected should not be allowed to sit upon the chamber-vessel and strain, but should lie upon the side or stand, while the nurse should be instructed to draw to one side one of the buttocks so as to tighten the anal orifice. After the motion the protruded part should be well washed in cold water, and afterward with some astringent solution of oak-bark, matico, or a weak solution of carbolic acid applied with a soft sponge. The bowel should then be gently returned and the child be allowed to lie at rest for a while. If there exists intestinal irritation, small doses of mercury with chalk, with rhubarb at night, with wine of iron three times daily, would be indicated. [p. 920] The application of an anal pad and a T-bandage will give sufficient support. If this treatment be carried out a cure usually results in a few weeks. Some cases do not yield to this mode, and then the surgeon has to make trial of ergotin given hypodermically, each injection representing a grain of ergot, which is to be thrown into the submucous tissue of the rectum every second day for two weeks. Should relief not follow its use, cauterization is to be tried. The cauterants usually applied are nitrate of silver, acid nitrate of mercury, and nitric acid. Of these, nitric acid is the best. After anæsthesia is complete every portion of the extrusion should be touched with the acid, care being taken not to bring it into contact with the skin; afterward the bowel is to be freely oiled and returned. To prevent its extrusion the bowel should be filled with soft cotton wool, a compress placed over the anus, and the buttocks strapped tightly together with adhesive plaster. For a general quieting effect the child should be given paregoric. About the fourth day the adhesive plaster may be removed and a dose of castor oil administered, which will bring away the cotton plug with the dejection.
Prolapsus and procidentia in the adult are much less manageable; indeed, these conditions are usually very obstinate. There may exist causes extraneous to the bowel, such as urethral stricture or enlarged prostate or an impacted renal calculus or a calculus of the prostate. The bowel should be searched for polypi or hemorrhoids, and the prolapse may be cured by the removal of the irritating cause. Failing to find any such cause, the surgeon has at his command either cauterization or a removal of redundancy. The former may be by nitrate of silver or acid nitrate of mercury or the actual cautery. It is well not to apply these strong acids to the aged or those who are broken down in health, as very destructive sloughing has followed their use in these cases. When these are used, the same plan as that mentioned in case of prolapse in children should be pursued. Strong carbolic acid may be used in these cases with much less risk of sloughing than when the acid is employed, and it may be applied oftener—indeed, daily if desirable. Van Buren has recommended linear cauterization with the hot iron to the mucous membrane, the bowel contracting as a result of cicatrization. In adults generally, and especially in the aged, all the forms of cauterization are less satisfactory as a means of relief than either of the various modifications of Copeland's operation, which consists in removing by ligation elliptical portions of the mucous and submucous tissues of the prolapsed bowel. The most satisfactory of these is either to excise two or three oval portions of the mucous membrane with flat-curved scissors and bring the edges together with interrupted suture, or to pinch up in several places the redundancy in a Smith's clamp and cut off the folds in advance of the instrument, applying to the stumps the hot iron. Allingham prefers ligatures of horsehair in these operations, and mentions the carbolized catgut in preference to silk. He cautions the operator not to carry his knife into the submucous tissue, as free hemorrhage would inevitably occur.
In old cases of prolapsus or of procidentia that are not amenable to operative treatment much can be done to render them comfortable: the air-dilated gum pessary will sometimes afford relief, or a pad and T-bandage will prevent the parts becoming ulcerated by friction. Neither gallic [p. 921] nor tannic acid answers the purpose so well as acorn flour. The frequent use of cold water to the part is always attended with comfort, and sometimes with relief. In these old cases of great relaxation Nélaton has used strychnia by the mouth, and Weber (of New York) hypodermically, with fair result. Vidal has cured three cases by the repeated use of ergotin locally, hypodermically. In order to bring about a radical cure in these very chronic cases, very decided means sometimes are justifiable. The late Mr. Hey of Leeds was the first to propose a plan by which, through cicatricial contraction and inflammatory gluing together of the various tissues composing the bowel, the anus and sphincter muscle might be strengthened and improved in tone; to which end he proposed to cut away the pendulous flaps of skin around the anus. In cases where these flaps are very redundant a cure is sometimes effected by this procedure alone. Other cases will be benefited by the operation proposed by Dupuytren, which consists in the removal of radiating folds of the skin and mucous membrane at the edge of the anus. To quote from Holmes's System of Surgery: "This operation is effected by laying hold of the fold of skin on each side of the anus with forceps, then with a sharp curved pair of scissors removing both skin and mucous membrane. In very severe cases four or six applications of the scissors may be necessary."
POLYPUS OF THE RECTUM.—The polypi of the rectum are the gelatinoid and the fibroid, but as a very rare occurrence a villous or warty polypus has been found. Polypoid growths are very different bodies, but they are too frequently confounded with true polypi. The only treatment is their removal, and the safest method is by ligation of the pedicle, and either cutting off the growth in advance of the knot or returning it into the bowel. The patient should remain quiet until the sloughing is complete, and his bowels must be confined, otherwise profuse and very troublesome hemorrhage might ensue. Their removal by the clamp and cautery is equally safe. Their removal by torsion or by the scissors is unsafe.
The peculiar villous polypus causes great and exhausting hemorrhage. A case was successfully treated by the application of fuming nitric acid.
FISTULA IN ANO.—In the palliative treatment of this very common malady no great amount of relief can be afforded. Those who are aged and feeble or those who are much broken down will find comfort to attend the free local use of warm water, and the sinuses should be injected with dilute solutions of one of the mineral astringents, the strength of these not exceeding two grains to the fluidounce of water. Cosmoline, simple cerate, ointment of the oxide of zinc, and even fresh lard, make the patient easier, as they prevent friction of the buttocks. One of the forms of the radical treatment consists in the division of all the structures between the fistulous tract and the surface. This may be accomplished either by the use of the knife or by seton. Stimulating injections or cauterization has been known occasionally to permanently close fistulæ in ano; but such plans of treatment are unreliable, and usually unjustifiable. When the fistula is not so high up in the bowel as to render the use of the knife unsafe, this plan of treatment should be adopted. As an invariable preliminary to all operations upon the rectum the bowels should be thoroughly emptied and the patient should be placed under the influence of [p. 922] an anæsthetic. A flexible grooved director should then be carried through the opening of the tract upon the surface and along the tract to its opening in the bowel, should such exist. The forefinger within the rectum will meet the point of the director as it emerges from the internal opening, and the director should be pushed onward and its extremity guided outward until it rests fairly upon the sound integument outside, and all the included structures should be divided along the groove of the director with a sharp-pointed curved bistoury. Should the fore finger in the rectum not discover an internal opening, one should be forced at the very bottom of the tract by rotating the point of the director while making counter-pressure with the end of the finger. Should several fistulæ be found, they should be treated in like manner. Sometimes it will be found that the incision is overlapped by the dusky-red flaps composing its margins, in which case they should be trimmed off with scissors. When the tract extends deeper than its internal opening, the latter should be ignored and the sinus laid open to its very bottom. When no external opening exists, one should be made, and the guide for this incision will be a point of induration felt by the finger at some point not far from the surface. The director entering at this point will find the tract, and should be pushed forward as described above. These opened sinuses should be packed with lint soaked in carbolized oil and confined by a pad and a T-bandage. It is the practice at the Pennsylvania Hospital to apply after division a stick of caustic potassa, allowing it to remain in contact with the cut surfaces for several seconds, after which the wounds are to be packed. This procedure ensures their healing from the bottom. The bowels should be confined for a few days, after which a dose of oil may be given. Besides attention to cleanliness and a daily renewing of the packing no further treatment will be demanded. The hemorrhage attending these operations is usually trifling. Should a vessel spring, a ligature may be thrown around it. When an abundant general oozing occurs, the rectum must be packed and a compress and bandage firmly applied. Should the surgeon prefer the seton operation, he should carry several threads of stout silk or a piece of rubber cord on an eyed probe into the fistula and out of its internal opening, and by tying their ends firmly down upon the enclosed tissues slowly effect the same result as in the cutting operation. When the seton used is silk, the ends should be carried through holes in a round leaden plate or through those of an ordinary button, and tied. These setons are to be drawn tighter every three or four days until the division of the enclosed tissues is complete. The subsequent treatment is the same as in the other operation.
A difference of opinion exists among surgeons as to the propriety of operating for fistula in ano in persons afflicted with tubercular disease of the lungs. The practice of the present day is decidedly in favor of operating, without reference to the condition of the lungs, provided the patient is not too much reduced in strength.
An operation for fistula in ano has been proposed and practised by Reeves, which is a compromise between cutting and ligation. He says: "It consisted in passing a strong and well-waxed silk ligature along the track of the fistula into the bowel. An ordinary surgical probe with an eye in its end carried this thread into the rectum. My bivalve expanding speculum was previously introduced, and by its use there was no difficulty [p. 923] in seeing and seizing the ligature and bringing it out through the anus. The probe was then withdrawn, and the ends of the silk were wound round two strong pieces of wood which were held between the fingers of each hand. An assistant passed a finger on either side of the track of the fistula to steady the tissues and to resist the traction which was put on the silk thread. The two pieces of wood were then drawn toward me with a rapid sawing motion, and the fistula was quickly divided, with the loss of scarcely any blood. Some oiled lint and a pad and bandage were applied in the usual way; and the wound healed well. No anæsthetic was administered, and although the patient did not relish the operation, still it was quite bearable, and what she felt most was a burning sensation, due, doubtless, to the friction of the silk."
HEMORRHOIDS.—The treatment of this form of rectal and anal disease is either medical or surgical according to the gravity of the case and according to the obstinacy with which it resists local and general therapeutic agents. An ordinary acute attack of external piles, such as is often produced by neglect of the bowels, causing constipation, may be treated in the following manner: The patient should rest and avoid stimulating food and beverages. He should employ cold bathing to the part frequently: indeed, great comfort and relief often follow this treatment alone. An ointment of tannic acid, glycerin, and simple cerate, or one containing calomel and extract of opium, will be found useful. Fresh lard, cosmoline, vaseline, cold cream, ointment of the oxide of zinc (benzoated) or an ointment containing extract of opium, extract of galls, and extract of belladonna or stramonium, are some among many agents that have been extolled for their relief. H. C. Wood46 recommends enemata of solution of chlorate of potassium and laudanum. Enemata of lime-water and linseed oil are recommended by Agnew: "One of the very best formulas for allaying the irritation incident to hemorrhoidal affections consists of the following combination: Acetate of lead and tannin, of each fifteen grains; carbonate of lead and extract of stramonium, of each thirty grains; creasote, five drops. With a sufficient quantity of cocoa-butter mould this into fifty suppositories."47 The internal exhibition of the balsam of copaiba, twenty drops in capsules taken four or five times daily, or the use of fifteen drops of liquor potassa rubbed up with half a drachm of the balsam into emulsion, taken three times a day, has been much extolled, as has also the confection of black pepper. Sometimes these various means will cure a chronic or long-standing case of piles, either internal or external. Wetherill has found that the topical application of rectified oil of amber has cured long-standing cases of piles. This oil should not be applied in cases where much inflammation exists, and where the piles are internal the best mode of bringing it in contact with them is to incorporate from three to five minims of the oil with sufficient cocoa-butter to make a suppository. One of these, pushed into the bowel night and morning for a week, will not infrequently cause the piles to shrink up and finally to disappear. The bowels should be kept open with the compound powder of licorice. It should be remembered that magnesia irritates hemorrhoids. Success has followed the internal use of ergotin, of the fluid extract of hamamelis virginica, of the corn blast (ustilago maidis), and of small doses of aloes combined with hyoscyamus. D. [p. 924] Young has had good results follow the internal use of glycerin. Chronic cases of piles have been cured by the application of ointments containing carbonate of lead, creasote, carbolic acid, or iodoform. Ergotin used hypodermically in the vicinity of the anus or injected into the piles has frequently resulted in a complete cure, and the same may be said of the injection of carbolic acid directly into the tumors. In the application of cold water to inflamed piles it should be borne in mind that its forcible impingement upon them in a fine stream acts far more efficiently than the mere bathing them. Some cases do better under the use of warm water or warm sedative and astringent lotions. A warm flaxseed poultice mixed with laudanum is a very comfortable application. In obstinate cases of prolapse Agnew48 recommends the use of a rectal obturator or the use of a hemorrhoidal truss.
46 Philada. Med. Times, Dec. 6, 1879.
47 Surgery in the Pennsylvania Hospital, p. 210.
48 Agnew's Surgery, vol. i. p. 445.
Those who suffer from prolapse of piles should avoid the habitual use of cushioned seats. They should assume a semi-erect posture during defecation, or, when this is attended with difficulty or inconvenience, they should contrive a portable water-closet seat by boring a hole an inch and a half in diameter through a piece of planed board, bevelling it so as to fit the person. These means will often prevent the extrusion of the tumors. After defecation the patient should rest for a little while in the recumbent attitude.
The careful touching of external piles with strong nitric acid is a mode of treatment that has been quite successful in the hands of some surgeons. The intolerable itching of these bodies can be allayed by touching them with tincture of aconite-root or with a concentrated tincture of prickly-ash bark. Freezing them with the ether spray allays the pain and itching for the time being, but these symptoms return with redoubled energy after the effect has subsided.
Should an attack of the external variety of piles not result in absorption, but leave an excrescence, painless but inconvenient, and liable at any time to become inflamed, excision would be in order. Divide the integument by an incision radiating from the anus, separate the skin from the tumor down to its base, and after seizing it with toothed forceps cut it off with scissors curved on the flat. Little flaps or tabs of skin remaining after piles may be snipped off with scissors. It is not well to operate upon external piles unless they obstinately resist all milder treatment. There are frequently venous enlargements containing blood-clot, and when this condition exists proceed as follows: Pinch up the little tumor between the thumb and finger of the left hand; transfix its base with a curved bistoury, and cut out; at the same time, by pressure with the thumb and finger, extrude the clot. Fill the bottom of the little sac with cotton wool, and the operation is complete. It is not necessary in these cases to wait until the inflammation subsides before operating.
The operative treatment of the internal variety may be by strangulation, by the cautery, by the écraseur, and by the use of caustics. The former of these is the safest and most convenient method, and the one usually employed in the Pennsylvania Hospital, and should be performed in the following manner: The lower bowel having been thoroughly evacuated and the patient etherized, the operator should gently but firmly stretch the sphincter. The patient should be placed upon the side, with [p. 925] the upper part of the body prone, the hips elevated, and the thighs flexed upon the abdomen. Transfix the largest tumor with a strong, long-handled tenaculum, cut through the skin at the base with a knife or scissors around its external half, and hand the hook to an assistant, instructing him to make gentle traction. Then encircle the mass with a stout cord if the mass is not too large, or pass a stout needle threaded with a double silk ligature, from without inward, deeply through the base of the pile, drawing it through the mucous membrane on the opposite side; cut loose the needle and tie tightly, so as to completely strangulate the included tissues on either side and leave the ends of the ligature long. Treat all the remaining tumors in a similar manner seriatim, and then with scissors cut away the strangulated bodies to within a safe distance of the ligatures, the ends of which are now to be cut off close. Place an opium suppository in the bowel, and the operation is complete.
When for any sufficiently good reason the patient will not bear the ordinary anæsthetics, it will become necessary to modify the operation as follows: The tumors having been well extruded by enema of warm water or by the efforts of the patient, bend him forward over a chair and direct an assistant to draw aside the buttocks. Then pass the double ligatures as before indicated, but refrain from tying until all the tumors are thus secured, as the operator will find it convenient to draw upon the ligatures to keep the mass of piles within view and working-distance. Then draw down each tumor, cut around its base, and tie as before; cut off the ends of the ligatures and the greater portion of each strangulated tumor, and return everything within the bowel, and follow with an opium suppository. In many cases Morton has used the nitrous oxide gas with the best results. The hook should then be withdrawn, and each knot should be drawn more firmly down prior to its reduplication. Following this procedure, if properly carried out, the tumors will change color, becoming blue, thus indicating complete strangulation.
The operation by the clamp and cautery is a good method when the hemorrhoidal tumors are small. The operation is that of Mr. Cusack of Dublin, and the clamp employed is that invented by Mr. H. Smith of London. This instrument is so well known that a detailed description of it would be unnecessary. In operating with it the tumor is to be drawn well out and the clamp applied close up to its attachment with the bowel. Strangulation is effected by means of the screw which runs through the shafts of the handles. This accomplished, the strangulated portion is cut off with scissors, which should leave a stump three-eighths of an inch long. To this stump apply the actual cautery at a dull red heat, touching its every portion, after which unscrew and remove the clamp and look for hemorrhage. Should any occur, touch the bleeding point with the hot iron. Confine the patient to bed for five or six days and give sufficient opium to confine the bowels. After this time has elapsed administer a dose of oil. Remember that but one pile should be clamped at one time. "The taking two piles into the clamp at once is sure to result in hemorrhage." Do not allow the cautery-iron to touch the clamp. After the operation return the parts within the sphincter and cut off any tabs of redundant integument with scissors.
The removal of internal piles by means of the écraseur was the favorite operation of Chassaignac, but it is a mode of procedure which is now [p. 926] regarded with disfavor by the best surgeons on account of the liability to hemorrhage, and from the fact that troublesome and injurious contractions of the anus have not infrequently followed its use. The employment of iron or copper wire instead of the usual chain has been recommended by those who prefer this mode of operation. The plan adopted by Chassaignac was to pedunculate the piles by tying a ligature around the base and drawing them down. The chain being then applied, the strangulation and crushing off was slowly accomplished by means of the lever of the instrument. It should take from twenty to twenty-five minutes' crushing to accomplish this object.
For the treatment of internal piles by caustics Houston of Dublin used strong nitric acid. A fenestrated speculum should be employed, and the acid should be applied with a piece of wood or with a glass brush, care being taken to limit its action to the tumors, the redundant liquid being mopped up with a swab of lint or prepared absorbent cotton. The entire surface should afterward be bathed in oil. The acid is relied upon to produce a granulating surface, by the healing of which and by the subsequent contraction a cure is sometimes achieved. At best, this plan of treatment has proved tedious and unsatisfactory.
Chloride of zinc and caustic potassa are even more unsatisfactory agents for this purpose than the acid, as they are very violent in local destruction and their action is very difficult to limit. The use of caustic potassa was last revived by Amussat, but failed to find favor from his contemporaries, and soon fell into merited disuse. Van Buren says: "From recent experience with the thermo-cautery of Paquelin, I am disposed to regard it as more manageable than nitric acid, and at least equally efficient." Allingham mentions favorably the strong carbolic acid as a substitute for the nitric as an application to vascular and granular surfaces. The reckless method employed by the older surgeons of cutting off internal piles with the knife or with scissors, without any precautions against bleeding, is merely mentioned in condemnation. Usually no serious symptoms are to be expected after operations for hemorrhoids, but to this general rule there are exceptions. Morton knows of two consecutive cases of tetanus after this operation performed in a hospital in this city, and both terminated fatally. One of the most common occurrences after the ligation of piles is retention of urine, generally lasting for a day or two and requiring the use of the catheter.
HEMORRHAGE FROM THE RECTUM.—Bleeding from these parts is more usually of a venous than an arterial character, but in some cases of hemorrhoids the bleeding is either arterial or arterio-venous. The latter occurs upon the detachment of a polypus, but not necessarily of a polypoid growth. Arterial or mixed bleeding occurs in carcinoma and in rodent ulcer, and also from the stumps of badly-occluded piles. In cases of vicarious menstruation from the rectum the venous blood simply oozes from the surface of the over-congested mucous membrane. This condition should be readily diagnosed by the physical properties of the blood and from the history of the patient. In almost all cases of bleeding near the anus it will be possible to pick up the vessel or the bleeding point on a tenaculum and ligate with silk, which is the most satisfactory method to the surgeon. The rectum has been dragged down with volsella forceps to apply a ligature to a point high up, but in some of these cases the acupressure pin [p. 927]with the twisted suture will be found more convenient. Should hemorrhage occur after the ligation of piles which cannot be checked by ligature, such as a general oozing, pass all the ligatures through a hole made in the centre of a small round sponge, then tie them across a piece of stick (thus constructing a sort of tourniquet), and twist this around. Van Buren cites a case in which a sudden laceration of the integument and sphincter occurred during forcible dilatation in a case of hemorrhoids in a very broken-down subject, with very copious hemorrhage. He passed a sponge armed with a double ligature into the bowel, and, directing an assistant to make traction upon the threads, the bleeding was checked. Injecting ice-water and perchloride of iron into the rectum will often check hemorrhage. Allingham prefers the persulphate of iron to any other styptic for this purpose. Passing fragments of ice into the bowel while holding a lump of ice upon the sacrum sometimes answers a good purpose. In many cases of secondary hemorrhage from large venous sinuses in a state of ulceration it will be impossible to ligate, and the use of the ordinary styptics will be but the waste of valuable time: the bowel must be tamponed as follows: Thread a strong silk ligature through near the apex of a cone-shaped sponge, and bring it back again, so that the apex of the sponge is held in a loop of thread. Wet the sponge, squeeze it dry, and fill its meshes with ferric alum or with persulphate of iron. Pass the left fore finger into the bowel, and upon it push up the sponge, apex first, by means of a metal rod or any other convenient body, fully five inches into the rectum. Now fill the rectum below this with cotton-wool filled with the styptic. The bowel having been completely filled, make traction upon the ligatures (thus spreading out the bell-shaped sponge), while with the other hand push up the packing. If this is carefully done no fear of bleeding need be apprehended. In these cases the patient often suffers from collections of flatus, which may be obviated at the time of packing by placing a flexible catheter in the bowel and packing around it. These plugs should remain for at least five or six days, and frequently eight or ten days are none too long. The packing must then be picked carefully away from the sponge. Agnew's rectal chemise answers the same purpose. In describing its application he says: "Through the openings at the end of the largest-sized gum catheter pass a strong silk thread; take three square pieces of the material usually known as mosquito-netting, placing them one on top of the other; at the centre of these squares or pieces make an opening, and pass the catheter through it, securing the two together by the threads. In applying the instrument the different layers of the chemise must be moistened with water, and afterward well filled with the persulphate of iron. It is then conducted some distance into the rectum on a finger previously inserted; after which it is expanded like a parachute by packing between the catheter and its hood with long strips of lint thrust up on the end of a bougie until the bowel is distended on every side. The catheter will serve to conduct away the flatus, and when, after eight or ten days, its removal becomes necessary, this is very easily effected by drawing out the ribbon-like pieces of lint which were used as packing." Another method is to stuff the bowel with fragments of sponge to which threads are tied, the ends of which, protruding from the anus, facilitate their withdrawal. In conjunction with these procedures the patient's pelvis should be elevated. [p. 928] After excision of portions of the mucous membrane the risk of hemorrhage will be lessened by the surgeon introducing through the edges of each incision a few fine sutures.
Enormous quantities of blood may escape into the bowel after operations without any external symptom being apparent until the patient becomes pallid and weak. In other cases the patient will complain of tenesmus and desire to go to stool, or of a sensation of something trickling into the bowel. Upon the recognition of these symptoms search should at once be made for internal hemorrhage.
Before taking leave of this very interesting class of diseases and of their modes of treatment, it seems proper to introduce a few remarks upon the subject of rectal alimentation, as it is now a well-recognized and much-practised means of sustaining those whose stomachs are unequal to the work which in health is so easily and unconsciously performed. In the use of the lower bowel as an absorbent surface of alimentary substances many failures have been reported, a fair proportion of which, it is safe to infer, are due to the methods employed, to the nutritive matters employed, and to the condition of the rectum at the time. Firstly, as to the state of the rectum, it must be empty. Wait a reasonable time, say an hour, after stool, so that the gut may be more passive; have the patient in the recumbent posture; direct him to resist tenesmus and to exert both the will and the muscular power to retain the aliment. The syringe must be of hard rubber, must be rectal-ended, and of the capacity of two fluidounces, and perfect in action.
The preparation to be introduced, after being warmed to a temperature of 98° or 99° F., should be very slowly injected with the syringe, which should be also warmed and oiled. The enema must never exceed in amount two fluidounces. If this be rejected, wait a reasonable time and try again, using a less amount. If tenesmus proves an insurmountable barrier to ordinary means, an opium suppository is to be introduced three hours prior to another attempt. It has been suggested, inasmuch as tenesmus is often relieved by the application of cold to the rectum, to introduce the aliment in that state; but this method is open to the objection that rectal digestion would be much less likely to take place under this condition, as the bowel would then have thrown upon it the additional work of warming up the substance prior to absorbing it.
The usual errors made in applying this means of sustaining the patient are, that the injections are too large, are too rapidly introduced, and are not of the proper temperature. Allowing an interval of eight hours between the enemata would afford three in the twenty-four hours, which method has been found to offer the best results. This must be persevered in at regular daily intervals for the patient to derive its full benefit, and there is reason to suppose that the nervous system gets expectant of these daily hours of support, as it does in the case of our ordinary meal-times. An examination of the well-formed daily stools of patients thus sustained will prove how close the analogy is between this and digestion proper.
[p. 929] Next, as to the substances to be employed. The best of these are milk, eggs, concentrated beef-extracts or beef or chicken peptones, and brandy or whiskey of good quality. These substances may be combined in various proportions to suit the individual requirements of the case. A very good mixture for this purpose is two tablespoonfuls of milk, one tablespoonful of whiskey, and an egg, using both the yelk and the albumen. To this add a little salt. This should be well beaten up and properly warmed.
It is well to persevere in the use of these enemata even though at first most of them appear to be rejected, as after a time, the rectum becoming accustomed to their presence, absorption or so-called rectal digestion may take place. This form of alimentation should be kept in reserve in a case of chronic illness until all other methods of sustaining the patient prove insufficient to support life. It is not contraindicated even in some cases of chronic diarrhoea with persistent vomiting and loss of peptic function, advantage being taken of the intervals between the evacuations to introduce a small and very concentrated nutrient enema. In ordinary cases not complicated by diarrhoea the most convenient times will be found to be about seven o'clock in the morning, three in the afternoon, and eleven at night. Wetherill suggests the possibility of forming with solid extract of beef, pepsin, and pure suet a nutrient suppository which might be retained and absorbed in some cases in which it has been found impossible to retain the enemata. A very small addition of white wax, he thinks, would keep these solid during warm weather; if not, the suet might be replaced by ol. theobroma (as in ordinary suppositories), which is probably as likely to be absorbed as the suet.
All animals, except in general the simple cell-forms constituting the sub-kingdom of protozoa, under ordinary circumstances are more or less liable to be infested with others, called parasites, which commonly live at the expense of their hosts, frequently with little or no inconvenience, but often causing discomfort and suffering even unto death. Parasites are distinguished as external and internal, the two being mostly of a widely different character. The former chiefly pertain to the division of arthropoda, or animals with jointed limbs, as exemplified by lice, fleas, and flies of the class of insects, mites of the class of arachnides, and epizoans and isopods of the class of crustaceans.
Internal parasites, from their usual habitation named entozoa, are commonly observed in the intestines of animals, and hence their distinction as intestinal worms. The name has proved to be appropriate, for investigations have shown that most entozoa, observed from time to time in other parts of the bodies of animals, pass part of their life in the intestinal canal of the same or of some other animal.
By far the greater number of entozoa are peculiar animals, constituting the chief part of the scolecides, an extensive group of the sub-kingdom of vermes or worms. Of this group they comprise the orders of CESTODES, or tape-worms; the ACANTHOCEPHALI, or thorn-headed worms; the TREMATODES, or fluke-worms; and the greater portion of the NEMATODES, or thread-worms. Many entozoa also belong to the protozoa, but these, so far as relates to man in a medical point of view, appear unimportant, and will therefore not here enter into consideration.
In the course of their life entozoa undergo changes of form and condition, and pass these in different organs of the same or of different animals, and it may be for a brief period externally or in a non-parasitic state. In many instances, as in the tape-worms and the fluke-worms, the transformations accompanying the changes are of so extraordinary a character that until their life-history was investigated the successive metamorphoses were viewed as distinct animals. Mostly, the entozoa pass one stage of existence within the intestine of some animal, and another stage in different organs of other animals. Many, perhaps most species, in each stage are peculiar to one or a few nearly-related animals, but others of the same kind infest a number of different animals. The animals infested by the same parasite may be remotely as well as nearly related. Thus the Tænia saginata, or beef tape-worm, in the mature state lives in the small intestine of man [p. 931] only, but in its juvenile or larval condition in the flesh meat of the ox. The Tænia elliptica, the common tape-worm of the intestine of the dog, in the larval condition lives in the louse of this animal. The liver-fluke, Distomum hepaticum, occasionally found in the liver of man, but of common occurrence in the sheep, to which it proves so destructive in the affection known as rot, in the juvenile condition lives in a little fresh-water snail of the genus Lymneus. The guinea-worm, Filaria medinensis, which in the mature state is found beneath the skin of man, in the larval condition inhabits the minute crustacean cyclops of stagnant waters.
As would be reasonably supposed, entozoa commonly gain access to their hosts through the food and drink, though in the case of aquatic animals they also obtain entrance directly through the integument from the surrounding medium. So long as they remain in the intestinal canal they may occasion little trouble or inconvenience. When they are numerous in this position or proportionately large, according to their peculiar nature they may produce more or less suffering and even the most serious consequences. Generally, however, it is when they occupy other positions, to which they have migrated from the intestine, that they induce aggravated symptoms proportioned to their numbers and the nature of the organs they infest.
Many species of entozoa have been discovered in man, and most of them are peculiar in kind. Many are common, and, while some are widely extended, others are more or less restricted to certain localities. They are variable in their frequency, largely proportioned to the prevalence of habits which are favorable to their transmission, and which, though under control, are more or less disregarded. Some species are so rare in their occurrence that they seem to be accidental, and therefore of comparatively little interest to the physician.
In general, the frequency of occurrence of intestinal worms is proportioned to the extent of use of uncooked or insufficiently cooked meats, the drinking of unfiltered standing waters, uncleanly habits, and the intimacy of association with domestic animals. It therefore follows that important prophylactics against infection by parasites are properly-cooked food, the use of spring or freely-running water or filtered standing water, cleanly habits, and the avoidance of intimacy with domestic animals.
Tape-worms in the mature condition inhabit the intestines of vertebrate animals, and are usually conspicuous for their long, tape-like appearance and jointed character. In the juvenile or larval state they infest the various organs, except the interior of the intestinal canal, of both vertebrates and invertebrates, and in this condition are so diminutive and inconspicuous that until a comparatively recent period they for the most part remained unnoticed, and when known their relationship with the mature forms was not recognized.
The mature tape-worm, as ordinarily observed, is a long, soft, flat, white worm, which from its resemblance has received its familiar name. [p. 932] It has a small head, succeeded by a short, more slender neck gradually widening into the body, which is divided transversely into segments. These, which are usually called joints or links, and also named proglottides, are so many individuals, and finally become separated to hold an independent existence. The tape-worm clings to the mucous membrane of the intestine by its head, which is provided for the purpose with suckers, and in many cases also with circlets of hooks. The segments of the body are incessantly produced by gradual growth and successive division of the neck, and as they enlarge they become more distinct and develop within a bisexual generative apparatus for each. The worm has neither mouth nor intestine, but is nourished by imbibition from the surrounding liquid in which it lies constantly bathed. A pair of longitudinal vessels commences in the head and extends throughout the body, one on each side, and in some genera is joined by a transverse vessel at the fore and back part of every segment. The mature segments have no body-cavity, but are occupied with a complex bisexual generative apparatus, which is self-impregnating. Finally the uterus, usually much ramified, becomes especially conspicuous through distension with eggs, and the rest of the organs for the most part become atrophied. The ripe segments successively detach themselves from those in advance, often singly and not infrequently several linked together. In this condition, often in lively movement, they are discharged with the feces, and thus commonly render themselves obvious to their host. Subsequently they may continue to live a brief period externally in a non-parasitic condition. Ordinarily, in moist excrement, or in water or similar materials, they will remain alive for several days.
After the discharge of the tape-worm segments, together with the eggs which had been previously laid by the latter and those still contained within them, any or all may be swallowed by animals feeding in places where the infected excrement has been deposited. When the proglottides and eggs are taken into the stomach they are digested and the embryos or proscolices are liberated.
The embryo or proscolex of the tape-worm is a microscopic spherical or oval body, provided at one pole with three pairs of divergent spicules, by which it is enabled to penetrate the walls of the stomach or intestine of its host. From these positions the embryo migrates either directly or through the blood-vessels to some other organ, most frequently the liver or the muscles. Having reached its destination, it becomes fixed in position, and for a time remains comparatively quiescent, but undergoes further development. The embryo loses its spicules and is transformed into the larval form or scolex. In most species of tape-worms the scolex is simple or individual in character, and consists of a head like that of the parent or mature worm, with a neck ending in a capacious cyst, within which the head and neck are inverted. In this form the scolex is contained in a sac of connective tissue induced by the presence of the parasite. Such sacs, frequently observed imbedded in the flesh, liver, lungs, and other organs of animals, are familiarly known as measles. In this condition the scolices of certain tape-worms have long been known, but as their relationship was not recognized, they were viewed as distinct species of parasites and described as cysticerci. In other species of tape-worms the scolex is of compound character; that is to say, the embryo [p. 933] in its further development gives rise to the production of one or more groups of individuals in conjunction. The compound scolex thus forms a sac or a group of sacs, the basis of hydatid tumors. These occur of various sizes, even up to that of a child's head, and may occupy any organ of the body. They consist of a spherical sac or group of sacs, simple in character or containing others, ranging in size from that of a mustard-seed to that of a marble, or larger to that of a walnut, enclosed in an envelope of connective tissue induced by the presence of the parasite. The sacs are filled with liquid, and have, attached within or free and floating, or less frequently attached without, variable numbers of little white grains, which on examination with the microscope exhibit the same constitution as the simple scolex above described. As in the case of the cysticerci of measles, the scolices of hydatids have long been known, but as their relationship with the mature forms was unrecognized until lately, they were regarded as distinct parasites and described as echinococci and coenuri. Sometimes the compound scolex fails in development further than the production of the sacs, which then constitute the so-called acephalocysts.
Measles with their occupants, when retained in the muscles or other organs, ordinarily undergo no further development, but ultimately, after some months to a year or two, undergo degradation. The larva or scolex dies and atrophies; the measle degenerates, and often becomes the focus of calcareous deposit, shrinks to a little cicatrix, and may finally disappear. Of a more serious nature is the tape-worm embryo which produces the hydatid tumor. With the increase of this, proportioned to the production of sacs and scolices, it may become so large as greatly to interfere with the function of the organ it occupies, and according to the nature of this organ will be the gravity of the affection.
When, however, the flesh or other parts of animals affected with measles or hydatids containing active scolices are used as food in a raw or insufficiently cooked state, the meats are digested in the stomach and the scolices liberated to pursue their further development. Passing into the small intestine, the active scolex everts its head from its caudal sac, which atrophies and disappears, and the parasite attaches itself to the mucous membrane, and rapidly develops and grows into the conspicuous and familiar form of the adult tape-worm. The duration of life of the latter while maintaining its position in the intestine is uncertain, but under favorable circumstances it commonly continues for years, and thus, with the incessant production of ripe segments charged with eggs, it becomes a constant focus of infection.
Three species of tape-worm in the mature condition are common parasites of man, living in the small intestine. They are the Tænia saginata, Tænia solium, and Bothriocephalus latus.
TÆNIA SAGINATA.—SYNONYMS: Tænia mediocanellata; Beef tape-worm; Unarmed tape-worm; Fat tape-worm.
Larval condition: Cysticercus saginata; Beef measle-worm.
This, which is now regarded as the most common tape-worm of man, is named the beef tape-worm because it is derived from the beef used as food. In the mature condition it lives only in the small intestine of [p. 934] man, and in the juvenile condition it lives in the ox. Its frequency is proportioned to the prevalence of the custom of eating beef in a raw or insufficiently cooked state, conjoined with the careless habit of leaving human excrement in pastures where it is accessible to cattle.
The mature beef tape-worm is commonly observed as a soft, yellowish-white, thickish, band-like worm, ranging from six to twenty feet or more in length. The head, about the size of a yellow mustard-seed, is rounded quadrate and provided with four equidistant hemispherical suckers. Succeeding the head is a short, slightly narrower, flattened neck, which merges into the gradually widening and segmented body. The segments, at first narrow fore and aft and several times wider than the length, become successively larger, proportionately longer, more distinct, and quadrate in outline; and finally the length may exceed the breadth two or three times. A full-grown tape-worm may possess twelve hundred segments and more, and specimens are recorded as reaching a length of thirty feet. The larger segments measure from a quarter of an inch to an inch long and from three to four lines wide. The larger or riper segments exhibit on one border, irregularly alternating on the two sides, at or near the middle, a papilla in which is the external aperture of the genital apparatus. In the fully-ripe segments the uterus, distended with eggs, may be obscurely seen through the wall of the body, but is rendered more visible by drying the segments, moderately compressed, between two pieces of glass. It appears as a long, narrow, white or brownish median line or tube, giving off laterally numerous short, transverse, more or less branching tubes.
The worm in its usual position lies along the course of the intestine in loose coils, and exhibits lively movements, alternately shortening and elongating, expanding and contracting the head, and protruding and retracting the suckers. The ripe segments spontaneously detach themselves, and may be found scattered along the large intestine ready to be discharged with the excrement, or, as is sometimes the case, they may spontaneously creep from the anus. Rarely more than a single worm infests a person at the time. The species is of rapid growth. According to Perroncito, quoted by Cobbold, a mature worm was reared from a beef measle, swallowed by a student, in fifty-four days.
It is estimated that the number of eggs in the mature segments of the beef tape-worm amounts to about 35,000. As the full-grown worm may consist of 1200 segments, and there is reason to believe these are renewed several times annually, we learn that the whole number of eggs produced by a single individual is enormous. The ripe segments, attached to the parent or becoming spontaneously detached, lay their eggs in the intestine to be discharged with the feces. When more or less emptied they shrink and appear reduced in size, and in this condition are expelled or spontaneously creep from the anus. If the ripe segments are forcibly expelled and are alive, they will lay their eggs in the feces externally. The ripe eggs are brown, oval, about 0.03 mm. long, and have a thick shell, with an outer vertically striated envelope.
As previously intimated, the common source of the beef tape-worm in man is the use of raw or insufficiently cooked beef affected with measles. The ox becomes infested by swallowing the eggs, or, it may be, even the entire segment, of a tape-worm deposited with feces in the [p. 935] pastures of cattle. The measles usually occur in the muscles, including the heart, though they have also been noticed in the liver and lungs. They appear, in beef, as oval, whitish bodies from the size of a mustard-seed to that of a pea. They consist of a sac of connective tissue containing the larval tape-worm or cysticercus. Measles under ordinary circumstances are seldom noticed in beef, and when they occur are commonly few in number.
According to the latest authorities—Leuckart, Cobbold, Stein, and others—the beef tape-worm is the most common of the cestodes which infest man. Until within about thirty years it was generally not distinguished from the pork tape-worm, and this was accordingly regarded as the most common human species. Since the writer distinctly recognized the beef tape-worm within the last twenty years, all the specimens of Tæniæ, from people of Philadelphia and its vicinity, that have been submitted to him for examination—perhaps in all about fifty—have appeared to belong solely to Tænia saginata. The prevalence of this species with us is no doubt due to the common custom of eating underdone or too rare beef, while the pork tape-worm is comparatively rare, as with us pork is only used in a well-cooked condition.
TÆNIA SOLIUM.—SYNONYMS: The Pork tape-worm; Solitary tape-worm; Armed tape-worm.
Larval condition: Cysticercus cellulosæ; Pork measle-worm.
Until a recent period this species was generally regarded as the most common tape-worm of man—a view which in great measure was due to the circumstance that the beef tape-worm was not distinguished from it. It was called the solitary tape-worm, still expressed by the specific name, from the impression that it rarely occurred otherwise than single at a time in a person. This has also proved to be incorrect, likewise due to the two kinds of tape-worms having been confounded together; for while the beef tape-worm most commonly occurs solitary, the pork tape-worm not unfrequently occurs with several together.
The species is now appropriately named the pork tape-worm, as indicating its common source—pork used as food. The frequency of the parasite is proportioned to the prevalence of the custom of using pork in a raw or imperfectly cooked state, conjoined with that of depositing excrement where it may be accessible to hogs. In the mature condition the pork tape-worm is peculiar to man and lives in the small intestine, but in the larval condition, though especially infesting the hog, it also occasionally infests man, and lives in any organs of the body, but mostly the muscles, liver, and lungs.
The mature pork tape-worm, as commonly seen, is a soft white, thin, band-like worm, from five to ten feet long and about four lines where widest. The head is spheroid, about the size of that of an ordinary pin, and smaller than that of the beef tape-worm. It is furnished with four hemispherical cup-like suckers, and the summit forms a blunt papilla armed with a double circle of twenty-five or twenty-six hooks. The neck is narrow, thread-like, about an inch long, and merges into the segmented body, which gradually widens to the extent mentioned. The segments, at first much wider than long, as they successively enlarge also become more distinct and proportionately longer, so that the more [p. 936] posterior ripe ones are as long as they are wide, and often longer, though not to the same degree as in the beef tape-worm. The genital papilla, with its external aperture, is marginal as in the latter. The fully-developed uterus is quite distinctive in character from that of the beef tape-worm. The median tube is coarser, and the lateral branches are likewise coarser, much fewer—half the number or fewer—less branched, and less crowded. The ripe and often spontaneously detached segments are commonly longer than broad, more or less elliptical in outline, with truncated ends, and usually measure about half an inch in length by about a third in breadth. The ripe eggs resemble those of the beef tape-worm, but are usually spheroid in shape.
The common source of the pork tape-worm is pork affected with measles eaten in the raw or insufficiently cooked state. The hog becomes affected with measles when it has access to human excrement containing eggs and ripe segments of the tape-worm, which it eats with avidity. The eggs, with their already developed embryos, when swallowed, undergo the same series of transformations and course as those indicated in the account of the beef tape-worm. Pork affected with measles is much more common than beef affected in the same way, and is frequently a subject of ordinary observation. From the difference in habit of the hog and ox this is what might have been suspected; and the fact that the beef tape-worm is more common than the pork tape-worm is to be explained from the circumstance that fresh beef is in more general use than pork, and is usually employed less thoroughly cooked.
The pork measles are commonly seen as round or oval, hard, whitish bodies, from the size of a hempseed to that of a pea, imbedded in the connective tissue of the muscles or flesh. The measle consists of a sac of connective tissue enclosing the scolex or larval tape-worm, which resembles that of the beef tape-worm, but differs especially in the possession of a double circlet of hooks to the head, as in the adult worm. The scolex has long been known, and was regarded as a distinct parasite, with the name of Cysticercus cellulosæ. When fresh pork measles are swallowed by man they are digested in the stomach, and the cysticercus or scolex is released and passes into the small intestine. Here, attaching itself to the mucous membrane by means of its suckers and crown of hooks, it rapidly develops and grows into the adult tape-worm. In this condition it lies in loose folds along the intestine, to which it clings so tenaciously that commonly the neck gives way when the greater part of the worm is forcibly detached by the use of medicines. Fragments, consisting of the more mature segments, frequently appear detached from the posterior part of the worm, and the fully-ripe segments may be seen scattered singly in the course of the large intestine. The isolated segments are thinner and more translucent than those of the beef tape-worm, and in this condition are discharged with the feces, but may also spontaneously creep from the anus, though seldom as compared with the other species.
Experiments repeatedly made by swallowing pork measles prove that the mature tape-worm may be developed in the course of three months. The length of life attained by it under favorable circumstances is uncertain, but it probably continues a dozen years or more.
The scolex of the pork tape-worm, or the cysticercus, so common in the hog, is also less frequently a parasite of man, and in this condition is a [p. 937] more potent agent of danger than in its ordinary or mature state. The infection is due to the introduction of eggs or mature segments of the tape-worm into the stomach—a circumstance which may readily occur through handling these objects and transferring them to the mouth, or more rarely perhaps by their transference from the intestine into the stomach through vomiting.
In the measle form the parasite may occur in any organ of the body, but is mostly found in the muscles and subcutaneous tissue. Its pathological significance depends on its number and position. Located in the nerve-centres, it may occasion the most serious consequences. Usually it occurs in small numbers and gives rise to no obvious inconvenience, and is only accidentally detected in dissection after death. It appears to maintain its vitality for some years, but finally dies, and undergoes degradation. Only when it can be detected in such position as the interior of the eye or beneath the conjunctiva can the patient be relieved by surgical aid. Elsewhere, even if its presence is suspected, it is ordinarily beyond the reach of medical treatment. The writer a few years since, in dissecting the body of a colored man to illustrate his lectures on the muscles, found two living measles, of which one was in the diaphragm and the other in the transversalis muscle of the abdomen, but none were detected elsewhere. The parasite unquestionably gave no inconvenience to its host during life.
Other species of Tænia which have been observed as parasitic in the human intestine are mostly of rare occurrence.
TÆNIA CUCUMERINA, the common tape-worm of the dog, and TÆNIA ELLIPTICA, the common tape-worm of the cat, are very much alike in appearance, and are regarded by many authorities as the same species. They occur frequently in considerable numbers in these animals, living in the small intestine. They have also been occasionally found in man, especially children.
It is a comparatively delicate worm, chain-like in appearance, ranging from four inches to a foot in length. The head is provided with four suckers and a prominent rostellum armed with about sixty hooks. The neck and anterior part of the body are thread-like. The mature segments are elliptical in outline or like a melon-seed, whence the name. There is a double set of sexual organs, and a genital orifice occupies the middle of both lateral margins of the segments. The ripe segments become readily detached and creep actively in the intestine, and are either expelled with the feces or they spontaneously creep from the anus. The eggs are comparatively few and measure 0.05 mm.
Late researches appear to show that the eggs adhering to the hair about the anus or elsewhere are eaten by lice of the same animals, and within these insects undergo further development. The dog and cat, subsequently swallowing the lice, infect themselves with the mature worms. Thus also persons, especially children, from too great familiarity with these animals, directly or through their food, may likewise become infected.
TÆNIA NANA, the Dwarf tape-worm, has been observed but once. It was discovered by Bilharz, in Egypt, in a boy who died of meningitis. It [p. 938] is a little worm, about half an inch in length, and occurred in large numbers in the duodenum.
TÆNIA TENELLA.—This is another small species, which has been but once observed. It is described by Cobbold, who suspects it to be derived from measles of the sheep.
TÆNIA FLAVOPUNCTATA is also a small species, from eight to ten inches long, with ripe joints about one millimeter long and from one and a half to two millimeters broad. It is described by Weinland, and has also been but once observed. A half-dozen specimens were discharged from a healthy child, of nineteen months, in Boston, Mass.
Since the above was written the author has had the opportunity of examining some little tape-worms which he suspects to be of the same kind as the former. They occurred in the practice of T. V. Crandall in Philadelphia, and were expelled from a child of three years of age after the use of santonin. About a dozen fragments appear to have pertained to three worms, from twelve to fifteen inches in length. The head in all was lost. The anterior part of the body is thread-like, the posterior part about two and a quarter millimeters wide. The width of the joints is more than twice the length. The ripe joints are pale brown, and are remarkable for the comparative simplicity of the uterus, which is distended with brown eggs. A peculiarity of the worm is the repeated but irregular alternation of fertile with sterile joints.1
1 Amer. Journ. of Medical Sciences, 1884, p. 110.
The species is probably more common than might be supposed, and from its small size, and perhaps harmless character, has generally escaped notice.
TÆNIA MADAGASCARIENSIS.—This species, described by Davaine, is imperfectly known. Fragments of the worm have been twice observed in the Comoro Islands.
BOTHRIOCEPHALUS LATUS.—SYNONYMS: Dibothrium latum; Tænia lata; Broad tape-worm.
This tape-worm, of another genus than the preceding, is a common parasite of man in certain localities of Europe, but has not been found as an indigenous product elsewhere. It occurs especially in Sweden and Russia, East Prussia, Poland, and West Switzerland. In the latter country it prevails to such an extent that it is reported that about one-fourth of the inhabitants of Geneva are thus infested. Among the tape-worms submitted to the writer from time to time for identification a few years ago was a large specimen of Bothriocephalus latus, but it proved to have been derived from a Swede who had arrived in this country only a few months previously.
There are many species of Bothriocephalus, which in the adult condition mainly live in fishes. The genus is distinguished from Tænia by many points, chiefly in the form and construction of the head, the form of the joints and uterus, and the position of the genital aperture, which is situated centrally on one of the broad surfaces instead of the lateral margin.
[p. 939] The broad tape-worm is the largest of the tape-worms infesting man, a full-grown specimen reaching to twenty-five feet in length with a breadth of three-fourths of an inch, and consisting of upward of four thousand segments. It is a soft, grayish, flat, band-like worm, with head, neck, and segmented body holding the same proportions as in the other tape-worms. The head is elongated, clavate, and is provided with a long, narrow, elliptical sucker on each side. The narrower neck is short and merges into the segmented body, which gradually widens to half an inch or more. As the segments successively enlarge, they increase proportionately to a greater extent in breadth, so that their width for the most part measures from two to four times their length. A few toward the end of the series become narrower and longer than those in advance. In the ripe segments the uterus, distended with brownish eggs, forms a central rosette-like group of pouches. The genital aperture is central in the broad surface of the segments, and is always on the same or ventral side.
The broad tape-worm inhabits the small intestine, and is usually found single, but occasionally several together, and sometimes also in association with one or both the other common tape-worms. The species is also reported to be not infrequent in the dog.
Ripe portions of the broad tape-worm become detached in fragments of variable length, to be discharged with the feces. The partially-emptied appearance of the uteri in these fragments indicates the laying of the eggs previous to the expulsion of the latter. The eggs are oval, of a light-brown color, and measure about 0.07 mm. long. The shell at one pole is furnished with an operculum or lid for the escape of the embryo. This is developed subsequently to the discharge of the eggs from the intestine. If the eggs are placed in water, in the course of some months the embryos are developed and escape from the shell. The embryo is a round or oval body furnished with three pairs of spicules, as in that of the Tæniæ, but differs in possessing a ciliated envelope, by means of which it freely swims about in the water. After some days the embryo discards its envelope and creeps about in an amoeboid manner. Further than this, until recently, the fate of the embryo was unknown. Braun of St. Petersburg, after determining the presence of scolices of Bothriocephalus in the muscles, liver, and organs of generation of the pike, trout, and eel-pout, by feeding these to cats and dogs succeeded in rearing worms which differed in no respect, except in being smaller, from the Bothriocephalus latus of man. Such being the case, it becomes evident that man may ordinarily become infested with the parasite by eating raw or insufficiently cooked fishes of the kind mentioned.
BOTHRIOCEPHALUS CORDATUS, described by Leuckart as a common species infesting the dog in Greenland, has been reported as having once been found in a woman. Böttger regards it as not distinct from Bothriocephalus latus.
BOTHRIOCEPHALUS CRISTATUS.—This species, but once observed, is described by Davaine. It was passed by a child in Paris, and the worm was upward of nine feet in length.
SYMPTOMS OF TAPE-WORMS.—Whichever may be the species of [p. 940] tape-worm infesting the human intestine, the symptoms to which it gives rise are mainly of the same character, modified of course in degree by the size and number of the parasites and the susceptibilities of the patient. Clinging by means of the head to the mucous membrane of the intestine, and involved among the valvulæ conniventes and villi, the worm may extend in loose folds along the greater part of the course of the intestine or lie coiled in an elongate mass. Besides being rendered evident from time to time by the discharge of segments or fragments, the beef tape-worm especially sometimes introduces itself to the notice of its host through the segments creeping from the anus. Sometimes segments of tape-worms are vomited, especially in women; and the exhibition in this way, especially of the pork tape-worm, is to be deplored, for should segments be retained in the stomach the patient becomes further liable to be affected with measles or cysticerci.
Some persons continue infested with a tape-worm a long time without suspecting its existence and with little or no inconvenience, and perhaps first become aware of its presence by the accidental discovery of segments discharged from the bowels. Usually, however, the parasite creates more or less disturbance, and not unfrequently occasions great discomfort. The symptoms are both local and of a general nature. Itching at the extremities of the alimentary canal and various dyspeptic symptoms are common; uncomfortable sensations in the abdomen, uneasiness, fulness or emptiness, feeling of movement attributed to the worm, and colicky pains; disordered appetite, sometimes deficient, oftener craving; paleness, discoloration around the eyes, furred tongue, fetid breath, and sometimes emaciation; fulness of the forehead, dull headache, buzzing in the ears, twitching of the face, and dizziness; often uncomfortable feelings in the abdomen increased by fasting, which are temporarily relieved by taking a full meal. Certain kinds of food also at times appear to produce greater uneasiness, apparently due to more than usual disturbance of the parasite. Symptoms of a more grave character are sensations of fainting, chorea, and epileptic fits. Others of a chlorotic and hysterical character are not unfrequent, especially in women, who also may suffer more or less from uterine disorder.
All the ordinary symptoms are quickly relieved by the expulsion of the tape-worm—permanently if it is entirely removed, but temporarily, as is frequently the case, when only the greater bulk of the parasite is discharged and the head continues to remain securely attached to the intestine and ready to renew its many-segmented body. The tape-worms are capable of a wonderful amount of extension from traction without detachment; and from the delicacy of the neck and the anterior part of the body, and the action of medicine on the peristaltic motion of the intestine, the posterior part of the worm, including its great bulk, is most apt to be torn away and discharged, while the head remains. So long as this is the case, and the worm has not been poisoned or killed, the anterior portion grows, and thus the parasite is renewed and accompanied by a return of all the former symptoms. Under the appropriate treatment the evacuations of the patient should be carefully inspected, so as to satisfy both physician and patient that the parasite has been completely expelled. To properly examine the evacuations, they should be repeatedly drenched with clear water, and the sediment, after the settling [p. 941]of the washings, must be inspected. It is only when the physician has seen the head of the parasite that he can reasonably ensure his patient a permanent cure.
TREATMENT.—To get rid of tape-worms many remedies have been employed, though comparatively few retain a reputation for positive success. Some act by powerfully operating on both bowels and worms, producing the detachment and discharge of the latter without killing them, as is often indicated in the lively movements they exhibit after their expulsion. Others poison and kill the worms, and also cause their detachment and expulsion from the bowel.
Before the administration of the appropriate medicine for tape-worms, with the object of rendering it more effective it is advisable to bring the alimentary canal into a condition which will render the parasites most vulnerable. For this purpose fasting is to be recommended for several days previously, and when food is used it should be in moderate quantity, and of such a character as to leave little residue to accumulate in the intestine. Wheat bread, the ordinary meats, milk and coffee, are best, while the usual vegetables should be avoided.
One of the most effective remedies is the oil of turpentine in the dose of one or two fluidounces, made into an emulsion with white of egg and sugar; children require about half the quantity. The large dose is less apt to produce the usual objectionable effects of that medicine than small ones. The only inconvenience caused by it is the heat of the stomach, some febrile excitement, and fulness of the head or headache lasting for one or two days. The effects are more apt to occur when the medicine does not act as a cathartic. The oil usually operates quickly, killing the worm and producing its discharge. If it does not act in the course of two or three hours, a full dose of castor oil may be given, and, if necessary to aid the action of this, enemata may be employed. To ensure the purgative action of the oil of turpentine it may be advantageously associated with the castor oil, of each a fluidounce made into an emulsion.
Another and effective remedy is the root of the male fern, Aspidium filix-mas, used in decoction or electuary. Stein of Frankfort recommends the ethereal extract as the best preparation, and prescribes it in doses of from seven to ten grammes, enclosed in half the number of gelatin capsules and administered at short intervals within half an hour. It should be taken in the morning fasting, after taking a cup of coffee, swallowing the capsules with the aid of a second cup. Half an hour after the capsules are taken a mixture of castor oil, brandy, and ginger syrup, of each fifteen grammes, should be administered. The treatment has proved all that could be desired, and the worm, including the head, is discharged altogether, rolled into a ball.
The bark of the pomegranate-root, Punica granatum, is also a powerful and efficient remedy, but often proves very disagreeable from its producing violent pains in the abdomen, with nausea and vomiting. It also generally purges, occasioning the discharge of the worm. Küchenmeister prefers it to any other medicine, given in the form of decoction prepared by macerating three ounces of the fresh bark in twelve fluidounces of water for twelve hours, and concentrating the infusion by gentle heat to one-half. He recommends it to be taken after fasting a day and the [p. 942] administration at night of two fluidounces of castor oil. It is to be given in three or four doses within an hour. Should the medicine not purge, it should be followed by another dose of castor oil.
Recently, Feraud has recommended the tannate of pelletierin, the alkaloid of which is derived from the pomegranate-root, as the most powerful of remedies for tape-worm, the dose for an adult being one-half to three-fourths of a grain. The patient should fast a day on bread and milk, and the following morning, before rising, take an infusion of one-third of an ounce of senna. This should be followed an hour later by half the medicine diffused in a little water, and the patient should remain quiet in bed to avoid nausea and vomiting. Half an hour later the rest of the medicine is to be given, followed in another half hour by a dose of castor oil. Should there be no stool after an hour, purgative enemata may be used. In one case twelve beef tape-worms were discharged together measuring, collectively, fifty meters.
Kousso, the flower of Brayera anthelmintica, an Abyssinian herb, has been of late much employed as a remedy for tape-worms, but with many physicians of experience it has lost favor. Heller speaks of it highly, and recommends it to be taken in the morning, an hour after the patient has taken coffee. The dose is from half an ounce to an ounce, and is conveniently taken in compressed balls or disks, coated with gelatin, and swallowed at intervals in the course of an hour, aided by mouthfuls of coffee. Any disposition to vomit should be repressed, which is rendered easier by taking small mouthfuls of strong coffee or pieces of ice.
Koussin, an alcoholic preparation of kousso, is also efficient, and has the advantage over the latter that it does not occasion nausea. It has been used in the medical clinic of Munich in the dose of 30 grains, and it has been a very rare occurrence that the result was not all that could be desired.
The seeds of the common pumpkin, Cucurbita pepo, are extolled by many physicians as a remedy for tape-worms; and the writer has twice had the opportunity of observing large specimens of the beef tape-worm which were expelled after the administration of this medicine. The dose is an ounce of the seeds bruised into a paste and made into an emulsion. It should be taken in the morning, fasting, and followed in an hour or two with a full dose of castor oil.
Santonin, a principle derived from santonica, Artemisia maritima, is reported as a remedy for tape-worms, but its efficacy has also been denied. The dose is from two to four grains for an adult, and from one-quarter to one-half a grain for children over two years. It is best administered in lozenges prepared with sugar and tragacanth.
The quinia sulphate has also been recommended as an effectual remedy both in tape- and seat-worms.
As regards the prophylaxis of tape-worms, there are some important points to which we direct attention.
The evacuations of patients containing tape-worms, their segments and eggs, should not be carelessly thrown away, at least in places accessible to animals which may become infected. They should be treated with boiling water, the heat of which is sufficient to kill all animal parasites. The handling of living tape-worms and segments should be avoided, as eggs [p. 943] which may adhere to the hands, if transferred to the mouth and swallowed, will produce infection.
Meats visibly infested with measles are not fit and should not be used as food. Raw meat should altogether be discarded as food, both for the sick and well, and all meats should be thoroughly cooked. As a rule, meat should not be used so long as it appears red or on cutting emits a bloody liquid. A large piece of meat requires long boiling or roasting for sufficient heat to penetrate to the interior to destroy any parasites that may be present. Even salted meats and hams should be cooked to ensure against parasitic infection. It is important also to avoid food prepared by uncleanly persons who may be infested with tape-worms.
As regards our domestic animals, which are the common source of the infection of man with tape-worms, they should also be protected from infection as far as possible. This is to be done by preventing them from having access to human excrement. As Heller remarks, with this object the barbarous custom of defecating in every place promiscuously should be put down with a high hand.2
2 Several years since a physician of Texas sent to the writer a piece of pork, making inquiry as to its condition, and stating that all the pigs of his vicinity were diseased and their flesh similarly affected. It contained a number of measles or larval tape-worms. On giving the information and the probable cause of the affection of the pigs, the doctor reported in return that there was not a privy in his village. Until our people are more careful with the raising of pigs, European governments will have reason for prohibiting the importation of our pork.
TÆNIA ECHINOCOCCUS.—SYNONYM: Hydatid tape-worm.
Larval condition: Echinococcus; E. hominis; E. veterinorum; E. granulosis; E. scolicipariens; E. altricipariens; E. hydatidosus; E. multilocularis; E. cyst; Hydatid; Hydatid cyst; Acephalocyst.
This tape-worm, in its mature state the most insignificant looking of its kind, though not strictly an intestinal worm of man, in the juvenile condition is one of his most dangerous parasites, as being the source of hydatid tumors. The adult tape-worm lives in the small intestine of the dog and wolf, in some localities often existing in these animals in thousands together. From its diminutive size it may be readily overlooked, concealed or obscured by the villi among which it is suspended to the mucous membrane. It is about a fourth of an inch in length, and consists of but four segments, of which the last alone exhibits the ripe condition. The head resembles in construction that of the pork tape-worm, being provided with four suckers and a prominent crown, with from thirty to fifty hooks arranged in a double circle. The terminal ripe segment exceeds in size all the preceding together, and before it separates from the series another is ready to take its place. The ripe eggs contain the usual six-spined embryo as in other tape-worms.
The mature worm is remarkable for the comparative shortness of its life, which, according to Siebold, is about seven weeks. Apparently to compensate for the small number of its segments, the larval form is endowed with the power of multiplying itself to a wonderful degree.
It is only in the larval condition that the hydatid tape-worm infests man, and in this state also it infests the ape, the ox and sheep and other ruminants, also the horse, hog, and indeed many other animals of the same class.
[p. 944] If the eggs of the tape-worm are swallowed, which may readily happen by too free intimacy or association with infested dogs, the liberated embryos obtain access to the intestine. Penetrating the mucous membrane, the embryos thence may migrate to any part of the body. From the comparative frequency of hydatid tumors in the liver we may suspect they mostly enter the portal venous system and take the course of the blood-current. It is, however, probable that they migrate directly to their destination, for hydatid tumors are also frequently seated in the neighboring organs and the abdominal walls. The embryo tape-worm, once fixed in position, becomes the starting-point of a hydatid tumor.
When dogs are fed on the liver, or other parts affected with hydatid tumors, from the sheep or other animals, the scolices are liberated, and, passing into the small intestine, are there developed into the mature tape-worms.
Hydatid tumors occur in any of the organs of the body, but are more frequent in the liver than in all others together. They are common in the lungs, kidneys, spleen, omentum, and subperitoneal tissue of the abdominal walls. They are less common in the heart, brain, spinal canal, the pelvic viscera, and the bones. Mostly but a single tumor is found in the same person, but occasionally several occur together in the same or in different organs.
There are several varieties of the hydatid tumor. In man the more common form consists of a cyst or a group of cysts enclosed in a connective-tissue envelope induced by the presence of the parasite. The simple cyst is produced through the transformation of the echinococcus embryo, and the group of cysts is derived from the former by proliferation; and hence the first has been called the parent cyst, and the others the daughter cysts. These also in the same manner may produce a third series, called granddaughter cysts. The parent cyst, at first spherical, becomes modified in shape according to the space it occupies and the resistance to which it is subjected, thus assuming an oval, lobulated, or other form. It may increase in size to that of a cocoanut or larger, and may remain simple, but usually is compounded by proliferation in the production of daughter cysts. These may be few or many up to hundreds, and range from a minute size up to that of a walnut, and are spherical or modified in shape by mutual pressure or other cause. The cysts are filled with a clear watery liquid of saline taste, but without albumen.
The hydatid cysts are usually composed of an outer thick, translucent, homogeneous, laminated, glistening, highly elastic membrane, the ectocyst, and an inner thin, granular, and cellular layer, the endocyst. From the endocyst originate minute buds, which become the brood-capsules of the larval worms or scolices. These form little groups of a few to a dozen individuals suspended within the brood-capsules, but capable of eversion from them. The individual scolices, which appear to the naked eye as mere white points, have the form and construction of the head-segment of the mature Tænia echinococcus. After death or by violence they become easily detached, and then float free in the liquid containing them. In some cases the echinococcus cysts develop no scolices, in which condition they constitute acephalocysts. Occasionally the echinococcus embryo undergoes imperfect development, constituting the multilocular hydatid tumor, rarely found elsewhere than in the liver.
[p. 945] Echinococcal tumors, especially those which have many daughter cysts, when accessible are remarkable for exhibiting a tremulous movement when grasped by the hand and quickly tapped with the finger.
Infection through the embryonic form of the Tænia echinococcus, as the source of hydatid tumors, is productive of the most disastrous consequences, and has ended in the destruction of many lives both of men and domestic animals. The parasite is not directly productive of suffering, but its effects and dangers are proportioned to the size of the tumor it occasions and the character and importance to life of the organ in which the latter is situated. With the increase of the hydatid tumor, usually of very slow growth, it encroaches upon the surrounding parts, and if these are not displaced they become disorganized and atrophied.
The liability and frequency of infection with the hydatid disease appear to be proportioned to the prevalence of intimate association with the dog. In Iceland, in which it is said every peasant owns half a dozen dogs, which share his dwelling with him, it is also reported that one-sixth of all the deaths are due to the hydatid parasite.
Ordinarily, the hydatid disease is beyond the reach of medical treatment. The mercurials and potassium iodide have been recommended, but the results are very doubtful. Apparently as an indication how little hydatid parasites may be influenced by medicine, the following incident will show: The writer once received for dissection the body of an English sailor which had been injected with zinc chloride for preservation. In the abdominal wall in the right iliac region there was a hydatid tumor the size of a fist. On examination of the tumor it was found full of daughter cysts, and these contained living scolices, though the man had been dead several days and the tissues were bleached by the zinc solution.
Favorable results in the treatment of hydatid tumors are only to be expected through surgical means when they are accessible.
As a prophylactic measure against infection the avoidance of too intimate association with dogs is especially to be recommended.
In concluding the chapter on Tænia echinococcus, as a prophylactic against this and other parasites Cobbold gives the advice that "all entozoa which are not preserved for scientific investigation or experiment should be destroyed by fire when practicable, and under no circumstances whatever should they be thrown aside as harmless refuse."
TÆNIA ACANTHOTRIAS.
Larval condition: Cysticercus acanthotrias.
This species has been but once observed, and only in the larval condition or that of the scolex, which was first described by Weinland. About a dozen specimens were found by Jefferies Wyman of Boston in the body of a woman of Virginia who died of phthisis. They were situated in the connective tissue beneath the skin and in the muscles, except one, which was attached to the dura mater. The scolex is distinguishable from that of the other human tape-worms in possessing a triple circle of hooks. The mature form of the worm remains unknown.
The trematodes or fluke-worms, though allied to the tape-worms, differ in many important characters. In the mature condition, like the latter, they are solid worms or are devoid of a body cavity or coelum, and are with rare exceptions hermaphroditic. They are, however, never compound, but simple or consist of single individuals, and are provided with a mouth and alimentary canal, but this is closed or is without an anal aperture. They have a water vascular system, communicating with the exterior by a pore at the posterior extremity of the body. They are commonly of flat, elliptical shape, with a sucker-like mouth at the fore end, and with a second sucker situated ventrally near the middle.
The fluke-worms are remarkable for their successive transformations and course of life, and, like the tape-worms, they pass the different stages of their existence in different animals. A number of species have been described as infesting man, but most of them are, fortunately, of rare occurrence.
DISTOMUM HEPATICUM.—SYNONYMS: Fasciola hepatica; Liver-fluke.
This species, the common liver-fluke, occasionally occurs in the human body, but is especially frequent in the sheep and other ruminating animals, as the ox, goat, and deer, and it likewise occurs in the horse, hog, and some other animals. It usually inhabits the liver, occupying the bile-ducts, but is also sometimes found in the portal and other veins and in the intestine, and more rarely in abscesses beneath the skin. It is the cause of the affection in sheep called rot, of which many thousands die annually.
The liver-fluke is a flat, tongue-shaped, brownish worm about an inch long and about half as wide. It is invested with minute scale-like spines. The head end is somewhat prolonged, and terminates in a small oral sucker, a short distance behind which is a small ventral sucker. The intestine is forked and much branched. The genital aperture is situated between the oral and ventral suckers. The commonly yellowish eggs are numerous and large, oval, and measure about 0.135 mm. long.
The common liver-fluke frequently occurs in large numbers, even hundreds, in the liver of the sheep, obstructing the bile-ducts and occasioning more or less destruction of the organ. The eggs pass off with the bile into the intestine, and are discharged with the excrement. In water the eggs are hatched, and deliver a ciliated and freely-swimming embryo. This in favorable positions, such as marshy pastures, obtains access to small fresh-water snails and penetrates to the interior of their body. Here the embryo sheds its ciliated integument and is transformed into a sporocyst. This is an elliptical pouch containing reproductive bodies, which become developed into individuals of more elongated form than the sporocyst, provided with a mouth and stomach, and named redias, or nurses. The nurse penetrates to the liver of the snail, and there develops within itself new forms called cercarias, which resemble the parent fluke-worm, but are provided with a long, powerful tail and have no apparent generative apparatus. The cercaria escapes through an aperture of the nurse, and makes its way out of the snail into the water, where it swims about actively by means of the tail, much in the manner of a tadpole. [p. 947] The cercaria after a time fixes itself to a submerged plant, becomes encysted, shakes off its tail, and remains in a quiescent state. If in this condition, in the feeding of sheep or other animals, the tailless cercaria or incipient fluke-worm is transferred to the stomach, it makes its way to the liver, and there grows and is developed into the sexually mature worm.
Recently it has been ascertained both in England and Germany that the juvenile state of the fluke-worm is passed especially in the little fresh-water snail Lymneus truncatulus. As, however, the common liver-fluke occurs in America, while the last-named species of Lymneus does not, it is rendered probable that the juvenile condition of the parasite also occurs in other species of snails. Incidentally, the writer may here mention that he has found certain of our smallest fresh-water snails, such as Planorbis parvus, frequenting meadows in the vicinity of our rivers and creeks, swarming with nurses of several different species of fluke-worms.
Notwithstanding the frequency of the common liver-fluke in the sheep and other domestic animals, its occurrence has been rare in man, and in all the cases reported it has been few in number, either single or from two to half a dozen. In man it has been found to occupy the bile-ducts, the portal vein, and abscesses beneath the skin.
DISTOMUM LANCEOLATUM.—SYNONYM: Smaller Liver-fluke.
This species, much smaller than the preceding, is of lanceolate form, acute behind, smooth, and about a third of an inch long. Its suckers are moderately large, and the bifurcate intestine is unbranched. It infests the liver of the sheep and ox and some other animals, and not unfrequently is found in association with the former species. It usually does not occur in such great numbers together as in the latter; from which and other circumstances, as the smaller size and smooth investment, it does not produce the same serious results. Its continuous history remains unknown, though it is probable that its course is similar to that of the common liver-fluke. Several cases are reported of its occurrence as a parasite in man.
DISTOMUM SINENSE.—Under this head Cobbold has recently described a species somewhat larger than the D. lanceolatum. It occurs in the liver of Chinese.
DISTOMUM CONJUNCTUM.—Another species described by Cobbold under this name, originally found in the liver of an American fox, has also been detected in man. The worm is about one-fourth of an inch long.
SYMPTOMS.—Cases of fluke-worms in the human liver have occurred so rarely that we are not prepared to indicate with certainty what may be the nature of the peculiar symptoms. If the parasites were numerous, they would give rise to more or less obstruction of the bile-ducts, with accumulation of bile, accompanied with jaundice and other symptoms usually attendant on functional disturbance of the liver. As in sheep, they would occasion dilatation of the bile-ducts, catarrhal inflammation, incrustation with biliary matters, hyperplasia of the surrounding [p. 948] tissues, and more or less disorganization and atrophy of the secretory structure.
TREATMENT.—As regards the treatment, we can say almost nothing. In the destructive disease of rot in sheep there are no known means to expel the parasites from the liver. If present in man, as they occur but few in number, we may hope for their spontaneous expulsion in due time without leaving any serious result. As a means of prophylaxis persons should carefully avoid salads prepared from subaquatic vegetables, like cress, which may harbor little fresh-water snails.
DISTOMUM HETEROPHYES.—This is a small species, about half a line long, with the fore part of the body covered with minute spines, and having a large, nearly central, ventral disk. It has been but once observed, and was reported by Bilharz, in Cairo, as having been found, in the post-mortem examination of a boy, in the small intestine, in which it existed in hundreds.
DISTOMUM CRASSUM.—This is the largest of the fluke-worms infesting man, and measures from one to three inches in length. It is elliptical, comparatively thick, and smooth. The two suckers have nearly the same relative size and position as in the D. hepaticum. It inhabits the duodenum, and has been observed a number of times infesting inhabitants of China and India.
DISTOMUM RINGERI.—A species by this name, about half an inch long, has recently been described by Cobbold as infesting the lungs of people in Formosa and China.
DISTOMUM OPHTHALMOBIUM.—A minute species, described under this name, has been detected several times in the human eye.
BILHARZIA HÆMATOBIA.—SYNONYM: Distomum hæmatobium.
As a human parasite this is the most important of the fluke-worms, being the most common and dangerous. It is apparently restricted to Africa and Arabia, and is especially frequent in Egypt, Abyssinia, the Cape of Good Hope, and Natal. So far as known, it is peculiar to man and monkeys, and inhabits the veins, especially those of the portal system, and it lives on the blood.
The blood fluke-worm is remarkable among its kind in having the sexes distinct. The female is slender, cylindrical, and tapering toward the ends, looking more like an ordinary thread-worm than a fluke-worm, and is about three-fourths of an inch long. The male is about half an inch long, but wider than the female, which it partially embraces at maturity by doubling upon it laterally.
This parasite, of the same essential nature as the more ordinary fluke-worms, is most probably introduced in the juvenile condition into the stomach by drinking unfiltered standing waters, and perhaps also by eating vegetables which grow in wet places and upon which the young fluke-worms may be encysted. From the stomach the worms gain access to the portal venous system, within which they undergo development to sexual maturity. The worms, proportioned to their number, [p. 949] occasion more or less sudden and dangerous hæmaturia. According to Bilharz, who first discovered the parasite, it also induces inflammation of the ureters, bladder, and rectum, accompanied with ulceration and incrustations and concretions in the same, due to the abundant deposit of eggs in the mucous membrane. The symptoms in the hæmaturia are obvious; all treatment fails, but the prophylaxis is evident.
AMPHISTOMUM HOMINIS.—The genus Amphistomum is distinguished from Distomum in having the ventral disk placed at the posterior extremity of the body.
A species has been recently described by Cobbold under the above name, and is reported as having been observed several times in natives of India. It is a red worm, about the fourth of an inch long, and inhabits the cæcum and ascending colon, in which it was found in hundreds together. The mucous membrane exhibited venous congestion and was marked with numerous red spots resembling leech-bites, produced by the parasites. One of the patients died of cholera.
We have too little information as to the symptoms induced by this parasite, and of its treatment, to say anything. It is probable that calomel, turpentine, and castor oil would be appropriate remedies.
Several other fluke-worms which have been reported as having been found in the human body are generally viewed with doubt as to their genuineness. Such are the Hexathyridium pinguicola, from a tumor of the ovary; the H. venarum, said to have been found in the blood and in the sputum of hæmoptysis; and the Tetrastomum renale, said to have been found in the urine.
The thorn-head worms in the mature condition are comparatively robust cylindrical worms, with a body-cavity or coelum, but devoid of mouth and alimentary canal. They are provided with a protrusile and retractile proboscis-like head armed with circular rows of recurved hooks, by which they firmly cling to the wall of the intestine of their host. The sexes are distinct. There are many species, which mostly in the mature state live in fishes. In the juvenile or larval condition they live in other animals, mostly crustaceans and insects. It is doubtful whether any species naturally infests man.
ECHINORHYNCHUS GIGAS.—The great thorn-head worm is a common parasite of the hog, living in the small intestine. It is a large white worm, the female of which reaches a foot in length, while the male is about one-third the size. It is doubtful whether it occurs as a human parasite, though a worm less than the fourth of an inch found in a man in Prague has been attributed to this species.
The nematodes, or thread-worms, are slender, cylindrical, and inarticulate, and usually more or less tapering toward one or both extremities. [p. 950] They have a distinct coelum or body-cavity, with thick muscular walls limited by a transparent elastic, chitinous integument, which is sometimes more or less distinctly and regularly transversely wrinkled. The alimentary canal extends the length of the coelum, with the mouth at the anterior extremity, and usually an anus at or near the posterior extremity. In some forms in the mature condition the intestine is atrophied and the anus absent. The sexes are distinct, and commonly the male is very much smaller than the female. The organs of generation occupy the coelum along the sides of the intestine. The female aperture is commonly situated ventrally near or in advance of the middle of the body, while the male aperture is at or in the vicinity of the anus. Mostly, the worms are oviparous, but many are viviparous. The development is direct, and usually the transformations are inconspicuous, so that the embryos mostly differ but little from the parent, except in the absence of the generative apparatus.
OXYURIS VERMICULARIS.—SYNONYMS: Ascaris vermicularis; Seat-worm; Pin-worm; Maw-worm; Maggot-worm; Thread-worm; Ascarides.
The seat-worm is the most common intestinal parasite of man, prevails everywhere, and is peculiar to him. It is a lively, wriggling creature which inhabits the small and large intestines and feeds on their contents. It frequently occurs in large numbers together, and in such cases incessantly makes its appearance, associated with multitudes of eggs, in the evacuations.
The female, which is ordinarily seen alone in the greatest abundance, is a white cylindrical worm tapering toward both extremities. The head end is thickened, and is provided with three prominent labial papillæ enclosing the mouth. The posterior end extends from the anal aperture in a long and straight, narrow, conical, sharp-pointed tail. The double uterine tube, distended with eggs, terminates in a vagina, the external aperture of which is situated ventrally near the anterior third of the body. The smaller male hardly tapers behind, but is incurved and ends in a short, blunt, conical tail. The penis is a single chitinous spicule, the end of which is usually seen projecting from the cloacal aperture.
The young seat-worms, in various degrees of growth and development, and the mature males are chiefly to be met in the lower portion of the small intestine, while the pregnant and mature females chiefly occupy the cæcum.
The seat-worm is exceedingly prolific, it being estimated that a single ripe female contains from 10,000 to 12,000 eggs, and these, it is suspected, may be renewed several times before her functions become exhausted. From time to time the ripe females proceed along the large intestine to the rectum, in which position they lay most of their eggs. These are discharged, together with many of the worms, in the feces.
The eggs are ovoid in shape and about 0.05 mm. long. After they are laid under favorable conditions the embryos are rapidly developed. Left in water, they soon die.
The investigations of the helminthologists of the day make it appear that it is necessary that the eggs of the seat-worm should be swallowed [p. 951] and pass through the stomach, in which the embryos are freed, before they can undergo development to sexual maturity. Moreover, observations go to show that infection may, and probably ordinarily does, occur from eggs scratched from the anus and conveyed to the mouth directly or by being applied to food from uncleanly hands. It is evident that itching of the anus, induced by the presence of the parasites in the rectum, often accompanied by itching of the nose and lips, may lead to alternate scratching of the parts and the transference of eggs from one to the other. Thus, too, uncleanly nurses who may be infested with seat-worms after scratching may handle food and infest children under their charge. Children are commonly more liable to the parasites than others, no doubt from the circumstance that they are less capable of avoiding the conditions favorable to infection. Seat-worms prevail in all conditions of society, but their prevalence is largely proportioned to the more or less uncleanly habits. Persons sleeping with others infested are liable to infection, especially if they are uncleanly and in the habit of eating in bed. Obvious hints to avoid the parasites are obtained by regarding the statements thus given.
SYMPTOMS.—The presence of a few seat-worms is usually attended with no obvious inconvenience, and they may remain unnoticed unless accidentally observed in the evacuations. The symptoms occasioned by them are in great measure proportioned to their quantity and the susceptibility of the patient. The most prominent symptom is excessive itching of the anus; often trifling or even absent during the day, it becomes very annoying and distressing in the evening or during the night. This periodic change appears to be due to the movement of the worms to the rectum, apparently induced by the position and repose of the patient and the increased warmth of the body in bed. Under these circumstances the patient attempts to relieve the incessant itching by scratching, and often by boring with the finger in the anus. In this way eggs become adherent to the finger-nails, under which they have been repeatedly detected, and may thus be inadvertently transferred to the mouth. Occasionally, some of the worms wander from the anus, and in women may thence penetrate into the vulva. The itching of the anus may induce more or less sexual irritation, which in the young may further lead to onanism and its attendant evils. Other symptoms of the presence of the parasites are itching of the nose and lips, restlessness in sleep, grinding of the teeth, startings, twitchings, and general nervous disturbance. When the worms are very numerous they may produce intestinal catarrh, with discharges of mucus, pain, and diarrhoea. In children especially they may give rise to more serious nervous symptoms, as epileptic fits and chorea.
TREATMENT.—Generally, persons are readily relieved of seat-worms. Epsom salt alone or with senna as a purgative, repeated once or twice, often answers to completely expel them. Castor oil, also alone or with a few drops of the oil of turpentine or of wormseed, is also an effectual remedy. The tincture of aloes, in the dose of from half a fluidounce to two fluidounces, once or twice repeated, the writer has found to fully answer the purpose. Besides the purgatives, medicated suppositories, in obstinate cases injections of olive oil, and enemata of a solution of castile soap introduced by means of an elastic tube, so as to wash out the entire length of the large intestine, may be employed.
[p. 952] ASCARIS LUMBRICOIDES.—SYNONYMS: Round-worm; Long round-worm; Maw-worm; Lumbricus.
The round-worm is the largest of the nematodes which ordinarily infest man, and is second only in frequency to the seat-worm. It is a well-known parasite, and prevails everywhere in all conditions of society. It is less lively in its movements than the seat-worm, and is remarkable for possessing a peculiar disagreeable odor, which is independent of the medium in which it lives. It inhabits the small intestine and feeds on the contents. It also infests the hog and the ox.
The round-worm is cylindrical, reddish or brownish, and tapering toward both extremities. The head end terminates in three prominent labial papillæ surrounding the mouth, and the tail end is short and conical. The female, as commonly seen, ranges from six inches to a foot in length, and is about a fourth of an inch in thickness. The ovarian tubes are long, thread-like, and tortuous, and, with the shorter, nearly straight, and wider uterine tubes, contain many millions of eggs. The genital aperture is situated ventrally near the anterior third of the body. The male is about half the size of the female, but is capable of considerable extension, and the tail end is incurved. The penis consists of a pair of slender, clavate, chitinous spicules, the ends of which protrude from the cloacal aperture at the root of the tail.
The round-worm is exceedingly prolific, it being estimated that the genital tubes of a large mature female contain the enormous number of 60,000,000 of eggs. The ripe eggs are laid in the intestine, and are discharged with the evacuations in great numbers, and often in considerable masses together. They are oval, about 0.05 mm. in length, and are provided with a thick shell and an additional tuberculate albuminoid envelope, usually colored by the intestinal contents.
The eggs of the round-worm after being expelled from the body are very tenacious of life, and under ordinary favorable circumstances they may remain in a condition capable of development for several years. Experiments have shown that they have great power in resisting the destructive influences of heat and cold, dryness, and the agencies of decomposition. In water and moist earth they have been retained alive for a year or two. When ripe eggs are placed in water the development of the embryo is observed to proceed very slowly, and is only completed after five or six months. The embryo while still contained within the egg sheds its skin and becomes provided with a tooth-like spine to the head end. The smallest examples of reputed round-worms found in the human intestine measured only about a line in length.
The further history of the round-worm is unknown, nor has it yet been positively ascertained in what manner man becomes infected with the parasite. Repeated experiments, not only on the hog and other animals, but on man himself, go to show that he is not directly infected by swallowing the recently-laid ripe eggs. It is rendered probable that the eggs are swallowed by some common but yet unknown minute aquatic animal, within which the embryo may undergo further development, and in this condition may be swallowed by man in drinking-water. In confirmation of the view that man becomes infected in the latter way, Davaine remarks that the "people of Paris, who drink only filtered [p. 953] water, are rarely infected with the round-worm, which is otherwise the case in the rural districts of France."
The round-worm is most prevalent in warm climates, and especially among the less-civilized peoples. The better classes among the more enlightened nations suffer comparatively little from the parasite, and it is the lower classes, especially the ill-fed and uncleanly, who are most afflicted. It is exceedingly frequent in the Orient, in Africa, the West Indies, and Brazil.
Most commonly, only a few round-worms—one, two, three, up to a dozen—occur together in the same person, but they often occur in considerable number, even to several hundreds. Not unfrequently they are found in association with seat-worms. They are more frequent and usually occur in greater abundance in children, perhaps in a measure due to the circumstance that they are less able to discriminate the conditions favorable to infection and avoided on other grounds by adults.
The natural and ordinary habitation of the round-worm is the small intestine, especially the jejunum, and it commonly only occurs in the large intestine, mostly dead, on the way to be discharged with the evacuations. Under disturbing circumstances, as the character of certain irritating food, the parasite is disposed to become restless and wander from its usual position. Not unfrequently it enters the stomach, and thence may ascend to the mouth or nose, and perhaps the first intimation of the presence of such an unwelcome guest is in its expulsion from the mouth. From the pharynx the worm may enter the larynx and trachea, or advance farther into the air-passages, giving rise to the usual symptoms of foreign bodies in these parts. Occasionally the parasite forces its way through the bile-ducts into the liver and gall-bladder, creating disturbance in those organs proportioned to the number and size of the worms and the extent of their progress. In the liver it may occasion inflammation and the formation of an abscess attended with all the usual symptoms of hepatitis. It has been reported that it may penetrate the intestinal wall and enter the peritoneal cavity, but it is generally regarded as doubtful whether the worm can do so in a healthy state of the intestine, but only where there may be ulceration or other similar condition.
SYMPTOMS.—The symptoms indicating the presence of the round-worm in the intestine vary with its numbers and with the age and susceptibility of the patient. In general, the presence of one or two worms is unattended with any marked disturbance, and is mostly unsuspected until the parasite is accidentally seen in the discharges. The ordinary symptoms are disordered appetite (usually increased), flatulence, hiccough, foul breath, dyspepsia, abdominal pains, itching at the extremities of the alimentary canal, furred tongue, darkening of the eyelids, and emaciation. The nervous symptoms are restlessness in sleep, unpleasant dreams, starting in fright, grating of the teeth, and muscular twitchings. In more aggravated cases, especially in children, epileptic fits may occur. If the parasites are numerous, they produce diarrhoea with copious mucus discharges, and may induce enteritis with all its attendant symptoms. When the worms wander into the stomach, they induce colic, nausea, retching, and vomiting, all of which disappear with the expulsion of the parasites.
TREATMENT.—The remedies employed for seat-worms often serve to [p. 954] expel the round-worm, and not unfrequently the two are discharged together. Wormseed, or the seed of Chenopodium anthelminticum, has been a favorite remedy for the round-worm, especially in children. The dose in these cases is one or two scruples of the powdered seeds in electuary with syrup or molasses, administered in the morning before breakfast and at bedtime for three or four days. It should be followed by calomel or other brisk cathartic. The volatile oil, in the dose of from five to ten drops in emulsion, may be used in the same manner.
A much-extolled remedy to destroy and get rid of the round-worm is santonin, given in doses of from one-third to one and a half grains three or four times a day, the larger dose being used only for adults. It should be followed by a purgative, for which a dose of castor oil answers a good purpose.
ASCARIS MYSTAX, the common round-worm of the cat and dog, has been reported as occasionally infesting man. It resembles the former species, but is much smaller, commonly from one to four inches in length, and has the head end furnished with a pair of lateral narrow, wing-like expansions of the integument. It inhabits the small intestine, and when present in man would no doubt induce symptoms like those of the ordinary round-worms which infest him.
TRIOCEPHALUS DISPAR.—SYNONYMS: Long thread-worm; Whip-worm.
The long thread-worm is a not unfrequent intestinal parasite of man, though rarely observed unless specially sought, as it ordinarily gives rise to little or no disturbance. It is common in England, Southern Europe, and the Orient. Davaine reports that half the cases of persons investigated in Paris were infested with it; it also occurs in this country. It inhabits the lower end of the ileum, the cæcum, and vermiform appendix, and feeds on the intestinal contents. It commonly occurs in small numbers, two or three to a dozen, occasions no evident inconvenience, and is rarely discharged with the evacuations.
The long thread-worm is yellowish-white and cylindrical, with the anterior half or more of the body attenuated in a hair-like manner. The female reaches about two inches in length, has the tail end conical, and the anus subterminal. The male is about two-thirds the length of the former, has the thicker portion of the body enrolled, and the tail end blunt. The eggs are laid in the intestine and discharged with the feces. The subsequent history of the parasite and its mode of infecting man remain unknown.
Only in cases where long thread-worms are numerous do they give rise to trouble. According to Leuckart, Pascal gives as constant symptoms of the presence of large numbers of the parasite, headache, redness of the face, prominence of the eyes, small, irregular, and intermittent pulse, and pains in the lower part of the abdomen.
The usual remedies addressed to the seat-worm and round-worm will most probably be equally applicable to the long thread-worm.
LEPTODERA STERCORALIS.—SYNONYMS: Anguillula stercoralis; Rhabditis stercoralis.
[p. 955] This is a minute nematode worm recently observed infesting French soldiers in Cochin China. It is about half a line in length, and inhabits the small and large intestine, and also penetrates into the biliary and pancreatic ducts. It occurs in myriads and occasions diarrhoea and dysentery. Another species, Leptodera intestinalis, nearly three times as large, has been noticed in smaller number associated with the former. The eggs of these worms are laid in the intestines, and both together are discharged in multitudes with the feces. They are probably introduced into man by drinking stagnant water, and undergo complete development after passing through the stomach.
It is probable that the remedies employed in the treatment of the familiar seat-worms and round-worms would be equally efficacious in the expulsion of these parasites.
ANCHYLOSTOMUM DUODENALE.—SYNONYMS: Strongylus duodenalis; Dochmius duodenalis; Sclerostoma duodenale.
This intestinal parasite, first noticed in Milan by Dubini in 1838, is of more dangerous character than any of the nematode worms previously described. In Europe, besides Italy, it was frequently observed among the workmen of the St. Gothard tunnel. It is exceedingly common in Egypt, and Bilharz found it in nearly all his post-mortem examinations of bodies. It probably prevails to a considerable extent in most tropical countries, including the East and West Indies and Brazil. There is also reason to suspect, from the nature of the affection it induces, that it may exist in the Southern States.
The Anchylostomum is a red, cylindrical worm, with the anterior extremity tapering and recurved. The head end, somewhat enlarged, encloses a capacious oral capsule armed with strong hook-like teeth. The caudal extremity of the female ends in a conical point, and the genital aperture is situated behind the middle of the body. The caudal extremity of the male ends in a trilobate pouch, within which projects the bispiculate penis. The female is from five lines to three-fourths of an inch long; the male is about half the size. The eggs are oval and measure 0.05 mm. long.
The worm inhabits the small intestine, especially the duodenum and jejunum, clinging tenaciously to the lining membrane by means of the armed mouth. It penetrates the mucous membrane to the submucous coat, from which it sucks the blood that forms its food. In the position of its attachment it gives rise to little ecchymoses. It often occurs in large numbers, even to hundreds and thousands. The eggs are laid in the intestine and are discharged with the evacuations. Externally, in water, the embryo undergoes development within the egg, and then escapes to lead for some time an independent existence. Subsequently, it is most probable that the worm obtains access to the human stomach by drinking standing water, and completes its development in the intestine.
The Anchylostomum proves to be a prolific source of wasting diseases in tropical countries, and is pernicious to an extent proportioned to the numbers infesting the intestine. By depriving the body of blood it produces a greater or less degree of anæmia. The affection begins very insidiously, and the general nutrition of the body may not be visibly disturbed [p. 956] until a late period. In moderate cases the disease is indicated by general paleness of the skin and mucous membranes, fatigue on slight exertion, and a tendency to palpitations and quickened pulse. In more severe cases there is constantly increasing debility, with increase of paleness, indisposition to exertion, excessive sleepiness, and feeling of coldness. Dyspeptic symptoms sometimes appear, and loss of appetite may alternate with ravenous hunger. Accompanying this there is often a disposition to eat innutritious articles, as coal, clay, wool, etc. Feeling of weight and oppression in the epigastrium and abdominal pains are frequent. In the advance of the affection shortness of breath appears, increased on exertion to violent dyspnoea. Emaciation becomes obvious in the later stage of the disease. In the worst cases the symptoms increase in severity, the patient becomes dropsical, is attacked with profuse diarrhoea and vomiting, and finally dies.
The severity of the affection is proportioned to the number of parasites present and the quantity of blood they consume and cause to be lost. Bad cases may end fatally in a few weeks, but generally the disease lasts for months, and where the patient is provided with abundance of good food it may continue for years.
The prognosis of the disease is rather unfavorable; if, however, the nature of the affection is ascertained before it has greatly exhausted the patient, and the parasites can be expelled, the result should be favorable.
We have thus far obtained but little information as to the best treatment for Anchylostomum. Calomel and turpentine have been recommended, and, as these are most powerful vermicides, we have reason to believe they would prove most effectual remedies.
In regard to the prophylaxis for Anchylostomum—and we may add in general for all parasites which gain entrance to man through drinking-water—all stagnant or standing waters should be filtered, so as to remove any source of infection, whether by eggs or free embryos of parasites or of larval forms existing within minute aquatic animals which serve as intermediate hosts to parasites. Standing waters, such as those of puddles, ditches, marshes, and ponds, more or less swarm with minute animals, all of which may be entirely removed by filtration. Even the water of cisterns and wells, if supplied from the free surface of the country, may not be free from minute animals, and especially eggs, and therefore requires filtration to be safe. Only spring and freely-running water of rivers and creeks and of lakes is commonly free from microscopic animals and their eggs, and therefore devoid of all danger in these respects.
STRONGYLUS LONGEVAGINATUS; S. bronchialis.—This nematode has been only once satisfactorily observed. Many occurred in the lungs of a boy in Germany, but the real cause of his death was not stated. The female worm is about an inch long, the male about five-eighths of an inch.
Certain worms previously discovered in the bronchial glands of a case of phthisis, and described under the name of Hamularia lymphatica, are regarded by Cobbold as the same with the former; but the descriptions of the two render this improbable. Treutler's drawing of Hamularia, as copied by Leuckart, looks like an Ascaris upside down.
[p. 957] EUSTRONGYLUS GIGAS; Strongylus gigas; Palisade-worm; Kidney-worm.—This worm, recorded in the catalogue of human parasites, is doubtful as such. Pertaining to the same family as Anchylostomum, as the common name indicates its usual habitation is the kidney. It is the largest of the nematodes, and is a long, cylindrical red worm, slightly tapering, and blunt at the ends. The mouth is enclosed by six rounded labial papillæ. The caudal extremity of the male ends in an inverted cup-like pouch, from which the penal spiculum protrudes. The female commonly ranges from one to three feet in length and from a fourth to nearly half an inch in thickness. The male ranges from six inches to a foot in length and from one to three lines in thickness.
The mature parasite is common in many fish-eating mammals, from which it is inferred that fishes are the intermediate host for the juvenile condition of the worm. It is frequent in the wolf, dog, mink, weasel, raccoon, otter, and seal. It also occurs in the hog, and is reported to have occurred in the horse, ox, and man. Usually it is solitary, and occupies one of the kidneys coiled upon itself. Under its influence the kidney is atrophied and reduced to the condition of a capsule of connective tissue, often containing bony spicules. It feeds on blood and on the purulent matter resulting from the inflammation it produces. The worm is occasionally found in other positions, as the mesentery, the abdominal cavity, the intestine, liver, urinary bladder, and lungs, but perhaps in most of these cases has been derived from its usual habitation. In this country the writer has repeatedly observed the kidney-worm in the mink, the dog, and the wolf. In one instance in the former animal he found a female and a male associated together in one kidney, which was reduced to the condition of a fibrous capsule containing in its wall a large radiated plate of bone.
The cases on record of the occurrence of this formidable parasite in man are of very early date, and are mostly doubtful as to the authentic nature of the worm, and are all unsatisfactory as to the attendant phenomena.
TRICHINA SPIRALIS.—The trichina, or flesh-worm, a minute nematode, is a common parasite of man, and from its wide prevalence and results may be regarded as the most dangerous of all. Perhaps from the earliest ages it has been dealing death freely and indiscriminately to our kind without its existence having been suspected until within the last half-century. Frequently, the affection, now named trichinosis, produced by its presence has been so prevalent in communities as to appear epidemic. The parasite was first discovered, and is commonly observed, as a little worm coiled up and imbedded in the flesh of man. In the same manner it is frequently seen in the flesh of the hog. In the adult or mature state it lives in the small intestine of both man and the hog, but its duration of life in this position is comparatively brief.
Trichinosis, or the disease induced by the introduction of trichinæ into the intestinal canal and the migration thence into the voluntary muscles, varies in symptoms and gravity with the number, condition, and position of the parasites and the susceptibility of the patient. The presence of trichinæ in the alimentary canal, though often accompanied by violent symptoms, is comparatively free from danger, whereas in the muscular [p. 958] system they not only produce the greatest suffering, but often the most disastrous results.
Man is ordinarily infected with the trichina by eating the raw or insufficiently cooked meat of the hog, or pork in any of its varieties of food. Infected meat often contains immense numbers of the parasite, a single ounce at times being estimated to contain from 50,000 to 100,000 worms.
The trichina was first distinctly noticed in the muscles of the human body by Paget in 1835, and was described by Owen with the name it now bears. It was subsequently observed under the same circumstances by other investigators. In 1846 the parasite was found by the writer in the muscles of the hog, but neither he nor others for some time afterward suspected the significance of the discovery. In 1860, Zenker of Dresden treated a supposed case of typhus complicated with excessive muscular pain and oedema. On post-mortem examination the muscles were found swarming with trichinæ, and to these the affection altogether was attributed. Nearly at the same time the investigations of Leuckart confirmed the relationship of the parasites as the cause of the disease. In 1862, Friederich first diagnosticated the affection and experimentally determined the presence of the worms in the living patient.
The trichina is also found infesting other animals of the same class besides man and the hog, especially the rat, mouse, rabbit, cat, and fox. Experiments further prove that mammals are generally more or less susceptible to infection with the parasite, though some appear to resist its extension to the muscular system, as in the case of the dog. The horse, ox, and sheep exhibit little disposition to artificial infection of the muscles, and hence from this circumstance and the nature of the food of these animals they are rarely found to be infested with trichinæ. In experiments on birds and lower classes of animals, though trichinæ were ascertained to advance in development in the intestine, they failed to invade the muscular system.
Ordinarily, it appears that while man is infected with trichinæ through the hog, this animal becomes infected by eating infested rats, mice, and cats, fragments of waste pork, and perhaps occasionally by feeding on the excrements of infested animals.
The trichinæ occupying the muscles are immature, and it is only after they are swallowed and the parasites are freed by digestion of the envelopes and pass into the intestine that they undergo development to sexual maturity. In this state the female is viviparous and gives birth to a multitude of active embryos, which immediately commence to migrate to the muscular system. As it is estimated that each female may give birth to upward of a thousand embryos, it is readily conceived to what an extent the body may become infested from eating a few ounces of trichinous pork.
The immature or larval trichinæ are also distinguished as muscular, and the sexually mature ones as intestinal, trichinæ, in accordance with their position in the two principal conditions.
Muscular trichinæ vary in condition from the embryo, which works its way among the muscular fibres or has obtained entrance into these, to the coiled-up worm lying quiescent in a capsule imbedded among the muscular fibres.
Infected flesh in the early state is scarcely distinguishable as such with [p. 959] the naked eye, but in old cases the trichina capsules become imbued with calcareous matter, and are thus rendered visible as minute white or grayish specks scattered through the red meat.
In the recent state of invasion the worms are found free among the muscular fibres or within these. Later, they appear mostly solitary and at rest, coiled within a fusiform mass of semi-liquid granular matter resulting from the degradation of the muscular substance. Subsequently, they become enclosed in an elliptical capsule, apparently derived from the myolemma of the muscular fibre they had entered. The capsules, situated among the bundles of sound muscular fibres, are arranged with their long diameter parallel with the latter. The trichina capsules commonly measure about one-fifth of a line long, and the coiled worm within is scarcely a half-line long.
If muscular trichinæ remain with their host, after a year or more they exhibit signs of decay. Commonly, little fat-globules appear at the poles of the capsules, and these become the seat of calcareous deposit. Finally, the worms die and undergo degeneration.
When meat with living trichina capsules is swallowed, the freed worms pass into the intestine, and here in the course of four or five days reach maturity.
The adult intestinal trichina is a minute, filiform white worm, thicker behind and tapering forward. The female is about an eighth of an inch long, and has the genital aperture at the anterior fourth of the body. The male is little more than half the length of the former, and has the caudal end provided with a pair of conical processes, between which is the genital aperture.
The ripe female trichinæ give birth to living embryos, and continue the function for about a month, after which they appear exhausted, ordinarily die, and disappear from the intestinal canal. The new-born embryos, about 1/200 of a line long, quickly leave the intestine to be disseminated throughout the body. Penetrating the mucous membrane, they probably enter the blood-vessels to be carried onward by the blood-currents, and perhaps also, in part, directly migrate to their destination in the muscles. The latter mode of progress is rendered the more probable from the circumstance that the muscles contiguous to the intestinal canal, as the diaphragm and those of the abdominal walls, are commonly most abundantly infested with the parasites. In the muscles of the limbs they are sometimes noticed to predominate toward the extremities of the former, as if retarded in their course by the tendinous connections.
It would appear that muscular trichinæ, to be capable of producing infection—that is to say, of further development—must have reached a certain stage, corresponding with the encapsulated condition, before they are swallowed. In this stage they may remain within their host probably for a year or two.
Children seem to suffer less in proportion to the quantity of trichinous meat they eat than adults, and they appear less susceptible to muscular invasion of the parasites. The difference is probably in a measure due to the greater susceptibility of the intestinal canal and the consequent production of more copious diarrhoea in children, with more complete expulsion of the worms.
SYMPTOMS.—In general, the effect produced by eating trichinous meat [p. 960] is proportioned to the number and condition of the trichinæ ingested and to the susceptibility of the patient. A few of the parasites may pursue their entire career and die within their host without ever exhibiting any obvious evidence of their presence. Sometimes the symptoms of trichinosis are obscure or trifling, sometimes sufficiently well marked, but moderate, and often they are more or less striking and violent. The period of incubation of the affection varies from a few hours to a week or more, and the duration of the disease also varies—both in a measure proportioned to the number and condition of the parasites.
In mild cases of trichinosis the patient may pass through the course of the disease without being confined to bed, and in a few weeks may be regarded as convalescent. The majority of cases pursue a slow course of from six or seven weeks to three or four months. A fatal termination is frequent, and is most common from the fourth to the sixth week, and appears mainly to be due to the loss of respiratory power. Fatal cases rarely happen after the seventh week.
From a few hours to a few days after eating trichinous meat the patient may be seized with dyspeptic symptoms—nausea, cardialgia, flatulence, eructations, and vomiting. These may be accompanied with complete loss of appetite, excessive thirst, bad taste, and fetid breath. There is also commonly a feeling of general uneasiness, with fulness of the forehead or headache, and feeling of weakness and fatigue to exhaustion or complete prostration. Neuralgic pains are felt in the abdomen and limbs, and the muscles generally are more or less relaxed and flabby.
Violent disturbance of the alimentary canal occurs only when large quantities of active trichinæ are taken with the food. The subsequent symptoms, due to invasion of the muscular system, may, but do not necessarily, accord in degree with the former.
Diarrhoea usually comes on early, and the evacuations, at first more consistent, become thin and clay-colored, like those of typhus or like the rice-water stools of cholera. In the severest cases the patient may die in this stage from extreme exhaustion and with all the appearance of cholera. Sometimes the diarrhoea subsides and gives place to obstinate constipation.
The muscular symptoms induced by the invasion of the trichinæ may be trifling or moderate, varying to a most violent character. They commonly appear after a week, and later up to the sixth week. The muscles become more or less swollen, hard and tender to the touch, or highly painful under pressure. Motion is extremely painful, and the patient usually lies in a helpless state with the limbs flexed—adults on the back, children on the side. Difficulty, with pain, in chewing and swallowing ensues, and even complete trismus, due to the presence of the parasites in the muscles of mastication and deglutition. Difficulty of breathing also arises from the presence of the trichinæ in the respiratory muscles, especially the diaphragm and those of the larynx. Even movement of the eyes is painful, due to the parasites in the orbital muscles. Bronchial catarrh comes on early, attended with hoarseness and asthmatic cough.
Fever may be absent in mild cases of trichinosis, but is considerable in the severer forms, though not in the first few days. The pulse accords with the increase of temperature.
Profuse sweating is a common symptom of the affection, commencing [p. 961] early and continuing throughout. Generally there is considerable decrease in the quantity of urine, which is highly colored.
Adults suffer with insomnia, while the reverse state prevails in children, who commonly lie in a soporose condition. Formication and dilatation of the pupils are frequent symptoms.
Oedema is a characteristic and pathognomonic symptom of trichinosis, and is seldom so slight as to escape attention. It commonly appears in the eyelids and face about the end of the first week, and may disappear after several days, to recur after several weeks. It usually commences in the limbs in the second week, and is more marked and persistent, and increases, especially in severe cases.
Peritoneal and pleuritic irritation and inflammation, with bronchitis and pneumonia, are not unfrequent complications in the more aggravated form of trichinosis.
Most cases of the disease reaching the seventh week advance in convalescence, while those of mild character by this time have recovered, except from the weakness and emaciation, which remain as evidences of serious illness.
Trichinosis in children is distinguished by greater mildness, less danger, abundant oedema, less muscular pain, a dormant condition, and more rapid convalescence.
The distinct recognition of trichinosis is difficult in isolated cases, but becomes more evident where it occurs in numbers, as in an entire family or in large portions of a community. The proof that the patient has partaken of trichinous pork helps to establish the diagnosis.
In the beginning of severe cases of the affection symptoms of a more or less violent gastro-intestinal catarrh are commonly present, often associated with slight fever and almost invariably excessive perspiration. Muscular lameness, both in mild and severe cases, is an early symptom. The disease is distinguished from cholera by the profuse perspiration and the peculiar muscular symptoms; from ordinary rheumatism by the gastro-intestinal catarrh and general exhaustion. With the appearance of oedema of the eyelids and face at the end of a week the diagnosis becomes more certain. The further progress of the affection is so characteristic that its distinction can scarcely remain in doubt. The general prostration, the violent muscular symptoms, the bronchial catarrh, the hoarseness and dyspnoea, the profuse sweating, and the sleeplessness, render the case pretty clear.
In the prognosis of the disease no positive conclusion can be derived from the severity or early appearance of the initial symptoms. Commonly, the more speedily they occur and the more violent they are, the less favorable will be the prognosis, while the later they appear, the more propitious it is. Long-continued diarrhoea is especially unfavorable, while a profuse diarrhoea at the beginning is to be viewed as a fortunate event. The prognosis is more favorable in cases in which sleep and the appetite are maintained, and in those in which the disturbance of the respiratory organs is slight. A favorable termination of the affection is the rule with children.
TREATMENT.—The treatment of trichinosis is not generally promising in favorable results. No means have yet been discovered to destroy or remove trichinæ which have migrated from the intestinal canal. While [p. 962] the parasites continue within the latter we may have reasonable hope of expelling them from the body by means of the usual remedies for intestinal worms. Experience, however, with these remedies has not been in accordance with expectations. In the mean time, until some more potent vermicide is discovered applicable to the destruction and removal of trichinæ from the intestine, we are disposed to place most reliance on such purgatives as oil of turpentine and castor oil and calomel and jalap. Subsequently, a good nutritive diet with wine is recommended to preserve the life of the patient until the affection has reached that period when the parasites become capsulated and there is no longer danger from them as irritants.
As a preventive of trichinosis, besides the avoidance of pork or its varied preparations of ham, sausages, etc. when it is known or suspected they may be infested, thorough cooking of meats is a certain means. A boiling temperature surely kills all animal parasites, but care is requisite that large pieces of meat should be cooked sufficiently long that the desired heat may extend to the interior throughout. The writer may add that it was in a slice of boiled ham, from which he had partly made his dinner, that he first discovered trichina in the hog.
Of the nematode worms there are many species of comparatively long, slender proportions, which constitute the family of Filaridæ. As parasites they rarely occupy the interior of the intestinal canal, except by way of transit, and live in most other organs and tissues of the body of both vertebrate and invertebrate animals.
FILARIA MEDINENSIS.—SYNONYMS: Dracunculus; D. medinensis; Medina-worm; Guinea-worm.
The Medina-worm has long been recognized as a parasite of man, and by competent authorities has been regarded as the fiery serpent which afflicted the children of Israel in the wilderness of Judea. It prevails in the tropical regions of Africa and Asia, and thence has been introduced into tropical America. It is ordinarily observed as a long, white, cord-like worm, situated beneath the skin in any part of the body, but mostly in the lower limbs, and especially in the vicinity of the ankle. Though a frequent parasite, only the female is known. In the mature condition it is nearly uniformly cylindrical, and ranges from eighteen inches to three or four feet in length and less than a line in thickness. The head end is rounded and furnished with a little papillate plate, in the centre of which is situated a minute oral aperture. The caudal end is conical and incurved. The intestinal canal is atrophied and without an anal aperture. The coelum is mainly occupied by a capacious uterus filled with free embryos. A generative aperture appears also to be absent, and the young can only escape by rupture of the parent.
Experiments made about a dozen years since in Turkestan by Fedschenko, at the suggestion of Leuckart, have shown that when the embryos of the Medina-worm are introduced into water containing the familiar little crustacean cyclops, they penetrate into this, and within it undergo transformation into the larval stage. The subsequent history of the larval worms remains unknown, but from what we have learned of the history of many parasitic worms it is reasonable to suppose that if [p. 963] the infested cyclops is swallowed in drinking-water, it may explain the presence of the mature worm in the human body. The young worms, liberated from their crustacean host by digestion in the stomach, probably enter the intestine, and thence migrate to their destination. In the young condition, advancing to maturity, the worms have been found in all parts of the body except within the cranium and eyeball. They appear to migrate in the course of the least-resisting connective tissues, along the route of the principal blood-vessels, until they reach the surface of the body.
Usually, a single worm is found in a person, though cases occur where several, to a dozen or more, are present. Commonly, the parasite is solitary, though two or three may be associated together. When deeply seated the Medina-worm ordinarily produces but little discomfort, though in some cases its movements are accompanied with more or less severe pain. It also gives rise to inflammation and the formation of an abscess, in the purulent matter of which the worm lies bathed. The removal of the worm, when accessible, by the proper surgical aid is followed by complete relief.
It is evident that filtration of the drinking-water would be a certain prophylaxis for the Medina-worm.
FILARIA SANGUINIS.—SYNONYMS: Filaria sanguinis hominis, Lewis; F. sanguinolenta; F. Bancrofti, Cobbold.
Another species of Filaria, a more dangerous parasite of man and indigenous to the tropics, is of frequent occurrence, though of comparatively recent discovery. It has been observed in India, Africa, Brazil, and the West Indies. It is commonly seen in the embryonic condition, living in the blood of patients affected with elephantiasis and certain other diseases, and is also found in the urine. In this early condition it is a minute worm, scarcely more than the 1/100 of an inch in length, and occurs together in immense numbers.
In the sexually mature condition the female filaria is a white hair-like worm three or four inches in length, living in the lymphatic vessels distally to the glands, especially in those of the lower limbs and scrotum. The embryos after leaving the parent pass into the lymphatic stream, and thence into the circulating blood. According to recent observations of Manson, they enter the blood in the evening and increase in number until midnight, after which they decrease and disappear by morning, from which time during the day they remain absent from the circulation. The investigations of the same authority have shown that when the blood of infected persons is sucked by mosquitoes these insects also imbibe the embryos, which subsequently undergo transformation in the mosquitoes into the larval state. In this condition the filariæ may be transferred to water, by drinking which man may become infected with the parasites. The larvæ introduced into the stomach appear thence to make their way to the lymphatics, within which they undergo further development to maturity, and thus remain a long time.
The presence of the worms in the lymphatics, with their numerous brood in the circulating blood, gives rise to hæmaturia and chyluria. As results of the obstruction of the lymphatic currents, the parasites induce inflammation, suppuration, lymphatic abscesses, buboes, lymphangiectasis, [p. 964] oedema, ascites, chylous hydrocele, elephantiasis,3 and certain cutaneous affections.
3 Several years since, with the view of ascertaining the presence of parasitic worms, the writer examined the blood of a case of elephantiasis under the charge of T. G. Morton, but none were detected. From what we have since been informed of the habits of Filaria sanguinis, the absence of the parasites may have its explanation in the circumstance that the blood examined was withdrawn in the daytime.
TREATMENT.—While the treatment of the affection induced by the Filaria sanguinis is varied and uncertain, the prophylactic measures are obvious and certain. Under favorable conditions of bright light, high temperature, and abundant food the stagnant waters of tropical countries are especially prolific of the minute forms of animals which harbor parasites. It hence becomes evident that all such waters, whether obtained from puddles, ponds, tanks, or cisterns, should be filtered before being used for drinking. Boiling is also effectual in destroying all the animal life of waters, and thus rendering them innocuous so far as parasites are concerned.
Several other species of Filaria have been found in the human body, but are little known and very rare in their occurrence.
FILARIA LOA.—This species occurs in Western Africa, on the Gaboon River, and is perhaps more frequent than now commonly supposed. It is an active worm, little more than an inch in length, and is usually found beneath the conjunctiva of the eye. It probably also occupies other positions, and a missionary on the Gaboon informed the writer that he had extracted one from the back of one of his own fingers. Its presence produced an intense burning pain. The negroes are reported to extract the worm by means of a thorn. The worm has also been observed in Brazil and the West Indies.
FILARIA RESTIFORMIS.—Under this name the writer recently described a large Filaria reported to have been withdrawn from the urethra of a man in West Virginia. It was obtained by C. L. Garnett, and sent, together with an account of the case, to the Army Medical Museum of Washington, where it is now preserved. It was a red cylindrical worm, twenty-six inches in length, tapering at the head, and thick, incurved, and obtusely rounded at the tail end.4
4 Proceedings of the Academy of Natural Sciences, Philada., 1880, p. 130.
FILARIA OCULI HUMANI; FILARIA LENTIS.—A few cases are on record of the occurrence of little worms in the aqueous humor and crystalline lens of the human eye, to which the accompanying names have been applied.
FILARIA TRACHEALIS.—Recently some minute worms found by Rainey in the trachea and lungs have been described under this name.
In conclusion, the writer acknowledges his indebtedness for much of the information of this article to the articles on "Intestinal Parasites" and "Diseases from Migratory Parasites" in Ziemssen's Cyclopædia of the Practice of Medicine, and to Glazier's Report on Trichina and Trichinosis.
DEFINITION.—The term biliousness is used to signify a disturbance of the gastro-intestinal digestion, with coincident excess in the production of bile. According to the popular conception, both lay and medical, the excess of bile is the cause of the symptoms; but when the whole subject is carefully examined it will be found that biliousness is made up of several factors, and that the hepatic disorder, if it exist at all, is a mere incident.
PATHOGENY.—From the time of Galen biliousness has been regarded as a morbid entity and the liver as the organ affected. Stoll, amongst moderns, first revived the Galenical doctrines. Abernethy1 was amongst English physicians the most conspicuous advocate of the condition called biliousness, and was the apostle of blue pill and black draught. Copland in his great dictionary2 more distinctly formulated the views of the English school—especially that portion of it influenced by the results of Indian practice—than had been previously attempted, and hence his work best represents the opinions and practice of the time amongst the English-speaking peoples. In this country the great Rush first promulgated the notions of biliousness which have since so dominated the medical opinion of this continent. A large part of the United States has proved a fruitful soil for the cultivation of theories of biliousness, since the condition known under this name is a frequent accompaniment of malarial poisoning. To this fact must be attributed the preponderating importance of biliary derangements in the practice of the physicians of India also.
1 Surgical Works, London, 1811, vol. i. p. 36.
2 A Dictionary of Practical Medicine, vol. ii. p. 723.
It is a fact which will be hereafter more fully developed that malarial infection may, and often does, derange the hepatic functions without producing fever. The malarial poison irritates the liver, and thus more bile is produced, but the quality deteriorates with the increase in quantity. The functions of the liver are more disturbed during an access of intermittent fever: the organ is swollen, the skin is muddy, the eyes yellow, the tongue coated with a thick yellow fur, and the urine is deeply tinged with bile-pigment.
Many of the metals employed as medicines and as poisons, as gold, [p. 966] silver, antimony, arsenic, phosphorus, etc., irritate the liver both in their entrance and in their exit from the organism, and cause biliousness; and the same fact is true of some vegetable alkaloids and animal poisons. The liver excretes many of these substances, and in their passage out from the blood the hepatic cells are irritated and an increased production of bile is a result. Improper food, indulgence in fats, sweets, condiments, and all kinds of fermented and alcoholic liquors, intestinal indigestion arising from any cause, and gastro-duodenal catarrh, are the most usual and obvious pathogenic factors. In respect to food and indigestion as etiological factors there are several points requiring more explicit statement. When nitrogenous elements (albuminoids) are in excess in quantity or as respects the power to digest and convert them, immature products, of which uric acid is the chief, accumulate in the blood. When the fats, sugars, and starches are in excess of the requirements of the organism or are imperfectly disposed of in the small intestines, a local irritation of the mucous membrane is produced, and various complicated, immature products enter the blood. With these troubles and faults of intestinal digestion a gastro-duodenal catarrh is usually associated. Without the production of catarrhal jaundice, gastro-duodenal catarrh, with the forms of indigestion accompanying it, keeps up a reflex irritation of the liver. Just as the presence of normal chyme induces the flow of bile, so the unhealthy products of intestinal indigestion excite an irritation of the liver. The continued operation of this cause maintains an abnormal activity of the liver, and more bile is produced than is easily disposed of.
SYMPTOMS.—The condition of biliousness, as now understood, is made up of derangement of the gastro-duodenal mucous membrane, with bile-production in excess and bile-absorption probably delayed. The symptoms are the product of these complicated conditions. The complexion is muddy; the conjunctivæ are yellow; the tongue is heavily coated with a yellowish-white fur; a bitter taste persists in the mouth; the breath is heavy in odor, even fetid; the appetite may be keen or there may be complete anorexia; a sensation of nausea, of heaviness, and fulness of the stomach is experienced, especially after eating; the bowels are confined usually, but occasionally the movements are relaxed, bilious in appearance, and cause heat and irritation about the anus; headache is constantly present to some extent, and there is a sense of fulness with more or less dizziness, and singing in the ears; vision is rather blurred, and there is a hebetude of mind; the urine is high-colored, high in specific gravity, and deposits lithates abundantly on cooling. When these symptoms are conjoined with hemicrania, nausea, and vomiting, the case is called bilious sick headache, and when diarrhoea supervenes, the discharges apparently containing much bile, it is bilious diarrhoea. The symptoms which above all others give the character to the morbid complexus are the muddy (bilious) complexion, the yellow-coated tongue, the yellow conjunctivæ, and the high-colored urine. The first departure from the normal may be scarcely observed. Gradually, owing chiefly to errors of diet, to climatic changes, or to malarial influences, or to these several factors combined, the affected person drifts into the condition of biliousness above described. Besides the general malaise, he experiences no little despondency, inaptitude for exertion, and indeed actual weakness. Finally, he is unable to apply himself to business, relinquishes the effort, and seeks advice.
[p. 967] COURSE, DURATION, AND TERMINATION.—Those who are accustomed to experience attacks of biliousness suffer from them at certain intervals which may be tolerably regular—at intervals of a few days, two, three, or four weeks—when the cause is uniform; but they may happen very irregularly when the conditions producing them are variable. The duration of an attack is from two days to a week or more, according to the severity of the symptoms and to the character of the measures instituted for relief. The termination is in a return to the normal state. If the conditions which produced it continue, when one attack is ended the preparations for another begin at once, and at length sufficient derangement of the organs concerned arises to constitute the morbid complexus of biliousness.
TREATMENT.—Prophylaxis has great importance, since the causes of the malady are to a considerable extent, at least, preventable. Errors of diet in respect to the use of condiments, fats, meat, pastry, etc. must be corrected. When there is pronounced gastro-duodenal catarrh and acid fermentation in the duodenum, the saccharine, fatty, and starchy elements of the food must rather be excluded and lean meats allowed. Abundant exercise, bathing, and an open-air life in general should be directed. Whenever a malarial infection is causative a change of climate becomes imperative. Heredity cannot, of course, be excluded, but the tendency to hepatic derangement can be rendered inoperative by an abstemious life.
The remedial management includes the dietetic as well as the medicinal treatment. When the distress has reached sufficient proportions to justify such an extreme measure, the patient should be restricted to a diet exclusively of skimmed milk, of which he is directed to take a gill or more every three hours. This serves a double purpose, as aliment and as a depurative agent, for this considerable quantity of fluid promotes the urinary excretion and the elimination of waste products. If the case is not severe enough to allow of such an expedient, the diet should in any event be restricted to skimmed milk hot, milk and hot water, hot lemonade, a little chicken or mutton broth, a bit of dry toast, etc. As a rule, although not so palatable, hot drinks are more beneficial than cold, but if the preference is decidedly for cold, they may be allowed. After the more severe symptoms have subsided a little lean meat broiled may be added, and as the cure proceeds the succulent vegetables and acid fruits may be permitted. Abstinence from potatoes, hominy, cracked wheat, and oatmeal should be enjoined during the convalescence of those who suffer from habitual attacks.
Medicines may not be necessary to those who have the resolution to adhere to skimmed milk for several days or who can abstain from food altogether for a day. Many experienced sufferers, especially through the South and West and in England, procure rather prompt relief from a blue pill of ten to fifteen grains or from one to five grains of calomel at night, followed by a Seidlitz powder, Rochelle or Epsom salts, or phosphate of soda on the following morning. Such patients find that no other treatment is as serviceable. They get relief from other measures, it is true, but neither as promptly nor as satisfactorily. It is held by the advocates of this practice that the mercurial acts on the liver—that the surplus bile is carried off; and they point to the peculiar stools and to [p. 968]the relief experienced in evidence of the truth of this theory. Without entering on the argument, which would occupy too much space, it must suffice here to state that calomel and blue pill do not increase bile-production,3 but they do stimulate the intestinal glands and increase excretion from them. The peculiar greenish stools produced by these mercurials do not owe their characteristic appearance to the presence of bile, but rather to the chemical transformations of the mercury itself and to the waste products excreted by the intestinal glands. Since the researches of Rutherford have been published, euonymin has been much prescribed in cases of biliousness. From three to five grains are taken at the bed-hour, and a mild laxative in the morning. In the same group of cholagogues are ipecac, iridin, sanguinarin, and especially podophyllin; but the serious objection to their use is that they stimulate the liver when this organ is in an irritable state. As calomel and blue pill have a sedative rather than a stimulant action on the liver, they are more useful in biliousness than are the true cholagogues. It should be borne in mind that one-half of a grain of calomel will have a distinct purgative action on many persons, and that one grain will rarely need to be exceeded.
3 That calomel, the type of a mercurial purgative, does not increase the discharge of bile has been demonstrated on dogs by Röhrig and Rutherford, and confirmed by observation of the effects of 20 grains on Westphalen's case of biliary fistula in man—a case in which, for a time, all the bile escaped externally, and none apparently entered the intestine (Deutsch. Archiv f. klin. Med., 1873, Band xi. pp. 598 and 600).
In general, notwithstanding the unquestionable utility of the mercurial, it is better to relieve cases of biliousness by less objectionable measures. A saline which acts at the same time on the intestines and kidneys, as Rochelle salts, is usually effective in bringing relief. A bottle of solution of magnesia citrate, of Saratoga water (Congress, Hathorn, or High Rock), and of Blue Lick, the famous sulphurous laxative of Kentucky, may remove the disorder in mild cases if at the same time a suitable diet is enjoined. Phosphate of soda in laxative doses, with or without Vichy water, is also a good remedy, if somewhat slow. The warm purgatives, rhubarb, colocynth, aloes, etc., are useful when there is pronounced constipation.
DEFINITION.—By the term lithæmia is meant a condition of the system in which uric (lithic) acid is produced in excess, and in which certain derangements occur in consequence of the accumulation of this material in the blood. Uricæmia was the term first suggested by Flint, Sr.,4 to express this state, and subsequently lithæmia was employed by Murchison.5 The latter has been more generally accepted. In one of the most recent and valuable contributions to this subject by DaCosta6 lithæmia is the term used to designate the complex of symptoms produced by uric acid in excess.
4 The Principles and Practice of Medicine, Philada., 1882.
5 Clinical Lectures on Diseases of the Liver, 2d ed., p. 565.
6 The Medical News, vol. ii., 1883.
PATHOGENY.—The ultimate product of albuminoid substances in the organism prepared for final excretion is urea. That this substance is [p. 969] finally formed in the liver, to be excreted by the kidneys, seems now well established.7 In acute yellow atrophy of the liver, with the disappearance of the proper structure of the organs urea ceases to be produced, and instead leucin and tyrosin are excreted. In certain states of the system characterized by deficient oxidation urea is not sufficiently formed, and instead uric acid, a lower grade of oxidation and a product of the disintegration of albuminoid substances, results. An excess of urates is not always pathological. Their excretion seems to be in a certain sense a safety-valve function. When albuminoid matters are taken in excess of the power of the system to convert them, or when the supply of oxygen to the blood is deficient from any cause, urea is not formed, but uric acid and urates are abundantly excreted by the urine.8 Imperfect digestion of the albuminoids when they are not taken in relatively too large an amount, and limitation below the normal of the oxidation process when the supply of oxygen is not insufficient, will have the same effect: in place of urea, uric acid and urates will be formed and excreted. One of the early results of the persistent presence of an excess of uric acid is the production of lithæmia, the morbid complexus of which this excess is at once the cause and the proof.
7 This proposition is not universally accepted. Valmont (Thèse de Paris, Étude sur les Causes des Variations de l'Urée dans quelques Maladies du Foie, 1879) has carefully studied the excretion of urea in several diseases in which the proper structure of the liver is damaged—in atrophic cirrhosis and in cancer. As in these maladies not all the secreting portion of the organ is destroyed, the argument is so far weakened. His conclusions are as follows: "1. Patients with cirrhosis or cancer of the liver who eat little excrete but little urea. If they eat and do not absorb, or vomit or have diarrhoea, the result is the same. When they partake largely of nitrogenous aliment the proportion of urea rapidly increases. 2. In a cachectic or simply anæmic patient the urea falls, apparently in proportion to the state of the general nutrition and of the work done by the organic functions. 3. Absolute immobility of the patient seems to have an influence on the amount of urea excreted. 4. In sclerosis or cancer the quantity of urea falls rapidly on the occurrence of ascites or oedema, when a notable quantity of urea is found in the fluid. 5. The digitalis often used in the treatment also contributed to the loss of urea." If these conclusions are verified, the formation of urea must depend on some other function.
8 Genevoix, Essai sur les Variations de l'Urée et de l'Acide urique dans les Maladies du Foie, Paris, 1876.
The persons who suffer from lithæmia are usually those who indulge in the pleasures of the table and habitually consume much meat, pastry, and highly-seasoned and rich food of all kinds. The idle, luxurious, and indolent, literary men of sedentary habits, men who have led active lives, but on retiring from business have continued to indulge in a full diet, are apt to suffer from this malady. Women are less disposed to it, but if subjected to the same conditions may also be similarly affected. Especially do those suffer from lithæmia who indulge in malt liquors or in alcoholic drinks of any kind. These substances act by deranging digestion, and thus preventing the proper conversion of the albuminoids, by inducing congestion of the liver, and also by interfering with the process of oxidation.
SYMPTOMS.—The symptoms of lithæmia include derangements of the digestive organs and of the liver, of the circulation, and of the nervous system. As these subjects suffer from gastric and gastro-duodenal catarrh, they present the usual symptomatology of these affections, as a sense of weight and oppression at the epigastrium, acidity, pyrosis, a capricious—sometimes voracious, sometimes good—appetite, a coated [p. 970]tongue, a bitter taste, etc. The bowels are irregular, sometimes constipated, occasionally relaxed, with scybalæ. The stools may be liquid, almost black or light-yellow and grayish. The motions are apt to be offensive, and a good deal of offensive gas is discharged with them. Hemorrhoids are often present, and there may be heat and irritation about the anus, and not unfrequently intolerable itching. After meals there is much depression, and often an insupportable drowsiness. Irregularity in the rhythm, even intermissions, of the pulse are not infrequent.
The nervous symptoms, as DaCosta has lately insisted on, are the most important and pronounced. The connection between oxaluria and mental despondency has long been known, but the nature of the relation remains undetermined. Headache, frontal and occipital, especially the former, dizziness, tinnitus aurium, suffusion of the eyes, ecchymoses of the conjunctiva, are usually present. Not unfrequently the subjects of this affection experience sudden attacks of vertigo, accompanied by dimness of vision and intense headache, and are supposed to have some organic lesion of the brain. They are irritable, despondent, and often intensely hypochondriacal, almost suicidal—are subject to neuralgic attacks, and have aching in the limbs, a sense of weariness, and more or less burning in the palms and soles.
The skin is rather dry and the complexion muddy. Urticaria is of frequent occurrence, and sudden attacks of nausea, vomiting, and intestinal pain coincide with the appearance of the eruption on the skin.
The urine is usually rather increased in amount, its color heightened, its acidity above normal, and floating in it, usually visible to the naked eye, are reddish masses composed of uric acid. More or less pain in the back, referable to the situation of the kidneys, and sometimes extending along the course of the ureters, is common. The bladder is rather irritable, and the passage of the urine produces heat and scalding. The testicles are apt to feel sore and are somewhat retracted. On standing, the urine may deposit uric acid and the urates copiously, or the acid may be seen to form a cloud which slowly subsides.
COURSE, DURATION, AND TERMINATION.—The course and duration of lithæmia are much influenced by the habits of life of the person affected. When unopposed by treatment and no change is made in the conditions producing it, a gradual increase in the various disturbances takes place. After a time structural changes occur in the liver; the organs of circulation early undergo atheromatous degeneration; various cerebral disorders due to degenerative changes arise; and acute intercurrent affections may terminate life. Amongst the secondary maladies due to lithæmia are gout, diabetes, renal calculi, and nephritic colic. If the cases are subjected to appropriate treatment, curative results may be certainly obtained. The prognosis, then, will be influenced materially by the moral strength of the patient. If he is one who can surrender his appetites and live abstemiously, a cure may be promised. The case is far different with those who will continue the use of malt, vinous, or alcoholic drinks, and will persist in indulging in the pleasures of the table.
DIAGNOSIS.—The differentiation of lithæmia from other affections offers no special difficulties. From gastro-duodenal catarrh it is separated by the [p. 971] excess of uric acid in the urine only, the other symptoms being for the most part the same. The cerebral symptoms—the vertigo, headache, etc.—are to be distinguished from the same due to actual disease of the brain by the previous history, by the absence of changes seen on ophthalmoscopic examination and of other signs of brain disease, and by the subsequent behavior. Cases of cerebral mischief producing such effects would rapidly develop into serious states, whereas in lithæmia there are great fluctuations, but no apparent progress in many months. In lithæmia also there are no changes in the fundus oculi, whereas in brain diseases choked disk, hemorrhage into the retina, white atrophy, etc. are often discovered. Further, in lithæmia there are no disorders of sensibility, of motility, or of intellection, whilst these are ordinary evidences of cerebral mischief.
TREATMENT.—Attention to diet is of the first importance. As uric acid is an intermediate product in the metamorphosis of albumen, it might be supposed that to diminish the quantity of this constituent of the food would be sufficient. In some cases this suffices, but usually attention must be given to the peculiarities of digestion characteristic of each patient. More frequently trouble arises from indulgence in the starchy and saccharine constituents of the diet; in some a very considerable gastro-duodenal catarrh exists, and the mucus, acting as a ferment, sets up an acetic fermentation in the starchy and saccharine substances, with the necessary production of much carbonic acid gas. If the fats disagree, the butyric fermentation also takes place, and very irritating fat acids result. In these cases there is usually much gas formed in the stomach and intestine, and an immediate ratio appears to exist between the degree of mental despondency and the quantity of gas in the intestinal canal. It follows, then, that in cases of lithæmia the saccharine, starchy, and fatty constituents of an ordinary diet should be omitted from the food of such subjects. Bread should be partaken of very sparingly, and the foods containing starch, sugar, and oil ought not to be partaken of at all. The succulent vegetables, as lettuce, spinach, celery, cole-slaw, tomatoes, etc., ought to be substituted. Lean fresh meats, poultry, game (plainly cooked), fresh fish, oysters, eggs, etc. should constitute the basis of the diet. On the other hand, there may be those who do better on a diet of vegetables and fruit, excluding meat. In such we may suppose the fault lies in the stomach digestion, where the albuminoids are converted into peptones, the intestinal digestion being active and normal. All kinds of wine and malt liquors should be prohibited. Coffee and tea must also be relinquished. Without the carefully-regulated diet medicines can accomplish but little; hence he who would obtain curative results must give careful attention to every dietetic detail.
As deficient oxidation is an important factor in developing lithæmia, active exercise must be enjoined. The amount of exercise must be determined by the condition of the individual and the time, regulated as far as may be by the period after meals. As when the food prepared for assimilation is entering the circulation oxygen is needed to perfect the final changes, it seems clear that exercise should be taken three or four hours after the process of digestion has begun. Walking exercise is better than any other for this purpose, but it should not be carried to the point of exhaustion from fatigue. Sea-air and sea-bathing are oxidizing agents of considerable value, and are especially useful to the [p. 972] subjects of lithæmia suffering at the same time from malarial infection.
Medicines are administered with the view to accomplish two purposes: to correct the disorders of digestion, to promote oxidation. One of the most useful remedies is nitric acid, five to ten minims of the official diluted acid being given before meals. It is more especially effective when there is an excessive production of acid. The fermentation which produces acid and the diffusion of acid-forming materials from the blood are alike prevented by it. The injunction to administer it before meals must be borne in mind when these purposes are to be subserved. Nitric acid, as well as the other mineral acids, but in a greater degree, promotes the flow of bile. This well-known clinical fact has been confirmed by experiments. Under the use of nitric acid, as above advised, uric acid and the urates disappear from the urine, being excreted as urea, and hence this remedy accomplishes both of the objects for which medicines are administered in this disorder. No other mineral acid can fill its place in this connection.
Alkalies possess very decidedly the power to promote oxidation. The soda salts are objectionable, for, combining with uric acid, they form the insoluble urate of soda. The salts of potash and lithium, on the other hand, form soluble combinations, and they also increase elimination. Much depends on the time at which they are administered, as Bence Jones,9 and since Ralfe10 especially, has shown. To increase the alkalinity of the blood and urine, they must be taken after meals, for then the acid materials of digestion are pouring into the blood. For the same reason, if alkalies are administered to neutralize the acidity of the intestinal canal, they must be given after meals. The most useful alkaline remedies are liquor potassæ, bicarbonate of potash, Rochelle salts, citrate of lithium, etc. The effervescing preparations of potash and of lithium are elegant and palatable forms in which to administer these remedies. They may also be taken dissolved in Vichy water, in our Saratoga Vichy, or in Carlsbad or Bethesda. When the use of mineral waters is not contraindicated in the state of the digestive organs, great good is accomplished by the persistent use of Vichy, foreign or domestic, of Carlsbad, and the alkaline waters of Wisconsin.
9 Lectures on Pathology and Therapeutics, by H. Bence Jones, London, pp. 90, 280.
10 Physiological Chemistry, by Charles Henry Ralfe, London, 1883.
The so-called cholagogues are unquestionably useful, but they become less and less necessary according to the success achieved in the dietetic course. Phosphate of soda is one of the most effective of this group of medicines. As it acts as a compound, and not as a salt of soda merely, it does not come within the prohibition against the use of soda salts. It promotes the flow of bile and appears to remove the catarrhal state of the mucous membrane. A teaspoonful three times a day is the quantity usually required. Under some circumstances it may be advantageously combined with arseniate of soda. Mercurials were formerly almost universally used, but they have been largely supplanted by podophyllin, euonymin, baptisin, etc., and by the phosphate of soda above mentioned. Podophyllin is indicated when constipation is a symptom. An efficient mode of giving it is in the form of granules, but it must be continued without intermission for some time or during the existence of [p. 973]the lithæmia. The quantity given should be sufficient to maintain the evacuations in a soluble state. Good results are obtained from a combination of podophyllin with extracts of physostigma, nux vomica, and belladonna. When distinct torpor of the liver without constipation exists, euonymin, combined with physostigma, may be advantageously used. For the vertigo and hypochondriasis no remedy is more beneficial than arsenic (Fowler's solution) in small doses kept up for some time, and it is also distinctly curative of the catarrhal state of the mucous membrane. When malarial infection is the cause of lithæmia, quinine becomes indispensable.
Topical agents in some cases render important aid to the other curative measures. A daily sponge-bath, the water made more stimulating by the addition of sea-salt, is very useful in the absence of sea-bathing. Friction of the hepatic region with the official ointment of the red iodide of mercury unquestionably stimulates the hepatic functions. General faradization and faradic and galvanic excitation of the chylopoietic system promotes activity of the digestive apparatus and of the organic functions in general.
DEFINITION.—By the term hepatic glycosuria in this connection is meant a temporary glycosuria due to excessive formation of glycogen. The liver, unduly stimulated, produces more glycogen than can be disposed of, and hence it is excreted by the kidneys as grape-sugar.
PATHOGENY.—In the normal condition it is supposed that the glycogen produced by the liver is converted into grape-sugar, and soon oxidized and thus consumed. One theory of diabetes maintained that in some way the conversion of glycogen into grape-sugar was excessive and beyond the oxidizing power of the blood, and hence this substance was discharged in the urine. The recent discovery by Pavy11 of glycogen in considerable amount in the blood of all parts of the body renders it certain that there are peculiar conditions necessary to the formation of grape-sugar in sufficient quantity to constitute diabetes. It is tolerably certain that an excess of acid in the intestinal canal, diminishing thus the alkalinity of the blood, will have as a symptom sugar in the urine. Persons disposed to the accumulation of fat, and eating freely of sugar and starchy food, are apt to have intestinal indigestion, and the acid produced by the fermentation of these substances will, after its absorption, hinder the conversion of any food-sugar. In such subjects also there may be an increased conversion of the glycogen of the blood into sugar under the same conditions. Such a glycosuria must necessarily be temporary and a purely functional disorder.
11 The Lancet, vol. ii., 1883.
SYMPTOMS.—The subjects of the malady under consideration are of full habit, even obese. They habitually consume considerable quantities of malt liquors and a diet composed largely of the starchy and saccharine foods. If not in malt liquors, they at least indulge freely in bread, potatoes, pastry, cakes—in all forms of farinaceous food, fats, and sweets. They have a keen appetite, eat largely, and drink freely of fluids. As [p. 974] a rule, these subjects are but little disposed to physical exercise and lead rather sedentary lives. Indulgence in such a mode of life tends to increase the accumulation of fat, weakens the muscles, and with them the heart-muscle, and slowly induces a gastro-intestinal catarrh accompanied by stomachal and intestinal indigestion. At first, heaviness, oppression, and drowsiness after meals are experienced; then acidity, pyrosis, and eructations follow; and ultimately the evidences of intestinal indigestion—flatulence, pain, irregular and unhealthy evacuations, etc.—come on. Meanwhile, the appetite is not usually impaired, and the disposition to drink fluids increases; the amount of urine voided is greater, and to rise during the night for the purpose of emptying the bladder comes to be a fixed habit. The urine under these circumstances is copious, high-colored, acid, and deposits on cooling abundantly of uric acid and urates. The amount passed in twenty-four hours will reach sixty, eighty, or more ounces, and the specific gravity will range from 1025 to 1035. On testing in the usual way, traces of sugar, more or less distinct, will appear,12 but not constantly, and hence repeated examinations are necessary to determine the quantity. As a rule, the evidence of the presence of sugar in small amount is satisfactory.
12 In testing for sugar, when the urine contains the urates in such abundance there is danger of error. In using Trommer's, Fehling's, or Moore's test, on heating, the urates will effect a reduction of the copper or bismuth. It is necessary, therefore, to separate them before applying the test. This is accomplished as follows: The urine is evaporated to dryness on a water-bath; the sugar in the evaporated residue is dissolved out by absolute alcohol, and then an aqueous solution is prepared, to which the test is applied. An experienced operator will not need to take such precautions, for, familiar with the reactions, he can readily judge of the results.
Various affections of the skin appear in the subjects of this malady, and urticaria, prurigo, eczema, and boils are the forms most usual.
COURSE, DURATION, AND TERMINATION.—Slow in developing, this temporary glycosuria is also slow in its course. It remains nearly stationary for months, even years. Meanwhile the degenerative changes associated with it slowly develop on all sides. The quantity of sugar does not greatly increase, for its amount, being apparently dependent on the quantity of acid entering the blood from the intestinal canal, must continue nearly at the same standard. It is comparatively rare for true diabetes to develop out of this state, although such a termination must be regarded as a natural outcome. One reason, it may be, why such a conclusion is not often reached is because of intercurrent maladies. It is an important fact that acute serous—less often parenchymatous—inflammations are very apt to occur during the existence of even temporary glycosuria. Under appropriate management this disorder is readily amenable to treatment. Hence the prognosis will be favorable or not according to the skill exhibited in its treatment.
DIAGNOSIS.—This malady offers no special difficulty in diagnosis. From gastro-duodenal catarrh and from lithæmia it is distinguished by the saccharine condition of the urine. From diabetes it is separated by the rate of progress, by the protracted duration of the case without any distinct advance, and by the temporary and fugitive character of the glycosuria.
TREATMENT.—To carefully regulate the diet is the first consideration. The traces of sugar and the excess of urates rapidly disappear when the [p. 975] starches, sugar, and fats are withdrawn from the diet. Indeed, the rule as to alimentation must be as rigidly enforced as in true diabetes, but after the gastro-intestinal catarrh has subsided the ordinary mixed diet—that before the disturbance began—may be returned to gradually. Active exercise must be enjoined under the same conditions and for the same purpose as in the treatment of lithæmia. In these obese subjects, unaccustomed to movement, exercise must be cautiously undertaken; beginning with short excursions, it must be gradually increased. Horseback riding is an excellent expedient, but should not take the place of walking.
The merely medical measures have a twofold direction: to remove the gastro-duodenal catarrh; to promote oxidation of the sugar in the blood or prevent the conversion of glycogen into grape-sugar. Vichy water, the potash salts, and alkalies generally serve to accomplish the latter, and phosphate and arseniate of soda, tinctures of nux vomica, and of physostigma, bismuth, and carbolic acid, relieve the former. Small doses of Fowler's solution (two drops ter in die), and a minim three times a day of a mixture in equal parts of tincture of iodine and carbolic acid, are effective remedies in gastro-duodenal catarrh.
DEFINITION.—The term jaundice has its origin in the French word jaune, yellow. Icterus, which has come to be a more technical word, is of uncertain Greek origin, and is much employed by French writers as ictère. The common German name is Gelbsucht, a highly expressive designation. Jaundice signifies a yellow discoloration of the skin caused by the presence of bile. It is a symptom rather than a disease. As a symptom it will receive much consideration in the pages to follow, but there is also a functional disorder—a jaundice due to a disturbance in the biliary functions, without evidences of structural change—which must be discussed here. This preliminary statement of our present knowledge of jaundice will facilitate the comprehension of it as a symptom, and will render unnecessary explanations that will be merely a repetition of previous ones.
CAUSES.—The theories of the causation of jaundice may be reduced to three: 1, that it is due to a disorganization of the blood in which the coloring matter is set free, and hence is known as hæmatogenous; 2, that the materials of the bile, which it is the office of the liver to remove from the blood, are not so disposed of; 3, that the bile, after being formed by the liver, is absorbed into the blood because of an obstacle to its escape, and hence this is called hepatogenous jaundice.
The modern view of hæmatogenous jaundice had its origin in the supposed discovery of the identity of hæmatoidin with bilirubin. If the pigment of the blood has the same composition as the pigment of the bile, hæmatogenous jaundice will be produced whenever hæmatoidin is set free in the blood. Virchow13 was the first investigator to show the close resemblance between these two pigments. Since his observation was made an identity of hæmatoidin and bilirubin has been maintained by Zenker, Valentiner, Kühne, and others, and as strenuously denied by [p. 976] Städeler, Preyer, Young, and others. At the present time it appears to be established that although the blood- and bile-pigments are closely related, they are not identical.14 Nevertheless, a hæmatogenous jaundice is still admitted to exist by Leyden,15 Immermann,16 Gubler,17 Ponfick,18 and some others. The existence or non-existence of this form of jaundice is, however, of little importance in this connection, since, if it ever occur, the malady of which it is a symptom is not an affection of the liver, but of the blood, as phosphorus-poisoning, pyæmia, etc.
13 Archiv für path. Anat., etc., Band i. p. 370, 1847.
14 Legg, J. Wickham, On the Bile, Jaundice, and Bilious Diseases, p. 243.
15 Beiträge zur Pathologie des Icterus, Berlin, 1866, p. 6.
16 Deutsch. Archiv für klin. Med., Band xii. p. 502.
17 Union médicale, 1857, p. 503.
18 Ziemssen's Cyclopædia, vol. ix. p. 24.
The second theory, that the bile is preformed in the blood and separated by the liver, and that jaundice results because of the failure of the liver to perform this office, is no longer entertained, although largely held down to within a very recent period. As the bile acids and bile-pigments are not to be found in the blood, chemistry lends no support to the theory of jaundice by suppression of the hepatic function. As they do not exist in the blood and are found in the secretion of the liver, there can be no other view held than that they are formed by this organ.19
19 The old doctrine of jaundice by suppression, which has always been maintained by Harley (On Jaundice, London, 1863, p. 20 et seq.), has been again restated and strongly advocated by him in his treatise on The Diseases of the Liver, p. 83, which was issued in 1883. In the two following postulates he formulates his view:
"1. The biliary secretion can be actually retarded, and even totally arrested, without alteration of hepatic tissue.
"2. When the liver strikes work and secretes no bile, the animal body becomes jaundiced as a direct consequence thereof."
This view, he affirms, "can be made comparatively easy of absolute proof."
The evidence on which he chiefly relies is exceedingly fallacious. It rests on two facts: the existence of a case of jaundice in which the ducts and gall-bladder contain no bile, but only ordinary mucus; the appearances presented by a liver in a case of jaundice due to obstruction of the common duct. The evidence afforded by the former is entirely fallacious, because in an old case of jaundice with catarrh of the bile-ducts such changes take place in the bile that it loses all of its distinctive characteristics. This may be seen in an ancient example of obstruction of the cystic duct, where the bile which the gall-bladder contained is ultimately transformed into a whitish or colorless mucus. The changes which occur in the so-called cysts of the arachnoid are comparable, and exhibit the entire transformation of blood-pigment, which is closely allied to bile-pigment.
The third theory of jaundice—that which refers the disease to an absorption of the bile into the blood after it has been formed by the liver—is the one now most generally held, and, indeed, as one of the causes is universally held. The bile is absorbed into the blood because an obstacle to its passage by the bile-ducts exists at some point in their course. This is the principal, but not the only, cause of absorption. When the pressure in the vessels falls below that in the ducts, bile will pass toward and into the vessels. Again, it sometimes happens that a considerable part of the bile discharged into the intestines is reabsorbed unchanged, and enters the portal vein and the general circulation, thus causing jaundice.
The disturbances of the liver causing jaundice are various. It sometimes occurs without cause, and the first intimation of it is the peculiar tint of the skin. It is certainly true that powerful emotions are causative; thus, a violent anger has brought on an attack. In such a case we must suppose a depression of the vaso-motor system, and such a lowering of the blood-pressure as to favor the passage of bile into the [p. 977] veins rather than into the bile-ducts. Thus, it has been abundantly shown that a slight difference in pressure will divert the bile in either direction. Heidenhain20 has demonstrated that the bile passes in the direction of least resistance, and in the case of the considerable vaso-motor depression caused by extreme emotion the least resistance is in the direction of the vessels. More frequently than moral emotion is catarrh of the bile-ducts. It is not necessary for the catarrhal swelling of the mucous membrane to close the ducts to have the bile pass into the veins; such a degree of swelling as to make the passage of the bile somewhat difficult suffices. A simple hyperæmia of the mucous membrane may cause sufficient obstruction of the bile-ducts to give rise to jaundice. Gastro-intestinal catarrh plays an important part in the production of simple jaundice. Frerichs21 ascertained that of 41 cases, gastro-duodenal catarrh existed in 34. Ponfick22 considers catarrh of the ducts the principal factor. In fact, at the present time there is but one dissenting voice on this point.23
20 Quoted by Legg, supra, p. 253.
21 Diseases of the Liver, Syd. Soc. ed., by Murchison.
22 Ziemssen's Cyclopædia, vol. ix., supra.
23 Harley, Diseases of the Liver, 1883, p. 440 et seq.
Gastro-duodenal catarrh extends by contiguity of tissue to the mucous lining of the bile-ducts. The catarrhal state of the mucous membrane is produced by errors of diet, acid indigestion, indulgence in condiments, wines, and rich foods in general. Climatic changes, malarial infection, exposure to cold and dampness, etc. are indirectly causative of jaundice through the intermediation of gastro-duodenal catarrh.
Formerly, obstruction of the gall-ducts was supposed to be caused sometimes by a spasmodic contraction of the organic muscular fibre assumed to exist in the walls of the ducts. Although the presence of these muscular elements has been denied, Heidenhain has lately, apparently, demonstrated them. Audigé has made observations confirmatory of those of Heidenhain, and Dujardin-Beaumetz24 has verified the statements of Audigé. It seems, therefore, in a high degree probable that organic muscular elements exist in the walls of the hepatic ducts, and that spasmodic icterus may therefore occur.
24 Bull. gén. de Thérapeutique, vol. lxxxv. p. 385, 1873.
SYMPTOMS.—Simple icterus may exist without any other obvious symptoms than the yellow discoloration of the skin. In most cases, however, the yellowness is preceded for a week or more by the symptoms of a gastro-intestinal catarrh, or these symptoms accompany the jaundice. There is much mental depression and a general malaise is experienced. Headache, mental hebetude, a total loss of appetite, a furred tongue, and a bitter taste, nausea and sometimes vomiting, constipation or diarrhoea, precede or accompany the jaundice. When these symptoms precede for some time the appearance of yellowness, it is probable that the biliary derangement is secondary to the gastro-duodenal catarrh, but when they occur with the jaundice it is probable that they are due to the absence of bile from the intestine.
The yellowness first appears in the conjunctiva for a day or two before the skin is tinted, and within forty-eight hours after the flow of bile into the intestine has ceased. The face next becomes yellow, then the body, [p. 978] and afterward the limbs, but in some cases the limbs remain free from discoloration. The lips do not exhibit any change of color, but the roof of the mouth, the palate, and the mucous membrane under the tongue are yellow. The saliva does not, as a rule, contain bile-pigment or exhibit any changes of color unless mercurial salivation is caused, when it becomes greenish in color and has a bitter taste.25 A yellow tint of the sweat, especially under the arm-pits, is common. The milk very often contains bile-pigment or is changed in color in some way.
25 Legg, On the Bile, etc., supra.
The feces are colorless or have a grayish or clay-colored tint, and are semi-solid, although sometimes hard and dry. In simple jaundice diarrhoea is very often present. There may be considerable flatulence, and more or less pain in consequence about the umbilicus, and the gas when discharged is very offensive. The stools also, in some cases, have an odor of decomposition, and if carefully examined particles of food, undigested and decomposing, will be found. The feces may have a parti-colored appearance—part whitish or grayish or clay-colored, and part of a normal color. This condition is not difficult of explanation. The obstruction to the flow of bile may be in a part, and indeed in a small part comparatively, of the liver, and hence there may be sufficient bile flow down to color the feces to a greater or less extent. But a small amount of bile-pigment in the blood suffices to tint the whole surface of the body.
The urine may exhibit changes in appearance before the conjunctiva becomes yellow. It is colored in all possible degrees, from a merely high normal hue to a deep brownish almost black tint. It may be deep red and clear like dark brandy or brown like porter, and thick with urates. Usually, the urine of jaundice deposits abundantly of urates, but this fact is more especially true of those patients retaining appetite or having a voracious appetite and indulging in a full diet without restraint. The reaction of the urine is acid, and the specific gravity does not often descend below 1010, and may be 1030. The amount passed in twenty-four hours varies, but does not differ materially from the normal. Toward the termination of some fatal cases the quantity of urine has greatly diminished, and in a few instances was suppressed, but in such examples other factors than hepatic disease were concerned. More or less albumen is nearly constantly present in the urine of jaundice, but the detection of a trace is very difficult when the urine, as is so often the case, is cloudy. The urine should be carefully filtered before applying the test, and a specimen for comparison should be placed alongside of that being examined. If on boiling no haze appears, it may be developed by dropping in some nitric acid. The nitric-acid test, so often employed by allowing some drops of urine to trickle down the test-tube and observing the reaction at the point of contact, is, in the writer's experience, very fallacious. The source of the albumen in jaundiced urine is obviously the blood-globules. As Von Dusch first demonstrated, and Kühne26 afterward clearly confirmed, the bile acids dissolve the red corpuscles. As the quantity of albumen in the urine is small, it is reasonable to conclude, as suggested by Legg, that the bile acids are not present in the blood in any considerable amount.
26 Archiv für path. Anat., Band xiv. p. 333.
When any large quantity of bile is contained in the urine, its detection is not difficult. A strip of muslin dipped in the urine will be stained, and the underclothing of the patient will have the yellowish spots [p. 979] caused by bile. Gmelin's test is the most convenient. This is applied as follows: Some nitric acid containing nitrous—which is the case of the ordinary commercial article—is put into a test-tube, and some of the suspected urine is allowed to trickle down the side of the tube to come in contact, but not mix, with the acid. At the point of contact, when the urine contains bile-pigment, first a zone of green, then blue, violet, and finally red color, develops. As this play of colors takes place on the instant, the attention must be sharply fixed to see the changes. Rosenbach27 suggests this test be applied by filtering some urine containing bile through filtering-paper and touching the paper with a drop of nitric acid. The result is, a green circle forms at the point of contact. The usual mode of applying Gmelin's test is to place on the bottom of a common white plate or on a porcelain dish a thin film of the urine, and carefully bring in contact with it a thin film of nitric acid. The color reaction mentioned above takes place at the margin of contact.
27 Centralblatt für die medicin Wissenschaft, 1876, p. 5.
Besides the presence of bile and albumen, and some fatty epithelium from the tubules, there is no material change in the composition of the urine. At one time it was supposed that the amount of urea was greatly lessened, but later and more accurate investigations have shown that this excretion is in greater or less quantity according to the food taken, and bears no relation to the jaundice. On the other hand, Genevoix28 maintains that the quantity of urea is increased in spasmodic icterus, and in the same ratio the uric acid declines. As regards the chlorides and other salts, there seems to be a tolerably constant ratio in their variations with the changes of quantity of urea and uric acid—are therefore nearly related to the amount of food taken.
28 Essai sur les Variations de l'Urée et de l'Acide urique dans les Maladies du Foie, Paris, 1876, p. 59 et seq.
As regards the condition of the liver, there is no apparent change. In topography, in the area of hepatic dulness, and in the dimensions of the right hypochondrium the local condition does not deviate from the normal in simple jaundice. There may be more or less tenderness over the epigastrium and along the inferior margin of the liver, but there is rarely any actual pain.
The circulation of bile in the blood and the action of the bile acids on the red corpuscles must have an influence on the functions of various organs. In some cases of jaundice, but by no means in all, the pulse is slow, in a few instances descending as low as 40 per minute, and, according to Frerichs,29 as low as 21 per minute. Usually, the pulse-rate is not lower than 60. To observe the slowing of the heart the patient must be recumbent, for the pulse rises to the normal or above on assuming the erect posture and moving about. The occurrence of fever also prevents the depression of the circulation. The slowing of the heart is found to be due to the action of the bile acids on the cardiac ganglia. The other elements of the bile were ascertained to have no influence on the circulation. As the heart may be slowed by an increase of inhibition through stimulation of the vagi or by a paralyzing action on the cardiac muscle, it was necessary to eliminate these effects to establish the influence of the bile acids on the ganglia. By exclusion, and by ascertaining the effects [p. 980]of the bile acids on a properly prepared Stannius heart, Steiner and Legg have succeeded in demonstrating this important point.30
29 Diseases of the Liver, Syd. Soc. ed., supra.
30 Archiv f. Anat. u. Physiol., 1874, p. 474; Legg, On the Bile, etc., loc. cit.
The temperature of jaundice is normal usually, sometimes below. When a febrile affection occurs during the course of jaundice, the rise of temperature belonging to it is prevented in considerable part, sometimes entirely. The depression of temperature is referred by Legg to the lessened activity of the hepatic functions; but it seems to the writer more satisfactory to refer it to the action of the bile acids on the red corpuscles, the conveyors of oxygen. Röhrig31 has shown experimentally that the injection of bile acids has this effect on the temperature of animals.
31 Archiv der Heilkunde, 1863, p. 418.
The nutrition of the body early suffers in jaundice; more or less loss of flesh soon occurs, and debility and languor are experienced. There are several factors concerned in this result. The diversion of the bile from the intestine interferes in the digestion of certain materials; when jaundice occurs, glycogen ceases to be formed—and this substance has an important office in nutrition and force-evolution—and the injury done to the red blood-globules interferes with oxidation processes.
The functions of the nervous system are variously disturbed in jaundice. Headache, frontal, occipital, or general, is present in most cases to a greater or less extent. Hebetude of mind and despondency are nearly if not quite invariable, although it is not unusual to see men with jaundice engaged in their ordinary avocations. Drowsiness is a common symptom. More or less wakefulness at night, or sleep with disturbing dreams, not unfrequently coincide with drowsiness during the waking moments. In severe cases of icterus dependent on structural changes the cholæmia may produce stupor, delirium, convulsions, etc., but such formidable symptoms do not belong to the simple and merely functional jaundice.
Vision is sometimes colored yellow, or, rather, white objects appear yellow, but this must be a rare symptom, since Frerichs never met with an example. Murchison32 narrates a case, and the writer has seen one. It is a fugitive symptom, rarely continuing longer than two or three days. The term xanthopsy has been applied to it.
32 Clinical Lectures on Diseases of the Liver, New York, 1877, p. 321.
A nervous symptom of common occurrence is pruritus of the skin. This may be so severe as to prevent sleep, and in any case is a disagreeable and persistent affection, always worse at night. It may appear before the jaundice so long a period as ten days, as in a case mentioned by Graves,33 and two months in a case narrated by Flint.34 It is most severe at the beginning of the jaundice, and usually disappears before the jaundice ceases, but it may continue to the end. It is not limited to any particular part of the body. Pruritus is sometimes accompanied by urticaria, and the irritation caused by the friction of the skin may set up an eczema. Occasionally boils, and more rarely carbuncles, appear during the course of jaundice. Another curious affection of the skin which occurs during chronic jaundice is xanthelasma or vitiligoidea. First mentioned by Rayer, this disease was afterward well described by Addison and Gull35 under the name vitiligoidea, and they recognized two varieties, v. plana and v. tuberosa. The plane variety is found on the [p. 981] mucous membrane of the mouth, the eyelids, the palms of the hands, and the flexures of the joints, and consists of a yellowish-white soft eruption slightly raised above the surrounding skin and varying in size from a pin's point to a dime in size. The color is described as like that of a dead leaf or chamois-skin. The tuberose variety consists of small tubercles from a millet-seed to a pea in size. They have a yellowish color, are tense and shining, and are placed on the ears, neck, knuckles, elbows, knees, and other parts. Whilst the plane variety gives little if any uneasiness, the tuberose is apt to become irritated and painful. From the pathological point of view this eruption consists of proliferating connective-tissue corpuscles, some of which have undergone fatty degeneration.36 The morbid process tends to occur symmetrically, as on the eyelids, to which it may be confined, but it usually develops in patches, and may indeed extend over the whole body, when it is called xanthelasma multiplex.
33 Clinical Lectures on the Practice of Medicine, 2d ed., by Neligan, p. 637.
34 Philada. Med. Times, 1878, p. 507.
35 Guy's Hospital Reports, 1851, p. 265.
36 Waldeyer, Archiv für path. Anatomie, etc., vol. lii. p. 318.
The disorganization of the blood caused by jaundice sets up a hemorrhagic diathesis. This result, however, is not usual in simple jaundice, but belongs rather to acute yellow atrophy, sclerosis, and other chronic affections of the liver. It will therefore be more appropriately considered in connection with those maladies.
COURSE, DURATION, AND TERMINATION.—When jaundice is a symptom merely, it pursues a course determined by the peculiarities of the disease. The duration of simple jaundice varies from one to four weeks, the average being about three weeks. If it continues longer than two months, suspicions may well be entertained that the case is of a more formidable character than simple jaundice. The termination of this form of the disease is always in health. A favorable prognosis can be given only in the case of an accurate diagnosis. Those cases may terminate more speedily which, being of malarial origin, are treated by efficient doses of quinine. If delirium and coma come on, the apparently mild case means, probably, acute yellow atrophy, which cannot at the onset be distinguished from simple jaundice. If any nervous symptoms occur or if hemorrhage appears, the case will prove to be serious. A rise of temperature usually indicates mischief. When the stools begin to exhibit the normal appearance from the presence of bile, a satisfactory termination of the case may be soon expected. The yellowness of the skin disappears slowly after the natural route of the bile has been restored, and the urine is the last to lose the pigment, as it was the first to exhibit its presence.
DIAGNOSIS.—The diagnosis of jaundice as a symptom is usually easy. It should be remembered that jaundice cannot be detected at night by any ordinary light, and when it is disappearing the tint varies, now being distinct, again absent. Mental emotion when the color is fading develops it. Browning by the sun's rays causes an appearance which might be mistaken by a superficial observer for jaundice, but it is only necessary to look at the parts protected and at the urine to discover the true state of the case. The detection of bile in the urine and the ocular evidence of its absence from the stools will be conclusive. In some cases of jaundice the stools are golden yellow, and in many instances they are offensive.
[p. 982] It is important to mark out the limits of the gall-bladder, if it is of sufficient size to do so, for any accumulation of bile in this sac signifies an obstruction of the ductus communis choledochus. If the jaundice has come on after the symptoms of gastro-duodenal catarrh, is recent, continues but two or three weeks, and then subsides without any nervous symptoms or hemorrhage, it is a case of simple jaundice, probably due to catarrh or spasm of the bile-ducts. If the jaundice be preceded by attacks of severe pain, nausea, and vomiting, and disappears after a week or two, the case is one of hepatic calculi. If the jaundice persists months after such an attack of acute pain, and does not disappear after a year or more, it is probably due to an impacted calculus. The other diagnostic relations of jaundice are more properly considered in connection with the malady of which jaundice is a symptom.
TREATMENT.—For jaundice the symptom the treatment is included in that of the disease. Here the treatment of simple jaundice, the functional disorder, is to be discussed. If there is much nausea, the tongue is heavily coated, and, especially if the seizure has followed dietetic excesses, an emetic of ipecac may be highly serviceable. Recent experiments have proved the accuracy of the clinical observations which recognized the cholagogue property of ipecac, and hence the emetic effect of this remedy is aided by its power to promote the discharge of bile. Emetics are of course contraindicated when jaundice is due to an impacted calculus, to malignant disease, to echinococci or other kinds of tumor. If there is much irritability of the gastro-intestinal mucous membrane, as shown in vomiting and diarrhoea, small doses of calomel (1/12 to ¼ grain) three or four times a day are highly useful. If calomel possessed the property ascribed to it of stimulating the liver, it would be injurious; it is beneficial here because it has a sedative effect at first, followed, when a sufficient amount has accumulated, by an eliminant action. Such hepatic stimulants as euonymin, sanguinarin, podophyllin, jalap, colocynth, rhubarb, etc. have long been used in cases of jaundice with the view that the liver is torpid and needs stimulating. It may be inquired, however, If the bile already formed has no outlet by the proper route, what utility can there be in making the organ produce more? The true reason for the administration of such remedies in any case of obstructive jaundice is to cause such downward pressure as to force out of the duct an obstructing plug of mucus. The writer has known this result to be accomplished by a dose of compound jalap powder when a great variety of remedies had been employed in vain. One of the most efficient remedies—in the writer's considerable experience the most efficient—is phosphate of sodium, of which a drachm or more is administered three times a day. This remedy liquefies mucous plugs and promotes the flow of bile without harshly and rudely forcing the biliary secretion, and it also has a marked curative effect in gastro-duodenal catarrh. It may be given advantageously with arseniate of soda—the latter in dose of 1/20 grain—and dissolved in a tumblerful of Vichy water or Saratoga Vichy water, or preferably in a wineglassful of hot water. Free use of alkaline and laxative mineral waters is desirable, for a double purpose—to act on the liver and on intestinal digestion, and to promote the excretion of biliary matters by the kidneys. In this country we have a number to select from—the Saratoga, Bethesda, Michigan, and others. Certain sulphurous waters, [p. 983] as the Blue Lick of Kentucky, are highly useful in the more chronic cases. Sulphur baths may be conjoined to the internal administration of the waters.
Nitric and nitro-muriatic acids have long been celebrated for their good effects in jaundice. It is the presence of the acid chyme in the duodenum which excites the normal flow of bile, and Bernard found that applying acid to the orifice of the common duct in the intestine has the same effect. There is then a rational reason for the administration of this remedy. A nitro-muriatic bath, both local and general, was formerly more used than now. Its utility is questionable, and the difficulties in the way of applying it great.
Recently, Gerhardt37 has proposed to faradize the gall-bladder, and by compression with the fingers to empty it, forcing the bile into the intestine, and thus clearing out obstructions. This seems to be very questionable if not dangerous practice, but repeated successes will justify it.
37 Sammlung klinische Vorträge, Volkmann, p. 112.
Regulation of the diet is of the first importance. Fats, starches, and sweets cannot be well digested when no bile enters the small intestine, where they undergo conversion. These substances fermenting, much acid results, and hence if a catarrh exist it is increased. An exclusive diet of skimmed milk, kept up for two weeks or as long as possible, is the best mode of alimentation for this part of the treatment. Afterward, the diet should be composed of milk, meat-broth, lemonade, and subsequently of the succulent vegetables, acid fruits, and fresh meat. Indulgence in malt liquors, wines, and spirits should be strictly prohibited.
A new method of treating jaundice has been lately proposed by Krull,38 which has the merit that no injury is done by it if no good is accomplished. It consists in injecting into the rectum from two to four pints of water at 60° F., which is retained as long as possible. Each time the injection is repeated the temperature is raised a little. Krull reports that he has uniformly succeeded, and has never found it necessary to repeat the injection more than seven times. It may be given twice or thrice a day.
38 Berliner klinische Wochenschrift, 1877, p. 159.
DEFINITION.—An abnormal quantity of blood in the liver, constantly present, constitutes hyperæmia or congestion. During the period of repose there is less, but during the period of activity more, blood circulating in the liver, but the physiological hyperæmia is not, nor does it contribute to, a diseased state unless abnormal conditions continue it beyond the proper limits. The term hyperæmia, here used, applies to a pathological state in which various structural alterations grow out of the continual congestion of the blood-vessels of the organ.
CAUSES.—A physiological congestion of the liver ensues when the [p. 984] process of digestion is going on. The afferent vessels dilate, and not only more blood, but various materials taken up from the foods and products of digestion, many of them having directly stimulating effects, also pass to the organ. Frequent and large indulgence in food, especially if rich in quality and highly seasoned with spices, mustard, etc., the consumption of malt liquors, wines, and alcoholic fluids in general, the habitual use of strong coffee and tea, gradually induce a state of hyperæmia. If to the consumption of a large quantity of highly-stimulating food there is added the mischief of insufficient waste, the danger of congestion of the liver is the greater. Persons addicted to the pleasures of the table are apt to pursue sedentary lives, and hence, besides the inappropriation of the material digested, the process of oxidation is insufficient to burn off the surplus. A sedentary life further tends to make the circulation in the hepatic veins sluggish by lessening the number and depth of the respirations, and with the obesity developed under these conditions the propelling power of the heart is diminished by fatty degeneration or fatty substitution of the cardiac muscle. Disease of the semilunar ganglion, the solar plexus, and of the splanchnics under circumstances and of a nature not now well understood may cause dilatation of the hepatic vessels.
Suppression of a long-existing hemorrhage from piles and from the uterine system has caused hyperæmia of the liver. Evidences of hepatic congestion are comparatively common about the menstrual period in consequence of the tardy appearance of the flow, of its insufficiency, or of its sudden suppression. There is a form of jaundice known as icterus menstrualis, and attacks of hepatic congestion are not uncommon at the climacteric period.
The most important causes of hyperæmia of the liver are mechanical, and consist in obstruction to the circulation in the ascending vena cava from disease of the heart or lungs. Dilatation of the right cavities, incompetence of the tricuspid, and stenosis of the mitral orifice are the usual cardiac changes leading to congestion of the liver. The same effect, to a much less extent, however, is produced by any cause which weakens the propelling power of the heart, as myocarditis, pericarditis, etc. Amongst the pulmonary lesions obstructing the venous circulation are emphysema, interstitial and croupous pneumonia, effusions into the pleura, intrathoracic aneurisms or tumors, etc. It should not be forgotten that effusions into the left pleura, as was demonstrated by Bartels39 and confirmed by Roser,40 so push over the mediastinum toward the right and bend the vena cava in the same direction, just as it emerges from the opening in the diaphragm, that the circulation in this vessel is impeded, and consequently congestion of the liver induced.
39 Deutsches Archiv für klin. Medicin, Band iv. p. 265.
40 Archiv der Heilkunde, Band vi. p. 40.
The influence of climate, especially of long-continued high temperature, has been warmly disputed. On the whole, it seems probable that in warm climates congestion of the liver is much more common. Malarial infection is an unquestionable cause. In the section on Jaundice it was stated that this symptom may occur without the phenomena of fever, and, indeed, without any other disturbance of the system. In a large proportion of cases of intermittent fever, probably in all, more or less congestion of the liver occurs.
[p. 985] PATHOLOGICAL ANATOMY.—Congestion may take place in the portal system, and be due to conditions of the gastro-intestinal mucous membrane, or in the hepatic vein and radicles, due to obstructive troubles in the heart or lungs. The appearances vary accordingly. Restricting the observations to the hyperæmia, and not including subsequent lesions, it suffices to say that the liver is somewhat enlarged, rather darker in color than the normal, and uniformly so; the radicles and branches of the portal vein in the liver, the trunk of the vein itself, and the veins of the spleen, stomach, intestines, mesentery, etc. are distended with black blood, and the tissue of the liver rather wet, inclined to soften, and here and there marked by minute hemorrhages from rupture of small vessels. The extravasations of blood accompany the hepatic congestion of hot climates, and probably are the preludes to suppurative inflammation. The portal system the more readily suffers from a passive congestion because of the provision for the alternate expansion and contraction of the tunics of the vessel, scantily supplied with contractile elements. An acute congestion of the liver produced by sudden dilatation of the capillaries of the hepatic artery has not been described, but it would appear to be possible.
The most important form of hepatic congestion is the mechanical, arising from obstruction of the circulation in the heart or lungs. In consequence of this obstruction the blood accumulates on the venous side, and there is in consequence an ischæmia of the arterial side. The hepatic vein becomes distended, and its terminal radicle in the centre of each acinus—the central vein—enlarges with the increased pressure. It follows that the minute capillaries emptying into the central vein are also distended with blood, and finally the portal vein and its radicles throughout are similarly affected. The same condition of the hepatic circulation was long ago observed by Virchow41 as a result of weakness of the muscular tissue of the heart, and consequently diminished propelling power of the organ. On section of the liver much black blood flows out; each central vein is a distinct dark object in the centre of each acinus, and contrasts strongly with the surrounding paler substance, whence the common term for this appearance is nutmeg liver. The long-continued distension of the central vein leads to sclerosis of its walls,42 and the neighboring hepatic cells undergo atrophy in consequence of the greater pressure. A relatively increased quantity of connective tissue seems to result, but whether hyperplasia occurs is disputed. By Talamon43 such increase of the connective tissue is denied, but Thierfelder44 admits that there is an apparent and also in some cases a real increase. The atrophy of the cells induces more or less shrinking and consolidation of the liver; it is therefore smaller in size and firmer in texture, and presents a brownish-red color. The atrophic change in the hepatic cells is represented finally by some brownish or black pigment, but it is rare, indeed, for all the cells of an acinus to disappear. To this change has been applied the term cyanotic atrophy. In some instances Liebermeister45 [p. 986]has found an increase of the connective tissue of the liver; and this opinion is confirmed by Legg.46 When this multiplication of the connective tissue occurs, the condition of the liver is entitled cyanotic induration. The sclerosis originating in this way is distinguished from true cirrhosis by its less extent, irregularity, situation, and the marked degree of hepatic congestion.
41 Archiv für path. Anat., etc., Band v. p. 289.
42 Talamon, Recherches anatomo-pathologiques et cliniques sur le Foie cardiaque, Paris, 1881 (pamphlet).
43 Ibid.
44 Atlas.
45 Beiträge zur path. Anat. u. Klinik der Leberkrankheiten, Tubingen, 1864, p. 209 et seq.
46 Medico-Chirurgical Transactions, vol. lviii. p. 345.
SYMPTOMS.—Hyperæmia of the liver is usually one of the complex conditions of a morbid state, and hence is associated in its symptomatology with the connected maladies. On the one hand associated with gastro-intestinal disorders, on the other with cardiac and pulmonary diseases, the symptoms must be varied accordingly. It is necessary, however, to indicate as clearly as may be those belonging to the hepatic circulation.
Congestion of the portal circulation is a condition to which frequent references are made, but which is rarely clearly defined. As seen in the West and South, it signifies a gastro-intestinal catarrh more or less acute, with an obvious condition of biliousness, as manifested in a faint jaundiced tint of the skin and of the conjunctivæ, uneasiness in the right hypochondrium, with enlargement of the area of hepatic dulness, the evacuations from the bowels being either grayish or clay-colored, or more frequently bilious, acrid, and offensive.
The gastro-intestinal disorder which initiates the hepatic disturbance should not be confounded with that which succeeds to congestion of the hepatic veins. The latter invariably comes on after the obstruction at the heart or lungs has continued for some time. There occurs in this state very extensive hyperæmia of the gastro-intestinal mucous membrane, and consequent disorders of stomachal and intestinal digestion. The former is a reflex cause of disturbance, probably through the intermediation of the solar plexus. The gastro-intestinal irritation, by depressing the functions of the hepatic through the solar plexus, induces a paresis of the muscular layer of the portal system, and thus congestion ensues. Such a result is aided by high temperature, but especially by the constitutional tendencies of some subjects to hepatic disturbances. In such examples of hyperæmia the symptoms consist of those belonging to gastro-intestinal catarrh, succeeded by those referable to the liver, consisting in uneasiness, heaviness, and fulness of the right hypochondrium, increase in the area of hepatic dulness, soreness on pressure along the inferior margin of the ribs and over the epigastric region, yellowness of the conjunctivæ, a fawn color of the skin generally, and high-colored rather scanty urine, depositing abundantly uric acid and urates. A liver considerably enlarged and projecting one or two fingers' breadths below the ribs may be quickly relieved and return to the normal size on the occurrence of hemorrhage from piles or after free watery evacuations produced by a hydragogue cathartic.
The form of hepatic congestion most usually observed is that of the hepatic vein, caused by obstructive troubles of the heart or lungs, and known as the nutmeg liver. The increase of size of the liver under these circumstances may be very considerable. To determine an increase in the area of hepatic dulness the position of the organ must be ascertained with reference to the position of the body, whether recumbent or erect. In the former position the liver gravitates toward the thorax; in the [p. 987] latter, downward into the abdomen. If palpation only were employed to detect an increase in the size of the organ, an error might readily be committed in this respect. Some congestion may doubtless exist without an actual increase of size recognizable by our means of investigation; there may be merely some distension manifested by a sense of increased resistance; the liver may project a hand's breadth below the ribs; and between these extremes there may be all possible degrees of enlargement. When the liver, in consequence of hyperæmia, projects below the ribs, it offers to the sense of touch the impression of a smooth, elastic, rather rounded surface, and not the hardness and nodular character of sclerosis, and not the sharpness of border and hardness of texture belonging to amyloid disease. The enlargement of the liver due to hyperæmia is further distinguished by the fact that it varies much in size at different times, and may be much reduced by hemorrhage from the portal system, and increased suddenly by an attack of dyspnoea.
When the liver is enlarged by hyperæmia the patient usually has a distinct appreciation of the fact, feels a sense of weight, tenderness, and oppression in the right hypochondrium, and experiences a painful dragging from the right toward the left when turned on the left side. In some cases pain is felt in the shoulder, or, if not pain, a feeling of weight. A slight icteroid hue of the conjunctiva, face, upper extremities, and trunk is often present, but the stools are not wanting in bile and the urine contains but little pigment—facts indicating that the obstruction is limited to a small number of ducts. If the jaundice is decided, the stools clay-colored, and the urine loaded with pigment, a catarrhal swelling of the common or hepatic duct exists.
As nutmeg liver is an incident in the course of the venous stasis from cardiac or pulmonary obstructive disease, it is not unusual to find ascites and general dropsy occur. When ascites precedes the other manifestations of dropsy, and is relatively more important, the hepatic congestion has led to atrophy of the cells and contraction of the organ, or to cyanotic induration, as it has been designated in contradistinction to cirrhotic induration.
The subjects of hepatic congestion, especially of that form of the malady due to gastro-intestinal irritation, are apt to experience no little mental depression, even hypochondriasis, as, indeed, is usual in most cases of hepatic disease.
COURSE, DURATION, AND TERMINATION.—The behavior of any case of hyperæmia of the liver is determined, first, by the character of the cause, and, secondly, by the extension of the mischief and the atrophic changes which ensue. The congestion arising from gastro-intestinal irritation is comparatively short-lived, since the causal conditions may usually be promptly removed. It is far different in the cases due to pulmonary or cardiac disease. If caused by a left pleuritic exudation, the congestion will disappear as soon as the bend in the ascending vena cava is removed by paracentesis. If, however, produced by a permanent pulmonary obstruction, the course of the hepatic disease is toward cyanotic induration. The same is true of obstructive cardiac lesions. If compensation—as, for example, of a mitral regurgitation—is not effected, the continual congestion must lead to the ultimate lesions of the liver; but if compensation can be brought about, the liver will be saved the irremediable [p. 988]changes. The prognosis, therapeutical and pathological, must necessarily be dependent on the lesions of which the hyperæmia of the liver is merely a symptom.
DIAGNOSIS.—The decision in any case of hyperæmia of the liver must rest on the determination of the gastro-intestinal, pulmonary, or cardiac diseases causative. When, for example, to the gastro-intestinal disturbance or cardiac disease there are added heaviness, uneasiness, increased area of dulness of the right hypochondrium, a hyperæmia of the liver may be concluded to exist. The extent to which the organ is damaged may be judged from its size, the duration of the congestion, and the character of the determining cause. If the area of hepatic dulness declines steadily after having been increased, the causative conditions continuing, the shrinking is due to atrophy. This view is confirmed if ascites has appeared and increased out of proportion to the general dropsy.
TREATMENT.—Those cases of hyperæmia dependent on excesses in eating and drinking require the substitution of a diet composed of lean meat, skimmed milk, acid fruits, and such succulent vegetables as lettuce, tomatoes, celery, etc. When there is a high degree of gastro-intestinal catarrh, an absolute milk diet may be enforced with great advantage. The diet, exercise, bathing, etc. enjoined in the section devoted to lithæmia are equally applicable here. Amongst the special plans of diet sometimes advocated in the condition of abdominal plethora or portal congestion are the grape cure, the whey cure, etc. Great good is accomplished by a simple diet and a course of the Saratoga saline laxative waters—the Congress, Hathorn, Geyser, etc. The alkaline waters of Wisconsin and Michigan, the White Sulphur of Virginia, and others having similar properties in this country may be employed for the same purpose. The saline laxatives, Pullna, Friedrichshall, and other purgative salines, may be used in robust, plethoric subjects with much portal congestion, hemorrhoids, etc. Phosphate of soda, given in sufficient quantity to maintain a soluble state of the bowels, is also a useful remedy. The resinous cathartics, podophyllin, jalap, rhubarb, aloes, euonymin, iridin, baptisin, etc., are all useful when the indication is to unload the portal circulation. The mercurials, formerly so much used, are now discredited to an unwarranted degree. In an irritable state of the gastro-intestinal mucous membrane calomel in small doses is remarkably useful.
The treatment of congestion of the hepatic vein is included in that of the lesion causing it. In some rather exceptional cases the liver enlarges considerably in consequence of incompetence of the mitral, without there being any other conspicuous evidence of the lesion. Remarkable relief is afforded to the hepatic symptoms by the administration of digitalis. The important point in all cases due to cardiac disease is to bring about compensation, and thus obviate the consequences of the lesion. Remediable pulmonary affections should be cured as promptly as possible, and the evil results of incurable affections lessened by efforts to remove the hepatic hyperæmia. Careful alimentation, saline laxatives, and diuretics are the most efficient measures. It would be encroaching on the subjects of pulmonary and of cardiac diseases to enter more minutely into the therapeutical questions connected with a symptom of these affections.
DEFINITION.—By the term perihepatitis is meant an acute inflammation of the serous envelope of the liver. It may be acute or chronic, very rarely the latter, and it is usually a secondary affection, although primary cases are not uncommon.
PATHOGENY.—Inflammation of the hepatic portion of the peritoneum may arise by an extension of the morbid process from neighboring parts, as in perforation of the stomach or duodenum, pleuritis of that part of the membrane reflected from the diaphragm, etc. More frequently it arises by contiguity from some disease of the liver itself, as chronic interstitial hepatitis, abscess, echinococci cysts, cancer, etc. The author has frequently (comparatively) seen perihepatitis follow the passage of gall-stones. It is usual to find considerable organized exudation at the hilus of the liver in the case of those who have had several attacks of hepatic colic, and attachments to various neighboring parts also. In those instances of secondary hepatitis there may be more or less extensive connective-tissue formation and compression of the hepatic substance (Budd).47
47 Diseases of the Liver; also, Bamberger, Krankheiten des Chlylopoietic Systems, p. 495, 2d ed.
Direct perihepatitis arises from traumatic causes—from contusions of the right hypochondrium by spent balls, blows and falls, etc. Tight-lacing and wearing a strap to support the trousers are supposed to excite a slow, chronic hepatitis, but the latter is more certain to bring about such a result than the former.
SYMPTOMS.—Acute perihepatitis, if of sufficient extent, causes more or less fever; pain is felt in the right hypochondrium, and is increased by pressure and by deep inspirations, and in some rare instances a friction murmur is audible synchronous with the respiratory movements. These symptoms succeed to attacks of hepatic colic, perforation of the stomach or intestine, and contusions of the abdominal wall. The chronic form is not febrile; there is a feeling of soreness instead of acute pain; pressure, the movements of the body, respiration, etc. increase the distress, and on turning on the left side a painful dragging is experienced. A slight degree of icterus may be present in both acute and chronic cases.
COURSE, DURATION, AND TERMINATION.—The course of the acute cases is toward recovery. In two or three days the inflammation reaches the maximum, adhesions form, and then the morbid process declines. The whole course of an acute perihepatitis caused by external injury or by the passage of gall-stones is terminated in a week or ten days. The mischief done may not be limited to the adhesions formed. The large quantity of newly-organized connective tissue may, in its subsequent contraction, compress the common, cystic, or hepatic duct, or the portal, or both ducts and vein. The course of the chronic cases is determined by the causative lesion. The contraction of the new-formed connective tissue may compress the organ and lead to sclerotic changes which cannot be distinguished from cirrhosis. In some instances contusions set up suppurative inflammation, and an abscess forms between the parietal and glandular layer of the peritoneum. Such a case will then present the phenomena of hepatic abscess.
DIAGNOSIS.—The determination of the character of the case will be [p. 990] largely influenced by the history. If the attack has followed a blow on the side or a paroxysm of hepatic colic or the symptoms of perforation, there will be no difficulty in determining its seat and character. In the absence of the history the differentiation must be made between perihepatitis and pleuritis. The distinction consists in the fact that in the former the pain and soreness are below the line of respiratory sounds, although synchronous with them. In chronic perihepatitis the symptoms come on in the course of the hepatic disorder, or are consequent on a local injury, as the pressure of stays or a band.
TREATMENT.—If the symptoms are acute and the subject robust, the local abstraction of blood by leeches affords relief and diminishes the violence of the disease. A bandage should be tightly applied around the body at the level of the hypochondrium to restrain the movements of the affected organ. A turpentine stupe may be confined in this way, or a compress of water may be utilized to serve the same purpose. If the pain is acute and the peritonitis due to perforation or to the passage of calculi, the hypodermatic injection of morphia is the most important resource.
DEFINITION.—The terms interstitial hepatitis and sclerosis of the liver express the nature of the malady: they signify an inflammation of the intervening connective tissue, resulting in a sclerosis—an induration of the organ. The term cirrhosis, now so largely in use, was originally proposed by Laennec48 because of the yellowish tint of the granulations, from the Greek word, [Greek: chirros], yellow. As Laennec's theory of cirrhosis was erroneous, having regarded these granulations as new formations, the word is a very faulty one, and hence it would be preferable to use the term sclerosis, since a similar change in other organs is thus designated, as sclerosis of the kidney, sclerosis of the lungs, etc. It is also called in England gin-drinker's liver, hobnail liver. Carswell49 first described the anatomical changes with accuracy, and illustrated them with correct drawings. The following year Hallmann50 confirmed the truth of Carswell's descriptions, and contributed a good account of the morbid anatomy; and subsequently French, German, and English authorities added new facts, which will be set forth in the further discussion of the subject.
48 Traité de l'Auscultatlon médiate, tome ii. p. 501.
49 Illustrations of the Elementary Form of Diseases, fasciculus 10, plate 2.
50 De Cirrhosi hep., Diss. Inaug., Berolini, 1839, quoted by Thierfelder.
CAUSES.—Sclerosis of the liver is, conspicuously, a disease of adult life and onward. Except the congenital example mentioned below, the earliest age at which the disease has occurred, so far as I am able to ascertain, is four years—a case reported by Wettergreen51 of hypertrophic sclerosis, in which neither a syphilitic nor paludal cause could be ascertained. Cayley52 reports a case in a child of six; Murchison,53 Frerichs,54 Griffith,55 one each at ten. After this period the increase relatively to age is rapid. The majority of cases occur between thirty [p. 991] and fifty years. Yet Virchow56 has given the details of a congenital example. According to Förster, of 31 cases of cirrhosis, 16 were between forty and sixty years. The preponderance of cases in the male sex is very decided. Of Bamberger's 51 cases, 39 were men, 12 were women; of Frerichs' 36 cases, 20 occurred in men and 16 in women—a larger proportion of women than any other author records; of 12 cases observed by myself, only 1 was a woman. Nationality does not affect the production of cirrhosis, except as regards the personal habits of the people. This disease is comparatively uncommon in wine- and beer-drinking countries, and frequent amongst a spirit-drinking people.57 The great etiological factor is the abuse, the habitual use, of spirits, and hence the number of cases observed in North Germany, England, Scotland, and the United States. Murchison affirms that he has never seen a case produced in any other way. Even in children of tender years the abuse of spirits can usually be traced. Nevertheless, there are instances of the disease the origin of which cannot be referred to alcoholic excess. The congenital cases, as that narrated by Virchow, and the instances occurring in children and adults not given to spirits in any form, indicate that there are other pathogenetic influences which may bring about a sclerosis of the liver. Virchow58 was one of the first to illuminate the subject of visceral syphilis and to demonstrate the occurrence of sclerosis of the liver from syphilitic infection. Very often the syphilitic cachexia coincides with alcoholic excess. There can be no doubt that chronic malarial poisoning causes, or powerfully predisposes to, cirrhosis. I have submitted elsewhere pathological evidence on this point,59 and the Italian physicians, who have the opportunity to obtain accurate data, maintain that malarial toxæmia does bring about this state. It is probable that the overgrowth of connective tissue is induced by the repeated congestions of the malarial attacks, and by the obstruction due to catarrh of the bile-ducts which so often occurs in the febrile paroxysms.
51 Hygeia, 1880, quoted by London Medical Record, March 15, 1881.
52 Transactions of the Path. Society of London, vol. xxvii., 1876, pp. 186, 194.
53 Clinical Lectures, loc. cit.
54 Clinical Treatise, etc., Syd. Soc. ed., by Murchison.
55 Clinical Lectures, loc. cit.
56 Archiv f. path. Anat., Band xxii. p. 426.
57 Baer, Der Alcoholismus, Berlin, 1878, p. 62 et seq.
58 Virchow's Archiv, vol. xv. p. 281; also, Lancereaux, A Treatise on Syphilis, Syd. Soc. ed.
59 Memoirs of the Sanitary Commission, medical volume.
J. Wickham Legg60 and Charcot61 nearly simultaneously discovered that obstruction of the bile-ducts, if continued a sufficient length of time, sets up a hyperplasia of the connective tissue of the liver. The evidence is pathological and experimental. Thus, Legg has seen a liver markedly cirrhotic in a case where a small cancer of the duodenum completely obstructed the flow of bile into the intestine.62 By tying the common duct in dogs it was found that a hyperplasia of the connective tissue very soon occurred, and this was followed, of course, by contraction of the new tissue and atrophy of the hepatic cells. Closure of the hepatic vein has the same effect, and also, as Solowieff63 has asserted, closure of the portal vein; on the other hand, by Frerichs and others the closure of the portal is attributed to the sclerosis.
60 On the Bile, Jaundice, etc., loc. cit., p. 351 et seq.
61 Leçons sur les Maladies du Foie, etc., p. 231 et seq.
62 On the Bile, Jaundice, etc., loc. cit., p. 355.
63 Arch. f. path. Anat., etc., Band lxii. p. 195.
Certain poisons, as antimony, arsenic, notably phosphorus, have the power to set up an irritative hyperplasia of the connective tissue of the [p. 992] liver. These metals accumulate in the liver in preparation for excretion. Wegner,64 in the study of the action of phosphorus on dogs, rabbits, and other animals, has induced a marked degree of sclerosis, but such results have not been observed in cases of poisoning by phosphorus in man, except in an instance reported by Küssner.
64 Virchow's Archiv, Band lv. p. 18.
Finally, a condition of the liver corresponding in all respects to cirrhosis has been induced by perihepatitis, by the organization of the exudation and its subsequent contraction, and by the extension of the morbid process from the capsule to the interlobular connective tissue (Poulin65).
65 Étude sur les Atrophies viscérales consécutives aux Inflammations chroniques du Sereuses, etc., Thèse de Paris, 1880.
PATHOLOGICAL ANATOMY.—Several forms of cirrhosis are recognized by the modern French school of pathologists. According to Sabourin,66 there is an annular, a monolobular, and a multilobular form. These differ merely in regard to the arrangement of the new connective tissue. At the outset of the disease the liver is increased in size and hyperæmic. Its consistence is also greater than normal. The outer surface is at this period smooth, but on section the islets of the parenchymatous tissue, yellowish in color, are distinctly visible between the grayish or pale-rose tint of the intervening or proliferating tissue. This reddish-gray material consists of fine connective-tissue elements containing spindle-shaped cells.67 The development of this material is such as to even exceed in quantity the proper glandular structure. The bands of newly-formed connective tissue extend between individual lobules (monolobular cirrhosis) or between groups of lobules (multilobular cirrhosis). A portion of the spindle-shaped cells form new vessels communicating with the branches of the hepatic artery.68 Coincidently with the formation of the new connective tissue ensues its contraction. The enlarged organ diminishes in size from a slight degree to one-half its original volume; especially in the left lobe is the diminution of size most marked. On the surface it exhibits a knobbed or nodular aspect (hobnail liver), and these knobs present through the capsule a yellow appearance. The granulations, so called, consist of small prominences corresponding to lobules or groups of lobules, and hence vary in size from that of a pinhead to that of a pea.69 Between these are the sharply-defined masses of connective tissue. On section the organ is found to be of firm almost cartilaginous hardness, and between the interlacing bundles of connective tissue are the small islands of parenchymatous tissue projecting above the cut surface and having a yellowish or brownish-yellow color. As the terminal branches of the portal are compressed in the process of shrinking undergone by the new connective tissue, they are destroyed. The result of this obliteration of the portal radicles is the impaired nutrition of the lobules and atrophy of the cells. Formerly it was held that the atrophy of the hepatic cells was due to the compression exercised by the contracting connective tissue, and Beale70 even maintained that the change began in [p. 993] the cells, the connective tissue contracting as the cells receded before them. This view has been reaffirmed by Ackermann in a paper read last year before the Congress of German Naturalists and Physicians, but without any acknowledgment, so far as I can ascertain, of Beale's long-before expressed opinions. In the discussion which followed the reading of Ackermann's paper the position of its author was supported by Aufrecht, Küssner, and others, but controverted by Rindfleisch. It has been demonstrated by Cohnheim and Litten71 that the lobule is nourished not only by the portal radicles, but by the branches of the hepatic artery, which enter, by the interlobular vein, the capillaries of the lobule, and hence the nutrition of the cells suffers in consequence of the lessened blood-supply; but it is probable also that more or less compression is exercised. When the cells are destroyed, their remains may be discerned in the mass of connective tissue as fine fat-granules or masses of pigment yellowish or brownish in color. The peculiar appearance to which the name cirrhosis is applied is due to the lobules or groups of lobules which project on section above the divided surface, and are colored yellowish by the bile-pigment, which here exists in an exaggerated quantity. The cells themselves are not normal: they are enlarged by compensatory hypertrophy, and they contain much bile-pigment and a considerable quantity of fat. The compression of the capillaries, especially their obliteration, leads to stasis of the blood and its consequences in the whole chylopoietic system.
66 Ch. Sabourin, "Du Rôle que joue le Système veineux sus-hépatique dans la topog. de la cirrhose du foie," Revue de Médecine, June, 1882.
67 Förster, Lehrbuch der pathologischen Anatomie, Jena, 1873, p. 264.
68 Cornil, "Note sur l'État anatomique des Canaux biliaires et des Vaisseaux sanguins dans la cirrhose du foie," Gaz. méd. de Paris, 1883.
69 Charcot, Leçons sur les Maladies du Foie, etc., p. 226.
70 Archives of Medicine, vol. ii. p. 82.
71 Archiv für path. Anat. (Virchow), Band lxvii. p. 153 et seq.
SYMPTOMS.—The development of sclerosis is usually very insidious. After some years' indulgence in spirit-drinking or affected for a length of time with the other causes of the malady, a gradual decline of vigor occurs. The complexion takes on a fawn color, stigmata slowly form on the face, there is more or less yellowness of the conjunctiva, and attacks of headache, giddiness, and even severe vertigo, are experienced. An increasing indisposition to mental effort, some hebetude of mind, and a gradually deepening despondency are felt. The appetite gradually fails, becomes capricious, and only highly-seasoned, rather odd, or unusual articles of food can be taken. Such subjects acquire a taste for condiments, for such uncooked vegetables as onions, celery, raw cabbage, etc., for fruits, and get a distaste for plainly-cooked meats and vegetables, for sweets, etc. The digestion is as capricious as the appetite: at first there are times of appetite, again of indifference, then of disgust; some heaviness is felt after meals; gaseous eructations, acidity, pyrosis, nausea, occur day after day as the case advances; and ultimately morning vomiting is regularly experienced. Nausea is felt on rising; then with much straining and distress a little glairy mucus and a teaspoonful of bile are brought up; after which, it may be, a little food can be taken. It is only after the case is fully declared that these troubles of stomach digestion become constant; previously they occur now and then in a paroxysmal way, whilst between there is only labored digestion.
As the compression of the portal radicles maintains, by reason of the obstruction, a constant hyperæmia of the intestinal mucous membrane, a catarrhal state, with fermentation of the fatty, starchy, and saccharine constituents of the food, and hence complicated products of an irritating kind, must result therefrom. Hemorrhoids, varying in size according to [p. 994] the degree of obstruction, form, sometimes bleeding more or less profusely, again being merely troublesome or painful. Fissures of the anus and fistula in ano not unfrequently complicate the case. The bowels are necessarily rather relaxed than confined, but at the onset of the malady they may be confined, afterward assuming more or less of the characteristics of diarrhoea. The stools may be offensive with the products of decomposition, rather clay-colored or golden, or brownish and almost black from the presence of blood. In some cases the stools are parti-colored—clay-colored in part, brownish in part—and in exceptional examples continue normal or nearly so until near the end. As the transudations from the portal vessels increase, the mucous membrane of the intestinal canal becomes oedematous, and, the normal secretions being arrested, the discharges finally consist of a watery fluid, whitish or grayish, dark-brown or blackish, and very offensive. The decomposition of foods instead of their proper digestion and solution, and especially the fermentation of the starchy and saccharine constituents of the aliment taken, produce a great quantity of gas; hence meteorism comes to be an ordinary symptom. The accumulation of gas is greatly promoted by the paretic state of the muscular layer and by the relaxation of the abdominal walls consequent on the oedema of the muscular tissue. A high degree of distress is sometimes caused by the great accumulation of flatus; the abdomen is greatly distended and the diaphragm is pushed up against the heart and lungs, compelling the patient at length to sit up to breathe with ease. Of course the accumulation of fluid may be greater, and the gas only add to the discomfort.
A very common symptom is hemorrhage. Sometimes it happens, indeed, that this is the only evidence of the portal obstruction at first observed. Hæmatemesis is more common than intestinal hemorrhage. Now the blood may be large in quantity, appear little changed from its usual coagulated state, and be brought up promptly with slight effort of vomiting; now it is passed by stool, is in coffee-colored, granular masses or in a tar-like, semifluid state; and again it appears in coffee-grounds mixed with the contents of the stomach. These variations are due to the character, seat, and extent of the hemorrhage and to the condition of the mucous membrane. Merely-distended capillaries, yielding, may furnish a little blood, which, acted on by the gastric juice, forms coffee-grounds, or, if not acted on in consequence of the failure of the gastric glands to functionate, appears as bloody streaks mixed with mucus. Enlarged veins, giving way, may furnish a large quantity of partly-coagulated venous blood, charred or not as the state of the juices will determine. In some cases hemorrhages into the submucous tissue or thromboses of the submucous veins lead to solution of the membrane thus deprived of its nutritional supply, and ulcers form. Two admirable examples of this kind have been seen by the writer in which large hæmatemesis occurred from ulcers near the pylorus. They were round, smooth ulcers, containing coagula, and the eroded vessels (veins) were readily seen opening into the cavity of each.
The obstruction to the portal circulation results also in an enlargement of the spleen. There may be a simple enlargement due to the hyperæmia merely; there may be an enlargement due to the hyperæmia and to a resulting hyperplasia of the connective tissue; there may be also, in [p. 995] addition to the second form of enlargement, amyloid degeneration, syphilitic hyperplasia, etc. The increased dimensions of the spleen are by no means always made out, and authorities differ greatly as to the proportion of cases in which the enlargement can be detected. The organ may indeed be considerably enlarged whilst pushed upward into the left hypochondrium by the effusion, and yet the attempt to measure and define its dimensions may be fruitless. From a slight increase due to the hyperæmia up to the enormous dimensions acquired by the added amyloid material there are all possible variations in size.
Partly in consequence of the increased blood-pressure in the vessels of the peritoneum, and partly in consequence of the watery condition of the blood itself, effusion takes place into the sac of the peritoneum. Such an accumulation is known as ascites, or dropsy of the abdomen. The time at which the effusion begins, the amount of it, and the degree of contraction of the liver necessary to produce it, vary in each case. Ascites may be the first symptom to announce the onset of cirrhosis; it is more frequently amongst the later symptoms, and is the evidence of much interference in the portal circulation. However, it is not due wholly to hepatic disease. The blood in cirrhosis is much reduced and watery, hence slight causes suffice to induce an outward diffusion. Given a certain obstacle to the passage of the blood through the liver, transudation will be the more prompt to appear the greater the anæmia. In some cases an enormous quantity of fluid collects: from ten to thirty pounds may be regarded as usual, and forty to sixty pounds as exceptional, although the highest amount just given is not rare. The fluid of ascites nearly represents the serum of the blood. It has a straw color and is clear, but it may have a reddish tint from the presence of blood, a greenish-yellow or brown from bile-pigment. The solids of the serum are in the proportion of from 1 to 3 per cent., and consist of albumen chiefly and salts, of which sodium chloride is the principal. Hoppe's72 analysis gives this result: 1.55 to 1.75 solids, of which 0.62 to 0.77 is albumen. According to Frerichs, the amounts of solids ranges from 2.04 to 2.48, and of these albumen constitutes 1.01 to 1.34.
72 Virchow's Archiv für path. Anat., etc., Band ix.
Oedema of the inferior extremities comes on after, usually—rarely with—the ascites. If the mechanism of this oedematous swelling be as supposed, the effusion into the areolar tissue necessarily succeeds to the abdominal effusion. The pressure of the fluid in the cavity on the ascending vena cava and iliac veins seems to be the principal factor; but to this must also be added the intestinal gas, which in some instances exerts a powerful force. The ankles have in rather rare cases appeared swollen before the abdomen, but the detection of fluid in the peritoneal cavity when in small quantity is not always easy. Obese women, with much accumulation of fat in the omentum and flatus in the intestines, have swollen feet and legs if erect for some time, the effusion being due to pressure on the vena cava. The legs may become enormously distended. The scrotum and penis in the male, the vulva in the female, the buttocks and the abdominal wall, also become oedematous, sometimes immensely. Walking grows increasingly difficult. Warmth and moisture and the friction of the sensitive surfaces excite vesicular and pustular eruptions where the [p. 996]scrotum and labiæ come in contact with the thighs. Urination may be impeded by the oedema of the prepuce.
An attempt at compensation for these evils growing out of the obstruction in the portal system is made by the natural powers. Anastomoses of veins through minute branches are made use of to convey the blood of the obstructed portal circulation into the general venous system, and to this end become greatly enlarged. The interlobular veins being obliterated by the contracting connective tissue, the pressure in the branches and trunk of the portal vein is much increased. Hence an outlet is sought for in the veins which communicate between the portal and the ascending vena cava. One of the most important of these is a vein in the round ligament, at one time supposed to be the closed umbilical vein, but proved by Sappey to be an accessory portal vein. Bamberger,73 however, has found the umbilical vein pervious, and since, Hoffmann74 has demonstrated the same fact. It is probable, indeed, that Sappey's observation is correct for some cases. In either event, the veins of the abdominal wall about the umbilicus communicating with the epigastric become enormously distended, and in some advanced cases of cirrhosis form a circle known as the caput Medusæ. Further communication between the portal and the veins of the diaphragm takes place by means of the veins in the coronary and suspensory ligaments. In some instances a new route is established between the veins of the diaphragm and the portal by means of new vessels formed in the organized connective tissue resulting from perihepatitis. Still another channel of communication exists between the inferior oesophageal veins, the azygos, and the coronary, and finally between the inferior hemorrhoidal and the hypogastric. The more completely can communication be established between these anastomosing veins the less severe the results of portal obstruction.
73 Krankheiten des Chylopoiet. Syst., loc. cit.
74 Quoted by Thierfelder, op. cit.
Besides these indirect evidences of portal obstruction and a contracting organ, there are direct means of ascertaining the condition of the liver. By the methods of physical diagnosis we may acquire much information. On auscultation, as our Jackson75 was the first to show, a grating or creaking like leather, or friction sound, is audible over the right hypochondrium synchronously with the respiratory movements or when produced by moving with the fingers the abdominal wall on the liver. This sound is caused by the bands of false membrane which extend between the two surfaces, and hence indicates a secondary perihepatitis.
75 The American Journal of the Medical Sciences, July, 1850.
To ascertain the dimensions of the liver—to mark out the area of hepatic dulness—with accuracy is a most necessary procedure. The period of the disease is an important element in the problem. When the new material is deposited and the congestion of the portal system first occurs, an increase in the dimensions of the organ is observed. This enlargement, of brief duration, must not be confounded with the hypertrophic sclerosis, another form of the malady. So considerable is the increase in the size of the liver that there is an evident enlargement of the right hypochondrium, and the whole abdomen seems fuller. The organ may be felt, on palpation, projecting one, two, or even three fingers' breadths below the margin of the ribs, and the left lobe extends well across the epigastrium, increasing the sense of resistance and the area [p. 997] of dulness in this direction. The enlarged liver, as felt below the ribs, appears firmer than is natural, is yet smooth, and the margin is sharply defined. The duration of this period of enlargement is indefinite, but it is rather brief, and is followed by the contracting and atrophic stage. It is not often, indeed, that the patient presents himself during the period of enlargement. Sometimes a perihepatitis or an unwonted tenderness in the right side compels attention during this stage, but more frequently it escapes notice. If perihepatitis occur, there will be fever, pain, and tenderness, a slight icterode hue of the skin, and possibly Jackson's76 friction sound. These symptoms, taken in conjunction with the history of the case and the obvious enlargement of the organ, will indicate the existence of the first stage of sclerosis.
76 The American Journal of the Medical Sciences, July, 1850, supra.
The contraction of the liver, or, as it may be expressed, the atrophy of the hepatic cells and the consequent shrinking of the interlobular connective tissue, goes on slowly. Several months may be occupied in an amount of atrophy distinct enough to be recognized by the narrowing of the area of hepatic dulness. Especially difficult is the recognition of the contraction when ascites has fully distended the abdomen. It may be necessary under such circumstances to postpone a decision until tapping has removed the fluid. If the organ can be felt by depressing the walls of the abdomen, more or less unevenness of surface may be detected, and the inferior margin may give the impression of hardness and sharpness of outline. At the same time, the increased dulness of the epigastric region observed during the hypertrophic stage will have gradually ceased because of the shrinking of the left lobe. The liver may be undergoing the atrophic degeneration to a marked extent and yet remain large—larger even than normal. Such a state of things may be due to conjoint amyloid or fatty degeneration of the organ, and, indeed, more or less fatty change occurs in all cases of cirrhosis. The shrinking of the liver persists until the area of dulness is not greater in area than two or three ribs.
The disturbances of function in sclerosis of the liver are not limited to the chylopoietic system. As the secreting structure of the liver is continually lessened in extent by the atrophy, symptoms result from the necessary interference in the hepatic functions. These symptoms are concerned with the liver, with the nutrition of the tissues of the body, and with the kidneys. As regards the biliary function of the liver, the quantity of bile acids and pigment is reduced below the normal in proportion to the damage done to the organ. As a rule, there is little jaundice in sclerosis, and very little bile-pigment present in the urine. Hence there must be little produced. Instead of a jaundiced hue of the skin, it has a fawn color—an earthy, sallow tint eminently characteristic of a chronic affection in which the power to produce bile is much impaired. Occasionally it happens, particularly in the early stages of cirrhosis, that a well-marked jaundice appears in the face and body, but this probably is due to a catarrh of the bile-ducts. In most cases the integument presents the earthy and sallow hue above mentioned. Graves77 appears to have been the first to interpret aright the greater significance of this appearance of the skin than the purely jaundiced tint. The glycogenic [p. 998]function of the liver must be impaired in the same ratio as the biliary. The nutrition of the body suffers; the skin becomes dry and harsh; the fat disappears; the temperature of the body, unless the conditions for producing fever are present, is barely up to normal, if not somewhat below; a marked degree of anæmia supervenes; and the action of the heart becomes feeble and rapid after a period of slowness. The blood is altered in quality, and hence hemorrhages—epistaxis especially—occur, petechiæ and ecchymoses appear in the skin, and stigmata are numerous about the face and nose.
77 Clinical Medicine, op. cit.
The urine in cirrhosis is high-colored because of the abundance of pigment, and in the early stages of the disease is increased in amount, although of lower specific gravity. When much effusion takes place into the peritoneal sac, the compression of the renal veins by the fluid lessens the activity of the kidneys and diminishes the urinary flow. Much discussion has taken place over the quantity of urea present in the urine in cases of cirrhosis, but it has been established that the relative quantity of urea lessens in proportion to the damage suffered by the liver.78 The urates are in excess.
78 Charcot, Leçons sur les Maladies du Foie, loc. cit., p. 252; also, Essai sur les Variations de l'Urée dans les Maladies du Foie, par F. Genevoix, Paris, 1876; Des Rapports de l'Urée avec le Foie, par A. Martin, Paris, 1877; Sur l'Urée et ces Variations dans la Cirrhose, Thèse de Paris, Audiguier; Contribution à l'Étude du Rôle du Foie dans la Product. de l'Urée, Reufflet.
COURSE, DURATION, AND TERMINATION.—There are enormous variations in the course of the disease as respects the rate of its progress. In general, it may be said that the whole duration is from three months to six years. The onset is often insidious, and little distress is occasioned until effusion begins in the abdomen. In other cases there is considerable pain in the right hypochondrium, severe disorders of digestion and intestinal derangements, rapid emaciation, ascites, and some intercurrent malady which terminates them, often quite unexpectedly. The usual course is as follows: After the protracted use of alcoholic stimulants the symptoms of gastro-intestinal catarrh appear; there occur acidity, pyrosis, morning vomiting, and distress after meals; the bowels are irregular, the stools rather dark and offensive; the bodily vigor declines and the mental condition is depressed and hypochondriacal; emaciation progresses; the skin becomes dry, harsh, and fawn-colored; stigmata appear on the face; some uneasiness is felt in the abdomen, through the right hypochondrium, and about the umbilicus; presently the abdomen enlarges and the feet and legs swell; after a time the abdominal enlargement is extreme and the walls become thin, the genitals and thighs are greatly distended, and the prepuce is so swollen that urination grows more and more difficult, the penis almost disappearing in the surrounding oedema; notwithstanding the immense size of the abdomen and lower extremities, the chest, face, and upper extremities are wasted away; to lie down is impossible, and only snatches of disturbed sleep are procured in the upright sitting posture; breathing grows more and more difficult, and a sense of suffocation is imminent; and, thus worn out by suffering and want of sleep, the patient at last sinks into a soporose state and dies comatose, if not cut off before by some acute serous inflammation—pleuritis, peritonitis, peri- or endocarditis, pneumonia, etc.
[p. 999] The course of any case of cirrhosis is much influenced by the amount of damage to the hepatic cells and by the extent of the compensatory changes in the circulation. Ulcers of the stomach or intestine, opening vessels, or hemorrhages from the mucous membranes may have a pronounced effect on the progress of any case. A fatal result was determined in a case under the writer's charge by hemorrhage from ulcers near the pylorus, which were caused by thromboses of the stomach veins at that point. Occasionally, the occurrence of thrombosis of the portal vein adds an embarrassing and dangerous complication. The liver, besides the change due to cirrhosis, may be affected by amyloid or fatty degeneration, or by both combined. It should not be forgotten that more or less fatty change takes place in the hepatic cells undergoing atrophy, whence the appearance called cirrhosis. Sclerosis may be a general condition in which several organs participate, the kidneys notably. These organs are changed by a hyperplasia of the connective tissue, and especially by fatty degeneration of the epithelium. In the brain the sclerosis consists in chronic pachymeningitis, adhesions of the dura, etc., and with these connective-tissue changes are often associated extravasations of blood. These lesions are probably due to chronic alcoholism rather than to the cirrhosis—are simultaneous lesions, instead of consecutive.
The duration of cirrhosis must necessarily depend largely on the occurrence of the complications above mentioned and on the appearance of intercurrent diseases. The most usual intercurrent maladies are peritonitis, pleuritis, and other serous inflammations. An attack of cerebral (meningeal) hemorrhage may occur. Failure of the heart may be due to fatty degeneration of its muscular tissue. Stupor, coma, and insensibility may come on toward the close in consequence of the retention of excrementitious matters. By Flint, Jr., these cerebral symptoms were referred to the retained cholesterin, and hence he designated this state cholesteræmia. Numerous experimentalists (Pagès,79 Chomjakow,80 Von Krusenstern,81 Koloman Müller82) have studied this question, and only Müller has been able to confirm Flint's theory. The condition is more suitably designated cholæmia, which signifies blood-poisoning from the excrementitious biliary matters retained in the system.
79 Quoted by Legg, p. 233.
80 Quoted by Krusenstern.
81 Virchow's Archiv, Band lxv. p. 412.
82 Archiv für experimentelle Pathologie und Pharmakologie, Band i. p. 213.
Any fully-developed case of cirrhosis can only terminate in one way, for we possess no means of restoring the hepatic cells when once destroyed. At the outset of the disease, before any serious changes have taken place, it is probable it may be arrested. Proceeding to its natural termination without complications or intercurrent affections, death finally occurs from exhaustion. The emaciation becomes extreme, the stomach gets to be excessively irritable, and an exhausting diarrhoea consumes the last remains of strength. Then an oedema of the lungs or failure of the heart or a deep coma ends the scene.
DIAGNOSIS.—Cirrhosis in its first stage is to be distinguished from diseases which cause enlargement of the liver, and in its second or contracting stage from diseases that induce contraction of the organ. The history of alcoholic excess is an important means of differentiating this [p. 1000] from other affections. The enlargement belonging to alcoholism is distinguished from that due to amyloid disease by the permanent character of the latter and by its history of chronic suppuration, in addition to, it may be, alcoholic excess; from cancer, by the character of the enlargement, by its permanence, by the secondary deposits in the mesentery and elsewhere, by the severe and persistent pain; from hydatids or echinococci cysts by the painless enlargement of the latter, by the absence, usually, of any interference with the hepatic functions, by the purring thrill, and by the presence of the characteristic hooklets in the fluid withdrawn. From the maladies characterized by the contraction of the organ it is distinguished by the rapidity with which the case is developed in acute yellow atrophy, and by the profound constitutional disturbance characteristic of this form of contraction. When the liver is lessened in size in consequence of the compression exercised by the contracting exudation of a local peritonitis, there is a history of pain and soreness of the right hypochondrium, followed by the symptoms of contraction—a very different history from that of cirrhosis, in which the local attacks of pain and distress succeed to or accompany the symptoms of contraction. Occlusion of the gall-ducts by a calculus may set up a slow atrophy having some points of resemblance to cirrhosis; but in this malady attacks of hepatic colic precede the signs of obstruction, the jaundice, and gray evacuations, and the evidences of contraction succeed to these very characteristic symptoms; whereas in cirrhosis paroxysms of pain followed by jaundice are not known. Occlusion of the portal vein may also be followed by atrophy, but this is usually due to some other affection of the abdominal organs, and the change in the condition of the liver occurs very promptly, there being neither the history nor the course of symptoms belonging to cirrhosis.
TREATMENT.—As the abuse of alcoholic liquors—even their habitual use in moderation—is the chief pathogenetic factor, they should be entirely given up. Condiments, coffee and tea, highly-seasoned animal foods, are of less importance as causes, but are sufficiently injurious to require them to be discontinued. The food of such subjects should not contain fat, because the bile is necessary to its right assimilation, and should have but a small proportion relatively of starch and sugar, since these articles readily ferment in the presence of an excess of mucus and in the absence of the bile. The succulent vegetables, as lettuce, celery, spinach, etc., should be substituted for the starchy and saccharine. A diet largely composed of skimmed milk renders an important service both as a nutrient and a diuretic and depurant. Lean meats, acid fruits, and the weak alkaline mineral waters should be the basis of a proper system of alimentation.
As malarial intoxication is a cause now distinctly recognized, patients should be removed from such influences. If this be impracticable, the effects of the poison should, as far as possible, be removed, especially the glandular complications. To this end, such remedies should be employed as will affect the overgrowth of the connective tissue, as the compound solution of iodine, the bichloride of mercury, and the chloride of gold (or gold and sodium). Quinine will be necessary, according to circumstances.
Do we possess any means to check the overgrowth of connective tissue [p. 1001] in cases of sclerosis? The writer believes that those remedies have this power to a less or greater extent which are separated by the liver from the blood. These are chiefly the salts of gold, silver, copper, arsenic, and mercury (chloride), and phosphorus. The most useful of these are the chloride of gold and sodium and the chloride of mercury, and some phosphates. The writer has had, he thinks, curative results in the commencement of the disease from the chloride of gold and sodium and the phosphate of sodium. German practitioners believe that the chloride of ammonium is a powerful alterant and deobstruent, and prescribe it in this affection to stop the overgrowth of connective tissue. That it does have this effect can hardly be disputed, but the daily quantity necessary is large, the taste very disagreeable, and the stomachal effect that of an irritant. Hence it is by no means so effective as the chlorides above mentioned. The chloride of gold and sodium (1/10 grain) can be given at the same time with chloride of mercury (1/20 grain) if it is desirable to combine their effects. The writer has seen what appeared to be cases of cirrhosis in the first stage yield to the persistent administration of phosphate of sodium—drachm j ter in die—and the chloride of gold and sodium.
When contraction of the liver has ensued, and hemorrhages, effusion into the cavity of the peritoneum, and a high degree of gastro-intestinal catarrh have occurred, the relief of the secondary symptoms takes the first place in importance. There are but three modes by which an effusion into the abdomen can be removed: by the skin, by the kidneys, by the intestinal canal. Each of these may be employed in turn. By the skin warm baths, vapor baths, digitalis stupes, and especially the subcutaneous injection of pilocarpin, may be employed. These alone may be sufficient in some cases—rather rarely, however. They may all be used simultaneously or in turn to effect the purpose. A digitalis stupe may be made to have the effect of a vapor bath: a large one is placed on the abdomen and the body is covered with blankets, which results in the production of abundant sweating. The vapor bath is applied in the ordinary way, so that no explanation is needed. If there be no contraindication in the state of the heart, pilocarpin salts can be injected in sufficient quantity to induce active diaphoresis. These measures proving inadequate, an attempt should be made to dispose of the fluid by acting on the kidneys and promoting diuresis. Amongst the diuretics in ascites, Wilks places the resin of copaiba first. The dose ranges from two to five grains, and it may be given in combination with gold or mercury chloride. When this remedy increases the flow of urine, it does good, but if the quantity of urine remains unchanged, it does no good, and should be discontinued.
As the effusion of fluid is due to the portal obstruction, it follows that depletion of the terminal radicles of this system will act most directly on the origin of the troubles. Hydragogue cathartics have, therefore, an important place in the treatment of ascites of hepatic origin. One of the most generally efficient of these remedies is the compound jalap powder, for whilst it produces free watery evacuations, it also stimulates the kidneys somewhat. It is generally better to give a full dose—one or two teaspoonfuls—in the early morning, so that the disturbance caused by it will subside before the time for taking food. Several free watery evacuations should be produced by it. Sometimes the resin or extract of podophyllin is added to the compound jalap powder to increase its activity. [p. 1002]Purgative combinations of colocynth, gamboge, and resin of podophyllin are also occasionally employed, but the most efficient hydragogue is elaterium. The last-mentioned may act very efficiently without causing any considerable depression, but the results obtained by it are usually fleeting. After even a very free discharge of fluid the effusion quickly increases, and further purgation is required. Tapping is a palliative expedient which must sometimes be considered. With the present improved aspirator and the antiseptic method the fluid may be withdrawn with ease and safety. It is not necessary in any case to remove all the fluid—merely that quantity which will relieve the pressure on the diaphragm and on the renal vessels. The author has seen general peritonitis result from tapping. As such a complication will increase all the difficulties of a case, it is very desirable to prevent it by careful application of the antiseptic method and sealing of the punctured orifice to prevent the entrance of germs.
In the protracted cases of cirrhosis there ensues, finally, a highly catarrhal state of the mucous membrane, the bowels become very irritable, and frequent offensive and watery discharges occur. If under these circumstances the abdominal effusion increases, the remedies must consist of diuretics and diaphoretics rather than purgatives. Indeed, an exhaustive colliquative diarrhoea may require bismuth, copper, and other astringents, combined with opium, to prevent the patient passing into the condition of collapse. Hemorrhage by vomiting or by stool will demand ice, subsulphate of iron, ipecac, ergotin in the form of subcutaneous injection especially, and other remedies which have been found useful in gastric or intestinal hemorrhage.
Topical remedies are not without utility if used early. When the changes in the liver are secondary to peritonitis of the hepatic portion, the application of leeches and cups renders an important service. At any time during the course of cirrhosis wet or dry cups may be used with advantage whenever local pain, tenderness, and a catching respiration indicate the extension of mischief to the peritoneum. The tincture of iodine or flying blisters, or both in turn, may be applied over the right hypochondrium after cups and leeches, or at any time when local distress indicates the need of counter-irritants. Probably the most efficient topical application during the hypertrophic stage of cirrhosis is the official ung. hydrarg. iodidi rubri. A piece the size of a large pea should be thoroughly rubbed in over the hepatic region daily until some irritation of the skin is produced. When this irritation has subsided the applications should be renewed.
DEFINITION.—Suppurative hepatitis is an acute inflammation of the hepatic parenchyma, terminating in suppuration. The inflammation may be primary or due to local conditions entirely, or it may arise from morbid processes occurring in parts or organs in anatomical relation to the liver.
CAUSES.—Climate exercises an unquestionable influence in the production of hepatic abscess. Those warm countries visited by dysentery, [p. 1003] says Lombard,83 are almost exclusively affected by this disease. Hirsch,84 whilst recognizing the influence of climate, shows that the natives are not affected to the same extent as are Europeans. Both writers maintain that hepatic abscess does not occur frequently in the corresponding parallels of latitude in the United States; which is true of the Atlantic border, but is not correct for the interior continent, the valley of the Mississippi, and its tributaries. In this vast region the conditions for the production of hepatitis exist abundantly. The mean annual temperature, the malaria-breeding soil, the social and personal habits of the people (males), combine to favor the production of hepatic abscess. As the native population and females in tropical countries are not affected, there must be other influences to the action of which the high temperature contributes. The rich and highly-seasoned food in which Europeans indulge and the large consumption of alcoholic drinks are doubtless responsible in a large measure for the occurrence of this malady in such excessive proportions amongst them.
83 Traité de Climatologie médicale, tome iv. p. 386.
84 Handbuch der historisch-geographischen Pathologie, Band ii. p. 300.
Sex has a remarkable influence in securing immunity against hepatic abscess. According to the statistics of Rouis,85 of 258 cases of hepatic abscess, only 8 were in women. He rightly enough attributes this exemption rather to the difference in habits of the two sexes than to any merely sexual peculiarity. In 12 cases observed by the writer, only 1 was in a woman. In Waring's86 collection of 300 fatal cases of tropical dysentery, only 9 occurred in women. These facts are most conclusive regarding the relatively greater frequency of the affection in men. As might be expected, the age at which this disease occurs is the period of adult life, when exposure to the conditions developing it is most likely to happen. In general, then, hepatic abscess may be referred to the period mentioned by Rouis—from twelve to seventy-five years of age. In my own cases the youngest was eleven years and the oldest fifty-four years of age. It is not the broken-down subject of mature age or the weakling of youth who is attacked by hepatic abscess, but the more vigorous and able-bodied, who have, because of their strength and activity, been exposed to the manifold conditions producing it.
85 Recherches sur les Suppurations endémiques du Foie d'apres des Observations recueilles dans le Nord de l'Afrique, par J. L. Rouis, Paris, 1860, p. 189.
86 An Inquiry into the Statistics and Pathology of Some Points connected with Abscess of the Liver, by Ed. John Waring, Resident Surgeon of Travancore, 1854, p. iii.
Rouis finds that a combination of the lymphatic and nervous temperaments seems most favorable to the production of this malady. It is certain that those who have the bodily conditions influential in the formation of gall-stones are not unfrequently attacked by abscess. The passage of the calculi may induce a local peritonitis of considerable severity; their arrest in the duct, with the result of ulcerating through, producing peritonitis and adhesions, are conditions eventuating in the formation of an abscess always large and sometimes of enormous size. Under such circumstances the element of temperament has a secondary place in the aggregate of causes.
Not very often hepatic abscess results from external blows, contusions, and from penetrating wounds. The liver is so placed as to glide aside when a blow is inflicted on the right hypochondrium, and thus escapes [p. 1004] direct compression. An injury which elsewhere would have but little effect may excite suppurative inflammation in the tropical—or, as it may be entitled, the hepatic—abscess zone. Climatic conditions, or the changed habits of Europeans in tropical and subtropical regions, exert a distinct influence in traumatic cases.
The most important causes of hepatic abscess exist in the state of the portal vein, hepatic artery, and the hepatic veins. In the valley of the Mississippi and its tributaries, where abscess of the liver is a comparatively common disease, it has been found that in a large proportion of the cases the initial stage is an affection of the rectum—a form of dysentery properly entitled proctitis. So far as this vast region is concerned, the intestinal disease which precedes abscess of the liver, and stands in a causative relation to it, is an affection of the mucous membrane from which the inferior hemorrhoidal veins arise. This disease, although having a dysenteric form, is not ordinary dysentery. The onset of the disease and its symptomatic expression are those of a mild affection of the mucous membrane of the rectum—so insignificant in some cases as to be recalled with difficulty. In tropical countries abscess of the liver may be associated with dysenteric ulcerations. This relation has been frequently observed, but is far from constant. In Waring's87 cases, which occurred in India, 31 per cent. of the fatal cases of hepatic abscess arose during the course of acute or chronic dysentery. De Castro of Alexandria88 finds that dysentery is the most frequent cause of abscess in that region, especially in the Greek hospital. Murchison89 considers tropical abscess of the liver as secondary to dysentery in a considerable proportion of the cases, but by no means in all. In non-tropical countries abscess of the liver is found to succeed to ulcerations of the stomach, the intestines, the bile-ducts, etc. In the case of ulceration of any part of the mucous membrane from which the portal vein receives branches a morbific material may be conveyed to the liver. This morbific material may be some unknown septic principle the presence of which in the liver will excite suppurative inflammation; it may consist of an embolus having septic power or a merely mechanical irritant; it may be micrococci or some other living organisms, which, arrested in the portal radicles, set up inflammatory foci, etc. There are many examples of hepatic abscess connected with dysenteric ulcerations of the intestine in which no embolus can be found. Admitting the presence of the embolus originally, its disappearance is readily understood by reference to the changes induced by suppuration. Excepting these cases there must be many in which no embolus can be found, because none existed; an unknown septic substance has excited the suppurative inflammation. Emboli may be lodged in the liver from thrombi formed in the peripheral distribution of the portal vein, or from distant parts of the systemic circulation, as in bone diseases. There has been no satisfactory explanation of the manner in which such emboli pass the pulmonary capillaries to be lodged in the liver. At one time there was supposed to be a special relation between injuries of the bones of the head and hepatic abscess, but it is now known [p. 1005]that these cases are not more numerous than those due to osteo-myelitis in any situation. Abscesses in the lungs are greatly more frequent than in the liver in cases of this kind. According to Waldeyer,90 whilst in two-thirds of the cases of death from surgical diseases and injuries there were abscesses in the lungs, in only 6 per cent. were there abscesses of the liver. It is evident that the emboli entering the systemic circulation are usually arrested in the pulmonary capillaries. Klebs maintains that such emboli consist of parasitic organisms.
87 On Abscess of the Liver, supra.
88 Des Abcès du Foie des Pays chauds, et de leur Traitement chirurgical, par le Dr. S. V. Castro (d'Alexandrie d'Egypte).
89 Clinical Lectures, loc. cit., p. 178.
90 Virchow's Archiv für path. Anat., etc., Band xl. pp. 380, 408.
Dilatation and ulceration of the bile-ducts were the principal causes of hepatic abscess, as ascertained by Von Baerensprung, in the Berlin Pathological Institute. Duodenal catarrh involving the orifice of the common duct, catarrh of the biliary passages leading to obstruction, and plugging with a gall-stone have resulted in abscess, the initial lesion being probably rupture of one or more of the finer tubes or inflammation leading to suppuration.91
91 Grainger Stewart, The Edinburgh Medical Journal, January, 1873.
Finally, a considerable proportion of cases of hepatic abscess arise under unknown conditions. In such cases, however, it is usually found that there has been more or less indulgence in alcoholic drinks, or the liver has been taxed by excesses in the use of rich foods and condiments, or exposure to extreme degrees of temperature has occurred. In the interior valley of this continent, where hepatic abscess is comparatively common, the causes are to be found in malarial influences, in alcoholic indulgence, in dysenteric attacks the product of climatic variations and improper alimentation, and in the formation and arrest in transitu of hepatic calculi also the result of long-continued gastro-duodenal and biliary catarrh.
PATHOLOGICAL ANATOMY.—Great differences of opinion have been expressed as to the initial lesions in hepatic abscess. It is probable, however, that these differences are due to the character of the abscess. Some have their origin in the hepatic cells, others in the connective tissue, and others still in the vessels. There may be a number of points at which the suppurative process begins, or it may be limited to one. Virchow92 describes the initial lesion as beginning in the cells, which first become coarsely granular, then opaque, and finally soften, and pus appears. Klebs, who maintains the constant agency of septic micrococci, affirms that the changes in the cells are due to compression exerted by the mass of these organisms distending the neighboring vessels, and then suppuration begins on the portal side of the lobules. Liebermeister originally held that the initial lesion is in the connective tissue; and this view is also supported by Köster, who brings to bear experimental data. In the walls of the vessels of the connective tissue and about them, between the hepatic cells, great numbers of lymphoid cells accumulate. The intercellular spaces are also distended with plasma and round cells, and in the vicinity of the central vein the swollen hepatic cells are pressed together; soon pus-corpuscles appear, and the proper anatomical elements are broken up into a diffluent mass composed of fat-granules, pus-corpuscles, and disintegrating hepatic cells.
92 Archiv für path. Anat., etc., Band iv. p. 314.
When suppurative hepatitis arises from an embolus, or emboli, the [p. 1006] first step is the change in the appearance of the acini, which are enlarged and grow softer by disintegration of their cells; then at the centre a yellowish spot appears, and is made up of the detritus, granules of fat, and pus. Surrounding such softening portions of the hepatic tissue is a zone of congestion. When the morbid processes are excited by emboli, there will be as many centres of pus-formation as there are particles distributed by the vessels—from two or three to fifty or more. They may be uniformly distributed through the organ or be collected in one part. Emboli conveyed by the portal vein will be arranged with a certain regularity and through the substance of the liver, whilst those coming from some part of the systemic circulation tend to form at the periphery under the capsule. Small abscesses in close proximity unite ultimately by the softening and disintegration of the intervening tissue.
In the so-called tropical abscess, which is the variety so frequently met with in the interior of this country, the mode of development is different from the embolic, above described. Owing to the deposit of some morbific matter whose nature is now unknown, the vessels dilate and hyperæmia of the part to become the seat of suppuration ensues. The cells become cloudy, granular, and opaque from the deposit of an albuminous matter in them. Within the area of congestion a yellowish spot soon appears, surrounded by a translucent, pale-gray ring, and here suppuration begins; the neighboring cells disintegrate and a purulent collection is formed, which enlarges by the destruction in succession of the adjacent portions of hepatic tissue. Whilst this process is going on there is a border of deep congestion about the abscess, fading off gradually into the normal tint of the hepatic parenchyma; the walls of the abscess are rough and irregular from projections of tissue just beginning to disintegrate, and the pus burrows in various directions more or less deeply into the softening parts. The size to which such purulent collections attain is largely determined by the condition of the liver as a whole. If the organ attacked is healthy otherwise and the general health is not deteriorated, the area of the abscess may be limited by a well-defined membrane and continue inactive for a long time. This limiting membrane is of inflammatory origin, developed from the connective tissue, and varies in thickness from a mere line to several. It was formerly called a pyogenic membrane, because the pus discharged was supposed to be formed by it. When such a limiting inflammation cannot take place, the abscess continually enlarges by the softening and destruction of the adjacent hepatic tissue, and may finally attain to enormous proportions. The embolic abscesses vary in size from that of a pea to that of an orange. The so-called tropical abscesses are usually single—in three-fourths of the cases, according to Rouis;93 in 62.1 per cent., according to Waring.94 Of the fatal cases collected by the latter author, 285 in number, a single abscess existed in 177, and multiple abscesses in 108. In 11 per cent. there were two abscesses; in 3.6 per cent., three; and in 5.6 per cent. there were four abscesses. As regards the part of the liver in which abscess occurs, the statistics show a great preponderance in favor of the right lobe. In Waring's collection of 300 cases the right lobe was the [p. 1007]seat of the abscess in 163, or 67.3 per cent.; the left lobe was affected in 16, or 6.6 per cent.; and both lobes in 35, or 14.4 per cent. The preponderance of cases affecting the right lobe is the more striking when it is understood that, other parts being invaded, the right is included with them in the morbid process. In my own cases the right lobe was the seat of the abscess in 70 per cent.
93 Recherches sur les Suppurations endémiques du Foie, loc. cit., p. 146.
94 An Inquiry into the Statistics and Pathology, etc. connected with Abscess of the Liver, loc. cit., p. 125.
The contents of the abscesses are affected in character by the form of the disease, whether embolic or tropical, by its rate of development, by the condition of the hepatic parenchyma, by the formation of a limiting membrane, etc. In the more chronic cases, surrounded by a dense membrane, the pus is usually laudable or dry and cheesy; in the acute embolic cases the pus is dark brown, ichorous or grumous, and contains a good deal of detritus of the hepatic parenchyma; and in the tropical cases it is of a sanguinolent, dark color, or more frequently of a grayish purulent fluid; and in the acute forms contains much broken-down tissue, whilst in the chronic cases, in direct ratio to their duration, the pus approaches the laudable character. The source of an abscess discharging from the neighborhood of the liver may be ascertained by a microscopical examination and the discovery of the hepatic elements (the cells) in the fluid. Bile may also be present in the pus.
The abscesses not confined by a limiting membrane constantly enlarge by the softening and disintegration of the adjacent liver substance, and those enclosed or encysted after a period of quiescence of variable duration begin active efforts to establish communication outwardly. The point to which a purulent collection in the liver tends becomes an important element in diagnosis and in treatment. As the abscess approaches the surface of the liver the capsule inflames, and if adhesions are not formed more or less sloughing occurs, and the contents are discharged into the abdominal cavity. Adhesions may form to the parietes, an external swelling appear, and after a time discharge take place in the right hypochondrium at some point. Pus may escape at the umbilicus, in the right inguinal region, posteriorly at the sacro-iliac junction, and in other situations. Adhesions may form to the stomach, duodenum, the ascending vena cava, to the diaphragm opening the thoracic cavity, the pericardium, or the mediastinum; and the accumulated pus may thus find a vent. According to Waring,95 the termination of hepatic abscess is as follows: Of 300 cases, 169, or 56.3 per cent., remained intact—that is, had not advanced beyond the liver; 48 were evacuated by operation, or 16 per cent.; 14, or 4.6 per cent., entered the thoracic cavity; 28, or 9.3 per cent., opened into the right lung; 15, or 5 per cent., entered the abdominal cavity; 7, or 2.3 per cent., opened into the colon; 1 entered the stomach; 3 entered the hepatic vein near the vena cava; 1 communicated with the hepatic ducts, 2 with the right kidney, etc. The termination of 162 fatal cases, according to Rouis,96 was as follows: 125 proved fatal in consequence of the extent of the abscess or of the severity of the accompanying dysentery; 3 terminated by gangrene of the walls of the abscess; 3 by peritonitis; 12 by opening of the abscess; 2 by rupture of adhesions; 11 by opening of the abscess into the pleura; 2 by intercurrent and 3 by secondary pneumonia. Notwithstanding the differences [p. 1008] in the mode of expressing the conditions, the general results are the same.
95 An Inquiry into the Statistics and Pathology, etc. of Abscess in the Liver, loc. cit.
96 Recherches sur les Suppurations endémiques, etc., p. 149.
An abscess of the liver having discharged in a favorable way, healing may take place. There may be such an extent of injury—the whole secreting structure of the liver being destroyed—that repair is beyond the power of the organism. The best results are attained when discharge occurs by the most direct route externally; the next, by way of the right lung; the third, by the stomach or intestine. Repair cannot be hoped for when a large part of the normal hepatic structure is destroyed. When the pus escapes the walls of the abscess approximate, and union takes place by connective tissue, leaving a radiated or a merely linear cicatrix to mark the site of the purulent collection. So perfectly does repair take place in suitable subjects that no trace of the lesion may remain.
Those portions of the liver outside the borders of the abscess, and beyond the vascular derangements produced by it, may be entirely healthy. In the cases terminating in recovery the portion of the liver unaffected by abscess continues to functionate normally. More or less of the liver may be destroyed; hence it follows that recovery may be partial. According to the damage done to the proper secreting structure of the organ will the recovery be partial, limited, or complete.
SYMPTOMS.—The existence of an abscess of the liver is determined by systemic or general and by local symptoms, and they may be acute or chronic.
Systemic.—In acute cases the beginning of mischief may be announced by a rigor, but more frequently this indicates the onset of suppuration, and is one of the phenomena of the chronic form. As the disease occurs in this country, a chill takes place suddenly in a case which presents the usual symptoms of proctitis (dysentery) during the course of this affection or soon after its apparent cure; then a febrile movement occurs, and subsequently an irregular intermittent, the rise of temperature being preceded by rigors or mere transient chilliness. With these febrile symptoms there may be associated uneasiness in the right hypochondrium, acute pain, or a feeling of weight and pressure, with jaundice, etc. The fever is septicæmic, intermittent, or remittent if it have any special type. In the septicæmic form the rigors are severe, occur irregularly, sometimes daily, sometimes twice a day, and at intervals of two or three days or longer; the fever rises to a high point—104°, 105°, or higher—and the sweats are profuse. In the intermittent form the fever usually has the quotidian type; some slight chilliness is experienced in the early morning as a rule, and the exacerbation occurs in the afternoon and evening, the sweating being slight toward the morning. More frequently, in the writer's observation, the type of fever has been remittent, with periodical, but not regularly so, exacerbations. In such cases the morning temperature has been at 99° or 100°, and the evening 102° or 103°. Such a range of temperature may be present during three or four weeks or even longer, the abscess gradually making its way outwardly. Conclusions may be drawn from the behavior of the febrile movement as to the character of the local affection, with the limitations imposed by the necessary uncertainty of the data. If the chills are decided rigors, the fever [p. 1009]high, and the sweats profuse, either pyæmic abscesses or large tropical abscesses implicating neighboring organs exist. The simple intermittent, especially the remittent, form of fever suggests abscesses of medium size making their way outwardly, with only partial injury to the parts traversed. In a certain portion of the cases the type of fever changes when a large accumulation of pus takes place; after several weeks of a mild remittent the fever becomes irregularly intermittent with rigors, strong exacerbations, and profuse sweats. In protracted cases the fever assumes the typhoid aspect; there is profound adynamia, dry tongue, sordes, diarrhoea, and the usual symptoms of this state. When the secreting structure of the liver is destroyed to a large extent, the condition of acholia is superadded to the typhoid state.
The pulse is irritable and quick from the beginning of the symptoms. In a few instances a slow pulse, such as occurs in jaundice, has been observed, but generally the number of cardiac contractions is in a direct ratio with the body temperature. When typhoid symptoms supervene in advanced cases the pulse becomes weak and dicrotic.
Not every case presents the symptom sweating. The chronic cases with mild remittent fever have little more than slight moisture of the surface, whilst the acute and pyæmic cases are characterized by profuse sweats. If to an irregular febrile movement, preceded by chills and followed by sweats, there is added the tendency to sweat on all occasions—on slight exertion, on sleeping, under any excitement—suppuration may be suspected.
General malaise, a sense of fatigue and exhaustion, and progressive decline in flesh and strength occur. It is remarkable, however, how some obese subjects preserve their roundness and apparent fulness of habit. Usually, however, emaciation advances pari passu with the progress of the suppuration. The more acute the symptoms, the more rapid the wasting. When an encysted abscess develops in the course of a chronic dysentery, there may be no appreciable change in the condition of the patient properly attributable to the additional lesion. The loss of appetite, the frequent vomiting, and often the dysenteric troubles, contribute materially to the exhaustion and the wasting of the tissues. The stomachal derangements may be present with the initial symptoms, but they are usually more pronounced when the abscess attains to considerable size.
A peculiar tint of the skin, especially of the face, is observed in those cases without jaundice. There is an earthy or sallow hue, which to the practised eye signifies suppuration. Jaundice is present in a less proportion of cases. In 13 of Waring's cases the skin is said to be sallow. In Rouis's collection icterus was present in 17 per cent., or 26 times in 155 patients. According to Waring, jaundice is rarely present. In the 12 cases in my own hands actual jaundice was not present in one, but 9 had an earthy hue or presented some yellowness of the conjunctiva. In fact, jaundice does not have the importance as a symptom which might, a priori, have been expected.
The mental condition of these subjects is that of depression. They sleep poorly, are disturbed by vivid dreams of a horrifying character, and the nocturnal sweats increase the tendency to wakefulness. Hypochondria, or at least marked symptoms of mental depression, as [p. 1010] Hammond97 has shown, are present in many cases. So frequent, indeed, seems to be the association of a depressed mental state with hepatic abscess that in every case of the former the liver should be carefully explored. Hammond goes so far as to say that in every case of hypochondriasis puncture of the liver with the aspirator needle should be practised when any symptom, however indefinite, indicates the existence of an abscess. Besides the condition of hypochondriasis in many cases, there may be stupor, hebetude of mind, confusion due to acholia, cholæmia (Flint's cholesteræmia), when a large part of the liver structure is destroyed.
97 Neurological Contributions, vol. i. No. 3, p. 68: "On Obscure Abscesses of the Liver, their association with Hypochondria and other Forms of Mental Derangement, and their Treatment."
Sweating has already been referred to as a phenomenon connected with the febrile movement. It is necessary to state further that this may vary in amount from a mere moisture of the surface connected with sleep, or it may be a profuse diaphoresis with which the febrile paroxysm terminates. As a systemic symptom, sweating is strongly suggestive of suppuration, and may therefore be extremely significant, in this connection, of suppuration in the liver. According to Waring, of 75 cases specifically interrogated on this point, 72 presented this symptom. Rouis refers (p. 123) to it as very constantly present, coming on chiefly at night—sometimes generally over the body, sometimes limited to the head, and always accompanied by an accelerated pulse.
The urine in cases of hepatic abscess varies; it is never normal. There may be merely an excess of urates—a symptom common enough in all febrile affections and in suppuration. It is usually high-colored, deficient in urea, and contains leucin and tyrosin, and not often bile-pigment, except when jaundice is present, which, as we have seen, is rather uncommon.
It should be borne in mind that whilst the above-described mental and cerebral and other symptoms are often present, they are by no means invariably so. There are cases, usually of encysted abscess, in which no functional disturbance of any kind exists. But the systemic symptoms are by no means so important as the local. To these we must now direct attention.
Local.—The position, size, and shape of the liver are not without significance, but it is strictly correct to say that an abscess of the liver may exist without any change in the size of the organ or in its relations to the surrounding organs. In 2 of 12 cases in the hands of the writer there was no evidence of enlargement of the right hypochondrium, but a difference in circumference of half an inch was ascertained in favor of the left side. In 4 cases there was no appreciable change in the size of the hepatic region; in one-half there was an increase in the area of hepatic dulness. In one of the cases in which the left side was the larger the abscess was of enormous extent, and discharged by the stomach and intestine. The enlargement of the liver may be very great. In one instance observed by the author the abscess reached to the upper border of the third rib. Rarely does the dulness extend more than two fingers' breadth below the inferior margin of the ribs, although cases are reported in which the enlarged organ reached to the crest of the ileum. As a rule, the diaphragm is pushed up and the lung displaced, rather than the dulness is extended downward. When the first tumefaction [p. 1011]due to the initial congestion takes place, the organ may be much larger than subsequently, the pus becoming encysted and the normal state outside of the area of suppuration being restored. The purulent collection in a large proportion of the cases taking place in the right lobe, the extension of dulness is in the same lines as the normal. When, however, the right lobe is the seat of abscess, or a purulent collection forms around an impacted calculus, the swelling may appear in the outer border of the epigastrium next the ribs, and the increased area of dulness will be across the epigastrium and occupying the superior portion of this region. The general experience on these points corresponds to my own. Thus, according to Waring, there was an evident enlargement of the liver in 90 cases, and no enlargement in 11. In most cases the increase in size gives the impression of a fulness or hardness of the liver or of a diffused swelling or tumor of the epigastrium. In some instances the right hypochondrium is bulged out, the intercostal spaces widened, and the side appears to be or is actually elevated, and occasionally enlarged veins form, as in cases of the obstructed portal circulation of cirrhosis. In a case recently presented at Jefferson College Hospital clinic by the author, a globular swelling formed in the walls of the abdomen just below the inferior margin of the ribs near the site of the gall-bladder, and was held by an eminent surgeon to be a tumor of this locality; but it had the history of an hepatic abscess, and ultimately proved to be one. Rouis furnishes statistical evidence of the time when the increase in size of the liver occurs with respect to the other symptoms. He has noted an enlargement of the organ 73 times in 122 cases. Of 51 cases, the liver was enlarged in 12 before suppuration, in 22 at the onset of suppuration, and in 17 after suppuration was established. In 49 examples the liver was enlarged in 2 before any other symptom was manifest, in 8 at the onset of symptoms, and in 39 after the symptoms were well declared.
Fluctuation is not referred to by the writers in general, and there are no statistical data on this symptom, so far as our observation extends. No symptom could be more uncertain in all doubtful cases. When a large accumulation has taken place and the parietes of the sac are thin, fluctuation may be detected, but it cannot then be regarded as decisive. When an abscess in the interior of the right lobe is encysted, no fluctuation can be effected. The best mode of eliciting fluctuation, according to Hammond, is to place the extremities of the fingers of the left hand in the depression between the ribs over the most prominent part of the right hypochondrium, and gently tap with the fingers of the right hand the right border of the epigastrium. In 3 out of 12 cases this method has apparently elicited fluctuation in my own experience. The elasticity of the hepatic structure is such that the method of palpation, however practised, must return a sensation nearly allied to that of fluctuation in a purulent accumulation. It is certain, therefore, that errors of observation are liable to occur, and hence conclusions based on an apparent fluctuation should be accepted with caution; under any circumstances it should be very distinct, and even then should not be acted on unless supported by other suggestive evidence.
The uneasiness or pain felt in the right hypochondrium varies greatly according to the position of the abscess, the degree and kind of pressure exerted on neighboring organs, and the period of its development. When [p. 1012] the peritoneal layer of the liver is involved, there will usually be acute pain, and this happens at two periods—when the abscess first forms from an impacted calculus or from any cause which includes the peritoneum, and subsequently when the pus, making its way from the liver, excites inflammation in the peritoneal investment of the liver, of the diaphragm, or affects ultimately the pleural membrane. In the so-called pyæmic abscesses there is very little pain, and in the case of the large single abscess in the interior of the right lobe there is rather a sensation of weight or of heaviness, of dragging than of acute pain. When the capsule of the liver is put on the stretch or the peritoneal investment is inflamed, then acute pain may be felt. More or less pain or local distress is, on the whole, a usual symptom. According to Rouis,98 local pain is present in 141 out of 177 cases, or in 85 per cent. The statistics of Waring99 closely correspond, for of 173 patients affected with this malady, in 153 there was more or less pain referable to the affected organ. The position of the pain has some influence in determining the seat of the malady, and often indicates the position of the abscess. As respects the character of the pain, there is little uniformity; in general it is a tensive, heavy, throbbing sensation, but under the circumstances above mentioned this may have an acute or lancinating character, as when the capsule or the peritoneal investment of the organ becomes involved.
98 Recherches, etc., loc. cit.
99 An Inquiry, etc. into Abscess of the Liver, loc. cit.
Besides the pain directly referable to the liver there are painful sensations felt in the neighboring parts, of very considerable significance. These are often described as sympathetic pains, and are referred to the shoulder—to the right shoulder when the right lobe is the seat of mischief, and to the left shoulder when the abscess forms in the left lobe of the liver. Although this statement has many limitations, it is not without diagnostic importance. Rouis ascertained the existence of the shoulder pain in 17 per cent. of the cases, or in 28 in a total of 163. Waring reports that this symptom was observed in 52 in a total of 76 cases. The right shoulder seems to be affected in about the same ratio as the right lobe of the liver in 25 times out of 26 cases, according to Rouis. The shoulder pain appears at the same time, in a majority of cases, as the hepatic pain, but it is very capricious. It is most frequently at the top of the shoulder, but it may be at the end of the clavicle, in the scapula, or extend down the arm. Its duration is very irregular, appearing occasionally during the existence of the disease, coming on at the outset, and lasting weeks or months, or only felt on pressure over the liver, on coughing, or on taking a full inspiration. The character of the pain is equally uncertain. It is usually heavy, tensive, stinging, or may be merely a sensation of soreness or of uneasiness or of weariness. The behavior of the shoulder pain is partly explicable by reference to the path by which the reflex is conveyed. As Luschka100 has shown, the filaments of the phrenic nerve supplied to the suspensory ligament and capsule of the liver, put on the stretch or irritated, convey the impression to the cord, and it is reflected over the sensory fibres of the fourth cervical distributed to the shoulder. Rouis reports an instance in which the deltoid was wasted.
100 Quoted by Thierfelder, op. cit.
The decubitus of patients affected with hepatic abscess is often [p. 1013] extremely characteristic. To obviate the pressure on the swollen and inflamed organ the position assumed is right lateral-dorsal, the body inclined to the right, the right thigh flexed on the pelvis, and the spinal column so curved as to relax the abdominal muscles of the right side. When the pain and tenderness are not great there may be frequent changes of position, but in repose the lateral-dorsal decubitus is assumed. When the suppuration is well advanced and the accumulation large, the patient keeps in that position nearly constantly. If pressure interferes with the normal play of the lungs, and dyspnoea is produced on assuming the recumbent posture, the attitude taken expresses this state also: then the decubitus is lateral and partly dorsal, but the body is raised to a half-upright. There are many exceptions to these rules. Some lie easiest on the back, some on the left side; but it is quite certain that much the largest number, when uninfluenced by special circumstances, naturally place themselves as above described.
Jaundice is amongst the rarer symptoms. Rouis finds it to be present in 17 per cent. of the cases, Thierfelder in 16 per cent., and Waring in somewhat less than 6 per cent. Referring to my own observation, jaundice has rarely been present, but some yellowness of the conjunctivæ and a faint yellow tint of the skin generally have been evident. The peculiar aspect of the countenance connected with suppuration has rarely been wanting. When jaundice does occur, it is referable to two conditions—to a catarrhal swelling of the bile-ducts, which may be coincident with the onset of the suppurative inflammation; to the pressure of the abscess on the hepatic or common duct, which must happen at a late period.
As an abscess of the liver forms and enlarges, pressure is exerted on neighboring organs, producing very decided disturbances. Nausea and vomiting, anorexia, a coated or glazed tongue, diarrhoea or dysentery, are amongst the disorders of this kind involving the digestive apparatus. Each of these symptoms will require examination.
There is nothing characteristic in the condition of the tongue which does not belong to suppuration in any situation. Nevertheless, there are some appearances that have a certain value in conjunction with other diagnostic signs. At the onset of the suppurative inflammation the tongue is more or less heavily coated, but as the case proceeds it becomes dry and glazed in parts, whilst covered with a well-defined membrane-like crust at the base and margins. This appearance is very characteristic of the cases of suppuration, the abscess enlarging. In a very important case observed by me lately there was a well-marked diphtheritic-like exudation of the tongue and fauces toward the termination of the case, the membrane forming as the pus accumulated. This appearance was coincident with a typhoid state.
Nausea and vomiting appear with the beginning of symptoms, are associated with the general signs of systemic disturbance, and are especially prominent when an accumulation of pus takes place, being due under these circumstances to pressure on the hepatic and solar plexuses or to direct encroachment on the stomach—probably to both causes. The frequency and persistence of the vomiting are points of much diagnostic importance, according to Maclean101 and Fayrer,102 which I [p. 1014] am able to fully confirm from my own experience. The matters ejected by vomiting consist of the contents of the stomach—glairy mucus, the accumulation in the gall-bladder, altered blood (coffee-grounds)—and the contents of the abscess if it discharge by the stomach. The vomiting is most apt to occur during the febrile exacerbation or at the time of sweating. The statistics are conclusive as to the frequency of vomiting as a symptom. Of 84 cases in which special reference was made to this point, in 74 nausea or vomiting existed. In my own experience this symptom has never been wanting.
101 "The Diagnostic Value of Uncontrollable Vomiting," by W. C. Maclean, Brit. Med. Journ., August 1, 1873.
102 Ibid., September 26, 1873.
The relation between abscess of the liver and dysentery has been much discussed. Under the head of Causes the influence of dysentery as a pathogenetic factor has already been examined. We have now to study its symptomatic relations. A considerable proportion of the cases occurring in this country have been preceded by proctitis—simple, sporadic dysentery affecting the rectum. In India a close relationship has been traced between ulcerations of the intestinal canal and abscess. According to Waring, 75 per cent. of the cases have occurred in those who were actually suffering from dysentery or recent or old ulcerations. As observed by Rouis in Algiers, out of 143 cases there were 128 with dysentery, or 90 per cent. Budd103 long ago maintained that a peculiar poison generated at an open ulceration in the intestine was the true cause. Moxon,104 Dickinson, and others have lately reaffirmed this explanation. A case by the latter105 casts a strong light on this question: A patient had extensive dysenteric ulceration of the intestine and an abscess of the liver, without any symptoms indicating their existence. Such a case teaches the instructive lesson that dysenteric ulcerations may escape detection, and hence the connection between abscess and the intestinal lesion remains unknown. In a small proportion of cases—about 5 per cent.—dysentery is a result, apparently, of hepatic abscess. Whether the relation is admitted to exist or not, it is a curious fact that in so many cases ulcerative disease of the intestinal canal accompanies the hepatic affection. Hemorrhoids, prolapse of the rectum, gastro-intestinal catarrh, etc. are produced by the pressure of an enlarging abscess on the portal vein.
103 Diseases of the Liver, 3d ed., p. 82.
104 Pathological Transactions, 1862 and subsequently. Numerous cases are recorded in the various volumes up to 1880.
105 Ibid., vol. xiii. p. 120.
The urine contains bile-pigment when jaundice is present, is usually loaded with urates, and the amount of urea may be deficient when much of the hepatic tissue is destroyed.
From the beginning of symptoms some cough is experienced: it is short and dry, but after a time in many cases the cough is catching and painful, and finally may be accompanied by profuse purulent expectoration. The breathing is short and catching when by the upward extension of the mischief the diaphragm is encroached on, and may become very painful when the pleura is inflamed. Ulceration of an abscess into the lungs is announced by the signs of a local pleuro-pneumonia—by the catching inspiration, the friction sound, the crepitant râle, the bronchophony and bronchial breathing, and bloody sputa usually, etc. Some time before the abscess really reaches the diaphragm, preparation is made in the lung for the discharge through a bronchus. The author has seen [p. 1015] many examples of this, and a very striking illustration of the same fact is afforded in a case by Dickinson,106 in which an abscess holding about four ounces was contained in the upper part of the right lobe; its walls were irregular and not lined by a limiting membrane. It is further stated that the "right pleura was coated with flocculent lymph, and the cavity contained serous fluid," etc. Here, in advance of the abscess, preparation was made for its discharge through the lung. The tendency of an abscess of the abdomen to external discharge is manifested in two directions: those of the upper part tend to discharge through the lungs, those of the lower part through the natural openings below. Abscesses of the liver come within the former rule, but it is not of invariable application, since some discharge by the stomach or intestine, some externally; yet a large proportion make their way through the lungs. Another symptom referable to the pulmonary organs in cases of hepatic abscess is singultus, or hiccough. This is a symptom of the period of discharge rather, and is often extremely protracted and exhausting. Pericarditis occurs in those cases in which discharge takes place in this direction, and it may develop, as does pleuritis, in advance of any change in the diaphragm. This preparation of the thoracic organs for external discharge seems almost like a conscious purpose, as if an intelligent supervision of these processes were exercised.
106 Transactions of the Pathological Society, vol. xxxii. p. 127.
COURSE, DURATION, AND TERMINATION.—As the facts already given have sufficiently shown, the course of abscess of the liver is extremely uncertain. From the beginning to the end there may not be a single indication of its presence. On the other hand, a well-marked case is perfectly characteristic. Abscesses of the liver are acute and chronic—the former of short duration, accompanying pyæmia, portal phlebitis, and similar conditions; the latter, arising in the course of chronic dysentery or from unknown causes, especially if encysted, remaining latent for weeks or months. The course of an abscess is much influenced by the direction taken by the pus in the attempt at discharge. This portion of the subject requires careful statement and thorough treatment, and we therefore present it somewhat in detail. Beginning with his individual observations, the abscess in the author's 12 cases discharged—3 externally, 5 by the lungs, and 4 by the stomach or intestines. In Waring's107 collection of 300 fatal cases, 169 remained intact at death, 48 were operated on; consequently, only 83 are left for the purpose of this comparison. Of 83 cases of hepatic abscess discharging spontaneously in some direction, 42 escaped into the thoracic cavity or by the right lung (in 28); into the abdominal cavity (15) or stomach (1) or intestine (7), 23; externally 2, besides in special directions to be hereafter referred to. Rouis108 has tabulated the results in 30 cases of abscess fatal without an operative influence. Of these, 2 discharged externally, 17 by the thorax (15 by the lung), 5 by the stomach, 4 by the intestine, and 2 by the biliary canals.
107 An Inquiry, etc. into Abscess of the Liver, loc. cit., p. 131.
108 Recherches sur les Suppurations endémiques du Foie, etc., loc. cit., p. 148.
The appearances presented when the discharge takes place through the external parts are by no means uniform. When the epigastric or umbilical region is the point of discharge, a globular tumor forms, which may [p. 1016] be mistaken for a fibroid or fatty growth; softening in the centre of the mass occurs, and ultimately the pus is discharged. If the pus makes its way outwardly through the right hypochondrium, the tumor formed is furrowed by the attachment to the ribs, and several openings usually occur. The pus may burrow under the skin for some distance and point in the axilla, or, making its way along the suspensory ligament, emerge at the navel, or, descending, appear in the lumbar region or under Poupart's ligament.
As the statistics prove, the most usual route for discharge to take place is by the thoracic cavity, especially the right lung. Some time in advance of an opening in the diaphragm a localized pleuro-pneumonia occurs, adhesions form between the pulmonary and costal pleura, and a channel is tunnelled out for the passage of the pus to a bronchus. The discharge of pus suddenly occurs after some days of cough and bloody expectoration. Even in favorable cases the amount is so large that the patient has extreme difficulty in disposing of it, and in unfavorable cases, the quantity being large, the patient's life is ended by apnoea. In still other cases an extensive purulent accumulation may form in the pleural cavity, the lung is compressed, and all the phenomena of an empyema superadded to those of a hepatic abscess. In a case reported by Westphalen109 all the bile secreted by the patient came out by an opening in the fifth intercostal space. The empyema thus induced may indeed be the principal lesion, as in the case of the late Gen. Breckenridge, on whom thoracentesis was performed by Sayre of New York, and in a case reported by Löwer.110 So far from this being uncommon, as asserted by Thierfelder, when an abscess of the liver approaches the diaphragm inflammatory symptoms begin on the pleural side, and thus pyothorax may occur in advance of the perforation of this septum.
109 Deutsches Archiv für klin. Med., 1873, Band xi. p. 588.
110 Berliner klinische Wochenschrift, 1864, p. 461.
The opening of an hepatic abscess into the pericardium is rare, since in Waring's collection of 300 fatal cases there was not one. When it does occur, pain is experienced about the heart; the action of the organ becomes irregular; præcordial anxiety and oppression are felt; suffocative attacks occur; and very soon the symptoms of pericarditis arise. Perforation of the ascending vena cava or of the hepatic vein happens in about 2 per cent. of the cases. When a quantity of pus is thus turned into the circulation, disastrous results follow, not so much from the infective nature of the pus as from the sudden increased pressure within the vascular system and the labor imposed on the heart, already failing.
The escape of the pus into the peritoneal cavity occurs in about 11 per cent. of the cases of spontaneous evacuation, according to Waring. Of the 162 fatal cases collected by Rouis, 14 opened into the peritoneum—about the same proportion as Waring gives. When discharge takes place into the peritoneum, the patient passes into a condition of collapse, or peritonitis is excited and rapidly proves fatal. In rare instances the inflammatory reaction is restricted to a small area, ulceration takes place through the abdominal parietes, and thus discharge is effected.
An opening may be made into the intestine or into the pelvis of the kidney. In the former case pus is discharged by stool or by vomit, and often in enormous quantity; in the latter by the urine, frequent and [p. 1017] painful micturition, with much pus, being the evidence of the accident. In either case communication may be kept up with the abscess, and the patient be worn out with the exhausting discharge maintained by the intercommunication between the abscess and the canal through which discharge takes place.
Cases of hepatic abscess prove fatal without perforation. In Waring's collection of 300 cases, 169 remained intact, in the words of the author—that is, did not extend beyond the boundaries of the liver. Of 203 cases collected by Rouis, 96 did not extend beyond the liver. According to Thierfelder, about one-half of the cases of hepatic abscess perforate the liver. These statistics therefore closely correspond, and the general conclusion is very nearly expressed in the formulated statement of Thierfelder.
The duration of hepatic abscess cannot readily be expressed in figures. The acute cases terminate early by reason of the various complicating conditions. The chronic cases are much influenced in their duration by the presence of a limiting membrane, for if this be formed the duration will be protracted over weeks or months; and those cases not thus confined are necessarily of shorter duration. A period of latency may result when the extension of the morbid process is thus hindered. Forming a conclusion from the general conduct of the cases, it may be said that the duration of hepatic abscess is from two weeks to six months. Of 220 cases collected by Waring, the average duration was 39 days. Rouis fixes the average duration in 179 cases at 60 days. Of Waring's cases, the largest number (59) terminated in from 10 to 20 days; whilst Rouis places the maximum number (104) at from 11 to 60 days, the shortest duration of any case being 10 days, and the longest 480 days.
The termination may be accelerated by the manner of discharge, as when the abscess opens into the ascending vena cava, into the sac of the pericardium, or into the peritoneal cavity. In my own cases, carefully selected for these observations, death occurred in one during discharge by the right lung, one within twelve hours after discharge by the intestine, and one within ten days after discharge by the stomach and intestine, the mortality of the whole being 75 per cent. In Waring's collection of 300 fatal cases, 169 died whilst the abscess was still intact—that is, in the liver.
The mortality from abscess of the liver is very large. In Rouis's collection of 203 cases, 162 died, 39 recovered entirely, and 2 improved; 80 per cent., therefore, proved fatal. According to De Castro,111 whose observations were made at Alexandria, Egypt, 93 in 208 cases died, this being 72.5 per cent. According to Ramirez,112 of 11 cases of which an account is given in his memoir, 10 died and 1 recovered—a mortality of 90 per cent. De Castro (p. 40) also gives the results arrived at by the Medico-chirurgical Society of Alexandria, who collected 72 cases of abscess, of which 58 died, making the percentage of deaths 80.5. Various circumstances besides the abscess affect the result. An early successful operation, the mode of discharge, the amount of hepatic tissue destroyed by the [p. 1018] suppuration, the extent of pre-existing lesions—especially ulcerations of the intestinal canal—are important factors in the result. In respect to some of these we have valuable statistical data. The discharge through the lungs is the most favorable route, next by the parietes of the abdomen, and lastly by the intestinal canal. One-half of those cases in which discharge is effected by the right lung get well. This is my own experience, and it accords with the observations of Rouis, of De Castro, and others. Rouis gives the result in 30 cases of hepatic abscess discharging by the right lung; of these 15 recovered. Of 25 cases observed by De Castro, discharging by the lungs, 19 recovered. Next to the discharge by the bronchi, the most favorable mode of exit is externally, through the parietes of the abdomen; much less favorable is by the stomach or intestine; but still more fatal is the discharge into the cavity of the peritoneum. When the abscesses are multiple and due to pyæmia, the termination is always in death. The numerous lesions besides the hepatic accelerate the fatal issue. In the case of large single abscesses the result is in a great measure due to exhaustion from protracted suppuration. When in addition to the formation of a great quantity of pus there is frequent vomiting and rejection of aliment, the failure of strength is proportionally rapid. In favorable cases, after an abscess is evacuated through the right lung, recovery takes place promptly. When the discharge occurs through the abdominal wall, the process is much slower, and often fistulous passages with several orifices, very slow to heal, are formed. Complete recovery may ultimately take place. The recovery will be incomplete in those cases with large loss of hepatic substance, especially when this coincides, as it usually does, with catarrh, ulceration, and other lesions of the intestinal tube. Again, the recovery will be incomplete in those cases where there are imperfect healing of the abscess site and a fistulous communication with the exterior.
111 Des Abcès du Foie des Pays chauds, et de leur Traitement chirurgical, loc. cit., p. 40, Paris, 1870.
112 Du Traitement des Abcès du Foie, Observations receuilles à Mexico et en Espagne, par Lino Ramirez, M.D., Paris, 1867, loc. cit.
It is possible for the arrest and healing of a suppurative inflammation of the liver to take place without discharge. Under such circumstances the watery part of the pus is absorbed, the solid constituents undergo a fatty metamorphosis, are emulsionized, and thus absorbed, and gradually closure of the damaged area is effected by a connective-tissue formation. We must, however, accept with caution those examples of this process which are supposed to have occurred because radiating cicatrices are discovered on the surface of the liver. In a case of hepatic abscess discharging through the lung, known to the writer, after death, which occurred fifteen years subsequently, there was no trace of the mischief, so perfectly had repair been effected. Radiating cicatrices are so often of syphilitic origin that they cannot be accepted as proof of the former existence of an abscess.
DIAGNOSIS.—He who finds the diagnosis of abscess of the liver easy under all circumstances can have had but little experience with the numerous difficulties in the way of a correct opinion. There are cases so plain that the most casual inspection suffices to form a conclusion; there are cases so difficult that the most elaborate study fails to unravel the mystery. The maladies with which hepatic abscess may be confounded are echinococcus of the liver, dropsy of the gall-bladder, cancer, abscess of the abdominal wall, empyema, or hydrothorax, etc. As regards echinococcus, the difference consists in the slow and painless enlargement characteristic of echinococcus, and the absence of any symptoms other than those [p. 1019]due to the mere pressure of the enlarging mass. In abscess there may be no apparent enlargement, or the increase in the area of dulness may be very great, or after a period of increase of size there may be contraction due to the formation of pus, and hence limitation of the inflammation; finally, the accumulation of fluid may be sufficient to cause dulness up to the inferior margin of the second rib. There are no corresponding changes of size in the echinococcus cyst. Furthermore, abscess of the liver large enough to be recognized by the increased dimensions of the organ will be accompanied by more or less pain in the right hypochondrium and by a septicæmic fever. On the other hand, an echinococcus tumor is not accompanied by fever, pain, or tenderness, and it has that peculiar elastic trembling known as the purring tremor. The most certain means of differential diagnosis is the use of an aspiration-needle and the withdrawal of a portion of the fluid. The presence of pus with hepatic cells will be conclusive of abscess, whilst a serous fluid with echinococci hooklets will prove the existence of the echinococcus cyst.
In cases of dropsy of the gall-bladder there are no febrile symptoms, no chills, and the tenderness when present is limited to the pyriform body, the seat of the accumulation of fluid, and no general enlargement of the liver can be made out. At the point of swelling fluctuation may be detected, or if the gall-bladder is filled with calculi the sensation imparted to the touch is that of a hard, nodular body of an area and position corresponding to that of the gall-bladder. Tapping the gall-bladder, an easy and safe procedure, will resolve all doubts. When an impaction of a gall-stone is the cause of abscess, the clinical history is eminently characteristic: there are attacks of hepatic colic, after one of which the chills, fever, and sweats belonging to hepatic abscess occur.
The differentiation of cancer of the liver from abscess rests on the following considerations: In cancer there is slow enlargement, with pain; a more or less nodular state of the organ without fluctuation; usually ascites; no rigors; no fever and sweats. In abscess the liver may or may not be enlarged; there are rigors, fever, and sweating, and the surface of the organ, so far as it can be reached, is smooth and elastic, and it may be fluctuating. Cancer happens in persons after middle life, develops very slowly, and is accompanied by a peculiar cachexia; abscess occurs at any period, very often succeeds to or is accompanied by dysentery and by the usual phenomena of suppuration.
It is extremely difficult to separate an abscess in the abdominal wall, in the right hypochondrium, or a tumor in this region, from an abscess of the liver. The history of the case, the existence of a dysentery or of an apparent intermittent or remittent fever before the appearance of a purulent collection, will indicate the liver as the probable source of the trouble. Attention has already been called to a case in which an abscess of the liver was supposed by an eminent surgeon to be a tumor of the abdominal wall. The history in this case of an obstinate remittent fever, followed by the appearance of a tumor of the hypochondrium and by a preliminary discharge at the umbilicus, clearly indicated the nature of the trouble. In the absence of any history of the case it is extremely difficult to fix the origin of a suppurating tumor originating, apparently, in the depth of the right hypochondrium.
Mistakes are frequently made in the case of an abscess developing in [p. 1020] the convexity of the right lobe of the liver and pushing the diaphragm up to the third, even to the second, rib, and thus producing conditions identical with empyema of the right thorax. Such instances of hepatic abscess are peculiarly difficult of recognition, because, the physical signs being the same as those of empyema, the differentiation must rest on the clinical history. In cases of empyema proper the effusion in the chest is preceded by pain and accompanied by an increasing difficulty of breathing; in hepatic abscess there are, as a rule, symptoms of disturbance in the hepatic functions, fluctuation in the hepatic region, dysentery, etc., long anterior to any disturbance in the thoracic organs. Again, empyema may be a latent affection, without any symptom except some obscure pain and a progressive increase in the difficulty of breathing; on the other hand, abscess of the liver is preceded by symptoms of liver disease and of associated maladies. A dry, purposeless cough is present in many cases of abscess; a painful cough with bloody expectoration occurs when preparation is making for discharge through the lungs.
Errors of diagnosis are liable to occur in the consideration of symptoms unquestionably hepatic in origin. Thus, the intermittent fever accompanying some cases of hepatic colic, like the shivering fits and fever which occur in cases of nephro-lithiasis, may be confounded with the septicæmic fever of hepatic abscess. An attentive examination of the attendant circumstances, especially a careful survey of the right hypochondrium, can alone determine the nature of the symptoms. In all doubtful cases the experimentum crucis of puncture with the exploring-needle becomes a measure of necessity. When all diagnostic indications are at fault, the needle of the aspirator may decide the issue. An abundant experience has shown that a needle of suitable size may be introduced into the right lobe without any ill result—often, indeed, with distinctly good effects when there is no suppuration or when pus cannot be detected. In the present state of our knowledge it cannot be determined why puncture of the organ should be beneficial in cases having the symptomatic type of hepatic abscess when none exists; but of this fact there is no doubt.
TREATMENT.—As the formation of pus is coincident with or causative of the first symptoms, it is obvious that treatment directed to prevent an abscess can rarely succeed. Yet it is probable that now and then an abscess just forming has been arrested and healing effected. At the onset of symptoms some large doses of quinine, with a little morphine (scruple j of the former and 1/8 gr. of the latter), every four or six hours, may have a decided curative effect. During the course of the septicæmic fever, with its chills and febrile exacerbations, quinine in full doses and alcohol according to the conditions present are necessary remedies. As the symptoms develop saline laxatives are useful until the formation of pus becomes evident, when all perturbating treatment of the intestinal canal should cease. If dysentery be present when the hepatic symptoms arise, it should be cured as promptly as possible; and of all remedies for this purpose, ipecac given in the usual antidysenteric quantity offers the best prospect of relief. For the dysentery which succeeds to abscess, and is probably, in part at least, dependent on portal obstruction, the mineral astringents, as copper sulphate, are the most effective remedies. As far as practicable, after an abscess has formed the intestinal canal should be kept quiet, for any considerable disturbance will [p. 1021] endanger the escape of pus into the peritoneal cavity. Persistent vomiting is very significant of pressure by an enlarging abscess in the stomach, and usually signifies an abscess associated with impacted calculus. It is important in such cases to maintain, as far as can be done, a quiescent condition of the stomach, for the purpose of preventing rupture into the peritoneal cavity and to favor the nutrition which is seriously endangered by the repeated vomiting. Effervescent soda powders are very useful; carbolic acid in solution, or creasote-water with or without bismuth, is beneficial; champagne, very dry and highly effervescent, has been, in the writer's hands, remarkably efficient. As food becomes a most important need in such cases, milk and lime-water, wine-whey, egg-nog, and similar aliments must be given in small doses and frequently. Nutrient enemata, prepared from eggs, milk, and beef-juice, with the materials for digestion—acid and pepsin—may be made to supplement the stomach, but such efforts have a very limited utility, owing to the state of the hepatic functions and to the obstruction of the portal circuit. In all cases it is necessary to maintain the strength by suitable aliment and the judicious use of stimulants. The long-continued and profuse suppuration makes an enormous demand on the vital resources of the patient, and this must be compensated by suitable food-supplies.
As the formation of pus has taken place in most cases when symptoms have begun, the question of highest importance is, Shall the pus be evacuated? The statistical evidence relating to this question becomes then an extremely valuable guide. As in almost all cases of puncture of the liver for the evacuation of an abscess some part of the liver substance must be passed through, it is necessary to note how far this can be done without inflicting permanent injury on the organ. Hammond has punctured the liver in eight cases without the presence of an abscess, and of these not one has presented any unfavorable symptom. The author has punctured the liver, penetrating well into the interior, in two cases in which no abscess was discovered, but the symptoms of hepatitis existed, with the effect to improve the symptoms. In Condon's113 collection of 11 cases there were 8 of abscess evacuated by the trocar, and 3 of acute hepatitis in which abscess had not formed, but in which the puncture procured the most decided amelioration of the symptoms. We have heretofore referred to Hammond's experience in the puncture of the liver in cases of hypochondriasis, this condition appearing to depend in some instances on the presence of abscess. In a number of instances abscesses did exist, but in many others there was no apparent lesion of the liver, but in these cases the puncture of the organ was without any ill result. Testimony to the same effect is given by Ramirez,114 who asserts that he had not known a single instance in which any ill result followed puncture of the liver. It may therefore be regarded as certain that exploratory puncture of the organ for the purpose of diagnosis as well as for treatment can at any time be performed with suitable precautions in respect to the size, condition, and character of the instrument.
113 "On the Use of the Aspirator in Hepatic Abscess," Dr. E. H. Condon, The Lancet (London), August, 1877.
114 Du Traitement des Abcès du Foie, Observations recueilles à Mexico et en Espagne, par Lino Ramirez, M.D., Paris, 1867, p. 65.
The authorities of most experience are agreed that, provided with the [p. 1022] aspirator, the abscess may be punctured as soon as a purulent collection can be ascertained to exist. The obvious reason for tapping the abscess is its tendency to extend in various directions, destroying the hepatic substance. In those examples confined by a limiting membrane, after a time of inactivity ulceration begins, and the pus seeks an outlet in some direction. The early evacuation by a suitable aspirator becomes then a measure of the highest necessity. The good effects of puncture with even such a crude instrument as the trocar is well exhibited in the statistics collected by Waring.115 In a collection of 81 cases opened by the knife or trocar there were 66 deaths, making the percentage of recoveries 18.5. In these cases the operative procedure was a final measure, and the mischief had been done almost if not quite in its entirety. The statistics of Waring are concerned with a period anterior to 1850. Although they demonstrate the value of the trocar and evacuation of the abscess, as compared with the results of the natural course of the disease, the far greater success of the treatment by the aspirator is shown by the statistics of recent times. Thus in McConnell's116 14 cases, also of India, in which the aspirator was used to empty the sac, 8 recovered and 6 died. The statistics of Waring may also be profitably compared with those of Condon,117 in which, of 8 cases of abscess evacuated by the aspirator, 4 recovered, or 50 per cent. They may also be compared with Sach's118 cases, 21 in number, of which 8 recovered, or 38 per cent., and with the cases of De Castro119 of Alexandria, who reports 22 large abscesses operated on, the proportion of cures being 31.8 per 100, and 10 small abscesses, the proportion of cures being 70 per 100. In a case seen in consultation with Collins, in this city, last year, the aspirator was used by us about three months after the symptoms of abscess declared themselves. About a quart of bloody pus was drawn off at once, the opening sealed, and no subsequent accumulation occurred, the patient entirely recovering, for after a year he was seen (December, 1884) in complete health. From these data we draw the important conclusion that early operation is desirable. This fact may be formulated in the expression: In all cases of hepatic abscess use the aspirator whenever the presence of pus is made out. When the abscess is large, and especially when communication is established with the parietes of the abdomen, a free opening, followed by the insertion of a drainage-tube, is the proper method to pursue. If the pus reaccumulates, it is good practice to inject the cavity with tincture or compound solution of iodine after the pus is drawn off, provided the dimensions of the abscess are not too great.
115 An Inquiry into the Statistics of Abscess of the Liver, loc. cit.
116 "Remarks on Pneumatic Aspiration, with Cases of Abscess of the Liver treated by this Method," Indian Annals of Medical Science, July, 1872, quoted.
117 Lancet, supra.
118 Ueber die Hepatitis der heissen Länder, etc., von Dr. Sachs in Cairo.
119 Des Abcès du Foie des Pays chauds, et de leur Traitement chirurgical, par le Docteur S. V. de Castro (d'Alexandrie d'Egypte), Paris, 1870, p. 59.
As regards the mode of proceeding, the following are useful rules: Ascertain, if possible, the existence of fluctuation; locate the point where the walls of the abscess are thinnest; insert an exploring-needle, and if the dépôt of pus is reached substitute a trocar having a sufficient calibre to evacuate the contents of the abscess; observe antiseptic precautions in respect to each detail of the operative procedure, and after the removal of the canula or needle, if a drainage-tube is not necessary, close the [p. 1023]wound antiseptically. If drainage is necessary, keep the cavity empty and use proper solutions to prevent septic decomposition. When an abscess of the liver is pointing, the best place to puncture is where the abscess is most prominent and it walls thinnest, but if the accumulation of pus is encysted and there is no attempt at effecting an exit, the exploring-needle should be passed into the interior of the right lobe, the most usual site of suppuration. If pus be reached, a larger trocar may be inserted to evacuate the cavity thoroughly. Repeated insertion of the needle-trocar is preferable when the abscess is small, but when the accumulation is large and sufficiently firm attachments to the abdominal parietes exist, a drainage-tube will be necessary.
In what direction soever discharge of an abscess may take place, the general indications are to support the powers of life by food and stimulants. The utmost quietude should be maintained. It is useful, by the application of a firm flannel bandage, to keep the liver in its proper position and maintain it there. When pointing of an abscess occurs, a large flaxseed poultice is a soothing and a mechanically supporting application.
DEFINITION.—By the term acute yellow atrophy is meant an acute affection of the liver, characterized by rapid wasting or degeneration of the organ, accompanied by the systemic symptoms belonging to an acute acholia or cholæmia. It is an acute, diffused inflammation, with atrophy of the proper gland-elements. It has been called icterus gravis, malignant icterus, hemorrhagic icterus, malignant jaundice, etc.
HISTORY.—Cases having a more or less exact resemblance to acute yellow atrophy have been occasionally reported from the earliest period. Amongst English physicians, Bright120 was one of the first to give an accurate account of the clinical history of some well-defined cases. Rokitansky121 was really the first to define the disease from the pathological standpoint, and it was he who designated it acute yellow atrophy, this term being intended to signify the nature of the objective changes. The first treatise ever published on the disease as a distinct morbid entity was the monograph of Horaezek,122 which appeared in 1843. Amongst the French, Ozonam in 1847 was the first to recognize and describe the disease as a distinct affection, although Andral123 had several years before mentioned an affection of the liver which corresponded in some of its features to this affection. In 1862, Wagner124 asserted that many of the cases of acute yellow atrophy were only examples of acute phosphorus-poisoning, and that no real distinction exists between the two affections. This statement has been warmly disputed by various German observers, but there is no doubt a close resemblance between the two affections.
120 Guy's Hospital Reports, 1836, vol. i. p. 621.
121 Handbook of Pathological Anatomy, Am. ed.
122 Quoted by Legg, On the Bile, Jaundice, and Bilious Diseases, loc. cit.
123 Clinique médicale, 1839, tome ii. p. 363.
124 Archiv der Heilkunde, 1862, p. 364.
CAUSES.—There can be no doubt that acute yellow atrophy is a very rare disease, since so few examples are found post-mortem. In the course of a very large experience in autopsical examinations I have met with but [p. 1024] one characteristic example.125 According to Legg, it is "one of the rarest diseases known to man."
125 General Field Hospital, December, 1863.
Several theories have been proposed to explain the occurrence of this affection, but without success. It has been ascribed to an excess in the production of bile, to stasis in the bile, and to a sudden saturation of the hepatic cells with biliary matters contained in the portal vein. That these supposed causes are really influential in producing the malady can hardly be entertained. That there is a peculiar poison which has a causative relation to the disease is rendered probable by the fact that a condition closely allied to this disease is produced by phosphorus, antimony, arsenic, and other poisons. Is it not a ptomaine generated under unknown conditions in the intestine? Especially does the morbid anatomy of phosphorus-poisoning nearly agree in all its details with icterus gravis—so nearly that by many German authorities they are held to be identical.
Age has a certain influence in the causation of this disease. It is rarely seen in early life, Lebert in a collection of 63 cases having found only 2 before ten years of age, yet there has been a well-marked case at three, and Hilton Fagge reports one at two and a half years of age. Nevertheless, much the largest number occur between fifteen and twenty-five years of age, and the maximum age may be fixed at sixty.
The influence of sex in the pathogeny is most remarkable. It is true in Lebert's collection of 72 cases there were 44 men and 28 women, but it is now known that he did not properly discriminate in his selection of supposed examples of the disease. The statistics of all other observers are opposed to those of Lebert. Thus, in Frerichs' collection of 31 cases, carefully sifted to eliminate error, there were 22 women and 9 men. Legg has also collected 100 cases of acute yellow atrophy, and of these 69 were women or girls. The most active period of life—from twenty to thirty years of age—is the usual period for the appearance of this disease. More than one-half of Lebert's cases occurred between fifteen and twenty-five; and of Frerichs', two-thirds happened between twenty and thirty years of age. In Legg's collection of 100 cases, 76 were between fifteen and thirty-five years of age. What is the condition of women at this period in life which renders them so susceptible to this malady? There can be no doubt that pregnancy is the great factor. Of 69 cases especially interrogated on this point, examined into by Legg, in 25 pregnancy was ascertained to exist. In Frerichs' collection one-half were women in the condition of pregnancy. The period of pregnancy at which the disease appears varies from the fourth to the ninth month, the greatest number occurring at the sixth month. So long ago as 1848, Virchow drew attention to the remarkable changes in the liver due to pregnancy. Sinety126 has studied the effect of lactation on the liver, and has ascertained the existence of fatty degeneration. There is a form of jaundice which accompanies menstruation, as shown by Senator,127 Hirschberg, and others. These facts indicate a certain relationship between the sexual system of the female and the liver, but they do not indicate the nature of the connection, if any exist, between this condition and acute yellow atrophy.
126 De l'État du Foie chez les Femelles en Lactation, Paris, 1873 (pamphlet).
127 Berliner klinische Wochenschrift, 1872, p. 615, "Ueber Menstruelle Gelbsucht."
The influence of depressing emotions has been supposed to be effective [p. 1025] in producing this disease, but it is more than doubtful if such a relationship exists. Lebert, however, refers 13 of his cases to this cause, but Legg, who bases his statements on the study of 100 carefully-recorded cases, is sceptical regarding the effect of such influences. Syphilis has in some instances appeared to be the principal, if not the only, pathogenetic factor, and Legg128 compares the action of the virus of syphilis to the effect of phosphorus, mercury, etc.
128 On the Bile, Jaundice, and Bilious Diseases, loc. cit.
PATHOLOGICAL ANATOMY.—The anatomical changes occurring in this disease indicate the existence of a systemic condition: the lesions are not limited to the liver, but involve various other organs. The changes in the liver should be first described, since the name of the disease is derived from the alterations in this organ. As the name indicates, the lesions are atrophic, but not all examples show this. In some cases there is little change in the size of the organ; in others the wasting is extreme; certainly in all typical examples the liver is reduced in size. The variations in size observed are probably due to the stage at which the inspection is made: if early, the organ may not be reduced in size, may be even somewhat enlarged by the deposition of new material; if later, the atrophic changes will be more or less pronounced. When the atrophy has taken place, the size of the liver is reduced to one-half, even to one-third, of its original dimensions; it is then soft, almost like pulp, and cannot maintain its shape, but flattens out on the table. The capsule is much wrinkled and the color of the organ is yellowish, variegated by islets of reddish or brownish-red color, these spots being somewhat depressed below the general surface and having a firm texture. On section the boundaries of the lobules are either lost or have become very indistinct, the line of section being bloodless. The knife with which the sections are made becomes greasy. In some instances ecchymoses are discovered under the capsule, and rarely hemorrhagic extravasations in the substance of the liver. The bile-ducts are found intact, as a rule. The greatest change in the size of the liver is observed in the left lobe. The duration of the disease, as has been indicated above, has a marked influence over the size and condition of the liver. The atrophic shrinking of the liver occurs more decidedly after the ninth day. In general, the tissue of the liver is soft and pulpy in consistence. On microscopic examination the most important alterations are seen to have occurred in the hepatic cells; ultimately, these cells disappear, being replaced by fatty and connective-tissue detritus; but before this stage is reached important alterations have taken place in the form and structure of these bodies: the cells become granular and fatty, and lose their sharpness and regularity of contour, especially at the periphery of the lobule, but ultimately all the cells within the lobule undergo atrophic degeneration. In this atrophic degeneration of the hepatic cells, in their fatty degeneration, and ultimately entire disappearance, consist the real proofs of the disease. The red islets of tissue already alluded to consist of the fatty detritus mixed with crystals of hæmatoidin.
More or less increase of the connective tissue is noted in many of the cases—increase of connective tissue with numerous young cells formed around the vessels and the bile-ducts (Waldeyer129). The changes in the [p. 1026] liver would surely be incomplete without some references to the minute organisms which play so important a part in modern pathology. Waldeyer was the first to demonstrate the presence of bacteria in the pigment-remains of the hepatic cells. Other observers have been unable to detect them, so that at present the parasitic origin of this affection remains sub judice.
129 Arch. für path. Anat., 1868, p. 536, Band xliii.
Important changes also take place in the spleen, but the opinions on this point are somewhat contradictory. Frerichs found the spleen enlarged in most of his cases; Liebermeister, on the other hand, and Legg,130 find that the spleen is enlarged in about one-third of the cases. When the atrophic changes occur in the liver, more or less swelling of the splenic veins must occur in consequence of portal obstruction. The peritoneum, especially the omental part, is the seat of multiple ecchymoses, and the endothelium is fatty. The mesenteric glands are usually swollen. More or less blackish or brownish fluid, consisting of altered blood, is usually found in the stomach, and the same, assuming a tar-like consistence, in the large intestine. Ecchymoses of rather small size are distributed over the stomach and intestines. The epithelium of the stomach-glands is found granular and disintegrating, and a catarrhal state of the gastro-intestinal mucous membrane exists throughout. The secretions are never normal, and the stools are wanting in bile or present a tarry appearance, due to the presence of blood.
130 On the Bile, Jaundice, and Bilious Diseases, supra.
Important changes take place in the kidneys. They consist essentially in a granular and fatty degeneration of the tubular epithelium, whence the altered appearance of the cortex. Multitudes of bacteria crowd the pyramids. Ecchymoses also are found in the mucous membrane of the pelvis of the kidney, in the bladder, and indeed all along the genito-urinary tract.
The muscular tissue of the heart is in a state of acute fatty degeneration, beginning with a granular change which may at the outset be of very limited extent and involve but few fibres. The endo- and pericardium are studded with ecchymoses or marked by hemorrhagic extravasations, and the pleura presents similar appearances, but not to the same extent.
The brain does not always show evidences of change, but in many instances there are ecchymoses of the meninges; the walls of the vessels are affected by fatty degeneration.
The tissues of the body are more or less deeply stained with bile. The pathological change on which the jaundice depends has been variously stated, but the most probable explanation is that which refers it to mechanical obstruction of the bile-ducts, either by catarrhal swelling or fatty degeneration of the epithelium. Notwithstanding the prominence of the hepatic symptoms, acute atrophy of the liver is probably only one element in a constitutional morbid complexus.
SYMPTOMS.—Acute yellow atrophy begins in two modes—the grave symptoms preceded by mild prodromes, or the most serious symptoms appear at the onset. The former mode is the more common. The usual prodromes are referable to the gastro-intestinal canal, and consist of loss of appetite, nausea, vomiting, a bitter taste in the mouth, headache, and general malaise. Indeed, the opening attack may be much like an [p. 1027] ordinary bilious seizure or acute gastro-duodenal catarrh or a sick headache. In some cases the initial symptoms—nausea and diarrhoea—appear to be induced by an indigestible article of food. Jaundice never fails to be present at some period, but is usually one of the prodromic symptoms. It has no special characteristics by which the gravity of the approaching seizure may be measured. It is usually rather deep, and all parts are deeply stained, but the coloration may be limited to the body and upper extremities. No change in pulse or temperature, except the usual depression of both functions, is to be observed; the urine is deeply stained with pigment, and the feces are grayish, colorless, or parti-colored.
The period of time elapsing before the serious symptoms come on is not constant; from one week to several months have been the variations observed. In a minority of the cases no prodromes have occurred, but the grave symptoms have declared themselves at once. From the appearance of the jaundice up to the onset of severe symptoms the time has varied from two weeks to several months, but has rarely exceeded three months. During this time there may be nothing to indicate the gravity of the approaching symptoms; in fact, the case then, as at the onset, seems to be one of simple gastro-duodenal catarrh associated with catarrhal jaundice. The onset of serious symptoms is most usually announced by dilatation of the pupil. If, therefore, in a case of apparently simple catarrhal jaundice, especially in a pregnant female, there should occur without apparent reason a marked and persistent dilatation of the pupil, the possibility of the case being one of acute atrophy should be apprehended. This symptom is not, alone, of sufficient value to decide the character of the case, but then an obstinate insomnia comes on, violent headache is experienced, there is more or less confusion of mind, and jactitations or an extreme restlessness occurs. When such pronounced nervous symptoms appear the character of the attack is explained.
Various divisions have been proposed to mark the type of the symptoms: thus, the icteric period embraces the prodromal symptoms with jaundice; the toxæmic period is that stage characterized by profound nervous disturbances. Ozonam has divided the symptoms into those of the prodromal period and those of the serious stage, the latter being subdivided into the symptoms of excitation and those of collapse. There may be no prodromal period, however; without any preliminary symptoms the patient is suddenly seized with delirium and passes into a condition of coma and insensibility, or the first evidence of serious illness may be convulsions. It is probable, however, that in even the most sudden cases mild prodromal symptoms had occurred, but were overlooked. There is much variability in the symptoms of the toxæmic period. There are three symptoms: excitement with delirium, sometimes delirium ferox; coma, less or more profound; and convulsions. Legg has numerically expressed the relative frequency of these symptoms thus: Of 100 cases of unquestionable acute atrophy, 76 had become comatose, 59 were delirious, and 32 had suffered convulsions.131 According to the same authority, delirium and coma were associated together in about one-half of the cases, but in pregnant women coma often occurs alone (Legg). Usually, when convulsions happen there has been either coma or delirium. With these cerebral symptoms there are often present various [p. 1028]disturbances of motility and sensibility, such as local convulsions, jactitations, hiccough, extreme restlessness, paralysis of the sphincters, and incontinence of urine and feces or retention, grinding of the teeth, exalted sensibility of the skin, or it may be complete anæsthesia, severe itching of the surface, etc.
131 On the Bile, Jaundice, and Bilious Diseases, loc. cit.
During the toxæmic period, and directly dependent on the retention of excrementitious matters in the blood, hemorrhages occur from the mucous surfaces, from wounds, and into the various serous membranes. A changed state of the blood being present in all cases of this disease, the proportion in which extravasations take place is high—in about 71.3 per cent. according to Liebermeister, and 80 per cent. according to Legg. The latter author regards these estimates as rather low. When hemorrhage occurs in the stomach in small amount, it presents itself as coffee-grounds or as black vomit, and in the intestine in the form of black, tarry stools or melæna. Hemorrhage may also occur from the surface of an ulcer, from a fresh wound, a leech-bite, etc.; but the most usual form of extravasation of blood after the gastro-intestinal is epistaxis or bleeding from the nose. Women who abort, as they are very apt to do when this disease comes on, may suffer from frightful hemorrhage, and deaths have been thus caused. Various opinions have been expressed as to the cause of the hemorrhagic condition—by some attributed to the changes in the composition of the blood; by others to the alterations of the vessel walls; both factors are doubtless concerned.
During the prodromic period the temperature of the body, as in the case of ordinary uncomplicated jaundice, is rather depressed below normal, sometimes as much as two degrees; but when the toxæmic stage comes on the body-heat rises to a variable extent, but usually over 100° F. In some cases no febrile movement can be detected; in others a very considerable elevation of temperature occurs, but very rarely attains to 105° or 106° F. The pulse becomes very rapid, in some instances rising to 140; but without any apparent cause it may fall suddenly to 70 or 80, and these fluctuations may take place several times a day. The rise of temperature and a very rapid pulse may come on in the final coma only; and immediately after death, as Legg points out, the body-heat may attain the maximum elevation.
As the toxæmic period develops the tongue becomes dry, glazed, fissured, sordes form on the teeth and lips, the breath becomes fetid, and the breathing may assume the Cheyne-Stokes type. The nausea and vomiting of the prodromal period persist, and the ominous coffee-grounds appear in the rejected matters, or grumous masses—clots acted on by the gastric juice—are brought up. Black, pitch-like, or tarry stools, the result of hemorrhage, are passed toward the end—involuntarily when liquid. When no blood is present the stools are grayish and without bile. Constipation may be the condition instead of diarrhoea in about one-third of the cases.
Various eruptions have been observed on the skin, such as petechiæ, roseola, eczema, etc., but their very variety, as their occasional appearance, indicates their accidental relationship to the disease.
The urine is much altered in character, but it is usually acid in reaction, although it has been observed neutral or alkaline. The specific gravity is at or nearly normal, and it has a deep-brownish or bilious hue [p. 1029] due to the presence of bile-pigment. The most important change in the composition of the urine is the diminished quantity of urea or its entire disappearance; the phosphates, and especially the chlorides, are also usually diminished in amount; and albumen and leucin and tyrosin appear to a lesser or greater extent, together with hyaline, fatty, and granular casts.
Although the observations are somewhat contradictory, it seems pretty definitely established that the blood is more or less altered in composition, morphological and chemical. The red corpuscles are diminished in amount, and often deformed; the white corpuscles are increased; and excrementitious products—urea, leucin, tyrosin, and cholesterin—are found in greater or less quantity.
COURSE, DURATION, AND TERMINATION.—Although, as a rule, the course of acute atrophy is rapid, it is not invariably so. In some instances the prodromic symptoms have continued through several months, but, according to Thierfelder, one-half of the cases terminate in from three to five weeks, and in only 10 per cent. is the duration continued into eight weeks. The course of the disease is extremely rapid in pregnant females, rarely extending beyond the second week. An extended course of the disease is due to delay in the prodromic stage, the toxæmic period being always absolutely and relatively shorter. In the condition of pregnancy the danger is increased by the hemorrhages, and the early termination is due chiefly to this factor. When the duration of the disease is protracted and its evolution normal, the accumulation of hepatic excrementitious matters sets up cerebral disturbance, which becomes a pronounced feature of the case.
The termination cannot probably be otherwise than fatal. As in the course of the disease the hepatic cells undergo solution and disintegration, their restoration can hardly be regarded as possible, certainly not probable. Any curative result must, then, be wrought in the prodromic period, when the diagnosis must be viewed with some mistrust.
DIAGNOSIS.—George Harley132 maintains the singular doctrine that acute yellow atrophy is only the "sporadic form of the contagious jaundice of the tropics," or yellow fever. He bases his opinion on the identity of their symptoms, pathological anatomy, mortality, and contagious character; for he affirms that acute yellow atrophy may exhibit contagious power in temperate climates.
132 Diseases of the Liver, Amer. ed., 1882, p. 255.
As acute yellow atrophy comes on as an ordinary catarrhal jaundice, it is impossible to distinguish it from the latter affection during the prodromal period. When cerebral symptoms, black vomit, and tarry stools appear, the area of hepatic dulness very decidedly diminishes, and leucin and tyrosin replace urea in the urine, acute atrophy may be suspected.
Acute phosphorus-poisoning, as regards its symptomatology and morbid anatomy, does not differ from acute yellow atrophy, and many cases of the latter have been mistaken, it is supposed, for the former. To distinguish between them the history of the case must be carefully ascertained.
When, after the prodromal symptoms, which may not be accurately diagnosticated, there occurs a rapid decline in the area of hepatic dulness, hemorrhages take place from the mucous surfaces, stupor and delirium [p. 1030] supervene, and urea disappears from the urine, being replaced by leucin and tyrosin, there can be no difficulty in coming to a conclusion: the case must be one of acute yellow atrophy.
TREATMENT.—It was formerly supposed that a case of acute yellow atrophy must necessarily prove fatal, but this opinion must now be modified, since examples of cure of supposed cases have been reported from Oppolzer's clinic,133 by Lebert,134 by Harley,135 and others. As at the onset the symptoms cannot be distinguished from a bilious attack or from catarrhal jaundice, the treatment must be appropriate to these states. When the serious symptoms begin, a large dose (scruple j) of quinine should be at once administered, and half the quantity at regular intervals to keep up the cinchonism. Phosphate of soda, with some arseniate and such mild hepatic stimulants as euonymin, iridin, etc., should be given to maintain a gentle aperient action. Experience has proved that active or drastic cathartics do harm rather than good; on the other hand, mild laxatives, especially those having cholagogue action, seem to do good.
133 Thierfelder, op. cit.
134 Ibid.
135 Diseases of the Liver, Amer. ed., supra.
Important symptoms arising during the toxæmic period require remedies to combat them. Nausea and vomiting, and also diarrhoea, are best relieved by carbolic acid and bismuth in combination. Hemorrhage requires, when intestinal, the chloride and perchloride of iron; when from other mucous surfaces, ergotin, gallic acid, and other hæmostatics. The depression of the vital forces should be treated by small and frequently-repeated doses of alcohol, by quinine, by iron, and, under some conditions, by digitalis. After the disintegration of the hepatic cells has been produced no remedies can be of any service. Until this occurs, however, it seems to the author well worth while to attempt to stay the destruction by the administration of those remedies which, by their accumulation in that organ, indicate a special affinity for its tissue. These drugs are phosphorus, antimony, gold, silver, and mercuric chloride. By the timely administration of one or more of these would it not be possible to stay the progress of the atrophic degeneration?
DEFINITION.—Poisoning by phosphorus may seem to be a toxicological question rather than a merely hepatic disease, but as the morbid complexus thus induced is so similar to acute yellow atrophy that the conditions are regarded as identical by many of our German colleagues, it is necessary to enter into some details regarding it.
PATHOGENY.—Phosphorus-poisoning occurs at any period from youth to old age, but is most common from twenty to thirty years of age. Women seem more inclined to effect self-destruction in this way than are men, probably because phosphorus matches are so readily obtained. Children may munch match-heads in a spirit of mischief. That form of chronic poisoning seen in workmen in match-factories, and consisting in necrosis of bone, etc., does not come within the scope of the present inquiry.
A body poisoned by phosphorus does not exhibit a tendency to putrefactive decomposition within the usual period. The tissues are more or less [p. 1031] deeply stained by bile-pigment, and this coloration extends to pathological fluids as well. The serous and mucous membranes contain points of blood-extravasation, but they are especially numerous in the serous membranes. Hemorrhages of this kind are due to two causes—to the disorganization of the blood, and to fatty degeneration of the arterioles. The heart is also more or less advanced in fatty degeneration, the muscles granular, the striations obscure or obliterated, and the whole soft and easily torn. The spleen is usually enlarged—often, indeed, to twice its natural size. The liver presents highly-characteristic alterations. When death occurs early the organ is generally enlarged, infiltrated with fat, the connective tissue undergoing hyperplasia; but in more advanced cases atrophy has taken place, the cells have disappeared and are replaced by fat-granules, crystals of leucin and tyrosin, connective tissue, etc.—in fact, the changes characteristic of acute yellow atrophy. The jaundice has been variously interpreted. As the bile-ducts in advanced cases are found to contain no bile, but only a colorless mucus, the advocates of a hæmatogenic jaundice hold that the jaundice is due to a failure of the liver to excrete the biliary principles in the blood; whilst the opponents of this view maintain the existence of an obstruction in the ultimate ducts. Harley136 has recently brought forward some strong facts and arguments—which we believe can be successfully controverted—maintaining the former view. The jaundice of phosphorus-poisoning, if Harley's opinion prove to be correct, must be regarded as a hæmatogenic jaundice.
136 Diseases of the Liver, loc. cit.
The mucous membrane of the stomach, as might be supposed, is more or less ulcerated or in an advanced state of catarrh, and the gastric glands are affected by fatty degeneration.
The kidneys are affected in a similar manner to the liver; the epithelium is fatty and sometimes detached, and the same process is found to occur in the vessels and epithelium of the cortex.
SYMPTOMS.—Not only in the morbid anatomy, but in the symptoms, do we find that a very remarkable resemblance exists between acute yellow atrophy and phosphorus-poisoning. As phosphorus is usually swallowed in bulk, some hours may elapse before the local symptoms begin, for the contents of the stomach and the tough mucus lining the mucous membrane may, and usually do, prevent immediate contact of the poison with the mucous membrane. When the stomach is entirely empty the symptoms may begin in an hour or two. The symptoms produced may be arranged in two groups—those due to the local irritation excited by the poison; those due to its systemic impression. In the first group belong burning in the gullet, pain, nausea, and vomiting. According to Lewin,137 who has collected a number of cases for analysis, vomiting occurs in 26 out of 32 instances of poisoning. Some hours—often, indeed, three or four days—then elapse before the systemic symptoms begin. Vomiting, which was for the time being suspended, occurs again, and instead of the mere contents of the stomach, containing more or less phosphorus, blood, somewhat changed by the gastric juice—chocolate-colored or as coffee-grounds—appears in the vomited matters. The evacuations from the bowels may at first, as the contents of the stomach, appear phosphorescent, and afterward exhibit the appearances due to the presence in them [p. 1032]of altered blood. At this time, if the liver be examined it will be found somewhat enlarged and tender to pressure, and on or about the third day jaundice appears; but it should not be overlooked that jaundice, as Bamberger138 has shown, may be postponed to the second or third week after the phosphorus has been taken.
137 Virchow's Archiv für path. Anat., etc., Band xxi. p. 514 et seq.
138 Legg, On the Bile, Jaundice, and Bilious Diseases, loc. cit.
In favorable cases the area of hepatic dulness decreases and the jaundice declines. In the fatal cases certain nervous phenomena become prominent. There occur drowsiness, developing into coma, with intercurrent attacks of delirium which may be of a maniacal character; convulsions, spasmodic attacks, dilated pupils, and involuntary evacuations. The disorganization of the blood and the fatty change in the vessels are exhibited in the hemorrhages from the gastro-intestinal mucous membrane. The nervous phenomena are due chiefly to the retention in the blood of various excrementitious matters which it is the function of the liver to separate from the blood. Flint's theory of cholesteræmia has been so abundantly disproved that no one upholds it at the present time, but the cerebral symptoms are properly referred to the retention of all hepatic excrement.
The temperature in phosphorus-poisoning rises from 99° to 102° F., but it may reach in severe cases to 103° to 105° F., and at death or immediately afterward to 105°, even to 107° F. The same fact is true of acute yellow atrophy. With the jaundice the pulse declines, but in the further progress of the case, especially toward the close, the pulse becomes rapid and small.
The changes occurring in the urine are highly significant. The amount of urea decreases as the symptoms increase in severity, and leucin and tyrosin take its place. If the case tends to recovery the urea again increases in amount, but if the tendency is in the opposite direction the quantity of urea steadily diminishes. Bile acids and bile-pigment are found in quantity, and albumen is present in small amount.
COURSE, DURATION, AND TERMINATION.—Phosphorus-poisoning is necessarily an acute affection, but the duration of cases is much influenced by the form in which the poison is taken. If in a liquid and diffusible form, as oleum phosphoratum, the local and systemic symptoms will develop in a few hours, but if in solid masses, as particles of match-heads, many hours (six to ten) may elapse before the local irritation begins. The proportion of cures in phosphorus-poisoning varies from one-fourth to one-half of the cases. Much depends, however, on the promptness and efficiency of the treatment. The prognosis is the more favorable the earlier proper measures of relief have been instituted. If the case has proceeded to jaundice, hemorrhages, black vomit, etc. without the administration of suitable antidotes, little can be expected from any kind of treatment.
DIAGNOSIS.—The history of any case involved in doubt is indispensable to a correct conclusion. The phosphorescent appearance of the matters vomited or passed by stool may make the differentiation comparatively easy; but if the case has passed beyond this stage, phosphorus-poisoning can be separated from acute yellow atrophy only by the history of the case. If the fact of the administration of phosphorus is successfully concealed, no differentiation can be made, since [p. 1033] even the best authorities hold to the identity of the toxic symptoms produced by this poison and of the morbid anatomy, with the symptoms and lesions of acute yellow atrophy.
TREATMENT.—The poison should be evacuated as quickly as possible by emetics and proper diluents. The best emetics are sulphate of copper, apomorphia, and ipecacuanha, the antimonial and mercurial emetics being unsuited, since their effects are similar to those of phosphorus. Oleaginous protectives do not prevent, but really favor, the absorption of phosphorus. Decoctions of flaxseed, slippery elm, acacia, etc. are suitable demulcents and protectives. The fatty matter in food, eggs, etc. will have an injurious effect by promoting the solution and absorption of the phosphorus, and should hence be excluded from the diet. The most effective antidote is oleum terebinthinæ, and the most suitable preparation is the French acid oil. Freshly-distilled turpentine appears to be almost if not entirely useless. It is probable that the American oil which is old and has been exposed to the air for many months will answer the purpose, but it cannot be too strongly insisted on that the turpentine which has proved to be efficient in phosphorus-poisoning is the French acid oil. Turpentine when exposed to the air absorbs oxygen as ozone, and to this principle are probably due the curative effects of old turpentine. Phosphorus when acted on by this agent is converted into a spermaceti-like substance entirely devoid of toxic power. As rapidly as possible the poison should be acted on by the antidote, and then the stomach should be evacuated, using, cæteris paribus, the sulphate of copper, since this forms an insoluble phosphide with any portion of free phosphorus, whilst at the same time it empties the stomach of its contents. Although the immediate results of the poison may be thus removed, the damage to the red corpuscles and to the whole mass of the blood requires special management. The success of transfusion, as practised by Jürgensen,139 proves that the substitution of fresh blood may save life when the existing blood-supply is inadequate to the performance of its proper functions. It follows that if the toxic effects of phosphorus have continued for several days, blood-transfusion will be necessary in those cases characterized by an inability to recuperate notwithstanding the successful removal of the poison.
139 Berliner klinische Wochenschrift, No. 21, 1871.
For the inflammatory symptoms produced by the local action of phosphorus, opium in some form is indispensable. This remedy is equally valuable as a means of maintaining the vital resources and to prevent the evil results of shock and inflammation.
DEFINITION.—Under the term carcinoma of the liver are included primary and secondary cancer of the liver. The malady with which we are now concerned is the primary affection, occurring in the organ proper or in some pathological new formation connected with it.
ETIOLOGY.—Heredity is the most important factor. A careful investigation of the reported examples demonstrates that from 15 to 20 per cent. owe their origin to hereditary influence clearly, and probably [p. 1034] considerably more are indirectly derived in this way when the immediate connection may not be demonstrable. Next to heredity, age must be regarded as the most important pathogenetic influence, much the largest number occurring at from forty to sixty years of age. It is a malady of advanced life, therefore, rather than of youth or middle age. Excluding the female organs from consideration, it is quite certain that sex has little special influence, and that males and females are affected about equally.
Primary cancer of the liver is comparatively infrequent, occurring in not more than one-fourth of the cases. Frerichs collected 91 cases, and of these 46 were secondary to cancer in organs having vascular communication with the liver.
PATHOLOGICAL ANATOMY.—Under the term cancer of the liver are included several distinct forms of morbid growth, but united in the characteristic of malignancy. From the merely clinical standpoint this characteristic is the most decisive bond of union between them, and serves as the point of departure in the study of this affection. Primary cancer of the liver is divisible into two forms: 1, as a single, defined tumor; 2, as an infiltration through the whole mass of the organ.140 Secondary cancer occurs in nodular masses, and with extreme rarity as an infiltration. The form of cancer is really the same; the differences in structure are only apparent, the variations being due to the relative proportion of cells, fibres, and vessels. If the fibrous stroma is abundant and the cells small in quantity, the form of structure approaches scirrhus; on the other hand, if the cells largely preponderate, the type is encephaloid; if vessels predominate, it is called telangiectatic. The usual form in cancer of the liver is the soft, cellular variety, encephaloid or medullary. When the cancerous new formation is nodular, the masses vary in size from a pea to a child's head,141 and are numerous inversely as their size. When the cancer occurs as a solitary tumor, it may attain to enormous dimensions. It has a spherical shape usually, protrudes from the surface of the organ somewhat irregularly, and the overlying peritoneum is thickened, cloudy, and adherent from a local inflammation. The central portion, whether there be one, several, or many nodules, is depressed, giving an umbilicated appearance to the tumor; and this central depression is found to be soft, almost diffluent, and full of juice. The fibrous stroma which extends through this central soft material has a reticulated arrangement and a shining, fibrous appearance. The cancerous masses are not confined to these nodules, but extend into the surrounding hepatic structure, push their way into the portal (especially the hepatic) veins, block the ducts, and invade the lymphatic glands in the fissure of the liver.
140 Virchow, Krankhaften Geschwülste, loc. cit.; Perls, Virchow's Archiv für path. Anat., etc., Band lvi. p. 448 et seq.; Frerichs, A Clinical Treatise, etc., Syd. Soc. ed., loc. cit., vol. ii. p. 281 et seq.
141 Förster, Lehrbuch der Pathologischen Anatomie, by Seibert, Jena, 1873.
When the cancerous new formation takes the form of an infiltration of the organ instead of distinct nodules, the liver is usually uniformly enlarged and its outlines preserved.142 The peritoneum is opaque, thickened, and adherent. The organ is traversed by fibrous bands, and the [p. 1035] intervening portion is a soft, juicy pulp, stained by the imbibition of bile. In extreme cases hardly any portion of the proper hepatic tissue remains, but is replaced by a cancerous new formation having the same shape.
142 Perls, Virchow's Archiv, Band lvi. p. 448 et seq.
As regards the minute structure of cancer of the liver, it may be regarded as a degeneration (cancerous) of the proper gland-cells and of the epithelium of the bile-ducts. As cancer develops in the liver it is to be noted that the cellular elements preponderate over the fibrous or the stroma, and hence the new formation presents the characteristics of softness, rapid growth, and a multitudinous cellular hyperplasia. As regards the form of the new cells, it cannot now be doubted that they are descendants of the secretory gland-cells and of the epithelial lining of the ducts. According to some observers, it is to the proliferation of the proper gland-cells that the new formations owe their origin; according to others, to the hyperplasia of the cells lining the ducts. As the growth of the new formation can take place only through an adequate blood-supply, it becomes very important to ascertain its source. There can be little doubt that primary cancer of the liver receives its nutrient supply through the hepatic artery, in connection with which new capillaries form in the pathological tissue.
Secondary cancer of the liver is the usual form of the specific manifestation. From the merely clinical standpoint the primary affection is the more important. From the pathological point of view the secondary implication of the liver may be a true metastasis or a mere communication by contiguity of tissue. The most usual metastasis occurs from epithelial cancer of the face (Schüppel), but the ordinary communication of the new formation is from primary cancer of the stomach, intestine, pancreas, mesentery, etc. The cancer elements, as the author has several times verified, crowd the lymphatics and veins, and through these channels reach the liver and other parts. As the cancer elements in the case of secondary implication of the liver are distributed chiefly by the portal vein, it follows that there must be numerous secondary foci and multiple nodes. Cancerous infiltration under these circumstances is the rarest possible form for the new growth to take. The size and number of nodes forming in these cases of secondary implication of the organ vary greatly—from two or three to twenty, or a hundred, or even more. As regards the form, structure, and ultimate behavior of the secondary formation, they do not differ from the primary. As respects the relative proportion of stroma and cellular elements—fibres and cells—they vary greatly, some presenting the firm texture of a predominating fibrous stroma, others the softness and ready diffluence of the excessive cellular production. The latter is undoubtedly the usual condition, and when the nodular masses are incised an abundant creamy juice exudes. With the development of these nodules an increase in the size of the liver takes place and the organ has an uneven and indurated feel. As the cancerous masses develop the proper hepatic structure undergoes atrophy, and finally little is left of the organ but the cancerous new formation. The blood-vessels, lymphatics, and peritoneal investment are invaded, the first mentioned most decidedly; and especially are organized exudations the favorite seats of cancer new formations, those, for example, about the gall-bladder and cystic duct resulting from repeated attacks of passage of calculi.
[p. 1036] Secondary changes take place in the cancerous nodes. As the cells develop pressure is brought to bear on the vessels supplying them and on each other, with the result of fatty degeneration of the central portion, which effects the change in the form of the nodules and in their consistence, already mentioned. The blood-supply to the cancerous nodes in the liver is derived from the hepatic artery, as Frerichs has determined by carefully-made injections; they also are new formations of exceedingly delicate structure, and form a network about the periphery of each mass or node. By reference to these anatomical considerations it is easy to understand the failure of nutrition of the central portions of the nodes.
Pigment cancers of the liver are rare as secondary formations, and excessively infrequent as primary formations. They are, properly speaking, melano-sarcomas (Schüppel). They are more often metastatic than merely secondary—that is, transferred from different parts, as in the case of melanotic sarcoma of the choroid—than due to neighboring disease transferred by contiguity of tissue. This variety of cancer, so called, takes the form of multiple nodes or of diffused infiltration, the former more frequently; but both modes of development may go on at the same time. The nodes vary in size from a pea to a child's head, have a grayish, brownish, or blackish tint, and exude on section a fluid not creamy like true cancer-juice, but rather watery and containing black particles floating in it. In the case of diffuse infiltration the pigment masses are thoroughly distributed through the original hepatic tissue. In both forms the size and weight of the organ are enormously increased. In the case of the melanotic infiltration the whole organ is uniformly enlarged, reaching in a few months the enormous size of twelve to twenty pounds.
Sarcomas also occur very rarely as primary growths in the liver, but secondary sarcomas are more frequent. There are fibro-sarcoma, lympho-sarcoma, and osteo-sarcoma as secondary deposits, the first being very firm in consistence, the second soft and medullary, and the last of hard, bony consistence.
SYMPTOMS.—We are especially concerned here with primary cancer of the liver. The secondary disease is so obscured by the main and primary lesion that a diagnosis may be impossible. Furthermore, the progress of the original disease is that which demands immediate consideration. As, therefore, the secondary implication of the liver is of relatively trifling importance, and only an incident in the course of the main disease, the matter for consideration now is primary cancer of the liver.
It is the fact that in some, even a considerable proportion, of the cases the onset and progress of cancer of the liver are very obscure. For some time the symptoms may be of the vaguest description. The usual history is this: A person of forty to sixty years begins to fail in flesh and strength, becomes sallow, has disorders of digestion, pain and uneasiness in the right hypochondrium, and the bowels are now confined, now relaxed. The abdomen, notwithstanding the general loss of flesh, increases in size, and the superficial veins are enlarged; very considerable pain is experienced in the right hypochondrium, and often extreme tenderness to pressure is a pronounced symptom. The pains are not limited to the hepatic region, out extend widely from this point in all directions. On palpation the [p. 1037]liver is found to be enlarged, its texture indurated, and its outline irregular and nodular, and pain—often, indeed, quite severe—is developed by pressure.
The condition of the liver on palpation is best ascertained by suddenly depressing the abdominal wall with the tips of the fingers arranged in a line. Displacing thus the movable bodies in the cavity, the liver is quickly reached, and nodules, if they exist, are readily felt. If the new formation has developed from exudations about the gall-bladder and cystic duct, it may be felt by suddenly depressing the walls of the abdomen over this organ in the usual position of the fissure.
In the case of general cancerous infiltration of the organ, with the remarkable enlargement which occurs in such cases, there will be present an obvious distension of the right hypochondrium; the intercostal spaces will be forced outward and the arches of the ribs rendered more prominent; the area of hepatic dulness, both vertical and transverse, will be increased; and the limits of dulness will move with a full inspiration downward, and with a full expiration upward. This mobility of cancer-nodules of the liver with the inspiratory and expiratory changes serves to distinguish them from tumors of the abdominal walls. Seen early, the changes in the size of a nodule or of the liver itself may be noted from week to week,143 especially in cases of rapidly-growing cancer.
143 Murchison, Clinical Lectures, p. 187.
As the cancerous new formations extend into the portal system within the liver, obstruction to the portal circulation results from the blocking of the blood-current. Also, interference in the portal circulation arises by compression of the vessels from without, either through the accumulation of cancer-products in the liver or by the enlargement of the lymphatics in the fissure of the organ. In what way soever it may be produced, the practical fact remains that ascites is a frequent symptom, occurring in somewhat more than one-half of the cases. The character of the fluid varies. It may be a clear serum containing a small proportion of albumen; it may be colored by bile or be of a deeper greenish or reddish hue; it may contain flocculi of lymph and numerous leucocytes floating in it; and the ordinary serum may be rendered cloudy and be filled with shreds of exudation in consequence of peritonitis, or bloody because of hemorrhage from a softening nodule. When the fluid is considerable in amount the difficulty of ascertaining the condition of the liver is greatly enhanced, and symptoms due to the interference of the fluid with the action of various organs are introduced into the complexus of morbid signs. Especially is the upward pressure of the ascitic fluid, and the consequent interference in the movements of the lungs and heart, a source of considerable distress. First, a local and afterward a general peritonitis ensues as a consequence of the extension outwardly of the new formations to the peritoneal layer, and its implication by contiguity of tissue or the rupture of a spreading fungous growth and hemorrhagic extravasation into the cavity. The peritoneal complication is not only a serious addition to the sufferings experienced by the patient, but it adds to the difficulties of a diagnosis. In the case of a celebrated savant who died of cancer of the liver (seen by the writer) there was such a pronounced peritonitis that the diagnosis made by the attending physician was chronic peritonitis. When this complication occurs, there takes place [p. 1038]a decided increase in the local tenderness, and this increased sensibility to pressure quickly extends over the abdomen, causing a general exquisite tenderness. Besides this tenderness characteristic of most cases of peritonitis, distension of the abdomen and the decubitus peculiar to this state are obvious symptoms. It is therefore clear that the occurrence of peritonitis not only contributes to the severity and painfulness of the case, but seriously complicates the diagnosis.
It has been already stated that pain in the right hypochondrium is a nearly constant symptom in cancer of the liver. With the initial symptoms, uneasiness, heaviness, a sense of pressure in the hepatic region are experienced, and as the case progresses more or less acute pain develops as a rule. But there are exceptions. In cases of cancer involving the deeper portion of the liver there may be little pain, and in some rare cases of cancer involving the external part of the liver—the capsule and peritoneum—but little pain is experienced. In much the largest proportion of cases the pain is severe, and the production of any considerable pain means the implication of the hepatic plexus of nerves or the hepatic peritoneum. It follows, then, that the pain in the former case is not limited to the locality of the disease, but is more or less widely distributed through the anatomical relations of the hepatic plexus, being felt in the epigastrium, the walls of the chest, the shoulders, etc.
In secondary cancer of the liver, following cancer of the stomach, vomiting is a constant symptom, but also in those cases of primary disease in which the left lobe is especially enlarged, relatively, are nausea and vomiting pronounced symptoms. At the onset of the malady the appetite fails and a gastro-intestinal catarrh is set up. More or less catarrh of the bile-ducts also ensues. The interference with nutrition thus occasioned is enhanced in those cases in which the obstruction of the ducts is sufficient to prevent the escape of bile into the intestine. Jaundice is not a constant symptom, occurring in little more than one-third of the cases. When it occurs, the peculiar stools are present and the intestinal digestion is deranged, as in cases of ordinary obstruction to the ducts. In two cases of cancer of the liver occurring in the writer's practice, and examined by post-mortem, there were calculi present in the gall-bladder; in one case the principal calculus was egg-shaped and the size of a pullet's egg.
The nutrition rapidly fails from the beginning of cancer of the liver. The downward pace is accelerated when the gastro-intestinal digestion fails and vomiting occurs after taking food. The skin becomes dry and wrinkled, and if not jaundiced has a peculiar tint, varying in depth of color from an earthy or fawn-like hue to a deep bronze. Failure of strength is a pronounced symptom from the beginning, and is out of proportion to the loss of flesh. As the wasting advances the decline of strength is accounted for, but the feeling of weakness and the distaste for exertion which occur so early are very significant signs of internal cancer, although they do not indicate the position of the neoplasm. Emaciation finally becomes extreme.
The urine declines in amount as the case progresses. It is usually very high-colored, contains bile-pigment when jaundice is present, and other forms of pigment produced by conditions not at present known. Sometimes albumen is present, and leucin and tyrosin rarely.
[p. 1039] COURSE, DURATION, AND TERMINATION.—As has been already set forth, cancer of the liver may present so few really distinctive symptoms as to escape recognition. Under favorable circumstances the diagnosis may be comparatively easy. In forming an opinion it is useful to review the whole course of the malady and draw conclusions not only from the characteristic signs, but from the development of the symptoms as a whole.
A case of cancer of the liver occurs usually after the middle period of life. The person so affected begins to decline in flesh and strength, has uneasiness in the right hypochondrium, disorders of digestion, and begins to have a pallid or earthy hue of the countenance. Presently, much pain is felt in the hepatic region, the organ distinctly enlarges, and some effusion of fluid and much flatus increase the dimensions of the abdomen. Much tenderness, often exquisite sensibility, is produced by pressure over the liver, and often over the whole abdomen. By careful palpation nodules can be made out and their growth noted in those cases free from peritoneal inflammation. The abdominal swelling and tenderness incommodes the lungs, and a semi-erect decubitus is assumed to relieve the pressure on them; the breathing becomes short, catching, hurried, and painful, and sometimes a most distressing hiccough is superadded to the other sufferings. Great wasting and weakness ensue. Jaundice appears, or the earthy hue of the skin deepens into a bronze discoloration. The case may be terminated by some intercurrent disease—by an attack of pleuritis, pneumonia, by peritonitis from rupture or perforation, by intra-peritoneal hemorrhage, by an exhausting diarrhoea. The natural termination is by gradual failure of the powers, by marasmus, the immediate cause of death being due to cerebral anæmia, to failure of the heart from fatty degeneration of the cardiac muscle, from thrombosis of the portal vein, from the development of a hemorrhagic state, and hemorrhages from the various mucous surfaces, etc. The duration is much influenced also by the character of the cancer, whether scirrhous or medullary. The latter are not only more rapidly growing, more destructive of the hepatic tissue, and more rapidly distributed to neighboring organs, but more quickly perforate the capsule and excite a fatal result by hemorrhage or by peritonitis. The average duration of cancer of the liver is variously stated. Having reference to my own personal observation, controlled by the experience of other observers, the duration is from three to nine months, one year being exceptional. There are cases in which the symptoms are very acute, the progress rapid, the whole course from the initial symptoms to the termination being completed in from two to three months. It need hardly be observed that no case of cancer of the liver has been cured. The invariable termination is in death. If any case has seemed to be cured, it may be asserted with confidence that cancer of the liver did not exist.
DIAGNOSIS.—The differential diagnosis is concerned, first, with the existence of cancer; second, with its form. As cancer causes enlargement of the liver in two textural conditions—namely, uniformly smooth, and nodular—it must be differentiated from other diseases producing similar results. Amyloid disease and echinococcus cysts present us types of the former; cirrhosis and syphilis, of the latter. The history of the amyloid disease and of the echinococcus cyst is very different, and both [p. 1040] develop much more slowly. Amyloid disease of the liver arises simultaneously with the same form of degeneration in other organs, and is connected with suppurative disease of some kind, with syphilis, with chronic malarial poisoning, etc., and may occur at any age. Echinococcus cysts enlarge painlessly and do not impair the vital forces; the liver is elastic, and under favorable circumstances presents by palpation the purring-tremor symptom. Cirrhosis may have to be differentiated at two periods—during the time of enlargement, which, however, is rather brief; and during the stage of contraction and nodulation. The history in cancer and in cirrhosis is different: the age, the habits of life, the rate of hepatic change, are opposed in the two diseases; the diminution in size with nodulation is characteristic of cirrhosis; enlargement with nodulation belongs to cancer. The rapid progress of cancer, the wasting, the debility, the cachexia, serve to distinguish it from all other affections of the liver except acute yellow atrophy and phosphorus-poisoning; both, however, are so different in history and development as not to require differentiation. It may be quite impossible in latent cases to distinguish primary cancer of the liver from secondary, but in those examples of the disease occurring in the stomach, intestines, and pancreas there is usually an antecedent history of the primary malady which distinctly separates it in point of time and the character of the symptoms from the secondary implication of the liver. Cancer of the gall-bladder, and especially of the organized exudation about it, may not be readily separated from cancer of the pancreas or of the duodenum. In doubtful cases the history of attacks of hepatic colic becomes an important element in making the differentiation.
TREATMENT.—As we are not in possession of a cure for cancer, the treatment of cancer of the liver must be palliative. Anodynes to relieve pain, paracentesis of the abdomen to remove accumulation of fluid which causes distress, carbolic acid to check nausea and vomiting, and the usual hæmostatics for hemorrhage, are the measures most necessary. In fact, the treatment must be throughout symptomatic—for the relief of symptoms as they arise.
DEFINITION.—By amyloid liver is meant a deposit in the cells of the organ, in its vessels and interstitial tissue, of a peculiar albuminoid matter called amyloid because of a superficial resemblance to starch-granules. Various designations have been applied to this condition of the organ; thus it has been entitled waxy liver and lardaceous liver, because of the apparent resemblance to wax and lard respectively.
CAUSES.—There exists in the blood a peculiar material, albuminoid in form, applied in the normal state to the structure of tissue—dystropodextrin, as it is called by Seegen—which, when precipitated under certain conditions not now known, assumes the peculiar appearance with which we are now familiar under the term amyloid. The character of the amyloid matter was first distinctly set forth in 1858 by Virchow, who also discovered the characteristic reaction by which it can always be detected. The reaction to iodine gave to the material the designation amyloid, or starch-like, by which it is chiefly known. The [p. 1041] circumstances inducing the deposit of this material are by no means clearly understood. It has long been known that suppuration, especially in connection with bone, has had a distinct influence. Syphilis, especially the tertiary lesions accompanied by pus-formation, has an evident causative relation. Chronic malarial infection has a more distant and doubtful, but still recognized, power to develop this morbid state. Of the various causes above mentioned, the most frequent is the suppuration of pulmonary cavities. In regard to the influence of this, however, it must be remembered that no form of suppurative disease is so common. The relative frequency of the association between suppurating cavities and amyloid disease is not greater than long-standing necrosis with an extensive sequestrum is with the same state; but the actual number of the former is greater. Amyloid disease of the liver is most frequent between the ages of ten and thirty, but it may occur at any age, the period in life being determined by the operation of the causes. Thus, Frerichs' statistics are: under ten there were 3 cases, from ten to twenty there were 19, and from twenty to fifty there were 37 cases. Men are, relatively to sex, more frequently attacked, and in the proportion of three-fourths, but this difference means, of course, the character of men's occupations and their greater liability thereby to the accidents and diseases incident to such employments.
Besides the pathogenetic factors above mentioned, it may be well to refer in this connection to the effect of long-standing neoplasms. It has been found that amyloid disease is produced in some subjects by the cachexia resulting from the slow development and persistence of such a new formation. The special character of the neoplasm is of less importance in respect to this condition than the constitutional condition—the cachexia—induced by its slow growth and interference with nutrition. Although long-standing disease, especially of a suppurative kind, is known to be necessary to cause amyloid disease, Cohnheim144 has lately published some facts which seem to prove that the degeneration may occur more speedily than has been heretofore supposed. He has shown, contrary to the previously-accepted view, that amyloid degeneration may follow in three months after the reception of a gunshot wound. He records three cases in which the amyloid deposits ensued in six, five, and three months, respectively.
144 Virchow's Archiv, vol. liv. p. 271 et seq., "Zur Kentniss der Amyloidentartung."
According to the author's observation, a peculiar somatic type is either necessary to, or at least is greatly promotive of, the amyloid degeneration. If, for example, the same suppurative process occurs in a person of a blond and lymphatic type and in another of brunette and nervo-muscular type, the former will be much more likely to suffer from amyloid change than the latter. "The gelatinous progeny of albuminous parents" is the mode of expression used to designate this particular type.
PATHOLOGICAL ANATOMY.—To use the term amyloid liver is rather misleading, since this indicates the restriction of the morbid process to the liver, whereas it is perfectly well known to be rather widely distributed through various organs and tissues of the body. The term amyloid is itself confusing, since the albuminoid material so designated is not really starch-like. The corpora amylacea, so called, differ materially from starch-granules, and still more from the amyloid matter. According to [p. 1042] Wagner,145 these substances "have nothing in common." In the study of the amyloid deposit it has not been possible to separate it from the tissue in which it is imbedded; hence the published analyses of this peculiar material are probably far from correct. However, it has been rendered probable that the amyloid deposit has close affinities with fibrin. One of the theories—that of Dickinson of London—assumes that this material is fibrin deprived of the potash associated intimately with it. According to Seegen, dystropodextrin, a material existing in normal blood, agrees with amyloid matter in its most essential characteristics. Although Dickinson's theory is not tenable, it has served a useful purpose in showing the close affinity of fibrin with this pathological product. What view soever may be entertained of its nature, it is certain that the material to which we apply the term amyloid is of albuminous origin. Under circumstances with which we are now unacquainted this material is deposited from the vessels, and, instead of undergoing organization and contributing to the structure of tissues, remains unorganized and unappropriated. It is known that this deposition of the amyloid material is related to the process of suppuration and to certain cachexiæ, but the intermediate steps remain unknown and inexplicable.
145 A Manual of General Pathology, by Prof. Dr. E. Wagner, p. 325 et seq.
The amyloid matter is first exuded into the coats of the finest ramifications of the hepatic artery, and therefore the first appearance of the disease is in the middle zone of the lobules. In this respect pathologists are agreed: that the amyloid deposits first appear in the walls of the vessels. Wagner maintained, in opposition to Virchow, that the exudation is limited to the vessels and does not extend to the hepatic cells, which perish by pressure and consequent atrophy. This point has not yet been decided. It seems most probable, however, that the ramifications of the hepatic artery and all the capillaries of the lobule are affected, and that the deposits in them lead to atrophic degeneration of the cells.
In consequence of this extensive implication of the vascular system of the liver important changes occur in the size, density, and appearance of the liver. The organ is greatly enlarged in all its diameters. When felt through the walls of the abdomen its outline is distinct, it is firm, even hard, to the sense of touch, and it projects from a finger's breadth to a hand's breadth below the margin of the ribs. The increase of size of the amyloid liver is very great, attaining in weight, on the average, twice that of the normal organ; but this size may be largely exceeded in exceptional instances. In respect to shape and outline the amyloid liver does not differ from the normal organ; for although its dimensions are increased, its relations to the parts adjacent are not altered. The weight of the amyloid liver may reach ten, twelve, even sixteen pounds avoirdupois. The color of the amyloid liver is very different from that of the normal organ: instead of having the reddish-brown tint, it becomes grayish, yellowish, or reddish-gray. In consistence the amyloid liver is firm and rather elastic and doughy, and on section the margins of the incision are well defined, even sharp. A very characteristic feature of the cut surface is its paleness, anæmia, or bloodlessness, and scarcely any blood is exuded, even from the large vessels. The appearance of the incised surface of the liver has been described by comparison with various substances: according to one, it is waxy; according to another, it is lardaceous. A thin [p. 1043]section of a part of the liver far advanced in the amyloid change is distinctly translucent, almost transparent; but a marked difference is observable between the amyloid matter and the lobules proper, even in the cases of extreme deposit. The lobules are separated by an opaque yellow border, and the centre of each is marked by a spot of a similar yellow color.
The amyloid material is remarkable for its power to resist the action of chemical agents and putrefactive decomposition. The test originally proposed by Virchow—iodine—continues to be the most characteristic. Orth146 suggests a method of applying it which is very excellent in respect to the clearness with which the reaction is shown: A large, thin section of the affected liver is placed in a saucer of water containing some iodine, and after the reaction has taken place is laid on a white plate. Iodine tincture, diluted or the compound solution, is brushed over the affected region, when the amyloid matter assumes a deep mahogany tint and the normal tissues a merely yellowish hue. The distinctness of the reaction may be increased by brushing over the iodized surface some dilute sulphuric acid, when the amyloid matter takes a deep violet, almost black, color.
146 Diagnosis in Pathological Anatomy, Riverside Press, 1878, p. 321.
Only a part of the organ—namely, the smaller vessels—may be involved in the degeneration, and this may be restricted to patches or parts of the organ. With the amyloid change there may be associated syphilitic gummata, or the liver may be more or less advanced in fatty degeneration or in cirrhosis. Those parts of the organ not invaded by the disease are not often entirely normal; they are more or less darkened in color by venous congestion, distinctly softer, etc. The amyloid change is not limited to the liver, but extends to the kidneys, lymphatic glands, the intestinal mucous membrane, etc.
SYMPTOMS.—As the amyloid change in the liver is usually coincident with a simultaneous alteration of other organs, and as the deposits characteristic of the affection are dependent on long-previous disease of an exhausting kind, it is not surprising that the subjects of this affection present the evidences of a cachexia. To the effects of a chronic malady we have added the complications growing out of the amyloid change in the liver, associated, as it usually is, with amyloid degeneration of other important organs.
The symptomatic expression of amyloid liver is therefore mixed up with various derangements that occur simultaneously, but especially with the causes inducing the existing cachexia, with chronic suppuration of pulmonary cavities, or in connection with diseased bone, with the syphilitic cachexia, or with chronic malarial toxæmia. With what cause soever the cachexia may be associated, the symptomatology of amyloid liver is secondary to, or ingrafted on, the conditions produced by the cachexia. The liver is enlarged in all well-marked cases from a finger's breadth to a hand's breadth or more below the inferior margin of the ribs; it is also firm to the touch, well defined, elastic, and its margin rounded, but yet well defined. There is usually no tenderness nor pain, and, without any uneasy sensations to indicate the change taking place, the organ is found to have slowly enlarged, sometimes to an extraordinary extent. Careful palpation may also demonstrate an enlargement of the spleen. When the abdominal muscles are relaxed and there is no swelling of the abdomen by flatus or peritoneal effusion, the very considerable enlargement of [p. 1044]the liver can be readily ascertained. If the effusion is not so great as to distend the abdomen unduly, the increased consistence and dimensions of the liver can still be made out with comparative ease. The hepatic functions are not always sufficiently disturbed to produce characteristic symptoms. In a small proportion—scarcely one-tenth—of the cases does jaundice appear, and when present it is due, usually, to enlargement of the lymphatics in the hilus of the organ, and thus directly compressing the hepatic duct. In the writer's experience, although jaundice has not occurred, there was present a peculiar dark earthy or bronzed tint of the skin, significant of chronic hepatic troubles. Obstruction of the portal circulation is rather unusual, and the explanation is to be found in the fact that the amyloid degeneration occurs first in the radicles of the hepatic artery. In about one-fourth of the cases ascites is present, but in a somewhat larger proportion hemorrhoids, blackish, tarry stools, and other evidences of portal congestion. When the intestinal arterioles are attacked, an intractable colliquative diarrhoea comes on; the stools are offensive, sometimes light from the absence of bile, sometimes dark from decomposition or the presence of blood. When the stomach arterioles are also involved, which is usual under these circumstances, the blandest and simplest articles of diet will pass unchanged or simply decomposed. Blood may be vomited sometimes in large quantity from thrombic ulcers, but the matter ejected from the stomach when the case is well advanced is a thin, watery fluid, faintly acid or neutral, and greenish or brownish in color.
An enlarged spleen is often present, produced by the same conditions—by amyloid degeneration. The same change taking place in the kidney, the urine becomes pale, abundant, of low specific gravity, and albuminous. General dropsy supervenes in a majority of the cases finally, due largely to the hydræmia; and of this condition ascites is a part. In some cases enlargement of the abdomen is the first step in the dropsical effusion, and may throughout be the most prominent, as the author has seen. In other cases oedema of the feet and legs is the first evidence of dropsy; in still others the dropsy is general from the beginning.
Amyloid liver may coexist with a fairly good state of the bodily nutrition, but if digestion and assimilation be interfered with by any of the causes above mentioned, the strength rapidly declines and emaciation reaches an extreme degree.
COURSE, DURATION, AND TERMINATION.—As amyloid liver is never a substantive affection, but secondary to some constitutional malady or to long-continued suppuration, its course must be considered in relation to the agency producing it. It is very silent in its origin and progress, and causes no pronounced symptoms until it attains considerable size and its functions are interfered with by the extent of the deposits. The history of the affection to which it is secondary therefore precedes the onset of the amyloid change and accompanies it throughout. The enlarged organ, with the results of its enlargement in altered functions of the abdominal organs, is a symptom superadded to existing disturbances. The period elapsing in the course of a chronic suppurative disease before the amyloid change occurs differs greatly in different cases, and may be stated as from three months (Cohnheim's case) to many years. Many of the cases terminate by an intercurrent disease; others by uræmic [p. 1045] convulsions; a very few by hemorrhage from the stomach or intestines; and those pursuing their course uninterruptedly, by exhaustion.
The prognosis is very unfavorable. By some a cure at the beginning of the morbid deposits is regarded as possible, and examples of cures have been reported. The writer has seen supposed cases of amyloid liver terminate in recovery. There must always remain an impression that in such instances an error of diagnosis was committed. Those of syphilitic origin are probably more curable, but syphiloma of the liver may be confounded with amyloid disease, and hence the cure may be referred to the latter.
DIAGNOSIS.—Amyloid degeneration of the liver may be confounded with the various non-febrile enlargements of the organ. An important element in making the differentiation is the history of suppuration in connection with bone, with lung cavities, with constitutional syphilis, with chronic malarial toxæmia, etc. From fatty liver, amyloid degeneration is distinguished by the history as just sketched; by the fatty tendencies of the body in the former, emaciation in the latter; by the concomitant changes in the spleen, kidneys, and elsewhere; and by the subsequent history, fatty liver terminating by a weak heart usually, whilst the amyloid disease ends in the modes described in the preceding paragraph. From hydatid disease, amyloid liver is differentiated by the history, by the difference in the physical characteristics of the enlargement, by the presence of the purring tremor in the one, its absence in the other, and especially by the subsequent course. In all doubtful cases the use of an aspirator-needle and the withdrawal of some fluid containing the characteristic hooklets of the echinococcus will serve to determine the nature of the growth. From cancer, amyloid liver is separated by the previous history, by the nodular character of the enlargement, by the pain, and by the cachexia and associated derangements. Whilst amyloid liver is secondary to suppurative diseases, cancer is usually secondary to cancer of the stomach or other organ within the limits of the portal circulation.
TREATMENT.—As amyloid disease owes its origin to syphilis, to chronic malarial toxæmia, to suppuration, these, so far as they are remediable conditions, should be cured as speedily as may be, to prevent the development of the amyloid disease or to arrest it if begun. Unfortunately, the condition of the liver is not recognized until the morbid change is effected, and therefore practically irremediable.
The treatment necessarily involves that of the morbid state to which the amyloid deposits are owing. The syphilitic disease requires iodine and mercury; the malarial, quinine, iodine and the iodides, eucalyptus, iron, etc., according to the state of each case; and surgical diseases, especially necrosis of bone, should be effectively treated by suitable surgical expedients. The cause being removed if possible, what means, if any, can be resorted to to cause the absorption of the amyloid matter? The only specific plan of treatment hitherto proposed is that of Dickinson,147 based on his theory of the constitution of amyloid matter; according to which the amyloid deposits consist of fibrin altered by the separation of the potash and soda salts, which have been eliminated in the pus. If this theory be admitted, the obvious indication is to supply the alkaline materials. The cases reported by Dickinson in which this theory was [p. 1046] practically demonstrated were not sufficiently improved to lend any empirical support to this method.
147 The Pathology and Treatment of Albuminuria, p. 214 et seq.
The medicinal remedies which do any good are the iodides—notably the iodides of ammonium, of iron, of manganese, etc., the compound solution of iodine, and the double iodide of iron and manganese. As the officinal ointment of the red iodide of mercury, rubbed in over the splenic region, does so much good in chronic enlargement of the spleen, it is probable that it will prove effective in this form of enlargement of the liver. The writer has observed results from it in such cases that justify him in strongly urging its employment. The method of its application consists in rubbing perseveringly a piece of the ointment, a large pea in size, over the whole hepatic area, and repeating it daily until some irritation and desquamation of the skin is produced, when it should be suspended until the parts will bear renewed applications. Besides the topical application of the red iodide, this remedy may be given internally with advantage without reference to syphilitic infection. It seems to the writer probable that bichloride of mercury may be as useful, as it is certainly more manageable. The chloride of gold and sodium, arsenic in small doses, and the metallic tonics, so called, may be useful carefully administered, especially the first mentioned, which the writer believes has some real power over the disease.
Dietetic rules are of great importance. As the hepatic functions are much disturbed, if not entirely suspended, it is necessary to give those foods which are converted into peptones in the stomach. As a rule, fats, starches, and sweets are mischievous, and milk, meats, oysters, and the nitrogenous foods best adapted to nourish the patient. If the diarrhoea should prove exhausting, the mineral acids, with opium, are the best remedies. Nausea and vomiting are best relieved by carbolic acid mixture, and hemorrhages by the solution of the chloride or subsulphate of iron.
DEFINITION.—By the term fatty liver is meant a change in the organ characterized by the excessive quantity of fat- or oil-globules contained in the cells of the parenchyma.
CAUSES.—The liver acts, under normal conditions, as a reservoir for the surplus fat, which it gives out as the demand is made. It is not only the fat brought to the liver by the blood which accumulates in the organ, but it apparently possesses the power to transform certain substances—albumen, for example—into fat. An important causative element, therefore, is the quantity of fat present in the food habitually consumed. This has been proved by the investigations of Radziejewsky148 and others, who have shown that the fat in the food is stored up in the normal places of deposit, one of which, of course, is the liver. Another causative element is the formation of fat from the albumen of the hepatic cells in consequence of diminished oxidation. In respect to both causes the consumption of oxygen is an important factor. The insufficient supply of oxygen [p. 1047]which is a necessary result of a sedentary life leads thus, directly, to the accumulation of fat in the liver-cells. A constitutional predisposition is also an important factor. There are those who under certain conditions of daily life store up large supplies of fat, and others who under the same conditions continue lean. Women more than men are subject to such inherited predispositions.
148 Virchow's Archiv für path. Anat., etc., Band lvi. p. 211.
Again, fatty liver occurs in the course of certain cachexiæ, notably phthisis. In this case the obstructive pulmonary lesions interfere with the process of oxidation, and also maintain a constant hyperæmia of the portal system. This condition of the liver also occurs in the cancerous cachexia, in anæmia and chlorosis of long standing, in chronic suppurative diseases, etc. The dyscrasia of chronic alcoholism is a very common cause of fatty liver. At the same time that hyperplasia of the connective tissue is taking place the fat is accumulating in the hepatic cells. So great is the accumulation of fat in the blood that the serum presents a milky appearance. This excess in the quantity of fat is rather due to diminished oxidation, to lessened combustion, than to increased production. Another causative element of the fat-production in cases of alcoholism is the interference of alcohol with the process of digestion and assimilation.
Poisoning by phosphorus, antimony, arsenic, and other metals sets up an acute fatty degeneration of the liver. Pregnancy, lactation, and suppuration also have the same effect, but to a slighter and less permanent extent.
PATHOLOGICAL ANATOMY.—Fatty liver agrees with amyloid liver in that the fatty deposits increase the size and weight of the organ. The surface is smooth, the peritoneal investment unaltered, and the margins rounded. Sometimes the organ is merely increased in thickness, sometimes in diameter. It has a greasy feel and cuts like a mass of fatty tissue. Examined at a low temperature—below freezing—it seems like a mass of suet, the proper structure being almost extinguished in the fatty metamorphosis. The outline of the lobules remains distinct even in cases far advanced in the fatty degeneration, but in the extreme cases it is obliterated, the cut surface presenting a uniformly yellowish or grayish-yellow tint. The fatty liver is also wanting in blood; it is dry, and on section only the largest vessels contain any blood. When cardiac disease of a kind to produce congestion of the venous system exists—for example, mitral or tricuspid lesions—the same relative decrease in the quantity of blood in the liver is observable after death, although during the life of the subject the opposite condition may have been present. The cause of this bloodlessness of the fatty liver is to be sought in the pressure exerted by the growing fat-cells.
Not all cases of fatty liver are advanced to the degree indicated in the above description. From the normal size up to the maximum attained by the most advanced fatty liver there are numerous gradations in the quantity of fat and in the dimensions of the organ. Fatty degeneration may accompany cirrhosis, in which the liver is contracted. The deposits of fat may take place in particular areas. In cases of fatty liver per se the deposit occurs within the liver-cells, as may be demonstrated on microscopic examination, the initial change consisting in the formation of granules in the protoplasm which ultimately coalesce, thus producing [p. 1048] fat-globules or cells. The fatty change in the hepatic cells proceeds in a certain methodical manner from the cells at the periphery of each lobule to the centre. The quantity of fat deposited in the liver in cases of fatty change is very great. In the normal condition of the organ fat exists, according to Perls,149 in the proportion of 3 per cent. of the weight of the liver. When the condition of fatty liver exists the quantity of fat rises to 40, even 45, per cent.—almost one-half. It is important to note, as was pointed out by Frerichs, that in an inverse ratio with the increase of fat was the quantity of water.
149 Virchow's Archiv, supra.
That more or less fatty change in the liver is not incompatible with a normal functional activity is quite certain, but the boundary between health and disease is by no means well defined in respect to the quantity of fatty change in the liver-cells. The liver, within certain limits, is a mere reservoir of the surplus fat of the body, and hence a variable, but not excessive, amount of accumulation of fat is not incompatible with a normal functional performance of the organ. The limits of a merely functional state and of a diseased state are not, therefore, very clearly defined. In certain inferior animals, as Frerichs has shown, a fatty condition of the liver is normal.
SYMPTOMS.—The signs and symptoms of fatty liver are by no means well defined. This state of the organ, as a rule, accompanies the general tendency to fatty metamorphosis and deposit in the body. It is a symptom in the course of phthisis, of chronic alcoholism, and of various forms of metallic poisoning, but under these circumstances there is no material change in the course of the symptoms produced by this complication. As an independent affection it rarely, if ever, exists alone. So far as its symptoms can be defined, they are referable to the organs of digestion and assimilation and to the liver itself.
The appetite is generally good, but distress after eating, acidity and heartburn, eructations of acid liquid and of certain articles of diet, are experienced. The stools are usually rather soft or liquid, wanting in color, whitish or pasty, and occasionally dark, almost black, owing to the presence of blood. Hemorrhoids are usually present. The discharges are often offensive from the decomposition of certain constituents of the food, acid and burning because of the presence of acetic, butyric, and other fat acids, or merely offensive because of the formation of hydrogen compounds with sulphur and phosphorus. Notwithstanding the derangement of the stomachal and intestinal digestion, the deposition of fat continues in an abnormal ratio. With the increase in body-weight a decline in muscular power takes place. The respiration is hurried on the slightest exertion, and dyspnoea is produced by any prolonged muscular effort. The circulation is feeble and the pulse slow in the state of repose, but on active exertion the pulse becomes rapid and at the same time feeble. The sleep is disturbed by horrifying dreams, and only on assuming a nearly sitting posture can the patient sleep with any degree of quietude.
In these cases of fatty liver a very considerable mental inquietude, despondency, even hypochondria and melancholia, result. The relation of insufficient hepatic excretion to the mental state is yet sub judice, but there can be no doubt that some connection exists. From the earliest [p. 1049] period hepatic derangements—as the term hypochondria denotes—have been associated with certain disorders of the mind. This relation certainly holds good in respect to the mental perturbation occurring in cases of fatty liver. With a rotund countenance and a well-nourished body there is associated very considerable mental despondency.
Without distinct jaundice the skin has an earthen or tallow-like hue, the conjunctiva is muddy or distinctly yellow, and now and then well-defined jaundice appears.
The urine is rather scanty, high-colored because of the presence of bile-pigments, and deposits urates abundantly. When jaundice accompanies fatty liver the urine will be very dark, muddy, thick, and will react to the usual tests for bile, urates, etc.
The area of hepatic dulness is, as a rule, enlarged in cases of fatty liver. The deposition of fat in the cells adds to the gross size of the organ, and hence the inferior margin extends below the border of the ribs to a degree determined by the amount of increase in its substance. If the liver can be felt, it is smooth, not hard and resisting, and is free from nodules. Usually, however, owing to deposits of fat in the omentum and in the abdominal walls, the outlines and condition of the liver cannot be ascertained, and must remain merely conjectural. Rather, therefore, by implication than by direct examination can the condition of the liver be ascertained.
COURSE, DURATION, AND TERMINATION.—The course of fatty liver, as an element in a general change not of a toxic character, is essentially of a chronic character. The fatty liver of acute phosphorus, antimonial, and other forms of poisoning is acute and fatal, but it is not these forms with which we are here concerned. Acting the part of a reservoir of the surplus fat stored up in the body, which may be disposed of under normal and physiological conditions, the fatty liver becomes by careful management a normal organ again. The course, duration, and termination will therefore largely depend on the nature of the management pursued. A fatty liver cannot, then, be regarded as fatal, or even as dangerous to life per se. The course and termination will therefore be those of the associated condition.
DIAGNOSIS.—The determination of the existence of fatty liver will not be difficult in all those cases in which this condition may properly be suspected; for example, in phthisis, in chronic alcoholismus, in obesity, and in cases of habitual indulgence in eating and drinking. If in these cases the organ is distinctly enlarged, is smooth, and is flabby in outline; if at the same time the digestion is deranged, the stools are light in color, there are hemorrhoids, flatulence, acid indigestion, and torpid bowels,—a fatty liver may be reasonably suspected. The subjects of fatty liver are usually obese, and present the characteristics typical of that condition, or they are the victims of alcoholismus or present the evidence of habitual indulgence in the pleasures of the table. The differentiation of fatty liver from amyloid degeneration, from cystic disease, and from other maladies causing enlargement of the organ is made by reference to these points in the etiological history—by a careful study of the condition of the organ itself and of the organs associated with it in function. As the amyloid liver is more likely to be confounded with the fatty liver, it should be noted that the former is an outgrowth of the process of suppuration, that the organ [p. 1050]is hard in texture, and that amyloid change occurs at the same time in other organs—conditions opposed to those characteristic of the fatty liver. Cancer of the liver is accompanied by a peculiar cachexia; the body wastes, and the enlarged liver is hard and nodular instead of being smooth and flabby.
TREATMENT.—When fatty liver is a symptom merely, its treatment is merged into that of the primary condition. Thus, in phthisis and in the various forms of metallic and phosphorus-poisoning the condition of the liver is quite secondary. There are cases of obesity, however, in which the fatty change in the liver is a part of the general morbid process, and must be treated accordingly. There are still other cases in which, without a decided tendency to obesity, the food habitually consumed is of a fatty or fat-forming nature. The first requisite in the treatment of fatty liver is to amend the diet. From the time of Hippocrates down to Mr. Banting it has been recognized that the starchy and saccharine constituents of the food, as well as the fatty, contribute to the formation of fat. In arranging a dietary in cases of fatty liver this fact should be regarded. Besides excluding the fats, saccharine and starchy substances should be cut off. The diet should be composed of fresh animal foods, game, fish, oysters, and such succulent vegetables as lettuce, celery, spinach, raw cabbage (cole-slaw), etc. Amongst the articles excluded should be bread, but the greatest difficulty is experienced in its withdrawal, many patients declaring themselves unable to live without it. In such instances a small biscuit (water-cracker) may be allowed, but, as far as may be accomplished, bread should be cut off from the diet.
If there are acidity, heartburn, pyrosis, and regurgitation of acid liquid, much good may be expected from the administration of diluted nitric acid before meals, especially if there be considerable uric acid in the urine. The simultaneous administration of tincture of nux vomica will prove useful if the appetite is poor and the digestion feeble. When the complexion is muddy, the conjunctivæ yellow, and the tongue coated, excellent results are had from the persistent use of phosphate of sodium. Under these circumstances also arsenic is very beneficial. Even better results may be had from a combination of the two agents, a teaspoonful of the pulverized phosphate being given with one-fortieth of a grain of the arseniate of sodium. Alkalies, as lithium citrate, solution of potassa, etc., are unquestionably useful as remedies for obesity and fatty liver, but they must be administered with a proper caution. Also, the permanganate of potassium has seemed to the author to be especially valuable as a remedy for these states.
Remedies to increase the activity of the portal circulation and diminish congestion of the hepatic vessels are useful at the outset, but the anæmia which succeeds renders their use improper at a later period. Amongst the hepatic stimulants of great use in those cases characterized by whitish, pasty stools, yellow conjunctivæ, etc., are resin of podophyllin, euonymin, baptisin, and others having the same powers. Saline laxatives are also useful, but to a less extent. It must be remembered, however, that these subjects are wanting in bodily vigor, often suffer from weak heart, and always have flabby muscles, so that they bear all depleting measures badly. The hepatic stimulant of greatest utility in these cases is sulphate of manganese. The writer has had excellent results from a [p. 1051]combination of quinine and manganese. For the general state, which denotes insufficient oxidation according to the chemical pathologists, permanganate of potassium is a remedy of value, as above mentioned. The best form in which to administer this is the compressed tablet, and the dose usually is two grains. As chalybeate tonics are indicated, the oxidizing power of the succinate of the ferric peroxide, the remedy so warmly advocated by Buckler, may be utilized with advantage. The combination of quinine, iron, and manganese in pill form, or the syrup of the iodides of iron and manganese, or the phosphate of iron, quinine, and strychnine, are tonics adapted to the relief of the depression accompanying this malady.
HISTORY AND DEFINITION.—Although catarrh of the bile-ducts had been incidentally referred to by some previous writers, notably by Stokes of Dublin, Virchow150 was the first to treat of this condition systematically. Amongst recent writers, Harley151 appears to be the only one disposed to question the importance of catarrh of the bile-ducts as a factor in the production of jaundice. Even in phosphorus-poisoning the appearance of jaundice, at one time supposed to be hæmatogenic in source, has been referred to a catarrh of the bile-ducts.152 It seems probable that opinions have too decidedly veered toward the importance of this condition as a factor in the production of jaundice.
150 Archiv für path. Anat., Band xxxii. p. 117 et seq.
151 Diseases of the Liver, supra.
152 Wyss, Archiv der Heilkunde, 1867, p. 469 (Legg).
CAUSES.—Catarrh of the bile-ducts has been referred to all those causes which can excite a catarrhal process in any situation. These are systemic and local. Amongst the systemic may be placed peculiarities of constitution or idiosyncrasy. A tendency to hepatic disorders is a feature in certain types of constitution, and, as such types are transmitted, the hepatic disorders seem to be inherited. In such persons, possessing the so-called bilious nature, catarrh of the biliary passages is not uncommon, and a special susceptibility to it apparently exists. The atmospherical and other causes which in some subjects will set up a catarrh of the bronchi will in the bilious type induce a catarrh of the duodenum and bile-ducts. The malady is not inherited; only the character of bodily structure which favors it under the necessary conditions.
Climatic changes and certain seasons, especially the autumn, are influential causes. Exposure to cold and dampness, the body warm and perspiring, will set up a catarrhal process in the bile-ducts and intestine, especially in those having the special susceptibility which belongs to certain bodily types. Malarial miasm is an especially active cause in malarial regions. The writer has seen many examples in various parts of the United States within the malaria-breeding zone. Other miasmatic agencies are not without importance. The exhalations from the [p. 1052] freshly-upturned soil of some cities, the gases from cesspools and sewers, and illuminating gas exert a causative influence. The bad air thus made up has been happily called civic malaria.
The most influential causes of catarrh of the biliary passages are local in origin and in action: they are the agencies which induce catarrh of the duodenum. Disturbances of the portal circulation should be first named. Whenever obstructive lesions of the cardiac orifices exist, whenever the pulmonary circulation is impeded by disease of the lungs, the portal vein is kept abnormally full, and as a necessary result of the stasis a catarrh of the mucous membrane follows. Congestion of the portal system may be a result of vaso-motor paresis. The abdominal sympathetic may be the seat of various reflex disturbances: those of a depressing kind induce stasis in the portal system. Certain medicinal agents have this effect, and prolonged and severe cutaneous irritation, it is probable, may act on the portal circulation in the same way. The action of cold on the peripheral nerves may be similarly explained.
Catarrh by contiguity of tissue is the most frequent factor. Catarrh of the duodenal mucous membrane is the initial condition, and from thence the process extends to the bile-ducts. Although the duodenum may be alone affected, the usual state of things is a gastro-intestinal catarrh, the stomach and the whole length of the small intestine being simultaneously diseased. When the catarrhal process is thus diffused the duodenal mucous membrane is most deranged, probably because the acid and fermenting chyme is first received here, and what acridity soever it may possess attacks this part in its greatest strength. It must be remembered that the secretion of the duodenal glands and of the pancreas and liver must also have an abnormal character; hence those foods which in the healthy condition of things are digested in this part of the canal undergo ordinary putrefactive decomposition and furnish very irritating products. This observation is especially true of the fats: the fat acids are in the highest degree irritating. The digestive fluid of the duodenum has a more or less pathological character, because the catarrhal process not only interferes with the habitually easy flow of the gland secretions, but, extending to the gland elements themselves, gradually alter their structure.
Gastro-intestinal catarrh results from the misuse of foods and the abuse of certain condiments and of spirits. Excess in the quantity of starchy, saccharine, and fatty foods which undergo conversion and absorption in the intestine, habitually consumed, decomposition of such portions as escape proper digestion ensues, and the products of this decomposition exercise an irritant influence on the mucous membrane. The daily consumption of sauces and condiments and of highly-seasoned foods has a constant irritating action; but more influential than any other causative agency is the abuse of malt liquors and spirit. Whilst the latter acts more on the stomach and the liver proper, the former affect more the duodenal mucous membrane and the bile-ducts.
To these causative agencies must be added a pathological state of the bile itself. Under conditions not now known the bile seems to acquire acrid properties and set up a catarrh in passing along the ducts.
PATHOLOGICAL ANATOMY.—The area affected by the catarrhal process varies greatly. The termination of the common duct for a short space may be the only part affected, but with this there is always more or less, [p. 1053] sometimes most extensive and severe, duodenal catarrh, followed by jaundice. The extent to which the common duct is affected may be exactly indicated by the staining with bile, which extends down to the point of obstruction. The catarrhal process may invade the whole extent of the common duct, the cystic duct, gall-bladder, and the ramifications of the tube throughout the organ. The resulting appearances will vary accordingly.
The first change observable is a more or less considerable hyperæmia of the mucous membrane; but this is rarely seen, because the examination cannot be made at the time when this condition is present. The epithelial layer is swollen, sodden, the cells cloudy, undergoing rapid multiplication and desquamating. The cast-off cylindrical epithelium, mucous cells, and serum make up a turbid mixture, which, with bile, fills the smaller ducts, and may in places, especially at the orifice of the common duct, form an obstruction sufficient to prevent the passage of the bile; which may, however, be readily pressed out with a little force. Especially near the end of the common duct the mucus is apt to accumulate, and a plug of it, often tenacious and somewhat consistent, obstructs the orifice. It is probable that whilst catarrh is the chief cause of jaundice, it may also, by a merely intermittent activity, cause the condition of biliousness—now so far relieved as to permit the bile to descend into the intestine, now so much obstruction as to prevent the escape of any considerable part of that formed. When the common duct is the seat of the catarrhal process, and the outflow of bile thus prevented, it accumulates in the gall-bladder, which may be so far distended as to present a recognizable tumor of pyriform shape through the abdominal parietes.
When the catarrhal process invades the finer ducts the appearances are somewhat different. There are no bile-stains along the course of the common and cystic ducts, and the gall-bladder is empty, or at most contains only some mucus, with altered bile. The tubes at or near their ultimate ramifications contain a turbid mucus composed of cylindrical epithelium and lymphoid cells, and tenacious enough to close them firmly. More or less hyperæmia of the liver-structures proper, and consequent increased dimensions of the organ, a more or less active catarrhal condition of the duodenal mucous membrane, accompany the changes in the finer ducts.
SYMPTOMS.—There are marked differences in the behavior of the more acute cases of catarrh of the bile-ducts and the chronic examples of the same disorder. The former is held to be the most frequent cause of jaundice, whilst the latter is an important element in the so-called bilious state, in lithæmia, and as a secondary condition in some cardiac and pulmonary diseases. Also, the morbid complexus of catarrh of the bile-ducts includes the symptoms of duodenal and gastro-duodenal catarrh.
The acute form of this disease sets in with the symptoms of gastro-duodenal catarrh. Usually, after indulgence in too highly stimulating food or in some article having a specially irritating character, an attack of acute indigestion supervenes. The tongue is more or less heavily coated, the breath heavy, the taste bitter, pasty, or sourish, the appetite poor or actual repugnance to food, especially to the offending articles, is experienced, and nausea, not unfrequently vomiting, ensues. The epigastrium and the hypochondriac regions have a heavy, overloaded, distressed, [p. 1054]and sore feeling; there is some tenderness to pressure; sometimes the gall-bladder, abnormally full, may be detected by careful palpation; and the area of hepatic dulness will usually be increased. The abdomen is more or less distended by gases, and eructations of offensive gases (hydrogen and sulphur compounds, volatile fat acids, etc.) occur. Constipation exists when the catarrhal process is limited to the duodenum, and the stools consist of hard lumps having a light yellow, clay-colored, or whitish appearance. When the whole extent of the small intestine is affected, the stools will be soft, liquid, or watery, and will vary in color from yellow to gray or white. In some cases the fecal matters will have an offensive odor—the odor of decomposition—and considerable discharges of very foul-smelling gas will attend the evacuations. This symptom will occur when the intestinal digestion is suspended and the contents of the bowel in consequence undergo putrefactive decomposition.
During the initial period of the disorder the urine will simply be high-colored and loaded with urates and uric acid, but when jaundice supervenes the pigment will convert the urine into a dark, coffee-colored, and somewhat thick liquid.
With the onset of the malady symptoms referable to the nervous system appear. Headache, dizziness, and hebetude of mind are present, and now and then an attack of catarrh of the bile-ducts will have the objective signs of an ordinary migraine or sick headache. Usually, however, as the intestinal and hepatic troubles develop, headache and some mental hebetude come on, but when jaundice supervenes the headache becomes more severe, and very considerable mental depression, irritability of temper, and moroseness are experienced. Chilly sensations, with flashes of heat, are felt at the outset, but with the appearance of jaundice the sensation of coldness predominates. In some cases, the intestinal catarrh being extensive, there will be, after some preliminary chilliness, a febrile movement, but this is never of a pronounced character, and in the slighter cases of the disease or when the catarrhal process is limited to the bile-ducts, there is no elevation of temperature. With the first symptoms the pulse is somewhat quickened, but as the bile acids accumulate in the blood they effect a decided slowing of the heart's action, the pulse falling as low, it may be, as 50 per minute. This lessened activity of the circulation is accompanied by corresponding reduction of temperature, the body-heat falling a degree or more.
The most distinctive symptom of catarrh of the bile-ducts is jaundice. In the acute or quickly-developing form above described of catarrhal icterus the symptoms of gastro-intestinal disturbance precede the first indication of jaundice from five to eight days. Yellowness of the conjunctiva and of those parts of the body exposed to the air is the first manifestation; afterward the jaundice hue becomes general. The tint varies in depth from a faint gamboge-yellow, only discernible in a favorable light, to a deep greenish- or brownish-yellow.
In the more chronic cases of catarrh of the bile-ducts the symptoms are simply those of a gastro-duodenal catarrh, to which some hepatic disturbances are superadded. Some abdominal uneasiness felt in the epigastrium and in the right hypochondrium, especially in two to three hours after meals; flatulence, sometimes accompanied by colic; [p. 1055] constipation, persistent or alternating with diarrhoea—in the one case in hard lumps with more or less mucus adherent, in the other soft or liquid, and in both cases having a rather golden-yellow color, grayish or black and tar-like appearance,—such are the symptoms referable to the intestinal canal. The disturbances in the hepatic functions produced by the catarrhal swelling of the mucous membrane of the ducts are further exhibited in a somewhat sallow, earthy, or muddy complexion, yellowish tint of the conjunctiva, high-colored, acid urine loaded with urates and phosphates. Such subjects, although having, it may be, a keen appetite, rather lose than gain in weight: they experience lassitude, headache, much depression of spirits, and the mental symptoms are most pronounced during the time intestinal digestion is going on. In fact, the morbid complexus is rather that of intestinal catarrh; nevertheless, the slight degree of obstruction to the outflow of bile occurring in these cases has an influence both in the intestinal digestion and in the nutritive functions. Any degree of obstruction, as has already been pointed out, leads to serious structural change of the liver, and this in turn produces well-defined symptoms.
Disturbances of the hepatic functions, even jaundice, accompany the paroxysms of malarial fever. Without the occurrence of fever, catarrhal jaundice may come on during the course of chronic malarial poisoning. Catarrh of the bile-ducts is the pathogenetic factor in these cases. More especially in malarial regions, but also in temperate and warm climates, paroxysmal attacks, with or without jaundice, are comparatively frequent. These acute seizures occur in those having the chronic form of the malady, and are excited by sudden climatic changes, by excesses in eating, especially by the use of improper articles of diet. Considerable nausea, flatulence, and constipation or diarrhoea, weight, tension, and soreness in the right hypochondrium and sometimes in the shoulder, chilliness, general malaise, headache, and an increasing icterode tint of the skin, constitute the complexus of symptoms belonging to these cases.
COURSE, DURATION, AND TERMINATION.—Acute catarrh of the bile-ducts with jaundice has a well-defined course—in its mildest form, with little gastric or gastro-intestinal disturbance—lasting ten days or two weeks; in the ordinary form, with the accompanying gastro-duodenal catarrh, running its course in a month to six weeks. In the chronic form, with acute exacerbations due to indiscretions in diet or to climatic influences, the course of the disease is chequered by vicissitudes, the result of the causes just mentioned, and its duration must therefore be indefinite and, as a rule, protracted. Catarrh of the bile-ducts, or catarrhal jaundice, usually terminates in health after a period of functional derangement of the intestines and liver. Without exhibiting any features of a special character, some cases do not pass through this benign course: the intestinal catarrh sets up an ulcerative process at one or more points in the duodenum; but more especially the obstruction to the free course of the bile caused by the catarrhal swelling of the mucous lining of the ducts induces structural changes in the liver—an hypertrophy of the connective-tissue elements, a sclerosis.
DIAGNOSIS.—There are but two signs which indicate the nature of the disorder, and only one that is really distinctive. Intestinal indigestion with slight coincident biliary derangement is one, and jaundice is the [p. 1056] other. When, after the signs and symptoms of gastro-duodenal catarrh have declared themselves, jaundice appears, there can be no question as to the nature of the case. The diagnosis is more difficult in the chronic cases with exacerbations due to the exciting causes above mentioned, for the persistence of the jaundice will suggest the occurrence of some permanent organic lesion. The differentiation of the various kinds of jaundice has already been made.
TREATMENT.—Regulation of the diet is of the first importance. Those foods requiring the intestinal juices for their solution and absorption, and which cannot be properly digested when a duodenal catarrh exists or when bile is absent, should of course be excluded from the diet. These articles are the fats, starches, and sweets. The mucus playing the part of a ferment, these substances are converted into various secondary products of an irritating character. Flatulence is caused by the evolution of carbonic acid gas and the hydrogen compounds of sulphur and phosphorus; and acetic, butyric, and other acids not only change the reaction of the intestinal juices, but are directly irritating to the mucous membrane. In the acute cases a diet of skimmed milk, taken hot and at three hours' interval, and after the acute symptoms have subsided, in conjunction with some other aliment, is the most appropriate mode of alimentation. Meats, fish, eggs, and oysters are the chief articles of diet, besides the milk, during the whole course of the more chronic cases; and to these may be added the succulent vegetables, as lettuce, spinach, celery, raw cabbage, and tomatoes. If, in consequence of irritability of the mucous membrane or of idiosyncrasy, any article occasions distress, it should be omitted from the diet.
The medicinal management includes the administration of remedies for gastro-intestinal catarrh. The treatment of catarrhal jaundice has been discussed. When constipation exists, saline laxatives, especially phosphate of sodium and Rochelle salt, are useful. If there be diarrhoea, the most appropriate remedies are bismuth, with or without carbolic acid, Hope's mixture, oxides of zinc and silver, and other mineral tonic astringents.
The propriety of the administration of special hepatic stimulants—cholagogues—has been much disputed. When the disorder consists merely in an obstruction to the outflow of bile, the utility of stimulating the production of this secretion seems more than doubtful. Much harm has been done by the indiscriminate use of mercury. Its power to increase the production of bile having been assumed, and the quantity of bile present in the feces being manifestly less in cases of catarrhal jaundice, it followed that mercury should be employed in this disorder. Modern experience has quite demonstrated its inutility in the mode and for the purpose to which it was formerly devoted. Nevertheless, good effects are had from calomel in small doses as a sedative to the mucous membrane. When there are nausea, headache, vertigo, and constipation present, excellent results may be had from the 1/20 gr. to 1/10 gr. of calomel, exhibited at short intervals until the bowels are moved. If calomel possessed the property formerly ascribed to it, of stimulating the hepatic functions, it would be contraindicated in catarrh of the bile-ducts. This contraindication exists in respect to all hepatic stimulants.
If there be decided irritability of the stomach and constipation, [p. 1057] Seidlitz powders may be given at regular intervals. Phosphate of sodium in drachm doses is highly useful for the double purpose of a laxative effect and to prevent the tendency to inspissation of the bile, which is one of the most important results of catarrh of the bile-ducts and gall-bladder. In the more chronic cases the persistent use of sodium phosphate is to be highly commended.
In this disease, especially as it occurs in gouty subjects, sulphate of manganese is often decidedly serviceable. If anæmia and debility coexist, this remedy can be combined with sulphate of iron and sulphate of quinine—a combination which the writer has found peculiarly effective under such circumstances. When oxidation is deficient and the urates are present in the urine in excessive quantity, good effects are had from the permanganate of potassium, a tablet containing two grains being given four times a day. In the more chronic cases the salts of silver, copper, and zinc are really very useful, especially the oxides of silver and zinc; and of these the former is more efficient. Better than any of those mentioned is arsenic, as arseniate of sodium or as Fowler's solution, but the best results are had from small or medium doses persistently used. If there be much intestinal catarrh and consequent diarrhoea, bismuth and aromatic powder, oxide of silver, Fowler's solution with a little opium, Hope's mixture, etc. are appropriate remedies.
It is in catarrh of the bile-ducts that nitric and nitro-muriatic acids have proved useful, rather than in cirrhosis and other diseases of the liver-tissues. They prevent fermentation, promote oxidation, and increase the activity of the assimilative functions. When there occurs active fermentation of certain foods, and consequently considerable flatulence, excellent results are obtained from the members of the antiseptic group—from creasote or carbolic acid, salicylic acid, biborate of sodium, the benzoates, etc. To these may be added quinine, the dose of which will be determined by the purpose for which it is prescribed. So often is catarrhal jaundice of malarial origin that quinine becomes a remedy of high importance in the cases occurring in the malarial-forming zone.
Certain special plans of treatment have been proposed for the cure of catarrhal jaundice. One of the most effective of these is enemata of cold water. By means of an irrigating apparatus the large intestine is well distended with water once a day for several days. The first enema has a temperature of 60° F., and subsequent injections are a little warmer. The increased peristalsis of the bowels and the reflex contractions of the gall-bladder dislodge the mucus lining and obstructing the gall-ducts. When the bile flows into the intestine, digestion is resumed and the catarrhal inflammation subsides. But with the irrigation method may be employed other remedies, as above indicated.
Faradization of the gall-bladder has been used successfully for the expulsion of the stored-up bile and the removal of the mucus obstructing the ducts. It is applied by means of one moistened sponge electrode placed directly over the gall-bladder, and the other on the opposite side of the body and posteriorly. A slowly-interrupted faradic current is then passed. This expedient is not suitable when the case is acute in character.
DEFINITION.—There are two classes of concretions which may occasion symptoms: inspissated bile and regularly-formed gall-stones. Slowly-developing symptoms of jaundice from obstruction may arise from the deposit of particles of inspissated bile in the hepatic ducts, or sudden attacks of hepatic colic be due to the passage of concretions. When biliary calculi reach the intestines, certain kinds of disturbance may be caused by their presence there. Under the term biliary concretions must be considered, therefore, the mechanism of their production, their composition, the symptoms caused by their passage through the ducts (hepatic colic), and the intestinal disturbance due to their retention in the bowel.
Formation: Inspissated Bile.—Those concretions consisting of inspissated bile are irregularly-shaped masses of a brownish, greenish-brown, or reddish-brown color, friable and crumbling into a gritty dust with slight pressure of the fingers. When recent and before drying, they are softer, almost pultaceous, and may take the form of the canal through which pressed. But as seen after drying they present the appearance of a dark vegetable extract, dried and partly pulverized. When examined as found in the gall-bladder or lodged in the larger hepatic ducts or distributed in irregular fragments (gall-sand) in the various hepatic passages, they present the shape, color, and general characteristics of a partly-dried vegetable extract roughly broken up, but still soft enough to take any shape from pressure. The writer has seen them thus in situ accompanying regularly-formed gall-stones in a case of gunshot wound of the liver. These masses of inspissated bile differ from gall-stones in composition; they consist of bile, but with a preponderance of the coloring matter. According to Harley,153 who has given a more correct account of these bodies than any other systematic writer, their composition is as follows:
| Water | 5.4 |
| Solids | 94.6 |
The contents of the solids are—
| Bile-pigment | 84.2 |
| Cholesterin | 0.6 |
| Salts (iron, potash, soda) | 15.2 |
153 The Diseases of the Liver, with and without Jaundice, etc., by George Harley, M.D., F.R.S., Philada., 1883, p. 349.
Some years ago, before I was aware of the nature of such concretions. I detected a number in examining the stools of a patient who had in quick succession many attacks of hepatic colic, but as the usual form of concretion was looked for and not found, the relation of these bodies to the symptoms in the case was not understood. I now recognize the value of Harley's observations on these bodies.
The biliary concretion which is properly a gall-stone has a definite form and a more or less well-defined crystalline structure. The forms taken are various. The most usual form is octagonal or hexagonal or polyangular, with smooth facets, corresponding to points of contact of other calculi. Instead of smooth facets and sharp angles, the concretion may be studded with irregularly-shaped masses. When there are numerous [p. 1059] calculi present, they have smooth surfaces and rather sharp angles, made, not by attrition, as has been supposed, but by deposition of the new material under pressure. When they have this form there are many present, but the number of facets does not indicate the number of calculi, and the absence of facets is not proof of the absence of other calculi. The smooth opposing surfaces are not always plane, but may be convex or concave to fit the shape of the adjacent bodies.
Calculi may be globular, ovoid, cylindrical, and truncated cones. The largest in my collection is egg-shaped, and nearly filled the gall-bladder which contained it, a little mucus free from bile-elements only being present. If a concretion forms in a duct or a single one is present in the gall-bladder, the shape is determined by the pressure of the walls of the duct or of the gall-bladder, respectively. As found in the stools, and still somewhat soft, the shape will represent the form of the common duct through which it has been pressed. Such a soft, recently-formed gall-stone will have the crystalline structure and chemical constitution of these bodies, and will therefore differ from, apparently, similar masses of inspissated bile. Although a round, ovoid, or cylindrical calculus indicates the absence of others because there are no evidences of mutual pressure and adaptation, a positive conclusion cannot be reached in that way, for the gall-bladder may contain numerous calculi of long-standing, and a recent concretion formed in a duct be discharged with the usual symptoms.
The number of calculi which may be present at any time or be produced in the course of years ranges from one to several thousand. The number is in inverse ratio to the size. One case154 is reported in which 7802 calculi were found in the gall-bladder, but they must have been very minute in size. Of the specimens now in my collection, there are 230 obtained from one gall-bladder, which they entirely filled; they are nearly uniform in size, have an average weight of two grains, and contain four, five, and six smooth facets. Another collection of calculi removed from a closed gall-bladder contains 45, of large size, distending the organ and forming a tumor which projected beyond the margin of the liver. Hepatic calculi are rarely solitary; hence if one attack of hepatic colic occur, others may be expected.
154 Frerichs, op. cit., vol. ii. p. 499.
In color gall-stones vary from a clear white to a dark-brown, almost black, tint. The most usual tint of the mature calculi in the gall-bladder is that of the ripe chestnut. Long stay in the intestines increases the depth of the color, until it becomes almost black; on the other hand, detention in the gall-bladder has a slightly bleaching action; but the real cause of difference of color is the presence or absence of pigment. If composed of pure cholesterin, the color will be whitish, opaque, or glistening and almost translucent.
In size gall-stones vary from the smallest pea up to a hen's egg. When several hundreds are contained in the gall-bladder, they will usually be of the dimension of a medium-sized pea. Two large solitary concretions in my possession are respectively 2 inches and 1½ inches in long diameter, and 1 inch and ¾ of an inch transversely. Very much larger calculi have, however, been recorded; thus, one mentioned by Frerichs is 5 inches in length and 4 inches in circumference. The most frequently [p. 1060] encountered calculus, at least in this country, is polyangular in shape and of the size of a large pea. Globular or ovoid seems to be the prevailing form, and the dimensions that of a small pea, in Germany, according to Frerichs and Von Schüppel, but this statement must refer to the initial shape of these bodies.
Not all hepatic calculi have defined mathematical forms, but may consist of branching cylinders composed of irregular nodular masses, not unlike the concretions of inspissated bile. As a rule, in each case where the calculi are multiple there is uniformity of color, shape, and composition. This feature is well exhibited in my collection. The calculi obtained from each subject are in one case white, polyangular, rather unctuous, and nearly equal in size; in another, chestnut-brown in color, polyangular in shape, and varying slightly in size, but uniformly characteristic in shape; and in a third, singular in number, ovoid in shape, dark-brown in color.
In composition gall-stones vary somewhat. When fresh they contain considerable water, and at all times are hygroscopic. Dried in the air, they are composed of—
| Water | 4 |
| Solids | 96 |
| 100 |
The solids consist of—
| Cholesterin | 98 |
| Pigment | 1 |
| Inorganic or mineral matter | 1 |
| 100 |
Such are the constituents, according to Harley, of the usual concretion, the cholesterin calculus. But as other varieties are encountered occasionally, it may be well to give the composition of these. The following table by Ritter, to be found in Robin's Journal for 1872 (p. 60), is a correct representation of the contents of different specimens:
| Composition of Different Kinds. | 1st. | 2d. | 3d. | 4th. | 5th. | 6th. | 7th. | 8th. |
| Cholesterin | 98.1 | 97.4 | 70.6 | 64.2 | 81.4 | 84.3 | trace. | 0 |
| Organic matter | 1.5 | 2.1 | 22.9 | 27.4 | 15.4 | 12.4 | 75.2 | 18.1 |
| Inorganic matter | 0.4 | 0.5 | 6.5 | 8.4 | 3.2 | 3.3 | 24.8 | 91.9 |
| Number of specimens | 28 | 16 | 580 | 94 | 220 | 16 | 3 | 1 |
The above may be regarded as the average composition, expressed in round numbers. The variations from these figures will be comprehended in two parts.
A calculus consists of three several parts: the nucleus, the body, the rind. A calculus of small or medium size may be a nucleus for the formation of a large one. Usually the nucleus consists of a bit of mucus, casts of the biliary ducts (Thudicum), inspissated bile, a blood-clot, a liver-fluke or other parasite, as a desiccated round-worm, or some foreign body, as a seed, or, as in one reported example, a globule of mercury.155 [p. 1061]The central mass of mucus may contain a large proportion of pigment or crystals of cholesterin or lime-salts, giving it special characteristics.156 There may be several nuclei. Fauconneau-Dufresne reports an instance in which a pyramidal concretion contained four, and Guilbert a globular stone with five, distinct nuclei. Such examples of calculi having multiple nuclei are produced by the adhesion whilst in a soft state of two or more, and the subsequent addition of material to the conjoint mass, welding it into a single stone. A few calculi are homogeneous throughout, composed of nearly pure cholesterin, mixed intimately with a little coloring matter and lime salts. The cholesterin calculus will have a somewhat translucent appearance, will be a dead white or a yellowish-white, or present a greenish- or brownish-yellow tint through the white. Even the white calculus, apparently composed of nearly pure cholesterin, will be found on section to contain traces of a nucleus. By long detention in a gall-bladder whose duct is permanently occluded, and is therefore free of fluid, the mucus nucleus may so shrivel as to leave a cavity which is merely stained. One of my specimens—a solitary calculus of large size—exhibits this peculiarity.
155 Thudicum, J. L., On Gall-stones, London, 1863; also Frerichs, op. cit., vol. ii. p. 503.
156 Cyr, Jules, Traité de l'Affection calculeuse du Foie, Paris, 1884, p. 11 et seq.
The body consists of cholesterin, nacreous or darkened by pigment, deposited in radiating lines or in concentric layers, or in both together. Pigment may be intimately incorporated with the cholesterin or deposited between the layers of this substance, pure or nearly pure, forming an alternating arrangement.
The crust or rind usually is smooth, unctuous to the touch, firm, but when broken with the finger-nail readily crumbles. When composed of lime salts, or when the cholesterin is mixed with varying proportions of these salts and of pigment, the surface is still smooth, but thicker, firmer, and darker in color. The rind may not be smooth, but studded with wart-like projections, or it may consist of several layers of earthy matter separated by pigment. These layers may be very friable, and readily crumble and fall off. In some instances the crust, several lines in thickness, is the body of the calculus, and the cavity contains only a light honeycomb of mucus and pigment.
The specific gravity of gall-stones composed of crystallized cholesterin is nearly that of water. Air-dried calculi will float on water, but the recent ones, full of moisture, sink. The relation of the weight of the calculus to that of the bile is more important. As the specific gravity of bile ranges from 1020 to 1026, it is obvious that on this fluid air-dried calculi will float, but, holding in the recent state much water, ordinary gall-stones will sink. Those containing much mineral matter will have a correspondingly high specific gravity—much higher than bile.
ORIGIN AND FORMATION OF HEPATIC CALCULI.—Certain conditions are necessary to the formation of these bodies on the part of the bile and on the part of the gall-bladder and ducts. Constituted for the most part of cholesterin, which exists in such small quantity in normal bile, there must be some change in the composition of this fluid to increase the quantity or to diminish the solubility of that constituent. It will conduce to a better understanding of the subject to premise the composition of the bile:
[p. 1062]| Bile contains, in 1000 parts, | |
| Water | 860 |
| Solids | 140 |
| The solids of bile are, | |
| Glycocholate and Taurocholate of soda | 90.8 |
| Fat | 9.2 |
| Cholesterin | 2.6 |
| Mucus | 1.4 |
| Pigment and extractive | 28.0 |
| Salts | 8.0 |
| 140.0 |
Normal bile is neutral or slightly alkaline in reaction. If the reaction become acid from any cause, the constituent cholesterin is precipitated; and this occurs the more readily the larger the proportion of this substance held in solution. Cholesterin is an excrementitious material found in the blood and excreted by the liver. It represents in part, probably, the waste of nervous matter, but more certainly of the fatty tissues in general. Conditions of the system in which the metamorphosis of the fatty elements occurs more freely—as obesity, advancing life, etc.—are accompanied by an increased production and excretion of cholesterin.
So long as the neutral state or the alkalinity of the bile is maintained, the cholesterin will be kept in solution, although its relative proportion may be in excess of the normal. A lack of the soda constituent of the system is one factor, but the most important is a catarrhal state of the mucous membrane of the bile-ducts and gall-bladder. The mucus formed plays a double rôle: it furnishes a nucleus about which cholesterin crystallizes; it acts as a ferment and inaugurates a process of acid fermentation which results in the precipitation of cholesterin. When all the conditions favorable to the separation and crystallization of cholesterin are present, any foreign body may serve the purpose of a nucleus. The articles which have thus served have been enumerated.
A by no means infrequent combination is that of bilirubin with calcium; and this may constitute the nucleus or form a part of the body or the crust of a calculus. The mechanism of its formation is not unlike that of the cholesterin concretion. Bilirubin is soluble in alkalies, and is precipitated from its solution by acids. It follows that when acid fermentation takes places under the influence of mucus, bilirubin may be precipitated in combination with calcium. The salts of sodium and potassium are much more abundant in bile than those of lime, but the latter much more often enter into the formation of calculi because of their slighter solubility. Other combinations of bile-pigments, mucus, and the salts of the bile take place, but they are relatively less frequent. The principal lime salt is the carbonate, and this combines in varying proportions with the bile acids, the fat acids, and bile-pigment.
Certain physical conditions are not less important than the chemical in the production of hepatic calculi. Accumulation of bile in the gall-bladder, stasis, and concentration are essential conditions. If bile remains long in the gall-bladder, it becomes darker in color and more viscid, its specific gravity rises, and the relative proportion of solids increases, doubtless because of the absorption of a part of the water. The reaction—which, as has been stated, is in the fresh state neutral or [p. 1063] alkaline—becomes acid in consequence of a fermentative change (Von Gorup-Besanez) set up by the mucus. If a catarrhal state of the mucous membrane exist, the mucus, epithelium, and lymphoid cells cast off play the part of a ferment. The lime which is so important a constituent of biliary concretions is not present even in concentrated bile in sufficient amount to account for its agency in the formation of these bodies, is furnished by the diseased mucous membrane (Frerichs). Indeed, numerous crystals of carbonate of lime have been seen in situ in contact with the mucous membrane in cases of chronic catarrh. It follows, then, that catarrh of the biliary passages has an important causative relation to that pathological condition of the bile which precedes the formation of calculi. In this connection we must not lose sight of the researches made by Ord157 on the action exerted by colloids on the formation of concretions. The mucus is the colloid; cholesterin, lime, and soda salts are the crystalloids. These latter diffusing through the colloid medium, the resulting combinations assume spheroidal forms. The union of bilirubin and lime salts illustrates the same principle.
157 On the Influence of Colloids upon Crystalline Forms and Cohesion, with Observations on the Structure and Mode of Formation of Urinary and other Calculi, by W. Miller Ord, M.D., F.R.C.P. Lond., etc., London, 1879.
CAUSES.—We have here to consider the external conditions and the general somatic influences which lead to the formation of biliary concretions. Age has an important causative action. Besides other agencies due to advancing life, the increase of cholesterin is an influential factor. The less active state of the functions in general, diminished oxidation, loss of water, and concentration of the bile are influential factors in determining the formation of hepatic calculi in advancing life, as the opposite conditions oppose their production in early life. Although not unknown in infancy, at this period in life and until twenty years of age they occur but rarely. Fauconneau-Dufresne,158 of 91 cases, had 4 in infants; Wolff159 had 1 in a collection of 45 cases; and Cyr,160 2 cases under ten in a group of 558 cases. The following table illustrates the influence of age on the productivity of gall-stones:
| AUTHORS. | |||||||||
| HEIN. | FAUCONNEAU-DUFRESNE. | WOLFF. | DURAND-FARDEL. | CYR. | |||||
| Whole No. | 395 | Whole No. | 91 | Whole No. | 45 | Whole No. | 230 | Whole No. | 558 |
| From infancy to 30 | 18 | Before 20 | 10 | Before 20 | 3 | Before 20 | 2 | Before 20 | 20 |
| From 30-70 | 377 | From 20-40 | 13 | From 30-60 | 42 | From 20-30 | 28 | From 21-30 | 208 |
| From 40-90 | 68 | From 30-60 | 162 | From 31-40 | 185 | ||||
| From 60-90 | 38 | From 41-50 | 91 | ||||||
| From 51-60 | 48 | ||||||||
| Above 60 | 6 | ||||||||
158 Traité de l'Affection calculeuse du Foie, Paris, 1851.
159 Virchow's Archiv f. path. Anat., etc., Band xx., 1861, p. 1.
160 Traité de l'Affection calculeuse du Foie, Paris, 1884, p. 53.
Although there is a general correspondence in the results of the observations on the age most liable, there are differences. Thus, Cyr, whose figures represent the experiences at Vichy, makes the age of maximum liability from twenty to forty years—distinctly earlier than any other observer; and hence it is necessary to bear in mind the extreme latitude of his diagnosis. Of my own collection, 30 in number, all doubtful cases [p. 1064] excluded, there were 20 between thirty and fifty years, and 10 between fifty and seventy. Of these, 22 occurred in subjects between forty and sixty. The period of maximum liability is about fifty years of age. Cyr refers the difference of his statistics from those of other observers to the character of the patients. The preponderance in the number of cases of hepatic calculi at or about the fiftieth year is referable to the lessened activity of the nutritive functions at this period, and to the increase in the relative proportion of cholesterin in the blood in advanced life (Luton161). Charcot162 maintains that after sixty biliary calculi are more frequent, but owing to the physiological conditions then existing the migration of these bodies is effected without notable inconvenience.
161 Jaccoud's Dictionnaire encyclopéd., art. "Voies Biliaires;" idem., Bull. gén. de Thérap., March 15, 1866.
162 Leçons sur les Maladies du Foie, etc., p. 145.
According to most authorities, females are more liable to the formation of gall-stones than are men. Thudicum, after an analysis of the statistics given by the most experienced and celebrated authorities, places the proportion at 3 to 2. Von Schüppel gives the same figures. Cyr, whilst recognizing this estimate as true of the great mass of observations on this point, finds that in his own cases the preponderance of females over males was even greater, being 4 to 1—inversely to the liability of the sexes to gout; but this excess is to be explained by the character of the subjects falling under his observation. Women are subjected to influences which favor the formation of these concretions, such as pregnancy, sedentary habits, diet of a restricted character, the use of corsets, and the somatic changes at the climacteric period.
The social state, by reason of the conditions associated with a good position in life, has an influence in the production of calculi. Luxurious habits and indulgence in the pleasures of the table are important factors, and hence this malady is encountered amongst the better class of patients in private practice rather than amongst laboring people in the hospitals.
As the somatic conditions which exert a predisposing action, and the social circumstances also favoring the formation of hepatic calculi, are transmitted, heredity is by some classed among the etiological factors, but it can only be regarded as indirect.
Malarial influences unquestionably exert a very powerful influence as this malady occurs in this country. Paroxysms of intermittent either induce or accompany the seizures of hepatic colic, and chronic malarial poisoning exerts a direct causative influence through the hepatic disturbances and the gastro-duodenal catarrh which are associated with it. Attacks of hepatic colic are extremely frequent in the malarial regions of the West and South. It may be, however, that this malady is frequent rather in consequence of the diet of pork than of climatic causes, for it is probable that indulgence in such food plays an important part in the formation of biliary concretions (Harley). Due allowance made for diet, climate is yet, no doubt, an influential factor. In warm, especially in malarial, regions the functions of the liver are taxed to compensate for the increased action of the skin and lungs; but this organ is, besides, affected by the poison of malaria, and to the congestion caused by it is superadded a catarrhal state of the bile-ducts and of the duodenum. A [p. 1065] pathological condition of the bile itself is first induced; then the fermentative changes set up by the mucus cause the separation and crystallization of pigment and cholesterin.
Certain seasons favor the formation of biliary concretions, because then the special influences which operate at all times are more active and persistent. These seasons are fall, winter, and early spring, and gall-stones are more numerous then in consequence of the activity of the malarial poison, the character of the diet then employed, and the lessened oxidation due to the more sedentary life. Climate is a factor of some consequence, but not in the direction that might have been supposed. Gall-stones are more common in temperate than in tropical climates—a statement confirmed by the observation of the physicians of India. They are, according to Harley, quite common in Russia, where also they attain to extraordinary dimensions; but these circumstances are not due to the climatic peculiarities of that country, so much as to the diet habitually consumed, consisting so largely of fatty substances.
Of all the conditions which favor the production of gall-stones, none are so influential as the bodily state and the associated dietetic peculiarities. Those troubled with these concretions, as they have occurred under my observation, have been either obese or have had a manifest tendency in that direction. They have had a strong inclination for the fat-forming foods, also for starchy, saccharine, and fatty articles, such as bread and butter, potatoes, beans and peas, pork, bacon, and fat poultry, etc. Harley thinks indulgence in bacon (p. 367) is a prime factor. Thudicum rejects this notion on chemical grounds, for obesity and the free consumption of fat cannot be concerned in the production of these bodies, because cholesterin is an alcohol.163 The agency of a fatty diet has been so strongly indicated in clinical observations, and the relation of cholesterin to the fats so obvious, that it can hardly be doubted the free consumption of fat in food contributes directly to the formation of calculi. An indirect relation may also be traced. A catarrhal state of the duodenal mucous membrane existing, and the bile excluded by swelling and obstruction of the bile-ducts, fats are decomposed, and the fat acids, absorbed into the portal blood, contribute to those chemical changes in the bile which result in the precipitation of cholesterin. Beneke164 traces a connection between atheromatous degeneration of the vessels and the formation of biliary concretions. A general increase in the amount of fat in the body is usually coincident with the atheromatous change, and at the same time the relative proportion of cholesterin in the bile becomes greater.
163 A Treatise on Gall-stones, p. 214.
164 Deut. Archiv für klin. Med., Band xviii.
Indulgence in the starchy and saccharine foods plays a part in the formation of gall-stones not less, if not more, important than the consumption of fats. A diet of such materials is highly fattening, and if the necessary local conditions exist they readily undergo fermentation, and thus cause or keep up a catarrh of the mucous membrane.
Too long intervals between meals, Frerichs165 thinks, is more influential than errors of diet in causing concretions. The bile accumulates in the gall-bladder, and the condition of repose favors the occurrence of those changes which induce the separation and crystallization of cholesterin. [p. 1066]Obstacles to outflow of every kind have the same effect. The largest calculus in my possession was obtained from a case of cancer of the gall-bladder which compressed, and finally closed, the cystic duct. Sedentary habits have the same mechanical effect, but, as already pointed out, insufficient air and exercise act by lessening oxidation. Corpulent persons indulging in rich food and avoiding all physical exertion, those of such habits confined to bed by illness or injury, the literary, the well-to-do, self-indulgent, lazy, are usual subjects of this malady. Any condition of things which causes a considerable retardation in the outflow of bile will have a pathogenetic importance, especially if the causes of chemical change, the lessened quantity of taurocholic and glycocholic acid, and an increased quantity of cholesterin, coexist. Moral causes, as fear, anxiety, chagrin, anger, etc., have seemed to exercise a causative influence in some instances (Cyr).
165 A Clinical Treatise on Disease of the Liver, Syd. Soc. ed., vol. ii. p. 511.
To the causes of retardation of the bile-flow mentioned above must be added catarrh of the bile-ducts. This acts in a twofold way—as an obstruction; a plug of mucus forming the nucleus. It has already been shown that fermentative changes may be set up by the mucus, which plays the part of a ferment, an acid state of the bile resulting.
Situation of Gall-stones, and their Destiny.—The gall-bladder is, of course, the chief site for these bodies, but biliary concretions and masses of inspissated bile may be found at any point in the course of the ducts. Single stones may be impacted at any point in the cystic, hepatic, or common duct, or masses composed of numerous small calculi may take the form of a duct and branches, making a branching calculus of the shape and size of the mould in which it is cast. Such casts may be hollow, thus permitting an outlet to the bile, or they may completely close the tube, and a cyst form, the walls of which grow thicker with connective-tissue deposits. Stones of very large size may be thus enclosed, Frerichs having seen one the size of a hen's egg formed about a plum-seed, which was the nucleus. In some rare instances the major part of the larger tubes have been filled with inspissated bile, through which the fluid bile could only be slowly filtered.
Calculi are not often found in the hepatic duct, since they can only lodge there in descending from the smaller tubes, and hence are too small to become wedged in. The usual site, as has been sufficiently explained, is the gall-bladder. At the entrance to the cystic duct and at the terminus of the common duct in the duodenum are the points where migrating calculi are most apt to be arrested.
Spontaneous disintegration of gall-stones sometimes occurs. Cholesterin being dissolved off of the corners and edges, the cohesion of the mass is impaired and it falls apart in several fragments. By very slight mechanical injury air-dried calculi will be broken up. In the gall-bladder two factors are in operation to effect the disintegration of the contained calculi: the movements of the body, by which the corners and the borders are crumbled; the solvent action of the alkaline bile on the cholesterin. When, however, these concretions are made up of lime and pigment, their integrity can be impaired only by the process of cleavage; no solvent action can take place.
Various changes occur in the ducts or in the gall-bladder in consequence of the presence of these concretions. Whilst a catarrhal state of the mucous [p. 1067] membrane of the ducts is an element of much importance in the process by which concretions are formed, on the other hand the presence of these bodies excites catarrh, ulceration, perforation, and, it may be, abscess of the liver. When concretions form or are deposited in the ducts, they cause inflammatory reaction, the walls yield, and the neighboring hepatic structures may also be affected by contiguity. The dilatation of the tube is usually cylindrical, much more rarely sacciform. The neighboring connective tissue may undergo hyperplasia and a more or less extensive sclerosis occur. More frequently the calculus ulcerates through, and an abscess is produced which will take the usual course of that malady. Very rarely a calculus is found enclosed in a separate sac and surrounded by healthy hepatic tissue (Roller).166
166 Berliner klin. Wochensch., No. 42, 1879; ibid., Nos. 16, 17, and 19 for 1877, Fargstein.
As the gall-bladder is the usual place for the formation and storage of gall-stones, the changes in connection with this organ are the most important. The calculi may be so numerous or so large as to distend the gall-bladder and cause it to project from under the inferior border of the liver, so as to be felt by palpation of the abdominal wall. The stones may be few in number and float in healthy bile, or they may fill the bladder to the exclusion of fluid, the cystic duct being closed permanently; or there may be, with one or more concretions, a fluid composed of mucus, muco-pus, serum, and bilious matter. The mucous membrane may be in a normal state, but this is rare; usually it is affected by the catarrhal process, and atrophic degeneration has taken place to a less or greater extent; the rugæ are obliterated, the muscular layer hypertrophied. When attacks of hepatic colic have occurred, more or less inflammation of the peritoneal layer of the gall-bladder and cystic duct is lighted up, and organized exudations form, changing the shape and position of the organs concerned. It is usual in old cases of hepatic colic to find the gall-bladder bound down by strong adhesions, the cavity much contracted or even obliterated, the cystic duct closed, and the neighboring portion of the liver the seat of sclerosis. Such inflammatory exudations about the gall-bladder may become the seat of malignant disease—of scirrhus. Several examples of this have been reported, and one has occurred in my own practice.
The contact of a gall-stone, especially of a polyangular stone, may cause ulceration of the mucous membrane. This is the more apt to occur if the muscular layer of the gall-bladder is hypertrophied, especially if certain fasciculi are thickened and overacting, leaving intervening parts weak and yielding to the pressure of the stone forced in by the spasmodically contracting muscles. Finally yielding, the stone and other contents of the gall-bladder escape into the cavity of the abdomen. Adhesions to neighboring parts may prevent rupture. Such adhesions are contracted with the colon, the duodenum, the stomach, and other organs. In some rare instances the closed gall-bladder has undergone a gradual process of calcification, the mucous membrane losing its proper structure, the muscular layer degenerating, and a slow deposit of lime salts taking place, the ultimate result being that the biliary concretions are enclosed in a permanent shell.
As above indicated, biliary concretions may remain where deposited for an indefinite period. Very often they migrate from the point of formation, the gall-bladder, into the duodenum, producing characteristic [p. 1068] symptoms called hepatic colic. As the size of the ducts increases from above downward, obviously but little vis a tergo is needed to propel the concretions onward. The chief agency in the migration of these bodies is the discharge of bile. Common observation shows that the symptoms of hepatic colic usually declare themselves in two or three hours after a meal—at that time when the presence of the chyme in the duodenum solicits the flow of bile. The gall-bladder contracts on its contents with an energy in direct ratio to the amount of bile present, and with the gush of fluid the concretion is whirled into the duct. Once there, the cystic duct being unprovided with muscular fibres, the onward progress of the stone must depend on the flow of bile; and, as the canal is devious, this may not always carry the concretion into the common duct. Just behind the neck of the gall-bladder the duct makes an angle somewhat abrupt, and here also its folds project into the canal, so that at this point the stone is apt to lodge; but much depends on the size and shape of the calculus. If it pass through the cystic duct, the inflammation resulting may close the canal, several instances of which have fallen under my observation. The next point where stoppage of the migrating calculus may, and frequently does, occur is the orifice of the common duct in the duodenum. This orifice has a funnel shape, the smaller extremity toward the intestine, the object of this being to prevent the entrance into the duct of foreign bodies from the intestine. A diverticulum is thereby made (Vater's) in which a concretion may lodge, partly or wholly preventing the escape of bile into the bowel. The various forces concerned in the propulsion of the concretion onward from the common duct into the intestine are the discharges of bile, the contraction of the few muscular fibres in the walls of the duct, the respiratory movements, especially forced expiration, coughing, sneezing, vomiting, defecation—in fact, all of those acts in which the abdominal muscles, the diaphragm, and the sphincters are simultaneously brought into strong contraction. The symptoms produced by the migration and stoppage of a concretion will vary according to the size and shape of the stone, and the consequent diminution in the amount of bile discharged or its complete arrest. In other words, the stone may be firmly wedged in, completely closing the canal against the passage of bile, or it may lie loosely in the diverticulum Vateri, acting as a sort of ball valve, now permitting a gush of bile, and now stopping the passage-way more or less tightly.
The migration of calculi may take place by ulcerating through into neighboring hollow organs. Usually the first step consists in stoppage of the bile. To the accumulating bile mucus is added, and the gall-bladder or the duct—usually the common or cystic duct—dilates, often to a considerable extent, and, adhesions forming, discharge ultimately takes place through some neighboring hollow organ. The routes pursued by such fistulous communications are various. The organs most frequently penetrated are the stomach, duodenum, and colon, less often the urinary passages, and very rarely the portal vein. Numerous examples of external discharge of calculi have been reported. The most usual, as it is the most direct, is the fistulous connection of the gall-bladder or common duct with the duodenum. Solitary stones of immense size have been thus discharged. Murchison167 gives references to many interesting [p. 1069]examples, and the various volumes of Transactions of the Pathological Society are rich in illustrative cases. The symptoms produced by the migration of calculi by the natural route and by ulceration into other organs will be hereafter considered.
167 Clinical Lectures on the Diseases of the Liver, 2d ed., p. 487 et seq.
SYMPTOMS DUE TO THE PRESENCE OF GALL-STONES AT THEIR ORIGINAL SITE.—Very large calculi or numerous small ones may be present in the biliary passages without causing any recognizable symptoms. The migration of these bodies by the natural channel and by ulceration into the duodenum may also be accomplished without any local or systemic disturbance.168 That the retention of calculi may not induce any characteristic reaction by which they may be recognized is probably due to the fact that the gall-bladder, in which they chiefly form, possesses but slight sensibility, and as it is in a constantly changing state of distension or emptiness according to the amount of bile present, it is obvious that a foreign body made up of the biliary constituents, and having nearly the same specific gravity as the bile, is not likely to cause any uneasiness or recognizable functional disturbances. Furthermore, the slowness with which biliary concretions form enables the organ to accommodate itself to the new conditions. The lack of sensibility which is a feature of the gall-bladder, and which I have had the opportunity to ascertain by actual puncture in an individual not anæsthetized, is in some instances supported by a general state of lowered acuteness of perception. There are great differences in respect to readiness of appreciation and promptness of response to all kinds of excitation in different individuals. To what cause soever we may ascribe the lack of sensibility, the fact remains that in not a few cases of gall-stones in the gall-bladder there are no symptoms to indicate their presence. On the other hand, there are some disturbances that have a certain significance.
168 Amongst the numerous examples of this kind to be found recorded may be mentioned the case reported by M. L. Garnier, Agrégé à la Faculté de Médecine de Nancy (Archives de Physiologie normale et pathologique, No. 6, 1884, p. 176): An hepatic calculus, weighing 24.5 grammes, was discharged without any symptoms or even consciousness on the part of the patient, a man of sixty years. He had had colic and jaundice, but these subsided entirely, and there was no further disturbance. As has happened in so many instances, this stone must have ulcerated through into the bowel without causing any recognizable symptoms.
The subjective signs are uneasiness—a deep-seated sensation of soreness—felt in the right hypochondrium, increased by taking a full inspiration and by decubitus on the left side. Pain or soreness, sometimes an acute pain, is experienced under the scapula near the angle, at or about the acromion process, and sometimes at the nape of the neck. In one case under my observation within the past year a patient who had had several attacks of hepatic colic, the usual polyangular stones having been recovered, had from time to time severe pain over the right side of the neck, shoulder, and scapula, accompanied by a severe herpes zoster in the district affected by the pain. This is of course an extreme example, but it is very suggestive of the relation which may exist between hepatic disturbances and shingles. Attacks of gastric pain coming on some time after food, and not soon after, as is the case in true gastralgia, are usual in the early stage of the disease—are constant, according to Cyr,169 who quotes approvingly an observation of Leared on this point. Migraine [p. 1070] or sick headache and vertigo occur in many cases, but it may well be doubted whether these symptoms are not due to the accompanying gastro-duodenal catarrh, which is a nearly constant symptom. Acidity, flatulence, epigastric oppression, a bitter taste, a muddy rather bilious complexion, and constipation are symptoms belonging to catarrh of the gastro-duodenal mucous membrane. Most of these symptoms are rather indefinite. Some additional information may be supplied by palpation. When the gall-bladder is distended with gall-stones, or is in the enlarged state which occurs when the common duct is obstructed, it may project beneath the inferior border of the liver far enough to be felt. In thin persons a grating sound, produced by the friction of the calculi, may be heard, the stethoscope being applied as palpation is made over the hypochondrium. It is rare that these symptoms can be elicited, since the calculous affection of the liver occurs for the most part in persons of full habit, in whom the abdominal walls are too thick to allow of the necessary manipulation. There may be also some tenderness on pressure along the inferior margin of the ribs, especially in the region of the gall-bladder.
169 Traité de l'Affection calculeuse du Foie, p. 71.
SYMPTOMS DUE TO THE MIGRATION OF GALL-STONES BY THE NATURAL CHANNELS.—A calculus passing into the cystic duct from the gall-bladder causes the disturbance known as hepatic colic or bilious colic, because of the jaundice which accompanies the major part of these seizures. But jaundice is not a necessary element in these cases; it is not until the concretion reaches the common duct that the passage of bile into the intestine is interfered with. The gall-bladder has a function rather conservative than essential, for its duct may be permanently closed without apparently affecting the health.
The time when an attack of hepatic colic is most likely to occur would seem to be determined by the flow of bile; for this, as has been stated, is the chief factor in moving calculi along the ducts. As, no doubt, the presence of the chyme in the duodenum is the stimulus for the production of bile and also for the contractions of the gall-bladder, it follows that a few hours after meals is the time when the attacks of hepatic colic would a priori be expected. This is in accord with experience, but there are exceptions. In one of the most formidable cases with which the writer has had to deal—the diagnosis confirmed by the recovery of the calculi—the most severe attacks occurred in the early morning. According to Harley,170 colic from the passage of inspissated bile occurs when the stomach and duodenum are most nearly empty—from ten at night until ten in the morning—and this he relies on as a means of diagnosis, but the exceptions are too numerous to assign much importance to this circumstance.
170 On Diseases of the Liver, p. 354.
The onset of pain is usually sudden, but it may develop slowly from a vague uneasiness in the region of the gall-bladder; or after some pain and soreness at this point, accompanied by nausea, even vomiting, the paroxysm will begin with very acute pain. The situation of the pain is by no means constant, and usually varies in position in the same case. The point of maximum intensity is near the ensiform cartilage, outward and downward two or three inches, about the point of junction of the cystic and common duct. From or about this region the pain radiates through the epigastrium, the right hypochondrium, upward into the chest, [p. 1071] backward under the scapula, and downward and inward toward the umbilicus. In some instances under my observation the most acute suffering was located in the right iliac region, in others in the lumbar region, and in still others in the epigastrium. The position of the pain may be such as to draw attention from the liver, and thus greatly confuse the diagnosis. In a well-defined attack the pain is intense, shooting, and boring, irregularly paroxysmal; the patient writhes in agony, screams and groans, rolls from side to side, or walks partly bent, holding the part with a gentle pressure or rubbing with an agonized tension of feeling. Meanwhile the countenance is expressive of the intensest suffering, is pallid and drawn, and the body is covered with a cold sweat. Nausea presently supervenes, and with the efforts to vomit a keen thrust of pain and a sense of cramp dart through the epigastrium and side. Very considerable depression of the vital powers occurs; the pulse becomes small, feeble, and slow, or very rapid and feeble. The patient may pass into a condition of collapse, and, indeed, the pain of hepatic colic may cause death by sudden arrest of the heart's action. The cases which prove fatal in this way are doubtless examples of fatty heart, the degeneration of the cardiac muscle being a result of the action of the same factors as those which cause gall-stones to form, if the relation of general steatosis to these bodies which I have set forth prove to be true. The pain is not continuously so violent as above expressed: it remits from time to time, and seems about to cease altogether when a sudden access of anguish is experienced and the former suffering is renewed, and, it may be, more savagely than before. The pain of an attack of hepatic colic has no fixed duration. It will depend on the size of the calculus, on the point where impacted, and on the impressionability of the subject. The severity of the seizures varies within very wide limits. The attack may consist in a transient colic-like pain, in a mere sense of soreness, in epigastric uneasiness with nausea, or it may be an agony sufficient to cause profound depression of the powers of life—to destroy life, indeed. The usual attack of hepatic colic is one in which severe suffering is experienced until relief is obtained by the exhibition of anodynes. Under these circumstances the subsidence of the pain may be rather gradual or it may be sudden: in the former case, as the effects of the anodyne are produced, we may suppose that the spasm subsides and the stone moves onward, at last dropping into the intestine: an enchanting sense of relief is at once experienced. Very serious nervous disturbances may accompany the pain. Paroxysms of hysteria may be excited in the hysterical; convulsions occur in those having the predisposition to them from any cause, and in the epileptic.
The onset of a severe seizure is announced by chilliness, sometimes by a severe chill. Now and then the paroxysms commence with the chill, and the pain follows. It occasionally happens that the attacks in respect to the order in which the symptoms occur, and in their regularity as to time, behave like an ordinary ague. In fact, there appear to be two modes or manifestations of the attacks of hepatic colic in malarious localities: those in which the phenomena are merely an outcome of the passage of the calculi; those in which an attack of intermittent fever is excited by the pain and disturbance of hepatic colic. To the first Charcot171 [p. 1072]has applied the phrase fièvre intermittente hépatique. It is supposed to correspond pathogenetically to urethral fever produced by the passage of a catheter. On the other hand, the second form of intermittent can occur only under the conditions producing ague. A calculus passing in a subject affected with chronic malarial poisoning, the latent malarial influence is aroused into full activity, and the resulting seizure is compounded of the two factors. The truly malarial form of calculus fever differs from the traumatic in its regular periodicity and the methodical sequence of the attacks, which occur in the order of an intermittent quotidian or tertian. During the attacks of hepatic colic, when protracted and severe, a sense of chilliness or distinct chills occur, sometimes with the regularity of an intermittent; but these differ from the seizures which the chill inaugurates at distinct times, the intervening period being free from disturbance.
171 Leçons sur la Maladies du Foie, p. 178.
The fever which accompanies some severe paroxysms of hepatic colic has a distinctly intermittent character, hence the name applied to it by Charcot. There are two forms of this calculus fever as it occurs in malarious localities: one intermittent, coming on during a protracted case, and immediately connected with and dependent on the passage of the stone; the other a regular intermittent quotidian or tertian, which determines and accompanies the paroxysm of colic. A case occurring under my observation very recently, in which these phenomena were exhibited and the calculi recovered, proves the existence of such a form of the malady. In this case with the onset of the pain a severe chill occurred; then the fever rose, followed by the sweat, during which the pain ceased, but much soreness and tenderness about the region of the gall-bladder, and jaundice, followed in the usual way. At the so-called septenary periods also attacks come on in accordance with the usual laws of recurrence of malarial fevers.
Not all cases are accompanied by fever. In many instances, probably a majority, the pulse is not accelerated, rather slowed, and the temperature does not rise above normal. The inflammation which follows an attack of hepatic colic will be accompanied by some elevation of the body-heat, and fever will occur when ulceration of the duct and perforation cause a local peritonitis; but these conditions are quite apart from those which obtain in the migration of calculi by the natural channel.
Nausea and vomiting are invariable symptoms of hepatic colic. First the contents of the stomach are brought up, then some glairy mucus only, with repeated and exhausting straining efforts; and with the sudden cessation of the pain there may appear in the vomit a quantity of bilious matter, the contents of the gall-bladder liberated by the passage of the stone into the intestine. If bile is present in the vomit from the beginning, it may be concluded that the obstruction is not complete.
Constipation is the rule. The abdomen may be distended with gas—is usually, indeed, when constipation exists. Free purgation gives great relief. The stools are composed of scybalæ chiefly at first, afterward of a brownish offensive liquid, and when jaundice supervenes they become whitish in color, pasty, and semi-solid. Now and then it happens that a copious movement of the bowels takes place as the attack is impending, but during the paroxysm no action occurs.
Jaundice is an important, but not an invariable, symptom. It comes on within the first twenty-four hours succeeding the paroxysm, and appears [p. 1073] first in the conjunctiva, thence spreading over the body generally. The intensity of the jaundice depends on the amount of the obstruction: if complete, the body is intensely yellow; and if partial, the tint may be very light. The very slight degree of obstruction which suffices to determine the flow of bile backward has been already stated. There may be no jaundice, although all the other symptoms of the passage of gall-stones may be present. Such is the state of the case when a calculus enters and is arrested in the cystic duct. Under these circumstances the natural history differs from that which obtains when the obstruction is in the common duct and ends abruptly by the discharge of the calculus into the intestine. After the persistence of the symptoms of hepatic colic for a variable period without jaundice, this sign of obstruction may appear, indicating the removal of the stone from the cystic into the common duct. The symptoms accompanying the jaundice—the hebetude of mind, the slow pulse, the itching of the skin, the dark-colored urine—have been sufficiently detailed in the section on that topic in another part of this article.
The duration of the jaundice is different in different cases, and is influenced by the degree and persistence of the obstruction. When the obstruction is partial and the stone is soon removed, the jaundice will be slight and will disappear in a day or two; on the other hand, when the stone completely blocks the passage and is slowly dislodged, the jaundice will be intense and will persist for ten days to two weeks.
After the paroxysm has passed, if severe, the liver will be swollen, more or less tenderness will be developed by pressure, and in some instances, a local peritonitis coming on, there will occur the usual symptoms of that condition.
Although all the symptoms produced by the passage of biliary calculi may be present, some uncertainty will always be felt unless the body causing the disturbance is recovered from the feces. A properly-conducted search is therefore necessary. As this is so often done inefficiently and the calculus not found, an error of diagnosis may seem to have occurred. Every stool should be examined in the mode hereinafter described for a number of days after the attack until the calculus is found. It should be remembered that only air-dried calculi float on water. The stool, as soon as passed, should be slowly stirred up in water sufficient to make a thin mixture, and all solid particles removed for further examination, the thinner portion poured off, and more water added from time to time until only solids remain at last. It should not be forgotten that masses of inspissated bile, biliary sand, may produce symptoms not unlike those due to gall-stones proper, and hence all particles having the appearance of this material should be examined chemically. Place some of the supposed bile on a white plate and pour over it some drops of strong sulphuric acid, when the biliverdin will take on a brilliant scarlet color.
The discharge of particles of inspissated bile causes symptoms not unlike those due to the migration of biliary calculi, but there are points of difference. A strongly-marked case diagnosticated biliary calculi, and in which masses of inspissated bile were discharged in great quantity, will furnish the symptomatology to be now described. The onset of the paroxysms of pain is less abrupt than is the case with gall-stones, and the attacks may occur at any time; the pain also subsides more gradually, and hardly [p. 1074]ceases at any time, but revives every now and then, so that several days, even weeks, may be occupied with one seizure. Jaundice is less apt to follow, and indeed well-defined jaundice rarely occurs in this affection. There is much swelling of the liver, also considerable tenderness, and relief is most certainly afforded by free purgation, anodynes seeming rather to keep up the disturbance, probably by checking the hepatic secretions.
Attacks of hepatic colic may be expected to recur when a calculus with multiple facets migrates, but the time when its associates may be expected to move cannot be predicated on any data now available. Single attacks may happen at intervals of weeks, months, or years. The migration of one large stone may so dilate the ducts as to facilitate the passage of those that remain behind, thus ensuring a recurrence of the seizures at an early period.
IMPACTION OF CALCULI AND MIGRATION BY ARTIFICIAL ROUTES.—The point at which impaction takes place is an element of great importance. The size of the calculus is far from being decisive as to the certainty of impaction or as to the untoward results. A not unfrequent accident is the blocking of the cystic duct at its opening, thus preventing the influx or outgo of bile from the gall-bladder. If the stone does not ulcerate through, in this position it does no damage, for the gall-bladder, as has been stated, may be closed without any apparent detriment. Just at the bend of the cystic duct, near its origin, is the point where arrest of a calculus is most likely to take place. The next most likely point is the duodenal end of the common duct. When impaction occurs a local inflammation comes on, an exudation is poured out, ulceration begins, and presently the peritoneum is reached. Adhesions usually form with the neighboring organs, but now and then perforation takes place, and bile, pus, and the calculus are precipitated into the peritoneal cavity. A fatal peritonitis follows, as a rule; but rarely the inflammation is localized, and an abscess forms which pursues the usual course of such accumulations; or adhesions may take place about the site of the perforation and prevent a general inflammation of the peritoneum. In this way a very large sac may be produced, with the ultimate result of rupture into the general cavity, although a fistulous communication may be established with some neighboring organ, permitting safe discharge in this direction.
A gall-stone impacted in one of the hepatic ducts or in the main duct, ulcerating through, may form an abscess not distinguishable from other solitary hepatic abscesses except by the presence of the concretion causing the mischief and the absence of the usual conditions giving rise to these accumulations of pus. It is probable that fatal abscesses of the liver not infrequently are caused in this way in extra-tropical countries. Adhesions forming to neighboring hollow organs or to the external integument, such abscesses discharge, carrying out the calculus with them. In this way may be explained the discharge by the intestine of calculi much too large to have passed by the natural route and unattended by the usual symptoms of hepatic colic. These gastro-intestinal biliary fistulæ extend from the gall-bladder and the larger ducts to the stomach, to the duodenum, and to the transverse colon; but of these the communication with the stomach is the least common. The adhesion of the gall-bladder or common duct to the duodenum or colon may be direct, exudations uniting [p. 1075] the two parts without the intervention of an abscess cavity, or such a sac or cavity may be interposed. In some cases the discharge of biliary calculi is effected through these routes with so little disturbance as to escape notice, or the symptoms may be only vague indications of a local inflammation in the neighborhood of the liver.
Biliary fistulæ communicating externally, caused by the migration of calculi, are comparatively common. They have the clinical history, and are usually treated as cases, of hepatic abscess. Sometimes hundreds of calculi are thus discharged. In such instances it may be assumed that communication has been established with the gall-bladder. Hepatic abscess thus due to the migration of calculi may discharge into the pelvis of the kidney, into the ascending vena cava, or through the lung, but these places of outlet are comparatively uncommon.
COURSES AND COMPLICATIONS.—Although symptoms cease for the time being when the calculus passes into the duodenum, and although in most instances no after unpleasant effects are experienced, there are cases in which the presence of the concretion in the intestine proves to be fruitful of mischief. Calculi of very large size—from a pigeon's to a hen's egg—are also found in the intestine, without the occurrence of symptoms indicative of their migration. It has been shown that this silent migration of calculi from the liver-passages to the intestinal is not uncommon. Hepatic concretions are distinguishable from the intestinal by their crystalline form and by their composition. The former are usually polyangular, and are composed of cholesterin crystallized about a nucleus of bile-pigment, inspissated bile, or mucus. After entrance into the intestine, lime salts and mucus are deposited in successive layers, so that the form of the calculus is modified and its size increased. The solitary ovoid concretion is most frequently found in the intestine, without previous symptoms of hepatic source, and, although increased in size in the intestine, it retains its original shape. A specimen of this kind now in my possession illustrates these points. It is composed of cholesterin crystallized in radiating lines and concentric rings about a central nucleus of inspissated bile. Around the hepatic concretion there have formed layers of lime and mucus since it has reached the intestine, and after drying this rind became brittle and was readily detached. The polyangular calculus is apt to form the nucleus of a scybala-like mass of feces; hence in the search for these bodies every such mass should be broken up. An example of this has recently come under my own observation. Concretions of all sizes, having reached the intestines, as a rule pass down without creating any commotion, and are silently discharged. But various disturbances occur in some instances. Obstruction of the bowels is one of the results. A great may cases have been collected by Murchison,172 as many more by Leichtenstern,173 of impaction of the intestine produced by an accumulation of feces about a biliary concretion. A calculus may be retained in a fold or diverticulum of the small intestine, and may indeed cause a loop to be formed which in turn readily twists, becoming an immovable obstruction. This mode of obstructing the bowels is less common than the simple impaction. It is affirmed by some authorities, especially by Von Schüppel, that obstruction of the bowels—impaction—is more often caused by stones that have ulcerated through into the [p. 1076] intestines than by those that have descended by the common duct; and this conclusion must be reached if jaundice has not been present. It is not only the size of the calculus which determines impaction, as has been stated: several may be agglutinated in one mass, and reflex spasm of the muscular layer may be induced by their presence in the bowel. Nevertheless, some enormous concretions have been found in the canal, and others have been discharged without special trouble. Hilton Fagge exhibited to the Pathological Society174 of London two gall-stones passed with the stools, measuring 2½ by 11/5 inches in long and short diameter, and Fauconneau-Dufresne175 refers to concretions of the size of a hen's egg. Mention has been made of one in the writer's possession of the size of a pullet's egg, which, until its discharge, caused a train of characteristic symptoms. These immense bodies may have ulcerated through from the gall-bladder or may have grown by successive deposits of carbonate and phosphate of lime after reaching the intestine.
172 Lectures on Diseases of the Liver, p. 573.
173 Ziemssen's Cyclopædia, vol. vii.
174 Transactions of the London Pathological Society, vol. xix. p. 254.
175 Op. cit.
The symptoms caused by the presence of concretions in the intestines are, when pronounced, sufficiently characteristic. At a variable period after an attack or attacks of hepatic colic the disturbance begins. The condition of impaction above referred to does not differ from ordinary fecal accumulation. It is true that occasionally the intestinal irritation due to the presence of these bodies in some instances preceded the symptoms of impaction, but usually there is no evidence to indicate that the stoppage of the bowel is due to anything else than feces. The irritability manifested by the intestinal mucous membrane when gall-stones are present varies remarkably. There may be only some ill-defined pain which, as a rule, indicates the position of the calculus, or it may be pain with a feeling of soreness, or it may take the form of violent colic, with nausea, vomiting, and depression. In my own cases pain was experienced at or near the ileo-cæcal valve, where one was lodged, and along the descending colon, where the others were; the pain and soreness ceased when these bodies were discharged.
In a few instances gall-stones are brought up by vomiting. The most remarkable example of this is a case to be found in the Transactions of the Pathological Society (vol. xii. p. 129): A woman ninety-four years of age vomited a stone the size of a nutmeg. In the reported examples violent pain, nausea, and much vomiting preceded the discharge of the calculus.
Like other foreign bodies, a gall-stone may ulcerate through the intestine, producing fatal peritonitis.
Many conditions due to the presence of biliary concretions, and which arise during their migrations, may be viewed as complications. Many of those produced directly have been described as a part of the proper course of the malady; others are local and reflex, and these may with propriety be considered as complications. First in importance are those due to obstruction and the local inflammation.
The passage of a calculus along the duct excites an inflammation of the mucous membrane, which by contiguity of tissue invades the peritoneal layer if the stone is retained for a sufficient time, and especially if it is immovably lodged. The stoppage in the flow of bile leads to dilatation of the ducts, and a change takes place in the character of that fluid, [p. 1077] owing to the admixture of mucus with the bile and to the pouring out of a pathological secretion: it loses the bilious appearance and becomes a merely sero-purulent fluid. Serious changes ensue in the structure of the liver, as was first suggested by O. Wyss and Leyden, and afterward more especially by Wickham Legg176 and Charcot.177 A ligature to the common duct in animals is followed in so short a time as two weeks by hyperplasia of the connective tissue and atrophy of the gland-elements. It has been ascertained that similar changes ensue in man from the impaction of a calculus in the common duct. Under these circumstances the size of the liver, as indicated by the area of hepatic dulness, at first enlarges, and subsequently more or less contraction, coincident with the atrophy, ensues. When the cystic duct is obstructed the contents of the gall-bladder increase, and become ultimately sero-purulent (dropsy). In some instances, the walls of the abdomen being thin, a globular elastic tumor may be felt projecting from beneath the liver.
176 St. Bartholomew's Hospital Reports for 1873. See also Treatise on Diseases of the Liver, by the same author, loc. cit.
177 Leçons.
Angiocholitis, or inflammation of the duct, is caused by the passage, especially by the impaction, of a calculus. The inflammation may extend by contiguity of tissue and involve the surrounding parts. Several cases have been examined by the writer in which the gall-bladder and the cystic and common duct were imbedded in a mass of organized exudation. An extension of inflammation may take place, and be confined to the hepatic peritoneum. Heavy organized exudations will form, adhesions be contracted to the diaphragm, to the parietal peritoneum, and to the neighboring organs, and the capsule, thickened and contracting, will ultimately induce changes in the structure of the adjacent part of the liver. When the inflammation extends to the peritoneum there are the usual systemic symptoms, and locally acute pain, increased by the respiratory movements and by pressure, and assuming a constrictive character; nausea and frequent vomiting, and often a very troublesome hiccough, caused, doubtless, by implication of some branches of the phrenic nerve; constipation, etc.
The relation of biliary colic to cancer of the biliary passages was first noted by Frerichs, who ascertained the occurrence of gall-stones in 9 out of 11 cases of cancer of these parts. Hilton Fagge178 reports a case of the kind, and the writer can add another from his own observations.
178 Guy's Hosp. Rep., 1875.
The most important of the reflex symptoms are those pertaining to the circulatory system. The action of the heart becomes irregular in rhythm and diminishes in force. The circulation of the bile acids in the blood causes slowing of the heart's action, as has been set forth in the section on jaundice; but that is a direct consequence, and is not a reflex impression. Potain was the first to show that the structure of the heart is affected. A mitral murmur is a recognized symptom in the icterus of gall-stones, but Potain179 has shown that the real seat of this murmur is the tricuspid, and that the affection of the heart is a dilatation of the right cavities. The physiological reason for this condition of the heart is the rise of tension in the pulmonary artery, which is secondary to irritation of the splanchnic nerves; and to this factor is also due the reduplication of the first sound and the accentuation of the second sound—characteristic signs of the cardiac change in these cases.
179 Cyr, Traité de l'Affec. calc. de Foie, loc. cit.
[p. 1078] There are certain reflex nervous troubles in cases of hepatic colic, some of them of great importance. One of the lesser troubles is herpes zoster. A very violent attack in the course of the distribution of the first, second, and third cervical nerves has happened in a case under the writer's observation. There have been reported from time to time cases of sudden death during the paroxysms of hepatic colic, in which a calculus lodged in Vater's diverticulum, at the intestinal extremity of the common duct, was the cause of the accident. An explanation of this result is to be found in the intimate nervous communications between the liver and the heart through the solar plexus and the large number of ganglia contained in Vater's diverticulum. The most severe pain is felt as the calculus is passing through the orifice of the common duct into the intestine, and here also the spasm of the muscular fibre is most tense. The so-called crushing-blow experiment of Goltz illustrates how intense suffering, such as the passage of a gall-stone, can paralyze the heart through the solar plexus. The depression of the heart's action does not always occur on the instant, but it may be gradual—several hours, even a day or two, being occupied in the suspension of activity. Leigh of Liverpool180 has reported an example of death in six hours in a female of thirty, previously in good health; Cornillon,181 another in a female of fifty-three, who died in twelve hours from the beginning of the paroxysm; Williamson,182 a female of fifty-one years, who expired on the fourth day; Habershon,183 two, who died during the paroxysms at a period not stated; and Brouardel, one which was the subject of a medico-legal investigation. In the first case the calculus was yet in the gall-bladder, the appearances indicating that persistent spasms had occurred to force the calculus into the cystic duct; in the others in which the position of the stone is mentioned, it was engaged in the orifice of the common duct or had reached the intestine.
180 Medical Times and Gazette, 1867, vol. i. p. 248.
181 Cyr, op. cit., p. 185.
182 The Lancet (London), vol. ii. p. 780.
183 Lectures on the Pneumogastric, 3d Lecture.
In several instances sudden death has resulted from uncontrollable vomiting induced by the paroxysms of hepatic colic. Trousseau184 mentions a case in which strangulated hernia and death ensued in consequence of the violent vomiting brought on by the passage of a calculus.
184 Clinique médicale.
DIAGNOSIS.—Unless the distension of the gall-bladder is sufficient to cause a recognizable tumor, gall-stones in that organ do not produce symptoms by which they can be diagnosticated. If sudden attacks of violent pain in the right hypochondrium, accompanied by nausea and vomiting and followed by jaundice, have occurred from time to time, then the presence of biliary concretions may be suspected if the symptoms belonging to them are present in the intervals between the seizures. The migrations of calculi produce symptoms so characteristic that error is hardly possible. The only disorders with which an attack of hepatic colic may be confounded are gastralgia and hepatalgia. As regards the first, the distinction is made by the seat of pain, by the absence of after jaundice, and by the lack of a concretion passed by stool. As the diagnosis may depend on the finding a concretion, the writer must again affirm the importance of a properly-conducted search of all the stools passed for several days after the paroxysm.
[p. 1079] Hepatalgia is diagnosticated with great difficulty, for the pain has the same seat, the same character, but as a rule it does not terminate so abruptly, is not accompanied by such severe vomiting and depression, jaundice is absent, and no stone can be found in the evacuations. Both gastralgia and hepatalgia occur in the subjects of neurotic disturbances—in the pale, delicate, and hysterical—whereas, as a rule, hepatic colic happens to the obese, to the persons of active digestion addicted to the pleasures of the table.
The passage of calculi may be confounded with flatulent colic, with the pain caused by lead and other mineral poisons, with impaction, internal strangulation, local peritonitis, and similar causes of sudden and violent pain. The differentiation is made by attention to the seat and character of the pain, by the previous history, and especially by the absence of jaundice and of a concretion. From renal colic the hepatic is separated by the position of the pain, by the direction taken by it, and by the retraction of the testicle, the irritability of the bladder, and the appearance of blood in the urine—all characteristic symptoms of the renal affection.
TREATMENT.—The treatment of biliary concretions includes the remedial management for the calculi in position, for the paroxysms of hepatic colic caused by the migration of these bodies, and for the results and complications.
Treatment of the Calculus State: Of Inspissated Bile.—As the particles of inspissated bile are deposited along the larger hepatic ducts, and form in consequence of a deficiency in the amount of glycocholate and taurocholate of soda, two methods of treatment are to be carried out: free purgation by an active cholagogue to wash out the offending substance, and the exhibition of a soda salt to promote the alkalinity of the bile and the consequent solution of the bile-pigment. Harley's method, which he strongly urges, consists in the administration of "one or two drachms of sulphate of soda in a bitter infusion every morning before breakfast, or from twenty to thirty grains of bicarbonate of soda, along with a drachm of taraxacum-juice in a bitter infusion, every night at bedtime at regulated intervals for a month or so, according to the constitution of the patient and the severity of the symptoms."
As persons who suffer from inspissation of the bile are naturally bilious, it is of the first importance in the prophylactic treatment to regulate the diet. Indulgence in malt liquors, in fatty and saccharine articles of food, must be forbidden. Acid fermentation in the course of duodenal digestion should be prevented by withholding the starches and sugars. Peptonized foods, given with an alkali, are highly useful. Milk, fresh meat, and the succulent vegetables are the proper constituents of a diet for these subjects. Bread is one of the most offending articles, and should be restricted in amount as much as possible.
Next to a suitable diet, systematic exercise is a measure of the highest utility in these cases. A daily morning sponge bath of a weak alkaline water not only maintains the skin in a healthy state, but also promotes the oxidation processes of the body. The alkaline mineral waters of Wisconsin, Michigan, Virginia, and other States, especially of the Bethesda Spring of Wisconsin, may be drunk with great advantage to accomplish the same purpose.
[p. 1080] We possess direct means for preventing inspissation of the bile—remedies which act in the physiological way by increasing the proportion of glycocholate and taurocholate of soda. Harley prefers the sulphate and bicarbonate for this purpose, but my experience is in favor of the cholate and phosphate of sodium, especially the latter; for, whilst it plays the part of a soda salt, it exerts a decided cholagogue action, thus effecting the results achieved by the combined use of sulphate of soda and taraxacum. A cure may be confidently looked for in this malady by the persistent use of sodium phosphate—drachm j ter in die. It seems to act more efficiently when given dissolved in hot water.
The paroxysms of hepatic colic due to the passage of inspissated bile are to be treated in the same way as when this condition of things is caused by the migration of formed calculi. The action of cholagogue purgatives is more decidedly beneficial in the attacks due to the passage of inspissated bile.
Biliary Calculi in Situ.—Notwithstanding their crystalline form and firmness of texture, it is possible to effect the gradual solution of biliary calculi. Outside of the body it is easy to dissolve a calculus in chloroform, in Durande's remedy, etc., if time enough be given, but the problem is a far more difficult one when the calculus is in position in the gall-bladder or in a hepatic duct. As Trousseau185 has wisely observed, it is not safe to apply to conditions within the body conclusions reached by experiments in the laboratory. Nevertheless, facts are known which justify the belief that an impression may be made on concretions in the gall-bladder. The motion of respiration and the voluntary actions of the abdominal muscles cause more or less attrition and breaking off of the angles and margins of the crystals, thus permitting the solvent action of the bile. If, however, the bile continues in the state in which it was at the time of the crystallization of the cholesterin, it will make no impression on this substance. We have now the means of restoring its power to dissolve crystallized cholesterin. As a necessary preliminary, fracture of the crystals must be effected. This may be accomplished, when the natural forces have failed to effect it, by manipulation of the gall-bladder through the walls of the abdomen, but especially by faradization. Excellent results have been achieved by this last-mentioned expedient, but no satisfactory explanation has been made of its methodus medendi, unless we accept the mechanical effect of the muscular movements. In applying the faradic current an electrode is introduced into the rectum, and the other, a sponge well moistened, is placed over the gall-bladder. An interrupted galvanic current is indicated, the electrodes in the position just mentioned, when a migrating calculus is stopped on its way. Such an application has rendered important service in a few cases.
185 Clinique médicale de l'Hôtel Dieu de Paris.
Except that calculi have been found in a state of decay, their angles and edges broken, divided by cleavage, there is no evidence that they have undergone solution when in situ, except the clinical evidence which consists in a disappearance of the symptoms. The remedy of Durande, which consists in a mixture of ether and turpentine—three parts of the former and two of the latter—has been celebrated since the close of the last century, and is yet much employed in France, notably at Vichy. It [p. 1081] is preferred by Cyr,186 who advises its administration in capsules taken immediately before meals. Chloroform readily dissolves calculi out of the body, and hence it has been proposed, and indeed much used, for the purpose of effecting their solution in the gall-bladder; but, as Trousseau urges, there is no warrant for the belief. Corlieu,187 who first proposed its use, and afterward Bouchut,188 maintained that chloroform does exert this solvent action, and reported cases in confirmation; but there are so many sources of fallacy that such evidence must be viewed with suspicion. It has usually been administered in small doses (five minims) three times a day for a long period. That it is beneficial by stimulating the flow of pancreatic secretion and by allaying spasms is probably true, but that any quantity which can be administered in safety will act as a solvent of cholesterin concretions cannot be believed.
186 Traité de l'Affection calculeuse du Foie, p. 287.
187 Gazette des Hôpitaux, 1856, June 19.
188 Bullétin gén. de Thérap., vol. lxi. p. 49.
If solution of hepatic calculi is possible under any circumstances, the most rational mode of effecting it would seem to be to restore that condition of the bile which in the normal state maintains cholesterin in the state of solution. Cholesterin is precipitated and crystallizes about a nucleus when the glycocholate and taurocholate of soda are deficient in amount. The agents most effective in restoring the solvent power of the bile are the salts of soda, of which the sulphate is preferred by Harley. In 1873 the cholate of soda was brought forward by Schiff, who prescribed it in doses of 50 centigrammes (8 grains nearly) three times a day, to be gradually increased until digestive or circulatory troubles arose. This remedy, which is eminently rational from the point of view above indicated, has apparently been of decided service in many published cases and in the writer's experience. It will be found, however, that five grains three times a day is as large a quantity as can be easily borne.
Another soda salt which in my own hands has proved in a high degree effective is the phosphate. As has been explained when referring to its use in cases of disorders due to inspissated bile, it has a distinct cholagogue action, but the chief sources of its utility in this affection are its chemical and resolvent powers. The usual quantity is one drachm three times a day, dissolved in sufficient warm water.
Bile itself, in the form of inspissated ox-gall, was formerly much used, a scruple to a drachm being given three times a day, and not without good results. It was also prescribed with chloride of ammonium. For the gastro-duodenal catarrh and the accompanying catarrh of the bile-ducts this combination is sometimes useful.
I have recently proposed a new expedient for effecting the solution of hepatic calculi. This method consists in puncture of the gall-bladder with a fine exploring-trocar, and the injection through the canula, after withdrawing the stylet, of a suitable solvent. Durande's remedy, chloroform, and other solvents can be introduced in this way without injury to the parts. I have punctured the gall-bladder, removed its contents, and explored its interior without damaging the organ in any way and without leaving after traces. The measure proposed offers no special difficulties in its execution.
The Paroxysms of Hepatic Colic.—The pain of hepatic colic being [p. 1082] the most acute suffering known to man—in its severest form at least—the most powerful anodynes are required. The measures employed for relief of pain happen to be the most efficient for promoting the expulsion of the calculus and for limiting, if not preventing, the subsequent inflammation. As soon as the character of the seizure is manifest a hypodermatic injection of morphine and atropine—1/8 to ½ grain of the former and 1/200 to 1/80 grain of the latter—should be given; ether administered by inhalation if necessary; and by the stomach chloroform, chlorodyne, or chloral. As the stomach is usually exceedingly irritable, the subcutaneous injection of remedies is a precious resource: this failing or contraindicated, relief may be given by the rectal injection of laudanum or chlorodyne. As relief is often afforded by the act of vomiting, the attempts to empty the stomach should be encouraged, and to this end large draughts of warm water should be given. Hot fomentations and mustard plaster should be applied over the right hypochondrium, and an entire warm bath may be used if available.
Great relief is usually afforded by the action of purgatives. The irritability of the stomach forbids the employment of drastic purgatives, yet podophyllin resin is warmly commended by Dobell. It must be given in small doses, and preferably dissolved in spirit. Calomel in one-grain doses, every four hours until it purges, allays nausea and lessens the after-uneasiness in the right hypochondrium, but mercurial treatment given with a view to a supposed cholagogue effect only does evil by prolonged administration, especially if ptyalism is induced. If evidences of portal congestion are present, such remedies as euonymin, iridin, baptisin, and others of the cholagogue group give good results. The most effective of the remedies of this kind is ipecacuanha, given in purgative doses: the emesis induced by it favors the extrusion of the stone, and the powerful cholagogue effect relieves the portal congestion. Twenty grains at once, and repeated if need be in three hours, is a suitable quantity.
The various complications which may occur, and the results which follow the migration of the calculus, require treatment adapted to the conditions existing, and will be mentioned in the sections devoted to these topics.
DEFINITION.—By occlusion of the biliary passages is meant an obstruction, internal or external, of the hepatic, cystic, or common duct. The causes of the obstruction are various, but the results are quite uniform; hence the term includes a complexus of symptoms of a very distinctive type. Occlusion may be congenital or acquired: it is the latter with which we have especially to deal.
Stenosis signifies a narrowing which in its extremest form produces a nearly complete obstruction; when the canal is entirely closed the term occlusion is applied. Stenosis also may be congenital or acquired.
PATHOGENY.—The conditions producing narrowing of a hepatic duct or its complete obstruction are numerous, and some of them complex in their relations. As regards the ducts themselves, the interference may [p. 1083] be entirely within the canal, or it may affect the walls, or it may be wholly extraneous; as, for example, when a cancer of the pancreas encroaches on the common duct. It will be convenient to consider the causes of stenosis and obstruction from these points of view: 1, internal; 2, of the duct walls; 3, extraneous.
The most usual situations for the occurrence of those changes that lead to occlusion by inflammatory adhesions are the beginning of the cystic duct, obstruction of which is of little moment, and the end of the common duct, which finally proves fatal.
The passage of a large polyangular calculus may cause such irritation, abrasion of the epithelium, and subsequent inflammatory exudation as to effect a direct union of the opposing sides of the canal. This takes place at the beginning of the cystic duct especially, since, owing to the spasm of the gall-bladder and the absence of muscular fibres in the walls of the duct, the stone crushes into, without passing through, the canal. The inflammatory exudation thus excited may close the duct. Not unfrequently the gall-bladder, full of calculi, is thus shut off from the liver permanently. In one instance the writer has seen a calculus wedged into the orifice of the cystic duct, whilst just beyond the lumen was permanently obstructed by an organized exudation. Permanent closure of the cystic duct is of far less consequence than of the common duct, and may, indeed, be a conservative condition, as in the case above mentioned, where numerous polyangular calculi may have migrated, except the closure of the passage.
The most usual point of obstruction in the course of the common duct is the intestinal end, but various processes are employed to effect it. The first in importance is catarrhal inflammation. This seems the more credible when it is remembered that to a simple catarrh of the mucous membrane is due the temporary stoppage of the duct, producing jaundice in much the largest proportion of cases. When the epithelium is detached and granulations spring up from the basement membrane, adhesions of the surfaces will readily take place, and the union may be so complete as that all traces of the duct will disappear. It is probable that in many, if not in most, of these cases the initial condition of the canal is that of simple catarrh, the more positive changes in the mucous membrane arising from peculiarities in the tissues of the individual affected, or from local injury caused by the passage of a concretion or irritation of pathological secretions of the duodenum.
Stenosis, and finally occlusion, of the common duct may arise from the cicatrization of an ulcer. Such ulcers may occur in several modes. They may result from catarrhal inflammation of a chronic type, much new connective-tissue material forming, and in the process of cicatrization, with the contraction belonging to it, the lumen of the canal is so far filled up that the passage of bile is effectually prevented. They may be produced in that state of the tissues which accompanies certain cachectic and profoundly adynamic conditions, as in severe typhoid fever. Such ulcers may also be due to the mechanical injury effected by the migration of a gall-stone. In cicatrizing, a tight stricture, impermeable to the passage of bile, may result, or the lumen of the canal be entirely obliterated. In the latter case the duct itself may disappear and leave no trace. An ulcer situated at the duodenal end of the common duct and extending into the [p. 1084]duodenum may also in the process of healing so contract as to render the orifice impermeable to bile. The same effect may follow the cicatrization of an ulcer of the duodenum in the immediate vicinity of the orifice of the common duct.
Without the intervention of an ulcer as a means of explaining closure of the common duct, this accident may be caused by a catarrhal inflammation which effects denudation of the basement membrane, and thence union may be produced by the mere contact of the freshly-granulating surfaces. Congenital occlusion of the bile-ducts or obstruction occurring in a few days after birth, it is probable, is effected in this way, but no direct evidence of the process has thus far been offered. During intra-uterine life, as at any period in after-life, it seems necessary to the production of such changes that a peculiar constitutional state must exist; otherwise, such a result might happen to every case of catarrhal inflammation of the bile-ducts. The extent of the changes is further evidence in the same direction; for not only are the walls of the duct in permanent apposition and adhesion, but the duct degenerates into a mere fibrous cord, and in some instances is nearly, even entirely, obliterated.189
189 Ziemssen's Cyclopædia, p. 589.
The cystic or common duct—the latter to be chiefly considered—may be occluded by the retention in its lumen of some foreign body. The impaction of a biliary calculus has already been repeatedly referred to, but there are some additional points demanding consideration. The larger concretions may be stopped in the neck of the gall-bladder; those small enough to enter the canal may be arrested at its bend behind the neck, and the very entrance of the cystic duct may be blocked, as in a case examined by the writer.
The hepatic duct is very rarely permanently occluded. As the calibre of this canal continuously enlarges downward, there is no point at which a stone is likely to be arrested; nevertheless, it occasionally happens that such an obstruction does occur. An example has occurred under the observation of the writer, but the cause was a gunshot wound of the liver.
The most usual, and for very obvious reasons the most important, of the sites where occlusion occurs is the common duct and at the termination of the duct in the small intestine, the intestinal orifice. Just behind and to the right of its orifice the duct is dilated into a fossa—the diverticulum Vateri; and here concretions of a size to pass along the common duct are stopped. It is not essential that the stone fit the canal: it may do so and prevent any bile passing into the duodenum; it may be a polyangular body, and, though wedged in, leave spaces through which more or less can slowly trickle. The symptoms will be modified accordingly. Again, the diverticulum may contain numerous concretions, which distend the canal greatly, but through the interstices of which some bile can flow.
Other foreign bodies very rarely close the intestinal end of the ductus communis; thus, for example, a cherry-seed, a plum-seed, a mass of raisin-seeds, may slip into the orifice after the passage of a gall-stone has stretched it sufficiently. A much more common cause of occlusion is an intestinal parasite, which crawls in and is fastened. The common round-worm is the most frequent offender, and much less often liver-flukes find a lodgment there.
[p. 1085] The ductus communis choledochus may be closed by agencies acting from without. They are various, but the most common are the carcinomata. Primary cancer of the gall-bladder and gall-ducts, although not of frequent occurrence, is by no means rare. It develops in connection with the connective-tissue new formations produced by the inflammation following the migration of large calculi. A very instructive example has been examined by the writer. The patient, a woman aged forty-eight, had had numerous paroxysms of hepatic colic, and after death, which followed a protracted stage of jaundice by obstruction, a large ovoid calculus, filling the gall-bladder, was found, and an extensive organized exudation of inflammatory origin was the seat of carcinomatous disease involving the cystic and common ducts and closing the lumen of both. Cancer of the pylorus, of the duodenum, of the pancreas, of the right kidney, and of the liver itself, not unfrequently by exterior pressure permanently occlude the common duct. To this category of obstructing causes must be added enlarged lymphatic glands of the transverse fissure, large fecal accumulations, tumors of the ovaries and uterus, aneurisms of the abdominal aorta, and especially aneurism of the hepatic artery, several examples of which have been reported, and one has occurred in a case seen by the writer.
The effects of obstruction are much less important when the cystic duct is closed. The contents of the gall-bladder accumulate, constituting the condition known as dropsy of the gall-bladder. A catarrhal state of the mucous membrane is set up; the muco-pus formed mixes with the bile, and the mixture undergoes fermentative changes which further alter its character and impart to it irritating qualities, in consequence of which the mucous membrane becomes more decidedly inflamed, and a still more purulent fluid forms, so that ultimately the contents of the gall-bladder are entirely purulent, and that organ may attain to enormous size. Instead of a catarrhal inflammation leading to suppuration, the mucous membrane may pour out serum abundantly, the biliary contents and mucus disappear by absorption, and finally the gall-bladder will be moderately distended by a serous-like fluid. No further disturbance ensues, and the gall-bladder, thus shut off from participation in the hepatic functions, ceases to give trouble.
The results are far different when the obstruction occurs in the hepatic or common duct, for then the bile can no longer perform its double function of secretion and excretion—of contributing materials necessary to digestion and assimilation, and excreting substances whose removal is necessary to health. The liver continuing to functionate after closure of the duct is effected, obviously the secretion of bile continues to accumulate, and the irritation of the mucous membrane causes a catarrhal state; mucus is poured out, and serum escapes from the distended vessels. If the hepatic duct only is obstructed, the dilatation will not involve the cystic duct and gall-bladder, but as the common duct at its termination is occluded, usually the whole system of tubes will be affected by the ensuing changes. The alterations already described as occurring in the gall-bladder take place in all the hepatic ducts. The bile-elements are absorbed, and the fluid distending the whole system of hepatic tubes becomes finally a semi-transparent serum or a very thin sero-mucus, having in bulk a pale sea-green color. Although an intense jaundice [p. 1086] coexists with the obstruction, no portion of the bile escapes into the ducts. At the beginning of the obstruction more or less bile is in the tubes, and then the fluid will have a distinct biliary character; but as it accumulates, first the bile-constituents disappear, then the mucus—which at the outset was formed freely—is absorbed, and at last only a colorless serum remains. This fluid, which has been examined chemically by Frerichs, is found to be slightly alkaline, to have only 2 per cent. of solids, and to present no trace of any biliary constituent. As the fluid accumulates the gall-bladder and ducts dilate, sometimes to an enormous extent, the fluid they contain amounting to several pints. The walls of the ducts grow thinner, and may finally give way with the pressure or from external violence, the fluid exciting an intense and quickly-fatal peritonitis. Important changes occur in the structure of the liver also. With the first retention of bile the liver conspicuously enlarges, and may indeed attain to twice its normal size, but it subsequently contracts, and may lessen in as great a degree as it had enlarged. Changes begin in the glandular structure as pressure is brought to bear on the cells by the enlarging ducts. The liver-cells become anæmic and the protoplasm cloudy, but granular and fatty degeneration does not take place. Even more important as an agency affecting the condition of the hepatic cells is the hyperplasia of the connective tissue, which ensues very promptly when an obstruction to the flow of bile arises from any cause, as has been shown by Legg190 and Charcot.191 The liver on section has a rather dark olive-green color, and is firmer in texture, owing to the increased development of the connective tissue; the cells are bile-stained and contain granules of coloring matter and crystals of bilirubin, and although they are at first not altered in outline, subsequently more or less atrophy is produced by the contraction of the newly-formed connective tissue and the pressure made by the dilated hepatic ducts.
190 On the Bile, Jaundice, and Bilious Diseases, p. 352 et seq.
191 Leçons sur les Maladies du Foie, etc., p. 205 et seq.
SYMPTOMS.—The symptoms produced by occlusion of the cystic duct are not sufficiently characteristic to be diagnosticated with any certainty. When an attack of hepatic colic has slowly subsided without jaundice, and an elastic tumor, globular or pyriform in shape, has appeared from under the inferior margin of the liver in the position of the gall-bladder, dropsy of that organ may then be suspected. As paracentesis of the gall-bladder may be performed with ease, safety, and little pain, the diagnosis may be rendered more certain by the use of the exploring-trocar.
Obstruction of the hepatic or common duct is accompanied by symptoms of a very pronounced and distinctly diagnostic character. Without referring now to the antecedent symptoms or to those belonging to the obstructing cause, the complexus of disturbances following the obstruction is the subject to which our attention must be directed. The great fact dominating all other considerations is the stoppage of the bile, whether this has occurred suddenly or slowly. Jaundice begins in a few hours after the canal is blocked. At first there is yellowness of the conjunctiva, then diffused jaundice, deepening into the intensest color in two or three weeks, or, when the obstruction is sudden and complete, in a few hours. At first the color is the vivid jaundice tint, a citron or salmon or yellow-saffron hue, but this gradually loses its bright appearance, grows darker, and passes successively into a brownish, bronze-like, and ultimately a [p. 1087] dark olive-green, which becomes the permanent color. Under some moral emotional influences there may be a sudden change to a brighter tint, lasting a few minutes, but otherwise the general dark olive-green hue persists throughout. In a few instances, after some weeks of jaundice, the abnormal coloration entirely disappears, signifying that the liver is too much damaged in its proper glandular structure to be in a condition to produce bile. Such a cessation of the jaundice is therefore of evil omen.
Pruritus, sometimes of a very intense character, accompanies the jaundice, in most cases appears with it, and in the supposed curable cases it has persisted after the cessation of the discoloration. The irritation may become intolerable, destroying all comfort, rendering sleep impossible, and so aggravating as to induce a highly nervous, hysterical state. The scratching sets up an inflammation of the skin, and presently a troublesome eczema is superadded. In some of the cases a peculiar eruption occurs on the skin and mucous membranes, entitled by Wilson192 xanthelasma. It has been carefully studied by Wickham Legg,193 who has ascertained the character of the changes occurring in the affected tissues, and also by Mr. Hutchinson.194 As a rule, this eruption appears after several months of jaundice, and manifests itself first on the eyelids, then on the palms of the hands, where it makes the most characteristic exhibit, and after a time on the lips and tongue. It occurs in irregular plaques of a yellowish tint slightly elevated above the general surface, and rarely assumes a tubercular form. As was shown by Hilton Fagge, xanthelasma occurs more especially in the milder cases of catarrhal icterus that had been protracted in duration, but it is also occasionally seen in the jaundice of obstruction.
192 Diseases of the Skin, 6th ed., Lond., p. 773.
193 On the Bile, Jaundice, and Bilious Diseases, p. 317 et seq.
194 Medico-Chirurgical Transactions, vol. liv. p. 171.
According to the stage of the disease during which the examination is made the liver will be enlarged or contracted; more or less tenderness may be developed by pressure in the area occupied by the ducts, and a tumor in a position to effect compression may possibly be detected. The area of hepatic dulness will be increased in the beginning of all the cases in which the obstruction is complete, but will remain normal so long as the flow of bile persists despite the obstruction. When enlarged, the liver can be felt projecting below the inferior margin of the ribs, and with it, in most cases, the elastic globular body, the gall-bladder. The state of the hepatic secretion, and in consequence the duration of the obstruction, may be ascertained by puncture of the gall-bladder and withdrawal of some of its contents for examination. The presence of unaltered bile will indicate recent obstruction; of serum, will prove long-standing interruption of bile-production. The presence of concretions in the gall-bladder will indicate the character of the obstructing cause, and an increased amount of bile of a normal or nearly normal kind will be conclusive evidence that the obstruction is in the course of the common duct. In a fatal case of permanent occlusion examined by myself the cystic duct was closed by inflammatory adhesions and the common duct was stopped up by a calculus.
The enlarged area of hepatic dulness will, in a protracted case, not continue. The proper secreting structure, the hepatic cells, undergo atrophy, [p. 1088] and the increased connective tissue—to the development of which enlargement of the organ is mainly due—contracts. The ultimate result is that the liver becomes sclerosed, and is distinctly smaller, the area of hepatic dulness diminishing to a greater relative extent than the area of dulness due to hypertrophic enlargement. The contraction of the liver goes on at the rate that several months are required to make the result evident on percussion and palpation. Not unfrequently, the contraction is too slight to affect the percussion note of the right hypochondrium, and then, to realize the condition of the organ, the history and rational signs must be closely studied.
Whilst the liver thus varies in size, the gall-bladder remains enlarged and projects from the under surface of the organ, elastic, globular, and distinctive. The shrinking of the liver from around it makes the impression of growing size; it may be increasing, indeed, but more frequently the enlargement is merely apparent.
Whether the liver be enlarging or diminishing in size, its functions are impaired, or indeed entirely suspended. As the digestive canal receives the bile immediately on its production, it will be best to begin with the gastro-intestinal disorders which accompany occlusion of the bile-ducts. The appetite is either wanting entirely and food is loathed, or an excessive or canine appetite is experienced. The latter belongs rather to an early stage of the disorder, and comes on after the first disturbance of the stomach belonging to the immediate effects of the occlusion. The former is the result of long-standing interference with the primary assimilation. The tongue is coated with a thick yellowish fur, which, drying, is detached in flakes, leaving the mucous membrane beneath red, raw, fissured, and easily bleeding. The taste is bitter, and the mouth has a pasty, greasy, and unclean feeling. There is much thirst, and as a rule the patient experiences a keen desire for acid drinks and for fresh fruits. The stomach is rather intolerant of food, and nausea comes on as soon as it enters the stomach. The mucus and stomach-juice accumulating over night, in the morning there is much retching and nausea until the acid and rather foul contents of the organ come up. When food is retained it causes much distress, gases of decomposition accumulate, distending the stomach and giving prominence to the epigastrium, and eructations of offensive gas, with some acid liquid, occur from time to time. Similarly, in the intestines the foods undergo decomposition instead of normal digestion; gases of putrefaction are evolved, the abdomen generally is swollen, and flatulent colic results. Very irritating fat acids are liberated by the decomposition of the fatty constituents of the food, which, with the acid products of the fermentation occurring in the starch and sugar of the diet, cause a sensation of heat and distress through the abdomen. Usually, the bowels are torpid, but in some cases the stools are relaxed, having the consistence and presenting somewhat the appearance of oatmeal porridge. They may be firm, moulded, even hard. The gas discharged and the stools are offensive, with a carrion-like odor. Sometimes decomposing articles of food can be detected in the stools by very casual inspection—always, indeed, when the examination is intimate. An excess of fat is also a characteristic of the condition induced by occlusion of the ducts, especially when the pancreatic duct is closed, as does happen in cancer of the head of the pancreas.
[p. 1089] A significant change in the color of the stools takes place. They lose their normal brownish-red tint and become yellowish or clay-colored or white, pasty, or grayish. Sometimes the stools are very dark, tar-like in color and consistence, or more thin like prune-juice, or in black scybalæ. The most usual appearance of the stools in occlusion is grayish, mush-like, and coarsely granular. The very dark hue assumed at times or in some cases signifies the presence of blood. A dark tint of the evacuations may be caused by articles of food, as a greenish hue may be due to the use of spinach; a clay-colored tint to the almost exclusive use of milk; a grayish tint to the action of bismuth; a bilious appearance to the action of rhubarb; and many others. When the occlusion is partial, although it be permanent, sufficient bile may descend into the duodenum to color the stools to the normal tint, and yet all the other signs of obstruction be present.
The bile-pigment, not having an outlet by the natural route, by the intestine, passes into the blood; all the tissues of the body and the various secretions and excretions, notably the urine, are stained by it, constituting the appearance known as jaundice or icterus. This malady has been described (see anté), but it is necessary now to give a more specialized account of those conditions due more especially to the prolonged obstruction of the biliary flow. These are a morbid state of the blood; changes in the kidneys and in the composition of the urine; a peculiar form of fever known as hepatic intermittent fever; and a group of nervous symptoms to which has been applied the term cholæmia.
It has already been shown that but little pressure is required to divert the flow of bile from the ducts backward into the blood. Changes consequently ensue in the constitution of the blood and in the action of the heart and of the vessels. The bile acids lower the heart's movements and lessen the arterial tension; hence the pulse is slower, softer, and feebler than the normal. Should fever arise, this depressing action of the bile acids is maintained; and hence, although the temperature becomes elevated, the pulse-rate does not increase correspondingly. There are exceptions to this, however, in so far that the heart and arteries are in some instances little affected, but it is probable under these circumstances that there are conditions present which induce decomposition of the bile acids.
The most important result of the action of the bile on the constitution of the blood is the hemorrhagic diathesis. Soon after the occlusion occurs in very young subjects—at a later period in adults—the occlusion having existed for many months, in some cases only near the end, the disposition to hemorrhagic extravasations and to hemorrhages manifests itself. From the surface of the mucous membranes, under the serous, in the substance of muscles, the hemorrhages occur. Epistaxis, or nasal hemorrhage, is usually the first to appear, and may be the most difficult to arrest. The gums transude blood, and wherever pressure is brought to bear on the integument ecchymoses follow. The conjunctiva may be disfigured and the eyelids swollen and blackened by extravasations, and the skin of the cheeks and nose marked by stigmata. Hæmatemesis sometimes occurs, but the extravasations into the intestinal canal more frequently—indeed, very constantly—take place in a gradual manner, and impart to the stools a dark, almost black, tar-like appearance. In the same way the urine may contain fluid blood and coagula, or it may have a merely smoky [p. 1090] appearance from intimate admixture with the blood at the moment of secretion.
Both the bile-pigment and bile acids exert an injurious action on the kidneys. In cases of prolonged obstruction not only are the tissues of the organ stained by pigment in common with the tissues of the body, but the epithelium of the tubules, of the straight and convoluted tubes, are, according to Moebius,195 infiltrated with pigment. In consequence of the size and number of the masses of pigment, the tubes may become obstructed and the secretion of urine much diminished. Other changes occur, due chiefly to the action of the bile acids, according to the same authority. These alterations consist in parenchymatous degeneration. The urine contains traces of albumen in most cases, and, according to Nothnägel,196 always casts of the hyaline and granular varieties stained with pigment. As the alterations in the structure of the kidneys progress, fatty epithelium is cast off, and thus the tubules come finally to be much obstructed and the function of the organ seriously impaired. To cholæmia then are superadded the peculiar disturbances belonging to retention of the urinary constituents.
195 Archiv der Heilkunde, vol. xviii. p. 83.
196 Deutsches Archiv für klin. Med., vol. xii. p. 326; also, Harley, op. cit., p. 503.
One of the most interesting complications which arises during the existence of obstruction of the bile-ducts is the form of fever entitled by Charcot197 intermittent hepatic fever. Although its character was first indicated by Monneret,198 we owe the present conception of its nature and its more accurate clinical history to Charcot. It does not occur in all cases. As has already been pointed out, the passage of a gall-stone may develop a latent malarial infection or a febrile movement comparable to that caused by the passage of a catheter, and known as urethral fever. Charcot supposes that true intermittent hepatic fever is septicæmic in character, and can therefore arise only in those cases accompanied by an angiocholitis of the suppurative variety—such, for example, as that which follows the passage of calculi. Illustrative cases of this fever, one of them confirmed by an autopsy, have been recently reported by E. Wagner,199 who is rather inclined to accept Charcot's view of the pathogeny. A remarkable case has been published by Regnard,200 in which the angiocholitis was induced by the extension of echinococcus cysts into the common duct. Whilst there are some objections to Charcot's theory, on the whole it is probably true that this intermittent hepatic fever is produced by the absorption from the inflamed surface of the ducts of a noxious material there produced. It may be likened to the fever which can be caused by the injection of putrid pus into the veins of animals.
197 Leçons sur les Maladies du Foie, etc., p. 178 et seq.
198 Cyr, Traité de l'Affection calculeuse du Foie, p. 193.
199 Deutsches Archiv für klin. Medicin, vol. xxxiv. p. 529.
200 Gazette méd. de Paris, No. 49, 1873, quoted by Wagner, supra.
Intermittent hepatic fever, as its name implies, is a paroxysmal fever, having a striking resemblance to malarial fever, but differs from it in less regularity of recurrence, in the fact that urea is below the normal amount instead of increased, and in the effect of quinine, which in the case of malarial fever is curative, but not curative in hepatic fever. The paroxysms are sometimes quotidian, rarely double quotidian, tertian, quartan, and even longer, and in the same case all of these varieties may occur; on [p. 1091]the other hand, there may be entire regularity of the seizures. The severity of the chill, the maximum temperature, and the amount of sweating vary within considerable limits; there may be merely a slight sense of chilliness or a severe rigor; the temperature may rise to 101° or to 104° F., and there may be a gentle moisture or a profuse sweat. There does not seem to be any relation between the extent and severity of the local mischief and the systemic condition.
The period of onset of intermittent hepatic fever, and its duration and mode of termination, are by no means readily determined. Cyr fixes on the paroxysms of colic as the beginning, but he obviously confounds the chill and fever caused by the passage of a calculus with the true intermittent hepatic fever. In a carefully-observed case, the facts confirmed by an autopsy, E. Wagner201 gives the clinical history of a typical example of this malady: Gall-stones were found in the duodenum, in the common and cystic ducts, but the most important one was a polyangular stone obstructing the hepatic duct. There was an ulcer with thickened margin at the entrance to the gall-bladder, and the mucous membrane of the common duct near the intestinal orifice had a smooth, cicatricial aspect of recent origin, indicating inflammatory ulceration. The conditions favorable to the production of a morbid material of a kind to induce septicæmic fever were therefore present. The onset of fever occurred ten days after the last seizure, time being thus afforded for the local changes necessary. The duration of the fever in this case was five months, but the existence of pulmonary phthisis with cavities will explain this apparently protracted hepatic intermittent fever. The duration of the disease in its usual form is uncertain, and ranges between a week and two months, or even three months, according to Charcot.202
201 Deutsches Archiv für klinische Medicin, Band xxxiv. p. 531, 1884.
202 Leçons sur les Maladies du Foie, p. 180.
Suspension of work by the liver necessarily involves retention in the blood of various excrementitious matters. The attempt of Flint203 to establish the doctrine of cholesteræmia has not been supported by the evidence of contemporary or subsequent physiologists. This theory denies to the other constituents of the bile any morbific action, and concentrates those disturbances known as cholæmia on the effects of cholesterin. As uræmia signifies not merely the presence of urea in the blood, but of all of the toxic substances excreted by the kidneys, so the word cholæmia comprehends all the constituents of bile having power to derange the organism by their presence in the blood.
203 The American Journal of the Medical Sciences, 1862, p. 349 et seq.
By cholæmia is meant those disturbances, chiefly nervous, which are due to the presence of biliary excrementitious matters in the blood, and not less to the effect on nutrition of the absence of bile from the process of digestion in the intestine. As the atrophic changes proceed in the liver, the quantity of urea and uric acid in the urine diminishes, and presently leucin and tyrosin appear. Amongst the means of differential diagnosis of hepatic intermittent fever from malarial fever Charcot mentions the quantity of urea present—in the former greatly lessened, in the latter much increased. There is, however, a source of fallacy here not mentioned by Charcot: that is, the variations in the amount of urea due to destruction of the hepatic secreting structure. It follows that as changes [p. 1092]occur in the kidneys, to the condition of cholæmia is superadded the derangements belonging to uræmia.
When the occlusion has existed for some time—a variable period, partly due to peculiarities of individual structure—there come on certain characteristic symptoms of nervous origin: headache, hebetude of mind, dull hearing, obscure or hazy vision, xanthopsia; somnolence and greatly increasing stupor, leading into coma; rambling and incoherence of mind, passing into delirium; muscular twitching, subsultus; muscular weakness, deepening into paralysis; and finally, it may be, general convulsions. As these derangements of the nervous system develop, a light febrile movement supervenes, so that the whole complexus has the typhoid type, or, as it can be more definitely expressed, the patient thus affected lapses into the typhoid state.
COURSE, DURATION, AND TERMINATION.—Occlusion of the gall-ducts is an essentially chronic malady in the greatest number of cases. As a rule, the causes of obstruction operate slowly, but to this rule there are exceptions. Permanent occlusion may take place suddenly, as when a gall-stone is impacted immovably in the common duct, or when a round-worm makes its way into the duct and is firmly fixed there, incapable of further movement.
When occlusion is once effected the gradual changes occurring in the liver lead to slow decline of the nutrition; the bile-elements circulating in the blood poison it and set up alterations in the structure of the kidney, and ultimately, the brain becoming affected, the end is reached by convulsions and coma. Although permanent occlusion, if unrelieved, terminates in death, a small proportion of cases get well, either in consequence of giving way of the obstructing cause or from the opening of a new route to the intestine. Thus, a calculus lodged in the fossa of Vater may suffer such injury to its outer shell as to yield to the action of solvents, or, suppuration occurring around it, the stone may be loosened and forced onward, or ulceration may open a channel into the bowel. An incurable malady causing the occlusion, the termination in death is only a question of time. The duration of any case must be indefinite. There are several factors, however, whose value can be approximately estimated. When the obstructing cause is merely local—as, for example, a gall-stone or the cicatrix of a simple ulcer—the duration of the case is determined by the mere effect of the suspension of the hepatic functions. As the eliminating action of the liver and the part played by the bile in the intestinal digestion are necessary to life, it follows that the complete cessation of these functions must lead to death. The rate at which decline takes place under these circumstances varies somewhat in different subjects. Probably two years may be regarded as the maximum, and three months the minimum, period at which death ensues when no other pathogenetic factor intervenes.
DIAGNOSIS.—To determine the fact of occlusion is by no means difficult: the persistent jaundice, the absence of bile in the stools, and the appearance of the bile-elements in the urine are sufficient. It is far different when the cause of the occlusion is to be ascertained.
The ease and safety with which the exploring-trocar can be used in cases of supposed obstruction of the cystic duct enable the physician to decide with confidence points which before could only be matters of mere [p. 1093] conjecture. The writer of these lines was the first to puncture the gall-bladder and to explore, by means of a flexible probe passed through the canula, the course of the duct.204 It is possible in this way to ascertain the existence of gall-stones in the gall-bladder, to find an obstruction at the entrance of the cystic duct, to demonstrate the presence of echinococci cysts, and to remove for microscopical examination pathological fluids of various kinds. More recently, Whittaker and Ransohoff205 of Cincinnati have attempted the detection of a gall-stone impacted at any point by the introduction of an exploring-needle; and this practice has been imitated by Harley206 of London, but without any reference to the pioneer and prior investigation of his American colleagues. The case of Whittaker and Ransohoff survived the exploratory puncture, but Harley's case proved fatal from traumatic peritonitis. Notwithstanding this untoward result, Harley persists in the advocacy of this method. It must appear to any one familiar with the intricate arrangement of the parts composing the anatomy of this region a most hazardous proceeding, and hardly to be justified in view of the superior safety and certainty of my method. To explore the interior of the gall-bladder an aspirator-trocar is introduced; any fluid intended for microscopical examination is then withdrawn, and through the canula a flexible whalebone bougie is passed.
204 The Cincinnati Lancet and Clinic for 1878-79; also, W. W. Keen, M.D., "On Cholecystotomy," The Medical News, Sept., 1884.
205 Lancet and Clinic, 1884.
206 Lancet (London), July, 1884.
When icterus comes on in a few days after birth and persists until death ensues by convulsions and coma, there can be no doubt regarding congenital absence or impermeability of the common duct. Permanent retention-jaundice, accompanied by the characteristic symptoms of that condition immediately succeeding an attack of hepatic colic, is probably due to impaction by a calculus. When, at or after middle life, in a patient with a history of former attacks due to gall-stones, there begins a fixed pain in the right hypochondrium, and subsequently retention-jaundice, the existence of a malignant growth in connection with the cicatricial tissue and ancient organized exudation should be suspected; and this suspicion will be confirmed if subsequently a tumor can be felt. If with a localized pain slowly-developing jaundice, intestinal indigestion, fats and oils appearing unchanged in the stools, and a condition of prostration more than is properly referable to the derangement of the hepatic functions, come on in a man or woman after thirty-five, cancer of the head of the pancreas should be suspected; and this suspicion will be confirmed if a tumor can be detected in that situation. It should not be forgotten, however, that in emaciated subjects the head of the pancreas may be so prominent as to be mistaken for a scirrhous growth.
A pulsating tumor of the right hypochondrium, accompanied by jaundice, may be an aneurism of the hepatic artery. Pulsation may be communicated to a bunch of enlarged portal lymphatic glands, which will compress the common duct, but in this case, as the increase in the size of the glands is due to caseous, amyloid, or cancerous deposits, there will be found a source whence these morbid products are derived, and will explain the nature of a tumor thus constituted.
The differentiation of hypertrophic cirrhosis from occlusion of a slowly-forming character is by no means easy. In both jaundice [p. 1094] gradually appears; in both the liver is enlarged, but in hypertrophic cirrhosis much more than in occlusion; and in the latter the gall-bladder is full—may indeed be distended—whilst in the former it is empty or contains but little bile. The history of the case may indicate the nature of the symptoms. Previous attacks of hepatic colic, and the symptoms of occlusion supervening on the last, are highly significant of calculous occlusion.
TREATMENT.—To ascertain the nature of the occlusion is a necessary preliminary to any exact treatment. In many cases this must remain a mere conjecture, when, of course, the treatment is only symptomatic. When it is probable or certain that the duct is obstructed by a calculus, two methods may be resorted to for its removal: one method is to break up the calculus by mechanical means; the other is to effect its solution by chemical agents.
Fracture of an impacted calculus is not a merely fanciful expedient. If the site of the obstruction is ascertained, an attempt may be made to penetrate the calculus by an aspirator-needle passed through the abdominal walls, according to the method of Whittaker and Ransohoff. The dangers attendant on this mere puncture are great, and a fatal result has occurred in one of the very few cases in which it has been done. Less severe and dangerous methods for attempting the disintegration of a calculus should be first tried, as follows: Make firm friction with the fingers along the inferior margin of the ribs and toward the epigastrium and umbilicus, whilst the opposite side posteriorly is supported by the hand spread out and applied firmly. A strong faradic current sent through the region of the gall-bladder and ducts has in several instances seemed to do good—indeed, to remove obstructions. A calculus impacted may be dislodged either by the fracture of its surfaces or by the strong muscular contractions of the abdominal walls and of the muscular layer of the duct. Most calculi are easily broken, and when the smallest breach is made in the external crust disintegration follows; and some calculi are so friable as to yield to slight pressure. Furthermore, the slightest solution in the continuity of the rind disposes the whole mass to dissolve in suitable menstrua. Mechanical rupture is so important a step in the process of disintegration of an impacted calculus that so serious an operation as section of the abdomen as a preliminary to it should be considered. The cavity exposed, the obstructed duct is found, and its retained calculus is mashed without section of the duct. I find one instance207 in which this was done as a subordinate part of a cholecystotomy, and the breaking up of the stone proved to be easy of accomplishment. It is also the method of Tait, who proposes to mash the calculus by means of suitable forceps fitted with padded blades.
207 Harley's case, op. cit.
I have suggested a means of effecting solution of an impacted calculus which seems, on further reflection, well worthy of consideration. The proposal is to inject, through a canula introduced into the gall-bladder, one of the solvents of the cholesterin calculus before mentioned. I have already used the canula as a duct for the passage of an exploring-sound, and have by means of it explored the interior of the gall-bladder. It is quite as feasible to inject through the canula a solvent, successive charges of which can be thrown in and withdrawn by the aspirator.
[p. 1095] That the usual solvents introduced by the stomach can effect the solution of impacted calculi has been declared impossible by Trousseau;208 and with this conclusion I unhesitatingly agree. I have already discussed this part of the subject, and need now only refer the reader to that section.
208 Clinique médicale, loc. cit.
The various causes of obstruction besides calculi do not offer an inviting field for the exercise of therapeutical skill. Each case must be treated according to the nature of the obstructing cause; hence to make an accurate diagnosis is an essential preliminary to suitable treatment.
DEFINITION.—By the terms at the head of this section are meant the various pathological processes which induce coagulation of the blood in some part of the portal system. As the portal vein is made up of many branches coming from the various organs of the abdominal cavity except the kidneys, and as it empties, so to speak, into the liver, it is obvious that various and complex derangements will ensue on the formation of thrombi.
CAUSES.—Thrombosis of the portal vein occurs under three general conditions: the blood is in a readily coagulable state; the action of the heart is weak and the blood-current sluggish; the circulation through the vein is impeded by external pressure. The coagulability of the blood is increased in diseases characterized by an excess of its fibrin-producing constituents, of which cirrhosis of the liver may be mentioned as one having this peculiarity. In chronic maladies of a depressing kind there may be simply a weak action of the heart, or the muscular tissue of the organ may be affected by a fatty and atrophic degeneration. The external pressure by which the blood-current through the vein is impeded may be caused by the newly-formed connective tissue of Glisson's capsule, by enlarged lymphatics in the hilus of the liver, or by tumors of various kinds. The first named of these causes of compression—atrophic cirrhosis—is most frequently acting. Very rarely, organized exudations of the peritoneum may be so situated as to compress the portal vein. This result can only happen when the hepatic portion of the peritoneum is involved.
Pylephlebitis exists in two forms: the adhesive and suppurative. The former results in changes not unlike those of simple thrombosis. The blood coagulates in the affected part of the vessel, the clot is organized, and the vessel ultimately forms a solid rounded cord which is permanently occluded. The suppurative variety is so different in its origin and in its results that it requires separate treatment, and I therefore postpone the consideration of it to the next section.
[p. 1096] SYMPTOMS OF THROMBOSIS AND ADHESIVE PYLEPHLEBITIS.—It is a remarkable fact that the biliary function of the liver is not necessarily affected in cases of occlusion of the portal vein. It is true, in advanced cases of cirrhosis, when the interlobular veins are obliterated by the pressure of the contracting newly-formed connective tissue, the functions of the liver are arrested in so far as the damage thus caused extends. Notwithstanding the blocking of the portal, sufficient blood reaches the hepatic cells by the anastomosis between the hepatic artery and the interlobular veins—an anatomical connection demonstrated by Cohnheim and Litten.209 So long as this anastomosis continues bile will be formed, although the portal vein is occluded.
209 Virchow's Archiv, Band lxvii. p. 153, "Ueber Circulationsstörungen in der Leber."
The most significant symptoms of thrombosis of the portal vein are the sudden formation of ascites, which quickly assumes a very high grade, and equally sudden passive congestion of the gastro-intestinal mucous membrane, enlargement of the spleen, and distension of the superficial veins of the abdominal parietes. When these symptoms succeed to cirrhosis of the liver, or appear after the formation of a tumor in the hepatic region, or come on in the course of phthisis or chronic inflammation of the hepatic peritoneum, the existence of thrombus of the portal vein may be reasonably suspected.
Coincidently with the occlusion of the portal vein the gastro-intestinal mucous membrane becomes the seat of a catarrhal process, and to the fluid thus produced is added a much more abundant transudation from the distended capillaries. Nausea, vomiting, and diarrhoea result, the rejected matters being serous, watery, and in many cases tinged with blood. Now and then quite a severe hemorrhage takes place, and the blood is brought up by vomiting (hæmatemesis) or is discharged by stool. Hemorrhoids form, and, in large masses protruding, much pain is experienced, and free bleeding may result from rupture of a distended vein.
The veins of the abdominal parietes, which in the normal state are invisible or at least not prominent, and which form anastomoses with the portal, when the obstruction occurs dilate, sometimes to a remarkable extent. The most important anastomosis is that between the femoral and saphena and internal mammary and epigastric veins. When the hepatic branches of the portal are closed, but the trunk remains pervious, the parumbilical vein enlarges greatly, and, communicating with the superficial veins of the anterior part of the abdominal walls, forms a radiating network of tortuous veins to which is given the striking title of caput Medusæ.
The most significant symptom of portal thrombosis is a quickly-forming ascites. It is true, ascites is a common symptom in advanced cirrhosis, but the rapid accumulation of fluid and the prompt filling of the cavity after tapping distinguish that which arises from portal thrombosis from all others. Besides its excessive extent, the ascites presents the usual symptoms.
Due to the same cause as the enlargement of the superficial veins, the hemorrhages, the ascites, etc., there occurs considerable hypertrophy of the spleen in many of the cases. It sometimes happens that the new compensatory circulation and the hemorrhages from some part in the [p. 1097] usual route of the portal so dispose of the blood that the spleen does not enlarge sufficiently to be readily made out.
COURSE AND TERMINATION.—It is obvious that a condition such as that induced by thrombosis of the portal must be comparatively quickly fatal; but the cases vary in duration as the compensatory circulation is more or less complete. Whilst the majority of cases terminate within two weeks, instances of several months' duration are not unknown, but a fatal termination, sooner or later, is inevitable in all cases.
Coming on in the course of some chronic affection of the liver or some obstructing cause exterior to the organ, there soon follow ascites, nausea and vomiting, hæmatemesis, bloody stools of a liquid character, enlargement of the spleen, distension of the abdominal veins, and the distressing symptoms produced by an excessive accumulation of fluid in the peritoneal cavity.
DIAGNOSIS.—As there is no symptom of thrombosis of the portal which may not be caused by advanced cirrhosis, the diagnosis rests on the rapid production of the attendant phenomena and their conjoint appearance.
TREATMENT.—A symptomatic treatment is alone possible. The highly irritable and congested intestinal mucous membrane precludes the employment of hydragogue cathartics. Salines which cause outward diffusion from the vessels are the only cathartics which can be used with propriety. Action of the kidneys and of the skin must be maintained. To this end the resin of copaiba in pilular form and pilocarpine subcutaneously may be used. If the strength of the patient will permit, leeches around the anus can be applied, and much relief may be expected from free bleeding. It is probable that opening a swollen hemorrhoid would give the same kind of relief as that caused by a free hemorrhage. In any case the benefit derived from treatment must be merely palliative and temporary.
PATHOGENY.—Primary pylephlebitis rarely if ever occurs. On the other hand, the secondary form is by no means uncommon; it succeeds to ulcerative or purulent inflammation at some point in the circuit of origin of the portal radicles. The most frequently-occurring cause is ulceration and suppuration of some part of the intestinal tube, and hence the most common result is multiple abscess of the liver. Pylephlebitis has often resulted from typhlitis; from ulcers of the large intestine, as in dysentery; from such traumatic injuries as tying hemorrhoids; from proctitis; from ulcers of the stomach and similar morbid processes elsewhere within the range of origin of the portal system. The pathogeny is clear. The inflammatory or ulcerative action extends to and involves the walls of the veins, or some morbid material diffuses through the vein walls. In either case coagulation of the blood in the vessel ensues, and the clot undergoes a series of changes resulting in the formation of emboli, which, carried into the main current, are subsequently lodged in the hepatic capillaries.
There are three steps in the morbid process: the changes in the vein wall; the production and transformation of the thrombus; and the formation of secondary suppurating foci in the liver.
[p. 1098] The appearance of the tunics of the inflamed vessels varies with the stage at which they are examined. At first the walls of the vessels are reddish from congestion, succulent, and swollen, infiltrated by leucocytes and inflammatory exudation and the cellular elements undergoing proliferation. The intima especially is much altered in its appearance and structure, becoming thick, opaque, grayish or yellowish in color, and having adherent to it a thrombus passing through its characteristic changes. Ulceration of the intima then occurs, and the purulent elements, with shreds of tissue, mingle with the degenerating blood-clot, and ultimately there remains a purulent dépôt lined with sloughing, even gangrenous, contents. Emboli detached from such decomposing thrombus are arrested in the vessels of the liver, and there set up a suppurating phlebitis, ending in an abscess formation, or a quantity of pus from the original point of ulcerative phlebitis passes into the portal vein, and is generally distributed through the hepatic branches, here and there foci of suppuration being established by the deposit of decomposing emboli. There may be numerous small abscesses irregularly distributed through the liver, or there may be one or two larger collections of pus. Very often the vessel whose occlusion by a suppurating embolus has caused the mischief is destroyed, and hence no communication with the abscess-cavity can then be traced. These abscesses are not limited by a line of inflammatory demarcation or by a limiting membrane, but the hepatic tissue adjacent is congested and infiltrated with pus.
Ulceration, abscesses, or purulent inflammation occurring at any point within the area of origin of the radicles of the portal vein may induce pylephlebitis and consequent hepatic abscess. There are two points at which, suppuration established, secondary pylephlebitis is most apt to occur: the cæcum; the rectum. As respects the former, the symptoms of typhlitis precede the hepatic disturbance; and as respects the latter, usually dysentery, or rather proctitis, is the initial disease. In both sources of the hepatic trouble the inferior hemorrhoidal veins are chiefly concerned—a fact explicable by reference to the sluggishness of the circulation and the distended condition of these veins, whence it is that thrombus is very readily induced. Numerous instances of pylephlebitis following suppurative lesions of the cæcum have been reported. One of the most recent, and at the same time typical, examples of such conditions is that published by Bradbury210 of Cambridge, England. The initial lesion was "an ulcer the size of a split pea" situated near "the junction of the vermiform appendix and cæcum." "The hemorrhoidal veins and the inferior mesenteric above were filled with breaking-down clot and pus," and "the liver contained many abscesses of various sizes, the largest about the size of a lemon, which had burst through the diaphragm." As is so often the case, the ulcer of the cæcum produced no recognizable disturbance, and important symptoms were manifest only when the emboli lodged in the liver set up suppuration, when there occurred the usual signs of hepatic abscess. In the West and South hepatic abscess due to pylephlebitis, induced by proctitis, with ulceration of the rectum, is a common incident. Various examples of this kind have fallen under my own observation. The relatively greater frequency of this form of pylephlebitis is due to the fact above [p. 1099] stated, that the inferior hemorrhoidal veins are voluminous, have a sluggish current, and are liable to over-distension by pressure of feces and by external abdominal bands and clothing. Cases of a corresponding character arise from suppuration and ulceration elsewhere within the portal circuit. Thus, Bristowe211 reports a case in which pylephlebitis resulted from an ulcer of the stomach, the neighboring veins becoming implicated and the usual results following.
210 The Medical Times and Gazette, Sept. 27, 1884, p. 450, "Proceedings of the Cambridge Medical Society."
211 Transactions of the Pathological Society of London, vol. ix. p. 278.
When inflammation has begun in a radicle of the portal vein, it may proceed to the liver by contiguity of tissue, the whole intervening portion of the vessel being affected. Probably more frequently the intra-hepatic portion of the portal is inflamed by emboli, and the adjacent hepatic tissue then undergoes suppuration, as has been already set forth.
SYMPTOMS.—There being two points of disease—the primary lesion of the peripheral vessel and the secondary results in the hepatic portion of the portal—the symptomatology must have a corresponding expression. The stomach, the cæcum, or the rectum, or some other organ or tissue, being occupied by a morbid process, there will be a characteristic complex of symptoms. Taking up the most usual primary disturbance, a typhlitis or an ulcer of the cæcum, there will be pain, tenderness, and possibly fever, occupying in point of time the period proper to such a malady and an amount of disturbance of function determined by the extent of the lesion. The symptoms caused by a single small ulcer of the cæcum, as in the example narrated by Bradbury, may present no characteristic features and may have little apparent importance, and yet the lesion is productive of very grave consequences.
When from any of the causes mentioned above a thrombus forms in a vein of the portal system in consequence of the extension of the inflammation about it, the case, what importance soever it previously had, now takes on new characters. The onset of the inflammation of the vein walls and the puriform degeneration of the thrombus is announced by a chill—a severe rigor, or chilly sensations at least. At the time of the chill, and sometimes before it, pain is felt, significant of the lesion in the vein. When proctitis or typhlitis precedes the pylephlebitis, pain appropriate to the malady is a significant symptom; but the pain which comes on with the beginning of the inflammation in the liver is a new sign. The most frequent sites of the pain are the right hypochondrium and the epigastrium, but it may also be felt in the left hypochondrium or in either iliac fossa. Unless there be diffuse peritonitis the pain is accompanied by a strictly-localized tenderness to pressure. The situation of the pain may afford an indication of the vein attacked, and when there are two points at which pain is experienced, one may originate at the first situation of the morbid action; the other will be due to pylephlebitis.
The fever succeeding the chill is decided, and in some cases may attain to extraordinary height—a manifestation indicative of the pyæmic character of the affection. The fever intermits or remits, with a more or less profuse perspiration. The febrile phenomena are similar in their objective expression to malarial fever, but there is an important difference in respect to the periods of recurrence of the chills. The paroxysms are very irregular as to time: there may a daily seizure at different hours, or there may be several chills on the same day. In other words, the [p. 1100]paroxysms have the pyæmic characteristics rather than the malarial. After a time the intermittent phenomenon ceases, and there occurs a remission merely, the exacerbation being preceded by chilliness and succeeded by sweating. The sweats are characteristically profuse and exhausting. During the sweating the temperature begins to decline, and reaches its lowest point just before the chilly sensations during the early morning announce the onset of the daily exacerbation of the afternoon and evening. The thermal line exhibits many irregularities until the febrile movement assumes the remittent type, when there occur the morning remission and nocturnal exacerbation. The maxima may be from 103° F. to 105°, even to 106°.
When the pain and chill come on, disturbances of the digestive organs ensue. When a large vein of the portal system is occluded, the remaining veins must be over-distended, and congestion of a part or of all of the digestive tract will be a result. An acute gastric catarrh is set up. The appetite is lost, the stomach becomes irritable, and vomiting is a usual incident. Sometimes the disgust for food is extreme, and the nausea and vomiting are almost incessant. The vomited matters consist of a watery mucus mixed with thin bile after a time, and now and then of a bloody mucus. Thrombosis of a stomach vein may occur, to be followed by an acute ulcer, and from this considerable hemorrhage may proceed, when the vomit will consist of blood. Such an accident, happening to the mucous membrane of the intestine, will be indicated by bloody stools if the ulceration is low down, or by brownish, blackish, or chocolate-colored stools if higher up in the small bowel.
The tongue has usually a characteristic coating in these cases. Large patches of a rather heavy and darkish fur form, and, cast off from time to time, leave a glazed and somewhat raw surface. Sometimes there is a profuse salivary flow, but more frequently the mouth is dry. The lips are fissured or contain patches of herpes, and the buccal cavity may be more or less completely lined by patches of aphthæ.
Diarrhoea is a usual symptom, the stools being dark when mixed with blood, or grayish and pasty or clay-colored when there is jaundice.
Three-fourths of the cases of pylephlebitis are free from jaundice. This symptom may occur at the onset when the common duct is obstructed by a calculus, but in other cases it appears when the formation of pus in the liver exerts sufficient compression of the hepatic ducts to prevent the passage of the bile.
When jaundice occurs, it is accompanied by the usual symptoms. The urine, previously unchanged, is now colored by bile-pigment, and the alterations in the renal structure and function belonging to jaundice also take place.
It sometimes happens that the obstruction of the portal vein is sufficient to cause enlargement of the superficial veins of the abdomen, but the duration of the disease is usually too brief to permit much deviation from the normal, except rarely. In the cases characterized by the occurrence of diffuse peritonitis the abdomen will present a swollen and tense appearance, and there will be acute tenderness to pressure. The area of hepatic and splenic dulness is not increased from the outset, but is evident, as respects the spleen, soon after the obstruction at the liver, and as respects the liver when the formation of abscesses occurs.
[p. 1101] COURSE, DURATION, AND TERMINATION.—The course of pylephlebitis is compounded of the disturbance at the original point of disease, and of the secondary inflammation at the several points in the liver where emboli set up purulent inflammation. There are, therefore, two distinct symptom-groups, and a short intervening period in which the first is being merged into the second. The duration is variable, but the extreme limits are not remote from each other, the condition of pylephlebitis terminating in from two weeks to three months, the shorter being the more usual. The termination is death, doubtless invariably; for, as in true pyæmia arising from other causes, the septic changes in the blood are such as to preclude the possibility of a return to the normal condition.
DIAGNOSIS.—The main point in the diagnosis consists in the occurrence of an evident local inflammation, followed by the signs of suppuration in the hepatic region coming on subsequent to ulceration and suppuration at some point in the peripheral expansion of the portal system. Thus, when a proctitis with ulceration of the rectum has been in existence for some time, there occur pain and tenderness in the hepatic region, accompanied by an irregularly intermittent fever and by profuse sweating, it can be assumed with considerable certainty that emboli have been deposited in some one or more of the terminal branches of the portal. The evidences of hepatic trouble—swelling of the organ, jaundice, etc.—and of portal obstruction, which then supervene, indicate with some precision the nature of the case.
TREATMENT.—Although pylephlebitis wears a most unfavorable aspect, the possibility of a favorable result should always be entertained by the therapeutist.
As absorption of medicaments must be slow—indeed, uncertain—by the gastro-intestinal mucous membrane when there is portal occlusion, it is well to attempt treatment by the skin and subcutaneous connective tissue. Gastro-intestinal disturbance—nausea, vomiting, and diarrhoea—should be treated by a combination of bismuth, creasote, and glycerin—remedies acting locally chiefly. Ammonia—the carbonate and solution of the acetate—is indicated, and should be given for the purpose of dissolving thrombi and emboli. Corrosive sublimate, carbolic acid, and quinine can be administered by the subcutaneous areolar tissue. Quinine may also be introduced by friction with lard, and in considerable quantity.
DEFINITION.—The echinococcus is the intermediate or larval stage in the development of the Tænia echinococcus—the completed parasite—whose chief habitat is the intestine of the dog. As the natural and clinical history of parasites is elsewhere treated of, the subject is here confined to the development of echinococci cysts in the liver, its ducts, and vessels.
CAUSES.—The presence of echinococcus vesicles in the liver is due to [p. 1102] the migration of the embryo from the intestinal canal. As Davaine212 has ascertained by analysis of all the recorded examples previous to the publication of his treatise, echinococci are found in as large a proportion in the liver as in all the other organs combined. This statement is repeated with approval by Cobbold213 and by Heller.214 The embryo, set free in the intestine from the food or drink containing the ova, starts on its migration. There are several reasons why the liver is selected for its habitat: it is the largest accessible organ; the common duct and the portal vein offer the most convenient roadway for reaching and penetrating its substance. The exact route or routes of which the parasite avails itself in migrating have not been definitely settled, although Friedreich has shown that the portal vein is the medium of transmission of the Echinococcus multilocularis. The comparative frequency with which the liver is entered indicates that the portal vein is the favorite route of migration.
212 Traité des Entozoaires et des Maladies vermineuses, etc., par C. Davaine, Paris, 1877, p. 383.
213 Entozoa, by T. Spencer Cobbold, M.D., F.R.S., London, 1874, p. 275.
214 In vol. iii of Ziemssen's Cyclopædia, p. 561.
PATHOLOGY AND SYMPTOMS.—The number of echinococci reaching the liver varies from one to ten or twelve or more. They increase in size from the time of their deposit in the organ, and ultimately attain to large proportions. The rapidity of growth depends somewhat on the character of the tissue in which imbedded, and the amount of disturbance of function is determined by the position of the parasite in the organ. Echinococci may be deposited in any part of the liver—in the substance of the organ, in the ducts, or in the vessels—but the most usual site is near the capsule, and, developing outwardly in the direction of least resistance, impart to the outline of the organ an irregular contour. As the echinococci develop, the adjacent parts of the liver pressed upon undergo atrophy, but the connective tissue of the organ contributes to the formation of the dense capsule which envelops them. But as the increase in size is not rapid, although continuous, if the cysts are situated at the periphery and adjacent to the capsule, they may be present for many months without causing any distinct symptoms. In a case occurring under my own observation last year the only symptom which attracted attention was an enlargement of the hepatic region, and on examination a characteristic elastic, irregular, and painless tumor could be readily detected by sight and touch occupying the right hypochondrium and extending into the epigastric and umbilical regions. When the echinococci cysts impinge on the portal vein or on the hepatic duct, there will be caused the usual results of such pressure—ascites or jaundice, or both conditions may occur simultaneously, with obstruction of both vein and duct. When the cysts develop downwardly, the stomach and intestines will be displaced, and nausea and vomiting, diarrhoea or constipation, and, it may be, considerable pain of a colic-like character, will be caused. An upward development of the cysts gives rise to more pronounced disturbances. The diaphragm is pushed upward, the heart displaced, and the lungs, especially the right, compressed. Occasionally the diaphragm is softened and perforated by the pressure of the enlarging cysts, and the lungs are ultimately tunnelled, the parasites being discharged by the bronchi.
[p. 1103] The growth of an echinococcus tumor may spontaneously cease, and then retrograde changes take place, leading to its final disappearance. This arrest of development may occur without any obvious cause, but now and then such a change from the ordinary course of tumors may be effected by an external injury, as a blow on the abdomen, but more frequently the death of the parasite is caused by ulceration into a bile-duct, and the entrance of bile, which is a poison to these hydatids. It sometimes happens that, opening into a duct of large size, the daughter and granddaughter vesicles are slowly discharged through it into the intestine, and thus a cure is effected. Inflammatory action occurring in the cysts, adhesions may form and rupture into a neighboring cavity take place. Direct communication may be established with the intestine, or the cavity of the pleura or peritoneum be entered, with results entirely disastrous.
A necessarily fatal termination must also ensue when the hydatids penetrate the ascending vena cava, but this accident is, fortunately, very rare.
The passage outward through the abdominal wall is an exceedingly uncommon but fortunate issue of echinococcus of the liver, for in this mode the hydatids may be discharged without much difficulty.
The echinococcus vesicle is enveloped in a dense, resisting, and elastic capsule, constructed out of the connective tissue of the part in which it is deposited. The innermost layer of the vesicle is the germinative (endocyst), and from its granular surface are developed the brood-capsules and their scolices—i.e. the head with its suckers and crown of hooklets.215 Each vesicle may contain not only daughter, but also granddaughter, progeny, numbering from a dozen up to many thousands, and they will vary in size from the head of a pin to a pullet's egg. It follows that the mother vesicles must also greatly vary in size: they range from a large pin's head to a child's head. The vesicles or sacs contain a clear, faintly yellowish, or opalescent fluid, neutral or slightly alkaline in reaction, and holding in solution a large per cent. of sodium chloride, but free from albumen. The specific gravity of the fluid ranges from 1007 to 1015, according to the quantity of sodium chloride present. Succinic acid and also hæmatoidin are usual constituents, besides the ingredients already mentioned.
215 Entozoa, Cobbold, p. 273 et seq., chapter viii.
Although the form of hydatid or echinococcus cyst above described is the usual one, there is occasionally produced an anomalous development of the parasite, which from its resemblance to colloid cancer was supposed to have this character until Virchow216 unravelled the mystery by demonstrating its true structure. This form of the parasite is designated Echinococcus multilocularis. Its resemblance to colloid cancer is the more striking because of the tendency of the interior of the mass to undergo degeneration, to disintegrate, and to break up into pus-sacs with greenish, cheesy, and bilious contents. An Echinococcus multilocularis tumor is of almost stony hardness; it has a very dense fibrous structure, intersected by cavities with thick gelatinous contents. These minor cavities217 are sacs of echinococci, but they depart widely from the typical form, well-defined scolices being seldom encountered.
216 Archiv für Anat., Virchow, vol. xi. p. 80.
217 Carrière, quoted by Davaine, op. cit., p. 961.
[p. 1104] Echinococci of the liver develop very slowly, and it is characteristic of them to attain to very large proportions in most cases without causing any very pronounced symptoms. There are certain signs common to hydatids in any situation; there are others which are due to particular circumstances.
A hydatid tumor of the liver is smooth but somewhat irregular in outline, and elastic, when it develops downward, extending below the margin of the ribs. If, however, it grows upward, the area of hepatic dulness extends in that direction beyond the usual limits; the diaphragm is pushed up, the lungs forced upward to the left and compressed, and the heart also displaced upward toward the left. The extension of the tumor downward, in the direction of least resistance, is more usual. If the walls of the abdomen are sufficiently thin, the tumor large enough, and if made up of many daughter vesicles, there may be evoked by palpation the very characteristic sign known as hydatid purring. To produce this effect an oscillation must be caused by a sudden impulse communicated to the tumor on one side, the hand resting against the other side. This sensation is likened to the impression on the eye of the vibration of a bowl of jelly. Even when there is a well-defined tumor this symptom is comparatively infrequent, but if present it is pathognomonic, since no other kind of tumor possesses the property of oscillation and elastic collision of its several constituents.
When the tumor is so situated as to occlude the hepatic or common duct, jaundice will be a symptom, and when the stomach is pressed upon there will be epigastric oppression and nausea. If the vena cava is impinged on or the portal vein, the usual results—ascites and oedema of the lower extremities and of the scrotum—will be manifest. There is, of course, nothing distinctive in these results.
The Echinococcus multilocularis, situated in the substance of the liver, causes the usual disturbances of a new formation in such a position. Much of the hepatic tissue is destroyed by its growth, and many of the minor ducts closed. Jaundice is an early symptom—the first, indeed, in many cases—and is also one of the most persistent. It is present, according to Griesinger, in 10 out of 13 cases. The usual gastro-intestinal disorders belonging to jaundice occur under these circumstances; also the nervous disturbances of cholæmia.218
218 Davaine, op. cit., p. 962.
Enlargement of the spleen is a very frequent symptom, being present, according to Davaine, in 11 out of 13 cases, and, according to Heller, in 25 out of 29 cases, in which this fact was made the subject of direct inquiry.
Pressure on the vena cava causes oedema of the inferior extremities in a small number of cases; and on the vena porta, ascites. There may occur thrombosis of the portal, in which event the ascites will form very quickly, and return as quickly after tapping.
The usually placid course pursued by echinococcus of the liver may be much modified by inflammation and suppuration. Some external injury may develop the inflammation. Having occurred, the clinical history corresponds to other cases of hepatic abscess, and the reader is therefore referred to the section on that topic for fuller information.
DIAGNOSIS.—At the outset of echinococcus of the liver the [p. 1105] differentiation of the tumor from other tumors, and of the disturbances produced by it as contrasted with the effects of other morbid growths, becomes exceedingly difficult, if not impossible. The size, painlessness, elasticity, the purring tremor of the echinococcus tumor, afford a sure basis for constructing a diagnosis, and as ultimately developed they become the means of accurate differentiation from other morbid growths of that locality. All doubt as to the nature of a given hydatid tumor of the liver may be set at rest by the use of the aspirator. The discovery of the characteristic hooklets of the scolex in the fluid withdrawn from the tumor will be conclusive as to the presence of echinococci. The hooklets may be absent, as in the case of acephalocysts, but the fluid is characteristic in other respects: it contains a large quantity of chloride of sodium and is free from albumen.
Very great difficulty is experienced in diagnosticating an echinococcus tumor developing from the upper surface of the liver, pushing the diaphragm and lungs upward and displacing the heart to the left. Whilst the physical signs may be, and are, usually alike when the condition calling for diagnosis has existed for some time, there are means of differentiating in the history of the cases and in the initial symptoms.
The origin and growth of the echinococcus tumor are obscure and free from constitutional disturbance; the onset of a pleuritic exudation is marked by pain, fever, and hurried respiration and by physical signs of a characteristic kind. It is true there are cases of so-called latent pleurisy in which a hydrothorax forms without any well-marked indications, but it will usually be found that some local pain, hurried breathing, or other symptoms existed from the beginning. Those cases of hydrothorax accompanying renal and cardiac diseases are readily enough associated with their original cause.
Echinococcus of the liver may be confounded with abscess of the liver, but a differentiation can be readily made by attention to a few considerations, except in the rare condition of the Echinococcus multilocularis which has proceeded to suppuration. In this latter condition there are no means of differentiation, since an abscess-formation has already occurred, nor is there any need to attempt a distinction without the occasion of a difference. Echinococcus differs from abscess in history, in the character of the swelling, and in progress. Abscess of the liver is preceded by paroxysms of hepatic colic, by inflammatory ulceration of some part of the intestinal tract, or by local injury—traumatism. The onset of a hydatid tumor is silent and painless. The swelling of the liver when an abscess forms is not considerable at any time, and appears to be a uniform enlargement of the organ, except when the pus tends to make its way through the walls of the abdomen externally. An enlarging echinococcus tumor is an obvious projection from the surface of the liver at some point, and it does not have the characteristic tenderness, the fluctuation of an abscess matured and ready to discharge, and the constitutional disturbance; but it does have a peculiar elasticity, and now and then may present that eminently characteristic sign, the purring tremor. The use of the exploring-trocar will usually suffice to clear up all doubts by the withdrawal of the characteristic fluid of the hydatid cyst or of pus.
DURATION AND TERMINATION.—The progress of an echinococcus [p. 1106] tumor is exceedingly slow, and the development of symptoms produced by its extension is early or late according to its position and to the nature of the parts impinged on. A spontaneous cure may take place under the rather rare circumstances of an opening into the hepatic duct or one of its principal divisions, and the gradual discharge of the cysts by this outlet into the intestine. Next to this mode of termination, the most fortunate direction taken by the enlarging cysts is through the walls of the abdomen externally. When the growth is upward through the lungs, the symptoms belonging to empyema or hydrothorax, with pulmonary abscess, ensue, and the termination is fatal after a protracted course. Rupture into the peritoneal cavity is a fatal event. Ulceration into the intestine, and the discharge of the cysts through the route thus made, may effect a cure, but more frequently the fistulous communication becomes a means of forming a fecal abscess.
The result in any case of hydatids of the liver is much influenced by the mode of treatment adopted and the period at which it is undertaken. As these parasites can be readily reached and destroyed by safe means, obviously the more early the diagnosis is made and the treatment carried out, the less the injury done to the hepatic structures and neighboring parts.
TREATMENT.—Prophylactic.—As the intestine of the dog is the natural habitat of the Tænia echinococcus, and as the hydatid is the first stage in the development of the ovum and the second in the life-history of the parasite, the means of prophylaxis consist in preventing contamination of human food and water with the dog's excrement, which contains the ova of the parasite. In Iceland, where hydatid disease is very prevalent, dogs and human beings living in the same huts and obtaining their water-supply by melting the snow just about them, contamination of food and drink must readily occur. In this country such conditions cannot exist; nevertheless, cases of hydatids are not infrequent. The chief, if not the only, source of contamination is through the consumption of such uncooked vegetables as lettuce, celery, cabbage, etc., in the folds of which the ova may be retained, and from which an ordinary washing does not suffice to detach them. It follows that such articles of food should be minutely inspected and cleansed before being placed on the table.
Boiling and filtration are the means of removing impurities of this kind from potable waters.
Therapeutical.—The remedial management of cases of Tænia echinococcus is necessarily restricted to that stage in their development when by increasing size the functions of organs begin to be affected. Internal medicines given with the view to arrest the growth of the parasite are useless. Formerly, such attempts were made and successes were claimed, but it is now known that no medicine can act on organisms enclosed as these are in a dense capsule. It is needless to occupy space with therapeutical details of this kind, but mention may be made of the agents that were supposed to be effective. Laennec held that baths of a solution of common salt had a distinct curative effect. The internal use of iodide of potassium and the local application of iodine paint were believed to cure a case in St. George's Hospital, London, in the practice of Mr. Cæsar Hawkins. Kameela was, in Iceland, supposed to have a curative effect, but notwithstanding this the physicians of that island resort to very heroical surgical methods in the treatment of this affection.
[p. 1107] The one means of relief consists in the removal of the vesicles, either by suitable incisions or by compassing the death of the parasite, after which the power of nature may be adequate to the cure. In Iceland large incisions are made into the tumor at its most prominent part, and, although accidents are not uncommon, the results in many cases are eminently satisfactory. The accidents are shock, hemorrhage, and especially peritonitis. Under favorable circumstances now no procedure is more satisfactory in its results than free incision and drainage. The tumor should be prominent, adherent all round to the peritoneum, and the walls of the abdomen thin to ensure complete success without accident. At the present time, so great have been the advances in abdominal surgery, this operative procedure may be preferable in some few cases presenting the favoring conditions above mentioned.
Very simple expedients, however, suffice in most cases. The most simple is puncture. This is now much practised in Iceland, and, as the statistics show, with considerable success. Thus, Hjaltelin219 reports 100 cases cured in this way, and in his own hands this expedient proved successful in 41 out of 50 cases operated on. In Australia, where hydatid disease is also quite common, simple puncture has effected a large proportion of cures,220 and is the method of treatment usually pursued. In England puncture has the approval of some of the best authorities.221
219 Davaine, op. cit., p. 605.
220 The Medical Times and Gazette, August, 1873, p. 164.
221 Transactions of the Clinical Society for 1872: discussion participated in by Gull, Bryant, Greenhow, etc.
The mode of performing this operation consists in the introduction of an exploring-trocar into the most prominent part of the tumor. It may be withdrawn at once or be permitted to remain for a few minutes to several hours. The dangers are suppuration in the sac and peritonitis; but the former, although sometimes accompanied by severe constitutional symptoms, is not likely to endanger life, and even formidable disturbances due to the latter are usually recovered from. The facts show that puncture very rarely indeed causes dangerous, especially fatal, symptoms. An eruption of urticaria has been observed to follow puncture with the trocar, and also aspiration, in a considerable proportion of the cases, but it has no special significance.
Since the introduction of the aspirateur, puncture and withdrawal of the fluid by means of this instrument has been practised more frequently, and this appears to be a more effective procedure, than simple puncture with an exploring-trocar, although in most cases the escape of the contained fluids suffices to destroy the parasite. The aspirateur is less likely to permit the escape of fluid into the peritoneal cavity or the entrance of air into a vein punctured by accident. If puncture with the trocar or aspiration be practised, shall all the fluid be withdrawn at once? The answer to this question may be decided by the character of the sac. Does it contain daughter and granddaughter vesicles? If so, one puncture may not permit the escape of much fluid; but in any event it is the practice of the most judicious and experienced authorities222 to withdraw as much as possible of the contents of the cysts at the first operation. Formerly, a method practised by some French surgeons consisted in successive tappings, a small quantity of fluid being drawn off each time.223 [p. 1108] There is no good reason for this method of treatment now, and it seems to have been discontinued.
222 Transactions of the Clinical Society, loc. cit.
223 Davaine, supra.
Yet another method of treatment, but less effective than puncture or aspiration, consists in injecting into the sac, after the removal of its contained fluid, certain agents toxic to hydatids. A solution of the extract of fern, alcohol, solution or tincture of iodine, and bile, are the chief remedies thus employed. It has long been known that bile is destructive of these parasites, and cases have occurred of spontaneous cure in which the opening of the growing cysts into a bile-duct has secured the entrance of bile and consequent arrest of growth and atrophy of the hydatids. Several successful cases have been reported in which the injection of aspidium (male fern) was the effective agent, but the threatening symptoms produced by it, and the comparative freedom of other methods of treatment from such disturbances, do not recommend the injections of fern. In the case reported by Pavy224 the extract of fern was mixed with a solution of potassa.
224 Lancet (London), July, 1865.
Injections of iodine in solution or in the form of tincture have been more frequently practised than of any other material. Davaine,225 who finds it less successful than simple puncture and aspiration, recommends, as affording the best results, a dilute aqueous solution of iodine. Alcohol, a solution of permanganate of potassium, and various antiseptic agents have been used to some extent, but none of them possess any advantages over more simple measures.
225 Op. cit., p. 650.
The latest proposal for the treatment of hydatid cysts, and probably the most effective consistent with entire safety, is electrolysis. Originally suggested by Althaus226 to those who first employed the measure on any considerable scale, it had been mentioned thirty years before by Budd, and appears to have been first practised in Iceland on a single case. The first elaborate attempt to establish electrolysis on a sound basis as a regular procedure was made by C. Hilton Fagge and Mr. Arthur E. Durham.227 They operated on eight cases, and all were successful. The method consists in the introduction of two needles connected with the negative pole, and the application of the positive—a moistened sponge—on the exterior in the neighborhood of the hepatic region. The strength of current employed by Fagge and Durham was that furnished by a battery of ten cells, and which by previous trial was found to decompose a saline solution. The two electrolytic needles, connected with wires attached to the negative pole, were introduced into the most prominent part of the tumor about two inches apart. The current was allowed to pass about ten minutes usually, sometimes a little longer, the sponge on the exterior—the positive pole—being shifted occasionally. The immediate effects are not considerable. The tumor may be rendered somewhat more tense and appear to be enlarged, but more frequently it becomes softer and is lessened in size, the increase of size being due to the disengagement of hydrogen gas, and the diminution caused by the escape of more or less fluid. The immediate effects of the operation varied. In one case no symptom followed, and in this the result was regarded as doubtful, although a cure was considered probable. In the others more or less [p. 1109] constitutional disturbance followed, the symptoms being pain and fever, the temperature ranging between 100° and 103° F. The duration of the fever was from two to nineteen days, the latter in one case only. As has been observed in some of the cases treated by puncture or by aspiration, a rash appeared on the skin—in some instances scarlatinous, in others of urticaria. It is a curious circumstance that an eruption of urticaria is reported to have appeared in one subject in whom a rupture of the sac into the peritoneal cavity is supposed to have occurred.
226 On the Electrolytic Treatment of Tumors, etc., London, 1867.
227 Medico-Chirurgical Transactions, 1871, p. 1 et seq.
Although so little change in the tumor occurs immediately after the operation, yet it undergoes slow absorption, and ultimately disappears. The time occupied in the disappearance of the tumor varies from a few weeks to many months, the difference being due probably to the situation of the growth, those occupying the substance of the liver requiring a longer time to fill up.
Fagge and Durham report a case in which simple acupuncture was followed by a result apparently as good as obtained by electrolysis, and other similar experiences have been published. If the simple introduction of a needle suffices to arrest the growth of a hydatid cyst and induce its atrophy, of course the more complex procedures will be abandoned.
The tendency of the treatment of hydatid cysts has constantly been toward simplicity, and the success occurs in a direct ratio thereto. In forming an estimate of the relative value of the methods of treatment, the average of mortality of each plan becomes the most important factor. Simple tapping and paracentesis, the most frequently adopted mode of treatment, is not without immediate and remote danger. Of 46 cases carefully tabulated by Murchison,228 there were 3 deaths properly attributable to the operation; but the after results—suppuration of the cyst and its consequences, peritonitis, etc.—cannot be measured so accurately. About two-thirds of the cases thus treated result in cure, and in a majority of these a single operation suffices. The injection of the various substances which have been employed for that purpose does not seem to increase the proportion of cures, and their use distinctly enhances the dangers of the treatment. At present, the decision as to the method of treatment to be employed in any case should be made between simple tapping, electrolysis, and acupuncture. Of these, the last mentioned, it can hardly be doubted, is the method which is most desirable, for although it has not been employed so largely as the others, thus far the results have been better: the percentage of recoveries without accident has been higher relatively than by other methods of treatment. As acupuncture presents no special difficulties or dangers, and is but little painful, it may be tried first, reserving more formidable measures for the failures by this simple expedient.
228 Clinical Lectures on Diseases of the Liver, loc. cit.
The Distoma hepaticum, entitled by Linnæus Fasciola hepatica, occurs very frequently in herbivorous animals and occasionally in the biliary [p. 1110] passages of man.229 It is, however, less important than the Distoma lanceolatum, which, although much smaller than the former, occurs in much larger numbers.
229 Davaine, Traité des Entozoaires, Paris, 1877, p. 240 et seq.; also, Cobbold, Entozoa, p. 148.
Distoma hepaticum is a leech-like parasite from 25 to 30 mm. in length, of a brownish color, smooth to the naked eye, but thickly covered with minute spikes or spines to be seen with a low power, and provided with a cephalic (entrance to oral cavity) and an abdominal sucking disk, which are also organs of locomotion. The Distoma lanceolatum owes its name to its lancet shape; it is smaller than D. hepaticum, measuring about 8 mm. in length and half this or less in width; it is unprovided with spines, but contains two suckers at the side. Both parasites are hermaphrodite; the ova, according to Cobbold (p. 166), have "an average longitudinal diameter of 1/180, whilst their greatest transversal measurement is about 1/270." These ova are capable of some movement, provided as they are with a ciliated envelope.
The disease known as the rot in sheep, and a peculiar cachexia entitled by Davaine la cachexie aqueuse, are caused by the presence of distoma. The ova gain access to man through the use of unwashed cress, lettuce, and similar vegetables eaten in the raw state, and in drinking-water. Fortunately, this accident is rare. The number of reported examples collected from all sources by the indefatigable Davaine is twelve.230
230 Ibid., p. 253 et seq.
The larger distoma passes into the common and hepatic duct and gall-bladder, whilst the smaller (lanceolatum) enters the finer ramifications, and, there multiplying, several consequences may ensue. The irritation caused by their presence and development will excite a more or less severe cholangitis, or, accumulating in sufficient numbers, an actual obstruction will be induced, and jaundice and structural alterations of the liver will in turn be brought on.
The DIAGNOSIS of such a malady is, in the very nature of the case, uncertain at best, and in most cases impossible. Nevertheless, it may be made in rare instances. The existence of the rot may cast suspicion on the mutton and kitchen vegetables so situated as to suggest the possibility of contamination with the ova of distoma. Definite and conclusive information will be afforded by the presence of the ova, still more of the more or less fully-developed parasite, in the feces of a patient effected by the symptoms of catarrhal jaundice or occlusion of the biliary passages. By tapping the gall-bladder parasites may be withdrawn.
The SYMPTOMS are those common to cases of catarrh of the bile-ducts (cholangitis), catarrhal jaundice, or occlusion of the passages, as may be. As these have been detailed under their respective heads, it is not necessary to repeat the observations already made.
As regards the TREATMENT, in addition to the methods of management recommended in such cases it may be stated that the use of certain parasiticides offers a reasonable prospect of good results. Creasote, bichloride of mercury, thymol, eucalyptol, oil of wintergreen (gaultheria), and similar agents are rational remedies and should be fairly tried.
The entozoön which by its presence in the blood causes the disease chyluria also inhabits the portal vein. In some parts of the world—Brazil more especially—this disease is exceedingly common. It has occurred also in two or three instances in England, and the writer has had a case within the past year (1884) in Philadelphia. The parasites in this case were found in immense numbers in the urine.
The blood of the portal vein sometimes is actually filled, and the liver substance itself is penetrated, by them, but nothing is known of the alterations they induce in these organs. When cases of hæmaturia or chylous urine due to the Filaria sanguinis hominis occur, the changes are not confined to the urinary organs, but often, doubtless, involve the liver. There are no signs in the present state of our knowledge by which the existence of these parasites in the portal vein and liver can be determined.
Until the middle of the seventeenth century the prevalent views upon the functions and diseases of the pancreas were vague in the extreme. By some the organ was regarded simply as a cushion provided for the protection of the neighboring blood-vessels and nerves; by others it was looked upon as the seat of lesion in many very diverse diseases, as ague, hypochondriasis, melancholia, and so on.
In 1642, Wirsung's discovery of an excretory duct demonstrated the fact that the pancreas was a special organ, and initiated the successful investigation of the physiology and pathology of the gland. For many years after this, however, little progress was made, and it is only comparatively recent investigations that have furnished definite and reliable information upon the subject. Even now our knowledge of the clinical and pathological features of diseases of the pancreas is far behind that of many of the other viscera of the body, the chief reasons for this being the uncertainty in regard to the physiology of the gland and the rarity with which its lesions are primary and uncomplicated.
ANATOMY AND PHYSIOLOGY.—The pancreas is a long, somewhat flattened, narrow, acinous gland, pinkish-white in color, and of looser texture than the salivary glands, which it otherwise closely resembles in structure. It is hammer-shaped, measures from six to eight inches in length, one and a half inches in breadth, and about three-fourths of an inch in thickness, and varies in weight from three to five ounces. The gland is situated in the upper part of the abdominal cavity; the expanded portion, or head, lies in the concavity of the duodenum; thence it extends transversely across the epigastric and both hypochondriac regions on a level with the first lumbar vertebra and in contact with the posterior abdominal wall. As it passes toward the left it gradually decreases in size, and the narrowest part, or tail, rests against the spleen. Behind the organ are the crura of the diaphragm, the aorta, the inferior cava, the superior mesenteric vessels, and the solar plexus; in front of it, the stomach and the left lobe of the liver. Its anterior surface alone is invested with peritoneum, being covered by the posterior layer of the lesser omentum. The ascending portion of the head is intimately connected with the duodenum by dense connective tissue, and at times the descending portion, by extending backward and outward, forms an almost complete ring around the gut; the body is loosely attached by connective tissue to the posterior abdominal wall, and the [p. 1113]left extremity and tail are joined to the left kidney and suprarenal capsule and to the spleen by loose areolar tissue. The gland is supplied with arterial blood by branches springing from the pancreatico-duodenal and splenic vessels; its veins join the splenic and superior mesenteric veins; its lymphatics communicate with the lumbar glands; and its nerves are branches from the solar plexus. The principal excretory duct, the canal of Wirsung, has at its widest part the calibre of a goose-quill. It begins by the union of five small branches at the tail, and extends transversely through the substance of the gland from left to right, nearer the lower than the upper border, and the anterior than the posterior surface; it is joined throughout its course by numerous small branches from the acini, which enter it at acute angles. In the head the duct curves slightly downward, and as a rule opens with the ductus choledochus into the ampulla of Vater in the second portion of the duodenum; sometimes, however, it has a separate opening into the intestine. A second, smaller, duct runs from the ascending portion of the head, and usually joins the main duct, but may also open independently.
The acini of the gland are from .045 mm. to .090 mm. in diameter, and are composed of a very thin membrane lined with pavement cells. The thin walls of the excretory ducts are formed of connective tissue and elastic fibres, and are lined by a single layer of small cylindrical epithelial cells. The terminal extremities of the ducts form a complete network around the glandular cells, resembling the intralobular biliary canaliculi. The acini are imbedded in a mass of adipose tissue which contains the vessels and nerves.
The topographical relation of the head of the pancreas to the ductus choledochus is of clinical importance. As a rule (fifteen times in twenty-two, Wyss), the bile-duct descends near the head, toward the duodenum; frequently it runs through this part of the organ, being either partially or entirely surrounded by the gland substance. Now, when the bile-duct merely passes over the pancreas, any enlargement, unless excessive, would simply push it aside, but when it passes through the head, a comparatively slight amount of disease is sufficient to close it entirely and cause jaundice.
It is only since the observations of Bernard in 1848 that the prominence of the pancreatic juice as a digestive fluid has been recognized. It fulfils several important purposes: in the first place, it emulsifies the fatty articles of food; secondly, it converts starch and cane-sugar into glucose; and, finally, it supplements the action of the gastric juice upon nitrogenous materials and completes their digestion. Each of these changes is probably brought about through the agency of a special ferment (Danilewsky). The pancreatic juice is not secreted continuously. According to the observations of Bernstein, there are two separate secretory flows following each ingestion of food—one occurring shortly after the food enters the stomach; the other a few hours later, corresponding in time to the passage of the food from the stomach into the intestine, the latter being followed by a period of rest until the next meal. Both the condition of nausea and the act of vomiting arrest the secretion. When the vagus is divided and the central extremity of the cut nerve is irritated, the secretion is also arrested, and remains checked [p. 1114]for a long time. The arrest in each instance is attributed to reflex action of the spinal cord and sympathetic nerve. At the same time, irritation of the mucous membrane of the stomach caused by the presence of food increases the flow of pancreatic juice, and so too does simple section of the nerves which accompany the arteries. It would seem, therefore, that the gland is under the influence of two sets of nerves from the vagus—one inhibiting, the other exciting, its secretion.
GENERAL ETIOLOGY.—Pancreatic disease occurs more frequently in men than in women. No period of life is exempt from it, but it is most commonly met with in the aged. The predisposing causes are constitutional syphilis, pregnancy, and hereditary tendency. Among the apparent exciting causes may be mentioned the habitual over-use of alcoholic drinks, gluttony, the excessive use of tobacco, suppression of the menstrual flux, the abuse of purgatives, excessive and prolonged mercurial medication, and mechanical injuries, either prolonged pressure or blows upon the epigastrium. As a secondary affection, disease of the pancreas is associated with chronic diseases of the heart, lungs, liver, alimentary canal, and abdominal glands, and the organ may be the seat of metastatic abscesses and tumors.
GENERAL SYMPTOMATOLOGY.—The objective symptoms are—rapid and extreme emaciation of the entire body; sialorrhoea; obstinate diarrhoea with viscid stools; fatty stools; lipuria; and the presence of masses of undigested striped muscular fibres in the stools.
The well-established fat-absorbing and peptonizing properties of the pancreatic juice furnish a ready explanation of the wasting of the body which occurs when this secretion is arrested, diminished in quantity, or altered in quality by disease. Emaciation is not a constant symptom of pancreatic disease. A number of cases are mentioned by Abercrombie, Claessen, and Schiff in which, notwithstanding disease of the gland and complete closure of the duct, revealed by post-mortem examination, the patients during life were not only well nourished, but even moderately corpulent. In such instances it is probable that the digestive functions of the absent pancreatic juice are more or less adequately performed by the bile and succus entericus. When present, emaciation is an early symptom; it is at the same time progressive, and is usually very intense in degree, being most marked in those cases where there is associated hepatic disease or obstruction to the passage of bile into the intestine, where the disease of the pancreas interferes mechanically with the processes of nutrition by pressing upon the pyloric extremity of the stomach or upon the duodenum, and when the organ is the seat of carcinomatous growths. In the last-named condition, in addition to the perversion or arrest of the secretion, the loss of flesh is attributable to the general causes of malnutrition attendant upon carcinoma wherever situated.
Sialorrhoea, or an excessive secretion from the salivary glands, is noticeable as a symptom of disease of the pancreas only when there is an associated lesion of the stomach, either of a catarrhal or cancerous nature. Under these circumstances a quantity—six or eight fluidounces—of a colorless, slightly opalescent, and adhesive and alkaline fluid may be expelled from the mouth at once as an early morning pyrosis; or by frequent and repeated acts of expectoration, following a sudden filling of the mouth with fluid, a large bulk of thin saliva may be expelled [p. 1115] during the day. This hypersecretion must not be looked upon as any indication of an especial sympathy existing between the salivary glands and the pancreas, neither can it be regarded as a pancreatic flux with a regurgitation of the fluid from the duodenum into the stomach and thence through the oesophagus into the mouth, since during the nausea that must always attend the passage of the intestinal contents into the stomach the pancreatic secretion is arrested, and since the liquid contains salivary, and not pancreatic, elements.
The diarrhoea pancreatica is the least constant of all the objective symptoms; in fact, constipation is present in many pancreatic affections, notably carcinoma. The fecal evacuations in this condition are frequent, thin, viscid, and contain an abundance of leucin. Under the microscope the leucin appears either in the form of concentrically sheathed globules, or as small crystalline rods and scales collected together in the form of wheels or aggregated in clusters. This form of diarrhoea may be attributed to a hypersecretion from the pancreas.
That the presence of fat in the stools is an important diagnostic symptom of pancreatic disease is proved both by clinical and experimental observations. The characters of these stools vary considerably. The fat may appear mixed with the feces in small lumps, ranging in size from a pea to a hazelnut, yellowish-white in color, soluble in æther, and easily melted and burned. Again, after the evacuation has become cool fat may be seen covering the fecal masses, collected into a thick cake around the edges of the containing vessel, or, when the feces are liquid, floating as free oil on the surface. Finally, the fat may be in a crystalline form, the crystals being needle-shaped and aggregated into sheaves and tufts. The quantity of fat also varies. It may be present only in small quantities, or may even be entirely absent from the evacuations in those cases in which the secretion from the pancreas is simply diminished, and the amount is greatest in those instances where there is a simultaneous arrest of the pancreatic and hepatic secretions. It must be remembered, too, that even in health the stools may contain fat; this occurs when an excess of oleaginous food is consumed and after the administration of castor oil or cod-liver oil. These conditions must be eliminated, therefore, in estimating the value of fatty stools as a diagnostic symptom; if, then, at the same time, coincident disease of the liver can be excluded, the symptom becomes almost pathognomonic. The appearance of fat in the stools may be due not only to an arrest of the pancreatic secretion, but also to pressure upon the large lymphatic trunks, interfering with the circulation of the chyle and checking the absorption of fat from the intestine.
Usually, the amount of fat expelled is in direct proportion to the quantity consumed, but occasionally the former greatly exceeds the latter. In such cases there must be some other source for the evacuated fat than the food; and it is probable that fat from the adipose tissue passes into the blood, and thence through the mesenteric vessels into the intestine. This theory would likewise account in part for the rapid and extreme wasting, and for another less frequently observed symptom—namely, lipuria. A case is recorded by Clark of medullary cancer of the pancreas with nutmeg liver, and another by Bowditch of cancer of the pancreas and liver in which lipuria was noted. The fat was observed, after the urine had cooled, floating about on the surface in masses or globules; differing, [p. 1116] therefore, from chyluria, for in this condition the fat is present in the form of an emulsion, and gives the urine either a uniform milk-like appearance, or, after it has been allowed to stand, rests upon the surface in a creamy layer.
When the pancreatic secretion is arrested, most of the animal food which has escaped gastric digestion will pass unchanged through the intestine and give rise to another characteristic condition of the evacuations—namely, the presence in the feces of undigested striped muscular fibres. The amount of these fibres, and indeed their appearance at all in any given case, will depend directly upon the nature of the food consumed.
SUBJECTIVE SYMPTOMS.—The subjective symptoms of disease of the pancreas are abnormal sensations in the epigastrium, and pain.
The abnormal sensations in the epigastrium are weight and pressure, attended at times by præcordial oppression and discomfort. The feeling of weight is usually deep-seated, may be intermittent or constant, and is generally increased or developed by pressure. It is often influenced by position, the assumption of the erect posture or turning from side to side giving rise to a stretching or dragging sensation, as if a heavy body were falling downward or moving about in the upper abdomen.
The pain may be due either to an inflammation of the peritoneum covering the gland or to pressure upon the solar plexus, and consequently varies in character. When it depends upon localized peritonitis, it is constant, circumscribed, and deeply seated in the epigastrium at a point midway between the tip of the ensiform cartilage and the umbilicus; it is rather acute, and is greatly augmented by pressure. The second variety occurs in paroxysms, and is neuralgic in character, the sharp, excessively severe lancinating pains extending from the epigastrium through to the back, upward into the thorax, and downward into the abdomen. These paroxysms—in reality attacks of coeliac neuralgia—are attended by great anxiety, restlessness, and oppression and a tendency to syncope. That calculi in the duct of Wirsung, tightly grasped at the position of arrest, may give rise to paroxysms of pain analogous to biliary colic, cannot be doubted, though there are no positive facts in support of this view.
PRESSURE SYMPTOMS.—When the pancreas becomes enlarged it encroaches upon the neighboring blood-vessels and viscera, interferes with their functions, and thus produces prominent symptoms.
The ductus choledochus from its close relation to the head of the gland is especially liable to become obstructed, with the consequent production of chronic jaundice and the general effects of the absence of bile from the intestinal canal. Pressure upon the portal vein gives rise to enlargement of the spleen; on the inferior cava, to oedema of the feet and legs; and on the aorta, occasionally, to aneurismal dilatation of the vessel above the point of obstruction and to subsequent alteration in the size of the heart. By encroaching on the stomach an enlarged pancreas may cause either displacement of the viscus or stenosis at its pyloric extremity, attended with occasional vomiting of large quantities of grumous, fermenting liquid, pain, constipation, general failure of health, and the distinctive physical signs of dilatation of the stomach. The duodenum may also be pressed upon and more or less occluded, and pain and vomiting occur several hours after food is taken. Occasionally hydronephrosis is [p. 1117] produced, the accumulation being usually in the right kidney and due to obstruction of the corresponding ureter.
A sufficient number of cases have been collected to show that there is an intimate connection between disease of the pancreas and diabetes mellitus. One or other condition may take the precedence, melituria occurring during the progress of pancreatic disease, demonstrating the onset of diabetes, and the appearance of fatty stools in diabetes a secondary involvement of the pancreas. Various theories have been advanced to account for this association, but the true explanation seems to be based upon the experiments of Munk and Klebs. By experimenting upon dogs these observers found that extirpation of the solar plexus produced either permanent or temporary diabetes, whereas section of the hepatic and splanchnic nerves, removal of the pancreas, or ligature of the duct of Wirsung was without effect. From the intimate anatomical relation of the pancreas to the solar plexus it is easy to understand how disease of the gland may give rise to alterations in the nerve-structure, either by direct pressure or by the extension of inflammation along the nerve-fibres connecting the gland with the ganglia; and these alterations in time produce diabetes. In the instances in which diabetes is the primary affection the condition of the pancreas, as proved by post-mortem section, is usually one of simple or fatty atrophy; and it may be assumed that a lesion of the solar plexus is the cause of both diseases, the changes in the pancreas being produced in a similar way to the atrophy of the submaxillary gland after section of the vaso-motor nerves in Bernard's experiments.
The same nerve-lesion may give rise to bronzing of the skin, and two cases are recorded in which disease of the pancreas (cheesy infiltration, cancer) was attended by this symptom.
PHYSICAL SIGNS.—To make a successful exploration of the pancreas the stomach and colon should be as far as possible empty, and the patient placed in a position, with the head and shoulders slightly elevated and the thighs drawn up toward the belly, to relax the abdominal muscles; or if necessary this relaxation must be brought about by the administration of æther. The knee-elbow position is often preferable to the dorsal position in practising palpation.
The condition of the gland giving rise to physical signs is one of enlargement, affecting chiefly and primarily its head, and due generally to the presence of some morbid growth.
Inspection reveals either a diffuse bulging of the upper third of the abdomen to the right of the median line, or a well-defined tumor situated beneath the right costal border, about the line of junction of the right hypochondriac and epigastric regions. Often the pancreatic tumor does not come in direct contact with the abdominal wall, but presses against and thrusts forward the left lobe of the liver, producing simply a prominence in the epigastrium. In the first condition palpation elicits an ill-defined sense of resistance; in the second, the fingers readily outline a tumor, which is slightly movable, rounded in shape, firm or fluctuating, with a smooth or nodulated surface, usually tender to the touch, and often giving a false impulse transmitted from the aorta lying beneath; and in the third, the smooth surface and the sharp edge of the left lobe of the liver are easily distinguishable.
[p. 1118] Percussion over a pancreatic tumor is commonly dully-tympanitic, absolute flatness occurring only when it is very large and comes directly in contact with the abdominal wall, pushing aside the stomach and intestines.
On auscultation a blowing murmur may, in some instances, be heard over the tumor. These murmurs are due to pressure upon the aorta, and must be distinguished from the sound produced in aneurism of this vessel.
The various complications of pancreatic disease, such as dilatation of the stomach, ascites, and secondary lesions of the liver, greatly modify the physical signs, and sometimes entirely prevent an exploration of the gland.
This is a rare disease. It occurs most frequently in males during and after adult life, and the strumous diathesis appears to predispose to it. Intemperance, the suppression of normal or morbid discharges, and traumatism act as exciting causes.
ANATOMICAL APPEARANCES.—The pathological changes may be divided into two stages. In the first the gland is deep red in color, intensely injected with blood, greatly increased in consistence, enlarged to the extent of two or three times its normal size, and when an incision is made the divided lobules feel firm and crisp. The interlobular tissue is sometimes dotted with bloody points, and the same hemorrhagic changes may occur in the connective tissue surrounding the gland. In this stage resolution may occur or the inflammation may pass into suppuration. At the beginning of the second, or suppurative, stage numerous minute collections of pus are seen scattered throughout the gland in the interacinous tissue; these gradually collect into a single large abscess, and at times the whole gland is converted into a mere pus-sac, the capsule being much thickened. In other instances the formation of pus is entirely peripancreatic. The pus is usually inodorous and creamy, but is sometimes grayish-white or greenish in color; it then has a faint disagreeable odor, and occasionally is very fetid. When mixed with pancreatic juice it becomes clear and yellowish in color, and contains numerous minute curd-like masses.
In the first stage secondary peritonitis may arise from a simple extension of the inflammatory process, and bands of lymph are formed, gluing the pancreas to the neighboring organs. In the second, fatal acute peritonitis may result from the bursting of an abscess into the peritoneal cavity. These abscesses also occasionally open into the duodenum or stomach. Gangrene and peripancreatic sloughing occur very exceptionally, and are probably due to extensive hemorrhagic changes.
SYMPTOMS AND COURSE.—The disease may be preceded for an indefinite period by symptoms of impaired gastric or intestinal digestion, but its onset is usually sudden. The attack begins with colic or continuous [p. 1119] deep-seated pain, starting in the epigastrium and extending toward the right shoulder or the back, and quickly becoming very intense. The pain is attended by pallor of the face, great restlessness, præcordial anxiety, dyspnoea, and faintness. The tongue is furred or dry and red; thirst is increased; the appetite is lost; there are frequent eructations, nausea, and constant vomiting of a clear, greenish, viscid fluid; the vomiting produces no sense of relief, and even increases the epigastric pain. The bowels are obstinately constipated. The epigastric region is tense, tumid, and excessively tender, so that it is usually impossible to elicit the physical signs of enlargement of the gland. There is moderate pyrexia, with evening exacerbations, and the pulse is increased in frequency. Jaundice does not occur.
These symptoms progressively increase in severity, and reach their maximum intensity in from three to five days. The pulse then becomes small, compressible, and irregular, the extremities cold, the face hippocratic, and death takes place in a state of collapse. The fatal termination is preceded by the symptoms of acute peritonitis in the cases which are complicated by an extension of inflammation or the rupture of an abscess into the peritoneal cavity.
Recovery is quite possible in the early stage of the disease. On the other hand, the course may be greatly protracted by a change in the type of the inflammation, resulting in induration and enlargement of the gland or in the formation of chronic abscesses. Again, when peritonitis from extension has been confined solely to the portion of the peritoneum that covers the gland, and has resulted in the formation of fibrinous bands binding the pancreas to the adjacent viscera, the symptoms of pancreatitis will on subsiding give place to those of obstruction of the stomach, duodenum, or bile-duct.
DIAGNOSIS.—The diseases most likely to be confounded with acute pancreatitis are biliary colic and the catarrhal form of acute gastritis.
From biliary colic it is distinguished by the absence of rigors, jaundice, enlargement of the liver, and a tender pyriform tumor corresponding in situation to the gall-bladder and due to its distension with accumulated bile. The pain in both affections is sudden in its onset, and very similar in character and distribution; but when caused by the passage of a gall-stone it usually begins either after a heavy meal or after some severe muscular exertion or shaking of the body—circumstances inoperative in the production of the pain of pancreatitis. The pain, too, in the former condition is less severe at first, increases gradually in severity, is more paroxysmal, is at the outset lessened by pressure, and is often temporarily relieved by the act of vomiting. The attacks at the same time are rarely isolated, and all doubt is removed when the pain ceases suddenly and a calculus is discovered in the feces.
Acute gastric catarrh is almost always traceable to the ingestion of some irritant substance, usually alcohol or food of bad quality. This history, together with the liability of the attack to occur during the course of chronic dyspepsia, the comparatively trifling severity of the pain, the headache, the irregularity of the bowels, the condition of the urine, which is either high-colored or deposits lithates abundantly, and the tendency of the affection to become chronic, are the points of distinction between this and the pancreatic disease.
[p. 1120] Acute inflammation of the stomach, or gastritis proper, resulting from corrosive poisons, presents a train of symptoms entirely different from those of acute pancreatitis.
TREATMENT.—Absolute rest is essential. The diet should consist of milk guarded by lime-water and of meat-broths, this food being administered in small quantities—one to two or three fluidounces of the milk and lime-water or half as much broth—at proper intervals. In the early stage an effort must be made to reduce the inflammation by the application of ice to the epigastrium or of leeches to the same region, or preferably to the anus. The excessive pain demands the free use of opium. The nausea and vomiting may be relieved to some extent by directing the patient to swallow small lumps of ice, and by the employment of iced carbonic-acid water and the effervescing draught; and the tendency to constipation may be overcome by enemata. Later in the course of the disease, if the epigastric tenderness permits of it, light linseed poultices should be placed over the upper abdomen. During the stage of collapse alcoholic stimulants and the application of heat to the extremities are necessary. The occurrence of acute peritonitis or other complications and sequelæ demand appropriate treatment.
In this condition the pancreas may be the seat of either acute parenchymatous inflammation or of metastatic abscesses.
Acute parenchymatous degeneration of the muscles, kidneys, liver, and so on is recognized as a frequent lesion in the acute infectious diseases, particularly typhoid fever; and it is under these circumstances, and in association always with similar changes in some of the organs mentioned, that parenchymatous degeneration of the pancreas takes place.
Metastatic suppurative inflammation is very rare: it has been observed in cases of disease of the testicles after the operation of extirpation of these organs, and occasionally in puerperal peritonitis.
ANATOMICAL APPEARANCES.—In parenchymatous inflammation the gland at first is hardened, swollen, and reddened, and on section presents a reddish-gray surface, with indistinctness of the glandular structure, due to the amount of swelling of the acini. Under the microscope the gland-cells are found to be enlarged; they contain several nuclei, their protoplasm is infiltrated with fatty granules, obscuring the nuclei to a certain extent, and their outline is well defined. These alterations are most marked in the head of the gland. After a time the hypertrophy of the cells, by pressing upon the blood-vessels, produces an anæmic condition and the organ becomes pale; in the advanced stages softening occurs.
Metastatic suppurative inflammation leads to the formation of a single large abscess or to multiple minute purulent collections.
SYMPTOMS AND COURSE.—Parenchymatous degeneration gives rise to no distinctive symptoms. Its occurrence in typhoid fever or other infectious disease may be suspected when after prolonged hyperpyrexia there are enlargement of the liver and spleen and albuminuria. The appearance of jaundice (from pressure) increases the probability of involvement of the pancreas in the general gland-change.
[p. 1121] The development of rigors, alternating with flushing, during the course of one of the lesions liable to be attended with metastatic abscesses in the pancreas might suggest the formation of pus in the gland, but an absolute diagnosis is impossible.
Several cases are on record pointing to the possibility of a metastasis of mumps from the parotid gland to the pancreas. In these the disappearance of the parotiditis was followed by symptoms resembling those of idiopathic pancreatitis—namely, thirst, fever, loss of appetite, anxiety, and burning in the epigastrium, with deep-seated pain extending toward the right side; in addition there was diarrhoea, with numerous, yellowish, watery stools. In one case that resulted fatally the secondary diarrhoea suddenly ceased and the parotid swelling reappeared. At the autopsy the pancreas was found to be swollen, reddened, engorged with blood, and indurated. Such a metastasis, however, must be very infrequent, and more extended observations are necessary to establish its course and clinical features.
The first form of acute secondary pancreatitis may be a comparatively unimportant complication of the acute infectious diseases, or, together with the parenchymatous degeneration of other organs, may form a distinct element in the fatal issue of these diseases.
Metastatic abscesses are prone to be followed by ulceration and the formation of fistulous communications with the neighboring viscera.
TREATMENT.—The management of secondary inflammation of the pancreas is regulated solely by the indications derived from the originating disease.
Inflammation of the connective tissue of the gland usually occurs after adult life, and depends upon a variety of causes.
The secondary form, due to long-continued venous engorgement resulting from lesions of the cardiac valves and from chronic disease of the lungs or liver, is the most frequently observed.
Other causes are closure of the duct of Wirsung, the retained secretion producing pressure upon the glandular tissue; the extension of inflammation from adjacent organs, as the bile-duct when there is an impacted gall-stone, or the stomach and duodenum, especially in cancer and perforating ulcer, where the floor of the ulcer is formed by the pancreas; the pressure of tumors, as aneurisms of the abdominal aorta and coeliac axis; chronic alcoholism; and syphilis.
ANATOMICAL APPEARANCES.—The lesion may be limited to the head or to isolated portions of the gland, or be uniformly distributed. The general changes are a hyperplasia of the interacinous connective tissue, with subsequent contraction and atrophy, or, in extreme instances, entire destruction of the glandular elements proper, the organ becoming granular and firmer and tougher than normal. A section shows a pale surface, studded at intervals with white spots, from which little cheese-like and fatty masses may be squeezed, and, when there has been intense hyperæmia, with minute collections of reddish pigment and small hemorrhagic cysts, indicating previous interstitial hemorrhages.
[p. 1122] When the contraction causes closure of the small excretory ducts or of the duct of Wirsung itself, the section shows secondary cysts and beaded canals.
In exceptional instances of acquired syphilis the pancreas is the seat of gummata or sclerosis, but in congenital syphilis hyperplasia of the glandular connective tissue frequently occurs, being usually associated with specific lesions of the lungs, liver, kidneys, and general glandular system.
SYMPTOMS AND COURSE.—As chronic pancreatitis rarely attains a sufficient degree of development to interfere seriously with the function of the organ, the disease is usually latent, or masked by the symptoms of the originating lesion in secondary hyperplasia, or by the associated diseases of the abdominal viscera in alcoholism and acquired syphilis.
When due to hereditary syphilis, the foetus is stillborn or death takes place soon after birth, and there are no characteristic symptoms.
Occasionally, however, especially when it depends upon a complete obstruction of the duct of Wirsung, a diagnosis may be made from the presence of emaciation, fatty stools, and melituria, with epigastric pain of a neuralgic character, and the discovery of a deep-seated, dense tumor extending transversely across the epigastrium.
The duration is indefinite, and varies greatly with the cause. While a return to the healthy condition is possible during the early stage of the lesion, the usual course is similar to that of chronic interstitial inflammation in other organs.
TREATMENT.—The management, when a diagnosis can be made, must be guided mainly by the etiological indications. The restoration of the functions of the heart, lungs, or liver when these organs are at fault, the abstinence from alcohol in the drunkard, and an energetic use of mercurials or iodide of potassium in syphilis, are of the first importance in arresting the disease. A persistent course of mild purgatives and of cathartic mineral waters is serviceable. Pain should be relieved by belladonna or opium. The diet must be simple and digestible, and if an arrest of the pancreatic secretion be indicated by the appearance of fat in the stools, an effort should be made to supply the deficiency. For this purpose pancreatin, prepared by precipitation by alcohol from a watery extract of a calf's or pig's pancreas, may be used.1 The pancreatin may be given in doses of from five to fifteen grains, in the form of a pill or in capsules, and at an interval of two hours after food is taken, or the same quantity of pancreatin may be added to the food a few moments before it is eaten. Probably the best substitute is a watery infusion of the gland containing all its soluble principles. To prepare an active infusion the pancreas must be taken from the animal during the act of digestion. It is then freed from its surrounding fat, and macerated for two hours in four times its weight of water at a temperature ranging between 25° and 30° C. (58.3° and 61.1° F.). Another plan is to beat a calf's pancreas in a mortar with six fluidounces of water until a milk-like fluid is obtained, and strain. One-third of the infusion obtained by either method is administered after each meal, an entire pancreas being thus used every twenty-four hours.
1 One gramme of pancreatin is sufficient to emulsify fifteen grammes of fatty substances, to convert eight grammes of starch into glucose, to digest fifty grammes of fibrin, twenty grammes of syntonine, and thirty-three grammes of boiled albumen (Raymond).
[p. 1123] The extractum pancreatis,2 as it is now furnished to the profession, is a very useful preparation. It may be employed to peptonize milk, milk-gruel, and broth, or be given in combination with bicarbonate of sodium at a fixed interval after each meal, as in the following formula:
| Rx. | Ext. pancreatis, | drachm j; |
| Sodii bicarbonatis, | drachm ij; | |
| M. et. ft. Chart No. XII. | ||
S. One powder to be taken two hours after each meal.
2 That prepared by Fairchild Brothers & Foster of New York has proved the best in my hands.
Peptonized milk is prepared by putting into a clean quart bottle 5 grains of extractum pancreatis, 15 grains of bicarbonate of sodium, and a gill of cool water; shake, and add a pint of fresh cool milk. Place the bottle in water not so hot but that the whole hand can be held in it without discomfort for a minute, and keep the bottle there for exactly thirty minutes. At the end of that time put the bottle on ice to check further digestion and keep the milk from spoiling.
Peptonized milk-gruel is made of equal parts of any farinaceous gruel and fresh cold milk. To a pint of this combination 5 grains of extractum pancreatis and 15 grains of bicarbonate of sodium are added, and the whole allowed to stand in a warm place for thirty minutes, when the process of digestion must be arrested by placing on ice.
Peptonized broth is made in the following way: Take one-fourth of a pound of finely-minced raw lean beef or mutton or chicken, and one-half pint of cold water; cook over a slow fire, stirring constantly, until it has boiled a few minutes. Then pour off the liquor, beat the meat to a paste, and put both into a bottle with a half pint of cold water. Add 30 grains of extractum pancreatis and 20 grains of bicarbonate of sodium; shake well, and set in a warm place (110-115°) for three hours, shaking occasionally; then boil quickly. Finally, strain or clarify in the usual way and season to taste.
Cancer is probably the most common of the chronic affections of the pancreas. It is usually secondary, being due to an extension of carcinoma of the stomach, duodenum, liver, or abdominal lymphatic glands, but there are enough cases on record to show that it may be primary. It has been discovered in the foetus at birth, but the vast majority of cases occur after the age of forty. Men are more frequently affected than women. Nothing is known as to the influence of inherited tendency in the production of the disease, and as little of the exciting causes, though some authors attach much importance to prolonged pressure upon the epigastrium and to blows and contusions on the upper part of the abdomen.
ANATOMICAL APPEARANCES.—Primary carcinoma may be either [p. 1124] scirrhous, encephaloid, or colloid, the first being the variety most frequently observed.
The lesion begins in the head of the gland in the form of several small nodules which gradually coalesce. Sometimes the whole gland becomes involved in the new formation; again, isolated nodules may be scattered throughout its substance, and exceptionally the growth is limited to the tail or middle portion. When the head alone is involved, the remainder of the gland either remains healthy, undergoes fatty degeneration, or becomes indurated. The tumor is rounded in outline and nodular, and varies in size, density, and color according to the form of carcinoma present. The duct of Wirsung is ordinarily obstructed, large retention cysts, containing a yellowish-red liquid, are formed, and the changes already described under the head of Chronic Interstitial Pancreatitis take place in those portions of the gland which are free from carcinoma. The disease is very prone to extend to the surrounding organs, particularly the neighboring lymphatic glands, the duodenum, and the liver, rarely to the stomach. When the contiguous organs are not directly implicated in the carcinomatous changes, they are subjected to pressure by the tumor, and in the case of the stomach and duodenum adhesions often form, and are followed by perforation. There seems to be a tendency also to infiltration of the adjacent subperitoneal connective tissue and to hyperplasia of the fibrous tissue of the viscera, even when they are not secondarily involved in the morbid growth, leading to narrowing of the aorta, thickening of the walls of the stomach and duodenum, and a sclerosis of the liver. Obstruction of the common bile-duct, with dilatation of the gall-bladder from retention of bile, is a frequent result of the disease.
Secondary carcinoma of the pancreas usually first appears in, and is limited to, the head of the gland. It seldom occurs in isolated nodules, but the growth is generally continuous with the primary cancerous mass. The form is either scirrhous or encephaloid. Wagner records a case of cylindrical-celled epithelioma following a simple epithelioma of the mucous membrane of the duodenum; and a similar instance has come under the author's own observation;3 but this variety of morbid growth is rare. The primary growth is almost uniformly situated in the stomach, duodenum, liver, or gall-bladder, though occasionally it may be seated in some distant organ; in such cases the pancreatic tumor appears as an isolated nodular mass.
3 Transactions of the Pathological Society of Philadelphia, vol. ix. 13.
SYMPTOMS AND COURSE.—The symptoms may be divided into two classes—namely, first, those which arise from the lesion of the gland itself; and, secondly, those which depend upon the effect of this lesion on the neighboring viscera.
The features belonging to the first class are general marasmus, pain, the appearance of fat and perhaps undigested muscular fibres in the fecal evacuations and of fat in the urine, and the physical signs of an abdominal tumor.
Loss of flesh is one of the earliest symptoms: it is generally progressive, and is at times so great that the spine can be distinctly traced through the abdominal walls. Together with this emaciation there is debility, often extreme, but sometimes not so marked as might be expected from the degree of wasting. The skin is commonly pale and dry, and before jaundice is [p. 1125] developed has the ordinary sallow hue of cancerous cachexia. The features are pinched, and the face wears an expression of anxiety and suffering. In cases uncomplicated by peritoneal inflammation the temperature remains about normal, or it may be lowered as the general exhaustion increases. The pulse is feeble and slightly increased in frequency.
Pain is the most uniformly present and the earliest symptom. It is always situated deep in the epigastrium, and from thence extends to the back, to the right or left side, downward to the umbilicus or lower part of the abdomen, and upward into the chest. It is generally continuous, but is subject to remissions and paroxysmal exacerbations. During the remissions sensations of distress, of burning, or of dull pain are experienced at the pit of the stomach; during the exacerbations, which may last several days, the pain becomes extremely acute and lancinating and extended in distribution. The ingestion of food and pressure upon the epigastrium have no constant effect upon the pain. Quick movements of the body from side to side often increase it and excite exacerbations. The suffering is greatest in the erect posture, and on this account the patient bends his body forward so as to relax the abdominal muscles. The paroxysmal and neuralgic character of the pain indicates implication of the coeliac plexus.
The appearance of fat in the stools is an important symptom, unless there be at the same time an obstruction to the passage of bile into the duodenum, indicated by jaundice. Lipuria has been noticed in a few cases only.
In many instances (nearly one-half of the number of recorded cases) physical exploration reveals the signs of enlargement of the organ. At times there is merely a sense of fulness and resistance to the touch, and a modified tympanitic percussion note in one of the three regions of the upper segment of the abdomen. But usually when a tumor is present it is readily mapped out by palpation. The tumor is seated in the epigastrium, and may extend into the right or left hypochondrium or downward into the umbilical region. It varies much in size, is rounded, nodulated, firm, slightly movable or fixed, and tender, though sometimes painless, to the touch. Percussion yields dulness or a dull-tympanitic sound. On auscultation a blowing murmur may be heard when the tumor presses upon the aorta; and when this murmur is present there is usually also transmitted pulsation.
The symptoms belonging to the second class arise when the adjacent viscera become involved in the cancerous disease, or when their functional activity is disturbed by the encroachment and pressure of the enlarged pancreas.
From the association of a catarrhal condition of the mucous membrane of the stomach, particularly when the pyloric orifice is obstructed, several prominent symptoms of gastric catarrh are frequently observed—namely, sialorrhoea, pyrosis, acid eructations, flatulence, abnormal sensations, such as burning, weight and oppression in the epigastrium after taking food, and increased thirst. The tongue varies in appearance: it may be dry and covered with a brown or yellow fur, but when the flow of saliva is increased it is peculiarly clean and moist; and this condition is rather characteristic. The appetite is also variable; sometimes it remains good [p. 1126]until the end, and occasionally it is perverted. Hiccough in some cases is an obstinate and annoying symptom.
Nausea and vomiting are late but moderately constant features. Their relation to the ingestion of food is not fixed. The vomited matter may consist of food, of glairy mucus more or less tinged with bile, of colorless liquid, or of a fluid resembling a mixture of bran and water. If there is marked pyloric obstruction with dilatation of the stomach, large quantities of frothy and fermenting material containing sarcina ventriculi are rejected at intervals. In the rare cases in which secondary sarcoma of the viscus is developed the ejecta are bloody or have the coffee-ground appearance, and the vomiting occurs several hours after eating, as the new growth is generally situated at the pylorus. When there is adhesion of the pancreatic tumor to the stomach, with perforation, both blood and pus are vomited. Dilatation of the stomach is attended by prominence of the epigastrium and an extended area of gastric tympany, and in cancer of the pylorus a tumor is often appreciable on palpation. The bowels are usually constipated. The fecal evacuations are hard, and when the biliary secretion is absent from the intestine they are clay-colored, and often contain fat. When there is ulceration of the mucous membrane of the duodenum following secondary cancer or adhesion, the stools become black and tar-like from the presence of altered blood. Complete obstipation occurs in mechanical obstruction of the gut from direct pressure or from bands of lymph. Occasionally, just before death there is diarrhoea, and there may be an alternation of vomiting and diarrhoea.
The symptoms and signs of secondary carcinoma or sclerosis of the liver may be present, but the most commonly observed indications of impaired hepatic function depend upon pressure-obstruction of the common bile-duct. These are jaundice, fatty and clay-colored stools, and the appearance of a tumor in the region of the gall-bladder. Jaundice is a very common symptom. It occurs late in the disease as a rule, is progressive and persistent, resisting all treatment, and is extreme in degree, the skin becoming deep-yellow or greenish in color. The tumor of the distended gall-bladder is pyriform in shape, firm and elastic to the touch, yields a dull percussion sound, and occupies a position opposite the extremity of the tenth rib on the right side of the abdomen.
Dropsy occurs in a large proportion of cases (nearly one-half) during the advanced stages of the disease. It is due to vascular obstruction occasioned by the pressure of the enlarged pancreas itself or of the secondarily degenerated coeliac glands, and finally by secondary lesions of the liver. The dropsy appears either in the form of ascites or anasarca, is not often extreme in degree, and is subject to variations, disappearing and reappearing at intervals. Ascites is the more common form, but both conditions may exist in the same patient.
It is impossible in the majority of instances to definitely fix the date of onset of a pancreatic cancer, but the average duration of the disease may be stated to be about one year. The uniformly fatal termination usually takes place slowly from gradual exhaustion or with the symptoms of an adynamic fever, but death may occur suddenly from hemorrhage.
DIAGNOSIS.—The principal features of carcinoma of the pancreas are extreme emaciation, loss of strength, dyspepsia, pain of a neuralgic [p. 1127] character in the epigastrium, constipation, obstinate jaundice, moderate ascites or anasarca, the appearance of fat in the stools, lipuria, occasional vomiting, and the physical signs of an epigastric tumor.
These symptoms are not pathognomonic, however, and the diagnosis can be certainly established only when it is possible to exclude primary disease of the surrounding organs, especially of the stomach and liver.
Cancer of the stomach may be excluded by the less-marked character of the functional disturbances of the viscus; by the absence of frequent vomiting, hæmatemesis, and the rejection of coffee-ground material; by the somewhat different situation and greater immobility of the tumor, by the seat, distribution, and constancy of the pain; and by the presence of jaundice and of fat in the stools and urine.
Diseases of the liver attended with alterations in the size of the organ, as cancer, abscess, albuminoid and fatty degeneration, sclerosis and hydatid tumor, have sufficiently characteristic physical signs and symptoms to be readily distinguished from cancer of the pancreas. On the other hand, the tumor of an enlarged gall-bladder is often confusing. The situation of this tumor opposite the tenth rib and its pyriform shape are important; other distinguishing points depend upon the cause of the enlargement. In enlargement from accumulated bile the tumor is elastic and fluctuating; from accumulation of gall-stones, hard and nodulated, movable, painless on palpation, and often the seat of crackling fremitus, produced by manipulation and due to the rubbing together of several calculi; from cancer, hard, nodular, the size of an orange, tender on pressure, rapid in growth, preceded by attacks of biliary colic, and attended by fistulous communications with the intestines and the passage of gall-stones per anum.
In aneurism of the aorta or coeliac axis the tumor may present in the epigastrium and produce analogous pressure symptoms. But the pain is more of the character described as wearing, and is usually augmented at night: on grasping the tumor a uniform expanding pulsation is felt in place of the to-and-fro movement appreciable in a tumor resting upon a healthy blood-vessel and receiving a transmitted impulse, while the constitutional symptoms and course are quite different.
The tumor of malignant disease of the omentum, although it appears in the epigastrium or upper part of the umbilical region, is much more movable, and is accompanied by ill-defined symptoms very dissimilar to those of pancreatic cancer.
In cancer of the transverse colon the mass may occupy nearly the same position as a pancreatic growth, but the pain occurs several hours after food is taken; vomiting is absent, and there is frequently hemorrhage from the bowels.
Chronic pancreatitis is accompanied by symptoms simulating those of cancer; the enlargement of the gland, however, is not so great, nor are the indications of pressure upon adjacent organs so prominent. The pain is less severe, the general failure in health more gradual, the progress slower, and constipation less common.
TREATMENT.—The indications are to maintain the strength of the patient, to provide a diet that is nutritious and at the same time easily digested, to allay pain by the employment of narcotics, and to relieve as far as possible the various symptoms as they arise. The plan of [p. 1128] administering a calf's pancreas or extractum pancreatis will prove serviceable when the fecal evacuations contain fat. Nutritious and peptonized enemata may be of service in some cases.
Sarcoma of the pancreas occurs with extreme rarity. It is impossible during life to distinguish it from carcinoma.
Tubercle of the gland is infrequently met with. Some pathologists deny its occurrence, and believe that the cases recorded as such are merely instances of caseous degeneration of the neighboring glands. When it does occur, it is always secondary, the primary disease being situated in the lungs or intestines. The alterations in the gland consist in the development of cheesy masses or of miliary granulations in the connective tissue between the acini. The condition gives rise to no definite symptoms, and its diagnosis during life is impossible.
Two forms of fatty degeneration occur, either separately or combined—namely, fatty infiltration and fatty metamorphosis.
Fatty infiltration consists of a true hypertrophy of the fat-tissue normally existing in the gland, or of an increase and extension into the gland of the peripancreatic adipose tissue. Yellow bands and masses of fat-tissue appear between the acini, and by constantly increasing in size lead gradually to a total atrophy of the cells of the acini. The canal of Wirsung contains a fatty liquid. These changes are found associated with fatty liver, heart, and omentum, in drunkards especially.
Fatty metamorphosis of the gland consists of a change analogous to fatty metamorphosis of other organs. When hyperplasia of the interstitial connective tissue is absent, the organ is flaccid, soft, and diminished in size; the acinous structure remains distinct, though the acini and ducts are filled with a fatty emulsion: after this is discharged or absorbed the gland appears as a flaccid band, and finally becomes entirely atrophied. Fatty metamorphosis occurs in drunkards, in diabetes, in advanced age, in cancer, phthisis, and other wasting diseases.
Neither form of fatty disease gives rise to symptoms by which it can be recognized during life.
This is only found in combination with amyloid change in other organs of the body, and a diagnosis cannot be made.
Hemorrhages into the pancreas may be divided into three classes.
The most common form depends upon passive hyperæmia, the result of chronic diseases of the heart, lungs, or liver. In this condition the effusion of blood coexists with chronic inflammatory changes in the interstitial connective tissue. The appearance at first is of minute bloody points scattered throughout the areolar tissue; later, these change into round or oval pigment masses, or spaces containing reddish serum and surrounded by thickened, rust-colored, irregular walls.
The second class includes the rare cases of hemorrhage resulting from the rupture of one of the large blood-vessels of the gland, and due to some pre-existing change in the vessel walls. In these the pancreas is enlarged, may be converted into a sac containing blood, either fluid or coagulated or partially crystallized according to the duration of life after the hemorrhage has taken place, and a ruptured blood-vessel may be readily discovered on dissection.
The condition in which, without any evidence of passive hyperæmia or gross vascular lesion, the entire pancreas become hemorrhagic, constitutes the third class. The gland is then dark-red or violet in color, the meshes of the interstitial tissue are filled with recent or altered blood, and the acini are stained of a dull-gray hue. The hemorrhage may extend to the connective tissue surrounding the gland. Finally, the organ becomes soft, the peritoneal covering sloughs, and fragments of broken-down gland-tissue escape into the peritoneal cavity. These lesions are so analogous to those which attend thrombosis occurring in other organs that their dependence upon the same cause seems probable.
The first form of hemorrhage is unattended by special symptoms. In the second a pulsating tumor may suddenly appear in the epigastrium, and the ordinary indications of hemorrhage—vomiting, fainting fits, cold extremities, feeble pulse, and general exhaustion—are present. Death may occur suddenly or the patient may linger on for months. In the third condition death usually occurs very suddenly, probably from pressure upon the sympathetic ganglia. There are no symptoms, and the rapid termination prevents the development of general peritonitis, which would otherwise occur from the sloughing of the peritoneum.
There are no indications for treatment.
Obstruction of the excretory duct is a frequent occurrence in pancreatic disease, and is due to two classes of causes—namely, 1st, pressure from without; and, 2d, closure of the canal by catarrhal swelling of its mucous membrane or by calculi.
In the first class may be placed obstruction depending upon contraction occurring in sclerosis of the gland, upon carcinoma of the head of the gland, upon peripancreatic adhesions and indurations, upon the [p. 1130] presence of large gall-stones in the ductus choledochus, and upon carcinoma of the pylorus and duodenum and enlargement of the neighboring lymphatic glands.
In catarrh of the canal of Wirsung the obstruction results either from simple swelling of the mucous membrane or from the presence of a plug of tough mucus.
The formation of pancreatic concretions is by no means a rare event, though these calculi are met with far less frequently than either gall-stones or salivary concretions. They result from precipitation of the inorganic ingredients of the pancreatic juice, and are usually seated in the main duct, although they may be situated in the smaller branches. They may be single or multiple, as many as twenty having been counted in one gland. In shape they are spherical, oval, or branched, with sometimes a smooth, at others a spiculated, surface; their size varies from that of a minute granule to a small walnut; they are usually white or grayish-white in color, but may be black; and are composed of the carbonate of lime or of a combination of the carbonate and phosphate with oxalate of lime. Coincidently with these calculi it is common to find concretions in the kidneys and gall-bladder.
Concretions composed of insoluble protein substances have also been found in the pancreatic ducts (Virchow).
The most probable causes of the formation of pancreatic calculi seem to be catarrhal conditions of the mucous membrane of the ducts and an alteration in the chemical composition of the secretion.
Whatever the cause, the obstruction, when complete, leads to retention of the secretion and the formation of retention cysts.
When the obstruction is situated at the duodenal extremity of the duct, the canal and its secondary branches are either uniformly dilated or sacculi are formed. These sacculi are round or oval, vary greatly in size, sometimes reaching the dimensions of the fist or of a child's head; they may be single, or several of them may be present, differing in size and causing irregular projections of the outer surface of the gland. When the obstruction occurs at some point in the course of the duct, the dilatations and sacculi are found only behind the point of occlusion. The small cysts contain a fluid resembling the pancreatic juice; the larger, a whitish, chalky fluid, which in old cases may contain white friable concretions composed of carbonate and phosphate of lime, and become purulent, or be stained bright red or chocolate-colored from the occurrence of hemorrhage. In such instances hæmatoidin crystals can be discovered by the microscope. The interior of the dilated ducts and of the retention cysts is lined by a single layer of thin flat cells, with irregular edges and with oval flat nuclei. The walls are thickened, and composed of superimposed layers of laminated connective tissue separated from one another by flat nucleated cells. The secreting structure of the gland undergoes atrophy from pressure, or fatty metamorphosis takes place, and, although the gland is increased in size from the presence of the cysts, its functional power is lost.
In addition to causing obstruction of the duct of Wirsung and the changes mentioned, pancreatic calculi may produce induration, atrophy, acute inflammation, or even suppuration of the surrounding glandular tissue.
[p. 1131] SYMPTOMS AND COURSE.—The main feature is the presence in the epigastrium of a rounded, smooth, fluctuating, painless tumor. There are also indications of the absence of the pancreatic secretion from the digestive tract—notably, emaciation, general debility, and the appearance of fat in the stools. Jaundice resulting from a coincident obstruction of the bile-duct is a frequent symptom, and melituria has been noted in some cases. It is probable, too, that the passage of a calculus along the duct may give rise to pain resembling in character and distribution the pain of hepatic colic.
The duration is indefinite. Sometimes the termination is sudden from the rupture of a cyst into the peritoneal cavity or into the stomach or duodenum, with hemorrhage.
DIAGNOSIS.—The absence of pain, of tenderness, and of cachexia, together with the physical characters of the tumor, distinguishes it from carcinoma of the gland.
Though not likely to be confounded with this disease, both hydatid tumor of the liver and distension of the gall-bladder must be borne in mind in making the diagnosis of a fluctuating tumor situated in the upper third of the abdomen.
TREATMENT must be entirely symptomatic. Attention to the general health, proper regulation of the diet, and the employment of pancreatin or an infusion of calf's pancreas to supply the place of the deficient pancreatic juice, are the important steps. Attacks of pancreatic colic indicate the use of anodynes.
In two reported cases in which the cysts were very large paracentesis for the removal of the fluid contents was resorted to, and there are two cases on record in which the cysts were extirpated after abdominal section. Kulenhampff of Bremen records a case of a man, thirty-nine years of age, in whom, after a succession of severe blows upon the abdomen, a tumor appeared in the epigastrium. An exploratory incision was made, and a few ounces of pancreatic fluid evacuated by aspiration. Six days afterward the abdomen was opened, the peritoneum united to the incision, and antiseptic gauze inserted to produce adhesive inflammation between the sac and the abdominal wall. Adhesion taking place after four days, the cyst was opened, a liter of fluid evacuated, a tent inserted, and an antiseptic dressing applied. For sixteen days fluid constantly escaped in slowly diminishing quantities, and the tumor disappeared, a fistulous tract remaining. This completely closed under the use of tincture of iodine and nitrate of silver at the end of the seventh week. Thiersch opened a pancreatic cyst and evacuated three liters of chocolate-colored fluid; recovery with a fistula followed.
From a patient supposed to be suffering from ovarian dropsy Rokitansky partially extirpated a cyst connected with the tail of the pancreas; death from suppurative peritonitis occurred on the tenth day.
N. Bozeman4 on December 2, 1880, successfully removed from a woman forty-one years old a pancreatic cyst weighing, with its contents, twenty and a half pounds. In this instance also the operation was undertaken for the removal of a supposed ovarian tumor, the diagnosis not being established until after the abdomen was opened.
4 New York Medical Record, Jan. 14, 1882.
Italian physicians in the later years of the seventeenth century and in the early ones of the eighteenth had acquired some knowledge of the symptoms of the disease we now call peritonitis, but known to them as inflammation of the intestines. Indeed, it is claimed by some of the admirers of Hippocrates that there are passages in his writings that indicate some knowledge of the disease. But this claim will probably be always received with many doubts as to its validity.
In confirmation of the first statement I will transcribe certain passages from Morgagni's thirty-fifth letter: In inflammation of the intestines "Albertini had observed the pulse to be low and rather weak, such as you will find it to have been in general in the foregoing letter under Nos. 9, 11, 18, and 25." He also observed the abdomen to be tense and hard, the face and eyes to have something unusual in their appearance. "Medical writers, indeed, agree in the tension of the abdomen, but they add many other symptoms, which prove beyond a doubt the intestines to be inflamed; yet they mean that evident inflammation which all may easily ascertain, and not that obscure disorder which we now speak of, and which few suspect" (gangrene of the intestines). "By the same writers it is also supposed that there is an obstinate costiveness and continual vomiting."
Morgagni refers to the assistance rendered by Albertini, Valsala, Van Swieten, Rosa, and others in elucidating this subject. It is singular, considering the clearness of his perception of the symptoms of inflammation of the intestines, that he should be so greatly confused regarding gangrene and sphacelus of the same parts. He looks on these as the result of inflammation, and when the two classes of cases are considered and compared, the result is a contrast and not a resemblance. Yet he supposes that the differences are to be accounted for by the different modes in which the same disease may be developed in different persons.
Another thing obtrudes itself on the attention in these letters: that while a number of post-mortem examinations are reported of those who had died of inflammation of the intestines, of gangrene and sphacelus of the intestines, of hepatic abscess opening into the peritoneal cavity, there is no record of finding in the abdomen anything corresponding to what is now known as the inflammatory effusions from serous membranes.
Sydenham died in 1689. I have searched his works, not for [p. 1133] peritonitis, for the word was not in use in his day, but for some account of inflammation of the intestines or of some disease in the description of which symptoms are named that distinguish or belong to peritonitis, and with the single exception of pain the search has been fruitless.
Cullen in 1775 mentions the disease, but says that so little is known about it that he will not attempt a description of it.
Bichat died in 1802 in the thirty-eighth year of his age. I am not able at present to lay my hand on his Pathological Anatomy; I therefore quote from Chomel's article on peritonitis in the Dictionnaire de Médecine to show his claim to important studies regarding that disease: "For a long time peritonitis was confounded under the name of inflammation du bas ventre with inflammations of the abdominal viscera; and it is to Bichat belongs the merit of having proved that inflammation of the peritoneum is a disease distinct, and that it ought to be separated from enteritis, gastritis, etc., as pleurisy is separate from pneumonia. The studies of Gasc and of Laennec soon confirmed the opinion of Bichat, and assured to peritonitis the important place which it ought to occupy in all nosological tables. It has become since then a subject of numerous observations and of interesting researches regarding the causes de sa marche and the lesions it causes."
The references are not given by Chomel, but they are probably these: Laennec, Histoire des Inflammations du Peritoine, 1804; and Gasc, Dictionnaire des Sciences Méd., p. 490, 1809.
Gasc says that the twenty years next preceding his publication witnessed the first stage of the true history of peritonitis. Walther in 1786 had contributed some facts, and S. G. Vogel in 1795, but the rounding off and completing their work was left for Bichat.
MORBID ANATOMY.—The first thing that strikes the observer in the post-mortem examination of a person who has died of this disease is the tendency of the intestines to protrude through the cut made in the abdominal wall. This is produced by their dilatation generally, both small and large, by gas. No gas, under these circumstances, ever escapes from the peritoneal cavity unless there has been perforation of the alimentary canal somewhere. While the intestines are in this manner dilated, the stomach is small and usually empty.
On the surface of the intestines there will be found a layer of coagulated fibrin, often very thin and delicate, requiring a scraping of the surface of the peritoneum to demonstrate it, but commonly obvious enough, and sometimes quite abundant. This same false membrane can be found on the viscera covered by the peritoneal membrane, on its anterior extension, and most at the point of contact of one coil of the intestine with another. Incorporated with this new membrane or lying under it will often be seen blood-spots, thin, translucent, diffused, and having ill-defined boundaries.
The blood-vessels themselves are not remarkably congested. Here and there may be spots where some redness remains, and the vessels are larger than natural. But the congestion and redness, which analogy leads us to [p. 1134] believe belong to the active stages of the disease, have in great degree disappeared after death.
The peritoneal membrane itself has hardly become thickened, certainly not in marked degree, but it has lost its lustrous surface, is, at least in parts, of an opaline color, as if it had absorbed diluted milk, and there is an effusion of serum or slight oedema on its attached surface. Whatever may be the popular opinion regarding the termination of inflammation of the bowels in mortification, whatever the opinion of the older physicians, it is safe to say that gangrene of the peritoneum has never been the result of uncomplicated, diffuse, acute peritonitis. Peritonitis from strangulation of the intestine or analogous causes is of course excepted. But in puerperal peritonitis I have noticed a fact to which I have nowhere seen an allusion. The parietal peritoneum is at two points in the abdomen but loosely attached to the wall. One of these is on the anterior wall, anterior to and a little above the iliac fossa; the other is above and below the kidney on each side of the body. In these parts I have seen the membrane forced off from its attachment to the walls, which with it made a sac containing pus. Such an abscess, if the patient live long enough, would doubtless cause the death of the membrane.
There is in almost every case of peritonitis more or less of serous effusion, commonly not seen at first on opening the abdomen, for it has sunk into the pelvis. It is transparent, of a yellowish hue, and sometimes flocculi of lymph are found in it.
Whether the inflammation of the peritoneum extends to organs covered by it is a question that has been much discussed; but it is admitted that these organs, to a shallow depth on their surface, have an unnatural color; and when it is remembered that the peritoneum is nourished by vessels not exclusively its own, but running along its attached surface, and distributed as well to the surface of the organs it covers, it is easy to admit that to a very limited depth the organs partake of the inflammatory disease. This supposition gives an easy explanation of the constipation which is so prominent a feature among the symptoms of the disease.
The manner in which the false membrane is disposed of in those who recover is an interesting question. Forty or more years ago Vogel described the process by which the new effusion became a living tissue, and the manner in which blood-corpuscles and blood-vessels were formed in it; and another author had found that the time needed to complete this vascularization was twenty days. But now Bauer and most of the German writers inform us that the coagulated fibrin is converted into fatty matter and is absorbed, and that when adhesions occur they result from the coalescence of a new formation of the connective-tissue elements built up into granules. The question, then, arises, Will the chemical constitution of fibrin permit its conversion into oil? If it will, then the further question presents itself, By what chemical action is the change effected within the body? I do not intend to discuss these questions, but propose them by way of expressing some doubt regarding the accuracy of this statement.
I have always supposed that the epithelial layer of the peritoneum was pushed off by the first of the effusions in peritonitis, and that this was one of the causes of the lustreless appearance of the membrane. This [p. 1135] opinion I have never attempted to confirm or correct by the microscope. Bauer confounds this idea. He says: "The deposition of fibrin occurs before the endothelium presents any changes. This fibrinous effusion encloses, primarily, hardly any cellular elements, and only a few cast-off endothelial cells are to be found in it. The endothelium itself is swollen and turbid; the cell-body is increased in size; the contents are granular; multiplication of the nuclei is apparent; the cells are, in fact, in active division. In the tissue of the serous membrane itself, soon after the deposition on its surface, an accumulation of indifferent (?) cells takes place, especially around the vessels, so that the spaces between the vessels are thus completely filled up. The fixed connective-tissue corpuscles take part in the inflammatory process."
Delafield says: "If the autopsy is made within a few hours after death, we find the entire peritoneum of a bright-red color from congestion of the blood-vessels; but that is all: there is no fibrin, no serum, no pus; epithelial cells are increased in size and number." For this kind of peritonitis he proposes the term cellular. He finds it in cases of local abscess of the abdominal cavity in which inflammatory action has extended over the whole membrane, and particularly on the omentum also, in the first two days of puerperal peritonitis. "The ordinary form of acute peritonitis is attended with changes in the endothelium and fixed connective tissue, and with the production of serum, fibrin, and pus." He describes the migration of white corpuscles of the blood through the walls of capillaries to become pus-cells, and then says: "Minute examination shows that two distinct sets of changes are going on at the same time: first, a production of fibrin, serum, and pus; second, swelling and multiplication of the endothelial cells. If the inflammation is very intense, the pus and fibrin are most abundant; if milder, the changes in the endothelium are more marked."
I have said above that the epithelium is early washed off by the inflammatory effusions. In opposition—or, perhaps better, in correction—of this idea, Delafield says: "There may be a considerable amount of pus produced, and yet the layer of endothelium remains in place." "If, however, the pus and fibrin are produced in large amounts, the endothelium falls off and leaves the surface of the peritoneum bare." The connective-tissue cells of peritoneum, he says, undergo but little change in the first three days of the inflammation, "but by the seventh day these cells are marked by increase in size and number in all parts of the peritoneum."
Two or three times in my life I have met with a peculiar arrangement of the false membrane and serum of peritoneal inflammation, of which I do not remember to have seen a description. It is this: the serum is enclosed or encysted in bladders, the walls of which are the false membrane. There may be two or three layers of these bladders, one upon another, all more or less flattened, and each holding from two to six ounces of fluid. It would seem that in these cases the inflammatory activity rose and fell in its progress, early reaching the point at which coagulable lymph was effused, then falling to the stage in which serum alone escaped. This serum lifted the false membrane irregularly, so that several pools were formed. After this the inflammation returns to the fibrous exudation stage, and gives to these bladders a floor which blends with the [p. 1136] roof at the edges, and thus makes a complete sac. Once more the inflammatory action is changed in its intensity, so that the only effusion is serum; and this serum again raises the new layer of false membrane into bladders—not always or generally in the exact position of the first series. Still again, the inflammation may be so changed as to make a fibrinous flow to this second series of bladders. I am not certain that I have seen a third series of these rare productions. They have doubtless been seen by other persons, and may have been described. I have not been an exhaustive reader on the subject, but I can well understand how they may have been called hydatids on examination of the sacs without looking at the contents. The fluid in the cysts is simply serum, with no echinococcus sacs, and then the number of these inflammatory sacs greatly exceeds the probable number of the fibrous sacs of hydatids.
Pus in large quantity is not often a product of simple acute diffusive peritonitis, although it is frequently found in that form of the disease that attends puerperal fever, septicæmia, or erysipelas. Yet I have seen it a few times. The pus is not generally pure, but is mixed with serum in different proportions, and there will be seen at the same time deposits of lymph attached to the peritoneum or scales of it floating in the fluid effusion, or both. There is reason to believe that in the cases of this class a very large proportion are fatal in the acute stages, but in the cases that live for a few weeks the pus is disposed to collect in pools and become abscesses by adhesions around them at their borders. These abscesses are disposed to find an exit from the body. In one case four abscesses that were found in this way in different parts of the abdominal cavity had each burrowed toward the umbilicus, and were actually discharging their contents at this point when I saw the case. In another case one abscess only was formed, and in four weeks it had perforated the colon. The opening was nearly an inch in diameter.
Kalantarians says, in eight examinations of the solar and hypogastric plexus in persons who had died of acute peritonitis changes which he regards as inflammatory had occurred, with subsequent opaque swelling of the nerve-cells, ultimate fatty degeneration, brown pigmentation, and atrophy. In chronic peritonitis the cells are often converted into amorphous pigment matter, with increase and sclerosis of the ganglionic connective tissue. Still, it is worthy of notice that these changes do not express themselves in symptoms in those that recover.
ETIOLOGY.—Numerous writers have expressed a doubt whether a spontaneous acute peritonitis ever occurs, or if it is ever primary its occurrence in this way is very rare. Habershon1 has presented the case with more apparent force than any other writer. He studied the record of five hundred autopsies of peritonitis made at Guy's Hospital during twenty-five years, but he "cannot find a single case thoroughly detailed where the disease could be correctly regarded as existing solely in the peritoneal serous membrane."
1 Medico-Chirurgical Trans., vol. xliii. p. 5.
This statement must be received with some caution. In twenty-five years the records were probably made by a number of different persons, and persons of varying views and varying capacity and judgment. It is possible that the quotation may embrace some of the changes already referred to as the consequences of peritonitis. It does embrace the cases [p. 1137] "when inflammation of the serous membrane occurs in the course of albuminuria, pyæmia, puerperal fever, erysipelas, etc." It also includes "peritonitis caused by general nutritive changes in the system," as seen "in struma, cancer, etc.," "comprising also those cases in which the circulation of the peritoneum has been so altered by continued hyperæmia (modifying its state of growth) that very slight existing causes suffice to excite mischief, as in peritonitis with cirrhosis, disease of the heart, etc."
With these explanations the statement differs widely from what it would seem to mean without them. It is far from saying that peritonitis always follows some abdominal lesion and is caused by that lesion.
Habershon's paper was published twenty-three years ago, and during all these years the curative treatment of peritonitis, to which the paper itself gave currency, has enabled us to study our cases after recovery as well as before the sickness, and it can hardly be doubted that a much larger proportion of the cases are primary and idiopathic than either Louis or Habershon found reason to admit. That a large number are produced by preceding lesions and constitutional conditions no one will be likely to doubt.
Among the 500 post-mortem examinations of peritonitis reported by Habershon, he found preceding disease or injury recognizable in the abdominal cavity in 261. The following is his table, viz.:
| From hernia, of which 19 were internal obstruction | 102 |
| From injuries or operations | 35 |
| From perforation of the stomach, ileum, cæcum and appendix, colon, etc. (other 13 mentioned with hernia, or with cæcal disease) | 43 |
| And leading to fecal abscess (2 otherwise mentioned) | 17 |
| From typhoid ulceration without perforation | 5 |
| From disease or operation on bladder and pelvis, viscera, etc. | 42 |
| From disease of the liver and gall-bladder | 11 |
| From acute disease of the colon (3 others enumerated with perforation) | 3 |
| From disease of the cæcum or appendix (9 others previously mentioned) | 3 |
| 261 |
Habershon says that in the (his) second and third divisions of the cases the causes were as follows:
| From Bright's disease | 63 |
| From pyæmia, 13; erysipelas, 5; puerperal fever, 10; with pneumonia, 3 | 31 |
| From strumous disease | 70 |
| From cancerous disease | 40 |
| From hepatic disease | 27 |
| From heart disease | 9 |
| 240 |
I have drawn thus liberally from Habershon's paper because it is the only paper that I know, in any language, founded on the analysis of a large number of cases (for five hundred post-mortem examinations is a large number for a disease no more frequent than peritonitis), in the belief that he dealt with facts and that his conclusions must be of great value. He may differ with other physicians regarding what constitutes strumous disease and in the agency of heart disease. He may have mistaken coincidence for consequence, but the paper bears the marks of honesty and good faith from the beginning to the end.
In Habershon's second division, under which he ranks the cases of [p. 1138] peritonitis caused by "a changed condition of the blood," he ascribes 63 to albuminuria. Every physician knows how often meningitis or pericarditis or pleurisy may occur under these circumstances, especially in young persons; but, for myself, I cannot but express surprise at these figures. In one capacity or another I have been connected with large hospitals for forty-eight years, and have seen many cases of albuminuria in private practice, and can recall but few instances in which kidney disease, excepting cancer and other tumors, has terminated in peritonitis. In modification of this statement, however, it is proper to add that the hospital physician cannot know how half the diseases he treats terminate, on account of the American plan of interrupted service, and even less can he know of the mode of death in cases which he sees in consultation. Even with this admission, from my standpoint it is not easy to believe that one-eighth of the cases of peritonitis are caused by albuminuria.
The word pyæmia used by Habershon, it seems to me, ought to be replaced by septicæmia, and it has been by many of the profession. Sédillot many years ago proved that laudable pus injected into the blood-vessels of the dog produced no signs of disease, but that septic pus, so used, was followed by grave symptoms, even death. Among the author's cases thirteen were associated with the septic poison. He also found five which he thinks were independent of erysipelas. One in one hundred is a proportion hardly large enough to establish the relation of cause and effect against the chances of concurrence.
I can make a remark with reference to the inquiry by C. Dubacy in the October number (1881) of the American Journal of Medical Sciences, whether diphtheria produces peritonitis. When diphtheria became epidemic among us in 1860 or 1861 for several years, I saw a great deal of it, but did not recognize any relation between it and peritonitis.
The relations of hernia, injuries, and operations to peritonitis need no commentary.
Perforations of the alimentary canal may require some illustrative statements. These occur most frequently in the vermiform appendix of the cæcum, and are almost invariably caused by some irritating substance imprisoned in its tube. In some cases it is a seed of some fruit, as the orange or lemon; in others, a cherry-pit; in one that I remember it was a small stone, such as is sometimes found in rice; in others, a hard fecal concretion; in one, a child, a singular formation: a strawberry-seed was the centre; around this a layer of fecal matter, around the fecal matter a calcareous layer, on this, again, a fecal layer, and so on to the number of six layers, the external one being calcareous. This body was about one-fourth of an inch in diameter, and may have been years in forming. In this connection I may state, per contra, that I am informed that in a pathological museum in Boston is preserved an appendix that contains, and did contain, a large number of bird-shot, which did no mischief except to enlarge the appendix. This was from the body of a man who had shot and eaten many birds. My observation has led me to the belief that a large proportion of the cases of peritonitis occurring in children are due to perforation of the appendix.
Of the diseases of the liver producing acute diffuse peritonitis, the foremost, I think, is abscess, single or multiple. The different modes in which gall-stones may produce it may be illustrated by the following [p. 1139] cases: (1) A lady died of acute peritonitis. At post-mortem examination a large abscess was found, bounded above by the liver, in other directions by adherent intestines; it contained nearly a quart of pus: at the bottom of the sac was a single gall-stone, very large and very black; the gall-bladder was perforated and very much shrunken. The gall-stone had caused an ulceration of the gall-bladder, but none of the intestines, in this respect differing from the process known as painless transit of a gall-stone. So the calculus caused the abscess, and the abscess caused the general peritonitis. (2) A lady between fifty and sixty years of age had an attack of gall-stone pains; she had had them before. In a few hours symptoms of peritonitis were manifest, and she died. The post-mortem examination showed the ductus cysticus was ulcerated and perforated. Two gall-stones of large size had been formed in the gall-bladder, and had been pushed forward into the duct about halfway to the common duct, leaving it enlarged as they advanced. The foremost one had caused an ulcer on the anterior or lower side of the duct, and bile had escaped, staining all the right half of the abdominal cavity, and throughout this half only the parts were covered with false membrane and stained with bile.
These cases are not so very uncommon. John Freeland of Antigua had a patient, a colored woman sixty-five years of age, who had been suffering from intermittent fever, gastric disorder, and retching. In one of the vomiting spells she experienced great pain, which, being relieved by an opiate, soon returned and was attended by tympanitic and tender abdomen. Death occurred in collapse about eight hours later. The cavity of the abdomen was found filled with blood and bile, the intestines inflamed and gangrenous in spots, and there was general peritonitis. The gall-bladder was empty; the hepatic duct was lacerated, and contained pouches in which gall-stones were encysted. One of these bags was lacerated. This laceration was surrounded by evidences of recent inflammation, and caused the general peritonitis.2
2 The Medical Record, Dec. 9, 1882.
The perforations of the stomach which I have seen have been attended by little inflammation of the peritoneum. Death has followed this accident in twenty to thirty-six hours. There has been little pain, little tumefaction of the bowels, little tenderness, but a sense of sinking and a peculiar feeling at the stomach which the patient finds it difficult to describe.
The ulcers of dysentery do at times perforate all the coats of the colon, and yet do not with any uniformity cause general peritonitis; but as the destructive process approaches the outer covering the latter becomes inflamed, and lymph enough is effused to close the opening and prevent the escape of the contents of the intestine; so that, while perforation is not uncommon, I have rarely seen diffuse peritonitis accompanying dysentery.
Habershon reports 5 cases in which incomplete typhoid ulcers of the intestines caused peritonitis, and 15 from the complete perforation. I believe that the physicians of this country and those of France have found the complete perforation much the most common.
I do not remember to have seen fecal accumulation in the intestines produce peritonitis at all general. I did see, years ago, a man of middle [p. 1140] age in whom fecal impaction in the ascending colon had caused destruction of all the layers of the abdominal wall on the right side, so that the contents of the intestine were exposed to view in a space of three inches by two. This implies that there had been peritoneal inflammation enough to seal the intestine to the abdominal wall on all the borders of this extraordinary ulcer. The man recovered in about six months, and returned to his business.
The inconsiderable operation of tapping for abdominal and ovarian dropsy has sometimes been followed by acute peritonitis. In the early part of my professional life I met with several such cases, and have witnessed the same from time to time since. These were mostly cases of dropsy from cirrhosis of the liver. Habershon found 5 such cases, and 7 in the tapping of ovarian cysts.
The rupture of ovarian cysts has produced peritonitis, but in a larger number of cases such rupture, even when the result of violence, has not led to inflammation; but the kidney secretion has been greatly augmented and the fluid absorbed, so that the rupture has been beneficial rather than harmful.
Tumors, particularly those of a malignant character, are apt to grow to the surrounding structures by adhesions the result of chronic inflammation, but now and then they provoke an acute attack which becomes general. Benign tumors may, in rare instances, do this. In one case a man died of acute peritonitis, and the examination showed that a tumor noticed before death, a very large serous cyst standing out of the left kidney, downward-forward, was the only lesion that antedated the inflammation.
Infiltration of urine, in any of the several ways in which it can reach the peritoneum, is a cause of peritonitis. Pelvic cellulitis may also be a cause, though twenty or thirty cases in succession may run a favorable course with no secondary lesions; it is still recognized as one of the occasional causes of peritonitis.
Among the rare causes of diffusive peritonitis is perforation of the intestine by lumbricoid worms. In such cases the product of the inflammatory action is apt to be sero-purulent, with but a limited amount of fibrin. E. Marcus reports such a perforation, and it was called by Peris ascaridophagie. The worms were apparently not found in the peritoneal cavity, but in the intestines. The perforation had bloodless edges, which lay quite close upon one another, as if they had been separated by a piercing action of the attenuated extremity of the parasite not eaten through.3
3 N.Y. Med. Journal, Jan. 27, 1883.
Lusk finds that certain vaginal injections excite a local peritonitis. Sentey gives the details of a case in which a midwife undertook to procure an abortion by the douche. She used a tube that was large with a spreading mouth or opening, which probably received the neck of the uterus in such a way as to prevent the return of the water. It was, in consequence, forced into the uterus and through one of the Fallopian tubes into the peritoneal cavity. By this a rapidly-fatal peritonitis was developed. He refers to two other similar cases. It would seem that this mode of procuring abortion can be frightfully misused, however safe it may be in skilful hands.
There is a word still to be said regarding the difference between peritonitis produced by wounds, operations, violence, and internal growths, or [p. 1141] what, with a little liberty, may be called traumatic causes, and that which arises spontaneously or without recognizable cause. The first shows a tendency to limit itself to the immediate neighborhood of the injury, and more frequently does not become general; while the latter spreads pretty quickly over the whole extent of the peritoneum.
SYMPTOMS.—There is, perhaps, no grave disease whose symptomatology is more easily interpreted, in which the diagnosis is more easily made, than the average case of acute diffuse peritonitis. Yet there are obscure cases which it is difficult to recognize.
In a well-marked case the first symptom is pain. Chomel and even some later writers believe that chill precedes the pain, but to the best of my recollection it has not generally so occurred to me; and the question arises, Have they kept the symptoms of puerperal peritonitis separated from those of simple peritonitis?
The pain is first felt in a somewhat limited space in the abdomen, and pretty rapidly spreads, so that it is soon felt in every part of the bowels. It may remain greatest in the part where it first began, but there are many exceptions to this statement. As the disease advances the pain and tenderness become more marked, and the patient will try to diminish the tension of the abdominal walls by lying on his back and by bending the hip- and knee-joints, often also for the additional purpose of lifting the bedclothes from his abdomen. Often the patient will resist the physician's movement to examine his bowel with the hand. In the last few hours of life the pain ceases.
The pulse in its frequency follows the advances in the disease. At the onset it is not much accelerated, but in two or three hours it may reach 100 to 120 in the minute. Besides becoming more frequent, it becomes smaller in volume and more tense. Toward the end of a fatal case it may reach 140 to 160 in the minute and be very small.
In the early hours of peritonitis the bowels begin to swell, and percussion shows that the swelling is caused by gaseous accumulation. This increases as the disease goes on, so that in some the bowels become greatly distended—so much, indeed, as to diminish the thoracic space and interfere with the respiration. As the disease advances the tympanitic resonance may give place to dulness on percussion on the sides and lower part of the abdomen. This is due to fluid effusion.
Before the introduction of opium in the treatment of peritonitis the green vomit was a marked feature of the disease. It occurs in other conditions, but rarely, and its occurrence in this disease was so common that it was regarded as almost diagnostic. The fluid vomited is of a spinach-green color, and the color is probably derived from the bile; at least, I have examined it repeatedly for the blood-elements, and have not found them. In these days this symptom of peritonitis is not often observed.
Constipation is absolute in uncomplicated peritonitis of ordinary severity, and I believe is caused by a temporary paralysis of the muscular layer of the intestine. It has already been stated that the blood-supply of the peritoneum is through vessels whose capillaries are shared by that membrane and the tissues which it covers. Inflammatory action in the peritoneum of average severity would naturally extend to this muscular layer and render it inactive. When the inflammation abates it recovers its contractile power. Thus, the intestines become entirely insensitive to [p. 1142]cathartic medicines. This fact is not observed in puerperal peritonitis, probably because the large share which the uterus takes of the disease may act, in some degree, as a derivative; and then, so far as I know, the muscular layer of the intestines does not undergo the change of color and appearance in the latter disease that has been observed in the former. This obstinate constipation has been noticed from the first discovery of the disease, and during forty years in the first part of this century many physicians believed that if they could overcome it their patients would recover. The present interpretation of this conviction is that if catharsis, which was very rarely effected, did precede recovery, the disease was not of a grave type—if, indeed, it was peritonitis at all.
Sometimes peritonitis occurs in the course of a diarrhoea; then the constipation is not at once established, but the symptoms of the two diseases concur for one or two days, when the diarrhoea ceases.
Abdominal respiration ceases when peritonitis is established, either because the movements of the diaphragm produce pain or because the diaphragm is partly paralyzed, as is the muscle of the intestines. Then the gaseous distension of the bowels obstructs the action of this muscle. As a clinical fact it is important, and has often helped me in a diagnosis. Another kindred fact is that all the indications of peristaltic action cease. I have a great many times placed my hand on the abdomen and patiently waited for a sensation that would be evidence of intestinal movements, but did not discover any—have placed my ear on the surface of the abdomen, and have long listened for the gurgling which is so constant in healthy bowels, and have listened in vain. In this respect my observations differ from those of Battey, who reports that he has heard the friction of the newly-made false membrane in respiration, while I concur with him in the statement that the sensation of friction can be felt by pressure of the ends of the fingers into the abdominal wall so as to produce indentation. It should be said regarding the friction sound in respiration that Battey has the support of Chomel, and he in his turn quotes Barth and Roger; so that there may be in this sign more than I have thus far found. (See case hereafter related.)
The temperature of the body is not, considering the extent of membrane involved, remarkably high. I have recently attended a most carefully-observed case in which the temperature never rose above 104° F. It falls below the temperature of health as the disease approaches a fatal termination.
From the time this disease was recognized as a separate and distinct affection the countenance has fixed the attention of writers. The face is pale and bloodless and the features pinched, and the general expression is one of anxiety and suffering. I do not remember to have seen a flushed face in peritonitis, although the degree of paleness differs in different patients.
The mind is almost always clear, unless disturbed by the medicines used in the treatment. Yet cases are recorded in which a mild, and still more rarely a violent, delirium has been noticed. Subsultus tendinum, and even convulsions, have been witnessed, but whether these symptoms belong to the peritonitis or to an accompanying uræmia has not received the attention of those who have witnessed them.
The urine is usually scanty and high-colored, but it does not often [p. 1143] contain either albumen or casts. This statement is presumably untrue of the cases in which Bright's disease preceded the peritonitis and is supposed to be the cause of it—a variety of the disease with which I have already declared my scanty acquaintance. The urine is often voided with difficulty, and sometimes retained, so that resort to a catheter becomes necessary.
The symptoms of this disease are not invariable. In one case the inflation of the bowels is only enough to be perceptible; in another, as I have said, it becomes a distressing symptom, while in most the bowels are obstinately constipated. A case may now and then occur in which evacuations can be procured by cathartics. Pain is regarded by all physicians as the most constant symptom, and it has existed in every case that I have seen, or at least tenderness; but the late Griscom stated to me that a man once came to his office for advice in whom he suspected peritonitis; but the man asserted that he had no pain, and the doctor placed his fist on the abdominal wall and pushed backward till he was resisted by the spinal column, the man asserting that the pressure did not hurt him; yet he died the next day, the doctor declared, of peritonitis. This may be credible in view of the fact that absence of pain in puerperal peritonitis is not very uncommon. The green vomit, which was expected in all cases forty years ago, for the most part, as I have intimated, disappears under the opium treatment. There are persons in whom peritonitis does not accelerate the pulse beyond 100 beats in the minute. The pain, in rare cases, remits and recurs with some degree of regularity, in this respect resembling intestinal colic. Andral reports such a case; I have also witnessed it.
MORTALITY.—Up to the time when the opium treatment was adopted, peritonitis was a fearful word; a large proportion of those attacked by it died of it. In 1832, I began to visit hospitals as a medical student, and for eight years, at home or abroad, was almost a daily attendant. The number of recoveries of those that I saw in that time can be counted on the fingers of one hand. This may be regarded as its natural mortality, for the treatment of that day seemed to exercise little or no control over it. (Farther on this matter will be referred to again.)
DURATION.—Chomel believed that the disease might prove fatal in eighteen hours, while he regards its average duration as seven or eight days. I very much doubt whether peritonitis, not caused by perforation, violence, or surgical operation, was ever fatal in eighteen hours. I do not remember any case of shorter duration than two or three days. Then, on the other hand, the period of seven or eight days in the fatal cases appears to me too long. In the early part of my professional life I remember to have looked for death in three or four days. At present, in the fatal cases, life is prolonged to double or more than double that time. In the majority of those that recover at present the duration of the symptoms is from two days to a week; in a few they have continued fourteen days; and lately I have assisted in the treatment of a case in which there was little amelioration for forty days, and yet the peritonitis was cured.
DIAGNOSIS.—When the symptoms are fully developed there are few diseases that are more easily recognized. It is when these symptoms are slowly or irregularly manifested, or when some other disease which may account for many of the symptoms occurs with it or precedes it, that there [p. 1144] should be any real difficulty. It is customary to regard the danger of confounding the transit of a renal or hepatic calculus with peritonitis as worthy of comment. But if the reader will turn to the articles in this work which relate to these topics, he will find the symptoms so widely different from those enumerated in this article as belonging to peritonitis that he will be surprised that this item in the diagnosis should have occupied so much room.
In a case already referred to, in which peritonitis followed gall-stone pains, the transition was so marked by the rapid acceleration of the pulse and swelling of the abdomen that each of the three physicians in attendance at once appreciated the significance of the change. A physician who resided in the country called on me to report his own case. He had a little before had a very painful affection of the abdomen which continued for three days. The pain was paroxysmal, confined to the region of the liver, back and front, for one day; after that there was some tenderness over most of the abdomen, but no tympanitis. His pulse became frequent and his temperature advanced to 103°. His physicians believed that these symptoms justified them in treating him for peritonitis. Yet his position in bed was constantly changed, and no one attitude long continued—a restlessness which never occurs in peritonitis, but is common in calculus transits. Add to this the absence of gaseous distension and of the green vomit, the paroxysmal character of the pain (though I remember one case in which peritoneal pain increased and diminished somewhat regularly, but only one), and, finally, the sudden cessation of the pain, such as often happens in calculus transit when the calculus passes into the intestine,—it is plain that his sufferings were caused by a gall-stone. The elevation of temperature was the result of a long-continued worry of the nervous system, and the abdominal tenderness came from the many times repeated contraction of the abdominal muscles which occurs in hepatic colic. And then, to make the diagnosis more complete, this gentleman, after twelve or fourteen hours of pain, became jaundiced—in the end very much so. There was no absolute constipation, and the stools were of the color of clay from the absence of bile.
The points of difference between renal colic and peritonitis are even better defined and easier recognized than those between it and hepatic colic.
In intestinal colic there may be some inflation of the bowels, and if it continues a day or two there may be some tenderness; but it is for the most part distinguished from peritonitis by the intermittent or remittent character of the pain, by its greater severity while it lasts, by its courting, rather than repulsing, pressure, by the moderate acceleration of the pulse, by no or only slight elevation of temperature (exception being made for long continuance), by the absence of the green vomit, by the absence of the fixed position of peritonitis, etc.
There does not seem to me any need of spending time to distinguish gastritis or enteritis or neuralgia from peritonitis, their symptoms are so wholly different; and if, as is said, the mucous inflammation can penetrate all the coats of the stomach or intestine, and so cause inflammation of the peritoneal layer, that is peritonitis, and will be distinguished by the proper symptoms of peritonitis.
TREATMENT.—Chomel4 says: "If general peritonitis is intense, it [p. 1145] should be attacked by the most powerful therapeutic agents. One should immediately prescribe a large bleeding from the arm—from 500 to 600 grammes, for example—and repeat according to the need once or even twice in the first twenty-four hours; apply to the abdomen, and particularly to the part of it where the pain was first felt, leeches in large number—fifty, even a hundred—as the violence of the disease may demand and the strength of the patient will permit." He recommends baths, presumably tepid, and describes an apparatus by which the patient can be put into the bath and lifted out of it without pain; prescribes a fixed posture, gentle laxatives, mercurial frictions, blisters; conditionally and doubtfully, paracentesis, emetics under certain circumstances—musk, etc. under others. In the treatment of general peritonitis there is no reference to opium. The word does not occur, but it does in the treatment of peritonitis following perforation. In this condition he would, among other things, give opium à haute dose, but he does not prescribe any repetition or give any details. It is probable that the idea was obtained from Graves, whose first use of opium in this accident was in 1821, although its first publication appears to have been by Stokes in 1832.
4 Dictionnaire de Médecine, 1841.
Wardell,5 who has written the latest treatise on the disease we are considering, relies greatly on bloodletting, but falls short of Chomel in the quantity of blood he would take—would bleed, not to withdraw a certain number of ounces, but to produce certain effects. The venesection is to be followed by the application of leeches—twenty, thirty, or forty—to the abdomen; after this turpentine applications to the bowels. After depletion, he says, opium should be given at once: "two or three grains may be given in urgent cases." Vesication he calls "another of our aids." He disapproves of cathartics, but when there is accumulation in the colon would use injections. "Opium in the asthenic form is the chief agent, and Graves and Stokes were among the first physicians who gave it very largely." "Two or three grains may at first be prescribed, and a grain every four or three, or even two, hours afterward." "In perforation there is sometimes great toleration of the drug. Murchison has known so large a quantity as sixty grains to be given in three days with impunity." Mercurials, he thinks, are of doubtful efficacy. In the paragraph devoted to the treatment of puerperal peritonitis the word opium does not occur, and it is only by a very doubtful inference that we can assume that he would ever use it. Chomel makes no allusion to the use of opium in the same disease.
5 Reynolds's System of Medicine.
For two years (1834-36) I was connected with the New York Hospital as house-physician or in positions by which that office is reached. The treatment of acute diffuse peritonitis then and there was formulated as follows: First, a full bleeding from the arm, commonly sixteen ounces, then a dozen or more leeches to the abdomen; following this, another bleeding or not, in the discretion of the physician. Meantime, the patient would take half a grain to a grain of calomel every two hours, with a little opium "to prevent the calomel acting on the bowels," of which there was no danger, in truth. Mercurial inunction was used at the same time. The belief was that after depletion the most important thing was "to establish mercurial action in the system;" in other words, [p. 1146] "to diminish the plasticity of the blood." Under this plan I saw one recovery in these two years.
In 1840, I went to Vermont to give a course of lectures in the Vermont Medical College, and while there was called by the physicians to see with them several cases of peritonitis. I found that they were treating the disease on the Armstrong plan; that is, bleeding freely, and then administering a full dose of opium, as they said, "to prolong the effects of the bleeding." In most cases there was a second bleeding and a second administration of opium. Leeches were also used, and irritating applications to the abdomen, and in some cases purges. I found they were getting better results than we were in New York, and I studied their cases as closely as I could, and reached the conclusion that opium was the curative agent, and that it would be safe to omit the abstraction of blood. This conviction grew in strength with every new case, and I saw, with different physicians, several cases, the disease being more prevalent among the mountains there than in the city—at least that year. The idea then formed was that to establish the narcotic effects of opium within safe limits, and continue them by repeated administration of the drug, would cure uncomplicated peritonitis—that a kind of saturation of the system with opium would be inconsistent with the progress of the inflammation, and would subdue it. There was no theory to build the treatment on, and no explanation of the action of the drug in my mind. What I saw of the action of two full doses of opium was the only foundation for the idea. I had in the course of two years after those observations in Vermont 9 cases of general acute peritonitis, 8 of which were cured. All these were reported in succession, as they occurred, to the medical societies and in my college lectures. The plan was adopted by many members of these societies and by others with whom I had opportunity of conversing on the subject, so that soon there were several—I may say many—workers in the field; and in all instances where the practitioner had the courage to carry out the treatment favorable reports were returned. Not that every case of peritonitis was cured, but the recoveries generally exceeded those that followed any other plan ever before used. No physician tried it with a proper understanding of its details, and with courage to execute them, who if living does not practise it to-day.
The treatment of puerperal peritonitis is not allotted to me, and I am very reluctent to encroach in any degree on the province of the very competent and highly-esteemed gentleman to whom that disease was assigned. But the history of the opium treatment is very incomplete without the statement I am about to make, and I trust to his generosity to forgive this encroachment; and all the more confidently because he was not at the time acquainted with the manner in which opium was first introduced into the treatment of puerperal fever.
After the curative action of the drug was demonstrated in general peritonitis, I was anxious to try it in puerperal fever, of which peritonitis forms a part. But I had no hospital and no obstetrical practice. In 1847, I was appointed one of the physicians to Bellevue Hospital, to which an obstetrical department was attached. After one or two years a single case occurred and was sent to my division. I gave her 100 grains of opium in four days, with more or less of calomel—I have [p. 1147] forgotten how much. She recovered, but after the symptoms of puerperal fever passed away she had secondary abscesses of the lungs. These kept her ill for several weeks. At length her recovery was complete.
In 1840 there was a very fatal visitation of puerperal fever in this hospital, and on invitation of Vaché, who then had charge of the whole institution, I was a daily visitor and took notes of all the cases. It was from these notes that Vaché compiled his report of the epidemic published in the Medical and Surgical Journal. The disease was fearfully fatal, although every known mode of treatment was tried in different cases, including Brenan's plan by turpentine, but all, with one or two exceptions, with the same result. At this time the opium plan was on its trial, and I had not acquired a confidence in it that authorized me to try it in these cases. The time for it came in 1851. Then a sudden, vigorous attack occurred. One woman was sent to me in whom the disease was well advanced. I instructed my house-physician not how much opium to give, but what effects to produce by it. I found this woman dying the next day, and that she had taken only three grains of opium in three doses. In three or four days seven cases were sent me from the lying-in wards. One was returned for error in diagnosis, and six put under treatment. Having found that prudence in my house-physician was so much more conspicuous than courage, another house-officer, who combined them both, was selected to be in almost constant attendance. The instruction I gave him was in these words: "I want you to narcotize those women to within an inch of their lives." He did it, and saved every one of them. This gentleman is now known over the whole land as a learned and distinguished surgeon. I feel called upon to give his name in this connection, that he may be a witness to the facts I state, and for the admiration with which his nerve and prudence impressed me. One of these patients took first two grains, then three grains, then four, and so on till she took twelve grains of opium at a dose, the intervals being two hours. The state into which the patient was to be brought I have denominated a state of semi-narcotism. The quantity of the drug necessary to produce this state varied surprisingly in different persons. One of these women was pretty fully narcotized by four grains every two hours. She was watched with anxiety; restoratives were kept in readiness, but nothing was done but to suspend the administration of the medicine and to wait. In seven hours the consciousness was fully restored, and the improvement in her condition was wonderful. The disease seemed to be cured. But in a few hours more the symptoms recurred, and the same medicine was again given in three-grain doses, and again narcotism was produced. Taught by the experience of the day before, we waited, and when she recovered from this second narcotism her disease was completely cured. She took no more medicine of any sort. This case was very instructive, as it taught me that over certain cases of puerperal fever opium has absolute control.
From the time here referred to, so long as the obstetrical service was maintained at Bellevue Hospital, a large proportion of cases of this fever, as they occurred, were sent to my wards, and in all these years I have not lost faith in opium. This statement, however, requires an explanation. Puerperal fever is a compound disease. Its great inflammatory lesions are found in the uterus and its appendages and in the peritoneum. [p. 1148] When the inflammation of the uterus is the dominant lesion, and is purulent, opium has little or perhaps no control over its fatality; but in the cases in which peritonitis is the ruling lesion, if begun early, it will show its power. In this connection I will only add that in private practice the drug has been perhaps more curative than in the hospital. I have seen many cases in consultation, and a decided majority have recovered. In some instances the patient has fallen into a pleasant sleep, only broken by some administration, and ending with her recovery. In one instance a very eminent physician had undertaken to treat a case by the opium plan, but he had administered the drug so timidly that for fourteen days he had done no more than hold the disease in check. After trial, I found that I could not induce him to give the drug in my way, and I asked him to give me sole charge of the patient for twenty-four hours. To this he assented, remarking, "If you cure her, doctor, I will have it announced to the profession that she was the sickest person I ever saw get well." In half the time allowed me I was able to establish the opium symptoms as given farther on, and the lady slowly recovered.
The treatment of any form of peritonitis by opium permits the use of the drug itself, or of any extract or preparation of it which contains its narcotic qualities, but it is wise to persevere with that one first chosen unless there is strong reason for a change. This caution is based on the fact that we cannot change from one to another and be certain to obtain the same drug activity. For example, we begin with laudanum, and find what it will do. We cannot take in its place the sulphate of morphia with the certainty that we can so graduate it as to get precisely the same effects. Then the quantity which will be effectual in one case may be quite inadequate for the next. The tolerance of opium in different persons varies remarkably, and probably the disease itself increases the tolerance in all. This will be illustrated by some of the details of this paper.
The drug symptoms to be produced are as follows: Subsidence or marked diminution of the pain; some or considerable tendency to sleep; contraction of the pupils; reduction of the breathing to twelve respirations in the minute; in the favorable cases a considerable reduction in the frequency of the pulse; a gentle perspiration; an itchy state of skin, or oftener of the nose; absolute inactivity of the bowels, and after a time a subsidence of the tumor and tenderness in them; some suffusion of the eyes.
Of these several signs of opiumism there is none more easily observed and none more valuable than the frequency of the respiration; and while the physician aims to reduce it to twelve in a minute, there are chances that he will see it fall to something below that. I have often counted it at seven, and in perhaps two cases it fell to seven in two minutes; and yet these cases of marked oppression from opium all recovered. In the cases in which the respiration has fallen so low there has been considerable obtuseness of the mind; but in no case except in the hospital patient already referred to have I seen unconsciousness. Then the sleepiness, so long as the patient is easily awakened, is wholly within the limits of safety.
As to the quantity of opium to be given, I have known two grains every two hours do the work, and in other cases many times this [p. 1149] quantity was necessary to produce this condition of semi-narcotism. The plan is to begin with a dose that is safe—say two or three grains of opium or its equivalent of sulphate of morphia—and in two hours notice its effects. If any of the opium symptoms have appeared, repeat the dose; if none, increase by one grain, and so on at intervals of two hours till the degree of tolerance in the patient is ascertained. After that the case can be treated by a diminished occupation of the physician's time—two or three visits a day. The dose is to be increased if the opium symptoms diminish before the disease yields, but always to be diminished or discontinued if narcotism is approaching. The duration of the treatment will be sometimes no more than two or three days; it may be a week, or even a fortnight, and in one case already mentioned the symptoms persisted mildly for forty days, and then yielded. In this case the medicine used was the sulphate of morphia, and the enormous dose reached by steady and graduated increase was one grain and a quarter every forty minutes in a boy ten years old.
In some puerperal cases the doses have been so large as to require witnesses to make the statement of them credible, and the administration of them criminal had not the effect of each dose been carefully studied and the amount of each measured by the action or inadequate action of the next preceding one.
Here are the doses given a woman who fell sick October 13, 1857; the record was made by C. H. Rawson during the treatment, and was kindly given me two or three years ago: On the first appearance of her disease, while the diagnosis was uncertain, 10 grains of Dover's powder gave her a quiet night. The next day the disease was more manifest, and she took of Magendie's solution (2 grains of sulphate of morphine to a drachm of water) x minims every hour; growing worse, at night she took xxx minims every hour; the next day, xl minims every hour, and no change of symptoms. She took in twenty-four hours 32 grains of sulphate of morphia; slept, but was awakened by the slightest noise. On the fourth day 31/3 drachms of the solution, and opium as follows: at 4 P.M., 3 gr.; at 5 P.M., 4 gr.; at 6 P.M., 5 gr.; at 7 P.M., 6 gr., and 6 gr. hourly after 7 P.M. Sleep light. Fifth day, in twenty-six hours took in opium and morphine the equivalent of 208 gr. of opium. The sixth day, 212 gr. of opium; on the seventh day, 221 gr. of opium; on the eighth, 224 gr.; on the ninth, the same quantity; on the tenth, the same; on the eleventh, 247 gr., pulse subsiding; on the twelfth, 261 gr., other symptoms better; on the thirteenth, 144 gr.; fourteenth day, 4 gr. hourly; slept for the first time heavily, all other symptoms improving, bowels moved freely, ate well, tympanites subsiding; fifteenth day, 1 gr. of opium every two hours, and at night the last dose. Recovery was complete. The woman denied the opium habit, and the medicines were tested by the apothecary. Such doses can only find their justification in the demonstrated fact that smaller doses will not produce the degree of narcotism desired.
In Keating's edition of Ramsbotham's Midwifery a case is reported by myself in which a woman, by pretty rapidly increasing doses, reached forty-eight grain doses of opium, with the effect of curing her disease and substituting a temporary active delirium.
A word of caution is probably necessary regarding the use of opium in high doses when peritonitis and Bright's disease coexist. I have [p. 1150] already said that I have but scanty personal knowledge of such a concurrence, but in Bright's disease alone I have known a large, non-heroic dose of an opiate fatal. For example: A young man had a felon on his finger, and did not sleep, so great was his pain. His physician prescribed 40 drops of laudanum at bedtime. Not sleeping on this, he took another portion of 40 drops, and in the morning he was found in a comatose condition, and in the course of the day he died. A post-mortem examination revealed Bright's disease, which was not before suspected. A woman took half a grain of the sulphate of morphine—for what reason I do not know. I was called to see her when she was in a semi-comatose state. The time between my seeing her and that of taking the morphine was fourteen or fifteen hours; its removal from the body was therefore hopeless. Her limbs were swollen with oedema, and the urine contained albumen and casts. Although the usual means of opposing the poisonous effects of opium were resorted to, they were of little use, and the patient died in the course of the day. These are selected from a considerable number of similar cases that show a similarity in their action on the brain of opium and urea. It seems that opium precipitates the uræmic coma, yet the coma produced by these agents combined is not so profound as that produced by opium alone. There is in it some movement of the limbs or body or some imperfect utterances, yet it seems to be more fatal than the coma of opium unaided. Notwithstanding all this, I have met with several cases of cardiac disease combined with Bright's—perhaps I should say many—in which half a grain of morphia sulphate has been taken every night to procure sleep with only beneficial results. This has been observed several times when physicians have been the patients.
These facts are stated to show the hesitation and prudence that should control the administration of opium when there is urea in the blood, whether there is peritonitis or not; but a case in which one form of Bright's disease preceded, and perhaps caused, peritonitis will be more instructive: A gentleman sixty-eight years of age was attacked by peritonitis on Thursday evening. There was a moderate chill at the onset (this being one of the few cases in which I have witnessed this occurrence). The diagnosis was then uncertain, and he took quieting doses of Dover's powder, which gave him sleep. The next day the diagnosis was easily made. The urine was examined for albumen, and none found. It was, however, scanty. He took only six-eighths of a grain of sulphate of morphine in the first twenty hours. It was then increased, so that in the next twenty-four hours he took two grains of the sulphate in divided doses—a quantity which has been greatly exceeded in hundreds of cases with the best results; but in this case coma was the result. At 10 A.M. on Sunday he was comatose, but not profoundly; he could be aroused. The breaths were five in the minute, the pulse increasing in frequency; secretion of urine next to none. The galvanic battery was used. After seven hours, while the respiration was growing more natural, the pulse grew more frequent and the stupor increased. At 8.30 P.M. the breathing was fifteen in the minute, and full and perfectly easy, but the pulse was running at 140, and the coma unbroken, and the pupils of good size. The effects of the opiate had passed off, but those of uræmia were profound. He died at 11 P.M. After the alarming symptoms occurred we tried to procure another specimen of the urine for fuller examination, but [p. 1151]could not. It was only after his death that we procured the evidences that he had shown symptoms of contracted kidney for months. The urine contained no albumen at the time of our examination, as very often happens in that disease.
Regarding other points in the opium treatment there is little to be said. Purgatives are entirely inadmissible. The bowels should be left entirely at rest till they recover their muscular tone; then they will expel first the gas, and then the feces; or if, after the inflammation is subdued, they do not move of their own accord, injections are admissible. I have often left the bowels absolutely inactive for fourteen days without any recognizable consequences. If I meet a physician who believes that leeches are essential, I yield him his point, but never advise them. I do this because a moderate bloodletting will do no harm, and little if any good. The same rule I apply to irritating applications to the surface of the abdomen. Mercurials, I think, are harmful, and therefore I object to them. As to food, it should be milk, fresh eggs beaten up with water and pleasantly flavored, peptones, etc. selected from among those that leave no refuse.
The testimony of physicians who have adopted this plan within my own circle is unanimously in favor of it. B. R. Palmer of Woodstock, Vt., afterward of Louisville, Ky., who was the first to test it, told me after a few years' trial that he used to dread peritonitis as he would dread the plague, but with opium in his pocket he met it cheerfully and hopefully, as he did a pneumonia. Chalmers of New York, who is known by many readers of this article, has a very extensive practice, and he told me lately that he had not had a fatal case of peritonitis in twenty-two years. He embraced the plan early.
Now, how did this treatment originate? From whom did the profession adopt it? In 1836-37, I visited daily the hospitals of London, Edinburgh, and Paris, was in frequent intercourse with the physicians of those cities, and never saw a patient anywhere treated by opium, and never heard the least allusion to it. I can safely appeal to any physician who was familiar with the history of the profession before the year 1840, or for two or three years later perhaps, to inquire whether anything was generally known regarding this treatment of peritonitis, or whether he himself ever heard of it. Let the inquiry be made of Willard Parker of New York or Alfred Stillé of Philadelphia—men of a degree of intelligence and learning that has made them leaders in the profession—and of all the profession at that time. I venture to assume that they were as ignorant as I was of what Graves and Stokes had done.
The following fact is significant: In 1843, Graves published A System of Clinical Medicine, the preface of which is dated January, 1843. In this he says he had previously published essays, lectures, and articles in several medical journals. In this volume he intends, he says, "to revise what I have written, and to compress the whole within the limits of a single volume." There is nothing in the table of contents or explanatory headings of the several chapters of this volume which alludes to treating peritonitis by opium. It is fair to infer that the cases treated in 1823 had made little impression on his mind, and that he did not think his treatment could take rank as a discovery; and yet Stokes had made favorable mention of it eleven years before this publication. Graves, then, did not [p. 1152]publish his cases, and the first knowledge which the profession could have of them was through Stokes's paper, published in the Dublin Journal of Medical and Chemical Science, No. 1, in 1832. Perhaps the reason why Stokes's paper produced so little impression on the profession may be found in the fact that first numbers of journals of every sort have few readers. Anyway, it was not till after the opium treatment had attracted much attention in this country that anybody here knew that Graves or Stokes had ever had anything to do with it. Besides, Graves and Stokes had only used opium in cases of perforation, and they had no plan or symptomatic guide in the use of the drug.
There is something new and strange in the following case copied from the Medical Record of May 12, 1883, under the heading, "Operative Measures in Acute Peritonitis:" "Dr. Reibel relates the case of a child, eight years old, suffering from acute idiopathic peritonitis. The disease had resisted all treatment, and the child being, apparently, about to die, it was determined to open the abdomen with a view to removing the fluid and washing out the peritoneal cavity with a solution of carbolic acid. The meteorism was intense. No fluid was found in the abdominal cavity. In prolonging the incision a loop of the intestine was punctured, as evidenced by the escape of gas and intestinal fluid. The wound was washed with carbolic acid and covered with a layer of antiseptic cotton. The following day the little patient was nearly free from pain, and was able to retain a little milk. The temperature had fallen from 104° to 101°, and the tympanitis was almost entirely gone. The (wounded) loop of intestine was adherent to the abdominal wall, and there had been no escape of fluid into the peritoneal cavity. The patient made an excellent recovery."
If the statements of this abstract are true, and the future supports the practice pursued in this case, acute peritonitis is likely to become a surgical rather than a medical disease. Reibel thinks that opening the intestine in the way he did is a better plan than the punctures with the exploring-needle to relieve the patient of the tympanitis. But it will require more facts than one to persuade the profession that this mishap of the scalpel can grow into a rule of practice. (The Record finds this report in the Journal de Médecine de Paris.)
I cannot say that I see the value of a distinction made in 1877 by Gubler between peritonitis and peritonism. By the latter term is meant the total of nervous and other symptoms that arise in the course of peritonitis. Trasour has lately revived this distinction, and thinks it important, and that a light peritonitis may be attended by a grave peritonism. He holds that the distinction is important, because "the treatment of peritonism consists in the administration of alcohol, chloral, and especially of opium in large doses. Of the latter fifteen grains may be given in twenty-four hours." "The symptoms [of peritonism] are produced through the agency of the great sympathetic."6
6 Med. Record, Aug. 28, 1883.
I cannot say that I have seen great effects follow small causes, but think that, in general, the effects of peritonitis on the pulse, strength, nervous tone, etc. are, to some extent at least, a measure of its severity.
CONSEQUENCES OF PERITONITIS.—These are usually nothing. When recovery takes place it is commonly complete, but cases have been known [p. 1153] in which the intestines have been left bound to the abdominal wall and to each other, and so made incapable of their natural action. The results of this are a swollen, tympanitic abdomen and impaction of the bowels, but the general health may be very good. A woman at Bellevue was left in this condition, yet she performed the duties of nurse in one of the wards for some years, and finally disappeared from the institution, and I do not know how it ended with her—probably by the breaking up of the adhesions and a return of the bowels to their natural condition.
In some few cases there remains new tissue, which in time is partly broken up and remains partly attached. In this manner strings and bands of considerable strength can be formed, and into these loops the intestine may pass, so as to form an internal hernia of a very dangerous character. In some bands are formed across the intestine, which by contraction flatten the tube and obstruct the fecal movement. There is reason to believe that such bands and bridles are formed by local inflammation of such imperfect manifestation by symptoms that the patient knows nothing about it. A very striking case illustrating the possible sequence of this inflammation came under my observation early in my professional life: A colored woman about twenty-five years of age gave a very clear history of a peritonitis from the consequences of which she had suffered two years before I saw her. About six months after recovery she began to have constipation and to suffer from small and frequent discharges of urine. The latter gradually grew milky and to have a bad odor; the constipation grew more and more, and at length came to be absolute for many days; then would come a diarrhoea of some hours' continuance, after which she would have a feeling of relief. This was her state when I saw her. She was emaciated, and so feeble as hardly able to leave her bed. She vomited occasionally, and her appetite for food was all gone. The urine was heavily loaded with pus, and was ammoniacal. She died after a few weeks. At post-mortem examination a firm membrane was found strained across the upper strait of the pelvis, wholly separating the abdominal cavity from the pelvic. It looked like a drum-head. The left posterior border was drawn very tensely over the colon where it passed into the pelvic cavity, flattening it down completely and making stricture. To the under or lower surface the fundus of the uterus and the base of the bladder were firmly adherent, and in this way both were suspended. The effect of this unnatural suspension of the inactive uterus did not seem to be noticeable, but with the bladder it was very different: it contained three to four ounces of water, ammoniacal and full of pus, and it could never have emptied itself. The explanation is very simple. During the peritonitis a false membrane was effused on the pelvic viscera in situ. When the period of contraction which is common to all such structures came, the new membrane was separated from the greater part of these two organs, but not from their bases. The firm attachment to the brim of the pelvis did the rest. So unusual a sequel of peritonitis I think deserves a record. I should add there were no adhesions above the pelvis. Such a structure as this, found long after the active symptoms of peritonitis have passed, as also the bands and cords before spoken of, does not give support to the doctrine that the false membranes are broken down into fatty matter, and in this condition absorbed.
[p. 1154] The possible remote effects of peritonitis are shown in a case reported by E. A. Mearns to the Medical Record, published Sept. 15, 1883: A young man, aged nineteen, four years after he had had acute general peritonitis was attacked with constipation, which was absolute. He had had before occasional attacks of pain in the bowels and constipation, which were overcome. But this was invincible. He had the train of symptoms usual in intestinal obstruction. There was no fever or tympanitis, and this time but little pain. He lived eight days. There was a tangle and a constriction of the intestines at the middle of the ileum, caused by the contraction and hardening of the effusion of the old peritonitis, and the intestine was very much softened.
H. B. Sands reports in another number of the same journal: "The patient was a man about thirty who had suffered from acute obstruction for a week. No exact diagnosis was made. When the abdomen was opened the intestinal coils were found extremely adherent one to another in consequence of a former peritonitis. A careful search failed to discover the nature or seat of the obstruction. The abdominal wound was closed, and the patient died soon after."
There is no part of the gastro-intestinal canal that may not, from one cause or another, become the seat of ulceration. The jejunum is the part of the tube long supposed to be an exception to this rule, but even in it one or two observers have found ulcers. These ulcers often exist without distinctive symptoms, and may go on to cicatrization without announcing themselves. In the stomach, however, there are commonly indications which will admit a conjecture of their existence, and perhaps a diagnosis. Sometimes these ulcers penetrate all the tissues of the tube and allow the contents of the intestine to escape into the peritoneal cavity, or they may have destroyed all but the external layer, and some succussion, as in coughing, sneezing, laughing, or perhaps straining at stool, may make the opening complete, with the same results. In these cases it seems to be inevitable that inflammation should follow, unless it has preceded, the complete opening and sealed it up by adhesions. The tendency of such an inflammation is to be local and limited, but when the contents of intestines escape into the peritoneal cavity it usually becomes general. These accidents are usually attended by the sudden development of local pain, by rapid increase in the frequency of the pulse, paleness, and prostration. The perforation of the vermiform appendix is often a partial exception to this statement, for, while the local symptoms are marked, the sympathy of the general system is not so quickly awakened. The same can be said of perityphlitis. The symptoms are often local for some time—a day or more; sometimes subside, as if the disease were cured, and then return in full form. This is produced by the tendency of the inflammation to limit itself to the immediate neighborhood of its cause. Lymph is effused at a short distance from the point of irritation, and seals the parts together, so as to shut in the offending substance; and though this substance may produce pus in contact with intestine or appendix, that [p. 1155] fluid is held for a time, as in abscess. It may be permanently held in its new-made sac till it burrows into some near part, as the intestine or bladder, or remain an abscess till opened by Willard Parker's puncture. On the other hand, the contents of this sac may be increased till it breaks bounds and causes extension of the peritoneal inflammation or general peritonitis. In one particular case this process of setting limits and breaking through them occurred in a young lady four times at intervals of from one to two days. When the limiting adhesions were established symptoms would subside, so as to encourage in her physicians the hope, even the expectation, of recovery; but again and again the fire was rekindled, and she died eight days after the first attack. In the greater number of cases the first breaking of the adhesions is followed by full peritonitis, and this often by death.
The perforations of the stomach which I have seen have not been attended by the severe pain described by most authors, but by a sudden prostration of strength and a feeling of disquiet and sinking at the stomach; more of collapse than of inflammation in the symptoms; no tumefaction of the bowels; almost nothing to indicate the nature of the accident, but a sudden new sensation in the bowels, a rapid increase in the frequency of the pulse, it growing small as it increases in rapidity, and a pale and shrunken countenance, and death in from twelve to thirty hours. Then, on inspection, hardly any signs of peritonitis are found. The peritoneal vessels are fuller and the membrane redder than in health, and its surface covered with the thinnest possible film of lymphy exudation, and some serum in the deeper parts of the cavity.
These ulcerations of the stomach are not always fatal by peritonitis. A few instances are recorded in which adhesions of the outer surface of the organ to adjoining organs have taken place, so as to protect the peritoneum almost wholly from the fatal contact with the gastric fluids, and death has occurred in some other way. I have a remarkable specimen illustrating this fact. It was taken from the body of a woman of about middle age who had long had symptoms of dyspepsia, and had from time to time vomited a little blood. It was not difficult to recognize ulcer, but the extent and peculiarities of it could be learned only by inspection. She died suddenly of copious hæmatemesis. On examination an ulcer two and a half to three inches in its several diameters was found, beginning near the pylorus and extending toward the left, which in this large space had destroyed all the coats of the stomach and exposed an inch and more of the right extremity of the pancreas and about the same extent of the liver. The liver and pancreas were both perceptibly eroded when exposed, and in the latter an artery that would admit the head of a large pin was opened. The stomach, outside of this extraordinary ulcer, was strongly attached to the adjacent organs.
The ulcerations of typhoid fever penetrate the intestine about three times in a hundred cases of the fever. This result is reached by the study of a large number of cases, and appears to be pretty generally admitted. The point where this perforation occurs is in the ileum, near the ileo-cæcal valve—within a foot or eighteen inches of it in the great majority of cases, although it has been known to occur seventy-two inches above the valve, and it has been seen very rarely in the cæcum. The fever itself may be either severe or mild. Suddenly severe pain [p. 1156] sets in, oftenest in the lower part of the abdomen, and spreads rapidly; the pulse is quickly accelerated and becomes small; and it has been lately stated that in this and other intestinal perforations the gases of the bowels, escaping into the peritoneal cavity, will give resonance to percussion over the lower part of the liver. Fetid gas found in this cavity after death is not without importance; for example, a distinguished Senator at Washington died not long ago of a very painful abdominal disease which his physicians declined to relieve with opium, though the patient pleaded for it. His family physician at home was summoned. Although the distance he had to travel was many hundred miles, he found the patient alive and still suffering. He at once gave morphine for the relief of the pain, but the patient died. Now, this gentleman had diabetes a year or more before his death, recognized by his physician at home and also by myself. While under my observation the urine ceased to contain sugar and its quantity became normal, but soon after this albumen was occasionally found in it. The quantity was generally small, and casts were only found now and then. This new disease was mild, and seemed to be, within certain limits, manageable. He went to Washington under injunction that he was not to let official and professional labors bear with any weight upon him. This last sickness and the death would naturally enough be supposed to be some new phase or consequence of the previous illness. But, while a post-mortem examination was not permitted, the family wished to have the body embalmed. The family physician accompanied the embalmer, and as the latter made a cut through the abdominal walls there was a gush of air laden with fecal odor, and he through this opening saw the intestines covered with false membrane. He satisfied himself that the intestine was not opened. This fetid gas came from the peritoneal cavity. An ulcer had perforated the intestine somewhere, and caused the death. The final disease could be only remotely dependent on the patient's previous illness, if at all. His impaired health may have made the ulcer possible.
All kinds of perforations in the bowels, except those of the stomach, cæcum, and appendix, even the cancerous, have one history and the same symptoms; and if treatment is ever successful in such occurrences it must all be based on one set of rules—absolute rest, no pressure on the bowels, and no movements of the muscles that will aggravate it; food that will be wholly digested and absorbed by the stomach; complete abstinence from cathartic and laxative medicines, and the free administration of opium or morphine. By these means, I fully believe, numbers have already been saved from the fatal consequences of peritonitis caused by perityphlitis and perforation of the vermiform appendix—some under my own observation and others under that of my friends. A boy fourteen years of age was brought to bed by a pain in the right iliac fossa. After a few hours his father, a physician, desired me to see him. There was already a perceptible fulness, with dulness on percussion, in the fossa, and some febrile excitement. I gave a portion of morphine, and promised to call the next morning. In the morning a message came from the father stating that the boy was better and there was no need of further attendance. In the evening I was recalled. The pain had returned, and had spread over most of the bowels. He had general peritonitis. He took tincture of opium, of which I believe the largest dose was 100 [p. 1157]drops, reached after three or four days of gradual but steady increase of dose. From that point the patient got better, and the quantity of the medicine was correspondingly reduced. There were a relapse and a repetition of the treatment, and again the disease yielded. During convalescence, about fourteen days from the attack, the boy, after emptying his bladder, was suddenly pressed to continue the discharge. Now he voided what appeared to be blood, two or three tablespoonfuls. It was, however, pus with blood enough to color it. This purulent discharge from the bladder continued for about three weeks, the boy steadily recovering his health. This occurred twenty or more years ago, and that boy is now a well-known physician. Similar cases could be recited.
In 1850, or thereabout, I attended a physician through an attack of typhoid fever. In the third week there was a sudden outbreak of peritonitis. The opium treatment was resorted to, and he recovered, and had good health for twenty years after. Peritonitis occurs rarely in typhoid fever from any other cause than perforation, and its occurrence in this case at this time, when perforation is more likely to occur, renders it probable, at least, that this attack was produced by that cause.
March 3, 1883, autopsy of Wm. Fletcher, age 59, iron-worker. On Friday last, Feb. 23d, he was attacked with pain in the region of the right iliac fossa; it was severe. There was no chill, but little fever, and only slight acceleration of the pulse. His stomach was a good deal disturbed, and the bowels were soon distended with flatus. I saw him on the Tuesday following, with James D. Elliott. The bowels were a good deal swollen and very resonant on percussion; pulse 84. His stomach was still greatly disturbed, so that he retained no food, yet there was no green vomit, but much flatulency. The movements in respiration were particularly noticeable, being nearly or quite as much abdominal as in health. There was a short friction sound in inspiration, but an entire absence of the sound produced by peristaltic action. There was no dulness on percussing over the iliac fossa, and no pain on pressure over any part of the abdomen. I was careful in examining the right fossa, for the first pain was there, and it was severe; but there was no physical sign by which the perforation could be ascertained. Still, my mind dwelt on the probability of perforation, and I expressed my fears to Elliott regarding it. The respiration was of natural frequency. The bowels had not moved for two or three days.
The next day Flint was added to the consultation. The symptoms had changed but little; the pulse was 102; no pain, no tenderness, no peristaltic action; slight friction at one point only; the abdominal respiration was as marked as before. Frequency of respiration, 18; patient sleepy; pupils only slightly contracted. When we were in consultation I again expressed my fear of perforation, but Flint expressed the most decided opinion as to its absence, because there was dulness to percussion over the liver. I had read his paper on the intrusion of gas between the ribs and liver in cases of intestinal perforation, and felt as if I were almost reproved for entertaining the thought without this physical corroboration.
Thursday, March 1st, the stomach had become much more retentive; there were no pain and no tenderness on pressure; pulse 109; no friction sound, no sound of peristaltic action, no dulness on percussion over right iliac fossa, but resonance over the whole abdomen, excepting over the [p. 1158] pubes; there the resonance was not clear; over a small space there was dulness; this was ascribed to moderate fulness of the bladder, and, as there had been no difficulty in emptying it, nothing was said of it. The abdominal respiratory movements were the same as before.
Friday morning, at 3 A.M., no marked change had occurred in the symptoms, but from this time onward there was a steady sinking of the vital powers. The pulse grew small and frequent, the hands became cool, the breathing more frequent, and without any sudden change or new symptom he died early in the morning. At the last visit there was no resonance on percussion over the liver.
Autopsy, Saturday, March 3d, 2 P.M. The bowels were distended, as they mostly are in peritonitis, but not extraordinarily. There was now pretty free resonance over the liver. The section to open the abdominal cavity was carefully made, with the aim of ascertaining whether there was air or gas in the peritoneal cavity. When a half-inch opening was made through the peritoneum, gas was forced out through it for some seconds with an unmistakable noise. The bowels were not opened by this cut. The bowels exposed, a very thin film of false membrane was found on all the middle and upper portions of the intestines, with a fringe of injection where the folds came in contact. But two or three inches above the symphysis pubis the section opened a collection of pus which extended downward into the pelvis. Somewhere hereabout—neither of us could say exactly where—was found a lump of fecal matter, not indurated, as large as a marrowfat pea, the intestine still unopened. Search was made for the vermiform appendix. At first it was not recognized on account of its remarkable shortness. It was found, however, pointing directly toward the median line of the body, and was short because a part had been separated from the rest by slough. The end of what remained was marked by a border, one-eighth of an inch deep, of a very dark-green gangrenous color. We did not attempt to measure the quantity of pus. It was six ounces or more. It was completely bounded and shut in by adhesions.
At no time during life was there resonance over the liver, but there was some at the time of post-mortem examination before the bowels were opened, due perhaps to the fact that at death the relaxation of the muscles allowed the gas to rise higher than it did during life. The unusual median position of the abscess is important in accounting for absence of dulness, when it is usually found in slough or ulcer of the vermiform appendix.
"A Fatal Case of Typhlitis without Recognizable Symptoms." Under this title José M. Fisser published a case of inflammation of the vermiform appendix causing general peritonitis in a young woman nineteen years of age. The peculiarities of the case were that the appendix was not perforated, and consequently there was no tumor in the right iliac fossa—that the symptoms were all referred to the epigastrium, without even tenderness in the fossa. She walked the floor and tossed about in bed; the highest temperature was 103°, and the most frequent pulse was 120, and these continued but a short time. Of tympanitis there was none till near death, and then but little. The obscurity in diagnosis led to the publication of the case. The cause of this disease was fecal matter, not very hard, in the appendix.7
7 Med. Record, Sept. 1, 1883.
[p. 1159] As much has been said in this article on the diagnosis of peritonitis, it may be well to introduce a case where that diagnosis was conjectural, and yet quite another state existed. I visited Mrs. H——, when her disease was advanced, twice. My impression was that she had peritonitis, but this opinion was held with grave doubt. After her death, Smith sent me the following record of the autopsy: "Mrs. H—— died Friday evening at ten o'clock; next day, at three in the afternoon, we made an autopsy. No gas or fluid in the peritoneal cavity; the small intestines inflated almost to bursting, with injection of the capillaries. In the left iliac region we at once discovered a portion of the intestine almost black, and on examination found a firm white band encircling and constricting that portion. Upon liberating the gas the intestines collapsed, and the constricted portion was released and easily removed. A further examination showed that two of the epiploic appendages, coming off from the colon above the sigmoid flexure, had united at their extreme points and formed a loop two and a half to three inches long, and through this loop or ring a portion of the ileum had passed, and was there constricted. The constricted intestine was about four feet in length. This examination has been gratifying to me. There was a small quantity of bloody serum in the peritoneal cavity low down in the pelvis. The dark grumous blood that passed the bowels on the second and third days can now be accounted for, and corroborates your remark that the hemorrhage looked like strangulation. This was at your first visit. This must be a new cause of strangulation, and one that we could not anticipate."
There was, before I saw her, a single vomit of a suspicious fluid, but the evidence was not strong enough to enable us to pronounce it stercoraceous. Some of the observers noticed bloody serum in the peritoneal cavity, and perhaps some shreds of lymph, but that was in consequence of the strangulation.
This may occur anywhere in the broad extent of the peritoneum, and will be more or less limited in different cases, or may be limited for a time, and then become general. It is either acute or chronic. The product of the diseased action may be serum or lymph or pus, or all of them. The cause of this local inflammation is sometimes very obvious, in other cases wholly unknown. The consequences vary all the way from harmlessness to death; the symptoms are as variable as the consequences, making the diagnosis easy in some cases, in others impossible. Some cases in which it was not difficult to recognize it have already been recorded—those caused by perityphlitis and perforation of the vermiform appendix, for example. In such cases the local pain, the swelling, the dulness or resonance on percussion, depending on whether the tumor is made by inflammatory exudation or gas, together with the general symptoms and the history, leave but little ground for doubt regarding the character of the disease. Perhaps one-half the local abscesses which form between the folds of the peritoneum are recognizable during life by the local, associated with the general, symptoms. When situated in the posterior and upper part of the abdominal cavity, the hand gives little, [p. 1160]perhaps no, assistance, as in the most widely-known case of abscess that has been recorded in all time. While the physicians were giving to the country hopeful reports day by day, thousands of medical men shook their heads and spoke sadly of the prospects. The illustrious patient was losing rather than gaining strength and flesh, his appetite poor, his digestion poor—a strong man growing helpless—and, above all, a pulse that for months never fell below 100. With an adequate cause of abscess, whether there were chills or not, what else could it be? Thus, in peritoneal abscesses that cannot be felt the general symptoms are of great importance to the diagnosis. When abscesses tend to discharge their contents soon or late—sometimes into the intestine, sometimes into the bladder, sometimes externally: in such cases there is a fair chance. Sometimes they burst into the peritoneum: such cases are almost inevitably fatal; even opium will not cure them. The pus of these abscesses often has the fecal odor, which it acquires by the transmission of the intestinal gases through the intestinal walls. I was attending, with the late James R. Wood, a young lady in whom peritoneal abscess had been recognized. It was anterior to the intestines. In the consultation, while we were discussing the propriety of using the trocar, the mother became alarmed at the odor and appearance of the urine just passed, and summoned the doctors back to the chamber. The abscess had opened into the bladder. The urine contained pus which gave off the fecal odor strongly. This patient recovered. It should be added that these abscesses, as well as those of the convex surface of the liver and those that are post-peritoneal, sometimes pierce the diaphragm and produce empyema, or by previous adhesion of the lung to its upper surface find a way into a bronchial tube, and so the pus is expectorated.
The history of local fibrinous exudations is not as easily told as that of the purulent. We find from time to time, on the peritoneum, bands, patches, or cords of false membrane, which were produced in so quiet a way that we can get no information regarding the time when they were formed, and perhaps the subject of them was not aware that anything was wrong with the bowels till he began to have the symptoms of obstruction. These unnatural structures are formed in great variety. The omentum is found thickened and contracted. The mesentery and mesocolon are seen in a similar condition, causing wrinkling and shortening of the bowels. The spleen has on its surface patches or even plates, or one great plate, of firm fibrinous deposit, often cartilaginous in density, sometimes calcareous; and we can rarely fix the time of these occurrences by any symptoms. It is not always so with the liver. We are acquainted with a perihepatitis which is acute, attended by pain in the right side, a febrile movement, and, if the inflammation reaches the under surface of the organ, by jaundice, and have learned to combat this with cups and opiates, the latter in rather free but not heroic doses, and to expect recovery in a few days. This may leave the liver wholly or partly invested with a layer of false membrane which may have a sequel of importance. Then, again, we find the organ invested with a thick contractile membrane, but cannot learn that the symptoms of perihepatitis have ever occurred. The diseased action which produced this bad investment appears to be analogous to that which not only covers the organ with a thinner coat of similar new tissue, but inlays it everywhere with the same material in cirrhosis. This also is [p. 1161] unattended by local pain. The effects that may result from this encasing of the liver in a strong contractile capsule may be illustrated by the following case (the late Buck was the physician): The patient was an unmarried lady of middle age who had consecrated her life to charitable works. In searching for the suffering poor she often had to ascend several flights of stairs. The time came when she found this fatiguing and a tax on her respiration. She observed at the same time that the bowels were enlarged. She called Buck, and he had no difficulty in discovering ascitic fluid. He was surprised, as he knew that her habits were perfectly good, and she had very little the appearance of an invalid. Notwithstanding the proper use of the usual remedies for dropsy, the fluid slowly increased, and at length he was obliged to draw it off. He found it to be a clear, yellowish serum. In the course of about two years she was tapped four times. I saw her, with Buck, after these tappings, when the fluid had again been effused in quantity that half filled the peritoneal cavity. The emaciation was not considerable; there was nothing of the semi-bronzed color of the skin so common in cirrhosis of similar duration; her appetite and digestion were not materially impaired; the temperature was natural; the pulse was increased in frequency only a few beats. The skin over the abdomen was in a soft, natural state, and there was nothing that suggested a hyperæmic or inflammatory dropsy. The liver on percussion appeared to be reduced in size. Taking all things into account, and especially the patient's habits and the absence cancerous cachexia, it seemed probable that the dropsy arose from atrophy of the liver, and that the atrophy was caused by an adventitious capsule of the organ, although the patient had never had symptoms of perihepatitis. From this point the fluid did not increase or diminish, but remained stationary till she died, perhaps two years after, of some other disease. Meanwhile, the lady resumed her favorite charity-work to a limited extent. At the post-mortem examination the capsule was found investing nearly the whole liver, but not materially obstructing the gall-duct. The new membrane was thick and strong, having a thickness of at least one-twentieth of an inch. The remaining liver structure was of natural appearance. The organ was reduced to one-half its natural size. No other cause of dropsy was found.
I have doubted whether any disease deserving this name really exists independent of such low inflammatory action as may arise from the irritations of tumors or heterologous deposits. This statement refers to general not local peritonitis. I have never seen anything that would lead me to believe that acute diffuse peritonitis can be deprived of its acute character and still continue an inflammation. With me it has always been death or cure. I have already referred to a case in which after recovery the bowels were greatly disturbed by tympanitis for years. But this came from adhesions: her general health was good. I have at long intervals met with cases of ascites in which the peritoneal membrane was redder than natural, and in which no obstruction to the portal [p. 1162] circulation was discovered. This, however, I have regarded as hyperæmia rather than inflammation.
Bauer,8 however, gives to these cases the title latent general peritonitis, especially when after death an abnormal adhesion is found here and there. In the cases that I have seen there was a peculiar state of the surface of the abdomen. The skin there was more or less scaly and dry, but I do not remember whether there were internal adhesions. Bauer regards the diagnosis of this form of disease as difficult, but refers to the constantly present meteorism as well as serous fluid. I have met with three or four instances in which at the time of puberty an abdominal dropsy has rather suddenly occurred, lasting one to three months, and disappearing on the use of diuretics. I have had no reason to attribute this effusion to inflammatory action, except in one case. A lady of extraordinary symmetry and beauty of form, in excellent health, whom I had treated for this disorder twelve years before, applied to know whether there was anything in that disease that would prevent her having children. She had been married seven or eight years, and had not been pregnant. The question then occurred to me, At the time of the dropsy could there have been lymphy exudation that has since confined the ovaries in an unnatural position? The question I could not answer. The treatment which Bauer prefers for his latent peritonitis consists in "painting with iodine, the use of diuretics, and the regulation of diaphoresis by means of Turkish baths."
8 Cyclopædia of the Practice, etc., vol. viii. pp. 297-302.
Another form of general chronic peritonitis is, according to Bauer, that which follows acute peritonitis. He quotes several authorities in support of his views. I must draw on him for a description of it, for, as I have said, practically I know nothing about it.
The symptoms of acute peritonitis are all toned down, but do not all disappear. Vomiting occurs occasionally; tenderness is diminished, but is quite perceptible; meteorism diminishes, but fluctuates greatly; appetite is poor or variable; constipation alternates with diarrhoea or is followed by dysentery; now there is a febrile heat, and then the temperature is normal—this fever is most likely to come in the evening; the pulse is frequent and varying; ultimately extreme emaciation and anæmia. The most striking feature of this condition appears to be sacculation of the fluid in the abdomen, wholly or partially; this fluid then is not freely movable, but will give dulness on percussion, which may contrast well with intestinal resonance in its immediate neighborhood. When the tension of the abdominal wall is diminished these sacs can be felt by the hand as uneven tumors. Colicky pains occur, and in a case cited it was at one time very severe, at another only slight. The majority of the cases terminate, after a protracted course, fatally. Recovery may occur by absorption or external evacuation of the fluid. He gives no special treatment.
Bauer makes still another class of cases of chronic peritonitis—those arising in the course of old ascites; he, however, does not make much out of it. He thinks the cases of this kind occur with cardiac and hepatic disease, and particularly with the nutmeg liver. The symptoms, he admits, are neither well defined nor severe, and the anatomical changes consist "in thickening of the serous membrane by a slight deposit of fibrin, [p. 1163] slight turbidity of the ascitic fluid, and a few flakes of fibrin suspended in it." He then, strangely, gives, as if they were illustrations of such a disease, two cases in which death by acute peritonitis followed the last of many tappings, in one of which a pool of pus was found encysted in front of the intestines. Both are borrowed.
Probably most practitioners who are in the habit of making post-mortem examinations have seen the flakes of lymph in the ascitic fluid, etc., but the German physicians have been the first, I believe, to regard such cases as belonging to separate forms of disease.
William Pepper has published9 a case observed by himself and G. A. Rex which shows non-malignant chronic peritonitis better than any I can recall to mind. The report forms the sequel to the case of the young woman on whom he successfully performed paracentesis of the pericardium.
9 Am. Journ. of Med. Sci., April, 1874.
This young woman began to have double pleuritic effusion, and this was soon followed by ascites three and a half months after the operation. From that time the ascites was better or worse, but did not wholly leave her, and became considerable before her death. This was sudden, she having some convulsive movements in extremis. Lesions were found in the thoracic cavity like those discovered in the abdominal, showing, it was believed, a special tendency in this person to plastic exudation on the serous membranes. "The lower part of the abdomen was found occupied by an extensive effusion. The intestines were floated upward. There were few if any signs of inflammation of the intestinal peritoneum, but marked changes were observed in the parietal peritoneum and in the capsules of the liver and spleen. The peritonitis was most marked in the upper segment of the abdomen, while the parietal membrane presented large patches of irregular thickening. No tubercles were found on any part of the peritoneum. The capsules of the liver and spleen were greatly thickened, whitish, opaque, and densely fibrous. The liver was enlarged and heavy, and so tightly bound by its thickened capsule that its shape was somewhat altered.
"The diaphragm, especially that part of it underlying the pericardial sacs, had undergone marked fibroid degeneration. The muscular tissue was much atrophied; many fasciculi had evidently disappeared, while many others were markedly narrowed, some of them shading off to a width of less than 1/3000 of an inch, and finally disappearing altogether. They retained, however, even in their narrowest dimensions, their transverse striæ."
(It may be remarked, in passing, that this substitution of fibrous for muscular tissue follows the same law that it does in the heart when that organ is the seat of fibrosis or fibrous degeneration. Here it was supposed to be the consequence of a low grade of inflammatory action. Is it when it occurs in the heart?)
In the abdomen these observers found nothing which suggested the possibility of tubercles or any obscure form of cancer. In the pericardium, on the heart side, were found numerous small nodular roughnesses. Irregularities of the pericardial false membrane are so common that nothing but the close and universal adhesions would raise any question of these relations. But tubercles would hardly be here and nowhere else.
[p. 1164] Delafield says that one form of the chronic disease is the continuance of his cellular peritonitis. In this, he says, the surface of the omentum is covered with cells which look as if they were derived from the endothelium and connective-tissue cells, although they differ from the normal shape of these. The new cells are for the most part polygonal, of different size, with one or several nuclei, and giant-cells—large granular masses filled with nuclei. Although these new cells are produced over the entire surface of the peritoneum, yet, as a rule, they are more numerous in little patches here and there. These little patches may be heaped together in such numbers as to form nodules visible to the naked eye. There is never any stroma between these cells.
This form of peritonitis occurs most frequently with organic heart disease, with cirrhosis of the liver, with chronic pulmonary phthisis, and with acute general tuberculosis. In the two latter diseases he thinks they have been improperly called tubercles.
He describes a form of chronic adhesion of peritoneal surfaces that occurs without the intervention of fibrin, but, as he supposes, by coalescence of the branching cells and a production from them of a fibrillated basement substance, the fibrils crossing in all directions. In the midst of these fibrils he finds the nuclei of these cells. He finds also in the immediate neighborhood of these adhesions thousands of branching cells that are attached one to another and float free in the water, the fixed end being attached to the peritoneum. He regards such a peritonitis with adhesions as a more advanced stage of the forms of cellular peritonitis already described, and the new cells are changed into membrane.
Sayre has published an extraordinary case in the Transactions of the Pathological Society. He calls it chronic proliferative peritonitis; it might be called more aptly the consequence of peritonitis.
A large, strong man fell from a hammock, the rope breaking, upon his shoulders, and felt a severe pain in his stomach, and soon developed symptoms of peritonitis. This pain never entirely subsided. The peritonitis was recognized. About one month after he was tapped, and 240 ounces of serum were drawn. He was tapped one hundred and eighty-seven times, and 12035/16 pounds of fluid were taken from him during the remainder of his life. At post-mortem examination 3000 cc. of yellow serum were found. The liver and spleen were covered by a thick layer of false membrane, intestines were glued together in the upper part of the abdomen, and the stomach was adherent to the lower surface of the liver. The portal vein was contracted by this membranous coating. There were numerous other lesions in the heart and pleura, but these will account for the dropsy.
This man was unusually strong and hearty until 1876, when he had an attack of double pleuro-pneumonia, and in 1878 he slipped on the front steps and fell, but seemed to recover from the effects of this. The fall from the swing occurred in July, 1879. He died in February, 1884.10
10 Med. Record, April 19, 1884.
This form of disease is by no means uniform in its first symptoms or in its progress. The only things uniformly attending it are tubercles on the peritoneum and more or less of inflammatory effusion, chiefly lymph and serum; tumor and hardness of the bowels, general or local; deranged function of the stomach and intestines; emaciation; and extreme fatality.
In some cases the invasion is acute and marked—a chill followed by fever, vomiting, early development of meteorism, and in a few days a point or points of resistance to pressure, but not necessarily dulness on percussion. In a few days the febrile action and the meteorism may subside, leaving the symptoms of local peritonitis. But we have not long to wait for a renewal of them and an evident extension of the inflammatory action. Remission and relapse alternate at varying intervals, until the whole extent of the peritoneal surface seems to be involved in inflammation. With this mode of development meteorism may not be renewed in the most common way. The lymphy product of inflammation may so bind the intestines to the posterior walls of the abdomen that they cannot extend forward, but are pushed upward against the liver and diaphragm, and so encroach on the thoracic space. But then the anterior parietes are tense and hard, and do not move in respiration. The febrile heat may not continue more than two or three months, but the pulse will be frequent to the end. There will be a thinning of bowel walls, and here and there a knuckle of adherent intestines may cause some prominence and give some resonance on percussion. There will be also occasional vomiting, and the dejections will be irregular—maybe only deficient or thin; there may be an alternation of constipation and diarrhoea.
Tuberculous ulcerations of the mucous layer of the bowels is not uncommon in tubercular peritonitis, and these ulcers have in rare cases perforated and allowed the fecal matter to accumulate in considerable quantity in a sac limited by previous adhesions. In all forms of tubercular peritonitis death is caused as often by grave complications as by what appears to be the primary disease. The affection occurs in probably every instance in those who had at the beginning, or had acquired in its progress, what we call the tubercular diathesis. We are not surprised, therefore, to find on inspection a wide diffusion of tubercles in the body, particularly on other serous membranes, and in the lungs. Death may occur, then, from phthisis pulmonalis or from pleurisy or meningitis, as well as from the exhaustion and accidents of the peritoneal disease. The effusion serum or turbid serum is very common in tubercular peritonitis, and can be recognized by the dulness it produces in part of the cavity, and sometimes by fluctuation. It is often sacculated, but it is not constantly found after death, it having been absorbed before, and perhaps long before, that event.
In other cases the invasion of the disease is stealthy and deceiving. It comes so quietly that the patient is not conscious of any local disorder beyond a dyspepsia and irregular action of the bowels. He has a pulse of growing frequency, but if he knows it he ascribes it to his dyspepsia. He is slowly losing flesh and strength; this he accounts for in the same way. At length a perceptible swelling of the bowels attracts his attention. At this stage the physician finds that the swollen bowels are tympanitic everywhere or only in the upper, while there is evidence of fluid [p. 1166] effusion in the more depending, parts. He discovers some, it may be little, tenderness on pressure, and a pulse of 85, or maybe 90, increasing in frequency toward evening. The appetite is poor, the digestion slow, and occasionally there is vomiting; the complexion is pale and a little dingy; the skin of the abdomen may be dry and rough or may be natural; some colicky pains have been or soon will be felt. From this point the disease gradually advances. The distension of the bowels slowly increases or they are firmly retracted; the emaciation increases; the strength diminishes; there is often cough, which is generally dry; the bowels are slow or diarrhoea alternates with constipation; with the distended bowels there is always more than natural resonance on percussion, except when there is fluid effusion, though not often the full tympanitic sound observed in acute diffuse peritonitis. This resonance is not equal, always, in different parts of the abdomen; the respiration is embarrassed and almost wholly thoracic. The abdomen is often as large as that of a female at full term of pregnancy, and indeed the condition has been mistaken for pregnancy. This is an inexcusable blunder in a case like that which I have in mind—a young unmarried woman. She had no dulness on percussion in the space that would be occupied by the gravid uterus, but rather resonance. The case might have been a little less clear if there had been fluid effusion in the abdominal cavity, but if this were not encysted it would flow from one side of the abdomen to the other when the patient turned correspondingly in bed; if it was encysted, there would be small chances that it would have the shape and position of the gravid uterus; if it had, there would be no chance of hearing in it the foetal heart or feeling the foetal movements; and after all this there remains the experimentum crucis—a vaginal examination.
At first the diagnosis is unavoidably uncertain. Some aid is found, possibly, in the medical history of the family, in tuberculous antecedents, yet I remember cases in which no phthisis could be found in any living or dead member of the family on the paternal or maternal side as far back as it could be traced. Some aid is found if the patient himself has any of the physical or rational indications of pulmonary phthisis, and yet there are recorded cases in which the abdominal symptoms were the first to appear. The prominent German physicians attach great importance to the pre-existence of a cheesy mass or degeneration somewhere in the body as the real parent of tubercles wherever they appear. The truth of this doctrine, I do not think, has received anything like universal recognition; and if it had, as this cheesy degeneration is often, perhaps commonly, only discoverable after death, it could rarely give any assistance in diagnosis, so that the early diagnosis is always difficult, and a very early one often impossible. But as time goes on, and the symptoms are better defined and show themselves one after another as they are above described, it seems as if a careful observer could not confound it with anything except perhaps one of the other forms of chronic peritonitis or cancerous peritonitis. As to the latter, the cough which exists in most cases of tubercular peritonitis will assist in the distinction, but a physical examination much more; for a cough does not always attend phthisis when this disease exists; for example, I visited a daughter of one of the distinguished gentlemen of Vermont. She had had the bowel symptoms that indicated tubercular peritonitis for eight or ten months, and the diagnosis was not [p. 1167]difficult. Remembering Louis's opinion that if tubercles invade any other part of the body, they are likely to be found at the same time in the lungs and in a more advanced condition, I examined the lungs, and found in the upper part of the right a cavity so large that it could have received a fist. I was only surprised by the fact that she did not cough, and had not coughed. She herself assured me of that (she was twenty-one years old); her physician, who was present at the visit, had never heard her cough, and had no suspicion of any pulmonary complication; but, more than all, her mother, who had walked with her, slept with her, eaten with her, travelled with her, and from the beginning of the illness had not been out of her company more than twenty minutes in any twenty-four hours since the disease began, had never heard her cough. Here, then, the nervous deviation to the abdomen, or whatever else it may have been, had so benumbed the sensibility of the pulmonary nerves that the alarm-bell of phthisis had never been sounded; but the cavity, had there been any doubt whether the bowel disease was cancerous or tuberculous, would have almost fully settled the question. But more of the peculiarities of cancerous peritonitis a little farther on.
The lesions of this disease (or its pathological anatomy) differ considerably, but the differences are in the amount of tuberculous deposit and the secondary results, not in the real nature of the disease. Lebert has published among his plates of pathological anatomy one which shows the peritoneum thickly sprinkled over with small tuberculous grains, and represents each particular grain surrounded by a little zone of inflammatory injection. There is yet no exudation, but that would soon follow. A fibrinous exudation will soon come over this primary deposit, and undergo a kind of organization, or at least get blood-vessels, which in their turn can furnish the material for a new crop of tubercles. These again provoke a new layer of fibrous tissue, which also becomes studded with tubercles, and so on, till a thick covering is formed over the intestines. But the same material is interposed between their folds, separating one from another and compressing them and diminishing their calibre; at the same time this agglomerated mass is firmly adherent to the abdominal walls everywhere. The new material may have a thickness of half an inch or even more. I remember how surprised and confused I was when I made my first inspection of such a case. The abdominal walls were cut through, but they could not be lifted from the intestines, but were firmly adherent to something. They were carefully dissected off and the bowel cavity (?) exposed; there was apparently an immense tumor filling the whole space: no intestines, no viscera, could be seen. A section was made through this mass from above downward, and another parallel with it and an inch distant from it, and this part removed. It appeared like a large, hard tumor, through which the intestine made several perforations. The new material appeared to be fibrous, with grayish-white tubercles sprinkled in through it everywhere, and pretty abundantly. In another case this fibro-tubercular material may occupy one part of the abdomen, and a large serous cyst or serous cysts another. The tuberculo-fibrous material may be found in markedly less quantity than is so far described, till there will be no more than in a case from Ziemssen's clinique, quoted by Bauer: "In the peritoneal cavity about four liters of yellowish-brown, slightly turbid fluid. Omentum [p. 1168] thickened, stretched, adherent to the anterior wall of the abdomen and beset with hemorrhages; the same was true of the parietal peritoneum; between the hemorrhages whitish-yellow and entirely white tubercles occur, varying in size from the head of a pin to a lentil. The intestinal serous membrane was similarly invaded. The intestines intensely inflated; a number of ulcers on the mucous membrane, one approaching perforation. Covering of the liver thickened by fibrinous deposition."
The lungs and serous membranes generally will, in all probability, show more or less of tubercular deposit, the pericardium less frequently than the others.
The result in this affection, after it is fully established, is believed to be uniformly fatal, and at its commencement the difficulty of diagnosis may lead one to doubt whether his apparent success is anything better than apparent. Still, a plan which I have relied on is, I believe, worth announcing. As soon as the disease is recognized the patient is put upon the use of the iodide of potassium and the iodide of iron, in full average doses, and a solution of iodine in olive oil is applied to the whole surface of the abdomen by such gentle friction as will produce no pain; and after a minute or two of such friction the oil is brushed thinly over the surface and the whole covered with oiled silk. This dressing is repeated twice a day. The quantity of iodine to an ounce of oil will vary considerably in different persons; for some, seven to ten grains will be enough; for others, thirty will be needed. The iron is to make the application moderately irritating, and if it produce pinhead blisters or blisters a little larger, all the better. When the application becomes painful the oil is washed off, and the application is not renewed for two or three days. In this manner it may be continued for two or three months. Meantime, the patient is put upon the diet and regimen of the consumptive, the appetite encouraged; he takes sustaining food, with plenty of milk and cream, or cod-liver oil, as much fresh air as possible, and friction is applied to other parts of the body with dry flannel.
Benign tumors of the abdomen are not frequently the cause of general peritonitis, and when they are, the grade of the disease is acute rather than chronic. They very often provoke local inflammation and become adherent to the neighboring structures. The same is true of malignant growths in the abdominal cavity, except that the adhesions are earlier formed and more likely to occur. Localized cancer, of whatever variety, is not very prone to produce general peritonitis, even though there be multiple developments of it. But when the disease takes the disseminated form, and is sprinkled over the whole extent of the peritoneum, then inflammation is almost certain to occur—not of high grade, and yet deserving the name subacute rather than chronic. A case which illustrates this statement has come under my observation within the last year. I will recite it with sufficient detail to make it intelligible.
A lady about forty years of age had, up to the summer of 1881, enjoyed very good health, though she was never robust. At that time she felt her strength abating and her stomach disordered. She sought [p. 1169] health in various places, and took professional advice in September. It availed her little; the bowels were gradually swelling and fluctuation could be felt. She was losing strength and flesh. There was not a cachectic countenance, but the features were growing sharp. She had suffered but little from pain till October. At that time she was at the family country home. Then she began to suffer from a severe pain in the left thigh; and this, it was noticed, increased as the accumulation in the bowels increased, and at length her physician felt compelled to tap her—not so much on account of great distension of the bowel as in the hope of relieving the pain. He drew off nine quarts of gluey, viscid fluid, and her pain was wholly relieved. Twelve or fifteen days after this she was brought to her city home, and her city physician, seeing that her case was a grave one, sought the aid of a distinguished gynæcologist. She was then again tapped to give him a more satisfactory examination. He found the ovaries considerably enlarged and hard. They could not, however, be felt by pressing the fingers into the pelvis from above—only by the vagina. I saw her on the 10th of November. The fluid had again made considerable tumefaction of the bowels, and she was again suffering great pain in the region of the right kidney and in the leg of the same side, together with cramps. The relief given by the first tapping induced us to propose its repetition. It was, however, delayed till the 14th, that the physician who had tapped her before might be present and assist. The quantity of water drawn was again nine quarts, and again the pains and spasms were quieted. The examination of the abdominal fluid was interesting. It was nearly clear, reddish, of syrupy flow and consistence, and so viscid that while a portion of it had remained on the slide of the microscope long enough for the examination of its constituents the thin cover became so firmly attached to the slide that it could not be removed without breaking or long maceration. The albumen was so abundant that the fluid was completely consolidated on boiling. Fibrinous threads were running through it in great numbers, and here and there was a cell of large size, round, granular, but not plumped up with granules, with a nucleus barely less in size than the cell itself; its outer border within, but only just within, the boundary or wall of the cell. It was the nucleus that was granular, for there was little room for granules between the nucleus and the cell wall. The vial containing the fluid had been standing three or four hours for a sediment. This in a vial four inches high occupied the lower half, and gave nothing to the dropping-tube till the sedimentary matter was drawn into it by suction. This matter consisted of fibrillated fibrin in large quantity; a great number of the cells just described, some grouped, but most separate or single. There were pus-cells in moderate quantity, each having the amoeboid movements, and a considerable number of red blood-corpuscles, some of natural form, some crenate.
Immediately after the tapping the flaccid condition of the abdominal walls admitted an examination. A solid, hard mass was found running across the upper part of the bowels, a nodule of which was lying on the stomach at the point of the ensiform cartilage. A harder mass of irregular shape was also found just above the pelvis on the right side, extending upward and to the right. This was in extent two by three inches. The ovary, however, could not be detected by pressure from above [p. 1170] downward. The diagnosis up to this time was hardly doubtful, but these revelations made it complete, and crushed any lingering hope of the patient's recovery.
While the pain and spasm ceased after the tapping, the oedema of the left leg, which came on some time before the last tapping, did not diminish. The hard spot near the right iliac fossa was tender on pressure, but otherwise hardly painful. While the fluid did not exceed six quarts or so, she had little pain anywhere. There were no external glandular swellings. Her appetite was poor, and she took but little food. She vomited very little till the end was approaching. The urine contained a few globules of pus, some pigment matter, two or three hyaline casts, but no trace of albumen. For sixteen days following November 14th the patient was comfortable, but the fluid was slowly filling the bowels again. At that time the pains already referred to began to return. On December 5th they required another tapping, and preparations were made for it, but vomiting, rather severe, led to its postponement to the next day. The quantity of fluid drawn was nine and a half quarts. It was of the same syrupy consistence as that previously drawn, and under the microscope showed exactly the same constituents and gave the same quantity of albumen. The next day stercoraceous vomiting commenced, with no movement of the bowels, except what was produced by 10 grains of calomel given on the second day of this vomiting. That acted well and produced a temporary relief. She after this took no food by the mouth, but milk and beef-tea were injected into the rectum. Still, the fecal vomiting returned, and she died on the 15th.
The post-mortem examination was made on the 17th by William H. Welch. I could not attend it. His report is complete as to the main features of the case, though it does not furnish an explanation of the spasms and the oedema of the left leg, regarding which Welch was not informed. The pain and spasm were doubtless due to backward pressure of a diseased part on a nerve or nerves, and the oedema to a narrowing of the iliac vein by pressure or constriction by fibro-cancerous matter on its outer sides. "The peritoneal cavity," he says, "contained somewhat over a gallon of clear, yellow serum. Both the visceral and parietal layers of the peritoneum were thickened, in some places more than in others; this was especially marked on the anterior of the stomach and on the lower part of the ileum and in the left iliac region. The omentum was greatly thickened and retracted into a firm mass (or roll), which extended somewhat obliquely across the body, more to the left than to the right. The mesentery was much thickened and contracted, drawing the intestines backward. In a few places only was the peritoneal surface coated with fibrin, and the intestines were mostly free from adhesions. The coils of the lower part of the ileum, however, were firmly matted together by organized connective tissue in such a way that they were twisted, often at a sharp angle, so as greatly to constrict the calibre of the gut. The serous and muscular layers of the intestine at this point were greatly thickened. By these causes there appeared to be a complete obstruction at a point about six inches above the ileo-cæcal valve. By careful dissection these coils were straightened out, so as to remove the main cause of obstruction. The peritoneal covering of the liver was adherent to the parietal layer.
[p. 1171] "The surface of both the visceral and parietal peritoneum was studded over with hundreds of small, firm, whitish nodules, generally not larger than a pea, and often not larger than a pin's head. In some places they had coalesced and made firm patches an inch in extent. This same material was found in the contracted omentum in considerable quantity. In a few places, particularly on the uterus, a blackish pigmented deposit appeared.
"The ovaries were not adherent, but both were enlarged to the size of a hen's egg. The outer surface of each was rough and corrugated. The new growth was deposited on the exterior and penetrated each a quarter to half an inch. It was of uniform white color and of firm consistence.
"The stomach wall was thickened nearly throughout its extent, but particularly in the anterior part, where it amounted to thrice the normal thickness. This consisted wholly of hypertrophy of the muscular coat and increase of fibrous tissue in the peritoneal layer. This new growth was traced, in the interlacing bands, from the surface into the muscular coat. In the outer layer of the stomach were found three small white nodules. The mucous membrane of the organ was healthy or a little pale.
"The retro-peritoneal glands along the aorta were enlarged, soft, and of a reddish-gray color. A nodule was found in the wall of the duodenum outside the mucous membrane, and one in the Fallopian tube."
Every organ in the abdomen and chest was examined, but nothing important found except what is here recorded. Welch concludes his record with the following diagnosis: "Primary scirrhous carcinoma of the ovaries. Secondary deposits in the peritoneum, in the outer layer of the right Fallopian tube, of the stomach and duodenum, and in the retro-peritoneal glands. Chronic peritonitis, intestinal obstruction."
This case presents to the reader so accurately the usual course of cancerous peritonitis, and the inspection its lesions, that a treatise on the subject is hardly called for. It often happens that cancerous antecedents in the patient or his relatives will lend an aid to the diagnosis, which this case did not present. To distinguish this disease from tubercular peritonitis no question can arise except in its dropsical form, and then the lungs in every case of the latter that I have met with have the physical signs of tubercles, though not always the rational indications. The pulse is much more accelerated in the tuberculous variety. I omitted to state that the temperature of this patient was often taken, and till the closing scene was never found more than one or two degrees above the healthy standard, and the morning and evening heat did not materially vary; the opposite of both, then, would be expected in a tuberculous case. The existence of meteorism is much more common in the tubercular disease; indeed, in the cancerous case recited there was none of it. The duration of the two is different—that of the cancerous kind is recorded in months, while the tuberculous variety may continue two years. The cancerous is more likely to be attended by alarming accidents, like the complete obstruction of the bowels, large hemorrhages, and a sudden lighting up of acute peritonitis. Finally, in the light of the case here recorded, it seems probable that the examination of the abdominal fluid will become of great importance. I have never carefully examined the fluid of tubercular dropsy, but it does not seem probable that it will have the syrupy [p. 1172] appearance, the large amount of albumen, the abundance of fibrin-fibres, and the granular large cells with nuclei only perceptibly less in size than the cells themselves, that were repeatedly found in this case—found by two observers, and at every tapping after the first.
TREATMENT cannot be curative; it therefore consists of such administrations as will relieve pain, give sleep, improve the appetite, increase the flow of urine if it be scanty, and relieve the bowels if there is a tendency to constipation. It is as much the duty of the physician to put off the fatal day, when he can, in incurable affections as it is to cure those that will yield to his prescription and advice. In the case just narrated opium or an opiate alone produced such unpleasant after-effects that she was unwilling to take it, but when the extract of belladonna was given with it she slept pleasantly, and could take her food the next day.
Bauer, in Ziemssen's Cyclopædia of Practice of Medicine, and Wardell, in Reynolds's System of Medicine, have each devoted a chapter to this form of disease. They refer to the fact that the foetus may have peritonitis before birth or be born with it, or may have it when a few days old. They say that this form of the disease occurs most frequently in lying-in asylums or foundling hospitals, and that it has been supposed to depend on a syphilitic taint. They say, too, that it follows erysipelas, scarlet fever, measles, etc. I do not perceive that the description of either of these authors makes any marked distinction between this and the same disease in adults, except what may arise from the inability of the infant to describe its sensations, and the more rapid course of the disease to a fatal result—in some cases twenty-four hours. Having myself had no obstetrical practice, or next to none, I have nothing to add to their statements, and can from my own knowledge abate nothing. I therefore refer the reader to these chapters, and to the references given by the first of these authors, for a fuller knowledge of the matter.
Regarding the comparative exemption of children, after the first few weeks of life, from spontaneous peritonitis, referred to by one of these authors, I can fully confirm his statement. Though I have assisted in the treatment of many children suffering from peritonitis, I have difficulty in recalling to mind a single case in which the disease was not caused by perforation of the intestine or vermiform appendix of the cæcum, and in much the greatest frequency perforation of the appendix.
B. F. Dawson,11 after reciting a case in which the liver had undergone a peculiar degeneration and was attended by peritonitis before birth, states that Sir J. Y. Simpson observed nine cases in his own practice "and notes more than a dozen from different sources." These cases seemed to have been caused by the ill-health of the mother during gestation, or excessive labor, injuries, venereal disease, and were mostly attended by grave disease; the viscera often, the liver; but sometimes the mother was perfectly healthy, and the peritonitis was the primary disease. Death almost always occurred in utero or shortly after birth. In one instance the child recovered.
11 N.Y. Med. Journ., Dec., 1882.
[p. 1173] The Med. Record takes the following from Schmidt's Jahrbucher for Jan. 7, 1883: "Dr. Oscar Silbermann recognizes two varieties of peritonitis in the new-born. The non-septic or chronic is developed usually in the first third of foetal life, and is generally syphilitic in origin. If the peritoneum covering the intestines be involved, as well as that over the liver and spleen, various forms of intestinal obstruction may result. Most frequently there is occlusion of the anus, less often stenosis or complete stricture of the small intestine. Of a number of cases of congenital occlusion of the intestine collected by the author, all ended fatally, only one living beyond twelve days.
"The second, acute or septic, form of peritonitis in the new-born the author divides into two varieties, according as the peritonitis is only a part of general infection or is the sole manifestation of the septic poison. In either case the point of entrance of the poison is always the navel wound. The symptoms, which need not all be present in a given case, are vomiting, watery stools, meteorism, ascites, abdominal tenderness, icterus, etc. The pulse and temperature may vary in degree in different cases. A cure of the septic form is possible; therefore the treatment should be carefully considered. The navel wound should be cleansed, and the child is to be isolated from its mother. To control the fever quinine may be given. Priessnitz's sheet is of value; vomiting may be checked by chloral (one-half to one grain in water). The strength should of course be maintained by stimulants if necessary."
The accumulation of fluid indicated by this name has already been referred to in its relations to several causes. There are, however, conditions producing it which have not been considered or only considered partially.
The most prolific source of abdominal dropsy is obstruction of the portal circulation on its way to or through the liver. Condensation of the liver structure in cirrhosis, with destruction of many of the portal capillaries and compression of many more, is prominent in this connection. The compression of the liver caused by an adventitious external covering, referred to under the head of Local Peritonitis, acts similarly, whether it compresses the vein at its entrance into the liver or not, although it is not known to produce any destruction of the portal capillaries. Some enlargements of the organ are attended by the same result, but they are always associated with a hardening of its structure. The disease lately called waxy liver, now often denominated lardaceous, belongs to this class, as does that condition in which the organ is enlarged, hardened, and fissured, regarded as syphilitic liver. That both these diseases may have a syphilitic and mercurial origin is not a point now under consideration. They both harden the hepatic structure and obstruct the portal circulation, while they may not in equal degree hinder the progress of arterial blood. This is explained when we remember the diminished force that propels the portal blood. Neither of these diseases produces dropsy early in its progress, but, as I have seen it, always before it reaches its fatal termination. Fatty liver has not, in my observation, produced dropsy, [p. 1174] although I have seen livers made very large by that disease, and the absence of dropsy when the liver has been large has aided me in distinguishing it from the waxy disease. Cancer of the liver in some instances does, and in others does not, produce dropsy of the bowels. It is only certain to have this result when a tumor is in position to press upon and obstruct the portal. Hypertrophy of the liver, caused by mitral regurgitation or other disease of the heart, does not generally produce dropsy, but, aided by anæmia or watery condition of the blood, such a result is possible. In children, however, it is not very rare to see the bowels distended by dropsy, and to discover that the liver is enlarged at the same time. It is common in such cases that the dropsy and the hypertrophy disappear after a few weeks of treatment. This may occur in a child that is anæmic, but without any disease of the heart. Such a case was brought to me two or three months ago, and after four weeks of treatment by tonics and diuretics the health was re-established. There is one point in these cases of some importance. When the child lies on his back, if the abdomen is much distended, the liver cannot be felt. It has sunk away into the fluid, and in this position ordinary percussion cannot ascertain its dimensions. In the July number (1840) of a quarterly journal edited by Swett and Watson, I published an article in which I reported the conjoined labors of the late Camman and myself on a new method of combining auscultation and percussion, with its results, under the heading "Auscultatory Percussion." By the method described in that article—viz. by placing a solid stethoscope, or for that Laennec's first stethoscope, a rolled-up pamphlet, on the chest at a point where the liver has not fallen away from its walls, and percussing on the abdomen from below upward—a point is reached whence the percussion sound is brought sharply to the ear, while half an inch below the sound is dull and distant. The lower edge of the liver is thus easily recognized, and its upper boundary is found in a similar manner or by ordinary percussion, so the difficulty of measurement disappears.
In such case, when the dropsy disappears and the liver recovers its natural dimensions at the same time, the inference is that the hypertrophy caused the dropsy, and that the hypertrophy was of the kind called simple. The nutmeg liver is thought to have an agency in producing dropsy, but as it is for the most part associated with diseases that have been called dropsy-producing, its bearing on this effusion may yet be regarded as uncertain.
It is common to speak of heart dropsy in such a way as to imply that disease of the heart alone can produce abdominal effusion. I doubt it. I even doubt whether the heart alone can cause the anasarca that is so often attributed to it. In following a great multitude of heart diseases from the time they were recognized to their termination, I have been struck with the ease with which the patients attend to their business, sometimes even laborious business, for years—in one instance fifty years—with almost no complaint, and how rapidly their condition changes as soon as albumen and casts appear in the urine. I have been compelled by these observations to ascribe the anasarca and oedema that makes this last stage of heart disease so distressing to the kidneys, and not to the heart. Double pleuritic effusion is not uncommon under these circumstances, but every physician must have noticed the rareness of troublesome abdominal [p. 1175]dropsy, while there is sometimes—perhaps often—a little effusion; and when in the exceptional cases there has been much, it was almost always accounted for by a dropsy-producing change in the abdominal organs, not, perhaps, discovered during life; so that for me, while they produce overwhelming effusions in other parts of the system, they are minor agents in the production of ascites. Phthisis is occasionally attended, toward its close, by oedematous legs and albuminous urine, but I cannot report any important relation between these and peritoneal effusion. I can say the same of chronic bronchitis. I record this negative testimony regarding the two last-named diseases, because I find them enumerated among the causes of abdominal dropsy.
Cancer may invade the portal vein, tumors of adjacent parts other than those of the liver, or an aneurism may compress it and cause dropsy. Hydatid tumors may do this. Diseases of the pelvic organs, both acute and chronic, may produce it, but then the disease would fall into the class of those produced by chronic or subacute peritonitis.
DaCosta thinks he has lately had a case of chronic peritonitis attended by ascites. It was in a woman thirty years of age, who had been thrown with force upon the frame of an iron bedstead, striking the lower part of the bowels. Pain and tenderness followed. These were not confined to the injured part, but extended to the whole abdomen; and there was menorrhagia. After a time there was fluid effusion in the peritoneal cavity, which slowly increased till her state demanded relief from tapping. The fluid after this operation did not return. The pain and tenderness were constant symptoms all through. She slowly improved, and at the time the case was reported it was believed that she would soon be discharged from the hospital. The only doubt which DaCosta finds regarding the diagnosis is in the facts that the liver was diminished in size and that the spleen was moderately enlarged, and he admits the possibility that an adventitious capsule of the liver may have caused the ascites, but believes that it was dependent on chronic peritonitis.
Acute peritonitis subsiding into chronic, with increase of fluid effusion, as I have already said, I am not familiar with. That occurring in cancerous and tuberculous peritonitis has already been considered. But in relation to these some facts regarding frequency of occurrence, collected by Bristowe, are worth quoting. He says that in 48 cases of tubercular peritonitis, dropsy was found in 12, and that in 22 of peritoneal cancer, 12 had more or less ascites. He further adds, regarding cirrhosis, that of 46 cases observed post-mortem, there was dropsy in only 20. This is not surprising, as in all the diseased conditions of the liver that produce dropsy the anatomical changes must reach the point at which there is considerable portal obstruction before the effusion will occur.
The amount of fluid found in ascites varies greatly. In some it may remain for a long time stationary at four or five quarts; in others the suffering caused by an accumulation of nine or ten quarts will demand its removal; and in a few cases twenty quarts have been removed in one operation. It is in cirrhosis that the largest quantity is found, and it is in this disease and in cancerous peritonitis that the most frequent tappings are required. The quality of the fluid also varies markedly: from being almost as clear and thin as spring-water it may be almost ropy, or in color greenish or yellowish or slightly red; it is very likely to contain [p. 1176] albumen; and it is probable that a further study of its microscopic elements may enable us to resolve doubts regarding the cause of the effusion. It very often contains blood-corpuscles.
Bristowe finds from hospital records that ascites occurs in about equal frequency in males and females, but, as everybody has noticed, that hepatic dropsy is much more frequent in men than in women. Ascites, he says, is most frequent between the ages of thirty and fifty, and next between twenty and thirty and between fifty and sixty, but is not uncommon above the latter age; and it occurs in children.
SYMPTOMS.—In general, ascites is easily recognized by the swollen state of the bowels: a well-rounded swelling when the patient stands or sits, but spread out in the flanks when he lies on his back; the fulness of the side on which the patient may be lying, and the flattened condition of the opposite side,—belong to this disease, and as a group to no other. The results of percussion are significant in the movement it causes in the fluid, and for the resonance or flatness it produces. When the patient lies on his back, tapping with the finger-ends on one side of the abdomen sends a wave of the fluid across to the other side, where it is perceived as a gentle blow by the applied fingers of the other hand. If the abdomen is not full, this wave will be produced at the upper level of the fluid, but not above that. If this wave cannot be sent across the body, it may be found on either side by percussing above and feeling for it below; percussion also teaches where the fluid is, and where it is not, by the dull sound it produces. It is rare in ascites that the intestines do not float on the surface of the fluid, at least from the umbilicus upward, and there give a loud percussion sound, while toward the back, and often toward the pelvis, it is dull, or even flat; changing the position of the body, the resonance will be uppermost and the dulness in the most dependent part. Then the softness or impressibility of the abdomen till the tension becomes great is noticeable. The changed position of the fluid as the body is turned from side to side is important. A very small quantity of fluid can be detected in this manner. The patient is placed on his right side and percussion is made in the right flank: there is dulness, while in the left flank there is resonance. The patient turns on to the left side: dulness now changes position, and is on the left, and on the right resonance. If it is feared that some undetected fluid remains in the pelvic cavity, the pelvis may be raised by pillows and the same examination repeated, or he may be placed in the knee-and-elbow position referred to by Bristowe, and the percussion will then be made upward in the umbilical region. In some cases the contraction of the mesentery will not allow the intestines to rise through a large amount of fluid and float on it; but such cases are almost confined to the cancerous and the tuberculous varieties of the disease; and as in these the symptoms are grave, the physician will probably have visited his patient many times before this contraction will embarrass him. Besides, when mesenteric contraction occurs there is a very strong probability that the omentum will also be contracted, be rolled up, and lumpy; as this can almost always be felt above the level of the umbilicus, he has in it an explanation of the absence of resonance on the fluid. It has happened that oedema of the abdominal walls or fatty accumulations there have given a delusive though feeble fluctuation on percussion. In such cases, if the patient make moderate pressure with the back of a small book in [p. 1177] the course of the median line, that kind of wave will be broken, while a wave in the abdominal cavity will not be prevented. When there is considerable distension of the abdomen by fluid, weak spots in the abdominal wall often yield and make a tumor. This is very common at the umbilicus, where a little bladder is lifted half an inch or more above the general curve of the abdomen. The fluid frequently follows the track of hernias. In females it has been known to press the anterior wall of the vagina backward and downward, so as to make it protrude at the vulva. It has, in one of my own cases, by downward pressure caused complete prolapse of the uterus. It is very often attended by oedema of the lower limbs. This is accounted for by the pressure of the abdominal fluid on the veins that return the blood from these parts, or in cirrhosis by contraction of the ring or notch through which the vena cava passes in the liver. If there is general oedema, the cause will probably be found in disease of the kidneys; or if in one limb, in pressure or thrombosis of one iliac vein. As the disease advances the accumulating fluid forces the diaphragm upward, diminishes the breathing room, and threatens the life still more. Then the patient cannot lie down in bed, but spends his nights as well as days in an easy-chair, and sleeps leaning forward on a support for his forehead. The veins on the abdominal surface will fix attention. With almost any large tumor in the cavity they become more or less enlarged. But in cirrhotic dropsy this becomes more striking than in any other affection. The enlargement is attended by a reversion of the blood-current on the lower half of the abdomen. This is early shown by emptying an inch or two of a vein with the finger, drawing it either upward or downward, and noticing from which direction it is refilled when the pressure is removed. The pelvic veins do not readily discharge their blood by the natural channels, and by anastomosing branches it is forced over the surface of the abdomen and into the thoracic veins, these latter becoming in turn greatly enlarged. The appetite is commonly poor, the digestion flatulent, the pulse accelerated. Emaciation is gradual or rapid. The urine is commonly scanty, and in cirrhosis of a reddish hue. The skin is apt to be dry, particularly so in simple chronic peritonitis. The tongue has no characteristic fur, and is often, almost always toward the close, dry. The mind is not affected till near the end; then often the patient is delirious, commonly mildly. Diarrhoea is not uncommon, and even dysentery has been observed. The result is almost always unfavorable, or, as has been said, lethal.
The diagnosis is not often difficult. When, as in chronic peritonitis and in tuberculous peritonitis, the fluid is confined in a sac or sacs, each particular pool will be yielding to pressure, but elastic, and will give the percussion wave, though it may extend but a short distance. To distinguish ovarian dropsy—ovarian cysts, as it is now called—from ascites may require a few words. Ovarian tumors of all kinds are found to be more prominent on one side when they rise from the pelvis than on the other. This is not the case with ascites. The uterus and its appendages lie in front of the pelvic intestine, and when any of them ascend above the pelvis they must occupy the same relative position. In other words, a large ovarian cyst must lie in front of the intestines, while intestinal resonance should be found behind and in the sides. But if the ovarian cyst does not occupy the whole height of the bowels, intestinal resonance [p. 1178]may exist above it, and the dulness may be found below, bounded by a portion of a circle, and sometimes the cyst walls are resisting enough to allow its boundaries to be ascertained by the fingers. This cyst can also be felt in the vagina; and the uterus, instead of being pressed down, is sometimes lifted upward, so that it cannot be reached in the vagina, but can be felt through the abdominal walls just above the pelvic bones. A condition more troublesome than this is when ovarian cyst and ascites occur together. Then the posterior or lateral resonance is lost when the patient lies on her back, but can be found on one side when she lies on the other. In that concurrence, in dorsal decubitus it is possible by pressure or a little blow to send a wave of the ascitic fluid over the front of the cyst. This can be seen as well as felt. Should the patient take the knee-and-elbow position, the intestinal resonance may be restored in both flanks.
TREATMENT.—In opening the chapter on the treatment of ascites it is usually said, Give principal consideration to the diseased conditions that have caused the dropsy; in other words, cure cirrhosis, cancerous peritonitis, tubercular peritonitis, heart disease, and the secondary affections of the abdominal organs, release the liver from the dangerous compression to which it is subjected, and all will go well. But they do not inform us how these impossibilities—at least in most cases impossibilities—are to be achieved. It is true that the physician would not shrink hopelessly from the treatment of simple chronic peritonitis. But this is one of the rarest causes of ascites. A physician in a long lifetime may not have seen a case. It is true, ascites is a symptom, always a secondary, or even a tertiary, affection; and theoretically there can be no better advice, but practically it cannot amount to much. Then, if the cause cannot be removed, it remains to do our best to relieve the patient of his load and strive to prolong his life to its utmost possible limit. In doing this the physician will often find himself able to give gratifying relief, and once in a great while to rejoice in a cure.
The three great emunctories, the skin, the bowels, and the kidneys, are chiefly appealed to for relief in this as in other serous accumulations. Most physicians prefer to use the diuretics—first, because if they will act at all, they act so quietly and produce so little debility that whatever can be gained by them is obtained at small cost to the system. The form of ascites that most resists diuretics is that which originates in cirrhosis. Often a full trial of them, with suitable changes from time to time, is of no avail, yet now and then the kidneys yield to persuasion and act freely. The saline diuretics and digitalis are most in favor with some. In the early part of the present century a pill composed of squill and digitalis in powder, and calomel, each one grain, given three times a day, was almost universally chosen. In place of the calomel the blue mass was often preferred. When this prescription had produced a little ptyalism the mercurial was omitted and the squill and digitalis continued. It has often been observed in dropsies of all kinds that diuretics act better after a little mercurial action is set up in the system. The diuretic that I most frequently prescribe is made of the carbonate of potass. ounce ss and water ounce vj; to a tablespoonful of this a tablespoonful of fresh lemon-juice is added. This is taken every two hours, and at the same time a dessertspoonful of the infusion of digitalis or more is taken three times a day. This is an [p. 1179]old prescription. Sometimes the old sal diureticus is used. This is the acetate of potassium. It is not always kindly received by the stomach. At Bellevue Hospital the following is much used: viz. infusion of digitalis, ounce iv; bitartrate of potash, ounce j; simple syrup, ounce ss; and water added to make a pint. This is taken pretty freely. But it would require many pages to exhaust the diuretics. I will only add that I have more confidence in the salts of potash and soda, singly or combined, aided by digitalis and a mercurial, than in any others.
The diaphoretics that are most efficient are warm water and steam. A foot-bath long continued and frequently repeated, the patient covered with blankets, and the water kept at 90° or warmer, are very effectual in producing perspiration. Bricks heated or hot water in bottles, or potatoes heated, and enveloped in damp cloths and laid alongside of the body and limbs, form an extemporaneous vapor-bath of considerable efficiency. A vapor-bath can be easily extemporized in the following way: Have a kitchen vessel furnished by the tinman with a cover which has an inch tube fitted to this and bent so as reach the floor six feet from the fire. The pot should have a capacity of a gallon or more, and should be kept boiling briskly. Meantime, the patient, in his night-dress, has a double blanket brought over his shoulders from behind, and another from before, and fastened. Now he takes a chair (wooden), under which the steam is delivered. The blanket from behind is kept off his body by the back of the chair, and the front one by his knees. The steam, shut in in this way, soon brings on a sweat, and when it is sufficiently active the front blanket is thrown off, and the patient wrapped in the rear one and put to bed, when the sweating can be regulated by blankets. This is better than what is called the alcohol sweat, for in that the patient is bathed in carbonic acid gas as well as heat. A patient is sometimes enveloped in a hot, wet blanket with good effect. Pilocarpine has come into use lately as a sudorific. I have witnessed its effects many times and can testify to its certainty as a sudorific; but it is too debilitating for common use. Digitalis has sometimes acted with extraordinary power in this way, but there are grave risks in administering large doses.
Among the cathartics that may be used in ascites, it has seemed to me that the milder hydragogues are safest. One ounce of Epsom salts with a drachm of the fluid extract of senna can be taken every second or third day for months, if need be, with little reduction of strength, and sometimes with an increase of it. I had charge of a young man in the hospital in whom cirrhosis was unquestionable, and dropsy at one time extreme, in whom the abdominal veins had made furrows that would receive the little finger, who was wholly relieved by a drastic dose of elaterium every second day. I saw him three years after his discharge, and then his health was good. Notwithstanding this, I prefer the milder medicines.
Bristowe has seen no cures from either sudorifics, diuretics, or purgatives. I have seen one or more from each of those agents, all cirrhotic. He "has seen cures occasionally from mercury, iodide and bromide of potash, copaiba, and a combination of fresh squills and crude mercury." I agree with him in his statement that counter-irritants are useless, making exception for chronic peritonitis and the early stage of the tubercular variety. He thinks quinia, iron, and cod-liver oil are useful.
[p. 1180] Paracentesis in almost every case will at length become necessary, and the question comes whether it should be practised early or late. If it be delayed till the oppression of the breathing makes it imperative, the walls of the abdomen will be so stretched as to present little resistance to the reaccumulation of the fluid, and a second tapping will be required in fifteen to twenty-five days. A bandage is a poor substitute for muscular contraction. If, on the other hand, the fluid is withdrawn before the muscularity is not stretched out of the muscles, then accumulation will be less rapid and the patient will be spared the suffering which large accumulations cause. But tapping is not always an innocent operation. It is sometimes followed by acute peritonitis. By the early tapping this risk is oftener taken. Reginald Smith suggests the use of a small canula by which only ten or twenty ounces of the fluid can escape each hour. This mode, he thinks, removes the danger of syncope and makes the bandage needless.
in the peritoneum is a topic on which there is little to be said. A primary effusion of this kind probably does not occur. In hæmatophilia, where the mucous membrane of the nose and wounds bleed dangerously, there is no record of spontaneous bleeding into the peritoneal cavity. The same thing can be said of that very rare disease which has been called bloody sweat. An unmarried lady applied to me fifteen years ago with this disorder. The blood would ooze out at hundreds of points on the inner face of the arm; these would run together and drop off the arm, or the same thing would occur on the chest and in the bend of the knee. This would continue for two or three minutes, and then cease of itself, but to recur in one or more, rarely several, places. For years this habit continued. There was no irregularity of the menses. I could find no visceral disease; there was no nose-bleed. She lost strength, but only moderately. This kind of bleeding continued for several years. She is now approaching fifty years of age, and for the last two or three years has had no recurrence of the bleeding. There was never anything in this case to lead to the suspicion of peritoneal or other serous hemorrhage. In the few similar cases on record there is the same absence of all evidence of internal bleeding.
It has already been said that a certain amount of blood, as shown by its corpuscles, is to be expected in cancerous ascites, and with less uniformity in tubercular ascites, and not unfrequently in hepatic dropsy, as well as in acute peritonitis. This may not deserve to be called hemorrhage, on account of the moderate quantity of blood that is effused; but aside from that which results from rupture of blood-vessels it is about the only kind of it with which we are familiar.
Scurvy, and conditions of the blood analogous to those produced by that disease, make it almost certain that if pleurisy or pericarditis occurs while these conditions exist, it will be hemorrhagic. I am not, personally, acquainted with a single instance in which peritonitis in this condition has occurred. Copeland, however, says that hemorrhage in peritonitis has been noticed by Broussais and others. The blood is mixed [p. 1181] with the serum and stains the surface of the false membrane, as in hemorrhagic pleurisy and pericarditis, and the disease is of an asthenic type, "occurring in the hemorrhagic diathesis." "The symptoms are inflammatory from the beginning, and rapidly pass into those indicating great depression; the pulse becomes rapid, small, and soft, death quickly supervening, with convulsions, cold and damp extremities and surface," etc.
Copeland has himself not seen a case, and regards its occurrence as very rare. Delafield states that "Friedreich describes two cases occurring in patients with ascites who had been frequently tapped. He says that both the parietal and visceral peritoneum was covered with a continuous membrane of a diffuse, yellowish-brown color, mottled with small and large extravasations of blood. The membrane was thickest over the anterior abdominal wall. It could be separated into a number of layers. These layers were composed of blood-vessels, masses of pigment, branching cells, and fibrillated basement substance. In many places the extravasated blood was coagulated in the shape of round, hard, black nodules. The new membrane could be readily stripped off from the peritoneum, and there were no adhesions between the visceral and parietal portions of the peritoneum."
The erosions of abdominal cancer sometimes open vessels of considerable size, causing large hemorrhage into this cavity and sudden death.
When aneurisms of the abdominal aorta rupture, they sometimes flood the abdominal cavity; oftener they open into the structures under the peritoneum on the left side, and make a large flat tumor extending from the point of rupture downward to the brim of the pelvis, and even beyond it.
A gentleman whose health was usually good, thirty-five years of age, felt an unwonted exhaustion and feebleness creeping over him. His countenance became pale, his pulse rapid, growing smaller and smaller. It seemed certain that there was hemorrhage somewhere, but until it was noticed that the bowels were growing tumid and hard there was nothing to guide us to its seat. Even then we were left to conjecture regarding the bleeding vessel. This sinking continued for thirty-six hours. After death it was found that a small aneurism had been formed on one of the vessels of the omentum, not larger than a small walnut, and had ruptured by a very small opening, and that it was by this small opening that life had oozed away.
Bleedings from stabs and other wounds of the bowels, from lacerations of the liver, spleen, uterus, and sometimes of the kidneys, should be mentioned in this connection; but as they, for the most part, fall into the hands of the surgeons, this is not the place to give the details regarding them.
DEFINITION.—Tabes mesenterica may be briefly defined to be tuberculosis of the mesenteric glands. This definition may seem too limited, because it recognizes the identity of tuberculosis and scrofulosis of the lymph-glands, and excludes those hyperplastic conditions which do not certainly undergo the cheesy degeneration. It is supported, however, by the absence of any essential difference in the histological changes which take place in tuberculous and scrofulous (Wagner) lymph-glands; by the frequent simultaneous occurrence of each in the same subject; by the secondary development of tubercles during the course of scrofulous affections; and by the fact that the cheesy transformation is alike common to both these conditions of new formations. Schüppel maintains that the presence of tubercles is necessary to the production of the cheesy metamorphosis of lymph-glands, and that "scrofulous glands are always tuberculous glands." In this view Rindfleisch coincides, and expresses the belief that the inflammatory and hyperplastic changes are secondary to the formation of the tubercles. Birch-Hirschfeld asserts that cheesy degeneration of the mesenteric glands is always accompanied by tubercular formations.
This definition is therefore adopted as the expression of the result of the most recent investigations. It must, nevertheless, be admitted that a few equally competent observers deny the identity of the tuberculous and scrofulous new formations in lymph-glands. It must also be conceded that occasionally hyperplastic processes in the lymph-glands undergo the cheesy metamorphosis independent of tubercular development.
SYNONYMS.—The differences of opinion, especially among the older authors, in regard to the nature of this disease are very distinctly indicated in the varying significance of the numerous synonyms, of which the following list is only a part: Atrophia mesenterica; Atrophia infantum (Hoffmann); Febris hectica infantum (Sydenham); Scrofula mesenterica (Sauvages); Paralysma mesentericum (Good); Physconia mesenterica (Baumes); Mesenteritis chronica (Stewart); Mesenteric fever, Hectic fever, Marasmus (Underwood); Carreau, Entero-mésentérite of the French; Darrsucht der Kinder and Gekröschwindsucht of the Germans; Tubercles of the mesentery; Tuberculous disease of the abdomen; Phthisis mesenterica; Tabes glandularis; Tabes scrofulosa; Macies infantum; Pædatrophia; and Rachialgia mesenterica.
[p. 1183] Some of these synonyms indicate the theoretical and unsupported opinions of their authors, and others refer merely to a symptom. The name carreau refers to a hardness of the abdomen; physconia, to the presence of a non-fluctuating and non-sonorous abdominal tumor; and that of entero-mésentérite presupposes a secondary origin from a primary enteritis. Good classes it among his numerous varieties of mesenteric turgescence, but characterizes this special form as a scrofulous turgescence always associated with the strumous diathesis. The terms tabes and atrophy originated when the nomenclature of disease was derived from symptoms, and not from pathology.
HISTORY AND PATHOLOGY.—The history of tabes mesenterica is coeval with that of scrofula and pulmonary consumption. The ancient authors recognized the existence of a chronic disease of the mesenteric glands, characterized by enlargement and induration, followed by destruction of the gland-parenchyma, which was associated with digestive disturbances, emaciation, hectic fever, and usually terminated in death. At first, the degenerative process was regarded as suppurative. But as the study of scrofula progressed, and frequent observations were made of the occurrence of disease of the external lymphatics and of the mesenteric glands in the same subject, disputes arose as to the identity of the two affections. These controversies led to the general acceptance of the belief that the scrofulous degeneration of lymph-glands and the process of destruction in tabes mesenterica were identical. Consentaneous with these investigations, and for a long time subsequent, even down to a very late period, which is, perhaps, not yet concluded, the relation of scrofulous disease of the lymph-glands to pulmonary consumption was discussed and studied with great assiduity. As the knowledge concerning these diseases advanced, and the results of investigations were accepted, the doctrine of the identity of the morbid processes in scrofulous disease of the external glands and mesenteric phthisis became firmly established. The history of scrofulosis and tuberculosis cannot be separated. The connection and identification of the two processes have been subjects of constant discussion from the discovery of tubercle to the present time. Occasionally, the dividing-line seemed definitely fixed. Then would follow the general acceptance of the doctrine of identity. With the discovery of miliary tubercle a determined reaction took place against this view, and for a while many regarded scrofulosis merely as a form or stage of tuberculosis. As the conclusions in regard to these questions changed, so did the opinions concerning the true nature of tabes mesenterica change, until, finally, the investigations of Rindfleisch, Schüppel, and others seem to have established the tuberculous nature of the disease. Many authors of a comparatively recent date have applied the term tuberculosis to this condition, not because they knew or believed the development of true tubercle was a constant or essential characteristic, but because they regarded the words scrofulosis and tuberculosis as synonymous.
Notwithstanding the obscurity in which, for so long a time, the pathology of this disease was involved, certain facts well known to the earliest writers have been confirmed by continuous observation down to the present. Its secondary character has been so uniformly recognized that some of the older authors based its origin upon the absorption and conveyance along the lymphatic vessels to the glands of some peccant material originating [p. 1184]in a primary focus of disease. The constant coexistence with scrofulous affections and pulmonary consumption had long ago established the direct and primary relation of these diseases to tabes mesenterica, and authors of recent date, though not so generally holding the opinion that it is always an intercurrent complication of these maladies, yet maintain its secondary development. Even Schüppel, whose investigations and conclusions lead in the direction of an idiopathic origin, admits that the only primary element is the tuberculosis, which finds its cause in some peripheral irritation.
In the earlier times, as now, tuberculosis of the mesenteric glands has been observed during every period of life from birth to advanced old age, but then, as at the present time, the greater number of cases were known to occur during infancy and childhood. But few cases have been observed during the earlier months of life or before weaning. Between the ages of two and eight years is the period of greatest frequency. Though rarer during the later years of childhood, the older the child the more rapid its progress to a fatal termination. Nursing infants are not exempt, but those nursed by healthy mothers are much less liable than the wet-nursed. Among hand-fed infants it is not an uncommon disease, but it is much more common among the farmed-out children. While, as has been stated, the greatest number of cases occur in those between two and eight years of age, statistics show that the liability to it increases from the age of two and a half years up to the eighth, and, according to some authors, up to the tenth year. At the latter age there is a remarkable diminution in the number of cases. This fact is probably due to the greater prevalence of the acute diseases of the respiratory organs and of the exanthematous diseases among children during this period of life. Some have attributed it to the more rapid development and increased functional activity of the mesenteric glands. This circumstance might afford a plausible explanation for the apparent sudden increase in frequency after the completion of the second year because of the independent subsistence of children at that age, and the additional duties imposed upon the alimentary tract and its dependencies; still, if this were so, the period of greatest frequency ought to begin at an earlier age and more nearly correspond with the time of weaning. It is, however, a fact that tubercularization of the mesenteric glands is more frequently associated with chronic intestinal inflammation in those over one year than in those under that age. This fact, together with the greater liability of artificially-fed infants, would seem to connect, at least in such cases, its secondary origin with some primary irritation of the intestinal canal.
Authors are not yet agreed in regard to the relative frequency of this disease in boys and girls, though opinions predominate in favor of the greater number among the males. The statistics of Rilliet and Barthez and Schmalz show a decidedly greater prevalence among boys.
The comparative frequency of tuberculosis of the mesenteric glands cannot be determined. Louis found disease of the mesenteric glands in one-fourth of the autopsies of persons dying of phthisis; in 100 adults dying of the same disease Lombard found tuberculosis of these glands in 10; and in the bodies of 100 tuberculous children he found the glands tuberculous in 34 cases. In the Hôpital des Enfants Maladies tubercles were found in the mesentery of one-half of the children dying of [p. 1185] tuberculous affections. In the bodies of children dying of tuberculous disease in the Children's Hospital of Washington tuberculous degeneration of the mesenteric glands has been found in two-thirds of the cases, and without a single exception in those dying of rickets. Authors differ also, and the statistics are equally unreliable, in regard to the relative frequency of tubercularization of the bronchial and mesenteric glands. The general opinion seems to be in favor of the greater frequency in the bronchial glands. In a majority of cases both sets of glands are found diseased.
The geographical distribution of tabes mesenterica is as universal as that of scrofula and pulmonary phthisis. No country or climate is exempt, yet there is no locality in which it is endemic. It has been observed among all civilized nations, in the cold regions as well as in the tropical countries. Wherever scrofulous and phthisical diseases are known, there also are found cases of tabes mesenterica. Livingstone has stated that scrofula is unknown in some regions in Central Africa, and other travellers have made similar statements in regard to some Indian tribes. The statistics of the Children's Hospital of Washington show a far greater frequency among the African race than among the whites. It belongs to no class or condition of life, but occurs more frequently among the children of the squalid than among the children of the affluent and well-to-do.
ETIOLOGY.—Predisposing Causes.—Modern as well as the older authors have very generally accepted the conclusion that a constitutional tendency or liability to this disease is its most frequent and potential etiological factor. This predisposition may be either inherited or acquired. The ancients called it the strumous, and the more recent writers the scrofulous or tuberculous, diathesis. Lugol maintained that this diathesis is begotten of old and syphilitic fathers, and others state that children of parents nearly related and of those broken down by disease and excesses may inherit it. That it is transmitted by scrofulous and phthisical parents no one can doubt, but as yet it cannot be defined to be anything more than a peculiarity of the constitution which may exhibit abnormal reactions against irritating influences. The scrofulous habit is believed to be indicated by physical appearances which represent two extremes. The erethic form is characterized by a feeble and delicate frame; deficient muscular development; transparent, smooth, and florid skin; light hair and blue eyes, large pupils; precocious intellect and sanguine temperament; the torpid form, by a large head; large and tumid upper lip; soft and flaccid flesh, bloated appearance; short and thick neck; muscular incapacity, tumid abdomen, and sluggish intellect. Some of these features are more frequently symptoms of the actual disease than of the existence of a predisposition to it, and, except so far as they may refer to a primary scrofulous or pulmonary disease, cannot be accepted as indicative of the presence of a constitutional tendency to tuberculosis of the mesenteric glands. A tumid abdomen, rapid emaciation, and anæmia are far more valuable signs of the disease of these glands.
Bad air and bad food are also important predisposing causes. They are conditions to which the children of the poor, especially in large cities, are constantly exposed. Insufficient protection from climatic influences, neglect of person, and unhygienic surroundings must be classed in the same category. It is claimed that vitiated air, unwholesome habitation, [p. 1186] insufficient or improper food, squalor and filth may cause the constitutional tendency, as they will certainly precipitate the development of the disease in those predisposed to it.
Exciting Causes.—The border-line between the predisposing and exciting causes cannot be positively fixed. The presence of tuberculosis or of some form of scrofulous disease in some other part of the body so constantly precedes the development of tuberculosis of the mesenteric glands, even in those who have not exhibited the characteristic phenomena of the scrofulous diathesis, that such affections must be regarded as exciting as well as predisposing causes. No one can doubt the frequent infection of the mesenteric glands in cases of pulmonary tuberculosis. The probability of systemic infection from a single focus is universally admitted. These facts and circumstances do not exclude the possibility of localized tuberculosis of the mesenteric glands. Whether such exclusively local development of tubercles ever occurs independent of the scrofulous diathesis cannot be determined, but that the disease does find its exciting cause in inflammatory conditions of the intestinal mucous membrane cannot be doubted. Schüppel, who asserts the primary development of the tubercle-formation in lymphatic glands, does not claim an idiopathic origin, but admits the necessity of a primary peripheral irritation in direct connection with the affected gland. The intimate connection between diseases of the intestinal mucous membrane and of the mesenteric glands is established beyond a doubt. Vogel and Steiner assert that tabes mesenterica is a common result of enteritis folliculosa. A primary inflammatory process may not contain any element which could be classed as tubercle, yet it may excite secondary tuberculosis of the glands. Whether such a result only occurs in those who may have acquired or inherited the predisposition is yet undecided. In many of the cases of tabes mesenterica tuberculous ulcers are found in the intestines, but it cannot be claimed that such ulcers are always the primary foci of tuberculous development. If primary, it is not difficult to understand how the virus may be transmitted to the glands.
It has been claimed that certain articles of food will produce the disease. Potatoes and rye bread in large quantities and a coarse vegetable diet have been mentioned among the exciting causes. Deficiency in the quantity of food is a much more frequent cause than inferiority in quality, yet there can be no doubt that any and every article of diet that will set up catarrhal inflammation of the intestinal mucous membrane may become a cause. Irritation of the mucous membrane of the alimentary tract, induced by coarse, stimulating, or imperfectly-digested food, or by the improper and frequent use of purgative medicines, may give rise to disease of the glands; and, even though the irritation may in itself be trivial, its long continuance or frequent renewal may prove sufficient, especially in those in whom the predisposition is present. Malarial and exanthematous diseases have also been considered exciting causes, and among the latter class measles and scarlet fever, because of the inflamed condition of the intestinal mucous membrane which they leave, are the most frequent. Difficult dentition and whooping cough must also be classed in this category.
Recently attention has been called to the probable transmission of the disease through the milk of diseased cows, but further investigation and [p. 1187] more reliable data are necessary to establish this connection. Klebs has deduced the conclusion from recent experiments that the use of the milk of cows in advanced phthisis will always produce tuberculosis, which begins as an intestinal catarrh and extends to the mesenteric glands.
Some of the older authors believed that the cure of some chronic diseases of the skin and mucous membranes and the suppression of chronic discharges might induce tuberculosis of the mesenteric glands; but these conditions are now known to be most frequently the initial manifestations of the scrofulous diathesis, and the mesenteric complications are far more likely to occur when these primary foci are neglected and the patient is left to suffer the unabated progress of the disease.
MORBID ANATOMY.—It is not usual to find all the glands of the mesentery affected at once, nor of those affected all in the same stage of disease. Newly-affected glands may be found alongside of others in an advanced condition. In the first stage the glands are enlarged, but rarely exceeding the size of a filbert; they are firm, but not inelastic. This change consists in hyperplasia of the gland-constituents. Microscopic examination shows abundant cell-proliferation, but the cells are badly constructed and prone to undergo retrogressive metamorphosis. The cells accumulate in clusters without any intercellular substance, and compress the lymph-sinuses and blood-vessels.
The second stage is characterized by the commencement of the cheesy degeneration. The glands enlarge and coalesce in clusters, sometimes forming large masses of hardened and inelastic glands. On section they exhibit in the beginning foci of cheesy material imbedded in the gland-parenchyma. In the further progress of the change the whole gland is transformed into a homogeneous yellowish substance. In this condition there are found on microscopic examination globular corpuscles, nuclei, shrivelled cells, sometimes giant-cells, and most frequently tubercles. The tubercles are usually found in the follicular substance. Birch-Hirschfield says the cheesy formations in secondary tuberculous mesenteric glands are only found in discrete foci, and the tubercles occur in the follicular substance imbedded in relatively normal tissue. The cheesy transformation is, according to Virchow, a necrobiosis of the hyperplastic gland-elements, but Schüppel insists that it is the result of tubercular development. After a time the cheesy masses soften, and the glands are converted into sacs containing a purulent fluid mixed with débris. In this condition they are most frequently coalesced in bunches, sometimes forming large tumors. The intervening walls may break down and the whole bunch be transformed into one large sac filled with purulent fluid and débris. Occasionally these masses of agglutinated glands become adherent to the abdominal parietes or to the intestines. Rupture of their walls may occur, and the contents may be emptied into either the peritoneal cavity or the intestines. When communication with the intestines takes place, it is usually through an ulcer on the mucous surface. It is probable that the cheesy substance may sometimes be absorbed, as Virchow thinks, by gradual softening proceeding from the surface toward the centre.
It is believed that these degenerated glands sometimes undergo the cretaceous transformation. Such an instance has been reported by Carswell: "The patient, who when a child had been affected with tabes [p. 1188] mesenterica and also with swellings of the cervical glands, some of which ulcerated, died at the age of twenty-one years of inflammation of the uterus seven days after delivery. Several of the mesenteric glands contained a dry cheesy matter mixed with a chalky-looking substance; others were composed of a cretaceous substance; and a tumor as large as a hen's egg, included within the folds of the peritoneum, and which appeared to be the remains of a large agglomerated mass of glands, was filled with a substance resembling a mixture of putty and dried mortar, moistened with a small quantity of serosity. In the neck, and immediately behind an old cicatrix in the skin, there were two glands containing, in several points of their substance, small masses of hard cretaceous matter." Calcareous concretions have been observed by Andral and others in the mesenteric glands in cases of chronic pulmonary disease; and Soemmering records several observations of a tartar-like substance found in devastated mesenteric glands in cases of rickets.
The morbid appearances in tabes mesenterica are not usually confined to the changes in the glands. In very many cases the evidences of disease of the peripheral glands are quite manifest, and in much the larger number of cases pulmonary phthisis and disease of the bronchial glands are present. The adjacent abdominal organs may also be involved. These consecutive morbid changes are succinctly set forth in the following notes of an autopsy taken from the records of the Children's Hospital of Washington, D.C. The subject was a negro boy aged ten, who had been taken sick a year previous to his death with a bad cold and cough, followed several months afterward by enlargement and suppuration of the cervical glands on both sides: "The body was greatly emaciated, the lips and teeth covered with sordes. Cheesy masses were scattered throughout the substance of both lungs. The right lung was firmly adherent to the thoracic walls, the left adherent at apex. The liver was enlarged and adherent to all adjacent tissues, and contained many cheesy nodules scattered throughout its substance and over the surface. The gall-bladder was distended with bile. The spleen was normal in size, very dark, and filled with cheesy masses. The pancreas contained many similar masses. The peritoneal cavity contained a quantity of muddy fluid. The peritoneum was dark in color, studded with tubercles, and ulcerated in a few places. The stomach and intestines were distended with gas; the walls of stomach thickened, the inner surface covered with a shiny mucus; in its lower wall was one large ulcer, penetrating to the peritoneal coat and measuring three-fourths of an inch in diameter. The peritoneal coat was thickly studded with nodules resembling tubercles. The small intestines were gangrenous in a few places; on the inner surface were found fourteen ulcers, varying in size from one-fourth to one and one-fourth inches in diameter, with elevated edges and red bases; two penetrated the peritoneal coat. This coat contained very many tubercles. On the mucous surface of the large intestines there were seven large ulcers, similar in appearance to those found in the small intestines. Some of Peyer's patches were ulcerated. The mesenteric glands, some as large as walnuts, were filled with cheesy material, and the mesentery was dotted over with small masses of similar matter."
In two of the reported cases of chylous effusion into the peritoneal cavity the rupture of the lacteals was caused by degeneration of the [p. 1189] mesenteric glands; and in several other cases the rupture was produced by the presence of tumors, apparently formed by the agglomeration of numerous degenerated glands.
Several cases of fatty diarrhoea from mesenteric phthisis have been reported. Of these the most conclusive is the case of Hall.1 The clinical history of the case and the detection of enlarged mesenteric glands in the umbilical and hypogastric regions placed the diagnosis beyond a doubt. It was, however, verified by the discovery of several vomicæ in the lungs, and of mesenteric glands "universally enlarged and affected with strumous disease. The intestinal mucous membrane was dotted with patches of ulceration, with here and there prominent masses of strumous deposit on the surface."
1 Guy's Hospital Reports, vol. i., 3d Series, 1855, p. 371.
SYMPTOMATOLOGY.—It is not possible to describe a definite and uniform clinical history of this disease. As a secondary complication of pulmonary phthisis and scrofulous affections the preliminary symptoms are so constantly identified with the development and progress of these maladies that, as a rule, the initial stage cannot be recognized by any special assemblage of symptoms. In any tuberculous or scrofulous child the possible implication of the mesenteric glands may be predicated upon any array of symptoms that would establish the presence of these classes of disease. And even in the absence of the rational and direct signs of such affections, in those exhibiting the physical evidences of the strumous diathesis, more especially when it is inherited, the symptoms of any trivial departure from health, such as the catching of cold, irritation of the alimentary tract, or protracted convalescence from any of the exanthematous or intestinal diseases, may constitute the initial history of tabes mesenterica. In such subjects debility and anæmia, from whatsoever cause they may apparently result—and, in fact, any manifest lowering of the standard of health, whether gradual or precipitate, and without assignable cause—may mark the beginning of the process of change in the parenchyma of the glands that will terminate in tuberculosis. The later as well as the earlier history may be completely masked by the symptomatology of other diseases belonging to the tuberculous class; and so grave, as a rule, are such primary and coexisting affections that definite recognition of this complication or localized extension of the systemic infection becomes more a matter of skilful diagnosis than of practical utility.
But in those cases where disease of the respiratory organs and of the bronchial glands can be excluded the general symptomatology becomes of paramount importance. And in view of the value of prophylactic measures which may be employed to arrest, limit, or delay the localized tuberculosis of these glands, the precursory symptoms may be of special significance. This condition may be characterized by languor and dulness or marked debility and anæmia, with loss of color, attended with flatulence, stomachal disturbance, frequent eructations consisting mainly of mucus, a sense of uneasiness in the abdomen after the ingestion of food, a variable appetite, sometimes voracious and occasionally depraved. Sometimes a dislike for fatty foods is a prominent symptom. The tongue may be coated, the breath is usually foul, and some have said the body emits an acid odor. If these symptoms occur in a child of the [p. 1190]scrofulous diathesis, or be directly or remotely associated with a previous gastro-intestinal disease, or occur or persist during the convalescence of some of the acute affections of infancy and childhood which stand in etiological relation to this disease, they may justify a reasonable presumption of commencing change in the mesenteric glands. This presumption will be strengthened by emaciation, a more marked disturbance of the digestive function, attended with fetid and occasionally whitish stools, a tumid belly, and deep, lancinating abdominal pains of short duration, recurring at long intervals and neither relieved nor aggravated by pressure or an evacuation. Some have attributed special importance to a chalky appearance and loss of consistency of the stools, indicating the suspension of absorption by the lacteals. There may also be slight evening fever. Later, the enlargement of the belly increases, the emaciation becomes more marked and rapid, the appetite more variable, sometimes very voracious, the alvine discharges more fetid or less consistent, sometimes putty-like, and generally irregular or constipated. The febrile exacerbations are more decided, and sometimes chills may occur at irregular intervals. When, in addition to these symptoms, either during the earlier or later stages, the enlargement of the glands can be detected, the clinical picture is complete. In consequence of the tympanitic distension of the abdomen, which usually increases with the progress of the disease, it is impossible in a majority of cases to detect the glandular enlargement; especially is this true when the affected glands are separate; but, as frequently happens during the last stage, when large tumors are formed by the coalescence of a number of diseased glands the diagnosis may be easily determined. In the absence of the discovery of enlarged glands the diagnosis cannot be considered positive. They are usually most readily found in the region of the umbilicus, and may in some cases, even when the tension of the abdomen is very great, be detected by grasping the abdomen with the hand and compressing it between the fingers and thumb so that the enlarged glands will be brought in close contiguity to the walls and be felt immediately under the fingers. If a tumor should be present and the peritoneal cavity be free from fluid, its locality may be recognized by a sense of resistance and circumscribed area of diminished resonance, and then definitely outlined by palpation. Underwood says: "Indigestion, costiveness or purging, irregular appetite, flushed cheeks or a total loss of color, impaired strength and spirits, remitting fever, and a hard and tumid belly, with emaciated limbs, are amongst the more common symptoms, attending at one period or other, of this disease."
When the diagnosis has been made out, it is not impossible to determine the stage of the disease. The progressive intensity of the symptoms, with rapid emaciation as a rule, bears a definite relation to the progress of the morbid changes taking place in the glands. It must, however, be borne in mind that children have died of tabes mesenterica who had enjoyed excellent health up to the moment of death, and the autopsy disclosed the condition of the glands, which had not been suspected during life. In the case previously cited, in which the autopsy exhibited such grave lesions of the stomach, liver, spleen, pancreas, and intestinal mucous membrane, the clinical phenomena were at no time commensurate with the gravity of the morbid changes.
[p. 1191] DIAGNOSIS.—In the absence of the proof of the presence of enlarged glands or of a tumor the diagnosis cannot be positively determined. The enlargement and tympanitic distension of the abdomen do not necessarily establish the existence of glandular disease, for they are present in a great many conditions of ill-health in children. Nor is the coexistence of a tumid belly, emaciation, and fever sufficient, for they are found in other tuberculous and in gastro-intestinal diseases. The discovery of enlarged discrete glands by palpation, as before described, in connection with such disturbances of nutrition as have been set forth, constitute the strongest presumption in favor of tabes mesenterica. The presence of enlarged glands unaccompanied by the ordinary symptoms of the tuberculous or scrofulous processes is inconclusive, because the glandular hypertrophy may be a simple hyperplasia, entirely independent of any tendency to retrogressive metamorphosis. There is usually some tenderness on pressure, but this may be present in any disease of the abdominal viscera. When the glands are of sufficient size, they may, by pressure, produce secondary derangements. Cramps in the legs may be caused by pressure on nerves. Oedema of the legs and dilatation of the superficial abdominal veins may result from compression of venous trunks. "If," says Eustace Smith, "these veins are seen to ramify on the abdominal surface and to join the veins on the thoracic walls, tabes may be suspected in the absence of chronic peritonitis and enlargement of the liver." Ascites may be present, but is not a necessary result of disease of the glands.
When a tumor has been discovered by palpation, it is necessary to determine its glandular nature. If situated about the umbilicus, in front of the spinal column, if irregular, hard, and feeling like a congeries of irregularly-rounded nodules, the evidence is very decided in favor of its glandular origin. But care must be taken to exclude tumors formed by fecal accumulations and masses attached to the omentum. Omental tumors are usually more movable, better defined, more superficial, and regular in form. Cancerous masses sometimes simulate glandular tumors. The general history of the case and the age of the patient are usually sufficient to make a diagnosis by exclusion. Rilliet and Barthez distinguished a cancerous pancreas by the presence of vomiting, jaundice, and abdominal pains.
The writer has many times based a conjectural diagnosis—which was verified by a post-mortem examination—upon the presence of a tumid abdomen, increasing emaciation, with the history of a protracted gastro-intestinal catarrh, and an irregular febrile curve characterized by frequent subnormal temperatures. He has also observed a number of cases of protracted diarrhoea in children, accompanied with extreme emaciation, notwithstanding the appetite was good, sometimes even voracious, and the food taken was ample, nutritious, and easily digested, in which the stools, varying from two to three, or twice as many, daily, were whitish, leaden, or slate-colored, sometimes semi-fluid, at other times containing lumps or masses of putty consistence, presenting to the naked eye a greasy appearance and to the touch a fatty feel, and at the autopsy has found only thinness and transparency of the coat of the small intestines and degenerated mesenteric glands.
PROGNOSIS.—The prognosis is decidedly unfavorable. So far as is known to the writer, there is but one recorded case of recovery in which the [p. 1192] diagnosis was indisputable and the fact of a cure was established by an autopsy. This was the case reported by Carswell, before referred to. The older and some of the modern authors have claimed many recoveries, but it must be manifest to every student of pathological anatomy that the mistaken diagnoses must have been nearly if not quite as numerous as the cases of cure. The writer has not witnessed a single case of recovery, but he has observed very many cured cases of disease which exhibited all the subjective and objective symptoms of tuberculosis of the mesenteric glands, save and except those by which its existence can alone be definitely and positively established. The case of Carswell demonstrates a remote possibility of cure by the cretaceous metamorphosis of the degenerated glands in a subject exhibiting the scrofulous diathesis. In view of this isolated observation, one cannot refuse to accept a similar possibility in cases in which the disease may be localized and confined to a few of the glands. In such cases, if recognized previous to the formation of cheesy foci, the possibility of staying, limiting, and perhaps occasionally curing, the disease should not be regarded as absolutely hopeless; yet the opportunities of examining the glands in the first stage of change has so rarely occurred that no one is authorized to assert that the hyperplasia is the true picture of the condition in which those in the advanced stage had its beginning; nor has any one claimed to have witnessed the progressive stages of resolution taking place in such glands.
The cretaceous transformation is an accepted though remote possibility, and absorption by means of gradual softening of the cheesy masses is perhaps a reasonable hypothesis. But even if either of these processes was an occasional termination of the disease, it could only lessen its gravity and prolong life, with an incomplete recovery, in those few cases in which the tuberculous or scrofulous changes were confined to a less number of glands than was necessary to maintain the nutrition of the body. For while there is no serious obstacle to the flow of chyle through the glands in the condition of simple hyperplasia, it is completely obstructed in those transformed into cheesy masses or purulent collections. The channels through the glands must sooner or later be obliterated by the presence of the abundant cell-proliferation which characterizes the initial stage of change in this disease. For if the compression is sufficient to cut off the supply of blood, it must prove equally destructive to the complex system of lymph-paths. To the impermeability of the glands must the emaciation and exhaustion which mark the course of the disease, to a greater or less degree according to the number of glands involved, be due.
If the investigations of Schüppel should be verified, and the primary tubercle-formations be accepted as the initial stage of change, the prognosis will be less favorable, but a distinct line of demarcation may be established between two classes of cases in each of which cheesy transformation may occur, but in one the tubercle-formations may be primary, and in the other secondary. In the latter class the prognosis may be more favorable, because treatment may be effective if commenced prior to the beginning of the retrogressive metamorphosis.
COURSE, DURATION, AND COMPLICATIONS.—When tabes is a complication of pulmonary or bronchial phthisis, or when either of the latter [p. 1193] diseases appears as an intercurrent affection during the course of a primary localized tuberculosis of these glands, the glandular degeneration runs a more rapid course. When it appears as an extension of external scrofulous affections or finds its cause in gastro-intestinal irritation, its course is usually less rapid. The number of glands involved greatly influences its duration. The mechanical impediment to nutrition offered by a large number of impermeable glands promotes rapid emaciation and exhaustion. The condition of the mucous coat of the alimentary tract offers many considerations that affect its course and duration. Follicular enteritis hastens, and tuberculous ulceration of the mucous membrane speedily brings, the case to a fatal termination.
Some of the older authors refer to the frequent complication of rickets with tabes mesenterica, and the writer in numerous post-mortem examinations of the bodies of children dying of rickets has invariably found cheesy mesenteric glands. In view of the fact that rickets is constantly associated with disturbance of the alimentary tract, it should not be a surprise to find the glands in such close contiguity to, and having vascular communication with, the diseased mucous surface in a condition of hyperplasia. Simple hypertrophy is probably a common complication in cases which terminate by recovery, but there must be some element of cause, other than inflammation of the mucous membrane of the intestines, that determines the retrogressive metamorphosis. Several of the older authors have classed rickets in the category of strumous diseases, and it may be that in the fatal cases tuberculosis of the mesenteric glands is a local expression of this diathesis.
TREATMENT.—The treatment consists, for the most part, in methods of prevention and palliation. The tendency to disease of the lymphatic glands in scrofulous children is so constant that it is important to remove all sources of irritation and to combat all influences likely to hasten or promote the localization of the constitutional condition. All chronic discharges and diseases of the skin and mucous membrane, the continuance of which might produce glandular complications, should be cured as speedily as possible, slight colds should receive prompt attention, and catarrhal inflammations of the respiratory organs should be arrested as quickly as the resources of science will permit. The alimentary tract demands constant and careful observation. Trivial disorders should not be neglected: the causes should be ascertained and removed. Digestion and nutrition should be maintained at a healthy standard. The hygiene of person, dwelling, and sleeping apartments merits constant and intelligent supervision.
As stated above, tabes of the mesenteric glands is so frequently secondary to other diseases of a scrofulous nature that the danger lies in the failure to arrest or cure such affections. It is unfortunately too true that some of them are often beyond the resources of medical skill, but in many cases the initial manifestations of the strumous diathesis are either entirely neglected or inappropriately treated. In many such cases the final and fatal complication of mesenteric phthisis could be prevented. The treatment of these affections belongs properly to the subjects of tuberculosis and scrofula, to be found in other parts of this System of Medicine.
Localized tuberculosis of the mesenteric glands is so often, either [p. 1194] directly or indirectly, connected with catarrhal inflammations of the gastro-intestinal mucous membrane that the cure of these affections cannot be too strongly insisted upon as an effective method of prevention. This is especially true with children exhibiting the physical signs of the strumous diathesis. When it is inherited from a diseased mother, it may be necessary to resort to artificial feeding before the proper time for weaning has been reached. In such cases no uniform rule can be arbitrarily followed. The condition of both mother and child must be considered, and cases will occur which will demand the exercise of the most cautious discretion and diligent observation.
When the disease has become established but little can be accomplished. In such cases the treatment refers to the palliation of symptoms and the maintenance of nutrition. Pain, when present, must be relieved—if necessary by anodynes, either given internally or applied in the form of cataplasms. Most often it is due to the coexisting disease of the intestinal mucous membrane or to the ingestion of unsuitable foods. The diet should be regulated and limited to nutritious and easily-digested articles. Sometimes, even in cases of advanced degeneration of the glands, great benefit may be temporarily obtained by attention to the diet. Diarrhoea should be controlled, but when dependent upon tuberculous ulcerations of the intestinal mucous membrane but little can be done toward delaying the fatal termination. When a large number of glands are affected, it will be necessary to limit the diet to such nutrient fluids as may be absorbed from the stomach.
The medical treatment is confined to a few remedies. Faulty nutrition is the predominant factor, and the drugs employed should be directed to the improvement of the assimilative functions. The lacto-phosphate of iron in the form of syrup, or the phosphates in the form of the compound syrup, sometimes prove valuable tonics. The lacto-phosphate may be given in combination with cod-liver oil. This latter, either internally or by inunction, is the most valuable and universally applicable of all remedies. The mistake is very frequently made of giving too large quantities. Few children can digest as much as a drachm administered three times a day. In Washington it is usually given in the form of the phosphatic emulsion, and has proved in the service of the Children's Hospital a valuable and effective remedy in the nutritional disorders of children. Of the chalybeates, the syrup of the iodide of iron is by far the most valuable; this may be given alone or in combination with cod-liver oil. It is specially indicated when anæmia is a marked characteristic. Some recent reports favor the employment of pancreatized foods. The ointment of the iodide of lead has been highly extolled as a local application to the belly. The nature of the disease should be constantly borne in mind, and all depressing agencies should be sedulously avoided.
End of the Project Gutenberg EBook of A System of Practical Medicine By
American Authors, Vol. II, by Various
*** END OF THIS PROJECT GUTENBERG EBOOK SYSTEM OF PRACTICAL MEDICINE, VOL II ***
***** This file should be named 45313-h.htm or 45313-h.zip *****
This and all associated files of various formats will be found in:
http://www.gutenberg.org/4/5/3/1/45313/
Produced by Ron Swanson
Updated editions will replace the previous one--the old editions
will be renamed.
Creating the works from public domain print editions means that no
one owns a United States copyright in these works, so the Foundation
(and you!) can copy and distribute it in the United States without
permission and without paying copyright royalties. Special rules,
set forth in the General Terms of Use part of this license, apply to
copying and distributing Project Gutenberg-tm electronic works to
protect the PROJECT GUTENBERG-tm concept and trademark. Project
Gutenberg is a registered trademark, and may not be used if you
charge for the eBooks, unless you receive specific permission. If you
do not charge anything for copies of this eBook, complying with the
rules is very easy. You may use this eBook for nearly any purpose
such as creation of derivative works, reports, performances and
research. They may be modified and printed and given away--you may do
practically ANYTHING with public domain eBooks. Redistribution is
subject to the trademark license, especially commercial
redistribution.
*** START: FULL LICENSE ***
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full Project
Gutenberg-tm License available with this file or online at
www.gutenberg.org/license.
Section 1. General Terms of Use and Redistributing Project Gutenberg-tm
electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or destroy
all copies of Project Gutenberg-tm electronic works in your possession.
If you paid a fee for obtaining a copy of or access to a Project
Gutenberg-tm electronic work and you do not agree to be bound by the
terms of this agreement, you may obtain a refund from the person or
entity to whom you paid the fee as set forth in paragraph 1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this agreement
and help preserve free future access to Project Gutenberg-tm electronic
works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the Foundation"
or PGLAF), owns a compilation copyright in the collection of Project
Gutenberg-tm electronic works. Nearly all the individual works in the
collection are in the public domain in the United States. If an
individual work is in the public domain in the United States and you are
located in the United States, we do not claim a right to prevent you from
copying, distributing, performing, displaying or creating derivative
works based on the work as long as all references to Project Gutenberg
are removed. Of course, we hope that you will support the Project
Gutenberg-tm mission of promoting free access to electronic works by
freely sharing Project Gutenberg-tm works in compliance with the terms of
this agreement for keeping the Project Gutenberg-tm name associated with
the work. You can easily comply with the terms of this agreement by
keeping this work in the same format with its attached full Project
Gutenberg-tm License when you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are in
a constant state of change. If you are outside the United States, check
the laws of your country in addition to the terms of this agreement
before downloading, copying, displaying, performing, distributing or
creating derivative works based on this work or any other Project
Gutenberg-tm work. The Foundation makes no representations concerning
the copyright status of any work in any country outside the United
States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other immediate
access to, the full Project Gutenberg-tm License must appear prominently
whenever any copy of a Project Gutenberg-tm work (any work on which the
phrase "Project Gutenberg" appears, or with which the phrase "Project
Gutenberg" is associated) is accessed, displayed, performed, viewed,
copied or distributed:
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
1.E.2. If an individual Project Gutenberg-tm electronic work is derived
from the public domain (does not contain a notice indicating that it is
posted with permission of the copyright holder), the work can be copied
and distributed to anyone in the United States without paying any fees
or charges. If you are redistributing or providing access to a work
with the phrase "Project Gutenberg" associated with or appearing on the
work, you must comply either with the requirements of paragraphs 1.E.1
through 1.E.7 or obtain permission for the use of the work and the
Project Gutenberg-tm trademark as set forth in paragraphs 1.E.8 or
1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any additional
terms imposed by the copyright holder. Additional terms will be linked
to the Project Gutenberg-tm License for all works posted with the
permission of the copyright holder found at the beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including any
word processing or hypertext form. However, if you provide access to or
distribute copies of a Project Gutenberg-tm work in a format other than
"Plain Vanilla ASCII" or other format used in the official version
posted on the official Project Gutenberg-tm web site (www.gutenberg.org),
you must, at no additional cost, fee or expense to the user, provide a
copy, a means of exporting a copy, or a means of obtaining a copy upon
request, of the work in its original "Plain Vanilla ASCII" or other
form. Any alternate format must include the full Project Gutenberg-tm
License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works provided
that
- You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is
owed to the owner of the Project Gutenberg-tm trademark, but he
has agreed to donate royalties under this paragraph to the
Project Gutenberg Literary Archive Foundation. Royalty payments
must be paid within 60 days following each date on which you
prepare (or are legally required to prepare) your periodic tax
returns. Royalty payments should be clearly marked as such and
sent to the Project Gutenberg Literary Archive Foundation at the
address specified in Section 4, "Information about donations to
the Project Gutenberg Literary Archive Foundation."
- You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or
destroy all copies of the works possessed in a physical medium
and discontinue all use of and all access to other copies of
Project Gutenberg-tm works.
- You provide, in accordance with paragraph 1.F.3, a full refund of any
money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days
of receipt of the work.
- You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project Gutenberg-tm
electronic work or group of works on different terms than are set
forth in this agreement, you must obtain permission in writing from
both the Project Gutenberg Literary Archive Foundation and Michael
Hart, the owner of the Project Gutenberg-tm trademark. Contact the
Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
public domain works in creating the Project Gutenberg-tm
collection. Despite these efforts, Project Gutenberg-tm electronic
works, and the medium on which they may be stored, may contain
"Defects," such as, but not limited to, incomplete, inaccurate or
corrupt data, transcription errors, a copyright or other intellectual
property infringement, a defective or damaged disk or other medium, a
computer virus, or computer codes that damage or cannot be read by
your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH 1.F.3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium with
your written explanation. The person or entity that provided you with
the defective work may elect to provide a replacement copy in lieu of a
refund. If you received the work electronically, the person or entity
providing it to you may choose to give you a second opportunity to
receive the work electronically in lieu of a refund. If the second copy
is also defective, you may demand a refund in writing without further
opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS', WITH NO OTHER
WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT LIMITED TO
WARRANTIES OF MERCHANTABILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of damages.
If any disclaimer or limitation set forth in this agreement violates the
law of the state applicable to this agreement, the agreement shall be
interpreted to make the maximum disclaimer or limitation permitted by
the applicable state law. The invalidity or unenforceability of any
provision of this agreement shall not void the remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in accordance
with this agreement, and any volunteers associated with the production,
promotion and distribution of Project Gutenberg-tm electronic works,
harmless from all liability, costs and expenses, including legal fees,
that arise directly or indirectly from any of the following which you do
or cause to occur: (a) distribution of this or any Project Gutenberg-tm
work, (b) alteration, modification, or additions or deletions to any
Project Gutenberg-tm work, and (c) any Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of computers
including obsolete, old, middle-aged and new computers. It exists
because of the efforts of hundreds of volunteers and donations from
people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need are critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future generations.
To learn more about the Project Gutenberg Literary Archive Foundation
and how your efforts and donations can help, see Sections 3 and 4
and the Foundation information page at www.gutenberg.org
Section 3. Information about the Project Gutenberg Literary Archive
Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Contributions to the Project Gutenberg
Literary Archive Foundation are tax deductible to the full extent
permitted by U.S. federal laws and your state's laws.
The Foundation's principal office is located at 4557 Melan Dr. S.
Fairbanks, AK, 99712., but its volunteers and employees are scattered
throughout numerous locations. Its business office is located at 809
North 1500 West, Salt Lake City, UT 84116, (801) 596-1887. Email
contact links and up to date contact information can be found at the
Foundation's web site and official page at www.gutenberg.org/contact
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
[email protected]
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To
SEND DONATIONS or determine the status of compliance for any
particular state visit www.gutenberg.org/donate
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including checks, online payments and credit card donations.
To donate, please visit: www.gutenberg.org/donate
Section 5. General Information About Project Gutenberg-tm electronic
works.
Professor Michael S. Hart was the originator of the Project Gutenberg-tm
concept of a library of electronic works that could be freely shared
with anyone. For forty years, he produced and distributed Project
Gutenberg-tm eBooks with only a loose network of volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as Public Domain in the U.S.
unless a copyright notice is included. Thus, we do not necessarily
keep eBooks in compliance with any particular paper edition.
Most people start at our Web site which has the main PG search facility:
www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.